User login
Oncology hospitalist field is small, but growing
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.

"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.

At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.

Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
On Twitter @maryellenny
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.
"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.
At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.
Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
On Twitter @maryellenny
Have you met an oncology hospitalist yet? If you haven’t, you probably will soon.
The latest offshoot of hospital medicine aims to take all the strengths of the hospitalist movement – increased efficiency and improved quality and safety – and apply them to inpatient cancer care.
While there is no typical oncology-hospitalist program, most manage the complications of a patient’s cancer and treatment, as well as providing some type of end-of-life services. Oncology hospitalists may be oncologists with an interest in taking care of hospitalized patients. Or they could be hospitalists trained in internal or family medicine, who have an interest in caring for cancer patients.
"People are very interested in this, and we really want to grow it," said Dr. Maria-Claudia Campagna, an oncology-hospitalist at the University of Texas MD Anderson Cancer Center in Houston.
Dr. Campagna is part of a nine-physician oncology-hospitalist program at MD Anderson. The program was launched in 2006 with just one hospitalist, but has grown to nine hospitalists over the last several years. And the program is in the process of recruiting three more physicians.
They are also piloting an observation unit geared toward oncology patients, she said.
Much like in the early days of hospital medicine, Dr. Campagna said the program initially got pushback from oncologists who didn’t want to give up care of their patients in the hospital. But over time, the hospitalists have proven their competence and oncologists have gotten even busier with their outpatient practices.
"They know we take good care of their patients, so ultimately they trust our criteria. And when we don’t know, we tell them," Dr. Campagna said. "So we have a very symbiotic relationship."
The experience at MD Anderson is being replicated at cancer centers and academic medical centers around the country. Even some community hospitals are exploring the idea.
The reason is simple, said Dr. Eddy Chen, an oncology hospitalist at Dana-Farber/Brigham and Women’s Cancer Center in Boston. The combination of a coming shortage of oncologists combined with an expected surge in cancer patients among aging baby boomers means that virtually every hospital will see a marked increase in cancer patients over the next several years.
"In the future, there are going to be a lot more patients with cancer who are going to be coming into the hospital," Dr. Chen said. "And who is going to take care of these patients?"
But I’m not an oncologist ...
At Dana-Farber/Brigham and Women’s, they have three oncology hospitalists, including Dr. Chen. Along with the regular cadre of oncologists, they manage all of the hospitalized cancer patients. What makes hospitalist management different from that of the oncologists, who are treating both inpatients and outpatients, is the focus on quality improvement, patient safety, and research, said Dr. Chen.
Dr. Chen, who is trained as an oncologist, said hospitalists don’t need to be oncologists to do this job. But as the field develops, there are likely to be some training or prerequisites that will develop. For now, Dr. Chen said hospitalists need to have an interest in treating complex patients and be willing to develop a deeper understanding of the principles of cancer medicine.
"We are now at a point in the road of this endeavor where best practices, and understanding these issues, can be further defined," Dr. Chen said.
As Dr. Chen proves, oncology hospitalists can be oncologists or traditional hospitalists trained in internal medicine or family medicine. But they must all be prepared to handle complex patients and take on end-of-life discussions.
At Memorial Sloan-Kettering Cancer Center in New York, where the oncology-hospitalist team works mainly with GI oncology and lymphoma patients, they treat patients with very advanced disease, many of whom are in the last 6 months of life.
"We’ve attained a lot of experience and expertise in end-of-life care, but it’s all been on-the-job training," said Dr. Barbara C. Egan, chief of the hospital medicine service at Sloan-Kettering.
Because of the heavy focus on end-of-life care, Dr. Egan and some of the other hospitalists in her group were recently board certified in hospice and palliative medicine based in part on their clinical experience working with cancer patients.
Emotional days
The work is very different from a general medicine hospitalist service. For oncology hospitalists, all of the patients have multisystem organ disease and also typically have complicated psychosocial dynamics end-of-life care. The result is a time-consuming, emotionally charged day that isn’t accurately measured by RVUs (relative value units) or the number of encounters per day, Dr. Egan said.
"It’s very different to round on a 25-year-old who’s dying of colon cancer, than in a general medicine hospital where you might have several patients on the service who are there for single issue, uncomplicated soft rule-out MI." she said. "It’s definitely very emotionally draining on the physicians."
To try to prevent burnout among their physicians, Sloan-Kettering’s program consists of seven daytime hospitalists who work a typical 2-week on/2-week off schedule. The other 10 hospitalists are dedicated nocturnalists. The model has resulted in virtually no turnover among the daytime hospitalists. The nocturnal group has high turnover, which is typical of most night-shift work. At this point, there’s no definitive count of the number of oncology hospitalists working in the United States today. But what is clear, is that the small niche is growing.
Dr. A. Charlotta Weaver, medical director of oncology hospitalists at Northwestern Memorial Hospital in Chicago, epitomizes the appeal for some young physicians.
Dr. Weaver graduated from residency in 2008, a year after Northwestern launched its oncology-hospitalist program. She had been considering a fellowship in hematology/oncology when she heard about the new program. "This little light went off in my head that that’s what I wanted to do," she said.
Initially, she thought about working as an oncology hospitalist for a few years as a bridge to fellowship, but ultimately decided to stay on with the program. The appeals, she said, was a combination of the hospitalist schedule and taking care of hematology/oncology patients.
"I think of it as real medicine. They are really sick," Dr. Weaver said. "There is something legitimately wrong with them and I can help; whereas in general medicine, you don’t always have that sense."
On Twitter @maryellenny

Communication and collaboration: An elusive goal
In recent months I’ve participated in several system-level efforts to reduce avoidable readmissions, with considerable focus placed upon handoff communication. Over the arc of my career, handoff communication has become increasingly important as inpatient care becomes more fragmented, resulting in several national initiatives. To date, there has been no such effort placed upon communication during the hospitalization.
The Joint Commission has estimated that up to 70% of sentinel events have poor interprofessional communication as a contributing factor. HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) domains emphasize communication between physicians, nurses, and patients. Patient care suffers when health care teams do not communicate effectively, and patient satisfaction follows suit.
A few recent examples from the palliative care service:
• A 54-year-old male hospitalized with cord compression secondary to malignancy and infection was evaluated by five different surgical subspecialists over a 6-day period. An additional 4 days passed before the surgeons were able to speak and agree upon a plan.
• A 16-year-old girl with epilepsy was admitted after elective orthognathic surgery. It took 2 weeks of effort (preoperatively) on the part of her parents to ensure that the surgeon and neurologist developed a plan for antiepileptic therapy while the patient was NPO for 5 days.
• An ethics case conference was called to discuss the case of a 62-year-old woman with cirrhosis and sepsis. Two of the providers involved disagreed over the patient’s prognosis and whether enteral nutrition should be continued. At the case conference, the providers were able to discuss the case face to face, and the issue was resolved. Prior to the meeting, they had not discussed the case except through progress notes.
It is curious that, in the age of nearly continuous communication via text, e-mail, Internet, and even wearable devices, we physicians have such difficulty having a quick conversation about a patient over the phone. How can this be? In my practice, I have almost no problem reaching my colleagues when there is an emergency. In the nonemergent situation, however, it is more complicated. I don’t want to pull my colleague away from a patient (whether office- or hospital-based) for an important, but nonurgent matter. For my hospital-based colleagues, there is no office staff with whom to leave a message.
As we are all being asked to see more patients, the time for reviewing charts and returning calls is progressively reduced. Standard text messaging is not HIPAA compliant; however, there are fee-based HIPAA-compliant text applications. Our local county medical society offers this as a benefit of membership, but to date only a minority of my colleagues are users.
As we move toward more team-based care and pay for performance, it is imperative for physicians to agree upon standards for communication and for health care systems to invest in infrastructure to facilitate effective communication and collaboration. If we fail to do so, it is likely that external forces (third-party payers, regulatory agencies, etc.) will impose their own standards, without our input.
Dr. Fredholm and colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog.
In recent months I’ve participated in several system-level efforts to reduce avoidable readmissions, with considerable focus placed upon handoff communication. Over the arc of my career, handoff communication has become increasingly important as inpatient care becomes more fragmented, resulting in several national initiatives. To date, there has been no such effort placed upon communication during the hospitalization.
The Joint Commission has estimated that up to 70% of sentinel events have poor interprofessional communication as a contributing factor. HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) domains emphasize communication between physicians, nurses, and patients. Patient care suffers when health care teams do not communicate effectively, and patient satisfaction follows suit.
A few recent examples from the palliative care service:
• A 54-year-old male hospitalized with cord compression secondary to malignancy and infection was evaluated by five different surgical subspecialists over a 6-day period. An additional 4 days passed before the surgeons were able to speak and agree upon a plan.
• A 16-year-old girl with epilepsy was admitted after elective orthognathic surgery. It took 2 weeks of effort (preoperatively) on the part of her parents to ensure that the surgeon and neurologist developed a plan for antiepileptic therapy while the patient was NPO for 5 days.
• An ethics case conference was called to discuss the case of a 62-year-old woman with cirrhosis and sepsis. Two of the providers involved disagreed over the patient’s prognosis and whether enteral nutrition should be continued. At the case conference, the providers were able to discuss the case face to face, and the issue was resolved. Prior to the meeting, they had not discussed the case except through progress notes.
It is curious that, in the age of nearly continuous communication via text, e-mail, Internet, and even wearable devices, we physicians have such difficulty having a quick conversation about a patient over the phone. How can this be? In my practice, I have almost no problem reaching my colleagues when there is an emergency. In the nonemergent situation, however, it is more complicated. I don’t want to pull my colleague away from a patient (whether office- or hospital-based) for an important, but nonurgent matter. For my hospital-based colleagues, there is no office staff with whom to leave a message.
As we are all being asked to see more patients, the time for reviewing charts and returning calls is progressively reduced. Standard text messaging is not HIPAA compliant; however, there are fee-based HIPAA-compliant text applications. Our local county medical society offers this as a benefit of membership, but to date only a minority of my colleagues are users.
As we move toward more team-based care and pay for performance, it is imperative for physicians to agree upon standards for communication and for health care systems to invest in infrastructure to facilitate effective communication and collaboration. If we fail to do so, it is likely that external forces (third-party payers, regulatory agencies, etc.) will impose their own standards, without our input.
Dr. Fredholm and colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog.
In recent months I’ve participated in several system-level efforts to reduce avoidable readmissions, with considerable focus placed upon handoff communication. Over the arc of my career, handoff communication has become increasingly important as inpatient care becomes more fragmented, resulting in several national initiatives. To date, there has been no such effort placed upon communication during the hospitalization.
The Joint Commission has estimated that up to 70% of sentinel events have poor interprofessional communication as a contributing factor. HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) domains emphasize communication between physicians, nurses, and patients. Patient care suffers when health care teams do not communicate effectively, and patient satisfaction follows suit.
A few recent examples from the palliative care service:
• A 54-year-old male hospitalized with cord compression secondary to malignancy and infection was evaluated by five different surgical subspecialists over a 6-day period. An additional 4 days passed before the surgeons were able to speak and agree upon a plan.
• A 16-year-old girl with epilepsy was admitted after elective orthognathic surgery. It took 2 weeks of effort (preoperatively) on the part of her parents to ensure that the surgeon and neurologist developed a plan for antiepileptic therapy while the patient was NPO for 5 days.
• An ethics case conference was called to discuss the case of a 62-year-old woman with cirrhosis and sepsis. Two of the providers involved disagreed over the patient’s prognosis and whether enteral nutrition should be continued. At the case conference, the providers were able to discuss the case face to face, and the issue was resolved. Prior to the meeting, they had not discussed the case except through progress notes.
It is curious that, in the age of nearly continuous communication via text, e-mail, Internet, and even wearable devices, we physicians have such difficulty having a quick conversation about a patient over the phone. How can this be? In my practice, I have almost no problem reaching my colleagues when there is an emergency. In the nonemergent situation, however, it is more complicated. I don’t want to pull my colleague away from a patient (whether office- or hospital-based) for an important, but nonurgent matter. For my hospital-based colleagues, there is no office staff with whom to leave a message.
As we are all being asked to see more patients, the time for reviewing charts and returning calls is progressively reduced. Standard text messaging is not HIPAA compliant; however, there are fee-based HIPAA-compliant text applications. Our local county medical society offers this as a benefit of membership, but to date only a minority of my colleagues are users.
As we move toward more team-based care and pay for performance, it is imperative for physicians to agree upon standards for communication and for health care systems to invest in infrastructure to facilitate effective communication and collaboration. If we fail to do so, it is likely that external forces (third-party payers, regulatory agencies, etc.) will impose their own standards, without our input.
Dr. Fredholm and colleague Dr. Stephen Bekanich are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin. They alternate contributions to the monthly Palliatively Speaking blog.

When death interrupts life
Death is no stranger to me. Like many my age, I have lost all my grandparents, but I also lost my dad early, when I was only 18. In my early 20s I saw death hundreds of times as an assistant to the medical examiner. Now, as part of my job, I routinely help families and patients approach this last and final stage of life.
Despite this familiarity, I somehow forget what the cold, harsh finality of death personally feels like; the incomprehensible irreversibility, the eerie emptiness. Patients often pass during the night, leaving me to find, the next day, their name off my list and their room being cleaned. I sign the death certificate and move on. It is, after all, part of my job.
Now and then death will touch me directly, and I am reminded anew what it is really like, beyond a "goals of care discussion" and a death certificate.
First there is the stunned knot in the stomach when you first hear the news; the pit of lost words and imploded emotions. Then comes the sadness followed by the unexpected and surreal work that has to be done. Emotions are briefly put on hold to "get things in order." Then, when all is said and done, you have to return to the empty nuances of life: work, bills, chores. You walk through the motions, trying to act the same. The world goes on.

Today I woke up to find that my friend and pet of 8 years had died in her sleep. She had been battling infections for a year and a half, had become incontinent, and was losing weight. I knew it was coming, I just didn’t know when. In evenings, I would find myself taking pause to look for respirations when she would rest in the shade. Then today, a day no different from any other, it just happened. Of course I knew instantly; there is such an indescribable difference between a lifeless body and one who still has even shallow breath. I just stood and stared. I told my wife and I watched the same helpless feelings pour over her.
This loyal rabbit, our friend, had been with me since I rescued her during medical school. At the time, I was not keen on owning any animal, let alone a little rabbit. But she needed rescuing and thus I adopted her. Then, through the loneliness of medical school clerkships and residency, she became my friend, often my only friend. She was a faithful companion that ran circles around my feet when I would come in the door after 30-hour shifts, and she would curl up next to me during post-call Netflix naps. When my wife moved to the United States in the middle of my residency, she was often her only companion for days at a time as I worked long hours in the ICU. She was with me through every relentless minute of studying for boards, sleeping quietly at my feet.
After we had a good cry came the cold requisite to "get things in order." We said our final good-byes just 2 hours ago, and we returned to the empty nuances of life: Fix the leaking faucet, eat dinner, do the dishes.
Working with patients who are sick and nearing the end of their lives can be part of our rhythm – monthly, weekly, or even daily. But for the patient and family, there is nothing rhythmic about it; death is a life event, perhaps the life event.
Quality of care can mean creating a temporal space of peace and honor, no matter the loss and however brief, that has a different tone from the rest of our day. It means never suggesting in word or deed that we are too busy to recognize the emptiness that the death will leave behind. It is understanding the initial thud that a palliative care/hospice referral makes on a loved-one’s soul. Even a novice physician or nurse should pause in recognition that though the hospital bed will be refilled and the hospital workload will continue, for families, nothing is ever quite the same.
Dr. Horton completed his residency in internal medicine and pediatrics at the University of Utah and Primary Children’s Medical Center, both in Salt Lake City, in July 2013, and joined the faculty there. He is sharing his new-career experiences with Hospitalist News.
Death is no stranger to me. Like many my age, I have lost all my grandparents, but I also lost my dad early, when I was only 18. In my early 20s I saw death hundreds of times as an assistant to the medical examiner. Now, as part of my job, I routinely help families and patients approach this last and final stage of life.
Despite this familiarity, I somehow forget what the cold, harsh finality of death personally feels like; the incomprehensible irreversibility, the eerie emptiness. Patients often pass during the night, leaving me to find, the next day, their name off my list and their room being cleaned. I sign the death certificate and move on. It is, after all, part of my job.
Now and then death will touch me directly, and I am reminded anew what it is really like, beyond a "goals of care discussion" and a death certificate.
First there is the stunned knot in the stomach when you first hear the news; the pit of lost words and imploded emotions. Then comes the sadness followed by the unexpected and surreal work that has to be done. Emotions are briefly put on hold to "get things in order." Then, when all is said and done, you have to return to the empty nuances of life: work, bills, chores. You walk through the motions, trying to act the same. The world goes on.
Today I woke up to find that my friend and pet of 8 years had died in her sleep. She had been battling infections for a year and a half, had become incontinent, and was losing weight. I knew it was coming, I just didn’t know when. In evenings, I would find myself taking pause to look for respirations when she would rest in the shade. Then today, a day no different from any other, it just happened. Of course I knew instantly; there is such an indescribable difference between a lifeless body and one who still has even shallow breath. I just stood and stared. I told my wife and I watched the same helpless feelings pour over her.
This loyal rabbit, our friend, had been with me since I rescued her during medical school. At the time, I was not keen on owning any animal, let alone a little rabbit. But she needed rescuing and thus I adopted her. Then, through the loneliness of medical school clerkships and residency, she became my friend, often my only friend. She was a faithful companion that ran circles around my feet when I would come in the door after 30-hour shifts, and she would curl up next to me during post-call Netflix naps. When my wife moved to the United States in the middle of my residency, she was often her only companion for days at a time as I worked long hours in the ICU. She was with me through every relentless minute of studying for boards, sleeping quietly at my feet.
After we had a good cry came the cold requisite to "get things in order." We said our final good-byes just 2 hours ago, and we returned to the empty nuances of life: Fix the leaking faucet, eat dinner, do the dishes.
Working with patients who are sick and nearing the end of their lives can be part of our rhythm – monthly, weekly, or even daily. But for the patient and family, there is nothing rhythmic about it; death is a life event, perhaps the life event.
Quality of care can mean creating a temporal space of peace and honor, no matter the loss and however brief, that has a different tone from the rest of our day. It means never suggesting in word or deed that we are too busy to recognize the emptiness that the death will leave behind. It is understanding the initial thud that a palliative care/hospice referral makes on a loved-one’s soul. Even a novice physician or nurse should pause in recognition that though the hospital bed will be refilled and the hospital workload will continue, for families, nothing is ever quite the same.
Dr. Horton completed his residency in internal medicine and pediatrics at the University of Utah and Primary Children’s Medical Center, both in Salt Lake City, in July 2013, and joined the faculty there. He is sharing his new-career experiences with Hospitalist News.
Death is no stranger to me. Like many my age, I have lost all my grandparents, but I also lost my dad early, when I was only 18. In my early 20s I saw death hundreds of times as an assistant to the medical examiner. Now, as part of my job, I routinely help families and patients approach this last and final stage of life.
Despite this familiarity, I somehow forget what the cold, harsh finality of death personally feels like; the incomprehensible irreversibility, the eerie emptiness. Patients often pass during the night, leaving me to find, the next day, their name off my list and their room being cleaned. I sign the death certificate and move on. It is, after all, part of my job.
Now and then death will touch me directly, and I am reminded anew what it is really like, beyond a "goals of care discussion" and a death certificate.
First there is the stunned knot in the stomach when you first hear the news; the pit of lost words and imploded emotions. Then comes the sadness followed by the unexpected and surreal work that has to be done. Emotions are briefly put on hold to "get things in order." Then, when all is said and done, you have to return to the empty nuances of life: work, bills, chores. You walk through the motions, trying to act the same. The world goes on.
Today I woke up to find that my friend and pet of 8 years had died in her sleep. She had been battling infections for a year and a half, had become incontinent, and was losing weight. I knew it was coming, I just didn’t know when. In evenings, I would find myself taking pause to look for respirations when she would rest in the shade. Then today, a day no different from any other, it just happened. Of course I knew instantly; there is such an indescribable difference between a lifeless body and one who still has even shallow breath. I just stood and stared. I told my wife and I watched the same helpless feelings pour over her.
This loyal rabbit, our friend, had been with me since I rescued her during medical school. At the time, I was not keen on owning any animal, let alone a little rabbit. But she needed rescuing and thus I adopted her. Then, through the loneliness of medical school clerkships and residency, she became my friend, often my only friend. She was a faithful companion that ran circles around my feet when I would come in the door after 30-hour shifts, and she would curl up next to me during post-call Netflix naps. When my wife moved to the United States in the middle of my residency, she was often her only companion for days at a time as I worked long hours in the ICU. She was with me through every relentless minute of studying for boards, sleeping quietly at my feet.
After we had a good cry came the cold requisite to "get things in order." We said our final good-byes just 2 hours ago, and we returned to the empty nuances of life: Fix the leaking faucet, eat dinner, do the dishes.
Working with patients who are sick and nearing the end of their lives can be part of our rhythm – monthly, weekly, or even daily. But for the patient and family, there is nothing rhythmic about it; death is a life event, perhaps the life event.
Quality of care can mean creating a temporal space of peace and honor, no matter the loss and however brief, that has a different tone from the rest of our day. It means never suggesting in word or deed that we are too busy to recognize the emptiness that the death will leave behind. It is understanding the initial thud that a palliative care/hospice referral makes on a loved-one’s soul. Even a novice physician or nurse should pause in recognition that though the hospital bed will be refilled and the hospital workload will continue, for families, nothing is ever quite the same.
Dr. Horton completed his residency in internal medicine and pediatrics at the University of Utah and Primary Children’s Medical Center, both in Salt Lake City, in July 2013, and joined the faculty there. He is sharing his new-career experiences with Hospitalist News.

