User login
Removing eyebrow and eyelid tattoos possible with laser, case series finds
SAN DIEGO – , results from a single-center retrospective study showed.
There is a market for these types of cosmetic tattoos today, “and a need for removal,” David Orbuch, MD, MBA, said during a clinical abstract session at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. Orbuch, a fellow at the Laser & Skin Surgery Center of New York, and his colleagues retrospectively reviewed the charts of 57 adults who underwent laser tattoo removal of eyebrow and eyelid tattoos at the center from January 2018 to December 2021. Data recorded included demographics, site location, initial parameters, colors treated, and clinical safety and efficacy. The mean age of the patients was 46 years, 98.8% were female, 50.9% were Fitzpatrick skin type I-II, and the remainder were types III-V.
Among the most common sites treated were the bilateral eyebrows (35%). Other common sites were the upper eyelids (21.1%), the lower eyelids (10.5%), and both the upper and lower eyelids (12%). Each patient underwent an average of 2.5 treatments (range, 1-11). The most common lasers used were a 755-nm picosecond laser (79%), a high‐power 1,064-nm picosecond laser (12.3%), a high‐power 532-nm picosecond laser (3.5%), and a 10,600-nm carbon dioxide laser (1.7%). The most common tattoo colors were black (94.7%), the far most common, followed by red (3.5%), and yellow (1.7%).
For removal of black tattoos, the most common treatment parameters for the 755 picosecond laser were a 2.5-mm spot size and a fluence of 3.36 J/cm2. For the 1,064-nm picosecond laser, the most common treatment parameters were a 2-mm spot size and a fluence of 4 J/cm2.
For removal of red tattoos, the most common treatment parameters for the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 2 J/cm2. For the 10,600-nm CO2 laser, the most common treatment parameters were a spot size of 7 mm and a fluence of 28.2 J/cm2.
As for removal of yellow tattoos, the most common treatment parameters with the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 0.5 J/cm2.
There were no documented cases of scarring, eyelash/eyebrow loss, necrosis, burns, prolonged erythema, prolonged swelling, or prolonged dyspigmentation noted.
“With all of these treatments, you can get a great effect, but you have to do it safely,” Dr. Orbuch said. “With all of these wavelengths, the 1,064 nm especially, there can be serious eye damage if done improperly,” he added. “As such, placement of the metallic eye shields is important. If they’re not properly placed, they can fall out. Make sure you are comfortable using these shields before doing these treatments.”
Pooja Sodha, MD, director of the Center for Laser and Cosmetic Dermatology at George Washington University, Washington, who was asked to comment on the study, said that cosmetic tattoos pose treatment challenges for several reasons. First, “there can be variability in the composition of the pigments since they are often tailored to fit the location and complexion of the patient,” she said. “Second, there can be placement of multiple layers of tattoo pigment to provide the final effect. Third, the pigment may contain two metal oxides (titanium dioxide and ferric oxide), which are often used to calibrate skin tone colors.”

Unfortunately, she noted, “these metal oxides are prone to reduction reactions with laser exposure, causing paradoxical darkening of tattoo pigment. In the past, these darker colors were treated with continued laser therapy and even fractional or fully ablative CO2/Er:YAG resurfacing.”
Dr. Sodha noted that prior studies have shown picosecond lasers to be effective cosmetic lasers, “and this study further supports this with a larger cohort of patients who were treated with the array of picosecond wavelengths (532, 755, and 1,064 nm) without long-term sequelae. Interestingly, there did not appear to be long-term sequelae with dyspigmentation or paradoxical darkening, with fewer than 2% necessitating treatment with a carbon dioxide laser.”
Neither Dr. Orbuch nor Dr. Sodha reported having financial disclosures.
SAN DIEGO – , results from a single-center retrospective study showed.
There is a market for these types of cosmetic tattoos today, “and a need for removal,” David Orbuch, MD, MBA, said during a clinical abstract session at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. Orbuch, a fellow at the Laser & Skin Surgery Center of New York, and his colleagues retrospectively reviewed the charts of 57 adults who underwent laser tattoo removal of eyebrow and eyelid tattoos at the center from January 2018 to December 2021. Data recorded included demographics, site location, initial parameters, colors treated, and clinical safety and efficacy. The mean age of the patients was 46 years, 98.8% were female, 50.9% were Fitzpatrick skin type I-II, and the remainder were types III-V.
Among the most common sites treated were the bilateral eyebrows (35%). Other common sites were the upper eyelids (21.1%), the lower eyelids (10.5%), and both the upper and lower eyelids (12%). Each patient underwent an average of 2.5 treatments (range, 1-11). The most common lasers used were a 755-nm picosecond laser (79%), a high‐power 1,064-nm picosecond laser (12.3%), a high‐power 532-nm picosecond laser (3.5%), and a 10,600-nm carbon dioxide laser (1.7%). The most common tattoo colors were black (94.7%), the far most common, followed by red (3.5%), and yellow (1.7%).
For removal of black tattoos, the most common treatment parameters for the 755 picosecond laser were a 2.5-mm spot size and a fluence of 3.36 J/cm2. For the 1,064-nm picosecond laser, the most common treatment parameters were a 2-mm spot size and a fluence of 4 J/cm2.
For removal of red tattoos, the most common treatment parameters for the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 2 J/cm2. For the 10,600-nm CO2 laser, the most common treatment parameters were a spot size of 7 mm and a fluence of 28.2 J/cm2.
As for removal of yellow tattoos, the most common treatment parameters with the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 0.5 J/cm2.
There were no documented cases of scarring, eyelash/eyebrow loss, necrosis, burns, prolonged erythema, prolonged swelling, or prolonged dyspigmentation noted.
“With all of these treatments, you can get a great effect, but you have to do it safely,” Dr. Orbuch said. “With all of these wavelengths, the 1,064 nm especially, there can be serious eye damage if done improperly,” he added. “As such, placement of the metallic eye shields is important. If they’re not properly placed, they can fall out. Make sure you are comfortable using these shields before doing these treatments.”
Pooja Sodha, MD, director of the Center for Laser and Cosmetic Dermatology at George Washington University, Washington, who was asked to comment on the study, said that cosmetic tattoos pose treatment challenges for several reasons. First, “there can be variability in the composition of the pigments since they are often tailored to fit the location and complexion of the patient,” she said. “Second, there can be placement of multiple layers of tattoo pigment to provide the final effect. Third, the pigment may contain two metal oxides (titanium dioxide and ferric oxide), which are often used to calibrate skin tone colors.”
Unfortunately, she noted, “these metal oxides are prone to reduction reactions with laser exposure, causing paradoxical darkening of tattoo pigment. In the past, these darker colors were treated with continued laser therapy and even fractional or fully ablative CO2/Er:YAG resurfacing.”
Dr. Sodha noted that prior studies have shown picosecond lasers to be effective cosmetic lasers, “and this study further supports this with a larger cohort of patients who were treated with the array of picosecond wavelengths (532, 755, and 1,064 nm) without long-term sequelae. Interestingly, there did not appear to be long-term sequelae with dyspigmentation or paradoxical darkening, with fewer than 2% necessitating treatment with a carbon dioxide laser.”
Neither Dr. Orbuch nor Dr. Sodha reported having financial disclosures.
SAN DIEGO – , results from a single-center retrospective study showed.
There is a market for these types of cosmetic tattoos today, “and a need for removal,” David Orbuch, MD, MBA, said during a clinical abstract session at the annual meeting of the American Society for Laser Medicine and Surgery.
Dr. Orbuch, a fellow at the Laser & Skin Surgery Center of New York, and his colleagues retrospectively reviewed the charts of 57 adults who underwent laser tattoo removal of eyebrow and eyelid tattoos at the center from January 2018 to December 2021. Data recorded included demographics, site location, initial parameters, colors treated, and clinical safety and efficacy. The mean age of the patients was 46 years, 98.8% were female, 50.9% were Fitzpatrick skin type I-II, and the remainder were types III-V.
Among the most common sites treated were the bilateral eyebrows (35%). Other common sites were the upper eyelids (21.1%), the lower eyelids (10.5%), and both the upper and lower eyelids (12%). Each patient underwent an average of 2.5 treatments (range, 1-11). The most common lasers used were a 755-nm picosecond laser (79%), a high‐power 1,064-nm picosecond laser (12.3%), a high‐power 532-nm picosecond laser (3.5%), and a 10,600-nm carbon dioxide laser (1.7%). The most common tattoo colors were black (94.7%), the far most common, followed by red (3.5%), and yellow (1.7%).
For removal of black tattoos, the most common treatment parameters for the 755 picosecond laser were a 2.5-mm spot size and a fluence of 3.36 J/cm2. For the 1,064-nm picosecond laser, the most common treatment parameters were a 2-mm spot size and a fluence of 4 J/cm2.
For removal of red tattoos, the most common treatment parameters for the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 2 J/cm2. For the 10,600-nm CO2 laser, the most common treatment parameters were a spot size of 7 mm and a fluence of 28.2 J/cm2.
As for removal of yellow tattoos, the most common treatment parameters with the 532-nm picosecond laser were a 3.3-mm spot size and a fluence of 0.5 J/cm2.
There were no documented cases of scarring, eyelash/eyebrow loss, necrosis, burns, prolonged erythema, prolonged swelling, or prolonged dyspigmentation noted.
“With all of these treatments, you can get a great effect, but you have to do it safely,” Dr. Orbuch said. “With all of these wavelengths, the 1,064 nm especially, there can be serious eye damage if done improperly,” he added. “As such, placement of the metallic eye shields is important. If they’re not properly placed, they can fall out. Make sure you are comfortable using these shields before doing these treatments.”
Pooja Sodha, MD, director of the Center for Laser and Cosmetic Dermatology at George Washington University, Washington, who was asked to comment on the study, said that cosmetic tattoos pose treatment challenges for several reasons. First, “there can be variability in the composition of the pigments since they are often tailored to fit the location and complexion of the patient,” she said. “Second, there can be placement of multiple layers of tattoo pigment to provide the final effect. Third, the pigment may contain two metal oxides (titanium dioxide and ferric oxide), which are often used to calibrate skin tone colors.”
Unfortunately, she noted, “these metal oxides are prone to reduction reactions with laser exposure, causing paradoxical darkening of tattoo pigment. In the past, these darker colors were treated with continued laser therapy and even fractional or fully ablative CO2/Er:YAG resurfacing.”
Dr. Sodha noted that prior studies have shown picosecond lasers to be effective cosmetic lasers, “and this study further supports this with a larger cohort of patients who were treated with the array of picosecond wavelengths (532, 755, and 1,064 nm) without long-term sequelae. Interestingly, there did not appear to be long-term sequelae with dyspigmentation or paradoxical darkening, with fewer than 2% necessitating treatment with a carbon dioxide laser.”
Neither Dr. Orbuch nor Dr. Sodha reported having financial disclosures.
AT ASLMS 2022
Transvaginal mesh, native tissue repair have similar outcomes in 3-year trial
Transvaginal mesh was found to be safe and effective for patients with pelvic organ prolapse (POP) when compared with native tissue repair (NTR) in a 3-year trial.
Researchers, led by Bruce S. Kahn, MD, with the department of obstetrics & gynecology at Scripps Clinic in San Diego evaluated the two surgical treatment methods and published their findings in Obstetrics & Gynecology.
At completion of the 3-year follow-up in 2016, there were 401 participants in the transvaginal mesh group and 171 in the NTR group.
The prospective, nonrandomized, parallel-cohort, 27-site trial used a primary composite endpoint of anatomical success; subjective success (vaginal bulging); retreatment measures; and serious device-related or serious procedure-related adverse events.
The secondary endpoint was a composite outcome similar to the primary composite outcome but with anatomical success more stringently defined as POP quantification (POP-Q) point Ba < 0 and/or C < 0.
The secondary outcome was added to this trial because investigators had criticized the primary endpoint, set by the Food and Drug Administration, because it included anatomic outcome measures that were the same for inclusion criteria (POP-Q point Ba < 0 and/or C < 0.)
The secondary-outcome composite also included quality-of-life measures, mesh exposure, and mesh- and procedure-related complications.
Outcomes similar for both groups
The primary outcome demonstrated transvaginal mesh was not superior to native tissue repair (P =.056).
In the secondary outcome, superiority of transvaginal mesh over native tissue repair was shown (P =.009), with a propensity score–adjusted difference of 10.6% (90% confidence interval, 3.3%-17.9%) in favor of transvaginal mesh.
The authors noted that subjective success regarding vaginal bulging, which is important in patient satisfaction, was high and not statistically different between the two groups.
Additionally, transvaginal mesh repair was as safe as NTR regarding serious device-related and/or serious procedure-related side effects.
For the primary safety endpoint, 3.1% in the mesh group and 2.7% in the native tissue repair group experienced serious adverse events, demonstrating that mesh was noninferior to NTR.
Research results have been mixed
Unanswered questions surround surgical options for POP, which, the authors wrote, “affects 3%-6% of women based on symptoms and up to 50% of women based on vaginal examination.”
The FDA in 2011 issued 522 postmarket surveillance study orders for companies that market transvaginal mesh for POP.
Research results have varied and contentious debate has continued in the field. Some studies have shown that mesh has better subjective and objective outcomes than NTR in the anterior compartment. Others have found more complications with transvaginal mesh, such as mesh exposure and painful intercourse.
Complicating comparisons, early versions of the mesh used were larger and denser than today’s versions.
In this postmarket study, patients received either the Uphold LITE brand of transvaginal mesh or native tissue repair for surgical treatment of POP.
Expert: This study unlikely to change minds
In an accompanying editorial, John O.L. DeLancey, MD, professor of gynecology at the University of Michigan, Ann Arbor, pointed out that so far there’s been a lack of randomized trials that could answer whether mesh surgeries result in fewer symptoms or result in sufficient improvements in anatomy to justify their additional risk.
This study may not help with the decision. Dr. DeLancey wrote: “Will this study change the minds of either side of this debate? Probably not. The two sides are deeply entrenched in their positions.”
Two considerations are important in thinking about the issue, he said. Surgical outcomes for POP are “not as good as we would hope.” Also, many women have had serious complications with mesh operations.
He wrote: “Mesh litigation has resulted in more $8 billion in settlements, which is many times the $1 billion annual national cost of providing care for prolapse. Those of us who practice in referral centers have seen women with devastating problems, even though they probably represent a small fraction of cases.”
Dr. DeLancey highlighted some limitations of the study by Dr. Kahn and colleagues, especially regarding differences in the groups studied and the design of the study.
