User login
Curbing Antibiotic Use Works
, revealed the fourth joint interagency antimicrobial consumption and resistance analysis report.
The report was published by the European Centre for Disease Prevention and Control, the European Food Safety Authority, and the European Medicines Agency. Its findings were derived from an integrated analysis of the potential relationship between antimicrobial consumption (AMC) by humans and animals and the occurrence of antimicrobial resistance (AMR) using data collected between 2019 and 2021.
A Real Threat
AMR poses a significant threat to public and animal health, causing more than 35,000 deaths annually in the European Union (EU) and the European Economic Area. It also imposes a substantial economic burden on European healthcare systems, amounting to approximately €11.7 billion per year.
To address this challenge, the Council of the European Union recommended concerted and sustained efforts to achieve a 20% reduction in AMC in humans (compared with 2019 levels) and a 50% reduction in food-producing animals (compared with 2018 levels) by 2030. These targets are outlined in the European Commission’s Farm to Fork strategy.
It Really Works
Analysis of the trends of AMC and AMR in Escherichia coli from humans and food-producing animals, conducted for the first time, revealed that the susceptibility of E coli to antimicrobials in humans and animals increases with an overall decrease in the consumption of antibiotics.
Concurrent trends in AMC and AMR from 2014 to 2021 were also assessed. AMC in both human and animal sectors, measured in mg/kg of estimated biomass, was compared at country and European levels. In 2021, human AMC totaled 125.0 mg/kg of biomass, while food-producing animals registered 92.6 mg/kg of biomass.
Over the 2014-2021 period, total AMC in food-producing animals decreased by 44%, while in humans, it remained relatively stable. The consumption of certain antimicrobials was positively associated with resistance to those substances in bacteria from both humans and food-producing animals.
The report also highlighted that E coli resistance is linked in humans to the use of carbapenems, third- and fourth-generation cephalosporins, and quinolones and in food-producing animals to the administration of quinolones, polymyxins, aminopenicillins, and tetracyclines. Further, a connection exists between bacterial resistance in humans and food-producing animals, particularly for bacterial species such as Campylobacter jejuni and C coli.
The findings suggest that measures to reduce AMC in both food-producing animals and humans have been effective in many countries. However, reinforcing these measures is crucial to maintain and further advance reductions in AMC.
More Work
Aligned with the European Commission’s One Health holistic and coordinated approach to managing the human and veterinary sectors together, the European agencies advocate for:
- Sustained efforts to combat AMR at national, EU, and global levels.
- Coordinated surveillance of antibiotic use and AMR in both human and animal sectors.
- Continued research in the field of AMR.
The statistical code used to conduct these analyses was made publicly available in order to support further research analyses.
A version of this article appeared on Medscape.com.
, revealed the fourth joint interagency antimicrobial consumption and resistance analysis report.
The report was published by the European Centre for Disease Prevention and Control, the European Food Safety Authority, and the European Medicines Agency. Its findings were derived from an integrated analysis of the potential relationship between antimicrobial consumption (AMC) by humans and animals and the occurrence of antimicrobial resistance (AMR) using data collected between 2019 and 2021.
A Real Threat
AMR poses a significant threat to public and animal health, causing more than 35,000 deaths annually in the European Union (EU) and the European Economic Area. It also imposes a substantial economic burden on European healthcare systems, amounting to approximately €11.7 billion per year.
To address this challenge, the Council of the European Union recommended concerted and sustained efforts to achieve a 20% reduction in AMC in humans (compared with 2019 levels) and a 50% reduction in food-producing animals (compared with 2018 levels) by 2030. These targets are outlined in the European Commission’s Farm to Fork strategy.
It Really Works
Analysis of the trends of AMC and AMR in Escherichia coli from humans and food-producing animals, conducted for the first time, revealed that the susceptibility of E coli to antimicrobials in humans and animals increases with an overall decrease in the consumption of antibiotics.
Concurrent trends in AMC and AMR from 2014 to 2021 were also assessed. AMC in both human and animal sectors, measured in mg/kg of estimated biomass, was compared at country and European levels. In 2021, human AMC totaled 125.0 mg/kg of biomass, while food-producing animals registered 92.6 mg/kg of biomass.
Over the 2014-2021 period, total AMC in food-producing animals decreased by 44%, while in humans, it remained relatively stable. The consumption of certain antimicrobials was positively associated with resistance to those substances in bacteria from both humans and food-producing animals.
The report also highlighted that E coli resistance is linked in humans to the use of carbapenems, third- and fourth-generation cephalosporins, and quinolones and in food-producing animals to the administration of quinolones, polymyxins, aminopenicillins, and tetracyclines. Further, a connection exists between bacterial resistance in humans and food-producing animals, particularly for bacterial species such as Campylobacter jejuni and C coli.
The findings suggest that measures to reduce AMC in both food-producing animals and humans have been effective in many countries. However, reinforcing these measures is crucial to maintain and further advance reductions in AMC.
More Work
Aligned with the European Commission’s One Health holistic and coordinated approach to managing the human and veterinary sectors together, the European agencies advocate for:
- Sustained efforts to combat AMR at national, EU, and global levels.
- Coordinated surveillance of antibiotic use and AMR in both human and animal sectors.
- Continued research in the field of AMR.
The statistical code used to conduct these analyses was made publicly available in order to support further research analyses.
A version of this article appeared on Medscape.com.
, revealed the fourth joint interagency antimicrobial consumption and resistance analysis report.
The report was published by the European Centre for Disease Prevention and Control, the European Food Safety Authority, and the European Medicines Agency. Its findings were derived from an integrated analysis of the potential relationship between antimicrobial consumption (AMC) by humans and animals and the occurrence of antimicrobial resistance (AMR) using data collected between 2019 and 2021.
A Real Threat
AMR poses a significant threat to public and animal health, causing more than 35,000 deaths annually in the European Union (EU) and the European Economic Area. It also imposes a substantial economic burden on European healthcare systems, amounting to approximately €11.7 billion per year.
To address this challenge, the Council of the European Union recommended concerted and sustained efforts to achieve a 20% reduction in AMC in humans (compared with 2019 levels) and a 50% reduction in food-producing animals (compared with 2018 levels) by 2030. These targets are outlined in the European Commission’s Farm to Fork strategy.
It Really Works
Analysis of the trends of AMC and AMR in Escherichia coli from humans and food-producing animals, conducted for the first time, revealed that the susceptibility of E coli to antimicrobials in humans and animals increases with an overall decrease in the consumption of antibiotics.
Concurrent trends in AMC and AMR from 2014 to 2021 were also assessed. AMC in both human and animal sectors, measured in mg/kg of estimated biomass, was compared at country and European levels. In 2021, human AMC totaled 125.0 mg/kg of biomass, while food-producing animals registered 92.6 mg/kg of biomass.
Over the 2014-2021 period, total AMC in food-producing animals decreased by 44%, while in humans, it remained relatively stable. The consumption of certain antimicrobials was positively associated with resistance to those substances in bacteria from both humans and food-producing animals.
The report also highlighted that E coli resistance is linked in humans to the use of carbapenems, third- and fourth-generation cephalosporins, and quinolones and in food-producing animals to the administration of quinolones, polymyxins, aminopenicillins, and tetracyclines. Further, a connection exists between bacterial resistance in humans and food-producing animals, particularly for bacterial species such as Campylobacter jejuni and C coli.
The findings suggest that measures to reduce AMC in both food-producing animals and humans have been effective in many countries. However, reinforcing these measures is crucial to maintain and further advance reductions in AMC.
More Work
Aligned with the European Commission’s One Health holistic and coordinated approach to managing the human and veterinary sectors together, the European agencies advocate for:
- Sustained efforts to combat AMR at national, EU, and global levels.
- Coordinated surveillance of antibiotic use and AMR in both human and animal sectors.
- Continued research in the field of AMR.
The statistical code used to conduct these analyses was made publicly available in order to support further research analyses.
A version of this article appeared on Medscape.com.
New Antibiotic Promising for Complicated UTIs
TOPLINE:
, according to a study published in The New England Journal of Medicine.
METHODOLOGY:
- Cefepime-taniborbactam is an antibiotic currently being explored as a treatment for antibiotic-resistant bacteria.
- The phase 3, double-blind, randomized trial included participants from 15 countries, including a safety group of 657 patients who were studied for adverse events and 436 in the micro intention-to-treat group who were studied for drug effectiveness.
- Each drug’s efficacy was measured as a combination of reduced bacteria levels and a resolution of symptoms and signs of infection.
- Patients in the study were over age 18; had a diagnosis of either complicated UTI or acute pyelonephritis; and had pyuria, at least one systemic sign, and at least one local sign or symptom. People were excluded if they had already received antibacterial drug therapy for more than 24 hours before randomization or had an infection with a meropenem-resistant pathogen.
TAKEAWAY:
- At days 19-23, 70.6% of patients in the cefepime-taniborbactam group showed a successful reduction in bacteria and symptoms compared with 58.0% in the meropenem group.
- Cefepime-taniborbactam was more effective than meropenem during follow-up, with 89.1% efficacy less than 24 hours after the last dose, compared to meropenem’s 86%. Cefepime-taniborbactam continued to have 63.8% efficacy up to 35 days after starting treatment, while meropenem was 51.7% during that timeframe.
- In the cefepime-taniborbactam group, 35.5% of patients experienced adverse effects that were mild to moderate, including headache, diarrhea, constipation, hypertension, and nausea, compared to 29% in the meropenem group.
- Overall, 3% of participants discontinued cefepime-taniborbactam and 1.8% discontinued meropenem, but reasons were heterogeneous.
IN PRACTICE:
“Cefepime-taniborbactam was superior to meropenem for the treatment of complicated UTI that included acute pyelonephritis, with a safety profile similar to that of meropenem,” the study authors wrote.
SOURCE:
Paul McGovern, MD, infectious disease specialist and senior vice president of Venatorx Pharmaceuticals, was the corresponding author of the study.
LIMITATIONS:
The authors reported no limitations.
DISCLOSURES:
The study was funded by Venatorx Pharmaceuticals, which received funding from the US Department of Health and Human Services, the Administration for Strategic Preparedness and Response, the Biomedical Advanced Research and Development Authority, the Global Antibiotic Research and Development Partnership, and Everest Medicines.
A version of this article appeared on Medscape.com.
TOPLINE:
, according to a study published in The New England Journal of Medicine.
METHODOLOGY:
- Cefepime-taniborbactam is an antibiotic currently being explored as a treatment for antibiotic-resistant bacteria.
- The phase 3, double-blind, randomized trial included participants from 15 countries, including a safety group of 657 patients who were studied for adverse events and 436 in the micro intention-to-treat group who were studied for drug effectiveness.
- Each drug’s efficacy was measured as a combination of reduced bacteria levels and a resolution of symptoms and signs of infection.
- Patients in the study were over age 18; had a diagnosis of either complicated UTI or acute pyelonephritis; and had pyuria, at least one systemic sign, and at least one local sign or symptom. People were excluded if they had already received antibacterial drug therapy for more than 24 hours before randomization or had an infection with a meropenem-resistant pathogen.
TAKEAWAY:
- At days 19-23, 70.6% of patients in the cefepime-taniborbactam group showed a successful reduction in bacteria and symptoms compared with 58.0% in the meropenem group.
- Cefepime-taniborbactam was more effective than meropenem during follow-up, with 89.1% efficacy less than 24 hours after the last dose, compared to meropenem’s 86%. Cefepime-taniborbactam continued to have 63.8% efficacy up to 35 days after starting treatment, while meropenem was 51.7% during that timeframe.
- In the cefepime-taniborbactam group, 35.5% of patients experienced adverse effects that were mild to moderate, including headache, diarrhea, constipation, hypertension, and nausea, compared to 29% in the meropenem group.
- Overall, 3% of participants discontinued cefepime-taniborbactam and 1.8% discontinued meropenem, but reasons were heterogeneous.
IN PRACTICE:
“Cefepime-taniborbactam was superior to meropenem for the treatment of complicated UTI that included acute pyelonephritis, with a safety profile similar to that of meropenem,” the study authors wrote.
SOURCE:
Paul McGovern, MD, infectious disease specialist and senior vice president of Venatorx Pharmaceuticals, was the corresponding author of the study.
LIMITATIONS:
The authors reported no limitations.
DISCLOSURES:
The study was funded by Venatorx Pharmaceuticals, which received funding from the US Department of Health and Human Services, the Administration for Strategic Preparedness and Response, the Biomedical Advanced Research and Development Authority, the Global Antibiotic Research and Development Partnership, and Everest Medicines.
A version of this article appeared on Medscape.com.
TOPLINE:
, according to a study published in The New England Journal of Medicine.
METHODOLOGY:
- Cefepime-taniborbactam is an antibiotic currently being explored as a treatment for antibiotic-resistant bacteria.
- The phase 3, double-blind, randomized trial included participants from 15 countries, including a safety group of 657 patients who were studied for adverse events and 436 in the micro intention-to-treat group who were studied for drug effectiveness.
- Each drug’s efficacy was measured as a combination of reduced bacteria levels and a resolution of symptoms and signs of infection.
- Patients in the study were over age 18; had a diagnosis of either complicated UTI or acute pyelonephritis; and had pyuria, at least one systemic sign, and at least one local sign or symptom. People were excluded if they had already received antibacterial drug therapy for more than 24 hours before randomization or had an infection with a meropenem-resistant pathogen.
TAKEAWAY:
- At days 19-23, 70.6% of patients in the cefepime-taniborbactam group showed a successful reduction in bacteria and symptoms compared with 58.0% in the meropenem group.
- Cefepime-taniborbactam was more effective than meropenem during follow-up, with 89.1% efficacy less than 24 hours after the last dose, compared to meropenem’s 86%. Cefepime-taniborbactam continued to have 63.8% efficacy up to 35 days after starting treatment, while meropenem was 51.7% during that timeframe.
- In the cefepime-taniborbactam group, 35.5% of patients experienced adverse effects that were mild to moderate, including headache, diarrhea, constipation, hypertension, and nausea, compared to 29% in the meropenem group.
- Overall, 3% of participants discontinued cefepime-taniborbactam and 1.8% discontinued meropenem, but reasons were heterogeneous.
IN PRACTICE:
“Cefepime-taniborbactam was superior to meropenem for the treatment of complicated UTI that included acute pyelonephritis, with a safety profile similar to that of meropenem,” the study authors wrote.
SOURCE:
Paul McGovern, MD, infectious disease specialist and senior vice president of Venatorx Pharmaceuticals, was the corresponding author of the study.
LIMITATIONS:
The authors reported no limitations.
DISCLOSURES:
The study was funded by Venatorx Pharmaceuticals, which received funding from the US Department of Health and Human Services, the Administration for Strategic Preparedness and Response, the Biomedical Advanced Research and Development Authority, the Global Antibiotic Research and Development Partnership, and Everest Medicines.
