User login
Isolated Sciatic Nerve Entrapment by Ectopic Bone After Femoral Head Fracture-Dislocation
Nonfatal Air Embolism During Shoulder Arthroscopy
Deep Vein Thrombosis and Pulmonary Embolism After Spine Surgery: Incidence and Patient Risk Factors
Vitamin D: When it helps, when it harms
Vitamin D is the new wonder cure and preventive for all kinds of ailments and chronic diseases. Or so it would seem from the popular press and Internet.1
But what do we actually know about the health benefits of vitamin D? Should we be screening patients for vitamin D deficiency? How much vitamin D should our patients consume daily? This Practice Alert answers these questions.
Vitamin D basics
Vitamin D is synthesized in the skin from cholesterol through sun exposure (vitamin D3) and consumed in food fortified with vitamin D2, such as milk, yogurt, and orange juice, or food that contains vitamin D3 (fatty fish and eggs). Both forms of vitamin D are inactive until metabolized in the liver to 25(OH)D (TABLE 1), which is further metabolized in the kidney to the biologically active calcitriol. The 25(OH)D circulates in the blood with a vitamin D–binding protein and is the basis of measurement of serum vitamin D levels.

The terminology of vitamin D
The metabolic actions of calcitriol include regulation of calcium and phosphate levels and maintenance of bone health. It also has a role in regulating cell proliferation and immune system functions. These last 2 activities are not well understood; still, they have led to the hypothesis that vitamin D may help prevent cancer, autoimmune conditions, and cardiovascular disease. Promotion of calcitriol for these purposes has yet to be supported by well-controlled clinical trials.
One more source…Vitamin D can also be found in multivitamin preparations at various dosages and is sold as a single vitamin supplement—sometimes in megadoses of up to 50,000 international units (IU).
How much vitamin D is enough?
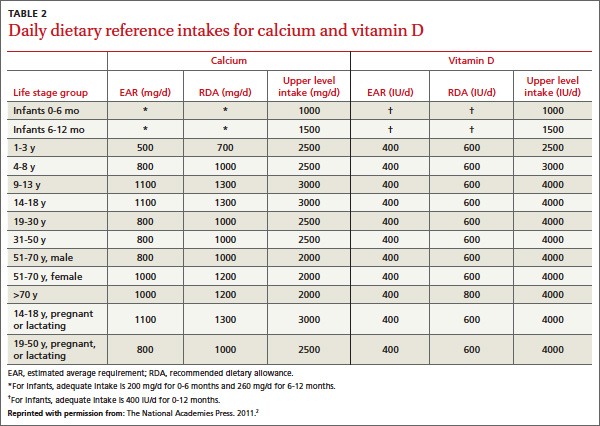
There is universal agreement that vitamin D and calcium are important for bone health. The Institute of Medicine (IOM) recently revised the recommended dietary allowance (RDA) of vitamin D, by age (TABLE 2).2 The IOM calculated the newer RDAs under the assumption that, in the United States and Canada, little or no vitamin D is obtained from sun exposure, particularly given anticancer campaigns that stress sun avoidance. The IOM committee also expressed concern, however, about high levels of vitamin D intake that have not been linked to any proven benefits but have been linked to harms.2 Excess vitamin D from oral intake (not from sun exposure, which is subject to autoregulatory mechanisms) can cause vitamin D intoxication, hypercalcemia, and kidney stones.
Daily dietary reference intakes for calcium and vitamin D
Recent systematic reviews and recommendations
The IOM reviewed the medical literature on the effects of vitamin D to prevent or treat cancer, cardiovascular disease, hypertension, diabetes, metabolic syndrome, falls, and preeclampsia; and to boost immune response, neuropsychological function, physical performance, and reproductive outcomes. The panel found that the evidence for all of these effects is mixed and inconclusive, even though the media often report a beneficial effect.2
Several Cochrane systematic reviews have yielded similar results. One looked at overall mortality in adults and found that vitamin D3 seems to decrease mortality, but mostly in elderly women in institutions and dependent-care settings. Vitamin D2 had no effect on mortality. Vitamin D3 and calcium significantly increased the incidence of kidney stones.3Another review examined the effect of vitamin D on chronic pain and concluded that there were only low-quality observational studies insufficient for drawing conclusions.4
The United States Preventive Services Task Force (USPSTF) recently released 2 recommendations related to vitamin D supplementation.5,6 It first recommends exercise or physical therapy and vitamin D supplementation (800 IU daily) to prevent falls in community-dwelling adults ≥65 years at increased risk for falls (described in a previous Practice Alert7). The second recommendation pertains to primary prevention of fractures and advises against daily supplementation with vitamin D and calcium at doses ≤400 IU and 1000 mg, respectively, for noninstitutionalized postmenopausal women. At these doses, supplementation with vitamin D and calcium does not prevent fractures but does cause kidney stones, with a number needed to harm of 273 over 7 years.6 The USPSTF concluded that the evidence is insufficient to assess the value of either vitamin D or calcium in men and premenopausal women at any dose, or daily supplementation with >400 IU of vitamin D3 and >1000 mg of calcium for the primary prevention of fractures in noninstitutionalized postmenopausal women.
What about screening for vitamin D deficiency?
The Endocrine Society recommends screening for vitamin D deficiency in individuals at risk FAST TRACK. The USPSTF recommends vitamin D supplementation at 800 IU/d to prevent falls in community-dwelling adults >65 years at increased risk for falls. for deficiency—ie, those who have darkly pigmented skin, live in northern latitudes, or receive little exposure to sun. It does not recommend population screening for vitamin D deficiency in individuals not at risk. It defines vitamin D deficiency as a 25(OH)D level <20 ng/mL (50 nmol/L) and vitamin D insufficiency as a 25(OH)D level of 21 to 29 ng/mL (52.5-72.5 nmol/L).8
The IOM expresses concern about testing for vitamin D levels because there is no validated cutoff, and some labs report cutoffs above what the IOM considers a deficient level, leading to inflated numbers of those labeled as deficient.2 The USPSTF is about to weigh in on this issue. It has posted a draft research plan that will guide its evidence report and recommendation considerations.9
Take-home message
Information on the health benefits of vitamin D is difficult to sort out. Evidence for anything other than bone health and fall prevention is problematic. Consider vitamin D supplements along with calcium for the frail elderly at risk for falls10and for those who have osteoporosis. Screening for vitamin D deficiency is of questionable value and the USPSTF will be producing an evidence-based report on this topic, which should be available in about a year. The IOM RDA tables are available to guide dietary advice.
1. Vitamin D Council. Available at: http://www.vitamindcouncil.org/health-conditions. Accessed May 7, 2013.
2. Institute of Medicine of the National Academies. Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press; 2011. Available at: http://www.nap.edu/catalog.php?record_id=13050. Accessed June 3, 2013.
3. Bjelakovic G, Gluud LL, Whitfield K, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2011;(7):CD007470.
4. Straube S, Derry S, Moore RA, et al. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst Rev. 2010;(1):CD007771.
5. USPSTF. Prevention of falls in community-dwelling older adults. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf/uspsfalls.htm. Accessed May 7, 2013.
6. USPSTF. Vitamin D and calcium supplementation to prevent fractures in adults. Available at: http://www.uspreventive
servicestaskforce.org/uspstf/uspsvitd.htm. Accessed May 7, 2013.
7. Campos-Outcalt D. The latest recommendations from the
USPSTF. J Fam Pract. 2013;62:249-252.
8. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency. J Clin Endocrinol Metab. 2011;96:1911-1930.
9. USPSTF. Draft research plan. Screening for vitamin D deficiency. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf13/vitddefic/vitddeficdraftresplan.htm. Accessed May 7, 2013.
10. Avenell A, Gillespie WJ, Gillespie LD, et al. Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis. Cochrane Database Syst Rev. 2009;(2):CD000227.
Vitamin D is the new wonder cure and preventive for all kinds of ailments and chronic diseases. Or so it would seem from the popular press and Internet.1
But what do we actually know about the health benefits of vitamin D? Should we be screening patients for vitamin D deficiency? How much vitamin D should our patients consume daily? This Practice Alert answers these questions.
Vitamin D basics
Vitamin D is synthesized in the skin from cholesterol through sun exposure (vitamin D3) and consumed in food fortified with vitamin D2, such as milk, yogurt, and orange juice, or food that contains vitamin D3 (fatty fish and eggs). Both forms of vitamin D are inactive until metabolized in the liver to 25(OH)D (TABLE 1), which is further metabolized in the kidney to the biologically active calcitriol. The 25(OH)D circulates in the blood with a vitamin D–binding protein and is the basis of measurement of serum vitamin D levels.
The terminology of vitamin D
The metabolic actions of calcitriol include regulation of calcium and phosphate levels and maintenance of bone health. It also has a role in regulating cell proliferation and immune system functions. These last 2 activities are not well understood; still, they have led to the hypothesis that vitamin D may help prevent cancer, autoimmune conditions, and cardiovascular disease. Promotion of calcitriol for these purposes has yet to be supported by well-controlled clinical trials.
One more source…Vitamin D can also be found in multivitamin preparations at various dosages and is sold as a single vitamin supplement—sometimes in megadoses of up to 50,000 international units (IU).
How much vitamin D is enough?
There is universal agreement that vitamin D and calcium are important for bone health. The Institute of Medicine (IOM) recently revised the recommended dietary allowance (RDA) of vitamin D, by age (TABLE 2).2 The IOM calculated the newer RDAs under the assumption that, in the United States and Canada, little or no vitamin D is obtained from sun exposure, particularly given anticancer campaigns that stress sun avoidance. The IOM committee also expressed concern, however, about high levels of vitamin D intake that have not been linked to any proven benefits but have been linked to harms.2 Excess vitamin D from oral intake (not from sun exposure, which is subject to autoregulatory mechanisms) can cause vitamin D intoxication, hypercalcemia, and kidney stones.
Daily dietary reference intakes for calcium and vitamin D
Recent systematic reviews and recommendations
The IOM reviewed the medical literature on the effects of vitamin D to prevent or treat cancer, cardiovascular disease, hypertension, diabetes, metabolic syndrome, falls, and preeclampsia; and to boost immune response, neuropsychological function, physical performance, and reproductive outcomes. The panel found that the evidence for all of these effects is mixed and inconclusive, even though the media often report a beneficial effect.2
Several Cochrane systematic reviews have yielded similar results. One looked at overall mortality in adults and found that vitamin D3 seems to decrease mortality, but mostly in elderly women in institutions and dependent-care settings. Vitamin D2 had no effect on mortality. Vitamin D3 and calcium significantly increased the incidence of kidney stones.3Another review examined the effect of vitamin D on chronic pain and concluded that there were only low-quality observational studies insufficient for drawing conclusions.4
The United States Preventive Services Task Force (USPSTF) recently released 2 recommendations related to vitamin D supplementation.5,6 It first recommends exercise or physical therapy and vitamin D supplementation (800 IU daily) to prevent falls in community-dwelling adults ≥65 years at increased risk for falls (described in a previous Practice Alert7). The second recommendation pertains to primary prevention of fractures and advises against daily supplementation with vitamin D and calcium at doses ≤400 IU and 1000 mg, respectively, for noninstitutionalized postmenopausal women. At these doses, supplementation with vitamin D and calcium does not prevent fractures but does cause kidney stones, with a number needed to harm of 273 over 7 years.6 The USPSTF concluded that the evidence is insufficient to assess the value of either vitamin D or calcium in men and premenopausal women at any dose, or daily supplementation with >400 IU of vitamin D3 and >1000 mg of calcium for the primary prevention of fractures in noninstitutionalized postmenopausal women.
What about screening for vitamin D deficiency?
The Endocrine Society recommends screening for vitamin D deficiency in individuals at risk FAST TRACK. The USPSTF recommends vitamin D supplementation at 800 IU/d to prevent falls in community-dwelling adults >65 years at increased risk for falls. for deficiency—ie, those who have darkly pigmented skin, live in northern latitudes, or receive little exposure to sun. It does not recommend population screening for vitamin D deficiency in individuals not at risk. It defines vitamin D deficiency as a 25(OH)D level <20 ng/mL (50 nmol/L) and vitamin D insufficiency as a 25(OH)D level of 21 to 29 ng/mL (52.5-72.5 nmol/L).8
The IOM expresses concern about testing for vitamin D levels because there is no validated cutoff, and some labs report cutoffs above what the IOM considers a deficient level, leading to inflated numbers of those labeled as deficient.2 The USPSTF is about to weigh in on this issue. It has posted a draft research plan that will guide its evidence report and recommendation considerations.9
Take-home message
Information on the health benefits of vitamin D is difficult to sort out. Evidence for anything other than bone health and fall prevention is problematic. Consider vitamin D supplements along with calcium for the frail elderly at risk for falls10and for those who have osteoporosis. Screening for vitamin D deficiency is of questionable value and the USPSTF will be producing an evidence-based report on this topic, which should be available in about a year. The IOM RDA tables are available to guide dietary advice.
Vitamin D is the new wonder cure and preventive for all kinds of ailments and chronic diseases. Or so it would seem from the popular press and Internet.1
But what do we actually know about the health benefits of vitamin D? Should we be screening patients for vitamin D deficiency? How much vitamin D should our patients consume daily? This Practice Alert answers these questions.
Vitamin D basics
Vitamin D is synthesized in the skin from cholesterol through sun exposure (vitamin D3) and consumed in food fortified with vitamin D2, such as milk, yogurt, and orange juice, or food that contains vitamin D3 (fatty fish and eggs). Both forms of vitamin D are inactive until metabolized in the liver to 25(OH)D (TABLE 1), which is further metabolized in the kidney to the biologically active calcitriol. The 25(OH)D circulates in the blood with a vitamin D–binding protein and is the basis of measurement of serum vitamin D levels.
The terminology of vitamin D
The metabolic actions of calcitriol include regulation of calcium and phosphate levels and maintenance of bone health. It also has a role in regulating cell proliferation and immune system functions. These last 2 activities are not well understood; still, they have led to the hypothesis that vitamin D may help prevent cancer, autoimmune conditions, and cardiovascular disease. Promotion of calcitriol for these purposes has yet to be supported by well-controlled clinical trials.
One more source…Vitamin D can also be found in multivitamin preparations at various dosages and is sold as a single vitamin supplement—sometimes in megadoses of up to 50,000 international units (IU).
How much vitamin D is enough?
There is universal agreement that vitamin D and calcium are important for bone health. The Institute of Medicine (IOM) recently revised the recommended dietary allowance (RDA) of vitamin D, by age (TABLE 2).2 The IOM calculated the newer RDAs under the assumption that, in the United States and Canada, little or no vitamin D is obtained from sun exposure, particularly given anticancer campaigns that stress sun avoidance. The IOM committee also expressed concern, however, about high levels of vitamin D intake that have not been linked to any proven benefits but have been linked to harms.2 Excess vitamin D from oral intake (not from sun exposure, which is subject to autoregulatory mechanisms) can cause vitamin D intoxication, hypercalcemia, and kidney stones.
Daily dietary reference intakes for calcium and vitamin D
Recent systematic reviews and recommendations
The IOM reviewed the medical literature on the effects of vitamin D to prevent or treat cancer, cardiovascular disease, hypertension, diabetes, metabolic syndrome, falls, and preeclampsia; and to boost immune response, neuropsychological function, physical performance, and reproductive outcomes. The panel found that the evidence for all of these effects is mixed and inconclusive, even though the media often report a beneficial effect.2
Several Cochrane systematic reviews have yielded similar results. One looked at overall mortality in adults and found that vitamin D3 seems to decrease mortality, but mostly in elderly women in institutions and dependent-care settings. Vitamin D2 had no effect on mortality. Vitamin D3 and calcium significantly increased the incidence of kidney stones.3Another review examined the effect of vitamin D on chronic pain and concluded that there were only low-quality observational studies insufficient for drawing conclusions.4
The United States Preventive Services Task Force (USPSTF) recently released 2 recommendations related to vitamin D supplementation.5,6 It first recommends exercise or physical therapy and vitamin D supplementation (800 IU daily) to prevent falls in community-dwelling adults ≥65 years at increased risk for falls (described in a previous Practice Alert7). The second recommendation pertains to primary prevention of fractures and advises against daily supplementation with vitamin D and calcium at doses ≤400 IU and 1000 mg, respectively, for noninstitutionalized postmenopausal women. At these doses, supplementation with vitamin D and calcium does not prevent fractures but does cause kidney stones, with a number needed to harm of 273 over 7 years.6 The USPSTF concluded that the evidence is insufficient to assess the value of either vitamin D or calcium in men and premenopausal women at any dose, or daily supplementation with >400 IU of vitamin D3 and >1000 mg of calcium for the primary prevention of fractures in noninstitutionalized postmenopausal women.
What about screening for vitamin D deficiency?
The Endocrine Society recommends screening for vitamin D deficiency in individuals at risk FAST TRACK. The USPSTF recommends vitamin D supplementation at 800 IU/d to prevent falls in community-dwelling adults >65 years at increased risk for falls. for deficiency—ie, those who have darkly pigmented skin, live in northern latitudes, or receive little exposure to sun. It does not recommend population screening for vitamin D deficiency in individuals not at risk. It defines vitamin D deficiency as a 25(OH)D level <20 ng/mL (50 nmol/L) and vitamin D insufficiency as a 25(OH)D level of 21 to 29 ng/mL (52.5-72.5 nmol/L).8
The IOM expresses concern about testing for vitamin D levels because there is no validated cutoff, and some labs report cutoffs above what the IOM considers a deficient level, leading to inflated numbers of those labeled as deficient.2 The USPSTF is about to weigh in on this issue. It has posted a draft research plan that will guide its evidence report and recommendation considerations.9
Take-home message
Information on the health benefits of vitamin D is difficult to sort out. Evidence for anything other than bone health and fall prevention is problematic. Consider vitamin D supplements along with calcium for the frail elderly at risk for falls10and for those who have osteoporosis. Screening for vitamin D deficiency is of questionable value and the USPSTF will be producing an evidence-based report on this topic, which should be available in about a year. The IOM RDA tables are available to guide dietary advice.