“For example,” he explained, “65% of individuals in the mesh-repair group had a prior hysterectomy as opposed to 30% in the native tissue repair group. In addition, some of the operations in the native tissue group are not typical choices; for example, hysteropexy was used for some patients and had a 47% failure rate.”
He said the all-or-nothing approach to surgical solutions may be clouding the debate – in other words mesh or no mesh for women as a group.
“Rather than asking whether mesh is better than no mesh, knowing which women (if any) stand to benefit from mesh is the critical question. We need to understand, for each woman, what structural failures exist so that we can target our interventions to correct them,” he wrote.
This study was sponsored by Boston Scientific. Dr. Kahn disclosed research support from Solaire, payments from AbbVie and Douchenay as a speaker, payments from Caldera and Cytuity (Boston Scientific) as a medical consultant, and payment from Johnson & Johnson as an expert witness. One coauthor disclosed that money was paid to her institution from Medtronic and Boston Scientific (both unrestricted educational grants for cadaveric lab). Another is chief medical officer at Axonics. One study coauthor receives research funding from Axonics and is a consultant for Group Dynamics, Medpace, and FirstThought. One coauthor received research support, is a consultant for Boston Scientific, and is an expert witness for Johnson & Johnson. Dr. DeLancey declared no relevant financial relationships.
Transvaginal mesh was found to be safe and effective for patients with pelvic organ prolapse (POP) when compared with native tissue repair (NTR) in a 3-year trial.
Researchers, led by Bruce S. Kahn, MD, with the department of obstetrics & gynecology at Scripps Clinic in San Diego evaluated the two surgical treatment methods and published their findings in Obstetrics & Gynecology.
At completion of the 3-year follow-up in 2016, there were 401 participants in the transvaginal mesh group and 171 in the NTR group.
The prospective, nonrandomized, parallel-cohort, 27-site trial used a primary composite endpoint of anatomical success; subjective success (vaginal bulging); retreatment measures; and serious device-related or serious procedure-related adverse events.
The secondary endpoint was a composite outcome similar to the primary composite outcome but with anatomical success more stringently defined as POP quantification (POP-Q) point Ba < 0 and/or C < 0.
The secondary outcome was added to this trial because investigators had criticized the primary endpoint, set by the Food and Drug Administration, because it included anatomic outcome measures that were the same for inclusion criteria (POP-Q point Ba < 0 and/or C < 0.)
The secondary-outcome composite also included quality-of-life measures, mesh exposure, and mesh- and procedure-related complications.
Outcomes similar for both groups
The primary outcome demonstrated transvaginal mesh was not superior to native tissue repair (P =.056).
In the secondary outcome, superiority of transvaginal mesh over native tissue repair was shown (P =.009), with a propensity score–adjusted difference of 10.6% (90% confidence interval, 3.3%-17.9%) in favor of transvaginal mesh.
The authors noted that subjective success regarding vaginal bulging, which is important in patient satisfaction, was high and not statistically different between the two groups.
Additionally, transvaginal mesh repair was as safe as NTR regarding serious device-related and/or serious procedure-related side effects.
For the primary safety endpoint, 3.1% in the mesh group and 2.7% in the native tissue repair group experienced serious adverse events, demonstrating that mesh was noninferior to NTR.
Research results have been mixed
Unanswered questions surround surgical options for POP, which, the authors wrote, “affects 3%-6% of women based on symptoms and up to 50% of women based on vaginal examination.”
The FDA in 2011 issued 522 postmarket surveillance study orders for companies that market transvaginal mesh for POP.
Research results have varied and contentious debate has continued in the field. Some studies have shown that mesh has better subjective and objective outcomes than NTR in the anterior compartment. Others have found more complications with transvaginal mesh, such as mesh exposure and painful intercourse.
Complicating comparisons, early versions of the mesh used were larger and denser than today’s versions.
In this postmarket study, patients received either the Uphold LITE brand of transvaginal mesh or native tissue repair for surgical treatment of POP.
Expert: This study unlikely to change minds
In an accompanying editorial, John O.L. DeLancey, MD, professor of gynecology at the University of Michigan, Ann Arbor, pointed out that so far there’s been a lack of randomized trials that could answer whether mesh surgeries result in fewer symptoms or result in sufficient improvements in anatomy to justify their additional risk.
This study may not help with the decision. Dr. DeLancey wrote: “Will this study change the minds of either side of this debate? Probably not. The two sides are deeply entrenched in their positions.”
Two considerations are important in thinking about the issue, he said. Surgical outcomes for POP are “not as good as we would hope.” Also, many women have had serious complications with mesh operations.
He wrote: “Mesh litigation has resulted in more $8 billion in settlements, which is many times the $1 billion annual national cost of providing care for prolapse. Those of us who practice in referral centers have seen women with devastating problems, even though they probably represent a small fraction of cases.”
Dr. DeLancey highlighted some limitations of the study by Dr. Kahn and colleagues, especially regarding differences in the groups studied and the design of the study.
“For example,” he explained, “65% of individuals in the mesh-repair group had a prior hysterectomy as opposed to 30% in the native tissue repair group. In addition, some of the operations in the native tissue group are not typical choices; for example, hysteropexy was used for some patients and had a 47% failure rate.”
He said the all-or-nothing approach to surgical solutions may be clouding the debate – in other words mesh or no mesh for women as a group.
“Rather than asking whether mesh is better than no mesh, knowing which women (if any) stand to benefit from mesh is the critical question. We need to understand, for each woman, what structural failures exist so that we can target our interventions to correct them,” he wrote.
This study was sponsored by Boston Scientific. Dr. Kahn disclosed research support from Solaire, payments from AbbVie and Douchenay as a speaker, payments from Caldera and Cytuity (Boston Scientific) as a medical consultant, and payment from Johnson & Johnson as an expert witness. One coauthor disclosed that money was paid to her institution from Medtronic and Boston Scientific (both unrestricted educational grants for cadaveric lab). Another is chief medical officer at Axonics. One study coauthor receives research funding from Axonics and is a consultant for Group Dynamics, Medpace, and FirstThought. One coauthor received research support, is a consultant for Boston Scientific, and is an expert witness for Johnson & Johnson. Dr. DeLancey declared no relevant financial relationships.
Transvaginal mesh was found to be safe and effective for patients with pelvic organ prolapse (POP) when compared with native tissue repair (NTR) in a 3-year trial.
Researchers, led by Bruce S. Kahn, MD, with the department of obstetrics & gynecology at Scripps Clinic in San Diego evaluated the two surgical treatment methods and published their findings in Obstetrics & Gynecology.
At completion of the 3-year follow-up in 2016, there were 401 participants in the transvaginal mesh group and 171 in the NTR group.
The prospective, nonrandomized, parallel-cohort, 27-site trial used a primary composite endpoint of anatomical success; subjective success (vaginal bulging); retreatment measures; and serious device-related or serious procedure-related adverse events.
The secondary endpoint was a composite outcome similar to the primary composite outcome but with anatomical success more stringently defined as POP quantification (POP-Q) point Ba < 0 and/or C < 0.
The secondary outcome was added to this trial because investigators had criticized the primary endpoint, set by the Food and Drug Administration, because it included anatomic outcome measures that were the same for inclusion criteria (POP-Q point Ba < 0 and/or C < 0.)
The secondary-outcome composite also included quality-of-life measures, mesh exposure, and mesh- and procedure-related complications.
Outcomes similar for both groups
The primary outcome demonstrated transvaginal mesh was not superior to native tissue repair (P =.056).
In the secondary outcome, superiority of transvaginal mesh over native tissue repair was shown (P =.009), with a propensity score–adjusted difference of 10.6% (90% confidence interval, 3.3%-17.9%) in favor of transvaginal mesh.
The authors noted that subjective success regarding vaginal bulging, which is important in patient satisfaction, was high and not statistically different between the two groups.
Additionally, transvaginal mesh repair was as safe as NTR regarding serious device-related and/or serious procedure-related side effects.
For the primary safety endpoint, 3.1% in the mesh group and 2.7% in the native tissue repair group experienced serious adverse events, demonstrating that mesh was noninferior to NTR.
Research results have been mixed
Unanswered questions surround surgical options for POP, which, the authors wrote, “affects 3%-6% of women based on symptoms and up to 50% of women based on vaginal examination.”
The FDA in 2011 issued 522 postmarket surveillance study orders for companies that market transvaginal mesh for POP.
Research results have varied and contentious debate has continued in the field. Some studies have shown that mesh has better subjective and objective outcomes than NTR in the anterior compartment. Others have found more complications with transvaginal mesh, such as mesh exposure and painful intercourse.
Complicating comparisons, early versions of the mesh used were larger and denser than today’s versions.
In this postmarket study, patients received either the Uphold LITE brand of transvaginal mesh or native tissue repair for surgical treatment of POP.
Expert: This study unlikely to change minds
In an accompanying editorial, John O.L. DeLancey, MD, professor of gynecology at the University of Michigan, Ann Arbor, pointed out that so far there’s been a lack of randomized trials that could answer whether mesh surgeries result in fewer symptoms or result in sufficient improvements in anatomy to justify their additional risk.
This study may not help with the decision. Dr. DeLancey wrote: “Will this study change the minds of either side of this debate? Probably not. The two sides are deeply entrenched in their positions.”
Two considerations are important in thinking about the issue, he said. Surgical outcomes for POP are “not as good as we would hope.” Also, many women have had serious complications with mesh operations.
He wrote: “Mesh litigation has resulted in more $8 billion in settlements, which is many times the $1 billion annual national cost of providing care for prolapse. Those of us who practice in referral centers have seen women with devastating problems, even though they probably represent a small fraction of cases.”
Dr. DeLancey highlighted some limitations of the study by Dr. Kahn and colleagues, especially regarding differences in the groups studied and the design of the study.
“For example,” he explained, “65% of individuals in the mesh-repair group had a prior hysterectomy as opposed to 30% in the native tissue repair group. In addition, some of the operations in the native tissue group are not typical choices; for example, hysteropexy was used for some patients and had a 47% failure rate.”
He said the all-or-nothing approach to surgical solutions may be clouding the debate – in other words mesh or no mesh for women as a group.
“Rather than asking whether mesh is better than no mesh, knowing which women (if any) stand to benefit from mesh is the critical question. We need to understand, for each woman, what structural failures exist so that we can target our interventions to correct them,” he wrote.
This study was sponsored by Boston Scientific. Dr. Kahn disclosed research support from Solaire, payments from AbbVie and Douchenay as a speaker, payments from Caldera and Cytuity (Boston Scientific) as a medical consultant, and payment from Johnson & Johnson as an expert witness. One coauthor disclosed that money was paid to her institution from Medtronic and Boston Scientific (both unrestricted educational grants for cadaveric lab). Another is chief medical officer at Axonics. One study coauthor receives research funding from Axonics and is a consultant for Group Dynamics, Medpace, and FirstThought. One coauthor received research support, is a consultant for Boston Scientific, and is an expert witness for Johnson & Johnson. Dr. DeLancey declared no relevant financial relationships.
FROM OBSTETRICS & GYNECOLOGY
Is it time to remove ‘cancer’ label from low-risk prostate tumors?
Physicians often advise that men with low-risk prostate tumors wait to see if the disease worsens – an approach called “active surveillance” – rather than rushing to treat the condition. After all, low-grade tumors rarely cause harm, and therapies such as radiation and surgery can carry serious side effects, including impotence and urinary leakage.
Yet doctors still label these lesions “cancer,” and as a result, some experts say, many men in the United States opt for treatment they don’t need.
In a new paper likely to stoke debate, experts from a range of disciplines, as well as one patient, argue that overtreatment could be reduced by removing the word “cancer” from low-risk disease. Tumors that rate 6 on the Gleason score (GS) cannot invade other organs but nonetheless scare patients into undergoing risky treatments, they argue. Fewer than 1% of men with GS6 prostate tumors experience metastatic disease or die from cancer within 15 years of the initial diagnosis, they report.
“No matter how much time a physician may spend downplaying the significance of a GS6 diagnosis or emphasizing the phrase low-risk, the words ‘you have cancer’ have a potent psychological effect on most men and their families,” they wrote in a paper published in the Journal of Clinical Oncology.
Dropping the C word for low-risk tumors, which make up about half of 268,000 prostate cancer diagnoses annually in the United States, is not a new idea. An independent panel convened by the National Institutes of Health proposed just that in 2011.
However, clinician support for the shift appears to be growing, said Scott Eggener, MD, a urologic oncologist and professor of surgery at the University of Chicago, and a coauthor of the new article.
Dr. Eggener said active surveillance has been increasing dramatically in the United States, to about 60% of patients with GS6. “We feel like the landscape is right now to be talking about this issue,” Dr. Eggener told this news organization.
Reducing unnecessary treatment, he and his coauthors argue, could reduce the cost of health care — and boost the benefit of prostate-specific antigen testing for prostate cancer, which the U.S. Preventive Services Task Force at the moment deems small.
In addition, patients with prostate cancer diagnoses encounter increased risk of depression and suicide, disqualification or higher rates for life insurance, and questions from family and friends if they choose active surveillance over treatment – all of which might be ameliorated by a change in terminology.
The word “cancer” has been dropped from bladder, cervical, and thyroid conditions and prostate abnormalities that used to be classified as Gleason 2 through 5, they noted.
Keeping the status quo
But some physicians say GS6 doesn’t need a name change.
From a scientific standpoint, GS6 disease has molecular hallmarks of cancer, according to Jonathan Epstein, MD, professor of pathology, urology, and oncology at Johns Hopkins University, Baltimore. More important, Dr. Epstein told Medscape, the classification does not guarantee that more serious cancer is not present, only that it has not been found yet in tissue samples.
Dr. Eggener acknowledged that while GS6 does have molecular markers associated with cancer – a fact that’s “challenging to reconcile with” – giving it another name “would still require surveillance, and since the window of opportunity for curing localized [prostate cancer] is typically measured in years or decades, evidence of histologic progression to a higher-grade cancer would far precede the potential time of future metastasis in the majority of cases.”
Still, Dr. Epstein worries that dropping the cancer designation may lead some patients to forgo active surveillance, which involves repeated imaging and biopsies to check for worse disease. Without such monitoring, he said, “if they do have higher grade cancer that’s unsampled, it will pose a threat to their life.”
Gleason 6 tumors “may progress, some significantly, or be incompletely sampled at the time of diagnosis. Both clinicians and patients need to understand such risk,” Peter Carroll, MD, MPH, a urologist at the University of California, San Francisco, who is critical of the proposed name change, told this news organization.
