User login
FAST trial clears febuxostat of increased mortality in gout
Febuxostat (Uloric) emerged as noninferior to allopurinol regarding risk of cardiovascular death among people 60 years and older with gout and at least one additional cardiovascular risk factor, results of the Febuxostat versus Allopurinol Streamlined Trial (FAST) suggest.

This primary outcome of the FAST trial stands in contrast to results of the CARES trial in 2018. The CARES researchers previously reported a 4.3% increased risk of cardiovascular death associated with febuxostat, compared with a 3.2% rate with allopurinol, a statistically significant 34% increase in the relative risk.
“In contrast to previous studies, there was no evidence of increased mortality with febuxostat, and we believe the regulators should review febuxostat licensing restrictions,” senior author Thomas MacDonald, MD, of the University of Dundee (Scotland), said during a late-breaking abstract session at the virtual annual meeting of the American College of Rheumatology.
The results of the FAST trial were simultaneously published online in The Lancet.
Both febuxostat and allopurinol treat gout by lowering urate levels. Concerns about the cardiovascular safety of febuxostat led to two post-licensing studies: the Cardiovascular Safety of Febuxostat and Allopurinol in Participants with Gout and Cardiovascular Comorbidities (CARES) study, mandated by the U.S. Food and Drug Administration, and FAST, requested by the European Medicines Agency. In February 2019, the FDA added a warning about elevated cardiovascular death and death risk associated with febuxostat.
“When CARES was published, it was somewhat of a threat to our study,” Dr. MacDonald said. “After hearing from our data-monitoring committee, we were told we could continue the trial.”
Some switched from allopurinol to febuxostat
So Dr. MacDonald, lead author Isla Mackenzie, MBChB, and their colleagues enrolled 6,128 people with gout in the United Kingdom, Sweden, and Denmark between December 2011 and January 2018. They followed patients for a median of 4 years. Participants had a mean age of 71 years, 85% were men, and 33% had a history of cardiovascular disease. The investigators excluded anyone with a stroke or myocardial infarction in the previous 6 months.
All participants were being treated with allopurinol. The investigators titrated those not at target up to an ideal dose that achieved a serum urate concentration of less than 0.357 mmol/L (< 6 mg/dL). Next, they randomly assigned 3,065 people to continue allopurinol and another 3,063 to switch to 80-120 mg of febuxostat.
The primary outcome of the multicenter, prospective, randomized, open-label FAST trial was a composite of hospitalization for nonfatal MI or biomarker positive for acute coronary syndrome, nonfatal stroke, or cardiovascular death.
Key findings
“There was definitely a noninferior primary outcome,” Dr. MacDonald said. In the on-treatment analysis, 172 patients in the febuxostat group reached the composite endpoint versus 241 patients in the allopurinol group. There were 1.72 events per 100 patient-years in the febuxostat group versus 2.05 events in the allopurinol group (adjusted hazard ratio, 0.85; 95% confidence interval, 0.70-1.03). An intent-to-treat analysis also found that febuxostat was noninferior to allopurinol on this measure.
Urate levels were approximately 80 micromoles lower in the febuxostat group versus the allopurinol group each year of the study, Dr. MacDonald said.
At least one gout flare was experienced by 1,017 patients in the febuxostat group and by 1,044 participants in the allopurinol group. “However, there was no placebo group, so we don’t know the effectiveness of either of these agents at preventing flares” based on this research, he said.
Both the on-treatment and intention-to-treat (ITT) secondary analyses demonstrated the noninferiority of febuxostat, compared with allopurinol, for all-cause death, each individual component of the composite primary outcome – cardiovascular death, hospitalization for heart failure, and hospitalization for new, unstable, or worsening angina.
In contrast, the ITT analysis revealed a “nominally significant increase” in hospitalization for arrhythmia with no evidence of ischemia in the febuxostat group. The 0.583 events per 100 patient-years in this group versus 0.385 events in the allopurinol cohort generated an adjusted HR of 1.51 (95% CI, 1.05-2.17).
In terms of all-cause mortality, 222 participants (7.2%) in the febuxostat group died, compared with 263 people (8.6%) in the allopurinol group.
Adverse events and withdrawals
A total 1,720 participants (57.3%) in the febuxostat group experienced at least one serious adverse event, as did 1,812 participants (59.4%) in the allopurinol group. Less than 1% of serious adverse events in each group were considered treatment-related.
Dr. MacDonald said that 6.2% of the febuxostat patients and 5.5% of the allopurinol group withdrew from the study. “We had pretty good follow-up [94%],” Dr. MacDonald said. “I don’t want to criticize CARES, but 47% did drop out of that study, and they could not follow them anymore.”
Limitations of FAST include its open-label design and lack of a placebo group, although Dr. MacDonald pointed out that a placebo group would have been unethical. Strengths included its large randomized trial design and good external validity, he added. “This is what will happen in clinical practice if you switch people from allopurinol to febuxostat.”
When asked how he would treat people with gout now given the FAST findings, Dr. MacDonald said, “I’m not a rheumatologist, I’m a cardiovascular physician. But I would say from the evidence from the FAST trial, it appears to be safe to give patients febuxostat whether or not they have cardiovascular risk factors or prior cardiovascular disease.”
“The FAST study indicates that febuxostat is similar to allopurinol in terms of cardiovascular events during the treatment period. The strengths of this study are its large sample size, excellent follow-up rate, and the relatively long follow-up time,” session moderator Shervin Assassi, MD, said when asked for comment. Dr. Assassi, director of the division of rheumatology at the University of Texas Health Science Center at Houston, was not involved in the research.
Menarini, Ipsen, and Teijin Pharma funded the study. The University of Dundee receives research funds from Menarini. Dr. MacDonald disclosed that he received speaker or consultant fees from Menarini. Dr. Assassi had no relevant disclosures.
SOURCE: MacDonald T et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract L08.
Febuxostat (Uloric) emerged as noninferior to allopurinol regarding risk of cardiovascular death among people 60 years and older with gout and at least one additional cardiovascular risk factor, results of the Febuxostat versus Allopurinol Streamlined Trial (FAST) suggest.
This primary outcome of the FAST trial stands in contrast to results of the CARES trial in 2018. The CARES researchers previously reported a 4.3% increased risk of cardiovascular death associated with febuxostat, compared with a 3.2% rate with allopurinol, a statistically significant 34% increase in the relative risk.
“In contrast to previous studies, there was no evidence of increased mortality with febuxostat, and we believe the regulators should review febuxostat licensing restrictions,” senior author Thomas MacDonald, MD, of the University of Dundee (Scotland), said during a late-breaking abstract session at the virtual annual meeting of the American College of Rheumatology.
The results of the FAST trial were simultaneously published online in The Lancet.
Both febuxostat and allopurinol treat gout by lowering urate levels. Concerns about the cardiovascular safety of febuxostat led to two post-licensing studies: the Cardiovascular Safety of Febuxostat and Allopurinol in Participants with Gout and Cardiovascular Comorbidities (CARES) study, mandated by the U.S. Food and Drug Administration, and FAST, requested by the European Medicines Agency. In February 2019, the FDA added a warning about elevated cardiovascular death and death risk associated with febuxostat.
“When CARES was published, it was somewhat of a threat to our study,” Dr. MacDonald said. “After hearing from our data-monitoring committee, we were told we could continue the trial.”
Some switched from allopurinol to febuxostat
So Dr. MacDonald, lead author Isla Mackenzie, MBChB, and their colleagues enrolled 6,128 people with gout in the United Kingdom, Sweden, and Denmark between December 2011 and January 2018. They followed patients for a median of 4 years. Participants had a mean age of 71 years, 85% were men, and 33% had a history of cardiovascular disease. The investigators excluded anyone with a stroke or myocardial infarction in the previous 6 months.
All participants were being treated with allopurinol. The investigators titrated those not at target up to an ideal dose that achieved a serum urate concentration of less than 0.357 mmol/L (< 6 mg/dL). Next, they randomly assigned 3,065 people to continue allopurinol and another 3,063 to switch to 80-120 mg of febuxostat.
The primary outcome of the multicenter, prospective, randomized, open-label FAST trial was a composite of hospitalization for nonfatal MI or biomarker positive for acute coronary syndrome, nonfatal stroke, or cardiovascular death.
Key findings
“There was definitely a noninferior primary outcome,” Dr. MacDonald said. In the on-treatment analysis, 172 patients in the febuxostat group reached the composite endpoint versus 241 patients in the allopurinol group. There were 1.72 events per 100 patient-years in the febuxostat group versus 2.05 events in the allopurinol group (adjusted hazard ratio, 0.85; 95% confidence interval, 0.70-1.03). An intent-to-treat analysis also found that febuxostat was noninferior to allopurinol on this measure.
Urate levels were approximately 80 micromoles lower in the febuxostat group versus the allopurinol group each year of the study, Dr. MacDonald said.
At least one gout flare was experienced by 1,017 patients in the febuxostat group and by 1,044 participants in the allopurinol group. “However, there was no placebo group, so we don’t know the effectiveness of either of these agents at preventing flares” based on this research, he said.
Both the on-treatment and intention-to-treat (ITT) secondary analyses demonstrated the noninferiority of febuxostat, compared with allopurinol, for all-cause death, each individual component of the composite primary outcome – cardiovascular death, hospitalization for heart failure, and hospitalization for new, unstable, or worsening angina.
In contrast, the ITT analysis revealed a “nominally significant increase” in hospitalization for arrhythmia with no evidence of ischemia in the febuxostat group. The 0.583 events per 100 patient-years in this group versus 0.385 events in the allopurinol cohort generated an adjusted HR of 1.51 (95% CI, 1.05-2.17).
In terms of all-cause mortality, 222 participants (7.2%) in the febuxostat group died, compared with 263 people (8.6%) in the allopurinol group.
Adverse events and withdrawals
A total 1,720 participants (57.3%) in the febuxostat group experienced at least one serious adverse event, as did 1,812 participants (59.4%) in the allopurinol group. Less than 1% of serious adverse events in each group were considered treatment-related.
Dr. MacDonald said that 6.2% of the febuxostat patients and 5.5% of the allopurinol group withdrew from the study. “We had pretty good follow-up [94%],” Dr. MacDonald said. “I don’t want to criticize CARES, but 47% did drop out of that study, and they could not follow them anymore.”
Limitations of FAST include its open-label design and lack of a placebo group, although Dr. MacDonald pointed out that a placebo group would have been unethical. Strengths included its large randomized trial design and good external validity, he added. “This is what will happen in clinical practice if you switch people from allopurinol to febuxostat.”
When asked how he would treat people with gout now given the FAST findings, Dr. MacDonald said, “I’m not a rheumatologist, I’m a cardiovascular physician. But I would say from the evidence from the FAST trial, it appears to be safe to give patients febuxostat whether or not they have cardiovascular risk factors or prior cardiovascular disease.”
“The FAST study indicates that febuxostat is similar to allopurinol in terms of cardiovascular events during the treatment period. The strengths of this study are its large sample size, excellent follow-up rate, and the relatively long follow-up time,” session moderator Shervin Assassi, MD, said when asked for comment. Dr. Assassi, director of the division of rheumatology at the University of Texas Health Science Center at Houston, was not involved in the research.
Menarini, Ipsen, and Teijin Pharma funded the study. The University of Dundee receives research funds from Menarini. Dr. MacDonald disclosed that he received speaker or consultant fees from Menarini. Dr. Assassi had no relevant disclosures.
SOURCE: MacDonald T et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract L08.
Febuxostat (Uloric) emerged as noninferior to allopurinol regarding risk of cardiovascular death among people 60 years and older with gout and at least one additional cardiovascular risk factor, results of the Febuxostat versus Allopurinol Streamlined Trial (FAST) suggest.
This primary outcome of the FAST trial stands in contrast to results of the CARES trial in 2018. The CARES researchers previously reported a 4.3% increased risk of cardiovascular death associated with febuxostat, compared with a 3.2% rate with allopurinol, a statistically significant 34% increase in the relative risk.
“In contrast to previous studies, there was no evidence of increased mortality with febuxostat, and we believe the regulators should review febuxostat licensing restrictions,” senior author Thomas MacDonald, MD, of the University of Dundee (Scotland), said during a late-breaking abstract session at the virtual annual meeting of the American College of Rheumatology.
The results of the FAST trial were simultaneously published online in The Lancet.
Both febuxostat and allopurinol treat gout by lowering urate levels. Concerns about the cardiovascular safety of febuxostat led to two post-licensing studies: the Cardiovascular Safety of Febuxostat and Allopurinol in Participants with Gout and Cardiovascular Comorbidities (CARES) study, mandated by the U.S. Food and Drug Administration, and FAST, requested by the European Medicines Agency. In February 2019, the FDA added a warning about elevated cardiovascular death and death risk associated with febuxostat.
“When CARES was published, it was somewhat of a threat to our study,” Dr. MacDonald said. “After hearing from our data-monitoring committee, we were told we could continue the trial.”
Some switched from allopurinol to febuxostat
So Dr. MacDonald, lead author Isla Mackenzie, MBChB, and their colleagues enrolled 6,128 people with gout in the United Kingdom, Sweden, and Denmark between December 2011 and January 2018. They followed patients for a median of 4 years. Participants had a mean age of 71 years, 85% were men, and 33% had a history of cardiovascular disease. The investigators excluded anyone with a stroke or myocardial infarction in the previous 6 months.
All participants were being treated with allopurinol. The investigators titrated those not at target up to an ideal dose that achieved a serum urate concentration of less than 0.357 mmol/L (< 6 mg/dL). Next, they randomly assigned 3,065 people to continue allopurinol and another 3,063 to switch to 80-120 mg of febuxostat.
The primary outcome of the multicenter, prospective, randomized, open-label FAST trial was a composite of hospitalization for nonfatal MI or biomarker positive for acute coronary syndrome, nonfatal stroke, or cardiovascular death.
Key findings
“There was definitely a noninferior primary outcome,” Dr. MacDonald said. In the on-treatment analysis, 172 patients in the febuxostat group reached the composite endpoint versus 241 patients in the allopurinol group. There were 1.72 events per 100 patient-years in the febuxostat group versus 2.05 events in the allopurinol group (adjusted hazard ratio, 0.85; 95% confidence interval, 0.70-1.03). An intent-to-treat analysis also found that febuxostat was noninferior to allopurinol on this measure.
Urate levels were approximately 80 micromoles lower in the febuxostat group versus the allopurinol group each year of the study, Dr. MacDonald said.
At least one gout flare was experienced by 1,017 patients in the febuxostat group and by 1,044 participants in the allopurinol group. “However, there was no placebo group, so we don’t know the effectiveness of either of these agents at preventing flares” based on this research, he said.
Both the on-treatment and intention-to-treat (ITT) secondary analyses demonstrated the noninferiority of febuxostat, compared with allopurinol, for all-cause death, each individual component of the composite primary outcome – cardiovascular death, hospitalization for heart failure, and hospitalization for new, unstable, or worsening angina.
In contrast, the ITT analysis revealed a “nominally significant increase” in hospitalization for arrhythmia with no evidence of ischemia in the febuxostat group. The 0.583 events per 100 patient-years in this group versus 0.385 events in the allopurinol cohort generated an adjusted HR of 1.51 (95% CI, 1.05-2.17).
In terms of all-cause mortality, 222 participants (7.2%) in the febuxostat group died, compared with 263 people (8.6%) in the allopurinol group.
Adverse events and withdrawals
A total 1,720 participants (57.3%) in the febuxostat group experienced at least one serious adverse event, as did 1,812 participants (59.4%) in the allopurinol group. Less than 1% of serious adverse events in each group were considered treatment-related.
Dr. MacDonald said that 6.2% of the febuxostat patients and 5.5% of the allopurinol group withdrew from the study. “We had pretty good follow-up [94%],” Dr. MacDonald said. “I don’t want to criticize CARES, but 47% did drop out of that study, and they could not follow them anymore.”
Limitations of FAST include its open-label design and lack of a placebo group, although Dr. MacDonald pointed out that a placebo group would have been unethical. Strengths included its large randomized trial design and good external validity, he added. “This is what will happen in clinical practice if you switch people from allopurinol to febuxostat.”
When asked how he would treat people with gout now given the FAST findings, Dr. MacDonald said, “I’m not a rheumatologist, I’m a cardiovascular physician. But I would say from the evidence from the FAST trial, it appears to be safe to give patients febuxostat whether or not they have cardiovascular risk factors or prior cardiovascular disease.”
“The FAST study indicates that febuxostat is similar to allopurinol in terms of cardiovascular events during the treatment period. The strengths of this study are its large sample size, excellent follow-up rate, and the relatively long follow-up time,” session moderator Shervin Assassi, MD, said when asked for comment. Dr. Assassi, director of the division of rheumatology at the University of Texas Health Science Center at Houston, was not involved in the research.
Menarini, Ipsen, and Teijin Pharma funded the study. The University of Dundee receives research funds from Menarini. Dr. MacDonald disclosed that he received speaker or consultant fees from Menarini. Dr. Assassi had no relevant disclosures.
SOURCE: MacDonald T et al. Arthritis Rheumatol. 2020;72(suppl 10). ACR 2020, Abstract L08.
FROM ACR 2020
RECIPE trial cooks up gout therapy improvement
Adding the immunomodulator mycophenolate mofetil (MMF) to therapy with pegloticase (Krystexxa) may improve outcomes in patients with refractory gout, results of the proof-of-concept RECIPE trial suggest.
In the phase 2 trial, 19 of 22 patients randomized to received pegloticase and MMF achieved the primary outcome of serum uric acid levels below 6 mg/dL at week 12, compared with 4 of 10 patients assigned to pegloticase and placebo, reported Puja Khanna MD, MPH, of the University of Michigan, Ann Arbor, and colleagues.
