User login
University of Washington, Harvard ranked top medical schools for second year
It may seem like déjà vu, as not much has changed regarding the rankings of top U.S. medical schools over the past 2 years.
The University of Washington, Seattle retained its ranking from the U.S. News & World Report as the top medical school for primary care for 2023. Also repeating its 2022 standing as the top medical school for research is Harvard University.
In the primary care ranking, the top 10 schools after the University of Washington were the University of California, San Francisco; the University of Minnesota; Oregon Health and Science University; the University of North Carolina at Chapel Hill; the University of Colorado; the University of Nebraska Medical Center; the University of California, Davis; and Harvard. Three schools tied for the no. 10 slot: the University of Kansas Medical Center, the University of Massachusetts Chan Medical Center, and the University of Pittsburgh.
The top five schools with the most graduates practicing in primary care specialties are Des Moines University, Iowa (50.6%); the University of Pikeville (Ky.) (46.8%); Western University of Health Sciences, Pomona, California (46%); William Carey University College of Osteopathic Medicine, Hattiesburg, Mississippi (44.7%); and A.T. Still University of Health Sciences, Kirksville, Missouri (44.3%).
Best for research
When it comes to schools ranking the highest for research, the Grossman School of Medicine at New York University takes the no. 2 spot after Harvard. Three schools were tied for the no. 3 spot: Columbia University, Johns Hopkins University, and the University of California, San Francisco; and two schools for no. 6: Duke University and the Perelman School of Medicine at the University of Pennsylvania, Philadelphia. No. 8 goes to Stanford University, followed by the University of Washington. Rounding out the top 10 is Yale University.
Specialty ranks
The top-ranked schools in eight specialties are as follows:
- Anesthesiology: Harvard
- Family medicine: the University of Washington
- Internal medicine: Johns Hopkins
- Obstetrics/gynecology: Harvard
- Pediatrics: the University of Pennsylvania (Perelman)
- Psychiatry: Harvard
- Radiology: Johns Hopkins
- Surgery: Harvard
Most diverse student body
If you’re looking for a school with significant minority representation, Howard University, Washington, D.C., ranked highest (76.8%), followed by the Wertheim College of Medicine at Florida International University, Miami (43.2%). The University of California, Davis (40%), Sacramento, California, and the University of Vermont (Larner), Burlington (14.1%), tied for third.
Three southern schools take top honors for the most graduates practicing in underserved areas, starting with the University of South Carolina (70.9%), followed by the University of Mississippi (66.2%), and East Tennessee State University (Quillen), Johnson City, Tennessee (65.8%).
The colleges with the most graduates practicing in rural areas are William Carey University College of Osteopathic Medicine (28%), the University of Pikesville (25.6%), and the University of Mississippi (22.1%).
College debt
The medical school where graduates have the most debt is Nova Southeastern University Patel College of Osteopathic Medicine, Fort Lauderdale, Florida. Graduates incurred an average debt of $309,206. Western University of Health Sciences graduates racked up $276,840 in debt, followed by graduates of West Virginia School of Osteopathic Medicine, owing $268,416.
Ranking criteria
Each year, U.S. News ranks hundreds of U.S. colleges and universities. Medical schools fall under the rankings for best graduate schools.
U.S. News surveyed 192 medical and osteopathic schools accredited in 2021 by the Liaison Committee on Medical Education or the American Osteopathic Association. Among the schools surveyed in fall 2021 and early 2022, 130 schools responded. Of those, 124 were included in both the research and primary care rankings.
The criteria for ranking include faculty resources, academic achievements of entering students, and qualitative assessments by schools and residency directors.
A version of this article first appeared on Medscape.com.
It may seem like déjà vu, as not much has changed regarding the rankings of top U.S. medical schools over the past 2 years.
The University of Washington, Seattle retained its ranking from the U.S. News & World Report as the top medical school for primary care for 2023. Also repeating its 2022 standing as the top medical school for research is Harvard University.
In the primary care ranking, the top 10 schools after the University of Washington were the University of California, San Francisco; the University of Minnesota; Oregon Health and Science University; the University of North Carolina at Chapel Hill; the University of Colorado; the University of Nebraska Medical Center; the University of California, Davis; and Harvard. Three schools tied for the no. 10 slot: the University of Kansas Medical Center, the University of Massachusetts Chan Medical Center, and the University of Pittsburgh.
