User login
The Affordable Care Act and the drive for electronic health records: Are small practices being squeezed?
Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.

Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
Two years ago, I zeroed in on the pressures straining small ObGyn practices in an article entitled, “Is private ObGyn practice on its way out?”1 The pressures haven’t eased in the interim. Today, small practices are still feeling squeezed to keep up with the many demands of modern specialty care. The push for electronic health records (EHRs), in particular, can profoundly affect physicians in private practice.
In this article, I outline some of the challenges facing small practices when they set out to implement EHRs, as well as the potential benefits they stand to gain a little farther down the road. Before we begin, however, let’s look at the latest trends in ObGyn practice, as they are related, in part, to the need to implement EHRs.
The exodus from private practice continues
A 2012 Accenture Physicians Alignment Survey shows an accelerating increase in physician employment. In 2000, 57% of all physicians were in independent practice; by the end of 2013, only 36% of physicians are projected to remain independent.2
The ObGyn specialty is a clear part of this trend, with both seasoned and incoming physicians finding hospital or other employment an attractive alternative to private practice. Fully one-third of ObGyn residents entering practice today sign hospital employment contracts. ObGyns who have made the switch from private to hospital practice, or who have become ObGyn hospitalists, often point to the difficulties of maintaining a solvent private practice, especially given the push toward EHRs and increasing regulatory and administrative burdens, as justification for their move.
The main reasons for the shift to employment. Top concerns influencing physicians’ decisions to opt for employment include:
- business expenses (87%)
- the dominance of managed care (61%)
- the requirement for EHRs (53%)
- the need to maintain and manage staff (53%)
- the increasing number of patients needed to break even (39%).2
A 2008 socioeconomic survey from ACOG revealed that 23.6% of ObGyn practices are solo practices, and 27.1% are single-specialty group practices. Many ObGyns—especially those in solo or small practices—are hesitant to make the large capital investment that is necessary to adopt EHRs.
EHRs offer benefits—and real costs
The system-wide benefits of health information technology (HIT), including EHRs, are many. Insurers stand to save money by reducing unnecessary tests, and patients will benefit from better coordination of their care and fewer medical errors. But these advantages don’t necessarily translate into savings or revenue for physician practices. Instead, physicians face payment cuts from Medicare and private insurance.
Although there’s wide agreement that HIT can improve quality of care and reduce health-care costs, fewer than one-quarter (22%) of office-based physicians had adopted EHRs by 2009. We know the main reasons why:
- upfront cost and maintenance expense
- uncertain return on investment
- fragmented business model in a high proportion of small and solo practices
- changing and inconsistent information technology (IT) systems.
What can a practice expect to fork over?
In 2011, the Agency for Healthcare Research and Quality (AHRQ) found that the “real-life” cost of implementing EHRs “in an average five-physician primary care practice, operating within a large physician network committed to network-wide implementation of electronic health records, is about $162,000, with an additional $85,500 in maintenance expenses during the first year.”3
These figures include an average of 134 hours needed per physician to prepare to use EHRs during patient visits.3
Fleming and colleagues investigated the cost associated with implementing EHRs within 26 primary care practices in Texas. They found the cost to be $32,409 per physician through the first 60 days after the EHR system was launched, with one-time costs for hardware of $25,000 per practice and an additional $7,000 per physician for personal computers, printers, and scanners. The annual cost of software and maintenance was approximately $17,100 per physician.4
Why physicians should hold out for the return on their investment
Despite these considerable expenses, EHRs hold promise over the long term. The Medical Group Management Association reported, through a 2009 survey of about 1,300 primary care and specialty practice members using EHRs, that efficiency gains from the elimination of paper charts, as well as transcription savings, better charge capturing, and reduced billing errors, resulted in a median revenue increase of $49,916 per full-time physician after operating costs.
After 5 years of EHR use, practices reported a median operating margin 10.1% higher than that of practices in the first year of EHR use.5
Trends in the adoption of EHRs
Private practice. An article in Health Affairs showed that, by 2011, only one in six office-based physicians was using an EHR system robust enough to approach “meaningful use”—that is, the use of EHRs to measurably improve the quality of health care.6 These robust systems offered physicians the ability to record information on patient demographics, view laboratory and imaging results, maintain patients’ problem lists, compile clinical notes, and manage prescription ordering. EHR adoption lagged among non−primary care physicians, physicians aged 55 and older, and physicians in small (1–2 providers) practices and physician-owned practices.6 (ObGyns were considered primary care providers in this survey.)
“Big” practice. By comparison, in 2011, 99% of physicians in health maintenance organizations, or HMOs, and 73% in academic health centers and other hospitals used EHR systems.6 The number of physicians in these practice settings is small but growing.
In 2011, only 17% of physicians were in large practices of 10 or more physicians; 40% were in practices of one or two physicians.6
Primary care. These practices lead others in the adoption of EHRs, in part because of federal assistance, including a nationwide system of regional HIT assistance centers established by the Health Information Technology for Economic and Clinical Health (HITECH) Act to help providers located in rural areas participate in the Centers for Medicare and Medicaid Services (CMS) programs in EHR. The goal of these programs is to provide HIT support to at least 100,000 primary care providers, including ObGyns, by 2014.
The numbers cited in the Health Affairs article largely mirror data developed by other research organizations, including the Deloitte Center for Health Solutions.6
The EHR incentive
The drive for EHRs started long before the Affordable Care Act (ACA) was passed in 2010. The US Congress took a first stab at encouraging the health-care community to embrace HIT in 1996, when it passed the Health Insurance Portability and Accountability Act (HIPAA). HIPAA created an electronic data interchange that health plans, health-care clearinghouses, and certain health-care providers, including pharmacists, are required to use for electronic transactions, including:
- claims and encounter information
- payment and remittance advice
- claims status
- eligibility
- enrollment and disenrollment
- referrals and authorizations
- coordination of benefits
- premium payment.
Congress stepped up its game in 2009, when it offered higher Medicare and Medicaid payments to physicians who adopt and “meaningfully use” EHRs. The HITECH Act included $30 billion in new Medicare and Medicaid incentive payments—as much as $44,000 under Medicare and $63,750 under Medicaid—as well as $500 million for states to develop health information exchanges.
The Act also established a government-led process for certification of electronic health records through a $35 billion appropriation for the Office of the National Coordinator for Health IT, housed in CMS.
Other programs designed to encourage use of EHRs
Other federal programs include the Physician Quality Reporting System (PQRS), which, when created in 2006, was a voluntary physician electronic reporting program. Under the ACA, however, it has become a mandate. Starting in 2015, Medicare payments will be reduced for nonparticipating physicians.
The Electronic Prescribing (eRx) Incentive Program, created in 2008 under the Medicare Improvements for Patients and Providers Act, provides incentives for eligible physicians who e-prescribe Medicare Part D medications through a qualified system. This program converted to a penalty program last year for physicians who don’t use eRx.
Grants were also provided under the HITECH Act to fund an HIT infrastructure and low-interest HIT loans. The AHRQ has awarded $300 million in federal grant money to more than 200 projects in 48 states to promote access to and encourage HIT adoption. Over $150 million in Medicaid transformation grants have been awarded to three states and territories for HIT in the Medicaid program under the 2005 Deficit Reduction Act.
The ACA carried these initiatives even further by establishing uniform standards that HIT systems must meet, including:
- automatic reconciliation of electronic fund transfers and HIPAA payment and remittance
- improved claims payment process
- consistent methods of health plan enrollment and claim edits
- simplified and improved routing of health-care transactions
- electronic claims attachments.
Clearly, a lot of effort and taxpayer dollars have been dedicated to drive efficient use of HIT and EHRs in the hopes that they can:
- help make sense of our increasingly fragmented health-care system
- improve patient safety
- increase efficiency
- reduce paperwork
- reduce unnecessary tests
- better coordinate patient care.
To see which providers are cashing in on the government’s incentives for EHRs, see “Some physicians are more likely to seek incentives for meaningful use of EHRs” on page 37.
The long view
HIT and EHRs are here to stay. Products are maturing and improving. Acceptance by large and small practices has gained traction. Are small practices being squeezed? No doubt.
