User login
Understanding the new CMS bundle model
Hospitalists have been among the highest-volume participants in Medicare’s Bundled Payments for Care Improvement (BPCI) demonstration model, initiating over 200,000 episodes representing $4.7 billion in spending since the model began.1 On Jan. 9, the Centers for Medicare & Medicaid Services announced BPCI’s follow-on model, “BPCI Advanced.”2
BPCI launched in October 2013 and sunsets at the end of Q3 2018. BPCI Advanced starts immediately upon conclusion of BPCI (Q4 2018) and is slated to finish at year-end 2023.
CMS intends for the program to qualify as an Advanced Alternative Payment Model (APM). As BPCI Advanced focuses on episodes of care involving an inpatient stay (It also includes three outpatient episodes.) and the subsequent 90-day recovery period, it represents the first large-scale opportunity for hospitalists to meet criteria for Advanced APM participation. Qualifying for the Advanced APM track of the Quality Payment Program – which involves meeting patient volume or payment thresholds3 – comes with a 5% lump-sum bonus based on Medicare Part B fees and avoids exposure to penalties and reporting requirements of the Merit-based Incentive Payment System (MIPS).
Key program features
Acute care hospitals and physician groups may initiate episodes under BPCI Advanced, assuming financial risk under the model. Similar to its predecessor, BPCI Advanced assigns a target price based on past claims payments associated with the “episode initiator.”
During the performance period, if the initiator can beat the price in the aggregate for its bundles, it can keep the difference, and if it comes in over the price, it must pay the difference back to Medicare. Medicare discounts the target price by 3%, effectively paying itself that amount. After that, there is no sharing of savings with Medicare, as opposed to the permanent ACO programs, where there is sharing after the ACO meets the minimum savings rate.
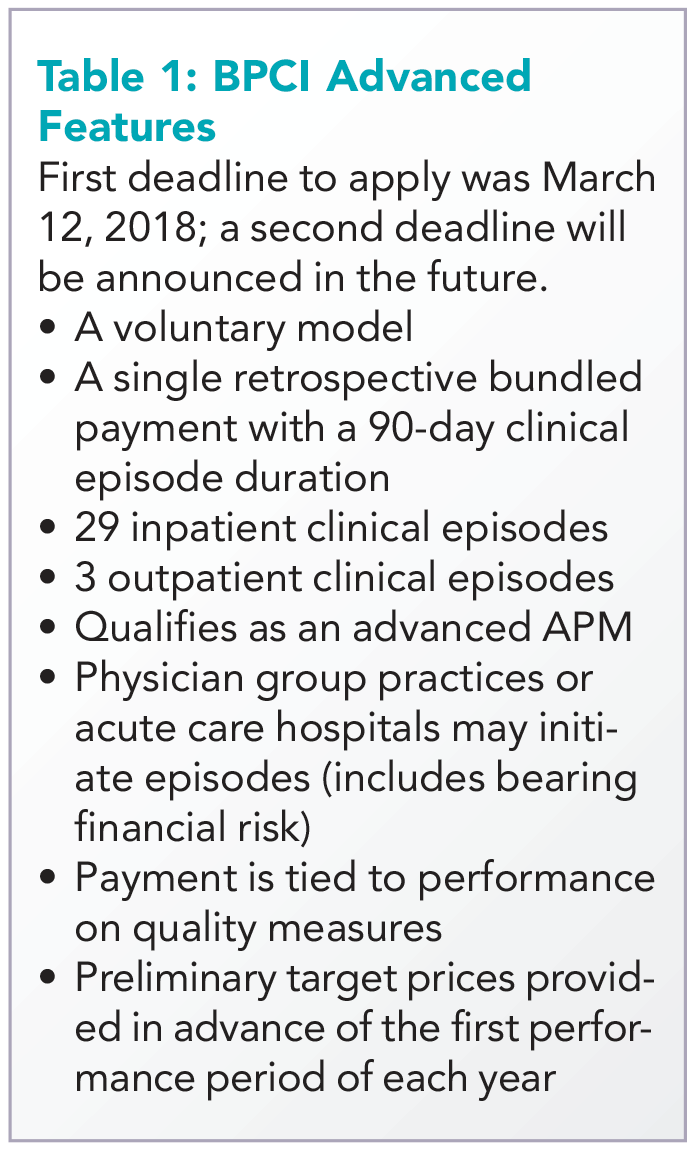
The program allows physician groups and hospital initiators to go it alone or to work with a “convener,” which may share risk and reward with initiators, and may provide software, analytics, networks of high-performing providers like nursing facilities, and knowledge of specific care redesign approaches to enable program success. See Table 1 for a listing of other notable features of BPCI Advanced.
Quality measures
BPCI Advanced qualifies as an Advanced APM in part because payment is tied to performance on a set of quality measures (see Table 2). There are two measures applied to all episodes: all-cause hospital readmissions and advance care plan. These are notable because hospitalists may be especially focused on improvement activities in these areas.
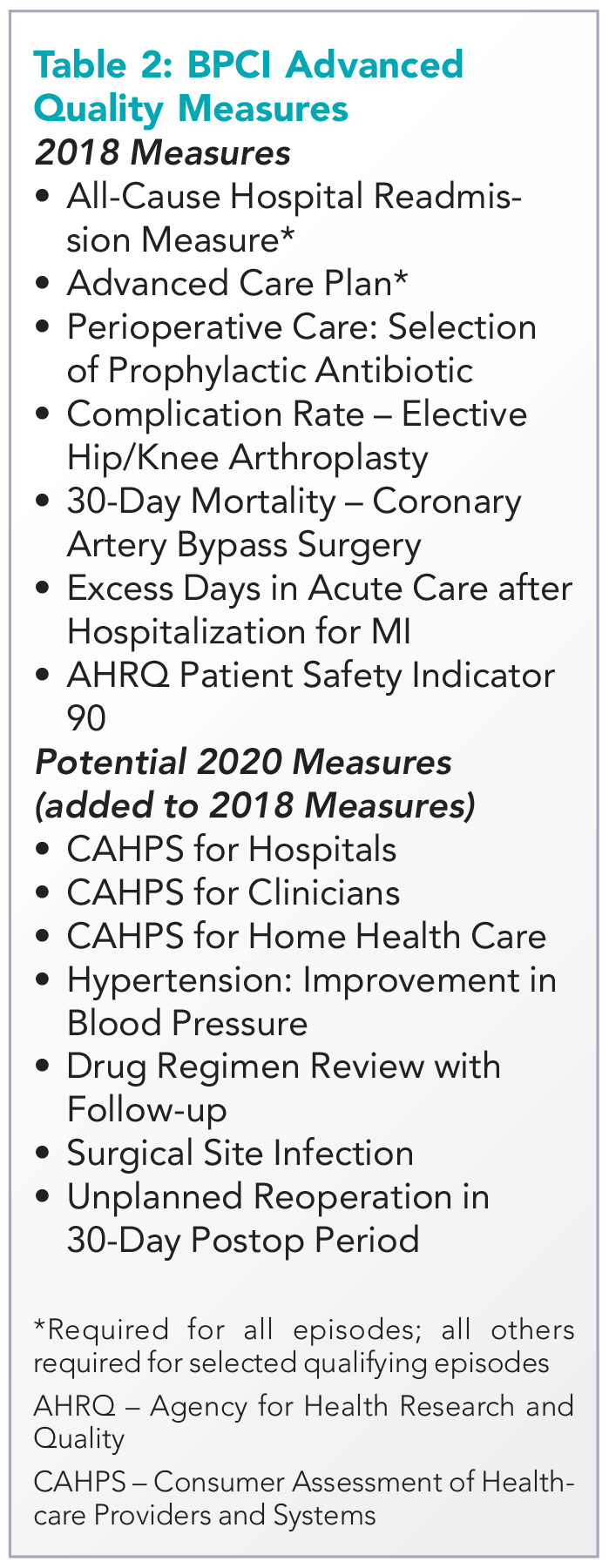
While the advance care plan measure refers to a process reflected by record documentation and is therefore directly under the control of hospitalists, readmissions – and most of the other measures – require a team approach. Because the outcome measures are risk adjusted, accurate and complete clinical documentation is crucial, as it drives how risk is adjusted. Of note, all the 2018 measures, collected directly through claims, will place no additional administrative burden for collection on providers.
Two ways for hospitalists to participate
Hospitalist groups – whether independent or employed – may be episode initiators in BPCI Advanced. In this case, any episodes in which the group participates that carry the name of a member of the hospitalist group in the “Attending Provider” field on the hospital bill claim form to Medicare (and the associated carrier claim) are attributed to that member’s physician group.
For example, if the group has chosen heart failure as an episode in which to participate at the program’s outset, a hospitalization is assigned the heart failure DRG (diagnosis-related group) and a group member is the Attending Provider on the claim form (and submits a claim for the physician services), then the episode is attributed to that group. This means that the group is responsible for payments represented by Medicare Part A and Part B claims (with a few exclusions like trauma and cancer) against the target price for the initial hospitalization and subsequent 90-day period. In practice, hospitalists are rewarded for actions aimed at optimizing location after discharge,4 avoiding readmissions, choosing efficient nursing facilities, and helping patients to maximize functional status.
The other way hospitalists may participate is through an agreement to share in savings with a hospital or physician group episode initiator. This requires hospitalist individuals or groups to enter into a contract with the initiator that meets certain program requirements – for example, report quality measures, engage in care redesign, use certified EHR technology (hospital-based clinicians automatically fulfill this criterion).
If there is broad participation, BPCI Advanced could represent a key milestone for hospitalists, as they seek to be recognized for the value they confer to the system as a whole instead of simply their professional billings. While there are legitimate concerns about the effect MIPS may have on health care value and the complexity of participation in APMs, barring a repeal of the law that created them, hospitalists now have the chance to extend their influence within and outside the hospital’s four walls and be more fairly rewarded for it.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected]. Disclosure: The author’s employer, Remedy Partners, is an Awardee Convener for the BPCI initiative and intends to apply as a Convener in BPCI Advanced.
References
1. Based on BPCI awardee convener Remedy Partners claims analysis.
2. https://innovation.cms.gov/initiatives/bpci-advanced.
3. https://qpp.cms.gov/apms/overview.
4. Whitcomb W. Choosing location after discharge wisely. The-hospitalist.org. 2018 Jan 3. Digital edition. Accessed Jan 13, 2018.
Hospitalists have been among the highest-volume participants in Medicare’s Bundled Payments for Care Improvement (BPCI) demonstration model, initiating over 200,000 episodes representing $4.7 billion in spending since the model began.1 On Jan. 9, the Centers for Medicare & Medicaid Services announced BPCI’s follow-on model, “BPCI Advanced.”2
BPCI launched in October 2013 and sunsets at the end of Q3 2018. BPCI Advanced starts immediately upon conclusion of BPCI (Q4 2018) and is slated to finish at year-end 2023.
CMS intends for the program to qualify as an Advanced Alternative Payment Model (APM). As BPCI Advanced focuses on episodes of care involving an inpatient stay (It also includes three outpatient episodes.) and the subsequent 90-day recovery period, it represents the first large-scale opportunity for hospitalists to meet criteria for Advanced APM participation. Qualifying for the Advanced APM track of the Quality Payment Program – which involves meeting patient volume or payment thresholds3 – comes with a 5% lump-sum bonus based on Medicare Part B fees and avoids exposure to penalties and reporting requirements of the Merit-based Incentive Payment System (MIPS).
Key program features
Acute care hospitals and physician groups may initiate episodes under BPCI Advanced, assuming financial risk under the model. Similar to its predecessor, BPCI Advanced assigns a target price based on past claims payments associated with the “episode initiator.”
During the performance period, if the initiator can beat the price in the aggregate for its bundles, it can keep the difference, and if it comes in over the price, it must pay the difference back to Medicare. Medicare discounts the target price by 3%, effectively paying itself that amount. After that, there is no sharing of savings with Medicare, as opposed to the permanent ACO programs, where there is sharing after the ACO meets the minimum savings rate.
The program allows physician groups and hospital initiators to go it alone or to work with a “convener,” which may share risk and reward with initiators, and may provide software, analytics, networks of high-performing providers like nursing facilities, and knowledge of specific care redesign approaches to enable program success. See Table 1 for a listing of other notable features of BPCI Advanced.
Quality measures
BPCI Advanced qualifies as an Advanced APM in part because payment is tied to performance on a set of quality measures (see Table 2). There are two measures applied to all episodes: all-cause hospital readmissions and advance care plan. These are notable because hospitalists may be especially focused on improvement activities in these areas.
While the advance care plan measure refers to a process reflected by record documentation and is therefore directly under the control of hospitalists, readmissions – and most of the other measures – require a team approach. Because the outcome measures are risk adjusted, accurate and complete clinical documentation is crucial, as it drives how risk is adjusted. Of note, all the 2018 measures, collected directly through claims, will place no additional administrative burden for collection on providers.
Two ways for hospitalists to participate
Hospitalist groups – whether independent or employed – may be episode initiators in BPCI Advanced. In this case, any episodes in which the group participates that carry the name of a member of the hospitalist group in the “Attending Provider” field on the hospital bill claim form to Medicare (and the associated carrier claim) are attributed to that member’s physician group.
For example, if the group has chosen heart failure as an episode in which to participate at the program’s outset, a hospitalization is assigned the heart failure DRG (diagnosis-related group) and a group member is the Attending Provider on the claim form (and submits a claim for the physician services), then the episode is attributed to that group. This means that the group is responsible for payments represented by Medicare Part A and Part B claims (with a few exclusions like trauma and cancer) against the target price for the initial hospitalization and subsequent 90-day period. In practice, hospitalists are rewarded for actions aimed at optimizing location after discharge,4 avoiding readmissions, choosing efficient nursing facilities, and helping patients to maximize functional status.
The other way hospitalists may participate is through an agreement to share in savings with a hospital or physician group episode initiator. This requires hospitalist individuals or groups to enter into a contract with the initiator that meets certain program requirements – for example, report quality measures, engage in care redesign, use certified EHR technology (hospital-based clinicians automatically fulfill this criterion).
If there is broad participation, BPCI Advanced could represent a key milestone for hospitalists, as they seek to be recognized for the value they confer to the system as a whole instead of simply their professional billings. While there are legitimate concerns about the effect MIPS may have on health care value and the complexity of participation in APMs, barring a repeal of the law that created them, hospitalists now have the chance to extend their influence within and outside the hospital’s four walls and be more fairly rewarded for it.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected]. Disclosure: The author’s employer, Remedy Partners, is an Awardee Convener for the BPCI initiative and intends to apply as a Convener in BPCI Advanced.
References
1. Based on BPCI awardee convener Remedy Partners claims analysis.
2. https://innovation.cms.gov/initiatives/bpci-advanced.
3. https://qpp.cms.gov/apms/overview.
4. Whitcomb W. Choosing location after discharge wisely. The-hospitalist.org. 2018 Jan 3. Digital edition. Accessed Jan 13, 2018.
Hospitalists have been among the highest-volume participants in Medicare’s Bundled Payments for Care Improvement (BPCI) demonstration model, initiating over 200,000 episodes representing $4.7 billion in spending since the model began.1 On Jan. 9, the Centers for Medicare & Medicaid Services announced BPCI’s follow-on model, “BPCI Advanced.”2
BPCI launched in October 2013 and sunsets at the end of Q3 2018. BPCI Advanced starts immediately upon conclusion of BPCI (Q4 2018) and is slated to finish at year-end 2023.
CMS intends for the program to qualify as an Advanced Alternative Payment Model (APM). As BPCI Advanced focuses on episodes of care involving an inpatient stay (It also includes three outpatient episodes.) and the subsequent 90-day recovery period, it represents the first large-scale opportunity for hospitalists to meet criteria for Advanced APM participation. Qualifying for the Advanced APM track of the Quality Payment Program – which involves meeting patient volume or payment thresholds3 – comes with a 5% lump-sum bonus based on Medicare Part B fees and avoids exposure to penalties and reporting requirements of the Merit-based Incentive Payment System (MIPS).
Key program features
Acute care hospitals and physician groups may initiate episodes under BPCI Advanced, assuming financial risk under the model. Similar to its predecessor, BPCI Advanced assigns a target price based on past claims payments associated with the “episode initiator.”
During the performance period, if the initiator can beat the price in the aggregate for its bundles, it can keep the difference, and if it comes in over the price, it must pay the difference back to Medicare. Medicare discounts the target price by 3%, effectively paying itself that amount. After that, there is no sharing of savings with Medicare, as opposed to the permanent ACO programs, where there is sharing after the ACO meets the minimum savings rate.
The program allows physician groups and hospital initiators to go it alone or to work with a “convener,” which may share risk and reward with initiators, and may provide software, analytics, networks of high-performing providers like nursing facilities, and knowledge of specific care redesign approaches to enable program success. See Table 1 for a listing of other notable features of BPCI Advanced.
Quality measures
BPCI Advanced qualifies as an Advanced APM in part because payment is tied to performance on a set of quality measures (see Table 2). There are two measures applied to all episodes: all-cause hospital readmissions and advance care plan. These are notable because hospitalists may be especially focused on improvement activities in these areas.
While the advance care plan measure refers to a process reflected by record documentation and is therefore directly under the control of hospitalists, readmissions – and most of the other measures – require a team approach. Because the outcome measures are risk adjusted, accurate and complete clinical documentation is crucial, as it drives how risk is adjusted. Of note, all the 2018 measures, collected directly through claims, will place no additional administrative burden for collection on providers.
Two ways for hospitalists to participate
Hospitalist groups – whether independent or employed – may be episode initiators in BPCI Advanced. In this case, any episodes in which the group participates that carry the name of a member of the hospitalist group in the “Attending Provider” field on the hospital bill claim form to Medicare (and the associated carrier claim) are attributed to that member’s physician group.
For example, if the group has chosen heart failure as an episode in which to participate at the program’s outset, a hospitalization is assigned the heart failure DRG (diagnosis-related group) and a group member is the Attending Provider on the claim form (and submits a claim for the physician services), then the episode is attributed to that group. This means that the group is responsible for payments represented by Medicare Part A and Part B claims (with a few exclusions like trauma and cancer) against the target price for the initial hospitalization and subsequent 90-day period. In practice, hospitalists are rewarded for actions aimed at optimizing location after discharge,4 avoiding readmissions, choosing efficient nursing facilities, and helping patients to maximize functional status.
The other way hospitalists may participate is through an agreement to share in savings with a hospital or physician group episode initiator. This requires hospitalist individuals or groups to enter into a contract with the initiator that meets certain program requirements – for example, report quality measures, engage in care redesign, use certified EHR technology (hospital-based clinicians automatically fulfill this criterion).
If there is broad participation, BPCI Advanced could represent a key milestone for hospitalists, as they seek to be recognized for the value they confer to the system as a whole instead of simply their professional billings. While there are legitimate concerns about the effect MIPS may have on health care value and the complexity of participation in APMs, barring a repeal of the law that created them, hospitalists now have the chance to extend their influence within and outside the hospital’s four walls and be more fairly rewarded for it.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected]. Disclosure: The author’s employer, Remedy Partners, is an Awardee Convener for the BPCI initiative and intends to apply as a Convener in BPCI Advanced.
References
1. Based on BPCI awardee convener Remedy Partners claims analysis.
2. https://innovation.cms.gov/initiatives/bpci-advanced.
3. https://qpp.cms.gov/apms/overview.
4. Whitcomb W. Choosing location after discharge wisely. The-hospitalist.org. 2018 Jan 3. Digital edition. Accessed Jan 13, 2018.
Federal budget grants $1.8 billion to Alzheimer’s and dementia research
Congress has appropriated an additional $414 million for research into Alzheimer’s disease and other dementias – the full increase requested by the National Institutes of Health for fiscal year 2018. The boost brings the total AD funding available this year to $1.8 billion.
Bolstered by the mandate of the National Plan to Address Alzheimer’s Disease, to prevent or treat AD by 2025, the NIH is aiming higher still. Its draft FY2019 AD appropriation asks for another $597 million; if passed, nearly $2.4 billion could be available for AD research as soon as next October.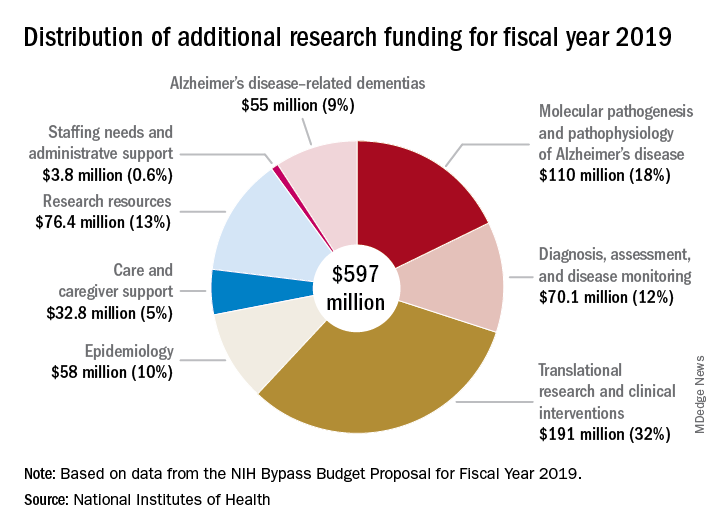
“For the third consecutive fiscal year, Congress has approved the Alzheimer’s Association’s appeal for a historic funding increase for Alzheimer’s and dementia research at the NIH,” Alzheimer’s Association president Harry Johns said in a press statement. “This decision demonstrates that Congress is deeply committed to providing the Alzheimer’s and dementia science community with the resources needed to move research forward.”
