User login
Getting the hypertension Dx right: Patient positioning matters
ABSTRACT
Purpose This study evaluated the effect of patient positioning on the diagnosis of hypertension in a clinic setting and the importance of following guidelines for measuring blood pressure (BP).
Methods In the trial part of this study, we recorded BP measurements by an aneroid sphygmomanometer with patients seated first on an examination table, a commonly observed practice, and second in the standard seated position as defined by the American Heart Association. Two measurements were obtained in each position for 204 patients, and we determined the difference between the average readings in the 2 positions. Factored into the comparison was an estimation of inherent variance of the device and observer achieved by repeated measurements on a healthy individual.
Results This investigation included an initial observational study of 25 regional primary care offices, the results of which showed frequent lack of adherence with accepted guidelines in patient positioning during BP measurement. The overall systolic and diastolic BPs were more than 2 mm Hg lower in the standard seated position compared with the examination table position (P<.001). Noncompliance with the position guideline resulted in misclassification of 15 patients (7.4%) as prehypertensive, when, in fact, they were normotensive. Misclassification of hypertension occurred in 12 patients (5.9%), when, in fact, they were normotensive. Logistic regression using relevant clinical factors did not identify those individuals who were misclassified.
Conclusion This study underscores the importance of patient positioning on BP determinations in order to accurately diagnose hypertension.
The high prevalence of hypertension and its burden of disease in the United States and worldwide are well known.1 Hypertension is a major risk factor for coronary heart disease, congestive heart failure, ischemic and hemorrhagic stroke, chronic kidney disease, and peripheral arterial disease.2 Among all risk factors, hypertension ranked first worldwide in disability-adjusted life-years.3 However, misclassification of an individual’s blood pressure (BP) as prehypertension or hypertension also confers significant health and financial burdens due to unnecessary medical encounters, testing, and treatment, and to increased cost of insurance coverage and out-of-pocket expenses. A correct assessment of BP in the outpatient setting depends on accurate measurement technique.
The diagnosis of hypertension is based on indirect measurement of BP using in-office, ambulatory, or home monitoring. Although office BP measurement is less than ideal, it is used most often to diagnose and monitor hypertension. Furthermore, most published trials of treatment recommendations are based on office BP measurements.4
Automated oscillometric and aneroid sphygmomanometers are common BP measurement devices. Proper technique is particularly important with the aneroid sphygmomanometer to obtain consistent and accurate results.5 Good training and an ability to hear the Korotkoff sounds are crucial.
Expert consensus groups such as the American Heart Association (AHA) publish recommendations for proper technique in reliably measuring BP,6-8 and they emphasize the importance of patient positioning during BP measurement. The individual should be seated comfortably in a chair with both arms and back supported, legs uncrossed, and feet flat on the floor. We’ll refer to this as the “standard position.” Although the proper technique for measuring BP has been widely advocated, a recent literature review for the US Preventive Services Task Force concluded that surprisingly few studies are available on the diagnostic accuracy of office BP practices.9
One paper evaluated the effect of leg crossing on accuracy of BP measurement. No subjects were reclassified as hypertensive, but the study lacked statistical rigor.10 Another study found variable BP readings regardless of body position.11
The purpose of our study was to compare BP measurement in 2 positions: the standard position described above, and the examination table position in which the patient is seated on the edge of the table with back, arms, and feet unsupported.
METHODS
We conducted our literature search across several scientific and medical literature databases, including PubMed, ScienceDirect, and CINAHL. Only English-language articles were reviewed.
We followed the BP measurement guidelines of the AHA. Prior to beginning the study, we provided instructions in proper BP measurement technique to the nurses who would obtain the data. The minimum sample size of patients needed to identify a difference of at least 2 mm Hg was 26, as estimated by power analysis. This was calculated using an alpha of .05 and a beta of .13.
The study population consisted of patients presenting consecutively to a teaching family medicine center. Adult patients, ages 18 and older, were informed about the study and invited to participate. Those who agreed were asked to read and sign an informed consent approved by a regional institutional review board for human subjects. We excluded patients who declined participation for any reason, who were in severe pain or distress that may have prevented them from completing the protocol, or who had limited mobility that could interfere with climbing onto the examination table. Patients considered for the study totaled 250, 28 of whom were ineligible. Another 18 patients declined participation, leaving 204 who completed the protocol.
Before testing began, we estimated the standard deviation of each aneroid sphygmomanometer and the assigned observer by repeatedly measuring the BP of a healthy normotensive individual sitting in the standard position. We obtained 46 measurements over 2 days to avoid subject and operator fatigue. Standard deviation for systolic BP was 3.6 mm Hg; for diastolic it was 3.8 mm Hg.
During testing, nurses recorded BP for each patient twice in the examination table position and twice in the standard position. They entered data into an Excel workbook for subsequent analysis. All examination rooms were equipped with newly purchased aneroid sphygmomanometers, and the appropriate cuff size was selected for each patient. Patients were instructed to remain quiet during the measurements. Patients sat first on the edge of the examination table. After a 5-minute rest, BP was measured twice in the same arm. Measurements were separated by 1 to 2 minutes. Patients then sat in the chair and rested another 2 minutes before BP was again measured twice in the same arm. The arms and back were supported in the chair and the stethoscope placed at heart level.
As per protocol, we obtained 4 BP readings on each patient and calculated the difference between the average systolic and diastolic BP values from the 2 positions. The standard error of the mean of this difference was determined using the equation, where Sd is the standard deviation of the aneroid sphygmomanometer and observer.12 A one-sided, 95% confidence upper bound for the standard error of the difference is 1.65 × SEd. We compared patient-specific differences against this upper bound to identify significant systolic and diastolic BP changes due to positioning. If the patient’s BP difference exceeded the upper bound, it was attributed to the positional change and not to variation inherent to the sphygmomanometer and observer.
As an example, consider a patient whose average systolic BP readings from the examination-table and standard positions, respectively, were 128 mm Hg and 120 mm Hg. Assuming an SEd of 3.55 and an upper bound of 5.86, the observed 8 mm Hg difference in average systolic BPs would be considered significant. The amount of random variation from the sphygmomanometer and observer would not be expected to exceed 5.86 mm Hg.
In accordance with accepted standards, prehypertension was defined as a BP between 120-139/80-89 mm Hg, and hypertension was defined as a BP ≥140/90 mm Hg.4 BP below 120/80 mm Hg was considered normal. We calculated each patient’s average systolic and diastolic BP values in the 2 positions and thereby classified the individual as normotensive, prehypertensive, or hypertensive. We regarded as misclassified any patient whose BP showed significant lowering between the examination-table and standard positions resulting in a change of classification from prehypertensive or hypertensive to normotensive. For example, a patient with an examination-table position average reading of 126/85 mm Hg and a standard position average reading of 118/78 mm Hg would have been misclassified as prehypertensive.
We reviewed charts and gathered data, including subject age, sex, obesity (defined as a body mass index of ≥30 kg/m2), and history of diabetes, hypertension, or smoking. Other than age, all data were binary. We performed logistic regression analysis using the Excel Add-in Real Statistics Resource Pack software (Release 4.3)13 to determine if these factors could predict significant lowering of BP due to positional change.
Our associated observational study. We also conducted a separate observational study of 25 regional primary care offices to evaluate compliance with the AHA guidelines for measuring BP. The office nurses taking measurements were not informed of the study’s purpose to prevent deviation from their common practice.
Data on 9 guideline criteria were collected to assess supervision of patients before and during measurements, including having the patient sit in a chair in quiet and comfortable surroundings with arms and back supported and feet on the ground. We also noted the type of BP measuring device used. Additionally, observers assessed the technique of the individuals using a manual device, including cuff placement and deflation rate. The observations were conducted during a clinic visit by a medical student knowledgeable in the AHA guidelines for measuring BP by automated oscillometric or aneroid sphygmomanometric devices. We conducted the study over a 2-week period in the second quarter of 2016.
RESULTS
Power analysis performed prior to the study showed that a minimum of 26 patients would be needed to predict a 2 mm Hg difference between BPs obtained in the 2 positions. Of the 204 patients used in the logistic regression analysis, 78 were men and 126 were women. Ages ranged from 18 to 101 years, yielding a mean of 54. One-hundred sixteen had previously received a diagnosis of hypertension, 39 had diabetes, 92 were obese, 22 were current smokers, and 68 were former smokers.
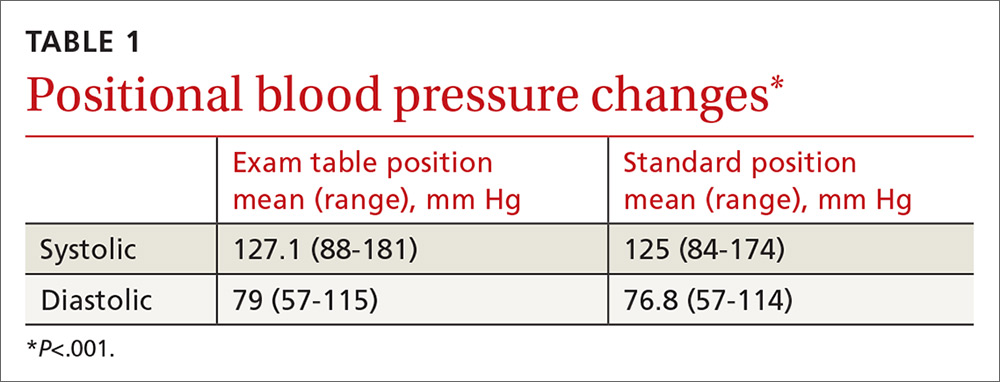
TABLE 1 shows the means and ranges of systolic and diastolic BP for both study positions. With this study population, mean BP recorded in the examination-table position decreased in the standard position by 2.1 and 2.2 mm Hg for systolic and diastolic BP, respectively (P<.001).