The top five schools with the most graduates practicing in primary care specialties are Des Moines University, Iowa (50.6%); the University of Pikeville (Ky.) (46.8%); Western University of Health Sciences, Pomona, California (46%); William Carey University College of Osteopathic Medicine, Hattiesburg, Mississippi (44.7%); and A.T. Still University of Health Sciences, Kirksville, Missouri (44.3%).
Best for research
When it comes to schools ranking the highest for research, the Grossman School of Medicine at New York University takes the no. 2 spot after Harvard. Three schools were tied for the no. 3 spot: Columbia University, Johns Hopkins University, and the University of California, San Francisco; and two schools for no. 6: Duke University and the Perelman School of Medicine at the University of Pennsylvania, Philadelphia. No. 8 goes to Stanford University, followed by the University of Washington. Rounding out the top 10 is Yale University.
Specialty ranks
The top-ranked schools in eight specialties are as follows:
- Anesthesiology: Harvard
- Family medicine: the University of Washington
- Internal medicine: Johns Hopkins
- Obstetrics/gynecology: Harvard
- Pediatrics: the University of Pennsylvania (Perelman)
- Psychiatry: Harvard
- Radiology: Johns Hopkins
- Surgery: Harvard
Most diverse student body
If you’re looking for a school with significant minority representation, Howard University, Washington, D.C., ranked highest (76.8%), followed by the Wertheim College of Medicine at Florida International University, Miami (43.2%). The University of California, Davis (40%), Sacramento, California, and the University of Vermont (Larner), Burlington (14.1%), tied for third.
Three southern schools take top honors for the most graduates practicing in underserved areas, starting with the University of South Carolina (70.9%), followed by the University of Mississippi (66.2%), and East Tennessee State University (Quillen), Johnson City, Tennessee (65.8%).
The colleges with the most graduates practicing in rural areas are William Carey University College of Osteopathic Medicine (28%), the University of Pikesville (25.6%), and the University of Mississippi (22.1%).
College debt
The medical school where graduates have the most debt is Nova Southeastern University Patel College of Osteopathic Medicine, Fort Lauderdale, Florida. Graduates incurred an average debt of $309,206. Western University of Health Sciences graduates racked up $276,840 in debt, followed by graduates of West Virginia School of Osteopathic Medicine, owing $268,416.
Ranking criteria
Each year, U.S. News ranks hundreds of U.S. colleges and universities. Medical schools fall under the rankings for best graduate schools.
U.S. News surveyed 192 medical and osteopathic schools accredited in 2021 by the Liaison Committee on Medical Education or the American Osteopathic Association. Among the schools surveyed in fall 2021 and early 2022, 130 schools responded. Of those, 124 were included in both the research and primary care rankings.
The criteria for ranking include faculty resources, academic achievements of entering students, and qualitative assessments by schools and residency directors.
A version of this article first appeared on Medscape.com.
It may seem like déjà vu, as not much has changed regarding the rankings of top U.S. medical schools over the past 2 years.
The University of Washington, Seattle retained its ranking from the U.S. News & World Report as the top medical school for primary care for 2023. Also repeating its 2022 standing as the top medical school for research is Harvard University.
In the primary care ranking, the top 10 schools after the University of Washington were the University of California, San Francisco; the University of Minnesota; Oregon Health and Science University; the University of North Carolina at Chapel Hill; the University of Colorado; the University of Nebraska Medical Center; the University of California, Davis; and Harvard. Three schools tied for the no. 10 slot: the University of Kansas Medical Center, the University of Massachusetts Chan Medical Center, and the University of Pittsburgh.
The top five schools with the most graduates practicing in primary care specialties are Des Moines University, Iowa (50.6%); the University of Pikeville (Ky.) (46.8%); Western University of Health Sciences, Pomona, California (46%); William Carey University College of Osteopathic Medicine, Hattiesburg, Mississippi (44.7%); and A.T. Still University of Health Sciences, Kirksville, Missouri (44.3%).
