User login
Which facts count?
Students who spend a month with me always want a session on topical steroids, that great undiscovered world they have to know but dread to explore. They’ve all seen those tables of steroid potency based on the rabbit-ear bioassay. These run to long columns (or several pages) of small print ordering the steroid universe from the aristocracy of Class 1 ("Supernovacort" 0.015%) down through the midrange ("Mediocricort" 0.026% ointment is Class 2, while Mediocricort 0.026% cream is only Class 3), down to the humble "Trivialicort" 32%, which on a good day is just a measly Class 6. All those multisyllabic names and numbers and classes bewilder and intimidate the poor kids. Even their earnest medical-student memorization skills leave them in despair of mastering all this stuff.
I ask them to ponder a mini-scenario: Your patient was given a topical steroid cream. He says it didn’t work. List all possible explanations.
The next day we discuss their answers. Most students manage to come up with several types of reasons. Maybe the steroid didn’t work because the diagnosis was wrong. (It was a fungus.) Perhaps the condition is inherently unresponsive (like knee psoriasis). Sometimes, the patient didn’t use the cream.
Then we break down that third category. Why would a patient not use the cream? Reasons include:
• The tube was too small (15 g for a full-body rash).
• The steroid did work, but the patient thought it didn’t because the eczema came back. (Eczema comes back.)
• The patient was afraid of steroids. ("I heard they thin your skin.")
I end our session by noting that this third group (the patient didn’t use the cream) is a) intellectually uninteresting; and b) the reason behind most cases were "the steroid didn’t work." By contrast, using the wrong steroid – as defined by the fine-grained distinctions on steroid potency tables – is rarely the difference between success and failure.
I give students a list of four generics, from weak to strong, and advise them not to clutter up their brains with any others. (Since most of them are headed for primary care, those four will be plenty, freeing brain space for board memorization.)
Ever since medical school, which is a rather long time ago by now, I’ve wondered why some things are taught and others left out. More particularly, why are some kinds of facts thought to be important (the ones you can quantify or put numbers next to, for instance) and others are too squishy to mention (such as knowing what the patient thinks about the treatment)?
After all, knowing what a patient thinks about what a treatment does – how it might harm them, and what a treatment "working" really means – has a lot to do with whether the treatment is used properly, or used at all. Why isn’t that important? Because you can’t put it into a table laced with decimal points and percentages?
The tendency to reduce everything to what you can measure has been around for a long time but seems to be getting worse. I read the other day about something called the Human Connectome Project, an effort to produce data to help answer the central question, "How do differences between you and me and how our brains are wired up, relate to differences in our behaviors, our thoughts, our emotions, our feelings, and our experiences?"
I am not the first to wonder whether functional MRIs, with those gaily colored snapshots of the brain in action, really tell us more about how the brain works than does talking with the people who own those brains. The assumption seems to be that pictures of brain circuits are "real," whereas mere talk is mush, not the stuff of science, whose fruits we physicians are supposed to apply. I am wired, therefore I am.
Suppose a patient thinks that topical steroids thin the skin? Suppose she expects your eczema cream to make the rash go away once and for all, and when it comes back, she takes that as proof that it "didn’t work" and stops using it because it’s clearly worthless? Would those opinions show up on a color photo of her amygdala?
Can my patients be the only ones whose opinions about health and disease matter more, and more often, than do the tabulated measures of clinical efficacy?
You know, the real stuff you have to memorize and document, to get in and to get by.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.
Students who spend a month with me always want a session on topical steroids, that great undiscovered world they have to know but dread to explore. They’ve all seen those tables of steroid potency based on the rabbit-ear bioassay. These run to long columns (or several pages) of small print ordering the steroid universe from the aristocracy of Class 1 ("Supernovacort" 0.015%) down through the midrange ("Mediocricort" 0.026% ointment is Class 2, while Mediocricort 0.026% cream is only Class 3), down to the humble "Trivialicort" 32%, which on a good day is just a measly Class 6. All those multisyllabic names and numbers and classes bewilder and intimidate the poor kids. Even their earnest medical-student memorization skills leave them in despair of mastering all this stuff.
I ask them to ponder a mini-scenario: Your patient was given a topical steroid cream. He says it didn’t work. List all possible explanations.
The next day we discuss their answers. Most students manage to come up with several types of reasons. Maybe the steroid didn’t work because the diagnosis was wrong. (It was a fungus.) Perhaps the condition is inherently unresponsive (like knee psoriasis). Sometimes, the patient didn’t use the cream.
Then we break down that third category. Why would a patient not use the cream? Reasons include:
• The tube was too small (15 g for a full-body rash).
• The steroid did work, but the patient thought it didn’t because the eczema came back. (Eczema comes back.)
• The patient was afraid of steroids. ("I heard they thin your skin.")
I end our session by noting that this third group (the patient didn’t use the cream) is a) intellectually uninteresting; and b) the reason behind most cases were "the steroid didn’t work." By contrast, using the wrong steroid – as defined by the fine-grained distinctions on steroid potency tables – is rarely the difference between success and failure.
I give students a list of four generics, from weak to strong, and advise them not to clutter up their brains with any others. (Since most of them are headed for primary care, those four will be plenty, freeing brain space for board memorization.)
Ever since medical school, which is a rather long time ago by now, I’ve wondered why some things are taught and others left out. More particularly, why are some kinds of facts thought to be important (the ones you can quantify or put numbers next to, for instance) and others are too squishy to mention (such as knowing what the patient thinks about the treatment)?
After all, knowing what a patient thinks about what a treatment does – how it might harm them, and what a treatment "working" really means – has a lot to do with whether the treatment is used properly, or used at all. Why isn’t that important? Because you can’t put it into a table laced with decimal points and percentages?
The tendency to reduce everything to what you can measure has been around for a long time but seems to be getting worse. I read the other day about something called the Human Connectome Project, an effort to produce data to help answer the central question, "How do differences between you and me and how our brains are wired up, relate to differences in our behaviors, our thoughts, our emotions, our feelings, and our experiences?"
I am not the first to wonder whether functional MRIs, with those gaily colored snapshots of the brain in action, really tell us more about how the brain works than does talking with the people who own those brains. The assumption seems to be that pictures of brain circuits are "real," whereas mere talk is mush, not the stuff of science, whose fruits we physicians are supposed to apply. I am wired, therefore I am.
Suppose a patient thinks that topical steroids thin the skin? Suppose she expects your eczema cream to make the rash go away once and for all, and when it comes back, she takes that as proof that it "didn’t work" and stops using it because it’s clearly worthless? Would those opinions show up on a color photo of her amygdala?
Can my patients be the only ones whose opinions about health and disease matter more, and more often, than do the tabulated measures of clinical efficacy?
You know, the real stuff you have to memorize and document, to get in and to get by.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.
Students who spend a month with me always want a session on topical steroids, that great undiscovered world they have to know but dread to explore. They’ve all seen those tables of steroid potency based on the rabbit-ear bioassay. These run to long columns (or several pages) of small print ordering the steroid universe from the aristocracy of Class 1 ("Supernovacort" 0.015%) down through the midrange ("Mediocricort" 0.026% ointment is Class 2, while Mediocricort 0.026% cream is only Class 3), down to the humble "Trivialicort" 32%, which on a good day is just a measly Class 6. All those multisyllabic names and numbers and classes bewilder and intimidate the poor kids. Even their earnest medical-student memorization skills leave them in despair of mastering all this stuff.
I ask them to ponder a mini-scenario: Your patient was given a topical steroid cream. He says it didn’t work. List all possible explanations.
The next day we discuss their answers. Most students manage to come up with several types of reasons. Maybe the steroid didn’t work because the diagnosis was wrong. (It was a fungus.) Perhaps the condition is inherently unresponsive (like knee psoriasis). Sometimes, the patient didn’t use the cream.
Then we break down that third category. Why would a patient not use the cream? Reasons include:
• The tube was too small (15 g for a full-body rash).
• The steroid did work, but the patient thought it didn’t because the eczema came back. (Eczema comes back.)
• The patient was afraid of steroids. ("I heard they thin your skin.")
I end our session by noting that this third group (the patient didn’t use the cream) is a) intellectually uninteresting; and b) the reason behind most cases were "the steroid didn’t work." By contrast, using the wrong steroid – as defined by the fine-grained distinctions on steroid potency tables – is rarely the difference between success and failure.
I give students a list of four generics, from weak to strong, and advise them not to clutter up their brains with any others. (Since most of them are headed for primary care, those four will be plenty, freeing brain space for board memorization.)
Ever since medical school, which is a rather long time ago by now, I’ve wondered why some things are taught and others left out. More particularly, why are some kinds of facts thought to be important (the ones you can quantify or put numbers next to, for instance) and others are too squishy to mention (such as knowing what the patient thinks about the treatment)?
After all, knowing what a patient thinks about what a treatment does – how it might harm them, and what a treatment "working" really means – has a lot to do with whether the treatment is used properly, or used at all. Why isn’t that important? Because you can’t put it into a table laced with decimal points and percentages?
The tendency to reduce everything to what you can measure has been around for a long time but seems to be getting worse. I read the other day about something called the Human Connectome Project, an effort to produce data to help answer the central question, "How do differences between you and me and how our brains are wired up, relate to differences in our behaviors, our thoughts, our emotions, our feelings, and our experiences?"
I am not the first to wonder whether functional MRIs, with those gaily colored snapshots of the brain in action, really tell us more about how the brain works than does talking with the people who own those brains. The assumption seems to be that pictures of brain circuits are "real," whereas mere talk is mush, not the stuff of science, whose fruits we physicians are supposed to apply. I am wired, therefore I am.
Suppose a patient thinks that topical steroids thin the skin? Suppose she expects your eczema cream to make the rash go away once and for all, and when it comes back, she takes that as proof that it "didn’t work" and stops using it because it’s clearly worthless? Would those opinions show up on a color photo of her amygdala?
Can my patients be the only ones whose opinions about health and disease matter more, and more often, than do the tabulated measures of clinical efficacy?
You know, the real stuff you have to memorize and document, to get in and to get by.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since 1997.

Report from the front line: A medical mission in Honduras
The poor are many
and so
impossible to forget.
Roberto Sosa, Honduran poet

In February, 20 physicians, nurses, and other health care personnel – including five members of the Family Medicine Residency Program at Abington (Pa.) Memorial Hospital – Dr. Kate Baranik, Dr. Magan Madsen, Dr. Margarita McDonald, Dr. John Russell, and Dr. Neil Skolnik – boarded a flight to Honduras for a medical mission to provide medical care to those in need there. Only 13% of people in the country have health insurance. The hospital bed ratio is 0.7 beds/1,000 people, as compared with the United States, where the ratio is 3 beds/1,000 people. These statistics make it evident that the health care system in Honduras needs restructuring. Although a group of Americans cannot restructure a whole health care system, the little steps we took in embarking on this journey to provide medical care has made a lasting impact on numerous lives, not least of which are our own.

Operation Heal Honduras was the culmination of 9 years of medical mission trips. What started as a small surgical team blossomed under the organizational leadership of an Abington Memorial Hospital general surgeon, Dr. Seth L. Newman, into a multidisciplinary group now including family medicine, general and trauma surgery, orthopedics, and ob.gyn. In addition to the five attending physicians, this year there were five residents-in-training, three certified registered nurse anesthetists, and multiple RNs and translators. While they vary in quality and cleanliness, Honduras has hospitals, operating rooms, and places to set up a clinic. More difficult is the job of obtaining the disposable items needed to perform operations and solve medical mysteries. Hospitals cannot afford to purchase these things. So the team brought gowns, gloves, sutures, gauze, mesh, casting material, ACE wraps, laparoscopic ports, drapes, and approximately $2,000 worth of medications.

While in Honduras, the team stayed at the Andrew Clinic located 15 miles north of El Progreso; the clinic is run by Dr. Florence Yoon and Dr. David Yoon. El Progreso is notable for its lush green mountains, palm trees, banana plants. On a typical day, the medical team set up a clinic in neighboring villages while the surgical team operated at the hospital in El Progreso.
One day specifically stands out in everyone’s mind. This day, like the others, started early, with a breakfast of scrambled eggs, beans, tortillas, mango, and cantaloupe, after which we left for the hospital and the mission medical clinic at 7 a.m. While driving to the hospital, it was impossible not to notice the poverty: the emaciated man walking on the side of the road with a plastic bag in hand; the muddy unpaved roads, branching off the side of the main road, each lined with wooden shacks with tin roofs; the rusted gutted cars on the side of the road; the Coca-Cola and Pepsi signs everywhere tempting people to spend money that they did not have on soda that they did not need. Everywhere we drove there were soldiers carrying machine guns to prevent crime, which is dramatically high in Honduras.

When we arrived at the hospital, the medical team consulted with the surgical team on a difficult case, and the surgeons were informed that the power to the hospital might be cut off at 8 a.m., as part of routine rotating power outages. It turned out that by 8:30, the power was still on, so the surgeons were able to operate in three operating rooms. The medical team then continued to the small village church where we were to stage a medical clinic. Pulling up to the church, we saw how the people lived in the village. They lived in small huts, with roosters, chickens, and dogs roaming freely in the muddy yards. Laundry was hanging outside each house, and smiling children played in the streets. Still, the medical team felt trepidation as we headed to care for the people in a neighborhood church built 3 years ago in a poor area of San Pedro Sula, the city known as the murder capital of the world.

Arriving, the bus turned into the narrow two-lane dirt street that was barely wider than the bus itself. When we disembarked the bus, we saw about a hundred people, young and old, waiting patiently for us in the church. The team saw about 400 people that day; we injected knees and shoulders, treated pneumonia in a young infant, gave prednisone for asthma, counseled an elderly woman with depression, gave antibiotics for wounds, saw a young child with clubfoot, and helped others who were tired, poor, and had headaches and joint pain. They waited a long time to be seen and receive the medical care we could give in the form of vitamins, antiparasite medications, antibiotics, skin creams, and others. That medical care that would not fix their lives, but it did make their lives a little better by virtue of medicines and knowing that someone cared enough to be there. Their smiles and their "gracias" connected them to us and told us a part of their story that could be told no other way.