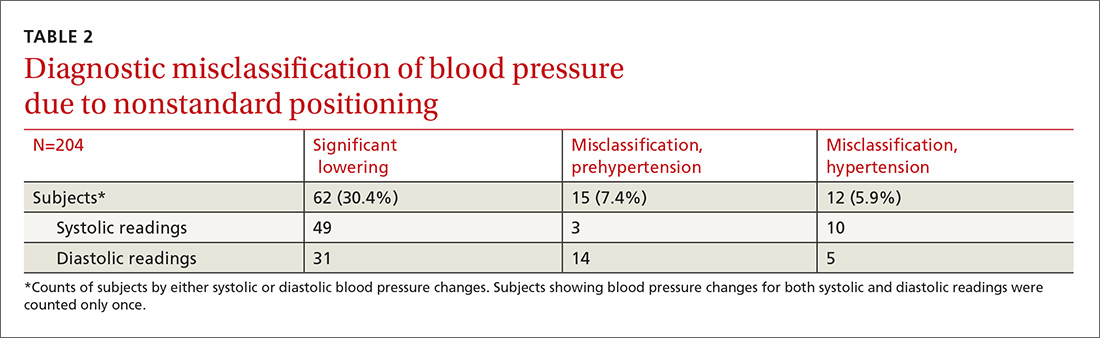
Significant BP lowering—as defined by a one-sided 95% confidence upper bound for the standard error of differences between study positions—was determined to be 5.86 and 6.22 mm Hg for systolic and diastolic pressures, respectively. Significant lowering of BP and misclassification due to positioning are summarized in TABLE 2. Significant lowering of mean systolic or diastolic BP with positional change from table to chair occurred in 62 subjects (30.4%). Misclassification of prehypertension occurred in 7.4% of subjects, and misclassification of hypertension occurred in 5.9%.
Logistic regression using patient age, sex, obesity, and history of diabetes, hypertension, and smoking as independent factors did not predict significant BP lowering with positional change.
Our observational study revealed that proper positioning in a chair was followed in only 10 of the 25 offices. In the remaining offices, patients were seated on the examination table. A 5-minute rest period before measuring BP was allowed in only 10 of the 25 offices. An automated oscillometric device was used in only 2 of the 25 offices.
DISCUSSION
In this study, 27 subjects (13.2%) were misclassified as prehypertensive or hypertensive as a result of deviating from the standard position in obtaining BP. Although the standard position is universally recommended, the guideline is not always followed in clinical practice.14
One study by Villegas et al found that 60% of physicians and nurses working in a major hospital were measuring BP inaccurately.15 In our initial observational study, 60% of primary care practices visited did not adhere to the recommended patient positioning. These medical offices are located in the community surrounding our facility and are operated by the same health care organization. The misclassification of prehypertension and hypertension observed in our prospective comparison of BP recordings in table and chair positions is, therefore, likely to occur to some degree at these practices, as well.
Similar diagnostic misclassifications have been reported in other medical settings. In a published survey of 114 medical offices, McKay and coworkers noted frequent inconsistencies with published guidelines in measuring BP.16
Common clinical demographic data obtained during this study showed no association with the positional BP change. Increased muscle tension due to lack of body support while sitting on the edge of the examination table could be the cause of elevated BP for this subgroup of individuals. Measuring muscle tension of the arms and back while seated on an exam table and chair was beyond the scope of this study.
In clinical practice, different types of BP measuring devices are used. Calibration and quality control of these devices is often lacking.17 Before starting our study, we determined the statistical variance of the aneroid sphygmomanometers and found it to approximate the manufacturer’s precision specification. Guidelines recommend using the mean of 2 BP readings as representing the patient’s BP for a given clinic visit. Additional readings are recommended if there is more than a 5 mm Hg difference between the initial 2 readings.4
In our study, we used sampling statistics of the BP readings and clinical guideline BP ranges in making diagnostic determinations. The inability to identify those patients whose BP will be affected by positional change highlights the importance of following standard BP measurement guidelines for all patients.
Study limitations. Positional change in BP from examination table to chair lacks a comparison to BP changes in positioning from chair to table. If similar BP changes in the reverse sequence were to be observed, this would add support to the hypothesis that muscle tension of the unsupported body is a cause of BP elevation in certain individuals. We believe, however, that the sequence of BP measurements (from table to chair) did not have a significant impact because all patients were allowed to rest in each position before the BP was measured. The BP was therefore measured in a steady-state in both positions.
Additionally, BP measurement by aneroid sphygmomanometry is highly dependent on observer skill and hearing ability. Furthermore, a disproportionate number of BP measurements recorded in the study ended in zero, suggesting terminal digit bias by the observer. These sources of error may be avoided using an automated oscillometric measuring device.18 Automated devices also allow for repeated independent measurements that minimize the white-coat effect. However, there are also limitations to the accuracy of oscillometric equipment. This is especially true when recording BP in the elderly, a group whose stiff arterial walls may cause erroneous measurements.19
Guideline justification. Nonadherence to standard positioning when measuring BP leads to certain individuals being misclassified as prehypertensive or hypertensive. Misclassification in turn leads to unnecessary medical encounters, testing, and treatment. Misdiagnosis is also likely to increase the cost of an individual’s insurance coverage and out-of-pocket health care expenses.
CORRESPONDENCE
Roy N. Morcos, MD, St. Elizabeth Family Medicine Residency Program, 8423 Market Street, Suite 101, Boardman, Ohio 44512; [email protected].
1. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217-223.
2. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224-2260.
3. Murray CJ, Lopez AD. Measuring the global burden of disease. New Engl J Med. 2013;369:448-457.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
5. Bailey RH, Bauer JH. A review of common errors in the indirect measurement of blood pressure. Sphygmomanometry. Arch Intern Med. 1993;153:2741-2748.
6. Padwal RS, Hemmelgarn BR, McAlister FA, et al. The 2007 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1- blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol. 2007;23:529-538.
7. Campbell NR, Chockalingam A, Fodor JG, et al. Accurate, reproducible measurement of blood pressure. CMAJ. 1990;143:19-24.
8. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens. 2005;7:102-109.
9. Piper MA, Evans CV, Burda BU, et al. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;162:192-204.
10. Peters GL, Binder SK, Campbell NR. The effect of crossing legs on blood pressure: a randomized single-blind cross-over study. Blood Press Monit. 1999;4:97-101.
11. Cicolini G, Pizzi C, Palma E, et al. Differences in blood pressure by body position (supine, Fowler’s, and sitting) in hypertensive subjects. Am J Hypertens. 2011;24:1073-1079.
12. Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences (10th Edition). Hoboken, NJ: John Wiley & Sons; 2013.
13. Zaiontz C. Real statistics using Excel. Available at: http://www.real-statistics.com/. Accessed February 20, 2018.
14. Burgess SE, MacLaughlin EJ, Smith PA, et al. Blood pressure rising: differences between current clinical and recommended measurement techniques. J Am Soc Hypertens. 2011;5:484-488.
15. Villegas I, Arias IC, Botero A, et al. Evaluation of the technique used by health-care workers for taking blood pressure. Hypertension. 1995;26:1204-1206.
16. McKay DW, Campbell NR, Parab LS, et al. Clinical assessment of blood pressure. J Hum Hypertens. 1990;4:639-645.
17. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
18. Leung AA, Nerenberg K, Daskalopoulou SS, et al. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can J Cardiol. 2016;32:569-588.
19. Raamat R, Talts J, Jagomägi K, et al. Errors of oscillometric blood pressure measurement as predicted by simulation. Blood Press Monit. 2011;16:238-245.
ABSTRACT
Purpose This study evaluated the effect of patient positioning on the diagnosis of hypertension in a clinic setting and the importance of following guidelines for measuring blood pressure (BP).
Methods In the trial part of this study, we recorded BP measurements by an aneroid sphygmomanometer with patients seated first on an examination table, a commonly observed practice, and second in the standard seated position as defined by the American Heart Association. Two measurements were obtained in each position for 204 patients, and we determined the difference between the average readings in the 2 positions. Factored into the comparison was an estimation of inherent variance of the device and observer achieved by repeated measurements on a healthy individual.
Results This investigation included an initial observational study of 25 regional primary care offices, the results of which showed frequent lack of adherence with accepted guidelines in patient positioning during BP measurement. The overall systolic and diastolic BPs were more than 2 mm Hg lower in the standard seated position compared with the examination table position (P<.001). Noncompliance with the position guideline resulted in misclassification of 15 patients (7.4%) as prehypertensive, when, in fact, they were normotensive. Misclassification of hypertension occurred in 12 patients (5.9%), when, in fact, they were normotensive. Logistic regression using relevant clinical factors did not identify those individuals who were misclassified.
Conclusion This study underscores the importance of patient positioning on BP determinations in order to accurately diagnose hypertension.
