User login
Overuse of Digital Devices in the Exam Room: A Teaching Opportunity
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.

At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.
At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
A 3-year-old presents to my clinic for evaluation of a possible autism spectrum disorder/difference. He has a history of severe emotional dysregulation, as well as reduced social skills and multiple sensory sensitivities. When I enter the exam room he is watching videos on his mom’s phone, and has some difficulty transitioning to play with toys when I encourage him to do so. He is eventually able to cooperate with my testing, though a bit reluctantly, and scores within the low average range for both language and pre-academic skills. His neurologic exam is within normal limits. He utilizes reasonably well-modulated eye contact paired with some typical use of gestures, and his affect is moderately directed and reactive. He displays typical intonation and prosody of speech, though engages in less spontaneous, imaginative, and reciprocal play than would be expected for his age. His mother reports decreased pretend play at home, minimal interest in toys, and difficulty playing cooperatively with other children.
Upon further history, it becomes apparent that the child spends a majority of his time on electronic devices, and has done so since early toddlerhood. Further dialogue suggests that the family became isolated during the COVID-19 pandemic, and has not yet re-engaged with the community in a meaningful way. The child has had rare opportunity for social interactions with other children, and minimal access to outdoor play. His most severe meltdowns generally involve transitions away from screens, and his overwhelmed parents often resort to use of additional screens to calm him once he is dysregulated.
At the end of the visit, through shared decision making, we agree that enrolling the child in a high-quality public preschool will help parents make a concerted effort towards a significant reduction in the hours per day in which the child utilizes electronic devices, while also providing him more exposure to peers. We plan for the child to return in 6 months for a re-evaluation around social-emotional skills, given his current limited exposure to peers and limited “unplugged” play-time.
Overutilization of Electronic Devices
As clinicians, we can all see how pervasive the use of electronic devices has become in the lives of the families we care for, as well as in our own lives, and how challenging some aspects of modern parenting have become. The developmental impact of early and excessive use of screens in young children is well documented,1 but as clinicians it can be tricky to help empower parents to find ways to limit screen time. When parents use screens to comfort and amuse their children during a clinic visit, this situation may serve as an excellent opportunity for a meaningful and respectful conversation around skill deficits which can result from overutilization of electronic devices in young children.
One scenario I often encounter during my patient evaluations as a developmental and behavioral pediatrician is children begging their parents for use of their phone throughout their visits with me. Not infrequently, a child is already on a screen when I enter the exam room, even when there has been a minimal wait time, which often leads to some resistance on behalf of the child as I explain to the family that a significant portion of the visit involves my interactions with the child, testing the child, and observing their child at play. I always provide ample amounts of age-appropriate art supplies, puzzles, fidgets, building toys, and imaginative play items to children during their 30 to 90 minute evaluations, but these are often not appealing to children when they have been very recently engaged with an electronic device. At times I also need to ask caretakers themselves to please disengage from their own electronic devices during the visit so that I can involve them in a detailed discussion about their child.
One challenge with the practice of allowing children access to entertainment on their parent’s smartphones in particular, lies in the fact that these devices are almost always present, meaning there is no natural boundary to inhibit access, in contrast to a television set or stationary computer parked in the family living room. Not dissimilar to candy visible in a parent’s purse, a cell phone becomes a constant temptation for children accustomed to utilizing them at home and public venues, and the incessant begging can wear down already stressed parents.
Children can become conditioned to utilize the distraction of screens to avoid feelings of discomfort or stress, and so can be very persistent and emotional when asking for the use of screens in public settings. Out in the community, I very frequently see young children and toddlers quietly staring at their phones and tablets while at restaurants and stores. While I have empathy for exhausted parents desperate for a moment of quiet, if this type of screen use is the rule rather than the exception for a child, there is risk for missed opportunities for the development of self-regulation skills.
Additionally, I have seen very young children present to my clinic with poor posture and neck pain secondary to chronic smartphone use, and young children who are getting minimal exercise or outdoor time due to excessive screen use, leading to concerns around fine and gross motor skills as well.
While allowing a child to stay occupied with or be soothed by a highly interesting digital experience can create a more calm environment for all, if habitual, this use can come at a cost regarding opportunities for the growth of executive functioning skills, general coping skills, general situational awareness, and experiential learning. Reliance on screens to decrease uncomfortable experiences decreases the opportunity for building distress tolerance, patience, and coping skills.
Of course there are times of extreme distress where a lollipop or bit of screen time might be reasonable to help keep a child safe or further avoid emotional trauma, but in general, other methods of soothing can very often be utilized, and in the long run would serve to increase the child’s general adaptive functioning.
A Teachable Moment
When clinicians encounter screens being used by parents to entertain their kids in clinic, it provides a valuable teaching moment around the risks of using screens to keep kids regulated and occupied during life’s less interesting or more anxiety provoking experiences. Having a meaningful conversation about the use of electronic devices with caregivers by clinicians in the exam room can be a delicate dance between providing supportive education while avoiding judgmental tones or verbiage. Normalizing and sympathizing with the difficulty of managing challenging behaviors from children in public spaces can help parents feel less desperate to keep their child quiet at all costs, and thus allow for greater development of coping skills.
Some parents may benefit from learning simple ideas for keeping a child regulated and occupied during times of waiting such as silly songs and dances, verbal games like “I spy,” and clapping routines. For a child with additional sensory or developmental needs, a referral to an occupational therapist to work on emotional regulation by way of specific sensory tools can be helpful. Parent-Child Interaction Therapy for kids ages 2 to 7 can also help build some relational activities and skills that can be utilized during trying situations to help keep a child settled and occupied.
If a child has qualified for Developmental Disability Services (DDS), medical providers can also write “prescriptions’ for sensory calming items which are often covered financially by DDS, such as chewies, weighted vests, stuffed animals, and fidgets. Encouraging parents to schedule allowed screen time at home in a very predictable and controlled manner is one method to help limit excessive use, as well as it’s utilization as an emotional regulation tool.
For public outings with children with special needs, and in particular in situations where meltdowns are likely to occur, some families find it helpful to dress their children in clothing or accessories that increase community awareness about their child’s condition (such as an autism awareness t-shirt). This effort can also help deflect unhelpful attention or advice from the public. Some parents choose to carry small cards explaining the child’s developmental differences, which can then be easily handed to unsupportive strangers in community settings during trying moments.
Clinicians can work to utilize even quick visits with families as an opportunity to review the American Academy of Pediatrics screen time recommendations with families, and also direct them to the Family Media Plan creation resources. Parenting in the modern era presents many challenges regarding choices around the use of electronic devices with children, and using the exam room experience as a teaching opportunity may be a helpful way to decrease utilization of screens as emotional regulation tools for children, while also providing general education around healthy use of screens.
Dr. Roth is a developmental and behavioral pediatrician in Eugene, Oregon.
Reference
1. Takahashi I et al. Screen Time at Age 1 Year and Communication and Problem-Solving Developmental Delays at 2 and 4 years. JAMA Pediatr. 2023 Oct 1;177(10):1039-1046. doi: 10.1001/jamapediatrics.2023.3057.
The New Cancer Stats Might Look Like a Death Sentence. They Aren’t.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Cancer is becoming more common in younger generations. Data show that people under 50 are experiencing higher rates of cancer than any generation before them. As a genetic counselor, I hoped these upward trends in early-onset malignancies would slow with a better understanding of risk factors and prevention strategies. Unfortunately, the opposite is happening. Recent findings from the American Cancer Society reveal that the incidence of at least 17 of 34 cancer types is rising among GenX and Millennials.
These statistics are alarming. I appreciate how easy it is for patients to get lost in the headlines about cancer, which may shape how they approach their healthcare. Each year, millions of Americans miss critical cancer screenings, with many citing fear of a positive test result as a leading reason. Others believe, despite the statistics, that cancer is not something they need to worry about until they are older. And then, of course, getting screened is not as easy as it should be.
In my work, I meet with people from both younger and older generations who have either faced cancer themselves or witnessed a loved one experience the disease. One of the most common sentiments I hear from these patients is the desire to catch cancer earlier. My answer is always this: The first and most important step everyone can take is understanding their risk.
For some, knowing they are at increased risk for cancer means starting screenings earlier — sometimes as early as age 25 — or getting screened with a more sensitive test.
This proactive approach is the right one. It also significantly reduces the burden of total and cancer-specific healthcare costs. While screening may carry some potential risks, clinicians can minimize these risks by adhering to evidence-based guidelines, such as those from the American Cancer Society, and ensuring there is appropriate discussion of treatment options when a diagnosis is made.
Normalizing Cancer Risk Assessment and Screening
A detailed cancer risk assessment and education about signs and symptoms should be part of every preventive care visit, regardless of someone’s age. Further, that cancer risk assessment should lead to clear recommendations and support for taking the next steps.
This is where care advocacy and patient navigation come in. Care advocacy can improve outcomes at every stage of the cancer journey, from increasing screening rates to improving quality of life for survivors. I’ve seen first-hand how care advocates help patients overcome hurdles like long wait times for appointments they need, making both screening and diagnostic care easier to access.
Now, with the finalization of a new rule from the Centers for Medicare & Medicaid Services, providers can bill for oncology navigation services that occur under their supervision. This formal recognition of care navigation affirms the value of these services not just clinically but financially as well. It will be through methods like care navigation, targeted outreach, and engaging educational resources — built into and covered by health plans — that patients will feel more in control over their health and have tools to help minimize the effects of cancer on the rest of their lives.
