User login
Combo can fight resistant lymphoma

Photo by Aaron Logan
Combining the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib with an anti-PD-L1 antibody can override resistance to ibrutinib, according to preclinical research.
Investigators found the combination of anti-PD-L1 and ibrutinib suppressed tumor growth in mouse models of lymphoma that are intrinsically insensitive to ibrutinib.
The combination also proved effective against 2 solid tumor malignancies—triple-negative breast cancer and colon cancer.
Ronald Levy, MD, of the Stanford University School of Medicine in California, and his colleagues described this work in PNAS.
The team first studied A20, a B-cell lymphoma in BALB/c mice that is insensitive to ibrutinib treatment even though A20 cells express BTK.
A20 cells also express high levels of PD-L1, so it follows that some of the mice responded to anti-PD-L1 treatment alone. However, the response eventually diminished over time.
When the investigators administered ibrutinib along with anti-PD-L1, half of the mice were cured. The other half experienced delays in tumor growth and prolonged survival.
Dr Levy and his colleagues also assessed ibrutinib plus anti-PD-L1 in 2 solid tumor models. They chose triple-negative breast cancer and colon cancer, which do not express BTK and have low levels of the PD-L1 protein.
When ibrutinib and the PD-L1 antibody were given as single agents, neither had any effect on tumor growth. However, combination treatment reduced the size of the primary tumors, improved survival, and resulted in fewer metastases in both breast and colon cancer.
In the case of the colon cancer model, approximately 30% of the mice were cured. The investigators decided to test whether these mice had developed long-term immune memory from the treatment.
So the team re-exposed the mice to colon cancer cells at 90 days post-cure. After 7 days of tumor growth, all the mice cleared the tumor by day 17 without any additional dosing of the ibrutinib and anti-PD-L1 combination.
“These findings are very encouraging and support our pursuit of a clinical development strategy that combines ibrutinib with anti-PD-L1 antibodies or other checkpoint inhibitors to maximize the effect that both drugs could have in treating cancer,” said Darrin Beaupre, MD, PhD, of Pharmacyclics, the company developing ibrutinib, which contributed funding for this research.
“Based on what we’ve seen preclinically, we are optimistic that combinations such as these may help to produce new treatment paradigms for patients with cancer.”
The investigators did not draw any conclusions about the safety of anti-PD-L1 and ibrutinib in combination.
They did note that both agents have been well-tolerated when given alone, but additional study of the combination is needed to fully understand the appropriate dosing, timing, and sequencing of combination treatment.
Investigators are planning clinical studies testing ibrutinib in combination with the anti-PD-L1 immune checkpoint inhibitor MEDI4736 (in hematologic and solid tumor malignancies) and with the PD-1-blocking antibody nivolumab (in hematologic malignancies). Enrollment is expected to begin in the coming months. ![]()
Photo by Aaron Logan
Combining the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib with an anti-PD-L1 antibody can override resistance to ibrutinib, according to preclinical research.
Investigators found the combination of anti-PD-L1 and ibrutinib suppressed tumor growth in mouse models of lymphoma that are intrinsically insensitive to ibrutinib.
The combination also proved effective against 2 solid tumor malignancies—triple-negative breast cancer and colon cancer.
Ronald Levy, MD, of the Stanford University School of Medicine in California, and his colleagues described this work in PNAS.
The team first studied A20, a B-cell lymphoma in BALB/c mice that is insensitive to ibrutinib treatment even though A20 cells express BTK.
A20 cells also express high levels of PD-L1, so it follows that some of the mice responded to anti-PD-L1 treatment alone. However, the response eventually diminished over time.
When the investigators administered ibrutinib along with anti-PD-L1, half of the mice were cured. The other half experienced delays in tumor growth and prolonged survival.
Dr Levy and his colleagues also assessed ibrutinib plus anti-PD-L1 in 2 solid tumor models. They chose triple-negative breast cancer and colon cancer, which do not express BTK and have low levels of the PD-L1 protein.
When ibrutinib and the PD-L1 antibody were given as single agents, neither had any effect on tumor growth. However, combination treatment reduced the size of the primary tumors, improved survival, and resulted in fewer metastases in both breast and colon cancer.
In the case of the colon cancer model, approximately 30% of the mice were cured. The investigators decided to test whether these mice had developed long-term immune memory from the treatment.
So the team re-exposed the mice to colon cancer cells at 90 days post-cure. After 7 days of tumor growth, all the mice cleared the tumor by day 17 without any additional dosing of the ibrutinib and anti-PD-L1 combination.
“These findings are very encouraging and support our pursuit of a clinical development strategy that combines ibrutinib with anti-PD-L1 antibodies or other checkpoint inhibitors to maximize the effect that both drugs could have in treating cancer,” said Darrin Beaupre, MD, PhD, of Pharmacyclics, the company developing ibrutinib, which contributed funding for this research.
“Based on what we’ve seen preclinically, we are optimistic that combinations such as these may help to produce new treatment paradigms for patients with cancer.”
The investigators did not draw any conclusions about the safety of anti-PD-L1 and ibrutinib in combination.
They did note that both agents have been well-tolerated when given alone, but additional study of the combination is needed to fully understand the appropriate dosing, timing, and sequencing of combination treatment.
Investigators are planning clinical studies testing ibrutinib in combination with the anti-PD-L1 immune checkpoint inhibitor MEDI4736 (in hematologic and solid tumor malignancies) and with the PD-1-blocking antibody nivolumab (in hematologic malignancies). Enrollment is expected to begin in the coming months. ![]()
Photo by Aaron Logan
Combining the Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib with an anti-PD-L1 antibody can override resistance to ibrutinib, according to preclinical research.
Investigators found the combination of anti-PD-L1 and ibrutinib suppressed tumor growth in mouse models of lymphoma that are intrinsically insensitive to ibrutinib.
The combination also proved effective against 2 solid tumor malignancies—triple-negative breast cancer and colon cancer.
Ronald Levy, MD, of the Stanford University School of Medicine in California, and his colleagues described this work in PNAS.
The team first studied A20, a B-cell lymphoma in BALB/c mice that is insensitive to ibrutinib treatment even though A20 cells express BTK.
A20 cells also express high levels of PD-L1, so it follows that some of the mice responded to anti-PD-L1 treatment alone. However, the response eventually diminished over time.
When the investigators administered ibrutinib along with anti-PD-L1, half of the mice were cured. The other half experienced delays in tumor growth and prolonged survival.
Dr Levy and his colleagues also assessed ibrutinib plus anti-PD-L1 in 2 solid tumor models. They chose triple-negative breast cancer and colon cancer, which do not express BTK and have low levels of the PD-L1 protein.
When ibrutinib and the PD-L1 antibody were given as single agents, neither had any effect on tumor growth. However, combination treatment reduced the size of the primary tumors, improved survival, and resulted in fewer metastases in both breast and colon cancer.
In the case of the colon cancer model, approximately 30% of the mice were cured. The investigators decided to test whether these mice had developed long-term immune memory from the treatment.
So the team re-exposed the mice to colon cancer cells at 90 days post-cure. After 7 days of tumor growth, all the mice cleared the tumor by day 17 without any additional dosing of the ibrutinib and anti-PD-L1 combination.
“These findings are very encouraging and support our pursuit of a clinical development strategy that combines ibrutinib with anti-PD-L1 antibodies or other checkpoint inhibitors to maximize the effect that both drugs could have in treating cancer,” said Darrin Beaupre, MD, PhD, of Pharmacyclics, the company developing ibrutinib, which contributed funding for this research.
“Based on what we’ve seen preclinically, we are optimistic that combinations such as these may help to produce new treatment paradigms for patients with cancer.”
The investigators did not draw any conclusions about the safety of anti-PD-L1 and ibrutinib in combination.
They did note that both agents have been well-tolerated when given alone, but additional study of the combination is needed to fully understand the appropriate dosing, timing, and sequencing of combination treatment.
Investigators are planning clinical studies testing ibrutinib in combination with the anti-PD-L1 immune checkpoint inhibitor MEDI4736 (in hematologic and solid tumor malignancies) and with the PD-1-blocking antibody nivolumab (in hematologic malignancies). Enrollment is expected to begin in the coming months. ![]()
Agent decreases use of pain meds in SCD patients

and a normal one
Image by Betty Pace
An investigational agent may be able to treat vaso-occlusive crises (VOC) in patients with sickle cell disease (SCD), according to research published in Blood.
The drug, rivipansel (formerly GMI-1070), is designed to prevent cells from sticking together to improve blood flow.
In a phase 2 study, SCD patients who received rivipansel used significantly less pain medication than those who received placebo.
However, rivipansel did not significantly reduce the time to resolution of VOC.
Researchers said the study’s small size, as well as the wide variability in the length of time that all patients suffered painful vascular obstruction, may explain the lack of statistical significance. A larger, international study is set to begin later this year to provide greater clarity.
“We have not had good therapies for people with [sickle cell] disease,” said study author Marilyn J. Telen, MD, of Duke University in Durham, North Carolina.
“But this approach shows more promise than anything else I’ve seen in 34 years of treating sickle cell disease.”
She and her colleagues analyzed 76 SCD patients from 17 sites in the US. The patients were randomized to receive placebo or rivipansel. All patients also received the standard treatment for pain and symptom management.
For patients who received rivipansel, the effects tended to begin within 24 hours, and their painful crises passed sooner than those receiving only treatment for pain, but the statistical difference was not significant.
The least-squares mean time to resolution of VOC was 103.64 hours in the rivipansel arm and 144.60 hours in the placebo arm (P=0.192). The median times were 69.6 hours and 132.9 hours, respectively (P=0.187).
The researchers said the improvements seen in the amount of time to resolution would likely be clinically meaningful if they were verified in a larger trial.
The team also said the findings demonstrating lower use of pain medication among patients was a critical step forward. The team assessed cumulative parenteral opioid use, and the least-squares mean dose was 9.62 mg/kg in the rivipansel arm and 55.59 mg/kg in the placebo arm (P=0.010).
“The difference in pain medication use was statistically significant, and it occurred in the first 24 hours, which implies that the therapy may be interfering with the mechanism of the vaso-occlusion,” Dr Telen said. “For these patients, having less pain is very important.”
In addition, there were no significant differences between the treatment arms with regard to adverse events.
Dr Telen said the larger study of rivipansel is set to begin later this year, with a goal of enrolling more than 300 patients.
The company developing rivipansel, GlycoMimetics, Inc., funded the current study. And Dr Telen has received consulting fees from the company. ![]()
and a normal one
Image by Betty Pace
An investigational agent may be able to treat vaso-occlusive crises (VOC) in patients with sickle cell disease (SCD), according to research published in Blood.
The drug, rivipansel (formerly GMI-1070), is designed to prevent cells from sticking together to improve blood flow.
In a phase 2 study, SCD patients who received rivipansel used significantly less pain medication than those who received placebo.
However, rivipansel did not significantly reduce the time to resolution of VOC.
Researchers said the study’s small size, as well as the wide variability in the length of time that all patients suffered painful vascular obstruction, may explain the lack of statistical significance. A larger, international study is set to begin later this year to provide greater clarity.
“We have not had good therapies for people with [sickle cell] disease,” said study author Marilyn J. Telen, MD, of Duke University in Durham, North Carolina.
“But this approach shows more promise than anything else I’ve seen in 34 years of treating sickle cell disease.”
She and her colleagues analyzed 76 SCD patients from 17 sites in the US. The patients were randomized to receive placebo or rivipansel. All patients also received the standard treatment for pain and symptom management.
For patients who received rivipansel, the effects tended to begin within 24 hours, and their painful crises passed sooner than those receiving only treatment for pain, but the statistical difference was not significant.
The least-squares mean time to resolution of VOC was 103.64 hours in the rivipansel arm and 144.60 hours in the placebo arm (P=0.192). The median times were 69.6 hours and 132.9 hours, respectively (P=0.187).
The researchers said the improvements seen in the amount of time to resolution would likely be clinically meaningful if they were verified in a larger trial.
The team also said the findings demonstrating lower use of pain medication among patients was a critical step forward. The team assessed cumulative parenteral opioid use, and the least-squares mean dose was 9.62 mg/kg in the rivipansel arm and 55.59 mg/kg in the placebo arm (P=0.010).
“The difference in pain medication use was statistically significant, and it occurred in the first 24 hours, which implies that the therapy may be interfering with the mechanism of the vaso-occlusion,” Dr Telen said. “For these patients, having less pain is very important.”
In addition, there were no significant differences between the treatment arms with regard to adverse events.
Dr Telen said the larger study of rivipansel is set to begin later this year, with a goal of enrolling more than 300 patients.
The company developing rivipansel, GlycoMimetics, Inc., funded the current study. And Dr Telen has received consulting fees from the company. ![]()
and a normal one
Image by Betty Pace
An investigational agent may be able to treat vaso-occlusive crises (VOC) in patients with sickle cell disease (SCD), according to research published in Blood.
The drug, rivipansel (formerly GMI-1070), is designed to prevent cells from sticking together to improve blood flow.
In a phase 2 study, SCD patients who received rivipansel used significantly less pain medication than those who received placebo.
However, rivipansel did not significantly reduce the time to resolution of VOC.
Researchers said the study’s small size, as well as the wide variability in the length of time that all patients suffered painful vascular obstruction, may explain the lack of statistical significance. A larger, international study is set to begin later this year to provide greater clarity.
“We have not had good therapies for people with [sickle cell] disease,” said study author Marilyn J. Telen, MD, of Duke University in Durham, North Carolina.
“But this approach shows more promise than anything else I’ve seen in 34 years of treating sickle cell disease.”
She and her colleagues analyzed 76 SCD patients from 17 sites in the US. The patients were randomized to receive placebo or rivipansel. All patients also received the standard treatment for pain and symptom management.
For patients who received rivipansel, the effects tended to begin within 24 hours, and their painful crises passed sooner than those receiving only treatment for pain, but the statistical difference was not significant.
The least-squares mean time to resolution of VOC was 103.64 hours in the rivipansel arm and 144.60 hours in the placebo arm (P=0.192). The median times were 69.6 hours and 132.9 hours, respectively (P=0.187).
The researchers said the improvements seen in the amount of time to resolution would likely be clinically meaningful if they were verified in a larger trial.
The team also said the findings demonstrating lower use of pain medication among patients was a critical step forward. The team assessed cumulative parenteral opioid use, and the least-squares mean dose was 9.62 mg/kg in the rivipansel arm and 55.59 mg/kg in the placebo arm (P=0.010).
“The difference in pain medication use was statistically significant, and it occurred in the first 24 hours, which implies that the therapy may be interfering with the mechanism of the vaso-occlusion,” Dr Telen said. “For these patients, having less pain is very important.”
In addition, there were no significant differences between the treatment arms with regard to adverse events.
Dr Telen said the larger study of rivipansel is set to begin later this year, with a goal of enrolling more than 300 patients.
The company developing rivipansel, GlycoMimetics, Inc., funded the current study. And Dr Telen has received consulting fees from the company. ![]()
Clinical follow-up data promising for EVAR in AAA with angulated aortic neck
SCOTTSDALE, ARIZ. – Endovascular abdominal aortic aneurysm repair using a flexible endovascular stent graft in patients with infrarenal aortic neck angles of sixty degrees or greater had more favorable survival and major adverse event rates when compared with open repair, although the difference was not statistically significant, according to clinical, 2-year, postmarketing data.

At this year’s annual Southern Association for Vascular Surgery meeting, Dr. Mahmoud B. Malas presented 2-year safety and efficacy follow-up data from the PYTHAGORAS trial to evaluate the Aorfix (Lombard Medical, U.K.). The device, approved in 2013 by the Food and Drug Administration, is an endovascular stent graft for use in patients whose aortic neck angulation of between 60 and 90 degrees typically has disqualified them from having endovascular aneurysm repair (EVAR) for AAA.
The device is placed within the aneurysm, where it conforms to the individual patient’s anatomy, creating an internal bypass of the aneurysm to reduce the risk of rupture.
“The freedom from major adverse events, despite this hostile neck anatomy, was excellent,” Dr. Malas said of the data.
The PYTHAGORAS study enrolled and treated 151 patients with aortic neck angles of 60 degrees or greater, and 67 patients with necks less than 60 degrees using EVAR. The primary control group consisted of 67 patients undergoing actual open surgical repair (OSR). A secondary control group was a meta-analysis of 323 patients taken from other U.S. EVAR studies (SVS Lifeline).
There were no statistically significant differences between major adverse event rates, nor 30-day and 1-year mortality rates between low- or high-angle EVAR groups when compared with controls. There also was no difference between low- and high-angle EVAR patients sac shrinkage, type I/III endoleaks, and endograft migration, according to Dr. Malas.
The median neck angle in the EVAR group was 71 degrees (standard deviation of ±23 degrees; P < .05), compared with 48 degrees (SD, ± 23 degrees; P < .05) in the OSR control group. There were twice as many women in the EVAR group (35% vs.17%; P < .0001). Patient demographics and comorbidities were similar between the entire EVAR cohort and control group, with the exception of age (76 years vs. 70 years, respectively; P < .05) and heart failure (13% vs. 7%, P = .015). Operative data favored EVAR for procedure duration, blood loss, and hospital length of stay (P < .05 for all).
Dr. Malas said that in the combined EVAR cohort, there was a tendency for the infrarenal area to dilate more rapidly than the suprarenal aorta. “If the neck dilated more than 10%, there was a significant increase in risk of migration and sac expansion, especially close to the renal, but it was not true as you went beyond 7 mm distal to the renal.”
He also noted that the suprarenal aorta does change in association with migration and that there is a “clear association between the degree of oversizing and neck dilation.”
The presentation’s discussant, Dr. Jean M. Panneton, a vascular surgeon at Sentara Heart Hospital in Norfolk, Va., challenged the findings.