The high prevalence of hypertension and its burden of disease in the United States and worldwide are well known.1 Hypertension is a major risk factor for coronary heart disease, congestive heart failure, ischemic and hemorrhagic stroke, chronic kidney disease, and peripheral arterial disease.2 Among all risk factors, hypertension ranked first worldwide in disability-adjusted life-years.3 However, misclassification of an individual’s blood pressure (BP) as prehypertension or hypertension also confers significant health and financial burdens due to unnecessary medical encounters, testing, and treatment, and to increased cost of insurance coverage and out-of-pocket expenses. A correct assessment of BP in the outpatient setting depends on accurate measurement technique.
The diagnosis of hypertension is based on indirect measurement of BP using in-office, ambulatory, or home monitoring. Although office BP measurement is less than ideal, it is used most often to diagnose and monitor hypertension. Furthermore, most published trials of treatment recommendations are based on office BP measurements.4
Automated oscillometric and aneroid sphygmomanometers are common BP measurement devices. Proper technique is particularly important with the aneroid sphygmomanometer to obtain consistent and accurate results.5 Good training and an ability to hear the Korotkoff sounds are crucial.
Expert consensus groups such as the American Heart Association (AHA) publish recommendations for proper technique in reliably measuring BP,6-8 and they emphasize the importance of patient positioning during BP measurement. The individual should be seated comfortably in a chair with both arms and back supported, legs uncrossed, and feet flat on the floor. We’ll refer to this as the “standard position.” Although the proper technique for measuring BP has been widely advocated, a recent literature review for the US Preventive Services Task Force concluded that surprisingly few studies are available on the diagnostic accuracy of office BP practices.9
One paper evaluated the effect of leg crossing on accuracy of BP measurement. No subjects were reclassified as hypertensive, but the study lacked statistical rigor.10 Another study found variable BP readings regardless of body position.11
The purpose of our study was to compare BP measurement in 2 positions: the standard position described above, and the examination table position in which the patient is seated on the edge of the table with back, arms, and feet unsupported.
METHODS
We conducted our literature search across several scientific and medical literature databases, including PubMed, ScienceDirect, and CINAHL. Only English-language articles were reviewed.
We followed the BP measurement guidelines of the AHA. Prior to beginning the study, we provided instructions in proper BP measurement technique to the nurses who would obtain the data. The minimum sample size of patients needed to identify a difference of at least 2 mm Hg was 26, as estimated by power analysis. This was calculated using an alpha of .05 and a beta of .13.
The study population consisted of patients presenting consecutively to a teaching family medicine center. Adult patients, ages 18 and older, were informed about the study and invited to participate. Those who agreed were asked to read and sign an informed consent approved by a regional institutional review board for human subjects. We excluded patients who declined participation for any reason, who were in severe pain or distress that may have prevented them from completing the protocol, or who had limited mobility that could interfere with climbing onto the examination table. Patients considered for the study totaled 250, 28 of whom were ineligible. Another 18 patients declined participation, leaving 204 who completed the protocol.
Before testing began, we estimated the standard deviation of each aneroid sphygmomanometer and the assigned observer by repeatedly measuring the BP of a healthy normotensive individual sitting in the standard position. We obtained 46 measurements over 2 days to avoid subject and operator fatigue. Standard deviation for systolic BP was 3.6 mm Hg; for diastolic it was 3.8 mm Hg.
During testing, nurses recorded BP for each patient twice in the examination table position and twice in the standard position. They entered data into an Excel workbook for subsequent analysis. All examination rooms were equipped with newly purchased aneroid sphygmomanometers, and the appropriate cuff size was selected for each patient. Patients were instructed to remain quiet during the measurements. Patients sat first on the edge of the examination table. After a 5-minute rest, BP was measured twice in the same arm. Measurements were separated by 1 to 2 minutes. Patients then sat in the chair and rested another 2 minutes before BP was again measured twice in the same arm. The arms and back were supported in the chair and the stethoscope placed at heart level.
As per protocol, we obtained 4 BP readings on each patient and calculated the difference between the average systolic and diastolic BP values from the 2 positions. The standard error of the mean of this difference was determined using the equation, where Sd is the standard deviation of the aneroid sphygmomanometer and observer.12 A one-sided, 95% confidence upper bound for the standard error of the difference is 1.65 × SEd. We compared patient-specific differences against this upper bound to identify significant systolic and diastolic BP changes due to positioning. If the patient’s BP difference exceeded the upper bound, it was attributed to the positional change and not to variation inherent to the sphygmomanometer and observer.
As an example, consider a patient whose average systolic BP readings from the examination-table and standard positions, respectively, were 128 mm Hg and 120 mm Hg. Assuming an SEd of 3.55 and an upper bound of 5.86, the observed 8 mm Hg difference in average systolic BPs would be considered significant. The amount of random variation from the sphygmomanometer and observer would not be expected to exceed 5.86 mm Hg.
In accordance with accepted standards, prehypertension was defined as a BP between 120-139/80-89 mm Hg, and hypertension was defined as a BP ≥140/90 mm Hg.4 BP below 120/80 mm Hg was considered normal. We calculated each patient’s average systolic and diastolic BP values in the 2 positions and thereby classified the individual as normotensive, prehypertensive, or hypertensive. We regarded as misclassified any patient whose BP showed significant lowering between the examination-table and standard positions resulting in a change of classification from prehypertensive or hypertensive to normotensive. For example, a patient with an examination-table position average reading of 126/85 mm Hg and a standard position average reading of 118/78 mm Hg would have been misclassified as prehypertensive.
We reviewed charts and gathered data, including subject age, sex, obesity (defined as a body mass index of ≥30 kg/m2), and history of diabetes, hypertension, or smoking. Other than age, all data were binary. We performed logistic regression analysis using the Excel Add-in Real Statistics Resource Pack software (Release 4.3)13 to determine if these factors could predict significant lowering of BP due to positional change.
Our associated observational study. We also conducted a separate observational study of 25 regional primary care offices to evaluate compliance with the AHA guidelines for measuring BP. The office nurses taking measurements were not informed of the study’s purpose to prevent deviation from their common practice.
Data on 9 guideline criteria were collected to assess supervision of patients before and during measurements, including having the patient sit in a chair in quiet and comfortable surroundings with arms and back supported and feet on the ground. We also noted the type of BP measuring device used. Additionally, observers assessed the technique of the individuals using a manual device, including cuff placement and deflation rate. The observations were conducted during a clinic visit by a medical student knowledgeable in the AHA guidelines for measuring BP by automated oscillometric or aneroid sphygmomanometric devices. We conducted the study over a 2-week period in the second quarter of 2016.
RESULTS
Power analysis performed prior to the study showed that a minimum of 26 patients would be needed to predict a 2 mm Hg difference between BPs obtained in the 2 positions. Of the 204 patients used in the logistic regression analysis, 78 were men and 126 were women. Ages ranged from 18 to 101 years, yielding a mean of 54. One-hundred sixteen had previously received a diagnosis of hypertension, 39 had diabetes, 92 were obese, 22 were current smokers, and 68 were former smokers.
TABLE 1 shows the means and ranges of systolic and diastolic BP for both study positions. With this study population, mean BP recorded in the examination-table position decreased in the standard position by 2.1 and 2.2 mm Hg for systolic and diastolic BP, respectively (P<.001).
Significant BP lowering—as defined by a one-sided 95% confidence upper bound for the standard error of differences between study positions—was determined to be 5.86 and 6.22 mm Hg for systolic and diastolic pressures, respectively. Significant lowering of BP and misclassification due to positioning are summarized in TABLE 2. Significant lowering of mean systolic or diastolic BP with positional change from table to chair occurred in 62 subjects (30.4%). Misclassification of prehypertension occurred in 7.4% of subjects, and misclassification of hypertension occurred in 5.9%.
Logistic regression using patient age, sex, obesity, and history of diabetes, hypertension, and smoking as independent factors did not predict significant BP lowering with positional change.
Our observational study revealed that proper positioning in a chair was followed in only 10 of the 25 offices. In the remaining offices, patients were seated on the examination table. A 5-minute rest period before measuring BP was allowed in only 10 of the 25 offices. An automated oscillometric device was used in only 2 of the 25 offices.
DISCUSSION
In this study, 27 subjects (13.2%) were misclassified as prehypertensive or hypertensive as a result of deviating from the standard position in obtaining BP. Although the standard position is universally recommended, the guideline is not always followed in clinical practice.14
One study by Villegas et al found that 60% of physicians and nurses working in a major hospital were measuring BP inaccurately.15 In our initial observational study, 60% of primary care practices visited did not adhere to the recommended patient positioning. These medical offices are located in the community surrounding our facility and are operated by the same health care organization. The misclassification of prehypertension and hypertension observed in our prospective comparison of BP recordings in table and chair positions is, therefore, likely to occur to some degree at these practices, as well.
Similar diagnostic misclassifications have been reported in other medical settings. In a published survey of 114 medical offices, McKay and coworkers noted frequent inconsistencies with published guidelines in measuring BP.16
Common clinical demographic data obtained during this study showed no association with the positional BP change. Increased muscle tension due to lack of body support while sitting on the edge of the examination table could be the cause of elevated BP for this subgroup of individuals. Measuring muscle tension of the arms and back while seated on an exam table and chair was beyond the scope of this study.
In clinical practice, different types of BP measuring devices are used. Calibration and quality control of these devices is often lacking.17 Before starting our study, we determined the statistical variance of the aneroid sphygmomanometers and found it to approximate the manufacturer’s precision specification. Guidelines recommend using the mean of 2 BP readings as representing the patient’s BP for a given clinic visit. Additional readings are recommended if there is more than a 5 mm Hg difference between the initial 2 readings.4
In our study, we used sampling statistics of the BP readings and clinical guideline BP ranges in making diagnostic determinations. The inability to identify those patients whose BP will be affected by positional change highlights the importance of following standard BP measurement guidelines for all patients.