Dr. Skolnik is professor of family and community medicine at, Temple University, Philadelphia, and associate director of the family medicine residency program there. Ms. Skolnik attends Drexel University and is a research assistant at the Children’s Hospital of Pennsylvania, both in Philadelphia. Ms. Ogen is a certified registered nurse anesthetist at Abington Memorial Hospital.
*Correction, 3/10/2014: An earlier version of this story misstated Ava Skolnik's name.
The poor are many
and so
impossible to forget.
Roberto Sosa, Honduran poet
In February, 20 physicians, nurses, and other health care personnel – including five members of the Family Medicine Residency Program at Abington (Pa.) Memorial Hospital – Dr. Kate Baranik, Dr. Magan Madsen, Dr. Margarita McDonald, Dr. John Russell, and Dr. Neil Skolnik – boarded a flight to Honduras for a medical mission to provide medical care to those in need there. Only 13% of people in the country have health insurance. The hospital bed ratio is 0.7 beds/1,000 people, as compared with the United States, where the ratio is 3 beds/1,000 people. These statistics make it evident that the health care system in Honduras needs restructuring. Although a group of Americans cannot restructure a whole health care system, the little steps we took in embarking on this journey to provide medical care has made a lasting impact on numerous lives, not least of which are our own.
Operation Heal Honduras was the culmination of 9 years of medical mission trips. What started as a small surgical team blossomed under the organizational leadership of an Abington Memorial Hospital general surgeon, Dr. Seth L. Newman, into a multidisciplinary group now including family medicine, general and trauma surgery, orthopedics, and ob.gyn. In addition to the five attending physicians, this year there were five residents-in-training, three certified registered nurse anesthetists, and multiple RNs and translators. While they vary in quality and cleanliness, Honduras has hospitals, operating rooms, and places to set up a clinic. More difficult is the job of obtaining the disposable items needed to perform operations and solve medical mysteries. Hospitals cannot afford to purchase these things. So the team brought gowns, gloves, sutures, gauze, mesh, casting material, ACE wraps, laparoscopic ports, drapes, and approximately $2,000 worth of medications.
While in Honduras, the team stayed at the Andrew Clinic located 15 miles north of El Progreso; the clinic is run by Dr. Florence Yoon and Dr. David Yoon. El Progreso is notable for its lush green mountains, palm trees, banana plants. On a typical day, the medical team set up a clinic in neighboring villages while the surgical team operated at the hospital in El Progreso.
One day specifically stands out in everyone’s mind. This day, like the others, started early, with a breakfast of scrambled eggs, beans, tortillas, mango, and cantaloupe, after which we left for the hospital and the mission medical clinic at 7 a.m. While driving to the hospital, it was impossible not to notice the poverty: the emaciated man walking on the side of the road with a plastic bag in hand; the muddy unpaved roads, branching off the side of the main road, each lined with wooden shacks with tin roofs; the rusted gutted cars on the side of the road; the Coca-Cola and Pepsi signs everywhere tempting people to spend money that they did not have on soda that they did not need. Everywhere we drove there were soldiers carrying machine guns to prevent crime, which is dramatically high in Honduras.
When we arrived at the hospital, the medical team consulted with the surgical team on a difficult case, and the surgeons were informed that the power to the hospital might be cut off at 8 a.m., as part of routine rotating power outages. It turned out that by 8:30, the power was still on, so the surgeons were able to operate in three operating rooms. The medical team then continued to the small village church where we were to stage a medical clinic. Pulling up to the church, we saw how the people lived in the village. They lived in small huts, with roosters, chickens, and dogs roaming freely in the muddy yards. Laundry was hanging outside each house, and smiling children played in the streets. Still, the medical team felt trepidation as we headed to care for the people in a neighborhood church built 3 years ago in a poor area of San Pedro Sula, the city known as the murder capital of the world.
Arriving, the bus turned into the narrow two-lane dirt street that was barely wider than the bus itself. When we disembarked the bus, we saw about a hundred people, young and old, waiting patiently for us in the church. The team saw about 400 people that day; we injected knees and shoulders, treated pneumonia in a young infant, gave prednisone for asthma, counseled an elderly woman with depression, gave antibiotics for wounds, saw a young child with clubfoot, and helped others who were tired, poor, and had headaches and joint pain. They waited a long time to be seen and receive the medical care we could give in the form of vitamins, antiparasite medications, antibiotics, skin creams, and others. That medical care that would not fix their lives, but it did make their lives a little better by virtue of medicines and knowing that someone cared enough to be there. Their smiles and their "gracias" connected them to us and told us a part of their story that could be told no other way.
Dr. Skolnik is professor of family and community medicine at, Temple University, Philadelphia, and associate director of the family medicine residency program there. Ms. Skolnik attends Drexel University and is a research assistant at the Children’s Hospital of Pennsylvania, both in Philadelphia. Ms. Ogen is a certified registered nurse anesthetist at Abington Memorial Hospital.
*Correction, 3/10/2014: An earlier version of this story misstated Ava Skolnik's name.
The poor are many
and so
impossible to forget.
Roberto Sosa, Honduran poet
In February, 20 physicians, nurses, and other health care personnel – including five members of the Family Medicine Residency Program at Abington (Pa.) Memorial Hospital – Dr. Kate Baranik, Dr. Magan Madsen, Dr. Margarita McDonald, Dr. John Russell, and Dr. Neil Skolnik – boarded a flight to Honduras for a medical mission to provide medical care to those in need there. Only 13% of people in the country have health insurance. The hospital bed ratio is 0.7 beds/1,000 people, as compared with the United States, where the ratio is 3 beds/1,000 people. These statistics make it evident that the health care system in Honduras needs restructuring. Although a group of Americans cannot restructure a whole health care system, the little steps we took in embarking on this journey to provide medical care has made a lasting impact on numerous lives, not least of which are our own.
Operation Heal Honduras was the culmination of 9 years of medical mission trips. What started as a small surgical team blossomed under the organizational leadership of an Abington Memorial Hospital general surgeon, Dr. Seth L. Newman, into a multidisciplinary group now including family medicine, general and trauma surgery, orthopedics, and ob.gyn. In addition to the five attending physicians, this year there were five residents-in-training, three certified registered nurse anesthetists, and multiple RNs and translators. While they vary in quality and cleanliness, Honduras has hospitals, operating rooms, and places to set up a clinic. More difficult is the job of obtaining the disposable items needed to perform operations and solve medical mysteries. Hospitals cannot afford to purchase these things. So the team brought gowns, gloves, sutures, gauze, mesh, casting material, ACE wraps, laparoscopic ports, drapes, and approximately $2,000 worth of medications.
While in Honduras, the team stayed at the Andrew Clinic located 15 miles north of El Progreso; the clinic is run by Dr. Florence Yoon and Dr. David Yoon. El Progreso is notable for its lush green mountains, palm trees, banana plants. On a typical day, the medical team set up a clinic in neighboring villages while the surgical team operated at the hospital in El Progreso.
One day specifically stands out in everyone’s mind. This day, like the others, started early, with a breakfast of scrambled eggs, beans, tortillas, mango, and cantaloupe, after which we left for the hospital and the mission medical clinic at 7 a.m. While driving to the hospital, it was impossible not to notice the poverty: the emaciated man walking on the side of the road with a plastic bag in hand; the muddy unpaved roads, branching off the side of the main road, each lined with wooden shacks with tin roofs; the rusted gutted cars on the side of the road; the Coca-Cola and Pepsi signs everywhere tempting people to spend money that they did not have on soda that they did not need. Everywhere we drove there were soldiers carrying machine guns to prevent crime, which is dramatically high in Honduras.
When we arrived at the hospital, the medical team consulted with the surgical team on a difficult case, and the surgeons were informed that the power to the hospital might be cut off at 8 a.m., as part of routine rotating power outages. It turned out that by 8:30, the power was still on, so the surgeons were able to operate in three operating rooms. The medical team then continued to the small village church where we were to stage a medical clinic. Pulling up to the church, we saw how the people lived in the village. They lived in small huts, with roosters, chickens, and dogs roaming freely in the muddy yards. Laundry was hanging outside each house, and smiling children played in the streets. Still, the medical team felt trepidation as we headed to care for the people in a neighborhood church built 3 years ago in a poor area of San Pedro Sula, the city known as the murder capital of the world.
Arriving, the bus turned into the narrow two-lane dirt street that was barely wider than the bus itself. When we disembarked the bus, we saw about a hundred people, young and old, waiting patiently for us in the church. The team saw about 400 people that day; we injected knees and shoulders, treated pneumonia in a young infant, gave prednisone for asthma, counseled an elderly woman with depression, gave antibiotics for wounds, saw a young child with clubfoot, and helped others who were tired, poor, and had headaches and joint pain. They waited a long time to be seen and receive the medical care we could give in the form of vitamins, antiparasite medications, antibiotics, skin creams, and others. That medical care that would not fix their lives, but it did make their lives a little better by virtue of medicines and knowing that someone cared enough to be there. Their smiles and their "gracias" connected them to us and told us a part of their story that could be told no other way.
Dr. Skolnik is professor of family and community medicine at, Temple University, Philadelphia, and associate director of the family medicine residency program there. Ms. Skolnik attends Drexel University and is a research assistant at the Children’s Hospital of Pennsylvania, both in Philadelphia. Ms. Ogen is a certified registered nurse anesthetist at Abington Memorial Hospital.
*Correction, 3/10/2014: An earlier version of this story misstated Ava Skolnik's name.

The demise of renal artery stenting
The announcement from Medtronic in January has apparently brought down the curtain on the much-heralded approach to the treatment of refractory hypertension using radio-frequency renal artery sympathetic nerve ablation (RASNA) applied through the tip of the Symplicity catheter.
This technology is being used widely around the world for the treatment of refractory hypertensive patients. The enthusiasm for RASNA was generated by a series of reports suggesting that an amazing decrease in systolic blood pressure of more than 30 mm Hg can be obtained in patients with resistant hypertension taking three or more antihypertensive drugs. However, the SYMPLICITY HTN-3 trial (Clin. Cardiol. 2012;35:528-35), which enrolled 535 patients with refractory hypertension, failed to achieve the primary endpoint of a significant decrease in systolic pressure in the radio-frequency (RF)-treated patients compared with the sham-operated patients. In the study, blinding was rigorously managed by renal artery catheterization of all 535 patients, with RF ablation instituted in two-thirds of the patients, and a sham operation conducted in one-third.
As a result of the observations in SYMPLICITY HTN-3, Medtronic is suspending enrollment in current trials using the Symplicity device throughout the world, and will "continue to ensure patients access to the Symplicity technology at the discretion of their physicians in countries where the device is approved," according to its statement.
Enthusiasm for RF ablation of the sympathetic nerves accompanying the renal artery was generated by a series of publications describing the physiologic and therapeutic effects. The first publications in this series described the metabolic changes that occurred after RF ablation carried out in one patient who experienced a decrease in systolic pressure of 20 mm Hg associated with modulation of sympathetic activity 30 days and 12 months after the procedure (N. Engl. J. Med. 2009;361:932-4). This study was followed by two subsequent reports of patients in whom RASNA was carried out. A proof-of-concept trial (SYMPLICITY HTN-1) in 153 patients reported a substantial decrease in blood pressure over a 2-year period (Hypertension 2011;57:911-7). A second trial (SYMPLICITY HTN-2) randomized 106 patients to either RASNA or standard therapy. That trial reported that 84% of the patients receiving RASNA had a reduction of blood pressure greater than 10 mm Hg within 6 months, compared with 35% of the control group (Lancet 2010;376:1903-9). Both studies reported a profound decrease in blood pressure that ensued over a 6-month period in 80%-90% of patients undergoing the therapy. In light of these reports, it is difficult to explain the fact that SYMPLICITY HTN-3 was a negative study.
Modulation of the sympathetic nervous system for the treatment of hypertension is not new. More than 60 years ago, Smithwick and colleagues carried out both surgical lumbar and sympathetic splanchnicectomy for its treatment with uncertain results (JAMA 1952;153:1501-4). In an era when all that we could offer hypertensive patients was a low-salt diet, the procedure became rather popular. However, the surgical risks, adverse side effects, and uncertainty of benefit led to both procedures being discontinued. Recently, there have been studies of the effect of stimulation of the carotid sinus nerve for the treatment of hypertension.
The potential benefit of modulation of the arterial sympathetic nerves, and particularly those located in the renal artery, became the focus of this recent interest. Nevertheless, a number of questions have arisen in regard to the mechanism of RASNA. And why does it take 6 months to achieve the blood pressure response? In addition, there is very little published data in regard to the changes in the renal artery and its adjacent tissue as a result of the RF ablation.
At the present, Medtronic has not provided any information beyond its indicating the lack of benefit. Further information will be reported at the upcoming American College of Cardiology scientific sessions. In the meantime, speculation is rampant as to whether the initial reports were purely placebo effects or if there is something intrinsically flawed in the SYMPLICITY HTN -3 trial.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The announcement from Medtronic in January has apparently brought down the curtain on the much-heralded approach to the treatment of refractory hypertension using radio-frequency renal artery sympathetic nerve ablation (RASNA) applied through the tip of the Symplicity catheter.
This technology is being used widely around the world for the treatment of refractory hypertensive patients. The enthusiasm for RASNA was generated by a series of reports suggesting that an amazing decrease in systolic blood pressure of more than 30 mm Hg can be obtained in patients with resistant hypertension taking three or more antihypertensive drugs. However, the SYMPLICITY HTN-3 trial (Clin. Cardiol. 2012;35:528-35), which enrolled 535 patients with refractory hypertension, failed to achieve the primary endpoint of a significant decrease in systolic pressure in the radio-frequency (RF)-treated patients compared with the sham-operated patients. In the study, blinding was rigorously managed by renal artery catheterization of all 535 patients, with RF ablation instituted in two-thirds of the patients, and a sham operation conducted in one-third.
As a result of the observations in SYMPLICITY HTN-3, Medtronic is suspending enrollment in current trials using the Symplicity device throughout the world, and will "continue to ensure patients access to the Symplicity technology at the discretion of their physicians in countries where the device is approved," according to its statement.
