User login
Coarctation of the Aorta
At age 27, a woman with no family history of hypertension was diagnosed with the disease, which was left untreated. Two years later—during her first pregnancy—she was still hypertensive and was prescribed methyldopa, which was switched to lisinopril in the postpartum period. Her blood pressure (BP) remained elevated, despite titration of lisinopril and the addition of a β-blocking agent.
In the same year, the woman went to the emergency department with a severe headache and near-syncope; her BP was 180/100 mm Hg. Her medications were changed, and she was discharged with a prescription for captopril 50 mg bid and the angiotensin receptor blocker (ARB) valsartan 80 mg bid. Over the following six years, her average BP remained around 140/90 mm Hg with no further medication adjustment.
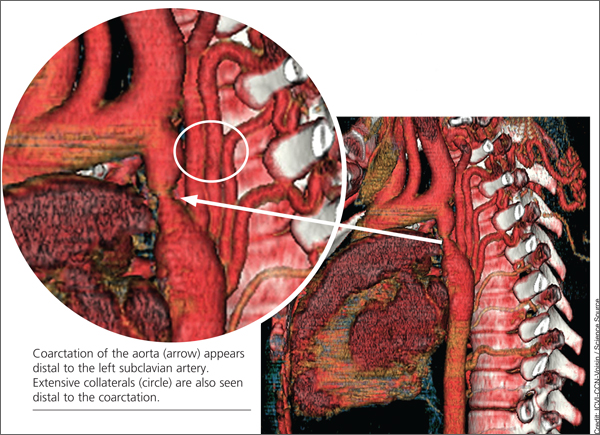
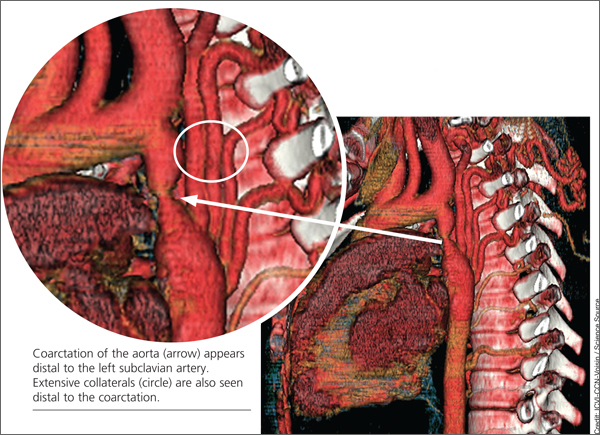
When the patient was 37, she underwent a chest x-ray (CXR), prompted by positive results on a purified protein derivative test at an employment physical; the CXR demonstrated a 3.6-cm mediastinal mass. This finding led to a chest CT exam that demonstrated a severe coarctation distal to the left subclavian artery with diffuse tubular hypoplasia, a collateral reconstitution of the descending aorta, and a true 2.7-cm aneurysm of one of the intercostal arteries.
The gradient between the ascending and descending aorta was 50 mm Hg, and the same wide pressure gradient was present between the upper and lower extremities (50 mm Hg).
Referral to pediatric cardiology was initiated. (It is not uncommon for an adult with a congenital heart lesion to be evaluated by a pediatric cardiologist in centers where adult congenital heart disease [ACHD] specialists are not available.) A cardiac MRI revealed a virtual interruption of the aortic arch in juxta-ductal position with multiple aortic collateral arteries. Subsequent cardiac catheterization demonstrated a transverse aortic arch at 1.2 cm and a narrowing to 7 mm just distal to the left subclavian artery, with a discrete coarctation of 2.5 mm.
With hypertension and a 50–mm Hg resting clinical gradient, corrective treatment was deemed necessary. Subsequently, balloon angioplasty was performed, and a drug-eluting stent was placed in the proximal distal aorta with dilation of the narrowing and a resultant decrease in BP gradient from 50 mm Hg to 7 mm Hg. Following stent placement, the aneurysm thrombosed secondary to reduced blood flow. Clinical reevaluation showed good dorsalis pedis and posterior tibial pulses with improved BP. The ARB was subsequently discontinued, and the patient continued to take captopril for mildly elevated BP (average, 130/85 mm Hg).
The patient did well until three years later, when she developed shortness of breath on exertion, claudication, and fatigue for a period of two weeks. On physical examination, her BP was noted to be elevated at 140/90 mm Hg with a clinical gradient of 20 mm between the upper and lower extremities and an increase in the gradient on echocardiogram to a peak of approximately 46 mm Hg and a mean of 21 mm Hg.
A subsequent chest CT demonstrated a narrowing of the previous stent site, and a right and left cardiac catheterization revealed neo-intimal proliferation affecting the stent with a 3–mm Hg gradient across the transverse arch and a 15–mm Hg gradient across the proximal descending aorta stent. The stent was subsequently redilated, and an additional stent was placed with no residual gradient.
The patient was discharged while taking clopidogrel 75 mg/d in addition to aspirin 325 mg/d for six months; antihypertensive medications were no longer necessary. Clinical evaluation with echocardiography was recommended every three months for the first year, and annually thereafter. At three-month and one-year follow-up, the patient was found to be symptom-free and normotensive (BP, 110/70 mm Hg).
DISCUSSION
Coarctation of the aorta (CoA) is a discrete narrowing of the thoracic aorta at the junction of the ductus arteriosus and the aortic arch, just distal to the subclavian artery. The specific anatomy, severity, and degree of hypoplasia proximal to the aortic coarctation are highly variable. For example, in some instances, coarctation presents as a long segment or a tubular hypoplasia.1
The defect is often associated with other congenital cardiovascular abnormalities, including bicuspid aortic valve (BAV; reported incidence, up to 85%),2,3 intracranial aneurysms (incidence, 3% to 10%),4 intrinsic abnormality in the aorta, aortic arch hypoplasia, ventricular septal defect, patent ductus arteriosus, aortic stenosis at different levels (valvular, subvalvular, or supravalvular), and mitral valve abnormalities.2,5 There is evidence of increased familial risk for CoA and increased prevalence with certain disorders, including Turner syndrome, maternal phenylketonuria syndrome, and Kabuki syndrome.6
CoA accounts for 5% to 8% of all congenital heart disease,2,3 and its incidence is 4 in 10,000 births.1 (Adults presenting with CoA represent either recoarctation or a missed diagnosis of native coarctation.) The mean life expectancy of untreated patients with aortic coarctation is 35 years; 90% die before age 50.1
Reduced life expectancy of patients with untreated CoA is due to systemic hypertension, accelerated coronary artery disease, stroke, heart failure, aortic rupture/dissection, cerebral hemorrhage, infective endarteritis/endocarditis, concomitant aortic valve disease (usually involving a BAV), and sudden cardiac death of presumed arrhythmogenic etiology.4 Even adults whose CoA has been detected early and managed with catheter-based and surgical interventions continue to face lifelong complications, including recoarctation, aneurysm formation, premature coronary artery disease, and cerebrovascular disease—mostly resulting from residual hypertension.3
Persistent hypertension has been reported in 68% of patients with repaired CoA at long-term follow-up. Hypertension may result in recurrence of CoA (incidence ranges from 5% to 50%), a residual CoA, or an idiopathic condition.7
The role of primary care providers is crucial in early detection and prompt referral to specialists in ACHD. For clinicians who manage these patients, increased morbidity and mortality from the associated cardiovascular sequelae pose an ongoing challenge.8
Presentation
Patients with hemodynamically stable coarctation in adolescence or adulthood are usually asymptomatic. Occasionally, a patient may be diagnosed with CoA based on its typical appearance on CXR or may come to medical attention because of an incidental murmur or management of hypertension.4 Symptoms vary in intensity and include headache, epistaxis, claudication, exertional fatigue, heart failure, aortic rupture, or dissection.7 Based on the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7), and the 2008 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for adults with congenital heart disease, patients with hypertension and/or a history of CoA repair should be evaluated periodically for coarctation.8
Physical Examination
Physical assessment should include simultaneous palpation of the brachial and femoral pulses to assess amplitude and timing, looking for diminished arterial pulses and brachial-femoral delay. Additionally, measurement of supine bilateral arm (brachial artery) BP and right or left supine leg BP is recommended to detect differing pressures.8
The following physical findings may be suggestive of CoA or recoarctation:
• Systolic BP in the right arm higher than in the lower extremities, unless the origin of the right subclavian artery is anomalous and thus is not reliable; the left arm BP may not always be reliable because of the origin of the left subclavian artery, which may vary and may or may not be hypertensive
• Hyperdynamic carotid pulsations
• A pulse delay between the right arm and the femoral or popliteal arteries
• A murmur or bruit heard in the left interscapular position; a systolic ejection click of moderate intensity heard along the left sternal border
• In cases of BAV, an early diastolic decrescendo murmur of aortic regurgitation
Diagnostic Workup
The diagnosis of CoA is usually confirmed by echocardiography or radiographic imaging, including cardiac MRI or CT angiography.8
The initial diagnostic workup should include echocardiography, which may demonstrate left ventricular hypertrophy and secondary ST-T wave abnormalities, and a two-dimensional Doppler echocardiogram, which can establish the diagnosis and severity of the CoA, with possible associated cardiac defects.9 Also recommended is a CXR, which may occasionally reveal rib notching (caused by erosion of the inferior border of the posterior ribs by enlarged intercostal arteries), also known as the 3 sign. Finally, cardiac MRI is used to delineate the coarctation anatomy and to determine whether collateral arteries and/or associated vascular anomalies and flow abnormalities exist.9 If MRI is not possible, CT angiography can be an alternate approach. Subsequently, invasive angiography is required for better assessment of the coarctation gradient and hemodynamic measurement.9
Treatment
Management of CoA requires treatment of hypertension with β-blockers, ACE inhibitors, and/or ARBs as first-line medications. Aortic root size, the presence of aortic regurgitation, or both may influence the choice of antihypertensive agents.3
Intervention is recommended if the peak-to-peak coarctation gradient is ≥ 20 mm Hg, or the peak-to-peak coarctation gradient is < 20 mm Hg, with evidence of significant coarctation and collateral flow on radiologic imaging.8 The choice of treatment (stenting or surgery) should be decided by a team of ACHD cardiologists, interventionalists, and surgeons at an ACHD center.
Surgical intervention via a lateral left thoracotomy approach was first performed in 1944. The most common surgical repair is resection with end-to-end anastomosis, which yields a low mortality and recoarctation rate. Other techniques such as resection with replacement by a tube graft, patch aortoplasty, and bypass graft are used less frequently.10-12 Postsurgical morbidity most commonly includes recoarctation and residual hypertension.
Thoracotomy was the only surgical treatment until 1982, when balloon angioplasty became available as an alternative.13 However, recoarctation, aneurysm formation, and aortic dissection are major disadvantages to balloon angioplasty.13
In the early 1990s, endovascular stents were introduced and have become an alternative approach to surgical repair.14 Aneurysms remain a significant complication in 4% to 7% of patients who undergo stent placement for CoA.14
Currently, there is insufficient evidence to indicate which is the best treatment for CoA: surgical or stent repair. Choice of treatment strategy will continue to depend on the operator’s skills or institutional preference until a prospective randomized controlled clinical trial is performed.13
Follow-Up
Based on recommendations from the ACC/AHA and the 2009 Canadian Cardiovascular Society Consensus Conference on the management of adults with congenital heart disease, lifelong follow-up is recommended for all patients with aortic coarctation (whether repaired or not), including an evaluation by a cardiologist with expertise in ACHD.4,8
A baseline cardiac MRI or CT for complete evaluation of the thoracic aorta and intracranial vessels is required for follow-up. Patients who have previously undergone surgical or interventional CoA repair should be followed annually with echocardiography to assess for potential late complications, such as aortic dilatation and aneurysm formation. Evaluation of the coarctation repair site by MRI and/or CT at intervals of five years or less is also recommended. Moreover, patients should be monitored for recurrent resting or exercise-induced hypertension, which should be treated aggressively after recoarctation is excluded.
The guidelines recommend that every patient with systemic arterial hypertension have the brachial and femoral pulses palpated simultaneously.4,8 This additional physical assessment will help detect significant aortic coarctation by assessing timing and amplitude of both pulses in search for a brachial-femoral delay. Moreover, measuring the differential pressure between bilateral arms (brachial artery) in a supine position and prone right or left supine leg (popliteal artery) BP should be performed.4,8 Initial imaging and hemodynamic evaluation by transthoracic echocardiogram is recommended in suspected aortic coarctation.
CONCLUSION
This case represents a missed CoA and provides an example of recoarctation as a late complication after repair. Unfortunately, the critical need to screen for coarctation was not recognized by the patient’s primary care providers in a timely manner. Had the guidelines for CoA screening been applied, this defect would have been detected earlier, avoiding many years of cardiovascular system stress from the sequelae of hypertension.
Measuring the BP gradient between the upper and lower extremities and searching for brachial-femoral timing delay are simple but crucial steps in the initial application of the clinical guidelines for early detection of CoA and recoarctation.
References
1. Jurcut R, Daraban AM, Lorber A, et al. Coarctation of the aorta in adults: what is the best treatment? Case report and literature review. J Med Life. 2011;4:189-195.
2. Teo LLS, Cannell T, Babu-Narayan SV, et al. Prevalence of associated cardiovascular abnormalities in 500 patients with aortic coarctation referred for cardiovascular magnetic resonance imaging to a tertiary center. Pediatr Cardiol. 2011;32:1120-1127.
3. Canniffe C. Hypertension after repair of aortic coarctation–a systematic review. Int J Cardiol. 2012;167:2456-2461.
4. Silversides CK, Kiess M, Beauchesne L, et al. Canadian Cardiovascular Society 2009 Consensus Conference on the management of adults with congenital heart disease: outflow tract obstruction, coarctation of the aorta, tetralogy of Fallot, Ebstein anomaly and Marfan’s syndrome. Can J Cardiol. 2010;26:e80-e97.
5. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for The Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease) Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e143-e263.
6. McBride KL, Pignatelli R, Lewin M, et al. Inheritance analysis of congenital left ventricular outflow tract obstruction malformations: segregation, multiplex relative risk, and heritability. Am J Med Genet. Part A. 2005;134:
180-186.
7. Brown JW, Ruzmetov M, Hoyer MH, et al. Recurrent coarctation: is surgical repair of recurrent coarctation of the aorta safe and effective? Ann Thorac Surg. 2009;88:1923-1931.
8. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: Executive Summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines for the management of adults with congenital heart disease). Circulation. 2008;118:2395-2451.
9. Darabian S, Zeb I, Rezaeian P, et al. Use of noninvasive imaging in the evaluation of coarctation of aorta. J Comput Assist Tomogr. 2013;37:75-78.
10. Backer CL, Mavroudis C, Zias EA, et al. Repair of coarctation with resection and extended end-to-end anastomosis. Ann Thorac Surg. 1998;66:1365-1370.
11. Cobanoglu A, Thyagarajan GK, Dobbs JL. Surgery for coarctation of the aorta in infants younger than 3 months: end-to-end repair versus subclavian flap angioplasty: is either operation better? Eur J Cardiothorac Surg. 1998;14:19-25.
12. Walhout RJ, Lekkerkerker JC, Oron GH, et al. Comparison of polytetrafluoroethylene patch aortoplasty and end-to-end anastomosis for coarctation of the aorta. J Thorac Cardiovasc Surg. 2003;126:521-528.
13. Pádua LM, Garcia LC, Rubira CJ, de Oliveira Carvalho PE. Stent placement versus surgery for coarctation of the thoracic aorta. Cochrane Database Syst Rev. 2012;5:CD008204.
14. Suárez de Lezo J, Pan M, Romero M, et al. Immediate and follow-up findings after stent treatment for severe coarctation of aorta. Am J Cardiol. 1999;83:400-406.
At age 27, a woman with no family history of hypertension was diagnosed with the disease, which was left untreated. Two years later—during her first pregnancy—she was still hypertensive and was prescribed methyldopa, which was switched to lisinopril in the postpartum period. Her blood pressure (BP) remained elevated, despite titration of lisinopril and the addition of a β-blocking agent.
In the same year, the woman went to the emergency department with a severe headache and near-syncope; her BP was 180/100 mm Hg. Her medications were changed, and she was discharged with a prescription for captopril 50 mg bid and the angiotensin receptor blocker (ARB) valsartan 80 mg bid. Over the following six years, her average BP remained around 140/90 mm Hg with no further medication adjustment.
When the patient was 37, she underwent a chest x-ray (CXR), prompted by positive results on a purified protein derivative test at an employment physical; the CXR demonstrated a 3.6-cm mediastinal mass. This finding led to a chest CT exam that demonstrated a severe coarctation distal to the left subclavian artery with diffuse tubular hypoplasia, a collateral reconstitution of the descending aorta, and a true 2.7-cm aneurysm of one of the intercostal arteries.
The gradient between the ascending and descending aorta was 50 mm Hg, and the same wide pressure gradient was present between the upper and lower extremities (50 mm Hg).
Referral to pediatric cardiology was initiated. (It is not uncommon for an adult with a congenital heart lesion to be evaluated by a pediatric cardiologist in centers where adult congenital heart disease [ACHD] specialists are not available.) A cardiac MRI revealed a virtual interruption of the aortic arch in juxta-ductal position with multiple aortic collateral arteries. Subsequent cardiac catheterization demonstrated a transverse aortic arch at 1.2 cm and a narrowing to 7 mm just distal to the left subclavian artery, with a discrete coarctation of 2.5 mm.
With hypertension and a 50–mm Hg resting clinical gradient, corrective treatment was deemed necessary. Subsequently, balloon angioplasty was performed, and a drug-eluting stent was placed in the proximal distal aorta with dilation of the narrowing and a resultant decrease in BP gradient from 50 mm Hg to 7 mm Hg. Following stent placement, the aneurysm thrombosed secondary to reduced blood flow. Clinical reevaluation showed good dorsalis pedis and posterior tibial pulses with improved BP. The ARB was subsequently discontinued, and the patient continued to take captopril for mildly elevated BP (average, 130/85 mm Hg).
The patient did well until three years later, when she developed shortness of breath on exertion, claudication, and fatigue for a period of two weeks. On physical examination, her BP was noted to be elevated at 140/90 mm Hg with a clinical gradient of 20 mm between the upper and lower extremities and an increase in the gradient on echocardiogram to a peak of approximately 46 mm Hg and a mean of 21 mm Hg.
A subsequent chest CT demonstrated a narrowing of the previous stent site, and a right and left cardiac catheterization revealed neo-intimal proliferation affecting the stent with a 3–mm Hg gradient across the transverse arch and a 15–mm Hg gradient across the proximal descending aorta stent. The stent was subsequently redilated, and an additional stent was placed with no residual gradient.
The patient was discharged while taking clopidogrel 75 mg/d in addition to aspirin 325 mg/d for six months; antihypertensive medications were no longer necessary. Clinical evaluation with echocardiography was recommended every three months for the first year, and annually thereafter. At three-month and one-year follow-up, the patient was found to be symptom-free and normotensive (BP, 110/70 mm Hg).
DISCUSSION
Coarctation of the aorta (CoA) is a discrete narrowing of the thoracic aorta at the junction of the ductus arteriosus and the aortic arch, just distal to the subclavian artery. The specific anatomy, severity, and degree of hypoplasia proximal to the aortic coarctation are highly variable. For example, in some instances, coarctation presents as a long segment or a tubular hypoplasia.1
The defect is often associated with other congenital cardiovascular abnormalities, including bicuspid aortic valve (BAV; reported incidence, up to 85%),2,3 intracranial aneurysms (incidence, 3% to 10%),4 intrinsic abnormality in the aorta, aortic arch hypoplasia, ventricular septal defect, patent ductus arteriosus, aortic stenosis at different levels (valvular, subvalvular, or supravalvular), and mitral valve abnormalities.2,5 There is evidence of increased familial risk for CoA and increased prevalence with certain disorders, including Turner syndrome, maternal phenylketonuria syndrome, and Kabuki syndrome.6
CoA accounts for 5% to 8% of all congenital heart disease,2,3 and its incidence is 4 in 10,000 births.1 (Adults presenting with CoA represent either recoarctation or a missed diagnosis of native coarctation.) The mean life expectancy of untreated patients with aortic coarctation is 35 years; 90% die before age 50.1
Reduced life expectancy of patients with untreated CoA is due to systemic hypertension, accelerated coronary artery disease, stroke, heart failure, aortic rupture/dissection, cerebral hemorrhage, infective endarteritis/endocarditis, concomitant aortic valve disease (usually involving a BAV), and sudden cardiac death of presumed arrhythmogenic etiology.4 Even adults whose CoA has been detected early and managed with catheter-based and surgical interventions continue to face lifelong complications, including recoarctation, aneurysm formation, premature coronary artery disease, and cerebrovascular disease—mostly resulting from residual hypertension.3
Persistent hypertension has been reported in 68% of patients with repaired CoA at long-term follow-up. Hypertension may result in recurrence of CoA (incidence ranges from 5% to 50%), a residual CoA, or an idiopathic condition.7
The role of primary care providers is crucial in early detection and prompt referral to specialists in ACHD. For clinicians who manage these patients, increased morbidity and mortality from the associated cardiovascular sequelae pose an ongoing challenge.8
Presentation
Patients with hemodynamically stable coarctation in adolescence or adulthood are usually asymptomatic. Occasionally, a patient may be diagnosed with CoA based on its typical appearance on CXR or may come to medical attention because of an incidental murmur or management of hypertension.4 Symptoms vary in intensity and include headache, epistaxis, claudication, exertional fatigue, heart failure, aortic rupture, or dissection.7 Based on the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7), and the 2008 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for adults with congenital heart disease, patients with hypertension and/or a history of CoA repair should be evaluated periodically for coarctation.8
Physical Examination
Physical assessment should include simultaneous palpation of the brachial and femoral pulses to assess amplitude and timing, looking for diminished arterial pulses and brachial-femoral delay. Additionally, measurement of supine bilateral arm (brachial artery) BP and right or left supine leg BP is recommended to detect differing pressures.8
The following physical findings may be suggestive of CoA or recoarctation:
• Systolic BP in the right arm higher than in the lower extremities, unless the origin of the right subclavian artery is anomalous and thus is not reliable; the left arm BP may not always be reliable because of the origin of the left subclavian artery, which may vary and may or may not be hypertensive
• Hyperdynamic carotid pulsations
• A pulse delay between the right arm and the femoral or popliteal arteries
• A murmur or bruit heard in the left interscapular position; a systolic ejection click of moderate intensity heard along the left sternal border
• In cases of BAV, an early diastolic decrescendo murmur of aortic regurgitation
Diagnostic Workup
The diagnosis of CoA is usually confirmed by echocardiography or radiographic imaging, including cardiac MRI or CT angiography.8
The initial diagnostic workup should include echocardiography, which may demonstrate left ventricular hypertrophy and secondary ST-T wave abnormalities, and a two-dimensional Doppler echocardiogram, which can establish the diagnosis and severity of the CoA, with possible associated cardiac defects.9 Also recommended is a CXR, which may occasionally reveal rib notching (caused by erosion of the inferior border of the posterior ribs by enlarged intercostal arteries), also known as the 3 sign. Finally, cardiac MRI is used to delineate the coarctation anatomy and to determine whether collateral arteries and/or associated vascular anomalies and flow abnormalities exist.9 If MRI is not possible, CT angiography can be an alternate approach. Subsequently, invasive angiography is required for better assessment of the coarctation gradient and hemodynamic measurement.9
Treatment
Management of CoA requires treatment of hypertension with β-blockers, ACE inhibitors, and/or ARBs as first-line medications. Aortic root size, the presence of aortic regurgitation, or both may influence the choice of antihypertensive agents.3
Intervention is recommended if the peak-to-peak coarctation gradient is ≥ 20 mm Hg, or the peak-to-peak coarctation gradient is < 20 mm Hg, with evidence of significant coarctation and collateral flow on radiologic imaging.8 The choice of treatment (stenting or surgery) should be decided by a team of ACHD cardiologists, interventionalists, and surgeons at an ACHD center.
Surgical intervention via a lateral left thoracotomy approach was first performed in 1944. The most common surgical repair is resection with end-to-end anastomosis, which yields a low mortality and recoarctation rate. Other techniques such as resection with replacement by a tube graft, patch aortoplasty, and bypass graft are used less frequently.10-12 Postsurgical morbidity most commonly includes recoarctation and residual hypertension.
Thoracotomy was the only surgical treatment until 1982, when balloon angioplasty became available as an alternative.13 However, recoarctation, aneurysm formation, and aortic dissection are major disadvantages to balloon angioplasty.13
In the early 1990s, endovascular stents were introduced and have become an alternative approach to surgical repair.14 Aneurysms remain a significant complication in 4% to 7% of patients who undergo stent placement for CoA.14
Currently, there is insufficient evidence to indicate which is the best treatment for CoA: surgical or stent repair. Choice of treatment strategy will continue to depend on the operator’s skills or institutional preference until a prospective randomized controlled clinical trial is performed.13
Follow-Up
Based on recommendations from the ACC/AHA and the 2009 Canadian Cardiovascular Society Consensus Conference on the management of adults with congenital heart disease, lifelong follow-up is recommended for all patients with aortic coarctation (whether repaired or not), including an evaluation by a cardiologist with expertise in ACHD.4,8
A baseline cardiac MRI or CT for complete evaluation of the thoracic aorta and intracranial vessels is required for follow-up. Patients who have previously undergone surgical or interventional CoA repair should be followed annually with echocardiography to assess for potential late complications, such as aortic dilatation and aneurysm formation. Evaluation of the coarctation repair site by MRI and/or CT at intervals of five years or less is also recommended. Moreover, patients should be monitored for recurrent resting or exercise-induced hypertension, which should be treated aggressively after recoarctation is excluded.
The guidelines recommend that every patient with systemic arterial hypertension have the brachial and femoral pulses palpated simultaneously.4,8 This additional physical assessment will help detect significant aortic coarctation by assessing timing and amplitude of both pulses in search for a brachial-femoral delay. Moreover, measuring the differential pressure between bilateral arms (brachial artery) in a supine position and prone right or left supine leg (popliteal artery) BP should be performed.4,8 Initial imaging and hemodynamic evaluation by transthoracic echocardiogram is recommended in suspected aortic coarctation.
CONCLUSION
This case represents a missed CoA and provides an example of recoarctation as a late complication after repair. Unfortunately, the critical need to screen for coarctation was not recognized by the patient’s primary care providers in a timely manner. Had the guidelines for CoA screening been applied, this defect would have been detected earlier, avoiding many years of cardiovascular system stress from the sequelae of hypertension.
Measuring the BP gradient between the upper and lower extremities and searching for brachial-femoral timing delay are simple but crucial steps in the initial application of the clinical guidelines for early detection of CoA and recoarctation.
References
1. Jurcut R, Daraban AM, Lorber A, et al. Coarctation of the aorta in adults: what is the best treatment? Case report and literature review. J Med Life. 2011;4:189-195.
2. Teo LLS, Cannell T, Babu-Narayan SV, et al. Prevalence of associated cardiovascular abnormalities in 500 patients with aortic coarctation referred for cardiovascular magnetic resonance imaging to a tertiary center. Pediatr Cardiol. 2011;32:1120-1127.
3. Canniffe C. Hypertension after repair of aortic coarctation–a systematic review. Int J Cardiol. 2012;167:2456-2461.
4. Silversides CK, Kiess M, Beauchesne L, et al. Canadian Cardiovascular Society 2009 Consensus Conference on the management of adults with congenital heart disease: outflow tract obstruction, coarctation of the aorta, tetralogy of Fallot, Ebstein anomaly and Marfan’s syndrome. Can J Cardiol. 2010;26:e80-e97.
5. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for The Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease) Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e143-e263.
6. McBride KL, Pignatelli R, Lewin M, et al. Inheritance analysis of congenital left ventricular outflow tract obstruction malformations: segregation, multiplex relative risk, and heritability. Am J Med Genet. Part A. 2005;134:
180-186.
7. Brown JW, Ruzmetov M, Hoyer MH, et al. Recurrent coarctation: is surgical repair of recurrent coarctation of the aorta safe and effective? Ann Thorac Surg. 2009;88:1923-1931.
8. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: Executive Summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines for the management of adults with congenital heart disease). Circulation. 2008;118:2395-2451.
9. Darabian S, Zeb I, Rezaeian P, et al. Use of noninvasive imaging in the evaluation of coarctation of aorta. J Comput Assist Tomogr. 2013;37:75-78.
10. Backer CL, Mavroudis C, Zias EA, et al. Repair of coarctation with resection and extended end-to-end anastomosis. Ann Thorac Surg. 1998;66:1365-1370.
11. Cobanoglu A, Thyagarajan GK, Dobbs JL. Surgery for coarctation of the aorta in infants younger than 3 months: end-to-end repair versus subclavian flap angioplasty: is either operation better? Eur J Cardiothorac Surg. 1998;14:19-25.
12. Walhout RJ, Lekkerkerker JC, Oron GH, et al. Comparison of polytetrafluoroethylene patch aortoplasty and end-to-end anastomosis for coarctation of the aorta. J Thorac Cardiovasc Surg. 2003;126:521-528.
13. Pádua LM, Garcia LC, Rubira CJ, de Oliveira Carvalho PE. Stent placement versus surgery for coarctation of the thoracic aorta. Cochrane Database Syst Rev. 2012;5:CD008204.
14. Suárez de Lezo J, Pan M, Romero M, et al. Immediate and follow-up findings after stent treatment for severe coarctation of aorta. Am J Cardiol. 1999;83:400-406.
At age 27, a woman with no family history of hypertension was diagnosed with the disease, which was left untreated. Two years later—during her first pregnancy—she was still hypertensive and was prescribed methyldopa, which was switched to lisinopril in the postpartum period. Her blood pressure (BP) remained elevated, despite titration of lisinopril and the addition of a β-blocking agent.