“The use of MMF was associated with statistically significant and clinically meaningful impact on the proportion of subjects who achieved and maintained a serum urate of less than 6 mg/dL. Short-term concomitant use of MMF with pegloticase was generally well tolerated, and the estimated rates of adverse events were comparable between the groups,” she said during the virtual annual meeting of the American College of Rheumatology.
Pegloticase is a pegylated recombinant form of porcine uricase that has been shown to be effective in the treatment of gout in patients for whom other therapies have failed.
The drug’s use is limited, however, by immunogenicity, with high antipegloticase antibody titers associated with a loss of response.
“The PEG portion of the molecule, the polyethylene glycol component, can initiate an immune response that would cause significant infusion reactions and preclude further use of the medication for our patients,” explained Suleman Bhana, MD, a rheumatologist with Crystal Run Healthcare in New York’s Hudson Valley, who was not involved in the study.
“By trying to attenuate that immune response by whatever means one can, that could reduce the risk of these infusion reactions and lead to longevity and continuing efficacy of the medication,” he said.
Study details
The RECIPE trial was designed to test whether concomitant immunomodulation could prolong the efficacy of pegloticase therapy by dampening immune reactions.
Investigators enrolled patients 18 years and older who met 2015 ACR/European League Against Rheumatism gout classification criteria and had chronic refractory disease, defined as having symptoms inadequately controlled with oral urate-lowering therapy or a contraindication to ULT.
A total of 42 patients from five rheumatology practices were screened, and 35 were randomized on a 3:1 basis. In the intention-to-treat analysis of the results, the investigators included 32 patients: 22 in the MMF/pegloticase group and 10 placebo-treated controls who had received at least one dose of pegloticase.
Men comprised approximately 90% of the patients in each study arm, with the mean patient age around 55 years. In both groups, patients had a median of one gout flare in the prior year, and a mean duration of gout of 13 years plus a few months.
The patients’ prior urate-lowering agents included allopurinol and febuxostat, and patients had received colchicine, NSAIDs, and corticosteroids for acute gout.
The mean serum urate levels at baseline were 8.9 mg/dL in the MMF group, and 9.8 mg/dL in the placebo group.
Patients were given either MMF 1 g twice daily or a placebo during a 2-week run-in, with the assigned medications continuing for the first 12 weeks concomitantly with pegloticase. The uricase was given intravenously at a dose of 8 mg every 2 weeks for a total of 12 infusions.
As noted before, 86% of patients in the MMF arm (19 of 22) reached the primary outcome of serum uric acid levels below 6 mg/dL by week 12, compared with 40% (4 of 10) in the placebo arm (P = .01).
Week 24 serum uric acid response, a secondary endpoint, was sustained in 68% of patients in the MMF arm, compared with 30% in the placebo arm (P = .03).
“We found no significant differences between the groups in the absolute change in serum urate from baseline to week 24, or from week 12 to 24. We also did not find any differences between the treatment arms for the PROMIS [Patient Reported Outcomes Measurement Information System] or for the Gout Impact Scale,” Dr. Khanna said.
The most commonly reported adverse events included gout flares in 13% of patients in the MMF group and 3% in the placebo group, cardiac disorders in 3% versus 2%, respectively, and gastrointestinal disorders in 9% versus 2%.
Adverse events that occurred only in the MMF group included infections (3%), musculoskeletal and connective tissue disorders (18%), and respiratory events.
Three patients in the placebo arm had infusion reactions, two of which occurred during the first infusion, and one during the second. One of the reactions was considered serious and required hospitalization, but all infusion reactions resolved and none were fatal. There were no infusion reactions in the MMF arm.
Maybe methotrexate instead?
“The efficacy data for mycophenolate in the RECIPE study are convincing, and suggest that this combination substantially increases the proportion of people who respond to pegloticase,” commented Nicola Dalbeth, MD, professor of medicine at the University of Auckland (New Zealand), who moderated the session where the RECIPE data were reported.
“Previous open-label studies of methotrexate with pegloticase [e.g., the MIRROR study] suggest that methotrexate is another effective option to increase the response to pegloticase. However, at this stage, placebo-controlled trials of methotrexate have not been reported. I think a key consideration will be safety, and which option [methotrexate vs. mycophenolate] is safer, noting that many patients with severe gout have important comorbidities, including chronic kidney disease, diabetes, and liver disease,” she said.
Dr. Bhana also noted that there are multiple factors that might determine the choice of MMF or methotrexate as an immunomodulatory partner for pegloticase.
“Some gout patients have chronic kidney disease or a variety of comorbidities – high uric acid can also cause kidney damage – and if they have a kidney illness, methotrexate may not be a safe medicine because there’s a risk of further toxicity that can lead to bone marrow suppression, which I have seen personally in patients, and in this case mycophenolate would be the preferred option,” he said.
The study was sponsored by the University of Alabama at Birmingham, with collaboration from the University of Michigan, as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases and Horizon, which makes pegloticase. Dr. Khanna disclosed grant and research support from Dyve, Selecta, and Sobi, and consulting for Sobi and Horizon. Dr. Dalbeth disclosed relationships with AstraZeneca, AbbVie, Arthrosi, Dyve, Selecta, and Janssen. Dr. Bhana disclosed nonbranded consulting work for Horizon.
SOURCE: Khanna P et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0952.
Adding the immunomodulator mycophenolate mofetil (MMF) to therapy with pegloticase (Krystexxa) may improve outcomes in patients with refractory gout, results of the proof-of-concept RECIPE trial suggest.
In the phase 2 trial, 19 of 22 patients randomized to received pegloticase and MMF achieved the primary outcome of serum uric acid levels below 6 mg/dL at week 12, compared with 4 of 10 patients assigned to pegloticase and placebo, reported Puja Khanna MD, MPH, of the University of Michigan, Ann Arbor, and colleagues.
“The use of MMF was associated with statistically significant and clinically meaningful impact on the proportion of subjects who achieved and maintained a serum urate of less than 6 mg/dL. Short-term concomitant use of MMF with pegloticase was generally well tolerated, and the estimated rates of adverse events were comparable between the groups,” she said during the virtual annual meeting of the American College of Rheumatology.
Pegloticase is a pegylated recombinant form of porcine uricase that has been shown to be effective in the treatment of gout in patients for whom other therapies have failed.
The drug’s use is limited, however, by immunogenicity, with high antipegloticase antibody titers associated with a loss of response.
“The PEG portion of the molecule, the polyethylene glycol component, can initiate an immune response that would cause significant infusion reactions and preclude further use of the medication for our patients,” explained Suleman Bhana, MD, a rheumatologist with Crystal Run Healthcare in New York’s Hudson Valley, who was not involved in the study.
“By trying to attenuate that immune response by whatever means one can, that could reduce the risk of these infusion reactions and lead to longevity and continuing efficacy of the medication,” he said.
Study details
The RECIPE trial was designed to test whether concomitant immunomodulation could prolong the efficacy of pegloticase therapy by dampening immune reactions.
Investigators enrolled patients 18 years and older who met 2015 ACR/European League Against Rheumatism gout classification criteria and had chronic refractory disease, defined as having symptoms inadequately controlled with oral urate-lowering therapy or a contraindication to ULT.
A total of 42 patients from five rheumatology practices were screened, and 35 were randomized on a 3:1 basis. In the intention-to-treat analysis of the results, the investigators included 32 patients: 22 in the MMF/pegloticase group and 10 placebo-treated controls who had received at least one dose of pegloticase.
Men comprised approximately 90% of the patients in each study arm, with the mean patient age around 55 years. In both groups, patients had a median of one gout flare in the prior year, and a mean duration of gout of 13 years plus a few months.
The patients’ prior urate-lowering agents included allopurinol and febuxostat, and patients had received colchicine, NSAIDs, and corticosteroids for acute gout.
The mean serum urate levels at baseline were 8.9 mg/dL in the MMF group, and 9.8 mg/dL in the placebo group.
Patients were given either MMF 1 g twice daily or a placebo during a 2-week run-in, with the assigned medications continuing for the first 12 weeks concomitantly with pegloticase. The uricase was given intravenously at a dose of 8 mg every 2 weeks for a total of 12 infusions.
As noted before, 86% of patients in the MMF arm (19 of 22) reached the primary outcome of serum uric acid levels below 6 mg/dL by week 12, compared with 40% (4 of 10) in the placebo arm (P = .01).
Week 24 serum uric acid response, a secondary endpoint, was sustained in 68% of patients in the MMF arm, compared with 30% in the placebo arm (P = .03).
“We found no significant differences between the groups in the absolute change in serum urate from baseline to week 24, or from week 12 to 24. We also did not find any differences between the treatment arms for the PROMIS [Patient Reported Outcomes Measurement Information System] or for the Gout Impact Scale,” Dr. Khanna said.
The most commonly reported adverse events included gout flares in 13% of patients in the MMF group and 3% in the placebo group, cardiac disorders in 3% versus 2%, respectively, and gastrointestinal disorders in 9% versus 2%.
Adverse events that occurred only in the MMF group included infections (3%), musculoskeletal and connective tissue disorders (18%), and respiratory events.
Three patients in the placebo arm had infusion reactions, two of which occurred during the first infusion, and one during the second. One of the reactions was considered serious and required hospitalization, but all infusion reactions resolved and none were fatal. There were no infusion reactions in the MMF arm.
Maybe methotrexate instead?
“The efficacy data for mycophenolate in the RECIPE study are convincing, and suggest that this combination substantially increases the proportion of people who respond to pegloticase,” commented Nicola Dalbeth, MD, professor of medicine at the University of Auckland (New Zealand), who moderated the session where the RECIPE data were reported.
“Previous open-label studies of methotrexate with pegloticase [e.g., the MIRROR study] suggest that methotrexate is another effective option to increase the response to pegloticase. However, at this stage, placebo-controlled trials of methotrexate have not been reported. I think a key consideration will be safety, and which option [methotrexate vs. mycophenolate] is safer, noting that many patients with severe gout have important comorbidities, including chronic kidney disease, diabetes, and liver disease,” she said.
Dr. Bhana also noted that there are multiple factors that might determine the choice of MMF or methotrexate as an immunomodulatory partner for pegloticase.
“Some gout patients have chronic kidney disease or a variety of comorbidities – high uric acid can also cause kidney damage – and if they have a kidney illness, methotrexate may not be a safe medicine because there’s a risk of further toxicity that can lead to bone marrow suppression, which I have seen personally in patients, and in this case mycophenolate would be the preferred option,” he said.
The study was sponsored by the University of Alabama at Birmingham, with collaboration from the University of Michigan, as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases and Horizon, which makes pegloticase. Dr. Khanna disclosed grant and research support from Dyve, Selecta, and Sobi, and consulting for Sobi and Horizon. Dr. Dalbeth disclosed relationships with AstraZeneca, AbbVie, Arthrosi, Dyve, Selecta, and Janssen. Dr. Bhana disclosed nonbranded consulting work for Horizon.
SOURCE: Khanna P et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0952.
Adding the immunomodulator mycophenolate mofetil (MMF) to therapy with pegloticase (Krystexxa) may improve outcomes in patients with refractory gout, results of the proof-of-concept RECIPE trial suggest.
In the phase 2 trial, 19 of 22 patients randomized to received pegloticase and MMF achieved the primary outcome of serum uric acid levels below 6 mg/dL at week 12, compared with 4 of 10 patients assigned to pegloticase and placebo, reported Puja Khanna MD, MPH, of the University of Michigan, Ann Arbor, and colleagues.
“The use of MMF was associated with statistically significant and clinically meaningful impact on the proportion of subjects who achieved and maintained a serum urate of less than 6 mg/dL. Short-term concomitant use of MMF with pegloticase was generally well tolerated, and the estimated rates of adverse events were comparable between the groups,” she said during the virtual annual meeting of the American College of Rheumatology.
Pegloticase is a pegylated recombinant form of porcine uricase that has been shown to be effective in the treatment of gout in patients for whom other therapies have failed.
The drug’s use is limited, however, by immunogenicity, with high antipegloticase antibody titers associated with a loss of response.
“The PEG portion of the molecule, the polyethylene glycol component, can initiate an immune response that would cause significant infusion reactions and preclude further use of the medication for our patients,” explained Suleman Bhana, MD, a rheumatologist with Crystal Run Healthcare in New York’s Hudson Valley, who was not involved in the study.
“By trying to attenuate that immune response by whatever means one can, that could reduce the risk of these infusion reactions and lead to longevity and continuing efficacy of the medication,” he said.
Study details
The RECIPE trial was designed to test whether concomitant immunomodulation could prolong the efficacy of pegloticase therapy by dampening immune reactions.
Investigators enrolled patients 18 years and older who met 2015 ACR/European League Against Rheumatism gout classification criteria and had chronic refractory disease, defined as having symptoms inadequately controlled with oral urate-lowering therapy or a contraindication to ULT.
A total of 42 patients from five rheumatology practices were screened, and 35 were randomized on a 3:1 basis. In the intention-to-treat analysis of the results, the investigators included 32 patients: 22 in the MMF/pegloticase group and 10 placebo-treated controls who had received at least one dose of pegloticase.
Men comprised approximately 90% of the patients in each study arm, with the mean patient age around 55 years. In both groups, patients had a median of one gout flare in the prior year, and a mean duration of gout of 13 years plus a few months.
The patients’ prior urate-lowering agents included allopurinol and febuxostat, and patients had received colchicine, NSAIDs, and corticosteroids for acute gout.
The mean serum urate levels at baseline were 8.9 mg/dL in the MMF group, and 9.8 mg/dL in the placebo group.
Patients were given either MMF 1 g twice daily or a placebo during a 2-week run-in, with the assigned medications continuing for the first 12 weeks concomitantly with pegloticase. The uricase was given intravenously at a dose of 8 mg every 2 weeks for a total of 12 infusions.
As noted before, 86% of patients in the MMF arm (19 of 22) reached the primary outcome of serum uric acid levels below 6 mg/dL by week 12, compared with 40% (4 of 10) in the placebo arm (P = .01).
Week 24 serum uric acid response, a secondary endpoint, was sustained in 68% of patients in the MMF arm, compared with 30% in the placebo arm (P = .03).
“We found no significant differences between the groups in the absolute change in serum urate from baseline to week 24, or from week 12 to 24. We also did not find any differences between the treatment arms for the PROMIS [Patient Reported Outcomes Measurement Information System] or for the Gout Impact Scale,” Dr. Khanna said.
The most commonly reported adverse events included gout flares in 13% of patients in the MMF group and 3% in the placebo group, cardiac disorders in 3% versus 2%, respectively, and gastrointestinal disorders in 9% versus 2%.
Adverse events that occurred only in the MMF group included infections (3%), musculoskeletal and connective tissue disorders (18%), and respiratory events.
Three patients in the placebo arm had infusion reactions, two of which occurred during the first infusion, and one during the second. One of the reactions was considered serious and required hospitalization, but all infusion reactions resolved and none were fatal. There were no infusion reactions in the MMF arm.
Maybe methotrexate instead?
“The efficacy data for mycophenolate in the RECIPE study are convincing, and suggest that this combination substantially increases the proportion of people who respond to pegloticase,” commented Nicola Dalbeth, MD, professor of medicine at the University of Auckland (New Zealand), who moderated the session where the RECIPE data were reported.
“Previous open-label studies of methotrexate with pegloticase [e.g., the MIRROR study] suggest that methotrexate is another effective option to increase the response to pegloticase. However, at this stage, placebo-controlled trials of methotrexate have not been reported. I think a key consideration will be safety, and which option [methotrexate vs. mycophenolate] is safer, noting that many patients with severe gout have important comorbidities, including chronic kidney disease, diabetes, and liver disease,” she said.
Dr. Bhana also noted that there are multiple factors that might determine the choice of MMF or methotrexate as an immunomodulatory partner for pegloticase.
“Some gout patients have chronic kidney disease or a variety of comorbidities – high uric acid can also cause kidney damage – and if they have a kidney illness, methotrexate may not be a safe medicine because there’s a risk of further toxicity that can lead to bone marrow suppression, which I have seen personally in patients, and in this case mycophenolate would be the preferred option,” he said.
The study was sponsored by the University of Alabama at Birmingham, with collaboration from the University of Michigan, as well as the National Institute of Arthritis and Musculoskeletal and Skin Diseases and Horizon, which makes pegloticase. Dr. Khanna disclosed grant and research support from Dyve, Selecta, and Sobi, and consulting for Sobi and Horizon. Dr. Dalbeth disclosed relationships with AstraZeneca, AbbVie, Arthrosi, Dyve, Selecta, and Janssen. Dr. Bhana disclosed nonbranded consulting work for Horizon.
SOURCE: Khanna P et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 0952.
FROM ACR 2020
Decline in febuxostat use trends with cardiovascular concerns
Use of febuxostat (Uloric) decreased among patients with gout in the United States following a Food and Drug Administration–mandated black-box warning that cited cardiovascular concerns, but overall use of urate-lowering therapy remained stable, according to data from a study of commercial insurance enrollees in the United States between 2009 and 2019.

Initiation of urate-lowering therapy (ULT) is recommended for gout patients, and allopurinol remains the first-line treatment, but it is not effective in all patients, and febuxostat was developed as an alternative, wrote Seoyoung C. Kim, MD, ScD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and colleagues.
However, based on data from a postmarketing safety trial (the CARES trial) mandated by the FDA, the agency first issued a safety announcement about an increased risk of cardiovascular mortality with febuxostat in November 2017, followed in February 2019 with a black-box warning after full CARES trial results were published in March 2018 showing a greater risk of cardiovascular and all-cause mortality in febuxostat versus allopurinol.
In a study published in Arthritis & Rheumatology, the researchers examined trends in the use of ULT before and after the FDA warning. They analyzed claims data from a national commercial health database that included 838,432 adult ULT users and 633,229 gout patients.
Overall, allopurinol accounted for the majority of ULT use between 2009 (95% in the first quarter) and 2019 (92% in the fourth quarter).