Enthusiasm for RF ablation of the sympathetic nerves accompanying the renal artery was generated by a series of publications describing the physiologic and therapeutic effects. The first publications in this series described the metabolic changes that occurred after RF ablation carried out in one patient who experienced a decrease in systolic pressure of 20 mm Hg associated with modulation of sympathetic activity 30 days and 12 months after the procedure (N. Engl. J. Med. 2009;361:932-4). This study was followed by two subsequent reports of patients in whom RASNA was carried out. A proof-of-concept trial (SYMPLICITY HTN-1) in 153 patients reported a substantial decrease in blood pressure over a 2-year period (Hypertension 2011;57:911-7). A second trial (SYMPLICITY HTN-2) randomized 106 patients to either RASNA or standard therapy. That trial reported that 84% of the patients receiving RASNA had a reduction of blood pressure greater than 10 mm Hg within 6 months, compared with 35% of the control group (Lancet 2010;376:1903-9). Both studies reported a profound decrease in blood pressure that ensued over a 6-month period in 80%-90% of patients undergoing the therapy. In light of these reports, it is difficult to explain the fact that SYMPLICITY HTN-3 was a negative study.
Modulation of the sympathetic nervous system for the treatment of hypertension is not new. More than 60 years ago, Smithwick and colleagues carried out both surgical lumbar and sympathetic splanchnicectomy for its treatment with uncertain results (JAMA 1952;153:1501-4). In an era when all that we could offer hypertensive patients was a low-salt diet, the procedure became rather popular. However, the surgical risks, adverse side effects, and uncertainty of benefit led to both procedures being discontinued. Recently, there have been studies of the effect of stimulation of the carotid sinus nerve for the treatment of hypertension.
The potential benefit of modulation of the arterial sympathetic nerves, and particularly those located in the renal artery, became the focus of this recent interest. Nevertheless, a number of questions have arisen in regard to the mechanism of RASNA. And why does it take 6 months to achieve the blood pressure response? In addition, there is very little published data in regard to the changes in the renal artery and its adjacent tissue as a result of the RF ablation.
At the present, Medtronic has not provided any information beyond its indicating the lack of benefit. Further information will be reported at the upcoming American College of Cardiology scientific sessions. In the meantime, speculation is rampant as to whether the initial reports were purely placebo effects or if there is something intrinsically flawed in the SYMPLICITY HTN -3 trial.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The announcement from Medtronic in January has apparently brought down the curtain on the much-heralded approach to the treatment of refractory hypertension using radio-frequency renal artery sympathetic nerve ablation (RASNA) applied through the tip of the Symplicity catheter.
This technology is being used widely around the world for the treatment of refractory hypertensive patients. The enthusiasm for RASNA was generated by a series of reports suggesting that an amazing decrease in systolic blood pressure of more than 30 mm Hg can be obtained in patients with resistant hypertension taking three or more antihypertensive drugs. However, the SYMPLICITY HTN-3 trial (Clin. Cardiol. 2012;35:528-35), which enrolled 535 patients with refractory hypertension, failed to achieve the primary endpoint of a significant decrease in systolic pressure in the radio-frequency (RF)-treated patients compared with the sham-operated patients. In the study, blinding was rigorously managed by renal artery catheterization of all 535 patients, with RF ablation instituted in two-thirds of the patients, and a sham operation conducted in one-third.
As a result of the observations in SYMPLICITY HTN-3, Medtronic is suspending enrollment in current trials using the Symplicity device throughout the world, and will "continue to ensure patients access to the Symplicity technology at the discretion of their physicians in countries where the device is approved," according to its statement.
Enthusiasm for RF ablation of the sympathetic nerves accompanying the renal artery was generated by a series of publications describing the physiologic and therapeutic effects. The first publications in this series described the metabolic changes that occurred after RF ablation carried out in one patient who experienced a decrease in systolic pressure of 20 mm Hg associated with modulation of sympathetic activity 30 days and 12 months after the procedure (N. Engl. J. Med. 2009;361:932-4). This study was followed by two subsequent reports of patients in whom RASNA was carried out. A proof-of-concept trial (SYMPLICITY HTN-1) in 153 patients reported a substantial decrease in blood pressure over a 2-year period (Hypertension 2011;57:911-7). A second trial (SYMPLICITY HTN-2) randomized 106 patients to either RASNA or standard therapy. That trial reported that 84% of the patients receiving RASNA had a reduction of blood pressure greater than 10 mm Hg within 6 months, compared with 35% of the control group (Lancet 2010;376:1903-9). Both studies reported a profound decrease in blood pressure that ensued over a 6-month period in 80%-90% of patients undergoing the therapy. In light of these reports, it is difficult to explain the fact that SYMPLICITY HTN-3 was a negative study.
Modulation of the sympathetic nervous system for the treatment of hypertension is not new. More than 60 years ago, Smithwick and colleagues carried out both surgical lumbar and sympathetic splanchnicectomy for its treatment with uncertain results (JAMA 1952;153:1501-4). In an era when all that we could offer hypertensive patients was a low-salt diet, the procedure became rather popular. However, the surgical risks, adverse side effects, and uncertainty of benefit led to both procedures being discontinued. Recently, there have been studies of the effect of stimulation of the carotid sinus nerve for the treatment of hypertension.
The potential benefit of modulation of the arterial sympathetic nerves, and particularly those located in the renal artery, became the focus of this recent interest. Nevertheless, a number of questions have arisen in regard to the mechanism of RASNA. And why does it take 6 months to achieve the blood pressure response? In addition, there is very little published data in regard to the changes in the renal artery and its adjacent tissue as a result of the RF ablation.
At the present, Medtronic has not provided any information beyond its indicating the lack of benefit. Further information will be reported at the upcoming American College of Cardiology scientific sessions. In the meantime, speculation is rampant as to whether the initial reports were purely placebo effects or if there is something intrinsically flawed in the SYMPLICITY HTN -3 trial.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Just in case
Uncertainty is one of the most difficult concepts to master in the art of medicine.
The prevailing paradigm, as portrayed on TV and feared by medical students, is that there must be some question to ask, or some exam finding to auscultate or palpate, or some lab test that could be ordered that will pinpoint the correct diagnosis and guide treatment. This mythos separates modern physicians from oracles reading entrails and shamans practicing magic.
It is a useful paradigm when it works. It fails rather frequently. An example is the teenage girl with chronic functional abdominal pain whose repeated blood tests and imaging have revealed no pathology. The paradigm of finding the root cause, choosing an appropriate treatment to remedy that cause, and then having the child return to school needs to be replaced by an alternative paradigm of managing symptoms, returning to the activities, and coping until the problem remits. In many cases, chronic pain won’t go away until regular activities have been resumed.
There is a third paradigm in the diagnostic regimen. It applies to an ever-increasing group of disorders. These disorders don’t have a pathognomonic finding or a gold standard test. Physicians have only a statistical probability that the patient has or will in the future get the disease. They must employ clinical judgment to weigh the risks and benefits of treatment.
Incomplete Kawasaki disease is one such diagnosis. A 5-year-old girl presents with 6 days of fever, chapped lips during the winter, and a rash. She is fussy. She has mild sterile pyuria, and her C-reactive protein level is elevated. Should she get intravenous immunoglobulin (IVIG)?
My approach is to explain to the parents that it is possible for me to both say, "I don’t think she has Kawasaki’s" and "I think we should treat." I find most parents, given a few extra minutes, grasp the general idea of number needed to treat [NNT] and number needed to harm [NNH], although I don’t use the jargon. This isn’t the first way in which most people approach decision making, but with explanation they can comprehend how, if there is a 10% risk of serious consequence and no perfect test to guide us, it makes sense to treat "just in case."
The concept is easier to understand if it is a test. ED doctors frequently state, "I don’t think it is broken, but we’ll get the x-ray to be sure." Concerns over radiation have reduced the number of head CTs performed for minor head bumps.
Although I find the general public can grasp the basics, they will depend on the physician to provide expertise in balancing the risks and consequences. Bayesian decision making is still an advanced concept for most medical students. When I assess the risks of sequelae from Kawasaki syndrome, I consider the risk that the patient really has Kawasaki times the risk of developing coronary changes times the risk those changes will progress to aneurysms times the risk aneurysms won’t heal spontaneously if ignored times the risk of an event happening because of the aneurysms times the risk that that event will be serious/catastrophic. It is a small number. This is analogous to the Drake equationin the search for extraterrestrial intelligence.
My first career experience with a patient receiving IVIG was a code blue featuring anaphylaxis, syncope, and apnea. My most recent was a patient who had 3 hours of excruciating headache during the infusion. The American Heart Association diagnostic criteria for Kawasakiemphasize high sensitivity, but they don’t adequately describe the NNT nor do they quantify the harms from overtreatment.
There is a bias to treat, even when the risk of adverse effects is greater than the risk of the disease. Factors include fear of malpractice, perceived culpability for errors of omission vs. commission, and economic gain. One of the most common error-producing biases I see in medicine is the response to a referral from an outlying hospital. I’ve worked both places. Tertiary centers find any possible reason to embark on diagnostic tests (particularly lucrative imaging) and treatment in order to justify or rationalize the transfer/admission and to keep the referring doctor happy and looking good in the patient’s/parent’s eyes. In low-risk, high-consequence Bayesian decision making, managing bias may be more important than improving the accuracy of the risk assessment.
Similar diagnostic and treatment dilemmas will occur even more frequently in the near future as genomic screening and exome sequencing become more common. Obstetrics has dealt with this for several years. Mothers are now frequently being confronted with low-specificity (positive predictive value of less than 5%) testing during pregnancy with triple and quad screens. Counseling for BRCA1 testing is the prototype for adult screening. In November 2013, the Food and Drug Administration cracked down on unregulated direct-to-consumer genomic screening. Pediatrics will soon see a large influx of this type of testing in the work-up of failure to thrive and developmental delay. Explaining these scenarios to parents will be a key, acquired professional skill.
Dr. Powell practices as a hospitalist at SSM Cardinal Glennon Children’s Medical Center in St. Louis. He is associate professor of pediatrics at St. Louis University. He is also listserv moderator for the American Academy of Pediatrics Section on Hospital Medicine and is a member of the Law and Bioethics Affinity Group of the American Society for Bioethics and Humanities. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].
Uncertainty is one of the most difficult concepts to master in the art of medicine.
The prevailing paradigm, as portrayed on TV and feared by medical students, is that there must be some question to ask, or some exam finding to auscultate or palpate, or some lab test that could be ordered that will pinpoint the correct diagnosis and guide treatment. This mythos separates modern physicians from oracles reading entrails and shamans practicing magic.
It is a useful paradigm when it works. It fails rather frequently. An example is the teenage girl with chronic functional abdominal pain whose repeated blood tests and imaging have revealed no pathology. The paradigm of finding the root cause, choosing an appropriate treatment to remedy that cause, and then having the child return to school needs to be replaced by an alternative paradigm of managing symptoms, returning to the activities, and coping until the problem remits. In many cases, chronic pain won’t go away until regular activities have been resumed.
There is a third paradigm in the diagnostic regimen. It applies to an ever-increasing group of disorders. These disorders don’t have a pathognomonic finding or a gold standard test. Physicians have only a statistical probability that the patient has or will in the future get the disease. They must employ clinical judgment to weigh the risks and benefits of treatment.
Incomplete Kawasaki disease is one such diagnosis. A 5-year-old girl presents with 6 days of fever, chapped lips during the winter, and a rash. She is fussy. She has mild sterile pyuria, and her C-reactive protein level is elevated. Should she get intravenous immunoglobulin (IVIG)?
My approach is to explain to the parents that it is possible for me to both say, "I don’t think she has Kawasaki’s" and "I think we should treat." I find most parents, given a few extra minutes, grasp the general idea of number needed to treat [NNT] and number needed to harm [NNH], although I don’t use the jargon. This isn’t the first way in which most people approach decision making, but with explanation they can comprehend how, if there is a 10% risk of serious consequence and no perfect test to guide us, it makes sense to treat "just in case."
The concept is easier to understand if it is a test. ED doctors frequently state, "I don’t think it is broken, but we’ll get the x-ray to be sure." Concerns over radiation have reduced the number of head CTs performed for minor head bumps.
Although I find the general public can grasp the basics, they will depend on the physician to provide expertise in balancing the risks and consequences. Bayesian decision making is still an advanced concept for most medical students. When I assess the risks of sequelae from Kawasaki syndrome, I consider the risk that the patient really has Kawasaki times the risk of developing coronary changes times the risk those changes will progress to aneurysms times the risk aneurysms won’t heal spontaneously if ignored times the risk of an event happening because of the aneurysms times the risk that that event will be serious/catastrophic. It is a small number. This is analogous to the Drake equationin the search for extraterrestrial intelligence.
My first career experience with a patient receiving IVIG was a code blue featuring anaphylaxis, syncope, and apnea. My most recent was a patient who had 3 hours of excruciating headache during the infusion. The American Heart Association diagnostic criteria for Kawasakiemphasize high sensitivity, but they don’t adequately describe the NNT nor do they quantify the harms from overtreatment.
There is a bias to treat, even when the risk of adverse effects is greater than the risk of the disease. Factors include fear of malpractice, perceived culpability for errors of omission vs. commission, and economic gain. One of the most common error-producing biases I see in medicine is the response to a referral from an outlying hospital. I’ve worked both places. Tertiary centers find any possible reason to embark on diagnostic tests (particularly lucrative imaging) and treatment in order to justify or rationalize the transfer/admission and to keep the referring doctor happy and looking good in the patient’s/parent’s eyes. In low-risk, high-consequence Bayesian decision making, managing bias may be more important than improving the accuracy of the risk assessment.
Similar diagnostic and treatment dilemmas will occur even more frequently in the near future as genomic screening and exome sequencing become more common. Obstetrics has dealt with this for several years. Mothers are now frequently being confronted with low-specificity (positive predictive value of less than 5%) testing during pregnancy with triple and quad screens. Counseling for BRCA1 testing is the prototype for adult screening. In November 2013, the Food and Drug Administration cracked down on unregulated direct-to-consumer genomic screening. Pediatrics will soon see a large influx of this type of testing in the work-up of failure to thrive and developmental delay. Explaining these scenarios to parents will be a key, acquired professional skill.
Dr. Powell practices as a hospitalist at SSM Cardinal Glennon Children’s Medical Center in St. Louis. He is associate professor of pediatrics at St. Louis University. He is also listserv moderator for the American Academy of Pediatrics Section on Hospital Medicine and is a member of the Law and Bioethics Affinity Group of the American Society for Bioethics and Humanities. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].
