User login
Immunotherapy demonstrates potential for T-cell lymphoma

Researchers have reported successful inhibition of the phosphatase SHIP1, which may be an effective approach for treating T-cell lymphoma.
The team found that intermittent treatment with a SHIP1 inhibitor prevented the immune exhaustion observed with SHIP1 deletion.
Intermittent SHIP1 inhibition enhanced the antitumor activity of natural killer (NK) cells and T cells in a mouse model of T-cell lymphoma.
The treatment also appeared to have a direct chemotherapeutic effect and induced immunological memory against lymphoma cells.
Matthew Gumbleton, MD, of SUNY Upstate Medical University in Syracuse, New York, and his colleagues reported these results in Science Signaling.
The researchers noted that previous efforts to inhibit SHIP1 have yielded disappointing results. Mice engineered to lack the SHIP1 gene had poorly responsive immune systems, potentially because overactivated cells became exhausted.
Dr Gumbleton and his colleagues found they could overcome this problem by administering a SHIP1 inhibitor—3-a-aminocholestane (3AC)—in a pulsed regimen of 2 consecutive treatment days per week.
The team tested this regimen in mouse models of colorectal cancer and T-cell lymphoma (RMA-Rae1).
In the lymphoma model, intermittent 3AC treatment increased the responsiveness of T cells and NK cells.
The treatment significantly increased the number of NK cells at the tumor site and the terminal maturation of the peripheral NK-cell compartment.
3AC also enhanced FasL-Fas–mediated killing of lymphoma cells. (NK cells induce apoptosis of target cells via Fas-FasL signaling.)
However, 3AC treatment reduced lymphoma burden in NK-cell-deficient mice as well. Therefore, the researchers believe 3AC may have a direct chemotherapeutic effect.
The team also found that intermittent 3AC treatment increased survival in lymphoma-bearing mice.
Treated mice had significantly longer survival than control mice. And some of the treated mice had long-term survival with no evidence of tumor burden, which suggests the treatment could be curative.
Additional experiments revealed that both NK cells and T cells were required to induce long-term survival in the lymphoma-bearing mice.
Finally, the researchers found evidence to suggest that 3AC treatment triggered “immunological memory capable of sustained and protective antitumor response that prevents relapse.”
The team infused hematolymphoid cells from either a naïve donor mouse or a lymphoma-challenged, 3AC-treated, long-term-surviving donor mouse into naïve host mice. The host mice were then challenged with RMA-Rae1 cells but didn’t receive 3AC.
Mice that received cells from the 3AC-treated donors had significantly better survival than mice that received cells from naive donors.
Based on these results, the researchers concluded that intermittent SHIP1 inhibition may be effective for treating and preventing relapse of T-cell lymphoma and other cancers. ![]()
Researchers have reported successful inhibition of the phosphatase SHIP1, which may be an effective approach for treating T-cell lymphoma.
The team found that intermittent treatment with a SHIP1 inhibitor prevented the immune exhaustion observed with SHIP1 deletion.
Intermittent SHIP1 inhibition enhanced the antitumor activity of natural killer (NK) cells and T cells in a mouse model of T-cell lymphoma.
The treatment also appeared to have a direct chemotherapeutic effect and induced immunological memory against lymphoma cells.
Matthew Gumbleton, MD, of SUNY Upstate Medical University in Syracuse, New York, and his colleagues reported these results in Science Signaling.
The researchers noted that previous efforts to inhibit SHIP1 have yielded disappointing results. Mice engineered to lack the SHIP1 gene had poorly responsive immune systems, potentially because overactivated cells became exhausted.
Dr Gumbleton and his colleagues found they could overcome this problem by administering a SHIP1 inhibitor—3-a-aminocholestane (3AC)—in a pulsed regimen of 2 consecutive treatment days per week.
The team tested this regimen in mouse models of colorectal cancer and T-cell lymphoma (RMA-Rae1).
In the lymphoma model, intermittent 3AC treatment increased the responsiveness of T cells and NK cells.
The treatment significantly increased the number of NK cells at the tumor site and the terminal maturation of the peripheral NK-cell compartment.
3AC also enhanced FasL-Fas–mediated killing of lymphoma cells. (NK cells induce apoptosis of target cells via Fas-FasL signaling.)
However, 3AC treatment reduced lymphoma burden in NK-cell-deficient mice as well. Therefore, the researchers believe 3AC may have a direct chemotherapeutic effect.
The team also found that intermittent 3AC treatment increased survival in lymphoma-bearing mice.
Treated mice had significantly longer survival than control mice. And some of the treated mice had long-term survival with no evidence of tumor burden, which suggests the treatment could be curative.
Additional experiments revealed that both NK cells and T cells were required to induce long-term survival in the lymphoma-bearing mice.
Finally, the researchers found evidence to suggest that 3AC treatment triggered “immunological memory capable of sustained and protective antitumor response that prevents relapse.”
The team infused hematolymphoid cells from either a naïve donor mouse or a lymphoma-challenged, 3AC-treated, long-term-surviving donor mouse into naïve host mice. The host mice were then challenged with RMA-Rae1 cells but didn’t receive 3AC.
Mice that received cells from the 3AC-treated donors had significantly better survival than mice that received cells from naive donors.
Based on these results, the researchers concluded that intermittent SHIP1 inhibition may be effective for treating and preventing relapse of T-cell lymphoma and other cancers. ![]()
Researchers have reported successful inhibition of the phosphatase SHIP1, which may be an effective approach for treating T-cell lymphoma.
The team found that intermittent treatment with a SHIP1 inhibitor prevented the immune exhaustion observed with SHIP1 deletion.
Intermittent SHIP1 inhibition enhanced the antitumor activity of natural killer (NK) cells and T cells in a mouse model of T-cell lymphoma.
The treatment also appeared to have a direct chemotherapeutic effect and induced immunological memory against lymphoma cells.
Matthew Gumbleton, MD, of SUNY Upstate Medical University in Syracuse, New York, and his colleagues reported these results in Science Signaling.
The researchers noted that previous efforts to inhibit SHIP1 have yielded disappointing results. Mice engineered to lack the SHIP1 gene had poorly responsive immune systems, potentially because overactivated cells became exhausted.
Dr Gumbleton and his colleagues found they could overcome this problem by administering a SHIP1 inhibitor—3-a-aminocholestane (3AC)—in a pulsed regimen of 2 consecutive treatment days per week.
The team tested this regimen in mouse models of colorectal cancer and T-cell lymphoma (RMA-Rae1).
In the lymphoma model, intermittent 3AC treatment increased the responsiveness of T cells and NK cells.
The treatment significantly increased the number of NK cells at the tumor site and the terminal maturation of the peripheral NK-cell compartment.
3AC also enhanced FasL-Fas–mediated killing of lymphoma cells. (NK cells induce apoptosis of target cells via Fas-FasL signaling.)
However, 3AC treatment reduced lymphoma burden in NK-cell-deficient mice as well. Therefore, the researchers believe 3AC may have a direct chemotherapeutic effect.
The team also found that intermittent 3AC treatment increased survival in lymphoma-bearing mice.
Treated mice had significantly longer survival than control mice. And some of the treated mice had long-term survival with no evidence of tumor burden, which suggests the treatment could be curative.
Additional experiments revealed that both NK cells and T cells were required to induce long-term survival in the lymphoma-bearing mice.
Finally, the researchers found evidence to suggest that 3AC treatment triggered “immunological memory capable of sustained and protective antitumor response that prevents relapse.”
The team infused hematolymphoid cells from either a naïve donor mouse or a lymphoma-challenged, 3AC-treated, long-term-surviving donor mouse into naïve host mice. The host mice were then challenged with RMA-Rae1 cells but didn’t receive 3AC.
Mice that received cells from the 3AC-treated donors had significantly better survival than mice that received cells from naive donors.
Based on these results, the researchers concluded that intermittent SHIP1 inhibition may be effective for treating and preventing relapse of T-cell lymphoma and other cancers. ![]()
AML trial placed on full clinical hold

The US Food and Drug Administration (FDA) has placed a full clinical hold on a phase 1/2 trial of SEL24, a dual PIM/FLT3 kinase inhibitor, in patients with relapsed/refractory acute myeloid leukemia (AML).
The hold is due to a fatal cerebral adverse event that is considered possibly related to SEL24.
The clinical hold means no new patients will be enrolled in the trial and enrolled patients will not receive SEL24 until the hold is lifted.
Selvita S.A., the company developing SEL24, received a clinical hold letter from the FDA on October 6 and said it plans to work with the agency to have the hold lifted.
As part of this process, Selvita will provide the FDA with additional data and analysis on patients treated with SEL24 as well as a proposed protocol amendment.
The trial began in the first quarter of 2017. The study is designed to determine the maximum tolerated dose and recommended dose of SEL24 in patients with relapsed and refractory AML. The study began with a 25 mg daily dose, which was then escalated following cohort reviews.
One AML patient started treatment with a 150 mg dose of SEL24 as the third patient in this dose cohort and received 4 doses of the drug. This patient developed a life-threatening, grade 4 venous thrombus in the brain with subsequent intracerebral hemorrhage, which required hospitalization.
The patient died in hospice 4 days later due to the cerebral event. The patient’s death was subsequently evaluated as possibly related to SEL24.
A safety report and a review of data by the trial’s data monitoring committee were submitted to the FDA. The agency then placed a clinical hold on the trial and requested more safety data on patients who have received SEL24, as well as specific protocol changes and additional guidance to the study staff.
Selvita said it plans to comply with the requests and provide additional information to the agency and clinical trial centers, in collaboration with the Menarini Group, its global development partner for SEL24.
The FDA has 30 days from the receipt of Selvita’s response to let the company know whether the clinical hold is lifted. ![]()
The US Food and Drug Administration (FDA) has placed a full clinical hold on a phase 1/2 trial of SEL24, a dual PIM/FLT3 kinase inhibitor, in patients with relapsed/refractory acute myeloid leukemia (AML).
The hold is due to a fatal cerebral adverse event that is considered possibly related to SEL24.
The clinical hold means no new patients will be enrolled in the trial and enrolled patients will not receive SEL24 until the hold is lifted.
Selvita S.A., the company developing SEL24, received a clinical hold letter from the FDA on October 6 and said it plans to work with the agency to have the hold lifted.
As part of this process, Selvita will provide the FDA with additional data and analysis on patients treated with SEL24 as well as a proposed protocol amendment.
The trial began in the first quarter of 2017. The study is designed to determine the maximum tolerated dose and recommended dose of SEL24 in patients with relapsed and refractory AML. The study began with a 25 mg daily dose, which was then escalated following cohort reviews.
One AML patient started treatment with a 150 mg dose of SEL24 as the third patient in this dose cohort and received 4 doses of the drug. This patient developed a life-threatening, grade 4 venous thrombus in the brain with subsequent intracerebral hemorrhage, which required hospitalization.
The patient died in hospice 4 days later due to the cerebral event. The patient’s death was subsequently evaluated as possibly related to SEL24.
A safety report and a review of data by the trial’s data monitoring committee were submitted to the FDA. The agency then placed a clinical hold on the trial and requested more safety data on patients who have received SEL24, as well as specific protocol changes and additional guidance to the study staff.
Selvita said it plans to comply with the requests and provide additional information to the agency and clinical trial centers, in collaboration with the Menarini Group, its global development partner for SEL24.
The FDA has 30 days from the receipt of Selvita’s response to let the company know whether the clinical hold is lifted. ![]()
The US Food and Drug Administration (FDA) has placed a full clinical hold on a phase 1/2 trial of SEL24, a dual PIM/FLT3 kinase inhibitor, in patients with relapsed/refractory acute myeloid leukemia (AML).
The hold is due to a fatal cerebral adverse event that is considered possibly related to SEL24.
The clinical hold means no new patients will be enrolled in the trial and enrolled patients will not receive SEL24 until the hold is lifted.
Selvita S.A., the company developing SEL24, received a clinical hold letter from the FDA on October 6 and said it plans to work with the agency to have the hold lifted.
As part of this process, Selvita will provide the FDA with additional data and analysis on patients treated with SEL24 as well as a proposed protocol amendment.
The trial began in the first quarter of 2017. The study is designed to determine the maximum tolerated dose and recommended dose of SEL24 in patients with relapsed and refractory AML. The study began with a 25 mg daily dose, which was then escalated following cohort reviews.
One AML patient started treatment with a 150 mg dose of SEL24 as the third patient in this dose cohort and received 4 doses of the drug. This patient developed a life-threatening, grade 4 venous thrombus in the brain with subsequent intracerebral hemorrhage, which required hospitalization.
The patient died in hospice 4 days later due to the cerebral event. The patient’s death was subsequently evaluated as possibly related to SEL24.
A safety report and a review of data by the trial’s data monitoring committee were submitted to the FDA. The agency then placed a clinical hold on the trial and requested more safety data on patients who have received SEL24, as well as specific protocol changes and additional guidance to the study staff.
Selvita said it plans to comply with the requests and provide additional information to the agency and clinical trial centers, in collaboration with the Menarini Group, its global development partner for SEL24.
The FDA has 30 days from the receipt of Selvita’s response to let the company know whether the clinical hold is lifted. ![]()
FDA rejects pegfilgrastim biosimilar

The US Food and Drug Administration (FDA) has issued a complete response letter saying the agency cannot approve MYL-1401H, a proposed biosimilar of pegfilgrastim (Neulasta).
Biocon and Mylan are seeking approval of MYL-1401H to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving chemotherapy to treat non-myeloid malignancies.
Biocon and Mylan filed the biologics license application for MYL-1401H in February.
The FDA had planned to issue a decision on the application by October 9.
Biocon and Mylan said the FDA’s complete response letter relates to a pending update to the application. The update involves chemistry manufacturing and control data from facility requalification activities after recent plant modifications.
The complete response letter did not raise any questions on the biosimilarity of MYL-1401H, pharmacokinetic/pharmacodynamic data, clinical data, or immunogenicity. (Results of a phase 3 study presented at ESMO 2016 Congress suggested MYL-1401H is equivalent to Neulasta.)
Biocon and Mylan said they do not expect the complete response letter for MYL-1401H to impact the commercial launch timing of the drug in the US. The companies said they are committed to working with the FDA to resolve the issues outlined in the letter. ![]()
The US Food and Drug Administration (FDA) has issued a complete response letter saying the agency cannot approve MYL-1401H, a proposed biosimilar of pegfilgrastim (Neulasta).
Biocon and Mylan are seeking approval of MYL-1401H to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving chemotherapy to treat non-myeloid malignancies.
Biocon and Mylan filed the biologics license application for MYL-1401H in February.
The FDA had planned to issue a decision on the application by October 9.
Biocon and Mylan said the FDA’s complete response letter relates to a pending update to the application. The update involves chemistry manufacturing and control data from facility requalification activities after recent plant modifications.
The complete response letter did not raise any questions on the biosimilarity of MYL-1401H, pharmacokinetic/pharmacodynamic data, clinical data, or immunogenicity. (Results of a phase 3 study presented at ESMO 2016 Congress suggested MYL-1401H is equivalent to Neulasta.)
Biocon and Mylan said they do not expect the complete response letter for MYL-1401H to impact the commercial launch timing of the drug in the US. The companies said they are committed to working with the FDA to resolve the issues outlined in the letter. ![]()
The US Food and Drug Administration (FDA) has issued a complete response letter saying the agency cannot approve MYL-1401H, a proposed biosimilar of pegfilgrastim (Neulasta).
Biocon and Mylan are seeking approval of MYL-1401H to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving chemotherapy to treat non-myeloid malignancies.
Biocon and Mylan filed the biologics license application for MYL-1401H in February.
The FDA had planned to issue a decision on the application by October 9.
Biocon and Mylan said the FDA’s complete response letter relates to a pending update to the application. The update involves chemistry manufacturing and control data from facility requalification activities after recent plant modifications.
The complete response letter did not raise any questions on the biosimilarity of MYL-1401H, pharmacokinetic/pharmacodynamic data, clinical data, or immunogenicity. (Results of a phase 3 study presented at ESMO 2016 Congress suggested MYL-1401H is equivalent to Neulasta.)
Biocon and Mylan said they do not expect the complete response letter for MYL-1401H to impact the commercial launch timing of the drug in the US. The companies said they are committed to working with the FDA to resolve the issues outlined in the letter. ![]()
Pelvic Inflammatory Disease: How to Recognize and Treat Revised
IN THIS ARTICLE
- Diagnostic tests
- Complications of PID
- CDC treatment regimens
Pelvic inflammatory disease (PID) is an ascending polymicrobial infection of the female upper reproductive tract that primarily affects sexually active women ages 15 to 29. Around 5% of sexually active women in the United States were treated for PID from 2011-2013.1 The rates and severity of PID have declined in North America and Western Europe due to overall decrease in sexually transmitted infection (STI) rates, improved screening initiatives for Chlamydia trachomatis, better treatment compliance secondary to increased access to antibiotics, and diagnostic tests with higher sensitivity.2 Despite this rate reduction, PID remains a major public health concern given the significant long-term complications, which include infertility, ectopic pregnancy, and chronic pelvic pain.3
EPIDEMIOLOGY AND PATHOGENESIS
PID is caused by sexually transmitted bacteria or enteric organisms that have spread to internal reproductive organs. Historically, the two most common pathogens identified in cases of PID have been Chlamydia trachomatis and Neisseria gonorrhoeae; however, the decline in rates of gonorrhea has led to a diminished role for N gonorrhoeae (though it continues to be associated with more severe cases).4,5
More recent studies have suggested a shift in the causative organisms; less than half of women diagnosed with acute PID test positive for either N gonorrhoeae or C trachomatis.6 Emerging infectious agents associated with PID include Mycoplasma genitalium, Gardnerella vaginalis, and bacterial vaginosis–associated bacteria.5,7,8-10
RISK FACTORS
Women ages 15 to 25 are at an increased risk for PID. The high prevalence in this age group may be attributable to high-risk behaviors, including a high number of sexual partners, high frequency of new sexual partners, and engagement in sexual intercourse without condoms.11
Taking an accurate sexual history is imperative. Clinicians should maintain a high level of suspicion for PID in women with a history of the disease, as 25% will experience recurrence.12
Clinicians should not be deterred from screening for STIs and cervical cancer in women who report having sex with other women. In addition, transgender patients should be assessed for STIs and HIV-related risks based on current anatomy sexual practices.13
PHYSICAL EXAM
While some cases of PID are asymptomatic, the typical presentation includes bilateral abdominal pain and/or pelvic pain, with onset during or shortly after menses. The pain often worsens with movement and coitus. Associated signs and symptoms include abnormal uterine bleeding or vaginal discharge; dysuria; fever and chills; frequent urination; lower back pain; and nausea and/or vomiting.14,15
All females suspected of having PID should undergo both a bimanual exam and a speculum exam. On bimanual examination, adnexal tenderness has the highest sensitivity (93% to 95.5%) for ruling out acute PID, whereas on speculum exam, purulent endocervical discharge has the highest specificity (93%).16,17 Bimanual exam findings suggestive of PID include cervical motion tenderness, uterine tenderness, and/or adnexal tenderness. Suggestive speculum exam findings include abnormal discoloration or texture of the cervix and/or endocervical mucopurulent discharge.5,16,17
One cardinal rule that should not be overlooked is that all females of reproductive age who present with abdominal pain and/or pelvic pain should take a pregnancy test to rule out ectopic pregnancy and any other pregnancy-related complications.

