User login
Clinical Images Capture Hospitalists’ Daily Rounds
EDITOR’S NOTE: Fourth in an occasional series of reviews of the Hospital Medicine: Current Concepts series by members of Team Hospitalist.
Summary
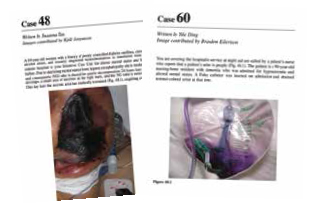
Hospital Images: A Clinical Atlas is a collection of 76 clinical cases discussing actual patient scenarios with accompanying clinical case questions, images, and evidence-based discussions. Cases are presented in the same manner a practicing hospitalist would encounter them during daily rounds—that is to say, randomly. Chosen cases vary widely, from aspiration pneumonitis to necrotizing fasciitis, and are also representative of a day in the life of most hospitalists. The clinical images are of excellent quality and accurately represent the conditions discussed. The case discussions are logical, clinically relevant, and evidence-based.
Analysis
In this reviewer’s opinion, Hospital Images: A Clinical Atlas is required reading for all practicing hospitalists. The full-color images are high resolution and presented as patients would be viewed from the bedside. The cases are diverse and absolutely pertinent to the practice of hospital medicine. I am confident even the most experienced reader will learn something that will quite probably improve his or her diagnostic capability.
Dr. Lindsey is a hospitalist and chief of staff at Victory Medical Center in McKinney, Texas. She has been a member of Team Hospitalist since 2013.

EDITOR’S NOTE: Fourth in an occasional series of reviews of the Hospital Medicine: Current Concepts series by members of Team Hospitalist.
Summary
Hospital Images: A Clinical Atlas is a collection of 76 clinical cases discussing actual patient scenarios with accompanying clinical case questions, images, and evidence-based discussions. Cases are presented in the same manner a practicing hospitalist would encounter them during daily rounds—that is to say, randomly. Chosen cases vary widely, from aspiration pneumonitis to necrotizing fasciitis, and are also representative of a day in the life of most hospitalists. The clinical images are of excellent quality and accurately represent the conditions discussed. The case discussions are logical, clinically relevant, and evidence-based.
Analysis
In this reviewer’s opinion, Hospital Images: A Clinical Atlas is required reading for all practicing hospitalists. The full-color images are high resolution and presented as patients would be viewed from the bedside. The cases are diverse and absolutely pertinent to the practice of hospital medicine. I am confident even the most experienced reader will learn something that will quite probably improve his or her diagnostic capability.
Dr. Lindsey is a hospitalist and chief of staff at Victory Medical Center in McKinney, Texas. She has been a member of Team Hospitalist since 2013.
EDITOR’S NOTE: Fourth in an occasional series of reviews of the Hospital Medicine: Current Concepts series by members of Team Hospitalist.
Summary
Hospital Images: A Clinical Atlas is a collection of 76 clinical cases discussing actual patient scenarios with accompanying clinical case questions, images, and evidence-based discussions. Cases are presented in the same manner a practicing hospitalist would encounter them during daily rounds—that is to say, randomly. Chosen cases vary widely, from aspiration pneumonitis to necrotizing fasciitis, and are also representative of a day in the life of most hospitalists. The clinical images are of excellent quality and accurately represent the conditions discussed. The case discussions are logical, clinically relevant, and evidence-based.
Analysis
In this reviewer’s opinion, Hospital Images: A Clinical Atlas is required reading for all practicing hospitalists. The full-color images are high resolution and presented as patients would be viewed from the bedside. The cases are diverse and absolutely pertinent to the practice of hospital medicine. I am confident even the most experienced reader will learn something that will quite probably improve his or her diagnostic capability.
Dr. Lindsey is a hospitalist and chief of staff at Victory Medical Center in McKinney, Texas. She has been a member of Team Hospitalist since 2013.
Hospitalists' Holistic Approach Draws Monal Shah, MD to Hospital Medicine
There was just something about hospitalized patients and the folks who cared for them that drew the attention of Monal Shah, MD. Midway through residency, he decided that the best word for it was respect. For the doctors and the people they treated—respect.
“I also liked that [the hospitalists] had a depth of knowledge outside of clinical care that was still important in managing patients: e.g. what insurance pays for what service, how to facilitate outpatient follow-up appointments, the importance of social factors in preventing a patient from returning to the hospital, etc.,” Dr. Shah says. “Even though we weren’t in an outpatient setting, I really appreciated that holistic approach and knowledge base required to care for inpatients.”
That was more than a decade ago at the University of Texas Health Science Center in San Antonio. In the intervening years, Dr. Shah has become involved in clinical informatics and works with a nonprofit company developing prediction models and surveillance analytics for healthcare systems. He also serves as a physician advisor for Parkland Health and Hospital System in Dallas.

Question: I have your CV, but tell me a little more about your training in medical school and residency. What did you like most [and] dislike during the process? Was there a single moment you knew “I can do this”?
Answer: I really enjoyed the camaraderie of residency, especially when I was on an inpatient service and worked with a team [residents, interns, students, and attending]. I was fortunate to have an amazing group of people who inspired me to become a better clinician. I liked clinic the least. I still have days when I’m not sure if “I can do this.”
Q: What’s the biggest change you would like to see in hospital medicine?
A: With information overload, I feel like it’s pretty easy to figure out how to clinically care for a patient. For example, knowing which antibiotic to give for a certain infection is pretty easy to figure out. But knowing which IV antibiotics can/should be given in a nursing facility or at home is more nuanced and forces providers to address and think about the financial and social implications of healthcare. I think that it’s helpful for all specialties to have understanding about this, so the earlier that this type of training occurs (i.e., medical school), the better.
Q: Clinical informatics is clearly a growing area of interest for many. What about it appeals to you? How would you like to apply that knowledge to HM?
A: I found the EHR [electronic health record] to be very valuable, and it’s become difficult to imagine what it was like practicing in the pre-electronic era, but, with it, there definitely is information overload. Specifically, there is lots of duplicative/repetitive information coupled with new information (e.g. labs, vitals, imaging, notes) continuously being generated. Unless you’re sitting at the EMR [electronic medical record] or being notified every time something new appears, it’s almost impossible to know what is going on with the patient in real time. Clinical informatics has the ability to look for the most salient pieces of information—for instance, specific labs or radiology findings or specific words a clinician/nurse might use through natural language processing, etc. [We can] synthesize that information in real time to identify patients with certain diseases—like sepsis, where treatment with antibiotics is time-sensitive, or those who are at risk for adverse events. [We can identify,] for example, those patients at risk for cardiopulmonary arrest, readmission, etc.
Q: You’ve talked about access to data. How do you access the technology? How often? What about it works best for you? Is it something you wish older docs used more?
A: There is so much information ... that is constantly being generated [that] it makes it almost impossible to stay up to date on everything. Rather than even attempt to memorize every single treatment, I make an effort to know where to look for standard of care treatment regimens (e.g. ACCP [American College of Chest Physicians] anticoagulation guidelines, IDSA [Infectious Diseases Society of America] guidelines, ACC/AHA [American College of Cardiology/American Heart Association] peri-operative guidelines). I use technology daily, probably looking up something on at least half of the patients I’m taking care of [on] a given day.
Q: What is your biggest professional challenge?
A: Being able to say no.
Q: What is your biggest professional reward?
A: Students and residents that I’ve worked with who choose a career in HM.
Q: What aspect of patient care is most rewarding?
A: Seeing a patient get well enough to be discharged home or to a lower level of care.
Q: What’s the best advice you ever received?
A: Say yes to anyone asking for help in managing a patient.
Q: What’s the worst advice you ever received?
A: Say yes to every job opportunity.
Q: Did you have a mentor during training or early career? If so, who was the mentor and what were the most important lessons you learned from him/her?
A: My division chief, although he probably didn’t know it. He was firm and had a clear direction for the division/program; however, he was very affable and had a delicate touch when dealing with the other physicians.
Richard Quinn is a freelance writer in New Jersey.
There was just something about hospitalized patients and the folks who cared for them that drew the attention of Monal Shah, MD. Midway through residency, he decided that the best word for it was respect. For the doctors and the people they treated—respect.
“I also liked that [the hospitalists] had a depth of knowledge outside of clinical care that was still important in managing patients: e.g. what insurance pays for what service, how to facilitate outpatient follow-up appointments, the importance of social factors in preventing a patient from returning to the hospital, etc.,” Dr. Shah says. “Even though we weren’t in an outpatient setting, I really appreciated that holistic approach and knowledge base required to care for inpatients.”
That was more than a decade ago at the University of Texas Health Science Center in San Antonio. In the intervening years, Dr. Shah has become involved in clinical informatics and works with a nonprofit company developing prediction models and surveillance analytics for healthcare systems. He also serves as a physician advisor for Parkland Health and Hospital System in Dallas.
Question: I have your CV, but tell me a little more about your training in medical school and residency. What did you like most [and] dislike during the process? Was there a single moment you knew “I can do this”?
Answer: I really enjoyed the camaraderie of residency, especially when I was on an inpatient service and worked with a team [residents, interns, students, and attending]. I was fortunate to have an amazing group of people who inspired me to become a better clinician. I liked clinic the least. I still have days when I’m not sure if “I can do this.”
Q: What’s the biggest change you would like to see in hospital medicine?
A: With information overload, I feel like it’s pretty easy to figure out how to clinically care for a patient. For example, knowing which antibiotic to give for a certain infection is pretty easy to figure out. But knowing which IV antibiotics can/should be given in a nursing facility or at home is more nuanced and forces providers to address and think about the financial and social implications of healthcare. I think that it’s helpful for all specialties to have understanding about this, so the earlier that this type of training occurs (i.e., medical school), the better.
Q: Clinical informatics is clearly a growing area of interest for many. What about it appeals to you? How would you like to apply that knowledge to HM?
A: I found the EHR [electronic health record] to be very valuable, and it’s become difficult to imagine what it was like practicing in the pre-electronic era, but, with it, there definitely is information overload. Specifically, there is lots of duplicative/repetitive information coupled with new information (e.g. labs, vitals, imaging, notes) continuously being generated. Unless you’re sitting at the EMR [electronic medical record] or being notified every time something new appears, it’s almost impossible to know what is going on with the patient in real time. Clinical informatics has the ability to look for the most salient pieces of information—for instance, specific labs or radiology findings or specific words a clinician/nurse might use through natural language processing, etc. [We can] synthesize that information in real time to identify patients with certain diseases—like sepsis, where treatment with antibiotics is time-sensitive, or those who are at risk for adverse events. [We can identify,] for example, those patients at risk for cardiopulmonary arrest, readmission, etc.
Q: You’ve talked about access to data. How do you access the technology? How often? What about it works best for you? Is it something you wish older docs used more?
A: There is so much information ... that is constantly being generated [that] it makes it almost impossible to stay up to date on everything. Rather than even attempt to memorize every single treatment, I make an effort to know where to look for standard of care treatment regimens (e.g. ACCP [American College of Chest Physicians] anticoagulation guidelines, IDSA [Infectious Diseases Society of America] guidelines, ACC/AHA [American College of Cardiology/American Heart Association] peri-operative guidelines). I use technology daily, probably looking up something on at least half of the patients I’m taking care of [on] a given day.
Q: What is your biggest professional challenge?
A: Being able to say no.
Q: What is your biggest professional reward?
A: Students and residents that I’ve worked with who choose a career in HM.
Q: What aspect of patient care is most rewarding?
A: Seeing a patient get well enough to be discharged home or to a lower level of care.
Q: What’s the best advice you ever received?
A: Say yes to anyone asking for help in managing a patient.
Q: What’s the worst advice you ever received?
A: Say yes to every job opportunity.
Q: Did you have a mentor during training or early career? If so, who was the mentor and what were the most important lessons you learned from him/her?
A: My division chief, although he probably didn’t know it. He was firm and had a clear direction for the division/program; however, he was very affable and had a delicate touch when dealing with the other physicians.
Richard Quinn is a freelance writer in New Jersey.
There was just something about hospitalized patients and the folks who cared for them that drew the attention of Monal Shah, MD. Midway through residency, he decided that the best word for it was respect. For the doctors and the people they treated—respect.
“I also liked that [the hospitalists] had a depth of knowledge outside of clinical care that was still important in managing patients: e.g. what insurance pays for what service, how to facilitate outpatient follow-up appointments, the importance of social factors in preventing a patient from returning to the hospital, etc.,” Dr. Shah says. “Even though we weren’t in an outpatient setting, I really appreciated that holistic approach and knowledge base required to care for inpatients.”
That was more than a decade ago at the University of Texas Health Science Center in San Antonio. In the intervening years, Dr. Shah has become involved in clinical informatics and works with a nonprofit company developing prediction models and surveillance analytics for healthcare systems. He also serves as a physician advisor for Parkland Health and Hospital System in Dallas.
Question: I have your CV, but tell me a little more about your training in medical school and residency. What did you like most [and] dislike during the process? Was there a single moment you knew “I can do this”?
Answer: I really enjoyed the camaraderie of residency, especially when I was on an inpatient service and worked with a team [residents, interns, students, and attending]. I was fortunate to have an amazing group of people who inspired me to become a better clinician. I liked clinic the least. I still have days when I’m not sure if “I can do this.”
Q: What’s the biggest change you would like to see in hospital medicine?
A: With information overload, I feel like it’s pretty easy to figure out how to clinically care for a patient. For example, knowing which antibiotic to give for a certain infection is pretty easy to figure out. But knowing which IV antibiotics can/should be given in a nursing facility or at home is more nuanced and forces providers to address and think about the financial and social implications of healthcare. I think that it’s helpful for all specialties to have understanding about this, so the earlier that this type of training occurs (i.e., medical school), the better.
Q: Clinical informatics is clearly a growing area of interest for many. What about it appeals to you? How would you like to apply that knowledge to HM?
