User login
Minimal residual disease could signify worse outcomes in acute myeloid leukemia treatment
Although peripheral count recovery and minimal residual disease level following induction therapy are linked, each is an independent prognostic factor for relapse and overall survival in patients with acute myeloid leukemia, investigators say in a report published online March 2 in Journal of Clinical Oncology. “Information about these post-treatment factors is likely more important than information about several traditional pretreatment prognostic factors and should play a major – and perhaps the dominant – role in planning postinduction therapy,” wrote Dr. Xueyan Chen and her associates.
The investigators retrospectively analyzed data from 245 adults with newly diagnosed, relapsed, or refractory acute myeloid leukemia (AML) who achieved either complete remission (CR), complete remission with incomplete platelet recovery (CRp), or complete remission with incomplete blood count recovery (CRi), after induction therapy. The 71% of patients who achieved CR had minimal residual disease (MRD) less frequently and had lower levels of MRD than the 19.6% of patients achieving CRp and 9.4% achieving CRi, suggesting that failure of blood count recovery may result from inadequate treatment of AML.
Read the entire article here: http://jco.ascopubs.org/content/early/2015/02/26/JCO.2014.58.3518
Although peripheral count recovery and minimal residual disease level following induction therapy are linked, each is an independent prognostic factor for relapse and overall survival in patients with acute myeloid leukemia, investigators say in a report published online March 2 in Journal of Clinical Oncology. “Information about these post-treatment factors is likely more important than information about several traditional pretreatment prognostic factors and should play a major – and perhaps the dominant – role in planning postinduction therapy,” wrote Dr. Xueyan Chen and her associates.
The investigators retrospectively analyzed data from 245 adults with newly diagnosed, relapsed, or refractory acute myeloid leukemia (AML) who achieved either complete remission (CR), complete remission with incomplete platelet recovery (CRp), or complete remission with incomplete blood count recovery (CRi), after induction therapy. The 71% of patients who achieved CR had minimal residual disease (MRD) less frequently and had lower levels of MRD than the 19.6% of patients achieving CRp and 9.4% achieving CRi, suggesting that failure of blood count recovery may result from inadequate treatment of AML.
Read the entire article here: http://jco.ascopubs.org/content/early/2015/02/26/JCO.2014.58.3518
Although peripheral count recovery and minimal residual disease level following induction therapy are linked, each is an independent prognostic factor for relapse and overall survival in patients with acute myeloid leukemia, investigators say in a report published online March 2 in Journal of Clinical Oncology. “Information about these post-treatment factors is likely more important than information about several traditional pretreatment prognostic factors and should play a major – and perhaps the dominant – role in planning postinduction therapy,” wrote Dr. Xueyan Chen and her associates.
The investigators retrospectively analyzed data from 245 adults with newly diagnosed, relapsed, or refractory acute myeloid leukemia (AML) who achieved either complete remission (CR), complete remission with incomplete platelet recovery (CRp), or complete remission with incomplete blood count recovery (CRi), after induction therapy. The 71% of patients who achieved CR had minimal residual disease (MRD) less frequently and had lower levels of MRD than the 19.6% of patients achieving CRp and 9.4% achieving CRi, suggesting that failure of blood count recovery may result from inadequate treatment of AML.
Read the entire article here: http://jco.ascopubs.org/content/early/2015/02/26/JCO.2014.58.3518
Studies of anesthesia’s effect on upper airway are limited
CORONADO, CALIF. – Studies of the most appropriate anesthetic agents for drug-induced sleep endoscopy are limited, but according to the best available evidence, local anesthetics appear to affect airway reflexes while inhalation anesthetics and opioids exaggerate dynamic airway collapse, so they may not be ideal.
Those are key conclusions from a systematic review of literature on the effects of commonly used anesthetic agents and opioids on the upper airway presented at the Triological Society’s Combined Sections meeting. Drug-induced sleep endoscopy (DISE) “is a great tool to assess upper airway dynamics in order to determine optimal surgical therapy for obstructive sleep apnea,” said Dr. Zarmina Ehsan, a pediatric pulmonary medicine fellow at Cincinnati Children’s Hospital Medical Center. “There’s a lack of understanding regarding how upper airway dynamics are altered by anesthetic agents, compared with normal sleep. This is important because this hinders the development of universal guidelines and protocols for the use of DISE.”

Using PubMed, EMBASE, and other sources, she and her associates conducted a qualitative systematic review of studies related to common anesthetic agents and opioids in the medical literature through September 2014. To be eligible for inclusion, a study must have evaluated the agent’s effect on the upper airway, must have contained an abstract, and must have been published in English. Studies with fewer than seven subjects, no original data, review articles, and those involving animals were excluded. The researchers reviewed 180 abstracts and included 56 full text articles in the final analysis, for a total study population of 8,540 patients. At the meeting Dr. Ehsan summarized the following findings by agent:
• Lidocaine. This agent is safe for topical use, has a rapid onset of action, and an intermediate duration of efficacy. Lidocaine acts on muscles “which are potent dilators and tensors of the pharyngeal and laryngeal structures,” she said. Of 10 studies included in the analysis, 7 assessed the impact of lidocaine on upper airway obstruction. Of these, three showed increased airway obstruction while four showed no significant effects. There were two studies on sleep parameters with conflicting results: One showed an increase in mean apnea duration with lidocaine use while the other did not. From this the researchers concluded that lidocaine does affect upper airway dynamics.
• Propofol. This lipophilic intravenous agent has a quick onset of action and acts by global central nervous system depression. Of 12 studies included in the analysis, 4 examined dose-response characteristics and showed a dose-dependent decrease in airway cross-sectional area with increased dosing of propofol. “So increasing your dose makes airway obstruction more likely,” Dr. Ehsan said. “The levels of obstruction were greatest at the base of tongue, and the closure was primarily in the anterior-posterior direction.” Three studies found that propofol caused a decrease in genioglossus electromyogram activity, while the remaining five studies assessed heterogeneous outcomes. “Overall, the studies showed that propofol had a dose-dependent effect on the upper airway with increasing doses making airway obstruction more likely,” she said.
• Dexmedetomidine (DEX). This agent is an alpha-2 adrenergic agonist with sedative, anxiolytic, and analgesic effects. It’s typically given as a 10-minute loading dose followed by a continuous infusion, and is recommended when you want to preserve spontaneous respiration. Of the four DEX-related studies that were included in the analysis, all demonstrated a minimal effect on upper airway cross-sectional area. “One of the studies looked at sleep parameters and concluded that DEX does approximate non-REM sleep without causing respiratory depression,” Dr. Ehsan added. “So overall, DEX was less likely to result in upper airway obstruction, compared with propofol.”
• Midazolam. This agent is commonly used for procedural sedation, with an onset of action within 1-3 minutes and a duration of 15-60 minutes. Of the six studies involving midazolam, two evaluated sleep staging. One reported lack of REM sleep and increased duration of stage N3 sleep, while the other study found that all sleep stages were observed at a lower dosage. The remaining four studies had heterogeneous outcomes. This led the researchers to conclude that midazolam “may lead to upper airway obstruction,” Dr. Ehsan said. “It’s unclear if this is dose dependent.”
• Pentobarbital. Of the two studies involving this short-acting barbiturate, one showed no effect on pharyngeal critical pressure or respiratory muscle function, while the other found that pentobarbital can increase the upper airway cross-sectional area. “So the effect of pentobarbital is unclear,” she said.
• Ketamine. This N-methyl-D-aspartate receptor has a rapid onset and a minimal effect on the central respiratory drive. Of the three studies involving ketamine, one found a 10% incidence of transient laryngospasm, one found that the incidence of transient laryngospasm was higher when it was delivered intramuscularly vs. intravenously, and one found that ketamine was safe in infants undergoing upper airway endoscopy. The researchers concluded that overall, ketamine “could be useful during DISE.”
• Inhalation anesthetics. There were 11 studies of these agents. Of these, six found that inhalation anesthetics caused upper airway collapse while five had heterogeneous outcomes. “Overall, a majority of studies found that inhalation anesthetics exaggerate dynamic airway collapse,” Dr. Ehsan said.
• Opioids. Of the nine studies involving these agents, six found that opioids caused upper airway obstruction; two found that they caused depression of upper airway reflexes, and one found that they caused a decrease in respiratory compliance. “Overall, opioids increase upper airway obstruction,” she said.
Dr. Ehsan acknowledged certain limitations of the analysis, including the fact that there was little information on sleep state approximated by many of these agents, “which makes it difficult to determine the ideal anesthetic protocol. There was substantial heterogeneity in outcomes, and few prospective studies comparing the ability of anesthetics to approximate natural sleep.” She recommended that future efforts focus on comparative effectiveness studies between the agents, as well as evaluate the impact of combining anesthetic agents. “This is important, because most DISE protocols use a combination of agents,” she said.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons
Dr. Ehsan reported having no relevant financial conflicts.
On Twitter @dougbrunk
CORONADO, CALIF. – Studies of the most appropriate anesthetic agents for drug-induced sleep endoscopy are limited, but according to the best available evidence, local anesthetics appear to affect airway reflexes while inhalation anesthetics and opioids exaggerate dynamic airway collapse, so they may not be ideal.
Those are key conclusions from a systematic review of literature on the effects of commonly used anesthetic agents and opioids on the upper airway presented at the Triological Society’s Combined Sections meeting. Drug-induced sleep endoscopy (DISE) “is a great tool to assess upper airway dynamics in order to determine optimal surgical therapy for obstructive sleep apnea,” said Dr. Zarmina Ehsan, a pediatric pulmonary medicine fellow at Cincinnati Children’s Hospital Medical Center. “There’s a lack of understanding regarding how upper airway dynamics are altered by anesthetic agents, compared with normal sleep. This is important because this hinders the development of universal guidelines and protocols for the use of DISE.”
Using PubMed, EMBASE, and other sources, she and her associates conducted a qualitative systematic review of studies related to common anesthetic agents and opioids in the medical literature through September 2014. To be eligible for inclusion, a study must have evaluated the agent’s effect on the upper airway, must have contained an abstract, and must have been published in English. Studies with fewer than seven subjects, no original data, review articles, and those involving animals were excluded. The researchers reviewed 180 abstracts and included 56 full text articles in the final analysis, for a total study population of 8,540 patients. At the meeting Dr. Ehsan summarized the following findings by agent:
• Lidocaine. This agent is safe for topical use, has a rapid onset of action, and an intermediate duration of efficacy. Lidocaine acts on muscles “which are potent dilators and tensors of the pharyngeal and laryngeal structures,” she said. Of 10 studies included in the analysis, 7 assessed the impact of lidocaine on upper airway obstruction. Of these, three showed increased airway obstruction while four showed no significant effects. There were two studies on sleep parameters with conflicting results: One showed an increase in mean apnea duration with lidocaine use while the other did not. From this the researchers concluded that lidocaine does affect upper airway dynamics.
• Propofol. This lipophilic intravenous agent has a quick onset of action and acts by global central nervous system depression. Of 12 studies included in the analysis, 4 examined dose-response characteristics and showed a dose-dependent decrease in airway cross-sectional area with increased dosing of propofol. “So increasing your dose makes airway obstruction more likely,” Dr. Ehsan said. “The levels of obstruction were greatest at the base of tongue, and the closure was primarily in the anterior-posterior direction.” Three studies found that propofol caused a decrease in genioglossus electromyogram activity, while the remaining five studies assessed heterogeneous outcomes. “Overall, the studies showed that propofol had a dose-dependent effect on the upper airway with increasing doses making airway obstruction more likely,” she said.
• Dexmedetomidine (DEX). This agent is an alpha-2 adrenergic agonist with sedative, anxiolytic, and analgesic effects. It’s typically given as a 10-minute loading dose followed by a continuous infusion, and is recommended when you want to preserve spontaneous respiration. Of the four DEX-related studies that were included in the analysis, all demonstrated a minimal effect on upper airway cross-sectional area. “One of the studies looked at sleep parameters and concluded that DEX does approximate non-REM sleep without causing respiratory depression,” Dr. Ehsan added. “So overall, DEX was less likely to result in upper airway obstruction, compared with propofol.”
• Midazolam. This agent is commonly used for procedural sedation, with an onset of action within 1-3 minutes and a duration of 15-60 minutes. Of the six studies involving midazolam, two evaluated sleep staging. One reported lack of REM sleep and increased duration of stage N3 sleep, while the other study found that all sleep stages were observed at a lower dosage. The remaining four studies had heterogeneous outcomes. This led the researchers to conclude that midazolam “may lead to upper airway obstruction,” Dr. Ehsan said. “It’s unclear if this is dose dependent.”
• Pentobarbital. Of the two studies involving this short-acting barbiturate, one showed no effect on pharyngeal critical pressure or respiratory muscle function, while the other found that pentobarbital can increase the upper airway cross-sectional area. “So the effect of pentobarbital is unclear,” she said.
• Ketamine. This N-methyl-D-aspartate receptor has a rapid onset and a minimal effect on the central respiratory drive. Of the three studies involving ketamine, one found a 10% incidence of transient laryngospasm, one found that the incidence of transient laryngospasm was higher when it was delivered intramuscularly vs. intravenously, and one found that ketamine was safe in infants undergoing upper airway endoscopy. The researchers concluded that overall, ketamine “could be useful during DISE.”
• Inhalation anesthetics. There were 11 studies of these agents. Of these, six found that inhalation anesthetics caused upper airway collapse while five had heterogeneous outcomes. “Overall, a majority of studies found that inhalation anesthetics exaggerate dynamic airway collapse,” Dr. Ehsan said.
• Opioids. Of the nine studies involving these agents, six found that opioids caused upper airway obstruction; two found that they caused depression of upper airway reflexes, and one found that they caused a decrease in respiratory compliance. “Overall, opioids increase upper airway obstruction,” she said.
Dr. Ehsan acknowledged certain limitations of the analysis, including the fact that there was little information on sleep state approximated by many of these agents, “which makes it difficult to determine the ideal anesthetic protocol. There was substantial heterogeneity in outcomes, and few prospective studies comparing the ability of anesthetics to approximate natural sleep.” She recommended that future efforts focus on comparative effectiveness studies between the agents, as well as evaluate the impact of combining anesthetic agents. “This is important, because most DISE protocols use a combination of agents,” she said.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons
Dr. Ehsan reported having no relevant financial conflicts.
On Twitter @dougbrunk
CORONADO, CALIF. – Studies of the most appropriate anesthetic agents for drug-induced sleep endoscopy are limited, but according to the best available evidence, local anesthetics appear to affect airway reflexes while inhalation anesthetics and opioids exaggerate dynamic airway collapse, so they may not be ideal.
Those are key conclusions from a systematic review of literature on the effects of commonly used anesthetic agents and opioids on the upper airway presented at the Triological Society’s Combined Sections meeting. Drug-induced sleep endoscopy (DISE) “is a great tool to assess upper airway dynamics in order to determine optimal surgical therapy for obstructive sleep apnea,” said Dr. Zarmina Ehsan, a pediatric pulmonary medicine fellow at Cincinnati Children’s Hospital Medical Center. “There’s a lack of understanding regarding how upper airway dynamics are altered by anesthetic agents, compared with normal sleep. This is important because this hinders the development of universal guidelines and protocols for the use of DISE.”
Using PubMed, EMBASE, and other sources, she and her associates conducted a qualitative systematic review of studies related to common anesthetic agents and opioids in the medical literature through September 2014. To be eligible for inclusion, a study must have evaluated the agent’s effect on the upper airway, must have contained an abstract, and must have been published in English. Studies with fewer than seven subjects, no original data, review articles, and those involving animals were excluded. The researchers reviewed 180 abstracts and included 56 full text articles in the final analysis, for a total study population of 8,540 patients. At the meeting Dr. Ehsan summarized the following findings by agent:
• Lidocaine. This agent is safe for topical use, has a rapid onset of action, and an intermediate duration of efficacy. Lidocaine acts on muscles “which are potent dilators and tensors of the pharyngeal and laryngeal structures,” she said. Of 10 studies included in the analysis, 7 assessed the impact of lidocaine on upper airway obstruction. Of these, three showed increased airway obstruction while four showed no significant effects. There were two studies on sleep parameters with conflicting results: One showed an increase in mean apnea duration with lidocaine use while the other did not. From this the researchers concluded that lidocaine does affect upper airway dynamics.
• Propofol. This lipophilic intravenous agent has a quick onset of action and acts by global central nervous system depression. Of 12 studies included in the analysis, 4 examined dose-response characteristics and showed a dose-dependent decrease in airway cross-sectional area with increased dosing of propofol. “So increasing your dose makes airway obstruction more likely,” Dr. Ehsan said. “The levels of obstruction were greatest at the base of tongue, and the closure was primarily in the anterior-posterior direction.” Three studies found that propofol caused a decrease in genioglossus electromyogram activity, while the remaining five studies assessed heterogeneous outcomes. “Overall, the studies showed that propofol had a dose-dependent effect on the upper airway with increasing doses making airway obstruction more likely,” she said.
• Dexmedetomidine (DEX). This agent is an alpha-2 adrenergic agonist with sedative, anxiolytic, and analgesic effects. It’s typically given as a 10-minute loading dose followed by a continuous infusion, and is recommended when you want to preserve spontaneous respiration. Of the four DEX-related studies that were included in the analysis, all demonstrated a minimal effect on upper airway cross-sectional area. “One of the studies looked at sleep parameters and concluded that DEX does approximate non-REM sleep without causing respiratory depression,” Dr. Ehsan added. “So overall, DEX was less likely to result in upper airway obstruction, compared with propofol.”
• Midazolam. This agent is commonly used for procedural sedation, with an onset of action within 1-3 minutes and a duration of 15-60 minutes. Of the six studies involving midazolam, two evaluated sleep staging. One reported lack of REM sleep and increased duration of stage N3 sleep, while the other study found that all sleep stages were observed at a lower dosage. The remaining four studies had heterogeneous outcomes. This led the researchers to conclude that midazolam “may lead to upper airway obstruction,” Dr. Ehsan said. “It’s unclear if this is dose dependent.”
• Pentobarbital. Of the two studies involving this short-acting barbiturate, one showed no effect on pharyngeal critical pressure or respiratory muscle function, while the other found that pentobarbital can increase the upper airway cross-sectional area. “So the effect of pentobarbital is unclear,” she said.
• Ketamine. This N-methyl-D-aspartate receptor has a rapid onset and a minimal effect on the central respiratory drive. Of the three studies involving ketamine, one found a 10% incidence of transient laryngospasm, one found that the incidence of transient laryngospasm was higher when it was delivered intramuscularly vs. intravenously, and one found that ketamine was safe in infants undergoing upper airway endoscopy. The researchers concluded that overall, ketamine “could be useful during DISE.”
• Inhalation anesthetics. There were 11 studies of these agents. Of these, six found that inhalation anesthetics caused upper airway collapse while five had heterogeneous outcomes. “Overall, a majority of studies found that inhalation anesthetics exaggerate dynamic airway collapse,” Dr. Ehsan said.
• Opioids. Of the nine studies involving these agents, six found that opioids caused upper airway obstruction; two found that they caused depression of upper airway reflexes, and one found that they caused a decrease in respiratory compliance. “Overall, opioids increase upper airway obstruction,” she said.
Dr. Ehsan acknowledged certain limitations of the analysis, including the fact that there was little information on sleep state approximated by many of these agents, “which makes it difficult to determine the ideal anesthetic protocol. There was substantial heterogeneity in outcomes, and few prospective studies comparing the ability of anesthetics to approximate natural sleep.” She recommended that future efforts focus on comparative effectiveness studies between the agents, as well as evaluate the impact of combining anesthetic agents. “This is important, because most DISE protocols use a combination of agents,” she said.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons
Dr. Ehsan reported having no relevant financial conflicts.
On Twitter @dougbrunk
AT THE COMBINED SECTIONS WINTER MEETING
Key clinical point: Choice of an appropriate anesthetic protocol for drug-induced sleep endoscopy must be based on a limited number of comparative studies.
Major finding: Local anesthetics appear to affect upper airway reflexes while inhalation anesthetics and opioids exaggerate dynamic airway collapse.
Data source: A qualitative systematic review of 56 studies related to common anesthetic agents and opioids published in the medical literature through September 2014.
Disclosures: Dr. Ehsan reported having no financial disclosures.

Smart diet remains potent cardiovascular medicine
SNOWMASS, COLO. – Cutting dietary fat intake remains a highly effective strategy for reducing coronary heart disease risk – but only so long as the replacement nutrients aren’t even bigger offenders, Dr. Robert A. Vogel said at the Annual Cardiovascular Conference at Snowmass.
In the face of decades of public health admonitions to reduce saturated fat intake, most Americans have increased their consumption of trans fats and simple carbohydrates, especially sugar. And therein lies a problem. Trans fats are far more harmful than saturated fats in terms of cardiovascular risk. And excessive sugar consumption is a major contributor to abdominal obesity, metabolic syndrome, hypertension, and endothelial dysfunction.
“In the United States, sugar is a bigger source of hypertension than is salt,” asserted Dr. Vogel, a cardiologist at the University of Colorado, Denver.
The editors of Time magazine ignited a public controversy last year with a cover story arrestingly titled, “Eat Butter – Scientists labelled fat the enemy. Why they were wrong.” The editors were picking up on a British meta-analysis of 32 observational studies that concluded there is no clear evidence to support the notion that saturated fats are harmful to cardiovascular health and that swapping them out for consumption of polyunsaturated fatty acids (PUFAs) is beneficial (Ann. Intern. Med. 2014;160:398-406).
Dr. Vogel said those investigators are in fact correct: Many of the observational studies – going all the way back to the pioneering work by Dr. Ancel Keys in the 1950s – are flawed. They don’t convincingly prove the case for PUFAs as a healthier alternative. But there is persuasive evidence from well-conducted, randomized, controlled trials that this is indeed so, he added.
Several of these studies were done in an earlier era when it was possible to slip around the challenges and limitations of dietary studies in free-living populations. These trials wouldn’t be possible today for ethical reasons involving lack of informed consent.

For example, in the Finnish Mental Hospital Study conducted during 1959-1971, the food served at two mental institutions was altered. Patients at one hospital got 6 years of a diet high in PUFAs, then were crossed over to a typical Finnish diet. At the other mental hospital, patients were fed a normal Finnish diet for 6 years, then crossed over to the high-PUFA diet for 6 years. During the experimental-diet years, the coronary heart disease event rate was reduced by nearly 60% (Int. J. Epidemiol. 1979;8:99-118).
Similarly, in a prospective randomized trial conducted at a Los Angeles Veterans Affairs institution for older, cognitively impaired men, a no-choice shift to a diet high in PUFAs with reduced saturated fats resulted in roughly a 30% reduction in CHD events compared to the usual institutional diet (Lancet 1968;2:1060-2). A similar magnitude of CHD event reduction was seen with a high-PUFA dietary intervention in the Oslo Diet-Heart Study, a prospective secondary prevention trial (Circulation 1970;42:935-42).
In the contemporary era, the standout randomized dietary intervention trial is the Lyon Diet Heart Study, a 46-month prospective secondary prevention trial in which a Mediterranean diet low in saturated fat and high in alpha-linoleic acid, a PUFA, reduced the combined endpoint of cardiac death and nonfatal MI by 70%, compared with the usual post-MI prudent diet recommended at that time. Yet total cholesterol levels in the two study arms did not differ (Circulation 1999;99:779-85).
To put these results into context, Dr. Vogel noted that the Cholesterol Treatment Trialists Collaboration headquartered at the University of Oxford (England) has shown that for every 40 mg/dL of LDL-lowering achieved with statin therapy, the result is roughly a 20% reduction in CHD. In contrast, the classic nonpharmacologic diet studies resulted in 30%-70% relative risk reductions.
“Heart disease is a dietary disease,” the cardiologist emphasized. “When you compare diet intervention to LDL lowering with statins, you see that diet is very, very effective. But you have to know the details of the diet. You can’t take something out and put just anything in. It doesn’t work like that.”
For example, an analysis of data from the National Health and Nutrition Examination Survey concluded that individuals who consumed 25% of their calories from added sugar – that’s the equivalent of three 12-oz cans of a sugary cola per day – had a 175% increased risk of cardiovascular mortality during a median 14.6 years of follow-up, compared with those who got less than 10% of their calories from added sugar (JAMA Intern. Med. 2014;174:516-24).
