User login
‘Perfect storm’ of depression, stress raises risk of MI, death
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Patients with coronary heart disease who have both depression and stress are at increased risk of myocardial infarction and death, according to findings from a large, prospective, cohort study.
Of 4,487 adults with CHD who were part of the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, 1,337 experienced MI or death during a median of nearly 6 years of follow-up. Those with both high depressive symptoms and high stress at baseline – about 6% of the study population – were at significantly increased risk of such events (adjusted hazard ratio, 1.48) during the first 2.5 years of follow-up, compared with those with low stress and low depressive symptoms. However, the association was not significant beyond the initial 2.5 years (HR, 0.89), Carmela Alcántara, Ph.D., of Columbia University, New York, and her colleagues reported.
Those with low stress and high depressive symptoms, and those with high stress and low depressive symptoms, were not at increased risk (HR, 0.92 and 0.86, respectively) at any point during follow-up (Circ. Cardiovasc. Qual. Outcomes 2015 March 10 [doi:10.1161/IRCOUTCOMES.114.001180]).
The findings provide initial empirical evidence to support a “psychosocial perfect storm conceptual model” based on the idea that it takes an underlying chronic psychosocial vulnerability such as depression along with a more transient state such as psychological stress to precipitate a clinical event. The confluence of these factors may be particularly destructive in the short term, the investigators concluded, noting that the findings could have implications for the development of preventive treatments that focus on depression and stress during this vulnerable period in CHD patients.
The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures, but two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
Key clinical point: Concurrent depression and stress in CHD patients may increase the early risk of MI and death.
Major finding: CHD patients with high depressive symptoms and high stress at baseline had an increased risk of MI and death early during follow-up (adjusted HR, 1.48).
Data source: A prospective cohort study of 4,487 adults.
Disclosures: The National Institute of Neurological Disorders and Stroke and the National Heart, Lung, and Blood Institute supported the study. Dr. Alcantara reported having no disclosures; two other authors received salary support from Amgen for research, and one served as a consultant for DiaDexus.
Venous thromboembolism common after heart transplant
For every 1,000 patients who underwent heart transplantation, about 45 had an episode of venous thromboembolism within a year after surgery, according to a retrospective study reported in the February issue of the Journal of Heart and Lung Transplantation.
Furthermore, patients who had a single VTE episode after transplant had a “high” risk of recurrent VTE, said Dr. Rolando Alvarez, a cardiologist at Complejo Hospitalario Universitario A Coruna in A Coruna, Spain, and his associates.
“Our opinion is that long-term oral anticoagulation should be maintained in these patients, especially if other risk factors are present and provided that the bleeding risk is not excessive,” said the researchers.
Venous thromboembolism is a common complication of lung, kidney, and liver transplantation, but less is known about VTE after heart transplant. The researchers found that “classic” risk factors for VTE, such as being older, obese, or having renal dysfunction, also increased the risk of VTE after heart transplant (J. Heart Lung Transplant. 2015;34:167-74).
The study included data from 635 consecutive patients who underwent heart transplantation at a single hospital between 1991 and 2013. During a median of 8.4 years of follow-up, the cumulative incidence of VTE was 8.5%, for an annual incidence rate of 12.7 episodes per year for every 1,000 patients, the researchers reported. The risk of VTE was far higher during the first year after transplant (45.1 episodes per 1,000 patients), but even after excluding these episodes, VTE was six times more common among heart transplant recipients than among the general population. Furthermore, VTE recurred an estimated 30.5 times/1,000 patient-years, and 50.8 times/1,000 patients-years among patients who had stopped anticoagulants.
The cumulative incidence rate of DVT and PE were 8.4 and 8.7 episodes per 1,000 patient-years.
In the multivariate analysis, significant risk factors for VTE at less than 1 year after transplantation included age, obesity, chronic kidney disease, and emergency transplantation, the investigators said. More than a year after transplantation, only use of the mammalian target of rapamycin (mTOR) inhibitors sirolimus and everolimus significantly increased VTE risk.
“The evidence that supports a potential association between mTOR inhibitors and an increased risk of VTE events is still weak, and might be confounded by a high prevalence of comorbid conditions such as chronic renal failure, dyslipidemia, or malignancy in patients taking these kinds of drugs,” the investigators cautioned.
The authors suggested that in view of the high recurrence rate, long-term anticoagulation should be considered in heart transplant patients after their first VTE episode.
The Fundacion BBVA-Carolina funded the study. Four coauthors reported receiving travel support from Novartis Pharma and Astellas Pharma. The other authors reported no relevant conflicts of interest.
For every 1,000 patients who underwent heart transplantation, about 45 had an episode of venous thromboembolism within a year after surgery, according to a retrospective study reported in the February issue of the Journal of Heart and Lung Transplantation.
Furthermore, patients who had a single VTE episode after transplant had a “high” risk of recurrent VTE, said Dr. Rolando Alvarez, a cardiologist at Complejo Hospitalario Universitario A Coruna in A Coruna, Spain, and his associates.
“Our opinion is that long-term oral anticoagulation should be maintained in these patients, especially if other risk factors are present and provided that the bleeding risk is not excessive,” said the researchers.
Venous thromboembolism is a common complication of lung, kidney, and liver transplantation, but less is known about VTE after heart transplant. The researchers found that “classic” risk factors for VTE, such as being older, obese, or having renal dysfunction, also increased the risk of VTE after heart transplant (J. Heart Lung Transplant. 2015;34:167-74).
The study included data from 635 consecutive patients who underwent heart transplantation at a single hospital between 1991 and 2013. During a median of 8.4 years of follow-up, the cumulative incidence of VTE was 8.5%, for an annual incidence rate of 12.7 episodes per year for every 1,000 patients, the researchers reported. The risk of VTE was far higher during the first year after transplant (45.1 episodes per 1,000 patients), but even after excluding these episodes, VTE was six times more common among heart transplant recipients than among the general population. Furthermore, VTE recurred an estimated 30.5 times/1,000 patient-years, and 50.8 times/1,000 patients-years among patients who had stopped anticoagulants.
The cumulative incidence rate of DVT and PE were 8.4 and 8.7 episodes per 1,000 patient-years.
In the multivariate analysis, significant risk factors for VTE at less than 1 year after transplantation included age, obesity, chronic kidney disease, and emergency transplantation, the investigators said. More than a year after transplantation, only use of the mammalian target of rapamycin (mTOR) inhibitors sirolimus and everolimus significantly increased VTE risk.
“The evidence that supports a potential association between mTOR inhibitors and an increased risk of VTE events is still weak, and might be confounded by a high prevalence of comorbid conditions such as chronic renal failure, dyslipidemia, or malignancy in patients taking these kinds of drugs,” the investigators cautioned.
The authors suggested that in view of the high recurrence rate, long-term anticoagulation should be considered in heart transplant patients after their first VTE episode.
The Fundacion BBVA-Carolina funded the study. Four coauthors reported receiving travel support from Novartis Pharma and Astellas Pharma. The other authors reported no relevant conflicts of interest.
For every 1,000 patients who underwent heart transplantation, about 45 had an episode of venous thromboembolism within a year after surgery, according to a retrospective study reported in the February issue of the Journal of Heart and Lung Transplantation.
Furthermore, patients who had a single VTE episode after transplant had a “high” risk of recurrent VTE, said Dr. Rolando Alvarez, a cardiologist at Complejo Hospitalario Universitario A Coruna in A Coruna, Spain, and his associates.
“Our opinion is that long-term oral anticoagulation should be maintained in these patients, especially if other risk factors are present and provided that the bleeding risk is not excessive,” said the researchers.
Venous thromboembolism is a common complication of lung, kidney, and liver transplantation, but less is known about VTE after heart transplant. The researchers found that “classic” risk factors for VTE, such as being older, obese, or having renal dysfunction, also increased the risk of VTE after heart transplant (J. Heart Lung Transplant. 2015;34:167-74).
The study included data from 635 consecutive patients who underwent heart transplantation at a single hospital between 1991 and 2013. During a median of 8.4 years of follow-up, the cumulative incidence of VTE was 8.5%, for an annual incidence rate of 12.7 episodes per year for every 1,000 patients, the researchers reported. The risk of VTE was far higher during the first year after transplant (45.1 episodes per 1,000 patients), but even after excluding these episodes, VTE was six times more common among heart transplant recipients than among the general population. Furthermore, VTE recurred an estimated 30.5 times/1,000 patient-years, and 50.8 times/1,000 patients-years among patients who had stopped anticoagulants.
The cumulative incidence rate of DVT and PE were 8.4 and 8.7 episodes per 1,000 patient-years.
In the multivariate analysis, significant risk factors for VTE at less than 1 year after transplantation included age, obesity, chronic kidney disease, and emergency transplantation, the investigators said. More than a year after transplantation, only use of the mammalian target of rapamycin (mTOR) inhibitors sirolimus and everolimus significantly increased VTE risk.
“The evidence that supports a potential association between mTOR inhibitors and an increased risk of VTE events is still weak, and might be confounded by a high prevalence of comorbid conditions such as chronic renal failure, dyslipidemia, or malignancy in patients taking these kinds of drugs,” the investigators cautioned.
The authors suggested that in view of the high recurrence rate, long-term anticoagulation should be considered in heart transplant patients after their first VTE episode.
The Fundacion BBVA-Carolina funded the study. Four coauthors reported receiving travel support from Novartis Pharma and Astellas Pharma. The other authors reported no relevant conflicts of interest.
Key clinical point: Venous thromboembolism (VTE) was common after heart transplant, especially when patients had relevant risk factors and were not on anticoagulants.
Major finding: Cumulative incidence of VTE was 8.5% during eight years of follow-up and was much higher during the first year after transplant.
Data source: Single-center retrospective cohort study of 635 heart transplant recipients.
Disclosures: The Fundacion BBVA-Carolina funded the study. Four coauthors reported receiving travel support from Novartis Pharma and Astellas Pharma. The other authors reported no relevant conflicts of interest.
Stroke ambulances speed treatment to U.S. patients
NASHVILLE, TENN. – Bringing a CT scanner and thrombolytic treatment directly to stroke patients in the field sped the time to thrombolysis, compared with waiting for the patient to arrive at the hospital.
Some U.S. stroke centers now send out a team that can immediately assess and start treating stroke patients in the community. In 2014, the first two U.S. mobile stroke-treatment units began operating, one in Houston and the second in Cleveland.