Several members of Congress championed the AD funding request, including Roy Blunt (R-Mo.), Patty Murray (D-Wash.), Nita Lowey (D-N.Y.), and Tom Cole (R-Okla.).
The forward momentum is on pace to continue into FY2019, according to Robert Egge, chief public policy officer and executive vice president of governmental affairs for the association. The NIH Bypass Budget, an estimate of how much additional funding is necessary to reach the 2025 goal, contains an additional $597 million appropriation for AD and other dementias.
“This is what we need to fund scientific projects that are meritorious and ready to go,” Mr. Egge said in an interview. “Congress has the assurance that this request is scientifically driven and that NIH is already thinking about how the money will be used.”
While a record-setting amount in the AD research world, this year’s $1.8 billion appropriation is a fraction of what other costly diseases receive. By comparison, the budget granted the National Cancer Institute $5.7 billion for its research programs.
“Compared to what the cost of the disease brings to Americans in terms of Medicare, Medicaid, and out of pocket expenses, it’s not that much,” Mr. Egge said. “But we have the opportunity to use this money to change these huge numbers that we’re facing.”

A 2013 report by the Rand Corporation found that, although Alzheimer’s affects fewer people than cancer or heart disease, the cost of treating and caring for those patients far outstrips spending in either of those other categories. The conclusions were perhaps even more startling, considering that it looked only at costs related solely to Alzheimer’s, not the cost of treating comorbid illnesses.
Long-term care was a key driver of the total cost in 2013, and remains the bulk of expenses today, Mr. Egge said. Transitions – going from home to nursing home to hospital – are terribly expensive, he noted. And although the Rand report didn’t include it, managing comorbid illnesses in Alzheimer’s is an enormous money drain. “Diabetes is just one example. It costs 80% more to manage diabetes in a patient with AD than in one without AD.”
The Facts and Figures report notes that the average 2017 per-person payout for Medicare beneficiaries was more than three times higher in AD patients than in those without the disease ($48,028 vs. $13,705). These are the kinds of numbers it takes to put partisan bickering on hold and grapple with tough decisions, Mr. Egge said.
“The fiscal argument is one thing that really impressed Congress. They do know how worried Americans are about this disease and how tough it is on families, but the growing fiscal impact has really focused them on addressing it.”
Congress has appropriated an additional $414 million for research into Alzheimer’s disease and other dementias – the full increase requested by the National Institutes of Health for fiscal year 2018. The boost brings the total AD funding available this year to $1.8 billion.
Bolstered by the mandate of the National Plan to Address Alzheimer’s Disease, to prevent or treat AD by 2025, the NIH is aiming higher still. Its draft FY2019 AD appropriation asks for another $597 million; if passed, nearly $2.4 billion could be available for AD research as soon as next October.
“For the third consecutive fiscal year, Congress has approved the Alzheimer’s Association’s appeal for a historic funding increase for Alzheimer’s and dementia research at the NIH,” Alzheimer’s Association president Harry Johns said in a press statement. “This decision demonstrates that Congress is deeply committed to providing the Alzheimer’s and dementia science community with the resources needed to move research forward.”
Several members of Congress championed the AD funding request, including Roy Blunt (R-Mo.), Patty Murray (D-Wash.), Nita Lowey (D-N.Y.), and Tom Cole (R-Okla.).
The forward momentum is on pace to continue into FY2019, according to Robert Egge, chief public policy officer and executive vice president of governmental affairs for the association. The NIH Bypass Budget, an estimate of how much additional funding is necessary to reach the 2025 goal, contains an additional $597 million appropriation for AD and other dementias.
“This is what we need to fund scientific projects that are meritorious and ready to go,” Mr. Egge said in an interview. “Congress has the assurance that this request is scientifically driven and that NIH is already thinking about how the money will be used.”
While a record-setting amount in the AD research world, this year’s $1.8 billion appropriation is a fraction of what other costly diseases receive. By comparison, the budget granted the National Cancer Institute $5.7 billion for its research programs.
“Compared to what the cost of the disease brings to Americans in terms of Medicare, Medicaid, and out of pocket expenses, it’s not that much,” Mr. Egge said. “But we have the opportunity to use this money to change these huge numbers that we’re facing.”
A 2013 report by the Rand Corporation found that, although Alzheimer’s affects fewer people than cancer or heart disease, the cost of treating and caring for those patients far outstrips spending in either of those other categories. The conclusions were perhaps even more startling, considering that it looked only at costs related solely to Alzheimer’s, not the cost of treating comorbid illnesses.
Long-term care was a key driver of the total cost in 2013, and remains the bulk of expenses today, Mr. Egge said. Transitions – going from home to nursing home to hospital – are terribly expensive, he noted. And although the Rand report didn’t include it, managing comorbid illnesses in Alzheimer’s is an enormous money drain. “Diabetes is just one example. It costs 80% more to manage diabetes in a patient with AD than in one without AD.”
The Facts and Figures report notes that the average 2017 per-person payout for Medicare beneficiaries was more than three times higher in AD patients than in those without the disease ($48,028 vs. $13,705). These are the kinds of numbers it takes to put partisan bickering on hold and grapple with tough decisions, Mr. Egge said.
“The fiscal argument is one thing that really impressed Congress. They do know how worried Americans are about this disease and how tough it is on families, but the growing fiscal impact has really focused them on addressing it.”
Congress has appropriated an additional $414 million for research into Alzheimer’s disease and other dementias – the full increase requested by the National Institutes of Health for fiscal year 2018. The boost brings the total AD funding available this year to $1.8 billion.
Bolstered by the mandate of the National Plan to Address Alzheimer’s Disease, to prevent or treat AD by 2025, the NIH is aiming higher still. Its draft FY2019 AD appropriation asks for another $597 million; if passed, nearly $2.4 billion could be available for AD research as soon as next October.
“For the third consecutive fiscal year, Congress has approved the Alzheimer’s Association’s appeal for a historic funding increase for Alzheimer’s and dementia research at the NIH,” Alzheimer’s Association president Harry Johns said in a press statement. “This decision demonstrates that Congress is deeply committed to providing the Alzheimer’s and dementia science community with the resources needed to move research forward.”
Several members of Congress championed the AD funding request, including Roy Blunt (R-Mo.), Patty Murray (D-Wash.), Nita Lowey (D-N.Y.), and Tom Cole (R-Okla.).
The forward momentum is on pace to continue into FY2019, according to Robert Egge, chief public policy officer and executive vice president of governmental affairs for the association. The NIH Bypass Budget, an estimate of how much additional funding is necessary to reach the 2025 goal, contains an additional $597 million appropriation for AD and other dementias.
“This is what we need to fund scientific projects that are meritorious and ready to go,” Mr. Egge said in an interview. “Congress has the assurance that this request is scientifically driven and that NIH is already thinking about how the money will be used.”
While a record-setting amount in the AD research world, this year’s $1.8 billion appropriation is a fraction of what other costly diseases receive. By comparison, the budget granted the National Cancer Institute $5.7 billion for its research programs.
“Compared to what the cost of the disease brings to Americans in terms of Medicare, Medicaid, and out of pocket expenses, it’s not that much,” Mr. Egge said. “But we have the opportunity to use this money to change these huge numbers that we’re facing.”
A 2013 report by the Rand Corporation found that, although Alzheimer’s affects fewer people than cancer or heart disease, the cost of treating and caring for those patients far outstrips spending in either of those other categories. The conclusions were perhaps even more startling, considering that it looked only at costs related solely to Alzheimer’s, not the cost of treating comorbid illnesses.
Long-term care was a key driver of the total cost in 2013, and remains the bulk of expenses today, Mr. Egge said. Transitions – going from home to nursing home to hospital – are terribly expensive, he noted. And although the Rand report didn’t include it, managing comorbid illnesses in Alzheimer’s is an enormous money drain. “Diabetes is just one example. It costs 80% more to manage diabetes in a patient with AD than in one without AD.”
The Facts and Figures report notes that the average 2017 per-person payout for Medicare beneficiaries was more than three times higher in AD patients than in those without the disease ($48,028 vs. $13,705). These are the kinds of numbers it takes to put partisan bickering on hold and grapple with tough decisions, Mr. Egge said.
“The fiscal argument is one thing that really impressed Congress. They do know how worried Americans are about this disease and how tough it is on families, but the growing fiscal impact has really focused them on addressing it.”
Fetal pathology exam performed without consent: $500,000 verdict
Fetal pathology exam performed without consent: $500,000 verdict

At 12 to 15 weeks' gestation, a fetus was found to have died. An ObGyn stimulated uterine contractions with misoprostol and the fetus was delivered.
The parents requested chromosomal testing to determine the cause of death. The ObGyn took samples of the baby's skin near the umbilical cord and from the placenta. He told the parents that the tests might come back as inconclusive, and that it may be necessary to take further samples. The couple was also told that, under hospital policy, the fetus must go to the pathology department before being taken to a funeral home. The parents told the ObGyn that they did not want further samples taken for any reason, and that nothing else should be done to their child before funeral preparations. The placenta, umbilical cord, and fetus were placed in 2 separate containers. The container with the placenta and umbilical cord had an anatomic pathology requisition form, indicating that a surgical pathology exam was to be performed. The container with the fetus did not have a requisition form. When the father accompanied the nurse who carried the containers to the pathology department, he told a general technologist that no additional tissue samples were to be taken from the fetus.
The next day, the pathologist made an incision on the fetus' left side and took a sample to create a slide for microscopic analysis. The parents discovered the incision at the funeral home.
PARENTS' CLAIM: The parents sued the hospital and pathologist. The pathologist was negligent in performing a surgical pathology examination without consent. The hospital had a duty to communicate the parents' desires to the pathologist.
According to hospital protocol, the nurse who attended the delivery was to fill out the proper forms and ensure that they were available to the pathologist. The container with the fetus should have had its own requisition form that instructed the pathologist to not perform any further testing. Every specimen that goes to pathology should have a requisition form, per guidelines from the College of American Pathologists (CAP). Without a form, the pathologist should not do anything with the sample.
The parents' verbal instructions not to take additional samples from the fetus were never relayed to the pathologist.
DEFENDANTS' DEFENSE: The hospital and pathologist denied negligence. A single requisition form was appropriate; the containers' labeling and the form made it clear that the placenta, umbilical cord, and fetus were from the same patient. CAP guidelines do not require separate forms. The remains were in the gross room at pathology, which is where specimens are taken for review and analysis. Therefore, the pathologist assumed he was to perform a standard pathology exam on both containers. The technologist with whom the father had spoken met the accepted standard of care.
VERDICT: A $500,000 Maine verdict was returned. The pathologist (through insurance) and the hospital equally shared payment of the award.
When should delivery have occurred? $4M verdict
Concerned that her fetus had stopped moving, a mother presented to the ED. Results of fetal heart-rate (FHR) monitoring ordered by the attending ObGyn (Dr. A) were nonreassuring. A second ObGyn (Dr. B) ordered a fetal biophysical profile (BPP); the score was 2 points. Although a low score usually results in immediate delivery, Dr. B consulted a maternal-fetal medicine (MFM) specialist. After another fetal BPP scored 8 points, the mother was discharged.
The next day, the mother called her ObGyn (Dr. C), who told her to immediately come to his office. A fetal BPP scored 4 points, with nonreassuring fetal heart sounds.
The mother was transported to the hospital for emergency cesarean delivery. At birth, the baby was blue, not breathing, and had meconium in his lungs. After 6 minutes' resuscitation, he began breathing. The child has an hypoxic brain injury.
PARENTS' CLAIM: Based on the nonreassuring FHR readings when the mother first reported lack of fetal movement, and a BPP of 2 points, an immediate cesarean delivery should have been performed. If the child had been delivered in a timely manner, he would have escaped a brain injury. At the very least, the mother should have been kept in the hospital for monitoring.
DEFENDANTS' DEFENSE: Drs. A and B and the hospital claimed that the child did not have a hypoxic injury; he had gastroschisis.
VERDICT: A $4,098,266 New York verdict was returned.
Second twin's birth delayed; brain damage: $1.5M settlement
A 35-year-old woman was 30 weeks' pregnant with twins when she was admitted to a hospital at high risk. At 36 weeks' gestation, she went into labor. A resident called the ObGyn to report that the patient was ready to deliver and waiting to push. The ObGyn advised that he was tied up in another procedure and for the mother to wait until he could get there.
Forty minutes later, the ObGyn arrived and the mother was allowed to push. A first-year resident delivered the first twin without incident. The second twin shifted from a cephalic presentation to a double foot- ling breech presentation and his FHR reflected severe bradycardia. Under the supervision of the ObGyn, a fourth-year resident managed the delivery, which took 28 minutes. The second twin's Apgar scores were low. He was intubated and transferred to a children's hospital for brain cooling.
PARENTS' CLAIM: Although excellent care following the birth reduced the degree of brain damage, the delay caused by the ObGyn's late arrival was responsible for the child's injuries.
PHYSICIAN'S DEFENSE: In pretrial findings, a panel of physicians reported that the child did not have a qualifying injury. However, the case settled before the trial began.
VERDICT: A $1.5 million Virginia settlement was reached.
Pregnant mother prepares for child's congenital heart disorder
A mother was told that her fetus had tricuspid atresia, a congenital defect. The mother and pediatric cardiologist developed a treatment plan to perform a balloon heart procedure at birth then transfer the baby to a specialized hospital.
After birth at a local hospital, the child was also found to have a lung disorder. He was promptly placed on a respirator. The hospital's pediatric cardiologist decided that the baby was too fragile to undergo the balloon procedure, and that the procedure could wait until the child was more stable. The baby died on his third day of life.
The neonatologists involved in treating the baby determined that the cause of death was tricuspid atresia. A pathologist reported that the death was due to a combination of congenital heart and lung disorders.
ESTATE'S CLAIM: The hospital team was sued for not following the prenatal plan. The baby's condition was serious but survivable if treated properly.
DEFENDANTS' DEFENSE: The hospital team made the correct decision to stabilize the baby's lung conditions before performing the balloon repair. The baby died because both his heart and lungs were compromised. The child's chance of survival was very small.
VERDICT: A Mississippi defense verdict was returned.
Severe uterine atony and PPH: hysterectomy
A 35-year-old woman at 41 weeks' gestation was admitted to the hospital in active labor at 5:45 am on July 26. At 2:45 pm, an ObGyn noted that she was 8+ cm dilated, 90% effaced, and that the baby's head was at -1 station. At 6:00 pm, the membranes were artificially ruptured. At 7:45 pm, examination revealed no change in her cervix. The ObGyn reviewed the options with the mother, including offering an epidural and cesarean delivery. At 8:30 pm, an intrauterine pressure catheter was placed. The ObGyn noted an inadequate labor pattern and ordered augmentation with oxytocin. On July 27 at 12:50 am, examination revealed that the cervix was completely dilated and the baby's head was at +1 station. At 2:30 am, oxytocin was infusing at 12 mU/m. At 2:30 am, the patient began to push. By 4:30 am, oxytocin was running at 14 mU/m and the patient continued to push. At 5:00 am, the ObGyn noted no further progression of labor and recommended a cesarean delivery, but the mother wanted to push a little longer. At 6:00 am, with no further progress, the decision was made to perform cesarean delivery. At 6:40 am, the patient was transferred to the operating room and delivery occurred at 7:08 am. The baby weighed 9.5 lb.
The mother's uterus was closed and hemostasis was reached. However, uterine atony was persistent and did not respond to multiple doses of medication or uterine massage. Persistent atony led to postpartum hemorrhaging (PPH). The ObGyn used conservative methods to control the hemorrhage, including medications and sutures. He then called for assistance from another ObGyn, and performed ligation of the utero-ovarian ligaments and additional suturing, which had no effect on the bleeding. They attempted an ovarian artery ligation and placed additional sutures, but the PPH continued. The ObGyn recommended a hysterectomy to the patient and her husband, who agreed. A supracervical hysterectomy was performed. During the procedure, the left ovary tore and was removed.
PARENTS' CLAIM: The patient and her husband spoke at trial of their intention to have more than one child. They sued the ObGyn, her practice, and the hospital. The ObGyn was negligent in allowing labor to continue for too long, for using oxytocin to stimulate contractions, and for allowing the patient to push for several hours, given that the baby was large. Oxytocin stimulation for so many hours without labor progression created an unacceptably high risk of uterine atony. This led to a nonreversible atonic state after delivery, which caused the patient to lose her uterus, left ovary, and her ability to reproduce.
DEFENDANTS' DEFENSE: The ObGyn was not negligent. The ObGyn met the standard of care in the management of labor and delivery. She was attentive, present at appropriate intervals, and there was no point at which a different decision should have been made. The ObGyn allowed the patient to have input in the decision-making process, as long as the ObGyn was comfortable that the decision was not compromising the safety of mother and baby. The length of labor and size of the fetus increased the risk of atony. However, in most cases, this does not occur; it can occur without those risk factors. PPH is a serious but frequently unavoidable complication of childbirth. The ObGyn's management was appropriate and prevented the patient's death.
VERDICT: A Pennsylvania defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Fetal pathology exam performed without consent: $500,000 verdict
At 12 to 15 weeks' gestation, a fetus was found to have died. An ObGyn stimulated uterine contractions with misoprostol and the fetus was delivered.
The parents requested chromosomal testing to determine the cause of death. The ObGyn took samples of the baby's skin near the umbilical cord and from the placenta. He told the parents that the tests might come back as inconclusive, and that it may be necessary to take further samples. The couple was also told that, under hospital policy, the fetus must go to the pathology department before being taken to a funeral home. The parents told the ObGyn that they did not want further samples taken for any reason, and that nothing else should be done to their child before funeral preparations. The placenta, umbilical cord, and fetus were placed in 2 separate containers. The container with the placenta and umbilical cord had an anatomic pathology requisition form, indicating that a surgical pathology exam was to be performed. The container with the fetus did not have a requisition form. When the father accompanied the nurse who carried the containers to the pathology department, he told a general technologist that no additional tissue samples were to be taken from the fetus.
The next day, the pathologist made an incision on the fetus' left side and took a sample to create a slide for microscopic analysis. The parents discovered the incision at the funeral home.
PARENTS' CLAIM: The parents sued the hospital and pathologist. The pathologist was negligent in performing a surgical pathology examination without consent. The hospital had a duty to communicate the parents' desires to the pathologist.
According to hospital protocol, the nurse who attended the delivery was to fill out the proper forms and ensure that they were available to the pathologist. The container with the fetus should have had its own requisition form that instructed the pathologist to not perform any further testing. Every specimen that goes to pathology should have a requisition form, per guidelines from the College of American Pathologists (CAP). Without a form, the pathologist should not do anything with the sample.
The parents' verbal instructions not to take additional samples from the fetus were never relayed to the pathologist.
DEFENDANTS' DEFENSE: The hospital and pathologist denied negligence. A single requisition form was appropriate; the containers' labeling and the form made it clear that the placenta, umbilical cord, and fetus were from the same patient. CAP guidelines do not require separate forms. The remains were in the gross room at pathology, which is where specimens are taken for review and analysis. Therefore, the pathologist assumed he was to perform a standard pathology exam on both containers. The technologist with whom the father had spoken met the accepted standard of care.
VERDICT: A $500,000 Maine verdict was returned. The pathologist (through insurance) and the hospital equally shared payment of the award.
When should delivery have occurred? $4M verdict
Concerned that her fetus had stopped moving, a mother presented to the ED. Results of fetal heart-rate (FHR) monitoring ordered by the attending ObGyn (Dr. A) were nonreassuring. A second ObGyn (Dr. B) ordered a fetal biophysical profile (BPP); the score was 2 points. Although a low score usually results in immediate delivery, Dr. B consulted a maternal-fetal medicine (MFM) specialist. After another fetal BPP scored 8 points, the mother was discharged.
The next day, the mother called her ObGyn (Dr. C), who told her to immediately come to his office. A fetal BPP scored 4 points, with nonreassuring fetal heart sounds.
The mother was transported to the hospital for emergency cesarean delivery. At birth, the baby was blue, not breathing, and had meconium in his lungs. After 6 minutes' resuscitation, he began breathing. The child has an hypoxic brain injury.