Best for research
When it comes to schools ranking the highest for research, the Grossman School of Medicine at New York University takes the no. 2 spot after Harvard. Three schools were tied for the no. 3 spot: Columbia University, Johns Hopkins University, and the University of California, San Francisco; and two schools for no. 6: Duke University and the Perelman School of Medicine at the University of Pennsylvania, Philadelphia. No. 8 goes to Stanford University, followed by the University of Washington. Rounding out the top 10 is Yale University.
Specialty ranks
The top-ranked schools in eight specialties are as follows:
- Anesthesiology: Harvard
- Family medicine: the University of Washington
- Internal medicine: Johns Hopkins
- Obstetrics/gynecology: Harvard
- Pediatrics: the University of Pennsylvania (Perelman)
- Psychiatry: Harvard
- Radiology: Johns Hopkins
- Surgery: Harvard
Most diverse student body
If you’re looking for a school with significant minority representation, Howard University, Washington, D.C., ranked highest (76.8%), followed by the Wertheim College of Medicine at Florida International University, Miami (43.2%). The University of California, Davis (40%), Sacramento, California, and the University of Vermont (Larner), Burlington (14.1%), tied for third.
Three southern schools take top honors for the most graduates practicing in underserved areas, starting with the University of South Carolina (70.9%), followed by the University of Mississippi (66.2%), and East Tennessee State University (Quillen), Johnson City, Tennessee (65.8%).
The colleges with the most graduates practicing in rural areas are William Carey University College of Osteopathic Medicine (28%), the University of Pikesville (25.6%), and the University of Mississippi (22.1%).
College debt
The medical school where graduates have the most debt is Nova Southeastern University Patel College of Osteopathic Medicine, Fort Lauderdale, Florida. Graduates incurred an average debt of $309,206. Western University of Health Sciences graduates racked up $276,840 in debt, followed by graduates of West Virginia School of Osteopathic Medicine, owing $268,416.
Ranking criteria
Each year, U.S. News ranks hundreds of U.S. colleges and universities. Medical schools fall under the rankings for best graduate schools.
U.S. News surveyed 192 medical and osteopathic schools accredited in 2021 by the Liaison Committee on Medical Education or the American Osteopathic Association. Among the schools surveyed in fall 2021 and early 2022, 130 schools responded. Of those, 124 were included in both the research and primary care rankings.
The criteria for ranking include faculty resources, academic achievements of entering students, and qualitative assessments by schools and residency directors.
A version of this article first appeared on Medscape.com.
Better survival in older cancer patients who take metformin
according to results of a retrospective study of patients with type 2 diabetes and stage IV cancer.
The analysis included 7,725 patients with lung, breast, colorectal, prostate, or pancreatic cancer identified through a search of a Surveillance, Epidemiology, and End Results (SEER)-Medicare dataset from 2007 to 2016.
Out of the full dataset, 2,981 patients (38.5%) had been prescribed metformin, and use was highest among patients with prostate cancer (46%).
Patients who took metformin versus those who did not had significantly better overall survival in both unadjusted (unadjusted hazard ratio [HR], 0.73; 95% confidence interval [CI], 0.69-0.76; P < .001) and adjusted models (adjusted HR, 0.77; 95% CI, 0.73-0.81; P < .001).
Lead author Lisa Scarton, PhD, RN, assistant professor, University of Florida College of Nursing, Gainesville, said that the “underlying mechanisms of metformin related to cancer are still not completely understood,” but many studies have shown metformin is associated with a reduction in the incidence of cancer, a reduction in cancer mortality, and an improvement in overall survival.
“As more evidence of anticancer benefit of metformin is emerging, it is important to explore optimal dosages that significantly improve cancer outcomes to boost anticancer effect,” she said in an interview.
Dr. Scarton presented the new data in a poster at the annual meeting of the American Association for Cancer Research.
The analysis found no significant difference in overall survival between patients who took metformin with average daily doses ≥ 1,000 mg or < 1,000 mg (aHR, 1.00; 95% CI, 0.93-1.08; P = .90).