Initial reports show both programs were successful in cutting the time to deliver thrombolytic treatment with intravenous tissue plasminogen activator (TPA) to appropriate patients.
In Houston, the active phase of the program started in May 2014, and by October 2014, 47 acute ischemic stroke patients had been treated with TPA. The mobile-unit crews started 43% of eligible patients on thrombolysis within 60 minutes of their symptom onset and another 31% were treated starting 61-80 minutes after symptom onset, said Stephanie A. Parker at the International Stroke Conference.

The unit also treats patients diagnosed with hemorrhagic stroke with intravenous nicardipine for rapid blood pressure reduction, said Ms. Parker, a critical care and emergency medicine–trained registered nurse who is project manager for the Houston mobile unit.
The Cleveland program began in July 2014; of the first 100 stroke patients seen by the mobile unit 16 of 19 eligible patients received tPA, with an average time of 56 minutes from symptom onset to treatment. This compared with an average 94 minutes to tPA onset in patients brought conventionally last year to a Cleveland-area hospital, Dr. M. Shazam Hussain said in a report at the meeting, sponsored by the American Heart Association.

The clinical impact and cost effectiveness of the pilot programs using the mobile units have not yet been assessed from the data, Dr. Hussain and Ms. Parker emphasized. Funding for the Cleveland and Houston vehicles came from local donors; the Houston program also received equipment donations from manufacturers.
The two mobile units are standard 12-foot, box-shaped ambulances outfitted with a CT scanner, a point-of-care lab, and telemedicine components as well as more standard emergency-vehicle equipment. The Houston vehicle contains “all the diagnostic equipment that is in our emergency room,” Ms. Parker said.
The concept behind both the Cleveland unit, operated by the Cleveland Clinic, and the Houston unit, operated by the University of Texas, Houston, is that the mobile stroke unit arrives to a patient with a suspected stroke, the unit is stationary while a CT scan and other diagnostic tests are run, diagnosis occurs with telemedicine assistance. If the patient is cleared for TPA treatment, the infusion starts and the vehicle carries the patient to an appropriate stroke center.

Currently, the Houston unit goes out with a vascular neurologist and a telemedicine physician on board, but plans are in place to test the feasibility of relying entirely on telemedicine when making diagnostic and treatment decisions. The Cleveland mobile unit already operates in this fashion, with no physician on board, and was the first mobile stroke unit in the world to depend completely on telemedicine, according to Dr. Hussain, a neurologist and head of the stroke program at the Cleveland Clinic.
The world’s first mobile stroke unit began operating in Saarland, Germany, in 2008 (Lancet Neurology 2012;11:397-404), and a second unit began running in Berlin after that, Dr. Hussain noted. Because of limited funding, the service he directs in Cleveland has been operating from 8 a.m.-8 p.m., 7 days a week. The program plans to expand to 24-hour coverage. The Houston mobile unit operates 24/7; it averages two runs per day and administers TPA on 1 of every 10 runs, Ms. Parker said. Both the Houston and Cleveland units tie into the local 911 emergency activation systems for their respective regions.
On Twitter @mitchelzoler
NASHVILLE, TENN. – Bringing a CT scanner and thrombolytic treatment directly to stroke patients in the field sped the time to thrombolysis, compared with waiting for the patient to arrive at the hospital.
Some U.S. stroke centers now send out a team that can immediately assess and start treating stroke patients in the community. In 2014, the first two U.S. mobile stroke-treatment units began operating, one in Houston and the second in Cleveland.
Initial reports show both programs were successful in cutting the time to deliver thrombolytic treatment with intravenous tissue plasminogen activator (TPA) to appropriate patients.
In Houston, the active phase of the program started in May 2014, and by October 2014, 47 acute ischemic stroke patients had been treated with TPA. The mobile-unit crews started 43% of eligible patients on thrombolysis within 60 minutes of their symptom onset and another 31% were treated starting 61-80 minutes after symptom onset, said Stephanie A. Parker at the International Stroke Conference.
The unit also treats patients diagnosed with hemorrhagic stroke with intravenous nicardipine for rapid blood pressure reduction, said Ms. Parker, a critical care and emergency medicine–trained registered nurse who is project manager for the Houston mobile unit.
The Cleveland program began in July 2014; of the first 100 stroke patients seen by the mobile unit 16 of 19 eligible patients received tPA, with an average time of 56 minutes from symptom onset to treatment. This compared with an average 94 minutes to tPA onset in patients brought conventionally last year to a Cleveland-area hospital, Dr. M. Shazam Hussain said in a report at the meeting, sponsored by the American Heart Association.
The clinical impact and cost effectiveness of the pilot programs using the mobile units have not yet been assessed from the data, Dr. Hussain and Ms. Parker emphasized. Funding for the Cleveland and Houston vehicles came from local donors; the Houston program also received equipment donations from manufacturers.
The two mobile units are standard 12-foot, box-shaped ambulances outfitted with a CT scanner, a point-of-care lab, and telemedicine components as well as more standard emergency-vehicle equipment. The Houston vehicle contains “all the diagnostic equipment that is in our emergency room,” Ms. Parker said.
The concept behind both the Cleveland unit, operated by the Cleveland Clinic, and the Houston unit, operated by the University of Texas, Houston, is that the mobile stroke unit arrives to a patient with a suspected stroke, the unit is stationary while a CT scan and other diagnostic tests are run, diagnosis occurs with telemedicine assistance. If the patient is cleared for TPA treatment, the infusion starts and the vehicle carries the patient to an appropriate stroke center.
Currently, the Houston unit goes out with a vascular neurologist and a telemedicine physician on board, but plans are in place to test the feasibility of relying entirely on telemedicine when making diagnostic and treatment decisions. The Cleveland mobile unit already operates in this fashion, with no physician on board, and was the first mobile stroke unit in the world to depend completely on telemedicine, according to Dr. Hussain, a neurologist and head of the stroke program at the Cleveland Clinic.
The world’s first mobile stroke unit began operating in Saarland, Germany, in 2008 (Lancet Neurology 2012;11:397-404), and a second unit began running in Berlin after that, Dr. Hussain noted. Because of limited funding, the service he directs in Cleveland has been operating from 8 a.m.-8 p.m., 7 days a week. The program plans to expand to 24-hour coverage. The Houston mobile unit operates 24/7; it averages two runs per day and administers TPA on 1 of every 10 runs, Ms. Parker said. Both the Houston and Cleveland units tie into the local 911 emergency activation systems for their respective regions.
On Twitter @mitchelzoler
NASHVILLE, TENN. – Bringing a CT scanner and thrombolytic treatment directly to stroke patients in the field sped the time to thrombolysis, compared with waiting for the patient to arrive at the hospital.
Some U.S. stroke centers now send out a team that can immediately assess and start treating stroke patients in the community. In 2014, the first two U.S. mobile stroke-treatment units began operating, one in Houston and the second in Cleveland.
Initial reports show both programs were successful in cutting the time to deliver thrombolytic treatment with intravenous tissue plasminogen activator (TPA) to appropriate patients.
In Houston, the active phase of the program started in May 2014, and by October 2014, 47 acute ischemic stroke patients had been treated with TPA. The mobile-unit crews started 43% of eligible patients on thrombolysis within 60 minutes of their symptom onset and another 31% were treated starting 61-80 minutes after symptom onset, said Stephanie A. Parker at the International Stroke Conference.
The unit also treats patients diagnosed with hemorrhagic stroke with intravenous nicardipine for rapid blood pressure reduction, said Ms. Parker, a critical care and emergency medicine–trained registered nurse who is project manager for the Houston mobile unit.
The Cleveland program began in July 2014; of the first 100 stroke patients seen by the mobile unit 16 of 19 eligible patients received tPA, with an average time of 56 minutes from symptom onset to treatment. This compared with an average 94 minutes to tPA onset in patients brought conventionally last year to a Cleveland-area hospital, Dr. M. Shazam Hussain said in a report at the meeting, sponsored by the American Heart Association.
The clinical impact and cost effectiveness of the pilot programs using the mobile units have not yet been assessed from the data, Dr. Hussain and Ms. Parker emphasized. Funding for the Cleveland and Houston vehicles came from local donors; the Houston program also received equipment donations from manufacturers.
The two mobile units are standard 12-foot, box-shaped ambulances outfitted with a CT scanner, a point-of-care lab, and telemedicine components as well as more standard emergency-vehicle equipment. The Houston vehicle contains “all the diagnostic equipment that is in our emergency room,” Ms. Parker said.
The concept behind both the Cleveland unit, operated by the Cleveland Clinic, and the Houston unit, operated by the University of Texas, Houston, is that the mobile stroke unit arrives to a patient with a suspected stroke, the unit is stationary while a CT scan and other diagnostic tests are run, diagnosis occurs with telemedicine assistance. If the patient is cleared for TPA treatment, the infusion starts and the vehicle carries the patient to an appropriate stroke center.
Currently, the Houston unit goes out with a vascular neurologist and a telemedicine physician on board, but plans are in place to test the feasibility of relying entirely on telemedicine when making diagnostic and treatment decisions. The Cleveland mobile unit already operates in this fashion, with no physician on board, and was the first mobile stroke unit in the world to depend completely on telemedicine, according to Dr. Hussain, a neurologist and head of the stroke program at the Cleveland Clinic.
The world’s first mobile stroke unit began operating in Saarland, Germany, in 2008 (Lancet Neurology 2012;11:397-404), and a second unit began running in Berlin after that, Dr. Hussain noted. Because of limited funding, the service he directs in Cleveland has been operating from 8 a.m.-8 p.m., 7 days a week. The program plans to expand to 24-hour coverage. The Houston mobile unit operates 24/7; it averages two runs per day and administers TPA on 1 of every 10 runs, Ms. Parker said. Both the Houston and Cleveland units tie into the local 911 emergency activation systems for their respective regions.
On Twitter @mitchelzoler
AT THE INTERNATIONAL STROKE CONFERENCE
Key clinical point: Dedicated stroke ambulances that bring a CT scanner and thrombolytic treatment to patients in the field speed thrombolytic therapy.
Major finding: In Cleveland, stroke patients received thrombolysis an average of 38 minutes sooner from the CT-equipped ambulance, compared with standard protocols.
Data source: Prospectively collected data on time-to-treatment from case series in Houston and in Cleveland.
Disclosures: Dr. Hussain and Ms. Parker had no disclosures.