And as for the impact of the trans fat that’s liberally present in many processed foods, the Nurses Health Study showed that for every 5% increase in energy intake from saturated fat – that’s equivalent to one 8-oz steak per day – the relative risk for CHD rose by a relatively modest 17%, while for a 5% increase in energy intake from trans fat – the equivalent of 4 oz of butter – CHD risk shot up by 382% (N. Engl. J. Med. 1997;337:1491-9).
Dr. Vogel reported serving as a paid consultant to the National Football League and the Pritikin Longevity Center and receiving a research grant from Sanofi.
SNOWMASS, COLO. – Cutting dietary fat intake remains a highly effective strategy for reducing coronary heart disease risk – but only so long as the replacement nutrients aren’t even bigger offenders, Dr. Robert A. Vogel said at the Annual Cardiovascular Conference at Snowmass.
In the face of decades of public health admonitions to reduce saturated fat intake, most Americans have increased their consumption of trans fats and simple carbohydrates, especially sugar. And therein lies a problem. Trans fats are far more harmful than saturated fats in terms of cardiovascular risk. And excessive sugar consumption is a major contributor to abdominal obesity, metabolic syndrome, hypertension, and endothelial dysfunction.
“In the United States, sugar is a bigger source of hypertension than is salt,” asserted Dr. Vogel, a cardiologist at the University of Colorado, Denver.
The editors of Time magazine ignited a public controversy last year with a cover story arrestingly titled, “Eat Butter – Scientists labelled fat the enemy. Why they were wrong.” The editors were picking up on a British meta-analysis of 32 observational studies that concluded there is no clear evidence to support the notion that saturated fats are harmful to cardiovascular health and that swapping them out for consumption of polyunsaturated fatty acids (PUFAs) is beneficial (Ann. Intern. Med. 2014;160:398-406).
Dr. Vogel said those investigators are in fact correct: Many of the observational studies – going all the way back to the pioneering work by Dr. Ancel Keys in the 1950s – are flawed. They don’t convincingly prove the case for PUFAs as a healthier alternative. But there is persuasive evidence from well-conducted, randomized, controlled trials that this is indeed so, he added.
Several of these studies were done in an earlier era when it was possible to slip around the challenges and limitations of dietary studies in free-living populations. These trials wouldn’t be possible today for ethical reasons involving lack of informed consent.
For example, in the Finnish Mental Hospital Study conducted during 1959-1971, the food served at two mental institutions was altered. Patients at one hospital got 6 years of a diet high in PUFAs, then were crossed over to a typical Finnish diet. At the other mental hospital, patients were fed a normal Finnish diet for 6 years, then crossed over to the high-PUFA diet for 6 years. During the experimental-diet years, the coronary heart disease event rate was reduced by nearly 60% (Int. J. Epidemiol. 1979;8:99-118).
Similarly, in a prospective randomized trial conducted at a Los Angeles Veterans Affairs institution for older, cognitively impaired men, a no-choice shift to a diet high in PUFAs with reduced saturated fats resulted in roughly a 30% reduction in CHD events compared to the usual institutional diet (Lancet 1968;2:1060-2). A similar magnitude of CHD event reduction was seen with a high-PUFA dietary intervention in the Oslo Diet-Heart Study, a prospective secondary prevention trial (Circulation 1970;42:935-42).
In the contemporary era, the standout randomized dietary intervention trial is the Lyon Diet Heart Study, a 46-month prospective secondary prevention trial in which a Mediterranean diet low in saturated fat and high in alpha-linoleic acid, a PUFA, reduced the combined endpoint of cardiac death and nonfatal MI by 70%, compared with the usual post-MI prudent diet recommended at that time. Yet total cholesterol levels in the two study arms did not differ (Circulation 1999;99:779-85).
To put these results into context, Dr. Vogel noted that the Cholesterol Treatment Trialists Collaboration headquartered at the University of Oxford (England) has shown that for every 40 mg/dL of LDL-lowering achieved with statin therapy, the result is roughly a 20% reduction in CHD. In contrast, the classic nonpharmacologic diet studies resulted in 30%-70% relative risk reductions.
“Heart disease is a dietary disease,” the cardiologist emphasized. “When you compare diet intervention to LDL lowering with statins, you see that diet is very, very effective. But you have to know the details of the diet. You can’t take something out and put just anything in. It doesn’t work like that.”
For example, an analysis of data from the National Health and Nutrition Examination Survey concluded that individuals who consumed 25% of their calories from added sugar – that’s the equivalent of three 12-oz cans of a sugary cola per day – had a 175% increased risk of cardiovascular mortality during a median 14.6 years of follow-up, compared with those who got less than 10% of their calories from added sugar (JAMA Intern. Med. 2014;174:516-24).
And as for the impact of the trans fat that’s liberally present in many processed foods, the Nurses Health Study showed that for every 5% increase in energy intake from saturated fat – that’s equivalent to one 8-oz steak per day – the relative risk for CHD rose by a relatively modest 17%, while for a 5% increase in energy intake from trans fat – the equivalent of 4 oz of butter – CHD risk shot up by 382% (N. Engl. J. Med. 1997;337:1491-9).
Dr. Vogel reported serving as a paid consultant to the National Football League and the Pritikin Longevity Center and receiving a research grant from Sanofi.
SNOWMASS, COLO. – Cutting dietary fat intake remains a highly effective strategy for reducing coronary heart disease risk – but only so long as the replacement nutrients aren’t even bigger offenders, Dr. Robert A. Vogel said at the Annual Cardiovascular Conference at Snowmass.
In the face of decades of public health admonitions to reduce saturated fat intake, most Americans have increased their consumption of trans fats and simple carbohydrates, especially sugar. And therein lies a problem. Trans fats are far more harmful than saturated fats in terms of cardiovascular risk. And excessive sugar consumption is a major contributor to abdominal obesity, metabolic syndrome, hypertension, and endothelial dysfunction.
“In the United States, sugar is a bigger source of hypertension than is salt,” asserted Dr. Vogel, a cardiologist at the University of Colorado, Denver.
The editors of Time magazine ignited a public controversy last year with a cover story arrestingly titled, “Eat Butter – Scientists labelled fat the enemy. Why they were wrong.” The editors were picking up on a British meta-analysis of 32 observational studies that concluded there is no clear evidence to support the notion that saturated fats are harmful to cardiovascular health and that swapping them out for consumption of polyunsaturated fatty acids (PUFAs) is beneficial (Ann. Intern. Med. 2014;160:398-406).
Dr. Vogel said those investigators are in fact correct: Many of the observational studies – going all the way back to the pioneering work by Dr. Ancel Keys in the 1950s – are flawed. They don’t convincingly prove the case for PUFAs as a healthier alternative. But there is persuasive evidence from well-conducted, randomized, controlled trials that this is indeed so, he added.
Several of these studies were done in an earlier era when it was possible to slip around the challenges and limitations of dietary studies in free-living populations. These trials wouldn’t be possible today for ethical reasons involving lack of informed consent.
For example, in the Finnish Mental Hospital Study conducted during 1959-1971, the food served at two mental institutions was altered. Patients at one hospital got 6 years of a diet high in PUFAs, then were crossed over to a typical Finnish diet. At the other mental hospital, patients were fed a normal Finnish diet for 6 years, then crossed over to the high-PUFA diet for 6 years. During the experimental-diet years, the coronary heart disease event rate was reduced by nearly 60% (Int. J. Epidemiol. 1979;8:99-118).
Similarly, in a prospective randomized trial conducted at a Los Angeles Veterans Affairs institution for older, cognitively impaired men, a no-choice shift to a diet high in PUFAs with reduced saturated fats resulted in roughly a 30% reduction in CHD events compared to the usual institutional diet (Lancet 1968;2:1060-2). A similar magnitude of CHD event reduction was seen with a high-PUFA dietary intervention in the Oslo Diet-Heart Study, a prospective secondary prevention trial (Circulation 1970;42:935-42).
In the contemporary era, the standout randomized dietary intervention trial is the Lyon Diet Heart Study, a 46-month prospective secondary prevention trial in which a Mediterranean diet low in saturated fat and high in alpha-linoleic acid, a PUFA, reduced the combined endpoint of cardiac death and nonfatal MI by 70%, compared with the usual post-MI prudent diet recommended at that time. Yet total cholesterol levels in the two study arms did not differ (Circulation 1999;99:779-85).
To put these results into context, Dr. Vogel noted that the Cholesterol Treatment Trialists Collaboration headquartered at the University of Oxford (England) has shown that for every 40 mg/dL of LDL-lowering achieved with statin therapy, the result is roughly a 20% reduction in CHD. In contrast, the classic nonpharmacologic diet studies resulted in 30%-70% relative risk reductions.
“Heart disease is a dietary disease,” the cardiologist emphasized. “When you compare diet intervention to LDL lowering with statins, you see that diet is very, very effective. But you have to know the details of the diet. You can’t take something out and put just anything in. It doesn’t work like that.”
For example, an analysis of data from the National Health and Nutrition Examination Survey concluded that individuals who consumed 25% of their calories from added sugar – that’s the equivalent of three 12-oz cans of a sugary cola per day – had a 175% increased risk of cardiovascular mortality during a median 14.6 years of follow-up, compared with those who got less than 10% of their calories from added sugar (JAMA Intern. Med. 2014;174:516-24).
And as for the impact of the trans fat that’s liberally present in many processed foods, the Nurses Health Study showed that for every 5% increase in energy intake from saturated fat – that’s equivalent to one 8-oz steak per day – the relative risk for CHD rose by a relatively modest 17%, while for a 5% increase in energy intake from trans fat – the equivalent of 4 oz of butter – CHD risk shot up by 382% (N. Engl. J. Med. 1997;337:1491-9).
Dr. Vogel reported serving as a paid consultant to the National Football League and the Pritikin Longevity Center and receiving a research grant from Sanofi.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Experimental vaccine may have worked on Ebola-exposed physician
A U.S. physician exposed to Ebola virus received an investigational vaccine afterward and didn’t contract the disease, but the vaccine’s effectiveness remains unknown, according to report published online March 5 in JAMA.
The vaccine, VSV[Delta]G-ZEBOV, is based on a vesicular stomatitis virus with the glycoprotein gene replaced by a Zaire Ebola glycoprotein gene.
The physician received the vaccine slightly less than 2 days after Ebola exposure. After 12 hours, symptoms appeared that are associated with vesicular stomatitis virus. Those dissipated after 3-4 days, noted Dr. Lilin Lai of Emory University, Atlanta, and her colleagues.
No Ebola symptoms were detected, but the patient tested positive for Ebola virus glycoprotein-specific antibodies and T cells, which was an intended effect of the vaccine.
A single case report cannot provide a definitive answer to the effectiveness of VSV[Delta]G-ZEBOV, noted Thomas W. Geisbert, Ph.D. of the Galveston National Laboratory, University of Texas Medical Branch, in a related editorial. However, “this incident serves as an example of how important it is to have safe and effective countermeasures available in sufficient quantities that can be rapidly deployed for emergency use for both medical workers and affected populations.”
Find the full study and editorial in JAMA: (doi: 10.1001/jama.2015.1995) and (doi: 10.1001/jama.2015.2057).
A U.S. physician exposed to Ebola virus received an investigational vaccine afterward and didn’t contract the disease, but the vaccine’s effectiveness remains unknown, according to report published online March 5 in JAMA.
The vaccine, VSV[Delta]G-ZEBOV, is based on a vesicular stomatitis virus with the glycoprotein gene replaced by a Zaire Ebola glycoprotein gene.
The physician received the vaccine slightly less than 2 days after Ebola exposure. After 12 hours, symptoms appeared that are associated with vesicular stomatitis virus. Those dissipated after 3-4 days, noted Dr. Lilin Lai of Emory University, Atlanta, and her colleagues.
No Ebola symptoms were detected, but the patient tested positive for Ebola virus glycoprotein-specific antibodies and T cells, which was an intended effect of the vaccine.
A single case report cannot provide a definitive answer to the effectiveness of VSV[Delta]G-ZEBOV, noted Thomas W. Geisbert, Ph.D. of the Galveston National Laboratory, University of Texas Medical Branch, in a related editorial. However, “this incident serves as an example of how important it is to have safe and effective countermeasures available in sufficient quantities that can be rapidly deployed for emergency use for both medical workers and affected populations.”
Find the full study and editorial in JAMA: (doi: 10.1001/jama.2015.1995) and (doi: 10.1001/jama.2015.2057).
A U.S. physician exposed to Ebola virus received an investigational vaccine afterward and didn’t contract the disease, but the vaccine’s effectiveness remains unknown, according to report published online March 5 in JAMA.
The vaccine, VSV[Delta]G-ZEBOV, is based on a vesicular stomatitis virus with the glycoprotein gene replaced by a Zaire Ebola glycoprotein gene.
The physician received the vaccine slightly less than 2 days after Ebola exposure. After 12 hours, symptoms appeared that are associated with vesicular stomatitis virus. Those dissipated after 3-4 days, noted Dr. Lilin Lai of Emory University, Atlanta, and her colleagues.
No Ebola symptoms were detected, but the patient tested positive for Ebola virus glycoprotein-specific antibodies and T cells, which was an intended effect of the vaccine.
A single case report cannot provide a definitive answer to the effectiveness of VSV[Delta]G-ZEBOV, noted Thomas W. Geisbert, Ph.D. of the Galveston National Laboratory, University of Texas Medical Branch, in a related editorial. However, “this incident serves as an example of how important it is to have safe and effective countermeasures available in sufficient quantities that can be rapidly deployed for emergency use for both medical workers and affected populations.”
Find the full study and editorial in JAMA: (doi: 10.1001/jama.2015.1995) and (doi: 10.1001/jama.2015.2057).
Regimen prolongs PFS, increases AEs in MCL

Results of a phase 3 study suggest the VR-CAP regimen is more effective but less safe than R-CHOP in patients with newly diagnosed mantle cell lymphoma (MCL).
Patients who received VR-CAP (bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone) had superior progression-free survival (PFS) when compared to patients who received R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
But VR-CAP was also associated with more adverse events (AEs), particularly hematologic toxicities.
Tadeusz Robak, MD, of the Medical University of Lodz in Poland, and his colleagues reported results from this trial, known as LYM-3002, in NEJM. The study was funded by Janssen Research and Development and Millennium Pharmaceuticals.
LYM-3002 included 487 patients newly diagnosed with MCL who were not eligible for stem cell transplant.
Patients were randomized to receive six to eight 21-day cycles of R-CHOP intravenously on day 1 (with prednisone administered orally on days 1 to 5) or VR-CAP (similar to the R-CHOP regimen, but replacing vincristine with bortezomib at a dose of 1.3 mg per square meter of body-surface area on days 1, 4, 8, and 11).
The median follow-up was 40 months. The VR-CAP regimen significantly improved PFS, the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio [HR]=0.63, P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (HR=0.51, P<0.001).
Patients in the VR-CAP arm also fared better with regard to some secondary endpoints. The complete response rate was higher in the VR-CAP arm than the R-CHOP arm—53% and 42%, respectively (HR=1.29, P=0.007).
And patients in the VR-CAP arm had a longer median treatment-free interval—40.6 months and 20.5 months, respectively (HR=0.50, P<0.001).
However, there was no significant difference in overall survival between the treatment arms. The median overall survival was not reached in the VR-CAP arm and was 56.3 months in the R-CHOP arm (HR=0.80, P=0.17). The 4-year overall survival rate was 64% and 54%, respectively.
The investigators said VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious AEs were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85% of patients, respectively.
Hematologic toxicity was more common in the VR-CAP arm than the R-CHOP arm. This included thrombocytopenia (72% vs 19%), neutropenia (88% vs 74%), anemia (51% vs 37%), leukopenia (50% vs 38%), lymphocytopenia (31% vs 13%), and febrile neutropenia (17% vs 14%).
Treatment discontinuation due to AEs occurred in 8% of patients in the VR-CAP arm and 6% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3% of patients, respectively.
It was based on these results that bortezomib was approved for use in patients with newly diagnosed MCL in the Europe Union and the US. ![]()
Results of a phase 3 study suggest the VR-CAP regimen is more effective but less safe than R-CHOP in patients with newly diagnosed mantle cell lymphoma (MCL).
Patients who received VR-CAP (bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone) had superior progression-free survival (PFS) when compared to patients who received R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
But VR-CAP was also associated with more adverse events (AEs), particularly hematologic toxicities.
Tadeusz Robak, MD, of the Medical University of Lodz in Poland, and his colleagues reported results from this trial, known as LYM-3002, in NEJM. The study was funded by Janssen Research and Development and Millennium Pharmaceuticals.
LYM-3002 included 487 patients newly diagnosed with MCL who were not eligible for stem cell transplant.
Patients were randomized to receive six to eight 21-day cycles of R-CHOP intravenously on day 1 (with prednisone administered orally on days 1 to 5) or VR-CAP (similar to the R-CHOP regimen, but replacing vincristine with bortezomib at a dose of 1.3 mg per square meter of body-surface area on days 1, 4, 8, and 11).
The median follow-up was 40 months. The VR-CAP regimen significantly improved PFS, the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio [HR]=0.63, P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (HR=0.51, P<0.001).
Patients in the VR-CAP arm also fared better with regard to some secondary endpoints. The complete response rate was higher in the VR-CAP arm than the R-CHOP arm—53% and 42%, respectively (HR=1.29, P=0.007).
And patients in the VR-CAP arm had a longer median treatment-free interval—40.6 months and 20.5 months, respectively (HR=0.50, P<0.001).
However, there was no significant difference in overall survival between the treatment arms. The median overall survival was not reached in the VR-CAP arm and was 56.3 months in the R-CHOP arm (HR=0.80, P=0.17). The 4-year overall survival rate was 64% and 54%, respectively.
The investigators said VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious AEs were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85% of patients, respectively.
Hematologic toxicity was more common in the VR-CAP arm than the R-CHOP arm. This included thrombocytopenia (72% vs 19%), neutropenia (88% vs 74%), anemia (51% vs 37%), leukopenia (50% vs 38%), lymphocytopenia (31% vs 13%), and febrile neutropenia (17% vs 14%).
Treatment discontinuation due to AEs occurred in 8% of patients in the VR-CAP arm and 6% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3% of patients, respectively.
It was based on these results that bortezomib was approved for use in patients with newly diagnosed MCL in the Europe Union and the US. ![]()
Results of a phase 3 study suggest the VR-CAP regimen is more effective but less safe than R-CHOP in patients with newly diagnosed mantle cell lymphoma (MCL).
Patients who received VR-CAP (bortezomib, rituximab, cyclophosphamide, doxorubicin, and prednisone) had superior progression-free survival (PFS) when compared to patients who received R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone).
But VR-CAP was also associated with more adverse events (AEs), particularly hematologic toxicities.
Tadeusz Robak, MD, of the Medical University of Lodz in Poland, and his colleagues reported results from this trial, known as LYM-3002, in NEJM. The study was funded by Janssen Research and Development and Millennium Pharmaceuticals.
LYM-3002 included 487 patients newly diagnosed with MCL who were not eligible for stem cell transplant.
Patients were randomized to receive six to eight 21-day cycles of R-CHOP intravenously on day 1 (with prednisone administered orally on days 1 to 5) or VR-CAP (similar to the R-CHOP regimen, but replacing vincristine with bortezomib at a dose of 1.3 mg per square meter of body-surface area on days 1, 4, 8, and 11).
The median follow-up was 40 months. The VR-CAP regimen significantly improved PFS, the primary endpoint, when compared to R-CHOP.
According to an independent review committee, there was a 59% improvement in PFS for the VR-CAP arm compared to the R-CHOP arm, with median PFS times of 24.7 months and 14.4 months, respectively (hazard ratio [HR]=0.63, P<0.001).
Study investigators reported a 96% increase in PFS with VR-CAP compared to R-CHOP, with median PFS times of 30.7 months and 16.1 months, respectively (HR=0.51, P<0.001).
Patients in the VR-CAP arm also fared better with regard to some secondary endpoints. The complete response rate was higher in the VR-CAP arm than the R-CHOP arm—53% and 42%, respectively (HR=1.29, P=0.007).
And patients in the VR-CAP arm had a longer median treatment-free interval—40.6 months and 20.5 months, respectively (HR=0.50, P<0.001).
However, there was no significant difference in overall survival between the treatment arms. The median overall survival was not reached in the VR-CAP arm and was 56.3 months in the R-CHOP arm (HR=0.80, P=0.17). The 4-year overall survival rate was 64% and 54%, respectively.
The investigators said VR-CAP was associated with additional, but manageable, toxicity when compared to R-CHOP. Serious AEs were reported in 38% and 30% of patients, respectively. And grade 3 or higher AEs were reported in 93% and 85% of patients, respectively.
Hematologic toxicity was more common in the VR-CAP arm than the R-CHOP arm. This included thrombocytopenia (72% vs 19%), neutropenia (88% vs 74%), anemia (51% vs 37%), leukopenia (50% vs 38%), lymphocytopenia (31% vs 13%), and febrile neutropenia (17% vs 14%).
Treatment discontinuation due to AEs occurred in 8% of patients in the VR-CAP arm and 6% in the R-CHOP arm. On-treatment, drug-related deaths occurred in 2% and 3% of patients, respectively.
It was based on these results that bortezomib was approved for use in patients with newly diagnosed MCL in the Europe Union and the US. ![]()
Placenta-derived cells may improve recovery after HSCT

Cells derived from placenta can increase blood counts after hematopoietic stem cell transplant (HSCT), preclinical research suggests.
Investigators evaluated PLX-R18, a product consisting of mesenchymal-like adherent stromal cells derived from full-term human placentas, in mice undergoing HSCT.
Mice that received PLX-R18 in conjunction with HSCT had significantly faster hematopoietic recovery than mice that received placebo with their transplants.
Pluristem Therapeutics, Inc., the company developing PLX-R18, recently announced these results.
The study included 78 irradiated mice divided into 4 groups. One group received a transplant of 4 million HSCs plus an intra-muscular (IM) injection of 1 million PLX-R18 cells on days 1 and 10. A second group received 8 million HSCs plus an IM injection of 1 million PLX-R18 cells on days 1 and 10.
The first control group received 4 million HSCs plus an IM injection of placebo on days 1 and 10. And the second control group received 8 million HSCs plus an IM injection of placebo on days 1 and 10.
The investigators performed complete blood counts on day 9 after HSCT and the first dose of PLX-R18 or placebo, on day 16 after the second dose of PLX-R18 or placebo, and on day 23.
Nine days after transplantation with a low dose of HSCs (4 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelets and granulocytes when compared to controls (P=0.0059 and P=0.0267, respectively).
PLX-R18-treated mice also had more lymphocytes and total white blood cells, but these increases were not statistically significant.
Nine days after transplantation with a high dose of HSCs (8 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelet levels (P=0.0015).
One week later, at 16 days after a low-dose HSCT, mice treated with PLX-R18 had more platelets than controls, although the difference wasn’t significant.
Also on day 16, mice treated with PLX-R18 and a high dose of HSCs had statistically significant increases in platelets, granulocytes, and total white blood cells compared to controls (P=0.0053, P=0.0122, and P=0.0262 respectively).
On day 23, there were no significant differences in the number of cells between the treatment groups.
Taking these results together, the investigators concluded that PLX-R18 cells can significantly accelerate the recovery of several components of normal blood counts.
“A statistically significant increase in blood counts soon after bone marrow transplant is very meaningful,” said Reuven Or, MD, of Hadassah Medical Center in Haifa, Israel.
“We were particularly encouraged to see that the administration of PLX-R18 cells resulted in the greatest early improvement when using a lower dose of bone marrow cells. This means we could one day potentially achieve success with lower bone marrow transplant doses, thus addressing both treatment costs and donor availability.” ![]()
Cells derived from placenta can increase blood counts after hematopoietic stem cell transplant (HSCT), preclinical research suggests.
Investigators evaluated PLX-R18, a product consisting of mesenchymal-like adherent stromal cells derived from full-term human placentas, in mice undergoing HSCT.
Mice that received PLX-R18 in conjunction with HSCT had significantly faster hematopoietic recovery than mice that received placebo with their transplants.
Pluristem Therapeutics, Inc., the company developing PLX-R18, recently announced these results.
The study included 78 irradiated mice divided into 4 groups. One group received a transplant of 4 million HSCs plus an intra-muscular (IM) injection of 1 million PLX-R18 cells on days 1 and 10. A second group received 8 million HSCs plus an IM injection of 1 million PLX-R18 cells on days 1 and 10.