A version of this article appeared on Medscape.com.
Hospital Adverse Events Rise After Private Equity Acquisition
Hospital-acquired adverse events or conditions including falls and infections increased by approximately 25% after hospitals’ acquisition by private equity compared with control hospitals, on the basis of a study of Medicare claims for more than 4,500,000 hospitalizations.
“Prior research on private equity in health care showed that acquisition is associated with higher charges, prices, and spending; however, the implications for quality of care and patient outcomes remained less understood,” corresponding author Zirui Song, MD, of Harvard Medical School, Boston, said in an interview. “This was particularly true for measures of clinical quality that were less susceptible to changes in patient mix or coding behavior, such as hospital-acquired adverse events.”
In the study, published in JAMA, the researchers compared data from 100% Medicare Part A claims for 662,095 hospitalizations at 51 hospitals acquired by private equities and 4,160,720 hospitalizations at 259 control hospitals. The hospitalizations occurred between 2009 and 2019. The researchers also used a difference-in-differences design to evaluate hospitalizations from 3 years before to 3 years after acquisition, controlling for patient and hospital attributes.
Hospital-acquired adverse events as defined by the US Centers for Medicare & Medicaid Services included falls, infections, stage III or IV pressure ulcers, foreign objects retained after surgery, air embolism, and blood incompatibility.
Overall, Medicare patients in private equity hospitals experienced a 25.4% increase in hospital-acquired conditions compared with those in control hospitals through a period of up to 3 years after acquisition, with a difference of 4.6 additional hospital-acquired conditions per 10,000 hospitalizations (P = .004). Central line-associated bloodstream infections accounted for 37.7% of the increase (P = .04), despite a 16.2% decrease in placement of central lines, and falls accounted for 27.3% (P = .02).
Notably, the incidence of surgical site infections increased from 10.8 per 10,000 hospitalizations before acquisition to 21.6 per 10,000 hospitalizations after acquisition, despite a reduction of 8.1% in surgical volume. By contrast, surgical site infections decreased at control hospitals over the study period.
In-hospital mortality decreased slightly at private equity hospitals compared with the control hospitals, but there was no differential change in mortality by 30 days after hospital discharge. The slight difference might be caused by the trend in slightly younger Medicare beneficiaries treated at private equity hospitals; these patients were less likely to be eligible for both Medicaid and Medicare and were more likely to be transferred to other hospitals, the researchers noted.
The findings were limited by several factors including the lack of generalizability to all private equity-acquired hospitals and to non-Medicare patients, the researchers noted. Other limitations include the use of the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes that might have failed to capture all hospital-acquired conditions and the inability to account for all confounding factors.
However, the results suggest that private equity acquisition was associated with increased hospital-acquired adverse events and highlight concerns about the impact of private equity ownership on healthcare delivery, the researchers concluded.
In a related story published in July 2023, this news organization described a report showing an association between private equity ownership of medical practices and increased consumer prices for multiple medical specialties.
“Medicare patients admitted to private equity-owned hospitals experienced, on average, an 25% increase in hospital-acquired adverse events after the hospital was bought compared to similar patients at hospitals not acquired by private equity firms. We were surprised by the extent of this change relative to the comparison (non-private equity) hospitals, including the sizable increase in central line-associated bloodstream infections and the doubling of surgical site infections at private equity hospitals — both of which went down at the comparison hospitals during the same period,” Dr. Song said in an interview.
“A key implication is that patients, providers, and policymakers might be more attuned to the potential clinical impact of private equity ownership in the delivery system. Given that a plausible explanation for these findings is reductions in clinician staffing, clinical organizations and policymakers might also be more aware of cost-cutting strategies after acquisition,” Dr. Song said. “Prior research has shown that hospitals, nursing homes, and physician practices experience staffing cuts after private equity acquisition, which is a common way to reduce operating costs and boost the profitability of acquired entities,” he noted.
“More research is needed to understand the impact of private equity acquisitions across health care settings and the potential effects of policy levers that aim to protect patients and societal resources,” said Dr. Song, who coauthored an article outlining a policy framework for addressing private equity in healthcare, published in JAMA in April 2023. “Potential regulatory remedies include minimum staffing ratios, antitrust enforcement, mitigating the financial risk of such acquisitions, increasing the transparency of these acquisitions, and protecting patients and society from the higher prices of care attributed to this model of provider ownership,” he said.
Patients Pay the Price of Private Equity Acquisition
“The exponential growth in private equity ownership in hospital and physician practices in the past few decades has left a majority of health care providers disillusioned with cost-cutting practices resulting in staffing reductions and ratios that sacrifice patient care as part of their approach to running clinical operations ‘lean,’ ” Robert Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, NY, said in an interview.
“While private equity companies argue that such practices are essential to meet their bottom line and increase operating margins, it doesn’t translate into ideal care for patients; lean practices in staffing which focus on profits at the expense of patient safety and quality of care.
“When you look at patient outcomes, it is the patients who ultimately pay the price — not the shareholders,” Dr. Glatter said. “This translates to higher risks of hospital-acquired complications including falls and blood-borne infections, including surgical site infections, as noted by the authors of the current study when private equity took over operations in hospitals.
Dr. Glatter said he was not surprised by the findings. “In my world, patient care and safety come first. Period,” he said. “Would you want your family’s health and well-being sacrificed in the name of company profits? I think it’s a rhetorical question, but one that every health care provider who works in a hospital or practice run by private equity must consider.”
Despite a decline in utilization at private equity hospitals as noted in the current study, hospital-acquired infections and adverse outcomes still increased, illustrating a decline in quality of care, said Dr. Glatter. “While these disparities were not evident when looking at 30-day outcomes, they demonstrate how operational changes impact patient outcomes in the near term. Having younger and healthier patients, and fewer Medicare and Medicaid patients combined with more hospital transfers to non–private equity run hospitals, resulted in lower in-hospital mortality in the near term, which was not apparent at 30 days post discharge,” he said.
“The explosion of hospital mergers and consolidation in the past several decades has led to skyrocketing health care costs at the expense of patient satisfaction, but also health care providers’ autonomy to manage and maintain quality care for their patients,” Dr. Glatter said.
“It’s important to understand that private equity’s interests are primarily aligned with their shareholder’s interests, as opposed to patients’ outcomes and interests,” Dr. Glatter told this news organization. “Within 5-7 years, the goal is to increase operating margins and profits and then sell a practice or hospital, which is ultimately part of a ‘health care portfolio,’ ” he said.
Additional research is needed to examine whether other hospital-acquired conditions including pressure sores, catheter-associated UTIs, methicillin-resistant Staphylococcus aureus infections, Clostridium difficile infections, and nosocomial pneumonia have increased in hospitals following private equity acquisition, given the overall national decline in these events, he said.
“At the same time, it is vital to also look at management and readmission rates for patients with strokes, heart attacks, and congestive heart failure in hospitals that are run by private equity,” Dr. Glatter noted. “These are important benchmarks of care monitored by CMS that reflect the quality of care that payers ultimately factor into reimbursement.”
Examining the metrics associated with these diagnoses will help in understanding whether private equity-managed facilities are leading to adverse outcomes and mortality, increased length of stay, hospital readmissions, and increased nosocomial infections, apart from other aspects of patient experience, Dr. Glatter added.
The study was supported by the National Heart, Lung, and Blood Institute, the National Institute on Aging, and Arnold Ventures. The researchers had no financial conflicts to disclose. Dr. Glatter had no financial conflicts to disclose and serves on the Medscape Emergency Medicine Editorial Board.
A version of this article appeared on Medscape.com.
Hospital-acquired adverse events or conditions including falls and infections increased by approximately 25% after hospitals’ acquisition by private equity compared with control hospitals, on the basis of a study of Medicare claims for more than 4,500,000 hospitalizations.
“Prior research on private equity in health care showed that acquisition is associated with higher charges, prices, and spending; however, the implications for quality of care and patient outcomes remained less understood,” corresponding author Zirui Song, MD, of Harvard Medical School, Boston, said in an interview. “This was particularly true for measures of clinical quality that were less susceptible to changes in patient mix or coding behavior, such as hospital-acquired adverse events.”
In the study, published in JAMA, the researchers compared data from 100% Medicare Part A claims for 662,095 hospitalizations at 51 hospitals acquired by private equities and 4,160,720 hospitalizations at 259 control hospitals. The hospitalizations occurred between 2009 and 2019. The researchers also used a difference-in-differences design to evaluate hospitalizations from 3 years before to 3 years after acquisition, controlling for patient and hospital attributes.
Hospital-acquired adverse events as defined by the US Centers for Medicare & Medicaid Services included falls, infections, stage III or IV pressure ulcers, foreign objects retained after surgery, air embolism, and blood incompatibility.
Overall, Medicare patients in private equity hospitals experienced a 25.4% increase in hospital-acquired conditions compared with those in control hospitals through a period of up to 3 years after acquisition, with a difference of 4.6 additional hospital-acquired conditions per 10,000 hospitalizations (P = .004). Central line-associated bloodstream infections accounted for 37.7% of the increase (P = .04), despite a 16.2% decrease in placement of central lines, and falls accounted for 27.3% (P = .02).
Notably, the incidence of surgical site infections increased from 10.8 per 10,000 hospitalizations before acquisition to 21.6 per 10,000 hospitalizations after acquisition, despite a reduction of 8.1% in surgical volume. By contrast, surgical site infections decreased at control hospitals over the study period.
In-hospital mortality decreased slightly at private equity hospitals compared with the control hospitals, but there was no differential change in mortality by 30 days after hospital discharge. The slight difference might be caused by the trend in slightly younger Medicare beneficiaries treated at private equity hospitals; these patients were less likely to be eligible for both Medicaid and Medicare and were more likely to be transferred to other hospitals, the researchers noted.
The findings were limited by several factors including the lack of generalizability to all private equity-acquired hospitals and to non-Medicare patients, the researchers noted. Other limitations include the use of the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes that might have failed to capture all hospital-acquired conditions and the inability to account for all confounding factors.
However, the results suggest that private equity acquisition was associated with increased hospital-acquired adverse events and highlight concerns about the impact of private equity ownership on healthcare delivery, the researchers concluded.
In a related story published in July 2023, this news organization described a report showing an association between private equity ownership of medical practices and increased consumer prices for multiple medical specialties.
“Medicare patients admitted to private equity-owned hospitals experienced, on average, an 25% increase in hospital-acquired adverse events after the hospital was bought compared to similar patients at hospitals not acquired by private equity firms. We were surprised by the extent of this change relative to the comparison (non-private equity) hospitals, including the sizable increase in central line-associated bloodstream infections and the doubling of surgical site infections at private equity hospitals — both of which went down at the comparison hospitals during the same period,” Dr. Song said in an interview.
“A key implication is that patients, providers, and policymakers might be more attuned to the potential clinical impact of private equity ownership in the delivery system. Given that a plausible explanation for these findings is reductions in clinician staffing, clinical organizations and policymakers might also be more aware of cost-cutting strategies after acquisition,” Dr. Song said. “Prior research has shown that hospitals, nursing homes, and physician practices experience staffing cuts after private equity acquisition, which is a common way to reduce operating costs and boost the profitability of acquired entities,” he noted.
“More research is needed to understand the impact of private equity acquisitions across health care settings and the potential effects of policy levers that aim to protect patients and societal resources,” said Dr. Song, who coauthored an article outlining a policy framework for addressing private equity in healthcare, published in JAMA in April 2023. “Potential regulatory remedies include minimum staffing ratios, antitrust enforcement, mitigating the financial risk of such acquisitions, increasing the transparency of these acquisitions, and protecting patients and society from the higher prices of care attributed to this model of provider ownership,” he said.
Patients Pay the Price of Private Equity Acquisition
“The exponential growth in private equity ownership in hospital and physician practices in the past few decades has left a majority of health care providers disillusioned with cost-cutting practices resulting in staffing reductions and ratios that sacrifice patient care as part of their approach to running clinical operations ‘lean,’ ” Robert Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, NY, said in an interview.
“While private equity companies argue that such practices are essential to meet their bottom line and increase operating margins, it doesn’t translate into ideal care for patients; lean practices in staffing which focus on profits at the expense of patient safety and quality of care.
“When you look at patient outcomes, it is the patients who ultimately pay the price — not the shareholders,” Dr. Glatter said. “This translates to higher risks of hospital-acquired complications including falls and blood-borne infections, including surgical site infections, as noted by the authors of the current study when private equity took over operations in hospitals.
Dr. Glatter said he was not surprised by the findings. “In my world, patient care and safety come first. Period,” he said. “Would you want your family’s health and well-being sacrificed in the name of company profits? I think it’s a rhetorical question, but one that every health care provider who works in a hospital or practice run by private equity must consider.”
Despite a decline in utilization at private equity hospitals as noted in the current study, hospital-acquired infections and adverse outcomes still increased, illustrating a decline in quality of care, said Dr. Glatter. “While these disparities were not evident when looking at 30-day outcomes, they demonstrate how operational changes impact patient outcomes in the near term. Having younger and healthier patients, and fewer Medicare and Medicaid patients combined with more hospital transfers to non–private equity run hospitals, resulted in lower in-hospital mortality in the near term, which was not apparent at 30 days post discharge,” he said.
“The explosion of hospital mergers and consolidation in the past several decades has led to skyrocketing health care costs at the expense of patient satisfaction, but also health care providers’ autonomy to manage and maintain quality care for their patients,” Dr. Glatter said.
“It’s important to understand that private equity’s interests are primarily aligned with their shareholder’s interests, as opposed to patients’ outcomes and interests,” Dr. Glatter told this news organization. “Within 5-7 years, the goal is to increase operating margins and profits and then sell a practice or hospital, which is ultimately part of a ‘health care portfolio,’ ” he said.
Additional research is needed to examine whether other hospital-acquired conditions including pressure sores, catheter-associated UTIs, methicillin-resistant Staphylococcus aureus infections, Clostridium difficile infections, and nosocomial pneumonia have increased in hospitals following private equity acquisition, given the overall national decline in these events, he said.
“At the same time, it is vital to also look at management and readmission rates for patients with strokes, heart attacks, and congestive heart failure in hospitals that are run by private equity,” Dr. Glatter noted. “These are important benchmarks of care monitored by CMS that reflect the quality of care that payers ultimately factor into reimbursement.”
Examining the metrics associated with these diagnoses will help in understanding whether private equity-managed facilities are leading to adverse outcomes and mortality, increased length of stay, hospital readmissions, and increased nosocomial infections, apart from other aspects of patient experience, Dr. Glatter added.