In 2011, I urged all ObGyns—especially those in private practice—to read an article written by President Barack Obama’s health-reform deputies on how physicians can be successful under the ACA.1 It reads, in part:
To realize the full benefits of the Affordable Care Act, physicians will need to embrace rather than resist change. The economic forces put in motion by the Act are likely to lead to vertical organization of providers and accelerate physician employment by hospitals and aggregation into larger physician groups. The most successful physicians will be those who most effectively collaborate with other providers to improve outcomes, care productivity, and patient experience.7
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.
1. DiVenere L, Yates J. Is private ObGyn practice on its way out? OBG Manage. 2011;23(10):42–54.
2. More US doctors leaving private practice due to rising costs and technology mandates, Accenture report finds [news release]. Arlington, Virginia: Accenture Newsroom; October 31, 2012. http://newsroom.accenture.com/news/more-us-doctors-leaving-private-practice-due-to-rising-costs-and-technology-mandates-accenture-report-finds.htm. Accessed June 5, 2013.
3. Study identifies costs of implementing electronic health records in network of physician practices: Research Activities October 2011, No. 374. Rockville, MD: Agency for Healthcare Research and Quality. http://www.ahrq.gov/news/newsletters/research-activities/oct11/1011RA15.html. Accessed June 5, 2013.
5. MGMA survey: Medical groups with EHRs report better financial performance than practices with paper medical records [news release]. New Orleans, Louisiana: Medical Group Management Association; October 25, 2010. http://www.mgma.com/press/default.aspx?id=39824. Accessed June 6, 2013.
8. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicaid Incentive Payments for 2011. GAO-13-146R. December 13, 2012. http://www.gao.gov/products/GAO-13-146R. Accessed June 6, 2013.
9. US Government Accountability Office. Electronic Health Records: Number and Characteristics of Providers Awarded Medicare Incentive Payments for 2011. GAO-12-778R. July 26, 2012. http://www.gao.gov/products/GAO-12-778R. Accessed June 6, 2013.
10. US Department of Health and Human Services. Doctors’ and hospitals’ use of health IT more than doubles since 2012 [news release]. Washington, DC: HHS.gov; May 22, 2013. http://www.hhs.gov/news/press/2013pres/05/20130522a.html. Accessed June 6, 2013.
Wound Hematoma After Anterior Cervical Spine Surgery: in vitro Study of the Pathophysiology of Airway Obstruction
Preventing Surgical Site Infection: Preoperative Bathing
Letters
Addressing biceps rupture, at what price?
I was glad to see you publish “When is a conservative approach best for proximal biceps tendon rupture?” (J Fam Pract. 2013;62:134-136), as it addressed an injury commonly seen in sports medicine practice, but one not often written about. However, I believe the approach the authors presented—which included both an MRI and specialty referral—is expensive and unnecessary.
Biceps tendon rupture is primarily a clinical diagnosis, and the findings are so classic that imaging is usually unnecessary. Adding a $750 MRI to the cost of treatment is wasteful, and not done by any of the orthopedists I work with. If imaging is "necessary" due to patient desire or diagnostic confusion (hard to imagine), an ultrasound has very high sensitivity and specificity.
Since the lesion is almost totally cosmetic, there is little reason to consider fixing it. The biceps is not really used in many sports activities, and strength is not impaired. In fact, John Elway, a prominent football player in the National Football League, played most of his games with this injury.
In 40 years of practice, I’ve seen about 15 patients with biceps tendon rupture. Only one opted for surgery, and that was because he wanted to look good at the gym. Usually, a careful discussion is adequate to manage this problem. Yet the authors noted that 2 orthopedic surgeons examined their patient. My concern is not about the accuracy of the data they presented, but about turning a $200 problem into a $1500 expenditure.
James Kennedy, MD
Winter Park, Colo
Drs. Sofya Pugach and Isaac Pugach respond:
We thank Dr. Kennedy for his letter. We’re glad our article prompted a discussion of different approaches to proximal biceps tendon rupture, including the conservative management (no MRI) he discusses as well as surgical repair. Treatment of this condition is still a subject of debate in the medical literature, and there is no one correct "recipe."
Sofya Pugach, MD, PhD, MPH
Isaac Z. Pugach, MD
Dallas, Tex
Saying No to EMRs
"End EMR tyranny!" (Editorial, J Fam Pract. 2013;62:173) reminded me of my own experience. As a solo practitioner, I began trying to implement my own EMR 13 years ago. I kept switching to bigger screens and newer computer system, but things just got worse.
Finally, I bought a top-rated pen-based tablet, but even then, voice and handwriting recognition didn’t work. I had to stay in the office until 9:30 pm just to type my notes. My children were asleep by the time I got home.
So I revolted. I went back to paper and pen and opted out of Medicare. Now I’m home at 5:30 every evening, seeing my children and enjoying my life—all because I got rid of this bureaucratic burden. I regret that I have only one practice to give to paper and pen!
Farid Taie, DO
Plano, Tex
… and saying Yes
For the past 2 years, our large multispecialty group has been in the throes of transitioning 250 doctors from the inadequate but familiar paper charts to the daunting EMR system.
I’ve been in practice for 36 years. Most of my colleagues are in my age group, and don’t take easily to change—or to computers. Three colleagues opted to retire rather than accommodate the changes, while others of us would never want to return to paper.
To be sure, it requires an investment of time to assimilate quick texts, problem lists, and myriad other details, but once that’s done, the EMR is a far superior system.
In a very few years, those of us who paved the way to EMRs will be retired, proud that we were the pioneers who brought about this important transition.
Cherry Brandstater, MD
Redlands, Calif
Addressing biceps rupture, at what price?
I was glad to see you publish “When is a conservative approach best for proximal biceps tendon rupture?” (J Fam Pract. 2013;62:134-136), as it addressed an injury commonly seen in sports medicine practice, but one not often written about. However, I believe the approach the authors presented—which included both an MRI and specialty referral—is expensive and unnecessary.
Biceps tendon rupture is primarily a clinical diagnosis, and the findings are so classic that imaging is usually unnecessary. Adding a $750 MRI to the cost of treatment is wasteful, and not done by any of the orthopedists I work with. If imaging is "necessary" due to patient desire or diagnostic confusion (hard to imagine), an ultrasound has very high sensitivity and specificity.
Since the lesion is almost totally cosmetic, there is little reason to consider fixing it. The biceps is not really used in many sports activities, and strength is not impaired. In fact, John Elway, a prominent football player in the National Football League, played most of his games with this injury.
In 40 years of practice, I’ve seen about 15 patients with biceps tendon rupture. Only one opted for surgery, and that was because he wanted to look good at the gym. Usually, a careful discussion is adequate to manage this problem. Yet the authors noted that 2 orthopedic surgeons examined their patient. My concern is not about the accuracy of the data they presented, but about turning a $200 problem into a $1500 expenditure.
James Kennedy, MD
Winter Park, Colo
Drs. Sofya Pugach and Isaac Pugach respond:
We thank Dr. Kennedy for his letter. We’re glad our article prompted a discussion of different approaches to proximal biceps tendon rupture, including the conservative management (no MRI) he discusses as well as surgical repair. Treatment of this condition is still a subject of debate in the medical literature, and there is no one correct "recipe."
Sofya Pugach, MD, PhD, MPH
Isaac Z. Pugach, MD
Dallas, Tex
Saying No to EMRs
"End EMR tyranny!" (Editorial, J Fam Pract. 2013;62:173) reminded me of my own experience. As a solo practitioner, I began trying to implement my own EMR 13 years ago. I kept switching to bigger screens and newer computer system, but things just got worse.
Finally, I bought a top-rated pen-based tablet, but even then, voice and handwriting recognition didn’t work. I had to stay in the office until 9:30 pm just to type my notes. My children were asleep by the time I got home.
So I revolted. I went back to paper and pen and opted out of Medicare. Now I’m home at 5:30 every evening, seeing my children and enjoying my life—all because I got rid of this bureaucratic burden. I regret that I have only one practice to give to paper and pen!
Farid Taie, DO
Plano, Tex
… and saying Yes
For the past 2 years, our large multispecialty group has been in the throes of transitioning 250 doctors from the inadequate but familiar paper charts to the daunting EMR system.
I’ve been in practice for 36 years. Most of my colleagues are in my age group, and don’t take easily to change—or to computers. Three colleagues opted to retire rather than accommodate the changes, while others of us would never want to return to paper.
To be sure, it requires an investment of time to assimilate quick texts, problem lists, and myriad other details, but once that’s done, the EMR is a far superior system.
In a very few years, those of us who paved the way to EMRs will be retired, proud that we were the pioneers who brought about this important transition.