Women having heart attacks face longer prehospital delay
When heart attack symptoms begin, women wait longer than do men to call for help, and it takes longer for them to arrive at a hospital that can care for them appropriately.
Further, statistical analysis suggests that this prehospital delay is a chief contributor to the higher in-hospital mortality rate for women who have sustained myocardial infarctions. Dr. Raffaele Bugiardini of the University of Bologna and his associates in the ISACS-TC study group examined data from a large international study to clarify gender disparities in heart attacks, and to identify more precisely where time is lost in caring for women.
They examined data from 2,282 women and 5,175 men who experienced ST-segment–elevation myocardial infarction (STEMI). Overall, female participants were older than males and were more likely to have diabetes, to be treated for hypertension, and to have experienced atypical chest pain – or no chest pain at all – during their heart attacks. The men were more likely to be smokers, to have chronic renal failure, and to have a prior history of angina.
The results were released in advance of the researchers’ presentation on March 14 at the annual meeting of the American College of Cardiology in San Diego.
Once symptoms began, women tended to wait significantly longer to call for help, a median 60.0 minutes, compared with 45.5 for men. Time to hospital admission was just a bit longer for women (60 minutes) compared to men (55 minutes). On admission, time to angioplasty or fibrinolysis did not vary significantly between the sexes. The likelihood of receiving appropriate medical treatment (aspirin, clopidogrel, heparin use) was also similar.
In outcome measures, 30% of women achieved hospital admission in 60 minutes or less from leaving home, compared with 70% of men. Dr. Bugiardini explained that the 60-minute admission marker is an important quality standard in the European framework. The odds ratio (OR) for a greater-than 60-minute time from home to hospital admission for women was 2.90 (95% CI, 1.52-5.82).
In-hospital mortality for women was nearly double that for men, at 11.8% compared to 6.3% for men (OR 1.34, 95% CI 1.01-1.77). However, after logistic regression analysis adjusted for the differences in time from home to hospital admission, the disparity in mortality disappeared (OR 0.90, 95% CI 0.31-2.56). Dr. Bugiardini emphasized that his analysis makes clear that delay in treatment is an important contributor to greater in-hospital mortality for women suffering heart attacks.
Though these finding were drawn from a large international study, American College of Cardiology Vice President Richard Chazal affirmed during a media briefing that the results are definitely applicable to the United States and other developed nations. “They are confirmatory,” said Dr. Chazal, “of other studies that have suggested this but have not shown this in such a complete and comprehensive way. This is very important information in this population.”
Heart disease kills more women than do all forms of cancer combined, but the varied presentation of heart attack symptoms in women is still underrecognized, noted Dr. Chazal of Lee Memorial Health System, Fort Myers, Fla. Raising awareness about heart disease risk and heart attack symptoms is critical to addressing the disparities identified in this study. “The delays in getting the patient to the hospital are really crucial in determining what the outcomes are,” he said.
“Time is still lost between contact with the system and arrival to the hospital” for women, he added. “There is less awareness not just by women, but in doctors in underestimating what’s going on with women. We are confused, so we stop and do one more EKG. We are losing time.”
Dr. Marija Vavlukis is on the speakers bureau for KRKA Macedonia. The other authors have no disclosures.
When heart attack symptoms begin, women wait longer than do men to call for help, and it takes longer for them to arrive at a hospital that can care for them appropriately.
Further, statistical analysis suggests that this prehospital delay is a chief contributor to the higher in-hospital mortality rate for women who have sustained myocardial infarctions. Dr. Raffaele Bugiardini of the University of Bologna and his associates in the ISACS-TC study group examined data from a large international study to clarify gender disparities in heart attacks, and to identify more precisely where time is lost in caring for women.
They examined data from 2,282 women and 5,175 men who experienced ST-segment–elevation myocardial infarction (STEMI). Overall, female participants were older than males and were more likely to have diabetes, to be treated for hypertension, and to have experienced atypical chest pain – or no chest pain at all – during their heart attacks. The men were more likely to be smokers, to have chronic renal failure, and to have a prior history of angina.
The results were released in advance of the researchers’ presentation on March 14 at the annual meeting of the American College of Cardiology in San Diego.
Once symptoms began, women tended to wait significantly longer to call for help, a median 60.0 minutes, compared with 45.5 for men. Time to hospital admission was just a bit longer for women (60 minutes) compared to men (55 minutes). On admission, time to angioplasty or fibrinolysis did not vary significantly between the sexes. The likelihood of receiving appropriate medical treatment (aspirin, clopidogrel, heparin use) was also similar.
In outcome measures, 30% of women achieved hospital admission in 60 minutes or less from leaving home, compared with 70% of men. Dr. Bugiardini explained that the 60-minute admission marker is an important quality standard in the European framework. The odds ratio (OR) for a greater-than 60-minute time from home to hospital admission for women was 2.90 (95% CI, 1.52-5.82).
In-hospital mortality for women was nearly double that for men, at 11.8% compared to 6.3% for men (OR 1.34, 95% CI 1.01-1.77). However, after logistic regression analysis adjusted for the differences in time from home to hospital admission, the disparity in mortality disappeared (OR 0.90, 95% CI 0.31-2.56). Dr. Bugiardini emphasized that his analysis makes clear that delay in treatment is an important contributor to greater in-hospital mortality for women suffering heart attacks.
Though these finding were drawn from a large international study, American College of Cardiology Vice President Richard Chazal affirmed during a media briefing that the results are definitely applicable to the United States and other developed nations. “They are confirmatory,” said Dr. Chazal, “of other studies that have suggested this but have not shown this in such a complete and comprehensive way. This is very important information in this population.”
Heart disease kills more women than do all forms of cancer combined, but the varied presentation of heart attack symptoms in women is still underrecognized, noted Dr. Chazal of Lee Memorial Health System, Fort Myers, Fla. Raising awareness about heart disease risk and heart attack symptoms is critical to addressing the disparities identified in this study. “The delays in getting the patient to the hospital are really crucial in determining what the outcomes are,” he said.
“Time is still lost between contact with the system and arrival to the hospital” for women, he added. “There is less awareness not just by women, but in doctors in underestimating what’s going on with women. We are confused, so we stop and do one more EKG. We are losing time.”
Dr. Marija Vavlukis is on the speakers bureau for KRKA Macedonia. The other authors have no disclosures.
When heart attack symptoms begin, women wait longer than do men to call for help, and it takes longer for them to arrive at a hospital that can care for them appropriately.
Further, statistical analysis suggests that this prehospital delay is a chief contributor to the higher in-hospital mortality rate for women who have sustained myocardial infarctions. Dr. Raffaele Bugiardini of the University of Bologna and his associates in the ISACS-TC study group examined data from a large international study to clarify gender disparities in heart attacks, and to identify more precisely where time is lost in caring for women.
They examined data from 2,282 women and 5,175 men who experienced ST-segment–elevation myocardial infarction (STEMI). Overall, female participants were older than males and were more likely to have diabetes, to be treated for hypertension, and to have experienced atypical chest pain – or no chest pain at all – during their heart attacks. The men were more likely to be smokers, to have chronic renal failure, and to have a prior history of angina.
The results were released in advance of the researchers’ presentation on March 14 at the annual meeting of the American College of Cardiology in San Diego.
Once symptoms began, women tended to wait significantly longer to call for help, a median 60.0 minutes, compared with 45.5 for men. Time to hospital admission was just a bit longer for women (60 minutes) compared to men (55 minutes). On admission, time to angioplasty or fibrinolysis did not vary significantly between the sexes. The likelihood of receiving appropriate medical treatment (aspirin, clopidogrel, heparin use) was also similar.
In outcome measures, 30% of women achieved hospital admission in 60 minutes or less from leaving home, compared with 70% of men. Dr. Bugiardini explained that the 60-minute admission marker is an important quality standard in the European framework. The odds ratio (OR) for a greater-than 60-minute time from home to hospital admission for women was 2.90 (95% CI, 1.52-5.82).
In-hospital mortality for women was nearly double that for men, at 11.8% compared to 6.3% for men (OR 1.34, 95% CI 1.01-1.77). However, after logistic regression analysis adjusted for the differences in time from home to hospital admission, the disparity in mortality disappeared (OR 0.90, 95% CI 0.31-2.56). Dr. Bugiardini emphasized that his analysis makes clear that delay in treatment is an important contributor to greater in-hospital mortality for women suffering heart attacks.
Though these finding were drawn from a large international study, American College of Cardiology Vice President Richard Chazal affirmed during a media briefing that the results are definitely applicable to the United States and other developed nations. “They are confirmatory,” said Dr. Chazal, “of other studies that have suggested this but have not shown this in such a complete and comprehensive way. This is very important information in this population.”
Heart disease kills more women than do all forms of cancer combined, but the varied presentation of heart attack symptoms in women is still underrecognized, noted Dr. Chazal of Lee Memorial Health System, Fort Myers, Fla. Raising awareness about heart disease risk and heart attack symptoms is critical to addressing the disparities identified in this study. “The delays in getting the patient to the hospital are really crucial in determining what the outcomes are,” he said.
“Time is still lost between contact with the system and arrival to the hospital” for women, he added. “There is less awareness not just by women, but in doctors in underestimating what’s going on with women. We are confused, so we stop and do one more EKG. We are losing time.”
Dr. Marija Vavlukis is on the speakers bureau for KRKA Macedonia. The other authors have no disclosures.
FROM ACC 15
Key clinical point: Women having heart attacks wait longer to call for help, and it takes longer to get them to a hospital.
Major findings: The median time from onset of symptoms to ambulance call was 45.5 minutes for men vs. 60.0 minutes for women; just 30% of women vs. 70% of men were admitted within 60 minutes of leaving home.
Data source: Multivariate analysis of data from 7,457 patients enrolled in the International Survey of Acute Coronary Syndromes in Transitional Countries (ISACS-TC).
Disclosures: Dr. Marija Vavlukis is on the speakers bureau for KRKA Macedonia. The other authors have no disclosures.
FDA approves first drug for high-risk neuroblastoma
The Food and Drug Administration has approved dinutuximab as part of a multimodality regimen, including surgery, chemotherapy, and radiation therapy, for pediatric patients with high-risk neuroblastoma.
The drug “marks the first approval for a therapy aimed specifically for the treatment of patients with high-risk neuroblastoma,” Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the March 10 FDA announcement.
Dinutuximab is a chimeric monoclonal antibody that targets GD2, a glycolipid on the surface of tumor cells, according to the manufacturer, United Therapeutics.
