User login
Toolkit Can Help Reduce Opioid-Related Adverse Events

The RADEO toolkit also provides strategies for facilitating policy formation, evaluating current processes, tracking progress against implementation goals, and identifying best practices. Although the RADEO toolkit is designed for the inpatient setting, it also discusses care transitions for patients on opioid therapy to the outpatient setting.
Download the toolkit today at www.hospitalmedicine.org/RADEO. Check out all available quality improvement and patient safety toolkits at www.hospitalmedicine.org/qi.
The RADEO toolkit also provides strategies for facilitating policy formation, evaluating current processes, tracking progress against implementation goals, and identifying best practices. Although the RADEO toolkit is designed for the inpatient setting, it also discusses care transitions for patients on opioid therapy to the outpatient setting.
Download the toolkit today at www.hospitalmedicine.org/RADEO. Check out all available quality improvement and patient safety toolkits at www.hospitalmedicine.org/qi.
The RADEO toolkit also provides strategies for facilitating policy formation, evaluating current processes, tracking progress against implementation goals, and identifying best practices. Although the RADEO toolkit is designed for the inpatient setting, it also discusses care transitions for patients on opioid therapy to the outpatient setting.
Download the toolkit today at www.hospitalmedicine.org/RADEO. Check out all available quality improvement and patient safety toolkits at www.hospitalmedicine.org/qi.
Submit Your Case Study on Promoting Antimicrobial Stewardship and “Fight the Resistance”


Commission on Care: Expand Community Care, Close Facilities
The Commission on Care has issued its final report, which called for the expansion of community care for all veterans through the creation of integrated community-based health care networks similar to TRICARE, expansion of eligibility for veterans, and the creation of a facility and capital asset realignment process based on the DoD Base Realignment and Closure Commission among its 18 recommendations.
Mandated by the Veterans Access, Choice and Accountability Act in the wake of the wait time, the 15-member Commission on Care was charged with providing recommendations for reforming veterans’ health care to President Obama. The commission’s recommendations carry considerable weight. The Choice Act mandated that the VA and other federal agencies “implement each recommendation that the President considers feasible, advisable, and able to implement without further legislation.”
The commission’s first recommendation was to scrap the Choice Program and establish the VHA Care System, a system of “integrated veteran-centric, community-based delivery networks that will optimize the balance of access, quality, and cost-effectiveness.” Local VHA leadership would develop the VHA Care System and base it on “local needs and veterans’ preferences.” The VHA would be mandated to furnish credentials to community providers, with the highest priority access given to service-connected veterans. The time and distance criteria used by the Choice Program would be eliminated, and veterans would be able to choose any primary care provider from within the system.
The Commission offered 4 possible models for implementing the VHA Care System. In the recommended option (an integrated network of VHA, DoD, other federally funded providers, and community providers, which requires a referral to access specialty care), the commission predicts as many as 60% of veterans would shift to community care for primary care needs, though far fewer would seek referrals in the community. The commission also predicted about a 15% increase in enrollment and an additional $5 billion in cost by FY 2019.
Another recommendation called for a “robust strategy for meeting and managing VHA’s facility and capital-asset needs.” According to the commission, the VA must reevaluate the future of individual facilities “in light of a transformative new delivery model.” A new commission, based on the military closure commissions, would help determine which facilities would remain open and which would close. “If VA could sell, repurpose, or otherwise divest itself of unused or underutilized buildings in a timely, cost-effective manner, it would free funds for the purposes for which they are appropriated,” the commission argued.
The commission also focused on personnel issues in a number of its recommendations, calling for the transformation of VHA culture and staff engagement, performance metrics for all employees, a new personnel system, and increased cultural and military competency, “to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.”
All but 2 commissioners signed the report. The commission charged that “many profound deficiencies in VHA operations require urgent reform, and that America’s veterans deserve a better organized, high-performing health care system.” While the changes may seem sweeping to many, the 2 dissenting commissioners urged even more significant changes. In a dissent letter acquired by the Washington Free Beacon, these commissioners argue that “the disappointing reality is that the commission’s final report is deeply compromised, disjointed, and incomplete. The report repeatedly invokes the need for a ‘bold transformation’ at the VHA. Yet, with a few exceptions, there is a decided lack of boldness in the Commission’s recommendations.”
Reaction has been slow as officials at the White House, VA, and veterans group digest the 308-page report. Some groups, however, already are raising concerns. The American Legion issued a statement: “Increased privatization of veteran health care services is not in the best interest of veterans or the American taxpayer. While we are still reviewing the complete report, we note that the commission had a very limited interaction with veterans who actually use VA health care, and even less time spent in VA facilities.”
The President also issued a brief noncommittal statement. “The commission's report includes a number of specific proposals that I look forward to reviewing closely over the coming weeks. We will continue to work with veterans, Congress, and our partners in the veteran advocacy community to further our ongoing transformation of the veterans’ health care system. Our veterans deserve nothing less for their sacrifices and their service.”
The VA offered a brief reaction to the report, finding commonalities in its current reform efforts. “While we will examine the report closely over the coming weeks and respond in a more detailed fashion, I am pleased to see that many of their recommendations are in line with our MyVA efforts to transform the VA into a veteran-centric organization,” Secretary of Veterans Affairs Robert A. McDonald said in the statement. “There are some things that can be done right now to help us continue our progress. Congress must act on our proposals to consolidate our Community Care programs, modernize and reform the claims appeals process, and pass the bi-partisan Veterans First Act.”
[Click through to the 18 recommendations offered by the commission.]
The full set of recommendations covers a broad range of issue for the VA:
Recommendation #1: Across the United States, with local input and knowledge, VHA should establish high-performing, integrated community health care networks, to be known as the VHA Care System, from which veterans will access high-quality health care services.
Recommendation #2: Enhance clinical operations through more effective use of providers and other health professionals, and improved data collection and management.
Recommendation #3: Develop a process for appealing clinical decisions that provides veterans protections at least comparable to those afforded patients under other federally supported programs.
Recommendation #4: Adopt a continuous improvement methodology to support VHA transformation, and consolidate best practices and continuous improvement efforts under the Veterans Engineering Resource Center.
Recommendation #5: Eliminate health care disparities among veterans treated in the VHA Care System by committing adequate personnel and monetary resources to address the causes of the problem and ensuring the VHA Health Equity Action Plan is fully implemented.
Recommendation #6: Develop and implement a robust strategy for meeting and managing VHA’s facility and capital-asset needs.
Recommendation #7: Modernize VA’s IT systems and infrastructure to improve veterans’ health and well-being and provide the foundation needed to transform VHA’s clinical and business processes.
Recommendation #8: Transform the management of the supply chain in VHA.
Recommendation #9: Establish a board of directors to provide overall VHA Care System governance, set long-term strategy, and direct and oversee the transformation process.
Recommendation #10: Require leaders at all levels of the organization to champion a focused, clear, benchmarked strategy to transform VHA culture and sustain staff engagement.
Recommendation #11: Rebuild a system for leadership succession based on a benchmarked health care competency model that is consistently applied to recruitment, development, and advancement within the leadership pipeline.
Recommendation #12: Transform organizational structures and management processes to ensure adherence to national VHA standards, while also promoting decision making at the lowest level of the organization, eliminating waste and redundancy, promoting innovation, and fostering the spread of best practices.
Recommendation #13: Streamline and focus organizational performance measurement in VHA using core metrics that are identical to those used in the private sector, and establish a personnel performance management system for health care leaders in VHA that is distinct from performance measurement, is based on the leadership competency model, assesses leadership ability, and measures the achievement of important organizational strategies.
Recommendation #14: Foster cultural and military competence among all VHA Care System leadership, providers, and staff to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.