Although the improvement in overall survival was seen in cancer subgroups, regardless of dose, Dr. Scarton noted the benefit was greatest among patients with breast cancer (aHR, 0.67; 95% CI, 0.56-0.82; P < .001). Hazard ratios among those who received metformin were 0.78 (95% CI, 0.69-0.88; P < .001) for colorectal cancer, 0.77 (95% CI, 0.72-0.82; P < .001) for lung cancer, 0.82 (95% CI, 0.72-0.93; P < .001) for pancreatic cancer, and 0.74 (95% CI, 0.62-0.88; P = .002) for prostate cancer. Also, she noted that race/ethnicity did not play a role as a significant factor for predicting better overall survival.
Among study limitations, Dr. Scarton said, was the advanced age of patients. “Our study population was 66 and older. It would be interesting to investigate this relationship among younger adults. We would also explore explicit benefits of metformin use in different racial and ethnic groups.”
The study was funded by the University of Florida. Dr. Scarton has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to results of a retrospective study of patients with type 2 diabetes and stage IV cancer.
The analysis included 7,725 patients with lung, breast, colorectal, prostate, or pancreatic cancer identified through a search of a Surveillance, Epidemiology, and End Results (SEER)-Medicare dataset from 2007 to 2016.
Out of the full dataset, 2,981 patients (38.5%) had been prescribed metformin, and use was highest among patients with prostate cancer (46%).
Patients who took metformin versus those who did not had significantly better overall survival in both unadjusted (unadjusted hazard ratio [HR], 0.73; 95% confidence interval [CI], 0.69-0.76; P < .001) and adjusted models (adjusted HR, 0.77; 95% CI, 0.73-0.81; P < .001).
Lead author Lisa Scarton, PhD, RN, assistant professor, University of Florida College of Nursing, Gainesville, said that the “underlying mechanisms of metformin related to cancer are still not completely understood,” but many studies have shown metformin is associated with a reduction in the incidence of cancer, a reduction in cancer mortality, and an improvement in overall survival.
“As more evidence of anticancer benefit of metformin is emerging, it is important to explore optimal dosages that significantly improve cancer outcomes to boost anticancer effect,” she said in an interview.
Dr. Scarton presented the new data in a poster at the annual meeting of the American Association for Cancer Research.
The analysis found no significant difference in overall survival between patients who took metformin with average daily doses ≥ 1,000 mg or < 1,000 mg (aHR, 1.00; 95% CI, 0.93-1.08; P = .90).
Although the improvement in overall survival was seen in cancer subgroups, regardless of dose, Dr. Scarton noted the benefit was greatest among patients with breast cancer (aHR, 0.67; 95% CI, 0.56-0.82; P < .001). Hazard ratios among those who received metformin were 0.78 (95% CI, 0.69-0.88; P < .001) for colorectal cancer, 0.77 (95% CI, 0.72-0.82; P < .001) for lung cancer, 0.82 (95% CI, 0.72-0.93; P < .001) for pancreatic cancer, and 0.74 (95% CI, 0.62-0.88; P = .002) for prostate cancer. Also, she noted that race/ethnicity did not play a role as a significant factor for predicting better overall survival.
Among study limitations, Dr. Scarton said, was the advanced age of patients. “Our study population was 66 and older. It would be interesting to investigate this relationship among younger adults. We would also explore explicit benefits of metformin use in different racial and ethnic groups.”
The study was funded by the University of Florida. Dr. Scarton has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to results of a retrospective study of patients with type 2 diabetes and stage IV cancer.
The analysis included 7,725 patients with lung, breast, colorectal, prostate, or pancreatic cancer identified through a search of a Surveillance, Epidemiology, and End Results (SEER)-Medicare dataset from 2007 to 2016.
Out of the full dataset, 2,981 patients (38.5%) had been prescribed metformin, and use was highest among patients with prostate cancer (46%).
Patients who took metformin versus those who did not had significantly better overall survival in both unadjusted (unadjusted hazard ratio [HR], 0.73; 95% confidence interval [CI], 0.69-0.76; P < .001) and adjusted models (adjusted HR, 0.77; 95% CI, 0.73-0.81; P < .001).
Lead author Lisa Scarton, PhD, RN, assistant professor, University of Florida College of Nursing, Gainesville, said that the “underlying mechanisms of metformin related to cancer are still not completely understood,” but many studies have shown metformin is associated with a reduction in the incidence of cancer, a reduction in cancer mortality, and an improvement in overall survival.
