User login
What AI can see in CT scans that humans can’t
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.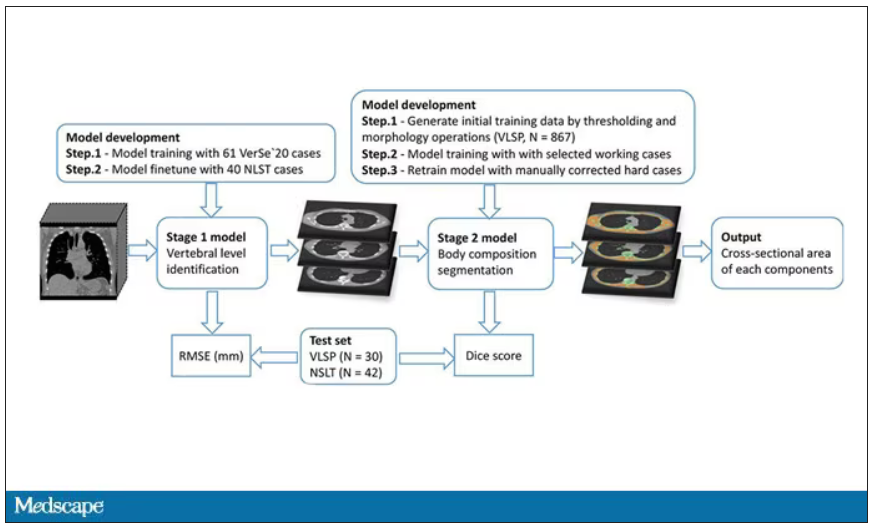
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.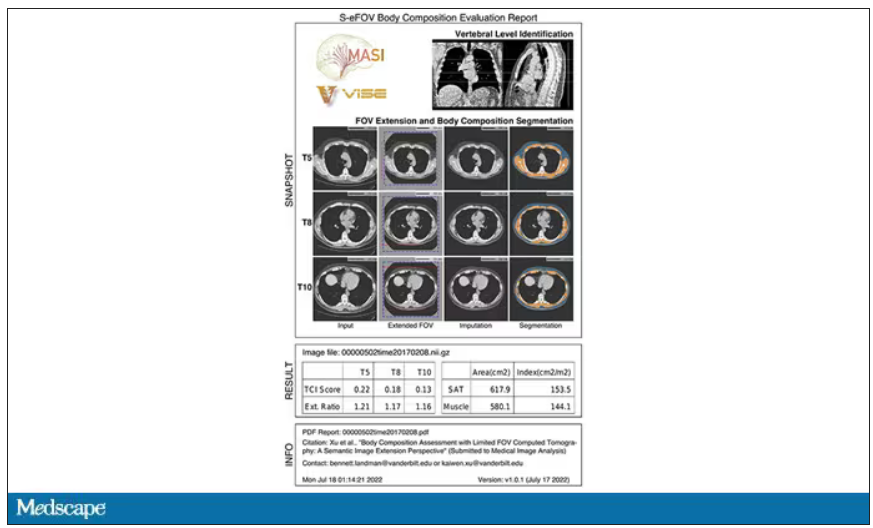
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.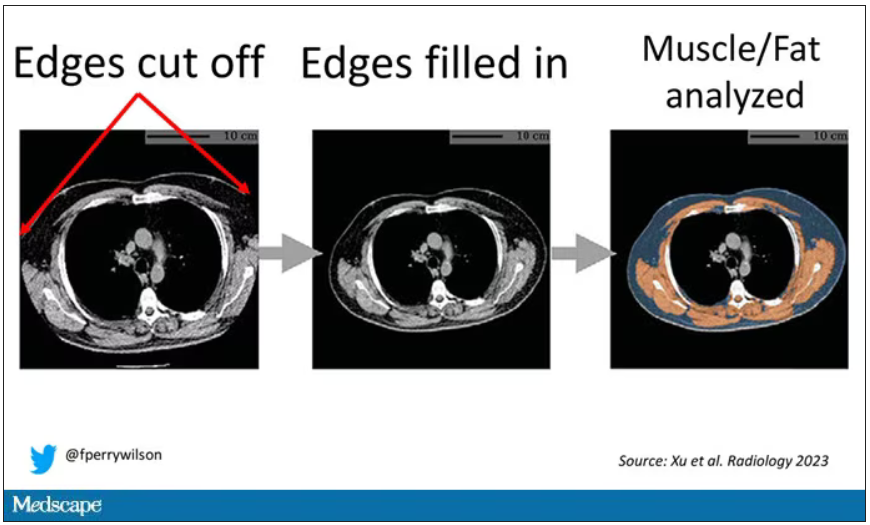
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.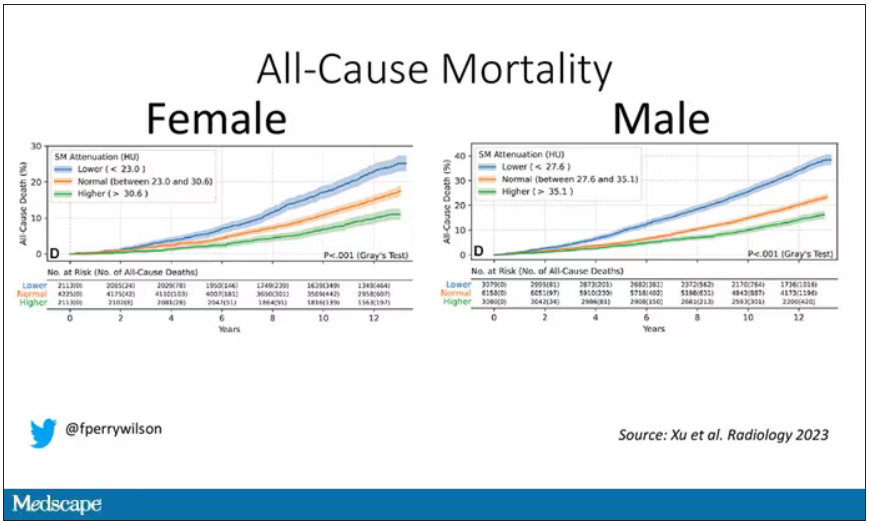
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.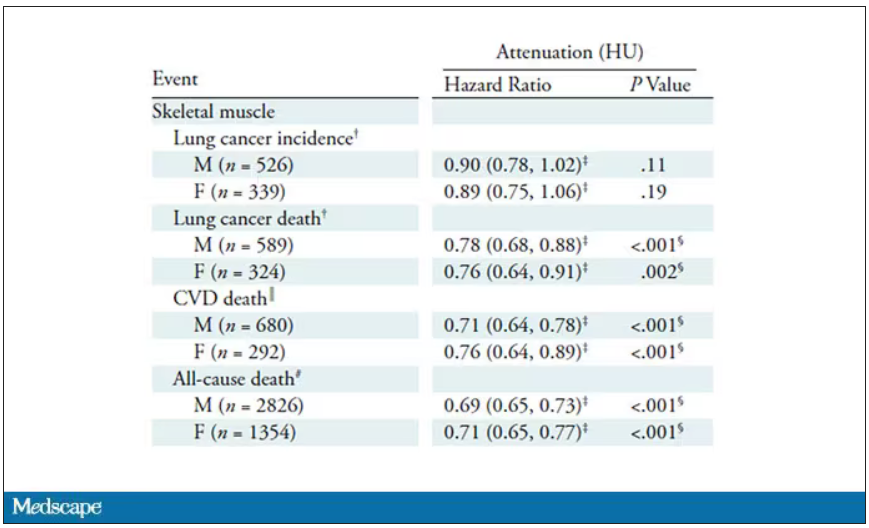
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.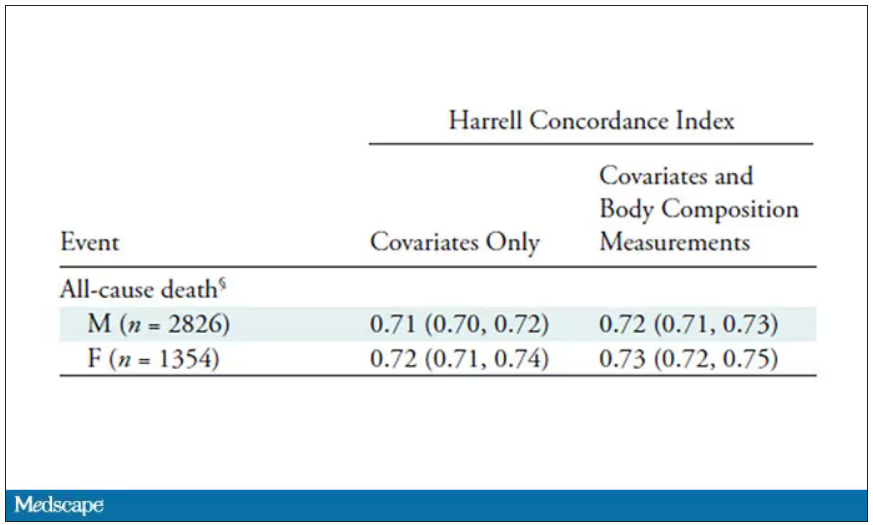
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If a picture is worth a thousand words, then a CT scan of the chest might as well be Atlas Shrugged. When you think of the sheer information content in one of those scans, it becomes immediately clear that our usual method of CT scan interpretation must be leaving a lot on the table. After all, we can go through all that information and come out with simply “normal” and call it a day.