These services benefit healthcare providers as well. Care navigation supports clinical care teams, from primary care providers to oncologists, by ensuring patients are seen before their cancer progresses to a more advanced stage. And even if patients follow screening recommendations for the rest of their lives and never get a positive result, they’ve still gained something invaluable: peace of mind, knowing they’ve taken an active role in their health.
Fighting Fear With Routine
Treating cancer as a normal part of young people’s healthcare means helping them envision the disease as a condition that can be treated, much like a diagnosis of diabetes or high cholesterol. This mindset shift means quickly following up on a concerning symptom or screening result and reducing the time to start treatment if needed. And with treatment options and success rates for some cancers being better than ever, survivorship support must be built into every treatment plan from the start. Before treatment begins, healthcare providers should make time to talk about sometimes-overlooked key topics, such as reproductive options for people whose fertility may be affected by their cancer treatment, about plans for returning to work during or after treatment, and finding the right mental health support.
Where we can’t prevent cancer, both primary care providers and oncologists can work together to help patients receive the right diagnosis and treatment as quickly as possible. Knowing insurance coverage has a direct effect on how early cancer is caught, for example, younger people need support in understanding and accessing benefits and resources that may be available through their existing healthcare channels, like some employer-sponsored health plans. Even if getting treated for cancer is inevitable for some, taking immediate action to get screened when it’s appropriate is the best thing we can do to lessen the impact of these rising cancer incidences across the country. At the end of the day, being afraid of cancer doesn’t decrease the chances of getting sick or dying from it. Proactive screening and early detection do.
Brockman, Genetic Counselor, Color Health, Buffalo, New York, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Mechanism of Action
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.

It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
MOA — Mechanism of action — gets bandied about a lot.
Drug reps love it. Saying your product is a “first-in-class MOA” sounds great as they hand you a glossy brochure. It also features prominently in print ads, usually with pics of smiling people.
It’s a good thing to know, too, both medically and in a cool-science-geeky way. We want to understand what we’re prescribing will do to patients. We want to explain it to them, too.
It certainly helps to know that what we’re doing when treating a disorder using rational polypharmacy.
But at the same time we face the realization that it may not mean as much as we think it should. I don’t have to go back very far in my career to find Food and Drug Administration–approved medications that worked, but we didn’t have a clear reason why. I mean, we had a vague idea on a scientific basis, but we’re still guessing.
This didn’t stop us from using them, which is nothing new. The ancients had learned certain plants reduced pain and fever long before they understood what aspirin (and its MOA) was.
At the same time we’re now using drugs, such as the anti-amyloid treatments for Alzheimer’s disease, that should be more effective than one would think. Pulling the damaged molecules out of the brain should, on paper, make a dramatic difference ... but it doesn’t. I’m not saying they don’t have some benefit, but certainly not as much as you’d think. Of course, that’s based on our understanding of the disease mechanism being correct. We find there’s a lot more going on than we know.
Like so much in science (and this aspect of medicine is a science) the answers often lead to more questions.
Observation takes the lead over understanding in most things. Our ancestors knew what fire was, and how to use it, without any idea of what rapid exothermic oxidation was. (Admittedly, I have a degree in chemistry and can’t explain it myself anymore.)
The glossy ads and scientific data about MOA doesn’t mean much in my world if they don’t work. My patients would say the same.
Clinical medicine, after all, is both an art and a science.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
What Should You Do When a Patient Asks for a PSA Test?
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Many patients ask us to request a prostate-specific antigen (PSA) test. According to the Brazilian Ministry of Health, prostate cancer is the second most common type of cancer in the male population in all regions of our country. It is the second-leading cause of cancer death in the male population, reaffirming its epidemiologic importance in Brazil. On the other hand, a Ministry of Health technical paper recommends against population-based screening for prostate cancer. So, what should we do?
First, it is important to distinguish early diagnosis from screening. Early diagnosis is the identification of cancer in early stages in people with signs and symptoms. Screening is characterized by the systematic application of exams — digital rectal exam and PSA test — in asymptomatic people, with the aim of identifying cancer in an early stage.
A recent European epidemiologic study reinforced this thesis and helps guide us.
The study included men aged 35-84 years from 26 European countries. Data on cancer incidence and mortality were collected between 1980 and 2017. The data suggested overdiagnosis of prostate cancer, which varied over time and among populations. The findings supported previous recommendations that any implementation of prostate cancer screening should be carefully designed, with an emphasis on minimizing the harms of overdiagnosis.
The clinical evolution of prostate cancer is still not well understood. Increasing age is associated with increased mortality. Many men with less aggressive disease tend to die with cancer rather than die of cancer. However, it is not always possible at the time of diagnosis to determine which tumors will be aggressive and which will grow slowly.
On the other hand, with screening, many of these indolent cancers are unnecessarily detected, generating excessive exams and treatments with negative repercussions (eg, pain, bleeding, infections, stress, and urinary and sexual dysfunction).
So, how should we as clinicians proceed regarding screening?
We should request the PSA test and emphasize the importance of digital rectal exam by a urologist for those at high risk for prostatic neoplasia (ie, those with family history) or those with urinary symptoms that may be associated with prostate cancer.
In general, we should draw attention to the possible risks and benefits of testing and adopt a shared decision-making approach with asymptomatic men or those at low risk who wish to have the screening exam. But achieving a shared decision is not a simple task.
I always have a thorough conversation with patients, but I confess that I request the exam in most cases.
Dr. Wajngarten is a professor of cardiology, Faculty of Medicine, at the University of São Paulo in Brazil. Dr. Wajngarten reported no conflicts of interest.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Are Targeted Drugs the Future in Colorectal Cancer?
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome back, everybody, from the European Society for Medical Oncology (ESMO) Congress in the wonderful city of Barcelona in Spain. I was coming from ESMO drenched in huge amounts of new data.
They looked at molecularly targeted drugs, some early-stage and a later-stage study in which there’s some evidence of promise.
She talked a little about the preliminary results from three trials suggesting some benefits, pretty marginal, of cetuximab plus irinotecan in patients who’d already had epidermal growth factor receptor (EGFR) receptor inhibitory treatment.
Amivantamab plus FOLFOX or FOLFIRI was also discussed. This is a bispecific antibody against EGFR and MET. Again, very early, but there are some potential marginal benefits coming through. She also discussed the results of a larger phase 3 randomized trial with an old friend, ramucirumab, the anti-angiogenic agent, in which the ramucirumab in combination with trifluridine-tipiracil failed to meet its primary endpoint of improving overall survival.
There were some interesting post hoc subgroup analyses showing potential benefits for women, left-sided tumors, and so on. She made an excellent presentation, which she summarized by saying that the future of colorectal cancer treatment lies in further defining molecularly targeted treatment.
Nobody would disagree with that. What is interesting, though, is that, if I were to use the analogy of mining, the more deeply we mine, perhaps the lower marginal the benefits are becoming. There’s no doubt that we’re understanding better the exquisite machinery of cell signaling. We understand that there’s redundancy, there’s repeatability, and the possibility of emergence of resistance can come quite quickly.
Although we can develop ever more precise molecularly targeted drugs, it does seem as if the clinical benefits of these, in some cases, are marginally small. I’d like to suggest that, in addition to Sara’s call for more molecularly targeted drugs, we should think about cellular targets.
We did a large amount of work (as have many others, of course) looking at the immune tumor microenvironment and trying to, in a way, separate and understand the contribution of the individual component cells — of which there are many, including cancer-associated fibroblasts, natural killer (NK) cells, whole hosts of different types of T-cell subsets, B cells, tumor-associated neutrophils, and so on — and how these interact together and of interact with the epithelial colorectal cancer cells.
We are collaborating with Patrick Soon-Shiong, a clever chap, who believes in combination immunotherapy, dissecting and understanding the individual role of these different cells, and coming up with cellular therapies or targeted therapies that either inhibit or stimulate some of the different cell components to be the way ahead for an immunologically cold tumor such as microsatellite-stable colorectal cancer.
For example, we’re looking at combinations of our histone deacetylase (HDAC) inhibitor, which switches on the machinery of antigen presentation, up-regulating major histocompatibility complex (MHC) class 1 and class 2, and some other of the molecules involved in antigen chopping and presentation; it’s like turning a microsatellite-stable immunologically cold tumor hot; an interleukin-15 superagonist that stimulates NK cells; and we’ve found a way to manipulate and reduce the number of Treg cells.
We have various approaches to reducing the microenvironment transforming growth factor beta and some of the downstream elements from that. We can look at combinatorial immunotherapy, but thinking at a cellular level and developing anticancer agents that either activate or inhibit these different cell components. I’d bring the two together.
Of course, the future has got to be better molecularly targeted drugs, but let’s think at a macro level as to how we can look at the different cellular interactions within the tumor microenvironment, and perhaps through that, come up with synergistic immunotherapeutic combinations.
Dr. Kerr is Professor, Nuffield Department of Clinical Laboratory Science, University of Oxford, and Professor of Cancer Medicine, Oxford Cancer Centre, both in England. He reported conflicts of interest with Celleron Therapeutics, Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Genomic Health, and Merck Serono.
A version of this article first appeared on Medscape.com.