Study limitations. Positional change in BP from examination table to chair lacks a comparison to BP changes in positioning from chair to table. If similar BP changes in the reverse sequence were to be observed, this would add support to the hypothesis that muscle tension of the unsupported body is a cause of BP elevation in certain individuals. We believe, however, that the sequence of BP measurements (from table to chair) did not have a significant impact because all patients were allowed to rest in each position before the BP was measured. The BP was therefore measured in a steady-state in both positions.
Additionally, BP measurement by aneroid sphygmomanometry is highly dependent on observer skill and hearing ability. Furthermore, a disproportionate number of BP measurements recorded in the study ended in zero, suggesting terminal digit bias by the observer. These sources of error may be avoided using an automated oscillometric measuring device.18 Automated devices also allow for repeated independent measurements that minimize the white-coat effect. However, there are also limitations to the accuracy of oscillometric equipment. This is especially true when recording BP in the elderly, a group whose stiff arterial walls may cause erroneous measurements.19
Guideline justification. Nonadherence to standard positioning when measuring BP leads to certain individuals being misclassified as prehypertensive or hypertensive. Misclassification in turn leads to unnecessary medical encounters, testing, and treatment. Misdiagnosis is also likely to increase the cost of an individual’s insurance coverage and out-of-pocket health care expenses.
CORRESPONDENCE
Roy N. Morcos, MD, St. Elizabeth Family Medicine Residency Program, 8423 Market Street, Suite 101, Boardman, Ohio 44512; [email protected].
ABSTRACT
Purpose This study evaluated the effect of patient positioning on the diagnosis of hypertension in a clinic setting and the importance of following guidelines for measuring blood pressure (BP).
Methods In the trial part of this study, we recorded BP measurements by an aneroid sphygmomanometer with patients seated first on an examination table, a commonly observed practice, and second in the standard seated position as defined by the American Heart Association. Two measurements were obtained in each position for 204 patients, and we determined the difference between the average readings in the 2 positions. Factored into the comparison was an estimation of inherent variance of the device and observer achieved by repeated measurements on a healthy individual.
Results This investigation included an initial observational study of 25 regional primary care offices, the results of which showed frequent lack of adherence with accepted guidelines in patient positioning during BP measurement. The overall systolic and diastolic BPs were more than 2 mm Hg lower in the standard seated position compared with the examination table position (P<.001). Noncompliance with the position guideline resulted in misclassification of 15 patients (7.4%) as prehypertensive, when, in fact, they were normotensive. Misclassification of hypertension occurred in 12 patients (5.9%), when, in fact, they were normotensive. Logistic regression using relevant clinical factors did not identify those individuals who were misclassified.
Conclusion This study underscores the importance of patient positioning on BP determinations in order to accurately diagnose hypertension.
The high prevalence of hypertension and its burden of disease in the United States and worldwide are well known.1 Hypertension is a major risk factor for coronary heart disease, congestive heart failure, ischemic and hemorrhagic stroke, chronic kidney disease, and peripheral arterial disease.2 Among all risk factors, hypertension ranked first worldwide in disability-adjusted life-years.3 However, misclassification of an individual’s blood pressure (BP) as prehypertension or hypertension also confers significant health and financial burdens due to unnecessary medical encounters, testing, and treatment, and to increased cost of insurance coverage and out-of-pocket expenses. A correct assessment of BP in the outpatient setting depends on accurate measurement technique.
The diagnosis of hypertension is based on indirect measurement of BP using in-office, ambulatory, or home monitoring. Although office BP measurement is less than ideal, it is used most often to diagnose and monitor hypertension. Furthermore, most published trials of treatment recommendations are based on office BP measurements.4
Automated oscillometric and aneroid sphygmomanometers are common BP measurement devices. Proper technique is particularly important with the aneroid sphygmomanometer to obtain consistent and accurate results.5 Good training and an ability to hear the Korotkoff sounds are crucial.
Expert consensus groups such as the American Heart Association (AHA) publish recommendations for proper technique in reliably measuring BP,6-8 and they emphasize the importance of patient positioning during BP measurement. The individual should be seated comfortably in a chair with both arms and back supported, legs uncrossed, and feet flat on the floor. We’ll refer to this as the “standard position.” Although the proper technique for measuring BP has been widely advocated, a recent literature review for the US Preventive Services Task Force concluded that surprisingly few studies are available on the diagnostic accuracy of office BP practices.9
One paper evaluated the effect of leg crossing on accuracy of BP measurement. No subjects were reclassified as hypertensive, but the study lacked statistical rigor.10 Another study found variable BP readings regardless of body position.11
The purpose of our study was to compare BP measurement in 2 positions: the standard position described above, and the examination table position in which the patient is seated on the edge of the table with back, arms, and feet unsupported.
METHODS
We conducted our literature search across several scientific and medical literature databases, including PubMed, ScienceDirect, and CINAHL. Only English-language articles were reviewed.
We followed the BP measurement guidelines of the AHA. Prior to beginning the study, we provided instructions in proper BP measurement technique to the nurses who would obtain the data. The minimum sample size of patients needed to identify a difference of at least 2 mm Hg was 26, as estimated by power analysis. This was calculated using an alpha of .05 and a beta of .13.
The study population consisted of patients presenting consecutively to a teaching family medicine center. Adult patients, ages 18 and older, were informed about the study and invited to participate. Those who agreed were asked to read and sign an informed consent approved by a regional institutional review board for human subjects. We excluded patients who declined participation for any reason, who were in severe pain or distress that may have prevented them from completing the protocol, or who had limited mobility that could interfere with climbing onto the examination table. Patients considered for the study totaled 250, 28 of whom were ineligible. Another 18 patients declined participation, leaving 204 who completed the protocol.
Before testing began, we estimated the standard deviation of each aneroid sphygmomanometer and the assigned observer by repeatedly measuring the BP of a healthy normotensive individual sitting in the standard position. We obtained 46 measurements over 2 days to avoid subject and operator fatigue. Standard deviation for systolic BP was 3.6 mm Hg; for diastolic it was 3.8 mm Hg.
During testing, nurses recorded BP for each patient twice in the examination table position and twice in the standard position. They entered data into an Excel workbook for subsequent analysis. All examination rooms were equipped with newly purchased aneroid sphygmomanometers, and the appropriate cuff size was selected for each patient. Patients were instructed to remain quiet during the measurements. Patients sat first on the edge of the examination table. After a 5-minute rest, BP was measured twice in the same arm. Measurements were separated by 1 to 2 minutes. Patients then sat in the chair and rested another 2 minutes before BP was again measured twice in the same arm. The arms and back were supported in the chair and the stethoscope placed at heart level.
As per protocol, we obtained 4 BP readings on each patient and calculated the difference between the average systolic and diastolic BP values from the 2 positions. The standard error of the mean of this difference was determined using the equation, where Sd is the standard deviation of the aneroid sphygmomanometer and observer.12 A one-sided, 95% confidence upper bound for the standard error of the difference is 1.65 × SEd. We compared patient-specific differences against this upper bound to identify significant systolic and diastolic BP changes due to positioning. If the patient’s BP difference exceeded the upper bound, it was attributed to the positional change and not to variation inherent to the sphygmomanometer and observer.
As an example, consider a patient whose average systolic BP readings from the examination-table and standard positions, respectively, were 128 mm Hg and 120 mm Hg. Assuming an SEd of 3.55 and an upper bound of 5.86, the observed 8 mm Hg difference in average systolic BPs would be considered significant. The amount of random variation from the sphygmomanometer and observer would not be expected to exceed 5.86 mm Hg.
In accordance with accepted standards, prehypertension was defined as a BP between 120-139/80-89 mm Hg, and hypertension was defined as a BP ≥140/90 mm Hg.4 BP below 120/80 mm Hg was considered normal. We calculated each patient’s average systolic and diastolic BP values in the 2 positions and thereby classified the individual as normotensive, prehypertensive, or hypertensive. We regarded as misclassified any patient whose BP showed significant lowering between the examination-table and standard positions resulting in a change of classification from prehypertensive or hypertensive to normotensive. For example, a patient with an examination-table position average reading of 126/85 mm Hg and a standard position average reading of 118/78 mm Hg would have been misclassified as prehypertensive.
We reviewed charts and gathered data, including subject age, sex, obesity (defined as a body mass index of ≥30 kg/m2), and history of diabetes, hypertension, or smoking. Other than age, all data were binary. We performed logistic regression analysis using the Excel Add-in Real Statistics Resource Pack software (Release 4.3)13 to determine if these factors could predict significant lowering of BP due to positional change.
Our associated observational study. We also conducted a separate observational study of 25 regional primary care offices to evaluate compliance with the AHA guidelines for measuring BP. The office nurses taking measurements were not informed of the study’s purpose to prevent deviation from their common practice.
Data on 9 guideline criteria were collected to assess supervision of patients before and during measurements, including having the patient sit in a chair in quiet and comfortable surroundings with arms and back supported and feet on the ground. We also noted the type of BP measuring device used. Additionally, observers assessed the technique of the individuals using a manual device, including cuff placement and deflation rate. The observations were conducted during a clinic visit by a medical student knowledgeable in the AHA guidelines for measuring BP by automated oscillometric or aneroid sphygmomanometric devices. We conducted the study over a 2-week period in the second quarter of 2016.
