User login
Hepatitis Outlook: April 2016
If you work on the front lines of medical care treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month covering a variety of the major hepatitis viruses.
Elderly patients with chronic hepatitis C disease are more likely to develop hepatocellular carcinoma (HCC) than younger patients, but they have traditionally received less antiviral treatment than younger patients, according to a study in the Journal of Viral Hepatitis. However, receipt of curative treatment is associated with a benefit in reducing cirrhosis, HCC, and overall mortality, irrespective of age, investigators said.

A report in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report from the Texas Department of State Health Services detailed how the agency dealt with a health care–associated hepatitis A outbreak in August 2015.
Researchers at McGill University in Montreal have developed a portable, paper-based electrochemical platform with multiplexing and telemedicine capabilities that may enable low-cost, point-of-care diagnosis of hepatitis C virus (HCV) and HIV co-infections within serum samples.
A study of patients at a gastroenterology clinic in Cameroon found that almost 40% of patients who were anti-hepatitis C virus antibody-positive were also asymptomatic, and some already presented with complications, including cirrhosis and hepatocellular carcinoma. The authors highlighted an urgent need to put in place programs to increase awareness and diagnosis of HCV infection in the country.
Chronic hepatitis C virus infection is an independent risk factor for osteoporosis and fractures among HIV-infected patients, even before the development of cirrhosis, according to a review of epidemiologic studies.
Quantitative maternal surface antigen (HBsAg) predicts hepatitis B virus infection in infants as well as maternal viral load does, according to a study in Hepatology. The authors conclude that antiviral therapy may be considered in pregnant women with an HBsAg level above 4-4.5 log10 IU/mL to interrupt mother-to-infant transmission.
A comprehensive literature review of cited WHO estimates for hepatitis B virus (HBV), HCV, and HIV co-infection between 2010 and 2014 showed that a wide range of co-infection estimates have been quoted using different WHO estimates. The authors detail the most recent, appropriate WHO estimates that should be used going forward.
A Chinese cohort study found that isolated anti-HBc–positive subjects can achieve good immune responses after hepatitis B vaccination, and the positive seroprotection rate and geometric mean titer (GMT) level for anti-HBs were lower than in a control group. Better responses were observed in young adults, the study authors said, and significant negative correlations were found between GMT of anti-HBc before vaccination and GMT of anti-HBs after vaccination.
New research indicates that evidence of long-lasting cellular immunity, regardless of anti-hepatitis B surface antigen level, suggests that protection afforded by primary immunization with plasma-derived hepatitis B vaccine during childhood and adulthood lasts at least 32 years.
Increased knowledge of hepatitis B cognition is an effective way for improving hepatitis B vaccination behavior and hepatitis B vaccination willingness of migrant workers, report the authors of a study in Human Vaccines & Immunotherapeutics. The researchers also found that health intervention policies should focus on older migrants (age at least 46 years) without medical insurance, with poorer self-reported health status, and poor health services accessibility.
Hepatitis B virus antibodies and galactomannan enzyme immunoassay (GM-EIA) positivity are common in patients receiving intravenous immunoglobulin and may confound diagnostic results, according to a study in Clinical Infectious Diseases.
Researchers in Niger have identified two recombinant hepatitis B virus forms and rare genotypic patterns that may affect hepatitis B surface antigen antigenicity and improve current knowledge of epidemiological, clinical, and virological patterns of hepatitis B in that country.
As viral hepatitis can be life threatening in patients with hematological malignancy, a new study suggests that all patients should be screened for hepatotropic viruses before hematological treatment, and that patients or hemopoietic stem cell donors with markers of past or current viral hepatitis should be assessed by an expert. The study also includes screening, vaccination, and treatment rules.
A study published in JAIDS suggests that lamivudine (3TC) monotherapy-based combination antiretroviral therapy is efficacious for hepatitis B virus treatment through 48 weeks in HIV/HBV coinfection, when baseline HBV DNA is less than 20,000 IU/mL.
Chinese researchers observed a significant elevation in CD4+Foxp3+ regulatory T-cells (Treg) in the peripheral blood of chronic hepatitis C patients, compared with healthy donors, in a study published in the International Journal of Infectious Diseases. The results demonstrate a decreasing trend in activated Treg cells after treatment with interferon alpha and ribavirin in vitro, the investigators also said.
Research published in Hepatology suggests hepatitis B virus e antigen (HBeAg) and its precursors promote HDM2-mediated degradation and impair the transcriptional activity of tumor suppressor p53 via interacting with the NUMB gene, consequently contributing to hepatocellular carcinoma development.
A systematic review of recent hepatitis B vaccine research highlighted the importance of introducing HBV vaccination not only for an infant universal vaccination program, but also for other settings in which patients are affected by communicable and noncommunicable diseases.
A “real-world” cohort study of 4,365 genotype 1 treatment-naïve hepatitis C virus–infected veterans treated with ledipasvir/sofosbuvir with or without ribavirin found that sustained virologic response (SVR) rates in the cohort nearly matched the SVR rates reported in clinical trials and were consistently high across all subgroups. Investigators found that noncirrhotics with HCV RNA less than 6,000,000 IU/mL were less likely to achieve SVR with 8 weeks, compared with 12 weeks of therapy, although the numeric difference in SVR rates was small.
A study in the Journal of Viral Hepatitis demonstrated that the DC-targeting protein has the ability to improve the immunogenicity and the antiviral activity of the hepatitis B DNA vaccine pSVK-HBVA, and that the DC-targeting protein can be a potential method for the delivery of DNA vaccines directly to DCs.
On Twitter @richpizzi
If you work on the front lines of medical care treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month covering a variety of the major hepatitis viruses.
Elderly patients with chronic hepatitis C disease are more likely to develop hepatocellular carcinoma (HCC) than younger patients, but they have traditionally received less antiviral treatment than younger patients, according to a study in the Journal of Viral Hepatitis. However, receipt of curative treatment is associated with a benefit in reducing cirrhosis, HCC, and overall mortality, irrespective of age, investigators said.
A report in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report from the Texas Department of State Health Services detailed how the agency dealt with a health care–associated hepatitis A outbreak in August 2015.
Researchers at McGill University in Montreal have developed a portable, paper-based electrochemical platform with multiplexing and telemedicine capabilities that may enable low-cost, point-of-care diagnosis of hepatitis C virus (HCV) and HIV co-infections within serum samples.
A study of patients at a gastroenterology clinic in Cameroon found that almost 40% of patients who were anti-hepatitis C virus antibody-positive were also asymptomatic, and some already presented with complications, including cirrhosis and hepatocellular carcinoma. The authors highlighted an urgent need to put in place programs to increase awareness and diagnosis of HCV infection in the country.
Chronic hepatitis C virus infection is an independent risk factor for osteoporosis and fractures among HIV-infected patients, even before the development of cirrhosis, according to a review of epidemiologic studies.
Quantitative maternal surface antigen (HBsAg) predicts hepatitis B virus infection in infants as well as maternal viral load does, according to a study in Hepatology. The authors conclude that antiviral therapy may be considered in pregnant women with an HBsAg level above 4-4.5 log10 IU/mL to interrupt mother-to-infant transmission.
A comprehensive literature review of cited WHO estimates for hepatitis B virus (HBV), HCV, and HIV co-infection between 2010 and 2014 showed that a wide range of co-infection estimates have been quoted using different WHO estimates. The authors detail the most recent, appropriate WHO estimates that should be used going forward.
A Chinese cohort study found that isolated anti-HBc–positive subjects can achieve good immune responses after hepatitis B vaccination, and the positive seroprotection rate and geometric mean titer (GMT) level for anti-HBs were lower than in a control group. Better responses were observed in young adults, the study authors said, and significant negative correlations were found between GMT of anti-HBc before vaccination and GMT of anti-HBs after vaccination.
New research indicates that evidence of long-lasting cellular immunity, regardless of anti-hepatitis B surface antigen level, suggests that protection afforded by primary immunization with plasma-derived hepatitis B vaccine during childhood and adulthood lasts at least 32 years.
Increased knowledge of hepatitis B cognition is an effective way for improving hepatitis B vaccination behavior and hepatitis B vaccination willingness of migrant workers, report the authors of a study in Human Vaccines & Immunotherapeutics. The researchers also found that health intervention policies should focus on older migrants (age at least 46 years) without medical insurance, with poorer self-reported health status, and poor health services accessibility.
Hepatitis B virus antibodies and galactomannan enzyme immunoassay (GM-EIA) positivity are common in patients receiving intravenous immunoglobulin and may confound diagnostic results, according to a study in Clinical Infectious Diseases.
Researchers in Niger have identified two recombinant hepatitis B virus forms and rare genotypic patterns that may affect hepatitis B surface antigen antigenicity and improve current knowledge of epidemiological, clinical, and virological patterns of hepatitis B in that country.
As viral hepatitis can be life threatening in patients with hematological malignancy, a new study suggests that all patients should be screened for hepatotropic viruses before hematological treatment, and that patients or hemopoietic stem cell donors with markers of past or current viral hepatitis should be assessed by an expert. The study also includes screening, vaccination, and treatment rules.
A study published in JAIDS suggests that lamivudine (3TC) monotherapy-based combination antiretroviral therapy is efficacious for hepatitis B virus treatment through 48 weeks in HIV/HBV coinfection, when baseline HBV DNA is less than 20,000 IU/mL.
Chinese researchers observed a significant elevation in CD4+Foxp3+ regulatory T-cells (Treg) in the peripheral blood of chronic hepatitis C patients, compared with healthy donors, in a study published in the International Journal of Infectious Diseases. The results demonstrate a decreasing trend in activated Treg cells after treatment with interferon alpha and ribavirin in vitro, the investigators also said.
Research published in Hepatology suggests hepatitis B virus e antigen (HBeAg) and its precursors promote HDM2-mediated degradation and impair the transcriptional activity of tumor suppressor p53 via interacting with the NUMB gene, consequently contributing to hepatocellular carcinoma development.
A systematic review of recent hepatitis B vaccine research highlighted the importance of introducing HBV vaccination not only for an infant universal vaccination program, but also for other settings in which patients are affected by communicable and noncommunicable diseases.
A “real-world” cohort study of 4,365 genotype 1 treatment-naïve hepatitis C virus–infected veterans treated with ledipasvir/sofosbuvir with or without ribavirin found that sustained virologic response (SVR) rates in the cohort nearly matched the SVR rates reported in clinical trials and were consistently high across all subgroups. Investigators found that noncirrhotics with HCV RNA less than 6,000,000 IU/mL were less likely to achieve SVR with 8 weeks, compared with 12 weeks of therapy, although the numeric difference in SVR rates was small.
A study in the Journal of Viral Hepatitis demonstrated that the DC-targeting protein has the ability to improve the immunogenicity and the antiviral activity of the hepatitis B DNA vaccine pSVK-HBVA, and that the DC-targeting protein can be a potential method for the delivery of DNA vaccines directly to DCs.
On Twitter @richpizzi
If you work on the front lines of medical care treating patients with hepatitis, you may not have time to review all the hepatitis research that enters the medical literature every month. Here’s a quick look at some notable news items and journal articles published over the past month covering a variety of the major hepatitis viruses.
Elderly patients with chronic hepatitis C disease are more likely to develop hepatocellular carcinoma (HCC) than younger patients, but they have traditionally received less antiviral treatment than younger patients, according to a study in the Journal of Viral Hepatitis. However, receipt of curative treatment is associated with a benefit in reducing cirrhosis, HCC, and overall mortality, irrespective of age, investigators said.
A report in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report from the Texas Department of State Health Services detailed how the agency dealt with a health care–associated hepatitis A outbreak in August 2015.
Researchers at McGill University in Montreal have developed a portable, paper-based electrochemical platform with multiplexing and telemedicine capabilities that may enable low-cost, point-of-care diagnosis of hepatitis C virus (HCV) and HIV co-infections within serum samples.
A study of patients at a gastroenterology clinic in Cameroon found that almost 40% of patients who were anti-hepatitis C virus antibody-positive were also asymptomatic, and some already presented with complications, including cirrhosis and hepatocellular carcinoma. The authors highlighted an urgent need to put in place programs to increase awareness and diagnosis of HCV infection in the country.
Chronic hepatitis C virus infection is an independent risk factor for osteoporosis and fractures among HIV-infected patients, even before the development of cirrhosis, according to a review of epidemiologic studies.
Quantitative maternal surface antigen (HBsAg) predicts hepatitis B virus infection in infants as well as maternal viral load does, according to a study in Hepatology. The authors conclude that antiviral therapy may be considered in pregnant women with an HBsAg level above 4-4.5 log10 IU/mL to interrupt mother-to-infant transmission.
A comprehensive literature review of cited WHO estimates for hepatitis B virus (HBV), HCV, and HIV co-infection between 2010 and 2014 showed that a wide range of co-infection estimates have been quoted using different WHO estimates. The authors detail the most recent, appropriate WHO estimates that should be used going forward.
A Chinese cohort study found that isolated anti-HBc–positive subjects can achieve good immune responses after hepatitis B vaccination, and the positive seroprotection rate and geometric mean titer (GMT) level for anti-HBs were lower than in a control group. Better responses were observed in young adults, the study authors said, and significant negative correlations were found between GMT of anti-HBc before vaccination and GMT of anti-HBs after vaccination.
New research indicates that evidence of long-lasting cellular immunity, regardless of anti-hepatitis B surface antigen level, suggests that protection afforded by primary immunization with plasma-derived hepatitis B vaccine during childhood and adulthood lasts at least 32 years.
Increased knowledge of hepatitis B cognition is an effective way for improving hepatitis B vaccination behavior and hepatitis B vaccination willingness of migrant workers, report the authors of a study in Human Vaccines & Immunotherapeutics. The researchers also found that health intervention policies should focus on older migrants (age at least 46 years) without medical insurance, with poorer self-reported health status, and poor health services accessibility.
Hepatitis B virus antibodies and galactomannan enzyme immunoassay (GM-EIA) positivity are common in patients receiving intravenous immunoglobulin and may confound diagnostic results, according to a study in Clinical Infectious Diseases.
Researchers in Niger have identified two recombinant hepatitis B virus forms and rare genotypic patterns that may affect hepatitis B surface antigen antigenicity and improve current knowledge of epidemiological, clinical, and virological patterns of hepatitis B in that country.
As viral hepatitis can be life threatening in patients with hematological malignancy, a new study suggests that all patients should be screened for hepatotropic viruses before hematological treatment, and that patients or hemopoietic stem cell donors with markers of past or current viral hepatitis should be assessed by an expert. The study also includes screening, vaccination, and treatment rules.
A study published in JAIDS suggests that lamivudine (3TC) monotherapy-based combination antiretroviral therapy is efficacious for hepatitis B virus treatment through 48 weeks in HIV/HBV coinfection, when baseline HBV DNA is less than 20,000 IU/mL.
Chinese researchers observed a significant elevation in CD4+Foxp3+ regulatory T-cells (Treg) in the peripheral blood of chronic hepatitis C patients, compared with healthy donors, in a study published in the International Journal of Infectious Diseases. The results demonstrate a decreasing trend in activated Treg cells after treatment with interferon alpha and ribavirin in vitro, the investigators also said.
Research published in Hepatology suggests hepatitis B virus e antigen (HBeAg) and its precursors promote HDM2-mediated degradation and impair the transcriptional activity of tumor suppressor p53 via interacting with the NUMB gene, consequently contributing to hepatocellular carcinoma development.
A systematic review of recent hepatitis B vaccine research highlighted the importance of introducing HBV vaccination not only for an infant universal vaccination program, but also for other settings in which patients are affected by communicable and noncommunicable diseases.
A “real-world” cohort study of 4,365 genotype 1 treatment-naïve hepatitis C virus–infected veterans treated with ledipasvir/sofosbuvir with or without ribavirin found that sustained virologic response (SVR) rates in the cohort nearly matched the SVR rates reported in clinical trials and were consistently high across all subgroups. Investigators found that noncirrhotics with HCV RNA less than 6,000,000 IU/mL were less likely to achieve SVR with 8 weeks, compared with 12 weeks of therapy, although the numeric difference in SVR rates was small.
A study in the Journal of Viral Hepatitis demonstrated that the DC-targeting protein has the ability to improve the immunogenicity and the antiviral activity of the hepatitis B DNA vaccine pSVK-HBVA, and that the DC-targeting protein can be a potential method for the delivery of DNA vaccines directly to DCs.
On Twitter @richpizzi