Recommendation #15: Create a simple-to-administer alternative personnel system, in law and regulation, which governs all VHA employees, applies best practices from the private sector to human capital management, and supports pay and benefits that are competitive with the private sector.
Recommendation #16: Require top executives to lead the transformation of HR, commit funds, and assign expert resources to achieve an effective human capital management system.
Recommendation #17: Provide a streamlined path to eligibility for health care for those with an other-than-honorable discharge who have substantial honorable service.
Recommendation #18: Establish an expert body to develop recommendations for VA care eligibility and benefit design.
The Commission on Care has issued its final report, which called for the expansion of community care for all veterans through the creation of integrated community-based health care networks similar to TRICARE, expansion of eligibility for veterans, and the creation of a facility and capital asset realignment process based on the DoD Base Realignment and Closure Commission among its 18 recommendations.
Mandated by the Veterans Access, Choice and Accountability Act in the wake of the wait time, the 15-member Commission on Care was charged with providing recommendations for reforming veterans’ health care to President Obama. The commission’s recommendations carry considerable weight. The Choice Act mandated that the VA and other federal agencies “implement each recommendation that the President considers feasible, advisable, and able to implement without further legislation.”
The commission’s first recommendation was to scrap the Choice Program and establish the VHA Care System, a system of “integrated veteran-centric, community-based delivery networks that will optimize the balance of access, quality, and cost-effectiveness.” Local VHA leadership would develop the VHA Care System and base it on “local needs and veterans’ preferences.” The VHA would be mandated to furnish credentials to community providers, with the highest priority access given to service-connected veterans. The time and distance criteria used by the Choice Program would be eliminated, and veterans would be able to choose any primary care provider from within the system.
The Commission offered 4 possible models for implementing the VHA Care System. In the recommended option (an integrated network of VHA, DoD, other federally funded providers, and community providers, which requires a referral to access specialty care), the commission predicts as many as 60% of veterans would shift to community care for primary care needs, though far fewer would seek referrals in the community. The commission also predicted about a 15% increase in enrollment and an additional $5 billion in cost by FY 2019.
Another recommendation called for a “robust strategy for meeting and managing VHA’s facility and capital-asset needs.” According to the commission, the VA must reevaluate the future of individual facilities “in light of a transformative new delivery model.” A new commission, based on the military closure commissions, would help determine which facilities would remain open and which would close. “If VA could sell, repurpose, or otherwise divest itself of unused or underutilized buildings in a timely, cost-effective manner, it would free funds for the purposes for which they are appropriated,” the commission argued.
The commission also focused on personnel issues in a number of its recommendations, calling for the transformation of VHA culture and staff engagement, performance metrics for all employees, a new personnel system, and increased cultural and military competency, “to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.”
All but 2 commissioners signed the report. The commission charged that “many profound deficiencies in VHA operations require urgent reform, and that America’s veterans deserve a better organized, high-performing health care system.” While the changes may seem sweeping to many, the 2 dissenting commissioners urged even more significant changes. In a dissent letter acquired by the Washington Free Beacon, these commissioners argue that “the disappointing reality is that the commission’s final report is deeply compromised, disjointed, and incomplete. The report repeatedly invokes the need for a ‘bold transformation’ at the VHA. Yet, with a few exceptions, there is a decided lack of boldness in the Commission’s recommendations.”
Reaction has been slow as officials at the White House, VA, and veterans group digest the 308-page report. Some groups, however, already are raising concerns. The American Legion issued a statement: “Increased privatization of veteran health care services is not in the best interest of veterans or the American taxpayer. While we are still reviewing the complete report, we note that the commission had a very limited interaction with veterans who actually use VA health care, and even less time spent in VA facilities.”
The President also issued a brief noncommittal statement. “The commission's report includes a number of specific proposals that I look forward to reviewing closely over the coming weeks. We will continue to work with veterans, Congress, and our partners in the veteran advocacy community to further our ongoing transformation of the veterans’ health care system. Our veterans deserve nothing less for their sacrifices and their service.”
The VA offered a brief reaction to the report, finding commonalities in its current reform efforts. “While we will examine the report closely over the coming weeks and respond in a more detailed fashion, I am pleased to see that many of their recommendations are in line with our MyVA efforts to transform the VA into a veteran-centric organization,” Secretary of Veterans Affairs Robert A. McDonald said in the statement. “There are some things that can be done right now to help us continue our progress. Congress must act on our proposals to consolidate our Community Care programs, modernize and reform the claims appeals process, and pass the bi-partisan Veterans First Act.”
[Click through to the 18 recommendations offered by the commission.]
The full set of recommendations covers a broad range of issue for the VA:
Recommendation #1: Across the United States, with local input and knowledge, VHA should establish high-performing, integrated community health care networks, to be known as the VHA Care System, from which veterans will access high-quality health care services.
Recommendation #2: Enhance clinical operations through more effective use of providers and other health professionals, and improved data collection and management.
Recommendation #3: Develop a process for appealing clinical decisions that provides veterans protections at least comparable to those afforded patients under other federally supported programs.
Recommendation #4: Adopt a continuous improvement methodology to support VHA transformation, and consolidate best practices and continuous improvement efforts under the Veterans Engineering Resource Center.
Recommendation #5: Eliminate health care disparities among veterans treated in the VHA Care System by committing adequate personnel and monetary resources to address the causes of the problem and ensuring the VHA Health Equity Action Plan is fully implemented.
Recommendation #6: Develop and implement a robust strategy for meeting and managing VHA’s facility and capital-asset needs.
Recommendation #7: Modernize VA’s IT systems and infrastructure to improve veterans’ health and well-being and provide the foundation needed to transform VHA’s clinical and business processes.
Recommendation #8: Transform the management of the supply chain in VHA.
Recommendation #9: Establish a board of directors to provide overall VHA Care System governance, set long-term strategy, and direct and oversee the transformation process.
Recommendation #10: Require leaders at all levels of the organization to champion a focused, clear, benchmarked strategy to transform VHA culture and sustain staff engagement.
Recommendation #11: Rebuild a system for leadership succession based on a benchmarked health care competency model that is consistently applied to recruitment, development, and advancement within the leadership pipeline.
Recommendation #12: Transform organizational structures and management processes to ensure adherence to national VHA standards, while also promoting decision making at the lowest level of the organization, eliminating waste and redundancy, promoting innovation, and fostering the spread of best practices.
Recommendation #13: Streamline and focus organizational performance measurement in VHA using core metrics that are identical to those used in the private sector, and establish a personnel performance management system for health care leaders in VHA that is distinct from performance measurement, is based on the leadership competency model, assesses leadership ability, and measures the achievement of important organizational strategies.
Recommendation #14: Foster cultural and military competence among all VHA Care System leadership, providers, and staff to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.
Recommendation #15: Create a simple-to-administer alternative personnel system, in law and regulation, which governs all VHA employees, applies best practices from the private sector to human capital management, and supports pay and benefits that are competitive with the private sector.
Recommendation #16: Require top executives to lead the transformation of HR, commit funds, and assign expert resources to achieve an effective human capital management system.
Recommendation #17: Provide a streamlined path to eligibility for health care for those with an other-than-honorable discharge who have substantial honorable service.
Recommendation #18: Establish an expert body to develop recommendations for VA care eligibility and benefit design.
The Commission on Care has issued its final report, which called for the expansion of community care for all veterans through the creation of integrated community-based health care networks similar to TRICARE, expansion of eligibility for veterans, and the creation of a facility and capital asset realignment process based on the DoD Base Realignment and Closure Commission among its 18 recommendations.