The study was supported by the National Heart, Lung, and Blood Institute, the National Institute on Aging, and Arnold Ventures. The researchers had no financial conflicts to disclose. Dr. Glatter had no financial conflicts to disclose and serves on the Medscape Emergency Medicine Editorial Board.
A version of this article appeared on Medscape.com.
Hospital-acquired adverse events or conditions including falls and infections increased by approximately 25% after hospitals’ acquisition by private equity compared with control hospitals, on the basis of a study of Medicare claims for more than 4,500,000 hospitalizations.
“Prior research on private equity in health care showed that acquisition is associated with higher charges, prices, and spending; however, the implications for quality of care and patient outcomes remained less understood,” corresponding author Zirui Song, MD, of Harvard Medical School, Boston, said in an interview. “This was particularly true for measures of clinical quality that were less susceptible to changes in patient mix or coding behavior, such as hospital-acquired adverse events.”
In the study, published in JAMA, the researchers compared data from 100% Medicare Part A claims for 662,095 hospitalizations at 51 hospitals acquired by private equities and 4,160,720 hospitalizations at 259 control hospitals. The hospitalizations occurred between 2009 and 2019. The researchers also used a difference-in-differences design to evaluate hospitalizations from 3 years before to 3 years after acquisition, controlling for patient and hospital attributes.
Hospital-acquired adverse events as defined by the US Centers for Medicare & Medicaid Services included falls, infections, stage III or IV pressure ulcers, foreign objects retained after surgery, air embolism, and blood incompatibility.
Overall, Medicare patients in private equity hospitals experienced a 25.4% increase in hospital-acquired conditions compared with those in control hospitals through a period of up to 3 years after acquisition, with a difference of 4.6 additional hospital-acquired conditions per 10,000 hospitalizations (P = .004). Central line-associated bloodstream infections accounted for 37.7% of the increase (P = .04), despite a 16.2% decrease in placement of central lines, and falls accounted for 27.3% (P = .02).
Notably, the incidence of surgical site infections increased from 10.8 per 10,000 hospitalizations before acquisition to 21.6 per 10,000 hospitalizations after acquisition, despite a reduction of 8.1% in surgical volume. By contrast, surgical site infections decreased at control hospitals over the study period.
In-hospital mortality decreased slightly at private equity hospitals compared with the control hospitals, but there was no differential change in mortality by 30 days after hospital discharge. The slight difference might be caused by the trend in slightly younger Medicare beneficiaries treated at private equity hospitals; these patients were less likely to be eligible for both Medicaid and Medicare and were more likely to be transferred to other hospitals, the researchers noted.
The findings were limited by several factors including the lack of generalizability to all private equity-acquired hospitals and to non-Medicare patients, the researchers noted. Other limitations include the use of the International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes that might have failed to capture all hospital-acquired conditions and the inability to account for all confounding factors.
However, the results suggest that private equity acquisition was associated with increased hospital-acquired adverse events and highlight concerns about the impact of private equity ownership on healthcare delivery, the researchers concluded.
In a related story published in July 2023, this news organization described a report showing an association between private equity ownership of medical practices and increased consumer prices for multiple medical specialties.
“Medicare patients admitted to private equity-owned hospitals experienced, on average, an 25% increase in hospital-acquired adverse events after the hospital was bought compared to similar patients at hospitals not acquired by private equity firms. We were surprised by the extent of this change relative to the comparison (non-private equity) hospitals, including the sizable increase in central line-associated bloodstream infections and the doubling of surgical site infections at private equity hospitals — both of which went down at the comparison hospitals during the same period,” Dr. Song said in an interview.
“A key implication is that patients, providers, and policymakers might be more attuned to the potential clinical impact of private equity ownership in the delivery system. Given that a plausible explanation for these findings is reductions in clinician staffing, clinical organizations and policymakers might also be more aware of cost-cutting strategies after acquisition,” Dr. Song said. “Prior research has shown that hospitals, nursing homes, and physician practices experience staffing cuts after private equity acquisition, which is a common way to reduce operating costs and boost the profitability of acquired entities,” he noted.
“More research is needed to understand the impact of private equity acquisitions across health care settings and the potential effects of policy levers that aim to protect patients and societal resources,” said Dr. Song, who coauthored an article outlining a policy framework for addressing private equity in healthcare, published in JAMA in April 2023. “Potential regulatory remedies include minimum staffing ratios, antitrust enforcement, mitigating the financial risk of such acquisitions, increasing the transparency of these acquisitions, and protecting patients and society from the higher prices of care attributed to this model of provider ownership,” he said.
Patients Pay the Price of Private Equity Acquisition
“The exponential growth in private equity ownership in hospital and physician practices in the past few decades has left a majority of health care providers disillusioned with cost-cutting practices resulting in staffing reductions and ratios that sacrifice patient care as part of their approach to running clinical operations ‘lean,’ ” Robert Glatter, MD, an emergency medicine physician at Lenox Hill Hospital, New York, NY, said in an interview.
“While private equity companies argue that such practices are essential to meet their bottom line and increase operating margins, it doesn’t translate into ideal care for patients; lean practices in staffing which focus on profits at the expense of patient safety and quality of care.
“When you look at patient outcomes, it is the patients who ultimately pay the price — not the shareholders,” Dr. Glatter said. “This translates to higher risks of hospital-acquired complications including falls and blood-borne infections, including surgical site infections, as noted by the authors of the current study when private equity took over operations in hospitals.
Dr. Glatter said he was not surprised by the findings. “In my world, patient care and safety come first. Period,” he said. “Would you want your family’s health and well-being sacrificed in the name of company profits? I think it’s a rhetorical question, but one that every health care provider who works in a hospital or practice run by private equity must consider.”
Despite a decline in utilization at private equity hospitals as noted in the current study, hospital-acquired infections and adverse outcomes still increased, illustrating a decline in quality of care, said Dr. Glatter. “While these disparities were not evident when looking at 30-day outcomes, they demonstrate how operational changes impact patient outcomes in the near term. Having younger and healthier patients, and fewer Medicare and Medicaid patients combined with more hospital transfers to non–private equity run hospitals, resulted in lower in-hospital mortality in the near term, which was not apparent at 30 days post discharge,” he said.
“The explosion of hospital mergers and consolidation in the past several decades has led to skyrocketing health care costs at the expense of patient satisfaction, but also health care providers’ autonomy to manage and maintain quality care for their patients,” Dr. Glatter said.
“It’s important to understand that private equity’s interests are primarily aligned with their shareholder’s interests, as opposed to patients’ outcomes and interests,” Dr. Glatter told this news organization. “Within 5-7 years, the goal is to increase operating margins and profits and then sell a practice or hospital, which is ultimately part of a ‘health care portfolio,’ ” he said.
Additional research is needed to examine whether other hospital-acquired conditions including pressure sores, catheter-associated UTIs, methicillin-resistant Staphylococcus aureus infections, Clostridium difficile infections, and nosocomial pneumonia have increased in hospitals following private equity acquisition, given the overall national decline in these events, he said.
“At the same time, it is vital to also look at management and readmission rates for patients with strokes, heart attacks, and congestive heart failure in hospitals that are run by private equity,” Dr. Glatter noted. “These are important benchmarks of care monitored by CMS that reflect the quality of care that payers ultimately factor into reimbursement.”
Examining the metrics associated with these diagnoses will help in understanding whether private equity-managed facilities are leading to adverse outcomes and mortality, increased length of stay, hospital readmissions, and increased nosocomial infections, apart from other aspects of patient experience, Dr. Glatter added.
The study was supported by the National Heart, Lung, and Blood Institute, the National Institute on Aging, and Arnold Ventures. The researchers had no financial conflicts to disclose. Dr. Glatter had no financial conflicts to disclose and serves on the Medscape Emergency Medicine Editorial Board.
A version of this article appeared on Medscape.com.
New antibiotic could combat multidrug-resistant superbugs
Antibiotic resistance is a major public health problem. Few new molecules are in development, but a new antibiotic called clovibactin brings hope.
The drug was discovered and has been studied by scientists from Utrecht University in the Netherlands, the University of Bonn in Germany, the German Center for Infection Research, Northeastern University in Boston, and NovoBiotic Pharmaceuticals in Cambridge, Mass.
Their research was published in Cell.
“Since clovibactin was isolated from bacteria that could not be grown before, pathogenic bacteria have not seen such an antibiotic before and had no time to develop resistance,” Markus Weingarth, MD, PhD, a researcher in Utrecht University’s chemistry department, said in a press release.
Microbial “dark matter”
Researchers isolated clovibactin from sandy soil from North Carolina and studied it using the iChip device, which was developed in 2015. This technique allowed them to grow “bacterial dark matter,” so-called unculturable bacteria, which compose a group to which 99% of bacteria belong.
This device also paved the way for the discovery of the antibiotic teixobactin in 2020. Teixobactin is effective against gram-positive bacteria and is one of the first truly new antibiotics in decades. Its mechanism of action is like that of clovibactin.
Combats resistant bacteria
In the Cell article, the researchers showed that clovibactin acts via several mechanisms and that it successfully treated mice infected with the superbug Staphylococcus aureus.
Clovibactin exhibited antibacterial activity against a broad range of gram-positive pathogens, including methicillin-resistant S. aureus, daptomycin-resistant and vancomycin-resistant S. aureus strains, and difficult-to-treat vancomycin-resistant Enterococcus faecalis and E faecium (vancomycin-resistant enterococci). Escherichia coli was only marginally affected “compared with an outer membrane deficient E. coli WO153 strain, probably reflecting insufficient penetration of the compound,” the authors wrote.
Original mechanism of action
Clovibactin acts not on one but three molecules, all of which are essential to the construction of bacterial walls: C55PP, lipid II, and lipid IIIWTA, which are from different cell wall biosynthetic pathways. Clovibactin binds to the pyrophosphate portion of these precursors.
“Clovibactin wraps around the pyrophosphate like [a] tight glove, like a cage that encloses its target,” said Dr. Weingarth. This is what gives clovibactin its name, which is derived from Greek word klouvi, meaning cage.
The remarkable aspect of clovibactin’s mechanism is that it only binds to the immutable pyrophosphate that is common to cell wall precursors, but it also ignores the variable sugar-peptide part of the targets. The bacteria therefore have a much harder time developing resistance against it. “In fact, we did not observe any resistance to clovibactin in our studies,” Dr. Weingarth confirmed.
Upon binding the target molecules, it self-assembles into large fibrils on the surface of bacterial membranes. These fibrils are stable for a long time and thereby ensure that the target molecules remain sequestered for as long as necessary to kill bacteria.
Few side effects
Because of the mechanism of action of the antibiotic, few side effects are predicted. Indeed, clovibactin targets bacteria cells but not human cells.
“Since these fibrils only form on bacterial membranes and not on human membranes, they are presumably also the reason why clovibactin selectively damages bacterial cells but is not toxic to human cells,” said Dr. Weingarth.
Other studies – in particular, studies in humans – are needed before the antibiotic can be considered a potential treatment. In the meantime, regulations regarding the proper use of antibiotics must continue to be applied to limit antibiotic resistance.
In 2019, 4.95 million deaths worldwide were associated with bacterial antimicrobial resistance, including 1.27 million deaths directly attributable to bacterial antimicrobial resistance. If this trend continues without new medicines becoming available to treat bacterial infections, it is estimated that by 2050, 10 million people will die every year from antimicrobial drug resistance.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
Antibiotic resistance is a major public health problem. Few new molecules are in development, but a new antibiotic called clovibactin brings hope.
The drug was discovered and has been studied by scientists from Utrecht University in the Netherlands, the University of Bonn in Germany, the German Center for Infection Research, Northeastern University in Boston, and NovoBiotic Pharmaceuticals in Cambridge, Mass.
Their research was published in Cell.
“Since clovibactin was isolated from bacteria that could not be grown before, pathogenic bacteria have not seen such an antibiotic before and had no time to develop resistance,” Markus Weingarth, MD, PhD, a researcher in Utrecht University’s chemistry department, said in a press release.
Microbial “dark matter”
Researchers isolated clovibactin from sandy soil from North Carolina and studied it using the iChip device, which was developed in 2015. This technique allowed them to grow “bacterial dark matter,” so-called unculturable bacteria, which compose a group to which 99% of bacteria belong.
This device also paved the way for the discovery of the antibiotic teixobactin in 2020. Teixobactin is effective against gram-positive bacteria and is one of the first truly new antibiotics in decades. Its mechanism of action is like that of clovibactin.
Combats resistant bacteria
In the Cell article, the researchers showed that clovibactin acts via several mechanisms and that it successfully treated mice infected with the superbug Staphylococcus aureus.
Clovibactin exhibited antibacterial activity against a broad range of gram-positive pathogens, including methicillin-resistant S. aureus, daptomycin-resistant and vancomycin-resistant S. aureus strains, and difficult-to-treat vancomycin-resistant Enterococcus faecalis and E faecium (vancomycin-resistant enterococci). Escherichia coli was only marginally affected “compared with an outer membrane deficient E. coli WO153 strain, probably reflecting insufficient penetration of the compound,” the authors wrote.
Original mechanism of action
Clovibactin acts not on one but three molecules, all of which are essential to the construction of bacterial walls: C55PP, lipid II, and lipid IIIWTA, which are from different cell wall biosynthetic pathways. Clovibactin binds to the pyrophosphate portion of these precursors.
“Clovibactin wraps around the pyrophosphate like [a] tight glove, like a cage that encloses its target,” said Dr. Weingarth. This is what gives clovibactin its name, which is derived from Greek word klouvi, meaning cage.
The remarkable aspect of clovibactin’s mechanism is that it only binds to the immutable pyrophosphate that is common to cell wall precursors, but it also ignores the variable sugar-peptide part of the targets. The bacteria therefore have a much harder time developing resistance against it. “In fact, we did not observe any resistance to clovibactin in our studies,” Dr. Weingarth confirmed.
Upon binding the target molecules, it self-assembles into large fibrils on the surface of bacterial membranes. These fibrils are stable for a long time and thereby ensure that the target molecules remain sequestered for as long as necessary to kill bacteria.
Few side effects
Because of the mechanism of action of the antibiotic, few side effects are predicted. Indeed, clovibactin targets bacteria cells but not human cells.
“Since these fibrils only form on bacterial membranes and not on human membranes, they are presumably also the reason why clovibactin selectively damages bacterial cells but is not toxic to human cells,” said Dr. Weingarth.
Other studies – in particular, studies in humans – are needed before the antibiotic can be considered a potential treatment. In the meantime, regulations regarding the proper use of antibiotics must continue to be applied to limit antibiotic resistance.
In 2019, 4.95 million deaths worldwide were associated with bacterial antimicrobial resistance, including 1.27 million deaths directly attributable to bacterial antimicrobial resistance. If this trend continues without new medicines becoming available to treat bacterial infections, it is estimated that by 2050, 10 million people will die every year from antimicrobial drug resistance.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
Antibiotic resistance is a major public health problem. Few new molecules are in development, but a new antibiotic called clovibactin brings hope.