Medical Mimics of Psychiatric Conditions, Part 1
The chaos of a busy ED can test the cognitive reserve of even the most focused practitioner. To streamline the challenge of serial diagnosis and treatment, clinicians employ heuristics while honing the skills of pattern recognition. However, by definition, heuristics employs shortcuts, leaving out information for the sake of efficiency—sometimes at the expense of accuracy. Whether a patient presents with chest pain, abdominal pain, headache, or (the dreaded) dizziness, emergency physicians (EPs) employ algorithms based on a combination of education and prior experience.
Most of the time, these models lead the EP along the correct path, but not always. For example, when a clinician evaluating a patient presenting with psychotic behavior assumes the patient has schizophrenia, he or she will be correct eight or nine times out of 10. However, in some cases, a patient’s bizarre behavior may not be due to a true psychiatric disorder but, for example, from ingestion of an illicit substance.
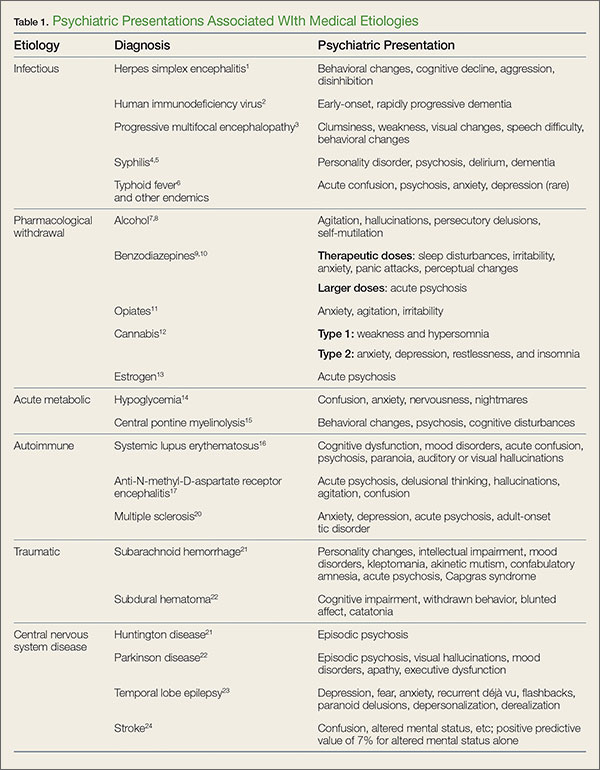
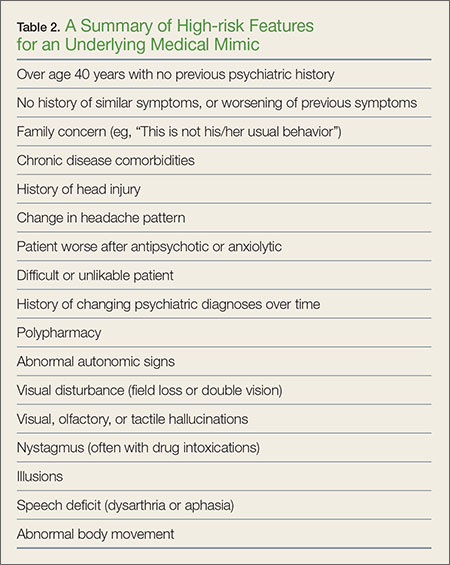
In addition, in such patients, psychiatric symptoms may be masking a serious acute, organic condition—one requiring prompt intervention and therapy to avoid morbidity or death. To help prevent diagnostic errors, this 2-part series reviews several of the most common medical mimics of psychiatric conditions. Part 1 of this series reviews the psychiatric presentations associated with medical conditions of an infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, or central nervous system etiology (Table 1). This article also discusses clinical signs and symptoms that suggest an increased likelihood that a patient’s psychiatric symptoms are from an underlying medical condition (Table 2).
Case Scenarios
Case 1
A 58-year-old woman with a history of smoking 40 packs of cigarettes per year presented to the ED 1 hour after onset of intermittent chest pain. Upon arrival at the ED, the patient stated that she had trouble catching her breath on and off throughout the day. The patient’s vital signs, electrocardiogram (ECG), and chest X-ray were all normal. The physical examination was unremarkable except for mild diaphoresis. The patient denied experiencing palpitations, recent travel, or previous episodes; she further stated that she was currently not on any medications. There was no previous history of visits to this hospital. The patient’s husband, who accompanied her to the ED, noted that his wife’s behavior had been atypical for approximately 1 week.
After receiving aspirin, the patient appeared symptom-free. Pending the results of another chest radiograph and laboratory evaluation, the EP anticipated moving her to the chest-pain observation unit.
Case 2
A 36-year-old woman presented with altered mental status to the ED via emergency medical services (EMS). Her vital signs, including temperature, were normal. Despite intermittently appearing to be asleep, the patient was alternatingly cooperative and combative. She repetitively whispered, “Who am I?” and randomly shouted at staff members as they walked by her room.
Her neurological examination was nonfocal. The hospital’s electronic medical record (EMR) for this patient showed nearly monthly ED visits for behavioral symptoms. Precipitating events noted in the EMR included job loss and separation from her husband. While waiting for the results of the basic laboratory work-up and toxicology screening to medically clear the patient for psychiatric evaluation, the EP contemplated a computed tomography (CT) study. Realizing the patient would not be able to remain still for the scan, the EP ordered 10 mg of intramuscular ziprasidone for sedation. When the patient’s husband arrived, the EP placed the CT scan on hold until she could obtain additional history from him.
Infections
Herpes Simplex Encephalitis
Herpes simplex encephalitis (HSE) is a serious but treatable disease—one that requires early detection and treatment to avoid severe morbidity. While the classic symptoms are fever and altered mental status, recent literature has noted that afebrile patients with HSE may present with behavioral changes, cognitive decline, aggression, and disinhibition. Therefore, diagnosis of a functional psychiatric complaint, if made initially, could delay appropriate treatment with acyclovir.1
Human Immunodeficiency Virus
Progression of human immunodeficiency virus (HIV) is a well-known cause of various neurocognitive disorders, including early-onset dementia. Since the availability of highly active antiretroviral therapy, the incidence of HIV dementia has decreased, but HIV remains the most common preventable cause of dementia in persons younger than age 50 years. Recent literature has described HIV dementia presenting as an early-onset, rapidly progressing dementia in a young person. Thus, the EP should consider early HIV testing in any young patient who presents with dementia, especially one with a history of fever of unknown origin.2
Progressive Multifocal Encephalopathy
Caused by reactivation of the John Cunningham virus, progressive multifocal encephalopathy has been classically described as a potentially lethal complication of a severely immunocompromised state, often presenting with clumsiness, weakness, visual changes, speech difficulty, and behavioral changes. Though typically described as occurring in the context of acquired immunodeficiency disease syndrome, hematological malignancy, or organ transplant, the condition can occur in the setting of minimal or occult immunosuppression—especially in patients with a history of cirrhosis. If the condition is detected early, immunotherapy can result in significant clinical improvement.3
Syphilis
Late stages of syphilis can present with a wide variety of psychiatric symptoms, including personality disorder, psychosis, delirium, and dementia. As with HIV, there has been a resurgence of syphilis cases, and screening is now often a routine part of a neuropsychiatric work-up. The EP should consider syphilis in the differential for any new-onset psychiatric complaint.4,5
Typhoid Fever
Although this severe febrile illness is uncommon in the United States, it is endemic to many tropical countries within Africa, Southeast Asia, and Central and South America. Typhoid is characterized by a stepwise fever that can progress to abdominal distension, toxemia, and potentially bowel perforation. It is also known to present with psychiatric symptoms such as acute confusion, psychosis, generalized anxiety disorder, and, though rare, depressive disorder. Physicians traveling to rural endemic areas should be aware of these neuropsychiatric presentations to avoid misdiagnosis and delay of treatment.6 Other infectious endemic diseases with reports of neuropsychiatric components are neurocystercercosis, Lyme disease, and African trypanosomiasis.
Pharmacological Withdrawal Syndromes
Alcohol
Alcohol withdrawal is a common presentation in the ED, and up to 24% of US adults brought to the ED by EMS suffer from alcoholism. Typically characterized by tachycardia, hypertension, and tremors, alcohol withdrawal syndrome can also feature psychiatric components such as agitation, hallucinations, persecutory delusions, and even self-mutilation.7 Evidence-based protocols indicate loading doses of benzodiazepines as a mainstay of treatment, with supplemental barbiturates or propofol in cases of treatment failure.8
Benzodiazepines
Withdrawal from therapeutic doses of benzodiazepines can potentially cause psychiatric symptoms, including sleep disturbances, irritability, anxiety, panic attacks, tremor, and perceptual changes. Withdrawal from higher doses of benzodiazepines can lead to more serious presentations, such as seizures and acute psychosis.9 Withdrawal symptoms can develop from discontinuation of the drug and with non-tapered switching between benzodiazepines.10
Opiates
Opiate withdrawal is an unpleasant experience characterized by generalized pain, nausea and vomiting, sweating, and tachycardia. Neuropsychiatric complaints such as anxiety, agitation, and irritability can also be present. More severe agitation has been described in naltrexone-accelerated detoxification.11
Cannabis
Recent literature on cannabis use indicates a high prevalence and clinical significance of associated withdrawal symptoms in frequent users. There appear to be two subsets of cannabis withdrawal—one characterized by weakness and hypersomnia, and the other by anxiety, depression, restlessness, and insomnia.12
Estrogen
Withdrawal from endogenous estrogen has been hypothesized as a possible cause of puerperal psychosis.13 Estrogen withdrawal outside of this setting, however, can and does occur, and recent literature has shown episodes of reversible psychosis associated with the discontinuation of both oral contraceptive regimens and hormonal therapy for menopausal symptoms.
Acute Metabolic Conditions
Hypoglycemia
Hypoglycemia, most often encountered as a side effect of insulin or oral hypoglycemic therapies, is a potentially lethal cause of confusion, anxiety, nervousness, and seizures. Nocturnal hypoglycemia can manifest as nightmares, crying out, and confusion upon awakening. A fingerstick blood-glucose test is an absolutely vital part of the initial work-up of any patient with an altered mental status or overt psychiatric complaint.14
Central Pontine Myelinolysis
A potentially devastating neurological condition associated with malnourishment and alcohol dependence, central pontine myelinolysis (CPM) is classically exacerbated by rapid overcorrection of hyponatremia. While the disease can manifest primarily with quadriplegia or pseudobulbar palsy and eventual progress to the dreaded “locked-in” syndrome, early presentations can include psychiatric symptoms such as behavioral changes, psychosis, and cognitive disturbances. Patients with early signs and symptoms of CPM have been misdiagnosed as having schizophrenia with catatonia, leading to delayed treatment and poor outcomes. The EP should remain vigilant when evaluating for this condition and consider a magnetic resonance imaging study in patients with psychiatric symptoms in the setting of fluctuating hyponatremia.15
Autoimmune Disorders
Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is one of the most common autoimmune disorders, and has a higher incidence in young women. The disease affects multiple organ systems. Though the classic initial presentation of SLE is fever, joint pain, and rash, the associated neuropsychiatric syndromes of this disease are diverse and surprisingly common, and can be the initial manifestation of the disease. Common psychiatric manifestations of SLE include cognitive dysfunction, anxiety, mood disorders such as depression, acute confusion, psychosis, paranoia, and auditory or visual hallucinations.16
Anti-N-methyl-D-Aspartate Receptor Encephalitis
Initially described as a paraneoplastic effect of ovarian teratomas, anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is actually an autoimmune disorder that can occur even in the absence of a primary tumor. As with SLE, the condition primarily occurs in young women. Antibodies in the cerebrospinal fluid cause prominent psychiatric symptoms such as acute psychosis, delusional thinking, hallucinations, agitation, and confusion. Although the disease can progress to seizures, movement disorders, autonomic dysregulation, and ultimately death, early recognition and treatment can lead to positive outcomes in up to 80% of cases.17 While the prevalence of anti-NMDAR antibodies in new-onset psychosis remains unclear, recent literature has suggested widespread screening for the disease in all first presentations of psychotic episodes.18,19
Multiple Sclerosis
Multiple sclerosis (MS) is another autoimmune disorder that has a higher prevalence in young women. The disease is characterized by central nervous system involvement that occurs over a period of months to years, with symptoms corresponding to different anatomic locations. Though the classic presenting symptom of MS is optic neuritis, neuropsychiatric syndromes are a common co-occurrence and can be the initial presenting symptom. The most commonly associated psychiatric complaints are anxiety, depression, and bipolar disorder, though case reports of SLE have described acute psychosis, psychotic depression, and adult-onset tic disorder.20
Trauma
Subarachnoid Hemorrhage
Long-term psychiatric sequelae from subarachnoid hemorrhage, either traumatic or aneurysmal, manifest most commonly as personality changes, intellectual impairment, depression, and anxiety. This condition is also known to cause a host of more bizarre psychiatric presentations, such as new-onset kleptomania, akinetic mutism, confabulatory amnesia, acute psychosis, and Capgras syndrome (the delusion that familiar individuals have been replaced by imposters). These symptoms can occur at initial presentation, and may show variable improvement with shunt surgery.21
Subdural Hematoma
Acute or chronic subdural hematoma can result from major head trauma, or even quite minor head trauma in an elderly or coagulopathic patient. Some common psychiatric manifestations of subdural hematoma include cognitive impairment, withdrawn behavior, blunted affect otherwise mimicking schizophrenic psychosis, and catatonia. The EP should consider early imaging studies in patients with new-onset psychotic symptoms—especially when they are refractory to typical antipsychotics.22
Central Nervous Symptom Diseases
Huntington Disease
Huntington disease (HD) is an autosomal dominant inherited, progressive neurodegenerative disorder characterized by mental decline, mood disorder, and muscle coordination problems that eventually become the classic involuntary writhing termed chorea. Due to its progressive nature, precise onset of the disease is difficult to describe; however, HD can manifest initially as schizophrenia-like psychotic episodes with only minimal apparent motor difficulty. Family history, including movement disorders and suicide, is important to obtain when available.23
Parkinson Disease
A progressive and disabling neurodegenerative disorder, Parkinson disease (PD) is classically characterized by fine resting tremor, cogwheeling rigidity, akinesia and mask-like facies, and postural instability. Comorbidity of psychiatric disorders is high, both as a result of the underlying disease process and as a side effect of dopaminergic treatment regimes. Common presentations of psychiatric disorders in PD include schizophrenia-like psychosis with visual hallucinations and mood disorders with prominent apathy and executive dysfunction. Recognition of the comorbidity is important because psychiatric disorders in PD respond differently to treatment than classic psychiatric disorders.24
Temporal Lobe Epilepsy
Epilepsy is a complex group of related neurological disorders involving unregulated nerve cell firing with a large variability in clinical presentation. Characteristically there is recurrent seizure activity. Temporal lobe epilepsy (TLE) is a subset of epilepsy known to present as a number of behavioral and neuropsychiatric complaints. Most presentations of TLE involve auras of emotional phenomena such as depression, fear, or anxiety, which can occur alone or with subsequent progression to complex partial or secondary generalized seizures.25 Many other bizarre presentations of TLE have been reported, including recurrent, potentially debilitating déjà vu, vivid recollection of past traumatic events mimicking posttraumatic stress disorder, paranoid delusions following olfactory triggers; and unprovoked attacks of depersonalization, derealization, anxiety, and dyspnea originally misdiagnosed as panic attack.
Stroke
The term “stroke chameleon” refers to presentations suggestive of other diseases that actually represent underlying strokes. Altered mental status is by far the largest block of these chameleons, with up to 30% of misdiagnosed strokes being misdiagnosed as altered mental status. The positive predictive value of altered mental status alone (ie, the chance that the diagnosis of altered mental status actually represents an undiagnosed acute stroke) is 7%.26
Case Scenarios Continued
Case 1
[The 58-year-old woman with intermittent chest pain.]
The patient’s D-dimer and troponin I levels were normal. Before the EP had an opportunity to discuss the results and next steps with the patient, the nurse asked him to see the patient immediately. Upon entering her room, the EP noted that the patient appeared anxious. The patient said the shortness of breath had returned, and also that she felt as if she were “floating” off the gurney, outside of her body. A check of her vital signs revealed a heart rate of 106 beats/minute and blood pressure of 160/100 mm Hg. A repeat ECG was significant only for sinus tachycardia. In an effort to calm the patient, the EP reassured her that the ECG, chest X-ray, and screening laboratory studies were normal, and that there was no evidence of a heart attack. Relieved, the patient asked for an Ativan to calm her nerves. Upon further questioning, the patient sheepishly reported that she had been taking 3 to 6 mg lorazepam for about 10 years, as prescribed by her family physician (FP) for anxiety. She further admitted that she abruptly discontinued taking the drug about one week before this ED visit after she’d heard on a daytime TV show that the medication was addictive.
After receiving lorazepam, the patient showed marked improvement. The EP’s final impressions were atypical chest pain and acute panic attack precipitated by abrupt benzodiazepine withdrawal. After discussing the case with the patient’s FP, the EP discharged the patient home with instructions to complete the cardiac evaluation as an outpatient. The EP also recommended that the patient resume taking lorazepam and follow-up with her FP within one week to discuss a benzodiazepine taper and alternative therapy for anxiety.
Case 2
[The 36-year-old woman with altered mental status.]
When the EP entered the patient’s room, he witnessed the patient staring at her husband and striking him repetitively with her right arm. When the EP asked the patient to stop hitting, her husband told the EP that everything was alright and that the patient’s neurologist had previously told them this behavior was caused by a seizure. While in the next examination room, one of the EP’s colleagues had overheard some of the patient’s history and recognized the name of the patient’s neurologist as a specialist in partial complex seizures—one who had retired from the local medical school about 10 years ago.
After records from the local university hospital confirmed the patient’s diagnosis of partial complex seizures, she was given intravenous lorazepam 2 mg; she became alert, conversational, and stopped flailing her right arm. She was then admitted to the hospital for medical stabilization of her frequent seizures.
Editor’s Note: Part 2 of this article will appear in the June 2016 issue of Emergency Medicine and will cover psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, and toxins.
1. Boyapati R, Papadopoulos G, Olver J, Geluk M, Johnson PD. An unusual presentation of herpes simplex virus encephalitis. Case Rep Med. 2012;241710.
2. Verma R, Anand KS. HIV presenting as young-onset dementia. J Int Assoc Provid AIDS Care. 2014;13(2):110-112.
3. Gheuens S, Pierone G, Peeters P, Koralnik IJ. Progressive multifocal leukoencephalopathy in individuals with minimal or occult immunosuppression. J Neurol Neurosurg Psychiatry. 2010;81(3):247-254.
4. Sobhan T, Rowe HM, Ryan WG, Munoz C. Unusual case report: three cases of psychiatric manifestations of neurosyphilis. Psychiatr Serv. 2004;55(7):830-832.
5. Noblett J, Roberts E. The importance of not jumping to conclusions: syphilis as an organic cause of neurological, psychiatric and endocrine presentations. BMJ Case Rep. 2015;25:2015.
6. Ukwaja KN. Typhoid fever presenting as a depressive disorder—a case report. Rural Remote Health. 2010;10(2):1276.
7. Patra BN, Sharma A, Mehra A, Singh S. Complicated alcohol withdrawal presenting as self mutilation. J Forensic Leg Med. 2014;21:46-47.
8. Stehman CR, Mycyk MB. A rational approach to the treatment of alcohol withdrawal in the ED. Am J Emerg Med. 2013;31(4):734-742.
9. Pétursson H. The benzodiazepine withdrawal syndrome. Addiction. 1994;89(11):1455-1459.
10. Bosshart H. Withdrawal-induced delirium associated with a benzodiazepine switch: a case report. J Med Case Rep. 2011;5:207207.
11. Hassanian-Moghaddam H, Afzali S, Pooya A. Withdrawal syndrome caused by naltrexone in opioid abusers. Hum Exp Toxicol. 2014;33(6):561-567. doi:10.1177/0960327112450901
12. Hasin DS, Keyes KM, Alderson D, Wang S, Aharonovich E, Grant BF. Cannabis withdrawal in the United States: results from NESARC. J Clin Psychiatry. 69(9):1354-1363.
13. Okazaki Y. The epidemiology and pathogenesis of postpartum depression. Nihon Rinsho. 2001;59(8):1555-1559.
14. Sinert R, Su M, Secko M, Zehtabchi S. The utility of routine laboratory testing in hypoglycaemic emergency department patients. Emerg Med J. 2009;26(1):28-31.
15. Schneider P, Nejtek VA, Hurd CL. A case of mistaken identity: alcohol withdrawal, schizophrenia, or central pontine myelinolysis? Neuropsychiatr Dis Treat. 2012;8:49-54.
16. Stojanovich L, Zandman-Goddard G, Pavlovich S, Sikanich N. Psychiatric manifestations in systemic lupus erythematosus. Autoimmun Rev. 2007;6(6):421-426.
17. Kayser MS, J Dalmau. Anti-NMDA receptor encephalitis, autoimmunity, and psychosis. Schizophr Res. 2014;pi:S0920-9964(14)00546-5.
18. Tidswell J, Kleinig T, Ash D, Thompson P, Galletly C. Early recognition of anti-N-methyl D-aspartate (NMDA) receptor encephalitis presenting as acute psychosis. Australas Psychiatry. 2013;21(6):596-599.
19. Masopust J, Andrýs C, Bažant J, Vyšata O, Kuca K, Vališ M. Anti-NMDA receptor antibodies in patients with a first episode of schizophrenia. Neuropsychiatr Dis Treat. 2015;11:619-623.
20. de Cerqueira AC, Semionato de Andrade P, Godoy Barreiros JM, Teixeira AL, Nardi AE. Psychiatric disorders in patients with multiple sclerosis. Compr Psychiatry. 2015;63:10-14.
21. Mobbs RJ, Chandran KN, Newcombe RL. Psychiatric presentation of aneurysmal subarachnoid haemorrhage. ANZ J Surg. 2001;71(1):69-70.
22. Kar SK, Kumar D, Singh P, Upadhyay PK. Psychiatric manifestation of chronic subdural hematoma: the unfolding of mystery in a homeless patient. Indian J Psychol Med. 2015;37(2):239-242.
23. Nagel M, Rumpf HJ, Kasten M. Acute psychosis in a verified Huntington disease gene carrier with subtle motor signs: psychiatric criteria should be considered for the diagnosis. Gen Hosp Psychiatry. 2014;36(3):361.e3-e4.
24. Buoli M, Caldiroli A, Altamura AC. Psychiatric conditions in Parkinson disease: a comparison with classical psychiatric disorders. J Geriatr Psychiatry Neurol. 2016;29(2):72-91.
25. Bortz JJ. Neuropsychiatric and memory issues in epilepsy.” Mayo Clin Proc. 2003;78(6):781-787.
26. Dupre CM, Libman R, Dupre SI, Katz JM, Rybinnik I, Kwiatkowski T. Stroke chameleons. J Stroke Cerebrovasc Dis. 2014;23(2):374-378.

