User login
Dermatoethics for Dermatology Residents
As dermatology residents, we have a lot on our plates. With so many diagnoses to learn and treatments to understand, the sheer volume of knowledge we are expected to be familiar with sometimes can be overwhelming. The thought of adding yet another thing to the list of many things we already need to know—least of all a topic such as dermatoethics—may be unappealing. This article will discuss the importance of ethics training in dermatology residency as well as provide helpful resources for how this training can be achieved.
Professionalism as a Core Competency
The Accreditation Council for Graduate Medical Education (ACGME) considers professionalism as 1 of its 6 core competencies.1 These competencies provide a conceptual framework detailing the domains physicians should be proficient in before they can enter autonomous practice. When it comes to professionalism, residents are expected to demonstrate compassion, integrity, and respect for others; honesty with patients; respect for patient confidentiality and autonomy; appropriate relationships with patients; accountability to patients, society, and the profession; and a sensitivity and responsiveness to diverse patient population.1
The ACGME milestones are intended to assess resident development within the 6 competencies with more specific parameters for evaluation.2 Those pertaining to professionalism evaluate a resident’s ability to demonstrate professional behavior, an understanding of ethical principles, accountability, and conscientiousness, as well as self-awareness and the ability to seek help for personal or professional well-being. The crux of the kinds of activities that constitute acquisition of these professional skills are specialty specific. The ACGME ultimately believes that having a working knowledge of professionalism and ethical principles prepares residents for practicing medicine in the real world. Because of these requirements, residency programs are expected to provide resources for residents to explore ethical problems faced by dermatologists.
Beyond “Passing” Residency
The reality is that learning about medical ethics and practicing professional behavior is not just about ticking boxes to get ACGME accreditation or to “pass” residency. The data suggest that having a strong foundation in these principles is good for overall personal well-being, job satisfaction, and patient care. Studies have shown that unprofessional behavior in medical school is correlated to disciplinary action by state licensing boards against practicing physicians.3,4 In fact, a study found that in one cohort of physicians (N=68), 95% of disciplinary actions were for lapses in professionalism, which included activities such as sexual misconduct and inappropriate prescribing.4 Behaving appropriately protects your license to practice medicine.
Thinking through these problematic ethical scenarios also goes beyond coming up with the right answer. Exploring ethical conundrums is thought to develop analytical skills that can help one navigate future tricky situations that can be morally distressing and can lead to burnout. Introspection and self-awareness coupled with these skills ideally will help physicians think through sensitive and difficult situations with the courage to hold true to their convictions and ultimately uphold the professionalism of the specialty.5
Self-awareness has the additional bonus of empowering physicians to acknowledge personal and professional limitations with the goal of seeking help when it is needed before it is too late. It comes as no surprise that how we feel as physicians directly impacts how we treat our patients. One study found that depressed residents were more than 6 times more likely to make medication errors compared to nondepressed colleagues.6 Regularly taking stock of our professional and personal reserves can go a long way to improving overall well-being.
Resources for Dermatoethics Training
The best starting point for developing a robust dermatoethics curriculum is the material provided by the American Board of Dermatology, which is available online.7 An ad hoc subcommittee of the American Board of Dermatology composed of experts in dermatoethics and resident education reviewed relevant ethics literature and identified 6 core domains considered fundamental to dermatology resident education in ethics and professionalism.8 This team also provided a thorough list of relevant background readings for each topic. To cover pertinent material, the subcommittee recommended a 60-minute teaching session every other month with the intent of covering all the material over a 3-year period. If your program directors are not aware of this great resource and you feel your own ethics training may be lacking, bringing this up as a template might be helpful. A detailed description of an innovative dermatoethics curriculum organized at the Department of Dermatology at the Warren Alpert Medical School of Brown University (Providence, Rhode Island) in 2001 also may serve as a guide for programs hoping to design their own approach.5
For those interested in self-study, there is an excellent text dedicated to dermatoethics, which is aptly entitled Dermatoethics: Contemporary Ethics and Professionalism in Dermatology.9 This book offers superb case-based discussions on a wide range of ethical quandaries that dermatologists may face, ranging from unsolicited dermatologic advice (eg, Is it wrong to tell the person next to you in the grocery store that they might have a melanoma?) to research and publication ethics. This text provides a toolkit for handling tough situations in the clinic and beyond. The Journal of the American Academy of Dermatology publishes an Ethics Journal Club for which contributors can submit real-life practical ethical dilemmas, and the journal solicits a resolution or response from a dermatoethicist.
Additionally, a pilot curriculum project out of the University of Utah (Salt Lake City, Utah), of which I am a team member, currently is designing and testing several dermatoethics PowerPoint modules with the intention of making this material widely available through medical education portals.
The Hidden Curriculum
A formal curriculum can only provide so much when it comes to ethics training. In truth, much of what we learn as ethically minded dermatologists comes from our day-to-day practice.10 Paying attention to the more informal curriculum that we are immersed in during routine as well as unusual encounters also is important for achieving milestones. Teaching moments for thinking through ethical dilemmas abound, and this approach easily can be incorporated into routine workflow.11 Next time you encounter an ethical situation that gives you pause (eg, Can I biopsy an intubated patient without getting appropriate consent?), talk it through with your supervisor. Gems of autonomous practice often can be mined from these off-the-cuff conversations.
Can Professionalism Be Taught?
Finally, it is worth mentioning that while the number of resources available to dermatology residents for honing their ethics skills is increasing, ways of measuring the impact of this additional training in vivo are not.12 There are no good tools available to determine how ethics training influences resident behaviors. Similarly, there is no good evidence for what constitutes the most effective method for teaching medical ethics to trainees. It is a growing field with lots of room for more robust research. For now, the overall goal of a dermatoethics curriculum is to provide a mix of curriculum opportunities, ranging from formal lectures and readings to more informal conversations, with the hope of providing residents a toolbox for dealing with ethical dilemmas and a working knowledge of professionalism.
Final Thoughts
There are several resources available for dermatology programs to provide quality dermatoethics training to their residents. These can be mixed and matched to create a tailored formal curriculum alongside the more informal ethics training that happens in the clinic and on the wards. Providing this education is about more than just fulfilling accreditation requirements. Understanding ethical principles and how they can be applied to navigate sensitive situations is ultimately good for both professional and personal well-being.
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (residency). ACGME website. Accessed June 10, 2021. https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResidency2020.pdf
- Edgar L, McLean S, Hogan SO, et al. The milestones guidebook. Accreditation Council for Graduate Medical Education website. Accessed June 10, 2021. acgme.org/portals/0/MilestonesGuidebook.pdf
- Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school. N Engl J Med. 2005;353:2673-2682.
- Papadakis MA, Hodgson CS, Teherani A, et al. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. Acad Med. 2004;79:244-249.
- Bercovitch L, Long TP. Dermatoethics: a curriculum in bioethics and professionalism for dermatology residents at Brown Medical School. J Am Acad Dermatol. 2007;56:679-682.
- Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
- Recommended topics for 3-year dermatoethics curricular cycle. American Board of Dermatology website. Accessed June 10, 2021. https://www.abderm.org/residents-and-fellows/dermatoethics.aspx
- Stoff BK, Grant-Kels JM, Brodell RT, et al. Introducing a curriculum in ethics and professionalism for dermatology residencies. J Am Acad Dermatol. 2018;78:1032-1034.
- Bercovitch L, Perlis C, Stoff BK, et al, eds. Dermatoethics: Contemporary Ethics and Professionalism in Dermatology. 2nd ed. Springer International Publishing; 2021.
- Hafferty FW, Franks R. The hidden curriculum, ethics teaching, and the structure of medical education. Acad Med. 1994;69:861-871.
- Aldrich N, Mostow E. Incorporating teaching dermatoethics in a busy outpatient clinic. J Am Acad Dermatol. 2011;65:423-424.
- de la Garza S, Phuoc V, Throneberry S, et al. Teaching medical ethics in graduate and undergraduate medical education: a systematic review of effectiveness. Acad Psychiatry. 2017;41:520-525.
As dermatology residents, we have a lot on our plates. With so many diagnoses to learn and treatments to understand, the sheer volume of knowledge we are expected to be familiar with sometimes can be overwhelming. The thought of adding yet another thing to the list of many things we already need to know—least of all a topic such as dermatoethics—may be unappealing. This article will discuss the importance of ethics training in dermatology residency as well as provide helpful resources for how this training can be achieved.
Professionalism as a Core Competency
The Accreditation Council for Graduate Medical Education (ACGME) considers professionalism as 1 of its 6 core competencies.1 These competencies provide a conceptual framework detailing the domains physicians should be proficient in before they can enter autonomous practice. When it comes to professionalism, residents are expected to demonstrate compassion, integrity, and respect for others; honesty with patients; respect for patient confidentiality and autonomy; appropriate relationships with patients; accountability to patients, society, and the profession; and a sensitivity and responsiveness to diverse patient population.1
The ACGME milestones are intended to assess resident development within the 6 competencies with more specific parameters for evaluation.2 Those pertaining to professionalism evaluate a resident’s ability to demonstrate professional behavior, an understanding of ethical principles, accountability, and conscientiousness, as well as self-awareness and the ability to seek help for personal or professional well-being. The crux of the kinds of activities that constitute acquisition of these professional skills are specialty specific. The ACGME ultimately believes that having a working knowledge of professionalism and ethical principles prepares residents for practicing medicine in the real world. Because of these requirements, residency programs are expected to provide resources for residents to explore ethical problems faced by dermatologists.
Beyond “Passing” Residency
The reality is that learning about medical ethics and practicing professional behavior is not just about ticking boxes to get ACGME accreditation or to “pass” residency. The data suggest that having a strong foundation in these principles is good for overall personal well-being, job satisfaction, and patient care. Studies have shown that unprofessional behavior in medical school is correlated to disciplinary action by state licensing boards against practicing physicians.3,4 In fact, a study found that in one cohort of physicians (N=68), 95% of disciplinary actions were for lapses in professionalism, which included activities such as sexual misconduct and inappropriate prescribing.4 Behaving appropriately protects your license to practice medicine.
Thinking through these problematic ethical scenarios also goes beyond coming up with the right answer. Exploring ethical conundrums is thought to develop analytical skills that can help one navigate future tricky situations that can be morally distressing and can lead to burnout. Introspection and self-awareness coupled with these skills ideally will help physicians think through sensitive and difficult situations with the courage to hold true to their convictions and ultimately uphold the professionalism of the specialty.5
Self-awareness has the additional bonus of empowering physicians to acknowledge personal and professional limitations with the goal of seeking help when it is needed before it is too late. It comes as no surprise that how we feel as physicians directly impacts how we treat our patients. One study found that depressed residents were more than 6 times more likely to make medication errors compared to nondepressed colleagues.6 Regularly taking stock of our professional and personal reserves can go a long way to improving overall well-being.