Mandated by the Veterans Access, Choice and Accountability Act in the wake of the wait time, the 15-member Commission on Care was charged with providing recommendations for reforming veterans’ health care to President Obama. The commission’s recommendations carry considerable weight. The Choice Act mandated that the VA and other federal agencies “implement each recommendation that the President considers feasible, advisable, and able to implement without further legislation.”
The commission’s first recommendation was to scrap the Choice Program and establish the VHA Care System, a system of “integrated veteran-centric, community-based delivery networks that will optimize the balance of access, quality, and cost-effectiveness.” Local VHA leadership would develop the VHA Care System and base it on “local needs and veterans’ preferences.” The VHA would be mandated to furnish credentials to community providers, with the highest priority access given to service-connected veterans. The time and distance criteria used by the Choice Program would be eliminated, and veterans would be able to choose any primary care provider from within the system.
The Commission offered 4 possible models for implementing the VHA Care System. In the recommended option (an integrated network of VHA, DoD, other federally funded providers, and community providers, which requires a referral to access specialty care), the commission predicts as many as 60% of veterans would shift to community care for primary care needs, though far fewer would seek referrals in the community. The commission also predicted about a 15% increase in enrollment and an additional $5 billion in cost by FY 2019.
Another recommendation called for a “robust strategy for meeting and managing VHA’s facility and capital-asset needs.” According to the commission, the VA must reevaluate the future of individual facilities “in light of a transformative new delivery model.” A new commission, based on the military closure commissions, would help determine which facilities would remain open and which would close. “If VA could sell, repurpose, or otherwise divest itself of unused or underutilized buildings in a timely, cost-effective manner, it would free funds for the purposes for which they are appropriated,” the commission argued.
The commission also focused on personnel issues in a number of its recommendations, calling for the transformation of VHA culture and staff engagement, performance metrics for all employees, a new personnel system, and increased cultural and military competency, “to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.”
All but 2 commissioners signed the report. The commission charged that “many profound deficiencies in VHA operations require urgent reform, and that America’s veterans deserve a better organized, high-performing health care system.” While the changes may seem sweeping to many, the 2 dissenting commissioners urged even more significant changes. In a dissent letter acquired by the Washington Free Beacon, these commissioners argue that “the disappointing reality is that the commission’s final report is deeply compromised, disjointed, and incomplete. The report repeatedly invokes the need for a ‘bold transformation’ at the VHA. Yet, with a few exceptions, there is a decided lack of boldness in the Commission’s recommendations.”
Reaction has been slow as officials at the White House, VA, and veterans group digest the 308-page report. Some groups, however, already are raising concerns. The American Legion issued a statement: “Increased privatization of veteran health care services is not in the best interest of veterans or the American taxpayer. While we are still reviewing the complete report, we note that the commission had a very limited interaction with veterans who actually use VA health care, and even less time spent in VA facilities.”
The President also issued a brief noncommittal statement. “The commission's report includes a number of specific proposals that I look forward to reviewing closely over the coming weeks. We will continue to work with veterans, Congress, and our partners in the veteran advocacy community to further our ongoing transformation of the veterans’ health care system. Our veterans deserve nothing less for their sacrifices and their service.”
The VA offered a brief reaction to the report, finding commonalities in its current reform efforts. “While we will examine the report closely over the coming weeks and respond in a more detailed fashion, I am pleased to see that many of their recommendations are in line with our MyVA efforts to transform the VA into a veteran-centric organization,” Secretary of Veterans Affairs Robert A. McDonald said in the statement. “There are some things that can be done right now to help us continue our progress. Congress must act on our proposals to consolidate our Community Care programs, modernize and reform the claims appeals process, and pass the bi-partisan Veterans First Act.”
[Click through to the 18 recommendations offered by the commission.]
The full set of recommendations covers a broad range of issue for the VA:
Recommendation #1: Across the United States, with local input and knowledge, VHA should establish high-performing, integrated community health care networks, to be known as the VHA Care System, from which veterans will access high-quality health care services.
Recommendation #2: Enhance clinical operations through more effective use of providers and other health professionals, and improved data collection and management.
Recommendation #3: Develop a process for appealing clinical decisions that provides veterans protections at least comparable to those afforded patients under other federally supported programs.
Recommendation #4: Adopt a continuous improvement methodology to support VHA transformation, and consolidate best practices and continuous improvement efforts under the Veterans Engineering Resource Center.
Recommendation #5: Eliminate health care disparities among veterans treated in the VHA Care System by committing adequate personnel and monetary resources to address the causes of the problem and ensuring the VHA Health Equity Action Plan is fully implemented.
Recommendation #6: Develop and implement a robust strategy for meeting and managing VHA’s facility and capital-asset needs.
Recommendation #7: Modernize VA’s IT systems and infrastructure to improve veterans’ health and well-being and provide the foundation needed to transform VHA’s clinical and business processes.
Recommendation #8: Transform the management of the supply chain in VHA.
Recommendation #9: Establish a board of directors to provide overall VHA Care System governance, set long-term strategy, and direct and oversee the transformation process.
Recommendation #10: Require leaders at all levels of the organization to champion a focused, clear, benchmarked strategy to transform VHA culture and sustain staff engagement.
Recommendation #11: Rebuild a system for leadership succession based on a benchmarked health care competency model that is consistently applied to recruitment, development, and advancement within the leadership pipeline.
Recommendation #12: Transform organizational structures and management processes to ensure adherence to national VHA standards, while also promoting decision making at the lowest level of the organization, eliminating waste and redundancy, promoting innovation, and fostering the spread of best practices.
Recommendation #13: Streamline and focus organizational performance measurement in VHA using core metrics that are identical to those used in the private sector, and establish a personnel performance management system for health care leaders in VHA that is distinct from performance measurement, is based on the leadership competency model, assesses leadership ability, and measures the achievement of important organizational strategies.
Recommendation #14: Foster cultural and military competence among all VHA Care System leadership, providers, and staff to embrace diversity, promote cultural sensitivity, and improve veteran health outcomes.
Recommendation #15: Create a simple-to-administer alternative personnel system, in law and regulation, which governs all VHA employees, applies best practices from the private sector to human capital management, and supports pay and benefits that are competitive with the private sector.
Recommendation #16: Require top executives to lead the transformation of HR, commit funds, and assign expert resources to achieve an effective human capital management system.
Recommendation #17: Provide a streamlined path to eligibility for health care for those with an other-than-honorable discharge who have substantial honorable service.
Recommendation #18: Establish an expert body to develop recommendations for VA care eligibility and benefit design.
Drugs produce comparable results in CP-CML
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm. ![]()
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm. ![]()
Long-term results from the DASISION trial suggest that dasatinib and imatinib produce similar outcomes in patients with newly diagnosed chronic phase chronic myeloid leukemia (CP-CML).
Although patients who received dasatinib experienced faster and deeper molecular responses than patients who received imatinib, the overall survival and progression-free survival rates were similar between the treatment arms.
Overall, adverse events (AEs) were similar between the arms as well.
Researchers said these results suggest that dasatinib should continue to be considered an option for patients with newly diagnosed CP-CML.
The team reported the results of this study in the Journal of Clinical Oncology. The research was sponsored by Bristol-Myers Squibb.
The trial enrolled 519 patients with newly diagnosed CP-CML. They were randomized to receive dasatinib at 100 mg once daily (n=259) or imatinib at 400 mg once daily (n=260). Baseline characteristics were well-balanced between the arms.
At 5 years of follow-up, 61% of patients in the dasatinib arm and 63% of patients in the imatinib arm remained on treatment.
Response and survival
The cumulative 5-year rate of major molecular response was 76% in the dasatinib arm and 64% in the imatinib arm (P=0.0022). The rates of MR4.5 were 42% and 33%, respectively (P=0.0251).