The drug was discovered and has been studied by scientists from Utrecht University in the Netherlands, the University of Bonn in Germany, the German Center for Infection Research, Northeastern University in Boston, and NovoBiotic Pharmaceuticals in Cambridge, Mass.
Their research was published in Cell.
“Since clovibactin was isolated from bacteria that could not be grown before, pathogenic bacteria have not seen such an antibiotic before and had no time to develop resistance,” Markus Weingarth, MD, PhD, a researcher in Utrecht University’s chemistry department, said in a press release.
Microbial “dark matter”
Researchers isolated clovibactin from sandy soil from North Carolina and studied it using the iChip device, which was developed in 2015. This technique allowed them to grow “bacterial dark matter,” so-called unculturable bacteria, which compose a group to which 99% of bacteria belong.
This device also paved the way for the discovery of the antibiotic teixobactin in 2020. Teixobactin is effective against gram-positive bacteria and is one of the first truly new antibiotics in decades. Its mechanism of action is like that of clovibactin.
Combats resistant bacteria
In the Cell article, the researchers showed that clovibactin acts via several mechanisms and that it successfully treated mice infected with the superbug Staphylococcus aureus.
Clovibactin exhibited antibacterial activity against a broad range of gram-positive pathogens, including methicillin-resistant S. aureus, daptomycin-resistant and vancomycin-resistant S. aureus strains, and difficult-to-treat vancomycin-resistant Enterococcus faecalis and E faecium (vancomycin-resistant enterococci). Escherichia coli was only marginally affected “compared with an outer membrane deficient E. coli WO153 strain, probably reflecting insufficient penetration of the compound,” the authors wrote.
Original mechanism of action
Clovibactin acts not on one but three molecules, all of which are essential to the construction of bacterial walls: C55PP, lipid II, and lipid IIIWTA, which are from different cell wall biosynthetic pathways. Clovibactin binds to the pyrophosphate portion of these precursors.
“Clovibactin wraps around the pyrophosphate like [a] tight glove, like a cage that encloses its target,” said Dr. Weingarth. This is what gives clovibactin its name, which is derived from Greek word klouvi, meaning cage.
The remarkable aspect of clovibactin’s mechanism is that it only binds to the immutable pyrophosphate that is common to cell wall precursors, but it also ignores the variable sugar-peptide part of the targets. The bacteria therefore have a much harder time developing resistance against it. “In fact, we did not observe any resistance to clovibactin in our studies,” Dr. Weingarth confirmed.
Upon binding the target molecules, it self-assembles into large fibrils on the surface of bacterial membranes. These fibrils are stable for a long time and thereby ensure that the target molecules remain sequestered for as long as necessary to kill bacteria.
Few side effects
Because of the mechanism of action of the antibiotic, few side effects are predicted. Indeed, clovibactin targets bacteria cells but not human cells.
“Since these fibrils only form on bacterial membranes and not on human membranes, they are presumably also the reason why clovibactin selectively damages bacterial cells but is not toxic to human cells,” said Dr. Weingarth.
Other studies – in particular, studies in humans – are needed before the antibiotic can be considered a potential treatment. In the meantime, regulations regarding the proper use of antibiotics must continue to be applied to limit antibiotic resistance.
In 2019, 4.95 million deaths worldwide were associated with bacterial antimicrobial resistance, including 1.27 million deaths directly attributable to bacterial antimicrobial resistance. If this trend continues without new medicines becoming available to treat bacterial infections, it is estimated that by 2050, 10 million people will die every year from antimicrobial drug resistance.
This article was translated from the Medscape French Edition. A version appeared on Medscape.com.
FROM CELL
How to optimize in-hospital antimicrobial prescribing?
Variability in antimicrobial prescribing among hospital-based physicians is not associated with patient characteristics or clinical outcomes, data suggest. The lowest level of such prescribing within each hospital could be considered a target for antimicrobial stewardship, according to the researchers.
In a multicenter study of 124 physicians responsible for more than 124,000 hospitalized patients, the difference in mean prescribing between the highest and lowest quartiles of prescription volume was 15.8 days of treatment per 100 patient-days.
Baseline patient characteristics were similar across the quartiles, and there were no differences in patient outcomes, including in-hospital deaths, hospital length of stay, intensive care unit transfer, and hospital readmission.
Although the investigators expected variation in prescribing, “what surprised us most was the limited association with any differences in clinical outcomes, particularly when it came to the amount of antimicrobials used,” study author Mark T. McIntyre, PharmD, pharmacotherapy specialist at the Sinai Health System in Toronto, told this news organization.
“Importantly, this is not a study that defines quality of care,” he said. “We looked at natural variation in practice and association with outcomes. So, I don’t want clinicians to think, ‘Well, I’m high, therefore I’m bad,’ or, ‘I’m low, therefore I’m good.’
“This is an early explanatory analysis that asks whether this is an opportunity to optimize prescribing in ways we hadn’t thought of before,” he said. “Now that we don’t have an association with higher or lower prescribing and outcomes, we can look at what else is driving that antimicrobial prescribing and what we can do about it. Comfort level, risk tolerance, and social, cultural, and contextual factors all likely play a role.”
The study was published online in the Canadian Medical Association Journal.
Antimicrobial reductions possible
The investigators conducted a retrospective cohort study using the General Medicine Inpatient Initiative database to assess physician-level volume and spectrum of antimicrobial prescribing in adult general medical wards. Four academic hospitals in Toronto were evaluated for the period 2010 to 2019.
The investigators stratified physicians into quartiles by hospital site on the basis of volume of antimicrobial prescribing (specifically, days of therapy per 100 patient-days and antimicrobial-free days) and antibacterial spectrum (modified spectrum score, which assigns a value to each antibacterial agent on the basis of its breadth of coverage).
They also examined potential differences between physician quartiles in patient characteristics, such as age, sex, the Laboratory-Based Acute Physiology Score, discharge diagnosis, and the Charlson Comorbidity Index.
Multilevel modeling allowed the investigators to evaluate the association between clinical outcomes and antimicrobial volume and spectrum.
The primary measure was days of therapy per 100 patient-days.
As noted, the cohort included 124 physicians who were responsible for 124,158 hospital admissions. The median physician-level volume of antimicrobial prescribing was 56.1 days of therapy per 100 patient-days. Patient characteristics were balanced across the quartiles of physician prescribing.
The difference in mean prescribing between physician quartile 4 and quartile 1 was 15.8 days of therapy per 100 patient-days, meaning the median physician in quartile 4 prescribed antimicrobials at a volume that was 30% higher than that of the median physician in quartile 1.
No significant differences were noted for any clinical outcome with regard to quartile of days of therapy, antimicrobial-free days, or modified spectrum score after adjustment for patient-level characteristics.
In addition, no significant differences in the case mix between quartile 4 and quartile 1 were found when the cohort was restricted to patients admitted and discharged by the same most responsible person, nor were differences found in an analysis that was restricted to those without a discharge diagnosis code of palliative care.
In-hospital mortality was higher among patients cared for by prescribers with higher modified spectrum scores (odds ratio, 1.13). “We still can’t fully explain this finding,” Dr. McIntyre acknowledged. “We only saw that in our primary analysis. When we did several sensitivity analyses, that finding didn’t appear.”
The authors concluded, “Ultimately, without discernible benefit in outcomes of patients of physicians who prescribe more frequently, less antimicrobial exposure may be possible, leading to lower risk of antimicrobial resistance.”
Decision-making support
Commenting on the study, Lawrence I. Kaplan, MD, section chief of general internal medicine and associate dean for interprofessional education at the Lewis Katz School of Medicine at Temple University in Philadelphia, said, “Trying to get to the lowest quartile would be a goal, and given that physician characteristics are involved, I think there needs to be much better training in clinical management decision-making: how you come about making a decision based on a diagnosis for a particular patient, in or out of the hospital.” Dr. Kaplan was not involved in the research.
“Clinical decision-making tools that can be plugged into the electronic health record can help,” he suggested. “The tools basically ask if a patient meets certain criteria and then might give a prompt that says, for example, ‘These symptoms are not consistent with bacterial sinusitis. The patient should be treated with decongestants, nasal steroids, et cetera, because antibiotics aren’t appropriate.’
“It’s a bit like checkbox medicine, which a lot of physicians bridle at,” he said. “But if it’s really based on evidence, I think that’s an appropriate use of evidence-based medicine.”
Dr. Kaplan said that more research is needed into the best way to get a physician or any provider to step back and say, “Is this the right decision?” or, “I’m doing this but I’m really on shaky ground. What am I missing?’” He noted that the Society for Medical Decision Making publishes research and resources in this area.
“I love the fact that the paper was authored by an interdisciplinary group,” Dr. Kaplan added. “A pharmacist embedded in the team can, for example, help with treatment decision-making and point out potential drug interactions that prescribers might not be aware of.
“We need to stop practicing medicine siloed, which is what we do a lot of ways, both in the hospital and out of the hospital, because it’s the path of least resistance,” Dr. Kaplan added. “But when we can say, ‘Hey, I have a question about this,’ be it to a computer or a colleague, I would argue that we come up with better care.”
No funding was provided for the study. Dr. McIntyre and Dr. Kaplan have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Variability in antimicrobial prescribing among hospital-based physicians is not associated with patient characteristics or clinical outcomes, data suggest. The lowest level of such prescribing within each hospital could be considered a target for antimicrobial stewardship, according to the researchers.
In a multicenter study of 124 physicians responsible for more than 124,000 hospitalized patients, the difference in mean prescribing between the highest and lowest quartiles of prescription volume was 15.8 days of treatment per 100 patient-days.
Baseline patient characteristics were similar across the quartiles, and there were no differences in patient outcomes, including in-hospital deaths, hospital length of stay, intensive care unit transfer, and hospital readmission.
Although the investigators expected variation in prescribing, “what surprised us most was the limited association with any differences in clinical outcomes, particularly when it came to the amount of antimicrobials used,” study author Mark T. McIntyre, PharmD, pharmacotherapy specialist at the Sinai Health System in Toronto, told this news organization.
“Importantly, this is not a study that defines quality of care,” he said. “We looked at natural variation in practice and association with outcomes. So, I don’t want clinicians to think, ‘Well, I’m high, therefore I’m bad,’ or, ‘I’m low, therefore I’m good.’
“This is an early explanatory analysis that asks whether this is an opportunity to optimize prescribing in ways we hadn’t thought of before,” he said. “Now that we don’t have an association with higher or lower prescribing and outcomes, we can look at what else is driving that antimicrobial prescribing and what we can do about it. Comfort level, risk tolerance, and social, cultural, and contextual factors all likely play a role.”
The study was published online in the Canadian Medical Association Journal.
Antimicrobial reductions possible
The investigators conducted a retrospective cohort study using the General Medicine Inpatient Initiative database to assess physician-level volume and spectrum of antimicrobial prescribing in adult general medical wards. Four academic hospitals in Toronto were evaluated for the period 2010 to 2019.
The investigators stratified physicians into quartiles by hospital site on the basis of volume of antimicrobial prescribing (specifically, days of therapy per 100 patient-days and antimicrobial-free days) and antibacterial spectrum (modified spectrum score, which assigns a value to each antibacterial agent on the basis of its breadth of coverage).
They also examined potential differences between physician quartiles in patient characteristics, such as age, sex, the Laboratory-Based Acute Physiology Score, discharge diagnosis, and the Charlson Comorbidity Index.
Multilevel modeling allowed the investigators to evaluate the association between clinical outcomes and antimicrobial volume and spectrum.
The primary measure was days of therapy per 100 patient-days.
As noted, the cohort included 124 physicians who were responsible for 124,158 hospital admissions. The median physician-level volume of antimicrobial prescribing was 56.1 days of therapy per 100 patient-days. Patient characteristics were balanced across the quartiles of physician prescribing.
The difference in mean prescribing between physician quartile 4 and quartile 1 was 15.8 days of therapy per 100 patient-days, meaning the median physician in quartile 4 prescribed antimicrobials at a volume that was 30% higher than that of the median physician in quartile 1.
No significant differences were noted for any clinical outcome with regard to quartile of days of therapy, antimicrobial-free days, or modified spectrum score after adjustment for patient-level characteristics.
In addition, no significant differences in the case mix between quartile 4 and quartile 1 were found when the cohort was restricted to patients admitted and discharged by the same most responsible person, nor were differences found in an analysis that was restricted to those without a discharge diagnosis code of palliative care.
In-hospital mortality was higher among patients cared for by prescribers with higher modified spectrum scores (odds ratio, 1.13). “We still can’t fully explain this finding,” Dr. McIntyre acknowledged. “We only saw that in our primary analysis. When we did several sensitivity analyses, that finding didn’t appear.”
The authors concluded, “Ultimately, without discernible benefit in outcomes of patients of physicians who prescribe more frequently, less antimicrobial exposure may be possible, leading to lower risk of antimicrobial resistance.”
Decision-making support
Commenting on the study, Lawrence I. Kaplan, MD, section chief of general internal medicine and associate dean for interprofessional education at the Lewis Katz School of Medicine at Temple University in Philadelphia, said, “Trying to get to the lowest quartile would be a goal, and given that physician characteristics are involved, I think there needs to be much better training in clinical management decision-making: how you come about making a decision based on a diagnosis for a particular patient, in or out of the hospital.” Dr. Kaplan was not involved in the research.
“Clinical decision-making tools that can be plugged into the electronic health record can help,” he suggested. “The tools basically ask if a patient meets certain criteria and then might give a prompt that says, for example, ‘These symptoms are not consistent with bacterial sinusitis. The patient should be treated with decongestants, nasal steroids, et cetera, because antibiotics aren’t appropriate.’
“It’s a bit like checkbox medicine, which a lot of physicians bridle at,” he said. “But if it’s really based on evidence, I think that’s an appropriate use of evidence-based medicine.”
Dr. Kaplan said that more research is needed into the best way to get a physician or any provider to step back and say, “Is this the right decision?” or, “I’m doing this but I’m really on shaky ground. What am I missing?’” He noted that the Society for Medical Decision Making publishes research and resources in this area.
“I love the fact that the paper was authored by an interdisciplinary group,” Dr. Kaplan added. “A pharmacist embedded in the team can, for example, help with treatment decision-making and point out potential drug interactions that prescribers might not be aware of.
“We need to stop practicing medicine siloed, which is what we do a lot of ways, both in the hospital and out of the hospital, because it’s the path of least resistance,” Dr. Kaplan added. “But when we can say, ‘Hey, I have a question about this,’ be it to a computer or a colleague, I would argue that we come up with better care.”