The FDA granted approval based on a clinical trial of 226 pediatric participants with high-risk neuroblastoma whose tumors shrunk or disappeared after treatment with multiple-drug chemotherapy and surgery followed by additional intensive chemotherapy and who subsequently received bone marrow transplantation support and radiation therapy. Three years after being randomly assigned to receive either isotretinoin or dinutuximab in combination with interleukin-2 and granulocyte macrophage colony-stimulating factor, 63% of participants receiving the combination were alive and free of tumor growth or recurrence, compared with 46% of participants treated with isotretinoin alone.
In an updated analysis, 73% of participants who received the combination were alive, compared with 58% of those receiving isotretinoin alone, the FDA said in the announcement.
The most common side effects were severe pain, fever, low platelet counts, infusion reactions, low blood pressure, hyponatremia, elevated liver enzymes, anemia, vomiting, diarrhea, low potassium levels in the blood, capillary leak syndrome, neutropenia and lymphopenia, hives, and low blood calcium levels, the statement said.
The drug carries a boxed warning that the drug can irritate nerve cells, causing severe pain that requires treatment with intravenous narcotics, and can cause nerve damage and life-threatening infusion reactions, including upper airway swelling, difficulty breathing, and low blood pressure, during or shortly following completion of the infusion. Dinutuximab may also cause other serious side effects, including infections, eye problems, electrolyte abnormalities, and bone marrow suppression.
The FDA granted approval of dinutuximab, to be marketed as Unituxin, following a priority review and orphan product designation.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has approved dinutuximab as part of a multimodality regimen, including surgery, chemotherapy, and radiation therapy, for pediatric patients with high-risk neuroblastoma.
The drug “marks the first approval for a therapy aimed specifically for the treatment of patients with high-risk neuroblastoma,” Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the March 10 FDA announcement.
Dinutuximab is a chimeric monoclonal antibody that targets GD2, a glycolipid on the surface of tumor cells, according to the manufacturer, United Therapeutics.
The FDA granted approval based on a clinical trial of 226 pediatric participants with high-risk neuroblastoma whose tumors shrunk or disappeared after treatment with multiple-drug chemotherapy and surgery followed by additional intensive chemotherapy and who subsequently received bone marrow transplantation support and radiation therapy. Three years after being randomly assigned to receive either isotretinoin or dinutuximab in combination with interleukin-2 and granulocyte macrophage colony-stimulating factor, 63% of participants receiving the combination were alive and free of tumor growth or recurrence, compared with 46% of participants treated with isotretinoin alone.
In an updated analysis, 73% of participants who received the combination were alive, compared with 58% of those receiving isotretinoin alone, the FDA said in the announcement.
The most common side effects were severe pain, fever, low platelet counts, infusion reactions, low blood pressure, hyponatremia, elevated liver enzymes, anemia, vomiting, diarrhea, low potassium levels in the blood, capillary leak syndrome, neutropenia and lymphopenia, hives, and low blood calcium levels, the statement said.
The drug carries a boxed warning that the drug can irritate nerve cells, causing severe pain that requires treatment with intravenous narcotics, and can cause nerve damage and life-threatening infusion reactions, including upper airway swelling, difficulty breathing, and low blood pressure, during or shortly following completion of the infusion. Dinutuximab may also cause other serious side effects, including infections, eye problems, electrolyte abnormalities, and bone marrow suppression.
The FDA granted approval of dinutuximab, to be marketed as Unituxin, following a priority review and orphan product designation.
[email protected]
On Twitter @nikolaideslaura
The Food and Drug Administration has approved dinutuximab as part of a multimodality regimen, including surgery, chemotherapy, and radiation therapy, for pediatric patients with high-risk neuroblastoma.
The drug “marks the first approval for a therapy aimed specifically for the treatment of patients with high-risk neuroblastoma,” Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the March 10 FDA announcement.
Dinutuximab is a chimeric monoclonal antibody that targets GD2, a glycolipid on the surface of tumor cells, according to the manufacturer, United Therapeutics.
The FDA granted approval based on a clinical trial of 226 pediatric participants with high-risk neuroblastoma whose tumors shrunk or disappeared after treatment with multiple-drug chemotherapy and surgery followed by additional intensive chemotherapy and who subsequently received bone marrow transplantation support and radiation therapy. Three years after being randomly assigned to receive either isotretinoin or dinutuximab in combination with interleukin-2 and granulocyte macrophage colony-stimulating factor, 63% of participants receiving the combination were alive and free of tumor growth or recurrence, compared with 46% of participants treated with isotretinoin alone.
In an updated analysis, 73% of participants who received the combination were alive, compared with 58% of those receiving isotretinoin alone, the FDA said in the announcement.
The most common side effects were severe pain, fever, low platelet counts, infusion reactions, low blood pressure, hyponatremia, elevated liver enzymes, anemia, vomiting, diarrhea, low potassium levels in the blood, capillary leak syndrome, neutropenia and lymphopenia, hives, and low blood calcium levels, the statement said.
The drug carries a boxed warning that the drug can irritate nerve cells, causing severe pain that requires treatment with intravenous narcotics, and can cause nerve damage and life-threatening infusion reactions, including upper airway swelling, difficulty breathing, and low blood pressure, during or shortly following completion of the infusion. Dinutuximab may also cause other serious side effects, including infections, eye problems, electrolyte abnormalities, and bone marrow suppression.
The FDA granted approval of dinutuximab, to be marketed as Unituxin, following a priority review and orphan product designation.
[email protected]
On Twitter @nikolaideslaura
Onchocerciasis
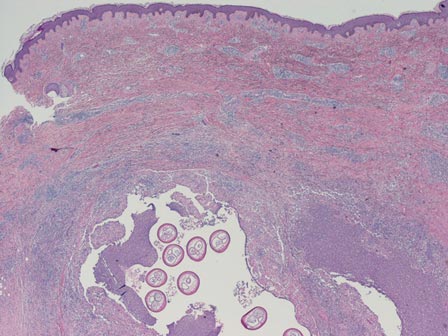
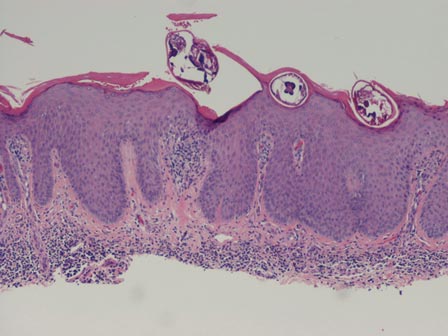
The larvae of Onchocerca volvulus, a nematode that is most commonly found in tropical Africa, Yemen, Central America, and South America, are transmitted by flies of the genus Simulium that breed near fast-flowing rivers.1 The flies bite the host and transmit the larvae, and the larvae then mature into adults within the skin and subcutis, forming nodules that typically are not painful. The worms may reside within the skin for years and produce microfilariae, which can migrate and cause visual impairment, blindness, or a pruritic papular rash.1
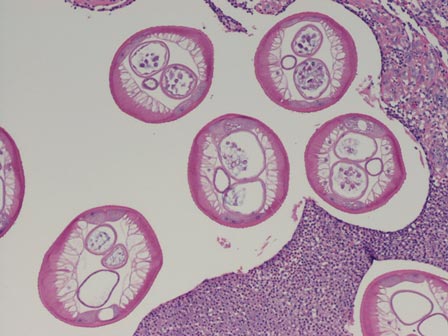
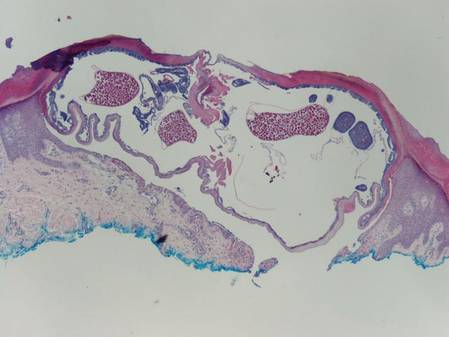
The nematode produces a nodule within the dermis or subcutis with surrounding fibrous tissue and a mixed inflammatory infiltrate with eosinophils (Figure 1). In some cases, microfilariae can be seen within the lymphatics or within the uteri of the worms.1 Male and female worms typically are present and have a corrugated cuticle with a thin underlying layer of striated muscle. The females have paired uteri, which usually contain microfilariae2 (Figure 2).
| 
|
Dirofilaria repens also is a nematode that produces a subcutaneous nodule with an inflammatory reaction. This worm typically has a thick cuticle with longitudinal ridges, long thick muscle, and lateral cords.3 Additionally, because humans are not the usual host, Dirofilaria species do not complete their lifecycle and typically are not gravid, unlike Onchocerca species.
Myiasis is the presence of fly larvae within the skin. The larvae demonstrate a thick hyaline cuticle with pigmented brown-yellow spikes (Figure 3). There is a thick muscular layer under the cuticle and a tubular tracheal system containing vertical striations. The digestive system has an epithelial lining with prominent vessels. Adipose tissue with granulated cytoplasm, prominent nuclei, and coarse chromatin also are present.4

Scabies mites (Figure 4), ova, and scybala are present within the stratum corneum. A mixed inflammatory infiltrate also can be present.1 Tungiasis is caused by burrowing fleas and typically occurs on acral skin; therefore, it is more frequently found in the superficial portion of the skin. Erythrocytes usually are present in the gastrointestinal tract, and the females usually are gravid.2 A surrounding mixed inflammatory infiltrate is present, and necrosis also can occur (Figure 5).1
| 
|
1. Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland: Churchill Livingstone Elsevier; 2010.
2. Elston DM, Ferringer T. Dermatopathology: Requisites in Dermatology. Edinburgh, Scotland: Saunders Elsevier; 2008.
3. Tzanetou K, Gasteratos S, Pantazopoulou A, et al. Subcutaneous dirofilariasis caused by Dirofilaria repens in Greece: a case report. J Cutan Pathol. 2009;36:892-895.
4. Fernandez-Flores A, Saeb-Lima M. Pulse granuloma of the lip: morphologic clues in its differential diagnosis. J Cutan Pathol. 2014;41:394-399.