Cherry Brandstater, MD
Redlands, Calif
Addressing biceps rupture, at what price?
I was glad to see you publish “When is a conservative approach best for proximal biceps tendon rupture?” (J Fam Pract. 2013;62:134-136), as it addressed an injury commonly seen in sports medicine practice, but one not often written about. However, I believe the approach the authors presented—which included both an MRI and specialty referral—is expensive and unnecessary.
Biceps tendon rupture is primarily a clinical diagnosis, and the findings are so classic that imaging is usually unnecessary. Adding a $750 MRI to the cost of treatment is wasteful, and not done by any of the orthopedists I work with. If imaging is "necessary" due to patient desire or diagnostic confusion (hard to imagine), an ultrasound has very high sensitivity and specificity.
Since the lesion is almost totally cosmetic, there is little reason to consider fixing it. The biceps is not really used in many sports activities, and strength is not impaired. In fact, John Elway, a prominent football player in the National Football League, played most of his games with this injury.
In 40 years of practice, I’ve seen about 15 patients with biceps tendon rupture. Only one opted for surgery, and that was because he wanted to look good at the gym. Usually, a careful discussion is adequate to manage this problem. Yet the authors noted that 2 orthopedic surgeons examined their patient. My concern is not about the accuracy of the data they presented, but about turning a $200 problem into a $1500 expenditure.
James Kennedy, MD
Winter Park, Colo
Drs. Sofya Pugach and Isaac Pugach respond:
We thank Dr. Kennedy for his letter. We’re glad our article prompted a discussion of different approaches to proximal biceps tendon rupture, including the conservative management (no MRI) he discusses as well as surgical repair. Treatment of this condition is still a subject of debate in the medical literature, and there is no one correct "recipe."
Sofya Pugach, MD, PhD, MPH
Isaac Z. Pugach, MD
Dallas, Tex
Saying No to EMRs
"End EMR tyranny!" (Editorial, J Fam Pract. 2013;62:173) reminded me of my own experience. As a solo practitioner, I began trying to implement my own EMR 13 years ago. I kept switching to bigger screens and newer computer system, but things just got worse.
Finally, I bought a top-rated pen-based tablet, but even then, voice and handwriting recognition didn’t work. I had to stay in the office until 9:30 pm just to type my notes. My children were asleep by the time I got home.
So I revolted. I went back to paper and pen and opted out of Medicare. Now I’m home at 5:30 every evening, seeing my children and enjoying my life—all because I got rid of this bureaucratic burden. I regret that I have only one practice to give to paper and pen!
Farid Taie, DO
Plano, Tex
… and saying Yes
For the past 2 years, our large multispecialty group has been in the throes of transitioning 250 doctors from the inadequate but familiar paper charts to the daunting EMR system.
I’ve been in practice for 36 years. Most of my colleagues are in my age group, and don’t take easily to change—or to computers. Three colleagues opted to retire rather than accommodate the changes, while others of us would never want to return to paper.
To be sure, it requires an investment of time to assimilate quick texts, problem lists, and myriad other details, but once that’s done, the EMR is a far superior system.
In a very few years, those of us who paved the way to EMRs will be retired, proud that we were the pioneers who brought about this important transition.
Cherry Brandstater, MD
Redlands, Calif
Words—not scores—inspire me
Being a physician does not seem as rewarding today as it did 30 years ago.
Under constant pressure to focus on production, meaningful use, and compliance with myriad regulations, it’s easy to lose sight of the most rewarding part of our work—caring for our patients. And most are highly satisfied with our care.
The modern rendition of patient satisfaction is the “patient experience” score, with the data tracked and disseminated by firms specializing in such reports. I do see some value in these reports, as they can help us pinpoint areas of our office operations or personal interactions that could be improved. But on an emotional level, they just don’t cut it. Patient experience scores, and the form in which they’re presented, are too much like report cards. They don’t inspire me.
What inspires me is receiving a heartfelt “thank you” from a grateful patient, and I’m reasonably sure the same is true for you. Which is why I offer the following excerpts from a truly inspiring “thank you” speech delivered by Sam Miller, an emeritus trustee of the Cleveland Clinic, at the clinic’s 2012 Professional Excellence Awards:
“You mean a lot to me personally and you mean a lot to each other, for you are, as far as I’m concerned, the veritable guardians of this community.
“Someday after enough DNA tests, they will discover the gene in doctors making you walking hearts, perennial consciences, and empathetic human beings. And when they do, they will look for this gene in all humanity, and we will have found the answer to wars and to peace and to love. Love means reaching towards neighbors and the world with the same care, regard, generosity and empathy we normally reserve for ourselves and those closest to us,” he said. “This is the gene that a doctor has inherited.”
“You will not have to wait for your reward in heaven,” Miller said. “Every day when you see the smiles of the sick, the poor, the look of hope and momentary happiness of that particular unfortunate that you’ve been able to help, that is heaven by itself. That is the magnificent gene that you possess.”
I offer heartfelt thanks to Mr. Miller for his deeply moving words, and I invite you, my fellow family physicians, to share your stories of patients whose expressions of appreciation have truly inspired you.
Being a physician does not seem as rewarding today as it did 30 years ago.
Under constant pressure to focus on production, meaningful use, and compliance with myriad regulations, it’s easy to lose sight of the most rewarding part of our work—caring for our patients. And most are highly satisfied with our care.
The modern rendition of patient satisfaction is the “patient experience” score, with the data tracked and disseminated by firms specializing in such reports. I do see some value in these reports, as they can help us pinpoint areas of our office operations or personal interactions that could be improved. But on an emotional level, they just don’t cut it. Patient experience scores, and the form in which they’re presented, are too much like report cards. They don’t inspire me.
What inspires me is receiving a heartfelt “thank you” from a grateful patient, and I’m reasonably sure the same is true for you. Which is why I offer the following excerpts from a truly inspiring “thank you” speech delivered by Sam Miller, an emeritus trustee of the Cleveland Clinic, at the clinic’s 2012 Professional Excellence Awards:
“You mean a lot to me personally and you mean a lot to each other, for you are, as far as I’m concerned, the veritable guardians of this community.
“Someday after enough DNA tests, they will discover the gene in doctors making you walking hearts, perennial consciences, and empathetic human beings. And when they do, they will look for this gene in all humanity, and we will have found the answer to wars and to peace and to love. Love means reaching towards neighbors and the world with the same care, regard, generosity and empathy we normally reserve for ourselves and those closest to us,” he said. “This is the gene that a doctor has inherited.”
“You will not have to wait for your reward in heaven,” Miller said. “Every day when you see the smiles of the sick, the poor, the look of hope and momentary happiness of that particular unfortunate that you’ve been able to help, that is heaven by itself. That is the magnificent gene that you possess.”
I offer heartfelt thanks to Mr. Miller for his deeply moving words, and I invite you, my fellow family physicians, to share your stories of patients whose expressions of appreciation have truly inspired you.
Being a physician does not seem as rewarding today as it did 30 years ago.
Under constant pressure to focus on production, meaningful use, and compliance with myriad regulations, it’s easy to lose sight of the most rewarding part of our work—caring for our patients. And most are highly satisfied with our care.
The modern rendition of patient satisfaction is the “patient experience” score, with the data tracked and disseminated by firms specializing in such reports. I do see some value in these reports, as they can help us pinpoint areas of our office operations or personal interactions that could be improved. But on an emotional level, they just don’t cut it. Patient experience scores, and the form in which they’re presented, are too much like report cards. They don’t inspire me.
What inspires me is receiving a heartfelt “thank you” from a grateful patient, and I’m reasonably sure the same is true for you. Which is why I offer the following excerpts from a truly inspiring “thank you” speech delivered by Sam Miller, an emeritus trustee of the Cleveland Clinic, at the clinic’s 2012 Professional Excellence Awards:
“You mean a lot to me personally and you mean a lot to each other, for you are, as far as I’m concerned, the veritable guardians of this community.
“Someday after enough DNA tests, they will discover the gene in doctors making you walking hearts, perennial consciences, and empathetic human beings. And when they do, they will look for this gene in all humanity, and we will have found the answer to wars and to peace and to love. Love means reaching towards neighbors and the world with the same care, regard, generosity and empathy we normally reserve for ourselves and those closest to us,” he said. “This is the gene that a doctor has inherited.”