No funding was provided for the study. Dr. McIntyre and Dr. Kaplan have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Variability in antimicrobial prescribing among hospital-based physicians is not associated with patient characteristics or clinical outcomes, data suggest. The lowest level of such prescribing within each hospital could be considered a target for antimicrobial stewardship, according to the researchers.
In a multicenter study of 124 physicians responsible for more than 124,000 hospitalized patients, the difference in mean prescribing between the highest and lowest quartiles of prescription volume was 15.8 days of treatment per 100 patient-days.
Baseline patient characteristics were similar across the quartiles, and there were no differences in patient outcomes, including in-hospital deaths, hospital length of stay, intensive care unit transfer, and hospital readmission.
Although the investigators expected variation in prescribing, “what surprised us most was the limited association with any differences in clinical outcomes, particularly when it came to the amount of antimicrobials used,” study author Mark T. McIntyre, PharmD, pharmacotherapy specialist at the Sinai Health System in Toronto, told this news organization.
“Importantly, this is not a study that defines quality of care,” he said. “We looked at natural variation in practice and association with outcomes. So, I don’t want clinicians to think, ‘Well, I’m high, therefore I’m bad,’ or, ‘I’m low, therefore I’m good.’
“This is an early explanatory analysis that asks whether this is an opportunity to optimize prescribing in ways we hadn’t thought of before,” he said. “Now that we don’t have an association with higher or lower prescribing and outcomes, we can look at what else is driving that antimicrobial prescribing and what we can do about it. Comfort level, risk tolerance, and social, cultural, and contextual factors all likely play a role.”
The study was published online in the Canadian Medical Association Journal.
Antimicrobial reductions possible
The investigators conducted a retrospective cohort study using the General Medicine Inpatient Initiative database to assess physician-level volume and spectrum of antimicrobial prescribing in adult general medical wards. Four academic hospitals in Toronto were evaluated for the period 2010 to 2019.
The investigators stratified physicians into quartiles by hospital site on the basis of volume of antimicrobial prescribing (specifically, days of therapy per 100 patient-days and antimicrobial-free days) and antibacterial spectrum (modified spectrum score, which assigns a value to each antibacterial agent on the basis of its breadth of coverage).
They also examined potential differences between physician quartiles in patient characteristics, such as age, sex, the Laboratory-Based Acute Physiology Score, discharge diagnosis, and the Charlson Comorbidity Index.
Multilevel modeling allowed the investigators to evaluate the association between clinical outcomes and antimicrobial volume and spectrum.
The primary measure was days of therapy per 100 patient-days.
As noted, the cohort included 124 physicians who were responsible for 124,158 hospital admissions. The median physician-level volume of antimicrobial prescribing was 56.1 days of therapy per 100 patient-days. Patient characteristics were balanced across the quartiles of physician prescribing.
The difference in mean prescribing between physician quartile 4 and quartile 1 was 15.8 days of therapy per 100 patient-days, meaning the median physician in quartile 4 prescribed antimicrobials at a volume that was 30% higher than that of the median physician in quartile 1.
No significant differences were noted for any clinical outcome with regard to quartile of days of therapy, antimicrobial-free days, or modified spectrum score after adjustment for patient-level characteristics.
In addition, no significant differences in the case mix between quartile 4 and quartile 1 were found when the cohort was restricted to patients admitted and discharged by the same most responsible person, nor were differences found in an analysis that was restricted to those without a discharge diagnosis code of palliative care.
In-hospital mortality was higher among patients cared for by prescribers with higher modified spectrum scores (odds ratio, 1.13). “We still can’t fully explain this finding,” Dr. McIntyre acknowledged. “We only saw that in our primary analysis. When we did several sensitivity analyses, that finding didn’t appear.”
The authors concluded, “Ultimately, without discernible benefit in outcomes of patients of physicians who prescribe more frequently, less antimicrobial exposure may be possible, leading to lower risk of antimicrobial resistance.”
Decision-making support
Commenting on the study, Lawrence I. Kaplan, MD, section chief of general internal medicine and associate dean for interprofessional education at the Lewis Katz School of Medicine at Temple University in Philadelphia, said, “Trying to get to the lowest quartile would be a goal, and given that physician characteristics are involved, I think there needs to be much better training in clinical management decision-making: how you come about making a decision based on a diagnosis for a particular patient, in or out of the hospital.” Dr. Kaplan was not involved in the research.
“Clinical decision-making tools that can be plugged into the electronic health record can help,” he suggested. “The tools basically ask if a patient meets certain criteria and then might give a prompt that says, for example, ‘These symptoms are not consistent with bacterial sinusitis. The patient should be treated with decongestants, nasal steroids, et cetera, because antibiotics aren’t appropriate.’
“It’s a bit like checkbox medicine, which a lot of physicians bridle at,” he said. “But if it’s really based on evidence, I think that’s an appropriate use of evidence-based medicine.”
Dr. Kaplan said that more research is needed into the best way to get a physician or any provider to step back and say, “Is this the right decision?” or, “I’m doing this but I’m really on shaky ground. What am I missing?’” He noted that the Society for Medical Decision Making publishes research and resources in this area.
“I love the fact that the paper was authored by an interdisciplinary group,” Dr. Kaplan added. “A pharmacist embedded in the team can, for example, help with treatment decision-making and point out potential drug interactions that prescribers might not be aware of.
“We need to stop practicing medicine siloed, which is what we do a lot of ways, both in the hospital and out of the hospital, because it’s the path of least resistance,” Dr. Kaplan added. “But when we can say, ‘Hey, I have a question about this,’ be it to a computer or a colleague, I would argue that we come up with better care.”
No funding was provided for the study. Dr. McIntyre and Dr. Kaplan have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
New and emerging options for treating recurrent C. difficile
This transcript has been edited for clarity.
Clostridioides difficile is a toxin-based infection that takes up residence in the colon due to disturbed normal bowel flora, usually after antibiotics.
Recurrent C. difficile can happen in up to a quarter of patients who receive oral vancomycin as a treatment for their infection. It can also occur with treatment with the newer agent, fidaxomicin, although possibly in fewer patients. In general, relapses are indeed common.
When I trained at Johns Hopkins under John Bartlett, he took the approach that after the second – and always after the third – relapse, an extended course of oral therapy with vancomycin could help get patients out of trouble. He used the so-called extended pulse method, where patients would take the drug for approximately 4-6 weeks and gradually reduce the dose.
This approach can also be done with fidaxomicin. However, I’m not sure it works much better than vancomycin, and there are often hurdles to using fidaxomicin because of insurers not approving it because of the expense.
What other therapies are there?
There is bezlotoxumab, which is a human monoclonal antibody targeting C. difficile toxin B. I’ve used it a few times. It is given as a one-time infusion, and there are challenges regarding cost, the logistics of setting up the infusion, and insurance approval.
Fecal microbiota transplant
In recent years, fecal microbiota transplants (FMT) have received a lot of attention as a different avenue of treatment that could lower the potential for relapses, with success rates usually around 80%-90%. However, in the past few years, there have been some serious safety signals because of possible transmission of dangerous pathogens, often with drug resistance, with FMT.
I’m therefore pleased to say that newer fecal microbiota products are coming in fast and furious. I thought I’d spend a few minutes speaking about these.
OpenBiome, an organization dedicated to microbiome research, offers an investigational product from screened donors that has not received Food and Drug Administration approval. It’s been around for some time. It can be used in either upper or lower GI applications, and the organization cites about an 84% success rate using this product.
There are also two new FDA-approved products I think are worth knowing about. They’ve just been approved recently and we’re a little uncertain of where they’re going to end up in the treatment landscape.
The first is from Ferring, and it goes by fecal microbiota, live-jslm (Rebyota). This is a product from qualified and screened donors, the main component of which is Bacteroides, which is given as a single dose by enema.
The company did a phase 3 trial with a Bayesian primary analysis, which I think convinced the FDA to approve this product. The success rate in people with multiple relapses was 70.6%, compared with 57.5% with placebo. The estimated treatment effect was 13.1%. Of those who did respond, over 90% were kept free of relapse over a 6-month period.
The other product, also FDA approved, is from Seres. It was previously called SER-109, and is now called fecal microbiota spores, live-brpk (Vowst). Unlike the previous product, this is orally administered, with patients taking four capsules daily for 3 days. Again, these donor-derived firmicutes have been appropriately screened and are free of potential pathogens.
The phase 3 randomized clinical trial results were published in the New England Journal of Medicine. They showed that 12% of those taking this product had a relapse, compared with 40% of those taking placebo, which is about the range we tend to see in people who have had multiple relapses. The safety profile was similar to placebo.
So, how will people use these treatments?
I think the FDA imprimatur will be attractive to people, but the products, I believe, will be priced fairly expensively, in the under $10,000 range. The first (Rebyota) is a rectal infusion; it is a one-and-done treatment but creates logistical issues. Interestingly, it could be a billable procedure for infectious disease clinicians. The ease of oral administration for Vowst, no doubt, will be very appealing. Both of these are given after completing a course of treatment with vancomycin or fidaxomicin so as not to interfere with the microbiome product.
I’ll also briefly mention a paper published in JAMA on yet another microbiome product, called VE303. This product was based on eight commensal strains of Clostridia and was given orally in a phase 2 trial. Interestingly, this worked about the same as the oral product that is already FDA approved. The study showed a recurrence rate of 13.8% in the high-dose group, compared with 45.5% in the placebo group.
I think this is exciting. And, of course, there is the expense.
But anything that can be done to help improve these patients is welcome, as once they get into the multiple-relapse phase, it is challenging to turn around. These commercialized products will hopefully become a bit more mainstream. Certainly, we’ll see how these will be utilized in the coming months and over the next few years.
Dr. Auwaerter is Clinical Director, Division of Infectious Diseases, Johns Hopkins University, Baltimore. He reported conflicts of interest with Gilead, Shionogi, and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Clostridioides difficile is a toxin-based infection that takes up residence in the colon due to disturbed normal bowel flora, usually after antibiotics.
Recurrent C. difficile can happen in up to a quarter of patients who receive oral vancomycin as a treatment for their infection. It can also occur with treatment with the newer agent, fidaxomicin, although possibly in fewer patients. In general, relapses are indeed common.
When I trained at Johns Hopkins under John Bartlett, he took the approach that after the second – and always after the third – relapse, an extended course of oral therapy with vancomycin could help get patients out of trouble. He used the so-called extended pulse method, where patients would take the drug for approximately 4-6 weeks and gradually reduce the dose.
This approach can also be done with fidaxomicin. However, I’m not sure it works much better than vancomycin, and there are often hurdles to using fidaxomicin because of insurers not approving it because of the expense.
What other therapies are there?
There is bezlotoxumab, which is a human monoclonal antibody targeting C. difficile toxin B. I’ve used it a few times. It is given as a one-time infusion, and there are challenges regarding cost, the logistics of setting up the infusion, and insurance approval.
Fecal microbiota transplant
In recent years, fecal microbiota transplants (FMT) have received a lot of attention as a different avenue of treatment that could lower the potential for relapses, with success rates usually around 80%-90%. However, in the past few years, there have been some serious safety signals because of possible transmission of dangerous pathogens, often with drug resistance, with FMT.
I’m therefore pleased to say that newer fecal microbiota products are coming in fast and furious. I thought I’d spend a few minutes speaking about these.
OpenBiome, an organization dedicated to microbiome research, offers an investigational product from screened donors that has not received Food and Drug Administration approval. It’s been around for some time. It can be used in either upper or lower GI applications, and the organization cites about an 84% success rate using this product.
There are also two new FDA-approved products I think are worth knowing about. They’ve just been approved recently and we’re a little uncertain of where they’re going to end up in the treatment landscape.
The first is from Ferring, and it goes by fecal microbiota, live-jslm (Rebyota). This is a product from qualified and screened donors, the main component of which is Bacteroides, which is given as a single dose by enema.
The company did a phase 3 trial with a Bayesian primary analysis, which I think convinced the FDA to approve this product. The success rate in people with multiple relapses was 70.6%, compared with 57.5% with placebo. The estimated treatment effect was 13.1%. Of those who did respond, over 90% were kept free of relapse over a 6-month period.
The other product, also FDA approved, is from Seres. It was previously called SER-109, and is now called fecal microbiota spores, live-brpk (Vowst). Unlike the previous product, this is orally administered, with patients taking four capsules daily for 3 days. Again, these donor-derived firmicutes have been appropriately screened and are free of potential pathogens.
The phase 3 randomized clinical trial results were published in the New England Journal of Medicine. They showed that 12% of those taking this product had a relapse, compared with 40% of those taking placebo, which is about the range we tend to see in people who have had multiple relapses. The safety profile was similar to placebo.
So, how will people use these treatments?
I think the FDA imprimatur will be attractive to people, but the products, I believe, will be priced fairly expensively, in the under $10,000 range. The first (Rebyota) is a rectal infusion; it is a one-and-done treatment but creates logistical issues. Interestingly, it could be a billable procedure for infectious disease clinicians. The ease of oral administration for Vowst, no doubt, will be very appealing. Both of these are given after completing a course of treatment with vancomycin or fidaxomicin so as not to interfere with the microbiome product.
I’ll also briefly mention a paper published in JAMA on yet another microbiome product, called VE303. This product was based on eight commensal strains of Clostridia and was given orally in a phase 2 trial. Interestingly, this worked about the same as the oral product that is already FDA approved. The study showed a recurrence rate of 13.8% in the high-dose group, compared with 45.5% in the placebo group.
I think this is exciting. And, of course, there is the expense.
But anything that can be done to help improve these patients is welcome, as once they get into the multiple-relapse phase, it is challenging to turn around. These commercialized products will hopefully become a bit more mainstream. Certainly, we’ll see how these will be utilized in the coming months and over the next few years.
Dr. Auwaerter is Clinical Director, Division of Infectious Diseases, Johns Hopkins University, Baltimore. He reported conflicts of interest with Gilead, Shionogi, and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Clostridioides difficile is a toxin-based infection that takes up residence in the colon due to disturbed normal bowel flora, usually after antibiotics.
Recurrent C. difficile can happen in up to a quarter of patients who receive oral vancomycin as a treatment for their infection. It can also occur with treatment with the newer agent, fidaxomicin, although possibly in fewer patients. In general, relapses are indeed common.
When I trained at Johns Hopkins under John Bartlett, he took the approach that after the second – and always after the third – relapse, an extended course of oral therapy with vancomycin could help get patients out of trouble. He used the so-called extended pulse method, where patients would take the drug for approximately 4-6 weeks and gradually reduce the dose.
This approach can also be done with fidaxomicin. However, I’m not sure it works much better than vancomycin, and there are often hurdles to using fidaxomicin because of insurers not approving it because of the expense.
What other therapies are there?