DIAGNOSIS
The diagnosis of PID relies on clinical judgement and a high index of suspicion.5,18 The CDC’s diagnostic criteria for acute PID include
- Sexually active female AND
- Pelvic or lower abdominal pain AND
- Cervical motion tenderness OR uterine tenderness OR adnexal tenderness.5
Additional findings that support the diagnosis include
- Abnormal cervical mucopurulent discharge or cervical friability
- Abundant white blood cells (WBCs) on saline microscopy of vaginal fluid
- Elevated C-reactive protein
- Elevated erythrocyte sedimentation rate
- Laboratory documentation of infection with C trachomatis or N gonorrhea
- Oral temperature > 101°F.5,18
The CDC notes that the first two findings (mucopurulent discharge and evidence of WBCs on microscopy) occur in most women with PID; in their absence, the diagnosis is unlikely and other sources of pain should be considered.5 The differential for PID includes acute appendicitis; adhesions; carcinoid tumor; cholecystitis; ectopic pregnancy; endometriosis; inflammatory bowel disease; and ovarian cyst.19
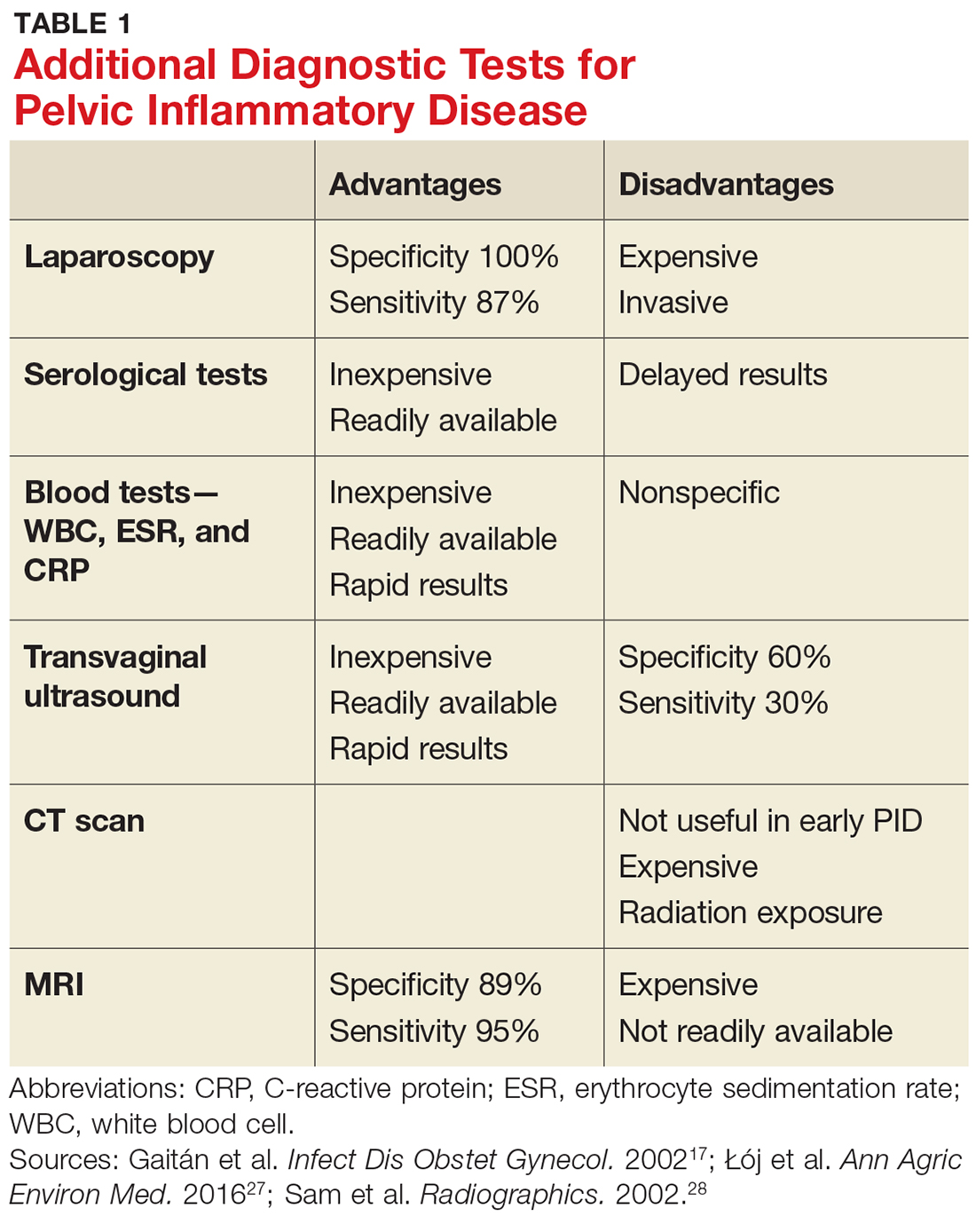
Given the variability in presentation, clinicians may find it useful to perform further diagnostic testing. There are additional laboratory tests that may be ordered for patients with a suspected diagnosis of PID (see Table 1).
TREATMENT
According to the CDC’s 2015 treatment guidelines for PID, a negative endocervical exam and negative microbial screening do not rule out an upper reproductive tract infection. Therefore, all sexually active women who present with lower abdominal pain and/or pelvic pain and have evidence of cervical motion, uterine, or adnexal tenderness on bimanual exam should be treated immediately.5
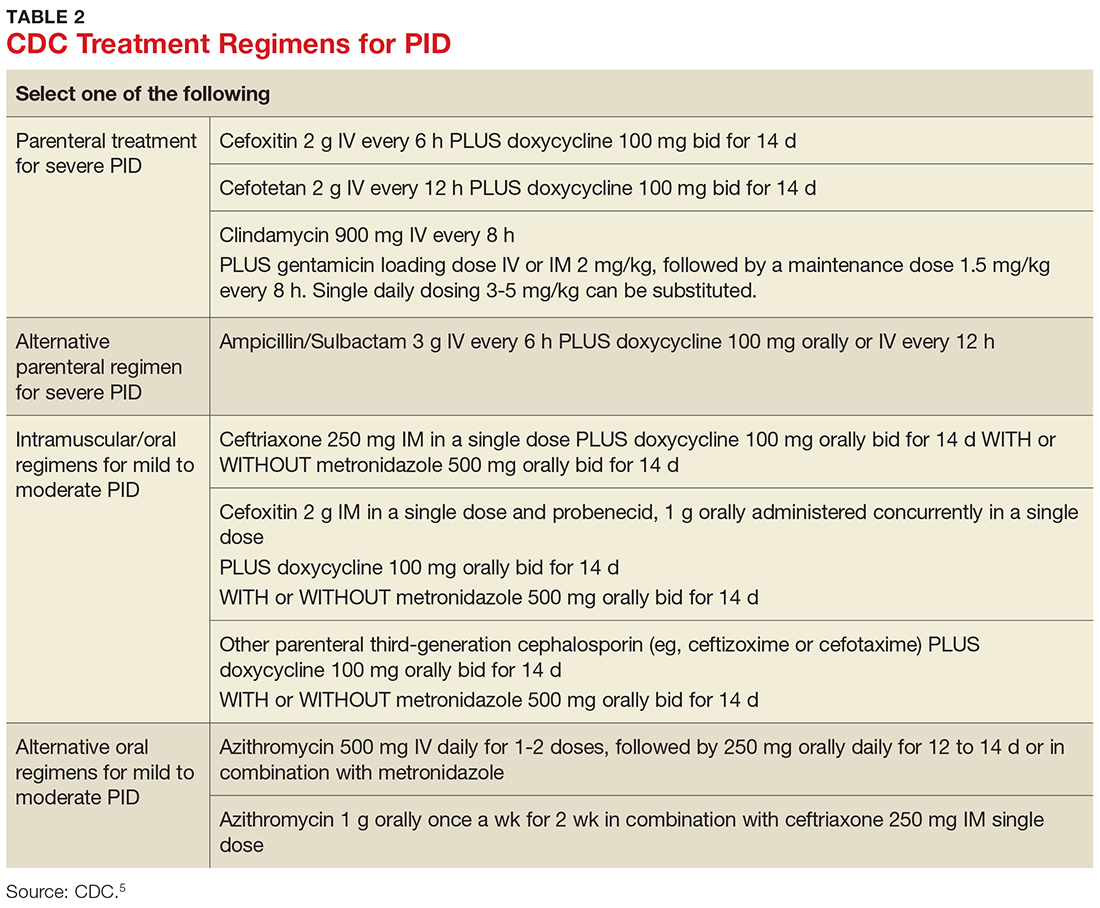
Treatment guidelines are outlined in Table 2. The polymicrobial nature of PID requires gram-negative antibiotic coverage, such as doxycycline plus a second/third-generation cephalosporin.5 Clinicians should note that cefoxitin, a second-generation cephalosporin, is recommended as firstline therapy for inpatients, as it has better anaerobic coverage than ceftriaxone.19 A targeted change in antibiotic coverage—such as inclusion of a macrolide and/or metronidazole—might be necessary if a causative organism is identified by culture.7
Treatment is indicated for all patients with a presumptive diagnosis of PID regardless of symptoms or exam findings, as PID may be asymptomatic and long-term sequelae (eg, infertility, ectopic pregnancy) are often irreversible. At-risk patients include sexually active adolescents, women with multiple sexual partners, women with a history of STI, those whose sexual partner has an STI, and women living in communities with a high prevalence of disease.20,21
Women being treated for PID should be advised to abstain from sexual intercourse until symptoms have resolved, treatment is completed, and any sexual partners have been treated as well. It is essential to emphasize to patients (and their partners) the importance of compliance to treatment regimens and the risk for PID co-infection and reinfection, as recurrence leads to an increase in long-term complications.5
Treatment of sexual partners. The CDC instructs that a woman’s most recent partner should be treated if she had sexual intercourse within 60 days of onset of symptoms or diagnosis. Furthermore, men who have had sexual contact with a woman who has PID in the 60 days prior to onset of her symptoms should be evaluated, tested, and treated for chlamydia and gonorrhea, regardless of the etiology of PID or the pathogens isolated from the woman.5
Admission criteria. Hospitalization should be based on provider judgment despite patient age. The suggested admission criteria include surgical emergency (eg, appendicitis), tubo-ovarian abscess, pregnancy, severe illness, nausea and vomiting, high fever, inability to follow or tolerate an outpatient oral regimen, and lack of clinical response to oral antimicrobial therapy.5
Follow-up care. Clinical improvement (ie, reduction in abdominal, uterine, adnexal, and cervical motion tenderness) should occur within 72 hours of antimicrobial therapy initiation. If it does not, hospital admission or adjustment in antimicrobial regimen should be considered, as well as additional diagnostic testing (eg, laparoscopy). In addition, all women with chlamydial- or gonococcal-related PID should return in three months for surveillance testing.22
COMPLICATIONS
Long-term complications—including infertility, chronic pelvic pain, and ectopic pregnancy—may occur, even when there has been a clinical response to adequate treatment. Data from the PID Evaluation and Clinical Health (PEACH) study were analyzed to assess long-term sequelae at seven years postdiagnosis and treatment. The researchers found that about 21% of women experienced recurrent PID, 19% developed infertility, and 42% reported chronic pelvic pain.3 Other research has also shown that repeat episodes of PID and delayed treatment increase the risk for long-term complications.23,24
SCREENING AND PREVENTION
Ten percent of women with an untreated STI will go on to develop PID.4 It is imperative to educate patients on the dangers and consequences of STIs when they become sexually active. Adolescents benefit the most from preventive education; this group is twice as likely as any other age group to be diagnosed with PID due to their inclination toward risky sexual behavior. Additionally, younger women tend to have a more friable cervix, increasing their risk for infection.25,26 Providers should promote safe sexual practices, such as condom use and less frequent partner exchange, in order to reduce STI exposure.
In 2015, the rate of reported cases of C trachomatis was 645.5 per 100,000 females, and of N gonorrheae, 107.2 per 100,000 females.23 The United States Preventive Services Task Force and the CDC recommend annual screening for chlamydia and gonorrhea in all sexually active women younger than 25, as well as sexually active women ages 25 and older who are considered at increased risk.5
CONCLUSION
PID is often difficult to diagnose, since patients may be asymptomatic or present with vague symptoms. Clinicians should maintain a high level of suspicion for PID in adolescent females due to the high incidence of STI exposure in this population. The best way to prevent long-term complications of PID is to prevent the first episode of PID and/or first exposure to STIs. Therefore, clinicians should be proactive in offering STI screenings to all sexually active patients younger than 25 who request care, regardless of their chief complaint, and educating patients on the potential long-term effects of PID and STIs.
1. Leichliter JS, Chandra A, Aral SO. Correlates of self-reported pelvic inflammatory disease treatment in sexually experienced reproductive-aged women in the United States, 1995 and 2006-2010. Sex Transm Dis. 2013;40(5):413-418.
2. Owusu-Edusei K Jr, Bohm MK, Chesson HW, Kent CK. Chlamydia screening and pelvic inflammatory disease: insights from exploratory time-series analyses. Am J Prev Med. 2010;38(6):652-657.
3. Trent M, Bass D, Ness RB, Haggerty C. Recurrent PID, subsequent STI, and reproductive health outcomes: findings from the PID evaluation and clinical health (PEACH) study. Sex Transm Dis. 2011;38(9):879-881.
4. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infect Dis Clin North Am. 2013;27(4):793-809.
5. CDC. Pelvic inflammatory disease (PID). www.cdc.gov/std/tg2015/pid.htm. Accessed July 13, 2017.
6. Burnett AM, Anderson CP, Zwank MD. Laboratory-confirmed gonorrhea and/or chlamydia rates in clinically diagnosed pelvic inflammatory disease and cervicitis. Am J Emerg Med. 2012;30:1114–1117.
7. Bjartling C, Osser S, Persson K. The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. BJOG. 2010;117(3):361-364.
8. Ness RB, Kip KE, Hillier SL, et al. A cluster analysis of bacterial vaginosis-associated microflora and pelvic inflammatory disease. Am J Epidemiol. 2005;162(6):585-590.
9. Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis and risk of pelvic inflammatory disease. Obstet Gynecol. 2004;104(4):761-769.
10. Cherpes TL, Wiesenfeld HC, Melan MA, et al. The associations between pelvic inflammatory disease, Trichomonas vaginalis infection, and positive herpes simplex virus type 2 serology. Sex Transm Dis. 2006;33(12):747-752.
11. Simms I, Stephenson JM, Mallinson H, et al. Risk factors associated with pelvic inflammatory disease. Sex Transm Infect. 2006;82(6):452-457.
12. Schindlbeck C, Dziura D, Mylonas I. Diagnosis of pelvic inflammatory disease (PID): intra-operative findings and comparison of vaginal and intra-abdominal cultures. Arch Gynecol Obstet. 2014;289(6):1263-1269.
13. CDC. 2015 sexually transmitted diseases treatment guidelines. www.cdc.gov/std/tg2015/default.htm. Accessed September 6, 2017.
14. Korn AP, Hessol NA, Padian NS, et al. Risk factors for plasma cell endometritis among women with cervical Neisseria gonorrhoeae, cervical Chlamydia trachomatis, or bacterial vaginosis. Am J Obstet Gynecol. 1998;178(5):987-990.
15. Wiesenfeld HC, Sweet RL, Ness RB, et al. Comparison of acute and subclinical pelvic inflammatory disease. Sex Transm Dis. 2005;32(7):400-405.
16. Peipert JF, Ness RB, Blume J, et al. Clinical predictors of endometritis in women with symptoms and signs of pelvic inflammatory disease. Am J Obstet Gynecol. 2001;184(5):856-864.
17. Gaitán H, Angel E, Diaz R, et al. Accuracy of five different diagnostic techniques in mild-to-moderate pelvic inflammatory disease. Infect Dis Obstet Gynecol. 2002;10(4):171-180.
18. Tukeva TA, Aronen HJ, Karjalainen PT, et al. MR imaging in pelvic inflammatory disease: comparison with laparoscopy and US. Radiology. 1999;210(1):209-216.
19. Morino M, Pellegrino L, Castagna E, et al. Acute nonspecific abdominal pain. Ann Surg. 2006;244(6):881-888.
20. Woods JL, Scurlock AM, Hensel DJ. Pelvic inflammatory disease in the adolescent: understanding diagnosis and treatment as a health care provider. Pediatric Emergency Care. 2013;29(6):720-725.
21. LeFevre ML; U.S. Preventive Services Task Force. Screening for chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902-910.
22. Hosenfeld CB, Workowski KA, Berman S, et al. Repeat infection with Chlamydia and gonorrhea among females: a systematic review of the literature. Sex Transm Dis. 2009;36(8):478-489.
23. CDC. Sexually transmitted disease surveillance. www.cdc.gov/std/stats15/STD-Surveillance-2015-print.pdf. Accessed July 13, 2017.
24. Hillis SD, Joesoef R, Marchbanks PA, et al. Delayed care of pelvic inflammatory disease as a risk factor for impaired fertility. Am J Obstet Gynecol. 1993;168(5):1503-1509.
25. Goyal M, Hersh A, Luan X, et al. National trends in pelvic inflammatory disease among adolescents in the emergency department. J Adolesc Health. 2013;53(2):249-252.
26. Gray-Swain MR, Peipert JF. Pelvic inflammatory disease in adolescents. Curr Opin Obstet Gynecol. 2006;18(5):503-510.
27. Łój B, Brodowska A, Ciecwiez S, et al. The role of serological testing for Chlamydia trachomatis in differential diagnosis of pelvic pain. Ann Agric Environ Med. 2016;23(3):506-510.