The larvae of Onchocerca volvulus, a nematode that is most commonly found in tropical Africa, Yemen, Central America, and South America, are transmitted by flies of the genus Simulium that breed near fast-flowing rivers.1 The flies bite the host and transmit the larvae, and the larvae then mature into adults within the skin and subcutis, forming nodules that typically are not painful. The worms may reside within the skin for years and produce microfilariae, which can migrate and cause visual impairment, blindness, or a pruritic papular rash.1
The nematode produces a nodule within the dermis or subcutis with surrounding fibrous tissue and a mixed inflammatory infiltrate with eosinophils (Figure 1). In some cases, microfilariae can be seen within the lymphatics or within the uteri of the worms.1 Male and female worms typically are present and have a corrugated cuticle with a thin underlying layer of striated muscle. The females have paired uteri, which usually contain microfilariae2 (Figure 2).
|
|
|
Dirofilaria repens also is a nematode that produces a subcutaneous nodule with an inflammatory reaction. This worm typically has a thick cuticle with longitudinal ridges, long thick muscle, and lateral cords.3 Additionally, because humans are not the usual host, Dirofilaria species do not complete their lifecycle and typically are not gravid, unlike Onchocerca species.
Myiasis is the presence of fly larvae within the skin. The larvae demonstrate a thick hyaline cuticle with pigmented brown-yellow spikes (Figure 3). There is a thick muscular layer under the cuticle and a tubular tracheal system containing vertical striations. The digestive system has an epithelial lining with prominent vessels. Adipose tissue with granulated cytoplasm, prominent nuclei, and coarse chromatin also are present.4
Scabies mites (Figure 4), ova, and scybala are present within the stratum corneum. A mixed inflammatory infiltrate also can be present.1 Tungiasis is caused by burrowing fleas and typically occurs on acral skin; therefore, it is more frequently found in the superficial portion of the skin. Erythrocytes usually are present in the gastrointestinal tract, and the females usually are gravid.2 A surrounding mixed inflammatory infiltrate is present, and necrosis also can occur (Figure 5).1
|
|
|
The larvae of Onchocerca volvulus, a nematode that is most commonly found in tropical Africa, Yemen, Central America, and South America, are transmitted by flies of the genus Simulium that breed near fast-flowing rivers.1 The flies bite the host and transmit the larvae, and the larvae then mature into adults within the skin and subcutis, forming nodules that typically are not painful. The worms may reside within the skin for years and produce microfilariae, which can migrate and cause visual impairment, blindness, or a pruritic papular rash.1
The nematode produces a nodule within the dermis or subcutis with surrounding fibrous tissue and a mixed inflammatory infiltrate with eosinophils (Figure 1). In some cases, microfilariae can be seen within the lymphatics or within the uteri of the worms.1 Male and female worms typically are present and have a corrugated cuticle with a thin underlying layer of striated muscle. The females have paired uteri, which usually contain microfilariae2 (Figure 2).
|
|
|
Dirofilaria repens also is a nematode that produces a subcutaneous nodule with an inflammatory reaction. This worm typically has a thick cuticle with longitudinal ridges, long thick muscle, and lateral cords.3 Additionally, because humans are not the usual host, Dirofilaria species do not complete their lifecycle and typically are not gravid, unlike Onchocerca species.
Myiasis is the presence of fly larvae within the skin. The larvae demonstrate a thick hyaline cuticle with pigmented brown-yellow spikes (Figure 3). There is a thick muscular layer under the cuticle and a tubular tracheal system containing vertical striations. The digestive system has an epithelial lining with prominent vessels. Adipose tissue with granulated cytoplasm, prominent nuclei, and coarse chromatin also are present.4
Scabies mites (Figure 4), ova, and scybala are present within the stratum corneum. A mixed inflammatory infiltrate also can be present.1 Tungiasis is caused by burrowing fleas and typically occurs on acral skin; therefore, it is more frequently found in the superficial portion of the skin. Erythrocytes usually are present in the gastrointestinal tract, and the females usually are gravid.2 A surrounding mixed inflammatory infiltrate is present, and necrosis also can occur (Figure 5).1
|
|
|
1. Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland: Churchill Livingstone Elsevier; 2010.
2. Elston DM, Ferringer T. Dermatopathology: Requisites in Dermatology. Edinburgh, Scotland: Saunders Elsevier; 2008.
3. Tzanetou K, Gasteratos S, Pantazopoulou A, et al. Subcutaneous dirofilariasis caused by Dirofilaria repens in Greece: a case report. J Cutan Pathol. 2009;36:892-895.
4. Fernandez-Flores A, Saeb-Lima M. Pulse granuloma of the lip: morphologic clues in its differential diagnosis. J Cutan Pathol. 2014;41:394-399.
1. Weedon D. Weedon’s Skin Pathology. 3rd ed. Edinburgh, Scotland: Churchill Livingstone Elsevier; 2010.
2. Elston DM, Ferringer T. Dermatopathology: Requisites in Dermatology. Edinburgh, Scotland: Saunders Elsevier; 2008.
3. Tzanetou K, Gasteratos S, Pantazopoulou A, et al. Subcutaneous dirofilariasis caused by Dirofilaria repens in Greece: a case report. J Cutan Pathol. 2009;36:892-895.
4. Fernandez-Flores A, Saeb-Lima M. Pulse granuloma of the lip: morphologic clues in its differential diagnosis. J Cutan Pathol. 2014;41:394-399.

Latest valvular disease guidelines bring big changes
SNOWMASS, COLO. – The 2014 American Heart Association/American College of Cardiology guidelines for the management of valvular heart disease break new ground in numerous ways, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
“We needed to do things differently. These guidelines were created in a different format from prior valvular heart disease guidelines. We wanted these guidelines to promote access to concise, relevant bytes of information at the point of care,” explained Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn., and cochair of the guidelines writing committee.
These guidelines – the first major revision in 8 years – introduce a new taxonomy and the first staging system for valvular heart disease. The guidelines also lower the threshold for intervention in asymptomatic patients, recommending surgical or catheter-based treatment at an earlier point in the disease process than ever before. And the guidelines introduce the concept of heart valve centers of excellence, offering a strong recommendation that patients be referred to those centers for procedures to be performed in the asymptomatic phase of disease (J. Am. Coll. Cardiol. 2014;63:2438-88).
These valvular heart disease guidelines place greater emphasis than before on the quality of the scientific evidence underlying recommendations. Since valvular heart disease is a field with a paucity of randomized trials, that meant cutting back.
“Our goal was, if there’s little evidence, don’t write a recommendation. So the number of recommendations went down, but at least the ones that were made were based on evidence,” the cardiologist noted.
Indeed, in the 2006 guidelines, more than 70% of the recommendations were Level of Evidence C and based solely upon expert opinion; in the new guidelines, that’s true for less than 50%. And the proportion of recommendations that are Level of Evidence B increased from 30% to 45%.
The 2014 update was prompted by huge changes in the field of valvular heart disease since 2006. For example, better data became available on the natural history of valvular heart disease. The old concept was not to operate on the asymptomatic patient with severe aortic stenosis and normal left ventricular function, but more recent natural history studies have shown that, left untreated, 72% of such patients will die or develop symptoms within 5 years.
So there has been a push to intervene earlier. Fortunately, that became doable, as recent years also brought improved noninvasive imaging, new catheter-based interventions, and refined surgical methods, enabling operators to safely lower the threshold for intervention in asymptomatic patients while at the same time extending procedural therapies to older, sicker populations.
Dr. Nishimura predicted that cardiologists and surgeons will find the new staging system clinically useful. The four stages, A-D, define the categories “at risk,” “progressive,” “asymptomatic severe,” and “symptomatic severe,” respectively. These categories are particularly helpful in determining how often to schedule patient follow-up and when to time intervention.
The guidelines recommend observation for patients who are Stage A or B and intervention when reasonable in patients who are Stage C2 or D. What bumps a patient with hemodynamically severe yet asymptomatic mitral regurgitation from Stage C1 to C2 is an left ventricular ejection fraction below 60% or a left ventricular end systolic dimension of 40 mm or more. In the setting of asymptomatic aortic stenosis, it’s a peak aortic valve velocity of 4.0 m/sec on Doppler echocardiography plus an LVEF of less than 50%.
The latest guidelines introduced the concept of heart valve centers of excellence in response to evidence of large variability across the country in terms of experience with valve operations. For example, the majority of centers perform fewer than 40 mitral valve repairs per year, and surgeons who perform mitral operations do a median of just five per year. The guideline committee, which included general and interventional cardiologists, surgeons, anesthesiologists, and imaging experts, was persuaded that those numbers are not sufficient to achieve optimal results in complex valve operations for asymptomatic patients.
The criteria for qualifying as a heart valve center of excellence, as defined in the guidelines, include having a multidisciplinary heart valve team, high patient volume, high-level surgical experience and expertise in complex valve procedures, and active participation in multicenter data registries and continuous quality improvement processes.
“The most important thing is you have to be very transparent with your data,” according to the cardiologist.
Ultimately, the most far-reaching change introduced in the current valvular heart disease guidelines is the switch from textbook format to what Dr. Nishimura calls structured data knowledge management.
“The AHA/ACC clinical practice guidelines are generally recognized as the flagship of U.S. cardiovascular medicine, but they’re like a library of old books. Clinically valuable knowledge is buried within documents that can be 200 pages long. What we need at the point of care is the gist: concise, relevant bytes of information that answer a specific clinical question, synthesized by experts,” Dr. Nishimura said.
The new approach is designed to counter the information overload that plagues contemporary medical practice. Each recommendation in the current valvular heart disease guidelines addresses a specific clinical question via a brief summary statement followed by a short explanatory paragraph, with accompanying references for those who seek additional details. This new format is designed to lead AHA/ACC clinical practice guidelines into the electronic information management future.
“In the future, you’ll go to your iPad or iPhone or whatever, type in search terms such as ‘anticoagulation for mechanical valves during pregnancy,’ and it will take you straight to the relevant knowledge byte. You can then click on ‘more’ and find out more and get to the supporting evidence tables. The knowledge chunks will be stored in a centralized knowledge management system. The nice thing about this is that it will be a living document that can easily be updated, instead of having to wait 8 years for a new version,” Dr. Nishimura explained.
He reported having no financial conflicts of interest.
SNOWMASS, COLO. – The 2014 American Heart Association/American College of Cardiology guidelines for the management of valvular heart disease break new ground in numerous ways, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
“We needed to do things differently. These guidelines were created in a different format from prior valvular heart disease guidelines. We wanted these guidelines to promote access to concise, relevant bytes of information at the point of care,” explained Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn., and cochair of the guidelines writing committee.