1. Vitamin D Council. Available at: http://www.vitamindcouncil.org/health-conditions. Accessed May 7, 2013.
2. Institute of Medicine of the National Academies. Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press; 2011. Available at: http://www.nap.edu/catalog.php?record_id=13050. Accessed June 3, 2013.
3. Bjelakovic G, Gluud LL, Whitfield K, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2011;(7):CD007470.
4. Straube S, Derry S, Moore RA, et al. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst Rev. 2010;(1):CD007771.
5. USPSTF. Prevention of falls in community-dwelling older adults. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf/uspsfalls.htm. Accessed May 7, 2013.
6. USPSTF. Vitamin D and calcium supplementation to prevent fractures in adults. Available at: http://www.uspreventive
servicestaskforce.org/uspstf/uspsvitd.htm. Accessed May 7, 2013.
7. Campos-Outcalt D. The latest recommendations from the
USPSTF. J Fam Pract. 2013;62:249-252.
8. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency. J Clin Endocrinol Metab. 2011;96:1911-1930.
9. USPSTF. Draft research plan. Screening for vitamin D deficiency. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf13/vitddefic/vitddeficdraftresplan.htm. Accessed May 7, 2013.
10. Avenell A, Gillespie WJ, Gillespie LD, et al. Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis. Cochrane Database Syst Rev. 2009;(2):CD000227.
1. Vitamin D Council. Available at: http://www.vitamindcouncil.org/health-conditions. Accessed May 7, 2013.
2. Institute of Medicine of the National Academies. Dietary reference intakes for calcium and vitamin D. Washington, DC: The National Academies Press; 2011. Available at: http://www.nap.edu/catalog.php?record_id=13050. Accessed June 3, 2013.
3. Bjelakovic G, Gluud LL, Whitfield K, et al. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst Rev. 2011;(7):CD007470.
4. Straube S, Derry S, Moore RA, et al. Vitamin D for the treatment of chronic painful conditions in adults. Cochrane Database Syst Rev. 2010;(1):CD007771.
5. USPSTF. Prevention of falls in community-dwelling older adults. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf/uspsfalls.htm. Accessed May 7, 2013.
6. USPSTF. Vitamin D and calcium supplementation to prevent fractures in adults. Available at: http://www.uspreventive
servicestaskforce.org/uspstf/uspsvitd.htm. Accessed May 7, 2013.
7. Campos-Outcalt D. The latest recommendations from the
USPSTF. J Fam Pract. 2013;62:249-252.
8. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency. J Clin Endocrinol Metab. 2011;96:1911-1930.
9. USPSTF. Draft research plan. Screening for vitamin D deficiency. Available at: http://www.uspreventiveservicestaskforce.org/
uspstf13/vitddefic/vitddeficdraftresplan.htm. Accessed May 7, 2013.
10. Avenell A, Gillespie WJ, Gillespie LD, et al. Vitamin D and vitamin D analogues for preventing fractures associated with involutional and post-menopausal osteoporosis. Cochrane Database Syst Rev. 2009;(2):CD000227.
How to manage emergencies associated with tocolysis for preterm labor
CASE 1: Preterm labor with cervical changes
Ms. M, a 42-year-old woman pregnant with her second child, begins having contractions at 30 weeks’ gestation. Examination reveals that her cervix is dilated 2 cm and effaced 50%. She is given subcutaneous terbutaline to suppress her contractions. Thirty minutes later, she complains of shortness of breath and chest pain. An electrocardiogram reveals depression of the ST segment, and a chest radiograph shows mild pulmonary edema.
How should her symptoms be managed?
Preterm labor precedes delivery in about 50% of preterm births. Approximately 33% of women who have preterm labor will experience spontaneous resolution, and more than 50% of women who have preterm labor will deliver at term. Although the use of tocolytic therapy has proved to be effective at temporarily suppressing uterine activity, it has not been shown to delay delivery for more than a few hours or days.1
The American College of Obstetricians and Gynecologists (ACOG) recommends the use of tocolytics only when a delay in labor for approximately 48 hours would improve outcome. Therefore, tocolytic therapy should be reserved for the following circumstances:
- to stop the progress of labor long enough to administer antenatal corticosteroid therapy
- to prolong pregnancy when there is an underlying self-limiting condition that can cause labor, such as pyelonephritis
- to provide time for safe transport to a facility with a higher level of neonatal care.2
Tocolytics are generally not indicated before the fetus is viable, although we lack data from randomized, controlled trials to support a specific recommendation. The approach is clearer when the fetus is near the upper limits of viability. Most studies suggest that 34 weeks’ gestation is the threshold at which the perinatal morbidity and mortality associated with delivery are too low to justify the cost and potential complications of tocolysis.3
Women who experience preterm labor without cervical changes generally should not be treated with tocolytics.2 Contraindications to tocolytic therapy include:
- lethal fetal anomaly
- nonreassuring fetal status
- maternal disease
- maternal hemorrhage with hemodynamic instability.
Beta-adrenergic agonists carry many risks
These agents have been studied in several randomized, controlled trials. Although ritodrine was approved as tocolytic therapy by the US Food and Drug Administration (FDA), it has since been removed from the US market. Terbutaline is still available but lacks FDA approval as a tocolytic.
Maternal side effects associated with beta-adrenergic agonists are thought to arise from stimulation of the beta-1 and beta-2 adrenergic receptors. Stimulation of the former increases maternal heart rate and stroke volume, whereas stimulation of the beta-2 adrenergic receptors causes the relaxation of smooth muscle, including the muscles of the myometrium, blood vessels, and bronchial tree. The resulting symptoms may include maternal tachycardia, cardiac arrhythmias, palpitations, and metabolic aberrations (including hyperglycemia, hypokalemia, and hypotension). Common symptoms associated with the administration of a beta-adrenergic agonist include tremor, shortness of breath, and chest discomfort.4 Although pulmonary edema and myocardial ischemia are uncommon, they can occur even when there is no history of underlying maternal disease.
Terbutaline has been linked to maternal deaths
Sixteen maternal deaths were reported following initial marketing of terbutaline in 1976 until 2009. Three of the 16 cases involved outpatient use of terbutaline administered by a subcutaneous pump, and nine cases involved use of oral terbutaline alone or in addition to subcutaneous or IV terbutaline. In addition, 12 cases of serious maternal cardiovascular events were reported in association with terbutaline. These events included cardiac arrhythmias, myocardial infarction, pulmonary edema, hypertension, and tachycardia.
Because of these events, the FDA issued a black box warning for terbutaline that prohibits its use in the treatment of preterm labor for longer than 48 to 72 hours in the inpatient or outpatient setting because of the potential for serious maternal heart problems and death.5 Oral terbutaline should be avoided entirely in the prevention and treatment of preterm labor. However, the use of terbutaline for the management of acute tachysystole with an abnormal fetal heart-rate (FHR) pattern remains a reasonable course of treatment.6
Fetal tachycardia is the most common side effect of beta-adrenergic receptor agonists. For this reason, use of these drugs is not recommended when changes in FHR may be the first sign of fetal compromise, such as in patients with hemorrhage or infection. Neonatal hypoglycemia may also occur if maternal hyperglycemia is not controlled.7
Case 1 Resolved
Terbutaline is discontinued, and the patient’s pulmonary edema is treated with a single dose of furosemide. Electrolyte abnormalities resolve with discontinuation of medication. The patient stabilizes. Once her cardiorespiratory status improves, her contractions lessen and the cervix remains unchanged. She requires no further tocolysis and is discharged home. She presents again at 38 weeks in spontaneous labor.
CASE 2: Preterm labor treated with indomethacin
Ms. J, age 23, is 26 weeks’ pregnant with her first child. When she experienced preterm labor at 24.5 weeks’ gestation, she was given indomethacin. Now, ultrasonographic imaging reveals decreased amniotic fluid volume.
How should she be managed?
Indomethacin is a cyclooxygenase (COX) inhibitor. These drugs reduce prostaglandin production through the general inhibition of cyclooxygenase or by a specific receptor.8 Indomethacin is the most commonly used tocolytic in this class. It is a nonspecific COX inhibitor, as opposed to a COX-2 inhibitor. The latter has been associated with serious adverse outcomes in the nonobstetric population. COX-2 inhibitors now carry a black box warning or are no longer available.
Maternal contraindications for COX inhibitors include asthma, bleeding disorders, and significant renal dysfunction.
Although maternal side effects with COX inhibitors are usually mild, fetal side effects may be serious enough to cause perinatal morbidity or death.9
How indomethacin can lead to oligohydramnios
Maternal administration of indomethacin or ibuprofen can reduce fetal urine output and decrease the volume of amniotic fluid. In most cases, oligohydramnios occurs when indomethacin or ibuprofen has been given for more than 72 hours. For this reason, long-term use of a COX inhibitor should be accompanied by frequent monitoring of amniotic fluid volume by ultrasonography.
The most serious fetal complication associated with prolonged indomethacin administration (longer than 72 hours) is premature constriction of the ductus arteriosus. Ductal constriction appears to be contingent on gestational age. It has been described as early as 24 weeks’ gestation but is most common after 31 or 32 weeks. Therefore, indomethacin is not recommended for use after 32 weeks’ gestation.10
CASE 2 Resolved
The indomethacin is discontinued as soon as the decreased amniotic fluid is noted. The fluid volume returns to normal over the next 3 to 5 days. Because of the early gestational age, nifedipine is given to suppress contractions, and the patient has no further complications.
CASE 3: Preterm labor and magnesium intoxication
Ms. K experiences contractions and rapid cervical change at 32 weeks’ gestation. She is given magnesium for the preterm labor and fetal neuroprophylaxis, with nifedipine, a calcium-channel blocker, added as second-line tocolysis. Approximately 8 hours later, she reports difficulty breathing and moving.
How should her obstetrician proceed?
Calcium-channel blockers such as nifedipine are used for acute and maintenance tocolysis. This class of drugs is often selected for its relative ease of use and safety, as it has few maternal and fetal side effects. However, concomitant use of a calcium-channel blocker and magnesium sulfate can sometimes lead to neuromuscular blockade and significant respiratory depression, even necessitating mechanical ventilation.9 Treatment of these effects includes IV administration of 10% calcium gluconate (5–10 mEq), which usually reverses respiratory depression and heart block caused by magnesium intoxication. In extreme cases, peritoneal dialysis or hemodialysis may be required.
CASE 3 Resolved
The patient is given 10% calcium gluconate in the dosage described above, and she stabilizes. However, her contractions continue and she delivers at 32 weeks’ gestation. The infant does well in the NICU.
CASE 4: Preterm labor in a woman with kidney dysfunction
Ms. F, age 40, presents at 30 weeks’ gestation with regular contractions and cervical dilation of more than 3 cm. She also reports a history of kidney disease.
What steps are recommended prior to the initiation of magnesium therapy?
Magnesium sulfate has been used for more than 40 years to treat preterm labor and is still considered a first-line therapy in many centers. Although maternal side effects usually are mild, an adverse event may occur if the patient is not monitored carefully. An absence of deep-tendon reflexes should alert the clinician that magnesium levels need to be measured. Reflexes usually are lost at a serum level of 10 mEq/L or higher. When the magnesium level exceeds 13 mEq/L, cardiac arrest is a risk. IV calcium should be administered immediately in such patients.
Magnesium should be used with caution in patients with myocardial compromise. Because magnesium is eliminated by the kidneys, women with impaired renal function may experience magnesium toxicity at normal doses. If a patient has a creatinine level above 1 mg/dL, consider alternative treatment for her preterm labor. If magnesium is given, the normal loading dose (4–6 g) is appropriate, but the maintenance dose should be reduced.11
Fetal effects of magnesium sulfate
Recent studies indicate that predelivery magnesium may offer fetal neuroprotection. The minimum duration of administration for such neuroprotection is unknown but is less than 24 hours.8
Although magnesium can alter FHR patterns slightly, these changes are not clinically significant. Magnesium can also cause mild neonatal suppression at the time of delivery, but its effects quickly resolve with appropriate neonatal resuscitation. Long-term (>5 days) therapy is not recommended.
In May 2013, the FDA issued a warning about the risk of neonatal complications with long-term maternal magnesium administration. These complications include osteopenia, low calcium, and bone fracture. The pregnancy category for magnesium sulfate will be changed from “A” to “D” because of these teratogenic effects.12
CASE 4 Resolved
Because magnesium is mainly cleared by renal excretion, the clinician administers the medication with caution in this patient with reduced renal function. The clinician administers the same 4- to 6-g bolus that would be given a patient with normal kidney function, but the maintenance dose is reduced to 1 g. Magnesium levels are obtained every 12 hours or when clinically indicated.
Bottom line: Be ready to act
The short-term use of tocolytic therapy usually is not associated with maternal or fetal complications. After initial administration, maintenance tocolytic therapy probably does not prolong gestation.
Given the potential for harm without additional fetal benefit associated with extended therapy, I recommend that clinicians follow current clinical guidelines from ACOG for use of tocolytic agents. In the process, be vigilant for complications and be ready to act appropriately. Keep maternal and fetal conditions in mind when selecting a tocolytic agent.
9. US Food and Drug Administration. Terbutaline: Label Change—Warnings Against Use for Treatment of Preterm Labor. Published February 17, 2011. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyalertsforHumanMedicalProducts/ucm243843.htm. Accessed June 17, 2013.
12. US Food and Drug Administration. Magnesium Sulfate: Drug Safety Communication—Recommendation against Prolonged Use in Preterm Labor. Published May 30, 2013. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm354603.htm. Accessed June 17, 2013.
CASE 1: Preterm labor with cervical changes
Ms. M, a 42-year-old woman pregnant with her second child, begins having contractions at 30 weeks’ gestation. Examination reveals that her cervix is dilated 2 cm and effaced 50%. She is given subcutaneous terbutaline to suppress her contractions. Thirty minutes later, she complains of shortness of breath and chest pain. An electrocardiogram reveals depression of the ST segment, and a chest radiograph shows mild pulmonary edema.
How should her symptoms be managed?
Preterm labor precedes delivery in about 50% of preterm births. Approximately 33% of women who have preterm labor will experience spontaneous resolution, and more than 50% of women who have preterm labor will deliver at term. Although the use of tocolytic therapy has proved to be effective at temporarily suppressing uterine activity, it has not been shown to delay delivery for more than a few hours or days.1
The American College of Obstetricians and Gynecologists (ACOG) recommends the use of tocolytics only when a delay in labor for approximately 48 hours would improve outcome. Therefore, tocolytic therapy should be reserved for the following circumstances:
- to stop the progress of labor long enough to administer antenatal corticosteroid therapy
- to prolong pregnancy when there is an underlying self-limiting condition that can cause labor, such as pyelonephritis
- to provide time for safe transport to a facility with a higher level of neonatal care.2
Tocolytics are generally not indicated before the fetus is viable, although we lack data from randomized, controlled trials to support a specific recommendation. The approach is clearer when the fetus is near the upper limits of viability. Most studies suggest that 34 weeks’ gestation is the threshold at which the perinatal morbidity and mortality associated with delivery are too low to justify the cost and potential complications of tocolysis.3
Women who experience preterm labor without cervical changes generally should not be treated with tocolytics.2 Contraindications to tocolytic therapy include:
- lethal fetal anomaly
- nonreassuring fetal status
- maternal disease
- maternal hemorrhage with hemodynamic instability.
Beta-adrenergic agonists carry many risks
These agents have been studied in several randomized, controlled trials. Although ritodrine was approved as tocolytic therapy by the US Food and Drug Administration (FDA), it has since been removed from the US market. Terbutaline is still available but lacks FDA approval as a tocolytic.
Maternal side effects associated with beta-adrenergic agonists are thought to arise from stimulation of the beta-1 and beta-2 adrenergic receptors. Stimulation of the former increases maternal heart rate and stroke volume, whereas stimulation of the beta-2 adrenergic receptors causes the relaxation of smooth muscle, including the muscles of the myometrium, blood vessels, and bronchial tree. The resulting symptoms may include maternal tachycardia, cardiac arrhythmias, palpitations, and metabolic aberrations (including hyperglycemia, hypokalemia, and hypotension). Common symptoms associated with the administration of a beta-adrenergic agonist include tremor, shortness of breath, and chest discomfort.4 Although pulmonary edema and myocardial ischemia are uncommon, they can occur even when there is no history of underlying maternal disease.
Terbutaline has been linked to maternal deaths
Sixteen maternal deaths were reported following initial marketing of terbutaline in 1976 until 2009. Three of the 16 cases involved outpatient use of terbutaline administered by a subcutaneous pump, and nine cases involved use of oral terbutaline alone or in addition to subcutaneous or IV terbutaline. In addition, 12 cases of serious maternal cardiovascular events were reported in association with terbutaline. These events included cardiac arrhythmias, myocardial infarction, pulmonary edema, hypertension, and tachycardia.