RESULTS
Power analysis performed prior to the study showed that a minimum of 26 patients would be needed to predict a 2 mm Hg difference between BPs obtained in the 2 positions. Of the 204 patients used in the logistic regression analysis, 78 were men and 126 were women. Ages ranged from 18 to 101 years, yielding a mean of 54. One-hundred sixteen had previously received a diagnosis of hypertension, 39 had diabetes, 92 were obese, 22 were current smokers, and 68 were former smokers.
TABLE 1 shows the means and ranges of systolic and diastolic BP for both study positions. With this study population, mean BP recorded in the examination-table position decreased in the standard position by 2.1 and 2.2 mm Hg for systolic and diastolic BP, respectively (P<.001).
Significant BP lowering—as defined by a one-sided 95% confidence upper bound for the standard error of differences between study positions—was determined to be 5.86 and 6.22 mm Hg for systolic and diastolic pressures, respectively. Significant lowering of BP and misclassification due to positioning are summarized in TABLE 2. Significant lowering of mean systolic or diastolic BP with positional change from table to chair occurred in 62 subjects (30.4%). Misclassification of prehypertension occurred in 7.4% of subjects, and misclassification of hypertension occurred in 5.9%.
Logistic regression using patient age, sex, obesity, and history of diabetes, hypertension, and smoking as independent factors did not predict significant BP lowering with positional change.
Our observational study revealed that proper positioning in a chair was followed in only 10 of the 25 offices. In the remaining offices, patients were seated on the examination table. A 5-minute rest period before measuring BP was allowed in only 10 of the 25 offices. An automated oscillometric device was used in only 2 of the 25 offices.
DISCUSSION
In this study, 27 subjects (13.2%) were misclassified as prehypertensive or hypertensive as a result of deviating from the standard position in obtaining BP. Although the standard position is universally recommended, the guideline is not always followed in clinical practice.14
One study by Villegas et al found that 60% of physicians and nurses working in a major hospital were measuring BP inaccurately.15 In our initial observational study, 60% of primary care practices visited did not adhere to the recommended patient positioning. These medical offices are located in the community surrounding our facility and are operated by the same health care organization. The misclassification of prehypertension and hypertension observed in our prospective comparison of BP recordings in table and chair positions is, therefore, likely to occur to some degree at these practices, as well.
Similar diagnostic misclassifications have been reported in other medical settings. In a published survey of 114 medical offices, McKay and coworkers noted frequent inconsistencies with published guidelines in measuring BP.16
Common clinical demographic data obtained during this study showed no association with the positional BP change. Increased muscle tension due to lack of body support while sitting on the edge of the examination table could be the cause of elevated BP for this subgroup of individuals. Measuring muscle tension of the arms and back while seated on an exam table and chair was beyond the scope of this study.
In clinical practice, different types of BP measuring devices are used. Calibration and quality control of these devices is often lacking.17 Before starting our study, we determined the statistical variance of the aneroid sphygmomanometers and found it to approximate the manufacturer’s precision specification. Guidelines recommend using the mean of 2 BP readings as representing the patient’s BP for a given clinic visit. Additional readings are recommended if there is more than a 5 mm Hg difference between the initial 2 readings.4
In our study, we used sampling statistics of the BP readings and clinical guideline BP ranges in making diagnostic determinations. The inability to identify those patients whose BP will be affected by positional change highlights the importance of following standard BP measurement guidelines for all patients.
Study limitations. Positional change in BP from examination table to chair lacks a comparison to BP changes in positioning from chair to table. If similar BP changes in the reverse sequence were to be observed, this would add support to the hypothesis that muscle tension of the unsupported body is a cause of BP elevation in certain individuals. We believe, however, that the sequence of BP measurements (from table to chair) did not have a significant impact because all patients were allowed to rest in each position before the BP was measured. The BP was therefore measured in a steady-state in both positions.
Additionally, BP measurement by aneroid sphygmomanometry is highly dependent on observer skill and hearing ability. Furthermore, a disproportionate number of BP measurements recorded in the study ended in zero, suggesting terminal digit bias by the observer. These sources of error may be avoided using an automated oscillometric measuring device.18 Automated devices also allow for repeated independent measurements that minimize the white-coat effect. However, there are also limitations to the accuracy of oscillometric equipment. This is especially true when recording BP in the elderly, a group whose stiff arterial walls may cause erroneous measurements.19
Guideline justification. Nonadherence to standard positioning when measuring BP leads to certain individuals being misclassified as prehypertensive or hypertensive. Misclassification in turn leads to unnecessary medical encounters, testing, and treatment. Misdiagnosis is also likely to increase the cost of an individual’s insurance coverage and out-of-pocket health care expenses.
CORRESPONDENCE
Roy N. Morcos, MD, St. Elizabeth Family Medicine Residency Program, 8423 Market Street, Suite 101, Boardman, Ohio 44512; [email protected].
1. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217-223.
2. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224-2260.
3. Murray CJ, Lopez AD. Measuring the global burden of disease. New Engl J Med. 2013;369:448-457.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
5. Bailey RH, Bauer JH. A review of common errors in the indirect measurement of blood pressure. Sphygmomanometry. Arch Intern Med. 1993;153:2741-2748.
6. Padwal RS, Hemmelgarn BR, McAlister FA, et al. The 2007 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1- blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol. 2007;23:529-538.
7. Campbell NR, Chockalingam A, Fodor JG, et al. Accurate, reproducible measurement of blood pressure. CMAJ. 1990;143:19-24.
8. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens. 2005;7:102-109.
9. Piper MA, Evans CV, Burda BU, et al. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;162:192-204.
10. Peters GL, Binder SK, Campbell NR. The effect of crossing legs on blood pressure: a randomized single-blind cross-over study. Blood Press Monit. 1999;4:97-101.
11. Cicolini G, Pizzi C, Palma E, et al. Differences in blood pressure by body position (supine, Fowler’s, and sitting) in hypertensive subjects. Am J Hypertens. 2011;24:1073-1079.
12. Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences (10th Edition). Hoboken, NJ: John Wiley & Sons; 2013.
13. Zaiontz C. Real statistics using Excel. Available at: http://www.real-statistics.com/. Accessed February 20, 2018.
14. Burgess SE, MacLaughlin EJ, Smith PA, et al. Blood pressure rising: differences between current clinical and recommended measurement techniques. J Am Soc Hypertens. 2011;5:484-488.
15. Villegas I, Arias IC, Botero A, et al. Evaluation of the technique used by health-care workers for taking blood pressure. Hypertension. 1995;26:1204-1206.
16. McKay DW, Campbell NR, Parab LS, et al. Clinical assessment of blood pressure. J Hum Hypertens. 1990;4:639-645.
17. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
18. Leung AA, Nerenberg K, Daskalopoulou SS, et al. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can J Cardiol. 2016;32:569-588.
19. Raamat R, Talts J, Jagomägi K, et al. Errors of oscillometric blood pressure measurement as predicted by simulation. Blood Press Monit. 2011;16:238-245.
1. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217-223.
2. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224-2260.
3. Murray CJ, Lopez AD. Measuring the global burden of disease. New Engl J Med. 2013;369:448-457.
4. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
5. Bailey RH, Bauer JH. A review of common errors in the indirect measurement of blood pressure. Sphygmomanometry. Arch Intern Med. 1993;153:2741-2748.
6. Padwal RS, Hemmelgarn BR, McAlister FA, et al. The 2007 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1- blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol. 2007;23:529-538.
7. Campbell NR, Chockalingam A, Fodor JG, et al. Accurate, reproducible measurement of blood pressure. CMAJ. 1990;143:19-24.
8. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J Clin Hypertens. 2005;7:102-109.
9. Piper MA, Evans CV, Burda BU, et al. Diagnostic and predictive accuracy of blood pressure screening methods with consideration of rescreening intervals: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2015;162:192-204.
10. Peters GL, Binder SK, Campbell NR. The effect of crossing legs on blood pressure: a randomized single-blind cross-over study. Blood Press Monit. 1999;4:97-101.
11. Cicolini G, Pizzi C, Palma E, et al. Differences in blood pressure by body position (supine, Fowler’s, and sitting) in hypertensive subjects. Am J Hypertens. 2011;24:1073-1079.
12. Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences (10th Edition). Hoboken, NJ: John Wiley & Sons; 2013.
13. Zaiontz C. Real statistics using Excel. Available at: http://www.real-statistics.com/. Accessed February 20, 2018.
14. Burgess SE, MacLaughlin EJ, Smith PA, et al. Blood pressure rising: differences between current clinical and recommended measurement techniques. J Am Soc Hypertens. 2011;5:484-488.
15. Villegas I, Arias IC, Botero A, et al. Evaluation of the technique used by health-care workers for taking blood pressure. Hypertension. 1995;26:1204-1206.
16. McKay DW, Campbell NR, Parab LS, et al. Clinical assessment of blood pressure. J Hum Hypertens. 1990;4:639-645.
17. Jones DW, Appel LJ, Sheps SG, et al. Measuring blood pressure accurately: new and persistent challenges. JAMA. 2003;289:1027-1030.
18. Leung AA, Nerenberg K, Daskalopoulou SS, et al. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood Pressure Measurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can J Cardiol. 2016;32:569-588.
19. Raamat R, Talts J, Jagomägi K, et al. Errors of oscillometric blood pressure measurement as predicted by simulation. Blood Press Monit. 2011;16:238-245.