“You will not have to wait for your reward in heaven,” Miller said. “Every day when you see the smiles of the sick, the poor, the look of hope and momentary happiness of that particular unfortunate that you’ve been able to help, that is heaven by itself. That is the magnificent gene that you possess.”
I offer heartfelt thanks to Mr. Miller for his deeply moving words, and I invite you, my fellow family physicians, to share your stories of patients whose expressions of appreciation have truly inspired you.
Finger injuries: 5 cases to test your skills
Some finger injuries require little more than icing; others are more serious, often emergent, conditions with outcomes that are dependent on an accurate diagnosis and rapid initiation of treatment.
The 5 cases that follow describe injuries with varying degrees of severity. Read each case and select the multiple-choice answer you think is most appropriate. Then read on to find out if you were right—and to learn more about the clinical presentation, diagnosis, and treatment for each type of injury.
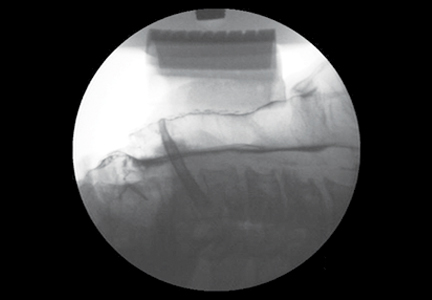
CASE 1 A 45-year-old auto body worker walks into your office at 5:30 pm, just as your staff is closing up for the day. A few hours ago, he reports, he was spray-painting a car with a paint gun when he felt a sudden pain in his right index finger. His immediate thought was that he had torn something, but the pain quickly subsided. So he continued to work—until about 45 minutes ago, when the pain became so intense that he knew he needed medical care right away.
Examination reveals redness and increased skin temperature on the radial palmar side of the proximal interphalangeal (PIP) joint of the index finger. Two-point discrimination is decreased to 10 mm, vs 5 mm on the same finger of the opposite hand. The patient can flex his PIP and distal interphalangeal (DIP) joints but complains of pain and stiffness. You obtain x-rays of the injured
finger (FIGURE 1).

WHAT'S YOUR NEXT STEP?
B. Update the patient’s tetanus immunization and start him on a broad-spectrum antibiotic.
C. Put a dorsal splint on the injured finger in the “safe hand” position and schedule a return visit in one week.
D. “Buddy tape” the index and long fingers and refer the patient to a hand surgeon.
Answer: Send the auto-body worker to the nearest ED and call ahead (A).
This patient sustained a high-pressure injection injury to the PIP joint of his right index finger. The patient’s description of how the injury occurred suggested this, and the radiograph confirmed it by showing some paint under the skin (See arrow, FIGURE 1). Such injuries occur when a high pressure (typically from a hose) forces air or a substance—eg, diesel fuel, paint, or solvent—through the skin into the finger.
Although high-pressure injection injury often has a benign presentation, it is actually a medical emergency. If aggressive surgical debridement does not occur within a 6-hour window, the patient runs a high risk for amputation of the digit.1 A hand surgeon should be contacted as soon as possible.
The severity of the injury varies, depending on the amount of pressure (amputation rates are as high as 43% when the pressure per square inch >1000), the type of material injected (diesel fuel is the most toxic), and the location.1,2
Instruct the patient to remove any jewelry, such as a wedding band or watch, on the affected hand or wrist, and to keep the hand elevated. Broad-spectrum antibiotics should be started right away, and a tetanus booster given, if needed. Do not apply heat or use local anesthesia, as both can increase the swelling.2
CASE 2 A 17-year-old cheerleader comes to see you on Monday afternoon, after injuring her left pinky during a Friday night game. The patient, who is right-handed, points to the left PIP joint when you ask where it hurts, and tells you that the finger is stiff. She has been icing it since the injury occurred, to make sure she is ready to cheer by next weekend.
The injury occurred when she was spotting another cheerleader during a routine, the patient reports, adding that the pinky was “dislocated.” The coach “popped” it back in place and buddy-taped the injured finger to her ring finger.
The patient is able to flex and extend the DIP joint on the pinky when the PIP joint is stabilized. She can also flex the PIP joint unassisted, but has difficulty extending it. The digit demonstrates slight flexion of the PIP joint. You note tenderness over both collateral ligaments and the dorsum of the PIP joint, but not over the volar aspect of the injured finger, and order x-rays (FIGURE 2).

WHAT'S YOUR NEXT STEP?
B. Refer the patient to a hand surgeon.
C. Apply an extension block splint so the patient can flex the finger but not extend it, and schedule a follow-up appointment in one to 2 weeks.
D. Apply an aluminum dorsal splint, allowing the DIP joint to be flexed and keeping the PIP joint in full extension for 4 weeks.
Answer: Refer the cheerleader to a hand surgeon (B).
This patient has a rupture of the central extensor tendon of the pinky finger at the PIP joint. The mechanism of injury and her inability to completely extend the injured finger at the PIP joint alert you to this type of injury. An x-ray may sometimes be normal but in this case, it shows the flexion of the PIP joint. Surgical repair of the rupture should be scheduled without delay.3
Most injuries at this joint occur from forced extension, not flexion, and result in a volar plate rupture.4 If swelling and pain make evaluation of an acute dislocation injury difficult, splinting in the “safe hand” position for 72 hours while icing the injured finger will make it possible to do a more detailed follow-up exam.3
Extended periods of splinting can make the PIP joint very stiff, however—and harder to treat than the original injury.5 If the rupture of the central extensor tendon is undetected or simply not treated, a Boutonniere deformity, in which the PIP joint is flexed and the DIP joint is hyperextended, is the likely result.3
CASE 3 A 24-year-old man “jammed” his right ring finger while trying to catch a ball that was passed to him during a pick-up basketball game. He has rested and iced the finger for a couple of days, but it’s still painful and hard to move. He has no significant medical history and has been taking only acetaminophen for the pain.
Examination reveals that the injured finger has good capillary refill, 2-point discrimination is intact at 5 mm, and the other fingers on his right hand have no deformities and a normal range of motion. On the injured finger, however, the DIP joint is swollen and tender; it cannot be fully extended (FiGURE 3).

WHAT'S YOUR DIAGNOSIS?
B. Distal tuft fracture.
C. Mallet finger.
D. Finger sprain.
E. Trigger finger.
Answer: The basketball player has mallet finger (C).
Mallet finger typically occurs on the dominant hand. The key physical finding is that the joint is “stuck” in flexion, which is evident during an exam and on x-ray. Although the DIP joint may be passively fully extended, the patient with mallet finger is unable to actively extend it.
Mallet injuries, which are common in sports and associated with minor trauma, are typically caused by sudden forced flexion of the DIP joint during active extension of the finger. This can either stretch or tear the extensor tendon or lead to avulsion of the tendon insertion from the dorsum of the distal phalanx, with or without a fragment of bone. The injury is called a “soft” mallet finger when there is no bone involvement and a “bony” mallet finger when an avulsion is present, like the one that is evident on the FIGURE 3 x-ray (see arrow).
On clinical examination, the finger may or may not have an obvious deformity; similarly, you won’t always see bruising, swelling, or tenderness over the DIP joint.6 The work-up should include posterior/anterior, oblique, and lateral x-rays, followed by an examination of the soft tissue and a range-of-motion evaluation of the metacarpophalangeal and PIP joints. In acute injuries, tenderness is elicited with palpation over the dorsal aspect of the DIP joint. Although most patients develop an extensor lag at the DIP joint immediately after injury, the deformity may be delayed by a few hours or even days.6,7
Nonsurgical management is the standard of care for most mallet injuries, including mallet fractures involving less than one-third of the articular surface with no associated DIP joint subluxation.7
If there is no displacement, round-the-clock splinting to keep the joint in extension for a minimum of 6 weeks is indicated, followed by 2 to 3 weeks of nighttime splinting. It is important that the splinting allow for complete extension of the DIP joint but flexion of the PIP joint. Keeping the PIP in extension for prolonged periods can lead to permanent stiffness of the joint, while failure to provide any immobilization may lead to permanent deformity.
Surgery is indicated for a fracture fragment involving >30% of the joint surface (as demonstrated in the radiograph), volar subluxation, or a swan neck deformity—and when conservative therapy fails.7
CASE 4 An 18-year-old high school football player presents with pain and swelling at the tip of his right ring finger from an injury that occurred a week ago. When the player he was trying to tackle broke away, the patient says, he immediately felt pain and a “pop” in the finger.