Uncertainty is one of the most difficult concepts to master in the art of medicine.
The prevailing paradigm, as portrayed on TV and feared by medical students, is that there must be some question to ask, or some exam finding to auscultate or palpate, or some lab test that could be ordered that will pinpoint the correct diagnosis and guide treatment. This mythos separates modern physicians from oracles reading entrails and shamans practicing magic.
It is a useful paradigm when it works. It fails rather frequently. An example is the teenage girl with chronic functional abdominal pain whose repeated blood tests and imaging have revealed no pathology. The paradigm of finding the root cause, choosing an appropriate treatment to remedy that cause, and then having the child return to school needs to be replaced by an alternative paradigm of managing symptoms, returning to the activities, and coping until the problem remits. In many cases, chronic pain won’t go away until regular activities have been resumed.
There is a third paradigm in the diagnostic regimen. It applies to an ever-increasing group of disorders. These disorders don’t have a pathognomonic finding or a gold standard test. Physicians have only a statistical probability that the patient has or will in the future get the disease. They must employ clinical judgment to weigh the risks and benefits of treatment.
Incomplete Kawasaki disease is one such diagnosis. A 5-year-old girl presents with 6 days of fever, chapped lips during the winter, and a rash. She is fussy. She has mild sterile pyuria, and her C-reactive protein level is elevated. Should she get intravenous immunoglobulin (IVIG)?
My approach is to explain to the parents that it is possible for me to both say, "I don’t think she has Kawasaki’s" and "I think we should treat." I find most parents, given a few extra minutes, grasp the general idea of number needed to treat [NNT] and number needed to harm [NNH], although I don’t use the jargon. This isn’t the first way in which most people approach decision making, but with explanation they can comprehend how, if there is a 10% risk of serious consequence and no perfect test to guide us, it makes sense to treat "just in case."
The concept is easier to understand if it is a test. ED doctors frequently state, "I don’t think it is broken, but we’ll get the x-ray to be sure." Concerns over radiation have reduced the number of head CTs performed for minor head bumps.
Although I find the general public can grasp the basics, they will depend on the physician to provide expertise in balancing the risks and consequences. Bayesian decision making is still an advanced concept for most medical students. When I assess the risks of sequelae from Kawasaki syndrome, I consider the risk that the patient really has Kawasaki times the risk of developing coronary changes times the risk those changes will progress to aneurysms times the risk aneurysms won’t heal spontaneously if ignored times the risk of an event happening because of the aneurysms times the risk that that event will be serious/catastrophic. It is a small number. This is analogous to the Drake equationin the search for extraterrestrial intelligence.
My first career experience with a patient receiving IVIG was a code blue featuring anaphylaxis, syncope, and apnea. My most recent was a patient who had 3 hours of excruciating headache during the infusion. The American Heart Association diagnostic criteria for Kawasakiemphasize high sensitivity, but they don’t adequately describe the NNT nor do they quantify the harms from overtreatment.
There is a bias to treat, even when the risk of adverse effects is greater than the risk of the disease. Factors include fear of malpractice, perceived culpability for errors of omission vs. commission, and economic gain. One of the most common error-producing biases I see in medicine is the response to a referral from an outlying hospital. I’ve worked both places. Tertiary centers find any possible reason to embark on diagnostic tests (particularly lucrative imaging) and treatment in order to justify or rationalize the transfer/admission and to keep the referring doctor happy and looking good in the patient’s/parent’s eyes. In low-risk, high-consequence Bayesian decision making, managing bias may be more important than improving the accuracy of the risk assessment.
Similar diagnostic and treatment dilemmas will occur even more frequently in the near future as genomic screening and exome sequencing become more common. Obstetrics has dealt with this for several years. Mothers are now frequently being confronted with low-specificity (positive predictive value of less than 5%) testing during pregnancy with triple and quad screens. Counseling for BRCA1 testing is the prototype for adult screening. In November 2013, the Food and Drug Administration cracked down on unregulated direct-to-consumer genomic screening. Pediatrics will soon see a large influx of this type of testing in the work-up of failure to thrive and developmental delay. Explaining these scenarios to parents will be a key, acquired professional skill.
Dr. Powell practices as a hospitalist at SSM Cardinal Glennon Children’s Medical Center in St. Louis. He is associate professor of pediatrics at St. Louis University. He is also listserv moderator for the American Academy of Pediatrics Section on Hospital Medicine and is a member of the Law and Bioethics Affinity Group of the American Society for Bioethics and Humanities. Dr. Powell said he had no relevant financial disclosures. E-mail him at [email protected].

Nicotinamide and Reflections on Alan Shalita and George Hambrick Jr
Counterphobia and Poor Sun Protection Practices in First-Degree Relatives of Melanoma Patients
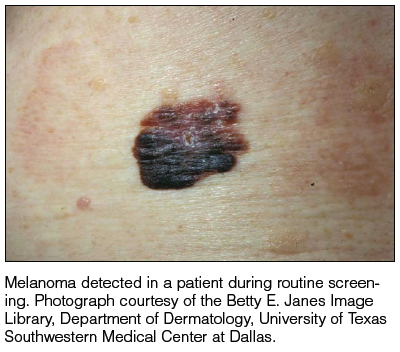
It is widely accepted that there are several factors that may independently elevate an individual’s risk for melanoma, such as a history of childhood sunburns, family history of melanoma, and poor sun protection practices. Several studies have examined risk behaviors in melanoma patients following their diagnosis and have reported findings such as increased UV exposure patterns, persistent tanning bed use, and sun-protective behaviors similar to those of the general population (Figure).1-4
Although first-degree relatives (FDRs) of melanoma patients are at an increased risk for melanoma, they also have been found to exhibit surprisingly poor sun protection practices. In one retrospective analysis, Geller et al5 found that frequent sunburns, high rates of tanning bed use, and low rates of sunscreen use were common among children of health care workers who reported a personal or family history of skin cancer. An independent study reported that merely 37% (37/100) of FDRs of melanoma patients use sunscreen more than half of the time, and considerably fewer wear protective clothing or seek shade while outdoors.6 Given their increased risk for developing melanoma, it is likely to be assumed that FDRs of melanoma patients practice diligent sun protection. The underlying reasons for the failure of this at-risk population to adhere strongly to sun protection practices warrants special attention.
Manne et al7 conducted a survey in a group of FDRs of melanoma patients with self-reported poor sun protection practices to evaluate the demographic, medical, psychological, educational (knowledge of sun protection guidelines), and social influences that correlate with sun protection and sunbathing practices. More effective sun protective behaviors were identified in FDRs with higher education, fewer perceived benefits of sunbathing, more prominent photoaging concerns, and greater sunscreen self-efficacy. The authors concluded that sun-protective behavior in FDRs was not associated with prior knowledge about sunscreen or UV exposure, their relative’s melanoma stage, or physician recommendations for sun protection.7
Factors that have been documented as influencing sun-protective behavior in the general population include knowledge of the benefits of sun protection; attitudes toward tanning and sun protection; subjective norms regarding the beauty and perceived health of a tan; and optimistic bias, which is a cognitive mechanism that causes a person to believe that he/she is at lesser risk for experiencing a negative outcome compared to others. Additionally, sun protection behaviors are influenced by the immediacy of getting the reward (the perceived benefits of tanning) versus the delayed punishment (development of skin cancer).6 Although all of these elements may be important for some individuals, we believe that a subset of FDRs of melanoma patients may be susceptible to the phenomenon known as counterphobia.
Counterphobia is a neurotic response to anxiety in which an individual actively pursues situations that heighten his/her fear rather than fleeing from a feared object or behavior.8 Most insight into counterphobia has come from the experiences of children who have parent(s) with a debilitating or fatal diagnosis. Due to their immature coping mechanisms, some children are at risk for maladaptive behavioral responses. The loss of a parent typically produces severe psychological trauma in all children, but in those who develop counterphobia, it manifests as a heightened fear of death and vulnerability to their parent’s illness. This maladaptive response is dependent on self-identification with the parent, especially among daughters of lost mothers and sons of lost fathers, and this fear remains with the child through adulthood. A survey of 154 motherless daughters found that women aged 19 to 35 years have the highest level of obsessive thoughts of mortality and more than 75% believe they will succumb to their mother’s illness (92% in the case of cancer).9 Despite this fear, children may exhibit health-compromising behaviors related to the diagnoses that led to their parents’ deaths; for example, counterphobia has been identified as a pathologic factor behind sexually promiscuous practices in the children of patients with AIDS, and it also may explain high-risk drinking behavior in a child whose parent died from hepatocellular carcinoma due to a history of alcoholic cirrhosis. Similarly, counterphobia can manifest as the deliberate refusal to undergo a mammogram in a woman whose mother died of breast cancer.9 Psychologists have hypothesized that counterphobic pursuits may result from attempts to master the anxiety associated with fear of injury or death as well as from the notion that attempts at risk-factor reduction are futile, as their death is certain.10
The strong influence of counterphobia on perspectives of health and mortality among individuals affected by early loss of a parent is well documented. An assessment of the subjective life expectancy, death anxiety, and health-related behaviors of college students who lost a parent revealed that these individuals estimated their own life spans to be shorter than college students with 2 living parents.11 Moreover, when students were explicitly instructed to predict their life expectancy based on a purely objective mentality rather than one influenced by personal feelings, the exclusion of emotion yielded a longer projected life span. This finding highlights the magnitude of the psychological forces influencing the ethos of individuals affected by premature parental loss. In the same study, individuals who had experienced early loss of a parent believed they would die of the same condition that caused their parent’s death, a finding accompanied by notably poorer diet and smoking behaviors, which might be expected among those with counterphobic defenses.11
Although Manne et al7 did not find an association between melanoma disease severity and sun-protective behavior in FDRs, the study design did not allow for assessment of potential counterphobic responses, which are most likely to develop in younger individuals who strongly identify with the family member whose disease was disabling or fatal. For example, the study included adult relatives (mean age, 46 years) of melanoma patients diagnosed in the preceding 4 years. Furthermore, fewer than 20% (108/545) of the patients had stage III or IV melanoma, and it was not known if melanoma patients communicated the diagnosis to their family members.7
A practice gap exists in FDRs of melanoma patients who are largely assumed to be practicing adequate, if not heightened, sun protection practices. Given that this group demonstrates poor sun protection practices, it is important to identify reasons for such behavior that may extend beyond what is currently known and may include counterphobia. Based on research performed in other medical conditions, the individuals most at risk for counterphobic responses are young children of patients diagnosed with a disabling or fatal condition, but whether in cases of melanoma counterphobia exists as a maladaptive response and whether such a response may occur in all close relatives, not just offspring, is unknown. Currently, the type of measure(s) that may mitigate poor risk factor modification due to counterphobia, including sun protection practices, is unknown. However, physician knowledge of counterphobic responses as a possibility in close relatives of melanoma patients may improve physician efforts to modify behavior in this unique, high-risk population.
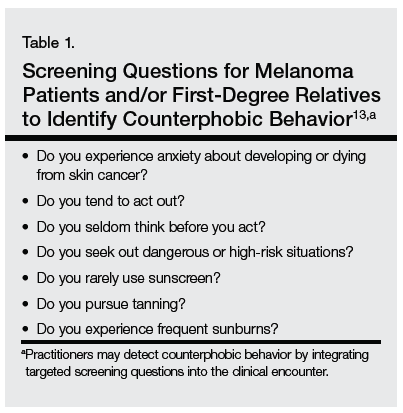
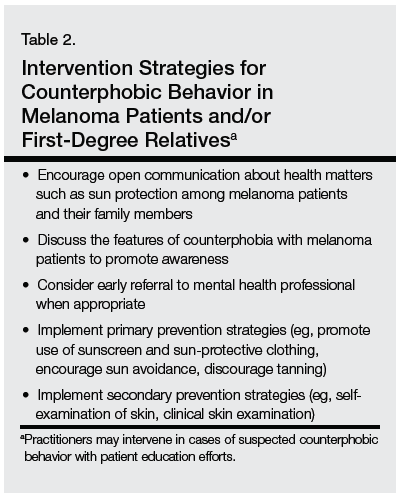
The multimodal pathway of melanoma development suggests that individuals with an underlying genetic predisposition for melanoma who also neglect sun-protective measures are an especially high-risk group.12 As such, targeted education and screening of this patient population may be warranted (Table 1). Although it is incumbent on physicians to incorporate concerted screening, counseling, and focused interventions for newly diagnosed melanoma patients, taking similar measures to counsel and educate immediate relatives who may be at high risk for poor sun protection practices also is encouraged (Table 2).
We believe that recognition of counterphobic behavior is critical in the evaluation of FDRs of melanoma patients. Heightened awareness may bolster primary prevention efforts, especially in our patients with genetic diatheses toward melanoma development.
1. Idorn L, Datta P, Heydenreich J, et al. A 3-year follow-up of sun behavior in patients with cutaneous malignant melanoma [published online ahead of print October 2, 2013]. JAMA Dermatol. doi:10.1001/jamadermatol.2013.5098.
2. Idorn LW, Datta P, Heydenreich J, et al. Sun behaviour after cutaneous malignant melanoma: a study based on ultraviolet radiation measurements and sun diary data [published online ahead of print]. Br J Dermatol. 2013;168:367-373.
3. Mayer D, Layman A, Carlson J. Sun-protection behaviors of melanoma survivors. J Am Acad Dermatol. 2012;66:e9-e10.
4. Lee TK, Brazier AS, Shoveller JA, et al. Sun-related behavior after a diagnosis of cutaneous malignant melanoma. Melanoma Res. 2007;17:51-55.
5. Geller AC, Brooks DR, Colditz GA, et al. Sun protection practices among offspring of women with personal or family history of skin cancer. Pediatrics. 2006;117:e688-e694.
6. Azzarello LM, Dessureault S, Jacobsen PB. Sun-protective behavior among individuals with a family history of melanoma. Cancer Epidemiol Boomarkers Prev. 2006;15:142-145.
7. Manne SL, Coups EJ, Jacobsen PB, et al. Sun protection and sunbathing practices among at-risk family members of patients with melanoma. BMC Public Health. 2011;11:122.