28. Sam JW, Jacobs JE, Birnbaum BA. Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics. 2002;22(6):1327-1 334.
IN THIS ARTICLE
- Diagnostic tests
- Complications of PID
- CDC treatment regimens
Pelvic inflammatory disease (PID) is an ascending polymicrobial infection of the female upper reproductive tract that primarily affects sexually active women ages 15 to 29. Around 5% of sexually active women in the United States were treated for PID from 2011-2013.1 The rates and severity of PID have declined in North America and Western Europe due to overall decrease in sexually transmitted infection (STI) rates, improved screening initiatives for Chlamydia trachomatis, better treatment compliance secondary to increased access to antibiotics, and diagnostic tests with higher sensitivity.2 Despite this rate reduction, PID remains a major public health concern given the significant long-term complications, which include infertility, ectopic pregnancy, and chronic pelvic pain.3
EPIDEMIOLOGY AND PATHOGENESIS
PID is caused by sexually transmitted bacteria or enteric organisms that have spread to internal reproductive organs. Historically, the two most common pathogens identified in cases of PID have been Chlamydia trachomatis and Neisseria gonorrhoeae; however, the decline in rates of gonorrhea has led to a diminished role for N gonorrhoeae (though it continues to be associated with more severe cases).4,5
More recent studies have suggested a shift in the causative organisms; less than half of women diagnosed with acute PID test positive for either N gonorrhoeae or C trachomatis.6 Emerging infectious agents associated with PID include Mycoplasma genitalium, Gardnerella vaginalis, and bacterial vaginosis–associated bacteria.5,7,8-10
RISK FACTORS
Women ages 15 to 25 are at an increased risk for PID. The high prevalence in this age group may be attributable to high-risk behaviors, including a high number of sexual partners, high frequency of new sexual partners, and engagement in sexual intercourse without condoms.11
Taking an accurate sexual history is imperative. Clinicians should maintain a high level of suspicion for PID in women with a history of the disease, as 25% will experience recurrence.12
Clinicians should not be deterred from screening for STIs and cervical cancer in women who report having sex with other women. In addition, transgender patients should be assessed for STIs and HIV-related risks based on current anatomy sexual practices.13
PHYSICAL EXAM
While some cases of PID are asymptomatic, the typical presentation includes bilateral abdominal pain and/or pelvic pain, with onset during or shortly after menses. The pain often worsens with movement and coitus. Associated signs and symptoms include abnormal uterine bleeding or vaginal discharge; dysuria; fever and chills; frequent urination; lower back pain; and nausea and/or vomiting.14,15
All females suspected of having PID should undergo both a bimanual exam and a speculum exam. On bimanual examination, adnexal tenderness has the highest sensitivity (93% to 95.5%) for ruling out acute PID, whereas on speculum exam, purulent endocervical discharge has the highest specificity (93%).16,17 Bimanual exam findings suggestive of PID include cervical motion tenderness, uterine tenderness, and/or adnexal tenderness. Suggestive speculum exam findings include abnormal discoloration or texture of the cervix and/or endocervical mucopurulent discharge.5,16,17
One cardinal rule that should not be overlooked is that all females of reproductive age who present with abdominal pain and/or pelvic pain should take a pregnancy test to rule out ectopic pregnancy and any other pregnancy-related complications.
DIAGNOSIS
The diagnosis of PID relies on clinical judgement and a high index of suspicion.5,18 The CDC’s diagnostic criteria for acute PID include
- Sexually active female AND
- Pelvic or lower abdominal pain AND
- Cervical motion tenderness OR uterine tenderness OR adnexal tenderness.5
Additional findings that support the diagnosis include
- Abnormal cervical mucopurulent discharge or cervical friability
- Abundant white blood cells (WBCs) on saline microscopy of vaginal fluid
- Elevated C-reactive protein
- Elevated erythrocyte sedimentation rate
- Laboratory documentation of infection with C trachomatis or N gonorrhea
- Oral temperature > 101°F.5,18
The CDC notes that the first two findings (mucopurulent discharge and evidence of WBCs on microscopy) occur in most women with PID; in their absence, the diagnosis is unlikely and other sources of pain should be considered.5 The differential for PID includes acute appendicitis; adhesions; carcinoid tumor; cholecystitis; ectopic pregnancy; endometriosis; inflammatory bowel disease; and ovarian cyst.19
Given the variability in presentation, clinicians may find it useful to perform further diagnostic testing. There are additional laboratory tests that may be ordered for patients with a suspected diagnosis of PID (see Table 1).
TREATMENT
According to the CDC’s 2015 treatment guidelines for PID, a negative endocervical exam and negative microbial screening do not rule out an upper reproductive tract infection. Therefore, all sexually active women who present with lower abdominal pain and/or pelvic pain and have evidence of cervical motion, uterine, or adnexal tenderness on bimanual exam should be treated immediately.5
Treatment guidelines are outlined in Table 2. The polymicrobial nature of PID requires gram-negative antibiotic coverage, such as doxycycline plus a second/third-generation cephalosporin.5 Clinicians should note that cefoxitin, a second-generation cephalosporin, is recommended as firstline therapy for inpatients, as it has better anaerobic coverage than ceftriaxone.19 A targeted change in antibiotic coverage—such as inclusion of a macrolide and/or metronidazole—might be necessary if a causative organism is identified by culture.7
Treatment is indicated for all patients with a presumptive diagnosis of PID regardless of symptoms or exam findings, as PID may be asymptomatic and long-term sequelae (eg, infertility, ectopic pregnancy) are often irreversible. At-risk patients include sexually active adolescents, women with multiple sexual partners, women with a history of STI, those whose sexual partner has an STI, and women living in communities with a high prevalence of disease.20,21
Women being treated for PID should be advised to abstain from sexual intercourse until symptoms have resolved, treatment is completed, and any sexual partners have been treated as well. It is essential to emphasize to patients (and their partners) the importance of compliance to treatment regimens and the risk for PID co-infection and reinfection, as recurrence leads to an increase in long-term complications.5
Treatment of sexual partners. The CDC instructs that a woman’s most recent partner should be treated if she had sexual intercourse within 60 days of onset of symptoms or diagnosis. Furthermore, men who have had sexual contact with a woman who has PID in the 60 days prior to onset of her symptoms should be evaluated, tested, and treated for chlamydia and gonorrhea, regardless of the etiology of PID or the pathogens isolated from the woman.5
Admission criteria. Hospitalization should be based on provider judgment despite patient age. The suggested admission criteria include surgical emergency (eg, appendicitis), tubo-ovarian abscess, pregnancy, severe illness, nausea and vomiting, high fever, inability to follow or tolerate an outpatient oral regimen, and lack of clinical response to oral antimicrobial therapy.5
Follow-up care. Clinical improvement (ie, reduction in abdominal, uterine, adnexal, and cervical motion tenderness) should occur within 72 hours of antimicrobial therapy initiation. If it does not, hospital admission or adjustment in antimicrobial regimen should be considered, as well as additional diagnostic testing (eg, laparoscopy). In addition, all women with chlamydial- or gonococcal-related PID should return in three months for surveillance testing.22
COMPLICATIONS
Long-term complications—including infertility, chronic pelvic pain, and ectopic pregnancy—may occur, even when there has been a clinical response to adequate treatment. Data from the PID Evaluation and Clinical Health (PEACH) study were analyzed to assess long-term sequelae at seven years postdiagnosis and treatment. The researchers found that about 21% of women experienced recurrent PID, 19% developed infertility, and 42% reported chronic pelvic pain.3 Other research has also shown that repeat episodes of PID and delayed treatment increase the risk for long-term complications.23,24
SCREENING AND PREVENTION
Ten percent of women with an untreated STI will go on to develop PID.4 It is imperative to educate patients on the dangers and consequences of STIs when they become sexually active. Adolescents benefit the most from preventive education; this group is twice as likely as any other age group to be diagnosed with PID due to their inclination toward risky sexual behavior. Additionally, younger women tend to have a more friable cervix, increasing their risk for infection.25,26 Providers should promote safe sexual practices, such as condom use and less frequent partner exchange, in order to reduce STI exposure.
In 2015, the rate of reported cases of C trachomatis was 645.5 per 100,000 females, and of N gonorrheae, 107.2 per 100,000 females.23 The United States Preventive Services Task Force and the CDC recommend annual screening for chlamydia and gonorrhea in all sexually active women younger than 25, as well as sexually active women ages 25 and older who are considered at increased risk.5
CONCLUSION
PID is often difficult to diagnose, since patients may be asymptomatic or present with vague symptoms. Clinicians should maintain a high level of suspicion for PID in adolescent females due to the high incidence of STI exposure in this population. The best way to prevent long-term complications of PID is to prevent the first episode of PID and/or first exposure to STIs. Therefore, clinicians should be proactive in offering STI screenings to all sexually active patients younger than 25 who request care, regardless of their chief complaint, and educating patients on the potential long-term effects of PID and STIs.
IN THIS ARTICLE
- Diagnostic tests
- Complications of PID
- CDC treatment regimens
Pelvic inflammatory disease (PID) is an ascending polymicrobial infection of the female upper reproductive tract that primarily affects sexually active women ages 15 to 29. Around 5% of sexually active women in the United States were treated for PID from 2011-2013.1 The rates and severity of PID have declined in North America and Western Europe due to overall decrease in sexually transmitted infection (STI) rates, improved screening initiatives for Chlamydia trachomatis, better treatment compliance secondary to increased access to antibiotics, and diagnostic tests with higher sensitivity.2 Despite this rate reduction, PID remains a major public health concern given the significant long-term complications, which include infertility, ectopic pregnancy, and chronic pelvic pain.3
EPIDEMIOLOGY AND PATHOGENESIS
PID is caused by sexually transmitted bacteria or enteric organisms that have spread to internal reproductive organs. Historically, the two most common pathogens identified in cases of PID have been Chlamydia trachomatis and Neisseria gonorrhoeae; however, the decline in rates of gonorrhea has led to a diminished role for N gonorrhoeae (though it continues to be associated with more severe cases).4,5
More recent studies have suggested a shift in the causative organisms; less than half of women diagnosed with acute PID test positive for either N gonorrhoeae or C trachomatis.6 Emerging infectious agents associated with PID include Mycoplasma genitalium, Gardnerella vaginalis, and bacterial vaginosis–associated bacteria.5,7,8-10
RISK FACTORS
Women ages 15 to 25 are at an increased risk for PID. The high prevalence in this age group may be attributable to high-risk behaviors, including a high number of sexual partners, high frequency of new sexual partners, and engagement in sexual intercourse without condoms.11
Taking an accurate sexual history is imperative. Clinicians should maintain a high level of suspicion for PID in women with a history of the disease, as 25% will experience recurrence.12
Clinicians should not be deterred from screening for STIs and cervical cancer in women who report having sex with other women. In addition, transgender patients should be assessed for STIs and HIV-related risks based on current anatomy sexual practices.13
PHYSICAL EXAM
While some cases of PID are asymptomatic, the typical presentation includes bilateral abdominal pain and/or pelvic pain, with onset during or shortly after menses. The pain often worsens with movement and coitus. Associated signs and symptoms include abnormal uterine bleeding or vaginal discharge; dysuria; fever and chills; frequent urination; lower back pain; and nausea and/or vomiting.14,15
All females suspected of having PID should undergo both a bimanual exam and a speculum exam. On bimanual examination, adnexal tenderness has the highest sensitivity (93% to 95.5%) for ruling out acute PID, whereas on speculum exam, purulent endocervical discharge has the highest specificity (93%).16,17 Bimanual exam findings suggestive of PID include cervical motion tenderness, uterine tenderness, and/or adnexal tenderness. Suggestive speculum exam findings include abnormal discoloration or texture of the cervix and/or endocervical mucopurulent discharge.5,16,17
One cardinal rule that should not be overlooked is that all females of reproductive age who present with abdominal pain and/or pelvic pain should take a pregnancy test to rule out ectopic pregnancy and any other pregnancy-related complications.
DIAGNOSIS
The diagnosis of PID relies on clinical judgement and a high index of suspicion.5,18 The CDC’s diagnostic criteria for acute PID include
- Sexually active female AND
- Pelvic or lower abdominal pain AND
- Cervical motion tenderness OR uterine tenderness OR adnexal tenderness.5
Additional findings that support the diagnosis include
- Abnormal cervical mucopurulent discharge or cervical friability
- Abundant white blood cells (WBCs) on saline microscopy of vaginal fluid
- Elevated C-reactive protein
- Elevated erythrocyte sedimentation rate
- Laboratory documentation of infection with C trachomatis or N gonorrhea
- Oral temperature > 101°F.5,18
The CDC notes that the first two findings (mucopurulent discharge and evidence of WBCs on microscopy) occur in most women with PID; in their absence, the diagnosis is unlikely and other sources of pain should be considered.5 The differential for PID includes acute appendicitis; adhesions; carcinoid tumor; cholecystitis; ectopic pregnancy; endometriosis; inflammatory bowel disease; and ovarian cyst.19
Given the variability in presentation, clinicians may find it useful to perform further diagnostic testing. There are additional laboratory tests that may be ordered for patients with a suspected diagnosis of PID (see Table 1).
TREATMENT
According to the CDC’s 2015 treatment guidelines for PID, a negative endocervical exam and negative microbial screening do not rule out an upper reproductive tract infection. Therefore, all sexually active women who present with lower abdominal pain and/or pelvic pain and have evidence of cervical motion, uterine, or adnexal tenderness on bimanual exam should be treated immediately.5
Treatment guidelines are outlined in Table 2. The polymicrobial nature of PID requires gram-negative antibiotic coverage, such as doxycycline plus a second/third-generation cephalosporin.5 Clinicians should note that cefoxitin, a second-generation cephalosporin, is recommended as firstline therapy for inpatients, as it has better anaerobic coverage than ceftriaxone.19 A targeted change in antibiotic coverage—such as inclusion of a macrolide and/or metronidazole—might be necessary if a causative organism is identified by culture.7
Treatment is indicated for all patients with a presumptive diagnosis of PID regardless of symptoms or exam findings, as PID may be asymptomatic and long-term sequelae (eg, infertility, ectopic pregnancy) are often irreversible. At-risk patients include sexually active adolescents, women with multiple sexual partners, women with a history of STI, those whose sexual partner has an STI, and women living in communities with a high prevalence of disease.20,21
Women being treated for PID should be advised to abstain from sexual intercourse until symptoms have resolved, treatment is completed, and any sexual partners have been treated as well. It is essential to emphasize to patients (and their partners) the importance of compliance to treatment regimens and the risk for PID co-infection and reinfection, as recurrence leads to an increase in long-term complications.5
Treatment of sexual partners. The CDC instructs that a woman’s most recent partner should be treated if she had sexual intercourse within 60 days of onset of symptoms or diagnosis. Furthermore, men who have had sexual contact with a woman who has PID in the 60 days prior to onset of her symptoms should be evaluated, tested, and treated for chlamydia and gonorrhea, regardless of the etiology of PID or the pathogens isolated from the woman.5
Admission criteria. Hospitalization should be based on provider judgment despite patient age. The suggested admission criteria include surgical emergency (eg, appendicitis), tubo-ovarian abscess, pregnancy, severe illness, nausea and vomiting, high fever, inability to follow or tolerate an outpatient oral regimen, and lack of clinical response to oral antimicrobial therapy.5
Follow-up care. Clinical improvement (ie, reduction in abdominal, uterine, adnexal, and cervical motion tenderness) should occur within 72 hours of antimicrobial therapy initiation. If it does not, hospital admission or adjustment in antimicrobial regimen should be considered, as well as additional diagnostic testing (eg, laparoscopy). In addition, all women with chlamydial- or gonococcal-related PID should return in three months for surveillance testing.22
COMPLICATIONS
Long-term complications—including infertility, chronic pelvic pain, and ectopic pregnancy—may occur, even when there has been a clinical response to adequate treatment. Data from the PID Evaluation and Clinical Health (PEACH) study were analyzed to assess long-term sequelae at seven years postdiagnosis and treatment. The researchers found that about 21% of women experienced recurrent PID, 19% developed infertility, and 42% reported chronic pelvic pain.3 Other research has also shown that repeat episodes of PID and delayed treatment increase the risk for long-term complications.23,24
SCREENING AND PREVENTION
Ten percent of women with an untreated STI will go on to develop PID.4 It is imperative to educate patients on the dangers and consequences of STIs when they become sexually active. Adolescents benefit the most from preventive education; this group is twice as likely as any other age group to be diagnosed with PID due to their inclination toward risky sexual behavior. Additionally, younger women tend to have a more friable cervix, increasing their risk for infection.25,26 Providers should promote safe sexual practices, such as condom use and less frequent partner exchange, in order to reduce STI exposure.
In 2015, the rate of reported cases of C trachomatis was 645.5 per 100,000 females, and of N gonorrheae, 107.2 per 100,000 females.23 The United States Preventive Services Task Force and the CDC recommend annual screening for chlamydia and gonorrhea in all sexually active women younger than 25, as well as sexually active women ages 25 and older who are considered at increased risk.5
CONCLUSION
PID is often difficult to diagnose, since patients may be asymptomatic or present with vague symptoms. Clinicians should maintain a high level of suspicion for PID in adolescent females due to the high incidence of STI exposure in this population. The best way to prevent long-term complications of PID is to prevent the first episode of PID and/or first exposure to STIs. Therefore, clinicians should be proactive in offering STI screenings to all sexually active patients younger than 25 who request care, regardless of their chief complaint, and educating patients on the potential long-term effects of PID and STIs.
1. Leichliter JS, Chandra A, Aral SO. Correlates of self-reported pelvic inflammatory disease treatment in sexually experienced reproductive-aged women in the United States, 1995 and 2006-2010. Sex Transm Dis. 2013;40(5):413-418.
2. Owusu-Edusei K Jr, Bohm MK, Chesson HW, Kent CK. Chlamydia screening and pelvic inflammatory disease: insights from exploratory time-series analyses. Am J Prev Med. 2010;38(6):652-657.
3. Trent M, Bass D, Ness RB, Haggerty C. Recurrent PID, subsequent STI, and reproductive health outcomes: findings from the PID evaluation and clinical health (PEACH) study. Sex Transm Dis. 2011;38(9):879-881.
4. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infect Dis Clin North Am. 2013;27(4):793-809.
5. CDC. Pelvic inflammatory disease (PID). www.cdc.gov/std/tg2015/pid.htm. Accessed July 13, 2017.
6. Burnett AM, Anderson CP, Zwank MD. Laboratory-confirmed gonorrhea and/or chlamydia rates in clinically diagnosed pelvic inflammatory disease and cervicitis. Am J Emerg Med. 2012;30:1114–1117.
7. Bjartling C, Osser S, Persson K. The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. BJOG. 2010;117(3):361-364.
8. Ness RB, Kip KE, Hillier SL, et al. A cluster analysis of bacterial vaginosis-associated microflora and pelvic inflammatory disease. Am J Epidemiol. 2005;162(6):585-590.
9. Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis and risk of pelvic inflammatory disease. Obstet Gynecol. 2004;104(4):761-769.
10. Cherpes TL, Wiesenfeld HC, Melan MA, et al. The associations between pelvic inflammatory disease, Trichomonas vaginalis infection, and positive herpes simplex virus type 2 serology. Sex Transm Dis. 2006;33(12):747-752.
11. Simms I, Stephenson JM, Mallinson H, et al. Risk factors associated with pelvic inflammatory disease. Sex Transm Infect. 2006;82(6):452-457.
12. Schindlbeck C, Dziura D, Mylonas I. Diagnosis of pelvic inflammatory disease (PID): intra-operative findings and comparison of vaginal and intra-abdominal cultures. Arch Gynecol Obstet. 2014;289(6):1263-1269.
13. CDC. 2015 sexually transmitted diseases treatment guidelines. www.cdc.gov/std/tg2015/default.htm. Accessed September 6, 2017.