The estimated 5-year overall survival was 91% in the dasatinib arm and 90% in the imatinib arm (hazard ratio=1.01; 95% CI, 0.58 to 1.73).
The estimated 5-year progression-free survival was 85% and 86%, respectively (hazard ratio=1.06; 95% CI, 0.68 to 1.66).
Safety
In both treatment arms, most AEs were grade 1 or 2. Grade 3/4 AEs occurred in 15% of patients in the dasatinib arm and 11% of patients in the imatinib arm.
Rates of grade 3/4 hematologic AEs tended to be higher in the dasatinib arm than the imatinib arm.
But the rates of most drug-related, nonhematologic AEs were lower in the dasatinib arm than the imatinib arm or were comparable between the arms.
The exception was drug-related pleural effusion, which was more common with dasatinib (28%) than with imatinib (0.8%).
Drug-related AEs were largely manageable, although they led to treatment discontinuation in 16% of dasatinib-treated patients and 7% of imatinib-treated patients.
By 5 years, 26 patients (10%) in each treatment arm had died. Nine patients in the dasatinib arm died of disease progression, as did 17 patients in the imatinib arm. ![]()
EC expands approved use of carfilzomib

Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan. ![]()
Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan. ![]()
Photo from Amgen
The European Commission (EC) has expanded the approved use of the proteasome inhibitor carfilzomib (Kyprolis).
The drug is now approved for use in combination with dexamethasone to treat adults with multiple myeloma (MM) who have received at least 1 prior therapy.
Carfilzomib was previously approved by the EC for use in combination with lenalidomide and dexamethasone to treat adult MM patients who have received at least 1 prior therapy.
The EC approved the extended indication for carfilzomib based on data from the phase 3 ENDEAVOR trial.
The trial included 929 MM patients whose disease had relapsed after 1 to 3 prior therapeutic regimens.
The patients received either carfilzomib plus dexamethasone (n=464) or bortezomib plus dexamethasone (n=465) until disease progression.
The primary endpoint was progression-free survival. The median progression-free survival was 18.7 months in the carfilzomib arm and 9.4 months in the bortezomib arm. The hazard ratio was 0.53 (P<0.0001).
Overall survival data were not yet mature at last follow-up.
Treatment discontinuation due to adverse events and on-study deaths were comparable between the 2 treatment arms.
However, a number of known adverse events were reported at a higher rate in the carfilzomib arm than the bortezomib arm, including dyspnea (28% vs 13%), hypertension (25% vs 3%), pyrexia (27% vs 14%), cough (25% vs 15%), cardiac failure (8% vs 3%), and acute renal failure (8% vs 5%).
Carfilzomib is marketed as Kyprolis by Onyx Pharmaceuticals, Inc., a subsidiary of Amgen that holds development and commercialization rights to the drug globally, with the exception of Japan. ![]()
How multiple infections make malaria worse
Image by Ute Frevert
and Margaret Shear
New research suggests that infections with 2 types of malaria parasite lead to greater health risks because 1 species helps the other thrive.
Investigators sought to understand what happens when the 2 most common malaria parasites cause infection at the same time, as they are known to attack the body in different ways.
The team found the first parasite helps provide the second with more of the resources it needs to prosper.
“Immune responses are assumed to determine the outcome of interactions between parasite species, but our study clearly shows that resources can be more important,” said Sarah Reece, of the University of Edinburgh in Scotland.
“Our findings also challenge ideas that 1 species will outcompete the other, which explains why infections involving 2 parasite species can pose a greater health risk to patients.”
Dr Reece and her colleagues recounted these findings in Ecology Letters.
In humans, the malaria parasite Plasmodium falciparum infects red blood cells of all ages, while the Plasmodium vivax parasite attacks only young red blood cells.
The current study, conducted in mice with equivalent malaria parasites (P chabaudi and P yoelii), showed that the body’s response to the first infection produces more of the type of red blood cell the second parasite needs.
In response to the first infection, millions of red blood cells are destroyed. The body responds by replenishing these cells.
The fresh cells then become infected by the second type of parasite, making the infection worse.
The investigators said these results appear to explain why infections with both P falciparum and P vivax often have worse outcomes for patients than infections with a single malaria parasite. ![]()
Image by Ute Frevert
and Margaret Shear
New research suggests that infections with 2 types of malaria parasite lead to greater health risks because 1 species helps the other thrive.
Investigators sought to understand what happens when the 2 most common malaria parasites cause infection at the same time, as they are known to attack the body in different ways.
The team found the first parasite helps provide the second with more of the resources it needs to prosper.
“Immune responses are assumed to determine the outcome of interactions between parasite species, but our study clearly shows that resources can be more important,” said Sarah Reece, of the University of Edinburgh in Scotland.
“Our findings also challenge ideas that 1 species will outcompete the other, which explains why infections involving 2 parasite species can pose a greater health risk to patients.”
Dr Reece and her colleagues recounted these findings in Ecology Letters.
In humans, the malaria parasite Plasmodium falciparum infects red blood cells of all ages, while the Plasmodium vivax parasite attacks only young red blood cells.
The current study, conducted in mice with equivalent malaria parasites (P chabaudi and P yoelii), showed that the body’s response to the first infection produces more of the type of red blood cell the second parasite needs.
In response to the first infection, millions of red blood cells are destroyed. The body responds by replenishing these cells.
The fresh cells then become infected by the second type of parasite, making the infection worse.
The investigators said these results appear to explain why infections with both P falciparum and P vivax often have worse outcomes for patients than infections with a single malaria parasite. ![]()
Image by Ute Frevert
and Margaret Shear
New research suggests that infections with 2 types of malaria parasite lead to greater health risks because 1 species helps the other thrive.
Investigators sought to understand what happens when the 2 most common malaria parasites cause infection at the same time, as they are known to attack the body in different ways.
The team found the first parasite helps provide the second with more of the resources it needs to prosper.
“Immune responses are assumed to determine the outcome of interactions between parasite species, but our study clearly shows that resources can be more important,” said Sarah Reece, of the University of Edinburgh in Scotland.
“Our findings also challenge ideas that 1 species will outcompete the other, which explains why infections involving 2 parasite species can pose a greater health risk to patients.”
Dr Reece and her colleagues recounted these findings in Ecology Letters.
In humans, the malaria parasite Plasmodium falciparum infects red blood cells of all ages, while the Plasmodium vivax parasite attacks only young red blood cells.
The current study, conducted in mice with equivalent malaria parasites (P chabaudi and P yoelii), showed that the body’s response to the first infection produces more of the type of red blood cell the second parasite needs.
In response to the first infection, millions of red blood cells are destroyed. The body responds by replenishing these cells.
The fresh cells then become infected by the second type of parasite, making the infection worse.
The investigators said these results appear to explain why infections with both P falciparum and P vivax often have worse outcomes for patients than infections with a single malaria parasite. ![]()
Study explains link between malignant hyperthermia and bleeding abnormalities

A new study helps explain why some patients with malignant hyperthermia may suffer from excessive bleeding.
The findings suggest a mutation that causes malignant hyperthermia can disrupt calcium signaling in vascular smooth muscle cells, leading to bleeding abnormalities.
What’s more, researchers found that a drug clinically approved to treat muscle-related symptoms in malignant hyperthermia helped stop bleeding.
Rubén Lopez, of Basel University Hospital in Switzerland, and his colleagues conducted this research and reported their findings in Science Signaling.
Patients with malignant hyperthermia experience dangerously high fever and severe muscle contractions when exposed to general anesthesia.
Malignant hyperthermia is often caused by mutations in the RYR1 gene, which encodes a calcium channel in skeletal muscle called ryanodine receptor type 1 (RyR1).