In the same year, the woman went to the emergency department with a severe headache and near-syncope; her BP was 180/100 mm Hg. Her medications were changed, and she was discharged with a prescription for captopril 50 mg bid and the angiotensin receptor blocker (ARB) valsartan 80 mg bid. Over the following six years, her average BP remained around 140/90 mm Hg with no further medication adjustment.
When the patient was 37, she underwent a chest x-ray (CXR), prompted by positive results on a purified protein derivative test at an employment physical; the CXR demonstrated a 3.6-cm mediastinal mass. This finding led to a chest CT exam that demonstrated a severe coarctation distal to the left subclavian artery with diffuse tubular hypoplasia, a collateral reconstitution of the descending aorta, and a true 2.7-cm aneurysm of one of the intercostal arteries.
The gradient between the ascending and descending aorta was 50 mm Hg, and the same wide pressure gradient was present between the upper and lower extremities (50 mm Hg).
Referral to pediatric cardiology was initiated. (It is not uncommon for an adult with a congenital heart lesion to be evaluated by a pediatric cardiologist in centers where adult congenital heart disease [ACHD] specialists are not available.) A cardiac MRI revealed a virtual interruption of the aortic arch in juxta-ductal position with multiple aortic collateral arteries. Subsequent cardiac catheterization demonstrated a transverse aortic arch at 1.2 cm and a narrowing to 7 mm just distal to the left subclavian artery, with a discrete coarctation of 2.5 mm.
With hypertension and a 50–mm Hg resting clinical gradient, corrective treatment was deemed necessary. Subsequently, balloon angioplasty was performed, and a drug-eluting stent was placed in the proximal distal aorta with dilation of the narrowing and a resultant decrease in BP gradient from 50 mm Hg to 7 mm Hg. Following stent placement, the aneurysm thrombosed secondary to reduced blood flow. Clinical reevaluation showed good dorsalis pedis and posterior tibial pulses with improved BP. The ARB was subsequently discontinued, and the patient continued to take captopril for mildly elevated BP (average, 130/85 mm Hg).
The patient did well until three years later, when she developed shortness of breath on exertion, claudication, and fatigue for a period of two weeks. On physical examination, her BP was noted to be elevated at 140/90 mm Hg with a clinical gradient of 20 mm between the upper and lower extremities and an increase in the gradient on echocardiogram to a peak of approximately 46 mm Hg and a mean of 21 mm Hg.
A subsequent chest CT demonstrated a narrowing of the previous stent site, and a right and left cardiac catheterization revealed neo-intimal proliferation affecting the stent with a 3–mm Hg gradient across the transverse arch and a 15–mm Hg gradient across the proximal descending aorta stent. The stent was subsequently redilated, and an additional stent was placed with no residual gradient.
The patient was discharged while taking clopidogrel 75 mg/d in addition to aspirin 325 mg/d for six months; antihypertensive medications were no longer necessary. Clinical evaluation with echocardiography was recommended every three months for the first year, and annually thereafter. At three-month and one-year follow-up, the patient was found to be symptom-free and normotensive (BP, 110/70 mm Hg).
DISCUSSION
Coarctation of the aorta (CoA) is a discrete narrowing of the thoracic aorta at the junction of the ductus arteriosus and the aortic arch, just distal to the subclavian artery. The specific anatomy, severity, and degree of hypoplasia proximal to the aortic coarctation are highly variable. For example, in some instances, coarctation presents as a long segment or a tubular hypoplasia.1
The defect is often associated with other congenital cardiovascular abnormalities, including bicuspid aortic valve (BAV; reported incidence, up to 85%),2,3 intracranial aneurysms (incidence, 3% to 10%),4 intrinsic abnormality in the aorta, aortic arch hypoplasia, ventricular septal defect, patent ductus arteriosus, aortic stenosis at different levels (valvular, subvalvular, or supravalvular), and mitral valve abnormalities.2,5 There is evidence of increased familial risk for CoA and increased prevalence with certain disorders, including Turner syndrome, maternal phenylketonuria syndrome, and Kabuki syndrome.6
CoA accounts for 5% to 8% of all congenital heart disease,2,3 and its incidence is 4 in 10,000 births.1 (Adults presenting with CoA represent either recoarctation or a missed diagnosis of native coarctation.) The mean life expectancy of untreated patients with aortic coarctation is 35 years; 90% die before age 50.1
Reduced life expectancy of patients with untreated CoA is due to systemic hypertension, accelerated coronary artery disease, stroke, heart failure, aortic rupture/dissection, cerebral hemorrhage, infective endarteritis/endocarditis, concomitant aortic valve disease (usually involving a BAV), and sudden cardiac death of presumed arrhythmogenic etiology.4 Even adults whose CoA has been detected early and managed with catheter-based and surgical interventions continue to face lifelong complications, including recoarctation, aneurysm formation, premature coronary artery disease, and cerebrovascular disease—mostly resulting from residual hypertension.3
Persistent hypertension has been reported in 68% of patients with repaired CoA at long-term follow-up. Hypertension may result in recurrence of CoA (incidence ranges from 5% to 50%), a residual CoA, or an idiopathic condition.7
The role of primary care providers is crucial in early detection and prompt referral to specialists in ACHD. For clinicians who manage these patients, increased morbidity and mortality from the associated cardiovascular sequelae pose an ongoing challenge.8
Presentation
Patients with hemodynamically stable coarctation in adolescence or adulthood are usually asymptomatic. Occasionally, a patient may be diagnosed with CoA based on its typical appearance on CXR or may come to medical attention because of an incidental murmur or management of hypertension.4 Symptoms vary in intensity and include headache, epistaxis, claudication, exertional fatigue, heart failure, aortic rupture, or dissection.7 Based on the Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7), and the 2008 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for adults with congenital heart disease, patients with hypertension and/or a history of CoA repair should be evaluated periodically for coarctation.8
Physical Examination
Physical assessment should include simultaneous palpation of the brachial and femoral pulses to assess amplitude and timing, looking for diminished arterial pulses and brachial-femoral delay. Additionally, measurement of supine bilateral arm (brachial artery) BP and right or left supine leg BP is recommended to detect differing pressures.8
The following physical findings may be suggestive of CoA or recoarctation:
• Systolic BP in the right arm higher than in the lower extremities, unless the origin of the right subclavian artery is anomalous and thus is not reliable; the left arm BP may not always be reliable because of the origin of the left subclavian artery, which may vary and may or may not be hypertensive
• Hyperdynamic carotid pulsations
• A pulse delay between the right arm and the femoral or popliteal arteries
• A murmur or bruit heard in the left interscapular position; a systolic ejection click of moderate intensity heard along the left sternal border
• In cases of BAV, an early diastolic decrescendo murmur of aortic regurgitation
Diagnostic Workup
The diagnosis of CoA is usually confirmed by echocardiography or radiographic imaging, including cardiac MRI or CT angiography.8
The initial diagnostic workup should include echocardiography, which may demonstrate left ventricular hypertrophy and secondary ST-T wave abnormalities, and a two-dimensional Doppler echocardiogram, which can establish the diagnosis and severity of the CoA, with possible associated cardiac defects.9 Also recommended is a CXR, which may occasionally reveal rib notching (caused by erosion of the inferior border of the posterior ribs by enlarged intercostal arteries), also known as the 3 sign. Finally, cardiac MRI is used to delineate the coarctation anatomy and to determine whether collateral arteries and/or associated vascular anomalies and flow abnormalities exist.9 If MRI is not possible, CT angiography can be an alternate approach. Subsequently, invasive angiography is required for better assessment of the coarctation gradient and hemodynamic measurement.9
Treatment
Management of CoA requires treatment of hypertension with β-blockers, ACE inhibitors, and/or ARBs as first-line medications. Aortic root size, the presence of aortic regurgitation, or both may influence the choice of antihypertensive agents.3
Intervention is recommended if the peak-to-peak coarctation gradient is ≥ 20 mm Hg, or the peak-to-peak coarctation gradient is < 20 mm Hg, with evidence of significant coarctation and collateral flow on radiologic imaging.8 The choice of treatment (stenting or surgery) should be decided by a team of ACHD cardiologists, interventionalists, and surgeons at an ACHD center.
Surgical intervention via a lateral left thoracotomy approach was first performed in 1944. The most common surgical repair is resection with end-to-end anastomosis, which yields a low mortality and recoarctation rate. Other techniques such as resection with replacement by a tube graft, patch aortoplasty, and bypass graft are used less frequently.10-12 Postsurgical morbidity most commonly includes recoarctation and residual hypertension.
Thoracotomy was the only surgical treatment until 1982, when balloon angioplasty became available as an alternative.13 However, recoarctation, aneurysm formation, and aortic dissection are major disadvantages to balloon angioplasty.13
In the early 1990s, endovascular stents were introduced and have become an alternative approach to surgical repair.14 Aneurysms remain a significant complication in 4% to 7% of patients who undergo stent placement for CoA.14
Currently, there is insufficient evidence to indicate which is the best treatment for CoA: surgical or stent repair. Choice of treatment strategy will continue to depend on the operator’s skills or institutional preference until a prospective randomized controlled clinical trial is performed.13
Follow-Up
Based on recommendations from the ACC/AHA and the 2009 Canadian Cardiovascular Society Consensus Conference on the management of adults with congenital heart disease, lifelong follow-up is recommended for all patients with aortic coarctation (whether repaired or not), including an evaluation by a cardiologist with expertise in ACHD.4,8
A baseline cardiac MRI or CT for complete evaluation of the thoracic aorta and intracranial vessels is required for follow-up. Patients who have previously undergone surgical or interventional CoA repair should be followed annually with echocardiography to assess for potential late complications, such as aortic dilatation and aneurysm formation. Evaluation of the coarctation repair site by MRI and/or CT at intervals of five years or less is also recommended. Moreover, patients should be monitored for recurrent resting or exercise-induced hypertension, which should be treated aggressively after recoarctation is excluded.
The guidelines recommend that every patient with systemic arterial hypertension have the brachial and femoral pulses palpated simultaneously.4,8 This additional physical assessment will help detect significant aortic coarctation by assessing timing and amplitude of both pulses in search for a brachial-femoral delay. Moreover, measuring the differential pressure between bilateral arms (brachial artery) in a supine position and prone right or left supine leg (popliteal artery) BP should be performed.4,8 Initial imaging and hemodynamic evaluation by transthoracic echocardiogram is recommended in suspected aortic coarctation.
CONCLUSION
This case represents a missed CoA and provides an example of recoarctation as a late complication after repair. Unfortunately, the critical need to screen for coarctation was not recognized by the patient’s primary care providers in a timely manner. Had the guidelines for CoA screening been applied, this defect would have been detected earlier, avoiding many years of cardiovascular system stress from the sequelae of hypertension.
Measuring the BP gradient between the upper and lower extremities and searching for brachial-femoral timing delay are simple but crucial steps in the initial application of the clinical guidelines for early detection of CoA and recoarctation.
References
1. Jurcut R, Daraban AM, Lorber A, et al. Coarctation of the aorta in adults: what is the best treatment? Case report and literature review. J Med Life. 2011;4:189-195.
2. Teo LLS, Cannell T, Babu-Narayan SV, et al. Prevalence of associated cardiovascular abnormalities in 500 patients with aortic coarctation referred for cardiovascular magnetic resonance imaging to a tertiary center. Pediatr Cardiol. 2011;32:1120-1127.
3. Canniffe C. Hypertension after repair of aortic coarctation–a systematic review. Int J Cardiol. 2012;167:2456-2461.
4. Silversides CK, Kiess M, Beauchesne L, et al. Canadian Cardiovascular Society 2009 Consensus Conference on the management of adults with congenital heart disease: outflow tract obstruction, coarctation of the aorta, tetralogy of Fallot, Ebstein anomaly and Marfan’s syndrome. Can J Cardiol. 2010;26:e80-e97.
5. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for The Management of Adults With Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease) Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e143-e263.
6. McBride KL, Pignatelli R, Lewin M, et al. Inheritance analysis of congenital left ventricular outflow tract obstruction malformations: segregation, multiplex relative risk, and heritability. Am J Med Genet. Part A. 2005;134:
180-186.
7. Brown JW, Ruzmetov M, Hoyer MH, et al. Recurrent coarctation: is surgical repair of recurrent coarctation of the aorta safe and effective? Ann Thorac Surg. 2009;88:1923-1931.
8. Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease: Executive Summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines for the management of adults with congenital heart disease). Circulation. 2008;118:2395-2451.
9. Darabian S, Zeb I, Rezaeian P, et al. Use of noninvasive imaging in the evaluation of coarctation of aorta. J Comput Assist Tomogr. 2013;37:75-78.
10. Backer CL, Mavroudis C, Zias EA, et al. Repair of coarctation with resection and extended end-to-end anastomosis. Ann Thorac Surg. 1998;66:1365-1370.
11. Cobanoglu A, Thyagarajan GK, Dobbs JL. Surgery for coarctation of the aorta in infants younger than 3 months: end-to-end repair versus subclavian flap angioplasty: is either operation better? Eur J Cardiothorac Surg. 1998;14:19-25.
12. Walhout RJ, Lekkerkerker JC, Oron GH, et al. Comparison of polytetrafluoroethylene patch aortoplasty and end-to-end anastomosis for coarctation of the aorta. J Thorac Cardiovasc Surg. 2003;126:521-528.
13. Pádua LM, Garcia LC, Rubira CJ, de Oliveira Carvalho PE. Stent placement versus surgery for coarctation of the thoracic aorta. Cochrane Database Syst Rev. 2012;5:CD008204.
14. Suárez de Lezo J, Pan M, Romero M, et al. Immediate and follow-up findings after stent treatment for severe coarctation of aorta. Am J Cardiol. 1999;83:400-406.
Helping Patients Navigate the Web
How often does this happen to you? You walk into an exam room and ask the patient what brings him in today, and the reply is something like, “Well, doc, I have stomach cancer.” You do a double-take and scan the patient’s chart, looking for test results or notes from a referring provider. Finding nothing, you ask the patient for more information on his diagnosis. To your surprise/dismay/frustration, he says, “Naw, I Googled my symptoms and that’s what I came up with.”
While you can’t control the Web-surfing your patients do before they present, you can influence their information-seeking behavior once you’ve delivered a diagnosis and/or treatment plan. You know they (and their family/caregivers) will have questions about the patient’s condition and how it can be managed for the long term. You hope they’ll come to you for answers. But since they are likely to use the resources at their fingertips, you at least want to ensure the information they receive is accurate and trustworthy.
With that in mind, we asked several Clinician Reviews board members to share the Web sites that they recommend to their patients. Some, including Cathy St. Pierre, PhD, APRN, FNP-BC, FAANP, and Ellen Mandel, DMH, MPA, PA-C, CDE, cited behemoths such as the Mayo Clinic Web site (www.mayoclinic.com/health-information), lauding it for being up to date, easy to access, and “clear and data-driven.” Other board members, as you’ll see below, suggested specialty-specific sites.
Freddi I. Segal-Gidan, PhD, PA, may speak for many clinicians when she explains, “We offer these [resources] to patients and families as part of health education, acknowledging that learning about someone’s condition is the first step to better understanding what they are experiencing and how this may change over time—since most of what we deal with are progressive, lengthy illnesses and chronic disease management.”
If you have reliable Web-based resources that you recommend to your patients, please visit us on Facebook (www.facebook.com/ClinRev) to share them!
Alzheimer’s Disease
ADEAR—Alzheimer’s Disease Education and Referral Center
www.nia.nih.gov/alzheimers
Who recommends it: Freddi I. Segal-Gidan, PA, PhD
Why: Operated by the NIH/National Institute on Aging specifically to provide consumers with current, accurate, state-of-the-art information about Alzheimer’s disease and dementing illness
Also recommended: Alzheimer’s Association (www.alz.org); Family Caregiver Alliance (www.caregiver.org); UCSF Memory Center for information on frontotemporal dementia (www.memory.ucsf.edu/ftd); Foundation for Health in Aging (www.healthinaging.org); Kaiser Family Foundation for information about Medicare, Medicaid, and health policy related to aging (www.kff.org)
Cardiology
Cardiac Arrhythmias Research and Education Foundation, Inc (CARE)
www.longqt.org
Who recommends it: Lyle W. Larson, PhD, PA-C
Why: Provides an overview of long QT syndrome (eg, management, genetics); includes links to a study registry for persons with implantable cardioverters-defibrillators who are participating in sports and a complete list of medications to avoid in this patient population. The information is collated and disseminated by health care experts in this field and is updated continuously as new data emerges.
Also recommended: CredibleMeds™ (www.crediblemeds.org)
Dermatology
American Academy of Dermatology: For the Public
www.aad.org/for-the-public
Who recommends it: Joe R. Monroe, MPAS, PA
Why: Provides patient information about a specific topic or diagnosis that is reliable, up to date, and in understandable language.
eMedicine
http://emedicine.medscape.com
Who recommends it: Joe R. Monroe, MPAS, PA
Why: The information is current and written by authoritative dermatologists or other relevant specialists. References are copious and relevant, and links in the text guide readers to equally good information on related topics.
Caveats: The only problem with eMedicine is that it’s jargon-heavy and meant only for those who are comfortable with the terminology. I reserve this suggestion for more medically erudite patients (eg, nurses or PAs).
Diabetes
DiabetesMine
www.diabetesmine.com/
Who recommends it: Christine Kessler, RN, MN, CNS, ANP, BC-ADM
Why: This is an award-winning blog by an individual with type 1 diabetes, but it has something for every diabetic patient and his/her family. Really awesome. I recommend it to my patients, and some of them blog for it!
Also recommended: American Diabetes Association (www.diabetes.org/)
Nephrology
American Association of Kidney Patients
www.aakp.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: Their information is written for and by kidney patients. It is for all patients with kidney disease, not just dialysis patients. They offer free publications that emphasize living with kidney disease; these pubs are attractive, with realistic information.
Kidney School
www.kidneyschool.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: This site offers about 16 modules, each on a different topic ranging from dialysis options to sexuality. It is for patients and allows them to pick the topic they want and view the module as often as they wish.
National Kidney Foundation
www.kidney.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: The patient section of this site contains recipes and health information. Patients can register for the Kidney Peers Program, in which they match up either as a mentor or a mentee with another kidney patient in the US. It covers the range from moderate kidney disease to kidney failure and transplant.
Also recommended: DaVita (www.davita.com); Fresenius Medical Care (www.ultracare-dialysis.com)
Orthopedics
OrthoInfo
orthoinfo.aaos.org/
Who recommends it: Mike Rudzinski, RPh, RPA-C
Why: Endorsed by the American Academy of Orthopedic Surgeons, this site offers patients information on the most common musculoskeletal conditions. Includes patient education materials with anatomic pictures and discussion. This is my “go to” site for these conditions; it offers an incredible, comprehensive overview of the condition, options for care including potential surgery, and what the patient can do to improve the condition. It is easy to use for the patient—they just click on the anatomic body part involved and a list of conditions comes up.
Rheumatology
American College of Rheumatology
www.rheumatology.org/Practice/Clinical/Patients/Information_for_Patients/
Who recommends it: Rick Pope, MPAS, PA-C, DFAAPA, CPAAPA
Why: Vetted by the American College of Rheumatologists, whose faculty is nationwide, altruistic, and collaborative, it is chock full of resources that are the standard of thinking and care for rheumatic conditions. It includes “scary” diagnoses such as lupus and rheumatoid arthritis, with short, patient-specific resources that can take the sting out of the perceived notions of these diseases. The information is available in Spanish and English. The Spanish information sheets can be provided to our Hispanic population and European populations that speak primarily Spanish. This is an awesome service for those of us on the East Coast and likely more helpful in parts of the country where Spanish is spoken more commonly.
How often does this happen to you? You walk into an exam room and ask the patient what brings him in today, and the reply is something like, “Well, doc, I have stomach cancer.” You do a double-take and scan the patient’s chart, looking for test results or notes from a referring provider. Finding nothing, you ask the patient for more information on his diagnosis. To your surprise/dismay/frustration, he says, “Naw, I Googled my symptoms and that’s what I came up with.”
While you can’t control the Web-surfing your patients do before they present, you can influence their information-seeking behavior once you’ve delivered a diagnosis and/or treatment plan. You know they (and their family/caregivers) will have questions about the patient’s condition and how it can be managed for the long term. You hope they’ll come to you for answers. But since they are likely to use the resources at their fingertips, you at least want to ensure the information they receive is accurate and trustworthy.
With that in mind, we asked several Clinician Reviews board members to share the Web sites that they recommend to their patients. Some, including Cathy St. Pierre, PhD, APRN, FNP-BC, FAANP, and Ellen Mandel, DMH, MPA, PA-C, CDE, cited behemoths such as the Mayo Clinic Web site (www.mayoclinic.com/health-information), lauding it for being up to date, easy to access, and “clear and data-driven.” Other board members, as you’ll see below, suggested specialty-specific sites.
Freddi I. Segal-Gidan, PhD, PA, may speak for many clinicians when she explains, “We offer these [resources] to patients and families as part of health education, acknowledging that learning about someone’s condition is the first step to better understanding what they are experiencing and how this may change over time—since most of what we deal with are progressive, lengthy illnesses and chronic disease management.”
If you have reliable Web-based resources that you recommend to your patients, please visit us on Facebook (www.facebook.com/ClinRev) to share them!
Alzheimer’s Disease
ADEAR—Alzheimer’s Disease Education and Referral Center
www.nia.nih.gov/alzheimers
Who recommends it: Freddi I. Segal-Gidan, PA, PhD
Why: Operated by the NIH/National Institute on Aging specifically to provide consumers with current, accurate, state-of-the-art information about Alzheimer’s disease and dementing illness
Also recommended: Alzheimer’s Association (www.alz.org); Family Caregiver Alliance (www.caregiver.org); UCSF Memory Center for information on frontotemporal dementia (www.memory.ucsf.edu/ftd); Foundation for Health in Aging (www.healthinaging.org); Kaiser Family Foundation for information about Medicare, Medicaid, and health policy related to aging (www.kff.org)
Cardiology
Cardiac Arrhythmias Research and Education Foundation, Inc (CARE)
www.longqt.org
Who recommends it: Lyle W. Larson, PhD, PA-C
Why: Provides an overview of long QT syndrome (eg, management, genetics); includes links to a study registry for persons with implantable cardioverters-defibrillators who are participating in sports and a complete list of medications to avoid in this patient population. The information is collated and disseminated by health care experts in this field and is updated continuously as new data emerges.
Also recommended: CredibleMeds™ (www.crediblemeds.org)
Dermatology
American Academy of Dermatology: For the Public
www.aad.org/for-the-public
Who recommends it: Joe R. Monroe, MPAS, PA
Why: Provides patient information about a specific topic or diagnosis that is reliable, up to date, and in understandable language.
eMedicine
http://emedicine.medscape.com
Who recommends it: Joe R. Monroe, MPAS, PA
Why: The information is current and written by authoritative dermatologists or other relevant specialists. References are copious and relevant, and links in the text guide readers to equally good information on related topics.
Caveats: The only problem with eMedicine is that it’s jargon-heavy and meant only for those who are comfortable with the terminology. I reserve this suggestion for more medically erudite patients (eg, nurses or PAs).
Diabetes
DiabetesMine
www.diabetesmine.com/
Who recommends it: Christine Kessler, RN, MN, CNS, ANP, BC-ADM
Why: This is an award-winning blog by an individual with type 1 diabetes, but it has something for every diabetic patient and his/her family. Really awesome. I recommend it to my patients, and some of them blog for it!
Also recommended: American Diabetes Association (www.diabetes.org/)
Nephrology
American Association of Kidney Patients
www.aakp.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: Their information is written for and by kidney patients. It is for all patients with kidney disease, not just dialysis patients. They offer free publications that emphasize living with kidney disease; these pubs are attractive, with realistic information.
Kidney School
www.kidneyschool.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: This site offers about 16 modules, each on a different topic ranging from dialysis options to sexuality. It is for patients and allows them to pick the topic they want and view the module as often as they wish.
National Kidney Foundation
www.kidney.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: The patient section of this site contains recipes and health information. Patients can register for the Kidney Peers Program, in which they match up either as a mentor or a mentee with another kidney patient in the US. It covers the range from moderate kidney disease to kidney failure and transplant.
Also recommended: DaVita (www.davita.com); Fresenius Medical Care (www.ultracare-dialysis.com)
Orthopedics
OrthoInfo
orthoinfo.aaos.org/
Who recommends it: Mike Rudzinski, RPh, RPA-C
Why: Endorsed by the American Academy of Orthopedic Surgeons, this site offers patients information on the most common musculoskeletal conditions. Includes patient education materials with anatomic pictures and discussion. This is my “go to” site for these conditions; it offers an incredible, comprehensive overview of the condition, options for care including potential surgery, and what the patient can do to improve the condition. It is easy to use for the patient—they just click on the anatomic body part involved and a list of conditions comes up.
Rheumatology
American College of Rheumatology
www.rheumatology.org/Practice/Clinical/Patients/Information_for_Patients/
Who recommends it: Rick Pope, MPAS, PA-C, DFAAPA, CPAAPA
Why: Vetted by the American College of Rheumatologists, whose faculty is nationwide, altruistic, and collaborative, it is chock full of resources that are the standard of thinking and care for rheumatic conditions. It includes “scary” diagnoses such as lupus and rheumatoid arthritis, with short, patient-specific resources that can take the sting out of the perceived notions of these diseases. The information is available in Spanish and English. The Spanish information sheets can be provided to our Hispanic population and European populations that speak primarily Spanish. This is an awesome service for those of us on the East Coast and likely more helpful in parts of the country where Spanish is spoken more commonly.
How often does this happen to you? You walk into an exam room and ask the patient what brings him in today, and the reply is something like, “Well, doc, I have stomach cancer.” You do a double-take and scan the patient’s chart, looking for test results or notes from a referring provider. Finding nothing, you ask the patient for more information on his diagnosis. To your surprise/dismay/frustration, he says, “Naw, I Googled my symptoms and that’s what I came up with.”
While you can’t control the Web-surfing your patients do before they present, you can influence their information-seeking behavior once you’ve delivered a diagnosis and/or treatment plan. You know they (and their family/caregivers) will have questions about the patient’s condition and how it can be managed for the long term. You hope they’ll come to you for answers. But since they are likely to use the resources at their fingertips, you at least want to ensure the information they receive is accurate and trustworthy.
With that in mind, we asked several Clinician Reviews board members to share the Web sites that they recommend to their patients. Some, including Cathy St. Pierre, PhD, APRN, FNP-BC, FAANP, and Ellen Mandel, DMH, MPA, PA-C, CDE, cited behemoths such as the Mayo Clinic Web site (www.mayoclinic.com/health-information), lauding it for being up to date, easy to access, and “clear and data-driven.” Other board members, as you’ll see below, suggested specialty-specific sites.
Freddi I. Segal-Gidan, PhD, PA, may speak for many clinicians when she explains, “We offer these [resources] to patients and families as part of health education, acknowledging that learning about someone’s condition is the first step to better understanding what they are experiencing and how this may change over time—since most of what we deal with are progressive, lengthy illnesses and chronic disease management.”
If you have reliable Web-based resources that you recommend to your patients, please visit us on Facebook (www.facebook.com/ClinRev) to share them!
Alzheimer’s Disease
ADEAR—Alzheimer’s Disease Education and Referral Center
www.nia.nih.gov/alzheimers
Who recommends it: Freddi I. Segal-Gidan, PA, PhD
Why: Operated by the NIH/National Institute on Aging specifically to provide consumers with current, accurate, state-of-the-art information about Alzheimer’s disease and dementing illness
Also recommended: Alzheimer’s Association (www.alz.org); Family Caregiver Alliance (www.caregiver.org); UCSF Memory Center for information on frontotemporal dementia (www.memory.ucsf.edu/ftd); Foundation for Health in Aging (www.healthinaging.org); Kaiser Family Foundation for information about Medicare, Medicaid, and health policy related to aging (www.kff.org)
Cardiology
Cardiac Arrhythmias Research and Education Foundation, Inc (CARE)
www.longqt.org
Who recommends it: Lyle W. Larson, PhD, PA-C
Why: Provides an overview of long QT syndrome (eg, management, genetics); includes links to a study registry for persons with implantable cardioverters-defibrillators who are participating in sports and a complete list of medications to avoid in this patient population. The information is collated and disseminated by health care experts in this field and is updated continuously as new data emerges.
Also recommended: CredibleMeds™ (www.crediblemeds.org)
Dermatology
American Academy of Dermatology: For the Public
www.aad.org/for-the-public
Who recommends it: Joe R. Monroe, MPAS, PA
Why: Provides patient information about a specific topic or diagnosis that is reliable, up to date, and in understandable language.
eMedicine
http://emedicine.medscape.com
Who recommends it: Joe R. Monroe, MPAS, PA
Why: The information is current and written by authoritative dermatologists or other relevant specialists. References are copious and relevant, and links in the text guide readers to equally good information on related topics.
Caveats: The only problem with eMedicine is that it’s jargon-heavy and meant only for those who are comfortable with the terminology. I reserve this suggestion for more medically erudite patients (eg, nurses or PAs).
Diabetes
DiabetesMine
www.diabetesmine.com/
Who recommends it: Christine Kessler, RN, MN, CNS, ANP, BC-ADM
Why: This is an award-winning blog by an individual with type 1 diabetes, but it has something for every diabetic patient and his/her family. Really awesome. I recommend it to my patients, and some of them blog for it!
Also recommended: American Diabetes Association (www.diabetes.org/)
Nephrology
American Association of Kidney Patients
www.aakp.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: Their information is written for and by kidney patients. It is for all patients with kidney disease, not just dialysis patients. They offer free publications that emphasize living with kidney disease; these pubs are attractive, with realistic information.
Kidney School
www.kidneyschool.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: This site offers about 16 modules, each on a different topic ranging from dialysis options to sexuality. It is for patients and allows them to pick the topic they want and view the module as often as they wish.