Resources for Dermatoethics Training
The best starting point for developing a robust dermatoethics curriculum is the material provided by the American Board of Dermatology, which is available online.7 An ad hoc subcommittee of the American Board of Dermatology composed of experts in dermatoethics and resident education reviewed relevant ethics literature and identified 6 core domains considered fundamental to dermatology resident education in ethics and professionalism.8 This team also provided a thorough list of relevant background readings for each topic. To cover pertinent material, the subcommittee recommended a 60-minute teaching session every other month with the intent of covering all the material over a 3-year period. If your program directors are not aware of this great resource and you feel your own ethics training may be lacking, bringing this up as a template might be helpful. A detailed description of an innovative dermatoethics curriculum organized at the Department of Dermatology at the Warren Alpert Medical School of Brown University (Providence, Rhode Island) in 2001 also may serve as a guide for programs hoping to design their own approach.5
For those interested in self-study, there is an excellent text dedicated to dermatoethics, which is aptly entitled Dermatoethics: Contemporary Ethics and Professionalism in Dermatology.9 This book offers superb case-based discussions on a wide range of ethical quandaries that dermatologists may face, ranging from unsolicited dermatologic advice (eg, Is it wrong to tell the person next to you in the grocery store that they might have a melanoma?) to research and publication ethics. This text provides a toolkit for handling tough situations in the clinic and beyond. The Journal of the American Academy of Dermatology publishes an Ethics Journal Club for which contributors can submit real-life practical ethical dilemmas, and the journal solicits a resolution or response from a dermatoethicist.
Additionally, a pilot curriculum project out of the University of Utah (Salt Lake City, Utah), of which I am a team member, currently is designing and testing several dermatoethics PowerPoint modules with the intention of making this material widely available through medical education portals.
The Hidden Curriculum
A formal curriculum can only provide so much when it comes to ethics training. In truth, much of what we learn as ethically minded dermatologists comes from our day-to-day practice.10 Paying attention to the more informal curriculum that we are immersed in during routine as well as unusual encounters also is important for achieving milestones. Teaching moments for thinking through ethical dilemmas abound, and this approach easily can be incorporated into routine workflow.11 Next time you encounter an ethical situation that gives you pause (eg, Can I biopsy an intubated patient without getting appropriate consent?), talk it through with your supervisor. Gems of autonomous practice often can be mined from these off-the-cuff conversations.
Can Professionalism Be Taught?
Finally, it is worth mentioning that while the number of resources available to dermatology residents for honing their ethics skills is increasing, ways of measuring the impact of this additional training in vivo are not.12 There are no good tools available to determine how ethics training influences resident behaviors. Similarly, there is no good evidence for what constitutes the most effective method for teaching medical ethics to trainees. It is a growing field with lots of room for more robust research. For now, the overall goal of a dermatoethics curriculum is to provide a mix of curriculum opportunities, ranging from formal lectures and readings to more informal conversations, with the hope of providing residents a toolbox for dealing with ethical dilemmas and a working knowledge of professionalism.
Final Thoughts
There are several resources available for dermatology programs to provide quality dermatoethics training to their residents. These can be mixed and matched to create a tailored formal curriculum alongside the more informal ethics training that happens in the clinic and on the wards. Providing this education is about more than just fulfilling accreditation requirements. Understanding ethical principles and how they can be applied to navigate sensitive situations is ultimately good for both professional and personal well-being.
As dermatology residents, we have a lot on our plates. With so many diagnoses to learn and treatments to understand, the sheer volume of knowledge we are expected to be familiar with sometimes can be overwhelming. The thought of adding yet another thing to the list of many things we already need to know—least of all a topic such as dermatoethics—may be unappealing. This article will discuss the importance of ethics training in dermatology residency as well as provide helpful resources for how this training can be achieved.
Professionalism as a Core Competency
The Accreditation Council for Graduate Medical Education (ACGME) considers professionalism as 1 of its 6 core competencies.1 These competencies provide a conceptual framework detailing the domains physicians should be proficient in before they can enter autonomous practice. When it comes to professionalism, residents are expected to demonstrate compassion, integrity, and respect for others; honesty with patients; respect for patient confidentiality and autonomy; appropriate relationships with patients; accountability to patients, society, and the profession; and a sensitivity and responsiveness to diverse patient population.1
The ACGME milestones are intended to assess resident development within the 6 competencies with more specific parameters for evaluation.2 Those pertaining to professionalism evaluate a resident’s ability to demonstrate professional behavior, an understanding of ethical principles, accountability, and conscientiousness, as well as self-awareness and the ability to seek help for personal or professional well-being. The crux of the kinds of activities that constitute acquisition of these professional skills are specialty specific. The ACGME ultimately believes that having a working knowledge of professionalism and ethical principles prepares residents for practicing medicine in the real world. Because of these requirements, residency programs are expected to provide resources for residents to explore ethical problems faced by dermatologists.
Beyond “Passing” Residency
The reality is that learning about medical ethics and practicing professional behavior is not just about ticking boxes to get ACGME accreditation or to “pass” residency. The data suggest that having a strong foundation in these principles is good for overall personal well-being, job satisfaction, and patient care. Studies have shown that unprofessional behavior in medical school is correlated to disciplinary action by state licensing boards against practicing physicians.3,4 In fact, a study found that in one cohort of physicians (N=68), 95% of disciplinary actions were for lapses in professionalism, which included activities such as sexual misconduct and inappropriate prescribing.4 Behaving appropriately protects your license to practice medicine.
Thinking through these problematic ethical scenarios also goes beyond coming up with the right answer. Exploring ethical conundrums is thought to develop analytical skills that can help one navigate future tricky situations that can be morally distressing and can lead to burnout. Introspection and self-awareness coupled with these skills ideally will help physicians think through sensitive and difficult situations with the courage to hold true to their convictions and ultimately uphold the professionalism of the specialty.5
Self-awareness has the additional bonus of empowering physicians to acknowledge personal and professional limitations with the goal of seeking help when it is needed before it is too late. It comes as no surprise that how we feel as physicians directly impacts how we treat our patients. One study found that depressed residents were more than 6 times more likely to make medication errors compared to nondepressed colleagues.6 Regularly taking stock of our professional and personal reserves can go a long way to improving overall well-being.
Resources for Dermatoethics Training
The best starting point for developing a robust dermatoethics curriculum is the material provided by the American Board of Dermatology, which is available online.7 An ad hoc subcommittee of the American Board of Dermatology composed of experts in dermatoethics and resident education reviewed relevant ethics literature and identified 6 core domains considered fundamental to dermatology resident education in ethics and professionalism.8 This team also provided a thorough list of relevant background readings for each topic. To cover pertinent material, the subcommittee recommended a 60-minute teaching session every other month with the intent of covering all the material over a 3-year period. If your program directors are not aware of this great resource and you feel your own ethics training may be lacking, bringing this up as a template might be helpful. A detailed description of an innovative dermatoethics curriculum organized at the Department of Dermatology at the Warren Alpert Medical School of Brown University (Providence, Rhode Island) in 2001 also may serve as a guide for programs hoping to design their own approach.5
For those interested in self-study, there is an excellent text dedicated to dermatoethics, which is aptly entitled Dermatoethics: Contemporary Ethics and Professionalism in Dermatology.9 This book offers superb case-based discussions on a wide range of ethical quandaries that dermatologists may face, ranging from unsolicited dermatologic advice (eg, Is it wrong to tell the person next to you in the grocery store that they might have a melanoma?) to research and publication ethics. This text provides a toolkit for handling tough situations in the clinic and beyond. The Journal of the American Academy of Dermatology publishes an Ethics Journal Club for which contributors can submit real-life practical ethical dilemmas, and the journal solicits a resolution or response from a dermatoethicist.
Additionally, a pilot curriculum project out of the University of Utah (Salt Lake City, Utah), of which I am a team member, currently is designing and testing several dermatoethics PowerPoint modules with the intention of making this material widely available through medical education portals.
The Hidden Curriculum
A formal curriculum can only provide so much when it comes to ethics training. In truth, much of what we learn as ethically minded dermatologists comes from our day-to-day practice.10 Paying attention to the more informal curriculum that we are immersed in during routine as well as unusual encounters also is important for achieving milestones. Teaching moments for thinking through ethical dilemmas abound, and this approach easily can be incorporated into routine workflow.11 Next time you encounter an ethical situation that gives you pause (eg, Can I biopsy an intubated patient without getting appropriate consent?), talk it through with your supervisor. Gems of autonomous practice often can be mined from these off-the-cuff conversations.
Can Professionalism Be Taught?
Finally, it is worth mentioning that while the number of resources available to dermatology residents for honing their ethics skills is increasing, ways of measuring the impact of this additional training in vivo are not.12 There are no good tools available to determine how ethics training influences resident behaviors. Similarly, there is no good evidence for what constitutes the most effective method for teaching medical ethics to trainees. It is a growing field with lots of room for more robust research. For now, the overall goal of a dermatoethics curriculum is to provide a mix of curriculum opportunities, ranging from formal lectures and readings to more informal conversations, with the hope of providing residents a toolbox for dealing with ethical dilemmas and a working knowledge of professionalism.
Final Thoughts
There are several resources available for dermatology programs to provide quality dermatoethics training to their residents. These can be mixed and matched to create a tailored formal curriculum alongside the more informal ethics training that happens in the clinic and on the wards. Providing this education is about more than just fulfilling accreditation requirements. Understanding ethical principles and how they can be applied to navigate sensitive situations is ultimately good for both professional and personal well-being.
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (residency). ACGME website. Accessed June 10, 2021. https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResidency2020.pdf
- Edgar L, McLean S, Hogan SO, et al. The milestones guidebook. Accreditation Council for Graduate Medical Education website. Accessed June 10, 2021. acgme.org/portals/0/MilestonesGuidebook.pdf
- Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school. N Engl J Med. 2005;353:2673-2682.
- Papadakis MA, Hodgson CS, Teherani A, et al. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. Acad Med. 2004;79:244-249.
- Bercovitch L, Long TP. Dermatoethics: a curriculum in bioethics and professionalism for dermatology residents at Brown Medical School. J Am Acad Dermatol. 2007;56:679-682.
- Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
- Recommended topics for 3-year dermatoethics curricular cycle. American Board of Dermatology website. Accessed June 10, 2021. https://www.abderm.org/residents-and-fellows/dermatoethics.aspx
- Stoff BK, Grant-Kels JM, Brodell RT, et al. Introducing a curriculum in ethics and professionalism for dermatology residencies. J Am Acad Dermatol. 2018;78:1032-1034.
- Bercovitch L, Perlis C, Stoff BK, et al, eds. Dermatoethics: Contemporary Ethics and Professionalism in Dermatology. 2nd ed. Springer International Publishing; 2021.
- Hafferty FW, Franks R. The hidden curriculum, ethics teaching, and the structure of medical education. Acad Med. 1994;69:861-871.
- Aldrich N, Mostow E. Incorporating teaching dermatoethics in a busy outpatient clinic. J Am Acad Dermatol. 2011;65:423-424.
- de la Garza S, Phuoc V, Throneberry S, et al. Teaching medical ethics in graduate and undergraduate medical education: a systematic review of effectiveness. Acad Psychiatry. 2017;41:520-525.
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (residency). ACGME website. Accessed June 10, 2021. https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResidency2020.pdf
- Edgar L, McLean S, Hogan SO, et al. The milestones guidebook. Accreditation Council for Graduate Medical Education website. Accessed June 10, 2021. acgme.org/portals/0/MilestonesGuidebook.pdf
- Papadakis MA, Teherani A, Banach MA, et al. Disciplinary action by medical boards and prior behavior in medical school. N Engl J Med. 2005;353:2673-2682.
- Papadakis MA, Hodgson CS, Teherani A, et al. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. Acad Med. 2004;79:244-249.
- Bercovitch L, Long TP. Dermatoethics: a curriculum in bioethics and professionalism for dermatology residents at Brown Medical School. J Am Acad Dermatol. 2007;56:679-682.
- Fahrenkopf AM, Sectish TC, Barger LK, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336:488-491.
- Recommended topics for 3-year dermatoethics curricular cycle. American Board of Dermatology website. Accessed June 10, 2021. https://www.abderm.org/residents-and-fellows/dermatoethics.aspx
- Stoff BK, Grant-Kels JM, Brodell RT, et al. Introducing a curriculum in ethics and professionalism for dermatology residencies. J Am Acad Dermatol. 2018;78:1032-1034.
- Bercovitch L, Perlis C, Stoff BK, et al, eds. Dermatoethics: Contemporary Ethics and Professionalism in Dermatology. 2nd ed. Springer International Publishing; 2021.
- Hafferty FW, Franks R. The hidden curriculum, ethics teaching, and the structure of medical education. Acad Med. 1994;69:861-871.
- Aldrich N, Mostow E. Incorporating teaching dermatoethics in a busy outpatient clinic. J Am Acad Dermatol. 2011;65:423-424.
- de la Garza S, Phuoc V, Throneberry S, et al. Teaching medical ethics in graduate and undergraduate medical education: a systematic review of effectiveness. Acad Psychiatry. 2017;41:520-525.
Resident Pearls
- Professionalism is one of the 6 core competencies used by the Accreditation Council for Graduate Medical Education (ACGME) to evaluate physician preparedness for autonomous practice. Dermatology residency programs are expected to provide resources for achieving this competency.
- Several resources for exploring ethical issues in dermatology are available and can be utilized to create a formal curriculum alongside the more tacit learning that takes place in daily practice.
- Learning about ethical principles and their application can ultimately help practicing physicians avoid disciplinary action and improve overall well-being.

Sotagliflozin use in T2D patients linked with posthospitalization benefits in analysis

The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
The outcome measure –days alive and out of the hospital – may be a meaningful, patient-centered way of capturing disease burden, the researchers wrote in their paper, published in Annals of Internal Medicine.
“The question was: Can we keep patients alive and out of the hospital for any reason, accounting for the duration of each hospitalization?” author Michael Szarek, PhD, a visiting professor in the division of cardiology at the University of Colorado at Denver, Aurora, said in an interview.
“For every 100 days of follow-up, patients in the sotagliflozin group were alive and out of the hospital 3% more days in relative terms or 2.9 days in absolute terms than those in the placebo group (91.8 vs. 88.9 days),” the researchers reported in their analysis of data from the SOLOIST-WHF trial.
“If you translate that to over the course of a year, that’s more than 10 days,” said Dr. Szarek, who is also a faculty member of CPC Clinical Research, an academic research organization affiliated with the University of Colorado.
Most patients in both groups survived to the end of the study without hospitalization, according to the paper.
Sotagliflozin, a sodium-glucose cotransporter 1 and SGLT2 inhibitor, is not approved in the United States. In 2019, the Food and Drug Administration rejected sotagliflozin as an adjunct to insulin for the treatment of type 1 diabetes after members of an advisory committee expressed concerns about an increased risk for diabetic ketoacidosis with the drug.
Methods and results
To examine whether sotagliflozin increased days alive and out of the hospital in the SOLOIST-WHF trial, Dr. Szarek and colleagues analyzed data from this randomized, double-blind, placebo-controlled study. The trial’s primary results were published in the New England Journal of Medicine in January 2021. Researchers conducted SOLOIST-WHF at more than 300 sites in 32 countries. The trial included 1,222 patients with type 2 diabetes and reduced or preserved ejection fraction who were recently hospitalized for worsening heart failure.
In the new analysis the researchers looked at hospitalizations for any reason and the duration of hospital admissions after randomization. They analyzed days alive and out of the hospital using prespecified models.
Similar proportions of patients who received sotagliflozin and placebo were hospitalized at least once (38.5% vs. 41.4%) during a median follow-up of 9 months. Fewer patients who received sotagliflozin were hospitalized more than once (16.3% vs. 22.1%). In all, 64 patients in the sotagliflozin group and 76 patients in the placebo group died.
The reason for each hospitalization was unspecified, except for cases of heart failure, the authors noted. About 62% of hospitalizations during the trial were for reasons other than heart failure.
Outside expert cites similarities to initial trial
The results for days alive and out of the hospital are “not particularly surprising given the previous publication” of the trial’s primary results, but the new analysis provides a “different view of outcomes that might be clinically meaningful for patients,” commented Frank Brosius, MD, a professor of medicine at the University of Arizona, Tucson.
The SOLOIST-WHF trial indicated that doctors may be able to effectively treat patients with relatively new heart failure with sotagliflozin as long as patients are relatively stable, said Dr. Brosius, who coauthored an editorial in the New England Journal of Medicine that accompanied the initial results from the SOLOIST-WHF trial. It appears that previously reported benefits with regard to heart failure outcomes “showed up in these other indicators” in the secondary analysis.
Still, the effect sizes in the new analysis were relatively small and “probably more studies will be necessary” to examine these end points, he added.
SOLOIST-WHF was funded by Sanofi at initiation and by Lexicon Pharmaceuticals at completion. Dr. Szarek disclosed grants from Lexicon and grants and personal fees from Sanofi, as well as personal fees from other companies. His coauthors included employees of Lexicon and other researchers with financial ties to Lexicon and other pharmaceutical companies. Dr. Brosius disclosed personal fees from the American Diabetes Association and is a member of the Diabetic Kidney Disease Collaborative task force for the American Society of Nephrology that is broadly advocating the use of SGLT2 inhibitors by patients with diabetic kidney diseases. He also has participated in an advisory group for treatment of diabetic kidney disease for Gilead.
FROM ANNALS OF INTERNAL MEDICINE
Tardive dyskinesia: The role of targeted therapy
Tardive dyskinesia is a movement disorder characterized by involuntary and repetitive movements of the tongue, lips, face, trunk, and extremities. It is caused by the use of dopamine receptor-blocking drugs, most often antipsychotics, but has also been associated with treatments for some gastrointestinal disorders.
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI, walks through some of the known causes of tardive dyskinesia as well as steps physicians can take in making a differential diagnosis.
Next, Dr. LeWitt dives into the role of targeted therapy in the management of tardive dyskinesia. VMAT2 (vesicular monoamine transporter type 2) inhibitors are emerging as a treatment class of choice that help suppress tardive dyskinesia symptoms by depleting presynaptic dopamine, while other patients may benefit more from benzodiazepines, botulinum toxin, or deep brain stimulation.
--
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI.
Peter A. LeWitt reports advisory roles for: Abide, Acorda Therapeutics, Adamas, Biogen, Cavion, Denali, Intec Pharma, Jazz Pharmaceuticals, Lundbeck, Neurocrine, Mitsubishi NeuroDerm Ltd, Prexton, Revance, Sage, and US WorldMeds.
Lecture fees from: Acorda, American Academy of Neurology, Kyowa Hakko Kirin, and US WorldMeds.
Research grant support from: Abide, Acorda, Amneal, Lundbeck, Michael J. Fox Foundation for Parkinson's Research, Mitsubishi NeuroDerm Ltd, Parkinson Study Group; Pharma 2B, Revance, Hoffmann-La Roche; Sunovion, Sun Pharma, and US WorldMeds.
Tardive dyskinesia is a movement disorder characterized by involuntary and repetitive movements of the tongue, lips, face, trunk, and extremities. It is caused by the use of dopamine receptor-blocking drugs, most often antipsychotics, but has also been associated with treatments for some gastrointestinal disorders.
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI, walks through some of the known causes of tardive dyskinesia as well as steps physicians can take in making a differential diagnosis.
Next, Dr. LeWitt dives into the role of targeted therapy in the management of tardive dyskinesia. VMAT2 (vesicular monoamine transporter type 2) inhibitors are emerging as a treatment class of choice that help suppress tardive dyskinesia symptoms by depleting presynaptic dopamine, while other patients may benefit more from benzodiazepines, botulinum toxin, or deep brain stimulation.
--
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI.
Peter A. LeWitt reports advisory roles for: Abide, Acorda Therapeutics, Adamas, Biogen, Cavion, Denali, Intec Pharma, Jazz Pharmaceuticals, Lundbeck, Neurocrine, Mitsubishi NeuroDerm Ltd, Prexton, Revance, Sage, and US WorldMeds.
Lecture fees from: Acorda, American Academy of Neurology, Kyowa Hakko Kirin, and US WorldMeds.
Research grant support from: Abide, Acorda, Amneal, Lundbeck, Michael J. Fox Foundation for Parkinson's Research, Mitsubishi NeuroDerm Ltd, Parkinson Study Group; Pharma 2B, Revance, Hoffmann-La Roche; Sunovion, Sun Pharma, and US WorldMeds.
Tardive dyskinesia is a movement disorder characterized by involuntary and repetitive movements of the tongue, lips, face, trunk, and extremities. It is caused by the use of dopamine receptor-blocking drugs, most often antipsychotics, but has also been associated with treatments for some gastrointestinal disorders.
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI, walks through some of the known causes of tardive dyskinesia as well as steps physicians can take in making a differential diagnosis.
Next, Dr. LeWitt dives into the role of targeted therapy in the management of tardive dyskinesia. VMAT2 (vesicular monoamine transporter type 2) inhibitors are emerging as a treatment class of choice that help suppress tardive dyskinesia symptoms by depleting presynaptic dopamine, while other patients may benefit more from benzodiazepines, botulinum toxin, or deep brain stimulation.
--
Dr. Peter LeWitt, Sastry Foundation Endowed Chair in Neurology at Wayne State University School of Medicine in Detroit, MI.
Peter A. LeWitt reports advisory roles for: Abide, Acorda Therapeutics, Adamas, Biogen, Cavion, Denali, Intec Pharma, Jazz Pharmaceuticals, Lundbeck, Neurocrine, Mitsubishi NeuroDerm Ltd, Prexton, Revance, Sage, and US WorldMeds.
Lecture fees from: Acorda, American Academy of Neurology, Kyowa Hakko Kirin, and US WorldMeds.
Research grant support from: Abide, Acorda, Amneal, Lundbeck, Michael J. Fox Foundation for Parkinson's Research, Mitsubishi NeuroDerm Ltd, Parkinson Study Group; Pharma 2B, Revance, Hoffmann-La Roche; Sunovion, Sun Pharma, and US WorldMeds.

Depression remains common among dystonia patients
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
About one-third of individuals with adult-onset idiopathic dystonia experience major depression or dysthymia, data from a meta-analysis of 54 studies show.
Adult-onset idiopathic dystonia (AOID) is the third-most common movement disorder after essential tremor and Parkinson’s disease, and data show that depression and anxiety are the largest contributors to reduced quality of life in these patients, wrote Alex Medina Escobar, MD, of the University of Calgary (Alta.), and colleagues. However, “the pathogenic mechanisms of depression and anxiety in AOID remain unclear” and might involve a combination of biologic factors, as well as social stigma.
In the meta-analysis, published in Neuroscience and Biobehavioral Reviews, the researchers examined the point prevalence of supraclinical threshold depressive symptoms/depressive disorders in AOID using 54 studies. The resulting study population included 12,635 patients: 6,977 with cervical dystonia, 732 with cranial dystonia, 4,504 with mixed forms, 303 with laryngeal dystonia, and 119 with upper-limb dystonia. The studies were published between 1988 and 2020, and included patients from 21 countries in 52 single-center studies and 2 multicenter studies.
Overall, the pooled prevalence of either supraclinical threshold depressive symptoms or depressive disorders was 31.5% for cervical dystonia, 29.2 % for cranial dystonia, and 33.6 % for clinical samples with mixed forms of AOID.
Among patients with cervical dystonia, major depressive disorder was more prevalent than dysthymia, but among patients with cranial dystonia, dysthymia was more prevalent. Among patients with mixed forms, the prevalence of major depressive disorder was higher than dysthymia. Heterogeneity varied among the studies but was higher in studies that used rating scales.
Treatment of patients with AOID does not take into account the impact of depression on quality of life, Dr. Escobar and colleagues reported.
“ Such model appears to be inefficient to guarantee resources to address these comorbidities within secondary or tertiary care, or through shared care pathways engaging both primary and hospital-based care.” They also said the use of antidepressants and cognitive-behavioral therapy as a way to target negative body concept or social stigma among these patients are “underexplored and underutilized.”
The study findings were limited by several factors, including the inclusion only of studies published in English. In addition, most of the studies were conducted at movement disorders clinics, which may have yielded a patient population with more severe AOID. Further limitations included the inability to perform subgroup analysis based on demographic and clinical factors, and the insufficient number of studies for meta-analysis of laryngeal and hand dystonia, Dr. Escobar and colleagues added.
However, the results represent the first pooled estimate of depression prevalence in AOID and confirm a high prevalence across different clinical forms, the researchers said. The heterogeneity across studies highlights the need for standardized screening for depression and improved diagnosis of mood disorders in AOID.
“The meta-analytic estimates provided here will be highly useful for the planning of future mechanistic and interventional studies, as well as for the redefinition of current models of care,” they concluded.
The study received no outside funding. Dr. Escobar and colleagues had no disclosures.
FROM NEUROSCIENCE AND BIOBEHAVIORAL REVIEWS
Children and COVID: Vaccination trends beginning to diverge
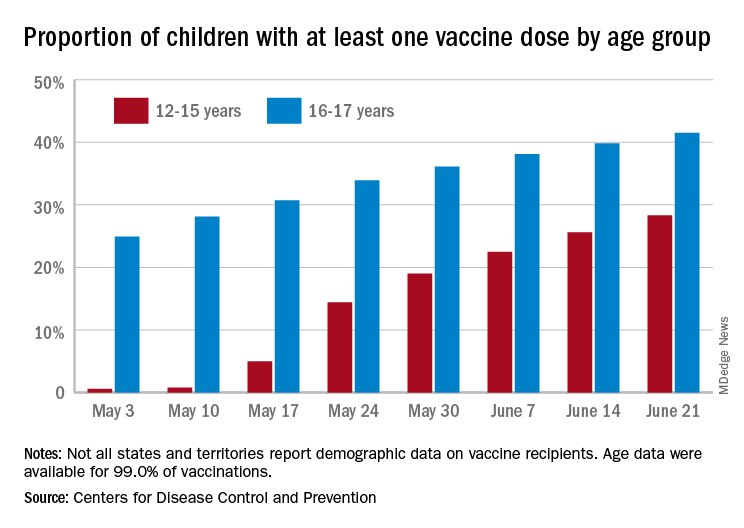
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
As more adolescents became eligible for a second dose of the Pfizer vaccine since it received approval from the Food and Drug Administration in mid-May, the share of 12- to 15-year-olds considered fully vaccinated rose from 11.4% on June 14 to 17.8% on June 28, an increase of 56%, the CDC’s COVID Data Tracker indicated June 22.
For children aged 16-17 years, who have been receiving the vaccine since early April, full vaccination rose by 9.6% in that same week, going from 29.1% on June 14 to 31.9% on June 21. The cumulative numbers for first vaccinations are higher, of course, but are rising more slowly in both age groups: 41.5% of those aged 16-17 had received at least one dose by June 21 (up by 4.3%), with the 12- to 15-year-olds at 28.3% (up by 10.5%), based on the CDC data.
Limiting the time frame to just the last 2 weeks, however, shows the opposite of rising among the younger children. During the 2 weeks ending June 7, 17.9% of those initiating a first dose were 12-15 years old, but that 2-week figure slipped to 17.1% as of June 14 and was down to 16.0% on June 21. The older group was slow but steady over that time: 4.8%, 4.7%, and 4.8%, the CDC said. To give those figures some context, those aged 25-39 years represented 23.7% of past-2-week initiations on June 7 and 24.3% on June 21.
Although no COVID-19 vaccine has been approved for children under 12 years, about 0.4% of that age group – just over 167,000 children – have received a first dose and almost 91,000 are fully vaccinated, according to CDC data.
Hard Nodular Plaque on the Scalp
The Diagnosis: Platelike Osteoma Cutis
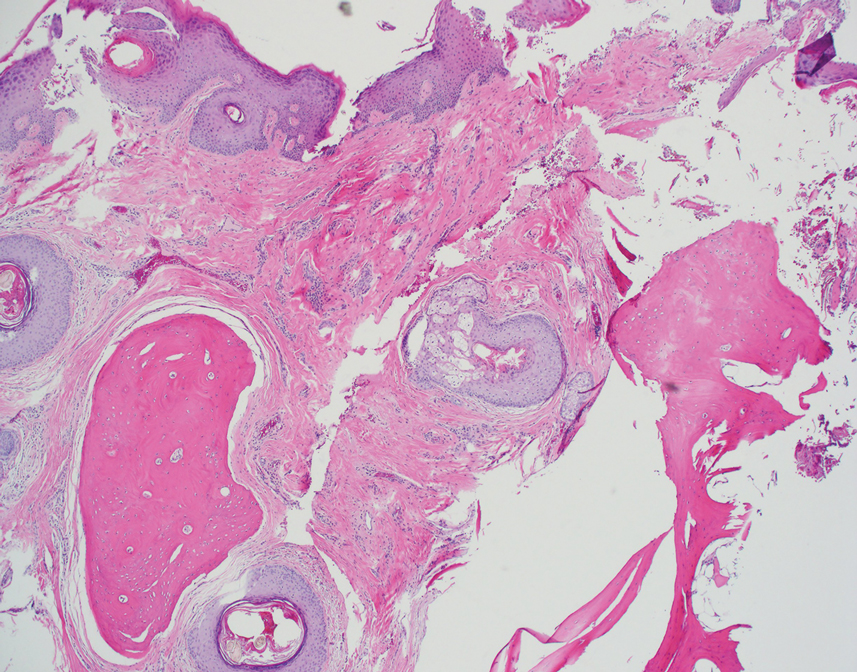
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).

Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.
The Diagnosis: Platelike Osteoma Cutis
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).
Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
The Diagnosis: Platelike Osteoma Cutis
Histopathologic examination revealed extensive cutaneous ossification in the dermis and subcutis with dermal fibrosis and minimal surrounding inflammation (Figure 1). There was no evidence of infection or neoplasm. Further evaluation did not demonstrate any additional physical dysmorphia, and there were no imbalances of calcium-phosphate metabolism or abnormalities in parathyroid hormone or thyroid hormone function. A diagnosis of platelike osteoma cutis (PLOC) was favored. Computed tomography of the head showed material at the posterior skull of similar density to the adjacent calvarial skull and centered within the dermis, consistent with osteoma cutis (Figure 2).
Osteoma cutis describes the formation of bone within the skin. It occurs when hydroxyapatite crystals in a proteinaceous matrix are deposited within the skin, ultimately leading to the formation of bone ultrastructure. Ossification of the skin most often occurs secondary to trauma, inflammation, or neoplasm; however, it rarely may be a primary event.1,2
Platelike osteoma cutis is a rare form of primary cutaneous ossification in which bone forms within the skin in a platelike manner. It most frequently affects the scalp but also has been observed on the trunk and extremities.1 A driving metabolic or endocrine abnormality typically is not identified.2
Platelike osteoma cutis can occur as an isolated finding or as a feature of Albright hereditary osteodystrophy (AHO) or progressive osseous heteroplasia (POH). In addition to cutaneous ossification, AHO involves short stature, endocrinopathy, obesity, shortened fourth and fifth metacarpals, and mental retardation. Progressive osseous heteroplasia is characterized by progressive ossification of the skin and deeper tissues such as muscle and fascia, leading to severe movement restriction; it is believed to be a localized nonprogressive variant of POH.3,4 Mutations in the guanine nucleotide binding protein, alpha stimulating activity polypeptide 1 gene, GNAS1, a key regulatory gene involved in AHO and POH, have been found in several cases of PLOC.3 Our patient lacked any dysmorphic features or laboratory abnormalities suggestive of AHO or POH. Moreover, testing of the tissue and blood for the GNAS1 mutation was negative. Treatment of PLOC often is difficult. Our patient underwent a trial of ablative fractional laser resurfacing, which failed to lead to perceivable improvement.
The differential diagnoses include a kerion, dissecting cellulitis of the scalp, folliculitis decalvans, and acne keloidalis nuchae. A kerion is a manifestation of tinea capitis characterized by an inflammatory plaque, often with pain or tenderness. Kerions most frequently occur in children aged 5 to 10 years.5 Failure to treat a kerion may result in scarring alopecia. Treatment consists of oral antifungals.
Dissecting cellulitis of the scalp is thought to occur secondary to follicular occlusion. It is characterized by boggy suppurative nodules primarily on the posterior and vertex scalp. Patchy hair loss is present and typically progresses to cicatricial alopecia. Histology characteristically shows areas of dense, predominantly neutrophilic, perifollicular dermal infiltrates.6
Folliculitis decalvans is a primary neutrophilic cicatricial alopecia that primarily occurs in adults. Patients with folliculitis decalvans tend to have multiple pustules on the periphery of confluent areas of scarring alopecia. It is theorized that an immune response to staphylococcal superantigens contributes to this disease process.7
The clinical findings of acne keloidalis nuchae include inflammatory pustules and papules with keloidlike plaques on the posterior neck and scalp. It occurs predominantly in teenaged and adult males of African ancestry.8 Treatment is aimed at reducing inflammation and preventing exacerbating factors. Severe disease courses may lead to scarring alopecia.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.
- Sanmartín O, Alegre V, Martinez-Aparicio A, et al. Congenital platelike osteoma cutis: case report and review of the literature. Pediatr Dermatol. 1993;10:182-186.
- Talsania N, Jolliffe V, O’Toole EA, et al. Platelike osteoma cutis. J Am Acad Dermatol. 2009;64:613-615.
- Yeh GL, Mathur S, Wivel A, et al. GNAS1 mutation and Cbfa1 misexpression in a child with severe congenital platelike osteoma cutis. J Bone Miner Res. 2000;15:2063-2073.
- Hernandez-Martin A, Perez-Mies B, Torrelo A. Congenital plate-like osteoma cutis in an infant. Pediatr Dermatol. 2009;26:479-481.
- Zaraa I, Hawilo A, Aounallah A, et al. Inflammatory tinea capitis: a 12-year study and a review of the literature. Mycoses. 2013;56:110-116.
- Scheinfeld N. Dissecting cellulitis (perifolliculitis capitis abscedens et suffodiens): a comprehensive review focusing on new treatments and findings of the last decade with commentary comparing the therapies and causes of dissecting cellulitis to hidradenitis suppurativa. Dermatol Online J. 2014;20:22692.
- Ross EK, Tan E, Shapiro J. Update on primary cicatricial alopecias. J Am Acad Dermatol. 2005;53:1-37.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574.

A 35-year-old man presented to the dermatology clinic with a slow-growing plaque on the scalp of 10 years’ duration. The lesion was mildly pruritic and was never associated with any pain or discharge. He denied antecedent trauma or infection. A hard, erythematous, nodular, alopecic plaque with punctate hyperkeratosis on the left posterior temporal and parietal scalp was noted on physical examination. The lesion was slightly tender to palpation.

AAP updates guidance for return to sports and physical activities
As pandemic restrictions ease and young athletes once again take to fields, courts, tracks, and rinks, doctors are sharing ways to help them get back to sports safely.
That means taking steps to prevent COVID-19.
It also means trying to avoid sports-related injuries, which may be more likely if young athletes didn’t move around so much during the pandemic.
For adolescents who are eligible, getting a COVID-19 vaccine may be the most important thing they can do, according to the American Academy of Pediatrics.
“The AAP encourages all people who are eligible to receive the COVID-19 vaccine as soon as it is available,” the organization wrote in updated guidance on returning to sports and physical activity.
“I don’t think it can be overemphasized how important these vaccines are, both for the individual and at the community level,” says Aaron L. Baggish, MD, an associate professor of medicine at Harvard Medical School, Boston, and director of the Cardiovascular Performance Program at Massachusetts General Hospital in Boston.
Dr. Baggish, team cardiologist for the New England Patriots, the Boston Bruins, the New England Revolution, U.S. Men’s and Women’s Soccer, and U.S. Rowing, as well as medical director for the Boston Marathon, has studied the effects of COVID-19 on the heart in college athletes and written return-to-play recommendations for athletes of high school age and older.
“Millions of people have received these vaccines from age 12 up,” Dr. Baggish says. “The efficacy continues to look very durable and near complete, and the risk associated with vaccination is incredibly low, to the point where the risk-benefit ratio across the age spectrum, whether you’re athletic or not, strongly favors getting vaccinated. There is really no reason to hold off at this point.”
While outdoor activities are lower-risk for spreading COVID-19 and many people have been vaccinated, masks still should be worn in certain settings, the AAP notes.
“Indoor spaces that are crowded are still high-risk for COVID-19 transmission. And we recognize that not everyone in these settings may be vaccinated,” says Susannah Briskin, MD, lead author of the AAP guidance.
“So for indoor sporting events with spectators, in locker rooms or other small spaces such as a training room, and during shared car rides or school transportation to and from events, individuals should continue to mask,” adds Dr. Briskin, a pediatrician in the Division of Sports Medicine and fellowship director for the Primary Care Sports Medicine program at University Hospitals Rainbow Babies & Children’s Hospital.
For outdoor sports, athletes who are not fully vaccinated should be encouraged to wear masks on the sidelines and during group training and competition when they are within 3 feet of others for sustained amounts of time, according to the AAP.
Get back into exercise gradually
In general, athletes who have not been active for more than a month should resume exercise gradually, Dr. Briskin says. Starting at 25% of normal volume and increasing slowly over time – with 10% increases each week – is one rule of thumb.
“Those who have taken a prolonged break from sports are at a higher risk of injury when they return,” she notes. “Families should also be aware of an increased risk for heat-related illness if they are not acclimated.”
Caitlyn Mooney, MD, a team doctor for the University of Texas, San Antonio, has heard reports of doctors seeing more injuries like stress fractures. Some cases may relate to people going from “months of doing nothing to all of a sudden going back to sports,” says Dr. Mooney, who is also a clinical assistant professor of pediatrics and orthopedics at UT Health San Antonio.
“The coaches, the parents, and the athletes themselves really need to keep in mind that it’s not like a regular season,” Dr. Mooney says. She suggests gradually ramping up activity and paying attention to any pain. “That’s a good indicator that maybe you’re going too fast,” she adds.
Athletes should be mindful of other symptoms too when restarting exercise, especially after illness.
It is “very important that any athlete with recent COVID-19 monitor for new symptoms when they return to exercise,” says Jonathan Drezner, MD, a professor of family medicine at the University of Washington, Seattle. “A little fatigue from detraining may be expected, but exertional chest pain deserves more evaluation.”
Dr. Drezner – editor-in-chief of the British Journal of Sports Medicine and team doctor for the Seattle Seahawks – along with Dr. Baggish and colleagues, found a low prevalence of cardiac involvement in a study of more than 3,000 college athletes with prior SARS-CoV-2 infection.
“Any athlete, despite their initial symptom course, who has cardiopulmonary symptoms on return to exercise, particularly chest pain, should see their physician for a comprehensive cardiac evaluation,” Dr. Drezner says. “Cardiac MRI should be reserved for athletes with abnormal testing or when clinical suspicion of myocardial involvement is high.”
If an athlete had COVID-19 with moderate symptoms (such as fever, chills, or a flu-like syndrome) or cardiopulmonary symptoms (such as chest pain or shortness of breath), cardiac testing should be considered, he notes.
These symptoms “were associated with a higher prevalence of cardiac involvement,” Dr. Drezner said in an email. “Testing may include an ECG, echocardiogram (ultrasound), and troponin (blood test).”
For kids who test positive for SARS-CoV-2 but do not have symptoms, or their symptoms last less than 4 days, a phone call or telemedicine visit with their doctor may be enough to clear them to play, says Dr. Briskin, who’s also an assistant professor of pediatrics at Case Western Reserve University, Cleveland.
“This will allow the physician an opportunity to screen for any concerning cardiac signs or symptoms, update the patient’s electronic medical record with the recent COVID-19 infection, and provide appropriate guidance back to exercise,” she adds.
Dr. Baggish, Dr. Briskin, Dr. Mooney, and Dr. Drezner had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
As pandemic restrictions ease and young athletes once again take to fields, courts, tracks, and rinks, doctors are sharing ways to help them get back to sports safely.
That means taking steps to prevent COVID-19.
It also means trying to avoid sports-related injuries, which may be more likely if young athletes didn’t move around so much during the pandemic.
For adolescents who are eligible, getting a COVID-19 vaccine may be the most important thing they can do, according to the American Academy of Pediatrics.
“The AAP encourages all people who are eligible to receive the COVID-19 vaccine as soon as it is available,” the organization wrote in updated guidance on returning to sports and physical activity.
“I don’t think it can be overemphasized how important these vaccines are, both for the individual and at the community level,” says Aaron L. Baggish, MD, an associate professor of medicine at Harvard Medical School, Boston, and director of the Cardiovascular Performance Program at Massachusetts General Hospital in Boston.
Dr. Baggish, team cardiologist for the New England Patriots, the Boston Bruins, the New England Revolution, U.S. Men’s and Women’s Soccer, and U.S. Rowing, as well as medical director for the Boston Marathon, has studied the effects of COVID-19 on the heart in college athletes and written return-to-play recommendations for athletes of high school age and older.
“Millions of people have received these vaccines from age 12 up,” Dr. Baggish says. “The efficacy continues to look very durable and near complete, and the risk associated with vaccination is incredibly low, to the point where the risk-benefit ratio across the age spectrum, whether you’re athletic or not, strongly favors getting vaccinated. There is really no reason to hold off at this point.”
While outdoor activities are lower-risk for spreading COVID-19 and many people have been vaccinated, masks still should be worn in certain settings, the AAP notes.
“Indoor spaces that are crowded are still high-risk for COVID-19 transmission. And we recognize that not everyone in these settings may be vaccinated,” says Susannah Briskin, MD, lead author of the AAP guidance.
“So for indoor sporting events with spectators, in locker rooms or other small spaces such as a training room, and during shared car rides or school transportation to and from events, individuals should continue to mask,” adds Dr. Briskin, a pediatrician in the Division of Sports Medicine and fellowship director for the Primary Care Sports Medicine program at University Hospitals Rainbow Babies & Children’s Hospital.
For outdoor sports, athletes who are not fully vaccinated should be encouraged to wear masks on the sidelines and during group training and competition when they are within 3 feet of others for sustained amounts of time, according to the AAP.
Get back into exercise gradually
In general, athletes who have not been active for more than a month should resume exercise gradually, Dr. Briskin says. Starting at 25% of normal volume and increasing slowly over time – with 10% increases each week – is one rule of thumb.
“Those who have taken a prolonged break from sports are at a higher risk of injury when they return,” she notes. “Families should also be aware of an increased risk for heat-related illness if they are not acclimated.”
Caitlyn Mooney, MD, a team doctor for the University of Texas, San Antonio, has heard reports of doctors seeing more injuries like stress fractures. Some cases may relate to people going from “months of doing nothing to all of a sudden going back to sports,” says Dr. Mooney, who is also a clinical assistant professor of pediatrics and orthopedics at UT Health San Antonio.
“The coaches, the parents, and the athletes themselves really need to keep in mind that it’s not like a regular season,” Dr. Mooney says. She suggests gradually ramping up activity and paying attention to any pain. “That’s a good indicator that maybe you’re going too fast,” she adds.
Athletes should be mindful of other symptoms too when restarting exercise, especially after illness.
It is “very important that any athlete with recent COVID-19 monitor for new symptoms when they return to exercise,” says Jonathan Drezner, MD, a professor of family medicine at the University of Washington, Seattle. “A little fatigue from detraining may be expected, but exertional chest pain deserves more evaluation.”
Dr. Drezner – editor-in-chief of the British Journal of Sports Medicine and team doctor for the Seattle Seahawks – along with Dr. Baggish and colleagues, found a low prevalence of cardiac involvement in a study of more than 3,000 college athletes with prior SARS-CoV-2 infection.
“Any athlete, despite their initial symptom course, who has cardiopulmonary symptoms on return to exercise, particularly chest pain, should see their physician for a comprehensive cardiac evaluation,” Dr. Drezner says. “Cardiac MRI should be reserved for athletes with abnormal testing or when clinical suspicion of myocardial involvement is high.”
If an athlete had COVID-19 with moderate symptoms (such as fever, chills, or a flu-like syndrome) or cardiopulmonary symptoms (such as chest pain or shortness of breath), cardiac testing should be considered, he notes.
These symptoms “were associated with a higher prevalence of cardiac involvement,” Dr. Drezner said in an email. “Testing may include an ECG, echocardiogram (ultrasound), and troponin (blood test).”
For kids who test positive for SARS-CoV-2 but do not have symptoms, or their symptoms last less than 4 days, a phone call or telemedicine visit with their doctor may be enough to clear them to play, says Dr. Briskin, who’s also an assistant professor of pediatrics at Case Western Reserve University, Cleveland.
“This will allow the physician an opportunity to screen for any concerning cardiac signs or symptoms, update the patient’s electronic medical record with the recent COVID-19 infection, and provide appropriate guidance back to exercise,” she adds.
Dr. Baggish, Dr. Briskin, Dr. Mooney, and Dr. Drezner had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
As pandemic restrictions ease and young athletes once again take to fields, courts, tracks, and rinks, doctors are sharing ways to help them get back to sports safely.
That means taking steps to prevent COVID-19.
It also means trying to avoid sports-related injuries, which may be more likely if young athletes didn’t move around so much during the pandemic.
For adolescents who are eligible, getting a COVID-19 vaccine may be the most important thing they can do, according to the American Academy of Pediatrics.
“The AAP encourages all people who are eligible to receive the COVID-19 vaccine as soon as it is available,” the organization wrote in updated guidance on returning to sports and physical activity.
“I don’t think it can be overemphasized how important these vaccines are, both for the individual and at the community level,” says Aaron L. Baggish, MD, an associate professor of medicine at Harvard Medical School, Boston, and director of the Cardiovascular Performance Program at Massachusetts General Hospital in Boston.
Dr. Baggish, team cardiologist for the New England Patriots, the Boston Bruins, the New England Revolution, U.S. Men’s and Women’s Soccer, and U.S. Rowing, as well as medical director for the Boston Marathon, has studied the effects of COVID-19 on the heart in college athletes and written return-to-play recommendations for athletes of high school age and older.
“Millions of people have received these vaccines from age 12 up,” Dr. Baggish says. “The efficacy continues to look very durable and near complete, and the risk associated with vaccination is incredibly low, to the point where the risk-benefit ratio across the age spectrum, whether you’re athletic or not, strongly favors getting vaccinated. There is really no reason to hold off at this point.”
While outdoor activities are lower-risk for spreading COVID-19 and many people have been vaccinated, masks still should be worn in certain settings, the AAP notes.
“Indoor spaces that are crowded are still high-risk for COVID-19 transmission. And we recognize that not everyone in these settings may be vaccinated,” says Susannah Briskin, MD, lead author of the AAP guidance.
“So for indoor sporting events with spectators, in locker rooms or other small spaces such as a training room, and during shared car rides or school transportation to and from events, individuals should continue to mask,” adds Dr. Briskin, a pediatrician in the Division of Sports Medicine and fellowship director for the Primary Care Sports Medicine program at University Hospitals Rainbow Babies & Children’s Hospital.
For outdoor sports, athletes who are not fully vaccinated should be encouraged to wear masks on the sidelines and during group training and competition when they are within 3 feet of others for sustained amounts of time, according to the AAP.
Get back into exercise gradually
In general, athletes who have not been active for more than a month should resume exercise gradually, Dr. Briskin says. Starting at 25% of normal volume and increasing slowly over time – with 10% increases each week – is one rule of thumb.
“Those who have taken a prolonged break from sports are at a higher risk of injury when they return,” she notes. “Families should also be aware of an increased risk for heat-related illness if they are not acclimated.”
Caitlyn Mooney, MD, a team doctor for the University of Texas, San Antonio, has heard reports of doctors seeing more injuries like stress fractures. Some cases may relate to people going from “months of doing nothing to all of a sudden going back to sports,” says Dr. Mooney, who is also a clinical assistant professor of pediatrics and orthopedics at UT Health San Antonio.
“The coaches, the parents, and the athletes themselves really need to keep in mind that it’s not like a regular season,” Dr. Mooney says. She suggests gradually ramping up activity and paying attention to any pain. “That’s a good indicator that maybe you’re going too fast,” she adds.
Athletes should be mindful of other symptoms too when restarting exercise, especially after illness.
It is “very important that any athlete with recent COVID-19 monitor for new symptoms when they return to exercise,” says Jonathan Drezner, MD, a professor of family medicine at the University of Washington, Seattle. “A little fatigue from detraining may be expected, but exertional chest pain deserves more evaluation.”
Dr. Drezner – editor-in-chief of the British Journal of Sports Medicine and team doctor for the Seattle Seahawks – along with Dr. Baggish and colleagues, found a low prevalence of cardiac involvement in a study of more than 3,000 college athletes with prior SARS-CoV-2 infection.
“Any athlete, despite their initial symptom course, who has cardiopulmonary symptoms on return to exercise, particularly chest pain, should see their physician for a comprehensive cardiac evaluation,” Dr. Drezner says. “Cardiac MRI should be reserved for athletes with abnormal testing or when clinical suspicion of myocardial involvement is high.”
If an athlete had COVID-19 with moderate symptoms (such as fever, chills, or a flu-like syndrome) or cardiopulmonary symptoms (such as chest pain or shortness of breath), cardiac testing should be considered, he notes.
These symptoms “were associated with a higher prevalence of cardiac involvement,” Dr. Drezner said in an email. “Testing may include an ECG, echocardiogram (ultrasound), and troponin (blood test).”
For kids who test positive for SARS-CoV-2 but do not have symptoms, or their symptoms last less than 4 days, a phone call or telemedicine visit with their doctor may be enough to clear them to play, says Dr. Briskin, who’s also an assistant professor of pediatrics at Case Western Reserve University, Cleveland.
“This will allow the physician an opportunity to screen for any concerning cardiac signs or symptoms, update the patient’s electronic medical record with the recent COVID-19 infection, and provide appropriate guidance back to exercise,” she adds.
Dr. Baggish, Dr. Briskin, Dr. Mooney, and Dr. Drezner had no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Rapid update to ASCO breast cancer guidelines after OlympiA data
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
The American Society of Clinical Oncology (ASCO) now recommends offering 1 year of adjuvant olaparib therapy to patients with early-stage HER2-negative, BRCA-mutated breast cancer who have completed chemotherapy and local treatment.
The change in management of hereditary breast cancer is outlined in an update to 2020 guidelines, and it comes as a “rapid recommendation” on the heels of the phase 3 OlympiA trial results, which indicated a 42% improvement in invasive and distant disease-free survival with the PARP inhibitor olaparib (Lynparza) in comparison with placebo.
The OlympiA trial results, as reported by this news organization, were presented during the plenary session of the ASCO 2021 annual meeting and were published June 3 in The New England Journal of Medicine.
“These clear and positive data prompted ASCO to issue a provisional update of the guideline recommendation focused specifically on the role of olaparib in this setting,” states an ASCO press release.
The previous 2020 guidelines stated: “There are insufficient data ... to recommend a PARP inhibitor for patients with nonmetastatic breast cancer.” The OlympiA trial changed that. ASCO now recommends that patients with early-stage, HER2-negative, BRCA-mutated breast cancer at high risk for recurrence be offered olaparib after completion of chemotherapy and local treatment, including radiotherapy.
The update states: “For those who had surgery first, adjuvant olaparib is recommended for patients with TNBC [triple-negative breast cancer] and tumor size greater than 2 cm or any involved axillary nodes. For patients with hormone receptor–positive disease, adjuvant olaparib is recommended for those with at least four involved axillary lymph nodes. For patients who had neoadjuvant chemotherapy, adjuvant olaparib is recommended for patients with TNBC and any residual cancer. Adjuvant olaparib is recommended for patients with residual disease and an estrogen receptor status and tumor grade (CSP+EG) score greater than or equal to 3.”
“The findings from the OlympiA trial – presented just last week – mark a significant improvement in the care of these patients,” Julie Garlow, MD, ASCO’s executive vice president and chief medical officer, states in the ASCO press release.
“ASCO’s Expert Guideline Panel and Evidence-based Medicine Committee noted this and then quickly produced and provisionally approved this guideline update to enable patients to begin to benefit from this research advance as quickly as possible,” she said.
A formal assessment and submission for publication in the Journal of Clinical Oncology will follow the release notes.
A version of this article first appeared on Medscape.com.
Stroke risk in new-onset atrial fib goes up with greater alcohol intake
There’s abundant evidence linking higher alcohol intake levels to greater stroke risk and, separately, increasing risk for new-onset atrial fibrillation (AFib). Less settled is whether moderate to heavy drinking worsens the risk for stroke in patients already in AFib and whether giving up alcohol can attenuate that risk. A new observational study suggests the answer to both questions is yes.
The risk for ischemic stroke was only around 1% over about 5 years in a Korean nationwide cohort of almost 98,000 patients with new-onset AFib. About half the patients followed were nondrinkers, as they had been before the study, 13% became abstinent soon after their AFib diagnosis, and 36% were currently drinkers.
But stroke risk went up about 30% with “moderate” current alcohol intake, compared with no intake, and by more than 40% for current drinkers reporting “heavy” alcohol intake, researchers found in an adjusted analysis.
However, abstainers who had mild to moderate alcohol-intake levels before their AFib diagnosis “had a similar risk of ischemic stroke as nondrinkers,” write the authors, led by So-Ryoung Lee, MD, PhD, and colleagues, Seoul National University Hospital, Republic of Korea, in their report published June 7 in the European Heart Journal. In a secondary analysis, binge drinking was also independently associated with risk for ischemic stroke.
The findings suggest that “alcohol abstinence after the diagnosis of AFib could reduce the risk of ischemic stroke,” they conclude. “Lifestyle interventions, including attention to alcohol consumption, should be encouraged as part of a comprehensive approach in the management of patients with a new diagnosis of AFib” for lowering the risk for stroke and other clinical outcomes.
“These results are pretty comparable to those obtained in the more general population,” David Conen, MD, MPH, not connected to the analysis, told this news organization.
In the study’s population with new-onset AFib, there is an alcohol-dependent risk for stroke “that goes up with increasing alcohol intake, which is more or less similar to that found without atrial fibrillation in previous studies,” said Dr. Conen, from the Population Health Research Institute, McMaster University, Hamilton, Ont.
The study, “which overall I think is very well done,” he said, is noteworthy for also suggesting that binge drinking, which was scrutinized in a secondary analysis, appeared independently to worsen the risk for stroke in its AFib population.
Dr. Conen said the observed 1% overall risk for stroke was very similar to the rate he and his colleagues saw in a recent combined analysis of two European cohorts with AFib that was usually longer standing; the median was 3 years. That analysis, in contrast, showed no significant association between increasing levels of alcohol intake and risk for stroke or systemic embolism.
However, “our confidence limits did not exclude the possibility of a small to moderate association,” he said. Given that, and the current study from Korea, there might indeed be “a weak association between alcohol consumption and stroke” in patients with AFib.
“Their results are just more precise because of the larger sample size. That’s why they were able to show those associations,” said Dr. Conen, who was senior author on the earlier report, which covered a pooled analysis of 3,852 patients with AFib in the BEAT-AF and SWISS-AF cohort studies. It was published January 25 in CMAJ, with lead author Philipp Reddiess, MD, Cardiovascular Research Institute Basel, Switzerland.
The two published studies contrast in other ways that are worth noting and together suggest the stroke rate might have been 1% in both by chance, Dr. Conen said. “The populations were pretty different.”
In the earlier study, for example, the overwhelmingly European patients had more comorbidities and had been in AFib for much longer; their mean age was 71 years; and 84% were on oral anticoagulation (OAC).
In contrast, the Korean cohort averaged 61 years in age and only about 24% were taking oral anticoagulants. Given their distribution of CHA2DS2-VASc scores and mean score of 2.3, more than twice as many should have been on OAC, Dr. Conen speculated. “Even if you take into account that some patients may have contraindications, this is clearly an underanticoagulated population.”
The European cohort might have been “a little bit more representative because atrial fibrillation is a disease of the elderly,” Dr. Conen said, but “the Korean paper has the advantage of being a population-based study.”
It involved 97,869 patients from a Korean national data base who were newly diagnosed with AFib from 2010 to 2016. Of the total, 49,781 (51%) were continuously nondrinkers before and after their diagnosis; 12,789 (13%) abstained from alcohol only after their AFib diagnosis; and 35,299 (36%) were drinkers during the follow-up, either because they continued to drink or newly started after their diagnosis.
Of the cohort, 3,120 were diagnosed with new ischemic stroke over a follow-up of 310,926 person-years, for a rate of 1 per 100 person-years.
The adjusted hazard ratio (HR) for ischemic stroke over a 5-year follow-up, compared with nondrinkers, was:
- 1.127 (95% confidence interval, 1.003-1.266) among abstainers
- 1.280 (95% CI, 1.166-1.405) for current drinkers
The corresponding HR, compared with current drinkers, was:
- 0.781 (95% CI, 0.712-0.858) for nondrinkers
- 0.880 (95% CI, 0.782-0.990) among abstainers
No significant interactions with ischemic stroke risk were observed in groups by sex, age, CHA2DS2-VASc score, or smoking status. The risk rose consistently with current drinking levels.
The overall stroke rate of 1% per year is “very low,” and “the absolute differences are small, even though there is a clear significant trend from nondrinking to drinking,” Dr. Conen said.
However, “the difference becomes more sizable when you compare heavy drinking to abstinence.”
Dr. Lee reports no conflicts of interest; disclosures for the other authors are in their report. Dr. Conen reports receiving speaker fees from Servier Canada; disclosures for the other authors are in their report.
A version of this article first appeared on Medscape.com.
There’s abundant evidence linking higher alcohol intake levels to greater stroke risk and, separately, increasing risk for new-onset atrial fibrillation (AFib). Less settled is whether moderate to heavy drinking worsens the risk for stroke in patients already in AFib and whether giving up alcohol can attenuate that risk. A new observational study suggests the answer to both questions is yes.
The risk for ischemic stroke was only around 1% over about 5 years in a Korean nationwide cohort of almost 98,000 patients with new-onset AFib. About half the patients followed were nondrinkers, as they had been before the study, 13% became abstinent soon after their AFib diagnosis, and 36% were currently drinkers.
But stroke risk went up about 30% with “moderate” current alcohol intake, compared with no intake, and by more than 40% for current drinkers reporting “heavy” alcohol intake, researchers found in an adjusted analysis.
However, abstainers who had mild to moderate alcohol-intake levels before their AFib diagnosis “had a similar risk of ischemic stroke as nondrinkers,” write the authors, led by So-Ryoung Lee, MD, PhD, and colleagues, Seoul National University Hospital, Republic of Korea, in their report published June 7 in the European Heart Journal. In a secondary analysis, binge drinking was also independently associated with risk for ischemic stroke.
The findings suggest that “alcohol abstinence after the diagnosis of AFib could reduce the risk of ischemic stroke,” they conclude. “Lifestyle interventions, including attention to alcohol consumption, should be encouraged as part of a comprehensive approach in the management of patients with a new diagnosis of AFib” for lowering the risk for stroke and other clinical outcomes.
“These results are pretty comparable to those obtained in the more general population,” David Conen, MD, MPH, not connected to the analysis, told this news organization.
In the study’s population with new-onset AFib, there is an alcohol-dependent risk for stroke “that goes up with increasing alcohol intake, which is more or less similar to that found without atrial fibrillation in previous studies,” said Dr. Conen, from the Population Health Research Institute, McMaster University, Hamilton, Ont.
The study, “which overall I think is very well done,” he said, is noteworthy for also suggesting that binge drinking, which was scrutinized in a secondary analysis, appeared independently to worsen the risk for stroke in its AFib population.
Dr. Conen said the observed 1% overall risk for stroke was very similar to the rate he and his colleagues saw in a recent combined analysis of two European cohorts with AFib that was usually longer standing; the median was 3 years. That analysis, in contrast, showed no significant association between increasing levels of alcohol intake and risk for stroke or systemic embolism.
However, “our confidence limits did not exclude the possibility of a small to moderate association,” he said. Given that, and the current study from Korea, there might indeed be “a weak association between alcohol consumption and stroke” in patients with AFib.
“Their results are just more precise because of the larger sample size. That’s why they were able to show those associations,” said Dr. Conen, who was senior author on the earlier report, which covered a pooled analysis of 3,852 patients with AFib in the BEAT-AF and SWISS-AF cohort studies. It was published January 25 in CMAJ, with lead author Philipp Reddiess, MD, Cardiovascular Research Institute Basel, Switzerland.
The two published studies contrast in other ways that are worth noting and together suggest the stroke rate might have been 1% in both by chance, Dr. Conen said. “The populations were pretty different.”
In the earlier study, for example, the overwhelmingly European patients had more comorbidities and had been in AFib for much longer; their mean age was 71 years; and 84% were on oral anticoagulation (OAC).
In contrast, the Korean cohort averaged 61 years in age and only about 24% were taking oral anticoagulants. Given their distribution of CHA2DS2-VASc scores and mean score of 2.3, more than twice as many should have been on OAC, Dr. Conen speculated. “Even if you take into account that some patients may have contraindications, this is clearly an underanticoagulated population.”
The European cohort might have been “a little bit more representative because atrial fibrillation is a disease of the elderly,” Dr. Conen said, but “the Korean paper has the advantage of being a population-based study.”
It involved 97,869 patients from a Korean national data base who were newly diagnosed with AFib from 2010 to 2016. Of the total, 49,781 (51%) were continuously nondrinkers before and after their diagnosis; 12,789 (13%) abstained from alcohol only after their AFib diagnosis; and 35,299 (36%) were drinkers during the follow-up, either because they continued to drink or newly started after their diagnosis.
Of the cohort, 3,120 were diagnosed with new ischemic stroke over a follow-up of 310,926 person-years, for a rate of 1 per 100 person-years.
The adjusted hazard ratio (HR) for ischemic stroke over a 5-year follow-up, compared with nondrinkers, was:
- 1.127 (95% confidence interval, 1.003-1.266) among abstainers
- 1.280 (95% CI, 1.166-1.405) for current drinkers
The corresponding HR, compared with current drinkers, was:
- 0.781 (95% CI, 0.712-0.858) for nondrinkers
- 0.880 (95% CI, 0.782-0.990) among abstainers
No significant interactions with ischemic stroke risk were observed in groups by sex, age, CHA2DS2-VASc score, or smoking status. The risk rose consistently with current drinking levels.
The overall stroke rate of 1% per year is “very low,” and “the absolute differences are small, even though there is a clear significant trend from nondrinking to drinking,” Dr. Conen said.
However, “the difference becomes more sizable when you compare heavy drinking to abstinence.”
Dr. Lee reports no conflicts of interest; disclosures for the other authors are in their report. Dr. Conen reports receiving speaker fees from Servier Canada; disclosures for the other authors are in their report.
A version of this article first appeared on Medscape.com.
There’s abundant evidence linking higher alcohol intake levels to greater stroke risk and, separately, increasing risk for new-onset atrial fibrillation (AFib). Less settled is whether moderate to heavy drinking worsens the risk for stroke in patients already in AFib and whether giving up alcohol can attenuate that risk. A new observational study suggests the answer to both questions is yes.
The risk for ischemic stroke was only around 1% over about 5 years in a Korean nationwide cohort of almost 98,000 patients with new-onset AFib. About half the patients followed were nondrinkers, as they had been before the study, 13% became abstinent soon after their AFib diagnosis, and 36% were currently drinkers.
But stroke risk went up about 30% with “moderate” current alcohol intake, compared with no intake, and by more than 40% for current drinkers reporting “heavy” alcohol intake, researchers found in an adjusted analysis.
However, abstainers who had mild to moderate alcohol-intake levels before their AFib diagnosis “had a similar risk of ischemic stroke as nondrinkers,” write the authors, led by So-Ryoung Lee, MD, PhD, and colleagues, Seoul National University Hospital, Republic of Korea, in their report published June 7 in the European Heart Journal. In a secondary analysis, binge drinking was also independently associated with risk for ischemic stroke.
The findings suggest that “alcohol abstinence after the diagnosis of AFib could reduce the risk of ischemic stroke,” they conclude. “Lifestyle interventions, including attention to alcohol consumption, should be encouraged as part of a comprehensive approach in the management of patients with a new diagnosis of AFib” for lowering the risk for stroke and other clinical outcomes.
“These results are pretty comparable to those obtained in the more general population,” David Conen, MD, MPH, not connected to the analysis, told this news organization.
In the study’s population with new-onset AFib, there is an alcohol-dependent risk for stroke “that goes up with increasing alcohol intake, which is more or less similar to that found without atrial fibrillation in previous studies,” said Dr. Conen, from the Population Health Research Institute, McMaster University, Hamilton, Ont.
The study, “which overall I think is very well done,” he said, is noteworthy for also suggesting that binge drinking, which was scrutinized in a secondary analysis, appeared independently to worsen the risk for stroke in its AFib population.
Dr. Conen said the observed 1% overall risk for stroke was very similar to the rate he and his colleagues saw in a recent combined analysis of two European cohorts with AFib that was usually longer standing; the median was 3 years. That analysis, in contrast, showed no significant association between increasing levels of alcohol intake and risk for stroke or systemic embolism.
However, “our confidence limits did not exclude the possibility of a small to moderate association,” he said. Given that, and the current study from Korea, there might indeed be “a weak association between alcohol consumption and stroke” in patients with AFib.
“Their results are just more precise because of the larger sample size. That’s why they were able to show those associations,” said Dr. Conen, who was senior author on the earlier report, which covered a pooled analysis of 3,852 patients with AFib in the BEAT-AF and SWISS-AF cohort studies. It was published January 25 in CMAJ, with lead author Philipp Reddiess, MD, Cardiovascular Research Institute Basel, Switzerland.
The two published studies contrast in other ways that are worth noting and together suggest the stroke rate might have been 1% in both by chance, Dr. Conen said. “The populations were pretty different.”
In the earlier study, for example, the overwhelmingly European patients had more comorbidities and had been in AFib for much longer; their mean age was 71 years; and 84% were on oral anticoagulation (OAC).
In contrast, the Korean cohort averaged 61 years in age and only about 24% were taking oral anticoagulants. Given their distribution of CHA2DS2-VASc scores and mean score of 2.3, more than twice as many should have been on OAC, Dr. Conen speculated. “Even if you take into account that some patients may have contraindications, this is clearly an underanticoagulated population.”
The European cohort might have been “a little bit more representative because atrial fibrillation is a disease of the elderly,” Dr. Conen said, but “the Korean paper has the advantage of being a population-based study.”
It involved 97,869 patients from a Korean national data base who were newly diagnosed with AFib from 2010 to 2016. Of the total, 49,781 (51%) were continuously nondrinkers before and after their diagnosis; 12,789 (13%) abstained from alcohol only after their AFib diagnosis; and 35,299 (36%) were drinkers during the follow-up, either because they continued to drink or newly started after their diagnosis.
Of the cohort, 3,120 were diagnosed with new ischemic stroke over a follow-up of 310,926 person-years, for a rate of 1 per 100 person-years.
The adjusted hazard ratio (HR) for ischemic stroke over a 5-year follow-up, compared with nondrinkers, was:
- 1.127 (95% confidence interval, 1.003-1.266) among abstainers
- 1.280 (95% CI, 1.166-1.405) for current drinkers
The corresponding HR, compared with current drinkers, was:
- 0.781 (95% CI, 0.712-0.858) for nondrinkers
- 0.880 (95% CI, 0.782-0.990) among abstainers
No significant interactions with ischemic stroke risk were observed in groups by sex, age, CHA2DS2-VASc score, or smoking status. The risk rose consistently with current drinking levels.
The overall stroke rate of 1% per year is “very low,” and “the absolute differences are small, even though there is a clear significant trend from nondrinking to drinking,” Dr. Conen said.
However, “the difference becomes more sizable when you compare heavy drinking to abstinence.”
Dr. Lee reports no conflicts of interest; disclosures for the other authors are in their report. Dr. Conen reports receiving speaker fees from Servier Canada; disclosures for the other authors are in their report.
A version of this article first appeared on Medscape.com.
New data on COVID-19’s cognitive fallout
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.
Investigators found cognitive changes, depression, and PTSD in infected patients, both in the subacute phase and 10 months after hospital discharge.
“We showed that cognitive and behavioral alterations are associated with COVID-19 infection within 2 months from hospital discharge and that they partially persist in the post-COVID phase,” study investigator Elisa Canu, PhD, neuroimaging research unit, division of neuroscience, IRCCS San Raffaele Scientific Institute, Milan, told a press briefing.
The findings were presented at the annual congress of the European Academy of Neurology.
Executive dysfunction
Previous research suggests about 30% of COVID-19 survivors have cognitive disturbances and 30%-40% have psychopathological disorders including anxiety and depression, said Dr. Canu.
These disturbances have been associated with the severity of acute-phase respiratory symptoms, infection-triggered neuroinflammation, cerebrovascular alterations, and/or neurodegeneration.
However, it’s unclear whether these disturbances persist in the post-COVID phase.
To investigate, the researchers explored cognitive and psychopathological features in 49 patients with confirmed COVID-19 admitted to a hospital ED. They examined these factors at 2 months (subacute phase) and at 10 months (post-COVID phase).
Participants had an average age of 61 years (age range, 40-75 years) and 73% were men. Most had at least one cardiovascular risk factor such as hypertension (55%), smoking (22%), and dyslipidemia (18%).
At hospital admission, 71% had an abnormal neurologic exam, 59% had hypogeusia (reduced sense of taste), 45% hyposmia (reduced sense of smell), 39% headache, and 20% confusion or drowsiness. During hospitalization, 27% had noninvasive ventilation.
In addition to cognitive and neurologic assessments, participants underwent MRI 2 months after hospital discharge. Researchers obtained data on gray matter, white matter, and total brain volume.
At 2 months post discharge, 53% of patients presented with at least one cognitive deficit. Many deficits related to executive function including difficulty planning, attention, and problem solving (16%).
However, some participants had memory issues (6%) or visuospatial disturbances (6%). Almost a quarter (23%) presented with a combination of symptoms related to executive dysfunction.
Low oxygen tied to more cognitive deficits
More than one-third of patients experienced symptoms of depression (16%) or PTSD (18%).
Patients younger than 50 years had more executive dysfunction, with these symptoms affecting 75% of younger patients. “Our explanation for that is that younger people had a milder clinical profile regarding COVID, so they were cared for at home,” said Dr. Canu.
While in hospital, patients may be on “continued alert” and receive structured interventions for cognitive and behavioral issues, she said.
More severe respiratory symptoms at hospital admission were significantly associated with deficits during the subacute phase (P = .002 for information processing).
“Low levels of oxygen in the brain could lead to confusion, headache, and brain fog, and cause the cognitive disturbances that we see,” said Dr. Canu.
White-matter hyperintensities were linked to cognitive deficits during this phase (P < .001 for verbal memory and delayed recall).
“These white-matter lesions are probably preexisting due to cardiovascular risk factors that were present in our population and may have amplified the memory disturbances we saw,” commented Dr. Canu.
The investigators did not find a significant relationship between cognitive performance and brain volume. Dr. Canu noted that cognitive and psychopathological disturbances are linked. For instance, she said, a patient with PTSD or depression may also have problems with attention or memory.
In the post-COVID phase, cognitive symptoms were reduced from 53% to 36%; again, the most common deficit was combined executive dysfunction symptoms. Depression persisted in 15% of patients and PTSD in 18%.
“We still don’t know if these alterations are a consequence of the infection,” said Dr. Canu. “And we don’t know whether the deficits are reversible or are part of a neurodegenerative process.”
The researchers plan to follow these patients further. “We definitely need longer follow-up and bigger populations, if possible, to see if these cognitive and psychopathological disturbances can improve in some way,” said Dr. Canu.
The study results underline the need for neuropsychological and neurologic monitoring in COVID patients. Cognitive stimulation training and physical activity, preferably outdoors, could be beneficial, Dr. Canu added.
A version of this article first appeared on Medscape.com.