J-Tip syringe cuts venipuncture pain in young kids
DALLAS – Jet-injected lidocaine is superior to vapocoolant spray in reducing venipuncture pain in children under 7 years of age, according to a randomized, double-blind clinical trial.
This form of needle-free local anesthesia, administered through what is popularly known as the J-Tip syringe, has been shown previously to decrease venipuncture pain in adults and older children. But data regarding the effectiveness of the J-Tip in young children has been scanty until now, Dr. Maren M. Lunoe noted at the annual meeting of the Society for Academic Emergency Medicine.

She presented the findings of a randomized, sham-controlled, double-blind clinical trial involving 205 children aged 1-6 years who presented for venipuncture. Ninety percent had undergone the procedure before.
The J-Tip device utilizes a cartridge of compressed carbon dioxide to drive buffered lidocaine into the skin. However, it does so with a loud "pop," which is why the study included a control arm featuring a sham J-Tip syringe with the compressed gas but no lidocaine, explained Dr. Lunoe of the Medical College of Wisconsin, Milwaukee.
Participants were randomized 2:1:1 to the J-Tip syringe deployed roughly 30 seconds prior to venipuncture; to a refrigerated vapocoolant spray, also applied immediately prior to venipuncture, which has been usual care for a blood draw at Children’s Hospital of Wisconsin; or to a second control group who received vapocoolant spray and a sham J-Tip.
The primary endpoint was the FLACC score at venipuncture as assessed by two blinded physicians viewing videotapes of every procedure. The FLACC (Face, Legs, Activity, Cry, and Consolability) scale is a validated pain assessment tool scored 0-10.
The median FLACC score while the young children were waiting for the nurse was 2.0. The score jumped by about 2 points in all three groups when the child saw the device. It climbed by another 5.5 points from that point to the actual venipuncture in controls who got vapocoolant spray only, and by 2.5 points in those who got vapocoolant spray plus a sham J-Tip. These increases in FLACC pain score at venipuncture were statistically significant and clinically meaningful. In contrast, patients who received needle-free lidocaine through a loaded J-Tip syringe did not experience a significant increase in FLACC scores at venipuncture.
Forty-five percent of patients in the J-Tip group had no or only mild pain at venipuncture as defined by a FLACC score of 0-3. This was the case in only 23% of the vapocoolant spray–only group and in 30% of controls who got vapocoolant spray and a sham J-Tip.
There were no between-group differences in adverse events, all of which were minor, consisting mostly of mild bruising.
Asked why the study didn’t include a comparison arm pretreated with EMLA cream, Dr. Lunoe said that topical agent takes 30 minutes to take effect, making it unattractive for use in an emergency department or busy clinic.
National Medical Products and Gebauer, which market the J-Tip syringe and the vapocoolant spray, respectively, provided those supplies for the study but had no further involvement. Dr. Lunoe reported no financial conflicts with regard to the investigation.
DALLAS – Jet-injected lidocaine is superior to vapocoolant spray in reducing venipuncture pain in children under 7 years of age, according to a randomized, double-blind clinical trial.
This form of needle-free local anesthesia, administered through what is popularly known as the J-Tip syringe, has been shown previously to decrease venipuncture pain in adults and older children. But data regarding the effectiveness of the J-Tip in young children has been scanty until now, Dr. Maren M. Lunoe noted at the annual meeting of the Society for Academic Emergency Medicine.
She presented the findings of a randomized, sham-controlled, double-blind clinical trial involving 205 children aged 1-6 years who presented for venipuncture. Ninety percent had undergone the procedure before.
The J-Tip device utilizes a cartridge of compressed carbon dioxide to drive buffered lidocaine into the skin. However, it does so with a loud "pop," which is why the study included a control arm featuring a sham J-Tip syringe with the compressed gas but no lidocaine, explained Dr. Lunoe of the Medical College of Wisconsin, Milwaukee.
Participants were randomized 2:1:1 to the J-Tip syringe deployed roughly 30 seconds prior to venipuncture; to a refrigerated vapocoolant spray, also applied immediately prior to venipuncture, which has been usual care for a blood draw at Children’s Hospital of Wisconsin; or to a second control group who received vapocoolant spray and a sham J-Tip.
The primary endpoint was the FLACC score at venipuncture as assessed by two blinded physicians viewing videotapes of every procedure. The FLACC (Face, Legs, Activity, Cry, and Consolability) scale is a validated pain assessment tool scored 0-10.
The median FLACC score while the young children were waiting for the nurse was 2.0. The score jumped by about 2 points in all three groups when the child saw the device. It climbed by another 5.5 points from that point to the actual venipuncture in controls who got vapocoolant spray only, and by 2.5 points in those who got vapocoolant spray plus a sham J-Tip. These increases in FLACC pain score at venipuncture were statistically significant and clinically meaningful. In contrast, patients who received needle-free lidocaine through a loaded J-Tip syringe did not experience a significant increase in FLACC scores at venipuncture.
Forty-five percent of patients in the J-Tip group had no or only mild pain at venipuncture as defined by a FLACC score of 0-3. This was the case in only 23% of the vapocoolant spray–only group and in 30% of controls who got vapocoolant spray and a sham J-Tip.
There were no between-group differences in adverse events, all of which were minor, consisting mostly of mild bruising.
Asked why the study didn’t include a comparison arm pretreated with EMLA cream, Dr. Lunoe said that topical agent takes 30 minutes to take effect, making it unattractive for use in an emergency department or busy clinic.
National Medical Products and Gebauer, which market the J-Tip syringe and the vapocoolant spray, respectively, provided those supplies for the study but had no further involvement. Dr. Lunoe reported no financial conflicts with regard to the investigation.
DALLAS – Jet-injected lidocaine is superior to vapocoolant spray in reducing venipuncture pain in children under 7 years of age, according to a randomized, double-blind clinical trial.
This form of needle-free local anesthesia, administered through what is popularly known as the J-Tip syringe, has been shown previously to decrease venipuncture pain in adults and older children. But data regarding the effectiveness of the J-Tip in young children has been scanty until now, Dr. Maren M. Lunoe noted at the annual meeting of the Society for Academic Emergency Medicine.
She presented the findings of a randomized, sham-controlled, double-blind clinical trial involving 205 children aged 1-6 years who presented for venipuncture. Ninety percent had undergone the procedure before.
The J-Tip device utilizes a cartridge of compressed carbon dioxide to drive buffered lidocaine into the skin. However, it does so with a loud "pop," which is why the study included a control arm featuring a sham J-Tip syringe with the compressed gas but no lidocaine, explained Dr. Lunoe of the Medical College of Wisconsin, Milwaukee.
Participants were randomized 2:1:1 to the J-Tip syringe deployed roughly 30 seconds prior to venipuncture; to a refrigerated vapocoolant spray, also applied immediately prior to venipuncture, which has been usual care for a blood draw at Children’s Hospital of Wisconsin; or to a second control group who received vapocoolant spray and a sham J-Tip.
The primary endpoint was the FLACC score at venipuncture as assessed by two blinded physicians viewing videotapes of every procedure. The FLACC (Face, Legs, Activity, Cry, and Consolability) scale is a validated pain assessment tool scored 0-10.
The median FLACC score while the young children were waiting for the nurse was 2.0. The score jumped by about 2 points in all three groups when the child saw the device. It climbed by another 5.5 points from that point to the actual venipuncture in controls who got vapocoolant spray only, and by 2.5 points in those who got vapocoolant spray plus a sham J-Tip. These increases in FLACC pain score at venipuncture were statistically significant and clinically meaningful. In contrast, patients who received needle-free lidocaine through a loaded J-Tip syringe did not experience a significant increase in FLACC scores at venipuncture.
Forty-five percent of patients in the J-Tip group had no or only mild pain at venipuncture as defined by a FLACC score of 0-3. This was the case in only 23% of the vapocoolant spray–only group and in 30% of controls who got vapocoolant spray and a sham J-Tip.
There were no between-group differences in adverse events, all of which were minor, consisting mostly of mild bruising.
Asked why the study didn’t include a comparison arm pretreated with EMLA cream, Dr. Lunoe said that topical agent takes 30 minutes to take effect, making it unattractive for use in an emergency department or busy clinic.
National Medical Products and Gebauer, which market the J-Tip syringe and the vapocoolant spray, respectively, provided those supplies for the study but had no further involvement. Dr. Lunoe reported no financial conflicts with regard to the investigation.
AT SAEM 2014
Key clinical point: Needle-free local anesthesia via jet-injected lidocaine is a fast and effective means of reducing venipuncture pain for young children.
Major finding: Forty-five percent of young children had no or mild pain at venipuncture if they received jet-injected lidocaine immediately beforehand, a rate twice that seen in controls pretreated with a vapocoolant spray.
Data source: A randomized, prospective, double-blind, sham procedure-controlled study involving 205 children aged 1-6 years undergoing venipuncture.
Disclosures: The presenter reported having no financial conflicts regarding this study, which was carried out with institutional funds.

Palliatively Speaking: Why consults don’t happen
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which physicians order palliative care consults in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, heart failure, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement screening tools on one unit at a time, or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day, leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at http://www.ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Dr. Jennifer Cox, FCCP, comments: Palliative care consults are a valuable, yet underutilized service. Palliative care programs, whether just beginning or well established, should place an emphasis on education of clinicians to the broad range of services they can provide. It’s not just for hospice anymore.
Dr. Jennifer Cox, FCCP, comments: Palliative care consults are a valuable, yet underutilized service. Palliative care programs, whether just beginning or well established, should place an emphasis on education of clinicians to the broad range of services they can provide. It’s not just for hospice anymore.
Dr. Jennifer Cox, FCCP, comments: Palliative care consults are a valuable, yet underutilized service. Palliative care programs, whether just beginning or well established, should place an emphasis on education of clinicians to the broad range of services they can provide. It’s not just for hospice anymore.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which physicians order palliative care consults in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, heart failure, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement screening tools on one unit at a time, or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day, leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at http://www.ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which physicians order palliative care consults in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, heart failure, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement screening tools on one unit at a time, or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day, leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at http://www.ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.