A: I found the EHR [electronic health record] to be very valuable, and it’s become difficult to imagine what it was like practicing in the pre-electronic era, but, with it, there definitely is information overload. Specifically, there is lots of duplicative/repetitive information coupled with new information (e.g. labs, vitals, imaging, notes) continuously being generated. Unless you’re sitting at the EMR [electronic medical record] or being notified every time something new appears, it’s almost impossible to know what is going on with the patient in real time. Clinical informatics has the ability to look for the most salient pieces of information—for instance, specific labs or radiology findings or specific words a clinician/nurse might use through natural language processing, etc. [We can] synthesize that information in real time to identify patients with certain diseases—like sepsis, where treatment with antibiotics is time-sensitive, or those who are at risk for adverse events. [We can identify,] for example, those patients at risk for cardiopulmonary arrest, readmission, etc.
Q: You’ve talked about access to data. How do you access the technology? How often? What about it works best for you? Is it something you wish older docs used more?
A: There is so much information ... that is constantly being generated [that] it makes it almost impossible to stay up to date on everything. Rather than even attempt to memorize every single treatment, I make an effort to know where to look for standard of care treatment regimens (e.g. ACCP [American College of Chest Physicians] anticoagulation guidelines, IDSA [Infectious Diseases Society of America] guidelines, ACC/AHA [American College of Cardiology/American Heart Association] peri-operative guidelines). I use technology daily, probably looking up something on at least half of the patients I’m taking care of [on] a given day.
Q: What is your biggest professional challenge?
A: Being able to say no.
Q: What is your biggest professional reward?
A: Students and residents that I’ve worked with who choose a career in HM.
Q: What aspect of patient care is most rewarding?
A: Seeing a patient get well enough to be discharged home or to a lower level of care.
Q: What’s the best advice you ever received?
A: Say yes to anyone asking for help in managing a patient.
Q: What’s the worst advice you ever received?
A: Say yes to every job opportunity.
Q: Did you have a mentor during training or early career? If so, who was the mentor and what were the most important lessons you learned from him/her?
A: My division chief, although he probably didn’t know it. He was firm and had a clear direction for the division/program; however, he was very affable and had a delicate touch when dealing with the other physicians.
Richard Quinn is a freelance writer in New Jersey.
How to Initiate a VTE Quality Improvement Project
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
- Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
- Patients are not optimally mobilized;
- Adherence to ordered mechanical prophylaxis is notoriously low; and
- Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
- Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
- Patients are not optimally mobilized;
- Adherence to ordered mechanical prophylaxis is notoriously low; and
- Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
While VTE sometimes occurs in spite of the best available prophylaxis, there are many lost opportunities to optimize prevention and reduce VTE risk factors in virtually every hospital. Reaching a meaningful improvement in VTE prevention requires an empowered, interdisciplinary team approach supported by the institution to standardize processes, monitor, and measure VTE process and outcomes, implement institutional policies, and educate providers and patients.
In particular, Greg Maynard, MD, MSc, SFHM, director of the University of California San Diego Center for Innovation and Improvement Science, and senior medical officer of the Society of Hospital Medicine’s Center for Hospital Innovation and Improvement, suggests reviewing guidelines and regulatory materials that focus on the implications for implementation. Then, summarize the evidence into a VTE prevention protocol.
A VTE prevention protocol includes a VTE risk assessment, bleeding risk assessment, and clinical decision support (CDS) on prophylactic choices based on this combination of VTE and bleeding risk factors. The VTE protocol CDS must be available at crucial junctures of care, such as admission to the hospital, transfer to different levels of care, and post-operatively.
“This VTE protocol guidance is most often embedded in order sets that are commonly used [or mandated for use] in these settings, essentially ‘hard-wiring’ the VTE risk assessment into the process,” Dr. Maynard says.
Risk assessment is essential, as there are harms, costs, and discomfort associated with prophylactic methods. For some inpatients, the risk of anticoagulant prophylaxis may outweigh the risk
of hospital-acquired VTE. No perfect VTE risk assessment tool exists, and there is always inherent tension between the desire to provide comprehensive, detailed guidance and the need to keep the process simple to understand and measure.
Principles for the effective implementation of reliable interventions generally favor simple models, with more complicated models reserved for settings with advanced methods to make the models easier for the end user.
“Order sets with CDS are of no use if they are not used correctly and reliably, so monitoring this process is crucial,” Dr. Maynard says.
No matter which VTE risk assessment model is used, every effort should be made to enhance ease of use for the ordering provider. This may include carving out special populations such as obstetric patients and major orthopedic, trauma, cardiovascular surgery, and neurosurgery patients for modified VTE risk assessment and order sets, Dr. Maynard says, which allows for streamlining and simplification of VTE prevention order sets.
Successful integration of a VTE prevention protocol into heavily utilized admission and transfer order sets serves as a foundational beginning point for VTE prevention efforts, rather than the end point.
“Even if every patient has the best prophylaxis ordered on admission, other problems can lead to VTE during the hospital stay or after discharge,”
Dr. Maynard says.
For example:
- Bleeding and VTE risk factors can change several times during a hospital stay, but reassessment does not occur;
- Patients are not optimally mobilized;
- Adherence to ordered mechanical prophylaxis is notoriously low; and
- Overutilization of peripherally inserted central catheter lines or other central venous catheters contributes to upper extremity DVT.
VTE prevention programs should address these pitfalls, in addition to implementing order sets.
Publicly reported measures and the CMS core measures set a relatively low bar for performance and are inadequate to drive breakthrough levels of improvement, Dr. Maynard adds. The adequacy of VTE prophylaxis should be assessed not only on admission or transfer to the intensive care unit but also across the hospital stay. Month-to-month reporting is important to follow progress, but at least some measures should drive concurrent intervention to address deficits in prophylaxis in real time. This method of active surveillance (also known as measure-vention), along with multiple other measurement methods that go beyond the core measures, is often necessary to secure real improvement.
An extensive update and revision of the Agency for Healthcare Research and Quality/Society of Hospital Medicine VTE Prevention Implementation Guide will be released by early spring. It will provide comprehensive coverage of these concepts.
Karen Appold is a freelance medical writer in Pennsylvania.
Advances in Medical Technology Encourage Hospitalist-Led Bedside Procedures
One trend working in favor of more hospitalist-led bedside procedures is the growing use of technology, particularly simulation models and ultrasound guidance. Simulators are “invaluable” teaching tools, says David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md.
“They’re easy. They’re inexpensive. You can poke them and poke them and poke them and they don’t scream. They’re not in pain,” he says. “ You’re not going to wind up hurting anybody by practicing on those simulation mannequins, simulators in the labs, and computer-based models.”
Lichtman says he’d also like to use Google Glass to create better training videos for central line placement from the point of view of the practitioner, particularly for cases that aren’t by the book.
As part of its procedure training, Northwestern University in Chicago includes simulation-based mastery learning, which assesses practitioners after a rigorous training regimen; those who don’t perform well receive more training and practice until they can meet the necessary testing benchmarks. The method ensures that on a simulator, everyone can perform the procedure competently. And in actual patient care, the strategy has been linked to decreased central line-related complications.5
Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, calls simulation training “absolutely necessary.” Hospitals that haven’t built their own simulation center, she says, are actively seeking out other simulation centers for training purposes. Checklists, proficiency guidelines, and more realistic simulation models are all being incorporated into training programs well before trainees start practicing on live patients, she says, as part of the necessary shift away from the old “see one, do one, teach one” model.
Beyond basic but effective “task trainers,” more advanced simulator models have heads that turn, anatomy similar to that of a live patient, and even “skin” that permits the use of ultrasound.

Even low-fidelity simulation training can be enormously helpful if it allows a provider to visualize a procedure’s steps before performing them on a patient, says Michelle Mourad, MD, director of quality improvement and patient safety for the division of hospital medicine at the University of California San Francisco. And research suggests that a significant amount of up-front simulation training can decrease the number of real-life procedures needed to achieve competency. The benefits of training fade over time, however, and accessing the sustained practice and simulation opportunities needed to maintain competencies could be a “big challenge,” she says.
Ultrasound is providing another potent—and increasingly portable—tool. Ultrasound guidance is now the standard of care for central lines, with paracentesis and thoracentesis following close behind. Imaging is used somewhat less often for lumbar puncture, but that too is trending in the direction of more ultrasound guidance. “I know of no interventional radiologist who would say that it’s OK on themselves or a family member to have any of these procedures done that weren’t imaging guided, because we’ve seen the outcomes when they’re not,” says Robert L. Vogelzang, MD, FSIR, professor of radiology at Northwestern University Feinberg School of Medicine in Chicago.
Enhanced safety, however, depends upon understanding how to use the tool and how to interpret the results. “The reality is, ultrasounds are great, but if you don’t know how to interpret the data, that information is worse than no information, and that can lead to worsening outcomes,” Lichtman says. A paracentesis that fails to draw any fluid from a patient’s belly, for example, may be due to the misreading of an ultrasound that actually indicated an absence of fluid. And accidentally sticking the needle into a patient’s bowel could cause a perforation or peritonitis.
Some institutions are now incorporating basic ultrasound training into medical school programs.
“It is going to be the way of the future,” Dr. Wang says. “I really think that we’re going to use ultrasound to replace the stethoscope even.” Doctors may instead perform ultrasound with probe-equipped smartphones.
Even then, she says, the technique will be effective only with the kind of advanced training that lets doctors know what they’re visualizing and whether they’re in an artery or vein, for example.
Amid mounting evidence that ultrasound use can improve outcomes, Melissa Tukey, MD, MSc, a pulmonology critical care physician at Lahey Clinic in Burlington, Mass., cautions that there may be other downsides. Cost, for example, may be a limiting factor for some hospitals. Another is physician training and comfort: Although younger physicians have grown up with the technology, she says, many older physicians lack exposure to and comfort using it. “Because ultrasound is now mandated as a quality measure for a number of the procedures, it really limits, by default, the performance of those procedures to a generation of clinicians that’s been trained in ultrasound,” she says.
Hospitals, then, need to ensure that an embrace of ultrasound technology doesn’t leave older physicians out in the cold.
One trend working in favor of more hospitalist-led bedside procedures is the growing use of technology, particularly simulation models and ultrasound guidance. Simulators are “invaluable” teaching tools, says David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md.
“They’re easy. They’re inexpensive. You can poke them and poke them and poke them and they don’t scream. They’re not in pain,” he says. “ You’re not going to wind up hurting anybody by practicing on those simulation mannequins, simulators in the labs, and computer-based models.”
Lichtman says he’d also like to use Google Glass to create better training videos for central line placement from the point of view of the practitioner, particularly for cases that aren’t by the book.
As part of its procedure training, Northwestern University in Chicago includes simulation-based mastery learning, which assesses practitioners after a rigorous training regimen; those who don’t perform well receive more training and practice until they can meet the necessary testing benchmarks. The method ensures that on a simulator, everyone can perform the procedure competently. And in actual patient care, the strategy has been linked to decreased central line-related complications.5
Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, calls simulation training “absolutely necessary.” Hospitals that haven’t built their own simulation center, she says, are actively seeking out other simulation centers for training purposes. Checklists, proficiency guidelines, and more realistic simulation models are all being incorporated into training programs well before trainees start practicing on live patients, she says, as part of the necessary shift away from the old “see one, do one, teach one” model.
Beyond basic but effective “task trainers,” more advanced simulator models have heads that turn, anatomy similar to that of a live patient, and even “skin” that permits the use of ultrasound.
Even low-fidelity simulation training can be enormously helpful if it allows a provider to visualize a procedure’s steps before performing them on a patient, says Michelle Mourad, MD, director of quality improvement and patient safety for the division of hospital medicine at the University of California San Francisco. And research suggests that a significant amount of up-front simulation training can decrease the number of real-life procedures needed to achieve competency. The benefits of training fade over time, however, and accessing the sustained practice and simulation opportunities needed to maintain competencies could be a “big challenge,” she says.
Ultrasound is providing another potent—and increasingly portable—tool. Ultrasound guidance is now the standard of care for central lines, with paracentesis and thoracentesis following close behind. Imaging is used somewhat less often for lumbar puncture, but that too is trending in the direction of more ultrasound guidance. “I know of no interventional radiologist who would say that it’s OK on themselves or a family member to have any of these procedures done that weren’t imaging guided, because we’ve seen the outcomes when they’re not,” says Robert L. Vogelzang, MD, FSIR, professor of radiology at Northwestern University Feinberg School of Medicine in Chicago.
Enhanced safety, however, depends upon understanding how to use the tool and how to interpret the results. “The reality is, ultrasounds are great, but if you don’t know how to interpret the data, that information is worse than no information, and that can lead to worsening outcomes,” Lichtman says. A paracentesis that fails to draw any fluid from a patient’s belly, for example, may be due to the misreading of an ultrasound that actually indicated an absence of fluid. And accidentally sticking the needle into a patient’s bowel could cause a perforation or peritonitis.
Some institutions are now incorporating basic ultrasound training into medical school programs.
“It is going to be the way of the future,” Dr. Wang says. “I really think that we’re going to use ultrasound to replace the stethoscope even.” Doctors may instead perform ultrasound with probe-equipped smartphones.
Even then, she says, the technique will be effective only with the kind of advanced training that lets doctors know what they’re visualizing and whether they’re in an artery or vein, for example.
Amid mounting evidence that ultrasound use can improve outcomes, Melissa Tukey, MD, MSc, a pulmonology critical care physician at Lahey Clinic in Burlington, Mass., cautions that there may be other downsides. Cost, for example, may be a limiting factor for some hospitals. Another is physician training and comfort: Although younger physicians have grown up with the technology, she says, many older physicians lack exposure to and comfort using it. “Because ultrasound is now mandated as a quality measure for a number of the procedures, it really limits, by default, the performance of those procedures to a generation of clinicians that’s been trained in ultrasound,” she says.
Hospitals, then, need to ensure that an embrace of ultrasound technology doesn’t leave older physicians out in the cold.
One trend working in favor of more hospitalist-led bedside procedures is the growing use of technology, particularly simulation models and ultrasound guidance. Simulators are “invaluable” teaching tools, says David Lichtman, PA, director of the Johns Hopkins Central Procedure Service in Baltimore, Md.