“As more evidence of anticancer benefit of metformin is emerging, it is important to explore optimal dosages that significantly improve cancer outcomes to boost anticancer effect,” she said in an interview.
Dr. Scarton presented the new data in a poster at the annual meeting of the American Association for Cancer Research.
The analysis found no significant difference in overall survival between patients who took metformin with average daily doses ≥ 1,000 mg or < 1,000 mg (aHR, 1.00; 95% CI, 0.93-1.08; P = .90).
Although the improvement in overall survival was seen in cancer subgroups, regardless of dose, Dr. Scarton noted the benefit was greatest among patients with breast cancer (aHR, 0.67; 95% CI, 0.56-0.82; P < .001). Hazard ratios among those who received metformin were 0.78 (95% CI, 0.69-0.88; P < .001) for colorectal cancer, 0.77 (95% CI, 0.72-0.82; P < .001) for lung cancer, 0.82 (95% CI, 0.72-0.93; P < .001) for pancreatic cancer, and 0.74 (95% CI, 0.62-0.88; P = .002) for prostate cancer. Also, she noted that race/ethnicity did not play a role as a significant factor for predicting better overall survival.
Among study limitations, Dr. Scarton said, was the advanced age of patients. “Our study population was 66 and older. It would be interesting to investigate this relationship among younger adults. We would also explore explicit benefits of metformin use in different racial and ethnic groups.”
The study was funded by the University of Florida. Dr. Scarton has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AACR 2022
COVID-19 cardiovascular complications in children: AHA statement
Cardiovascular complications are uncommon for children and young adults after COVID-19 disease or SARS-CoV-2 infection, according to a new scientific statement from the American Heart Association.
However, the infection can cause some children and young people to experience arrhythmias, myocarditis, pericarditis, or multisystem inflammatory syndrome (MIS-C), a new condition identified during the pandemic, it notes.
The statement details what has been learned about how to treat, manage, and prevent cardiovascular complications associated with COVID-19 in children and young adults and calls for more research, including studies following the short- and long-term cardiovascular effects.
It also reports that COVID-19 vaccines have been found to prevent severe COVID-19 disease and decrease the risk of developing MIS-C by 91% among children ages 12-18 years.
On returning to sports, it says data suggest it is safe for young people with mild or asymptomatic COVID-19 to resume exercise after recovery from symptoms. For those with more serious infections, it recommends additional tests, including cardiac enzyme levels, electrocardiogram, and echocardiogram, before returning to sports or strenuous physical exercise.
The scientific statement was published online on in Circulation.
“Two years into the pandemic and with vast amounts of research conducted in children with COVID-19, this statement summarizes what we know so far related to COVID-19 in children,” said chair of the statement writing group Pei-Ni Jone, MD, from the Children’s Hospital Colorado, Aurora.
Analysis of the latest research indicates children generally have mild symptoms from SARS-CoV-2 infection. In the U.S., as of Feb. 24, 2022, children under 18 years of age have accounted for 17.6% of total COVID-19 cases and about 0.1% of deaths from the virus, the report states.
In addition, young adults, ages 18-29 years, have accounted for 21.3% of cases and 0.8% of deaths from COVID-19.
Like adults, children with underlying medical conditions such as chronic lung disease or obesity and those who are immunocompromised are more likely to be hospitalized, to be admitted to an intensive care unit, and to die of COVID-19, the statement notes. There are conflicting reports on the risk of severe COVID-19 in children and young adults with congenital heart disease, with some reports suggesting a slightly increased risk of severe COVID-19.
In terms of cardiovascular complications of COVID-19 in children, arrhythmias have included ventricular tachycardia and atrial tachycardia, as well as first-degree atrioventricular block. Although arrhythmias generally self-resolve without the need for treatment, prophylactic antiarrhythmics have been administered in some cases, and death caused by recurrent ventricular tachycardia in an adolescent with hypertrophic cardiomyopathy has been described.
Elevations of troponin, electrocardiographic abnormalities, including ST-segment changes, and delayed gadolinium enhancement on cardiac magnetic resonance imaging have been seen in those with myocardial involvement. Although death is rare, both sudden cardiac death and death after intensive medical and supportive therapies have occurred in children with severe myocardial involvement.
In a large retrospective pediatric case series of SARS-CoV-2–associated deaths in individuals under 21 years of age, the median age at death was 17 years, 63% were male, 28% were Black, and 46% were Hispanic. Of those who died, 86% had a comorbid condition, with obesity (42%) and asthma (29%) being the most common.
But the report concludes that: “Although children with comorbidities are at increased risk for symptomatic SARS-CoV-2 infection, compared with healthy children, cardiovascular complications, severe illness, and death are uncommon.”
MIS-C: Rare but severe
The authors of the statement explain that children and some young adults may develop MIS-C, a relatively rare but severe inflammatory syndrome generally occurring 2-6 weeks after infection with SARS-CoV-2 that can affect the heart and multiple organ systems.
In the first year of the pandemic, more than 2,600 cases of MIS-C were reported to the Centers for Disease Control and Prevention, at an estimated rate of 1 case per 3,164 cases of SARS-CoV-2 infection in children, with MIS-C disproportionately affecting Hispanic and Black children.
As many as 50% of children with MIS-C have myocardial involvement, including decreased left ventricular function, coronary artery dilation or aneurysms, myocarditis, elevated troponin and BNP or NT-proBNP, or pericardial effusion. Acute-phase reactants, including C-reactive protein, D-dimer, ferritin, and fibrinogen, can be significantly elevated in MIS-C, neutrophil/lymphocyte ratio may be higher, and platelet counts lower than those with non–MIS-C febrile illnesses.
Fortunately, the outcome of MIS-C is generally very good, with resolution of inflammation and cardiovascular abnormalities within 1-4 weeks of diagnosis, the report says.
However, there have been reports of progression of coronary artery aneurysms after discharge, highlighting the potential for long-term complications. Death resulting from MIS-C is rare, with a mortality rate of 1.4%-1.9%.
Compared with children and young adults who died of acute SARS-CoV-2 infection, most of the fatalities from MIS-C were in previously healthy individuals without comorbidities.
The authors recommend structured follow-up of patients with MIS-C because of concern about progression of cardiac complications and an unclear long-term prognosis.
The statement notes that the first-line treatment for MIS-C is typically intravenous immunoglobulin (IVIG) and patients with poor ventricular function may need to have IVIG in divided doses to tolerate the fluid load.
Supportive treatment for heart failure and vasoplegic shock often requires aggressive management in an ICU for administration of inotropes and vasoactive medications. Antiplatelet therapy with low-dose aspirin is considered in patients with coronary artery involvement, and anticoagulation is added, depending on the degree of coronary artery dilation.
COVID-19 vaccination
The statement notes that vaccines can prevent patients from getting COVID-19 and decrease the risk of MIS-C by 91% among children 12-18 years of age.
On vaccine-associated myocarditis, it concludes the benefits of getting the vaccines outweigh the risks.
For example, for every 1 million doses of the mRNA COVID-19 vaccines in males ages 12-29 years (the highest risk group for vaccine-associated myocarditis), it is estimated that 11,000 COVID-19 cases, 560 hospitalizations, and six deaths would be prevented, whereas 39-47 cases of myocarditis would be expected.
But it adds that the CDC is continuing to follow myocarditis in children and young adults closely, particularly a possible connection to the mRNA COVID-19 vaccines.
The statement says that more research is needed to better understand the mechanisms and optimal treatment approaches for SARS-CoV-2 infection, vaccine-associated myocarditis, the long-term outcomes of both COVID-19 and MIS-C, and the impact of these various conditions on the heart in children and young adults. In addition, any new antiviral therapies need to be tested in clinical trials focused on children.
“Although much has been learned about how the virus impacts children’s and young adult’s hearts, how to best treat cardiovascular complications, and prevent severe illness, continued clinical research trials are needed to better understand the long-term cardiovascular impacts,” Dr. Jone said. “It is also important to address health disparities that have become more apparent during the pandemic. We must work to ensure all children receive equal access to vaccination and high-quality care.”
A version of this article first appeared on Medscape.com.