For some patients with these mutations, malignant hyperthermia is accompanied by a mild bleeding disorder, but whether the 2 conditions are connected has not been clear.
Working in a mouse model of malignant hyperthermia, researchers found that vascular smooth muscle cells with mutated RyR1 displayed frequent spikes in calcium levels, known as calcium sparks. These sparks led to excessive vasodilation and prolonged bleeding.
Blocking the receptor with dantrolene, a drug used to treat malignant hyperthermia, helped reduce bleeding in the mice and in a single human patient, pointing to an unexpected benefit from the drug.
The findings suggest that mutations in RyR1, which is also found in other types of smooth muscle cells such as those in the bladder and uterus, may have a wider range of effects than previously thought. ![]()
A new study helps explain why some patients with malignant hyperthermia may suffer from excessive bleeding.
The findings suggest a mutation that causes malignant hyperthermia can disrupt calcium signaling in vascular smooth muscle cells, leading to bleeding abnormalities.
What’s more, researchers found that a drug clinically approved to treat muscle-related symptoms in malignant hyperthermia helped stop bleeding.
Rubén Lopez, of Basel University Hospital in Switzerland, and his colleagues conducted this research and reported their findings in Science Signaling.
Patients with malignant hyperthermia experience dangerously high fever and severe muscle contractions when exposed to general anesthesia.
Malignant hyperthermia is often caused by mutations in the RYR1 gene, which encodes a calcium channel in skeletal muscle called ryanodine receptor type 1 (RyR1).
For some patients with these mutations, malignant hyperthermia is accompanied by a mild bleeding disorder, but whether the 2 conditions are connected has not been clear.
Working in a mouse model of malignant hyperthermia, researchers found that vascular smooth muscle cells with mutated RyR1 displayed frequent spikes in calcium levels, known as calcium sparks. These sparks led to excessive vasodilation and prolonged bleeding.
Blocking the receptor with dantrolene, a drug used to treat malignant hyperthermia, helped reduce bleeding in the mice and in a single human patient, pointing to an unexpected benefit from the drug.
The findings suggest that mutations in RyR1, which is also found in other types of smooth muscle cells such as those in the bladder and uterus, may have a wider range of effects than previously thought. ![]()
A new study helps explain why some patients with malignant hyperthermia may suffer from excessive bleeding.
The findings suggest a mutation that causes malignant hyperthermia can disrupt calcium signaling in vascular smooth muscle cells, leading to bleeding abnormalities.
What’s more, researchers found that a drug clinically approved to treat muscle-related symptoms in malignant hyperthermia helped stop bleeding.
Rubén Lopez, of Basel University Hospital in Switzerland, and his colleagues conducted this research and reported their findings in Science Signaling.
Patients with malignant hyperthermia experience dangerously high fever and severe muscle contractions when exposed to general anesthesia.
Malignant hyperthermia is often caused by mutations in the RYR1 gene, which encodes a calcium channel in skeletal muscle called ryanodine receptor type 1 (RyR1).
For some patients with these mutations, malignant hyperthermia is accompanied by a mild bleeding disorder, but whether the 2 conditions are connected has not been clear.
Working in a mouse model of malignant hyperthermia, researchers found that vascular smooth muscle cells with mutated RyR1 displayed frequent spikes in calcium levels, known as calcium sparks. These sparks led to excessive vasodilation and prolonged bleeding.
Blocking the receptor with dantrolene, a drug used to treat malignant hyperthermia, helped reduce bleeding in the mice and in a single human patient, pointing to an unexpected benefit from the drug.
The findings suggest that mutations in RyR1, which is also found in other types of smooth muscle cells such as those in the bladder and uterus, may have a wider range of effects than previously thought. ![]()
David Henry's JCSO podcast, July 2016
In the July podcast for The Journal of Community and Supportive Oncology, Dr David Henry discusses an editorial by Dr Linda bosserman, in which she presents the case for pathways and the importance of processes and team work in paving the way for value-based care. Survivor care is the focus of 2 Original Reports in which investigators report on adolescent and young adult perceptions of cancer survivor care and supportive programming and on the symptoms, unmet need, and quality of life among recent breast cancer survivors. Also in the Original Report section are reports on the impact of loss of income and medicine costs on the financial burden for cancer patients in Australia and the use of a gene-panel for testing for hereditary ovarian cancer. Dr Henry also looks at 2 Case Reports, one in which a patient undergoes multivisceral resection for growing teratoma syndrome and another in which a patient presents with aleukemic acute lymphoblastic leukemia with unusual clinical features. Diabetes management in cancer patients is the topic of a lengthy and informative interview between Dr Henry and Dr Todd Brown.
Listen to the podcast below.
In the July podcast for The Journal of Community and Supportive Oncology, Dr David Henry discusses an editorial by Dr Linda bosserman, in which she presents the case for pathways and the importance of processes and team work in paving the way for value-based care. Survivor care is the focus of 2 Original Reports in which investigators report on adolescent and young adult perceptions of cancer survivor care and supportive programming and on the symptoms, unmet need, and quality of life among recent breast cancer survivors. Also in the Original Report section are reports on the impact of loss of income and medicine costs on the financial burden for cancer patients in Australia and the use of a gene-panel for testing for hereditary ovarian cancer. Dr Henry also looks at 2 Case Reports, one in which a patient undergoes multivisceral resection for growing teratoma syndrome and another in which a patient presents with aleukemic acute lymphoblastic leukemia with unusual clinical features. Diabetes management in cancer patients is the topic of a lengthy and informative interview between Dr Henry and Dr Todd Brown.
Listen to the podcast below.
In the July podcast for The Journal of Community and Supportive Oncology, Dr David Henry discusses an editorial by Dr Linda bosserman, in which she presents the case for pathways and the importance of processes and team work in paving the way for value-based care. Survivor care is the focus of 2 Original Reports in which investigators report on adolescent and young adult perceptions of cancer survivor care and supportive programming and on the symptoms, unmet need, and quality of life among recent breast cancer survivors. Also in the Original Report section are reports on the impact of loss of income and medicine costs on the financial burden for cancer patients in Australia and the use of a gene-panel for testing for hereditary ovarian cancer. Dr Henry also looks at 2 Case Reports, one in which a patient undergoes multivisceral resection for growing teratoma syndrome and another in which a patient presents with aleukemic acute lymphoblastic leukemia with unusual clinical features. Diabetes management in cancer patients is the topic of a lengthy and informative interview between Dr Henry and Dr Todd Brown.
Listen to the podcast below.
Absorb bioresorbable vascular scaffold wins FDA approval
The Food and Drug Administration approved the first fully absorbable vascular scaffold designed for use in coronary arteries, the Absorb GT1 bioresorbable vascular scaffold system, made by Abbott.
Concurrent with the FDA’s announcement on July 5, the company said that it plans to start immediate commercial rollout of the Absorb bioresorbable vascular scaffold (BVS). Initial availability will be limited to the roughly 100 most active sites that participated in the ABSORB III trial, the pivotal study that established noninferiority of the BVS, compared with a state-of-the-art metallic coronary stent during 1-year follow-up, according to a company spokesman.

However, the ABSORB III results, reported in October 2015, failed to document any superiority of the BVS, compared with a metallic stent. The potential advantages of a BVS remain for now unproven, and are based on the potential long-term advantages of using devices in percutaneous coronary interventions that slowly degrade away and thereby eliminate a residual metallic structure in a patient’s coronaries and the long-term threat they could pose for thrombosis or interference with subsequent coronary procedures.