8. Fenichel O. The Psychoanalytic Theory of Neurosis. Oxford, United Kingdom: Taylor & Francis; 1999.
9. Edelman H. Motherless Daughters: The Legacy of Loss. 2nd ed. Cambridge, MA: Da Capo Press; 2006.
10. Poznanski E, Arthur B. The counterphobic defense in children. Child Psychiatry Hum Dev. 1971;1:178-191.
11. Denes-Raj V, Ehrlichman H. Effects of premature parental death on subjective life expectancy, death anxiety, and health behavior. Omega: Journal of Death and Dying. 1991;23:309-321.
12. Hayward NK. Genetics of melanoma predisposition. Oncogene. 2003;22:3053-3062.
13. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychologial literature. Soc Sci Med. 1995;40:265-274.
It is widely accepted that there are several factors that may independently elevate an individual’s risk for melanoma, such as a history of childhood sunburns, family history of melanoma, and poor sun protection practices. Several studies have examined risk behaviors in melanoma patients following their diagnosis and have reported findings such as increased UV exposure patterns, persistent tanning bed use, and sun-protective behaviors similar to those of the general population (Figure).1-4
Although first-degree relatives (FDRs) of melanoma patients are at an increased risk for melanoma, they also have been found to exhibit surprisingly poor sun protection practices. In one retrospective analysis, Geller et al5 found that frequent sunburns, high rates of tanning bed use, and low rates of sunscreen use were common among children of health care workers who reported a personal or family history of skin cancer. An independent study reported that merely 37% (37/100) of FDRs of melanoma patients use sunscreen more than half of the time, and considerably fewer wear protective clothing or seek shade while outdoors.6 Given their increased risk for developing melanoma, it is likely to be assumed that FDRs of melanoma patients practice diligent sun protection. The underlying reasons for the failure of this at-risk population to adhere strongly to sun protection practices warrants special attention.
Manne et al7 conducted a survey in a group of FDRs of melanoma patients with self-reported poor sun protection practices to evaluate the demographic, medical, psychological, educational (knowledge of sun protection guidelines), and social influences that correlate with sun protection and sunbathing practices. More effective sun protective behaviors were identified in FDRs with higher education, fewer perceived benefits of sunbathing, more prominent photoaging concerns, and greater sunscreen self-efficacy. The authors concluded that sun-protective behavior in FDRs was not associated with prior knowledge about sunscreen or UV exposure, their relative’s melanoma stage, or physician recommendations for sun protection.7
Factors that have been documented as influencing sun-protective behavior in the general population include knowledge of the benefits of sun protection; attitudes toward tanning and sun protection; subjective norms regarding the beauty and perceived health of a tan; and optimistic bias, which is a cognitive mechanism that causes a person to believe that he/she is at lesser risk for experiencing a negative outcome compared to others. Additionally, sun protection behaviors are influenced by the immediacy of getting the reward (the perceived benefits of tanning) versus the delayed punishment (development of skin cancer).6 Although all of these elements may be important for some individuals, we believe that a subset of FDRs of melanoma patients may be susceptible to the phenomenon known as counterphobia.
Counterphobia is a neurotic response to anxiety in which an individual actively pursues situations that heighten his/her fear rather than fleeing from a feared object or behavior.8 Most insight into counterphobia has come from the experiences of children who have parent(s) with a debilitating or fatal diagnosis. Due to their immature coping mechanisms, some children are at risk for maladaptive behavioral responses. The loss of a parent typically produces severe psychological trauma in all children, but in those who develop counterphobia, it manifests as a heightened fear of death and vulnerability to their parent’s illness. This maladaptive response is dependent on self-identification with the parent, especially among daughters of lost mothers and sons of lost fathers, and this fear remains with the child through adulthood. A survey of 154 motherless daughters found that women aged 19 to 35 years have the highest level of obsessive thoughts of mortality and more than 75% believe they will succumb to their mother’s illness (92% in the case of cancer).9 Despite this fear, children may exhibit health-compromising behaviors related to the diagnoses that led to their parents’ deaths; for example, counterphobia has been identified as a pathologic factor behind sexually promiscuous practices in the children of patients with AIDS, and it also may explain high-risk drinking behavior in a child whose parent died from hepatocellular carcinoma due to a history of alcoholic cirrhosis. Similarly, counterphobia can manifest as the deliberate refusal to undergo a mammogram in a woman whose mother died of breast cancer.9 Psychologists have hypothesized that counterphobic pursuits may result from attempts to master the anxiety associated with fear of injury or death as well as from the notion that attempts at risk-factor reduction are futile, as their death is certain.10
The strong influence of counterphobia on perspectives of health and mortality among individuals affected by early loss of a parent is well documented. An assessment of the subjective life expectancy, death anxiety, and health-related behaviors of college students who lost a parent revealed that these individuals estimated their own life spans to be shorter than college students with 2 living parents.11 Moreover, when students were explicitly instructed to predict their life expectancy based on a purely objective mentality rather than one influenced by personal feelings, the exclusion of emotion yielded a longer projected life span. This finding highlights the magnitude of the psychological forces influencing the ethos of individuals affected by premature parental loss. In the same study, individuals who had experienced early loss of a parent believed they would die of the same condition that caused their parent’s death, a finding accompanied by notably poorer diet and smoking behaviors, which might be expected among those with counterphobic defenses.11
Although Manne et al7 did not find an association between melanoma disease severity and sun-protective behavior in FDRs, the study design did not allow for assessment of potential counterphobic responses, which are most likely to develop in younger individuals who strongly identify with the family member whose disease was disabling or fatal. For example, the study included adult relatives (mean age, 46 years) of melanoma patients diagnosed in the preceding 4 years. Furthermore, fewer than 20% (108/545) of the patients had stage III or IV melanoma, and it was not known if melanoma patients communicated the diagnosis to their family members.7
A practice gap exists in FDRs of melanoma patients who are largely assumed to be practicing adequate, if not heightened, sun protection practices. Given that this group demonstrates poor sun protection practices, it is important to identify reasons for such behavior that may extend beyond what is currently known and may include counterphobia. Based on research performed in other medical conditions, the individuals most at risk for counterphobic responses are young children of patients diagnosed with a disabling or fatal condition, but whether in cases of melanoma counterphobia exists as a maladaptive response and whether such a response may occur in all close relatives, not just offspring, is unknown. Currently, the type of measure(s) that may mitigate poor risk factor modification due to counterphobia, including sun protection practices, is unknown. However, physician knowledge of counterphobic responses as a possibility in close relatives of melanoma patients may improve physician efforts to modify behavior in this unique, high-risk population.
The multimodal pathway of melanoma development suggests that individuals with an underlying genetic predisposition for melanoma who also neglect sun-protective measures are an especially high-risk group.12 As such, targeted education and screening of this patient population may be warranted (Table 1). Although it is incumbent on physicians to incorporate concerted screening, counseling, and focused interventions for newly diagnosed melanoma patients, taking similar measures to counsel and educate immediate relatives who may be at high risk for poor sun protection practices also is encouraged (Table 2).
We believe that recognition of counterphobic behavior is critical in the evaluation of FDRs of melanoma patients. Heightened awareness may bolster primary prevention efforts, especially in our patients with genetic diatheses toward melanoma development.
It is widely accepted that there are several factors that may independently elevate an individual’s risk for melanoma, such as a history of childhood sunburns, family history of melanoma, and poor sun protection practices. Several studies have examined risk behaviors in melanoma patients following their diagnosis and have reported findings such as increased UV exposure patterns, persistent tanning bed use, and sun-protective behaviors similar to those of the general population (Figure).1-4
Although first-degree relatives (FDRs) of melanoma patients are at an increased risk for melanoma, they also have been found to exhibit surprisingly poor sun protection practices. In one retrospective analysis, Geller et al5 found that frequent sunburns, high rates of tanning bed use, and low rates of sunscreen use were common among children of health care workers who reported a personal or family history of skin cancer. An independent study reported that merely 37% (37/100) of FDRs of melanoma patients use sunscreen more than half of the time, and considerably fewer wear protective clothing or seek shade while outdoors.6 Given their increased risk for developing melanoma, it is likely to be assumed that FDRs of melanoma patients practice diligent sun protection. The underlying reasons for the failure of this at-risk population to adhere strongly to sun protection practices warrants special attention.
Manne et al7 conducted a survey in a group of FDRs of melanoma patients with self-reported poor sun protection practices to evaluate the demographic, medical, psychological, educational (knowledge of sun protection guidelines), and social influences that correlate with sun protection and sunbathing practices. More effective sun protective behaviors were identified in FDRs with higher education, fewer perceived benefits of sunbathing, more prominent photoaging concerns, and greater sunscreen self-efficacy. The authors concluded that sun-protective behavior in FDRs was not associated with prior knowledge about sunscreen or UV exposure, their relative’s melanoma stage, or physician recommendations for sun protection.7
Factors that have been documented as influencing sun-protective behavior in the general population include knowledge of the benefits of sun protection; attitudes toward tanning and sun protection; subjective norms regarding the beauty and perceived health of a tan; and optimistic bias, which is a cognitive mechanism that causes a person to believe that he/she is at lesser risk for experiencing a negative outcome compared to others. Additionally, sun protection behaviors are influenced by the immediacy of getting the reward (the perceived benefits of tanning) versus the delayed punishment (development of skin cancer).6 Although all of these elements may be important for some individuals, we believe that a subset of FDRs of melanoma patients may be susceptible to the phenomenon known as counterphobia.
Counterphobia is a neurotic response to anxiety in which an individual actively pursues situations that heighten his/her fear rather than fleeing from a feared object or behavior.8 Most insight into counterphobia has come from the experiences of children who have parent(s) with a debilitating or fatal diagnosis. Due to their immature coping mechanisms, some children are at risk for maladaptive behavioral responses. The loss of a parent typically produces severe psychological trauma in all children, but in those who develop counterphobia, it manifests as a heightened fear of death and vulnerability to their parent’s illness. This maladaptive response is dependent on self-identification with the parent, especially among daughters of lost mothers and sons of lost fathers, and this fear remains with the child through adulthood. A survey of 154 motherless daughters found that women aged 19 to 35 years have the highest level of obsessive thoughts of mortality and more than 75% believe they will succumb to their mother’s illness (92% in the case of cancer).9 Despite this fear, children may exhibit health-compromising behaviors related to the diagnoses that led to their parents’ deaths; for example, counterphobia has been identified as a pathologic factor behind sexually promiscuous practices in the children of patients with AIDS, and it also may explain high-risk drinking behavior in a child whose parent died from hepatocellular carcinoma due to a history of alcoholic cirrhosis. Similarly, counterphobia can manifest as the deliberate refusal to undergo a mammogram in a woman whose mother died of breast cancer.9 Psychologists have hypothesized that counterphobic pursuits may result from attempts to master the anxiety associated with fear of injury or death as well as from the notion that attempts at risk-factor reduction are futile, as their death is certain.10
The strong influence of counterphobia on perspectives of health and mortality among individuals affected by early loss of a parent is well documented. An assessment of the subjective life expectancy, death anxiety, and health-related behaviors of college students who lost a parent revealed that these individuals estimated their own life spans to be shorter than college students with 2 living parents.11 Moreover, when students were explicitly instructed to predict their life expectancy based on a purely objective mentality rather than one influenced by personal feelings, the exclusion of emotion yielded a longer projected life span. This finding highlights the magnitude of the psychological forces influencing the ethos of individuals affected by premature parental loss. In the same study, individuals who had experienced early loss of a parent believed they would die of the same condition that caused their parent’s death, a finding accompanied by notably poorer diet and smoking behaviors, which might be expected among those with counterphobic defenses.11
Although Manne et al7 did not find an association between melanoma disease severity and sun-protective behavior in FDRs, the study design did not allow for assessment of potential counterphobic responses, which are most likely to develop in younger individuals who strongly identify with the family member whose disease was disabling or fatal. For example, the study included adult relatives (mean age, 46 years) of melanoma patients diagnosed in the preceding 4 years. Furthermore, fewer than 20% (108/545) of the patients had stage III or IV melanoma, and it was not known if melanoma patients communicated the diagnosis to their family members.7
A practice gap exists in FDRs of melanoma patients who are largely assumed to be practicing adequate, if not heightened, sun protection practices. Given that this group demonstrates poor sun protection practices, it is important to identify reasons for such behavior that may extend beyond what is currently known and may include counterphobia. Based on research performed in other medical conditions, the individuals most at risk for counterphobic responses are young children of patients diagnosed with a disabling or fatal condition, but whether in cases of melanoma counterphobia exists as a maladaptive response and whether such a response may occur in all close relatives, not just offspring, is unknown. Currently, the type of measure(s) that may mitigate poor risk factor modification due to counterphobia, including sun protection practices, is unknown. However, physician knowledge of counterphobic responses as a possibility in close relatives of melanoma patients may improve physician efforts to modify behavior in this unique, high-risk population.
The multimodal pathway of melanoma development suggests that individuals with an underlying genetic predisposition for melanoma who also neglect sun-protective measures are an especially high-risk group.12 As such, targeted education and screening of this patient population may be warranted (Table 1). Although it is incumbent on physicians to incorporate concerted screening, counseling, and focused interventions for newly diagnosed melanoma patients, taking similar measures to counsel and educate immediate relatives who may be at high risk for poor sun protection practices also is encouraged (Table 2).
We believe that recognition of counterphobic behavior is critical in the evaluation of FDRs of melanoma patients. Heightened awareness may bolster primary prevention efforts, especially in our patients with genetic diatheses toward melanoma development.
1. Idorn L, Datta P, Heydenreich J, et al. A 3-year follow-up of sun behavior in patients with cutaneous malignant melanoma [published online ahead of print October 2, 2013]. JAMA Dermatol. doi:10.1001/jamadermatol.2013.5098.
2. Idorn LW, Datta P, Heydenreich J, et al. Sun behaviour after cutaneous malignant melanoma: a study based on ultraviolet radiation measurements and sun diary data [published online ahead of print]. Br J Dermatol. 2013;168:367-373.
3. Mayer D, Layman A, Carlson J. Sun-protection behaviors of melanoma survivors. J Am Acad Dermatol. 2012;66:e9-e10.
4. Lee TK, Brazier AS, Shoveller JA, et al. Sun-related behavior after a diagnosis of cutaneous malignant melanoma. Melanoma Res. 2007;17:51-55.