“Unfortunately, this trial did suffer from a slow accrual. As a result, only a small proportion of patients have reached the 5-year follow-up, and any subanalysis of such a small study population divided into three groups reduces the n value to the point that a type II error can easily be introduced into your analysis.”
Among the issues he raised was that the mortality data at 30 days, 1 year, and 2 years for the patients with the highest neck angulations could be misleading. “The patients in this group had a threefold increase [in mortality] compared with the standard group. Could this difference have been significant with a larger number?”
To overcome the lack of follow-up time, Dr. Malas said he and his colleagues used statistical modeling that gave them 500 data points on which they based their analysis.
Dr. Panneton also wondered if in the realm of EVAR AAA outside of the study, patients whose aortic neck lengths he said would average between 10 and 15 mm, would enjoy the same success rates as those EVAR patients in the study whose median aortic neck size was 20 mm-25 mm. “Do you think that this long seal zone accounted partially for the performance of the Aorfix? And will this performance hold up in real life?”
Dr. Malas responded that the investigators mandated at least a 15-mm neck for patients in the EVAR arms “because the way the seal zone is in a severely angulated neck means the effective seal zone will be on the inner curve of the neck, which might end up being only 4 or 5 mm, even if you have a 15-mm neck. So, it is very important to get the message out that if you’re going to use the Aorfix in a standard neck – less than 60 degrees – that you have zero migration. If you’re going to place this at a 90-degree angle, it’s very important you do not put it in a patient who doesn’t have a 15-mm neck.”
Dr. Mahmoud was one of the lead site investigators for the PYTHAGORAS trial, sponsored by Lombard Medical.
On Twitter @whitneymcknight
SCOTTSDALE, ARIZ. – Endovascular abdominal aortic aneurysm repair using a flexible endovascular stent graft in patients with infrarenal aortic neck angles of sixty degrees or greater had more favorable survival and major adverse event rates when compared with open repair, although the difference was not statistically significant, according to clinical, 2-year, postmarketing data.
At this year’s annual Southern Association for Vascular Surgery meeting, Dr. Mahmoud B. Malas presented 2-year safety and efficacy follow-up data from the PYTHAGORAS trial to evaluate the Aorfix (Lombard Medical, U.K.). The device, approved in 2013 by the Food and Drug Administration, is an endovascular stent graft for use in patients whose aortic neck angulation of between 60 and 90 degrees typically has disqualified them from having endovascular aneurysm repair (EVAR) for AAA.
The device is placed within the aneurysm, where it conforms to the individual patient’s anatomy, creating an internal bypass of the aneurysm to reduce the risk of rupture.
“The freedom from major adverse events, despite this hostile neck anatomy, was excellent,” Dr. Malas said of the data.
The PYTHAGORAS study enrolled and treated 151 patients with aortic neck angles of 60 degrees or greater, and 67 patients with necks less than 60 degrees using EVAR. The primary control group consisted of 67 patients undergoing actual open surgical repair (OSR). A secondary control group was a meta-analysis of 323 patients taken from other U.S. EVAR studies (SVS Lifeline).
There were no statistically significant differences between major adverse event rates, nor 30-day and 1-year mortality rates between low- or high-angle EVAR groups when compared with controls. There also was no difference between low- and high-angle EVAR patients sac shrinkage, type I/III endoleaks, and endograft migration, according to Dr. Malas.
The median neck angle in the EVAR group was 71 degrees (standard deviation of ±23 degrees; P < .05), compared with 48 degrees (SD, ± 23 degrees; P < .05) in the OSR control group. There were twice as many women in the EVAR group (35% vs.17%; P < .0001). Patient demographics and comorbidities were similar between the entire EVAR cohort and control group, with the exception of age (76 years vs. 70 years, respectively; P < .05) and heart failure (13% vs. 7%, P = .015). Operative data favored EVAR for procedure duration, blood loss, and hospital length of stay (P < .05 for all).
Dr. Malas said that in the combined EVAR cohort, there was a tendency for the infrarenal area to dilate more rapidly than the suprarenal aorta. “If the neck dilated more than 10%, there was a significant increase in risk of migration and sac expansion, especially close to the renal, but it was not true as you went beyond 7 mm distal to the renal.”
He also noted that the suprarenal aorta does change in association with migration and that there is a “clear association between the degree of oversizing and neck dilation.”
The presentation’s discussant, Dr. Jean M. Panneton, a vascular surgeon at Sentara Heart Hospital in Norfolk, Va., challenged the findings.
“Unfortunately, this trial did suffer from a slow accrual. As a result, only a small proportion of patients have reached the 5-year follow-up, and any subanalysis of such a small study population divided into three groups reduces the n value to the point that a type II error can easily be introduced into your analysis.”
Among the issues he raised was that the mortality data at 30 days, 1 year, and 2 years for the patients with the highest neck angulations could be misleading. “The patients in this group had a threefold increase [in mortality] compared with the standard group. Could this difference have been significant with a larger number?”
To overcome the lack of follow-up time, Dr. Malas said he and his colleagues used statistical modeling that gave them 500 data points on which they based their analysis.
Dr. Panneton also wondered if in the realm of EVAR AAA outside of the study, patients whose aortic neck lengths he said would average between 10 and 15 mm, would enjoy the same success rates as those EVAR patients in the study whose median aortic neck size was 20 mm-25 mm. “Do you think that this long seal zone accounted partially for the performance of the Aorfix? And will this performance hold up in real life?”
Dr. Malas responded that the investigators mandated at least a 15-mm neck for patients in the EVAR arms “because the way the seal zone is in a severely angulated neck means the effective seal zone will be on the inner curve of the neck, which might end up being only 4 or 5 mm, even if you have a 15-mm neck. So, it is very important to get the message out that if you’re going to use the Aorfix in a standard neck – less than 60 degrees – that you have zero migration. If you’re going to place this at a 90-degree angle, it’s very important you do not put it in a patient who doesn’t have a 15-mm neck.”
Dr. Mahmoud was one of the lead site investigators for the PYTHAGORAS trial, sponsored by Lombard Medical.
On Twitter @whitneymcknight
SCOTTSDALE, ARIZ. – Endovascular abdominal aortic aneurysm repair using a flexible endovascular stent graft in patients with infrarenal aortic neck angles of sixty degrees or greater had more favorable survival and major adverse event rates when compared with open repair, although the difference was not statistically significant, according to clinical, 2-year, postmarketing data.
At this year’s annual Southern Association for Vascular Surgery meeting, Dr. Mahmoud B. Malas presented 2-year safety and efficacy follow-up data from the PYTHAGORAS trial to evaluate the Aorfix (Lombard Medical, U.K.). The device, approved in 2013 by the Food and Drug Administration, is an endovascular stent graft for use in patients whose aortic neck angulation of between 60 and 90 degrees typically has disqualified them from having endovascular aneurysm repair (EVAR) for AAA.
The device is placed within the aneurysm, where it conforms to the individual patient’s anatomy, creating an internal bypass of the aneurysm to reduce the risk of rupture.
“The freedom from major adverse events, despite this hostile neck anatomy, was excellent,” Dr. Malas said of the data.
The PYTHAGORAS study enrolled and treated 151 patients with aortic neck angles of 60 degrees or greater, and 67 patients with necks less than 60 degrees using EVAR. The primary control group consisted of 67 patients undergoing actual open surgical repair (OSR). A secondary control group was a meta-analysis of 323 patients taken from other U.S. EVAR studies (SVS Lifeline).
There were no statistically significant differences between major adverse event rates, nor 30-day and 1-year mortality rates between low- or high-angle EVAR groups when compared with controls. There also was no difference between low- and high-angle EVAR patients sac shrinkage, type I/III endoleaks, and endograft migration, according to Dr. Malas.
The median neck angle in the EVAR group was 71 degrees (standard deviation of ±23 degrees; P < .05), compared with 48 degrees (SD, ± 23 degrees; P < .05) in the OSR control group. There were twice as many women in the EVAR group (35% vs.17%; P < .0001). Patient demographics and comorbidities were similar between the entire EVAR cohort and control group, with the exception of age (76 years vs. 70 years, respectively; P < .05) and heart failure (13% vs. 7%, P = .015). Operative data favored EVAR for procedure duration, blood loss, and hospital length of stay (P < .05 for all).
Dr. Malas said that in the combined EVAR cohort, there was a tendency for the infrarenal area to dilate more rapidly than the suprarenal aorta. “If the neck dilated more than 10%, there was a significant increase in risk of migration and sac expansion, especially close to the renal, but it was not true as you went beyond 7 mm distal to the renal.”
He also noted that the suprarenal aorta does change in association with migration and that there is a “clear association between the degree of oversizing and neck dilation.”
The presentation’s discussant, Dr. Jean M. Panneton, a vascular surgeon at Sentara Heart Hospital in Norfolk, Va., challenged the findings.
“Unfortunately, this trial did suffer from a slow accrual. As a result, only a small proportion of patients have reached the 5-year follow-up, and any subanalysis of such a small study population divided into three groups reduces the n value to the point that a type II error can easily be introduced into your analysis.”
Among the issues he raised was that the mortality data at 30 days, 1 year, and 2 years for the patients with the highest neck angulations could be misleading. “The patients in this group had a threefold increase [in mortality] compared with the standard group. Could this difference have been significant with a larger number?”
To overcome the lack of follow-up time, Dr. Malas said he and his colleagues used statistical modeling that gave them 500 data points on which they based their analysis.
Dr. Panneton also wondered if in the realm of EVAR AAA outside of the study, patients whose aortic neck lengths he said would average between 10 and 15 mm, would enjoy the same success rates as those EVAR patients in the study whose median aortic neck size was 20 mm-25 mm. “Do you think that this long seal zone accounted partially for the performance of the Aorfix? And will this performance hold up in real life?”
Dr. Malas responded that the investigators mandated at least a 15-mm neck for patients in the EVAR arms “because the way the seal zone is in a severely angulated neck means the effective seal zone will be on the inner curve of the neck, which might end up being only 4 or 5 mm, even if you have a 15-mm neck. So, it is very important to get the message out that if you’re going to use the Aorfix in a standard neck – less than 60 degrees – that you have zero migration. If you’re going to place this at a 90-degree angle, it’s very important you do not put it in a patient who doesn’t have a 15-mm neck.”
Dr. Mahmoud was one of the lead site investigators for the PYTHAGORAS trial, sponsored by Lombard Medical.
On Twitter @whitneymcknight
AT THE SAVS ANNUAL MEETING 2015
Key clinical point: AAA patients with 60 degree or greater aortic neck angles may benefit from EVAR with flexible stent graft instead of open surgical repair.
Major finding: There was no statistical difference in rates of major adverse events between open repair and EVAR in AAA patients with a 60-90 degree aortic neck angulation .
Data source: Postmarketing safety and efficacy data from the controlled, prospective, nonrandomized, multicenter PYTHAGORAS study of 218 patients.
Disclosures: Dr. Mahmoud was one of the lead site investigators for the PYTHAGORAS trial, sponsored by Lombard Medical.

POINT/COUNTERPOINT: Renal artery occlusive disease – To treat or not to treat? ASTRAL and CORAL trials show no indication to treat percutaneously. There are still indications to treat renal artery occlusive disease.
Percutaneous treatment of renal artery occlusive disease is unnecessary and should be abandoned, except in pediatric cases.
BY GEORGE HAMILTON, M.D.
This position is supported by findings from both the ASTRAL trial (N. Engl. J. Med. 2009;361:1953-62) and the CORAL trial (N. Engl. J. Med. 2013 Nov. 18 [doi:10.1056/NEJMoa1310753]).
The ASTRAL trial, a prospective, randomized comparison of best medical therapy with and without stent angioplasty in more than 800 patients, was the largest trial to date when it began back in the 1990s. The well-known results showed no difference in time to first renal event, first vascular and cardiovascular events, and overall survival. Furthermore, there was no difference in these outcomes among patients with greater than 90% stenosis, with the exception of a possible difference in mortality, which trended toward improvement among those with high-grade stenosis.
We concluded that revascularization in the vast majority of patients is unlikely to improve hypertension control or renal function, and that renal artery stenosis is not pathophysiologically important. We also concluded that there is no point in screening for asymptomatic disease; this was back when every patient was getting screened, and treated primarily on the basis of finding a renal arterial stenosis.
Finally, we concluded that properly applied best medical therapy alone was an extremely good treatment.
Several flaws in the trial garnered extensive criticism, however, and the more rigidly designed CORAL trial was expected to address them. The findings confirmed those of the ASTRAL trial. In more than 900 patients from 88 centers, there was absolutely no benefit of intervention with respect to primary and secondary outcomes, including among those with high-grade stenosis.
We can now see on the basis of extensive level 1 evidence that when added to comprehensive, multifactorial medical therapy, intervention yielded no benefit.
So are there certain patient groups who might benefit more from intervention? Among listed indications are high-grade stenosis (which doesn’t apply any longer); short history of progressive failure (which is quite rare); ACE-induced renal failure (which is also quite rare); difficult-to-control hypertension (there really is no such thing now, except in a tiny percentage of patients); and – the least challenged indication – flash pulmonary edema. These remaining indications move our interventions into a very high risk group of patients.
The current debate is focused almost entirely on endovascular intervention, but a systematic review showed that there is long-term benefit in terms of renal function and hypertension with open procedures. Although overall there is increased mortality, this risk is minimized – and not significantly different from endovascular procedures – in those having only renal revascularization vs. those having concomitant aortic procedures. So open surgery remains a possible treatment option, indeed a recent level 1 study comparing stenting and open surgery, showed better long-term results with open surgery (J. Vasc. Surg. 2009;49:667-75). The authors concluded that surgical reconstruction remains the gold standard in treating renal artery stenosis. Although national data suggest an overall mortality of about 10%, it is much lower at specialist, high-volume centers with mortality rates similar to those of stent angioplasty.
Renal stenting is not a low-risk procedure. In all-comers the complication rates, serious complication rates, and mortality rates are significant with short-term equivalence between focused renal arterial surgery and percutaneous intervention.
Returning to the debate, are either methods of revascularization appropriate? Probably not.
Even in flash pulmonary edema, there is little evidence to support revascularization. Few papers exist suggesting a benefit of revascularization in reduction of flash pulmonary edema, but the patient numbers were small, and there was no benefit in terms of preservation of renal function.
The history of evolution and evaluation of the role of renal revascularization is remarkably similar to that of renal denervation, initially and with considerable conviction thought to be a cure for hypertension. However, when properly assessed by prospective randomized comparison there was found to be absolutely no benefit.
So, given the considerable objective evidence from two major trials and revisiting the basics of the pathophysiology of atherosclerotic renovascular disease, to expect benefit from treating the osteal component of renal artery occlusive disease is at best naive, in my opinion. There remains little clinical evidence of benefit for any indication, with the possible exceptions of ACE-induced renal failure and possibly flash pulmonary edema in the presence of bilateral renal arterial stenoses.
Dr. Hamilton is a professor at the Royal Free London Hospital, University College London, United Kingdom.
There are still indications to treat renal artery occlusive disease
BY MATTHEW A. CORRIERE, M.D.
Although renal artery revascularization has been grossly overutilized and is not indicated in the majority of patients with renal artery stenosis, I perform renal artery revascularization as part of my routine clinical practice and believe that there are many instances where revascularization should be considered, particularly when patients have severe symptoms despite aggressive medical therapy. While neither ASTRAL nor CORAL observed any benefit associated with revascularization, both have important limitations that should be kept in mind when interpreting the results of these trials.
These limitations can be broadly categorized as mismatch between indications for revascularization and clinical endpoints, selection biases favoring enrollment of patients with relatively mild symptoms, and inconsistencies between study protocols and contemporary decision-making strategies.
Given that ASTRAL’s primary outcome was change in renal function (defined by a 20% or greater reduction in the mean slope of the reciprocal of serum creatinine), it is important to remember that the inclusion criteria were renal artery stenosis with unexplained renal dysfunction or poorly controlled hypertension. Patients who had hypertension in the absence of significant renal dysfunction were therefore eligible, and 40% of the randomized participants had preserved baseline renal function (based on a serum creatinine of < 150 micromol/liter). Unlike patients with baseline renal dysfunction (which, in theory, might improve with revascularization), these patients with normal renal function who were treated with revascularization risked decline in renal function resulting from procedure-related adverse events without any real chance of renal function improvement. It would certainly be difficult to justify revascularization for the sake of renal function salvage in these patients, and their inclusion within a randomized trial with change in renal function as its primary outcome is problematic for the same reason.
ASTRAL also had an additional, somewhat unorthodox inclusion criterion: uncertainty on the part of the treating physician that the patient “definitely would have a worthwhile clinical benefit from revascularization.” Exclusion of patients considered likely to benefit from revascularization would seem to ensure a selection bias favoring the null hypothesis; this approach may also explain the large proportion of participants with relatively mild occlusive disease (40% had stenotic lesions that were < 70% in severity).
A high rate of both technical failure (12%) and adverse events (20%) associated with revascularization, asymmetric crossover between treatment groups (86 of the 110 patients who did not receive their randomized intervention were in the revascularization group), and lack of standardized protocol for medical therapy further limit the conclusions that can be drawn from the ASTRAL results.
Although this trial does not provide us with compelling evidence that renal revascularization should be abandoned for patients failing appropriate medical therapy, ASTRAL demonstrated that no benefit should be expected from nonselective use of revascularization, which can be associated with significant rates of both technical failure and major adverse events.
The CORAL trial overcame many of the design limitations for which ASTRAL drew criticism. CORAL’s primary endpoint (freedom from major adverse cardiovascular or renal events) allowed potential benefit for participants with either systolic hypertension or chronic kidney disease as their indication for treatment. Although participants with systolic hypertension as their inclusion criterion had to be on at least two antihypertensive medications, it is important to acknowledge the growing number of indications for these medications related to cardiovascular risk reduction in the setting of diabetes, heart disease, and other diagnoses that may be unrelated to any specific blood pressure target. Number of antihypertensive medications is therefore often a crude and potentially invalid indicator of hypertension severity or control.