Of course, radiologists can glean a lot from a CT scan, but they are trained to look for abnormalities. They can find pneumonia, emboli, fractures, and pneumothoraces, but the presence or absence of life-threatening abnormalities is still just a fraction of the data contained within a CT scan.
Pulling out more data from those images – data that may not indicate disease per se, but nevertheless tell us something important about patients and their risks – might just fall to those entities that are primed to take a bunch of data and interpret it in new ways: artificial intelligence (AI).
I’m thinking about AI and CT scans this week thanks to this study, appearing in the journal Radiology, from Kaiwen Xu and colleagues at Vanderbilt.
In a previous study, the team had developed an AI algorithm to take chest CT images and convert that data into information about body composition: skeletal muscle mass, fat mass, muscle lipid content – that sort of thing.
While the radiologists are busy looking for cancer or pneumonia, the AI can create a body composition report – two results from one data stream.
Here’s an example of a report generated from a CT scan from the authors’ GitHub page.
The cool thing here is that this is a clinically collected CT scan of the chest, not a special protocol designed to assess body composition. In fact, this comes from the low-dose lung cancer screening trial dataset.
As you may know, the U.S. Preventive Services Task Force recommends low-dose CT screening of the chest every year for those aged 50-80 with at least a 20 pack-year smoking history. These CT scans form an incredible dataset, actually, as they are all collected with nearly the same parameters. Obviously, the important thing to look for in these CT scans is whether there is early lung cancer. But the new paper asks, as long as we can get information about body composition from these scans, why don’t we? Can it help to risk-stratify these patients?
They took 20,768 individuals with CT scans done as part of the low-dose lung cancer screening trial and passed their scans through their automated data pipeline.
One cool feature here: Depending on body size, sometimes the edges of people in CT scans are not visible. That’s not a big deal for lung-cancer screening as long as you can see both lungs. But it does matter for assessment of muscle and body fat because that stuff lives on the edges of the thoracic cavity. The authors’ data pipeline actually accounts for this, extrapolating what the missing pieces look like from what is able to be seen. It’s quite clever.
On to some results. Would knowledge about the patient’s body composition help predict their ultimate outcome?
It would. And the best single predictor found was skeletal muscle attenuation – lower levels of skeletal muscle attenuation mean more fat infiltrating the muscle – so lower is worse here. You can see from these all-cause mortality curves that lower levels were associated with substantially worse life expectancy.
It’s worth noting that these are unadjusted curves. While AI prediction from CT images is very cool, we might be able to make similar predictions knowing, for example, the age of the patient. To account for this, the authors adjusted the findings for age, diabetes, heart disease, stroke, and coronary calcium score (also calculated from those same CT scans). Even after adjustment, skeletal muscle attenuation was significantly associated with all-cause mortality, cardiovascular mortality, and lung-cancer mortality – but not lung cancer incidence.
Those results tell us that there is likely a physiologic significance to skeletal muscle attenuation, and they provide a great proof-of-concept that automated data extraction techniques can be applied broadly to routinely collected radiology images.
That said, it’s one thing to show that something is physiologically relevant. In terms of actually predicting outcomes, adding this information to a model that contains just those clinical factors like age and diabetes doesn’t actually improve things very much. We measure this with something called the concordance index. This tells us the probability, given two individuals, of how often we can identify the person who has the outcome of interest sooner – if at all. (You can probably guess that the worst possible score is thus 0.5 and the best is 1.) A model without the AI data gives a concordance index for all-cause mortality of 0.71 or 0.72, depending on sex. Adding in the body composition data bumps that up only by a percent or so.
This honestly feels a bit like a missed opportunity to me. The authors pass the imaging data through an AI to get body composition data and then see how that predicts death.
Why not skip the middleman? Train a model using the imaging data to predict death directly, using whatever signal the AI chooses: body composition, lung size, rib thickness – whatever.
I’d be very curious to see how that model might improve our ability to predict these outcomes. In the end, this is a space where AI can make some massive gains – not by trying to do radiologists’ jobs better than radiologists, but by extracting information that radiologists aren’t looking for in the first place.
F. Perry Wilson, MD, MSCE, is associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Time to end direct-to-consumer ads, says physician
One has to be living off the grid to not be bombarded with direct-to-consumer (DTC) pharmaceutical advertising. Since 1997, when the Food and Drug Administration eased restrictions on this prohibition and allowed pharmaceutical companies to promote prescription-only medications to the public, there has been a deluge of ads in magazines, on the Internet, and, most annoying, on commercial television.
These television ads are quite formulaic:
We are initially introduced to a number of highly functioning patients (typically actors) who are engaged in rewarding pursuits. A voiceover narration then presents the pharmaceutical to be promoted, suggesting (not so subtly) to consumers that taking the advertised drug will improve one’s disease outlook or quality of life such that they too, just like the actors in the minidrama, can lead such highly productive lives.
The potential best-case scenarios of these new treatments may be stated. There then follows a litany of side effects – some of them life threatening – warnings, and contraindications. We’re again treated to another 5 or 10 seconds of patients leading “the good life,” and almost all of the ads end with the narrator concluding: “Ask your doctor (sometimes ‘provider’) if _____ is right for you.”
Americans spend more money on their prescriptions than do citizens of any other highly developed nation. I have personally heard from patients who get their prescriptions from other countries, where they are more affordable. These patients will also cut their pills in half or take a medication every other day instead of every day, to economize on drug costs.
Another “trick” they use to save money – and I have heard pharmacists and pharmaceutical reps themselves recommend this – is to ask for a higher dose of a medication, usually double, and then use a pill cutter to divide a tablet in half, thus making their prescription last twice as long. Why do Americans have to resort to such “workarounds”?
Many of the medications advertised are for relatively rare conditions, such as thyroid eye disease or myasthenia gravis (which affects up to about 60,000 patients in the United States). Why not spend these advertising dollars on programs to make drugs taken by the millions of Americans with common conditions (for example, hypertension, diabetes, heart failure) more affordable?
Very often the television ads contain medical jargon, such as: “If you have the EGFR mutation, or if your cancer is HER2 negative ...”
Do most patients truly understand what these terms mean? And what happens when a patient’s physician doesn’t prescribe a medication that a patient has seen on TV and asks for, or when the physician believes that a generic (nonadvertised) medication might work just as well? This creates conflict and potential discord, adversely affecting the doctor-patient relationship.