Time-Restricted Eating Is Not a Metabolic Magic Bullet
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia. 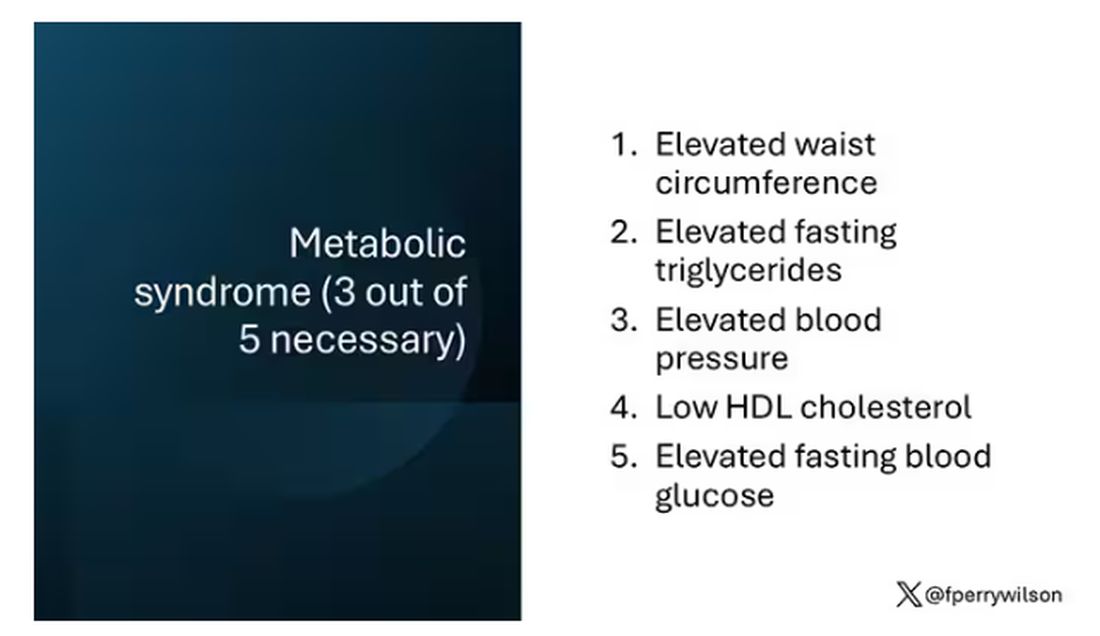
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.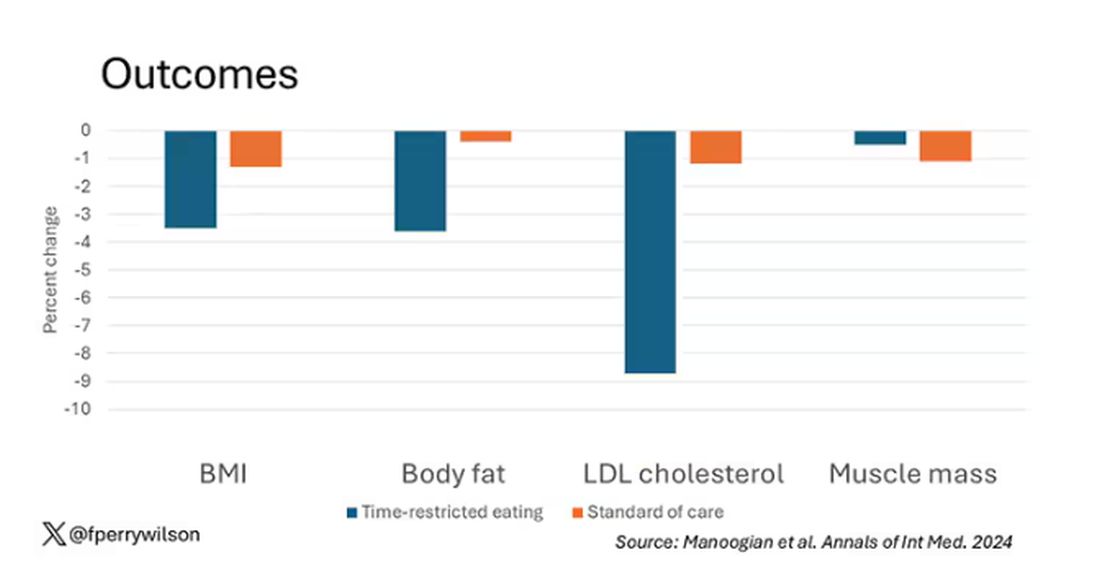
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.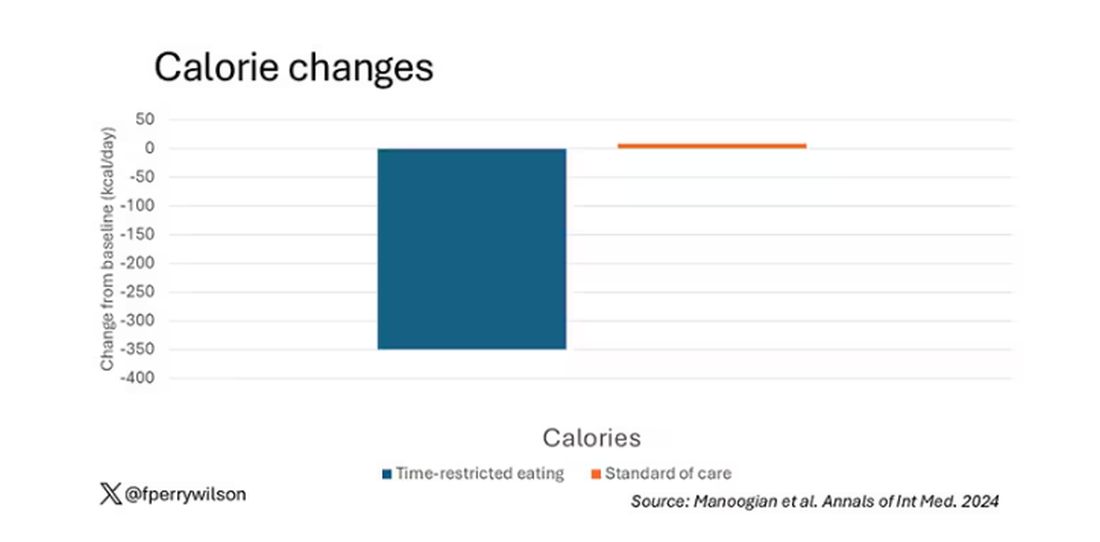
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial. 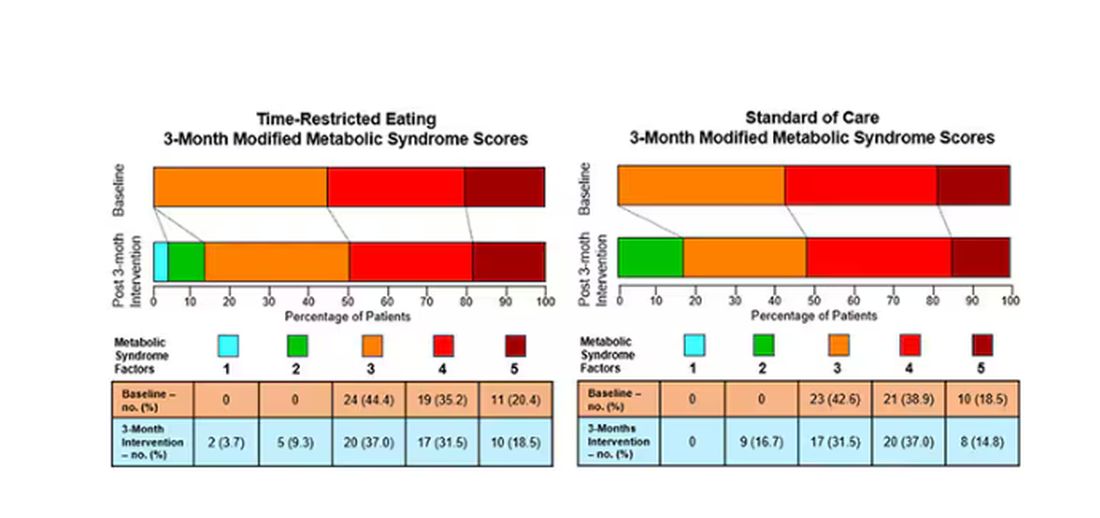
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia.
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial.
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
One out of three American adults — about 100 million people in this country — have the metabolic syndrome. I’m showing you the official criteria here, but essentially this is a syndrome of insulin resistance and visceral adiposity that predisposes us to a host of chronic diseases such as diabetes, heart disease, and even dementia.
The metabolic syndrome is, fundamentally, a lifestyle disease. There is a direct line between our dietary habits and the wide availability of carbohydrate-rich, highly processed foods, and the rise in the syndrome in the population.
A saying I learned from one of my epidemiology teachers comes to mind: “Lifestyle diseases require lifestyle reinterventions.” But you know what? I’m not so sure anymore.
I’ve been around long enough to see multiple dietary fads come and go with varying efficacy. I grew up in the low-fat era, probably the most detrimental time to our national health as food manufacturers started replacing fats with carbohydrates, driving much of the problem we’re faced with today.
But I was also around for the Atkins diet and the low-carb craze — a healthier approach, all things being equal. And I’ve seen variants of these: the paleo diet (essentially a low-carb, high-protein diet based on minimally processed foods) and the Mediterranean diet, which sought to replace some percentage of fats with healthier fats.
And, of course, there is time-restricted eating.