PARENTS' CLAIM: Based on the nonreassuring FHR readings when the mother first reported lack of fetal movement, and a BPP of 2 points, an immediate cesarean delivery should have been performed. If the child had been delivered in a timely manner, he would have escaped a brain injury. At the very least, the mother should have been kept in the hospital for monitoring.
DEFENDANTS' DEFENSE: Drs. A and B and the hospital claimed that the child did not have a hypoxic injury; he had gastroschisis.
VERDICT: A $4,098,266 New York verdict was returned.
Second twin's birth delayed; brain damage: $1.5M settlement
A 35-year-old woman was 30 weeks' pregnant with twins when she was admitted to a hospital at high risk. At 36 weeks' gestation, she went into labor. A resident called the ObGyn to report that the patient was ready to deliver and waiting to push. The ObGyn advised that he was tied up in another procedure and for the mother to wait until he could get there.
Forty minutes later, the ObGyn arrived and the mother was allowed to push. A first-year resident delivered the first twin without incident. The second twin shifted from a cephalic presentation to a double foot- ling breech presentation and his FHR reflected severe bradycardia. Under the supervision of the ObGyn, a fourth-year resident managed the delivery, which took 28 minutes. The second twin's Apgar scores were low. He was intubated and transferred to a children's hospital for brain cooling.
PARENTS' CLAIM: Although excellent care following the birth reduced the degree of brain damage, the delay caused by the ObGyn's late arrival was responsible for the child's injuries.
PHYSICIAN'S DEFENSE: In pretrial findings, a panel of physicians reported that the child did not have a qualifying injury. However, the case settled before the trial began.
VERDICT: A $1.5 million Virginia settlement was reached.
Pregnant mother prepares for child's congenital heart disorder
A mother was told that her fetus had tricuspid atresia, a congenital defect. The mother and pediatric cardiologist developed a treatment plan to perform a balloon heart procedure at birth then transfer the baby to a specialized hospital.
After birth at a local hospital, the child was also found to have a lung disorder. He was promptly placed on a respirator. The hospital's pediatric cardiologist decided that the baby was too fragile to undergo the balloon procedure, and that the procedure could wait until the child was more stable. The baby died on his third day of life.
The neonatologists involved in treating the baby determined that the cause of death was tricuspid atresia. A pathologist reported that the death was due to a combination of congenital heart and lung disorders.
ESTATE'S CLAIM: The hospital team was sued for not following the prenatal plan. The baby's condition was serious but survivable if treated properly.
DEFENDANTS' DEFENSE: The hospital team made the correct decision to stabilize the baby's lung conditions before performing the balloon repair. The baby died because both his heart and lungs were compromised. The child's chance of survival was very small.
VERDICT: A Mississippi defense verdict was returned.
Severe uterine atony and PPH: hysterectomy
A 35-year-old woman at 41 weeks' gestation was admitted to the hospital in active labor at 5:45 am on July 26. At 2:45 pm, an ObGyn noted that she was 8+ cm dilated, 90% effaced, and that the baby's head was at -1 station. At 6:00 pm, the membranes were artificially ruptured. At 7:45 pm, examination revealed no change in her cervix. The ObGyn reviewed the options with the mother, including offering an epidural and cesarean delivery. At 8:30 pm, an intrauterine pressure catheter was placed. The ObGyn noted an inadequate labor pattern and ordered augmentation with oxytocin. On July 27 at 12:50 am, examination revealed that the cervix was completely dilated and the baby's head was at +1 station. At 2:30 am, oxytocin was infusing at 12 mU/m. At 2:30 am, the patient began to push. By 4:30 am, oxytocin was running at 14 mU/m and the patient continued to push. At 5:00 am, the ObGyn noted no further progression of labor and recommended a cesarean delivery, but the mother wanted to push a little longer. At 6:00 am, with no further progress, the decision was made to perform cesarean delivery. At 6:40 am, the patient was transferred to the operating room and delivery occurred at 7:08 am. The baby weighed 9.5 lb.
The mother's uterus was closed and hemostasis was reached. However, uterine atony was persistent and did not respond to multiple doses of medication or uterine massage. Persistent atony led to postpartum hemorrhaging (PPH). The ObGyn used conservative methods to control the hemorrhage, including medications and sutures. He then called for assistance from another ObGyn, and performed ligation of the utero-ovarian ligaments and additional suturing, which had no effect on the bleeding. They attempted an ovarian artery ligation and placed additional sutures, but the PPH continued. The ObGyn recommended a hysterectomy to the patient and her husband, who agreed. A supracervical hysterectomy was performed. During the procedure, the left ovary tore and was removed.
PARENTS' CLAIM: The patient and her husband spoke at trial of their intention to have more than one child. They sued the ObGyn, her practice, and the hospital. The ObGyn was negligent in allowing labor to continue for too long, for using oxytocin to stimulate contractions, and for allowing the patient to push for several hours, given that the baby was large. Oxytocin stimulation for so many hours without labor progression created an unacceptably high risk of uterine atony. This led to a nonreversible atonic state after delivery, which caused the patient to lose her uterus, left ovary, and her ability to reproduce.
DEFENDANTS' DEFENSE: The ObGyn was not negligent. The ObGyn met the standard of care in the management of labor and delivery. She was attentive, present at appropriate intervals, and there was no point at which a different decision should have been made. The ObGyn allowed the patient to have input in the decision-making process, as long as the ObGyn was comfortable that the decision was not compromising the safety of mother and baby. The length of labor and size of the fetus increased the risk of atony. However, in most cases, this does not occur; it can occur without those risk factors. PPH is a serious but frequently unavoidable complication of childbirth. The ObGyn's management was appropriate and prevented the patient's death.
VERDICT: A Pennsylvania defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Fetal pathology exam performed without consent: $500,000 verdict
At 12 to 15 weeks' gestation, a fetus was found to have died. An ObGyn stimulated uterine contractions with misoprostol and the fetus was delivered.
The parents requested chromosomal testing to determine the cause of death. The ObGyn took samples of the baby's skin near the umbilical cord and from the placenta. He told the parents that the tests might come back as inconclusive, and that it may be necessary to take further samples. The couple was also told that, under hospital policy, the fetus must go to the pathology department before being taken to a funeral home. The parents told the ObGyn that they did not want further samples taken for any reason, and that nothing else should be done to their child before funeral preparations. The placenta, umbilical cord, and fetus were placed in 2 separate containers. The container with the placenta and umbilical cord had an anatomic pathology requisition form, indicating that a surgical pathology exam was to be performed. The container with the fetus did not have a requisition form. When the father accompanied the nurse who carried the containers to the pathology department, he told a general technologist that no additional tissue samples were to be taken from the fetus.
The next day, the pathologist made an incision on the fetus' left side and took a sample to create a slide for microscopic analysis. The parents discovered the incision at the funeral home.
PARENTS' CLAIM: The parents sued the hospital and pathologist. The pathologist was negligent in performing a surgical pathology examination without consent. The hospital had a duty to communicate the parents' desires to the pathologist.
According to hospital protocol, the nurse who attended the delivery was to fill out the proper forms and ensure that they were available to the pathologist. The container with the fetus should have had its own requisition form that instructed the pathologist to not perform any further testing. Every specimen that goes to pathology should have a requisition form, per guidelines from the College of American Pathologists (CAP). Without a form, the pathologist should not do anything with the sample.
The parents' verbal instructions not to take additional samples from the fetus were never relayed to the pathologist.
DEFENDANTS' DEFENSE: The hospital and pathologist denied negligence. A single requisition form was appropriate; the containers' labeling and the form made it clear that the placenta, umbilical cord, and fetus were from the same patient. CAP guidelines do not require separate forms. The remains were in the gross room at pathology, which is where specimens are taken for review and analysis. Therefore, the pathologist assumed he was to perform a standard pathology exam on both containers. The technologist with whom the father had spoken met the accepted standard of care.
VERDICT: A $500,000 Maine verdict was returned. The pathologist (through insurance) and the hospital equally shared payment of the award.
When should delivery have occurred? $4M verdict
Concerned that her fetus had stopped moving, a mother presented to the ED. Results of fetal heart-rate (FHR) monitoring ordered by the attending ObGyn (Dr. A) were nonreassuring. A second ObGyn (Dr. B) ordered a fetal biophysical profile (BPP); the score was 2 points. Although a low score usually results in immediate delivery, Dr. B consulted a maternal-fetal medicine (MFM) specialist. After another fetal BPP scored 8 points, the mother was discharged.
The next day, the mother called her ObGyn (Dr. C), who told her to immediately come to his office. A fetal BPP scored 4 points, with nonreassuring fetal heart sounds.
The mother was transported to the hospital for emergency cesarean delivery. At birth, the baby was blue, not breathing, and had meconium in his lungs. After 6 minutes' resuscitation, he began breathing. The child has an hypoxic brain injury.
PARENTS' CLAIM: Based on the nonreassuring FHR readings when the mother first reported lack of fetal movement, and a BPP of 2 points, an immediate cesarean delivery should have been performed. If the child had been delivered in a timely manner, he would have escaped a brain injury. At the very least, the mother should have been kept in the hospital for monitoring.
DEFENDANTS' DEFENSE: Drs. A and B and the hospital claimed that the child did not have a hypoxic injury; he had gastroschisis.
VERDICT: A $4,098,266 New York verdict was returned.
Second twin's birth delayed; brain damage: $1.5M settlement
A 35-year-old woman was 30 weeks' pregnant with twins when she was admitted to a hospital at high risk. At 36 weeks' gestation, she went into labor. A resident called the ObGyn to report that the patient was ready to deliver and waiting to push. The ObGyn advised that he was tied up in another procedure and for the mother to wait until he could get there.
Forty minutes later, the ObGyn arrived and the mother was allowed to push. A first-year resident delivered the first twin without incident. The second twin shifted from a cephalic presentation to a double foot- ling breech presentation and his FHR reflected severe bradycardia. Under the supervision of the ObGyn, a fourth-year resident managed the delivery, which took 28 minutes. The second twin's Apgar scores were low. He was intubated and transferred to a children's hospital for brain cooling.
PARENTS' CLAIM: Although excellent care following the birth reduced the degree of brain damage, the delay caused by the ObGyn's late arrival was responsible for the child's injuries.
PHYSICIAN'S DEFENSE: In pretrial findings, a panel of physicians reported that the child did not have a qualifying injury. However, the case settled before the trial began.
VERDICT: A $1.5 million Virginia settlement was reached.
Pregnant mother prepares for child's congenital heart disorder
A mother was told that her fetus had tricuspid atresia, a congenital defect. The mother and pediatric cardiologist developed a treatment plan to perform a balloon heart procedure at birth then transfer the baby to a specialized hospital.
After birth at a local hospital, the child was also found to have a lung disorder. He was promptly placed on a respirator. The hospital's pediatric cardiologist decided that the baby was too fragile to undergo the balloon procedure, and that the procedure could wait until the child was more stable. The baby died on his third day of life.
The neonatologists involved in treating the baby determined that the cause of death was tricuspid atresia. A pathologist reported that the death was due to a combination of congenital heart and lung disorders.
ESTATE'S CLAIM: The hospital team was sued for not following the prenatal plan. The baby's condition was serious but survivable if treated properly.
DEFENDANTS' DEFENSE: The hospital team made the correct decision to stabilize the baby's lung conditions before performing the balloon repair. The baby died because both his heart and lungs were compromised. The child's chance of survival was very small.
VERDICT: A Mississippi defense verdict was returned.
Severe uterine atony and PPH: hysterectomy
A 35-year-old woman at 41 weeks' gestation was admitted to the hospital in active labor at 5:45 am on July 26. At 2:45 pm, an ObGyn noted that she was 8+ cm dilated, 90% effaced, and that the baby's head was at -1 station. At 6:00 pm, the membranes were artificially ruptured. At 7:45 pm, examination revealed no change in her cervix. The ObGyn reviewed the options with the mother, including offering an epidural and cesarean delivery. At 8:30 pm, an intrauterine pressure catheter was placed. The ObGyn noted an inadequate labor pattern and ordered augmentation with oxytocin. On July 27 at 12:50 am, examination revealed that the cervix was completely dilated and the baby's head was at +1 station. At 2:30 am, oxytocin was infusing at 12 mU/m. At 2:30 am, the patient began to push. By 4:30 am, oxytocin was running at 14 mU/m and the patient continued to push. At 5:00 am, the ObGyn noted no further progression of labor and recommended a cesarean delivery, but the mother wanted to push a little longer. At 6:00 am, with no further progress, the decision was made to perform cesarean delivery. At 6:40 am, the patient was transferred to the operating room and delivery occurred at 7:08 am. The baby weighed 9.5 lb.
The mother's uterus was closed and hemostasis was reached. However, uterine atony was persistent and did not respond to multiple doses of medication or uterine massage. Persistent atony led to postpartum hemorrhaging (PPH). The ObGyn used conservative methods to control the hemorrhage, including medications and sutures. He then called for assistance from another ObGyn, and performed ligation of the utero-ovarian ligaments and additional suturing, which had no effect on the bleeding. They attempted an ovarian artery ligation and placed additional sutures, but the PPH continued. The ObGyn recommended a hysterectomy to the patient and her husband, who agreed. A supracervical hysterectomy was performed. During the procedure, the left ovary tore and was removed.
PARENTS' CLAIM: The patient and her husband spoke at trial of their intention to have more than one child. They sued the ObGyn, her practice, and the hospital. The ObGyn was negligent in allowing labor to continue for too long, for using oxytocin to stimulate contractions, and for allowing the patient to push for several hours, given that the baby was large. Oxytocin stimulation for so many hours without labor progression created an unacceptably high risk of uterine atony. This led to a nonreversible atonic state after delivery, which caused the patient to lose her uterus, left ovary, and her ability to reproduce.
DEFENDANTS' DEFENSE: The ObGyn was not negligent. The ObGyn met the standard of care in the management of labor and delivery. She was attentive, present at appropriate intervals, and there was no point at which a different decision should have been made. The ObGyn allowed the patient to have input in the decision-making process, as long as the ObGyn was comfortable that the decision was not compromising the safety of mother and baby. The length of labor and size of the fetus increased the risk of atony. However, in most cases, this does not occur; it can occur without those risk factors. PPH is a serious but frequently unavoidable complication of childbirth. The ObGyn's management was appropriate and prevented the patient's death.
VERDICT: A Pennsylvania defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
From the Editors: “Okay” is not good enough
Keeping up with refinements in old procedures and adopting new procedures throughout one’s surgical career has always been a challenge.
That challenge has grown as advancements in technology have become ever more disruptive, requiring the learning of radically different skills. Surgeons are highly motivated to learn new procedures, lest they become extinct like professional “dodo birds.” But doing so requires a considerable expenditure of time and money to attend courses and then a period of being proctored in the new procedure once it has been learned.

The acquisition of technical skill in surgery is well recognized as a primary responsibility of surgical residency training programs. Surgical meetings and surgical journals have recently given a lot of space to the question of whether training programs are imparting adequate surgical skill to their learners and whether new graduates have achieved surgical competence at graduation. Some highly cited articles, having surveyed surgical teachers, maintain that a significant percentage of the new graduates have not achieved the needed skills to practice independently.1,2 Many place the blame at the feet of the much-maligned restriction in the resident work week to 80 hours, a limitation imposed by the Accreditation Council of Graduate Medical Education in 2003.
The reasons for the perceived decline in competence are many, including an increase in the number and complexity of surgical procedures, as well as institutional expectations for increased involvement of attendings in procedures. Recommended solutions include lengthening training, encouraging increased and earlier specialization, and proctoring by senior surgeons in the first year of a surgeon’s practice. Less frequently mentioned is the fact that, although the work hours are shorter and the surgery more complex, we have not compensated for these factors by appreciably changing the methods used to teach surgical technique. In many programs, faculty are performing an increasing proportion of procedures: doing more and teaching less.
Mandated surgical skills labs may be helpful to teach a basic level of skill. Simulation can be helpful in imparting the ability to perform more complex procedures and quickly adapt to unexpected intraoperative findings or occurrences. Virtual reality simulators are available, but they’re very expensive and often beyond the budgets of most residency programs. While simulation can help, it is not the whole solution to learning surgical skills.
It is now long past due for surgical training programs to rethink the process of teaching surgical skill in a more deliberate way to residents. One way to accomplish this might be through utilizing “master teachers” or “coaches” who are trained specifically to impart not only skill in performing a given procedure but also an understanding of how to critically assess one’s own performance in practice and learn how to improve that performance through self-reflection and self-assessment. Some very thoughtful and compelling studies have described how coaching might aid performance improvement of both residents and of surgeons already in practice.3,4,5
The process involves a review of videotaped procedures by both the operating surgeon (or surgical resident) and the coach to recognize points at which performance was subpar and to have a discussion about steps needed for improvement. Through further reviews of videotapes of subsequent procedures, the surgeon or resident learns to internalize the techniques of performance improvement.
While ideal in a perfect world, such a schema is far from universally feasible in our current surgical culture. Although master classes and coaching are accepted as the norm in other fields that also require technical excellence, such as classical music and athletics, our surgical culture does not readily accept that our surgical technique might be less than perfect. We tend to downplay the notion that we (and our patients) might benefit from improving our surgical skills beyond mere competence to the point of mastery. A culture change in this regard will not occur overnight and most likely must begin by making coaching a standard and accepted part of surgical training programs, both for the residents and for the teachers themselves.
We make the tacit assumption that attending surgeons are teachers, but we rarely teach them how to teach. The fact that many attendings don’t know how to give effective feedback to residents may be a reason that they fail to give specific coaching on how their learners might improve and why these attendings take over an increasing portion of the procedures themselves. In order for faculty to improve the quality of their teaching, they need training of their own. The training should be a mandatory, “protected” part of their day or it will not occur, and the “teaching the teachers” must be done by master teachers who are respected for their skill not only as a surgeons but also as a surgical educators. This role is an appropriate one for Associate Members of the new ACS Academy of Master Surgeon Educators to assume (see https://www.facs.org/education/academy/membership).
Coaching by master surgeons should become a professional norm. It is only after surgical education and coaching are incorporated all along the training continuum – from novice to competent to master during residency training – that surgeons already in practice will accept it as a regular part of their work. Refinements in procedures and new procedures would be met by continued professional improvement that would be enhanced by master surgeon coaching. We owe it to ourselves and our patients to achieve excellence, not mere competence. “Okay” is not good enough.
Dr. Deveney is a professor of surgery and the vice chair of education in the department of surgery at Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
1. Mattar SG et al. General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg. 2013;258(3):440-9.
2. Damewood RB et al. “Taking training to the next level”: The American College of Surgeons Committee on residency training survey. J Surg Educ. 2017;74(6):e95-e105.
3. Gawande A. Coaching a surgeon: What makes top performers better? The New Yorker, Oct. 3, 2011.
4. Bonrath EM et al. Comprehensive surgical coaching enhances surgical skill in the operating room: a randomized controlled trial. Ann Surg. 2015;262:205-12.
5. Greenberg CC et al. Surgical coaching for individual performance improvement. Ann Surg. 2015;261(1):32-4.
Keeping up with refinements in old procedures and adopting new procedures throughout one’s surgical career has always been a challenge.
That challenge has grown as advancements in technology have become ever more disruptive, requiring the learning of radically different skills. Surgeons are highly motivated to learn new procedures, lest they become extinct like professional “dodo birds.” But doing so requires a considerable expenditure of time and money to attend courses and then a period of being proctored in the new procedure once it has been learned.
The acquisition of technical skill in surgery is well recognized as a primary responsibility of surgical residency training programs. Surgical meetings and surgical journals have recently given a lot of space to the question of whether training programs are imparting adequate surgical skill to their learners and whether new graduates have achieved surgical competence at graduation. Some highly cited articles, having surveyed surgical teachers, maintain that a significant percentage of the new graduates have not achieved the needed skills to practice independently.1,2 Many place the blame at the feet of the much-maligned restriction in the resident work week to 80 hours, a limitation imposed by the Accreditation Council of Graduate Medical Education in 2003.
The reasons for the perceived decline in competence are many, including an increase in the number and complexity of surgical procedures, as well as institutional expectations for increased involvement of attendings in procedures. Recommended solutions include lengthening training, encouraging increased and earlier specialization, and proctoring by senior surgeons in the first year of a surgeon’s practice. Less frequently mentioned is the fact that, although the work hours are shorter and the surgery more complex, we have not compensated for these factors by appreciably changing the methods used to teach surgical technique. In many programs, faculty are performing an increasing proportion of procedures: doing more and teaching less.
Mandated surgical skills labs may be helpful to teach a basic level of skill. Simulation can be helpful in imparting the ability to perform more complex procedures and quickly adapt to unexpected intraoperative findings or occurrences. Virtual reality simulators are available, but they’re very expensive and often beyond the budgets of most residency programs. While simulation can help, it is not the whole solution to learning surgical skills.