“All the potential advantages are hypothetical at this point,” said Hiram G. Bezerra, MD, an investigator in the ABSORB III trial and director of the cardiac catheterization laboratory at University Hospitals Case Medical Center in Cleveland. However, “if you have a metallic stent it lasts a lifetime, creating a metallic cage” that could interfere with a possible later coronary procedure or be the site for thrombus formation. Disappearance of the BVS also creates the possibility for eventual restoration of more normal vasomotion in the coronary wall, said Dr. Bezerra, a self-professed “enthusiast” for the BVS alternative.
A major limiting factor for BVS use today is coronary diameter because the Absorb BVS is bulkier than metallic stents. The ABSORB III trial limited use of the BVS to coronary vessels with a reference-vessel diameter by visual assessment of at least 2.5 mm, with an upper limit of 3.75 mm. Other limiting factors can be coronary calcification and tortuosity, although Dr. Bezerra said that these obstacles are usually overcome with a more time-consuming procedure if the operator is committed to placing a BVS.
Another variable will be the cost of the BVS. According to the Abbott spokesman, the device “will be priced so that it will be broadly accessible to hospitals.” Also, the Absorb BVS will receive payer reimbursement comparable to a drug-eluting stent using existing reimbursement codes, the spokesman said. Abbott will require inexperienced operators to take a training course to learn proper placement technique.
Dr. Bezerra admitted that he is probably an outlier in his plan to quickly make the BVS a mainstay of his practice. “I think adoption will be slow in the beginning” for most U.S. operators, he predicted. One of his Cleveland colleagues who spoke about the near-term prospects BVS use last October when the ABSORB III results came out predicted that immediate use might occur in about 10%-15% of patients undergoing percutaneous coronary interventions, similar to the usage level in Europe where this BVS has been available for several years.
Dr. Bezerra has been a consultant to Abbott and St. Jude. He was an investigator on the ABSORB III trial.
On Twitter @mitchelzoler
The Food and Drug Administration approved the first fully absorbable vascular scaffold designed for use in coronary arteries, the Absorb GT1 bioresorbable vascular scaffold system, made by Abbott.
Concurrent with the FDA’s announcement on July 5, the company said that it plans to start immediate commercial rollout of the Absorb bioresorbable vascular scaffold (BVS). Initial availability will be limited to the roughly 100 most active sites that participated in the ABSORB III trial, the pivotal study that established noninferiority of the BVS, compared with a state-of-the-art metallic coronary stent during 1-year follow-up, according to a company spokesman.
However, the ABSORB III results, reported in October 2015, failed to document any superiority of the BVS, compared with a metallic stent. The potential advantages of a BVS remain for now unproven, and are based on the potential long-term advantages of using devices in percutaneous coronary interventions that slowly degrade away and thereby eliminate a residual metallic structure in a patient’s coronaries and the long-term threat they could pose for thrombosis or interference with subsequent coronary procedures.
“All the potential advantages are hypothetical at this point,” said Hiram G. Bezerra, MD, an investigator in the ABSORB III trial and director of the cardiac catheterization laboratory at University Hospitals Case Medical Center in Cleveland. However, “if you have a metallic stent it lasts a lifetime, creating a metallic cage” that could interfere with a possible later coronary procedure or be the site for thrombus formation. Disappearance of the BVS also creates the possibility for eventual restoration of more normal vasomotion in the coronary wall, said Dr. Bezerra, a self-professed “enthusiast” for the BVS alternative.
A major limiting factor for BVS use today is coronary diameter because the Absorb BVS is bulkier than metallic stents. The ABSORB III trial limited use of the BVS to coronary vessels with a reference-vessel diameter by visual assessment of at least 2.5 mm, with an upper limit of 3.75 mm. Other limiting factors can be coronary calcification and tortuosity, although Dr. Bezerra said that these obstacles are usually overcome with a more time-consuming procedure if the operator is committed to placing a BVS.
Another variable will be the cost of the BVS. According to the Abbott spokesman, the device “will be priced so that it will be broadly accessible to hospitals.” Also, the Absorb BVS will receive payer reimbursement comparable to a drug-eluting stent using existing reimbursement codes, the spokesman said. Abbott will require inexperienced operators to take a training course to learn proper placement technique.
Dr. Bezerra admitted that he is probably an outlier in his plan to quickly make the BVS a mainstay of his practice. “I think adoption will be slow in the beginning” for most U.S. operators, he predicted. One of his Cleveland colleagues who spoke about the near-term prospects BVS use last October when the ABSORB III results came out predicted that immediate use might occur in about 10%-15% of patients undergoing percutaneous coronary interventions, similar to the usage level in Europe where this BVS has been available for several years.
Dr. Bezerra has been a consultant to Abbott and St. Jude. He was an investigator on the ABSORB III trial.
On Twitter @mitchelzoler
The Food and Drug Administration approved the first fully absorbable vascular scaffold designed for use in coronary arteries, the Absorb GT1 bioresorbable vascular scaffold system, made by Abbott.
Concurrent with the FDA’s announcement on July 5, the company said that it plans to start immediate commercial rollout of the Absorb bioresorbable vascular scaffold (BVS). Initial availability will be limited to the roughly 100 most active sites that participated in the ABSORB III trial, the pivotal study that established noninferiority of the BVS, compared with a state-of-the-art metallic coronary stent during 1-year follow-up, according to a company spokesman.
However, the ABSORB III results, reported in October 2015, failed to document any superiority of the BVS, compared with a metallic stent. The potential advantages of a BVS remain for now unproven, and are based on the potential long-term advantages of using devices in percutaneous coronary interventions that slowly degrade away and thereby eliminate a residual metallic structure in a patient’s coronaries and the long-term threat they could pose for thrombosis or interference with subsequent coronary procedures.
“All the potential advantages are hypothetical at this point,” said Hiram G. Bezerra, MD, an investigator in the ABSORB III trial and director of the cardiac catheterization laboratory at University Hospitals Case Medical Center in Cleveland. However, “if you have a metallic stent it lasts a lifetime, creating a metallic cage” that could interfere with a possible later coronary procedure or be the site for thrombus formation. Disappearance of the BVS also creates the possibility for eventual restoration of more normal vasomotion in the coronary wall, said Dr. Bezerra, a self-professed “enthusiast” for the BVS alternative.
A major limiting factor for BVS use today is coronary diameter because the Absorb BVS is bulkier than metallic stents. The ABSORB III trial limited use of the BVS to coronary vessels with a reference-vessel diameter by visual assessment of at least 2.5 mm, with an upper limit of 3.75 mm. Other limiting factors can be coronary calcification and tortuosity, although Dr. Bezerra said that these obstacles are usually overcome with a more time-consuming procedure if the operator is committed to placing a BVS.
Another variable will be the cost of the BVS. According to the Abbott spokesman, the device “will be priced so that it will be broadly accessible to hospitals.” Also, the Absorb BVS will receive payer reimbursement comparable to a drug-eluting stent using existing reimbursement codes, the spokesman said. Abbott will require inexperienced operators to take a training course to learn proper placement technique.
Dr. Bezerra admitted that he is probably an outlier in his plan to quickly make the BVS a mainstay of his practice. “I think adoption will be slow in the beginning” for most U.S. operators, he predicted. One of his Cleveland colleagues who spoke about the near-term prospects BVS use last October when the ABSORB III results came out predicted that immediate use might occur in about 10%-15% of patients undergoing percutaneous coronary interventions, similar to the usage level in Europe where this BVS has been available for several years.
Dr. Bezerra has been a consultant to Abbott and St. Jude. He was an investigator on the ABSORB III trial.