Because of these events, the FDA issued a black box warning for terbutaline that prohibits its use in the treatment of preterm labor for longer than 48 to 72 hours in the inpatient or outpatient setting because of the potential for serious maternal heart problems and death.5 Oral terbutaline should be avoided entirely in the prevention and treatment of preterm labor. However, the use of terbutaline for the management of acute tachysystole with an abnormal fetal heart-rate (FHR) pattern remains a reasonable course of treatment.6
Fetal tachycardia is the most common side effect of beta-adrenergic receptor agonists. For this reason, use of these drugs is not recommended when changes in FHR may be the first sign of fetal compromise, such as in patients with hemorrhage or infection. Neonatal hypoglycemia may also occur if maternal hyperglycemia is not controlled.7
Case 1 Resolved
Terbutaline is discontinued, and the patient’s pulmonary edema is treated with a single dose of furosemide. Electrolyte abnormalities resolve with discontinuation of medication. The patient stabilizes. Once her cardiorespiratory status improves, her contractions lessen and the cervix remains unchanged. She requires no further tocolysis and is discharged home. She presents again at 38 weeks in spontaneous labor.
CASE 2: Preterm labor treated with indomethacin
Ms. J, age 23, is 26 weeks’ pregnant with her first child. When she experienced preterm labor at 24.5 weeks’ gestation, she was given indomethacin. Now, ultrasonographic imaging reveals decreased amniotic fluid volume.
How should she be managed?
Indomethacin is a cyclooxygenase (COX) inhibitor. These drugs reduce prostaglandin production through the general inhibition of cyclooxygenase or by a specific receptor.8 Indomethacin is the most commonly used tocolytic in this class. It is a nonspecific COX inhibitor, as opposed to a COX-2 inhibitor. The latter has been associated with serious adverse outcomes in the nonobstetric population. COX-2 inhibitors now carry a black box warning or are no longer available.
Maternal contraindications for COX inhibitors include asthma, bleeding disorders, and significant renal dysfunction.
Although maternal side effects with COX inhibitors are usually mild, fetal side effects may be serious enough to cause perinatal morbidity or death.9
How indomethacin can lead to oligohydramnios
Maternal administration of indomethacin or ibuprofen can reduce fetal urine output and decrease the volume of amniotic fluid. In most cases, oligohydramnios occurs when indomethacin or ibuprofen has been given for more than 72 hours. For this reason, long-term use of a COX inhibitor should be accompanied by frequent monitoring of amniotic fluid volume by ultrasonography.
The most serious fetal complication associated with prolonged indomethacin administration (longer than 72 hours) is premature constriction of the ductus arteriosus. Ductal constriction appears to be contingent on gestational age. It has been described as early as 24 weeks’ gestation but is most common after 31 or 32 weeks. Therefore, indomethacin is not recommended for use after 32 weeks’ gestation.10
CASE 2 Resolved
The indomethacin is discontinued as soon as the decreased amniotic fluid is noted. The fluid volume returns to normal over the next 3 to 5 days. Because of the early gestational age, nifedipine is given to suppress contractions, and the patient has no further complications.
CASE 3: Preterm labor and magnesium intoxication
Ms. K experiences contractions and rapid cervical change at 32 weeks’ gestation. She is given magnesium for the preterm labor and fetal neuroprophylaxis, with nifedipine, a calcium-channel blocker, added as second-line tocolysis. Approximately 8 hours later, she reports difficulty breathing and moving.
How should her obstetrician proceed?
Calcium-channel blockers such as nifedipine are used for acute and maintenance tocolysis. This class of drugs is often selected for its relative ease of use and safety, as it has few maternal and fetal side effects. However, concomitant use of a calcium-channel blocker and magnesium sulfate can sometimes lead to neuromuscular blockade and significant respiratory depression, even necessitating mechanical ventilation.9 Treatment of these effects includes IV administration of 10% calcium gluconate (5–10 mEq), which usually reverses respiratory depression and heart block caused by magnesium intoxication. In extreme cases, peritoneal dialysis or hemodialysis may be required.
CASE 3 Resolved
The patient is given 10% calcium gluconate in the dosage described above, and she stabilizes. However, her contractions continue and she delivers at 32 weeks’ gestation. The infant does well in the NICU.
CASE 4: Preterm labor in a woman with kidney dysfunction
Ms. F, age 40, presents at 30 weeks’ gestation with regular contractions and cervical dilation of more than 3 cm. She also reports a history of kidney disease.
What steps are recommended prior to the initiation of magnesium therapy?
Magnesium sulfate has been used for more than 40 years to treat preterm labor and is still considered a first-line therapy in many centers. Although maternal side effects usually are mild, an adverse event may occur if the patient is not monitored carefully. An absence of deep-tendon reflexes should alert the clinician that magnesium levels need to be measured. Reflexes usually are lost at a serum level of 10 mEq/L or higher. When the magnesium level exceeds 13 mEq/L, cardiac arrest is a risk. IV calcium should be administered immediately in such patients.
Magnesium should be used with caution in patients with myocardial compromise. Because magnesium is eliminated by the kidneys, women with impaired renal function may experience magnesium toxicity at normal doses. If a patient has a creatinine level above 1 mg/dL, consider alternative treatment for her preterm labor. If magnesium is given, the normal loading dose (4–6 g) is appropriate, but the maintenance dose should be reduced.11
Fetal effects of magnesium sulfate
Recent studies indicate that predelivery magnesium may offer fetal neuroprotection. The minimum duration of administration for such neuroprotection is unknown but is less than 24 hours.8
Although magnesium can alter FHR patterns slightly, these changes are not clinically significant. Magnesium can also cause mild neonatal suppression at the time of delivery, but its effects quickly resolve with appropriate neonatal resuscitation. Long-term (>5 days) therapy is not recommended.
In May 2013, the FDA issued a warning about the risk of neonatal complications with long-term maternal magnesium administration. These complications include osteopenia, low calcium, and bone fracture. The pregnancy category for magnesium sulfate will be changed from “A” to “D” because of these teratogenic effects.12
CASE 4 Resolved
Because magnesium is mainly cleared by renal excretion, the clinician administers the medication with caution in this patient with reduced renal function. The clinician administers the same 4- to 6-g bolus that would be given a patient with normal kidney function, but the maintenance dose is reduced to 1 g. Magnesium levels are obtained every 12 hours or when clinically indicated.
Bottom line: Be ready to act
The short-term use of tocolytic therapy usually is not associated with maternal or fetal complications. After initial administration, maintenance tocolytic therapy probably does not prolong gestation.
Given the potential for harm without additional fetal benefit associated with extended therapy, I recommend that clinicians follow current clinical guidelines from ACOG for use of tocolytic agents. In the process, be vigilant for complications and be ready to act appropriately. Keep maternal and fetal conditions in mind when selecting a tocolytic agent.
CASE 1: Preterm labor with cervical changes
Ms. M, a 42-year-old woman pregnant with her second child, begins having contractions at 30 weeks’ gestation. Examination reveals that her cervix is dilated 2 cm and effaced 50%. She is given subcutaneous terbutaline to suppress her contractions. Thirty minutes later, she complains of shortness of breath and chest pain. An electrocardiogram reveals depression of the ST segment, and a chest radiograph shows mild pulmonary edema.
How should her symptoms be managed?
Preterm labor precedes delivery in about 50% of preterm births. Approximately 33% of women who have preterm labor will experience spontaneous resolution, and more than 50% of women who have preterm labor will deliver at term. Although the use of tocolytic therapy has proved to be effective at temporarily suppressing uterine activity, it has not been shown to delay delivery for more than a few hours or days.1
The American College of Obstetricians and Gynecologists (ACOG) recommends the use of tocolytics only when a delay in labor for approximately 48 hours would improve outcome. Therefore, tocolytic therapy should be reserved for the following circumstances:
- to stop the progress of labor long enough to administer antenatal corticosteroid therapy
- to prolong pregnancy when there is an underlying self-limiting condition that can cause labor, such as pyelonephritis
- to provide time for safe transport to a facility with a higher level of neonatal care.2
Tocolytics are generally not indicated before the fetus is viable, although we lack data from randomized, controlled trials to support a specific recommendation. The approach is clearer when the fetus is near the upper limits of viability. Most studies suggest that 34 weeks’ gestation is the threshold at which the perinatal morbidity and mortality associated with delivery are too low to justify the cost and potential complications of tocolysis.3
Women who experience preterm labor without cervical changes generally should not be treated with tocolytics.2 Contraindications to tocolytic therapy include:
- lethal fetal anomaly
- nonreassuring fetal status
- maternal disease
- maternal hemorrhage with hemodynamic instability.
Beta-adrenergic agonists carry many risks
These agents have been studied in several randomized, controlled trials. Although ritodrine was approved as tocolytic therapy by the US Food and Drug Administration (FDA), it has since been removed from the US market. Terbutaline is still available but lacks FDA approval as a tocolytic.
Maternal side effects associated with beta-adrenergic agonists are thought to arise from stimulation of the beta-1 and beta-2 adrenergic receptors. Stimulation of the former increases maternal heart rate and stroke volume, whereas stimulation of the beta-2 adrenergic receptors causes the relaxation of smooth muscle, including the muscles of the myometrium, blood vessels, and bronchial tree. The resulting symptoms may include maternal tachycardia, cardiac arrhythmias, palpitations, and metabolic aberrations (including hyperglycemia, hypokalemia, and hypotension). Common symptoms associated with the administration of a beta-adrenergic agonist include tremor, shortness of breath, and chest discomfort.4 Although pulmonary edema and myocardial ischemia are uncommon, they can occur even when there is no history of underlying maternal disease.
Terbutaline has been linked to maternal deaths
Sixteen maternal deaths were reported following initial marketing of terbutaline in 1976 until 2009. Three of the 16 cases involved outpatient use of terbutaline administered by a subcutaneous pump, and nine cases involved use of oral terbutaline alone or in addition to subcutaneous or IV terbutaline. In addition, 12 cases of serious maternal cardiovascular events were reported in association with terbutaline. These events included cardiac arrhythmias, myocardial infarction, pulmonary edema, hypertension, and tachycardia.
Because of these events, the FDA issued a black box warning for terbutaline that prohibits its use in the treatment of preterm labor for longer than 48 to 72 hours in the inpatient or outpatient setting because of the potential for serious maternal heart problems and death.5 Oral terbutaline should be avoided entirely in the prevention and treatment of preterm labor. However, the use of terbutaline for the management of acute tachysystole with an abnormal fetal heart-rate (FHR) pattern remains a reasonable course of treatment.6
Fetal tachycardia is the most common side effect of beta-adrenergic receptor agonists. For this reason, use of these drugs is not recommended when changes in FHR may be the first sign of fetal compromise, such as in patients with hemorrhage or infection. Neonatal hypoglycemia may also occur if maternal hyperglycemia is not controlled.7
Case 1 Resolved
Terbutaline is discontinued, and the patient’s pulmonary edema is treated with a single dose of furosemide. Electrolyte abnormalities resolve with discontinuation of medication. The patient stabilizes. Once her cardiorespiratory status improves, her contractions lessen and the cervix remains unchanged. She requires no further tocolysis and is discharged home. She presents again at 38 weeks in spontaneous labor.
CASE 2: Preterm labor treated with indomethacin
Ms. J, age 23, is 26 weeks’ pregnant with her first child. When she experienced preterm labor at 24.5 weeks’ gestation, she was given indomethacin. Now, ultrasonographic imaging reveals decreased amniotic fluid volume.
How should she be managed?
Indomethacin is a cyclooxygenase (COX) inhibitor. These drugs reduce prostaglandin production through the general inhibition of cyclooxygenase or by a specific receptor.8 Indomethacin is the most commonly used tocolytic in this class. It is a nonspecific COX inhibitor, as opposed to a COX-2 inhibitor. The latter has been associated with serious adverse outcomes in the nonobstetric population. COX-2 inhibitors now carry a black box warning or are no longer available.
Maternal contraindications for COX inhibitors include asthma, bleeding disorders, and significant renal dysfunction.
Although maternal side effects with COX inhibitors are usually mild, fetal side effects may be serious enough to cause perinatal morbidity or death.9
How indomethacin can lead to oligohydramnios
Maternal administration of indomethacin or ibuprofen can reduce fetal urine output and decrease the volume of amniotic fluid. In most cases, oligohydramnios occurs when indomethacin or ibuprofen has been given for more than 72 hours. For this reason, long-term use of a COX inhibitor should be accompanied by frequent monitoring of amniotic fluid volume by ultrasonography.
The most serious fetal complication associated with prolonged indomethacin administration (longer than 72 hours) is premature constriction of the ductus arteriosus. Ductal constriction appears to be contingent on gestational age. It has been described as early as 24 weeks’ gestation but is most common after 31 or 32 weeks. Therefore, indomethacin is not recommended for use after 32 weeks’ gestation.10
CASE 2 Resolved
The indomethacin is discontinued as soon as the decreased amniotic fluid is noted. The fluid volume returns to normal over the next 3 to 5 days. Because of the early gestational age, nifedipine is given to suppress contractions, and the patient has no further complications.
CASE 3: Preterm labor and magnesium intoxication
Ms. K experiences contractions and rapid cervical change at 32 weeks’ gestation. She is given magnesium for the preterm labor and fetal neuroprophylaxis, with nifedipine, a calcium-channel blocker, added as second-line tocolysis. Approximately 8 hours later, she reports difficulty breathing and moving.
How should her obstetrician proceed?
Calcium-channel blockers such as nifedipine are used for acute and maintenance tocolysis. This class of drugs is often selected for its relative ease of use and safety, as it has few maternal and fetal side effects. However, concomitant use of a calcium-channel blocker and magnesium sulfate can sometimes lead to neuromuscular blockade and significant respiratory depression, even necessitating mechanical ventilation.9 Treatment of these effects includes IV administration of 10% calcium gluconate (5–10 mEq), which usually reverses respiratory depression and heart block caused by magnesium intoxication. In extreme cases, peritoneal dialysis or hemodialysis may be required.
CASE 3 Resolved
The patient is given 10% calcium gluconate in the dosage described above, and she stabilizes. However, her contractions continue and she delivers at 32 weeks’ gestation. The infant does well in the NICU.
CASE 4: Preterm labor in a woman with kidney dysfunction
Ms. F, age 40, presents at 30 weeks’ gestation with regular contractions and cervical dilation of more than 3 cm. She also reports a history of kidney disease.
What steps are recommended prior to the initiation of magnesium therapy?
Magnesium sulfate has been used for more than 40 years to treat preterm labor and is still considered a first-line therapy in many centers. Although maternal side effects usually are mild, an adverse event may occur if the patient is not monitored carefully. An absence of deep-tendon reflexes should alert the clinician that magnesium levels need to be measured. Reflexes usually are lost at a serum level of 10 mEq/L or higher. When the magnesium level exceeds 13 mEq/L, cardiac arrest is a risk. IV calcium should be administered immediately in such patients.
Magnesium should be used with caution in patients with myocardial compromise. Because magnesium is eliminated by the kidneys, women with impaired renal function may experience magnesium toxicity at normal doses. If a patient has a creatinine level above 1 mg/dL, consider alternative treatment for her preterm labor. If magnesium is given, the normal loading dose (4–6 g) is appropriate, but the maintenance dose should be reduced.11
Fetal effects of magnesium sulfate
Recent studies indicate that predelivery magnesium may offer fetal neuroprotection. The minimum duration of administration for such neuroprotection is unknown but is less than 24 hours.8
Although magnesium can alter FHR patterns slightly, these changes are not clinically significant. Magnesium can also cause mild neonatal suppression at the time of delivery, but its effects quickly resolve with appropriate neonatal resuscitation. Long-term (>5 days) therapy is not recommended.
In May 2013, the FDA issued a warning about the risk of neonatal complications with long-term maternal magnesium administration. These complications include osteopenia, low calcium, and bone fracture. The pregnancy category for magnesium sulfate will be changed from “A” to “D” because of these teratogenic effects.12
CASE 4 Resolved
Because magnesium is mainly cleared by renal excretion, the clinician administers the medication with caution in this patient with reduced renal function. The clinician administers the same 4- to 6-g bolus that would be given a patient with normal kidney function, but the maintenance dose is reduced to 1 g. Magnesium levels are obtained every 12 hours or when clinically indicated.
Bottom line: Be ready to act
The short-term use of tocolytic therapy usually is not associated with maternal or fetal complications. After initial administration, maintenance tocolytic therapy probably does not prolong gestation.
Given the potential for harm without additional fetal benefit associated with extended therapy, I recommend that clinicians follow current clinical guidelines from ACOG for use of tocolytic agents. In the process, be vigilant for complications and be ready to act appropriately. Keep maternal and fetal conditions in mind when selecting a tocolytic agent.
9. US Food and Drug Administration. Terbutaline: Label Change—Warnings Against Use for Treatment of Preterm Labor. Published February 17, 2011. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyalertsforHumanMedicalProducts/ucm243843.htm. Accessed June 17, 2013.
12. US Food and Drug Administration. Magnesium Sulfate: Drug Safety Communication—Recommendation against Prolonged Use in Preterm Labor. Published May 30, 2013. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm354603.htm. Accessed June 17, 2013.
9. US Food and Drug Administration. Terbutaline: Label Change—Warnings Against Use for Treatment of Preterm Labor. Published February 17, 2011. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyalertsforHumanMedicalProducts/ucm243843.htm. Accessed June 17, 2013.
12. US Food and Drug Administration. Magnesium Sulfate: Drug Safety Communication—Recommendation against Prolonged Use in Preterm Labor. Published May 30, 2013. http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm354603.htm. Accessed June 17, 2013.
Beta-adrenergic agonists carry many risks
Fetal effects of magnesium sulfate
Do cosmetic breast implants hinder the detection of malignancy and reduce breast cancer–specific survival?
Most epidemiologic studies have found no elevated risk of breast cancer among women who undergo cosmetic breast augmentation. However, there is concern that implants, which are radio-opaque, may limit our ability to diagnose malignancies at an early stage using screening mammography.