An oncologist colleague related to me that he often has to spend time correcting patients’ misperceptions of potential miracle cures offered by these ads, and that several patients have left his practice because he would not prescribe a drug they saw advertised.
Further, while these ads urge patients to try expensive “newest and latest” treatments, pharmacy benefit plans are working with health care insurance conglomerates to reduce costs of pharmaceuticals.
How does this juxtaposition of opposing forces make any sense?
It is time for us to put an end to DTC advertising, at least on television. It will require legislative action by our federal government to end this practice (legal, by the way, only in the United States and New Zealand), and hence the willingness of our politicians to get behind legislation to do so.
Just as a law was passed to prohibit tobacco advertising on television, so should a law be passed to regulate DTC pharmaceutical advertising.
The time to end DTC advertising has come!
Lloyd Alterman, MD, is a retired physician and chairman of the New Jersey Universal Healthcare Coalition. He disclosed having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
One has to be living off the grid to not be bombarded with direct-to-consumer (DTC) pharmaceutical advertising. Since 1997, when the Food and Drug Administration eased restrictions on this prohibition and allowed pharmaceutical companies to promote prescription-only medications to the public, there has been a deluge of ads in magazines, on the Internet, and, most annoying, on commercial television.
These television ads are quite formulaic:
We are initially introduced to a number of highly functioning patients (typically actors) who are engaged in rewarding pursuits. A voiceover narration then presents the pharmaceutical to be promoted, suggesting (not so subtly) to consumers that taking the advertised drug will improve one’s disease outlook or quality of life such that they too, just like the actors in the minidrama, can lead such highly productive lives.
The potential best-case scenarios of these new treatments may be stated. There then follows a litany of side effects – some of them life threatening – warnings, and contraindications. We’re again treated to another 5 or 10 seconds of patients leading “the good life,” and almost all of the ads end with the narrator concluding: “Ask your doctor (sometimes ‘provider’) if _____ is right for you.”
Americans spend more money on their prescriptions than do citizens of any other highly developed nation. I have personally heard from patients who get their prescriptions from other countries, where they are more affordable. These patients will also cut their pills in half or take a medication every other day instead of every day, to economize on drug costs.
Another “trick” they use to save money – and I have heard pharmacists and pharmaceutical reps themselves recommend this – is to ask for a higher dose of a medication, usually double, and then use a pill cutter to divide a tablet in half, thus making their prescription last twice as long. Why do Americans have to resort to such “workarounds”?
Many of the medications advertised are for relatively rare conditions, such as thyroid eye disease or myasthenia gravis (which affects up to about 60,000 patients in the United States). Why not spend these advertising dollars on programs to make drugs taken by the millions of Americans with common conditions (for example, hypertension, diabetes, heart failure) more affordable?
Very often the television ads contain medical jargon, such as: “If you have the EGFR mutation, or if your cancer is HER2 negative ...”
Do most patients truly understand what these terms mean? And what happens when a patient’s physician doesn’t prescribe a medication that a patient has seen on TV and asks for, or when the physician believes that a generic (nonadvertised) medication might work just as well? This creates conflict and potential discord, adversely affecting the doctor-patient relationship.
An oncologist colleague related to me that he often has to spend time correcting patients’ misperceptions of potential miracle cures offered by these ads, and that several patients have left his practice because he would not prescribe a drug they saw advertised.
Further, while these ads urge patients to try expensive “newest and latest” treatments, pharmacy benefit plans are working with health care insurance conglomerates to reduce costs of pharmaceuticals.
How does this juxtaposition of opposing forces make any sense?
It is time for us to put an end to DTC advertising, at least on television. It will require legislative action by our federal government to end this practice (legal, by the way, only in the United States and New Zealand), and hence the willingness of our politicians to get behind legislation to do so.
Just as a law was passed to prohibit tobacco advertising on television, so should a law be passed to regulate DTC pharmaceutical advertising.
The time to end DTC advertising has come!
Lloyd Alterman, MD, is a retired physician and chairman of the New Jersey Universal Healthcare Coalition. He disclosed having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
One has to be living off the grid to not be bombarded with direct-to-consumer (DTC) pharmaceutical advertising. Since 1997, when the Food and Drug Administration eased restrictions on this prohibition and allowed pharmaceutical companies to promote prescription-only medications to the public, there has been a deluge of ads in magazines, on the Internet, and, most annoying, on commercial television.
These television ads are quite formulaic:
We are initially introduced to a number of highly functioning patients (typically actors) who are engaged in rewarding pursuits. A voiceover narration then presents the pharmaceutical to be promoted, suggesting (not so subtly) to consumers that taking the advertised drug will improve one’s disease outlook or quality of life such that they too, just like the actors in the minidrama, can lead such highly productive lives.
The potential best-case scenarios of these new treatments may be stated. There then follows a litany of side effects – some of them life threatening – warnings, and contraindications. We’re again treated to another 5 or 10 seconds of patients leading “the good life,” and almost all of the ads end with the narrator concluding: “Ask your doctor (sometimes ‘provider’) if _____ is right for you.”
Americans spend more money on their prescriptions than do citizens of any other highly developed nation. I have personally heard from patients who get their prescriptions from other countries, where they are more affordable. These patients will also cut their pills in half or take a medication every other day instead of every day, to economize on drug costs.
Another “trick” they use to save money – and I have heard pharmacists and pharmaceutical reps themselves recommend this – is to ask for a higher dose of a medication, usually double, and then use a pill cutter to divide a tablet in half, thus making their prescription last twice as long. Why do Americans have to resort to such “workarounds”?
Many of the medications advertised are for relatively rare conditions, such as thyroid eye disease or myasthenia gravis (which affects up to about 60,000 patients in the United States). Why not spend these advertising dollars on programs to make drugs taken by the millions of Americans with common conditions (for example, hypertension, diabetes, heart failure) more affordable?
Very often the television ads contain medical jargon, such as: “If you have the EGFR mutation, or if your cancer is HER2 negative ...”
Do most patients truly understand what these terms mean? And what happens when a patient’s physician doesn’t prescribe a medication that a patient has seen on TV and asks for, or when the physician believes that a generic (nonadvertised) medication might work just as well? This creates conflict and potential discord, adversely affecting the doctor-patient relationship.
An oncologist colleague related to me that he often has to spend time correcting patients’ misperceptions of potential miracle cures offered by these ads, and that several patients have left his practice because he would not prescribe a drug they saw advertised.
Further, while these ads urge patients to try expensive “newest and latest” treatments, pharmacy benefit plans are working with health care insurance conglomerates to reduce costs of pharmaceuticals.
How does this juxtaposition of opposing forces make any sense?
It is time for us to put an end to DTC advertising, at least on television. It will require legislative action by our federal government to end this practice (legal, by the way, only in the United States and New Zealand), and hence the willingness of our politicians to get behind legislation to do so.
Just as a law was passed to prohibit tobacco advertising on television, so should a law be passed to regulate DTC pharmaceutical advertising.
The time to end DTC advertising has come!
Lloyd Alterman, MD, is a retired physician and chairman of the New Jersey Universal Healthcare Coalition. He disclosed having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Just a simple country doctor
Whenever someone asks me what I do, I happily reply, “I’m just a simple country doctor.” That is, in part, why I am honored to be granted the opportunity to serve as editor-in-chief of The Journal of Family Practice (JFP). As our late colleague Dr. John Hickner noted in his first JFP editorial, he and the 2 editors-in-chief before him (Drs. Jeff Susman and Mark Ebell) were also of the small-town family doc tradition.1
My small-town roots trace back to rural South Carolina. I am a first-generation college student and attended medical school on a Navy Health Professions Scholarship. After completing my residency training, I had the privilege of serving for 5 years in the Navy (2 of those years were overseas), where I practiced and taught full-scope family medicine. I saw patients of all ages, attended deliveries, and provided inpatient hospital care, as well as performed a full range of procedures and tests, including colposcopies, skin procedures, vasectomies, flexible sigmoidoscopies, and exercise treadmill testing.