Regardless of what it’s called, Gleason 6 disease warrants close monitoring, said Joe Gallo, a 77-year-old Pennsylvania man whose high-risk cancer was detected during active surveillance. “If I had taken a laid-back, or less, approach” to monitoring, Mr. Gallo said, “necessary treatment may have been delayed and my condition may have become more serious.”
Some advocates say patients and their families need to be educated that cancer exists on a spectrum of severity.
Mark Lichty, 73, chairman of a support group called Active Surveillance Patients International, received a Gleason 6 diagnosis 17 years ago. He resisted treatment against medical advice, and the cancer never progressed.
Mr. Lichty said active surveillance has been more widely adopted in Sweden, where physicians assure patients that treatment is unnecessary and support systems exist. “Yes, a diagnosis of cancer is frightening,” he said in an interview. But “we can do a lot better in how we communicate the diagnosis.”
Dr. Eggener reported consulting or advisory roles with Sophiris Bio, Francis Medical, Insightec, Profound Medical, and Candel Therapeutics; speakers bureau at Janssen; and fees for travel, accommodations, and expenses from Janssen Biotech and Insightec; as well as an uncompensated relationship with Steba Biotech. The remaining coauthors reported several financial relationships, which are listed in the paper. Dr. Epstein and Dr. Carroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physicians often advise that men with low-risk prostate tumors wait to see if the disease worsens – an approach called “active surveillance” – rather than rushing to treat the condition. After all, low-grade tumors rarely cause harm, and therapies such as radiation and surgery can carry serious side effects, including impotence and urinary leakage.
Yet doctors still label these lesions “cancer,” and as a result, some experts say, many men in the United States opt for treatment they don’t need.
In a new paper likely to stoke debate, experts from a range of disciplines, as well as one patient, argue that overtreatment could be reduced by removing the word “cancer” from low-risk disease. Tumors that rate 6 on the Gleason score (GS) cannot invade other organs but nonetheless scare patients into undergoing risky treatments, they argue. Fewer than 1% of men with GS6 prostate tumors experience metastatic disease or die from cancer within 15 years of the initial diagnosis, they report.
“No matter how much time a physician may spend downplaying the significance of a GS6 diagnosis or emphasizing the phrase low-risk, the words ‘you have cancer’ have a potent psychological effect on most men and their families,” they wrote in a paper published in the Journal of Clinical Oncology.
Dropping the C word for low-risk tumors, which make up about half of 268,000 prostate cancer diagnoses annually in the United States, is not a new idea. An independent panel convened by the National Institutes of Health proposed just that in 2011.
However, clinician support for the shift appears to be growing, said Scott Eggener, MD, a urologic oncologist and professor of surgery at the University of Chicago, and a coauthor of the new article.
Dr. Eggener said active surveillance has been increasing dramatically in the United States, to about 60% of patients with GS6. “We feel like the landscape is right now to be talking about this issue,” Dr. Eggener told this news organization.
Reducing unnecessary treatment, he and his coauthors argue, could reduce the cost of health care — and boost the benefit of prostate-specific antigen testing for prostate cancer, which the U.S. Preventive Services Task Force at the moment deems small.
In addition, patients with prostate cancer diagnoses encounter increased risk of depression and suicide, disqualification or higher rates for life insurance, and questions from family and friends if they choose active surveillance over treatment – all of which might be ameliorated by a change in terminology.
The word “cancer” has been dropped from bladder, cervical, and thyroid conditions and prostate abnormalities that used to be classified as Gleason 2 through 5, they noted.
Keeping the status quo
But some physicians say GS6 doesn’t need a name change.
From a scientific standpoint, GS6 disease has molecular hallmarks of cancer, according to Jonathan Epstein, MD, professor of pathology, urology, and oncology at Johns Hopkins University, Baltimore. More important, Dr. Epstein told Medscape, the classification does not guarantee that more serious cancer is not present, only that it has not been found yet in tissue samples.
Dr. Eggener acknowledged that while GS6 does have molecular markers associated with cancer – a fact that’s “challenging to reconcile with” – giving it another name “would still require surveillance, and since the window of opportunity for curing localized [prostate cancer] is typically measured in years or decades, evidence of histologic progression to a higher-grade cancer would far precede the potential time of future metastasis in the majority of cases.”
Still, Dr. Epstein worries that dropping the cancer designation may lead some patients to forgo active surveillance, which involves repeated imaging and biopsies to check for worse disease. Without such monitoring, he said, “if they do have higher grade cancer that’s unsampled, it will pose a threat to their life.”
Gleason 6 tumors “may progress, some significantly, or be incompletely sampled at the time of diagnosis. Both clinicians and patients need to understand such risk,” Peter Carroll, MD, MPH, a urologist at the University of California, San Francisco, who is critical of the proposed name change, told this news organization.
Regardless of what it’s called, Gleason 6 disease warrants close monitoring, said Joe Gallo, a 77-year-old Pennsylvania man whose high-risk cancer was detected during active surveillance. “If I had taken a laid-back, or less, approach” to monitoring, Mr. Gallo said, “necessary treatment may have been delayed and my condition may have become more serious.”
Some advocates say patients and their families need to be educated that cancer exists on a spectrum of severity.
Mark Lichty, 73, chairman of a support group called Active Surveillance Patients International, received a Gleason 6 diagnosis 17 years ago. He resisted treatment against medical advice, and the cancer never progressed.
Mr. Lichty said active surveillance has been more widely adopted in Sweden, where physicians assure patients that treatment is unnecessary and support systems exist. “Yes, a diagnosis of cancer is frightening,” he said in an interview. But “we can do a lot better in how we communicate the diagnosis.”
Dr. Eggener reported consulting or advisory roles with Sophiris Bio, Francis Medical, Insightec, Profound Medical, and Candel Therapeutics; speakers bureau at Janssen; and fees for travel, accommodations, and expenses from Janssen Biotech and Insightec; as well as an uncompensated relationship with Steba Biotech. The remaining coauthors reported several financial relationships, which are listed in the paper. Dr. Epstein and Dr. Carroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Physicians often advise that men with low-risk prostate tumors wait to see if the disease worsens – an approach called “active surveillance” – rather than rushing to treat the condition. After all, low-grade tumors rarely cause harm, and therapies such as radiation and surgery can carry serious side effects, including impotence and urinary leakage.
Yet doctors still label these lesions “cancer,” and as a result, some experts say, many men in the United States opt for treatment they don’t need.
In a new paper likely to stoke debate, experts from a range of disciplines, as well as one patient, argue that overtreatment could be reduced by removing the word “cancer” from low-risk disease. Tumors that rate 6 on the Gleason score (GS) cannot invade other organs but nonetheless scare patients into undergoing risky treatments, they argue. Fewer than 1% of men with GS6 prostate tumors experience metastatic disease or die from cancer within 15 years of the initial diagnosis, they report.
“No matter how much time a physician may spend downplaying the significance of a GS6 diagnosis or emphasizing the phrase low-risk, the words ‘you have cancer’ have a potent psychological effect on most men and their families,” they wrote in a paper published in the Journal of Clinical Oncology.
Dropping the C word for low-risk tumors, which make up about half of 268,000 prostate cancer diagnoses annually in the United States, is not a new idea. An independent panel convened by the National Institutes of Health proposed just that in 2011.
However, clinician support for the shift appears to be growing, said Scott Eggener, MD, a urologic oncologist and professor of surgery at the University of Chicago, and a coauthor of the new article.
Dr. Eggener said active surveillance has been increasing dramatically in the United States, to about 60% of patients with GS6. “We feel like the landscape is right now to be talking about this issue,” Dr. Eggener told this news organization.
Reducing unnecessary treatment, he and his coauthors argue, could reduce the cost of health care — and boost the benefit of prostate-specific antigen testing for prostate cancer, which the U.S. Preventive Services Task Force at the moment deems small.
In addition, patients with prostate cancer diagnoses encounter increased risk of depression and suicide, disqualification or higher rates for life insurance, and questions from family and friends if they choose active surveillance over treatment – all of which might be ameliorated by a change in terminology.
The word “cancer” has been dropped from bladder, cervical, and thyroid conditions and prostate abnormalities that used to be classified as Gleason 2 through 5, they noted.
Keeping the status quo
But some physicians say GS6 doesn’t need a name change.
From a scientific standpoint, GS6 disease has molecular hallmarks of cancer, according to Jonathan Epstein, MD, professor of pathology, urology, and oncology at Johns Hopkins University, Baltimore. More important, Dr. Epstein told Medscape, the classification does not guarantee that more serious cancer is not present, only that it has not been found yet in tissue samples.
Dr. Eggener acknowledged that while GS6 does have molecular markers associated with cancer – a fact that’s “challenging to reconcile with” – giving it another name “would still require surveillance, and since the window of opportunity for curing localized [prostate cancer] is typically measured in years or decades, evidence of histologic progression to a higher-grade cancer would far precede the potential time of future metastasis in the majority of cases.”
Still, Dr. Epstein worries that dropping the cancer designation may lead some patients to forgo active surveillance, which involves repeated imaging and biopsies to check for worse disease. Without such monitoring, he said, “if they do have higher grade cancer that’s unsampled, it will pose a threat to their life.”
Gleason 6 tumors “may progress, some significantly, or be incompletely sampled at the time of diagnosis. Both clinicians and patients need to understand such risk,” Peter Carroll, MD, MPH, a urologist at the University of California, San Francisco, who is critical of the proposed name change, told this news organization.
Regardless of what it’s called, Gleason 6 disease warrants close monitoring, said Joe Gallo, a 77-year-old Pennsylvania man whose high-risk cancer was detected during active surveillance. “If I had taken a laid-back, or less, approach” to monitoring, Mr. Gallo said, “necessary treatment may have been delayed and my condition may have become more serious.”
Some advocates say patients and their families need to be educated that cancer exists on a spectrum of severity.
Mark Lichty, 73, chairman of a support group called Active Surveillance Patients International, received a Gleason 6 diagnosis 17 years ago. He resisted treatment against medical advice, and the cancer never progressed.
Mr. Lichty said active surveillance has been more widely adopted in Sweden, where physicians assure patients that treatment is unnecessary and support systems exist. “Yes, a diagnosis of cancer is frightening,” he said in an interview. But “we can do a lot better in how we communicate the diagnosis.”
Dr. Eggener reported consulting or advisory roles with Sophiris Bio, Francis Medical, Insightec, Profound Medical, and Candel Therapeutics; speakers bureau at Janssen; and fees for travel, accommodations, and expenses from Janssen Biotech and Insightec; as well as an uncompensated relationship with Steba Biotech. The remaining coauthors reported several financial relationships, which are listed in the paper. Dr. Epstein and Dr. Carroll have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Could a common cold virus be causing severe hepatitis in kids?
This is a transcript of a video that first appeared on Medscape.com. It has been edited for clarity.
On April 21, 2022, the Centers for Disease Control and Prevention released a Health Alert Network advisory regarding a cluster of nine cases of acute hepatitis in children in Alabama over a 5-month period from October 2021 to February 2022 – a rate substantially higher than what would be expected, given the relative rarity of hepatitis in children.
Standard workup was negative for the common causative agents – hepatitis A, B, and C – and no toxic exposures were identified. But there was one common thread among all these kids: They all tested positive for adenovirus.
And that is really strange.
There are about 100 circulating adenoviruses in the world that we know of, and around 50 of them infect humans. If you are an adult, it’s a virtual certainty that you have been infected with an adenovirus in the past. Most strains cause symptoms we would describe as the common cold: runny nose, sore throat. Some strains cause conjunctivitis (pink eye). Some cause gastrointestinal illness – the stomach bugs that kids get.
It’s the banality of adenovirus that makes this hepatitis finding so surprising.
The United States is not alone in reporting this new hepatitis syndrome. As of April 21, 169 cases have been reported across the world, including 114 in the United Kingdom.
Of the 169 cases reported worldwide, 74 had evidence of adenovirus infection. On molecular testing, 18 of those were adenovirus 41.
What I wanted to do today was go through the various hypotheses for what could be going on with these hepatitis cases, one by one, and highlight the evidence supporting them. We won’t reach a conclusion, but hopefully by the end, the path forward will be more clear. OK, let’s get started.
Hypothesis 1: Nothing is happening.
It’s worth noting that “clusters” of disease occur all the time, even when no relevant epidemiologic process has occurred. If there is some baseline rate of hepatitis, every once in a while, through bad luck alone, you’d see a group of cases all at once. This is known as the clustering illusion. And I’m quite confident in saying that this is not the case here.
For one, this phenomenon is worldwide, as we know from the World Health Organization report. In fact, the CDC didn’t provide the most detailed data about the nine (now 12) cases in the United States. This study from Scotland is the first to give a detailed accounting of cases, reporting on 13 cases of acute hepatitis of unknown cause in kids at a single hospital from January to April. Typically, the hospital sees fewer than four cases of hepatitis per year. Five of these 13 kids tested positive for adenovirus. So let’s take the clustering illusion off the list.
Hypothesis 2: It’s adenovirus.
The major evidence supporting adenovirus as the causative agent here is that a lot of these kids had adenovirus, and adenovirus 41 – a gut-tropic strain – in particular. This is important, because stool testing might be necessary for diagnosis and lots of kids with this condition didn’t get that. In other words, we have hard evidence of adenovirus infection in about 40% of the cases so far, but the true number might be substantially higher.
That said, adenovirus is seasonal, and we are in adenovirus season. Granted, 40% seems quite a bit higher than the background infection rate, but we have to be careful not to assume that correlation means causation.
The evidence against adenovirus, even adenovirus 41, is that this acute hepatitis syndrome is new, and adenovirus 41 is not. To be fair, we know adenoviruses can cause acute hepatitis, but the vast majority of reports are in immunocompromised individuals – organ transplant recipients and those with HIV. I was able to find just a handful of cases of immunocompetent kids developing hepatitis from adenovirus prior to this current outbreak.
The current outbreak would exceed the published literature by nearly two orders of magnitude. It feels like something else has to be going on.
Hypothesis 3: It’s coronavirus.
SARS-CoV-2 is a strange virus, both in its acute presentation and its long-term outcomes. It was clear early in the pandemic that some children infected by the coronavirus would develop MIS-C – multisystem inflammatory syndrome in children. MIS-C is associated with hepatitis in about 10% of children, according to this New England Journal of Medicine
But the presentation of these kids is quite different from MIS-C; fever is rare, for example. The WHO reports that of the 169 identified cases so far, 20 had active COVID infection. The Scotland cohort suggests that a similar proportion had past COVID infections. In other times, we might consider this a smoking gun, but at this point a history of COVID is not remarkable – after the Omicron wave, it’s about as common to have a history of COVID as it is not to have a history of COVID.