In CORAL, the initial hypertension inclusion criterion of 155 mm Hg was subsequently abandoned during the trial, suggesting that hypertension in many of these patients may have been mild and/or well controlled. Although medical therapy in CORAL was standardized, it also is notable that all patients had their medical therapy adjusted prior to randomization during a roll-in phase to achieve target blood pressure goals of 130/80 in patients with CKD and/or diabetes or 140/90 otherwise. I would suggest that achievement of these blood pressure targets on the study medications (candesartan ± hydrochlorothiazide plus amlodipine-atorvastatin) might be appropriately considered success of medical therapy for patients with hypertension in the absence of renal dysfunction, making it challenging to defend proceeding with revascularization in this scenario.
The study protocol, although well designed from the perspective of attempting to isolate the effect of renal artery angioplasty and stenting, therefore did not uniformly reflect what would be considered responsible utilization of renal revascularization in a real-world environment.
Patient enrollment in CORAL was also very selective; only 947 of the 5,322 patients who were screened went on to be enrolled and randomized. It is likely that at least some of those patients who were not enrolled (especially those who declined to participate or were withdrawn by their physicians) were failing aggressive medical therapy and therefore unwilling to being excluded from angioplasty and stenting through randomization. These limitations aside, however, CORAL does provide some very useful observations that should inform treatment decisions. The results demonstrate the efficacy of contemporary medical therapy for many patients, and show that revascularization offers no additional benefit when medical therapy achieves an acceptable clinical response (defined by stable renal function and reasonable blood pressure control). Additional subgroup analyses of the CORAL data are anticipated, but will likely be underpowered to draw conclusions in the absence of identified revascularization effects.
So when should revascularization be considered for patients with atherosclerotic renal artery stenosis? In general, medical therapy is adequate for most patients and should be implemented prior to any consideration of procedural intervention. Revascularization should be considered only for patients who have failed appropriate, aggressive medical therapy; the medications used in CORAL can certainly be regarded as adequate initial therapy for symptomatic renal artery stenosis, but many providers (including myself) would argue that additional agents should be considered before proceeding with revascularization.
When decline in renal function is the indication for considering revascularization, alternative causes (such as intrinsic renal disease) should diminish enthusiasm for proceeding with angioplasty and stenting, particularly when the anatomic disease distribution does not affect the entire renal mass (as in patients with two kidneys and unilateral stenosis). Appropriate candidates for revascularization include patients with severely impaired renal function (particularly in the setting of a precipitous functional decline) or severe acute blood pressure elevation associated with hypertensive emergency (such as acute congestive heart failure, encephalopathy, acute coronary syndrome, or other signs and symptoms of target organ damage resulting from hypertension and/or volume overload). Continuation of failed medical therapy is often unacceptable to these “no-options” patients as well as their providers, both of whom presumably would be unlikely to accept randomization to ongoing medical management.
Other populations that are not represented within these trials include patients with renal artery restenosis and those with nonatherosclerotic disease; it is therefore important to exercise caution when generalizing these study results to these distinct groups of patients. Enrolling patients with severe symptoms who have failed medical therapy will likely remain challenging for future randomized studies in the absence of alternative treatment options. Although the benefits of renal angioplasty and stenting for these “no-options” patients remain to be proved, the uncertainty of response to revascularization is often easier to accept than the ongoing morbidity and mortality associated with staying the course when medical therapy has failed.
Dr. Matthew A. Corriere is a vascular surgeon at Wake Forest University School of Medicine, Winston-Salem, N.C.
This article developed from a debate held at the 2014 Vascular Annual Meeting.
Percutaneous treatment of renal artery occlusive disease is unnecessary and should be abandoned, except in pediatric cases.
BY GEORGE HAMILTON, M.D.
This position is supported by findings from both the ASTRAL trial (N. Engl. J. Med. 2009;361:1953-62) and the CORAL trial (N. Engl. J. Med. 2013 Nov. 18 [doi:10.1056/NEJMoa1310753]).
The ASTRAL trial, a prospective, randomized comparison of best medical therapy with and without stent angioplasty in more than 800 patients, was the largest trial to date when it began back in the 1990s. The well-known results showed no difference in time to first renal event, first vascular and cardiovascular events, and overall survival. Furthermore, there was no difference in these outcomes among patients with greater than 90% stenosis, with the exception of a possible difference in mortality, which trended toward improvement among those with high-grade stenosis.
We concluded that revascularization in the vast majority of patients is unlikely to improve hypertension control or renal function, and that renal artery stenosis is not pathophysiologically important. We also concluded that there is no point in screening for asymptomatic disease; this was back when every patient was getting screened, and treated primarily on the basis of finding a renal arterial stenosis.
Finally, we concluded that properly applied best medical therapy alone was an extremely good treatment.
Several flaws in the trial garnered extensive criticism, however, and the more rigidly designed CORAL trial was expected to address them. The findings confirmed those of the ASTRAL trial. In more than 900 patients from 88 centers, there was absolutely no benefit of intervention with respect to primary and secondary outcomes, including among those with high-grade stenosis.
We can now see on the basis of extensive level 1 evidence that when added to comprehensive, multifactorial medical therapy, intervention yielded no benefit.
So are there certain patient groups who might benefit more from intervention? Among listed indications are high-grade stenosis (which doesn’t apply any longer); short history of progressive failure (which is quite rare); ACE-induced renal failure (which is also quite rare); difficult-to-control hypertension (there really is no such thing now, except in a tiny percentage of patients); and – the least challenged indication – flash pulmonary edema. These remaining indications move our interventions into a very high risk group of patients.
The current debate is focused almost entirely on endovascular intervention, but a systematic review showed that there is long-term benefit in terms of renal function and hypertension with open procedures. Although overall there is increased mortality, this risk is minimized – and not significantly different from endovascular procedures – in those having only renal revascularization vs. those having concomitant aortic procedures. So open surgery remains a possible treatment option, indeed a recent level 1 study comparing stenting and open surgery, showed better long-term results with open surgery (J. Vasc. Surg. 2009;49:667-75). The authors concluded that surgical reconstruction remains the gold standard in treating renal artery stenosis. Although national data suggest an overall mortality of about 10%, it is much lower at specialist, high-volume centers with mortality rates similar to those of stent angioplasty.
Renal stenting is not a low-risk procedure. In all-comers the complication rates, serious complication rates, and mortality rates are significant with short-term equivalence between focused renal arterial surgery and percutaneous intervention.
Returning to the debate, are either methods of revascularization appropriate? Probably not.
Even in flash pulmonary edema, there is little evidence to support revascularization. Few papers exist suggesting a benefit of revascularization in reduction of flash pulmonary edema, but the patient numbers were small, and there was no benefit in terms of preservation of renal function.
The history of evolution and evaluation of the role of renal revascularization is remarkably similar to that of renal denervation, initially and with considerable conviction thought to be a cure for hypertension. However, when properly assessed by prospective randomized comparison there was found to be absolutely no benefit.
So, given the considerable objective evidence from two major trials and revisiting the basics of the pathophysiology of atherosclerotic renovascular disease, to expect benefit from treating the osteal component of renal artery occlusive disease is at best naive, in my opinion. There remains little clinical evidence of benefit for any indication, with the possible exceptions of ACE-induced renal failure and possibly flash pulmonary edema in the presence of bilateral renal arterial stenoses.
Dr. Hamilton is a professor at the Royal Free London Hospital, University College London, United Kingdom.
There are still indications to treat renal artery occlusive disease
BY MATTHEW A. CORRIERE, M.D.
Although renal artery revascularization has been grossly overutilized and is not indicated in the majority of patients with renal artery stenosis, I perform renal artery revascularization as part of my routine clinical practice and believe that there are many instances where revascularization should be considered, particularly when patients have severe symptoms despite aggressive medical therapy. While neither ASTRAL nor CORAL observed any benefit associated with revascularization, both have important limitations that should be kept in mind when interpreting the results of these trials.
These limitations can be broadly categorized as mismatch between indications for revascularization and clinical endpoints, selection biases favoring enrollment of patients with relatively mild symptoms, and inconsistencies between study protocols and contemporary decision-making strategies.
Given that ASTRAL’s primary outcome was change in renal function (defined by a 20% or greater reduction in the mean slope of the reciprocal of serum creatinine), it is important to remember that the inclusion criteria were renal artery stenosis with unexplained renal dysfunction or poorly controlled hypertension. Patients who had hypertension in the absence of significant renal dysfunction were therefore eligible, and 40% of the randomized participants had preserved baseline renal function (based on a serum creatinine of < 150 micromol/liter). Unlike patients with baseline renal dysfunction (which, in theory, might improve with revascularization), these patients with normal renal function who were treated with revascularization risked decline in renal function resulting from procedure-related adverse events without any real chance of renal function improvement. It would certainly be difficult to justify revascularization for the sake of renal function salvage in these patients, and their inclusion within a randomized trial with change in renal function as its primary outcome is problematic for the same reason.
ASTRAL also had an additional, somewhat unorthodox inclusion criterion: uncertainty on the part of the treating physician that the patient “definitely would have a worthwhile clinical benefit from revascularization.” Exclusion of patients considered likely to benefit from revascularization would seem to ensure a selection bias favoring the null hypothesis; this approach may also explain the large proportion of participants with relatively mild occlusive disease (40% had stenotic lesions that were < 70% in severity).
A high rate of both technical failure (12%) and adverse events (20%) associated with revascularization, asymmetric crossover between treatment groups (86 of the 110 patients who did not receive their randomized intervention were in the revascularization group), and lack of standardized protocol for medical therapy further limit the conclusions that can be drawn from the ASTRAL results.
Although this trial does not provide us with compelling evidence that renal revascularization should be abandoned for patients failing appropriate medical therapy, ASTRAL demonstrated that no benefit should be expected from nonselective use of revascularization, which can be associated with significant rates of both technical failure and major adverse events.
The CORAL trial overcame many of the design limitations for which ASTRAL drew criticism. CORAL’s primary endpoint (freedom from major adverse cardiovascular or renal events) allowed potential benefit for participants with either systolic hypertension or chronic kidney disease as their indication for treatment. Although participants with systolic hypertension as their inclusion criterion had to be on at least two antihypertensive medications, it is important to acknowledge the growing number of indications for these medications related to cardiovascular risk reduction in the setting of diabetes, heart disease, and other diagnoses that may be unrelated to any specific blood pressure target. Number of antihypertensive medications is therefore often a crude and potentially invalid indicator of hypertension severity or control.
In CORAL, the initial hypertension inclusion criterion of 155 mm Hg was subsequently abandoned during the trial, suggesting that hypertension in many of these patients may have been mild and/or well controlled. Although medical therapy in CORAL was standardized, it also is notable that all patients had their medical therapy adjusted prior to randomization during a roll-in phase to achieve target blood pressure goals of 130/80 in patients with CKD and/or diabetes or 140/90 otherwise. I would suggest that achievement of these blood pressure targets on the study medications (candesartan ± hydrochlorothiazide plus amlodipine-atorvastatin) might be appropriately considered success of medical therapy for patients with hypertension in the absence of renal dysfunction, making it challenging to defend proceeding with revascularization in this scenario.
The study protocol, although well designed from the perspective of attempting to isolate the effect of renal artery angioplasty and stenting, therefore did not uniformly reflect what would be considered responsible utilization of renal revascularization in a real-world environment.
Patient enrollment in CORAL was also very selective; only 947 of the 5,322 patients who were screened went on to be enrolled and randomized. It is likely that at least some of those patients who were not enrolled (especially those who declined to participate or were withdrawn by their physicians) were failing aggressive medical therapy and therefore unwilling to being excluded from angioplasty and stenting through randomization. These limitations aside, however, CORAL does provide some very useful observations that should inform treatment decisions. The results demonstrate the efficacy of contemporary medical therapy for many patients, and show that revascularization offers no additional benefit when medical therapy achieves an acceptable clinical response (defined by stable renal function and reasonable blood pressure control). Additional subgroup analyses of the CORAL data are anticipated, but will likely be underpowered to draw conclusions in the absence of identified revascularization effects.
So when should revascularization be considered for patients with atherosclerotic renal artery stenosis? In general, medical therapy is adequate for most patients and should be implemented prior to any consideration of procedural intervention. Revascularization should be considered only for patients who have failed appropriate, aggressive medical therapy; the medications used in CORAL can certainly be regarded as adequate initial therapy for symptomatic renal artery stenosis, but many providers (including myself) would argue that additional agents should be considered before proceeding with revascularization.
When decline in renal function is the indication for considering revascularization, alternative causes (such as intrinsic renal disease) should diminish enthusiasm for proceeding with angioplasty and stenting, particularly when the anatomic disease distribution does not affect the entire renal mass (as in patients with two kidneys and unilateral stenosis). Appropriate candidates for revascularization include patients with severely impaired renal function (particularly in the setting of a precipitous functional decline) or severe acute blood pressure elevation associated with hypertensive emergency (such as acute congestive heart failure, encephalopathy, acute coronary syndrome, or other signs and symptoms of target organ damage resulting from hypertension and/or volume overload). Continuation of failed medical therapy is often unacceptable to these “no-options” patients as well as their providers, both of whom presumably would be unlikely to accept randomization to ongoing medical management.
Other populations that are not represented within these trials include patients with renal artery restenosis and those with nonatherosclerotic disease; it is therefore important to exercise caution when generalizing these study results to these distinct groups of patients. Enrolling patients with severe symptoms who have failed medical therapy will likely remain challenging for future randomized studies in the absence of alternative treatment options. Although the benefits of renal angioplasty and stenting for these “no-options” patients remain to be proved, the uncertainty of response to revascularization is often easier to accept than the ongoing morbidity and mortality associated with staying the course when medical therapy has failed.
Dr. Matthew A. Corriere is a vascular surgeon at Wake Forest University School of Medicine, Winston-Salem, N.C.
This article developed from a debate held at the 2014 Vascular Annual Meeting.
Percutaneous treatment of renal artery occlusive disease is unnecessary and should be abandoned, except in pediatric cases.
BY GEORGE HAMILTON, M.D.
This position is supported by findings from both the ASTRAL trial (N. Engl. J. Med. 2009;361:1953-62) and the CORAL trial (N. Engl. J. Med. 2013 Nov. 18 [doi:10.1056/NEJMoa1310753]).
The ASTRAL trial, a prospective, randomized comparison of best medical therapy with and without stent angioplasty in more than 800 patients, was the largest trial to date when it began back in the 1990s. The well-known results showed no difference in time to first renal event, first vascular and cardiovascular events, and overall survival. Furthermore, there was no difference in these outcomes among patients with greater than 90% stenosis, with the exception of a possible difference in mortality, which trended toward improvement among those with high-grade stenosis.
We concluded that revascularization in the vast majority of patients is unlikely to improve hypertension control or renal function, and that renal artery stenosis is not pathophysiologically important. We also concluded that there is no point in screening for asymptomatic disease; this was back when every patient was getting screened, and treated primarily on the basis of finding a renal arterial stenosis.
Finally, we concluded that properly applied best medical therapy alone was an extremely good treatment.
Several flaws in the trial garnered extensive criticism, however, and the more rigidly designed CORAL trial was expected to address them. The findings confirmed those of the ASTRAL trial. In more than 900 patients from 88 centers, there was absolutely no benefit of intervention with respect to primary and secondary outcomes, including among those with high-grade stenosis.
We can now see on the basis of extensive level 1 evidence that when added to comprehensive, multifactorial medical therapy, intervention yielded no benefit.
So are there certain patient groups who might benefit more from intervention? Among listed indications are high-grade stenosis (which doesn’t apply any longer); short history of progressive failure (which is quite rare); ACE-induced renal failure (which is also quite rare); difficult-to-control hypertension (there really is no such thing now, except in a tiny percentage of patients); and – the least challenged indication – flash pulmonary edema. These remaining indications move our interventions into a very high risk group of patients.
The current debate is focused almost entirely on endovascular intervention, but a systematic review showed that there is long-term benefit in terms of renal function and hypertension with open procedures. Although overall there is increased mortality, this risk is minimized – and not significantly different from endovascular procedures – in those having only renal revascularization vs. those having concomitant aortic procedures. So open surgery remains a possible treatment option, indeed a recent level 1 study comparing stenting and open surgery, showed better long-term results with open surgery (J. Vasc. Surg. 2009;49:667-75). The authors concluded that surgical reconstruction remains the gold standard in treating renal artery stenosis. Although national data suggest an overall mortality of about 10%, it is much lower at specialist, high-volume centers with mortality rates similar to those of stent angioplasty.
Renal stenting is not a low-risk procedure. In all-comers the complication rates, serious complication rates, and mortality rates are significant with short-term equivalence between focused renal arterial surgery and percutaneous intervention.
Returning to the debate, are either methods of revascularization appropriate? Probably not.
Even in flash pulmonary edema, there is little evidence to support revascularization. Few papers exist suggesting a benefit of revascularization in reduction of flash pulmonary edema, but the patient numbers were small, and there was no benefit in terms of preservation of renal function.
The history of evolution and evaluation of the role of renal revascularization is remarkably similar to that of renal denervation, initially and with considerable conviction thought to be a cure for hypertension. However, when properly assessed by prospective randomized comparison there was found to be absolutely no benefit.
So, given the considerable objective evidence from two major trials and revisiting the basics of the pathophysiology of atherosclerotic renovascular disease, to expect benefit from treating the osteal component of renal artery occlusive disease is at best naive, in my opinion. There remains little clinical evidence of benefit for any indication, with the possible exceptions of ACE-induced renal failure and possibly flash pulmonary edema in the presence of bilateral renal arterial stenoses.