The chaos of a busy ED can test the cognitive reserve of even the most focused practitioner. To streamline the challenge of serial diagnosis and treatment, clinicians employ heuristics while honing the skills of pattern recognition. However, by definition, heuristics employs shortcuts, leaving out information for the sake of efficiency—sometimes at the expense of accuracy. Whether a patient presents with chest pain, abdominal pain, headache, or (the dreaded) dizziness, emergency physicians (EPs) employ algorithms based on a combination of education and prior experience.
Most of the time, these models lead the EP along the correct path, but not always. For example, when a clinician evaluating a patient presenting with psychotic behavior assumes the patient has schizophrenia, he or she will be correct eight or nine times out of 10. However, in some cases, a patient’s bizarre behavior may not be due to a true psychiatric disorder but, for example, from ingestion of an illicit substance.
In addition, in such patients, psychiatric symptoms may be masking a serious acute, organic condition—one requiring prompt intervention and therapy to avoid morbidity or death. To help prevent diagnostic errors, this 2-part series reviews several of the most common medical mimics of psychiatric conditions. Part 1 of this series reviews the psychiatric presentations associated with medical conditions of an infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, or central nervous system etiology (Table 1). This article also discusses clinical signs and symptoms that suggest an increased likelihood that a patient’s psychiatric symptoms are from an underlying medical condition (Table 2).
Case Scenarios
Case 1
A 58-year-old woman with a history of smoking 40 packs of cigarettes per year presented to the ED 1 hour after onset of intermittent chest pain. Upon arrival at the ED, the patient stated that she had trouble catching her breath on and off throughout the day. The patient’s vital signs, electrocardiogram (ECG), and chest X-ray were all normal. The physical examination was unremarkable except for mild diaphoresis. The patient denied experiencing palpitations, recent travel, or previous episodes; she further stated that she was currently not on any medications. There was no previous history of visits to this hospital. The patient’s husband, who accompanied her to the ED, noted that his wife’s behavior had been atypical for approximately 1 week.
After receiving aspirin, the patient appeared symptom-free. Pending the results of another chest radiograph and laboratory evaluation, the EP anticipated moving her to the chest-pain observation unit.
Case 2
A 36-year-old woman presented with altered mental status to the ED via emergency medical services (EMS). Her vital signs, including temperature, were normal. Despite intermittently appearing to be asleep, the patient was alternatingly cooperative and combative. She repetitively whispered, “Who am I?” and randomly shouted at staff members as they walked by her room.
Her neurological examination was nonfocal. The hospital’s electronic medical record (EMR) for this patient showed nearly monthly ED visits for behavioral symptoms. Precipitating events noted in the EMR included job loss and separation from her husband. While waiting for the results of the basic laboratory work-up and toxicology screening to medically clear the patient for psychiatric evaluation, the EP contemplated a computed tomography (CT) study. Realizing the patient would not be able to remain still for the scan, the EP ordered 10 mg of intramuscular ziprasidone for sedation. When the patient’s husband arrived, the EP placed the CT scan on hold until she could obtain additional history from him.
Infections
Herpes Simplex Encephalitis
Herpes simplex encephalitis (HSE) is a serious but treatable disease—one that requires early detection and treatment to avoid severe morbidity. While the classic symptoms are fever and altered mental status, recent literature has noted that afebrile patients with HSE may present with behavioral changes, cognitive decline, aggression, and disinhibition. Therefore, diagnosis of a functional psychiatric complaint, if made initially, could delay appropriate treatment with acyclovir.1
Human Immunodeficiency Virus
Progression of human immunodeficiency virus (HIV) is a well-known cause of various neurocognitive disorders, including early-onset dementia. Since the availability of highly active antiretroviral therapy, the incidence of HIV dementia has decreased, but HIV remains the most common preventable cause of dementia in persons younger than age 50 years. Recent literature has described HIV dementia presenting as an early-onset, rapidly progressing dementia in a young person. Thus, the EP should consider early HIV testing in any young patient who presents with dementia, especially one with a history of fever of unknown origin.2
Progressive Multifocal Encephalopathy
Caused by reactivation of the John Cunningham virus, progressive multifocal encephalopathy has been classically described as a potentially lethal complication of a severely immunocompromised state, often presenting with clumsiness, weakness, visual changes, speech difficulty, and behavioral changes. Though typically described as occurring in the context of acquired immunodeficiency disease syndrome, hematological malignancy, or organ transplant, the condition can occur in the setting of minimal or occult immunosuppression—especially in patients with a history of cirrhosis. If the condition is detected early, immunotherapy can result in significant clinical improvement.3
Syphilis
Late stages of syphilis can present with a wide variety of psychiatric symptoms, including personality disorder, psychosis, delirium, and dementia. As with HIV, there has been a resurgence of syphilis cases, and screening is now often a routine part of a neuropsychiatric work-up. The EP should consider syphilis in the differential for any new-onset psychiatric complaint.4,5
Typhoid Fever
Although this severe febrile illness is uncommon in the United States, it is endemic to many tropical countries within Africa, Southeast Asia, and Central and South America. Typhoid is characterized by a stepwise fever that can progress to abdominal distension, toxemia, and potentially bowel perforation. It is also known to present with psychiatric symptoms such as acute confusion, psychosis, generalized anxiety disorder, and, though rare, depressive disorder. Physicians traveling to rural endemic areas should be aware of these neuropsychiatric presentations to avoid misdiagnosis and delay of treatment.6 Other infectious endemic diseases with reports of neuropsychiatric components are neurocystercercosis, Lyme disease, and African trypanosomiasis.
Pharmacological Withdrawal Syndromes
Alcohol
Alcohol withdrawal is a common presentation in the ED, and up to 24% of US adults brought to the ED by EMS suffer from alcoholism. Typically characterized by tachycardia, hypertension, and tremors, alcohol withdrawal syndrome can also feature psychiatric components such as agitation, hallucinations, persecutory delusions, and even self-mutilation.7 Evidence-based protocols indicate loading doses of benzodiazepines as a mainstay of treatment, with supplemental barbiturates or propofol in cases of treatment failure.8
Benzodiazepines
Withdrawal from therapeutic doses of benzodiazepines can potentially cause psychiatric symptoms, including sleep disturbances, irritability, anxiety, panic attacks, tremor, and perceptual changes. Withdrawal from higher doses of benzodiazepines can lead to more serious presentations, such as seizures and acute psychosis.9 Withdrawal symptoms can develop from discontinuation of the drug and with non-tapered switching between benzodiazepines.10
Opiates
Opiate withdrawal is an unpleasant experience characterized by generalized pain, nausea and vomiting, sweating, and tachycardia. Neuropsychiatric complaints such as anxiety, agitation, and irritability can also be present. More severe agitation has been described in naltrexone-accelerated detoxification.11
Cannabis
Recent literature on cannabis use indicates a high prevalence and clinical significance of associated withdrawal symptoms in frequent users. There appear to be two subsets of cannabis withdrawal—one characterized by weakness and hypersomnia, and the other by anxiety, depression, restlessness, and insomnia.12
Estrogen
Withdrawal from endogenous estrogen has been hypothesized as a possible cause of puerperal psychosis.13 Estrogen withdrawal outside of this setting, however, can and does occur, and recent literature has shown episodes of reversible psychosis associated with the discontinuation of both oral contraceptive regimens and hormonal therapy for menopausal symptoms.
Acute Metabolic Conditions
Hypoglycemia
Hypoglycemia, most often encountered as a side effect of insulin or oral hypoglycemic therapies, is a potentially lethal cause of confusion, anxiety, nervousness, and seizures. Nocturnal hypoglycemia can manifest as nightmares, crying out, and confusion upon awakening. A fingerstick blood-glucose test is an absolutely vital part of the initial work-up of any patient with an altered mental status or overt psychiatric complaint.14
Central Pontine Myelinolysis
A potentially devastating neurological condition associated with malnourishment and alcohol dependence, central pontine myelinolysis (CPM) is classically exacerbated by rapid overcorrection of hyponatremia. While the disease can manifest primarily with quadriplegia or pseudobulbar palsy and eventual progress to the dreaded “locked-in” syndrome, early presentations can include psychiatric symptoms such as behavioral changes, psychosis, and cognitive disturbances. Patients with early signs and symptoms of CPM have been misdiagnosed as having schizophrenia with catatonia, leading to delayed treatment and poor outcomes. The EP should remain vigilant when evaluating for this condition and consider a magnetic resonance imaging study in patients with psychiatric symptoms in the setting of fluctuating hyponatremia.15
Autoimmune Disorders
Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is one of the most common autoimmune disorders, and has a higher incidence in young women. The disease affects multiple organ systems. Though the classic initial presentation of SLE is fever, joint pain, and rash, the associated neuropsychiatric syndromes of this disease are diverse and surprisingly common, and can be the initial manifestation of the disease. Common psychiatric manifestations of SLE include cognitive dysfunction, anxiety, mood disorders such as depression, acute confusion, psychosis, paranoia, and auditory or visual hallucinations.16
Anti-N-methyl-D-Aspartate Receptor Encephalitis
Initially described as a paraneoplastic effect of ovarian teratomas, anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is actually an autoimmune disorder that can occur even in the absence of a primary tumor. As with SLE, the condition primarily occurs in young women. Antibodies in the cerebrospinal fluid cause prominent psychiatric symptoms such as acute psychosis, delusional thinking, hallucinations, agitation, and confusion. Although the disease can progress to seizures, movement disorders, autonomic dysregulation, and ultimately death, early recognition and treatment can lead to positive outcomes in up to 80% of cases.17 While the prevalence of anti-NMDAR antibodies in new-onset psychosis remains unclear, recent literature has suggested widespread screening for the disease in all first presentations of psychotic episodes.18,19
Multiple Sclerosis
Multiple sclerosis (MS) is another autoimmune disorder that has a higher prevalence in young women. The disease is characterized by central nervous system involvement that occurs over a period of months to years, with symptoms corresponding to different anatomic locations. Though the classic presenting symptom of MS is optic neuritis, neuropsychiatric syndromes are a common co-occurrence and can be the initial presenting symptom. The most commonly associated psychiatric complaints are anxiety, depression, and bipolar disorder, though case reports of SLE have described acute psychosis, psychotic depression, and adult-onset tic disorder.20
Trauma
Subarachnoid Hemorrhage
Long-term psychiatric sequelae from subarachnoid hemorrhage, either traumatic or aneurysmal, manifest most commonly as personality changes, intellectual impairment, depression, and anxiety. This condition is also known to cause a host of more bizarre psychiatric presentations, such as new-onset kleptomania, akinetic mutism, confabulatory amnesia, acute psychosis, and Capgras syndrome (the delusion that familiar individuals have been replaced by imposters). These symptoms can occur at initial presentation, and may show variable improvement with shunt surgery.21
Subdural Hematoma
Acute or chronic subdural hematoma can result from major head trauma, or even quite minor head trauma in an elderly or coagulopathic patient. Some common psychiatric manifestations of subdural hematoma include cognitive impairment, withdrawn behavior, blunted affect otherwise mimicking schizophrenic psychosis, and catatonia. The EP should consider early imaging studies in patients with new-onset psychotic symptoms—especially when they are refractory to typical antipsychotics.22
Central Nervous Symptom Diseases
Huntington Disease
Huntington disease (HD) is an autosomal dominant inherited, progressive neurodegenerative disorder characterized by mental decline, mood disorder, and muscle coordination problems that eventually become the classic involuntary writhing termed chorea. Due to its progressive nature, precise onset of the disease is difficult to describe; however, HD can manifest initially as schizophrenia-like psychotic episodes with only minimal apparent motor difficulty. Family history, including movement disorders and suicide, is important to obtain when available.23
Parkinson Disease
A progressive and disabling neurodegenerative disorder, Parkinson disease (PD) is classically characterized by fine resting tremor, cogwheeling rigidity, akinesia and mask-like facies, and postural instability. Comorbidity of psychiatric disorders is high, both as a result of the underlying disease process and as a side effect of dopaminergic treatment regimes. Common presentations of psychiatric disorders in PD include schizophrenia-like psychosis with visual hallucinations and mood disorders with prominent apathy and executive dysfunction. Recognition of the comorbidity is important because psychiatric disorders in PD respond differently to treatment than classic psychiatric disorders.24
Temporal Lobe Epilepsy
Epilepsy is a complex group of related neurological disorders involving unregulated nerve cell firing with a large variability in clinical presentation. Characteristically there is recurrent seizure activity. Temporal lobe epilepsy (TLE) is a subset of epilepsy known to present as a number of behavioral and neuropsychiatric complaints. Most presentations of TLE involve auras of emotional phenomena such as depression, fear, or anxiety, which can occur alone or with subsequent progression to complex partial or secondary generalized seizures.25 Many other bizarre presentations of TLE have been reported, including recurrent, potentially debilitating déjà vu, vivid recollection of past traumatic events mimicking posttraumatic stress disorder, paranoid delusions following olfactory triggers; and unprovoked attacks of depersonalization, derealization, anxiety, and dyspnea originally misdiagnosed as panic attack.
Stroke
The term “stroke chameleon” refers to presentations suggestive of other diseases that actually represent underlying strokes. Altered mental status is by far the largest block of these chameleons, with up to 30% of misdiagnosed strokes being misdiagnosed as altered mental status. The positive predictive value of altered mental status alone (ie, the chance that the diagnosis of altered mental status actually represents an undiagnosed acute stroke) is 7%.26
Case Scenarios Continued
Case 1
[The 58-year-old woman with intermittent chest pain.]
The patient’s D-dimer and troponin I levels were normal. Before the EP had an opportunity to discuss the results and next steps with the patient, the nurse asked him to see the patient immediately. Upon entering her room, the EP noted that the patient appeared anxious. The patient said the shortness of breath had returned, and also that she felt as if she were “floating” off the gurney, outside of her body. A check of her vital signs revealed a heart rate of 106 beats/minute and blood pressure of 160/100 mm Hg. A repeat ECG was significant only for sinus tachycardia. In an effort to calm the patient, the EP reassured her that the ECG, chest X-ray, and screening laboratory studies were normal, and that there was no evidence of a heart attack. Relieved, the patient asked for an Ativan to calm her nerves. Upon further questioning, the patient sheepishly reported that she had been taking 3 to 6 mg lorazepam for about 10 years, as prescribed by her family physician (FP) for anxiety. She further admitted that she abruptly discontinued taking the drug about one week before this ED visit after she’d heard on a daytime TV show that the medication was addictive.
After receiving lorazepam, the patient showed marked improvement. The EP’s final impressions were atypical chest pain and acute panic attack precipitated by abrupt benzodiazepine withdrawal. After discussing the case with the patient’s FP, the EP discharged the patient home with instructions to complete the cardiac evaluation as an outpatient. The EP also recommended that the patient resume taking lorazepam and follow-up with her FP within one week to discuss a benzodiazepine taper and alternative therapy for anxiety.
Case 2
[The 36-year-old woman with altered mental status.]
When the EP entered the patient’s room, he witnessed the patient staring at her husband and striking him repetitively with her right arm. When the EP asked the patient to stop hitting, her husband told the EP that everything was alright and that the patient’s neurologist had previously told them this behavior was caused by a seizure. While in the next examination room, one of the EP’s colleagues had overheard some of the patient’s history and recognized the name of the patient’s neurologist as a specialist in partial complex seizures—one who had retired from the local medical school about 10 years ago.
After records from the local university hospital confirmed the patient’s diagnosis of partial complex seizures, she was given intravenous lorazepam 2 mg; she became alert, conversational, and stopped flailing her right arm. She was then admitted to the hospital for medical stabilization of her frequent seizures.
Editor’s Note: Part 2 of this article will appear in the June 2016 issue of Emergency Medicine and will cover psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, and toxins.
The chaos of a busy ED can test the cognitive reserve of even the most focused practitioner. To streamline the challenge of serial diagnosis and treatment, clinicians employ heuristics while honing the skills of pattern recognition. However, by definition, heuristics employs shortcuts, leaving out information for the sake of efficiency—sometimes at the expense of accuracy. Whether a patient presents with chest pain, abdominal pain, headache, or (the dreaded) dizziness, emergency physicians (EPs) employ algorithms based on a combination of education and prior experience.
Most of the time, these models lead the EP along the correct path, but not always. For example, when a clinician evaluating a patient presenting with psychotic behavior assumes the patient has schizophrenia, he or she will be correct eight or nine times out of 10. However, in some cases, a patient’s bizarre behavior may not be due to a true psychiatric disorder but, for example, from ingestion of an illicit substance.
In addition, in such patients, psychiatric symptoms may be masking a serious acute, organic condition—one requiring prompt intervention and therapy to avoid morbidity or death. To help prevent diagnostic errors, this 2-part series reviews several of the most common medical mimics of psychiatric conditions. Part 1 of this series reviews the psychiatric presentations associated with medical conditions of an infectious, pharmacological withdrawal, metabolic, autoimmune, traumatic, or central nervous system etiology (Table 1). This article also discusses clinical signs and symptoms that suggest an increased likelihood that a patient’s psychiatric symptoms are from an underlying medical condition (Table 2).
Case Scenarios
Case 1
A 58-year-old woman with a history of smoking 40 packs of cigarettes per year presented to the ED 1 hour after onset of intermittent chest pain. Upon arrival at the ED, the patient stated that she had trouble catching her breath on and off throughout the day. The patient’s vital signs, electrocardiogram (ECG), and chest X-ray were all normal. The physical examination was unremarkable except for mild diaphoresis. The patient denied experiencing palpitations, recent travel, or previous episodes; she further stated that she was currently not on any medications. There was no previous history of visits to this hospital. The patient’s husband, who accompanied her to the ED, noted that his wife’s behavior had been atypical for approximately 1 week.
After receiving aspirin, the patient appeared symptom-free. Pending the results of another chest radiograph and laboratory evaluation, the EP anticipated moving her to the chest-pain observation unit.
Case 2
A 36-year-old woman presented with altered mental status to the ED via emergency medical services (EMS). Her vital signs, including temperature, were normal. Despite intermittently appearing to be asleep, the patient was alternatingly cooperative and combative. She repetitively whispered, “Who am I?” and randomly shouted at staff members as they walked by her room.
Her neurological examination was nonfocal. The hospital’s electronic medical record (EMR) for this patient showed nearly monthly ED visits for behavioral symptoms. Precipitating events noted in the EMR included job loss and separation from her husband. While waiting for the results of the basic laboratory work-up and toxicology screening to medically clear the patient for psychiatric evaluation, the EP contemplated a computed tomography (CT) study. Realizing the patient would not be able to remain still for the scan, the EP ordered 10 mg of intramuscular ziprasidone for sedation. When the patient’s husband arrived, the EP placed the CT scan on hold until she could obtain additional history from him.
Infections
Herpes Simplex Encephalitis
Herpes simplex encephalitis (HSE) is a serious but treatable disease—one that requires early detection and treatment to avoid severe morbidity. While the classic symptoms are fever and altered mental status, recent literature has noted that afebrile patients with HSE may present with behavioral changes, cognitive decline, aggression, and disinhibition. Therefore, diagnosis of a functional psychiatric complaint, if made initially, could delay appropriate treatment with acyclovir.1