14. Korn AP, Hessol NA, Padian NS, et al. Risk factors for plasma cell endometritis among women with cervical Neisseria gonorrhoeae, cervical Chlamydia trachomatis, or bacterial vaginosis. Am J Obstet Gynecol. 1998;178(5):987-990.
15. Wiesenfeld HC, Sweet RL, Ness RB, et al. Comparison of acute and subclinical pelvic inflammatory disease. Sex Transm Dis. 2005;32(7):400-405.
16. Peipert JF, Ness RB, Blume J, et al. Clinical predictors of endometritis in women with symptoms and signs of pelvic inflammatory disease. Am J Obstet Gynecol. 2001;184(5):856-864.
17. Gaitán H, Angel E, Diaz R, et al. Accuracy of five different diagnostic techniques in mild-to-moderate pelvic inflammatory disease. Infect Dis Obstet Gynecol. 2002;10(4):171-180.
18. Tukeva TA, Aronen HJ, Karjalainen PT, et al. MR imaging in pelvic inflammatory disease: comparison with laparoscopy and US. Radiology. 1999;210(1):209-216.
19. Morino M, Pellegrino L, Castagna E, et al. Acute nonspecific abdominal pain. Ann Surg. 2006;244(6):881-888.
20. Woods JL, Scurlock AM, Hensel DJ. Pelvic inflammatory disease in the adolescent: understanding diagnosis and treatment as a health care provider. Pediatric Emergency Care. 2013;29(6):720-725.
21. LeFevre ML; U.S. Preventive Services Task Force. Screening for chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902-910.
22. Hosenfeld CB, Workowski KA, Berman S, et al. Repeat infection with Chlamydia and gonorrhea among females: a systematic review of the literature. Sex Transm Dis. 2009;36(8):478-489.
23. CDC. Sexually transmitted disease surveillance. www.cdc.gov/std/stats15/STD-Surveillance-2015-print.pdf. Accessed July 13, 2017.
24. Hillis SD, Joesoef R, Marchbanks PA, et al. Delayed care of pelvic inflammatory disease as a risk factor for impaired fertility. Am J Obstet Gynecol. 1993;168(5):1503-1509.
25. Goyal M, Hersh A, Luan X, et al. National trends in pelvic inflammatory disease among adolescents in the emergency department. J Adolesc Health. 2013;53(2):249-252.
26. Gray-Swain MR, Peipert JF. Pelvic inflammatory disease in adolescents. Curr Opin Obstet Gynecol. 2006;18(5):503-510.
27. Łój B, Brodowska A, Ciecwiez S, et al. The role of serological testing for Chlamydia trachomatis in differential diagnosis of pelvic pain. Ann Agric Environ Med. 2016;23(3):506-510.
28. Sam JW, Jacobs JE, Birnbaum BA. Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics. 2002;22(6):1327-1 334.
1. Leichliter JS, Chandra A, Aral SO. Correlates of self-reported pelvic inflammatory disease treatment in sexually experienced reproductive-aged women in the United States, 1995 and 2006-2010. Sex Transm Dis. 2013;40(5):413-418.
2. Owusu-Edusei K Jr, Bohm MK, Chesson HW, Kent CK. Chlamydia screening and pelvic inflammatory disease: insights from exploratory time-series analyses. Am J Prev Med. 2010;38(6):652-657.
3. Trent M, Bass D, Ness RB, Haggerty C. Recurrent PID, subsequent STI, and reproductive health outcomes: findings from the PID evaluation and clinical health (PEACH) study. Sex Transm Dis. 2011;38(9):879-881.
4. Mitchell C, Prabhu M. Pelvic inflammatory disease: current concepts in pathogenesis, diagnosis and treatment. Infect Dis Clin North Am. 2013;27(4):793-809.
5. CDC. Pelvic inflammatory disease (PID). www.cdc.gov/std/tg2015/pid.htm. Accessed July 13, 2017.
6. Burnett AM, Anderson CP, Zwank MD. Laboratory-confirmed gonorrhea and/or chlamydia rates in clinically diagnosed pelvic inflammatory disease and cervicitis. Am J Emerg Med. 2012;30:1114–1117.
7. Bjartling C, Osser S, Persson K. The association between Mycoplasma genitalium and pelvic inflammatory disease after termination of pregnancy. BJOG. 2010;117(3):361-364.
8. Ness RB, Kip KE, Hillier SL, et al. A cluster analysis of bacterial vaginosis-associated microflora and pelvic inflammatory disease. Am J Epidemiol. 2005;162(6):585-590.
9. Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis and risk of pelvic inflammatory disease. Obstet Gynecol. 2004;104(4):761-769.
10. Cherpes TL, Wiesenfeld HC, Melan MA, et al. The associations between pelvic inflammatory disease, Trichomonas vaginalis infection, and positive herpes simplex virus type 2 serology. Sex Transm Dis. 2006;33(12):747-752.
11. Simms I, Stephenson JM, Mallinson H, et al. Risk factors associated with pelvic inflammatory disease. Sex Transm Infect. 2006;82(6):452-457.
12. Schindlbeck C, Dziura D, Mylonas I. Diagnosis of pelvic inflammatory disease (PID): intra-operative findings and comparison of vaginal and intra-abdominal cultures. Arch Gynecol Obstet. 2014;289(6):1263-1269.
13. CDC. 2015 sexually transmitted diseases treatment guidelines. www.cdc.gov/std/tg2015/default.htm. Accessed September 6, 2017.
14. Korn AP, Hessol NA, Padian NS, et al. Risk factors for plasma cell endometritis among women with cervical Neisseria gonorrhoeae, cervical Chlamydia trachomatis, or bacterial vaginosis. Am J Obstet Gynecol. 1998;178(5):987-990.
15. Wiesenfeld HC, Sweet RL, Ness RB, et al. Comparison of acute and subclinical pelvic inflammatory disease. Sex Transm Dis. 2005;32(7):400-405.
16. Peipert JF, Ness RB, Blume J, et al. Clinical predictors of endometritis in women with symptoms and signs of pelvic inflammatory disease. Am J Obstet Gynecol. 2001;184(5):856-864.
17. Gaitán H, Angel E, Diaz R, et al. Accuracy of five different diagnostic techniques in mild-to-moderate pelvic inflammatory disease. Infect Dis Obstet Gynecol. 2002;10(4):171-180.
18. Tukeva TA, Aronen HJ, Karjalainen PT, et al. MR imaging in pelvic inflammatory disease: comparison with laparoscopy and US. Radiology. 1999;210(1):209-216.
19. Morino M, Pellegrino L, Castagna E, et al. Acute nonspecific abdominal pain. Ann Surg. 2006;244(6):881-888.
20. Woods JL, Scurlock AM, Hensel DJ. Pelvic inflammatory disease in the adolescent: understanding diagnosis and treatment as a health care provider. Pediatric Emergency Care. 2013;29(6):720-725.
21. LeFevre ML; U.S. Preventive Services Task Force. Screening for chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902-910.
22. Hosenfeld CB, Workowski KA, Berman S, et al. Repeat infection with Chlamydia and gonorrhea among females: a systematic review of the literature. Sex Transm Dis. 2009;36(8):478-489.
23. CDC. Sexually transmitted disease surveillance. www.cdc.gov/std/stats15/STD-Surveillance-2015-print.pdf. Accessed July 13, 2017.
24. Hillis SD, Joesoef R, Marchbanks PA, et al. Delayed care of pelvic inflammatory disease as a risk factor for impaired fertility. Am J Obstet Gynecol. 1993;168(5):1503-1509.
25. Goyal M, Hersh A, Luan X, et al. National trends in pelvic inflammatory disease among adolescents in the emergency department. J Adolesc Health. 2013;53(2):249-252.
26. Gray-Swain MR, Peipert JF. Pelvic inflammatory disease in adolescents. Curr Opin Obstet Gynecol. 2006;18(5):503-510.
27. Łój B, Brodowska A, Ciecwiez S, et al. The role of serological testing for Chlamydia trachomatis in differential diagnosis of pelvic pain. Ann Agric Environ Med. 2016;23(3):506-510.
28. Sam JW, Jacobs JE, Birnbaum BA. Spectrum of CT findings in acute pyogenic pelvic inflammatory disease. Radiographics. 2002;22(6):1327-1 334.
Can we stop worrying about the age of blood?
Blood transfusions are common in critically ill patients; two in five adults admitted to an ICU receive at least one transfusion during their hospitalization (Corwin HL, et al. Crit Care Med. 2004;32[1]:39). Recently, there has been growing concern about the potential dangers involved with prolonged blood storage. Several provocative observational and retrospective studies found that prolonged storage time (ie, the age of the blood being transfused) negatively affects clinical outcomes (Wang D, et al. Transfusion. 2012;52[6]:1184). But now, some newly published trials on blood transfusion practice, including one published in late September 2017 (Cooper DJ, et al. N Engl J Med. Published online, September 27, 2017) seem to debunk much of this literature. Was all of the concern about age of blood overblown?
The appeal of “fresh” blood is intuitive. As consumers, we’re conditioned that the fresher the better. Fresh food tastes best. Carbonated beverages go “flat” over time. The newest iPhone® device is superior to your old one. So, of course, it follows that fresh blood is also better for your health than older blood.
But, in order to have a viable transfusion service, blood has to be stored. Blood is a scarce resource, and blood banks need to keep an adequate supply on hand for expected clinical necessities, as well as for emergencies. Donors can’t be on standby, waiting in the hospital to provide immediate whole blood transfusion. Also, blood needs to be tested for infections and for potential interactions with the patient, and whole blood must be broken down into individual components for transfusion. All of this requires time and storage.![]()
In a randomized study of 100 critically ill adults supported by mechanical ventilation, 50 were randomized to receive “fresh” blood (median storage age 4 days, interquartile range 3-5 days) and 50 were randomized to receive “standard” blood (median storage age 26.5 days, interquartile range 21-36 days) (Kor DJ, et al. Am J Respir Crit Care Med. 2012;185[8]:842). The primary outcome was gas exchange, as prolonged storage of red blood cells could potentially lead to an increased inflammatory response in patients. However, the authors found no difference in gas exchange between the two groups, and there were no differences in immunologic function or coagulation status.
The ABLE (Age of Blood Evaluation) trial was a randomized, blinded trial of transfusion practices in critically ill patients (Lacroix J, et al. N Engl J Med. 2015;372:1410). In 64 centers in Canada and Europe, 2,430 critically ill adults were randomized to receive either “fresh” blood (mean storage age 6.1 ± 4.9 days) or “standard” blood (mean storage age 22.0 ± 8.4 days). The primary outcome was 90-day mortality, with a power of 90% to detect a 5% change in mortality between the two groups. The investigators found no statistically significant difference in 90-day mortality between the “fresh” and “standard” groups (37% vs 35.3%; hazard ratio 1.1; 95% CI 0.9 – 1.2). Additionally, there were no differences in secondary outcomes, including multiorgan system dysfunction, duration of supportive care, or development of nosocomial infections.
The INFORM (Informing Fresh versus Old Red Cell Management) trial was a randomized study of patients hospitalized in six centers in Canada, Australia, Israel, and the United States (Heddle NM, et al. N Engl J Med. 2016;375[2]:1937). A total of 24,736 patients received transfusions with either “fresh” blood (median storage age 11 days) or “standard” blood (median storage age 23 days). The primary outcome was in-hospital death, with a 90% power to detect a 15% lower relative risk. When comparing the 8,215 patients who received “fresh” blood and the 16,521 patients who received “standard” blood, the authors found no difference in mortality between the two groups (9.1% vs 8.8%; odds ratio 1.04; 95% CI 0.95 to 1.14). Furthermore, there were no differences in outcomes in the high-risk subgroups that included patients with cancer, patients in the ICU, and patients undergoing cardiovascular surgery.
A meta-analysis examined 12 trials of patients who received “fresh” blood compared with those who received “older” or “standard” blood (Alexander PE, et al. Blood. 2016;127[4]:400); 5,229 patients were included in these trials, in which “fresh” blood was defined as blood stored for 3 to 10 days and “older” blood was stored for longer durations. There was no difference in mortality between the two groups (relative risk 1.04; 95% CI 0.94 - 1.14), and no difference in adverse events (relative risk 1.02; 95% CI 0.91 - 1.14). However, perhaps surprisingly, “fresh” blood was associated with an increased risk of nosocomial infections (relative risk 1.09; 95% CI 1.00 - 1.18).

So, can we stop worrying about the age of the blood that we are about to transfuse? Probably. Taken together, these studies suggest that differences in the duration of red blood cell storage allowed within current US FDA standards aren’t clinically relevant, even in critically ill patients. At least, for now, the current practices for age of blood and duration of storage appear unrelated to adverse clinical outcomes.
Dr. Carroll is Professor of Pediatrics, University of Connecticut, Division of Critical Care, Connecticut Children’s Medical Center, Hartford, Connecticut.
Blood transfusions are common in critically ill patients; two in five adults admitted to an ICU receive at least one transfusion during their hospitalization (Corwin HL, et al. Crit Care Med. 2004;32[1]:39). Recently, there has been growing concern about the potential dangers involved with prolonged blood storage. Several provocative observational and retrospective studies found that prolonged storage time (ie, the age of the blood being transfused) negatively affects clinical outcomes (Wang D, et al. Transfusion. 2012;52[6]:1184). But now, some newly published trials on blood transfusion practice, including one published in late September 2017 (Cooper DJ, et al. N Engl J Med. Published online, September 27, 2017) seem to debunk much of this literature. Was all of the concern about age of blood overblown?
The appeal of “fresh” blood is intuitive. As consumers, we’re conditioned that the fresher the better. Fresh food tastes best. Carbonated beverages go “flat” over time. The newest iPhone® device is superior to your old one. So, of course, it follows that fresh blood is also better for your health than older blood.
But, in order to have a viable transfusion service, blood has to be stored. Blood is a scarce resource, and blood banks need to keep an adequate supply on hand for expected clinical necessities, as well as for emergencies. Donors can’t be on standby, waiting in the hospital to provide immediate whole blood transfusion. Also, blood needs to be tested for infections and for potential interactions with the patient, and whole blood must be broken down into individual components for transfusion. All of this requires time and storage.![]()
In a randomized study of 100 critically ill adults supported by mechanical ventilation, 50 were randomized to receive “fresh” blood (median storage age 4 days, interquartile range 3-5 days) and 50 were randomized to receive “standard” blood (median storage age 26.5 days, interquartile range 21-36 days) (Kor DJ, et al. Am J Respir Crit Care Med. 2012;185[8]:842). The primary outcome was gas exchange, as prolonged storage of red blood cells could potentially lead to an increased inflammatory response in patients. However, the authors found no difference in gas exchange between the two groups, and there were no differences in immunologic function or coagulation status.
The ABLE (Age of Blood Evaluation) trial was a randomized, blinded trial of transfusion practices in critically ill patients (Lacroix J, et al. N Engl J Med. 2015;372:1410). In 64 centers in Canada and Europe, 2,430 critically ill adults were randomized to receive either “fresh” blood (mean storage age 6.1 ± 4.9 days) or “standard” blood (mean storage age 22.0 ± 8.4 days). The primary outcome was 90-day mortality, with a power of 90% to detect a 5% change in mortality between the two groups. The investigators found no statistically significant difference in 90-day mortality between the “fresh” and “standard” groups (37% vs 35.3%; hazard ratio 1.1; 95% CI 0.9 – 1.2). Additionally, there were no differences in secondary outcomes, including multiorgan system dysfunction, duration of supportive care, or development of nosocomial infections.
The INFORM (Informing Fresh versus Old Red Cell Management) trial was a randomized study of patients hospitalized in six centers in Canada, Australia, Israel, and the United States (Heddle NM, et al. N Engl J Med. 2016;375[2]:1937). A total of 24,736 patients received transfusions with either “fresh” blood (median storage age 11 days) or “standard” blood (median storage age 23 days). The primary outcome was in-hospital death, with a 90% power to detect a 15% lower relative risk. When comparing the 8,215 patients who received “fresh” blood and the 16,521 patients who received “standard” blood, the authors found no difference in mortality between the two groups (9.1% vs 8.8%; odds ratio 1.04; 95% CI 0.95 to 1.14). Furthermore, there were no differences in outcomes in the high-risk subgroups that included patients with cancer, patients in the ICU, and patients undergoing cardiovascular surgery.
A meta-analysis examined 12 trials of patients who received “fresh” blood compared with those who received “older” or “standard” blood (Alexander PE, et al. Blood. 2016;127[4]:400); 5,229 patients were included in these trials, in which “fresh” blood was defined as blood stored for 3 to 10 days and “older” blood was stored for longer durations. There was no difference in mortality between the two groups (relative risk 1.04; 95% CI 0.94 - 1.14), and no difference in adverse events (relative risk 1.02; 95% CI 0.91 - 1.14). However, perhaps surprisingly, “fresh” blood was associated with an increased risk of nosocomial infections (relative risk 1.09; 95% CI 1.00 - 1.18).
So, can we stop worrying about the age of the blood that we are about to transfuse? Probably. Taken together, these studies suggest that differences in the duration of red blood cell storage allowed within current US FDA standards aren’t clinically relevant, even in critically ill patients. At least, for now, the current practices for age of blood and duration of storage appear unrelated to adverse clinical outcomes.
Dr. Carroll is Professor of Pediatrics, University of Connecticut, Division of Critical Care, Connecticut Children’s Medical Center, Hartford, Connecticut.
Blood transfusions are common in critically ill patients; two in five adults admitted to an ICU receive at least one transfusion during their hospitalization (Corwin HL, et al. Crit Care Med. 2004;32[1]:39). Recently, there has been growing concern about the potential dangers involved with prolonged blood storage. Several provocative observational and retrospective studies found that prolonged storage time (ie, the age of the blood being transfused) negatively affects clinical outcomes (Wang D, et al. Transfusion. 2012;52[6]:1184). But now, some newly published trials on blood transfusion practice, including one published in late September 2017 (Cooper DJ, et al. N Engl J Med. Published online, September 27, 2017) seem to debunk much of this literature. Was all of the concern about age of blood overblown?
The appeal of “fresh” blood is intuitive. As consumers, we’re conditioned that the fresher the better. Fresh food tastes best. Carbonated beverages go “flat” over time. The newest iPhone® device is superior to your old one. So, of course, it follows that fresh blood is also better for your health than older blood.
But, in order to have a viable transfusion service, blood has to be stored. Blood is a scarce resource, and blood banks need to keep an adequate supply on hand for expected clinical necessities, as well as for emergencies. Donors can’t be on standby, waiting in the hospital to provide immediate whole blood transfusion. Also, blood needs to be tested for infections and for potential interactions with the patient, and whole blood must be broken down into individual components for transfusion. All of this requires time and storage.![]()
In a randomized study of 100 critically ill adults supported by mechanical ventilation, 50 were randomized to receive “fresh” blood (median storage age 4 days, interquartile range 3-5 days) and 50 were randomized to receive “standard” blood (median storage age 26.5 days, interquartile range 21-36 days) (Kor DJ, et al. Am J Respir Crit Care Med. 2012;185[8]:842). The primary outcome was gas exchange, as prolonged storage of red blood cells could potentially lead to an increased inflammatory response in patients. However, the authors found no difference in gas exchange between the two groups, and there were no differences in immunologic function or coagulation status.