The first control group received 4 million HSCs plus an IM injection of placebo on days 1 and 10. And the second control group received 8 million HSCs plus an IM injection of placebo on days 1 and 10.
The investigators performed complete blood counts on day 9 after HSCT and the first dose of PLX-R18 or placebo, on day 16 after the second dose of PLX-R18 or placebo, and on day 23.
Nine days after transplantation with a low dose of HSCs (4 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelets and granulocytes when compared to controls (P=0.0059 and P=0.0267, respectively).
PLX-R18-treated mice also had more lymphocytes and total white blood cells, but these increases were not statistically significant.
Nine days after transplantation with a high dose of HSCs (8 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelet levels (P=0.0015).
One week later, at 16 days after a low-dose HSCT, mice treated with PLX-R18 had more platelets than controls, although the difference wasn’t significant.
Also on day 16, mice treated with PLX-R18 and a high dose of HSCs had statistically significant increases in platelets, granulocytes, and total white blood cells compared to controls (P=0.0053, P=0.0122, and P=0.0262 respectively).
On day 23, there were no significant differences in the number of cells between the treatment groups.
Taking these results together, the investigators concluded that PLX-R18 cells can significantly accelerate the recovery of several components of normal blood counts.
“A statistically significant increase in blood counts soon after bone marrow transplant is very meaningful,” said Reuven Or, MD, of Hadassah Medical Center in Haifa, Israel.
“We were particularly encouraged to see that the administration of PLX-R18 cells resulted in the greatest early improvement when using a lower dose of bone marrow cells. This means we could one day potentially achieve success with lower bone marrow transplant doses, thus addressing both treatment costs and donor availability.” ![]()
Cells derived from placenta can increase blood counts after hematopoietic stem cell transplant (HSCT), preclinical research suggests.
Investigators evaluated PLX-R18, a product consisting of mesenchymal-like adherent stromal cells derived from full-term human placentas, in mice undergoing HSCT.
Mice that received PLX-R18 in conjunction with HSCT had significantly faster hematopoietic recovery than mice that received placebo with their transplants.
Pluristem Therapeutics, Inc., the company developing PLX-R18, recently announced these results.
The study included 78 irradiated mice divided into 4 groups. One group received a transplant of 4 million HSCs plus an intra-muscular (IM) injection of 1 million PLX-R18 cells on days 1 and 10. A second group received 8 million HSCs plus an IM injection of 1 million PLX-R18 cells on days 1 and 10.
The first control group received 4 million HSCs plus an IM injection of placebo on days 1 and 10. And the second control group received 8 million HSCs plus an IM injection of placebo on days 1 and 10.
The investigators performed complete blood counts on day 9 after HSCT and the first dose of PLX-R18 or placebo, on day 16 after the second dose of PLX-R18 or placebo, and on day 23.
Nine days after transplantation with a low dose of HSCs (4 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelets and granulocytes when compared to controls (P=0.0059 and P=0.0267, respectively).
PLX-R18-treated mice also had more lymphocytes and total white blood cells, but these increases were not statistically significant.
Nine days after transplantation with a high dose of HSCs (8 million) and concurrent administration of either PLX-R18 or placebo, mice treated with PLX-R18 had statistically significant increases in platelet levels (P=0.0015).
One week later, at 16 days after a low-dose HSCT, mice treated with PLX-R18 had more platelets than controls, although the difference wasn’t significant.
Also on day 16, mice treated with PLX-R18 and a high dose of HSCs had statistically significant increases in platelets, granulocytes, and total white blood cells compared to controls (P=0.0053, P=0.0122, and P=0.0262 respectively).
On day 23, there were no significant differences in the number of cells between the treatment groups.
Taking these results together, the investigators concluded that PLX-R18 cells can significantly accelerate the recovery of several components of normal blood counts.
“A statistically significant increase in blood counts soon after bone marrow transplant is very meaningful,” said Reuven Or, MD, of Hadassah Medical Center in Haifa, Israel.
“We were particularly encouraged to see that the administration of PLX-R18 cells resulted in the greatest early improvement when using a lower dose of bone marrow cells. This means we could one day potentially achieve success with lower bone marrow transplant doses, thus addressing both treatment costs and donor availability.” ![]()
New radiation guidelines for pediatric HL

New guidelines on radiation therapy aim to help physicians more effectively treat pediatric Hodgkin lymphoma (HL) while reducing the radiation dose to normal tissue.
Previous guidelines for pediatric HL have focused on 2D imaging and bony landmarks to define dose volumes for radiation therapy, and they’ve recommended treating large volumes of normal tissue, in part, because of uncertainty about which lymph node areas were involved.
The new guidelines, published in Practical Radiation Oncology, describe how to use modern imaging and advances in radiation therapy planning technology to treat patients with pediatric HL while decreasing the risk of late side effects, including second cancers and heart disease.
The authors describe methods for identifying target volumes for radiation therapy and how to implement the concept of involved-site radiation to define radiation target volumes and limit the dose to normal organs at risk.
According to the guidelines, accurate assessment of the extent and location of disease requires both contrast-enhanced CT as well as FDG-PET.
The document describes how the evaluation of response to chemotherapy influences the targeting of the lymphoma and the volume of normal tissue treated, by fusing CT and FDG-PET images taken before and after chemotherapy to CT imaging taken for radiation therapy planning.
“The emergence of new imaging technologies, more accurate ways of delivering radiation therapy, and more detailed patient selection criteria have made a significant change in our ability to customize treatment for many cancer patients,” said lead guideline author David C. Hodgson, MD, of the University of Toronto in Ontario, Canada.
“This guideline has the potential to reduce the radiation therapy breast dose by about 80% and the heart dose by about 65% for an adolescent girl with Hodgkin lymphoma. This shift in more personalized treatment planning tailored to the individual patient’s disease will optimize risk-benefit considerations for our patients and reduce the likelihood that they will suffer late effects from radiation therapy.” ![]()
New guidelines on radiation therapy aim to help physicians more effectively treat pediatric Hodgkin lymphoma (HL) while reducing the radiation dose to normal tissue.
Previous guidelines for pediatric HL have focused on 2D imaging and bony landmarks to define dose volumes for radiation therapy, and they’ve recommended treating large volumes of normal tissue, in part, because of uncertainty about which lymph node areas were involved.
The new guidelines, published in Practical Radiation Oncology, describe how to use modern imaging and advances in radiation therapy planning technology to treat patients with pediatric HL while decreasing the risk of late side effects, including second cancers and heart disease.
The authors describe methods for identifying target volumes for radiation therapy and how to implement the concept of involved-site radiation to define radiation target volumes and limit the dose to normal organs at risk.
According to the guidelines, accurate assessment of the extent and location of disease requires both contrast-enhanced CT as well as FDG-PET.
The document describes how the evaluation of response to chemotherapy influences the targeting of the lymphoma and the volume of normal tissue treated, by fusing CT and FDG-PET images taken before and after chemotherapy to CT imaging taken for radiation therapy planning.
“The emergence of new imaging technologies, more accurate ways of delivering radiation therapy, and more detailed patient selection criteria have made a significant change in our ability to customize treatment for many cancer patients,” said lead guideline author David C. Hodgson, MD, of the University of Toronto in Ontario, Canada.
“This guideline has the potential to reduce the radiation therapy breast dose by about 80% and the heart dose by about 65% for an adolescent girl with Hodgkin lymphoma. This shift in more personalized treatment planning tailored to the individual patient’s disease will optimize risk-benefit considerations for our patients and reduce the likelihood that they will suffer late effects from radiation therapy.” ![]()
New guidelines on radiation therapy aim to help physicians more effectively treat pediatric Hodgkin lymphoma (HL) while reducing the radiation dose to normal tissue.
Previous guidelines for pediatric HL have focused on 2D imaging and bony landmarks to define dose volumes for radiation therapy, and they’ve recommended treating large volumes of normal tissue, in part, because of uncertainty about which lymph node areas were involved.
The new guidelines, published in Practical Radiation Oncology, describe how to use modern imaging and advances in radiation therapy planning technology to treat patients with pediatric HL while decreasing the risk of late side effects, including second cancers and heart disease.
The authors describe methods for identifying target volumes for radiation therapy and how to implement the concept of involved-site radiation to define radiation target volumes and limit the dose to normal organs at risk.
According to the guidelines, accurate assessment of the extent and location of disease requires both contrast-enhanced CT as well as FDG-PET.
The document describes how the evaluation of response to chemotherapy influences the targeting of the lymphoma and the volume of normal tissue treated, by fusing CT and FDG-PET images taken before and after chemotherapy to CT imaging taken for radiation therapy planning.
“The emergence of new imaging technologies, more accurate ways of delivering radiation therapy, and more detailed patient selection criteria have made a significant change in our ability to customize treatment for many cancer patients,” said lead guideline author David C. Hodgson, MD, of the University of Toronto in Ontario, Canada.
“This guideline has the potential to reduce the radiation therapy breast dose by about 80% and the heart dose by about 65% for an adolescent girl with Hodgkin lymphoma. This shift in more personalized treatment planning tailored to the individual patient’s disease will optimize risk-benefit considerations for our patients and reduce the likelihood that they will suffer late effects from radiation therapy.” ![]()
Parasite discovery could aid malaria treatment
Image by Ke Hu & John Murray
Researchers say they have gained new insight into how malaria-related parasites spread inside humans and other animals.
The team discovered how the malaria relative Toxoplasma gondii manages to replicate its chromosomes up to thousands of times before spinning off into daughter cells—all while avoiding cell death.
The findings, published in PLOS Biology, may have implications for malaria treatment, according to the researchers.
Once transmitted into an animal or human, malaria-related parasites can hide out in a single cell in many different tissues, replicating thousands of times before the host’s immune system can detect them.
Then, they burst forth as daughter cells, which are unleashed in massive quantities, quickly overwhelming the body’s immune response.
The researchers found that Toxoplasma parasites pull this off thanks to the centrosome, which imposes order on the replication chaos.
“Unlike the comparatively simple centrosome present in human cells, the parasite [centrosome] has 2 distinct operating machines,” said study author Michael White, PhD, of the University of South Florida in Tampa.
“One machine controls chromosome copying, while the other machine regulates when to form daughter cell bodies. Working together, but with independent responsibilities, parasite centrosome machines can dictate the scale and timing of pathogen replication.”
This discovery of the centrosome’s function leads to a critical conclusion, Dr White said. Disrupting the centrosome machines kills the parasite. Breaking any part of the highly efficient but highly fragile replication function shuts everything down.
With these findings and the new knowledge of the parasites’ vulnerabilities, Dr White and his fellow researchers are planning to explore drug development for malaria. Whether the team is able to find an already-approved drug or must develop one from scratch, they said the drug will need to be used in conjunction with other therapies.
Dr White noted that current drugs used to treat malaria target the pathogen’s metabolism. But the goal of the new drug will be to undermine the parasite’s foundation in enough of the spreading cells to allow the immune system to fight back and not become overwhelmed. ![]()
Image by Ke Hu & John Murray
Researchers say they have gained new insight into how malaria-related parasites spread inside humans and other animals.
The team discovered how the malaria relative Toxoplasma gondii manages to replicate its chromosomes up to thousands of times before spinning off into daughter cells—all while avoiding cell death.
The findings, published in PLOS Biology, may have implications for malaria treatment, according to the researchers.
Once transmitted into an animal or human, malaria-related parasites can hide out in a single cell in many different tissues, replicating thousands of times before the host’s immune system can detect them.
Then, they burst forth as daughter cells, which are unleashed in massive quantities, quickly overwhelming the body’s immune response.
The researchers found that Toxoplasma parasites pull this off thanks to the centrosome, which imposes order on the replication chaos.
“Unlike the comparatively simple centrosome present in human cells, the parasite [centrosome] has 2 distinct operating machines,” said study author Michael White, PhD, of the University of South Florida in Tampa.
“One machine controls chromosome copying, while the other machine regulates when to form daughter cell bodies. Working together, but with independent responsibilities, parasite centrosome machines can dictate the scale and timing of pathogen replication.”
This discovery of the centrosome’s function leads to a critical conclusion, Dr White said. Disrupting the centrosome machines kills the parasite. Breaking any part of the highly efficient but highly fragile replication function shuts everything down.
With these findings and the new knowledge of the parasites’ vulnerabilities, Dr White and his fellow researchers are planning to explore drug development for malaria. Whether the team is able to find an already-approved drug or must develop one from scratch, they said the drug will need to be used in conjunction with other therapies.
Dr White noted that current drugs used to treat malaria target the pathogen’s metabolism. But the goal of the new drug will be to undermine the parasite’s foundation in enough of the spreading cells to allow the immune system to fight back and not become overwhelmed. ![]()
Image by Ke Hu & John Murray
Researchers say they have gained new insight into how malaria-related parasites spread inside humans and other animals.
The team discovered how the malaria relative Toxoplasma gondii manages to replicate its chromosomes up to thousands of times before spinning off into daughter cells—all while avoiding cell death.
The findings, published in PLOS Biology, may have implications for malaria treatment, according to the researchers.
Once transmitted into an animal or human, malaria-related parasites can hide out in a single cell in many different tissues, replicating thousands of times before the host’s immune system can detect them.
Then, they burst forth as daughter cells, which are unleashed in massive quantities, quickly overwhelming the body’s immune response.
The researchers found that Toxoplasma parasites pull this off thanks to the centrosome, which imposes order on the replication chaos.
“Unlike the comparatively simple centrosome present in human cells, the parasite [centrosome] has 2 distinct operating machines,” said study author Michael White, PhD, of the University of South Florida in Tampa.
“One machine controls chromosome copying, while the other machine regulates when to form daughter cell bodies. Working together, but with independent responsibilities, parasite centrosome machines can dictate the scale and timing of pathogen replication.”
This discovery of the centrosome’s function leads to a critical conclusion, Dr White said. Disrupting the centrosome machines kills the parasite. Breaking any part of the highly efficient but highly fragile replication function shuts everything down.
With these findings and the new knowledge of the parasites’ vulnerabilities, Dr White and his fellow researchers are planning to explore drug development for malaria. Whether the team is able to find an already-approved drug or must develop one from scratch, they said the drug will need to be used in conjunction with other therapies.
Dr White noted that current drugs used to treat malaria target the pathogen’s metabolism. But the goal of the new drug will be to undermine the parasite’s foundation in enough of the spreading cells to allow the immune system to fight back and not become overwhelmed. ![]()
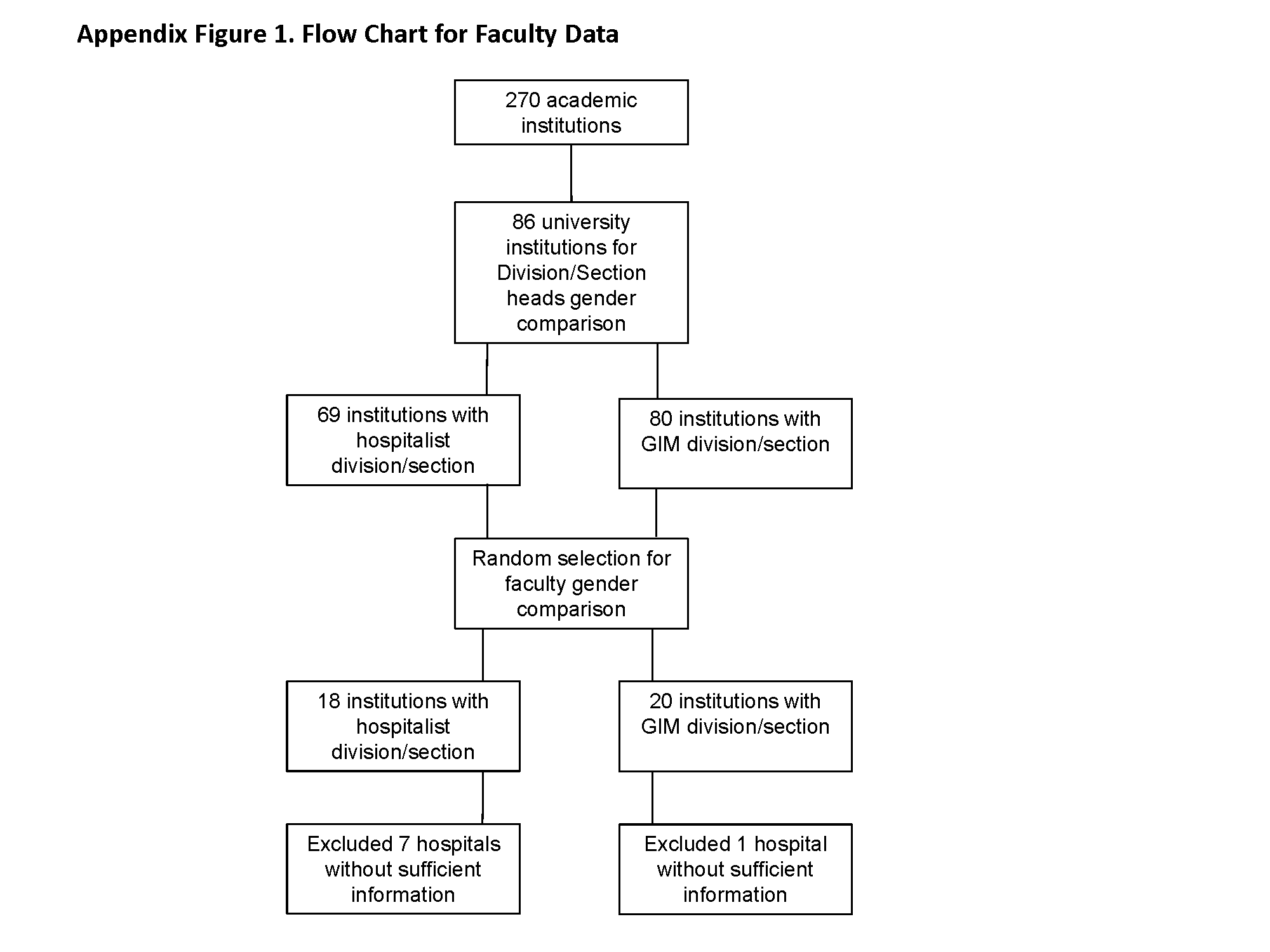
OUs and Patient Outcomes
Many pediatric hospitalizations are of short duration, and more than half of short‐stay hospitalizations are designated as observation status.[1, 2] Observation status is an administrative label assigned to patients who do not meet hospital or payer criteria for inpatient‐status care. Short‐stay observation‐status patients do not fit in traditional models of emergency department (ED) or inpatient care. EDs often focus on discharging or admitting patients within a matter of hours, whereas inpatient units tend to measure length of stay (LOS) in terms of days[3] and may not have systems in place to facilitate rapid discharge of short‐stay patients.[4] Observation units (OUs) have been established in some hospitals to address the unique care needs of short‐stay patients.[5, 6, 7]
Single‐site reports from children's hospitals with successful OUs have demonstrated shorter LOS and lower costs compared with inpatient settings.[6, 8, 9, 10, 11, 12, 13, 14] No prior study has examined hospital‐level effects of an OU on observation‐status patient outcomes. The Pediatric Health Information System (PHIS) database provides a unique opportunity to explore this question, because unlike other national hospital administrative databases,[15, 16] the PHIS dataset contains information about children under observation status. In addition, we know which PHIS hospitals had a dedicated OU in 2011.7
We hypothesized that overall observation‐status stays in hospitals with a dedicated OU would be of shorter duration with earlier discharges at lower cost than observation‐status stays in hospitals without a dedicated OU. We compared hospitals with and without a dedicated OU on secondary outcomes including rates of conversion to inpatient status and return care for any reason.
METHODS
We conducted a cross‐sectional analysis of hospital administrative data using the 2011 PHIS databasea national administrative database that contains resource utilization data from 43 participating hospitals located in 26 states plus the District of Columbia. These hospitals account for approximately 20% of pediatric hospitalizations in the United States.
For each hospital encounter, PHIS includes patient demographics, up to 41 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) diagnoses, up to 41 ICD‐9‐CM procedures, and hospital charges for services. Data are deidentified prior to inclusion, but unique identifiers allow for determination of return visits and readmissions following an index visit for an individual patient. Data quality and reliability are assured jointly by the Children's Hospital Association (formerly Child Health Corporation of America, Overland Park, KS), participating hospitals, and Truven Health Analytics (New York, NY). This study, using administrative data, was not considered human subjects research by the policies of the Cincinnati Children's Hospital Medical Center Institutional Review Board.
Hospital Selection and Hospital Characteristics
The study sample was drawn from the 31 hospitals that reported observation‐status patient data to PHIS in 2011. Analyses were conducted in 2013, at which time 2011 was the most recent year of data. We categorized 14 hospitals as having a dedicated OU during 2011 based on information collected in 2013.7 To summarize briefly, we interviewed by telephone representatives of hospitals responding to an email query as to the presence of a geographically distinct OU for the care of unscheduled patients from the ED. Three of the 14 representatives reported their hospital had 2 OUs, 1 of which was a separate surgical OU. Ten OUs cared for both ED patients and patients with scheduled procedures; 8 units received patients from non‐ED sources. Hospitalists provided staffing in more than half of the OUs.
We attempted to identify administrative data that would signal care delivered in a dedicated OU using hospital charge codes reported to PHIS, but learned this was not possible due to between‐hospital variation in the specificity of the charge codes. Therefore, we were unable to determine if patient care was delivered in a dedicated OU or another setting, such as a general inpatient unit or the ED. Other hospital characteristics available from the PHIS dataset included the number of inpatient beds, ED visits, inpatient admissions, observation‐status stays, and payer mix. We calculated the percentage of ED visits resulting in admission by dividing the number of ED visits with associated inpatient or observation status by the total number of ED visits and the percentage of admissions under observation status by dividing the number of observation‐status stays by the total number of admissions under observation or inpatient status.
Visit Selection and Patient Characteristics
All observation‐status stays regardless of the point of entry into the hospital were eligible for this study. We excluded stays that were birth‐related, included intensive care, or resulted in transfer or death. Patient demographic characteristics used to describe the cohort included age, gender, race/ethnicity, and primary payer. Stays that began in the ED were identified by an emergency room charge within PHIS. Eligible stays were categorized using All Patient Refined Diagnosis Related Groups (APR‐DRGs) version 24 using the ICD‐9‐CM code‐based proprietary 3M software (3M Health Information Systems, St. Paul, MN). We determined the 15 top‐ranking APR‐DRGs among observation‐status stays in hospitals with a dedicated OU and hospitals without. Procedural stays were identified based on procedural APR‐DRGs (eg, tonsil and adenoid procedures) or the presence of an ICD‐9‐CM procedure code (eg, 331 spinal tap).
Measured Outcomes
Outcomes of observation‐status stays were determined within 4 categories: (1) LOS, (2) standardized costs, (3) conversion to inpatient status, and (4) return visits and readmissions. LOS was calculated in terms of nights spent in hospital for all stays by subtracting the discharge date from the admission date and in terms of hours for stays in the 28 hospitals that report admission and discharge hour to the PHIS database. Discharge timing was examined in 4, 6‐hour blocks starting at midnight. Standardized costs were derived from a charge master index that was created by taking the median costs from all PHIS hospitals for each charged service.[17] Standardized costs represent the estimated cost of providing any particular clinical activity but are not the cost to patients, nor do they represent the actual cost to any given hospital. This approach allows for cost comparisons across hospitals, without biases arising from using charges or from deriving costs using hospitals' ratios of costs to charges.[18] Conversion from observation to inpatient status was calculated by dividing the number of inpatient‐status stays with observation codes by the number of observation‐statusonly stays plus the number of inpatient‐status stays with observation codes. All‐cause 3‐day ED return visits and 30‐day readmissions to the same hospital were assessed using patient‐specific identifiers that allowed for tracking of ED return visits and readmissions following the index observation stay.
Data Analysis
Descriptive statistics were calculated for hospital and patient characteristics using medians and interquartile ranges (IQRs) for continuous factors and frequencies with percentages for categorical factors. Comparisons of these factors between hospitals with dedicated OUs and without were made using [2] and Wilcoxon rank sum tests as appropriate. Multivariable regression was performed using generalized linear mixed models treating hospital as a random effect and used patient age, the case‐mix index based on the APR‐DRG severity of illness, ED visit, and procedures associated with the index observation‐status stay. For continuous outcomes, we performed a log transformation on the outcome, confirmed the normality assumption, and back transformed the results. Sensitivity analyses were conducted to compare LOS, standardized costs, and conversation rates by hospital type for 10 of the 15 top‐ranking APR‐DRGs commonly cared for by pediatric hospitalists and to compare hospitals that reported the presence of an OU that was consistently open (24 hours per day, 7 days per week) and operating during the entire 2011 calendar year, and those without. Based on information gathered from the telephone interviews, hospitals with partially open OUs were similar to hospitals with continuously open OUs, such that they were included in our main analyses. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC). P values <0.05 were considered statistically significant.