Human Immunodeficiency Virus
Progression of human immunodeficiency virus (HIV) is a well-known cause of various neurocognitive disorders, including early-onset dementia. Since the availability of highly active antiretroviral therapy, the incidence of HIV dementia has decreased, but HIV remains the most common preventable cause of dementia in persons younger than age 50 years. Recent literature has described HIV dementia presenting as an early-onset, rapidly progressing dementia in a young person. Thus, the EP should consider early HIV testing in any young patient who presents with dementia, especially one with a history of fever of unknown origin.2
Progressive Multifocal Encephalopathy
Caused by reactivation of the John Cunningham virus, progressive multifocal encephalopathy has been classically described as a potentially lethal complication of a severely immunocompromised state, often presenting with clumsiness, weakness, visual changes, speech difficulty, and behavioral changes. Though typically described as occurring in the context of acquired immunodeficiency disease syndrome, hematological malignancy, or organ transplant, the condition can occur in the setting of minimal or occult immunosuppression—especially in patients with a history of cirrhosis. If the condition is detected early, immunotherapy can result in significant clinical improvement.3
Syphilis
Late stages of syphilis can present with a wide variety of psychiatric symptoms, including personality disorder, psychosis, delirium, and dementia. As with HIV, there has been a resurgence of syphilis cases, and screening is now often a routine part of a neuropsychiatric work-up. The EP should consider syphilis in the differential for any new-onset psychiatric complaint.4,5
Typhoid Fever
Although this severe febrile illness is uncommon in the United States, it is endemic to many tropical countries within Africa, Southeast Asia, and Central and South America. Typhoid is characterized by a stepwise fever that can progress to abdominal distension, toxemia, and potentially bowel perforation. It is also known to present with psychiatric symptoms such as acute confusion, psychosis, generalized anxiety disorder, and, though rare, depressive disorder. Physicians traveling to rural endemic areas should be aware of these neuropsychiatric presentations to avoid misdiagnosis and delay of treatment.6 Other infectious endemic diseases with reports of neuropsychiatric components are neurocystercercosis, Lyme disease, and African trypanosomiasis.
Pharmacological Withdrawal Syndromes
Alcohol
Alcohol withdrawal is a common presentation in the ED, and up to 24% of US adults brought to the ED by EMS suffer from alcoholism. Typically characterized by tachycardia, hypertension, and tremors, alcohol withdrawal syndrome can also feature psychiatric components such as agitation, hallucinations, persecutory delusions, and even self-mutilation.7 Evidence-based protocols indicate loading doses of benzodiazepines as a mainstay of treatment, with supplemental barbiturates or propofol in cases of treatment failure.8
Benzodiazepines
Withdrawal from therapeutic doses of benzodiazepines can potentially cause psychiatric symptoms, including sleep disturbances, irritability, anxiety, panic attacks, tremor, and perceptual changes. Withdrawal from higher doses of benzodiazepines can lead to more serious presentations, such as seizures and acute psychosis.9 Withdrawal symptoms can develop from discontinuation of the drug and with non-tapered switching between benzodiazepines.10
Opiates
Opiate withdrawal is an unpleasant experience characterized by generalized pain, nausea and vomiting, sweating, and tachycardia. Neuropsychiatric complaints such as anxiety, agitation, and irritability can also be present. More severe agitation has been described in naltrexone-accelerated detoxification.11
Cannabis
Recent literature on cannabis use indicates a high prevalence and clinical significance of associated withdrawal symptoms in frequent users. There appear to be two subsets of cannabis withdrawal—one characterized by weakness and hypersomnia, and the other by anxiety, depression, restlessness, and insomnia.12
Estrogen
Withdrawal from endogenous estrogen has been hypothesized as a possible cause of puerperal psychosis.13 Estrogen withdrawal outside of this setting, however, can and does occur, and recent literature has shown episodes of reversible psychosis associated with the discontinuation of both oral contraceptive regimens and hormonal therapy for menopausal symptoms.
Acute Metabolic Conditions
Hypoglycemia
Hypoglycemia, most often encountered as a side effect of insulin or oral hypoglycemic therapies, is a potentially lethal cause of confusion, anxiety, nervousness, and seizures. Nocturnal hypoglycemia can manifest as nightmares, crying out, and confusion upon awakening. A fingerstick blood-glucose test is an absolutely vital part of the initial work-up of any patient with an altered mental status or overt psychiatric complaint.14
Central Pontine Myelinolysis
A potentially devastating neurological condition associated with malnourishment and alcohol dependence, central pontine myelinolysis (CPM) is classically exacerbated by rapid overcorrection of hyponatremia. While the disease can manifest primarily with quadriplegia or pseudobulbar palsy and eventual progress to the dreaded “locked-in” syndrome, early presentations can include psychiatric symptoms such as behavioral changes, psychosis, and cognitive disturbances. Patients with early signs and symptoms of CPM have been misdiagnosed as having schizophrenia with catatonia, leading to delayed treatment and poor outcomes. The EP should remain vigilant when evaluating for this condition and consider a magnetic resonance imaging study in patients with psychiatric symptoms in the setting of fluctuating hyponatremia.15
Autoimmune Disorders
Systemic Lupus Erythematosus
Systemic lupus erythematosus (SLE) is one of the most common autoimmune disorders, and has a higher incidence in young women. The disease affects multiple organ systems. Though the classic initial presentation of SLE is fever, joint pain, and rash, the associated neuropsychiatric syndromes of this disease are diverse and surprisingly common, and can be the initial manifestation of the disease. Common psychiatric manifestations of SLE include cognitive dysfunction, anxiety, mood disorders such as depression, acute confusion, psychosis, paranoia, and auditory or visual hallucinations.16
Anti-N-methyl-D-Aspartate Receptor Encephalitis
Initially described as a paraneoplastic effect of ovarian teratomas, anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis is actually an autoimmune disorder that can occur even in the absence of a primary tumor. As with SLE, the condition primarily occurs in young women. Antibodies in the cerebrospinal fluid cause prominent psychiatric symptoms such as acute psychosis, delusional thinking, hallucinations, agitation, and confusion. Although the disease can progress to seizures, movement disorders, autonomic dysregulation, and ultimately death, early recognition and treatment can lead to positive outcomes in up to 80% of cases.17 While the prevalence of anti-NMDAR antibodies in new-onset psychosis remains unclear, recent literature has suggested widespread screening for the disease in all first presentations of psychotic episodes.18,19
Multiple Sclerosis
Multiple sclerosis (MS) is another autoimmune disorder that has a higher prevalence in young women. The disease is characterized by central nervous system involvement that occurs over a period of months to years, with symptoms corresponding to different anatomic locations. Though the classic presenting symptom of MS is optic neuritis, neuropsychiatric syndromes are a common co-occurrence and can be the initial presenting symptom. The most commonly associated psychiatric complaints are anxiety, depression, and bipolar disorder, though case reports of SLE have described acute psychosis, psychotic depression, and adult-onset tic disorder.20
Trauma
Subarachnoid Hemorrhage
Long-term psychiatric sequelae from subarachnoid hemorrhage, either traumatic or aneurysmal, manifest most commonly as personality changes, intellectual impairment, depression, and anxiety. This condition is also known to cause a host of more bizarre psychiatric presentations, such as new-onset kleptomania, akinetic mutism, confabulatory amnesia, acute psychosis, and Capgras syndrome (the delusion that familiar individuals have been replaced by imposters). These symptoms can occur at initial presentation, and may show variable improvement with shunt surgery.21
Subdural Hematoma
Acute or chronic subdural hematoma can result from major head trauma, or even quite minor head trauma in an elderly or coagulopathic patient. Some common psychiatric manifestations of subdural hematoma include cognitive impairment, withdrawn behavior, blunted affect otherwise mimicking schizophrenic psychosis, and catatonia. The EP should consider early imaging studies in patients with new-onset psychotic symptoms—especially when they are refractory to typical antipsychotics.22
Central Nervous Symptom Diseases
Huntington Disease
Huntington disease (HD) is an autosomal dominant inherited, progressive neurodegenerative disorder characterized by mental decline, mood disorder, and muscle coordination problems that eventually become the classic involuntary writhing termed chorea. Due to its progressive nature, precise onset of the disease is difficult to describe; however, HD can manifest initially as schizophrenia-like psychotic episodes with only minimal apparent motor difficulty. Family history, including movement disorders and suicide, is important to obtain when available.23
Parkinson Disease
A progressive and disabling neurodegenerative disorder, Parkinson disease (PD) is classically characterized by fine resting tremor, cogwheeling rigidity, akinesia and mask-like facies, and postural instability. Comorbidity of psychiatric disorders is high, both as a result of the underlying disease process and as a side effect of dopaminergic treatment regimes. Common presentations of psychiatric disorders in PD include schizophrenia-like psychosis with visual hallucinations and mood disorders with prominent apathy and executive dysfunction. Recognition of the comorbidity is important because psychiatric disorders in PD respond differently to treatment than classic psychiatric disorders.24
Temporal Lobe Epilepsy
Epilepsy is a complex group of related neurological disorders involving unregulated nerve cell firing with a large variability in clinical presentation. Characteristically there is recurrent seizure activity. Temporal lobe epilepsy (TLE) is a subset of epilepsy known to present as a number of behavioral and neuropsychiatric complaints. Most presentations of TLE involve auras of emotional phenomena such as depression, fear, or anxiety, which can occur alone or with subsequent progression to complex partial or secondary generalized seizures.25 Many other bizarre presentations of TLE have been reported, including recurrent, potentially debilitating déjà vu, vivid recollection of past traumatic events mimicking posttraumatic stress disorder, paranoid delusions following olfactory triggers; and unprovoked attacks of depersonalization, derealization, anxiety, and dyspnea originally misdiagnosed as panic attack.
Stroke
The term “stroke chameleon” refers to presentations suggestive of other diseases that actually represent underlying strokes. Altered mental status is by far the largest block of these chameleons, with up to 30% of misdiagnosed strokes being misdiagnosed as altered mental status. The positive predictive value of altered mental status alone (ie, the chance that the diagnosis of altered mental status actually represents an undiagnosed acute stroke) is 7%.26
Case Scenarios Continued
Case 1
[The 58-year-old woman with intermittent chest pain.]
The patient’s D-dimer and troponin I levels were normal. Before the EP had an opportunity to discuss the results and next steps with the patient, the nurse asked him to see the patient immediately. Upon entering her room, the EP noted that the patient appeared anxious. The patient said the shortness of breath had returned, and also that she felt as if she were “floating” off the gurney, outside of her body. A check of her vital signs revealed a heart rate of 106 beats/minute and blood pressure of 160/100 mm Hg. A repeat ECG was significant only for sinus tachycardia. In an effort to calm the patient, the EP reassured her that the ECG, chest X-ray, and screening laboratory studies were normal, and that there was no evidence of a heart attack. Relieved, the patient asked for an Ativan to calm her nerves. Upon further questioning, the patient sheepishly reported that she had been taking 3 to 6 mg lorazepam for about 10 years, as prescribed by her family physician (FP) for anxiety. She further admitted that she abruptly discontinued taking the drug about one week before this ED visit after she’d heard on a daytime TV show that the medication was addictive.
After receiving lorazepam, the patient showed marked improvement. The EP’s final impressions were atypical chest pain and acute panic attack precipitated by abrupt benzodiazepine withdrawal. After discussing the case with the patient’s FP, the EP discharged the patient home with instructions to complete the cardiac evaluation as an outpatient. The EP also recommended that the patient resume taking lorazepam and follow-up with her FP within one week to discuss a benzodiazepine taper and alternative therapy for anxiety.
Case 2
[The 36-year-old woman with altered mental status.]
When the EP entered the patient’s room, he witnessed the patient staring at her husband and striking him repetitively with her right arm. When the EP asked the patient to stop hitting, her husband told the EP that everything was alright and that the patient’s neurologist had previously told them this behavior was caused by a seizure. While in the next examination room, one of the EP’s colleagues had overheard some of the patient’s history and recognized the name of the patient’s neurologist as a specialist in partial complex seizures—one who had retired from the local medical school about 10 years ago.
After records from the local university hospital confirmed the patient’s diagnosis of partial complex seizures, she was given intravenous lorazepam 2 mg; she became alert, conversational, and stopped flailing her right arm. She was then admitted to the hospital for medical stabilization of her frequent seizures.
Editor’s Note: Part 2 of this article will appear in the June 2016 issue of Emergency Medicine and will cover psychiatric presentations related to dementia, cancer, cardiac disease, nutritional deficiencies, endocrine disorders, and toxins.
1. Boyapati R, Papadopoulos G, Olver J, Geluk M, Johnson PD. An unusual presentation of herpes simplex virus encephalitis. Case Rep Med. 2012;241710.
2. Verma R, Anand KS. HIV presenting as young-onset dementia. J Int Assoc Provid AIDS Care. 2014;13(2):110-112.
3. Gheuens S, Pierone G, Peeters P, Koralnik IJ. Progressive multifocal leukoencephalopathy in individuals with minimal or occult immunosuppression. J Neurol Neurosurg Psychiatry. 2010;81(3):247-254.
4. Sobhan T, Rowe HM, Ryan WG, Munoz C. Unusual case report: three cases of psychiatric manifestations of neurosyphilis. Psychiatr Serv. 2004;55(7):830-832.
5. Noblett J, Roberts E. The importance of not jumping to conclusions: syphilis as an organic cause of neurological, psychiatric and endocrine presentations. BMJ Case Rep. 2015;25:2015.
6. Ukwaja KN. Typhoid fever presenting as a depressive disorder—a case report. Rural Remote Health. 2010;10(2):1276.
7. Patra BN, Sharma A, Mehra A, Singh S. Complicated alcohol withdrawal presenting as self mutilation. J Forensic Leg Med. 2014;21:46-47.
8. Stehman CR, Mycyk MB. A rational approach to the treatment of alcohol withdrawal in the ED. Am J Emerg Med. 2013;31(4):734-742.
9. Pétursson H. The benzodiazepine withdrawal syndrome. Addiction. 1994;89(11):1455-1459.
10. Bosshart H. Withdrawal-induced delirium associated with a benzodiazepine switch: a case report. J Med Case Rep. 2011;5:207207.
11. Hassanian-Moghaddam H, Afzali S, Pooya A. Withdrawal syndrome caused by naltrexone in opioid abusers. Hum Exp Toxicol. 2014;33(6):561-567. doi:10.1177/0960327112450901
12. Hasin DS, Keyes KM, Alderson D, Wang S, Aharonovich E, Grant BF. Cannabis withdrawal in the United States: results from NESARC. J Clin Psychiatry. 69(9):1354-1363.
13. Okazaki Y. The epidemiology and pathogenesis of postpartum depression. Nihon Rinsho. 2001;59(8):1555-1559.
14. Sinert R, Su M, Secko M, Zehtabchi S. The utility of routine laboratory testing in hypoglycaemic emergency department patients. Emerg Med J. 2009;26(1):28-31.
15. Schneider P, Nejtek VA, Hurd CL. A case of mistaken identity: alcohol withdrawal, schizophrenia, or central pontine myelinolysis? Neuropsychiatr Dis Treat. 2012;8:49-54.
16. Stojanovich L, Zandman-Goddard G, Pavlovich S, Sikanich N. Psychiatric manifestations in systemic lupus erythematosus. Autoimmun Rev. 2007;6(6):421-426.
17. Kayser MS, J Dalmau. Anti-NMDA receptor encephalitis, autoimmunity, and psychosis. Schizophr Res. 2014;pi:S0920-9964(14)00546-5.
18. Tidswell J, Kleinig T, Ash D, Thompson P, Galletly C. Early recognition of anti-N-methyl D-aspartate (NMDA) receptor encephalitis presenting as acute psychosis. Australas Psychiatry. 2013;21(6):596-599.
19. Masopust J, Andrýs C, Bažant J, Vyšata O, Kuca K, Vališ M. Anti-NMDA receptor antibodies in patients with a first episode of schizophrenia. Neuropsychiatr Dis Treat. 2015;11:619-623.
20. de Cerqueira AC, Semionato de Andrade P, Godoy Barreiros JM, Teixeira AL, Nardi AE. Psychiatric disorders in patients with multiple sclerosis. Compr Psychiatry. 2015;63:10-14.
21. Mobbs RJ, Chandran KN, Newcombe RL. Psychiatric presentation of aneurysmal subarachnoid haemorrhage. ANZ J Surg. 2001;71(1):69-70.
22. Kar SK, Kumar D, Singh P, Upadhyay PK. Psychiatric manifestation of chronic subdural hematoma: the unfolding of mystery in a homeless patient. Indian J Psychol Med. 2015;37(2):239-242.
23. Nagel M, Rumpf HJ, Kasten M. Acute psychosis in a verified Huntington disease gene carrier with subtle motor signs: psychiatric criteria should be considered for the diagnosis. Gen Hosp Psychiatry. 2014;36(3):361.e3-e4.
24. Buoli M, Caldiroli A, Altamura AC. Psychiatric conditions in Parkinson disease: a comparison with classical psychiatric disorders. J Geriatr Psychiatry Neurol. 2016;29(2):72-91.
25. Bortz JJ. Neuropsychiatric and memory issues in epilepsy.” Mayo Clin Proc. 2003;78(6):781-787.
26. Dupre CM, Libman R, Dupre SI, Katz JM, Rybinnik I, Kwiatkowski T. Stroke chameleons. J Stroke Cerebrovasc Dis. 2014;23(2):374-378.
1. Boyapati R, Papadopoulos G, Olver J, Geluk M, Johnson PD. An unusual presentation of herpes simplex virus encephalitis. Case Rep Med. 2012;241710.
2. Verma R, Anand KS. HIV presenting as young-onset dementia. J Int Assoc Provid AIDS Care. 2014;13(2):110-112.
3. Gheuens S, Pierone G, Peeters P, Koralnik IJ. Progressive multifocal leukoencephalopathy in individuals with minimal or occult immunosuppression. J Neurol Neurosurg Psychiatry. 2010;81(3):247-254.
4. Sobhan T, Rowe HM, Ryan WG, Munoz C. Unusual case report: three cases of psychiatric manifestations of neurosyphilis. Psychiatr Serv. 2004;55(7):830-832.
5. Noblett J, Roberts E. The importance of not jumping to conclusions: syphilis as an organic cause of neurological, psychiatric and endocrine presentations. BMJ Case Rep. 2015;25:2015.
6. Ukwaja KN. Typhoid fever presenting as a depressive disorder—a case report. Rural Remote Health. 2010;10(2):1276.
7. Patra BN, Sharma A, Mehra A, Singh S. Complicated alcohol withdrawal presenting as self mutilation. J Forensic Leg Med. 2014;21:46-47.
8. Stehman CR, Mycyk MB. A rational approach to the treatment of alcohol withdrawal in the ED. Am J Emerg Med. 2013;31(4):734-742.
9. Pétursson H. The benzodiazepine withdrawal syndrome. Addiction. 1994;89(11):1455-1459.
10. Bosshart H. Withdrawal-induced delirium associated with a benzodiazepine switch: a case report. J Med Case Rep. 2011;5:207207.
11. Hassanian-Moghaddam H, Afzali S, Pooya A. Withdrawal syndrome caused by naltrexone in opioid abusers. Hum Exp Toxicol. 2014;33(6):561-567. doi:10.1177/0960327112450901
12. Hasin DS, Keyes KM, Alderson D, Wang S, Aharonovich E, Grant BF. Cannabis withdrawal in the United States: results from NESARC. J Clin Psychiatry. 69(9):1354-1363.
13. Okazaki Y. The epidemiology and pathogenesis of postpartum depression. Nihon Rinsho. 2001;59(8):1555-1559.
14. Sinert R, Su M, Secko M, Zehtabchi S. The utility of routine laboratory testing in hypoglycaemic emergency department patients. Emerg Med J. 2009;26(1):28-31.
15. Schneider P, Nejtek VA, Hurd CL. A case of mistaken identity: alcohol withdrawal, schizophrenia, or central pontine myelinolysis? Neuropsychiatr Dis Treat. 2012;8:49-54.
16. Stojanovich L, Zandman-Goddard G, Pavlovich S, Sikanich N. Psychiatric manifestations in systemic lupus erythematosus. Autoimmun Rev. 2007;6(6):421-426.
17. Kayser MS, J Dalmau. Anti-NMDA receptor encephalitis, autoimmunity, and psychosis. Schizophr Res. 2014;pi:S0920-9964(14)00546-5.
18. Tidswell J, Kleinig T, Ash D, Thompson P, Galletly C. Early recognition of anti-N-methyl D-aspartate (NMDA) receptor encephalitis presenting as acute psychosis. Australas Psychiatry. 2013;21(6):596-599.
19. Masopust J, Andrýs C, Bažant J, Vyšata O, Kuca K, Vališ M. Anti-NMDA receptor antibodies in patients with a first episode of schizophrenia. Neuropsychiatr Dis Treat. 2015;11:619-623.
20. de Cerqueira AC, Semionato de Andrade P, Godoy Barreiros JM, Teixeira AL, Nardi AE. Psychiatric disorders in patients with multiple sclerosis. Compr Psychiatry. 2015;63:10-14.
21. Mobbs RJ, Chandran KN, Newcombe RL. Psychiatric presentation of aneurysmal subarachnoid haemorrhage. ANZ J Surg. 2001;71(1):69-70.
22. Kar SK, Kumar D, Singh P, Upadhyay PK. Psychiatric manifestation of chronic subdural hematoma: the unfolding of mystery in a homeless patient. Indian J Psychol Med. 2015;37(2):239-242.
23. Nagel M, Rumpf HJ, Kasten M. Acute psychosis in a verified Huntington disease gene carrier with subtle motor signs: psychiatric criteria should be considered for the diagnosis. Gen Hosp Psychiatry. 2014;36(3):361.e3-e4.
24. Buoli M, Caldiroli A, Altamura AC. Psychiatric conditions in Parkinson disease: a comparison with classical psychiatric disorders. J Geriatr Psychiatry Neurol. 2016;29(2):72-91.
25. Bortz JJ. Neuropsychiatric and memory issues in epilepsy.” Mayo Clin Proc. 2003;78(6):781-787.
26. Dupre CM, Libman R, Dupre SI, Katz JM, Rybinnik I, Kwiatkowski T. Stroke chameleons. J Stroke Cerebrovasc Dis. 2014;23(2):374-378.