Dr. Hamilton is a professor at the Royal Free London Hospital, University College London, United Kingdom.
There are still indications to treat renal artery occlusive disease
BY MATTHEW A. CORRIERE, M.D.
Although renal artery revascularization has been grossly overutilized and is not indicated in the majority of patients with renal artery stenosis, I perform renal artery revascularization as part of my routine clinical practice and believe that there are many instances where revascularization should be considered, particularly when patients have severe symptoms despite aggressive medical therapy. While neither ASTRAL nor CORAL observed any benefit associated with revascularization, both have important limitations that should be kept in mind when interpreting the results of these trials.
These limitations can be broadly categorized as mismatch between indications for revascularization and clinical endpoints, selection biases favoring enrollment of patients with relatively mild symptoms, and inconsistencies between study protocols and contemporary decision-making strategies.
Given that ASTRAL’s primary outcome was change in renal function (defined by a 20% or greater reduction in the mean slope of the reciprocal of serum creatinine), it is important to remember that the inclusion criteria were renal artery stenosis with unexplained renal dysfunction or poorly controlled hypertension. Patients who had hypertension in the absence of significant renal dysfunction were therefore eligible, and 40% of the randomized participants had preserved baseline renal function (based on a serum creatinine of < 150 micromol/liter). Unlike patients with baseline renal dysfunction (which, in theory, might improve with revascularization), these patients with normal renal function who were treated with revascularization risked decline in renal function resulting from procedure-related adverse events without any real chance of renal function improvement. It would certainly be difficult to justify revascularization for the sake of renal function salvage in these patients, and their inclusion within a randomized trial with change in renal function as its primary outcome is problematic for the same reason.
ASTRAL also had an additional, somewhat unorthodox inclusion criterion: uncertainty on the part of the treating physician that the patient “definitely would have a worthwhile clinical benefit from revascularization.” Exclusion of patients considered likely to benefit from revascularization would seem to ensure a selection bias favoring the null hypothesis; this approach may also explain the large proportion of participants with relatively mild occlusive disease (40% had stenotic lesions that were < 70% in severity).
A high rate of both technical failure (12%) and adverse events (20%) associated with revascularization, asymmetric crossover between treatment groups (86 of the 110 patients who did not receive their randomized intervention were in the revascularization group), and lack of standardized protocol for medical therapy further limit the conclusions that can be drawn from the ASTRAL results.
Although this trial does not provide us with compelling evidence that renal revascularization should be abandoned for patients failing appropriate medical therapy, ASTRAL demonstrated that no benefit should be expected from nonselective use of revascularization, which can be associated with significant rates of both technical failure and major adverse events.
The CORAL trial overcame many of the design limitations for which ASTRAL drew criticism. CORAL’s primary endpoint (freedom from major adverse cardiovascular or renal events) allowed potential benefit for participants with either systolic hypertension or chronic kidney disease as their indication for treatment. Although participants with systolic hypertension as their inclusion criterion had to be on at least two antihypertensive medications, it is important to acknowledge the growing number of indications for these medications related to cardiovascular risk reduction in the setting of diabetes, heart disease, and other diagnoses that may be unrelated to any specific blood pressure target. Number of antihypertensive medications is therefore often a crude and potentially invalid indicator of hypertension severity or control.
In CORAL, the initial hypertension inclusion criterion of 155 mm Hg was subsequently abandoned during the trial, suggesting that hypertension in many of these patients may have been mild and/or well controlled. Although medical therapy in CORAL was standardized, it also is notable that all patients had their medical therapy adjusted prior to randomization during a roll-in phase to achieve target blood pressure goals of 130/80 in patients with CKD and/or diabetes or 140/90 otherwise. I would suggest that achievement of these blood pressure targets on the study medications (candesartan ± hydrochlorothiazide plus amlodipine-atorvastatin) might be appropriately considered success of medical therapy for patients with hypertension in the absence of renal dysfunction, making it challenging to defend proceeding with revascularization in this scenario.
The study protocol, although well designed from the perspective of attempting to isolate the effect of renal artery angioplasty and stenting, therefore did not uniformly reflect what would be considered responsible utilization of renal revascularization in a real-world environment.
Patient enrollment in CORAL was also very selective; only 947 of the 5,322 patients who were screened went on to be enrolled and randomized. It is likely that at least some of those patients who were not enrolled (especially those who declined to participate or were withdrawn by their physicians) were failing aggressive medical therapy and therefore unwilling to being excluded from angioplasty and stenting through randomization. These limitations aside, however, CORAL does provide some very useful observations that should inform treatment decisions. The results demonstrate the efficacy of contemporary medical therapy for many patients, and show that revascularization offers no additional benefit when medical therapy achieves an acceptable clinical response (defined by stable renal function and reasonable blood pressure control). Additional subgroup analyses of the CORAL data are anticipated, but will likely be underpowered to draw conclusions in the absence of identified revascularization effects.
So when should revascularization be considered for patients with atherosclerotic renal artery stenosis? In general, medical therapy is adequate for most patients and should be implemented prior to any consideration of procedural intervention. Revascularization should be considered only for patients who have failed appropriate, aggressive medical therapy; the medications used in CORAL can certainly be regarded as adequate initial therapy for symptomatic renal artery stenosis, but many providers (including myself) would argue that additional agents should be considered before proceeding with revascularization.
When decline in renal function is the indication for considering revascularization, alternative causes (such as intrinsic renal disease) should diminish enthusiasm for proceeding with angioplasty and stenting, particularly when the anatomic disease distribution does not affect the entire renal mass (as in patients with two kidneys and unilateral stenosis). Appropriate candidates for revascularization include patients with severely impaired renal function (particularly in the setting of a precipitous functional decline) or severe acute blood pressure elevation associated with hypertensive emergency (such as acute congestive heart failure, encephalopathy, acute coronary syndrome, or other signs and symptoms of target organ damage resulting from hypertension and/or volume overload). Continuation of failed medical therapy is often unacceptable to these “no-options” patients as well as their providers, both of whom presumably would be unlikely to accept randomization to ongoing medical management.
Other populations that are not represented within these trials include patients with renal artery restenosis and those with nonatherosclerotic disease; it is therefore important to exercise caution when generalizing these study results to these distinct groups of patients. Enrolling patients with severe symptoms who have failed medical therapy will likely remain challenging for future randomized studies in the absence of alternative treatment options. Although the benefits of renal angioplasty and stenting for these “no-options” patients remain to be proved, the uncertainty of response to revascularization is often easier to accept than the ongoing morbidity and mortality associated with staying the course when medical therapy has failed.
Dr. Matthew A. Corriere is a vascular surgeon at Wake Forest University School of Medicine, Winston-Salem, N.C.
This article developed from a debate held at the 2014 Vascular Annual Meeting.
FDA: Limit testosterone use to men with specific medical conditions
Testosterone therapy is not appropriate for men with age-related low testosterone because it may be associated with an increased risk of cardiovascular events, the Food and Drug Administration has determined.
The agency will now require labeling changes to all prescription testosterone products, clarifying their appropriate use, and warning about a possible increased risk of heart attack and stroke in any patient taking the hormone. Testosterone is approved only for men with specific medical conditions, but is widely used off label for men with age-related low testosterone.
“Health care professionals should make patients aware of this possible risk when deciding whether to start or continue a patient on testosterone therapy,” an FDA statement said. “We are also requiring manufacturers of approved testosterone products to conduct a well-designed clinical trial to more clearly address the question of whether an increased risk of heart attack or stroke exists among users of these products. We are encouraging these manufacturers to work together on a clinical trial, but they are allowed to work separately if they so choose.”
The statement arose from a September 2014 recommendation by the FDA’s Bone, Reproductive, and Urologic Drugs Advisory Committee and Drug Safety and Risk Management Advisory Committee. The groups reviewed studies of aging men using testosterone – some of which reported an increased risk of heart attack, stroke, or death associated with testosterone treatment – and voted 20-1 that the current indication, as worded in the labeling for all testosterone products, should be tightened to make it clear that testosterone therapy is not indicated for men with age-related reductions in testosterone.
Any clinician who prescribes testosterone to a patient who later experiences a cardiovascular event should report that toFDA’s MedWatch Safety Information and Adverse Event Reporting Program.
On Twitter @alz_gal
Testosterone therapy is not appropriate for men with age-related low testosterone because it may be associated with an increased risk of cardiovascular events, the Food and Drug Administration has determined.
The agency will now require labeling changes to all prescription testosterone products, clarifying their appropriate use, and warning about a possible increased risk of heart attack and stroke in any patient taking the hormone. Testosterone is approved only for men with specific medical conditions, but is widely used off label for men with age-related low testosterone.
“Health care professionals should make patients aware of this possible risk when deciding whether to start or continue a patient on testosterone therapy,” an FDA statement said. “We are also requiring manufacturers of approved testosterone products to conduct a well-designed clinical trial to more clearly address the question of whether an increased risk of heart attack or stroke exists among users of these products. We are encouraging these manufacturers to work together on a clinical trial, but they are allowed to work separately if they so choose.”
The statement arose from a September 2014 recommendation by the FDA’s Bone, Reproductive, and Urologic Drugs Advisory Committee and Drug Safety and Risk Management Advisory Committee. The groups reviewed studies of aging men using testosterone – some of which reported an increased risk of heart attack, stroke, or death associated with testosterone treatment – and voted 20-1 that the current indication, as worded in the labeling for all testosterone products, should be tightened to make it clear that testosterone therapy is not indicated for men with age-related reductions in testosterone.
Any clinician who prescribes testosterone to a patient who later experiences a cardiovascular event should report that toFDA’s MedWatch Safety Information and Adverse Event Reporting Program.
On Twitter @alz_gal
Testosterone therapy is not appropriate for men with age-related low testosterone because it may be associated with an increased risk of cardiovascular events, the Food and Drug Administration has determined.
The agency will now require labeling changes to all prescription testosterone products, clarifying their appropriate use, and warning about a possible increased risk of heart attack and stroke in any patient taking the hormone. Testosterone is approved only for men with specific medical conditions, but is widely used off label for men with age-related low testosterone.
“Health care professionals should make patients aware of this possible risk when deciding whether to start or continue a patient on testosterone therapy,” an FDA statement said. “We are also requiring manufacturers of approved testosterone products to conduct a well-designed clinical trial to more clearly address the question of whether an increased risk of heart attack or stroke exists among users of these products. We are encouraging these manufacturers to work together on a clinical trial, but they are allowed to work separately if they so choose.”
The statement arose from a September 2014 recommendation by the FDA’s Bone, Reproductive, and Urologic Drugs Advisory Committee and Drug Safety and Risk Management Advisory Committee. The groups reviewed studies of aging men using testosterone – some of which reported an increased risk of heart attack, stroke, or death associated with testosterone treatment – and voted 20-1 that the current indication, as worded in the labeling for all testosterone products, should be tightened to make it clear that testosterone therapy is not indicated for men with age-related reductions in testosterone.
Any clinician who prescribes testosterone to a patient who later experiences a cardiovascular event should report that toFDA’s MedWatch Safety Information and Adverse Event Reporting Program.
On Twitter @alz_gal
LISTEN NOW: Highlights of the March 2015 issue of The Hospitalist
http://www.the-hospitalist.org/wp-content/uploads/2015/03/2015-March-Hospitalist-Highlights.mp3
http://www.the-hospitalist.org/wp-content/uploads/2015/03/2015-March-Hospitalist-Highlights.mp3
http://www.the-hospitalist.org/wp-content/uploads/2015/03/2015-March-Hospitalist-Highlights.mp3
What Is the Best Approach to a Cavitary Lung Lesion?
Case
A 66-year-old homeless man with a history of smoking and cirrhosis due to alcoholism presents to the hospital with a productive cough and fever for one month. He has traveled around Arizona and New Mexico but has never left the country. His complete blood count (CBC) is notable for a white blood cell count of 13,000. His chest X-ray reveals a 1.7-cm right upper lobe cavitary lung lesion (see Figure 1). What is the best approach to this patient’s cavitary lung lesion?
Overview
Cavitary lung lesions are relatively common findings on chest imaging and often pose a diagnostic challenge to the hospitalist. Having a standard approach to the evaluation of a cavitary lung lesion can facilitate an expedited workup.

A lung cavity is defined radiographically as a lucent area contained within a consolidation, mass, or nodule.1 Cavities usually are accompanied by thick walls, greater than 4 mm. These should be differentiated from cysts, which are not surrounded by consolidation, mass, or nodule, and are accompanied by a thinner wall.2
The differential diagnosis of a cavitary lung lesion is broad and can be delineated into categories of infectious and noninfectious etiologies (see Figure 2). Infectious causes include bacterial, fungal, and, rarely, parasitic agents. Noninfectious causes encompass malignant, rheumatologic, and other less common etiologies such as infarct related to pulmonary embolism.
The clinical presentation and assessment of risk factors for a particular patient are of the utmost importance in delineating next steps for evaluation and management (see Table 1). For those patients of older age with smoking history, specific occupational or environmental exposures, and weight loss, the most common etiology is neoplasm. Common infectious causes include lung abscess and necrotizing pneumonia, as well as tuberculosis. The approach to diagnosis should be based on a composite of the clinical presentation, patient characteristics, and radiographic appearance of the cavity.
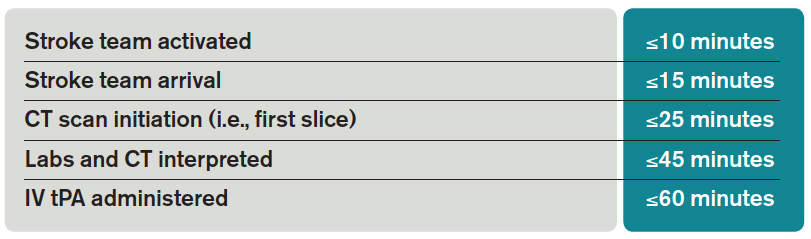
Guidelines for the approach to cavitary lung lesions are lacking, yet a thorough understanding of the initial approach is important for those practicing hospital medicine. Key components in the approach to diagnosis of a solitary cavitary lesion are outlined in this article.
Diagnosis of Infectious Causes
In the initial evaluation of a cavitary lung lesion, it is important to first determine if the cause is an infectious process. The infectious etiologies to consider include lung abscess and necrotizing pneumonia, tuberculosis, and septic emboli. Important components in the clinical presentation include presence of cough, fever, night sweats, chills, and symptoms that have lasted less than one month, as well as comorbid conditions, drug or alcohol abuse, and history of immunocompromise (e.g. HIV, immunosuppressive therapy, or organ transplant).
Given the public health considerations and impact of treatment, tuberculosis (TB) will be discussed in its own category.
Tuberculosis. Given the fact that TB patients require airborne isolation, the disease must be considered early in the evaluation of a cavitary lung lesion. Patients with TB often present with more chronic symptoms, such as fevers, night sweats, weight loss, and hemoptysis. Immunocompromised state, travel to endemic regions, and incarceration increase the likelihood of TB. Nontuberculous mycobacterium (i.e., M. kansasii) should also be considered in endemic areas.
For those patients in whom TB is suspected, airborne isolation must be initiated promptly. The provider should obtain three sputum samples for acid-fast bacillus (AFB) smear and culture when risk factors are present. Most patients with reactivation TB have abnormal chest X-rays, with approximately 20% of those patients having air-fluid levels and the majority of cases affecting the upper lobes.3 Cavities may be seen in patients with primary or reactivation TB.3
Lung abscess and necrotizing pneumonia. Lung abscesses are cavities associated with necrosis caused by a microbial infection. The term necrotizing pneumonia typically is used when there are multiple smaller (smaller than 2 cm) associated lung abscesses, although both lung abscess and necrotizing pneumonia represent a similar pathophysiologic process and are along the same continuum. Lung abscess is suspected with the presence of predisposing risk factors to aspiration (e.g. alcoholism) and poor dentition. History of cough, fever, putrid sputum, night sweats, and weight loss may indicate subacute or chronic development of a lung abscess. Physical examination might be significant for signs of pneumonia and gingivitis.
Organisms that cause lung abscesses include anaerobes (most common), TB, methicillin-resistant Staphylococcus aureus (MRSA), post-influenza illness, endemic fungi, and Nocardia, among others.4 In immunocompromised patients, more common considerations include TB, Mycobacterium avium complex, other mycobacteria, Pseudomonas aeruginosa, Nocardia, Cryptococcus, Aspergillus, endemic fungi (e.g. Coccidiodes in the Southwest and Histoplasma in the Midwest), and, less commonly, Pneumocystis jiroveci.4 The likelihood of each organism is dependent on the patient’s risk factors. Initial laboratory testing includes sputum and blood cultures, as well as serologic testing for endemic fungi, especially in immunocompromised patients.
Imaging may reveal a cavitary lesion in the dependent pulmonary segments (posterior segments of the upper lobes or superior segments of the lower lobes), at times associated with a pleural effusion or infiltrate. The most common appearance of a lung abscess is an asymmetric cavity with an air-fluid level and a wall with a ragged or smooth border. CT scan is often indicated when X-rays are equivocal and when cases are of uncertain cause or are unresponsive to antibiotic therapy. Bronchoscopy is reserved for patients with an immunocompromising condition, atypical presentation, or lack of response to treatment.
For those cavitary lesions in which there is a high degree of suspicion for lung abscess, empiric treatment should include antibiotics active against anaerobes and MRSA if the patient has risk factors. Patients often receive an empiric trial of antibiotics prior to biopsy unless there are clear indications that the cavitary lung lesion is related to cancer. Lung abscesses typically drain spontaneously, and transthoracic or endobronchial drainage is not usually recommended as initial management due to risk of pneumothorax and formation of bronchopleural fistula.
Lung abscesses should be followed to resolution with serial chest imaging. If the lung abscess does not resolve, it would be appropriate to consult thoracic surgery, interventional radiology, or pulmonary, depending on the location of the abscess and the local expertise with transthoracic or endobronchial drainage and surgical resection.