Time-restricted eating, a variant of intermittent fasting, has the advantage of being very simple. No cookbooks, no recipes. Eat what you want — but limit it to certain hours in the day, ideally a window of less than 10 hours, such as 8 a.m. to 6 p.m.
When it comes to weight loss, the diets that work tend to work because they reduce calorie intake. I know, people will get angry about this, but thermodynamics is not just a good idea, it’s the law.
But weight loss is not the only reason we need to eat healthier. What we eat can impact our health in multiple ways; certain foods lead to more atherosclerosis, more inflammation, increased strain on the kidney and liver, and can affect our glucose homeostasis.
So I was really interested when I saw this article, “Time-Restricted Eating in Adults With Metabolic Syndrome,” appearing in Annals of Internal Medicine October 1, which examined the effect of time-restricted eating on the metabolic syndrome itself. Could this lifestyle intervention cure this lifestyle disease?
In the study, 108 individuals, all of whom had the metabolic syndrome but not full-blown diabetes, were randomized to usual care — basically, nutrition education — vs time-restricted eating. In that group, participants were instructed to reduce their window of eating by at least 4 hours to achieve an 8- to 10-hour eating window. The groups were followed for 3 months.
Now, before we get to the results, it’s important to remember that the success of a lifestyle intervention trial is quite dependent on how well people adhere to the lifestyle intervention. Time-restricted eating is not as easy as taking a pill once a day.
The researchers had participants log their consumption using a smartphone app to confirm whether they were adhering to that restricted eating window.
Broadly speaking, they did. At baseline, both groups had an eating window of about 14 hours a day — think 7 a.m. to 9 p.m. The intervention group reduced that to just under 10 hours, with 10% of days falling outside of the target window.
Lifestyle change achieved, the primary outcome was the change in hemoglobin A1c at 3 months. A1c integrates the serum glucose over time and is thus a good indicator of the success of the intervention in terms of insulin resistance. But the effect was, honestly, disappointing.
Technically, the time-restricted-eating group had a greater A1c change than the control group — by 0.1 percentage points. On average, they went from a baseline A1c of 5.87 to a 3-month A1c of 5.75.
Other metabolic syndrome markers were equally lackluster: no difference in fasting glucose, mean glucose, or fasting insulin.
There was some weight change. The control group, which got that dietary education, lost 1.5% of body weight over the 3 months. The time-restricted-eating group lost 3.3% — about 7 pounds, which is reasonable.
With that weight loss came statistically significant, albeit modest improvements in BMI, body fat percentage, and LDL cholesterol.
Of interest, despite the larger weight loss in the intermittent-fasting group, there was no difference in muscle mass loss, which is encouraging.
Taken together, we can say that, yes, it seems like time-restricted eating can help people lose some weight. This is essentially due to the fact that people eat fewer calories when they do time-restricted eating, as you can see here.
But, in the end, this trial examined whether this relatively straightforward lifestyle intervention would move the needle in terms of metabolic syndrome, and the data are not very compelling for that.
This graph shows how many of those five factors for metabolic syndrome the individuals in this trial had from the start to the end. You see that, over the 3 months, seven people in the time-restricted-eating group moved from having three criteria to two or one — being “cured” of metabolic syndrome, if you will. Nine people in the standard group were cured by that definition. Remember, they had to have at least three to have the syndrome and thus be eligible for the trial.
So If it just leads to weight loss by forcing people to consume less calories, then we need to acknowledge that we probably have better methods to achieve this same end. Ten years ago, I would have said that lifestyle change is the only way to end the epidemic of the metabolic syndrome in this country. Today, well, we live in a world of GLP-1 weight loss drugs. It is simply a different world now. Yes, they are expensive. Yes, they have side effects. But we need to evaluate them against the comparison. And so far, lifestyle changes alone are really no comparison.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Flash Drive Versus Paper
“Here’s my records.”
I hear that a lot, usually in the context of a patient handing me a flash drive or (less commonly) trying to plug it into my computer. (I have the USB ports turned toward me to keep that from happening.)
Uh, no.
I love flash drives. They definitely make data transfer easy, compared with the CDs, ZIPs, JAZZ, floppies, paper, and punch cards of past years (I should also, as a childhood TRS-80 user, include cassette tapes).
At this point an encrypted flash drive is pretty much the entire briefcase I carry back and forth to work each day.
But there is no patient I trust enough to plug in one they handed me.
I’m sure most, if not all, are well meaning. But look at how many large corporations have been damaged by someone slipping in a flash drive with a malicious program somewhere in their network. Once in, it’s almost impossible to get out, and can spread quickly.
Even if the patient is benign, I have no idea who formatted the gadget, or put the records on. It could be a relative, or friend, with other motives. It could even be a random flash drive and they don’t even know what else is on it.
My desktop is my chart system. I have to protect the data of all my patients, so I exercise caution about what emails I open and what I plug into it. Even the person offering me the flash drive wants the info guarded.
So I don’t, as a rule, plug in anything a patient hands me. All it takes is one malicious file to compromise it all. Yeah, I pay for software to watch for that sort of thing, but you still can’t be too careful.
This is where paper still shines. It’s readable and it’s transportable (at least for small things like an MRI report and lab results). I can scan it into a PDF without risking any damage to my computer. And it definitely shouldn’t be plugged into a USB drive unless you’re trying to start a fire.
Of course, paper isn’t secure, either. If you have it piled up everywhere it’s pretty easy for an unsupervised person to walk off with it. That actually happened to a doctor I shared space with 20 years ago, albeit unintentionally. A patient had brought in a bunch of his records in a folder and set them down on the counter. When he left he grabbed another patient’s chart by mistake and didn’t realize it until the next day. Fortunately he returned them promptly, and there were no issues. But it had the potential to be worse.
Today my charts on roughly 20,000 patients can all fit on a gadget the size of my thumb instead of a multi-room shelving system and storage closet. That’s pretty cool, actually. But it also opens other vulnerabilities.
It ticks some patients off that I won’t plug in their flash drives, but I don’t care. Most of them understand when I explain it, because it’s to protect them, too.
The odds are that they don’t mean any harm, but I can’t take that chance.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
“Here’s my records.”
I hear that a lot, usually in the context of a patient handing me a flash drive or (less commonly) trying to plug it into my computer. (I have the USB ports turned toward me to keep that from happening.)
Uh, no.
I love flash drives. They definitely make data transfer easy, compared with the CDs, ZIPs, JAZZ, floppies, paper, and punch cards of past years (I should also, as a childhood TRS-80 user, include cassette tapes).
At this point an encrypted flash drive is pretty much the entire briefcase I carry back and forth to work each day.
But there is no patient I trust enough to plug in one they handed me.
I’m sure most, if not all, are well meaning. But look at how many large corporations have been damaged by someone slipping in a flash drive with a malicious program somewhere in their network. Once in, it’s almost impossible to get out, and can spread quickly.
Even if the patient is benign, I have no idea who formatted the gadget, or put the records on. It could be a relative, or friend, with other motives. It could even be a random flash drive and they don’t even know what else is on it.
My desktop is my chart system. I have to protect the data of all my patients, so I exercise caution about what emails I open and what I plug into it. Even the person offering me the flash drive wants the info guarded.
So I don’t, as a rule, plug in anything a patient hands me. All it takes is one malicious file to compromise it all. Yeah, I pay for software to watch for that sort of thing, but you still can’t be too careful.
This is where paper still shines. It’s readable and it’s transportable (at least for small things like an MRI report and lab results). I can scan it into a PDF without risking any damage to my computer. And it definitely shouldn’t be plugged into a USB drive unless you’re trying to start a fire.
Of course, paper isn’t secure, either. If you have it piled up everywhere it’s pretty easy for an unsupervised person to walk off with it. That actually happened to a doctor I shared space with 20 years ago, albeit unintentionally. A patient had brought in a bunch of his records in a folder and set them down on the counter. When he left he grabbed another patient’s chart by mistake and didn’t realize it until the next day. Fortunately he returned them promptly, and there were no issues. But it had the potential to be worse.
Today my charts on roughly 20,000 patients can all fit on a gadget the size of my thumb instead of a multi-room shelving system and storage closet. That’s pretty cool, actually. But it also opens other vulnerabilities.
It ticks some patients off that I won’t plug in their flash drives, but I don’t care. Most of them understand when I explain it, because it’s to protect them, too.
The odds are that they don’t mean any harm, but I can’t take that chance.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
“Here’s my records.”
I hear that a lot, usually in the context of a patient handing me a flash drive or (less commonly) trying to plug it into my computer. (I have the USB ports turned toward me to keep that from happening.)
Uh, no.
I love flash drives. They definitely make data transfer easy, compared with the CDs, ZIPs, JAZZ, floppies, paper, and punch cards of past years (I should also, as a childhood TRS-80 user, include cassette tapes).
At this point an encrypted flash drive is pretty much the entire briefcase I carry back and forth to work each day.
But there is no patient I trust enough to plug in one they handed me.
I’m sure most, if not all, are well meaning. But look at how many large corporations have been damaged by someone slipping in a flash drive with a malicious program somewhere in their network. Once in, it’s almost impossible to get out, and can spread quickly.
Even if the patient is benign, I have no idea who formatted the gadget, or put the records on. It could be a relative, or friend, with other motives. It could even be a random flash drive and they don’t even know what else is on it.
My desktop is my chart system. I have to protect the data of all my patients, so I exercise caution about what emails I open and what I plug into it. Even the person offering me the flash drive wants the info guarded.