“They’re easy. They’re inexpensive. You can poke them and poke them and poke them and they don’t scream. They’re not in pain,” he says. “ You’re not going to wind up hurting anybody by practicing on those simulation mannequins, simulators in the labs, and computer-based models.”
Lichtman says he’d also like to use Google Glass to create better training videos for central line placement from the point of view of the practitioner, particularly for cases that aren’t by the book.
As part of its procedure training, Northwestern University in Chicago includes simulation-based mastery learning, which assesses practitioners after a rigorous training regimen; those who don’t perform well receive more training and practice until they can meet the necessary testing benchmarks. The method ensures that on a simulator, everyone can perform the procedure competently. And in actual patient care, the strategy has been linked to decreased central line-related complications.5
Sally Wang, MD, FHM, director of procedure education at Brigham and Women’s Hospital and a clinical instructor at Harvard Medical School in Boston, calls simulation training “absolutely necessary.” Hospitals that haven’t built their own simulation center, she says, are actively seeking out other simulation centers for training purposes. Checklists, proficiency guidelines, and more realistic simulation models are all being incorporated into training programs well before trainees start practicing on live patients, she says, as part of the necessary shift away from the old “see one, do one, teach one” model.
Beyond basic but effective “task trainers,” more advanced simulator models have heads that turn, anatomy similar to that of a live patient, and even “skin” that permits the use of ultrasound.
Even low-fidelity simulation training can be enormously helpful if it allows a provider to visualize a procedure’s steps before performing them on a patient, says Michelle Mourad, MD, director of quality improvement and patient safety for the division of hospital medicine at the University of California San Francisco. And research suggests that a significant amount of up-front simulation training can decrease the number of real-life procedures needed to achieve competency. The benefits of training fade over time, however, and accessing the sustained practice and simulation opportunities needed to maintain competencies could be a “big challenge,” she says.
Ultrasound is providing another potent—and increasingly portable—tool. Ultrasound guidance is now the standard of care for central lines, with paracentesis and thoracentesis following close behind. Imaging is used somewhat less often for lumbar puncture, but that too is trending in the direction of more ultrasound guidance. “I know of no interventional radiologist who would say that it’s OK on themselves or a family member to have any of these procedures done that weren’t imaging guided, because we’ve seen the outcomes when they’re not,” says Robert L. Vogelzang, MD, FSIR, professor of radiology at Northwestern University Feinberg School of Medicine in Chicago.
Enhanced safety, however, depends upon understanding how to use the tool and how to interpret the results. “The reality is, ultrasounds are great, but if you don’t know how to interpret the data, that information is worse than no information, and that can lead to worsening outcomes,” Lichtman says. A paracentesis that fails to draw any fluid from a patient’s belly, for example, may be due to the misreading of an ultrasound that actually indicated an absence of fluid. And accidentally sticking the needle into a patient’s bowel could cause a perforation or peritonitis.
Some institutions are now incorporating basic ultrasound training into medical school programs.
“It is going to be the way of the future,” Dr. Wang says. “I really think that we’re going to use ultrasound to replace the stethoscope even.” Doctors may instead perform ultrasound with probe-equipped smartphones.
Even then, she says, the technique will be effective only with the kind of advanced training that lets doctors know what they’re visualizing and whether they’re in an artery or vein, for example.
Amid mounting evidence that ultrasound use can improve outcomes, Melissa Tukey, MD, MSc, a pulmonology critical care physician at Lahey Clinic in Burlington, Mass., cautions that there may be other downsides. Cost, for example, may be a limiting factor for some hospitals. Another is physician training and comfort: Although younger physicians have grown up with the technology, she says, many older physicians lack exposure to and comfort using it. “Because ultrasound is now mandated as a quality measure for a number of the procedures, it really limits, by default, the performance of those procedures to a generation of clinicians that’s been trained in ultrasound,” she says.
Hospitals, then, need to ensure that an embrace of ultrasound technology doesn’t leave older physicians out in the cold.
De-Escalation Training Prepares Hospitalists to Calm Agitated Patients

If a patient shows signs of agitation, Aaron Gottesman, MD, SFHM, says the best way to handle it is to stay calm. It may sound simple, but, in the heat of the moment, people tend to become defensive and on guard rather than acting composed and sympathetic. He suggests trying to speak softly and evenly to the patient, make eye contact, keep your arms at your side, and ask opened-ended questions such as, “How can I help you?” in a genuine manner.

Dr. Gottesman, director of hospitalist services at Staten Island (N.Y.) University Hospital (SIUH), learned these strategies in a voluntary one-hour course on de-escalation training. Although he says he feels fortunate that he has never had to deal with a physically volatile patient, he has used the verbal de-escalation training. In some cases, he believes that employing it may have prevented a physically violent situation from occurring.
Specifically, de-escalation training teaches how to respond to individuals who are acting aggressive or agitated in a verbal or physical manner. The techniques focus on how to calm someone down, while also teaching basic self-defense skills.
Various companies offer this type of training; some will train staff onsite.
“It is money well-spent,” says Scott Zeller, MD, chief of psychiatric emergency services at Alameda Health System in Oakland, Calif. “This is truly a situation where an ounce of prevention is worth a pound of cure. It only takes one unfortunate episode to result in a serious injury, where a healthcare professional will have to miss work or go on disability, which results in a far greater cost than that of the training.”
Appropriate Responses

By the nature of their work, hospitalists regularly come into contact with agitated patients. “Knowing how to safely help a patient calm down will result in better outcomes for the patient, the physicians, and everyone nearby,” Dr. Zeller says.
“Hospitalists should focus on what they can control,” says Judith Schubert, president of Crisis Prevention Institute (CPI), a Milwaukee, Wis.-based company that offers de-escalation training in 400 cities annually. This includes physicians’ own behavior/demeanor, responsiveness, environmental factors, communication protocols, and a continuous assessment of risk and an understanding of how to balance duty of care with responsibilities to maintain safety.
Hospitalists should be aware of behaviors that could lead to volatility.
“Challenging or oppositional questions and emotional release or intimidating comments often mark the beginning stages of loss of rationality. These are behaviors that warrant specific, directive intervention aimed at stimulating a rational response and diffusing tension,” Schubert says. “Before it even gets to that point, empathy, demonstrated with the patient and family members, can reduce contagion of emotional displays that are likely rooted in fear and anxiety.”
Agitation usually doesn’t arise out of the blue.
“It is typically seen over a spectrum of behaviors, from merely restless and irritable up to sarcastic and demeaning, pacing, unable to sit still, all the way up to screaming, combative, and violent to persons and property,” Dr. Zeller says. “It is best to intervene in the earlier stages and help a person to calm before a situation gets out of hand.”
Thus, hospitalists should be wary of people who are increasingly hostile and energetic and should seek help or work to de-escalate promptly.
Although you may suspect that patients with mental illnesses are more prone to volatility, Dr. Zeller says that isn’t necessarily the case. The most common psychiatric illnesses that can lead to agitation are schizophrenia and bipolar mania. In addition, being intoxicated—especially with alcohol and stimulants—can predispose someone to agitation. Many other medical conditions can cause someone to become agitated, such as confusion, a postictal state, hypoglycemia, or a head injury.

How Bad Is It?
According to the Emergency Nurses Association’s Institute for Emergency Nursing Research, violence is especially prevalent in the ED; about 11% of ED nurses report being physically assaulted each week. The agency states that the data is most likely grossly underreported, since reporting is voluntary.1
Healthcare workers in psychiatric wards are the most likely to suffer an injury caused by an agitated patient, Dr. Zeller says. Of those, nurses are the ones most commonly affected, followed by physicians.
“But agitation-related assaults and injuries can happen just about anywhere in a hospital,” he adds.
According to a study conducted by the Emergency Nurses Association, pushing/grabbing and yelling/shouting were the most prevalent types of violence. Eighty percent of cases occurred in the patient’s room.2 Dr. Zeller says that the most common injuries are those resulting from being struck, kicked or punched, or knocked down. Injuries include heavy bruising, sprains, and broken bones.
Dr. Zeller says it’s difficult to quantify exactly what types and costs of injuries occur. Injuries related to agitation are known to cause staff to miss work frequently. “That can cost a lot in terms of lost hours and replacement wages, as well as medical care for the injured party,” he says.
The Most Dangerous Circumstances
According to a series of 2012 articles on best practices guidelines for the evaluation and treatment of agitation published in Western Journal of Emergency Medicine, two-thirds of all staff injuries occur during the “takedown,” which is when staff attempt to tackle and restrain an agitated patient.3
“If interactions with a patient could help the person to regain control without needing the takedown or restraints, there would be fewer injuries and better outcomes,” says Dr. Zeller, who co-authored the article. “To help these patients in a collaborative and noncoercive way, and avoid restraints, verbal de-escalation is the necessary approach.”
As part of the study, a team of more than 40 experts nationwide was established to create Project BETA (Best practices in Evaluation and Treatment of Agitation). Participants were divided into five workgroups: triage and medical evaluation, psychiatric evaluation, de-escalation techniques, psychopharmacology of agitation, and use and avoidance of seclusion and restraint.
The guidelines were intended to cover all aspects of working with an agitated individual, with a focus on safety and outcomes, but also had a goal of being as patient-centric, collaborative, and noncoercive as possible.
“Every part of Project BETA revolves around verbal de-escalation, which can be done in a very short amount of time while simultaneously doing an assessment and offering medications,” Dr. Zeller says.
As a result of incorporating the guidelines in Project BETA, the psychiatric emergency room at Alameda Health System—which deals with a highly acute, emergency population of patients with serious mental illnesses—restrains less than 0.5% of patients seen. Dr. Zeller points out that this is much lower than the numbers restrained at other institutions. For instance, an article published in October 2013 reported several studies showing that 8% to 24% of patients in psychiatric EDs were placed into physical restraints or seclusion.4
What’s Required of Hospital Administration?
Under its Environment of Care standards, The Joint Commission requires accredited healthcare facilities to address workplace violence risk. The requirements mandate facilities to maintain a written plan describing how the security of patients, staff, and facility visitors will be ensured, to conduct proactive risk assessments considering the potential for workplace violence, and to determine a means for identifying individuals on their premises and controlling access to and egress from security-sensitive areas.1
The standard states that “staff are trained in the use of nonphysical intervention skills,” says Cynthia Leslie, APRN, BC, MSN, associate director of the Standards Interpretation Group at The Joint Commission, which is based in Oakbrook Terrace, Ill. “These skills may assist the patient in calming down and prevent the use of restraints and/or seclusion.”
In addition, staff must be trained before they participate in a restraint or seclusion episode and must have periodic training thereafter.
Anyone who wants de-escalation training can contact a company like CPI directly or establish in-house training teams (CPI offers an Instructor Certification Program). “This allows a cost-effective way [approximately $10 per person] to cascade training to others within the hospital who are part of care teams,” Schubert says.
In Sum
Providing for the care and welfare of patients while maintaining a safe and secure environment for everyone is a balancing act that requires the involvement of a multidisciplinary hospital team, Schubert says.
“Coordination, communication, and continuity among all members of a hospital team are crucial to minimize conflict, avoid chaos, and reduce risks,” she explains. “By being armed with information and skills, hospitalists are less likely to isolate themselves from other team members or react in a nonproductive way when crisis situations emerge.
“Training will help staff to take steps to ensure that their behavior and attitudes don’t become part of the problem and increase risks for others involved. Care team perceptions of physician involvement in solution-focused interventions are important for hospitalists to fully understand so risks can be avoided.”
Karen Appold is a freelance medical writer in Pennsylvania.
References
- ECRI Institute. Healthcare Risk, Quality, and Safety Guidance. Violence in healthcare facilities. March 1, 2011. Available at: https://www.ecri.org/components/HRC/Pages/SafSec3.aspx?tab=1. Accessed February 11, 2015.
- Emergency Nurses Association. Emergency department violence surveillance study. November 2011. Available at: http://www.ena.org/practice-research/research/Documents/ENAEDVSReportNovember2011.pdf. Accessed February 11, 2015.
- Richmond JS, Berlin JS, Fishkind AB, et al. Verbal de-escalation of the agitated patient: consensus statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2012;13(1):17-25.
- Simpson SA, Joesch JM, West II, Pasic J. Risk for physical restraint or seclusion in the psychiatric emergency service (PES). Gen Hosp Psychiatry. 2014;36(1):113-118.
If a patient shows signs of agitation, Aaron Gottesman, MD, SFHM, says the best way to handle it is to stay calm. It may sound simple, but, in the heat of the moment, people tend to become defensive and on guard rather than acting composed and sympathetic. He suggests trying to speak softly and evenly to the patient, make eye contact, keep your arms at your side, and ask opened-ended questions such as, “How can I help you?” in a genuine manner.
Dr. Gottesman, director of hospitalist services at Staten Island (N.Y.) University Hospital (SIUH), learned these strategies in a voluntary one-hour course on de-escalation training. Although he says he feels fortunate that he has never had to deal with a physically volatile patient, he has used the verbal de-escalation training. In some cases, he believes that employing it may have prevented a physically violent situation from occurring.
Specifically, de-escalation training teaches how to respond to individuals who are acting aggressive or agitated in a verbal or physical manner. The techniques focus on how to calm someone down, while also teaching basic self-defense skills.
Various companies offer this type of training; some will train staff onsite.
“It is money well-spent,” says Scott Zeller, MD, chief of psychiatric emergency services at Alameda Health System in Oakland, Calif. “This is truly a situation where an ounce of prevention is worth a pound of cure. It only takes one unfortunate episode to result in a serious injury, where a healthcare professional will have to miss work or go on disability, which results in a far greater cost than that of the training.”
Appropriate Responses
By the nature of their work, hospitalists regularly come into contact with agitated patients. “Knowing how to safely help a patient calm down will result in better outcomes for the patient, the physicians, and everyone nearby,” Dr. Zeller says.