It is now long past due for surgical training programs to rethink the process of teaching surgical skill in a more deliberate way to residents. One way to accomplish this might be through utilizing “master teachers” or “coaches” who are trained specifically to impart not only skill in performing a given procedure but also an understanding of how to critically assess one’s own performance in practice and learn how to improve that performance through self-reflection and self-assessment. Some very thoughtful and compelling studies have described how coaching might aid performance improvement of both residents and of surgeons already in practice.3,4,5
The process involves a review of videotaped procedures by both the operating surgeon (or surgical resident) and the coach to recognize points at which performance was subpar and to have a discussion about steps needed for improvement. Through further reviews of videotapes of subsequent procedures, the surgeon or resident learns to internalize the techniques of performance improvement.
While ideal in a perfect world, such a schema is far from universally feasible in our current surgical culture. Although master classes and coaching are accepted as the norm in other fields that also require technical excellence, such as classical music and athletics, our surgical culture does not readily accept that our surgical technique might be less than perfect. We tend to downplay the notion that we (and our patients) might benefit from improving our surgical skills beyond mere competence to the point of mastery. A culture change in this regard will not occur overnight and most likely must begin by making coaching a standard and accepted part of surgical training programs, both for the residents and for the teachers themselves.
We make the tacit assumption that attending surgeons are teachers, but we rarely teach them how to teach. The fact that many attendings don’t know how to give effective feedback to residents may be a reason that they fail to give specific coaching on how their learners might improve and why these attendings take over an increasing portion of the procedures themselves. In order for faculty to improve the quality of their teaching, they need training of their own. The training should be a mandatory, “protected” part of their day or it will not occur, and the “teaching the teachers” must be done by master teachers who are respected for their skill not only as a surgeons but also as a surgical educators. This role is an appropriate one for Associate Members of the new ACS Academy of Master Surgeon Educators to assume (see https://www.facs.org/education/academy/membership).
Coaching by master surgeons should become a professional norm. It is only after surgical education and coaching are incorporated all along the training continuum – from novice to competent to master during residency training – that surgeons already in practice will accept it as a regular part of their work. Refinements in procedures and new procedures would be met by continued professional improvement that would be enhanced by master surgeon coaching. We owe it to ourselves and our patients to achieve excellence, not mere competence. “Okay” is not good enough.
Dr. Deveney is a professor of surgery and the vice chair of education in the department of surgery at Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
Keeping up with refinements in old procedures and adopting new procedures throughout one’s surgical career has always been a challenge.
That challenge has grown as advancements in technology have become ever more disruptive, requiring the learning of radically different skills. Surgeons are highly motivated to learn new procedures, lest they become extinct like professional “dodo birds.” But doing so requires a considerable expenditure of time and money to attend courses and then a period of being proctored in the new procedure once it has been learned.
The acquisition of technical skill in surgery is well recognized as a primary responsibility of surgical residency training programs. Surgical meetings and surgical journals have recently given a lot of space to the question of whether training programs are imparting adequate surgical skill to their learners and whether new graduates have achieved surgical competence at graduation. Some highly cited articles, having surveyed surgical teachers, maintain that a significant percentage of the new graduates have not achieved the needed skills to practice independently.1,2 Many place the blame at the feet of the much-maligned restriction in the resident work week to 80 hours, a limitation imposed by the Accreditation Council of Graduate Medical Education in 2003.
The reasons for the perceived decline in competence are many, including an increase in the number and complexity of surgical procedures, as well as institutional expectations for increased involvement of attendings in procedures. Recommended solutions include lengthening training, encouraging increased and earlier specialization, and proctoring by senior surgeons in the first year of a surgeon’s practice. Less frequently mentioned is the fact that, although the work hours are shorter and the surgery more complex, we have not compensated for these factors by appreciably changing the methods used to teach surgical technique. In many programs, faculty are performing an increasing proportion of procedures: doing more and teaching less.
Mandated surgical skills labs may be helpful to teach a basic level of skill. Simulation can be helpful in imparting the ability to perform more complex procedures and quickly adapt to unexpected intraoperative findings or occurrences. Virtual reality simulators are available, but they’re very expensive and often beyond the budgets of most residency programs. While simulation can help, it is not the whole solution to learning surgical skills.
It is now long past due for surgical training programs to rethink the process of teaching surgical skill in a more deliberate way to residents. One way to accomplish this might be through utilizing “master teachers” or “coaches” who are trained specifically to impart not only skill in performing a given procedure but also an understanding of how to critically assess one’s own performance in practice and learn how to improve that performance through self-reflection and self-assessment. Some very thoughtful and compelling studies have described how coaching might aid performance improvement of both residents and of surgeons already in practice.3,4,5
The process involves a review of videotaped procedures by both the operating surgeon (or surgical resident) and the coach to recognize points at which performance was subpar and to have a discussion about steps needed for improvement. Through further reviews of videotapes of subsequent procedures, the surgeon or resident learns to internalize the techniques of performance improvement.
While ideal in a perfect world, such a schema is far from universally feasible in our current surgical culture. Although master classes and coaching are accepted as the norm in other fields that also require technical excellence, such as classical music and athletics, our surgical culture does not readily accept that our surgical technique might be less than perfect. We tend to downplay the notion that we (and our patients) might benefit from improving our surgical skills beyond mere competence to the point of mastery. A culture change in this regard will not occur overnight and most likely must begin by making coaching a standard and accepted part of surgical training programs, both for the residents and for the teachers themselves.
We make the tacit assumption that attending surgeons are teachers, but we rarely teach them how to teach. The fact that many attendings don’t know how to give effective feedback to residents may be a reason that they fail to give specific coaching on how their learners might improve and why these attendings take over an increasing portion of the procedures themselves. In order for faculty to improve the quality of their teaching, they need training of their own. The training should be a mandatory, “protected” part of their day or it will not occur, and the “teaching the teachers” must be done by master teachers who are respected for their skill not only as a surgeons but also as a surgical educators. This role is an appropriate one for Associate Members of the new ACS Academy of Master Surgeon Educators to assume (see https://www.facs.org/education/academy/membership).
Coaching by master surgeons should become a professional norm. It is only after surgical education and coaching are incorporated all along the training continuum – from novice to competent to master during residency training – that surgeons already in practice will accept it as a regular part of their work. Refinements in procedures and new procedures would be met by continued professional improvement that would be enhanced by master surgeon coaching. We owe it to ourselves and our patients to achieve excellence, not mere competence. “Okay” is not good enough.
Dr. Deveney is a professor of surgery and the vice chair of education in the department of surgery at Oregon Health & Science University, Portland. She is the coeditor of ACS Surgery News.
1. Mattar SG et al. General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg. 2013;258(3):440-9.
2. Damewood RB et al. “Taking training to the next level”: The American College of Surgeons Committee on residency training survey. J Surg Educ. 2017;74(6):e95-e105.
3. Gawande A. Coaching a surgeon: What makes top performers better? The New Yorker, Oct. 3, 2011.
4. Bonrath EM et al. Comprehensive surgical coaching enhances surgical skill in the operating room: a randomized controlled trial. Ann Surg. 2015;262:205-12.
5. Greenberg CC et al. Surgical coaching for individual performance improvement. Ann Surg. 2015;261(1):32-4.
1. Mattar SG et al. General surgery residency inadequately prepares trainees for fellowship: results of a survey of fellowship program directors. Ann Surg. 2013;258(3):440-9.
2. Damewood RB et al. “Taking training to the next level”: The American College of Surgeons Committee on residency training survey. J Surg Educ. 2017;74(6):e95-e105.
3. Gawande A. Coaching a surgeon: What makes top performers better? The New Yorker, Oct. 3, 2011.
4. Bonrath EM et al. Comprehensive surgical coaching enhances surgical skill in the operating room: a randomized controlled trial. Ann Surg. 2015;262:205-12.
5. Greenberg CC et al. Surgical coaching for individual performance improvement. Ann Surg. 2015;261(1):32-4.
‘Aggressive’ new advance directive would let dementia patients refuse food
Treading into ethically and legally uncertain territory, .
The directive, finalized this month by the board for End of Life Choices New York, aims to provide patients a way to hasten death in late-stage dementia, if they choose.
Dementia is a terminal illness, but even in the seven U.S. jurisdictions that allow medical aid-in-dying, it’s not a condition covered by the laws. Increasingly, patients are seeking other options, said Timothy Quill, MD, a palliative care expert at the University of Rochester (N.Y.) and an advocate of the practice.
“Developing incapacitating dementia is certainly my and a lot of people’s worst nightmare,” he said. “This is an aggressive document. It’s a way of addressing a real problem, which is the prospect of advanced dementia.”
The document offers two options: one that requests “comfort feeding” – providing oral food and water if a patient appears to enjoy or allows it during the final stages of the disease – and one that would halt all assisted eating and drinking, even if a patient seems willing to accept it.
Supporters say it’s the strongest effort to date to allow people who want to avoid the ravages of advanced dementia to make their final wishes known – while they still have the ability to do so.
“They do not want their dying prolonged,” said Judith Schwarz, who drafted the document as clinical director for the advocacy group. “This is an informed and thoughtful choice that needs a great deal of reflection and discussion.”
But critics say it’s a disturbing effort to allow withdrawal of basic sustenance from the most vulnerable in society.
“I think oral feeding is basic care,” said Richard Doerflinger, an associate scholar with the Charlotte Lozier Institute, which opposes abortion and euthanasia. “It’s what they want here and now that matters. If they start taking food, you give them food.”
Advance directives are legally recognized documents that specify care if a person is incapacitated. They can confirm that a patient doesn’t want to be resuscitated or kept on life support, such as a ventilator or feeding tube, if they have a terminal condition from which they’re not likely to recover.
However, the documents typically say nothing about withdrawing hand-feeding of food or fluids.
The New York directive, in contrast, offers option A, which allows refusal of all oral assisted feeding. Option B permits comfort-focused feeding.
Both options would be invoked only when a patient is diagnosed with moderate or severe dementia, defined as stages 6 or 7 of a widely used test known as the Functional Assessment Staging Test (FAST). At those stages, patients would be unable to feed themselves or make health care decisions.
The new form goes further than a similar dementia directive introduced last year by another group that supports aid-in-dying, End of Life Washington. That document says that a person with dementia who accepts food or drink should receive oral nourishment until he or she is unwilling or unable to do so.
The New York document says, “My instructions are that I do NOT want to be fed by hand even if I appear to cooperate in being fed by opening my mouth.”
Whether the new directive will be honored in New York – or anywhere else – is unclear. Legal scholars and ethicists say directives withdrawing oral assisted feeding are prohibited in several states. Many care facilities are unlikely to cooperate, said Thaddeus Pope, director of the Health Law Institute at Hamline University, St. Paul, Minn., and an expert on end-of-life law. Doctors have a duty to honor patient wishes, but they can refuse if they have medical or moral qualms.
“Even solidly legal advance directives do not and cannot ENSURE that wishes are respected,” Pope said in an email. “They can only ‘help assure’ that.”
Directors at End of Life Choices New York consider the document “legally sturdy,” Schwarz said, adding, “Of course it’s going to end up in court.”
Whether assisted feeding can be withdrawn was at the center of recent high-profile cases in which patients with dementia were spoon-fed against their documented wishes because they continued to open their mouths. In a case in Canada, a court ruled that such feeding is basic care that can’t be withdrawn.
People who fill out the directives may be more likely to have them honored if they remain at home, Schwarz said. She stressed that patients should make their wishes known far in advance and choose health care agents who will be strong advocates. Legal experts say the documents should be updated regularly.
Doerflinger, however, said creating the directive and making it available misses a crucial point: People who don’t have dementia now can’t know how they’ll feel later, yet they’re deciding in advance to forgo nourishment.
“The question is: Do we, the able-bodied, have a right to discriminate against the disabled people we will later become?” Doerflinger said.
Already, though, Schwarz has heard from people determined to put the new directive in place.
Janet Dwyer, 59, of New York, said her family was horrified by her father’s lingering death after a heart attack 4 years ago and mindful of a family history of dementia. When Dwyer learned there was a directive to address terminal illness and dementia, she signed it. So did her husband, John Harney, also 59.
“Judith informed me of the Option A or Option B scenarios,” said Dwyer, who opted for A. “I said, ‘Well, that is just perfect.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation, which is not affiliated with Kaiser Permanente. KHN’s coverage of end-of-life and serious illness issues is supported in part by the Gordon and Betty Moore Foundation.
Treading into ethically and legally uncertain territory, .
The directive, finalized this month by the board for End of Life Choices New York, aims to provide patients a way to hasten death in late-stage dementia, if they choose.
Dementia is a terminal illness, but even in the seven U.S. jurisdictions that allow medical aid-in-dying, it’s not a condition covered by the laws. Increasingly, patients are seeking other options, said Timothy Quill, MD, a palliative care expert at the University of Rochester (N.Y.) and an advocate of the practice.
“Developing incapacitating dementia is certainly my and a lot of people’s worst nightmare,” he said. “This is an aggressive document. It’s a way of addressing a real problem, which is the prospect of advanced dementia.”
The document offers two options: one that requests “comfort feeding” – providing oral food and water if a patient appears to enjoy or allows it during the final stages of the disease – and one that would halt all assisted eating and drinking, even if a patient seems willing to accept it.
Supporters say it’s the strongest effort to date to allow people who want to avoid the ravages of advanced dementia to make their final wishes known – while they still have the ability to do so.
“They do not want their dying prolonged,” said Judith Schwarz, who drafted the document as clinical director for the advocacy group. “This is an informed and thoughtful choice that needs a great deal of reflection and discussion.”
But critics say it’s a disturbing effort to allow withdrawal of basic sustenance from the most vulnerable in society.
“I think oral feeding is basic care,” said Richard Doerflinger, an associate scholar with the Charlotte Lozier Institute, which opposes abortion and euthanasia. “It’s what they want here and now that matters. If they start taking food, you give them food.”
Advance directives are legally recognized documents that specify care if a person is incapacitated. They can confirm that a patient doesn’t want to be resuscitated or kept on life support, such as a ventilator or feeding tube, if they have a terminal condition from which they’re not likely to recover.
However, the documents typically say nothing about withdrawing hand-feeding of food or fluids.
The New York directive, in contrast, offers option A, which allows refusal of all oral assisted feeding. Option B permits comfort-focused feeding.
Both options would be invoked only when a patient is diagnosed with moderate or severe dementia, defined as stages 6 or 7 of a widely used test known as the Functional Assessment Staging Test (FAST). At those stages, patients would be unable to feed themselves or make health care decisions.
The new form goes further than a similar dementia directive introduced last year by another group that supports aid-in-dying, End of Life Washington. That document says that a person with dementia who accepts food or drink should receive oral nourishment until he or she is unwilling or unable to do so.
The New York document says, “My instructions are that I do NOT want to be fed by hand even if I appear to cooperate in being fed by opening my mouth.”
Whether the new directive will be honored in New York – or anywhere else – is unclear. Legal scholars and ethicists say directives withdrawing oral assisted feeding are prohibited in several states. Many care facilities are unlikely to cooperate, said Thaddeus Pope, director of the Health Law Institute at Hamline University, St. Paul, Minn., and an expert on end-of-life law. Doctors have a duty to honor patient wishes, but they can refuse if they have medical or moral qualms.
“Even solidly legal advance directives do not and cannot ENSURE that wishes are respected,” Pope said in an email. “They can only ‘help assure’ that.”
Directors at End of Life Choices New York consider the document “legally sturdy,” Schwarz said, adding, “Of course it’s going to end up in court.”
Whether assisted feeding can be withdrawn was at the center of recent high-profile cases in which patients with dementia were spoon-fed against their documented wishes because they continued to open their mouths. In a case in Canada, a court ruled that such feeding is basic care that can’t be withdrawn.
People who fill out the directives may be more likely to have them honored if they remain at home, Schwarz said. She stressed that patients should make their wishes known far in advance and choose health care agents who will be strong advocates. Legal experts say the documents should be updated regularly.
Doerflinger, however, said creating the directive and making it available misses a crucial point: People who don’t have dementia now can’t know how they’ll feel later, yet they’re deciding in advance to forgo nourishment.
“The question is: Do we, the able-bodied, have a right to discriminate against the disabled people we will later become?” Doerflinger said.
Already, though, Schwarz has heard from people determined to put the new directive in place.
Janet Dwyer, 59, of New York, said her family was horrified by her father’s lingering death after a heart attack 4 years ago and mindful of a family history of dementia. When Dwyer learned there was a directive to address terminal illness and dementia, she signed it. So did her husband, John Harney, also 59.
“Judith informed me of the Option A or Option B scenarios,” said Dwyer, who opted for A. “I said, ‘Well, that is just perfect.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation, which is not affiliated with Kaiser Permanente. KHN’s coverage of end-of-life and serious illness issues is supported in part by the Gordon and Betty Moore Foundation.
Treading into ethically and legally uncertain territory, .
The directive, finalized this month by the board for End of Life Choices New York, aims to provide patients a way to hasten death in late-stage dementia, if they choose.
Dementia is a terminal illness, but even in the seven U.S. jurisdictions that allow medical aid-in-dying, it’s not a condition covered by the laws. Increasingly, patients are seeking other options, said Timothy Quill, MD, a palliative care expert at the University of Rochester (N.Y.) and an advocate of the practice.
“Developing incapacitating dementia is certainly my and a lot of people’s worst nightmare,” he said. “This is an aggressive document. It’s a way of addressing a real problem, which is the prospect of advanced dementia.”
The document offers two options: one that requests “comfort feeding” – providing oral food and water if a patient appears to enjoy or allows it during the final stages of the disease – and one that would halt all assisted eating and drinking, even if a patient seems willing to accept it.
Supporters say it’s the strongest effort to date to allow people who want to avoid the ravages of advanced dementia to make their final wishes known – while they still have the ability to do so.
“They do not want their dying prolonged,” said Judith Schwarz, who drafted the document as clinical director for the advocacy group. “This is an informed and thoughtful choice that needs a great deal of reflection and discussion.”
But critics say it’s a disturbing effort to allow withdrawal of basic sustenance from the most vulnerable in society.
“I think oral feeding is basic care,” said Richard Doerflinger, an associate scholar with the Charlotte Lozier Institute, which opposes abortion and euthanasia. “It’s what they want here and now that matters. If they start taking food, you give them food.”
Advance directives are legally recognized documents that specify care if a person is incapacitated. They can confirm that a patient doesn’t want to be resuscitated or kept on life support, such as a ventilator or feeding tube, if they have a terminal condition from which they’re not likely to recover.
However, the documents typically say nothing about withdrawing hand-feeding of food or fluids.
The New York directive, in contrast, offers option A, which allows refusal of all oral assisted feeding. Option B permits comfort-focused feeding.
Both options would be invoked only when a patient is diagnosed with moderate or severe dementia, defined as stages 6 or 7 of a widely used test known as the Functional Assessment Staging Test (FAST). At those stages, patients would be unable to feed themselves or make health care decisions.
The new form goes further than a similar dementia directive introduced last year by another group that supports aid-in-dying, End of Life Washington. That document says that a person with dementia who accepts food or drink should receive oral nourishment until he or she is unwilling or unable to do so.
The New York document says, “My instructions are that I do NOT want to be fed by hand even if I appear to cooperate in being fed by opening my mouth.”
Whether the new directive will be honored in New York – or anywhere else – is unclear. Legal scholars and ethicists say directives withdrawing oral assisted feeding are prohibited in several states. Many care facilities are unlikely to cooperate, said Thaddeus Pope, director of the Health Law Institute at Hamline University, St. Paul, Minn., and an expert on end-of-life law. Doctors have a duty to honor patient wishes, but they can refuse if they have medical or moral qualms.
“Even solidly legal advance directives do not and cannot ENSURE that wishes are respected,” Pope said in an email. “They can only ‘help assure’ that.”
Directors at End of Life Choices New York consider the document “legally sturdy,” Schwarz said, adding, “Of course it’s going to end up in court.”
Whether assisted feeding can be withdrawn was at the center of recent high-profile cases in which patients with dementia were spoon-fed against their documented wishes because they continued to open their mouths. In a case in Canada, a court ruled that such feeding is basic care that can’t be withdrawn.
People who fill out the directives may be more likely to have them honored if they remain at home, Schwarz said. She stressed that patients should make their wishes known far in advance and choose health care agents who will be strong advocates. Legal experts say the documents should be updated regularly.
Doerflinger, however, said creating the directive and making it available misses a crucial point: People who don’t have dementia now can’t know how they’ll feel later, yet they’re deciding in advance to forgo nourishment.
“The question is: Do we, the able-bodied, have a right to discriminate against the disabled people we will later become?” Doerflinger said.
Already, though, Schwarz has heard from people determined to put the new directive in place.