There is bezlotoxumab, which is a human monoclonal antibody targeting C. difficile toxin B. I’ve used it a few times. It is given as a one-time infusion, and there are challenges regarding cost, the logistics of setting up the infusion, and insurance approval.
Fecal microbiota transplant
In recent years, fecal microbiota transplants (FMT) have received a lot of attention as a different avenue of treatment that could lower the potential for relapses, with success rates usually around 80%-90%. However, in the past few years, there have been some serious safety signals because of possible transmission of dangerous pathogens, often with drug resistance, with FMT.
I’m therefore pleased to say that newer fecal microbiota products are coming in fast and furious. I thought I’d spend a few minutes speaking about these.
OpenBiome, an organization dedicated to microbiome research, offers an investigational product from screened donors that has not received Food and Drug Administration approval. It’s been around for some time. It can be used in either upper or lower GI applications, and the organization cites about an 84% success rate using this product.
There are also two new FDA-approved products I think are worth knowing about. They’ve just been approved recently and we’re a little uncertain of where they’re going to end up in the treatment landscape.
The first is from Ferring, and it goes by fecal microbiota, live-jslm (Rebyota). This is a product from qualified and screened donors, the main component of which is Bacteroides, which is given as a single dose by enema.
The company did a phase 3 trial with a Bayesian primary analysis, which I think convinced the FDA to approve this product. The success rate in people with multiple relapses was 70.6%, compared with 57.5% with placebo. The estimated treatment effect was 13.1%. Of those who did respond, over 90% were kept free of relapse over a 6-month period.
The other product, also FDA approved, is from Seres. It was previously called SER-109, and is now called fecal microbiota spores, live-brpk (Vowst). Unlike the previous product, this is orally administered, with patients taking four capsules daily for 3 days. Again, these donor-derived firmicutes have been appropriately screened and are free of potential pathogens.
The phase 3 randomized clinical trial results were published in the New England Journal of Medicine. They showed that 12% of those taking this product had a relapse, compared with 40% of those taking placebo, which is about the range we tend to see in people who have had multiple relapses. The safety profile was similar to placebo.
So, how will people use these treatments?
I think the FDA imprimatur will be attractive to people, but the products, I believe, will be priced fairly expensively, in the under $10,000 range. The first (Rebyota) is a rectal infusion; it is a one-and-done treatment but creates logistical issues. Interestingly, it could be a billable procedure for infectious disease clinicians. The ease of oral administration for Vowst, no doubt, will be very appealing. Both of these are given after completing a course of treatment with vancomycin or fidaxomicin so as not to interfere with the microbiome product.
I’ll also briefly mention a paper published in JAMA on yet another microbiome product, called VE303. This product was based on eight commensal strains of Clostridia and was given orally in a phase 2 trial. Interestingly, this worked about the same as the oral product that is already FDA approved. The study showed a recurrence rate of 13.8% in the high-dose group, compared with 45.5% in the placebo group.
I think this is exciting. And, of course, there is the expense.
But anything that can be done to help improve these patients is welcome, as once they get into the multiple-relapse phase, it is challenging to turn around. These commercialized products will hopefully become a bit more mainstream. Certainly, we’ll see how these will be utilized in the coming months and over the next few years.
Dr. Auwaerter is Clinical Director, Division of Infectious Diseases, Johns Hopkins University, Baltimore. He reported conflicts of interest with Gilead, Shionogi, and Medscape.
A version of this article first appeared on Medscape.com.
The antimicrobial peptide that even Pharma can love
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.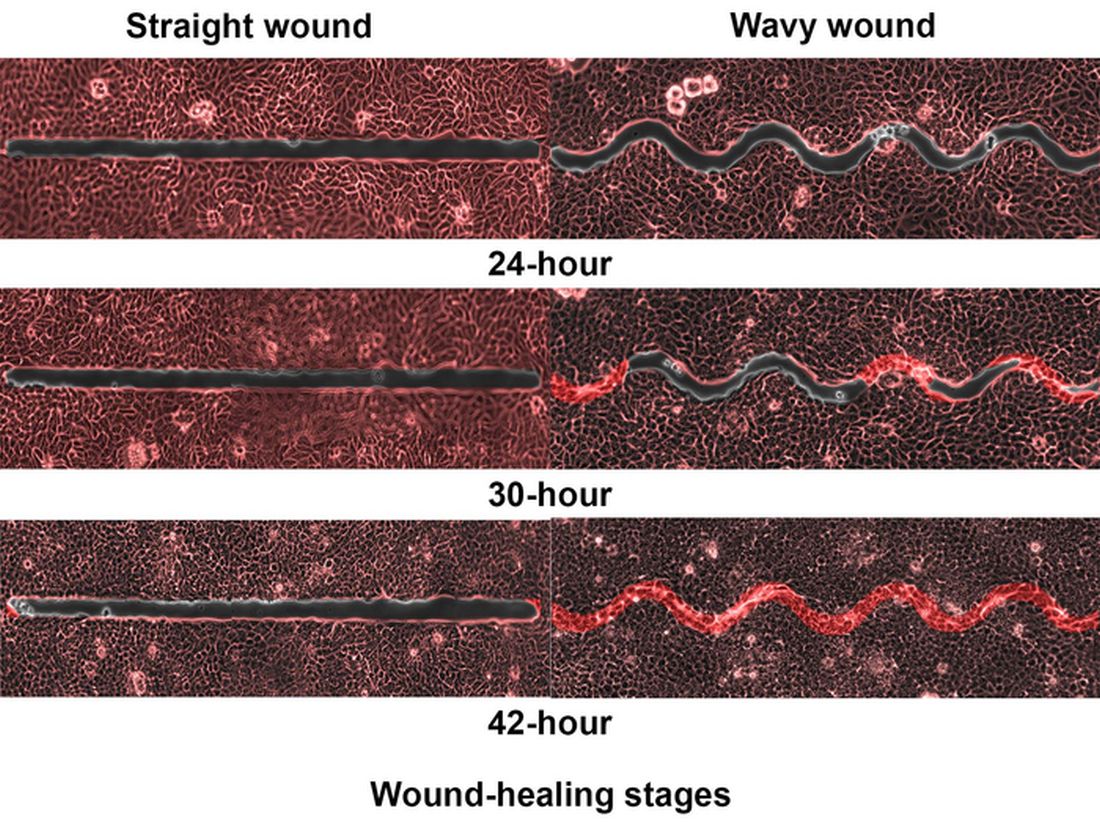
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
FMT in a pill: FDA approves second product to prevent C. diff recurrence
The recent approval of the first oral fecal-derived microbiota therapy to prevent the recurrence of Clostridioides difficile (C. diff) infection in patients was welcome news for physicians who’ve struggled under the weight of having too few treatment options for the prevention of C. diff recurrence.

The product, developed by Massachusetts-based Seres Therepeutics and marketed as Vowst, was approved by the U.S. Food and Drug Administration on April 26. It is approved for use in adults who have already been treated with antibiotics for a recurrent infection with C. diff bacteria.
and is designed to be delivered in four capsules taken daily for 3 days.
Gastroenterologist Phillip I. Tarr, MD, division chief of gastroenterology at Washington University, St. Louis, and chair of the American Gastroenterological Association Center for Gut Microbiome Research and Education, said that prevention of recurrent C. diff infection “remains challenging,” and that Vowst “provides the first FDA-approved, orally administered microbiome therapeutic with which to achieve this goal. This advance also makes us optimistic we might soon be able to prevent other disorders by managing gut microbial communities.”
Vowst is the second therapy derived from human stool to be approved for the indication in less than 6 months. In December, the FDA approved Rebyota (Ferring), a rectally delivered treatment that also uses microbes from donor feces. Both products were given priority review, orphan drug, and breakthrough therapy designations by the agency.
C. diff infection can be aggravated by an alteration of normal gut flora associated with antibiotics treatment, leading to cycles of repeated infections. Infection can produce diarrhea, abdominal pain, fever, and severe morbidity. In the United States, an estimated 15,000 to 30,000 deaths per year are linked to C. diff. Risk factors for recurrent infection include being 65 or older, hospitalization, being in a nursing home, a weakened immune system, and previous infection with C. diff.
Therapies transplanting fecal microbiota from donors have been used since the 1950s as treatments for recurrent C. diff infection, and in the past decade, as stool banks recruiting screened donors have made fecal microbiota transplants, or FMT, standard of care. However, only in recent years have fecal-derived therapies become subject to standardized safety and efficacy testing.
Both the current FDA-approved products, Rebyota and Vowst, were shown in randomized controlled trials to reduce recurrence of C. diff infection, compared with placebo. In a phase 3 clinical trial of Rebyota (n = 262) in antibiotic-treated patients, one rectally administered dose reduced recurrence of C. diff infection by 70.6% at 8 weeks, compared with 57.5% for placebo. A phase 3 study of Vowst (n = 281) showed recurrence in treated subjects to be 12.4% at 8 weeks, compared with nearly 40% of those receiving placebo (relative risk, 0.32; 95% confidence interval, 0.18-0.58; P less than .001).
Despite screening protocols that have become increasingly homogenized and rigorous, FMT is associated with the risk of introducing pathogens. Vowst is manufactured with purified bacterial spores derived from donor feces, not whole stool. Nonetheless, FDA noted in its statement that Vowst could still potentially introduce infectious agents or allergens.
Antibiotics are still first-line treatment
In an interview, Jessica Allegretti, MD, MPH, AGAF, medical director of the Crohn’s and Colitis Center at Brigham & Women’s Hospital, Boston, said that having two FDA-approved therapies with different means of administration “is great for the field and great for patients. These are both meant to be used after a course of antibiotics, so antibiotics are still the mainstay of treatment for C. diff and recurrent C. diff, but we now have more options to prevent recurrence.”
The convenience of an oral therapy that can be taken at home is “very attractive,” Dr. Allegretti added, noting that there will also be patients “who either don’t want to or can’t take capsules, for whom a rectal administration [in a health care setting] may be preferred.”
Dr. Allegretti, who has used FMT to treat recurrent C. difficile for more than a decade, said that she expected traditional FMT using screened donor stool to remain available even as the new products are adopted by clinicians. FMT centers like OpenBiome “will continue to provide access for patients who either don’t have the ability to get the FDA-approved products because of insurance coverage, or for financial reasons, or maybe neither of the new products is appropriate for them,” she said. “I do think there will always be a need for the traditional option. The more options that we have available the better.”
TD Cowen analyst Joseph Thome told Reuters that the drug could be priced close to $20,000 per course, expecting peak sales of $750 million in the U.S. in 2033.
Dr. Allegretti disclosed consulting work for Seres Therapeutics, Ferring, and other manufacturers. She is a member of OpenBiome’s clinical advisory board.
The recent approval of the first oral fecal-derived microbiota therapy to prevent the recurrence of Clostridioides difficile (C. diff) infection in patients was welcome news for physicians who’ve struggled under the weight of having too few treatment options for the prevention of C. diff recurrence.
The product, developed by Massachusetts-based Seres Therepeutics and marketed as Vowst, was approved by the U.S. Food and Drug Administration on April 26. It is approved for use in adults who have already been treated with antibiotics for a recurrent infection with C. diff bacteria.
and is designed to be delivered in four capsules taken daily for 3 days.
Gastroenterologist Phillip I. Tarr, MD, division chief of gastroenterology at Washington University, St. Louis, and chair of the American Gastroenterological Association Center for Gut Microbiome Research and Education, said that prevention of recurrent C. diff infection “remains challenging,” and that Vowst “provides the first FDA-approved, orally administered microbiome therapeutic with which to achieve this goal. This advance also makes us optimistic we might soon be able to prevent other disorders by managing gut microbial communities.”
Vowst is the second therapy derived from human stool to be approved for the indication in less than 6 months. In December, the FDA approved Rebyota (Ferring), a rectally delivered treatment that also uses microbes from donor feces. Both products were given priority review, orphan drug, and breakthrough therapy designations by the agency.
C. diff infection can be aggravated by an alteration of normal gut flora associated with antibiotics treatment, leading to cycles of repeated infections. Infection can produce diarrhea, abdominal pain, fever, and severe morbidity. In the United States, an estimated 15,000 to 30,000 deaths per year are linked to C. diff. Risk factors for recurrent infection include being 65 or older, hospitalization, being in a nursing home, a weakened immune system, and previous infection with C. diff.
Therapies transplanting fecal microbiota from donors have been used since the 1950s as treatments for recurrent C. diff infection, and in the past decade, as stool banks recruiting screened donors have made fecal microbiota transplants, or FMT, standard of care. However, only in recent years have fecal-derived therapies become subject to standardized safety and efficacy testing.
Both the current FDA-approved products, Rebyota and Vowst, were shown in randomized controlled trials to reduce recurrence of C. diff infection, compared with placebo. In a phase 3 clinical trial of Rebyota (n = 262) in antibiotic-treated patients, one rectally administered dose reduced recurrence of C. diff infection by 70.6% at 8 weeks, compared with 57.5% for placebo. A phase 3 study of Vowst (n = 281) showed recurrence in treated subjects to be 12.4% at 8 weeks, compared with nearly 40% of those receiving placebo (relative risk, 0.32; 95% confidence interval, 0.18-0.58; P less than .001).
Despite screening protocols that have become increasingly homogenized and rigorous, FMT is associated with the risk of introducing pathogens. Vowst is manufactured with purified bacterial spores derived from donor feces, not whole stool. Nonetheless, FDA noted in its statement that Vowst could still potentially introduce infectious agents or allergens.
Antibiotics are still first-line treatment
In an interview, Jessica Allegretti, MD, MPH, AGAF, medical director of the Crohn’s and Colitis Center at Brigham & Women’s Hospital, Boston, said that having two FDA-approved therapies with different means of administration “is great for the field and great for patients. These are both meant to be used after a course of antibiotics, so antibiotics are still the mainstay of treatment for C. diff and recurrent C. diff, but we now have more options to prevent recurrence.”
The convenience of an oral therapy that can be taken at home is “very attractive,” Dr. Allegretti added, noting that there will also be patients “who either don’t want to or can’t take capsules, for whom a rectal administration [in a health care setting] may be preferred.”
Dr. Allegretti, who has used FMT to treat recurrent C. difficile for more than a decade, said that she expected traditional FMT using screened donor stool to remain available even as the new products are adopted by clinicians. FMT centers like OpenBiome “will continue to provide access for patients who either don’t have the ability to get the FDA-approved products because of insurance coverage, or for financial reasons, or maybe neither of the new products is appropriate for them,” she said. “I do think there will always be a need for the traditional option. The more options that we have available the better.”
TD Cowen analyst Joseph Thome told Reuters that the drug could be priced close to $20,000 per course, expecting peak sales of $750 million in the U.S. in 2033.
Dr. Allegretti disclosed consulting work for Seres Therapeutics, Ferring, and other manufacturers. She is a member of OpenBiome’s clinical advisory board.