Home Hospice Providers Offer Best Practices for End-of-Life Care

New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
New research from the Birmingham, Ala., Veterans Affairs Medical Center and the University of Alabama-Birmingham, published in the Journal of General Internal Medicine, finds that clinical techniques and care processes imported from home-based hospice professionals improved outcomes for hospitalized patients approaching the end of their lives.1
The project, conducted in six VA medical centers, employed a multi-modal strategy for improving end-of-life care processes, with staff training for all hospital providers in how to identify actively dying patients and then communicate this information to their families. Best clinical practices, supported by electronic order sets and paper-based educational materials, were implemented. Patients also were encouraged to eat what—and when—they wanted, to sit up in bed, and to receive family visitors at all hours.
“I started the project years ago, when I noticed that patients on hospice care at home often seemed more comfortable, while if I brought them into the hospital, they sometimes got worse,” says lead author F. Amos Bailey, MD. “We went out to the home to observe what the hospice nurses were doing and then came back to the hospital to write order sets to reflect that practice.”
Key quality endpoints included:
- Rates of orders for opioid pain medications;
- Anti-psychotic medications and scopolamine for death rattle;
- Completion of advance directives; and
- Consultations for palliative care and pastoral care.
Patients were more likely to have their pain relieved and symptoms addressed, according to chart reviews of 6,066 patients who died before or after the intervention was launched.
“All of the processes we measured moved in the direction of increased comfort,” Dr. Bailey says.
This is the first study to show that palliative care techniques developed in the home setting can have an impact on end-of-life care. That’s important, he adds, because most patients die in hospitals or nursing homes.
Larry Beresford is a freelance writer in Alameda, Calif.
References
- Bailey FA, Williams BR, Woodby LL, et al. Intervention to improve care at life's end in inpatient settings: The BEACON trial. J Gen Intern Med. 2014;29(6):836-843.
- Burling S. Yogurt a solution to hospital infection? Philadelphia Inquirer website. December 10, 2013. Available at: http://articles.philly.com/2013-12-10/news/44946926_1_holy-redeemer-probiotics-yogurt. Accessed June 5, 2014.
- Landelle C, Verachten M, Legrand P, Girou E, Barbut F, Buisson CB. Contamination of healthcare workers’ hands with Clostridium difficile spores after caring for patients with C. difficile infection. Infect Control Hosp Epidemiol. 2014;35(1):10-15.
- Lewis K, Walker C. Development and application of information technology solutions to improve the quality and availability of discharge summaries. Journal of Hospital Medicine RIV abstracts website. Available at: http://www.shmabstracts.com/abstract.asp?MeetingID=793&id=104276&meeting=JHM201305. Published May 2013. Accessed June 14, 2014.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement. American College of Physicians; Society of General Internal Medicine; Society of Hospital Medicine; American Geriatrics Society; American College of Emergency Physicians; Society of Academic Emergency Medicine. J Gen Intern Med. 2009;24(8):971-976.
- American Hospital Association: Uncompensated hospital care cost fact sheet. January 2014. Available at: http://www.aha.org/content/14/14uncompensatedcare.pdf. Accessed June 5, 2014.
Promoting higher blood pressure targets for frail older adults: A consensus guideline from Canada
Frail older adults deserve guidelines that take frailty into account while assessing the potential benefit and risks of treatment.
Specifically, our group—the Dalhousie Academic Detailing Service (ADS) and the Palliative and Therapeutic Harmonization (PATH) program—recommends that physicians strive to achieve more liberal treatment targets for elderly frail patients who have high blood pressure,1 as evidence does not support an aggressive approach in the frail elderly and the potential exists for harm.
This article reviews the evidence and reasoning that were used to develop and promote a guideline for drug treatment of hypertension in frail older adults. Our recommendations differ from other guidelines in that they focus as much on stopping or decreasing therapy as on starting or increasing it.
FRAILTY INCREASES THE RISK OF ADVERSE EFFECTS
The word frail, applied to older adults, describes those who have complex medical illnesses severe enough to compromise their ability to live independently.2 Many have multiple coexisting medical problems for which they take numerous drugs, in addition to dementia, impaired mobility, compromised functional ability, or a history of falling.
Frailty denotes vulnerability; it increases the risk of adverse effects from medical and surgical procedures,3 complicates drug therapy,4 prolongs hospital length of stay,5 leads to functional and cognitive decline,6 increases the risk of institutionalization,7 and reduces life expectancy8—all of which affect the benefit and harm of medical treatments.
Guidelines for treating hypertension9–11 now acknowledge that little evidence exists to support starting treatment for systolic blood pressure between 140 and 160 mm Hg or aiming for a target of less than 140 mm Hg for “very old” adults, commonly defined as over the age of 80. New guidelines loosen the treatment targets for the very old, but they do not specify targets for the frail and do not describe how to recognize or measure frailty.
RECOGNIZING AND MEASURING FRAILTY
A number of tools are available to recognize and measure frailty.12
The Fried frailty assessment13 has five items:
- Unintentional weight loss
- Self-reported exhaustion
- Weakness in grip
- Slow walking speed
- Low physical activity and energy expenditure.
People are deemed frail if they have three or more of these five. However, experts disagree about whether this system is too sensitive14 or not sensitive enough.15,16
The FRAIL questionnaire17 also has five items:
- Fatigue
- Resistance (inability to climb stairs)
- Ambulation (inability to walk 1 city block)
- Illness (more than 5 major illnesses)
- Weight loss.
People are deemed frail if they have at least three of these five items, and “prefrail” if they have two.
These and other tools are limited by being dichotomous: they classify people as being either frail or not frail18–20 but do not define the spectrum of frailty.
Other frailty assessments such as the Frailty Index21 identify frailty based on the number of accumulated health deficits but take a long time to complete, making them difficult to use in busy clinical settings.22–24
The Clinical Frailty Scale7 is a validated scale that categorizes frailty based on physical and functional indicators of health, such as cognition, function, and mobility, with scores that range from 1 (very fit) to 9 (terminally ill).7,12
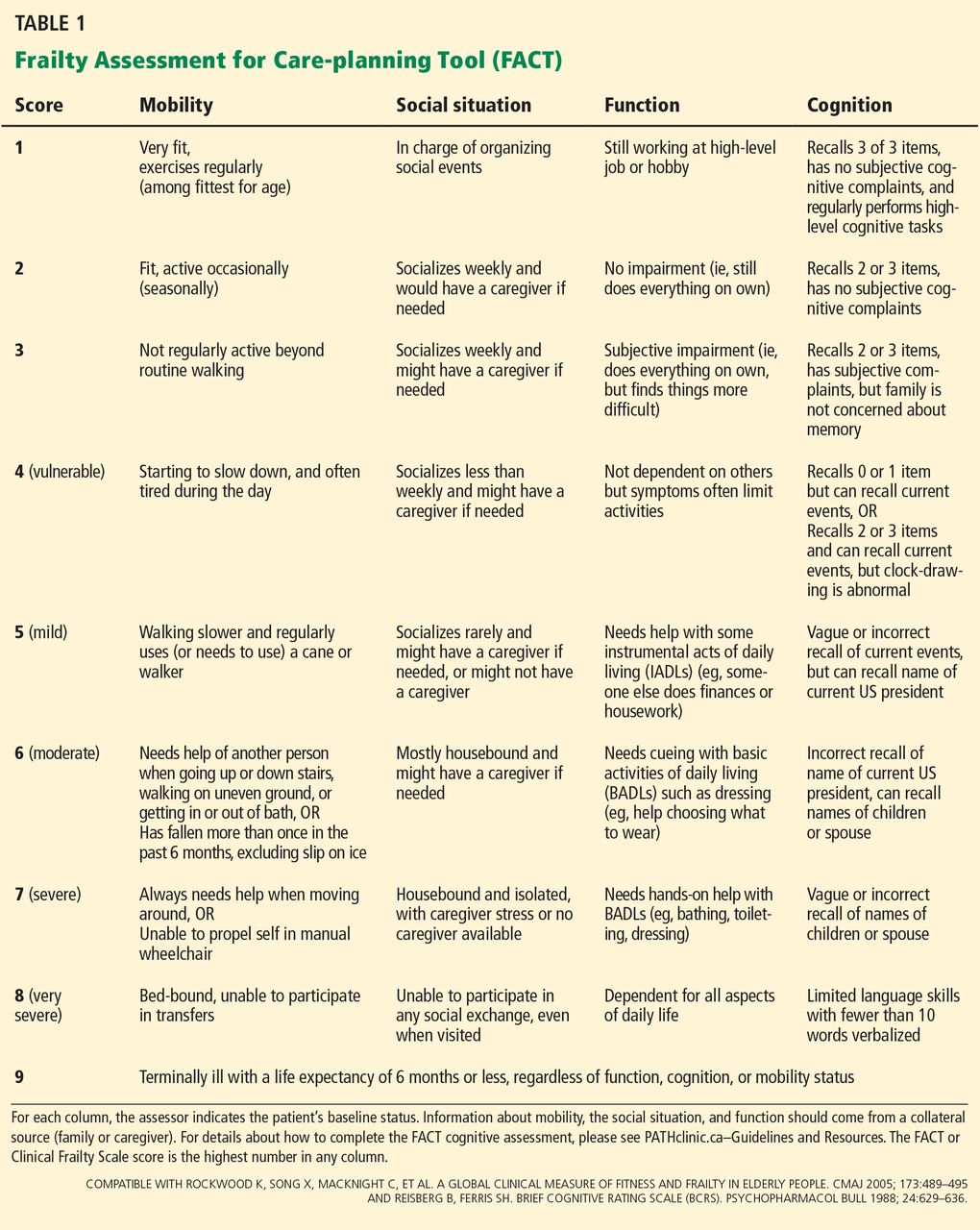
The Frailty Assessment for Care-planning Tool (FACT) uses scaling compatible with the Clinical Frailty Scale but has been developed for use as a practical and interpretable frailty screening tool for nonexperts (Table 1). The FACT assesses cognition, mobility, function, and the social situation, using a combination of caregiver report and objective measures. To assess cognition, a health care professional uses items from the Mini-Cog25 (ie, the ability to draw an analog clock face and then recall three unrelated items following the clock-drawing test) and the memory axis of the Brief Cognitive Rating Scale26 (ie, the ability to recall current events, the current US president, and the names of children or spouse). Mobility, function, and social circumstance scores are assigned according to the caregiver report of the patient’s baseline status.
The FACT can be completed in busy clinical settings. Once a caregiver is identified, it takes about 5 minutes to complete.
Our guideline27–31 is intended for those with a score of 7 or more on the Clinical Frailty Scale or FACT,7,12 a score we chose because it describes people who are severely frail with shortened life expectancy.8 At this level, people need help with all instrumental activities of daily living (eg, handling finances, medication management, household chores, and shopping) as well as with basic activities of daily living such as bathing or dressing.
REVIEWING THE LIMITED EVIDENCE
We found no studies that addressed the risks and benefits of treating hypertension in frail older adults; therefore, we concentrated on studies that enrolled individuals who were chronologically old but not frail. We reviewed prominent guidelines,9–11,32,33 the evidence base for these guidelines,34–44 and Cochrane reviews.45,46 A detailed description of the evidence used to build our recommendation can be found online.31
When we deliberated on treatment targets, we reviewed evidence from two types of randomized controlled trials47:
Drug treatment trials randomize patients to different treatments, such as placebo versus a drug or one drug compared with another drug. Patients in different treatment groups may achieve different blood pressures and clinical outcomes, and this information is then used to define optimal targets. However, it may be difficult to determine if the benefit came from lowering blood pressure or from some other effect of the drug, which can be independent of blood pressure lowering.
Treat-to-target trials randomize patients to different blood pressure goals, but the groups are treated with the same or similar drugs. Therefore, any identified benefit can be attributed to the differences in blood pressure rather than the medications used. Compared with a drug treatment trial, this type of trial provides stronger evidence about optimal targets.
We also considered the characteristics of frailty, the dilemma of polypharmacy, and the relevance of the available scientific evidence to those who are frail.
Drug treatment trials
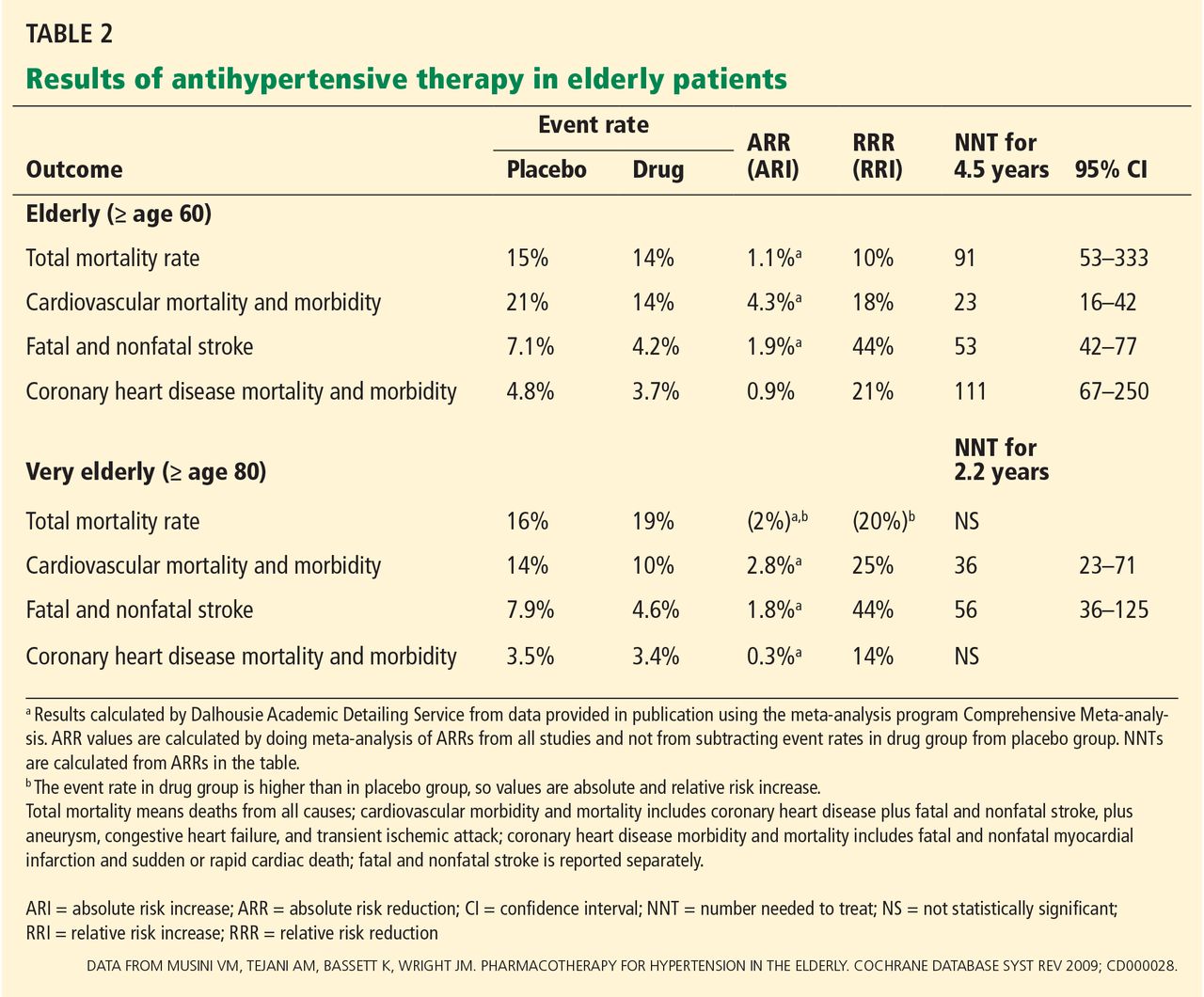
A Cochrane review45 of 15 studies with approximately 24,000 elderly participants found that treating hypertension decreased the rates of cardiovascular morbidity and mortality as well as fatal and nonfatal stroke in the “elderly” (defined as age ≥ 60) and “very elderly” (age ≥ 80). However, in the very elderly, all-cause mortality rates were not statistically significantly different with treatment compared with placebo. The mean duration of treatment was 4.5 years in the elderly and 2.2 years in the very elderly (Table 2). Of importance, all the trials enrolled only those individuals whose systolic blood pressure was at least 160 mm Hg at baseline.
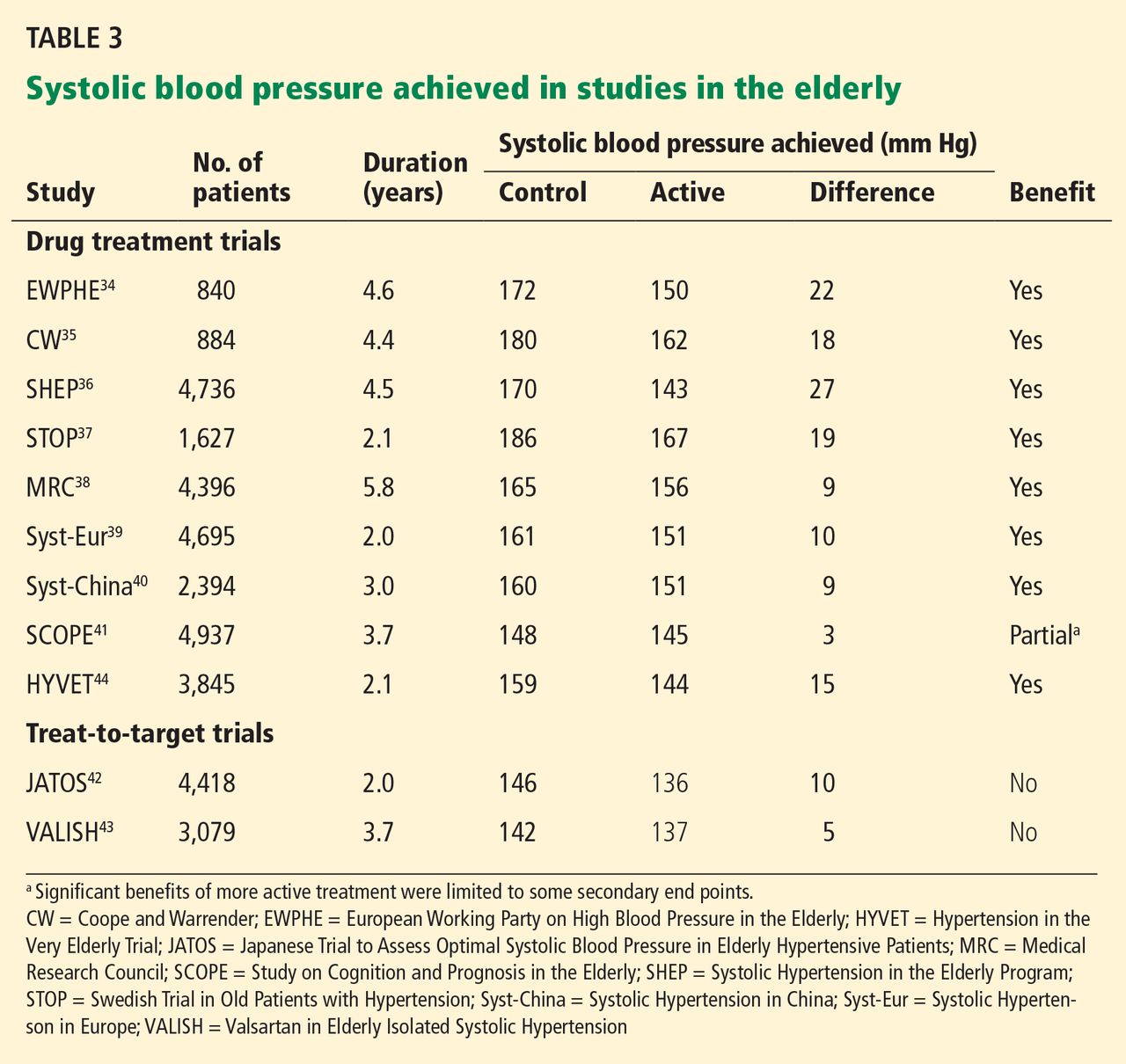
None of the studies were treat-to-target trials—patients were assigned either active medication or placebo. Thus, these trials provide evidence of benefit for treating hypertension in the elderly and very elderly but do not identify the optimal target. All of the drug treatment trials showed benefit, but none achieved a systolic pressure lower than 140 mm Hg with active treatment (Table 3). Therefore, these studies do not support a systolic target of less than 140 mm Hg in the elderly.
Treat-to-target trials: JATOS and VALISH
The Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients (JATOS)42 and the Valsartan in Elderly Isolated Systolic Hypertension (VALISH) study43 each enrolled more than 3,000 people age 65 or older (mean age approximately 75). Patients were randomized to either a strict systolic target of less than 140 mm Hg or a higher (more permissive) target of 140 to 160 mm Hg in JATOS and 140 to 149 mm Hg in VALISH.
In both trials, the group with strict targets achieved a systolic pressure of approximately 136 mm Hg, while the group with higher blood pressure targets achieved a systolic pressure of 146 mm Hg in JATOS and 142 mm Hg in VALISH. Despite these differences, there was no statistically significant difference in the primary outcome.
Thus, treat-to-target studies also fail to support a systolic target of less than 140 mm Hg in the elderly, although it is important to recognize the limitations of the studies. Approximately 15% of the participants had cardiovascular disease, so the applicability of the findings to patients with target-organ damage is uncertain. In addition, there were fewer efficacy outcome events than expected, which suggests that the studies were underpowered.
When to start drug treatment
In each of the drug treatment and treat-to-target trials, the inclusion criterion for study entry was a systolic blood pressure above 160 mm Hg, with a mean blood pressure at entry into the drug treatment trials of 182/95 mm Hg.46 Thus, data support starting treatment if the systolic blood pressure is above 160 mm Hg, but not lower.
Notably, in all but one study,46 at least two-thirds of the participants took no more than two antihypertensive medications. Since adverse events become more common as the number of medications increases, the benefit of adding a third drug to lower blood pressure is uncertain.
Evidence in the ‘very elderly’: HYVET
With the exception of the Hypertension in the Very Elderly Trial (HYVET),44 the mean age of elderly patients in the reported studies was between 67 and 76.
HYVET patients were age 80 and older (mean age 84) and were randomized to receive either indapamide (with or without perindopril) or placebo. The trial was stopped early at 2 years because the mortality rate was lower in the treatment group (10.1%) than in the placebo group (12.3%) (number needed to treat 46, 95% confidence interval 24–637, P = .02). There was no significant difference in the primary outcome of fatal and nonfatal stroke.
Notably, trials that are stopped early may overestimate treatment benefit.48
Evidence in frail older adults
While the above studies provide some information about managing hypertension in the elderly, the participants were generally healthy. HYVET44 specifically excluded those with a standing systolic blood pressure of less than 140 mm Hg and enrolled few patients with orthostasis (7.9% in the placebo group and 8.8% in the treatment group), a condition commonly associated with frailty. As such, these studies may be less relevant to the frail elderly, who are at higher risk of adverse drug events and have competing risks for morbidity and mortality.
Observational studies, in fact, raise questions about whether tight blood pressure control improves clinical outcomes for the very elderly. In the Leiden 85-plus study, lower systolic blood pressure was associated with lower cognitive scores, worse functional ability,49,50 and a higher mortality rate51 compared with higher systolic pressure, although it is uncertain whether these outcomes were indicative of underlying disease that could result in lower blood pressure or an effect of blood pressure-lowering.
The National Health and Nutrition Examination Survey52 found an association between blood pressure and mortality rate that varied by walking speed. For slower walkers (based on the 6-minute walk test), higher systolic pressures were not associated with a higher risk of death, suggesting that when older adults are frail (as indicated by their slow walking speed) they are less likely to benefit from aggressive treatment of hypertension.
People at high risk because of stroke
Because the evidence is limited, it is even more difficult to judge whether lowering blood pressure below 140 mm Hg is beneficial for frail patients who have a history of stroke, compared with the possibility that medications will cause adverse effects such as weakness, orthostasis, and falls. When reviewing the evidence to answer this question, we especially looked at outcomes that affect quality of life, such as nonfatal stroke leading to disability. In contrast, because the frail elderly have competing causes of mortality, we could not assume that a mortality benefit shown in nonfrail populations could be applied to frail populations.
The PROGRESS trial (Perindopril Protection Against Recurrent Stroke Study)53 was in patients with a history of stroke or transient ischemic attack and a mean age of 64, who were treated with either perindopril (with or without indapamide) or placebo.
At almost 4 years, the rate of disabling stroke was 2.7% in the treatment group and 4.3% in the placebo group, a relative risk reduction of 38% and an absolute risk reduction of 1.64% (number needed to treat 61, 95% confidence interval 39–139). The relative risk reduction for all strokes (fatal and nonfatal) was similar across a range of baseline systolic pressures, but the absolute risk reduction was greater in the prespecified subgroup that had hypertension at baseline (mean blood pressure 159/94 mm Hg) than in the normotensive subgroup (mean blood pressure 136/79 mm Hg), suggesting that treatment is most beneficial for those with higher systolic blood pressures. Also, the benefit was only demonstrated in the subgroup that received two antihypertensive medications; those who received perindopril alone showed no benefit.
This study involved relatively young patients in relatively good health except for their strokes. The extent to which the results can be extrapolated to older, frail adults is uncertain because of the time needed to achieve benefit and because of the added vulnerability of frailty, which could make treatment with two antihypertensive medications riskier.
PRoFESS (Prevention Regimen for Effectively Avoiding Second Strokes),54 another study in patients with previous stroke (mean age 66) showed no benefit over 2.5 years in the primary outcome of stroke using telmesartan 80 mg daily compared with placebo. This result is concordant with that of PROGRESS,53 in which patients who took only one medication did not show a significant decrease in the rate of stroke.
A possible reason for the lack of benefit from monotherapy was that the differences in blood pressure between the placebo group and the treatment group on monotherapy were small in both studies (3.8/2.0 mm Hg in PRoFESS, 5/3 mm Hg in PROGRESS). In contrast, patients on dual therapy in PROGRESS decreased their blood pressure by 12/5 mm Hg compared with placebo.
CURRENT HYPERTENSION GUIDELINES
Current guidelines make reference to the elderly, but we found none that made specific recommendations for the frail elderly.
JNC 8
In December 2013, members of the Eighth Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) released new recommendations.32 One significant revision was to support higher blood pressure targets for older adults (age 60 and older). Whereas JNC 7 stated that lowering blood pressure below 140/90 mm Hg reduced cardiovascular complications,33 JNC 8 now acknowledges that there is no strong evidence to support blood pressure targets below 150/90 mm Hg for hypertensive persons without kidney disease or diabetes age 60 and older. Thus, in the general population age 60 and older, JNC 8 recommends starting antihypertensive treatment when blood pressure is 150/90 mm Hg or higher, and treating to a goal blood pressure of less than 150/90 mm Hg. JNC 8 makes no recommendation about how to adjust blood pressure targets for frailty or how to measure blood pressure.
American College of Cardiology and American Heart Association
In 2011, the American College of Cardiology and American Heart Association published a consensus document on the management of hypertension in the elderly.9
They acknowledged that the generally recommended blood pressure goal of lower than 140/90 mm Hg in uncomplicated elderly patients is based on expert opinion rather than on data from randomized controlled trials, but nevertheless recommended a target systolic pressure lower than 140 mm Hg for older adults, except for octogenarians.
For those over age 80, systolic levels of 140 to 145 mm Hg can be acceptable if tolerated and if the patient does not experience orthostasis when standing. Systolic pressure lower than 130 mm Hg and diastolic pressures lower than 65 mm Hg should be avoided in this age group.
The document acknowledges that systolic pressure may have to remain above 150 mm Hg if there is no response to four “well-selected drugs” or if there are unacceptable side effects. In these cases, the lowest “safely achieved” systolic blood pressure should be the goal.
Canadian Hypertension Education Program
The 2014 Canadian Hypertension Education Program (CHEP) report makes several recommendations for the “very elderly,” a group they define as over the age of 80. The CHEP website and resources include the following recommendations10:
- For the very elderly without diabetes or target-organ damage, drug therapy should be initiated when systolic blood pressure is higher than 160 mm Hg to reach a systolic blood pressure target lower than 150 mm Hg. This is a grade C level recommendation, indicating that it is based on low-quality trials, unvalidated surrogate outcomes, or results from nonrandomized observational studies.
- For the very elderly with macrovascular target-organ damage, antihypertensive therapy should be considered if systolic blood pressure readings average 140 mm Hg or higher (grade D for 140 to 160 mm Hg; grade A for higher than 160 mm Hg), although caution should be exercised in elderly patients who are frail. (Grade D recommendations are the weakest, as they are based on low-powered, imprecise studies or expert opinion, whereas grade A recommendations are based on the strongest evidence from high-quality randomized clinical trials.)
- Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based on an individualized risk-benefit analysis.
The European Society of Hypertension and European Society of Cardiology
The 2013 guidelines from the European Society of Hypertension and the European Society of Cardiology11 recommend that for elderly patients under age 80, antihypertensive treatment may be considered at systolic values higher than 140 mm Hg and aimed at values lower than 140 mm Hg if the patient is fit and treatment is well tolerated.
For those over age 80 with an initial systolic pressure of 160 mm Hg or higher, the guidelines recommend lowering systolic pressure to between 150 and 140 mm Hg, provided the patient is in good physical and mental condition. In frail elderly patients, they recommend leaving decisions on antihypertensive therapy to the treating physician, based on monitoring of the clinical effects of treatment.11
The ADS/PATH guidelines
When finalizing our recommendations,1 we considered the characteristics of frailty and the following key points from the evidence:
- Although evidence from drug treatment trials indicates that there is benefit in treating healthy older adults who have hypertension, the benefit of treating frail older adults is unknown.
- Major trials enrolled elderly patients only if they had systolic blood pressures of at least 160 mm Hg. Therefore, evidence supports initiating pharmacotherapy at a systolic pressure of 160 mm Hg or higher.
- No evidence from randomized controlled trials supports a systolic target lower than 140 mm Hg in the elderly, and there is some evidence that such a target does not benefit.
- The benefit of adding a third medication to lower blood pressure has not been studied.
- Frailty makes the potential benefits of strict blood pressure targets even less certain and increases the possibility of harm from adverse drug events.
- The only study of very old adults, HYVET,44 enrolled relatively healthy older adults and few with orthostasis, while excluding those with a standing systolic blood pressure lower than 140 mm Hg.
OUR RECOMMENDATIONS
Based on the above, we advise against unnecessarily strict targets and recommend stopping antihypertensive medications that are used for the sole purpose of keeping the systolic blood pressure below 140 mm Hg. Our guidelines are unique in that they focus equally on when to stop and when to start medications. We concluded that without evidence of definitive benefit, “less is more” with frailty.55 We believe that if physicians and health professionals understand the limitations of the evidence, they can be more confident in stopping medications that lower blood pressure to an unnecessarily low level.
We recommend the following (Table 4):
Before treating
- Carefully review the risks and the potential but unproven benefits of treatment.
- To avoid overtreatment, treatment decisions should be based on blood pressure measurements in the seated (not supine) position, while also considering the presence of orthostasis.
- To evaluate orthostasis, measure blood pressure in the supine position, then immediately on standing, and again after 2 minutes. Ask the patient if he or she feels light-headed or dizzy when standing.
Stop treatment
- If the seated systolic blood pressure is less than 140 mm Hg, medications can be tapered and discontinued to achieve the targets described below.
- Before discontinuation, consider whether the medications are treating additional conditions such as rate control for atrial fibrillation or symptomatic management of heart failure.
- It is uncertain whether to discontinue treatment when there is a history of stroke. Consider that treatment with two medications resulted in an absolute risk reduction for disabling stroke of 1.64% over approximately 4 years for adults with previous stroke and a mean age of 64,57 an effect that may be more prominent at higher systolic pressures.
Start treatment
- Consider starting treatment when systolic pressure is 160 mm Hg or higher.
- Aim for a seated systolic pressure between 140 and 160 mm Hg if there are no adverse effects from treatment that affect quality of life.
- If there is symptomatic orthostasis or if standing systolic pressure is lower than 140 mm Hg, the target seated systolic pressure can be adjusted upwards.
- In the severely frail nearing the end of life, a target systolic pressure of 160 to 190 mm Hg is reasonable.
- The blood pressure target is the same in people with diabetes.
- In general, use no more than two medications.
Dissemination and implementation
The ADS/PATH guideline is intended for use by physicians and other health professionals (eg, pharmacists and nurses) who care for frail older adults or who work in long-term care facilities. Since creating our guideline, we have disseminated it to physicians, pharmacists, and other health professionals through academic detailing, large conferences, and interactive webinars.
While we do not have objective evidence of practice change, our evaluation data found that 34% of 403 family physicians who received academic detailing indicated that the guideline would change their practice, while 36% stated that the guideline confirmed their practice, an indication that family physicians are sensitive to the needs of the frail elderly.
Because health professionals may be wary of stopping medications and not meeting recommended targets, there may be barriers to adopting this guideline. However, our experience with the PATH program indicates that these barriers can be overcome using effective communication strategies between health professionals and consumers.
AN APPROACH APPROPRIATE TO FRAILTY
There is no direct evidence for systolic blood pressure targets in the frail elderly, so we applied evidence from the nonfrail elderly. Our recommendations differ somewhat from those of other groups, which recommend targets below 140 to 150 mm Hg for older adults, although some do advise caution in the elderly for whom a substantial fall in blood pressure might be poorly tolerated. Despite these messages, we believe that clearer guidance is needed to direct health practitioners toward models that acknowledge that frail patients are in a precarious balance of health and may be harmed by treatments that strive to lower blood pressure to unproven targets. For this reason, our guideline clearly indicates when to decrease or stop drug treatment.
After physicians and health professionals examine the evidence and more fully understand the benefits and harms of treating frail older adults, we are confident that they will be more comfortable stopping medications that lower blood pressure to an unnecessarily low level and instead use an approach that is more appropriate to frailty. We hope clinicians can use this guideline with the same enthusiasm applied to other guidelines, and we welcome discussion.
Acknowledgments: We would like to thank and acknowledge Tanya MacLeod and Kathryn Yuill for their review of and advice about the manuscript.
- Palliative and Therapeutic Harmonization program. Hypertension guidelines. Treating hypertension in frailty. http://pathclinic.ca/resources/hypertension/. Accessed May 2, 2014.
- Theou O, Rockwood MR, Mitnitski A, Rockwood K. Disability and co-morbidity in relation to frailty: how much do they overlap? Arch Gerontol Geriatr 2012; 55:e1–e8.
- Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg 2010; 210:901–908.
- Tinetti ME, Bogardus ST, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004; 351:2870–2874.
- Ekerstad N, Swahn E, Janzon M, et al. Frailty is independently associated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation 2011; 124:2397–2404.
- Theou O, Rockwood K. Should frailty status always be considered when treating the elderly patient? Aging Health 2012; 8:261–271.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173:489–495.
- Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr 2008; 8:24.
- Aronow WS, Fleg JL, Pepine CJ, et al; ACCF Task Force. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2011; 123:2434–2506.
- The Canadian Hypertension Education Program (CHEP). 2014 CHEP recommendations. www.hypertension.ca/en/. Accessed May 2, 2014.
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013; 34:2159–2219.
- Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14:392–397.
- Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56:M146–M156.
- Ensrud KE, Ewing SK, Cawthon PM, et al; Osteoporotic Fractures in Men Research Group. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J Am Geriatr Soc 2009; 57:492–498.
- Avila-Funes JA, Amieva H, Barberger-Gateau P, et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: the three-city study. J Am Geriatr Soc 2009; 57:453–461.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging 2012; 16:601–608.
- Strawbridge WJ, Shema SJ, Balfour JL, Higby HR, Kaplan GA. Antecedents of frailty over three decades in an older cohort. J Gerontol B Psychol Sci Soc Sci 1998; 53:S9–S16.
- Matthews M, Lucas A, Boland R, et al. Use of a questionnaire to screen for frailty in the elderly: an exploratory study. Aging Clin Exp Res 2004; 16:34–40.
- Salvi F, Morichi V, Grilli A, et al. Screening for frailty in elderly emergency department patients by using the Identification of Seniors At Risk (ISAR). J Nutr Health Aging 2012; 16:313–318.
- Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal 2001; 1:323–336.
- Kellen E, Bulens P, Deckx L, et al. Identifying an accurate pre-screening tool in geriatric oncology. Crit Rev Oncol Hematol 2010; 75:243–248.
- Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006; 35:526–529.
- Martin FC, Brighton P. Frailty: different tools for different purposes? Age Ageing 2008; 37:129–131.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Reisberg B, Ferris SH. Brief Cognitive Rating Scale (BCRS). Psychopharmacol Bull 1988; 24:629–636.
- Moorhouse P, Mallery LH. Palliative and therapeutic harmonization: a model for appropriate decision-making in frail older adults. J Am Geriatr Soc 2012; 60:2326–2332.
- Palliative and Therapeutic Harmonization Clinic (PATH). www.pathclinic.ca. Accessed May 2, 2014.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. http://cme.medicine.dal.ca/ADS.htm. Accessed January 8, 2014.
- Mallery LH, Moorhouse P. Respecting frailty. J Med Ethics 2011; 37:126–128.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. Issues in hypertension 2011. http://cme.medicine.dal.ca/files/Hypertension%20book.pdf. Accessed May 2, 2014.
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
- Amery A, Birkenhäger W, Brixko P, et al. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet 1985; 1:1349–1354.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. Br Med J (Clin Res Ed) 1986; 293:1145–1151.
- SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
- Dahlöf B, Lindholm LH, Hansson L, Scherstén B, Ekbom T, Wester PO. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- Medical Research Council trial of treatment of hypertension in older adults: principal results. MRC Working Party. BMJ 1992; 304:405–412.
- Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
- Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertens 1998; 16:1823–1829.
- Lithell H, Hansson L, Skoog I, et al; SCOPE Study Group. The Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trial. J Hypertens 2003; 21:875–886.
- JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
- Oparil S, Yarows SA, Patel S, Fang H, Zhang J, Satlin A. Efficacy and safety of combined use of aliskiren and valsartan in patients with hypertension: a randomised, double-blind trial. Lancet 2007; 370:221–229.
- Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
- Musini VM, Tejani AM, Bassett K, Wright JM. Pharmacotherapy for hypertension in the elderly. Cochrane Database Syst Rev 2009;CD000028.
- He FJ, MacGregor GA. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database Syst Rev 2004;CD004937.
- Allen M, Kelly K, Fleming I. Hypertension in elderly patients: recommended systolic targets are not evidence based [in French]. Can Fam Physician 2013; 59:19–24.
- Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ 2012; 344:e3863.
- Sabayan B, Oleksik AM, Maier AB, et al. High blood pressure and resilience to physical and cognitive decline in the oldest old: the Leiden 85-plus Study. J Am Geriatr Soc 2012; 60:2014–2019.
- Sabayan B, van Vliet P, de Ruijter W, Gussekloo J, de Craen AJ, Westendorp RG. High blood pressure, physical and cognitive function, and risk of stroke in the oldest old: the Leiden 85-plus Study. Stroke 2013; 44:15–20.
- Poortvliet RK, Blom JW, de Craen AJ, et al. Low blood pressure predicts increased mortality in very old age even without heart failure: the Leiden 85-plus Study. Eur J Heart Fail 2013; 15:528–533.
- Odden MC, Peralta CA, Haan MN, Covinsky KE. Rethinking the association of high blood pressure with mortality in elderly adults: the impact of frailty. Arch Intern Med 2012; 172:1162–1168.
- PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001; 358:1033–1041.
- Yusuf S, Diener HC, Sacco RL, et al; PRoFESS Study Group. Telmisartan to prevent recurrent stroke and cardiovascular events. N Engl J Med 2008; 359:1225–1237.
- Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010; 170:1648–1654.
Frail older adults deserve guidelines that take frailty into account while assessing the potential benefit and risks of treatment.
Specifically, our group—the Dalhousie Academic Detailing Service (ADS) and the Palliative and Therapeutic Harmonization (PATH) program—recommends that physicians strive to achieve more liberal treatment targets for elderly frail patients who have high blood pressure,1 as evidence does not support an aggressive approach in the frail elderly and the potential exists for harm.
This article reviews the evidence and reasoning that were used to develop and promote a guideline for drug treatment of hypertension in frail older adults. Our recommendations differ from other guidelines in that they focus as much on stopping or decreasing therapy as on starting or increasing it.
FRAILTY INCREASES THE RISK OF ADVERSE EFFECTS
The word frail, applied to older adults, describes those who have complex medical illnesses severe enough to compromise their ability to live independently.2 Many have multiple coexisting medical problems for which they take numerous drugs, in addition to dementia, impaired mobility, compromised functional ability, or a history of falling.
Frailty denotes vulnerability; it increases the risk of adverse effects from medical and surgical procedures,3 complicates drug therapy,4 prolongs hospital length of stay,5 leads to functional and cognitive decline,6 increases the risk of institutionalization,7 and reduces life expectancy8—all of which affect the benefit and harm of medical treatments.
Guidelines for treating hypertension9–11 now acknowledge that little evidence exists to support starting treatment for systolic blood pressure between 140 and 160 mm Hg or aiming for a target of less than 140 mm Hg for “very old” adults, commonly defined as over the age of 80. New guidelines loosen the treatment targets for the very old, but they do not specify targets for the frail and do not describe how to recognize or measure frailty.
RECOGNIZING AND MEASURING FRAILTY
A number of tools are available to recognize and measure frailty.12
The Fried frailty assessment13 has five items:
- Unintentional weight loss
- Self-reported exhaustion
- Weakness in grip
- Slow walking speed
- Low physical activity and energy expenditure.
People are deemed frail if they have three or more of these five. However, experts disagree about whether this system is too sensitive14 or not sensitive enough.15,16
The FRAIL questionnaire17 also has five items:
- Fatigue
- Resistance (inability to climb stairs)
- Ambulation (inability to walk 1 city block)
- Illness (more than 5 major illnesses)
- Weight loss.
People are deemed frail if they have at least three of these five items, and “prefrail” if they have two.
These and other tools are limited by being dichotomous: they classify people as being either frail or not frail18–20 but do not define the spectrum of frailty.
Other frailty assessments such as the Frailty Index21 identify frailty based on the number of accumulated health deficits but take a long time to complete, making them difficult to use in busy clinical settings.22–24
The Clinical Frailty Scale7 is a validated scale that categorizes frailty based on physical and functional indicators of health, such as cognition, function, and mobility, with scores that range from 1 (very fit) to 9 (terminally ill).7,12
The Frailty Assessment for Care-planning Tool (FACT) uses scaling compatible with the Clinical Frailty Scale but has been developed for use as a practical and interpretable frailty screening tool for nonexperts (Table 1). The FACT assesses cognition, mobility, function, and the social situation, using a combination of caregiver report and objective measures. To assess cognition, a health care professional uses items from the Mini-Cog25 (ie, the ability to draw an analog clock face and then recall three unrelated items following the clock-drawing test) and the memory axis of the Brief Cognitive Rating Scale26 (ie, the ability to recall current events, the current US president, and the names of children or spouse). Mobility, function, and social circumstance scores are assigned according to the caregiver report of the patient’s baseline status.
The FACT can be completed in busy clinical settings. Once a caregiver is identified, it takes about 5 minutes to complete.
Our guideline27–31 is intended for those with a score of 7 or more on the Clinical Frailty Scale or FACT,7,12 a score we chose because it describes people who are severely frail with shortened life expectancy.8 At this level, people need help with all instrumental activities of daily living (eg, handling finances, medication management, household chores, and shopping) as well as with basic activities of daily living such as bathing or dressing.
REVIEWING THE LIMITED EVIDENCE
We found no studies that addressed the risks and benefits of treating hypertension in frail older adults; therefore, we concentrated on studies that enrolled individuals who were chronologically old but not frail. We reviewed prominent guidelines,9–11,32,33 the evidence base for these guidelines,34–44 and Cochrane reviews.45,46 A detailed description of the evidence used to build our recommendation can be found online.31
When we deliberated on treatment targets, we reviewed evidence from two types of randomized controlled trials47:
Drug treatment trials randomize patients to different treatments, such as placebo versus a drug or one drug compared with another drug. Patients in different treatment groups may achieve different blood pressures and clinical outcomes, and this information is then used to define optimal targets. However, it may be difficult to determine if the benefit came from lowering blood pressure or from some other effect of the drug, which can be independent of blood pressure lowering.
Treat-to-target trials randomize patients to different blood pressure goals, but the groups are treated with the same or similar drugs. Therefore, any identified benefit can be attributed to the differences in blood pressure rather than the medications used. Compared with a drug treatment trial, this type of trial provides stronger evidence about optimal targets.
We also considered the characteristics of frailty, the dilemma of polypharmacy, and the relevance of the available scientific evidence to those who are frail.
Drug treatment trials
A Cochrane review45 of 15 studies with approximately 24,000 elderly participants found that treating hypertension decreased the rates of cardiovascular morbidity and mortality as well as fatal and nonfatal stroke in the “elderly” (defined as age ≥ 60) and “very elderly” (age ≥ 80). However, in the very elderly, all-cause mortality rates were not statistically significantly different with treatment compared with placebo. The mean duration of treatment was 4.5 years in the elderly and 2.2 years in the very elderly (Table 2). Of importance, all the trials enrolled only those individuals whose systolic blood pressure was at least 160 mm Hg at baseline.
None of the studies were treat-to-target trials—patients were assigned either active medication or placebo. Thus, these trials provide evidence of benefit for treating hypertension in the elderly and very elderly but do not identify the optimal target. All of the drug treatment trials showed benefit, but none achieved a systolic pressure lower than 140 mm Hg with active treatment (Table 3). Therefore, these studies do not support a systolic target of less than 140 mm Hg in the elderly.
Treat-to-target trials: JATOS and VALISH
The Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients (JATOS)42 and the Valsartan in Elderly Isolated Systolic Hypertension (VALISH) study43 each enrolled more than 3,000 people age 65 or older (mean age approximately 75). Patients were randomized to either a strict systolic target of less than 140 mm Hg or a higher (more permissive) target of 140 to 160 mm Hg in JATOS and 140 to 149 mm Hg in VALISH.
In both trials, the group with strict targets achieved a systolic pressure of approximately 136 mm Hg, while the group with higher blood pressure targets achieved a systolic pressure of 146 mm Hg in JATOS and 142 mm Hg in VALISH. Despite these differences, there was no statistically significant difference in the primary outcome.
Thus, treat-to-target studies also fail to support a systolic target of less than 140 mm Hg in the elderly, although it is important to recognize the limitations of the studies. Approximately 15% of the participants had cardiovascular disease, so the applicability of the findings to patients with target-organ damage is uncertain. In addition, there were fewer efficacy outcome events than expected, which suggests that the studies were underpowered.
When to start drug treatment
In each of the drug treatment and treat-to-target trials, the inclusion criterion for study entry was a systolic blood pressure above 160 mm Hg, with a mean blood pressure at entry into the drug treatment trials of 182/95 mm Hg.46 Thus, data support starting treatment if the systolic blood pressure is above 160 mm Hg, but not lower.
Notably, in all but one study,46 at least two-thirds of the participants took no more than two antihypertensive medications. Since adverse events become more common as the number of medications increases, the benefit of adding a third drug to lower blood pressure is uncertain.
Evidence in the ‘very elderly’: HYVET
With the exception of the Hypertension in the Very Elderly Trial (HYVET),44 the mean age of elderly patients in the reported studies was between 67 and 76.
HYVET patients were age 80 and older (mean age 84) and were randomized to receive either indapamide (with or without perindopril) or placebo. The trial was stopped early at 2 years because the mortality rate was lower in the treatment group (10.1%) than in the placebo group (12.3%) (number needed to treat 46, 95% confidence interval 24–637, P = .02). There was no significant difference in the primary outcome of fatal and nonfatal stroke.
Notably, trials that are stopped early may overestimate treatment benefit.48
Evidence in frail older adults
While the above studies provide some information about managing hypertension in the elderly, the participants were generally healthy. HYVET44 specifically excluded those with a standing systolic blood pressure of less than 140 mm Hg and enrolled few patients with orthostasis (7.9% in the placebo group and 8.8% in the treatment group), a condition commonly associated with frailty. As such, these studies may be less relevant to the frail elderly, who are at higher risk of adverse drug events and have competing risks for morbidity and mortality.
Observational studies, in fact, raise questions about whether tight blood pressure control improves clinical outcomes for the very elderly. In the Leiden 85-plus study, lower systolic blood pressure was associated with lower cognitive scores, worse functional ability,49,50 and a higher mortality rate51 compared with higher systolic pressure, although it is uncertain whether these outcomes were indicative of underlying disease that could result in lower blood pressure or an effect of blood pressure-lowering.
The National Health and Nutrition Examination Survey52 found an association between blood pressure and mortality rate that varied by walking speed. For slower walkers (based on the 6-minute walk test), higher systolic pressures were not associated with a higher risk of death, suggesting that when older adults are frail (as indicated by their slow walking speed) they are less likely to benefit from aggressive treatment of hypertension.
People at high risk because of stroke
Because the evidence is limited, it is even more difficult to judge whether lowering blood pressure below 140 mm Hg is beneficial for frail patients who have a history of stroke, compared with the possibility that medications will cause adverse effects such as weakness, orthostasis, and falls. When reviewing the evidence to answer this question, we especially looked at outcomes that affect quality of life, such as nonfatal stroke leading to disability. In contrast, because the frail elderly have competing causes of mortality, we could not assume that a mortality benefit shown in nonfrail populations could be applied to frail populations.
The PROGRESS trial (Perindopril Protection Against Recurrent Stroke Study)53 was in patients with a history of stroke or transient ischemic attack and a mean age of 64, who were treated with either perindopril (with or without indapamide) or placebo.
At almost 4 years, the rate of disabling stroke was 2.7% in the treatment group and 4.3% in the placebo group, a relative risk reduction of 38% and an absolute risk reduction of 1.64% (number needed to treat 61, 95% confidence interval 39–139). The relative risk reduction for all strokes (fatal and nonfatal) was similar across a range of baseline systolic pressures, but the absolute risk reduction was greater in the prespecified subgroup that had hypertension at baseline (mean blood pressure 159/94 mm Hg) than in the normotensive subgroup (mean blood pressure 136/79 mm Hg), suggesting that treatment is most beneficial for those with higher systolic blood pressures. Also, the benefit was only demonstrated in the subgroup that received two antihypertensive medications; those who received perindopril alone showed no benefit.
This study involved relatively young patients in relatively good health except for their strokes. The extent to which the results can be extrapolated to older, frail adults is uncertain because of the time needed to achieve benefit and because of the added vulnerability of frailty, which could make treatment with two antihypertensive medications riskier.
PRoFESS (Prevention Regimen for Effectively Avoiding Second Strokes),54 another study in patients with previous stroke (mean age 66) showed no benefit over 2.5 years in the primary outcome of stroke using telmesartan 80 mg daily compared with placebo. This result is concordant with that of PROGRESS,53 in which patients who took only one medication did not show a significant decrease in the rate of stroke.
A possible reason for the lack of benefit from monotherapy was that the differences in blood pressure between the placebo group and the treatment group on monotherapy were small in both studies (3.8/2.0 mm Hg in PRoFESS, 5/3 mm Hg in PROGRESS). In contrast, patients on dual therapy in PROGRESS decreased their blood pressure by 12/5 mm Hg compared with placebo.
CURRENT HYPERTENSION GUIDELINES
Current guidelines make reference to the elderly, but we found none that made specific recommendations for the frail elderly.
JNC 8
In December 2013, members of the Eighth Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) released new recommendations.32 One significant revision was to support higher blood pressure targets for older adults (age 60 and older). Whereas JNC 7 stated that lowering blood pressure below 140/90 mm Hg reduced cardiovascular complications,33 JNC 8 now acknowledges that there is no strong evidence to support blood pressure targets below 150/90 mm Hg for hypertensive persons without kidney disease or diabetes age 60 and older. Thus, in the general population age 60 and older, JNC 8 recommends starting antihypertensive treatment when blood pressure is 150/90 mm Hg or higher, and treating to a goal blood pressure of less than 150/90 mm Hg. JNC 8 makes no recommendation about how to adjust blood pressure targets for frailty or how to measure blood pressure.
American College of Cardiology and American Heart Association
In 2011, the American College of Cardiology and American Heart Association published a consensus document on the management of hypertension in the elderly.9
They acknowledged that the generally recommended blood pressure goal of lower than 140/90 mm Hg in uncomplicated elderly patients is based on expert opinion rather than on data from randomized controlled trials, but nevertheless recommended a target systolic pressure lower than 140 mm Hg for older adults, except for octogenarians.
For those over age 80, systolic levels of 140 to 145 mm Hg can be acceptable if tolerated and if the patient does not experience orthostasis when standing. Systolic pressure lower than 130 mm Hg and diastolic pressures lower than 65 mm Hg should be avoided in this age group.
The document acknowledges that systolic pressure may have to remain above 150 mm Hg if there is no response to four “well-selected drugs” or if there are unacceptable side effects. In these cases, the lowest “safely achieved” systolic blood pressure should be the goal.
Canadian Hypertension Education Program
The 2014 Canadian Hypertension Education Program (CHEP) report makes several recommendations for the “very elderly,” a group they define as over the age of 80. The CHEP website and resources include the following recommendations10:
- For the very elderly without diabetes or target-organ damage, drug therapy should be initiated when systolic blood pressure is higher than 160 mm Hg to reach a systolic blood pressure target lower than 150 mm Hg. This is a grade C level recommendation, indicating that it is based on low-quality trials, unvalidated surrogate outcomes, or results from nonrandomized observational studies.
- For the very elderly with macrovascular target-organ damage, antihypertensive therapy should be considered if systolic blood pressure readings average 140 mm Hg or higher (grade D for 140 to 160 mm Hg; grade A for higher than 160 mm Hg), although caution should be exercised in elderly patients who are frail. (Grade D recommendations are the weakest, as they are based on low-powered, imprecise studies or expert opinion, whereas grade A recommendations are based on the strongest evidence from high-quality randomized clinical trials.)
- Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based on an individualized risk-benefit analysis.
The European Society of Hypertension and European Society of Cardiology
The 2013 guidelines from the European Society of Hypertension and the European Society of Cardiology11 recommend that for elderly patients under age 80, antihypertensive treatment may be considered at systolic values higher than 140 mm Hg and aimed at values lower than 140 mm Hg if the patient is fit and treatment is well tolerated.
For those over age 80 with an initial systolic pressure of 160 mm Hg or higher, the guidelines recommend lowering systolic pressure to between 150 and 140 mm Hg, provided the patient is in good physical and mental condition. In frail elderly patients, they recommend leaving decisions on antihypertensive therapy to the treating physician, based on monitoring of the clinical effects of treatment.11
The ADS/PATH guidelines
When finalizing our recommendations,1 we considered the characteristics of frailty and the following key points from the evidence:
- Although evidence from drug treatment trials indicates that there is benefit in treating healthy older adults who have hypertension, the benefit of treating frail older adults is unknown.
- Major trials enrolled elderly patients only if they had systolic blood pressures of at least 160 mm Hg. Therefore, evidence supports initiating pharmacotherapy at a systolic pressure of 160 mm Hg or higher.
- No evidence from randomized controlled trials supports a systolic target lower than 140 mm Hg in the elderly, and there is some evidence that such a target does not benefit.
- The benefit of adding a third medication to lower blood pressure has not been studied.
- Frailty makes the potential benefits of strict blood pressure targets even less certain and increases the possibility of harm from adverse drug events.
- The only study of very old adults, HYVET,44 enrolled relatively healthy older adults and few with orthostasis, while excluding those with a standing systolic blood pressure lower than 140 mm Hg.
OUR RECOMMENDATIONS
Based on the above, we advise against unnecessarily strict targets and recommend stopping antihypertensive medications that are used for the sole purpose of keeping the systolic blood pressure below 140 mm Hg. Our guidelines are unique in that they focus equally on when to stop and when to start medications. We concluded that without evidence of definitive benefit, “less is more” with frailty.55 We believe that if physicians and health professionals understand the limitations of the evidence, they can be more confident in stopping medications that lower blood pressure to an unnecessarily low level.
We recommend the following (Table 4):
Before treating
- Carefully review the risks and the potential but unproven benefits of treatment.
- To avoid overtreatment, treatment decisions should be based on blood pressure measurements in the seated (not supine) position, while also considering the presence of orthostasis.
- To evaluate orthostasis, measure blood pressure in the supine position, then immediately on standing, and again after 2 minutes. Ask the patient if he or she feels light-headed or dizzy when standing.
Stop treatment
- If the seated systolic blood pressure is less than 140 mm Hg, medications can be tapered and discontinued to achieve the targets described below.
- Before discontinuation, consider whether the medications are treating additional conditions such as rate control for atrial fibrillation or symptomatic management of heart failure.
- It is uncertain whether to discontinue treatment when there is a history of stroke. Consider that treatment with two medications resulted in an absolute risk reduction for disabling stroke of 1.64% over approximately 4 years for adults with previous stroke and a mean age of 64,57 an effect that may be more prominent at higher systolic pressures.
Start treatment
- Consider starting treatment when systolic pressure is 160 mm Hg or higher.
- Aim for a seated systolic pressure between 140 and 160 mm Hg if there are no adverse effects from treatment that affect quality of life.
- If there is symptomatic orthostasis or if standing systolic pressure is lower than 140 mm Hg, the target seated systolic pressure can be adjusted upwards.
- In the severely frail nearing the end of life, a target systolic pressure of 160 to 190 mm Hg is reasonable.
- The blood pressure target is the same in people with diabetes.
- In general, use no more than two medications.
Dissemination and implementation
The ADS/PATH guideline is intended for use by physicians and other health professionals (eg, pharmacists and nurses) who care for frail older adults or who work in long-term care facilities. Since creating our guideline, we have disseminated it to physicians, pharmacists, and other health professionals through academic detailing, large conferences, and interactive webinars.
While we do not have objective evidence of practice change, our evaluation data found that 34% of 403 family physicians who received academic detailing indicated that the guideline would change their practice, while 36% stated that the guideline confirmed their practice, an indication that family physicians are sensitive to the needs of the frail elderly.
Because health professionals may be wary of stopping medications and not meeting recommended targets, there may be barriers to adopting this guideline. However, our experience with the PATH program indicates that these barriers can be overcome using effective communication strategies between health professionals and consumers.
AN APPROACH APPROPRIATE TO FRAILTY
There is no direct evidence for systolic blood pressure targets in the frail elderly, so we applied evidence from the nonfrail elderly. Our recommendations differ somewhat from those of other groups, which recommend targets below 140 to 150 mm Hg for older adults, although some do advise caution in the elderly for whom a substantial fall in blood pressure might be poorly tolerated. Despite these messages, we believe that clearer guidance is needed to direct health practitioners toward models that acknowledge that frail patients are in a precarious balance of health and may be harmed by treatments that strive to lower blood pressure to unproven targets. For this reason, our guideline clearly indicates when to decrease or stop drug treatment.
After physicians and health professionals examine the evidence and more fully understand the benefits and harms of treating frail older adults, we are confident that they will be more comfortable stopping medications that lower blood pressure to an unnecessarily low level and instead use an approach that is more appropriate to frailty. We hope clinicians can use this guideline with the same enthusiasm applied to other guidelines, and we welcome discussion.
Acknowledgments: We would like to thank and acknowledge Tanya MacLeod and Kathryn Yuill for their review of and advice about the manuscript.
Frail older adults deserve guidelines that take frailty into account while assessing the potential benefit and risks of treatment.
Specifically, our group—the Dalhousie Academic Detailing Service (ADS) and the Palliative and Therapeutic Harmonization (PATH) program—recommends that physicians strive to achieve more liberal treatment targets for elderly frail patients who have high blood pressure,1 as evidence does not support an aggressive approach in the frail elderly and the potential exists for harm.
This article reviews the evidence and reasoning that were used to develop and promote a guideline for drug treatment of hypertension in frail older adults. Our recommendations differ from other guidelines in that they focus as much on stopping or decreasing therapy as on starting or increasing it.
FRAILTY INCREASES THE RISK OF ADVERSE EFFECTS
The word frail, applied to older adults, describes those who have complex medical illnesses severe enough to compromise their ability to live independently.2 Many have multiple coexisting medical problems for which they take numerous drugs, in addition to dementia, impaired mobility, compromised functional ability, or a history of falling.
Frailty denotes vulnerability; it increases the risk of adverse effects from medical and surgical procedures,3 complicates drug therapy,4 prolongs hospital length of stay,5 leads to functional and cognitive decline,6 increases the risk of institutionalization,7 and reduces life expectancy8—all of which affect the benefit and harm of medical treatments.
Guidelines for treating hypertension9–11 now acknowledge that little evidence exists to support starting treatment for systolic blood pressure between 140 and 160 mm Hg or aiming for a target of less than 140 mm Hg for “very old” adults, commonly defined as over the age of 80. New guidelines loosen the treatment targets for the very old, but they do not specify targets for the frail and do not describe how to recognize or measure frailty.
RECOGNIZING AND MEASURING FRAILTY
A number of tools are available to recognize and measure frailty.12
The Fried frailty assessment13 has five items:
- Unintentional weight loss
- Self-reported exhaustion
- Weakness in grip
- Slow walking speed
- Low physical activity and energy expenditure.
People are deemed frail if they have three or more of these five. However, experts disagree about whether this system is too sensitive14 or not sensitive enough.15,16
The FRAIL questionnaire17 also has five items:
- Fatigue
- Resistance (inability to climb stairs)
- Ambulation (inability to walk 1 city block)
- Illness (more than 5 major illnesses)
- Weight loss.
People are deemed frail if they have at least three of these five items, and “prefrail” if they have two.
These and other tools are limited by being dichotomous: they classify people as being either frail or not frail18–20 but do not define the spectrum of frailty.
Other frailty assessments such as the Frailty Index21 identify frailty based on the number of accumulated health deficits but take a long time to complete, making them difficult to use in busy clinical settings.22–24
The Clinical Frailty Scale7 is a validated scale that categorizes frailty based on physical and functional indicators of health, such as cognition, function, and mobility, with scores that range from 1 (very fit) to 9 (terminally ill).7,12
The Frailty Assessment for Care-planning Tool (FACT) uses scaling compatible with the Clinical Frailty Scale but has been developed for use as a practical and interpretable frailty screening tool for nonexperts (Table 1). The FACT assesses cognition, mobility, function, and the social situation, using a combination of caregiver report and objective measures. To assess cognition, a health care professional uses items from the Mini-Cog25 (ie, the ability to draw an analog clock face and then recall three unrelated items following the clock-drawing test) and the memory axis of the Brief Cognitive Rating Scale26 (ie, the ability to recall current events, the current US president, and the names of children or spouse). Mobility, function, and social circumstance scores are assigned according to the caregiver report of the patient’s baseline status.
The FACT can be completed in busy clinical settings. Once a caregiver is identified, it takes about 5 minutes to complete.
Our guideline27–31 is intended for those with a score of 7 or more on the Clinical Frailty Scale or FACT,7,12 a score we chose because it describes people who are severely frail with shortened life expectancy.8 At this level, people need help with all instrumental activities of daily living (eg, handling finances, medication management, household chores, and shopping) as well as with basic activities of daily living such as bathing or dressing.
REVIEWING THE LIMITED EVIDENCE
We found no studies that addressed the risks and benefits of treating hypertension in frail older adults; therefore, we concentrated on studies that enrolled individuals who were chronologically old but not frail. We reviewed prominent guidelines,9–11,32,33 the evidence base for these guidelines,34–44 and Cochrane reviews.45,46 A detailed description of the evidence used to build our recommendation can be found online.31
When we deliberated on treatment targets, we reviewed evidence from two types of randomized controlled trials47:
Drug treatment trials randomize patients to different treatments, such as placebo versus a drug or one drug compared with another drug. Patients in different treatment groups may achieve different blood pressures and clinical outcomes, and this information is then used to define optimal targets. However, it may be difficult to determine if the benefit came from lowering blood pressure or from some other effect of the drug, which can be independent of blood pressure lowering.
Treat-to-target trials randomize patients to different blood pressure goals, but the groups are treated with the same or similar drugs. Therefore, any identified benefit can be attributed to the differences in blood pressure rather than the medications used. Compared with a drug treatment trial, this type of trial provides stronger evidence about optimal targets.