A brief aside here. This is not because of coronavirus vaccination. Of the more than 100 cases reported in the United Kingdom, none of these kids were vaccinated. So let’s put aside the possibility that this is a vaccine effect – there’s no real evidence to support that.
Which brings us to …
Hypothesis 4: It’s coronavirus and adenovirus.
This is sort of intriguing and can work a few different ways, via a direct and indirect path.
In the direct path, we posit that COVID infection does something to kids’ immune systems – something we don’t yet understand that limits their ability to fight off adenovirus. There is some support for this idea. This study in Immunity found that COVID infection can functionally impair dendritic cells and T-cells, including natural killer cells. These cells are important components of our innate antiviral immunity.
There’s an indirect path as well. COVID has led to lockdowns, distancing, masking – stuff that prevents kids from being exposed to germs from other kids. Could a lack of exposure to adenovirus or other viruses because of distancing increase the risk for severe disease when restrictions are lifted? Also possible – the severity of respiratory syncytial virus (RSV) infections this year is substantially higher than what we’ve seen in the past, for example.
And finally, hypothesis 5: This is something new.
We can’t ignore the possibility that this is simply a new disease-causing agent. Toxicology studies so far have been negative, and we wouldn’t expect hepatitis from a chemical toxin to appear in multiple countries around the world; this is almost certainly a biological phenomenon. It is possible that this is a new strain of adenovirus 41, or that adenovirus is a red herring altogether. Remember, we knew about “non-A/non-B viral hepatitis” for more than 2 decades before hepatitis C was discovered.
The pace of science is faster now, fortunately, and information is coming out quickly. As we learn more, we’ll share it with you.
Dr. Wilson, MD, MSCE, is an associate professor of medicine at Yale University, New Haven, Conn., and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. Dr. Wilson has disclosed no relevant financial relationships.
This is a transcript of a video that first appeared on Medscape.com. It has been edited for clarity.
On April 21, 2022, the Centers for Disease Control and Prevention released a Health Alert Network advisory regarding a cluster of nine cases of acute hepatitis in children in Alabama over a 5-month period from October 2021 to February 2022 – a rate substantially higher than what would be expected, given the relative rarity of hepatitis in children.
Standard workup was negative for the common causative agents – hepatitis A, B, and C – and no toxic exposures were identified. But there was one common thread among all these kids: They all tested positive for adenovirus.
And that is really strange.
There are about 100 circulating adenoviruses in the world that we know of, and around 50 of them infect humans. If you are an adult, it’s a virtual certainty that you have been infected with an adenovirus in the past. Most strains cause symptoms we would describe as the common cold: runny nose, sore throat. Some strains cause conjunctivitis (pink eye). Some cause gastrointestinal illness – the stomach bugs that kids get.
It’s the banality of adenovirus that makes this hepatitis finding so surprising.
The United States is not alone in reporting this new hepatitis syndrome. As of April 21, 169 cases have been reported across the world, including 114 in the United Kingdom.
Of the 169 cases reported worldwide, 74 had evidence of adenovirus infection. On molecular testing, 18 of those were adenovirus 41.
What I wanted to do today was go through the various hypotheses for what could be going on with these hepatitis cases, one by one, and highlight the evidence supporting them. We won’t reach a conclusion, but hopefully by the end, the path forward will be more clear. OK, let’s get started.
Hypothesis 1: Nothing is happening.
It’s worth noting that “clusters” of disease occur all the time, even when no relevant epidemiologic process has occurred. If there is some baseline rate of hepatitis, every once in a while, through bad luck alone, you’d see a group of cases all at once. This is known as the clustering illusion. And I’m quite confident in saying that this is not the case here.
For one, this phenomenon is worldwide, as we know from the World Health Organization report. In fact, the CDC didn’t provide the most detailed data about the nine (now 12) cases in the United States. This study from Scotland is the first to give a detailed accounting of cases, reporting on 13 cases of acute hepatitis of unknown cause in kids at a single hospital from January to April. Typically, the hospital sees fewer than four cases of hepatitis per year. Five of these 13 kids tested positive for adenovirus. So let’s take the clustering illusion off the list.
Hypothesis 2: It’s adenovirus.
The major evidence supporting adenovirus as the causative agent here is that a lot of these kids had adenovirus, and adenovirus 41 – a gut-tropic strain – in particular. This is important, because stool testing might be necessary for diagnosis and lots of kids with this condition didn’t get that. In other words, we have hard evidence of adenovirus infection in about 40% of the cases so far, but the true number might be substantially higher.
That said, adenovirus is seasonal, and we are in adenovirus season. Granted, 40% seems quite a bit higher than the background infection rate, but we have to be careful not to assume that correlation means causation.
The evidence against adenovirus, even adenovirus 41, is that this acute hepatitis syndrome is new, and adenovirus 41 is not. To be fair, we know adenoviruses can cause acute hepatitis, but the vast majority of reports are in immunocompromised individuals – organ transplant recipients and those with HIV. I was able to find just a handful of cases of immunocompetent kids developing hepatitis from adenovirus prior to this current outbreak.
The current outbreak would exceed the published literature by nearly two orders of magnitude. It feels like something else has to be going on.
Hypothesis 3: It’s coronavirus.
SARS-CoV-2 is a strange virus, both in its acute presentation and its long-term outcomes. It was clear early in the pandemic that some children infected by the coronavirus would develop MIS-C – multisystem inflammatory syndrome in children. MIS-C is associated with hepatitis in about 10% of children, according to this New England Journal of Medicine
But the presentation of these kids is quite different from MIS-C; fever is rare, for example. The WHO reports that of the 169 identified cases so far, 20 had active COVID infection. The Scotland cohort suggests that a similar proportion had past COVID infections. In other times, we might consider this a smoking gun, but at this point a history of COVID is not remarkable – after the Omicron wave, it’s about as common to have a history of COVID as it is not to have a history of COVID.
A brief aside here. This is not because of coronavirus vaccination. Of the more than 100 cases reported in the United Kingdom, none of these kids were vaccinated. So let’s put aside the possibility that this is a vaccine effect – there’s no real evidence to support that.
Which brings us to …
Hypothesis 4: It’s coronavirus and adenovirus.
This is sort of intriguing and can work a few different ways, via a direct and indirect path.
In the direct path, we posit that COVID infection does something to kids’ immune systems – something we don’t yet understand that limits their ability to fight off adenovirus. There is some support for this idea. This study in Immunity found that COVID infection can functionally impair dendritic cells and T-cells, including natural killer cells. These cells are important components of our innate antiviral immunity.
There’s an indirect path as well. COVID has led to lockdowns, distancing, masking – stuff that prevents kids from being exposed to germs from other kids. Could a lack of exposure to adenovirus or other viruses because of distancing increase the risk for severe disease when restrictions are lifted? Also possible – the severity of respiratory syncytial virus (RSV) infections this year is substantially higher than what we’ve seen in the past, for example.
And finally, hypothesis 5: This is something new.
We can’t ignore the possibility that this is simply a new disease-causing agent. Toxicology studies so far have been negative, and we wouldn’t expect hepatitis from a chemical toxin to appear in multiple countries around the world; this is almost certainly a biological phenomenon. It is possible that this is a new strain of adenovirus 41, or that adenovirus is a red herring altogether. Remember, we knew about “non-A/non-B viral hepatitis” for more than 2 decades before hepatitis C was discovered.
The pace of science is faster now, fortunately, and information is coming out quickly. As we learn more, we’ll share it with you.
Dr. Wilson, MD, MSCE, is an associate professor of medicine at Yale University, New Haven, Conn., and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. Dr. Wilson has disclosed no relevant financial relationships.
This is a transcript of a video that first appeared on Medscape.com. It has been edited for clarity.
On April 21, 2022, the Centers for Disease Control and Prevention released a Health Alert Network advisory regarding a cluster of nine cases of acute hepatitis in children in Alabama over a 5-month period from October 2021 to February 2022 – a rate substantially higher than what would be expected, given the relative rarity of hepatitis in children.
Standard workup was negative for the common causative agents – hepatitis A, B, and C – and no toxic exposures were identified. But there was one common thread among all these kids: They all tested positive for adenovirus.
And that is really strange.
There are about 100 circulating adenoviruses in the world that we know of, and around 50 of them infect humans. If you are an adult, it’s a virtual certainty that you have been infected with an adenovirus in the past. Most strains cause symptoms we would describe as the common cold: runny nose, sore throat. Some strains cause conjunctivitis (pink eye). Some cause gastrointestinal illness – the stomach bugs that kids get.
It’s the banality of adenovirus that makes this hepatitis finding so surprising.
The United States is not alone in reporting this new hepatitis syndrome. As of April 21, 169 cases have been reported across the world, including 114 in the United Kingdom.
Of the 169 cases reported worldwide, 74 had evidence of adenovirus infection. On molecular testing, 18 of those were adenovirus 41.
What I wanted to do today was go through the various hypotheses for what could be going on with these hepatitis cases, one by one, and highlight the evidence supporting them. We won’t reach a conclusion, but hopefully by the end, the path forward will be more clear. OK, let’s get started.
Hypothesis 1: Nothing is happening.
It’s worth noting that “clusters” of disease occur all the time, even when no relevant epidemiologic process has occurred. If there is some baseline rate of hepatitis, every once in a while, through bad luck alone, you’d see a group of cases all at once. This is known as the clustering illusion. And I’m quite confident in saying that this is not the case here.
For one, this phenomenon is worldwide, as we know from the World Health Organization report. In fact, the CDC didn’t provide the most detailed data about the nine (now 12) cases in the United States. This study from Scotland is the first to give a detailed accounting of cases, reporting on 13 cases of acute hepatitis of unknown cause in kids at a single hospital from January to April. Typically, the hospital sees fewer than four cases of hepatitis per year. Five of these 13 kids tested positive for adenovirus. So let’s take the clustering illusion off the list.
Hypothesis 2: It’s adenovirus.
The major evidence supporting adenovirus as the causative agent here is that a lot of these kids had adenovirus, and adenovirus 41 – a gut-tropic strain – in particular. This is important, because stool testing might be necessary for diagnosis and lots of kids with this condition didn’t get that. In other words, we have hard evidence of adenovirus infection in about 40% of the cases so far, but the true number might be substantially higher.
That said, adenovirus is seasonal, and we are in adenovirus season. Granted, 40% seems quite a bit higher than the background infection rate, but we have to be careful not to assume that correlation means causation.
The evidence against adenovirus, even adenovirus 41, is that this acute hepatitis syndrome is new, and adenovirus 41 is not. To be fair, we know adenoviruses can cause acute hepatitis, but the vast majority of reports are in immunocompromised individuals – organ transplant recipients and those with HIV. I was able to find just a handful of cases of immunocompetent kids developing hepatitis from adenovirus prior to this current outbreak.
The current outbreak would exceed the published literature by nearly two orders of magnitude. It feels like something else has to be going on.
Hypothesis 3: It’s coronavirus.
SARS-CoV-2 is a strange virus, both in its acute presentation and its long-term outcomes. It was clear early in the pandemic that some children infected by the coronavirus would develop MIS-C – multisystem inflammatory syndrome in children. MIS-C is associated with hepatitis in about 10% of children, according to this New England Journal of Medicine
But the presentation of these kids is quite different from MIS-C; fever is rare, for example. The WHO reports that of the 169 identified cases so far, 20 had active COVID infection. The Scotland cohort suggests that a similar proportion had past COVID infections. In other times, we might consider this a smoking gun, but at this point a history of COVID is not remarkable – after the Omicron wave, it’s about as common to have a history of COVID as it is not to have a history of COVID.
A brief aside here. This is not because of coronavirus vaccination. Of the more than 100 cases reported in the United Kingdom, none of these kids were vaccinated. So let’s put aside the possibility that this is a vaccine effect – there’s no real evidence to support that.
Which brings us to …
Hypothesis 4: It’s coronavirus and adenovirus.
This is sort of intriguing and can work a few different ways, via a direct and indirect path.
In the direct path, we posit that COVID infection does something to kids’ immune systems – something we don’t yet understand that limits their ability to fight off adenovirus. There is some support for this idea. This study in Immunity found that COVID infection can functionally impair dendritic cells and T-cells, including natural killer cells. These cells are important components of our innate antiviral immunity.
There’s an indirect path as well. COVID has led to lockdowns, distancing, masking – stuff that prevents kids from being exposed to germs from other kids. Could a lack of exposure to adenovirus or other viruses because of distancing increase the risk for severe disease when restrictions are lifted? Also possible – the severity of respiratory syncytial virus (RSV) infections this year is substantially higher than what we’ve seen in the past, for example.
And finally, hypothesis 5: This is something new.
We can’t ignore the possibility that this is simply a new disease-causing agent. Toxicology studies so far have been negative, and we wouldn’t expect hepatitis from a chemical toxin to appear in multiple countries around the world; this is almost certainly a biological phenomenon. It is possible that this is a new strain of adenovirus 41, or that adenovirus is a red herring altogether. Remember, we knew about “non-A/non-B viral hepatitis” for more than 2 decades before hepatitis C was discovered.
The pace of science is faster now, fortunately, and information is coming out quickly. As we learn more, we’ll share it with you.
Dr. Wilson, MD, MSCE, is an associate professor of medicine at Yale University, New Haven, Conn., and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com. Dr. Wilson has disclosed no relevant financial relationships.
Expanded Treatment Options for Lupus Nephritis
Lupus nephritis (LN) affects approximately 25%-60% of patients with systemic lupus erythematosus. Currently, guideline-directed therapy recommends a combination of steroids plus either mycophenolate mofetil or cyclophosphamide. Despite treatment, about 10%-30% of LN patients will progress to end-stage kidney disease.
Fortunately, over the past 2 years, the FDA approved two novel agents that expand treatment options for patients with active disease who have received standard-of-care therapy.
In this ReCAP, Dr Joan Merrill, of the University of Oklahoma Health Sciences Center, reports on the B-lymphocyte stimulator–specific inhibitor belimumab, which was evaluated in the BLISS-LN trial, and the oral calcineurin inhibitor voclosporin, which was assessed in the AURORA trials.
Dr Merrill discusses how these recently approved medications fit into the standard of care for LN patients.