Why you shouldn’t screen for ovarian cancer in asymptomatic women
Resources
- US Preventive Services Task Force. Screening for ovarian cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;319:588-594.
- Henderson JT, Webber EM, Sawaya GF. Screening for ovarian cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;319:595-606.
Resources
- US Preventive Services Task Force. Screening for ovarian cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;319:588-594.
- Henderson JT, Webber EM, Sawaya GF. Screening for ovarian cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;319:595-606.
Resources
- US Preventive Services Task Force. Screening for ovarian cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2018;319:588-594.
- Henderson JT, Webber EM, Sawaya GF. Screening for ovarian cancer: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;319:595-606.

David Henry's JCSO podcast, March-April 2018
In his bimonthly podcast, Dr David Henry, the JCSO Editor-in-Chief, discusses the approval of the biosimilars, bevacizumab-awwb and trastuzumab-dkst, and new therapies for virally associated cancers. Also in the line-up are an interview with Dr Daniel Haller on the latest advances in treating gastrointestinal cancers, and an article on hands-on advice on integrating survivorship care planning in a radiation oncology workflow. Research topics incude how to improve communication between oncology care providers and patient caregivers during hospice; the impact of patient education on enrollment in clinical trials; and organizational barriers to optimal lung cancer care in the community setting. A series of Case Reports that highlight some of the clincial challenges in treating patients with cancer round out the issue.
Listen to the podcast below
In his bimonthly podcast, Dr David Henry, the JCSO Editor-in-Chief, discusses the approval of the biosimilars, bevacizumab-awwb and trastuzumab-dkst, and new therapies for virally associated cancers. Also in the line-up are an interview with Dr Daniel Haller on the latest advances in treating gastrointestinal cancers, and an article on hands-on advice on integrating survivorship care planning in a radiation oncology workflow. Research topics incude how to improve communication between oncology care providers and patient caregivers during hospice; the impact of patient education on enrollment in clinical trials; and organizational barriers to optimal lung cancer care in the community setting. A series of Case Reports that highlight some of the clincial challenges in treating patients with cancer round out the issue.
Listen to the podcast below
In his bimonthly podcast, Dr David Henry, the JCSO Editor-in-Chief, discusses the approval of the biosimilars, bevacizumab-awwb and trastuzumab-dkst, and new therapies for virally associated cancers. Also in the line-up are an interview with Dr Daniel Haller on the latest advances in treating gastrointestinal cancers, and an article on hands-on advice on integrating survivorship care planning in a radiation oncology workflow. Research topics incude how to improve communication between oncology care providers and patient caregivers during hospice; the impact of patient education on enrollment in clinical trials; and organizational barriers to optimal lung cancer care in the community setting. A series of Case Reports that highlight some of the clincial challenges in treating patients with cancer round out the issue.
Listen to the podcast below
Opioid Use Disorder: Challenges and Solutions to a Rising Epidemic
Click here to read the supplement
CME: Opioid Use Disorder: Challenges and Solutions to a Rising Epidemic
Earn 1.25 CME Credits.

- Introduction and 2 Case Studies by Genie L. Bailey, MD
- Opioid Use Disorder: The Epidemic is Real by Kevin P. Hill, MD, MHS
- Managing the Opioid Use Disorder Crisis by Richard N. Rosenthal, MD
Click here to read the supplement
Click here to read the supplement
CME: Opioid Use Disorder: Challenges and Solutions to a Rising Epidemic
Earn 1.25 CME Credits.
- Introduction and 2 Case Studies by Genie L. Bailey, MD
- Opioid Use Disorder: The Epidemic is Real by Kevin P. Hill, MD, MHS
- Managing the Opioid Use Disorder Crisis by Richard N. Rosenthal, MD
Click here to read the supplement
Click here to read the supplement
CME: Opioid Use Disorder: Challenges and Solutions to a Rising Epidemic
Earn 1.25 CME Credits.
- Introduction and 2 Case Studies by Genie L. Bailey, MD
- Opioid Use Disorder: The Epidemic is Real by Kevin P. Hill, MD, MHS
- Managing the Opioid Use Disorder Crisis by Richard N. Rosenthal, MD
Click here to read the supplement
DDSEP® 8 Quick Quiz - April 2018 Question 2
Q2. Correct Answer: C
Rationale
The patient presents with acute gallstone pancreatitis. In patients with gallstone pancreatitis and evidence of cholangitis, ERCP with sphincterotomy and stone extraction should be performed. The patients fever, jaundice, and right upper quadrant pain are sufficient to make the diagnosis of cholangitis. It is too early in the course of the disease to evaluate for pancreatic necrosis. Typically, triglyceride levels above 1,000 mg/dL are required to induce pancreatitis. Finally, while the patient has cholelithiasis, there is no evidence of cholecystitis. Therefore, a HIDA scan is not warranted.
Reference
1. Behrns KE, Ashley SW, Hunter JG, Carr-Locke D. Early ERCP for gallstone pancreatitis: for whom and when? J Gastrointestinal Surgery. 2008;12(4):629-33.
Q2. Correct Answer: C
Rationale
The patient presents with acute gallstone pancreatitis. In patients with gallstone pancreatitis and evidence of cholangitis, ERCP with sphincterotomy and stone extraction should be performed. The patients fever, jaundice, and right upper quadrant pain are sufficient to make the diagnosis of cholangitis. It is too early in the course of the disease to evaluate for pancreatic necrosis. Typically, triglyceride levels above 1,000 mg/dL are required to induce pancreatitis. Finally, while the patient has cholelithiasis, there is no evidence of cholecystitis. Therefore, a HIDA scan is not warranted.
Reference
1. Behrns KE, Ashley SW, Hunter JG, Carr-Locke D. Early ERCP for gallstone pancreatitis: for whom and when? J Gastrointestinal Surgery. 2008;12(4):629-33.
Q2. Correct Answer: C
Rationale
The patient presents with acute gallstone pancreatitis. In patients with gallstone pancreatitis and evidence of cholangitis, ERCP with sphincterotomy and stone extraction should be performed. The patients fever, jaundice, and right upper quadrant pain are sufficient to make the diagnosis of cholangitis. It is too early in the course of the disease to evaluate for pancreatic necrosis. Typically, triglyceride levels above 1,000 mg/dL are required to induce pancreatitis. Finally, while the patient has cholelithiasis, there is no evidence of cholecystitis. Therefore, a HIDA scan is not warranted.
Reference
1. Behrns KE, Ashley SW, Hunter JG, Carr-Locke D. Early ERCP for gallstone pancreatitis: for whom and when? J Gastrointestinal Surgery. 2008;12(4):629-33.
A 50-year-old woman with no past medical history presents to the emergency department with the acute onset of severe epigastric pain and vomiting. She is afebrile with a blood pressure of 100/50 mm Hg, and pulse of 110 bpm. Physical exam shows right upper quadrant and epigastric tenderness to palpation without rebound. Labs demonstrate a white blood cell count of 17,000/mm3, hemoglobin of 16 g/dL, creatinine of 1.4 mg/dL, alanine aminotransferase of 215 U/L, aspartate aminotransferase of 190 U/L, a total bilirubin of 2.1 mg/dL, and triglycerides of 492 mg/dL. Right upper quadrant ultrasound reveals gallstones and a 1.2-cm common bile duct. The following day, despite being hydrated aggressively, the patient develops a fever and becomes jaundiced with worsening abdominal pain.
What would be the next step in the patient's management?
DDSEP® 8 Quick Quiz - April 2018 Question 1
Q1. Correct Answer: C
Rationale
The CagA strain of H. pylori has been found to be associated with an increased risk of gastric adenocarcinoma and MALT lymphoma. CagA-producing H. pylori infection also cause more severe mucosal inflammation and is associated with higher incidences of gastric and duodenal ulcers. A protective effect of CagA+ H. pylori against gastroesophageal reflux disease, reflux esophagitis, Barrett's esophagus, and esophageal adenocarcinoma has been suggested, as some epidemiologic studies have shown a decreased prevalence of these disorders. Although further studies are needed to verify these relationships, no studies to date have demonstrated an increased risk of esophageal carcinoma associated with H. pylori. CagA-producing H. pylori has not been associated with gastric carcinoid tumor.
References
1. Fallone CA, Barkun AN, Göttke MU, et al. Association of Helicobacter pylori genotype with gastroesophageal reflux disease and other upper gastrointestinal diseases. Am J Gastroenterol. 2000;95(3):659-69.
2. Huang JQ, Zheng GF, Sumanac K, et al. Meta-analysis of the relationship between cagA seropositivity and gastric cancer. Gastroenterology 2003;125(6):1636-44.
3. Islami F, Kamangar F. Helicobacter pylori and esophageal cancer risk: a meta-analysis. Cancer Prev Res. 2008;1:329-38.
Q1. Correct Answer: C
Rationale
The CagA strain of H. pylori has been found to be associated with an increased risk of gastric adenocarcinoma and MALT lymphoma. CagA-producing H. pylori infection also cause more severe mucosal inflammation and is associated with higher incidences of gastric and duodenal ulcers. A protective effect of CagA+ H. pylori against gastroesophageal reflux disease, reflux esophagitis, Barrett's esophagus, and esophageal adenocarcinoma has been suggested, as some epidemiologic studies have shown a decreased prevalence of these disorders. Although further studies are needed to verify these relationships, no studies to date have demonstrated an increased risk of esophageal carcinoma associated with H. pylori. CagA-producing H. pylori has not been associated with gastric carcinoid tumor.