We also considered the characteristics of frailty, the dilemma of polypharmacy, and the relevance of the available scientific evidence to those who are frail.
Drug treatment trials
A Cochrane review45 of 15 studies with approximately 24,000 elderly participants found that treating hypertension decreased the rates of cardiovascular morbidity and mortality as well as fatal and nonfatal stroke in the “elderly” (defined as age ≥ 60) and “very elderly” (age ≥ 80). However, in the very elderly, all-cause mortality rates were not statistically significantly different with treatment compared with placebo. The mean duration of treatment was 4.5 years in the elderly and 2.2 years in the very elderly (Table 2). Of importance, all the trials enrolled only those individuals whose systolic blood pressure was at least 160 mm Hg at baseline.
None of the studies were treat-to-target trials—patients were assigned either active medication or placebo. Thus, these trials provide evidence of benefit for treating hypertension in the elderly and very elderly but do not identify the optimal target. All of the drug treatment trials showed benefit, but none achieved a systolic pressure lower than 140 mm Hg with active treatment (Table 3). Therefore, these studies do not support a systolic target of less than 140 mm Hg in the elderly.
Treat-to-target trials: JATOS and VALISH
The Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients (JATOS)42 and the Valsartan in Elderly Isolated Systolic Hypertension (VALISH) study43 each enrolled more than 3,000 people age 65 or older (mean age approximately 75). Patients were randomized to either a strict systolic target of less than 140 mm Hg or a higher (more permissive) target of 140 to 160 mm Hg in JATOS and 140 to 149 mm Hg in VALISH.
In both trials, the group with strict targets achieved a systolic pressure of approximately 136 mm Hg, while the group with higher blood pressure targets achieved a systolic pressure of 146 mm Hg in JATOS and 142 mm Hg in VALISH. Despite these differences, there was no statistically significant difference in the primary outcome.
Thus, treat-to-target studies also fail to support a systolic target of less than 140 mm Hg in the elderly, although it is important to recognize the limitations of the studies. Approximately 15% of the participants had cardiovascular disease, so the applicability of the findings to patients with target-organ damage is uncertain. In addition, there were fewer efficacy outcome events than expected, which suggests that the studies were underpowered.
When to start drug treatment
In each of the drug treatment and treat-to-target trials, the inclusion criterion for study entry was a systolic blood pressure above 160 mm Hg, with a mean blood pressure at entry into the drug treatment trials of 182/95 mm Hg.46 Thus, data support starting treatment if the systolic blood pressure is above 160 mm Hg, but not lower.
Notably, in all but one study,46 at least two-thirds of the participants took no more than two antihypertensive medications. Since adverse events become more common as the number of medications increases, the benefit of adding a third drug to lower blood pressure is uncertain.
Evidence in the ‘very elderly’: HYVET
With the exception of the Hypertension in the Very Elderly Trial (HYVET),44 the mean age of elderly patients in the reported studies was between 67 and 76.
HYVET patients were age 80 and older (mean age 84) and were randomized to receive either indapamide (with or without perindopril) or placebo. The trial was stopped early at 2 years because the mortality rate was lower in the treatment group (10.1%) than in the placebo group (12.3%) (number needed to treat 46, 95% confidence interval 24–637, P = .02). There was no significant difference in the primary outcome of fatal and nonfatal stroke.
Notably, trials that are stopped early may overestimate treatment benefit.48
Evidence in frail older adults
While the above studies provide some information about managing hypertension in the elderly, the participants were generally healthy. HYVET44 specifically excluded those with a standing systolic blood pressure of less than 140 mm Hg and enrolled few patients with orthostasis (7.9% in the placebo group and 8.8% in the treatment group), a condition commonly associated with frailty. As such, these studies may be less relevant to the frail elderly, who are at higher risk of adverse drug events and have competing risks for morbidity and mortality.
Observational studies, in fact, raise questions about whether tight blood pressure control improves clinical outcomes for the very elderly. In the Leiden 85-plus study, lower systolic blood pressure was associated with lower cognitive scores, worse functional ability,49,50 and a higher mortality rate51 compared with higher systolic pressure, although it is uncertain whether these outcomes were indicative of underlying disease that could result in lower blood pressure or an effect of blood pressure-lowering.
The National Health and Nutrition Examination Survey52 found an association between blood pressure and mortality rate that varied by walking speed. For slower walkers (based on the 6-minute walk test), higher systolic pressures were not associated with a higher risk of death, suggesting that when older adults are frail (as indicated by their slow walking speed) they are less likely to benefit from aggressive treatment of hypertension.
People at high risk because of stroke
Because the evidence is limited, it is even more difficult to judge whether lowering blood pressure below 140 mm Hg is beneficial for frail patients who have a history of stroke, compared with the possibility that medications will cause adverse effects such as weakness, orthostasis, and falls. When reviewing the evidence to answer this question, we especially looked at outcomes that affect quality of life, such as nonfatal stroke leading to disability. In contrast, because the frail elderly have competing causes of mortality, we could not assume that a mortality benefit shown in nonfrail populations could be applied to frail populations.
The PROGRESS trial (Perindopril Protection Against Recurrent Stroke Study)53 was in patients with a history of stroke or transient ischemic attack and a mean age of 64, who were treated with either perindopril (with or without indapamide) or placebo.
At almost 4 years, the rate of disabling stroke was 2.7% in the treatment group and 4.3% in the placebo group, a relative risk reduction of 38% and an absolute risk reduction of 1.64% (number needed to treat 61, 95% confidence interval 39–139). The relative risk reduction for all strokes (fatal and nonfatal) was similar across a range of baseline systolic pressures, but the absolute risk reduction was greater in the prespecified subgroup that had hypertension at baseline (mean blood pressure 159/94 mm Hg) than in the normotensive subgroup (mean blood pressure 136/79 mm Hg), suggesting that treatment is most beneficial for those with higher systolic blood pressures. Also, the benefit was only demonstrated in the subgroup that received two antihypertensive medications; those who received perindopril alone showed no benefit.
This study involved relatively young patients in relatively good health except for their strokes. The extent to which the results can be extrapolated to older, frail adults is uncertain because of the time needed to achieve benefit and because of the added vulnerability of frailty, which could make treatment with two antihypertensive medications riskier.
PRoFESS (Prevention Regimen for Effectively Avoiding Second Strokes),54 another study in patients with previous stroke (mean age 66) showed no benefit over 2.5 years in the primary outcome of stroke using telmesartan 80 mg daily compared with placebo. This result is concordant with that of PROGRESS,53 in which patients who took only one medication did not show a significant decrease in the rate of stroke.
A possible reason for the lack of benefit from monotherapy was that the differences in blood pressure between the placebo group and the treatment group on monotherapy were small in both studies (3.8/2.0 mm Hg in PRoFESS, 5/3 mm Hg in PROGRESS). In contrast, patients on dual therapy in PROGRESS decreased their blood pressure by 12/5 mm Hg compared with placebo.
CURRENT HYPERTENSION GUIDELINES
Current guidelines make reference to the elderly, but we found none that made specific recommendations for the frail elderly.
JNC 8
In December 2013, members of the Eighth Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8) released new recommendations.32 One significant revision was to support higher blood pressure targets for older adults (age 60 and older). Whereas JNC 7 stated that lowering blood pressure below 140/90 mm Hg reduced cardiovascular complications,33 JNC 8 now acknowledges that there is no strong evidence to support blood pressure targets below 150/90 mm Hg for hypertensive persons without kidney disease or diabetes age 60 and older. Thus, in the general population age 60 and older, JNC 8 recommends starting antihypertensive treatment when blood pressure is 150/90 mm Hg or higher, and treating to a goal blood pressure of less than 150/90 mm Hg. JNC 8 makes no recommendation about how to adjust blood pressure targets for frailty or how to measure blood pressure.
American College of Cardiology and American Heart Association
In 2011, the American College of Cardiology and American Heart Association published a consensus document on the management of hypertension in the elderly.9
They acknowledged that the generally recommended blood pressure goal of lower than 140/90 mm Hg in uncomplicated elderly patients is based on expert opinion rather than on data from randomized controlled trials, but nevertheless recommended a target systolic pressure lower than 140 mm Hg for older adults, except for octogenarians.
For those over age 80, systolic levels of 140 to 145 mm Hg can be acceptable if tolerated and if the patient does not experience orthostasis when standing. Systolic pressure lower than 130 mm Hg and diastolic pressures lower than 65 mm Hg should be avoided in this age group.
The document acknowledges that systolic pressure may have to remain above 150 mm Hg if there is no response to four “well-selected drugs” or if there are unacceptable side effects. In these cases, the lowest “safely achieved” systolic blood pressure should be the goal.
Canadian Hypertension Education Program
The 2014 Canadian Hypertension Education Program (CHEP) report makes several recommendations for the “very elderly,” a group they define as over the age of 80. The CHEP website and resources include the following recommendations10:
- For the very elderly without diabetes or target-organ damage, drug therapy should be initiated when systolic blood pressure is higher than 160 mm Hg to reach a systolic blood pressure target lower than 150 mm Hg. This is a grade C level recommendation, indicating that it is based on low-quality trials, unvalidated surrogate outcomes, or results from nonrandomized observational studies.
- For the very elderly with macrovascular target-organ damage, antihypertensive therapy should be considered if systolic blood pressure readings average 140 mm Hg or higher (grade D for 140 to 160 mm Hg; grade A for higher than 160 mm Hg), although caution should be exercised in elderly patients who are frail. (Grade D recommendations are the weakest, as they are based on low-powered, imprecise studies or expert opinion, whereas grade A recommendations are based on the strongest evidence from high-quality randomized clinical trials.)
- Decisions regarding initiating and intensifying pharmacotherapy in the very elderly should be based on an individualized risk-benefit analysis.
The European Society of Hypertension and European Society of Cardiology
The 2013 guidelines from the European Society of Hypertension and the European Society of Cardiology11 recommend that for elderly patients under age 80, antihypertensive treatment may be considered at systolic values higher than 140 mm Hg and aimed at values lower than 140 mm Hg if the patient is fit and treatment is well tolerated.
For those over age 80 with an initial systolic pressure of 160 mm Hg or higher, the guidelines recommend lowering systolic pressure to between 150 and 140 mm Hg, provided the patient is in good physical and mental condition. In frail elderly patients, they recommend leaving decisions on antihypertensive therapy to the treating physician, based on monitoring of the clinical effects of treatment.11
The ADS/PATH guidelines
When finalizing our recommendations,1 we considered the characteristics of frailty and the following key points from the evidence:
- Although evidence from drug treatment trials indicates that there is benefit in treating healthy older adults who have hypertension, the benefit of treating frail older adults is unknown.
- Major trials enrolled elderly patients only if they had systolic blood pressures of at least 160 mm Hg. Therefore, evidence supports initiating pharmacotherapy at a systolic pressure of 160 mm Hg or higher.
- No evidence from randomized controlled trials supports a systolic target lower than 140 mm Hg in the elderly, and there is some evidence that such a target does not benefit.
- The benefit of adding a third medication to lower blood pressure has not been studied.
- Frailty makes the potential benefits of strict blood pressure targets even less certain and increases the possibility of harm from adverse drug events.
- The only study of very old adults, HYVET,44 enrolled relatively healthy older adults and few with orthostasis, while excluding those with a standing systolic blood pressure lower than 140 mm Hg.
OUR RECOMMENDATIONS
Based on the above, we advise against unnecessarily strict targets and recommend stopping antihypertensive medications that are used for the sole purpose of keeping the systolic blood pressure below 140 mm Hg. Our guidelines are unique in that they focus equally on when to stop and when to start medications. We concluded that without evidence of definitive benefit, “less is more” with frailty.55 We believe that if physicians and health professionals understand the limitations of the evidence, they can be more confident in stopping medications that lower blood pressure to an unnecessarily low level.
We recommend the following (Table 4):
Before treating
- Carefully review the risks and the potential but unproven benefits of treatment.
- To avoid overtreatment, treatment decisions should be based on blood pressure measurements in the seated (not supine) position, while also considering the presence of orthostasis.
- To evaluate orthostasis, measure blood pressure in the supine position, then immediately on standing, and again after 2 minutes. Ask the patient if he or she feels light-headed or dizzy when standing.
Stop treatment
- If the seated systolic blood pressure is less than 140 mm Hg, medications can be tapered and discontinued to achieve the targets described below.
- Before discontinuation, consider whether the medications are treating additional conditions such as rate control for atrial fibrillation or symptomatic management of heart failure.
- It is uncertain whether to discontinue treatment when there is a history of stroke. Consider that treatment with two medications resulted in an absolute risk reduction for disabling stroke of 1.64% over approximately 4 years for adults with previous stroke and a mean age of 64,57 an effect that may be more prominent at higher systolic pressures.
Start treatment
- Consider starting treatment when systolic pressure is 160 mm Hg or higher.
- Aim for a seated systolic pressure between 140 and 160 mm Hg if there are no adverse effects from treatment that affect quality of life.
- If there is symptomatic orthostasis or if standing systolic pressure is lower than 140 mm Hg, the target seated systolic pressure can be adjusted upwards.
- In the severely frail nearing the end of life, a target systolic pressure of 160 to 190 mm Hg is reasonable.
- The blood pressure target is the same in people with diabetes.
- In general, use no more than two medications.
Dissemination and implementation
The ADS/PATH guideline is intended for use by physicians and other health professionals (eg, pharmacists and nurses) who care for frail older adults or who work in long-term care facilities. Since creating our guideline, we have disseminated it to physicians, pharmacists, and other health professionals through academic detailing, large conferences, and interactive webinars.
While we do not have objective evidence of practice change, our evaluation data found that 34% of 403 family physicians who received academic detailing indicated that the guideline would change their practice, while 36% stated that the guideline confirmed their practice, an indication that family physicians are sensitive to the needs of the frail elderly.
Because health professionals may be wary of stopping medications and not meeting recommended targets, there may be barriers to adopting this guideline. However, our experience with the PATH program indicates that these barriers can be overcome using effective communication strategies between health professionals and consumers.
AN APPROACH APPROPRIATE TO FRAILTY
There is no direct evidence for systolic blood pressure targets in the frail elderly, so we applied evidence from the nonfrail elderly. Our recommendations differ somewhat from those of other groups, which recommend targets below 140 to 150 mm Hg for older adults, although some do advise caution in the elderly for whom a substantial fall in blood pressure might be poorly tolerated. Despite these messages, we believe that clearer guidance is needed to direct health practitioners toward models that acknowledge that frail patients are in a precarious balance of health and may be harmed by treatments that strive to lower blood pressure to unproven targets. For this reason, our guideline clearly indicates when to decrease or stop drug treatment.
After physicians and health professionals examine the evidence and more fully understand the benefits and harms of treating frail older adults, we are confident that they will be more comfortable stopping medications that lower blood pressure to an unnecessarily low level and instead use an approach that is more appropriate to frailty. We hope clinicians can use this guideline with the same enthusiasm applied to other guidelines, and we welcome discussion.
Acknowledgments: We would like to thank and acknowledge Tanya MacLeod and Kathryn Yuill for their review of and advice about the manuscript.
- Palliative and Therapeutic Harmonization program. Hypertension guidelines. Treating hypertension in frailty. http://pathclinic.ca/resources/hypertension/. Accessed May 2, 2014.
- Theou O, Rockwood MR, Mitnitski A, Rockwood K. Disability and co-morbidity in relation to frailty: how much do they overlap? Arch Gerontol Geriatr 2012; 55:e1–e8.
- Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg 2010; 210:901–908.
- Tinetti ME, Bogardus ST, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004; 351:2870–2874.
- Ekerstad N, Swahn E, Janzon M, et al. Frailty is independently associated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation 2011; 124:2397–2404.
- Theou O, Rockwood K. Should frailty status always be considered when treating the elderly patient? Aging Health 2012; 8:261–271.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173:489–495.
- Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr 2008; 8:24.
- Aronow WS, Fleg JL, Pepine CJ, et al; ACCF Task Force. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2011; 123:2434–2506.
- The Canadian Hypertension Education Program (CHEP). 2014 CHEP recommendations. www.hypertension.ca/en/. Accessed May 2, 2014.
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013; 34:2159–2219.
- Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14:392–397.
- Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56:M146–M156.
- Ensrud KE, Ewing SK, Cawthon PM, et al; Osteoporotic Fractures in Men Research Group. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J Am Geriatr Soc 2009; 57:492–498.
- Avila-Funes JA, Amieva H, Barberger-Gateau P, et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: the three-city study. J Am Geriatr Soc 2009; 57:453–461.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging 2012; 16:601–608.
- Strawbridge WJ, Shema SJ, Balfour JL, Higby HR, Kaplan GA. Antecedents of frailty over three decades in an older cohort. J Gerontol B Psychol Sci Soc Sci 1998; 53:S9–S16.
- Matthews M, Lucas A, Boland R, et al. Use of a questionnaire to screen for frailty in the elderly: an exploratory study. Aging Clin Exp Res 2004; 16:34–40.
- Salvi F, Morichi V, Grilli A, et al. Screening for frailty in elderly emergency department patients by using the Identification of Seniors At Risk (ISAR). J Nutr Health Aging 2012; 16:313–318.
- Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal 2001; 1:323–336.
- Kellen E, Bulens P, Deckx L, et al. Identifying an accurate pre-screening tool in geriatric oncology. Crit Rev Oncol Hematol 2010; 75:243–248.
- Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006; 35:526–529.
- Martin FC, Brighton P. Frailty: different tools for different purposes? Age Ageing 2008; 37:129–131.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Reisberg B, Ferris SH. Brief Cognitive Rating Scale (BCRS). Psychopharmacol Bull 1988; 24:629–636.
- Moorhouse P, Mallery LH. Palliative and therapeutic harmonization: a model for appropriate decision-making in frail older adults. J Am Geriatr Soc 2012; 60:2326–2332.
- Palliative and Therapeutic Harmonization Clinic (PATH). www.pathclinic.ca. Accessed May 2, 2014.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. http://cme.medicine.dal.ca/ADS.htm. Accessed January 8, 2014.
- Mallery LH, Moorhouse P. Respecting frailty. J Med Ethics 2011; 37:126–128.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. Issues in hypertension 2011. http://cme.medicine.dal.ca/files/Hypertension%20book.pdf. Accessed May 2, 2014.
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
- Amery A, Birkenhäger W, Brixko P, et al. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet 1985; 1:1349–1354.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. Br Med J (Clin Res Ed) 1986; 293:1145–1151.
- SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
- Dahlöf B, Lindholm LH, Hansson L, Scherstén B, Ekbom T, Wester PO. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- Medical Research Council trial of treatment of hypertension in older adults: principal results. MRC Working Party. BMJ 1992; 304:405–412.
- Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
- Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertens 1998; 16:1823–1829.
- Lithell H, Hansson L, Skoog I, et al; SCOPE Study Group. The Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trial. J Hypertens 2003; 21:875–886.
- JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
- Oparil S, Yarows SA, Patel S, Fang H, Zhang J, Satlin A. Efficacy and safety of combined use of aliskiren and valsartan in patients with hypertension: a randomised, double-blind trial. Lancet 2007; 370:221–229.
- Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
- Musini VM, Tejani AM, Bassett K, Wright JM. Pharmacotherapy for hypertension in the elderly. Cochrane Database Syst Rev 2009;CD000028.
- He FJ, MacGregor GA. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database Syst Rev 2004;CD004937.
- Allen M, Kelly K, Fleming I. Hypertension in elderly patients: recommended systolic targets are not evidence based [in French]. Can Fam Physician 2013; 59:19–24.
- Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ 2012; 344:e3863.
- Sabayan B, Oleksik AM, Maier AB, et al. High blood pressure and resilience to physical and cognitive decline in the oldest old: the Leiden 85-plus Study. J Am Geriatr Soc 2012; 60:2014–2019.
- Sabayan B, van Vliet P, de Ruijter W, Gussekloo J, de Craen AJ, Westendorp RG. High blood pressure, physical and cognitive function, and risk of stroke in the oldest old: the Leiden 85-plus Study. Stroke 2013; 44:15–20.
- Poortvliet RK, Blom JW, de Craen AJ, et al. Low blood pressure predicts increased mortality in very old age even without heart failure: the Leiden 85-plus Study. Eur J Heart Fail 2013; 15:528–533.
- Odden MC, Peralta CA, Haan MN, Covinsky KE. Rethinking the association of high blood pressure with mortality in elderly adults: the impact of frailty. Arch Intern Med 2012; 172:1162–1168.
- PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001; 358:1033–1041.
- Yusuf S, Diener HC, Sacco RL, et al; PRoFESS Study Group. Telmisartan to prevent recurrent stroke and cardiovascular events. N Engl J Med 2008; 359:1225–1237.
- Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010; 170:1648–1654.
- Palliative and Therapeutic Harmonization program. Hypertension guidelines. Treating hypertension in frailty. http://pathclinic.ca/resources/hypertension/. Accessed May 2, 2014.
- Theou O, Rockwood MR, Mitnitski A, Rockwood K. Disability and co-morbidity in relation to frailty: how much do they overlap? Arch Gerontol Geriatr 2012; 55:e1–e8.
- Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg 2010; 210:901–908.
- Tinetti ME, Bogardus ST, Agostini JV. Potential pitfalls of disease-specific guidelines for patients with multiple conditions. N Engl J Med 2004; 351:2870–2874.
- Ekerstad N, Swahn E, Janzon M, et al. Frailty is independently associated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation 2011; 124:2397–2404.
- Theou O, Rockwood K. Should frailty status always be considered when treating the elderly patient? Aging Health 2012; 8:261–271.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005; 173:489–495.
- Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr 2008; 8:24.
- Aronow WS, Fleg JL, Pepine CJ, et al; ACCF Task Force. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2011; 123:2434–2506.
- The Canadian Hypertension Education Program (CHEP). 2014 CHEP recommendations. www.hypertension.ca/en/. Accessed May 2, 2014.
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013; 34:2159–2219.
- Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14:392–397.
- Fried LP, Tangen CM, Walston J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56:M146–M156.
- Ensrud KE, Ewing SK, Cawthon PM, et al; Osteoporotic Fractures in Men Research Group. A comparison of frailty indexes for the prediction of falls, disability, fractures, and mortality in older men. J Am Geriatr Soc 2009; 57:492–498.
- Avila-Funes JA, Amieva H, Barberger-Gateau P, et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: the three-city study. J Am Geriatr Soc 2009; 57:453–461.
- Bergman H, Ferrucci L, Guralnik J, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol A Biol Sci Med Sci 2007; 62:731–737.
- Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging 2012; 16:601–608.
- Strawbridge WJ, Shema SJ, Balfour JL, Higby HR, Kaplan GA. Antecedents of frailty over three decades in an older cohort. J Gerontol B Psychol Sci Soc Sci 1998; 53:S9–S16.
- Matthews M, Lucas A, Boland R, et al. Use of a questionnaire to screen for frailty in the elderly: an exploratory study. Aging Clin Exp Res 2004; 16:34–40.
- Salvi F, Morichi V, Grilli A, et al. Screening for frailty in elderly emergency department patients by using the Identification of Seniors At Risk (ISAR). J Nutr Health Aging 2012; 16:313–318.
- Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal 2001; 1:323–336.
- Kellen E, Bulens P, Deckx L, et al. Identifying an accurate pre-screening tool in geriatric oncology. Crit Rev Oncol Hematol 2010; 75:243–248.
- Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006; 35:526–529.
- Martin FC, Brighton P. Frailty: different tools for different purposes? Age Ageing 2008; 37:129–131.
- Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry 2000; 15:1021–1027.
- Reisberg B, Ferris SH. Brief Cognitive Rating Scale (BCRS). Psychopharmacol Bull 1988; 24:629–636.
- Moorhouse P, Mallery LH. Palliative and therapeutic harmonization: a model for appropriate decision-making in frail older adults. J Am Geriatr Soc 2012; 60:2326–2332.
- Palliative and Therapeutic Harmonization Clinic (PATH). www.pathclinic.ca. Accessed May 2, 2014.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. http://cme.medicine.dal.ca/ADS.htm. Accessed January 8, 2014.
- Mallery LH, Moorhouse P. Respecting frailty. J Med Ethics 2011; 37:126–128.
- Dalhousie University Faculty of Medicine: Continuing Medical Education. Issues in hypertension 2011. http://cme.medicine.dal.ca/files/Hypertension%20book.pdf. Accessed May 2, 2014.
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520.
- Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560–2572.
- Amery A, Birkenhäger W, Brixko P, et al. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet 1985; 1:1349–1354.
- Coope J, Warrender TS. Randomised trial of treatment of hypertension in elderly patients in primary care. Br Med J (Clin Res Ed) 1986; 293:1145–1151.
- SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
- Dahlöf B, Lindholm LH, Hansson L, Scherstén B, Ekbom T, Wester PO. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991; 338:1281–1285.
- Medical Research Council trial of treatment of hypertension in older adults: principal results. MRC Working Party. BMJ 1992; 304:405–412.
- Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
- Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertens 1998; 16:1823–1829.
- Lithell H, Hansson L, Skoog I, et al; SCOPE Study Group. The Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trial. J Hypertens 2003; 21:875–886.
- JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
- Oparil S, Yarows SA, Patel S, Fang H, Zhang J, Satlin A. Efficacy and safety of combined use of aliskiren and valsartan in patients with hypertension: a randomised, double-blind trial. Lancet 2007; 370:221–229.
- Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
- Musini VM, Tejani AM, Bassett K, Wright JM. Pharmacotherapy for hypertension in the elderly. Cochrane Database Syst Rev 2009;CD000028.
- He FJ, MacGregor GA. Effect of longer-term modest salt reduction on blood pressure. Cochrane Database Syst Rev 2004;CD004937.
- Allen M, Kelly K, Fleming I. Hypertension in elderly patients: recommended systolic targets are not evidence based [in French]. Can Fam Physician 2013; 59:19–24.
- Guyatt GH, Briel M, Glasziou P, Bassler D, Montori VM. Problems of stopping trials early. BMJ 2012; 344:e3863.
- Sabayan B, Oleksik AM, Maier AB, et al. High blood pressure and resilience to physical and cognitive decline in the oldest old: the Leiden 85-plus Study. J Am Geriatr Soc 2012; 60:2014–2019.
- Sabayan B, van Vliet P, de Ruijter W, Gussekloo J, de Craen AJ, Westendorp RG. High blood pressure, physical and cognitive function, and risk of stroke in the oldest old: the Leiden 85-plus Study. Stroke 2013; 44:15–20.
- Poortvliet RK, Blom JW, de Craen AJ, et al. Low blood pressure predicts increased mortality in very old age even without heart failure: the Leiden 85-plus Study. Eur J Heart Fail 2013; 15:528–533.
- Odden MC, Peralta CA, Haan MN, Covinsky KE. Rethinking the association of high blood pressure with mortality in elderly adults: the impact of frailty. Arch Intern Med 2012; 172:1162–1168.
- PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001; 358:1033–1041.
- Yusuf S, Diener HC, Sacco RL, et al; PRoFESS Study Group. Telmisartan to prevent recurrent stroke and cardiovascular events. N Engl J Med 2008; 359:1225–1237.
- Garfinkel D, Mangin D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: addressing polypharmacy. Arch Intern Med 2010; 170:1648–1654.
KEY POINTS
- For frail elderly patients, consider starting treatment if the systolic blood pressure is 160 mm Hg or higher.
- An appropriate target in this population is a seated systolic pressure between 140 and 160 mm Hg, as long as there is no orthostatic drop to less than 140 mm Hg upon standing from a lying position and treatment does not adversely affect quality of life.
- The blood pressure target does not need to be lower if the patient has diabetes. If the patient is severely frail and has a short life expectancy, a systolic target of 160 to 190 mm Hg may be reasonable.
- If the systolic pressure is below 140 mm Hg, antihypertensive medications can be reduced as long as they are not indicated for other conditions.
- In general, one should prescribe no more than two antihypertensive medications.
Palliative care at time of cancer diagnosis improves survival
CHICAGO – Early palliative care delivered almost exclusively by telephone improved survival among patients with advanced cancer in the ENABLE III study.
After a median follow-up of a little more than 1 year, 46% of patients receiving palliative care from the time of cancer diagnosis and 54% of those with delayed palliative care had died.