Febuxostat use peaked at 10% of all ULT use in 2013 and 2014, after a gradual increase following its introduction into the market in 2009, the researchers noted, but decreased to 6% of all ULT use in the fourth quarter of 2019. Other medications, including probenecid, lesinurad (Zurampic), and pegloticase (Krystexxa), accounted for no more than 5% of ULT use.
When the researchers examined gout patients in particular, they found a slight increase in any ULT use from 567 per 1,000 patients in the first quarter of 2009 to 656 per 1,000 patients in the fourth quarter of 2019.
The study findings were limited by several factors, including potential lack of generalizability to other health plans and lack of adjustment for comorbid conditions, the researchers noted.
However, the results highlight the suboptimal use of ULT as a class and the need to address the treatment gap in gout patients “with appropriate ULT prescribing and monitoring,” they said. “While the decrease in febuxostat use was accompanied by a compensatory increase in allopurinol use, the proportion of patients with gout without any ULT remained high throughout the study period,” they concluded.
The study was supported by the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital. Dr. Kim disclosed receiving research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb for research unrelated to the current study.
SOURCE: Kim SC et al. Arthritis Rheumatol. 2020 Oct 7. doi: 10.1002/art.41550.
Use of febuxostat (Uloric) decreased among patients with gout in the United States following a Food and Drug Administration–mandated black-box warning that cited cardiovascular concerns, but overall use of urate-lowering therapy remained stable, according to data from a study of commercial insurance enrollees in the United States between 2009 and 2019.
Initiation of urate-lowering therapy (ULT) is recommended for gout patients, and allopurinol remains the first-line treatment, but it is not effective in all patients, and febuxostat was developed as an alternative, wrote Seoyoung C. Kim, MD, ScD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and colleagues.
However, based on data from a postmarketing safety trial (the CARES trial) mandated by the FDA, the agency first issued a safety announcement about an increased risk of cardiovascular mortality with febuxostat in November 2017, followed in February 2019 with a black-box warning after full CARES trial results were published in March 2018 showing a greater risk of cardiovascular and all-cause mortality in febuxostat versus allopurinol.
In a study published in Arthritis & Rheumatology, the researchers examined trends in the use of ULT before and after the FDA warning. They analyzed claims data from a national commercial health database that included 838,432 adult ULT users and 633,229 gout patients.
Overall, allopurinol accounted for the majority of ULT use between 2009 (95% in the first quarter) and 2019 (92% in the fourth quarter).
Febuxostat use peaked at 10% of all ULT use in 2013 and 2014, after a gradual increase following its introduction into the market in 2009, the researchers noted, but decreased to 6% of all ULT use in the fourth quarter of 2019. Other medications, including probenecid, lesinurad (Zurampic), and pegloticase (Krystexxa), accounted for no more than 5% of ULT use.
When the researchers examined gout patients in particular, they found a slight increase in any ULT use from 567 per 1,000 patients in the first quarter of 2009 to 656 per 1,000 patients in the fourth quarter of 2019.
The study findings were limited by several factors, including potential lack of generalizability to other health plans and lack of adjustment for comorbid conditions, the researchers noted.
However, the results highlight the suboptimal use of ULT as a class and the need to address the treatment gap in gout patients “with appropriate ULT prescribing and monitoring,” they said. “While the decrease in febuxostat use was accompanied by a compensatory increase in allopurinol use, the proportion of patients with gout without any ULT remained high throughout the study period,” they concluded.
The study was supported by the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital. Dr. Kim disclosed receiving research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb for research unrelated to the current study.
SOURCE: Kim SC et al. Arthritis Rheumatol. 2020 Oct 7. doi: 10.1002/art.41550.
Use of febuxostat (Uloric) decreased among patients with gout in the United States following a Food and Drug Administration–mandated black-box warning that cited cardiovascular concerns, but overall use of urate-lowering therapy remained stable, according to data from a study of commercial insurance enrollees in the United States between 2009 and 2019.
Initiation of urate-lowering therapy (ULT) is recommended for gout patients, and allopurinol remains the first-line treatment, but it is not effective in all patients, and febuxostat was developed as an alternative, wrote Seoyoung C. Kim, MD, ScD, of Brigham and Women’s Hospital and Harvard Medical School, Boston, and colleagues.
However, based on data from a postmarketing safety trial (the CARES trial) mandated by the FDA, the agency first issued a safety announcement about an increased risk of cardiovascular mortality with febuxostat in November 2017, followed in February 2019 with a black-box warning after full CARES trial results were published in March 2018 showing a greater risk of cardiovascular and all-cause mortality in febuxostat versus allopurinol.
In a study published in Arthritis & Rheumatology, the researchers examined trends in the use of ULT before and after the FDA warning. They analyzed claims data from a national commercial health database that included 838,432 adult ULT users and 633,229 gout patients.
Overall, allopurinol accounted for the majority of ULT use between 2009 (95% in the first quarter) and 2019 (92% in the fourth quarter).
Febuxostat use peaked at 10% of all ULT use in 2013 and 2014, after a gradual increase following its introduction into the market in 2009, the researchers noted, but decreased to 6% of all ULT use in the fourth quarter of 2019. Other medications, including probenecid, lesinurad (Zurampic), and pegloticase (Krystexxa), accounted for no more than 5% of ULT use.
When the researchers examined gout patients in particular, they found a slight increase in any ULT use from 567 per 1,000 patients in the first quarter of 2009 to 656 per 1,000 patients in the fourth quarter of 2019.
The study findings were limited by several factors, including potential lack of generalizability to other health plans and lack of adjustment for comorbid conditions, the researchers noted.
However, the results highlight the suboptimal use of ULT as a class and the need to address the treatment gap in gout patients “with appropriate ULT prescribing and monitoring,” they said. “While the decrease in febuxostat use was accompanied by a compensatory increase in allopurinol use, the proportion of patients with gout without any ULT remained high throughout the study period,” they concluded.
The study was supported by the division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital. Dr. Kim disclosed receiving research grants to Brigham and Women’s Hospital from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb for research unrelated to the current study.
SOURCE: Kim SC et al. Arthritis Rheumatol. 2020 Oct 7. doi: 10.1002/art.41550.
FROM ARTHRITIS & RHEUMATOLOGY
Dr. Brian Mandell gives his take on ACR’s newest gout guideline
Guidance on the initiation and use of urate-lowering therapies was among the strong recommendations in the updated gout guideline recently issued by the American College of Rheumatology, said Brian F. Mandell, MD, PhD, in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.

The 2020 American College of Rheumatology Guideline for the Management of Gout is “intended to provide guidance for particular patterns of practice and not to dictate the care of a particular patient,” said Dr. Mandell, chair of academic medicine at the Cleveland Clinic in Ohio and cochair of the conference. However, “there was a hope that, with additional evidence since the previous guideline issued in 2012, the recommendations are more firmly based and will improve care,” he said.
Of 42 recommendations, 16 were strong, and these included guidance on several points: when to initiate urate-lowering therapy and using a treat-to-target strategy for lowering serum uric acid to less than 6 mg/dL; prophylaxis against attacks; the use of allopurinol as the first-choice drug and how to avoid hypersensitivity reactions; the use of pegloticase (Krystexxa); and treating flares.
Hyperuricemia does not automatically equal gout, Dr. Mandell said. A 2018 published analysis of data from several large cohorts including 18,889 adults who were gout-free at baseline showed that serum uric acid levels could not accurately predict an initial gout attack. Therefore, the guideline conditionally recommends against initiating any pharmacologic urate-lowering therapy in patients with asymptomatic hyperuricemia. The guideline authors intentionally did not include the presence of comorbidities or deposits of uric acid in making their recommendation. But when advising an individual patient, these factors plus the patient’s age and family history should be considered, he said. “Individualize the decision to use ULT [urate-lowering therapy] to prevent possible future flares,” he advised, with consideration of age, the effects of the flare on the patient’s life, and challenges in treating flares.
For patients who are being treated with urate-lowering therapy, a published study indicated that if treatment is discontinued, “gout attacks will recur, depending on the new serum urate level,” Dr. Mandell said. “Maintenance of low SUA [serum uric acid] must be lifelong to stop attacks,” he emphasized, noting that this is counter to a management guideline published by the American College of Physicians in 2017.
“For patients starting any ULT, we strongly recommend allopurinol over all other urate-lowering therapies as the preferred first-line agent for all patients, including those with CKD [chronic kidney disease] stage 3 or higher,” according to the new guideline, which also recommends starting at a low dose followed by dose titration to target versus starting at a higher dose.
Two reasons in support of a slow up-titration of urate-lowering therapy are a lower frequency of mobilization flares and a possibly lower chance of allopurinol hypersensitivity reactions, Dr. Mandell said.
Although the guideline recommends allopurinol over probenecid, “probenecid works well as monotherapy and effectively as add-on therapy to a xanthine oxidase inhibitor, and it is cheap,” Dr. Mandell said.
Allopurinol can be associated with life-threatening hypersensitivity reactions, but most of these have been associated with a higher-than-recommended starting dose, according to the literature, he noted. The new guideline suggests checking for the HLA-B*5801 haplotype in high-risk demographic groups, and if it is present, to use an alternative to allopurinol if possible
The updated guideline also carries a strong recommendation for the use of pegloticase for patients with frequent gout flares and nonresolving subcutaneous tophi, but it strongly recommends against switching to pegloticase for patients with infrequent gout flares and no tophi.
However, Dr. Mandell said that he will consider off-label treatment of gout with pegloticase “in patients where a shorter time to response really matters,” which is consistent with his belief that, within these treatment principles, the management of gout must be individualized to the specific patient.
For treating acute gout flares, the guideline recommendations strongly supports the use of oral colchicine, NSAIDs, or glucocorticoids as an appropriate first-line therapy, based on patient factors and preferences, instead of using interleukin-1 inhibitors or adrenocorticotropic hormone. However, the interleukin-1 inhibitor anakinra has shown relatively rapid and successful response in treating patients hospitalized with acute gout, Dr. Mandell said. No large, randomized, trials have been conducted, but he cited his experience at the Cleveland Clinic in Ohio, where anakinra is the most common treatment for acute gout on inpatient consults, and he cited a representative small study of 26 patients in which 73% showed “significant response” within 5 days of treatment, which meant that they were able to move and bear weight without pain. In addition, a more recent study of 100 hospitalized patients in the Journal of Rheumatology, found that 75% showed a rapid response to anakinra and improvement or resolution of flares within 4 days, Dr. Mandell said.
Dr. Mandell disclosed relationships with companies including Horizon, Ardea/AstraZeneca/Ironwood, and Takeda. He served as coauthor on the 2012 American College of Rheumatology gout guideline.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Guidance on the initiation and use of urate-lowering therapies was among the strong recommendations in the updated gout guideline recently issued by the American College of Rheumatology, said Brian F. Mandell, MD, PhD, in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
The 2020 American College of Rheumatology Guideline for the Management of Gout is “intended to provide guidance for particular patterns of practice and not to dictate the care of a particular patient,” said Dr. Mandell, chair of academic medicine at the Cleveland Clinic in Ohio and cochair of the conference. However, “there was a hope that, with additional evidence since the previous guideline issued in 2012, the recommendations are more firmly based and will improve care,” he said.
Of 42 recommendations, 16 were strong, and these included guidance on several points: when to initiate urate-lowering therapy and using a treat-to-target strategy for lowering serum uric acid to less than 6 mg/dL; prophylaxis against attacks; the use of allopurinol as the first-choice drug and how to avoid hypersensitivity reactions; the use of pegloticase (Krystexxa); and treating flares.
Hyperuricemia does not automatically equal gout, Dr. Mandell said. A 2018 published analysis of data from several large cohorts including 18,889 adults who were gout-free at baseline showed that serum uric acid levels could not accurately predict an initial gout attack. Therefore, the guideline conditionally recommends against initiating any pharmacologic urate-lowering therapy in patients with asymptomatic hyperuricemia. The guideline authors intentionally did not include the presence of comorbidities or deposits of uric acid in making their recommendation. But when advising an individual patient, these factors plus the patient’s age and family history should be considered, he said. “Individualize the decision to use ULT [urate-lowering therapy] to prevent possible future flares,” he advised, with consideration of age, the effects of the flare on the patient’s life, and challenges in treating flares.
For patients who are being treated with urate-lowering therapy, a published study indicated that if treatment is discontinued, “gout attacks will recur, depending on the new serum urate level,” Dr. Mandell said. “Maintenance of low SUA [serum uric acid] must be lifelong to stop attacks,” he emphasized, noting that this is counter to a management guideline published by the American College of Physicians in 2017.
“For patients starting any ULT, we strongly recommend allopurinol over all other urate-lowering therapies as the preferred first-line agent for all patients, including those with CKD [chronic kidney disease] stage 3 or higher,” according to the new guideline, which also recommends starting at a low dose followed by dose titration to target versus starting at a higher dose.
Two reasons in support of a slow up-titration of urate-lowering therapy are a lower frequency of mobilization flares and a possibly lower chance of allopurinol hypersensitivity reactions, Dr. Mandell said.
Although the guideline recommends allopurinol over probenecid, “probenecid works well as monotherapy and effectively as add-on therapy to a xanthine oxidase inhibitor, and it is cheap,” Dr. Mandell said.
Allopurinol can be associated with life-threatening hypersensitivity reactions, but most of these have been associated with a higher-than-recommended starting dose, according to the literature, he noted. The new guideline suggests checking for the HLA-B*5801 haplotype in high-risk demographic groups, and if it is present, to use an alternative to allopurinol if possible
The updated guideline also carries a strong recommendation for the use of pegloticase for patients with frequent gout flares and nonresolving subcutaneous tophi, but it strongly recommends against switching to pegloticase for patients with infrequent gout flares and no tophi.
However, Dr. Mandell said that he will consider off-label treatment of gout with pegloticase “in patients where a shorter time to response really matters,” which is consistent with his belief that, within these treatment principles, the management of gout must be individualized to the specific patient.
For treating acute gout flares, the guideline recommendations strongly supports the use of oral colchicine, NSAIDs, or glucocorticoids as an appropriate first-line therapy, based on patient factors and preferences, instead of using interleukin-1 inhibitors or adrenocorticotropic hormone. However, the interleukin-1 inhibitor anakinra has shown relatively rapid and successful response in treating patients hospitalized with acute gout, Dr. Mandell said. No large, randomized, trials have been conducted, but he cited his experience at the Cleveland Clinic in Ohio, where anakinra is the most common treatment for acute gout on inpatient consults, and he cited a representative small study of 26 patients in which 73% showed “significant response” within 5 days of treatment, which meant that they were able to move and bear weight without pain. In addition, a more recent study of 100 hospitalized patients in the Journal of Rheumatology, found that 75% showed a rapid response to anakinra and improvement or resolution of flares within 4 days, Dr. Mandell said.
Dr. Mandell disclosed relationships with companies including Horizon, Ardea/AstraZeneca/Ironwood, and Takeda. He served as coauthor on the 2012 American College of Rheumatology gout guideline.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Guidance on the initiation and use of urate-lowering therapies was among the strong recommendations in the updated gout guideline recently issued by the American College of Rheumatology, said Brian F. Mandell, MD, PhD, in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
The 2020 American College of Rheumatology Guideline for the Management of Gout is “intended to provide guidance for particular patterns of practice and not to dictate the care of a particular patient,” said Dr. Mandell, chair of academic medicine at the Cleveland Clinic in Ohio and cochair of the conference. However, “there was a hope that, with additional evidence since the previous guideline issued in 2012, the recommendations are more firmly based and will improve care,” he said.
Of 42 recommendations, 16 were strong, and these included guidance on several points: when to initiate urate-lowering therapy and using a treat-to-target strategy for lowering serum uric acid to less than 6 mg/dL; prophylaxis against attacks; the use of allopurinol as the first-choice drug and how to avoid hypersensitivity reactions; the use of pegloticase (Krystexxa); and treating flares.
Hyperuricemia does not automatically equal gout, Dr. Mandell said. A 2018 published analysis of data from several large cohorts including 18,889 adults who were gout-free at baseline showed that serum uric acid levels could not accurately predict an initial gout attack. Therefore, the guideline conditionally recommends against initiating any pharmacologic urate-lowering therapy in patients with asymptomatic hyperuricemia. The guideline authors intentionally did not include the presence of comorbidities or deposits of uric acid in making their recommendation. But when advising an individual patient, these factors plus the patient’s age and family history should be considered, he said. “Individualize the decision to use ULT [urate-lowering therapy] to prevent possible future flares,” he advised, with consideration of age, the effects of the flare on the patient’s life, and challenges in treating flares.
For patients who are being treated with urate-lowering therapy, a published study indicated that if treatment is discontinued, “gout attacks will recur, depending on the new serum urate level,” Dr. Mandell said. “Maintenance of low SUA [serum uric acid] must be lifelong to stop attacks,” he emphasized, noting that this is counter to a management guideline published by the American College of Physicians in 2017.
“For patients starting any ULT, we strongly recommend allopurinol over all other urate-lowering therapies as the preferred first-line agent for all patients, including those with CKD [chronic kidney disease] stage 3 or higher,” according to the new guideline, which also recommends starting at a low dose followed by dose titration to target versus starting at a higher dose.
Two reasons in support of a slow up-titration of urate-lowering therapy are a lower frequency of mobilization flares and a possibly lower chance of allopurinol hypersensitivity reactions, Dr. Mandell said.
Although the guideline recommends allopurinol over probenecid, “probenecid works well as monotherapy and effectively as add-on therapy to a xanthine oxidase inhibitor, and it is cheap,” Dr. Mandell said.
Allopurinol can be associated with life-threatening hypersensitivity reactions, but most of these have been associated with a higher-than-recommended starting dose, according to the literature, he noted. The new guideline suggests checking for the HLA-B*5801 haplotype in high-risk demographic groups, and if it is present, to use an alternative to allopurinol if possible
The updated guideline also carries a strong recommendation for the use of pegloticase for patients with frequent gout flares and nonresolving subcutaneous tophi, but it strongly recommends against switching to pegloticase for patients with infrequent gout flares and no tophi.