“Hospitalists should focus on what they can control,” says Judith Schubert, president of Crisis Prevention Institute (CPI), a Milwaukee, Wis.-based company that offers de-escalation training in 400 cities annually. This includes physicians’ own behavior/demeanor, responsiveness, environmental factors, communication protocols, and a continuous assessment of risk and an understanding of how to balance duty of care with responsibilities to maintain safety.
Hospitalists should be aware of behaviors that could lead to volatility.
“Challenging or oppositional questions and emotional release or intimidating comments often mark the beginning stages of loss of rationality. These are behaviors that warrant specific, directive intervention aimed at stimulating a rational response and diffusing tension,” Schubert says. “Before it even gets to that point, empathy, demonstrated with the patient and family members, can reduce contagion of emotional displays that are likely rooted in fear and anxiety.”
Agitation usually doesn’t arise out of the blue.
“It is typically seen over a spectrum of behaviors, from merely restless and irritable up to sarcastic and demeaning, pacing, unable to sit still, all the way up to screaming, combative, and violent to persons and property,” Dr. Zeller says. “It is best to intervene in the earlier stages and help a person to calm before a situation gets out of hand.”
Thus, hospitalists should be wary of people who are increasingly hostile and energetic and should seek help or work to de-escalate promptly.
Although you may suspect that patients with mental illnesses are more prone to volatility, Dr. Zeller says that isn’t necessarily the case. The most common psychiatric illnesses that can lead to agitation are schizophrenia and bipolar mania. In addition, being intoxicated—especially with alcohol and stimulants—can predispose someone to agitation. Many other medical conditions can cause someone to become agitated, such as confusion, a postictal state, hypoglycemia, or a head injury.
How Bad Is It?
According to the Emergency Nurses Association’s Institute for Emergency Nursing Research, violence is especially prevalent in the ED; about 11% of ED nurses report being physically assaulted each week. The agency states that the data is most likely grossly underreported, since reporting is voluntary.1
Healthcare workers in psychiatric wards are the most likely to suffer an injury caused by an agitated patient, Dr. Zeller says. Of those, nurses are the ones most commonly affected, followed by physicians.
“But agitation-related assaults and injuries can happen just about anywhere in a hospital,” he adds.
According to a study conducted by the Emergency Nurses Association, pushing/grabbing and yelling/shouting were the most prevalent types of violence. Eighty percent of cases occurred in the patient’s room.2 Dr. Zeller says that the most common injuries are those resulting from being struck, kicked or punched, or knocked down. Injuries include heavy bruising, sprains, and broken bones.
Dr. Zeller says it’s difficult to quantify exactly what types and costs of injuries occur. Injuries related to agitation are known to cause staff to miss work frequently. “That can cost a lot in terms of lost hours and replacement wages, as well as medical care for the injured party,” he says.
The Most Dangerous Circumstances
According to a series of 2012 articles on best practices guidelines for the evaluation and treatment of agitation published in Western Journal of Emergency Medicine, two-thirds of all staff injuries occur during the “takedown,” which is when staff attempt to tackle and restrain an agitated patient.3
“If interactions with a patient could help the person to regain control without needing the takedown or restraints, there would be fewer injuries and better outcomes,” says Dr. Zeller, who co-authored the article. “To help these patients in a collaborative and noncoercive way, and avoid restraints, verbal de-escalation is the necessary approach.”
As part of the study, a team of more than 40 experts nationwide was established to create Project BETA (Best practices in Evaluation and Treatment of Agitation). Participants were divided into five workgroups: triage and medical evaluation, psychiatric evaluation, de-escalation techniques, psychopharmacology of agitation, and use and avoidance of seclusion and restraint.
The guidelines were intended to cover all aspects of working with an agitated individual, with a focus on safety and outcomes, but also had a goal of being as patient-centric, collaborative, and noncoercive as possible.
“Every part of Project BETA revolves around verbal de-escalation, which can be done in a very short amount of time while simultaneously doing an assessment and offering medications,” Dr. Zeller says.
As a result of incorporating the guidelines in Project BETA, the psychiatric emergency room at Alameda Health System—which deals with a highly acute, emergency population of patients with serious mental illnesses—restrains less than 0.5% of patients seen. Dr. Zeller points out that this is much lower than the numbers restrained at other institutions. For instance, an article published in October 2013 reported several studies showing that 8% to 24% of patients in psychiatric EDs were placed into physical restraints or seclusion.4
What’s Required of Hospital Administration?
Under its Environment of Care standards, The Joint Commission requires accredited healthcare facilities to address workplace violence risk. The requirements mandate facilities to maintain a written plan describing how the security of patients, staff, and facility visitors will be ensured, to conduct proactive risk assessments considering the potential for workplace violence, and to determine a means for identifying individuals on their premises and controlling access to and egress from security-sensitive areas.1
The standard states that “staff are trained in the use of nonphysical intervention skills,” says Cynthia Leslie, APRN, BC, MSN, associate director of the Standards Interpretation Group at The Joint Commission, which is based in Oakbrook Terrace, Ill. “These skills may assist the patient in calming down and prevent the use of restraints and/or seclusion.”
In addition, staff must be trained before they participate in a restraint or seclusion episode and must have periodic training thereafter.
Anyone who wants de-escalation training can contact a company like CPI directly or establish in-house training teams (CPI offers an Instructor Certification Program). “This allows a cost-effective way [approximately $10 per person] to cascade training to others within the hospital who are part of care teams,” Schubert says.
In Sum
Providing for the care and welfare of patients while maintaining a safe and secure environment for everyone is a balancing act that requires the involvement of a multidisciplinary hospital team, Schubert says.
“Coordination, communication, and continuity among all members of a hospital team are crucial to minimize conflict, avoid chaos, and reduce risks,” she explains. “By being armed with information and skills, hospitalists are less likely to isolate themselves from other team members or react in a nonproductive way when crisis situations emerge.
“Training will help staff to take steps to ensure that their behavior and attitudes don’t become part of the problem and increase risks for others involved. Care team perceptions of physician involvement in solution-focused interventions are important for hospitalists to fully understand so risks can be avoided.”
Karen Appold is a freelance medical writer in Pennsylvania.
References
- ECRI Institute. Healthcare Risk, Quality, and Safety Guidance. Violence in healthcare facilities. March 1, 2011. Available at: https://www.ecri.org/components/HRC/Pages/SafSec3.aspx?tab=1. Accessed February 11, 2015.
- Emergency Nurses Association. Emergency department violence surveillance study. November 2011. Available at: http://www.ena.org/practice-research/research/Documents/ENAEDVSReportNovember2011.pdf. Accessed February 11, 2015.
- Richmond JS, Berlin JS, Fishkind AB, et al. Verbal de-escalation of the agitated patient: consensus statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2012;13(1):17-25.
- Simpson SA, Joesch JM, West II, Pasic J. Risk for physical restraint or seclusion in the psychiatric emergency service (PES). Gen Hosp Psychiatry. 2014;36(1):113-118.
If a patient shows signs of agitation, Aaron Gottesman, MD, SFHM, says the best way to handle it is to stay calm. It may sound simple, but, in the heat of the moment, people tend to become defensive and on guard rather than acting composed and sympathetic. He suggests trying to speak softly and evenly to the patient, make eye contact, keep your arms at your side, and ask opened-ended questions such as, “How can I help you?” in a genuine manner.
Dr. Gottesman, director of hospitalist services at Staten Island (N.Y.) University Hospital (SIUH), learned these strategies in a voluntary one-hour course on de-escalation training. Although he says he feels fortunate that he has never had to deal with a physically volatile patient, he has used the verbal de-escalation training. In some cases, he believes that employing it may have prevented a physically violent situation from occurring.
Specifically, de-escalation training teaches how to respond to individuals who are acting aggressive or agitated in a verbal or physical manner. The techniques focus on how to calm someone down, while also teaching basic self-defense skills.
Various companies offer this type of training; some will train staff onsite.
“It is money well-spent,” says Scott Zeller, MD, chief of psychiatric emergency services at Alameda Health System in Oakland, Calif. “This is truly a situation where an ounce of prevention is worth a pound of cure. It only takes one unfortunate episode to result in a serious injury, where a healthcare professional will have to miss work or go on disability, which results in a far greater cost than that of the training.”
Appropriate Responses
By the nature of their work, hospitalists regularly come into contact with agitated patients. “Knowing how to safely help a patient calm down will result in better outcomes for the patient, the physicians, and everyone nearby,” Dr. Zeller says.
“Hospitalists should focus on what they can control,” says Judith Schubert, president of Crisis Prevention Institute (CPI), a Milwaukee, Wis.-based company that offers de-escalation training in 400 cities annually. This includes physicians’ own behavior/demeanor, responsiveness, environmental factors, communication protocols, and a continuous assessment of risk and an understanding of how to balance duty of care with responsibilities to maintain safety.
Hospitalists should be aware of behaviors that could lead to volatility.
“Challenging or oppositional questions and emotional release or intimidating comments often mark the beginning stages of loss of rationality. These are behaviors that warrant specific, directive intervention aimed at stimulating a rational response and diffusing tension,” Schubert says. “Before it even gets to that point, empathy, demonstrated with the patient and family members, can reduce contagion of emotional displays that are likely rooted in fear and anxiety.”
Agitation usually doesn’t arise out of the blue.
“It is typically seen over a spectrum of behaviors, from merely restless and irritable up to sarcastic and demeaning, pacing, unable to sit still, all the way up to screaming, combative, and violent to persons and property,” Dr. Zeller says. “It is best to intervene in the earlier stages and help a person to calm before a situation gets out of hand.”
Thus, hospitalists should be wary of people who are increasingly hostile and energetic and should seek help or work to de-escalate promptly.
Although you may suspect that patients with mental illnesses are more prone to volatility, Dr. Zeller says that isn’t necessarily the case. The most common psychiatric illnesses that can lead to agitation are schizophrenia and bipolar mania. In addition, being intoxicated—especially with alcohol and stimulants—can predispose someone to agitation. Many other medical conditions can cause someone to become agitated, such as confusion, a postictal state, hypoglycemia, or a head injury.
How Bad Is It?
According to the Emergency Nurses Association’s Institute for Emergency Nursing Research, violence is especially prevalent in the ED; about 11% of ED nurses report being physically assaulted each week. The agency states that the data is most likely grossly underreported, since reporting is voluntary.1
Healthcare workers in psychiatric wards are the most likely to suffer an injury caused by an agitated patient, Dr. Zeller says. Of those, nurses are the ones most commonly affected, followed by physicians.
“But agitation-related assaults and injuries can happen just about anywhere in a hospital,” he adds.
According to a study conducted by the Emergency Nurses Association, pushing/grabbing and yelling/shouting were the most prevalent types of violence. Eighty percent of cases occurred in the patient’s room.2 Dr. Zeller says that the most common injuries are those resulting from being struck, kicked or punched, or knocked down. Injuries include heavy bruising, sprains, and broken bones.
Dr. Zeller says it’s difficult to quantify exactly what types and costs of injuries occur. Injuries related to agitation are known to cause staff to miss work frequently. “That can cost a lot in terms of lost hours and replacement wages, as well as medical care for the injured party,” he says.
The Most Dangerous Circumstances
According to a series of 2012 articles on best practices guidelines for the evaluation and treatment of agitation published in Western Journal of Emergency Medicine, two-thirds of all staff injuries occur during the “takedown,” which is when staff attempt to tackle and restrain an agitated patient.3
“If interactions with a patient could help the person to regain control without needing the takedown or restraints, there would be fewer injuries and better outcomes,” says Dr. Zeller, who co-authored the article. “To help these patients in a collaborative and noncoercive way, and avoid restraints, verbal de-escalation is the necessary approach.”
As part of the study, a team of more than 40 experts nationwide was established to create Project BETA (Best practices in Evaluation and Treatment of Agitation). Participants were divided into five workgroups: triage and medical evaluation, psychiatric evaluation, de-escalation techniques, psychopharmacology of agitation, and use and avoidance of seclusion and restraint.
The guidelines were intended to cover all aspects of working with an agitated individual, with a focus on safety and outcomes, but also had a goal of being as patient-centric, collaborative, and noncoercive as possible.
“Every part of Project BETA revolves around verbal de-escalation, which can be done in a very short amount of time while simultaneously doing an assessment and offering medications,” Dr. Zeller says.
As a result of incorporating the guidelines in Project BETA, the psychiatric emergency room at Alameda Health System—which deals with a highly acute, emergency population of patients with serious mental illnesses—restrains less than 0.5% of patients seen. Dr. Zeller points out that this is much lower than the numbers restrained at other institutions. For instance, an article published in October 2013 reported several studies showing that 8% to 24% of patients in psychiatric EDs were placed into physical restraints or seclusion.4
What’s Required of Hospital Administration?
Under its Environment of Care standards, The Joint Commission requires accredited healthcare facilities to address workplace violence risk. The requirements mandate facilities to maintain a written plan describing how the security of patients, staff, and facility visitors will be ensured, to conduct proactive risk assessments considering the potential for workplace violence, and to determine a means for identifying individuals on their premises and controlling access to and egress from security-sensitive areas.1
The standard states that “staff are trained in the use of nonphysical intervention skills,” says Cynthia Leslie, APRN, BC, MSN, associate director of the Standards Interpretation Group at The Joint Commission, which is based in Oakbrook Terrace, Ill. “These skills may assist the patient in calming down and prevent the use of restraints and/or seclusion.”
In addition, staff must be trained before they participate in a restraint or seclusion episode and must have periodic training thereafter.
Anyone who wants de-escalation training can contact a company like CPI directly or establish in-house training teams (CPI offers an Instructor Certification Program). “This allows a cost-effective way [approximately $10 per person] to cascade training to others within the hospital who are part of care teams,” Schubert says.
In Sum
Providing for the care and welfare of patients while maintaining a safe and secure environment for everyone is a balancing act that requires the involvement of a multidisciplinary hospital team, Schubert says.
“Coordination, communication, and continuity among all members of a hospital team are crucial to minimize conflict, avoid chaos, and reduce risks,” she explains. “By being armed with information and skills, hospitalists are less likely to isolate themselves from other team members or react in a nonproductive way when crisis situations emerge.