U.S. official raises concerns over Zika readiness
The ability of the United States to respond to a potential spike in Zika virus infection rates is a cause for concern, according to a top federal health official.
“The big question is will we get local transmission, and my response to that is very likely we will,” Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, told reporters during a joint media briefing with the Pan American Health Organization (PAHO) on May 3.
As many as 500 million people in the Americas are at risk for being infected by the Zika virus, PAHO’s Zika incident manager, Dr. Sylvain Aldighieri, said during the briefing.
In the continental United States to date, there have been about 400 travel-related cases of infection. In Puerto Rico, there have been nearly 700 locally reported cases, and one Zika-related death.
Countries at highest risk for Zika include those that have experienced any outbreaks of dengue fever or chikungunya in the past 15 years, Dr. Aldighieri said. Hawaii and U.S. territories in the Caribbean have experienced local dengue outbreaks during that time. Florida has had local outbreaks of both illnesses.
In the United States, Zika is poised to gain a stronger foothold even as funding for the study and prevention of the virus remains stalled in Congress, and a lack of cohesive public health messaging leaves the public vulnerable to misunderstanding the potential threat of the disease, according to Dr. Fauci.

A vaccine to fight Zika virus is currently under development. “Don’t confuse that with readiness,” Dr. Fauci cautioned.
Dr. Fauci said he believes the disbursement by Congress of President Obama’s requested $1.9 billion in Zika-related funds would facilitate a more comprehensive approach to preventing and treating the virus’s spread, but so far, the funding remains stalled.
As a result, Dr. Fauci said he has reallocated funds intended for other infectious disease research needs to cover Zika-related costs, but is concerned that continued congressional inaction could mean he is left with holes across many budgets. “That 1.9 billion dollars is essential,” he said.
Vaccine progress
In April, $589 millionin funds primarily earmarked for the Ebola crisis were redirected by the Obama administration to fight the Zika virus. That money is now being used in part to fund development of a vaccine that is expected to be ready for a phase I study of 80 people by September 2016. If successful, a phase II-b efficacy study of the vaccine would be conducted in the first quarter of 2017 in a country or region that has a high rate of infection.
Dr. Fauci said that although the study is not be as high-powered as would be ideal, researchers might be able to determine the vaccine’s efficacy with several thousand volunteers, taking into consideration that during the 1-3 years needed to gather conclusive data, herd immunity could skew rates of infection downward, bringing into question the vaccine’s actual efficacy.
“That’s just something we have to deal with,” Dr. Fauci said, saying that fewer people being infected is a good thing, either way.
Research gaps
Other pressing Zika research needs to include learning more about the virus’s impact on a developing fetus.
“We don’t know exactly what the percentage is of [infants born with] microcephaly,” Dr. Fauci said. “We don’t know beyond microcephaly what the long-range effects are on babies that look like they were born [without microcephaly] but might have other defects that are more subtle.”
Dr. Fauci said current data are unhelpful in that they show anywhere from 1% to 29% of infected mothers will give birth to children with congenital defects. However, he said that a coalition of nations affected by the virus is currently enrolling thousands of pregnant women in a cohort study to determine risk ratios.
“When we get the data from that study, we will be able to answer precisely what the percentage is, but today in May 2016, we don’t know the answer,” he said.
Predicting which infants are most susceptible, and at what point in utero abnormalities develop, are questions still under investigation, although a study published earlier this year supports the theory that infection during the first trimester poses the highest risk to a developing fetus.
Communicating risk
Another problem facing health officials is how to communicate the potential seriousness of an illness that, if it presents at all, does so only mildly, Dr. Fauci said. “In general, it’s a disease in which 80% of people don’t have any symptoms.”
The World Health Organization advises physicians to suspect Zika – particularly if a person has been in Zika-affected regions – if clinical symptoms include rash, fever, or both, plus at least one of these: arthralgia, arthritis, or conjunctivitis. Aside from bed rest, hydration, and over-the-counter analgesics, there are no specific treatments for the virus.
How to counsel women about avoiding pregnancy where Zika is a concern also poses challenges, particularly if the pregnancy is unintended, as about half of all American pregnancies are, or if, as Dr. Fauci told reporters, pregnancy is “guided by laws and religion.”
Although federal policy has not been to advise persons about whether to delay pregnancy, Dr. Fauci said U.S. officials are unwilling to contradict authorities in local regions such as Puerto Rico where such statements have been issued.
On April 28, the Food and Drug Administration authorized the emergency use of a commercial in vitro diagnostic test for use in individuals with symptoms of the virus, or those who have traveled to affected regions. Earlier this year, the FDA granted emergency authorization for use of a single test that can detect Zika, dengue, and chikungunya. Still, serology tests for Zika are often inconclusive, since the virus can mimic dengue or chikungunya, according to Dr. Aldighieri. “It can be complex to know if there is a Zika or dengue or chikungunya outbreak,” he said.
On Twitter @whitneymcknight
The ability of the United States to respond to a potential spike in Zika virus infection rates is a cause for concern, according to a top federal health official.
“The big question is will we get local transmission, and my response to that is very likely we will,” Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, told reporters during a joint media briefing with the Pan American Health Organization (PAHO) on May 3.
As many as 500 million people in the Americas are at risk for being infected by the Zika virus, PAHO’s Zika incident manager, Dr. Sylvain Aldighieri, said during the briefing.
In the continental United States to date, there have been about 400 travel-related cases of infection. In Puerto Rico, there have been nearly 700 locally reported cases, and one Zika-related death.
Countries at highest risk for Zika include those that have experienced any outbreaks of dengue fever or chikungunya in the past 15 years, Dr. Aldighieri said. Hawaii and U.S. territories in the Caribbean have experienced local dengue outbreaks during that time. Florida has had local outbreaks of both illnesses.
In the United States, Zika is poised to gain a stronger foothold even as funding for the study and prevention of the virus remains stalled in Congress, and a lack of cohesive public health messaging leaves the public vulnerable to misunderstanding the potential threat of the disease, according to Dr. Fauci.
A vaccine to fight Zika virus is currently under development. “Don’t confuse that with readiness,” Dr. Fauci cautioned.
Dr. Fauci said he believes the disbursement by Congress of President Obama’s requested $1.9 billion in Zika-related funds would facilitate a more comprehensive approach to preventing and treating the virus’s spread, but so far, the funding remains stalled.
As a result, Dr. Fauci said he has reallocated funds intended for other infectious disease research needs to cover Zika-related costs, but is concerned that continued congressional inaction could mean he is left with holes across many budgets. “That 1.9 billion dollars is essential,” he said.
Vaccine progress
In April, $589 millionin funds primarily earmarked for the Ebola crisis were redirected by the Obama administration to fight the Zika virus. That money is now being used in part to fund development of a vaccine that is expected to be ready for a phase I study of 80 people by September 2016. If successful, a phase II-b efficacy study of the vaccine would be conducted in the first quarter of 2017 in a country or region that has a high rate of infection.
Dr. Fauci said that although the study is not be as high-powered as would be ideal, researchers might be able to determine the vaccine’s efficacy with several thousand volunteers, taking into consideration that during the 1-3 years needed to gather conclusive data, herd immunity could skew rates of infection downward, bringing into question the vaccine’s actual efficacy.
“That’s just something we have to deal with,” Dr. Fauci said, saying that fewer people being infected is a good thing, either way.
Research gaps
Other pressing Zika research needs to include learning more about the virus’s impact on a developing fetus.
“We don’t know exactly what the percentage is of [infants born with] microcephaly,” Dr. Fauci said. “We don’t know beyond microcephaly what the long-range effects are on babies that look like they were born [without microcephaly] but might have other defects that are more subtle.”
Dr. Fauci said current data are unhelpful in that they show anywhere from 1% to 29% of infected mothers will give birth to children with congenital defects. However, he said that a coalition of nations affected by the virus is currently enrolling thousands of pregnant women in a cohort study to determine risk ratios.
“When we get the data from that study, we will be able to answer precisely what the percentage is, but today in May 2016, we don’t know the answer,” he said.
Predicting which infants are most susceptible, and at what point in utero abnormalities develop, are questions still under investigation, although a study published earlier this year supports the theory that infection during the first trimester poses the highest risk to a developing fetus.
Communicating risk
Another problem facing health officials is how to communicate the potential seriousness of an illness that, if it presents at all, does so only mildly, Dr. Fauci said. “In general, it’s a disease in which 80% of people don’t have any symptoms.”
The World Health Organization advises physicians to suspect Zika – particularly if a person has been in Zika-affected regions – if clinical symptoms include rash, fever, or both, plus at least one of these: arthralgia, arthritis, or conjunctivitis. Aside from bed rest, hydration, and over-the-counter analgesics, there are no specific treatments for the virus.
How to counsel women about avoiding pregnancy where Zika is a concern also poses challenges, particularly if the pregnancy is unintended, as about half of all American pregnancies are, or if, as Dr. Fauci told reporters, pregnancy is “guided by laws and religion.”
Although federal policy has not been to advise persons about whether to delay pregnancy, Dr. Fauci said U.S. officials are unwilling to contradict authorities in local regions such as Puerto Rico where such statements have been issued.
On April 28, the Food and Drug Administration authorized the emergency use of a commercial in vitro diagnostic test for use in individuals with symptoms of the virus, or those who have traveled to affected regions. Earlier this year, the FDA granted emergency authorization for use of a single test that can detect Zika, dengue, and chikungunya. Still, serology tests for Zika are often inconclusive, since the virus can mimic dengue or chikungunya, according to Dr. Aldighieri. “It can be complex to know if there is a Zika or dengue or chikungunya outbreak,” he said.
On Twitter @whitneymcknight
The ability of the United States to respond to a potential spike in Zika virus infection rates is a cause for concern, according to a top federal health official.
“The big question is will we get local transmission, and my response to that is very likely we will,” Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, told reporters during a joint media briefing with the Pan American Health Organization (PAHO) on May 3.
As many as 500 million people in the Americas are at risk for being infected by the Zika virus, PAHO’s Zika incident manager, Dr. Sylvain Aldighieri, said during the briefing.
In the continental United States to date, there have been about 400 travel-related cases of infection. In Puerto Rico, there have been nearly 700 locally reported cases, and one Zika-related death.
Countries at highest risk for Zika include those that have experienced any outbreaks of dengue fever or chikungunya in the past 15 years, Dr. Aldighieri said. Hawaii and U.S. territories in the Caribbean have experienced local dengue outbreaks during that time. Florida has had local outbreaks of both illnesses.
In the United States, Zika is poised to gain a stronger foothold even as funding for the study and prevention of the virus remains stalled in Congress, and a lack of cohesive public health messaging leaves the public vulnerable to misunderstanding the potential threat of the disease, according to Dr. Fauci.
A vaccine to fight Zika virus is currently under development. “Don’t confuse that with readiness,” Dr. Fauci cautioned.
Dr. Fauci said he believes the disbursement by Congress of President Obama’s requested $1.9 billion in Zika-related funds would facilitate a more comprehensive approach to preventing and treating the virus’s spread, but so far, the funding remains stalled.
As a result, Dr. Fauci said he has reallocated funds intended for other infectious disease research needs to cover Zika-related costs, but is concerned that continued congressional inaction could mean he is left with holes across many budgets. “That 1.9 billion dollars is essential,” he said.
Vaccine progress
In April, $589 millionin funds primarily earmarked for the Ebola crisis were redirected by the Obama administration to fight the Zika virus. That money is now being used in part to fund development of a vaccine that is expected to be ready for a phase I study of 80 people by September 2016. If successful, a phase II-b efficacy study of the vaccine would be conducted in the first quarter of 2017 in a country or region that has a high rate of infection.
Dr. Fauci said that although the study is not be as high-powered as would be ideal, researchers might be able to determine the vaccine’s efficacy with several thousand volunteers, taking into consideration that during the 1-3 years needed to gather conclusive data, herd immunity could skew rates of infection downward, bringing into question the vaccine’s actual efficacy.
“That’s just something we have to deal with,” Dr. Fauci said, saying that fewer people being infected is a good thing, either way.
Research gaps
Other pressing Zika research needs to include learning more about the virus’s impact on a developing fetus.
“We don’t know exactly what the percentage is of [infants born with] microcephaly,” Dr. Fauci said. “We don’t know beyond microcephaly what the long-range effects are on babies that look like they were born [without microcephaly] but might have other defects that are more subtle.”
Dr. Fauci said current data are unhelpful in that they show anywhere from 1% to 29% of infected mothers will give birth to children with congenital defects. However, he said that a coalition of nations affected by the virus is currently enrolling thousands of pregnant women in a cohort study to determine risk ratios.
“When we get the data from that study, we will be able to answer precisely what the percentage is, but today in May 2016, we don’t know the answer,” he said.
Predicting which infants are most susceptible, and at what point in utero abnormalities develop, are questions still under investigation, although a study published earlier this year supports the theory that infection during the first trimester poses the highest risk to a developing fetus.
Communicating risk
Another problem facing health officials is how to communicate the potential seriousness of an illness that, if it presents at all, does so only mildly, Dr. Fauci said. “In general, it’s a disease in which 80% of people don’t have any symptoms.”
The World Health Organization advises physicians to suspect Zika – particularly if a person has been in Zika-affected regions – if clinical symptoms include rash, fever, or both, plus at least one of these: arthralgia, arthritis, or conjunctivitis. Aside from bed rest, hydration, and over-the-counter analgesics, there are no specific treatments for the virus.
How to counsel women about avoiding pregnancy where Zika is a concern also poses challenges, particularly if the pregnancy is unintended, as about half of all American pregnancies are, or if, as Dr. Fauci told reporters, pregnancy is “guided by laws and religion.”
Although federal policy has not been to advise persons about whether to delay pregnancy, Dr. Fauci said U.S. officials are unwilling to contradict authorities in local regions such as Puerto Rico where such statements have been issued.
On April 28, the Food and Drug Administration authorized the emergency use of a commercial in vitro diagnostic test for use in individuals with symptoms of the virus, or those who have traveled to affected regions. Earlier this year, the FDA granted emergency authorization for use of a single test that can detect Zika, dengue, and chikungunya. Still, serology tests for Zika are often inconclusive, since the virus can mimic dengue or chikungunya, according to Dr. Aldighieri. “It can be complex to know if there is a Zika or dengue or chikungunya outbreak,” he said.
On Twitter @whitneymcknight

N-Acetylcysteine, Statins May Prevent Contrast-Induced Nephropathy, but Strength of Evidence is Low
Clinical question: What strategies are effective in reducing contrast-induced nephropathy?
Bottom line: N-acetylcysteine plus intravenous fluids alone or in combination with a statin can prevent contrast-induced nephropathy (CIN). However, the strength of the evidence for these interventions is low. (LOE = 1b)
Reference: Subramaniam RM, Suarez-Cuervo C, Wilson RF, et al. Effectiveness of prevention strategies for contrast-induced nephropathy. Ann Intern Med 2016;164(6):406-416.
Study design: Systematic review
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis
CIN is defined as an increase in serum creatinine of more than 25% or 0.5 mg/dL (44.2 umol/L) within 3 days of intravenous contrast administration. These investigators searched MEDLINE, EMBASE, and the Cochrane Library along with reference lists of relevant articles to find studies that evaluated use of N-acetylcysteine, sodium bicarbonate, sodium chloride, statins, or ascorbic acid to prevent CIN.
Two reviewers independently screened articles for eligibility, assessed each study's risk of bias, and graded the strength of evidence (SOE) for different comparisons. A total of 86 randomized controlled trials examining different strategies for CIN prevention were included. Ultimately, only 3 strategies were shown to have both a clinically important and statistically significant benefit: (1) low-dose N-acetylcysteine plus intravenous (IV) saline versus IV saline alone (pooled relative risk [RR] 0.75; 95% CI 0.63-0.89; low SOE), (2) N-acetylcysteine plus IV saline versus IV saline alone in patients receiving low-osmolar contrast media (pooled RR 0.69; 0.58-0.84; moderate SOE), and (3) statin plus N-acetylcysteine versus N-acetylcysteine alone (pooled RR 0.52; 0.29-0.93; low SOE). There were no statistically significant benefits seen with sodium bicarbonate or ascorbic acid.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What strategies are effective in reducing contrast-induced nephropathy?
Bottom line: N-acetylcysteine plus intravenous fluids alone or in combination with a statin can prevent contrast-induced nephropathy (CIN). However, the strength of the evidence for these interventions is low. (LOE = 1b)
Reference: Subramaniam RM, Suarez-Cuervo C, Wilson RF, et al. Effectiveness of prevention strategies for contrast-induced nephropathy. Ann Intern Med 2016;164(6):406-416.
Study design: Systematic review
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis
CIN is defined as an increase in serum creatinine of more than 25% or 0.5 mg/dL (44.2 umol/L) within 3 days of intravenous contrast administration. These investigators searched MEDLINE, EMBASE, and the Cochrane Library along with reference lists of relevant articles to find studies that evaluated use of N-acetylcysteine, sodium bicarbonate, sodium chloride, statins, or ascorbic acid to prevent CIN.
Two reviewers independently screened articles for eligibility, assessed each study's risk of bias, and graded the strength of evidence (SOE) for different comparisons. A total of 86 randomized controlled trials examining different strategies for CIN prevention were included. Ultimately, only 3 strategies were shown to have both a clinically important and statistically significant benefit: (1) low-dose N-acetylcysteine plus intravenous (IV) saline versus IV saline alone (pooled relative risk [RR] 0.75; 95% CI 0.63-0.89; low SOE), (2) N-acetylcysteine plus IV saline versus IV saline alone in patients receiving low-osmolar contrast media (pooled RR 0.69; 0.58-0.84; moderate SOE), and (3) statin plus N-acetylcysteine versus N-acetylcysteine alone (pooled RR 0.52; 0.29-0.93; low SOE). There were no statistically significant benefits seen with sodium bicarbonate or ascorbic acid.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What strategies are effective in reducing contrast-induced nephropathy?
Bottom line: N-acetylcysteine plus intravenous fluids alone or in combination with a statin can prevent contrast-induced nephropathy (CIN). However, the strength of the evidence for these interventions is low. (LOE = 1b)
Reference: Subramaniam RM, Suarez-Cuervo C, Wilson RF, et al. Effectiveness of prevention strategies for contrast-induced nephropathy. Ann Intern Med 2016;164(6):406-416.
Study design: Systematic review
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis
CIN is defined as an increase in serum creatinine of more than 25% or 0.5 mg/dL (44.2 umol/L) within 3 days of intravenous contrast administration. These investigators searched MEDLINE, EMBASE, and the Cochrane Library along with reference lists of relevant articles to find studies that evaluated use of N-acetylcysteine, sodium bicarbonate, sodium chloride, statins, or ascorbic acid to prevent CIN.
Two reviewers independently screened articles for eligibility, assessed each study's risk of bias, and graded the strength of evidence (SOE) for different comparisons. A total of 86 randomized controlled trials examining different strategies for CIN prevention were included. Ultimately, only 3 strategies were shown to have both a clinically important and statistically significant benefit: (1) low-dose N-acetylcysteine plus intravenous (IV) saline versus IV saline alone (pooled relative risk [RR] 0.75; 95% CI 0.63-0.89; low SOE), (2) N-acetylcysteine plus IV saline versus IV saline alone in patients receiving low-osmolar contrast media (pooled RR 0.69; 0.58-0.84; moderate SOE), and (3) statin plus N-acetylcysteine versus N-acetylcysteine alone (pooled RR 0.52; 0.29-0.93; low SOE). There were no statistically significant benefits seen with sodium bicarbonate or ascorbic acid.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Short-Term High-Flow Oxygen Therapy for Low-Risk Patients Decreases Reintubation Rates
Clinical question: Does the use of high-flow oxygen therapy for 24 hours following extubation reduce the risk of reintubation in low-risk patients?
Bottom line: Using high-flow nasal cannula oxygen therapy for 24 hours following extubation of patients who are already at low risk of reintubation further reduces the risk of reintubation. You would need to treat 14 patients with high-flow therapy to prevent reintubation in one patient. (LOE = 1b)
Reference: Hernandez G, Vaquero C, Gonzalez P, et al. Effect of postextubation high-flow nasal cannula vs conventional oxygen therapy on reintubation in low-risk patients. JAMA 2016;315(13):1354-1361.
Study design: Randomized controlled trial (nonblinded)
Funding source: Self-funded or unfunded
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators recruited mechanically ventilated adult patients who were ready for extubation and who met the criteria for low risk for reintubation. Low risk was defined as: younger than 65 years; Acute Physiology and Chronic Health Evaluation (APACHE) II score of less than 12; fewer than 2 comorbidities; body mass index of less than 30; ability to manage secretions; simple weaning; and the absence of heart failure, moderate-to-severe chronic obstructive pulmonary disease, airway patency issues, and prolonged mechanical ventilation.
Using concealed allocation, these patients were randomized to receive either conventional oxygen therapy or high-flow oxygen therapy for 24 hours following extubation. Conventional oxygen therapy was continued in both groups after 24 hours as needed. The 2 groups had a mean age of 51 years and similar APACHE scores at baseline. The use of high-flow oxygen therapy reduced the rate of reintubation within 72 hours from 12.2% to 4.9% (absolute difference 7.2%; 95% CI 2.5%-12.2%; number needed to treat [NNT] = 14; P = .004). There were no significant differences detected in the 2 groups in secondary outcomes including time to reintubation or hospital length of stay. Notably, the study population had a high proportion of surgical and neurocritical patients, resulting in one-third of the reintubations occurring because of nonrespiratory causes such as repeat surgery or altered mental status. When the analysis was limited to only the respiratory-related intubations, the reduced risk of reintubation persisted in the high-flow oxygen group (1.5% vs 8.7%; NNT = 14; P = .001).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of high-flow oxygen therapy for 24 hours following extubation reduce the risk of reintubation in low-risk patients?
Bottom line: Using high-flow nasal cannula oxygen therapy for 24 hours following extubation of patients who are already at low risk of reintubation further reduces the risk of reintubation. You would need to treat 14 patients with high-flow therapy to prevent reintubation in one patient. (LOE = 1b)
Reference: Hernandez G, Vaquero C, Gonzalez P, et al. Effect of postextubation high-flow nasal cannula vs conventional oxygen therapy on reintubation in low-risk patients. JAMA 2016;315(13):1354-1361.
Study design: Randomized controlled trial (nonblinded)
Funding source: Self-funded or unfunded
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators recruited mechanically ventilated adult patients who were ready for extubation and who met the criteria for low risk for reintubation. Low risk was defined as: younger than 65 years; Acute Physiology and Chronic Health Evaluation (APACHE) II score of less than 12; fewer than 2 comorbidities; body mass index of less than 30; ability to manage secretions; simple weaning; and the absence of heart failure, moderate-to-severe chronic obstructive pulmonary disease, airway patency issues, and prolonged mechanical ventilation.
Using concealed allocation, these patients were randomized to receive either conventional oxygen therapy or high-flow oxygen therapy for 24 hours following extubation. Conventional oxygen therapy was continued in both groups after 24 hours as needed. The 2 groups had a mean age of 51 years and similar APACHE scores at baseline. The use of high-flow oxygen therapy reduced the rate of reintubation within 72 hours from 12.2% to 4.9% (absolute difference 7.2%; 95% CI 2.5%-12.2%; number needed to treat [NNT] = 14; P = .004). There were no significant differences detected in the 2 groups in secondary outcomes including time to reintubation or hospital length of stay. Notably, the study population had a high proportion of surgical and neurocritical patients, resulting in one-third of the reintubations occurring because of nonrespiratory causes such as repeat surgery or altered mental status. When the analysis was limited to only the respiratory-related intubations, the reduced risk of reintubation persisted in the high-flow oxygen group (1.5% vs 8.7%; NNT = 14; P = .001).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of high-flow oxygen therapy for 24 hours following extubation reduce the risk of reintubation in low-risk patients?
Bottom line: Using high-flow nasal cannula oxygen therapy for 24 hours following extubation of patients who are already at low risk of reintubation further reduces the risk of reintubation. You would need to treat 14 patients with high-flow therapy to prevent reintubation in one patient. (LOE = 1b)
Reference: Hernandez G, Vaquero C, Gonzalez P, et al. Effect of postextubation high-flow nasal cannula vs conventional oxygen therapy on reintubation in low-risk patients. JAMA 2016;315(13):1354-1361.
Study design: Randomized controlled trial (nonblinded)
Funding source: Self-funded or unfunded
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators recruited mechanically ventilated adult patients who were ready for extubation and who met the criteria for low risk for reintubation. Low risk was defined as: younger than 65 years; Acute Physiology and Chronic Health Evaluation (APACHE) II score of less than 12; fewer than 2 comorbidities; body mass index of less than 30; ability to manage secretions; simple weaning; and the absence of heart failure, moderate-to-severe chronic obstructive pulmonary disease, airway patency issues, and prolonged mechanical ventilation.
Using concealed allocation, these patients were randomized to receive either conventional oxygen therapy or high-flow oxygen therapy for 24 hours following extubation. Conventional oxygen therapy was continued in both groups after 24 hours as needed. The 2 groups had a mean age of 51 years and similar APACHE scores at baseline. The use of high-flow oxygen therapy reduced the rate of reintubation within 72 hours from 12.2% to 4.9% (absolute difference 7.2%; 95% CI 2.5%-12.2%; number needed to treat [NNT] = 14; P = .004). There were no significant differences detected in the 2 groups in secondary outcomes including time to reintubation or hospital length of stay. Notably, the study population had a high proportion of surgical and neurocritical patients, resulting in one-third of the reintubations occurring because of nonrespiratory causes such as repeat surgery or altered mental status. When the analysis was limited to only the respiratory-related intubations, the reduced risk of reintubation persisted in the high-flow oxygen group (1.5% vs 8.7%; NNT = 14; P = .001).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
AF and stroke may be temporally related
CHICAGO – One-third of a large cohort of patients with an implantable cardiac device in place at the time of an ischemic stroke had one or more episodes of atrial fibrillation within the prior 30 days, Dr. Rhea C. Pimentel reported at the annual meeting of the American College of Cardiology.
The in-hospital mortality rate of these atrial fibrillation–related strokes was high: 11 of 42 (26%) such patients died during their stroke hospitalization, compared with 6 of 83 (7%) whose strokes were not temporally related to atrial fibrillation (AF), noted Dr. Pimentel, an electrophysiologist at the University of Kansas Medical Center in Kansas City.