5. Geller AC, Brooks DR, Colditz GA, et al. Sun protection practices among offspring of women with personal or family history of skin cancer. Pediatrics. 2006;117:e688-e694.
6. Azzarello LM, Dessureault S, Jacobsen PB. Sun-protective behavior among individuals with a family history of melanoma. Cancer Epidemiol Boomarkers Prev. 2006;15:142-145.
7. Manne SL, Coups EJ, Jacobsen PB, et al. Sun protection and sunbathing practices among at-risk family members of patients with melanoma. BMC Public Health. 2011;11:122.
8. Fenichel O. The Psychoanalytic Theory of Neurosis. Oxford, United Kingdom: Taylor & Francis; 1999.
9. Edelman H. Motherless Daughters: The Legacy of Loss. 2nd ed. Cambridge, MA: Da Capo Press; 2006.
10. Poznanski E, Arthur B. The counterphobic defense in children. Child Psychiatry Hum Dev. 1971;1:178-191.
11. Denes-Raj V, Ehrlichman H. Effects of premature parental death on subjective life expectancy, death anxiety, and health behavior. Omega: Journal of Death and Dying. 1991;23:309-321.
12. Hayward NK. Genetics of melanoma predisposition. Oncogene. 2003;22:3053-3062.
13. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychologial literature. Soc Sci Med. 1995;40:265-274.
1. Idorn L, Datta P, Heydenreich J, et al. A 3-year follow-up of sun behavior in patients with cutaneous malignant melanoma [published online ahead of print October 2, 2013]. JAMA Dermatol. doi:10.1001/jamadermatol.2013.5098.
2. Idorn LW, Datta P, Heydenreich J, et al. Sun behaviour after cutaneous malignant melanoma: a study based on ultraviolet radiation measurements and sun diary data [published online ahead of print]. Br J Dermatol. 2013;168:367-373.
3. Mayer D, Layman A, Carlson J. Sun-protection behaviors of melanoma survivors. J Am Acad Dermatol. 2012;66:e9-e10.
4. Lee TK, Brazier AS, Shoveller JA, et al. Sun-related behavior after a diagnosis of cutaneous malignant melanoma. Melanoma Res. 2007;17:51-55.
5. Geller AC, Brooks DR, Colditz GA, et al. Sun protection practices among offspring of women with personal or family history of skin cancer. Pediatrics. 2006;117:e688-e694.
6. Azzarello LM, Dessureault S, Jacobsen PB. Sun-protective behavior among individuals with a family history of melanoma. Cancer Epidemiol Boomarkers Prev. 2006;15:142-145.
7. Manne SL, Coups EJ, Jacobsen PB, et al. Sun protection and sunbathing practices among at-risk family members of patients with melanoma. BMC Public Health. 2011;11:122.
8. Fenichel O. The Psychoanalytic Theory of Neurosis. Oxford, United Kingdom: Taylor & Francis; 1999.
9. Edelman H. Motherless Daughters: The Legacy of Loss. 2nd ed. Cambridge, MA: Da Capo Press; 2006.
10. Poznanski E, Arthur B. The counterphobic defense in children. Child Psychiatry Hum Dev. 1971;1:178-191.
11. Denes-Raj V, Ehrlichman H. Effects of premature parental death on subjective life expectancy, death anxiety, and health behavior. Omega: Journal of Death and Dying. 1991;23:309-321.
12. Hayward NK. Genetics of melanoma predisposition. Oncogene. 2003;22:3053-3062.
13. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychologial literature. Soc Sci Med. 1995;40:265-274.

Truly connected health care
For years, we have all been promised interconnected electronic patient records – the concept that information would follow patients and be available across all care settings. Unfortunately, this reality has yet to materialize.
Regional Health Information Organizations (RHIOs) exist all over (these are hospitals, physician practices, and health networks that exchange data on a local level), but they typically present a "brick wall" at their borders where the information sharing stops. Thankfully, that is poised to change, with a new push toward meaningful interconnectedness.
Finally, health information technology (HIT) thought leaders and electronic health records (EHR) vendors are homing in on standards that will allow physicians and other healthcare providers to exchange information seamlessly regardless of EHR system or geographical location. The goal, as usual, is to improve patient care and outcomes. In this column, we felt it would be useful to highlight some of the ideas driving this effort, as there is good reason to be optimistic about the possibility of true interoperability.
A view from the top
Recently, at the annual meeting of the Health Information Management Systems Society (HIMSS) in Orlando, Dr. Karen DeSalvo, national health IT coordinator, made a strong plea for interoperability by 2017. She said "We can do national health care exchange in 3 years. ... I want this as a doctor, I want this as patient, I want this as a daughter."
Dr. DeSalvo’s words resonate because this is a concept we all expected from the earliest days of electronic records. Unfortunately, barriers – both real and artificial – have stood in the way. First and foremost are patient privacy and information security. It is essential that patient data are protected and maintained as the data pass from one system to the next, but often, even the basic function of matching patients with the right records can be challenging. Many identifiers exist, including various medical record numbers and insurance codes. If a name is misspelled or middle initial omitted, this can also create significant chaos and allow sensitive data to file into the wrong place, creating HIPAA violations and distrust among patients.
In addition to concerns over data security, the lack of standard formatting for storing and sharing records has been a huge hurdle for EHR vendors. Not surprisingly, the simultaneous development of dozens of competing EHR products has created significant fragmentation throughout the market. Instead of starting from a common set of data elements, each EHR was essentially designed "in a vacuum," and only now are their creators attempting to find a way to get them to communicate. A number of cross-platform projects currently underway highlight this effort.
VHS or Betamax?
On Feb. 25, 2014, NextGen Healthcare and Cerner announced bilateral certification of their EHR products and affirmed their commitment to interoperability. According to the press release, they are committed to "creating proactive working relationships, expanding the boundaries of current interoperability ... and supporting the efforts of [their] clients to advance the health of their communities." These may not be novel goals, but at least both vendors have demonstrated their best attempt to achieve them. Also, both companies have a huge footprint in the market, so their collaboration is certain to raise the level of attention being paid to this topic. But this isn’t the only attempt at broad-based interoperability.
EClinicalWorks (eCW), another large player in the ambulatory EHR market, has developed a product know as P2P, or Provider to Provider. Originally conceived as a way to communicate between different users of the eCW platform, it has now been expanded to all providers, regardless of their EHR, as a secure communication tool. This new product is known as P2POpen and is free to any health care professional wishing to join "the network." According to their website, P2POpen now boasts close to 22,000 users and facilitates "improved quality, safety, and efficiency of care." Like the collaboration mentioned above, P2POpen has a shot at success, but both of these efforts may also portend more debate over standardization moving forward. Will the disparity in how each company addresses the issue of interoperability lead to further fragmentation? And how can we be sure that embracing one of these ideas won’t severely limit us in the future?
Setting the standard
The only way to answer these and other looming concerns over developing a consistent interoperability protocol is to start at the top and rapidly build consensus. In other words, Dr. DeSalvo’s words need to be quickly translated into action, as she and other thought leaders agree – not only on a standard – but also on a way to properly motivate EHR vendors to adopt that standard.
One possible opportunity to enforce this as Meaningful Use stage III. The requirements for stage III EHR certification, which have yet to be finalized, should include a necessity for every vendor to adopt a consistent format for information exchange and data transmission. Making this a certification requirement will ensure that all EHR products remain cooperative if they plan to stay competitive.
Another solution being considered involves the use of centralized "Health Information Exchanges," which could collect and warehouse data from multiple sources and then retransmit those data in a universally readable format. Either way, if a consensus can be reached and issues over privacy and security addressed, it will only spell a victory for physicians and patients and truly get us on the road to improved patient care and outcomes. We tend to agree with Dr. DeSalvo, and believe that victory is well within reach.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
For years, we have all been promised interconnected electronic patient records – the concept that information would follow patients and be available across all care settings. Unfortunately, this reality has yet to materialize.
Regional Health Information Organizations (RHIOs) exist all over (these are hospitals, physician practices, and health networks that exchange data on a local level), but they typically present a "brick wall" at their borders where the information sharing stops. Thankfully, that is poised to change, with a new push toward meaningful interconnectedness.
Finally, health information technology (HIT) thought leaders and electronic health records (EHR) vendors are homing in on standards that will allow physicians and other healthcare providers to exchange information seamlessly regardless of EHR system or geographical location. The goal, as usual, is to improve patient care and outcomes. In this column, we felt it would be useful to highlight some of the ideas driving this effort, as there is good reason to be optimistic about the possibility of true interoperability.
A view from the top
Recently, at the annual meeting of the Health Information Management Systems Society (HIMSS) in Orlando, Dr. Karen DeSalvo, national health IT coordinator, made a strong plea for interoperability by 2017. She said "We can do national health care exchange in 3 years. ... I want this as a doctor, I want this as patient, I want this as a daughter."
Dr. DeSalvo’s words resonate because this is a concept we all expected from the earliest days of electronic records. Unfortunately, barriers – both real and artificial – have stood in the way. First and foremost are patient privacy and information security. It is essential that patient data are protected and maintained as the data pass from one system to the next, but often, even the basic function of matching patients with the right records can be challenging. Many identifiers exist, including various medical record numbers and insurance codes. If a name is misspelled or middle initial omitted, this can also create significant chaos and allow sensitive data to file into the wrong place, creating HIPAA violations and distrust among patients.
In addition to concerns over data security, the lack of standard formatting for storing and sharing records has been a huge hurdle for EHR vendors. Not surprisingly, the simultaneous development of dozens of competing EHR products has created significant fragmentation throughout the market. Instead of starting from a common set of data elements, each EHR was essentially designed "in a vacuum," and only now are their creators attempting to find a way to get them to communicate. A number of cross-platform projects currently underway highlight this effort.
VHS or Betamax?
On Feb. 25, 2014, NextGen Healthcare and Cerner announced bilateral certification of their EHR products and affirmed their commitment to interoperability. According to the press release, they are committed to "creating proactive working relationships, expanding the boundaries of current interoperability ... and supporting the efforts of [their] clients to advance the health of their communities." These may not be novel goals, but at least both vendors have demonstrated their best attempt to achieve them. Also, both companies have a huge footprint in the market, so their collaboration is certain to raise the level of attention being paid to this topic. But this isn’t the only attempt at broad-based interoperability.
EClinicalWorks (eCW), another large player in the ambulatory EHR market, has developed a product know as P2P, or Provider to Provider. Originally conceived as a way to communicate between different users of the eCW platform, it has now been expanded to all providers, regardless of their EHR, as a secure communication tool. This new product is known as P2POpen and is free to any health care professional wishing to join "the network." According to their website, P2POpen now boasts close to 22,000 users and facilitates "improved quality, safety, and efficiency of care." Like the collaboration mentioned above, P2POpen has a shot at success, but both of these efforts may also portend more debate over standardization moving forward. Will the disparity in how each company addresses the issue of interoperability lead to further fragmentation? And how can we be sure that embracing one of these ideas won’t severely limit us in the future?
Setting the standard
The only way to answer these and other looming concerns over developing a consistent interoperability protocol is to start at the top and rapidly build consensus. In other words, Dr. DeSalvo’s words need to be quickly translated into action, as she and other thought leaders agree – not only on a standard – but also on a way to properly motivate EHR vendors to adopt that standard.
One possible opportunity to enforce this as Meaningful Use stage III. The requirements for stage III EHR certification, which have yet to be finalized, should include a necessity for every vendor to adopt a consistent format for information exchange and data transmission. Making this a certification requirement will ensure that all EHR products remain cooperative if they plan to stay competitive.
Another solution being considered involves the use of centralized "Health Information Exchanges," which could collect and warehouse data from multiple sources and then retransmit those data in a universally readable format. Either way, if a consensus can be reached and issues over privacy and security addressed, it will only spell a victory for physicians and patients and truly get us on the road to improved patient care and outcomes. We tend to agree with Dr. DeSalvo, and believe that victory is well within reach.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.
For years, we have all been promised interconnected electronic patient records – the concept that information would follow patients and be available across all care settings. Unfortunately, this reality has yet to materialize.
Regional Health Information Organizations (RHIOs) exist all over (these are hospitals, physician practices, and health networks that exchange data on a local level), but they typically present a "brick wall" at their borders where the information sharing stops. Thankfully, that is poised to change, with a new push toward meaningful interconnectedness.
Finally, health information technology (HIT) thought leaders and electronic health records (EHR) vendors are homing in on standards that will allow physicians and other healthcare providers to exchange information seamlessly regardless of EHR system or geographical location. The goal, as usual, is to improve patient care and outcomes. In this column, we felt it would be useful to highlight some of the ideas driving this effort, as there is good reason to be optimistic about the possibility of true interoperability.
A view from the top
Recently, at the annual meeting of the Health Information Management Systems Society (HIMSS) in Orlando, Dr. Karen DeSalvo, national health IT coordinator, made a strong plea for interoperability by 2017. She said "We can do national health care exchange in 3 years. ... I want this as a doctor, I want this as patient, I want this as a daughter."
Dr. DeSalvo’s words resonate because this is a concept we all expected from the earliest days of electronic records. Unfortunately, barriers – both real and artificial – have stood in the way. First and foremost are patient privacy and information security. It is essential that patient data are protected and maintained as the data pass from one system to the next, but often, even the basic function of matching patients with the right records can be challenging. Many identifiers exist, including various medical record numbers and insurance codes. If a name is misspelled or middle initial omitted, this can also create significant chaos and allow sensitive data to file into the wrong place, creating HIPAA violations and distrust among patients.
In addition to concerns over data security, the lack of standard formatting for storing and sharing records has been a huge hurdle for EHR vendors. Not surprisingly, the simultaneous development of dozens of competing EHR products has created significant fragmentation throughout the market. Instead of starting from a common set of data elements, each EHR was essentially designed "in a vacuum," and only now are their creators attempting to find a way to get them to communicate. A number of cross-platform projects currently underway highlight this effort.
VHS or Betamax?