References
1. Fallone CA, Barkun AN, Göttke MU, et al. Association of Helicobacter pylori genotype with gastroesophageal reflux disease and other upper gastrointestinal diseases. Am J Gastroenterol. 2000;95(3):659-69.
2. Huang JQ, Zheng GF, Sumanac K, et al. Meta-analysis of the relationship between cagA seropositivity and gastric cancer. Gastroenterology 2003;125(6):1636-44.
3. Islami F, Kamangar F. Helicobacter pylori and esophageal cancer risk: a meta-analysis. Cancer Prev Res. 2008;1:329-38.
Q1. Correct Answer: C
Rationale
The CagA strain of H. pylori has been found to be associated with an increased risk of gastric adenocarcinoma and MALT lymphoma. CagA-producing H. pylori infection also cause more severe mucosal inflammation and is associated with higher incidences of gastric and duodenal ulcers. A protective effect of CagA+ H. pylori against gastroesophageal reflux disease, reflux esophagitis, Barrett's esophagus, and esophageal adenocarcinoma has been suggested, as some epidemiologic studies have shown a decreased prevalence of these disorders. Although further studies are needed to verify these relationships, no studies to date have demonstrated an increased risk of esophageal carcinoma associated with H. pylori. CagA-producing H. pylori has not been associated with gastric carcinoid tumor.
References
1. Fallone CA, Barkun AN, Göttke MU, et al. Association of Helicobacter pylori genotype with gastroesophageal reflux disease and other upper gastrointestinal diseases. Am J Gastroenterol. 2000;95(3):659-69.
2. Huang JQ, Zheng GF, Sumanac K, et al. Meta-analysis of the relationship between cagA seropositivity and gastric cancer. Gastroenterology 2003;125(6):1636-44.
3. Islami F, Kamangar F. Helicobacter pylori and esophageal cancer risk: a meta-analysis. Cancer Prev Res. 2008;1:329-38.
The CagA strain of Helicobacter pylori is associated with which of the following?
The role of defensins in treating skin aging
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.

Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.
Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.
Most skin-aging treatments work by prodding old fibroblasts and keratinocytes to accelerate the production of important cellular components. For example, retinoids act on retinoic acid receptors to activate collagen genes and deactivate collagenase genes. Glycolic acid, ascorbic acid, and certain growth factors stimulate synthesis of collagen by fibroblasts. Older fibroblasts and keratinocytes are sluggish for many reasons; they do not “hear” signals as well as younger cells do. Glycosaminoglycans such as heparan sulfate can help cells hear these signals. Heparan sulfate, for example, assists in the delivery of growth factors to cells, stabilizes them, and presents them to the receptors on the keratinocytes and fibroblasts, and amplifies cellular response to these factors.
A new angle in antiaging skin care is to create new keratinocytes rather than to stimulate old cells. For the last decade, personal care companies have touted the benefit of putting stem cells in cosmeceuticals, claiming that these cells would rejuvenate skin. However, this proved to be unsubstantiated marketing hype because the stem cells were plant derived (often from apples), had poor shelf life, and could not intercalate between the native skin cells and work with them to have any effect. Stems cells in cosmeceuticals became a point of disdain for savvy scientists.
Stem cells
Wounding the skin stimulates LGR6+ stem cells. This occurs when neutrophils in the immune system release defensins in response to injury, and, in turn, defensins activate LGR6+ stem cells. Situated above the follicular bulge, these cells are reported to have the capacity to synthesize all cutaneous cell lineages, including sebaceous gland and interfollicular epidermal cells.1,2 There are no specific studies that show that the LGR6+ cells generate new fibroblasts, but it seems likely. Transplantation of LGR6+ stem cells into the skin results in increased wound healing, hair follicle genesis, and angiogenesis.3 LGR6+ stem cells repopulate the epidermis by creating new basal stem cells. In regards to skin rejuvenation, it is clear that activated LGR6+ stems cells produce new, younger-acting keratinocytes in the epidermis.
Peptides
Defensin is a peptide. Peptides are short amino acid chains. These important substances are challenging to incorporate into topical formulations for various reasons, including stabilization difficulty, interaction with other molecules, and poor penetration (greater than 500 Dalton molecular weight). For these reasons, many peptide-containing formulations do not have efficacy. Attempts are underway to better develop or modify peptide products to enhance solubility, achieve better penetration, and target increased receptor activity. Defensins are peptides, which makes them difficult to formulate in a topical product. Special steps must be taken in the formulation process to stabilize defensin and allow penetration into the hair follicle where the LGR6+ cells reside. Fortunately, it is easier for a peptide to target the hair follicle because it can traverse through the “pore” – than it is to get a peptide to reach the fibroblasts in the dermis.
Defensins
Defensins, or human beta-defensins, are host defense peptides that exhibit antimicrobial activities against numerous bacteria.4 LGR6+ stem cells, which are dormant until they are activated to respond to damage, are stimulated by defensins. Defensins have been shown to stimulate keratinocyte proliferation, migration, and wound healing. (3) **Human alpha-defensin 5 peptide has also been shown to enhance wound healing, increasing LGR5+ and LGR6+ stem cell migration in the wound bed.(1)***
When formulated in a manner that allows for stability and penetration into the hair follicle where the LGR6+ stem cells reside, defensin formulations can be applied topically. A product sold as DefenAge uses a patented formulation that uses albumin, a large and stable protein, to stabilize defensin and act as a carrier molecule while helping the defensin maintain its integrity and extend shelf life in the serum base. The albumin/defensin complex is incorporated into liposomes to prevent other ingredients in the cosmetic base from interacting with the peptide and to enhance delivery to the LGR6+ target cell.
The role of defensins in treating skin aging
- Old fibroblast and keratinocytes are sluggish and lazy.
- Old cells do not “hear” signals as well as younger cells.
- LGR6+ stem cells repopulate the epidermis with new, young keratinocytes.
- Defensin stimulates LGR6+ stem cells.
- The defensin/LGR6+ pathway plays a role in keratinization.
- Using topical defensin can improve the skin’s appearance.
Studying DefenAge
At this time, there is only one small multicenter, double-blind, placebo-controlled clinical study completed at three locations by investigators who are stockholders in the company and an independent dermatologic histopathologist who has no relation with the company; results have been reported in aesthetic dermatology industry newsletters. Each site had 15 patients for a total of 45 patients; all were women, aged 41-70 years (average age, 60 years), with little or no history of “quality” skin care. The study regimen used a system that contained alpha- and beta-defensins developed by Progenitor Biologics. Thirty patients used the three products in the DefenAge line: the 2-Minute Reveal Masque Exfoliator, 24/7 Barrier Balance Cream, and 8-in-1 BioSerum. The remaining patients received a three-part placebo system. Baseline biopsies were obtained to evaluate underlying conditions in the patients’ skin, and their skin was evaluated at 6 and 12 weeks, when additional biopsies were taken. Data analysis indicated that patients using DefenAge experienced significant improvement in coarse and fine wrinkles, pigmentation, pore prominence, epidermal thickness, as well as skin texture and evenness.
My personal opinion
I have never been a fan of formulations containing stem cells or peptides for the reasons listed above. DefenAge is unique in the way it has been stabilized, by penetrating the hair follicle rather than through the dermis and because defensin has very well-documented effects on the important LGR6+ stem cells. The effects of defensin on LGR6+ stem cells intrigue me. I do not intend to stop recommending retinoids for antiaging, but rather will add DefenAge to the antiaging regimen. In the past year, I have used DefenAge on many patients and have had many observations. I do not recommend starting retinoids and DefenAge at the same time because I have seen increased retinoid dermatitis. I suggest starting one the first month and then introducing the other product during the second month. Although no studies have been performed on this, my impression is that the DefenAge gives a quick result that helps improve patient compliance with the entire skin care regimen, but the effects reach a point at which no further improvement is seen. Combining DefenAge with a skin care regimen (targeted specifically to their Baumann Skin Type of course!) that includes a retinoid will increase efficacy. For wrinkle-prone skin types, I combine DefenAge with a retinoid, vitamin C, and heparan sulfate. After cleansing in the morning, I have them apply vitamin C followed by the DefenAge and an SPF. In the evening after cleansing, I have them apply a retinoid followed by a heparan sulfate analogue.
Conclusion
DefenAge offers a new approach to skin aging. At this time, there is much basic science research about the benefits of LGR6+ and that uses defensin to stimulate these stem cells; however, only one small clinical trial using defensin topically for antiaging has been published. It is doubtful that many studies will be performed because cosmetic companies are not allowed to make biologic claims so they have little incentive to demonstrate biologic changes. For this reason, we have to rely upon anecdotal reports from physicians such as the information that I have shared here.
Conflict of interest note: I have no financial relationship (no honorarium, stocks, or research funding) with Progenitor Biologics. I was asked to lecture in a DefenAge Symposium at the Vegas Cosmetic Surgery meeting but received no compensation. DefenAge products are sold through doctors, with my company, Skin Type Solutions Franchise Systems, as are heparan sulfate analogues, multiple brands of retinol, and 40 other product brands.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann wrote two textbooks: “Cosmetic Dermatology: Principles and Practice” (New York: McGraw-Hill, 2002) and “Cosmeceuticals and Cosmetic Ingredients” (New York: McGraw-Hill, 2014); she also authored a New York Times Best Seller for consumers, “The Skin Type Solution” (New York: Bantam Dell, 2006). Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Evolus, Galderma, and Revance Therapeutics. She is the founder and CEO of Skin Type Solutions Franchise Systems LLC.