The ABLE (Age of Blood Evaluation) trial was a randomized, blinded trial of transfusion practices in critically ill patients (Lacroix J, et al. N Engl J Med. 2015;372:1410). In 64 centers in Canada and Europe, 2,430 critically ill adults were randomized to receive either “fresh” blood (mean storage age 6.1 ± 4.9 days) or “standard” blood (mean storage age 22.0 ± 8.4 days). The primary outcome was 90-day mortality, with a power of 90% to detect a 5% change in mortality between the two groups. The investigators found no statistically significant difference in 90-day mortality between the “fresh” and “standard” groups (37% vs 35.3%; hazard ratio 1.1; 95% CI 0.9 – 1.2). Additionally, there were no differences in secondary outcomes, including multiorgan system dysfunction, duration of supportive care, or development of nosocomial infections.
The INFORM (Informing Fresh versus Old Red Cell Management) trial was a randomized study of patients hospitalized in six centers in Canada, Australia, Israel, and the United States (Heddle NM, et al. N Engl J Med. 2016;375[2]:1937). A total of 24,736 patients received transfusions with either “fresh” blood (median storage age 11 days) or “standard” blood (median storage age 23 days). The primary outcome was in-hospital death, with a 90% power to detect a 15% lower relative risk. When comparing the 8,215 patients who received “fresh” blood and the 16,521 patients who received “standard” blood, the authors found no difference in mortality between the two groups (9.1% vs 8.8%; odds ratio 1.04; 95% CI 0.95 to 1.14). Furthermore, there were no differences in outcomes in the high-risk subgroups that included patients with cancer, patients in the ICU, and patients undergoing cardiovascular surgery.
A meta-analysis examined 12 trials of patients who received “fresh” blood compared with those who received “older” or “standard” blood (Alexander PE, et al. Blood. 2016;127[4]:400); 5,229 patients were included in these trials, in which “fresh” blood was defined as blood stored for 3 to 10 days and “older” blood was stored for longer durations. There was no difference in mortality between the two groups (relative risk 1.04; 95% CI 0.94 - 1.14), and no difference in adverse events (relative risk 1.02; 95% CI 0.91 - 1.14). However, perhaps surprisingly, “fresh” blood was associated with an increased risk of nosocomial infections (relative risk 1.09; 95% CI 1.00 - 1.18).
So, can we stop worrying about the age of the blood that we are about to transfuse? Probably. Taken together, these studies suggest that differences in the duration of red blood cell storage allowed within current US FDA standards aren’t clinically relevant, even in critically ill patients. At least, for now, the current practices for age of blood and duration of storage appear unrelated to adverse clinical outcomes.
Dr. Carroll is Professor of Pediatrics, University of Connecticut, Division of Critical Care, Connecticut Children’s Medical Center, Hartford, Connecticut.
Ribaxamase reduced new CDI infection by 71%
SAN DIEGO – , results from a phase 2b study showed.
At an annual scientific meeting on infectious diseases, lead investigator John F. Kokai-Kun, PhD, said that the finding represents a paradigm shift in the use of intravenous beta-lactam antibiotics to prevent opportunistic infections. “We currently treat Clostridium difficile infection (CDI) with antibiotics, which attack the vegetative cells,” said Dr. Kokai-Kun, vice president of nonclinical affairs for Rockville, Md.–based Synthetic Biologics, which is developing ribaxamase. “Since C. diff. is primarily a toxin-mediated disease, certain products seem to neutralize the toxin. There’s also been work with probiotics and prebiotics to try to strengthen and repair the dysbiotic colon. Fecal replacement therapy has been shown to be fairly effective for treatment of recurrent C. diff. infection. What if we could simply block the initial insult that leads to this cascade? That’s the damage caused to the gut microbiome by the antibiotic that’s excreted to the intestine.”

That’s where ribaxamase comes in, he said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. Ribaxamase is an orally administered beta-lactamase designed to degrade penicillin and cephalosporins in the intestinal lumen. It’s formulated for release in the proximal small intestine and is expected to be given during or a short time after administration of IV beta-lactam antibiotics such as ceftriaxone. “This is expected to degrade the excess antibiotics that are excreted into the small intestine via the bile,” Dr. Kokai-Kun explained. “It’s designed to prevent disruption of the gut microbiome and thus protect from opportunistic GI infections like CDI.” Early-stage clinical studies demonstrated that ribaxamase was well tolerated and that it is not systemically absorbed, while phase 2 studies showed that ribaxamase degrades ceftriaxone in the intestine to below the level of detection while not affecting the pharmacokinetics of ceftriaxone in the plasma.
For the current study, 412 patients were enrolled at 84 multinational clinical sites. These patients were admitted to the hospital for treatment of a lower respiratory tract infection and were randomized 1:1 to receive ceftriaxone plus 150 mg ribaxamase or ceftriaxone plus placebo. Patients in both groups could also receive an oral macrolide at the discretion of the clinical investigator. The researchers also obtained fecal samples at screening, 72 hours post antibiotic treatment, and at the end of a 4-week follow-up visit, to determine colonization by opportunistic pathogens and to examine changes in the gut microbiome. Patients were monitored for 6 weeks for diarrhea and CDI. Diarrhea was defined as three or more loose or watery stools in a 24-hour period. “If that occurred, then we collected a sample, which was sent to the local lab to determine the presence of C. difficile toxins,” Dr. Kokai-Kun said.
The average age of study participants was 70 years, and about one-third in each arm received oral macrolides. The number of adverse events and serious adverse events were similar between active and placebo arms, and there was no trend associated with ribaxamase use. The lower respiratory tract infection cure rate to the ceftriaxone treatment was about 99% in both arms at 72 hours post treatment and at 2 weeks post treatment.
To analyze changes in the gut microbiome, the researchers conducted 16S rRNA sequencing of DNA extracted from fecal samples. In all, 652 samples were sequenced from 229 patients. Results from that analysis suggests that ribaxamase “appears to protect the gut microbiome from the onslaught of the ceftriaxone,” he said.
Ribaxamase reduced the incidence of new-onset CDI by 71%, compared with placebo (P = .045). “It apparently did this by protecting the integrity of the gut microbiome,” Dr. Kokai-Kun said. “There was also a significant reduction of new colonization by vancomycin-resistant enterococci at 72 hours and 4 weeks (P = .0001 and P = .0002, respectively) which is an opportunistic pathogen that is known to be able to inhabit gut microbiome when there is dysbiosis.”
The study was sponsored by Synthetic Biologics. Dr. Kokai-Kun is an employee of the company.
SAN DIEGO – , results from a phase 2b study showed.
At an annual scientific meeting on infectious diseases, lead investigator John F. Kokai-Kun, PhD, said that the finding represents a paradigm shift in the use of intravenous beta-lactam antibiotics to prevent opportunistic infections. “We currently treat Clostridium difficile infection (CDI) with antibiotics, which attack the vegetative cells,” said Dr. Kokai-Kun, vice president of nonclinical affairs for Rockville, Md.–based Synthetic Biologics, which is developing ribaxamase. “Since C. diff. is primarily a toxin-mediated disease, certain products seem to neutralize the toxin. There’s also been work with probiotics and prebiotics to try to strengthen and repair the dysbiotic colon. Fecal replacement therapy has been shown to be fairly effective for treatment of recurrent C. diff. infection. What if we could simply block the initial insult that leads to this cascade? That’s the damage caused to the gut microbiome by the antibiotic that’s excreted to the intestine.”
That’s where ribaxamase comes in, he said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. Ribaxamase is an orally administered beta-lactamase designed to degrade penicillin and cephalosporins in the intestinal lumen. It’s formulated for release in the proximal small intestine and is expected to be given during or a short time after administration of IV beta-lactam antibiotics such as ceftriaxone. “This is expected to degrade the excess antibiotics that are excreted into the small intestine via the bile,” Dr. Kokai-Kun explained. “It’s designed to prevent disruption of the gut microbiome and thus protect from opportunistic GI infections like CDI.” Early-stage clinical studies demonstrated that ribaxamase was well tolerated and that it is not systemically absorbed, while phase 2 studies showed that ribaxamase degrades ceftriaxone in the intestine to below the level of detection while not affecting the pharmacokinetics of ceftriaxone in the plasma.
For the current study, 412 patients were enrolled at 84 multinational clinical sites. These patients were admitted to the hospital for treatment of a lower respiratory tract infection and were randomized 1:1 to receive ceftriaxone plus 150 mg ribaxamase or ceftriaxone plus placebo. Patients in both groups could also receive an oral macrolide at the discretion of the clinical investigator. The researchers also obtained fecal samples at screening, 72 hours post antibiotic treatment, and at the end of a 4-week follow-up visit, to determine colonization by opportunistic pathogens and to examine changes in the gut microbiome. Patients were monitored for 6 weeks for diarrhea and CDI. Diarrhea was defined as three or more loose or watery stools in a 24-hour period. “If that occurred, then we collected a sample, which was sent to the local lab to determine the presence of C. difficile toxins,” Dr. Kokai-Kun said.
The average age of study participants was 70 years, and about one-third in each arm received oral macrolides. The number of adverse events and serious adverse events were similar between active and placebo arms, and there was no trend associated with ribaxamase use. The lower respiratory tract infection cure rate to the ceftriaxone treatment was about 99% in both arms at 72 hours post treatment and at 2 weeks post treatment.
To analyze changes in the gut microbiome, the researchers conducted 16S rRNA sequencing of DNA extracted from fecal samples. In all, 652 samples were sequenced from 229 patients. Results from that analysis suggests that ribaxamase “appears to protect the gut microbiome from the onslaught of the ceftriaxone,” he said.
Ribaxamase reduced the incidence of new-onset CDI by 71%, compared with placebo (P = .045). “It apparently did this by protecting the integrity of the gut microbiome,” Dr. Kokai-Kun said. “There was also a significant reduction of new colonization by vancomycin-resistant enterococci at 72 hours and 4 weeks (P = .0001 and P = .0002, respectively) which is an opportunistic pathogen that is known to be able to inhabit gut microbiome when there is dysbiosis.”
The study was sponsored by Synthetic Biologics. Dr. Kokai-Kun is an employee of the company.
SAN DIEGO – , results from a phase 2b study showed.
At an annual scientific meeting on infectious diseases, lead investigator John F. Kokai-Kun, PhD, said that the finding represents a paradigm shift in the use of intravenous beta-lactam antibiotics to prevent opportunistic infections. “We currently treat Clostridium difficile infection (CDI) with antibiotics, which attack the vegetative cells,” said Dr. Kokai-Kun, vice president of nonclinical affairs for Rockville, Md.–based Synthetic Biologics, which is developing ribaxamase. “Since C. diff. is primarily a toxin-mediated disease, certain products seem to neutralize the toxin. There’s also been work with probiotics and prebiotics to try to strengthen and repair the dysbiotic colon. Fecal replacement therapy has been shown to be fairly effective for treatment of recurrent C. diff. infection. What if we could simply block the initial insult that leads to this cascade? That’s the damage caused to the gut microbiome by the antibiotic that’s excreted to the intestine.”
That’s where ribaxamase comes in, he said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. Ribaxamase is an orally administered beta-lactamase designed to degrade penicillin and cephalosporins in the intestinal lumen. It’s formulated for release in the proximal small intestine and is expected to be given during or a short time after administration of IV beta-lactam antibiotics such as ceftriaxone. “This is expected to degrade the excess antibiotics that are excreted into the small intestine via the bile,” Dr. Kokai-Kun explained. “It’s designed to prevent disruption of the gut microbiome and thus protect from opportunistic GI infections like CDI.” Early-stage clinical studies demonstrated that ribaxamase was well tolerated and that it is not systemically absorbed, while phase 2 studies showed that ribaxamase degrades ceftriaxone in the intestine to below the level of detection while not affecting the pharmacokinetics of ceftriaxone in the plasma.
For the current study, 412 patients were enrolled at 84 multinational clinical sites. These patients were admitted to the hospital for treatment of a lower respiratory tract infection and were randomized 1:1 to receive ceftriaxone plus 150 mg ribaxamase or ceftriaxone plus placebo. Patients in both groups could also receive an oral macrolide at the discretion of the clinical investigator. The researchers also obtained fecal samples at screening, 72 hours post antibiotic treatment, and at the end of a 4-week follow-up visit, to determine colonization by opportunistic pathogens and to examine changes in the gut microbiome. Patients were monitored for 6 weeks for diarrhea and CDI. Diarrhea was defined as three or more loose or watery stools in a 24-hour period. “If that occurred, then we collected a sample, which was sent to the local lab to determine the presence of C. difficile toxins,” Dr. Kokai-Kun said.
The average age of study participants was 70 years, and about one-third in each arm received oral macrolides. The number of adverse events and serious adverse events were similar between active and placebo arms, and there was no trend associated with ribaxamase use. The lower respiratory tract infection cure rate to the ceftriaxone treatment was about 99% in both arms at 72 hours post treatment and at 2 weeks post treatment.
To analyze changes in the gut microbiome, the researchers conducted 16S rRNA sequencing of DNA extracted from fecal samples. In all, 652 samples were sequenced from 229 patients. Results from that analysis suggests that ribaxamase “appears to protect the gut microbiome from the onslaught of the ceftriaxone,” he said.
Ribaxamase reduced the incidence of new-onset CDI by 71%, compared with placebo (P = .045). “It apparently did this by protecting the integrity of the gut microbiome,” Dr. Kokai-Kun said. “There was also a significant reduction of new colonization by vancomycin-resistant enterococci at 72 hours and 4 weeks (P = .0001 and P = .0002, respectively) which is an opportunistic pathogen that is known to be able to inhabit gut microbiome when there is dysbiosis.”
The study was sponsored by Synthetic Biologics. Dr. Kokai-Kun is an employee of the company.
REPORTING FROM ID WEEK 2017
Key clinical point: Ribaxamase reduced new colonization with C. diff. and vancomycin-resistant enterococci.
Major finding: Ribaxamase reduced the incidence of new onset CDI by 71%, compared with placebo (P = 0.045).
Study details: A trial of 412 patients admitted to the hospital for treatment of a lower respiratory tract infection who were randomized to receive ceftriaxone plus 150 mg ribaxamase or ceftriaxone plus placebo.
Disclosures: The study was sponsored by Synthetic Biologics. Dr. Kokai-Kun is an employee of the company.
New App Aims to Bring Personalized Headache Medicine One Step Closer
STANFORD, CA—Headache specialists have created a new app intended to support patients with headache pain. Developed by board-certified headache specialists in collaboration with a machine learning and artificial intelligence professional, the BonTriage Headache Compass may help patients with headache better manage and improve their condition. When used consistently over time, this app is intended to help patients reduce the frequency, severity, and duration of headaches, as well as the disability they cause.
“The BonTriage Headache Compass provides a diagnostic clinical impression and monitoring, which patients can take to their doctor or just use to gain insight into their condition,” said Robert Cowan, MD, Professor of Neurology and Chief of the Division of Headache Medicine at Stanford University and a co-creator of the new app.

Personalized Data
The BonTriage Headache Compass app is the second product developed by BonTriage. The first is a detailed web-based questionnaire, available at www.bontriage.com, that creates a detailed report about a patient’s headache. The questionnaire has been validated and its accuracy is greater than 90%. Once completed, the questionnaire can be printed and shared with the patient’s physician.
The app works together with the questionnaire, but can be used independently. “When you first download the app, it asks the questions that are necessary to make the diagnostic clinical impression,” Dr. Cowan said. After asking basic demographic questions, the app poses specific questions about the characteristics of typical and current headaches and other related conditions. This information, which takes about 10 minutes to enter, will populate the app and generate a clinical impression similar to one formed at an initial clinical presentation.
The BonTriage Headache Compass then prompts users daily for data on headaches, medications, triggers, and lifestyle factors. Based on these data, the app can predict headache frequency; report the effect of treatment strategies on headache frequency, severity, and duration in real time; and answer questions based on personalized data. Users can thus see potential connections between their headaches, triggers, and behaviors. Data entry requires a minute or two each day.

Individualized Advice
The app’s internal analytics analyze data to interpret the personalized information that it collects. This analysis is intended to help patients with headache avoid factors (behaviors, triggers, etc) that worsen their headaches and enhance behaviors that reduce their headaches. The app also provides feedback to indicate which management strategies are working. “One critical piece of information we want to feed back to patients is whether they are getting better or not, based on how they are treating their headaches,” said Dr. Cowan. The data that the BonTriage Headache Compass app collects can inform patients about their specific headache triggers, lifestyle choices, medication, or environmental factors, and about how they influence their headache. After a month of consistent data entry … the app can begin to predict headaches. With continued use, the app could, for example, send a text message advising the user that a storm is coming to their area and he orshe did not sleep well the night before, so he or she should skip wine with dinner because of an increased risk of headache on that particular night.

Users of the BonTriage Headache Compass can query the app for data on areas of personal concern. For example, it can compare headache severity or frequency between months or examine the relationship between exercise or sleep and headache duration or frequency. The Headache Compass tool can provide visual representations and headache indices (ie, scores) to compare a current headache with previous headaches.
The BonTriage Headache Compass is available for free in the iPhone App Store.
—Glenn S. Williams
STANFORD, CA—Headache specialists have created a new app intended to support patients with headache pain. Developed by board-certified headache specialists in collaboration with a machine learning and artificial intelligence professional, the BonTriage Headache Compass may help patients with headache better manage and improve their condition. When used consistently over time, this app is intended to help patients reduce the frequency, severity, and duration of headaches, as well as the disability they cause.
“The BonTriage Headache Compass provides a diagnostic clinical impression and monitoring, which patients can take to their doctor or just use to gain insight into their condition,” said Robert Cowan, MD, Professor of Neurology and Chief of the Division of Headache Medicine at Stanford University and a co-creator of the new app.
Personalized Data
The BonTriage Headache Compass app is the second product developed by BonTriage. The first is a detailed web-based questionnaire, available at www.bontriage.com, that creates a detailed report about a patient’s headache. The questionnaire has been validated and its accuracy is greater than 90%. Once completed, the questionnaire can be printed and shared with the patient’s physician.
The app works together with the questionnaire, but can be used independently. “When you first download the app, it asks the questions that are necessary to make the diagnostic clinical impression,” Dr. Cowan said. After asking basic demographic questions, the app poses specific questions about the characteristics of typical and current headaches and other related conditions. This information, which takes about 10 minutes to enter, will populate the app and generate a clinical impression similar to one formed at an initial clinical presentation.