The recent approval of the first oral fecal-derived microbiota therapy to prevent the recurrence of Clostridioides difficile (C. diff) infection in patients was welcome news for physicians who’ve struggled under the weight of having too few treatment options for the prevention of C. diff recurrence.
The product, developed by Massachusetts-based Seres Therepeutics and marketed as Vowst, was approved by the U.S. Food and Drug Administration on April 26. It is approved for use in adults who have already been treated with antibiotics for a recurrent infection with C. diff bacteria.
and is designed to be delivered in four capsules taken daily for 3 days.
Gastroenterologist Phillip I. Tarr, MD, division chief of gastroenterology at Washington University, St. Louis, and chair of the American Gastroenterological Association Center for Gut Microbiome Research and Education, said that prevention of recurrent C. diff infection “remains challenging,” and that Vowst “provides the first FDA-approved, orally administered microbiome therapeutic with which to achieve this goal. This advance also makes us optimistic we might soon be able to prevent other disorders by managing gut microbial communities.”
Vowst is the second therapy derived from human stool to be approved for the indication in less than 6 months. In December, the FDA approved Rebyota (Ferring), a rectally delivered treatment that also uses microbes from donor feces. Both products were given priority review, orphan drug, and breakthrough therapy designations by the agency.
C. diff infection can be aggravated by an alteration of normal gut flora associated with antibiotics treatment, leading to cycles of repeated infections. Infection can produce diarrhea, abdominal pain, fever, and severe morbidity. In the United States, an estimated 15,000 to 30,000 deaths per year are linked to C. diff. Risk factors for recurrent infection include being 65 or older, hospitalization, being in a nursing home, a weakened immune system, and previous infection with C. diff.
Therapies transplanting fecal microbiota from donors have been used since the 1950s as treatments for recurrent C. diff infection, and in the past decade, as stool banks recruiting screened donors have made fecal microbiota transplants, or FMT, standard of care. However, only in recent years have fecal-derived therapies become subject to standardized safety and efficacy testing.
Both the current FDA-approved products, Rebyota and Vowst, were shown in randomized controlled trials to reduce recurrence of C. diff infection, compared with placebo. In a phase 3 clinical trial of Rebyota (n = 262) in antibiotic-treated patients, one rectally administered dose reduced recurrence of C. diff infection by 70.6% at 8 weeks, compared with 57.5% for placebo. A phase 3 study of Vowst (n = 281) showed recurrence in treated subjects to be 12.4% at 8 weeks, compared with nearly 40% of those receiving placebo (relative risk, 0.32; 95% confidence interval, 0.18-0.58; P less than .001).
Despite screening protocols that have become increasingly homogenized and rigorous, FMT is associated with the risk of introducing pathogens. Vowst is manufactured with purified bacterial spores derived from donor feces, not whole stool. Nonetheless, FDA noted in its statement that Vowst could still potentially introduce infectious agents or allergens.
Antibiotics are still first-line treatment
In an interview, Jessica Allegretti, MD, MPH, AGAF, medical director of the Crohn’s and Colitis Center at Brigham & Women’s Hospital, Boston, said that having two FDA-approved therapies with different means of administration “is great for the field and great for patients. These are both meant to be used after a course of antibiotics, so antibiotics are still the mainstay of treatment for C. diff and recurrent C. diff, but we now have more options to prevent recurrence.”
The convenience of an oral therapy that can be taken at home is “very attractive,” Dr. Allegretti added, noting that there will also be patients “who either don’t want to or can’t take capsules, for whom a rectal administration [in a health care setting] may be preferred.”
Dr. Allegretti, who has used FMT to treat recurrent C. difficile for more than a decade, said that she expected traditional FMT using screened donor stool to remain available even as the new products are adopted by clinicians. FMT centers like OpenBiome “will continue to provide access for patients who either don’t have the ability to get the FDA-approved products because of insurance coverage, or for financial reasons, or maybe neither of the new products is appropriate for them,” she said. “I do think there will always be a need for the traditional option. The more options that we have available the better.”
TD Cowen analyst Joseph Thome told Reuters that the drug could be priced close to $20,000 per course, expecting peak sales of $750 million in the U.S. in 2033.
Dr. Allegretti disclosed consulting work for Seres Therapeutics, Ferring, and other manufacturers. She is a member of OpenBiome’s clinical advisory board.
Are delayed antibiotic prescriptions futile?
I recently posted a case about a smoker who became angry when I hesitated to prescribe antibiotics for his self-diagnosed bronchitis. He even threatened to retaliate by posting negative online reviews of my practice. In the end, I decided to use the strategy of a delayed prescription for antibiotics, instructing him to fill the prescription only if his symptoms worsened. I asked whether readers agreed with this approach. Thank you for the thoughtful comments regarding a case that certainly seemed familiar to many of you. I very much appreciate the chance to interact and share perspectives in a challenging clinical dilemma.
One theme that emerged through several comments was the perceived futility of the delayed prescriptions for antibiotics. To summarize, the collective logic stated that there is no point in delaying a prescription, because the patient will be very likely to fill that prescription right away despite counseling from the health care provider (HCP).
However, studies of delayed antibiotic prescriptions show that patients generally honor the advice to only fill the prescription if they are not improving clinically. In a study comparing immediate, delayed, or no antibiotic prescriptions among a cohort of children with uncomplicated respiratory infections, the overall rates of use of antibiotics in the three respective groups were 96%, 25.3%, and 12.0%. In another randomized trial exploring different strategies for delayed prescriptions among adults with upper respiratory infections, the rate of antibiotic use was 37% with delayed prescription strategies vs. 97% of patients prescribed antibiotics immediately. Neither of these prospective studies found a significant difference in clinical symptoms or complications in comparing the delayed and immediate antibiotic prescription groups.
Another common theme in the comments on this case focused on the challenge of online reviews of HCPs by patients. Multiple popular websites are devoted to patients’ unedited comments on HCPs and their practices, but there are still certain patterns to the comments. Some reviews describe the professionalism or empathy of the HCP, but others might focus more attention on the overall practice or office. These latter comments might emphasize issues such as timeliness of appointments, interactions with staff, or even parking and traffic. These are issues over which the HCP usually has little control.
HCPs are quite human, and therefore we might feel great about positive comments and dispirited or even angry with negative comments. So what is the best practice for HCPs in managing these online comments? A review by Dr Rebekah Bernard, which was published in the Sept. 25, 2018, issue of Medical Economics, offered some pragmatic advice:
Do not perseverate on one or two negative reviews. In fact, they might help! Dr. Bernard describes the psychological theory of the “pratfall effect,” in which people are more likely to prefer someone who is generally very good but not perfect to someone with nothing but exceptional reviews. HCPs with perfect reviews every time may be seen as intimidating or unapproachable.
Satisfied patients will frequently rally to support an HCP with an unfavorable review. This group may not be very motivated to complete online reviews until they see a comment which does at all match their own experience with the HCP.
Most importantly, HCPs can take an active role in minimizing the impact of negative online reviews while also enhancing their business model. Increasing your presence on the Internet and social media can help dilute negative reviews and push them down the list when someone performs a search on your name or practice. Creating a website for your practice is an effective means to be first on search engine lists, and HCPs should seek search-engine optimization features that promote this outcome. Adding social media contacts for yourself and/or your practice, as many as you can tolerate and maintain, allows HCPs to further control the narrative regarding their practice and central messaging to patients and the community.
In conclusion, delayed antibiotic prescriptions can reduce the use of unnecessary antibiotics for upper respiratory infections among children and adults, and they are not associated with worse clinical outcomes vs. immediate antibiotic prescriptions. They can also improve patient satisfaction for these visits, which can minimize the challenging issue of negative reviews of HCPs. HCPs should therefore consider delayed prescriptions as a strong option among patients without an indication for an antibiotic prescription.
A version of this article first appeared on Medscape.com.
I recently posted a case about a smoker who became angry when I hesitated to prescribe antibiotics for his self-diagnosed bronchitis. He even threatened to retaliate by posting negative online reviews of my practice. In the end, I decided to use the strategy of a delayed prescription for antibiotics, instructing him to fill the prescription only if his symptoms worsened. I asked whether readers agreed with this approach. Thank you for the thoughtful comments regarding a case that certainly seemed familiar to many of you. I very much appreciate the chance to interact and share perspectives in a challenging clinical dilemma.
One theme that emerged through several comments was the perceived futility of the delayed prescriptions for antibiotics. To summarize, the collective logic stated that there is no point in delaying a prescription, because the patient will be very likely to fill that prescription right away despite counseling from the health care provider (HCP).
However, studies of delayed antibiotic prescriptions show that patients generally honor the advice to only fill the prescription if they are not improving clinically. In a study comparing immediate, delayed, or no antibiotic prescriptions among a cohort of children with uncomplicated respiratory infections, the overall rates of use of antibiotics in the three respective groups were 96%, 25.3%, and 12.0%. In another randomized trial exploring different strategies for delayed prescriptions among adults with upper respiratory infections, the rate of antibiotic use was 37% with delayed prescription strategies vs. 97% of patients prescribed antibiotics immediately. Neither of these prospective studies found a significant difference in clinical symptoms or complications in comparing the delayed and immediate antibiotic prescription groups.
Another common theme in the comments on this case focused on the challenge of online reviews of HCPs by patients. Multiple popular websites are devoted to patients’ unedited comments on HCPs and their practices, but there are still certain patterns to the comments. Some reviews describe the professionalism or empathy of the HCP, but others might focus more attention on the overall practice or office. These latter comments might emphasize issues such as timeliness of appointments, interactions with staff, or even parking and traffic. These are issues over which the HCP usually has little control.
HCPs are quite human, and therefore we might feel great about positive comments and dispirited or even angry with negative comments. So what is the best practice for HCPs in managing these online comments? A review by Dr Rebekah Bernard, which was published in the Sept. 25, 2018, issue of Medical Economics, offered some pragmatic advice:
Do not perseverate on one or two negative reviews. In fact, they might help! Dr. Bernard describes the psychological theory of the “pratfall effect,” in which people are more likely to prefer someone who is generally very good but not perfect to someone with nothing but exceptional reviews. HCPs with perfect reviews every time may be seen as intimidating or unapproachable.
Satisfied patients will frequently rally to support an HCP with an unfavorable review. This group may not be very motivated to complete online reviews until they see a comment which does at all match their own experience with the HCP.
Most importantly, HCPs can take an active role in minimizing the impact of negative online reviews while also enhancing their business model. Increasing your presence on the Internet and social media can help dilute negative reviews and push them down the list when someone performs a search on your name or practice. Creating a website for your practice is an effective means to be first on search engine lists, and HCPs should seek search-engine optimization features that promote this outcome. Adding social media contacts for yourself and/or your practice, as many as you can tolerate and maintain, allows HCPs to further control the narrative regarding their practice and central messaging to patients and the community.
In conclusion, delayed antibiotic prescriptions can reduce the use of unnecessary antibiotics for upper respiratory infections among children and adults, and they are not associated with worse clinical outcomes vs. immediate antibiotic prescriptions. They can also improve patient satisfaction for these visits, which can minimize the challenging issue of negative reviews of HCPs. HCPs should therefore consider delayed prescriptions as a strong option among patients without an indication for an antibiotic prescription.
A version of this article first appeared on Medscape.com.
I recently posted a case about a smoker who became angry when I hesitated to prescribe antibiotics for his self-diagnosed bronchitis. He even threatened to retaliate by posting negative online reviews of my practice. In the end, I decided to use the strategy of a delayed prescription for antibiotics, instructing him to fill the prescription only if his symptoms worsened. I asked whether readers agreed with this approach. Thank you for the thoughtful comments regarding a case that certainly seemed familiar to many of you. I very much appreciate the chance to interact and share perspectives in a challenging clinical dilemma.
One theme that emerged through several comments was the perceived futility of the delayed prescriptions for antibiotics. To summarize, the collective logic stated that there is no point in delaying a prescription, because the patient will be very likely to fill that prescription right away despite counseling from the health care provider (HCP).
However, studies of delayed antibiotic prescriptions show that patients generally honor the advice to only fill the prescription if they are not improving clinically. In a study comparing immediate, delayed, or no antibiotic prescriptions among a cohort of children with uncomplicated respiratory infections, the overall rates of use of antibiotics in the three respective groups were 96%, 25.3%, and 12.0%. In another randomized trial exploring different strategies for delayed prescriptions among adults with upper respiratory infections, the rate of antibiotic use was 37% with delayed prescription strategies vs. 97% of patients prescribed antibiotics immediately. Neither of these prospective studies found a significant difference in clinical symptoms or complications in comparing the delayed and immediate antibiotic prescription groups.
Another common theme in the comments on this case focused on the challenge of online reviews of HCPs by patients. Multiple popular websites are devoted to patients’ unedited comments on HCPs and their practices, but there are still certain patterns to the comments. Some reviews describe the professionalism or empathy of the HCP, but others might focus more attention on the overall practice or office. These latter comments might emphasize issues such as timeliness of appointments, interactions with staff, or even parking and traffic. These are issues over which the HCP usually has little control.
HCPs are quite human, and therefore we might feel great about positive comments and dispirited or even angry with negative comments. So what is the best practice for HCPs in managing these online comments? A review by Dr Rebekah Bernard, which was published in the Sept. 25, 2018, issue of Medical Economics, offered some pragmatic advice:
Do not perseverate on one or two negative reviews. In fact, they might help! Dr. Bernard describes the psychological theory of the “pratfall effect,” in which people are more likely to prefer someone who is generally very good but not perfect to someone with nothing but exceptional reviews. HCPs with perfect reviews every time may be seen as intimidating or unapproachable.
Satisfied patients will frequently rally to support an HCP with an unfavorable review. This group may not be very motivated to complete online reviews until they see a comment which does at all match their own experience with the HCP.
Most importantly, HCPs can take an active role in minimizing the impact of negative online reviews while also enhancing their business model. Increasing your presence on the Internet and social media can help dilute negative reviews and push them down the list when someone performs a search on your name or practice. Creating a website for your practice is an effective means to be first on search engine lists, and HCPs should seek search-engine optimization features that promote this outcome. Adding social media contacts for yourself and/or your practice, as many as you can tolerate and maintain, allows HCPs to further control the narrative regarding their practice and central messaging to patients and the community.
In conclusion, delayed antibiotic prescriptions can reduce the use of unnecessary antibiotics for upper respiratory infections among children and adults, and they are not associated with worse clinical outcomes vs. immediate antibiotic prescriptions. They can also improve patient satisfaction for these visits, which can minimize the challenging issue of negative reviews of HCPs. HCPs should therefore consider delayed prescriptions as a strong option among patients without an indication for an antibiotic prescription.
A version of this article first appeared on Medscape.com.