RESULTS
Hospital Characteristics
Dedicated OUs were present in 14 of the 31 hospitals that reported observation‐status patient data to PHIS (Figure 1). Three of these hospitals had OUs that were open for 5 months or less in 2011; 1 unit opened, 1 unit closed, and 1 hospital operated a seasonal unit. The remaining 17 hospitals reported no OU that admitted unscheduled patients from the ED during 2011. Hospitals with a dedicated OU had more inpatient beds and higher median number of inpatient admissions than those without (Table 1). Hospitals were statistically similar in terms of total volume of ED visits, percentage of ED visits resulting in admission, total number of observation‐status stays, percentage of admissions under observation status, and payer mix.
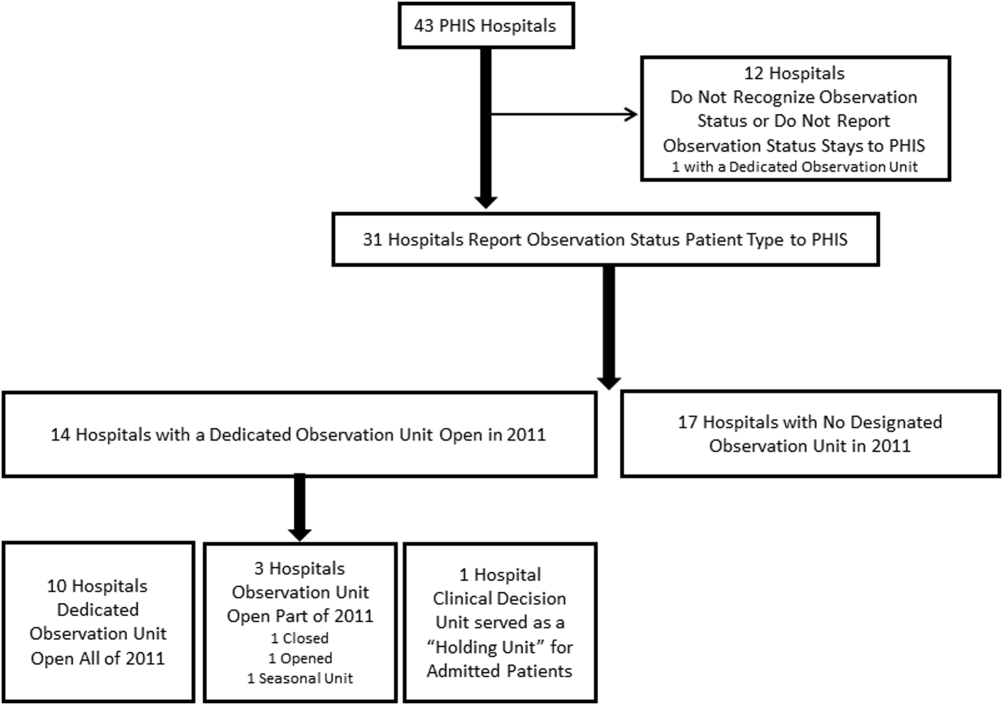
| Overall, Median (IQR) | Hospitals With a Dedicated Observation Unit, Median (IQR) | Hospitals Without a Dedicated Observation Unit, Median (IQR) | P Value | |
|---|---|---|---|---|
| ||||
| No. of hospitals | 31 | 14 | 17 | |
| Total no. of inpatient beds | 273 (213311) | 304 (269425) | 246 (175293) | 0.006 |
| Total no. ED visits | 62971 (47,50497,723) | 87,892 (55,102117,119) | 53,151 (4750470,882) | 0.21 |
| ED visits resulting in admission, % | 13.1 (9.715.0) | 13.8 (10.5, 19.1) | 12.5 (9.714.5) | 0.31 |
| Total no. of inpatient admissions | 11,537 (9,26814,568) | 13,206 (11,32517,869) | 10,207 (8,64013,363) | 0.04 |
| Admissions under observation status, % | 25.7 (19.733.8) | 25.5 (21.431.4) | 26.0 (16.935.1) | 0.98 |
| Total no. of observation stays | 3,820 (27935672) | 4,850 (3,309 6,196) | 3,141 (2,3654,616) | 0.07 |
| Government payer, % | 60.2 (53.371.2) | 62.1 (54.9, 65.9) | 59.2 (53.373.7) | 0.89 |
Observation‐Status Patients by Hospital Type
In 2011, there were a total of 136,239 observation‐status stays69,983 (51.4%) within the 14 hospitals with a dedicated OU and 66,256 (48.6%) within the 17 hospitals without. Patient care originated in the ED for 57.8% observation‐status stays in hospitals with an OU compared with 53.0% of observation‐status stays in hospitals without (P<0.001). Compared with hospitals with a dedicated OU, those without a dedicated OU had higher percentages of observation‐status patients older than 12 years and non‐Hispanic and a higher percentage of observation‐status patients with private payer type (Table 2). The 15 top‐ranking APR‐DRGs accounted for roughly half of all observation‐status stays and were relatively consistent between hospitals with and without a dedicated OU (Table 3). Procedural care was frequently associated with observation‐status stays.
| Overall, No. (%) | Hospitals With a Dedicated Observation Unit, No. (%)* | Hospitals Without a Dedicated Observation Unit, No. (%) | P Value | |
|---|---|---|---|---|
| ||||
| Age | ||||
| <1 year | 23,845 (17.5) | 12,101 (17.3) | 11,744 (17.7) | <0.001 |
| 15 years | 53,405 (38.5) | 28,052 (40.1) | 24,353 (36.8) | |
| 612 years | 33,674 (24.7) | 17,215 (24.6) | 16,459 (24.8) | |
| 1318 years | 23,607 (17.3) | 11,472 (16.4) | 12,135 (18.3) | |
| >18 years | 2,708 (2) | 1,143 (1.6) | 1,565 (2.4) | |
| Gender | ||||
| Male | 76,142 (55.9) | 39,178 (56) | 36,964 (55.8) | 0.43 |
| Female | 60,025 (44.1) | 30,756 (44) | 29,269 (44.2) | |
| Race/ethnicity | ||||
| Non‐Hispanic white | 72,183 (53.0) | 30,653 (43.8) | 41,530 (62.7) | <0.001 |
| Non‐Hispanic black | 30,995 (22.8) | 16,314 (23.3) | 14,681 (22.2) | |
| Hispanic | 21,255 (15.6) | 16,583 (23.7) | 4,672 (7.1) | |
| Asian | 2,075 (1.5) | 1,313 (1.9) | 762 (1.2) | |
| Non‐Hispanic other | 9,731 (7.1) | 5,120 (7.3) | 4,611 (7.0) | |
| Payer | ||||
| Government | 68,725 (50.4) | 36,967 (52.8) | 31,758 (47.9) | <0.001 |
| Private | 48,416 (35.5) | 21,112 (30.2) | 27,304 (41.2) | |
| Other | 19,098 (14.0) | 11,904 (17) | 7,194 (10.9) | |
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit* | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED | Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED |
| |||||||||
| 1 | Tonsil and adenoid procedures | 4,621 | 6.6 | 1.3 | 1 | Tonsil and adenoid procedures | 3,806 | 5.7 | 1.6 |
| 2 | Asthma | 4,246 | 6.1 | 85.3 | 2 | Asthma | 3,756 | 5.7 | 79.0 |
| 3 | Seizure | 3,516 | 5.0 | 52.0 | 3 | Seizure | 2,846 | 4.3 | 54.9 |
| 4 | Nonbacterial gastroenteritis | 3,286 | 4.7 | 85.8 | 4 | Upper respiratory infections | 2,733 | 4.1 | 69.6 |
| 5 | Bronchiolitis, RSV pneumonia | 3,093 | 4.4 | 78.5 | 5 | Nonbacterial gastroenteritis | 2,682 | 4.0 | 74.5 |
| 6 | Upper respiratory infections | 2,923 | 4.2 | 80.0 | 6 | Other digestive system diagnoses | 2,545 | 3.8 | 66.3 |
| 7 | Other digestive system diagnoses | 2,064 | 2.9 | 74.0 | 7 | Bronchiolitis, RSV pneumonia | 2,544 | 3.8 | 69.2 |
| 8 | Respiratory signs, symptoms, diagnoses | 2,052 | 2.9 | 81.6 | 8 | Shoulder and arm procedures | 1,862 | 2.8 | 72.6 |
| 9 | Other ENT/cranial/facial diagnoses | 1,684 | 2.4 | 43.6 | 9 | Appendectomy | 1,785 | 2.7 | 79.2 |
| 10 | Shoulder and arm procedures | 1,624 | 2.3 | 79.1 | 10 | Other ENT/cranial/facial diagnoses | 1,624 | 2.5 | 29.9 |
| 11 | Abdominal pain | 1,612 | 2.3 | 86.2 | 11 | Abdominal pain | 1,461 | 2.2 | 82.3 |
| 12 | Fever | 1,494 | 2.1 | 85.1 | 12 | Other factors influencing health status | 1,461 | 2.2 | 66.3 |
| 13 | Appendectomy | 1,465 | 2.1 | 66.4 | 13 | Cellulitis/other bacterial skin infections | 1,383 | 2.1 | 84.2 |
| 14 | Cellulitis/other bacterial skin infections | 1,393 | 2.0 | 86.4 | 14 | Respiratory signs, symptoms, diagnoses | 1,308 | 2.0 | 39.1 |
| 15 | Pneumonia NEC | 1,356 | 1.9 | 79.1 | 15 | Pneumonia NEC | 1,245 | 1.9 | 73.1 |
| Total | 36,429 | 52.0 | 57.8 | Total | 33,041 | 49.87 | 53.0 | ||
Outcomes of Observation‐Status Stays
A greater percentage of observation‐status stays in hospitals with a dedicated OU experienced a same‐day discharge (Table 4). In addition, a higher percentage of discharges occurred between midnight and 11 am in hospitals with a dedicated OU. However, overall risk‐adjusted LOS in hours (12.8 vs 12.2 hours, P=0.90) and risk‐adjusted total standardized costs ($2551 vs $2433, P=0.75) were similar between hospital types. These findings were consistent within the 1 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Overall, conversion from observation to inpatient status was significantly higher in hospitals with a dedicated OU compared with hospitals without; however, this pattern was not consistent across the 10 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Adjusted odds of 3‐day ED return visits and 30‐day readmissions were comparable between hospital groups.
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | P Value | |
|---|---|---|---|
| |||
| No. of hospitals | 14 | 17 | |
| Length of stay, h, median (IQR) | 12.8 (6.923.7) | 12.2 (721.3) | 0.90 |
| 0 midnights, no. (%) | 16,678 (23.8) | 14,648 (22.1) | <.001 |
| 1 midnight, no. (%) | 46,144 (65.9) | 44,559 (67.3) | |
| 2 midnights or more, no. (%) | 7,161 (10.2) | 7,049 (10.6) | |
| Discharge timing, no. (%) | |||
| Midnight5 am | 1,223 (1.9) | 408 (0.7) | <0.001 |
| 6 am11 am | 18,916 (29.3) | 15,914 (27.1) | |
| Noon5 pm | 32,699 (50.7) | 31,619 (53.9) | |
| 6 pm11 pm | 11,718 (18.2) | 10,718 (18.3) | |
| Total standardized costs, $, median (IQR) | 2,551.3 (2,053.93,169.1) | 2,433.4 (1,998.42,963) | 0.75 |
| Conversion to inpatient status | 11.06% | 9.63% | <0.01 |
| Return care, AOR (95% CI) | |||
| 3‐day ED return visit | 0.93 (0.77‐1.12) | Referent | 0.46 |
| 30‐day readmission | 0.88 (0.67‐1.15) | Referent | 0.36 |
We found similar results in sensitivity analyses comparing observation‐status stays in hospitals with a continuously open OU (open 24 hours per day, 7 days per week, for all of 2011 [n=10 hospitals]) to those without(see Supporting Information, Appendix 2, in the online version of this article). However, there were, on average, more observation‐status stays in hospitals with a continuously open OU (median 5605, IQR 42077089) than hospitals without (median 3309, IQR 26784616) (P=0.04). In contrast to our main results, conversion to inpatient status was lower in hospitals with a continuously open OU compared with hospitals without (8.52% vs 11.57%, P<0.01).
DISCUSSION
Counter to our hypothesis, we did not find hospital‐level differences in length of stay or costs for observation‐status patients cared for in hospitals with and without a dedicated OU, though hospitals with dedicated OUs did have more same‐day discharges and more morning discharges. The lack of observed differences in LOS and costs may reflect the fact that many children under observation status are treated throughout the hospital, even in facilities with a dedicated OU. Access to a dedicated OU is limited by factors including small numbers of OU beds and specific low acuity/low complexity OU admission criteria.[7] The inclusion of all children admitted under observation status in our analyses may have diluted any effect of dedicated OUs at the hospital level, but was necessary due to the inability to identify location of care for children admitted under observation status. Location of care is an important variable that should be incorporated into administrative databases to allow for comparative effectiveness research designs. Until such data are available, chart review at individual hospitals would be necessary to determine which patients received care in an OU.
We did find that discharges for observation‐status patients occurred earlier in the day in hospitals with a dedicated OU when compared with observation‐status patients in hospitals without a dedicated OU. In addition, the percentage of same‐day discharges was higher among observation‐status patients treated in hospitals with a dedicated OU. These differences may stem from policies and procedures that encourage rapid discharge in dedicated OUs, and those practices may affect other care areas. For example, OUs may enforce policies requiring family presence at the bedside or utilize staffing models where doctors and nurses are in frequent communication, both of which would facilitate discharge as soon as a patient no longer required hospital‐based care.[7] A retrospective chart review study design could be used to identify discharge processes and other key characteristics of highly performing OUs.
We found conflicting results in our main and sensitivity analyses related to conversion to inpatient status. Lower percentages of observation‐status patients converting to inpatient status indicates greater success in the delivery of observation care based on established performance metrics.[19] Lower rates of conversion to inpatient status may be the result of stricter admission criteria for some diagnosis and in hospitals with a continuously open dedicate OU, more refined processes for utilization review that allow for patients to be placed into the correct status (observation vs inpatient) at the time of admission, or efforts to educate providers about the designation of observation status.[7] It is also possible that fewer observation‐status patients convert to inpatient status in hospitals with a continuously open dedicated OU because such a change would require movement of the patient to an inpatient bed.
These analyses were more comprehensive than our prior studies[2, 20] in that we included both patients who were treated first in the ED and those who were not. In addition to the APR‐DRGs representative of conditions that have been successfully treated in ED‐based pediatric OUs (eg, asthma, seizures, gastroenteritis, cellulitis),[8, 9, 21, 22] we found observation‐status was commonly associated with procedural care. This population of patients may be relevant to hospitalists who staff OUs that provide both unscheduled and postprocedural care. The colocation of medical and postprocedural patients has been described by others[8, 23] and was reported to occur in over half of the OUs included in this study.[7] The extent to which postprocedure observation care is provided in general OUs staffed by hospitalists represents another opportunity for further study.
Hospitals face many considerations when determining if and how they will provide observation services to patients expected to experience short stays.[7] Some hospitals may be unable to justify an OU for all or part of the year based on the volume of admissions or the costs to staff an OU.[24, 25] Other hospitals may open an OU to promote patient flow and reduce ED crowding.[26] Hospitals may also be influenced by reimbursement policies related to observation‐status stays. Although we did not observe differences in overall payer mix, we did find higher percentages of observation‐status patients in hospitals with dedicated OUs to have public insurance. Although hospital contracts with payers around observation status patients are complex and beyond the scope of this analysis, it is possible that hospitals have established OUs because of increasingly stringent rules or criteria to meet inpatient status or experiences with high volumes of observation‐status patients covered by a particular payer. Nevertheless, the brief nature of many pediatric hospitalizations and the scarcity of pediatric OU beds must be considered in policy changes that result from national discussions about the appropriateness of inpatient stays shorter than 2 nights in duration.[27]
Limitations
The primary limitation to our analyses is the lack of ability to identify patients who were treated in a dedicated OU because few hospitals provided data to PHIS that allowed for the identification of the unit or location of care. Second, it is possible that some hospitals were misclassified as not having a dedicated OU based on our survey, which initially inquired about OUs that provided care to patients first treated in the ED. Therefore, OUs that exclusively care for postoperative patients or patients with scheduled treatments may be present in hospitals that we have labeled as not having a dedicated OU. This potential misclassification would bias our results toward finding no differences. Third, in any study of administrative data there is potential that diagnosis codes are incomplete or inaccurately capture the underlying reason for the episode of care. Fourth, the experiences of the free‐standing children's hospitals that contribute data to PHIS may not be generalizable to other hospitals that provide observation care to children. Finally, return care may be underestimated, as children could receive treatment at another hospital following discharge from a PHIS hospital. Care outside of PHIS hospitals would not be captured, but we do not expect this to differ for hospitals with and without dedicated OUs. It is possible that health information exchanges will permit more comprehensive analyses of care across different hospitals in the future.
CONCLUSION
Observation status patients are similar in hospitals with and without dedicated observation units that admit children from the ED. The presence of a dedicated OU appears to have an influence on same‐day and morning discharges across all observation‐status stays without impacting other hospital‐level outcomes. Inclusion of location of care (eg, geographically distinct dedicated OU vs general inpatient unit vs ED) in hospital administrative datasets would allow for meaningful comparisons of different models of care for short‐stay observation‐status patients.
Acknowledgements
The authors thank John P. Harding, MBA, FACHE, Children's Hospital of the King's Daughters, Norfolk, Virginia for his input on the study design.
Disclosures: Dr. Hall had full access to the data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Internal funds from the Children's Hospital Association supported the conduct of this work. The authors have no financial relationships or conflicts of interest to disclose.
Many pediatric hospitalizations are of short duration, and more than half of short‐stay hospitalizations are designated as observation status.[1, 2] Observation status is an administrative label assigned to patients who do not meet hospital or payer criteria for inpatient‐status care. Short‐stay observation‐status patients do not fit in traditional models of emergency department (ED) or inpatient care. EDs often focus on discharging or admitting patients within a matter of hours, whereas inpatient units tend to measure length of stay (LOS) in terms of days[3] and may not have systems in place to facilitate rapid discharge of short‐stay patients.[4] Observation units (OUs) have been established in some hospitals to address the unique care needs of short‐stay patients.[5, 6, 7]
Single‐site reports from children's hospitals with successful OUs have demonstrated shorter LOS and lower costs compared with inpatient settings.[6, 8, 9, 10, 11, 12, 13, 14] No prior study has examined hospital‐level effects of an OU on observation‐status patient outcomes. The Pediatric Health Information System (PHIS) database provides a unique opportunity to explore this question, because unlike other national hospital administrative databases,[15, 16] the PHIS dataset contains information about children under observation status. In addition, we know which PHIS hospitals had a dedicated OU in 2011.7
We hypothesized that overall observation‐status stays in hospitals with a dedicated OU would be of shorter duration with earlier discharges at lower cost than observation‐status stays in hospitals without a dedicated OU. We compared hospitals with and without a dedicated OU on secondary outcomes including rates of conversion to inpatient status and return care for any reason.
METHODS
We conducted a cross‐sectional analysis of hospital administrative data using the 2011 PHIS databasea national administrative database that contains resource utilization data from 43 participating hospitals located in 26 states plus the District of Columbia. These hospitals account for approximately 20% of pediatric hospitalizations in the United States.
For each hospital encounter, PHIS includes patient demographics, up to 41 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) diagnoses, up to 41 ICD‐9‐CM procedures, and hospital charges for services. Data are deidentified prior to inclusion, but unique identifiers allow for determination of return visits and readmissions following an index visit for an individual patient. Data quality and reliability are assured jointly by the Children's Hospital Association (formerly Child Health Corporation of America, Overland Park, KS), participating hospitals, and Truven Health Analytics (New York, NY). This study, using administrative data, was not considered human subjects research by the policies of the Cincinnati Children's Hospital Medical Center Institutional Review Board.
Hospital Selection and Hospital Characteristics
The study sample was drawn from the 31 hospitals that reported observation‐status patient data to PHIS in 2011. Analyses were conducted in 2013, at which time 2011 was the most recent year of data. We categorized 14 hospitals as having a dedicated OU during 2011 based on information collected in 2013.7 To summarize briefly, we interviewed by telephone representatives of hospitals responding to an email query as to the presence of a geographically distinct OU for the care of unscheduled patients from the ED. Three of the 14 representatives reported their hospital had 2 OUs, 1 of which was a separate surgical OU. Ten OUs cared for both ED patients and patients with scheduled procedures; 8 units received patients from non‐ED sources. Hospitalists provided staffing in more than half of the OUs.
We attempted to identify administrative data that would signal care delivered in a dedicated OU using hospital charge codes reported to PHIS, but learned this was not possible due to between‐hospital variation in the specificity of the charge codes. Therefore, we were unable to determine if patient care was delivered in a dedicated OU or another setting, such as a general inpatient unit or the ED. Other hospital characteristics available from the PHIS dataset included the number of inpatient beds, ED visits, inpatient admissions, observation‐status stays, and payer mix. We calculated the percentage of ED visits resulting in admission by dividing the number of ED visits with associated inpatient or observation status by the total number of ED visits and the percentage of admissions under observation status by dividing the number of observation‐status stays by the total number of admissions under observation or inpatient status.
Visit Selection and Patient Characteristics
All observation‐status stays regardless of the point of entry into the hospital were eligible for this study. We excluded stays that were birth‐related, included intensive care, or resulted in transfer or death. Patient demographic characteristics used to describe the cohort included age, gender, race/ethnicity, and primary payer. Stays that began in the ED were identified by an emergency room charge within PHIS. Eligible stays were categorized using All Patient Refined Diagnosis Related Groups (APR‐DRGs) version 24 using the ICD‐9‐CM code‐based proprietary 3M software (3M Health Information Systems, St. Paul, MN). We determined the 15 top‐ranking APR‐DRGs among observation‐status stays in hospitals with a dedicated OU and hospitals without. Procedural stays were identified based on procedural APR‐DRGs (eg, tonsil and adenoid procedures) or the presence of an ICD‐9‐CM procedure code (eg, 331 spinal tap).
Measured Outcomes
Outcomes of observation‐status stays were determined within 4 categories: (1) LOS, (2) standardized costs, (3) conversion to inpatient status, and (4) return visits and readmissions. LOS was calculated in terms of nights spent in hospital for all stays by subtracting the discharge date from the admission date and in terms of hours for stays in the 28 hospitals that report admission and discharge hour to the PHIS database. Discharge timing was examined in 4, 6‐hour blocks starting at midnight. Standardized costs were derived from a charge master index that was created by taking the median costs from all PHIS hospitals for each charged service.[17] Standardized costs represent the estimated cost of providing any particular clinical activity but are not the cost to patients, nor do they represent the actual cost to any given hospital. This approach allows for cost comparisons across hospitals, without biases arising from using charges or from deriving costs using hospitals' ratios of costs to charges.[18] Conversion from observation to inpatient status was calculated by dividing the number of inpatient‐status stays with observation codes by the number of observation‐statusonly stays plus the number of inpatient‐status stays with observation codes. All‐cause 3‐day ED return visits and 30‐day readmissions to the same hospital were assessed using patient‐specific identifiers that allowed for tracking of ED return visits and readmissions following the index observation stay.
Data Analysis
Descriptive statistics were calculated for hospital and patient characteristics using medians and interquartile ranges (IQRs) for continuous factors and frequencies with percentages for categorical factors. Comparisons of these factors between hospitals with dedicated OUs and without were made using [2] and Wilcoxon rank sum tests as appropriate. Multivariable regression was performed using generalized linear mixed models treating hospital as a random effect and used patient age, the case‐mix index based on the APR‐DRG severity of illness, ED visit, and procedures associated with the index observation‐status stay. For continuous outcomes, we performed a log transformation on the outcome, confirmed the normality assumption, and back transformed the results. Sensitivity analyses were conducted to compare LOS, standardized costs, and conversation rates by hospital type for 10 of the 15 top‐ranking APR‐DRGs commonly cared for by pediatric hospitalists and to compare hospitals that reported the presence of an OU that was consistently open (24 hours per day, 7 days per week) and operating during the entire 2011 calendar year, and those without. Based on information gathered from the telephone interviews, hospitals with partially open OUs were similar to hospitals with continuously open OUs, such that they were included in our main analyses. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC). P values <0.05 were considered statistically significant.