On Twitter @mitchelzoler

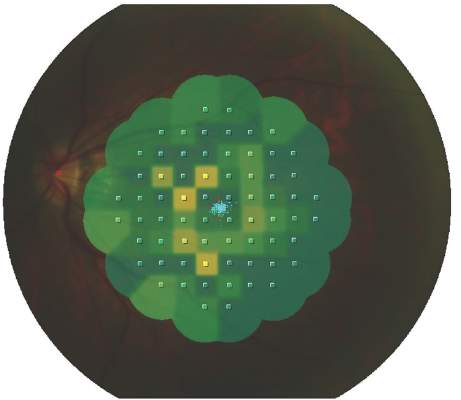
HCQ eye toxicity needs experience to assess
LONDON – Retinopathy in patients taking long-term hydroxychloroquine for rheumatic conditions requires assessment by those experienced with specialized ophthalmic imaging, according to study findings presented at the European Congress of Rheumatology.
Nonspecific abnormalities, which often are unrelated to hydroxychloroquine (HCQ), can be seen with many of the tests recommended by current ophthalmology guidelines. These changes need “careful interpretation by retina specialists,” the study’s investigators wrote in a poster presentation.
HCQ is used widely for the treatment of systemic lupus erythematosus (SLE), rheumatoid arthritis, and many other inflammatory or autoimmune conditions, but it can cause irreversible eye damage and is often associated with prolonged (greater than 5 years) use. Specifically, it can cause a type of end-stage retinopathy called bull’s-eye maculopathy, which is where the fovea becomes hyperpigmented, much like the bull’s-eye on a dartboard. This can lead to substantial vision loss (blind spots) if not caught early.

Although it is reasonably rare to develop end-stage retinopathy, there is currently no treatment for HCQ-induced retinopathy. Stopping the drug may not necessarily stop the retinal damage, and drug withdrawal may not be an option in many patients given the lack of alternative options to treat the symptoms of SLE, study author and ophthalmologist Syed Mahmood Ali Shah, MBBS, MD, said in an interview.
Dr. Shah and his associates at Johns Hopkins University in Baltimore reported on applying the 2011 American Academy of Ophthalmology (AAO) guidelines on screening for HCQ retinopathy (Ophthalmology. 2011;118:415-22) to an academic practice. They also estimated the prevalence of HCQ retinopathy among 135 consecutively treated patients with SLE using recommended tests. The mean duration of HCQ use was 12.5 years.
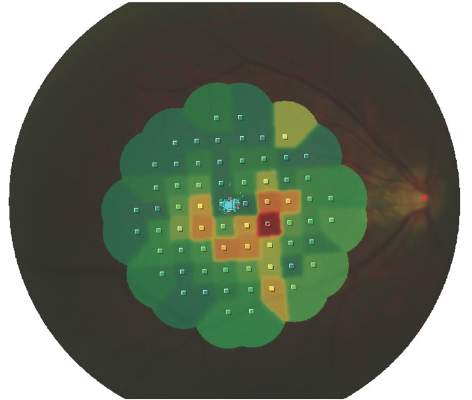
The 2011 AAO guidelines – which in March 2016 were updated (Ophthalmology 2016 Jun;123:1386-94) – recommended the use of three “ancillary” tests in addition to the usual clinical ophthalmic examination and assessment of visual fields: optical coherence tomography (OCT), fundus autofluorescence (FAF), and multifocal electroretinography (mfERG). Dr. Shah and his colleagues used these three tests together with eye-tracking microperimetry (MP) as a substitute for Humphrey Visual Fields (HVF), which is a common visual field test used in the United States.
One difference between the 2011 guidelines and 2016 revision is that “the baseline exam can now be performed relying [only] on the fundus exam, with additional imaging required only for abnormal patients,” Dr. Shah said. “Overall, the guidelines have not changed on how often and how much you follow up,” he added. “The change is that there is no need to do these tests at baseline unless changes of the fundus are present.” However, OCT has become more widely used in many offices and has been recognized as the most useful objective test and shall be performed if there are any abnormal findings of the fundus.
A total of 266 eyes were examined using these imaging methods and interpreted by experienced retina specialists. Overall, HCQ-related abnormalities were noted in 14 (5%) eyes using OCT, 18 (7%) using FAF, 27 (10%) eyes using mfERG, and 20 (7%) using MP.
MP had the lowest discrepancy between the overall number of eyes with abnormalities (72 [27%] of 266) detected and the number of eyes with abnormalities related to HCQ (20 [28%] of 72), followed by OCT (21% and 25%, respectively), FAF (19% and 35%) and mfERG (37% and 28%). Only four patients (3%) showed changes in all four tests suggestive of HCQ retinopathy.
In the absence of baseline data from the AAO recommended ancillary tests before the use of HCQ, “it may be difficult to interpret changes seen on these tests since most of the screenings are done by regular ophthalmologists who lack the equipment and experience with specialized testing such as mfERG, FAF, and OCT,” Dr. Shah and his coauthors noted. “We found a substantial number of cases with abnormalities unrelated to HCQ.”
Giving some practical advice, Dr. Shah noted that “before a patient starts treatment with HCQ, they should undergo a baseline ophthalmic assessment. Then if the patient complains of any vision changes, even if they have been taking the drug for less than 5 years, they should be reassessed.”
While repeat follow-up is, of course, necessary, he intimated that it is necessary to find a balance of risk and cost in regard to the frequency of screening for drug-related damage. “The American Academy of Ophthalmology currently recommends that a baseline fundus exam be performed shortly after starting HCQ. Ancillary OCT and visual fields shall only be performed if the fundus is abnormal at this baseline exam. However, since most retina specialists get OCT and visual field testing anyway it is wise to look at these as well,” he suggested. After 5 years of using the drug, they must be seen more regularly, and this is the point when ophthalmologists can decide if this should be every 6 months or annually, with the latter recommended by the AAO guidelines for patients with no additional risk factors.
The study was supported by noncommercial grants. Dr. Shah had no conflicts of interest to disclose.
LONDON – Retinopathy in patients taking long-term hydroxychloroquine for rheumatic conditions requires assessment by those experienced with specialized ophthalmic imaging, according to study findings presented at the European Congress of Rheumatology.
Nonspecific abnormalities, which often are unrelated to hydroxychloroquine (HCQ), can be seen with many of the tests recommended by current ophthalmology guidelines. These changes need “careful interpretation by retina specialists,” the study’s investigators wrote in a poster presentation.
HCQ is used widely for the treatment of systemic lupus erythematosus (SLE), rheumatoid arthritis, and many other inflammatory or autoimmune conditions, but it can cause irreversible eye damage and is often associated with prolonged (greater than 5 years) use. Specifically, it can cause a type of end-stage retinopathy called bull’s-eye maculopathy, which is where the fovea becomes hyperpigmented, much like the bull’s-eye on a dartboard. This can lead to substantial vision loss (blind spots) if not caught early.
Although it is reasonably rare to develop end-stage retinopathy, there is currently no treatment for HCQ-induced retinopathy. Stopping the drug may not necessarily stop the retinal damage, and drug withdrawal may not be an option in many patients given the lack of alternative options to treat the symptoms of SLE, study author and ophthalmologist Syed Mahmood Ali Shah, MBBS, MD, said in an interview.
Dr. Shah and his associates at Johns Hopkins University in Baltimore reported on applying the 2011 American Academy of Ophthalmology (AAO) guidelines on screening for HCQ retinopathy (Ophthalmology. 2011;118:415-22) to an academic practice. They also estimated the prevalence of HCQ retinopathy among 135 consecutively treated patients with SLE using recommended tests. The mean duration of HCQ use was 12.5 years.
The 2011 AAO guidelines – which in March 2016 were updated (Ophthalmology 2016 Jun;123:1386-94) – recommended the use of three “ancillary” tests in addition to the usual clinical ophthalmic examination and assessment of visual fields: optical coherence tomography (OCT), fundus autofluorescence (FAF), and multifocal electroretinography (mfERG). Dr. Shah and his colleagues used these three tests together with eye-tracking microperimetry (MP) as a substitute for Humphrey Visual Fields (HVF), which is a common visual field test used in the United States.