The BonTriage Headache Compass then prompts users daily for data on headaches, medications, triggers, and lifestyle factors. Based on these data, the app can predict headache frequency; report the effect of treatment strategies on headache frequency, severity, and duration in real time; and answer questions based on personalized data. Users can thus see potential connections between their headaches, triggers, and behaviors. Data entry requires a minute or two each day.
Individualized Advice
The app’s internal analytics analyze data to interpret the personalized information that it collects. This analysis is intended to help patients with headache avoid factors (behaviors, triggers, etc) that worsen their headaches and enhance behaviors that reduce their headaches. The app also provides feedback to indicate which management strategies are working. “One critical piece of information we want to feed back to patients is whether they are getting better or not, based on how they are treating their headaches,” said Dr. Cowan. The data that the BonTriage Headache Compass app collects can inform patients about their specific headache triggers, lifestyle choices, medication, or environmental factors, and about how they influence their headache. After a month of consistent data entry … the app can begin to predict headaches. With continued use, the app could, for example, send a text message advising the user that a storm is coming to their area and he orshe did not sleep well the night before, so he or she should skip wine with dinner because of an increased risk of headache on that particular night.
Users of the BonTriage Headache Compass can query the app for data on areas of personal concern. For example, it can compare headache severity or frequency between months or examine the relationship between exercise or sleep and headache duration or frequency. The Headache Compass tool can provide visual representations and headache indices (ie, scores) to compare a current headache with previous headaches.
The BonTriage Headache Compass is available for free in the iPhone App Store.
—Glenn S. Williams
STANFORD, CA—Headache specialists have created a new app intended to support patients with headache pain. Developed by board-certified headache specialists in collaboration with a machine learning and artificial intelligence professional, the BonTriage Headache Compass may help patients with headache better manage and improve their condition. When used consistently over time, this app is intended to help patients reduce the frequency, severity, and duration of headaches, as well as the disability they cause.
“The BonTriage Headache Compass provides a diagnostic clinical impression and monitoring, which patients can take to their doctor or just use to gain insight into their condition,” said Robert Cowan, MD, Professor of Neurology and Chief of the Division of Headache Medicine at Stanford University and a co-creator of the new app.
Personalized Data
The BonTriage Headache Compass app is the second product developed by BonTriage. The first is a detailed web-based questionnaire, available at www.bontriage.com, that creates a detailed report about a patient’s headache. The questionnaire has been validated and its accuracy is greater than 90%. Once completed, the questionnaire can be printed and shared with the patient’s physician.
The app works together with the questionnaire, but can be used independently. “When you first download the app, it asks the questions that are necessary to make the diagnostic clinical impression,” Dr. Cowan said. After asking basic demographic questions, the app poses specific questions about the characteristics of typical and current headaches and other related conditions. This information, which takes about 10 minutes to enter, will populate the app and generate a clinical impression similar to one formed at an initial clinical presentation.
The BonTriage Headache Compass then prompts users daily for data on headaches, medications, triggers, and lifestyle factors. Based on these data, the app can predict headache frequency; report the effect of treatment strategies on headache frequency, severity, and duration in real time; and answer questions based on personalized data. Users can thus see potential connections between their headaches, triggers, and behaviors. Data entry requires a minute or two each day.
Individualized Advice
The app’s internal analytics analyze data to interpret the personalized information that it collects. This analysis is intended to help patients with headache avoid factors (behaviors, triggers, etc) that worsen their headaches and enhance behaviors that reduce their headaches. The app also provides feedback to indicate which management strategies are working. “One critical piece of information we want to feed back to patients is whether they are getting better or not, based on how they are treating their headaches,” said Dr. Cowan. The data that the BonTriage Headache Compass app collects can inform patients about their specific headache triggers, lifestyle choices, medication, or environmental factors, and about how they influence their headache. After a month of consistent data entry … the app can begin to predict headaches. With continued use, the app could, for example, send a text message advising the user that a storm is coming to their area and he orshe did not sleep well the night before, so he or she should skip wine with dinner because of an increased risk of headache on that particular night.
Users of the BonTriage Headache Compass can query the app for data on areas of personal concern. For example, it can compare headache severity or frequency between months or examine the relationship between exercise or sleep and headache duration or frequency. The Headache Compass tool can provide visual representations and headache indices (ie, scores) to compare a current headache with previous headaches.
The BonTriage Headache Compass is available for free in the iPhone App Store.
—Glenn S. Williams
Transbronchial cryobiopsy, updated guidelines for chronic cough in children, PD-1 inhibition
Interventional Chest/Diagnostic Procedures
Cryobiopsy for ILD: Careful stewardship needed
Interest in transbronchial cryobiopsy has accelerated rapidly in recent years. This procedure is performed by advancing a cryoprobe into the peripheral lung via flexible bronchoscopy, where lung tissue freezes and adheres to the probe and is subsequently extracted as a cryobiopsy. The number of cryobiopsy-related publications has increased exponentially since it was described in 2009 (Babiak A, et al. Respiration. 2009;78[2]:203). This interest stems from reports of high diagnostic yields in patients with interstitial lung disease (ILD) while maintaining complication rates similar to that of conventional bronchoscopic biopsy.
Traditional bronchoscopic biopsies are notoriously insensitive; a specific diagnosis can be established in fewer than a third of cases (Sheth JS, et al. Chest. 2017;151[2]:389). As such, surgical lung biopsy continues to be recommended but is associated with significant mortality (2%) and morbidity (30%) in patients with ILD (Hutchinson JP, et al. ARJCCM. 2016;193[10]:1161). Cryobiopsy, which appears to rival surgical lung biopsy in terms of ability to contribute to a specific diagnosis, is, therefore, a highly promising alternative (Tomassetti S, et al. AJRCCM. 2016;193[7]:745).
As cryobiopsy is increasingly adopted around the world, however, troubling reports of serious complications have surfaced. Most notable is the recently reported experience of the initial 25 cases performed at the University of Pennsylvania, in which almost one in four patients suffered serious complications (DiBardino DM, et al. Ann Am Thorac Soc. 2017;14[6]:851). The authors pointed to lack of a predefined procedural protocol, as well as several choices relating to the specific technique used, including inconsistent use of fluoroscopy, lack of prophylactic bronchial blocker placement, and predominant use of laryngeal mask airways as potential contributing factors. Indeed, many variations of the basic cryobiopsy procedure have been described (Lentz RJ, et al. J Thoracic Dis. 2017;9[7]:2186), with no formal guidance or training available to inform advanced bronchoscopists interested in this procedure.

It is incumbent on the interventional pulmonology and ILD specialist communities to be responsible stewards of this promising procedure. Implementation of three parallel efforts to standardize and rigorously study this procedure should be considered as soon as possible: creation of expert consensus guidelines establishing best-practices for safe and effective biopsy technique; a training requirement before independent performance of the procedure; and creation of an international cryobiopsy registry to facilitate higher-quality research into optimal technique and outcomes. We owe this to our patients.
Robert J. Lentz, MD
NetWork Member
Fabien Maldonado, MD, FCCP
NetWork Member
Pediatric Chest Medicine
Chronic cough in children: New guidelines
A chronic cough is a common complaint among children whose parents seek medical evaluation. Chronic wet cough can indicate an underlying illness; therefore, an early diagnosis can lead to prevention of complications of the disease and improvement in quality of life.
CHEST is a leading resource in evidence and consensus-based guidelines on important topics affecting children. The most recent guidelines entitled Management of Children with Chronic Wet Cough and Protracted Bacterial Bronchitis (Chest. 2017;151(4):884-890) and Use of Management Pathways or Algorithms in Children with Chronic Cough (Chest. 2017;151(4):875-873) are updates from the 2006 CHEST guidelines on chronic cough in children.
The present updates utilized the CHEST methodological guidelines with chronic wet or productive cough and Grading of Recommendations Assessment, Development, and Evaluation framework and also performed a systematic review addressing key questions concerning the management of childhood disease for children 14 years and younger.
Guidance provided by the expert panel focused on recommendations to answer six key questions concerning the management of children 14 years and younger with a chronic wet cough unrelated to established chronic lung disease. The recommendations are:
1. Chronic cough is defined as the presence of a cough 4 weeks or longer in duration.
2. Assessment of the effect of the cough on the child and the family be undertaken as part of clinical consultation.
3. Evaluation of a chronic cough should be done with a systematic approach with pediatric-specific cough management protocols or algorithms.
4. Chest radiograph and, when age appropriate, spirometry with bronchodilator be undertaken as evaluation; tests for pertussis infection only to be performed if clinically suspected.
5. Chronic wet cough with no specific clinical features should receive antibiotics for 2 weeks targeted for common respiratory bacteria (Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis).
6. When cough persists despite 2 weeks of appropriate antibiotics, it is recommended to continue for an additional 2 weeks.
7. Additional tests (eg skin prick test, Mantoux, bronchoscopy, chest CT scan) should be individualized in accordance with the clinical setting and child’s clinical symptoms and signs.
The panel recognizes the need for prospective studies to assess current algorithms outcomes of children with chronic cough. Both articles can be found on the guidelines section of the CHEST site.
John Bishara, DO
Fellow-in-Training Member
Pulmonary Physiology, Function, and Rehabilitation
Functional imaging of the lung
Quantifying heterogeneity of ventilation and gas exchange in lung diseases remains a clinical challenge. Conventional pulmonary function test is insensitive to regional changes. The multiple inert gas elimination technique can quantify ventilation-perfusion distribution, but it requires invasive instrumentation (eg, pulmonary artery catheterization) and is not practical for clinical use. Computed tomography (CT) scans delineate spatial changes in lung structures but do not directly measure changes in ventilation and gas exchange. With its radiation, it is difficult to apply CT scanning repeatedly in patients. More recently, MR imaging techniques have been developed to directly “visualize” and quantify regional lung function (Kruger SJ, et al. J Magn Reson Imaging. 2016;43(2):295; Roos JE, et al. Magn Reson Imaging Clin N Am. 2015;23(2):217). These techniques employ inhalation of gases, such as oxygen, perfluorinated gases, and hyperpolarized 3He and 129Xe. Hyperpolarized 3He has been studied the most; however, the dwindling supply of 3He gas and its rising cost have prevented its further development. 129Xe has abundant supply and has emerged to be the inert gas of choice for MR imaging. Hyperpolarized 129Xe can measure ventilation, like hyperpolarized 3He. In addition, Xe diffuses into alveolar barrier (interstitium and plasma) and red blood cells, where it exhibits distinct resonant frequency shifts that can be captured by MR. Therefore, in one test, information on pulmonary ventilation and gas transfer can be obtained. To date, the results from MR imaging studies have provided new insights into the pathophysiology of obstructive and restrictive lung diseases. With continuous development, MR imaging of the lung could become a clinically useful tool in the near future.
Yuh-Chin T. Huang, MD, MHS, FCCP
Steering Committee Member
Thoracic Oncology
Immune-mediated pneumonitis and PD-1 inhibition
Inhibitors of the programmed cell death 1 receptor (PD-1) have shown significant promise in the treatment of advanced stage malignancy. With the recent expansion of indications for use of these agents, the number of patients treated will continue to grow. Clinicians must be aware of their potential for serious adverse side effects, including dermatitis, colitis, and potentially life-threatening pneumonitis.
The development of pneumonitis secondary to PD-1 inhibitions is reported to occur in 2% to 5% of patients and can present at any time during therapy, with 1% of patients developing grade 3 or higher pneumonitis.1,2 The most common symptoms are dyspnea and cough, though one-third of patients are asymptomatic at presentation.2 Radiographic and pathologic features vary greatly and include organizing pneumonia, interstitial pneumonitis, hypersensitivity pneumonitis, or diffuse alveolar damage.3 While pneumonitis due to PD-1 inhibition is reportedly uncommon, the increasing number of patients expected to receive these medications will predictably result in increasing overall frequency of pneumonitis cases. In addition, the lack of large prospective randomized trials and reliance on radiographic rather than pathologic data in diagnosing immune-mediated pneumonitis gives one pause. Given the variability of presentation, lack of routine pathologic data, and increasing use of dual agents (eg, PD-1 and CTLA-4), chest physicians and medical oncologists should have a high index of suspicion yet practice equipoise in patients receiving immunotherapy who develop unexplained pulmonary symptoms or infiltrates. More research is needed to help improve the multidisciplinary diagnosis and treatment of this potentially serious complication.
David Maurice Chambers, MD
Fellow-in-Training Member
Jason Atticus Akulian, MD, MPH
Steering Committee Member
References
1. Nishino M, et al. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncology. 2016;2(12):1607.
2. Naidoo J, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol. 2017;35(7):709.
3. Nishino M, et al. PD-1 inhibitor-related pneumonitis in advanced cancer patients: radiographic patterns and clinical course. Clin Cancer Res. 2016;22(24):6051.
Pulmonary Vascular Disease
Pulmonary Arterial Hypertension Associated With SLE
While pulmonary arterial hypertension (PAH) commonly complicates scleroderma (SSc), it is a rare complication of other connective tissue diseases (CTD), such as systemic lupus erythematosus (SLE). In the few prospective studies that utilize right-sided heart catheterization (RHC), the estimated prevalence of PAH in SLE is about 4%. However, since the prevalence of SLE is 10 to 15 times greater than SSc in the United States, the true prevalence of SLE-PAH may be higher than previously thought, and, thus, clinically relevant. Despite this, little is known about SLE-PAH.
A recent retrospective study from the French Pulmonary Hypertension Registry has added significantly to our understanding of this complication of SLE. Hachulla and colleagues studied 51 patients with RHC-proven SLE-PAH compared with 101 SLE control subjects without PAH. While the authors did not find any relevant differences in the demographics between groups, they did find a significantly higher prevalence of SSA and SSB antibodies in SLE-PAH. Interestingly, the presence of anti-U1 RNP antibody appeared to be less common in SLE-PAH patients; this lack of association is in contrast to prior studies in mixed CTD patients with anti-U1 RNP antibodies in which the prevalence of PAH can be as high as 60%. Further, none of the SLE-PAH patients demonstrated an acute response to vasodilator challenge during RHC, emphasizing that this maneuver does not need to be performed in SLE patients at risk of PAH. Trends toward improved survival in SLE-PAH patients treated with hydroxychloroquine are preliminary and hypothesis-generating but require confirmation in larger clinical studies.
Stephen Mathai, MD, FCCP
Chair
Leena Palwar, MD
Fellow-in-Training Member
References
Hachulla E, Jais X, Cinquetti G, et al. Pulmonary arterial hypertension associated with SLE: Results from the French pulmonary hypertension registry. Chest. 2017 Aug 26. pii: S0012-3692(17)31430-7. doi: 10.1016/j.chest.2017.08.014. [Epub ahead of print]
Chung L, Liu J, Parsons L, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138:1383-1394.
Shirai Y, Yasuoka H, Okano Y, Takeuchi T, Satoh T, Kuwana M. Clinical characteristics and survival of Japanese patients with connective tissue disease and pulmonary arterial hypertension: a singlecentre cohort. Rheumatology. 2012;51:1846-1854.
Hao YJ, Jiang X, Zhou W, et al. Connective tissue disease-associated pulmonary arterial hypertension in Chinese patients. Eur Respir J. 2014;44: 963-972.
Huang C, Li M, Liu Y, et al. Baseline characteristics and risk factors of pulmonary arterial hypertension in systemic lupus erythematosus patients. Medicine. 2016;95:e2761.
Pérez-Peñate GM, Rúa-Figueroa I, Juliá- Serdá G, et al. Pulmonary arterial hypertension in systemic lupus erythematosus: prevalence and predictors. J Rheumatol. 2016;43:323-329.
Alpert MA, Goldberg SH, Sindem BH, et al. Cardiovascular manifestations of mixed connective tissue disease in adults. Circulation. 1983;63:1182-1193.
Interventional Chest/Diagnostic Procedures
Cryobiopsy for ILD: Careful stewardship needed
Interest in transbronchial cryobiopsy has accelerated rapidly in recent years. This procedure is performed by advancing a cryoprobe into the peripheral lung via flexible bronchoscopy, where lung tissue freezes and adheres to the probe and is subsequently extracted as a cryobiopsy. The number of cryobiopsy-related publications has increased exponentially since it was described in 2009 (Babiak A, et al. Respiration. 2009;78[2]:203). This interest stems from reports of high diagnostic yields in patients with interstitial lung disease (ILD) while maintaining complication rates similar to that of conventional bronchoscopic biopsy.
Traditional bronchoscopic biopsies are notoriously insensitive; a specific diagnosis can be established in fewer than a third of cases (Sheth JS, et al. Chest. 2017;151[2]:389). As such, surgical lung biopsy continues to be recommended but is associated with significant mortality (2%) and morbidity (30%) in patients with ILD (Hutchinson JP, et al. ARJCCM. 2016;193[10]:1161). Cryobiopsy, which appears to rival surgical lung biopsy in terms of ability to contribute to a specific diagnosis, is, therefore, a highly promising alternative (Tomassetti S, et al. AJRCCM. 2016;193[7]:745).
As cryobiopsy is increasingly adopted around the world, however, troubling reports of serious complications have surfaced. Most notable is the recently reported experience of the initial 25 cases performed at the University of Pennsylvania, in which almost one in four patients suffered serious complications (DiBardino DM, et al. Ann Am Thorac Soc. 2017;14[6]:851). The authors pointed to lack of a predefined procedural protocol, as well as several choices relating to the specific technique used, including inconsistent use of fluoroscopy, lack of prophylactic bronchial blocker placement, and predominant use of laryngeal mask airways as potential contributing factors. Indeed, many variations of the basic cryobiopsy procedure have been described (Lentz RJ, et al. J Thoracic Dis. 2017;9[7]:2186), with no formal guidance or training available to inform advanced bronchoscopists interested in this procedure.
It is incumbent on the interventional pulmonology and ILD specialist communities to be responsible stewards of this promising procedure. Implementation of three parallel efforts to standardize and rigorously study this procedure should be considered as soon as possible: creation of expert consensus guidelines establishing best-practices for safe and effective biopsy technique; a training requirement before independent performance of the procedure; and creation of an international cryobiopsy registry to facilitate higher-quality research into optimal technique and outcomes. We owe this to our patients.
Robert J. Lentz, MD
NetWork Member
Fabien Maldonado, MD, FCCP
NetWork Member
Pediatric Chest Medicine
Chronic cough in children: New guidelines
A chronic cough is a common complaint among children whose parents seek medical evaluation. Chronic wet cough can indicate an underlying illness; therefore, an early diagnosis can lead to prevention of complications of the disease and improvement in quality of life.
CHEST is a leading resource in evidence and consensus-based guidelines on important topics affecting children. The most recent guidelines entitled Management of Children with Chronic Wet Cough and Protracted Bacterial Bronchitis (Chest. 2017;151(4):884-890) and Use of Management Pathways or Algorithms in Children with Chronic Cough (Chest. 2017;151(4):875-873) are updates from the 2006 CHEST guidelines on chronic cough in children.
The present updates utilized the CHEST methodological guidelines with chronic wet or productive cough and Grading of Recommendations Assessment, Development, and Evaluation framework and also performed a systematic review addressing key questions concerning the management of childhood disease for children 14 years and younger.