These guidelines – the first major revision in 8 years – introduce a new taxonomy and the first staging system for valvular heart disease. The guidelines also lower the threshold for intervention in asymptomatic patients, recommending surgical or catheter-based treatment at an earlier point in the disease process than ever before. And the guidelines introduce the concept of heart valve centers of excellence, offering a strong recommendation that patients be referred to those centers for procedures to be performed in the asymptomatic phase of disease (J. Am. Coll. Cardiol. 2014;63:2438-88).
These valvular heart disease guidelines place greater emphasis than before on the quality of the scientific evidence underlying recommendations. Since valvular heart disease is a field with a paucity of randomized trials, that meant cutting back.
“Our goal was, if there’s little evidence, don’t write a recommendation. So the number of recommendations went down, but at least the ones that were made were based on evidence,” the cardiologist noted.
Indeed, in the 2006 guidelines, more than 70% of the recommendations were Level of Evidence C and based solely upon expert opinion; in the new guidelines, that’s true for less than 50%. And the proportion of recommendations that are Level of Evidence B increased from 30% to 45%.
The 2014 update was prompted by huge changes in the field of valvular heart disease since 2006. For example, better data became available on the natural history of valvular heart disease. The old concept was not to operate on the asymptomatic patient with severe aortic stenosis and normal left ventricular function, but more recent natural history studies have shown that, left untreated, 72% of such patients will die or develop symptoms within 5 years.
So there has been a push to intervene earlier. Fortunately, that became doable, as recent years also brought improved noninvasive imaging, new catheter-based interventions, and refined surgical methods, enabling operators to safely lower the threshold for intervention in asymptomatic patients while at the same time extending procedural therapies to older, sicker populations.
Dr. Nishimura predicted that cardiologists and surgeons will find the new staging system clinically useful. The four stages, A-D, define the categories “at risk,” “progressive,” “asymptomatic severe,” and “symptomatic severe,” respectively. These categories are particularly helpful in determining how often to schedule patient follow-up and when to time intervention.
The guidelines recommend observation for patients who are Stage A or B and intervention when reasonable in patients who are Stage C2 or D. What bumps a patient with hemodynamically severe yet asymptomatic mitral regurgitation from Stage C1 to C2 is an left ventricular ejection fraction below 60% or a left ventricular end systolic dimension of 40 mm or more. In the setting of asymptomatic aortic stenosis, it’s a peak aortic valve velocity of 4.0 m/sec on Doppler echocardiography plus an LVEF of less than 50%.
The latest guidelines introduced the concept of heart valve centers of excellence in response to evidence of large variability across the country in terms of experience with valve operations. For example, the majority of centers perform fewer than 40 mitral valve repairs per year, and surgeons who perform mitral operations do a median of just five per year. The guideline committee, which included general and interventional cardiologists, surgeons, anesthesiologists, and imaging experts, was persuaded that those numbers are not sufficient to achieve optimal results in complex valve operations for asymptomatic patients.
The criteria for qualifying as a heart valve center of excellence, as defined in the guidelines, include having a multidisciplinary heart valve team, high patient volume, high-level surgical experience and expertise in complex valve procedures, and active participation in multicenter data registries and continuous quality improvement processes.
“The most important thing is you have to be very transparent with your data,” according to the cardiologist.
Ultimately, the most far-reaching change introduced in the current valvular heart disease guidelines is the switch from textbook format to what Dr. Nishimura calls structured data knowledge management.
“The AHA/ACC clinical practice guidelines are generally recognized as the flagship of U.S. cardiovascular medicine, but they’re like a library of old books. Clinically valuable knowledge is buried within documents that can be 200 pages long. What we need at the point of care is the gist: concise, relevant bytes of information that answer a specific clinical question, synthesized by experts,” Dr. Nishimura said.
The new approach is designed to counter the information overload that plagues contemporary medical practice. Each recommendation in the current valvular heart disease guidelines addresses a specific clinical question via a brief summary statement followed by a short explanatory paragraph, with accompanying references for those who seek additional details. This new format is designed to lead AHA/ACC clinical practice guidelines into the electronic information management future.
“In the future, you’ll go to your iPad or iPhone or whatever, type in search terms such as ‘anticoagulation for mechanical valves during pregnancy,’ and it will take you straight to the relevant knowledge byte. You can then click on ‘more’ and find out more and get to the supporting evidence tables. The knowledge chunks will be stored in a centralized knowledge management system. The nice thing about this is that it will be a living document that can easily be updated, instead of having to wait 8 years for a new version,” Dr. Nishimura explained.
He reported having no financial conflicts of interest.
SNOWMASS, COLO. – The 2014 American Heart Association/American College of Cardiology guidelines for the management of valvular heart disease break new ground in numerous ways, Dr. Rick A. Nishimura said at the Annual Cardiovascular Conference at Snowmass.
“We needed to do things differently. These guidelines were created in a different format from prior valvular heart disease guidelines. We wanted these guidelines to promote access to concise, relevant bytes of information at the point of care,” explained Dr. Nishimura, professor of medicine at the Mayo Clinic in Rochester, Minn., and cochair of the guidelines writing committee.
These guidelines – the first major revision in 8 years – introduce a new taxonomy and the first staging system for valvular heart disease. The guidelines also lower the threshold for intervention in asymptomatic patients, recommending surgical or catheter-based treatment at an earlier point in the disease process than ever before. And the guidelines introduce the concept of heart valve centers of excellence, offering a strong recommendation that patients be referred to those centers for procedures to be performed in the asymptomatic phase of disease (J. Am. Coll. Cardiol. 2014;63:2438-88).
These valvular heart disease guidelines place greater emphasis than before on the quality of the scientific evidence underlying recommendations. Since valvular heart disease is a field with a paucity of randomized trials, that meant cutting back.
“Our goal was, if there’s little evidence, don’t write a recommendation. So the number of recommendations went down, but at least the ones that were made were based on evidence,” the cardiologist noted.
Indeed, in the 2006 guidelines, more than 70% of the recommendations were Level of Evidence C and based solely upon expert opinion; in the new guidelines, that’s true for less than 50%. And the proportion of recommendations that are Level of Evidence B increased from 30% to 45%.
The 2014 update was prompted by huge changes in the field of valvular heart disease since 2006. For example, better data became available on the natural history of valvular heart disease. The old concept was not to operate on the asymptomatic patient with severe aortic stenosis and normal left ventricular function, but more recent natural history studies have shown that, left untreated, 72% of such patients will die or develop symptoms within 5 years.
So there has been a push to intervene earlier. Fortunately, that became doable, as recent years also brought improved noninvasive imaging, new catheter-based interventions, and refined surgical methods, enabling operators to safely lower the threshold for intervention in asymptomatic patients while at the same time extending procedural therapies to older, sicker populations.
Dr. Nishimura predicted that cardiologists and surgeons will find the new staging system clinically useful. The four stages, A-D, define the categories “at risk,” “progressive,” “asymptomatic severe,” and “symptomatic severe,” respectively. These categories are particularly helpful in determining how often to schedule patient follow-up and when to time intervention.
The guidelines recommend observation for patients who are Stage A or B and intervention when reasonable in patients who are Stage C2 or D. What bumps a patient with hemodynamically severe yet asymptomatic mitral regurgitation from Stage C1 to C2 is an left ventricular ejection fraction below 60% or a left ventricular end systolic dimension of 40 mm or more. In the setting of asymptomatic aortic stenosis, it’s a peak aortic valve velocity of 4.0 m/sec on Doppler echocardiography plus an LVEF of less than 50%.
The latest guidelines introduced the concept of heart valve centers of excellence in response to evidence of large variability across the country in terms of experience with valve operations. For example, the majority of centers perform fewer than 40 mitral valve repairs per year, and surgeons who perform mitral operations do a median of just five per year. The guideline committee, which included general and interventional cardiologists, surgeons, anesthesiologists, and imaging experts, was persuaded that those numbers are not sufficient to achieve optimal results in complex valve operations for asymptomatic patients.
The criteria for qualifying as a heart valve center of excellence, as defined in the guidelines, include having a multidisciplinary heart valve team, high patient volume, high-level surgical experience and expertise in complex valve procedures, and active participation in multicenter data registries and continuous quality improvement processes.
“The most important thing is you have to be very transparent with your data,” according to the cardiologist.
Ultimately, the most far-reaching change introduced in the current valvular heart disease guidelines is the switch from textbook format to what Dr. Nishimura calls structured data knowledge management.
“The AHA/ACC clinical practice guidelines are generally recognized as the flagship of U.S. cardiovascular medicine, but they’re like a library of old books. Clinically valuable knowledge is buried within documents that can be 200 pages long. What we need at the point of care is the gist: concise, relevant bytes of information that answer a specific clinical question, synthesized by experts,” Dr. Nishimura said.
The new approach is designed to counter the information overload that plagues contemporary medical practice. Each recommendation in the current valvular heart disease guidelines addresses a specific clinical question via a brief summary statement followed by a short explanatory paragraph, with accompanying references for those who seek additional details. This new format is designed to lead AHA/ACC clinical practice guidelines into the electronic information management future.
“In the future, you’ll go to your iPad or iPhone or whatever, type in search terms such as ‘anticoagulation for mechanical valves during pregnancy,’ and it will take you straight to the relevant knowledge byte. You can then click on ‘more’ and find out more and get to the supporting evidence tables. The knowledge chunks will be stored in a centralized knowledge management system. The nice thing about this is that it will be a living document that can easily be updated, instead of having to wait 8 years for a new version,” Dr. Nishimura explained.
He reported having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
26% 1-year death, stroke rate after TAVR
One year after transcatheter aortic valve replacement in the United States, the overall mortality was 23.7%, the stroke rate was 4.1%, and the composite outcome of death and stroke was 26.0%, according to a report published online March 10 in JAMA.
Long-term outcomes for TAVR haven’t been well studied until now, yet the procedure is being performed with increasing frequency for aortic stenosis in patients who are too high risk to undergo conventional surgical aortic valve replacement, said Dr. David R. Holmes Jr. of the Mayo Clinic, Rochester, Minn., and his associates.
They assessed 1-year outcomes by analyzing administrative data from the Centers for Medicare & Medicaid Services and clinical data from the Transcatheter Valve Therapies Registry, an initiative of the Society of Thoracic Surgeons and the American College of Cardiology. The study involved 12,182 patients who underwent TAVR at 299 medical centers across the country during a 19-month period. The patients’ median age was 84 years; 95% were white and 52% were women. The transfemoral approach was used in most patients, but alternative approaches were used in roughly 44%. As expected for an elderly, high-risk study population, baseline functional status was poor and comorbidities were common. They included reduced left ventricular ejection fraction (26% of patients), prior stroke (12%), moderate or severe lung disease (28%), renal failure (16%), peripheral vascular disease (32%), and atrial fibrillation (42%), Dr. Holmes and his associates reported (JAMA 2015 March 10 [doi:10.1001/jama.2015.1474]).