Following military service and completion of a 2-year fellowship and Master of Public Health degree (while working nights at a rural emergency department), I began work at the University of North Carolina at Chapel Hill. I had the good fortune of spending the next 11 years as a faculty member there, where I advanced my research and teaching career. In 2017, I was named the Chair of Family Medicine and Community Health at Duke University School of Medicine, where I continue to have an active outpatient practice.
My experiences have shaped my belief that it is critical that family medicine maintain its presence (and advance its prominence) both in our communities and at our large academic medicine centers, championing service to rural areas, promoting health equity, and advocating for the importance of high-quality primary care delivery and training. No matter where we are, our work is valuable, and we make a difference. Like my predecessors, I have a love of evidence-based medicine. I also have a love of writing, which I can trace back to my days as an intern. I am excited to be able to apply what I have learned over the years to help maintain the rigor, practicality, and relevance of JFP while simultaneously helping to nurture new authors and peer reviewers.
My goal as this journal’s editor-in-chief will be to continue its high academic standing while maintaining its utility for busy clinicians. The provision of evidence-based clinical review articles that are succinct and practical, along with departments (eg, Photo Rounds, Behavioral Health Consult, Practice Alert, PURLs), will remain the journal’s major focus. Within this framework, I also want to share the best evidence and ideas on other aspects of practicing medicine, such as quality improvement, population health, and health equity. I’ll be looking to increase recruitment and mentorship of authors from diverse backgrounds, including those historically underrepresented in medicine.
I look forward to working with the editorial board, associate and assistant editors, and staff of JFP to serve the diverse interests and needs of our readers. To that end, we’ll be looking for your guidance. How else can JFP help you in your day-to-day practice? Please let us know your ideas. Drop us a line at [email protected].
Finally, please join me in thanking Drs. Henry Barry and Kate Rowland for all of their work this past year in keeping JFP going strong!
1. Hickner J. Meet JFP’s new editor-in-chief. J Fam Pract. 2012;61: 581.

Editor-in-Chief
[email protected]
Editor-in-Chief
[email protected]
Editor-in-Chief
[email protected]
Whenever someone asks me what I do, I happily reply, “I’m just a simple country doctor.” That is, in part, why I am honored to be granted the opportunity to serve as editor-in-chief of The Journal of Family Practice (JFP). As our late colleague Dr. John Hickner noted in his first JFP editorial, he and the 2 editors-in-chief before him (Drs. Jeff Susman and Mark Ebell) were also of the small-town family doc tradition.1
My small-town roots trace back to rural South Carolina. I am a first-generation college student and attended medical school on a Navy Health Professions Scholarship. After completing my residency training, I had the privilege of serving for 5 years in the Navy (2 of those years were overseas), where I practiced and taught full-scope family medicine. I saw patients of all ages, attended deliveries, and provided inpatient hospital care, as well as performed a full range of procedures and tests, including colposcopies, skin procedures, vasectomies, flexible sigmoidoscopies, and exercise treadmill testing.
Following military service and completion of a 2-year fellowship and Master of Public Health degree (while working nights at a rural emergency department), I began work at the University of North Carolina at Chapel Hill. I had the good fortune of spending the next 11 years as a faculty member there, where I advanced my research and teaching career. In 2017, I was named the Chair of Family Medicine and Community Health at Duke University School of Medicine, where I continue to have an active outpatient practice.
My experiences have shaped my belief that it is critical that family medicine maintain its presence (and advance its prominence) both in our communities and at our large academic medicine centers, championing service to rural areas, promoting health equity, and advocating for the importance of high-quality primary care delivery and training. No matter where we are, our work is valuable, and we make a difference. Like my predecessors, I have a love of evidence-based medicine. I also have a love of writing, which I can trace back to my days as an intern. I am excited to be able to apply what I have learned over the years to help maintain the rigor, practicality, and relevance of JFP while simultaneously helping to nurture new authors and peer reviewers.
My goal as this journal’s editor-in-chief will be to continue its high academic standing while maintaining its utility for busy clinicians. The provision of evidence-based clinical review articles that are succinct and practical, along with departments (eg, Photo Rounds, Behavioral Health Consult, Practice Alert, PURLs), will remain the journal’s major focus. Within this framework, I also want to share the best evidence and ideas on other aspects of practicing medicine, such as quality improvement, population health, and health equity. I’ll be looking to increase recruitment and mentorship of authors from diverse backgrounds, including those historically underrepresented in medicine.
I look forward to working with the editorial board, associate and assistant editors, and staff of JFP to serve the diverse interests and needs of our readers. To that end, we’ll be looking for your guidance. How else can JFP help you in your day-to-day practice? Please let us know your ideas. Drop us a line at [email protected].
Finally, please join me in thanking Drs. Henry Barry and Kate Rowland for all of their work this past year in keeping JFP going strong!
Whenever someone asks me what I do, I happily reply, “I’m just a simple country doctor.” That is, in part, why I am honored to be granted the opportunity to serve as editor-in-chief of The Journal of Family Practice (JFP). As our late colleague Dr. John Hickner noted in his first JFP editorial, he and the 2 editors-in-chief before him (Drs. Jeff Susman and Mark Ebell) were also of the small-town family doc tradition.1
My small-town roots trace back to rural South Carolina. I am a first-generation college student and attended medical school on a Navy Health Professions Scholarship. After completing my residency training, I had the privilege of serving for 5 years in the Navy (2 of those years were overseas), where I practiced and taught full-scope family medicine. I saw patients of all ages, attended deliveries, and provided inpatient hospital care, as well as performed a full range of procedures and tests, including colposcopies, skin procedures, vasectomies, flexible sigmoidoscopies, and exercise treadmill testing.
Following military service and completion of a 2-year fellowship and Master of Public Health degree (while working nights at a rural emergency department), I began work at the University of North Carolina at Chapel Hill. I had the good fortune of spending the next 11 years as a faculty member there, where I advanced my research and teaching career. In 2017, I was named the Chair of Family Medicine and Community Health at Duke University School of Medicine, where I continue to have an active outpatient practice.
My experiences have shaped my belief that it is critical that family medicine maintain its presence (and advance its prominence) both in our communities and at our large academic medicine centers, championing service to rural areas, promoting health equity, and advocating for the importance of high-quality primary care delivery and training. No matter where we are, our work is valuable, and we make a difference. Like my predecessors, I have a love of evidence-based medicine. I also have a love of writing, which I can trace back to my days as an intern. I am excited to be able to apply what I have learned over the years to help maintain the rigor, practicality, and relevance of JFP while simultaneously helping to nurture new authors and peer reviewers.
My goal as this journal’s editor-in-chief will be to continue its high academic standing while maintaining its utility for busy clinicians. The provision of evidence-based clinical review articles that are succinct and practical, along with departments (eg, Photo Rounds, Behavioral Health Consult, Practice Alert, PURLs), will remain the journal’s major focus. Within this framework, I also want to share the best evidence and ideas on other aspects of practicing medicine, such as quality improvement, population health, and health equity. I’ll be looking to increase recruitment and mentorship of authors from diverse backgrounds, including those historically underrepresented in medicine.
I look forward to working with the editorial board, associate and assistant editors, and staff of JFP to serve the diverse interests and needs of our readers. To that end, we’ll be looking for your guidance. How else can JFP help you in your day-to-day practice? Please let us know your ideas. Drop us a line at [email protected].
Finally, please join me in thanking Drs. Henry Barry and Kate Rowland for all of their work this past year in keeping JFP going strong!
1. Hickner J. Meet JFP’s new editor-in-chief. J Fam Pract. 2012;61: 581.
1. Hickner J. Meet JFP’s new editor-in-chief. J Fam Pract. 2012;61: 581.
25 years of Viagra: A huge change in attitudes about ED
This transcript has been edited for clarity.