In this study, investigators compared the stage distribution of breast cancers at diagnosis and documented breast cancer–specific survival among women with and without cosmetic breast implants. Twelve cross-sectional studies published after 2000 in the United States had evaluated stage distribution of breast cancer among women with and without cosmetic implants. As stated above, investigators found an elevated risk of nonlocalized breast cancer among women with implants in their meta-analysis of these studies (OR, 1.26), but this elevated risk did not achieve statistical significance. A second analysis of five studies found an elevated risk of breast cancer–specific mortality (OR, 1.38), compared with the general population (no implants), which did achieve significance.
MRI may be helpful—but is the expense justified?
More than 300,000 women underwent cosmetic breast augmentation in 2011 in the United States, an increase of roughly 800% since the early 1990s. The impaired visualization of breast tissue via mammography in these women ranges from 22% to 83%. In addition, the implants limit compression of the breasts during mammography, and capsular contraction further contributes to this problem.
Magnetic resonance imaging (MRI) may be helpful in screening women with cosmetic breast implants, but this technology is expensive, and evidence supporting its routine use in this population is limited.
Some mammographers use special techniques to better visualize the breast tissue of women with implants. These techniques include displacing the implant posteriorly and pulling the breast tissue in front of it. However, even with such strategies, as much as one-third of the breast tissue may be inadequately assessed.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
These findings underscore the importance of sharing the risks of nonlocalized breast malignancy and increased breast cancer mortality with patients who are considering cosmetic breast implants, as well as with women who have already undergone this common procedure. Future studies are needed to address relevant issues, including the role of 3-D (tomosynthesis) technology in screening women with breast implants and optimal screening intervals in this subgroup.
ANDREW M. KAUNITZ, MD
We want to hear from you. Tell us what you think.
Most epidemiologic studies have found no elevated risk of breast cancer among women who undergo cosmetic breast augmentation. However, there is concern that implants, which are radio-opaque, may limit our ability to diagnose malignancies at an early stage using screening mammography.
In this study, investigators compared the stage distribution of breast cancers at diagnosis and documented breast cancer–specific survival among women with and without cosmetic breast implants. Twelve cross-sectional studies published after 2000 in the United States had evaluated stage distribution of breast cancer among women with and without cosmetic implants. As stated above, investigators found an elevated risk of nonlocalized breast cancer among women with implants in their meta-analysis of these studies (OR, 1.26), but this elevated risk did not achieve statistical significance. A second analysis of five studies found an elevated risk of breast cancer–specific mortality (OR, 1.38), compared with the general population (no implants), which did achieve significance.
MRI may be helpful—but is the expense justified?
More than 300,000 women underwent cosmetic breast augmentation in 2011 in the United States, an increase of roughly 800% since the early 1990s. The impaired visualization of breast tissue via mammography in these women ranges from 22% to 83%. In addition, the implants limit compression of the breasts during mammography, and capsular contraction further contributes to this problem.
Magnetic resonance imaging (MRI) may be helpful in screening women with cosmetic breast implants, but this technology is expensive, and evidence supporting its routine use in this population is limited.
Some mammographers use special techniques to better visualize the breast tissue of women with implants. These techniques include displacing the implant posteriorly and pulling the breast tissue in front of it. However, even with such strategies, as much as one-third of the breast tissue may be inadequately assessed.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
These findings underscore the importance of sharing the risks of nonlocalized breast malignancy and increased breast cancer mortality with patients who are considering cosmetic breast implants, as well as with women who have already undergone this common procedure. Future studies are needed to address relevant issues, including the role of 3-D (tomosynthesis) technology in screening women with breast implants and optimal screening intervals in this subgroup.
ANDREW M. KAUNITZ, MD
We want to hear from you. Tell us what you think.
Most epidemiologic studies have found no elevated risk of breast cancer among women who undergo cosmetic breast augmentation. However, there is concern that implants, which are radio-opaque, may limit our ability to diagnose malignancies at an early stage using screening mammography.
In this study, investigators compared the stage distribution of breast cancers at diagnosis and documented breast cancer–specific survival among women with and without cosmetic breast implants. Twelve cross-sectional studies published after 2000 in the United States had evaluated stage distribution of breast cancer among women with and without cosmetic implants. As stated above, investigators found an elevated risk of nonlocalized breast cancer among women with implants in their meta-analysis of these studies (OR, 1.26), but this elevated risk did not achieve statistical significance. A second analysis of five studies found an elevated risk of breast cancer–specific mortality (OR, 1.38), compared with the general population (no implants), which did achieve significance.
MRI may be helpful—but is the expense justified?
More than 300,000 women underwent cosmetic breast augmentation in 2011 in the United States, an increase of roughly 800% since the early 1990s. The impaired visualization of breast tissue via mammography in these women ranges from 22% to 83%. In addition, the implants limit compression of the breasts during mammography, and capsular contraction further contributes to this problem.
Magnetic resonance imaging (MRI) may be helpful in screening women with cosmetic breast implants, but this technology is expensive, and evidence supporting its routine use in this population is limited.
Some mammographers use special techniques to better visualize the breast tissue of women with implants. These techniques include displacing the implant posteriorly and pulling the breast tissue in front of it. However, even with such strategies, as much as one-third of the breast tissue may be inadequately assessed.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
These findings underscore the importance of sharing the risks of nonlocalized breast malignancy and increased breast cancer mortality with patients who are considering cosmetic breast implants, as well as with women who have already undergone this common procedure. Future studies are needed to address relevant issues, including the role of 3-D (tomosynthesis) technology in screening women with breast implants and optimal screening intervals in this subgroup.
ANDREW M. KAUNITZ, MD
We want to hear from you. Tell us what you think.
The “Canoe” Technique to Insert Lumbar Pedicle Screws: Consistent, Safe, and Simple
Successful treatment of chronic vaginitis
Gadzooks! In preparing for the morning office practice session you notice that two patients with chronic vaginitis have been scheduled back to back in 15-minute slots.
Ms. A has chronic bacterial vaginosis. Ms. B has chronic yeast vaginitis. What are you going to do?
Chronic bacterial vaginosis
The normal vaginal microbiome is dominated by Lactobacillus crispatus and Lactobacillus jensenii. These organisms produce hydrogen peroxide and keep the vaginal pH ≤4.5. When Gardnerella vaginalis and associated anaerobic bacteria gain dominance in the vagina, bacterial vaginosis ensues. This infection is characterized by1:
- homogenous, thin, grayish-white discharge that smoothly coats the vaginal epithelium
- pH >4.5
- fishy odor when potassium hydroxide is added to a sample of the discharge
- clue cells on a saline wet mount.
Why is it prone to recur? If bacterial vaginosis was a simple infection, treatment with metronidazole or clindamycin should be very effective. But in many women the relief from symptoms provided by a single course of antibiotics is short-lived, and many patients experience recurrent bacterial vaginosis in the next few months.
The cause of this resistance to antibiotic treatment may be that G vaginalis and other anaerobes, such as Atopobium species, aggregate in vaginal biofilms that prevent the antibiotic from reaching the organism.2 The biofilm provides a safe haven for the bacteria to regrow following a single course of treatment.3 In addition, the nutrient-limited environment inside the encapsulated biofilm helps the bacteria to resist the toxic effects of the antibiotic.4
Another potential mechanism for bacterial vaginosis recurrence is that women destined to develop repeat infection often harbor G vaginalis encapsulated in biofilms in the mouth. These extravaginal bacteria often are found again in the vagina, suggesting that bacterial vaginosis can be acquired from extravaginal bacterial reservoirs.5 Investigators are developing approaches, such as intravaginal treatment with DNase, to destroy the vaginal biofilm in order to enhance the efficacy of antibiotic treatment.6
Treatment
Options for initial infection. There are three treatments for an initial occurrence of bacterial vaginosis7:
- oral metronidazole 500 mg twice daily for 7 days
- 0.75% metronidazole gel one applicator intravaginally once daily for 5 days, or
- 2% clindamycin cream one applicator intravaginally at bedtime for 7 days.
Long-term metronidazole for recurrence. Approximately half of women who respond to initial treatment will have bacterial vaginosis again within 1 year. If vaginitis caused by recurrent bacterial vaginosisis diagnosed, a prolonged course of antibiotic treatment is warranted. Treatment starts with an induction regimen of the standard treatments listed in the paragraph above. This is followed by a long-term maintenance regimen using 0.75% metronidazole vaginal gel one applicator twice weekly for 4 to 6 months.8
Recurrent Candida vulvovaginitis
Four or more occurrences of symptomatic Candida vulvovaginitis in 12 months indicates recurrent infection. Recurrence is usually caused by reinfection with the same organism from a vaginal reservoir. For women with such repeat infection, vaginal cultures should be obtained to confirm Candida and to search for treatment-resistant species, such as Candida glabrata. (Many C glabrata organisms are resistant to standard fluconazole treatment.)
Treatment options
Long courses of oral or vaginal antimycotic agents can be effective treatment for recurrent Candida vulvovaginitis.
Fluconazole. One regimen is fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg once weekly for 6 months.9 If patients relapse from this regimen, then the vaginitis should be retreated with fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg weekly for 12 months.
Boric acid. If C glabrata is thought to be the cause of the infection, it may be difficult to eradicate with fluconazole. A regimen to treat recurrent vaginitis caused by C glabrata is intravaginal boric acid, a 600 mg capsule once nightly for 14 days.10,11This medication is not FDA-approved for this purpose and must be made by a compounding pharmacy. Boric acid can be fatal if swallowed rather than used intravaginally. Care must be taken to avoid access to these capsules by children.
Boric acid vaginal capsules also can be used to treat chronic bacterial vaginosis in combination with antibiotic therapy.12
Flucytosine. An alternative regimen to treat C glabrata is flucytosine vaginal cream one applicator nightly for 14 days. This vaginal cream must be compounded because it is not available as a commercial medication.
You are armed and ready
In retrospect, you realize that the morning office session schedule is going to be fine. You will treat Ms. A with a long course of metronidazole and Ms. B with a long course of fluconazole. Hopefully, they will both find relief from their symptoms.
Tell us what you think, at [email protected]. Please include your name and city and state.
- Eschenbach DA, Hillier S, Critchlow C, Stevens C, DeRouen T, Holmes KK. Diagnosis and clinical manifestations of bacterial vaginosis. Am J Obstet Gynecol. 1988;158(4):819–828.
- Swidinski A, Mendling W, Loening-Baucke V, et al. Adherent biofilms in bacterial vaginosis.Obstet Gynecol. 2005;106(5 pt 1):1013–1023.
- Swidinski A, Mendling W, Loening-Baucke V, et al. An adherent Gardnerella vaginalis biofilm persists on the vaginal epithelium after standard therapy with oral metronidazole. Am J Obstet Gynecol. 2008;198(1):97e1–e6.
- Monds RD, O’Toole GA. The developmental model of microbial biofilm: ten years of a paradigm up for review. Trends Microbiol. 2009;17(2):73–87.
- Marrazzo JM, Friedler TL, Srinivasan S, et al. Extravaginal reservoirs of vaginal bacteria as risk factors for incident bacterial vaginosis. J Infect Dis. 2012;205(10):1580–1588.
- Hymes SR, Randis TM, Sun TY, Ratner AJ. DNase inhibits Gardnerella vaginalis biofilms in vitro and in vivo. J Infect Dis. 2013;207(10):1491–1497.
- Workowski KA, Berman S; Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010; 59(RR-12):1–110.
- Sobel JD, Ferris D, Schwebke J, et al. Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am J Obstet Gynecol. 2006;194(5):1283–1289.
- Sobel JD, Wiesenfeld HC, Martens M, et al. Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. N Engl J Med. 2004;351(9):876–883.
- Savini V, Catavitello C, Bianco A, Balbinot A, D’Antonio F, D’Antonio D. Azole resistant Candida glabrata vulvovaginitis treated with boric acid. Eur J Obstet Gynecol Reprod Biol. 2009;147(1):112.
- Iavazzo C, Gkegkes ID, Zarkada IM, Falagas ME. Boric acid for recurrent vulvovaginal candidiasis: the clinical evidence. J Womens Health(Larchmt). 2011;20(8):1245–1255.
- Reichman O, Akins R, Sobel JD. Boric acid addition to suppressive antimicrobial therapy for recurrent bacterial vaginosis. Sex Transm Dis. 2009;36(11):732–734.

Robert L. Barbieri, MD, Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD, Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD, Editor in Chief
Dr. Barbieri reports no financial relationships relevant to this article.
Gadzooks! In preparing for the morning office practice session you notice that two patients with chronic vaginitis have been scheduled back to back in 15-minute slots.
Ms. A has chronic bacterial vaginosis. Ms. B has chronic yeast vaginitis. What are you going to do?
Chronic bacterial vaginosis
The normal vaginal microbiome is dominated by Lactobacillus crispatus and Lactobacillus jensenii. These organisms produce hydrogen peroxide and keep the vaginal pH ≤4.5. When Gardnerella vaginalis and associated anaerobic bacteria gain dominance in the vagina, bacterial vaginosis ensues. This infection is characterized by1:
- homogenous, thin, grayish-white discharge that smoothly coats the vaginal epithelium
- pH >4.5
- fishy odor when potassium hydroxide is added to a sample of the discharge
- clue cells on a saline wet mount.
Why is it prone to recur? If bacterial vaginosis was a simple infection, treatment with metronidazole or clindamycin should be very effective. But in many women the relief from symptoms provided by a single course of antibiotics is short-lived, and many patients experience recurrent bacterial vaginosis in the next few months.
The cause of this resistance to antibiotic treatment may be that G vaginalis and other anaerobes, such as Atopobium species, aggregate in vaginal biofilms that prevent the antibiotic from reaching the organism.2 The biofilm provides a safe haven for the bacteria to regrow following a single course of treatment.3 In addition, the nutrient-limited environment inside the encapsulated biofilm helps the bacteria to resist the toxic effects of the antibiotic.4
Another potential mechanism for bacterial vaginosis recurrence is that women destined to develop repeat infection often harbor G vaginalis encapsulated in biofilms in the mouth. These extravaginal bacteria often are found again in the vagina, suggesting that bacterial vaginosis can be acquired from extravaginal bacterial reservoirs.5 Investigators are developing approaches, such as intravaginal treatment with DNase, to destroy the vaginal biofilm in order to enhance the efficacy of antibiotic treatment.6
Treatment
Options for initial infection. There are three treatments for an initial occurrence of bacterial vaginosis7:
- oral metronidazole 500 mg twice daily for 7 days
- 0.75% metronidazole gel one applicator intravaginally once daily for 5 days, or
- 2% clindamycin cream one applicator intravaginally at bedtime for 7 days.
Long-term metronidazole for recurrence. Approximately half of women who respond to initial treatment will have bacterial vaginosis again within 1 year. If vaginitis caused by recurrent bacterial vaginosisis diagnosed, a prolonged course of antibiotic treatment is warranted. Treatment starts with an induction regimen of the standard treatments listed in the paragraph above. This is followed by a long-term maintenance regimen using 0.75% metronidazole vaginal gel one applicator twice weekly for 4 to 6 months.8
Recurrent Candida vulvovaginitis
Four or more occurrences of symptomatic Candida vulvovaginitis in 12 months indicates recurrent infection. Recurrence is usually caused by reinfection with the same organism from a vaginal reservoir. For women with such repeat infection, vaginal cultures should be obtained to confirm Candida and to search for treatment-resistant species, such as Candida glabrata. (Many C glabrata organisms are resistant to standard fluconazole treatment.)
Treatment options
Long courses of oral or vaginal antimycotic agents can be effective treatment for recurrent Candida vulvovaginitis.
Fluconazole. One regimen is fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg once weekly for 6 months.9 If patients relapse from this regimen, then the vaginitis should be retreated with fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg weekly for 12 months.
Boric acid. If C glabrata is thought to be the cause of the infection, it may be difficult to eradicate with fluconazole. A regimen to treat recurrent vaginitis caused by C glabrata is intravaginal boric acid, a 600 mg capsule once nightly for 14 days.10,11This medication is not FDA-approved for this purpose and must be made by a compounding pharmacy. Boric acid can be fatal if swallowed rather than used intravaginally. Care must be taken to avoid access to these capsules by children.
Boric acid vaginal capsules also can be used to treat chronic bacterial vaginosis in combination with antibiotic therapy.12
Flucytosine. An alternative regimen to treat C glabrata is flucytosine vaginal cream one applicator nightly for 14 days. This vaginal cream must be compounded because it is not available as a commercial medication.
You are armed and ready
In retrospect, you realize that the morning office session schedule is going to be fine. You will treat Ms. A with a long course of metronidazole and Ms. B with a long course of fluconazole. Hopefully, they will both find relief from their symptoms.
Tell us what you think, at [email protected]. Please include your name and city and state.
Gadzooks! In preparing for the morning office practice session you notice that two patients with chronic vaginitis have been scheduled back to back in 15-minute slots.
Ms. A has chronic bacterial vaginosis. Ms. B has chronic yeast vaginitis. What are you going to do?
Chronic bacterial vaginosis
The normal vaginal microbiome is dominated by Lactobacillus crispatus and Lactobacillus jensenii. These organisms produce hydrogen peroxide and keep the vaginal pH ≤4.5. When Gardnerella vaginalis and associated anaerobic bacteria gain dominance in the vagina, bacterial vaginosis ensues. This infection is characterized by1:
- homogenous, thin, grayish-white discharge that smoothly coats the vaginal epithelium
- pH >4.5
- fishy odor when potassium hydroxide is added to a sample of the discharge
- clue cells on a saline wet mount.
Why is it prone to recur? If bacterial vaginosis was a simple infection, treatment with metronidazole or clindamycin should be very effective. But in many women the relief from symptoms provided by a single course of antibiotics is short-lived, and many patients experience recurrent bacterial vaginosis in the next few months.