Data from the Framingham Heart Study and other sources suggest that stroke in patients who have AF carries about double the mortality rate of strokes in patients without AF. Mortality associated with AF-related stroke in the Kansas study was probably so much higher because the hospital serves as a comprehensive stroke center, drawing patients from considerable distances across the Midwest, she said.
Dr. Pimentel reported on 125 patients who presented with an ischemic stroke when a cardiac monitoring device was in place. This is believed to be the largest such patient series ever reported. Their mean age was 73 years, and 41% were women. The mean CHADS2 score was 3.96, with a CHA2DS2-VASc score of 5.28. Of the patients, 62% had a pacemaker; the rest had an implantable cardioverter-defibrillator or cardiac resynchronization device. One-quarter of the group had a prior history of AF, and a fifth were on an oral anticoagulant – warfarin, in 70% of cases – at the time of their stroke.
The investigators defined a stroke-related AF episode as a total of at least 1 hour spent in AF during the 30 days preceding the stroke. Eighty percent of affected patients had paroxysmal AF. They typically fulfilled the 1-hour AF requirement via multiple short, self-terminated episodes rather than in an hour-long episode.
Being on an oral anticoagulant had no impact on in-hospital mortality, which was 14.2% in patients on warfarin or a newer anticoagulant and 14.3% in those who were not. Dr. Pimentel noted that she was presenting the results of the investigators’ initial look at the data. They are in the process of obtaining the patients’ international normalized ratio data, which “should be very enlightening,” she said.
She and her coinvestigators also plan to subdivide their 30-day study period into 5-day segments to learn just how soon after an AF episode the strokes occurred. Researchers at Stanford (Calif.) University have reported that the greatest stroke risk in patients with AF is in the first 5 days after an AF episode, and the Kansas group would like to confirm that observation.
In addition, because it remains an unresolved question whether any amount of AF is safe, Dr. Pimentel and her coworkers are considering reanalyzing their data using a cutoff of 6 minutes of AF rather than 1 hour during the 30 days prior to stroke.
The study was conducted free of commercial support. Dr. Pimentel reported having no relevant financial conflicts.
CHICAGO – One-third of a large cohort of patients with an implantable cardiac device in place at the time of an ischemic stroke had one or more episodes of atrial fibrillation within the prior 30 days, Dr. Rhea C. Pimentel reported at the annual meeting of the American College of Cardiology.
The in-hospital mortality rate of these atrial fibrillation–related strokes was high: 11 of 42 (26%) such patients died during their stroke hospitalization, compared with 6 of 83 (7%) whose strokes were not temporally related to atrial fibrillation (AF), noted Dr. Pimentel, an electrophysiologist at the University of Kansas Medical Center in Kansas City.
Data from the Framingham Heart Study and other sources suggest that stroke in patients who have AF carries about double the mortality rate of strokes in patients without AF. Mortality associated with AF-related stroke in the Kansas study was probably so much higher because the hospital serves as a comprehensive stroke center, drawing patients from considerable distances across the Midwest, she said.
Dr. Pimentel reported on 125 patients who presented with an ischemic stroke when a cardiac monitoring device was in place. This is believed to be the largest such patient series ever reported. Their mean age was 73 years, and 41% were women. The mean CHADS2 score was 3.96, with a CHA2DS2-VASc score of 5.28. Of the patients, 62% had a pacemaker; the rest had an implantable cardioverter-defibrillator or cardiac resynchronization device. One-quarter of the group had a prior history of AF, and a fifth were on an oral anticoagulant – warfarin, in 70% of cases – at the time of their stroke.
The investigators defined a stroke-related AF episode as a total of at least 1 hour spent in AF during the 30 days preceding the stroke. Eighty percent of affected patients had paroxysmal AF. They typically fulfilled the 1-hour AF requirement via multiple short, self-terminated episodes rather than in an hour-long episode.
Being on an oral anticoagulant had no impact on in-hospital mortality, which was 14.2% in patients on warfarin or a newer anticoagulant and 14.3% in those who were not. Dr. Pimentel noted that she was presenting the results of the investigators’ initial look at the data. They are in the process of obtaining the patients’ international normalized ratio data, which “should be very enlightening,” she said.
She and her coinvestigators also plan to subdivide their 30-day study period into 5-day segments to learn just how soon after an AF episode the strokes occurred. Researchers at Stanford (Calif.) University have reported that the greatest stroke risk in patients with AF is in the first 5 days after an AF episode, and the Kansas group would like to confirm that observation.
In addition, because it remains an unresolved question whether any amount of AF is safe, Dr. Pimentel and her coworkers are considering reanalyzing their data using a cutoff of 6 minutes of AF rather than 1 hour during the 30 days prior to stroke.
The study was conducted free of commercial support. Dr. Pimentel reported having no relevant financial conflicts.
CHICAGO – One-third of a large cohort of patients with an implantable cardiac device in place at the time of an ischemic stroke had one or more episodes of atrial fibrillation within the prior 30 days, Dr. Rhea C. Pimentel reported at the annual meeting of the American College of Cardiology.
The in-hospital mortality rate of these atrial fibrillation–related strokes was high: 11 of 42 (26%) such patients died during their stroke hospitalization, compared with 6 of 83 (7%) whose strokes were not temporally related to atrial fibrillation (AF), noted Dr. Pimentel, an electrophysiologist at the University of Kansas Medical Center in Kansas City.
Data from the Framingham Heart Study and other sources suggest that stroke in patients who have AF carries about double the mortality rate of strokes in patients without AF. Mortality associated with AF-related stroke in the Kansas study was probably so much higher because the hospital serves as a comprehensive stroke center, drawing patients from considerable distances across the Midwest, she said.
Dr. Pimentel reported on 125 patients who presented with an ischemic stroke when a cardiac monitoring device was in place. This is believed to be the largest such patient series ever reported. Their mean age was 73 years, and 41% were women. The mean CHADS2 score was 3.96, with a CHA2DS2-VASc score of 5.28. Of the patients, 62% had a pacemaker; the rest had an implantable cardioverter-defibrillator or cardiac resynchronization device. One-quarter of the group had a prior history of AF, and a fifth were on an oral anticoagulant – warfarin, in 70% of cases – at the time of their stroke.
The investigators defined a stroke-related AF episode as a total of at least 1 hour spent in AF during the 30 days preceding the stroke. Eighty percent of affected patients had paroxysmal AF. They typically fulfilled the 1-hour AF requirement via multiple short, self-terminated episodes rather than in an hour-long episode.
Being on an oral anticoagulant had no impact on in-hospital mortality, which was 14.2% in patients on warfarin or a newer anticoagulant and 14.3% in those who were not. Dr. Pimentel noted that she was presenting the results of the investigators’ initial look at the data. They are in the process of obtaining the patients’ international normalized ratio data, which “should be very enlightening,” she said.
She and her coinvestigators also plan to subdivide their 30-day study period into 5-day segments to learn just how soon after an AF episode the strokes occurred. Researchers at Stanford (Calif.) University have reported that the greatest stroke risk in patients with AF is in the first 5 days after an AF episode, and the Kansas group would like to confirm that observation.
In addition, because it remains an unresolved question whether any amount of AF is safe, Dr. Pimentel and her coworkers are considering reanalyzing their data using a cutoff of 6 minutes of AF rather than 1 hour during the 30 days prior to stroke.
The study was conducted free of commercial support. Dr. Pimentel reported having no relevant financial conflicts.
AT ACC 16
Key clinical point: One-third of patients with an ischemic stroke while they had an implantable cardiac device had atrial fibrillation in the 30 days prior.
Major finding: The in-hospital mortality rate was 26% in patients with AF-related stroke, compared with 7% in those without AF.
Data source: A single-center, retrospective study of 125 patients who had an ischemic stroke while wearing a pacemaker or other implanted cardiac device.
Disclosures: The study was conducted free of commercial support. The presenter reported having no financial conflicts of interest.

Make the Diagnosis - May 2016
Diagnosis: Perforating disorder
Histology on this patient revealed compact hyperkeratosis and parakeratosis with an entrapped neutrophilic crust and invaginated epidermis. The epidermis showed collagen fibers and the underlying dermis was fibrotic with inflammatory cells. PAS was negative. A Verhoeff-Van Gieson (VVG) stain failed to reveal elastic tissue fibers within the crusted stratum corneum. The results were consistent with a perforating disorder.
Perforating dermatoses result from the extrusion of dermal substances through epidermal channels without any alteration of nearby histologic structures. The substances in the upper dermis induce epidermal hyperplasia that results in the epidermis surrounding the dermal materials, with eventual elimination secondary to keratinocyte maturation and sloughing. Several different forms of perforating dermatoses exist, including reactive perforating collagenosis and the acquired perforating dermatosis diagnostic group (often associated with diabetes mellitus or chronic renal disease), which includes acquired reactive perforating collagenosis (RPC), elastosis perforans serpiginosa, perforating folliculitis, and Kyrle’s disease. Both RPC and perforating folliculitis may demonstrate koebnerization (a phenomenon in which superficial trauma induces lesion formation), which may help a clinician further delineate the specific perforating dermatosis diagnosis.
Reactive perforating collagenosis (RPC) consists of both a familial and an acquired form. The familial form is typically autosomal recessive and presents in childhood but may persist into adulthood. The acquired form develops in adulthood. Clinically, RPC presents as pruritic papules (1-3 mm) with a central dark keratotic plug, which enlarge but often regress after 2 months. Lesions often occur on the extremities and face with onset after superficial trauma (associated with scratching, arthropod bites, etc.). With acquired RPC, underlying systemic diseases are often present, including renal failure, diabetes, and occasionally liver disease or malignant neoplasm. Laboratory tests to screen for these conditions should be ordered as appropriate. In managing RPC, avoiding skin trauma and controlling itching appear to be the most important interventions. Lesions may resolve without treatment, but topical retinoids also may be useful.
Elastosis perforans serpiginosa (EPS) results from changes in both elastic and collagen fibers within the dermis, resulting in a foreign body reaction with transepidermal elimination. Clinically, EPS presents around the second decade of life as erythematous umbilicated papules (2-3 mm) with a central keratin plug arranged in an annular or serpiginous pattern. Lesions usually only involve one anatomic area (frequently the neck and upper extremities). Some of the associated conditions can be remembered with the mnemonic MADPPORES: Marfan syndrome, Acrogeria, Down syndrome, Penicillamine, Pseudoxanthoma elasticum, Osteogenesis imperfecta, Rothmund-Thomson syndrome, Ehlers-Danlos (some forms), and Scleroderma. Regression of lesions often leaves hypopigmented scars. Treatment with cryotherapy may be useful, but electrocautery, dermabrasion, and surgery should be avoided.
Perforating folliculitis is characterized by adult-onset scaly follicular papules with a white central keratotic plug (may contain curled hair) on the extensor surfaces of the extremities and buttocks. Lesions may be pruritic but are more often asymptomatic. The pathophysiology includes the transfollicular extrusion of dermal debris (keratin, cellular debris, degenerated collagen, or degenerated elastic fibers), which may be expressed when the papule is compressed. Perforating folliculitis is often associated with chronic renal failure, diabetes mellitus, and other systemic diseases. The lesions may resolve after stabilization of the underlying disease, including renal transplantation. Management focuses on controlling pruritus with oral antihistamines and topical soothing lotions (menthol, phenol, or camphor), but other unsubstantiated treatments have been tried, including UVB, oral retinoids, and topical retinoids.
Kyrle’s disease (hyperkeratosis folliculitis) may have both an acquired and autosomal recessive form. In the inherited form, a genetic disturbance may accelerate epidermal keratinization, resulting in dyskeratotic foci and parakeratosis that penetrate the dermis and induce a granulomatous inflammatory reaction. The acquired form may be associated with diabetic nephropathy, hemodialysis secondary to diabetic nephropathy, congestive heart failure, and liver disease. In contrast to other perforating disorders, the extruded material is predominantly keratin rather than elastic fibers or collagen. Clinically, Kyrle’s disease presents around age 30 years as discrete, pruritic, and scaly folliculocentric papules (1-8 mm) with a hyperkeratotic plug (one-third of diameter). With removal of the plug, a cutaneous depression remains (Kyrle’s phenomenon). The lesions also may coalesce into plaques. Typically, the bilateral lower extremities and extensor surfaces are involved, but lesions may present on any area except for plantar, palmar, and mucosal surfaces. Management should focus on treating the associated medical condition, but UVB and tretinoin also have been used. Other treatment options include allopurinol, psoralen plus UVA, acitretin, phenol, doxycycline, surgical debridement, and topical corticosteroids. Regardless, lesions may resolve and leave atrophic scars.
This case and photo were submitted by Dr. Damon McClain of Three Rivers Dermatology in Coraopolis, Pa., and Mark Ash, a medical student at East Carolina University, Greenville, N.C.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to [email protected].
Diagnosis: Perforating disorder
Histology on this patient revealed compact hyperkeratosis and parakeratosis with an entrapped neutrophilic crust and invaginated epidermis. The epidermis showed collagen fibers and the underlying dermis was fibrotic with inflammatory cells. PAS was negative. A Verhoeff-Van Gieson (VVG) stain failed to reveal elastic tissue fibers within the crusted stratum corneum. The results were consistent with a perforating disorder.
Perforating dermatoses result from the extrusion of dermal substances through epidermal channels without any alteration of nearby histologic structures. The substances in the upper dermis induce epidermal hyperplasia that results in the epidermis surrounding the dermal materials, with eventual elimination secondary to keratinocyte maturation and sloughing. Several different forms of perforating dermatoses exist, including reactive perforating collagenosis and the acquired perforating dermatosis diagnostic group (often associated with diabetes mellitus or chronic renal disease), which includes acquired reactive perforating collagenosis (RPC), elastosis perforans serpiginosa, perforating folliculitis, and Kyrle’s disease. Both RPC and perforating folliculitis may demonstrate koebnerization (a phenomenon in which superficial trauma induces lesion formation), which may help a clinician further delineate the specific perforating dermatosis diagnosis.
Reactive perforating collagenosis (RPC) consists of both a familial and an acquired form. The familial form is typically autosomal recessive and presents in childhood but may persist into adulthood. The acquired form develops in adulthood. Clinically, RPC presents as pruritic papules (1-3 mm) with a central dark keratotic plug, which enlarge but often regress after 2 months. Lesions often occur on the extremities and face with onset after superficial trauma (associated with scratching, arthropod bites, etc.). With acquired RPC, underlying systemic diseases are often present, including renal failure, diabetes, and occasionally liver disease or malignant neoplasm. Laboratory tests to screen for these conditions should be ordered as appropriate. In managing RPC, avoiding skin trauma and controlling itching appear to be the most important interventions. Lesions may resolve without treatment, but topical retinoids also may be useful.
Elastosis perforans serpiginosa (EPS) results from changes in both elastic and collagen fibers within the dermis, resulting in a foreign body reaction with transepidermal elimination. Clinically, EPS presents around the second decade of life as erythematous umbilicated papules (2-3 mm) with a central keratin plug arranged in an annular or serpiginous pattern. Lesions usually only involve one anatomic area (frequently the neck and upper extremities). Some of the associated conditions can be remembered with the mnemonic MADPPORES: Marfan syndrome, Acrogeria, Down syndrome, Penicillamine, Pseudoxanthoma elasticum, Osteogenesis imperfecta, Rothmund-Thomson syndrome, Ehlers-Danlos (some forms), and Scleroderma. Regression of lesions often leaves hypopigmented scars. Treatment with cryotherapy may be useful, but electrocautery, dermabrasion, and surgery should be avoided.
Perforating folliculitis is characterized by adult-onset scaly follicular papules with a white central keratotic plug (may contain curled hair) on the extensor surfaces of the extremities and buttocks. Lesions may be pruritic but are more often asymptomatic. The pathophysiology includes the transfollicular extrusion of dermal debris (keratin, cellular debris, degenerated collagen, or degenerated elastic fibers), which may be expressed when the papule is compressed. Perforating folliculitis is often associated with chronic renal failure, diabetes mellitus, and other systemic diseases. The lesions may resolve after stabilization of the underlying disease, including renal transplantation. Management focuses on controlling pruritus with oral antihistamines and topical soothing lotions (menthol, phenol, or camphor), but other unsubstantiated treatments have been tried, including UVB, oral retinoids, and topical retinoids.
Kyrle’s disease (hyperkeratosis folliculitis) may have both an acquired and autosomal recessive form. In the inherited form, a genetic disturbance may accelerate epidermal keratinization, resulting in dyskeratotic foci and parakeratosis that penetrate the dermis and induce a granulomatous inflammatory reaction. The acquired form may be associated with diabetic nephropathy, hemodialysis secondary to diabetic nephropathy, congestive heart failure, and liver disease. In contrast to other perforating disorders, the extruded material is predominantly keratin rather than elastic fibers or collagen. Clinically, Kyrle’s disease presents around age 30 years as discrete, pruritic, and scaly folliculocentric papules (1-8 mm) with a hyperkeratotic plug (one-third of diameter). With removal of the plug, a cutaneous depression remains (Kyrle’s phenomenon). The lesions also may coalesce into plaques. Typically, the bilateral lower extremities and extensor surfaces are involved, but lesions may present on any area except for plantar, palmar, and mucosal surfaces. Management should focus on treating the associated medical condition, but UVB and tretinoin also have been used. Other treatment options include allopurinol, psoralen plus UVA, acitretin, phenol, doxycycline, surgical debridement, and topical corticosteroids. Regardless, lesions may resolve and leave atrophic scars.
This case and photo were submitted by Dr. Damon McClain of Three Rivers Dermatology in Coraopolis, Pa., and Mark Ash, a medical student at East Carolina University, Greenville, N.C.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to [email protected].
Diagnosis: Perforating disorder
Histology on this patient revealed compact hyperkeratosis and parakeratosis with an entrapped neutrophilic crust and invaginated epidermis. The epidermis showed collagen fibers and the underlying dermis was fibrotic with inflammatory cells. PAS was negative. A Verhoeff-Van Gieson (VVG) stain failed to reveal elastic tissue fibers within the crusted stratum corneum. The results were consistent with a perforating disorder.
Perforating dermatoses result from the extrusion of dermal substances through epidermal channels without any alteration of nearby histologic structures. The substances in the upper dermis induce epidermal hyperplasia that results in the epidermis surrounding the dermal materials, with eventual elimination secondary to keratinocyte maturation and sloughing. Several different forms of perforating dermatoses exist, including reactive perforating collagenosis and the acquired perforating dermatosis diagnostic group (often associated with diabetes mellitus or chronic renal disease), which includes acquired reactive perforating collagenosis (RPC), elastosis perforans serpiginosa, perforating folliculitis, and Kyrle’s disease. Both RPC and perforating folliculitis may demonstrate koebnerization (a phenomenon in which superficial trauma induces lesion formation), which may help a clinician further delineate the specific perforating dermatosis diagnosis.
Reactive perforating collagenosis (RPC) consists of both a familial and an acquired form. The familial form is typically autosomal recessive and presents in childhood but may persist into adulthood. The acquired form develops in adulthood. Clinically, RPC presents as pruritic papules (1-3 mm) with a central dark keratotic plug, which enlarge but often regress after 2 months. Lesions often occur on the extremities and face with onset after superficial trauma (associated with scratching, arthropod bites, etc.). With acquired RPC, underlying systemic diseases are often present, including renal failure, diabetes, and occasionally liver disease or malignant neoplasm. Laboratory tests to screen for these conditions should be ordered as appropriate. In managing RPC, avoiding skin trauma and controlling itching appear to be the most important interventions. Lesions may resolve without treatment, but topical retinoids also may be useful.
Elastosis perforans serpiginosa (EPS) results from changes in both elastic and collagen fibers within the dermis, resulting in a foreign body reaction with transepidermal elimination. Clinically, EPS presents around the second decade of life as erythematous umbilicated papules (2-3 mm) with a central keratin plug arranged in an annular or serpiginous pattern. Lesions usually only involve one anatomic area (frequently the neck and upper extremities). Some of the associated conditions can be remembered with the mnemonic MADPPORES: Marfan syndrome, Acrogeria, Down syndrome, Penicillamine, Pseudoxanthoma elasticum, Osteogenesis imperfecta, Rothmund-Thomson syndrome, Ehlers-Danlos (some forms), and Scleroderma. Regression of lesions often leaves hypopigmented scars. Treatment with cryotherapy may be useful, but electrocautery, dermabrasion, and surgery should be avoided.
Perforating folliculitis is characterized by adult-onset scaly follicular papules with a white central keratotic plug (may contain curled hair) on the extensor surfaces of the extremities and buttocks. Lesions may be pruritic but are more often asymptomatic. The pathophysiology includes the transfollicular extrusion of dermal debris (keratin, cellular debris, degenerated collagen, or degenerated elastic fibers), which may be expressed when the papule is compressed. Perforating folliculitis is often associated with chronic renal failure, diabetes mellitus, and other systemic diseases. The lesions may resolve after stabilization of the underlying disease, including renal transplantation. Management focuses on controlling pruritus with oral antihistamines and topical soothing lotions (menthol, phenol, or camphor), but other unsubstantiated treatments have been tried, including UVB, oral retinoids, and topical retinoids.
Kyrle’s disease (hyperkeratosis folliculitis) may have both an acquired and autosomal recessive form. In the inherited form, a genetic disturbance may accelerate epidermal keratinization, resulting in dyskeratotic foci and parakeratosis that penetrate the dermis and induce a granulomatous inflammatory reaction. The acquired form may be associated with diabetic nephropathy, hemodialysis secondary to diabetic nephropathy, congestive heart failure, and liver disease. In contrast to other perforating disorders, the extruded material is predominantly keratin rather than elastic fibers or collagen. Clinically, Kyrle’s disease presents around age 30 years as discrete, pruritic, and scaly folliculocentric papules (1-8 mm) with a hyperkeratotic plug (one-third of diameter). With removal of the plug, a cutaneous depression remains (Kyrle’s phenomenon). The lesions also may coalesce into plaques. Typically, the bilateral lower extremities and extensor surfaces are involved, but lesions may present on any area except for plantar, palmar, and mucosal surfaces. Management should focus on treating the associated medical condition, but UVB and tretinoin also have been used. Other treatment options include allopurinol, psoralen plus UVA, acitretin, phenol, doxycycline, surgical debridement, and topical corticosteroids. Regardless, lesions may resolve and leave atrophic scars.
This case and photo were submitted by Dr. Damon McClain of Three Rivers Dermatology in Coraopolis, Pa., and Mark Ash, a medical student at East Carolina University, Greenville, N.C.
Dr. Bilu Martin is in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit your case for possible publication, send an email to [email protected].