Incredibly, 25 years ago, Bob Dole, a senator from Kansas at the time and former presidential candidate, went on national television in a commercial and discussed the fact that he was sexually impotent. You might be thinking, “What was happening then? Was this an early Jerry Springer experience or reality TV gone haywire?” No. Viagra was approved as a treatment 25 years ago this year.
Bob Dole was recruited by Pfizer, the manufacturer of Viagra, to do commercials in which he discussed his sexual dysfunction. He was recruited for a very specific set of reasons. First, he was a distinguished, prominent, respected national figure. Second, he was conservative.
For those of you who don’t remember, when 25 years ago Viagra first appeared, Pfizer was terrified that they would get attacked for promoting promiscuity by introducing a sex pill onto the market. Bob Dole was basically saying, “I have a medical problem. It’s tough to talk about, but there is a treatment. I’m going to discuss the fact that I, among many other men, could use this to help that problem.”
He was used in a way to deflect conservative or religious critics worried about the promotion of sex outside of marriage. Bob Dole was also well known to be married to Elizabeth Dole. This wasn’t somebody who was out on the dating market. Bob Dole was a family man, and his selection was no accident. For all these reasons, Bob Dole was the first spokesperson for Viagra.
Now, as it happens, I had a role to play with this drug. Pfizer called me up and asked me to come and do a consult with them about the ethics of this brand-new treatment. I had never been asked by a drug company to do anything like this. I didn’t know what I was doing. I thought about it and said: “I’ll do it if you let me sit in on discussions and meetings at your New York headquarters about this drug. I want open access.”
I assume they gave me open access. I went to many meetings before the Food and Drug Administration approved Viagra, and many discussions took place about how to roll it out. Once I got there, the one thing I insisted upon was that they had to be treating a disease. If they didn’t want to get involved in criticisms about this new miracle solution to the age-old problem of sexual dysfunction, impotence wouldn’t do. It wasn’t a medical diagnosis, and it was kind of a very undefined situation.
Erectile dysfunction was the answer. They met with urologists, sex experts, and individuals within the company and came up with the idea that if you were unable to have an erection after trying for 6 months or more, you suffered from erectile dysfunction, and that was the group for whom they should market Viagra. I fully agreed with that.
What happened was that probably hundreds of millions of men worldwide came forward for the first time and said, “I’m ashamed and guilty. I feel stigmatized. Now, with something that might help me, I’m going to say to my doctor, I have this problem.”
It’s a very important lesson because 25 years later, it’s still difficult for people – men and women – to discuss sexual problems, sexual dysfunction, and unhappiness with their sex life. I know we’ve gotten better at asking about this, but it’s still difficult for patients to go into it, bring it up, and talk about it. It’s something that we have to think hard about how we bring forward, honest, frank conversation and make people comfortable so they can tell us.
One thing that Viagra proved to the world is that not only is there a large amount of sexual dysfunction – some numbers as high as 35% of men over age 65 – but that sexual dysfunction is related to diseases. It’s caused by hypertension, hardening of the arteries, and diabetes. It may be caused by psychological anxiety or even just a poor relationship where things are falling apart.
I think it’s important that, when Viagra first appeared, what Pfizer tried to do and with the marketing oriented around it was treating it as a disease, trying to treat erectile dysfunction as a symptom, and then trying to explore the underlying possible causes for that symptom.
Sadly, if we look today, we have come a long way – and not always a good way – from where Viagra started. Viagra is easily available online. Many companies say, just get online and a doctor will talk with you about a prescription. They do, but they don’t explore the underlying causes anymore online of what might be causing the erectile dysfunction. They certainly may have a checkbox and ask somebody about this or that, but I’ve gone and tested the sites, and you can get a prescription in about 30 seconds.
It’s not really gone with the old medical model that accompanied the appearance of Viagra. We now treat it as a recreational drug or an aphrodisiac, none of which is true. If your body is working properly, blood will flow where it’s going to go. Taking Viagra or any of the other treatments will not help improve that or enhance that.
The other problem I see today with where we are with these impotence and erectile dysfunction drugs is that we still have not developed a full array of interventions for women. It’s true that men have Viagra, and it’s true that that’s often reimbursed. We still have women complaining that they have sexual dysfunction or loss of interest or whatever the problem might be, and we haven’t been able to develop drugs that will help them.
Since Viagra’s approval 25 years ago until the patent ran out in 2019, $40 billion worth of the drug has been sold. Its advertising has shifted so that
Doctors always need to be thinking about exploring that and trying to get a vision or a view of the health of their patients. It’s still hard for many people to speak up and say if they’re having problems in bed, and we want to make sure that we try our best to make that happen.
Overall, I think the approval of Viagra 25 years ago was a very good thing. It brought a terrible problem out into the open. It helped enhance the quality of life for many men. Despite where we are today, I think the introduction of that pill was actually a major achievement in pharmacology.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported conflicts of interest with Johnson & Johnson, Medscape, and Pfizer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Incredibly, 25 years ago, Bob Dole, a senator from Kansas at the time and former presidential candidate, went on national television in a commercial and discussed the fact that he was sexually impotent. You might be thinking, “What was happening then? Was this an early Jerry Springer experience or reality TV gone haywire?” No. Viagra was approved as a treatment 25 years ago this year.
Bob Dole was recruited by Pfizer, the manufacturer of Viagra, to do commercials in which he discussed his sexual dysfunction. He was recruited for a very specific set of reasons. First, he was a distinguished, prominent, respected national figure. Second, he was conservative.
For those of you who don’t remember, when 25 years ago Viagra first appeared, Pfizer was terrified that they would get attacked for promoting promiscuity by introducing a sex pill onto the market. Bob Dole was basically saying, “I have a medical problem. It’s tough to talk about, but there is a treatment. I’m going to discuss the fact that I, among many other men, could use this to help that problem.”
He was used in a way to deflect conservative or religious critics worried about the promotion of sex outside of marriage. Bob Dole was also well known to be married to Elizabeth Dole. This wasn’t somebody who was out on the dating market. Bob Dole was a family man, and his selection was no accident. For all these reasons, Bob Dole was the first spokesperson for Viagra.
Now, as it happens, I had a role to play with this drug. Pfizer called me up and asked me to come and do a consult with them about the ethics of this brand-new treatment. I had never been asked by a drug company to do anything like this. I didn’t know what I was doing. I thought about it and said: “I’ll do it if you let me sit in on discussions and meetings at your New York headquarters about this drug. I want open access.”
I assume they gave me open access. I went to many meetings before the Food and Drug Administration approved Viagra, and many discussions took place about how to roll it out. Once I got there, the one thing I insisted upon was that they had to be treating a disease. If they didn’t want to get involved in criticisms about this new miracle solution to the age-old problem of sexual dysfunction, impotence wouldn’t do. It wasn’t a medical diagnosis, and it was kind of a very undefined situation.
Erectile dysfunction was the answer. They met with urologists, sex experts, and individuals within the company and came up with the idea that if you were unable to have an erection after trying for 6 months or more, you suffered from erectile dysfunction, and that was the group for whom they should market Viagra. I fully agreed with that.
What happened was that probably hundreds of millions of men worldwide came forward for the first time and said, “I’m ashamed and guilty. I feel stigmatized. Now, with something that might help me, I’m going to say to my doctor, I have this problem.”
It’s a very important lesson because 25 years later, it’s still difficult for people – men and women – to discuss sexual problems, sexual dysfunction, and unhappiness with their sex life. I know we’ve gotten better at asking about this, but it’s still difficult for patients to go into it, bring it up, and talk about it. It’s something that we have to think hard about how we bring forward, honest, frank conversation and make people comfortable so they can tell us.
One thing that Viagra proved to the world is that not only is there a large amount of sexual dysfunction – some numbers as high as 35% of men over age 65 – but that sexual dysfunction is related to diseases. It’s caused by hypertension, hardening of the arteries, and diabetes. It may be caused by psychological anxiety or even just a poor relationship where things are falling apart.