--
Joan Merrill, MD, Professor, Department of Medicine, Division of Rheumatology, University of Oklahoma Health Sciences Center; Director of Clinical Projects, Arthritis & Clinical Immunology Program, Oklahoma Medical Research Foundation, Oklahoma City, Oklahoma
Joan Merrill, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Biogen
Received research grant from: Bristol-Myers Squibb; GlaxoSmithKline
Received income in an amount equal to or greater than $250 from: AbbVie; Alexion; Amgen; AstraZeneca; Aurinia; Bristol-Myers Squibb; EMD Serono; Genentech; Gilead; GlaxoSmithKline; Lilly; Merck; Provention; RemeGen; Sanofi; UCB; Zenas
Received research grant from: AbbVie; AstraZeneca; BeiGene; Pharmacyclics; TG Therapeutics
Lupus nephritis (LN) affects approximately 25%-60% of patients with systemic lupus erythematosus. Currently, guideline-directed therapy recommends a combination of steroids plus either mycophenolate mofetil or cyclophosphamide. Despite treatment, about 10%-30% of LN patients will progress to end-stage kidney disease.
Fortunately, over the past 2 years, the FDA approved two novel agents that expand treatment options for patients with active disease who have received standard-of-care therapy.
In this ReCAP, Dr Joan Merrill, of the University of Oklahoma Health Sciences Center, reports on the B-lymphocyte stimulator–specific inhibitor belimumab, which was evaluated in the BLISS-LN trial, and the oral calcineurin inhibitor voclosporin, which was assessed in the AURORA trials.
Dr Merrill discusses how these recently approved medications fit into the standard of care for LN patients.
--
Joan Merrill, MD, Professor, Department of Medicine, Division of Rheumatology, University of Oklahoma Health Sciences Center; Director of Clinical Projects, Arthritis & Clinical Immunology Program, Oklahoma Medical Research Foundation, Oklahoma City, Oklahoma
Joan Merrill, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Biogen
Received research grant from: Bristol-Myers Squibb; GlaxoSmithKline
Received income in an amount equal to or greater than $250 from: AbbVie; Alexion; Amgen; AstraZeneca; Aurinia; Bristol-Myers Squibb; EMD Serono; Genentech; Gilead; GlaxoSmithKline; Lilly; Merck; Provention; RemeGen; Sanofi; UCB; Zenas
Received research grant from: AbbVie; AstraZeneca; BeiGene; Pharmacyclics; TG Therapeutics
Lupus nephritis (LN) affects approximately 25%-60% of patients with systemic lupus erythematosus. Currently, guideline-directed therapy recommends a combination of steroids plus either mycophenolate mofetil or cyclophosphamide. Despite treatment, about 10%-30% of LN patients will progress to end-stage kidney disease.
Fortunately, over the past 2 years, the FDA approved two novel agents that expand treatment options for patients with active disease who have received standard-of-care therapy.
In this ReCAP, Dr Joan Merrill, of the University of Oklahoma Health Sciences Center, reports on the B-lymphocyte stimulator–specific inhibitor belimumab, which was evaluated in the BLISS-LN trial, and the oral calcineurin inhibitor voclosporin, which was assessed in the AURORA trials.
Dr Merrill discusses how these recently approved medications fit into the standard of care for LN patients.
--
Joan Merrill, MD, Professor, Department of Medicine, Division of Rheumatology, University of Oklahoma Health Sciences Center; Director of Clinical Projects, Arthritis & Clinical Immunology Program, Oklahoma Medical Research Foundation, Oklahoma City, Oklahoma
Joan Merrill, MD, has disclosed the following relevant financial relationships:
Serve(d) as a speaker or a member of a speakers bureau for: Biogen
Received research grant from: Bristol-Myers Squibb; GlaxoSmithKline
Received income in an amount equal to or greater than $250 from: AbbVie; Alexion; Amgen; AstraZeneca; Aurinia; Bristol-Myers Squibb; EMD Serono; Genentech; Gilead; GlaxoSmithKline; Lilly; Merck; Provention; RemeGen; Sanofi; UCB; Zenas
Received research grant from: AbbVie; AstraZeneca; BeiGene; Pharmacyclics; TG Therapeutics

Clinical Edge Journal Scan Commentary: Migraine May 2022
Cefaly is a commonly used nonprescription device that uses external trigeminal nerve stimulation (e-TNS) to either abort or prevent migraine attacks. The pivotal Cefaly study was published about 10 years ago, and Cefaly was the first US Food and Drug Administration–cleared neurostimulation device for headache. The initial acute data were gathered primarily in the hospital setting, and the investigators in the study by Kuruvilla and colleagues intended to replicate a more real-world scenario for the acute use of Cefaly.
This was a prospective, multicenter, sham-controlled study. Patients were enrolled if they developed migraine prior to age 50 years and experienced two to eight attacks per month of moderate to severe intensity. Patients were randomized to either Cefaly or a sham device. The Cefaly device itself has two setting: acute and preventive. For this study, the acute setting was used for 2 hours at a time during an acute attack (within the first 4 hours). The supraorbital and supratrochlear branches of trigeminal nerves bilaterally are stimulated with a continuous stimulation via a self-adhesive electrode. This has previously been shown to be safe and effective with the most common side effect noted to be skin irritation at the electrode site.
Patients collected data about their headaches in an e-diary and continued to treat for 2 months. The co-primary outcomes were headache freedom and resolution of most bothersome syndrome at 2 hours. Secondary outcomes were pain relief at 2 hours, resolution of any migraine-associated symptom at 2 hours after beginning e-TNS treatment, sustained pain freedom (defined as pain freedom at 2 hours and pain freedom at 24 hours without the use of antimigraine medication during those 24 hours), and use of a rescue medication between 2 and 24 hours after beginning an e-TNS session.
A total of 538 patients were enrolled. The percentage of patients with both freedom from pain and resolution of the most bothersome symptoms were statistically different in the intervention and sham groups. The secondary outcomes were also statistically improved in the device group, with the exception of use of rescue medications between 2 and 24 hours. The most common adverse events were forehead discomfort and paresthesia.
This study does show the effectiveness of Cefaly, especially when used for longer periods of time than had been previously recommended. The outcomes were all met with the exception of rescue medication use, and there is no contraindication to using any rescue medication while using the Cefaly device. Cefaly can be an excellent add-on for acute treatment, especially in patients that may need to use more than one intervention acutely for their migraine attacks.
Providers often discuss when to start medications but do not as often discuss when to stop medications. This is especially true for preventive medications for migraine. The best-case scenario is that a preventive medication is so effective that it is no longer necessary; but in other circumstances, preventive medications have to be stopped, for instance, during pregnancy planning. One concern especially when starting and stopping a monoclonal antibody (mAb) medication is the development of neutralizing antibodies to negate the effect of restarting the medication. This study was designed to determine whether restarting calcitonin gene-related peptide (CGRP)–mAb medications was still effective after having been previously stopped.
Raffaelli and colleagues managed a small (39 patients) open-label prospective study. Patients either had a diagnosis of episodic or chronic migraine and were initially given CGRP-mAbs for at least 8 months. They then stopped the therapy for at least 3 months and were restarted on the same mAb that they had initially used. They tracked their headache symptoms for 3 months after restarting therapy. If another treatment had been started in between, those patients were excluded.
The primary outcome was change in mean monthly migraine days between the last 4 weeks of treatment discontinuation and weeks 9-12 after restarting therapy. Secondary endpoints were the changes in mean monthly headache days across the other observation points and Headache Impact Test-6 (HIT-6) sum scores. Of the 39 patients enrolled, 16 were given erenumab, 15 galcanezumab, and 8 fremanezumab.
Mean migraine days and mean headache days were shown to have a statistically significant decrease after resumption of therapy. Restarting CGRP medications was not associated with other adverse events associated with these medications. This gives us evidence in favor of restarting the same CGRP medication when a patient's symptoms start to worsen after they have discontinued because of improvement or after pregnancy and breastfeeding.
The use of implanted devices for migraine treatment is considered somewhat controversial. Surgical interventions and implantations for migraine have not been well studied; however small case series have been published, and non-neurologists report anecdotally that these interventions can be helpful for refractory headache disorders. The study by Evans and colleagues reviewed via meta-analysis much of the prior data for nerve stimulation in migraine.
Studies included in this meta-analysis were English-language, peer-reviewed articles of prospective studies with patients over age 18 years for migraine diagnosed according to International Classification of Headache Disorders (ICHD) criteria. The devices were transcutaneous nerve stimulator devices in a single region of the head (occipital, supraorbital/supratrochlear areas) and enrolled a minimum of 10 patients in the treatment groups. A total of 14 studies were identified; 13 of the studies did report significant adverse events related to treatment.
Regarding migraine frequency, only four of the studies were considered comparable, investigating episodic migraine with 2-3 months of transcutaneous stimulation, and two were comparable in investigating chronic migraine. The episodic migraine studies had a pooled reduction by 2.8 days of migraine per month; chronic migraine was noted to be 2.97 days fewer per month. Three comparable studies for episodic migraine showed a pooled reduction in severity by 2.23 points after 3 months.
Occipital and other trigeminal branch stimulation implants are invasive and associated with risk, most prominently leading to migration and worsening headache and neck pain. This meta-analysis did reveal important pooled data, but it becomes less impressive when considering the published data for standard oral or injection therapies. The fact that there can be long-term worsening and adverse events with surgical implantation makes this choice a higher risk. Of note, there are now neurostimulation devices, such as Cefaly, that allow similar transcutaneous stimulation without the risk of surgery.
Cefaly is a commonly used nonprescription device that uses external trigeminal nerve stimulation (e-TNS) to either abort or prevent migraine attacks. The pivotal Cefaly study was published about 10 years ago, and Cefaly was the first US Food and Drug Administration–cleared neurostimulation device for headache. The initial acute data were gathered primarily in the hospital setting, and the investigators in the study by Kuruvilla and colleagues intended to replicate a more real-world scenario for the acute use of Cefaly.
This was a prospective, multicenter, sham-controlled study. Patients were enrolled if they developed migraine prior to age 50 years and experienced two to eight attacks per month of moderate to severe intensity. Patients were randomized to either Cefaly or a sham device. The Cefaly device itself has two setting: acute and preventive. For this study, the acute setting was used for 2 hours at a time during an acute attack (within the first 4 hours). The supraorbital and supratrochlear branches of trigeminal nerves bilaterally are stimulated with a continuous stimulation via a self-adhesive electrode. This has previously been shown to be safe and effective with the most common side effect noted to be skin irritation at the electrode site.
Patients collected data about their headaches in an e-diary and continued to treat for 2 months. The co-primary outcomes were headache freedom and resolution of most bothersome syndrome at 2 hours. Secondary outcomes were pain relief at 2 hours, resolution of any migraine-associated symptom at 2 hours after beginning e-TNS treatment, sustained pain freedom (defined as pain freedom at 2 hours and pain freedom at 24 hours without the use of antimigraine medication during those 24 hours), and use of a rescue medication between 2 and 24 hours after beginning an e-TNS session.
A total of 538 patients were enrolled. The percentage of patients with both freedom from pain and resolution of the most bothersome symptoms were statistically different in the intervention and sham groups. The secondary outcomes were also statistically improved in the device group, with the exception of use of rescue medications between 2 and 24 hours. The most common adverse events were forehead discomfort and paresthesia.
This study does show the effectiveness of Cefaly, especially when used for longer periods of time than had been previously recommended. The outcomes were all met with the exception of rescue medication use, and there is no contraindication to using any rescue medication while using the Cefaly device. Cefaly can be an excellent add-on for acute treatment, especially in patients that may need to use more than one intervention acutely for their migraine attacks.
Providers often discuss when to start medications but do not as often discuss when to stop medications. This is especially true for preventive medications for migraine. The best-case scenario is that a preventive medication is so effective that it is no longer necessary; but in other circumstances, preventive medications have to be stopped, for instance, during pregnancy planning. One concern especially when starting and stopping a monoclonal antibody (mAb) medication is the development of neutralizing antibodies to negate the effect of restarting the medication. This study was designed to determine whether restarting calcitonin gene-related peptide (CGRP)–mAb medications was still effective after having been previously stopped.
Raffaelli and colleagues managed a small (39 patients) open-label prospective study. Patients either had a diagnosis of episodic or chronic migraine and were initially given CGRP-mAbs for at least 8 months. They then stopped the therapy for at least 3 months and were restarted on the same mAb that they had initially used. They tracked their headache symptoms for 3 months after restarting therapy. If another treatment had been started in between, those patients were excluded.
The primary outcome was change in mean monthly migraine days between the last 4 weeks of treatment discontinuation and weeks 9-12 after restarting therapy. Secondary endpoints were the changes in mean monthly headache days across the other observation points and Headache Impact Test-6 (HIT-6) sum scores. Of the 39 patients enrolled, 16 were given erenumab, 15 galcanezumab, and 8 fremanezumab.
Mean migraine days and mean headache days were shown to have a statistically significant decrease after resumption of therapy. Restarting CGRP medications was not associated with other adverse events associated with these medications. This gives us evidence in favor of restarting the same CGRP medication when a patient's symptoms start to worsen after they have discontinued because of improvement or after pregnancy and breastfeeding.
The use of implanted devices for migraine treatment is considered somewhat controversial. Surgical interventions and implantations for migraine have not been well studied; however small case series have been published, and non-neurologists report anecdotally that these interventions can be helpful for refractory headache disorders. The study by Evans and colleagues reviewed via meta-analysis much of the prior data for nerve stimulation in migraine.
Studies included in this meta-analysis were English-language, peer-reviewed articles of prospective studies with patients over age 18 years for migraine diagnosed according to International Classification of Headache Disorders (ICHD) criteria. The devices were transcutaneous nerve stimulator devices in a single region of the head (occipital, supraorbital/supratrochlear areas) and enrolled a minimum of 10 patients in the treatment groups. A total of 14 studies were identified; 13 of the studies did report significant adverse events related to treatment.
Regarding migraine frequency, only four of the studies were considered comparable, investigating episodic migraine with 2-3 months of transcutaneous stimulation, and two were comparable in investigating chronic migraine. The episodic migraine studies had a pooled reduction by 2.8 days of migraine per month; chronic migraine was noted to be 2.97 days fewer per month. Three comparable studies for episodic migraine showed a pooled reduction in severity by 2.23 points after 3 months.
Occipital and other trigeminal branch stimulation implants are invasive and associated with risk, most prominently leading to migration and worsening headache and neck pain. This meta-analysis did reveal important pooled data, but it becomes less impressive when considering the published data for standard oral or injection therapies. The fact that there can be long-term worsening and adverse events with surgical implantation makes this choice a higher risk. Of note, there are now neurostimulation devices, such as Cefaly, that allow similar transcutaneous stimulation without the risk of surgery.