The DIP joint of his right ring finger is swollen (FIGURE 4), but appears normal otherwise. When you isolate the joint, however, the patient is unable to flex it. You can palpate a stump on the volar surface of the finger.

What’s your next step?
B. Treat with splinting, RICE (rest, ice, compression, and elevation), and nonsteroidal anti-inflammatory drugs.
C. Order an ultrasound of the finger and palm.
D. Order magnetic resonance imaging (MRI) of the hand.
Answer: Order an ultrasound of the football player’s finger and palm (C).
This patient has Jersey finger, caused by a traumatic avulsion of the flexor digitorum profundus (FDP) from the distal phalanx and diagnosed based on the mechanism of injury and the patient’s inability to flex the DIP joint. The injury often does not show on x-rays, and the diagnosis may be missed for several weeks.
Jersey finger usually happens in sports like football or rugby, where players tackle each other, and involves forced, passive extension of the DIP joint at a time of active flexion. Management of Jersey finger starts with splinting, with both the DIP and PIP in slight flexion. Surgical reattachment of the flexor tendon is needed, with best results when it is done within 7 to 10 days of injury.4
You may be able to palpate the tendon stump in the palm or along the digit; bony avulsions can be trapped at the flexor sheath. Soft tissue swelling can be misleading, however, and the point of maximal tenderness is not an accurate means of identifying the avulsed tendon stump.8
Ultrasound is effective in differentiating between a partial and full thickness rupture and in localizing the distal tendon stump.8 MRI is usually reserved for precise evaluation of the tendon edges, to aid in operative planning. If the tendon is retracted to the palm, scarring may be irreversible because of the lack of blood supply.
Athletes typically return to play 12 weeks after injury, starting with protected activity and progressing to full gripping/grasping. Physical therapy and/or occupational therapy will be needed after the surgical wound has healed.
CASE 5 A 40-year-old construction worker who smashed his left index finger with a hammer one day ago presents with severe pain in his fingertip, which he is unable to move. On examination, you find that the distal finger is swollen and there is extensive ecchymosis and swelling underneath the nail. The finger has normal sensation, but you are unable to see capillary refill due to a large hematoma.
X-rays (FIGURE 5) reveal a distal tuft fracture. The patient’s main concern is the pain, and he asks what you can do to relieve it.

What’s your next step?
B. Perform fenestration of the nail.
C. Refer the patient to a hand surgeon.
D. Order computed tomography of the hand.
Answer: Perform fenestration of the construction worker’s nail (B).
This patient has a closed fracture of the distal phalanx, called a tuft fracture, and a sub-ungual hematoma, evident from the x-ray and the physical presentation.
Subungual hematoma requires fenestration with a needle to create small holes in the nail. If the nail bed is lacerated, the nail is removed and the injured nail bed repaired with sutures.
Tuft fractures sometimes require reduction. More often, they are stable and minimally displaced and can be managed conservatively, with splinting with a padded aluminum splint or a fingertip guard (Stax splint) for 3 to 4 weeks. Antibiotics are not indicated unless there is suspicion of an overlying or secondary infection. Referral to a hand surgeon is required for severe crush injuries, avulsion of the nail matrix, and open fractures of the distal phalanx.5,6
1. Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma. 2006;20:503-511.
2. Gonzalez R, Kasdan ML. High pressure injection injuries of the hand. Clin Occup Environ Med. 2006;5:407-411.
3. Freiberg A. Management of proximal interphalangeal joint injuries. Can J Plast Surg. 2007;15:199-203.
4. Perron AD, Brady WJ, Keats TE, et al. Orthopedic pitfalls in the emergency department: closed tendon injuries of the hand. Am J Emerg Med. 2001;19:76-80.
5. Oetgen ME, Dodds SD. Non-operative treatment of common finger injuries. Curr Rev Musculoskel Med. 2008;1:97-102.
6. Anderson D. Mallet finger. Aust Fam Physician. 2011;40:91-92.
7. Smit JM, Beets MR. Treatment options for mallet finger: a review. Plast Reconstr Surg. 2010;126:1624-1629.
8. Goodson A, Morgan M. Current management of Jersey finger in rugby players: cases series and literature review. Hand Surg. 2010;15:103-107.
Some finger injuries require little more than icing; others are more serious, often emergent, conditions with outcomes that are dependent on an accurate diagnosis and rapid initiation of treatment.
The 5 cases that follow describe injuries with varying degrees of severity. Read each case and select the multiple-choice answer you think is most appropriate. Then read on to find out if you were right—and to learn more about the clinical presentation, diagnosis, and treatment for each type of injury.
CASE 1 A 45-year-old auto body worker walks into your office at 5:30 pm, just as your staff is closing up for the day. A few hours ago, he reports, he was spray-painting a car with a paint gun when he felt a sudden pain in his right index finger. His immediate thought was that he had torn something, but the pain quickly subsided. So he continued to work—until about 45 minutes ago, when the pain became so intense that he knew he needed medical care right away.
Examination reveals redness and increased skin temperature on the radial palmar side of the proximal interphalangeal (PIP) joint of the index finger. Two-point discrimination is decreased to 10 mm, vs 5 mm on the same finger of the opposite hand. The patient can flex his PIP and distal interphalangeal (DIP) joints but complains of pain and stiffness. You obtain x-rays of the injured
finger (FIGURE 1).
WHAT'S YOUR NEXT STEP?
B. Update the patient’s tetanus immunization and start him on a broad-spectrum antibiotic.
C. Put a dorsal splint on the injured finger in the “safe hand” position and schedule a return visit in one week.
D. “Buddy tape” the index and long fingers and refer the patient to a hand surgeon.
Answer: Send the auto-body worker to the nearest ED and call ahead (A).
This patient sustained a high-pressure injection injury to the PIP joint of his right index finger. The patient’s description of how the injury occurred suggested this, and the radiograph confirmed it by showing some paint under the skin (See arrow, FIGURE 1). Such injuries occur when a high pressure (typically from a hose) forces air or a substance—eg, diesel fuel, paint, or solvent—through the skin into the finger.
Although high-pressure injection injury often has a benign presentation, it is actually a medical emergency. If aggressive surgical debridement does not occur within a 6-hour window, the patient runs a high risk for amputation of the digit.1 A hand surgeon should be contacted as soon as possible.
The severity of the injury varies, depending on the amount of pressure (amputation rates are as high as 43% when the pressure per square inch >1000), the type of material injected (diesel fuel is the most toxic), and the location.1,2
Instruct the patient to remove any jewelry, such as a wedding band or watch, on the affected hand or wrist, and to keep the hand elevated. Broad-spectrum antibiotics should be started right away, and a tetanus booster given, if needed. Do not apply heat or use local anesthesia, as both can increase the swelling.2
CASE 2 A 17-year-old cheerleader comes to see you on Monday afternoon, after injuring her left pinky during a Friday night game. The patient, who is right-handed, points to the left PIP joint when you ask where it hurts, and tells you that the finger is stiff. She has been icing it since the injury occurred, to make sure she is ready to cheer by next weekend.
The injury occurred when she was spotting another cheerleader during a routine, the patient reports, adding that the pinky was “dislocated.” The coach “popped” it back in place and buddy-taped the injured finger to her ring finger.
The patient is able to flex and extend the DIP joint on the pinky when the PIP joint is stabilized. She can also flex the PIP joint unassisted, but has difficulty extending it. The digit demonstrates slight flexion of the PIP joint. You note tenderness over both collateral ligaments and the dorsum of the PIP joint, but not over the volar aspect of the injured finger, and order x-rays (FIGURE 2).
WHAT'S YOUR NEXT STEP?
B. Refer the patient to a hand surgeon.
C. Apply an extension block splint so the patient can flex the finger but not extend it, and schedule a follow-up appointment in one to 2 weeks.
D. Apply an aluminum dorsal splint, allowing the DIP joint to be flexed and keeping the PIP joint in full extension for 4 weeks.
Answer: Refer the cheerleader to a hand surgeon (B).