However, Dr. Mandell said that he will consider off-label treatment of gout with pegloticase “in patients where a shorter time to response really matters,” which is consistent with his belief that, within these treatment principles, the management of gout must be individualized to the specific patient.
For treating acute gout flares, the guideline recommendations strongly supports the use of oral colchicine, NSAIDs, or glucocorticoids as an appropriate first-line therapy, based on patient factors and preferences, instead of using interleukin-1 inhibitors or adrenocorticotropic hormone. However, the interleukin-1 inhibitor anakinra has shown relatively rapid and successful response in treating patients hospitalized with acute gout, Dr. Mandell said. No large, randomized, trials have been conducted, but he cited his experience at the Cleveland Clinic in Ohio, where anakinra is the most common treatment for acute gout on inpatient consults, and he cited a representative small study of 26 patients in which 73% showed “significant response” within 5 days of treatment, which meant that they were able to move and bear weight without pain. In addition, a more recent study of 100 hospitalized patients in the Journal of Rheumatology, found that 75% showed a rapid response to anakinra and improvement or resolution of flares within 4 days, Dr. Mandell said.
Dr. Mandell disclosed relationships with companies including Horizon, Ardea/AstraZeneca/Ironwood, and Takeda. He served as coauthor on the 2012 American College of Rheumatology gout guideline.
Global Academy for Medical Education and this news organization are owned by the same parent company.
FROM PRD 2020
Dr. Len Calabrese gives advice on vaccinating adult patients with rheumatic disease
When it comes to preventing infection in rheumatology patients, “vaccination is the best mode of infection protection” and works synergistically with masks and hand washing, according to Leonard H. Calabrese, DO.
“Patients with rheumatic diseases have increased morbidity and mortality [from infection] and a lot of risk factors, including age, comorbidities, cytopenias, and extra-articular disease immunosuppression,” he said in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
Unfortunately, vaccination uptake remains “much lower than we would like in this country,” he said. Notably, influenza vaccination remains well below the World Health Organization target of 75%, he said.
Influenza vaccination
Flu vaccination will be even more important this year in the context of the COVID-19 pandemic, said Dr. Calabrese, professor of medicine and the RJ Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio. “For everyone who comes in with a respiratory illness, we will have to figure out whether it is flu or COVID,” he emphasized.
The Centers for Disease Control and Prevention recommendations include a detailed special considerations section for patients with immunocompromising conditions; “the notes have everything you need to know” about advising rheumatology patients, most of whom can safely receive a flu vaccine, he said.
One concern that always comes up is whether an antibody response will be suppressed based on therapy, Dr. Calabrese noted. Two major drugs with the greatest ability to reduce response are methotrexate and rituximab, he said. His tip: “Withhold methotrexate for two doses following seasonal flu vaccination.” This advice stems from a series of “practice-changing” studies by Park et al. published in 2017, 2018, and 2019 that showed benefit in withholding methotrexate for two doses following vaccination.
In the past, high-dose trivalent flu vaccines have been more expensive, and not necessarily practice changing, with studies showing varying clinical effectiveness and cost-effectiveness, Dr. Calabrese said. This year, a high-dose quadrivalent vaccine should be available that showed a 24% improvement in protection from all strains of influenza, compared with the standard vaccine in a head-to-head, randomized, controlled trial, he noted.
“All patients in rheumatology practices should get a flu vaccine,” with a 2-week hold on methotrexate following vaccination, he advised, and those aged 65 years and older should receive the high-dose quadrivalent. Younger patients on immunosuppressive therapy also might be considered for the high-dose vaccine, he said.
Pneumococcal vaccination
Dr. Calabrese also emphasized the value of pneumococcal vaccines for rheumatology patients. “The mortality for invasive disease ranges from 5% to 32%, but patients with immunocompromising conditions are at increased risk.”
Dr. Calabrese added a note on safety: Patients with cryopyrin-associated periodic syndrome (CAPS), a rare hereditary inflammatory disorder with cutaneous, neurologic, ophthalmologic, and rheumatologic manifestations, may have severe local and systemic reactions to the 23-valent polysaccharide vaccine (PPSV23), he said.
However, immunization against pneumococcal disease is safe and effective for most patients with autoimmune and inflammatory disorders regardless of their current therapy, he said. As with influenza, the CDC’s vaccination recommendations provide details for special situations, including immunocompromised individuals, he noted.
Dr. Calabrese recommended the 13-valent pneumococcal conjugate vaccine (PCV13) as soon as possible for rheumatology patients who have never been vaccinated, with follow-up doses of the 23-valent polysaccharide vaccine (PPSV23) at least 8 weeks later, and a PPSV23 booster 5 years after the first PPSV23 dose.
Protecting against shingles
When it comes to managing the varicella zoster virus (VZV) in immunocompromised patients, “prevention is preferable to treatment, as our patients are particularly vulnerable because of age and declining immunity,” Dr. Calabrese said.
Prevention is important because “once herpes zoster develops, the available treatments, including antiviral therapy, do not prevent postherpetic neuralgia in all patients,” he emphasized. “The treatments are complicated and not always effective,” he added.
The complications of zoster are well known, but recent data show an increased risk of cardiovascular disease as well, Dr. Calabrese said. “All the more reason to protect rheumatology patients from incident zoster,” he said.
Currently, the nonlive recombinant subunit zoster vaccine (Shingrix) is the preferred option for VZV vaccination according to the CDC’s Advisory Committee on Immunization Practices, Dr. Calabrese said. The CDC initially recommended its use to prevent herpes zoster and related complications in all immunocompetent adults aged 50 years and older; in an update, a C-level recommendation extends to “all patients aged 50 with or without immunosuppressive illnesses regardless of previous Zostavax exposure,” Dr. Calabrese said. “All patients on or starting [Janus] kinase inhibitors, regardless of age, should be considered” to receive the herpes zoster vaccine, he noted.
In general, promoting vaccination for rheumatology patients and for all patients is a multipronged effort that might include reminders, rewards, education, and standing orders, Dr. Calabrese said. Clinicians must continue to educate patients not only by strongly recommending the appropriate vaccines, but dispelling myths about vaccination, addressing fears, and providing current and accurate information, he said.
Dr. Calabrese disclosed relationships with AbbVie, Bristol-Myers Squibb, Crescendo, Genentech, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Sanofi-Regeneron, and UCB.
Global Academy for Medical Education and this news organization are owned by the same parent company.
When it comes to preventing infection in rheumatology patients, “vaccination is the best mode of infection protection” and works synergistically with masks and hand washing, according to Leonard H. Calabrese, DO.
“Patients with rheumatic diseases have increased morbidity and mortality [from infection] and a lot of risk factors, including age, comorbidities, cytopenias, and extra-articular disease immunosuppression,” he said in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
Unfortunately, vaccination uptake remains “much lower than we would like in this country,” he said. Notably, influenza vaccination remains well below the World Health Organization target of 75%, he said.
Influenza vaccination
Flu vaccination will be even more important this year in the context of the COVID-19 pandemic, said Dr. Calabrese, professor of medicine and the RJ Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio. “For everyone who comes in with a respiratory illness, we will have to figure out whether it is flu or COVID,” he emphasized.
The Centers for Disease Control and Prevention recommendations include a detailed special considerations section for patients with immunocompromising conditions; “the notes have everything you need to know” about advising rheumatology patients, most of whom can safely receive a flu vaccine, he said.
One concern that always comes up is whether an antibody response will be suppressed based on therapy, Dr. Calabrese noted. Two major drugs with the greatest ability to reduce response are methotrexate and rituximab, he said. His tip: “Withhold methotrexate for two doses following seasonal flu vaccination.” This advice stems from a series of “practice-changing” studies by Park et al. published in 2017, 2018, and 2019 that showed benefit in withholding methotrexate for two doses following vaccination.
In the past, high-dose trivalent flu vaccines have been more expensive, and not necessarily practice changing, with studies showing varying clinical effectiveness and cost-effectiveness, Dr. Calabrese said. This year, a high-dose quadrivalent vaccine should be available that showed a 24% improvement in protection from all strains of influenza, compared with the standard vaccine in a head-to-head, randomized, controlled trial, he noted.
“All patients in rheumatology practices should get a flu vaccine,” with a 2-week hold on methotrexate following vaccination, he advised, and those aged 65 years and older should receive the high-dose quadrivalent. Younger patients on immunosuppressive therapy also might be considered for the high-dose vaccine, he said.
Pneumococcal vaccination
Dr. Calabrese also emphasized the value of pneumococcal vaccines for rheumatology patients. “The mortality for invasive disease ranges from 5% to 32%, but patients with immunocompromising conditions are at increased risk.”
Dr. Calabrese added a note on safety: Patients with cryopyrin-associated periodic syndrome (CAPS), a rare hereditary inflammatory disorder with cutaneous, neurologic, ophthalmologic, and rheumatologic manifestations, may have severe local and systemic reactions to the 23-valent polysaccharide vaccine (PPSV23), he said.
However, immunization against pneumococcal disease is safe and effective for most patients with autoimmune and inflammatory disorders regardless of their current therapy, he said. As with influenza, the CDC’s vaccination recommendations provide details for special situations, including immunocompromised individuals, he noted.
Dr. Calabrese recommended the 13-valent pneumococcal conjugate vaccine (PCV13) as soon as possible for rheumatology patients who have never been vaccinated, with follow-up doses of the 23-valent polysaccharide vaccine (PPSV23) at least 8 weeks later, and a PPSV23 booster 5 years after the first PPSV23 dose.
Protecting against shingles
When it comes to managing the varicella zoster virus (VZV) in immunocompromised patients, “prevention is preferable to treatment, as our patients are particularly vulnerable because of age and declining immunity,” Dr. Calabrese said.
Prevention is important because “once herpes zoster develops, the available treatments, including antiviral therapy, do not prevent postherpetic neuralgia in all patients,” he emphasized. “The treatments are complicated and not always effective,” he added.
The complications of zoster are well known, but recent data show an increased risk of cardiovascular disease as well, Dr. Calabrese said. “All the more reason to protect rheumatology patients from incident zoster,” he said.
Currently, the nonlive recombinant subunit zoster vaccine (Shingrix) is the preferred option for VZV vaccination according to the CDC’s Advisory Committee on Immunization Practices, Dr. Calabrese said. The CDC initially recommended its use to prevent herpes zoster and related complications in all immunocompetent adults aged 50 years and older; in an update, a C-level recommendation extends to “all patients aged 50 with or without immunosuppressive illnesses regardless of previous Zostavax exposure,” Dr. Calabrese said. “All patients on or starting [Janus] kinase inhibitors, regardless of age, should be considered” to receive the herpes zoster vaccine, he noted.
In general, promoting vaccination for rheumatology patients and for all patients is a multipronged effort that might include reminders, rewards, education, and standing orders, Dr. Calabrese said. Clinicians must continue to educate patients not only by strongly recommending the appropriate vaccines, but dispelling myths about vaccination, addressing fears, and providing current and accurate information, he said.
Dr. Calabrese disclosed relationships with AbbVie, Bristol-Myers Squibb, Crescendo, Genentech, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Sanofi-Regeneron, and UCB.
Global Academy for Medical Education and this news organization are owned by the same parent company.
When it comes to preventing infection in rheumatology patients, “vaccination is the best mode of infection protection” and works synergistically with masks and hand washing, according to Leonard H. Calabrese, DO.
“Patients with rheumatic diseases have increased morbidity and mortality [from infection] and a lot of risk factors, including age, comorbidities, cytopenias, and extra-articular disease immunosuppression,” he said in a virtual presentation at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
Unfortunately, vaccination uptake remains “much lower than we would like in this country,” he said. Notably, influenza vaccination remains well below the World Health Organization target of 75%, he said.
Influenza vaccination
Flu vaccination will be even more important this year in the context of the COVID-19 pandemic, said Dr. Calabrese, professor of medicine and the RJ Fasenmyer Chair of Clinical Immunology at the Cleveland Clinic in Ohio. “For everyone who comes in with a respiratory illness, we will have to figure out whether it is flu or COVID,” he emphasized.
The Centers for Disease Control and Prevention recommendations include a detailed special considerations section for patients with immunocompromising conditions; “the notes have everything you need to know” about advising rheumatology patients, most of whom can safely receive a flu vaccine, he said.
One concern that always comes up is whether an antibody response will be suppressed based on therapy, Dr. Calabrese noted. Two major drugs with the greatest ability to reduce response are methotrexate and rituximab, he said. His tip: “Withhold methotrexate for two doses following seasonal flu vaccination.” This advice stems from a series of “practice-changing” studies by Park et al. published in 2017, 2018, and 2019 that showed benefit in withholding methotrexate for two doses following vaccination.
In the past, high-dose trivalent flu vaccines have been more expensive, and not necessarily practice changing, with studies showing varying clinical effectiveness and cost-effectiveness, Dr. Calabrese said. This year, a high-dose quadrivalent vaccine should be available that showed a 24% improvement in protection from all strains of influenza, compared with the standard vaccine in a head-to-head, randomized, controlled trial, he noted.
“All patients in rheumatology practices should get a flu vaccine,” with a 2-week hold on methotrexate following vaccination, he advised, and those aged 65 years and older should receive the high-dose quadrivalent. Younger patients on immunosuppressive therapy also might be considered for the high-dose vaccine, he said.
Pneumococcal vaccination
Dr. Calabrese also emphasized the value of pneumococcal vaccines for rheumatology patients. “The mortality for invasive disease ranges from 5% to 32%, but patients with immunocompromising conditions are at increased risk.”
Dr. Calabrese added a note on safety: Patients with cryopyrin-associated periodic syndrome (CAPS), a rare hereditary inflammatory disorder with cutaneous, neurologic, ophthalmologic, and rheumatologic manifestations, may have severe local and systemic reactions to the 23-valent polysaccharide vaccine (PPSV23), he said.
However, immunization against pneumococcal disease is safe and effective for most patients with autoimmune and inflammatory disorders regardless of their current therapy, he said. As with influenza, the CDC’s vaccination recommendations provide details for special situations, including immunocompromised individuals, he noted.
Dr. Calabrese recommended the 13-valent pneumococcal conjugate vaccine (PCV13) as soon as possible for rheumatology patients who have never been vaccinated, with follow-up doses of the 23-valent polysaccharide vaccine (PPSV23) at least 8 weeks later, and a PPSV23 booster 5 years after the first PPSV23 dose.
Protecting against shingles
When it comes to managing the varicella zoster virus (VZV) in immunocompromised patients, “prevention is preferable to treatment, as our patients are particularly vulnerable because of age and declining immunity,” Dr. Calabrese said.
Prevention is important because “once herpes zoster develops, the available treatments, including antiviral therapy, do not prevent postherpetic neuralgia in all patients,” he emphasized. “The treatments are complicated and not always effective,” he added.
The complications of zoster are well known, but recent data show an increased risk of cardiovascular disease as well, Dr. Calabrese said. “All the more reason to protect rheumatology patients from incident zoster,” he said.
Currently, the nonlive recombinant subunit zoster vaccine (Shingrix) is the preferred option for VZV vaccination according to the CDC’s Advisory Committee on Immunization Practices, Dr. Calabrese said. The CDC initially recommended its use to prevent herpes zoster and related complications in all immunocompetent adults aged 50 years and older; in an update, a C-level recommendation extends to “all patients aged 50 with or without immunosuppressive illnesses regardless of previous Zostavax exposure,” Dr. Calabrese said. “All patients on or starting [Janus] kinase inhibitors, regardless of age, should be considered” to receive the herpes zoster vaccine, he noted.
In general, promoting vaccination for rheumatology patients and for all patients is a multipronged effort that might include reminders, rewards, education, and standing orders, Dr. Calabrese said. Clinicians must continue to educate patients not only by strongly recommending the appropriate vaccines, but dispelling myths about vaccination, addressing fears, and providing current and accurate information, he said.
Dr. Calabrese disclosed relationships with AbbVie, Bristol-Myers Squibb, Crescendo, Genentech, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Sanofi-Regeneron, and UCB.
Global Academy for Medical Education and this news organization are owned by the same parent company.
FROM PRD 2020
The earlier the better for colchicine post-MI: COLCOT
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
The earlier the anti-inflammatory drug colchicine is initiated after a myocardial infarction (MI) the greater the benefit, a new COLCOT analysis suggests.
The parent trial was conducted in patients with a recent MI because of the intense inflammation present at that time, and added colchicine 0.5 mg daily to standard care within 30 days following MI.
As previously reported, colchicine significantly reduced the risk of the primary end point – a composite of cardiovascular (CV) death, resuscitated cardiac arrest, MI, stroke, or urgent hospitalization for angina requiring revascularization – by 23% compared with placebo.
This new analysis shows the risk was reduced by 48% in patients receiving colchicine within 3 days of an MI (4.3% vs. 8.3%; adjusted hazard ratio, 0.52; 95% confidence interval, 0.32-0.84, P = .007).
Risk of a secondary efficacy end point – CV death, resuscitated cardiac arrest, MI, or stroke – was reduced by 45% over an average follow up of 22.7 months (3.3% vs 6.1%; adjusted HR, 0.55; 95% CI, 0.32-0.95, P = .031).
“We believe that our results support an early, in-hospital initiation of adjunctive colchicine for post-MI prevention,” Nadia Bouabdallaoui, MD, Montreal Heart Institute, Quebec, Canada, said during an online session devoted to colchicine at the European Society of Cardiology Congress 2020.
Session moderator Massimo Imazio, MD, professor of cardiology at the University of Turin, Italy, said the improved outcomes suggest that earlier treatment is better – a finding that parallels his own experience using colchicine in patients with pericarditis.
“This substudy is very important because this is probably also the year in cardiovascular applications [that] early use of the drug could improve outcomes,” he said.