So I don’t, as a rule, plug in anything a patient hands me. All it takes is one malicious file to compromise it all. Yeah, I pay for software to watch for that sort of thing, but you still can’t be too careful.
This is where paper still shines. It’s readable and it’s transportable (at least for small things like an MRI report and lab results). I can scan it into a PDF without risking any damage to my computer. And it definitely shouldn’t be plugged into a USB drive unless you’re trying to start a fire.
Of course, paper isn’t secure, either. If you have it piled up everywhere it’s pretty easy for an unsupervised person to walk off with it. That actually happened to a doctor I shared space with 20 years ago, albeit unintentionally. A patient had brought in a bunch of his records in a folder and set them down on the counter. When he left he grabbed another patient’s chart by mistake and didn’t realize it until the next day. Fortunately he returned them promptly, and there were no issues. But it had the potential to be worse.
Today my charts on roughly 20,000 patients can all fit on a gadget the size of my thumb instead of a multi-room shelving system and storage closet. That’s pretty cool, actually. But it also opens other vulnerabilities.
It ticks some patients off that I won’t plug in their flash drives, but I don’t care. Most of them understand when I explain it, because it’s to protect them, too.
The odds are that they don’t mean any harm, but I can’t take that chance.
Dr. Block has a solo neurology practice in Scottsdale, Arizona.
The Patient Encounter Is Changing
Over the last few decades the patient encounter has changed dramatically. Most recently fueled by the COVID pandemic, face-to-face events between patients and providers have become less frequent. The shift began years before with the slow acceptance of telemedicine by third-party payers.
, often leaving both providers and patients with more questions than answers. Even more recently, the explosive arrival of generative artificial intelligence (AI) has promised, some might say threatened, to add a whole new complexity and uncertainty to patient encounters regardless of the venue or platform.

Still, among the growing collection of options, I think it is fair to say that a live face-to-face encounter remains the gold standard in the opinions of both patients and providers. Patients may have become increasingly critical and vocal when they feel their provider appears rushed or is over focused on the desktop computer screen. However, given all of the options, I suspect that for the moment patients feel a face-to-face meeting continues to offer them the best chance of being heard and their concerns answered.
Even when the image on the video screen is sharp and the intelligibility of the audio feed is crystal clear, I bet most providers feel they can learn more about the patient during a live face-to-face encounter than a Zoom-style encounter.
Nonetheless, there are hints that face-to-face visits maybe losing their place in the pantheon of patient-provider encounters. A recent study from England found that there were a significant number of patients who were more forthcoming in reporting their preferences for social care-related quality of life when they were surveyed by internet rather than face-to-face. It is unclear what was behind this observation, however it may be that patients were embarrassed and viewed these questions about their social neediness as too sensitive to share face-to-face.
There is ample evidence of situations in which the internet can provide a level of anonymity that emboldens the user to say things that are cruel and hurtful, using words they might be afraid to voice in a live setting. This license to act in an uncivil manner is behind much of the harm generated by chat rooms and other social media sites. While in these cases the ability to hide behind the video screen is a negative, this study from England suggests that we should be looking for more opportunities to use this emboldening feature with certain individuals and populations who may be intimidated during a face-to-face encounter. It is likely a hybrid approach may be the most beneficial strategy tailored to the individual patient.
One advantage of a face-to-face visit is that each participant can read the body language of the other. This, of course, can be a disadvantage for the provider who has failed to master the art of disguising his “I’m running behind” stress level, when he should be replacing it with an “I’m ready to listen” posture.
Portals have opened up a whole other can of worms, particularly when the provider has failed to clearly delineate what sort of questions are appropriate for an online forum, not informed the patient who will be providing the answer, and a rough idea of when this will happen. It may take several trips up the learning curve for patients and providers to develop a style of writing that make optimal use of the portal format and make it fit the needs of the practice and the patients.
Regardless of what kind of visit platform we are talking about, a lot hinges on the providers choice of words. I recently reviewed some of the work of Jeffrey D. Robinson, PhD, a professor of communication at the Portland State University, Portland, Oregon. He offers the example of the difference between “some” and “any.” When the patient was asked “Is there something else you would like to address today” almost 80% of the patient’s unmet questions were addressed. However, when the question was “Is there anything else ...” very few of the patient’s unmet questions were addressed. Dr. Robinson has also found that when the question is posed early in the visit rather than at the end, it improves the chances of having the patient’s unmet concerns addressed.
I suspect that the face-to-face patient encounter will survive, but it will continue to lose its market share as other platforms emerge. We can be sure there will be change. We need look no further than generative AI to look for the next step. A well-crafted question could help the patient and the provider choose the most appropriate patient encounter format given the patient’s demographic, chief complaint, and prior history, and match this with the provider’s background and strengths.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Over the last few decades the patient encounter has changed dramatically. Most recently fueled by the COVID pandemic, face-to-face events between patients and providers have become less frequent. The shift began years before with the slow acceptance of telemedicine by third-party payers.
, often leaving both providers and patients with more questions than answers. Even more recently, the explosive arrival of generative artificial intelligence (AI) has promised, some might say threatened, to add a whole new complexity and uncertainty to patient encounters regardless of the venue or platform.
Still, among the growing collection of options, I think it is fair to say that a live face-to-face encounter remains the gold standard in the opinions of both patients and providers. Patients may have become increasingly critical and vocal when they feel their provider appears rushed or is over focused on the desktop computer screen. However, given all of the options, I suspect that for the moment patients feel a face-to-face meeting continues to offer them the best chance of being heard and their concerns answered.
Even when the image on the video screen is sharp and the intelligibility of the audio feed is crystal clear, I bet most providers feel they can learn more about the patient during a live face-to-face encounter than a Zoom-style encounter.
Nonetheless, there are hints that face-to-face visits maybe losing their place in the pantheon of patient-provider encounters. A recent study from England found that there were a significant number of patients who were more forthcoming in reporting their preferences for social care-related quality of life when they were surveyed by internet rather than face-to-face. It is unclear what was behind this observation, however it may be that patients were embarrassed and viewed these questions about their social neediness as too sensitive to share face-to-face.
There is ample evidence of situations in which the internet can provide a level of anonymity that emboldens the user to say things that are cruel and hurtful, using words they might be afraid to voice in a live setting. This license to act in an uncivil manner is behind much of the harm generated by chat rooms and other social media sites. While in these cases the ability to hide behind the video screen is a negative, this study from England suggests that we should be looking for more opportunities to use this emboldening feature with certain individuals and populations who may be intimidated during a face-to-face encounter. It is likely a hybrid approach may be the most beneficial strategy tailored to the individual patient.
One advantage of a face-to-face visit is that each participant can read the body language of the other. This, of course, can be a disadvantage for the provider who has failed to master the art of disguising his “I’m running behind” stress level, when he should be replacing it with an “I’m ready to listen” posture.
Portals have opened up a whole other can of worms, particularly when the provider has failed to clearly delineate what sort of questions are appropriate for an online forum, not informed the patient who will be providing the answer, and a rough idea of when this will happen. It may take several trips up the learning curve for patients and providers to develop a style of writing that make optimal use of the portal format and make it fit the needs of the practice and the patients.
Regardless of what kind of visit platform we are talking about, a lot hinges on the providers choice of words. I recently reviewed some of the work of Jeffrey D. Robinson, PhD, a professor of communication at the Portland State University, Portland, Oregon. He offers the example of the difference between “some” and “any.” When the patient was asked “Is there something else you would like to address today” almost 80% of the patient’s unmet questions were addressed. However, when the question was “Is there anything else ...” very few of the patient’s unmet questions were addressed. Dr. Robinson has also found that when the question is posed early in the visit rather than at the end, it improves the chances of having the patient’s unmet concerns addressed.
I suspect that the face-to-face patient encounter will survive, but it will continue to lose its market share as other platforms emerge. We can be sure there will be change. We need look no further than generative AI to look for the next step. A well-crafted question could help the patient and the provider choose the most appropriate patient encounter format given the patient’s demographic, chief complaint, and prior history, and match this with the provider’s background and strengths.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Over the last few decades the patient encounter has changed dramatically. Most recently fueled by the COVID pandemic, face-to-face events between patients and providers have become less frequent. The shift began years before with the slow acceptance of telemedicine by third-party payers.
, often leaving both providers and patients with more questions than answers. Even more recently, the explosive arrival of generative artificial intelligence (AI) has promised, some might say threatened, to add a whole new complexity and uncertainty to patient encounters regardless of the venue or platform.
Still, among the growing collection of options, I think it is fair to say that a live face-to-face encounter remains the gold standard in the opinions of both patients and providers. Patients may have become increasingly critical and vocal when they feel their provider appears rushed or is over focused on the desktop computer screen. However, given all of the options, I suspect that for the moment patients feel a face-to-face meeting continues to offer them the best chance of being heard and their concerns answered.
Even when the image on the video screen is sharp and the intelligibility of the audio feed is crystal clear, I bet most providers feel they can learn more about the patient during a live face-to-face encounter than a Zoom-style encounter.
Nonetheless, there are hints that face-to-face visits maybe losing their place in the pantheon of patient-provider encounters. A recent study from England found that there were a significant number of patients who were more forthcoming in reporting their preferences for social care-related quality of life when they were surveyed by internet rather than face-to-face. It is unclear what was behind this observation, however it may be that patients were embarrassed and viewed these questions about their social neediness as too sensitive to share face-to-face.