National Kidney Foundation
www.kidney.org
Who recommends it: Jane S. Davis, DNP, CRNP
Why: The patient section of this site contains recipes and health information. Patients can register for the Kidney Peers Program, in which they match up either as a mentor or a mentee with another kidney patient in the US. It covers the range from moderate kidney disease to kidney failure and transplant.
Also recommended: DaVita (www.davita.com); Fresenius Medical Care (www.ultracare-dialysis.com)
Orthopedics
OrthoInfo
orthoinfo.aaos.org/
Who recommends it: Mike Rudzinski, RPh, RPA-C
Why: Endorsed by the American Academy of Orthopedic Surgeons, this site offers patients information on the most common musculoskeletal conditions. Includes patient education materials with anatomic pictures and discussion. This is my “go to” site for these conditions; it offers an incredible, comprehensive overview of the condition, options for care including potential surgery, and what the patient can do to improve the condition. It is easy to use for the patient—they just click on the anatomic body part involved and a list of conditions comes up.
Rheumatology
American College of Rheumatology
www.rheumatology.org/Practice/Clinical/Patients/Information_for_Patients/
Who recommends it: Rick Pope, MPAS, PA-C, DFAAPA, CPAAPA
Why: Vetted by the American College of Rheumatologists, whose faculty is nationwide, altruistic, and collaborative, it is chock full of resources that are the standard of thinking and care for rheumatic conditions. It includes “scary” diagnoses such as lupus and rheumatoid arthritis, with short, patient-specific resources that can take the sting out of the perceived notions of these diseases. The information is available in Spanish and English. The Spanish information sheets can be provided to our Hispanic population and European populations that speak primarily Spanish. This is an awesome service for those of us on the East Coast and likely more helpful in parts of the country where Spanish is spoken more commonly.
Update on pelvic floor dysfunction: Focus on urinary incontinence
Urinary incontinence (UI) affects almost half of all women in the United States.1,2 Estimates suggest that the prevalence of UI gradually rises during young adult life, comes to a broad plateau in middle age, and then steadily increases from that plateau after age 65. Therefore, over the next 40 years, as the elderly population expands in size, the number of women affected by UI will significantly grow.3
For patients with UI, a multitude of therapeutic options are available. Which option is the best for your patient? In this article, we aim to answer that question by interpreting the results of four randomized trials, each of which directly compare two available treatment options. The first study examines patients with stress urinary incontinence (SUI), comparing the patients’ subjective improvement in urinary leakage and bladder function at 12 months after randomization to treatment with physiotherapy or midurethral sling surgery.
The three other trials examine patients with overactive bladder (OAB) and urgency urinary incontinence (UUI). Each trial directly compares the use of anticholinergic medications to an alternate treatment modality. Currently, anticholinergic medications and behavioral therapy are the recommended first-line therapies for OAB. Unfortunately, anticholinergic medications have poor patient compliance and significant systemic side effects.4 Caution should be used when considering anticholinergic medications in patients with impaired gastric emptying or a history of urinary retention. They also should be used with caution in elderly patients who are extremely frail. Additionally, clearance from an ophthalmologist must be obtained prior to starting anticholinergic medication in patients with narrow-angle glaucoma.5 Due to poor adherence and potential side effects, there is a growing effort to discover alternative treatment modalities that are safe and effective. Therefore, we chose to examine trials comparing: mirabegron versus tolterodine, percutaneous tibial nerve stimulation versus tolterodine, and onabotulinumtoxinA versus anticholingeric medications.
UI defined
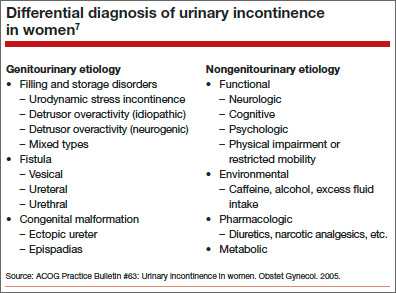
Before discussing treatment options, we want to clarify the main types of UI (FIGURE). UI is defined as the complaint of involuntary loss of urine. UI can be subdivided into SUI, OAB/UUI, or mixed urinary incontinence.6 While there are other less common genitourinary etiologies that can lead to UI, nongenitourinary etiologies are prevalent and can aggravate existing SUI or OAB (TABLE).
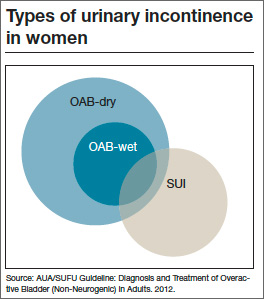
SUI is the complaint of involuntary loss of urine on effort or physical exertion (such as during sporting activities) or on sneezing or coughing. Often, SUI can be diagnosed by patient report alone and surgery can be considered in symptomatic patients who demonstrate cough leakage on physical examination and normal postvoid residual volumes.
UUI is the involuntary loss of urine associated with urgency; it often occurs in the setting of OAB, which is defined as the syndrome of urinary urgency, usually accompanied by frequency and nocturia, with or without UUI, in the absence of urinary tract infection or other obvious pathology (such as neurologic dysfunction, infection, or urologic neoplasm). OAB-dry is present when patients do not have leakage with urgency, but are bothered by urgency, frequency, and/or nocturia. OAB-wet occurs when a patient has urgencyincontinence.
The presence of both SUI and OAB/UUI is known as mixed urinary incontinence. Stress and urgency urinary symptoms often present together. In fact, 10% to 30% of women with stress symptoms are found to have bladder overactivity on subsequent evaluation.2,7 Therefore, it is important to take a good history and consider urodynamic evaluation to confirm the diagnosis of SUI prior to surgery in women with mixed stress and urge symptoms, a history of a previous surgery for incontinence, or when there is a poor correlation of physical examination findings to reported symptoms.
Is surgery a first-line option for patients with SUI?
Labrie J, Berghmans BL, Fischer K, et al. Surgery versus physiotherapy for stress urinary incontinence. NEJM. 2013;369(12):1124−1133.
Physiotherapy, including pelvic floor muscle training (“Kegel exercises”), is utilized as a first-line treatment option for women with SUI that carries minimal risk for the patient. Midurethral sling surgery is often recommended if an initial trial of conservative treatment fails.7 Up to 50% of women treated with pelvic floor physiotherapy will ultimately undergo surgery to treat their SUI.8
Related article: Does urodynamic testing before surgery for stress incontinence improve outcomes? G. Willy Davila, MD (Examining the Evidence, December 2012)
Details of the study
This was a randomized, multicenter trial of women aged 35 to 80 years with moderate to severe SUI. After excluding women with previous incontinence surgery and stage 2 or higher pelvic organ prolapse, 460 participants were randomly assigned to undergo either a midurethral sling surgery or physiotherapy (pelvic floor muscle training). The primary outcome was subjective improvement in urinary leakage and bladder function at 12 months, as measured by the Patient Global Impression of Improvement (PGI-I), a 7-point Likert scale ranging from “very much worse” to “very much better.”
In an intention-to-treat analysis, subjective improvement at 12 months was significantly higher in women randomized to midurethral sling surgery than in women randomized to physiotherapy (91% vs 64%, respectively).
Ten percent of patients had adverse events (AEs); all were related to surgery. The most common AEs were hematoma, vaginal epithelial perforation, and bladder perforation.
Notably, women had the option to cross over to the other treatment modality if they desired. In the physiotherapy group, 49% of women elected to cross over to surgery, while 11% of those who underwent midurethral sling surgery elected to cross over to physiotherapy during the 12-month follow-up period. When analyzing results by treatment received, the investigators found that the proportion of women who reported improvement was significantly lower among women who underwent physiotherapy only (32%), versus sling only (94%), or sling after physiotherapy (91%).
This randomized trial was well-designed and included a variety of treatment centers (university and general hospitals) with interventions performed by experienced surgeons (all of whom had performed at least 20 sling surgeries) and physiotherapists educated specifically in pelvic floor physiotherapy. The study population was limited to patients with moderate to severe SUI as defined by the Sandvik severity index.9 Therefore, these results may not be applicable to patients with milder symptoms, for whom physiotherapy has been recommended as first-line therapy with consideration of surgery if physiotherapy fails to sufficiently improve symptoms.7
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women with moderate to severe SUI without significant prolapse or a history of prior incontinence surgery have significantly better outcomes at 12 months after undergoing midurethral sling surgery versus physiotherapy. Physiotherapy carries little to no risk of adverse effects. Women with moderate to severe SUI should be counseled regarding the risks and benefits of both physiotherapy and midurethral sling surgery as initial treatment options.
Because stress and urgency urinary symptoms often present together, it is important to consider urodynamic evaluation to confirm SUI prior to surgery in women with:
• mixed stress and urge symptoms
• a history of a previous surgery for incontinence, or
• poor correlation of physical examination findings to reported symptoms.
Safety and tolerability of mirabegron versus tolterodine for OAB
Chapple CR, Kaplan SA, Mitcheson D, et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a beta(3)-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013;63(2):296−305.
In the bladder, beta3-receptors located within the detrusor smooth muscle facilitate urine storage by relaxing the detrusor, enabling the bladder to fill.10 The activation of beta3-receptors is thought to increase the bladder’s ability to store urine, with the goal of decreasing urgency, frequency, nocturia, and urgency incontinence. An alternative to anticholinergic medications, mirabegron is a beta3-agonist approved by the US Food and Drug Administration (FDA) in 2012 for clinical use in the treatment of OAB.
Details of the study
Chapple and colleagues aimed to assess the 12-month efficacy and safety of mirabegron in a randomized, double-blind active controlled trial. The primary outcome was incidence and severity of treatment-emergent adverse effects (TEAEs); the secondary outcome was the change in OAB symptoms from baseline to up to 12 months. Patients experiencing OAB symptoms for more than 3 months were eligible and were subsequently enrolled if they averaged 8 or more voids per day and 3 or more episodes of urgency with or without incontinence on a 3-day bladder diary. A total of 2,444 patients were randomly assigned in a 1:1:1 fashion to mirabegron 50 mg daily, mirabegron 100 mg daily, or tolterodine extended release (ER) 4 mg daily.
There was a similar incidence (60% to 63%) of TEAEs across all three groups. The most common TEAEs were hypertension (defined as average systolic blood pressure [BP] >140 mm Hg or average diastolic BP >90 mm Hg at two consecutive visits), UTI, headache, nasopharyngitis, and constipation. The adjusted mean changes in BP from baseline to final visit were less than 1 mm Hg for both systolic and diastolic BP for patients taking both doses of mirabegron, as well as for patients taking tolterodine. The incidence of dry mouth was higher in the tolterodine group than the mirabegron groups. Mirabegron 50 mg daily and 100 mg daily improved incontinence symptoms within 1 month of starting therapy; the degree of improvement was similar to that seen in the patients taking tolterodine ER 4 mg daily.
Related article: New overactive bladder treatment approved by the FDA (August 2012)
Some caveats
This study was well-designed to assess the safety and tolerability of mirabegron versus tolterodine. The doses utilized in the study were at or above the FDA-approved dosage of 25 mg to 50 mg daily for OAB treatment. Although investigators found mirabegron to be a safe alternative to anticholinergic medication, the study was not designed or powered to examine the efficacy of mirabegron versus tolterodine. No formal comparison of efficacy was made between mirabegron or tolterodine, or between the 50-mg and 100-mg doses of mirabegron. Moreover, 81% of participants had been treated with mirabegron in earlier Phase 3 studies, so most were not treatment naïve, limiting the applicability of results.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Mirabegron should be considered as a potential treatment option for patients who demonstrate poor tolerance of or response to anticholinergic medications; however, caution should be used in patients with severe uncontrolled high BP, end-stage kidney disease, or severe liver impairment.
Consider percutaneous tibial nerve stimulation over tolterodine for OAB in select patients
Peters KM, Macdiarmid SA, Wooldridge LS, et al. Randomized trial of percutaneous tibial nerve stimulation versus extended-release tolterodine: Results from the overactive bladder innovative therapy trial. J Urol. 2009;182(3):1055−1061.
Neuromodulation utilizes electrical stimulation to improve bladder function and decrease OAB symptoms. First developed in the early 1980s by McGuire and colleagues, percutaneous tibial nerve stimulation (PTNS) was approved by the FDA in 2000 as Urgent PC and provides an outpatient, nonimplantable neuromodulation alternative to medication therapy for patients with OAB.11,12 By directly stimulating the posterior tibial nerve, PTNS works via the S3 sacral nerve plexus to alter the micturition reflex and improve bladder function.
Details of the study
Patients were eligible for the study if they demonstrated 8 or more voids per day on a 3-day bladder diary (whether or not they had a history of previous anticholinergic drug use). A total of 100 ambulatory adults with OAB symptoms were enrolled and randomly assigned to PTNS 30-minutes per week or tolterodine ER 4 mg daily.
At 12 weeks, both groups demonstrated a significant improvement in OAB measures as well as validated symptom severity and quality-of-life questionnaire scores. Subjective assessment of improvement in OAB symptoms was significantly greater in the PTNS group than in the tolterodine group (79.5% vs 54.8%, respectively; P = .01). However, mean reduction of voids for 24 hours was not significantly different between the two groups.
Both treatments were well tolerated, with only 15% to 16% of patients in both groups reporting mild to moderate side effects. The tolterodine group did have a significantly higher risk of dry mouth; however, the risk of constipation was not significantly different between the groups.
Study limitations
The authors performed an important multicenter, nonblinded, randomized, controlled trial, which was one of the first trials to directly compare two OAB therapies. The generalizability of the findings were limited, as the cohort included mostly patients with dry OAB who had no objective measures on UUI episodes. In addition, this trial had a limited observation period of only 12 weeks. Information regarding the effect of treatment after cessation of weekly PTNS therapy was not examined. Therefore, we are not able to determine whether repeat sessions provide adequate maintenance in the long term.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
PTNS 30 minutes daily is as effective as tolterodine ER 4 mg daily for 12 weeks in reducing OAB symptoms. PTNS is a safe alternative that should be considered in patients with OAB who poorly tolerate or have contraindications to medication therapy.
OnabotulinumtoxinA is an effective therapy for OAB
Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. NEJM. 2012;367(19):1803−1813.
The newest therapy for OAB is onabotulinumtoxinA, or Botox, which was FDA approved this year for the treatment of OAB in adults who cannot use or do not tolerate anticholinergic medications. Recommended doses are 100 U onabotulinumtoxinA in patients with idiopathic refractory OAB and 200 U onabotulinumtoxinA for patients with neurogenic OAB.
OnabotulinumtoxinA is a neurotoxin that blocks synaptic transmission at the neuromuscular junction to cause muscle paralysis and atrophy.13 Injecting onabotulinumtoxinA into the detrusor smooth muscle should relax the bladder and decrease sensations of urgency and frequency to achieve a longer duration of time for bladder filling and reduce the risk of urgency incontinence.
Effects of onabotulinumtoxinA appear to wear off over time, and patients may require repeat injections. Side effects of onabotulinumtoxinA therapy include an increased risk of UTI and the potential for urinary retention requiring intermittent self-catheterization.
Related article: Update on Pelvic Floor Dysfunction Autumn L. Edenfield, MD, and Cindy L. Amundsen, MD (October 2012)
Details of the study
The Anticholinergic Versus Botulinum Toxin Comparison (ABC) study was a multicenter, randomized, double-blind, double-placebo–controlled trial conducted in women without known neurologic disease with moderate to severe UUI (defined as >5 UUI episodes on a 3-day bladder diary). Women were randomly assigned to a single intradetrusor injection of 100 U onabotulinumtoxinA plus oral placebo or to a single intradetrusor injection of saline plus solifenacin 5 mg daily (with the option of dose escalation and then switching to trospium XR if no improvement was seen).
Of the 241 women included in the final analysis, approximately 70% in each group reported adequate control of symptoms at 6 months. Adequate control was defined as a response of “agree strongly” or “agree” to the statement: “This treatment has given me adequate control of my urinary leakage.” Women in the onabotulinumtoxinA group were significantly more likely than women in the anticholinergic medication group to report complete resolution of UUI at 6 months (27% vs 13%, P = .003). However, the mean reduction in episodes of UUI per day and the improvements in quality-of-life questionnaire scores were found to be similar. Interestingly, worse baseline UUI was associated with greater reduction in episodes of UUI for both therapies.
This was a rigorous and well-executed double-blind, double-placebo−controlled randomized trial. By utilizing broad inclusion criteria and enrolling patients both with and without previous exposure to anticholinergic medications, the generalizability of study findings are greatly improved. Because this study did not examine the effect or efficacy of repeat injections, these findings have limited applicability to patients undergoing multiple onabotulinumtoxinA injections.
When considering use in your patient population, keep the possible side effects in mind.There were important differences in the side effects experienced with each therapy. Specifically, while the anticholinergic group had a higher frequency of dry mouth (46% anticholinergic vs 31% onabotulinumtoxinA, P = .02), the onabotulinumtoxinA group demonstrated higher rates of incomplete bladder emptying requiring catheterization (peak of 5% at 2 months) and greater risk of UTI (33% onabotulinumtoxinA vs 13% anticholinergic, P <.001).
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This study showed that, among women with UUI, anticholinergic medication and onabotulinumtoxinA are equally effective in reducing UUI episodes and improving quality of life. It is important to consider the side effect profile, determine the patient’s preferences, and weigh the risks and benefits of each therapy when deciding what is the best treatment for your individual patient.
We want to hear from you! Tell us what you think.
- Anger JT, Saigal CS, Litwin MS. The prevalence of urinary incontinence among community dwelling adult women: Results from the National Health and Nutrition Examination Survey. J Urol. 2006;175(2):601–604.
- Dooley Y, Kenton K, Cao G, et al. Urinary incontinence prevalence: Results from the National Health and Nutrition Examination Survey. J Urol. 2008;179(2):656–661.
- Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstetr Gynecol. 2009;114(6):1278–1283.
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU Guideline. Americal Urological Association. http://www.auanet.org/common/pdf/education/clinical-guidance/Overactive-Bladder.pdf. Published 2012. Revised June 11, 2013. Accessed October 21, 2013.
- Yu YF, Nichol MB, Yu AP, Ahn J. Persistence and adherence of medications for chronic overactive bladder/urinary incontinence in the California Medicaid program. Value Health. 2005;8(4):495–505.
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26.
- ACOG Practice Bulletin No. 63: Urinary incontinence in women. American College of Obstetricians and Gynecologists. Obstetr Gynecol. 2005;105(6):1533–1545.
- Bo K, Kvarstein B, Nygaard I. Lower urinary tract symptoms and pelvic floor muscle exercise adherence after 15 years. Obstetr Gynecol. 2005;105(5 Pt 1):999–1005.
- Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health. 1993;47(6):497–499.
- Fowler CJ, Griffiths D, de Groat WC. The neural control of micturition. Nat Rev Neurosci. 2008;9(6):453–466.
- Levin PJ, Wu JM, Kawasaki A, Weidner AC, Amundsen CL. The efficacy of posterior tibial nerve stimulation for the treatment of overactive bladder in women: a systematic review. Int Urogynecol J. 2012;23(11):1591–1597.
- McGuire EJ, Zhang SC, Horwinski ER, Lytton B. Treatment of motor and sensory detrusor instability by electrical stimulation. J Urol. 1983;129(1):78–79.
- Schiavo G, Santucci A, Dasgupta BR, et al. Botulinum neurotoxins serotypes A and E cleave SNAP-25 at distinct COOH-terminal peptide bonds. FEBS Lett. 1993;335(1):99–103.

Alexis A. Dieter, MD, is a Fellow in the Division of Female Pelvic and Reconstructive Pelvic Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University in Durham, NC.

Cindy L. Amundsen, MD, is Professor and Fellowship Director of the Division of Female Pelvic and Reconstructive Pelvic Surgery, Department of Obstetrics and Gynecology, at Duke University in Durham, NC.
Dr. Dieter reports that she received the American Urogynecologic Society (AUGS) Foundation Thomas Benson Award, and participates in the NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Loan Repayment Program. Dr. Amundsen reports no financial relationships relevant to this article.
Alexis A. Dieter, MD, is a Fellow in the Division of Female Pelvic and Reconstructive Pelvic Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University in Durham, NC.
Cindy L. Amundsen, MD, is Professor and Fellowship Director of the Division of Female Pelvic and Reconstructive Pelvic Surgery, Department of Obstetrics and Gynecology, at Duke University in Durham, NC.
Dr. Dieter reports that she received the American Urogynecologic Society (AUGS) Foundation Thomas Benson Award, and participates in the NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Loan Repayment Program. Dr. Amundsen reports no financial relationships relevant to this article.
Alexis A. Dieter, MD, is a Fellow in the Division of Female Pelvic and Reconstructive Pelvic Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University in Durham, NC.
Cindy L. Amundsen, MD, is Professor and Fellowship Director of the Division of Female Pelvic and Reconstructive Pelvic Surgery, Department of Obstetrics and Gynecology, at Duke University in Durham, NC.
Dr. Dieter reports that she received the American Urogynecologic Society (AUGS) Foundation Thomas Benson Award, and participates in the NIH National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Loan Repayment Program. Dr. Amundsen reports no financial relationships relevant to this article.
Urinary incontinence (UI) affects almost half of all women in the United States.1,2 Estimates suggest that the prevalence of UI gradually rises during young adult life, comes to a broad plateau in middle age, and then steadily increases from that plateau after age 65. Therefore, over the next 40 years, as the elderly population expands in size, the number of women affected by UI will significantly grow.3
For patients with UI, a multitude of therapeutic options are available. Which option is the best for your patient? In this article, we aim to answer that question by interpreting the results of four randomized trials, each of which directly compare two available treatment options. The first study examines patients with stress urinary incontinence (SUI), comparing the patients’ subjective improvement in urinary leakage and bladder function at 12 months after randomization to treatment with physiotherapy or midurethral sling surgery.
The three other trials examine patients with overactive bladder (OAB) and urgency urinary incontinence (UUI). Each trial directly compares the use of anticholinergic medications to an alternate treatment modality. Currently, anticholinergic medications and behavioral therapy are the recommended first-line therapies for OAB. Unfortunately, anticholinergic medications have poor patient compliance and significant systemic side effects.4 Caution should be used when considering anticholinergic medications in patients with impaired gastric emptying or a history of urinary retention. They also should be used with caution in elderly patients who are extremely frail. Additionally, clearance from an ophthalmologist must be obtained prior to starting anticholinergic medication in patients with narrow-angle glaucoma.5 Due to poor adherence and potential side effects, there is a growing effort to discover alternative treatment modalities that are safe and effective. Therefore, we chose to examine trials comparing: mirabegron versus tolterodine, percutaneous tibial nerve stimulation versus tolterodine, and onabotulinumtoxinA versus anticholingeric medications.
UI defined
Before discussing treatment options, we want to clarify the main types of UI (FIGURE). UI is defined as the complaint of involuntary loss of urine. UI can be subdivided into SUI, OAB/UUI, or mixed urinary incontinence.6 While there are other less common genitourinary etiologies that can lead to UI, nongenitourinary etiologies are prevalent and can aggravate existing SUI or OAB (TABLE).
SUI is the complaint of involuntary loss of urine on effort or physical exertion (such as during sporting activities) or on sneezing or coughing. Often, SUI can be diagnosed by patient report alone and surgery can be considered in symptomatic patients who demonstrate cough leakage on physical examination and normal postvoid residual volumes.
UUI is the involuntary loss of urine associated with urgency; it often occurs in the setting of OAB, which is defined as the syndrome of urinary urgency, usually accompanied by frequency and nocturia, with or without UUI, in the absence of urinary tract infection or other obvious pathology (such as neurologic dysfunction, infection, or urologic neoplasm). OAB-dry is present when patients do not have leakage with urgency, but are bothered by urgency, frequency, and/or nocturia. OAB-wet occurs when a patient has urgencyincontinence.
The presence of both SUI and OAB/UUI is known as mixed urinary incontinence. Stress and urgency urinary symptoms often present together. In fact, 10% to 30% of women with stress symptoms are found to have bladder overactivity on subsequent evaluation.2,7 Therefore, it is important to take a good history and consider urodynamic evaluation to confirm the diagnosis of SUI prior to surgery in women with mixed stress and urge symptoms, a history of a previous surgery for incontinence, or when there is a poor correlation of physical examination findings to reported symptoms.
Is surgery a first-line option for patients with SUI?
Labrie J, Berghmans BL, Fischer K, et al. Surgery versus physiotherapy for stress urinary incontinence. NEJM. 2013;369(12):1124−1133.
Physiotherapy, including pelvic floor muscle training (“Kegel exercises”), is utilized as a first-line treatment option for women with SUI that carries minimal risk for the patient. Midurethral sling surgery is often recommended if an initial trial of conservative treatment fails.7 Up to 50% of women treated with pelvic floor physiotherapy will ultimately undergo surgery to treat their SUI.8
Related article: Does urodynamic testing before surgery for stress incontinence improve outcomes? G. Willy Davila, MD (Examining the Evidence, December 2012)
Details of the study
This was a randomized, multicenter trial of women aged 35 to 80 years with moderate to severe SUI. After excluding women with previous incontinence surgery and stage 2 or higher pelvic organ prolapse, 460 participants were randomly assigned to undergo either a midurethral sling surgery or physiotherapy (pelvic floor muscle training). The primary outcome was subjective improvement in urinary leakage and bladder function at 12 months, as measured by the Patient Global Impression of Improvement (PGI-I), a 7-point Likert scale ranging from “very much worse” to “very much better.”
In an intention-to-treat analysis, subjective improvement at 12 months was significantly higher in women randomized to midurethral sling surgery than in women randomized to physiotherapy (91% vs 64%, respectively).
Ten percent of patients had adverse events (AEs); all were related to surgery. The most common AEs were hematoma, vaginal epithelial perforation, and bladder perforation.
Notably, women had the option to cross over to the other treatment modality if they desired. In the physiotherapy group, 49% of women elected to cross over to surgery, while 11% of those who underwent midurethral sling surgery elected to cross over to physiotherapy during the 12-month follow-up period. When analyzing results by treatment received, the investigators found that the proportion of women who reported improvement was significantly lower among women who underwent physiotherapy only (32%), versus sling only (94%), or sling after physiotherapy (91%).
This randomized trial was well-designed and included a variety of treatment centers (university and general hospitals) with interventions performed by experienced surgeons (all of whom had performed at least 20 sling surgeries) and physiotherapists educated specifically in pelvic floor physiotherapy. The study population was limited to patients with moderate to severe SUI as defined by the Sandvik severity index.9 Therefore, these results may not be applicable to patients with milder symptoms, for whom physiotherapy has been recommended as first-line therapy with consideration of surgery if physiotherapy fails to sufficiently improve symptoms.7
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women with moderate to severe SUI without significant prolapse or a history of prior incontinence surgery have significantly better outcomes at 12 months after undergoing midurethral sling surgery versus physiotherapy. Physiotherapy carries little to no risk of adverse effects. Women with moderate to severe SUI should be counseled regarding the risks and benefits of both physiotherapy and midurethral sling surgery as initial treatment options.
Because stress and urgency urinary symptoms often present together, it is important to consider urodynamic evaluation to confirm SUI prior to surgery in women with:
• mixed stress and urge symptoms
• a history of a previous surgery for incontinence, or
• poor correlation of physical examination findings to reported symptoms.
Safety and tolerability of mirabegron versus tolterodine for OAB
Chapple CR, Kaplan SA, Mitcheson D, et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a beta(3)-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013;63(2):296−305.
In the bladder, beta3-receptors located within the detrusor smooth muscle facilitate urine storage by relaxing the detrusor, enabling the bladder to fill.10 The activation of beta3-receptors is thought to increase the bladder’s ability to store urine, with the goal of decreasing urgency, frequency, nocturia, and urgency incontinence. An alternative to anticholinergic medications, mirabegron is a beta3-agonist approved by the US Food and Drug Administration (FDA) in 2012 for clinical use in the treatment of OAB.
Details of the study
Chapple and colleagues aimed to assess the 12-month efficacy and safety of mirabegron in a randomized, double-blind active controlled trial. The primary outcome was incidence and severity of treatment-emergent adverse effects (TEAEs); the secondary outcome was the change in OAB symptoms from baseline to up to 12 months. Patients experiencing OAB symptoms for more than 3 months were eligible and were subsequently enrolled if they averaged 8 or more voids per day and 3 or more episodes of urgency with or without incontinence on a 3-day bladder diary. A total of 2,444 patients were randomly assigned in a 1:1:1 fashion to mirabegron 50 mg daily, mirabegron 100 mg daily, or tolterodine extended release (ER) 4 mg daily.
There was a similar incidence (60% to 63%) of TEAEs across all three groups. The most common TEAEs were hypertension (defined as average systolic blood pressure [BP] >140 mm Hg or average diastolic BP >90 mm Hg at two consecutive visits), UTI, headache, nasopharyngitis, and constipation. The adjusted mean changes in BP from baseline to final visit were less than 1 mm Hg for both systolic and diastolic BP for patients taking both doses of mirabegron, as well as for patients taking tolterodine. The incidence of dry mouth was higher in the tolterodine group than the mirabegron groups. Mirabegron 50 mg daily and 100 mg daily improved incontinence symptoms within 1 month of starting therapy; the degree of improvement was similar to that seen in the patients taking tolterodine ER 4 mg daily.
Related article: New overactive bladder treatment approved by the FDA (August 2012)
Some caveats
This study was well-designed to assess the safety and tolerability of mirabegron versus tolterodine. The doses utilized in the study were at or above the FDA-approved dosage of 25 mg to 50 mg daily for OAB treatment. Although investigators found mirabegron to be a safe alternative to anticholinergic medication, the study was not designed or powered to examine the efficacy of mirabegron versus tolterodine. No formal comparison of efficacy was made between mirabegron or tolterodine, or between the 50-mg and 100-mg doses of mirabegron. Moreover, 81% of participants had been treated with mirabegron in earlier Phase 3 studies, so most were not treatment naïve, limiting the applicability of results.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Mirabegron should be considered as a potential treatment option for patients who demonstrate poor tolerance of or response to anticholinergic medications; however, caution should be used in patients with severe uncontrolled high BP, end-stage kidney disease, or severe liver impairment.