Cardiovascular complications are uncommon for children and young adults after COVID-19 disease or SARS-CoV-2 infection, according to a new scientific statement from the American Heart Association.
However, the infection can cause some children and young people to experience arrhythmias, myocarditis, pericarditis, or multisystem inflammatory syndrome (MIS-C), a new condition identified during the pandemic, it notes.
The statement details what has been learned about how to treat, manage, and prevent cardiovascular complications associated with COVID-19 in children and young adults and calls for more research, including studies following the short- and long-term cardiovascular effects.
It also reports that COVID-19 vaccines have been found to prevent severe COVID-19 disease and decrease the risk of developing MIS-C by 91% among children ages 12-18 years.
On returning to sports, it says data suggest it is safe for young people with mild or asymptomatic COVID-19 to resume exercise after recovery from symptoms. For those with more serious infections, it recommends additional tests, including cardiac enzyme levels, electrocardiogram, and echocardiogram, before returning to sports or strenuous physical exercise.
The scientific statement was published online on in Circulation.
“Two years into the pandemic and with vast amounts of research conducted in children with COVID-19, this statement summarizes what we know so far related to COVID-19 in children,” said chair of the statement writing group Pei-Ni Jone, MD, from the Children’s Hospital Colorado, Aurora.
Analysis of the latest research indicates children generally have mild symptoms from SARS-CoV-2 infection. In the U.S., as of Feb. 24, 2022, children under 18 years of age have accounted for 17.6% of total COVID-19 cases and about 0.1% of deaths from the virus, the report states.
In addition, young adults, ages 18-29 years, have accounted for 21.3% of cases and 0.8% of deaths from COVID-19.
Like adults, children with underlying medical conditions such as chronic lung disease or obesity and those who are immunocompromised are more likely to be hospitalized, to be admitted to an intensive care unit, and to die of COVID-19, the statement notes. There are conflicting reports on the risk of severe COVID-19 in children and young adults with congenital heart disease, with some reports suggesting a slightly increased risk of severe COVID-19.
In terms of cardiovascular complications of COVID-19 in children, arrhythmias have included ventricular tachycardia and atrial tachycardia, as well as first-degree atrioventricular block. Although arrhythmias generally self-resolve without the need for treatment, prophylactic antiarrhythmics have been administered in some cases, and death caused by recurrent ventricular tachycardia in an adolescent with hypertrophic cardiomyopathy has been described.
Elevations of troponin, electrocardiographic abnormalities, including ST-segment changes, and delayed gadolinium enhancement on cardiac magnetic resonance imaging have been seen in those with myocardial involvement. Although death is rare, both sudden cardiac death and death after intensive medical and supportive therapies have occurred in children with severe myocardial involvement.
In a large retrospective pediatric case series of SARS-CoV-2–associated deaths in individuals under 21 years of age, the median age at death was 17 years, 63% were male, 28% were Black, and 46% were Hispanic. Of those who died, 86% had a comorbid condition, with obesity (42%) and asthma (29%) being the most common.
But the report concludes that: “Although children with comorbidities are at increased risk for symptomatic SARS-CoV-2 infection, compared with healthy children, cardiovascular complications, severe illness, and death are uncommon.”
MIS-C: Rare but severe
The authors of the statement explain that children and some young adults may develop MIS-C, a relatively rare but severe inflammatory syndrome generally occurring 2-6 weeks after infection with SARS-CoV-2 that can affect the heart and multiple organ systems.
In the first year of the pandemic, more than 2,600 cases of MIS-C were reported to the Centers for Disease Control and Prevention, at an estimated rate of 1 case per 3,164 cases of SARS-CoV-2 infection in children, with MIS-C disproportionately affecting Hispanic and Black children.
As many as 50% of children with MIS-C have myocardial involvement, including decreased left ventricular function, coronary artery dilation or aneurysms, myocarditis, elevated troponin and BNP or NT-proBNP, or pericardial effusion. Acute-phase reactants, including C-reactive protein, D-dimer, ferritin, and fibrinogen, can be significantly elevated in MIS-C, neutrophil/lymphocyte ratio may be higher, and platelet counts lower than those with non–MIS-C febrile illnesses.