The cause of this resistance to antibiotic treatment may be that G vaginalis and other anaerobes, such as Atopobium species, aggregate in vaginal biofilms that prevent the antibiotic from reaching the organism.2 The biofilm provides a safe haven for the bacteria to regrow following a single course of treatment.3 In addition, the nutrient-limited environment inside the encapsulated biofilm helps the bacteria to resist the toxic effects of the antibiotic.4
Another potential mechanism for bacterial vaginosis recurrence is that women destined to develop repeat infection often harbor G vaginalis encapsulated in biofilms in the mouth. These extravaginal bacteria often are found again in the vagina, suggesting that bacterial vaginosis can be acquired from extravaginal bacterial reservoirs.5 Investigators are developing approaches, such as intravaginal treatment with DNase, to destroy the vaginal biofilm in order to enhance the efficacy of antibiotic treatment.6
Treatment
Options for initial infection. There are three treatments for an initial occurrence of bacterial vaginosis7:
- oral metronidazole 500 mg twice daily for 7 days
- 0.75% metronidazole gel one applicator intravaginally once daily for 5 days, or
- 2% clindamycin cream one applicator intravaginally at bedtime for 7 days.
Long-term metronidazole for recurrence. Approximately half of women who respond to initial treatment will have bacterial vaginosis again within 1 year. If vaginitis caused by recurrent bacterial vaginosisis diagnosed, a prolonged course of antibiotic treatment is warranted. Treatment starts with an induction regimen of the standard treatments listed in the paragraph above. This is followed by a long-term maintenance regimen using 0.75% metronidazole vaginal gel one applicator twice weekly for 4 to 6 months.8
Recurrent Candida vulvovaginitis
Four or more occurrences of symptomatic Candida vulvovaginitis in 12 months indicates recurrent infection. Recurrence is usually caused by reinfection with the same organism from a vaginal reservoir. For women with such repeat infection, vaginal cultures should be obtained to confirm Candida and to search for treatment-resistant species, such as Candida glabrata. (Many C glabrata organisms are resistant to standard fluconazole treatment.)
Treatment options
Long courses of oral or vaginal antimycotic agents can be effective treatment for recurrent Candida vulvovaginitis.
Fluconazole. One regimen is fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg once weekly for 6 months.9 If patients relapse from this regimen, then the vaginitis should be retreated with fluconazole 150 mg orally every 72 hours for 3 doses, followed by fluconazole 150 mg weekly for 12 months.
Boric acid. If C glabrata is thought to be the cause of the infection, it may be difficult to eradicate with fluconazole. A regimen to treat recurrent vaginitis caused by C glabrata is intravaginal boric acid, a 600 mg capsule once nightly for 14 days.10,11This medication is not FDA-approved for this purpose and must be made by a compounding pharmacy. Boric acid can be fatal if swallowed rather than used intravaginally. Care must be taken to avoid access to these capsules by children.
Boric acid vaginal capsules also can be used to treat chronic bacterial vaginosis in combination with antibiotic therapy.12
Flucytosine. An alternative regimen to treat C glabrata is flucytosine vaginal cream one applicator nightly for 14 days. This vaginal cream must be compounded because it is not available as a commercial medication.
You are armed and ready
In retrospect, you realize that the morning office session schedule is going to be fine. You will treat Ms. A with a long course of metronidazole and Ms. B with a long course of fluconazole. Hopefully, they will both find relief from their symptoms.
Tell us what you think, at [email protected]. Please include your name and city and state.
- Eschenbach DA, Hillier S, Critchlow C, Stevens C, DeRouen T, Holmes KK. Diagnosis and clinical manifestations of bacterial vaginosis. Am J Obstet Gynecol. 1988;158(4):819–828.
- Swidinski A, Mendling W, Loening-Baucke V, et al. Adherent biofilms in bacterial vaginosis.Obstet Gynecol. 2005;106(5 pt 1):1013–1023.
- Swidinski A, Mendling W, Loening-Baucke V, et al. An adherent Gardnerella vaginalis biofilm persists on the vaginal epithelium after standard therapy with oral metronidazole. Am J Obstet Gynecol. 2008;198(1):97e1–e6.
- Monds RD, O’Toole GA. The developmental model of microbial biofilm: ten years of a paradigm up for review. Trends Microbiol. 2009;17(2):73–87.
- Marrazzo JM, Friedler TL, Srinivasan S, et al. Extravaginal reservoirs of vaginal bacteria as risk factors for incident bacterial vaginosis. J Infect Dis. 2012;205(10):1580–1588.
- Hymes SR, Randis TM, Sun TY, Ratner AJ. DNase inhibits Gardnerella vaginalis biofilms in vitro and in vivo. J Infect Dis. 2013;207(10):1491–1497.
- Workowski KA, Berman S; Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010; 59(RR-12):1–110.
- Sobel JD, Ferris D, Schwebke J, et al. Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am J Obstet Gynecol. 2006;194(5):1283–1289.
- Sobel JD, Wiesenfeld HC, Martens M, et al. Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. N Engl J Med. 2004;351(9):876–883.
- Savini V, Catavitello C, Bianco A, Balbinot A, D’Antonio F, D’Antonio D. Azole resistant Candida glabrata vulvovaginitis treated with boric acid. Eur J Obstet Gynecol Reprod Biol. 2009;147(1):112.
- Iavazzo C, Gkegkes ID, Zarkada IM, Falagas ME. Boric acid for recurrent vulvovaginal candidiasis: the clinical evidence. J Womens Health(Larchmt). 2011;20(8):1245–1255.
- Reichman O, Akins R, Sobel JD. Boric acid addition to suppressive antimicrobial therapy for recurrent bacterial vaginosis. Sex Transm Dis. 2009;36(11):732–734.
- Eschenbach DA, Hillier S, Critchlow C, Stevens C, DeRouen T, Holmes KK. Diagnosis and clinical manifestations of bacterial vaginosis. Am J Obstet Gynecol. 1988;158(4):819–828.
- Swidinski A, Mendling W, Loening-Baucke V, et al. Adherent biofilms in bacterial vaginosis.Obstet Gynecol. 2005;106(5 pt 1):1013–1023.
- Swidinski A, Mendling W, Loening-Baucke V, et al. An adherent Gardnerella vaginalis biofilm persists on the vaginal epithelium after standard therapy with oral metronidazole. Am J Obstet Gynecol. 2008;198(1):97e1–e6.
- Monds RD, O’Toole GA. The developmental model of microbial biofilm: ten years of a paradigm up for review. Trends Microbiol. 2009;17(2):73–87.
- Marrazzo JM, Friedler TL, Srinivasan S, et al. Extravaginal reservoirs of vaginal bacteria as risk factors for incident bacterial vaginosis. J Infect Dis. 2012;205(10):1580–1588.
- Hymes SR, Randis TM, Sun TY, Ratner AJ. DNase inhibits Gardnerella vaginalis biofilms in vitro and in vivo. J Infect Dis. 2013;207(10):1491–1497.
- Workowski KA, Berman S; Centers for Disease Control and Prevention (CDC). Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010; 59(RR-12):1–110.
- Sobel JD, Ferris D, Schwebke J, et al. Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am J Obstet Gynecol. 2006;194(5):1283–1289.
- Sobel JD, Wiesenfeld HC, Martens M, et al. Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. N Engl J Med. 2004;351(9):876–883.
- Savini V, Catavitello C, Bianco A, Balbinot A, D’Antonio F, D’Antonio D. Azole resistant Candida glabrata vulvovaginitis treated with boric acid. Eur J Obstet Gynecol Reprod Biol. 2009;147(1):112.
- Iavazzo C, Gkegkes ID, Zarkada IM, Falagas ME. Boric acid for recurrent vulvovaginal candidiasis: the clinical evidence. J Womens Health(Larchmt). 2011;20(8):1245–1255.
- Reichman O, Akins R, Sobel JD. Boric acid addition to suppressive antimicrobial therapy for recurrent bacterial vaginosis. Sex Transm Dis. 2009;36(11):732–734.
Type IIb Bony Mallet Finger: Is Anatomical Reduction of the Fracture Necessary?
Travelers' diarrhea: Prevention, treatment, and post-trip evaluation
1. Recommend antibiotic chemoprophylaxis for travelers at high risk for travelers’ diarrhea (TD) and those at high risk for complications. It is also appropriate for travelers who have an inflexible itinerary. B
2. Recommend bismuth subsalicylate chemoprophylaxis for travelers at high risk for TD who are willing to comply with the regimen and want to avoid antibiotic prophylaxis. B
3. Advise travelers to initiate self-treatment for TD with a fluoroquinolone (or azithromycin, if in South or Southeast Asia) at the onset of diarrhea if it is bloody or accompanied by fever. A
NOTE: This practice recommendation in the print version of this article stated that travelers should also take loperamide; however, both the Centers for Disease Control and Prevention and the Infectious Diseases Society of America advise against the use of loperamide by travelers with fever or bloody diarrhea [corrected August 27, 2013].
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 40-year-old female patient, a childhood immigrant from India, is seeking advice regarding her upcoming 2-week trip to Mumbai. She is taking her 2 children, ages 16 years and 16 months, to visit their grandparents for the first time. She has made this trip alone a few times and has invariably experienced short bouts of self-limited diarrheal illness. She wonders what she might do to prevent travelers’ diarrhea. Her only medical problem is rheumatoid arthritis, which has been well controlled with methotrexate. Her children are healthy. What would you recommend?
Recommendations regarding travelers’ diarrhea (TD) address prevention and management. Prevention encompasses advice about personal behaviors and the use of chemoprophylaxis (antimicrobial and non-antimicrobial) and vaccinations. Since international travelers are known to treat themselves for diarrheal illnesses during their trips,1 recommendations regarding management should assume self-treatment and include the use of both antibiotics and non-antibiotic remedies. Pretravel recommendations will of course be most effective if they account for the individual’s risk for TD.
Innate patient susceptibility, destination, and dietary choices determine TD risk
TD is generally defined as the passage of 3 of more loose stools in a 24-hour period, with associated symptoms of enteric infection—eg, fever, nausea, vomiting, or abdominal cramping. Defined in this manner, TD is thought to occur in 60% to 70% of individuals who travel from developed countries to less-developed countries.2,4 Risk of TD is influenced both by intrinsic personal factors and by factors specific to the trip.
Personal risk factorsIndividual variation in susceptibility to TD might result from a genetic predisposition arising from single nucleotide polymorphisms governing various inflammatory marker proteins.5 A history of multiple episodes of TD, especially if fellow travelers were spared, can suggest this kind of individual susceptibility. Other factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.6,7 However, the trip itself is much more important in assessing risk for TD.
Trip-related risk factors
The destination. The most salient risk factor for TD is the geographic destination. Regions of the world can be divided into TD risk strata:2
- Very high: South Asia
- High: South America, Sub-Saharan Africa
- Medium: Central America, Mexico, Caribbean, Middle East, North Africa, Southeast Asia, Oceania
- Low: Europe, North America (excluding Mexico), Australasia, Northeast Asia.
Particularly notable countries, in descending order of risk, are Nepal, India, Myanmar, Bolivia, Sri Lanka, Ecuador, Peru, Kenya, and Guatemala.2
Dietary choices. Additionally, since travelers acquire TD by ingesting food or beverages contaminated with pathogenic fecal microbes, dietary behaviors during the trip affect their susceptibility. At least risk are business travelers and tourists who confine their activities to more affluent settings in which food and beverages are prepared and stored hygienically.1,4,8,9 At greater risk are travelers who immerse themselves in local culture, visiting locations that are more impoverished and not as well equipped with sanitation systems, especially if their stay is at least 2 to 3 weeks.1,4,8,9
Also, the older a traveler is, the lower his or her risk of TD.1,9 An exception to this might be infants whose diet consists solely of breast milk or formula prepared under sanitary conditions.
Mandates and options for preventing TD
Emphasize food and beverage precautions
It might be reasonable to expect that travelers who are circumspect about their food and beverage choices on trips will be able to avoid TD. Indeed, this is the basis for the aphorism, “Boil it, peel it, or forget it.” Guidelines routinely recommend that travelers restrict their selection of foods to those that have been well cooked and are served while still very hot, and to fruits and vegetables that they peel themselves. Likewise, they should drink only beverages that have been boiled or are in sealed bottles or under carbonation and served without ice.10-12 Many travelers might find these recommendations too restrictive to follow faithfully. Moreover, studies suggest it may not be possible for even the most assiduous traveler to fully avoid the risk of TD.13,14 The hygienic characteristics of the travel destination may be more determinative, as illustrated by the successful reduction of TD rates in Jamaica by improving sanitation in tourist resorts.15
Antibiotic chemoprophylaxis: A debated practice with limited consensusThe etiologic agents of TD are multiple and vary somewhat in predominance according to geographic region.3,16,17 TABLE 1 depicts variance by region.16 The most common pathogens are strains of the bacterium Escherichia coli, particularly enterotoxigenic (ETEC), enteroaggregative (EAEC), and enteropathogenic (EPEC) strains.16 Other bacteria of importance are Campylobacter, Salmonella, and Shigella. Viruses, particularly norovirus (notably connected with cruise ships), can also cause TD, although it is implicated in no more than 17% of cases.18 Parasitic pathogens are even less common causes of TD (4%-10%) and mainly involve the protozoa, Giardia lamblia, and, to a lesser extent, Entamoeba histolytica and Cryptosporidium.
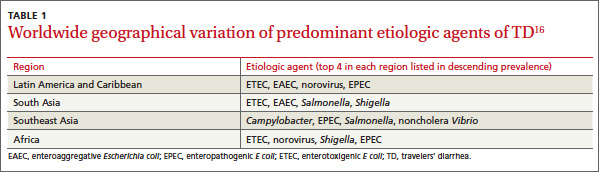
Although some pathogens often have a characteristic presentation—such as frothy, greasy diarrhea in the case of G lamblia—they generally cannot be reliably distinguished from one another clinically. Notably, up to 50% of stool samples from TD patients do not yield any pathogen,16 raising the suspicion that current diagnostic technology is not sufficiently sensitive to routinely identify certain bacteria.
There is no consensus on recommending antibiotic chemoprophylaxis against TD.
Opponents of this practice10-12,19,20 point out that TD is generally a brief (3-5 days), self-limited illness. Moreover, concerns about antibiotic resistance have come to pass. Previously used agents, trimethoprim-sulfamethoxazole and doxycycline, are no longer effective in preventing or treating TD. In addition, antibiotic use carries the risk of allergic reactions as well as other adverse effects including, ironically, the development of antibiotic-associated diarrhea and Clostridium difficile diarrhea.
Proponents of antibiotic chemoprophylaxis21,22 point to its demonstrated efficacy in reducing the risk of TD by 4% to 40%.11 They also argue that at least 20% to 25% of travelers who get TD must significantly curtail their activities for a day or more.1,23 This change in travel plans is associated not only with significant personal loss but also imposes a financial burden.23 Furthermore, TD is known to have longer-term effects. Up to 10% of sufferers develop postinfectious irritable bowel syndrome (PI-IBS) that can last for 5 or 6 years.21,22,24,25 It is not known, however, whether the use of antibiotic chemoprophylaxis significantly reduces the incidence of PI-IBS.
Finally, the luminal antibiotic, rifaximin, nonabsorbable as it is, is very well-tolerated and holds promise for not inciting antibiotic resistance.22 However, while its efficacy in preventing TD has been demonstrated in various settings,22,26,27 it is not approved by the US Food and Drug Administration for this indication. Also, concerns persist that it might not be effective in preventing TD caused by invasive pathogens.19
Indications on which all agree. Even opponents of antibiotic chemoprophylaxis grant that it is probably warranted for 2 groups of travelers.10-12 The first is those whose trip schedule is of such importance that any deviation would be intolerable. The second is travelers with comorbidities that would render them at high risk for serious inconvenience or illness if they developed TD. Examples of the latter include patients with enterostomies, mobility impairments, immune suppression, inflammatory bowel disease, and renal or metabolic diseases.
Chemoprophylaxis regimens. If you prescribe an antibiotic prophylactically, consider daily doses of a fluoroquinolone (eg, ciprofloxacin 500 mg orally once daily, not twice daily as for treatment) or rifaximin 200 mg orally once or twice a day, for no longer than 2 to 3 weeks.10
Non-antimicrobial chemoprophylaxis
Bismuth subsalicylate has reduced the incidence of TD from 40% to just 14% when taken in doses of 2 chewable tablets or 60 mL of liquid 4 times daily. 11,19,22 However, the dosing frequency can hinder adherence. Moreover, the relatively high doses required raise the risk of adverse drug reactions such as blackening of the tongue and stool, nausea, constipation, Reye syndrome (in children under 12 years), and possibly tinnitus. The salicylate component of the drug poses a threat to patients with aspirin allergy, renal disease, and those taking anticoagulants. Drug interactions with probenecid and methotrexate are also possible. Bismuth is not recommended for use for longer than 3 weeks, or for children younger than 3 years or pregnant women in their third trimester.
Other non-antimicrobial chemoprophylaxis agents include probiotics such as Lactobacillus andSaccharomyces. These preparations of bacteria and fungi are marketed either singly or in blends of varying composition and proportion. The evidence is divided on their efficacy, and even though some meta-analyses have concluded probiotics such as Saccharomyces boulardii are useful in preventing TD, endorsement in clinical guidelines is muted.10-12,28-30
Immunizations have limited value so farNatural immunity to E coli gastrointestinal infection among indigenous people in less developed countries has raised the possibility of a role for vaccines in preventing TD. Some strains of ETEC produce a heat-labile toxin (LT) that bears significant resemblance to the toxin produced by Vibrio cholerae. Therefore, the oral cholera vaccine, Dukoral, has been marketed outside the United States for the prevention of TD.19,22 However, only ≤7% of TD cases worldwide would be prevented by routine use of this vaccine.31 A transdermal LT vaccine, which involves the antigen-presenting Langerhans cells in the superficial skin layers, is promising but not yet available for routine use.19,22
Treating TD and associated symptoms
Antibiotic treatment
Given that most cases of TD are caused by bacterial pathogens, antibiotics are considered the mainstay of treatment. Concerns about the ill effects of antibiotic use in the case of enterohemorrhagic E coli(EHEC O157:H7) can be allayed because this strain is rarely a cause of TD.9Patient factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.