There is ample evidence of situations in which the internet can provide a level of anonymity that emboldens the user to say things that are cruel and hurtful, using words they might be afraid to voice in a live setting. This license to act in an uncivil manner is behind much of the harm generated by chat rooms and other social media sites. While in these cases the ability to hide behind the video screen is a negative, this study from England suggests that we should be looking for more opportunities to use this emboldening feature with certain individuals and populations who may be intimidated during a face-to-face encounter. It is likely a hybrid approach may be the most beneficial strategy tailored to the individual patient.
One advantage of a face-to-face visit is that each participant can read the body language of the other. This, of course, can be a disadvantage for the provider who has failed to master the art of disguising his “I’m running behind” stress level, when he should be replacing it with an “I’m ready to listen” posture.
Portals have opened up a whole other can of worms, particularly when the provider has failed to clearly delineate what sort of questions are appropriate for an online forum, not informed the patient who will be providing the answer, and a rough idea of when this will happen. It may take several trips up the learning curve for patients and providers to develop a style of writing that make optimal use of the portal format and make it fit the needs of the practice and the patients.
Regardless of what kind of visit platform we are talking about, a lot hinges on the providers choice of words. I recently reviewed some of the work of Jeffrey D. Robinson, PhD, a professor of communication at the Portland State University, Portland, Oregon. He offers the example of the difference between “some” and “any.” When the patient was asked “Is there something else you would like to address today” almost 80% of the patient’s unmet questions were addressed. However, when the question was “Is there anything else ...” very few of the patient’s unmet questions were addressed. Dr. Robinson has also found that when the question is posed early in the visit rather than at the end, it improves the chances of having the patient’s unmet concerns addressed.
I suspect that the face-to-face patient encounter will survive, but it will continue to lose its market share as other platforms emerge. We can be sure there will be change. We need look no further than generative AI to look for the next step. A well-crafted question could help the patient and the provider choose the most appropriate patient encounter format given the patient’s demographic, chief complaint, and prior history, and match this with the provider’s background and strengths.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Five Essential Nutrients for Patients on GLP-1s
Fatigue, nausea, acid reflux, muscle loss, and the dreaded “Ozempic face” are side effects from using glucagon-like peptide 1 (GLP-1) receptor agonists (RAs) such as semaglutide or the dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA tirzepatide to control blood sugar and promote weight loss.
But what I’ve learned from working with hundreds of patients on these medications, and others, is that most (if not all) of these side effects can be minimized by ensuring proper nutrition.
Setting patients up for success requires dietary education and counseling, along with regular monitoring to determine any nutritional deficiencies. Although adequate intake of all the macro and micronutrients is obviously important,
Protein
My patients are probably sick of hearing me talk about protein, but without the constant reinforcement, many of them wouldn’t consume enough of this macronutrient to maintain their baseline lean body mass. The recommended dietary allowance (RDA) for protein (0.8 g/kg bodyweight) doesn’t cut it, especially for older, obese patients, who need closer to 1.0-1.2 g/kg bodyweight to maintain their muscle mass. For example, for a 250-lb patient, I would recommend 114-136 g protein per day. This is equivalent to roughly 15 oz of cooked animal protein. It’s important to note, though, that individuals with kidney disease must limit their protein intake to 0.6-0.8 g/kg bodyweight per day, to avoid overtaxing their kidneys. In this situation, the benefit of increased protein intake does not outweigh the risk of harming the kidneys.
It’s often challenging for patients with suppressed appetites to even think about eating a large hunk of meat or fish, let alone consume it. Plus, eating more than 3-4 oz of protein in one meal can make some patients extremely uncomfortable, owing to the medication’s effect on gastric emptying. This means that daily protein intake must be spread out over multiple mini-meals.
For patients who need more than 100 g of protein per day, protein powders and premade protein shakes can provide 20-30 g protein to fill in the gaps. Although I always try to promote food first, protein supplements have been game changers for my patients, especially those who find solid food less appealing on the medication, or those who avoid animal protein.
Clinicians should have their patients monitor changes in their lean body mass using a dual-energy x-ray absorptiometry scan or a bioelectrical impedance scale; this can be a helpful tool in assessing whether protein intake is sufficient.
Fiber
Even my most knowledgeable and compliant patients will experience some constipation. Generally speaking, when you eat less, you will have fewer bowel movements. Combine that with delayed gastric emptying and reduced fiber intake, and you have a perfect storm. Many patients are simply not able to get in the recommended 25-35 g fiber per day through food, because fibrous foods are filling. If they are prioritizing the protein in their meal, they will not have enough room for all the vegetables on their plate.
To ensure that patients are getting sufficient fiber, clinicians should push consumption of certain vegetables and fruits, such as carrots, broccoli, Brussels sprouts, raspberries, blackberries, and apples, as well as beans and legumes. (Salads are great, but greens like spinach are not as fibrous as one might think.) If the fruit and veggie intake isn’t up to par, a fiber supplement such as psyllium husk can provide an effective boost.
Vitamin B12
Use of these medications is associated with a reduction in vitamin B12 levels, in part because delayed gastric emptying may affect B12 absorption. Low dietary intake of B12 while on the medications can also be to blame, though. The best food sources are animal proteins, so if possible, patients should prioritize having fish, lean meat, eggs, and dairy daily.
Vegetarians and vegans, who are at an increased risk for deficiency, can incorporate nutritional yeast, an excellent source of vitamin B12, into their daily routine. It is beneficial for patients to get blood work periodically to check on B12 status, because insufficient B12 can contribute to the fatigue patients experience while on the medication.
Calcium
Individuals should have calcium on their radar, because weight loss is associated with a decrease in bone mineral density. Adequate intake of the mineral is crucial for optimal bone health, particularly among postmenopausal women and those who are at risk of developing osteoporosis. The RDA for calcium is 1000-1200 mg/d, which an estimated 50% of obese individuals do not take in.
Although dairy products are well-known for being rich in calcium, there are other great sources. Dark green leafy vegetables, such as cooked collard greens and spinach, provide nearly 300 mg per cup. Tofu and sardines are also calcium powerhouses. Despite the plethora of calcium-rich foods, however, some patients may need a calcium supplement.
Vitamin D
Vitamin D deficiency or insufficiency is common among individuals with obesity, so even before these patients start the medications, supplementation may be warranted. The vitamin’s role in promoting calcium absorption, as well as in bone remodeling, make adequate intake essential for patients experiencing significant weight loss.
Clinicians should emphasize regular consumption of fatty fish, such as salmon, as well as eggs, mushrooms, and vitamin D–fortified milks. But unfortunately, that’s where the list of vitamin D–rich foods ends, so taking a vitamin D supplement will be necessary for many patients.
Regularly monitoring patients on GLP-1 RAs through blood work to check vitamin levels and body composition analysis can be helpful in assessing nutritional status while losing weight. Clinicians can also encourage their patients to work with a registered dietitian who is familiar with these medications, so they can develop optimal eating habits throughout their health journey.
Ms. Hanks, a registered dietitian in New York City, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Fatigue, nausea, acid reflux, muscle loss, and the dreaded “Ozempic face” are side effects from using glucagon-like peptide 1 (GLP-1) receptor agonists (RAs) such as semaglutide or the dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA tirzepatide to control blood sugar and promote weight loss.
But what I’ve learned from working with hundreds of patients on these medications, and others, is that most (if not all) of these side effects can be minimized by ensuring proper nutrition.
Setting patients up for success requires dietary education and counseling, along with regular monitoring to determine any nutritional deficiencies. Although adequate intake of all the macro and micronutrients is obviously important,
Protein
My patients are probably sick of hearing me talk about protein, but without the constant reinforcement, many of them wouldn’t consume enough of this macronutrient to maintain their baseline lean body mass. The recommended dietary allowance (RDA) for protein (0.8 g/kg bodyweight) doesn’t cut it, especially for older, obese patients, who need closer to 1.0-1.2 g/kg bodyweight to maintain their muscle mass. For example, for a 250-lb patient, I would recommend 114-136 g protein per day. This is equivalent to roughly 15 oz of cooked animal protein. It’s important to note, though, that individuals with kidney disease must limit their protein intake to 0.6-0.8 g/kg bodyweight per day, to avoid overtaxing their kidneys. In this situation, the benefit of increased protein intake does not outweigh the risk of harming the kidneys.
It’s often challenging for patients with suppressed appetites to even think about eating a large hunk of meat or fish, let alone consume it. Plus, eating more than 3-4 oz of protein in one meal can make some patients extremely uncomfortable, owing to the medication’s effect on gastric emptying. This means that daily protein intake must be spread out over multiple mini-meals.
For patients who need more than 100 g of protein per day, protein powders and premade protein shakes can provide 20-30 g protein to fill in the gaps. Although I always try to promote food first, protein supplements have been game changers for my patients, especially those who find solid food less appealing on the medication, or those who avoid animal protein.
Clinicians should have their patients monitor changes in their lean body mass using a dual-energy x-ray absorptiometry scan or a bioelectrical impedance scale; this can be a helpful tool in assessing whether protein intake is sufficient.
Fiber
Even my most knowledgeable and compliant patients will experience some constipation. Generally speaking, when you eat less, you will have fewer bowel movements. Combine that with delayed gastric emptying and reduced fiber intake, and you have a perfect storm. Many patients are simply not able to get in the recommended 25-35 g fiber per day through food, because fibrous foods are filling. If they are prioritizing the protein in their meal, they will not have enough room for all the vegetables on their plate.