Consider percutaneous tibial nerve stimulation over tolterodine for OAB in select patients
Peters KM, Macdiarmid SA, Wooldridge LS, et al. Randomized trial of percutaneous tibial nerve stimulation versus extended-release tolterodine: Results from the overactive bladder innovative therapy trial. J Urol. 2009;182(3):1055−1061.
Neuromodulation utilizes electrical stimulation to improve bladder function and decrease OAB symptoms. First developed in the early 1980s by McGuire and colleagues, percutaneous tibial nerve stimulation (PTNS) was approved by the FDA in 2000 as Urgent PC and provides an outpatient, nonimplantable neuromodulation alternative to medication therapy for patients with OAB.11,12 By directly stimulating the posterior tibial nerve, PTNS works via the S3 sacral nerve plexus to alter the micturition reflex and improve bladder function.
Details of the study
Patients were eligible for the study if they demonstrated 8 or more voids per day on a 3-day bladder diary (whether or not they had a history of previous anticholinergic drug use). A total of 100 ambulatory adults with OAB symptoms were enrolled and randomly assigned to PTNS 30-minutes per week or tolterodine ER 4 mg daily.
At 12 weeks, both groups demonstrated a significant improvement in OAB measures as well as validated symptom severity and quality-of-life questionnaire scores. Subjective assessment of improvement in OAB symptoms was significantly greater in the PTNS group than in the tolterodine group (79.5% vs 54.8%, respectively; P = .01). However, mean reduction of voids for 24 hours was not significantly different between the two groups.
Both treatments were well tolerated, with only 15% to 16% of patients in both groups reporting mild to moderate side effects. The tolterodine group did have a significantly higher risk of dry mouth; however, the risk of constipation was not significantly different between the groups.
Study limitations
The authors performed an important multicenter, nonblinded, randomized, controlled trial, which was one of the first trials to directly compare two OAB therapies. The generalizability of the findings were limited, as the cohort included mostly patients with dry OAB who had no objective measures on UUI episodes. In addition, this trial had a limited observation period of only 12 weeks. Information regarding the effect of treatment after cessation of weekly PTNS therapy was not examined. Therefore, we are not able to determine whether repeat sessions provide adequate maintenance in the long term.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
PTNS 30 minutes daily is as effective as tolterodine ER 4 mg daily for 12 weeks in reducing OAB symptoms. PTNS is a safe alternative that should be considered in patients with OAB who poorly tolerate or have contraindications to medication therapy.
OnabotulinumtoxinA is an effective therapy for OAB
Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. NEJM. 2012;367(19):1803−1813.
The newest therapy for OAB is onabotulinumtoxinA, or Botox, which was FDA approved this year for the treatment of OAB in adults who cannot use or do not tolerate anticholinergic medications. Recommended doses are 100 U onabotulinumtoxinA in patients with idiopathic refractory OAB and 200 U onabotulinumtoxinA for patients with neurogenic OAB.
OnabotulinumtoxinA is a neurotoxin that blocks synaptic transmission at the neuromuscular junction to cause muscle paralysis and atrophy.13 Injecting onabotulinumtoxinA into the detrusor smooth muscle should relax the bladder and decrease sensations of urgency and frequency to achieve a longer duration of time for bladder filling and reduce the risk of urgency incontinence.
Effects of onabotulinumtoxinA appear to wear off over time, and patients may require repeat injections. Side effects of onabotulinumtoxinA therapy include an increased risk of UTI and the potential for urinary retention requiring intermittent self-catheterization.
Related article: Update on Pelvic Floor Dysfunction Autumn L. Edenfield, MD, and Cindy L. Amundsen, MD (October 2012)
Details of the study
The Anticholinergic Versus Botulinum Toxin Comparison (ABC) study was a multicenter, randomized, double-blind, double-placebo–controlled trial conducted in women without known neurologic disease with moderate to severe UUI (defined as >5 UUI episodes on a 3-day bladder diary). Women were randomly assigned to a single intradetrusor injection of 100 U onabotulinumtoxinA plus oral placebo or to a single intradetrusor injection of saline plus solifenacin 5 mg daily (with the option of dose escalation and then switching to trospium XR if no improvement was seen).
Of the 241 women included in the final analysis, approximately 70% in each group reported adequate control of symptoms at 6 months. Adequate control was defined as a response of “agree strongly” or “agree” to the statement: “This treatment has given me adequate control of my urinary leakage.” Women in the onabotulinumtoxinA group were significantly more likely than women in the anticholinergic medication group to report complete resolution of UUI at 6 months (27% vs 13%, P = .003). However, the mean reduction in episodes of UUI per day and the improvements in quality-of-life questionnaire scores were found to be similar. Interestingly, worse baseline UUI was associated with greater reduction in episodes of UUI for both therapies.
This was a rigorous and well-executed double-blind, double-placebo−controlled randomized trial. By utilizing broad inclusion criteria and enrolling patients both with and without previous exposure to anticholinergic medications, the generalizability of study findings are greatly improved. Because this study did not examine the effect or efficacy of repeat injections, these findings have limited applicability to patients undergoing multiple onabotulinumtoxinA injections.
When considering use in your patient population, keep the possible side effects in mind.There were important differences in the side effects experienced with each therapy. Specifically, while the anticholinergic group had a higher frequency of dry mouth (46% anticholinergic vs 31% onabotulinumtoxinA, P = .02), the onabotulinumtoxinA group demonstrated higher rates of incomplete bladder emptying requiring catheterization (peak of 5% at 2 months) and greater risk of UTI (33% onabotulinumtoxinA vs 13% anticholinergic, P <.001).
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This study showed that, among women with UUI, anticholinergic medication and onabotulinumtoxinA are equally effective in reducing UUI episodes and improving quality of life. It is important to consider the side effect profile, determine the patient’s preferences, and weigh the risks and benefits of each therapy when deciding what is the best treatment for your individual patient.
We want to hear from you! Tell us what you think.
Urinary incontinence (UI) affects almost half of all women in the United States.1,2 Estimates suggest that the prevalence of UI gradually rises during young adult life, comes to a broad plateau in middle age, and then steadily increases from that plateau after age 65. Therefore, over the next 40 years, as the elderly population expands in size, the number of women affected by UI will significantly grow.3
For patients with UI, a multitude of therapeutic options are available. Which option is the best for your patient? In this article, we aim to answer that question by interpreting the results of four randomized trials, each of which directly compare two available treatment options. The first study examines patients with stress urinary incontinence (SUI), comparing the patients’ subjective improvement in urinary leakage and bladder function at 12 months after randomization to treatment with physiotherapy or midurethral sling surgery.
The three other trials examine patients with overactive bladder (OAB) and urgency urinary incontinence (UUI). Each trial directly compares the use of anticholinergic medications to an alternate treatment modality. Currently, anticholinergic medications and behavioral therapy are the recommended first-line therapies for OAB. Unfortunately, anticholinergic medications have poor patient compliance and significant systemic side effects.4 Caution should be used when considering anticholinergic medications in patients with impaired gastric emptying or a history of urinary retention. They also should be used with caution in elderly patients who are extremely frail. Additionally, clearance from an ophthalmologist must be obtained prior to starting anticholinergic medication in patients with narrow-angle glaucoma.5 Due to poor adherence and potential side effects, there is a growing effort to discover alternative treatment modalities that are safe and effective. Therefore, we chose to examine trials comparing: mirabegron versus tolterodine, percutaneous tibial nerve stimulation versus tolterodine, and onabotulinumtoxinA versus anticholingeric medications.
UI defined
Before discussing treatment options, we want to clarify the main types of UI (FIGURE). UI is defined as the complaint of involuntary loss of urine. UI can be subdivided into SUI, OAB/UUI, or mixed urinary incontinence.6 While there are other less common genitourinary etiologies that can lead to UI, nongenitourinary etiologies are prevalent and can aggravate existing SUI or OAB (TABLE).
SUI is the complaint of involuntary loss of urine on effort or physical exertion (such as during sporting activities) or on sneezing or coughing. Often, SUI can be diagnosed by patient report alone and surgery can be considered in symptomatic patients who demonstrate cough leakage on physical examination and normal postvoid residual volumes.
UUI is the involuntary loss of urine associated with urgency; it often occurs in the setting of OAB, which is defined as the syndrome of urinary urgency, usually accompanied by frequency and nocturia, with or without UUI, in the absence of urinary tract infection or other obvious pathology (such as neurologic dysfunction, infection, or urologic neoplasm). OAB-dry is present when patients do not have leakage with urgency, but are bothered by urgency, frequency, and/or nocturia. OAB-wet occurs when a patient has urgencyincontinence.
The presence of both SUI and OAB/UUI is known as mixed urinary incontinence. Stress and urgency urinary symptoms often present together. In fact, 10% to 30% of women with stress symptoms are found to have bladder overactivity on subsequent evaluation.2,7 Therefore, it is important to take a good history and consider urodynamic evaluation to confirm the diagnosis of SUI prior to surgery in women with mixed stress and urge symptoms, a history of a previous surgery for incontinence, or when there is a poor correlation of physical examination findings to reported symptoms.
Is surgery a first-line option for patients with SUI?
Labrie J, Berghmans BL, Fischer K, et al. Surgery versus physiotherapy for stress urinary incontinence. NEJM. 2013;369(12):1124−1133.
Physiotherapy, including pelvic floor muscle training (“Kegel exercises”), is utilized as a first-line treatment option for women with SUI that carries minimal risk for the patient. Midurethral sling surgery is often recommended if an initial trial of conservative treatment fails.7 Up to 50% of women treated with pelvic floor physiotherapy will ultimately undergo surgery to treat their SUI.8
Related article: Does urodynamic testing before surgery for stress incontinence improve outcomes? G. Willy Davila, MD (Examining the Evidence, December 2012)
Details of the study
This was a randomized, multicenter trial of women aged 35 to 80 years with moderate to severe SUI. After excluding women with previous incontinence surgery and stage 2 or higher pelvic organ prolapse, 460 participants were randomly assigned to undergo either a midurethral sling surgery or physiotherapy (pelvic floor muscle training). The primary outcome was subjective improvement in urinary leakage and bladder function at 12 months, as measured by the Patient Global Impression of Improvement (PGI-I), a 7-point Likert scale ranging from “very much worse” to “very much better.”
In an intention-to-treat analysis, subjective improvement at 12 months was significantly higher in women randomized to midurethral sling surgery than in women randomized to physiotherapy (91% vs 64%, respectively).
Ten percent of patients had adverse events (AEs); all were related to surgery. The most common AEs were hematoma, vaginal epithelial perforation, and bladder perforation.
Notably, women had the option to cross over to the other treatment modality if they desired. In the physiotherapy group, 49% of women elected to cross over to surgery, while 11% of those who underwent midurethral sling surgery elected to cross over to physiotherapy during the 12-month follow-up period. When analyzing results by treatment received, the investigators found that the proportion of women who reported improvement was significantly lower among women who underwent physiotherapy only (32%), versus sling only (94%), or sling after physiotherapy (91%).
This randomized trial was well-designed and included a variety of treatment centers (university and general hospitals) with interventions performed by experienced surgeons (all of whom had performed at least 20 sling surgeries) and physiotherapists educated specifically in pelvic floor physiotherapy. The study population was limited to patients with moderate to severe SUI as defined by the Sandvik severity index.9 Therefore, these results may not be applicable to patients with milder symptoms, for whom physiotherapy has been recommended as first-line therapy with consideration of surgery if physiotherapy fails to sufficiently improve symptoms.7
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Women with moderate to severe SUI without significant prolapse or a history of prior incontinence surgery have significantly better outcomes at 12 months after undergoing midurethral sling surgery versus physiotherapy. Physiotherapy carries little to no risk of adverse effects. Women with moderate to severe SUI should be counseled regarding the risks and benefits of both physiotherapy and midurethral sling surgery as initial treatment options.
Because stress and urgency urinary symptoms often present together, it is important to consider urodynamic evaluation to confirm SUI prior to surgery in women with:
• mixed stress and urge symptoms
• a history of a previous surgery for incontinence, or
• poor correlation of physical examination findings to reported symptoms.
Safety and tolerability of mirabegron versus tolterodine for OAB
Chapple CR, Kaplan SA, Mitcheson D, et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a beta(3)-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013;63(2):296−305.
In the bladder, beta3-receptors located within the detrusor smooth muscle facilitate urine storage by relaxing the detrusor, enabling the bladder to fill.10 The activation of beta3-receptors is thought to increase the bladder’s ability to store urine, with the goal of decreasing urgency, frequency, nocturia, and urgency incontinence. An alternative to anticholinergic medications, mirabegron is a beta3-agonist approved by the US Food and Drug Administration (FDA) in 2012 for clinical use in the treatment of OAB.
Details of the study
Chapple and colleagues aimed to assess the 12-month efficacy and safety of mirabegron in a randomized, double-blind active controlled trial. The primary outcome was incidence and severity of treatment-emergent adverse effects (TEAEs); the secondary outcome was the change in OAB symptoms from baseline to up to 12 months. Patients experiencing OAB symptoms for more than 3 months were eligible and were subsequently enrolled if they averaged 8 or more voids per day and 3 or more episodes of urgency with or without incontinence on a 3-day bladder diary. A total of 2,444 patients were randomly assigned in a 1:1:1 fashion to mirabegron 50 mg daily, mirabegron 100 mg daily, or tolterodine extended release (ER) 4 mg daily.
There was a similar incidence (60% to 63%) of TEAEs across all three groups. The most common TEAEs were hypertension (defined as average systolic blood pressure [BP] >140 mm Hg or average diastolic BP >90 mm Hg at two consecutive visits), UTI, headache, nasopharyngitis, and constipation. The adjusted mean changes in BP from baseline to final visit were less than 1 mm Hg for both systolic and diastolic BP for patients taking both doses of mirabegron, as well as for patients taking tolterodine. The incidence of dry mouth was higher in the tolterodine group than the mirabegron groups. Mirabegron 50 mg daily and 100 mg daily improved incontinence symptoms within 1 month of starting therapy; the degree of improvement was similar to that seen in the patients taking tolterodine ER 4 mg daily.
Related article: New overactive bladder treatment approved by the FDA (August 2012)
Some caveats
This study was well-designed to assess the safety and tolerability of mirabegron versus tolterodine. The doses utilized in the study were at or above the FDA-approved dosage of 25 mg to 50 mg daily for OAB treatment. Although investigators found mirabegron to be a safe alternative to anticholinergic medication, the study was not designed or powered to examine the efficacy of mirabegron versus tolterodine. No formal comparison of efficacy was made between mirabegron or tolterodine, or between the 50-mg and 100-mg doses of mirabegron. Moreover, 81% of participants had been treated with mirabegron in earlier Phase 3 studies, so most were not treatment naïve, limiting the applicability of results.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
Mirabegron should be considered as a potential treatment option for patients who demonstrate poor tolerance of or response to anticholinergic medications; however, caution should be used in patients with severe uncontrolled high BP, end-stage kidney disease, or severe liver impairment.
Consider percutaneous tibial nerve stimulation over tolterodine for OAB in select patients
Peters KM, Macdiarmid SA, Wooldridge LS, et al. Randomized trial of percutaneous tibial nerve stimulation versus extended-release tolterodine: Results from the overactive bladder innovative therapy trial. J Urol. 2009;182(3):1055−1061.
Neuromodulation utilizes electrical stimulation to improve bladder function and decrease OAB symptoms. First developed in the early 1980s by McGuire and colleagues, percutaneous tibial nerve stimulation (PTNS) was approved by the FDA in 2000 as Urgent PC and provides an outpatient, nonimplantable neuromodulation alternative to medication therapy for patients with OAB.11,12 By directly stimulating the posterior tibial nerve, PTNS works via the S3 sacral nerve plexus to alter the micturition reflex and improve bladder function.
Details of the study
Patients were eligible for the study if they demonstrated 8 or more voids per day on a 3-day bladder diary (whether or not they had a history of previous anticholinergic drug use). A total of 100 ambulatory adults with OAB symptoms were enrolled and randomly assigned to PTNS 30-minutes per week or tolterodine ER 4 mg daily.
At 12 weeks, both groups demonstrated a significant improvement in OAB measures as well as validated symptom severity and quality-of-life questionnaire scores. Subjective assessment of improvement in OAB symptoms was significantly greater in the PTNS group than in the tolterodine group (79.5% vs 54.8%, respectively; P = .01). However, mean reduction of voids for 24 hours was not significantly different between the two groups.
Both treatments were well tolerated, with only 15% to 16% of patients in both groups reporting mild to moderate side effects. The tolterodine group did have a significantly higher risk of dry mouth; however, the risk of constipation was not significantly different between the groups.
Study limitations
The authors performed an important multicenter, nonblinded, randomized, controlled trial, which was one of the first trials to directly compare two OAB therapies. The generalizability of the findings were limited, as the cohort included mostly patients with dry OAB who had no objective measures on UUI episodes. In addition, this trial had a limited observation period of only 12 weeks. Information regarding the effect of treatment after cessation of weekly PTNS therapy was not examined. Therefore, we are not able to determine whether repeat sessions provide adequate maintenance in the long term.
WHAT THIS EVIDENCE MEANS FOR PRACTICE
PTNS 30 minutes daily is as effective as tolterodine ER 4 mg daily for 12 weeks in reducing OAB symptoms. PTNS is a safe alternative that should be considered in patients with OAB who poorly tolerate or have contraindications to medication therapy.
OnabotulinumtoxinA is an effective therapy for OAB
Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs onabotulinumtoxinA for urgency urinary incontinence. NEJM. 2012;367(19):1803−1813.
The newest therapy for OAB is onabotulinumtoxinA, or Botox, which was FDA approved this year for the treatment of OAB in adults who cannot use or do not tolerate anticholinergic medications. Recommended doses are 100 U onabotulinumtoxinA in patients with idiopathic refractory OAB and 200 U onabotulinumtoxinA for patients with neurogenic OAB.
OnabotulinumtoxinA is a neurotoxin that blocks synaptic transmission at the neuromuscular junction to cause muscle paralysis and atrophy.13 Injecting onabotulinumtoxinA into the detrusor smooth muscle should relax the bladder and decrease sensations of urgency and frequency to achieve a longer duration of time for bladder filling and reduce the risk of urgency incontinence.
Effects of onabotulinumtoxinA appear to wear off over time, and patients may require repeat injections. Side effects of onabotulinumtoxinA therapy include an increased risk of UTI and the potential for urinary retention requiring intermittent self-catheterization.
Related article: Update on Pelvic Floor Dysfunction Autumn L. Edenfield, MD, and Cindy L. Amundsen, MD (October 2012)
Details of the study
The Anticholinergic Versus Botulinum Toxin Comparison (ABC) study was a multicenter, randomized, double-blind, double-placebo–controlled trial conducted in women without known neurologic disease with moderate to severe UUI (defined as >5 UUI episodes on a 3-day bladder diary). Women were randomly assigned to a single intradetrusor injection of 100 U onabotulinumtoxinA plus oral placebo or to a single intradetrusor injection of saline plus solifenacin 5 mg daily (with the option of dose escalation and then switching to trospium XR if no improvement was seen).
Of the 241 women included in the final analysis, approximately 70% in each group reported adequate control of symptoms at 6 months. Adequate control was defined as a response of “agree strongly” or “agree” to the statement: “This treatment has given me adequate control of my urinary leakage.” Women in the onabotulinumtoxinA group were significantly more likely than women in the anticholinergic medication group to report complete resolution of UUI at 6 months (27% vs 13%, P = .003). However, the mean reduction in episodes of UUI per day and the improvements in quality-of-life questionnaire scores were found to be similar. Interestingly, worse baseline UUI was associated with greater reduction in episodes of UUI for both therapies.
This was a rigorous and well-executed double-blind, double-placebo−controlled randomized trial. By utilizing broad inclusion criteria and enrolling patients both with and without previous exposure to anticholinergic medications, the generalizability of study findings are greatly improved. Because this study did not examine the effect or efficacy of repeat injections, these findings have limited applicability to patients undergoing multiple onabotulinumtoxinA injections.
When considering use in your patient population, keep the possible side effects in mind.There were important differences in the side effects experienced with each therapy. Specifically, while the anticholinergic group had a higher frequency of dry mouth (46% anticholinergic vs 31% onabotulinumtoxinA, P = .02), the onabotulinumtoxinA group demonstrated higher rates of incomplete bladder emptying requiring catheterization (peak of 5% at 2 months) and greater risk of UTI (33% onabotulinumtoxinA vs 13% anticholinergic, P <.001).
WHAT THIS EVIDENCE MEANS FOR PRACTICE
This study showed that, among women with UUI, anticholinergic medication and onabotulinumtoxinA are equally effective in reducing UUI episodes and improving quality of life. It is important to consider the side effect profile, determine the patient’s preferences, and weigh the risks and benefits of each therapy when deciding what is the best treatment for your individual patient.
We want to hear from you! Tell us what you think.
- Anger JT, Saigal CS, Litwin MS. The prevalence of urinary incontinence among community dwelling adult women: Results from the National Health and Nutrition Examination Survey. J Urol. 2006;175(2):601–604.
- Dooley Y, Kenton K, Cao G, et al. Urinary incontinence prevalence: Results from the National Health and Nutrition Examination Survey. J Urol. 2008;179(2):656–661.
- Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstetr Gynecol. 2009;114(6):1278–1283.
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU Guideline. Americal Urological Association. http://www.auanet.org/common/pdf/education/clinical-guidance/Overactive-Bladder.pdf. Published 2012. Revised June 11, 2013. Accessed October 21, 2013.
- Yu YF, Nichol MB, Yu AP, Ahn J. Persistence and adherence of medications for chronic overactive bladder/urinary incontinence in the California Medicaid program. Value Health. 2005;8(4):495–505.
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26.
- ACOG Practice Bulletin No. 63: Urinary incontinence in women. American College of Obstetricians and Gynecologists. Obstetr Gynecol. 2005;105(6):1533–1545.
- Bo K, Kvarstein B, Nygaard I. Lower urinary tract symptoms and pelvic floor muscle exercise adherence after 15 years. Obstetr Gynecol. 2005;105(5 Pt 1):999–1005.
- Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health. 1993;47(6):497–499.
- Fowler CJ, Griffiths D, de Groat WC. The neural control of micturition. Nat Rev Neurosci. 2008;9(6):453–466.
- Levin PJ, Wu JM, Kawasaki A, Weidner AC, Amundsen CL. The efficacy of posterior tibial nerve stimulation for the treatment of overactive bladder in women: a systematic review. Int Urogynecol J. 2012;23(11):1591–1597.
- McGuire EJ, Zhang SC, Horwinski ER, Lytton B. Treatment of motor and sensory detrusor instability by electrical stimulation. J Urol. 1983;129(1):78–79.
- Schiavo G, Santucci A, Dasgupta BR, et al. Botulinum neurotoxins serotypes A and E cleave SNAP-25 at distinct COOH-terminal peptide bonds. FEBS Lett. 1993;335(1):99–103.
- Anger JT, Saigal CS, Litwin MS. The prevalence of urinary incontinence among community dwelling adult women: Results from the National Health and Nutrition Examination Survey. J Urol. 2006;175(2):601–604.
- Dooley Y, Kenton K, Cao G, et al. Urinary incontinence prevalence: Results from the National Health and Nutrition Examination Survey. J Urol. 2008;179(2):656–661.
- Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstetr Gynecol. 2009;114(6):1278–1283.
- Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU Guideline. Americal Urological Association. http://www.auanet.org/common/pdf/education/clinical-guidance/Overactive-Bladder.pdf. Published 2012. Revised June 11, 2013. Accessed October 21, 2013.
- Yu YF, Nichol MB, Yu AP, Ahn J. Persistence and adherence of medications for chronic overactive bladder/urinary incontinence in the California Medicaid program. Value Health. 2005;8(4):495–505.
- Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26.
- ACOG Practice Bulletin No. 63: Urinary incontinence in women. American College of Obstetricians and Gynecologists. Obstetr Gynecol. 2005;105(6):1533–1545.
- Bo K, Kvarstein B, Nygaard I. Lower urinary tract symptoms and pelvic floor muscle exercise adherence after 15 years. Obstetr Gynecol. 2005;105(5 Pt 1):999–1005.
- Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. J Epidemiol Community Health. 1993;47(6):497–499.
- Fowler CJ, Griffiths D, de Groat WC. The neural control of micturition. Nat Rev Neurosci. 2008;9(6):453–466.
- Levin PJ, Wu JM, Kawasaki A, Weidner AC, Amundsen CL. The efficacy of posterior tibial nerve stimulation for the treatment of overactive bladder in women: a systematic review. Int Urogynecol J. 2012;23(11):1591–1597.
- McGuire EJ, Zhang SC, Horwinski ER, Lytton B. Treatment of motor and sensory detrusor instability by electrical stimulation. J Urol. 1983;129(1):78–79.
- Schiavo G, Santucci A, Dasgupta BR, et al. Botulinum neurotoxins serotypes A and E cleave SNAP-25 at distinct COOH-terminal peptide bonds. FEBS Lett. 1993;335(1):99–103.
Morphea: From a Rash to Atrophy
Safety and Efficacy Comparison of Maximum Dose Simvastatin vs Rosuvastatin
Intraocular Pressure and Metabolic Syndrome After Menopause
Endometrial Cancer Update: The move toward personalized cancer care
Endometrial cancer is the most common malignancy of the female reproductive tract in the United States, and its incidence continues to rise, with an estimated 49,560 new cases predicted for 2013.1 If we are to successfully traverse the pathway from molecular cell genetics to the development of targeted therapies and personalized cancer care, we need to meet a few benchmarks:
- We need to enhance our understanding of the molecular changes that lead to endometrial cancer. Of particular interest are nonendometrioid tumors. Increased mortality from endometrial cancer appears to be related to the growing number of uterine papillary serous carcinomas and clear-cell cancers. Although these cancers constitute less than 10% of all endometrial cancers, they account for a disproportionately high number of recurrences and cancer-related deaths.2,3 Do recent studies validate the original classification of endometrial cancers as Type I (endometrioid) or Type II (serous and clear cell), or is there more heterogeneity than was originally thought? How do recent studies affect treatment options?
- We need to establish a genomic characterization of endometrial cancer to supplement clinical research data. The identification of novel mutations specific to each histologic type has the potential to improve adjuvant therapy. How close are we to performing a comprehensive genomic analysis of endometrial cancer?
- We need to develop new adjuvant treatment options for recurrent and advanced disease. When clinical symptoms of endometrial cancer are overt, as they often are, early diagnosis is possible, with a 5-year survival rate of 80% to 90%. The prognosis declines dramatically in women with advanced-stage disease or high-risk histologies, with a 5-year survival rate of 57% and 19% for Stage III and Stage IV disease, respectively.1 Adjuvant treatment options are limited in the setting of recurrent or advanced disease. Do any biologic agents increase survival?
In this article, we highlight the historical foundation and newest advances in the field of endometrial cancer, focusing on:
- histologic classification
- etiologic heterogeneity and molecular biology
- genome-guided clinical trials involving targeted therapy, with the ultimate goal of achieving individualized cancer care.
Should we reclassify endometrial cancers to reflect molecular characteristics of tumors?
Brinton LA, Felix AS, McMeekin DS, et al. Etiologic heterogeneity in endometrial cancer: evidence from a Gynecologic Oncology Group trial. Gynecol Oncol. 2013;129(2):277–284.
Cancer Genome Atlas Research Network, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
Uterine papillary serous carcinoma (UPSC) was first established as a distinct subtype of endometrial cancer in the early 1980s, when teams led by Lauchlan4 and Hendrickson5 described it as histologically similar to serous epithelial ovarian carcinoma. Shortly thereafter, Bokhman proposed two broad categories of endometrial carcinoma characterized by distinct microscopic appearance, epidemiology, and endocrine and metabolic functioning (TABLE, page 28).6
More recently, research has focused on expanding this histologic classification system to encompass molecular differences. Brinton and colleagues conducted a study within Gynecologic Oncology Group 210, investigating the etiologic heterogeneity of endometrial cancers by comparing risk factors for different histologies. They found that risk factors for aggressive endometrial cancers, including Grade 3 endometrioid and nonendometrioid tumors, appear to differ from those of lower-grade endometrioid carcinomas.
Details of the study by Brinton and colleagues
A total of 3,434 women were included, representing endometrioid (78%) and serous (9%) carcinomas. Grade 3 endometrioid tumors resembled Type II endometrial cancers more closely than did Grade 1–2 endometrioid tumors. Patients with Grade 3 endometrioid and Type II cancers were diagnosed at a significantly older age than patients with Grades 1–2 endometrioid cancers (eg, diagnosis of serous cancers: median age, 67.4 years; Grade 3 endometrioid cancers: median age, 61.9 years; Grade 1–2 endometrioid cancers: median age, 59.6 years). They also were more likely to be nonwhite than patients with Grades 1–2 endometrioid histology. Specifically, black patients were rarely diagnosed with Grades 1–2 endometrioid cancers (5% vs 9% for Grade 3 endometrioid cancers; 20% for serous cancers, 23% for carcinosarcomas, and 12% for clear-cell cancers).
After adjustments for age, enrollment year, and race, patients with Type II tumors (serous, carcinosarcomas, or clear-cell tumors) were much more likely to be multiparous or smokers or to have a history of breast cancer treated with tamoxifen, compared with women with Grade 1–2 endometrioid cancers. An adequately powered subanalysis of serous carcinomas and Grades 1–2 endometrioid cancers revealed that associations persisted between serous carcinomas and multiparity, body mass index, and a history of breast cancer treated with tamoxifen.
Related article: The future of the Pap test: Identifying endometrial and ovarian cancers (Janelle Yates, August 2013)
Overall, this study provides some of the strongest epidemiologic support we have that endometrial cancers are heterogeneous, with evidence to suggest that we might classify Grade 3 endometrioid carcinomas as Type II cancers. These findings paved the way for molecular profiling of endometrial cancers.