One difference between the 2011 guidelines and 2016 revision is that “the baseline exam can now be performed relying [only] on the fundus exam, with additional imaging required only for abnormal patients,” Dr. Shah said. “Overall, the guidelines have not changed on how often and how much you follow up,” he added. “The change is that there is no need to do these tests at baseline unless changes of the fundus are present.” However, OCT has become more widely used in many offices and has been recognized as the most useful objective test and shall be performed if there are any abnormal findings of the fundus.
A total of 266 eyes were examined using these imaging methods and interpreted by experienced retina specialists. Overall, HCQ-related abnormalities were noted in 14 (5%) eyes using OCT, 18 (7%) using FAF, 27 (10%) eyes using mfERG, and 20 (7%) using MP.
MP had the lowest discrepancy between the overall number of eyes with abnormalities (72 [27%] of 266) detected and the number of eyes with abnormalities related to HCQ (20 [28%] of 72), followed by OCT (21% and 25%, respectively), FAF (19% and 35%) and mfERG (37% and 28%). Only four patients (3%) showed changes in all four tests suggestive of HCQ retinopathy.
In the absence of baseline data from the AAO recommended ancillary tests before the use of HCQ, “it may be difficult to interpret changes seen on these tests since most of the screenings are done by regular ophthalmologists who lack the equipment and experience with specialized testing such as mfERG, FAF, and OCT,” Dr. Shah and his coauthors noted. “We found a substantial number of cases with abnormalities unrelated to HCQ.”
Giving some practical advice, Dr. Shah noted that “before a patient starts treatment with HCQ, they should undergo a baseline ophthalmic assessment. Then if the patient complains of any vision changes, even if they have been taking the drug for less than 5 years, they should be reassessed.”
While repeat follow-up is, of course, necessary, he intimated that it is necessary to find a balance of risk and cost in regard to the frequency of screening for drug-related damage. “The American Academy of Ophthalmology currently recommends that a baseline fundus exam be performed shortly after starting HCQ. Ancillary OCT and visual fields shall only be performed if the fundus is abnormal at this baseline exam. However, since most retina specialists get OCT and visual field testing anyway it is wise to look at these as well,” he suggested. After 5 years of using the drug, they must be seen more regularly, and this is the point when ophthalmologists can decide if this should be every 6 months or annually, with the latter recommended by the AAO guidelines for patients with no additional risk factors.
The study was supported by noncommercial grants. Dr. Shah had no conflicts of interest to disclose.
LONDON – Retinopathy in patients taking long-term hydroxychloroquine for rheumatic conditions requires assessment by those experienced with specialized ophthalmic imaging, according to study findings presented at the European Congress of Rheumatology.
Nonspecific abnormalities, which often are unrelated to hydroxychloroquine (HCQ), can be seen with many of the tests recommended by current ophthalmology guidelines. These changes need “careful interpretation by retina specialists,” the study’s investigators wrote in a poster presentation.
HCQ is used widely for the treatment of systemic lupus erythematosus (SLE), rheumatoid arthritis, and many other inflammatory or autoimmune conditions, but it can cause irreversible eye damage and is often associated with prolonged (greater than 5 years) use. Specifically, it can cause a type of end-stage retinopathy called bull’s-eye maculopathy, which is where the fovea becomes hyperpigmented, much like the bull’s-eye on a dartboard. This can lead to substantial vision loss (blind spots) if not caught early.
Although it is reasonably rare to develop end-stage retinopathy, there is currently no treatment for HCQ-induced retinopathy. Stopping the drug may not necessarily stop the retinal damage, and drug withdrawal may not be an option in many patients given the lack of alternative options to treat the symptoms of SLE, study author and ophthalmologist Syed Mahmood Ali Shah, MBBS, MD, said in an interview.
Dr. Shah and his associates at Johns Hopkins University in Baltimore reported on applying the 2011 American Academy of Ophthalmology (AAO) guidelines on screening for HCQ retinopathy (Ophthalmology. 2011;118:415-22) to an academic practice. They also estimated the prevalence of HCQ retinopathy among 135 consecutively treated patients with SLE using recommended tests. The mean duration of HCQ use was 12.5 years.
The 2011 AAO guidelines – which in March 2016 were updated (Ophthalmology 2016 Jun;123:1386-94) – recommended the use of three “ancillary” tests in addition to the usual clinical ophthalmic examination and assessment of visual fields: optical coherence tomography (OCT), fundus autofluorescence (FAF), and multifocal electroretinography (mfERG). Dr. Shah and his colleagues used these three tests together with eye-tracking microperimetry (MP) as a substitute for Humphrey Visual Fields (HVF), which is a common visual field test used in the United States.
One difference between the 2011 guidelines and 2016 revision is that “the baseline exam can now be performed relying [only] on the fundus exam, with additional imaging required only for abnormal patients,” Dr. Shah said. “Overall, the guidelines have not changed on how often and how much you follow up,” he added. “The change is that there is no need to do these tests at baseline unless changes of the fundus are present.” However, OCT has become more widely used in many offices and has been recognized as the most useful objective test and shall be performed if there are any abnormal findings of the fundus.
A total of 266 eyes were examined using these imaging methods and interpreted by experienced retina specialists. Overall, HCQ-related abnormalities were noted in 14 (5%) eyes using OCT, 18 (7%) using FAF, 27 (10%) eyes using mfERG, and 20 (7%) using MP.
MP had the lowest discrepancy between the overall number of eyes with abnormalities (72 [27%] of 266) detected and the number of eyes with abnormalities related to HCQ (20 [28%] of 72), followed by OCT (21% and 25%, respectively), FAF (19% and 35%) and mfERG (37% and 28%). Only four patients (3%) showed changes in all four tests suggestive of HCQ retinopathy.
In the absence of baseline data from the AAO recommended ancillary tests before the use of HCQ, “it may be difficult to interpret changes seen on these tests since most of the screenings are done by regular ophthalmologists who lack the equipment and experience with specialized testing such as mfERG, FAF, and OCT,” Dr. Shah and his coauthors noted. “We found a substantial number of cases with abnormalities unrelated to HCQ.”
Giving some practical advice, Dr. Shah noted that “before a patient starts treatment with HCQ, they should undergo a baseline ophthalmic assessment. Then if the patient complains of any vision changes, even if they have been taking the drug for less than 5 years, they should be reassessed.”
While repeat follow-up is, of course, necessary, he intimated that it is necessary to find a balance of risk and cost in regard to the frequency of screening for drug-related damage. “The American Academy of Ophthalmology currently recommends that a baseline fundus exam be performed shortly after starting HCQ. Ancillary OCT and visual fields shall only be performed if the fundus is abnormal at this baseline exam. However, since most retina specialists get OCT and visual field testing anyway it is wise to look at these as well,” he suggested. After 5 years of using the drug, they must be seen more regularly, and this is the point when ophthalmologists can decide if this should be every 6 months or annually, with the latter recommended by the AAO guidelines for patients with no additional risk factors.
The study was supported by noncommercial grants. Dr. Shah had no conflicts of interest to disclose.
AT THE EULAR 2016 CONGRESS
Key clinical point: Several eye abnormalities can be mistaken for hydroxychloroquine-related eye toxicity, making specialist ophthalmic assessment paramount.
Major finding: Only four patients (3%) showed changes in all four tests suggestive of HCQ retinopathy.
Data source: Observational study of 135 patients with SLE being seen for suspected hydroxychloroquine-related retinopathy at an academic practice
Disclosures: The study was supported by noncommercial grants. Dr. Shah had no conflicts of interest to disclose.