Consider local resistance patterns and risk of invasive infection. Which antibiotic to recommend is governed by the antibiotic resistance patterns prevalent in the travel destinations and by the risk of infection by invasive pathogens. Invasive TD is generally caused by Campylobacter, Shigella, or Salmonella and manifests clinically with bloody diarrhea, fever, or both. Rifaximin at a dose of 200 mg orally 3 times daily is effective for noninvasive TD.31,32 However, travelers who develop invasive TD need an alternative to rifaximin. (Those who advocate reserving antibiotic treatment only for invasive diarrhea will not see a role for rifaximin in the first place.) In most invasive cases, a fluoroquinolone will suffice.10-12,19,32 However, increasing prevalence of fluoroquinolone-resistantCampylobacter species has been reported in South and Southeast Asia. In those locations, azithromycin is an effective alternative, albeit with risk of nausea.33TABLE 212 provides details of recommended antibiotic dosages for adults and children. The duration of treatment is generally 1 day unless symptoms persist, in which case a 3-day course is recommended.10-12,19,32 If the traveler experiences persistent, new, or worsening symptoms beyond this point, immediate evaluation by a physician is required.
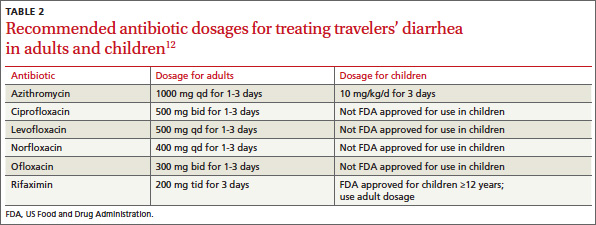
Non-antibiotic treatment
The antimotility agent loperamide is a well-established antidiarrheal agent. Its effective and safe use as an adjunct to antibiotics in the treatment of TD has been demonstrated in several studies.10-12,19,32,34 It is generally not used to treat children with TD9
No other non-antibiotic treatment for TD has significant guideline or clinical trial support. Bismuth subsalicylate can be helpful as an antidiarrheal agent,35 but is not often recommended because the regimen makes adherence difficult and because antibiotics and loperamide are effective.
Oral rehydration is usually a mainstay of treating gastrointestinal disease among infants and children. However, it, too, has a limited role in cases of TD because dehydration is not usually a significant part of the clinical presentation, perhaps because vomiting is not often prominent.
CASE Advice regarding safe food and beverage choices is essential for the patient and her children. Despite the increased risk for TD due to her history and her use of the immunosuppressant methotrexate, she decides not to pursue antibiotic prophylaxis. Bismuth is also contraindicated because of the methotrexate. Her teenage daughter declines bismuth prophylaxis, and her toddler is too young for it.
The patient does accept a prescription for azithromycin for her and her daughters in case they experience TD. This choice is appropriate given the destination of India and concern about Campylobacterresistance to fluoroquinolones. You also recommend loperamide for use by the mother and older child, in conjunction with the antibiotic.
Two weeks after their trip abroad, the travelers return for an office visit. On the trip, the mother and toddler suffered diarrhea, which responded well to your recommended management. The older child was well during the trip, but she developed diarrhea, abdominal pain, and anorexia one week after returning to the United States. These symptoms have persisted despite a 3-day course of azithromycin and loperamide.
Post-travel evaluation
TD generally occurs within one to 2 weeks of arrival at the travel destination and usually lasts no longer than 4 to 5 days.19 This scenario is typical of a bacterial infection. When it occurs later or lasts longer, or both, consider several alternative possibilities.19,36 First, the likelihood of a protozoal parasitic infection is increased. Although giardiasis is most likely, other protozoa such as Entamoeba, Cyclospora, Isospora, and Cryptosporidium are also possibilities. Second, if diarrhea persists, it might be due, not to continued infection, but to a self-limited post-infectious enteropathy or to PI-IBS. Third, TD is known to precipitate the clinical manifestation of underlying gastrointestinal disorders such as inflammatory bowel disease (IBD), celiac disease, or even cancer.37
With an atypical disease course, it’s advisable to send 3 stool samples for laboratory evaluation for ova and parasites and for antigen assays for Giardia. If results of these tests are negative, given the difficulty inherent in diagnosing Giardia, consider empiric treatment with metronidazole in lieu of duodenal sampling.36 If the diarrhea persists, investigate serologic markers for celiac disease and IBD. If these are not revealing, referral for colonoscopy is prudent.
CASE The teenager’s 3 stool samples were negative for ova and parasites and for Giardia antigen. Following empirical treatment with oral metronidazole 250 mg, 3 times daily for 7 days, the diarrhea resolved.
CORRESPONDENCE Dilip Nair, MD, Joan C. Edwards School of Medicine at Marshall University, 1600 Medical Center Drive, Suite 1500, Huntington, WV 25701; [email protected]
1. Hill DR. Occurrence and self-treatment of diarrhea in a large cohort of Americans traveling to developing countries. Am J Trop Med Hyg. 2000;62:585–589.
2. Greenwood Z, Black J, Weld L, et al. for the GeoSentinel Surveillance Network. Gastrointestinal infection among international travelers globally. J Travel Med. 2008;15:221–228.
3. DuPont HL. Systematic review: the epidemiology and clinical features of travellers’ diarrhoea. Aliment Pharmacol Ther. 2009;30:187–196.
4. Steffen R, Tornieporth N, Clemens SA, et al. Epidemiology of travelers’ diarrhea: details of a global survey. J Travel Med. 2004;11:231–237.
5. de la Cabada Bauche J, DuPont HL. New developments in traveler’s diarrhea. Gastroenterol Hepatol. 2011;7:88–95.
6. Cabada MM, White AC. Travelers’ diarrhea: an update on susceptibility, prevention, and treatment. Curr Gastroenterol Rep. 2008;10:473–479.
7. Ericsson CD. Travellers with pre-existing medical conditions. Int J Antimicrob Agents. 2003;21:181–188.
8. Cabada MM, Maldonado F, Quispe W, et al. Risk factors associated with diarrhea among international visitors to Cuzco, Peru. Am J Trop Med Hyg. 2006;75:968–972.
9. Mackell S. Traveler’s diarrhea in the pediatric population: etiology and impact. Clin Infect Dis. 2005;41(suppl 8):S547–S552.
10. Hill DR, Ericsson CD, Pearson RD, et al. The practice of travel medicine: guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1499–1539.
11. Connor BA. Travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-2-the-pre-travel-consultation/travelers-diarrhea.htm. Accessed August 20, 2012.
12. Advice for travelers. Treat Guidel Med Lett. 2012;10:45–56.
13. Shlim DR. Looking for evidence that personal hygiene precautions prevent travelers’ diarrhea. Clin Infect Dis. 2005;41(suppl 8):S531–S535.
14. Laverone E, Boccalini S, Bechini A, et al. Travelers’ compliance to prophylactic measures and behavior during stay abroad: results of a retrospective study of subjects returning to a travel medicine center in Italy. J Travel Med. 2006;13:338–344.
15. Ashley DV, Walters C, Dockery-Brown C, et al. Interventions to prevent and control food-borne diseases associated with a reduction in traveler’s diarrhea in tourists to Jamaica. J Travel Med. 2004;11:364–367.
16. Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers’ diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg. 2009;80:609–614.
17. Riddle MS, Sanders JW, Putnam SD, et al. Incidence, etiology, and impact of diarrhea among long-term travelers (US military and similar populations): a systematic review. Am J Trop Med Hyg. 2006;74:891–900.
18. Koo HL, Ajami NJ, Jiang ZD, et al. Noroviruses as a cause of diarrhea in travelers to Guatemala, India, and Mexico. J Clin Microbiol. 2010;48:1673–1676.
19. Hill DR, Ryan ET. Management of travellers’ diarrhoea. BMJ. 2008;337:863–867.
20. Rendi-Wagner P, Kollaritsch H. Drug prophylaxis for travelers’ diarrhea. Clin Infect Dis. 2002;34:628–633.
21. Pimentel M, Riddle MS. Prevention of traveler’s diarrhea: a call to reconvene. Clin Infect Dis. 2008;46:151–152.
22. DuPont HL. Systematic review: prevention of travellers’ diarrhoea. Aliment Pharmacol Ther. 2008;27:741–751.
23. Wang M, Szucs TD, Steffen R. Economic aspects of travelers’ diarrhea. J Travel Med. 2008;15:110–118.
24. Neal KR, Barker L, Spiller RC. Prognosis in post-infective irritable bowel syndrome: a six year follow up study. Gut. 2002;51:410–413.
25. Tornblom H, Holmvall P, Svenungsson B, et al. Gastrointestinal symptoms after infectious diarrhea: a five-year follow-up in a Swedish cohort of adults. Clin Gastroenterol Hepatol. 2007;5:461–464.
26. DuPont HL, Jiang ZD, Okhuysen PC, et al. A randomized, double-blind, placebo-controlled trial of rifaximin to prevent travelers’ diarrhea. Ann Intern Med. 2005;142:805–812.
27. Taylor DN, McKenzie R, Durbin A, et al. Rifaximin, a nonabsorbed oral antibiotic, prevents shigellosis after experimental challenge. Clin Infect Dis. 2006;42:1283–1288.
28. Sazawal S, Hiremath G, Dhingra U, et al. Efficacy of probiotics in prevention of acute diarrhoea: a meta-analysis of masked, randomised, placebo-controlled trials. Lancet Infect Dis. 2006;6:374–382.
29. Bri V, Buffet P, Genty S, et al. Absence of efficacy of nonviable Lactobacillus acidophilus for the prevention of traveler’s diarrhea: a randomized, double-blind, controlled study. Clin Infect Dis. 2006;43:1170–1175.
30. Hill DR, Ford L, Lalloo DG. Oral cholera vaccines—use in clinical practice. Lancet Infect Dis. 2006;6:361–373.
31. Taylor DN, Bourgeois AL, Ericsson CD, et al. A randomized double-blind, multicenter study of rifaximin compared with placebo and with ciprofloxacin in the treatment of travelers’ diarrhea. Am J Trop Med Hyg. 2006;74:1060–1066.
32. DuPont HL, Ericsson CD, Farthing MJG, et al. Expert review of the evidence base for self-therapy of travelers’ diarrhea. J Travel Med. 2009;16:161–171.
33. Tribble DR, Sanders JW, Pang LW, et al. Traveler’s diarrhea in Thailand: randomized, double-blind trial comparing single-dose and 3-day azithromycin-based regimens with a 3-day levofloxacin regimen. Clin Infect Dis. 2007;44:338–346.
34. Riddle MS, Arnold S, Tribble DR. Effect of adjunctive loperamide in combination with antibiotics on treatment outcomes in travelers’ diarrhea: a systematic review and meta-analysis. Clin Infect Dis. 2008;47:1007–1014.
35. Steffen R. Worldwide efficacy of bismuth subsalicylate in the treatment of travelers’ diarrhea. Rev Infect Dis. 1990;12(suppl 1):S80–S86.
36. Connor BA. Persistent travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/persistent-travelers-diarrhea.htm. Accessed August 20, 2012.
37.Landzberg BR, Connor BA. Persistent diarrhea in the returning traveler: think beyond persistent infection. Scand J Gastroenterol. 2005;40:112–114.
1. Recommend antibiotic chemoprophylaxis for travelers at high risk for travelers’ diarrhea (TD) and those at high risk for complications. It is also appropriate for travelers who have an inflexible itinerary. B
2. Recommend bismuth subsalicylate chemoprophylaxis for travelers at high risk for TD who are willing to comply with the regimen and want to avoid antibiotic prophylaxis. B
3. Advise travelers to initiate self-treatment for TD with a fluoroquinolone (or azithromycin, if in South or Southeast Asia) at the onset of diarrhea if it is bloody or accompanied by fever. A
NOTE: This practice recommendation in the print version of this article stated that travelers should also take loperamide; however, both the Centers for Disease Control and Prevention and the Infectious Diseases Society of America advise against the use of loperamide by travelers with fever or bloody diarrhea [corrected August 27, 2013].
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 40-year-old female patient, a childhood immigrant from India, is seeking advice regarding her upcoming 2-week trip to Mumbai. She is taking her 2 children, ages 16 years and 16 months, to visit their grandparents for the first time. She has made this trip alone a few times and has invariably experienced short bouts of self-limited diarrheal illness. She wonders what she might do to prevent travelers’ diarrhea. Her only medical problem is rheumatoid arthritis, which has been well controlled with methotrexate. Her children are healthy. What would you recommend?
Recommendations regarding travelers’ diarrhea (TD) address prevention and management. Prevention encompasses advice about personal behaviors and the use of chemoprophylaxis (antimicrobial and non-antimicrobial) and vaccinations. Since international travelers are known to treat themselves for diarrheal illnesses during their trips,1 recommendations regarding management should assume self-treatment and include the use of both antibiotics and non-antibiotic remedies. Pretravel recommendations will of course be most effective if they account for the individual’s risk for TD.
Innate patient susceptibility, destination, and dietary choices determine TD risk
TD is generally defined as the passage of 3 of more loose stools in a 24-hour period, with associated symptoms of enteric infection—eg, fever, nausea, vomiting, or abdominal cramping. Defined in this manner, TD is thought to occur in 60% to 70% of individuals who travel from developed countries to less-developed countries.2,4 Risk of TD is influenced both by intrinsic personal factors and by factors specific to the trip.
Personal risk factorsIndividual variation in susceptibility to TD might result from a genetic predisposition arising from single nucleotide polymorphisms governing various inflammatory marker proteins.5 A history of multiple episodes of TD, especially if fellow travelers were spared, can suggest this kind of individual susceptibility. Other factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.6,7 However, the trip itself is much more important in assessing risk for TD.
Trip-related risk factors
The destination. The most salient risk factor for TD is the geographic destination. Regions of the world can be divided into TD risk strata:2
- Very high: South Asia
- High: South America, Sub-Saharan Africa
- Medium: Central America, Mexico, Caribbean, Middle East, North Africa, Southeast Asia, Oceania
- Low: Europe, North America (excluding Mexico), Australasia, Northeast Asia.
Particularly notable countries, in descending order of risk, are Nepal, India, Myanmar, Bolivia, Sri Lanka, Ecuador, Peru, Kenya, and Guatemala.2
Dietary choices. Additionally, since travelers acquire TD by ingesting food or beverages contaminated with pathogenic fecal microbes, dietary behaviors during the trip affect their susceptibility. At least risk are business travelers and tourists who confine their activities to more affluent settings in which food and beverages are prepared and stored hygienically.1,4,8,9 At greater risk are travelers who immerse themselves in local culture, visiting locations that are more impoverished and not as well equipped with sanitation systems, especially if their stay is at least 2 to 3 weeks.1,4,8,9
Also, the older a traveler is, the lower his or her risk of TD.1,9 An exception to this might be infants whose diet consists solely of breast milk or formula prepared under sanitary conditions.
Mandates and options for preventing TD
Emphasize food and beverage precautions
It might be reasonable to expect that travelers who are circumspect about their food and beverage choices on trips will be able to avoid TD. Indeed, this is the basis for the aphorism, “Boil it, peel it, or forget it.” Guidelines routinely recommend that travelers restrict their selection of foods to those that have been well cooked and are served while still very hot, and to fruits and vegetables that they peel themselves. Likewise, they should drink only beverages that have been boiled or are in sealed bottles or under carbonation and served without ice.10-12 Many travelers might find these recommendations too restrictive to follow faithfully. Moreover, studies suggest it may not be possible for even the most assiduous traveler to fully avoid the risk of TD.13,14 The hygienic characteristics of the travel destination may be more determinative, as illustrated by the successful reduction of TD rates in Jamaica by improving sanitation in tourist resorts.15
Antibiotic chemoprophylaxis: A debated practice with limited consensusThe etiologic agents of TD are multiple and vary somewhat in predominance according to geographic region.3,16,17 TABLE 1 depicts variance by region.16 The most common pathogens are strains of the bacterium Escherichia coli, particularly enterotoxigenic (ETEC), enteroaggregative (EAEC), and enteropathogenic (EPEC) strains.16 Other bacteria of importance are Campylobacter, Salmonella, and Shigella. Viruses, particularly norovirus (notably connected with cruise ships), can also cause TD, although it is implicated in no more than 17% of cases.18 Parasitic pathogens are even less common causes of TD (4%-10%) and mainly involve the protozoa, Giardia lamblia, and, to a lesser extent, Entamoeba histolytica and Cryptosporidium.
Although some pathogens often have a characteristic presentation—such as frothy, greasy diarrhea in the case of G lamblia—they generally cannot be reliably distinguished from one another clinically. Notably, up to 50% of stool samples from TD patients do not yield any pathogen,16 raising the suspicion that current diagnostic technology is not sufficiently sensitive to routinely identify certain bacteria.
There is no consensus on recommending antibiotic chemoprophylaxis against TD.
Opponents of this practice10-12,19,20 point out that TD is generally a brief (3-5 days), self-limited illness. Moreover, concerns about antibiotic resistance have come to pass. Previously used agents, trimethoprim-sulfamethoxazole and doxycycline, are no longer effective in preventing or treating TD. In addition, antibiotic use carries the risk of allergic reactions as well as other adverse effects including, ironically, the development of antibiotic-associated diarrhea and Clostridium difficile diarrhea.