Janet Dwyer, 59, of New York, said her family was horrified by her father’s lingering death after a heart attack 4 years ago and mindful of a family history of dementia. When Dwyer learned there was a directive to address terminal illness and dementia, she signed it. So did her husband, John Harney, also 59.
“Judith informed me of the Option A or Option B scenarios,” said Dwyer, who opted for A. “I said, ‘Well, that is just perfect.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation, which is not affiliated with Kaiser Permanente. KHN’s coverage of end-of-life and serious illness issues is supported in part by the Gordon and Betty Moore Foundation.
A public health approach to gun violence
In 2014, 33,594 people were killed by firearms in the United States. More than 21,000 of these deaths were suicides. The rest were primarily homicides and accidental shootings. Meanwhile, firearm deaths represented nearly 17% of injury deaths that year.1,2
In a 2015 Perspective published in the New England Journal of Medicine, author Chana Sacks, MD, pointed out that 20 children and adolescents are sent to the hospital daily for firearm injuries and 2,000 people each year suffer gunshot-related spinal cord injuries and “become lifelong patients.”3
At the same time, Federal Bureau of Investigation data show that the number of active shooter situations rose between 2000 and 2013, with an average of 6.4 incidents a year for the first 7 years of the study, conducted in 2013, and an average of 16.4 in the last 7 years of the study. More than 1,000 people were wounded or killed across 160 active shooter incidents, defined as an individual or individuals actively engaged in killing or trying to kill people in a populous area.4
“Gun violence is undeniably a public health issue,” said Dr. Sacks, a hospitalist at Massachusetts General Hospital and instructor at Harvard Medical School, both in Boston, and a vocal proponent of addressing firearms in the public health sphere. Her cousin’s 7-year-old son, Daniel Barden, was fatally shot at Sandy Hook Elementary School in Newtown, Conn., in December 2012.
Yet, the notion of firearm injuries and deaths as a public health issue is, in America, an issue of contention. How can hospitalists and other health care providers avoid wading into the political thicket while also looking out for their patients?
For one, it’s not the only controversial issue with which providers are confronted, Dr. Sacks and others say. From taking sexual histories, counseling patients about abortion and adoption, and discussing end-of-life issues, clinicians may routinely face uncomfortable interactions in the name of patient care.
“It’s not a question about their right to a weapon; it’s about how individuals can stay as safe as possible and keep their families as safe as possible,” said Dr. Sacks, who also wrote in a January 2017 opinion for the American Medical Association that: “Counseling about gun safety is not political – no more so than a physician counseling a patient about cutting down on sugary beverages is an act of declaring support for New York City’s attempted ban on large-sized sodas.”5
This idea is echoed by David Hemenway, PhD, director of the Harvard Injury Control Research Center, Boston. “You can talk about wearing your seat belt without advocating for mandatory seat belt laws,” he said.

Yet in a 2014 survey of internist members of the American College of Physicians, only 66% of respondents said they believed physicians have the right to counsel patients on gun violence prevention and 58% said they never ask patients about guns in their home. That same survey showed the public is also split: While two-thirds of respondents said it was at least sometimes appropriate for providers to ask about firearms during a visit, one-third believed it was never appropriate.6
In fact, Barbara Meyer, MD, MPH, a family physician in Seattle, said she once had a patient walk out of the office when he encountered a question about firearms on the intake forms for the health system at which she was employed at the time. Today, at NeighborCare Health, the presence of firearms in the home is a question in the well-child electronic health record.
The Harvard Injury Control Research Center runs a campaign called Means Matter, designed to address suicide by firearm, the most common method of suicide in America. The campaign – backed by decades of some of the best research available – reports that people die of suicide by gun more than all other methods combined, that suicide attempts using a firearm are almost always fatal, and that firearms used by youths who commit suicide almost always belong to a parent.
“Suicide is often an impulsive act,” said Dr. Sacks, which means preventing access to firearms for patients at risk can be a matter of life and death. “There is potential for intervention there … what can be more clearly medical than suicide prevention?”
For her, that means eliminating the partisan component and equipping providers with the best evidence-based research available and with best practices. Reliable studies show that having guns at home increases the danger to families, said Dr. Hemenway, and places with fewer guns and stronger gun laws are correlated with fewer gun fatalities.7,8
“In accordance with guidelines and the best evidence out there, we should be screening patients who might be at risk for gun violence,” he said. “In some cases, interventions can be as simple and straightforward as informing patients where to get gun locks and talking to them about how to store firearms safely.”
At Massachusetts General Hospital, Dr. Sacks helped found the Gun Violence Prevention Coalition, an interdisciplinary group of physicians, nurses, physical therapists, and others committed to raising awareness and preparing providers to address gun violence. She believes strongly that physicians can act locally to help address the issue.
In Seattle, Dr. Meyer has been involved with a local group called Washington Ceasefire, prompted both by her experience as a resident in Detroit – where she was routinely exposed to the traumas of gun violence – as well as a shooting that occurred outside her daughter’s high school in Seattle years ago. The group has recently begun advocating for smart guns, which are designed to be fired only by an authorized user.
Indeed, Dr. Hemenway said research by his group suggests 300,000-500,000 guns are stolen every year, though he points out that we know almost nothing about “who, what, when, why, and where.” That’s largely because of an effective ban on gun violence research, enacted by Congress in the 1990s.9
“It’s not like there’s no evidence, but compared to the size of the problem, you want good evidence,” Dr. Hemenway said. “America has lots of guns. How can we learn to live with them?”
Gun violence affects not just those shot and killed by firearms, but also those affected by the trauma it can leave in its wake. Dr. Sacks recounts a recent visit to Massachusetts General by survivors of the Pulse Nightclub shooting in Orlando, Fla., which took place on June 12, 2016.
“It was a moving, intense event where we all sat around and talked about this issue,” Dr. Sacks said. “The number of people dying is horrific enough, but it’s not just that. Here were a number of young people who survived and yet whose lives will never be the same. We are undercounting the number of people affected by gun violence.”
Studies also estimate the cost of medical care related to gun violence to be roughly $620 million per year, averaging between $9,000 and $18,000 per patient in 2014.10
Despite some arguments to the contrary, addressing gun violence as a public health issue is not a distraction from other important public health issues such as opioid abuse. “It is entirely a false choice that we must only take on one issue or another,” Dr. Sacks said.
Nor should efforts to address gun violence focus only on individuals, said Dr. Hemenway, who told the Harvard T.H. Chan School of Public Health in October 2017 that: “A lesson from public health is that it is usually more effective to change the environment than to try to change people. The U.S. should use the same harm reduction approach to gun violence that it uses to treat other public health threats, like automobile crashes or air pollution, employing a wide variety of methods to reduce the problem.”
The issue must be reframed, said Dr. Sacks. This remains one of her biggest goals. “If we can find a way to act and intervene and lower [the] number [of people affected by gun violence], what could be more fundamentally in line with what we try to do every day as physicians?” she asked. “How can we reduce morbidity and mortality? That’s an answerable question and we can make sure we have pathways and approaches we can put in place to understand this. This is a solvable problem.”
1. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Injuries. https://www.cdc.gov/nchs/fastats/injury.htm. Accessed Nov 20, 2017.
2. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Suicide. https://www.cdc.gov/nchs/fastats/suicide.htm. Accessed Nov 20, 2017.
3. Sacks CA. In memory of Daniel – Reviving research to prevent gun violence. N Engl J Med. 2015; 372:800-801. doi: 10.1056/NEJMp1415128.
4. U.S. Department of Justice, Federal Bureau of Investigation. A study of active shooter incidents in the United States between 2000 and 2013. Published Sept 16, 2013. Accessed Nov 20, 2017.
5. Sacks CA. The role of physicians in preventing firearm suicides. JAMA Int Med. doi: 10.001/jamainternmed.2016.6715. Published Nov 14, 2016. Accessed Nov 20, 2017.
6. Butkus R, Weissman A. Internists’ attitudes toward prevention of firearm injury. Ann Intern Med. 2014;160(12):821-827. doi: 10.7326/M13-1960.
7. Fleegler EW, Lee LK, Monuteaux MC, et al. Firearm Legislation and Firearm-Related Fatalities in the United States. JAMA Intern Med. 2013; 173(9):732-740. doi: 10.1001/jamaimternmed.2013.1286.
8. American Academy of Pediatricians. Addressing gun violence. The federal level. https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Pages/Gun-Violence-Matrix--Intentional-(Federal).aspx. Accessed Nov 20, 2017.
9. Rubin R. Tale of 2 agencies: CDC avoids gun violence research bit NIH funds it. JAMA. 2016;315(16):1689-1692. doi:10.1001/jama.2016.1707.
10. Howell E and Gangopadhyaya A. State variation in the hospital costs of gun violence, 2010 and 2014. The Urban Institute, Health Policy Center.
In 2014, 33,594 people were killed by firearms in the United States. More than 21,000 of these deaths were suicides. The rest were primarily homicides and accidental shootings. Meanwhile, firearm deaths represented nearly 17% of injury deaths that year.1,2
In a 2015 Perspective published in the New England Journal of Medicine, author Chana Sacks, MD, pointed out that 20 children and adolescents are sent to the hospital daily for firearm injuries and 2,000 people each year suffer gunshot-related spinal cord injuries and “become lifelong patients.”3
At the same time, Federal Bureau of Investigation data show that the number of active shooter situations rose between 2000 and 2013, with an average of 6.4 incidents a year for the first 7 years of the study, conducted in 2013, and an average of 16.4 in the last 7 years of the study. More than 1,000 people were wounded or killed across 160 active shooter incidents, defined as an individual or individuals actively engaged in killing or trying to kill people in a populous area.4
“Gun violence is undeniably a public health issue,” said Dr. Sacks, a hospitalist at Massachusetts General Hospital and instructor at Harvard Medical School, both in Boston, and a vocal proponent of addressing firearms in the public health sphere. Her cousin’s 7-year-old son, Daniel Barden, was fatally shot at Sandy Hook Elementary School in Newtown, Conn., in December 2012.
Yet, the notion of firearm injuries and deaths as a public health issue is, in America, an issue of contention. How can hospitalists and other health care providers avoid wading into the political thicket while also looking out for their patients?
For one, it’s not the only controversial issue with which providers are confronted, Dr. Sacks and others say. From taking sexual histories, counseling patients about abortion and adoption, and discussing end-of-life issues, clinicians may routinely face uncomfortable interactions in the name of patient care.
“It’s not a question about their right to a weapon; it’s about how individuals can stay as safe as possible and keep their families as safe as possible,” said Dr. Sacks, who also wrote in a January 2017 opinion for the American Medical Association that: “Counseling about gun safety is not political – no more so than a physician counseling a patient about cutting down on sugary beverages is an act of declaring support for New York City’s attempted ban on large-sized sodas.”5
This idea is echoed by David Hemenway, PhD, director of the Harvard Injury Control Research Center, Boston. “You can talk about wearing your seat belt without advocating for mandatory seat belt laws,” he said.
Yet in a 2014 survey of internist members of the American College of Physicians, only 66% of respondents said they believed physicians have the right to counsel patients on gun violence prevention and 58% said they never ask patients about guns in their home. That same survey showed the public is also split: While two-thirds of respondents said it was at least sometimes appropriate for providers to ask about firearms during a visit, one-third believed it was never appropriate.6
In fact, Barbara Meyer, MD, MPH, a family physician in Seattle, said she once had a patient walk out of the office when he encountered a question about firearms on the intake forms for the health system at which she was employed at the time. Today, at NeighborCare Health, the presence of firearms in the home is a question in the well-child electronic health record.
The Harvard Injury Control Research Center runs a campaign called Means Matter, designed to address suicide by firearm, the most common method of suicide in America. The campaign – backed by decades of some of the best research available – reports that people die of suicide by gun more than all other methods combined, that suicide attempts using a firearm are almost always fatal, and that firearms used by youths who commit suicide almost always belong to a parent.
“Suicide is often an impulsive act,” said Dr. Sacks, which means preventing access to firearms for patients at risk can be a matter of life and death. “There is potential for intervention there … what can be more clearly medical than suicide prevention?”
For her, that means eliminating the partisan component and equipping providers with the best evidence-based research available and with best practices. Reliable studies show that having guns at home increases the danger to families, said Dr. Hemenway, and places with fewer guns and stronger gun laws are correlated with fewer gun fatalities.7,8
“In accordance with guidelines and the best evidence out there, we should be screening patients who might be at risk for gun violence,” he said. “In some cases, interventions can be as simple and straightforward as informing patients where to get gun locks and talking to them about how to store firearms safely.”
At Massachusetts General Hospital, Dr. Sacks helped found the Gun Violence Prevention Coalition, an interdisciplinary group of physicians, nurses, physical therapists, and others committed to raising awareness and preparing providers to address gun violence. She believes strongly that physicians can act locally to help address the issue.
In Seattle, Dr. Meyer has been involved with a local group called Washington Ceasefire, prompted both by her experience as a resident in Detroit – where she was routinely exposed to the traumas of gun violence – as well as a shooting that occurred outside her daughter’s high school in Seattle years ago. The group has recently begun advocating for smart guns, which are designed to be fired only by an authorized user.
Indeed, Dr. Hemenway said research by his group suggests 300,000-500,000 guns are stolen every year, though he points out that we know almost nothing about “who, what, when, why, and where.” That’s largely because of an effective ban on gun violence research, enacted by Congress in the 1990s.9
“It’s not like there’s no evidence, but compared to the size of the problem, you want good evidence,” Dr. Hemenway said. “America has lots of guns. How can we learn to live with them?”
Gun violence affects not just those shot and killed by firearms, but also those affected by the trauma it can leave in its wake. Dr. Sacks recounts a recent visit to Massachusetts General by survivors of the Pulse Nightclub shooting in Orlando, Fla., which took place on June 12, 2016.
“It was a moving, intense event where we all sat around and talked about this issue,” Dr. Sacks said. “The number of people dying is horrific enough, but it’s not just that. Here were a number of young people who survived and yet whose lives will never be the same. We are undercounting the number of people affected by gun violence.”
Studies also estimate the cost of medical care related to gun violence to be roughly $620 million per year, averaging between $9,000 and $18,000 per patient in 2014.10
Despite some arguments to the contrary, addressing gun violence as a public health issue is not a distraction from other important public health issues such as opioid abuse. “It is entirely a false choice that we must only take on one issue or another,” Dr. Sacks said.
Nor should efforts to address gun violence focus only on individuals, said Dr. Hemenway, who told the Harvard T.H. Chan School of Public Health in October 2017 that: “A lesson from public health is that it is usually more effective to change the environment than to try to change people. The U.S. should use the same harm reduction approach to gun violence that it uses to treat other public health threats, like automobile crashes or air pollution, employing a wide variety of methods to reduce the problem.”
The issue must be reframed, said Dr. Sacks. This remains one of her biggest goals. “If we can find a way to act and intervene and lower [the] number [of people affected by gun violence], what could be more fundamentally in line with what we try to do every day as physicians?” she asked. “How can we reduce morbidity and mortality? That’s an answerable question and we can make sure we have pathways and approaches we can put in place to understand this. This is a solvable problem.”
In 2014, 33,594 people were killed by firearms in the United States. More than 21,000 of these deaths were suicides. The rest were primarily homicides and accidental shootings. Meanwhile, firearm deaths represented nearly 17% of injury deaths that year.1,2
In a 2015 Perspective published in the New England Journal of Medicine, author Chana Sacks, MD, pointed out that 20 children and adolescents are sent to the hospital daily for firearm injuries and 2,000 people each year suffer gunshot-related spinal cord injuries and “become lifelong patients.”3
At the same time, Federal Bureau of Investigation data show that the number of active shooter situations rose between 2000 and 2013, with an average of 6.4 incidents a year for the first 7 years of the study, conducted in 2013, and an average of 16.4 in the last 7 years of the study. More than 1,000 people were wounded or killed across 160 active shooter incidents, defined as an individual or individuals actively engaged in killing or trying to kill people in a populous area.4
“Gun violence is undeniably a public health issue,” said Dr. Sacks, a hospitalist at Massachusetts General Hospital and instructor at Harvard Medical School, both in Boston, and a vocal proponent of addressing firearms in the public health sphere. Her cousin’s 7-year-old son, Daniel Barden, was fatally shot at Sandy Hook Elementary School in Newtown, Conn., in December 2012.
Yet, the notion of firearm injuries and deaths as a public health issue is, in America, an issue of contention. How can hospitalists and other health care providers avoid wading into the political thicket while also looking out for their patients?
For one, it’s not the only controversial issue with which providers are confronted, Dr. Sacks and others say. From taking sexual histories, counseling patients about abortion and adoption, and discussing end-of-life issues, clinicians may routinely face uncomfortable interactions in the name of patient care.
“It’s not a question about their right to a weapon; it’s about how individuals can stay as safe as possible and keep their families as safe as possible,” said Dr. Sacks, who also wrote in a January 2017 opinion for the American Medical Association that: “Counseling about gun safety is not political – no more so than a physician counseling a patient about cutting down on sugary beverages is an act of declaring support for New York City’s attempted ban on large-sized sodas.”5
This idea is echoed by David Hemenway, PhD, director of the Harvard Injury Control Research Center, Boston. “You can talk about wearing your seat belt without advocating for mandatory seat belt laws,” he said.
Yet in a 2014 survey of internist members of the American College of Physicians, only 66% of respondents said they believed physicians have the right to counsel patients on gun violence prevention and 58% said they never ask patients about guns in their home. That same survey showed the public is also split: While two-thirds of respondents said it was at least sometimes appropriate for providers to ask about firearms during a visit, one-third believed it was never appropriate.6
In fact, Barbara Meyer, MD, MPH, a family physician in Seattle, said she once had a patient walk out of the office when he encountered a question about firearms on the intake forms for the health system at which she was employed at the time. Today, at NeighborCare Health, the presence of firearms in the home is a question in the well-child electronic health record.
The Harvard Injury Control Research Center runs a campaign called Means Matter, designed to address suicide by firearm, the most common method of suicide in America. The campaign – backed by decades of some of the best research available – reports that people die of suicide by gun more than all other methods combined, that suicide attempts using a firearm are almost always fatal, and that firearms used by youths who commit suicide almost always belong to a parent.
“Suicide is often an impulsive act,” said Dr. Sacks, which means preventing access to firearms for patients at risk can be a matter of life and death. “There is potential for intervention there … what can be more clearly medical than suicide prevention?”
For her, that means eliminating the partisan component and equipping providers with the best evidence-based research available and with best practices. Reliable studies show that having guns at home increases the danger to families, said Dr. Hemenway, and places with fewer guns and stronger gun laws are correlated with fewer gun fatalities.7,8
“In accordance with guidelines and the best evidence out there, we should be screening patients who might be at risk for gun violence,” he said. “In some cases, interventions can be as simple and straightforward as informing patients where to get gun locks and talking to them about how to store firearms safely.”
At Massachusetts General Hospital, Dr. Sacks helped found the Gun Violence Prevention Coalition, an interdisciplinary group of physicians, nurses, physical therapists, and others committed to raising awareness and preparing providers to address gun violence. She believes strongly that physicians can act locally to help address the issue.
In Seattle, Dr. Meyer has been involved with a local group called Washington Ceasefire, prompted both by her experience as a resident in Detroit – where she was routinely exposed to the traumas of gun violence – as well as a shooting that occurred outside her daughter’s high school in Seattle years ago. The group has recently begun advocating for smart guns, which are designed to be fired only by an authorized user.
Indeed, Dr. Hemenway said research by his group suggests 300,000-500,000 guns are stolen every year, though he points out that we know almost nothing about “who, what, when, why, and where.” That’s largely because of an effective ban on gun violence research, enacted by Congress in the 1990s.9
“It’s not like there’s no evidence, but compared to the size of the problem, you want good evidence,” Dr. Hemenway said. “America has lots of guns. How can we learn to live with them?”
Gun violence affects not just those shot and killed by firearms, but also those affected by the trauma it can leave in its wake. Dr. Sacks recounts a recent visit to Massachusetts General by survivors of the Pulse Nightclub shooting in Orlando, Fla., which took place on June 12, 2016.
“It was a moving, intense event where we all sat around and talked about this issue,” Dr. Sacks said. “The number of people dying is horrific enough, but it’s not just that. Here were a number of young people who survived and yet whose lives will never be the same. We are undercounting the number of people affected by gun violence.”
Studies also estimate the cost of medical care related to gun violence to be roughly $620 million per year, averaging between $9,000 and $18,000 per patient in 2014.10
Despite some arguments to the contrary, addressing gun violence as a public health issue is not a distraction from other important public health issues such as opioid abuse. “It is entirely a false choice that we must only take on one issue or another,” Dr. Sacks said.