To ensure that patients are getting sufficient fiber, clinicians should push consumption of certain vegetables and fruits, such as carrots, broccoli, Brussels sprouts, raspberries, blackberries, and apples, as well as beans and legumes. (Salads are great, but greens like spinach are not as fibrous as one might think.) If the fruit and veggie intake isn’t up to par, a fiber supplement such as psyllium husk can provide an effective boost.
Vitamin B12
Use of these medications is associated with a reduction in vitamin B12 levels, in part because delayed gastric emptying may affect B12 absorption. Low dietary intake of B12 while on the medications can also be to blame, though. The best food sources are animal proteins, so if possible, patients should prioritize having fish, lean meat, eggs, and dairy daily.
Vegetarians and vegans, who are at an increased risk for deficiency, can incorporate nutritional yeast, an excellent source of vitamin B12, into their daily routine. It is beneficial for patients to get blood work periodically to check on B12 status, because insufficient B12 can contribute to the fatigue patients experience while on the medication.
Calcium
Individuals should have calcium on their radar, because weight loss is associated with a decrease in bone mineral density. Adequate intake of the mineral is crucial for optimal bone health, particularly among postmenopausal women and those who are at risk of developing osteoporosis. The RDA for calcium is 1000-1200 mg/d, which an estimated 50% of obese individuals do not take in.
Although dairy products are well-known for being rich in calcium, there are other great sources. Dark green leafy vegetables, such as cooked collard greens and spinach, provide nearly 300 mg per cup. Tofu and sardines are also calcium powerhouses. Despite the plethora of calcium-rich foods, however, some patients may need a calcium supplement.
Vitamin D
Vitamin D deficiency or insufficiency is common among individuals with obesity, so even before these patients start the medications, supplementation may be warranted. The vitamin’s role in promoting calcium absorption, as well as in bone remodeling, make adequate intake essential for patients experiencing significant weight loss.
Clinicians should emphasize regular consumption of fatty fish, such as salmon, as well as eggs, mushrooms, and vitamin D–fortified milks. But unfortunately, that’s where the list of vitamin D–rich foods ends, so taking a vitamin D supplement will be necessary for many patients.
Regularly monitoring patients on GLP-1 RAs through blood work to check vitamin levels and body composition analysis can be helpful in assessing nutritional status while losing weight. Clinicians can also encourage their patients to work with a registered dietitian who is familiar with these medications, so they can develop optimal eating habits throughout their health journey.
Ms. Hanks, a registered dietitian in New York City, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Fatigue, nausea, acid reflux, muscle loss, and the dreaded “Ozempic face” are side effects from using glucagon-like peptide 1 (GLP-1) receptor agonists (RAs) such as semaglutide or the dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 RA tirzepatide to control blood sugar and promote weight loss.
But what I’ve learned from working with hundreds of patients on these medications, and others, is that most (if not all) of these side effects can be minimized by ensuring proper nutrition.
Setting patients up for success requires dietary education and counseling, along with regular monitoring to determine any nutritional deficiencies. Although adequate intake of all the macro and micronutrients is obviously important,
Protein
My patients are probably sick of hearing me talk about protein, but without the constant reinforcement, many of them wouldn’t consume enough of this macronutrient to maintain their baseline lean body mass. The recommended dietary allowance (RDA) for protein (0.8 g/kg bodyweight) doesn’t cut it, especially for older, obese patients, who need closer to 1.0-1.2 g/kg bodyweight to maintain their muscle mass. For example, for a 250-lb patient, I would recommend 114-136 g protein per day. This is equivalent to roughly 15 oz of cooked animal protein. It’s important to note, though, that individuals with kidney disease must limit their protein intake to 0.6-0.8 g/kg bodyweight per day, to avoid overtaxing their kidneys. In this situation, the benefit of increased protein intake does not outweigh the risk of harming the kidneys.
It’s often challenging for patients with suppressed appetites to even think about eating a large hunk of meat or fish, let alone consume it. Plus, eating more than 3-4 oz of protein in one meal can make some patients extremely uncomfortable, owing to the medication’s effect on gastric emptying. This means that daily protein intake must be spread out over multiple mini-meals.
For patients who need more than 100 g of protein per day, protein powders and premade protein shakes can provide 20-30 g protein to fill in the gaps. Although I always try to promote food first, protein supplements have been game changers for my patients, especially those who find solid food less appealing on the medication, or those who avoid animal protein.
Clinicians should have their patients monitor changes in their lean body mass using a dual-energy x-ray absorptiometry scan or a bioelectrical impedance scale; this can be a helpful tool in assessing whether protein intake is sufficient.
Fiber
Even my most knowledgeable and compliant patients will experience some constipation. Generally speaking, when you eat less, you will have fewer bowel movements. Combine that with delayed gastric emptying and reduced fiber intake, and you have a perfect storm. Many patients are simply not able to get in the recommended 25-35 g fiber per day through food, because fibrous foods are filling. If they are prioritizing the protein in their meal, they will not have enough room for all the vegetables on their plate.
To ensure that patients are getting sufficient fiber, clinicians should push consumption of certain vegetables and fruits, such as carrots, broccoli, Brussels sprouts, raspberries, blackberries, and apples, as well as beans and legumes. (Salads are great, but greens like spinach are not as fibrous as one might think.) If the fruit and veggie intake isn’t up to par, a fiber supplement such as psyllium husk can provide an effective boost.
Vitamin B12
Use of these medications is associated with a reduction in vitamin B12 levels, in part because delayed gastric emptying may affect B12 absorption. Low dietary intake of B12 while on the medications can also be to blame, though. The best food sources are animal proteins, so if possible, patients should prioritize having fish, lean meat, eggs, and dairy daily.
Vegetarians and vegans, who are at an increased risk for deficiency, can incorporate nutritional yeast, an excellent source of vitamin B12, into their daily routine. It is beneficial for patients to get blood work periodically to check on B12 status, because insufficient B12 can contribute to the fatigue patients experience while on the medication.
Calcium
Individuals should have calcium on their radar, because weight loss is associated with a decrease in bone mineral density. Adequate intake of the mineral is crucial for optimal bone health, particularly among postmenopausal women and those who are at risk of developing osteoporosis. The RDA for calcium is 1000-1200 mg/d, which an estimated 50% of obese individuals do not take in.
Although dairy products are well-known for being rich in calcium, there are other great sources. Dark green leafy vegetables, such as cooked collard greens and spinach, provide nearly 300 mg per cup. Tofu and sardines are also calcium powerhouses. Despite the plethora of calcium-rich foods, however, some patients may need a calcium supplement.
Vitamin D
Vitamin D deficiency or insufficiency is common among individuals with obesity, so even before these patients start the medications, supplementation may be warranted. The vitamin’s role in promoting calcium absorption, as well as in bone remodeling, make adequate intake essential for patients experiencing significant weight loss.
Clinicians should emphasize regular consumption of fatty fish, such as salmon, as well as eggs, mushrooms, and vitamin D–fortified milks. But unfortunately, that’s where the list of vitamin D–rich foods ends, so taking a vitamin D supplement will be necessary for many patients.
Regularly monitoring patients on GLP-1 RAs through blood work to check vitamin levels and body composition analysis can be helpful in assessing nutritional status while losing weight. Clinicians can also encourage their patients to work with a registered dietitian who is familiar with these medications, so they can develop optimal eating habits throughout their health journey.
Ms. Hanks, a registered dietitian in New York City, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Burnout and Vacations
How many weeks of vacation do you take each year? Does it feel like enough? What prevents you from taking more time off? Is it a contractual obligation to your employer? Or a concern about the lack of income while your are away? Is it the difficulty of finding coverage for your patient care responsibilities? How much of it is the dread of facing your unattended or poorly attended EHR box when you return?
A recent survey of more than 3000 US physicians found that almost 60% took 3 weeks or less vacation per year? The investigators also learned that 70% of the respondents did patient-related tasks while they were on vacation and less than half had full EHR coverage while they were away. Not surprisingly, providers who expressed concerns about finding someone to cover clinical responsibilities and financial concerns were less likely to take more than 3 weeks’ vacation.
As one might hope, taking more than 3 weeks’ vacation and having full EHR coverage were associated with decreased rates of burnout. On the other hand, spending more than 30 minutes per day doing patient-related work while on vacation was associated with higher rates of burnout.
In their conclusion, the authors suggest that if we hope to reduce physician burnout, employers should introduce system-level initiatives to ensure that physicians take adequate vacation and have adequate coverage for their clinical responsibilities — including EHR inbox management.
I will readily admit that I was one of those physicians who took less than 3 weeks of vacation and can’t recall ever taking more than 2 weeks. Since most of our vacations were staycations, I would usually round on the newborns first thing in the morning when I was in town to keep the flow of new patients coming into the practice.
I’m sure there was some collateral damage to my family, but our children continue to reassure me that they weren’t envious of their peers who went away on “real” vacations. As adults two of them take their families on the kind of vacations that make me envious. The third has married someone who shares, what I might call, a “robust commitment” to showing up in the office. But they seem to be a happy couple.
At the root of my vacation style was an egotistical delusion that there weren’t any clinicians in the community who could look after my patients as well as I did. Unfortunately, I had done little to discourage those patients who shared my distorted view.