RESULTS
Hospital Characteristics
Dedicated OUs were present in 14 of the 31 hospitals that reported observation‐status patient data to PHIS (Figure 1). Three of these hospitals had OUs that were open for 5 months or less in 2011; 1 unit opened, 1 unit closed, and 1 hospital operated a seasonal unit. The remaining 17 hospitals reported no OU that admitted unscheduled patients from the ED during 2011. Hospitals with a dedicated OU had more inpatient beds and higher median number of inpatient admissions than those without (Table 1). Hospitals were statistically similar in terms of total volume of ED visits, percentage of ED visits resulting in admission, total number of observation‐status stays, percentage of admissions under observation status, and payer mix.
| Overall, Median (IQR) | Hospitals With a Dedicated Observation Unit, Median (IQR) | Hospitals Without a Dedicated Observation Unit, Median (IQR) | P Value | |
|---|---|---|---|---|
| ||||
| No. of hospitals | 31 | 14 | 17 | |
| Total no. of inpatient beds | 273 (213311) | 304 (269425) | 246 (175293) | 0.006 |
| Total no. ED visits | 62971 (47,50497,723) | 87,892 (55,102117,119) | 53,151 (4750470,882) | 0.21 |
| ED visits resulting in admission, % | 13.1 (9.715.0) | 13.8 (10.5, 19.1) | 12.5 (9.714.5) | 0.31 |
| Total no. of inpatient admissions | 11,537 (9,26814,568) | 13,206 (11,32517,869) | 10,207 (8,64013,363) | 0.04 |
| Admissions under observation status, % | 25.7 (19.733.8) | 25.5 (21.431.4) | 26.0 (16.935.1) | 0.98 |
| Total no. of observation stays | 3,820 (27935672) | 4,850 (3,309 6,196) | 3,141 (2,3654,616) | 0.07 |
| Government payer, % | 60.2 (53.371.2) | 62.1 (54.9, 65.9) | 59.2 (53.373.7) | 0.89 |
Observation‐Status Patients by Hospital Type
In 2011, there were a total of 136,239 observation‐status stays69,983 (51.4%) within the 14 hospitals with a dedicated OU and 66,256 (48.6%) within the 17 hospitals without. Patient care originated in the ED for 57.8% observation‐status stays in hospitals with an OU compared with 53.0% of observation‐status stays in hospitals without (P<0.001). Compared with hospitals with a dedicated OU, those without a dedicated OU had higher percentages of observation‐status patients older than 12 years and non‐Hispanic and a higher percentage of observation‐status patients with private payer type (Table 2). The 15 top‐ranking APR‐DRGs accounted for roughly half of all observation‐status stays and were relatively consistent between hospitals with and without a dedicated OU (Table 3). Procedural care was frequently associated with observation‐status stays.
| Overall, No. (%) | Hospitals With a Dedicated Observation Unit, No. (%)* | Hospitals Without a Dedicated Observation Unit, No. (%) | P Value | |
|---|---|---|---|---|
| ||||
| Age | ||||
| <1 year | 23,845 (17.5) | 12,101 (17.3) | 11,744 (17.7) | <0.001 |
| 15 years | 53,405 (38.5) | 28,052 (40.1) | 24,353 (36.8) | |
| 612 years | 33,674 (24.7) | 17,215 (24.6) | 16,459 (24.8) | |
| 1318 years | 23,607 (17.3) | 11,472 (16.4) | 12,135 (18.3) | |
| >18 years | 2,708 (2) | 1,143 (1.6) | 1,565 (2.4) | |
| Gender | ||||
| Male | 76,142 (55.9) | 39,178 (56) | 36,964 (55.8) | 0.43 |
| Female | 60,025 (44.1) | 30,756 (44) | 29,269 (44.2) | |
| Race/ethnicity | ||||
| Non‐Hispanic white | 72,183 (53.0) | 30,653 (43.8) | 41,530 (62.7) | <0.001 |
| Non‐Hispanic black | 30,995 (22.8) | 16,314 (23.3) | 14,681 (22.2) | |
| Hispanic | 21,255 (15.6) | 16,583 (23.7) | 4,672 (7.1) | |
| Asian | 2,075 (1.5) | 1,313 (1.9) | 762 (1.2) | |
| Non‐Hispanic other | 9,731 (7.1) | 5,120 (7.3) | 4,611 (7.0) | |
| Payer | ||||
| Government | 68,725 (50.4) | 36,967 (52.8) | 31,758 (47.9) | <0.001 |
| Private | 48,416 (35.5) | 21,112 (30.2) | 27,304 (41.2) | |
| Other | 19,098 (14.0) | 11,904 (17) | 7,194 (10.9) | |
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit* | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED | Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED |
| |||||||||
| 1 | Tonsil and adenoid procedures | 4,621 | 6.6 | 1.3 | 1 | Tonsil and adenoid procedures | 3,806 | 5.7 | 1.6 |
| 2 | Asthma | 4,246 | 6.1 | 85.3 | 2 | Asthma | 3,756 | 5.7 | 79.0 |
| 3 | Seizure | 3,516 | 5.0 | 52.0 | 3 | Seizure | 2,846 | 4.3 | 54.9 |
| 4 | Nonbacterial gastroenteritis | 3,286 | 4.7 | 85.8 | 4 | Upper respiratory infections | 2,733 | 4.1 | 69.6 |
| 5 | Bronchiolitis, RSV pneumonia | 3,093 | 4.4 | 78.5 | 5 | Nonbacterial gastroenteritis | 2,682 | 4.0 | 74.5 |
| 6 | Upper respiratory infections | 2,923 | 4.2 | 80.0 | 6 | Other digestive system diagnoses | 2,545 | 3.8 | 66.3 |
| 7 | Other digestive system diagnoses | 2,064 | 2.9 | 74.0 | 7 | Bronchiolitis, RSV pneumonia | 2,544 | 3.8 | 69.2 |
| 8 | Respiratory signs, symptoms, diagnoses | 2,052 | 2.9 | 81.6 | 8 | Shoulder and arm procedures | 1,862 | 2.8 | 72.6 |
| 9 | Other ENT/cranial/facial diagnoses | 1,684 | 2.4 | 43.6 | 9 | Appendectomy | 1,785 | 2.7 | 79.2 |
| 10 | Shoulder and arm procedures | 1,624 | 2.3 | 79.1 | 10 | Other ENT/cranial/facial diagnoses | 1,624 | 2.5 | 29.9 |
| 11 | Abdominal pain | 1,612 | 2.3 | 86.2 | 11 | Abdominal pain | 1,461 | 2.2 | 82.3 |
| 12 | Fever | 1,494 | 2.1 | 85.1 | 12 | Other factors influencing health status | 1,461 | 2.2 | 66.3 |
| 13 | Appendectomy | 1,465 | 2.1 | 66.4 | 13 | Cellulitis/other bacterial skin infections | 1,383 | 2.1 | 84.2 |
| 14 | Cellulitis/other bacterial skin infections | 1,393 | 2.0 | 86.4 | 14 | Respiratory signs, symptoms, diagnoses | 1,308 | 2.0 | 39.1 |
| 15 | Pneumonia NEC | 1,356 | 1.9 | 79.1 | 15 | Pneumonia NEC | 1,245 | 1.9 | 73.1 |
| Total | 36,429 | 52.0 | 57.8 | Total | 33,041 | 49.87 | 53.0 | ||
Outcomes of Observation‐Status Stays
A greater percentage of observation‐status stays in hospitals with a dedicated OU experienced a same‐day discharge (Table 4). In addition, a higher percentage of discharges occurred between midnight and 11 am in hospitals with a dedicated OU. However, overall risk‐adjusted LOS in hours (12.8 vs 12.2 hours, P=0.90) and risk‐adjusted total standardized costs ($2551 vs $2433, P=0.75) were similar between hospital types. These findings were consistent within the 1 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Overall, conversion from observation to inpatient status was significantly higher in hospitals with a dedicated OU compared with hospitals without; however, this pattern was not consistent across the 10 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Adjusted odds of 3‐day ED return visits and 30‐day readmissions were comparable between hospital groups.
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | P Value | |
|---|---|---|---|
| |||
| No. of hospitals | 14 | 17 | |
| Length of stay, h, median (IQR) | 12.8 (6.923.7) | 12.2 (721.3) | 0.90 |
| 0 midnights, no. (%) | 16,678 (23.8) | 14,648 (22.1) | <.001 |
| 1 midnight, no. (%) | 46,144 (65.9) | 44,559 (67.3) | |
| 2 midnights or more, no. (%) | 7,161 (10.2) | 7,049 (10.6) | |
| Discharge timing, no. (%) | |||
| Midnight5 am | 1,223 (1.9) | 408 (0.7) | <0.001 |
| 6 am11 am | 18,916 (29.3) | 15,914 (27.1) | |
| Noon5 pm | 32,699 (50.7) | 31,619 (53.9) | |
| 6 pm11 pm | 11,718 (18.2) | 10,718 (18.3) | |
| Total standardized costs, $, median (IQR) | 2,551.3 (2,053.93,169.1) | 2,433.4 (1,998.42,963) | 0.75 |
| Conversion to inpatient status | 11.06% | 9.63% | <0.01 |
| Return care, AOR (95% CI) | |||
| 3‐day ED return visit | 0.93 (0.77‐1.12) | Referent | 0.46 |
| 30‐day readmission | 0.88 (0.67‐1.15) | Referent | 0.36 |
We found similar results in sensitivity analyses comparing observation‐status stays in hospitals with a continuously open OU (open 24 hours per day, 7 days per week, for all of 2011 [n=10 hospitals]) to those without(see Supporting Information, Appendix 2, in the online version of this article). However, there were, on average, more observation‐status stays in hospitals with a continuously open OU (median 5605, IQR 42077089) than hospitals without (median 3309, IQR 26784616) (P=0.04). In contrast to our main results, conversion to inpatient status was lower in hospitals with a continuously open OU compared with hospitals without (8.52% vs 11.57%, P<0.01).
DISCUSSION
Counter to our hypothesis, we did not find hospital‐level differences in length of stay or costs for observation‐status patients cared for in hospitals with and without a dedicated OU, though hospitals with dedicated OUs did have more same‐day discharges and more morning discharges. The lack of observed differences in LOS and costs may reflect the fact that many children under observation status are treated throughout the hospital, even in facilities with a dedicated OU. Access to a dedicated OU is limited by factors including small numbers of OU beds and specific low acuity/low complexity OU admission criteria.[7] The inclusion of all children admitted under observation status in our analyses may have diluted any effect of dedicated OUs at the hospital level, but was necessary due to the inability to identify location of care for children admitted under observation status. Location of care is an important variable that should be incorporated into administrative databases to allow for comparative effectiveness research designs. Until such data are available, chart review at individual hospitals would be necessary to determine which patients received care in an OU.
We did find that discharges for observation‐status patients occurred earlier in the day in hospitals with a dedicated OU when compared with observation‐status patients in hospitals without a dedicated OU. In addition, the percentage of same‐day discharges was higher among observation‐status patients treated in hospitals with a dedicated OU. These differences may stem from policies and procedures that encourage rapid discharge in dedicated OUs, and those practices may affect other care areas. For example, OUs may enforce policies requiring family presence at the bedside or utilize staffing models where doctors and nurses are in frequent communication, both of which would facilitate discharge as soon as a patient no longer required hospital‐based care.[7] A retrospective chart review study design could be used to identify discharge processes and other key characteristics of highly performing OUs.
We found conflicting results in our main and sensitivity analyses related to conversion to inpatient status. Lower percentages of observation‐status patients converting to inpatient status indicates greater success in the delivery of observation care based on established performance metrics.[19] Lower rates of conversion to inpatient status may be the result of stricter admission criteria for some diagnosis and in hospitals with a continuously open dedicate OU, more refined processes for utilization review that allow for patients to be placed into the correct status (observation vs inpatient) at the time of admission, or efforts to educate providers about the designation of observation status.[7] It is also possible that fewer observation‐status patients convert to inpatient status in hospitals with a continuously open dedicated OU because such a change would require movement of the patient to an inpatient bed.
These analyses were more comprehensive than our prior studies[2, 20] in that we included both patients who were treated first in the ED and those who were not. In addition to the APR‐DRGs representative of conditions that have been successfully treated in ED‐based pediatric OUs (eg, asthma, seizures, gastroenteritis, cellulitis),[8, 9, 21, 22] we found observation‐status was commonly associated with procedural care. This population of patients may be relevant to hospitalists who staff OUs that provide both unscheduled and postprocedural care. The colocation of medical and postprocedural patients has been described by others[8, 23] and was reported to occur in over half of the OUs included in this study.[7] The extent to which postprocedure observation care is provided in general OUs staffed by hospitalists represents another opportunity for further study.
Hospitals face many considerations when determining if and how they will provide observation services to patients expected to experience short stays.[7] Some hospitals may be unable to justify an OU for all or part of the year based on the volume of admissions or the costs to staff an OU.[24, 25] Other hospitals may open an OU to promote patient flow and reduce ED crowding.[26] Hospitals may also be influenced by reimbursement policies related to observation‐status stays. Although we did not observe differences in overall payer mix, we did find higher percentages of observation‐status patients in hospitals with dedicated OUs to have public insurance. Although hospital contracts with payers around observation status patients are complex and beyond the scope of this analysis, it is possible that hospitals have established OUs because of increasingly stringent rules or criteria to meet inpatient status or experiences with high volumes of observation‐status patients covered by a particular payer. Nevertheless, the brief nature of many pediatric hospitalizations and the scarcity of pediatric OU beds must be considered in policy changes that result from national discussions about the appropriateness of inpatient stays shorter than 2 nights in duration.[27]
Limitations
The primary limitation to our analyses is the lack of ability to identify patients who were treated in a dedicated OU because few hospitals provided data to PHIS that allowed for the identification of the unit or location of care. Second, it is possible that some hospitals were misclassified as not having a dedicated OU based on our survey, which initially inquired about OUs that provided care to patients first treated in the ED. Therefore, OUs that exclusively care for postoperative patients or patients with scheduled treatments may be present in hospitals that we have labeled as not having a dedicated OU. This potential misclassification would bias our results toward finding no differences. Third, in any study of administrative data there is potential that diagnosis codes are incomplete or inaccurately capture the underlying reason for the episode of care. Fourth, the experiences of the free‐standing children's hospitals that contribute data to PHIS may not be generalizable to other hospitals that provide observation care to children. Finally, return care may be underestimated, as children could receive treatment at another hospital following discharge from a PHIS hospital. Care outside of PHIS hospitals would not be captured, but we do not expect this to differ for hospitals with and without dedicated OUs. It is possible that health information exchanges will permit more comprehensive analyses of care across different hospitals in the future.
CONCLUSION
Observation status patients are similar in hospitals with and without dedicated observation units that admit children from the ED. The presence of a dedicated OU appears to have an influence on same‐day and morning discharges across all observation‐status stays without impacting other hospital‐level outcomes. Inclusion of location of care (eg, geographically distinct dedicated OU vs general inpatient unit vs ED) in hospital administrative datasets would allow for meaningful comparisons of different models of care for short‐stay observation‐status patients.
Acknowledgements
The authors thank John P. Harding, MBA, FACHE, Children's Hospital of the King's Daughters, Norfolk, Virginia for his input on the study design.
Disclosures: Dr. Hall had full access to the data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Internal funds from the Children's Hospital Association supported the conduct of this work. The authors have no financial relationships or conflicts of interest to disclose.
Many pediatric hospitalizations are of short duration, and more than half of short‐stay hospitalizations are designated as observation status.[1, 2] Observation status is an administrative label assigned to patients who do not meet hospital or payer criteria for inpatient‐status care. Short‐stay observation‐status patients do not fit in traditional models of emergency department (ED) or inpatient care. EDs often focus on discharging or admitting patients within a matter of hours, whereas inpatient units tend to measure length of stay (LOS) in terms of days[3] and may not have systems in place to facilitate rapid discharge of short‐stay patients.[4] Observation units (OUs) have been established in some hospitals to address the unique care needs of short‐stay patients.[5, 6, 7]
Single‐site reports from children's hospitals with successful OUs have demonstrated shorter LOS and lower costs compared with inpatient settings.[6, 8, 9, 10, 11, 12, 13, 14] No prior study has examined hospital‐level effects of an OU on observation‐status patient outcomes. The Pediatric Health Information System (PHIS) database provides a unique opportunity to explore this question, because unlike other national hospital administrative databases,[15, 16] the PHIS dataset contains information about children under observation status. In addition, we know which PHIS hospitals had a dedicated OU in 2011.7
We hypothesized that overall observation‐status stays in hospitals with a dedicated OU would be of shorter duration with earlier discharges at lower cost than observation‐status stays in hospitals without a dedicated OU. We compared hospitals with and without a dedicated OU on secondary outcomes including rates of conversion to inpatient status and return care for any reason.
METHODS
We conducted a cross‐sectional analysis of hospital administrative data using the 2011 PHIS databasea national administrative database that contains resource utilization data from 43 participating hospitals located in 26 states plus the District of Columbia. These hospitals account for approximately 20% of pediatric hospitalizations in the United States.
For each hospital encounter, PHIS includes patient demographics, up to 41 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD‐9‐CM) diagnoses, up to 41 ICD‐9‐CM procedures, and hospital charges for services. Data are deidentified prior to inclusion, but unique identifiers allow for determination of return visits and readmissions following an index visit for an individual patient. Data quality and reliability are assured jointly by the Children's Hospital Association (formerly Child Health Corporation of America, Overland Park, KS), participating hospitals, and Truven Health Analytics (New York, NY). This study, using administrative data, was not considered human subjects research by the policies of the Cincinnati Children's Hospital Medical Center Institutional Review Board.
Hospital Selection and Hospital Characteristics
The study sample was drawn from the 31 hospitals that reported observation‐status patient data to PHIS in 2011. Analyses were conducted in 2013, at which time 2011 was the most recent year of data. We categorized 14 hospitals as having a dedicated OU during 2011 based on information collected in 2013.7 To summarize briefly, we interviewed by telephone representatives of hospitals responding to an email query as to the presence of a geographically distinct OU for the care of unscheduled patients from the ED. Three of the 14 representatives reported their hospital had 2 OUs, 1 of which was a separate surgical OU. Ten OUs cared for both ED patients and patients with scheduled procedures; 8 units received patients from non‐ED sources. Hospitalists provided staffing in more than half of the OUs.
We attempted to identify administrative data that would signal care delivered in a dedicated OU using hospital charge codes reported to PHIS, but learned this was not possible due to between‐hospital variation in the specificity of the charge codes. Therefore, we were unable to determine if patient care was delivered in a dedicated OU or another setting, such as a general inpatient unit or the ED. Other hospital characteristics available from the PHIS dataset included the number of inpatient beds, ED visits, inpatient admissions, observation‐status stays, and payer mix. We calculated the percentage of ED visits resulting in admission by dividing the number of ED visits with associated inpatient or observation status by the total number of ED visits and the percentage of admissions under observation status by dividing the number of observation‐status stays by the total number of admissions under observation or inpatient status.
Visit Selection and Patient Characteristics
All observation‐status stays regardless of the point of entry into the hospital were eligible for this study. We excluded stays that were birth‐related, included intensive care, or resulted in transfer or death. Patient demographic characteristics used to describe the cohort included age, gender, race/ethnicity, and primary payer. Stays that began in the ED were identified by an emergency room charge within PHIS. Eligible stays were categorized using All Patient Refined Diagnosis Related Groups (APR‐DRGs) version 24 using the ICD‐9‐CM code‐based proprietary 3M software (3M Health Information Systems, St. Paul, MN). We determined the 15 top‐ranking APR‐DRGs among observation‐status stays in hospitals with a dedicated OU and hospitals without. Procedural stays were identified based on procedural APR‐DRGs (eg, tonsil and adenoid procedures) or the presence of an ICD‐9‐CM procedure code (eg, 331 spinal tap).
Measured Outcomes
Outcomes of observation‐status stays were determined within 4 categories: (1) LOS, (2) standardized costs, (3) conversion to inpatient status, and (4) return visits and readmissions. LOS was calculated in terms of nights spent in hospital for all stays by subtracting the discharge date from the admission date and in terms of hours for stays in the 28 hospitals that report admission and discharge hour to the PHIS database. Discharge timing was examined in 4, 6‐hour blocks starting at midnight. Standardized costs were derived from a charge master index that was created by taking the median costs from all PHIS hospitals for each charged service.[17] Standardized costs represent the estimated cost of providing any particular clinical activity but are not the cost to patients, nor do they represent the actual cost to any given hospital. This approach allows for cost comparisons across hospitals, without biases arising from using charges or from deriving costs using hospitals' ratios of costs to charges.[18] Conversion from observation to inpatient status was calculated by dividing the number of inpatient‐status stays with observation codes by the number of observation‐statusonly stays plus the number of inpatient‐status stays with observation codes. All‐cause 3‐day ED return visits and 30‐day readmissions to the same hospital were assessed using patient‐specific identifiers that allowed for tracking of ED return visits and readmissions following the index observation stay.
Data Analysis
Descriptive statistics were calculated for hospital and patient characteristics using medians and interquartile ranges (IQRs) for continuous factors and frequencies with percentages for categorical factors. Comparisons of these factors between hospitals with dedicated OUs and without were made using [2] and Wilcoxon rank sum tests as appropriate. Multivariable regression was performed using generalized linear mixed models treating hospital as a random effect and used patient age, the case‐mix index based on the APR‐DRG severity of illness, ED visit, and procedures associated with the index observation‐status stay. For continuous outcomes, we performed a log transformation on the outcome, confirmed the normality assumption, and back transformed the results. Sensitivity analyses were conducted to compare LOS, standardized costs, and conversation rates by hospital type for 10 of the 15 top‐ranking APR‐DRGs commonly cared for by pediatric hospitalists and to compare hospitals that reported the presence of an OU that was consistently open (24 hours per day, 7 days per week) and operating during the entire 2011 calendar year, and those without. Based on information gathered from the telephone interviews, hospitals with partially open OUs were similar to hospitals with continuously open OUs, such that they were included in our main analyses. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC). P values <0.05 were considered statistically significant.