Nor should efforts to address gun violence focus only on individuals, said Dr. Hemenway, who told the Harvard T.H. Chan School of Public Health in October 2017 that: “A lesson from public health is that it is usually more effective to change the environment than to try to change people. The U.S. should use the same harm reduction approach to gun violence that it uses to treat other public health threats, like automobile crashes or air pollution, employing a wide variety of methods to reduce the problem.”
The issue must be reframed, said Dr. Sacks. This remains one of her biggest goals. “If we can find a way to act and intervene and lower [the] number [of people affected by gun violence], what could be more fundamentally in line with what we try to do every day as physicians?” she asked. “How can we reduce morbidity and mortality? That’s an answerable question and we can make sure we have pathways and approaches we can put in place to understand this. This is a solvable problem.”
1. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Injuries. https://www.cdc.gov/nchs/fastats/injury.htm. Accessed Nov 20, 2017.
2. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Suicide. https://www.cdc.gov/nchs/fastats/suicide.htm. Accessed Nov 20, 2017.
3. Sacks CA. In memory of Daniel – Reviving research to prevent gun violence. N Engl J Med. 2015; 372:800-801. doi: 10.1056/NEJMp1415128.
4. U.S. Department of Justice, Federal Bureau of Investigation. A study of active shooter incidents in the United States between 2000 and 2013. Published Sept 16, 2013. Accessed Nov 20, 2017.
5. Sacks CA. The role of physicians in preventing firearm suicides. JAMA Int Med. doi: 10.001/jamainternmed.2016.6715. Published Nov 14, 2016. Accessed Nov 20, 2017.
6. Butkus R, Weissman A. Internists’ attitudes toward prevention of firearm injury. Ann Intern Med. 2014;160(12):821-827. doi: 10.7326/M13-1960.
7. Fleegler EW, Lee LK, Monuteaux MC, et al. Firearm Legislation and Firearm-Related Fatalities in the United States. JAMA Intern Med. 2013; 173(9):732-740. doi: 10.1001/jamaimternmed.2013.1286.
8. American Academy of Pediatricians. Addressing gun violence. The federal level. https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Pages/Gun-Violence-Matrix--Intentional-(Federal).aspx. Accessed Nov 20, 2017.
9. Rubin R. Tale of 2 agencies: CDC avoids gun violence research bit NIH funds it. JAMA. 2016;315(16):1689-1692. doi:10.1001/jama.2016.1707.
10. Howell E and Gangopadhyaya A. State variation in the hospital costs of gun violence, 2010 and 2014. The Urban Institute, Health Policy Center.
1. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Injuries. https://www.cdc.gov/nchs/fastats/injury.htm. Accessed Nov 20, 2017.
2. Centers for Disease Control and Prevention, National Center for Health Statistics. FastStats. Suicide. https://www.cdc.gov/nchs/fastats/suicide.htm. Accessed Nov 20, 2017.
3. Sacks CA. In memory of Daniel – Reviving research to prevent gun violence. N Engl J Med. 2015; 372:800-801. doi: 10.1056/NEJMp1415128.
4. U.S. Department of Justice, Federal Bureau of Investigation. A study of active shooter incidents in the United States between 2000 and 2013. Published Sept 16, 2013. Accessed Nov 20, 2017.
5. Sacks CA. The role of physicians in preventing firearm suicides. JAMA Int Med. doi: 10.001/jamainternmed.2016.6715. Published Nov 14, 2016. Accessed Nov 20, 2017.
6. Butkus R, Weissman A. Internists’ attitudes toward prevention of firearm injury. Ann Intern Med. 2014;160(12):821-827. doi: 10.7326/M13-1960.
7. Fleegler EW, Lee LK, Monuteaux MC, et al. Firearm Legislation and Firearm-Related Fatalities in the United States. JAMA Intern Med. 2013; 173(9):732-740. doi: 10.1001/jamaimternmed.2013.1286.
8. American Academy of Pediatricians. Addressing gun violence. The federal level. https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Pages/Gun-Violence-Matrix--Intentional-(Federal).aspx. Accessed Nov 20, 2017.
9. Rubin R. Tale of 2 agencies: CDC avoids gun violence research bit NIH funds it. JAMA. 2016;315(16):1689-1692. doi:10.1001/jama.2016.1707.
10. Howell E and Gangopadhyaya A. State variation in the hospital costs of gun violence, 2010 and 2014. The Urban Institute, Health Policy Center.
Bedside Ultrasound for Pulsatile Hand Mass
Case
A 23-year-old man presented to an outside hospital’s ED for evaluation of a wound on his right hand, which he sustained after he accidentally stabbed himself with a steak knife. At presentation, the patient’s vital signs were: heart rate, 90 beats/min; respiratory rate, 16 breaths/min; blood pressure, 150/92 mm Hg; and temperature, 98.1°F. Oxygen saturation was 98% on room air. Examination revealed a laceration on the patient’s right hand measuring 2 cm in length. The emergency physician (EP) closed the wound using four nylon sutures and administered a Boostrix shot. The patient was discharged home with a prescription for cephalexin capsule 500 mg to be taken four times daily for 5 days. He was instructed to return in 10 days for suture removal, but failed to follow-up.
The patient presented to our ED two months after the initial injury for evaluation of a 1.5-cm round pulsatile mass on his right palm, at the base of the middle finger, from which exuded a small amount of sanguineous fluid. The patient complained of numbness and difficulty extending his right index and middle fingers.

Discussion
Palmar Pseudoaneurysms
A pseudoaneurysm, also referred to as a traumatic aneurysm, develops when a tear of the vessel wall and hemorrhage is contained by a thin-walled capsule, typically following traumatic perforation of the arterial wall. Unlike a true aneurysm, a pseudoaneurysm does not contain all three layers of intima, media, and adventitia. Thin walls lead to inevitable expansion over time; in some cases, a patient will present with a soft-tissue mass years after the initial injury. Compression of nearby structures can cause neuropathy, peripheral edema, venous thrombosis, arterial occlusion or emboli, and even bone erosion.1,2
Hand pseudoaneurysms are more likely to occur on the palmar surface, involving the superficial palmar arch,3 and are due to a penetrating injury or repetitive microtrauma. Hypothenar hammer syndrome occurs when repetitive microtrauma is applied to the ulnar artery as it passes under the hook of the hamate bone into the hand. This condition is also referred to as “hammer hand syndrome” because it frequently occurs in laborers such as mechanics, carpenters, and machinists as a result of repetitive palm trauma. Cases have also been reported in baseball players and cooks who also expose their hands to repetitive trauma.3 Likewise, elderly patients who use walking canes can also present with bilateral hammer hand syndrome,3 and patients who need crutches for a prolonged period of time may also develop axillary artery aneurysms.1,2
Although rare, there have also been cases of spontaneous hand pseudoaneurysms in patients on anticoagulation therapy;4,5 however, pseudoaneurysms are not an absolute contraindication to initiating or continuing use of anticoagulants.
Evaluation
Physical Examination. The patient’s mass in this case was clearly pulsatile on examination, but physical examination alone is not a reliable indicator of pseudoaneurysm, as patients may present only with soft-tissue swelling, pain, erythema, or neurological symptoms.3,6,7
Ultrasound Imaging. In the emergency setting, POC ultrasound should be performed to evaluate any soft-tissue hand mass, especially in the context of trauma or any neurovascular findings, since palmar pseudoaneurysms can easily be confused with an abscess, foreign body, cyst, or even a tendon tear.6 Ultrasound studies using the linear vascular probe should always be done before any attempt to incise and drain the mass.
Three ultrasound characteristics of pseudoaneurysms include expansile pulsatility, turbulent flow with a classic yin-yang sign on Doppler, and a hematoma with variable echogenicity. Variable echogenicity may represent separate episodes of bleeding and rebleeding.8 A “to-and-fro” spectral waveform is pathognomonic for palmar pseudoaneurysms.8
Computed Tomography and Magnetic Resonance Angiography. Definitive imaging for operative management includes computed tomography or magnetic resonance angiography to assess for the exact location and presence of collateral circulation.
Treatment
Treatment of pseudoaneurysms includes conservative compression therapy, surgical excision, or anastomosis, and more recently, ultrasound-guided thrombin injection (UGTI).
Compression Therapy. Compression therapy is often used for femoral artery pseudoaneurysms that develop after iatrogenic injury. However, this technique is time consuming, is uncomfortable for patients, is not effective in treating large pseudoaneurysms, and is contraindicated in patients on anticoagulation therapy. Compression therapy also has a high-failure rate of resolving pseudoaneurysms. Traditionally, surgical excision or anastomosis has been the definitive treatment for palmar pseudoaneurysms.
Ultrasound-Guided Thrombin Injection. A more recent treatment option is UGTI, which is usually performed by an interventional radiologist. Although there is no consensus on exact dose of thrombin for this procedure, the literature describes UGTI to treat both the radial and ulnar arteries.9,10 One study of 83 pseudoaneurysms demonstrated a relationship between the size of the palmar pseudoaneurysm and the number of thrombin injections required to resolve it. Depending on the size of the palmar pseudoaneurysm, the effective thrombin doses ranged from 200 to 2,500 U. Regarding adverse effects and events from treatment, this study reported one case of transient distal ischemia.11
Intravascular balloon occlusion of the pseudoaneurysm neck has also been recommended for UGTI in the femoral artery if the neck is greater than 1 mm, but there is currently nothing in the literature describing its use in palmar pseudoaneurysms.12
Complications
There are more descriptions of palmar, radial, and ulnar pseudoaneurysms in critical care patients due to the frequent, but necessary, use of invasive lines. Emergency physicians frequently place radial or femoral arterial lines for hemodynamic monitoring in critically ill patients. However, the incidence of pseudoaneurysms and its sequelae from these lines are not usually observed in the ED setting.
Radial arterial lines may cause thrombosis in 19% to 57% of cases, and local infection in 1% to 18% of cases.10 In a study of 12,500 patients with radial artery catheters, the rate of radial pseudoaneurysm was only 0.05%.11 Although this is a small complication rate, pseudoaneurysms can lead to significant loss of function. To decrease the number of attempts and penetrating injuries to the arteries, ultrasound guidance for these procedures in the ED is strongly recommended. In addition to decreasing the risk of developing a pseudoaneurysm, ultrasound-guidance decreases the discomfort level of the patient and reduces the risk of bleeding, hematoma formation, and infection. Arterial line placement in the ED using ultrasound guidance decreases the risk of developing pseudoaneurysms and their sequelae, such as distal embolization.
Case Conclusion
The patient in this case underwent an arterial duplex study, which found a partially thrombosed right superficial palmar arch pseudoaneurysm measuring 1.91 cm x 2.08 cm, with an active flow area measuring 0.58 cm x 0.68 cm. The flow to the index finger medial artery and middle finger lateral artery was also diminished. The patient was discharged home with a bulky soft dressing and underwent excision and repair by hand surgery 3 days later. At the 1-month postoperative follow-up visit, the patient had full sensation but mildly decreased range of motion in his fingers.
Summary
Hand pseudoaneurysms are often associated with penetrating injuries—as demonstrated in our case—or repetitive microtrauma. Hand pseudoaneurysms can present with minimal findings such as isolated soft-tissue swelling, pain, or neuropathy. The EP should consider vascular pathology in the differential for patients who present with posttraumatic neuropathy. Regarding imaging studies, ultrasound is the best imaging modality to assess for pseudoaneurysms, and EPs should have a low threshold for its use at bedside—especially prior to attempting any invasive procedure. Patients with a confirmed pseudoaneurysm should be referred to a hand or vascular surgeon for surgical repair, or to an interventional radiologist for UGTI.
1. Newton EJ, Arora S. Peripheral vascular injury. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:502.
2. Aufderheide TP. Peripheral arteriovascular disease. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. 2014:1147-1149.
3. Anderson SE, De Monaco D, Buechler U, et al. Imaging features of pseudoaneurysms of the hand in children and adults. AJR Am J Roentgenol. 2003;180(3):659-664. doi:10.2214/ajr.180.3.1800659.
4. Shah S, Powell-Brett S, Garnham A. Pseudoaneurysm: an unusual cause of post-traumatic hand swelling. BMJ Case Rep. 2015;2015. pii: bcr2014208750. doi:10.1136/bcr-2014-208750.
5. Kitamura A, Mukohara N. Spontaneous pseudoaneurysm of the hand. Ann Vasc Surg. 2014;28(3):739.e1-e3. doi:10.1016/j.avsg.2013.04.033.
6. Huang SW, Wei TS, Liu SY, Wang WT. Spontaneous totally thrombosed pseudoaneurysm mimicking a tendon tear of the wrist. Orthopedics. 2010;33(10):776. doi:10.3928/01477447-20100826-23.
7. Belyayev L, Rich NM, McKay P, Nesti L, Wind G. Traumatic ulnar artery pseudoaneurysm following a grenade blast: report of a case. Mil Med. 2015;180(6):e725-e727. doi:10.7205/MILMED-D-14-00400.
8. Pero T, Herrick J. Pseudoaneurysm of the radial artery diagnosed by bedside ultrasound. West J Emerg Med. 2009;10(2):89-91.
9. Bosman A, Veger HTC, Doornink F, Hedeman Joosten PPA. A pseudoaneurysm of the deep palmar arch after penetrating trauma to the hand: successful exclusion by ultrasound guided percutaneous thrombin injection. EJVES Short Rep. 2016;31:9-11. doi:10.1016/j.ejvssr.2016.03.002.
10. Komorowska-Timek E, Teruya TH, Abou-Zamzam AM Jr, Papa D, Ballard JL. Treatment of radial and ulnar artery pseudoaneurysms using percutaneous thrombin injection. J Hand Surg. 2004;29A(5):936-942. doi:10.1016/j.jhsa.2004.05.009.
11. Falk PS, Scuderi PE, Sherertz RJ, Motsinger SM. Infected radial artery pseudoaneurysms occurring after percutaneous cannulation. Chest. 1992;101(2):490-495.
12. Kang SS, Labropoulos N, Mansour MA, et al. Expanded indications for ultrasound-guided thrombin injection of pseudoaneurysms. J Vasc Surg. 2000;31(2):289-298.
Case
A 23-year-old man presented to an outside hospital’s ED for evaluation of a wound on his right hand, which he sustained after he accidentally stabbed himself with a steak knife. At presentation, the patient’s vital signs were: heart rate, 90 beats/min; respiratory rate, 16 breaths/min; blood pressure, 150/92 mm Hg; and temperature, 98.1°F. Oxygen saturation was 98% on room air. Examination revealed a laceration on the patient’s right hand measuring 2 cm in length. The emergency physician (EP) closed the wound using four nylon sutures and administered a Boostrix shot. The patient was discharged home with a prescription for cephalexin capsule 500 mg to be taken four times daily for 5 days. He was instructed to return in 10 days for suture removal, but failed to follow-up.
The patient presented to our ED two months after the initial injury for evaluation of a 1.5-cm round pulsatile mass on his right palm, at the base of the middle finger, from which exuded a small amount of sanguineous fluid. The patient complained of numbness and difficulty extending his right index and middle fingers.
Discussion
Palmar Pseudoaneurysms
A pseudoaneurysm, also referred to as a traumatic aneurysm, develops when a tear of the vessel wall and hemorrhage is contained by a thin-walled capsule, typically following traumatic perforation of the arterial wall. Unlike a true aneurysm, a pseudoaneurysm does not contain all three layers of intima, media, and adventitia. Thin walls lead to inevitable expansion over time; in some cases, a patient will present with a soft-tissue mass years after the initial injury. Compression of nearby structures can cause neuropathy, peripheral edema, venous thrombosis, arterial occlusion or emboli, and even bone erosion.1,2
Hand pseudoaneurysms are more likely to occur on the palmar surface, involving the superficial palmar arch,3 and are due to a penetrating injury or repetitive microtrauma. Hypothenar hammer syndrome occurs when repetitive microtrauma is applied to the ulnar artery as it passes under the hook of the hamate bone into the hand. This condition is also referred to as “hammer hand syndrome” because it frequently occurs in laborers such as mechanics, carpenters, and machinists as a result of repetitive palm trauma. Cases have also been reported in baseball players and cooks who also expose their hands to repetitive trauma.3 Likewise, elderly patients who use walking canes can also present with bilateral hammer hand syndrome,3 and patients who need crutches for a prolonged period of time may also develop axillary artery aneurysms.1,2
Although rare, there have also been cases of spontaneous hand pseudoaneurysms in patients on anticoagulation therapy;4,5 however, pseudoaneurysms are not an absolute contraindication to initiating or continuing use of anticoagulants.
Evaluation
Physical Examination. The patient’s mass in this case was clearly pulsatile on examination, but physical examination alone is not a reliable indicator of pseudoaneurysm, as patients may present only with soft-tissue swelling, pain, erythema, or neurological symptoms.3,6,7
Ultrasound Imaging. In the emergency setting, POC ultrasound should be performed to evaluate any soft-tissue hand mass, especially in the context of trauma or any neurovascular findings, since palmar pseudoaneurysms can easily be confused with an abscess, foreign body, cyst, or even a tendon tear.6 Ultrasound studies using the linear vascular probe should always be done before any attempt to incise and drain the mass.
Three ultrasound characteristics of pseudoaneurysms include expansile pulsatility, turbulent flow with a classic yin-yang sign on Doppler, and a hematoma with variable echogenicity. Variable echogenicity may represent separate episodes of bleeding and rebleeding.8 A “to-and-fro” spectral waveform is pathognomonic for palmar pseudoaneurysms.8
Computed Tomography and Magnetic Resonance Angiography. Definitive imaging for operative management includes computed tomography or magnetic resonance angiography to assess for the exact location and presence of collateral circulation.
Treatment
Treatment of pseudoaneurysms includes conservative compression therapy, surgical excision, or anastomosis, and more recently, ultrasound-guided thrombin injection (UGTI).
Compression Therapy. Compression therapy is often used for femoral artery pseudoaneurysms that develop after iatrogenic injury. However, this technique is time consuming, is uncomfortable for patients, is not effective in treating large pseudoaneurysms, and is contraindicated in patients on anticoagulation therapy. Compression therapy also has a high-failure rate of resolving pseudoaneurysms. Traditionally, surgical excision or anastomosis has been the definitive treatment for palmar pseudoaneurysms.
Ultrasound-Guided Thrombin Injection. A more recent treatment option is UGTI, which is usually performed by an interventional radiologist. Although there is no consensus on exact dose of thrombin for this procedure, the literature describes UGTI to treat both the radial and ulnar arteries.9,10 One study of 83 pseudoaneurysms demonstrated a relationship between the size of the palmar pseudoaneurysm and the number of thrombin injections required to resolve it. Depending on the size of the palmar pseudoaneurysm, the effective thrombin doses ranged from 200 to 2,500 U. Regarding adverse effects and events from treatment, this study reported one case of transient distal ischemia.11
Intravascular balloon occlusion of the pseudoaneurysm neck has also been recommended for UGTI in the femoral artery if the neck is greater than 1 mm, but there is currently nothing in the literature describing its use in palmar pseudoaneurysms.12
Complications
There are more descriptions of palmar, radial, and ulnar pseudoaneurysms in critical care patients due to the frequent, but necessary, use of invasive lines. Emergency physicians frequently place radial or femoral arterial lines for hemodynamic monitoring in critically ill patients. However, the incidence of pseudoaneurysms and its sequelae from these lines are not usually observed in the ED setting.
Radial arterial lines may cause thrombosis in 19% to 57% of cases, and local infection in 1% to 18% of cases.10 In a study of 12,500 patients with radial artery catheters, the rate of radial pseudoaneurysm was only 0.05%.11 Although this is a small complication rate, pseudoaneurysms can lead to significant loss of function. To decrease the number of attempts and penetrating injuries to the arteries, ultrasound guidance for these procedures in the ED is strongly recommended. In addition to decreasing the risk of developing a pseudoaneurysm, ultrasound-guidance decreases the discomfort level of the patient and reduces the risk of bleeding, hematoma formation, and infection. Arterial line placement in the ED using ultrasound guidance decreases the risk of developing pseudoaneurysms and their sequelae, such as distal embolization.
Case Conclusion
The patient in this case underwent an arterial duplex study, which found a partially thrombosed right superficial palmar arch pseudoaneurysm measuring 1.91 cm x 2.08 cm, with an active flow area measuring 0.58 cm x 0.68 cm. The flow to the index finger medial artery and middle finger lateral artery was also diminished. The patient was discharged home with a bulky soft dressing and underwent excision and repair by hand surgery 3 days later. At the 1-month postoperative follow-up visit, the patient had full sensation but mildly decreased range of motion in his fingers.
Summary
Hand pseudoaneurysms are often associated with penetrating injuries—as demonstrated in our case—or repetitive microtrauma. Hand pseudoaneurysms can present with minimal findings such as isolated soft-tissue swelling, pain, or neuropathy. The EP should consider vascular pathology in the differential for patients who present with posttraumatic neuropathy. Regarding imaging studies, ultrasound is the best imaging modality to assess for pseudoaneurysms, and EPs should have a low threshold for its use at bedside—especially prior to attempting any invasive procedure. Patients with a confirmed pseudoaneurysm should be referred to a hand or vascular surgeon for surgical repair, or to an interventional radiologist for UGTI.