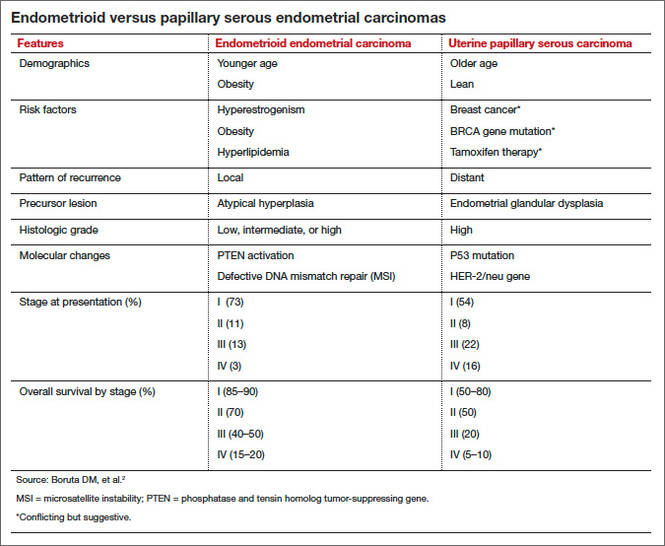
Details of the study by the Cancer Genome Atlas Research Network
The Cancer Genome Atlas Research Network recently published an integrated genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas using array- and sequencing-based technologies. The goal was to provide better insight into disease biology and tumor classification to help guide clinical trials and drug development, with the ultimate goal of achieving personalized cancer care.
The group classified endometrial cancers into four new categories:
- polymerase (DNA-directed) epsilon catalytic subunit (POLE) ultramutated
- microsatellite instability (MSI) hypermutated
- somatic copy number alterations (SCNA) low
- SCNA high.
Most endometrioid tumors had few SCNA or P53 mutations but frequent mutations in PTEN, CTNNB1, PIK3CA, ARID1A, and KRAS genes. Novel mutations also were discovered in the SWI/SNF chromatin remodeling complex gene ARID5B. About 10% of endometrioid tumors had markedly increased transversion mutations and newly identified mutations in POLE, a gene involved in nuclear DNA replication and repair.
As expected, serous tumors had significantly worse progression-free survival (PFS) than endometrioid tumors (P = .003, log-rank). A subset (25%) of high-grade endometrioid tumors had SCNAs and mutation spectra similar to those of uterine serous carcinomas, suggesting that patients with such tumors might benefit from treatment options that parallel those for serous tumors.
Other overlapping treatment paradigms existed between different organ systems. For example, some molecular features were similar in uterine serous carcinomas, basal-like breast carcinomas, and high-grade serous ovarian carcinomas. All three carcinomas displayed a high frequency of P53 mutations, very low frequency of PTEN mutations, similar focal SCNA patterns, and minimal DNA methylation changes. However, investigators also found several mutations that are unique to uterine serous carcinomas (eg, PIK3CA, FBXW7, PPP2R1A, and ARID1A), providing potential opportunities for targeted pharmacotherapy.
What this evidence means for practice
These studies highlight the etiologic heterogeneity of endometrial cancer. The histologic groundwork laid by Bokhman was not only correct but provided a foundation for molecular characterization of endometrial cancers to drive translational science into targeted therapeutics.
The similar molecular phenotypes of high-grade endometrioid carcinomas and serous endometrial carcinomas strengthens existing evidence that chemotherapy may be preferable to adjuvant radiotherapy for patients with highly mutated endometrioid cancers (eg, SCNA). Current chemotherapy regimens for serous endometrial cancers remain appropriate, given the compelling similarities between these cancers and serous ovarian and basal-like breast cancers. However, the identification of unique molecular features not shared by breast or ovarian cancer may expand standard options to include more targeted therapy.
Overall, this type of research, which encompasses proper histologic classification refined by genomics, has the potential to achieve personalized cancer care.
How we are achieving individualized cancer care: 3 genome-guided clinical trials
Oza AM, Elit L, Tsao MS, et al. Phase II study of temsirolimus in women with recurrent or metastatic endometrial cancer: a trial of the NCIC Clinical Trials Group. J Clin Oncol. 2011;29(24):3278–3285.
Aghajanian C, Sill MW, Darcy KM, et al. Phase II trial of bevacizumab in recurrent or persistent endometrial cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2011;29(16):2259–2265.
Alvarez EA, Brady WE, Walker JL, et al. Phase II trial of combination bevacizumab and temsirolimus in the treatment of recurrent or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2013;129(1):22–27.
Women with locally recurrent, advanced, or metastatic endometrial cancer have limited options for treatment. Hormonal therapies have modest effects at best, with a median survival rate of 7 to 12 months.7–9 To address this lack of options, researchers have begun to focus on targeted therapies directed at molecular pathways of cellular proliferation. These therapies include but are not limited to inhibitors of:
- mammalian target of rapamycin (mTOR)
- human epidermal growth factor receptor 2
- epidermal growth factor receptor
- vascular endothelial growth factor (VEGF).
Several studies have produced promising findings in recent years. They involve investigations of temsirolimus and bevacizumab as single agents in two independent clinical trials, and a study of the drugs in combination in women with recurrent or persistent endometrial carcinoma.
mTOR inhibitors elicited a greater response in chemotherapy-naïve women
Phosphatase and tensin homolog (PTEN) is a tumor-suppressor gene more commonly associated with endometrioid endometrial cancers (26%–80%) than with Type II cancers.10 Loss of PTEN expression leads to deregulated signaling of the phosphatidylinositol-3 kinase (PI3K)/serine-threonine kinase (Akt)/mTOR pathway. Disruption of this pathway is thought to provide cells with a selective survival advantage by enhancing angiogenesis, protein translation, and cell-cycle progression.10
Temsirolimus is an mTOR inhibitor recently explored by Oza and colleagues. They performed a multicenter, Phase II study involving 62 patients with recurrent and/or metastatic endometrial cancer as part of the National Cancer Institute of Canada (NCIC) Clinical Trials Group. Patients were divided into two groups on the basis of their treatment history:
- chemotherapy-naïve women, with no more than one prior hormonal treatment (n = 33)
- chemotherapy-treated women (n = 27).
Temsirolimus was given weekly in 4-week cycles at an intravenous (IV) dose of 25 mg over 30 minutes.
The drug elicited a response regardless of the histologic type of cancer. That response was more pronounced in chemotherapy-naïve women and not limited to patients with PTEN loss. In the chemotherapy-naïve group, four women (14%) had a partial response, 20 (69%) had stable disease, and five (18%) had progressive disease. Median PFS was 7.33 months (95% confidence interval [CI], 3.61–9.86), compared with 3.25 months (95% CI, 1.97–3.84) in chemotherapy-treated women. Among chemotherapy-treated women, one (4%) had a partial response and 12 (48%) had stable disease.
An angiogenesis inhibitor alone was well tolerated
VEGF is the principal growth factor responsible for angiogenesis, initiating the process of neovascularization. Bevacizumab is a humanized monoclonal antibody that binds to circulating VEGF-A, stimulating clinical effects in multiple tumor types, including persistent or recurrent ovarian and cervical cancers.
Aghajanian and colleagues conducted a Phase II trial of single-agent bevacizumab in women with recurrent or persistent endometrial cancer to assess the drug’s activity and tolerability. Eligible patients had histologic confirmation by central pathology review, recurrent or persistent disease after one or two cytotoxic regimens, and a Gynecologic Oncology Group performance score of 2 or lower. They received IV bevacizumab 15 mg/kg every 3 weeks until the disease progressed or toxicity became prohibitive. Fifty-two women participated.
Seven women (13.5%) experienced a clinical response (one complete response and six partial responses), and 21 (40%) had PFS of at least 6 months. Median PFS and overall survival were 4.2 and 10.5 months, respectively.
Combined with temsirolimus, bevacizumab increased overall survival
Alvarez and colleagues conducted a Phase II trial of combination bevacizumab and temsirolimus in women with recurrent or persistent endometrial carcinoma. Forty-nine patients participated.
These women had undergone earlier treatment with one (82%) or two (18%) chemotherapy regimens and radiation (41%). Median PFS and overall survival were 5.6 and 16.9 months, respectively. Toxicity was significant, with 38.8% of women withdrawn from the study due to toxicity.
What this evidence means for practice
Given the findings regarding temsirolimus and bevacizumab as single agents, their use in combination was expected to produce a robust effect. The 6-month PFS rate is similar for all three regimens, but for overall survival, combination therapy had a 6.4-month advantage over bevacizumab alone.
Given the significant toxicity associated with the combination of bevacizumab and temsirolimus, further study is needed to develop biomarkers to predict response and toxicity. Other areas meriting future research include optimal timing of angiogenesis and mTOR pathway inhibitors, different combinations of agents, and the identification, through genomic analysis, of patient populations most likely to benefit from these drugs with minimal toxicity.
The studies presented here show promise in the area of genomics and represent the beginning of our movement toward personalized cancer care.
We want to hear from you! Tell us what you think.
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30.
- Boruta DM 2nd, Gehrig PA, Fader AN, Olawaiye AB. Management of women with uterine papillary serous cancer: a Society of Gynecologic Oncology (SGO) review. Gynecol Oncol. 2009;115(1):142–153.
- Ueda SM, Kapp DS, Cheung MK, et al. Trends in demographic and clinical characteristics in women diagnosed with corpus cancer and their potential impact on the increasing number of deaths. Am J Obstet Gynecol. 2008;198(2):218.e1–e6.
- Lauchlan SC. Tubal (serous) carcinoma of the endometrium. Arch Pathol Lab Med. 1981;105(11):615–618.
- Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol. 1982;6(2):93–108.
- Bokhman JV. Two pathogenetic types of endometrial
carcinoma. Gynecol Oncol. 1983;15(1):10–17. - Bellone S, Shah HR, McKenney JK, Stone PJ, Santin AD. Recurrent endometrial carcinoma regression with the use of the aromatase inhibitor anastrozole. Am J Obstet Gynecol. 2008;199(3):e7–e10.
- Rose PG, Brunetto VL, VanLe L, Bell J, Walker JL, Lee
RB. A phase II trial of anastrozole in advanced recurrent
or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2000;78(2):212–216. - Thigpen T, Brady MF, Homesley HD, Soper JT, Bell J. Tamoxifen in the treatment of advanced or recurrent endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2001;19(2):364–367.
- Kanamori Y, Kigawa J, Itamochi H, et al. Correlation between loss of PTEN expression and Akt phosphorylation in endometrial carcinoma. Clin Cancer Res. 2001; 7(4):892–895.

Lindsay M. Kuroki, MD
Dr. Kuroki is a Fellow in the Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, at Washington University School of Medicine in St. Louis, Missouri.

David G. Mutch, MD
Dr. Mutch is Ira C. and Judith Gall Professor of Obstetrics and Gynecology and Chief of Gynecologic Oncology at Washington University School of Medicine in St. Louis, Missouri. He serves on the OBG Management Board of Editors.
Dr. Kuroki reports no financial relationships relevant to this article. Dr. Mutch reports that he has received research support from the National Institutes of Health and the Gynecologic Oncology Group, with no financial relationships relevant to this article.
Lindsay M. Kuroki, MD
Dr. Kuroki is a Fellow in the Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, at Washington University School of Medicine in St. Louis, Missouri.
David G. Mutch, MD
Dr. Mutch is Ira C. and Judith Gall Professor of Obstetrics and Gynecology and Chief of Gynecologic Oncology at Washington University School of Medicine in St. Louis, Missouri. He serves on the OBG Management Board of Editors.
Dr. Kuroki reports no financial relationships relevant to this article. Dr. Mutch reports that he has received research support from the National Institutes of Health and the Gynecologic Oncology Group, with no financial relationships relevant to this article.
Lindsay M. Kuroki, MD
Dr. Kuroki is a Fellow in the Department of Obstetrics and Gynecology, Division of Gynecologic Oncology, at Washington University School of Medicine in St. Louis, Missouri.
David G. Mutch, MD
Dr. Mutch is Ira C. and Judith Gall Professor of Obstetrics and Gynecology and Chief of Gynecologic Oncology at Washington University School of Medicine in St. Louis, Missouri. He serves on the OBG Management Board of Editors.
Dr. Kuroki reports no financial relationships relevant to this article. Dr. Mutch reports that he has received research support from the National Institutes of Health and the Gynecologic Oncology Group, with no financial relationships relevant to this article.
Endometrial cancer is the most common malignancy of the female reproductive tract in the United States, and its incidence continues to rise, with an estimated 49,560 new cases predicted for 2013.1 If we are to successfully traverse the pathway from molecular cell genetics to the development of targeted therapies and personalized cancer care, we need to meet a few benchmarks:
- We need to enhance our understanding of the molecular changes that lead to endometrial cancer. Of particular interest are nonendometrioid tumors. Increased mortality from endometrial cancer appears to be related to the growing number of uterine papillary serous carcinomas and clear-cell cancers. Although these cancers constitute less than 10% of all endometrial cancers, they account for a disproportionately high number of recurrences and cancer-related deaths.2,3 Do recent studies validate the original classification of endometrial cancers as Type I (endometrioid) or Type II (serous and clear cell), or is there more heterogeneity than was originally thought? How do recent studies affect treatment options?
- We need to establish a genomic characterization of endometrial cancer to supplement clinical research data. The identification of novel mutations specific to each histologic type has the potential to improve adjuvant therapy. How close are we to performing a comprehensive genomic analysis of endometrial cancer?
- We need to develop new adjuvant treatment options for recurrent and advanced disease. When clinical symptoms of endometrial cancer are overt, as they often are, early diagnosis is possible, with a 5-year survival rate of 80% to 90%. The prognosis declines dramatically in women with advanced-stage disease or high-risk histologies, with a 5-year survival rate of 57% and 19% for Stage III and Stage IV disease, respectively.1 Adjuvant treatment options are limited in the setting of recurrent or advanced disease. Do any biologic agents increase survival?
In this article, we highlight the historical foundation and newest advances in the field of endometrial cancer, focusing on:
- histologic classification
- etiologic heterogeneity and molecular biology
- genome-guided clinical trials involving targeted therapy, with the ultimate goal of achieving individualized cancer care.
Should we reclassify endometrial cancers to reflect molecular characteristics of tumors?
Brinton LA, Felix AS, McMeekin DS, et al. Etiologic heterogeneity in endometrial cancer: evidence from a Gynecologic Oncology Group trial. Gynecol Oncol. 2013;129(2):277–284.
Cancer Genome Atlas Research Network, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
Uterine papillary serous carcinoma (UPSC) was first established as a distinct subtype of endometrial cancer in the early 1980s, when teams led by Lauchlan4 and Hendrickson5 described it as histologically similar to serous epithelial ovarian carcinoma. Shortly thereafter, Bokhman proposed two broad categories of endometrial carcinoma characterized by distinct microscopic appearance, epidemiology, and endocrine and metabolic functioning (TABLE, page 28).6
More recently, research has focused on expanding this histologic classification system to encompass molecular differences. Brinton and colleagues conducted a study within Gynecologic Oncology Group 210, investigating the etiologic heterogeneity of endometrial cancers by comparing risk factors for different histologies. They found that risk factors for aggressive endometrial cancers, including Grade 3 endometrioid and nonendometrioid tumors, appear to differ from those of lower-grade endometrioid carcinomas.
Details of the study by Brinton and colleagues
A total of 3,434 women were included, representing endometrioid (78%) and serous (9%) carcinomas. Grade 3 endometrioid tumors resembled Type II endometrial cancers more closely than did Grade 1–2 endometrioid tumors. Patients with Grade 3 endometrioid and Type II cancers were diagnosed at a significantly older age than patients with Grades 1–2 endometrioid cancers (eg, diagnosis of serous cancers: median age, 67.4 years; Grade 3 endometrioid cancers: median age, 61.9 years; Grade 1–2 endometrioid cancers: median age, 59.6 years). They also were more likely to be nonwhite than patients with Grades 1–2 endometrioid histology. Specifically, black patients were rarely diagnosed with Grades 1–2 endometrioid cancers (5% vs 9% for Grade 3 endometrioid cancers; 20% for serous cancers, 23% for carcinosarcomas, and 12% for clear-cell cancers).
After adjustments for age, enrollment year, and race, patients with Type II tumors (serous, carcinosarcomas, or clear-cell tumors) were much more likely to be multiparous or smokers or to have a history of breast cancer treated with tamoxifen, compared with women with Grade 1–2 endometrioid cancers. An adequately powered subanalysis of serous carcinomas and Grades 1–2 endometrioid cancers revealed that associations persisted between serous carcinomas and multiparity, body mass index, and a history of breast cancer treated with tamoxifen.
Related article: The future of the Pap test: Identifying endometrial and ovarian cancers (Janelle Yates, August 2013)
Overall, this study provides some of the strongest epidemiologic support we have that endometrial cancers are heterogeneous, with evidence to suggest that we might classify Grade 3 endometrioid carcinomas as Type II cancers. These findings paved the way for molecular profiling of endometrial cancers.
Details of the study by the Cancer Genome Atlas Research Network
The Cancer Genome Atlas Research Network recently published an integrated genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas using array- and sequencing-based technologies. The goal was to provide better insight into disease biology and tumor classification to help guide clinical trials and drug development, with the ultimate goal of achieving personalized cancer care.
The group classified endometrial cancers into four new categories:
- polymerase (DNA-directed) epsilon catalytic subunit (POLE) ultramutated
- microsatellite instability (MSI) hypermutated
- somatic copy number alterations (SCNA) low
- SCNA high.
Most endometrioid tumors had few SCNA or P53 mutations but frequent mutations in PTEN, CTNNB1, PIK3CA, ARID1A, and KRAS genes. Novel mutations also were discovered in the SWI/SNF chromatin remodeling complex gene ARID5B. About 10% of endometrioid tumors had markedly increased transversion mutations and newly identified mutations in POLE, a gene involved in nuclear DNA replication and repair.
As expected, serous tumors had significantly worse progression-free survival (PFS) than endometrioid tumors (P = .003, log-rank). A subset (25%) of high-grade endometrioid tumors had SCNAs and mutation spectra similar to those of uterine serous carcinomas, suggesting that patients with such tumors might benefit from treatment options that parallel those for serous tumors.
Other overlapping treatment paradigms existed between different organ systems. For example, some molecular features were similar in uterine serous carcinomas, basal-like breast carcinomas, and high-grade serous ovarian carcinomas. All three carcinomas displayed a high frequency of P53 mutations, very low frequency of PTEN mutations, similar focal SCNA patterns, and minimal DNA methylation changes. However, investigators also found several mutations that are unique to uterine serous carcinomas (eg, PIK3CA, FBXW7, PPP2R1A, and ARID1A), providing potential opportunities for targeted pharmacotherapy.
What this evidence means for practice
These studies highlight the etiologic heterogeneity of endometrial cancer. The histologic groundwork laid by Bokhman was not only correct but provided a foundation for molecular characterization of endometrial cancers to drive translational science into targeted therapeutics.
The similar molecular phenotypes of high-grade endometrioid carcinomas and serous endometrial carcinomas strengthens existing evidence that chemotherapy may be preferable to adjuvant radiotherapy for patients with highly mutated endometrioid cancers (eg, SCNA). Current chemotherapy regimens for serous endometrial cancers remain appropriate, given the compelling similarities between these cancers and serous ovarian and basal-like breast cancers. However, the identification of unique molecular features not shared by breast or ovarian cancer may expand standard options to include more targeted therapy.
Overall, this type of research, which encompasses proper histologic classification refined by genomics, has the potential to achieve personalized cancer care.
How we are achieving individualized cancer care: 3 genome-guided clinical trials
Oza AM, Elit L, Tsao MS, et al. Phase II study of temsirolimus in women with recurrent or metastatic endometrial cancer: a trial of the NCIC Clinical Trials Group. J Clin Oncol. 2011;29(24):3278–3285.
Aghajanian C, Sill MW, Darcy KM, et al. Phase II trial of bevacizumab in recurrent or persistent endometrial cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2011;29(16):2259–2265.
Alvarez EA, Brady WE, Walker JL, et al. Phase II trial of combination bevacizumab and temsirolimus in the treatment of recurrent or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2013;129(1):22–27.
Women with locally recurrent, advanced, or metastatic endometrial cancer have limited options for treatment. Hormonal therapies have modest effects at best, with a median survival rate of 7 to 12 months.7–9 To address this lack of options, researchers have begun to focus on targeted therapies directed at molecular pathways of cellular proliferation. These therapies include but are not limited to inhibitors of:
- mammalian target of rapamycin (mTOR)
- human epidermal growth factor receptor 2
- epidermal growth factor receptor
- vascular endothelial growth factor (VEGF).
Several studies have produced promising findings in recent years. They involve investigations of temsirolimus and bevacizumab as single agents in two independent clinical trials, and a study of the drugs in combination in women with recurrent or persistent endometrial carcinoma.
mTOR inhibitors elicited a greater response in chemotherapy-naïve women
Phosphatase and tensin homolog (PTEN) is a tumor-suppressor gene more commonly associated with endometrioid endometrial cancers (26%–80%) than with Type II cancers.10 Loss of PTEN expression leads to deregulated signaling of the phosphatidylinositol-3 kinase (PI3K)/serine-threonine kinase (Akt)/mTOR pathway. Disruption of this pathway is thought to provide cells with a selective survival advantage by enhancing angiogenesis, protein translation, and cell-cycle progression.10
Temsirolimus is an mTOR inhibitor recently explored by Oza and colleagues. They performed a multicenter, Phase II study involving 62 patients with recurrent and/or metastatic endometrial cancer as part of the National Cancer Institute of Canada (NCIC) Clinical Trials Group. Patients were divided into two groups on the basis of their treatment history:
- chemotherapy-naïve women, with no more than one prior hormonal treatment (n = 33)
- chemotherapy-treated women (n = 27).
Temsirolimus was given weekly in 4-week cycles at an intravenous (IV) dose of 25 mg over 30 minutes.
The drug elicited a response regardless of the histologic type of cancer. That response was more pronounced in chemotherapy-naïve women and not limited to patients with PTEN loss. In the chemotherapy-naïve group, four women (14%) had a partial response, 20 (69%) had stable disease, and five (18%) had progressive disease. Median PFS was 7.33 months (95% confidence interval [CI], 3.61–9.86), compared with 3.25 months (95% CI, 1.97–3.84) in chemotherapy-treated women. Among chemotherapy-treated women, one (4%) had a partial response and 12 (48%) had stable disease.
An angiogenesis inhibitor alone was well tolerated
VEGF is the principal growth factor responsible for angiogenesis, initiating the process of neovascularization. Bevacizumab is a humanized monoclonal antibody that binds to circulating VEGF-A, stimulating clinical effects in multiple tumor types, including persistent or recurrent ovarian and cervical cancers.
Aghajanian and colleagues conducted a Phase II trial of single-agent bevacizumab in women with recurrent or persistent endometrial cancer to assess the drug’s activity and tolerability. Eligible patients had histologic confirmation by central pathology review, recurrent or persistent disease after one or two cytotoxic regimens, and a Gynecologic Oncology Group performance score of 2 or lower. They received IV bevacizumab 15 mg/kg every 3 weeks until the disease progressed or toxicity became prohibitive. Fifty-two women participated.
Seven women (13.5%) experienced a clinical response (one complete response and six partial responses), and 21 (40%) had PFS of at least 6 months. Median PFS and overall survival were 4.2 and 10.5 months, respectively.
Combined with temsirolimus, bevacizumab increased overall survival
Alvarez and colleagues conducted a Phase II trial of combination bevacizumab and temsirolimus in women with recurrent or persistent endometrial carcinoma. Forty-nine patients participated.
These women had undergone earlier treatment with one (82%) or two (18%) chemotherapy regimens and radiation (41%). Median PFS and overall survival were 5.6 and 16.9 months, respectively. Toxicity was significant, with 38.8% of women withdrawn from the study due to toxicity.
What this evidence means for practice
Given the findings regarding temsirolimus and bevacizumab as single agents, their use in combination was expected to produce a robust effect. The 6-month PFS rate is similar for all three regimens, but for overall survival, combination therapy had a 6.4-month advantage over bevacizumab alone.
Given the significant toxicity associated with the combination of bevacizumab and temsirolimus, further study is needed to develop biomarkers to predict response and toxicity. Other areas meriting future research include optimal timing of angiogenesis and mTOR pathway inhibitors, different combinations of agents, and the identification, through genomic analysis, of patient populations most likely to benefit from these drugs with minimal toxicity.
The studies presented here show promise in the area of genomics and represent the beginning of our movement toward personalized cancer care.
We want to hear from you! Tell us what you think.
Endometrial cancer is the most common malignancy of the female reproductive tract in the United States, and its incidence continues to rise, with an estimated 49,560 new cases predicted for 2013.1 If we are to successfully traverse the pathway from molecular cell genetics to the development of targeted therapies and personalized cancer care, we need to meet a few benchmarks:
- We need to enhance our understanding of the molecular changes that lead to endometrial cancer. Of particular interest are nonendometrioid tumors. Increased mortality from endometrial cancer appears to be related to the growing number of uterine papillary serous carcinomas and clear-cell cancers. Although these cancers constitute less than 10% of all endometrial cancers, they account for a disproportionately high number of recurrences and cancer-related deaths.2,3 Do recent studies validate the original classification of endometrial cancers as Type I (endometrioid) or Type II (serous and clear cell), or is there more heterogeneity than was originally thought? How do recent studies affect treatment options?
- We need to establish a genomic characterization of endometrial cancer to supplement clinical research data. The identification of novel mutations specific to each histologic type has the potential to improve adjuvant therapy. How close are we to performing a comprehensive genomic analysis of endometrial cancer?
- We need to develop new adjuvant treatment options for recurrent and advanced disease. When clinical symptoms of endometrial cancer are overt, as they often are, early diagnosis is possible, with a 5-year survival rate of 80% to 90%. The prognosis declines dramatically in women with advanced-stage disease or high-risk histologies, with a 5-year survival rate of 57% and 19% for Stage III and Stage IV disease, respectively.1 Adjuvant treatment options are limited in the setting of recurrent or advanced disease. Do any biologic agents increase survival?
In this article, we highlight the historical foundation and newest advances in the field of endometrial cancer, focusing on:
- histologic classification
- etiologic heterogeneity and molecular biology
- genome-guided clinical trials involving targeted therapy, with the ultimate goal of achieving individualized cancer care.
Should we reclassify endometrial cancers to reflect molecular characteristics of tumors?
Brinton LA, Felix AS, McMeekin DS, et al. Etiologic heterogeneity in endometrial cancer: evidence from a Gynecologic Oncology Group trial. Gynecol Oncol. 2013;129(2):277–284.
Cancer Genome Atlas Research Network, et al. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67–73.
Uterine papillary serous carcinoma (UPSC) was first established as a distinct subtype of endometrial cancer in the early 1980s, when teams led by Lauchlan4 and Hendrickson5 described it as histologically similar to serous epithelial ovarian carcinoma. Shortly thereafter, Bokhman proposed two broad categories of endometrial carcinoma characterized by distinct microscopic appearance, epidemiology, and endocrine and metabolic functioning (TABLE, page 28).6
More recently, research has focused on expanding this histologic classification system to encompass molecular differences. Brinton and colleagues conducted a study within Gynecologic Oncology Group 210, investigating the etiologic heterogeneity of endometrial cancers by comparing risk factors for different histologies. They found that risk factors for aggressive endometrial cancers, including Grade 3 endometrioid and nonendometrioid tumors, appear to differ from those of lower-grade endometrioid carcinomas.
Details of the study by Brinton and colleagues
A total of 3,434 women were included, representing endometrioid (78%) and serous (9%) carcinomas. Grade 3 endometrioid tumors resembled Type II endometrial cancers more closely than did Grade 1–2 endometrioid tumors. Patients with Grade 3 endometrioid and Type II cancers were diagnosed at a significantly older age than patients with Grades 1–2 endometrioid cancers (eg, diagnosis of serous cancers: median age, 67.4 years; Grade 3 endometrioid cancers: median age, 61.9 years; Grade 1–2 endometrioid cancers: median age, 59.6 years). They also were more likely to be nonwhite than patients with Grades 1–2 endometrioid histology. Specifically, black patients were rarely diagnosed with Grades 1–2 endometrioid cancers (5% vs 9% for Grade 3 endometrioid cancers; 20% for serous cancers, 23% for carcinosarcomas, and 12% for clear-cell cancers).
After adjustments for age, enrollment year, and race, patients with Type II tumors (serous, carcinosarcomas, or clear-cell tumors) were much more likely to be multiparous or smokers or to have a history of breast cancer treated with tamoxifen, compared with women with Grade 1–2 endometrioid cancers. An adequately powered subanalysis of serous carcinomas and Grades 1–2 endometrioid cancers revealed that associations persisted between serous carcinomas and multiparity, body mass index, and a history of breast cancer treated with tamoxifen.
Related article: The future of the Pap test: Identifying endometrial and ovarian cancers (Janelle Yates, August 2013)
Overall, this study provides some of the strongest epidemiologic support we have that endometrial cancers are heterogeneous, with evidence to suggest that we might classify Grade 3 endometrioid carcinomas as Type II cancers. These findings paved the way for molecular profiling of endometrial cancers.
Details of the study by the Cancer Genome Atlas Research Network
The Cancer Genome Atlas Research Network recently published an integrated genomic, transcriptomic, and proteomic characterization of 373 endometrial carcinomas using array- and sequencing-based technologies. The goal was to provide better insight into disease biology and tumor classification to help guide clinical trials and drug development, with the ultimate goal of achieving personalized cancer care.
The group classified endometrial cancers into four new categories:
- polymerase (DNA-directed) epsilon catalytic subunit (POLE) ultramutated
- microsatellite instability (MSI) hypermutated
- somatic copy number alterations (SCNA) low
- SCNA high.