Cefaly is a commonly used nonprescription device that uses external trigeminal nerve stimulation (e-TNS) to either abort or prevent migraine attacks. The pivotal Cefaly study was published about 10 years ago, and Cefaly was the first US Food and Drug Administration–cleared neurostimulation device for headache. The initial acute data were gathered primarily in the hospital setting, and the investigators in the study by Kuruvilla and colleagues intended to replicate a more real-world scenario for the acute use of Cefaly.
This was a prospective, multicenter, sham-controlled study. Patients were enrolled if they developed migraine prior to age 50 years and experienced two to eight attacks per month of moderate to severe intensity. Patients were randomized to either Cefaly or a sham device. The Cefaly device itself has two setting: acute and preventive. For this study, the acute setting was used for 2 hours at a time during an acute attack (within the first 4 hours). The supraorbital and supratrochlear branches of trigeminal nerves bilaterally are stimulated with a continuous stimulation via a self-adhesive electrode. This has previously been shown to be safe and effective with the most common side effect noted to be skin irritation at the electrode site.
Patients collected data about their headaches in an e-diary and continued to treat for 2 months. The co-primary outcomes were headache freedom and resolution of most bothersome syndrome at 2 hours. Secondary outcomes were pain relief at 2 hours, resolution of any migraine-associated symptom at 2 hours after beginning e-TNS treatment, sustained pain freedom (defined as pain freedom at 2 hours and pain freedom at 24 hours without the use of antimigraine medication during those 24 hours), and use of a rescue medication between 2 and 24 hours after beginning an e-TNS session.
A total of 538 patients were enrolled. The percentage of patients with both freedom from pain and resolution of the most bothersome symptoms were statistically different in the intervention and sham groups. The secondary outcomes were also statistically improved in the device group, with the exception of use of rescue medications between 2 and 24 hours. The most common adverse events were forehead discomfort and paresthesia.
This study does show the effectiveness of Cefaly, especially when used for longer periods of time than had been previously recommended. The outcomes were all met with the exception of rescue medication use, and there is no contraindication to using any rescue medication while using the Cefaly device. Cefaly can be an excellent add-on for acute treatment, especially in patients that may need to use more than one intervention acutely for their migraine attacks.
Providers often discuss when to start medications but do not as often discuss when to stop medications. This is especially true for preventive medications for migraine. The best-case scenario is that a preventive medication is so effective that it is no longer necessary; but in other circumstances, preventive medications have to be stopped, for instance, during pregnancy planning. One concern especially when starting and stopping a monoclonal antibody (mAb) medication is the development of neutralizing antibodies to negate the effect of restarting the medication. This study was designed to determine whether restarting calcitonin gene-related peptide (CGRP)–mAb medications was still effective after having been previously stopped.
Raffaelli and colleagues managed a small (39 patients) open-label prospective study. Patients either had a diagnosis of episodic or chronic migraine and were initially given CGRP-mAbs for at least 8 months. They then stopped the therapy for at least 3 months and were restarted on the same mAb that they had initially used. They tracked their headache symptoms for 3 months after restarting therapy. If another treatment had been started in between, those patients were excluded.
The primary outcome was change in mean monthly migraine days between the last 4 weeks of treatment discontinuation and weeks 9-12 after restarting therapy. Secondary endpoints were the changes in mean monthly headache days across the other observation points and Headache Impact Test-6 (HIT-6) sum scores. Of the 39 patients enrolled, 16 were given erenumab, 15 galcanezumab, and 8 fremanezumab.
Mean migraine days and mean headache days were shown to have a statistically significant decrease after resumption of therapy. Restarting CGRP medications was not associated with other adverse events associated with these medications. This gives us evidence in favor of restarting the same CGRP medication when a patient's symptoms start to worsen after they have discontinued because of improvement or after pregnancy and breastfeeding.
The use of implanted devices for migraine treatment is considered somewhat controversial. Surgical interventions and implantations for migraine have not been well studied; however small case series have been published, and non-neurologists report anecdotally that these interventions can be helpful for refractory headache disorders. The study by Evans and colleagues reviewed via meta-analysis much of the prior data for nerve stimulation in migraine.
Studies included in this meta-analysis were English-language, peer-reviewed articles of prospective studies with patients over age 18 years for migraine diagnosed according to International Classification of Headache Disorders (ICHD) criteria. The devices were transcutaneous nerve stimulator devices in a single region of the head (occipital, supraorbital/supratrochlear areas) and enrolled a minimum of 10 patients in the treatment groups. A total of 14 studies were identified; 13 of the studies did report significant adverse events related to treatment.
Regarding migraine frequency, only four of the studies were considered comparable, investigating episodic migraine with 2-3 months of transcutaneous stimulation, and two were comparable in investigating chronic migraine. The episodic migraine studies had a pooled reduction by 2.8 days of migraine per month; chronic migraine was noted to be 2.97 days fewer per month. Three comparable studies for episodic migraine showed a pooled reduction in severity by 2.23 points after 3 months.
Occipital and other trigeminal branch stimulation implants are invasive and associated with risk, most prominently leading to migration and worsening headache and neck pain. This meta-analysis did reveal important pooled data, but it becomes less impressive when considering the published data for standard oral or injection therapies. The fact that there can be long-term worsening and adverse events with surgical implantation makes this choice a higher risk. Of note, there are now neurostimulation devices, such as Cefaly, that allow similar transcutaneous stimulation without the risk of surgery.
Most at-home STI testing kits fail to meet young people’s needs
The wide majority of at-home sexually transmitted infection testing kits in the United States appear to be limited to use by adults, a new study finds, and many have limitations that make them less than ideal for young people to use.
While at-home kits do allow more access to STI testing, “we need to create programs that are specific for youth because they have extra needs,” said lead author Saumya Sao, a research assistant at the department of gynecology & obstetrics at Johns Hopkins University, Baltimore, in an interview. “The only platform that did meet our needs was the program that we developed specifically.”
The findings were released ahead of the study’s scheduled presentation at the 2022 annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (Session A117).
According to Ms. Sao, companies began to offer more at-home testing kits during the pandemic as in-person STI clinics shut down. Still, “the fact that we only found 13 self-collect mail-in STI programs shows you that this is pretty new,” she said. “There are not too many companies that do it. We found a lot more platforms that allow users to place orders for testing online, but you’re still required to go into a lab and actually do the testing.”
The researchers gathered information about 13 programs, including the one that they developed at Johns Hopkins known as Violet. Of those, seven limited testing to adults aged 18 and up, and one didn’t list an age requirement. The rest had some age requirements (such as 14 and up) or no age requirements.
The lack of full access for teens is problematic, Ms. Sao said. According to the study, “access to testing among young people is especially important because youth (ages 13-24) bear a disproportionate burden of sexually transmitted infection, accounting for 50% of cases but only 25% of the sexually active population.”
Research has suggested that young people are often wary of visiting STI clinics because they fear stigma from medical professionals or worry about being seen there, Ms. Sao said.
Tests are free in only three of the programs analyzed in the new study. Among the other programs, tests for Chlamydia trachomatis and Neisseria gonorrhoeae cost $45-$179; only two accepted insurance. “These out-of-pocket costs are really high in regard to what a young person might be able to afford for testing, especially if they would need to do repeat testing between partners, or 3 months after testing positive,” Ms. Sao said.
Most of the programs will link users to medical professionals if they test positive. This is a key feature, Ms. Sao said, in order to make sure young people have support.
As for location, most of the programs – including all those that offer free testing – are limited to certain states. Planned Parenthood, for example, only offers at-home STI testing in Maine, New Hampshire, and Vermont. The program charges patients on a sliding scale, accepts insurance, and is available for ages 14 and up. It connects users who test positive to physicians.
Another free program, TakeMeHome, is restricted to 16 states. It includes an HIV panel for ages 17+ (although it doesn’t have vaginal swab testing). It recommends that patients who are positive consult a doctor.
The researchers also found that some, but not all, of the programs send testing material in discreet packaging. This is important to young people because they may not want their parents to know that they’re getting tested.
Some of the testing programs analyzed don’t make it clear on their web sites whether their packaging is discreet, Ms. Sao said.
At Johns Hopkins, Ms. Sao has helped develop the Violet Project, which is designed to meet the needs of young people and offers free STI testing to residents of Maryland of any age for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis. Mailing packages are discreet, and physicians reach out to those who test positive. Fees are covered.
“We don’t have money yet to expand beyond Maryland, but we’re hopeful,” she said.
In an interview, Loma Linda (Calif.) University Health maternal-fetal medicine specialist Sarah Smithson, DO, MS, praised the study and said she supports optimizing at-home testing for young people. It may be useful for youths who first get tested in a clinic but then need follow-up testing or testing of their partners, she said.
Dr. Smithson added that transportation is often a challenge for young people. At her pregnancy clinic in California’s Inland Empire, she said, some patients live in remote areas and make virtual doctor visits because of the distance. STI testing is crucial for pregnant women, she said, “and this could be a game changer for them.”
The wide majority of at-home sexually transmitted infection testing kits in the United States appear to be limited to use by adults, a new study finds, and many have limitations that make them less than ideal for young people to use.
While at-home kits do allow more access to STI testing, “we need to create programs that are specific for youth because they have extra needs,” said lead author Saumya Sao, a research assistant at the department of gynecology & obstetrics at Johns Hopkins University, Baltimore, in an interview. “The only platform that did meet our needs was the program that we developed specifically.”
The findings were released ahead of the study’s scheduled presentation at the 2022 annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (Session A117).
According to Ms. Sao, companies began to offer more at-home testing kits during the pandemic as in-person STI clinics shut down. Still, “the fact that we only found 13 self-collect mail-in STI programs shows you that this is pretty new,” she said. “There are not too many companies that do it. We found a lot more platforms that allow users to place orders for testing online, but you’re still required to go into a lab and actually do the testing.”
The researchers gathered information about 13 programs, including the one that they developed at Johns Hopkins known as Violet. Of those, seven limited testing to adults aged 18 and up, and one didn’t list an age requirement. The rest had some age requirements (such as 14 and up) or no age requirements.
The lack of full access for teens is problematic, Ms. Sao said. According to the study, “access to testing among young people is especially important because youth (ages 13-24) bear a disproportionate burden of sexually transmitted infection, accounting for 50% of cases but only 25% of the sexually active population.”
Research has suggested that young people are often wary of visiting STI clinics because they fear stigma from medical professionals or worry about being seen there, Ms. Sao said.
Tests are free in only three of the programs analyzed in the new study. Among the other programs, tests for Chlamydia trachomatis and Neisseria gonorrhoeae cost $45-$179; only two accepted insurance. “These out-of-pocket costs are really high in regard to what a young person might be able to afford for testing, especially if they would need to do repeat testing between partners, or 3 months after testing positive,” Ms. Sao said.
Most of the programs will link users to medical professionals if they test positive. This is a key feature, Ms. Sao said, in order to make sure young people have support.
As for location, most of the programs – including all those that offer free testing – are limited to certain states. Planned Parenthood, for example, only offers at-home STI testing in Maine, New Hampshire, and Vermont. The program charges patients on a sliding scale, accepts insurance, and is available for ages 14 and up. It connects users who test positive to physicians.
Another free program, TakeMeHome, is restricted to 16 states. It includes an HIV panel for ages 17+ (although it doesn’t have vaginal swab testing). It recommends that patients who are positive consult a doctor.
The researchers also found that some, but not all, of the programs send testing material in discreet packaging. This is important to young people because they may not want their parents to know that they’re getting tested.
Some of the testing programs analyzed don’t make it clear on their web sites whether their packaging is discreet, Ms. Sao said.
At Johns Hopkins, Ms. Sao has helped develop the Violet Project, which is designed to meet the needs of young people and offers free STI testing to residents of Maryland of any age for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis. Mailing packages are discreet, and physicians reach out to those who test positive. Fees are covered.
“We don’t have money yet to expand beyond Maryland, but we’re hopeful,” she said.
In an interview, Loma Linda (Calif.) University Health maternal-fetal medicine specialist Sarah Smithson, DO, MS, praised the study and said she supports optimizing at-home testing for young people. It may be useful for youths who first get tested in a clinic but then need follow-up testing or testing of their partners, she said.
Dr. Smithson added that transportation is often a challenge for young people. At her pregnancy clinic in California’s Inland Empire, she said, some patients live in remote areas and make virtual doctor visits because of the distance. STI testing is crucial for pregnant women, she said, “and this could be a game changer for them.”
The wide majority of at-home sexually transmitted infection testing kits in the United States appear to be limited to use by adults, a new study finds, and many have limitations that make them less than ideal for young people to use.
While at-home kits do allow more access to STI testing, “we need to create programs that are specific for youth because they have extra needs,” said lead author Saumya Sao, a research assistant at the department of gynecology & obstetrics at Johns Hopkins University, Baltimore, in an interview. “The only platform that did meet our needs was the program that we developed specifically.”
The findings were released ahead of the study’s scheduled presentation at the 2022 annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists (Session A117).
According to Ms. Sao, companies began to offer more at-home testing kits during the pandemic as in-person STI clinics shut down. Still, “the fact that we only found 13 self-collect mail-in STI programs shows you that this is pretty new,” she said. “There are not too many companies that do it. We found a lot more platforms that allow users to place orders for testing online, but you’re still required to go into a lab and actually do the testing.”
The researchers gathered information about 13 programs, including the one that they developed at Johns Hopkins known as Violet. Of those, seven limited testing to adults aged 18 and up, and one didn’t list an age requirement. The rest had some age requirements (such as 14 and up) or no age requirements.
The lack of full access for teens is problematic, Ms. Sao said. According to the study, “access to testing among young people is especially important because youth (ages 13-24) bear a disproportionate burden of sexually transmitted infection, accounting for 50% of cases but only 25% of the sexually active population.”
Research has suggested that young people are often wary of visiting STI clinics because they fear stigma from medical professionals or worry about being seen there, Ms. Sao said.
Tests are free in only three of the programs analyzed in the new study. Among the other programs, tests for Chlamydia trachomatis and Neisseria gonorrhoeae cost $45-$179; only two accepted insurance. “These out-of-pocket costs are really high in regard to what a young person might be able to afford for testing, especially if they would need to do repeat testing between partners, or 3 months after testing positive,” Ms. Sao said.
Most of the programs will link users to medical professionals if they test positive. This is a key feature, Ms. Sao said, in order to make sure young people have support.
As for location, most of the programs – including all those that offer free testing – are limited to certain states. Planned Parenthood, for example, only offers at-home STI testing in Maine, New Hampshire, and Vermont. The program charges patients on a sliding scale, accepts insurance, and is available for ages 14 and up. It connects users who test positive to physicians.