A 41-year-old black male with a past medical history of a kidney transplant, currently on dialysis and waiting for another kidney transplant, presented with a 2-month history of a pruritic rash on the upper body consisting of erythematous papules with central erosions.

Using videos to educate your ObGyn patients
Patient barriers to optimal health-care outcomes are well documented. According to a 2003 estimate from the National Center for Education Statistics, 9 in 10 individuals do not know how to adequately access information readily available for their own health care.1 A December 7, 2013, report in Modern Healthcare stated, “When patients are in doctors’ offices, they (might) hear 50% of what’s being said and maybe their relative hears another 30%, but they walk away without 20%.”2
In addition, patients often do not fill or refill their prescriptions. More than 31% of about 37,000 prescriptions written in a primary care setting for nearly 16,000 patients were not filled.3 Reasons may be poor health literacy, a medication’s expense, or disappointment with lack of drug efficacy. In a 2010 Commonwealth Fund survey, 23.1% of US patients reported not filling a drug prescription in the previous 12 months due to cost,4 and in 2012, 27% did not follow through with recommended testing or treatment.5
On the physician side, the advent of managed care, electronic health records, and requirements to document extraneous information have shortened “face time” with patients. This means less time to educate patients about their conditions and treatments. And patients who have insufficient information may have trouble adhering with recommendations and experience unsatisfactory outcomes.
Using focused patient-education videos can help you circumvent in-office time constraints and inform patients of their conditions and your recommendations, thereby increasing practice efficiency and improving patient outcomes. There are certain considerations you should keep in mind when implementing and executing videos for patients.
Planning your video
With videos, you can convey to patients the exact message you want them to receive. This is far more effective and more appreciatedthan videos distributed by pharmaceutical companies and vendors of equipment used in your office or hospital. If you do not have the time to create patient videos, purchasing professionally created videos could be worth the cost; however, those created by physicians are far better and can be a source of enhanced communication when patients see their own physician on the screen discussing the condition, procedure, or medications prescribed.
We suggest selecting topics you regularly discuss with patients. If the topic of prolapse arises several times a day or week, a video presentation about it would be appropriate. Other topics of interest to gynecology patients are shown in the TABLE. The topics included are those that many of our colleagues find that they discuss with patients frequently and are in need of an instructional video.
Example video topics for patient viewing
• Evaluation of urinary incontinence
• Recurrent urinary tract infection
• Infertility evaluation
• Options for hysterectomy
• Management of menometrorrhagia
• Contraception options (including bilateral tubal ligation)
• Pros and cons of hormone replacement therapy
• Breast self examination
One of us (NB) likes to select topics that are receiving lots of publicity. For example, when flibanserin was approved by the US Food and Drug Administration in 2015 and patients were asking about it, we created a video with a handout that summarized the drug’s actions and its adverse effects and that emphasized the precaution about using flibanserin in conjunction with alcohol.
Production elements
The script.
- Define the problem/condition
- Offer how the problem is evaluated
- Discuss treatment options
- Go over risks and complications
- Include a summary.
Embedding details of these bullet points into a PowerPoint presentation can serve as your teleprompter. Each video might end with the statement, “I hope you have found this video on <name of topic> informative. If you open the door at the end of the video, I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have.” We refer to this as the “sandwich technique,” in which the physician interacts with the patient first and performs the examination, invites the patient to watch the video, and returns to the room to conclude the patient visit.
The recording device. Recording can be accomplished easily with technology available in nearly every ObGyn office. You can use a video camera, the webcam on your computer, or a smart phone (probably the easiest choice). The quality of video created with the Apple, Samsung, or Motorola devices is excellent. The only other piece of equipment we recommend is a flexible tripod to hold the phone. Several such tripod stands are available for purchase, but the type with a flexible stand can be beneficial (FIGURE 1). These are available for purchase on Amazon.
| FIGURE 1 Our recommended tripod stand | ||
| ||
The TriFlex Mini Phone Tripod Stand, available for purchase at retailers and at Amazon (http://www.amazon.com/dp/B017NA7V1U?psc=1). | ||

Putting it all together. With the smartphone in the tripod attached to the computer and the PowerPoint program serving as your notes, you are ready to create a video. We suggest limiting the recording to 5 to 7 minutes, the attention span of most patients. Those who want to produce a more professional looking video can use the editing programs iMovie on the Mac or Movie Maker on the PC.
Videos can be uploaded to your website, your EMR, or onto separate computers in each of your examination rooms. Depending on where you upload your videos (your own website or YouTube), patients can access them from home. An advantage of your own website and YouTube is that the videos can be viewed again and by patients’ significant others (which patients often inquire about the ability to do).
Other considerations
Videos that are conversational in nature, using the pronouns “I” and “we” and using such language as “my opinion” and “our patients” may hold the attention of viewers more than didactic “talking head” videos. In addition, creating videos on controversial topics that patients are interested in and need more information about can benefit patients and your practice.
Creating videos in other languages for your patients is an option as well. If you speak the language, then create your video in both English and the other language. Or you can create the script and ask a patient who speaks the non-English language to assist with the video production or voiceover. Also, there are other language videos for patients on YouTube. An excellent example of a Spanish-language gynecologic video on the pelvic examination is available (https://www.youtube.com/watch?v=IKsGYc-dCSI). It is easy to create a link from your website to a YouTube video. This requires requesting permission from the creator of the video. (We do not recommend showcasing another physician on your website.)
Example Patient education videos
Examples of videos on stress urinary incontinence and treatment with a midurethral sling can be viewed at: https://www.youtube.com/watch?v=BFZj8x3-oCA and https://www.youtube.com/watch?v=-gnOqkXiye0.
Dr. Neil Baum is the author of Social Media for the Healthcare Professional (Greenbranch Publishing, 2012).
Advantages of creating videos
When patients are watching the video, you can conduct visits with other patients and even perform brief office procedures. You can anticipate an up to 15% to 20% improvement in office efficiency by using educational videos. And patients will appreciate the information and the written summary accompanying each video.
Videos and medical-legal protection
Documentation is necessary to protect yourself from litigation. Record the viewing of a video in a patient’s chart, as well as the receipt of pertinent written information. We suggest you also note that all of the patient’s questions were answered before the patient left the office. To confirm that the patient understood the condition, procedure, or surgery, you can ask the patient to fill out a true/false questionnaire after watching the video and also include it in the chart. A questionnaire I (NB) use after the patient watches a video on stress incontinence is shown in FIGURE 2.
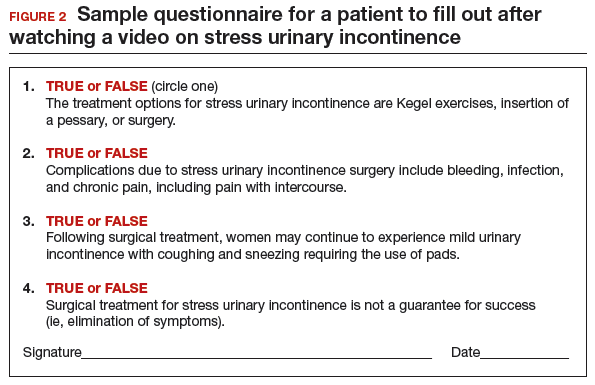
A statement to accompany the questionnaire is also a good idea. Example: “<name of patient> watched a video on the treatment of stress incontinence. The video discussed the procedure and its risks and complications, and alternate treatments, including the option to have no treatment. She agrees to proceeding with a midurethral sling using synthetic mesh and understands the risks and complications associated with the use of mesh.”
An additional helpful option is to end your videos with a comment that addresses the statement and consent form you will ask the patient to sign. For instance, “I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have. I also will ask you to sign a procedure or operative consent form as well as sign a statement that says you have watched the video, understand the content, and have had your questions answered.”
We believe that this makes the video an excellent medical-legal protection tool for the physician and that the video enhances the informed consent process.
Bottom line
We are challenged today to provide quality care in an efficient and cost-effective manner. This is a concern for every ObGyn practice regardless of its size or location or whether it is a solo or group practice or academic or private. We can improve our efficiency and our productivity, maintain quality of care, improve patient adherence, and even improve outcomes using patient videos. So get ready for lights, camera, and action!
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kutner M, Greenberg E, Jin Y, et al. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy. Washington, DC: National Center for Education Statistics, US Dept of Education, 2006.
- 1NCES publication 2006-483.2. Modern Healthcare. Providers help patients address emotion, money, health literacy. Available at: http://www.modernhealthcare.com/article/20131207/MAGAZINE/312079983. Accessed April 15, 2016.
- Tamblyn R, Eguale T, Huang A, Winsdale N, Doran P. The incidence and determinants of primary nonadherence with prescribed medication in primary care: a cohort study. Ann Intern Med. 2014;160(7):441–450.
- Morgan S, Kennedy J. Prescription drug accessibility and affordability in the United States and abroad. Issue Brief (Commonw Fund). 2010;89:1012.
- Collins SR, Robertson R, Garber T, et al. Insuring the future. Current trends in health coverage and the effects of implementing the Affordable Care Act. Available at: http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2013/Apr/1681_Collins_insuring_future_biennial_survey_2012_FINAL.pdf. Accessed April 15, 2016.
Neil H. Baum, MD, and Mickey M. Karram, MD

Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.

Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
The authors report no financial relationships relevant to this article.
Neil H. Baum, MD, and Mickey M. Karram, MD
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
The authors report no financial relationships relevant to this article.
Neil H. Baum, MD, and Mickey M. Karram, MD
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
The authors report no financial relationships relevant to this article.
Patient barriers to optimal health-care outcomes are well documented. According to a 2003 estimate from the National Center for Education Statistics, 9 in 10 individuals do not know how to adequately access information readily available for their own health care.1 A December 7, 2013, report in Modern Healthcare stated, “When patients are in doctors’ offices, they (might) hear 50% of what’s being said and maybe their relative hears another 30%, but they walk away without 20%.”2
In addition, patients often do not fill or refill their prescriptions. More than 31% of about 37,000 prescriptions written in a primary care setting for nearly 16,000 patients were not filled.3 Reasons may be poor health literacy, a medication’s expense, or disappointment with lack of drug efficacy. In a 2010 Commonwealth Fund survey, 23.1% of US patients reported not filling a drug prescription in the previous 12 months due to cost,4 and in 2012, 27% did not follow through with recommended testing or treatment.5
On the physician side, the advent of managed care, electronic health records, and requirements to document extraneous information have shortened “face time” with patients. This means less time to educate patients about their conditions and treatments. And patients who have insufficient information may have trouble adhering with recommendations and experience unsatisfactory outcomes.
Using focused patient-education videos can help you circumvent in-office time constraints and inform patients of their conditions and your recommendations, thereby increasing practice efficiency and improving patient outcomes. There are certain considerations you should keep in mind when implementing and executing videos for patients.
Planning your video
With videos, you can convey to patients the exact message you want them to receive. This is far more effective and more appreciatedthan videos distributed by pharmaceutical companies and vendors of equipment used in your office or hospital. If you do not have the time to create patient videos, purchasing professionally created videos could be worth the cost; however, those created by physicians are far better and can be a source of enhanced communication when patients see their own physician on the screen discussing the condition, procedure, or medications prescribed.
We suggest selecting topics you regularly discuss with patients. If the topic of prolapse arises several times a day or week, a video presentation about it would be appropriate. Other topics of interest to gynecology patients are shown in the TABLE. The topics included are those that many of our colleagues find that they discuss with patients frequently and are in need of an instructional video.
Example video topics for patient viewing
• Evaluation of urinary incontinence
• Recurrent urinary tract infection
• Infertility evaluation
• Options for hysterectomy
• Management of menometrorrhagia
• Contraception options (including bilateral tubal ligation)
• Pros and cons of hormone replacement therapy
• Breast self examination
One of us (NB) likes to select topics that are receiving lots of publicity. For example, when flibanserin was approved by the US Food and Drug Administration in 2015 and patients were asking about it, we created a video with a handout that summarized the drug’s actions and its adverse effects and that emphasized the precaution about using flibanserin in conjunction with alcohol.
Production elements
The script.
- Define the problem/condition
- Offer how the problem is evaluated
- Discuss treatment options
- Go over risks and complications
- Include a summary.
Embedding details of these bullet points into a PowerPoint presentation can serve as your teleprompter. Each video might end with the statement, “I hope you have found this video on <name of topic> informative. If you open the door at the end of the video, I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have.” We refer to this as the “sandwich technique,” in which the physician interacts with the patient first and performs the examination, invites the patient to watch the video, and returns to the room to conclude the patient visit.
The recording device. Recording can be accomplished easily with technology available in nearly every ObGyn office. You can use a video camera, the webcam on your computer, or a smart phone (probably the easiest choice). The quality of video created with the Apple, Samsung, or Motorola devices is excellent. The only other piece of equipment we recommend is a flexible tripod to hold the phone. Several such tripod stands are available for purchase, but the type with a flexible stand can be beneficial (FIGURE 1). These are available for purchase on Amazon.
| FIGURE 1 Our recommended tripod stand | ||
| ||
The TriFlex Mini Phone Tripod Stand, available for purchase at retailers and at Amazon (http://www.amazon.com/dp/B017NA7V1U?psc=1). | ||
Putting it all together. With the smartphone in the tripod attached to the computer and the PowerPoint program serving as your notes, you are ready to create a video. We suggest limiting the recording to 5 to 7 minutes, the attention span of most patients. Those who want to produce a more professional looking video can use the editing programs iMovie on the Mac or Movie Maker on the PC.
Videos can be uploaded to your website, your EMR, or onto separate computers in each of your examination rooms. Depending on where you upload your videos (your own website or YouTube), patients can access them from home. An advantage of your own website and YouTube is that the videos can be viewed again and by patients’ significant others (which patients often inquire about the ability to do).
Other considerations
Videos that are conversational in nature, using the pronouns “I” and “we” and using such language as “my opinion” and “our patients” may hold the attention of viewers more than didactic “talking head” videos. In addition, creating videos on controversial topics that patients are interested in and need more information about can benefit patients and your practice.
Creating videos in other languages for your patients is an option as well. If you speak the language, then create your video in both English and the other language. Or you can create the script and ask a patient who speaks the non-English language to assist with the video production or voiceover. Also, there are other language videos for patients on YouTube. An excellent example of a Spanish-language gynecologic video on the pelvic examination is available (https://www.youtube.com/watch?v=IKsGYc-dCSI). It is easy to create a link from your website to a YouTube video. This requires requesting permission from the creator of the video. (We do not recommend showcasing another physician on your website.)
Example Patient education videos
Examples of videos on stress urinary incontinence and treatment with a midurethral sling can be viewed at: https://www.youtube.com/watch?v=BFZj8x3-oCA and https://www.youtube.com/watch?v=-gnOqkXiye0.
Dr. Neil Baum is the author of Social Media for the Healthcare Professional (Greenbranch Publishing, 2012).
Advantages of creating videos
When patients are watching the video, you can conduct visits with other patients and even perform brief office procedures. You can anticipate an up to 15% to 20% improvement in office efficiency by using educational videos. And patients will appreciate the information and the written summary accompanying each video.
Videos and medical-legal protection
Documentation is necessary to protect yourself from litigation. Record the viewing of a video in a patient’s chart, as well as the receipt of pertinent written information. We suggest you also note that all of the patient’s questions were answered before the patient left the office. To confirm that the patient understood the condition, procedure, or surgery, you can ask the patient to fill out a true/false questionnaire after watching the video and also include it in the chart. A questionnaire I (NB) use after the patient watches a video on stress incontinence is shown in FIGURE 2.
A statement to accompany the questionnaire is also a good idea. Example: “<name of patient> watched a video on the treatment of stress incontinence. The video discussed the procedure and its risks and complications, and alternate treatments, including the option to have no treatment. She agrees to proceeding with a midurethral sling using synthetic mesh and understands the risks and complications associated with the use of mesh.”
An additional helpful option is to end your videos with a comment that addresses the statement and consent form you will ask the patient to sign. For instance, “I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have. I also will ask you to sign a procedure or operative consent form as well as sign a statement that says you have watched the video, understand the content, and have had your questions answered.”
We believe that this makes the video an excellent medical-legal protection tool for the physician and that the video enhances the informed consent process.
Bottom line
We are challenged today to provide quality care in an efficient and cost-effective manner. This is a concern for every ObGyn practice regardless of its size or location or whether it is a solo or group practice or academic or private. We can improve our efficiency and our productivity, maintain quality of care, improve patient adherence, and even improve outcomes using patient videos. So get ready for lights, camera, and action!
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Patient barriers to optimal health-care outcomes are well documented. According to a 2003 estimate from the National Center for Education Statistics, 9 in 10 individuals do not know how to adequately access information readily available for their own health care.1 A December 7, 2013, report in Modern Healthcare stated, “When patients are in doctors’ offices, they (might) hear 50% of what’s being said and maybe their relative hears another 30%, but they walk away without 20%.”2
In addition, patients often do not fill or refill their prescriptions. More than 31% of about 37,000 prescriptions written in a primary care setting for nearly 16,000 patients were not filled.3 Reasons may be poor health literacy, a medication’s expense, or disappointment with lack of drug efficacy. In a 2010 Commonwealth Fund survey, 23.1% of US patients reported not filling a drug prescription in the previous 12 months due to cost,4 and in 2012, 27% did not follow through with recommended testing or treatment.5
On the physician side, the advent of managed care, electronic health records, and requirements to document extraneous information have shortened “face time” with patients. This means less time to educate patients about their conditions and treatments. And patients who have insufficient information may have trouble adhering with recommendations and experience unsatisfactory outcomes.
Using focused patient-education videos can help you circumvent in-office time constraints and inform patients of their conditions and your recommendations, thereby increasing practice efficiency and improving patient outcomes. There are certain considerations you should keep in mind when implementing and executing videos for patients.
Planning your video
With videos, you can convey to patients the exact message you want them to receive. This is far more effective and more appreciatedthan videos distributed by pharmaceutical companies and vendors of equipment used in your office or hospital. If you do not have the time to create patient videos, purchasing professionally created videos could be worth the cost; however, those created by physicians are far better and can be a source of enhanced communication when patients see their own physician on the screen discussing the condition, procedure, or medications prescribed.
We suggest selecting topics you regularly discuss with patients. If the topic of prolapse arises several times a day or week, a video presentation about it would be appropriate. Other topics of interest to gynecology patients are shown in the TABLE. The topics included are those that many of our colleagues find that they discuss with patients frequently and are in need of an instructional video.
Example video topics for patient viewing
• Evaluation of urinary incontinence
• Recurrent urinary tract infection
• Infertility evaluation
• Options for hysterectomy
• Management of menometrorrhagia
• Contraception options (including bilateral tubal ligation)
• Pros and cons of hormone replacement therapy
• Breast self examination
One of us (NB) likes to select topics that are receiving lots of publicity. For example, when flibanserin was approved by the US Food and Drug Administration in 2015 and patients were asking about it, we created a video with a handout that summarized the drug’s actions and its adverse effects and that emphasized the precaution about using flibanserin in conjunction with alcohol.
Production elements
The script.
- Define the problem/condition
- Offer how the problem is evaluated
- Discuss treatment options
- Go over risks and complications
- Include a summary.
Embedding details of these bullet points into a PowerPoint presentation can serve as your teleprompter. Each video might end with the statement, “I hope you have found this video on <name of topic> informative. If you open the door at the end of the video, I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have.” We refer to this as the “sandwich technique,” in which the physician interacts with the patient first and performs the examination, invites the patient to watch the video, and returns to the room to conclude the patient visit.
The recording device. Recording can be accomplished easily with technology available in nearly every ObGyn office. You can use a video camera, the webcam on your computer, or a smart phone (probably the easiest choice). The quality of video created with the Apple, Samsung, or Motorola devices is excellent. The only other piece of equipment we recommend is a flexible tripod to hold the phone. Several such tripod stands are available for purchase, but the type with a flexible stand can be beneficial (FIGURE 1). These are available for purchase on Amazon.
| FIGURE 1 Our recommended tripod stand | ||
| ||
The TriFlex Mini Phone Tripod Stand, available for purchase at retailers and at Amazon (http://www.amazon.com/dp/B017NA7V1U?psc=1). | ||
Putting it all together. With the smartphone in the tripod attached to the computer and the PowerPoint program serving as your notes, you are ready to create a video. We suggest limiting the recording to 5 to 7 minutes, the attention span of most patients. Those who want to produce a more professional looking video can use the editing programs iMovie on the Mac or Movie Maker on the PC.
Videos can be uploaded to your website, your EMR, or onto separate computers in each of your examination rooms. Depending on where you upload your videos (your own website or YouTube), patients can access them from home. An advantage of your own website and YouTube is that the videos can be viewed again and by patients’ significant others (which patients often inquire about the ability to do).
Other considerations
Videos that are conversational in nature, using the pronouns “I” and “we” and using such language as “my opinion” and “our patients” may hold the attention of viewers more than didactic “talking head” videos. In addition, creating videos on controversial topics that patients are interested in and need more information about can benefit patients and your practice.
Creating videos in other languages for your patients is an option as well. If you speak the language, then create your video in both English and the other language. Or you can create the script and ask a patient who speaks the non-English language to assist with the video production or voiceover. Also, there are other language videos for patients on YouTube. An excellent example of a Spanish-language gynecologic video on the pelvic examination is available (https://www.youtube.com/watch?v=IKsGYc-dCSI). It is easy to create a link from your website to a YouTube video. This requires requesting permission from the creator of the video. (We do not recommend showcasing another physician on your website.)
Example Patient education videos
Examples of videos on stress urinary incontinence and treatment with a midurethral sling can be viewed at: https://www.youtube.com/watch?v=BFZj8x3-oCA and https://www.youtube.com/watch?v=-gnOqkXiye0.
Dr. Neil Baum is the author of Social Media for the Healthcare Professional (Greenbranch Publishing, 2012).
Advantages of creating videos
When patients are watching the video, you can conduct visits with other patients and even perform brief office procedures. You can anticipate an up to 15% to 20% improvement in office efficiency by using educational videos. And patients will appreciate the information and the written summary accompanying each video.
Videos and medical-legal protection
Documentation is necessary to protect yourself from litigation. Record the viewing of a video in a patient’s chart, as well as the receipt of pertinent written information. We suggest you also note that all of the patient’s questions were answered before the patient left the office. To confirm that the patient understood the condition, procedure, or surgery, you can ask the patient to fill out a true/false questionnaire after watching the video and also include it in the chart. A questionnaire I (NB) use after the patient watches a video on stress incontinence is shown in FIGURE 2.
A statement to accompany the questionnaire is also a good idea. Example: “<name of patient> watched a video on the treatment of stress incontinence. The video discussed the procedure and its risks and complications, and alternate treatments, including the option to have no treatment. She agrees to proceeding with a midurethral sling using synthetic mesh and understands the risks and complications associated with the use of mesh.”
An additional helpful option is to end your videos with a comment that addresses the statement and consent form you will ask the patient to sign. For instance, “I will return to the examination room and provide you with a summary of the <topic> and answer any questions you may have. I also will ask you to sign a procedure or operative consent form as well as sign a statement that says you have watched the video, understand the content, and have had your questions answered.”
We believe that this makes the video an excellent medical-legal protection tool for the physician and that the video enhances the informed consent process.
Bottom line
We are challenged today to provide quality care in an efficient and cost-effective manner. This is a concern for every ObGyn practice regardless of its size or location or whether it is a solo or group practice or academic or private. We can improve our efficiency and our productivity, maintain quality of care, improve patient adherence, and even improve outcomes using patient videos. So get ready for lights, camera, and action!
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kutner M, Greenberg E, Jin Y, et al. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy. Washington, DC: National Center for Education Statistics, US Dept of Education, 2006.
- 1NCES publication 2006-483.2. Modern Healthcare. Providers help patients address emotion, money, health literacy. Available at: http://www.modernhealthcare.com/article/20131207/MAGAZINE/312079983. Accessed April 15, 2016.
- Tamblyn R, Eguale T, Huang A, Winsdale N, Doran P. The incidence and determinants of primary nonadherence with prescribed medication in primary care: a cohort study. Ann Intern Med. 2014;160(7):441–450.
- Morgan S, Kennedy J. Prescription drug accessibility and affordability in the United States and abroad. Issue Brief (Commonw Fund). 2010;89:1012.
- Collins SR, Robertson R, Garber T, et al. Insuring the future. Current trends in health coverage and the effects of implementing the Affordable Care Act. Available at: http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2013/Apr/1681_Collins_insuring_future_biennial_survey_2012_FINAL.pdf. Accessed April 15, 2016.
- Kutner M, Greenberg E, Jin Y, et al. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy. Washington, DC: National Center for Education Statistics, US Dept of Education, 2006.
- 1NCES publication 2006-483.2. Modern Healthcare. Providers help patients address emotion, money, health literacy. Available at: http://www.modernhealthcare.com/article/20131207/MAGAZINE/312079983. Accessed April 15, 2016.
- Tamblyn R, Eguale T, Huang A, Winsdale N, Doran P. The incidence and determinants of primary nonadherence with prescribed medication in primary care: a cohort study. Ann Intern Med. 2014;160(7):441–450.
- Morgan S, Kennedy J. Prescription drug accessibility and affordability in the United States and abroad. Issue Brief (Commonw Fund). 2010;89:1012.
- Collins SR, Robertson R, Garber T, et al. Insuring the future. Current trends in health coverage and the effects of implementing the Affordable Care Act. Available at: http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2013/Apr/1681_Collins_insuring_future_biennial_survey_2012_FINAL.pdf. Accessed April 15, 2016.
In this article
• Videos and medical-legal protection
• Patient questionnaire post-video viewing