Septic emboli. Septic emboli are a less common cause of cavitary lung lesions. This entity should be considered in patients with a history of IV drug use or infected indwelling devices (central venous catheters, pacemaker wires, and right-sided prosthetic heart valves). Physical examination should include an assessment for signs of endocarditis and inspection for infected indwelling devices. In patients with IV drug use, the likely pathogen is S. aureus.
Oropharyngeal infection or indwelling catheters may predispose patients to septic thrombophlebitis of the internal jugular vein, also known as Lemierre’s syndrome, a rare but important cause of septic emboli.5 Laboratory testing includes culture for sputum and blood and culture of the infected device if applicable. On chest X-ray, septic emboli commonly appear as nodules located in the lung periphery. CT scan is more sensitive for detecting cavitation associated with septic emboli.
Diagnosis of Noninfectious Causes
Upon identification of a cavitary lung lesion, noninfectious etiologies must also be entertained. Noninfectious etiologies include malignancy, rheumatologic diseases, pulmonary embolism, and other causes. Important components in the clinical presentation include the presence of constitutional symptoms (fevers, weight loss, night sweats), smoking history, family history, and an otherwise complete review of systems. Physical exam should include evaluation for lymphadenopathy, cachexia, rash, clubbing, and other symptoms pertinent to the suspected etiology.
Malignancy. Perhaps most important among noninfectious causes of cavitary lung lesions is malignancy, and a high index of suspicion is warranted given that it is commonly the first diagnosis to consider overall.2 Cavities can form in primary lung cancers (e.g. bronchogenic carcinomas), lung tumors such as lymphoma or Kaposi’s sarcoma, or in metastatic disease. Cavitation has been detected in 7%-11% of primary lung cancers by plain radiography and in 22% by computed tomography.5 Cancers of squamous cell origin are the most likely to cavitate; this holds true for both primary lung tumors and metastatic tumors.6 Additionally, cavitation portends a worse prognosis.7
Clinicians should review any available prior chest imaging studies to look for a change in the quality or size of a cavitary lung lesion. Neoplasms are typically of variable size with irregular thick walls (greater than 4 mm) on CT scan, with higher specificity for neoplasm in those with a wall thickness greater than 15 mm.2
When the diagnosis is less clear, the decision to embark on more advanced diagnostic methods, such as biopsy, should rest on the provider’s clinical suspicion for a certain disease process. When a lung cancer is suspected, consultation with pulmonary and interventional radiology should be obtained to determine the best approach for biopsy.
Rheumatologic. Less common causes of cavitary lesions include those related to rheumatologic diseases (e.g. granulomatosis with polyangiitis, formerly known as Wegener’s granulomatosis). One study demonstrated that cavitary lung nodules occur in 37% of patients with granulomatosis with polyangiitis.8
Although uncommon, cavitary nodules can also be seen in rheumatoid arthritis and sarcoidosis. Given that patients with rheumatologic diseases are often treated with immunosuppressive agents, infection must remain high on the differential. Suspicion of a rheumatologic cause should prompt the clinician to obtain appropriate serologic testing and consultation as needed.

Pulmonary embolism. Although often not considered in the evaluation of cavitary lung lesions, pulmonary embolism (PE) can lead to infarction and the formation of a cavitary lesion. Pulmonary infarction has been reported to occur in as many as one third of cases of PE.9 Cavitary lesions also have been described in chronic thromboembolic disease.10
Other. Uncommon causes of cavitary lesions include bronchiolitis obliterans with organizing pneumonia, Langerhans cell histiocytosis, and amyloidosis, among others. The hospitalist should keep a broad differential and involve consultants if the diagnosis remains unclear after initial diagnostic evaluation.
Back to the Case
The patient’s fever and productive cough, in combination with recent travel and location of the cavitary lesion, increase his risk for tuberculosis and endemic fungi, such as Coccidioides. This patient was placed on respiratory isolation with AFBs obtained to rule out TB, with Coccidioides antibodies, Cyptococcal antigen titers, and sputum for fungus sent to evaluate for an endemic fungus. He had a chest CT, which revealed a 17-mm cavitary mass within the right upper lobe that contained an air-fluid level indicating lung abscess. Coccidioides, cryptococcal, fungal sputum, and TB studies were negative.
The patient was treated empirically with clindamycin given the high prevalence of anaerobes in lung abscess. He was followed as an outpatient and had a chest X-ray showing resolution of the lesion at six months. The purpose of the X-ray was two-fold: to monitor the effect of antibiotic treatment and to evaluate for persistence of the cavitation given the neoplastic risk factors of older age and smoking.
Bottom Line
The best approach to a patient with a cavitary lung lesion includes assessing the clinical presentation and risk factors, differentiating infectious from noninfectious causes, and then utilizing this information to further direct the diagnostic evaluation. Consultation with a subspecialist or further testing such as biopsy should be considered if the etiology remains undefined after the initial evaluation.
Drs. Rendon, Pizanis, Montanaro, and Kraai are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque.
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722.
- Ryu JH, Swensen SJ. Cystic and cavitary lung diseases: focal and diffuse. Mayo Clin Proc. 2003;78(6):744-752.
- Barnes PF, Verdegem TD, Vachon LA, Leedom JM, Overturf GD. Chest roentgenogram in pulmonary tuberculosis. New data on an old test. Chest. 1988;94(2):316-320.
- Yazbeck MF, Dahdel M, Kalra A, Browne AS, Pratter MR. Lung abscess: update on microbiology and management. Am J Ther. 2012;21(3):217-221. doi: 10.1097/MJT.0b013e3182383c9b.
- Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-333.
- Chiu FT. Cavitation in lung cancers. Aust N Z J Med. 1975;5(6):523-530.
- Kolodziejski LS, Dyczek S, Duda K, Góralczyk J, Wysocki WM, Lobaziewicz W. Cavitated tumor as a clinical subentity in squamous cell lung cancer patients. Neoplasma. 2003;50(1):66-73.
- Cordier JF, Valeyre D, Guillevin L, Loire R, Brechot JM. Pulmonary Wegener’s granulomatosis. A clinical and imaging study of 77 cases. Chest. 1990;97(4):906-912.
- He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006;21(1):1-7.
- Harris H, Barraclough R, Davies C, Armstrong I, Kiely DG, van Beek E Jr. Cavitating lung lesions in chronic thromboembolic pulmonary hypertension. J Radiol Case Rep. 2008;2(3):11-21.
- Woodring JH, Fried AM, Chuang VP. Solitary cavities of the lung: diagnostic implications of cavity wall thickness. AJR Am J Roentgenol. 1980;135(6):1269-1271.
Case
A 66-year-old homeless man with a history of smoking and cirrhosis due to alcoholism presents to the hospital with a productive cough and fever for one month. He has traveled around Arizona and New Mexico but has never left the country. His complete blood count (CBC) is notable for a white blood cell count of 13,000. His chest X-ray reveals a 1.7-cm right upper lobe cavitary lung lesion (see Figure 1). What is the best approach to this patient’s cavitary lung lesion?
Overview
Cavitary lung lesions are relatively common findings on chest imaging and often pose a diagnostic challenge to the hospitalist. Having a standard approach to the evaluation of a cavitary lung lesion can facilitate an expedited workup.
A lung cavity is defined radiographically as a lucent area contained within a consolidation, mass, or nodule.1 Cavities usually are accompanied by thick walls, greater than 4 mm. These should be differentiated from cysts, which are not surrounded by consolidation, mass, or nodule, and are accompanied by a thinner wall.2
The differential diagnosis of a cavitary lung lesion is broad and can be delineated into categories of infectious and noninfectious etiologies (see Figure 2). Infectious causes include bacterial, fungal, and, rarely, parasitic agents. Noninfectious causes encompass malignant, rheumatologic, and other less common etiologies such as infarct related to pulmonary embolism.
The clinical presentation and assessment of risk factors for a particular patient are of the utmost importance in delineating next steps for evaluation and management (see Table 1). For those patients of older age with smoking history, specific occupational or environmental exposures, and weight loss, the most common etiology is neoplasm. Common infectious causes include lung abscess and necrotizing pneumonia, as well as tuberculosis. The approach to diagnosis should be based on a composite of the clinical presentation, patient characteristics, and radiographic appearance of the cavity.
Guidelines for the approach to cavitary lung lesions are lacking, yet a thorough understanding of the initial approach is important for those practicing hospital medicine. Key components in the approach to diagnosis of a solitary cavitary lesion are outlined in this article.
Diagnosis of Infectious Causes
In the initial evaluation of a cavitary lung lesion, it is important to first determine if the cause is an infectious process. The infectious etiologies to consider include lung abscess and necrotizing pneumonia, tuberculosis, and septic emboli. Important components in the clinical presentation include presence of cough, fever, night sweats, chills, and symptoms that have lasted less than one month, as well as comorbid conditions, drug or alcohol abuse, and history of immunocompromise (e.g. HIV, immunosuppressive therapy, or organ transplant).
Given the public health considerations and impact of treatment, tuberculosis (TB) will be discussed in its own category.
Tuberculosis. Given the fact that TB patients require airborne isolation, the disease must be considered early in the evaluation of a cavitary lung lesion. Patients with TB often present with more chronic symptoms, such as fevers, night sweats, weight loss, and hemoptysis. Immunocompromised state, travel to endemic regions, and incarceration increase the likelihood of TB. Nontuberculous mycobacterium (i.e., M. kansasii) should also be considered in endemic areas.
For those patients in whom TB is suspected, airborne isolation must be initiated promptly. The provider should obtain three sputum samples for acid-fast bacillus (AFB) smear and culture when risk factors are present. Most patients with reactivation TB have abnormal chest X-rays, with approximately 20% of those patients having air-fluid levels and the majority of cases affecting the upper lobes.3 Cavities may be seen in patients with primary or reactivation TB.3
Lung abscess and necrotizing pneumonia. Lung abscesses are cavities associated with necrosis caused by a microbial infection. The term necrotizing pneumonia typically is used when there are multiple smaller (smaller than 2 cm) associated lung abscesses, although both lung abscess and necrotizing pneumonia represent a similar pathophysiologic process and are along the same continuum. Lung abscess is suspected with the presence of predisposing risk factors to aspiration (e.g. alcoholism) and poor dentition. History of cough, fever, putrid sputum, night sweats, and weight loss may indicate subacute or chronic development of a lung abscess. Physical examination might be significant for signs of pneumonia and gingivitis.
Organisms that cause lung abscesses include anaerobes (most common), TB, methicillin-resistant Staphylococcus aureus (MRSA), post-influenza illness, endemic fungi, and Nocardia, among others.4 In immunocompromised patients, more common considerations include TB, Mycobacterium avium complex, other mycobacteria, Pseudomonas aeruginosa, Nocardia, Cryptococcus, Aspergillus, endemic fungi (e.g. Coccidiodes in the Southwest and Histoplasma in the Midwest), and, less commonly, Pneumocystis jiroveci.4 The likelihood of each organism is dependent on the patient’s risk factors. Initial laboratory testing includes sputum and blood cultures, as well as serologic testing for endemic fungi, especially in immunocompromised patients.
Imaging may reveal a cavitary lesion in the dependent pulmonary segments (posterior segments of the upper lobes or superior segments of the lower lobes), at times associated with a pleural effusion or infiltrate. The most common appearance of a lung abscess is an asymmetric cavity with an air-fluid level and a wall with a ragged or smooth border. CT scan is often indicated when X-rays are equivocal and when cases are of uncertain cause or are unresponsive to antibiotic therapy. Bronchoscopy is reserved for patients with an immunocompromising condition, atypical presentation, or lack of response to treatment.
For those cavitary lesions in which there is a high degree of suspicion for lung abscess, empiric treatment should include antibiotics active against anaerobes and MRSA if the patient has risk factors. Patients often receive an empiric trial of antibiotics prior to biopsy unless there are clear indications that the cavitary lung lesion is related to cancer. Lung abscesses typically drain spontaneously, and transthoracic or endobronchial drainage is not usually recommended as initial management due to risk of pneumothorax and formation of bronchopleural fistula.
Lung abscesses should be followed to resolution with serial chest imaging. If the lung abscess does not resolve, it would be appropriate to consult thoracic surgery, interventional radiology, or pulmonary, depending on the location of the abscess and the local expertise with transthoracic or endobronchial drainage and surgical resection.
Septic emboli. Septic emboli are a less common cause of cavitary lung lesions. This entity should be considered in patients with a history of IV drug use or infected indwelling devices (central venous catheters, pacemaker wires, and right-sided prosthetic heart valves). Physical examination should include an assessment for signs of endocarditis and inspection for infected indwelling devices. In patients with IV drug use, the likely pathogen is S. aureus.
Oropharyngeal infection or indwelling catheters may predispose patients to septic thrombophlebitis of the internal jugular vein, also known as Lemierre’s syndrome, a rare but important cause of septic emboli.5 Laboratory testing includes culture for sputum and blood and culture of the infected device if applicable. On chest X-ray, septic emboli commonly appear as nodules located in the lung periphery. CT scan is more sensitive for detecting cavitation associated with septic emboli.
Diagnosis of Noninfectious Causes
Upon identification of a cavitary lung lesion, noninfectious etiologies must also be entertained. Noninfectious etiologies include malignancy, rheumatologic diseases, pulmonary embolism, and other causes. Important components in the clinical presentation include the presence of constitutional symptoms (fevers, weight loss, night sweats), smoking history, family history, and an otherwise complete review of systems. Physical exam should include evaluation for lymphadenopathy, cachexia, rash, clubbing, and other symptoms pertinent to the suspected etiology.
Malignancy. Perhaps most important among noninfectious causes of cavitary lung lesions is malignancy, and a high index of suspicion is warranted given that it is commonly the first diagnosis to consider overall.2 Cavities can form in primary lung cancers (e.g. bronchogenic carcinomas), lung tumors such as lymphoma or Kaposi’s sarcoma, or in metastatic disease. Cavitation has been detected in 7%-11% of primary lung cancers by plain radiography and in 22% by computed tomography.5 Cancers of squamous cell origin are the most likely to cavitate; this holds true for both primary lung tumors and metastatic tumors.6 Additionally, cavitation portends a worse prognosis.7
Clinicians should review any available prior chest imaging studies to look for a change in the quality or size of a cavitary lung lesion. Neoplasms are typically of variable size with irregular thick walls (greater than 4 mm) on CT scan, with higher specificity for neoplasm in those with a wall thickness greater than 15 mm.2
When the diagnosis is less clear, the decision to embark on more advanced diagnostic methods, such as biopsy, should rest on the provider’s clinical suspicion for a certain disease process. When a lung cancer is suspected, consultation with pulmonary and interventional radiology should be obtained to determine the best approach for biopsy.
Rheumatologic. Less common causes of cavitary lesions include those related to rheumatologic diseases (e.g. granulomatosis with polyangiitis, formerly known as Wegener’s granulomatosis). One study demonstrated that cavitary lung nodules occur in 37% of patients with granulomatosis with polyangiitis.8
Although uncommon, cavitary nodules can also be seen in rheumatoid arthritis and sarcoidosis. Given that patients with rheumatologic diseases are often treated with immunosuppressive agents, infection must remain high on the differential. Suspicion of a rheumatologic cause should prompt the clinician to obtain appropriate serologic testing and consultation as needed.
Pulmonary embolism. Although often not considered in the evaluation of cavitary lung lesions, pulmonary embolism (PE) can lead to infarction and the formation of a cavitary lesion. Pulmonary infarction has been reported to occur in as many as one third of cases of PE.9 Cavitary lesions also have been described in chronic thromboembolic disease.10
Other. Uncommon causes of cavitary lesions include bronchiolitis obliterans with organizing pneumonia, Langerhans cell histiocytosis, and amyloidosis, among others. The hospitalist should keep a broad differential and involve consultants if the diagnosis remains unclear after initial diagnostic evaluation.
Back to the Case
The patient’s fever and productive cough, in combination with recent travel and location of the cavitary lesion, increase his risk for tuberculosis and endemic fungi, such as Coccidioides. This patient was placed on respiratory isolation with AFBs obtained to rule out TB, with Coccidioides antibodies, Cyptococcal antigen titers, and sputum for fungus sent to evaluate for an endemic fungus. He had a chest CT, which revealed a 17-mm cavitary mass within the right upper lobe that contained an air-fluid level indicating lung abscess. Coccidioides, cryptococcal, fungal sputum, and TB studies were negative.
The patient was treated empirically with clindamycin given the high prevalence of anaerobes in lung abscess. He was followed as an outpatient and had a chest X-ray showing resolution of the lesion at six months. The purpose of the X-ray was two-fold: to monitor the effect of antibiotic treatment and to evaluate for persistence of the cavitation given the neoplastic risk factors of older age and smoking.
Bottom Line
The best approach to a patient with a cavitary lung lesion includes assessing the clinical presentation and risk factors, differentiating infectious from noninfectious causes, and then utilizing this information to further direct the diagnostic evaluation. Consultation with a subspecialist or further testing such as biopsy should be considered if the etiology remains undefined after the initial evaluation.
Drs. Rendon, Pizanis, Montanaro, and Kraai are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque.
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722.
- Ryu JH, Swensen SJ. Cystic and cavitary lung diseases: focal and diffuse. Mayo Clin Proc. 2003;78(6):744-752.
- Barnes PF, Verdegem TD, Vachon LA, Leedom JM, Overturf GD. Chest roentgenogram in pulmonary tuberculosis. New data on an old test. Chest. 1988;94(2):316-320.
- Yazbeck MF, Dahdel M, Kalra A, Browne AS, Pratter MR. Lung abscess: update on microbiology and management. Am J Ther. 2012;21(3):217-221. doi: 10.1097/MJT.0b013e3182383c9b.
- Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-333.