“Training will help staff to take steps to ensure that their behavior and attitudes don’t become part of the problem and increase risks for others involved. Care team perceptions of physician involvement in solution-focused interventions are important for hospitalists to fully understand so risks can be avoided.”
Karen Appold is a freelance medical writer in Pennsylvania.
References
- ECRI Institute. Healthcare Risk, Quality, and Safety Guidance. Violence in healthcare facilities. March 1, 2011. Available at: https://www.ecri.org/components/HRC/Pages/SafSec3.aspx?tab=1. Accessed February 11, 2015.
- Emergency Nurses Association. Emergency department violence surveillance study. November 2011. Available at: http://www.ena.org/practice-research/research/Documents/ENAEDVSReportNovember2011.pdf. Accessed February 11, 2015.
- Richmond JS, Berlin JS, Fishkind AB, et al. Verbal de-escalation of the agitated patient: consensus statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2012;13(1):17-25.
- Simpson SA, Joesch JM, West II, Pasic J. Risk for physical restraint or seclusion in the psychiatric emergency service (PES). Gen Hosp Psychiatry. 2014;36(1):113-118.
Hospitalists Should Lead Training, Preparedness for Hospital Violence Prevention
On Jan. 20, a 44-year old surgeon was shot and killed in the middle of the day at one of the country’s top hospitals. Michael Davidson, MD, an endovascular surgeon at Brigham and Women’s Hospital in Boston, was in a second-floor hospital clinic when 55-year-old Stephen Pasceri asked for him by name. Dr. Davidson, the division director of endovascular cardiac surgery and assistant professor at Harvard Medical School, had taken care of Pasceri’s mother before her death in November 2014. Witnesses reported that Dr. Davidson came out to talk to Pasceri; during that conversation, Pasceri shot Dr. Davidson twice.
Dr. Davidson was quickly taken to the ED but died 12 hours later.
The shooter died of a self-inflicted gunshot wound to the head.
The motive is not clear, but Pasceri had voiced frustrations with the medical industry during the care of both his father and his mother. In addition, his mother seemed to have suffered some type of complication after a surgery performed by Dr. Davidson. Interviews of Pasceri’s relatives, friends, and neighbors found they were all shocked and dismayed. The shooter was, by all accounts, an upstanding citizen in his work, home, church, and community; he was an accountant with four children, with no past history of criminal or violent activity.1
A Disheartening Trend
Two other fatal events in medical centers occurred within weeks of the Davidson shooting. In December 2014, at Wentworth-Douglass Hospital in Dover, N.H., a man shot and killed his wife before killing himself.
Days later, at a Veterans Hospital clinic in El Paso, Texas, another shooting left both the perpetrator and a psychologist dead.2
In the healthcare setting, providers encounter many types of violence. Nonfatal violence, ranging from physical aggression to various levels of physical harm, has become commonplace. Inciters of such violence tend to be those who “can’t help themselves,” often patients with primary psychiatric illness or those with medically induced mental impairment, such as delirium or withdrawal. For these patients, there is at least some level of compassion and tolerance for their behavior, and because they tend to be relatively predictable, preparedness and mitigation of such acts can give providers some sense of control over the situation.
But the Davidson event represents a type of violence that is frightening, unpredictable, and very difficult to prevent, prepare for, or adequately handle.
Actual shootings on medical campuses are, fortunately, rare. A recent study by the Johns Hopkins Office of Critical Event Preparedness and Response found 154 hospital shootings between 2000 and 2011, resulting in 235 injured or dead victims. The most commonly occurring scenario is that of people acting against family members, with healthcare workers getting caught in the crosshairs. The most common victim is the shooter (45% of the time), and the least common victims are physicians and nurses. Over half (59%) of medical center shootings occur within the hospital; the other 41% occur somewhere else on the hospital grounds.3
So what can hospitalists and hospitals do about the real threat of physical violence and shootings within medical centers? Some have recommended metal detectors as effective barriers for preventing weapons from entering medical centers. The primary problem with this solution is that the majority of medical centers have found this plan impossible to implement, given the number of entrances in typical hospitals; Johns Hopkins for example, has more than 80 entrances. Metal detectors also require security staffing at each entrance 24/7.4
Because of the barriers, metal detectors present an insurmountable financial obstacle for most hospitals. In addition, they present an issue with public perception. Many would argue that hospitals are (and should be) places of healing and sanctuary (e.g. “safe havens”), not places for suspicion and searches. In addition, although there is evidence that the use of metal detectors results in increased confiscation of weapons, there is no evidence that they result in fewer on-site assaults.5 Further complicating matters, almost a quarter of the shootings that occur in EDs result from the perpetrator grabbing a weapon from a security guard.3
Others advocate for stricter gun control laws and enforcement, an argument that has vehement advocates and critics on both sides and is unlikely to be resolved in the near future.
Take Action: Be Prepared
In the meantime, hospitalists are left with preparedness tactics that range from situational awareness to active shooter drills. Both are equally important and should be a part of disaster preparedness at any medical center regardless of size, type, or location. Hospitalists can and should take a lead in such preparedness. Current statistics show that hospitalists are employed in at least 85% of all U.S. hospitals. With such widespread penetration, hospitalists can have a huge impact on the preparedness efforts that can prevent such acts from occurring, as well as on organizational resilience and recovery if such an act does occur.
Such training is more important in healthcare settings than other workplaces, as medical personnel have to be specially trained to resist the temptation to help. For example, active shooter training instructs personnel to run, hide, or fight, none of which come “naturally” to those trained to save and rescue for a living. This training instructs anyone in the “Hot Zone” (where life is in direct danger) to run away from the scene (always preferred if feasible), hide (barricade the door, silence any devices, and stay still), or fight (use anything in sight to fight the shooter, and work as a team if feasible). These responses are the exact opposite of what most trained healthcare personnel are accustomed to doing in cases of emergency.
In Sum
The Michael Davidson story is very sobering by all accounts. Healthcare violence such as this, while rare, is devastating.
Hospitalists should lead the way in training and preparedness for violence prevention and mitigation, including active shooter simulation scenarios. We can all have a huge impact in reducing the risk of casualties should such an unpredictable event occur in our hospital.

References
- Freyer FJ, Kowalczyk L, Murphy SP. Surgeon slain, gunman found dead in day of crisis at Brigham. January 20, 2015. The Boston Globe online. Available at: http://www.bostonglobe.com/metro/2015/01/20/boston-police-investigate-report-shooting-brigham-and-women/Jhig9z8LO8A5PH9Er4vTiP/story.html?rss_id=Top-GNP&utm_source=Managed&utm_campaign=386d2ff709-Quality+%26+Patient+Safety+Update&utm_medium=email&utm_term=0_ebe1fa6178-386d2ff709-319388717. Accessed February 5, 2015.
- Barnet S. Gun violence in hospitals: how much of a threat is it really? January 21, 2015. Becker’s Hospital Review. Available at: http://www.beckershospitalreview.com/healthcare-blog/gun-violence-in-hospitals-how-much-of-a-threat-is-it-really.html. Accessed February 5, 2015.
- Kelen GD, Catlett CL, Kubit JG, Hsieh Y-H. Hospital-based shootings in the United States: 2000 to 2011. Annals of Emergency Medicine online. September 20, 2012. Available at: http://www.annemergmed.com/article/S0196-0644%2812%2901408-4/abstract. Accessed February 5, 2015.
- Calvert S, Scharper J, Roylance F. Experts: no need for metal detectors at Hopkins. September 17, 2010. The Baltimore Sun online. Available at: http://articles.baltimoresun.com/2010-09-17/business/bs-md-hopkins-hospital-security-20100916_1_metal-detectors-healthcare-security-and-safety-hospital-security-experts. Accessed February 5, 2015.
- Rankins RC, Hendey GW. Effect of a security system on violent incidents and hidden weapons in the emergency department. Ann Emerg Med. 1999;33(6):676-679.
On Jan. 20, a 44-year old surgeon was shot and killed in the middle of the day at one of the country’s top hospitals. Michael Davidson, MD, an endovascular surgeon at Brigham and Women’s Hospital in Boston, was in a second-floor hospital clinic when 55-year-old Stephen Pasceri asked for him by name. Dr. Davidson, the division director of endovascular cardiac surgery and assistant professor at Harvard Medical School, had taken care of Pasceri’s mother before her death in November 2014. Witnesses reported that Dr. Davidson came out to talk to Pasceri; during that conversation, Pasceri shot Dr. Davidson twice.
Dr. Davidson was quickly taken to the ED but died 12 hours later.
The shooter died of a self-inflicted gunshot wound to the head.
The motive is not clear, but Pasceri had voiced frustrations with the medical industry during the care of both his father and his mother. In addition, his mother seemed to have suffered some type of complication after a surgery performed by Dr. Davidson. Interviews of Pasceri’s relatives, friends, and neighbors found they were all shocked and dismayed. The shooter was, by all accounts, an upstanding citizen in his work, home, church, and community; he was an accountant with four children, with no past history of criminal or violent activity.1
A Disheartening Trend
Two other fatal events in medical centers occurred within weeks of the Davidson shooting. In December 2014, at Wentworth-Douglass Hospital in Dover, N.H., a man shot and killed his wife before killing himself.
Days later, at a Veterans Hospital clinic in El Paso, Texas, another shooting left both the perpetrator and a psychologist dead.2
In the healthcare setting, providers encounter many types of violence. Nonfatal violence, ranging from physical aggression to various levels of physical harm, has become commonplace. Inciters of such violence tend to be those who “can’t help themselves,” often patients with primary psychiatric illness or those with medically induced mental impairment, such as delirium or withdrawal. For these patients, there is at least some level of compassion and tolerance for their behavior, and because they tend to be relatively predictable, preparedness and mitigation of such acts can give providers some sense of control over the situation.
But the Davidson event represents a type of violence that is frightening, unpredictable, and very difficult to prevent, prepare for, or adequately handle.
Actual shootings on medical campuses are, fortunately, rare. A recent study by the Johns Hopkins Office of Critical Event Preparedness and Response found 154 hospital shootings between 2000 and 2011, resulting in 235 injured or dead victims. The most commonly occurring scenario is that of people acting against family members, with healthcare workers getting caught in the crosshairs. The most common victim is the shooter (45% of the time), and the least common victims are physicians and nurses. Over half (59%) of medical center shootings occur within the hospital; the other 41% occur somewhere else on the hospital grounds.3
So what can hospitalists and hospitals do about the real threat of physical violence and shootings within medical centers? Some have recommended metal detectors as effective barriers for preventing weapons from entering medical centers. The primary problem with this solution is that the majority of medical centers have found this plan impossible to implement, given the number of entrances in typical hospitals; Johns Hopkins for example, has more than 80 entrances. Metal detectors also require security staffing at each entrance 24/7.4
Because of the barriers, metal detectors present an insurmountable financial obstacle for most hospitals. In addition, they present an issue with public perception. Many would argue that hospitals are (and should be) places of healing and sanctuary (e.g. “safe havens”), not places for suspicion and searches. In addition, although there is evidence that the use of metal detectors results in increased confiscation of weapons, there is no evidence that they result in fewer on-site assaults.5 Further complicating matters, almost a quarter of the shootings that occur in EDs result from the perpetrator grabbing a weapon from a security guard.3
Others advocate for stricter gun control laws and enforcement, an argument that has vehement advocates and critics on both sides and is unlikely to be resolved in the near future.
Take Action: Be Prepared
In the meantime, hospitalists are left with preparedness tactics that range from situational awareness to active shooter drills. Both are equally important and should be a part of disaster preparedness at any medical center regardless of size, type, or location. Hospitalists can and should take a lead in such preparedness. Current statistics show that hospitalists are employed in at least 85% of all U.S. hospitals. With such widespread penetration, hospitalists can have a huge impact on the preparedness efforts that can prevent such acts from occurring, as well as on organizational resilience and recovery if such an act does occur.
Such training is more important in healthcare settings than other workplaces, as medical personnel have to be specially trained to resist the temptation to help. For example, active shooter training instructs personnel to run, hide, or fight, none of which come “naturally” to those trained to save and rescue for a living. This training instructs anyone in the “Hot Zone” (where life is in direct danger) to run away from the scene (always preferred if feasible), hide (barricade the door, silence any devices, and stay still), or fight (use anything in sight to fight the shooter, and work as a team if feasible). These responses are the exact opposite of what most trained healthcare personnel are accustomed to doing in cases of emergency.
In Sum
The Michael Davidson story is very sobering by all accounts. Healthcare violence such as this, while rare, is devastating.
Hospitalists should lead the way in training and preparedness for violence prevention and mitigation, including active shooter simulation scenarios. We can all have a huge impact in reducing the risk of casualties should such an unpredictable event occur in our hospital.
References
- Freyer FJ, Kowalczyk L, Murphy SP. Surgeon slain, gunman found dead in day of crisis at Brigham. January 20, 2015. The Boston Globe online. Available at: http://www.bostonglobe.com/metro/2015/01/20/boston-police-investigate-report-shooting-brigham-and-women/Jhig9z8LO8A5PH9Er4vTiP/story.html?rss_id=Top-GNP&utm_source=Managed&utm_campaign=386d2ff709-Quality+%26+Patient+Safety+Update&utm_medium=email&utm_term=0_ebe1fa6178-386d2ff709-319388717. Accessed February 5, 2015.
- Barnet S. Gun violence in hospitals: how much of a threat is it really? January 21, 2015. Becker’s Hospital Review. Available at: http://www.beckershospitalreview.com/healthcare-blog/gun-violence-in-hospitals-how-much-of-a-threat-is-it-really.html. Accessed February 5, 2015.
- Kelen GD, Catlett CL, Kubit JG, Hsieh Y-H. Hospital-based shootings in the United States: 2000 to 2011. Annals of Emergency Medicine online. September 20, 2012. Available at: http://www.annemergmed.com/article/S0196-0644%2812%2901408-4/abstract. Accessed February 5, 2015.