I think it’s important that, when Viagra first appeared, what Pfizer tried to do and with the marketing oriented around it was treating it as a disease, trying to treat erectile dysfunction as a symptom, and then trying to explore the underlying possible causes for that symptom.
Sadly, if we look today, we have come a long way – and not always a good way – from where Viagra started. Viagra is easily available online. Many companies say, just get online and a doctor will talk with you about a prescription. They do, but they don’t explore the underlying causes anymore online of what might be causing the erectile dysfunction. They certainly may have a checkbox and ask somebody about this or that, but I’ve gone and tested the sites, and you can get a prescription in about 30 seconds.
It’s not really gone with the old medical model that accompanied the appearance of Viagra. We now treat it as a recreational drug or an aphrodisiac, none of which is true. If your body is working properly, blood will flow where it’s going to go. Taking Viagra or any of the other treatments will not help improve that or enhance that.
The other problem I see today with where we are with these impotence and erectile dysfunction drugs is that we still have not developed a full array of interventions for women. It’s true that men have Viagra, and it’s true that that’s often reimbursed. We still have women complaining that they have sexual dysfunction or loss of interest or whatever the problem might be, and we haven’t been able to develop drugs that will help them.
Since Viagra’s approval 25 years ago until the patent ran out in 2019, $40 billion worth of the drug has been sold. Its advertising has shifted so that
Doctors always need to be thinking about exploring that and trying to get a vision or a view of the health of their patients. It’s still hard for many people to speak up and say if they’re having problems in bed, and we want to make sure that we try our best to make that happen.
Overall, I think the approval of Viagra 25 years ago was a very good thing. It brought a terrible problem out into the open. It helped enhance the quality of life for many men. Despite where we are today, I think the introduction of that pill was actually a major achievement in pharmacology.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported conflicts of interest with Johnson & Johnson, Medscape, and Pfizer.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Incredibly, 25 years ago, Bob Dole, a senator from Kansas at the time and former presidential candidate, went on national television in a commercial and discussed the fact that he was sexually impotent. You might be thinking, “What was happening then? Was this an early Jerry Springer experience or reality TV gone haywire?” No. Viagra was approved as a treatment 25 years ago this year.
Bob Dole was recruited by Pfizer, the manufacturer of Viagra, to do commercials in which he discussed his sexual dysfunction. He was recruited for a very specific set of reasons. First, he was a distinguished, prominent, respected national figure. Second, he was conservative.
For those of you who don’t remember, when 25 years ago Viagra first appeared, Pfizer was terrified that they would get attacked for promoting promiscuity by introducing a sex pill onto the market. Bob Dole was basically saying, “I have a medical problem. It’s tough to talk about, but there is a treatment. I’m going to discuss the fact that I, among many other men, could use this to help that problem.”
He was used in a way to deflect conservative or religious critics worried about the promotion of sex outside of marriage. Bob Dole was also well known to be married to Elizabeth Dole. This wasn’t somebody who was out on the dating market. Bob Dole was a family man, and his selection was no accident. For all these reasons, Bob Dole was the first spokesperson for Viagra.
Now, as it happens, I had a role to play with this drug. Pfizer called me up and asked me to come and do a consult with them about the ethics of this brand-new treatment. I had never been asked by a drug company to do anything like this. I didn’t know what I was doing. I thought about it and said: “I’ll do it if you let me sit in on discussions and meetings at your New York headquarters about this drug. I want open access.”
I assume they gave me open access. I went to many meetings before the Food and Drug Administration approved Viagra, and many discussions took place about how to roll it out. Once I got there, the one thing I insisted upon was that they had to be treating a disease. If they didn’t want to get involved in criticisms about this new miracle solution to the age-old problem of sexual dysfunction, impotence wouldn’t do. It wasn’t a medical diagnosis, and it was kind of a very undefined situation.
Erectile dysfunction was the answer. They met with urologists, sex experts, and individuals within the company and came up with the idea that if you were unable to have an erection after trying for 6 months or more, you suffered from erectile dysfunction, and that was the group for whom they should market Viagra. I fully agreed with that.
What happened was that probably hundreds of millions of men worldwide came forward for the first time and said, “I’m ashamed and guilty. I feel stigmatized. Now, with something that might help me, I’m going to say to my doctor, I have this problem.”
It’s a very important lesson because 25 years later, it’s still difficult for people – men and women – to discuss sexual problems, sexual dysfunction, and unhappiness with their sex life. I know we’ve gotten better at asking about this, but it’s still difficult for patients to go into it, bring it up, and talk about it. It’s something that we have to think hard about how we bring forward, honest, frank conversation and make people comfortable so they can tell us.
One thing that Viagra proved to the world is that not only is there a large amount of sexual dysfunction – some numbers as high as 35% of men over age 65 – but that sexual dysfunction is related to diseases. It’s caused by hypertension, hardening of the arteries, and diabetes. It may be caused by psychological anxiety or even just a poor relationship where things are falling apart.
I think it’s important that, when Viagra first appeared, what Pfizer tried to do and with the marketing oriented around it was treating it as a disease, trying to treat erectile dysfunction as a symptom, and then trying to explore the underlying possible causes for that symptom.
Sadly, if we look today, we have come a long way – and not always a good way – from where Viagra started. Viagra is easily available online. Many companies say, just get online and a doctor will talk with you about a prescription. They do, but they don’t explore the underlying causes anymore online of what might be causing the erectile dysfunction. They certainly may have a checkbox and ask somebody about this or that, but I’ve gone and tested the sites, and you can get a prescription in about 30 seconds.
It’s not really gone with the old medical model that accompanied the appearance of Viagra. We now treat it as a recreational drug or an aphrodisiac, none of which is true. If your body is working properly, blood will flow where it’s going to go. Taking Viagra or any of the other treatments will not help improve that or enhance that.
The other problem I see today with where we are with these impotence and erectile dysfunction drugs is that we still have not developed a full array of interventions for women. It’s true that men have Viagra, and it’s true that that’s often reimbursed. We still have women complaining that they have sexual dysfunction or loss of interest or whatever the problem might be, and we haven’t been able to develop drugs that will help them.
Since Viagra’s approval 25 years ago until the patent ran out in 2019, $40 billion worth of the drug has been sold. Its advertising has shifted so that
Doctors always need to be thinking about exploring that and trying to get a vision or a view of the health of their patients. It’s still hard for many people to speak up and say if they’re having problems in bed, and we want to make sure that we try our best to make that happen.
Overall, I think the approval of Viagra 25 years ago was a very good thing. It brought a terrible problem out into the open. It helped enhance the quality of life for many men. Despite where we are today, I think the introduction of that pill was actually a major achievement in pharmacology.
Dr. Kaplan is director, division of medical ethics, New York University Langone Medical Center, New York. He reported conflicts of interest with Johnson & Johnson, Medscape, and Pfizer.
A version of this article first appeared on Medscape.com.
Goodbye, finger sticks; hello, CGMs
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
Nearly 90% of diabetes management in the United States is provided by primary care clinicians; diabetes is the fifth most common reason for a primary care visit. State-of-the-art technology such as continuous glucose monitors (CGMs) will inevitably transform the management of diabetes in primary care. Clinicians and staff must be ready to educate, counsel, and support primary care patients in the use of CGMs.
CGMs (also called glucose sensors) are small, minimally invasive devices that attach to the skin of the upper arm or trunk. A tiny electrode in the subcutaneous space prompts an enzyme reaction that measures the interstitial (rather than blood) glucose concentration, typically every 5 minutes. The results are displayed on an accompanying reader or transmitted to an app on the user’s mobile phone.
CGMs could eliminate the need for finger-stick blood glucose testing, which until now, has been the much-despised gold standard for self-monitoring of glucose levels in diabetes. Despite being relatively inexpensive and accurate, finger-stick glucose tests are inconvenient and often painful. But of greater significance is this downside: Finger-stick monitoring reveals the patient’s blood glucose concentration at a single point in time, which can be difficult to interpret. Is the blood glucose rising or falling? Multiple finger-stick tests are required to determine the trend of a patient’s glucose levels or the response to food or exercise.