- Chiu FT. Cavitation in lung cancers. Aust N Z J Med. 1975;5(6):523-530.
- Kolodziejski LS, Dyczek S, Duda K, Góralczyk J, Wysocki WM, Lobaziewicz W. Cavitated tumor as a clinical subentity in squamous cell lung cancer patients. Neoplasma. 2003;50(1):66-73.
- Cordier JF, Valeyre D, Guillevin L, Loire R, Brechot JM. Pulmonary Wegener’s granulomatosis. A clinical and imaging study of 77 cases. Chest. 1990;97(4):906-912.
- He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006;21(1):1-7.
- Harris H, Barraclough R, Davies C, Armstrong I, Kiely DG, van Beek E Jr. Cavitating lung lesions in chronic thromboembolic pulmonary hypertension. J Radiol Case Rep. 2008;2(3):11-21.
- Woodring JH, Fried AM, Chuang VP. Solitary cavities of the lung: diagnostic implications of cavity wall thickness. AJR Am J Roentgenol. 1980;135(6):1269-1271.
Case
A 66-year-old homeless man with a history of smoking and cirrhosis due to alcoholism presents to the hospital with a productive cough and fever for one month. He has traveled around Arizona and New Mexico but has never left the country. His complete blood count (CBC) is notable for a white blood cell count of 13,000. His chest X-ray reveals a 1.7-cm right upper lobe cavitary lung lesion (see Figure 1). What is the best approach to this patient’s cavitary lung lesion?
Overview
Cavitary lung lesions are relatively common findings on chest imaging and often pose a diagnostic challenge to the hospitalist. Having a standard approach to the evaluation of a cavitary lung lesion can facilitate an expedited workup.
A lung cavity is defined radiographically as a lucent area contained within a consolidation, mass, or nodule.1 Cavities usually are accompanied by thick walls, greater than 4 mm. These should be differentiated from cysts, which are not surrounded by consolidation, mass, or nodule, and are accompanied by a thinner wall.2
The differential diagnosis of a cavitary lung lesion is broad and can be delineated into categories of infectious and noninfectious etiologies (see Figure 2). Infectious causes include bacterial, fungal, and, rarely, parasitic agents. Noninfectious causes encompass malignant, rheumatologic, and other less common etiologies such as infarct related to pulmonary embolism.
The clinical presentation and assessment of risk factors for a particular patient are of the utmost importance in delineating next steps for evaluation and management (see Table 1). For those patients of older age with smoking history, specific occupational or environmental exposures, and weight loss, the most common etiology is neoplasm. Common infectious causes include lung abscess and necrotizing pneumonia, as well as tuberculosis. The approach to diagnosis should be based on a composite of the clinical presentation, patient characteristics, and radiographic appearance of the cavity.
Guidelines for the approach to cavitary lung lesions are lacking, yet a thorough understanding of the initial approach is important for those practicing hospital medicine. Key components in the approach to diagnosis of a solitary cavitary lesion are outlined in this article.
Diagnosis of Infectious Causes
In the initial evaluation of a cavitary lung lesion, it is important to first determine if the cause is an infectious process. The infectious etiologies to consider include lung abscess and necrotizing pneumonia, tuberculosis, and septic emboli. Important components in the clinical presentation include presence of cough, fever, night sweats, chills, and symptoms that have lasted less than one month, as well as comorbid conditions, drug or alcohol abuse, and history of immunocompromise (e.g. HIV, immunosuppressive therapy, or organ transplant).
Given the public health considerations and impact of treatment, tuberculosis (TB) will be discussed in its own category.
Tuberculosis. Given the fact that TB patients require airborne isolation, the disease must be considered early in the evaluation of a cavitary lung lesion. Patients with TB often present with more chronic symptoms, such as fevers, night sweats, weight loss, and hemoptysis. Immunocompromised state, travel to endemic regions, and incarceration increase the likelihood of TB. Nontuberculous mycobacterium (i.e., M. kansasii) should also be considered in endemic areas.
For those patients in whom TB is suspected, airborne isolation must be initiated promptly. The provider should obtain three sputum samples for acid-fast bacillus (AFB) smear and culture when risk factors are present. Most patients with reactivation TB have abnormal chest X-rays, with approximately 20% of those patients having air-fluid levels and the majority of cases affecting the upper lobes.3 Cavities may be seen in patients with primary or reactivation TB.3
Lung abscess and necrotizing pneumonia. Lung abscesses are cavities associated with necrosis caused by a microbial infection. The term necrotizing pneumonia typically is used when there are multiple smaller (smaller than 2 cm) associated lung abscesses, although both lung abscess and necrotizing pneumonia represent a similar pathophysiologic process and are along the same continuum. Lung abscess is suspected with the presence of predisposing risk factors to aspiration (e.g. alcoholism) and poor dentition. History of cough, fever, putrid sputum, night sweats, and weight loss may indicate subacute or chronic development of a lung abscess. Physical examination might be significant for signs of pneumonia and gingivitis.
Organisms that cause lung abscesses include anaerobes (most common), TB, methicillin-resistant Staphylococcus aureus (MRSA), post-influenza illness, endemic fungi, and Nocardia, among others.4 In immunocompromised patients, more common considerations include TB, Mycobacterium avium complex, other mycobacteria, Pseudomonas aeruginosa, Nocardia, Cryptococcus, Aspergillus, endemic fungi (e.g. Coccidiodes in the Southwest and Histoplasma in the Midwest), and, less commonly, Pneumocystis jiroveci.4 The likelihood of each organism is dependent on the patient’s risk factors. Initial laboratory testing includes sputum and blood cultures, as well as serologic testing for endemic fungi, especially in immunocompromised patients.
Imaging may reveal a cavitary lesion in the dependent pulmonary segments (posterior segments of the upper lobes or superior segments of the lower lobes), at times associated with a pleural effusion or infiltrate. The most common appearance of a lung abscess is an asymmetric cavity with an air-fluid level and a wall with a ragged or smooth border. CT scan is often indicated when X-rays are equivocal and when cases are of uncertain cause or are unresponsive to antibiotic therapy. Bronchoscopy is reserved for patients with an immunocompromising condition, atypical presentation, or lack of response to treatment.
For those cavitary lesions in which there is a high degree of suspicion for lung abscess, empiric treatment should include antibiotics active against anaerobes and MRSA if the patient has risk factors. Patients often receive an empiric trial of antibiotics prior to biopsy unless there are clear indications that the cavitary lung lesion is related to cancer. Lung abscesses typically drain spontaneously, and transthoracic or endobronchial drainage is not usually recommended as initial management due to risk of pneumothorax and formation of bronchopleural fistula.
Lung abscesses should be followed to resolution with serial chest imaging. If the lung abscess does not resolve, it would be appropriate to consult thoracic surgery, interventional radiology, or pulmonary, depending on the location of the abscess and the local expertise with transthoracic or endobronchial drainage and surgical resection.
Septic emboli. Septic emboli are a less common cause of cavitary lung lesions. This entity should be considered in patients with a history of IV drug use or infected indwelling devices (central venous catheters, pacemaker wires, and right-sided prosthetic heart valves). Physical examination should include an assessment for signs of endocarditis and inspection for infected indwelling devices. In patients with IV drug use, the likely pathogen is S. aureus.
Oropharyngeal infection or indwelling catheters may predispose patients to septic thrombophlebitis of the internal jugular vein, also known as Lemierre’s syndrome, a rare but important cause of septic emboli.5 Laboratory testing includes culture for sputum and blood and culture of the infected device if applicable. On chest X-ray, septic emboli commonly appear as nodules located in the lung periphery. CT scan is more sensitive for detecting cavitation associated with septic emboli.
Diagnosis of Noninfectious Causes
Upon identification of a cavitary lung lesion, noninfectious etiologies must also be entertained. Noninfectious etiologies include malignancy, rheumatologic diseases, pulmonary embolism, and other causes. Important components in the clinical presentation include the presence of constitutional symptoms (fevers, weight loss, night sweats), smoking history, family history, and an otherwise complete review of systems. Physical exam should include evaluation for lymphadenopathy, cachexia, rash, clubbing, and other symptoms pertinent to the suspected etiology.
Malignancy. Perhaps most important among noninfectious causes of cavitary lung lesions is malignancy, and a high index of suspicion is warranted given that it is commonly the first diagnosis to consider overall.2 Cavities can form in primary lung cancers (e.g. bronchogenic carcinomas), lung tumors such as lymphoma or Kaposi’s sarcoma, or in metastatic disease. Cavitation has been detected in 7%-11% of primary lung cancers by plain radiography and in 22% by computed tomography.5 Cancers of squamous cell origin are the most likely to cavitate; this holds true for both primary lung tumors and metastatic tumors.6 Additionally, cavitation portends a worse prognosis.7
Clinicians should review any available prior chest imaging studies to look for a change in the quality or size of a cavitary lung lesion. Neoplasms are typically of variable size with irregular thick walls (greater than 4 mm) on CT scan, with higher specificity for neoplasm in those with a wall thickness greater than 15 mm.2
When the diagnosis is less clear, the decision to embark on more advanced diagnostic methods, such as biopsy, should rest on the provider’s clinical suspicion for a certain disease process. When a lung cancer is suspected, consultation with pulmonary and interventional radiology should be obtained to determine the best approach for biopsy.
Rheumatologic. Less common causes of cavitary lesions include those related to rheumatologic diseases (e.g. granulomatosis with polyangiitis, formerly known as Wegener’s granulomatosis). One study demonstrated that cavitary lung nodules occur in 37% of patients with granulomatosis with polyangiitis.8
Although uncommon, cavitary nodules can also be seen in rheumatoid arthritis and sarcoidosis. Given that patients with rheumatologic diseases are often treated with immunosuppressive agents, infection must remain high on the differential. Suspicion of a rheumatologic cause should prompt the clinician to obtain appropriate serologic testing and consultation as needed.
Pulmonary embolism. Although often not considered in the evaluation of cavitary lung lesions, pulmonary embolism (PE) can lead to infarction and the formation of a cavitary lesion. Pulmonary infarction has been reported to occur in as many as one third of cases of PE.9 Cavitary lesions also have been described in chronic thromboembolic disease.10
Other. Uncommon causes of cavitary lesions include bronchiolitis obliterans with organizing pneumonia, Langerhans cell histiocytosis, and amyloidosis, among others. The hospitalist should keep a broad differential and involve consultants if the diagnosis remains unclear after initial diagnostic evaluation.
Back to the Case
The patient’s fever and productive cough, in combination with recent travel and location of the cavitary lesion, increase his risk for tuberculosis and endemic fungi, such as Coccidioides. This patient was placed on respiratory isolation with AFBs obtained to rule out TB, with Coccidioides antibodies, Cyptococcal antigen titers, and sputum for fungus sent to evaluate for an endemic fungus. He had a chest CT, which revealed a 17-mm cavitary mass within the right upper lobe that contained an air-fluid level indicating lung abscess. Coccidioides, cryptococcal, fungal sputum, and TB studies were negative.
The patient was treated empirically with clindamycin given the high prevalence of anaerobes in lung abscess. He was followed as an outpatient and had a chest X-ray showing resolution of the lesion at six months. The purpose of the X-ray was two-fold: to monitor the effect of antibiotic treatment and to evaluate for persistence of the cavitation given the neoplastic risk factors of older age and smoking.
Bottom Line
The best approach to a patient with a cavitary lung lesion includes assessing the clinical presentation and risk factors, differentiating infectious from noninfectious causes, and then utilizing this information to further direct the diagnostic evaluation. Consultation with a subspecialist or further testing such as biopsy should be considered if the etiology remains undefined after the initial evaluation.
Drs. Rendon, Pizanis, Montanaro, and Kraai are hospitalists in the department of internal medicine at the University of New Mexico School of Medicine in Albuquerque.
References
- Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008;246(3):697-722.
- Ryu JH, Swensen SJ. Cystic and cavitary lung diseases: focal and diffuse. Mayo Clin Proc. 2003;78(6):744-752.
- Barnes PF, Verdegem TD, Vachon LA, Leedom JM, Overturf GD. Chest roentgenogram in pulmonary tuberculosis. New data on an old test. Chest. 1988;94(2):316-320.
- Yazbeck MF, Dahdel M, Kalra A, Browne AS, Pratter MR. Lung abscess: update on microbiology and management. Am J Ther. 2012;21(3):217-221. doi: 10.1097/MJT.0b013e3182383c9b.
- Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-333.
- Chiu FT. Cavitation in lung cancers. Aust N Z J Med. 1975;5(6):523-530.
- Kolodziejski LS, Dyczek S, Duda K, Góralczyk J, Wysocki WM, Lobaziewicz W. Cavitated tumor as a clinical subentity in squamous cell lung cancer patients. Neoplasma. 2003;50(1):66-73.
- Cordier JF, Valeyre D, Guillevin L, Loire R, Brechot JM. Pulmonary Wegener’s granulomatosis. A clinical and imaging study of 77 cases. Chest. 1990;97(4):906-912.
- He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006;21(1):1-7.
- Harris H, Barraclough R, Davies C, Armstrong I, Kiely DG, van Beek E Jr. Cavitating lung lesions in chronic thromboembolic pulmonary hypertension. J Radiol Case Rep. 2008;2(3):11-21.
- Woodring JH, Fried AM, Chuang VP. Solitary cavities of the lung: diagnostic implications of cavity wall thickness. AJR Am J Roentgenol. 1980;135(6):1269-1271.
Hospitalists Are Frontline Providers in Treating Venous Thromboembolism

“While VTE may not be the No. 1 reason for hospitalization, hospitalists very frequently care for patients with VTE,” says Sowmya Kanikkannan, MD, FACP, SFHM, hospitalist medical director and assistant professor of medicine at Rowan University School of Osteopathic Medicine in Stratford, N.J. “Hospitalists usually are the frontline providers that diagnose and manage hospital-acquired VTEs in hospitalized patients.”
Dr. Kanikkannan, a member of Team Hospitalist, sees a wide range of VTE cases caused by two related conditions—deep vein thrombosis (DVT) and pulmonary embolism (PE).
“Some patients present with a straightforward diagnosis of DVT, while others have extensive DVT,” she says. “In other instances, patients present with acute PE with or without hemodynamic compromise. I’ve also diagnosed and managed hospital-acquired VTEs in medical patients, as well as post-operatively in surgical co-management.”

It is estimated that between 350,000 to 900,000 Americans are affected by DVT or PE each year, with up to 100,000 dying as a result. Twenty to 50% of people who experience DVT develop long-term complications.1VTE costs the U.S. healthcare system more than $1.5 billion annually.2
As lieutenants in the war against VTE, hospitalists are finding that new treatments, continued efforts to standardize VTE prophylaxis, and increased transparency in performance reporting are the tools needed to combat these common conditions—and hospitalists are being held accountable for optimal patient care.
New Treatments Show Promise
Diagnosing and treating VTE early helps to prevent progression and hemodynamic instability. Although the accepted treatment for VTE used to be heparin, or a low molecular weight heparin (LMWH) (Fragmin, Innohep and Lovenox) with a transition to warfarin, three target-specific oral anticoagulants (TSOACs)—dabigatran, rivaroxaban, and apixaban—are now being prescribed. The FDA has approved rivaroxaban and apixaban for the prevention of VTE after knee and hip surgery and for treatment of VTE, while dabigatran is FDA approved only for the treatment of VTE. All three are approved for use in nonvalvular atrial fibrillation (Afib). A fourth TSOAC, edoxaban, received FDA approval in January for VTE treatment and nonvalvular atrial fibrillation.
“The drawback of warfarin is that patients need frequent international normalized ratio (INR) monitoring,” Dr. Kanikkannan says. “Discharge planning is time consuming because patients need to be educated on warfarin, and follow-up appointments need to be arranged before discharge to ensure patient safety.”
“Their [TSOACs] ease of administration and easy dosing helps hospitalists to manage patients with VTE more efficiently,” Dr. Kanikkannan says. “Patients like having lab testing less frequently but equal efficacy in treatment.”
Rivaroxaban used to have the most approved indications by the FDA; however, based on three clinical trials—ADVANCE-1, 2, and 3—apixaban has the same six FDA indications as rivaroxaban.
The majority of clinical trials suggest noninferiority or superiority of the oral agents compared to LMWH, and safety appears to be similar across treatment groups, other than an increased risk in bleeding with oral agents (see Table 1).
“The increased risk of bleeding seen in trials is something hospitalists need to consider,” says Yong Lee, PharmD, BCPS, clinical pharmacy specialist at Parkland Health and Hospital System in Dallas, Texas. Warfarin is easily reversed; the new anticoagulants don’t have any specific reversal agent (see new table about reversal options). Consequently, the American College of Chest Physicians still recommends unfractionated heparin or a LMWH for VTE prophylaxis. “These agents will still likely remain the best available options to hospitalists for VTE prevention,” he adds.
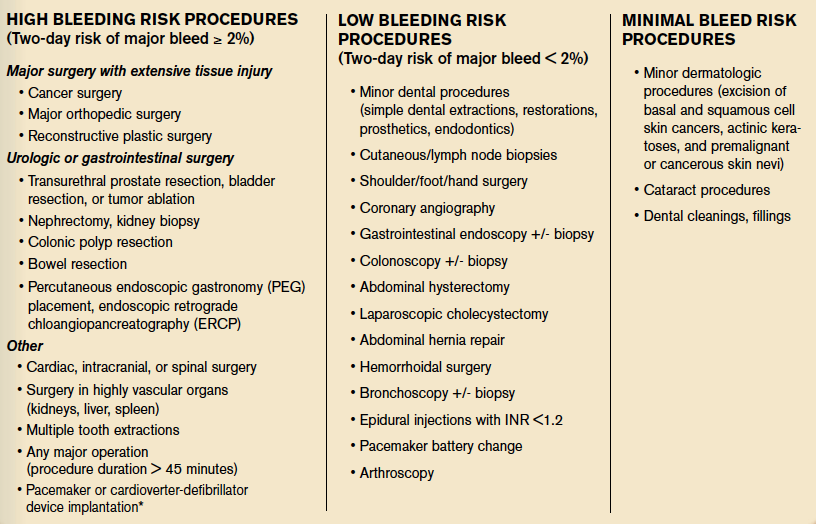
Julianna Lindsey, MD, MBA, FACP, FHM, chief of staff and hospitalist at Victory Medical Center in McKinney, Texas, says there are instances when it would be helpful to know what the therapeutic level of a TSOAC’s anticoagulation effect is, such as in a patient with active bleeding or one who requires major emergent surgery. But there is no coagulation assay to date that is readily available to test the effect of apixaban; the anticoagulation effect for dabigatran can be roughly estimated by the activated partial thromboplastin time (aPTT) and thrombin time (TT), and the anticoagulation effect for rivaroxaban can be roughly estimated by the prothrombin time (PT).