Case
A 23-year-old man presented to an outside hospital’s ED for evaluation of a wound on his right hand, which he sustained after he accidentally stabbed himself with a steak knife. At presentation, the patient’s vital signs were: heart rate, 90 beats/min; respiratory rate, 16 breaths/min; blood pressure, 150/92 mm Hg; and temperature, 98.1°F. Oxygen saturation was 98% on room air. Examination revealed a laceration on the patient’s right hand measuring 2 cm in length. The emergency physician (EP) closed the wound using four nylon sutures and administered a Boostrix shot. The patient was discharged home with a prescription for cephalexin capsule 500 mg to be taken four times daily for 5 days. He was instructed to return in 10 days for suture removal, but failed to follow-up.
The patient presented to our ED two months after the initial injury for evaluation of a 1.5-cm round pulsatile mass on his right palm, at the base of the middle finger, from which exuded a small amount of sanguineous fluid. The patient complained of numbness and difficulty extending his right index and middle fingers.
Discussion
Palmar Pseudoaneurysms
A pseudoaneurysm, also referred to as a traumatic aneurysm, develops when a tear of the vessel wall and hemorrhage is contained by a thin-walled capsule, typically following traumatic perforation of the arterial wall. Unlike a true aneurysm, a pseudoaneurysm does not contain all three layers of intima, media, and adventitia. Thin walls lead to inevitable expansion over time; in some cases, a patient will present with a soft-tissue mass years after the initial injury. Compression of nearby structures can cause neuropathy, peripheral edema, venous thrombosis, arterial occlusion or emboli, and even bone erosion.1,2
Hand pseudoaneurysms are more likely to occur on the palmar surface, involving the superficial palmar arch,3 and are due to a penetrating injury or repetitive microtrauma. Hypothenar hammer syndrome occurs when repetitive microtrauma is applied to the ulnar artery as it passes under the hook of the hamate bone into the hand. This condition is also referred to as “hammer hand syndrome” because it frequently occurs in laborers such as mechanics, carpenters, and machinists as a result of repetitive palm trauma. Cases have also been reported in baseball players and cooks who also expose their hands to repetitive trauma.3 Likewise, elderly patients who use walking canes can also present with bilateral hammer hand syndrome,3 and patients who need crutches for a prolonged period of time may also develop axillary artery aneurysms.1,2
Although rare, there have also been cases of spontaneous hand pseudoaneurysms in patients on anticoagulation therapy;4,5 however, pseudoaneurysms are not an absolute contraindication to initiating or continuing use of anticoagulants.
Evaluation
Physical Examination. The patient’s mass in this case was clearly pulsatile on examination, but physical examination alone is not a reliable indicator of pseudoaneurysm, as patients may present only with soft-tissue swelling, pain, erythema, or neurological symptoms.3,6,7
Ultrasound Imaging. In the emergency setting, POC ultrasound should be performed to evaluate any soft-tissue hand mass, especially in the context of trauma or any neurovascular findings, since palmar pseudoaneurysms can easily be confused with an abscess, foreign body, cyst, or even a tendon tear.6 Ultrasound studies using the linear vascular probe should always be done before any attempt to incise and drain the mass.
Three ultrasound characteristics of pseudoaneurysms include expansile pulsatility, turbulent flow with a classic yin-yang sign on Doppler, and a hematoma with variable echogenicity. Variable echogenicity may represent separate episodes of bleeding and rebleeding.8 A “to-and-fro” spectral waveform is pathognomonic for palmar pseudoaneurysms.8
Computed Tomography and Magnetic Resonance Angiography. Definitive imaging for operative management includes computed tomography or magnetic resonance angiography to assess for the exact location and presence of collateral circulation.
Treatment
Treatment of pseudoaneurysms includes conservative compression therapy, surgical excision, or anastomosis, and more recently, ultrasound-guided thrombin injection (UGTI).
Compression Therapy. Compression therapy is often used for femoral artery pseudoaneurysms that develop after iatrogenic injury. However, this technique is time consuming, is uncomfortable for patients, is not effective in treating large pseudoaneurysms, and is contraindicated in patients on anticoagulation therapy. Compression therapy also has a high-failure rate of resolving pseudoaneurysms. Traditionally, surgical excision or anastomosis has been the definitive treatment for palmar pseudoaneurysms.
Ultrasound-Guided Thrombin Injection. A more recent treatment option is UGTI, which is usually performed by an interventional radiologist. Although there is no consensus on exact dose of thrombin for this procedure, the literature describes UGTI to treat both the radial and ulnar arteries.9,10 One study of 83 pseudoaneurysms demonstrated a relationship between the size of the palmar pseudoaneurysm and the number of thrombin injections required to resolve it. Depending on the size of the palmar pseudoaneurysm, the effective thrombin doses ranged from 200 to 2,500 U. Regarding adverse effects and events from treatment, this study reported one case of transient distal ischemia.11
Intravascular balloon occlusion of the pseudoaneurysm neck has also been recommended for UGTI in the femoral artery if the neck is greater than 1 mm, but there is currently nothing in the literature describing its use in palmar pseudoaneurysms.12
Complications
There are more descriptions of palmar, radial, and ulnar pseudoaneurysms in critical care patients due to the frequent, but necessary, use of invasive lines. Emergency physicians frequently place radial or femoral arterial lines for hemodynamic monitoring in critically ill patients. However, the incidence of pseudoaneurysms and its sequelae from these lines are not usually observed in the ED setting.
Radial arterial lines may cause thrombosis in 19% to 57% of cases, and local infection in 1% to 18% of cases.10 In a study of 12,500 patients with radial artery catheters, the rate of radial pseudoaneurysm was only 0.05%.11 Although this is a small complication rate, pseudoaneurysms can lead to significant loss of function. To decrease the number of attempts and penetrating injuries to the arteries, ultrasound guidance for these procedures in the ED is strongly recommended. In addition to decreasing the risk of developing a pseudoaneurysm, ultrasound-guidance decreases the discomfort level of the patient and reduces the risk of bleeding, hematoma formation, and infection. Arterial line placement in the ED using ultrasound guidance decreases the risk of developing pseudoaneurysms and their sequelae, such as distal embolization.
Case Conclusion
The patient in this case underwent an arterial duplex study, which found a partially thrombosed right superficial palmar arch pseudoaneurysm measuring 1.91 cm x 2.08 cm, with an active flow area measuring 0.58 cm x 0.68 cm. The flow to the index finger medial artery and middle finger lateral artery was also diminished. The patient was discharged home with a bulky soft dressing and underwent excision and repair by hand surgery 3 days later. At the 1-month postoperative follow-up visit, the patient had full sensation but mildly decreased range of motion in his fingers.
Summary
Hand pseudoaneurysms are often associated with penetrating injuries—as demonstrated in our case—or repetitive microtrauma. Hand pseudoaneurysms can present with minimal findings such as isolated soft-tissue swelling, pain, or neuropathy. The EP should consider vascular pathology in the differential for patients who present with posttraumatic neuropathy. Regarding imaging studies, ultrasound is the best imaging modality to assess for pseudoaneurysms, and EPs should have a low threshold for its use at bedside—especially prior to attempting any invasive procedure. Patients with a confirmed pseudoaneurysm should be referred to a hand or vascular surgeon for surgical repair, or to an interventional radiologist for UGTI.
1. Newton EJ, Arora S. Peripheral vascular injury. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:502.
2. Aufderheide TP. Peripheral arteriovascular disease. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. 2014:1147-1149.
3. Anderson SE, De Monaco D, Buechler U, et al. Imaging features of pseudoaneurysms of the hand in children and adults. AJR Am J Roentgenol. 2003;180(3):659-664. doi:10.2214/ajr.180.3.1800659.
4. Shah S, Powell-Brett S, Garnham A. Pseudoaneurysm: an unusual cause of post-traumatic hand swelling. BMJ Case Rep. 2015;2015. pii: bcr2014208750. doi:10.1136/bcr-2014-208750.
5. Kitamura A, Mukohara N. Spontaneous pseudoaneurysm of the hand. Ann Vasc Surg. 2014;28(3):739.e1-e3. doi:10.1016/j.avsg.2013.04.033.
6. Huang SW, Wei TS, Liu SY, Wang WT. Spontaneous totally thrombosed pseudoaneurysm mimicking a tendon tear of the wrist. Orthopedics. 2010;33(10):776. doi:10.3928/01477447-20100826-23.
7. Belyayev L, Rich NM, McKay P, Nesti L, Wind G. Traumatic ulnar artery pseudoaneurysm following a grenade blast: report of a case. Mil Med. 2015;180(6):e725-e727. doi:10.7205/MILMED-D-14-00400.
8. Pero T, Herrick J. Pseudoaneurysm of the radial artery diagnosed by bedside ultrasound. West J Emerg Med. 2009;10(2):89-91.
9. Bosman A, Veger HTC, Doornink F, Hedeman Joosten PPA. A pseudoaneurysm of the deep palmar arch after penetrating trauma to the hand: successful exclusion by ultrasound guided percutaneous thrombin injection. EJVES Short Rep. 2016;31:9-11. doi:10.1016/j.ejvssr.2016.03.002.
10. Komorowska-Timek E, Teruya TH, Abou-Zamzam AM Jr, Papa D, Ballard JL. Treatment of radial and ulnar artery pseudoaneurysms using percutaneous thrombin injection. J Hand Surg. 2004;29A(5):936-942. doi:10.1016/j.jhsa.2004.05.009.
11. Falk PS, Scuderi PE, Sherertz RJ, Motsinger SM. Infected radial artery pseudoaneurysms occurring after percutaneous cannulation. Chest. 1992;101(2):490-495.
12. Kang SS, Labropoulos N, Mansour MA, et al. Expanded indications for ultrasound-guided thrombin injection of pseudoaneurysms. J Vasc Surg. 2000;31(2):289-298.
1. Newton EJ, Arora S. Peripheral vascular injury. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. Philadelphia, PA: Elsevier Saunders; 2014:502.
2. Aufderheide TP. Peripheral arteriovascular disease. In: Marx JA, Hockberger RS, Walls RM, et al, eds. Rosen’s Emergency Medicine Concepts and Clinical Practice. Vol 1. 8th ed. 2014:1147-1149.
3. Anderson SE, De Monaco D, Buechler U, et al. Imaging features of pseudoaneurysms of the hand in children and adults. AJR Am J Roentgenol. 2003;180(3):659-664. doi:10.2214/ajr.180.3.1800659.
4. Shah S, Powell-Brett S, Garnham A. Pseudoaneurysm: an unusual cause of post-traumatic hand swelling. BMJ Case Rep. 2015;2015. pii: bcr2014208750. doi:10.1136/bcr-2014-208750.
5. Kitamura A, Mukohara N. Spontaneous pseudoaneurysm of the hand. Ann Vasc Surg. 2014;28(3):739.e1-e3. doi:10.1016/j.avsg.2013.04.033.
6. Huang SW, Wei TS, Liu SY, Wang WT. Spontaneous totally thrombosed pseudoaneurysm mimicking a tendon tear of the wrist. Orthopedics. 2010;33(10):776. doi:10.3928/01477447-20100826-23.
7. Belyayev L, Rich NM, McKay P, Nesti L, Wind G. Traumatic ulnar artery pseudoaneurysm following a grenade blast: report of a case. Mil Med. 2015;180(6):e725-e727. doi:10.7205/MILMED-D-14-00400.
8. Pero T, Herrick J. Pseudoaneurysm of the radial artery diagnosed by bedside ultrasound. West J Emerg Med. 2009;10(2):89-91.
9. Bosman A, Veger HTC, Doornink F, Hedeman Joosten PPA. A pseudoaneurysm of the deep palmar arch after penetrating trauma to the hand: successful exclusion by ultrasound guided percutaneous thrombin injection. EJVES Short Rep. 2016;31:9-11. doi:10.1016/j.ejvssr.2016.03.002.
10. Komorowska-Timek E, Teruya TH, Abou-Zamzam AM Jr, Papa D, Ballard JL. Treatment of radial and ulnar artery pseudoaneurysms using percutaneous thrombin injection. J Hand Surg. 2004;29A(5):936-942. doi:10.1016/j.jhsa.2004.05.009.
11. Falk PS, Scuderi PE, Sherertz RJ, Motsinger SM. Infected radial artery pseudoaneurysms occurring after percutaneous cannulation. Chest. 1992;101(2):490-495.
12. Kang SS, Labropoulos N, Mansour MA, et al. Expanded indications for ultrasound-guided thrombin injection of pseudoaneurysms. J Vasc Surg. 2000;31(2):289-298.
Balloon pulmonary angioplasty for CTEPH improves heart failure symptoms
WASHINGTON – Balloon pulmonary angioplasty provides meaningful improvements in functional capacity for patients with chronic thromboembolic pulmonary hypertension (CTEPH) who are not candidates for surgical pulmonary thromboendarterectomy, according to a single-center experience with 15 consecutive patients that was presented at CRT 2018 sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
The treatment of choice for CTEPH is pulmonary thromboendarterectomy (PTE), but “a huge percentage of the population with CTEPH” is not eligible or does not undergo surgical treatment, which was the impetus to initiate this intervention, reported Riyaz Bashir, MD, director of vascular and endovascular medicine at Temple University Hospital and professor of medicine at Temple University, Philadelphia.

There have now been 15 CTEPH patients treated with BPA by Dr. Bashir and his team at Temple University. He reported 6-month outcome data on the first 13 patients, all of whom had a history of pulmonary embolism. Three of the patients had a prior PTE.
The primary outcome of interest in this series was functional improvement. Unlike PTE, immediate improvement in hemodynamics is not typically observed immediately after the procedure, but these measures do improve incrementally over time, Dr. Bashir reported. This is reflected in progressive improvements in the 6-minute walk test and in New York Heart Association (NYHA) functional class.
Of the 13 patients treated so far, 6 (46%) were in NYHA class IV and only 2 (15%) were in NYHA class II prior to BPA. Six months after BPA, the proportions had reversed. At that point, seven patients (54%) were in class II and two (15%) in class IV. The remaining patients at both time points were in NYHA class III. Similar improvements were seen in the 6-minute walk test, which typically tracks with NYHA class.
Describing the first case, performed about 2 years ago, Dr. Bashir explained that a tight stenosis in the right lower pulmonary artery of a 44-year-old woman was reached with a multipurpose guiding catheter through femoral access. A 5-mm balloon was used to dilate the stenosis and create a pulsatile flow.
“The goal is not to raise the mean arterial pressure above 35 mm Hg, because this has been associated with significant peripheral edema,” Dr. Bashir explained.
In this patient, progressive improvements in pulmonary pressure, cardiac index, and other hemodynamics were associated with progressive shrinking of the right ventricle over 6 months of follow-up. The walk test improved from 216 m prior to BPA to 421 m at her most recent evaluation.
The average age in the 13 patients treated so far was 55 years, and 75% are males. The mean left ventricular ejection fraction (LVEF) was 55%. According to Dr. Bashir, most patients required at least two treatment sessions and some have required up to four.
There have been two complications – one patient developed hemoptysis that required a brief intubation and the other involved perfusion edema – and no deaths in this series so far, he said.
The outcomes so far, which Dr. Bashir characterized as “an early experience,” provide evidence that BPA is “safe and feasible” for patients with CTEPH who are not surgical candidates. At Dr. Bashir’s institution, where PTE is commonly performed in patients with CTEPH (Dr. Bashir reported that 134 cases were performed over the period of time in which these 15 cases of BPA were performed), there is a plan to compare functional outcomes in CTEPH patients managed with these two different approaches.
Dr. Bashir reported no financial relationships relevant to this study.
SOURCE: Bashir R. CRT 2018
WASHINGTON – Balloon pulmonary angioplasty provides meaningful improvements in functional capacity for patients with chronic thromboembolic pulmonary hypertension (CTEPH) who are not candidates for surgical pulmonary thromboendarterectomy, according to a single-center experience with 15 consecutive patients that was presented at CRT 2018 sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
The treatment of choice for CTEPH is pulmonary thromboendarterectomy (PTE), but “a huge percentage of the population with CTEPH” is not eligible or does not undergo surgical treatment, which was the impetus to initiate this intervention, reported Riyaz Bashir, MD, director of vascular and endovascular medicine at Temple University Hospital and professor of medicine at Temple University, Philadelphia.
There have now been 15 CTEPH patients treated with BPA by Dr. Bashir and his team at Temple University. He reported 6-month outcome data on the first 13 patients, all of whom had a history of pulmonary embolism. Three of the patients had a prior PTE.
The primary outcome of interest in this series was functional improvement. Unlike PTE, immediate improvement in hemodynamics is not typically observed immediately after the procedure, but these measures do improve incrementally over time, Dr. Bashir reported. This is reflected in progressive improvements in the 6-minute walk test and in New York Heart Association (NYHA) functional class.
Of the 13 patients treated so far, 6 (46%) were in NYHA class IV and only 2 (15%) were in NYHA class II prior to BPA. Six months after BPA, the proportions had reversed. At that point, seven patients (54%) were in class II and two (15%) in class IV. The remaining patients at both time points were in NYHA class III. Similar improvements were seen in the 6-minute walk test, which typically tracks with NYHA class.
Describing the first case, performed about 2 years ago, Dr. Bashir explained that a tight stenosis in the right lower pulmonary artery of a 44-year-old woman was reached with a multipurpose guiding catheter through femoral access. A 5-mm balloon was used to dilate the stenosis and create a pulsatile flow.
“The goal is not to raise the mean arterial pressure above 35 mm Hg, because this has been associated with significant peripheral edema,” Dr. Bashir explained.
In this patient, progressive improvements in pulmonary pressure, cardiac index, and other hemodynamics were associated with progressive shrinking of the right ventricle over 6 months of follow-up. The walk test improved from 216 m prior to BPA to 421 m at her most recent evaluation.
The average age in the 13 patients treated so far was 55 years, and 75% are males. The mean left ventricular ejection fraction (LVEF) was 55%. According to Dr. Bashir, most patients required at least two treatment sessions and some have required up to four.
There have been two complications – one patient developed hemoptysis that required a brief intubation and the other involved perfusion edema – and no deaths in this series so far, he said.
The outcomes so far, which Dr. Bashir characterized as “an early experience,” provide evidence that BPA is “safe and feasible” for patients with CTEPH who are not surgical candidates. At Dr. Bashir’s institution, where PTE is commonly performed in patients with CTEPH (Dr. Bashir reported that 134 cases were performed over the period of time in which these 15 cases of BPA were performed), there is a plan to compare functional outcomes in CTEPH patients managed with these two different approaches.
Dr. Bashir reported no financial relationships relevant to this study.
SOURCE: Bashir R. CRT 2018
WASHINGTON – Balloon pulmonary angioplasty provides meaningful improvements in functional capacity for patients with chronic thromboembolic pulmonary hypertension (CTEPH) who are not candidates for surgical pulmonary thromboendarterectomy, according to a single-center experience with 15 consecutive patients that was presented at CRT 2018 sponsored by the Cardiovascular Research Institute at Washington Hospital Center.
The treatment of choice for CTEPH is pulmonary thromboendarterectomy (PTE), but “a huge percentage of the population with CTEPH” is not eligible or does not undergo surgical treatment, which was the impetus to initiate this intervention, reported Riyaz Bashir, MD, director of vascular and endovascular medicine at Temple University Hospital and professor of medicine at Temple University, Philadelphia.
There have now been 15 CTEPH patients treated with BPA by Dr. Bashir and his team at Temple University. He reported 6-month outcome data on the first 13 patients, all of whom had a history of pulmonary embolism. Three of the patients had a prior PTE.
The primary outcome of interest in this series was functional improvement. Unlike PTE, immediate improvement in hemodynamics is not typically observed immediately after the procedure, but these measures do improve incrementally over time, Dr. Bashir reported. This is reflected in progressive improvements in the 6-minute walk test and in New York Heart Association (NYHA) functional class.
Of the 13 patients treated so far, 6 (46%) were in NYHA class IV and only 2 (15%) were in NYHA class II prior to BPA. Six months after BPA, the proportions had reversed. At that point, seven patients (54%) were in class II and two (15%) in class IV. The remaining patients at both time points were in NYHA class III. Similar improvements were seen in the 6-minute walk test, which typically tracks with NYHA class.
Describing the first case, performed about 2 years ago, Dr. Bashir explained that a tight stenosis in the right lower pulmonary artery of a 44-year-old woman was reached with a multipurpose guiding catheter through femoral access. A 5-mm balloon was used to dilate the stenosis and create a pulsatile flow.
“The goal is not to raise the mean arterial pressure above 35 mm Hg, because this has been associated with significant peripheral edema,” Dr. Bashir explained.