Overall median survival was 18.3 months for the immediate group and 11.9 months for the delayed group (P = .17).
In preplanned analyses, the risk of death at 1 year was significantly lower in the immediate group (hazard ratio 0.72; P = .003), with a catch-up effect thereafter, Marie Bakitas, DNSc, reported at the annual meeting of the American Society of Clinical Oncology.
"Enhanced medical care, reduced aggressive care and chemotherapy use, longer access to hospice, and biologic impacts of improved quality of life have all been proposed as mechanisms to explain this survival advantage," Dr. Bakitas said. "However, at the present time, we do not have the data to support a particular mechanism and we are actively exploring this question through secondary analyses."
ENABLE (Educate, Nurture, Advise, Before Life Ends) III is the first study to examine the timing of early palliative care, but not the first to identify a survival advantage.
A recent study (N. Engl. J. Med. 2010:363:733-42) found that patients with metastatic non–small cell lung cancer (NSCLC) who received palliative care at the time of randomization lived a significant 2.7 months longer than did those receiving standard oncologic care, despite receiving significantly less aggressive end-of-life care (33% vs. 54%).
In ENABLE III, 207 patients with advanced cancer, and their caregivers, were randomized as a dyad to begin usual cancer care plus the intervention at the time of diagnosis (immediate group) or usual care alone for 3 months followed by the intervention (delayed group).
The intervention consisted of a traditional outpatient palliative care consult and six weekly structured telephone calls with a nurse coach using a guidebook that covers such topics as problem solving, symptom management, communication, and advanced care planning, explained Dr. Bakitas, the Marie O’Koren Endowed Chair and Professor, School of Nursing, and associate director of the Center for Palliative and Supportive Care, University of Alabama, Birmingham.
Usual care included the clinical consult, but not the telephone intervention.
The participants’ mean age was 64 years, half were male, 60% lived in a rural area, and 65% were married or living with a partner. Lung cancer was the most common diagnosis at 42%.
At baseline, 75% of patients were receiving chemotherapy, 19% were undergoing radiation, and 43% had an advanced directive completed at diagnosis.
Unlike the group’s prior trial comparing palliative care to usual care at 3 months, immediate versus delayed palliative care did not lead to significant improvements in quality of life on the Functional Assessment of Chronic Illness Therapy-Palliative care scale (129.9 vs. 127.2; P = .34), mood on the Center for Epidemiologic Studies Depression scale (11.2 vs. 10.8; P = .33), or symptom impact on the Quality of Life at the End of Life symptom impact subscale (11.4 vs. 12.2; P = .09).
One plausible reason for the findings is that there may not have been enough care differences between the two groups, with 40% of the delayed group receiving their first palliative care contact an average of 30 days before they were scheduled to do so on day 84, Dr. Bakitas said.
Second, difficulties in accrual and decreased study power may have made it difficult to pick up between-group differences on the subjective instruments, resulting in a type 2 error.
"A 3-month delay is still very early," Dr. Bakitas said.
She noted that early intervention allowed the palliative care team to have contact with patients for 1 year on average (range 240-493 days), compared with a median of 41-90 days from referral to death reported for outpatient clinics in a national survey of 142 National Cancer Institute and non-NCI cancer centers (JAMA 2010;303:1054-61).
Resource and chemotherapy use in ENABLE III was also comparable in both groups. Decedents in the immediate and delayed groups spent a median of 5 and 6 days, respectively, in hospital in the 7-9 months preceding death, while 8% and 5% received chemotherapy in the last 2 weeks of life.
This compares favorably with a national average of more than 8 hospital days in the last 6 months of life observed in the 2014 Dartmouth Atlas of Health Care, and a chemotherapy rate of 17.5% reported in the previously noted NSCLC study, Dr. Bakitas said.
She called for more studies of early palliative care to determine the optimal timing, personnel, essential elements, and mechanisms of improved survival.
"While the benefits of these approaches have been demonstrated when provided early after a cancer diagnosis, in practice these potentially beneficial palliative care services are often provided very late, sometimes hours or weeks before death," Dr. Bakitas said. "This trend is likely to continue in the absence of clear direction on the very pragmatic questions of who, what, and when."
The study was funded by National Institute for Nursing Research. Dr. Bakitas reported having no relevant disclosures.
Palliative care support buoys caregivers of advanced cancer patients
Providing early palliative care support to caregivers of advanced cancer patients improves their quality of life, depression, and stress burden, the ENABLE III study found.
"Similar to patients, waiting to provide these caregiver services until patients are in their last weeks to days of life may not adequately address the distress that they experience," Nick Dionne-Odom, Ph.D., RN, said at the meeting.
Caregivers for the 13 million cancer patients in the United States living with advanced disease can spend up to 8 hours per day providing assistance in activities that include symptom management, emotional and spiritual support, meal preparation, arranging medical appointments, and transportation.
The combination of this burden and witnessing someone close to you struggle with illness can cause psychological distress equal to or sometimes greater than that experienced by the patient, said Dr. Dionne-Odom, a postdoctoral fellow at the University of Alabama at Birmingham.
In ENABLE III, 122 caregivers were randomized at the time of the patient’s cancer diagnosis or 12 weeks later to a palliative care intervention that consisted of three weekly structured educational telephone calls from an advanced practice nurse coach, monthly check-in calls to address new or ongoing issues, and a bereavement call for caregivers whose loved ones died.
Caregivers were not restricted to family members, but could include close friends and even neighbors. Their mean age was 60 years, 79% were female, 75% were spouses, and all had at least a high school education.
At 12 weeks from the start of the intervention, caregivers in the immediate versus delayed group had significantly better quality of life on the Caregiver Quality of Life Index–Cancer scale (mean 50.2 vs. 56.1; P = .02) and less depressive symptoms on the Center for Epidemiologic Studies Depression (CESD) scale (10.2 vs. 16.6; P = .0006), Dr. Dionne-Odom said. Notably, the delayed group surpassed the clinical cutoff for depression of 16 on the CESD scale, he added.
The intervention did not appear to change the perception among caregivers of what was demanded of them by the patient or their objective burden, though there was a trend among the immediate group for improved caregiver stress burden on the Montgomery Borgatta Caregiver Burden Scale (13.2 vs. 13.8; P = .10).
There was no significant difference between groups in depression or grief scores for caregivers of decedents. A difference may have been detected with a larger sample size, he said, adding that prior studies have shown that reducing caregiver stress before patients’ death is associated with better bereavement adjustment.
As for why caregivers appear to benefit more than the patients from the parallel palliative care interventions, Dr. Bakitas said in an interview it may be the timing of the assessments, adding that other studies have shown an impact of palliative care at 4 months, but not at 3 months.
CHICAGO – Early palliative care delivered almost exclusively by telephone improved survival among patients with advanced cancer in the ENABLE III study.
After a median follow-up of a little more than 1 year, 46% of patients receiving palliative care from the time of cancer diagnosis and 54% of those with delayed palliative care had died.
Overall median survival was 18.3 months for the immediate group and 11.9 months for the delayed group (P = .17).
In preplanned analyses, the risk of death at 1 year was significantly lower in the immediate group (hazard ratio 0.72; P = .003), with a catch-up effect thereafter, Marie Bakitas, DNSc, reported at the annual meeting of the American Society of Clinical Oncology.
"Enhanced medical care, reduced aggressive care and chemotherapy use, longer access to hospice, and biologic impacts of improved quality of life have all been proposed as mechanisms to explain this survival advantage," Dr. Bakitas said. "However, at the present time, we do not have the data to support a particular mechanism and we are actively exploring this question through secondary analyses."
ENABLE (Educate, Nurture, Advise, Before Life Ends) III is the first study to examine the timing of early palliative care, but not the first to identify a survival advantage.
A recent study (N. Engl. J. Med. 2010:363:733-42) found that patients with metastatic non–small cell lung cancer (NSCLC) who received palliative care at the time of randomization lived a significant 2.7 months longer than did those receiving standard oncologic care, despite receiving significantly less aggressive end-of-life care (33% vs. 54%).
In ENABLE III, 207 patients with advanced cancer, and their caregivers, were randomized as a dyad to begin usual cancer care plus the intervention at the time of diagnosis (immediate group) or usual care alone for 3 months followed by the intervention (delayed group).
The intervention consisted of a traditional outpatient palliative care consult and six weekly structured telephone calls with a nurse coach using a guidebook that covers such topics as problem solving, symptom management, communication, and advanced care planning, explained Dr. Bakitas, the Marie O’Koren Endowed Chair and Professor, School of Nursing, and associate director of the Center for Palliative and Supportive Care, University of Alabama, Birmingham.
Usual care included the clinical consult, but not the telephone intervention.
The participants’ mean age was 64 years, half were male, 60% lived in a rural area, and 65% were married or living with a partner. Lung cancer was the most common diagnosis at 42%.
At baseline, 75% of patients were receiving chemotherapy, 19% were undergoing radiation, and 43% had an advanced directive completed at diagnosis.
Unlike the group’s prior trial comparing palliative care to usual care at 3 months, immediate versus delayed palliative care did not lead to significant improvements in quality of life on the Functional Assessment of Chronic Illness Therapy-Palliative care scale (129.9 vs. 127.2; P = .34), mood on the Center for Epidemiologic Studies Depression scale (11.2 vs. 10.8; P = .33), or symptom impact on the Quality of Life at the End of Life symptom impact subscale (11.4 vs. 12.2; P = .09).
One plausible reason for the findings is that there may not have been enough care differences between the two groups, with 40% of the delayed group receiving their first palliative care contact an average of 30 days before they were scheduled to do so on day 84, Dr. Bakitas said.
Second, difficulties in accrual and decreased study power may have made it difficult to pick up between-group differences on the subjective instruments, resulting in a type 2 error.
"A 3-month delay is still very early," Dr. Bakitas said.
She noted that early intervention allowed the palliative care team to have contact with patients for 1 year on average (range 240-493 days), compared with a median of 41-90 days from referral to death reported for outpatient clinics in a national survey of 142 National Cancer Institute and non-NCI cancer centers (JAMA 2010;303:1054-61).
Resource and chemotherapy use in ENABLE III was also comparable in both groups. Decedents in the immediate and delayed groups spent a median of 5 and 6 days, respectively, in hospital in the 7-9 months preceding death, while 8% and 5% received chemotherapy in the last 2 weeks of life.
This compares favorably with a national average of more than 8 hospital days in the last 6 months of life observed in the 2014 Dartmouth Atlas of Health Care, and a chemotherapy rate of 17.5% reported in the previously noted NSCLC study, Dr. Bakitas said.
She called for more studies of early palliative care to determine the optimal timing, personnel, essential elements, and mechanisms of improved survival.
"While the benefits of these approaches have been demonstrated when provided early after a cancer diagnosis, in practice these potentially beneficial palliative care services are often provided very late, sometimes hours or weeks before death," Dr. Bakitas said. "This trend is likely to continue in the absence of clear direction on the very pragmatic questions of who, what, and when."
The study was funded by National Institute for Nursing Research. Dr. Bakitas reported having no relevant disclosures.
Palliative care support buoys caregivers of advanced cancer patients
Providing early palliative care support to caregivers of advanced cancer patients improves their quality of life, depression, and stress burden, the ENABLE III study found.
"Similar to patients, waiting to provide these caregiver services until patients are in their last weeks to days of life may not adequately address the distress that they experience," Nick Dionne-Odom, Ph.D., RN, said at the meeting.
Caregivers for the 13 million cancer patients in the United States living with advanced disease can spend up to 8 hours per day providing assistance in activities that include symptom management, emotional and spiritual support, meal preparation, arranging medical appointments, and transportation.
The combination of this burden and witnessing someone close to you struggle with illness can cause psychological distress equal to or sometimes greater than that experienced by the patient, said Dr. Dionne-Odom, a postdoctoral fellow at the University of Alabama at Birmingham.
In ENABLE III, 122 caregivers were randomized at the time of the patient’s cancer diagnosis or 12 weeks later to a palliative care intervention that consisted of three weekly structured educational telephone calls from an advanced practice nurse coach, monthly check-in calls to address new or ongoing issues, and a bereavement call for caregivers whose loved ones died.
Caregivers were not restricted to family members, but could include close friends and even neighbors. Their mean age was 60 years, 79% were female, 75% were spouses, and all had at least a high school education.
At 12 weeks from the start of the intervention, caregivers in the immediate versus delayed group had significantly better quality of life on the Caregiver Quality of Life Index–Cancer scale (mean 50.2 vs. 56.1; P = .02) and less depressive symptoms on the Center for Epidemiologic Studies Depression (CESD) scale (10.2 vs. 16.6; P = .0006), Dr. Dionne-Odom said. Notably, the delayed group surpassed the clinical cutoff for depression of 16 on the CESD scale, he added.
The intervention did not appear to change the perception among caregivers of what was demanded of them by the patient or their objective burden, though there was a trend among the immediate group for improved caregiver stress burden on the Montgomery Borgatta Caregiver Burden Scale (13.2 vs. 13.8; P = .10).
There was no significant difference between groups in depression or grief scores for caregivers of decedents. A difference may have been detected with a larger sample size, he said, adding that prior studies have shown that reducing caregiver stress before patients’ death is associated with better bereavement adjustment.
As for why caregivers appear to benefit more than the patients from the parallel palliative care interventions, Dr. Bakitas said in an interview it may be the timing of the assessments, adding that other studies have shown an impact of palliative care at 4 months, but not at 3 months.
CHICAGO – Early palliative care delivered almost exclusively by telephone improved survival among patients with advanced cancer in the ENABLE III study.
After a median follow-up of a little more than 1 year, 46% of patients receiving palliative care from the time of cancer diagnosis and 54% of those with delayed palliative care had died.
Overall median survival was 18.3 months for the immediate group and 11.9 months for the delayed group (P = .17).
In preplanned analyses, the risk of death at 1 year was significantly lower in the immediate group (hazard ratio 0.72; P = .003), with a catch-up effect thereafter, Marie Bakitas, DNSc, reported at the annual meeting of the American Society of Clinical Oncology.
"Enhanced medical care, reduced aggressive care and chemotherapy use, longer access to hospice, and biologic impacts of improved quality of life have all been proposed as mechanisms to explain this survival advantage," Dr. Bakitas said. "However, at the present time, we do not have the data to support a particular mechanism and we are actively exploring this question through secondary analyses."
ENABLE (Educate, Nurture, Advise, Before Life Ends) III is the first study to examine the timing of early palliative care, but not the first to identify a survival advantage.
A recent study (N. Engl. J. Med. 2010:363:733-42) found that patients with metastatic non–small cell lung cancer (NSCLC) who received palliative care at the time of randomization lived a significant 2.7 months longer than did those receiving standard oncologic care, despite receiving significantly less aggressive end-of-life care (33% vs. 54%).
In ENABLE III, 207 patients with advanced cancer, and their caregivers, were randomized as a dyad to begin usual cancer care plus the intervention at the time of diagnosis (immediate group) or usual care alone for 3 months followed by the intervention (delayed group).
The intervention consisted of a traditional outpatient palliative care consult and six weekly structured telephone calls with a nurse coach using a guidebook that covers such topics as problem solving, symptom management, communication, and advanced care planning, explained Dr. Bakitas, the Marie O’Koren Endowed Chair and Professor, School of Nursing, and associate director of the Center for Palliative and Supportive Care, University of Alabama, Birmingham.
Usual care included the clinical consult, but not the telephone intervention.
The participants’ mean age was 64 years, half were male, 60% lived in a rural area, and 65% were married or living with a partner. Lung cancer was the most common diagnosis at 42%.
At baseline, 75% of patients were receiving chemotherapy, 19% were undergoing radiation, and 43% had an advanced directive completed at diagnosis.
Unlike the group’s prior trial comparing palliative care to usual care at 3 months, immediate versus delayed palliative care did not lead to significant improvements in quality of life on the Functional Assessment of Chronic Illness Therapy-Palliative care scale (129.9 vs. 127.2; P = .34), mood on the Center for Epidemiologic Studies Depression scale (11.2 vs. 10.8; P = .33), or symptom impact on the Quality of Life at the End of Life symptom impact subscale (11.4 vs. 12.2; P = .09).
One plausible reason for the findings is that there may not have been enough care differences between the two groups, with 40% of the delayed group receiving their first palliative care contact an average of 30 days before they were scheduled to do so on day 84, Dr. Bakitas said.
Second, difficulties in accrual and decreased study power may have made it difficult to pick up between-group differences on the subjective instruments, resulting in a type 2 error.
"A 3-month delay is still very early," Dr. Bakitas said.
She noted that early intervention allowed the palliative care team to have contact with patients for 1 year on average (range 240-493 days), compared with a median of 41-90 days from referral to death reported for outpatient clinics in a national survey of 142 National Cancer Institute and non-NCI cancer centers (JAMA 2010;303:1054-61).
Resource and chemotherapy use in ENABLE III was also comparable in both groups. Decedents in the immediate and delayed groups spent a median of 5 and 6 days, respectively, in hospital in the 7-9 months preceding death, while 8% and 5% received chemotherapy in the last 2 weeks of life.
This compares favorably with a national average of more than 8 hospital days in the last 6 months of life observed in the 2014 Dartmouth Atlas of Health Care, and a chemotherapy rate of 17.5% reported in the previously noted NSCLC study, Dr. Bakitas said.
She called for more studies of early palliative care to determine the optimal timing, personnel, essential elements, and mechanisms of improved survival.
"While the benefits of these approaches have been demonstrated when provided early after a cancer diagnosis, in practice these potentially beneficial palliative care services are often provided very late, sometimes hours or weeks before death," Dr. Bakitas said. "This trend is likely to continue in the absence of clear direction on the very pragmatic questions of who, what, and when."
The study was funded by National Institute for Nursing Research. Dr. Bakitas reported having no relevant disclosures.
Palliative care support buoys caregivers of advanced cancer patients
Providing early palliative care support to caregivers of advanced cancer patients improves their quality of life, depression, and stress burden, the ENABLE III study found.
"Similar to patients, waiting to provide these caregiver services until patients are in their last weeks to days of life may not adequately address the distress that they experience," Nick Dionne-Odom, Ph.D., RN, said at the meeting.
Caregivers for the 13 million cancer patients in the United States living with advanced disease can spend up to 8 hours per day providing assistance in activities that include symptom management, emotional and spiritual support, meal preparation, arranging medical appointments, and transportation.
The combination of this burden and witnessing someone close to you struggle with illness can cause psychological distress equal to or sometimes greater than that experienced by the patient, said Dr. Dionne-Odom, a postdoctoral fellow at the University of Alabama at Birmingham.
In ENABLE III, 122 caregivers were randomized at the time of the patient’s cancer diagnosis or 12 weeks later to a palliative care intervention that consisted of three weekly structured educational telephone calls from an advanced practice nurse coach, monthly check-in calls to address new or ongoing issues, and a bereavement call for caregivers whose loved ones died.
Caregivers were not restricted to family members, but could include close friends and even neighbors. Their mean age was 60 years, 79% were female, 75% were spouses, and all had at least a high school education.
At 12 weeks from the start of the intervention, caregivers in the immediate versus delayed group had significantly better quality of life on the Caregiver Quality of Life Index–Cancer scale (mean 50.2 vs. 56.1; P = .02) and less depressive symptoms on the Center for Epidemiologic Studies Depression (CESD) scale (10.2 vs. 16.6; P = .0006), Dr. Dionne-Odom said. Notably, the delayed group surpassed the clinical cutoff for depression of 16 on the CESD scale, he added.
The intervention did not appear to change the perception among caregivers of what was demanded of them by the patient or their objective burden, though there was a trend among the immediate group for improved caregiver stress burden on the Montgomery Borgatta Caregiver Burden Scale (13.2 vs. 13.8; P = .10).
There was no significant difference between groups in depression or grief scores for caregivers of decedents. A difference may have been detected with a larger sample size, he said, adding that prior studies have shown that reducing caregiver stress before patients’ death is associated with better bereavement adjustment.
As for why caregivers appear to benefit more than the patients from the parallel palliative care interventions, Dr. Bakitas said in an interview it may be the timing of the assessments, adding that other studies have shown an impact of palliative care at 4 months, but not at 3 months.
AT THE ASCO ANNUAL MEETING 2014
Key clinical point: Palliative care delivered at the time of cancer diagnosis improves survival.
Major finding: The risk of death at 1 year was significantly lower in the immediate palliative care group versus the delayed palliative care group (hazard ratio 0.72; P = .003).
Data source: A randomized trial of palliative oncology care in 207 patients with advanced cancer and their caregivers.
Disclosures: The National Institute for Nursing Research funded the study. Dr. Bakitas reported having no relevant disclosures.