I was lucky to have spent nearly all my career without the added burden of an EHR inbox. However, in the lead up to our infrequent vacations, the rush to tie up the loose ends of those patients for whom we had not achieved diagnostic closure was stressful and time consuming. Luckily, as a primary care pediatrician most of their problems were short lived. But, leaving the ship battened down could be exhausting.
I can fully understand why the physicians who are taking less than 3 weeks’ vacation and continue to be burdened by patient-related tasks while they are “away” are more likely to experience burnout. However, I wonder why I seemed to have been resistant considering my vacation style, which the authors of the above-mentioned article feel would have placed me at high risk.
I think the answer may lie in my commitment to making decisions that allowed me to maintain equilibrium in my life. In other words, if there were things in my day-to-day activities that were so taxing or distasteful that I am counting the hours and days until I can escape them, then I needed to make the necessary changes promptly and not count on a vacation to repair the accumulating damage. That may have required cutting back some responsibilities or it may have meant that I needed to be in better mental and physical shape to be able to maintain that equilibrium. Maybe it was more sleep, more exercise, less television, not investing as much in time-wasting meetings. This doesn’t mean that I didn’t have bad days. Stuff happens. But if I was putting together two or three bad days a week, something had to change. A vacation wasn’t going solve the inherent or systemic problems that are making day-to-day life so intolerable that I needed to escape for some respite.
In full disclosure, I will share that at age 55 I took a leave of 2 1/2 months and with my wife and another couple bicycled across America. This was a goal I had harbored since childhood and in anticipation over several decades had banked considerable coverage equity by doing extra coverage for other providers to minimize my guilt feelings at being away. This was not an escape from I job I didn’t enjoy going to everyday. It was an exercise in goal fulfillment.
I think the authors of this recent study should be applauded for providing some numbers to support the obvious. However,
Encouraging a clinician to take a bit more vacation may help. But, having someone to properly manage the EHR inbox would do a lot more. If your coverage is telling everyone to “Wait until Dr. Away has returned” it is only going to make things worse.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
How many weeks of vacation do you take each year? Does it feel like enough? What prevents you from taking more time off? Is it a contractual obligation to your employer? Or a concern about the lack of income while your are away? Is it the difficulty of finding coverage for your patient care responsibilities? How much of it is the dread of facing your unattended or poorly attended EHR box when you return?
A recent survey of more than 3000 US physicians found that almost 60% took 3 weeks or less vacation per year? The investigators also learned that 70% of the respondents did patient-related tasks while they were on vacation and less than half had full EHR coverage while they were away. Not surprisingly, providers who expressed concerns about finding someone to cover clinical responsibilities and financial concerns were less likely to take more than 3 weeks’ vacation.
As one might hope, taking more than 3 weeks’ vacation and having full EHR coverage were associated with decreased rates of burnout. On the other hand, spending more than 30 minutes per day doing patient-related work while on vacation was associated with higher rates of burnout.
In their conclusion, the authors suggest that if we hope to reduce physician burnout, employers should introduce system-level initiatives to ensure that physicians take adequate vacation and have adequate coverage for their clinical responsibilities — including EHR inbox management.
I will readily admit that I was one of those physicians who took less than 3 weeks of vacation and can’t recall ever taking more than 2 weeks. Since most of our vacations were staycations, I would usually round on the newborns first thing in the morning when I was in town to keep the flow of new patients coming into the practice.
I’m sure there was some collateral damage to my family, but our children continue to reassure me that they weren’t envious of their peers who went away on “real” vacations. As adults two of them take their families on the kind of vacations that make me envious. The third has married someone who shares, what I might call, a “robust commitment” to showing up in the office. But they seem to be a happy couple.
At the root of my vacation style was an egotistical delusion that there weren’t any clinicians in the community who could look after my patients as well as I did. Unfortunately, I had done little to discourage those patients who shared my distorted view.
I was lucky to have spent nearly all my career without the added burden of an EHR inbox. However, in the lead up to our infrequent vacations, the rush to tie up the loose ends of those patients for whom we had not achieved diagnostic closure was stressful and time consuming. Luckily, as a primary care pediatrician most of their problems were short lived. But, leaving the ship battened down could be exhausting.
I can fully understand why the physicians who are taking less than 3 weeks’ vacation and continue to be burdened by patient-related tasks while they are “away” are more likely to experience burnout. However, I wonder why I seemed to have been resistant considering my vacation style, which the authors of the above-mentioned article feel would have placed me at high risk.
I think the answer may lie in my commitment to making decisions that allowed me to maintain equilibrium in my life. In other words, if there were things in my day-to-day activities that were so taxing or distasteful that I am counting the hours and days until I can escape them, then I needed to make the necessary changes promptly and not count on a vacation to repair the accumulating damage. That may have required cutting back some responsibilities or it may have meant that I needed to be in better mental and physical shape to be able to maintain that equilibrium. Maybe it was more sleep, more exercise, less television, not investing as much in time-wasting meetings. This doesn’t mean that I didn’t have bad days. Stuff happens. But if I was putting together two or three bad days a week, something had to change. A vacation wasn’t going solve the inherent or systemic problems that are making day-to-day life so intolerable that I needed to escape for some respite.
In full disclosure, I will share that at age 55 I took a leave of 2 1/2 months and with my wife and another couple bicycled across America. This was a goal I had harbored since childhood and in anticipation over several decades had banked considerable coverage equity by doing extra coverage for other providers to minimize my guilt feelings at being away. This was not an escape from I job I didn’t enjoy going to everyday. It was an exercise in goal fulfillment.
I think the authors of this recent study should be applauded for providing some numbers to support the obvious. However,
Encouraging a clinician to take a bit more vacation may help. But, having someone to properly manage the EHR inbox would do a lot more. If your coverage is telling everyone to “Wait until Dr. Away has returned” it is only going to make things worse.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
How many weeks of vacation do you take each year? Does it feel like enough? What prevents you from taking more time off? Is it a contractual obligation to your employer? Or a concern about the lack of income while your are away? Is it the difficulty of finding coverage for your patient care responsibilities? How much of it is the dread of facing your unattended or poorly attended EHR box when you return?
A recent survey of more than 3000 US physicians found that almost 60% took 3 weeks or less vacation per year? The investigators also learned that 70% of the respondents did patient-related tasks while they were on vacation and less than half had full EHR coverage while they were away. Not surprisingly, providers who expressed concerns about finding someone to cover clinical responsibilities and financial concerns were less likely to take more than 3 weeks’ vacation.
As one might hope, taking more than 3 weeks’ vacation and having full EHR coverage were associated with decreased rates of burnout. On the other hand, spending more than 30 minutes per day doing patient-related work while on vacation was associated with higher rates of burnout.
In their conclusion, the authors suggest that if we hope to reduce physician burnout, employers should introduce system-level initiatives to ensure that physicians take adequate vacation and have adequate coverage for their clinical responsibilities — including EHR inbox management.
I will readily admit that I was one of those physicians who took less than 3 weeks of vacation and can’t recall ever taking more than 2 weeks. Since most of our vacations were staycations, I would usually round on the newborns first thing in the morning when I was in town to keep the flow of new patients coming into the practice.
I’m sure there was some collateral damage to my family, but our children continue to reassure me that they weren’t envious of their peers who went away on “real” vacations. As adults two of them take their families on the kind of vacations that make me envious. The third has married someone who shares, what I might call, a “robust commitment” to showing up in the office. But they seem to be a happy couple.
At the root of my vacation style was an egotistical delusion that there weren’t any clinicians in the community who could look after my patients as well as I did. Unfortunately, I had done little to discourage those patients who shared my distorted view.
I was lucky to have spent nearly all my career without the added burden of an EHR inbox. However, in the lead up to our infrequent vacations, the rush to tie up the loose ends of those patients for whom we had not achieved diagnostic closure was stressful and time consuming. Luckily, as a primary care pediatrician most of their problems were short lived. But, leaving the ship battened down could be exhausting.
I can fully understand why the physicians who are taking less than 3 weeks’ vacation and continue to be burdened by patient-related tasks while they are “away” are more likely to experience burnout. However, I wonder why I seemed to have been resistant considering my vacation style, which the authors of the above-mentioned article feel would have placed me at high risk.
I think the answer may lie in my commitment to making decisions that allowed me to maintain equilibrium in my life. In other words, if there were things in my day-to-day activities that were so taxing or distasteful that I am counting the hours and days until I can escape them, then I needed to make the necessary changes promptly and not count on a vacation to repair the accumulating damage. That may have required cutting back some responsibilities or it may have meant that I needed to be in better mental and physical shape to be able to maintain that equilibrium. Maybe it was more sleep, more exercise, less television, not investing as much in time-wasting meetings. This doesn’t mean that I didn’t have bad days. Stuff happens. But if I was putting together two or three bad days a week, something had to change. A vacation wasn’t going solve the inherent or systemic problems that are making day-to-day life so intolerable that I needed to escape for some respite.
In full disclosure, I will share that at age 55 I took a leave of 2 1/2 months and with my wife and another couple bicycled across America. This was a goal I had harbored since childhood and in anticipation over several decades had banked considerable coverage equity by doing extra coverage for other providers to minimize my guilt feelings at being away. This was not an escape from I job I didn’t enjoy going to everyday. It was an exercise in goal fulfillment.
I think the authors of this recent study should be applauded for providing some numbers to support the obvious. However,
Encouraging a clinician to take a bit more vacation may help. But, having someone to properly manage the EHR inbox would do a lot more. If your coverage is telling everyone to “Wait until Dr. Away has returned” it is only going to make things worse.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].