Most endometrioid tumors had few SCNA or P53 mutations but frequent mutations in PTEN, CTNNB1, PIK3CA, ARID1A, and KRAS genes. Novel mutations also were discovered in the SWI/SNF chromatin remodeling complex gene ARID5B. About 10% of endometrioid tumors had markedly increased transversion mutations and newly identified mutations in POLE, a gene involved in nuclear DNA replication and repair.
As expected, serous tumors had significantly worse progression-free survival (PFS) than endometrioid tumors (P = .003, log-rank). A subset (25%) of high-grade endometrioid tumors had SCNAs and mutation spectra similar to those of uterine serous carcinomas, suggesting that patients with such tumors might benefit from treatment options that parallel those for serous tumors.
Other overlapping treatment paradigms existed between different organ systems. For example, some molecular features were similar in uterine serous carcinomas, basal-like breast carcinomas, and high-grade serous ovarian carcinomas. All three carcinomas displayed a high frequency of P53 mutations, very low frequency of PTEN mutations, similar focal SCNA patterns, and minimal DNA methylation changes. However, investigators also found several mutations that are unique to uterine serous carcinomas (eg, PIK3CA, FBXW7, PPP2R1A, and ARID1A), providing potential opportunities for targeted pharmacotherapy.
What this evidence means for practice
These studies highlight the etiologic heterogeneity of endometrial cancer. The histologic groundwork laid by Bokhman was not only correct but provided a foundation for molecular characterization of endometrial cancers to drive translational science into targeted therapeutics.
The similar molecular phenotypes of high-grade endometrioid carcinomas and serous endometrial carcinomas strengthens existing evidence that chemotherapy may be preferable to adjuvant radiotherapy for patients with highly mutated endometrioid cancers (eg, SCNA). Current chemotherapy regimens for serous endometrial cancers remain appropriate, given the compelling similarities between these cancers and serous ovarian and basal-like breast cancers. However, the identification of unique molecular features not shared by breast or ovarian cancer may expand standard options to include more targeted therapy.
Overall, this type of research, which encompasses proper histologic classification refined by genomics, has the potential to achieve personalized cancer care.
How we are achieving individualized cancer care: 3 genome-guided clinical trials
Oza AM, Elit L, Tsao MS, et al. Phase II study of temsirolimus in women with recurrent or metastatic endometrial cancer: a trial of the NCIC Clinical Trials Group. J Clin Oncol. 2011;29(24):3278–3285.
Aghajanian C, Sill MW, Darcy KM, et al. Phase II trial of bevacizumab in recurrent or persistent endometrial cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2011;29(16):2259–2265.
Alvarez EA, Brady WE, Walker JL, et al. Phase II trial of combination bevacizumab and temsirolimus in the treatment of recurrent or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2013;129(1):22–27.
Women with locally recurrent, advanced, or metastatic endometrial cancer have limited options for treatment. Hormonal therapies have modest effects at best, with a median survival rate of 7 to 12 months.7–9 To address this lack of options, researchers have begun to focus on targeted therapies directed at molecular pathways of cellular proliferation. These therapies include but are not limited to inhibitors of:
- mammalian target of rapamycin (mTOR)
- human epidermal growth factor receptor 2
- epidermal growth factor receptor
- vascular endothelial growth factor (VEGF).
Several studies have produced promising findings in recent years. They involve investigations of temsirolimus and bevacizumab as single agents in two independent clinical trials, and a study of the drugs in combination in women with recurrent or persistent endometrial carcinoma.
mTOR inhibitors elicited a greater response in chemotherapy-naïve women
Phosphatase and tensin homolog (PTEN) is a tumor-suppressor gene more commonly associated with endometrioid endometrial cancers (26%–80%) than with Type II cancers.10 Loss of PTEN expression leads to deregulated signaling of the phosphatidylinositol-3 kinase (PI3K)/serine-threonine kinase (Akt)/mTOR pathway. Disruption of this pathway is thought to provide cells with a selective survival advantage by enhancing angiogenesis, protein translation, and cell-cycle progression.10
Temsirolimus is an mTOR inhibitor recently explored by Oza and colleagues. They performed a multicenter, Phase II study involving 62 patients with recurrent and/or metastatic endometrial cancer as part of the National Cancer Institute of Canada (NCIC) Clinical Trials Group. Patients were divided into two groups on the basis of their treatment history:
- chemotherapy-naïve women, with no more than one prior hormonal treatment (n = 33)
- chemotherapy-treated women (n = 27).
Temsirolimus was given weekly in 4-week cycles at an intravenous (IV) dose of 25 mg over 30 minutes.
The drug elicited a response regardless of the histologic type of cancer. That response was more pronounced in chemotherapy-naïve women and not limited to patients with PTEN loss. In the chemotherapy-naïve group, four women (14%) had a partial response, 20 (69%) had stable disease, and five (18%) had progressive disease. Median PFS was 7.33 months (95% confidence interval [CI], 3.61–9.86), compared with 3.25 months (95% CI, 1.97–3.84) in chemotherapy-treated women. Among chemotherapy-treated women, one (4%) had a partial response and 12 (48%) had stable disease.
An angiogenesis inhibitor alone was well tolerated
VEGF is the principal growth factor responsible for angiogenesis, initiating the process of neovascularization. Bevacizumab is a humanized monoclonal antibody that binds to circulating VEGF-A, stimulating clinical effects in multiple tumor types, including persistent or recurrent ovarian and cervical cancers.
Aghajanian and colleagues conducted a Phase II trial of single-agent bevacizumab in women with recurrent or persistent endometrial cancer to assess the drug’s activity and tolerability. Eligible patients had histologic confirmation by central pathology review, recurrent or persistent disease after one or two cytotoxic regimens, and a Gynecologic Oncology Group performance score of 2 or lower. They received IV bevacizumab 15 mg/kg every 3 weeks until the disease progressed or toxicity became prohibitive. Fifty-two women participated.
Seven women (13.5%) experienced a clinical response (one complete response and six partial responses), and 21 (40%) had PFS of at least 6 months. Median PFS and overall survival were 4.2 and 10.5 months, respectively.
Combined with temsirolimus, bevacizumab increased overall survival
Alvarez and colleagues conducted a Phase II trial of combination bevacizumab and temsirolimus in women with recurrent or persistent endometrial carcinoma. Forty-nine patients participated.
These women had undergone earlier treatment with one (82%) or two (18%) chemotherapy regimens and radiation (41%). Median PFS and overall survival were 5.6 and 16.9 months, respectively. Toxicity was significant, with 38.8% of women withdrawn from the study due to toxicity.
What this evidence means for practice
Given the findings regarding temsirolimus and bevacizumab as single agents, their use in combination was expected to produce a robust effect. The 6-month PFS rate is similar for all three regimens, but for overall survival, combination therapy had a 6.4-month advantage over bevacizumab alone.
Given the significant toxicity associated with the combination of bevacizumab and temsirolimus, further study is needed to develop biomarkers to predict response and toxicity. Other areas meriting future research include optimal timing of angiogenesis and mTOR pathway inhibitors, different combinations of agents, and the identification, through genomic analysis, of patient populations most likely to benefit from these drugs with minimal toxicity.
The studies presented here show promise in the area of genomics and represent the beginning of our movement toward personalized cancer care.
We want to hear from you! Tell us what you think.
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30.
- Boruta DM 2nd, Gehrig PA, Fader AN, Olawaiye AB. Management of women with uterine papillary serous cancer: a Society of Gynecologic Oncology (SGO) review. Gynecol Oncol. 2009;115(1):142–153.
- Ueda SM, Kapp DS, Cheung MK, et al. Trends in demographic and clinical characteristics in women diagnosed with corpus cancer and their potential impact on the increasing number of deaths. Am J Obstet Gynecol. 2008;198(2):218.e1–e6.
- Lauchlan SC. Tubal (serous) carcinoma of the endometrium. Arch Pathol Lab Med. 1981;105(11):615–618.
- Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol. 1982;6(2):93–108.
- Bokhman JV. Two pathogenetic types of endometrial
carcinoma. Gynecol Oncol. 1983;15(1):10–17. - Bellone S, Shah HR, McKenney JK, Stone PJ, Santin AD. Recurrent endometrial carcinoma regression with the use of the aromatase inhibitor anastrozole. Am J Obstet Gynecol. 2008;199(3):e7–e10.
- Rose PG, Brunetto VL, VanLe L, Bell J, Walker JL, Lee
RB. A phase II trial of anastrozole in advanced recurrent
or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2000;78(2):212–216. - Thigpen T, Brady MF, Homesley HD, Soper JT, Bell J. Tamoxifen in the treatment of advanced or recurrent endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2001;19(2):364–367.
- Kanamori Y, Kigawa J, Itamochi H, et al. Correlation between loss of PTEN expression and Akt phosphorylation in endometrial carcinoma. Clin Cancer Res. 2001; 7(4):892–895.
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30.
- Boruta DM 2nd, Gehrig PA, Fader AN, Olawaiye AB. Management of women with uterine papillary serous cancer: a Society of Gynecologic Oncology (SGO) review. Gynecol Oncol. 2009;115(1):142–153.
- Ueda SM, Kapp DS, Cheung MK, et al. Trends in demographic and clinical characteristics in women diagnosed with corpus cancer and their potential impact on the increasing number of deaths. Am J Obstet Gynecol. 2008;198(2):218.e1–e6.
- Lauchlan SC. Tubal (serous) carcinoma of the endometrium. Arch Pathol Lab Med. 1981;105(11):615–618.
- Hendrickson M, Ross J, Eifel P, Martinez A, Kempson R. Uterine papillary serous carcinoma: a highly malignant form of endometrial adenocarcinoma. Am J Surg Pathol. 1982;6(2):93–108.
- Bokhman JV. Two pathogenetic types of endometrial
carcinoma. Gynecol Oncol. 1983;15(1):10–17. - Bellone S, Shah HR, McKenney JK, Stone PJ, Santin AD. Recurrent endometrial carcinoma regression with the use of the aromatase inhibitor anastrozole. Am J Obstet Gynecol. 2008;199(3):e7–e10.
- Rose PG, Brunetto VL, VanLe L, Bell J, Walker JL, Lee
RB. A phase II trial of anastrozole in advanced recurrent
or persistent endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2000;78(2):212–216. - Thigpen T, Brady MF, Homesley HD, Soper JT, Bell J. Tamoxifen in the treatment of advanced or recurrent endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2001;19(2):364–367.
- Kanamori Y, Kigawa J, Itamochi H, et al. Correlation between loss of PTEN expression and Akt phosphorylation in endometrial carcinoma. Clin Cancer Res. 2001; 7(4):892–895.
A stepwise approach to managing eclampsia and other hypertensive emergencies
CASE: MISSED PREECLAMPSIA
At her first prenatal visit at 14 weeks’ gestation, a 41-year-old woman (G2P1) presents with a dichorionic twin gestation, blood pressure (BP) of 105/68 mm Hg, and a body mass index (BMI) of 40 kg/m2. The pregnancy was achieved through in vitro fertilization. Ten years earlier, the patient’s first pregnancy was complicated by preeclampsia, requiring preterm delivery at 33 weeks’ gestation.
By 28 weeks’ gestation, the patient has gained 26 lb. Her BP is 120/70 mm Hg, with no proteinuria detected by urine dipstick. By 30 weeks, she has gained an additional 8 lb, her BP is 142/84 mm Hg, and no proteinuria is detected. At 32 weeks, her BP is 140/92 mm Hg, she has gained another 8 lb, and no proteinuria is present. She also reports new-onset headaches that do not respond to over-the-counter analgesics. She is sent to the obstetric triage area for BP monitoring, blood testing for preeclampsia and nonstress test fetal monitoring.
During the 2-hour observation period, the patient continues to report headaches, and swelling of her face and hands is present. Her systolic BP values range from 132 to 152 mm Hg, and diastolic values range from 80 to 96 mm Hg. No proteinuria is detected, blood testing results for preeclampsia (complete blood count, liver enzymes, serum creatinine, and uric acid) are normal, and the nonstress tests are reactive in both fetuses.
The patient is given a diagnosis of gestational hypertension, along with a prescription for oral labetalol 200 mg daily and two tablets of acetaminophen with codeine for the headaches (to be taken every 6 hours as needed). She is sent home with instructions to return to her physician’s office in 1 week.
Two days later, she wakes in the middle of the night with a severe headache, blurred vision, and vomiting. Her husband calls the obstetrician’s answering service and is instructed to call 911 immediately. While waiting for an ambulance, the patient experiences a grand mal eclamptic convulsion. A second convulsion occurs during her transfer to the ED.
This scenario could have been avoided.
The obstetrician in this case was negligent for failing to recognize preeclampsia in a patient who had two clear risk factors for it: multifetal gestation and a history of early-onset (<37 weeks) preeclampsia in an earlier pregnancy (other risk factors are listed in TABLE 1).
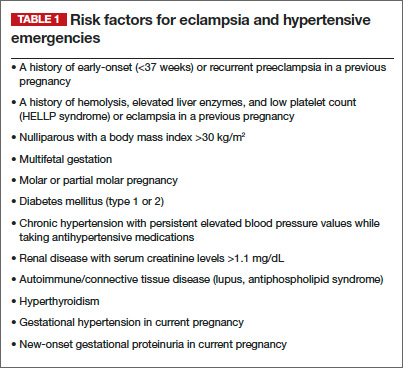
As a result, the patient developed eclampsia, a serious condition that can lead to grave maternal complications (TABLE 2), including death. It also can cause fetal complications, including growth restriction, hypoxia, acidosis, preterm birth, long-term developmental deficits, and death.1,2
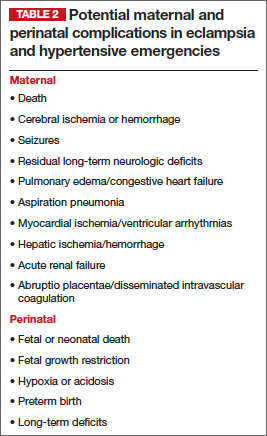
The obstetrician in this case also overlooked published evidence indicating that, in the setting of hypertension and headaches, as many as 20% to 30% of pregnant women whose tests for proteinuria show a negative or trace result via dipstick will develop eclampsia.3 Instead of initiating outpatient administration of oral antihypertensive agents, the obstetrician should have hospitalized this patient for at least 48 hours, with steroid administration, to determine whether outpatient management was feasible.
Related article: 10 practical, evidence-based recommendations to improve outcomes in women who have eclampsia Baha Sibai, MD (November 2011)
Defining eclampsia
Eclampsia is marked by the onset of convulsions (during pregnancy or postpartum) in association with gestational hypertension alone, proteinuria, preeclampsia, or superimposed preeclampsia. Although it is rare, eclampsia is potentially life-threatening. For that reason, obstetricians, anesthesiologists, ED physicians, neurologists, and critical-care physicians should be well versed in its diagnosis and management. In this article, I focus on management.
A few preliminary points
Eclampsia can develop any time during the antenatal period (>16 weeks’ gestation), during labor and delivery, and as long as 6 weeks after delivery. Therefore, we should be vigilant for preeclampsia whenever a pregnant patient visits our office, as well as when she makes unscheduled visits to the ED or obstetric triage area or is hospitalized.
Early recognition of women at high risk for preeclampsia and eclampsia may allow for prompt intervention, including early hospitalization for close observation prior to delivery and postpartum.1,2,4–10
Hospitalization of high-risk women allows for use of antihypertensive agents to treat severe BP, administration of magnesium sulfate to prevent convulsions, and timely delivery of the infant. It also allows for intensive maternal support during and after an eclamptic seizure.
Hospitalization is essential for women who exhibit features that suggest severe disease. More specifically, the presence of gestational hypertension with any of the following features is an indication for immediate hospitalization for evaluation and management:
- persistent severe hypertension (systolic
BP ≥160 mm Hg or diastolic BP ≥110 mm Hg) for at least 1 hour - gestational hypertension requiring oral antihypertensive therapy
- progressive and excessive weight gain (≥20 lb prior to 28 weeks’ gestation)
- generalized swelling (edema of hands or face)
- new-onset or persistent headaches despite analgesics
- persistent visual changes (blurred vision, scotomata, photophobia, double vision)
- shortness of breath, dyspnea, orthopnea, or tightness in the chest
- persistent retrosternal chest pain, severe epigastric or right upper quadrant pain
- persistent nausea, vomiting, malaise
- altered mental state, confusion, numbness, tingling, or motor weakness
- platelet count below 100 3 103 µL
- aspartate aminotransferase (AST), alanine aminotransferase (ALT), or lactic acid dehydrogenase (LDH) levels more than twice the upper limit of normal
- serum creatinine level >1.1 mg/dL
- suspected abruptio placentae.
A stepwise approach to eclampsia
Eclampsia is an obstetric emergency. Inadequate preparation for it or an inappropriate response to maternal and fetal conditions during and after an eclamptic convulsion can be detrimental to the mother and fetus. All obstetric units should have up-to-date protocols in place and should conduct mandatory drills to prepare nursing staff, obstetric providers, and anesthesia staff working in these units to manage eclampsia.
Step 1: Let the seizure run its course
During a seizure, resist the impulse to administer anticonvulsive drugs, including intravenous (IV) magnesium sulfate, because most eclamptic convulsions are self-limiting. Also abstain from administering medications such as IV phenytoin, diazepam, or midazolam, as these drugs are less effective than magnesium sulfate, and some can suppress the laryngeal reflex, increasing the risk of aspiration.
If the patient develops status epilepticus, initiate muscle paralysis and intubate her.
Step 2: Support the maternal condition
It is vital to support maternal respiratory and cardiovascular functions to prevent hypoxia, acidosis, and cardiorespiratory arrest.
Begin by establishing airway patency and maternal oxygenation during and after the convulsion. Administer oxygen via a face mask, with or without a reservoir, at a rate of 8 to 10 L/min.
During the apneic period (see “Profile of an eclamptic seizure” on page 46), the patient will develop hypoxia. Use pulse oximetry to monitor oxygen saturation, with the goal of keeping it above 94%. Arterial blood gas analysis is required if oxygen saturation remains below 92% or if pulmonary edema or aspiration is suspected.
If the patient develops recurrent seizures, status epilepticus, florid alveolar pulmonary edema, or respiratory arrest, intubate her immediately.
Step 3: Prevent maternal injury and aspiration
Secure the side rails of the patient’s bed by elevating them to prevent a fall, and make sure they are padded to prevent trauma during convulsions and afterward, when some women become combative and agitated. Position the patient in a lateral decubitus position to minimize aspiration of oral secretions. If any secretions or vomitus are present, remove them via suction.
Step 4: After the convulsion, give magnesium sulfate
Magnesium is the drug of choice for seizure prophylaxis in women with preeclampsia and severe symptoms, and to prevent recurrent seizures in women with eclampsia.
In the latter group, once the eclamptic convulsion has ended, give a loading dose of IV magnesium (6 g/100 mL over 20 minutes), followed by a continuous infusion of 2 g/h for at least 24 hours. If the patient develops a second seizure during the maintenance infusion, administer another bolus of magnesium (2 g/100 mL over 3–5 minutes).
Step 5: Treat severe hypertension
If severe hypertension persists for 60 minutes or longer, it can lead to injury of the brain, heart, and kidneys. To avoid these complications, it is essential to reduce BP to a safe range and maintain that level without compromising cerebral perfusion pressure and uteroplacental blood flow (which already may be reduced in some patients).
The goal of antihypertensive therapy is to keep systolic BP between 140 and 155 mm Hg and diastolic values between 90 and 105 mm Hg.9 Several agents are available for the treatment of severe hypertension during pregnancy and postpartum. The most commonly used IV medications for this purpose are labetalol and hydralazine. Another option is oral, rapidly acting
nifedipine.
Several randomized trials have compared efficacy and side effects between IV bolus injections of hydralazine; IV labetalol; and oral, rapidly acting nifedipine. In general, the findings of these studies suggest that either IV hydralazine or labetalol or oral nifedipine can be used to treat severe hypertension in pregnancy, as long as the provider is familiar with the dose to be used, the expected onset of action, and potential side effects (TABLE 3).
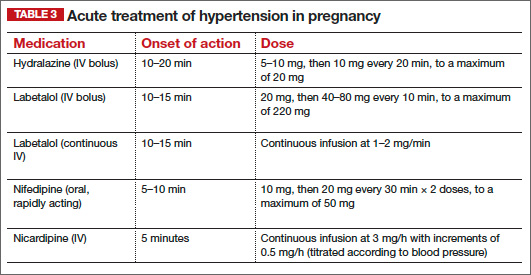
Women who develop generalized swelling or hemoconcentration (hematocrit ≥40%), or both, usually experience markedly reduced plasma volume. For this reason, these women will benefit from treatment with labetalol. If this is ineffective, then add IV hydralazine. However, delay administration of a rapidly acting vasodilator such as hydralazine to prevent an excessive hypotensive response and a secondary reduction in tissue perfusion and uteroplacental blood flow. Rather, administer a bolus infusion of 250 to 500 mL of isotonic saline before giving a vasodilator.
Additional details about the use of antihypertensive drugs are given in the section on other hypertensive emergencies below.
Step 6: Evaluate the patient for complications
Pulmonary edema can develop in patients with eclampsia or another hypertensive emergency. Suspect it if the patient has respiratory symptoms in association with tachypnea, tachycardia, or sustained oxygen saturation values below 93%, as well as when the patient exhibits basal rales during auscultation of the lungs. Treatment involves the administration of oxygen and IV furosemide (20–40 mg push), repeated as needed.
Some women with eclampsia may develop severe cerebral edema, hemorrhage, or both. The edema can be vasogenic or cytotoxic, leading to increased intracerebral pressure. Suspect edema or hemorrhage if the patient remains unresponsive, continues to experience convulsions despite therapy, or exhibits sensory or motor neurologic deficits. In such cases, neuroimaging is indicated, and the patient should be managed in consultation with neurology or neurosurgery.
Step 7: Begin the process of induction and delivery
Once the patient has been stabilized—and not before—initiate the induction process. Be aware that during and after the convulsion, changes in fetal heart rate (FHR) and uterine monitoring will usually be evident:
- prolonged deceleration or bradycardia (3–10 minutes)
- compensatory tachycardia, decreased beat-to-beat variability
- transient recurrent decelerations
- increased uterine tone and greater frequency of uterine activity.
These changes in FHR and uterine activity usually last 3 to 15 minutes. For this reason, it is important to avoid rushing the patient for cesarean delivery, as FHR and uterine activity are likely to return to normal after maternal resuscitation and stabilization. If not, consider other causes, such as abruptio placentae.
Eclampsia itself is not an indication for cesarean delivery. The selection of mode of delivery should be based on the presence or absence of labor, the cervical Bishop score, fetal gestational age, fetal presentation, and overall fetal condition.
Choosing an anesthetic
Regional analgesia/anesthesia is the method of choice for most women with eclampsia. However, regional anesthesia is to be avoided in the presence of disseminated intravascular coagulation or thrombocytopenia (the threshold platelet count is usually less than 75 x 103 µL. In such a case, IV analgesia can be used during labor, and general anesthesia may be appropriate for cesarean delivery. Both spinal and epidural analgesia and anesthesia are appropriate for women with eclampsia.
How to manage other hypertensive emergencies
A hypertensive emergency during pregnancy or postpartum involves acute-onset, persistent (>15 minutes), severe systolic BP (≥160 mm Hg) or severe diastolic BP (≥110 mm Hg), or both. The first step in such an emergency is to ensure the accurate measurement of BP using standard techniques.
Patients with acute-onset, persistent, severe BP should be hospitalized promptly for evaluation and treatment to prevent organ damage. Once such a patient is hospitalized, BP should be recorded every 15 minutes, with continuous FHR monitoring to ensure fetal viability.
Related article: Failure to diagnose preeclampsia and more (Medical Verdicts, February 2013)
The timing of initiation of antihypertensive medications, as well as determination of the type of medication best suited for the patient, should be based on:
- systolic and diastolic BP levels
- maternal clinical and laboratory findings
- presence of associated symptoms
- preexisting medical comorbidities
- whether the patient is antepartum or postpartum.
For example, a sustained BP level of 200/120 mm Hg requires therapy after 15 minutes, whereas observation may be suitable for as long as 60 minutes for a sustained BP of 160/72 mm Hg during labor.
Rapid reduction of systolic BP can lead to marked reductions in uteroplacental blood flow and a nonreassuring FHR tracing. Moreover, a rapid reduction of severe systolic BP in patients who have constricted plasma volume can reduce perfusion to the kidney, brain, and placenta. However, sustained BP of 165/100 mm Hg in association with central nervous system signs or symptoms, congestive heart failure, thrombocytopenia, or postpartum status requires therapy within 1 hour.
In general, it is difficult to obtain accurate BP recordings using noninvasive electronic instruments during labor because of the effects of labor on systolic BP and the lack of standardized methods for positioning of the arm cuff and the patient.
For these reasons, the decision about when to start acute antihypertensive therapy, based on systolic or diastolic BP, or both, should be individualized. And the choice of antihypertensive agent should be based on maternal clinical findings.
Choosing an antihypertensive agent
Because both hydralazine and nifedipine are associated with tachycardia, avoid them in patients with a heart rate above 110 bpm, using labetalol instead.10
In patients with bradycardia (heart rate <60 bpm), asthma, or congestive heart failure, however, labetalol should be avoided. In these populations, hydralazine or nifedipine is the drug of choice. Nifedipine is associated with improved renal blood flow and a resultant increase in urine output, making it preferable for patients with decreased urine output or severe postpartum hypertension.10
One theoretical concern is that the combined use of nifedipine and magnesium sulfate can cause excessive hypotension and neuromuscular blockage. As a result, some experts recommend that nifedipine be avoided in patients receiving magnesium sulfate. However, a recent review of this subject concluded that combined use of these drugs does not increase the risks of excessive hypotension and neuromuscular blockage in patients with severe hypertension or preeclampsia.
The initial dose of labetalol, when it is your chosen agent, is 20 mg IV, with BP measured 10 minutes later. If the target BP threshold is not achieved, administer 40 mg, 80 mg, and 80 mg at 10-minute intervals, as needed, again measuring BP 10 minutes after every dose. If, after a maximum dose of 240 mg, the desired BP threshold still has not been reached, give 5 to 10 mg IV hydralazine and measure BP 20 minutes later. If the target BP threshold still has not been achieved, it is essential to obtain consultation on the need for continuous infusion of labetalol, nicardipine, or sodium nitroprusside.
The initial dose of hydralazine, when it is your chosen agent, is 5 to 10 mg IV, with BP measured 20 minutes later. If needed, give another 10 mg and measure BP after another 20-minute interval. After a maximum dose of hydralazine 20 mg, switch to IV labetalol, using the regimen described above for labetalol, if the BP threshold still has not been achieved.
Nitroglycerin may be helpful in carefully selected patients
This drug is an arterial—but mostly venous—dilator. It is administered via IV infusion at an initial rate of 5 µg/min, with the rate gradually increased every 3 to 5 minutes (titrated to BP) to a maximum dose of 100 µg/min. It is the drug of choice in any hypertensive emergency associated with pulmonary edema and for control of hypertension associated with tracheal manipulation during intubation and extubation with general anesthesia.
Nitroglycerin is contraindicated in hypertensive encephalopathy because it increases cerebral blood flow and intracranial pressure. This drug should be administered only under the supervision of an experienced obstetric intensivist.
Sodium nitroprusside: Only in an ICU
This agent causes arterial and venous relaxation by interfering with the influx and intracellular activation of calcium. It is the drug of choice in hypertensive encephalopathy because it controls both afterload (vascular resistance) and preload (fluid status). It should be used only in the setting of intensive care.
The recommended dose is IV infusion at a rate of 0.25 to 5.00 µg/kg/min. Sodium nitroprusside has an immediate onset of action and may continue to exert an effect 3 to 5 minutes after discontinuation. Any hypotension caused by the drug should subside within minutes after discontinuation of the drip, due to the drug’s short half-life.
Nitroprusside is metabolized into thiocyanate and excreted in the urine. Cyanide can accumulate with large doses (>10 µg/kg/min) or prolonged administration (>48 hours), or if the patient has renal insufficiency or decreased hepatic metabolism. Signs of toxicity include anorexia, disorientation, headache, fatigue, restlessness, tinnitus, delirium, hallucinations, nausea, vomiting, and metabolic acidosis. When infused at a rate of less than 2 µg/kg/min, however, cyanide toxicity is unlikely.
As is the case with nitroglycerin, this drug should be administered only under the supervision of an experienced obstetric intensivist.
Case: Resolved
Upon arrival at the ED, the patient exhibits shallow, rapid breathing and foaming from the mouth. She is placed in a lateral decubitus position, an oral airway is established, and all secretions are suctioned. Oxygen is administered via face mask at a rate of 8 L/min. Her initial oxygen saturation level is 92%. IV access is secured, and a loading dose of magnesium sulfate 6 g is given over 20 minutes. Oxygen saturation increases to 94% to 96%. Auscultation of both lungs is normal.
The patient remains in a postictal state for about 15 minutes, but then orients to name, place, and time. FHR monitoring of both fetuses reveals a normal baseline with moderate variability, as well as variable decelerations in the presenting twin.
A maintenance dose of magnesium sulfate is initiated at a rate of 2 g/h, with the BP level recorded every 15 minutes. Systolic values remain between 170 and 180 mm Hg, and diastolic values between 108 and 112 mm Hg for 60 minutes. The obstetrician administers IV labetalol (20 mg) over 2 minutes. About 15 minutes later, the BP level is 154/100 mm Hg, with values remaining in the range of 150 to 156 mm Hg systolic and 92 to 104 mm Hg diastolic.