Why consults don’t happen
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.
Today our team saw an 89-year-old gentleman on the hospitalist service with dementia, heart failure, atrial fibrillation, chronic kidney disease, and problems falling. His last known fall was less than 3 months ago and resulted in a broken hip requiring surgical intervention. This was his fourth hospitalization in 6 months, yet it was the first time he was seen by our service.
The frequency at which palliative care (PC) consults are ordered in a particular hospital varies widely. Some reasons for this are not easy fixes – PC is not available in each hospital (as was the case in two of this gentleman’s four hospitalizations), many PC teams are available only Monday-Friday, and patient volumes within a hospital ebb and flow with much less predictability than the tides.
However, some of the reasons are amenable to change. These might include the particular group of hospitalists, or one attending physician, utilizing PC consults less frequently than another. Or it may simply be that the connection was not made between the patient’s experience and the usefulness of an early PC consults. Screening tools are one method of decreasing variability in PC involvement as well as increasing the appropriateness of our service for a particular patient.
There are quite a few palliative care screening tools available. Many of them focus on what most of us would expect, which are the most common diagnoses we see (late-stage cancer, HF, cirrhosis, end-stage renal disease, dementia, etc.). Multiple studies have estimated that mature PC programs in large hospitals are consulted on 1%-2% of live discharges. However, we estimate that more than 10% of these discharged patients have palliative needs that go unmet. While it is true that we wish PC could be involved in all of these lives, this large number of people who spend time in the hospital with these diagnoses, coupled with a national shortage of PC providers, translates into an unbalanced equation.
Rather than looking at a specific diagnosis, we suggest incorporating inquiries on the presence of "palliative care–related problems." While these might require more thought or investigation into a patient’s situation, we find them to be more fruitful than using diagnosis alone.
Some examples? Mismatch between the expectations of the medical team vs. patient/family when it comes to prognosis or the goals of care would be one of them. Another might be persistent uncontrolled symptoms despite usual medical management. Family members disagreeing or demonstrating concerns about the goals of care is still another.
Having used various screening tools in multiple hospitals and clinical settings, we suggest the following considerations in setting up your own:
• Stakeholder management: The right services and staff need to agree on this being a way to improve quality of care (we always provide an "opt-out" option for those who don’t want us involved for some reason).
• Start small: Implement these on one unit at a time or limit the diagnoses to one or two conditions only. You can make the criteria less stringent if the PC team’s bandwidth is not too narrow.
• Be flexible: Even by starting small, there will be times that the PC teams are overwhelmed on a particular day leaving the occasional patient who meets criteria unseen. If the consult is urgent, a phone call is appropriate so that an assumption isn’t made that the screening tool will catch 100% of the patients.
• Track data: When using these tools, palliative care teams have been able to show things such as improved Hospital Consumer Assessment of Healthcare Providers and Systems survey results and decreased readmissions. Demonstrate what you’re doing for your institution so that you can expand the units or patients served.
PC screening tools are an effective way to decrease variability and improve quality. For examples of tools that we use, please get in touch. Find our contact info and read earlier columns at ehospitalistnews/Palliatively.
Dr. Bekanich and Dr. Fredholm are codirectors of Seton Palliative Care, part of the University of Texas Southwestern Residency Programs in Austin.