RESULTS
Hospital Characteristics
Dedicated OUs were present in 14 of the 31 hospitals that reported observation‐status patient data to PHIS (Figure 1). Three of these hospitals had OUs that were open for 5 months or less in 2011; 1 unit opened, 1 unit closed, and 1 hospital operated a seasonal unit. The remaining 17 hospitals reported no OU that admitted unscheduled patients from the ED during 2011. Hospitals with a dedicated OU had more inpatient beds and higher median number of inpatient admissions than those without (Table 1). Hospitals were statistically similar in terms of total volume of ED visits, percentage of ED visits resulting in admission, total number of observation‐status stays, percentage of admissions under observation status, and payer mix.
| Overall, Median (IQR) | Hospitals With a Dedicated Observation Unit, Median (IQR) | Hospitals Without a Dedicated Observation Unit, Median (IQR) | P Value | |
|---|---|---|---|---|
| ||||
| No. of hospitals | 31 | 14 | 17 | |
| Total no. of inpatient beds | 273 (213311) | 304 (269425) | 246 (175293) | 0.006 |
| Total no. ED visits | 62971 (47,50497,723) | 87,892 (55,102117,119) | 53,151 (4750470,882) | 0.21 |
| ED visits resulting in admission, % | 13.1 (9.715.0) | 13.8 (10.5, 19.1) | 12.5 (9.714.5) | 0.31 |
| Total no. of inpatient admissions | 11,537 (9,26814,568) | 13,206 (11,32517,869) | 10,207 (8,64013,363) | 0.04 |
| Admissions under observation status, % | 25.7 (19.733.8) | 25.5 (21.431.4) | 26.0 (16.935.1) | 0.98 |
| Total no. of observation stays | 3,820 (27935672) | 4,850 (3,309 6,196) | 3,141 (2,3654,616) | 0.07 |
| Government payer, % | 60.2 (53.371.2) | 62.1 (54.9, 65.9) | 59.2 (53.373.7) | 0.89 |
Observation‐Status Patients by Hospital Type
In 2011, there were a total of 136,239 observation‐status stays69,983 (51.4%) within the 14 hospitals with a dedicated OU and 66,256 (48.6%) within the 17 hospitals without. Patient care originated in the ED for 57.8% observation‐status stays in hospitals with an OU compared with 53.0% of observation‐status stays in hospitals without (P<0.001). Compared with hospitals with a dedicated OU, those without a dedicated OU had higher percentages of observation‐status patients older than 12 years and non‐Hispanic and a higher percentage of observation‐status patients with private payer type (Table 2). The 15 top‐ranking APR‐DRGs accounted for roughly half of all observation‐status stays and were relatively consistent between hospitals with and without a dedicated OU (Table 3). Procedural care was frequently associated with observation‐status stays.
| Overall, No. (%) | Hospitals With a Dedicated Observation Unit, No. (%)* | Hospitals Without a Dedicated Observation Unit, No. (%) | P Value | |
|---|---|---|---|---|
| ||||
| Age | ||||
| <1 year | 23,845 (17.5) | 12,101 (17.3) | 11,744 (17.7) | <0.001 |
| 15 years | 53,405 (38.5) | 28,052 (40.1) | 24,353 (36.8) | |
| 612 years | 33,674 (24.7) | 17,215 (24.6) | 16,459 (24.8) | |
| 1318 years | 23,607 (17.3) | 11,472 (16.4) | 12,135 (18.3) | |
| >18 years | 2,708 (2) | 1,143 (1.6) | 1,565 (2.4) | |
| Gender | ||||
| Male | 76,142 (55.9) | 39,178 (56) | 36,964 (55.8) | 0.43 |
| Female | 60,025 (44.1) | 30,756 (44) | 29,269 (44.2) | |
| Race/ethnicity | ||||
| Non‐Hispanic white | 72,183 (53.0) | 30,653 (43.8) | 41,530 (62.7) | <0.001 |
| Non‐Hispanic black | 30,995 (22.8) | 16,314 (23.3) | 14,681 (22.2) | |
| Hispanic | 21,255 (15.6) | 16,583 (23.7) | 4,672 (7.1) | |
| Asian | 2,075 (1.5) | 1,313 (1.9) | 762 (1.2) | |
| Non‐Hispanic other | 9,731 (7.1) | 5,120 (7.3) | 4,611 (7.0) | |
| Payer | ||||
| Government | 68,725 (50.4) | 36,967 (52.8) | 31,758 (47.9) | <0.001 |
| Private | 48,416 (35.5) | 21,112 (30.2) | 27,304 (41.2) | |
| Other | 19,098 (14.0) | 11,904 (17) | 7,194 (10.9) | |
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit* | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED | Rank | APR‐DRG | No. | % of All Observation Status Stays | % Began in ED |
| |||||||||
| 1 | Tonsil and adenoid procedures | 4,621 | 6.6 | 1.3 | 1 | Tonsil and adenoid procedures | 3,806 | 5.7 | 1.6 |
| 2 | Asthma | 4,246 | 6.1 | 85.3 | 2 | Asthma | 3,756 | 5.7 | 79.0 |
| 3 | Seizure | 3,516 | 5.0 | 52.0 | 3 | Seizure | 2,846 | 4.3 | 54.9 |
| 4 | Nonbacterial gastroenteritis | 3,286 | 4.7 | 85.8 | 4 | Upper respiratory infections | 2,733 | 4.1 | 69.6 |
| 5 | Bronchiolitis, RSV pneumonia | 3,093 | 4.4 | 78.5 | 5 | Nonbacterial gastroenteritis | 2,682 | 4.0 | 74.5 |
| 6 | Upper respiratory infections | 2,923 | 4.2 | 80.0 | 6 | Other digestive system diagnoses | 2,545 | 3.8 | 66.3 |
| 7 | Other digestive system diagnoses | 2,064 | 2.9 | 74.0 | 7 | Bronchiolitis, RSV pneumonia | 2,544 | 3.8 | 69.2 |
| 8 | Respiratory signs, symptoms, diagnoses | 2,052 | 2.9 | 81.6 | 8 | Shoulder and arm procedures | 1,862 | 2.8 | 72.6 |
| 9 | Other ENT/cranial/facial diagnoses | 1,684 | 2.4 | 43.6 | 9 | Appendectomy | 1,785 | 2.7 | 79.2 |
| 10 | Shoulder and arm procedures | 1,624 | 2.3 | 79.1 | 10 | Other ENT/cranial/facial diagnoses | 1,624 | 2.5 | 29.9 |
| 11 | Abdominal pain | 1,612 | 2.3 | 86.2 | 11 | Abdominal pain | 1,461 | 2.2 | 82.3 |
| 12 | Fever | 1,494 | 2.1 | 85.1 | 12 | Other factors influencing health status | 1,461 | 2.2 | 66.3 |
| 13 | Appendectomy | 1,465 | 2.1 | 66.4 | 13 | Cellulitis/other bacterial skin infections | 1,383 | 2.1 | 84.2 |
| 14 | Cellulitis/other bacterial skin infections | 1,393 | 2.0 | 86.4 | 14 | Respiratory signs, symptoms, diagnoses | 1,308 | 2.0 | 39.1 |
| 15 | Pneumonia NEC | 1,356 | 1.9 | 79.1 | 15 | Pneumonia NEC | 1,245 | 1.9 | 73.1 |
| Total | 36,429 | 52.0 | 57.8 | Total | 33,041 | 49.87 | 53.0 | ||
Outcomes of Observation‐Status Stays
A greater percentage of observation‐status stays in hospitals with a dedicated OU experienced a same‐day discharge (Table 4). In addition, a higher percentage of discharges occurred between midnight and 11 am in hospitals with a dedicated OU. However, overall risk‐adjusted LOS in hours (12.8 vs 12.2 hours, P=0.90) and risk‐adjusted total standardized costs ($2551 vs $2433, P=0.75) were similar between hospital types. These findings were consistent within the 1 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Overall, conversion from observation to inpatient status was significantly higher in hospitals with a dedicated OU compared with hospitals without; however, this pattern was not consistent across the 10 APR‐DRGs commonly cared for by pediatric hospitalists (see Supporting Information, Appendix 1, in the online version of this article). Adjusted odds of 3‐day ED return visits and 30‐day readmissions were comparable between hospital groups.
| Observation‐Status Patients in Hospitals With a Dedicated Observation Unit | Observation‐Status Patients in Hospitals Without a Dedicated Observation Unit | P Value | |
|---|---|---|---|
| |||
| No. of hospitals | 14 | 17 | |
| Length of stay, h, median (IQR) | 12.8 (6.923.7) | 12.2 (721.3) | 0.90 |
| 0 midnights, no. (%) | 16,678 (23.8) | 14,648 (22.1) | <.001 |
| 1 midnight, no. (%) | 46,144 (65.9) | 44,559 (67.3) | |
| 2 midnights or more, no. (%) | 7,161 (10.2) | 7,049 (10.6) | |
| Discharge timing, no. (%) | |||
| Midnight5 am | 1,223 (1.9) | 408 (0.7) | <0.001 |
| 6 am11 am | 18,916 (29.3) | 15,914 (27.1) | |
| Noon5 pm | 32,699 (50.7) | 31,619 (53.9) | |
| 6 pm11 pm | 11,718 (18.2) | 10,718 (18.3) | |
| Total standardized costs, $, median (IQR) | 2,551.3 (2,053.93,169.1) | 2,433.4 (1,998.42,963) | 0.75 |
| Conversion to inpatient status | 11.06% | 9.63% | <0.01 |
| Return care, AOR (95% CI) | |||
| 3‐day ED return visit | 0.93 (0.77‐1.12) | Referent | 0.46 |
| 30‐day readmission | 0.88 (0.67‐1.15) | Referent | 0.36 |
We found similar results in sensitivity analyses comparing observation‐status stays in hospitals with a continuously open OU (open 24 hours per day, 7 days per week, for all of 2011 [n=10 hospitals]) to those without(see Supporting Information, Appendix 2, in the online version of this article). However, there were, on average, more observation‐status stays in hospitals with a continuously open OU (median 5605, IQR 42077089) than hospitals without (median 3309, IQR 26784616) (P=0.04). In contrast to our main results, conversion to inpatient status was lower in hospitals with a continuously open OU compared with hospitals without (8.52% vs 11.57%, P<0.01).
DISCUSSION
Counter to our hypothesis, we did not find hospital‐level differences in length of stay or costs for observation‐status patients cared for in hospitals with and without a dedicated OU, though hospitals with dedicated OUs did have more same‐day discharges and more morning discharges. The lack of observed differences in LOS and costs may reflect the fact that many children under observation status are treated throughout the hospital, even in facilities with a dedicated OU. Access to a dedicated OU is limited by factors including small numbers of OU beds and specific low acuity/low complexity OU admission criteria.[7] The inclusion of all children admitted under observation status in our analyses may have diluted any effect of dedicated OUs at the hospital level, but was necessary due to the inability to identify location of care for children admitted under observation status. Location of care is an important variable that should be incorporated into administrative databases to allow for comparative effectiveness research designs. Until such data are available, chart review at individual hospitals would be necessary to determine which patients received care in an OU.
We did find that discharges for observation‐status patients occurred earlier in the day in hospitals with a dedicated OU when compared with observation‐status patients in hospitals without a dedicated OU. In addition, the percentage of same‐day discharges was higher among observation‐status patients treated in hospitals with a dedicated OU. These differences may stem from policies and procedures that encourage rapid discharge in dedicated OUs, and those practices may affect other care areas. For example, OUs may enforce policies requiring family presence at the bedside or utilize staffing models where doctors and nurses are in frequent communication, both of which would facilitate discharge as soon as a patient no longer required hospital‐based care.[7] A retrospective chart review study design could be used to identify discharge processes and other key characteristics of highly performing OUs.
We found conflicting results in our main and sensitivity analyses related to conversion to inpatient status. Lower percentages of observation‐status patients converting to inpatient status indicates greater success in the delivery of observation care based on established performance metrics.[19] Lower rates of conversion to inpatient status may be the result of stricter admission criteria for some diagnosis and in hospitals with a continuously open dedicate OU, more refined processes for utilization review that allow for patients to be placed into the correct status (observation vs inpatient) at the time of admission, or efforts to educate providers about the designation of observation status.[7] It is also possible that fewer observation‐status patients convert to inpatient status in hospitals with a continuously open dedicated OU because such a change would require movement of the patient to an inpatient bed.
These analyses were more comprehensive than our prior studies[2, 20] in that we included both patients who were treated first in the ED and those who were not. In addition to the APR‐DRGs representative of conditions that have been successfully treated in ED‐based pediatric OUs (eg, asthma, seizures, gastroenteritis, cellulitis),[8, 9, 21, 22] we found observation‐status was commonly associated with procedural care. This population of patients may be relevant to hospitalists who staff OUs that provide both unscheduled and postprocedural care. The colocation of medical and postprocedural patients has been described by others[8, 23] and was reported to occur in over half of the OUs included in this study.[7] The extent to which postprocedure observation care is provided in general OUs staffed by hospitalists represents another opportunity for further study.
Hospitals face many considerations when determining if and how they will provide observation services to patients expected to experience short stays.[7] Some hospitals may be unable to justify an OU for all or part of the year based on the volume of admissions or the costs to staff an OU.[24, 25] Other hospitals may open an OU to promote patient flow and reduce ED crowding.[26] Hospitals may also be influenced by reimbursement policies related to observation‐status stays. Although we did not observe differences in overall payer mix, we did find higher percentages of observation‐status patients in hospitals with dedicated OUs to have public insurance. Although hospital contracts with payers around observation status patients are complex and beyond the scope of this analysis, it is possible that hospitals have established OUs because of increasingly stringent rules or criteria to meet inpatient status or experiences with high volumes of observation‐status patients covered by a particular payer. Nevertheless, the brief nature of many pediatric hospitalizations and the scarcity of pediatric OU beds must be considered in policy changes that result from national discussions about the appropriateness of inpatient stays shorter than 2 nights in duration.[27]
Limitations
The primary limitation to our analyses is the lack of ability to identify patients who were treated in a dedicated OU because few hospitals provided data to PHIS that allowed for the identification of the unit or location of care. Second, it is possible that some hospitals were misclassified as not having a dedicated OU based on our survey, which initially inquired about OUs that provided care to patients first treated in the ED. Therefore, OUs that exclusively care for postoperative patients or patients with scheduled treatments may be present in hospitals that we have labeled as not having a dedicated OU. This potential misclassification would bias our results toward finding no differences. Third, in any study of administrative data there is potential that diagnosis codes are incomplete or inaccurately capture the underlying reason for the episode of care. Fourth, the experiences of the free‐standing children's hospitals that contribute data to PHIS may not be generalizable to other hospitals that provide observation care to children. Finally, return care may be underestimated, as children could receive treatment at another hospital following discharge from a PHIS hospital. Care outside of PHIS hospitals would not be captured, but we do not expect this to differ for hospitals with and without dedicated OUs. It is possible that health information exchanges will permit more comprehensive analyses of care across different hospitals in the future.
CONCLUSION
Observation status patients are similar in hospitals with and without dedicated observation units that admit children from the ED. The presence of a dedicated OU appears to have an influence on same‐day and morning discharges across all observation‐status stays without impacting other hospital‐level outcomes. Inclusion of location of care (eg, geographically distinct dedicated OU vs general inpatient unit vs ED) in hospital administrative datasets would allow for meaningful comparisons of different models of care for short‐stay observation‐status patients.
Acknowledgements
The authors thank John P. Harding, MBA, FACHE, Children's Hospital of the King's Daughters, Norfolk, Virginia for his input on the study design.
Disclosures: Dr. Hall had full access to the data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Internal funds from the Children's Hospital Association supported the conduct of this work. The authors have no financial relationships or conflicts of interest to disclose.
© 2015 Society of Hospital Medicine
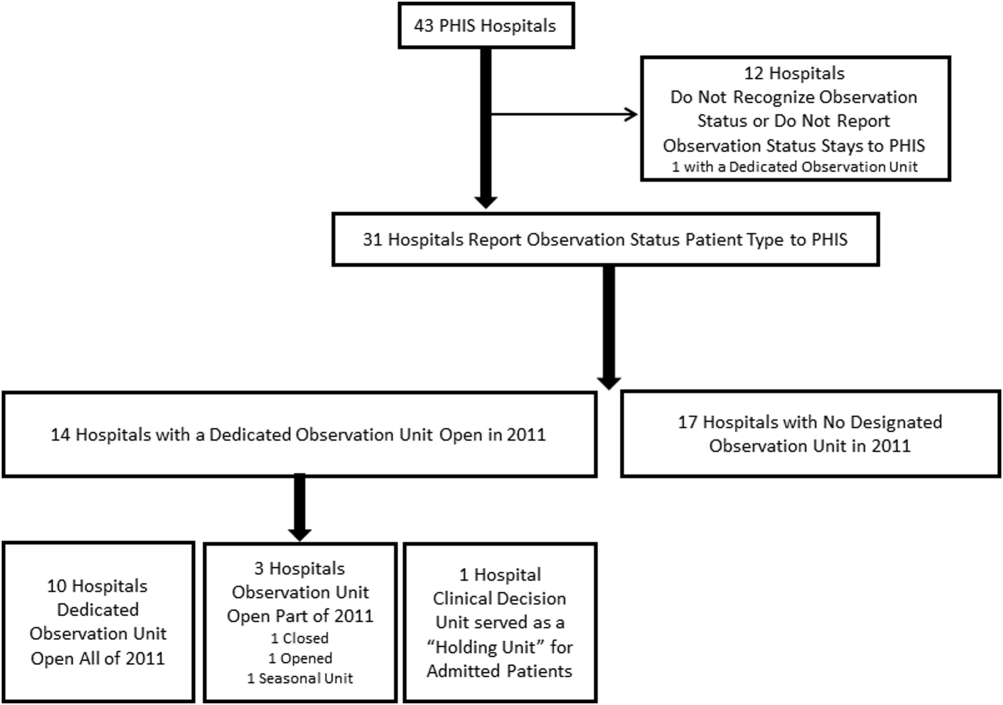
Gender Disparities for Academic Hospitalists
Gender disparities still exist for women in academic medicine.[1, 2, 3, 4, 5, 6, 7, 8, 9] The most recent data from the Association of American Medical Colleges (AAMC) show that although gender disparities are decreasing, women are still under‐represented in the assistant, associate, and full‐professor ranks as well as in leadership positions.[1]
Some studies indicate that gender differences are less evident when examining younger cohorts.[1, 10, 11, 12, 13] Hospital medicine emerged around 1996, when the term hospitalist was first coined.[14] The gender distribution of academic hospitalists is likely nearly equal,[15, 16] and they are generally younger physicians.[15, 17, 18, 19, 20] Accordingly, we questioned whether gender disparities existed in academic hospital medicine (HM) and, if so, whether these disparities were greater than those that might exist in academic general internal medicine (GIM).
METHODS
This study consisted of both prospective and retrospective observation of data collected for academic adult hospitalists and general internists who practice in the United States. It was approved by the Colorado Multiple Institutional Review Board.
Gender distribution was assessed with respect to: (1) academic HM and GIM faculty, (2) leadership (ie, division or section heads), and (3) scholarly work (ie, speaking opportunities and publications). Data were collected between October 1, 2012 and August 31, 2014.
Gender Distribution of Faculty and Division/Section Heads
All US internal medicine residency programs were identified from the list of members or affiliates of the AAMC that were fully accredited by the Liaison Committee on Medical Education[21] using the Graduate Medical Education Directory.[22] We then determined the primary training hospital(s) affiliated with each program and selected those that were considered to be university hospitals and eliminated those that did not have divisions or sections of HM or GIM. We determined the gender of the respective division/section heads on the basis of the faculty member's first name (and often from accompanying photos) as well as from information obtained via Internet searches and, if necessary, contacted the individual institutions via email or phone call(s). We also determined the number and gender of all of the HM and GIM faculty members in a random sample of 25% of these hospitals from information on their respective websites.
Gender Distribution for Scholarly Productivity
We determined the gender and specialty of all speakers at the Society of Hospital Medicine and the Society of General Internal Medicine national conferences from 2006 to 2012. A list of speakers at each conference was obtained from conference pamphlets or agendas that were available via Internet searches or obtained directly from the organization. We also determined whether each presenter was a featured speaker (defined as one whose talk was unopposed by other sessions), plenary speaker (defined as such in the conference pamphlets), or if they spoke in a group format (also as indicated in the conference pamphlets). Because of the low number of featured and plenary speakers, these data were combined. Faculty labeled as additional faculty when presenting in a group format were excluded as were speakers at precourses, those presenting abstracts, and those participating in interest group sessions.
For authorship, a PubMed search was used to identify all articles published in the Journal of Hospital Medicine (JHM) and the Journal of General Internal Medicine (JGIM) from January 1, 2006 through December 31, 2012, and the gender and specialty of all the first and last authors were determined as described above. Specialty was determined from the division, section or department affiliation indicated for each author and by Internet searches. In some instances, it was necessary to contact the authors or their departments directly to verify their specialty. When articles had only 1 author, the author was considered a first author.
Duplicate records (eg, same author, same journal) and articles without an author were excluded, as were authors who did not have an MD, DO, or MBBS degree and those who were not affiliated with an institution in the United States. All manuscripts, with the exception of errata, were analyzed together as well as in 3 subgroups: original research, editorials, and others.
A second investigator corroborated data regarding gender and specialty for all speakers and authors to strengthen data integrity. On the rare occasion when discrepancies were found, a third investigator adjudicated the results.
Definitions
Physicians were defined as being hospitalists if they were listed as a member of a division or section of HM on their publications or if Internet searches indicated that they were a hospitalist or primarily worked on inpatient medical services. Physicians were considered to be general internists if they were listed as such on their publications and their specialty could be verified in Web‐based searches. If physicians appeared to have changing roles over time, we attempted to assign their specialty based upon their role at the time the article was published or the presentation was delivered. If necessary, phone calls and/or emails were also done to determine the physician's specialty.
Analysis
REDCap, a secure, Web‐based application for building and managing online surveys and databases, was used to collect and manage all study data.[23] All analyses were performed using SAS Enterprise Guide 4.3 (SAS Institute, Inc., Cary, NC). A [2] test was used to compare proportions of male versus female physicians, and data from hospitalists versus general internists. Because we performed multiple comparisons when analyzing presentations and publications, a Bonferroni adjustment was made such that a P<0.0125 for presentations and P<0.006 (within specialty) or P<0.0125 (between specialty) for the publication analyses were considered significant. P<0.05 was considered significant for all other comparisons.
RESULTS
Gender Distribution of Faculty
Eighteen HM and 20 GIM programs from university hospitals were randomly selected for review (see Supporting Figure 1 in the online version of this article). Seven of the HM programs and 1 of the GIM programs did not have a website, did not differentiate hospitalists from other faculty, or did not list their faculty on the website and were excluded from the analysis. In the remaining 11 HM programs and 19 GIM programs, women made up 277/568 (49%) and 555/1099 (51%) of the faculty, respectively (P=0.50).
Gender Distribution of Division/Section Heads
Eighty‐six of the programs were classified as university hospitals (see Supporting Figure 1 in the online version of this article), and in these, women led 11/69 (16%) of the HM divisions or sections and 28/80 (35%) of the GIM divisions (P=0.008).
Gender Distribution for Scholarly Productivity
Speaking Opportunities
A total of 1227 presentations were given at the 2 conferences from 2006 to 2012, with 1343 of the speakers meeting inclusion criteria (see Supporting Figure 2 in the online version of this article). Hospitalists accounted for 557 of the speakers, of which 146 (26%) were women. General internists accounted for 580 of the speakers, of which 291 (50%) were women (P<0.0001) (Table 1).
| Male, N (%) | Female, N (%) | |
|---|---|---|
| ||
| Hospitalists | ||
| All presentations | 411 (74) | 146 (26)* |
| Featured or plenary presentations | 49 (91) | 5 (9)* |
| General internists | ||
| All presentations | 289 (50) | 291 (50) |
| Featured or plenary presentations | 27 (55) | 22 (45) |
Of the 117 featured or plenary speakers, 54 were hospitalists and 5 (9%) of these were women. Of the 49 who were general internists, 22 (45%) were women (P<0.0001).
Authorship
The PubMed search identified a total of 3285 articles published in the JHM and the JGIM from 2006 to 2012, and 2172 first authors and 1869 last authors met inclusion criteria (see Supporting Figure 3 in the online version of this article). Hospitalists were listed as first or last authors on 464 and 305 articles, respectively, and of these, women were first authors on 153 (33%) and last authors on 63 (21%). General internists were listed as first or last authors on 895 and 769 articles, respectively, with women as first authors on 423 (47%) and last authors on 265 (34%). Compared with general internists, fewer women hospitalists were listed as either first or last authors (both P<0.0001) (Table 2).
| First Author | Last Author | |||
|---|---|---|---|---|
| Male, N (%) | Female, N (%) | Male, N (%) | Female, N (%) | |
| ||||
| Hospitalists | ||||
| All publications | 311 (67) | 153 (33)* | 242 (79) | 63 (21)* |
| Original investigations/brief reports | 124 (61) | 79 (39)* | 96 (76) | 30 (24)* |
| Editorials | 34 (77) | 10 (23)* | 18 (86) | 3 (14)* |
| Other | 153 (71) | 64 (29)* | 128 (81) | 30 (19)* |
| General internists | ||||
| All publications | 472 (53) | 423 (47) | 504 (66) | 265 (34)* |
| Original investigations/brief reports | 218 (46) | 261 (54) | 310 (65) | 170 (35)* |
| Editorial | 98 (68) | 46 (32)* | 43 (73) | 16 (27)* |
| Other | 156 (57) | 116 (43) | 151 (66) | 79 (34)* |
Fewer women hospitalists were listed as first or last authors on all article types. For original research articles written by general internists, there was a trend for more women to be listed as first authors than men (261/479, 54%), but this difference was not statistically significant.
DISCUSSION
The important findings of this study are that, despite an equal gender distribution of academic HM and GIM faculty, fewer women were HM division/section chiefs, fewer women were speakers at the 2 selected national meetings, and fewer women were first or last authors of publications in 2 selected journals in comparison with general internists.