Positive data have been accumulating for colchicine from COLCOT, LoDoCo, and, most recently, the LoDoCo2 trial, even as another anti-inflammatory drug, methotrexate, flamed out as secondary prevention in the CIRT trial.
The new COLCOT substudy included 4,661 of the 4,745 original patients and examined treatment initiation using three strata: within 0-3 days (n = 1,193), 4-7 days (n = 720), and 8-30 days (n = 2,748). Patients who received treatment within 3 days were slightly younger, more likely to be smokers, and to have a shorter time from MI to randomization (2.1 days vs 5.1 days vs. 20.8 days, respectively).
In the subset receiving treatment within 3 days, those assigned to colchicine had the same number of cardiac deaths as those given placebo (2 vs. 2) but fewer resuscitated cardiac arrests (1 vs. 3), MIs (17 vs. 29), strokes (1 vs. 5), and urgent hospitalizations for angina requiring revascularization (6 vs. 17).
“A larger trial might have allowed for a better assessment of individual endpoints and subgroups,” observed Bouabdallaoui.
Although there is growing support for colchicine, experts caution that the drug many not be for everyone. In COLCOT, 1 in 10 patients were unable to tolerate the drug, largely because of gastrointestinal (GI) issues.
Pharmacogenomics substudy
A second COLCOT substudy aimed to identify genetic markers predictive of colchicine response and to gain insights into the mechanisms behind this response. It included 767 patients treated with colchicine and another 755 treated with placebo – or about one-third the patients in the original trial.
A genome-wide association study did not find a significant association for the primary CV endpoint, although a prespecified subgroup analysis in men identified an interesting region on chromosome 9 (variant: rs10811106), which just missed reaching genomewide significance, said Marie-Pierre Dubé, PhD, director of the Université de Montréal Beaulieu-Saucier Pharmacogenomics Centre at the Montreal Heart Institute.
In addition, the genomewide analysis found two significant regions for GI events: one on chromosome 6 (variant: rs6916345) and one on chromosome 10 (variant: rs74795203).
For each of the identified regions, the researchers then tested the effect of the allele in the placebo group and the interaction between the genetic variant and treatment with colchicine. For the chromosome 9 region in males, there was no effect in the placebo group and a significant interaction in the colchicine group.
For the significant GI event findings, there was a small effect for the chromosome 6 region in the placebo group and a very significant interaction with colchicine, Dubé said. Similarly, there was no effect for the chromosome 10 region in the placebo group and a significant interaction with colchicine.
Additional analyses in stratified patient populations showed that males with the protective allele (CC) for the chromosome 9 region represented 83% of the population. The primary CV endpoint occurred in 3.2% of these men treated with colchicine and 6.3% treated with placebo (HR, 0.46; 95% CI, 0.24 - 0.86).
For the gastrointestinal events, 25% of patients carried the risk allele (AA) for the chromosome 6 region and 36.9% of these had GI events when treated with colchicine versus 18.6% when treated with placebo (HR, 2.42; 95% CI, 1.57-3.72).
Similarly, 13% of individuals carried one or two copies of the risk allele (AG+GG) for the chromosome 10 region and the risk of GI events in these was nearly four times higher with colchicine (47.1% vs. 18.9%; HR, 3.98; 95% CI 2.24-7.07).
Functional genomic analyses of the identified regions were also performed and showed that the chromosome 9 locus overlaps with the SAXO1 gene, a stabilizer of axonemal microtubules 1.
“The leading variant at this locus (rs10811106 C allele) correlated with the expression of the HAUS6 gene, which is involved in microtubule generation from existing microtubules, and may interact with the effect of colchicine, which is known to inhibit microtubule formation,” observed Dubé.
Also, the chromosome 6 locus associated with gastrointestinal events was colocalizing with the Crohn’s disease locus, adding further support for this region.
“The results support potential personalized approaches to inflammation reduction for cardiovascular prevention,” Dubé said.
This is a post hoc subgroup analysis, however, and replication is necessary, ideally in prospective randomized trials, she noted.
The substudy is important because it provides further insights into the link between colchicine and microtubule polymerization, affecting the activation of the inflammasome, session moderator Imazio said.
“Second, it is important because pharmacogenomics can help us to better understand the optimal responder to colchicine and colchicine resistance,” he said. “So it can be useful for personalized medicine, leading to the proper use of the drug for the proper patient.”
COLCOT was supported by the government of Quebec, the Canadian Institutes of Health Research, and philanthropic foundations. Bouabdallaoui has disclosed no relevant financial relationships. Dubé reported grants from the government of Quebec; personal fees from DalCor and GlaxoSmithKline; research support from AstraZeneca, Pfizer, Servier, Sanofi; and minor equity interest in DalCor. Dubé is also coauthor of patents on pharmacogenomics-guided CETP inhibition, and pharmacogenomics markers of response to colchicine.
This article first appeared on Medscape.com.
LoDoCo2: Added steam for colchicine as secondary prevention
The anti-inflammatory drug colchicine picked up new support as secondary prevention in chronic coronary disease, cutting the risk of cardiovascular events by one-third when added to standard prevention therapies in the double-blind LoDoCo2 study.
Across a median follow up of 29 months in more than 5,000 patients, almost 1 in 10 patients assigned to placebo experienced the primary endpoint of cardiovascular death, myocardial infarction (MI), ischemic stroke, or ischemia-driven coronary revascularization. That risk was 31% lower and resulted in 77 fewer events in those assigned to colchicine (hazard ratio, 0.69; 95% confidence interval, 0.57-0.83).
The beneficial effect of low-dose colchicine 0.5 mg daily was seen early on and accrued over time, extending to five of the eight secondary end points, including a near 30% reduction in the composite of major adverse cardiac events, as well as reductions in the individual endpoints of MI and ischemia-driven revascularization.
“It did that with broadly consistent effects across a range of clinical subgroups, which together speak to the strength of the effect of colchicine on cardiovascular outcomes in the sort of patients we routinely see in our clinics,” primary investigator Mark Nidorf, MD, MBBS, GenesisCare Western Australia, Perth, said at the virtual annual congress of the European Society of Cardiology.
The results were published simultaneously in the New England Journal of Medicine (2020 Aug 31. doi: 10.1056/NEJMoa2021372).
“The totality of evidence from the big three double-blind placebo controlled trials – CANTOS, COLCOT, and LoDoCo2 – are highly consistent and should be practice changing,” Paul Ridker, MD, MPH, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, said in an interview.
Massimo Imazio, MD, the formal discussant for the study and professor of cardiology at the University of Turin, Italy, also called for repurposing the inexpensive gout medication for cardiovascular patients.
“I would like to congratulate the authors for a well-designed, large, randomized trial that in my view provides convincing evidence that colchicine is safe and efficacious for secondary prevention in chronic coronary syndrome, of course if tolerated,” he said.
Dr. Imazio noted that colchicine demonstrated similar benefits in the smaller, open-label LoDoCo trial, but that 1 in 10 patients couldn’t tolerate the drug, largely because of gastrointestinal issues. The LoCoDo2 investigators very wisely opted for a 30-day run-in period for tolerance without a loading dose, and 90% of patients in each arm continued study medication while 3.4% stopped because of perceived effects.
Clinicians should bear in mind the potential for side effects and interactions with other medications, particularly statins, observed Dr. Imazio. “So monitoring of repeat blood tests is indicated, especially blood cell count, transaminase, and [creatine kinase] CK.”
Colchicine can be problematic in patients with chronic kidney disease because it is renally excreted, particularly if patients also take some common antibiotics such as clarithromycin, said Dr. Ridker, who led the landmark CANTOS trial. “So while these data are exciting and confirm the importance of inflammation inhibition in stable coronary disease, colchicine is not for all patients.”
During the discussion of the results, Dr. Nidorf said: “We were very concerned at the outset that there would be an interaction because there is certainly literature there, particularly in renal patients. But as the data showed, the incidence of myotoxicity was decidedly rare.”
Further, myotoxic episodes were independently assessed by a blinded reviewer, and although there was one case of mild rhabdomyolysis in the treatment group, it was considered not primarily caused by colchicine, he said. “So we’re fairly comfortable that you can use colchicine at a low dose quite comfortably with full-dose statins.”
Notably, 94% of patients in both groups were taking statins, and two-thirds were on moderate- or high-dose statins. About one-quarter were on dual-antiplatelet therapy, and 12% were on an anticoagulant.
In all, 5,522 patients aged 35-82 years (mean, 66 years) were randomly assigned to colchicine 0.5 mg once daily or placebo on top of proven secondary prevention therapies, and all but one was available for analysis.
Most were male (85%), one-half had hypertension, 18% had diabetes, and 84% had a history of acute coronary syndrome, with an equal number having undergone revascularization. Patients with advanced renal disease, severe heart failure, or severe valvular heart disease were excluded.
Colchicine, when compared with placebo, was associated with significantly lower incidence rates of the top five ranked secondary endpoints:
- Cardiovascular death, MI, or ischemic stroke (4.2% vs. 5.7%; HR, 0.72).
- MI or ischemia-driven revascularization (5.6% vs. 8.1%; HR, 0.67).
- Cardiovascular death or MI (3.6% vs. 5.0%; HR, 0.71).
- Ischemia-driven revascularization (4.9% vs. 6.4%; HR, 0.75).
- MI (3.0% vs. 4.2%; HR, 0.70).
The incidence rates were similar among the remaining three secondary outcomes: ischemic stroke (0.6% vs. 0.9%), all-cause death (2.6% vs. 2.2%), and CV death (0.7% vs. 0.9%), Dr. Nidorf reported.
The effect of colchicine was consistent in 13 subgroups, including those with and without hypertension, diabetes, or prior acute coronary syndrome. Patients in Australia appeared to do better with colchicine than did those in the Netherlands, which was a bit unexpected but likely caused by the play of chance, Dr. Nidorf said.
“Importantly, the effect when we looked at the predictors of outcome of our patients in this trial, they related to factors such as age and diabetes, which were included in both populations. So we believe the effect of therapy to be universal,” he added.
Session moderator Stephan Achenbach, MD, chair of cardiology at the University of Erlangen (Germany), however, noted that event rates were about 3% per year and many patients had undergone coronary revascularizations for acute coronary syndromes, suggesting this may be a preselected, somewhat higher-risk cohort. “Do you think we can transfer these findings to the just-average patient who comes in with chest pain and gets an elective [percutaneous coronary intervention]?” he asked.
Dr. Nidorf replied that, unlike the patients in COLCOT, who were randomized to colchicine within 30 days of an MI, acute events occurred more than 24 months before randomization in most (68.2%) patients. As such, patients were quite stable, and major adverse cardiac event and cardiovascular death rates were also exceedingly low.
“We did not see them as a particularly high-risk group, which I think is one of the beauties of this study,” Dr. Nidorf said. “It looks at people that are very similar to those who come and meet us in our clinics for regular review and follow-up.”
“And in that regard, I think the next time we’re faced with patients in our rooms, we have to ask the question: Are we doing enough for this patient beyond aspirin and statins? Should we be considering treating the inflammatory axis? And now we have an opportunity to do that,” he said.
Serious adverse effects were similar in the colchicine and placebo groups, including hospitalizations for infection (5.0% vs. 5.2%), pneumonia (1.7% vs. 2.0%), or gastrointestinal reasons (1.9% vs. 1.8%). Myotoxicity occurred in four and three patients, respectively.
Although the signal for increased risk of infection observed in CANTOS and COLCOT was not borne out, Dr. Nidorf observed that chest infections can occur frequently in these patients and echoed cautions about a potential unfavorable interaction between clarithromycin and colchicine.
“If we are to use this drug widely, clinicians will need to learn how to use this drug and what drugs to avoid, and that’s an important teaching point,” he said.
Limitations of the study are the small number of women and lack of routine measurement of C-reactive protein or other inflammatory markers at baseline.
The study was supported by the National Health Medical Research Council of Australia, a grant from the Sir Charles Gairdner Research Advisory Committee, the Withering Foundation the Netherlands, the Netherlands Heart Foundation, the Netherlands Organization for Health Research and Development, and a consortium of Teva, Disphar, and Tiofarma in the Netherlands. The authors’ disclosures are listed in the article.
A version of this article originally appeared on Medscape.com.
The anti-inflammatory drug colchicine picked up new support as secondary prevention in chronic coronary disease, cutting the risk of cardiovascular events by one-third when added to standard prevention therapies in the double-blind LoDoCo2 study.
Across a median follow up of 29 months in more than 5,000 patients, almost 1 in 10 patients assigned to placebo experienced the primary endpoint of cardiovascular death, myocardial infarction (MI), ischemic stroke, or ischemia-driven coronary revascularization. That risk was 31% lower and resulted in 77 fewer events in those assigned to colchicine (hazard ratio, 0.69; 95% confidence interval, 0.57-0.83).
The beneficial effect of low-dose colchicine 0.5 mg daily was seen early on and accrued over time, extending to five of the eight secondary end points, including a near 30% reduction in the composite of major adverse cardiac events, as well as reductions in the individual endpoints of MI and ischemia-driven revascularization.
“It did that with broadly consistent effects across a range of clinical subgroups, which together speak to the strength of the effect of colchicine on cardiovascular outcomes in the sort of patients we routinely see in our clinics,” primary investigator Mark Nidorf, MD, MBBS, GenesisCare Western Australia, Perth, said at the virtual annual congress of the European Society of Cardiology.
The results were published simultaneously in the New England Journal of Medicine (2020 Aug 31. doi: 10.1056/NEJMoa2021372).
“The totality of evidence from the big three double-blind placebo controlled trials – CANTOS, COLCOT, and LoDoCo2 – are highly consistent and should be practice changing,” Paul Ridker, MD, MPH, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, said in an interview.
Massimo Imazio, MD, the formal discussant for the study and professor of cardiology at the University of Turin, Italy, also called for repurposing the inexpensive gout medication for cardiovascular patients.
“I would like to congratulate the authors for a well-designed, large, randomized trial that in my view provides convincing evidence that colchicine is safe and efficacious for secondary prevention in chronic coronary syndrome, of course if tolerated,” he said.
Dr. Imazio noted that colchicine demonstrated similar benefits in the smaller, open-label LoDoCo trial, but that 1 in 10 patients couldn’t tolerate the drug, largely because of gastrointestinal issues. The LoCoDo2 investigators very wisely opted for a 30-day run-in period for tolerance without a loading dose, and 90% of patients in each arm continued study medication while 3.4% stopped because of perceived effects.
Clinicians should bear in mind the potential for side effects and interactions with other medications, particularly statins, observed Dr. Imazio. “So monitoring of repeat blood tests is indicated, especially blood cell count, transaminase, and [creatine kinase] CK.”
Colchicine can be problematic in patients with chronic kidney disease because it is renally excreted, particularly if patients also take some common antibiotics such as clarithromycin, said Dr. Ridker, who led the landmark CANTOS trial. “So while these data are exciting and confirm the importance of inflammation inhibition in stable coronary disease, colchicine is not for all patients.”
During the discussion of the results, Dr. Nidorf said: “We were very concerned at the outset that there would be an interaction because there is certainly literature there, particularly in renal patients. But as the data showed, the incidence of myotoxicity was decidedly rare.”
Further, myotoxic episodes were independently assessed by a blinded reviewer, and although there was one case of mild rhabdomyolysis in the treatment group, it was considered not primarily caused by colchicine, he said. “So we’re fairly comfortable that you can use colchicine at a low dose quite comfortably with full-dose statins.”
Notably, 94% of patients in both groups were taking statins, and two-thirds were on moderate- or high-dose statins. About one-quarter were on dual-antiplatelet therapy, and 12% were on an anticoagulant.
In all, 5,522 patients aged 35-82 years (mean, 66 years) were randomly assigned to colchicine 0.5 mg once daily or placebo on top of proven secondary prevention therapies, and all but one was available for analysis.
Most were male (85%), one-half had hypertension, 18% had diabetes, and 84% had a history of acute coronary syndrome, with an equal number having undergone revascularization. Patients with advanced renal disease, severe heart failure, or severe valvular heart disease were excluded.
Colchicine, when compared with placebo, was associated with significantly lower incidence rates of the top five ranked secondary endpoints:
- Cardiovascular death, MI, or ischemic stroke (4.2% vs. 5.7%; HR, 0.72).
- MI or ischemia-driven revascularization (5.6% vs. 8.1%; HR, 0.67).
- Cardiovascular death or MI (3.6% vs. 5.0%; HR, 0.71).
- Ischemia-driven revascularization (4.9% vs. 6.4%; HR, 0.75).
- MI (3.0% vs. 4.2%; HR, 0.70).
The incidence rates were similar among the remaining three secondary outcomes: ischemic stroke (0.6% vs. 0.9%), all-cause death (2.6% vs. 2.2%), and CV death (0.7% vs. 0.9%), Dr. Nidorf reported.
The effect of colchicine was consistent in 13 subgroups, including those with and without hypertension, diabetes, or prior acute coronary syndrome. Patients in Australia appeared to do better with colchicine than did those in the Netherlands, which was a bit unexpected but likely caused by the play of chance, Dr. Nidorf said.
“Importantly, the effect when we looked at the predictors of outcome of our patients in this trial, they related to factors such as age and diabetes, which were included in both populations. So we believe the effect of therapy to be universal,” he added.
Session moderator Stephan Achenbach, MD, chair of cardiology at the University of Erlangen (Germany), however, noted that event rates were about 3% per year and many patients had undergone coronary revascularizations for acute coronary syndromes, suggesting this may be a preselected, somewhat higher-risk cohort. “Do you think we can transfer these findings to the just-average patient who comes in with chest pain and gets an elective [percutaneous coronary intervention]?” he asked.
Dr. Nidorf replied that, unlike the patients in COLCOT, who were randomized to colchicine within 30 days of an MI, acute events occurred more than 24 months before randomization in most (68.2%) patients. As such, patients were quite stable, and major adverse cardiac event and cardiovascular death rates were also exceedingly low.