Ultrasonography reveals that the presenting twin is in a breech position, with estimated fetal weight below the 10th percentile and oligohydramnios. As a result, the obstetrician elects to proceed to cesarean delivery. The twins are delivered by cesarean section using spinal anesthesia. Although the infants are premature, there are no complications.Profile of an eclamptic seizure
Witnessing an eclamptic convulsion can be a frightening experience for nurses and medical providers. The convulsion usually lasts 60 to 90 seconds and occurs in two phases:
- Phase 1 (15–25 seconds) involves facial twitching, rolling of the eyes, and stiffening of the body, with generalized muscular contractions.
- Phase 2 (20–50 seconds) involves alternate contraction and relaxation of the muscles of the body in rapid succession, starting in the face and spreading throughout the body. Foaming at the mouth also occurs, and the patient may bite her tongue if it isn’t protected.
Apnea develops during and immediately after the convulsion, lasting about 120 seconds. A period of hyperventilation follows to compensate for the respiratory acidosis during the apneic period.
A postictal state follows the convulsion, and the patient usually remembers nothing of the episode. Some patients also become restless, combative, and agitated, requiring sedation. Aspiration is possible during or after the convulsion.
We want to hear from you! Tell us what you think.
- Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005;105(2):402–410.
- Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):182–192.
- Meyer NL, Mercer BM, Friedman SA, Sibai BM. Urinary dipstick protein: a poor predictor of absent or severe proteinuria. Am J Obstet Gynecol. 1994;170(1 Pt 1):137–141.
- Knight M; UK Obstetric Surveillance System (UKOSS). Eclampsia in the United Kingdom 2005. BJOG. 2007;114(9):1072–1078.
- ACOG Practice Bulletin #33: Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99:159–167.
- Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia–eclampsia. Am J Obstet Gynecol. 2009;200(5):481.e1–e7.
- Sibai BM. Etiology and management of postpartum hypertension-preeclampsia. Am J Obstet Gynecol. 2012;206(6):470–475.
- ACOG Committee Opinion #514: Emergent therapy for acute-onset, severe hypertension with preeclampsia or eclampsia. Obstet Gynecol. 2011;118:1465–1468.
- Liu S, Joseph KS, Liston RM, et al. Incidence, risk factors, and associated complications of eclampsia. Obstet Gynecol. 2011;118(5):987–994.
- Raheem IA, Saaid R, Omar Sz, Tan PC. Oral nifedipine versus intravenous labetalol for acute blood pressure control in hypertensive emergencies of pregnancy: a randomized trial. BJOG. 2012;119(1):78–85.

Baha M. Sibai, MD
Dr. Sibai is Professor and Director of the Maternal-Fetal Medicine Fellowshp Program in the Department of Obstetrics, Gynecology, and Reproductive Sciences at the University of Texas at Houston.
Dr. Sibai reports no financial relationships relevant to this article.
Baha M. Sibai, MD
Dr. Sibai is Professor and Director of the Maternal-Fetal Medicine Fellowshp Program in the Department of Obstetrics, Gynecology, and Reproductive Sciences at the University of Texas at Houston.
Dr. Sibai reports no financial relationships relevant to this article.
Baha M. Sibai, MD
Dr. Sibai is Professor and Director of the Maternal-Fetal Medicine Fellowshp Program in the Department of Obstetrics, Gynecology, and Reproductive Sciences at the University of Texas at Houston.
Dr. Sibai reports no financial relationships relevant to this article.
CASE: MISSED PREECLAMPSIA
At her first prenatal visit at 14 weeks’ gestation, a 41-year-old woman (G2P1) presents with a dichorionic twin gestation, blood pressure (BP) of 105/68 mm Hg, and a body mass index (BMI) of 40 kg/m2. The pregnancy was achieved through in vitro fertilization. Ten years earlier, the patient’s first pregnancy was complicated by preeclampsia, requiring preterm delivery at 33 weeks’ gestation.
By 28 weeks’ gestation, the patient has gained 26 lb. Her BP is 120/70 mm Hg, with no proteinuria detected by urine dipstick. By 30 weeks, she has gained an additional 8 lb, her BP is 142/84 mm Hg, and no proteinuria is detected. At 32 weeks, her BP is 140/92 mm Hg, she has gained another 8 lb, and no proteinuria is present. She also reports new-onset headaches that do not respond to over-the-counter analgesics. She is sent to the obstetric triage area for BP monitoring, blood testing for preeclampsia and nonstress test fetal monitoring.
During the 2-hour observation period, the patient continues to report headaches, and swelling of her face and hands is present. Her systolic BP values range from 132 to 152 mm Hg, and diastolic values range from 80 to 96 mm Hg. No proteinuria is detected, blood testing results for preeclampsia (complete blood count, liver enzymes, serum creatinine, and uric acid) are normal, and the nonstress tests are reactive in both fetuses.
The patient is given a diagnosis of gestational hypertension, along with a prescription for oral labetalol 200 mg daily and two tablets of acetaminophen with codeine for the headaches (to be taken every 6 hours as needed). She is sent home with instructions to return to her physician’s office in 1 week.
Two days later, she wakes in the middle of the night with a severe headache, blurred vision, and vomiting. Her husband calls the obstetrician’s answering service and is instructed to call 911 immediately. While waiting for an ambulance, the patient experiences a grand mal eclamptic convulsion. A second convulsion occurs during her transfer to the ED.
This scenario could have been avoided.
The obstetrician in this case was negligent for failing to recognize preeclampsia in a patient who had two clear risk factors for it: multifetal gestation and a history of early-onset (<37 weeks) preeclampsia in an earlier pregnancy (other risk factors are listed in TABLE 1).
As a result, the patient developed eclampsia, a serious condition that can lead to grave maternal complications (TABLE 2), including death. It also can cause fetal complications, including growth restriction, hypoxia, acidosis, preterm birth, long-term developmental deficits, and death.1,2
The obstetrician in this case also overlooked published evidence indicating that, in the setting of hypertension and headaches, as many as 20% to 30% of pregnant women whose tests for proteinuria show a negative or trace result via dipstick will develop eclampsia.3 Instead of initiating outpatient administration of oral antihypertensive agents, the obstetrician should have hospitalized this patient for at least 48 hours, with steroid administration, to determine whether outpatient management was feasible.
Related article: 10 practical, evidence-based recommendations to improve outcomes in women who have eclampsia Baha Sibai, MD (November 2011)
Defining eclampsia
Eclampsia is marked by the onset of convulsions (during pregnancy or postpartum) in association with gestational hypertension alone, proteinuria, preeclampsia, or superimposed preeclampsia. Although it is rare, eclampsia is potentially life-threatening. For that reason, obstetricians, anesthesiologists, ED physicians, neurologists, and critical-care physicians should be well versed in its diagnosis and management. In this article, I focus on management.
A few preliminary points
Eclampsia can develop any time during the antenatal period (>16 weeks’ gestation), during labor and delivery, and as long as 6 weeks after delivery. Therefore, we should be vigilant for preeclampsia whenever a pregnant patient visits our office, as well as when she makes unscheduled visits to the ED or obstetric triage area or is hospitalized.
Early recognition of women at high risk for preeclampsia and eclampsia may allow for prompt intervention, including early hospitalization for close observation prior to delivery and postpartum.1,2,4–10
Hospitalization of high-risk women allows for use of antihypertensive agents to treat severe BP, administration of magnesium sulfate to prevent convulsions, and timely delivery of the infant. It also allows for intensive maternal support during and after an eclamptic seizure.
Hospitalization is essential for women who exhibit features that suggest severe disease. More specifically, the presence of gestational hypertension with any of the following features is an indication for immediate hospitalization for evaluation and management:
- persistent severe hypertension (systolic
BP ≥160 mm Hg or diastolic BP ≥110 mm Hg) for at least 1 hour - gestational hypertension requiring oral antihypertensive therapy
- progressive and excessive weight gain (≥20 lb prior to 28 weeks’ gestation)
- generalized swelling (edema of hands or face)
- new-onset or persistent headaches despite analgesics
- persistent visual changes (blurred vision, scotomata, photophobia, double vision)
- shortness of breath, dyspnea, orthopnea, or tightness in the chest
- persistent retrosternal chest pain, severe epigastric or right upper quadrant pain
- persistent nausea, vomiting, malaise
- altered mental state, confusion, numbness, tingling, or motor weakness
- platelet count below 100 3 103 µL
- aspartate aminotransferase (AST), alanine aminotransferase (ALT), or lactic acid dehydrogenase (LDH) levels more than twice the upper limit of normal
- serum creatinine level >1.1 mg/dL
- suspected abruptio placentae.
A stepwise approach to eclampsia
Eclampsia is an obstetric emergency. Inadequate preparation for it or an inappropriate response to maternal and fetal conditions during and after an eclamptic convulsion can be detrimental to the mother and fetus. All obstetric units should have up-to-date protocols in place and should conduct mandatory drills to prepare nursing staff, obstetric providers, and anesthesia staff working in these units to manage eclampsia.
Step 1: Let the seizure run its course
During a seizure, resist the impulse to administer anticonvulsive drugs, including intravenous (IV) magnesium sulfate, because most eclamptic convulsions are self-limiting. Also abstain from administering medications such as IV phenytoin, diazepam, or midazolam, as these drugs are less effective than magnesium sulfate, and some can suppress the laryngeal reflex, increasing the risk of aspiration.
If the patient develops status epilepticus, initiate muscle paralysis and intubate her.
Step 2: Support the maternal condition
It is vital to support maternal respiratory and cardiovascular functions to prevent hypoxia, acidosis, and cardiorespiratory arrest.
Begin by establishing airway patency and maternal oxygenation during and after the convulsion. Administer oxygen via a face mask, with or without a reservoir, at a rate of 8 to 10 L/min.
During the apneic period (see “Profile of an eclamptic seizure” on page 46), the patient will develop hypoxia. Use pulse oximetry to monitor oxygen saturation, with the goal of keeping it above 94%. Arterial blood gas analysis is required if oxygen saturation remains below 92% or if pulmonary edema or aspiration is suspected.
If the patient develops recurrent seizures, status epilepticus, florid alveolar pulmonary edema, or respiratory arrest, intubate her immediately.
Step 3: Prevent maternal injury and aspiration
Secure the side rails of the patient’s bed by elevating them to prevent a fall, and make sure they are padded to prevent trauma during convulsions and afterward, when some women become combative and agitated. Position the patient in a lateral decubitus position to minimize aspiration of oral secretions. If any secretions or vomitus are present, remove them via suction.
Step 4: After the convulsion, give magnesium sulfate
Magnesium is the drug of choice for seizure prophylaxis in women with preeclampsia and severe symptoms, and to prevent recurrent seizures in women with eclampsia.
In the latter group, once the eclamptic convulsion has ended, give a loading dose of IV magnesium (6 g/100 mL over 20 minutes), followed by a continuous infusion of 2 g/h for at least 24 hours. If the patient develops a second seizure during the maintenance infusion, administer another bolus of magnesium (2 g/100 mL over 3–5 minutes).
Step 5: Treat severe hypertension
If severe hypertension persists for 60 minutes or longer, it can lead to injury of the brain, heart, and kidneys. To avoid these complications, it is essential to reduce BP to a safe range and maintain that level without compromising cerebral perfusion pressure and uteroplacental blood flow (which already may be reduced in some patients).
The goal of antihypertensive therapy is to keep systolic BP between 140 and 155 mm Hg and diastolic values between 90 and 105 mm Hg.9 Several agents are available for the treatment of severe hypertension during pregnancy and postpartum. The most commonly used IV medications for this purpose are labetalol and hydralazine. Another option is oral, rapidly acting
nifedipine.
Several randomized trials have compared efficacy and side effects between IV bolus injections of hydralazine; IV labetalol; and oral, rapidly acting nifedipine. In general, the findings of these studies suggest that either IV hydralazine or labetalol or oral nifedipine can be used to treat severe hypertension in pregnancy, as long as the provider is familiar with the dose to be used, the expected onset of action, and potential side effects (TABLE 3).
Women who develop generalized swelling or hemoconcentration (hematocrit ≥40%), or both, usually experience markedly reduced plasma volume. For this reason, these women will benefit from treatment with labetalol. If this is ineffective, then add IV hydralazine. However, delay administration of a rapidly acting vasodilator such as hydralazine to prevent an excessive hypotensive response and a secondary reduction in tissue perfusion and uteroplacental blood flow. Rather, administer a bolus infusion of 250 to 500 mL of isotonic saline before giving a vasodilator.
Additional details about the use of antihypertensive drugs are given in the section on other hypertensive emergencies below.
Step 6: Evaluate the patient for complications
Pulmonary edema can develop in patients with eclampsia or another hypertensive emergency. Suspect it if the patient has respiratory symptoms in association with tachypnea, tachycardia, or sustained oxygen saturation values below 93%, as well as when the patient exhibits basal rales during auscultation of the lungs. Treatment involves the administration of oxygen and IV furosemide (20–40 mg push), repeated as needed.
Some women with eclampsia may develop severe cerebral edema, hemorrhage, or both. The edema can be vasogenic or cytotoxic, leading to increased intracerebral pressure. Suspect edema or hemorrhage if the patient remains unresponsive, continues to experience convulsions despite therapy, or exhibits sensory or motor neurologic deficits. In such cases, neuroimaging is indicated, and the patient should be managed in consultation with neurology or neurosurgery.
Step 7: Begin the process of induction and delivery
Once the patient has been stabilized—and not before—initiate the induction process. Be aware that during and after the convulsion, changes in fetal heart rate (FHR) and uterine monitoring will usually be evident:
- prolonged deceleration or bradycardia (3–10 minutes)
- compensatory tachycardia, decreased beat-to-beat variability
- transient recurrent decelerations
- increased uterine tone and greater frequency of uterine activity.
These changes in FHR and uterine activity usually last 3 to 15 minutes. For this reason, it is important to avoid rushing the patient for cesarean delivery, as FHR and uterine activity are likely to return to normal after maternal resuscitation and stabilization. If not, consider other causes, such as abruptio placentae.
Eclampsia itself is not an indication for cesarean delivery. The selection of mode of delivery should be based on the presence or absence of labor, the cervical Bishop score, fetal gestational age, fetal presentation, and overall fetal condition.
Choosing an anesthetic
Regional analgesia/anesthesia is the method of choice for most women with eclampsia. However, regional anesthesia is to be avoided in the presence of disseminated intravascular coagulation or thrombocytopenia (the threshold platelet count is usually less than 75 x 103 µL. In such a case, IV analgesia can be used during labor, and general anesthesia may be appropriate for cesarean delivery. Both spinal and epidural analgesia and anesthesia are appropriate for women with eclampsia.
How to manage other hypertensive emergencies
A hypertensive emergency during pregnancy or postpartum involves acute-onset, persistent (>15 minutes), severe systolic BP (≥160 mm Hg) or severe diastolic BP (≥110 mm Hg), or both. The first step in such an emergency is to ensure the accurate measurement of BP using standard techniques.
Patients with acute-onset, persistent, severe BP should be hospitalized promptly for evaluation and treatment to prevent organ damage. Once such a patient is hospitalized, BP should be recorded every 15 minutes, with continuous FHR monitoring to ensure fetal viability.
Related article: Failure to diagnose preeclampsia and more (Medical Verdicts, February 2013)
The timing of initiation of antihypertensive medications, as well as determination of the type of medication best suited for the patient, should be based on:
- systolic and diastolic BP levels
- maternal clinical and laboratory findings
- presence of associated symptoms
- preexisting medical comorbidities
- whether the patient is antepartum or postpartum.
For example, a sustained BP level of 200/120 mm Hg requires therapy after 15 minutes, whereas observation may be suitable for as long as 60 minutes for a sustained BP of 160/72 mm Hg during labor.
Rapid reduction of systolic BP can lead to marked reductions in uteroplacental blood flow and a nonreassuring FHR tracing. Moreover, a rapid reduction of severe systolic BP in patients who have constricted plasma volume can reduce perfusion to the kidney, brain, and placenta. However, sustained BP of 165/100 mm Hg in association with central nervous system signs or symptoms, congestive heart failure, thrombocytopenia, or postpartum status requires therapy within 1 hour.
In general, it is difficult to obtain accurate BP recordings using noninvasive electronic instruments during labor because of the effects of labor on systolic BP and the lack of standardized methods for positioning of the arm cuff and the patient.
For these reasons, the decision about when to start acute antihypertensive therapy, based on systolic or diastolic BP, or both, should be individualized. And the choice of antihypertensive agent should be based on maternal clinical findings.
Choosing an antihypertensive agent
Because both hydralazine and nifedipine are associated with tachycardia, avoid them in patients with a heart rate above 110 bpm, using labetalol instead.10
In patients with bradycardia (heart rate <60 bpm), asthma, or congestive heart failure, however, labetalol should be avoided. In these populations, hydralazine or nifedipine is the drug of choice. Nifedipine is associated with improved renal blood flow and a resultant increase in urine output, making it preferable for patients with decreased urine output or severe postpartum hypertension.10
One theoretical concern is that the combined use of nifedipine and magnesium sulfate can cause excessive hypotension and neuromuscular blockage. As a result, some experts recommend that nifedipine be avoided in patients receiving magnesium sulfate. However, a recent review of this subject concluded that combined use of these drugs does not increase the risks of excessive hypotension and neuromuscular blockage in patients with severe hypertension or preeclampsia.
The initial dose of labetalol, when it is your chosen agent, is 20 mg IV, with BP measured 10 minutes later. If the target BP threshold is not achieved, administer 40 mg, 80 mg, and 80 mg at 10-minute intervals, as needed, again measuring BP 10 minutes after every dose. If, after a maximum dose of 240 mg, the desired BP threshold still has not been reached, give 5 to 10 mg IV hydralazine and measure BP 20 minutes later. If the target BP threshold still has not been achieved, it is essential to obtain consultation on the need for continuous infusion of labetalol, nicardipine, or sodium nitroprusside.
The initial dose of hydralazine, when it is your chosen agent, is 5 to 10 mg IV, with BP measured 20 minutes later. If needed, give another 10 mg and measure BP after another 20-minute interval. After a maximum dose of hydralazine 20 mg, switch to IV labetalol, using the regimen described above for labetalol, if the BP threshold still has not been achieved.
Nitroglycerin may be helpful in carefully selected patients
This drug is an arterial—but mostly venous—dilator. It is administered via IV infusion at an initial rate of 5 µg/min, with the rate gradually increased every 3 to 5 minutes (titrated to BP) to a maximum dose of 100 µg/min. It is the drug of choice in any hypertensive emergency associated with pulmonary edema and for control of hypertension associated with tracheal manipulation during intubation and extubation with general anesthesia.
Nitroglycerin is contraindicated in hypertensive encephalopathy because it increases cerebral blood flow and intracranial pressure. This drug should be administered only under the supervision of an experienced obstetric intensivist.
Sodium nitroprusside: Only in an ICU
This agent causes arterial and venous relaxation by interfering with the influx and intracellular activation of calcium. It is the drug of choice in hypertensive encephalopathy because it controls both afterload (vascular resistance) and preload (fluid status). It should be used only in the setting of intensive care.
The recommended dose is IV infusion at a rate of 0.25 to 5.00 µg/kg/min. Sodium nitroprusside has an immediate onset of action and may continue to exert an effect 3 to 5 minutes after discontinuation. Any hypotension caused by the drug should subside within minutes after discontinuation of the drip, due to the drug’s short half-life.
Nitroprusside is metabolized into thiocyanate and excreted in the urine. Cyanide can accumulate with large doses (>10 µg/kg/min) or prolonged administration (>48 hours), or if the patient has renal insufficiency or decreased hepatic metabolism. Signs of toxicity include anorexia, disorientation, headache, fatigue, restlessness, tinnitus, delirium, hallucinations, nausea, vomiting, and metabolic acidosis. When infused at a rate of less than 2 µg/kg/min, however, cyanide toxicity is unlikely.
As is the case with nitroglycerin, this drug should be administered only under the supervision of an experienced obstetric intensivist.
Case: Resolved
Upon arrival at the ED, the patient exhibits shallow, rapid breathing and foaming from the mouth. She is placed in a lateral decubitus position, an oral airway is established, and all secretions are suctioned. Oxygen is administered via face mask at a rate of 8 L/min. Her initial oxygen saturation level is 92%. IV access is secured, and a loading dose of magnesium sulfate 6 g is given over 20 minutes. Oxygen saturation increases to 94% to 96%. Auscultation of both lungs is normal.
The patient remains in a postictal state for about 15 minutes, but then orients to name, place, and time. FHR monitoring of both fetuses reveals a normal baseline with moderate variability, as well as variable decelerations in the presenting twin.
A maintenance dose of magnesium sulfate is initiated at a rate of 2 g/h, with the BP level recorded every 15 minutes. Systolic values remain between 170 and 180 mm Hg, and diastolic values between 108 and 112 mm Hg for 60 minutes. The obstetrician administers IV labetalol (20 mg) over 2 minutes. About 15 minutes later, the BP level is 154/100 mm Hg, with values remaining in the range of 150 to 156 mm Hg systolic and 92 to 104 mm Hg diastolic.
Ultrasonography reveals that the presenting twin is in a breech position, with estimated fetal weight below the 10th percentile and oligohydramnios. As a result, the obstetrician elects to proceed to cesarean delivery. The twins are delivered by cesarean section using spinal anesthesia. Although the infants are premature, there are no complications.Profile of an eclamptic seizure
Witnessing an eclamptic convulsion can be a frightening experience for nurses and medical providers. The convulsion usually lasts 60 to 90 seconds and occurs in two phases:
- Phase 1 (15–25 seconds) involves facial twitching, rolling of the eyes, and stiffening of the body, with generalized muscular contractions.
- Phase 2 (20–50 seconds) involves alternate contraction and relaxation of the muscles of the body in rapid succession, starting in the face and spreading throughout the body. Foaming at the mouth also occurs, and the patient may bite her tongue if it isn’t protected.
Apnea develops during and immediately after the convulsion, lasting about 120 seconds. A period of hyperventilation follows to compensate for the respiratory acidosis during the apneic period.
A postictal state follows the convulsion, and the patient usually remembers nothing of the episode. Some patients also become restless, combative, and agitated, requiring sedation. Aspiration is possible during or after the convulsion.
We want to hear from you! Tell us what you think.
CASE: MISSED PREECLAMPSIA
At her first prenatal visit at 14 weeks’ gestation, a 41-year-old woman (G2P1) presents with a dichorionic twin gestation, blood pressure (BP) of 105/68 mm Hg, and a body mass index (BMI) of 40 kg/m2. The pregnancy was achieved through in vitro fertilization. Ten years earlier, the patient’s first pregnancy was complicated by preeclampsia, requiring preterm delivery at 33 weeks’ gestation.
By 28 weeks’ gestation, the patient has gained 26 lb. Her BP is 120/70 mm Hg, with no proteinuria detected by urine dipstick. By 30 weeks, she has gained an additional 8 lb, her BP is 142/84 mm Hg, and no proteinuria is detected. At 32 weeks, her BP is 140/92 mm Hg, she has gained another 8 lb, and no proteinuria is present. She also reports new-onset headaches that do not respond to over-the-counter analgesics. She is sent to the obstetric triage area for BP monitoring, blood testing for preeclampsia and nonstress test fetal monitoring.
During the 2-hour observation period, the patient continues to report headaches, and swelling of her face and hands is present. Her systolic BP values range from 132 to 152 mm Hg, and diastolic values range from 80 to 96 mm Hg. No proteinuria is detected, blood testing results for preeclampsia (complete blood count, liver enzymes, serum creatinine, and uric acid) are normal, and the nonstress tests are reactive in both fetuses.
The patient is given a diagnosis of gestational hypertension, along with a prescription for oral labetalol 200 mg daily and two tablets of acetaminophen with codeine for the headaches (to be taken every 6 hours as needed). She is sent home with instructions to return to her physician’s office in 1 week.
Two days later, she wakes in the middle of the night with a severe headache, blurred vision, and vomiting. Her husband calls the obstetrician’s answering service and is instructed to call 911 immediately. While waiting for an ambulance, the patient experiences a grand mal eclamptic convulsion. A second convulsion occurs during her transfer to the ED.
This scenario could have been avoided.
The obstetrician in this case was negligent for failing to recognize preeclampsia in a patient who had two clear risk factors for it: multifetal gestation and a history of early-onset (<37 weeks) preeclampsia in an earlier pregnancy (other risk factors are listed in TABLE 1).
As a result, the patient developed eclampsia, a serious condition that can lead to grave maternal complications (TABLE 2), including death. It also can cause fetal complications, including growth restriction, hypoxia, acidosis, preterm birth, long-term developmental deficits, and death.1,2
The obstetrician in this case also overlooked published evidence indicating that, in the setting of hypertension and headaches, as many as 20% to 30% of pregnant women whose tests for proteinuria show a negative or trace result via dipstick will develop eclampsia.3 Instead of initiating outpatient administration of oral antihypertensive agents, the obstetrician should have hospitalized this patient for at least 48 hours, with steroid administration, to determine whether outpatient management was feasible.
Related article: 10 practical, evidence-based recommendations to improve outcomes in women who have eclampsia Baha Sibai, MD (November 2011)
Defining eclampsia
Eclampsia is marked by the onset of convulsions (during pregnancy or postpartum) in association with gestational hypertension alone, proteinuria, preeclampsia, or superimposed preeclampsia. Although it is rare, eclampsia is potentially life-threatening. For that reason, obstetricians, anesthesiologists, ED physicians, neurologists, and critical-care physicians should be well versed in its diagnosis and management. In this article, I focus on management.
A few preliminary points
Eclampsia can develop any time during the antenatal period (>16 weeks’ gestation), during labor and delivery, and as long as 6 weeks after delivery. Therefore, we should be vigilant for preeclampsia whenever a pregnant patient visits our office, as well as when she makes unscheduled visits to the ED or obstetric triage area or is hospitalized.
Early recognition of women at high risk for preeclampsia and eclampsia may allow for prompt intervention, including early hospitalization for close observation prior to delivery and postpartum.1,2,4–10
Hospitalization of high-risk women allows for use of antihypertensive agents to treat severe BP, administration of magnesium sulfate to prevent convulsions, and timely delivery of the infant. It also allows for intensive maternal support during and after an eclamptic seizure.
Hospitalization is essential for women who exhibit features that suggest severe disease. More specifically, the presence of gestational hypertension with any of the following features is an indication for immediate hospitalization for evaluation and management:
- persistent severe hypertension (systolic
BP ≥160 mm Hg or diastolic BP ≥110 mm Hg) for at least 1 hour - gestational hypertension requiring oral antihypertensive therapy
- progressive and excessive weight gain (≥20 lb prior to 28 weeks’ gestation)
- generalized swelling (edema of hands or face)
- new-onset or persistent headaches despite analgesics
- persistent visual changes (blurred vision, scotomata, photophobia, double vision)
- shortness of breath, dyspnea, orthopnea, or tightness in the chest
- persistent retrosternal chest pain, severe epigastric or right upper quadrant pain
- persistent nausea, vomiting, malaise
- altered mental state, confusion, numbness, tingling, or motor weakness
- platelet count below 100 3 103 µL
- aspartate aminotransferase (AST), alanine aminotransferase (ALT), or lactic acid dehydrogenase (LDH) levels more than twice the upper limit of normal
- serum creatinine level >1.1 mg/dL
- suspected abruptio placentae.
A stepwise approach to eclampsia
Eclampsia is an obstetric emergency. Inadequate preparation for it or an inappropriate response to maternal and fetal conditions during and after an eclamptic convulsion can be detrimental to the mother and fetus. All obstetric units should have up-to-date protocols in place and should conduct mandatory drills to prepare nursing staff, obstetric providers, and anesthesia staff working in these units to manage eclampsia.
Step 1: Let the seizure run its course
During a seizure, resist the impulse to administer anticonvulsive drugs, including intravenous (IV) magnesium sulfate, because most eclamptic convulsions are self-limiting. Also abstain from administering medications such as IV phenytoin, diazepam, or midazolam, as these drugs are less effective than magnesium sulfate, and some can suppress the laryngeal reflex, increasing the risk of aspiration.
If the patient develops status epilepticus, initiate muscle paralysis and intubate her.
Step 2: Support the maternal condition
It is vital to support maternal respiratory and cardiovascular functions to prevent hypoxia, acidosis, and cardiorespiratory arrest.
Begin by establishing airway patency and maternal oxygenation during and after the convulsion. Administer oxygen via a face mask, with or without a reservoir, at a rate of 8 to 10 L/min.
During the apneic period (see “Profile of an eclamptic seizure” on page 46), the patient will develop hypoxia. Use pulse oximetry to monitor oxygen saturation, with the goal of keeping it above 94%. Arterial blood gas analysis is required if oxygen saturation remains below 92% or if pulmonary edema or aspiration is suspected.
If the patient develops recurrent seizures, status epilepticus, florid alveolar pulmonary edema, or respiratory arrest, intubate her immediately.
Step 3: Prevent maternal injury and aspiration
Secure the side rails of the patient’s bed by elevating them to prevent a fall, and make sure they are padded to prevent trauma during convulsions and afterward, when some women become combative and agitated. Position the patient in a lateral decubitus position to minimize aspiration of oral secretions. If any secretions or vomitus are present, remove them via suction.
Step 4: After the convulsion, give magnesium sulfate
Magnesium is the drug of choice for seizure prophylaxis in women with preeclampsia and severe symptoms, and to prevent recurrent seizures in women with eclampsia.
In the latter group, once the eclamptic convulsion has ended, give a loading dose of IV magnesium (6 g/100 mL over 20 minutes), followed by a continuous infusion of 2 g/h for at least 24 hours. If the patient develops a second seizure during the maintenance infusion, administer another bolus of magnesium (2 g/100 mL over 3–5 minutes).
Step 5: Treat severe hypertension
If severe hypertension persists for 60 minutes or longer, it can lead to injury of the brain, heart, and kidneys. To avoid these complications, it is essential to reduce BP to a safe range and maintain that level without compromising cerebral perfusion pressure and uteroplacental blood flow (which already may be reduced in some patients).