In addition to the mortality and stroke rates listed above, the 1-year rate of one rehospitalization was 24.4%, that of two rehospitalizations was 12.5%, and that of three or more rehospitalizations was 11.6%. The 1-year readmission rate specifically for stroke, heart failure, or repeat aortic valve intervention was 18.6%. These are important considerations for elderly, fragile patients because rehospitalizations indicate “an unacceptable quality-of-life outcome” and are very costly, the investigators noted.
Several baseline characteristics, including male sex, severe chronic obstructive pulmonary disease, dialysis-dependent end-stage renal disease, older age, higher STS Predicted Risk of Operative Mortality (PROM) score, a history of atrial fibrillation/flutter, and use of an access route (other than transfemoral), were found to be independently associated with higher 1-year mortality. Thus, “It may be possible to identify patients who may not benefit from this procedure and who should be counseled accordingly.” For example, in this study there was a small (77 patients) very high-risk subset of patients – aged 85-94 years, dependent on dialysis, and having an STS PROM score greater than 15% – whose 1-year mortality was 53.5%.
The STS and the ACC supported this study, and support the Transcatheter Valve Therapies Registry. Dr. Holmes reported having no relevant financial disclosures; his associates reported ties to Boston Scientific, Edwards Lifesciences, Janssen, Eli Lilly, Boehringer Ingelheim, Bayer, and AstraZeneca.
One year after transcatheter aortic valve replacement in the United States, the overall mortality was 23.7%, the stroke rate was 4.1%, and the composite outcome of death and stroke was 26.0%, according to a report published online March 10 in JAMA.
Long-term outcomes for TAVR haven’t been well studied until now, yet the procedure is being performed with increasing frequency for aortic stenosis in patients who are too high risk to undergo conventional surgical aortic valve replacement, said Dr. David R. Holmes Jr. of the Mayo Clinic, Rochester, Minn., and his associates.
They assessed 1-year outcomes by analyzing administrative data from the Centers for Medicare & Medicaid Services and clinical data from the Transcatheter Valve Therapies Registry, an initiative of the Society of Thoracic Surgeons and the American College of Cardiology. The study involved 12,182 patients who underwent TAVR at 299 medical centers across the country during a 19-month period. The patients’ median age was 84 years; 95% were white and 52% were women. The transfemoral approach was used in most patients, but alternative approaches were used in roughly 44%. As expected for an elderly, high-risk study population, baseline functional status was poor and comorbidities were common. They included reduced left ventricular ejection fraction (26% of patients), prior stroke (12%), moderate or severe lung disease (28%), renal failure (16%), peripheral vascular disease (32%), and atrial fibrillation (42%), Dr. Holmes and his associates reported (JAMA 2015 March 10 [doi:10.1001/jama.2015.1474]).
In addition to the mortality and stroke rates listed above, the 1-year rate of one rehospitalization was 24.4%, that of two rehospitalizations was 12.5%, and that of three or more rehospitalizations was 11.6%. The 1-year readmission rate specifically for stroke, heart failure, or repeat aortic valve intervention was 18.6%. These are important considerations for elderly, fragile patients because rehospitalizations indicate “an unacceptable quality-of-life outcome” and are very costly, the investigators noted.
Several baseline characteristics, including male sex, severe chronic obstructive pulmonary disease, dialysis-dependent end-stage renal disease, older age, higher STS Predicted Risk of Operative Mortality (PROM) score, a history of atrial fibrillation/flutter, and use of an access route (other than transfemoral), were found to be independently associated with higher 1-year mortality. Thus, “It may be possible to identify patients who may not benefit from this procedure and who should be counseled accordingly.” For example, in this study there was a small (77 patients) very high-risk subset of patients – aged 85-94 years, dependent on dialysis, and having an STS PROM score greater than 15% – whose 1-year mortality was 53.5%.
The STS and the ACC supported this study, and support the Transcatheter Valve Therapies Registry. Dr. Holmes reported having no relevant financial disclosures; his associates reported ties to Boston Scientific, Edwards Lifesciences, Janssen, Eli Lilly, Boehringer Ingelheim, Bayer, and AstraZeneca.
One year after transcatheter aortic valve replacement in the United States, the overall mortality was 23.7%, the stroke rate was 4.1%, and the composite outcome of death and stroke was 26.0%, according to a report published online March 10 in JAMA.
Long-term outcomes for TAVR haven’t been well studied until now, yet the procedure is being performed with increasing frequency for aortic stenosis in patients who are too high risk to undergo conventional surgical aortic valve replacement, said Dr. David R. Holmes Jr. of the Mayo Clinic, Rochester, Minn., and his associates.
They assessed 1-year outcomes by analyzing administrative data from the Centers for Medicare & Medicaid Services and clinical data from the Transcatheter Valve Therapies Registry, an initiative of the Society of Thoracic Surgeons and the American College of Cardiology. The study involved 12,182 patients who underwent TAVR at 299 medical centers across the country during a 19-month period. The patients’ median age was 84 years; 95% were white and 52% were women. The transfemoral approach was used in most patients, but alternative approaches were used in roughly 44%. As expected for an elderly, high-risk study population, baseline functional status was poor and comorbidities were common. They included reduced left ventricular ejection fraction (26% of patients), prior stroke (12%), moderate or severe lung disease (28%), renal failure (16%), peripheral vascular disease (32%), and atrial fibrillation (42%), Dr. Holmes and his associates reported (JAMA 2015 March 10 [doi:10.1001/jama.2015.1474]).
In addition to the mortality and stroke rates listed above, the 1-year rate of one rehospitalization was 24.4%, that of two rehospitalizations was 12.5%, and that of three or more rehospitalizations was 11.6%. The 1-year readmission rate specifically for stroke, heart failure, or repeat aortic valve intervention was 18.6%. These are important considerations for elderly, fragile patients because rehospitalizations indicate “an unacceptable quality-of-life outcome” and are very costly, the investigators noted.
Several baseline characteristics, including male sex, severe chronic obstructive pulmonary disease, dialysis-dependent end-stage renal disease, older age, higher STS Predicted Risk of Operative Mortality (PROM) score, a history of atrial fibrillation/flutter, and use of an access route (other than transfemoral), were found to be independently associated with higher 1-year mortality. Thus, “It may be possible to identify patients who may not benefit from this procedure and who should be counseled accordingly.” For example, in this study there was a small (77 patients) very high-risk subset of patients – aged 85-94 years, dependent on dialysis, and having an STS PROM score greater than 15% – whose 1-year mortality was 53.5%.
The STS and the ACC supported this study, and support the Transcatheter Valve Therapies Registry. Dr. Holmes reported having no relevant financial disclosures; his associates reported ties to Boston Scientific, Edwards Lifesciences, Janssen, Eli Lilly, Boehringer Ingelheim, Bayer, and AstraZeneca.
FROM JAMA
Key clinical point: Severe chronic obstructive pulmonary disease, end-stage renal disease, older age, higher STS PROM score, and use of an access route (other than transfemoral) are among the baseline characteristics linked with higher 1-year mortality after TAVR.
Major finding: The overall mortality was 23.7%, the stroke rate was 4.1%, and the composite rate of death and stroke was 26% 1 year after TAVR.
Data source: An analysis of data from the Transcatheter Valve Therapies Registry for 12,182 patients who underwent TAVR procedures at 299 U.S. hospitals during a 19-month period.
Disclosures: The Society of Thoracic Surgeons and the American College of Cardiology supported this study, and support the Transcatheter Valve Therapies Registry. Dr. Holmes reported having no relevant financial disclosures; his associates reported ties to Boston Scientific, Edwards Lifesciences, Janssen, Eli Lilly, Boehringer Ingelheim, Bayer, and AstraZeneca.
Leadership 101: Basic skills for early-career hospitalists

Early career hospitalists may think leadership roles automatically yield more money and free time, Dr. Gundersen says. Actually, being a leader requires stamina and the ability to weather the ups and downs that come with the leadership role. For example, will you be able to handle situations in which your decisions make others unhappy?
Deliver on Promises
Honest self-assessment is one of the most critical elements in becoming a leader, agrees Steven Deitelzweig, MD, MMM, FACP, FSVMB, RVT, VPMA, system chairman of hospital medicine and medical director of regional business development for Ochsner Health System in the greater New Orleans area. In addition to having good interpersonal skills, showing enthusiasm, and promoting your organization sincerely—what Dr. Deitelzweig labels “emotional intelligence”—prospective leaders need to be cognizant of delivering on promises.
“This is something I call a high ‘say/do’ ratio,” he explains, “and, simply put, it means that you accomplish what you say you will. At the end of the day, the only way anybody moves up is by being good at achieving results.”
If you start missing deadlines, you communicate that you are not reliable. Not all project implementation goes according to plan, of course, so when you encounter difficulties, early communication about obstacles is also key, he says.
Nuts and Bolts
Through SHM’s Leadership Academy, hospitalists can be trained in team management and other key leadership skills. An October 2015 session is scheduled in Austin.
Having trusted mentors is crucial, agreed both physicians, so that you can keep polishing your skill set and obtain honest feedback. These mentors should not be people to whom you directly report, and they need not be in the healthcare industry.
In fact, Dr. Gundersen says he’s known mentors for years “who have not been in the same specialty or even the same field, but who give me guidance and have helped make me into the leader I am.”
How do you assert your desire to be a leader? Dr. Deitelzweig suggests making your aspirations clear to your own group leaders. The annual review is an excellent juncture at which to discuss this, he says.
If you do not yet have project management or communications experience, ask your leaders whether they are familiar with training to help you develop those skills. In the current healthcare environment, the Affordable Care Act and reimbursement regulations mean that change will continue to be part of the leadership challenge.
“If you really want to be a leader,” Dr. Deitelzweig says, “you cannot be a naysayer. Make change work for you, look at it as an opportunity for you to innovate, and then show how valuable you can be.”
Gretchen Henkel is a freelance writer in California.