Critical Care Commentary: Brain death – patient, law, and family
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.

Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
|
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
|
|
|
In this thorough and somber commentary, Dr. Bowton clearly points out how much gray remains in a world that demands black and white certainty.
Brain death, and its implication, is not an exact diagnosis, which impacts the family, society, and the care-giving team, but most of all, the patient.
As there are times that brain death cannot be truly determined, we must be mindful that our primary goal is always the patient, then the families, society, and others. As a practitioner in New York, where family discussion is the law, I have not found this to be a great impediment; with palliative care and pastoral support, most issues can be resolved. As we progress in our knowledge, a more global unified approach would be welcomed.
Dr. Peter Spiro, FCCP Section Editor
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.
Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.
Perhaps no other concept in modern medicine is surrounded by as much misunderstanding and controversy as that of death by neurologic criteria, or brain death.
Legal challenges to brain death have spanned the gamut of continuing life support for a legally dead patient to denying a family’s request to continue support for their dead child.
Two recent, highly publicized cases highlight the poles of these controversies and concerns. In November 2013, Marlise Muñoz was declared brain dead. She was 33 years old and 14 weeks’ pregnant. Concordant with the patient’s wishes, the husband requested that the hospital remove the patient from mechanical ventilatory support. Citing Texas law that precludes the withholding of life-sustaining treatment to a pregnant patient, the hospital refused, despite the logical fallacy of withholding life support from a person declared dead.
In December 2013, 13-year-old Jahi McMath was declared brain dead. Her parents obtained a court order to prevent the hospital from discontinuing ventilatory support. A better understanding of the development of the concept of brain death and the incorporation of recent evidence into its determination may reduce the confusion and misunderstandings surrounding the determination of brain death.
Three reports in 1959 describe death of the nervous system and brain death (coma dépassé) building upon clinical and laboratory data from the 1930s relating the cessation of brain blood flow and EEG activity to ensuing apnea and subsequent cardiac arrest (Machado et al. J Med Ethics. 2007;33[4]:197). With the increasing sophistication of critical care support, especially mechanical ventilation, the loss of central respiratory drive no longer meant imminent death, and patients could be supported for long periods of time without recovery of brain function.
In 1968, an ad hoc committee at Harvard Medical School proposed a definition of irreversible coma and brain death (Beecher et al. JAMA. 1968;205[6]:337). They posited that any organ that no longer functions and has no possibility of functioning again was "for all practical purposes dead." The goals of the committee were (1) to reduce the suffering of patients and families and the care burden of hospitals; and (2) mitigate the controversies that surrounded obtaining organs for transplantation.
The committee then set out their rationale for their proposed characteristics of the permanently nonfunctioning brain. Subsequently, in 1976, The Conference of the Medical Royal Colleges and their Faculties in the United Kingdom required a deeply comatose state, irremediable structural brain damage, and irreversible cessation of brain stem function to ascertain brain death (Spinello. J Intensive Care Med. May 2014, in press).
In 1981, the National Conference of Commissioners on Uniform State Laws approved the Uniform Determination of Death Act (UDDA), codifying the legal concept of brain death. Thirty-six states and the District of Columbia have enacted the UDDA, but legal precedent and statutes in the remaining states are consistent with the UDDA. New York and New Jersey require that a family’s religious or moral views be considered in the process following the determination of brain death (Gostin. JAMA. 2014;311[9]:903); in all other states, clinicians are not required to consult with family prior to withdrawing ventilatory support from the brain dead patient.
‘No reports of clinical recovery’
However, the UDDA does not define brain death but rather states that "a determination of death must be made with accepted medical standards" (Wijdicks et al. Neurology. 2010;74[23]:1911). The American Academy of Neurology (AAN) published a practice parameter in 1995 to guide clinicians in the determination of brain death; this was updated by their Quality Standards Committee in 2010 (Wijdicks et al. Neurology. 2010;74[23]:1911). In the updated guidance document, the committee stated: "There are no reports of clinical recovery in patients after the clinical diagnosis of brain death has been determined using the AAN practice parameter."
It is striking, however, that there appears to be an inconsistent approach and criteria for the determination of brain death across hospitals, and even amongst specialties within a hospital (Powner et al. Crit Care Med. 2004;32[6]:1284). Further, in most states, any physician is permitted to ascertain brain death, though some states have now added requirements for specific qualifications and/or confirmation by a second physician (Spinello IM. J Intensive Care Med. May 2014, in press).
These inconsistencies in criteria, process, and experience may be responsible for reports in the lay press of recovery following pronouncement of brain death. Every hospital should have a validated, well-defined process for the evaluation of brain death guided by the AAN practice parameter.
A single exam
In most states, a single exam is required to determine brain death. The clinical setting and the results of imaging studies should be used to determine the duration of observation needed to exclude the possibility of recovery. Given that the patient should be normothermic, have a normal systolic blood pressure, have both a history and imaging studies supporting an irreversible cause of coma, and that drugs and toxins must be excluded as a cause of coma, this observation period is uncommonly less than several hours.
Confounded by movement
Movement of the patient with devastating brain injury is often a confounder in the determination of brain death.
This is also a source of confusion and concern for the family. Plantar reflexes have been commonly reported in patients pronounced brain dead. Head turning in response to noxious stimuli, repetitive leg movements, facial myokymia, and other movements have been observed (Wu et al. Crit Care. 2013;17[4]:440; Wijdicks et al. Neurology. 2010;74[23]:1911). When this is observed, knowledge of the potential reflex arcs is needed, and consultation with a neurologist or other physician skilled in brain death determination is usually appropriate.
Movement can sometimes extend to apparent respiratory activity. This can be caused by ventilator autocycling due to variations in circuit pressure (especially in a noncompliant lung or with large tidal volumes) or triggering due to cardiac-induced alterations in transpulmonary pressure. The latter is most common in a hyperdynamic circulatory state.
Apnea is a critical criterion for the determination of brain death and is most reliably assessed when the patient has been removed from the mechanical ventilator. During testing, apnea should be present despite achieving a PaCO2 of greater than or equal to 60 mm Hg, or 20 mm Hg above the baseline to support the diagnosis of brain death.
Some patients, especially those who are hemodynamically unstable or who require high levels of PEEP to support oxygenation, may not tolerate the apnea test without oxygen desaturation or hypotension.
Most commonly, the apnea test is performed with the patient off the ventilator and 6 L/min of oxygen flowing through an insufflation catheter placed near the carina. We prefer to use a modified Mapleson circuit with enough flow to only partially distend the anesthesia bag in the circuit. With this arrangement, one can look not only at the patient’s chest wall and abdomen for signs of respiratory activity but also look for cyclic changes in the level of bag inflation.
In patients with ARDS, trauma involving the chest or other causes of oxygenation failure, CPAP, with or without an antecedent recruitment maneuver may facilitate successful completion of the apnea test (Hocker et al. Neurocrit Care. 2014;20[2]:298).
Controversy over ancillary testing
There are no well-designed prospective studies examining the accuracy of ancillary tests for the determination of brain death using the appropriate control group of patients with coma but who are not brain dead and with blinding of the interpretation of the study results to the clinical setting.
Brain death is not synonymous with complete neuronal death. While cortical areas exhibit moderate to severe histopathologic ischemic changes in the large majority (but not all) of brain dead patients, the basal ganglia and diencephalon inconsistently demonstrate these changes (Wijdicks et al. Neurology. 2008;70[15]:1234). Thus, it may not be surprising that both false-positive (test positive for brain death – clinically not brain dead) and false-negative (test negative for brain death – clinically brain dead) results have been reported for virtually all tests proposed for confirmatory testing, including CT angiography, transcranial Doppler, and nuclear brain scan. Confirmatory testing is most commonly used in patients who cannot complete an apnea test.
It has been forcefully argued that, in adults, confirmatory tests should not be done (Wijdicks. Neurology. 2010;75[1]:77). There will be some patients in whom brain death cannot be definitively determined. When all criteria of the AAN guidelines cannot be fulfilled, clinicians should err on the side of concluding that the patient is not brain dead and turn their efforts toward counseling the family regarding the likelihood of neurologic recovery and assisting the family in ascertaining the desires of the patient under these circumstances.
It is vital that care providers not lose perspective on the plight of the family in these settings. The symbolic power of a beating heart to a parent, spouse, or loved one cannot be underestimated. Family members who observe resuscitation efforts have been shown to have a lower incidence of posttraumatic stress disorder symptoms (Jabre et al. N Engl J Med. 2013;368[11]:1008).
A recent trial demonstrated that family presence during the brain death determination had an increased understanding of brain death without an adverse impact on emotional well being (Tawil et al. Crit Care Med. 2013;42[4]:934). A consistent process for determination of brain death, engagement of the family in the brain death evaluation and helping them understand the meaning of patient movements that can be distressingly misinterpreted, and honesty when a definitive determination of brain death cannot be determined will not remove the misunderstanding or controversy surrounding a diagnosis of brain death but will serve to ensure its accurate and humane application.
Dr. Bowton is Professor, Section on Critical Care, Department of Anesthesiology, Wake Forest Baptist Health, Winston-Salem, North Carolina. Read previous Critical Care Commentaries online.