The goal of antihypertensive therapy is to keep systolic BP between 140 and 155 mm Hg and diastolic values between 90 and 105 mm Hg.9 Several agents are available for the treatment of severe hypertension during pregnancy and postpartum. The most commonly used IV medications for this purpose are labetalol and hydralazine. Another option is oral, rapidly acting
nifedipine.
Several randomized trials have compared efficacy and side effects between IV bolus injections of hydralazine; IV labetalol; and oral, rapidly acting nifedipine. In general, the findings of these studies suggest that either IV hydralazine or labetalol or oral nifedipine can be used to treat severe hypertension in pregnancy, as long as the provider is familiar with the dose to be used, the expected onset of action, and potential side effects (TABLE 3).
Women who develop generalized swelling or hemoconcentration (hematocrit ≥40%), or both, usually experience markedly reduced plasma volume. For this reason, these women will benefit from treatment with labetalol. If this is ineffective, then add IV hydralazine. However, delay administration of a rapidly acting vasodilator such as hydralazine to prevent an excessive hypotensive response and a secondary reduction in tissue perfusion and uteroplacental blood flow. Rather, administer a bolus infusion of 250 to 500 mL of isotonic saline before giving a vasodilator.
Additional details about the use of antihypertensive drugs are given in the section on other hypertensive emergencies below.
Step 6: Evaluate the patient for complications
Pulmonary edema can develop in patients with eclampsia or another hypertensive emergency. Suspect it if the patient has respiratory symptoms in association with tachypnea, tachycardia, or sustained oxygen saturation values below 93%, as well as when the patient exhibits basal rales during auscultation of the lungs. Treatment involves the administration of oxygen and IV furosemide (20–40 mg push), repeated as needed.
Some women with eclampsia may develop severe cerebral edema, hemorrhage, or both. The edema can be vasogenic or cytotoxic, leading to increased intracerebral pressure. Suspect edema or hemorrhage if the patient remains unresponsive, continues to experience convulsions despite therapy, or exhibits sensory or motor neurologic deficits. In such cases, neuroimaging is indicated, and the patient should be managed in consultation with neurology or neurosurgery.
Step 7: Begin the process of induction and delivery
Once the patient has been stabilized—and not before—initiate the induction process. Be aware that during and after the convulsion, changes in fetal heart rate (FHR) and uterine monitoring will usually be evident:
- prolonged deceleration or bradycardia (3–10 minutes)
- compensatory tachycardia, decreased beat-to-beat variability
- transient recurrent decelerations
- increased uterine tone and greater frequency of uterine activity.
These changes in FHR and uterine activity usually last 3 to 15 minutes. For this reason, it is important to avoid rushing the patient for cesarean delivery, as FHR and uterine activity are likely to return to normal after maternal resuscitation and stabilization. If not, consider other causes, such as abruptio placentae.
Eclampsia itself is not an indication for cesarean delivery. The selection of mode of delivery should be based on the presence or absence of labor, the cervical Bishop score, fetal gestational age, fetal presentation, and overall fetal condition.
Choosing an anesthetic
Regional analgesia/anesthesia is the method of choice for most women with eclampsia. However, regional anesthesia is to be avoided in the presence of disseminated intravascular coagulation or thrombocytopenia (the threshold platelet count is usually less than 75 x 103 µL. In such a case, IV analgesia can be used during labor, and general anesthesia may be appropriate for cesarean delivery. Both spinal and epidural analgesia and anesthesia are appropriate for women with eclampsia.
How to manage other hypertensive emergencies
A hypertensive emergency during pregnancy or postpartum involves acute-onset, persistent (>15 minutes), severe systolic BP (≥160 mm Hg) or severe diastolic BP (≥110 mm Hg), or both. The first step in such an emergency is to ensure the accurate measurement of BP using standard techniques.
Patients with acute-onset, persistent, severe BP should be hospitalized promptly for evaluation and treatment to prevent organ damage. Once such a patient is hospitalized, BP should be recorded every 15 minutes, with continuous FHR monitoring to ensure fetal viability.
Related article: Failure to diagnose preeclampsia and more (Medical Verdicts, February 2013)
The timing of initiation of antihypertensive medications, as well as determination of the type of medication best suited for the patient, should be based on:
- systolic and diastolic BP levels
- maternal clinical and laboratory findings
- presence of associated symptoms
- preexisting medical comorbidities
- whether the patient is antepartum or postpartum.
For example, a sustained BP level of 200/120 mm Hg requires therapy after 15 minutes, whereas observation may be suitable for as long as 60 minutes for a sustained BP of 160/72 mm Hg during labor.
Rapid reduction of systolic BP can lead to marked reductions in uteroplacental blood flow and a nonreassuring FHR tracing. Moreover, a rapid reduction of severe systolic BP in patients who have constricted plasma volume can reduce perfusion to the kidney, brain, and placenta. However, sustained BP of 165/100 mm Hg in association with central nervous system signs or symptoms, congestive heart failure, thrombocytopenia, or postpartum status requires therapy within 1 hour.
In general, it is difficult to obtain accurate BP recordings using noninvasive electronic instruments during labor because of the effects of labor on systolic BP and the lack of standardized methods for positioning of the arm cuff and the patient.
For these reasons, the decision about when to start acute antihypertensive therapy, based on systolic or diastolic BP, or both, should be individualized. And the choice of antihypertensive agent should be based on maternal clinical findings.
Choosing an antihypertensive agent
Because both hydralazine and nifedipine are associated with tachycardia, avoid them in patients with a heart rate above 110 bpm, using labetalol instead.10
In patients with bradycardia (heart rate <60 bpm), asthma, or congestive heart failure, however, labetalol should be avoided. In these populations, hydralazine or nifedipine is the drug of choice. Nifedipine is associated with improved renal blood flow and a resultant increase in urine output, making it preferable for patients with decreased urine output or severe postpartum hypertension.10
One theoretical concern is that the combined use of nifedipine and magnesium sulfate can cause excessive hypotension and neuromuscular blockage. As a result, some experts recommend that nifedipine be avoided in patients receiving magnesium sulfate. However, a recent review of this subject concluded that combined use of these drugs does not increase the risks of excessive hypotension and neuromuscular blockage in patients with severe hypertension or preeclampsia.
The initial dose of labetalol, when it is your chosen agent, is 20 mg IV, with BP measured 10 minutes later. If the target BP threshold is not achieved, administer 40 mg, 80 mg, and 80 mg at 10-minute intervals, as needed, again measuring BP 10 minutes after every dose. If, after a maximum dose of 240 mg, the desired BP threshold still has not been reached, give 5 to 10 mg IV hydralazine and measure BP 20 minutes later. If the target BP threshold still has not been achieved, it is essential to obtain consultation on the need for continuous infusion of labetalol, nicardipine, or sodium nitroprusside.
The initial dose of hydralazine, when it is your chosen agent, is 5 to 10 mg IV, with BP measured 20 minutes later. If needed, give another 10 mg and measure BP after another 20-minute interval. After a maximum dose of hydralazine 20 mg, switch to IV labetalol, using the regimen described above for labetalol, if the BP threshold still has not been achieved.
Nitroglycerin may be helpful in carefully selected patients
This drug is an arterial—but mostly venous—dilator. It is administered via IV infusion at an initial rate of 5 µg/min, with the rate gradually increased every 3 to 5 minutes (titrated to BP) to a maximum dose of 100 µg/min. It is the drug of choice in any hypertensive emergency associated with pulmonary edema and for control of hypertension associated with tracheal manipulation during intubation and extubation with general anesthesia.
Nitroglycerin is contraindicated in hypertensive encephalopathy because it increases cerebral blood flow and intracranial pressure. This drug should be administered only under the supervision of an experienced obstetric intensivist.
Sodium nitroprusside: Only in an ICU
This agent causes arterial and venous relaxation by interfering with the influx and intracellular activation of calcium. It is the drug of choice in hypertensive encephalopathy because it controls both afterload (vascular resistance) and preload (fluid status). It should be used only in the setting of intensive care.
The recommended dose is IV infusion at a rate of 0.25 to 5.00 µg/kg/min. Sodium nitroprusside has an immediate onset of action and may continue to exert an effect 3 to 5 minutes after discontinuation. Any hypotension caused by the drug should subside within minutes after discontinuation of the drip, due to the drug’s short half-life.
Nitroprusside is metabolized into thiocyanate and excreted in the urine. Cyanide can accumulate with large doses (>10 µg/kg/min) or prolonged administration (>48 hours), or if the patient has renal insufficiency or decreased hepatic metabolism. Signs of toxicity include anorexia, disorientation, headache, fatigue, restlessness, tinnitus, delirium, hallucinations, nausea, vomiting, and metabolic acidosis. When infused at a rate of less than 2 µg/kg/min, however, cyanide toxicity is unlikely.
As is the case with nitroglycerin, this drug should be administered only under the supervision of an experienced obstetric intensivist.
Case: Resolved
Upon arrival at the ED, the patient exhibits shallow, rapid breathing and foaming from the mouth. She is placed in a lateral decubitus position, an oral airway is established, and all secretions are suctioned. Oxygen is administered via face mask at a rate of 8 L/min. Her initial oxygen saturation level is 92%. IV access is secured, and a loading dose of magnesium sulfate 6 g is given over 20 minutes. Oxygen saturation increases to 94% to 96%. Auscultation of both lungs is normal.
The patient remains in a postictal state for about 15 minutes, but then orients to name, place, and time. FHR monitoring of both fetuses reveals a normal baseline with moderate variability, as well as variable decelerations in the presenting twin.
A maintenance dose of magnesium sulfate is initiated at a rate of 2 g/h, with the BP level recorded every 15 minutes. Systolic values remain between 170 and 180 mm Hg, and diastolic values between 108 and 112 mm Hg for 60 minutes. The obstetrician administers IV labetalol (20 mg) over 2 minutes. About 15 minutes later, the BP level is 154/100 mm Hg, with values remaining in the range of 150 to 156 mm Hg systolic and 92 to 104 mm Hg diastolic.
Ultrasonography reveals that the presenting twin is in a breech position, with estimated fetal weight below the 10th percentile and oligohydramnios. As a result, the obstetrician elects to proceed to cesarean delivery. The twins are delivered by cesarean section using spinal anesthesia. Although the infants are premature, there are no complications.Profile of an eclamptic seizure
Witnessing an eclamptic convulsion can be a frightening experience for nurses and medical providers. The convulsion usually lasts 60 to 90 seconds and occurs in two phases:
- Phase 1 (15–25 seconds) involves facial twitching, rolling of the eyes, and stiffening of the body, with generalized muscular contractions.
- Phase 2 (20–50 seconds) involves alternate contraction and relaxation of the muscles of the body in rapid succession, starting in the face and spreading throughout the body. Foaming at the mouth also occurs, and the patient may bite her tongue if it isn’t protected.
Apnea develops during and immediately after the convulsion, lasting about 120 seconds. A period of hyperventilation follows to compensate for the respiratory acidosis during the apneic period.
A postictal state follows the convulsion, and the patient usually remembers nothing of the episode. Some patients also become restless, combative, and agitated, requiring sedation. Aspiration is possible during or after the convulsion.
We want to hear from you! Tell us what you think.
- Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005;105(2):402–410.
- Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):182–192.
- Meyer NL, Mercer BM, Friedman SA, Sibai BM. Urinary dipstick protein: a poor predictor of absent or severe proteinuria. Am J Obstet Gynecol. 1994;170(1 Pt 1):137–141.
- Knight M; UK Obstetric Surveillance System (UKOSS). Eclampsia in the United Kingdom 2005. BJOG. 2007;114(9):1072–1078.
- ACOG Practice Bulletin #33: Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99:159–167.
- Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia–eclampsia. Am J Obstet Gynecol. 2009;200(5):481.e1–e7.
- Sibai BM. Etiology and management of postpartum hypertension-preeclampsia. Am J Obstet Gynecol. 2012;206(6):470–475.
- ACOG Committee Opinion #514: Emergent therapy for acute-onset, severe hypertension with preeclampsia or eclampsia. Obstet Gynecol. 2011;118:1465–1468.
- Liu S, Joseph KS, Liston RM, et al. Incidence, risk factors, and associated complications of eclampsia. Obstet Gynecol. 2011;118(5):987–994.
- Raheem IA, Saaid R, Omar Sz, Tan PC. Oral nifedipine versus intravenous labetalol for acute blood pressure control in hypertensive emergencies of pregnancy: a randomized trial. BJOG. 2012;119(1):78–85.
- Sibai BM. Diagnosis, prevention, and management of eclampsia. Obstet Gynecol. 2005;105(2):402–410.
- Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):182–192.
- Meyer NL, Mercer BM, Friedman SA, Sibai BM. Urinary dipstick protein: a poor predictor of absent or severe proteinuria. Am J Obstet Gynecol. 1994;170(1 Pt 1):137–141.
- Knight M; UK Obstetric Surveillance System (UKOSS). Eclampsia in the United Kingdom 2005. BJOG. 2007;114(9):1072–1078.
- ACOG Practice Bulletin #33: Diagnosis and management of preeclampsia and eclampsia. Obstet Gynecol. 2002;99:159–167.
- Sibai BM, Stella CL. Diagnosis and management of atypical preeclampsia–eclampsia. Am J Obstet Gynecol. 2009;200(5):481.e1–e7.
- Sibai BM. Etiology and management of postpartum hypertension-preeclampsia. Am J Obstet Gynecol. 2012;206(6):470–475.
- ACOG Committee Opinion #514: Emergent therapy for acute-onset, severe hypertension with preeclampsia or eclampsia. Obstet Gynecol. 2011;118:1465–1468.
- Liu S, Joseph KS, Liston RM, et al. Incidence, risk factors, and associated complications of eclampsia. Obstet Gynecol. 2011;118(5):987–994.
- Raheem IA, Saaid R, Omar Sz, Tan PC. Oral nifedipine versus intravenous labetalol for acute blood pressure control in hypertensive emergencies of pregnancy: a randomized trial. BJOG. 2012;119(1):78–85.

5 Points on Unicompartmental Knee Arthroplasty
Despite the long-term survivorship and clinical effectiveness of total knee arthroplasty (TKA), the percentage of patients who indicate dissatisfaction with their procedures (little improvement in pain and function) can be as high as 15% to 30%.1-3 Although early reports on survivorship of unicompartmental knee arthroplasty (UKA) were discouraging, recent studies assessing modern implant designs and surgical techniques have found 10-year survival rates of 90% to 98%.4 The number of UKAs performed over the past decade has increased by 30%, as numerous studies have demonstrated shorter hospital stays, decreased perioperative morbidity, faster functional recovery, increased range of motion (ROM), and improved knee kinematics compared with TKA.4
[Introductory paragraph provided in lieu of abstract]
Despite the long-term survivorship and clinical effectiveness of total knee arthroplasty (TKA), the percentage of patients who indicate dissatisfaction with their procedures (little improvement in pain and function) can be as high as 15% to 30%.1-3 Although early reports on survivorship of unicompartmental knee arthroplasty (UKA) were discouraging, recent studies assessing modern implant designs and surgical techniques have found 10-year survival rates of 90% to 98%.4 The number of UKAs performed over the past decade has increased by 30%, as numerous studies have demonstrated shorter hospital stays, decreased perioperative morbidity, faster functional recovery, increased range of motion (ROM), and improved knee kinematics compared with TKA.4
[Introductory paragraph provided in lieu of abstract]
Despite the long-term survivorship and clinical effectiveness of total knee arthroplasty (TKA), the percentage of patients who indicate dissatisfaction with their procedures (little improvement in pain and function) can be as high as 15% to 30%.1-3 Although early reports on survivorship of unicompartmental knee arthroplasty (UKA) were discouraging, recent studies assessing modern implant designs and surgical techniques have found 10-year survival rates of 90% to 98%.4 The number of UKAs performed over the past decade has increased by 30%, as numerous studies have demonstrated shorter hospital stays, decreased perioperative morbidity, faster functional recovery, increased range of motion (ROM), and improved knee kinematics compared with TKA.4
[Introductory paragraph provided in lieu of abstract]
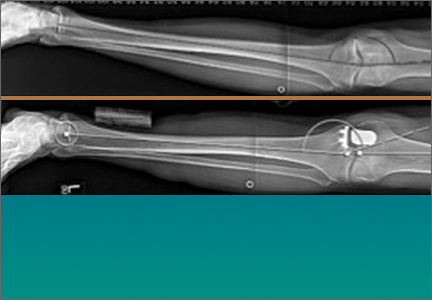
Banish ‘obesity’ from your vocabulary when counseling about weight loss
SAN DIEGO – If you’re skeptical about the impact that you as a primary care provider can make on patients who seek assistance from you with weight loss, think again, advised Dr. Lindsay Botsford.
"You can really make a big difference in your office," Dr. Botsford, a family physician who practices in Sugar Land, Tex., said at the annual meeting of the American Academy of Family Physicians.
During her presentation, she spotlighted the success of Practice-Based Opportunities for Weight Reduction (POWER-UP), a 2-year randomized controlled trial of obesity treatment in the primary care setting. For the trial, 390 patients at six primary care practices were randomized to one of three interventions: usual care, which consisted of quarterly visits that included education about weight management; brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control; and enhanced brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control, plus meal replacements or orlistat or sibutramine to potentially increase weight loss (N. Engl. J. Med. 2011;365[2]:1969-79).
At the end of the second year, patients in the enhanced lifestyle counseling group lost an average of 4.6 kg, which exceeded the average weight loss experienced by patients in the brief lifestyle counseling and usual care groups (an average of 2.9 kg and 1.7 kg, respectively). The proportion of patients who achieved a weight loss of more than 5% at the end of the second year was also greatest in the enhanced lifestyle group (34.9% vs. 26% and 21.5% in the other two groups, respectively).
Some patients harbor sensitivity about their weight, so if they want to talk about the issue, Dr. Botsford recommended avoiding the term "obesity" and instead using terms such as "weight," "excess weight," "unhealthy body weight," and "BMI." She also recommended involving other members of the staff. For example, front desk staff can ask patients to fill out a fitness inventory and medical assistants can check BMI, measure waist circumference, and provide basic counseling advice about weight loss strategies such as keeping a food journal and portion control.
Regarding how patients perceive overweight physicians, Dr. Botsford noted, "In general, patients find overweight physicians less credible. I find that a little sad, but your view on the subject can influence patients. If you are not at your healthy weight, try to overcome this by sharing personal stories with them."
In counseling patients who express interest in losing weight, she said she begins with a 24-hour dietary recall and then reviews the U.S. Preventive Services Task Force’s "5 A’s" framework to create goals. The five A’s include assess (ask about or assess behavioral health risk[s] and factors affecting choice of behavior change goals); advise (give clear, specific, and personalized behavior change advice, including information about harms and benefits); agree (collaboratively select treatment goals and methods based on interest and willingness to change); assist (using behavior change techniques, help patient to acquire the skills, confidence, and social or environmental supports for behavior change, supplemented with medical treatments when needed); and arrange (schedule follow-up to provide ongoing assistance or support and to adjust the treatment plan as needed).
Other evidence-based counseling tips include recommending that patients avoid artificial sweetener, eating out of a bag, eating in front of the television, eating bread when dining out, and being mindful of liquid calorie intake. She also said she advises patients to stay hydrated, leave one-third of the portion on the plate when dining out, order "small" sizes when possible, and use small plates and bowls at home.
"Study after study has shown that low-calorie diets – 1,000-1,200 kcal/day for women and 1,200-1,600 kcal/day for men are the most successful for maintaining weight loss in the long term," Dr. Botsford said. "Adherence is a big thing when it comes to diets. The most common thing is that people stop. They can’t stick with it. Low glycemic load may help adherence. That’s still within the context of a low-calorie diet. There is certain evidence that having more fiber and more protein will make you feel fuller along the way, but in the end, a low-calorie diet is best."
Tools that can help patients keep a handle on food intake include the AAFP\'s initiative Americans in Motion Healthy Interventions and smartphone apps such as Lose It!, Calorie Counter and Diet Tracker by MyFitnessPal.com, healthfinder.gov, and Weight Watchers Mobile. "Exercise alone is better than nothing, but it only translates into a small weight loss," Dr. Botsford said. "However, exercise reduces blood pressure, triglycerides, and fasting glucose, and it decreases abdominal adipose tissue. To make the real difference you need exercise and diet. You also improve your strength, balance, and peak oxygen consumption. The more intense your exercise, [the more] you will increase your weight loss."
Medicare will reimburse for obesity counseling, but the patient’s BMI has to be greater than 30 kg/m2; the patient has to be competent and alert, and the counseling has to be done in a primary care setting or by the primary care provider. "Medicare will cover up to 22 visits in 12 months in a staged way," Dr. Botsford said, noting that the ICD-9 code for a BMI of 30 or more is G0447. "For the first month they’ll cover once a week. The only caveat is that you cannot bill for any other services on the same day as the visit for obesity counseling."
Dr. Botsford said she had no relevant financial conflicts to disclose.
SAN DIEGO – If you’re skeptical about the impact that you as a primary care provider can make on patients who seek assistance from you with weight loss, think again, advised Dr. Lindsay Botsford.
"You can really make a big difference in your office," Dr. Botsford, a family physician who practices in Sugar Land, Tex., said at the annual meeting of the American Academy of Family Physicians.
During her presentation, she spotlighted the success of Practice-Based Opportunities for Weight Reduction (POWER-UP), a 2-year randomized controlled trial of obesity treatment in the primary care setting. For the trial, 390 patients at six primary care practices were randomized to one of three interventions: usual care, which consisted of quarterly visits that included education about weight management; brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control; and enhanced brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control, plus meal replacements or orlistat or sibutramine to potentially increase weight loss (N. Engl. J. Med. 2011;365[2]:1969-79).
At the end of the second year, patients in the enhanced lifestyle counseling group lost an average of 4.6 kg, which exceeded the average weight loss experienced by patients in the brief lifestyle counseling and usual care groups (an average of 2.9 kg and 1.7 kg, respectively). The proportion of patients who achieved a weight loss of more than 5% at the end of the second year was also greatest in the enhanced lifestyle group (34.9% vs. 26% and 21.5% in the other two groups, respectively).
Some patients harbor sensitivity about their weight, so if they want to talk about the issue, Dr. Botsford recommended avoiding the term "obesity" and instead using terms such as "weight," "excess weight," "unhealthy body weight," and "BMI." She also recommended involving other members of the staff. For example, front desk staff can ask patients to fill out a fitness inventory and medical assistants can check BMI, measure waist circumference, and provide basic counseling advice about weight loss strategies such as keeping a food journal and portion control.
Regarding how patients perceive overweight physicians, Dr. Botsford noted, "In general, patients find overweight physicians less credible. I find that a little sad, but your view on the subject can influence patients. If you are not at your healthy weight, try to overcome this by sharing personal stories with them."
In counseling patients who express interest in losing weight, she said she begins with a 24-hour dietary recall and then reviews the U.S. Preventive Services Task Force’s "5 A’s" framework to create goals. The five A’s include assess (ask about or assess behavioral health risk[s] and factors affecting choice of behavior change goals); advise (give clear, specific, and personalized behavior change advice, including information about harms and benefits); agree (collaboratively select treatment goals and methods based on interest and willingness to change); assist (using behavior change techniques, help patient to acquire the skills, confidence, and social or environmental supports for behavior change, supplemented with medical treatments when needed); and arrange (schedule follow-up to provide ongoing assistance or support and to adjust the treatment plan as needed).
Other evidence-based counseling tips include recommending that patients avoid artificial sweetener, eating out of a bag, eating in front of the television, eating bread when dining out, and being mindful of liquid calorie intake. She also said she advises patients to stay hydrated, leave one-third of the portion on the plate when dining out, order "small" sizes when possible, and use small plates and bowls at home.
"Study after study has shown that low-calorie diets – 1,000-1,200 kcal/day for women and 1,200-1,600 kcal/day for men are the most successful for maintaining weight loss in the long term," Dr. Botsford said. "Adherence is a big thing when it comes to diets. The most common thing is that people stop. They can’t stick with it. Low glycemic load may help adherence. That’s still within the context of a low-calorie diet. There is certain evidence that having more fiber and more protein will make you feel fuller along the way, but in the end, a low-calorie diet is best."
Tools that can help patients keep a handle on food intake include the AAFP\'s initiative Americans in Motion Healthy Interventions and smartphone apps such as Lose It!, Calorie Counter and Diet Tracker by MyFitnessPal.com, healthfinder.gov, and Weight Watchers Mobile. "Exercise alone is better than nothing, but it only translates into a small weight loss," Dr. Botsford said. "However, exercise reduces blood pressure, triglycerides, and fasting glucose, and it decreases abdominal adipose tissue. To make the real difference you need exercise and diet. You also improve your strength, balance, and peak oxygen consumption. The more intense your exercise, [the more] you will increase your weight loss."
Medicare will reimburse for obesity counseling, but the patient’s BMI has to be greater than 30 kg/m2; the patient has to be competent and alert, and the counseling has to be done in a primary care setting or by the primary care provider. "Medicare will cover up to 22 visits in 12 months in a staged way," Dr. Botsford said, noting that the ICD-9 code for a BMI of 30 or more is G0447. "For the first month they’ll cover once a week. The only caveat is that you cannot bill for any other services on the same day as the visit for obesity counseling."
Dr. Botsford said she had no relevant financial conflicts to disclose.
SAN DIEGO – If you’re skeptical about the impact that you as a primary care provider can make on patients who seek assistance from you with weight loss, think again, advised Dr. Lindsay Botsford.
"You can really make a big difference in your office," Dr. Botsford, a family physician who practices in Sugar Land, Tex., said at the annual meeting of the American Academy of Family Physicians.
During her presentation, she spotlighted the success of Practice-Based Opportunities for Weight Reduction (POWER-UP), a 2-year randomized controlled trial of obesity treatment in the primary care setting. For the trial, 390 patients at six primary care practices were randomized to one of three interventions: usual care, which consisted of quarterly visits that included education about weight management; brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control; and enhanced brief lifestyle counseling, which consisted of quarterly primary care visits combined with short monthly sessions with lifestyle coaches who instructed patients about behavioral control, plus meal replacements or orlistat or sibutramine to potentially increase weight loss (N. Engl. J. Med. 2011;365[2]:1969-79).
At the end of the second year, patients in the enhanced lifestyle counseling group lost an average of 4.6 kg, which exceeded the average weight loss experienced by patients in the brief lifestyle counseling and usual care groups (an average of 2.9 kg and 1.7 kg, respectively). The proportion of patients who achieved a weight loss of more than 5% at the end of the second year was also greatest in the enhanced lifestyle group (34.9% vs. 26% and 21.5% in the other two groups, respectively).
Some patients harbor sensitivity about their weight, so if they want to talk about the issue, Dr. Botsford recommended avoiding the term "obesity" and instead using terms such as "weight," "excess weight," "unhealthy body weight," and "BMI." She also recommended involving other members of the staff. For example, front desk staff can ask patients to fill out a fitness inventory and medical assistants can check BMI, measure waist circumference, and provide basic counseling advice about weight loss strategies such as keeping a food journal and portion control.
Regarding how patients perceive overweight physicians, Dr. Botsford noted, "In general, patients find overweight physicians less credible. I find that a little sad, but your view on the subject can influence patients. If you are not at your healthy weight, try to overcome this by sharing personal stories with them."
In counseling patients who express interest in losing weight, she said she begins with a 24-hour dietary recall and then reviews the U.S. Preventive Services Task Force’s "5 A’s" framework to create goals. The five A’s include assess (ask about or assess behavioral health risk[s] and factors affecting choice of behavior change goals); advise (give clear, specific, and personalized behavior change advice, including information about harms and benefits); agree (collaboratively select treatment goals and methods based on interest and willingness to change); assist (using behavior change techniques, help patient to acquire the skills, confidence, and social or environmental supports for behavior change, supplemented with medical treatments when needed); and arrange (schedule follow-up to provide ongoing assistance or support and to adjust the treatment plan as needed).
Other evidence-based counseling tips include recommending that patients avoid artificial sweetener, eating out of a bag, eating in front of the television, eating bread when dining out, and being mindful of liquid calorie intake. She also said she advises patients to stay hydrated, leave one-third of the portion on the plate when dining out, order "small" sizes when possible, and use small plates and bowls at home.
"Study after study has shown that low-calorie diets – 1,000-1,200 kcal/day for women and 1,200-1,600 kcal/day for men are the most successful for maintaining weight loss in the long term," Dr. Botsford said. "Adherence is a big thing when it comes to diets. The most common thing is that people stop. They can’t stick with it. Low glycemic load may help adherence. That’s still within the context of a low-calorie diet. There is certain evidence that having more fiber and more protein will make you feel fuller along the way, but in the end, a low-calorie diet is best."
Tools that can help patients keep a handle on food intake include the AAFP\'s initiative Americans in Motion Healthy Interventions and smartphone apps such as Lose It!, Calorie Counter and Diet Tracker by MyFitnessPal.com, healthfinder.gov, and Weight Watchers Mobile. "Exercise alone is better than nothing, but it only translates into a small weight loss," Dr. Botsford said. "However, exercise reduces blood pressure, triglycerides, and fasting glucose, and it decreases abdominal adipose tissue. To make the real difference you need exercise and diet. You also improve your strength, balance, and peak oxygen consumption. The more intense your exercise, [the more] you will increase your weight loss."
Medicare will reimburse for obesity counseling, but the patient’s BMI has to be greater than 30 kg/m2; the patient has to be competent and alert, and the counseling has to be done in a primary care setting or by the primary care provider. "Medicare will cover up to 22 visits in 12 months in a staged way," Dr. Botsford said, noting that the ICD-9 code for a BMI of 30 or more is G0447. "For the first month they’ll cover once a week. The only caveat is that you cannot bill for any other services on the same day as the visit for obesity counseling."
Dr. Botsford said she had no relevant financial conflicts to disclose.
EXPERT ANALYSIS FROM THE AAFP SCIENTIFIC ASSEMBLY