“We did not see them as a particularly high-risk group, which I think is one of the beauties of this study,” Dr. Nidorf said. “It looks at people that are very similar to those who come and meet us in our clinics for regular review and follow-up.”
“And in that regard, I think the next time we’re faced with patients in our rooms, we have to ask the question: Are we doing enough for this patient beyond aspirin and statins? Should we be considering treating the inflammatory axis? And now we have an opportunity to do that,” he said.
Serious adverse effects were similar in the colchicine and placebo groups, including hospitalizations for infection (5.0% vs. 5.2%), pneumonia (1.7% vs. 2.0%), or gastrointestinal reasons (1.9% vs. 1.8%). Myotoxicity occurred in four and three patients, respectively.
Although the signal for increased risk of infection observed in CANTOS and COLCOT was not borne out, Dr. Nidorf observed that chest infections can occur frequently in these patients and echoed cautions about a potential unfavorable interaction between clarithromycin and colchicine.
“If we are to use this drug widely, clinicians will need to learn how to use this drug and what drugs to avoid, and that’s an important teaching point,” he said.
Limitations of the study are the small number of women and lack of routine measurement of C-reactive protein or other inflammatory markers at baseline.
The study was supported by the National Health Medical Research Council of Australia, a grant from the Sir Charles Gairdner Research Advisory Committee, the Withering Foundation the Netherlands, the Netherlands Heart Foundation, the Netherlands Organization for Health Research and Development, and a consortium of Teva, Disphar, and Tiofarma in the Netherlands. The authors’ disclosures are listed in the article.
A version of this article originally appeared on Medscape.com.
The anti-inflammatory drug colchicine picked up new support as secondary prevention in chronic coronary disease, cutting the risk of cardiovascular events by one-third when added to standard prevention therapies in the double-blind LoDoCo2 study.
Across a median follow up of 29 months in more than 5,000 patients, almost 1 in 10 patients assigned to placebo experienced the primary endpoint of cardiovascular death, myocardial infarction (MI), ischemic stroke, or ischemia-driven coronary revascularization. That risk was 31% lower and resulted in 77 fewer events in those assigned to colchicine (hazard ratio, 0.69; 95% confidence interval, 0.57-0.83).
The beneficial effect of low-dose colchicine 0.5 mg daily was seen early on and accrued over time, extending to five of the eight secondary end points, including a near 30% reduction in the composite of major adverse cardiac events, as well as reductions in the individual endpoints of MI and ischemia-driven revascularization.
“It did that with broadly consistent effects across a range of clinical subgroups, which together speak to the strength of the effect of colchicine on cardiovascular outcomes in the sort of patients we routinely see in our clinics,” primary investigator Mark Nidorf, MD, MBBS, GenesisCare Western Australia, Perth, said at the virtual annual congress of the European Society of Cardiology.
The results were published simultaneously in the New England Journal of Medicine (2020 Aug 31. doi: 10.1056/NEJMoa2021372).
“The totality of evidence from the big three double-blind placebo controlled trials – CANTOS, COLCOT, and LoDoCo2 – are highly consistent and should be practice changing,” Paul Ridker, MD, MPH, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital in Boston, said in an interview.
Massimo Imazio, MD, the formal discussant for the study and professor of cardiology at the University of Turin, Italy, also called for repurposing the inexpensive gout medication for cardiovascular patients.
“I would like to congratulate the authors for a well-designed, large, randomized trial that in my view provides convincing evidence that colchicine is safe and efficacious for secondary prevention in chronic coronary syndrome, of course if tolerated,” he said.
Dr. Imazio noted that colchicine demonstrated similar benefits in the smaller, open-label LoDoCo trial, but that 1 in 10 patients couldn’t tolerate the drug, largely because of gastrointestinal issues. The LoCoDo2 investigators very wisely opted for a 30-day run-in period for tolerance without a loading dose, and 90% of patients in each arm continued study medication while 3.4% stopped because of perceived effects.
Clinicians should bear in mind the potential for side effects and interactions with other medications, particularly statins, observed Dr. Imazio. “So monitoring of repeat blood tests is indicated, especially blood cell count, transaminase, and [creatine kinase] CK.”
Colchicine can be problematic in patients with chronic kidney disease because it is renally excreted, particularly if patients also take some common antibiotics such as clarithromycin, said Dr. Ridker, who led the landmark CANTOS trial. “So while these data are exciting and confirm the importance of inflammation inhibition in stable coronary disease, colchicine is not for all patients.”
During the discussion of the results, Dr. Nidorf said: “We were very concerned at the outset that there would be an interaction because there is certainly literature there, particularly in renal patients. But as the data showed, the incidence of myotoxicity was decidedly rare.”
Further, myotoxic episodes were independently assessed by a blinded reviewer, and although there was one case of mild rhabdomyolysis in the treatment group, it was considered not primarily caused by colchicine, he said. “So we’re fairly comfortable that you can use colchicine at a low dose quite comfortably with full-dose statins.”
Notably, 94% of patients in both groups were taking statins, and two-thirds were on moderate- or high-dose statins. About one-quarter were on dual-antiplatelet therapy, and 12% were on an anticoagulant.
In all, 5,522 patients aged 35-82 years (mean, 66 years) were randomly assigned to colchicine 0.5 mg once daily or placebo on top of proven secondary prevention therapies, and all but one was available for analysis.
Most were male (85%), one-half had hypertension, 18% had diabetes, and 84% had a history of acute coronary syndrome, with an equal number having undergone revascularization. Patients with advanced renal disease, severe heart failure, or severe valvular heart disease were excluded.
Colchicine, when compared with placebo, was associated with significantly lower incidence rates of the top five ranked secondary endpoints:
- Cardiovascular death, MI, or ischemic stroke (4.2% vs. 5.7%; HR, 0.72).
- MI or ischemia-driven revascularization (5.6% vs. 8.1%; HR, 0.67).
- Cardiovascular death or MI (3.6% vs. 5.0%; HR, 0.71).
- Ischemia-driven revascularization (4.9% vs. 6.4%; HR, 0.75).
- MI (3.0% vs. 4.2%; HR, 0.70).
The incidence rates were similar among the remaining three secondary outcomes: ischemic stroke (0.6% vs. 0.9%), all-cause death (2.6% vs. 2.2%), and CV death (0.7% vs. 0.9%), Dr. Nidorf reported.
The effect of colchicine was consistent in 13 subgroups, including those with and without hypertension, diabetes, or prior acute coronary syndrome. Patients in Australia appeared to do better with colchicine than did those in the Netherlands, which was a bit unexpected but likely caused by the play of chance, Dr. Nidorf said.
“Importantly, the effect when we looked at the predictors of outcome of our patients in this trial, they related to factors such as age and diabetes, which were included in both populations. So we believe the effect of therapy to be universal,” he added.
Session moderator Stephan Achenbach, MD, chair of cardiology at the University of Erlangen (Germany), however, noted that event rates were about 3% per year and many patients had undergone coronary revascularizations for acute coronary syndromes, suggesting this may be a preselected, somewhat higher-risk cohort. “Do you think we can transfer these findings to the just-average patient who comes in with chest pain and gets an elective [percutaneous coronary intervention]?” he asked.
Dr. Nidorf replied that, unlike the patients in COLCOT, who were randomized to colchicine within 30 days of an MI, acute events occurred more than 24 months before randomization in most (68.2%) patients. As such, patients were quite stable, and major adverse cardiac event and cardiovascular death rates were also exceedingly low.
“We did not see them as a particularly high-risk group, which I think is one of the beauties of this study,” Dr. Nidorf said. “It looks at people that are very similar to those who come and meet us in our clinics for regular review and follow-up.”
“And in that regard, I think the next time we’re faced with patients in our rooms, we have to ask the question: Are we doing enough for this patient beyond aspirin and statins? Should we be considering treating the inflammatory axis? And now we have an opportunity to do that,” he said.
Serious adverse effects were similar in the colchicine and placebo groups, including hospitalizations for infection (5.0% vs. 5.2%), pneumonia (1.7% vs. 2.0%), or gastrointestinal reasons (1.9% vs. 1.8%). Myotoxicity occurred in four and three patients, respectively.
Although the signal for increased risk of infection observed in CANTOS and COLCOT was not borne out, Dr. Nidorf observed that chest infections can occur frequently in these patients and echoed cautions about a potential unfavorable interaction between clarithromycin and colchicine.
“If we are to use this drug widely, clinicians will need to learn how to use this drug and what drugs to avoid, and that’s an important teaching point,” he said.
Limitations of the study are the small number of women and lack of routine measurement of C-reactive protein or other inflammatory markers at baseline.
The study was supported by the National Health Medical Research Council of Australia, a grant from the Sir Charles Gairdner Research Advisory Committee, the Withering Foundation the Netherlands, the Netherlands Heart Foundation, the Netherlands Organization for Health Research and Development, and a consortium of Teva, Disphar, and Tiofarma in the Netherlands. The authors’ disclosures are listed in the article.
A version of this article originally appeared on Medscape.com.
DECT has mixed performance in differentiating gout vs. CPPD
Dual-energy computed tomography (DECT) appears to have limited utility for differentiating between gout and calcium pyrophosphate deposition disease (CPPD), according to a German prospective cohort study. Findings were reported at the annual European Congress of Rheumatology, held online this year because of COVID-19.
“Differentiation of gout and pseudogout, or CPPD, is sometimes difficult,” said presenting investigator Valentin S. Schäfer, MD, associate professor of internal medicine and head of the department of rheumatology and clinical immunology at University Hospital Bonn (Germany).
“Arthrocentesis and subsequent polarization microscopy remains the gold standard,” he noted. “Novel diagnostic approaches, such as DECT, have recently been validated for gout, but limited data [are] available on the use of DECT in patients with CPPD.”
The investigators studied 30 patients: 22 with suspected gout and 8 with suspected CPPD. All underwent arthrocentesis with subsequent polarization microscopy for definitive diagnosis, plus clinical examination, ultrasound examination, conventional radiography, DECT, and assessment of 12 laboratory parameters.
For diagnosis of gout, DECT had a sensitivity and specificity of 59.1% and 100%, respectively, Dr. Schäfer reported, noting that this sensitivity falls considerably short of the 90% previously reported for gout.
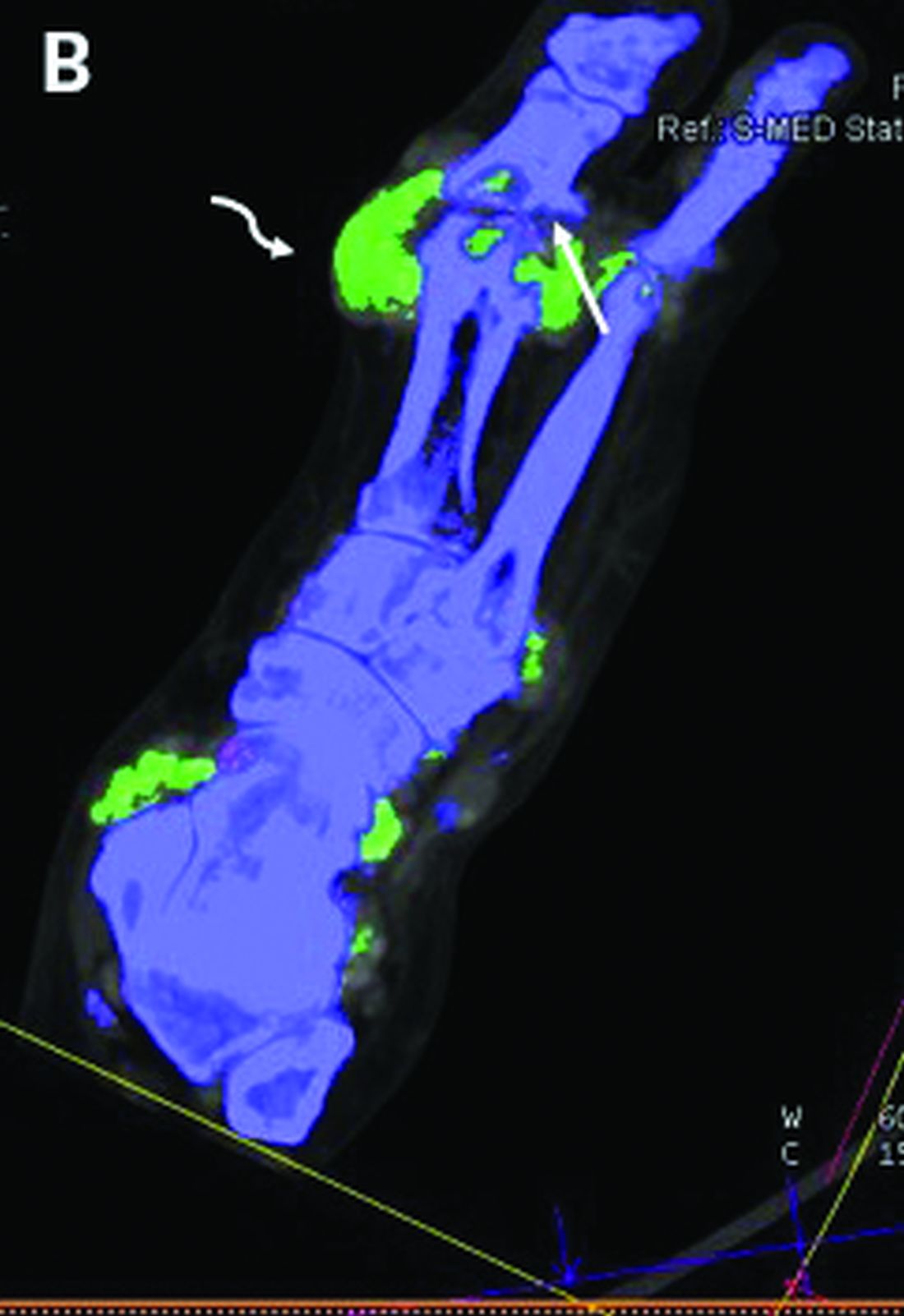
Corresponding sensitivity and specificity were 90.9% and 75% for ultrasound, 58.8% and 100% for conventional radiography, and 81.8% and 87.5% for the rheumatologists’ suspected clinical diagnosis.
For diagnosis of CPPD, DECT had sensitivity of 37.5% and specificity of 81.8%. Corresponding values were 87.5% and 91% for ultrasound, 0% and 94.1% for conventional radiography, and 75.0% and 100% for suspected clinical diagnosis.

None of the 12 laboratory parameters studied – uric acid, C-reactive protein, organic phosphate, and leukocytes, among others – significantly differentiated between conditions.

“Both ultrasound and suspected clinical diagnosis had higher sensitivities than DECT for gout and CPPD,” Dr. Schäfer concluded. “Further studies with larger patient cohorts and perhaps modified scan protocols are needed in order to determine the diagnostic utility of DECT in CPPD.”
Findings in context
“Noninvasive, accurate methods for distinguishing between gout and CPPD will improve clinical care,” Sara K. Tedeschi, MD, MPH, predicted in an interview.
“Arthrocentesis is painful in an acutely inflamed joint, can be difficult to perform on small joints, and is underutilized in clinical practice,” she elaborated. And ultrasound is operator dependent and does not quantify crystal volume in and around the joint.
The question addressed by the study is therefore clinically relevant, according to Dr. Tedeschi, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston.
However, among the patients with CPPD, the study did not report specific phenotypes (acute inflammatory arthritis, chronic inflammatory arthritis, and osteoarthritis with calcium pyrophosphate deposits), she noted. “It is difficult to draw conclusions about the sensitivity or specificity of DECT for CPPD without this information, especially among just 8 CPPD patients.”
In addition, among the patients with gout, the proportion having new-onset disease with flare duration less than 6 weeks and the proportion with tophi were unknown, both of which affected DECT sensitivity in the previous study that reported 90% sensitivity. “Based on the 95% confidence interval in the present study, it is possible that with a larger sample size, DECT sensitivity for gout would have been higher,” she pointed out. “We also do not know the DECT software settings, which impact DECT interpretation as positive or negative for the crystal of interest.”
Finally, “it would be relevant to know what joints were aspirated and imaged in each group,” Dr. Tedeschi said. “For example, if the first metatarsophalangeal (MTP) joint was aspirated and imaged for half of the gout patients but for none of the CPPD patients, that may affect the study interpretation.”
The study did not receive any specific funding. Dr. Schäfer disclosed a variety of financial relationships with multiple pharmaceutical companies. Dr. Tedeschi disclosed receiving grant support from the National Institutes of Health to study imaging modalities for CPPD, and being first author on a study comparing the sensitivity of DECT, ultrasound, and x-ray for acute CPP crystal arthritis.
SOURCE: Kravchenko D et al. Ann Rheum Dis. 2020 Jun;79[suppl 1]:196.
Dual-energy computed tomography (DECT) appears to have limited utility for differentiating between gout and calcium pyrophosphate deposition disease (CPPD), according to a German prospective cohort study. Findings were reported at the annual European Congress of Rheumatology, held online this year because of COVID-19.
“Differentiation of gout and pseudogout, or CPPD, is sometimes difficult,” said presenting investigator Valentin S. Schäfer, MD, associate professor of internal medicine and head of the department of rheumatology and clinical immunology at University Hospital Bonn (Germany).
“Arthrocentesis and subsequent polarization microscopy remains the gold standard,” he noted. “Novel diagnostic approaches, such as DECT, have recently been validated for gout, but limited data [are] available on the use of DECT in patients with CPPD.”
The investigators studied 30 patients: 22 with suspected gout and 8 with suspected CPPD. All underwent arthrocentesis with subsequent polarization microscopy for definitive diagnosis, plus clinical examination, ultrasound examination, conventional radiography, DECT, and assessment of 12 laboratory parameters.