Antimicrobial resistance requires a manifold response
BUENOS AIRES – Antimicrobial resistance (AMR) has become a global concern. And while one issue to be addressed is the deficit in research and development for new antibiotics, efforts to tackle this public health threat also should be directed toward promoting more rational prescription practices and strengthening the ability to identify the microorganisms responsible for infections, according to the World Health Organization. This was the conclusion reached at the fourth meeting of the WHO AMR Surveillance and Quality Assessment Collaborating Centres Network, which was held in Buenos Aires.
“We have to provide assistance to countries to ensure that the drugs are being used responsibly. We can come up with new antibiotics, but the issue at hand is not simply one of innovation: If nothing is done to correct inappropriate prescription practices and to overcome the lack of diagnostic laboratories at the country level, we’re going to miss out on those drugs as soon as they become available,” Kitty van Weezenbeek, MD, PhD, MPH, director of the AMR Surveillance, Prevention, and Control (AMR/SPC) Department at the WHO’s headquarters in Geneva, told this news organization.
Dr. van Weezenbeek pointed out that although there are currently no shortages of antimicrobials, the development and launch of new drugs that fight multidrug-resistant infections – infections for which there are few therapeutic options – has proceeded slowly. “It takes 10 to 15 years to develop a new antibiotic,” she said, adding that “the majority of pharmaceutical companies that had been engaged in the development of antimicrobials have filed for bankruptcy.”
In 2019, more people died – 1.2 million – from AMR than from malaria, tuberculosis, and HIV combined. Why are there so few market incentives when there is such a great need for those drugs? “One reason is that the pharmaceutical industry makes more money with long-term treatments, such as those for cancer and respiratory diseases. The other problem is that people everywhere are told not to use antibiotics,” said Dr. van Weezenbeek.
“A course of antibiotics lasts a few days, especially because we’re promoting rational use. Therefore, the trend is for the total amount of antimicrobials being used to be lower. So, it’s not as profitable,” added Carmem Lucia Pessoa-Silva, MD, PhD, head of the Surveillance, Evidence, and Laboratory Strengthening Unit of the WHO’s AMR/SPC Department.
On that note, Dr. van Weezenbeek mentioned that member countries are working with pharmaceutical companies and universities to address this problem. The WHO, for its part, has responded by implementing a global mechanism with a public health approach to create a “healthy” and equitable market for these medicines.
AMR is one of the top 10 global threats to human health. But it also has an impact on animal production, agricultural production, and the environment. Strategies to tackle AMR based on the One Health approach should involve all actors, social sectors, and citizens, according to Eva Jané Llopis, PhD, the representative of the Pan American Health Organization/WHO in Argentina.
At the root of the AMR problem is the widespread use of these drugs as growth promoters in animal production – for which several countries have enacted regulations – as well as “misunderstandings” between patients and physicians when there is not sufficient, timely access to laboratory diagnostics, especially in low- and middle-income countries.
“People think that if they’re given broad-spectrum antibiotics, they’re being prescribed the best antibiotics; and doctors, because there are no laboratory services, prescribe broad-spectrum antibiotics because they want to help patients. But that ends up causing more resistance to drugs, and thus, those antibiotics aren’t good for the patients,” said Dr. van Weezenbeek.
The WHO Global AMR and Use Surveillance System (GLASS) was launched in 2015. Its 2022 report, which marked the end of the system’s early implementation period, noted that the reported AMR rates are often lower in countries, territories, and areas with better testing coverage for most pathogen-drug-infection site combinations. However, as Dr. Pessoa-Silva acknowledged, monitoring “has not yet generated representative data,” because in many cases, countries either do not have surveillance systems or have only recently started implementing them.
Even so, the indicators that are available paint an increasingly worrisome picture. “For example, in many countries, resistance rates to first-line antibiotics were around 10%-20% with respect to Escherichia coli urinary tract infections and bloodstream bacteriologically confirmed infections. So, the risk of treatment failure is very high,” explained Dr. Pessoa-Silva.
The latest estimates indicate that every 2 or 3 minutes, somewhere in the world, a child dies from AMR. And the situation is particularly “dramatic” in neonatal intensive care units, where outbreaks of multidrug-resistant infections have a mortality rate of 50%, said Pilar Ramón-Pardo, MD, PhD, lead of the Special Program on AMR at the Pan American Health Organization, the WHO Regional Office for the Americas.
AMR rates also got worse during the pandemic because of the inappropriate prescription of massive amounts of antibiotics to hospitalized patients – something that was not in compliance with guidelines or protocols. Silvia Bertagnolio, MD, is an infectious disease specialist and the head of the Control and Response Strategies Unit in the WHO’s AMR Division. She spoke about the global clinical platform data pertaining to more than 1,500,000 patients who were hospitalized for COVID-19. Since 2020, 85% received antimicrobial treatment, despite the fact that only 5% had a concomitant infection at admission. “It’s easier to give antibiotics than to make a proper diagnosis,” said Dr. Bertagnolio.
This article was translated from Medscape’s Spanish edition and a version appeared on Medscape.com.
BUENOS AIRES – Antimicrobial resistance (AMR) has become a global concern. And while one issue to be addressed is the deficit in research and development for new antibiotics, efforts to tackle this public health threat also should be directed toward promoting more rational prescription practices and strengthening the ability to identify the microorganisms responsible for infections, according to the World Health Organization. This was the conclusion reached at the fourth meeting of the WHO AMR Surveillance and Quality Assessment Collaborating Centres Network, which was held in Buenos Aires.
“We have to provide assistance to countries to ensure that the drugs are being used responsibly. We can come up with new antibiotics, but the issue at hand is not simply one of innovation: If nothing is done to correct inappropriate prescription practices and to overcome the lack of diagnostic laboratories at the country level, we’re going to miss out on those drugs as soon as they become available,” Kitty van Weezenbeek, MD, PhD, MPH, director of the AMR Surveillance, Prevention, and Control (AMR/SPC) Department at the WHO’s headquarters in Geneva, told this news organization.
Dr. van Weezenbeek pointed out that although there are currently no shortages of antimicrobials, the development and launch of new drugs that fight multidrug-resistant infections – infections for which there are few therapeutic options – has proceeded slowly. “It takes 10 to 15 years to develop a new antibiotic,” she said, adding that “the majority of pharmaceutical companies that had been engaged in the development of antimicrobials have filed for bankruptcy.”
In 2019, more people died – 1.2 million – from AMR than from malaria, tuberculosis, and HIV combined. Why are there so few market incentives when there is such a great need for those drugs? “One reason is that the pharmaceutical industry makes more money with long-term treatments, such as those for cancer and respiratory diseases. The other problem is that people everywhere are told not to use antibiotics,” said Dr. van Weezenbeek.
“A course of antibiotics lasts a few days, especially because we’re promoting rational use. Therefore, the trend is for the total amount of antimicrobials being used to be lower. So, it’s not as profitable,” added Carmem Lucia Pessoa-Silva, MD, PhD, head of the Surveillance, Evidence, and Laboratory Strengthening Unit of the WHO’s AMR/SPC Department.
On that note, Dr. van Weezenbeek mentioned that member countries are working with pharmaceutical companies and universities to address this problem. The WHO, for its part, has responded by implementing a global mechanism with a public health approach to create a “healthy” and equitable market for these medicines.
AMR is one of the top 10 global threats to human health. But it also has an impact on animal production, agricultural production, and the environment. Strategies to tackle AMR based on the One Health approach should involve all actors, social sectors, and citizens, according to Eva Jané Llopis, PhD, the representative of the Pan American Health Organization/WHO in Argentina.
At the root of the AMR problem is the widespread use of these drugs as growth promoters in animal production – for which several countries have enacted regulations – as well as “misunderstandings” between patients and physicians when there is not sufficient, timely access to laboratory diagnostics, especially in low- and middle-income countries.
“People think that if they’re given broad-spectrum antibiotics, they’re being prescribed the best antibiotics; and doctors, because there are no laboratory services, prescribe broad-spectrum antibiotics because they want to help patients. But that ends up causing more resistance to drugs, and thus, those antibiotics aren’t good for the patients,” said Dr. van Weezenbeek.
The WHO Global AMR and Use Surveillance System (GLASS) was launched in 2015. Its 2022 report, which marked the end of the system’s early implementation period, noted that the reported AMR rates are often lower in countries, territories, and areas with better testing coverage for most pathogen-drug-infection site combinations. However, as Dr. Pessoa-Silva acknowledged, monitoring “has not yet generated representative data,” because in many cases, countries either do not have surveillance systems or have only recently started implementing them.
Even so, the indicators that are available paint an increasingly worrisome picture. “For example, in many countries, resistance rates to first-line antibiotics were around 10%-20% with respect to Escherichia coli urinary tract infections and bloodstream bacteriologically confirmed infections. So, the risk of treatment failure is very high,” explained Dr. Pessoa-Silva.
The latest estimates indicate that every 2 or 3 minutes, somewhere in the world, a child dies from AMR. And the situation is particularly “dramatic” in neonatal intensive care units, where outbreaks of multidrug-resistant infections have a mortality rate of 50%, said Pilar Ramón-Pardo, MD, PhD, lead of the Special Program on AMR at the Pan American Health Organization, the WHO Regional Office for the Americas.
AMR rates also got worse during the pandemic because of the inappropriate prescription of massive amounts of antibiotics to hospitalized patients – something that was not in compliance with guidelines or protocols. Silvia Bertagnolio, MD, is an infectious disease specialist and the head of the Control and Response Strategies Unit in the WHO’s AMR Division. She spoke about the global clinical platform data pertaining to more than 1,500,000 patients who were hospitalized for COVID-19. Since 2020, 85% received antimicrobial treatment, despite the fact that only 5% had a concomitant infection at admission. “It’s easier to give antibiotics than to make a proper diagnosis,” said Dr. Bertagnolio.
This article was translated from Medscape’s Spanish edition and a version appeared on Medscape.com.
BUENOS AIRES – Antimicrobial resistance (AMR) has become a global concern. And while one issue to be addressed is the deficit in research and development for new antibiotics, efforts to tackle this public health threat also should be directed toward promoting more rational prescription practices and strengthening the ability to identify the microorganisms responsible for infections, according to the World Health Organization. This was the conclusion reached at the fourth meeting of the WHO AMR Surveillance and Quality Assessment Collaborating Centres Network, which was held in Buenos Aires.
“We have to provide assistance to countries to ensure that the drugs are being used responsibly. We can come up with new antibiotics, but the issue at hand is not simply one of innovation: If nothing is done to correct inappropriate prescription practices and to overcome the lack of diagnostic laboratories at the country level, we’re going to miss out on those drugs as soon as they become available,” Kitty van Weezenbeek, MD, PhD, MPH, director of the AMR Surveillance, Prevention, and Control (AMR/SPC) Department at the WHO’s headquarters in Geneva, told this news organization.
Dr. van Weezenbeek pointed out that although there are currently no shortages of antimicrobials, the development and launch of new drugs that fight multidrug-resistant infections – infections for which there are few therapeutic options – has proceeded slowly. “It takes 10 to 15 years to develop a new antibiotic,” she said, adding that “the majority of pharmaceutical companies that had been engaged in the development of antimicrobials have filed for bankruptcy.”
In 2019, more people died – 1.2 million – from AMR than from malaria, tuberculosis, and HIV combined. Why are there so few market incentives when there is such a great need for those drugs? “One reason is that the pharmaceutical industry makes more money with long-term treatments, such as those for cancer and respiratory diseases. The other problem is that people everywhere are told not to use antibiotics,” said Dr. van Weezenbeek.
“A course of antibiotics lasts a few days, especially because we’re promoting rational use. Therefore, the trend is for the total amount of antimicrobials being used to be lower. So, it’s not as profitable,” added Carmem Lucia Pessoa-Silva, MD, PhD, head of the Surveillance, Evidence, and Laboratory Strengthening Unit of the WHO’s AMR/SPC Department.
On that note, Dr. van Weezenbeek mentioned that member countries are working with pharmaceutical companies and universities to address this problem. The WHO, for its part, has responded by implementing a global mechanism with a public health approach to create a “healthy” and equitable market for these medicines.
AMR is one of the top 10 global threats to human health. But it also has an impact on animal production, agricultural production, and the environment. Strategies to tackle AMR based on the One Health approach should involve all actors, social sectors, and citizens, according to Eva Jané Llopis, PhD, the representative of the Pan American Health Organization/WHO in Argentina.
At the root of the AMR problem is the widespread use of these drugs as growth promoters in animal production – for which several countries have enacted regulations – as well as “misunderstandings” between patients and physicians when there is not sufficient, timely access to laboratory diagnostics, especially in low- and middle-income countries.
“People think that if they’re given broad-spectrum antibiotics, they’re being prescribed the best antibiotics; and doctors, because there are no laboratory services, prescribe broad-spectrum antibiotics because they want to help patients. But that ends up causing more resistance to drugs, and thus, those antibiotics aren’t good for the patients,” said Dr. van Weezenbeek.
The WHO Global AMR and Use Surveillance System (GLASS) was launched in 2015. Its 2022 report, which marked the end of the system’s early implementation period, noted that the reported AMR rates are often lower in countries, territories, and areas with better testing coverage for most pathogen-drug-infection site combinations. However, as Dr. Pessoa-Silva acknowledged, monitoring “has not yet generated representative data,” because in many cases, countries either do not have surveillance systems or have only recently started implementing them.
Even so, the indicators that are available paint an increasingly worrisome picture. “For example, in many countries, resistance rates to first-line antibiotics were around 10%-20% with respect to Escherichia coli urinary tract infections and bloodstream bacteriologically confirmed infections. So, the risk of treatment failure is very high,” explained Dr. Pessoa-Silva.
The latest estimates indicate that every 2 or 3 minutes, somewhere in the world, a child dies from AMR. And the situation is particularly “dramatic” in neonatal intensive care units, where outbreaks of multidrug-resistant infections have a mortality rate of 50%, said Pilar Ramón-Pardo, MD, PhD, lead of the Special Program on AMR at the Pan American Health Organization, the WHO Regional Office for the Americas.
AMR rates also got worse during the pandemic because of the inappropriate prescription of massive amounts of antibiotics to hospitalized patients – something that was not in compliance with guidelines or protocols. Silvia Bertagnolio, MD, is an infectious disease specialist and the head of the Control and Response Strategies Unit in the WHO’s AMR Division. She spoke about the global clinical platform data pertaining to more than 1,500,000 patients who were hospitalized for COVID-19. Since 2020, 85% received antimicrobial treatment, despite the fact that only 5% had a concomitant infection at admission. “It’s easier to give antibiotics than to make a proper diagnosis,” said Dr. Bertagnolio.
This article was translated from Medscape’s Spanish edition and a version appeared on Medscape.com.