Previous studies have found that women lag behind their male counterparts with respect to academic productivity, leadership, and promotion.[1, 5, 7] Some studies suggest, however, that gender differences are reduced when younger cohorts are examined.[1, 10, 11, 12, 13] Surveys indicate that that the mean age of hospitalists is younger than most other specialties.[15, 19, 20, 24] The mean age of academic GIM physicians is unknown, but surveys of GIM (not differentiating academic from nonacademic) suggest that it is an older cohort than that of HM.[24] Despite hospitalists being a younger cohort, we found gender disparities in all areas investigated.
Our findings with respect to gender disparities in HM division or section leadership are consistent with the annual AAMC Women in US Academic Medicine and Science Benchmarking Report that found only 22% of all permanent division or section heads were women.[1]
Gender disparities with respect to authorship of medical publications have been previously noted,[3, 6, 15, 25] but to our knowledge, this is the first study to investigate the gender of authors who were hospitalists. Although we found a higher proportion of women hospitalists who were first or last authors than was observed by Jagsi and colleagues,[3] women hospitalists were still under‐represented with respect to this measure of academic productivity. Erren et al. reviewed 6 major journals from 2010 and 2011, and found that first authorship of original research by women ranged from 23.7% to 46.7%, and for last authorship from 18.3% to 28.8%.[25] Interestingly, we found no significant gender difference for first authors who were general internists, and there was a trend toward more women general internists being first authors than men for original research, reviews, and brief reports (data not shown).
Our study did not attempt to answer the question of why gender disparities persist, but many previous studies have explored this issue.[4, 8, 12, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42] Issues raised by others include the quantity of academic work (ie, publications and grants obtained), differences in hours worked and allocation of time, lack of mentorship, family responsibilities, discrimination, differences in career motivation, and levels of institutional support, to name a few.
The under‐representation of women hospitalists in leadership, authorship, and speaking opportunities may be consistent with gender‐related differences in research productivity. Fewer publications could lead to fewer national presentations, which could lead to fewer leadership opportunities. Our findings with respect to general internists are not consistent with this idea, however, as whereas women were under‐represented in GIM leadership positions, we found no disparities with respect to the gender of first authors or speakers at national meetings for general internists. The finding that hospitalists had gender disparities with respect to first authors and national speakers but general internists did not, argues against several hypotheses (ie, that women lack mentorship, have less career motivation, fewer career building opportunities).
One notable hypothesis, and perhaps one that is often discussed in the literature, is that women shoulder the majority of family responsibilities, and this may result in women having less time for their careers. Jolly and colleagues studied physician‐researchers and noted that women were more likely than men to have spouses or domestic partners who were fully employed, spent 8.5 more hours per week on domestic activities, and were more likely to take time off during disruptions of usual child care.[33] Carr and colleagues found that women with children (compared to men with children) had fewer publications, slower self‐perceived career progress, and lower career satisfaction, but having children had little effect on faculty aspirations and goals.[2] Kaplan et al., however, found that family responsibilities do not appear to account for sex differences in academic advancement.[4] Interestingly, in a study comparing physicians from Generation X to those of the Baby Boomer age, Generation X women reported working more than their male Generation X counterparts, and both had more of a focus on worklife balance than the older generation.[12]
The nature the of 2 specialties' work environment and job requirements could have also resulted in some of the differences seen. Primary care clinical work is typically conducted Monday through Friday, and hospitalist work frequently includes some weekend, evening, night, and holiday coverage. Although these are known differences, both specialties have also been noted to offer many advantages to women and men alike, including collaborative working environments and flexible work hours.[16]
Finally, finding disparity in leadership positions in both specialties supports the possibility that those responsible for hiring could have implicit gender biases. Under‐representation in entry‐level positions is also not a likely explanation for the differences we observed, because nearly an equal number of men and women graduate from medical school, pursue residency training in internal medicine, and become either academic hospitalists or general internists at university settings.[1, 15, 24] This hypothesis could, however, explain why disparities exist with respect to senior authorship and leadership positions, as typically, these individuals have been in practice longer and the current trends of improved gender equality have not always been the case.
Our study has a number of limitations. First, we only examined publications in 2 journals and presentations at 2 national conferences, although the journals and conferences selected are considered to be the major ones in the 2 specialties. Second, using Internet searches may have resulted in inaccurate gender and specialty assignment, but previous studies have used similar methodology.[3, 43] Additionally, we also attempted to contact individuals for direct confirmation when the information we obtained was not clear and had a second investigator independently verify the gender and specialty data. Third, we utilized division/department websites when available to determine the gender of HM divisions/sections. If not recently updated, these websites may not have reflected the most current leader of the unit, but this concern would seemingly pertain to both hospitalists and general internists. Fourth, we opted to only study faculty and division/section heads at university hospitals, as typically these institutions had GIM and hospitalist groups and also typically had websites. Because we only studied faculty and leadership at university hospitals, our data are not generalizable to all hospitalist and GIM groups. Finally, we excluded pediatric hospitalists, and thus, this study is representative of adult hospitalists only. Including pediatric hospitalists was out of the scope of this project.
Our study also had a number of strengths. To our knowledge, this is the first study to provide an estimate of the gender distribution in academic HM, of hospitalists as speakers at national meetings, as first and last authors, and of HM division or section heads, and is the first to compare these results with those observed for general internists. In addition, we examined 7 years of data from 2 of the major journals and national conferences for these specialties.
In summary, despite HM being a newer field with a younger cohort of physicians, we found that gender disparities exist for women with respect to authorship, national speaking opportunities, and division or section leadership. Identifying why these gender differences exist presents an important next step.
Disclosures: Nothing to report. Marisha Burden, MD and Maria G. Frank, MD are coprincipal authors.
- Association of American Medical Colleges. Women in U.S. academic medicine and science: Statistics and benchmarking report. 2012. Available at: https://members.aamc.org/eweb/upload/Women%20in%20U%20S%20%20Academic%20Medicine%20Statistics%20and%20Benchmarking%20Report%202011-20123.pdf. Accessed September 1, 2014.
- , , , et al. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Intern Med. 1998;129:532–538.
- , , , et al. The “gender gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355:281–287.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335:1282–1289.
- . Women physicians in academic medicine: new insights from cohort studies. N Engl J Med. 2000;342:399–405.
- , , , , . Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad Med. 2011;86:43–47.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273:1022–1025.
- , , , . Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141:205–212.
- , , . Women physicians: choosing a career in academic medicine. Acad Med. 2012;87:105–114.
- , , , . The status of women at one academic medical center. Breaking through the glass ceiling. JAMA. 1990;264:1813–1817.
- , . Status of women in academic anesthesiology. Anesthesiology. 1986;64:496–500.
- , , . The generation and gender shifts in medicine: an exploratory survey of internal medicine physicians. BMC Health Serv Res. 2006;6:55.
- Pew Research Center. On pay gap, millenial women near parity—for now. December 2013. Available at: http://www.pewsocialtrends.org/files/2013/12/gender-and-work_final.pdf. Published December 11, 2013. Accessed February 5, 2015.
- , . The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514–517.
- , , , , , . Mentorship, productivity, and promotion among academic hospitalists. J Gen Intern Med. 2012;27:23–27.
- . The gender factor. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/the‐gender‐factor. Published March 1, 2006. Accessed September 1, 2014.
- Association of American Medical Colleges. Analysis in brief: Supplemental information for estimating the number and characteristics of hospitalist physicians in the United States and their possible workforce implications. Available at: https://www.aamc.org/download/300686/data/aibvol12_no3-supplemental.pdf. Published August 2012. Accessed September 1, 2014.
- , , , . Survey of US academic hospitalist leaders about mentorship and academic activities in hospitalist groups. J Hosp Med. 2011;6:5–9.
- State of Hospital Medicine: 2011 Report Based on 2010 Data. Medical Group Management Association and Society of Hospital Medicine. www.mgma.com, www.hospitalmedicine.org.
- Today's Hospitalist Survey. Compensation and Career Survey Results. 2013. Available at: http://www.todayshospitalist.com/index.php?b=salary_survey_results. Accessed January 11, 2015.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report. 2009–2010. Available at: https://www.aamc.org/download/182674/data/gwims_stats_2009‐2010.pdf. Accessed September 1, 2014.
- American Medical Association. Graduate Medical Education Directory 2012–2013. Chicago, IL: American Medical Association; 2012:182–203.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- Association of American Medical Colleges. 2012 Physician Specialty Data Book. Center for Workforce Studies. Available at: https://www.aamc.org/download/313228/data/2012physicianspecialtydatabook.pdf. Published November 2012. Accessed September 1, 2014.
- , , , . Representation of women as authors, reviewers, editors in chief, and editorial board members at 6 general medical journals in 2010 and 2011. JAMA Intern Med. 2014;174:633–635.
- , , , et al. Relationships of gender and career motivation to medical faculty members' production of academic publications. Acad Med. 1998;73:180–186.
- , , , et al. Faculty perceptions of gender discrimination and sexual harassment in academic medicine. Ann Intern Med. 2000;132:889–896.
- , , , . Attitudes of clinical faculty about career progress, career success and recognition, and commitment to academic medicine. Results of a survey. Arch Intern Med. 2000;160:2625–2629.
- , , , , . A "ton of feathers": gender discrimination in academic medical careers and how to manage it. J Womens Health (Larchmt). 2003;12:1009–1018.
- , , . Perceived obstacles to career success for women in academic surgery. Arch Surg. 2000;135:972–977.
- , , , . Career satisfaction of US women physicians: results from the Women Physicians' Health Study. Society of General Internal Medicine Career Satisfaction Study Group. Arch Intern Med. 1999;159:1417–1426.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301–315.
- , , , , , . Gender differences in time spent on parenting and domestic responsibilities by high‐achieving young physician‐researchers. Ann Intern Med. 2014;160:344–353.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86:752–758.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28:201–207.
- . Gender pay gaps in hospital medicine. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/gender‐pay‐gaps‐in‐hospital‐medicine. Published February 29, 2012. Accessed September 1, 2014.
- , , . Mentoring in academic medicine: a systematic review. JAMA. 2006;296:1103–1115.
- . Inequality quantified: mind the gender gap. Nature. 2013;495:22–24.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78:500–508.
- , . Why aren't there more women leaders in academic medicine? The views of clinical department chairs. Acad Med. 2001;76:453–465.
- . Gender factors in reviewer recommendations for manuscript publication. J Appl Behav Anal. 1990;23:539–543.
- , , , . Scientific impact of women in academic surgery. J Surg Res. 2008;148:13–16.
Gender disparities still exist for women in academic medicine.[1, 2, 3, 4, 5, 6, 7, 8, 9] The most recent data from the Association of American Medical Colleges (AAMC) show that although gender disparities are decreasing, women are still under‐represented in the assistant, associate, and full‐professor ranks as well as in leadership positions.[1]
Some studies indicate that gender differences are less evident when examining younger cohorts.[1, 10, 11, 12, 13] Hospital medicine emerged around 1996, when the term hospitalist was first coined.[14] The gender distribution of academic hospitalists is likely nearly equal,[15, 16] and they are generally younger physicians.[15, 17, 18, 19, 20] Accordingly, we questioned whether gender disparities existed in academic hospital medicine (HM) and, if so, whether these disparities were greater than those that might exist in academic general internal medicine (GIM).
METHODS
This study consisted of both prospective and retrospective observation of data collected for academic adult hospitalists and general internists who practice in the United States. It was approved by the Colorado Multiple Institutional Review Board.
Gender distribution was assessed with respect to: (1) academic HM and GIM faculty, (2) leadership (ie, division or section heads), and (3) scholarly work (ie, speaking opportunities and publications). Data were collected between October 1, 2012 and August 31, 2014.
Gender Distribution of Faculty and Division/Section Heads
All US internal medicine residency programs were identified from the list of members or affiliates of the AAMC that were fully accredited by the Liaison Committee on Medical Education[21] using the Graduate Medical Education Directory.[22] We then determined the primary training hospital(s) affiliated with each program and selected those that were considered to be university hospitals and eliminated those that did not have divisions or sections of HM or GIM. We determined the gender of the respective division/section heads on the basis of the faculty member's first name (and often from accompanying photos) as well as from information obtained via Internet searches and, if necessary, contacted the individual institutions via email or phone call(s). We also determined the number and gender of all of the HM and GIM faculty members in a random sample of 25% of these hospitals from information on their respective websites.
Gender Distribution for Scholarly Productivity
We determined the gender and specialty of all speakers at the Society of Hospital Medicine and the Society of General Internal Medicine national conferences from 2006 to 2012. A list of speakers at each conference was obtained from conference pamphlets or agendas that were available via Internet searches or obtained directly from the organization. We also determined whether each presenter was a featured speaker (defined as one whose talk was unopposed by other sessions), plenary speaker (defined as such in the conference pamphlets), or if they spoke in a group format (also as indicated in the conference pamphlets). Because of the low number of featured and plenary speakers, these data were combined. Faculty labeled as additional faculty when presenting in a group format were excluded as were speakers at precourses, those presenting abstracts, and those participating in interest group sessions.
For authorship, a PubMed search was used to identify all articles published in the Journal of Hospital Medicine (JHM) and the Journal of General Internal Medicine (JGIM) from January 1, 2006 through December 31, 2012, and the gender and specialty of all the first and last authors were determined as described above. Specialty was determined from the division, section or department affiliation indicated for each author and by Internet searches. In some instances, it was necessary to contact the authors or their departments directly to verify their specialty. When articles had only 1 author, the author was considered a first author.
Duplicate records (eg, same author, same journal) and articles without an author were excluded, as were authors who did not have an MD, DO, or MBBS degree and those who were not affiliated with an institution in the United States. All manuscripts, with the exception of errata, were analyzed together as well as in 3 subgroups: original research, editorials, and others.
A second investigator corroborated data regarding gender and specialty for all speakers and authors to strengthen data integrity. On the rare occasion when discrepancies were found, a third investigator adjudicated the results.
Definitions
Physicians were defined as being hospitalists if they were listed as a member of a division or section of HM on their publications or if Internet searches indicated that they were a hospitalist or primarily worked on inpatient medical services. Physicians were considered to be general internists if they were listed as such on their publications and their specialty could be verified in Web‐based searches. If physicians appeared to have changing roles over time, we attempted to assign their specialty based upon their role at the time the article was published or the presentation was delivered. If necessary, phone calls and/or emails were also done to determine the physician's specialty.
Analysis
REDCap, a secure, Web‐based application for building and managing online surveys and databases, was used to collect and manage all study data.[23] All analyses were performed using SAS Enterprise Guide 4.3 (SAS Institute, Inc., Cary, NC). A [2] test was used to compare proportions of male versus female physicians, and data from hospitalists versus general internists. Because we performed multiple comparisons when analyzing presentations and publications, a Bonferroni adjustment was made such that a P<0.0125 for presentations and P<0.006 (within specialty) or P<0.0125 (between specialty) for the publication analyses were considered significant. P<0.05 was considered significant for all other comparisons.
RESULTS
Gender Distribution of Faculty
Eighteen HM and 20 GIM programs from university hospitals were randomly selected for review (see Supporting Figure 1 in the online version of this article). Seven of the HM programs and 1 of the GIM programs did not have a website, did not differentiate hospitalists from other faculty, or did not list their faculty on the website and were excluded from the analysis. In the remaining 11 HM programs and 19 GIM programs, women made up 277/568 (49%) and 555/1099 (51%) of the faculty, respectively (P=0.50).
Gender Distribution of Division/Section Heads
Eighty‐six of the programs were classified as university hospitals (see Supporting Figure 1 in the online version of this article), and in these, women led 11/69 (16%) of the HM divisions or sections and 28/80 (35%) of the GIM divisions (P=0.008).
Gender Distribution for Scholarly Productivity
Speaking Opportunities
A total of 1227 presentations were given at the 2 conferences from 2006 to 2012, with 1343 of the speakers meeting inclusion criteria (see Supporting Figure 2 in the online version of this article). Hospitalists accounted for 557 of the speakers, of which 146 (26%) were women. General internists accounted for 580 of the speakers, of which 291 (50%) were women (P<0.0001) (Table 1).
| Male, N (%) | Female, N (%) | |
|---|---|---|
| ||
| Hospitalists | ||
| All presentations | 411 (74) | 146 (26)* |
| Featured or plenary presentations | 49 (91) | 5 (9)* |
| General internists | ||
| All presentations | 289 (50) | 291 (50) |
| Featured or plenary presentations | 27 (55) | 22 (45) |
Of the 117 featured or plenary speakers, 54 were hospitalists and 5 (9%) of these were women. Of the 49 who were general internists, 22 (45%) were women (P<0.0001).
Authorship
The PubMed search identified a total of 3285 articles published in the JHM and the JGIM from 2006 to 2012, and 2172 first authors and 1869 last authors met inclusion criteria (see Supporting Figure 3 in the online version of this article). Hospitalists were listed as first or last authors on 464 and 305 articles, respectively, and of these, women were first authors on 153 (33%) and last authors on 63 (21%). General internists were listed as first or last authors on 895 and 769 articles, respectively, with women as first authors on 423 (47%) and last authors on 265 (34%). Compared with general internists, fewer women hospitalists were listed as either first or last authors (both P<0.0001) (Table 2).
| First Author | Last Author | |||
|---|---|---|---|---|
| Male, N (%) | Female, N (%) | Male, N (%) | Female, N (%) | |
| ||||
| Hospitalists | ||||
| All publications | 311 (67) | 153 (33)* | 242 (79) | 63 (21)* |
| Original investigations/brief reports | 124 (61) | 79 (39)* | 96 (76) | 30 (24)* |
| Editorials | 34 (77) | 10 (23)* | 18 (86) | 3 (14)* |
| Other | 153 (71) | 64 (29)* | 128 (81) | 30 (19)* |
| General internists | ||||
| All publications | 472 (53) | 423 (47) | 504 (66) | 265 (34)* |
| Original investigations/brief reports | 218 (46) | 261 (54) | 310 (65) | 170 (35)* |
| Editorial | 98 (68) | 46 (32)* | 43 (73) | 16 (27)* |
| Other | 156 (57) | 116 (43) | 151 (66) | 79 (34)* |
Fewer women hospitalists were listed as first or last authors on all article types. For original research articles written by general internists, there was a trend for more women to be listed as first authors than men (261/479, 54%), but this difference was not statistically significant.
DISCUSSION
The important findings of this study are that, despite an equal gender distribution of academic HM and GIM faculty, fewer women were HM division/section chiefs, fewer women were speakers at the 2 selected national meetings, and fewer women were first or last authors of publications in 2 selected journals in comparison with general internists.
Previous studies have found that women lag behind their male counterparts with respect to academic productivity, leadership, and promotion.[1, 5, 7] Some studies suggest, however, that gender differences are reduced when younger cohorts are examined.[1, 10, 11, 12, 13] Surveys indicate that that the mean age of hospitalists is younger than most other specialties.[15, 19, 20, 24] The mean age of academic GIM physicians is unknown, but surveys of GIM (not differentiating academic from nonacademic) suggest that it is an older cohort than that of HM.[24] Despite hospitalists being a younger cohort, we found gender disparities in all areas investigated.
Our findings with respect to gender disparities in HM division or section leadership are consistent with the annual AAMC Women in US Academic Medicine and Science Benchmarking Report that found only 22% of all permanent division or section heads were women.[1]
Gender disparities with respect to authorship of medical publications have been previously noted,[3, 6, 15, 25] but to our knowledge, this is the first study to investigate the gender of authors who were hospitalists. Although we found a higher proportion of women hospitalists who were first or last authors than was observed by Jagsi and colleagues,[3] women hospitalists were still under‐represented with respect to this measure of academic productivity. Erren et al. reviewed 6 major journals from 2010 and 2011, and found that first authorship of original research by women ranged from 23.7% to 46.7%, and for last authorship from 18.3% to 28.8%.[25] Interestingly, we found no significant gender difference for first authors who were general internists, and there was a trend toward more women general internists being first authors than men for original research, reviews, and brief reports (data not shown).
Our study did not attempt to answer the question of why gender disparities persist, but many previous studies have explored this issue.[4, 8, 12, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42] Issues raised by others include the quantity of academic work (ie, publications and grants obtained), differences in hours worked and allocation of time, lack of mentorship, family responsibilities, discrimination, differences in career motivation, and levels of institutional support, to name a few.
The under‐representation of women hospitalists in leadership, authorship, and speaking opportunities may be consistent with gender‐related differences in research productivity. Fewer publications could lead to fewer national presentations, which could lead to fewer leadership opportunities. Our findings with respect to general internists are not consistent with this idea, however, as whereas women were under‐represented in GIM leadership positions, we found no disparities with respect to the gender of first authors or speakers at national meetings for general internists. The finding that hospitalists had gender disparities with respect to first authors and national speakers but general internists did not, argues against several hypotheses (ie, that women lack mentorship, have less career motivation, fewer career building opportunities).
One notable hypothesis, and perhaps one that is often discussed in the literature, is that women shoulder the majority of family responsibilities, and this may result in women having less time for their careers. Jolly and colleagues studied physician‐researchers and noted that women were more likely than men to have spouses or domestic partners who were fully employed, spent 8.5 more hours per week on domestic activities, and were more likely to take time off during disruptions of usual child care.[33] Carr and colleagues found that women with children (compared to men with children) had fewer publications, slower self‐perceived career progress, and lower career satisfaction, but having children had little effect on faculty aspirations and goals.[2] Kaplan et al., however, found that family responsibilities do not appear to account for sex differences in academic advancement.[4] Interestingly, in a study comparing physicians from Generation X to those of the Baby Boomer age, Generation X women reported working more than their male Generation X counterparts, and both had more of a focus on worklife balance than the older generation.[12]
The nature the of 2 specialties' work environment and job requirements could have also resulted in some of the differences seen. Primary care clinical work is typically conducted Monday through Friday, and hospitalist work frequently includes some weekend, evening, night, and holiday coverage. Although these are known differences, both specialties have also been noted to offer many advantages to women and men alike, including collaborative working environments and flexible work hours.[16]
Finally, finding disparity in leadership positions in both specialties supports the possibility that those responsible for hiring could have implicit gender biases. Under‐representation in entry‐level positions is also not a likely explanation for the differences we observed, because nearly an equal number of men and women graduate from medical school, pursue residency training in internal medicine, and become either academic hospitalists or general internists at university settings.[1, 15, 24] This hypothesis could, however, explain why disparities exist with respect to senior authorship and leadership positions, as typically, these individuals have been in practice longer and the current trends of improved gender equality have not always been the case.
Our study has a number of limitations. First, we only examined publications in 2 journals and presentations at 2 national conferences, although the journals and conferences selected are considered to be the major ones in the 2 specialties. Second, using Internet searches may have resulted in inaccurate gender and specialty assignment, but previous studies have used similar methodology.[3, 43] Additionally, we also attempted to contact individuals for direct confirmation when the information we obtained was not clear and had a second investigator independently verify the gender and specialty data. Third, we utilized division/department websites when available to determine the gender of HM divisions/sections. If not recently updated, these websites may not have reflected the most current leader of the unit, but this concern would seemingly pertain to both hospitalists and general internists. Fourth, we opted to only study faculty and division/section heads at university hospitals, as typically these institutions had GIM and hospitalist groups and also typically had websites. Because we only studied faculty and leadership at university hospitals, our data are not generalizable to all hospitalist and GIM groups. Finally, we excluded pediatric hospitalists, and thus, this study is representative of adult hospitalists only. Including pediatric hospitalists was out of the scope of this project.
Our study also had a number of strengths. To our knowledge, this is the first study to provide an estimate of the gender distribution in academic HM, of hospitalists as speakers at national meetings, as first and last authors, and of HM division or section heads, and is the first to compare these results with those observed for general internists. In addition, we examined 7 years of data from 2 of the major journals and national conferences for these specialties.
In summary, despite HM being a newer field with a younger cohort of physicians, we found that gender disparities exist for women with respect to authorship, national speaking opportunities, and division or section leadership. Identifying why these gender differences exist presents an important next step.
Disclosures: Nothing to report. Marisha Burden, MD and Maria G. Frank, MD are coprincipal authors.