Guidance provided by the expert panel focused on recommendations to answer six key questions concerning the management of children 14 years and younger with a chronic wet cough unrelated to established chronic lung disease. The recommendations are:
1. Chronic cough is defined as the presence of a cough 4 weeks or longer in duration.
2. Assessment of the effect of the cough on the child and the family be undertaken as part of clinical consultation.
3. Evaluation of a chronic cough should be done with a systematic approach with pediatric-specific cough management protocols or algorithms.
4. Chest radiograph and, when age appropriate, spirometry with bronchodilator be undertaken as evaluation; tests for pertussis infection only to be performed if clinically suspected.
5. Chronic wet cough with no specific clinical features should receive antibiotics for 2 weeks targeted for common respiratory bacteria (Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis).
6. When cough persists despite 2 weeks of appropriate antibiotics, it is recommended to continue for an additional 2 weeks.
7. Additional tests (eg skin prick test, Mantoux, bronchoscopy, chest CT scan) should be individualized in accordance with the clinical setting and child’s clinical symptoms and signs.
The panel recognizes the need for prospective studies to assess current algorithms outcomes of children with chronic cough. Both articles can be found on the guidelines section of the CHEST site.
John Bishara, DO
Fellow-in-Training Member
Pulmonary Physiology, Function, and Rehabilitation
Functional imaging of the lung
Quantifying heterogeneity of ventilation and gas exchange in lung diseases remains a clinical challenge. Conventional pulmonary function test is insensitive to regional changes. The multiple inert gas elimination technique can quantify ventilation-perfusion distribution, but it requires invasive instrumentation (eg, pulmonary artery catheterization) and is not practical for clinical use. Computed tomography (CT) scans delineate spatial changes in lung structures but do not directly measure changes in ventilation and gas exchange. With its radiation, it is difficult to apply CT scanning repeatedly in patients. More recently, MR imaging techniques have been developed to directly “visualize” and quantify regional lung function (Kruger SJ, et al. J Magn Reson Imaging. 2016;43(2):295; Roos JE, et al. Magn Reson Imaging Clin N Am. 2015;23(2):217). These techniques employ inhalation of gases, such as oxygen, perfluorinated gases, and hyperpolarized 3He and 129Xe. Hyperpolarized 3He has been studied the most; however, the dwindling supply of 3He gas and its rising cost have prevented its further development. 129Xe has abundant supply and has emerged to be the inert gas of choice for MR imaging. Hyperpolarized 129Xe can measure ventilation, like hyperpolarized 3He. In addition, Xe diffuses into alveolar barrier (interstitium and plasma) and red blood cells, where it exhibits distinct resonant frequency shifts that can be captured by MR. Therefore, in one test, information on pulmonary ventilation and gas transfer can be obtained. To date, the results from MR imaging studies have provided new insights into the pathophysiology of obstructive and restrictive lung diseases. With continuous development, MR imaging of the lung could become a clinically useful tool in the near future.
Yuh-Chin T. Huang, MD, MHS, FCCP
Steering Committee Member
Thoracic Oncology
Immune-mediated pneumonitis and PD-1 inhibition
Inhibitors of the programmed cell death 1 receptor (PD-1) have shown significant promise in the treatment of advanced stage malignancy. With the recent expansion of indications for use of these agents, the number of patients treated will continue to grow. Clinicians must be aware of their potential for serious adverse side effects, including dermatitis, colitis, and potentially life-threatening pneumonitis.
The development of pneumonitis secondary to PD-1 inhibitions is reported to occur in 2% to 5% of patients and can present at any time during therapy, with 1% of patients developing grade 3 or higher pneumonitis.1,2 The most common symptoms are dyspnea and cough, though one-third of patients are asymptomatic at presentation.2 Radiographic and pathologic features vary greatly and include organizing pneumonia, interstitial pneumonitis, hypersensitivity pneumonitis, or diffuse alveolar damage.3 While pneumonitis due to PD-1 inhibition is reportedly uncommon, the increasing number of patients expected to receive these medications will predictably result in increasing overall frequency of pneumonitis cases. In addition, the lack of large prospective randomized trials and reliance on radiographic rather than pathologic data in diagnosing immune-mediated pneumonitis gives one pause. Given the variability of presentation, lack of routine pathologic data, and increasing use of dual agents (eg, PD-1 and CTLA-4), chest physicians and medical oncologists should have a high index of suspicion yet practice equipoise in patients receiving immunotherapy who develop unexplained pulmonary symptoms or infiltrates. More research is needed to help improve the multidisciplinary diagnosis and treatment of this potentially serious complication.
David Maurice Chambers, MD
Fellow-in-Training Member
Jason Atticus Akulian, MD, MPH
Steering Committee Member
References
1. Nishino M, et al. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncology. 2016;2(12):1607.
2. Naidoo J, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol. 2017;35(7):709.
3. Nishino M, et al. PD-1 inhibitor-related pneumonitis in advanced cancer patients: radiographic patterns and clinical course. Clin Cancer Res. 2016;22(24):6051.
Pulmonary Vascular Disease
Pulmonary Arterial Hypertension Associated With SLE
While pulmonary arterial hypertension (PAH) commonly complicates scleroderma (SSc), it is a rare complication of other connective tissue diseases (CTD), such as systemic lupus erythematosus (SLE). In the few prospective studies that utilize right-sided heart catheterization (RHC), the estimated prevalence of PAH in SLE is about 4%. However, since the prevalence of SLE is 10 to 15 times greater than SSc in the United States, the true prevalence of SLE-PAH may be higher than previously thought, and, thus, clinically relevant. Despite this, little is known about SLE-PAH.
A recent retrospective study from the French Pulmonary Hypertension Registry has added significantly to our understanding of this complication of SLE. Hachulla and colleagues studied 51 patients with RHC-proven SLE-PAH compared with 101 SLE control subjects without PAH. While the authors did not find any relevant differences in the demographics between groups, they did find a significantly higher prevalence of SSA and SSB antibodies in SLE-PAH. Interestingly, the presence of anti-U1 RNP antibody appeared to be less common in SLE-PAH patients; this lack of association is in contrast to prior studies in mixed CTD patients with anti-U1 RNP antibodies in which the prevalence of PAH can be as high as 60%. Further, none of the SLE-PAH patients demonstrated an acute response to vasodilator challenge during RHC, emphasizing that this maneuver does not need to be performed in SLE patients at risk of PAH. Trends toward improved survival in SLE-PAH patients treated with hydroxychloroquine are preliminary and hypothesis-generating but require confirmation in larger clinical studies.
Stephen Mathai, MD, FCCP
Chair
Leena Palwar, MD
Fellow-in-Training Member
References
Hachulla E, Jais X, Cinquetti G, et al. Pulmonary arterial hypertension associated with SLE: Results from the French pulmonary hypertension registry. Chest. 2017 Aug 26. pii: S0012-3692(17)31430-7. doi: 10.1016/j.chest.2017.08.014. [Epub ahead of print]
Chung L, Liu J, Parsons L, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138:1383-1394.
Shirai Y, Yasuoka H, Okano Y, Takeuchi T, Satoh T, Kuwana M. Clinical characteristics and survival of Japanese patients with connective tissue disease and pulmonary arterial hypertension: a singlecentre cohort. Rheumatology. 2012;51:1846-1854.
Hao YJ, Jiang X, Zhou W, et al. Connective tissue disease-associated pulmonary arterial hypertension in Chinese patients. Eur Respir J. 2014;44: 963-972.
Huang C, Li M, Liu Y, et al. Baseline characteristics and risk factors of pulmonary arterial hypertension in systemic lupus erythematosus patients. Medicine. 2016;95:e2761.
Pérez-Peñate GM, Rúa-Figueroa I, Juliá- Serdá G, et al. Pulmonary arterial hypertension in systemic lupus erythematosus: prevalence and predictors. J Rheumatol. 2016;43:323-329.
Alpert MA, Goldberg SH, Sindem BH, et al. Cardiovascular manifestations of mixed connective tissue disease in adults. Circulation. 1983;63:1182-1193.
Interventional Chest/Diagnostic Procedures
Cryobiopsy for ILD: Careful stewardship needed
Interest in transbronchial cryobiopsy has accelerated rapidly in recent years. This procedure is performed by advancing a cryoprobe into the peripheral lung via flexible bronchoscopy, where lung tissue freezes and adheres to the probe and is subsequently extracted as a cryobiopsy. The number of cryobiopsy-related publications has increased exponentially since it was described in 2009 (Babiak A, et al. Respiration. 2009;78[2]:203). This interest stems from reports of high diagnostic yields in patients with interstitial lung disease (ILD) while maintaining complication rates similar to that of conventional bronchoscopic biopsy.
Traditional bronchoscopic biopsies are notoriously insensitive; a specific diagnosis can be established in fewer than a third of cases (Sheth JS, et al. Chest. 2017;151[2]:389). As such, surgical lung biopsy continues to be recommended but is associated with significant mortality (2%) and morbidity (30%) in patients with ILD (Hutchinson JP, et al. ARJCCM. 2016;193[10]:1161). Cryobiopsy, which appears to rival surgical lung biopsy in terms of ability to contribute to a specific diagnosis, is, therefore, a highly promising alternative (Tomassetti S, et al. AJRCCM. 2016;193[7]:745).
As cryobiopsy is increasingly adopted around the world, however, troubling reports of serious complications have surfaced. Most notable is the recently reported experience of the initial 25 cases performed at the University of Pennsylvania, in which almost one in four patients suffered serious complications (DiBardino DM, et al. Ann Am Thorac Soc. 2017;14[6]:851). The authors pointed to lack of a predefined procedural protocol, as well as several choices relating to the specific technique used, including inconsistent use of fluoroscopy, lack of prophylactic bronchial blocker placement, and predominant use of laryngeal mask airways as potential contributing factors. Indeed, many variations of the basic cryobiopsy procedure have been described (Lentz RJ, et al. J Thoracic Dis. 2017;9[7]:2186), with no formal guidance or training available to inform advanced bronchoscopists interested in this procedure.
It is incumbent on the interventional pulmonology and ILD specialist communities to be responsible stewards of this promising procedure. Implementation of three parallel efforts to standardize and rigorously study this procedure should be considered as soon as possible: creation of expert consensus guidelines establishing best-practices for safe and effective biopsy technique; a training requirement before independent performance of the procedure; and creation of an international cryobiopsy registry to facilitate higher-quality research into optimal technique and outcomes. We owe this to our patients.
Robert J. Lentz, MD
NetWork Member
Fabien Maldonado, MD, FCCP
NetWork Member
Pediatric Chest Medicine
Chronic cough in children: New guidelines
A chronic cough is a common complaint among children whose parents seek medical evaluation. Chronic wet cough can indicate an underlying illness; therefore, an early diagnosis can lead to prevention of complications of the disease and improvement in quality of life.
CHEST is a leading resource in evidence and consensus-based guidelines on important topics affecting children. The most recent guidelines entitled Management of Children with Chronic Wet Cough and Protracted Bacterial Bronchitis (Chest. 2017;151(4):884-890) and Use of Management Pathways or Algorithms in Children with Chronic Cough (Chest. 2017;151(4):875-873) are updates from the 2006 CHEST guidelines on chronic cough in children.
The present updates utilized the CHEST methodological guidelines with chronic wet or productive cough and Grading of Recommendations Assessment, Development, and Evaluation framework and also performed a systematic review addressing key questions concerning the management of childhood disease for children 14 years and younger.
Guidance provided by the expert panel focused on recommendations to answer six key questions concerning the management of children 14 years and younger with a chronic wet cough unrelated to established chronic lung disease. The recommendations are:
1. Chronic cough is defined as the presence of a cough 4 weeks or longer in duration.
2. Assessment of the effect of the cough on the child and the family be undertaken as part of clinical consultation.
3. Evaluation of a chronic cough should be done with a systematic approach with pediatric-specific cough management protocols or algorithms.
4. Chest radiograph and, when age appropriate, spirometry with bronchodilator be undertaken as evaluation; tests for pertussis infection only to be performed if clinically suspected.
5. Chronic wet cough with no specific clinical features should receive antibiotics for 2 weeks targeted for common respiratory bacteria (Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis).
6. When cough persists despite 2 weeks of appropriate antibiotics, it is recommended to continue for an additional 2 weeks.
7. Additional tests (eg skin prick test, Mantoux, bronchoscopy, chest CT scan) should be individualized in accordance with the clinical setting and child’s clinical symptoms and signs.
The panel recognizes the need for prospective studies to assess current algorithms outcomes of children with chronic cough. Both articles can be found on the guidelines section of the CHEST site.
John Bishara, DO
Fellow-in-Training Member
Pulmonary Physiology, Function, and Rehabilitation
Functional imaging of the lung
Quantifying heterogeneity of ventilation and gas exchange in lung diseases remains a clinical challenge. Conventional pulmonary function test is insensitive to regional changes. The multiple inert gas elimination technique can quantify ventilation-perfusion distribution, but it requires invasive instrumentation (eg, pulmonary artery catheterization) and is not practical for clinical use. Computed tomography (CT) scans delineate spatial changes in lung structures but do not directly measure changes in ventilation and gas exchange. With its radiation, it is difficult to apply CT scanning repeatedly in patients. More recently, MR imaging techniques have been developed to directly “visualize” and quantify regional lung function (Kruger SJ, et al. J Magn Reson Imaging. 2016;43(2):295; Roos JE, et al. Magn Reson Imaging Clin N Am. 2015;23(2):217). These techniques employ inhalation of gases, such as oxygen, perfluorinated gases, and hyperpolarized 3He and 129Xe. Hyperpolarized 3He has been studied the most; however, the dwindling supply of 3He gas and its rising cost have prevented its further development. 129Xe has abundant supply and has emerged to be the inert gas of choice for MR imaging. Hyperpolarized 129Xe can measure ventilation, like hyperpolarized 3He. In addition, Xe diffuses into alveolar barrier (interstitium and plasma) and red blood cells, where it exhibits distinct resonant frequency shifts that can be captured by MR. Therefore, in one test, information on pulmonary ventilation and gas transfer can be obtained. To date, the results from MR imaging studies have provided new insights into the pathophysiology of obstructive and restrictive lung diseases. With continuous development, MR imaging of the lung could become a clinically useful tool in the near future.
Yuh-Chin T. Huang, MD, MHS, FCCP
Steering Committee Member
Thoracic Oncology
Immune-mediated pneumonitis and PD-1 inhibition
Inhibitors of the programmed cell death 1 receptor (PD-1) have shown significant promise in the treatment of advanced stage malignancy. With the recent expansion of indications for use of these agents, the number of patients treated will continue to grow. Clinicians must be aware of their potential for serious adverse side effects, including dermatitis, colitis, and potentially life-threatening pneumonitis.
The development of pneumonitis secondary to PD-1 inhibitions is reported to occur in 2% to 5% of patients and can present at any time during therapy, with 1% of patients developing grade 3 or higher pneumonitis.1,2 The most common symptoms are dyspnea and cough, though one-third of patients are asymptomatic at presentation.2 Radiographic and pathologic features vary greatly and include organizing pneumonia, interstitial pneumonitis, hypersensitivity pneumonitis, or diffuse alveolar damage.3 While pneumonitis due to PD-1 inhibition is reportedly uncommon, the increasing number of patients expected to receive these medications will predictably result in increasing overall frequency of pneumonitis cases. In addition, the lack of large prospective randomized trials and reliance on radiographic rather than pathologic data in diagnosing immune-mediated pneumonitis gives one pause. Given the variability of presentation, lack of routine pathologic data, and increasing use of dual agents (eg, PD-1 and CTLA-4), chest physicians and medical oncologists should have a high index of suspicion yet practice equipoise in patients receiving immunotherapy who develop unexplained pulmonary symptoms or infiltrates. More research is needed to help improve the multidisciplinary diagnosis and treatment of this potentially serious complication.
David Maurice Chambers, MD
Fellow-in-Training Member
Jason Atticus Akulian, MD, MPH
Steering Committee Member
References
1. Nishino M, et al. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncology. 2016;2(12):1607.
2. Naidoo J, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol. 2017;35(7):709.
3. Nishino M, et al. PD-1 inhibitor-related pneumonitis in advanced cancer patients: radiographic patterns and clinical course. Clin Cancer Res. 2016;22(24):6051.
Pulmonary Vascular Disease
Pulmonary Arterial Hypertension Associated With SLE
While pulmonary arterial hypertension (PAH) commonly complicates scleroderma (SSc), it is a rare complication of other connective tissue diseases (CTD), such as systemic lupus erythematosus (SLE). In the few prospective studies that utilize right-sided heart catheterization (RHC), the estimated prevalence of PAH in SLE is about 4%. However, since the prevalence of SLE is 10 to 15 times greater than SSc in the United States, the true prevalence of SLE-PAH may be higher than previously thought, and, thus, clinically relevant. Despite this, little is known about SLE-PAH.
A recent retrospective study from the French Pulmonary Hypertension Registry has added significantly to our understanding of this complication of SLE. Hachulla and colleagues studied 51 patients with RHC-proven SLE-PAH compared with 101 SLE control subjects without PAH. While the authors did not find any relevant differences in the demographics between groups, they did find a significantly higher prevalence of SSA and SSB antibodies in SLE-PAH. Interestingly, the presence of anti-U1 RNP antibody appeared to be less common in SLE-PAH patients; this lack of association is in contrast to prior studies in mixed CTD patients with anti-U1 RNP antibodies in which the prevalence of PAH can be as high as 60%. Further, none of the SLE-PAH patients demonstrated an acute response to vasodilator challenge during RHC, emphasizing that this maneuver does not need to be performed in SLE patients at risk of PAH. Trends toward improved survival in SLE-PAH patients treated with hydroxychloroquine are preliminary and hypothesis-generating but require confirmation in larger clinical studies.
Stephen Mathai, MD, FCCP
Chair
Leena Palwar, MD
Fellow-in-Training Member
References
Hachulla E, Jais X, Cinquetti G, et al. Pulmonary arterial hypertension associated with SLE: Results from the French pulmonary hypertension registry. Chest. 2017 Aug 26. pii: S0012-3692(17)31430-7. doi: 10.1016/j.chest.2017.08.014. [Epub ahead of print]
Chung L, Liu J, Parsons L, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138:1383-1394.
Shirai Y, Yasuoka H, Okano Y, Takeuchi T, Satoh T, Kuwana M. Clinical characteristics and survival of Japanese patients with connective tissue disease and pulmonary arterial hypertension: a singlecentre cohort. Rheumatology. 2012;51:1846-1854.
Hao YJ, Jiang X, Zhou W, et al. Connective tissue disease-associated pulmonary arterial hypertension in Chinese patients. Eur Respir J. 2014;44: 963-972.
Huang C, Li M, Liu Y, et al. Baseline characteristics and risk factors of pulmonary arterial hypertension in systemic lupus erythematosus patients. Medicine. 2016;95:e2761.