In this patient, progressive improvements in pulmonary pressure, cardiac index, and other hemodynamics were associated with progressive shrinking of the right ventricle over 6 months of follow-up. The walk test improved from 216 m prior to BPA to 421 m at her most recent evaluation.
The average age in the 13 patients treated so far was 55 years, and 75% are males. The mean left ventricular ejection fraction (LVEF) was 55%. According to Dr. Bashir, most patients required at least two treatment sessions and some have required up to four.
There have been two complications – one patient developed hemoptysis that required a brief intubation and the other involved perfusion edema – and no deaths in this series so far, he said.
The outcomes so far, which Dr. Bashir characterized as “an early experience,” provide evidence that BPA is “safe and feasible” for patients with CTEPH who are not surgical candidates. At Dr. Bashir’s institution, where PTE is commonly performed in patients with CTEPH (Dr. Bashir reported that 134 cases were performed over the period of time in which these 15 cases of BPA were performed), there is a plan to compare functional outcomes in CTEPH patients managed with these two different approaches.
Dr. Bashir reported no financial relationships relevant to this study.
SOURCE: Bashir R. CRT 2018
REPORTING FROM CRT 2018
Key clinical point: Balloon pulmonary angioplasty has clinical benefits in chronic thromboembolic pulmonary hypertension (CTEPH) patients not candidates for surgery.
Major finding: At baseline, only 30% of CTEPH patients were at or below NYHA class II, rising to 65% 6 months after balloon pulmonary angioplasty.
Data source: Single-center review of 15 patients.
Disclosures: Dr. Bashir reports no financial relationships relevant to this study.
Source: Bashir R. CRT 2018
Failure to find cancer earlier; patient dies: $4.69M verdict
Failure to find cancer earlier; patient dies: $4.69M verdict

On July 19, a 26-year-old woman presented to the emergency department (ED) with abnormal vaginal bleeding 3 months after giving birth. She was found to have endometrial thickening and an elevated ß human chorionic gonadotropin level. An ObGyn (Dr. A) assumed that the patient was having a miscarriage and sent her home.
On July 30, when the patient returned to the ED with continued bleeding, lesions on her cervix and urethra were discovered. A second ObGyn, Dr. B, addressed the bleeding, removed the lesion, and ordered testing. On August 17, the patient saw a third ObGyn (Dr. C), who did not conduct an examination.
Days later, the patient suffered a brain hemorrhage that was suspicious for hemorrhagic metastasis. After that, stage IV choriocarcinoma was identified. Although she underwent chemotherapy, the patient died 18 months later.
ESTATE'S CLAIM: All 3 ObGyns failed to take a proper history, conduct adequate examinations, and order appropriate testing. Even at stage IV, 75% of patients with choriocarcinoma survive past 5 years. The stroke rendered chemotherapy less effective and substantially contributed to the patient's death. Failure to diagnose the cancer before the stroke allowed the disease to progress beyond the point at which the patient's life could be saved.
DEFENDANTS' DEFENSE: The ObGyns and hospital claimed that appropriate care was provided and that they were not negligent in failing to consider the diagnosis of a very rare form of cancer.
VERDICT: A $4.69 million New Jersey verdict was returned, with all 3 physicians held partially liable.
Hot speculum burns patient: $547,090 award
A 54-year-old woman underwent a hysterectomy performed at a government-operated hospital. After she was anesthetized and unconscious, a second-year resident took a speculum that had been placed in the sterile field by a nurse, and inserted it in the patient's vagina.
When the patient awoke from surgery, she discovered significant burns to her vaginal area, perineum, anus, and buttocks.
PATIENT'S CLAIM: The speculum had just been removed from the autoclave and was very hot. The patient incurred substantial medical bills to treat her injuries and was unable to work for several months. She sued the hospital and resident, alleging error by the nurse in placing the hot speculum in the sterile field without cooling it or advising the resident that it was still hot. The resident was blamed for using the speculum without confirming that it was hot.
DEFENDANTS' DEFENSE: The resident claimed that she reasonably relied on the nurse to not place a hot instrument in the surgical field without first cooling it. The hospital, representing the nurse, denied fault, blaming the resident for not checking the speculum.
VERDICT: A $547,090 Louisiana verdict was awarded by a judge against the resident and the hospital, but it was halved by comparative fault to $273,545.
Surgeon's breast exam insufficient: $375,000 verdict
After a woman in her early 40s found a lump in her left breast, she underwent a radiographic study, which a radiologist interpreted as showing a 3-mm cyst. Without performing additional tests, a general surgeon immediately scheduled her for surgery.
On May 17, the radiologist performed an ultrasound-guided needle-localized biopsy and found a nodule. The patient was immediately sent to the operating room where the surgeon performed a segmental resection of the nodule.
On May 24, the patient presented to the surgeon's office for a postoperative visit. She told the nurse that the palpable mass was still there. The nurse examined the mass, told the patient that the incision was healing nicely, and suggested follow-up in a month.
Four months later, the patient sought a second opinion. On September 15, she underwent a diagnostic mammogram, ultrasound, and biopsy. The biopsy was positive for invasive ductal carcinoma. On September 30, magnetic resonance imaging and a second biopsy further confirmed the diagnosis. On November 2, she underwent a segmental mastectomy with sentinel lymph node biopsy. The pathology report noted a 3-cm invasive ductal carcinoma with necrosis. The patient underwent chemotherapy and radiation treatment.
PATIENT'S CLAIM: She sued the general surgeon, radiologist, and surgical center, alleging that her breast cancer went undiagnosed. Prior to trial, the radiologist and surgical center were dismissed from the case.
The surgeon failed to perform a thorough physical examination and nodal evaluation of the left breast and axilla. His substandard methods to diagnose and treat the patient's breast cancer delayed proper treatment and significantly altered the outcome.
PHYSICIAN'S CLAIM: The surgeon's treatment met the standard of care. The outcome and treatment were not significantly changed by the delay.
VERDICT: A $375,000 Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Failure to find cancer earlier; patient dies: $4.69M verdict
On July 19, a 26-year-old woman presented to the emergency department (ED) with abnormal vaginal bleeding 3 months after giving birth. She was found to have endometrial thickening and an elevated ß human chorionic gonadotropin level. An ObGyn (Dr. A) assumed that the patient was having a miscarriage and sent her home.
On July 30, when the patient returned to the ED with continued bleeding, lesions on her cervix and urethra were discovered. A second ObGyn, Dr. B, addressed the bleeding, removed the lesion, and ordered testing. On August 17, the patient saw a third ObGyn (Dr. C), who did not conduct an examination.
Days later, the patient suffered a brain hemorrhage that was suspicious for hemorrhagic metastasis. After that, stage IV choriocarcinoma was identified. Although she underwent chemotherapy, the patient died 18 months later.
ESTATE'S CLAIM: All 3 ObGyns failed to take a proper history, conduct adequate examinations, and order appropriate testing. Even at stage IV, 75% of patients with choriocarcinoma survive past 5 years. The stroke rendered chemotherapy less effective and substantially contributed to the patient's death. Failure to diagnose the cancer before the stroke allowed the disease to progress beyond the point at which the patient's life could be saved.
DEFENDANTS' DEFENSE: The ObGyns and hospital claimed that appropriate care was provided and that they were not negligent in failing to consider the diagnosis of a very rare form of cancer.
VERDICT: A $4.69 million New Jersey verdict was returned, with all 3 physicians held partially liable.
Hot speculum burns patient: $547,090 award
A 54-year-old woman underwent a hysterectomy performed at a government-operated hospital. After she was anesthetized and unconscious, a second-year resident took a speculum that had been placed in the sterile field by a nurse, and inserted it in the patient's vagina.
When the patient awoke from surgery, she discovered significant burns to her vaginal area, perineum, anus, and buttocks.
PATIENT'S CLAIM: The speculum had just been removed from the autoclave and was very hot. The patient incurred substantial medical bills to treat her injuries and was unable to work for several months. She sued the hospital and resident, alleging error by the nurse in placing the hot speculum in the sterile field without cooling it or advising the resident that it was still hot. The resident was blamed for using the speculum without confirming that it was hot.
DEFENDANTS' DEFENSE: The resident claimed that she reasonably relied on the nurse to not place a hot instrument in the surgical field without first cooling it. The hospital, representing the nurse, denied fault, blaming the resident for not checking the speculum.
VERDICT: A $547,090 Louisiana verdict was awarded by a judge against the resident and the hospital, but it was halved by comparative fault to $273,545.
Surgeon's breast exam insufficient: $375,000 verdict
After a woman in her early 40s found a lump in her left breast, she underwent a radiographic study, which a radiologist interpreted as showing a 3-mm cyst. Without performing additional tests, a general surgeon immediately scheduled her for surgery.
On May 17, the radiologist performed an ultrasound-guided needle-localized biopsy and found a nodule. The patient was immediately sent to the operating room where the surgeon performed a segmental resection of the nodule.
On May 24, the patient presented to the surgeon's office for a postoperative visit. She told the nurse that the palpable mass was still there. The nurse examined the mass, told the patient that the incision was healing nicely, and suggested follow-up in a month.
Four months later, the patient sought a second opinion. On September 15, she underwent a diagnostic mammogram, ultrasound, and biopsy. The biopsy was positive for invasive ductal carcinoma. On September 30, magnetic resonance imaging and a second biopsy further confirmed the diagnosis. On November 2, she underwent a segmental mastectomy with sentinel lymph node biopsy. The pathology report noted a 3-cm invasive ductal carcinoma with necrosis. The patient underwent chemotherapy and radiation treatment.
PATIENT'S CLAIM: She sued the general surgeon, radiologist, and surgical center, alleging that her breast cancer went undiagnosed. Prior to trial, the radiologist and surgical center were dismissed from the case.
The surgeon failed to perform a thorough physical examination and nodal evaluation of the left breast and axilla. His substandard methods to diagnose and treat the patient's breast cancer delayed proper treatment and significantly altered the outcome.
PHYSICIAN'S CLAIM: The surgeon's treatment met the standard of care. The outcome and treatment were not significantly changed by the delay.
VERDICT: A $375,000 Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Failure to find cancer earlier; patient dies: $4.69M verdict
On July 19, a 26-year-old woman presented to the emergency department (ED) with abnormal vaginal bleeding 3 months after giving birth. She was found to have endometrial thickening and an elevated ß human chorionic gonadotropin level. An ObGyn (Dr. A) assumed that the patient was having a miscarriage and sent her home.
On July 30, when the patient returned to the ED with continued bleeding, lesions on her cervix and urethra were discovered. A second ObGyn, Dr. B, addressed the bleeding, removed the lesion, and ordered testing. On August 17, the patient saw a third ObGyn (Dr. C), who did not conduct an examination.
Days later, the patient suffered a brain hemorrhage that was suspicious for hemorrhagic metastasis. After that, stage IV choriocarcinoma was identified. Although she underwent chemotherapy, the patient died 18 months later.
ESTATE'S CLAIM: All 3 ObGyns failed to take a proper history, conduct adequate examinations, and order appropriate testing. Even at stage IV, 75% of patients with choriocarcinoma survive past 5 years. The stroke rendered chemotherapy less effective and substantially contributed to the patient's death. Failure to diagnose the cancer before the stroke allowed the disease to progress beyond the point at which the patient's life could be saved.
DEFENDANTS' DEFENSE: The ObGyns and hospital claimed that appropriate care was provided and that they were not negligent in failing to consider the diagnosis of a very rare form of cancer.
VERDICT: A $4.69 million New Jersey verdict was returned, with all 3 physicians held partially liable.
Hot speculum burns patient: $547,090 award
A 54-year-old woman underwent a hysterectomy performed at a government-operated hospital. After she was anesthetized and unconscious, a second-year resident took a speculum that had been placed in the sterile field by a nurse, and inserted it in the patient's vagina.
When the patient awoke from surgery, she discovered significant burns to her vaginal area, perineum, anus, and buttocks.
PATIENT'S CLAIM: The speculum had just been removed from the autoclave and was very hot. The patient incurred substantial medical bills to treat her injuries and was unable to work for several months. She sued the hospital and resident, alleging error by the nurse in placing the hot speculum in the sterile field without cooling it or advising the resident that it was still hot. The resident was blamed for using the speculum without confirming that it was hot.
DEFENDANTS' DEFENSE: The resident claimed that she reasonably relied on the nurse to not place a hot instrument in the surgical field without first cooling it. The hospital, representing the nurse, denied fault, blaming the resident for not checking the speculum.
VERDICT: A $547,090 Louisiana verdict was awarded by a judge against the resident and the hospital, but it was halved by comparative fault to $273,545.
Surgeon's breast exam insufficient: $375,000 verdict
After a woman in her early 40s found a lump in her left breast, she underwent a radiographic study, which a radiologist interpreted as showing a 3-mm cyst. Without performing additional tests, a general surgeon immediately scheduled her for surgery.
On May 17, the radiologist performed an ultrasound-guided needle-localized biopsy and found a nodule. The patient was immediately sent to the operating room where the surgeon performed a segmental resection of the nodule.
On May 24, the patient presented to the surgeon's office for a postoperative visit. She told the nurse that the palpable mass was still there. The nurse examined the mass, told the patient that the incision was healing nicely, and suggested follow-up in a month.
Four months later, the patient sought a second opinion. On September 15, she underwent a diagnostic mammogram, ultrasound, and biopsy. The biopsy was positive for invasive ductal carcinoma. On September 30, magnetic resonance imaging and a second biopsy further confirmed the diagnosis. On November 2, she underwent a segmental mastectomy with sentinel lymph node biopsy. The pathology report noted a 3-cm invasive ductal carcinoma with necrosis. The patient underwent chemotherapy and radiation treatment.
PATIENT'S CLAIM: She sued the general surgeon, radiologist, and surgical center, alleging that her breast cancer went undiagnosed. Prior to trial, the radiologist and surgical center were dismissed from the case.
The surgeon failed to perform a thorough physical examination and nodal evaluation of the left breast and axilla. His substandard methods to diagnose and treat the patient's breast cancer delayed proper treatment and significantly altered the outcome.
PHYSICIAN'S CLAIM: The surgeon's treatment met the standard of care. The outcome and treatment were not significantly changed by the delay.
VERDICT: A $375,000 Pennsylvania verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Checkpoint inhibition less toxic than antiangiogenic therapy in NSCLC
ORLANDO – , a systematic review and meta-analysis suggests.
In 16,810 patients from 37 trials included in the analysis, first-line treatment with nivolumab or pembrolizumab, compared with first-line sorafenib plus platinum doublets, for example, was associated with less combined direct and indirect toxicity (odds ratios, 0.08 and 0.12, respectively), Chin-Chuan Hung, MD, and her colleagues reported in a poster at the annual conference of the National Comprehensive Cancer Network.
For subsequent therapy, nivolumab showed lower risk than most antiangiogenic therapies, particularly combination ramucirumab and docetaxel (OR, 0.06), said Dr. Hung of China Medical University Hospital in Taichung, Taiwan.
The findings are notable because tolerability is an essential selection criterion for patients with advanced stage disease, and while checkpoint inhibitors – including nivolumab, pembrolizumab, and atezolizumab – and antiangiogenic agents – including bevacizumab, ramucirumab, and nintedanib – have become the treatments of choice, direct comparisons with respect to tolerability are lacking, she noted.
The investigators performed a systematic review using Bayesian-model network meta-analysis of studies conducted through July 2017 comparing first-line and subsequent regimens containing chemotherapy, antiangiogenic therapy, and/or immune checkpoint inhibitors. Chemotherapy agents studied included cisplatin, carboplatin, oxaliplatin, gemcitabine, paclitaxel, docetaxel, and pemetrexed; antiangiogenic agents included bevacizumab, aflibercept, ramucirumab, nintedanib, axitinib, sorafenib, vandetanib, and sunitinib; and immune checkpoint inhibitors included ipilimumab, pembrolizumab, nivolumab, and atezolizumab.
Direct and indirect data for all grade 3-5 adverse events were combined using random-effects network meta-analysis.
“The results indicated that [checkpoint] inhibitors can be preferred choices for less toxicity to treat advanced stage NSCLC compared with antiangiogenic therapies in first-line and subsequent settings,” Dr. Hung and her associates concluded.
This study was supported by the China Medical University Beigang Hospital.
SOURCE: Hsu C et al. NCCN poster 13
ORLANDO – , a systematic review and meta-analysis suggests.
In 16,810 patients from 37 trials included in the analysis, first-line treatment with nivolumab or pembrolizumab, compared with first-line sorafenib plus platinum doublets, for example, was associated with less combined direct and indirect toxicity (odds ratios, 0.08 and 0.12, respectively), Chin-Chuan Hung, MD, and her colleagues reported in a poster at the annual conference of the National Comprehensive Cancer Network.
For subsequent therapy, nivolumab showed lower risk than most antiangiogenic therapies, particularly combination ramucirumab and docetaxel (OR, 0.06), said Dr. Hung of China Medical University Hospital in Taichung, Taiwan.
The findings are notable because tolerability is an essential selection criterion for patients with advanced stage disease, and while checkpoint inhibitors – including nivolumab, pembrolizumab, and atezolizumab – and antiangiogenic agents – including bevacizumab, ramucirumab, and nintedanib – have become the treatments of choice, direct comparisons with respect to tolerability are lacking, she noted.
The investigators performed a systematic review using Bayesian-model network meta-analysis of studies conducted through July 2017 comparing first-line and subsequent regimens containing chemotherapy, antiangiogenic therapy, and/or immune checkpoint inhibitors. Chemotherapy agents studied included cisplatin, carboplatin, oxaliplatin, gemcitabine, paclitaxel, docetaxel, and pemetrexed; antiangiogenic agents included bevacizumab, aflibercept, ramucirumab, nintedanib, axitinib, sorafenib, vandetanib, and sunitinib; and immune checkpoint inhibitors included ipilimumab, pembrolizumab, nivolumab, and atezolizumab.
Direct and indirect data for all grade 3-5 adverse events were combined using random-effects network meta-analysis.
“The results indicated that [checkpoint] inhibitors can be preferred choices for less toxicity to treat advanced stage NSCLC compared with antiangiogenic therapies in first-line and subsequent settings,” Dr. Hung and her associates concluded.
This study was supported by the China Medical University Beigang Hospital.
SOURCE: Hsu C et al. NCCN poster 13
ORLANDO – , a systematic review and meta-analysis suggests.
In 16,810 patients from 37 trials included in the analysis, first-line treatment with nivolumab or pembrolizumab, compared with first-line sorafenib plus platinum doublets, for example, was associated with less combined direct and indirect toxicity (odds ratios, 0.08 and 0.12, respectively), Chin-Chuan Hung, MD, and her colleagues reported in a poster at the annual conference of the National Comprehensive Cancer Network.
For subsequent therapy, nivolumab showed lower risk than most antiangiogenic therapies, particularly combination ramucirumab and docetaxel (OR, 0.06), said Dr. Hung of China Medical University Hospital in Taichung, Taiwan.
The findings are notable because tolerability is an essential selection criterion for patients with advanced stage disease, and while checkpoint inhibitors – including nivolumab, pembrolizumab, and atezolizumab – and antiangiogenic agents – including bevacizumab, ramucirumab, and nintedanib – have become the treatments of choice, direct comparisons with respect to tolerability are lacking, she noted.
The investigators performed a systematic review using Bayesian-model network meta-analysis of studies conducted through July 2017 comparing first-line and subsequent regimens containing chemotherapy, antiangiogenic therapy, and/or immune checkpoint inhibitors. Chemotherapy agents studied included cisplatin, carboplatin, oxaliplatin, gemcitabine, paclitaxel, docetaxel, and pemetrexed; antiangiogenic agents included bevacizumab, aflibercept, ramucirumab, nintedanib, axitinib, sorafenib, vandetanib, and sunitinib; and immune checkpoint inhibitors included ipilimumab, pembrolizumab, nivolumab, and atezolizumab.
Direct and indirect data for all grade 3-5 adverse events were combined using random-effects network meta-analysis.
“The results indicated that [checkpoint] inhibitors can be preferred choices for less toxicity to treat advanced stage NSCLC compared with antiangiogenic therapies in first-line and subsequent settings,” Dr. Hung and her associates concluded.
This study was supported by the China Medical University Beigang Hospital.
SOURCE: Hsu C et al. NCCN poster 13
REPORTING FROM THE NCCN ANNUAL CONFERENCE
Key clinical point: Checkpoint blockade appears less toxic than antiangiogenic therapies in advanced NSCLC
Major finding: Less toxicity was seen with first-line nivolumab or pembrolizumab vs. sorafenib + platinum doublets (odds ratios, 0.08 and 0.12, respectively).
Study details: A systematic review and meta-analysis of 37 trials involving 16,810 patients.
Disclosures: The study was supported by the China Medical University Beigang Hospital.
Source: Hsu C et al. NCCN poster 13.