Proponents of antibiotic chemoprophylaxis21,22 point to its demonstrated efficacy in reducing the risk of TD by 4% to 40%.11 They also argue that at least 20% to 25% of travelers who get TD must significantly curtail their activities for a day or more.1,23 This change in travel plans is associated not only with significant personal loss but also imposes a financial burden.23 Furthermore, TD is known to have longer-term effects. Up to 10% of sufferers develop postinfectious irritable bowel syndrome (PI-IBS) that can last for 5 or 6 years.21,22,24,25 It is not known, however, whether the use of antibiotic chemoprophylaxis significantly reduces the incidence of PI-IBS.
Finally, the luminal antibiotic, rifaximin, nonabsorbable as it is, is very well-tolerated and holds promise for not inciting antibiotic resistance.22 However, while its efficacy in preventing TD has been demonstrated in various settings,22,26,27 it is not approved by the US Food and Drug Administration for this indication. Also, concerns persist that it might not be effective in preventing TD caused by invasive pathogens.19
Indications on which all agree. Even opponents of antibiotic chemoprophylaxis grant that it is probably warranted for 2 groups of travelers.10-12 The first is those whose trip schedule is of such importance that any deviation would be intolerable. The second is travelers with comorbidities that would render them at high risk for serious inconvenience or illness if they developed TD. Examples of the latter include patients with enterostomies, mobility impairments, immune suppression, inflammatory bowel disease, and renal or metabolic diseases.
Chemoprophylaxis regimens. If you prescribe an antibiotic prophylactically, consider daily doses of a fluoroquinolone (eg, ciprofloxacin 500 mg orally once daily, not twice daily as for treatment) or rifaximin 200 mg orally once or twice a day, for no longer than 2 to 3 weeks.10
Non-antimicrobial chemoprophylaxis
Bismuth subsalicylate has reduced the incidence of TD from 40% to just 14% when taken in doses of 2 chewable tablets or 60 mL of liquid 4 times daily. 11,19,22 However, the dosing frequency can hinder adherence. Moreover, the relatively high doses required raise the risk of adverse drug reactions such as blackening of the tongue and stool, nausea, constipation, Reye syndrome (in children under 12 years), and possibly tinnitus. The salicylate component of the drug poses a threat to patients with aspirin allergy, renal disease, and those taking anticoagulants. Drug interactions with probenecid and methotrexate are also possible. Bismuth is not recommended for use for longer than 3 weeks, or for children younger than 3 years or pregnant women in their third trimester.
Other non-antimicrobial chemoprophylaxis agents include probiotics such as Lactobacillus andSaccharomyces. These preparations of bacteria and fungi are marketed either singly or in blends of varying composition and proportion. The evidence is divided on their efficacy, and even though some meta-analyses have concluded probiotics such as Saccharomyces boulardii are useful in preventing TD, endorsement in clinical guidelines is muted.10-12,28-30
Immunizations have limited value so farNatural immunity to E coli gastrointestinal infection among indigenous people in less developed countries has raised the possibility of a role for vaccines in preventing TD. Some strains of ETEC produce a heat-labile toxin (LT) that bears significant resemblance to the toxin produced by Vibrio cholerae. Therefore, the oral cholera vaccine, Dukoral, has been marketed outside the United States for the prevention of TD.19,22 However, only ≤7% of TD cases worldwide would be prevented by routine use of this vaccine.31 A transdermal LT vaccine, which involves the antigen-presenting Langerhans cells in the superficial skin layers, is promising but not yet available for routine use.19,22
Treating TD and associated symptoms
Antibiotic treatment
Given that most cases of TD are caused by bacterial pathogens, antibiotics are considered the mainstay of treatment. Concerns about the ill effects of antibiotic use in the case of enterohemorrhagic E coli(EHEC O157:H7) can be allayed because this strain is rarely a cause of TD.9Patient factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.
Consider local resistance patterns and risk of invasive infection. Which antibiotic to recommend is governed by the antibiotic resistance patterns prevalent in the travel destinations and by the risk of infection by invasive pathogens. Invasive TD is generally caused by Campylobacter, Shigella, or Salmonella and manifests clinically with bloody diarrhea, fever, or both. Rifaximin at a dose of 200 mg orally 3 times daily is effective for noninvasive TD.31,32 However, travelers who develop invasive TD need an alternative to rifaximin. (Those who advocate reserving antibiotic treatment only for invasive diarrhea will not see a role for rifaximin in the first place.) In most invasive cases, a fluoroquinolone will suffice.10-12,19,32 However, increasing prevalence of fluoroquinolone-resistantCampylobacter species has been reported in South and Southeast Asia. In those locations, azithromycin is an effective alternative, albeit with risk of nausea.33TABLE 212 provides details of recommended antibiotic dosages for adults and children. The duration of treatment is generally 1 day unless symptoms persist, in which case a 3-day course is recommended.10-12,19,32 If the traveler experiences persistent, new, or worsening symptoms beyond this point, immediate evaluation by a physician is required.
Non-antibiotic treatment
The antimotility agent loperamide is a well-established antidiarrheal agent. Its effective and safe use as an adjunct to antibiotics in the treatment of TD has been demonstrated in several studies.10-12,19,32,34 It is generally not used to treat children with TD9
No other non-antibiotic treatment for TD has significant guideline or clinical trial support. Bismuth subsalicylate can be helpful as an antidiarrheal agent,35 but is not often recommended because the regimen makes adherence difficult and because antibiotics and loperamide are effective.
Oral rehydration is usually a mainstay of treating gastrointestinal disease among infants and children. However, it, too, has a limited role in cases of TD because dehydration is not usually a significant part of the clinical presentation, perhaps because vomiting is not often prominent.
CASE Advice regarding safe food and beverage choices is essential for the patient and her children. Despite the increased risk for TD due to her history and her use of the immunosuppressant methotrexate, she decides not to pursue antibiotic prophylaxis. Bismuth is also contraindicated because of the methotrexate. Her teenage daughter declines bismuth prophylaxis, and her toddler is too young for it.
The patient does accept a prescription for azithromycin for her and her daughters in case they experience TD. This choice is appropriate given the destination of India and concern about Campylobacterresistance to fluoroquinolones. You also recommend loperamide for use by the mother and older child, in conjunction with the antibiotic.
Two weeks after their trip abroad, the travelers return for an office visit. On the trip, the mother and toddler suffered diarrhea, which responded well to your recommended management. The older child was well during the trip, but she developed diarrhea, abdominal pain, and anorexia one week after returning to the United States. These symptoms have persisted despite a 3-day course of azithromycin and loperamide.
Post-travel evaluation
TD generally occurs within one to 2 weeks of arrival at the travel destination and usually lasts no longer than 4 to 5 days.19 This scenario is typical of a bacterial infection. When it occurs later or lasts longer, or both, consider several alternative possibilities.19,36 First, the likelihood of a protozoal parasitic infection is increased. Although giardiasis is most likely, other protozoa such as Entamoeba, Cyclospora, Isospora, and Cryptosporidium are also possibilities. Second, if diarrhea persists, it might be due, not to continued infection, but to a self-limited post-infectious enteropathy or to PI-IBS. Third, TD is known to precipitate the clinical manifestation of underlying gastrointestinal disorders such as inflammatory bowel disease (IBD), celiac disease, or even cancer.37
With an atypical disease course, it’s advisable to send 3 stool samples for laboratory evaluation for ova and parasites and for antigen assays for Giardia. If results of these tests are negative, given the difficulty inherent in diagnosing Giardia, consider empiric treatment with metronidazole in lieu of duodenal sampling.36 If the diarrhea persists, investigate serologic markers for celiac disease and IBD. If these are not revealing, referral for colonoscopy is prudent.
CASE The teenager’s 3 stool samples were negative for ova and parasites and for Giardia antigen. Following empirical treatment with oral metronidazole 250 mg, 3 times daily for 7 days, the diarrhea resolved.
CORRESPONDENCE Dilip Nair, MD, Joan C. Edwards School of Medicine at Marshall University, 1600 Medical Center Drive, Suite 1500, Huntington, WV 25701; [email protected]
1. Recommend antibiotic chemoprophylaxis for travelers at high risk for travelers’ diarrhea (TD) and those at high risk for complications. It is also appropriate for travelers who have an inflexible itinerary. B
2. Recommend bismuth subsalicylate chemoprophylaxis for travelers at high risk for TD who are willing to comply with the regimen and want to avoid antibiotic prophylaxis. B
3. Advise travelers to initiate self-treatment for TD with a fluoroquinolone (or azithromycin, if in South or Southeast Asia) at the onset of diarrhea if it is bloody or accompanied by fever. A
NOTE: This practice recommendation in the print version of this article stated that travelers should also take loperamide; however, both the Centers for Disease Control and Prevention and the Infectious Diseases Society of America advise against the use of loperamide by travelers with fever or bloody diarrhea [corrected August 27, 2013].
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A 40-year-old female patient, a childhood immigrant from India, is seeking advice regarding her upcoming 2-week trip to Mumbai. She is taking her 2 children, ages 16 years and 16 months, to visit their grandparents for the first time. She has made this trip alone a few times and has invariably experienced short bouts of self-limited diarrheal illness. She wonders what she might do to prevent travelers’ diarrhea. Her only medical problem is rheumatoid arthritis, which has been well controlled with methotrexate. Her children are healthy. What would you recommend?
Recommendations regarding travelers’ diarrhea (TD) address prevention and management. Prevention encompasses advice about personal behaviors and the use of chemoprophylaxis (antimicrobial and non-antimicrobial) and vaccinations. Since international travelers are known to treat themselves for diarrheal illnesses during their trips,1 recommendations regarding management should assume self-treatment and include the use of both antibiotics and non-antibiotic remedies. Pretravel recommendations will of course be most effective if they account for the individual’s risk for TD.
Innate patient susceptibility, destination, and dietary choices determine TD risk
TD is generally defined as the passage of 3 of more loose stools in a 24-hour period, with associated symptoms of enteric infection—eg, fever, nausea, vomiting, or abdominal cramping. Defined in this manner, TD is thought to occur in 60% to 70% of individuals who travel from developed countries to less-developed countries.2,4 Risk of TD is influenced both by intrinsic personal factors and by factors specific to the trip.
Personal risk factorsIndividual variation in susceptibility to TD might result from a genetic predisposition arising from single nucleotide polymorphisms governing various inflammatory marker proteins.5 A history of multiple episodes of TD, especially if fellow travelers were spared, can suggest this kind of individual susceptibility. Other factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.6,7 However, the trip itself is much more important in assessing risk for TD.
Trip-related risk factors
The destination. The most salient risk factor for TD is the geographic destination. Regions of the world can be divided into TD risk strata:2
- Very high: South Asia
- High: South America, Sub-Saharan Africa
- Medium: Central America, Mexico, Caribbean, Middle East, North Africa, Southeast Asia, Oceania
- Low: Europe, North America (excluding Mexico), Australasia, Northeast Asia.
Particularly notable countries, in descending order of risk, are Nepal, India, Myanmar, Bolivia, Sri Lanka, Ecuador, Peru, Kenya, and Guatemala.2
Dietary choices. Additionally, since travelers acquire TD by ingesting food or beverages contaminated with pathogenic fecal microbes, dietary behaviors during the trip affect their susceptibility. At least risk are business travelers and tourists who confine their activities to more affluent settings in which food and beverages are prepared and stored hygienically.1,4,8,9 At greater risk are travelers who immerse themselves in local culture, visiting locations that are more impoverished and not as well equipped with sanitation systems, especially if their stay is at least 2 to 3 weeks.1,4,8,9
Also, the older a traveler is, the lower his or her risk of TD.1,9 An exception to this might be infants whose diet consists solely of breast milk or formula prepared under sanitary conditions.
Mandates and options for preventing TD
Emphasize food and beverage precautions
It might be reasonable to expect that travelers who are circumspect about their food and beverage choices on trips will be able to avoid TD. Indeed, this is the basis for the aphorism, “Boil it, peel it, or forget it.” Guidelines routinely recommend that travelers restrict their selection of foods to those that have been well cooked and are served while still very hot, and to fruits and vegetables that they peel themselves. Likewise, they should drink only beverages that have been boiled or are in sealed bottles or under carbonation and served without ice.10-12 Many travelers might find these recommendations too restrictive to follow faithfully. Moreover, studies suggest it may not be possible for even the most assiduous traveler to fully avoid the risk of TD.13,14 The hygienic characteristics of the travel destination may be more determinative, as illustrated by the successful reduction of TD rates in Jamaica by improving sanitation in tourist resorts.15
Antibiotic chemoprophylaxis: A debated practice with limited consensusThe etiologic agents of TD are multiple and vary somewhat in predominance according to geographic region.3,16,17 TABLE 1 depicts variance by region.16 The most common pathogens are strains of the bacterium Escherichia coli, particularly enterotoxigenic (ETEC), enteroaggregative (EAEC), and enteropathogenic (EPEC) strains.16 Other bacteria of importance are Campylobacter, Salmonella, and Shigella. Viruses, particularly norovirus (notably connected with cruise ships), can also cause TD, although it is implicated in no more than 17% of cases.18 Parasitic pathogens are even less common causes of TD (4%-10%) and mainly involve the protozoa, Giardia lamblia, and, to a lesser extent, Entamoeba histolytica and Cryptosporidium.
Although some pathogens often have a characteristic presentation—such as frothy, greasy diarrhea in the case of G lamblia—they generally cannot be reliably distinguished from one another clinically. Notably, up to 50% of stool samples from TD patients do not yield any pathogen,16 raising the suspicion that current diagnostic technology is not sufficiently sensitive to routinely identify certain bacteria.
There is no consensus on recommending antibiotic chemoprophylaxis against TD.
Opponents of this practice10-12,19,20 point out that TD is generally a brief (3-5 days), self-limited illness. Moreover, concerns about antibiotic resistance have come to pass. Previously used agents, trimethoprim-sulfamethoxazole and doxycycline, are no longer effective in preventing or treating TD. In addition, antibiotic use carries the risk of allergic reactions as well as other adverse effects including, ironically, the development of antibiotic-associated diarrhea and Clostridium difficile diarrhea.
Proponents of antibiotic chemoprophylaxis21,22 point to its demonstrated efficacy in reducing the risk of TD by 4% to 40%.11 They also argue that at least 20% to 25% of travelers who get TD must significantly curtail their activities for a day or more.1,23 This change in travel plans is associated not only with significant personal loss but also imposes a financial burden.23 Furthermore, TD is known to have longer-term effects. Up to 10% of sufferers develop postinfectious irritable bowel syndrome (PI-IBS) that can last for 5 or 6 years.21,22,24,25 It is not known, however, whether the use of antibiotic chemoprophylaxis significantly reduces the incidence of PI-IBS.
Finally, the luminal antibiotic, rifaximin, nonabsorbable as it is, is very well-tolerated and holds promise for not inciting antibiotic resistance.22 However, while its efficacy in preventing TD has been demonstrated in various settings,22,26,27 it is not approved by the US Food and Drug Administration for this indication. Also, concerns persist that it might not be effective in preventing TD caused by invasive pathogens.19
Indications on which all agree. Even opponents of antibiotic chemoprophylaxis grant that it is probably warranted for 2 groups of travelers.10-12 The first is those whose trip schedule is of such importance that any deviation would be intolerable. The second is travelers with comorbidities that would render them at high risk for serious inconvenience or illness if they developed TD. Examples of the latter include patients with enterostomies, mobility impairments, immune suppression, inflammatory bowel disease, and renal or metabolic diseases.
Chemoprophylaxis regimens. If you prescribe an antibiotic prophylactically, consider daily doses of a fluoroquinolone (eg, ciprofloxacin 500 mg orally once daily, not twice daily as for treatment) or rifaximin 200 mg orally once or twice a day, for no longer than 2 to 3 weeks.10
Non-antimicrobial chemoprophylaxis
Bismuth subsalicylate has reduced the incidence of TD from 40% to just 14% when taken in doses of 2 chewable tablets or 60 mL of liquid 4 times daily. 11,19,22 However, the dosing frequency can hinder adherence. Moreover, the relatively high doses required raise the risk of adverse drug reactions such as blackening of the tongue and stool, nausea, constipation, Reye syndrome (in children under 12 years), and possibly tinnitus. The salicylate component of the drug poses a threat to patients with aspirin allergy, renal disease, and those taking anticoagulants. Drug interactions with probenecid and methotrexate are also possible. Bismuth is not recommended for use for longer than 3 weeks, or for children younger than 3 years or pregnant women in their third trimester.
Other non-antimicrobial chemoprophylaxis agents include probiotics such as Lactobacillus andSaccharomyces. These preparations of bacteria and fungi are marketed either singly or in blends of varying composition and proportion. The evidence is divided on their efficacy, and even though some meta-analyses have concluded probiotics such as Saccharomyces boulardii are useful in preventing TD, endorsement in clinical guidelines is muted.10-12,28-30
Immunizations have limited value so farNatural immunity to E coli gastrointestinal infection among indigenous people in less developed countries has raised the possibility of a role for vaccines in preventing TD. Some strains of ETEC produce a heat-labile toxin (LT) that bears significant resemblance to the toxin produced by Vibrio cholerae. Therefore, the oral cholera vaccine, Dukoral, has been marketed outside the United States for the prevention of TD.19,22 However, only ≤7% of TD cases worldwide would be prevented by routine use of this vaccine.31 A transdermal LT vaccine, which involves the antigen-presenting Langerhans cells in the superficial skin layers, is promising but not yet available for routine use.19,22
Treating TD and associated symptoms
Antibiotic treatment
Given that most cases of TD are caused by bacterial pathogens, antibiotics are considered the mainstay of treatment. Concerns about the ill effects of antibiotic use in the case of enterohemorrhagic E coli(EHEC O157:H7) can be allayed because this strain is rarely a cause of TD.9Patient factors that increase vulnerability to TD are immunodeficiency, achlorhydric states such as atrophic gastritis, and chronic use of proton pump inhibitors.