For diagnosis of gout, DECT had a sensitivity and specificity of 59.1% and 100%, respectively, Dr. Schäfer reported, noting that this sensitivity falls considerably short of the 90% previously reported for gout.
Corresponding sensitivity and specificity were 90.9% and 75% for ultrasound, 58.8% and 100% for conventional radiography, and 81.8% and 87.5% for the rheumatologists’ suspected clinical diagnosis.
For diagnosis of CPPD, DECT had sensitivity of 37.5% and specificity of 81.8%. Corresponding values were 87.5% and 91% for ultrasound, 0% and 94.1% for conventional radiography, and 75.0% and 100% for suspected clinical diagnosis.
None of the 12 laboratory parameters studied – uric acid, C-reactive protein, organic phosphate, and leukocytes, among others – significantly differentiated between conditions.
“Both ultrasound and suspected clinical diagnosis had higher sensitivities than DECT for gout and CPPD,” Dr. Schäfer concluded. “Further studies with larger patient cohorts and perhaps modified scan protocols are needed in order to determine the diagnostic utility of DECT in CPPD.”
Findings in context
“Noninvasive, accurate methods for distinguishing between gout and CPPD will improve clinical care,” Sara K. Tedeschi, MD, MPH, predicted in an interview.
“Arthrocentesis is painful in an acutely inflamed joint, can be difficult to perform on small joints, and is underutilized in clinical practice,” she elaborated. And ultrasound is operator dependent and does not quantify crystal volume in and around the joint.
The question addressed by the study is therefore clinically relevant, according to Dr. Tedeschi, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston.
However, among the patients with CPPD, the study did not report specific phenotypes (acute inflammatory arthritis, chronic inflammatory arthritis, and osteoarthritis with calcium pyrophosphate deposits), she noted. “It is difficult to draw conclusions about the sensitivity or specificity of DECT for CPPD without this information, especially among just 8 CPPD patients.”
In addition, among the patients with gout, the proportion having new-onset disease with flare duration less than 6 weeks and the proportion with tophi were unknown, both of which affected DECT sensitivity in the previous study that reported 90% sensitivity. “Based on the 95% confidence interval in the present study, it is possible that with a larger sample size, DECT sensitivity for gout would have been higher,” she pointed out. “We also do not know the DECT software settings, which impact DECT interpretation as positive or negative for the crystal of interest.”
Finally, “it would be relevant to know what joints were aspirated and imaged in each group,” Dr. Tedeschi said. “For example, if the first metatarsophalangeal (MTP) joint was aspirated and imaged for half of the gout patients but for none of the CPPD patients, that may affect the study interpretation.”
The study did not receive any specific funding. Dr. Schäfer disclosed a variety of financial relationships with multiple pharmaceutical companies. Dr. Tedeschi disclosed receiving grant support from the National Institutes of Health to study imaging modalities for CPPD, and being first author on a study comparing the sensitivity of DECT, ultrasound, and x-ray for acute CPP crystal arthritis.
SOURCE: Kravchenko D et al. Ann Rheum Dis. 2020 Jun;79[suppl 1]:196.
Dual-energy computed tomography (DECT) appears to have limited utility for differentiating between gout and calcium pyrophosphate deposition disease (CPPD), according to a German prospective cohort study. Findings were reported at the annual European Congress of Rheumatology, held online this year because of COVID-19.
“Differentiation of gout and pseudogout, or CPPD, is sometimes difficult,” said presenting investigator Valentin S. Schäfer, MD, associate professor of internal medicine and head of the department of rheumatology and clinical immunology at University Hospital Bonn (Germany).
“Arthrocentesis and subsequent polarization microscopy remains the gold standard,” he noted. “Novel diagnostic approaches, such as DECT, have recently been validated for gout, but limited data [are] available on the use of DECT in patients with CPPD.”
The investigators studied 30 patients: 22 with suspected gout and 8 with suspected CPPD. All underwent arthrocentesis with subsequent polarization microscopy for definitive diagnosis, plus clinical examination, ultrasound examination, conventional radiography, DECT, and assessment of 12 laboratory parameters.
For diagnosis of gout, DECT had a sensitivity and specificity of 59.1% and 100%, respectively, Dr. Schäfer reported, noting that this sensitivity falls considerably short of the 90% previously reported for gout.
Corresponding sensitivity and specificity were 90.9% and 75% for ultrasound, 58.8% and 100% for conventional radiography, and 81.8% and 87.5% for the rheumatologists’ suspected clinical diagnosis.
For diagnosis of CPPD, DECT had sensitivity of 37.5% and specificity of 81.8%. Corresponding values were 87.5% and 91% for ultrasound, 0% and 94.1% for conventional radiography, and 75.0% and 100% for suspected clinical diagnosis.
None of the 12 laboratory parameters studied – uric acid, C-reactive protein, organic phosphate, and leukocytes, among others – significantly differentiated between conditions.
“Both ultrasound and suspected clinical diagnosis had higher sensitivities than DECT for gout and CPPD,” Dr. Schäfer concluded. “Further studies with larger patient cohorts and perhaps modified scan protocols are needed in order to determine the diagnostic utility of DECT in CPPD.”
Findings in context
“Noninvasive, accurate methods for distinguishing between gout and CPPD will improve clinical care,” Sara K. Tedeschi, MD, MPH, predicted in an interview.
“Arthrocentesis is painful in an acutely inflamed joint, can be difficult to perform on small joints, and is underutilized in clinical practice,” she elaborated. And ultrasound is operator dependent and does not quantify crystal volume in and around the joint.
The question addressed by the study is therefore clinically relevant, according to Dr. Tedeschi, a rheumatologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston.
However, among the patients with CPPD, the study did not report specific phenotypes (acute inflammatory arthritis, chronic inflammatory arthritis, and osteoarthritis with calcium pyrophosphate deposits), she noted. “It is difficult to draw conclusions about the sensitivity or specificity of DECT for CPPD without this information, especially among just 8 CPPD patients.”
In addition, among the patients with gout, the proportion having new-onset disease with flare duration less than 6 weeks and the proportion with tophi were unknown, both of which affected DECT sensitivity in the previous study that reported 90% sensitivity. “Based on the 95% confidence interval in the present study, it is possible that with a larger sample size, DECT sensitivity for gout would have been higher,” she pointed out. “We also do not know the DECT software settings, which impact DECT interpretation as positive or negative for the crystal of interest.”
Finally, “it would be relevant to know what joints were aspirated and imaged in each group,” Dr. Tedeschi said. “For example, if the first metatarsophalangeal (MTP) joint was aspirated and imaged for half of the gout patients but for none of the CPPD patients, that may affect the study interpretation.”
The study did not receive any specific funding. Dr. Schäfer disclosed a variety of financial relationships with multiple pharmaceutical companies. Dr. Tedeschi disclosed receiving grant support from the National Institutes of Health to study imaging modalities for CPPD, and being first author on a study comparing the sensitivity of DECT, ultrasound, and x-ray for acute CPP crystal arthritis.
SOURCE: Kravchenko D et al. Ann Rheum Dis. 2020 Jun;79[suppl 1]:196.
FROM THE EULAR 2020 E-CONGRESS
EULAR gives pointers on intra-articular injection best practices
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
New EULAR recommendations for the intra-articular (IA) treatment of arthropathies aim to facilitate uniformity and quality of care for this mainstay of rheumatologic practice, according to a report on the new guidance that was presented at the annual European Congress of Rheumatology, held online this year due to COVID-19.
Until now there were no official recommendations on how best to use it in everyday practice. “This is the first time that there’s been a joint effort to develop evidence-based recommendations,” Jacqueline Usón, MD, PhD, associate professor medicine at Rey Juan Carlos University in Madrid, said in an interview. “Everything that we are saying is pretty logical, but it’s nice to see it put in recommendations based on evidence.”
IA therapy has been around for decades and is key for treating adults with a number of different conditions where synovitis, effusion, pain, or all three, are present, such as inflammatory arthritis and osteoarthritis, Dr. Usón observed during her presentation.
“Today, commonly used injectables are not only corticosteroids but also local anesthetics, hyaluronic acid, blood products, and maybe pharmaceuticals,” she said, adding that “there is a wide variation in the way intra-articular therapies are used and delivered to patients.” Health professionals also have very different views and habits depending on geographic locations and health care systems, she observed. Ironing out the variation was one of the main objectives of the recommendations.
As one of the two conveners of the EULAR task force behind the recommendations, Dr. Usón, herself a rheumatologist at University Hospital of Móstoles, pointed out that the task force brought together a range of specialties – rheumatologists, orthopedic surgeons, radiologists, nuclear medicine specialists, among others, as well as patients – to ensure that the best advice could be given.
The task force followed EULAR standard operating procedures for developing recommendations, with discussion groups, systematic literature reviews, and Delphi technique-based consensus all being employed. The literature search considered publications from 1946 up until 2019.
“We agreed on the need for more background information from health professionals and patients, so we developed two surveys: One for health professionals with 160 items, [for which] we obtained 186 responses from 26 countries; and the patient survey was made up of 44 items, translated into 10 different languages, and we obtained 200 responses,” she said.
The results of the systematic literature review and surveys were used to help form expert consensus, leading to 5 overarching principles and 11 recommendations that look at before, during, and after intra-articular therapy.
Five overarching principles
The first overarching principle recognizes the widespread use of IA therapies and that their use is specific to the disease that is being treated and “may not be interchangeable across indications,” Dr. Usón said. The second principle concerns improving patient-centered outcomes, which are “those that are relevant to the patient,” and include the benefits, harms, preferences, or implications for self-management.
“Contextual factors are important and contribute to the effect of IAT [intra-articular treatment],” she said, discussing the third principle. “These include effective communication, patient expectations, or settings [where the procedure takes place]. In addition, one should take into account that the route of delivery has in itself a placebo effect. We found that in different RCTs [randomized controlled trials], the pooled placebo effect of IA saline is moderate to large.”
The fourth principle looks at ensuring that patients and clinicians make an informed and shared decision, which is again highlighted by the first recommendation. The fifth, and last, overarching principle acknowledges that IA injections may be given by a range of health care professionals.
Advice for before, during, and after injection
Patients need to be “fully informed of the nature of the procedure, the injectable used, and potential effects – benefits and risks – [and] informed consent should be obtained and documented,” said Dr. Usón, outlining the first recommendation. “That seems common,” she said in the interview, “but when we did the survey, we realize that many patients didn’t [give consent], and the doctors didn’t even ask for it. This is why it’s a very general statement, and it’s our first recommendation. The agreement was 99%!”
The recommendations also look at the optimal settings for performing injections, such as providing a professional and private, well-lighted room, and having a resuscitation kit nearby in case patients faint. Accuracy is important, Dr. Usón said, and imaging, such as ultrasound, should be used where available to ensure accurate injection into the joint. This is an area where further research could be performed, she said, urging young rheumatologists and health professionals to consider this. “Intra-articular therapy is something that you learn and do, but you never really investigate in it,” she said.
One recommendation states that when intra-articular injections are being given to pregnant patients, the safety of injected compound must be considered, both for the mother and for the fetus. There is another recommendation on the need to perform IA injections under aseptic conditions, and another stating that patients should be offered local anesthetics, after explaining the pros and cons.
Special populations of patients are also considered, Dr. Usón said. For example, the guidance advises warning patients with diabetes of the risk of transient glycemia after IA glucocorticoids and the need to monitor their blood glucose levels carefully for a couple of days afterward.
As a rule, “IAT is not a contraindication to people with clotting or bleeding disorders, or taking antithrombotic medications,” she said, unless they are at a high risk of bleeding.
Importantly, the recommendations cover when IAT can be performed after joint replacement surgery (after at least 3 months), and the need to “avoid overuse of injected joints” while also avoiding complete immobilization for at least 24 hours afterward. The recommendations very generally cover re-injections, but not how long intervals between injections should be. When asked about interval duration after her presentation, Dr. Usón said that the usual advice is to give IA injections no more than 2-3 times a year, but it depends on the injectable.
“It wasn’t our intention to review the efficacy and the safety of the different injectables, nor to review the use of IAT in different types of joint diseases,” she said. “We do lack a lot of information, a lot of evidence in this, and I really would hope that new rheumatologists start looking into and start investigating in this topic,” she added.
Recommendations will increase awareness of good clinical practice
“IA injections are commonly administered in the rheumatology setting. This is because [IA injection] is often a useful treatment for acute flare of arthritis, particularly when it is limited to a few joints,” observed Ai Lyn Tan, MD, associate professor and honorary consultant rheumatologist at the Leeds (England) Institute of Rheumatic and Musculoskeletal Medicine.
IA injection “also relieves symptoms relatively quickly for patients; however, the response can be variable, and there are side effects associated with IA injections,” Dr. Tan added in an interview.
There is a lack of universally accepted recommendations, Dr. Tan observed, noting that while there might be some local guidelines on how to safely perform IA injections these were often not standardized and were subject to being continually updated to try to improve the experience for patients.
“It is therefore timely to learn about the new EULAR recommendations for IA injections. The advantage of this will be to increase awareness of good clinical practice for performing IA injections.”
Dr. Tan had no relevant conflicts of interest.
SOURCE: EULAR COVID-19 Recommendations. E-congress content available until Sept. 1, 2020.
FROM THE EULAR 2020 E-CONGRESS
Advice on treating rheumatic diseases from a COVID-19 epicenter
The COVID-19 pandemic continues to pose an unprecedented challenge to health care systems worldwide. In addition to the direct impact of the disease itself, there is a growing concern related to ensuring adequate health care utilization and addressing the needs of vulnerable populations, such as those with chronic illness.
Emanuel et al. have advocated a framework of fair allocation of resources, led by the principles of equity, maximizing benefits, and prioritizing the vulnerable. In these uncertain times, patients with rheumatic diseases represent a vulnerable population whose health and wellness are particularly threatened, not only by the risk of COVID-19, but also by reduced access to usual medical care (e.g., in-person clinic visits), potential treatment interruptions (e.g., planned infusion therapies), and the ongoing shortage of hydroxychloroquine, to name a few.
As rheumatologists, we are now tasked with the development of best practices for caring for patients with rheumatic conditions in this uncertain, evolving, and nearly data-free landscape. We also must maintain an active role as advocates for our patients to help them navigate this pandemic. Herein, we discuss our approach to caring for patients with rheumatic diseases within our practice in New York City, an epicenter of the COVID-19 pandemic.
Communication with patients
Maintaining an open line of communication with our patients (by phone, patient portal, telemedicine, and so on) has become more essential than ever. It is through these communications that we best understand our patients’ concerns and provide support and personalized treatment decisions. The most common questions we have received during recent weeks are:
- Should I stop my medication to lower my risk for infection?
- Are my current symptoms caused by coronavirus, and what should I do next?
- Where can I fill my hydroxychloroquine prescription?
The American College of Rheumatology has deployed a number of task forces aimed at advocating for rheumatologists and patients with rheumatic diseases and is doing an exemplary job guiding us. For patients, several other organizations (e.g., CreakyJoints, Arthritis Foundation, Lupus Research Alliance, Vasculitis Foundation, and Scleroderma Foundation) are also providing accurate information regarding hygiene practices, social distancing, management of medications, and other guidance related to specific rheumatic diseases. In line with ACR recommendations, we encourage a personalized, shared decision-making process with each of our patients.
Patients with rheumatic disease at risk for COVID-19 infection
First, for rheumatology patients who have no COVID-19 symptoms, our management approach is individualized. For patients who are able to maintain social distancing, we have not routinely stopped immunosuppressive medications, including disease-modifying antirheumatic drugs (DMARDs) and biologic agents. However, we discuss the risks and benefits of continuing immunosuppressive therapy during this time with all of our patients.
In certain cases of stable, non–life-threatening disease, we may consider spacing or temporarily interrupting immunosuppressive therapy, using individualized, shared decision making. Yet, it is important to recognize that, for some patients, achieving adequate disease control can require a substantial amount of time.
Furthermore, it is important to acknowledge that disease flares requiring steroid therapy may increase the risk for infection even more, keeping in mind that, in some rheumatic diseases, high disease activity itself can increase infection risk. We advise patients who are continuing therapy to maintain at least a 1-month supply of their medications.
Decisions regarding infusions in the hospital and outpatient settings are similarly made on an individual basis, weighing the risk for virus exposure against that of disease flare. The more limited availability of appropriately distanced infusion chairs in some already overburdened systems must be considered in this discussion. We agree with the ACR, whose infusion guidance recommends that “possible changes might include temporary interruption of therapy, temporary initiation of a bridge therapy such as a less potent anti-inflammatory or immune-modulating agent, or temporary change to an alternative therapy.”
We also reinforce recommended behaviors for preventing infection, including social distancing, frequent handwashing, and avoiding touching one’s face.
Patients with rheumatic disease and confirmed or suspected COVID-19 infection
With the worldwide spread of COVID-19, patients with rheumatic diseases will undoubtedly be among those exposed and infected. Though current data are limited, within a cohort from China, 1% had an autoimmune disease. Testing recommendations to confirm COVID-19 and decision guidelines for outpatient versus inpatient management are evolving, and we consult the most up-to-date, local information regarding testing as individual potential cases arise.
For patients who develop COVID-19 and are currently taking DMARDs and biologics, we recommend that they discontinue these medications, with the exception of hydroxychloroquine (HCQ). HCQ may be continued because its mechanism is not expected to worsen infection, and it plays a key role in the management of patients with systemic lupus erythematosus (SLE). In addition, in vitro antiviral effects have been reported and there is growing interest for its use in the management of COVID-19. However, there are conflicting data and methodological concerns about the nonrandomized human studies that suggest a benefit of HCQ against COVID-19.
The decision regarding management of glucocorticoids in the setting of new COVID-19 infection is challenging and should be individualized. At present, expert panels recommend against the use of glucocorticoids among individuals with COVID-19 who do not have acute respiratory distress syndrome. However, adrenal insufficiency must be considered among patients with COVID-19 who are treated with chronic glucocorticoids. Again, these decisions should be made on an individual, case-by-case basis.