This patient has a rupture of the central extensor tendon of the pinky finger at the PIP joint. The mechanism of injury and her inability to completely extend the injured finger at the PIP joint alert you to this type of injury. An x-ray may sometimes be normal but in this case, it shows the flexion of the PIP joint. Surgical repair of the rupture should be scheduled without delay.3
Most injuries at this joint occur from forced extension, not flexion, and result in a volar plate rupture.4 If swelling and pain make evaluation of an acute dislocation injury difficult, splinting in the “safe hand” position for 72 hours while icing the injured finger will make it possible to do a more detailed follow-up exam.3
Extended periods of splinting can make the PIP joint very stiff, however—and harder to treat than the original injury.5 If the rupture of the central extensor tendon is undetected or simply not treated, a Boutonniere deformity, in which the PIP joint is flexed and the DIP joint is hyperextended, is the likely result.3
CASE 3 A 24-year-old man “jammed” his right ring finger while trying to catch a ball that was passed to him during a pick-up basketball game. He has rested and iced the finger for a couple of days, but it’s still painful and hard to move. He has no significant medical history and has been taking only acetaminophen for the pain.
Examination reveals that the injured finger has good capillary refill, 2-point discrimination is intact at 5 mm, and the other fingers on his right hand have no deformities and a normal range of motion. On the injured finger, however, the DIP joint is swollen and tender; it cannot be fully extended (FiGURE 3).
WHAT'S YOUR DIAGNOSIS?
B. Distal tuft fracture.
C. Mallet finger.
D. Finger sprain.
E. Trigger finger.
Answer: The basketball player has mallet finger (C).
Mallet finger typically occurs on the dominant hand. The key physical finding is that the joint is “stuck” in flexion, which is evident during an exam and on x-ray. Although the DIP joint may be passively fully extended, the patient with mallet finger is unable to actively extend it.
Mallet injuries, which are common in sports and associated with minor trauma, are typically caused by sudden forced flexion of the DIP joint during active extension of the finger. This can either stretch or tear the extensor tendon or lead to avulsion of the tendon insertion from the dorsum of the distal phalanx, with or without a fragment of bone. The injury is called a “soft” mallet finger when there is no bone involvement and a “bony” mallet finger when an avulsion is present, like the one that is evident on the FIGURE 3 x-ray (see arrow).
On clinical examination, the finger may or may not have an obvious deformity; similarly, you won’t always see bruising, swelling, or tenderness over the DIP joint.6 The work-up should include posterior/anterior, oblique, and lateral x-rays, followed by an examination of the soft tissue and a range-of-motion evaluation of the metacarpophalangeal and PIP joints. In acute injuries, tenderness is elicited with palpation over the dorsal aspect of the DIP joint. Although most patients develop an extensor lag at the DIP joint immediately after injury, the deformity may be delayed by a few hours or even days.6,7
Nonsurgical management is the standard of care for most mallet injuries, including mallet fractures involving less than one-third of the articular surface with no associated DIP joint subluxation.7
If there is no displacement, round-the-clock splinting to keep the joint in extension for a minimum of 6 weeks is indicated, followed by 2 to 3 weeks of nighttime splinting. It is important that the splinting allow for complete extension of the DIP joint but flexion of the PIP joint. Keeping the PIP in extension for prolonged periods can lead to permanent stiffness of the joint, while failure to provide any immobilization may lead to permanent deformity.
Surgery is indicated for a fracture fragment involving >30% of the joint surface (as demonstrated in the radiograph), volar subluxation, or a swan neck deformity—and when conservative therapy fails.7
CASE 4 An 18-year-old high school football player presents with pain and swelling at the tip of his right ring finger from an injury that occurred a week ago. When the player he was trying to tackle broke away, the patient says, he immediately felt pain and a “pop” in the finger.
The DIP joint of his right ring finger is swollen (FIGURE 4), but appears normal otherwise. When you isolate the joint, however, the patient is unable to flex it. You can palpate a stump on the volar surface of the finger.
What’s your next step?
B. Treat with splinting, RICE (rest, ice, compression, and elevation), and nonsteroidal anti-inflammatory drugs.
C. Order an ultrasound of the finger and palm.
D. Order magnetic resonance imaging (MRI) of the hand.
Answer: Order an ultrasound of the football player’s finger and palm (C).
This patient has Jersey finger, caused by a traumatic avulsion of the flexor digitorum profundus (FDP) from the distal phalanx and diagnosed based on the mechanism of injury and the patient’s inability to flex the DIP joint. The injury often does not show on x-rays, and the diagnosis may be missed for several weeks.
Jersey finger usually happens in sports like football or rugby, where players tackle each other, and involves forced, passive extension of the DIP joint at a time of active flexion. Management of Jersey finger starts with splinting, with both the DIP and PIP in slight flexion. Surgical reattachment of the flexor tendon is needed, with best results when it is done within 7 to 10 days of injury.4
You may be able to palpate the tendon stump in the palm or along the digit; bony avulsions can be trapped at the flexor sheath. Soft tissue swelling can be misleading, however, and the point of maximal tenderness is not an accurate means of identifying the avulsed tendon stump.8
Ultrasound is effective in differentiating between a partial and full thickness rupture and in localizing the distal tendon stump.8 MRI is usually reserved for precise evaluation of the tendon edges, to aid in operative planning. If the tendon is retracted to the palm, scarring may be irreversible because of the lack of blood supply.
Athletes typically return to play 12 weeks after injury, starting with protected activity and progressing to full gripping/grasping. Physical therapy and/or occupational therapy will be needed after the surgical wound has healed.
CASE 5 A 40-year-old construction worker who smashed his left index finger with a hammer one day ago presents with severe pain in his fingertip, which he is unable to move. On examination, you find that the distal finger is swollen and there is extensive ecchymosis and swelling underneath the nail. The finger has normal sensation, but you are unable to see capillary refill due to a large hematoma.
X-rays (FIGURE 5) reveal a distal tuft fracture. The patient’s main concern is the pain, and he asks what you can do to relieve it.
What’s your next step?
B. Perform fenestration of the nail.
C. Refer the patient to a hand surgeon.
D. Order computed tomography of the hand.
Answer: Perform fenestration of the construction worker’s nail (B).
This patient has a closed fracture of the distal phalanx, called a tuft fracture, and a sub-ungual hematoma, evident from the x-ray and the physical presentation.
Subungual hematoma requires fenestration with a needle to create small holes in the nail. If the nail bed is lacerated, the nail is removed and the injured nail bed repaired with sutures.
Tuft fractures sometimes require reduction. More often, they are stable and minimally displaced and can be managed conservatively, with splinting with a padded aluminum splint or a fingertip guard (Stax splint) for 3 to 4 weeks. Antibiotics are not indicated unless there is suspicion of an overlying or secondary infection. Referral to a hand surgeon is required for severe crush injuries, avulsion of the nail matrix, and open fractures of the distal phalanx.5,6
Some finger injuries require little more than icing; others are more serious, often emergent, conditions with outcomes that are dependent on an accurate diagnosis and rapid initiation of treatment.
The 5 cases that follow describe injuries with varying degrees of severity. Read each case and select the multiple-choice answer you think is most appropriate. Then read on to find out if you were right—and to learn more about the clinical presentation, diagnosis, and treatment for each type of injury.
CASE 1 A 45-year-old auto body worker walks into your office at 5:30 pm, just as your staff is closing up for the day. A few hours ago, he reports, he was spray-painting a car with a paint gun when he felt a sudden pain in his right index finger. His immediate thought was that he had torn something, but the pain quickly subsided. So he continued to work—until about 45 minutes ago, when the pain became so intense that he knew he needed medical care right away.
Examination reveals redness and increased skin temperature on the radial palmar side of the proximal interphalangeal (PIP) joint of the index finger. Two-point discrimination is decreased to 10 mm, vs 5 mm on the same finger of the opposite hand. The patient can flex his PIP and distal interphalangeal (DIP) joints but complains of pain and stiffness. You obtain x-rays of the injured
finger (FIGURE 1).
WHAT'S YOUR NEXT STEP?
B. Update the patient’s tetanus immunization and start him on a broad-spectrum antibiotic.
C. Put a dorsal splint on the injured finger in the “safe hand” position and schedule a return visit in one week.
D. “Buddy tape” the index and long fingers and refer the patient to a hand surgeon.
Answer: Send the auto-body worker to the nearest ED and call ahead (A).
This patient sustained a high-pressure injection injury to the PIP joint of his right index finger. The patient’s description of how the injury occurred suggested this, and the radiograph confirmed it by showing some paint under the skin (See arrow, FIGURE 1). Such injuries occur when a high pressure (typically from a hose) forces air or a substance—eg, diesel fuel, paint, or solvent—through the skin into the finger.