In contrast, the graphic display from a CGM sensor is more like a movie, telling a story as it unfolds. Uninterrupted data provide valuable feedback to patients about the effects of diet, physical activity, stress, or pain on their glucose levels. And for the first time, it’s easy to determine the proportion of time the patient spends in or out of the target glucose range.
Incorporating new technology into your practice may seem like a burden, but the reward is better information that leads to better management of diabetes. If you’re new to glucose sensors, many excellent resources are available to learn how to use them.
I recommend starting with a website called diabeteswise.org, which has both a patient-facing and clinician-facing version. This unbranded site serves as a kind of Consumer Reports for diabetes technology, allowing both patients and professionals to compare and contrast currently available CGM devices.
DiabetesWisePro has information ranging from CGM device fundamentals and best practices to CGM prescribing and reimbursement.
Clinical Diabetes also provides multiple tools to help incorporate these devices into primary care clinical practice, including:
• Continuous Glucose Monitoring: Optimizing Diabetes Care (CME course).
• Diabetes Technology in Primary Care.
The next article in this series will cover two types of CGMs used in primary care: professional and personal devices.
Dr. Shubrook is a professor in the department of primary care, Touro University California College of Osteopathic Medicine, Vallejo, Calif., and director of diabetes services, Solano County Family Health Services, Fairfield, Calif. He disclosed ties with Abbott, Astra Zeneca, Bayer, Nevro, and Novo Nordisk.
A version of this article first appeared on Medscape.com.
The sacred office space
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.

Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.

Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.
Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.
Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Church architecture describes visually the idea of the sacred, which is a fundamental need of man.
– Mario Botta, Swiss architect
My parents are visiting the Holy See today – prima volta in Italia! My mom waited years for this. She isn’t meeting the Pope or attending Mass. Yet, in the Whatsapp pics they sent me, you can see tears well up as she experiences St. Peter’s Basilica. It’s a visceral response to what is just a building and a poignant example of the significance of spaces.
More than just appreciating an edifice’s grandeur or exquisiteness, we are wired to connect with spaces emotionally. Beautiful or significant buildings move us, they make us feel something. Churches, synagogues, or mosques are good examples. They combine spiritual and aesthetic allure. But so too do gorgeous hotels, Apple stores, and posh restaurants. We crave the richness of an environment experienced through our five senses. The glory of sunlight through stained glass, the smell of luxurious scent pumped into a lobby, the weight of a silky new iPhone in your hand. We also have a sixth sense, that feeling we get from knowing that we are standing in a sacred place. A physical space that connects us with something wider and deeper than ourselves.
Virtual may be the peak of convenience, but in-real-life is the pinnacle of experience. Patients will be inconvenienced and pay higher costs to experience their appointment in person. This should not be surprising. Contemplate this: Every year, millions of people will travel across the globe to stand before a wall or walk seven times around a stone building. And millions everyday will perambulate around an Apple Store, willingly paying a higher price for the same product they can buy for less elsewhere. The willingness to pay for certain experiences is remarkably high.
Every day when I cover patient messages, I offer some patients an immediate, free solution to their problem. Just today I exchanged emails with a patient thinking I had addressed her concern by reassuring her that it was a benign seborrheic keratosis. Done. She then replied, “Thanks so much, Dr. Benabio! I still would like to schedule an appointment to come in person.” So much for the efficiency of digital medicine.
Before dismissing these patients as Luddites, understand what they want is the doctor’s office experience. The sights, the smells, the sacredness of what happens here. It is no coincidence that the first clinics were temples. In ancient Greece and Rome, the sick and the gashed made pilgrimages to one of at least 300 Asclepieia, temples of healing. During the medieval period, monasteries doubled as housing for the sick until the church began constructing stand-alone hospitals, often in cross-shaped design with an altar in the middle (eventually that became the nurses station, but without the wine).
Patients entrust us with their lives and their loved ones’ lives and a visit takes on far more significance than a simple service transaction. Forty years on, I can recall visits to Dr. Bellin’s office. He saw pediatric patients out of his Victorian home office with broad, creaky hardwood floors, stained glass, and cast iron radiators. The scent of isopropyl soaked cotton balls and typewriter ink is unforgettable. Far from sterile, it was warm, safe. It was a sacred place, one for which we still sometimes drive by when doing the tour of where I grew up.
We shall forge ahead and continue to offer virtual channels to serve our patients just as any service industry. But don’t force them there. At the same time Starbucks has been building its digital app, it is also building Starbucks Reserve Roasteries. Immense cathedral edifices with warm woods and luxurious brass, the smell of roasting coffee and warm leather perfuming the air. It is where patrons will travel long distances and endure long waits to pay a lot more for a cup of coffee.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Creating a fair time-off policy
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?

First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
It’s interesting how questions often arrive in clusters. This week, my inbox is packed with queries about paid sick leave and paid time off (PTO); what is the difference, which is preferable, what is required, and how does one implement a fair and legal time-off policy for a medical office?
First, the difference: Paid sick leave is the time off allotted to each employee for illness or injury, whereas PTO is an all-encompassing bundle that includes vacation and any other miscellaneous time benefits in addition to sick leave.
Which is preferable? That depends on whom you ask, and sometimes, on the legal situation in your state. Employees generally like the PTO concept, because most never use all of their sick leave. The ability to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate making their own decisions about taking time off.
. Reasons for absences are now irrelevant, so feigned illnesses are a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee’s duties, you don’t need to know (or care) about the reason for the request.
Critics of PTO say employees are absent more often, since employees who never used their full allotment of sick leave will typically use all of their PTO; but that, in a sense, is the idea. Time off is necessary and important for good office morale, and should be taken by all employees, as well as by all employers. (Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.”)
Moreover, you should be suspicious of any employee who refuses to take vacations. They may be embezzlers who fear that their illicit modus operandi will be discovered during their absence.
Another common criticism of PTO is the possibility that employees will not stay home when they are truly sick because some employees may view all PTO as vacation time, and don’t want to “waste” any of it on illness. You should make it very clear that sick employees should stay home – and will be sent home if they come to work sick. You have an obligation to protect your other employees – and of course your patients, particularly those who are elderly or immunocompromised – from a staff member with a potentially communicable illness.
The legal requirements of time off are variable. There are currently no federal laws requiring employers to offer paid time off, but each state has its own PTO and sick leave requirements, so you will need to check your state’s specific guidelines before creating or updating a time off policy.
When drafting your policy, make sure everyone knows they will have to request PTO in advance, except for emergencies. Start with defining “in advance” (72 hours? A week?), and then “emergency”; and put these definitions in writing. Illnesses are emergencies, of course, but what about waking up with a bad hangover? A sick child qualifies if your employee is the only available caregiver, but what if the employee’s car has broken down? Some circumstances will have to be decided on a case-by-case basis; but you will have fewer hassles if you anticipate and settle more situations in advance.
What about allowing employees to take salary in exchange for unused PTO, or to roll it over into the next year? We don’t permit either in my office, but some states (for instance, California, Montana, and Nebraska) prohibit use-it-or-lose-it policies.
When an employee leaves or is terminated, do you have to pay accrued PTO? No federal law requires it, but some states do.
What about employees who use up their allotted PTO and request unpaid time off? In my office, we require employees to submit a written request, explaining why they need it, and why it’s a special situation and won’t be a regular occurrence. Even if you (almost) always approve such requests, forcing your employees to jump through a hoop or two makes it less likely that anyone will abuse the privilege. Moreover, this allows you to make judgments on a case-by-case basis, while still being able to honestly say you offer it as a blanket policy to all your employees.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Alzheimer’s disease and the primary care physician
Recent news highlights advancements in the understanding of Alzheimer’s disease: Increased information on biomarkers to be used for evaluation and diagnosis and recent studies on lifestyle factors or medications that do and do not correlate with Alzheimer’s disease.