Implications of a hydroxychloroquine shortage
The use of HCQ in rheumatology is supported by years of research. Particularly in SLE, HCQ has been shown to reduce disease activity and damage and to improve survival. Furthermore, for pregnant patients with SLE, numerous studies have demonstrated the safety and benefit of HCQ for both the mother and fetus; thus, it is strongly recommended. By contrast, despite the growing interest for HCQ in patients with COVID-19, the evidence is inconclusive and limited.
The ACR suggests that decisions regarding HCQ dose reductions to extend individual patients supplies should be tailored to each patient’s need and risk in the unfortunate setting of medication shortages. Even in patients with stable SLE, however, disease flares at 6 months are more common among individuals who discontinue HCQ. Of note, these flares may incorporate novel and severe disease manifestations.
Unfortunately, other therapeutic options for SLE are associated with more adverse effects (including increased susceptibility to infection) or are largely unavailable (e.g., quinacrine). Thus, we strive to continue standard dosing of HCQ for patients who are currently flaring or recently flared, and we make shared, individualized decisions for those patients with stable disease as the HCQ shortage evolves.
Future research on COVID-19 and rheumatic disease
While we might expect that an underlying rheumatic disease and associated treatments may predispose individuals to developing COVID-19, current data do not indicate which, if any, rheumatic diseases and associated therapies convey the greatest risk.
To address this uncertainty, the rheumatology community created the COVID-19 Global Rheumatology Alliance, an international effort to initiate and maintain a deidentified patient registry for individuals with rheumatic disease who develop COVID-19. These efforts will allow us to gain essential insights regarding which patient demographics, underlying diseases, and medications are most common among patients who develop COVID-19.
This alliance encourages rheumatologists and those caring for patients with rheumatic diseases to report their patient cases to this registry. As we are confronted with making management decisions with a scarcity of supporting data, efforts like these will improve our ability to make individualized treatment recommendations.
The COVID-19 pandemic has presented us all with unprecedented challenges. As rheumatologists, it is our duty to lead our patients through this uncharted territory with close communication, information, advocacy, and personalized treatment decisions. Each of these is central to the management of rheumatology patients during the COVID-19 pandemic.
With the growing interest in immunomodulatory therapies for the complications of this infection, we have the unique opportunity to share our expertise, recommendations, and caution with our colleagues. As clinicians and scientists, we must advocate for data collection and studies that will allow us to develop novel, data-driven disease management approaches while providing the best care possible for our patients.
Stephen Paget, MD, is physician in chief emeritus for the Center for Rheumatology at Hospital for Special Surgery in New York. Kimberly Showalter, MD, is a third-year rheumatology fellow at Hospital for Special Surgery. Sebastian E. Sattui, MD, is a third-year rheumatology and 1-year vasculitis fellow at Hospital for Special Surgery.
A version of this article originally appeared on Medscape.com.
The COVID-19 pandemic continues to pose an unprecedented challenge to health care systems worldwide. In addition to the direct impact of the disease itself, there is a growing concern related to ensuring adequate health care utilization and addressing the needs of vulnerable populations, such as those with chronic illness.
Emanuel et al. have advocated a framework of fair allocation of resources, led by the principles of equity, maximizing benefits, and prioritizing the vulnerable. In these uncertain times, patients with rheumatic diseases represent a vulnerable population whose health and wellness are particularly threatened, not only by the risk of COVID-19, but also by reduced access to usual medical care (e.g., in-person clinic visits), potential treatment interruptions (e.g., planned infusion therapies), and the ongoing shortage of hydroxychloroquine, to name a few.
As rheumatologists, we are now tasked with the development of best practices for caring for patients with rheumatic conditions in this uncertain, evolving, and nearly data-free landscape. We also must maintain an active role as advocates for our patients to help them navigate this pandemic. Herein, we discuss our approach to caring for patients with rheumatic diseases within our practice in New York City, an epicenter of the COVID-19 pandemic.
Communication with patients
Maintaining an open line of communication with our patients (by phone, patient portal, telemedicine, and so on) has become more essential than ever. It is through these communications that we best understand our patients’ concerns and provide support and personalized treatment decisions. The most common questions we have received during recent weeks are:
- Should I stop my medication to lower my risk for infection?
- Are my current symptoms caused by coronavirus, and what should I do next?
- Where can I fill my hydroxychloroquine prescription?
The American College of Rheumatology has deployed a number of task forces aimed at advocating for rheumatologists and patients with rheumatic diseases and is doing an exemplary job guiding us. For patients, several other organizations (e.g., CreakyJoints, Arthritis Foundation, Lupus Research Alliance, Vasculitis Foundation, and Scleroderma Foundation) are also providing accurate information regarding hygiene practices, social distancing, management of medications, and other guidance related to specific rheumatic diseases. In line with ACR recommendations, we encourage a personalized, shared decision-making process with each of our patients.
Patients with rheumatic disease at risk for COVID-19 infection
First, for rheumatology patients who have no COVID-19 symptoms, our management approach is individualized. For patients who are able to maintain social distancing, we have not routinely stopped immunosuppressive medications, including disease-modifying antirheumatic drugs (DMARDs) and biologic agents. However, we discuss the risks and benefits of continuing immunosuppressive therapy during this time with all of our patients.
In certain cases of stable, non–life-threatening disease, we may consider spacing or temporarily interrupting immunosuppressive therapy, using individualized, shared decision making. Yet, it is important to recognize that, for some patients, achieving adequate disease control can require a substantial amount of time.
Furthermore, it is important to acknowledge that disease flares requiring steroid therapy may increase the risk for infection even more, keeping in mind that, in some rheumatic diseases, high disease activity itself can increase infection risk. We advise patients who are continuing therapy to maintain at least a 1-month supply of their medications.
Decisions regarding infusions in the hospital and outpatient settings are similarly made on an individual basis, weighing the risk for virus exposure against that of disease flare. The more limited availability of appropriately distanced infusion chairs in some already overburdened systems must be considered in this discussion. We agree with the ACR, whose infusion guidance recommends that “possible changes might include temporary interruption of therapy, temporary initiation of a bridge therapy such as a less potent anti-inflammatory or immune-modulating agent, or temporary change to an alternative therapy.”
We also reinforce recommended behaviors for preventing infection, including social distancing, frequent handwashing, and avoiding touching one’s face.
Patients with rheumatic disease and confirmed or suspected COVID-19 infection
With the worldwide spread of COVID-19, patients with rheumatic diseases will undoubtedly be among those exposed and infected. Though current data are limited, within a cohort from China, 1% had an autoimmune disease. Testing recommendations to confirm COVID-19 and decision guidelines for outpatient versus inpatient management are evolving, and we consult the most up-to-date, local information regarding testing as individual potential cases arise.
For patients who develop COVID-19 and are currently taking DMARDs and biologics, we recommend that they discontinue these medications, with the exception of hydroxychloroquine (HCQ). HCQ may be continued because its mechanism is not expected to worsen infection, and it plays a key role in the management of patients with systemic lupus erythematosus (SLE). In addition, in vitro antiviral effects have been reported and there is growing interest for its use in the management of COVID-19. However, there are conflicting data and methodological concerns about the nonrandomized human studies that suggest a benefit of HCQ against COVID-19.
The decision regarding management of glucocorticoids in the setting of new COVID-19 infection is challenging and should be individualized. At present, expert panels recommend against the use of glucocorticoids among individuals with COVID-19 who do not have acute respiratory distress syndrome. However, adrenal insufficiency must be considered among patients with COVID-19 who are treated with chronic glucocorticoids. Again, these decisions should be made on an individual, case-by-case basis.
Implications of a hydroxychloroquine shortage
The use of HCQ in rheumatology is supported by years of research. Particularly in SLE, HCQ has been shown to reduce disease activity and damage and to improve survival. Furthermore, for pregnant patients with SLE, numerous studies have demonstrated the safety and benefit of HCQ for both the mother and fetus; thus, it is strongly recommended. By contrast, despite the growing interest for HCQ in patients with COVID-19, the evidence is inconclusive and limited.
The ACR suggests that decisions regarding HCQ dose reductions to extend individual patients supplies should be tailored to each patient’s need and risk in the unfortunate setting of medication shortages. Even in patients with stable SLE, however, disease flares at 6 months are more common among individuals who discontinue HCQ. Of note, these flares may incorporate novel and severe disease manifestations.
Unfortunately, other therapeutic options for SLE are associated with more adverse effects (including increased susceptibility to infection) or are largely unavailable (e.g., quinacrine). Thus, we strive to continue standard dosing of HCQ for patients who are currently flaring or recently flared, and we make shared, individualized decisions for those patients with stable disease as the HCQ shortage evolves.
Future research on COVID-19 and rheumatic disease
While we might expect that an underlying rheumatic disease and associated treatments may predispose individuals to developing COVID-19, current data do not indicate which, if any, rheumatic diseases and associated therapies convey the greatest risk.
To address this uncertainty, the rheumatology community created the COVID-19 Global Rheumatology Alliance, an international effort to initiate and maintain a deidentified patient registry for individuals with rheumatic disease who develop COVID-19. These efforts will allow us to gain essential insights regarding which patient demographics, underlying diseases, and medications are most common among patients who develop COVID-19.
This alliance encourages rheumatologists and those caring for patients with rheumatic diseases to report their patient cases to this registry. As we are confronted with making management decisions with a scarcity of supporting data, efforts like these will improve our ability to make individualized treatment recommendations.
The COVID-19 pandemic has presented us all with unprecedented challenges. As rheumatologists, it is our duty to lead our patients through this uncharted territory with close communication, information, advocacy, and personalized treatment decisions. Each of these is central to the management of rheumatology patients during the COVID-19 pandemic.
With the growing interest in immunomodulatory therapies for the complications of this infection, we have the unique opportunity to share our expertise, recommendations, and caution with our colleagues. As clinicians and scientists, we must advocate for data collection and studies that will allow us to develop novel, data-driven disease management approaches while providing the best care possible for our patients.
Stephen Paget, MD, is physician in chief emeritus for the Center for Rheumatology at Hospital for Special Surgery in New York. Kimberly Showalter, MD, is a third-year rheumatology fellow at Hospital for Special Surgery. Sebastian E. Sattui, MD, is a third-year rheumatology and 1-year vasculitis fellow at Hospital for Special Surgery.
A version of this article originally appeared on Medscape.com.
The COVID-19 pandemic continues to pose an unprecedented challenge to health care systems worldwide. In addition to the direct impact of the disease itself, there is a growing concern related to ensuring adequate health care utilization and addressing the needs of vulnerable populations, such as those with chronic illness.
Emanuel et al. have advocated a framework of fair allocation of resources, led by the principles of equity, maximizing benefits, and prioritizing the vulnerable. In these uncertain times, patients with rheumatic diseases represent a vulnerable population whose health and wellness are particularly threatened, not only by the risk of COVID-19, but also by reduced access to usual medical care (e.g., in-person clinic visits), potential treatment interruptions (e.g., planned infusion therapies), and the ongoing shortage of hydroxychloroquine, to name a few.
As rheumatologists, we are now tasked with the development of best practices for caring for patients with rheumatic conditions in this uncertain, evolving, and nearly data-free landscape. We also must maintain an active role as advocates for our patients to help them navigate this pandemic. Herein, we discuss our approach to caring for patients with rheumatic diseases within our practice in New York City, an epicenter of the COVID-19 pandemic.
Communication with patients
Maintaining an open line of communication with our patients (by phone, patient portal, telemedicine, and so on) has become more essential than ever. It is through these communications that we best understand our patients’ concerns and provide support and personalized treatment decisions. The most common questions we have received during recent weeks are:
- Should I stop my medication to lower my risk for infection?
- Are my current symptoms caused by coronavirus, and what should I do next?
- Where can I fill my hydroxychloroquine prescription?
The American College of Rheumatology has deployed a number of task forces aimed at advocating for rheumatologists and patients with rheumatic diseases and is doing an exemplary job guiding us. For patients, several other organizations (e.g., CreakyJoints, Arthritis Foundation, Lupus Research Alliance, Vasculitis Foundation, and Scleroderma Foundation) are also providing accurate information regarding hygiene practices, social distancing, management of medications, and other guidance related to specific rheumatic diseases. In line with ACR recommendations, we encourage a personalized, shared decision-making process with each of our patients.
Patients with rheumatic disease at risk for COVID-19 infection
First, for rheumatology patients who have no COVID-19 symptoms, our management approach is individualized. For patients who are able to maintain social distancing, we have not routinely stopped immunosuppressive medications, including disease-modifying antirheumatic drugs (DMARDs) and biologic agents. However, we discuss the risks and benefits of continuing immunosuppressive therapy during this time with all of our patients.
In certain cases of stable, non–life-threatening disease, we may consider spacing or temporarily interrupting immunosuppressive therapy, using individualized, shared decision making. Yet, it is important to recognize that, for some patients, achieving adequate disease control can require a substantial amount of time.
Furthermore, it is important to acknowledge that disease flares requiring steroid therapy may increase the risk for infection even more, keeping in mind that, in some rheumatic diseases, high disease activity itself can increase infection risk. We advise patients who are continuing therapy to maintain at least a 1-month supply of their medications.
Decisions regarding infusions in the hospital and outpatient settings are similarly made on an individual basis, weighing the risk for virus exposure against that of disease flare. The more limited availability of appropriately distanced infusion chairs in some already overburdened systems must be considered in this discussion. We agree with the ACR, whose infusion guidance recommends that “possible changes might include temporary interruption of therapy, temporary initiation of a bridge therapy such as a less potent anti-inflammatory or immune-modulating agent, or temporary change to an alternative therapy.”
We also reinforce recommended behaviors for preventing infection, including social distancing, frequent handwashing, and avoiding touching one’s face.
Patients with rheumatic disease and confirmed or suspected COVID-19 infection
With the worldwide spread of COVID-19, patients with rheumatic diseases will undoubtedly be among those exposed and infected. Though current data are limited, within a cohort from China, 1% had an autoimmune disease. Testing recommendations to confirm COVID-19 and decision guidelines for outpatient versus inpatient management are evolving, and we consult the most up-to-date, local information regarding testing as individual potential cases arise.
For patients who develop COVID-19 and are currently taking DMARDs and biologics, we recommend that they discontinue these medications, with the exception of hydroxychloroquine (HCQ). HCQ may be continued because its mechanism is not expected to worsen infection, and it plays a key role in the management of patients with systemic lupus erythematosus (SLE). In addition, in vitro antiviral effects have been reported and there is growing interest for its use in the management of COVID-19. However, there are conflicting data and methodological concerns about the nonrandomized human studies that suggest a benefit of HCQ against COVID-19.
The decision regarding management of glucocorticoids in the setting of new COVID-19 infection is challenging and should be individualized. At present, expert panels recommend against the use of glucocorticoids among individuals with COVID-19 who do not have acute respiratory distress syndrome. However, adrenal insufficiency must be considered among patients with COVID-19 who are treated with chronic glucocorticoids. Again, these decisions should be made on an individual, case-by-case basis.
Implications of a hydroxychloroquine shortage
The use of HCQ in rheumatology is supported by years of research. Particularly in SLE, HCQ has been shown to reduce disease activity and damage and to improve survival. Furthermore, for pregnant patients with SLE, numerous studies have demonstrated the safety and benefit of HCQ for both the mother and fetus; thus, it is strongly recommended. By contrast, despite the growing interest for HCQ in patients with COVID-19, the evidence is inconclusive and limited.
The ACR suggests that decisions regarding HCQ dose reductions to extend individual patients supplies should be tailored to each patient’s need and risk in the unfortunate setting of medication shortages. Even in patients with stable SLE, however, disease flares at 6 months are more common among individuals who discontinue HCQ. Of note, these flares may incorporate novel and severe disease manifestations.
Unfortunately, other therapeutic options for SLE are associated with more adverse effects (including increased susceptibility to infection) or are largely unavailable (e.g., quinacrine). Thus, we strive to continue standard dosing of HCQ for patients who are currently flaring or recently flared, and we make shared, individualized decisions for those patients with stable disease as the HCQ shortage evolves.
Future research on COVID-19 and rheumatic disease
While we might expect that an underlying rheumatic disease and associated treatments may predispose individuals to developing COVID-19, current data do not indicate which, if any, rheumatic diseases and associated therapies convey the greatest risk.
To address this uncertainty, the rheumatology community created the COVID-19 Global Rheumatology Alliance, an international effort to initiate and maintain a deidentified patient registry for individuals with rheumatic disease who develop COVID-19. These efforts will allow us to gain essential insights regarding which patient demographics, underlying diseases, and medications are most common among patients who develop COVID-19.
This alliance encourages rheumatologists and those caring for patients with rheumatic diseases to report their patient cases to this registry. As we are confronted with making management decisions with a scarcity of supporting data, efforts like these will improve our ability to make individualized treatment recommendations.
The COVID-19 pandemic has presented us all with unprecedented challenges. As rheumatologists, it is our duty to lead our patients through this uncharted territory with close communication, information, advocacy, and personalized treatment decisions. Each of these is central to the management of rheumatology patients during the COVID-19 pandemic.
With the growing interest in immunomodulatory therapies for the complications of this infection, we have the unique opportunity to share our expertise, recommendations, and caution with our colleagues. As clinicians and scientists, we must advocate for data collection and studies that will allow us to develop novel, data-driven disease management approaches while providing the best care possible for our patients.
Stephen Paget, MD, is physician in chief emeritus for the Center for Rheumatology at Hospital for Special Surgery in New York. Kimberly Showalter, MD, is a third-year rheumatology fellow at Hospital for Special Surgery. Sebastian E. Sattui, MD, is a third-year rheumatology and 1-year vasculitis fellow at Hospital for Special Surgery.
A version of this article originally appeared on Medscape.com.