References
1. Lough D et al. Plast Reconstr Surg. 2013 Nov;132(5):1159-71.
2. Snippert HJ et al. Science. 2010 Mar 12;327(5971):1385-9.
3. Lough DM et al. Plast Reconstr Surg. 2014 Mar;133(3):579-90.
4. Kiatsurayanon C et al. J Invest Dermatol. 2014 Aug;134(8):2163-73.

April 2018 Digital Edition
Click here to access the April 2018 Digital Edition.
Table of Contents
- Understanding, Assessing, and Conceptualizing Suicide Risk Among Veterans With PTSD
- Reducing the Expenditures and Workload Associated With VA Partial-Fill Prescription Processing
- Acute Exertional Upper-Extremity Rhabdomyolysis in 3 Female Trainees
- A Practical Guide to Urine Drug Monitoring
- Synovial Chondromatosis: An Unusual Case of Knee Pain and Swelling
- Complementary and Integrative Health Therapies for Opioid Overuse
Click here to access the April 2018 Digital Edition.
Table of Contents
- Understanding, Assessing, and Conceptualizing Suicide Risk Among Veterans With PTSD
- Reducing the Expenditures and Workload Associated With VA Partial-Fill Prescription Processing
- Acute Exertional Upper-Extremity Rhabdomyolysis in 3 Female Trainees
- A Practical Guide to Urine Drug Monitoring
- Synovial Chondromatosis: An Unusual Case of Knee Pain and Swelling
- Complementary and Integrative Health Therapies for Opioid Overuse
Click here to access the April 2018 Digital Edition.
Table of Contents
- Understanding, Assessing, and Conceptualizing Suicide Risk Among Veterans With PTSD
- Reducing the Expenditures and Workload Associated With VA Partial-Fill Prescription Processing
- Acute Exertional Upper-Extremity Rhabdomyolysis in 3 Female Trainees
- A Practical Guide to Urine Drug Monitoring
- Synovial Chondromatosis: An Unusual Case of Knee Pain and Swelling
- Complementary and Integrative Health Therapies for Opioid Overuse
Neurologic and Spinal Cord Disorders in Federal Health Care System (April 2018)
Click here to access Neurologic and Spinal Cord Disorders in Federal Health Care System Digital Edition.
Table of Contents
- Neurology Research News
- Self-Management in Epilepsy Care: Untapped Opportunities
- Restless Legs Syndrome Among Veterans With Spinal Cord Lesions
- A Robotic Hand Device Safety Study for People With Cervical Spinal Cord Injury
Click here to access Neurologic and Spinal Cord Disorders in Federal Health Care System Digital Edition.
Table of Contents
- Neurology Research News
- Self-Management in Epilepsy Care: Untapped Opportunities
- Restless Legs Syndrome Among Veterans With Spinal Cord Lesions
- A Robotic Hand Device Safety Study for People With Cervical Spinal Cord Injury
Click here to access Neurologic and Spinal Cord Disorders in Federal Health Care System Digital Edition.
Table of Contents
- Neurology Research News
- Self-Management in Epilepsy Care: Untapped Opportunities
- Restless Legs Syndrome Among Veterans With Spinal Cord Lesions
- A Robotic Hand Device Safety Study for People With Cervical Spinal Cord Injury
Hyponatremia After Traumatic Brain Injury
Hyponatremia is a dangerous complication of major head trauma, and timely diagnosis and treatment can be fraught with “confounding factors” and complexity, say clinicians from the University of Newcastle and John Hunter Hospital in Australia. They reported a case of hyponatremia that required some clinical tightrope walking.
The patient, a 20-year-old university student, had fractured his skull in a skateboard fall while intoxicated. He was started on dexamethasone to reduce the risk of worsening cerebral edema. On day 3, he developed hypo-osmolar hyponatremia, which was worse on day 4, despite treatment, including IV fluid therapy, fluid restriction, and oral salt tablets. Although cognitively the patient was deteriorating, he seemed clinically euvolemic. However, the patient was in negative fluid balance, suggesting renal salt wasting (RSW). After a trial of isotonic normal saline, the patient’s serum sodium level fell further. The patient was then treated for suspected syndrome of inappropriate antidiuretic hormone (SIADH) with a hypertonic saline infusion. The rise in sodium was carefully controlled to avoid rapid overcorrection, which can lead to irreversible neurologic symptoms. Finally, the patient’s sodium level and neurologic status improved.
The clinicians say the case demonstrates the complexity of differentiating between the causes of hyponatremia after head injury. Volume status may be an indicator, they say, but current clinical and laboratory markers of volume status are often limited in accuracy. The hallmark of RSW is volume depletion, whereas diagnosis of SIADH depends on a coexisting euvolemic state (as with the patient).
As many as 10% of victims of traumatic brain injury develop hyponatremia, and it is associated with a worse prognosis, even in mild cases, the clinicians note. Making the right diagnosis is critical—the treatment chosen can easily compromise the outcome. Patients with neurosurgical conditions are often treated with considerable volumes of saline-containing fluid, with consequent dynamic changes in blood and extracellular volumes. Moreover, the patients have elevated levels of adrenergic hormones with their own confounding effects.
In the long term, the patient experienced significant neurologic sequelae, including prolonged posttraumatic amnesia. After extensive rehabilitation he was able to return to the university.
Hyponatremia is a dangerous complication of major head trauma, and timely diagnosis and treatment can be fraught with “confounding factors” and complexity, say clinicians from the University of Newcastle and John Hunter Hospital in Australia. They reported a case of hyponatremia that required some clinical tightrope walking.
The patient, a 20-year-old university student, had fractured his skull in a skateboard fall while intoxicated. He was started on dexamethasone to reduce the risk of worsening cerebral edema. On day 3, he developed hypo-osmolar hyponatremia, which was worse on day 4, despite treatment, including IV fluid therapy, fluid restriction, and oral salt tablets. Although cognitively the patient was deteriorating, he seemed clinically euvolemic. However, the patient was in negative fluid balance, suggesting renal salt wasting (RSW). After a trial of isotonic normal saline, the patient’s serum sodium level fell further. The patient was then treated for suspected syndrome of inappropriate antidiuretic hormone (SIADH) with a hypertonic saline infusion. The rise in sodium was carefully controlled to avoid rapid overcorrection, which can lead to irreversible neurologic symptoms. Finally, the patient’s sodium level and neurologic status improved.
The clinicians say the case demonstrates the complexity of differentiating between the causes of hyponatremia after head injury. Volume status may be an indicator, they say, but current clinical and laboratory markers of volume status are often limited in accuracy. The hallmark of RSW is volume depletion, whereas diagnosis of SIADH depends on a coexisting euvolemic state (as with the patient).
As many as 10% of victims of traumatic brain injury develop hyponatremia, and it is associated with a worse prognosis, even in mild cases, the clinicians note. Making the right diagnosis is critical—the treatment chosen can easily compromise the outcome. Patients with neurosurgical conditions are often treated with considerable volumes of saline-containing fluid, with consequent dynamic changes in blood and extracellular volumes. Moreover, the patients have elevated levels of adrenergic hormones with their own confounding effects.
In the long term, the patient experienced significant neurologic sequelae, including prolonged posttraumatic amnesia. After extensive rehabilitation he was able to return to the university.
Hyponatremia is a dangerous complication of major head trauma, and timely diagnosis and treatment can be fraught with “confounding factors” and complexity, say clinicians from the University of Newcastle and John Hunter Hospital in Australia. They reported a case of hyponatremia that required some clinical tightrope walking.
The patient, a 20-year-old university student, had fractured his skull in a skateboard fall while intoxicated. He was started on dexamethasone to reduce the risk of worsening cerebral edema. On day 3, he developed hypo-osmolar hyponatremia, which was worse on day 4, despite treatment, including IV fluid therapy, fluid restriction, and oral salt tablets. Although cognitively the patient was deteriorating, he seemed clinically euvolemic. However, the patient was in negative fluid balance, suggesting renal salt wasting (RSW). After a trial of isotonic normal saline, the patient’s serum sodium level fell further. The patient was then treated for suspected syndrome of inappropriate antidiuretic hormone (SIADH) with a hypertonic saline infusion. The rise in sodium was carefully controlled to avoid rapid overcorrection, which can lead to irreversible neurologic symptoms. Finally, the patient’s sodium level and neurologic status improved.
The clinicians say the case demonstrates the complexity of differentiating between the causes of hyponatremia after head injury. Volume status may be an indicator, they say, but current clinical and laboratory markers of volume status are often limited in accuracy. The hallmark of RSW is volume depletion, whereas diagnosis of SIADH depends on a coexisting euvolemic state (as with the patient).
As many as 10% of victims of traumatic brain injury develop hyponatremia, and it is associated with a worse prognosis, even in mild cases, the clinicians note. Making the right diagnosis is critical—the treatment chosen can easily compromise the outcome. Patients with neurosurgical conditions are often treated with considerable volumes of saline-containing fluid, with consequent dynamic changes in blood and extracellular volumes. Moreover, the patients have elevated levels of adrenergic hormones with their own confounding effects.
In the long term, the patient experienced significant neurologic sequelae, including prolonged posttraumatic amnesia. After extensive rehabilitation he was able to return to the university.