Another free program, TakeMeHome, is restricted to 16 states. It includes an HIV panel for ages 17+ (although it doesn’t have vaginal swab testing). It recommends that patients who are positive consult a doctor.
The researchers also found that some, but not all, of the programs send testing material in discreet packaging. This is important to young people because they may not want their parents to know that they’re getting tested.
Some of the testing programs analyzed don’t make it clear on their web sites whether their packaging is discreet, Ms. Sao said.
At Johns Hopkins, Ms. Sao has helped develop the Violet Project, which is designed to meet the needs of young people and offers free STI testing to residents of Maryland of any age for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis. Mailing packages are discreet, and physicians reach out to those who test positive. Fees are covered.
“We don’t have money yet to expand beyond Maryland, but we’re hopeful,” she said.
In an interview, Loma Linda (Calif.) University Health maternal-fetal medicine specialist Sarah Smithson, DO, MS, praised the study and said she supports optimizing at-home testing for young people. It may be useful for youths who first get tested in a clinic but then need follow-up testing or testing of their partners, she said.
Dr. Smithson added that transportation is often a challenge for young people. At her pregnancy clinic in California’s Inland Empire, she said, some patients live in remote areas and make virtual doctor visits because of the distance. STI testing is crucial for pregnant women, she said, “and this could be a game changer for them.”
FROM ACOG 2022
Topline results for dapagliflozin in HFpEF: DELIVER
Topline results from the phase 3 DELIVER trial show dapagliflozin (Farxiga) significantly reduced the primary endpoint of cardiovascular death or worsening heart failure in patients with mildly reduced or preserved ejection fraction, AstraZeneca announced today.
The sodium-glucose cotransporter 2 (SGLT2) inhibitor is not approved in this setting but is already approved for treatment of type 2 diabetes, chronic kidney disease, and heart failure with reduced ejection fraction.
“The results of DELIVER extend the benefit of dapagliflozin to the full spectrum of patients with heart failure,” principal investigator of the trial, Scott Solomon, MD, Harvard Medical School and Brigham and Women’s Hospital, Boston, said in the news release.
The safety and tolerability of dapagliflozin in the trial were consistent with its established safety profile, the company says.
The full trial results will be submitted for presentation at a forthcoming medical meeting, and regulatory submissions will be made in the coming months, it notes.
A version of this article first appeared on Medscape.com.
Topline results from the phase 3 DELIVER trial show dapagliflozin (Farxiga) significantly reduced the primary endpoint of cardiovascular death or worsening heart failure in patients with mildly reduced or preserved ejection fraction, AstraZeneca announced today.
The sodium-glucose cotransporter 2 (SGLT2) inhibitor is not approved in this setting but is already approved for treatment of type 2 diabetes, chronic kidney disease, and heart failure with reduced ejection fraction.
“The results of DELIVER extend the benefit of dapagliflozin to the full spectrum of patients with heart failure,” principal investigator of the trial, Scott Solomon, MD, Harvard Medical School and Brigham and Women’s Hospital, Boston, said in the news release.
The safety and tolerability of dapagliflozin in the trial were consistent with its established safety profile, the company says.
The full trial results will be submitted for presentation at a forthcoming medical meeting, and regulatory submissions will be made in the coming months, it notes.
A version of this article first appeared on Medscape.com.
Topline results from the phase 3 DELIVER trial show dapagliflozin (Farxiga) significantly reduced the primary endpoint of cardiovascular death or worsening heart failure in patients with mildly reduced or preserved ejection fraction, AstraZeneca announced today.
The sodium-glucose cotransporter 2 (SGLT2) inhibitor is not approved in this setting but is already approved for treatment of type 2 diabetes, chronic kidney disease, and heart failure with reduced ejection fraction.
“The results of DELIVER extend the benefit of dapagliflozin to the full spectrum of patients with heart failure,” principal investigator of the trial, Scott Solomon, MD, Harvard Medical School and Brigham and Women’s Hospital, Boston, said in the news release.
The safety and tolerability of dapagliflozin in the trial were consistent with its established safety profile, the company says.
The full trial results will be submitted for presentation at a forthcoming medical meeting, and regulatory submissions will be made in the coming months, it notes.
A version of this article first appeared on Medscape.com.
Bone, breath, heart, guts: Eight essential papers in primary care
1. Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults: A Retrospective Observational Study
Roughly one in three adults with hypertension have inadequate blood pressure control, and clinicians have two options for intensifying treatment: “The dose of the current drug regimen can be maximized, or a new drug can be added,” said deputy editor Christina C. Wee, MD, MPH, at the annual meeting of the American College of Physicians.
Data from randomized controlled trials suggest treatment with lower doses of combination therapy may be more effective, with fewer side effects – although the best strategy in older adults remains unclear.
To answer that question, researchers conducted a large-scale, population-based, retrospective cohort study, and observational data were used to emulate a target trial with two groups: new medication and maximizing dose.
The cohort comprised people aged 65 years or older with hypertension and was limited to those with a systolic blood pressure of 130 mm Hg or higher. Two intensification approaches were used: adding a new medication, defined as a total dose increase with a new medication; and maximizing dose, defined as a total dose increase without new medication.
A total of 178,562 patients were included in the study, and 45,575 (25.5%) had intensification by adding a new medication and 132,987 (74.5%) by maximizing dose.
“Both produced systolic blood pressure reduction with a slight advantage in the ‘add a new medication’ group,” Dr. Wee said. “That group reduced their systolic blood pressure by over 4.5 points as compared to 3.8 points in the maximized [dose] group.”
At 12 months the results were similar, but only 50% of patients in the new medication group were able to sustain that strategy, compared with two-thirds of patients who had their dose increased.
“This suggests that, in older adults, adding a new antihypertensive medication versus maximizing dosing of existing regimen is less common, only minimally more effective, and less sustainable,” Dr. Wee said. “Maximizing dose of antihypertensive medication is a reasonable approach [and] may be easier to sustain.”
2. Cost-Effectiveness of Screening Mammography Beyond Age 75 Years: A Cost-Effectiveness Analysis
The U.S. Preventive Services Task Force recommends biennial screening mammograms through the age of 74 years, and a meta-analysis of randomized controlled trials suggests mortality is reduced among women with at least a 10-year life expectancy, Dr. Wee said.
However, whether screening beyond age 75 years is cost effective, especially among women with comorbidities, is unclear.
To address that question, researchers estimated benefits, harms, and cost-effectiveness of extending mammography to age 80, 85, or 90 years according to comorbidity burden, using data from the Surveillance, Epidemiology, and End Results program and the Breast Cancer Surveillance Consortium.
The results showed that extending annual mammography beyond age 75 years was not cost effective, but biennial mammography was. “It was cost effective to age 80 regardless of baseline comorbidity score, but it averted only small, absolute numbers of breast cancer deaths – especially for women with comorbidities,” Dr. Wee said. “It was not cost effective beyond age 80.”
3. Prediction of End-Stage Kidney Disease Using Estimated Glomerular Filtration Rate With and Without Race: A Prospective Cohort Study
Estimated glomerular filtration rate (eGFR) is associated with end-stage kidney disease (ESKD) and is used to make dialysis and transplant decisions. “However, the accuracy of using eGFR alone has been questioned and, previously, some eGFR equations included a correction for race and this has been quite controversial,” Dr. Wee said. “And just last year, the Chronic Kidney Disease Epidemiology Collaboration released their new equations, removing the adjustment for race.”
The study authors posed two questions:
- How well does eGFR alone predict risk of ESKD, compared with Kidney Function Risk Equation (KFRE)?
- Does using different eGFR equations affect performance of either eGFR alone or KFRE in predicting the risk of ESKD?
During a maximum 16 years of follow-up, 856 participants (n = 3,873) developed ESKD. Across all eGFR equations, the KFRE score was superior for predicting 2-year incidence of end-stage kidney disease, compared with eGFR alone.
“KFRE score better predicted 2-year risk of ESKD than eGFR alone regardless of eGFR equations used,” Dr. Wee said. “Correcting eGFR equations for race did not improve performance and validates recent guidelines.”
4. Comparative Fracture Risk During Osteoporosis Drug Holidays After Long-Term Risedronate Versus Alendronate Therapy: A Propensity Score-Matched Cohort Study
The study looked at the comparative risks of drug holidays after long-term (≥ 3 years) risedronate versus alendronate therapy in a cohort of individuals aged 66 years or older. The primary outcome was hip fracture within 3 years after a 120-day ascertainment period.
The cohort included 25,077 propensity score–matched pairs (81% female) with a mean age of 81 years. Hip fracture rates were higher among risedronate than alendronate drug holidays, although this association was attenuated when any fracture was included as the outcome.
Overall, risedronate treatment before a drug holiday was associated with an 18% greater risk of hip fractures than alendronate, and this relative increase translated to a small absolute increase of 0.6%.
“These differences primarily manifested after 24 months, but given these small differences, I’m not sure if we need to change our current management strategy,” Dr. Wee said. “But further study is warranted.”
5. The Effects of Four Doses of Vitamin D Supplements on Falls in Older Adults: A Response-Adaptive, Randomized Clinical Trial
This study assessed the effects of four doses of vitamin D3 supplements on the risk of falls.
The cohort included 688 participants, aged 70 years and older, with an elevated fall risk and a serum 25-hydroxyvitamin D level of 25-72.5 nmol/L. The intervention was 200 (control), 1,000, 2,000, or 4,000 IU of vitamin D3 per day.
“Their results showed that supplementation at doses of 1,000 IU/day or higher did not prevent falls compared with 200 IU/day,” said deputy editor Stephanie Chang, MD, MPH. “Several analyses raised safety concerns about vitamin D3 doses of 1,000 IU/day or higher.”
6. Postdiagnosis Smoking Cessation and Reduced Risk for Lung Cancer Progression and Mortality: A Prospective Cohort Study
This study sought to determine if quitting smoking after a diagnosis of lung cancer reduced the risk for disease progression and mortality. Researchers prospectively analyzed patients with non–small cell lung cancer (NSCLC) who were recruited between 2007 and 2016 and followed annually through 2020. The cohort comprised 517 current smokers who were diagnosed with early-stage (IA-IIIA) NSCLC.
The adjusted median overall survival time was 21.6 months higher among patients who quit smoking versus those who continued smoking, and a higher 5-year overall and progression-free survival were observed among patients who quit than those who continued smoking. After adjusting for confounders, smoking cessation remained associated with a lower risk for all-cause mortality, cancer-specific mortality, and disease progression.
7. Acute Consumption of Alcohol and Discrete Atrial Fibrillation Events
This study sought to determine if alcohol consumption heightened the risk for an episode of atrial fibrillation (AFib). The cohort included 100 individuals with paroxysmal AFib who were fitted with a continuous electrocardiogram monitor and an ankle-worn transdermal ethanol sensor for 4 weeks. Real-time documentation of each alcoholic drink consumed was self-recorded and finger-stick blood tests for phosphatidylethanol were used to corroborate ascertainments of drinking events.
Phosphatidylethanol testing correlated with the number of real-time recorded drinks and with the transdermal alcohol sensor. Consuming one alcoholic drink was associated with a twofold increased risk of AFib over the next 4 hours. The risk rose threefold with the consumption of two drinks.
“There is evidence of dose-response relationship with higher risk with more drinks,” Dr. Chang said. “Even one drink may predispose to an acute episode of AF[ib] in those so predisposed.”
8. Evaluation and Management After Acute Left-Sided Colonic Diverticulitis: A Systematic Review
Management of uncomplicated diverticulitis is usually conservative and includes bowel rest and fluids. However, uncertainty remains about the role of hospitalization and antibiotics, Dr. Chang said. The new review included 51 studies looking at colonoscopy, nonsurgical treatments, and elective surgery for patients with diverticulitis.
It was unclear if patients with recent acute diverticulitis are at increased risk for colorectal cancer, although those with complicated diverticulitis do appear to be at a higher risk of the disease. Treatment with mesalamine was shown to be ineffective in preventing recurrence, and other nonsurgical treatments lacked adequate evidence.
As for surgery, elective procedures reduce recurrence in patients with prior complicated or smoldering or frequently recurrent diverticulitis, but it is unclear which of these patients may benefit most.
“The ACP recommends initial management without antibiotics,” said Dr. Chang, adding that other questions need to be addressed, such as inpatient versus outpatient management and elective surgery after an acute episode.
Dr. Wee and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
1. Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults: A Retrospective Observational Study
Roughly one in three adults with hypertension have inadequate blood pressure control, and clinicians have two options for intensifying treatment: “The dose of the current drug regimen can be maximized, or a new drug can be added,” said deputy editor Christina C. Wee, MD, MPH, at the annual meeting of the American College of Physicians.
Data from randomized controlled trials suggest treatment with lower doses of combination therapy may be more effective, with fewer side effects – although the best strategy in older adults remains unclear.
To answer that question, researchers conducted a large-scale, population-based, retrospective cohort study, and observational data were used to emulate a target trial with two groups: new medication and maximizing dose.
The cohort comprised people aged 65 years or older with hypertension and was limited to those with a systolic blood pressure of 130 mm Hg or higher. Two intensification approaches were used: adding a new medication, defined as a total dose increase with a new medication; and maximizing dose, defined as a total dose increase without new medication.
A total of 178,562 patients were included in the study, and 45,575 (25.5%) had intensification by adding a new medication and 132,987 (74.5%) by maximizing dose.
“Both produced systolic blood pressure reduction with a slight advantage in the ‘add a new medication’ group,” Dr. Wee said. “That group reduced their systolic blood pressure by over 4.5 points as compared to 3.8 points in the maximized [dose] group.”
At 12 months the results were similar, but only 50% of patients in the new medication group were able to sustain that strategy, compared with two-thirds of patients who had their dose increased.
“This suggests that, in older adults, adding a new antihypertensive medication versus maximizing dosing of existing regimen is less common, only minimally more effective, and less sustainable,” Dr. Wee said. “Maximizing dose of antihypertensive medication is a reasonable approach [and] may be easier to sustain.”
2. Cost-Effectiveness of Screening Mammography Beyond Age 75 Years: A Cost-Effectiveness Analysis
The U.S. Preventive Services Task Force recommends biennial screening mammograms through the age of 74 years, and a meta-analysis of randomized controlled trials suggests mortality is reduced among women with at least a 10-year life expectancy, Dr. Wee said.
However, whether screening beyond age 75 years is cost effective, especially among women with comorbidities, is unclear.
To address that question, researchers estimated benefits, harms, and cost-effectiveness of extending mammography to age 80, 85, or 90 years according to comorbidity burden, using data from the Surveillance, Epidemiology, and End Results program and the Breast Cancer Surveillance Consortium.