- Calvert S, Scharper J, Roylance F. Experts: no need for metal detectors at Hopkins. September 17, 2010. The Baltimore Sun online. Available at: http://articles.baltimoresun.com/2010-09-17/business/bs-md-hopkins-hospital-security-20100916_1_metal-detectors-healthcare-security-and-safety-hospital-security-experts. Accessed February 5, 2015.
- Rankins RC, Hendey GW. Effect of a security system on violent incidents and hidden weapons in the emergency department. Ann Emerg Med. 1999;33(6):676-679.
On Jan. 20, a 44-year old surgeon was shot and killed in the middle of the day at one of the country’s top hospitals. Michael Davidson, MD, an endovascular surgeon at Brigham and Women’s Hospital in Boston, was in a second-floor hospital clinic when 55-year-old Stephen Pasceri asked for him by name. Dr. Davidson, the division director of endovascular cardiac surgery and assistant professor at Harvard Medical School, had taken care of Pasceri’s mother before her death in November 2014. Witnesses reported that Dr. Davidson came out to talk to Pasceri; during that conversation, Pasceri shot Dr. Davidson twice.
Dr. Davidson was quickly taken to the ED but died 12 hours later.
The shooter died of a self-inflicted gunshot wound to the head.
The motive is not clear, but Pasceri had voiced frustrations with the medical industry during the care of both his father and his mother. In addition, his mother seemed to have suffered some type of complication after a surgery performed by Dr. Davidson. Interviews of Pasceri’s relatives, friends, and neighbors found they were all shocked and dismayed. The shooter was, by all accounts, an upstanding citizen in his work, home, church, and community; he was an accountant with four children, with no past history of criminal or violent activity.1
A Disheartening Trend
Two other fatal events in medical centers occurred within weeks of the Davidson shooting. In December 2014, at Wentworth-Douglass Hospital in Dover, N.H., a man shot and killed his wife before killing himself.
Days later, at a Veterans Hospital clinic in El Paso, Texas, another shooting left both the perpetrator and a psychologist dead.2
In the healthcare setting, providers encounter many types of violence. Nonfatal violence, ranging from physical aggression to various levels of physical harm, has become commonplace. Inciters of such violence tend to be those who “can’t help themselves,” often patients with primary psychiatric illness or those with medically induced mental impairment, such as delirium or withdrawal. For these patients, there is at least some level of compassion and tolerance for their behavior, and because they tend to be relatively predictable, preparedness and mitigation of such acts can give providers some sense of control over the situation.
But the Davidson event represents a type of violence that is frightening, unpredictable, and very difficult to prevent, prepare for, or adequately handle.
Actual shootings on medical campuses are, fortunately, rare. A recent study by the Johns Hopkins Office of Critical Event Preparedness and Response found 154 hospital shootings between 2000 and 2011, resulting in 235 injured or dead victims. The most commonly occurring scenario is that of people acting against family members, with healthcare workers getting caught in the crosshairs. The most common victim is the shooter (45% of the time), and the least common victims are physicians and nurses. Over half (59%) of medical center shootings occur within the hospital; the other 41% occur somewhere else on the hospital grounds.3
So what can hospitalists and hospitals do about the real threat of physical violence and shootings within medical centers? Some have recommended metal detectors as effective barriers for preventing weapons from entering medical centers. The primary problem with this solution is that the majority of medical centers have found this plan impossible to implement, given the number of entrances in typical hospitals; Johns Hopkins for example, has more than 80 entrances. Metal detectors also require security staffing at each entrance 24/7.4
Because of the barriers, metal detectors present an insurmountable financial obstacle for most hospitals. In addition, they present an issue with public perception. Many would argue that hospitals are (and should be) places of healing and sanctuary (e.g. “safe havens”), not places for suspicion and searches. In addition, although there is evidence that the use of metal detectors results in increased confiscation of weapons, there is no evidence that they result in fewer on-site assaults.5 Further complicating matters, almost a quarter of the shootings that occur in EDs result from the perpetrator grabbing a weapon from a security guard.3
Others advocate for stricter gun control laws and enforcement, an argument that has vehement advocates and critics on both sides and is unlikely to be resolved in the near future.
Take Action: Be Prepared
In the meantime, hospitalists are left with preparedness tactics that range from situational awareness to active shooter drills. Both are equally important and should be a part of disaster preparedness at any medical center regardless of size, type, or location. Hospitalists can and should take a lead in such preparedness. Current statistics show that hospitalists are employed in at least 85% of all U.S. hospitals. With such widespread penetration, hospitalists can have a huge impact on the preparedness efforts that can prevent such acts from occurring, as well as on organizational resilience and recovery if such an act does occur.
Such training is more important in healthcare settings than other workplaces, as medical personnel have to be specially trained to resist the temptation to help. For example, active shooter training instructs personnel to run, hide, or fight, none of which come “naturally” to those trained to save and rescue for a living. This training instructs anyone in the “Hot Zone” (where life is in direct danger) to run away from the scene (always preferred if feasible), hide (barricade the door, silence any devices, and stay still), or fight (use anything in sight to fight the shooter, and work as a team if feasible). These responses are the exact opposite of what most trained healthcare personnel are accustomed to doing in cases of emergency.
In Sum
The Michael Davidson story is very sobering by all accounts. Healthcare violence such as this, while rare, is devastating.
Hospitalists should lead the way in training and preparedness for violence prevention and mitigation, including active shooter simulation scenarios. We can all have a huge impact in reducing the risk of casualties should such an unpredictable event occur in our hospital.
References
- Freyer FJ, Kowalczyk L, Murphy SP. Surgeon slain, gunman found dead in day of crisis at Brigham. January 20, 2015. The Boston Globe online. Available at: http://www.bostonglobe.com/metro/2015/01/20/boston-police-investigate-report-shooting-brigham-and-women/Jhig9z8LO8A5PH9Er4vTiP/story.html?rss_id=Top-GNP&utm_source=Managed&utm_campaign=386d2ff709-Quality+%26+Patient+Safety+Update&utm_medium=email&utm_term=0_ebe1fa6178-386d2ff709-319388717. Accessed February 5, 2015.
- Barnet S. Gun violence in hospitals: how much of a threat is it really? January 21, 2015. Becker’s Hospital Review. Available at: http://www.beckershospitalreview.com/healthcare-blog/gun-violence-in-hospitals-how-much-of-a-threat-is-it-really.html. Accessed February 5, 2015.
- Kelen GD, Catlett CL, Kubit JG, Hsieh Y-H. Hospital-based shootings in the United States: 2000 to 2011. Annals of Emergency Medicine online. September 20, 2012. Available at: http://www.annemergmed.com/article/S0196-0644%2812%2901408-4/abstract. Accessed February 5, 2015.
- Calvert S, Scharper J, Roylance F. Experts: no need for metal detectors at Hopkins. September 17, 2010. The Baltimore Sun online. Available at: http://articles.baltimoresun.com/2010-09-17/business/bs-md-hopkins-hospital-security-20100916_1_metal-detectors-healthcare-security-and-safety-hospital-security-experts. Accessed February 5, 2015.
- Rankins RC, Hendey GW. Effect of a security system on violent incidents and hidden weapons in the emergency department. Ann Emerg Med. 1999;33(6):676-679.
Geographic Rounding of Hospital Nurses Challenges Unit-Based Theory
Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
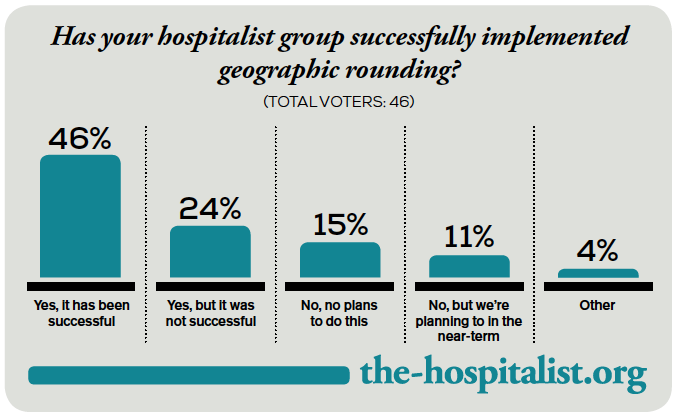
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.

Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.
Nurses, of course, have always been assigned by unit—that is, geographically. So it should come as no surprise that searching “unit-based” at the-hospitalist.org returns many articles about assigning hospitalists geographically, but not nurses, partly because few would consider it a new idea. But this article is about a new wrinkle in assigning nurses.
Although there likely are a number of hospitals doing something similar, I’ll describe a place I was lucky enough to see up close.
Bassett Medical Center
On a cold day last December, I was part of a team that spent a few days in Cooperstown, N.Y. This is a place that is so pretty that I didn’t immediately recognize we had arrived at the Bassett Medical Center Campus, since the entrance we used looked more like a library topped by a pretty cupola and warmly decorated for the holidays. We met so many nice people, including Kai Mebust, MD, FHM, who I’m convinced works full-time for the local Chamber of Commerce and tourism industry. If he doesn’t, then they should put him on their payroll.
Not long after our arrival, Dr. Mebust led us outside in the winter air without our coats to see the very beautiful view from the patio adjacent to the hospital cafeteria. And before we left for home he climbed in our car to direct us on a tour of the town. I’m sold. What a beautiful place. So much more than the Baseball Hall of Fame for which Cooperstown is known.
When not promoting his town’s tourism or enthusiastically describing his eighth-grade son playing with the Preservation Hall Jazz Band in New Orleans, he seems to find time to serve as the chief of this academic hospital’s hospital medicine practice. He was the principal engineer of the geographic assignment of nurses and describes it with an enthusiasm that matches his service as tour guide.
Geographic Care: Single RN Caring for Five Adjacent Patients
The idea is simple and best described using an illustration. A single nurse cares for five patients in adjacent rooms referred to as a “pod.” A second nurse is responsible for the next pod of five consecutive patients, and a single hospitalist cares for all 10 in both pods. There are currently four pods on a single floor of 36 beds; however, they hope to expand this system to most of the medical-surgical beds in the hospital.
The nurses eligible to care for patients in these pods are all trained to be able to provide “step down” level of care, meaning patients don’t need to transfer to a different location for more frequent monitoring and such therapies as vasopressors, mask ventilation, and the like.
Each hospitalist caring for two pods of 10 adjacent patients will typically have additional patients in other locations. This is the hospital’s way of finding the sweet spot between the competing interests of “load leveling” patient volume across hospitalists and rigidly assigning each doctor to a single location, though if they succeed in expanding the model through most of the hospital, the hospitalists will likely need to figure out how to assign themselves more rigidly to three or four pods.
Additional Components
Each morning, the hospitalist meets with the two pod nurses. They briefly discuss overnight events and plans for the day.
Much later in the morning, they also conduct daily multidisciplinary rounds involving nurse, case manager, pharmacist, dietician, social worker, respiratory therapist, and hospitalist. These follow a standard format, which is posted on the wall, and are done in a workroom that allows most participants to be in front of a computer, so they can enter notes and orders into the electronic health record (EHR) as they discuss patients.
What Is the Big Deal Here?
A lot of smart people have developed and written about systems that assign hospitalists geographically, but in most cases this has not been accompanied by adjustments in the way nurses are assigned. On nursing units at most hospitals, this means that even if a hospitalist has all of her patients on the same floor, she is still interacting with five to seven nurses caring for her patients. That usually means the hospitalist and nurse have less awareness of each other’s thinking and doing than if the ratio is reduced to no more than three or four nurses for a single hospitalist.
Dr. Mebust provided a document enumerating the goals for the program:
- Improve communication;
- Reduce patient bed moves;
- Improve patient and staff satisfaction; and
- Provide more efficient care as measured in time-of-discharge, decreased physician time-per-patient, and possibly length of stay.
Because of a number of problems teasing out the effects of this program and its limited duration to this point, Dr. Mebust and staff can’t provide robust statistics to document success in these goals. But anecdotal information is very encouraging, and clearly the nurses love it.
A major barrier to assigning nurses based rigidly on patients in adjacent rooms is the inability to ensure that each nurse has a workload of roughly equivalent complexity, but they’ve found this is a much less significant problem than feared. The nurse I spoke with said any risk of ending up with unusually complex and time-consuming patients is essentially offset by the efficiency gained by having the same attending hospitalist for all of her patients.
In fact, the nurses love it so much that they much prefer being assigned to a pod rather than a traditional assortment of patients with different attending physicians, even if the latter offers a chance to address uneven acuity.
The Big Picture
I’ve often wished that I could incorporate into hospitalist work some of the efficient ways a doctor and nurse can work together seeing scheduled patients in an outpatient setting. Surely assigning hospitalists geographically does this to some degree and has a number of advantages that others have written about. But it comes at the cost of difficult tradeoffs for hospitalists, and I know of many groups that have abandoned it after concluding that the challenges of the system exceeded its benefits.
But when it is coupled with assigning nurses geographically, I think the benefits are even greater, not only for the hospitalists, but also for patients, nurses, and other hospital staff.
Next time you’re in Cooperstown, be sure you don’t just visit the Baseball Hall of Fame. Look up Dr. Mebust, Komron Ostovar, MD, and their colleagues at Bassett Medical Center. I betcha you’ll be persuaded to see the value of their geographic model.
And maybe you’ll even fall so far under the spell of how they all talk about where they work and live that you’ll be ready to move there and join them.
Little Progress Made Training Hospitalists to Stem Shortage of Intensivists
What would the status be for a hospitalist who could train for one year to become a critical care intensivist to address the shortage of intensivists? I’m one of the hospitalists who love critical care but cannot do two more years out for critical care training.
—Amadeo Rivera, MD
Has there been any progress in the 2012 SCCM/SHM proposal to train hospitalists as intensivists?
—Stephen M. Pastores, MD, Memorial
Sloan-Kettering Cancer Center, New York, N.Y.
Dr. Hospitalist responds:

As you may recall, SHM and the Society of Critical Care Medicine (SCCM) published a joint position paper in the Journal of Hospital Medicine in June 2012 in which they proposed a one-year critical care fellowship for hospitalists with at least three years of experience.