Gender disparities still exist for women in academic medicine.[1, 2, 3, 4, 5, 6, 7, 8, 9] The most recent data from the Association of American Medical Colleges (AAMC) show that although gender disparities are decreasing, women are still under‐represented in the assistant, associate, and full‐professor ranks as well as in leadership positions.[1]
Some studies indicate that gender differences are less evident when examining younger cohorts.[1, 10, 11, 12, 13] Hospital medicine emerged around 1996, when the term hospitalist was first coined.[14] The gender distribution of academic hospitalists is likely nearly equal,[15, 16] and they are generally younger physicians.[15, 17, 18, 19, 20] Accordingly, we questioned whether gender disparities existed in academic hospital medicine (HM) and, if so, whether these disparities were greater than those that might exist in academic general internal medicine (GIM).
METHODS
This study consisted of both prospective and retrospective observation of data collected for academic adult hospitalists and general internists who practice in the United States. It was approved by the Colorado Multiple Institutional Review Board.
Gender distribution was assessed with respect to: (1) academic HM and GIM faculty, (2) leadership (ie, division or section heads), and (3) scholarly work (ie, speaking opportunities and publications). Data were collected between October 1, 2012 and August 31, 2014.
Gender Distribution of Faculty and Division/Section Heads
All US internal medicine residency programs were identified from the list of members or affiliates of the AAMC that were fully accredited by the Liaison Committee on Medical Education[21] using the Graduate Medical Education Directory.[22] We then determined the primary training hospital(s) affiliated with each program and selected those that were considered to be university hospitals and eliminated those that did not have divisions or sections of HM or GIM. We determined the gender of the respective division/section heads on the basis of the faculty member's first name (and often from accompanying photos) as well as from information obtained via Internet searches and, if necessary, contacted the individual institutions via email or phone call(s). We also determined the number and gender of all of the HM and GIM faculty members in a random sample of 25% of these hospitals from information on their respective websites.
Gender Distribution for Scholarly Productivity
We determined the gender and specialty of all speakers at the Society of Hospital Medicine and the Society of General Internal Medicine national conferences from 2006 to 2012. A list of speakers at each conference was obtained from conference pamphlets or agendas that were available via Internet searches or obtained directly from the organization. We also determined whether each presenter was a featured speaker (defined as one whose talk was unopposed by other sessions), plenary speaker (defined as such in the conference pamphlets), or if they spoke in a group format (also as indicated in the conference pamphlets). Because of the low number of featured and plenary speakers, these data were combined. Faculty labeled as additional faculty when presenting in a group format were excluded as were speakers at precourses, those presenting abstracts, and those participating in interest group sessions.
For authorship, a PubMed search was used to identify all articles published in the Journal of Hospital Medicine (JHM) and the Journal of General Internal Medicine (JGIM) from January 1, 2006 through December 31, 2012, and the gender and specialty of all the first and last authors were determined as described above. Specialty was determined from the division, section or department affiliation indicated for each author and by Internet searches. In some instances, it was necessary to contact the authors or their departments directly to verify their specialty. When articles had only 1 author, the author was considered a first author.
Duplicate records (eg, same author, same journal) and articles without an author were excluded, as were authors who did not have an MD, DO, or MBBS degree and those who were not affiliated with an institution in the United States. All manuscripts, with the exception of errata, were analyzed together as well as in 3 subgroups: original research, editorials, and others.
A second investigator corroborated data regarding gender and specialty for all speakers and authors to strengthen data integrity. On the rare occasion when discrepancies were found, a third investigator adjudicated the results.
Definitions
Physicians were defined as being hospitalists if they were listed as a member of a division or section of HM on their publications or if Internet searches indicated that they were a hospitalist or primarily worked on inpatient medical services. Physicians were considered to be general internists if they were listed as such on their publications and their specialty could be verified in Web‐based searches. If physicians appeared to have changing roles over time, we attempted to assign their specialty based upon their role at the time the article was published or the presentation was delivered. If necessary, phone calls and/or emails were also done to determine the physician's specialty.
Analysis
REDCap, a secure, Web‐based application for building and managing online surveys and databases, was used to collect and manage all study data.[23] All analyses were performed using SAS Enterprise Guide 4.3 (SAS Institute, Inc., Cary, NC). A [2] test was used to compare proportions of male versus female physicians, and data from hospitalists versus general internists. Because we performed multiple comparisons when analyzing presentations and publications, a Bonferroni adjustment was made such that a P<0.0125 for presentations and P<0.006 (within specialty) or P<0.0125 (between specialty) for the publication analyses were considered significant. P<0.05 was considered significant for all other comparisons.
RESULTS
Gender Distribution of Faculty
Eighteen HM and 20 GIM programs from university hospitals were randomly selected for review (see Supporting Figure 1 in the online version of this article). Seven of the HM programs and 1 of the GIM programs did not have a website, did not differentiate hospitalists from other faculty, or did not list their faculty on the website and were excluded from the analysis. In the remaining 11 HM programs and 19 GIM programs, women made up 277/568 (49%) and 555/1099 (51%) of the faculty, respectively (P=0.50).
Gender Distribution of Division/Section Heads
Eighty‐six of the programs were classified as university hospitals (see Supporting Figure 1 in the online version of this article), and in these, women led 11/69 (16%) of the HM divisions or sections and 28/80 (35%) of the GIM divisions (P=0.008).
Gender Distribution for Scholarly Productivity
Speaking Opportunities
A total of 1227 presentations were given at the 2 conferences from 2006 to 2012, with 1343 of the speakers meeting inclusion criteria (see Supporting Figure 2 in the online version of this article). Hospitalists accounted for 557 of the speakers, of which 146 (26%) were women. General internists accounted for 580 of the speakers, of which 291 (50%) were women (P<0.0001) (Table 1).
| Male, N (%) | Female, N (%) | |
|---|---|---|
| ||
| Hospitalists | ||
| All presentations | 411 (74) | 146 (26)* |
| Featured or plenary presentations | 49 (91) | 5 (9)* |
| General internists | ||
| All presentations | 289 (50) | 291 (50) |
| Featured or plenary presentations | 27 (55) | 22 (45) |
Of the 117 featured or plenary speakers, 54 were hospitalists and 5 (9%) of these were women. Of the 49 who were general internists, 22 (45%) were women (P<0.0001).
Authorship
The PubMed search identified a total of 3285 articles published in the JHM and the JGIM from 2006 to 2012, and 2172 first authors and 1869 last authors met inclusion criteria (see Supporting Figure 3 in the online version of this article). Hospitalists were listed as first or last authors on 464 and 305 articles, respectively, and of these, women were first authors on 153 (33%) and last authors on 63 (21%). General internists were listed as first or last authors on 895 and 769 articles, respectively, with women as first authors on 423 (47%) and last authors on 265 (34%). Compared with general internists, fewer women hospitalists were listed as either first or last authors (both P<0.0001) (Table 2).
| First Author | Last Author | |||
|---|---|---|---|---|
| Male, N (%) | Female, N (%) | Male, N (%) | Female, N (%) | |
| ||||
| Hospitalists | ||||
| All publications | 311 (67) | 153 (33)* | 242 (79) | 63 (21)* |
| Original investigations/brief reports | 124 (61) | 79 (39)* | 96 (76) | 30 (24)* |
| Editorials | 34 (77) | 10 (23)* | 18 (86) | 3 (14)* |
| Other | 153 (71) | 64 (29)* | 128 (81) | 30 (19)* |
| General internists | ||||
| All publications | 472 (53) | 423 (47) | 504 (66) | 265 (34)* |
| Original investigations/brief reports | 218 (46) | 261 (54) | 310 (65) | 170 (35)* |
| Editorial | 98 (68) | 46 (32)* | 43 (73) | 16 (27)* |
| Other | 156 (57) | 116 (43) | 151 (66) | 79 (34)* |
Fewer women hospitalists were listed as first or last authors on all article types. For original research articles written by general internists, there was a trend for more women to be listed as first authors than men (261/479, 54%), but this difference was not statistically significant.
DISCUSSION
The important findings of this study are that, despite an equal gender distribution of academic HM and GIM faculty, fewer women were HM division/section chiefs, fewer women were speakers at the 2 selected national meetings, and fewer women were first or last authors of publications in 2 selected journals in comparison with general internists.
Previous studies have found that women lag behind their male counterparts with respect to academic productivity, leadership, and promotion.[1, 5, 7] Some studies suggest, however, that gender differences are reduced when younger cohorts are examined.[1, 10, 11, 12, 13] Surveys indicate that that the mean age of hospitalists is younger than most other specialties.[15, 19, 20, 24] The mean age of academic GIM physicians is unknown, but surveys of GIM (not differentiating academic from nonacademic) suggest that it is an older cohort than that of HM.[24] Despite hospitalists being a younger cohort, we found gender disparities in all areas investigated.
Our findings with respect to gender disparities in HM division or section leadership are consistent with the annual AAMC Women in US Academic Medicine and Science Benchmarking Report that found only 22% of all permanent division or section heads were women.[1]
Gender disparities with respect to authorship of medical publications have been previously noted,[3, 6, 15, 25] but to our knowledge, this is the first study to investigate the gender of authors who were hospitalists. Although we found a higher proportion of women hospitalists who were first or last authors than was observed by Jagsi and colleagues,[3] women hospitalists were still under‐represented with respect to this measure of academic productivity. Erren et al. reviewed 6 major journals from 2010 and 2011, and found that first authorship of original research by women ranged from 23.7% to 46.7%, and for last authorship from 18.3% to 28.8%.[25] Interestingly, we found no significant gender difference for first authors who were general internists, and there was a trend toward more women general internists being first authors than men for original research, reviews, and brief reports (data not shown).
Our study did not attempt to answer the question of why gender disparities persist, but many previous studies have explored this issue.[4, 8, 12, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42] Issues raised by others include the quantity of academic work (ie, publications and grants obtained), differences in hours worked and allocation of time, lack of mentorship, family responsibilities, discrimination, differences in career motivation, and levels of institutional support, to name a few.
The under‐representation of women hospitalists in leadership, authorship, and speaking opportunities may be consistent with gender‐related differences in research productivity. Fewer publications could lead to fewer national presentations, which could lead to fewer leadership opportunities. Our findings with respect to general internists are not consistent with this idea, however, as whereas women were under‐represented in GIM leadership positions, we found no disparities with respect to the gender of first authors or speakers at national meetings for general internists. The finding that hospitalists had gender disparities with respect to first authors and national speakers but general internists did not, argues against several hypotheses (ie, that women lack mentorship, have less career motivation, fewer career building opportunities).
One notable hypothesis, and perhaps one that is often discussed in the literature, is that women shoulder the majority of family responsibilities, and this may result in women having less time for their careers. Jolly and colleagues studied physician‐researchers and noted that women were more likely than men to have spouses or domestic partners who were fully employed, spent 8.5 more hours per week on domestic activities, and were more likely to take time off during disruptions of usual child care.[33] Carr and colleagues found that women with children (compared to men with children) had fewer publications, slower self‐perceived career progress, and lower career satisfaction, but having children had little effect on faculty aspirations and goals.[2] Kaplan et al., however, found that family responsibilities do not appear to account for sex differences in academic advancement.[4] Interestingly, in a study comparing physicians from Generation X to those of the Baby Boomer age, Generation X women reported working more than their male Generation X counterparts, and both had more of a focus on worklife balance than the older generation.[12]
The nature the of 2 specialties' work environment and job requirements could have also resulted in some of the differences seen. Primary care clinical work is typically conducted Monday through Friday, and hospitalist work frequently includes some weekend, evening, night, and holiday coverage. Although these are known differences, both specialties have also been noted to offer many advantages to women and men alike, including collaborative working environments and flexible work hours.[16]
Finally, finding disparity in leadership positions in both specialties supports the possibility that those responsible for hiring could have implicit gender biases. Under‐representation in entry‐level positions is also not a likely explanation for the differences we observed, because nearly an equal number of men and women graduate from medical school, pursue residency training in internal medicine, and become either academic hospitalists or general internists at university settings.[1, 15, 24] This hypothesis could, however, explain why disparities exist with respect to senior authorship and leadership positions, as typically, these individuals have been in practice longer and the current trends of improved gender equality have not always been the case.
Our study has a number of limitations. First, we only examined publications in 2 journals and presentations at 2 national conferences, although the journals and conferences selected are considered to be the major ones in the 2 specialties. Second, using Internet searches may have resulted in inaccurate gender and specialty assignment, but previous studies have used similar methodology.[3, 43] Additionally, we also attempted to contact individuals for direct confirmation when the information we obtained was not clear and had a second investigator independently verify the gender and specialty data. Third, we utilized division/department websites when available to determine the gender of HM divisions/sections. If not recently updated, these websites may not have reflected the most current leader of the unit, but this concern would seemingly pertain to both hospitalists and general internists. Fourth, we opted to only study faculty and division/section heads at university hospitals, as typically these institutions had GIM and hospitalist groups and also typically had websites. Because we only studied faculty and leadership at university hospitals, our data are not generalizable to all hospitalist and GIM groups. Finally, we excluded pediatric hospitalists, and thus, this study is representative of adult hospitalists only. Including pediatric hospitalists was out of the scope of this project.
Our study also had a number of strengths. To our knowledge, this is the first study to provide an estimate of the gender distribution in academic HM, of hospitalists as speakers at national meetings, as first and last authors, and of HM division or section heads, and is the first to compare these results with those observed for general internists. In addition, we examined 7 years of data from 2 of the major journals and national conferences for these specialties.
In summary, despite HM being a newer field with a younger cohort of physicians, we found that gender disparities exist for women with respect to authorship, national speaking opportunities, and division or section leadership. Identifying why these gender differences exist presents an important next step.
Disclosures: Nothing to report. Marisha Burden, MD and Maria G. Frank, MD are coprincipal authors.
- Association of American Medical Colleges. Women in U.S. academic medicine and science: Statistics and benchmarking report. 2012. Available at: https://members.aamc.org/eweb/upload/Women%20in%20U%20S%20%20Academic%20Medicine%20Statistics%20and%20Benchmarking%20Report%202011-20123.pdf. Accessed September 1, 2014.
- , , , et al. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Intern Med. 1998;129:532–538.
- , , , et al. The “gender gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355:281–287.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335:1282–1289.
- . Women physicians in academic medicine: new insights from cohort studies. N Engl J Med. 2000;342:399–405.
- , , , , . Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad Med. 2011;86:43–47.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273:1022–1025.
- , , , . Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141:205–212.
- , , . Women physicians: choosing a career in academic medicine. Acad Med. 2012;87:105–114.
- , , , . The status of women at one academic medical center. Breaking through the glass ceiling. JAMA. 1990;264:1813–1817.
- , . Status of women in academic anesthesiology. Anesthesiology. 1986;64:496–500.
- , , . The generation and gender shifts in medicine: an exploratory survey of internal medicine physicians. BMC Health Serv Res. 2006;6:55.
- Pew Research Center. On pay gap, millenial women near parity—for now. December 2013. Available at: http://www.pewsocialtrends.org/files/2013/12/gender-and-work_final.pdf. Published December 11, 2013. Accessed February 5, 2015.
- , . The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514–517.
- , , , , , . Mentorship, productivity, and promotion among academic hospitalists. J Gen Intern Med. 2012;27:23–27.
- . The gender factor. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/the‐gender‐factor. Published March 1, 2006. Accessed September 1, 2014.
- Association of American Medical Colleges. Analysis in brief: Supplemental information for estimating the number and characteristics of hospitalist physicians in the United States and their possible workforce implications. Available at: https://www.aamc.org/download/300686/data/aibvol12_no3-supplemental.pdf. Published August 2012. Accessed September 1, 2014.
- , , , . Survey of US academic hospitalist leaders about mentorship and academic activities in hospitalist groups. J Hosp Med. 2011;6:5–9.
- State of Hospital Medicine: 2011 Report Based on 2010 Data. Medical Group Management Association and Society of Hospital Medicine. www.mgma.com, www.hospitalmedicine.org.
- Today's Hospitalist Survey. Compensation and Career Survey Results. 2013. Available at: http://www.todayshospitalist.com/index.php?b=salary_survey_results. Accessed January 11, 2015.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report. 2009–2010. Available at: https://www.aamc.org/download/182674/data/gwims_stats_2009‐2010.pdf. Accessed September 1, 2014.
- American Medical Association. Graduate Medical Education Directory 2012–2013. Chicago, IL: American Medical Association; 2012:182–203.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- Association of American Medical Colleges. 2012 Physician Specialty Data Book. Center for Workforce Studies. Available at: https://www.aamc.org/download/313228/data/2012physicianspecialtydatabook.pdf. Published November 2012. Accessed September 1, 2014.
- , , , . Representation of women as authors, reviewers, editors in chief, and editorial board members at 6 general medical journals in 2010 and 2011. JAMA Intern Med. 2014;174:633–635.
- , , , et al. Relationships of gender and career motivation to medical faculty members' production of academic publications. Acad Med. 1998;73:180–186.
- , , , et al. Faculty perceptions of gender discrimination and sexual harassment in academic medicine. Ann Intern Med. 2000;132:889–896.
- , , , . Attitudes of clinical faculty about career progress, career success and recognition, and commitment to academic medicine. Results of a survey. Arch Intern Med. 2000;160:2625–2629.
- , , , , . A "ton of feathers": gender discrimination in academic medical careers and how to manage it. J Womens Health (Larchmt). 2003;12:1009–1018.
- , , . Perceived obstacles to career success for women in academic surgery. Arch Surg. 2000;135:972–977.
- , , , . Career satisfaction of US women physicians: results from the Women Physicians' Health Study. Society of General Internal Medicine Career Satisfaction Study Group. Arch Intern Med. 1999;159:1417–1426.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301–315.
- , , , , , . Gender differences in time spent on parenting and domestic responsibilities by high‐achieving young physician‐researchers. Ann Intern Med. 2014;160:344–353.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86:752–758.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28:201–207.
- . Gender pay gaps in hospital medicine. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/gender‐pay‐gaps‐in‐hospital‐medicine. Published February 29, 2012. Accessed September 1, 2014.
- , , . Mentoring in academic medicine: a systematic review. JAMA. 2006;296:1103–1115.
- . Inequality quantified: mind the gender gap. Nature. 2013;495:22–24.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78:500–508.
- , . Why aren't there more women leaders in academic medicine? The views of clinical department chairs. Acad Med. 2001;76:453–465.
- . Gender factors in reviewer recommendations for manuscript publication. J Appl Behav Anal. 1990;23:539–543.
- , , , . Scientific impact of women in academic surgery. J Surg Res. 2008;148:13–16.
- Association of American Medical Colleges. Women in U.S. academic medicine and science: Statistics and benchmarking report. 2012. Available at: https://members.aamc.org/eweb/upload/Women%20in%20U%20S%20%20Academic%20Medicine%20Statistics%20and%20Benchmarking%20Report%202011-20123.pdf. Accessed September 1, 2014.
- , , , et al. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Intern Med. 1998;129:532–538.
- , , , et al. The “gender gap” in authorship of academic medical literature—a 35‐year perspective. N Engl J Med. 2006;355:281–287.
- , , , , , . Sex differences in academic advancement. Results of a national study of pediatricians. N Engl J Med. 1996;335:1282–1289.
- . Women physicians in academic medicine: new insights from cohort studies. N Engl J Med. 2000;342:399–405.
- , , , , . Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad Med. 2011;86:43–47.
- , , , . Promotion of women physicians in academic medicine. Glass ceiling or sticky floor? JAMA. 1995;273:1022–1025.
- , , , . Compensation and advancement of women in academic medicine: is there equity? Ann Intern Med. 2004;141:205–212.
- , , . Women physicians: choosing a career in academic medicine. Acad Med. 2012;87:105–114.
- , , , . The status of women at one academic medical center. Breaking through the glass ceiling. JAMA. 1990;264:1813–1817.
- , . Status of women in academic anesthesiology. Anesthesiology. 1986;64:496–500.
- , , . The generation and gender shifts in medicine: an exploratory survey of internal medicine physicians. BMC Health Serv Res. 2006;6:55.
- Pew Research Center. On pay gap, millenial women near parity—for now. December 2013. Available at: http://www.pewsocialtrends.org/files/2013/12/gender-and-work_final.pdf. Published December 11, 2013. Accessed February 5, 2015.
- , . The emerging role of "hospitalists" in the American health care system. N Engl J Med. 1996;335:514–517.
- , , , , , . Mentorship, productivity, and promotion among academic hospitalists. J Gen Intern Med. 2012;27:23–27.
- . The gender factor. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/the‐gender‐factor. Published March 1, 2006. Accessed September 1, 2014.
- Association of American Medical Colleges. Analysis in brief: Supplemental information for estimating the number and characteristics of hospitalist physicians in the United States and their possible workforce implications. Available at: https://www.aamc.org/download/300686/data/aibvol12_no3-supplemental.pdf. Published August 2012. Accessed September 1, 2014.
- , , , . Survey of US academic hospitalist leaders about mentorship and academic activities in hospitalist groups. J Hosp Med. 2011;6:5–9.
- State of Hospital Medicine: 2011 Report Based on 2010 Data. Medical Group Management Association and Society of Hospital Medicine. www.mgma.com, www.hospitalmedicine.org.
- Today's Hospitalist Survey. Compensation and Career Survey Results. 2013. Available at: http://www.todayshospitalist.com/index.php?b=salary_survey_results. Accessed January 11, 2015.
- Association of American Medical Colleges. Women in U.S. Academic Medicine: Statistics and Benchmarking Report. 2009–2010. Available at: https://www.aamc.org/download/182674/data/gwims_stats_2009‐2010.pdf. Accessed September 1, 2014.
- American Medical Association. Graduate Medical Education Directory 2012–2013. Chicago, IL: American Medical Association; 2012:182–203.
- , , , , , . Research electronic data capture (REDCap)—a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381.
- Association of American Medical Colleges. 2012 Physician Specialty Data Book. Center for Workforce Studies. Available at: https://www.aamc.org/download/313228/data/2012physicianspecialtydatabook.pdf. Published November 2012. Accessed September 1, 2014.
- , , , . Representation of women as authors, reviewers, editors in chief, and editorial board members at 6 general medical journals in 2010 and 2011. JAMA Intern Med. 2014;174:633–635.
- , , , et al. Relationships of gender and career motivation to medical faculty members' production of academic publications. Acad Med. 1998;73:180–186.
- , , , et al. Faculty perceptions of gender discrimination and sexual harassment in academic medicine. Ann Intern Med. 2000;132:889–896.
- , , , . Attitudes of clinical faculty about career progress, career success and recognition, and commitment to academic medicine. Results of a survey. Arch Intern Med. 2000;160:2625–2629.
- , , , , . A "ton of feathers": gender discrimination in academic medical careers and how to manage it. J Womens Health (Larchmt). 2003;12:1009–1018.
- , , . Perceived obstacles to career success for women in academic surgery. Arch Surg. 2000;135:972–977.
- , , , . Career satisfaction of US women physicians: results from the Women Physicians' Health Study. Society of General Internal Medicine Career Satisfaction Study Group. Arch Intern Med. 1999;159:1417–1426.
- . Doing the same and earning less: male and female physicians in a new medical specialty. Inquiry. 2004;41:301–315.
- , , , , , . Gender differences in time spent on parenting and domestic responsibilities by high‐achieving young physician‐researchers. Ann Intern Med. 2014;160:344–353.
- , , , , . Stories from early‐career women physicians who have left academic medicine: a qualitative study at a single institution. Acad Med. 2011;86:752–758.
- , , , . The $16,819 pay gap for newly trained physicians: the unexplained trend of men earning more than women. Health Aff (Millwood). 2011;30:193–201.
- , , , , . Experiencing the culture of academic medicine: gender matters, a national study. J Gen Intern Med. 2013;28:201–207.
- . Gender pay gaps in hospital medicine. The Hospitalist. Available at: http://www.the‐hospitalist.org/article/gender‐pay‐gaps‐in‐hospital‐medicine. Published February 29, 2012. Accessed September 1, 2014.
- , , . Mentoring in academic medicine: a systematic review. JAMA. 2006;296:1103–1115.
- . Inequality quantified: mind the gender gap. Nature. 2013;495:22–24.
- , , , et al. Gender differences in academic advancement: patterns, causes, and potential solutions in one US College of Medicine. Acad Med. 2003;78:500–508.
- , . Why aren't there more women leaders in academic medicine? The views of clinical department chairs. Acad Med. 2001;76:453–465.
- . Gender factors in reviewer recommendations for manuscript publication. J Appl Behav Anal. 1990;23:539–543.
- , , , . Scientific impact of women in academic surgery. J Surg Res. 2008;148:13–16.
© 2015 Society of Hospital Medicine