Although high-pressure injection injury often has a benign presentation, it is actually a medical emergency. If aggressive surgical debridement does not occur within a 6-hour window, the patient runs a high risk for amputation of the digit.1 A hand surgeon should be contacted as soon as possible.
The severity of the injury varies, depending on the amount of pressure (amputation rates are as high as 43% when the pressure per square inch >1000), the type of material injected (diesel fuel is the most toxic), and the location.1,2
Instruct the patient to remove any jewelry, such as a wedding band or watch, on the affected hand or wrist, and to keep the hand elevated. Broad-spectrum antibiotics should be started right away, and a tetanus booster given, if needed. Do not apply heat or use local anesthesia, as both can increase the swelling.2
CASE 2 A 17-year-old cheerleader comes to see you on Monday afternoon, after injuring her left pinky during a Friday night game. The patient, who is right-handed, points to the left PIP joint when you ask where it hurts, and tells you that the finger is stiff. She has been icing it since the injury occurred, to make sure she is ready to cheer by next weekend.
The injury occurred when she was spotting another cheerleader during a routine, the patient reports, adding that the pinky was “dislocated.” The coach “popped” it back in place and buddy-taped the injured finger to her ring finger.
The patient is able to flex and extend the DIP joint on the pinky when the PIP joint is stabilized. She can also flex the PIP joint unassisted, but has difficulty extending it. The digit demonstrates slight flexion of the PIP joint. You note tenderness over both collateral ligaments and the dorsum of the PIP joint, but not over the volar aspect of the injured finger, and order x-rays (FIGURE 2).
WHAT'S YOUR NEXT STEP?
B. Refer the patient to a hand surgeon.
C. Apply an extension block splint so the patient can flex the finger but not extend it, and schedule a follow-up appointment in one to 2 weeks.
D. Apply an aluminum dorsal splint, allowing the DIP joint to be flexed and keeping the PIP joint in full extension for 4 weeks.
Answer: Refer the cheerleader to a hand surgeon (B).
This patient has a rupture of the central extensor tendon of the pinky finger at the PIP joint. The mechanism of injury and her inability to completely extend the injured finger at the PIP joint alert you to this type of injury. An x-ray may sometimes be normal but in this case, it shows the flexion of the PIP joint. Surgical repair of the rupture should be scheduled without delay.3
Most injuries at this joint occur from forced extension, not flexion, and result in a volar plate rupture.4 If swelling and pain make evaluation of an acute dislocation injury difficult, splinting in the “safe hand” position for 72 hours while icing the injured finger will make it possible to do a more detailed follow-up exam.3
Extended periods of splinting can make the PIP joint very stiff, however—and harder to treat than the original injury.5 If the rupture of the central extensor tendon is undetected or simply not treated, a Boutonniere deformity, in which the PIP joint is flexed and the DIP joint is hyperextended, is the likely result.3
CASE 3 A 24-year-old man “jammed” his right ring finger while trying to catch a ball that was passed to him during a pick-up basketball game. He has rested and iced the finger for a couple of days, but it’s still painful and hard to move. He has no significant medical history and has been taking only acetaminophen for the pain.
Examination reveals that the injured finger has good capillary refill, 2-point discrimination is intact at 5 mm, and the other fingers on his right hand have no deformities and a normal range of motion. On the injured finger, however, the DIP joint is swollen and tender; it cannot be fully extended (FiGURE 3).
WHAT'S YOUR DIAGNOSIS?
B. Distal tuft fracture.
C. Mallet finger.
D. Finger sprain.
E. Trigger finger.
Answer: The basketball player has mallet finger (C).
Mallet finger typically occurs on the dominant hand. The key physical finding is that the joint is “stuck” in flexion, which is evident during an exam and on x-ray. Although the DIP joint may be passively fully extended, the patient with mallet finger is unable to actively extend it.
Mallet injuries, which are common in sports and associated with minor trauma, are typically caused by sudden forced flexion of the DIP joint during active extension of the finger. This can either stretch or tear the extensor tendon or lead to avulsion of the tendon insertion from the dorsum of the distal phalanx, with or without a fragment of bone. The injury is called a “soft” mallet finger when there is no bone involvement and a “bony” mallet finger when an avulsion is present, like the one that is evident on the FIGURE 3 x-ray (see arrow).
On clinical examination, the finger may or may not have an obvious deformity; similarly, you won’t always see bruising, swelling, or tenderness over the DIP joint.6 The work-up should include posterior/anterior, oblique, and lateral x-rays, followed by an examination of the soft tissue and a range-of-motion evaluation of the metacarpophalangeal and PIP joints. In acute injuries, tenderness is elicited with palpation over the dorsal aspect of the DIP joint. Although most patients develop an extensor lag at the DIP joint immediately after injury, the deformity may be delayed by a few hours or even days.6,7
Nonsurgical management is the standard of care for most mallet injuries, including mallet fractures involving less than one-third of the articular surface with no associated DIP joint subluxation.7
If there is no displacement, round-the-clock splinting to keep the joint in extension for a minimum of 6 weeks is indicated, followed by 2 to 3 weeks of nighttime splinting. It is important that the splinting allow for complete extension of the DIP joint but flexion of the PIP joint. Keeping the PIP in extension for prolonged periods can lead to permanent stiffness of the joint, while failure to provide any immobilization may lead to permanent deformity.
Surgery is indicated for a fracture fragment involving >30% of the joint surface (as demonstrated in the radiograph), volar subluxation, or a swan neck deformity—and when conservative therapy fails.7
CASE 4 An 18-year-old high school football player presents with pain and swelling at the tip of his right ring finger from an injury that occurred a week ago. When the player he was trying to tackle broke away, the patient says, he immediately felt pain and a “pop” in the finger.
The DIP joint of his right ring finger is swollen (FIGURE 4), but appears normal otherwise. When you isolate the joint, however, the patient is unable to flex it. You can palpate a stump on the volar surface of the finger.
What’s your next step?
B. Treat with splinting, RICE (rest, ice, compression, and elevation), and nonsteroidal anti-inflammatory drugs.
C. Order an ultrasound of the finger and palm.
D. Order magnetic resonance imaging (MRI) of the hand.
Answer: Order an ultrasound of the football player’s finger and palm (C).
This patient has Jersey finger, caused by a traumatic avulsion of the flexor digitorum profundus (FDP) from the distal phalanx and diagnosed based on the mechanism of injury and the patient’s inability to flex the DIP joint. The injury often does not show on x-rays, and the diagnosis may be missed for several weeks.
Jersey finger usually happens in sports like football or rugby, where players tackle each other, and involves forced, passive extension of the DIP joint at a time of active flexion. Management of Jersey finger starts with splinting, with both the DIP and PIP in slight flexion. Surgical reattachment of the flexor tendon is needed, with best results when it is done within 7 to 10 days of injury.4
You may be able to palpate the tendon stump in the palm or along the digit; bony avulsions can be trapped at the flexor sheath. Soft tissue swelling can be misleading, however, and the point of maximal tenderness is not an accurate means of identifying the avulsed tendon stump.8
Ultrasound is effective in differentiating between a partial and full thickness rupture and in localizing the distal tendon stump.8 MRI is usually reserved for precise evaluation of the tendon edges, to aid in operative planning. If the tendon is retracted to the palm, scarring may be irreversible because of the lack of blood supply.
Athletes typically return to play 12 weeks after injury, starting with protected activity and progressing to full gripping/grasping. Physical therapy and/or occupational therapy will be needed after the surgical wound has healed.
CASE 5 A 40-year-old construction worker who smashed his left index finger with a hammer one day ago presents with severe pain in his fingertip, which he is unable to move. On examination, you find that the distal finger is swollen and there is extensive ecchymosis and swelling underneath the nail. The finger has normal sensation, but you are unable to see capillary refill due to a large hematoma.
X-rays (FIGURE 5) reveal a distal tuft fracture. The patient’s main concern is the pain, and he asks what you can do to relieve it.
What’s your next step?
B. Perform fenestration of the nail.
C. Refer the patient to a hand surgeon.
D. Order computed tomography of the hand.
Answer: Perform fenestration of the construction worker’s nail (B).
This patient has a closed fracture of the distal phalanx, called a tuft fracture, and a sub-ungual hematoma, evident from the x-ray and the physical presentation.
Subungual hematoma requires fenestration with a needle to create small holes in the nail. If the nail bed is lacerated, the nail is removed and the injured nail bed repaired with sutures.