The results showed that extending annual mammography beyond age 75 years was not cost effective, but biennial mammography was. “It was cost effective to age 80 regardless of baseline comorbidity score, but it averted only small, absolute numbers of breast cancer deaths – especially for women with comorbidities,” Dr. Wee said. “It was not cost effective beyond age 80.”
3. Prediction of End-Stage Kidney Disease Using Estimated Glomerular Filtration Rate With and Without Race: A Prospective Cohort Study
Estimated glomerular filtration rate (eGFR) is associated with end-stage kidney disease (ESKD) and is used to make dialysis and transplant decisions. “However, the accuracy of using eGFR alone has been questioned and, previously, some eGFR equations included a correction for race and this has been quite controversial,” Dr. Wee said. “And just last year, the Chronic Kidney Disease Epidemiology Collaboration released their new equations, removing the adjustment for race.”
The study authors posed two questions:
- How well does eGFR alone predict risk of ESKD, compared with Kidney Function Risk Equation (KFRE)?
- Does using different eGFR equations affect performance of either eGFR alone or KFRE in predicting the risk of ESKD?
During a maximum 16 years of follow-up, 856 participants (n = 3,873) developed ESKD. Across all eGFR equations, the KFRE score was superior for predicting 2-year incidence of end-stage kidney disease, compared with eGFR alone.
“KFRE score better predicted 2-year risk of ESKD than eGFR alone regardless of eGFR equations used,” Dr. Wee said. “Correcting eGFR equations for race did not improve performance and validates recent guidelines.”
4. Comparative Fracture Risk During Osteoporosis Drug Holidays After Long-Term Risedronate Versus Alendronate Therapy: A Propensity Score-Matched Cohort Study
The study looked at the comparative risks of drug holidays after long-term (≥ 3 years) risedronate versus alendronate therapy in a cohort of individuals aged 66 years or older. The primary outcome was hip fracture within 3 years after a 120-day ascertainment period.
The cohort included 25,077 propensity score–matched pairs (81% female) with a mean age of 81 years. Hip fracture rates were higher among risedronate than alendronate drug holidays, although this association was attenuated when any fracture was included as the outcome.
Overall, risedronate treatment before a drug holiday was associated with an 18% greater risk of hip fractures than alendronate, and this relative increase translated to a small absolute increase of 0.6%.
“These differences primarily manifested after 24 months, but given these small differences, I’m not sure if we need to change our current management strategy,” Dr. Wee said. “But further study is warranted.”
5. The Effects of Four Doses of Vitamin D Supplements on Falls in Older Adults: A Response-Adaptive, Randomized Clinical Trial
This study assessed the effects of four doses of vitamin D3 supplements on the risk of falls.
The cohort included 688 participants, aged 70 years and older, with an elevated fall risk and a serum 25-hydroxyvitamin D level of 25-72.5 nmol/L. The intervention was 200 (control), 1,000, 2,000, or 4,000 IU of vitamin D3 per day.
“Their results showed that supplementation at doses of 1,000 IU/day or higher did not prevent falls compared with 200 IU/day,” said deputy editor Stephanie Chang, MD, MPH. “Several analyses raised safety concerns about vitamin D3 doses of 1,000 IU/day or higher.”
6. Postdiagnosis Smoking Cessation and Reduced Risk for Lung Cancer Progression and Mortality: A Prospective Cohort Study
This study sought to determine if quitting smoking after a diagnosis of lung cancer reduced the risk for disease progression and mortality. Researchers prospectively analyzed patients with non–small cell lung cancer (NSCLC) who were recruited between 2007 and 2016 and followed annually through 2020. The cohort comprised 517 current smokers who were diagnosed with early-stage (IA-IIIA) NSCLC.
The adjusted median overall survival time was 21.6 months higher among patients who quit smoking versus those who continued smoking, and a higher 5-year overall and progression-free survival were observed among patients who quit than those who continued smoking. After adjusting for confounders, smoking cessation remained associated with a lower risk for all-cause mortality, cancer-specific mortality, and disease progression.
7. Acute Consumption of Alcohol and Discrete Atrial Fibrillation Events
This study sought to determine if alcohol consumption heightened the risk for an episode of atrial fibrillation (AFib). The cohort included 100 individuals with paroxysmal AFib who were fitted with a continuous electrocardiogram monitor and an ankle-worn transdermal ethanol sensor for 4 weeks. Real-time documentation of each alcoholic drink consumed was self-recorded and finger-stick blood tests for phosphatidylethanol were used to corroborate ascertainments of drinking events.
Phosphatidylethanol testing correlated with the number of real-time recorded drinks and with the transdermal alcohol sensor. Consuming one alcoholic drink was associated with a twofold increased risk of AFib over the next 4 hours. The risk rose threefold with the consumption of two drinks.
“There is evidence of dose-response relationship with higher risk with more drinks,” Dr. Chang said. “Even one drink may predispose to an acute episode of AF[ib] in those so predisposed.”
8. Evaluation and Management After Acute Left-Sided Colonic Diverticulitis: A Systematic Review
Management of uncomplicated diverticulitis is usually conservative and includes bowel rest and fluids. However, uncertainty remains about the role of hospitalization and antibiotics, Dr. Chang said. The new review included 51 studies looking at colonoscopy, nonsurgical treatments, and elective surgery for patients with diverticulitis.
It was unclear if patients with recent acute diverticulitis are at increased risk for colorectal cancer, although those with complicated diverticulitis do appear to be at a higher risk of the disease. Treatment with mesalamine was shown to be ineffective in preventing recurrence, and other nonsurgical treatments lacked adequate evidence.
As for surgery, elective procedures reduce recurrence in patients with prior complicated or smoldering or frequently recurrent diverticulitis, but it is unclear which of these patients may benefit most.
“The ACP recommends initial management without antibiotics,” said Dr. Chang, adding that other questions need to be addressed, such as inpatient versus outpatient management and elective surgery after an acute episode.
Dr. Wee and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
1. Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults: A Retrospective Observational Study
Roughly one in three adults with hypertension have inadequate blood pressure control, and clinicians have two options for intensifying treatment: “The dose of the current drug regimen can be maximized, or a new drug can be added,” said deputy editor Christina C. Wee, MD, MPH, at the annual meeting of the American College of Physicians.
Data from randomized controlled trials suggest treatment with lower doses of combination therapy may be more effective, with fewer side effects – although the best strategy in older adults remains unclear.
To answer that question, researchers conducted a large-scale, population-based, retrospective cohort study, and observational data were used to emulate a target trial with two groups: new medication and maximizing dose.
The cohort comprised people aged 65 years or older with hypertension and was limited to those with a systolic blood pressure of 130 mm Hg or higher. Two intensification approaches were used: adding a new medication, defined as a total dose increase with a new medication; and maximizing dose, defined as a total dose increase without new medication.
A total of 178,562 patients were included in the study, and 45,575 (25.5%) had intensification by adding a new medication and 132,987 (74.5%) by maximizing dose.
“Both produced systolic blood pressure reduction with a slight advantage in the ‘add a new medication’ group,” Dr. Wee said. “That group reduced their systolic blood pressure by over 4.5 points as compared to 3.8 points in the maximized [dose] group.”
At 12 months the results were similar, but only 50% of patients in the new medication group were able to sustain that strategy, compared with two-thirds of patients who had their dose increased.
“This suggests that, in older adults, adding a new antihypertensive medication versus maximizing dosing of existing regimen is less common, only minimally more effective, and less sustainable,” Dr. Wee said. “Maximizing dose of antihypertensive medication is a reasonable approach [and] may be easier to sustain.”
2. Cost-Effectiveness of Screening Mammography Beyond Age 75 Years: A Cost-Effectiveness Analysis
The U.S. Preventive Services Task Force recommends biennial screening mammograms through the age of 74 years, and a meta-analysis of randomized controlled trials suggests mortality is reduced among women with at least a 10-year life expectancy, Dr. Wee said.
However, whether screening beyond age 75 years is cost effective, especially among women with comorbidities, is unclear.
To address that question, researchers estimated benefits, harms, and cost-effectiveness of extending mammography to age 80, 85, or 90 years according to comorbidity burden, using data from the Surveillance, Epidemiology, and End Results program and the Breast Cancer Surveillance Consortium.
The results showed that extending annual mammography beyond age 75 years was not cost effective, but biennial mammography was. “It was cost effective to age 80 regardless of baseline comorbidity score, but it averted only small, absolute numbers of breast cancer deaths – especially for women with comorbidities,” Dr. Wee said. “It was not cost effective beyond age 80.”
3. Prediction of End-Stage Kidney Disease Using Estimated Glomerular Filtration Rate With and Without Race: A Prospective Cohort Study
Estimated glomerular filtration rate (eGFR) is associated with end-stage kidney disease (ESKD) and is used to make dialysis and transplant decisions. “However, the accuracy of using eGFR alone has been questioned and, previously, some eGFR equations included a correction for race and this has been quite controversial,” Dr. Wee said. “And just last year, the Chronic Kidney Disease Epidemiology Collaboration released their new equations, removing the adjustment for race.”
The study authors posed two questions:
- How well does eGFR alone predict risk of ESKD, compared with Kidney Function Risk Equation (KFRE)?
- Does using different eGFR equations affect performance of either eGFR alone or KFRE in predicting the risk of ESKD?
During a maximum 16 years of follow-up, 856 participants (n = 3,873) developed ESKD. Across all eGFR equations, the KFRE score was superior for predicting 2-year incidence of end-stage kidney disease, compared with eGFR alone.
“KFRE score better predicted 2-year risk of ESKD than eGFR alone regardless of eGFR equations used,” Dr. Wee said. “Correcting eGFR equations for race did not improve performance and validates recent guidelines.”
4. Comparative Fracture Risk During Osteoporosis Drug Holidays After Long-Term Risedronate Versus Alendronate Therapy: A Propensity Score-Matched Cohort Study
The study looked at the comparative risks of drug holidays after long-term (≥ 3 years) risedronate versus alendronate therapy in a cohort of individuals aged 66 years or older. The primary outcome was hip fracture within 3 years after a 120-day ascertainment period.
The cohort included 25,077 propensity score–matched pairs (81% female) with a mean age of 81 years. Hip fracture rates were higher among risedronate than alendronate drug holidays, although this association was attenuated when any fracture was included as the outcome.
Overall, risedronate treatment before a drug holiday was associated with an 18% greater risk of hip fractures than alendronate, and this relative increase translated to a small absolute increase of 0.6%.
“These differences primarily manifested after 24 months, but given these small differences, I’m not sure if we need to change our current management strategy,” Dr. Wee said. “But further study is warranted.”
5. The Effects of Four Doses of Vitamin D Supplements on Falls in Older Adults: A Response-Adaptive, Randomized Clinical Trial
This study assessed the effects of four doses of vitamin D3 supplements on the risk of falls.
The cohort included 688 participants, aged 70 years and older, with an elevated fall risk and a serum 25-hydroxyvitamin D level of 25-72.5 nmol/L. The intervention was 200 (control), 1,000, 2,000, or 4,000 IU of vitamin D3 per day.
“Their results showed that supplementation at doses of 1,000 IU/day or higher did not prevent falls compared with 200 IU/day,” said deputy editor Stephanie Chang, MD, MPH. “Several analyses raised safety concerns about vitamin D3 doses of 1,000 IU/day or higher.”
6. Postdiagnosis Smoking Cessation and Reduced Risk for Lung Cancer Progression and Mortality: A Prospective Cohort Study
This study sought to determine if quitting smoking after a diagnosis of lung cancer reduced the risk for disease progression and mortality. Researchers prospectively analyzed patients with non–small cell lung cancer (NSCLC) who were recruited between 2007 and 2016 and followed annually through 2020. The cohort comprised 517 current smokers who were diagnosed with early-stage (IA-IIIA) NSCLC.
The adjusted median overall survival time was 21.6 months higher among patients who quit smoking versus those who continued smoking, and a higher 5-year overall and progression-free survival were observed among patients who quit than those who continued smoking. After adjusting for confounders, smoking cessation remained associated with a lower risk for all-cause mortality, cancer-specific mortality, and disease progression.
7. Acute Consumption of Alcohol and Discrete Atrial Fibrillation Events
This study sought to determine if alcohol consumption heightened the risk for an episode of atrial fibrillation (AFib). The cohort included 100 individuals with paroxysmal AFib who were fitted with a continuous electrocardiogram monitor and an ankle-worn transdermal ethanol sensor for 4 weeks. Real-time documentation of each alcoholic drink consumed was self-recorded and finger-stick blood tests for phosphatidylethanol were used to corroborate ascertainments of drinking events.
Phosphatidylethanol testing correlated with the number of real-time recorded drinks and with the transdermal alcohol sensor. Consuming one alcoholic drink was associated with a twofold increased risk of AFib over the next 4 hours. The risk rose threefold with the consumption of two drinks.
“There is evidence of dose-response relationship with higher risk with more drinks,” Dr. Chang said. “Even one drink may predispose to an acute episode of AF[ib] in those so predisposed.”
8. Evaluation and Management After Acute Left-Sided Colonic Diverticulitis: A Systematic Review
Management of uncomplicated diverticulitis is usually conservative and includes bowel rest and fluids. However, uncertainty remains about the role of hospitalization and antibiotics, Dr. Chang said. The new review included 51 studies looking at colonoscopy, nonsurgical treatments, and elective surgery for patients with diverticulitis.
It was unclear if patients with recent acute diverticulitis are at increased risk for colorectal cancer, although those with complicated diverticulitis do appear to be at a higher risk of the disease. Treatment with mesalamine was shown to be ineffective in preventing recurrence, and other nonsurgical treatments lacked adequate evidence.
As for surgery, elective procedures reduce recurrence in patients with prior complicated or smoldering or frequently recurrent diverticulitis, but it is unclear which of these patients may benefit most.
“The ACP recommends initial management without antibiotics,” said Dr. Chang, adding that other questions need to be addressed, such as inpatient versus outpatient management and elective surgery after an acute episode.
Dr. Wee and Dr. Chang disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM INTERNAL MEDICINE 2022
Adherence to ADHD meds may lower unemployment risk
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.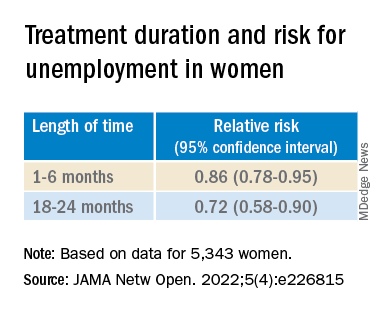
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN