User login
Tenalisib receives orphan designation for CTCL

The US Food and Drug Administration (FDA) has granted orphan drug designation to tenalisib for treatment of cutaneous T-cell lymphoma (CTCL).
Tenalisib (formerly RP6530) is a dual PI3K delta/gamma inhibitor under development by Rhizen Pharmaceuticals SA.
The FDA previously granted tenalisib fast track and orphan drug designations for the treatment of peripheral T-cell lymphoma (PTCL).
Tenalisib has been investigated in a phase 1 trial of patients with relapsed/refractory PTCL and CTCL. Results from this trial were presented at the 10th Annual T-cell Lymphoma Forum in February.
The data included 55 patients—28 with CTCL and 27 with PTCL—who received varying doses of tenalisib. The maximum tolerated dose was an 800 mg daily fasting dose.
Fourteen PTCL patients were evaluable for efficacy, and 7 responded (50%) to treatment. Three patients had a complete response, and 4 had a partial response.
Eighteen CTCL patients were evaluable for efficacy. Eight patients responded (44%), all with partial responses.
In the entire cohort, treatment-related adverse events (AEs) of grade 3 or higher included transaminitis (20%), rash (5%), neutropenia (2%), hypophosphatemia (2%), international normalized ratio increase (2%), sepsis (2%), pyrexia (2%), and diplopia secondary to neuropathy (2%).
Four CTCL patients stopped tenalisib due to a treatment-related AE—transaminitis, sepsis, diarrhea, and diplopia secondary to neuropathy. One PTCL patient stopped treatment due to a related AE, which was transaminitis.
About orphan and fast track designations
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
The US Food and Drug Administration (FDA) has granted orphan drug designation to tenalisib for treatment of cutaneous T-cell lymphoma (CTCL).
Tenalisib (formerly RP6530) is a dual PI3K delta/gamma inhibitor under development by Rhizen Pharmaceuticals SA.
The FDA previously granted tenalisib fast track and orphan drug designations for the treatment of peripheral T-cell lymphoma (PTCL).
Tenalisib has been investigated in a phase 1 trial of patients with relapsed/refractory PTCL and CTCL. Results from this trial were presented at the 10th Annual T-cell Lymphoma Forum in February.
The data included 55 patients—28 with CTCL and 27 with PTCL—who received varying doses of tenalisib. The maximum tolerated dose was an 800 mg daily fasting dose.
Fourteen PTCL patients were evaluable for efficacy, and 7 responded (50%) to treatment. Three patients had a complete response, and 4 had a partial response.
Eighteen CTCL patients were evaluable for efficacy. Eight patients responded (44%), all with partial responses.
In the entire cohort, treatment-related adverse events (AEs) of grade 3 or higher included transaminitis (20%), rash (5%), neutropenia (2%), hypophosphatemia (2%), international normalized ratio increase (2%), sepsis (2%), pyrexia (2%), and diplopia secondary to neuropathy (2%).
Four CTCL patients stopped tenalisib due to a treatment-related AE—transaminitis, sepsis, diarrhea, and diplopia secondary to neuropathy. One PTCL patient stopped treatment due to a related AE, which was transaminitis.
About orphan and fast track designations
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
The US Food and Drug Administration (FDA) has granted orphan drug designation to tenalisib for treatment of cutaneous T-cell lymphoma (CTCL).
Tenalisib (formerly RP6530) is a dual PI3K delta/gamma inhibitor under development by Rhizen Pharmaceuticals SA.
The FDA previously granted tenalisib fast track and orphan drug designations for the treatment of peripheral T-cell lymphoma (PTCL).
Tenalisib has been investigated in a phase 1 trial of patients with relapsed/refractory PTCL and CTCL. Results from this trial were presented at the 10th Annual T-cell Lymphoma Forum in February.
The data included 55 patients—28 with CTCL and 27 with PTCL—who received varying doses of tenalisib. The maximum tolerated dose was an 800 mg daily fasting dose.
Fourteen PTCL patients were evaluable for efficacy, and 7 responded (50%) to treatment. Three patients had a complete response, and 4 had a partial response.
Eighteen CTCL patients were evaluable for efficacy. Eight patients responded (44%), all with partial responses.
In the entire cohort, treatment-related adverse events (AEs) of grade 3 or higher included transaminitis (20%), rash (5%), neutropenia (2%), hypophosphatemia (2%), international normalized ratio increase (2%), sepsis (2%), pyrexia (2%), and diplopia secondary to neuropathy (2%).
Four CTCL patients stopped tenalisib due to a treatment-related AE—transaminitis, sepsis, diarrhea, and diplopia secondary to neuropathy. One PTCL patient stopped treatment due to a related AE, which was transaminitis.
About orphan and fast track designations
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved.
The FDA’s fast track drug development program is designed to expedite clinical development and submission of new drug applications for medicines with the potential to treat serious or life-threatening conditions and address unmet medical needs.
Fast track designation facilitates frequent interactions with the FDA review team, including meetings to discuss all aspects of development to support a drug’s approval, and also provides the opportunity to submit sections of a new drug application on a rolling basis as data become available.
Duvelisib NDA granted priority review

The US Food and Drug Administration (FDA) has accepted for priority review the new drug application (NDA) for duvelisib, a dual PI3K delta/gamma inhibitor.
With this NDA, Verastem, Inc., is seeking full approval of duvelisib for the treatment of relapsed or refractory chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and accelerated approval of the drug for the treatment of relapsed or refractory follicular lymphoma (FL).
The FDA expects to make a decision on the NDA by October 5, 2018.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The application for duvelisib is supported by data from DUO™, a randomized, phase 3 study of patients with relapsed or refractory CLL/SLL, and DYNAMO™, a phase 2 study of patients with refractory indolent non-Hodgkin lymphoma.
Phase 3 DUO trial
Results from DUO were presented at the 2017 ASH Annual Meeting in December.
This study included 319 CLL/SLL patients who were randomized 1:1 to receive either duvelisib (25 mg orally twice daily) or ofatumumab (initial infusion of 300 mg followed by 7 weekly infusions and 4 monthly infusions of 2000 mg).
The study’s primary endpoint was met, as duvelisib conferred a significant improvement in median progression-free survival (PFS) over ofatumumab.
Per an independent review committee, the median PFS was 13.3 months with duvelisib and 9.9 months with ofatumumab (hazard ratio=0.52; P<0.0001). Duvelisib maintained a PFS advantage in all patient subgroups analyzed.
The overall response rate was 73.8% with duvelisib and 45.3% with ofatumumab (P<0.0001). The complete response rate was 0.6% in both arms.
Overall survival (OS) was similar in the duvelisib and ofatumumab arms (hazard ratio=0.99; P=0.4807). The median OS was not reached in either arm.
The most common grade 3 or higher adverse events (AEs)—in the duvelisib and ofatumumab arms, respectively—were neutropenia (30% vs 17%), anemia (13% vs 5%), diarrhea (15% vs 1%), pneumonia (14% vs 1%), and colitis (12% vs 1%).
Thirty-five percent of patients discontinued duvelisib due to an AE.
Severe opportunistic infections occurred in 6% of duvelisib recipients—bronchopulmonary aspergillosis (n=4), fungal infection (n=2), Pneumocystis jirovecii pneumonia (n=2), and cytomegalovirus colitis (n=1).
There were 4 deaths related to duvelisib—staphylococcal pneumonia (n=2), general physical health deterioration (n=1), and sepsis (n=1).
Phase 2 DYNAMO trial
Results from DYNAMO were presented at the 22nd EHA Congress (abstract S777) in June 2017.
This trial enrolled patients with indolent non-Hodgkin lymphoma whose disease was refractory to both rituximab and chemotherapy or radioimmunotherapy.
There were 83 patients with FL. They had a median of 3 prior anticancer regimens (range, 1-10).
The patients received duvelisib at 25 mg orally twice daily until disease progression or unacceptable toxicity.
The overall response rate, per an independent review committee, was 43%. One patient achieved a complete response, and 35 had a partial response. The median duration of response was 7.9 months.
The median PFS was 8.3 months, and the median OS was 27.8 months.
The most common grade 3 or higher AEs were neutropenia (22%), anemia (13%), diarrhea (16%), lipase increase (10%), and thrombocytopenia (9%).
There were 2 serious opportunistic infections—Pneumocystis pneumonia and fungal pneumonia.
There were 3 deaths attributed to duvelisib—toxic epidermal necrolysis/sepsis syndrome (n=1), drug reaction/eosinophilia/systemic symptoms (n=1), and pneumonitis/pneumonia (n=1).
The US Food and Drug Administration (FDA) has accepted for priority review the new drug application (NDA) for duvelisib, a dual PI3K delta/gamma inhibitor.
With this NDA, Verastem, Inc., is seeking full approval of duvelisib for the treatment of relapsed or refractory chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and accelerated approval of the drug for the treatment of relapsed or refractory follicular lymphoma (FL).
The FDA expects to make a decision on the NDA by October 5, 2018.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The application for duvelisib is supported by data from DUO™, a randomized, phase 3 study of patients with relapsed or refractory CLL/SLL, and DYNAMO™, a phase 2 study of patients with refractory indolent non-Hodgkin lymphoma.
Phase 3 DUO trial
Results from DUO were presented at the 2017 ASH Annual Meeting in December.
This study included 319 CLL/SLL patients who were randomized 1:1 to receive either duvelisib (25 mg orally twice daily) or ofatumumab (initial infusion of 300 mg followed by 7 weekly infusions and 4 monthly infusions of 2000 mg).
The study’s primary endpoint was met, as duvelisib conferred a significant improvement in median progression-free survival (PFS) over ofatumumab.
Per an independent review committee, the median PFS was 13.3 months with duvelisib and 9.9 months with ofatumumab (hazard ratio=0.52; P<0.0001). Duvelisib maintained a PFS advantage in all patient subgroups analyzed.
The overall response rate was 73.8% with duvelisib and 45.3% with ofatumumab (P<0.0001). The complete response rate was 0.6% in both arms.
Overall survival (OS) was similar in the duvelisib and ofatumumab arms (hazard ratio=0.99; P=0.4807). The median OS was not reached in either arm.
The most common grade 3 or higher adverse events (AEs)—in the duvelisib and ofatumumab arms, respectively—were neutropenia (30% vs 17%), anemia (13% vs 5%), diarrhea (15% vs 1%), pneumonia (14% vs 1%), and colitis (12% vs 1%).
Thirty-five percent of patients discontinued duvelisib due to an AE.
Severe opportunistic infections occurred in 6% of duvelisib recipients—bronchopulmonary aspergillosis (n=4), fungal infection (n=2), Pneumocystis jirovecii pneumonia (n=2), and cytomegalovirus colitis (n=1).
There were 4 deaths related to duvelisib—staphylococcal pneumonia (n=2), general physical health deterioration (n=1), and sepsis (n=1).
Phase 2 DYNAMO trial
Results from DYNAMO were presented at the 22nd EHA Congress (abstract S777) in June 2017.
This trial enrolled patients with indolent non-Hodgkin lymphoma whose disease was refractory to both rituximab and chemotherapy or radioimmunotherapy.
There were 83 patients with FL. They had a median of 3 prior anticancer regimens (range, 1-10).
The patients received duvelisib at 25 mg orally twice daily until disease progression or unacceptable toxicity.
The overall response rate, per an independent review committee, was 43%. One patient achieved a complete response, and 35 had a partial response. The median duration of response was 7.9 months.
The median PFS was 8.3 months, and the median OS was 27.8 months.
The most common grade 3 or higher AEs were neutropenia (22%), anemia (13%), diarrhea (16%), lipase increase (10%), and thrombocytopenia (9%).
There were 2 serious opportunistic infections—Pneumocystis pneumonia and fungal pneumonia.
There were 3 deaths attributed to duvelisib—toxic epidermal necrolysis/sepsis syndrome (n=1), drug reaction/eosinophilia/systemic symptoms (n=1), and pneumonitis/pneumonia (n=1).
The US Food and Drug Administration (FDA) has accepted for priority review the new drug application (NDA) for duvelisib, a dual PI3K delta/gamma inhibitor.
With this NDA, Verastem, Inc., is seeking full approval of duvelisib for the treatment of relapsed or refractory chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and accelerated approval of the drug for the treatment of relapsed or refractory follicular lymphoma (FL).
The FDA expects to make a decision on the NDA by October 5, 2018.
The FDA aims to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The agency grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The application for duvelisib is supported by data from DUO™, a randomized, phase 3 study of patients with relapsed or refractory CLL/SLL, and DYNAMO™, a phase 2 study of patients with refractory indolent non-Hodgkin lymphoma.
Phase 3 DUO trial
Results from DUO were presented at the 2017 ASH Annual Meeting in December.
This study included 319 CLL/SLL patients who were randomized 1:1 to receive either duvelisib (25 mg orally twice daily) or ofatumumab (initial infusion of 300 mg followed by 7 weekly infusions and 4 monthly infusions of 2000 mg).
The study’s primary endpoint was met, as duvelisib conferred a significant improvement in median progression-free survival (PFS) over ofatumumab.
Per an independent review committee, the median PFS was 13.3 months with duvelisib and 9.9 months with ofatumumab (hazard ratio=0.52; P<0.0001). Duvelisib maintained a PFS advantage in all patient subgroups analyzed.
The overall response rate was 73.8% with duvelisib and 45.3% with ofatumumab (P<0.0001). The complete response rate was 0.6% in both arms.
Overall survival (OS) was similar in the duvelisib and ofatumumab arms (hazard ratio=0.99; P=0.4807). The median OS was not reached in either arm.
The most common grade 3 or higher adverse events (AEs)—in the duvelisib and ofatumumab arms, respectively—were neutropenia (30% vs 17%), anemia (13% vs 5%), diarrhea (15% vs 1%), pneumonia (14% vs 1%), and colitis (12% vs 1%).
Thirty-five percent of patients discontinued duvelisib due to an AE.
Severe opportunistic infections occurred in 6% of duvelisib recipients—bronchopulmonary aspergillosis (n=4), fungal infection (n=2), Pneumocystis jirovecii pneumonia (n=2), and cytomegalovirus colitis (n=1).
There were 4 deaths related to duvelisib—staphylococcal pneumonia (n=2), general physical health deterioration (n=1), and sepsis (n=1).
Phase 2 DYNAMO trial
Results from DYNAMO were presented at the 22nd EHA Congress (abstract S777) in June 2017.
This trial enrolled patients with indolent non-Hodgkin lymphoma whose disease was refractory to both rituximab and chemotherapy or radioimmunotherapy.
There were 83 patients with FL. They had a median of 3 prior anticancer regimens (range, 1-10).
The patients received duvelisib at 25 mg orally twice daily until disease progression or unacceptable toxicity.
The overall response rate, per an independent review committee, was 43%. One patient achieved a complete response, and 35 had a partial response. The median duration of response was 7.9 months.
The median PFS was 8.3 months, and the median OS was 27.8 months.
The most common grade 3 or higher AEs were neutropenia (22%), anemia (13%), diarrhea (16%), lipase increase (10%), and thrombocytopenia (9%).
There were 2 serious opportunistic infections—Pneumocystis pneumonia and fungal pneumonia.
There were 3 deaths attributed to duvelisib—toxic epidermal necrolysis/sepsis syndrome (n=1), drug reaction/eosinophilia/systemic symptoms (n=1), and pneumonitis/pneumonia (n=1).
Alzheimer’s: Biomarkers, not cognition, will now define disorder
A new definition of Alzheimer’s disease based solely on biomarkers has the potential to strengthen clinical trials and change the way physicians talk to patients.
AB is the key to this classification paradigm – any patient with it (A+) is on the Alzheimer’s continuum. But only those with both amyloid and tau in the brain (A+T+) receive the “Alzheimer’s disease” classification. A third biomarker, neurodegeneration, may be either present or absent for an Alzheimer’s disease profile (N+ or N-). Cognitive staging adds important details, but remains secondary to the biomarker classification.

Jointly created by National Institute on Aging and the Alzheimer’s Association, the system – dubbed the NIA-AA Research Framework – represents a new, common language that researchers around the world may now use to generate and test Alzheimer’s hypotheses, and to optimize both epidemiologic studies and interventional trials. It will be especially important as Alzheimer’s prevention trials seek to target patients who are cognitively normal, yet harbor the neuropathological hallmarks of the disease.
This recasting adds Alzheimer’s to the list of biomarker-defined disorders, including hypertension, diabetes, and hyperlipidemia. It is a timely and necessary reframing, said Clifford Jack, MD, chair of the 20-member committee that created the paradigm. It appears in the April 10 issue of Alzheimer’s & Dementia.
“This is a fundamental change in the definition of Alzheimer’s disease,” Dr. Jack said in an interview. “We are advocating the disease be defined by its neuropathology [of plaques and tangles], which is specific to Alzheimer’s, and no longer by clinical symptoms which are not specific for any disease.”
One of the primary intents is to refine AD research cohorts, allowing pure stratification of patients who actually have the intended therapeutic targets of amyloid beta or tau. Without biomarker screening, up to 30% of subjects who enroll in AD drug trials don’t have the target pathologies – a situation researchers say contributes to the long string of failed Alzheimer’s drug studies.
For now, the system is intended only for research settings said Dr. Jack, an Alzheimer’s investigator at the Mayo Clinic, Rochester, Minn. But as biomarker testing comes of age and new less-expensive markers are discovered, the paradigm will likely be incorporated into clinical practice. The process can begin even now with a simple change in the way doctors talk to patients about Alzheimer’s, he said in an interview.
“We advocate people stop using the terms ‘probable or possible AD.’ A better term is ‘Alzheimer’s clinical syndrome.’ Without biomarkers, the clinical syndrome is the only thing you can know. What you can’t know is whether they do or don’t have Alzheimer’s disease. When I’m asked by physicians, ‘What do I tell my patients now?’ my very direct answer is ‘Tell them the truth.’ And the truth is that they have Alzheimer’s clinical syndrome and may or may not have Alzheimer’s disease.”
A reflection of evolving science
The research framework reflects advances in Alzheimer’s science that have occurred since the NIA last updated it AD diagnostic criteria in 2011. Those criteria divided the disease continuum into three phases largely based on cognitive symptoms, but were the first to recognize a presymptomatic AD phase.
- Preclinical: Brain changes, including amyloid buildup and other nerve cell changes already may be in progress but significant clinical symptoms are not yet evident.
- Mild cognitive impairment (MCI): A stage marked by symptoms of memory and/or other thinking problems that are greater than normal for a person’s age and education but that do not interfere with his or her independence. MCI may or may not progress to Alzheimer’s dementia.
- Alzheimer’s dementia: The final stage of the disease in which the symptoms of Alzheimer’s, such as memory loss, word-finding difficulties, and visual/spatial problems, are significant enough to impair a person’s ability to function independently.
The next 6 years brought striking advances in understanding the biology and pathology of AD, as well as technical advances in biomarker measurements. It became possible not only to measure AB and tau in cerebrospinal fluid but also to see these proteins in living brains with specialized PET ligands. It also became obvious that about a third of subjects in any given AD study didn’t have the disease-defining brain plaques and tangles – the therapeutic targets of all the largest drug studies to date. And while it’s clear that none of the interventions that have been through trials have exerted a significant benefit yet, “Treating people for a disease they don’t have can’t possibly help the results,” Dr. Jack said.
These research observations and revolutionary biomarker advances have reshaped the way researchers think about AD. To maximize research potential and to create a global classification standard that would unify studies as well, NIA and the Alzheimer’s Association convened several meetings to redefine Alzheimer’s disease biologically, by pathologic brain changes as measured by biomarkers. In this paradigm, cognitive dysfunction steps aside as the primary classification driver, becoming a symptom of AD rather than its definition.
“The way AD has historically been defined is by clinical symptoms: a progressive amnestic dementia was Alzheimer’s, and if there was no progressive amnestic dementia, it wasn’t,” Dr. Jack said. “Well, it turns out that both of those statements are wrong. About 30% of people with progressive amnestic dementia have other things causing it.”
It makes much more sense, he said, to define the disease based on its unique neuropathologic signature: amyloid beta plaques and tau neurofibrillary tangles in the brain.
The three-part key: A/T(N)
The NIA-AA research framework yields eight biomarker profiles with different combinations of amyloid (A), tau (T), and neuropathologic damage (N).
“Different measures have different roles,” Dr. Jack and his colleagues wrote in Alzheimer’s & Dementia. “Amyloid beta biomarkers determine whether or not an individual is in the Alzheimer’s continuum. Pathologic tau biomarkers determine if someone who is in the Alzheimer’s continuum has AD, because both amyloid beta and tau are required for a neuropathologic diagnosis of the disease. Neurodegenerative/neuronal injury biomarkers and cognitive symptoms, neither of which is specific for AD, are used only to stage severity not to define the presence of the Alzheimer’s continuum.”
The “N” category is not as cut and dried at the other biomarkers, the paper noted.
“Biomarkers in the (N) group are indicators of neurodegeneration or neuronal injury resulting from many causes; they are not specific for neurodegeneration due to AD. In any individual, the proportion of observed neurodegeneration/injury that can be attributed to AD versus other possible comorbid conditions (most of which have no extant biomarker) is unknown.”
The biomarker profiles are:
- A-T-(N): Normal AD biomarkers
- A+T-(N): Alzheimer’s pathologic change; Alzheimer’s continuum
- A+T+(N): Alzheimer’s disease; Alzheimer’s continuum
- A+T-(N)+: Alzheimer’s with suspected non Alzheimer’s pathologic change; Alzheimer’s continuum
- A-T+(N)-: Non-AD pathologic change
- A-T-(N)+: Non-AD pathologic change
- A-T+(N)+: Non-AD pathologic change
“This latter biomarker profile implies evidence of one or more neuropathologic processes other than AD and has been labeled ‘suspected non-Alzheimer’s pathophysiology, or SNAP,” according to the paper.
Cognitive staging further refines each person’s status. There are two clinical staging schemes in the framework. One is the familiar syndromal staging system of cognitively unimpaired, MCI, and dementia, which can be subdivided into mild, moderate, and severe. This can be applied to anyone with a biomarker profile.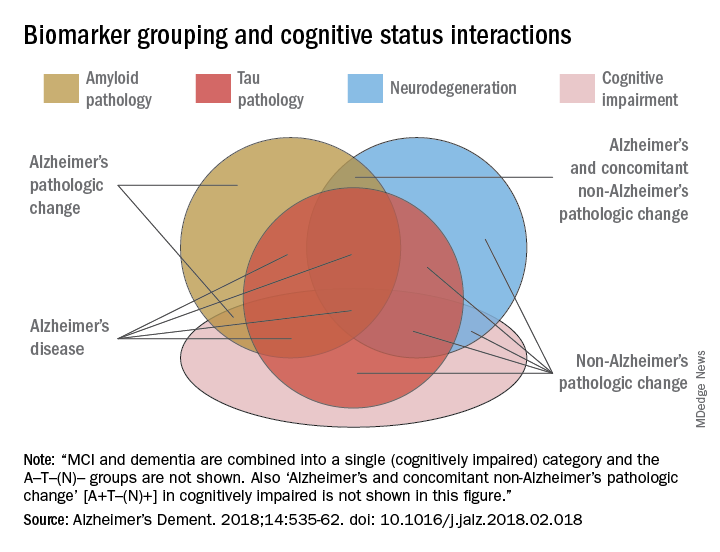
The second, a six-stage numerical clinical staging scheme, will apply only to those who are amyloid-positive and on the Alzheimer’s continuum. Stages run from 1 (unimpaired) to 6 (severe dementia). The numeric staging does not concentrate solely on cognition but also takes into account neurobehavioral and functional symptoms. It includes a transitional stage during which measures may be within population norms but have declined relative to the individual’s past performance.
The numeric staging scheme is intended to mesh with FDA guidance for clinical trials outcomes, the committee noted.
“A useful application envisioned for this numeric cognitive staging scheme is interventional trials. Indeed, the NIA-AA numeric staging scheme is intentionally very similar to the categorical system for staging AD outlined in recent FDA guidance for industry pertaining to developing drugs for treatment of early AD … it was our belief that harmonizing this aspect of the framework with FDA guidance would enhance cross fertilization between observational and interventional studies, which in turn would facilitate conduct of interventional clinical trials early in the disease process.”
The entire system yields a shorthand biomarker profile entirely unique to each subject. For example an A+T-(N)+ MCI profile suggests that both Alzheimer’s and non-Alzheimer’s pathologic change may be contributing to the cognitive impairment. A cognitive staging number could also be added.
This biomarker profile introduces the option of completely avoiding traditional AD nomenclature, the committee noted.
“Some investigators may prefer to not use the biomarker category terminology but instead simply report biomarker profile, i.e., A+T+(N)+ instead of ‘Alzheimer’s disease.’ An alternative is to combine the biomarker profile with a descriptive term – for example, ‘A+T+(N)+ with dementia’ instead of ‘Alzheimer’s disease with dementia’.”
Again, Dr. Jack cautioned, the paradigm is not intended for clinical use – at least not now. It relies entirely on biomarkers obtained by methods that are either invasive (lumbar puncture), unavailable outside research settings (tau scans), or very expensive when privately obtained (amyloid scans). Until this situation changes, the biomarker profile paradigm has little clinical impact.
IDEAS on the horizon
Change may be coming, however. The Alzheimer’s Association-sponsored Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) study is assessing the clinical usefulness of amyloid PET scans and their impact on patient outcomes. The goal is to accumulate enough data to prove that amyloid scans are a cost-effective addition to the management of dementia patients. If federal payers agree and decide to cover amyloid scans, advocates hope that private insurers might follow suit.
An interim analysis of 4,000 scans, presented at the 2017 Alzheimer’s Association International Conference, was quite positive. Scan results changed patient management in 68% of cases, including refining dementia diagnoses, adding, stopping, or switching medications, and altering patient counseling.
IDEAS uses an FDA-approved amyloid imaging agent. But although several are under investigation, there are no approved tau PET ligands. However, other less-invasive and less-costly options may soon be developed, the committee noted. The search continues for a validated blood-based biomarker, including neurofilament light protein, plasma amyloid beta, and plasma tau.
“In the future, less-invasive/less-expensive blood-based biomarker tests - along with genetics, clinical, and demographic information - will likely play an important screening role in selecting individuals for more-expensive/more-invasive biomarker testing. This has been the history in other biologically defined diseases such as cardiovascular disease,” Dr. Jack and his colleagues noted in the paper.
In any case, however, without an effective treatment, much of the information conveyed by the biomarker profile paradigm remains, literally, academic, Dr. Jack said.
“If [the biomarker profile] were easy to determine and inexpensive, I imagine a lot of people would ask for it. Certainly many people would want to know, especially if they have a cognitive problem. People who have a family history, who may have Alzheimer’s pathology without the symptoms, might want to know. But the reality is that, until there’s a treatment that alters the course of this disease, finding out that you actually have Alzheimer’s is not going to enable you to change anything.”
The editors of Alzheimer’s & Dementia are seeking comment on the research framework. Letters and commentary can be submitted through June and will be considered for publication in an e-book, to be published sometime this summer, according to an accompanying editorial (https://doi.org/10/1016/j.jalz.2018.03.003).
Alzheimer’s & Dementia is the official journal of the Alzheimer’s Association. Dr. Jack has served on scientific advisory boards for Elan/Janssen AI, Bristol-Meyers Squibb, Eli Lilly, GE Healthcare, Siemens, and Eisai; received research support from Baxter International, Allon Therapeutics; and holds stock in Johnson & Johnson. Disclosures for other committee members can be found here.
SOURCE: Jack CR et al. Alzheimer’s Dement. 2018;14:535-62. doi: 10.1016/j.jalz.2018.02.018.
The biologically defined amyloid beta–tau–neuronal damage (ATN) framework is a logical and modern approach to Alzheimer’s disease (AD) diagnosis. It is hard to argue that more data are bad. Having such data on every patient would certainly be a luxury, but, with a few notable exceptions, the context in which this will most frequently occur is within the context of clinical trials.
While having this information does provide a biological basis for diagnosis, it does not account for non-AD contributions to the patient’s symptoms, which are found in more than half of all AD patients at autopsy; these non-AD pathologies also can influence clinical trial outcomes.

It also seems a bit ironic that the only meaningful manifestation of AD is now essentially left out of the diagnostic framework or relegated to nothing more than an adjective. Yet having a head full of amyloid means little if a person does not express symptoms (and vice versa), and we know that all people do not progress in the same way.
In the future, genomic and exposomic profiles may provide an even-more-nuanced picture, but further work is needed before that becomes a clinical reality. For now, the ATN biomarker framework represents the state of the art, though not an end.
Richard J. Caselli, MD, is professor of neurology at the Mayo Clinic Arizona in Scottsdale. He is also associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
The biologically defined amyloid beta–tau–neuronal damage (ATN) framework is a logical and modern approach to Alzheimer’s disease (AD) diagnosis. It is hard to argue that more data are bad. Having such data on every patient would certainly be a luxury, but, with a few notable exceptions, the context in which this will most frequently occur is within the context of clinical trials.
While having this information does provide a biological basis for diagnosis, it does not account for non-AD contributions to the patient’s symptoms, which are found in more than half of all AD patients at autopsy; these non-AD pathologies also can influence clinical trial outcomes.
It also seems a bit ironic that the only meaningful manifestation of AD is now essentially left out of the diagnostic framework or relegated to nothing more than an adjective. Yet having a head full of amyloid means little if a person does not express symptoms (and vice versa), and we know that all people do not progress in the same way.
In the future, genomic and exposomic profiles may provide an even-more-nuanced picture, but further work is needed before that becomes a clinical reality. For now, the ATN biomarker framework represents the state of the art, though not an end.
Richard J. Caselli, MD, is professor of neurology at the Mayo Clinic Arizona in Scottsdale. He is also associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
The biologically defined amyloid beta–tau–neuronal damage (ATN) framework is a logical and modern approach to Alzheimer’s disease (AD) diagnosis. It is hard to argue that more data are bad. Having such data on every patient would certainly be a luxury, but, with a few notable exceptions, the context in which this will most frequently occur is within the context of clinical trials.
While having this information does provide a biological basis for diagnosis, it does not account for non-AD contributions to the patient’s symptoms, which are found in more than half of all AD patients at autopsy; these non-AD pathologies also can influence clinical trial outcomes.
It also seems a bit ironic that the only meaningful manifestation of AD is now essentially left out of the diagnostic framework or relegated to nothing more than an adjective. Yet having a head full of amyloid means little if a person does not express symptoms (and vice versa), and we know that all people do not progress in the same way.
In the future, genomic and exposomic profiles may provide an even-more-nuanced picture, but further work is needed before that becomes a clinical reality. For now, the ATN biomarker framework represents the state of the art, though not an end.
Richard J. Caselli, MD, is professor of neurology at the Mayo Clinic Arizona in Scottsdale. He is also associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
A new definition of Alzheimer’s disease based solely on biomarkers has the potential to strengthen clinical trials and change the way physicians talk to patients.
AB is the key to this classification paradigm – any patient with it (A+) is on the Alzheimer’s continuum. But only those with both amyloid and tau in the brain (A+T+) receive the “Alzheimer’s disease” classification. A third biomarker, neurodegeneration, may be either present or absent for an Alzheimer’s disease profile (N+ or N-). Cognitive staging adds important details, but remains secondary to the biomarker classification.
Jointly created by National Institute on Aging and the Alzheimer’s Association, the system – dubbed the NIA-AA Research Framework – represents a new, common language that researchers around the world may now use to generate and test Alzheimer’s hypotheses, and to optimize both epidemiologic studies and interventional trials. It will be especially important as Alzheimer’s prevention trials seek to target patients who are cognitively normal, yet harbor the neuropathological hallmarks of the disease.
This recasting adds Alzheimer’s to the list of biomarker-defined disorders, including hypertension, diabetes, and hyperlipidemia. It is a timely and necessary reframing, said Clifford Jack, MD, chair of the 20-member committee that created the paradigm. It appears in the April 10 issue of Alzheimer’s & Dementia.
“This is a fundamental change in the definition of Alzheimer’s disease,” Dr. Jack said in an interview. “We are advocating the disease be defined by its neuropathology [of plaques and tangles], which is specific to Alzheimer’s, and no longer by clinical symptoms which are not specific for any disease.”
One of the primary intents is to refine AD research cohorts, allowing pure stratification of patients who actually have the intended therapeutic targets of amyloid beta or tau. Without biomarker screening, up to 30% of subjects who enroll in AD drug trials don’t have the target pathologies – a situation researchers say contributes to the long string of failed Alzheimer’s drug studies.
For now, the system is intended only for research settings said Dr. Jack, an Alzheimer’s investigator at the Mayo Clinic, Rochester, Minn. But as biomarker testing comes of age and new less-expensive markers are discovered, the paradigm will likely be incorporated into clinical practice. The process can begin even now with a simple change in the way doctors talk to patients about Alzheimer’s, he said in an interview.
“We advocate people stop using the terms ‘probable or possible AD.’ A better term is ‘Alzheimer’s clinical syndrome.’ Without biomarkers, the clinical syndrome is the only thing you can know. What you can’t know is whether they do or don’t have Alzheimer’s disease. When I’m asked by physicians, ‘What do I tell my patients now?’ my very direct answer is ‘Tell them the truth.’ And the truth is that they have Alzheimer’s clinical syndrome and may or may not have Alzheimer’s disease.”
A reflection of evolving science
The research framework reflects advances in Alzheimer’s science that have occurred since the NIA last updated it AD diagnostic criteria in 2011. Those criteria divided the disease continuum into three phases largely based on cognitive symptoms, but were the first to recognize a presymptomatic AD phase.
- Preclinical: Brain changes, including amyloid buildup and other nerve cell changes already may be in progress but significant clinical symptoms are not yet evident.
- Mild cognitive impairment (MCI): A stage marked by symptoms of memory and/or other thinking problems that are greater than normal for a person’s age and education but that do not interfere with his or her independence. MCI may or may not progress to Alzheimer’s dementia.
- Alzheimer’s dementia: The final stage of the disease in which the symptoms of Alzheimer’s, such as memory loss, word-finding difficulties, and visual/spatial problems, are significant enough to impair a person’s ability to function independently.
The next 6 years brought striking advances in understanding the biology and pathology of AD, as well as technical advances in biomarker measurements. It became possible not only to measure AB and tau in cerebrospinal fluid but also to see these proteins in living brains with specialized PET ligands. It also became obvious that about a third of subjects in any given AD study didn’t have the disease-defining brain plaques and tangles – the therapeutic targets of all the largest drug studies to date. And while it’s clear that none of the interventions that have been through trials have exerted a significant benefit yet, “Treating people for a disease they don’t have can’t possibly help the results,” Dr. Jack said.
These research observations and revolutionary biomarker advances have reshaped the way researchers think about AD. To maximize research potential and to create a global classification standard that would unify studies as well, NIA and the Alzheimer’s Association convened several meetings to redefine Alzheimer’s disease biologically, by pathologic brain changes as measured by biomarkers. In this paradigm, cognitive dysfunction steps aside as the primary classification driver, becoming a symptom of AD rather than its definition.
“The way AD has historically been defined is by clinical symptoms: a progressive amnestic dementia was Alzheimer’s, and if there was no progressive amnestic dementia, it wasn’t,” Dr. Jack said. “Well, it turns out that both of those statements are wrong. About 30% of people with progressive amnestic dementia have other things causing it.”
It makes much more sense, he said, to define the disease based on its unique neuropathologic signature: amyloid beta plaques and tau neurofibrillary tangles in the brain.
The three-part key: A/T(N)
The NIA-AA research framework yields eight biomarker profiles with different combinations of amyloid (A), tau (T), and neuropathologic damage (N).
“Different measures have different roles,” Dr. Jack and his colleagues wrote in Alzheimer’s & Dementia. “Amyloid beta biomarkers determine whether or not an individual is in the Alzheimer’s continuum. Pathologic tau biomarkers determine if someone who is in the Alzheimer’s continuum has AD, because both amyloid beta and tau are required for a neuropathologic diagnosis of the disease. Neurodegenerative/neuronal injury biomarkers and cognitive symptoms, neither of which is specific for AD, are used only to stage severity not to define the presence of the Alzheimer’s continuum.”
The “N” category is not as cut and dried at the other biomarkers, the paper noted.
“Biomarkers in the (N) group are indicators of neurodegeneration or neuronal injury resulting from many causes; they are not specific for neurodegeneration due to AD. In any individual, the proportion of observed neurodegeneration/injury that can be attributed to AD versus other possible comorbid conditions (most of which have no extant biomarker) is unknown.”
The biomarker profiles are:
- A-T-(N): Normal AD biomarkers
- A+T-(N): Alzheimer’s pathologic change; Alzheimer’s continuum
- A+T+(N): Alzheimer’s disease; Alzheimer’s continuum
- A+T-(N)+: Alzheimer’s with suspected non Alzheimer’s pathologic change; Alzheimer’s continuum
- A-T+(N)-: Non-AD pathologic change
- A-T-(N)+: Non-AD pathologic change
- A-T+(N)+: Non-AD pathologic change
“This latter biomarker profile implies evidence of one or more neuropathologic processes other than AD and has been labeled ‘suspected non-Alzheimer’s pathophysiology, or SNAP,” according to the paper.
Cognitive staging further refines each person’s status. There are two clinical staging schemes in the framework. One is the familiar syndromal staging system of cognitively unimpaired, MCI, and dementia, which can be subdivided into mild, moderate, and severe. This can be applied to anyone with a biomarker profile.
The second, a six-stage numerical clinical staging scheme, will apply only to those who are amyloid-positive and on the Alzheimer’s continuum. Stages run from 1 (unimpaired) to 6 (severe dementia). The numeric staging does not concentrate solely on cognition but also takes into account neurobehavioral and functional symptoms. It includes a transitional stage during which measures may be within population norms but have declined relative to the individual’s past performance.
The numeric staging scheme is intended to mesh with FDA guidance for clinical trials outcomes, the committee noted.
“A useful application envisioned for this numeric cognitive staging scheme is interventional trials. Indeed, the NIA-AA numeric staging scheme is intentionally very similar to the categorical system for staging AD outlined in recent FDA guidance for industry pertaining to developing drugs for treatment of early AD … it was our belief that harmonizing this aspect of the framework with FDA guidance would enhance cross fertilization between observational and interventional studies, which in turn would facilitate conduct of interventional clinical trials early in the disease process.”
The entire system yields a shorthand biomarker profile entirely unique to each subject. For example an A+T-(N)+ MCI profile suggests that both Alzheimer’s and non-Alzheimer’s pathologic change may be contributing to the cognitive impairment. A cognitive staging number could also be added.
This biomarker profile introduces the option of completely avoiding traditional AD nomenclature, the committee noted.
“Some investigators may prefer to not use the biomarker category terminology but instead simply report biomarker profile, i.e., A+T+(N)+ instead of ‘Alzheimer’s disease.’ An alternative is to combine the biomarker profile with a descriptive term – for example, ‘A+T+(N)+ with dementia’ instead of ‘Alzheimer’s disease with dementia’.”
Again, Dr. Jack cautioned, the paradigm is not intended for clinical use – at least not now. It relies entirely on biomarkers obtained by methods that are either invasive (lumbar puncture), unavailable outside research settings (tau scans), or very expensive when privately obtained (amyloid scans). Until this situation changes, the biomarker profile paradigm has little clinical impact.
IDEAS on the horizon
Change may be coming, however. The Alzheimer’s Association-sponsored Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) study is assessing the clinical usefulness of amyloid PET scans and their impact on patient outcomes. The goal is to accumulate enough data to prove that amyloid scans are a cost-effective addition to the management of dementia patients. If federal payers agree and decide to cover amyloid scans, advocates hope that private insurers might follow suit.
An interim analysis of 4,000 scans, presented at the 2017 Alzheimer’s Association International Conference, was quite positive. Scan results changed patient management in 68% of cases, including refining dementia diagnoses, adding, stopping, or switching medications, and altering patient counseling.
IDEAS uses an FDA-approved amyloid imaging agent. But although several are under investigation, there are no approved tau PET ligands. However, other less-invasive and less-costly options may soon be developed, the committee noted. The search continues for a validated blood-based biomarker, including neurofilament light protein, plasma amyloid beta, and plasma tau.
“In the future, less-invasive/less-expensive blood-based biomarker tests - along with genetics, clinical, and demographic information - will likely play an important screening role in selecting individuals for more-expensive/more-invasive biomarker testing. This has been the history in other biologically defined diseases such as cardiovascular disease,” Dr. Jack and his colleagues noted in the paper.
In any case, however, without an effective treatment, much of the information conveyed by the biomarker profile paradigm remains, literally, academic, Dr. Jack said.
“If [the biomarker profile] were easy to determine and inexpensive, I imagine a lot of people would ask for it. Certainly many people would want to know, especially if they have a cognitive problem. People who have a family history, who may have Alzheimer’s pathology without the symptoms, might want to know. But the reality is that, until there’s a treatment that alters the course of this disease, finding out that you actually have Alzheimer’s is not going to enable you to change anything.”
The editors of Alzheimer’s & Dementia are seeking comment on the research framework. Letters and commentary can be submitted through June and will be considered for publication in an e-book, to be published sometime this summer, according to an accompanying editorial (https://doi.org/10/1016/j.jalz.2018.03.003).
Alzheimer’s & Dementia is the official journal of the Alzheimer’s Association. Dr. Jack has served on scientific advisory boards for Elan/Janssen AI, Bristol-Meyers Squibb, Eli Lilly, GE Healthcare, Siemens, and Eisai; received research support from Baxter International, Allon Therapeutics; and holds stock in Johnson & Johnson. Disclosures for other committee members can be found here.
SOURCE: Jack CR et al. Alzheimer’s Dement. 2018;14:535-62. doi: 10.1016/j.jalz.2018.02.018.
A new definition of Alzheimer’s disease based solely on biomarkers has the potential to strengthen clinical trials and change the way physicians talk to patients.
AB is the key to this classification paradigm – any patient with it (A+) is on the Alzheimer’s continuum. But only those with both amyloid and tau in the brain (A+T+) receive the “Alzheimer’s disease” classification. A third biomarker, neurodegeneration, may be either present or absent for an Alzheimer’s disease profile (N+ or N-). Cognitive staging adds important details, but remains secondary to the biomarker classification.
Jointly created by National Institute on Aging and the Alzheimer’s Association, the system – dubbed the NIA-AA Research Framework – represents a new, common language that researchers around the world may now use to generate and test Alzheimer’s hypotheses, and to optimize both epidemiologic studies and interventional trials. It will be especially important as Alzheimer’s prevention trials seek to target patients who are cognitively normal, yet harbor the neuropathological hallmarks of the disease.
This recasting adds Alzheimer’s to the list of biomarker-defined disorders, including hypertension, diabetes, and hyperlipidemia. It is a timely and necessary reframing, said Clifford Jack, MD, chair of the 20-member committee that created the paradigm. It appears in the April 10 issue of Alzheimer’s & Dementia.
“This is a fundamental change in the definition of Alzheimer’s disease,” Dr. Jack said in an interview. “We are advocating the disease be defined by its neuropathology [of plaques and tangles], which is specific to Alzheimer’s, and no longer by clinical symptoms which are not specific for any disease.”
One of the primary intents is to refine AD research cohorts, allowing pure stratification of patients who actually have the intended therapeutic targets of amyloid beta or tau. Without biomarker screening, up to 30% of subjects who enroll in AD drug trials don’t have the target pathologies – a situation researchers say contributes to the long string of failed Alzheimer’s drug studies.
For now, the system is intended only for research settings said Dr. Jack, an Alzheimer’s investigator at the Mayo Clinic, Rochester, Minn. But as biomarker testing comes of age and new less-expensive markers are discovered, the paradigm will likely be incorporated into clinical practice. The process can begin even now with a simple change in the way doctors talk to patients about Alzheimer’s, he said in an interview.
“We advocate people stop using the terms ‘probable or possible AD.’ A better term is ‘Alzheimer’s clinical syndrome.’ Without biomarkers, the clinical syndrome is the only thing you can know. What you can’t know is whether they do or don’t have Alzheimer’s disease. When I’m asked by physicians, ‘What do I tell my patients now?’ my very direct answer is ‘Tell them the truth.’ And the truth is that they have Alzheimer’s clinical syndrome and may or may not have Alzheimer’s disease.”
A reflection of evolving science
The research framework reflects advances in Alzheimer’s science that have occurred since the NIA last updated it AD diagnostic criteria in 2011. Those criteria divided the disease continuum into three phases largely based on cognitive symptoms, but were the first to recognize a presymptomatic AD phase.
- Preclinical: Brain changes, including amyloid buildup and other nerve cell changes already may be in progress but significant clinical symptoms are not yet evident.
- Mild cognitive impairment (MCI): A stage marked by symptoms of memory and/or other thinking problems that are greater than normal for a person’s age and education but that do not interfere with his or her independence. MCI may or may not progress to Alzheimer’s dementia.
- Alzheimer’s dementia: The final stage of the disease in which the symptoms of Alzheimer’s, such as memory loss, word-finding difficulties, and visual/spatial problems, are significant enough to impair a person’s ability to function independently.
The next 6 years brought striking advances in understanding the biology and pathology of AD, as well as technical advances in biomarker measurements. It became possible not only to measure AB and tau in cerebrospinal fluid but also to see these proteins in living brains with specialized PET ligands. It also became obvious that about a third of subjects in any given AD study didn’t have the disease-defining brain plaques and tangles – the therapeutic targets of all the largest drug studies to date. And while it’s clear that none of the interventions that have been through trials have exerted a significant benefit yet, “Treating people for a disease they don’t have can’t possibly help the results,” Dr. Jack said.
These research observations and revolutionary biomarker advances have reshaped the way researchers think about AD. To maximize research potential and to create a global classification standard that would unify studies as well, NIA and the Alzheimer’s Association convened several meetings to redefine Alzheimer’s disease biologically, by pathologic brain changes as measured by biomarkers. In this paradigm, cognitive dysfunction steps aside as the primary classification driver, becoming a symptom of AD rather than its definition.
“The way AD has historically been defined is by clinical symptoms: a progressive amnestic dementia was Alzheimer’s, and if there was no progressive amnestic dementia, it wasn’t,” Dr. Jack said. “Well, it turns out that both of those statements are wrong. About 30% of people with progressive amnestic dementia have other things causing it.”
It makes much more sense, he said, to define the disease based on its unique neuropathologic signature: amyloid beta plaques and tau neurofibrillary tangles in the brain.
The three-part key: A/T(N)
The NIA-AA research framework yields eight biomarker profiles with different combinations of amyloid (A), tau (T), and neuropathologic damage (N).
“Different measures have different roles,” Dr. Jack and his colleagues wrote in Alzheimer’s & Dementia. “Amyloid beta biomarkers determine whether or not an individual is in the Alzheimer’s continuum. Pathologic tau biomarkers determine if someone who is in the Alzheimer’s continuum has AD, because both amyloid beta and tau are required for a neuropathologic diagnosis of the disease. Neurodegenerative/neuronal injury biomarkers and cognitive symptoms, neither of which is specific for AD, are used only to stage severity not to define the presence of the Alzheimer’s continuum.”
The “N” category is not as cut and dried at the other biomarkers, the paper noted.
“Biomarkers in the (N) group are indicators of neurodegeneration or neuronal injury resulting from many causes; they are not specific for neurodegeneration due to AD. In any individual, the proportion of observed neurodegeneration/injury that can be attributed to AD versus other possible comorbid conditions (most of which have no extant biomarker) is unknown.”
The biomarker profiles are:
- A-T-(N): Normal AD biomarkers
- A+T-(N): Alzheimer’s pathologic change; Alzheimer’s continuum
- A+T+(N): Alzheimer’s disease; Alzheimer’s continuum
- A+T-(N)+: Alzheimer’s with suspected non Alzheimer’s pathologic change; Alzheimer’s continuum
- A-T+(N)-: Non-AD pathologic change
- A-T-(N)+: Non-AD pathologic change
- A-T+(N)+: Non-AD pathologic change
“This latter biomarker profile implies evidence of one or more neuropathologic processes other than AD and has been labeled ‘suspected non-Alzheimer’s pathophysiology, or SNAP,” according to the paper.
Cognitive staging further refines each person’s status. There are two clinical staging schemes in the framework. One is the familiar syndromal staging system of cognitively unimpaired, MCI, and dementia, which can be subdivided into mild, moderate, and severe. This can be applied to anyone with a biomarker profile.
The second, a six-stage numerical clinical staging scheme, will apply only to those who are amyloid-positive and on the Alzheimer’s continuum. Stages run from 1 (unimpaired) to 6 (severe dementia). The numeric staging does not concentrate solely on cognition but also takes into account neurobehavioral and functional symptoms. It includes a transitional stage during which measures may be within population norms but have declined relative to the individual’s past performance.
The numeric staging scheme is intended to mesh with FDA guidance for clinical trials outcomes, the committee noted.
“A useful application envisioned for this numeric cognitive staging scheme is interventional trials. Indeed, the NIA-AA numeric staging scheme is intentionally very similar to the categorical system for staging AD outlined in recent FDA guidance for industry pertaining to developing drugs for treatment of early AD … it was our belief that harmonizing this aspect of the framework with FDA guidance would enhance cross fertilization between observational and interventional studies, which in turn would facilitate conduct of interventional clinical trials early in the disease process.”
The entire system yields a shorthand biomarker profile entirely unique to each subject. For example an A+T-(N)+ MCI profile suggests that both Alzheimer’s and non-Alzheimer’s pathologic change may be contributing to the cognitive impairment. A cognitive staging number could also be added.
This biomarker profile introduces the option of completely avoiding traditional AD nomenclature, the committee noted.
“Some investigators may prefer to not use the biomarker category terminology but instead simply report biomarker profile, i.e., A+T+(N)+ instead of ‘Alzheimer’s disease.’ An alternative is to combine the biomarker profile with a descriptive term – for example, ‘A+T+(N)+ with dementia’ instead of ‘Alzheimer’s disease with dementia’.”
Again, Dr. Jack cautioned, the paradigm is not intended for clinical use – at least not now. It relies entirely on biomarkers obtained by methods that are either invasive (lumbar puncture), unavailable outside research settings (tau scans), or very expensive when privately obtained (amyloid scans). Until this situation changes, the biomarker profile paradigm has little clinical impact.
IDEAS on the horizon
Change may be coming, however. The Alzheimer’s Association-sponsored Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) study is assessing the clinical usefulness of amyloid PET scans and their impact on patient outcomes. The goal is to accumulate enough data to prove that amyloid scans are a cost-effective addition to the management of dementia patients. If federal payers agree and decide to cover amyloid scans, advocates hope that private insurers might follow suit.
An interim analysis of 4,000 scans, presented at the 2017 Alzheimer’s Association International Conference, was quite positive. Scan results changed patient management in 68% of cases, including refining dementia diagnoses, adding, stopping, or switching medications, and altering patient counseling.
IDEAS uses an FDA-approved amyloid imaging agent. But although several are under investigation, there are no approved tau PET ligands. However, other less-invasive and less-costly options may soon be developed, the committee noted. The search continues for a validated blood-based biomarker, including neurofilament light protein, plasma amyloid beta, and plasma tau.
“In the future, less-invasive/less-expensive blood-based biomarker tests - along with genetics, clinical, and demographic information - will likely play an important screening role in selecting individuals for more-expensive/more-invasive biomarker testing. This has been the history in other biologically defined diseases such as cardiovascular disease,” Dr. Jack and his colleagues noted in the paper.
In any case, however, without an effective treatment, much of the information conveyed by the biomarker profile paradigm remains, literally, academic, Dr. Jack said.
“If [the biomarker profile] were easy to determine and inexpensive, I imagine a lot of people would ask for it. Certainly many people would want to know, especially if they have a cognitive problem. People who have a family history, who may have Alzheimer’s pathology without the symptoms, might want to know. But the reality is that, until there’s a treatment that alters the course of this disease, finding out that you actually have Alzheimer’s is not going to enable you to change anything.”
The editors of Alzheimer’s & Dementia are seeking comment on the research framework. Letters and commentary can be submitted through June and will be considered for publication in an e-book, to be published sometime this summer, according to an accompanying editorial (https://doi.org/10/1016/j.jalz.2018.03.003).
Alzheimer’s & Dementia is the official journal of the Alzheimer’s Association. Dr. Jack has served on scientific advisory boards for Elan/Janssen AI, Bristol-Meyers Squibb, Eli Lilly, GE Healthcare, Siemens, and Eisai; received research support from Baxter International, Allon Therapeutics; and holds stock in Johnson & Johnson. Disclosures for other committee members can be found here.
SOURCE: Jack CR et al. Alzheimer’s Dement. 2018;14:535-62. doi: 10.1016/j.jalz.2018.02.018.
FROM ALZHEIMER’S & DEMENTIA
An Easy Approach to Obtaining Clean-catch Urine From Infants
A fussy 6-month-old infant is brought to the emergency department (ED) with a rectal temperature of 101.5°F. She is consolable,
A febrile infant in a family practice office or ED is a familiar clinical situation that may require an invasive diagnostic workup. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre–toilet-trained children can be time consuming. In fact, in one RCT, obtaining a clean-catch urine sample in this age group took more than an hour, on average.3 But more convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
In its guidelines for evaluating possible UTI in a febrile child younger than age 2, the American Academy of Pediatrics (AAP) recommends obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 6 months or younger.7 Within five minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants younger than 30 days old showed similar results.8 There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation triggers faster samples
A nonblinded, single-center RCT conducted in Australia compared two methods for obtaining a clean-catch urine sample within five minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 A total of 354 infants (ages 1-12 mo) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within five minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8°C). At five minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within five minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within five minutes, compared with 9% in the usual-care group (number needed to treat, 4.7).
Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is “most satisfied”). There was no difference when results were adjusted for age or sex. No adverse events occurred.
Continue to: WHAT'S NEW
WHAT’S NEW
Method could reduce need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within five minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.

CAVEATS
Complete age range & ideal storage temperature are unknown
Neonates and precontinent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups. The intervention period lasted only five minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8°C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[3]: 166, 168-169).
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27(4):302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93(5):423-424.
4. Al-Orifi F, McGillivray D, Tange S, Kramer MS. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137(2):221-226.
5. Roberts KB, Downs SM, Finnell SM, et al; Subcommittee on Urinary Tract Infection. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138(6): e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management [clinical guideline CG54]. www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed March 1, 2018.
7. Labrosse M, Levy A, Autmizguine J, Gravel J. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138(3):e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98(1):27-29.
A fussy 6-month-old infant is brought to the emergency department (ED) with a rectal temperature of 101.5°F. She is consolable,
A febrile infant in a family practice office or ED is a familiar clinical situation that may require an invasive diagnostic workup. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre–toilet-trained children can be time consuming. In fact, in one RCT, obtaining a clean-catch urine sample in this age group took more than an hour, on average.3 But more convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
In its guidelines for evaluating possible UTI in a febrile child younger than age 2, the American Academy of Pediatrics (AAP) recommends obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 6 months or younger.7 Within five minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants younger than 30 days old showed similar results.8 There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation triggers faster samples
A nonblinded, single-center RCT conducted in Australia compared two methods for obtaining a clean-catch urine sample within five minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 A total of 354 infants (ages 1-12 mo) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within five minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8°C). At five minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within five minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within five minutes, compared with 9% in the usual-care group (number needed to treat, 4.7).
Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is “most satisfied”). There was no difference when results were adjusted for age or sex. No adverse events occurred.
Continue to: WHAT'S NEW
WHAT’S NEW
Method could reduce need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within five minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.
CAVEATS
Complete age range & ideal storage temperature are unknown
Neonates and precontinent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups. The intervention period lasted only five minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8°C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[3]: 166, 168-169).
A fussy 6-month-old infant is brought to the emergency department (ED) with a rectal temperature of 101.5°F. She is consolable,
A febrile infant in a family practice office or ED is a familiar clinical situation that may require an invasive diagnostic workup. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre–toilet-trained children can be time consuming. In fact, in one RCT, obtaining a clean-catch urine sample in this age group took more than an hour, on average.3 But more convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
In its guidelines for evaluating possible UTI in a febrile child younger than age 2, the American Academy of Pediatrics (AAP) recommends obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 6 months or younger.7 Within five minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants younger than 30 days old showed similar results.8 There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation triggers faster samples
A nonblinded, single-center RCT conducted in Australia compared two methods for obtaining a clean-catch urine sample within five minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 A total of 354 infants (ages 1-12 mo) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within five minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8°C). At five minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within five minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within five minutes, compared with 9% in the usual-care group (number needed to treat, 4.7).
Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is “most satisfied”). There was no difference when results were adjusted for age or sex. No adverse events occurred.
Continue to: WHAT'S NEW
WHAT’S NEW
Method could reduce need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within five minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.
CAVEATS
Complete age range & ideal storage temperature are unknown
Neonates and precontinent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups. The intervention period lasted only five minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8°C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
Reprinted with permission from the Family Physicians Inquiries Network and The Journal of Family Practice (2018;67[3]: 166, 168-169).
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27(4):302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93(5):423-424.
4. Al-Orifi F, McGillivray D, Tange S, Kramer MS. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137(2):221-226.
5. Roberts KB, Downs SM, Finnell SM, et al; Subcommittee on Urinary Tract Infection. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138(6): e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management [clinical guideline CG54]. www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed March 1, 2018.
7. Labrosse M, Levy A, Autmizguine J, Gravel J. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138(3):e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98(1):27-29.
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27(4):302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93(5):423-424.
4. Al-Orifi F, McGillivray D, Tange S, Kramer MS. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137(2):221-226.
5. Roberts KB, Downs SM, Finnell SM, et al; Subcommittee on Urinary Tract Infection. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138(6): e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management [clinical guideline CG54]. www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed March 1, 2018.
7. Labrosse M, Levy A, Autmizguine J, Gravel J. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138(3):e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98(1):27-29.

Why do people act that way?
You can try all you want, but you never really figure people out.
Take Brendan. He spent a good few minutes chewing out my front desk staffer Linda. “You’re incompetent!” he shouted at her.
Linda tried to explain. “We can’t administer the Botox for your sweating today,” she said, “because it hasn’t come in yet.”
No, Brendan certainly didn’t want to hear that. Nor did he want to hear that we had called in advance to ask him to actually wait until we let him know that the Botox was in. But here he was, hyperinflating his lungs.
“You’re just damned useless!” he explained.
OK, we all have unreasonable patients from time to time. But what I’m describing is behavior that’s not just aggressive and unpleasant but incomprehensible. Would you like to know why I call it incomprehensible?
Because Brendan has been coming in for axillary Botox injections every 6 months for 5 years! He knows the drill. He knows the staff. He’s always pleasant as punch. Just not today. Why? Who knows?
What’s true for patients can of course also be true for employees. Model workers, superb team players, reliable folks who show up in snowstorms, who come right back to work after major surgery, who deliver heartfelt speeches at holiday parties about their good luck in overcoming adversity to be able to work. Contributors who share their pleasant disposition and can-do energy year after year ...
Until one day that they don’t show up, send a text to say they quit, no warning or explanation, then apply for Workmen’s Compensation, and at the magistrate’s hearing to which they’ve dragged my staff and our HR attorney, lie right to the face of the manager who was their best friend and confidante until the day before yesterday.
Get it? I don’t. Never will.
Two pieces of advice: 1) Don’t ever take things like that personally; and 2) Hire a good human resources attorney.
**********************
On the other hand ...
Jeralyn is 27 years old. She lists her chief complaint as “dark spots on my back.”
“How did you notice these?” I ask. “Did you see them, or did you doctor point them out?”
“It was when I tried on my wedding dress,” she says.
I understand, or think I do. Her dress exposed her back, her mother noticed the spots ...
“When is the wedding?” I ask.
“The wedding? Oh, the wedding already was. A year and a half ago.”
“You saw the spots when you tried on your wedding dress, and you’re coming in a year and half later?” I ask, trying not to sound incredulous. I’ve met enough nervous brides – and brides’ mothers – to find her account astonishing. “You must be a very patient person,” I say.
“Well,” says Jeralyn, “the spots didn’t spread or get any worse. And I am patient. I teach kindergarten. You have to be patient with little ones.”
“If you decide to have children, they’ll benefit from that,” I reply.
“That’s actually why I’m here,” says Jeralyn. “My husband and I want to start a family, and we want to be sure my skin condition wouldn’t affect that.”
A bride so unconcerned with herself that she wears a wedding dress that reveals a rash she doesn’t go running to a doctor to fix? Who comes only when the rash might affect someone else?
What is the matter with Jeralyn? Doesn’t she know she’s a millennial?
**********************
Kidding aside, wouldn’t it be nice if everyone acted like Jeralyn, and acted in a measured manner, appropriate to the concerns and circumstances? Wouldn’t it be nice if no one acted like Brendan?
That’s not how it is, though, is it? As professionals who deal with the public (as patients, coworkers, employees), we take all comers and roll with them: tolerate the annoyances and celebrate the (much larger, if less individually memorable) group who are pleasant, often delightful, sometimes inspiring.
And every once in a while, someone like Jeralyn comes along, upending all those negative expectations and reminding us that even if you can never really figure people out, it’s still worth the effort to keep trying.

Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
You can try all you want, but you never really figure people out.
Take Brendan. He spent a good few minutes chewing out my front desk staffer Linda. “You’re incompetent!” he shouted at her.
Linda tried to explain. “We can’t administer the Botox for your sweating today,” she said, “because it hasn’t come in yet.”
No, Brendan certainly didn’t want to hear that. Nor did he want to hear that we had called in advance to ask him to actually wait until we let him know that the Botox was in. But here he was, hyperinflating his lungs.
“You’re just damned useless!” he explained.
OK, we all have unreasonable patients from time to time. But what I’m describing is behavior that’s not just aggressive and unpleasant but incomprehensible. Would you like to know why I call it incomprehensible?
Because Brendan has been coming in for axillary Botox injections every 6 months for 5 years! He knows the drill. He knows the staff. He’s always pleasant as punch. Just not today. Why? Who knows?
What’s true for patients can of course also be true for employees. Model workers, superb team players, reliable folks who show up in snowstorms, who come right back to work after major surgery, who deliver heartfelt speeches at holiday parties about their good luck in overcoming adversity to be able to work. Contributors who share their pleasant disposition and can-do energy year after year ...
Until one day that they don’t show up, send a text to say they quit, no warning or explanation, then apply for Workmen’s Compensation, and at the magistrate’s hearing to which they’ve dragged my staff and our HR attorney, lie right to the face of the manager who was their best friend and confidante until the day before yesterday.
Get it? I don’t. Never will.
Two pieces of advice: 1) Don’t ever take things like that personally; and 2) Hire a good human resources attorney.
**********************
On the other hand ...
Jeralyn is 27 years old. She lists her chief complaint as “dark spots on my back.”
“How did you notice these?” I ask. “Did you see them, or did you doctor point them out?”
“It was when I tried on my wedding dress,” she says.
I understand, or think I do. Her dress exposed her back, her mother noticed the spots ...
“When is the wedding?” I ask.
“The wedding? Oh, the wedding already was. A year and a half ago.”
“You saw the spots when you tried on your wedding dress, and you’re coming in a year and half later?” I ask, trying not to sound incredulous. I’ve met enough nervous brides – and brides’ mothers – to find her account astonishing. “You must be a very patient person,” I say.
“Well,” says Jeralyn, “the spots didn’t spread or get any worse. And I am patient. I teach kindergarten. You have to be patient with little ones.”
“If you decide to have children, they’ll benefit from that,” I reply.
“That’s actually why I’m here,” says Jeralyn. “My husband and I want to start a family, and we want to be sure my skin condition wouldn’t affect that.”
A bride so unconcerned with herself that she wears a wedding dress that reveals a rash she doesn’t go running to a doctor to fix? Who comes only when the rash might affect someone else?
What is the matter with Jeralyn? Doesn’t she know she’s a millennial?
**********************
Kidding aside, wouldn’t it be nice if everyone acted like Jeralyn, and acted in a measured manner, appropriate to the concerns and circumstances? Wouldn’t it be nice if no one acted like Brendan?
That’s not how it is, though, is it? As professionals who deal with the public (as patients, coworkers, employees), we take all comers and roll with them: tolerate the annoyances and celebrate the (much larger, if less individually memorable) group who are pleasant, often delightful, sometimes inspiring.
And every once in a while, someone like Jeralyn comes along, upending all those negative expectations and reminding us that even if you can never really figure people out, it’s still worth the effort to keep trying.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
You can try all you want, but you never really figure people out.
Take Brendan. He spent a good few minutes chewing out my front desk staffer Linda. “You’re incompetent!” he shouted at her.
Linda tried to explain. “We can’t administer the Botox for your sweating today,” she said, “because it hasn’t come in yet.”
No, Brendan certainly didn’t want to hear that. Nor did he want to hear that we had called in advance to ask him to actually wait until we let him know that the Botox was in. But here he was, hyperinflating his lungs.
“You’re just damned useless!” he explained.
OK, we all have unreasonable patients from time to time. But what I’m describing is behavior that’s not just aggressive and unpleasant but incomprehensible. Would you like to know why I call it incomprehensible?
Because Brendan has been coming in for axillary Botox injections every 6 months for 5 years! He knows the drill. He knows the staff. He’s always pleasant as punch. Just not today. Why? Who knows?
What’s true for patients can of course also be true for employees. Model workers, superb team players, reliable folks who show up in snowstorms, who come right back to work after major surgery, who deliver heartfelt speeches at holiday parties about their good luck in overcoming adversity to be able to work. Contributors who share their pleasant disposition and can-do energy year after year ...
Until one day that they don’t show up, send a text to say they quit, no warning or explanation, then apply for Workmen’s Compensation, and at the magistrate’s hearing to which they’ve dragged my staff and our HR attorney, lie right to the face of the manager who was their best friend and confidante until the day before yesterday.
Get it? I don’t. Never will.
Two pieces of advice: 1) Don’t ever take things like that personally; and 2) Hire a good human resources attorney.
**********************
On the other hand ...
Jeralyn is 27 years old. She lists her chief complaint as “dark spots on my back.”
“How did you notice these?” I ask. “Did you see them, or did you doctor point them out?”
“It was when I tried on my wedding dress,” she says.
I understand, or think I do. Her dress exposed her back, her mother noticed the spots ...
“When is the wedding?” I ask.
“The wedding? Oh, the wedding already was. A year and a half ago.”
“You saw the spots when you tried on your wedding dress, and you’re coming in a year and half later?” I ask, trying not to sound incredulous. I’ve met enough nervous brides – and brides’ mothers – to find her account astonishing. “You must be a very patient person,” I say.
“Well,” says Jeralyn, “the spots didn’t spread or get any worse. And I am patient. I teach kindergarten. You have to be patient with little ones.”
“If you decide to have children, they’ll benefit from that,” I reply.
“That’s actually why I’m here,” says Jeralyn. “My husband and I want to start a family, and we want to be sure my skin condition wouldn’t affect that.”
A bride so unconcerned with herself that she wears a wedding dress that reveals a rash she doesn’t go running to a doctor to fix? Who comes only when the rash might affect someone else?
What is the matter with Jeralyn? Doesn’t she know she’s a millennial?
**********************
Kidding aside, wouldn’t it be nice if everyone acted like Jeralyn, and acted in a measured manner, appropriate to the concerns and circumstances? Wouldn’t it be nice if no one acted like Brendan?
That’s not how it is, though, is it? As professionals who deal with the public (as patients, coworkers, employees), we take all comers and roll with them: tolerate the annoyances and celebrate the (much larger, if less individually memorable) group who are pleasant, often delightful, sometimes inspiring.
And every once in a while, someone like Jeralyn comes along, upending all those negative expectations and reminding us that even if you can never really figure people out, it’s still worth the effort to keep trying.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
Treating female-to-male transgender adolescents with acne presents unique concerns with depression
according to the results of a case series.
“Acne is a foreseeable adverse effect of testosterone treatment in transgender adolescents, and it may be advisable that, once such treatment has begun, they be monitored for the appearance of acne,” Lucia Campos-Munoz, MD, of the Hospital Clinico San Carlos in Madrid wrote in Pediatric Dermatology. “Even if only mild, treatment should be provided.”
Dr. Campos-Munoz and her colleagues examined five female-to-male transgender patients who were admitted to their clinic from 2016-2017. All five patients presented with testosterone-associated acne. Two patients with severe acne were treated with 20 mg/day of isotretinoin. While one patient tolerated this well and discontinued treatment after 4 months, another patient stopped treatment because of a bout of depression at 3 months. The remaining patients received other treatments, including doxycycline, 0.05 topical tretinoin, and 3% benzoyl peroxide.
This case study highlights the unique role that dermatologists and primary care providers play in treating acne in female-to-male transgender patients. Using the proper pronouns and recognizing that physical examinations of the chest and thorax may be especially embarrassing for these patients are important considerations, according to Dr. Campos-Munoz and her colleagues. Also, neither antiandrogenic agents nor contraceptives can be given because “this would conflict with the masculinization sought.”
Apart from being aware of the patients’ feelings, there are real medical concerns associated with dermatologic treatment of acne in female-to-male transgender patients. One of these risks is depression, which several studies have shown to be associated with severe acne. This is compounded by higher rates of depression and suicidal ideation in transgender adolescents, they said.
An additional concern is the teratogenic effects of isotretinoin in patients with natal female internal genitalia. While these patients may not think they can get pregnant because of testosterone-associated amenorrhea, the potential is still present and pregnancy should be avoided, Dr. Campos-Munoz and her colleagues warned.
No funding or conflicts of interest were disclosed.
SOURCE: Campos-Munoz L et al. Pediatr Dermatol. 2018 Mar 25. doi: 10.1111/pde.13448.
according to the results of a case series.
“Acne is a foreseeable adverse effect of testosterone treatment in transgender adolescents, and it may be advisable that, once such treatment has begun, they be monitored for the appearance of acne,” Lucia Campos-Munoz, MD, of the Hospital Clinico San Carlos in Madrid wrote in Pediatric Dermatology. “Even if only mild, treatment should be provided.”
Dr. Campos-Munoz and her colleagues examined five female-to-male transgender patients who were admitted to their clinic from 2016-2017. All five patients presented with testosterone-associated acne. Two patients with severe acne were treated with 20 mg/day of isotretinoin. While one patient tolerated this well and discontinued treatment after 4 months, another patient stopped treatment because of a bout of depression at 3 months. The remaining patients received other treatments, including doxycycline, 0.05 topical tretinoin, and 3% benzoyl peroxide.
This case study highlights the unique role that dermatologists and primary care providers play in treating acne in female-to-male transgender patients. Using the proper pronouns and recognizing that physical examinations of the chest and thorax may be especially embarrassing for these patients are important considerations, according to Dr. Campos-Munoz and her colleagues. Also, neither antiandrogenic agents nor contraceptives can be given because “this would conflict with the masculinization sought.”
Apart from being aware of the patients’ feelings, there are real medical concerns associated with dermatologic treatment of acne in female-to-male transgender patients. One of these risks is depression, which several studies have shown to be associated with severe acne. This is compounded by higher rates of depression and suicidal ideation in transgender adolescents, they said.
An additional concern is the teratogenic effects of isotretinoin in patients with natal female internal genitalia. While these patients may not think they can get pregnant because of testosterone-associated amenorrhea, the potential is still present and pregnancy should be avoided, Dr. Campos-Munoz and her colleagues warned.
No funding or conflicts of interest were disclosed.
SOURCE: Campos-Munoz L et al. Pediatr Dermatol. 2018 Mar 25. doi: 10.1111/pde.13448.
according to the results of a case series.
“Acne is a foreseeable adverse effect of testosterone treatment in transgender adolescents, and it may be advisable that, once such treatment has begun, they be monitored for the appearance of acne,” Lucia Campos-Munoz, MD, of the Hospital Clinico San Carlos in Madrid wrote in Pediatric Dermatology. “Even if only mild, treatment should be provided.”
Dr. Campos-Munoz and her colleagues examined five female-to-male transgender patients who were admitted to their clinic from 2016-2017. All five patients presented with testosterone-associated acne. Two patients with severe acne were treated with 20 mg/day of isotretinoin. While one patient tolerated this well and discontinued treatment after 4 months, another patient stopped treatment because of a bout of depression at 3 months. The remaining patients received other treatments, including doxycycline, 0.05 topical tretinoin, and 3% benzoyl peroxide.
This case study highlights the unique role that dermatologists and primary care providers play in treating acne in female-to-male transgender patients. Using the proper pronouns and recognizing that physical examinations of the chest and thorax may be especially embarrassing for these patients are important considerations, according to Dr. Campos-Munoz and her colleagues. Also, neither antiandrogenic agents nor contraceptives can be given because “this would conflict with the masculinization sought.”
Apart from being aware of the patients’ feelings, there are real medical concerns associated with dermatologic treatment of acne in female-to-male transgender patients. One of these risks is depression, which several studies have shown to be associated with severe acne. This is compounded by higher rates of depression and suicidal ideation in transgender adolescents, they said.
An additional concern is the teratogenic effects of isotretinoin in patients with natal female internal genitalia. While these patients may not think they can get pregnant because of testosterone-associated amenorrhea, the potential is still present and pregnancy should be avoided, Dr. Campos-Munoz and her colleagues warned.
No funding or conflicts of interest were disclosed.
SOURCE: Campos-Munoz L et al. Pediatr Dermatol. 2018 Mar 25. doi: 10.1111/pde.13448.
FROM PEDIATRIC DERMATOLOGY
Key clinical point: Being transgender and severe acne both are related to higher rates of depression and suicide.
Major finding: In the case study, one of the five patients discontinued use of isotretinoin because of a bout of depression.
Study details: A 2016-2017 case series of five female-to-male transgender adolescents (aged 16-18 years) who had testosterone-associated acne.
Disclosures: No funding or conflicts of interest were disclosed.
Source: Campos-Munoz L et al. Pediatr Dermatol. 2018 Mar 25. doi: 10.1111/pde.13448.
Winners chosen at the SHM Clinical Vignettes competition
ORLANDO – Researchers presenting a case of starving ketoacidosis in a woman who was on a “Paleo” diet while breastfeeding won the Clinical Vignettes competition held Monday at HM18. The announcement capped a flurry of presenting and judging of posters on single cases that were captivating in both the stories they told and the lessons they taught.
The trainee award winner in the competition were presenters of a case of licorice-induced hypokalemia that, clinicians learned, was brought about by the drinking of an obscure kind of tea. The two others that made it into the final round of judging were on cases of syphilitic hepatitis and cardiac amyloidosis.
By chance, both of the winners highlighted dietary triggers, said Stephanie Sherman, MD, chair of the annual meeting’s clinical vignettes committee.
“The common themes in both of these were the importance of dietary history when interviewing patients,” Dr. Sherman said. “And then both had a beautiful review of the physiology that’s normal and how it gets broken in these situations.”
The Clinical Vignettes portion of the RIV competition, which also includes research and innovations categories, was separate this year because of space constraints, Dr. Sherman said.
Judges said they looked not only at how interesting and applicable each case was, but also the quality of the oral presentation and the poster’s visual appeal and clarity.
The ketoacidosis case, presented by Timothy Judson, MD, a resident at University of California, San Francisco, involved a 40-year-old woman who was previously healthy and had given birth 9 weeks earlier. Since the birth, the woman had been on a Paleo diet, a low-carbohydrate, ketogenic diet. She also was breastfeeding her newborn and continuing to breastfeed her 2-year-old son.
She presented with nonbilious, nonbloody emesis. On physical exam, she was found to be tachycardic, with diffuse tenderness of the abdomen. She was positive for ketones and had an elevated acetone level and elevated osmolar gap, the difference between the measured and calculated solutes in the serum.
Clinicians identified that low carbohydrate intake, high fat intake, and a high metabolic state, such as that brought on by breastfeeding, can contribute to ketoacidosis. She was treated with IV glucose-containing fluids, bicarbonate, fomepizole, and thiamine.
The case shows that patients should be warned about ketoacidosis risk when they start an ultra-low carbohydrate diet, especially if they are breastfeeding or lactating, Dr. Hudson said.
“Usually they’re safe, but they may not be if you’re in a high metabolic state,” he told judges.
“We take care of so many patients on a daily basis and we rarely get to tell their stories,” he said. “To be able to tell the story of the patients and give the learning points that we took away to others, I think is very rewarding.”
The winner of the trainee award, Maxwell Bressman, MD, a resident at Montefiore Medical Center in New York, presented the case of a 62-year-old woman with hypertension who had profound generalized weakness and an inability to walk.
“She actually came to the hospital because she couldn’t lift a cup of tea,” Dr. Bressman told judges.
Clinicians traced her problem to that very tea – a licorice-containing brew – after an ECG indicated hypokalemia. A breakdown product of licorice, glycyrrhizic acid, can prevent the breakdown of cortisol into cortisone, causing increased absorption of sodium in exchange for potassium, he explained.
“I really like interesting cases – it’s something I’ve thought about throughout medical school,” Dr. Bressman said. “It’s been incredibly fun. We have great cases at Montefiore. ... It’s taught me to think very broadly and with an expansive differential.”
ORLANDO – Researchers presenting a case of starving ketoacidosis in a woman who was on a “Paleo” diet while breastfeeding won the Clinical Vignettes competition held Monday at HM18. The announcement capped a flurry of presenting and judging of posters on single cases that were captivating in both the stories they told and the lessons they taught.
The trainee award winner in the competition were presenters of a case of licorice-induced hypokalemia that, clinicians learned, was brought about by the drinking of an obscure kind of tea. The two others that made it into the final round of judging were on cases of syphilitic hepatitis and cardiac amyloidosis.
By chance, both of the winners highlighted dietary triggers, said Stephanie Sherman, MD, chair of the annual meeting’s clinical vignettes committee.
“The common themes in both of these were the importance of dietary history when interviewing patients,” Dr. Sherman said. “And then both had a beautiful review of the physiology that’s normal and how it gets broken in these situations.”
The Clinical Vignettes portion of the RIV competition, which also includes research and innovations categories, was separate this year because of space constraints, Dr. Sherman said.
Judges said they looked not only at how interesting and applicable each case was, but also the quality of the oral presentation and the poster’s visual appeal and clarity.
The ketoacidosis case, presented by Timothy Judson, MD, a resident at University of California, San Francisco, involved a 40-year-old woman who was previously healthy and had given birth 9 weeks earlier. Since the birth, the woman had been on a Paleo diet, a low-carbohydrate, ketogenic diet. She also was breastfeeding her newborn and continuing to breastfeed her 2-year-old son.
She presented with nonbilious, nonbloody emesis. On physical exam, she was found to be tachycardic, with diffuse tenderness of the abdomen. She was positive for ketones and had an elevated acetone level and elevated osmolar gap, the difference between the measured and calculated solutes in the serum.
Clinicians identified that low carbohydrate intake, high fat intake, and a high metabolic state, such as that brought on by breastfeeding, can contribute to ketoacidosis. She was treated with IV glucose-containing fluids, bicarbonate, fomepizole, and thiamine.
The case shows that patients should be warned about ketoacidosis risk when they start an ultra-low carbohydrate diet, especially if they are breastfeeding or lactating, Dr. Hudson said.
“Usually they’re safe, but they may not be if you’re in a high metabolic state,” he told judges.
“We take care of so many patients on a daily basis and we rarely get to tell their stories,” he said. “To be able to tell the story of the patients and give the learning points that we took away to others, I think is very rewarding.”
The winner of the trainee award, Maxwell Bressman, MD, a resident at Montefiore Medical Center in New York, presented the case of a 62-year-old woman with hypertension who had profound generalized weakness and an inability to walk.
“She actually came to the hospital because she couldn’t lift a cup of tea,” Dr. Bressman told judges.
Clinicians traced her problem to that very tea – a licorice-containing brew – after an ECG indicated hypokalemia. A breakdown product of licorice, glycyrrhizic acid, can prevent the breakdown of cortisol into cortisone, causing increased absorption of sodium in exchange for potassium, he explained.
“I really like interesting cases – it’s something I’ve thought about throughout medical school,” Dr. Bressman said. “It’s been incredibly fun. We have great cases at Montefiore. ... It’s taught me to think very broadly and with an expansive differential.”
ORLANDO – Researchers presenting a case of starving ketoacidosis in a woman who was on a “Paleo” diet while breastfeeding won the Clinical Vignettes competition held Monday at HM18. The announcement capped a flurry of presenting and judging of posters on single cases that were captivating in both the stories they told and the lessons they taught.
The trainee award winner in the competition were presenters of a case of licorice-induced hypokalemia that, clinicians learned, was brought about by the drinking of an obscure kind of tea. The two others that made it into the final round of judging were on cases of syphilitic hepatitis and cardiac amyloidosis.
By chance, both of the winners highlighted dietary triggers, said Stephanie Sherman, MD, chair of the annual meeting’s clinical vignettes committee.
“The common themes in both of these were the importance of dietary history when interviewing patients,” Dr. Sherman said. “And then both had a beautiful review of the physiology that’s normal and how it gets broken in these situations.”
The Clinical Vignettes portion of the RIV competition, which also includes research and innovations categories, was separate this year because of space constraints, Dr. Sherman said.
Judges said they looked not only at how interesting and applicable each case was, but also the quality of the oral presentation and the poster’s visual appeal and clarity.
The ketoacidosis case, presented by Timothy Judson, MD, a resident at University of California, San Francisco, involved a 40-year-old woman who was previously healthy and had given birth 9 weeks earlier. Since the birth, the woman had been on a Paleo diet, a low-carbohydrate, ketogenic diet. She also was breastfeeding her newborn and continuing to breastfeed her 2-year-old son.
She presented with nonbilious, nonbloody emesis. On physical exam, she was found to be tachycardic, with diffuse tenderness of the abdomen. She was positive for ketones and had an elevated acetone level and elevated osmolar gap, the difference between the measured and calculated solutes in the serum.
Clinicians identified that low carbohydrate intake, high fat intake, and a high metabolic state, such as that brought on by breastfeeding, can contribute to ketoacidosis. She was treated with IV glucose-containing fluids, bicarbonate, fomepizole, and thiamine.
The case shows that patients should be warned about ketoacidosis risk when they start an ultra-low carbohydrate diet, especially if they are breastfeeding or lactating, Dr. Hudson said.
“Usually they’re safe, but they may not be if you’re in a high metabolic state,” he told judges.
“We take care of so many patients on a daily basis and we rarely get to tell their stories,” he said. “To be able to tell the story of the patients and give the learning points that we took away to others, I think is very rewarding.”
The winner of the trainee award, Maxwell Bressman, MD, a resident at Montefiore Medical Center in New York, presented the case of a 62-year-old woman with hypertension who had profound generalized weakness and an inability to walk.
“She actually came to the hospital because she couldn’t lift a cup of tea,” Dr. Bressman told judges.
Clinicians traced her problem to that very tea – a licorice-containing brew – after an ECG indicated hypokalemia. A breakdown product of licorice, glycyrrhizic acid, can prevent the breakdown of cortisol into cortisone, causing increased absorption of sodium in exchange for potassium, he explained.
“I really like interesting cases – it’s something I’ve thought about throughout medical school,” Dr. Bressman said. “It’s been incredibly fun. We have great cases at Montefiore. ... It’s taught me to think very broadly and with an expansive differential.”
REPORTING FROM HOSPITAL MEDICINE 2018
New guidance for inpatient opioid prescribing
ORLANDO – A new guidance statement for opioid prescribing for hospitalized adults who have acute noncancer pain has been issued by the Society for Hospital Medicine.
The statement comes after an exhaustive systematic review that found just four existing guidelines met inclusion criteria, though none focused specifically on acute pain in hospitalized adults.
Among the key issues taken from the existing guidelines and addressed in the new SHM guidance statement are deciding when opioids – or a nonopioid alternative – should be used, as well as selection of appropriate dose, route, and duration of administration. The guidance statement advises that clinicians prescribe the lowest effective opioid dose for the shortest duration possible.
Best practices for screening and monitoring before and during opioid initiation is another major focus, as is minimizing opioid-related adverse events, both by careful patient selection and by judicious prescribing.
Finally, the statement acknowledges that, when a discharge medication list includes an opioid prescription, there is potential risk for misuse or diversion. Accordingly, the recommendation is to limit the duration of outpatient prescribing to 7 days of medication, with consideration of a 3-5 day prescription.
An interactive session at the 2018 SHM annual meeting presenting the guidance statement focused less on marching through the guidance’s 16 specific statements, and more on teasing out the why, when, how – and how long – of inpatient opioid prescribing.
The well-attended session, led by two of the guideline authors, Shoshana Herzig, MD, MPH, and Teryl K. Nuckols, MD, FHM, began with Dr. Herzig, director of hospital medicine research at Beth Israel Deaconess Medical Center, Boston, making a compelling case for why guidance is needed for inpatient opioid prescribing for acute pain.
“Few would disagree that, at the end of the day, we are the final common pathway” for hospitalized patients who receive opioids, said Dr. Herzig. And there’s ample evidence that troublesome opioid prescribing is widespread, she said, adding that associated problems aren’t limited to such inpatient adverse events as falls, respiratory arrest, and acute kidney injury; plenty of opioid-exposed patients who leave the hospital continue to use opioids in problematic ways after discharge.
Of patients who were opioid naive and filled outpatient opioid prescriptions on discharge, “Almost half of patients were still using opioids 90 days later,” Dr. Herzig said. “Hospitals contribute to opioid initiation in millions of patients each year, so our prescribing patterns in the hospital do matter.”
“We tend to prescribe high doses,” said Dr. Herzig – an average of a 68-mg oral morphine equivalent (OME) dose on days that opioids were received, according to a 2014 study she coauthored. Overall, Dr. Herzig and her colleagues found that about 40% of patients who received opioids had a daily dose of at least 50 mg OME, and about a quarter received a daily dose at or exceeding 100 mg OME (Herzig et al. J Hosp Med. 2014 Feb;9[2]:73-81).
Further, she said, “We tend to prescribe a bit haphazardly.” The same study found wide variation in regional inpatient opioid-prescribing practices, with inpatients in the U.S. Midwest, South, and West seeing adjusted relative rates of exposure to opioids of 1.26, 1.33, and 1.37, compared with the Northeast, she said.
Among the more concerning findings, she said, was that “hospitals that prescribe opioids more frequently appear to do so less safely.” In hospitals that fell into the top quartile for inpatient opioid exposure, the overall rate of opioid-related adverse events was 0.39%, compared with 0.21% for hospitals in the bottom quartile of opioid prescribing, for an overall adjusted relative risk of 1.23 in opioid-exposed patients in the hospitals with the highest prescribing, said Dr. Herzig.
Dr. Nuckols, director of the division of general internal medicine at Cedars-Sinai Medical Center, Los Angeles, engaged attendees to identify challenges in acute pain management among hospitalized adults.
The audience was quick and prolific with answers, which included varying physician standards for opioid prescribing; patient expectations for pain management – and sometimes denial that opioid use has become a disorder; varying expectations for pain management among care team members who may be reluctant to let go of pain as “the fifth vital sign;” difficulty accessing and being reimbursed for nonpharmacologic strategies; and, acknowledged by all, patient satisfaction scores.
To this last point, Dr. Nuckols said that there have been “a few recent changes for the better.” The Joint Commission is revising its standards to move away from pain as a vital sign, toward a focused assessment of pain that considers how patients are responding to pain, as well as functional status. However, she said, “There aren’t any validated measures yet for how we’re going to do this.”
Similar shifts are underway with pain-related HCAHPS (the Hospital Consumer Assessment of Healthcare Providers and Systems) questions, which have undergone a “big pullback” from an emphasis on complete control of pain, and now put more focus on whether caregivers asked about pain and talked with inpatients about ways to treat pain, said Dr. Nuckols.
Speaking to the process of developing the guidance statement, Dr. Nuckols said that “I think it’s important to note that the empirical literature about managing pain for inpatients … is almost nonexistent.” Of the four criteria that met inclusion criteria – “and we were tough raters when it comes to the guidelines” – most were based on expert consensus, she said, and most had primarily an outpatient focus.
Themes that emerged from the review process included consideration of a nonopioid strategy before initiating an opioid. These might include pharmacologic interventions such as acetaminophen or a nonsteroidal anti-inflammatory for nociceptive pain, pregabalin, gabapentin, or other medication to manage neuropathic pain, or nonpharmacologic interventions such as heat, ice, or distraction. All of these should also be considered as adjuncts to minimize opioid dosing as well, said Dr. Nuckols, citing well-documented synergy with multiple modalities of pain treatment.
Careful patient selection is also key, said Dr. Nuckols. She noted that she asks herself, “How likely is this patient to get into trouble?” with inpatient opioid administration. A concept that goes hand-in-hand, she said, is choosing the appropriate dose and route.
Dr. Herzig picked up this theme, noting that route of administration matters. A speedy route, such as intravenous administration, has been shown to reinforce the potentially addictive effect of opioids. There are times when IV is the route to use, such as when the patient can’t take medication by mouth or when immediate pain control truly is needed. However, oral medication is just as effective, albeit slightly slower acting, she said.
Conversion from IV to oral opioids is a potential time for trouble, said Dr. Herzig. “Always use an opioid conversion chart,” she said. Cross-tolerance can be incomplete between opioids, so safe practice is to begin with about 50% of the OME dose with the new medication and titrate up. And don’t use a long-acting opioid for acute pain, she said, noting that not only will there be a long half-life and washout period if the dose is too high, but patient risk for later opioid use disorder is also upped with this strategy. “You can always add more, but it’s hard to take away,” said Dr. Herzig.
On discharge, consider whether an opioid should be prescribed at all, said Dr. Herzig. The guidance statement advises generally prescribing less than a 7-day supply, with the rationale that, if posthospitalization acute pain is severe enough to require an opioid at that point, the patient should have outpatient follow-up.
This approach doesn’t undertreat outpatient pain, said Dr. Herzig, pointing to studies that show that, at discharge, “the majority of opioids that patients are getting, they are not taking – which tells us that by definition we are overprescribing.”
The authors of the guidance statement wanted to address two important topics that were not sufficiently evidence backed, Dr. Herzig said. They had hoped to give clear guidance about best practices for communication and follow-up with outpatient providers after hospital discharge. Though they didn’t find clear guidance in this area, “We do believe that outpatient providers need to be kept in the loop.”
A second area, currently a hot button topic both in the medical community and in the lay press, is whether a naloxone prescription should accompany an opioid prescription at discharge. “There just aren’t studies for this,” said Dr. Herzig.
The full text of the guidance statement may be found here: https://www.journalofhospitalmedicine.com/jhospmed/article/161927/hospital-medicine/improving-safety-opioid-use-acute-noncancer-pain.
ORLANDO – A new guidance statement for opioid prescribing for hospitalized adults who have acute noncancer pain has been issued by the Society for Hospital Medicine.
The statement comes after an exhaustive systematic review that found just four existing guidelines met inclusion criteria, though none focused specifically on acute pain in hospitalized adults.
Among the key issues taken from the existing guidelines and addressed in the new SHM guidance statement are deciding when opioids – or a nonopioid alternative – should be used, as well as selection of appropriate dose, route, and duration of administration. The guidance statement advises that clinicians prescribe the lowest effective opioid dose for the shortest duration possible.
Best practices for screening and monitoring before and during opioid initiation is another major focus, as is minimizing opioid-related adverse events, both by careful patient selection and by judicious prescribing.
Finally, the statement acknowledges that, when a discharge medication list includes an opioid prescription, there is potential risk for misuse or diversion. Accordingly, the recommendation is to limit the duration of outpatient prescribing to 7 days of medication, with consideration of a 3-5 day prescription.
An interactive session at the 2018 SHM annual meeting presenting the guidance statement focused less on marching through the guidance’s 16 specific statements, and more on teasing out the why, when, how – and how long – of inpatient opioid prescribing.
The well-attended session, led by two of the guideline authors, Shoshana Herzig, MD, MPH, and Teryl K. Nuckols, MD, FHM, began with Dr. Herzig, director of hospital medicine research at Beth Israel Deaconess Medical Center, Boston, making a compelling case for why guidance is needed for inpatient opioid prescribing for acute pain.
“Few would disagree that, at the end of the day, we are the final common pathway” for hospitalized patients who receive opioids, said Dr. Herzig. And there’s ample evidence that troublesome opioid prescribing is widespread, she said, adding that associated problems aren’t limited to such inpatient adverse events as falls, respiratory arrest, and acute kidney injury; plenty of opioid-exposed patients who leave the hospital continue to use opioids in problematic ways after discharge.
Of patients who were opioid naive and filled outpatient opioid prescriptions on discharge, “Almost half of patients were still using opioids 90 days later,” Dr. Herzig said. “Hospitals contribute to opioid initiation in millions of patients each year, so our prescribing patterns in the hospital do matter.”
“We tend to prescribe high doses,” said Dr. Herzig – an average of a 68-mg oral morphine equivalent (OME) dose on days that opioids were received, according to a 2014 study she coauthored. Overall, Dr. Herzig and her colleagues found that about 40% of patients who received opioids had a daily dose of at least 50 mg OME, and about a quarter received a daily dose at or exceeding 100 mg OME (Herzig et al. J Hosp Med. 2014 Feb;9[2]:73-81).
Further, she said, “We tend to prescribe a bit haphazardly.” The same study found wide variation in regional inpatient opioid-prescribing practices, with inpatients in the U.S. Midwest, South, and West seeing adjusted relative rates of exposure to opioids of 1.26, 1.33, and 1.37, compared with the Northeast, she said.
Among the more concerning findings, she said, was that “hospitals that prescribe opioids more frequently appear to do so less safely.” In hospitals that fell into the top quartile for inpatient opioid exposure, the overall rate of opioid-related adverse events was 0.39%, compared with 0.21% for hospitals in the bottom quartile of opioid prescribing, for an overall adjusted relative risk of 1.23 in opioid-exposed patients in the hospitals with the highest prescribing, said Dr. Herzig.
Dr. Nuckols, director of the division of general internal medicine at Cedars-Sinai Medical Center, Los Angeles, engaged attendees to identify challenges in acute pain management among hospitalized adults.
The audience was quick and prolific with answers, which included varying physician standards for opioid prescribing; patient expectations for pain management – and sometimes denial that opioid use has become a disorder; varying expectations for pain management among care team members who may be reluctant to let go of pain as “the fifth vital sign;” difficulty accessing and being reimbursed for nonpharmacologic strategies; and, acknowledged by all, patient satisfaction scores.
To this last point, Dr. Nuckols said that there have been “a few recent changes for the better.” The Joint Commission is revising its standards to move away from pain as a vital sign, toward a focused assessment of pain that considers how patients are responding to pain, as well as functional status. However, she said, “There aren’t any validated measures yet for how we’re going to do this.”
Similar shifts are underway with pain-related HCAHPS (the Hospital Consumer Assessment of Healthcare Providers and Systems) questions, which have undergone a “big pullback” from an emphasis on complete control of pain, and now put more focus on whether caregivers asked about pain and talked with inpatients about ways to treat pain, said Dr. Nuckols.
Speaking to the process of developing the guidance statement, Dr. Nuckols said that “I think it’s important to note that the empirical literature about managing pain for inpatients … is almost nonexistent.” Of the four criteria that met inclusion criteria – “and we were tough raters when it comes to the guidelines” – most were based on expert consensus, she said, and most had primarily an outpatient focus.
Themes that emerged from the review process included consideration of a nonopioid strategy before initiating an opioid. These might include pharmacologic interventions such as acetaminophen or a nonsteroidal anti-inflammatory for nociceptive pain, pregabalin, gabapentin, or other medication to manage neuropathic pain, or nonpharmacologic interventions such as heat, ice, or distraction. All of these should also be considered as adjuncts to minimize opioid dosing as well, said Dr. Nuckols, citing well-documented synergy with multiple modalities of pain treatment.
Careful patient selection is also key, said Dr. Nuckols. She noted that she asks herself, “How likely is this patient to get into trouble?” with inpatient opioid administration. A concept that goes hand-in-hand, she said, is choosing the appropriate dose and route.
Dr. Herzig picked up this theme, noting that route of administration matters. A speedy route, such as intravenous administration, has been shown to reinforce the potentially addictive effect of opioids. There are times when IV is the route to use, such as when the patient can’t take medication by mouth or when immediate pain control truly is needed. However, oral medication is just as effective, albeit slightly slower acting, she said.
Conversion from IV to oral opioids is a potential time for trouble, said Dr. Herzig. “Always use an opioid conversion chart,” she said. Cross-tolerance can be incomplete between opioids, so safe practice is to begin with about 50% of the OME dose with the new medication and titrate up. And don’t use a long-acting opioid for acute pain, she said, noting that not only will there be a long half-life and washout period if the dose is too high, but patient risk for later opioid use disorder is also upped with this strategy. “You can always add more, but it’s hard to take away,” said Dr. Herzig.
On discharge, consider whether an opioid should be prescribed at all, said Dr. Herzig. The guidance statement advises generally prescribing less than a 7-day supply, with the rationale that, if posthospitalization acute pain is severe enough to require an opioid at that point, the patient should have outpatient follow-up.
This approach doesn’t undertreat outpatient pain, said Dr. Herzig, pointing to studies that show that, at discharge, “the majority of opioids that patients are getting, they are not taking – which tells us that by definition we are overprescribing.”
The authors of the guidance statement wanted to address two important topics that were not sufficiently evidence backed, Dr. Herzig said. They had hoped to give clear guidance about best practices for communication and follow-up with outpatient providers after hospital discharge. Though they didn’t find clear guidance in this area, “We do believe that outpatient providers need to be kept in the loop.”
A second area, currently a hot button topic both in the medical community and in the lay press, is whether a naloxone prescription should accompany an opioid prescription at discharge. “There just aren’t studies for this,” said Dr. Herzig.
The full text of the guidance statement may be found here: https://www.journalofhospitalmedicine.com/jhospmed/article/161927/hospital-medicine/improving-safety-opioid-use-acute-noncancer-pain.
ORLANDO – A new guidance statement for opioid prescribing for hospitalized adults who have acute noncancer pain has been issued by the Society for Hospital Medicine.
The statement comes after an exhaustive systematic review that found just four existing guidelines met inclusion criteria, though none focused specifically on acute pain in hospitalized adults.
Among the key issues taken from the existing guidelines and addressed in the new SHM guidance statement are deciding when opioids – or a nonopioid alternative – should be used, as well as selection of appropriate dose, route, and duration of administration. The guidance statement advises that clinicians prescribe the lowest effective opioid dose for the shortest duration possible.
Best practices for screening and monitoring before and during opioid initiation is another major focus, as is minimizing opioid-related adverse events, both by careful patient selection and by judicious prescribing.
Finally, the statement acknowledges that, when a discharge medication list includes an opioid prescription, there is potential risk for misuse or diversion. Accordingly, the recommendation is to limit the duration of outpatient prescribing to 7 days of medication, with consideration of a 3-5 day prescription.
An interactive session at the 2018 SHM annual meeting presenting the guidance statement focused less on marching through the guidance’s 16 specific statements, and more on teasing out the why, when, how – and how long – of inpatient opioid prescribing.
The well-attended session, led by two of the guideline authors, Shoshana Herzig, MD, MPH, and Teryl K. Nuckols, MD, FHM, began with Dr. Herzig, director of hospital medicine research at Beth Israel Deaconess Medical Center, Boston, making a compelling case for why guidance is needed for inpatient opioid prescribing for acute pain.
“Few would disagree that, at the end of the day, we are the final common pathway” for hospitalized patients who receive opioids, said Dr. Herzig. And there’s ample evidence that troublesome opioid prescribing is widespread, she said, adding that associated problems aren’t limited to such inpatient adverse events as falls, respiratory arrest, and acute kidney injury; plenty of opioid-exposed patients who leave the hospital continue to use opioids in problematic ways after discharge.
Of patients who were opioid naive and filled outpatient opioid prescriptions on discharge, “Almost half of patients were still using opioids 90 days later,” Dr. Herzig said. “Hospitals contribute to opioid initiation in millions of patients each year, so our prescribing patterns in the hospital do matter.”
“We tend to prescribe high doses,” said Dr. Herzig – an average of a 68-mg oral morphine equivalent (OME) dose on days that opioids were received, according to a 2014 study she coauthored. Overall, Dr. Herzig and her colleagues found that about 40% of patients who received opioids had a daily dose of at least 50 mg OME, and about a quarter received a daily dose at or exceeding 100 mg OME (Herzig et al. J Hosp Med. 2014 Feb;9[2]:73-81).
Further, she said, “We tend to prescribe a bit haphazardly.” The same study found wide variation in regional inpatient opioid-prescribing practices, with inpatients in the U.S. Midwest, South, and West seeing adjusted relative rates of exposure to opioids of 1.26, 1.33, and 1.37, compared with the Northeast, she said.
Among the more concerning findings, she said, was that “hospitals that prescribe opioids more frequently appear to do so less safely.” In hospitals that fell into the top quartile for inpatient opioid exposure, the overall rate of opioid-related adverse events was 0.39%, compared with 0.21% for hospitals in the bottom quartile of opioid prescribing, for an overall adjusted relative risk of 1.23 in opioid-exposed patients in the hospitals with the highest prescribing, said Dr. Herzig.
Dr. Nuckols, director of the division of general internal medicine at Cedars-Sinai Medical Center, Los Angeles, engaged attendees to identify challenges in acute pain management among hospitalized adults.
The audience was quick and prolific with answers, which included varying physician standards for opioid prescribing; patient expectations for pain management – and sometimes denial that opioid use has become a disorder; varying expectations for pain management among care team members who may be reluctant to let go of pain as “the fifth vital sign;” difficulty accessing and being reimbursed for nonpharmacologic strategies; and, acknowledged by all, patient satisfaction scores.
To this last point, Dr. Nuckols said that there have been “a few recent changes for the better.” The Joint Commission is revising its standards to move away from pain as a vital sign, toward a focused assessment of pain that considers how patients are responding to pain, as well as functional status. However, she said, “There aren’t any validated measures yet for how we’re going to do this.”
Similar shifts are underway with pain-related HCAHPS (the Hospital Consumer Assessment of Healthcare Providers and Systems) questions, which have undergone a “big pullback” from an emphasis on complete control of pain, and now put more focus on whether caregivers asked about pain and talked with inpatients about ways to treat pain, said Dr. Nuckols.
Speaking to the process of developing the guidance statement, Dr. Nuckols said that “I think it’s important to note that the empirical literature about managing pain for inpatients … is almost nonexistent.” Of the four criteria that met inclusion criteria – “and we were tough raters when it comes to the guidelines” – most were based on expert consensus, she said, and most had primarily an outpatient focus.
Themes that emerged from the review process included consideration of a nonopioid strategy before initiating an opioid. These might include pharmacologic interventions such as acetaminophen or a nonsteroidal anti-inflammatory for nociceptive pain, pregabalin, gabapentin, or other medication to manage neuropathic pain, or nonpharmacologic interventions such as heat, ice, or distraction. All of these should also be considered as adjuncts to minimize opioid dosing as well, said Dr. Nuckols, citing well-documented synergy with multiple modalities of pain treatment.
Careful patient selection is also key, said Dr. Nuckols. She noted that she asks herself, “How likely is this patient to get into trouble?” with inpatient opioid administration. A concept that goes hand-in-hand, she said, is choosing the appropriate dose and route.
Dr. Herzig picked up this theme, noting that route of administration matters. A speedy route, such as intravenous administration, has been shown to reinforce the potentially addictive effect of opioids. There are times when IV is the route to use, such as when the patient can’t take medication by mouth or when immediate pain control truly is needed. However, oral medication is just as effective, albeit slightly slower acting, she said.
Conversion from IV to oral opioids is a potential time for trouble, said Dr. Herzig. “Always use an opioid conversion chart,” she said. Cross-tolerance can be incomplete between opioids, so safe practice is to begin with about 50% of the OME dose with the new medication and titrate up. And don’t use a long-acting opioid for acute pain, she said, noting that not only will there be a long half-life and washout period if the dose is too high, but patient risk for later opioid use disorder is also upped with this strategy. “You can always add more, but it’s hard to take away,” said Dr. Herzig.
On discharge, consider whether an opioid should be prescribed at all, said Dr. Herzig. The guidance statement advises generally prescribing less than a 7-day supply, with the rationale that, if posthospitalization acute pain is severe enough to require an opioid at that point, the patient should have outpatient follow-up.
This approach doesn’t undertreat outpatient pain, said Dr. Herzig, pointing to studies that show that, at discharge, “the majority of opioids that patients are getting, they are not taking – which tells us that by definition we are overprescribing.”
The authors of the guidance statement wanted to address two important topics that were not sufficiently evidence backed, Dr. Herzig said. They had hoped to give clear guidance about best practices for communication and follow-up with outpatient providers after hospital discharge. Though they didn’t find clear guidance in this area, “We do believe that outpatient providers need to be kept in the loop.”
A second area, currently a hot button topic both in the medical community and in the lay press, is whether a naloxone prescription should accompany an opioid prescription at discharge. “There just aren’t studies for this,” said Dr. Herzig.
The full text of the guidance statement may be found here: https://www.journalofhospitalmedicine.com/jhospmed/article/161927/hospital-medicine/improving-safety-opioid-use-acute-noncancer-pain.
REPORTING FROM HM18
Chikungunya infection in children masquerades as SJS-TEN
Chikungunya infections in young children resemble skin symptoms characteristic of Stevens-Johnson syndrome and toxic epidermal necrolysis, (SJS-TEN), according to data from a case series of 21 children seen during a chikungunya outbreak in India in August and September 2016.
The researchers described their observations of 13 boys and eight girls aged 1-36 months in Pediatric Dermatology. All 21 children presented with vesiculobullous and necrotic lesions and mild to moderate fever; 16 children (76%) had large erosions, purpuric macules, and necrosis. Most of the lesions occurred on the extremities.
The time from the onset of illness to presentation ranged from 1 to 9 days, and the skin lesions resolved in 5-7 days. The lesions resolved with no sequelae in 11 patients, with hyperpigmentation in seven (33%) , and with hypopigmentation in three patients (14%).
In addition, three patients (14%) developed minor oral erosions, and four (19%) developed palmoplantar erythema, which also may be associated with SJS-TEN. However, none of the patients experienced the severe mucositis and ocular and genital involvement common to SJS-TEN, Dr. Garg and associates noted. A total of seven children tested positive for chikungunya based on enzyme-linked immunosorbent assay results.
Severity of illness can be helpful to distinguish chikungunya from SJS-TEN, the researchers said. Based on the Nelson severity index, 11 children in this series met the criteria for “not sick,” nine were “moderately sick,” and one was “very sick.”
It is key “to be aware of SJS-TEN–like presentation of chikungunya and not to misinterpret it as true SJS-TEN, which will lead to unnecessary intervention and management,” Dr. Garg and associates said.
The researchers had no financial conflicts to disclose.
SOURCE: Garg T et al. Pediatr Dermatol. 2018 Mar 24. doi: 10.1111/pde.13450.
Chikungunya infections in young children resemble skin symptoms characteristic of Stevens-Johnson syndrome and toxic epidermal necrolysis, (SJS-TEN), according to data from a case series of 21 children seen during a chikungunya outbreak in India in August and September 2016.
The researchers described their observations of 13 boys and eight girls aged 1-36 months in Pediatric Dermatology. All 21 children presented with vesiculobullous and necrotic lesions and mild to moderate fever; 16 children (76%) had large erosions, purpuric macules, and necrosis. Most of the lesions occurred on the extremities.
The time from the onset of illness to presentation ranged from 1 to 9 days, and the skin lesions resolved in 5-7 days. The lesions resolved with no sequelae in 11 patients, with hyperpigmentation in seven (33%) , and with hypopigmentation in three patients (14%).
In addition, three patients (14%) developed minor oral erosions, and four (19%) developed palmoplantar erythema, which also may be associated with SJS-TEN. However, none of the patients experienced the severe mucositis and ocular and genital involvement common to SJS-TEN, Dr. Garg and associates noted. A total of seven children tested positive for chikungunya based on enzyme-linked immunosorbent assay results.
Severity of illness can be helpful to distinguish chikungunya from SJS-TEN, the researchers said. Based on the Nelson severity index, 11 children in this series met the criteria for “not sick,” nine were “moderately sick,” and one was “very sick.”
It is key “to be aware of SJS-TEN–like presentation of chikungunya and not to misinterpret it as true SJS-TEN, which will lead to unnecessary intervention and management,” Dr. Garg and associates said.
The researchers had no financial conflicts to disclose.
SOURCE: Garg T et al. Pediatr Dermatol. 2018 Mar 24. doi: 10.1111/pde.13450.
Chikungunya infections in young children resemble skin symptoms characteristic of Stevens-Johnson syndrome and toxic epidermal necrolysis, (SJS-TEN), according to data from a case series of 21 children seen during a chikungunya outbreak in India in August and September 2016.
The researchers described their observations of 13 boys and eight girls aged 1-36 months in Pediatric Dermatology. All 21 children presented with vesiculobullous and necrotic lesions and mild to moderate fever; 16 children (76%) had large erosions, purpuric macules, and necrosis. Most of the lesions occurred on the extremities.
The time from the onset of illness to presentation ranged from 1 to 9 days, and the skin lesions resolved in 5-7 days. The lesions resolved with no sequelae in 11 patients, with hyperpigmentation in seven (33%) , and with hypopigmentation in three patients (14%).
In addition, three patients (14%) developed minor oral erosions, and four (19%) developed palmoplantar erythema, which also may be associated with SJS-TEN. However, none of the patients experienced the severe mucositis and ocular and genital involvement common to SJS-TEN, Dr. Garg and associates noted. A total of seven children tested positive for chikungunya based on enzyme-linked immunosorbent assay results.
Severity of illness can be helpful to distinguish chikungunya from SJS-TEN, the researchers said. Based on the Nelson severity index, 11 children in this series met the criteria for “not sick,” nine were “moderately sick,” and one was “very sick.”
It is key “to be aware of SJS-TEN–like presentation of chikungunya and not to misinterpret it as true SJS-TEN, which will lead to unnecessary intervention and management,” Dr. Garg and associates said.
The researchers had no financial conflicts to disclose.
SOURCE: Garg T et al. Pediatr Dermatol. 2018 Mar 24. doi: 10.1111/pde.13450.
FROM PEDIATRIC DERMATOLOGY
Key clinical point:
Major finding: Of 21 children with chikungunya, 76% had developed vesicles and bullae with purpuric macules and necrosis.
Study details: A case series of 21 children with chikungunya fever in India.
Disclosures: The researchers had no financial conflicts to disclose.
Source: Garg T et al. Pediatr Dermatol. 2018 Mar 24. doi: 10.1111/pde.13450.
Video : The SHM Research Committee: Expanding the role and footprint of research in hospital medicine
ORLANDO – In a video interview, Stephanie Mueller, MD, SFHM, of Brigham and Women’s Hospital, Boston, discusses the scope and importance of the SHM Research Committee.
One of its most important roles is overseeing the yearly Scientific Abstract and Poster Competition, known as the Research, Innovations and Clinical Vignettes (RIV) portion of the annual conference, which brings the best of current research in hospital medicine, especially in the increasingly important area of value in patient care, to the members.
In discussing the work of the committee, Dr. Mueller – who is in her third year as a member – adds that they “are working to expand the research footprint within the Society of Hospital Medicine,” including implementing initiatives such as the VIP program, which is a visiting professorship in which junior and mid-level faculty can do an exchange program between institutions.
ORLANDO – In a video interview, Stephanie Mueller, MD, SFHM, of Brigham and Women’s Hospital, Boston, discusses the scope and importance of the SHM Research Committee.
One of its most important roles is overseeing the yearly Scientific Abstract and Poster Competition, known as the Research, Innovations and Clinical Vignettes (RIV) portion of the annual conference, which brings the best of current research in hospital medicine, especially in the increasingly important area of value in patient care, to the members.
In discussing the work of the committee, Dr. Mueller – who is in her third year as a member – adds that they “are working to expand the research footprint within the Society of Hospital Medicine,” including implementing initiatives such as the VIP program, which is a visiting professorship in which junior and mid-level faculty can do an exchange program between institutions.
ORLANDO – In a video interview, Stephanie Mueller, MD, SFHM, of Brigham and Women’s Hospital, Boston, discusses the scope and importance of the SHM Research Committee.
One of its most important roles is overseeing the yearly Scientific Abstract and Poster Competition, known as the Research, Innovations and Clinical Vignettes (RIV) portion of the annual conference, which brings the best of current research in hospital medicine, especially in the increasingly important area of value in patient care, to the members.
In discussing the work of the committee, Dr. Mueller – who is in her third year as a member – adds that they “are working to expand the research footprint within the Society of Hospital Medicine,” including implementing initiatives such as the VIP program, which is a visiting professorship in which junior and mid-level faculty can do an exchange program between institutions.
REPORTING FROM HOSPITAL MEDICINE 2018