Since only one year of clinical rotations is required for critical care board eligibility, and there already exists a one-year track for other medical subspecialists (e.g. nephrology, infectious disease), most of us in hospital medicine thought the recommendation would have been much better received. Well, you guessed it. The following month, the leadership of the American College of Chest Physicians and the American Association of Critical-Care Nurses wrote in an editorial that a one-year fellowship was inadequate for hospitalists to gain competence in critical care medicine. Since then, there has not been much progress, at least not publicly, toward a standardized, streamlined, and accredited process for hospitalists to achieve critical care certification in one year.
Nevertheless, employing a standard search engine (Google) and terminology, I was able to locate one U.S.-based training program offering a one-year critical care medicine fellowship program recognized by the Accreditation Council for Graduate Medical Education for candidates with a background in anesthesiology, surgery, or internal medicine.
What would the status be for a hospitalist who could train for one year to become a critical care intensivist to address the shortage of intensivists? I’m one of the hospitalists who love critical care but cannot do two more years out for critical care training.
—Amadeo Rivera, MD
Has there been any progress in the 2012 SCCM/SHM proposal to train hospitalists as intensivists?
—Stephen M. Pastores, MD, Memorial
Sloan-Kettering Cancer Center, New York, N.Y.
Dr. Hospitalist responds:
As you may recall, SHM and the Society of Critical Care Medicine (SCCM) published a joint position paper in the Journal of Hospital Medicine in June 2012 in which they proposed a one-year critical care fellowship for hospitalists with at least three years of experience.
Since only one year of clinical rotations is required for critical care board eligibility, and there already exists a one-year track for other medical subspecialists (e.g. nephrology, infectious disease), most of us in hospital medicine thought the recommendation would have been much better received. Well, you guessed it. The following month, the leadership of the American College of Chest Physicians and the American Association of Critical-Care Nurses wrote in an editorial that a one-year fellowship was inadequate for hospitalists to gain competence in critical care medicine. Since then, there has not been much progress, at least not publicly, toward a standardized, streamlined, and accredited process for hospitalists to achieve critical care certification in one year.
Nevertheless, employing a standard search engine (Google) and terminology, I was able to locate one U.S.-based training program offering a one-year critical care medicine fellowship program recognized by the Accreditation Council for Graduate Medical Education for candidates with a background in anesthesiology, surgery, or internal medicine.
What would the status be for a hospitalist who could train for one year to become a critical care intensivist to address the shortage of intensivists? I’m one of the hospitalists who love critical care but cannot do two more years out for critical care training.
—Amadeo Rivera, MD
Has there been any progress in the 2012 SCCM/SHM proposal to train hospitalists as intensivists?
—Stephen M. Pastores, MD, Memorial
Sloan-Kettering Cancer Center, New York, N.Y.
Dr. Hospitalist responds:
As you may recall, SHM and the Society of Critical Care Medicine (SCCM) published a joint position paper in the Journal of Hospital Medicine in June 2012 in which they proposed a one-year critical care fellowship for hospitalists with at least three years of experience.
Since only one year of clinical rotations is required for critical care board eligibility, and there already exists a one-year track for other medical subspecialists (e.g. nephrology, infectious disease), most of us in hospital medicine thought the recommendation would have been much better received. Well, you guessed it. The following month, the leadership of the American College of Chest Physicians and the American Association of Critical-Care Nurses wrote in an editorial that a one-year fellowship was inadequate for hospitalists to gain competence in critical care medicine. Since then, there has not been much progress, at least not publicly, toward a standardized, streamlined, and accredited process for hospitalists to achieve critical care certification in one year.
Nevertheless, employing a standard search engine (Google) and terminology, I was able to locate one U.S.-based training program offering a one-year critical care medicine fellowship program recognized by the Accreditation Council for Graduate Medical Education for candidates with a background in anesthesiology, surgery, or internal medicine.
Billing for Hospital Admission, Discharge in Same 24-Hour Period
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
Should the admitting physician or the discharge physician bill the CPT code (99234-99236) for a patient who is admitted and discharged in the same 24-hour period?
—Charlette
Dr. Hospitalist responds:
Assuming both physicians are part of the same group and specialty, they are considered one physician. Since it appears that both face-to-face encounters are separated by eight hours, you’re correct, only one physician can bill the bundled care code 99234-99236. The group must decide which physician gets the RVU credit for the bundled code. Our group gives the credit to the admitting physician.
Hospital Violence Hits Home
Hospitalists could hardly be faulted for wondering: Am I safe? After all, the inpatient setting can be a tense place, and it’s where hospitalists work day in and day out.
David Pressel, MD, PhD, FHM, a pediatric hospitalist and medical director of inpatient services at Nemours Children’s Health System, which has locations in Delaware, New Jersey, Pennsylvania, and Florida, says it’s no wonder violence can erupt in the hospital setting.
“Violence is an issue in hospitals that is a reflection of our society, unfortunately,” says Dr. Pressel, a member of Team Hospitalist. “And it happens because these are very stressful places where people’s behavior can get outside the norm given the stress of the problems.”
Dr. Pressel, in collaboration with many others, has developed a workplace violence prevention program at Nemours aimed at de-escalating situations to avoid physical violence. The program teaches providers how to respond when something violent does happen. It’s a tiered training regimen that involves more training for those most involved in handling violent situations.
Dr. Pressel is no stranger to violence himself. Although he is a pediatric hospitalist and his patients are younger, some adolescent patients can have the physical presence of adults and pose just as serious a threat. He said that before the training program was put into place about a year ago, an episode of violence every month or two would require a patient to be placed in restraints.
“Staff has been hurt,” he explains. “I’ve been bitten twice by a patient. I have a scar on my arm that will be with me for life from one episode.”
A Slow, Disheartening, Upward Trend
Whether violence in hospitals and medical facilities is really a growing problem—or whether awareness of the issue is simply greater given these recent, high profile incidents—is not entirely known.
But according to the latest figures available from the Bureau of Labor Statistics (BLS), provided by the Occupational Safety and Health Administration (OSHA), violent incidents in hospitals did appear to be on the rise through 2013. The number of hospital assaults rose from 5,030 in 2011 to 5,500 in 2012 to 5,660 in 2013.
The number of assaults rose across all private sector industries over that span, but the percentage of those assaults that occurred in hospitals grew greater during that time—an indication that hospitals might be getting more violent at a faster pace than other workplaces. In 2011, according to BLS data, 21.4% of all assaults in private sector industries occurred in hospitals. That number rose to 21.8% in 2012 and to 22.1% in 2013.
According to the 2014 Healthcare Crime Survey, published by the International Association for Healthcare Security and Safety (IAHSS)—an organization of hospital security officials and administrators—violent crime at U.S. facilities rose from two incidents per 100 beds in 2012 to 2.5 incidents per 100 beds in 2013. That category includes murder, rape, aggravated assault, and robbery.
Assaults rose from 10.7 incidents per 100 beds in 2012 to 11.1 incidents per 100 beds in 2013.
BLS data also show that more injuries in hospitals are due to assaults compared with the private sector overall. In 2011, 2.6% of all private sector injuries were due to assault; in 2012, the number rose to 2.8%; and, in 2013, it was 2.8%. In hospitals in 2011, 8.6% of all injuries resulted from assaults. That percentage rose to 9.5% in 2012 and to 9.8% in 2013.
“BLS data show that nonfatal injuries due to violence are greater in the healthcare/social assistance setting than in other workplaces,” an OSHA spokesperson says. “Assaults represent a serious safety and health hazard within healthcare, and data indicate that hospitals comprise a large percentage of workplace assaults.”
Incident Prevention
Programs aimed at preventing violence can reduce these incidents.
“How well prepared hospital workers are in dealing with violent situations depends on the workplace violence prevention program implemented at a facility,” the OSHA spokesperson says. “Some states have passed legislation that specifically requires workplace violence prevention programs in the healthcare setting.”
These programs should address management commitment and employee participation, worksite analysis, hazard prevention and control, safety and health training, and recordkeeping and program evaluation. These elements should be assessed regularly, with changes made to respond to changing conditions, OSHA says.
A large number of OSHA inspections in the healthcare setting occur because of complaints regarding lack of protections against workplace violence. In 2014, the agency did 35 inspections in response to such complaints; 25 of those were in a healthcare setting, with 12 specifically at hospitals. As a result, five citations were issued, all of which were in healthcare, including two at hospitals.
Last year, Brookdale University Hospital and Medical Center in Brooklyn, N.Y., was fined $78,000 after an OSHA inspection found 40 incidents of workplace violence between Feb. 7 and April 12. They included employees who were threatened or verbally or physically assaulted by patients and visitors or while breaking up fights between patients. In the worst attack, a nurse sustained severe brain injuries.
The bulk of the hospital’s fines came as a result of a willful violation—an intentional or voluntary disregard for laws meant to protect workers against hospital violence.
While data from IAHSS and the BLS show an increase in hospital violence, those national figures aren’t as important as what is happening at your own facility, says David LaRose, MS, CHPA, CPP, the president of IAHSS and director of safety, security, and emergency management at Lakeland Regional Medical Center in Florida.
“You have to do a vulnerability assessment, and you specifically have to look at your demographic,” he says. “You specifically have to look at what is the history and the culture of the facility” to determine a hospital’s specific risk factors.
Although it’s crucial that a hospital track its own statistics on violence, that’s not to say that incidents elsewhere are irrelevant.
“You also want to look at what’s happening in the real world,” he says. “Somebody else’s unfortunate (occurrence) is a learning experience for my system, so we can try to be proactively preventing that.”
Educate, Recognize, React
At Nemours, Dr. Pressel didn’t develop the training in response to a perceived rise in incidents there. It was apparent, he says, that deficiencies in readiness needed to be addressed.
In the Nemours program, every staff member with some level of patient care responsibility gets basic training in aggressive child emergencies: identifying these situations, responding appropriately, and keeping safe. This group includes doctors, nurses, and nurse’s aids. The training involves actually playing out scenarios of violence, with staff members attempting to subdue a would-be attacker.
Depending on the job, each worker receives extra training that is specific to the role he or she would play in handling violent scenarios.
The training is designed to help individuals respond to such situations with “the same alacrity and acuity as they would respond to a Code Blue,” Dr. Pressel says. “Drop what you’re doing and run. These events are dangerous. That’s what they teach people. They’re dangerous and they’re scary and they’re chaotic, just like a Code Blue. That’s how people need to treat it.”
The goal is to de-escalate a situation, verbally or physically, without more aggressive means. But if that doesn’t work, physical restraints, medication, or both are used.
Throughout the medical field, training in this area is scarce, Dr. Pressel says. In nursing school and medical school, “for the most part, it’s zero,” he says.
“If you’re in a psychiatric facility, these events happen,” he adds. “And then you get a lot of enhanced training.” But, he notes, “I had no formal training until I became tasked with dealing with this.”
Since the program was implemented at Nemours, it seems to have worked.
“We have had many of these episodes that have been resolved by verbal de-escalation, as opposed to physical restraints or medication,” he says.
His hospital has also made other changes. The facility used to have multiple entrances and exits that were unsecured, and anybody could walk into any unit “with no challenge whatsoever.” Now, everyone entering has to pass hospital personnel. And, to get into a patient unit, visitors have to check in and be issued a photo ID. Also, in response to an incident in 2013, the hospital now has “constables” who are trained and licensed to carry firearms, Dr. Pressel says.
Above all, he notes, is personal safety. If you yourself are hurt, you won’t be able to help anyone else.
“That’s absolutely the first thing that people hear, the last thing that people hear, and it’s repeated over and over again,” he says.
Both Dr. Pressel and LaRose say that even with the drumbeat of high profile incidents, they haven’t heard from colleagues that health professionals are concerned about people losing interest in entering the field or are feeling burned out because of safety concerns. Being prepared is the key, and the level of preparedness varies by facility, LaRose says. The IAHSS provides security and healthcare safety guidelines at iahss.org.
“We recognize that we are in an occupation that tends to be on the receiving end of more aggression and more violence than the average worker,” LaRose says. “Therefore, how proactively does the organization or the institution take that knowledge and provide the tools and the training to the staff?
“What can we do as a team to increase our sense of security and safety and make this a great place to continue your career?”
Tom Collins is a freelance writer in South Florida.
Hospitalists could hardly be faulted for wondering: Am I safe? After all, the inpatient setting can be a tense place, and it’s where hospitalists work day in and day out.
David Pressel, MD, PhD, FHM, a pediatric hospitalist and medical director of inpatient services at Nemours Children’s Health System, which has locations in Delaware, New Jersey, Pennsylvania, and Florida, says it’s no wonder violence can erupt in the hospital setting.
“Violence is an issue in hospitals that is a reflection of our society, unfortunately,” says Dr. Pressel, a member of Team Hospitalist. “And it happens because these are very stressful places where people’s behavior can get outside the norm given the stress of the problems.”
Dr. Pressel, in collaboration with many others, has developed a workplace violence prevention program at Nemours aimed at de-escalating situations to avoid physical violence. The program teaches providers how to respond when something violent does happen. It’s a tiered training regimen that involves more training for those most involved in handling violent situations.
Dr. Pressel is no stranger to violence himself. Although he is a pediatric hospitalist and his patients are younger, some adolescent patients can have the physical presence of adults and pose just as serious a threat. He said that before the training program was put into place about a year ago, an episode of violence every month or two would require a patient to be placed in restraints.
“Staff has been hurt,” he explains. “I’ve been bitten twice by a patient. I have a scar on my arm that will be with me for life from one episode.”
A Slow, Disheartening, Upward Trend
Whether violence in hospitals and medical facilities is really a growing problem—or whether awareness of the issue is simply greater given these recent, high profile incidents—is not entirely known.
But according to the latest figures available from the Bureau of Labor Statistics (BLS), provided by the Occupational Safety and Health Administration (OSHA), violent incidents in hospitals did appear to be on the rise through 2013. The number of hospital assaults rose from 5,030 in 2011 to 5,500 in 2012 to 5,660 in 2013.