Tuft fractures sometimes require reduction. More often, they are stable and minimally displaced and can be managed conservatively, with splinting with a padded aluminum splint or a fingertip guard (Stax splint) for 3 to 4 weeks. Antibiotics are not indicated unless there is suspicion of an overlying or secondary infection. Referral to a hand surgeon is required for severe crush injuries, avulsion of the nail matrix, and open fractures of the distal phalanx.5,6
1. Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma. 2006;20:503-511.
2. Gonzalez R, Kasdan ML. High pressure injection injuries of the hand. Clin Occup Environ Med. 2006;5:407-411.
3. Freiberg A. Management of proximal interphalangeal joint injuries. Can J Plast Surg. 2007;15:199-203.
4. Perron AD, Brady WJ, Keats TE, et al. Orthopedic pitfalls in the emergency department: closed tendon injuries of the hand. Am J Emerg Med. 2001;19:76-80.
5. Oetgen ME, Dodds SD. Non-operative treatment of common finger injuries. Curr Rev Musculoskel Med. 2008;1:97-102.
6. Anderson D. Mallet finger. Aust Fam Physician. 2011;40:91-92.
7. Smit JM, Beets MR. Treatment options for mallet finger: a review. Plast Reconstr Surg. 2010;126:1624-1629.
8. Goodson A, Morgan M. Current management of Jersey finger in rugby players: cases series and literature review. Hand Surg. 2010;15:103-107.
1. Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma. 2006;20:503-511.
2. Gonzalez R, Kasdan ML. High pressure injection injuries of the hand. Clin Occup Environ Med. 2006;5:407-411.
3. Freiberg A. Management of proximal interphalangeal joint injuries. Can J Plast Surg. 2007;15:199-203.
4. Perron AD, Brady WJ, Keats TE, et al. Orthopedic pitfalls in the emergency department: closed tendon injuries of the hand. Am J Emerg Med. 2001;19:76-80.
5. Oetgen ME, Dodds SD. Non-operative treatment of common finger injuries. Curr Rev Musculoskel Med. 2008;1:97-102.
6. Anderson D. Mallet finger. Aust Fam Physician. 2011;40:91-92.
7. Smit JM, Beets MR. Treatment options for mallet finger: a review. Plast Reconstr Surg. 2010;126:1624-1629.
8. Goodson A, Morgan M. Current management of Jersey finger in rugby players: cases series and literature review. Hand Surg. 2010;15:103-107.
Cartilage Defect of Lunate Facet of Distal Radius After Fracture Treated With Osteochondral Autograft From Knee
Irreducible Longitudinal Distraction-Dislocation of the Hallux Interphalangeal Joint
Disk Degeneration in Lumbar Spine Precedes Osteoarthritic Changes in Hip
Pituitary tumor size not definitive for Cushing's
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.

Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.
Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
SAN FRANCISCO – The size of a pituitary tumor on magnetic resonance imaging in a patient with ACTH-dependent Cushing’s syndrome can’t differentiate between etiologies, but combining that information with biochemical test results could help avoid costly and difficult inferior petrosal sinus sampling in some patients, a study of 131 cases suggests.
If MRI shows a pituitary tumor larger than 6 mm in size, the finding is 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of adrenocorticotropic hormone (ACTH)-dependent Cushing’s syndrome, and additional information from biochemical testing may help further differentiate this from ectopic ACTH secretion, Dr. Divya Yogi-Morren and her associates reported at the Endocrine Society’s Annual Meeting.
Pituitary tumors were seen on MRI in 6 of 26 patients with ectopic ACTH secretion (23%) and 73 of 105 patients with Cushing’s disease (69%), with mean measurements of 4.5 mm in the ectopic ACTH secretion group and 8 mm in the Cushing’s disease group. All but one tumor in the ectopic ACTH secretion group were 6 mm or smaller in diameter, but one was 14 mm.
Because pituitary "incidentalomas" as large as 14 mm can be seen in patients with ectopic ACTH secretion, the presence of a pituitary tumor can’t definitively discriminate between ectopic ACTH secretion and Cushing’s disease, said Dr. Yogi-Morren, a fellow at the Cleveland Clinic.
That finding contradicts part of a 2003 consensus statement that said the presence of a focal pituitary lesion larger than 6 mm on MRI could provide a definitive diagnosis of Cushing’s disease, with no further evaluation needed in patients who have a classic clinical presentation and dynamic biochemical testing results that are compatible with a pituitary etiology (J. Clin. Endocrinol. Metab. 2003;88:5593-602). The 6-mm cutoff, said Dr. Yogi-Morren, came from an earlier study reporting that 10% of 100 normal, healthy adults had focal pituitary abnormalities on MRI ranging from 3 to 6 mm in diameter that were consistent with a diagnosis of asymptomatic pituitary adenomas (Ann. Intern. Med. 1994;120:817-20).
A traditional workup of a patient with ACTH-dependent Cushing’s syndrome might include a clinical history, biochemical testing, neuroimaging, and an inferior petrosal sinus sampling (IPSS). Biochemical testing typically includes tests for hypokalemia, measurement of cortisol and ACTH levels, a high-dose dexamethasone suppression test, and a corticotropin-releasing hormone (CRH) stimulation test. Although IPSS is the gold standard for differentiating between the two etiologies, it is expensive and technically difficult, especially in institutions that don’t regularly do the procedure, so it would be desirable to avoid IPSS if it’s not needed in a subset of patients, Dr. Yogi-Morren said.
The investigators reviewed charts from two centers (the Cleveland Clinic and the M.D. Anderson Cancer Center, Houston) for patients with ACTH-dependent Cushing’s syndrome seen during 2000-2012.
ACTH levels were significantly different between groups, averaging 162 pg/mL (range, 58-671 pg/mL) in patients with ectopic ACTH secretion, compared with a mean 71 pg/mL in patients with Cushing’s disease (range, 16-209 pg/mL), she reported. Although there was some overlap between groups in the range of ACTH levels, all patients with an ACTH level higher than 210 pg/mL had ectopic ACTH secretion.
Median serum potassium levels at baseline were 2.9 mmol/L in the ectopic ACTH secretion group and 3.8 mmol/L in the Cushing’s disease group, a significant difference. Again, there was some overlap between groups in the range of potassium levels, but all patients with a baseline potassium level lower than 2.7 mmol/L had ectopic ACTH secretion, she said.
Among patients who underwent a high-dose dexamethasone suppression test, cortisol levels decreased by less than 50% in 88% of patients with ectopic ACTH secretion and in 26% of patients with Cushing’s disease.
Most patients did not undergo a standardized, formal CRH stimulation test, so investigators extracted the ACTH response to CRH in peripheral plasma during the IPSS test. As expected, they found a significantly higher percent increase in ACTH in response to CRH during IPSS in the Cushing’s disease group, ranging up to more than a 1,000% increase. In the ectopic ACTH secretion group, 40% of patients did have an ACTH increase greater than 50%, ranging as high as a 200%-300% increase in ACTH in a couple of patients.
"Although there was some overlap in the biochemical testing, it is possible that it provides some additional proof to differentiate between ectopic ACTH secretion and Cushing’s disease," Dr. Yogi-Morren said.
In the ectopic ACTH secretion group, the source of the secretion remained occult in seven patients. The most common identifiable cause was a bronchial carcinoid tumor, in six patients. Three patients each had small cell lung cancer, a thymic carcinoid tumor, or a pancreatic neuroendocrine tumor. One patient each had a bladder neuroendocrine tumor, ovarian endometrioid cancer, medullary thyroid cancer, or a metastatic neuroendocrine tumor from an unknown primary cancer.
The ectopic ACTH secretion group had a median age of 41 years and was 63% female. The Cushing’s disease group had a median age of 46 years and was 76% female.
Dr. Yogi-Morren reported having no financial disclosures.
[email protected]
On Twitter @sherryboschert
AT ENDO 2013
Major finding: A pituitary tumor larger than 6 mm on MRI was 40% sensitive and 96% specific for a diagnosis of Cushing’s disease as the cause of ACTH-dependent Cushing’s syndrome.
Data source: Retrospective study of 131 patients with ACTH-dependent Cushing’s syndrome, 26 from ectopic ACTH secretion and 105 from Cushing’s disease.
Disclosures: Dr. Yogi-Morren reported having no financial disclosures.