It is helpful for family medicine physicians and other primary care physicians to be aware of this information to better help our patients and their families. When we have patients with strong family history of cognitive decline, they often will ask us for an early assessment or help with next steps and requests for treatment. Patients and their families want to understand what testing will be done by the neurologist they will likely be seeing.

An article published in Alzheimer’s and Dementia put forward a consensus statement by 11 European scientific societies on diagnosis and management of the disease. These societies defined work flows for processes to utilize biomarkers to diagnose Alzheimer’s disease. Although these work flows may help with diagnosis, they are not able to definitively rule out other causes of dementia. However, they may lead to consistency in how treatments are determined.1 More consistency will be helpful in counseling patients and their families on the next steps in the treatment plan.
Another study evaluated the correlation between lean mass and dementia. This study demonstrated a decreased risk of dementia in patients with higher lean mass. It is unclear from this study whether the higher lean mass is protective or if decreased cognitive function decreases the amount of lean mass. However, this study does provide hope in two possible ways: it provides potentially predictive information on who may be more at risk of declining cognitive function as well as a modifiable risk factor to address.2 Family physicians may use this as part of their counseling for patients who are concerned about their potential risk of dementia. It is yet another reason why we may counsel on healthy diet and weight-bearing exercise to help maintain lean mass.
Other associations related to dementia have been disproven. An article in Gastroenterology discussed the association between cognitive decline and use of proton pump inhibitors and H2 blockers – indicating that there is no association.3 Although there are reasons why we want to limit the use of these medications – particularly when they are not needed, it is a relief that they are not causing cognitive decline in patients.
Most of these studies provide information that is helpful for both family medicine physicians and patients. We are learning more about cognitive decline and Alzheimer’s disease. This gives hope to patients with strong family history that we may be able to reduce their risks. These studies also give us possible risk factors on which we can counsel our patients.
Developments in Alzheimer’s disease research are speeding ahead and give family physicians a bit more information to discuss with patients and their families as they face the challenging symptoms of cognitive decline. Future research, it is hoped, will help with treatment plans and modifiable risk factors to improve the outcomes for patients at high risk of cognitive decline.
Dr. Wheat is associate professor of family and community medicine at Northwestern University in Chicago. She has no conflicts of interest.
References
1. Massa F et al. Alzheimer’s and Dementia. 2023;19(S2):e062216.
2. Daghlas I et al. BMJ Medicine. 2023;2(1):e000354.
3. Mehta R et al. Gastroenterology. 2023 Jun 12. doi: 10.1053/j.gastro.2023.05.052.
Recent news highlights advancements in the understanding of Alzheimer’s disease: Increased information on biomarkers to be used for evaluation and diagnosis and recent studies on lifestyle factors or medications that do and do not correlate with Alzheimer’s disease.
It is helpful for family medicine physicians and other primary care physicians to be aware of this information to better help our patients and their families. When we have patients with strong family history of cognitive decline, they often will ask us for an early assessment or help with next steps and requests for treatment. Patients and their families want to understand what testing will be done by the neurologist they will likely be seeing.
An article published in Alzheimer’s and Dementia put forward a consensus statement by 11 European scientific societies on diagnosis and management of the disease. These societies defined work flows for processes to utilize biomarkers to diagnose Alzheimer’s disease. Although these work flows may help with diagnosis, they are not able to definitively rule out other causes of dementia. However, they may lead to consistency in how treatments are determined.1 More consistency will be helpful in counseling patients and their families on the next steps in the treatment plan.
Another study evaluated the correlation between lean mass and dementia. This study demonstrated a decreased risk of dementia in patients with higher lean mass. It is unclear from this study whether the higher lean mass is protective or if decreased cognitive function decreases the amount of lean mass. However, this study does provide hope in two possible ways: it provides potentially predictive information on who may be more at risk of declining cognitive function as well as a modifiable risk factor to address.2 Family physicians may use this as part of their counseling for patients who are concerned about their potential risk of dementia. It is yet another reason why we may counsel on healthy diet and weight-bearing exercise to help maintain lean mass.
Other associations related to dementia have been disproven. An article in Gastroenterology discussed the association between cognitive decline and use of proton pump inhibitors and H2 blockers – indicating that there is no association.3 Although there are reasons why we want to limit the use of these medications – particularly when they are not needed, it is a relief that they are not causing cognitive decline in patients.
Most of these studies provide information that is helpful for both family medicine physicians and patients. We are learning more about cognitive decline and Alzheimer’s disease. This gives hope to patients with strong family history that we may be able to reduce their risks. These studies also give us possible risk factors on which we can counsel our patients.
Developments in Alzheimer’s disease research are speeding ahead and give family physicians a bit more information to discuss with patients and their families as they face the challenging symptoms of cognitive decline. Future research, it is hoped, will help with treatment plans and modifiable risk factors to improve the outcomes for patients at high risk of cognitive decline.
Dr. Wheat is associate professor of family and community medicine at Northwestern University in Chicago. She has no conflicts of interest.
References
1. Massa F et al. Alzheimer’s and Dementia. 2023;19(S2):e062216.
2. Daghlas I et al. BMJ Medicine. 2023;2(1):e000354.
3. Mehta R et al. Gastroenterology. 2023 Jun 12. doi: 10.1053/j.gastro.2023.05.052.
Recent news highlights advancements in the understanding of Alzheimer’s disease: Increased information on biomarkers to be used for evaluation and diagnosis and recent studies on lifestyle factors or medications that do and do not correlate with Alzheimer’s disease.
It is helpful for family medicine physicians and other primary care physicians to be aware of this information to better help our patients and their families. When we have patients with strong family history of cognitive decline, they often will ask us for an early assessment or help with next steps and requests for treatment. Patients and their families want to understand what testing will be done by the neurologist they will likely be seeing.
An article published in Alzheimer’s and Dementia put forward a consensus statement by 11 European scientific societies on diagnosis and management of the disease. These societies defined work flows for processes to utilize biomarkers to diagnose Alzheimer’s disease. Although these work flows may help with diagnosis, they are not able to definitively rule out other causes of dementia. However, they may lead to consistency in how treatments are determined.1 More consistency will be helpful in counseling patients and their families on the next steps in the treatment plan.
Another study evaluated the correlation between lean mass and dementia. This study demonstrated a decreased risk of dementia in patients with higher lean mass. It is unclear from this study whether the higher lean mass is protective or if decreased cognitive function decreases the amount of lean mass. However, this study does provide hope in two possible ways: it provides potentially predictive information on who may be more at risk of declining cognitive function as well as a modifiable risk factor to address.2 Family physicians may use this as part of their counseling for patients who are concerned about their potential risk of dementia. It is yet another reason why we may counsel on healthy diet and weight-bearing exercise to help maintain lean mass.
Other associations related to dementia have been disproven. An article in Gastroenterology discussed the association between cognitive decline and use of proton pump inhibitors and H2 blockers – indicating that there is no association.3 Although there are reasons why we want to limit the use of these medications – particularly when they are not needed, it is a relief that they are not causing cognitive decline in patients.
Most of these studies provide information that is helpful for both family medicine physicians and patients. We are learning more about cognitive decline and Alzheimer’s disease. This gives hope to patients with strong family history that we may be able to reduce their risks. These studies also give us possible risk factors on which we can counsel our patients.
Developments in Alzheimer’s disease research are speeding ahead and give family physicians a bit more information to discuss with patients and their families as they face the challenging symptoms of cognitive decline. Future research, it is hoped, will help with treatment plans and modifiable risk factors to improve the outcomes for patients at high risk of cognitive decline.
Dr. Wheat is associate professor of family and community medicine at Northwestern University in Chicago. She has no conflicts of interest.
References
1. Massa F et al. Alzheimer’s and Dementia. 2023;19(S2):e062216.
2. Daghlas I et al. BMJ Medicine. 2023;2(1):e000354.
3. Mehta R et al. Gastroenterology. 2023 Jun 12. doi: 10.1053/j.gastro.2023.05.052.