The number of assaults rose across all private sector industries over that span, but the percentage of those assaults that occurred in hospitals grew greater during that time—an indication that hospitals might be getting more violent at a faster pace than other workplaces. In 2011, according to BLS data, 21.4% of all assaults in private sector industries occurred in hospitals. That number rose to 21.8% in 2012 and to 22.1% in 2013.
According to the 2014 Healthcare Crime Survey, published by the International Association for Healthcare Security and Safety (IAHSS)—an organization of hospital security officials and administrators—violent crime at U.S. facilities rose from two incidents per 100 beds in 2012 to 2.5 incidents per 100 beds in 2013. That category includes murder, rape, aggravated assault, and robbery.
Assaults rose from 10.7 incidents per 100 beds in 2012 to 11.1 incidents per 100 beds in 2013.
BLS data also show that more injuries in hospitals are due to assaults compared with the private sector overall. In 2011, 2.6% of all private sector injuries were due to assault; in 2012, the number rose to 2.8%; and, in 2013, it was 2.8%. In hospitals in 2011, 8.6% of all injuries resulted from assaults. That percentage rose to 9.5% in 2012 and to 9.8% in 2013.
“BLS data show that nonfatal injuries due to violence are greater in the healthcare/social assistance setting than in other workplaces,” an OSHA spokesperson says. “Assaults represent a serious safety and health hazard within healthcare, and data indicate that hospitals comprise a large percentage of workplace assaults.”
Incident Prevention
Programs aimed at preventing violence can reduce these incidents.
“How well prepared hospital workers are in dealing with violent situations depends on the workplace violence prevention program implemented at a facility,” the OSHA spokesperson says. “Some states have passed legislation that specifically requires workplace violence prevention programs in the healthcare setting.”
These programs should address management commitment and employee participation, worksite analysis, hazard prevention and control, safety and health training, and recordkeeping and program evaluation. These elements should be assessed regularly, with changes made to respond to changing conditions, OSHA says.
A large number of OSHA inspections in the healthcare setting occur because of complaints regarding lack of protections against workplace violence. In 2014, the agency did 35 inspections in response to such complaints; 25 of those were in a healthcare setting, with 12 specifically at hospitals. As a result, five citations were issued, all of which were in healthcare, including two at hospitals.
Last year, Brookdale University Hospital and Medical Center in Brooklyn, N.Y., was fined $78,000 after an OSHA inspection found 40 incidents of workplace violence between Feb. 7 and April 12. They included employees who were threatened or verbally or physically assaulted by patients and visitors or while breaking up fights between patients. In the worst attack, a nurse sustained severe brain injuries.
The bulk of the hospital’s fines came as a result of a willful violation—an intentional or voluntary disregard for laws meant to protect workers against hospital violence.
While data from IAHSS and the BLS show an increase in hospital violence, those national figures aren’t as important as what is happening at your own facility, says David LaRose, MS, CHPA, CPP, the president of IAHSS and director of safety, security, and emergency management at Lakeland Regional Medical Center in Florida.
“You have to do a vulnerability assessment, and you specifically have to look at your demographic,” he says. “You specifically have to look at what is the history and the culture of the facility” to determine a hospital’s specific risk factors.
Although it’s crucial that a hospital track its own statistics on violence, that’s not to say that incidents elsewhere are irrelevant.
“You also want to look at what’s happening in the real world,” he says. “Somebody else’s unfortunate (occurrence) is a learning experience for my system, so we can try to be proactively preventing that.”
Educate, Recognize, React
At Nemours, Dr. Pressel didn’t develop the training in response to a perceived rise in incidents there. It was apparent, he says, that deficiencies in readiness needed to be addressed.
In the Nemours program, every staff member with some level of patient care responsibility gets basic training in aggressive child emergencies: identifying these situations, responding appropriately, and keeping safe. This group includes doctors, nurses, and nurse’s aids. The training involves actually playing out scenarios of violence, with staff members attempting to subdue a would-be attacker.
Depending on the job, each worker receives extra training that is specific to the role he or she would play in handling violent scenarios.
The training is designed to help individuals respond to such situations with “the same alacrity and acuity as they would respond to a Code Blue,” Dr. Pressel says. “Drop what you’re doing and run. These events are dangerous. That’s what they teach people. They’re dangerous and they’re scary and they’re chaotic, just like a Code Blue. That’s how people need to treat it.”
The goal is to de-escalate a situation, verbally or physically, without more aggressive means. But if that doesn’t work, physical restraints, medication, or both are used.
Throughout the medical field, training in this area is scarce, Dr. Pressel says. In nursing school and medical school, “for the most part, it’s zero,” he says.
“If you’re in a psychiatric facility, these events happen,” he adds. “And then you get a lot of enhanced training.” But, he notes, “I had no formal training until I became tasked with dealing with this.”
Since the program was implemented at Nemours, it seems to have worked.
“We have had many of these episodes that have been resolved by verbal de-escalation, as opposed to physical restraints or medication,” he says.
His hospital has also made other changes. The facility used to have multiple entrances and exits that were unsecured, and anybody could walk into any unit “with no challenge whatsoever.” Now, everyone entering has to pass hospital personnel. And, to get into a patient unit, visitors have to check in and be issued a photo ID. Also, in response to an incident in 2013, the hospital now has “constables” who are trained and licensed to carry firearms, Dr. Pressel says.
Above all, he notes, is personal safety. If you yourself are hurt, you won’t be able to help anyone else.
“That’s absolutely the first thing that people hear, the last thing that people hear, and it’s repeated over and over again,” he says.
Both Dr. Pressel and LaRose say that even with the drumbeat of high profile incidents, they haven’t heard from colleagues that health professionals are concerned about people losing interest in entering the field or are feeling burned out because of safety concerns. Being prepared is the key, and the level of preparedness varies by facility, LaRose says. The IAHSS provides security and healthcare safety guidelines at iahss.org.
“We recognize that we are in an occupation that tends to be on the receiving end of more aggression and more violence than the average worker,” LaRose says. “Therefore, how proactively does the organization or the institution take that knowledge and provide the tools and the training to the staff?
“What can we do as a team to increase our sense of security and safety and make this a great place to continue your career?”
Tom Collins is a freelance writer in South Florida.
Hospitalists could hardly be faulted for wondering: Am I safe? After all, the inpatient setting can be a tense place, and it’s where hospitalists work day in and day out.
David Pressel, MD, PhD, FHM, a pediatric hospitalist and medical director of inpatient services at Nemours Children’s Health System, which has locations in Delaware, New Jersey, Pennsylvania, and Florida, says it’s no wonder violence can erupt in the hospital setting.
“Violence is an issue in hospitals that is a reflection of our society, unfortunately,” says Dr. Pressel, a member of Team Hospitalist. “And it happens because these are very stressful places where people’s behavior can get outside the norm given the stress of the problems.”
Dr. Pressel, in collaboration with many others, has developed a workplace violence prevention program at Nemours aimed at de-escalating situations to avoid physical violence. The program teaches providers how to respond when something violent does happen. It’s a tiered training regimen that involves more training for those most involved in handling violent situations.
Dr. Pressel is no stranger to violence himself. Although he is a pediatric hospitalist and his patients are younger, some adolescent patients can have the physical presence of adults and pose just as serious a threat. He said that before the training program was put into place about a year ago, an episode of violence every month or two would require a patient to be placed in restraints.
“Staff has been hurt,” he explains. “I’ve been bitten twice by a patient. I have a scar on my arm that will be with me for life from one episode.”
A Slow, Disheartening, Upward Trend
Whether violence in hospitals and medical facilities is really a growing problem—or whether awareness of the issue is simply greater given these recent, high profile incidents—is not entirely known.
But according to the latest figures available from the Bureau of Labor Statistics (BLS), provided by the Occupational Safety and Health Administration (OSHA), violent incidents in hospitals did appear to be on the rise through 2013. The number of hospital assaults rose from 5,030 in 2011 to 5,500 in 2012 to 5,660 in 2013.
The number of assaults rose across all private sector industries over that span, but the percentage of those assaults that occurred in hospitals grew greater during that time—an indication that hospitals might be getting more violent at a faster pace than other workplaces. In 2011, according to BLS data, 21.4% of all assaults in private sector industries occurred in hospitals. That number rose to 21.8% in 2012 and to 22.1% in 2013.
According to the 2014 Healthcare Crime Survey, published by the International Association for Healthcare Security and Safety (IAHSS)—an organization of hospital security officials and administrators—violent crime at U.S. facilities rose from two incidents per 100 beds in 2012 to 2.5 incidents per 100 beds in 2013. That category includes murder, rape, aggravated assault, and robbery.
Assaults rose from 10.7 incidents per 100 beds in 2012 to 11.1 incidents per 100 beds in 2013.
BLS data also show that more injuries in hospitals are due to assaults compared with the private sector overall. In 2011, 2.6% of all private sector injuries were due to assault; in 2012, the number rose to 2.8%; and, in 2013, it was 2.8%. In hospitals in 2011, 8.6% of all injuries resulted from assaults. That percentage rose to 9.5% in 2012 and to 9.8% in 2013.
“BLS data show that nonfatal injuries due to violence are greater in the healthcare/social assistance setting than in other workplaces,” an OSHA spokesperson says. “Assaults represent a serious safety and health hazard within healthcare, and data indicate that hospitals comprise a large percentage of workplace assaults.”
Incident Prevention
Programs aimed at preventing violence can reduce these incidents.
“How well prepared hospital workers are in dealing with violent situations depends on the workplace violence prevention program implemented at a facility,” the OSHA spokesperson says. “Some states have passed legislation that specifically requires workplace violence prevention programs in the healthcare setting.”
These programs should address management commitment and employee participation, worksite analysis, hazard prevention and control, safety and health training, and recordkeeping and program evaluation. These elements should be assessed regularly, with changes made to respond to changing conditions, OSHA says.
A large number of OSHA inspections in the healthcare setting occur because of complaints regarding lack of protections against workplace violence. In 2014, the agency did 35 inspections in response to such complaints; 25 of those were in a healthcare setting, with 12 specifically at hospitals. As a result, five citations were issued, all of which were in healthcare, including two at hospitals.
Last year, Brookdale University Hospital and Medical Center in Brooklyn, N.Y., was fined $78,000 after an OSHA inspection found 40 incidents of workplace violence between Feb. 7 and April 12. They included employees who were threatened or verbally or physically assaulted by patients and visitors or while breaking up fights between patients. In the worst attack, a nurse sustained severe brain injuries.
The bulk of the hospital’s fines came as a result of a willful violation—an intentional or voluntary disregard for laws meant to protect workers against hospital violence.
While data from IAHSS and the BLS show an increase in hospital violence, those national figures aren’t as important as what is happening at your own facility, says David LaRose, MS, CHPA, CPP, the president of IAHSS and director of safety, security, and emergency management at Lakeland Regional Medical Center in Florida.
“You have to do a vulnerability assessment, and you specifically have to look at your demographic,” he says. “You specifically have to look at what is the history and the culture of the facility” to determine a hospital’s specific risk factors.
Although it’s crucial that a hospital track its own statistics on violence, that’s not to say that incidents elsewhere are irrelevant.
“You also want to look at what’s happening in the real world,” he says. “Somebody else’s unfortunate (occurrence) is a learning experience for my system, so we can try to be proactively preventing that.”
Educate, Recognize, React
At Nemours, Dr. Pressel didn’t develop the training in response to a perceived rise in incidents there. It was apparent, he says, that deficiencies in readiness needed to be addressed.
In the Nemours program, every staff member with some level of patient care responsibility gets basic training in aggressive child emergencies: identifying these situations, responding appropriately, and keeping safe. This group includes doctors, nurses, and nurse’s aids. The training involves actually playing out scenarios of violence, with staff members attempting to subdue a would-be attacker.
Depending on the job, each worker receives extra training that is specific to the role he or she would play in handling violent scenarios.
The training is designed to help individuals respond to such situations with “the same alacrity and acuity as they would respond to a Code Blue,” Dr. Pressel says. “Drop what you’re doing and run. These events are dangerous. That’s what they teach people. They’re dangerous and they’re scary and they’re chaotic, just like a Code Blue. That’s how people need to treat it.”
The goal is to de-escalate a situation, verbally or physically, without more aggressive means. But if that doesn’t work, physical restraints, medication, or both are used.
Throughout the medical field, training in this area is scarce, Dr. Pressel says. In nursing school and medical school, “for the most part, it’s zero,” he says.
“If you’re in a psychiatric facility, these events happen,” he adds. “And then you get a lot of enhanced training.” But, he notes, “I had no formal training until I became tasked with dealing with this.”
Since the program was implemented at Nemours, it seems to have worked.
“We have had many of these episodes that have been resolved by verbal de-escalation, as opposed to physical restraints or medication,” he says.
His hospital has also made other changes. The facility used to have multiple entrances and exits that were unsecured, and anybody could walk into any unit “with no challenge whatsoever.” Now, everyone entering has to pass hospital personnel. And, to get into a patient unit, visitors have to check in and be issued a photo ID. Also, in response to an incident in 2013, the hospital now has “constables” who are trained and licensed to carry firearms, Dr. Pressel says.
Above all, he notes, is personal safety. If you yourself are hurt, you won’t be able to help anyone else.
“That’s absolutely the first thing that people hear, the last thing that people hear, and it’s repeated over and over again,” he says.
Both Dr. Pressel and LaRose say that even with the drumbeat of high profile incidents, they haven’t heard from colleagues that health professionals are concerned about people losing interest in entering the field or are feeling burned out because of safety concerns. Being prepared is the key, and the level of preparedness varies by facility, LaRose says. The IAHSS provides security and healthcare safety guidelines at iahss.org.
“We recognize that we are in an occupation that tends to be on the receiving end of more aggression and more violence than the average worker,” LaRose says. “Therefore, how proactively does the organization or the institution take that knowledge and provide the tools and the training to the staff?
“What can we do as a team to increase our sense of security and safety and make this a great place to continue your career?”
Tom Collins is a freelance writer in South Florida.