Pérez-Peñate GM, Rúa-Figueroa I, Juliá- Serdá G, et al. Pulmonary arterial hypertension in systemic lupus erythematosus: prevalence and predictors. J Rheumatol. 2016;43:323-329.
Alpert MA, Goldberg SH, Sindem BH, et al. Cardiovascular manifestations of mixed connective tissue disease in adults. Circulation. 1983;63:1182-1193.
CDC: Forty percent of cancers linked to overweight or obesity
Being overweight or obese significantly increased the risk of developing at least 13 types of cancer, according to a report by the Centers for Disease Control and Prevention.
Now that a larger proportion of the American population is overweight or obese, the rates of obesity-related cancers have increased. Between 2005 and 2014, the rate of obesity-related cancers, excluding colorectal cancer, increased by 7%. Over the same period, non–obesity-related cancers declined, according to C. Brooke Steele, DO, of the CDC’s Division of Cancer Prevention and Control, and her associates (MMWR Morb Mortal Wkly Rep. 2017 Oct 3;66[39]:1052-8).![]()
They found that 631,604 people were diagnosed with an overweight- or obesity-related cancer, 40% of nearly 1.6 million of all cancer diagnoses in 2014. The effect was more pronounced in older people (age at least 50 years), compared with younger people, with two-thirds of cases occurring in the 50- to 74-year-old age range.
Women were much more likely to have overweight- and obesity-related cancers, with higher incidence rates (218.1 per 100,000 population) than those of men (115.0 per 100,000). A contributing factor for this difference between men and women was female-specific cancers such as endometrial, ovarian, and postmenopausal breast cancers, which accounted for 42% (268,091) of overweight- and obesity-related cancers.
Researchers found that, between 2005 and 2014, the overall incidence of overweight- and obesity-related cancers (including colorectal cancer) decreased by 2%, colorectal cancer decreased by 23%, and cancers unrelated to body weight decreased by 13%. A contributing factor to the decrease in colorectal cancer was most likely cancer screening tests, which can detect and lead to the removal of precancerous polyps.
“A majority of American adults weigh more than recommended – and being overweight or obese puts people at higher risk for a number of cancers – so these findings are a cause for concern,” CDC Director Brenda Fitzgerald, MD, said in a statement. “By getting to and keeping a healthy weight, we all can play a role in cancer prevention.”
The researchers had no conflicts of interest to report.
Being overweight or obese significantly increased the risk of developing at least 13 types of cancer, according to a report by the Centers for Disease Control and Prevention.
Now that a larger proportion of the American population is overweight or obese, the rates of obesity-related cancers have increased. Between 2005 and 2014, the rate of obesity-related cancers, excluding colorectal cancer, increased by 7%. Over the same period, non–obesity-related cancers declined, according to C. Brooke Steele, DO, of the CDC’s Division of Cancer Prevention and Control, and her associates (MMWR Morb Mortal Wkly Rep. 2017 Oct 3;66[39]:1052-8).![]()
They found that 631,604 people were diagnosed with an overweight- or obesity-related cancer, 40% of nearly 1.6 million of all cancer diagnoses in 2014. The effect was more pronounced in older people (age at least 50 years), compared with younger people, with two-thirds of cases occurring in the 50- to 74-year-old age range.
Women were much more likely to have overweight- and obesity-related cancers, with higher incidence rates (218.1 per 100,000 population) than those of men (115.0 per 100,000). A contributing factor for this difference between men and women was female-specific cancers such as endometrial, ovarian, and postmenopausal breast cancers, which accounted for 42% (268,091) of overweight- and obesity-related cancers.
Researchers found that, between 2005 and 2014, the overall incidence of overweight- and obesity-related cancers (including colorectal cancer) decreased by 2%, colorectal cancer decreased by 23%, and cancers unrelated to body weight decreased by 13%. A contributing factor to the decrease in colorectal cancer was most likely cancer screening tests, which can detect and lead to the removal of precancerous polyps.
“A majority of American adults weigh more than recommended – and being overweight or obese puts people at higher risk for a number of cancers – so these findings are a cause for concern,” CDC Director Brenda Fitzgerald, MD, said in a statement. “By getting to and keeping a healthy weight, we all can play a role in cancer prevention.”
The researchers had no conflicts of interest to report.
Being overweight or obese significantly increased the risk of developing at least 13 types of cancer, according to a report by the Centers for Disease Control and Prevention.
Now that a larger proportion of the American population is overweight or obese, the rates of obesity-related cancers have increased. Between 2005 and 2014, the rate of obesity-related cancers, excluding colorectal cancer, increased by 7%. Over the same period, non–obesity-related cancers declined, according to C. Brooke Steele, DO, of the CDC’s Division of Cancer Prevention and Control, and her associates (MMWR Morb Mortal Wkly Rep. 2017 Oct 3;66[39]:1052-8).![]()
They found that 631,604 people were diagnosed with an overweight- or obesity-related cancer, 40% of nearly 1.6 million of all cancer diagnoses in 2014. The effect was more pronounced in older people (age at least 50 years), compared with younger people, with two-thirds of cases occurring in the 50- to 74-year-old age range.
Women were much more likely to have overweight- and obesity-related cancers, with higher incidence rates (218.1 per 100,000 population) than those of men (115.0 per 100,000). A contributing factor for this difference between men and women was female-specific cancers such as endometrial, ovarian, and postmenopausal breast cancers, which accounted for 42% (268,091) of overweight- and obesity-related cancers.
Researchers found that, between 2005 and 2014, the overall incidence of overweight- and obesity-related cancers (including colorectal cancer) decreased by 2%, colorectal cancer decreased by 23%, and cancers unrelated to body weight decreased by 13%. A contributing factor to the decrease in colorectal cancer was most likely cancer screening tests, which can detect and lead to the removal of precancerous polyps.
“A majority of American adults weigh more than recommended – and being overweight or obese puts people at higher risk for a number of cancers – so these findings are a cause for concern,” CDC Director Brenda Fitzgerald, MD, said in a statement. “By getting to and keeping a healthy weight, we all can play a role in cancer prevention.”
The researchers had no conflicts of interest to report.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Key clinical point:
Major finding: In the United States, more than 631,000 patients received cancer diagnoses related to overweight or obesity, representing 40% of nearly 1.6 million cancer diagnoses in 2014.
Data source: An analysis of United States Cancer Statistics data from 2005 to 2014.
Disclosures: The researchers had no conflicts of interest to report.
Don't just blame Facebook for fake news: It's us, too
Critics such as Zeynep Tufekci are quite right to take Facebook and Twitter to task for allowing nefarious and hostile actors, likely including the Russian state, to hold sway on social media (“Facebook’s Ad Scandal Isn’t a ‘Fail,’ It’s a Feature,” New York Times, Sept. 23, 2017).
These actors must be reined in online, for the very simple reason that so many of us are immersed in our news feeds and Twitter streams, and thus susceptible to whatever toxins are allowed to proliferate there.

Some have called apps, including social media, “the race to the bottom of the brainstem.” The most primitive parts of our brain, responsible for fight-flight and survival, are always on the lookout for perceived threats. In our restless, clicking and scrolling state, we are often naturally attracted to and activated by tantalizing, titillating, and emotionally charged posts that are lacking in reason, but are inflammatory and viscerally captivating. Viral news, click bait, gossip, rumors, and scandals get a disproportionate share of our attention. And since we become what we do, our reason is overwhelmed by reaction. In fact, a recent 60 Minutes segment demonstrated how President Trump’s political operatives optimized Facebook ads for reaction, not thought. As we engage in social media, we may become less reasonable, and prone to reacting out of our most base and primal fears.
The late neurologist and psychiatrist Viktor E. Frankl pointed out our freedom lies in our ability to put space between stimulus and response. In this space lies our freedom to choose, he wrote. Online, this inner life can shrink. Our wandering minds look for cheap thrills and anything that confirms our biases of threat. We reduce the world to simplistic one-size-fits-all narratives, and heap blame on our usual suspects. I call the Internet the angernet. Anger is the most viral and contagious emotion on social networks, and as we use social media, we deepen the groove of anger – making our anger more likely and the most readily shared.
But we’ve been racing to the bottom of the brainstem, where fear, anger, hatred, and reactivity reside, for decades in this country. Again, we can’t simply blame social media. Trust has been eroding for decades, for many reasons. No matter the generation, only a minority of us trust each other, according to the Pew Research Center’s surveys. Millennials are the least trusting of all: Only 19% of them agree that “generally speaking, people are to be trusted.” Any scroll of the news feed quickly confirms this dangerous bias to mistrust, as we are besieged by a near cataclysmic barrage of traumatic events. We are also more polarized than ever, with a great percentage of partisans believing that the other side aims at the destruction of all they hold dear in America. As we feel more vulnerable, we are more likely to mistrust and become further polarized, and the cycle continues.
More importantly, as we flee real-world relationships and interaction for the ease and seeming reach of the online world, we lose subtle cues and important connections that would normally soothe our reactivity. Humanity has evolved and progressed precisely because of our social connections. We are who happens to us, and what we make of the happening. When we connect in more superficial ways, we endanger our very identities. As a nation, we are having an identity crisis: We have not worked out who we are in relation to one another, and to ourselves. This is expressed politically, and in our confused and fearful opinions and appraisals of each other and government. Without the good graces that come out of shared presence in real-world relationships, we are more likely to think badly of each other. We are more likely to retreat into narrow and tribal identities where we think safety resides, and deemphasize communal identity. In this space of narrow identity, ideological self-righteousness and dogma prevail, and we are less likely to listen and cultivate curiosity, understanding, and empathy for others. One example lies in how representatives and senators spend less time socializing with each other than in years past, and are thus less likely to forge compromise. Online, we are all refugees from the real world, and we fall to building our own personal walls and exiling those with whom we disagree – who then become those we hate, fear, blame, and fight.
We have met the enemy, and it is us.
The antidote to mistrust is in cultivating the top of our nervous systems, where long-term planning and positive emotions reside. We can only do this through real-world relationships. Social media will not ultimately take us to a feeling of society. It might provide a glimmer of connection, but its inherent vectors of disconnection and division are proving deadly, from Internet radicalization, to the increased levels of depression, anxiety, loneliness, and suicidality noted with increasing Internet and social media use.
We each have incredible human possibilities, but to reach them, we have to transcend the biases and reactivity of our habitually and usually unconsciously self-centered egos. We can start with awareness of what the Internet siren is doing to us and steer our ships in a more fruitful direction. Toward home, toward our hearts, and toward each other.
Dr. Chandra is a psychiatrist and writer in San Francisco. He is the author of Facebuddha: Transcendence in the Age of Social Networks (Pacific Heart Books, 2017).
Critics such as Zeynep Tufekci are quite right to take Facebook and Twitter to task for allowing nefarious and hostile actors, likely including the Russian state, to hold sway on social media (“Facebook’s Ad Scandal Isn’t a ‘Fail,’ It’s a Feature,” New York Times, Sept. 23, 2017).
These actors must be reined in online, for the very simple reason that so many of us are immersed in our news feeds and Twitter streams, and thus susceptible to whatever toxins are allowed to proliferate there.
Some have called apps, including social media, “the race to the bottom of the brainstem.” The most primitive parts of our brain, responsible for fight-flight and survival, are always on the lookout for perceived threats. In our restless, clicking and scrolling state, we are often naturally attracted to and activated by tantalizing, titillating, and emotionally charged posts that are lacking in reason, but are inflammatory and viscerally captivating. Viral news, click bait, gossip, rumors, and scandals get a disproportionate share of our attention. And since we become what we do, our reason is overwhelmed by reaction. In fact, a recent 60 Minutes segment demonstrated how President Trump’s political operatives optimized Facebook ads for reaction, not thought. As we engage in social media, we may become less reasonable, and prone to reacting out of our most base and primal fears.
The late neurologist and psychiatrist Viktor E. Frankl pointed out our freedom lies in our ability to put space between stimulus and response. In this space lies our freedom to choose, he wrote. Online, this inner life can shrink. Our wandering minds look for cheap thrills and anything that confirms our biases of threat. We reduce the world to simplistic one-size-fits-all narratives, and heap blame on our usual suspects. I call the Internet the angernet. Anger is the most viral and contagious emotion on social networks, and as we use social media, we deepen the groove of anger – making our anger more likely and the most readily shared.
But we’ve been racing to the bottom of the brainstem, where fear, anger, hatred, and reactivity reside, for decades in this country. Again, we can’t simply blame social media. Trust has been eroding for decades, for many reasons. No matter the generation, only a minority of us trust each other, according to the Pew Research Center’s surveys. Millennials are the least trusting of all: Only 19% of them agree that “generally speaking, people are to be trusted.” Any scroll of the news feed quickly confirms this dangerous bias to mistrust, as we are besieged by a near cataclysmic barrage of traumatic events. We are also more polarized than ever, with a great percentage of partisans believing that the other side aims at the destruction of all they hold dear in America. As we feel more vulnerable, we are more likely to mistrust and become further polarized, and the cycle continues.
More importantly, as we flee real-world relationships and interaction for the ease and seeming reach of the online world, we lose subtle cues and important connections that would normally soothe our reactivity. Humanity has evolved and progressed precisely because of our social connections. We are who happens to us, and what we make of the happening. When we connect in more superficial ways, we endanger our very identities. As a nation, we are having an identity crisis: We have not worked out who we are in relation to one another, and to ourselves. This is expressed politically, and in our confused and fearful opinions and appraisals of each other and government. Without the good graces that come out of shared presence in real-world relationships, we are more likely to think badly of each other. We are more likely to retreat into narrow and tribal identities where we think safety resides, and deemphasize communal identity. In this space of narrow identity, ideological self-righteousness and dogma prevail, and we are less likely to listen and cultivate curiosity, understanding, and empathy for others. One example lies in how representatives and senators spend less time socializing with each other than in years past, and are thus less likely to forge compromise. Online, we are all refugees from the real world, and we fall to building our own personal walls and exiling those with whom we disagree – who then become those we hate, fear, blame, and fight.
We have met the enemy, and it is us.
The antidote to mistrust is in cultivating the top of our nervous systems, where long-term planning and positive emotions reside. We can only do this through real-world relationships. Social media will not ultimately take us to a feeling of society. It might provide a glimmer of connection, but its inherent vectors of disconnection and division are proving deadly, from Internet radicalization, to the increased levels of depression, anxiety, loneliness, and suicidality noted with increasing Internet and social media use.
We each have incredible human possibilities, but to reach them, we have to transcend the biases and reactivity of our habitually and usually unconsciously self-centered egos. We can start with awareness of what the Internet siren is doing to us and steer our ships in a more fruitful direction. Toward home, toward our hearts, and toward each other.
Dr. Chandra is a psychiatrist and writer in San Francisco. He is the author of Facebuddha: Transcendence in the Age of Social Networks (Pacific Heart Books, 2017).
Critics such as Zeynep Tufekci are quite right to take Facebook and Twitter to task for allowing nefarious and hostile actors, likely including the Russian state, to hold sway on social media (“Facebook’s Ad Scandal Isn’t a ‘Fail,’ It’s a Feature,” New York Times, Sept. 23, 2017).
These actors must be reined in online, for the very simple reason that so many of us are immersed in our news feeds and Twitter streams, and thus susceptible to whatever toxins are allowed to proliferate there.
Some have called apps, including social media, “the race to the bottom of the brainstem.” The most primitive parts of our brain, responsible for fight-flight and survival, are always on the lookout for perceived threats. In our restless, clicking and scrolling state, we are often naturally attracted to and activated by tantalizing, titillating, and emotionally charged posts that are lacking in reason, but are inflammatory and viscerally captivating. Viral news, click bait, gossip, rumors, and scandals get a disproportionate share of our attention. And since we become what we do, our reason is overwhelmed by reaction. In fact, a recent 60 Minutes segment demonstrated how President Trump’s political operatives optimized Facebook ads for reaction, not thought. As we engage in social media, we may become less reasonable, and prone to reacting out of our most base and primal fears.
The late neurologist and psychiatrist Viktor E. Frankl pointed out our freedom lies in our ability to put space between stimulus and response. In this space lies our freedom to choose, he wrote. Online, this inner life can shrink. Our wandering minds look for cheap thrills and anything that confirms our biases of threat. We reduce the world to simplistic one-size-fits-all narratives, and heap blame on our usual suspects. I call the Internet the angernet. Anger is the most viral and contagious emotion on social networks, and as we use social media, we deepen the groove of anger – making our anger more likely and the most readily shared.
But we’ve been racing to the bottom of the brainstem, where fear, anger, hatred, and reactivity reside, for decades in this country. Again, we can’t simply blame social media. Trust has been eroding for decades, for many reasons. No matter the generation, only a minority of us trust each other, according to the Pew Research Center’s surveys. Millennials are the least trusting of all: Only 19% of them agree that “generally speaking, people are to be trusted.” Any scroll of the news feed quickly confirms this dangerous bias to mistrust, as we are besieged by a near cataclysmic barrage of traumatic events. We are also more polarized than ever, with a great percentage of partisans believing that the other side aims at the destruction of all they hold dear in America. As we feel more vulnerable, we are more likely to mistrust and become further polarized, and the cycle continues.
More importantly, as we flee real-world relationships and interaction for the ease and seeming reach of the online world, we lose subtle cues and important connections that would normally soothe our reactivity. Humanity has evolved and progressed precisely because of our social connections. We are who happens to us, and what we make of the happening. When we connect in more superficial ways, we endanger our very identities. As a nation, we are having an identity crisis: We have not worked out who we are in relation to one another, and to ourselves. This is expressed politically, and in our confused and fearful opinions and appraisals of each other and government. Without the good graces that come out of shared presence in real-world relationships, we are more likely to think badly of each other. We are more likely to retreat into narrow and tribal identities where we think safety resides, and deemphasize communal identity. In this space of narrow identity, ideological self-righteousness and dogma prevail, and we are less likely to listen and cultivate curiosity, understanding, and empathy for others. One example lies in how representatives and senators spend less time socializing with each other than in years past, and are thus less likely to forge compromise. Online, we are all refugees from the real world, and we fall to building our own personal walls and exiling those with whom we disagree – who then become those we hate, fear, blame, and fight.
We have met the enemy, and it is us.
The antidote to mistrust is in cultivating the top of our nervous systems, where long-term planning and positive emotions reside. We can only do this through real-world relationships. Social media will not ultimately take us to a feeling of society. It might provide a glimmer of connection, but its inherent vectors of disconnection and division are proving deadly, from Internet radicalization, to the increased levels of depression, anxiety, loneliness, and suicidality noted with increasing Internet and social media use.
We each have incredible human possibilities, but to reach them, we have to transcend the biases and reactivity of our habitually and usually unconsciously self-centered egos. We can start with awareness of what the Internet siren is doing to us and steer our ships in a more fruitful direction. Toward home, toward our hearts, and toward each other.
Dr. Chandra is a psychiatrist and writer in San Francisco. He is the author of Facebuddha: Transcendence in the Age of Social Networks (Pacific Heart Books, 2017).