Aprepitant Protects Against Chemo-Induced Nausea and Vomiting
According to international guidelines, > 90% of patients on a cisplatin regimen experience chemotherapy-induced nausea and vomiting (CINV). Antiemetic prophylaxis with a 5 hydroxytryptamine receptor-3 antagonist (5-HT3RA) plus dexamethasone still leaves about 20% of patients with acute or delayed vomiting and nausea during the first cycle of chemotherapy. However, researchers from Chang Gung University in Taiwan found that adding aprepitant provided about 70% complete protection against emesis when the primary prophylaxis did not work. Those findings led them to conduct a study that evaluated the antiemetic efficacy of a combination of 3 drugs: palonosetron (a long-acting second-generation 5-HT3RA), 3-day oral aprepitant (a neurokinin-1 receptor antagonist), and dexamethasone.
Related: Delayed Adjuvant Chemotherapy Significantly Affects Breast Cancer Recovery
Patients in the study were scheduled to receive at least 50 mg/m2 cisplatin followed by a continuous infusion of 5-fluorouracil (5-FU) with or without other chemotherapeutic agents. Cisplatin was given on day 1; the other drugs were given on day 1 and subsequent days. All 69 patients who received palonosetron, aprepitant, and dexamethasone were evaluated in the first cycle of chemotherapy.
No patients experienced acute vomiting; nearly all (98.6%) were protected against nausea. Moreover, 97.1% had no delayed vomiting, and 87% had no delayed nausea. Most episodes of delayed nausea were rated as mild. Overall, 97.1% of patients had no vomiting, and 85.5% of patients had no nausea.
Related: FDA Approves Rescue Drug for Chemotherapy Overdose
The effects were sustained. In the second cycle of chemotherapy, again, none of 61 evaluated patients experienced acute vomiting, and 96.7% were free of nausea. Most patients also were protected against delayed vomiting or nausea (96.7% and 83.6%, respectively). Of patients who underwent 2 cycles, 45 did not experience nausea or vomiting in either cycle.
The combination of drugs was generally well tolerated; most adverse events were mild.
Yang C-K, Wu C-E, Liaw C-C. Biomed J. 2016;39(1):60-66.
doi: 10.1016/j.bj.2015.08.006.
According to international guidelines, > 90% of patients on a cisplatin regimen experience chemotherapy-induced nausea and vomiting (CINV). Antiemetic prophylaxis with a 5 hydroxytryptamine receptor-3 antagonist (5-HT3RA) plus dexamethasone still leaves about 20% of patients with acute or delayed vomiting and nausea during the first cycle of chemotherapy. However, researchers from Chang Gung University in Taiwan found that adding aprepitant provided about 70% complete protection against emesis when the primary prophylaxis did not work. Those findings led them to conduct a study that evaluated the antiemetic efficacy of a combination of 3 drugs: palonosetron (a long-acting second-generation 5-HT3RA), 3-day oral aprepitant (a neurokinin-1 receptor antagonist), and dexamethasone.
Related: Delayed Adjuvant Chemotherapy Significantly Affects Breast Cancer Recovery
Patients in the study were scheduled to receive at least 50 mg/m2 cisplatin followed by a continuous infusion of 5-fluorouracil (5-FU) with or without other chemotherapeutic agents. Cisplatin was given on day 1; the other drugs were given on day 1 and subsequent days. All 69 patients who received palonosetron, aprepitant, and dexamethasone were evaluated in the first cycle of chemotherapy.
No patients experienced acute vomiting; nearly all (98.6%) were protected against nausea. Moreover, 97.1% had no delayed vomiting, and 87% had no delayed nausea. Most episodes of delayed nausea were rated as mild. Overall, 97.1% of patients had no vomiting, and 85.5% of patients had no nausea.
Related: FDA Approves Rescue Drug for Chemotherapy Overdose
The effects were sustained. In the second cycle of chemotherapy, again, none of 61 evaluated patients experienced acute vomiting, and 96.7% were free of nausea. Most patients also were protected against delayed vomiting or nausea (96.7% and 83.6%, respectively). Of patients who underwent 2 cycles, 45 did not experience nausea or vomiting in either cycle.
The combination of drugs was generally well tolerated; most adverse events were mild.
Yang C-K, Wu C-E, Liaw C-C. Biomed J. 2016;39(1):60-66.
doi: 10.1016/j.bj.2015.08.006.
According to international guidelines, > 90% of patients on a cisplatin regimen experience chemotherapy-induced nausea and vomiting (CINV). Antiemetic prophylaxis with a 5 hydroxytryptamine receptor-3 antagonist (5-HT3RA) plus dexamethasone still leaves about 20% of patients with acute or delayed vomiting and nausea during the first cycle of chemotherapy. However, researchers from Chang Gung University in Taiwan found that adding aprepitant provided about 70% complete protection against emesis when the primary prophylaxis did not work. Those findings led them to conduct a study that evaluated the antiemetic efficacy of a combination of 3 drugs: palonosetron (a long-acting second-generation 5-HT3RA), 3-day oral aprepitant (a neurokinin-1 receptor antagonist), and dexamethasone.
Related: Delayed Adjuvant Chemotherapy Significantly Affects Breast Cancer Recovery
Patients in the study were scheduled to receive at least 50 mg/m2 cisplatin followed by a continuous infusion of 5-fluorouracil (5-FU) with or without other chemotherapeutic agents. Cisplatin was given on day 1; the other drugs were given on day 1 and subsequent days. All 69 patients who received palonosetron, aprepitant, and dexamethasone were evaluated in the first cycle of chemotherapy.
No patients experienced acute vomiting; nearly all (98.6%) were protected against nausea. Moreover, 97.1% had no delayed vomiting, and 87% had no delayed nausea. Most episodes of delayed nausea were rated as mild. Overall, 97.1% of patients had no vomiting, and 85.5% of patients had no nausea.
Related: FDA Approves Rescue Drug for Chemotherapy Overdose
The effects were sustained. In the second cycle of chemotherapy, again, none of 61 evaluated patients experienced acute vomiting, and 96.7% were free of nausea. Most patients also were protected against delayed vomiting or nausea (96.7% and 83.6%, respectively). Of patients who underwent 2 cycles, 45 did not experience nausea or vomiting in either cycle.
The combination of drugs was generally well tolerated; most adverse events were mild.
Yang C-K, Wu C-E, Liaw C-C. Biomed J. 2016;39(1):60-66.
doi: 10.1016/j.bj.2015.08.006.
Baseline King-Devick concussion score skewed by English proficiency issues
VANCOUVER – In a study at New York University, it took 27 healthy, native English–speaking volunteers 42.8 seconds to complete the King-Devick concussion screening test, which is about average for nonconcussed subjects.
However, it took 27 other volunteers with English as a second language 54.4 seconds (P = .001). Had the test been given on the sidelines instead of in a laboratory, the extra 12 seconds might easily have been mistaken as a sign of serious concussion because concussions generally add about 5 seconds to the King-Devick score.

“A prolongation of 12 seconds in non-native English speakers has real clinical implications,” said lead investigator Katharine Dempsey, a medical student and member of the eye movement research team in the department of neurology at New York University.
King-Devick (KD) is an increasingly popular sideline screening tool used widely in professional sports. Subjects are timed on how long it takes to read out loud and in English three sets of 40 numbers, with each set progressively more difficult to read. It’s administered by flashcards or, as in the study, by computer screen.
All of the non-native speakers at NYU were largely proficient in English, but their native languages – 18 in total, most often Spanish or Chinese – were often dominant, meaning they were used at home and to work out mental arithmetic. Some subjects did not use Roman numerals or right-to-left reading in their native tongues.
KD instructions recommend testing subjects against their own preseason baseline scores; the NYU findings emphasize how important that is when subjects aren’t native English speakers. The investigators are concerned that when baseline scores are unavailable, non-native English speakers will be scored against reference ranges for native speakers.
“There’s incredible utility in using a sideline concussion screening test, but we definitely have to get out the message that the best practice is to take an athlete’s own preseason baseline. We have to be incredibly cautious when comparing test times of non-native English speakers to a normative database for native speakers,” Ms. Dempsey said at the annual meeting of the American Academy of Neurology.
The participants were in their early 30s, on average, and had no histories of concussion. The majority were women, and most were NYU employees or their friends.
The team also tracked eye movements during testing. Non-native speakers had more quick eye movement (149 vs. 135; P = .03), but also fixated longer on numbers before initiating eye movement (345.4 milliseconds vs. 288.0; P = .007). Lag time correlated with native language dominance and suggests longer processing time.
The next step is to test how well patients do with KD testing in their native language, Ms. Dempsey said.
Ms. Dempsey had no disclosures.
VANCOUVER – In a study at New York University, it took 27 healthy, native English–speaking volunteers 42.8 seconds to complete the King-Devick concussion screening test, which is about average for nonconcussed subjects.
However, it took 27 other volunteers with English as a second language 54.4 seconds (P = .001). Had the test been given on the sidelines instead of in a laboratory, the extra 12 seconds might easily have been mistaken as a sign of serious concussion because concussions generally add about 5 seconds to the King-Devick score.
“A prolongation of 12 seconds in non-native English speakers has real clinical implications,” said lead investigator Katharine Dempsey, a medical student and member of the eye movement research team in the department of neurology at New York University.
King-Devick (KD) is an increasingly popular sideline screening tool used widely in professional sports. Subjects are timed on how long it takes to read out loud and in English three sets of 40 numbers, with each set progressively more difficult to read. It’s administered by flashcards or, as in the study, by computer screen.
All of the non-native speakers at NYU were largely proficient in English, but their native languages – 18 in total, most often Spanish or Chinese – were often dominant, meaning they were used at home and to work out mental arithmetic. Some subjects did not use Roman numerals or right-to-left reading in their native tongues.
KD instructions recommend testing subjects against their own preseason baseline scores; the NYU findings emphasize how important that is when subjects aren’t native English speakers. The investigators are concerned that when baseline scores are unavailable, non-native English speakers will be scored against reference ranges for native speakers.
“There’s incredible utility in using a sideline concussion screening test, but we definitely have to get out the message that the best practice is to take an athlete’s own preseason baseline. We have to be incredibly cautious when comparing test times of non-native English speakers to a normative database for native speakers,” Ms. Dempsey said at the annual meeting of the American Academy of Neurology.
The participants were in their early 30s, on average, and had no histories of concussion. The majority were women, and most were NYU employees or their friends.
The team also tracked eye movements during testing. Non-native speakers had more quick eye movement (149 vs. 135; P = .03), but also fixated longer on numbers before initiating eye movement (345.4 milliseconds vs. 288.0; P = .007). Lag time correlated with native language dominance and suggests longer processing time.
The next step is to test how well patients do with KD testing in their native language, Ms. Dempsey said.
Ms. Dempsey had no disclosures.
VANCOUVER – In a study at New York University, it took 27 healthy, native English–speaking volunteers 42.8 seconds to complete the King-Devick concussion screening test, which is about average for nonconcussed subjects.
However, it took 27 other volunteers with English as a second language 54.4 seconds (P = .001). Had the test been given on the sidelines instead of in a laboratory, the extra 12 seconds might easily have been mistaken as a sign of serious concussion because concussions generally add about 5 seconds to the King-Devick score.
“A prolongation of 12 seconds in non-native English speakers has real clinical implications,” said lead investigator Katharine Dempsey, a medical student and member of the eye movement research team in the department of neurology at New York University.
King-Devick (KD) is an increasingly popular sideline screening tool used widely in professional sports. Subjects are timed on how long it takes to read out loud and in English three sets of 40 numbers, with each set progressively more difficult to read. It’s administered by flashcards or, as in the study, by computer screen.
All of the non-native speakers at NYU were largely proficient in English, but their native languages – 18 in total, most often Spanish or Chinese – were often dominant, meaning they were used at home and to work out mental arithmetic. Some subjects did not use Roman numerals or right-to-left reading in their native tongues.
KD instructions recommend testing subjects against their own preseason baseline scores; the NYU findings emphasize how important that is when subjects aren’t native English speakers. The investigators are concerned that when baseline scores are unavailable, non-native English speakers will be scored against reference ranges for native speakers.
“There’s incredible utility in using a sideline concussion screening test, but we definitely have to get out the message that the best practice is to take an athlete’s own preseason baseline. We have to be incredibly cautious when comparing test times of non-native English speakers to a normative database for native speakers,” Ms. Dempsey said at the annual meeting of the American Academy of Neurology.
The participants were in their early 30s, on average, and had no histories of concussion. The majority were women, and most were NYU employees or their friends.
The team also tracked eye movements during testing. Non-native speakers had more quick eye movement (149 vs. 135; P = .03), but also fixated longer on numbers before initiating eye movement (345.4 milliseconds vs. 288.0; P = .007). Lag time correlated with native language dominance and suggests longer processing time.
The next step is to test how well patients do with KD testing in their native language, Ms. Dempsey said.
Ms. Dempsey had no disclosures.
AT THE AAN 2016 ANNUAL MEETING
Key clinical point: King-Devick instructions recommend testing subjects against their own preseason baseline scores; the NYU findings emphasize how important that is when subjects aren’t native English speakers.
Major finding: It took 27 healthy, native English–speaking volunteers 42.8 seconds to complete the King-Devick concussion screening test, but 27 other volunteers with English as a second language 54.4 seconds (P = .001).
Data source: Prospective screening of 54 healthy volunteers.
Disclosures: The presenter had no disclosures.