Dr. Lee expects the new FDA approvals to expand the utilization of oral anti-Xa inhibitors in practice. “This will, hopefully, make the new oral anticoagulant market more competitive, driving down their costs,” he says, referring to one of the biggest barriers to current use of these agents. Warfarin still remains the most cost-effective option, despite the need for regular INR monitoring.
“Studies are looking not only at effectiveness but also the safety profile of these anticoagulants,” Dr. Kanikkannan says, as long-term safety data is not yet available on these oral agents.8,9

Researchers also are looking at the comparative effects of other medications. For example, a Journal of Hospital Medicine study concluded that, compared with other anticoagulants, aspirin is associated with a higher risk of DVT following hip fracture repair but similar rates of DVT risk following hip-knee arthroplasty. Bleeding rates with aspirin, however, were substantially lower.10

Improvement Efforts
In an effort to improve VTE prophylaxis in hospitalized patients, The Joint Commission developed a VTE standardized performance measure set in 2009, which has been reported on www.qualitycheck.org since then. The VTE measure set comprises six different measures evaluating the prophylaxis of VTE, treatment of VTE, warfarin discharge education, and hospital-acquired VTE. Since reporting started, most hospitals have implemented VTE risk assessment models and VTE process improvement programs; data trends have shown improvement, says Denise Krusenoski, MSN, RN, CMSRN, CHTS-CP, associate project director at The Joint Commission, which is based in Oakbrook Terrace, Ill.
“While a lot of good, evidence-based data is available, no single VTE risk assessment tool has been prospectively validated as superior,” she says. “Involving key members of medical staff to create and approve protocols based on proven data will increase the buy-in and adoption for using these tools.”
E-Measures Promote Excellence
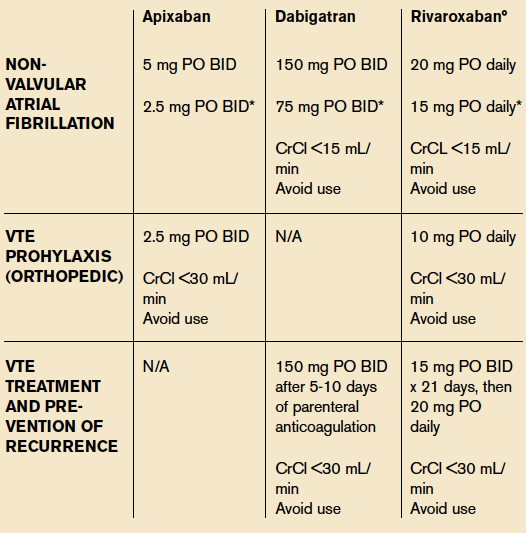
Many hospitals are now moving from traditional chart abstracting for VTE measures to electronic measures (e-measures), which allow for more rapid and automated reporting of these quality metrics. In order for e-measures to be accurate, documentation necessary for measure computation must be present in defined standardized fields in the medical record. “With no human interpretation, data must be documented in a precise fashion,” Krusenoski says. “Providers will need to be flexible in learning new documentation skills.”
Dr. Lindsey, a member of Team Hospitalist, cautions that e-measures have the potential to increase unwanted events by overutilization of pharmacologic VTE prophylaxis and associated hemorrhagic events.
“We have to continue to make sure that our practice of medicine remains based in evidence and not succumb to the pull of getting a check-box ticked,” she warns.
VTE remains a significant problem in hospitalized patients today. Hospitalists should consider the pros and cons of using newer treatment methods over traditional agents. Efforts are under way to improve VTE prophylaxis by standardizing best practice and moving from traditional chart abstracting to using e-measures for performance reporting.
Karen Appold is a freelance medical writer in Pennsylvania.
Bringing Awareness to VTE
Thromboembolisms (VTEs) are the most common cause of preventable death in the hospitalized patient. Given the adverse outcomes and economic burden associated with VTEs, it is truly a public health concern. As Dr. Kanikkannan suggests, “Why not use the month of March—VTE awareness month—as an opportunity to educate patients about healthy lifestyle practices to prevent VTE?
“Patients can learn to identify their risk factors and become aware of symptoms that may be a cause for concern, prompting them to seek medical attention,” she says.

Hospitalists could also organize or participate in community health fairs—a great venue to spread the word about VTE and create awareness among the public. Because hospitalists frequently sit on VTE task forces in hospitals and take a lead role in implementing VTE prophylaxis efforts, they are in a prime position to implement a hospital campaign during VTE awareness month.
Keeping staff abreast of advancements is also advisable.
“It might be helpful for hospitals to arrange review sessions for VTE prophylaxis for providers and staff,” says Klaus Suehler, MD, FHM, hospitalist at Mercy Hospital Allina Health in Coon Rapids, Minn., who believes that creating awareness makes a 0% failure rate on VTE prophylaxis achievable.
—Karen Appold
References
- Centers for Disease Control and Prevention. Public Health Grand Rounds. Preventing venous thromboembolism. January 15, 2013. Available at: http://www.cdc.gov/cdcgrandrounds/archives/2013/january2013.htm. Accessed February 12, 2015.
- Dobesh PP. Economic burden of venous thromboembolism in hospitalized patients. Pharmacotherapy. 2009;29(8):943-953.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): a randomised double-blind trial. Lancet. 2010;375(9717):807-815.
- Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
- Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368(6):513-523.
- Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med. 2011;365(23):2167-2177.
- Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013;88(5):495-511.
- Holster IL, Valkoff VE, Kuipers EJ, Tjwa ET. New oral anticoagulants increase risk for gastrointestinal bleeding: a systematic review and meta-analysis. Gastroenterology. 2013;145(1):105-112.
- Drescher FS, Sirovich BE, Lee A, Morrison DH, Chiang WH, Larson RJ. Aspirin versus anticoagulation for prevention of venous thromboembolism major lower extremity orthopedic surgery: a systematic review and meta-analysis. J Hosp Med. 2014;9(9):579-585.
- Bullock-Palmer RP, Weiss S, Hyman C. Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital-acquired deep vein thrombosis at a tertiary-care teaching hospital. J Hosp Med. 2008;3(2):148-155.
“While VTE may not be the No. 1 reason for hospitalization, hospitalists very frequently care for patients with VTE,” says Sowmya Kanikkannan, MD, FACP, SFHM, hospitalist medical director and assistant professor of medicine at Rowan University School of Osteopathic Medicine in Stratford, N.J. “Hospitalists usually are the frontline providers that diagnose and manage hospital-acquired VTEs in hospitalized patients.”
Dr. Kanikkannan, a member of Team Hospitalist, sees a wide range of VTE cases caused by two related conditions—deep vein thrombosis (DVT) and pulmonary embolism (PE).
“Some patients present with a straightforward diagnosis of DVT, while others have extensive DVT,” she says. “In other instances, patients present with acute PE with or without hemodynamic compromise. I’ve also diagnosed and managed hospital-acquired VTEs in medical patients, as well as post-operatively in surgical co-management.”
It is estimated that between 350,000 to 900,000 Americans are affected by DVT or PE each year, with up to 100,000 dying as a result. Twenty to 50% of people who experience DVT develop long-term complications.1VTE costs the U.S. healthcare system more than $1.5 billion annually.2
As lieutenants in the war against VTE, hospitalists are finding that new treatments, continued efforts to standardize VTE prophylaxis, and increased transparency in performance reporting are the tools needed to combat these common conditions—and hospitalists are being held accountable for optimal patient care.
New Treatments Show Promise
Diagnosing and treating VTE early helps to prevent progression and hemodynamic instability. Although the accepted treatment for VTE used to be heparin, or a low molecular weight heparin (LMWH) (Fragmin, Innohep and Lovenox) with a transition to warfarin, three target-specific oral anticoagulants (TSOACs)—dabigatran, rivaroxaban, and apixaban—are now being prescribed. The FDA has approved rivaroxaban and apixaban for the prevention of VTE after knee and hip surgery and for treatment of VTE, while dabigatran is FDA approved only for the treatment of VTE. All three are approved for use in nonvalvular atrial fibrillation (Afib). A fourth TSOAC, edoxaban, received FDA approval in January for VTE treatment and nonvalvular atrial fibrillation.
“The drawback of warfarin is that patients need frequent international normalized ratio (INR) monitoring,” Dr. Kanikkannan says. “Discharge planning is time consuming because patients need to be educated on warfarin, and follow-up appointments need to be arranged before discharge to ensure patient safety.”
“Their [TSOACs] ease of administration and easy dosing helps hospitalists to manage patients with VTE more efficiently,” Dr. Kanikkannan says. “Patients like having lab testing less frequently but equal efficacy in treatment.”
Rivaroxaban used to have the most approved indications by the FDA; however, based on three clinical trials—ADVANCE-1, 2, and 3—apixaban has the same six FDA indications as rivaroxaban.
The majority of clinical trials suggest noninferiority or superiority of the oral agents compared to LMWH, and safety appears to be similar across treatment groups, other than an increased risk in bleeding with oral agents (see Table 1).
“The increased risk of bleeding seen in trials is something hospitalists need to consider,” says Yong Lee, PharmD, BCPS, clinical pharmacy specialist at Parkland Health and Hospital System in Dallas, Texas. Warfarin is easily reversed; the new anticoagulants don’t have any specific reversal agent (see new table about reversal options). Consequently, the American College of Chest Physicians still recommends unfractionated heparin or a LMWH for VTE prophylaxis. “These agents will still likely remain the best available options to hospitalists for VTE prevention,” he adds.
Julianna Lindsey, MD, MBA, FACP, FHM, chief of staff and hospitalist at Victory Medical Center in McKinney, Texas, says there are instances when it would be helpful to know what the therapeutic level of a TSOAC’s anticoagulation effect is, such as in a patient with active bleeding or one who requires major emergent surgery. But there is no coagulation assay to date that is readily available to test the effect of apixaban; the anticoagulation effect for dabigatran can be roughly estimated by the activated partial thromboplastin time (aPTT) and thrombin time (TT), and the anticoagulation effect for rivaroxaban can be roughly estimated by the prothrombin time (PT).
Dr. Lee expects the new FDA approvals to expand the utilization of oral anti-Xa inhibitors in practice. “This will, hopefully, make the new oral anticoagulant market more competitive, driving down their costs,” he says, referring to one of the biggest barriers to current use of these agents. Warfarin still remains the most cost-effective option, despite the need for regular INR monitoring.
“Studies are looking not only at effectiveness but also the safety profile of these anticoagulants,” Dr. Kanikkannan says, as long-term safety data is not yet available on these oral agents.8,9
Researchers also are looking at the comparative effects of other medications. For example, a Journal of Hospital Medicine study concluded that, compared with other anticoagulants, aspirin is associated with a higher risk of DVT following hip fracture repair but similar rates of DVT risk following hip-knee arthroplasty. Bleeding rates with aspirin, however, were substantially lower.10
Improvement Efforts
In an effort to improve VTE prophylaxis in hospitalized patients, The Joint Commission developed a VTE standardized performance measure set in 2009, which has been reported on www.qualitycheck.org since then. The VTE measure set comprises six different measures evaluating the prophylaxis of VTE, treatment of VTE, warfarin discharge education, and hospital-acquired VTE. Since reporting started, most hospitals have implemented VTE risk assessment models and VTE process improvement programs; data trends have shown improvement, says Denise Krusenoski, MSN, RN, CMSRN, CHTS-CP, associate project director at The Joint Commission, which is based in Oakbrook Terrace, Ill.
“While a lot of good, evidence-based data is available, no single VTE risk assessment tool has been prospectively validated as superior,” she says. “Involving key members of medical staff to create and approve protocols based on proven data will increase the buy-in and adoption for using these tools.”
E-Measures Promote Excellence
Many hospitals are now moving from traditional chart abstracting for VTE measures to electronic measures (e-measures), which allow for more rapid and automated reporting of these quality metrics. In order for e-measures to be accurate, documentation necessary for measure computation must be present in defined standardized fields in the medical record. “With no human interpretation, data must be documented in a precise fashion,” Krusenoski says. “Providers will need to be flexible in learning new documentation skills.”
Dr. Lindsey, a member of Team Hospitalist, cautions that e-measures have the potential to increase unwanted events by overutilization of pharmacologic VTE prophylaxis and associated hemorrhagic events.
“We have to continue to make sure that our practice of medicine remains based in evidence and not succumb to the pull of getting a check-box ticked,” she warns.
VTE remains a significant problem in hospitalized patients today. Hospitalists should consider the pros and cons of using newer treatment methods over traditional agents. Efforts are under way to improve VTE prophylaxis by standardizing best practice and moving from traditional chart abstracting to using e-measures for performance reporting.
Karen Appold is a freelance medical writer in Pennsylvania.
Bringing Awareness to VTE
Thromboembolisms (VTEs) are the most common cause of preventable death in the hospitalized patient. Given the adverse outcomes and economic burden associated with VTEs, it is truly a public health concern. As Dr. Kanikkannan suggests, “Why not use the month of March—VTE awareness month—as an opportunity to educate patients about healthy lifestyle practices to prevent VTE?
“Patients can learn to identify their risk factors and become aware of symptoms that may be a cause for concern, prompting them to seek medical attention,” she says.
Hospitalists could also organize or participate in community health fairs—a great venue to spread the word about VTE and create awareness among the public. Because hospitalists frequently sit on VTE task forces in hospitals and take a lead role in implementing VTE prophylaxis efforts, they are in a prime position to implement a hospital campaign during VTE awareness month.
Keeping staff abreast of advancements is also advisable.
“It might be helpful for hospitals to arrange review sessions for VTE prophylaxis for providers and staff,” says Klaus Suehler, MD, FHM, hospitalist at Mercy Hospital Allina Health in Coon Rapids, Minn., who believes that creating awareness makes a 0% failure rate on VTE prophylaxis achievable.
—Karen Appold
References
- Centers for Disease Control and Prevention. Public Health Grand Rounds. Preventing venous thromboembolism. January 15, 2013. Available at: http://www.cdc.gov/cdcgrandrounds/archives/2013/january2013.htm. Accessed February 12, 2015.
- Dobesh PP. Economic burden of venous thromboembolism in hospitalized patients. Pharmacotherapy. 2009;29(8):943-953.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): a randomised double-blind trial. Lancet. 2010;375(9717):807-815.
- Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
- Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368(6):513-523.
- Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med. 2011;365(23):2167-2177.
- Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013;88(5):495-511.
- Holster IL, Valkoff VE, Kuipers EJ, Tjwa ET. New oral anticoagulants increase risk for gastrointestinal bleeding: a systematic review and meta-analysis. Gastroenterology. 2013;145(1):105-112.
- Drescher FS, Sirovich BE, Lee A, Morrison DH, Chiang WH, Larson RJ. Aspirin versus anticoagulation for prevention of venous thromboembolism major lower extremity orthopedic surgery: a systematic review and meta-analysis. J Hosp Med. 2014;9(9):579-585.
- Bullock-Palmer RP, Weiss S, Hyman C. Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital-acquired deep vein thrombosis at a tertiary-care teaching hospital. J Hosp Med. 2008;3(2):148-155.
“While VTE may not be the No. 1 reason for hospitalization, hospitalists very frequently care for patients with VTE,” says Sowmya Kanikkannan, MD, FACP, SFHM, hospitalist medical director and assistant professor of medicine at Rowan University School of Osteopathic Medicine in Stratford, N.J. “Hospitalists usually are the frontline providers that diagnose and manage hospital-acquired VTEs in hospitalized patients.”
Dr. Kanikkannan, a member of Team Hospitalist, sees a wide range of VTE cases caused by two related conditions—deep vein thrombosis (DVT) and pulmonary embolism (PE).
“Some patients present with a straightforward diagnosis of DVT, while others have extensive DVT,” she says. “In other instances, patients present with acute PE with or without hemodynamic compromise. I’ve also diagnosed and managed hospital-acquired VTEs in medical patients, as well as post-operatively in surgical co-management.”
It is estimated that between 350,000 to 900,000 Americans are affected by DVT or PE each year, with up to 100,000 dying as a result. Twenty to 50% of people who experience DVT develop long-term complications.1VTE costs the U.S. healthcare system more than $1.5 billion annually.2
As lieutenants in the war against VTE, hospitalists are finding that new treatments, continued efforts to standardize VTE prophylaxis, and increased transparency in performance reporting are the tools needed to combat these common conditions—and hospitalists are being held accountable for optimal patient care.
New Treatments Show Promise
Diagnosing and treating VTE early helps to prevent progression and hemodynamic instability. Although the accepted treatment for VTE used to be heparin, or a low molecular weight heparin (LMWH) (Fragmin, Innohep and Lovenox) with a transition to warfarin, three target-specific oral anticoagulants (TSOACs)—dabigatran, rivaroxaban, and apixaban—are now being prescribed. The FDA has approved rivaroxaban and apixaban for the prevention of VTE after knee and hip surgery and for treatment of VTE, while dabigatran is FDA approved only for the treatment of VTE. All three are approved for use in nonvalvular atrial fibrillation (Afib). A fourth TSOAC, edoxaban, received FDA approval in January for VTE treatment and nonvalvular atrial fibrillation.