On Feb. 25, 2014, NextGen Healthcare and Cerner announced bilateral certification of their EHR products and affirmed their commitment to interoperability. According to the press release, they are committed to "creating proactive working relationships, expanding the boundaries of current interoperability ... and supporting the efforts of [their] clients to advance the health of their communities." These may not be novel goals, but at least both vendors have demonstrated their best attempt to achieve them. Also, both companies have a huge footprint in the market, so their collaboration is certain to raise the level of attention being paid to this topic. But this isn’t the only attempt at broad-based interoperability.
EClinicalWorks (eCW), another large player in the ambulatory EHR market, has developed a product know as P2P, or Provider to Provider. Originally conceived as a way to communicate between different users of the eCW platform, it has now been expanded to all providers, regardless of their EHR, as a secure communication tool. This new product is known as P2POpen and is free to any health care professional wishing to join "the network." According to their website, P2POpen now boasts close to 22,000 users and facilitates "improved quality, safety, and efficiency of care." Like the collaboration mentioned above, P2POpen has a shot at success, but both of these efforts may also portend more debate over standardization moving forward. Will the disparity in how each company addresses the issue of interoperability lead to further fragmentation? And how can we be sure that embracing one of these ideas won’t severely limit us in the future?
Setting the standard
The only way to answer these and other looming concerns over developing a consistent interoperability protocol is to start at the top and rapidly build consensus. In other words, Dr. DeSalvo’s words need to be quickly translated into action, as she and other thought leaders agree – not only on a standard – but also on a way to properly motivate EHR vendors to adopt that standard.
One possible opportunity to enforce this as Meaningful Use stage III. The requirements for stage III EHR certification, which have yet to be finalized, should include a necessity for every vendor to adopt a consistent format for information exchange and data transmission. Making this a certification requirement will ensure that all EHR products remain cooperative if they plan to stay competitive.
Another solution being considered involves the use of centralized "Health Information Exchanges," which could collect and warehouse data from multiple sources and then retransmit those data in a universally readable format. Either way, if a consensus can be reached and issues over privacy and security addressed, it will only spell a victory for physicians and patients and truly get us on the road to improved patient care and outcomes. We tend to agree with Dr. DeSalvo, and believe that victory is well within reach.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. An avid programmer, he has published software for handheld devices in partnership with national organizations, and he is always looking for new ways to bring evidence-based medicine to the point of care. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. He is also editor-in-chief of Redi-Reference Inc., a software company that creates mobile apps.

Scribes
I’m willing to give the Affordable Care Act several more months before I finally decide that it is as poorly conceived and executed as it appears to be at the moment. However, when it comes to the efforts by the federal government to speed the adoption of electronic health records, I’m sure that the result has been several giant steps backward for both the quality of medical care and the level of satisfaction for the physicians in this country.
Doctors who have begun to use electronic health records (EHRs) are finding that they are spending more hours of their day in front of a computer screen doing clerical work. If they can’t afford to see fewer patients, the result is an extra hour or two at the end of the day catching up with the paperless work. This means that hours of family and rejuvenation time that were already in short supply are lost. A recent survey by Mark William Friedberg of the Rand Corp. and his associates listed the burden caused by electronic health records as the leading contributor to physician dissatisfaction. Neither physicians nor their patients are happy with the loss of eye to eye contact that also accompanies the adoption of EHRs.
I suspect that most physicians continue to hold out hope that computerized medical records will prove to benefit patient care in the long run. But, their patience has worn so thin it is easy to see the frustration on their faces and hear it in their voices. Those of us who have already endured more than once the steep learning curve that comes with a new computer system have found that at the top of the curve is a plateau – a plateau that leaves us no more productive than we were when we started the painful and expensive climb, despite promises from the vendors and administrators who bought their sales pitches.
But, there may be a solution to at least some of the downside to electronic health records, namely, scribes. A scribe is an assistant who accompanies the physician as he sees patients and records the pertinent information generated from the visit in real time. The result is a completed medical record and a bill for services without the physician having to lift a pen, move a cursor, or take her eyes off the patient. It is estimated that there are nearly 10,000 scribes working in this country, and there are companies who promise to provide a turnkey operation that includes hiring, training, and updating skills. The charge for the service runs about $20-$25 per hour, with the scribe receiving $8-$16 per hour.
Scribes have been most popular in hospitals and emergency departments where the expense may be less of a hurdle than elsewhere, but they work in outpatient settings as well. The issue of confidentiality has been raised, but it doesn’t seem to have been a problem. Patients are accustomed to having a nurse or chaperone, and for many years haven’t expressed much concern about having their medical records read or listened to by transcriptionists.
If I were still in practice, I think I could easily rationalize the cost of a scribe if he or she allowed me to get home an hour or two earlier. I suspect my children would even have been willing to chip in some of their allowance to fund the service if it allowed their father to show up for dinner and in a sunnier frame of mind.
Two little wrinkles come to mind, but I think they could be easily ironed out. My exam rooms have never been terribly spacious, and now that two parents and a grandparent often accompany the patient, I wonder where we would put another warm body. And, with the increasing volume of mental health–related visits that pediatricians are seeing, I can imagine a few situations in which the presence of a scribe might be a deterrent to effective communication. However, I am sure that it would be easy to arrange a system in which the physician wore a microphone that would connect to the scribe in another room. A prominently displayed sign reminding the patient that a scribe was listening and recording would blend in with the other informational signs that paper the walls of most examining rooms and are being ignored.
So what do you think? Would a scribe system work for you? Would it be worth the expense? Can you imagine some downsides that I haven’t considered?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at pdnews@ frontlinemedcom.com. Scan this QR code or go to pediatricnews.com to read similar columns.
I’m willing to give the Affordable Care Act several more months before I finally decide that it is as poorly conceived and executed as it appears to be at the moment. However, when it comes to the efforts by the federal government to speed the adoption of electronic health records, I’m sure that the result has been several giant steps backward for both the quality of medical care and the level of satisfaction for the physicians in this country.
Doctors who have begun to use electronic health records (EHRs) are finding that they are spending more hours of their day in front of a computer screen doing clerical work. If they can’t afford to see fewer patients, the result is an extra hour or two at the end of the day catching up with the paperless work. This means that hours of family and rejuvenation time that were already in short supply are lost. A recent survey by Mark William Friedberg of the Rand Corp. and his associates listed the burden caused by electronic health records as the leading contributor to physician dissatisfaction. Neither physicians nor their patients are happy with the loss of eye to eye contact that also accompanies the adoption of EHRs.
I suspect that most physicians continue to hold out hope that computerized medical records will prove to benefit patient care in the long run. But, their patience has worn so thin it is easy to see the frustration on their faces and hear it in their voices. Those of us who have already endured more than once the steep learning curve that comes with a new computer system have found that at the top of the curve is a plateau – a plateau that leaves us no more productive than we were when we started the painful and expensive climb, despite promises from the vendors and administrators who bought their sales pitches.
But, there may be a solution to at least some of the downside to electronic health records, namely, scribes. A scribe is an assistant who accompanies the physician as he sees patients and records the pertinent information generated from the visit in real time. The result is a completed medical record and a bill for services without the physician having to lift a pen, move a cursor, or take her eyes off the patient. It is estimated that there are nearly 10,000 scribes working in this country, and there are companies who promise to provide a turnkey operation that includes hiring, training, and updating skills. The charge for the service runs about $20-$25 per hour, with the scribe receiving $8-$16 per hour.
Scribes have been most popular in hospitals and emergency departments where the expense may be less of a hurdle than elsewhere, but they work in outpatient settings as well. The issue of confidentiality has been raised, but it doesn’t seem to have been a problem. Patients are accustomed to having a nurse or chaperone, and for many years haven’t expressed much concern about having their medical records read or listened to by transcriptionists.
If I were still in practice, I think I could easily rationalize the cost of a scribe if he or she allowed me to get home an hour or two earlier. I suspect my children would even have been willing to chip in some of their allowance to fund the service if it allowed their father to show up for dinner and in a sunnier frame of mind.
Two little wrinkles come to mind, but I think they could be easily ironed out. My exam rooms have never been terribly spacious, and now that two parents and a grandparent often accompany the patient, I wonder where we would put another warm body. And, with the increasing volume of mental health–related visits that pediatricians are seeing, I can imagine a few situations in which the presence of a scribe might be a deterrent to effective communication. However, I am sure that it would be easy to arrange a system in which the physician wore a microphone that would connect to the scribe in another room. A prominently displayed sign reminding the patient that a scribe was listening and recording would blend in with the other informational signs that paper the walls of most examining rooms and are being ignored.
So what do you think? Would a scribe system work for you? Would it be worth the expense? Can you imagine some downsides that I haven’t considered?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at pdnews@ frontlinemedcom.com. Scan this QR code or go to pediatricnews.com to read similar columns.
I’m willing to give the Affordable Care Act several more months before I finally decide that it is as poorly conceived and executed as it appears to be at the moment. However, when it comes to the efforts by the federal government to speed the adoption of electronic health records, I’m sure that the result has been several giant steps backward for both the quality of medical care and the level of satisfaction for the physicians in this country.
Doctors who have begun to use electronic health records (EHRs) are finding that they are spending more hours of their day in front of a computer screen doing clerical work. If they can’t afford to see fewer patients, the result is an extra hour or two at the end of the day catching up with the paperless work. This means that hours of family and rejuvenation time that were already in short supply are lost. A recent survey by Mark William Friedberg of the Rand Corp. and his associates listed the burden caused by electronic health records as the leading contributor to physician dissatisfaction. Neither physicians nor their patients are happy with the loss of eye to eye contact that also accompanies the adoption of EHRs.
I suspect that most physicians continue to hold out hope that computerized medical records will prove to benefit patient care in the long run. But, their patience has worn so thin it is easy to see the frustration on their faces and hear it in their voices. Those of us who have already endured more than once the steep learning curve that comes with a new computer system have found that at the top of the curve is a plateau – a plateau that leaves us no more productive than we were when we started the painful and expensive climb, despite promises from the vendors and administrators who bought their sales pitches.
But, there may be a solution to at least some of the downside to electronic health records, namely, scribes. A scribe is an assistant who accompanies the physician as he sees patients and records the pertinent information generated from the visit in real time. The result is a completed medical record and a bill for services without the physician having to lift a pen, move a cursor, or take her eyes off the patient. It is estimated that there are nearly 10,000 scribes working in this country, and there are companies who promise to provide a turnkey operation that includes hiring, training, and updating skills. The charge for the service runs about $20-$25 per hour, with the scribe receiving $8-$16 per hour.
Scribes have been most popular in hospitals and emergency departments where the expense may be less of a hurdle than elsewhere, but they work in outpatient settings as well. The issue of confidentiality has been raised, but it doesn’t seem to have been a problem. Patients are accustomed to having a nurse or chaperone, and for many years haven’t expressed much concern about having their medical records read or listened to by transcriptionists.
If I were still in practice, I think I could easily rationalize the cost of a scribe if he or she allowed me to get home an hour or two earlier. I suspect my children would even have been willing to chip in some of their allowance to fund the service if it allowed their father to show up for dinner and in a sunnier frame of mind.
Two little wrinkles come to mind, but I think they could be easily ironed out. My exam rooms have never been terribly spacious, and now that two parents and a grandparent often accompany the patient, I wonder where we would put another warm body. And, with the increasing volume of mental health–related visits that pediatricians are seeing, I can imagine a few situations in which the presence of a scribe might be a deterrent to effective communication. However, I am sure that it would be easy to arrange a system in which the physician wore a microphone that would connect to the scribe in another room. A prominently displayed sign reminding the patient that a scribe was listening and recording would blend in with the other informational signs that paper the walls of most examining rooms and are being ignored.
So what do you think? Would a scribe system work for you? Would it be worth the expense? Can you imagine some downsides that I haven’t considered?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at pdnews@ frontlinemedcom.com. Scan this QR code or go to pediatricnews.com to read similar columns.
Would you?
Would you tell your children to eliminate the practice of medicine from their list of potential career paths? It’s not a question I ever needed to consider. Although my three children are bright and have a good work ethic, none of them considered becoming a doctor. At least if they did, I wasn’t consulted. Two of them have always been squeamish about body fluids, and that was probably a deal breaker for them. It certainly wasn’t because I complained about my job. I don’t recall ever grumbling about being a pediatrician. Although my considerably less-than-perfect attendance at dinner and their sporting events may have prompted them to seek a more family-friendly profession.
In a recent column, Dr. Allan M. Block wrote a piece titled "Why I’m happy my kids don’t want to be doctors"(January 2014, p. 16). In his sad-but-true commentary, he imagines how uncomfortable it must be to leave medical school with nearly a quarter of a million dollars in debt, a burden that must affect how young doctors choose what and how they practice. While none of us planned to practice rogue medicine, Dr. Block also bemoans the fact that "people who know nothing about medicine try to tell us what we can or can’t do."
Is his commentary merely a burnout candidate’s last rant before the flames reach his vital organs? Or, is he speaking for the many physicians who have worked long enough to realize that the practice of medicine has moved perilously close to the point where the cost/benefit ratio has tipped to the "it-isn’t-worth-it" side?
While none of my children sought my opinion on medicine as a career path, scores of my patients have shared their dreams of becoming physicians. Whenever this has happened, I egotistically hope that in some way I may have served as a positive role model they wish to emulate. But, I have learned that there are usually more potent motivators lurking in the background. While still puffed up with undeserved pride, I also assume that they are asking for my opinion on their plans . . . which of course they are not.
I ignore the obvious and offer, "Well, it may not be as much fun as it was 20 years ago, but being a pediatrician is still a lot of fun." Of course, this begs the question, If I were in their shoes today, would I apply to medical school?
Hesitant to throw too much cold water on their enthusiasm, I am sure to reassure them that I think they would make wonderful doctors. But, I add that becoming a physician is a long and expensive process. I hope that they are still listening when I add, "You know that nurse practitioners and physician assistants get to do almost all of the cool things I enjoy the most about being a pediatrician, . . . and the training is certainly shorter and less costly."
Of course, choosing either of these nonphysician career paths will rob their parents of the opportunity to introduce them at cocktail parties as "Our daughter, the doctor." But, the trade-off is that they will be more likely to be content with their jobs.
While my observations may be good advice for some of my patients, it leaves unanswered what to do about the malaise that hangs over Dr. Block and many of our colleagues. Educational debt has robbed some young doctors of their entrepreneurial spirit. Pressures from the government and third-party payers have nibbled away at our autonomy. And, the threat of malpractice action has smothered many of us in a blanket of fear.