Listen Now
Listen to Dr. Gundersen dive further into the importance of mentors and assessing your personal qualities to be a good leader.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/03/Gundersen_CareerCenter1_FINAL_012515.mp3"][/audio]
Early career hospitalists may think leadership roles automatically yield more money and free time, Dr. Gundersen says. Actually, being a leader requires stamina and the ability to weather the ups and downs that come with the leadership role. For example, will you be able to handle situations in which your decisions make others unhappy?
Deliver on Promises
Honest self-assessment is one of the most critical elements in becoming a leader, agrees Steven Deitelzweig, MD, MMM, FACP, FSVMB, RVT, VPMA, system chairman of hospital medicine and medical director of regional business development for Ochsner Health System in the greater New Orleans area. In addition to having good interpersonal skills, showing enthusiasm, and promoting your organization sincerely—what Dr. Deitelzweig labels “emotional intelligence”—prospective leaders need to be cognizant of delivering on promises.
“This is something I call a high ‘say/do’ ratio,” he explains, “and, simply put, it means that you accomplish what you say you will. At the end of the day, the only way anybody moves up is by being good at achieving results.”
If you start missing deadlines, you communicate that you are not reliable. Not all project implementation goes according to plan, of course, so when you encounter difficulties, early communication about obstacles is also key, he says.
Nuts and Bolts
Through SHM’s Leadership Academy, hospitalists can be trained in team management and other key leadership skills. An October 2015 session is scheduled in Austin.
Having trusted mentors is crucial, agreed both physicians, so that you can keep polishing your skill set and obtain honest feedback. These mentors should not be people to whom you directly report, and they need not be in the healthcare industry.
In fact, Dr. Gundersen says he’s known mentors for years “who have not been in the same specialty or even the same field, but who give me guidance and have helped make me into the leader I am.”
How do you assert your desire to be a leader? Dr. Deitelzweig suggests making your aspirations clear to your own group leaders. The annual review is an excellent juncture at which to discuss this, he says.
If you do not yet have project management or communications experience, ask your leaders whether they are familiar with training to help you develop those skills. In the current healthcare environment, the Affordable Care Act and reimbursement regulations mean that change will continue to be part of the leadership challenge.
“If you really want to be a leader,” Dr. Deitelzweig says, “you cannot be a naysayer. Make change work for you, look at it as an opportunity for you to innovate, and then show how valuable you can be.”
Gretchen Henkel is a freelance writer in California.
Listen Now
Listen to Dr. Gundersen dive further into the importance of mentors and assessing your personal qualities to be a good leader.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/03/Gundersen_CareerCenter1_FINAL_012515.mp3"][/audio]
Early career hospitalists may think leadership roles automatically yield more money and free time, Dr. Gundersen says. Actually, being a leader requires stamina and the ability to weather the ups and downs that come with the leadership role. For example, will you be able to handle situations in which your decisions make others unhappy?
Deliver on Promises
Honest self-assessment is one of the most critical elements in becoming a leader, agrees Steven Deitelzweig, MD, MMM, FACP, FSVMB, RVT, VPMA, system chairman of hospital medicine and medical director of regional business development for Ochsner Health System in the greater New Orleans area. In addition to having good interpersonal skills, showing enthusiasm, and promoting your organization sincerely—what Dr. Deitelzweig labels “emotional intelligence”—prospective leaders need to be cognizant of delivering on promises.
“This is something I call a high ‘say/do’ ratio,” he explains, “and, simply put, it means that you accomplish what you say you will. At the end of the day, the only way anybody moves up is by being good at achieving results.”
If you start missing deadlines, you communicate that you are not reliable. Not all project implementation goes according to plan, of course, so when you encounter difficulties, early communication about obstacles is also key, he says.
Nuts and Bolts
Through SHM’s Leadership Academy, hospitalists can be trained in team management and other key leadership skills. An October 2015 session is scheduled in Austin.
Having trusted mentors is crucial, agreed both physicians, so that you can keep polishing your skill set and obtain honest feedback. These mentors should not be people to whom you directly report, and they need not be in the healthcare industry.
In fact, Dr. Gundersen says he’s known mentors for years “who have not been in the same specialty or even the same field, but who give me guidance and have helped make me into the leader I am.”
How do you assert your desire to be a leader? Dr. Deitelzweig suggests making your aspirations clear to your own group leaders. The annual review is an excellent juncture at which to discuss this, he says.
If you do not yet have project management or communications experience, ask your leaders whether they are familiar with training to help you develop those skills. In the current healthcare environment, the Affordable Care Act and reimbursement regulations mean that change will continue to be part of the leadership challenge.
“If you really want to be a leader,” Dr. Deitelzweig says, “you cannot be a naysayer. Make change work for you, look at it as an opportunity for you to innovate, and then show how valuable you can be.”
Gretchen Henkel is a freelance writer in California.
Listen Now
Listen to Dr. Gundersen dive further into the importance of mentors and assessing your personal qualities to be a good leader.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/03/Gundersen_CareerCenter1_FINAL_012515.mp3"][/audio]

Federal Program to Cut Hospital Readmissions Turns Out Modest Results
A new report has found that only a small number of groups included in a government-funded experiment to cut Medicare readmissions actually produced results. However, the less-than-hoped-for results don't necessarily indicate failure, a hospitalist and readmissions expert says.
The Community-based Care Transitions Program (CCTP) is one of several test care-delivery models created by the Affordable Care Act. Its main goal is to improve transitions of Medicare patients from the hospital to community-based settings, such as nursing homes, rehabilitation facilities, and government agencies that provide services to the elderly, and thereby reduce readmissions.
However, a new report [PDF] commissioned by the Centers for Medicare & Medicaid Services found that only four CCTP groups of the 48 studied significantly cut readmissions compared with those of a control group. The report was finished in May 2014 but wasn't made public until January.
"There are so few examples in healthcare where resource alignment makes sense with what we believe are the ideal ways of practicing," says Jeffrey L. Greenwald, MD, associate professor of medicine at Harvard Medical School and a member of the Inpatient Clinician Educator Service at Massachusetts General Hospital, both in Boston. "Things like CCTP, where you have an opportunity to partner a hospital with a community-based organization that can help to support patient transitions still looks promising despite its warts."
CCTP, funded with $300 million over five years, signed its first round of deals with community agencies in late 2011. The report covered partial 2012 results from groups participating in the early rounds.
Dr. Greenwald is one of the cofounders of SHM's Project BOOST, a yearlong QI program in which hospital teams are paired with mentors to help them improve care transitions. He explained that BOOST teams typically need at least 18-24 months to show positive results on length-of-stay or readmissions reductions.
"These are long processes that don't turn around overnight," Dr. Greenwald adds. "If they do, it's probably because [the hospital team] put in place something that is not sustainable, and the minute they stop measuring and keeping an eye on it, it will likely deteriorate.
"There's no magic bullet in care transitions."
Visit our website for more information on ways hospitals can reduce readmissions.
A new report has found that only a small number of groups included in a government-funded experiment to cut Medicare readmissions actually produced results. However, the less-than-hoped-for results don't necessarily indicate failure, a hospitalist and readmissions expert says.
The Community-based Care Transitions Program (CCTP) is one of several test care-delivery models created by the Affordable Care Act. Its main goal is to improve transitions of Medicare patients from the hospital to community-based settings, such as nursing homes, rehabilitation facilities, and government agencies that provide services to the elderly, and thereby reduce readmissions.
However, a new report [PDF] commissioned by the Centers for Medicare & Medicaid Services found that only four CCTP groups of the 48 studied significantly cut readmissions compared with those of a control group. The report was finished in May 2014 but wasn't made public until January.
"There are so few examples in healthcare where resource alignment makes sense with what we believe are the ideal ways of practicing," says Jeffrey L. Greenwald, MD, associate professor of medicine at Harvard Medical School and a member of the Inpatient Clinician Educator Service at Massachusetts General Hospital, both in Boston. "Things like CCTP, where you have an opportunity to partner a hospital with a community-based organization that can help to support patient transitions still looks promising despite its warts."
CCTP, funded with $300 million over five years, signed its first round of deals with community agencies in late 2011. The report covered partial 2012 results from groups participating in the early rounds.
Dr. Greenwald is one of the cofounders of SHM's Project BOOST, a yearlong QI program in which hospital teams are paired with mentors to help them improve care transitions. He explained that BOOST teams typically need at least 18-24 months to show positive results on length-of-stay or readmissions reductions.
"These are long processes that don't turn around overnight," Dr. Greenwald adds. "If they do, it's probably because [the hospital team] put in place something that is not sustainable, and the minute they stop measuring and keeping an eye on it, it will likely deteriorate.
"There's no magic bullet in care transitions."
Visit our website for more information on ways hospitals can reduce readmissions.
A new report has found that only a small number of groups included in a government-funded experiment to cut Medicare readmissions actually produced results. However, the less-than-hoped-for results don't necessarily indicate failure, a hospitalist and readmissions expert says.
The Community-based Care Transitions Program (CCTP) is one of several test care-delivery models created by the Affordable Care Act. Its main goal is to improve transitions of Medicare patients from the hospital to community-based settings, such as nursing homes, rehabilitation facilities, and government agencies that provide services to the elderly, and thereby reduce readmissions.
However, a new report [PDF] commissioned by the Centers for Medicare & Medicaid Services found that only four CCTP groups of the 48 studied significantly cut readmissions compared with those of a control group. The report was finished in May 2014 but wasn't made public until January.
"There are so few examples in healthcare where resource alignment makes sense with what we believe are the ideal ways of practicing," says Jeffrey L. Greenwald, MD, associate professor of medicine at Harvard Medical School and a member of the Inpatient Clinician Educator Service at Massachusetts General Hospital, both in Boston. "Things like CCTP, where you have an opportunity to partner a hospital with a community-based organization that can help to support patient transitions still looks promising despite its warts."
CCTP, funded with $300 million over five years, signed its first round of deals with community agencies in late 2011. The report covered partial 2012 results from groups participating in the early rounds.
Dr. Greenwald is one of the cofounders of SHM's Project BOOST, a yearlong QI program in which hospital teams are paired with mentors to help them improve care transitions. He explained that BOOST teams typically need at least 18-24 months to show positive results on length-of-stay or readmissions reductions.
"These are long processes that don't turn around overnight," Dr. Greenwald adds. "If they do, it's probably because [the hospital team] put in place something that is not sustainable, and the minute they stop measuring and keeping an eye on it, it will likely deteriorate.
"There's no magic bullet in care transitions."
Visit our website for more information on ways hospitals can reduce readmissions.