“The drawback of warfarin is that patients need frequent international normalized ratio (INR) monitoring,” Dr. Kanikkannan says. “Discharge planning is time consuming because patients need to be educated on warfarin, and follow-up appointments need to be arranged before discharge to ensure patient safety.”
“Their [TSOACs] ease of administration and easy dosing helps hospitalists to manage patients with VTE more efficiently,” Dr. Kanikkannan says. “Patients like having lab testing less frequently but equal efficacy in treatment.”
Rivaroxaban used to have the most approved indications by the FDA; however, based on three clinical trials—ADVANCE-1, 2, and 3—apixaban has the same six FDA indications as rivaroxaban.
The majority of clinical trials suggest noninferiority or superiority of the oral agents compared to LMWH, and safety appears to be similar across treatment groups, other than an increased risk in bleeding with oral agents (see Table 1).
“The increased risk of bleeding seen in trials is something hospitalists need to consider,” says Yong Lee, PharmD, BCPS, clinical pharmacy specialist at Parkland Health and Hospital System in Dallas, Texas. Warfarin is easily reversed; the new anticoagulants don’t have any specific reversal agent (see new table about reversal options). Consequently, the American College of Chest Physicians still recommends unfractionated heparin or a LMWH for VTE prophylaxis. “These agents will still likely remain the best available options to hospitalists for VTE prevention,” he adds.
Julianna Lindsey, MD, MBA, FACP, FHM, chief of staff and hospitalist at Victory Medical Center in McKinney, Texas, says there are instances when it would be helpful to know what the therapeutic level of a TSOAC’s anticoagulation effect is, such as in a patient with active bleeding or one who requires major emergent surgery. But there is no coagulation assay to date that is readily available to test the effect of apixaban; the anticoagulation effect for dabigatran can be roughly estimated by the activated partial thromboplastin time (aPTT) and thrombin time (TT), and the anticoagulation effect for rivaroxaban can be roughly estimated by the prothrombin time (PT).
Dr. Lee expects the new FDA approvals to expand the utilization of oral anti-Xa inhibitors in practice. “This will, hopefully, make the new oral anticoagulant market more competitive, driving down their costs,” he says, referring to one of the biggest barriers to current use of these agents. Warfarin still remains the most cost-effective option, despite the need for regular INR monitoring.
“Studies are looking not only at effectiveness but also the safety profile of these anticoagulants,” Dr. Kanikkannan says, as long-term safety data is not yet available on these oral agents.8,9
Researchers also are looking at the comparative effects of other medications. For example, a Journal of Hospital Medicine study concluded that, compared with other anticoagulants, aspirin is associated with a higher risk of DVT following hip fracture repair but similar rates of DVT risk following hip-knee arthroplasty. Bleeding rates with aspirin, however, were substantially lower.10
Improvement Efforts
In an effort to improve VTE prophylaxis in hospitalized patients, The Joint Commission developed a VTE standardized performance measure set in 2009, which has been reported on www.qualitycheck.org since then. The VTE measure set comprises six different measures evaluating the prophylaxis of VTE, treatment of VTE, warfarin discharge education, and hospital-acquired VTE. Since reporting started, most hospitals have implemented VTE risk assessment models and VTE process improvement programs; data trends have shown improvement, says Denise Krusenoski, MSN, RN, CMSRN, CHTS-CP, associate project director at The Joint Commission, which is based in Oakbrook Terrace, Ill.
“While a lot of good, evidence-based data is available, no single VTE risk assessment tool has been prospectively validated as superior,” she says. “Involving key members of medical staff to create and approve protocols based on proven data will increase the buy-in and adoption for using these tools.”
E-Measures Promote Excellence
Many hospitals are now moving from traditional chart abstracting for VTE measures to electronic measures (e-measures), which allow for more rapid and automated reporting of these quality metrics. In order for e-measures to be accurate, documentation necessary for measure computation must be present in defined standardized fields in the medical record. “With no human interpretation, data must be documented in a precise fashion,” Krusenoski says. “Providers will need to be flexible in learning new documentation skills.”
Dr. Lindsey, a member of Team Hospitalist, cautions that e-measures have the potential to increase unwanted events by overutilization of pharmacologic VTE prophylaxis and associated hemorrhagic events.
“We have to continue to make sure that our practice of medicine remains based in evidence and not succumb to the pull of getting a check-box ticked,” she warns.
VTE remains a significant problem in hospitalized patients today. Hospitalists should consider the pros and cons of using newer treatment methods over traditional agents. Efforts are under way to improve VTE prophylaxis by standardizing best practice and moving from traditional chart abstracting to using e-measures for performance reporting.
Karen Appold is a freelance medical writer in Pennsylvania.
Bringing Awareness to VTE
Thromboembolisms (VTEs) are the most common cause of preventable death in the hospitalized patient. Given the adverse outcomes and economic burden associated with VTEs, it is truly a public health concern. As Dr. Kanikkannan suggests, “Why not use the month of March—VTE awareness month—as an opportunity to educate patients about healthy lifestyle practices to prevent VTE?
“Patients can learn to identify their risk factors and become aware of symptoms that may be a cause for concern, prompting them to seek medical attention,” she says.
Hospitalists could also organize or participate in community health fairs—a great venue to spread the word about VTE and create awareness among the public. Because hospitalists frequently sit on VTE task forces in hospitals and take a lead role in implementing VTE prophylaxis efforts, they are in a prime position to implement a hospital campaign during VTE awareness month.
Keeping staff abreast of advancements is also advisable.
“It might be helpful for hospitals to arrange review sessions for VTE prophylaxis for providers and staff,” says Klaus Suehler, MD, FHM, hospitalist at Mercy Hospital Allina Health in Coon Rapids, Minn., who believes that creating awareness makes a 0% failure rate on VTE prophylaxis achievable.
—Karen Appold
References
- Centers for Disease Control and Prevention. Public Health Grand Rounds. Preventing venous thromboembolism. January 15, 2013. Available at: http://www.cdc.gov/cdcgrandrounds/archives/2013/january2013.htm. Accessed February 12, 2015.
- Dobesh PP. Economic burden of venous thromboembolism in hospitalized patients. Pharmacotherapy. 2009;29(8):943-953.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Portman RJ. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. N Engl J Med. 2009;361(6):594-604.
- Lassen MR, Raskob GE, Gallus A, Pineo G, Chen D, Hornick P; ADVANCE-2 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after knee replacement (ADVANCE-2): a randomised double-blind trial. Lancet. 2010;375(9717):807-815.
- Lassen MR, Gallus A, Raskob GE, Pineo G, Chen D, Ramirez LM; ADVANCE-3 Investigators. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. N Engl J Med. 2010;363(26):2487-2498.
- Cohen AT, Spiro TE, Büller HR, et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N Engl J Med. 2013;368(6):513-523.
- Goldhaber SZ, Leizorovicz A, Kakkar AK, et al. Apixaban versus enoxaparin for thromboprophylaxis in medically ill patients. N Engl J Med. 2011;365(23):2167-2177.
- Gonsalves WI, Pruthi RK, Patnaik MM. The new oral anticoagulants in clinical practice. Mayo Clin Proc. 2013;88(5):495-511.
- Holster IL, Valkoff VE, Kuipers EJ, Tjwa ET. New oral anticoagulants increase risk for gastrointestinal bleeding: a systematic review and meta-analysis. Gastroenterology. 2013;145(1):105-112.
- Drescher FS, Sirovich BE, Lee A, Morrison DH, Chiang WH, Larson RJ. Aspirin versus anticoagulation for prevention of venous thromboembolism major lower extremity orthopedic surgery: a systematic review and meta-analysis. J Hosp Med. 2014;9(9):579-585.
- Bullock-Palmer RP, Weiss S, Hyman C. Innovative approaches to increase deep vein thrombosis prophylaxis rate resulting in a decrease in hospital-acquired deep vein thrombosis at a tertiary-care teaching hospital. J Hosp Med. 2008;3(2):148-155.
{kind=link}
Left Atrial Appendage Closure Noninferior to Warfain for Cardioembolic Event Prophylaxis in Nonvalvular Afibrillation
Clinical question: Is mechanical, left atrial appendage (LAA) closure as effective as warfarin therapy in preventing cardioembolic events in patients with nonvalvular atrial fibrillation (Afib)?
Background: Anticoagulation with warfarin has long been the standard therapy for prevention of thromboembolic complications of nonvalvular Afib; however, its use is limited by the need for monitoring and lifelong adherence, as well as its many dietary and medication interactions. Prior studies investigating the efficacy of a deployable device intended to close the LAA have shown noninferiority of the device when compared with standard warfarin anticoagulation. This study evaluated LAA closure device efficacy after a 3.8-year interval.
Study design: Randomized, unblinded controlled trial.
Setting: Fifty-nine centers in the U.S. and Europe.
Synopsis: Authors randomized 707 participants 18 years or older with nonvalvular Afib and CHADS2 score ≥1 in a 2:1 fashion to the intervention and warfarin therapy groups. The primary outcome was a composite endpoint including stroke, systemic embolism, and cardiovascular or unexplained death. The event rate in the device group was 2.3 per 100 patient-years, compared with 3.8 in the warfarin group. Rate ratio was 0.60, meeting noninferiority criteria. Primary safety events were not statistically different.
Although the authors concluded that LAA device closure was noninferior to warfarin therapy, it should be noted that there was a high dropout rate, especially in the warfarin group, motivated either by a desire to try a novel oral anticoagulant or the perception that warfarin therapy was not beneficial. It should also be noted that device placement involved not only a percutaneous procedure, but also 45 days of aspirin and warfarin therapy initially to promote endothelization, followed by six months of clopidogrel.
Bottom line: Percutaneous device closure of the LAA appears to be noninferior to warfarin therapy in the prevention of cardioembolic events over a period of several years, and might be superior.
Clinical question: Is mechanical, left atrial appendage (LAA) closure as effective as warfarin therapy in preventing cardioembolic events in patients with nonvalvular atrial fibrillation (Afib)?
Background: Anticoagulation with warfarin has long been the standard therapy for prevention of thromboembolic complications of nonvalvular Afib; however, its use is limited by the need for monitoring and lifelong adherence, as well as its many dietary and medication interactions. Prior studies investigating the efficacy of a deployable device intended to close the LAA have shown noninferiority of the device when compared with standard warfarin anticoagulation. This study evaluated LAA closure device efficacy after a 3.8-year interval.
Study design: Randomized, unblinded controlled trial.
Setting: Fifty-nine centers in the U.S. and Europe.
Synopsis: Authors randomized 707 participants 18 years or older with nonvalvular Afib and CHADS2 score ≥1 in a 2:1 fashion to the intervention and warfarin therapy groups. The primary outcome was a composite endpoint including stroke, systemic embolism, and cardiovascular or unexplained death. The event rate in the device group was 2.3 per 100 patient-years, compared with 3.8 in the warfarin group. Rate ratio was 0.60, meeting noninferiority criteria. Primary safety events were not statistically different.
Although the authors concluded that LAA device closure was noninferior to warfarin therapy, it should be noted that there was a high dropout rate, especially in the warfarin group, motivated either by a desire to try a novel oral anticoagulant or the perception that warfarin therapy was not beneficial. It should also be noted that device placement involved not only a percutaneous procedure, but also 45 days of aspirin and warfarin therapy initially to promote endothelization, followed by six months of clopidogrel.
Bottom line: Percutaneous device closure of the LAA appears to be noninferior to warfarin therapy in the prevention of cardioembolic events over a period of several years, and might be superior.
Clinical question: Is mechanical, left atrial appendage (LAA) closure as effective as warfarin therapy in preventing cardioembolic events in patients with nonvalvular atrial fibrillation (Afib)?
Background: Anticoagulation with warfarin has long been the standard therapy for prevention of thromboembolic complications of nonvalvular Afib; however, its use is limited by the need for monitoring and lifelong adherence, as well as its many dietary and medication interactions. Prior studies investigating the efficacy of a deployable device intended to close the LAA have shown noninferiority of the device when compared with standard warfarin anticoagulation. This study evaluated LAA closure device efficacy after a 3.8-year interval.
Study design: Randomized, unblinded controlled trial.
Setting: Fifty-nine centers in the U.S. and Europe.
Synopsis: Authors randomized 707 participants 18 years or older with nonvalvular Afib and CHADS2 score ≥1 in a 2:1 fashion to the intervention and warfarin therapy groups. The primary outcome was a composite endpoint including stroke, systemic embolism, and cardiovascular or unexplained death. The event rate in the device group was 2.3 per 100 patient-years, compared with 3.8 in the warfarin group. Rate ratio was 0.60, meeting noninferiority criteria. Primary safety events were not statistically different.
Although the authors concluded that LAA device closure was noninferior to warfarin therapy, it should be noted that there was a high dropout rate, especially in the warfarin group, motivated either by a desire to try a novel oral anticoagulant or the perception that warfarin therapy was not beneficial. It should also be noted that device placement involved not only a percutaneous procedure, but also 45 days of aspirin and warfarin therapy initially to promote endothelization, followed by six months of clopidogrel.
Bottom line: Percutaneous device closure of the LAA appears to be noninferior to warfarin therapy in the prevention of cardioembolic events over a period of several years, and might be superior.
Tramadol Associated with Increased Rate of Hypoglycemia
Clinical question: Does tramadol increase rates of hospitalization from hypoglycemia compared to other opioids?
Background: As tramadol use has increased in the general population, there have been multiple reports of hypoglycemia after initiation of the painkiller, including in patients with no other known risk factors, such as diabetes mellitus.
Study design: Case control study.
Setting: United Kingdom.
Synopsis: Using the United Kingdom’s Clinical Practice Research Datalink, a cohort of 334,034 patients was identified, including 1,105 hospitalized for hypoglycemia. To compare incidence of hypoglycemia in patients taking tramadol versus nontramadol opioids, patients newly treated with tramadol for noncancer pain were compared with those treated with codeine.
Use of tramadol was associated with increase in hospitalization for treatment of hypoglycemia compared with codeine. Specifically, tramadol use had an odds ratio (OR) of 1.52 (95% confidence interval, 1.09-2.10). The risk of hypoglycemia was higher in the first 30 days of use, with an OR of 2.61 (95% confidence interval, 1.61-4.23).
Since tramadol prescribing has increased over the past 10 years, clinicians should be mindful of the potential association between tramadol and severe hypoglycemia requiring hospitalization. Although the details of the pathophysiology leading to this outcome remain unclear, evidence of a causal relationship is mounting. The association with hypoglycemia was seen particularly in the first 30 days of therapy. The incidence of less severe hypoglycemia not requiring hospitalization remains unknown.
Bottom line: Tramadol use is associated with increased rates of hypoglycemia requiring hospitalization.
Clinical question: Does tramadol increase rates of hospitalization from hypoglycemia compared to other opioids?
Background: As tramadol use has increased in the general population, there have been multiple reports of hypoglycemia after initiation of the painkiller, including in patients with no other known risk factors, such as diabetes mellitus.
Study design: Case control study.
Setting: United Kingdom.
Synopsis: Using the United Kingdom’s Clinical Practice Research Datalink, a cohort of 334,034 patients was identified, including 1,105 hospitalized for hypoglycemia. To compare incidence of hypoglycemia in patients taking tramadol versus nontramadol opioids, patients newly treated with tramadol for noncancer pain were compared with those treated with codeine.
Use of tramadol was associated with increase in hospitalization for treatment of hypoglycemia compared with codeine. Specifically, tramadol use had an odds ratio (OR) of 1.52 (95% confidence interval, 1.09-2.10). The risk of hypoglycemia was higher in the first 30 days of use, with an OR of 2.61 (95% confidence interval, 1.61-4.23).
Since tramadol prescribing has increased over the past 10 years, clinicians should be mindful of the potential association between tramadol and severe hypoglycemia requiring hospitalization. Although the details of the pathophysiology leading to this outcome remain unclear, evidence of a causal relationship is mounting. The association with hypoglycemia was seen particularly in the first 30 days of therapy. The incidence of less severe hypoglycemia not requiring hospitalization remains unknown.
Bottom line: Tramadol use is associated with increased rates of hypoglycemia requiring hospitalization.
Clinical question: Does tramadol increase rates of hospitalization from hypoglycemia compared to other opioids?
Background: As tramadol use has increased in the general population, there have been multiple reports of hypoglycemia after initiation of the painkiller, including in patients with no other known risk factors, such as diabetes mellitus.
Study design: Case control study.
Setting: United Kingdom.
Synopsis: Using the United Kingdom’s Clinical Practice Research Datalink, a cohort of 334,034 patients was identified, including 1,105 hospitalized for hypoglycemia. To compare incidence of hypoglycemia in patients taking tramadol versus nontramadol opioids, patients newly treated with tramadol for noncancer pain were compared with those treated with codeine.
Use of tramadol was associated with increase in hospitalization for treatment of hypoglycemia compared with codeine. Specifically, tramadol use had an odds ratio (OR) of 1.52 (95% confidence interval, 1.09-2.10). The risk of hypoglycemia was higher in the first 30 days of use, with an OR of 2.61 (95% confidence interval, 1.61-4.23).
Since tramadol prescribing has increased over the past 10 years, clinicians should be mindful of the potential association between tramadol and severe hypoglycemia requiring hospitalization. Although the details of the pathophysiology leading to this outcome remain unclear, evidence of a causal relationship is mounting. The association with hypoglycemia was seen particularly in the first 30 days of therapy. The incidence of less severe hypoglycemia not requiring hospitalization remains unknown.
Bottom line: Tramadol use is associated with increased rates of hypoglycemia requiring hospitalization.