Even in the face of all this gloom, if one of my grandchildren told me that they really wanted to be a pediatrician and expressed no interest in the nurse practitioner option, I would be candid in describing the erosion that has occurred over the course of my career. But, I would challenge them to tell me another job that could offer them even half of the opportunities to feel needed and appreciated that I have enjoyed. Hopefully, at least some of the frustrating downsides of medicine today will be reversed by the time they enter practice.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Would you tell your children to eliminate the practice of medicine from their list of potential career paths? It’s not a question I ever needed to consider. Although my three children are bright and have a good work ethic, none of them considered becoming a doctor. At least if they did, I wasn’t consulted. Two of them have always been squeamish about body fluids, and that was probably a deal breaker for them. It certainly wasn’t because I complained about my job. I don’t recall ever grumbling about being a pediatrician. Although my considerably less-than-perfect attendance at dinner and their sporting events may have prompted them to seek a more family-friendly profession.
In a recent column, Dr. Allan M. Block wrote a piece titled "Why I’m happy my kids don’t want to be doctors"(January 2014, p. 16). In his sad-but-true commentary, he imagines how uncomfortable it must be to leave medical school with nearly a quarter of a million dollars in debt, a burden that must affect how young doctors choose what and how they practice. While none of us planned to practice rogue medicine, Dr. Block also bemoans the fact that "people who know nothing about medicine try to tell us what we can or can’t do."
Is his commentary merely a burnout candidate’s last rant before the flames reach his vital organs? Or, is he speaking for the many physicians who have worked long enough to realize that the practice of medicine has moved perilously close to the point where the cost/benefit ratio has tipped to the "it-isn’t-worth-it" side?
While none of my children sought my opinion on medicine as a career path, scores of my patients have shared their dreams of becoming physicians. Whenever this has happened, I egotistically hope that in some way I may have served as a positive role model they wish to emulate. But, I have learned that there are usually more potent motivators lurking in the background. While still puffed up with undeserved pride, I also assume that they are asking for my opinion on their plans . . . which of course they are not.
I ignore the obvious and offer, "Well, it may not be as much fun as it was 20 years ago, but being a pediatrician is still a lot of fun." Of course, this begs the question, If I were in their shoes today, would I apply to medical school?
Hesitant to throw too much cold water on their enthusiasm, I am sure to reassure them that I think they would make wonderful doctors. But, I add that becoming a physician is a long and expensive process. I hope that they are still listening when I add, "You know that nurse practitioners and physician assistants get to do almost all of the cool things I enjoy the most about being a pediatrician, . . . and the training is certainly shorter and less costly."
Of course, choosing either of these nonphysician career paths will rob their parents of the opportunity to introduce them at cocktail parties as "Our daughter, the doctor." But, the trade-off is that they will be more likely to be content with their jobs.
While my observations may be good advice for some of my patients, it leaves unanswered what to do about the malaise that hangs over Dr. Block and many of our colleagues. Educational debt has robbed some young doctors of their entrepreneurial spirit. Pressures from the government and third-party payers have nibbled away at our autonomy. And, the threat of malpractice action has smothered many of us in a blanket of fear.
Even in the face of all this gloom, if one of my grandchildren told me that they really wanted to be a pediatrician and expressed no interest in the nurse practitioner option, I would be candid in describing the erosion that has occurred over the course of my career. But, I would challenge them to tell me another job that could offer them even half of the opportunities to feel needed and appreciated that I have enjoyed. Hopefully, at least some of the frustrating downsides of medicine today will be reversed by the time they enter practice.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Would you tell your children to eliminate the practice of medicine from their list of potential career paths? It’s not a question I ever needed to consider. Although my three children are bright and have a good work ethic, none of them considered becoming a doctor. At least if they did, I wasn’t consulted. Two of them have always been squeamish about body fluids, and that was probably a deal breaker for them. It certainly wasn’t because I complained about my job. I don’t recall ever grumbling about being a pediatrician. Although my considerably less-than-perfect attendance at dinner and their sporting events may have prompted them to seek a more family-friendly profession.
In a recent column, Dr. Allan M. Block wrote a piece titled "Why I’m happy my kids don’t want to be doctors"(January 2014, p. 16). In his sad-but-true commentary, he imagines how uncomfortable it must be to leave medical school with nearly a quarter of a million dollars in debt, a burden that must affect how young doctors choose what and how they practice. While none of us planned to practice rogue medicine, Dr. Block also bemoans the fact that "people who know nothing about medicine try to tell us what we can or can’t do."
Is his commentary merely a burnout candidate’s last rant before the flames reach his vital organs? Or, is he speaking for the many physicians who have worked long enough to realize that the practice of medicine has moved perilously close to the point where the cost/benefit ratio has tipped to the "it-isn’t-worth-it" side?
While none of my children sought my opinion on medicine as a career path, scores of my patients have shared their dreams of becoming physicians. Whenever this has happened, I egotistically hope that in some way I may have served as a positive role model they wish to emulate. But, I have learned that there are usually more potent motivators lurking in the background. While still puffed up with undeserved pride, I also assume that they are asking for my opinion on their plans . . . which of course they are not.
I ignore the obvious and offer, "Well, it may not be as much fun as it was 20 years ago, but being a pediatrician is still a lot of fun." Of course, this begs the question, If I were in their shoes today, would I apply to medical school?
Hesitant to throw too much cold water on their enthusiasm, I am sure to reassure them that I think they would make wonderful doctors. But, I add that becoming a physician is a long and expensive process. I hope that they are still listening when I add, "You know that nurse practitioners and physician assistants get to do almost all of the cool things I enjoy the most about being a pediatrician, . . . and the training is certainly shorter and less costly."
Of course, choosing either of these nonphysician career paths will rob their parents of the opportunity to introduce them at cocktail parties as "Our daughter, the doctor." But, the trade-off is that they will be more likely to be content with their jobs.
While my observations may be good advice for some of my patients, it leaves unanswered what to do about the malaise that hangs over Dr. Block and many of our colleagues. Educational debt has robbed some young doctors of their entrepreneurial spirit. Pressures from the government and third-party payers have nibbled away at our autonomy. And, the threat of malpractice action has smothered many of us in a blanket of fear.
Even in the face of all this gloom, if one of my grandchildren told me that they really wanted to be a pediatrician and expressed no interest in the nurse practitioner option, I would be candid in describing the erosion that has occurred over the course of my career. But, I would challenge them to tell me another job that could offer them even half of the opportunities to feel needed and appreciated that I have enjoyed. Hopefully, at least some of the frustrating downsides of medicine today will be reversed by the time they enter practice.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including "How to Say No to Your Toddler." E-mail him at [email protected].
Gabapentin for alcohol use disorder
Two-thirds of U.S. adults currently consume alcohol, according to the National Health Interview Survey. While most are infrequent or light drinkers, 8% are problem drinkers (more than 14 drinks per week for men and more than 7 drinks per week for women).
Alcohol consumption is the second-leading cause of preventable death and disability in the United States. Annually, excessive alcohol consumption costs us almost a quarter of a trillion dollars in lost productivity, health care, law enforcement, and motor vehicle collisions.
Alcoholism is a relapsing and remitting disease characterized by psychosocial impairment and drug craving and withdrawal. Challenged by access inequalities to formal treatment services, few alcoholics, when interacting with the medical setting for other reasons, are offered or receive treatment. Some patients may be open to receiving treatment by primary care providers, but few drugs are available (naltrexone, acamprosate, and disulfiram). Clinicians may be unconvinced of their efficacy or uncomfortable with their use.
Gabapentin is an antiepileptic used commonly in primary care settings, mostly for neuropathic pain. Gabapentin is well tolerated, with a favorable pharmacokinetic profile and a broad therapeutic index. Preclinical data suggest that gabapentin normalizes stress-induced GABA (gamma-aminobutyric acid) activation associated with alcohol use disorder. Human data suggest that gabapentin reduces alcohol craving and alcohol-associated sleep and mood problems.
Mason and colleagues published the results from a randomized controlled clinical trial evaluating the efficacy and safety of different doses of gabapentin for increasing alcohol abstinence and reducing heavy drinking, insomnia, dysphoria, and craving. Potential participants were eligible for enrollment if they were aged 18 years or older, met criteria for alcohol dependence, and were recently abstinent from alcohol (at least 3 days). Participants were randomized to gabapentin 900 mg/day, gabapentin 1,800 mg/day, or placebo. Treatment was received for 12 weeks with titration and tapering (JAMA Intern. Med. 2014;174:70-7).
A total of 150 patients were randomized, and the groups were similar at baseline. Abstinence rates were 17%, 11.1%, and 4.1% in the 1,800-mg, 900-mg, and placebo groups (P = .04 for linear dose effect), respectively. The no-heavy-drinking rates were 44.7%, 29.6%, and 22.5% (P = .02 for linear dose effect). A dose effect was also observed for reductions in mood disturbance, sleep problems, and craving. No serious adverse events were reported.
We need to try to meet patients where they are. Patients should be directed to alcohol treatment services if they are willing to go. In my experience, many of them are not. In these cases, recommending an Alcoholics Anonymous group, trying gabapentin, and following them up in a clinic is a harm-reduction strategy worth trying.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
Two-thirds of U.S. adults currently consume alcohol, according to the National Health Interview Survey. While most are infrequent or light drinkers, 8% are problem drinkers (more than 14 drinks per week for men and more than 7 drinks per week for women).
Alcohol consumption is the second-leading cause of preventable death and disability in the United States. Annually, excessive alcohol consumption costs us almost a quarter of a trillion dollars in lost productivity, health care, law enforcement, and motor vehicle collisions.
Alcoholism is a relapsing and remitting disease characterized by psychosocial impairment and drug craving and withdrawal. Challenged by access inequalities to formal treatment services, few alcoholics, when interacting with the medical setting for other reasons, are offered or receive treatment. Some patients may be open to receiving treatment by primary care providers, but few drugs are available (naltrexone, acamprosate, and disulfiram). Clinicians may be unconvinced of their efficacy or uncomfortable with their use.
Gabapentin is an antiepileptic used commonly in primary care settings, mostly for neuropathic pain. Gabapentin is well tolerated, with a favorable pharmacokinetic profile and a broad therapeutic index. Preclinical data suggest that gabapentin normalizes stress-induced GABA (gamma-aminobutyric acid) activation associated with alcohol use disorder. Human data suggest that gabapentin reduces alcohol craving and alcohol-associated sleep and mood problems.
Mason and colleagues published the results from a randomized controlled clinical trial evaluating the efficacy and safety of different doses of gabapentin for increasing alcohol abstinence and reducing heavy drinking, insomnia, dysphoria, and craving. Potential participants were eligible for enrollment if they were aged 18 years or older, met criteria for alcohol dependence, and were recently abstinent from alcohol (at least 3 days). Participants were randomized to gabapentin 900 mg/day, gabapentin 1,800 mg/day, or placebo. Treatment was received for 12 weeks with titration and tapering (JAMA Intern. Med. 2014;174:70-7).
A total of 150 patients were randomized, and the groups were similar at baseline. Abstinence rates were 17%, 11.1%, and 4.1% in the 1,800-mg, 900-mg, and placebo groups (P = .04 for linear dose effect), respectively. The no-heavy-drinking rates were 44.7%, 29.6%, and 22.5% (P = .02 for linear dose effect). A dose effect was also observed for reductions in mood disturbance, sleep problems, and craving. No serious adverse events were reported.
We need to try to meet patients where they are. Patients should be directed to alcohol treatment services if they are willing to go. In my experience, many of them are not. In these cases, recommending an Alcoholics Anonymous group, trying gabapentin, and following them up in a clinic is a harm-reduction strategy worth trying.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
Two-thirds of U.S. adults currently consume alcohol, according to the National Health Interview Survey. While most are infrequent or light drinkers, 8% are problem drinkers (more than 14 drinks per week for men and more than 7 drinks per week for women).
Alcohol consumption is the second-leading cause of preventable death and disability in the United States. Annually, excessive alcohol consumption costs us almost a quarter of a trillion dollars in lost productivity, health care, law enforcement, and motor vehicle collisions.
Alcoholism is a relapsing and remitting disease characterized by psychosocial impairment and drug craving and withdrawal. Challenged by access inequalities to formal treatment services, few alcoholics, when interacting with the medical setting for other reasons, are offered or receive treatment. Some patients may be open to receiving treatment by primary care providers, but few drugs are available (naltrexone, acamprosate, and disulfiram). Clinicians may be unconvinced of their efficacy or uncomfortable with their use.
Gabapentin is an antiepileptic used commonly in primary care settings, mostly for neuropathic pain. Gabapentin is well tolerated, with a favorable pharmacokinetic profile and a broad therapeutic index. Preclinical data suggest that gabapentin normalizes stress-induced GABA (gamma-aminobutyric acid) activation associated with alcohol use disorder. Human data suggest that gabapentin reduces alcohol craving and alcohol-associated sleep and mood problems.
Mason and colleagues published the results from a randomized controlled clinical trial evaluating the efficacy and safety of different doses of gabapentin for increasing alcohol abstinence and reducing heavy drinking, insomnia, dysphoria, and craving. Potential participants were eligible for enrollment if they were aged 18 years or older, met criteria for alcohol dependence, and were recently abstinent from alcohol (at least 3 days). Participants were randomized to gabapentin 900 mg/day, gabapentin 1,800 mg/day, or placebo. Treatment was received for 12 weeks with titration and tapering (JAMA Intern. Med. 2014;174:70-7).
A total of 150 patients were randomized, and the groups were similar at baseline. Abstinence rates were 17%, 11.1%, and 4.1% in the 1,800-mg, 900-mg, and placebo groups (P = .04 for linear dose effect), respectively. The no-heavy-drinking rates were 44.7%, 29.6%, and 22.5% (P = .02 for linear dose effect). A dose effect was also observed for reductions in mood disturbance, sleep problems, and craving. No serious adverse events were reported.
We need to try to meet patients where they are. Patients should be directed to alcohol treatment services if they are willing to go. In my experience, many of them are not. In these cases, recommending an Alcoholics Anonymous group, trying gabapentin, and following them up in a clinic is a harm-reduction strategy worth trying.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author. He reports no conflicts of interest.