Consider local resistance patterns and risk of invasive infection. Which antibiotic to recommend is governed by the antibiotic resistance patterns prevalent in the travel destinations and by the risk of infection by invasive pathogens. Invasive TD is generally caused by Campylobacter, Shigella, or Salmonella and manifests clinically with bloody diarrhea, fever, or both. Rifaximin at a dose of 200 mg orally 3 times daily is effective for noninvasive TD.31,32 However, travelers who develop invasive TD need an alternative to rifaximin. (Those who advocate reserving antibiotic treatment only for invasive diarrhea will not see a role for rifaximin in the first place.) In most invasive cases, a fluoroquinolone will suffice.10-12,19,32 However, increasing prevalence of fluoroquinolone-resistantCampylobacter species has been reported in South and Southeast Asia. In those locations, azithromycin is an effective alternative, albeit with risk of nausea.33TABLE 212 provides details of recommended antibiotic dosages for adults and children. The duration of treatment is generally 1 day unless symptoms persist, in which case a 3-day course is recommended.10-12,19,32 If the traveler experiences persistent, new, or worsening symptoms beyond this point, immediate evaluation by a physician is required.
Non-antibiotic treatment
The antimotility agent loperamide is a well-established antidiarrheal agent. Its effective and safe use as an adjunct to antibiotics in the treatment of TD has been demonstrated in several studies.10-12,19,32,34 It is generally not used to treat children with TD9
No other non-antibiotic treatment for TD has significant guideline or clinical trial support. Bismuth subsalicylate can be helpful as an antidiarrheal agent,35 but is not often recommended because the regimen makes adherence difficult and because antibiotics and loperamide are effective.
Oral rehydration is usually a mainstay of treating gastrointestinal disease among infants and children. However, it, too, has a limited role in cases of TD because dehydration is not usually a significant part of the clinical presentation, perhaps because vomiting is not often prominent.
CASE Advice regarding safe food and beverage choices is essential for the patient and her children. Despite the increased risk for TD due to her history and her use of the immunosuppressant methotrexate, she decides not to pursue antibiotic prophylaxis. Bismuth is also contraindicated because of the methotrexate. Her teenage daughter declines bismuth prophylaxis, and her toddler is too young for it.
The patient does accept a prescription for azithromycin for her and her daughters in case they experience TD. This choice is appropriate given the destination of India and concern about Campylobacterresistance to fluoroquinolones. You also recommend loperamide for use by the mother and older child, in conjunction with the antibiotic.
Two weeks after their trip abroad, the travelers return for an office visit. On the trip, the mother and toddler suffered diarrhea, which responded well to your recommended management. The older child was well during the trip, but she developed diarrhea, abdominal pain, and anorexia one week after returning to the United States. These symptoms have persisted despite a 3-day course of azithromycin and loperamide.
Post-travel evaluation
TD generally occurs within one to 2 weeks of arrival at the travel destination and usually lasts no longer than 4 to 5 days.19 This scenario is typical of a bacterial infection. When it occurs later or lasts longer, or both, consider several alternative possibilities.19,36 First, the likelihood of a protozoal parasitic infection is increased. Although giardiasis is most likely, other protozoa such as Entamoeba, Cyclospora, Isospora, and Cryptosporidium are also possibilities. Second, if diarrhea persists, it might be due, not to continued infection, but to a self-limited post-infectious enteropathy or to PI-IBS. Third, TD is known to precipitate the clinical manifestation of underlying gastrointestinal disorders such as inflammatory bowel disease (IBD), celiac disease, or even cancer.37
With an atypical disease course, it’s advisable to send 3 stool samples for laboratory evaluation for ova and parasites and for antigen assays for Giardia. If results of these tests are negative, given the difficulty inherent in diagnosing Giardia, consider empiric treatment with metronidazole in lieu of duodenal sampling.36 If the diarrhea persists, investigate serologic markers for celiac disease and IBD. If these are not revealing, referral for colonoscopy is prudent.
CASE The teenager’s 3 stool samples were negative for ova and parasites and for Giardia antigen. Following empirical treatment with oral metronidazole 250 mg, 3 times daily for 7 days, the diarrhea resolved.
CORRESPONDENCE Dilip Nair, MD, Joan C. Edwards School of Medicine at Marshall University, 1600 Medical Center Drive, Suite 1500, Huntington, WV 25701; [email protected]
1. Hill DR. Occurrence and self-treatment of diarrhea in a large cohort of Americans traveling to developing countries. Am J Trop Med Hyg. 2000;62:585–589.
2. Greenwood Z, Black J, Weld L, et al. for the GeoSentinel Surveillance Network. Gastrointestinal infection among international travelers globally. J Travel Med. 2008;15:221–228.
3. DuPont HL. Systematic review: the epidemiology and clinical features of travellers’ diarrhoea. Aliment Pharmacol Ther. 2009;30:187–196.
4. Steffen R, Tornieporth N, Clemens SA, et al. Epidemiology of travelers’ diarrhea: details of a global survey. J Travel Med. 2004;11:231–237.
5. de la Cabada Bauche J, DuPont HL. New developments in traveler’s diarrhea. Gastroenterol Hepatol. 2011;7:88–95.
6. Cabada MM, White AC. Travelers’ diarrhea: an update on susceptibility, prevention, and treatment. Curr Gastroenterol Rep. 2008;10:473–479.
7. Ericsson CD. Travellers with pre-existing medical conditions. Int J Antimicrob Agents. 2003;21:181–188.
8. Cabada MM, Maldonado F, Quispe W, et al. Risk factors associated with diarrhea among international visitors to Cuzco, Peru. Am J Trop Med Hyg. 2006;75:968–972.
9. Mackell S. Traveler’s diarrhea in the pediatric population: etiology and impact. Clin Infect Dis. 2005;41(suppl 8):S547–S552.
10. Hill DR, Ericsson CD, Pearson RD, et al. The practice of travel medicine: guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1499–1539.
11. Connor BA. Travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-2-the-pre-travel-consultation/travelers-diarrhea.htm. Accessed August 20, 2012.
12. Advice for travelers. Treat Guidel Med Lett. 2012;10:45–56.
13. Shlim DR. Looking for evidence that personal hygiene precautions prevent travelers’ diarrhea. Clin Infect Dis. 2005;41(suppl 8):S531–S535.
14. Laverone E, Boccalini S, Bechini A, et al. Travelers’ compliance to prophylactic measures and behavior during stay abroad: results of a retrospective study of subjects returning to a travel medicine center in Italy. J Travel Med. 2006;13:338–344.
15. Ashley DV, Walters C, Dockery-Brown C, et al. Interventions to prevent and control food-borne diseases associated with a reduction in traveler’s diarrhea in tourists to Jamaica. J Travel Med. 2004;11:364–367.
16. Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers’ diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg. 2009;80:609–614.
17. Riddle MS, Sanders JW, Putnam SD, et al. Incidence, etiology, and impact of diarrhea among long-term travelers (US military and similar populations): a systematic review. Am J Trop Med Hyg. 2006;74:891–900.
18. Koo HL, Ajami NJ, Jiang ZD, et al. Noroviruses as a cause of diarrhea in travelers to Guatemala, India, and Mexico. J Clin Microbiol. 2010;48:1673–1676.
19. Hill DR, Ryan ET. Management of travellers’ diarrhoea. BMJ. 2008;337:863–867.
20. Rendi-Wagner P, Kollaritsch H. Drug prophylaxis for travelers’ diarrhea. Clin Infect Dis. 2002;34:628–633.
21. Pimentel M, Riddle MS. Prevention of traveler’s diarrhea: a call to reconvene. Clin Infect Dis. 2008;46:151–152.
22. DuPont HL. Systematic review: prevention of travellers’ diarrhoea. Aliment Pharmacol Ther. 2008;27:741–751.
23. Wang M, Szucs TD, Steffen R. Economic aspects of travelers’ diarrhea. J Travel Med. 2008;15:110–118.
24. Neal KR, Barker L, Spiller RC. Prognosis in post-infective irritable bowel syndrome: a six year follow up study. Gut. 2002;51:410–413.
25. Tornblom H, Holmvall P, Svenungsson B, et al. Gastrointestinal symptoms after infectious diarrhea: a five-year follow-up in a Swedish cohort of adults. Clin Gastroenterol Hepatol. 2007;5:461–464.
26. DuPont HL, Jiang ZD, Okhuysen PC, et al. A randomized, double-blind, placebo-controlled trial of rifaximin to prevent travelers’ diarrhea. Ann Intern Med. 2005;142:805–812.
27. Taylor DN, McKenzie R, Durbin A, et al. Rifaximin, a nonabsorbed oral antibiotic, prevents shigellosis after experimental challenge. Clin Infect Dis. 2006;42:1283–1288.
28. Sazawal S, Hiremath G, Dhingra U, et al. Efficacy of probiotics in prevention of acute diarrhoea: a meta-analysis of masked, randomised, placebo-controlled trials. Lancet Infect Dis. 2006;6:374–382.
29. Bri V, Buffet P, Genty S, et al. Absence of efficacy of nonviable Lactobacillus acidophilus for the prevention of traveler’s diarrhea: a randomized, double-blind, controlled study. Clin Infect Dis. 2006;43:1170–1175.
30. Hill DR, Ford L, Lalloo DG. Oral cholera vaccines—use in clinical practice. Lancet Infect Dis. 2006;6:361–373.
31. Taylor DN, Bourgeois AL, Ericsson CD, et al. A randomized double-blind, multicenter study of rifaximin compared with placebo and with ciprofloxacin in the treatment of travelers’ diarrhea. Am J Trop Med Hyg. 2006;74:1060–1066.
32. DuPont HL, Ericsson CD, Farthing MJG, et al. Expert review of the evidence base for self-therapy of travelers’ diarrhea. J Travel Med. 2009;16:161–171.
33. Tribble DR, Sanders JW, Pang LW, et al. Traveler’s diarrhea in Thailand: randomized, double-blind trial comparing single-dose and 3-day azithromycin-based regimens with a 3-day levofloxacin regimen. Clin Infect Dis. 2007;44:338–346.
34. Riddle MS, Arnold S, Tribble DR. Effect of adjunctive loperamide in combination with antibiotics on treatment outcomes in travelers’ diarrhea: a systematic review and meta-analysis. Clin Infect Dis. 2008;47:1007–1014.
35. Steffen R. Worldwide efficacy of bismuth subsalicylate in the treatment of travelers’ diarrhea. Rev Infect Dis. 1990;12(suppl 1):S80–S86.
36. Connor BA. Persistent travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/persistent-travelers-diarrhea.htm. Accessed August 20, 2012.
37.Landzberg BR, Connor BA. Persistent diarrhea in the returning traveler: think beyond persistent infection. Scand J Gastroenterol. 2005;40:112–114.
1. Hill DR. Occurrence and self-treatment of diarrhea in a large cohort of Americans traveling to developing countries. Am J Trop Med Hyg. 2000;62:585–589.
2. Greenwood Z, Black J, Weld L, et al. for the GeoSentinel Surveillance Network. Gastrointestinal infection among international travelers globally. J Travel Med. 2008;15:221–228.
3. DuPont HL. Systematic review: the epidemiology and clinical features of travellers’ diarrhoea. Aliment Pharmacol Ther. 2009;30:187–196.
4. Steffen R, Tornieporth N, Clemens SA, et al. Epidemiology of travelers’ diarrhea: details of a global survey. J Travel Med. 2004;11:231–237.
5. de la Cabada Bauche J, DuPont HL. New developments in traveler’s diarrhea. Gastroenterol Hepatol. 2011;7:88–95.
6. Cabada MM, White AC. Travelers’ diarrhea: an update on susceptibility, prevention, and treatment. Curr Gastroenterol Rep. 2008;10:473–479.
7. Ericsson CD. Travellers with pre-existing medical conditions. Int J Antimicrob Agents. 2003;21:181–188.
8. Cabada MM, Maldonado F, Quispe W, et al. Risk factors associated with diarrhea among international visitors to Cuzco, Peru. Am J Trop Med Hyg. 2006;75:968–972.
9. Mackell S. Traveler’s diarrhea in the pediatric population: etiology and impact. Clin Infect Dis. 2005;41(suppl 8):S547–S552.
10. Hill DR, Ericsson CD, Pearson RD, et al. The practice of travel medicine: guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1499–1539.
11. Connor BA. Travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-2-the-pre-travel-consultation/travelers-diarrhea.htm. Accessed August 20, 2012.
12. Advice for travelers. Treat Guidel Med Lett. 2012;10:45–56.
13. Shlim DR. Looking for evidence that personal hygiene precautions prevent travelers’ diarrhea. Clin Infect Dis. 2005;41(suppl 8):S531–S535.
14. Laverone E, Boccalini S, Bechini A, et al. Travelers’ compliance to prophylactic measures and behavior during stay abroad: results of a retrospective study of subjects returning to a travel medicine center in Italy. J Travel Med. 2006;13:338–344.
15. Ashley DV, Walters C, Dockery-Brown C, et al. Interventions to prevent and control food-borne diseases associated with a reduction in traveler’s diarrhea in tourists to Jamaica. J Travel Med. 2004;11:364–367.
16. Shah N, DuPont HL, Ramsey DJ. Global etiology of travelers’ diarrhea: systematic review from 1973 to the present. Am J Trop Med Hyg. 2009;80:609–614.
17. Riddle MS, Sanders JW, Putnam SD, et al. Incidence, etiology, and impact of diarrhea among long-term travelers (US military and similar populations): a systematic review. Am J Trop Med Hyg. 2006;74:891–900.
18. Koo HL, Ajami NJ, Jiang ZD, et al. Noroviruses as a cause of diarrhea in travelers to Guatemala, India, and Mexico. J Clin Microbiol. 2010;48:1673–1676.
19. Hill DR, Ryan ET. Management of travellers’ diarrhoea. BMJ. 2008;337:863–867.
20. Rendi-Wagner P, Kollaritsch H. Drug prophylaxis for travelers’ diarrhea. Clin Infect Dis. 2002;34:628–633.
21. Pimentel M, Riddle MS. Prevention of traveler’s diarrhea: a call to reconvene. Clin Infect Dis. 2008;46:151–152.
22. DuPont HL. Systematic review: prevention of travellers’ diarrhoea. Aliment Pharmacol Ther. 2008;27:741–751.
23. Wang M, Szucs TD, Steffen R. Economic aspects of travelers’ diarrhea. J Travel Med. 2008;15:110–118.
24. Neal KR, Barker L, Spiller RC. Prognosis in post-infective irritable bowel syndrome: a six year follow up study. Gut. 2002;51:410–413.
25. Tornblom H, Holmvall P, Svenungsson B, et al. Gastrointestinal symptoms after infectious diarrhea: a five-year follow-up in a Swedish cohort of adults. Clin Gastroenterol Hepatol. 2007;5:461–464.
26. DuPont HL, Jiang ZD, Okhuysen PC, et al. A randomized, double-blind, placebo-controlled trial of rifaximin to prevent travelers’ diarrhea. Ann Intern Med. 2005;142:805–812.
27. Taylor DN, McKenzie R, Durbin A, et al. Rifaximin, a nonabsorbed oral antibiotic, prevents shigellosis after experimental challenge. Clin Infect Dis. 2006;42:1283–1288.
28. Sazawal S, Hiremath G, Dhingra U, et al. Efficacy of probiotics in prevention of acute diarrhoea: a meta-analysis of masked, randomised, placebo-controlled trials. Lancet Infect Dis. 2006;6:374–382.
29. Bri V, Buffet P, Genty S, et al. Absence of efficacy of nonviable Lactobacillus acidophilus for the prevention of traveler’s diarrhea: a randomized, double-blind, controlled study. Clin Infect Dis. 2006;43:1170–1175.
30. Hill DR, Ford L, Lalloo DG. Oral cholera vaccines—use in clinical practice. Lancet Infect Dis. 2006;6:361–373.
31. Taylor DN, Bourgeois AL, Ericsson CD, et al. A randomized double-blind, multicenter study of rifaximin compared with placebo and with ciprofloxacin in the treatment of travelers’ diarrhea. Am J Trop Med Hyg. 2006;74:1060–1066.
32. DuPont HL, Ericsson CD, Farthing MJG, et al. Expert review of the evidence base for self-therapy of travelers’ diarrhea. J Travel Med. 2009;16:161–171.
33. Tribble DR, Sanders JW, Pang LW, et al. Traveler’s diarrhea in Thailand: randomized, double-blind trial comparing single-dose and 3-day azithromycin-based regimens with a 3-day levofloxacin regimen. Clin Infect Dis. 2007;44:338–346.
34. Riddle MS, Arnold S, Tribble DR. Effect of adjunctive loperamide in combination with antibiotics on treatment outcomes in travelers’ diarrhea: a systematic review and meta-analysis. Clin Infect Dis. 2008;47:1007–1014.
35. Steffen R. Worldwide efficacy of bismuth subsalicylate in the treatment of travelers’ diarrhea. Rev Infect Dis. 1990;12(suppl 1):S80–S86.
36. Connor BA. Persistent travelers’ diarrhea. Available at:http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/persistent-travelers-diarrhea.htm. Accessed August 20, 2012.
37.Landzberg BR, Connor BA. Persistent diarrhea in the returning traveler: think beyond persistent infection. Scand J Gastroenterol. 2005;40:112–114.