Fortunately, the outcome of MIS-C is generally very good, with resolution of inflammation and cardiovascular abnormalities within 1-4 weeks of diagnosis, the report says.
However, there have been reports of progression of coronary artery aneurysms after discharge, highlighting the potential for long-term complications. Death resulting from MIS-C is rare, with a mortality rate of 1.4%-1.9%.
Compared with children and young adults who died of acute SARS-CoV-2 infection, most of the fatalities from MIS-C were in previously healthy individuals without comorbidities.
The authors recommend structured follow-up of patients with MIS-C because of concern about progression of cardiac complications and an unclear long-term prognosis.
The statement notes that the first-line treatment for MIS-C is typically intravenous immunoglobulin (IVIG) and patients with poor ventricular function may need to have IVIG in divided doses to tolerate the fluid load.
Supportive treatment for heart failure and vasoplegic shock often requires aggressive management in an ICU for administration of inotropes and vasoactive medications. Antiplatelet therapy with low-dose aspirin is considered in patients with coronary artery involvement, and anticoagulation is added, depending on the degree of coronary artery dilation.
COVID-19 vaccination
The statement notes that vaccines can prevent patients from getting COVID-19 and decrease the risk of MIS-C by 91% among children 12-18 years of age.
On vaccine-associated myocarditis, it concludes the benefits of getting the vaccines outweigh the risks.
For example, for every 1 million doses of the mRNA COVID-19 vaccines in males ages 12-29 years (the highest risk group for vaccine-associated myocarditis), it is estimated that 11,000 COVID-19 cases, 560 hospitalizations, and six deaths would be prevented, whereas 39-47 cases of myocarditis would be expected.
But it adds that the CDC is continuing to follow myocarditis in children and young adults closely, particularly a possible connection to the mRNA COVID-19 vaccines.
The statement says that more research is needed to better understand the mechanisms and optimal treatment approaches for SARS-CoV-2 infection, vaccine-associated myocarditis, the long-term outcomes of both COVID-19 and MIS-C, and the impact of these various conditions on the heart in children and young adults. In addition, any new antiviral therapies need to be tested in clinical trials focused on children.
“Although much has been learned about how the virus impacts children’s and young adult’s hearts, how to best treat cardiovascular complications, and prevent severe illness, continued clinical research trials are needed to better understand the long-term cardiovascular impacts,” Dr. Jone said. “It is also important to address health disparities that have become more apparent during the pandemic. We must work to ensure all children receive equal access to vaccination and high-quality care.”
A version of this article first appeared on Medscape.com.
Cardiovascular complications are uncommon for children and young adults after COVID-19 disease or SARS-CoV-2 infection, according to a new scientific statement from the American Heart Association.
However, the infection can cause some children and young people to experience arrhythmias, myocarditis, pericarditis, or multisystem inflammatory syndrome (MIS-C), a new condition identified during the pandemic, it notes.
The statement details what has been learned about how to treat, manage, and prevent cardiovascular complications associated with COVID-19 in children and young adults and calls for more research, including studies following the short- and long-term cardiovascular effects.
It also reports that COVID-19 vaccines have been found to prevent severe COVID-19 disease and decrease the risk of developing MIS-C by 91% among children ages 12-18 years.
On returning to sports, it says data suggest it is safe for young people with mild or asymptomatic COVID-19 to resume exercise after recovery from symptoms. For those with more serious infections, it recommends additional tests, including cardiac enzyme levels, electrocardiogram, and echocardiogram, before returning to sports or strenuous physical exercise.
The scientific statement was published online on in Circulation.
“Two years into the pandemic and with vast amounts of research conducted in children with COVID-19, this statement summarizes what we know so far related to COVID-19 in children,” said chair of the statement writing group Pei-Ni Jone, MD, from the Children’s Hospital Colorado, Aurora.
Analysis of the latest research indicates children generally have mild symptoms from SARS-CoV-2 infection. In the U.S., as of Feb. 24, 2022, children under 18 years of age have accounted for 17.6% of total COVID-19 cases and about 0.1% of deaths from the virus, the report states.
In addition, young adults, ages 18-29 years, have accounted for 21.3% of cases and 0.8% of deaths from COVID-19.
Like adults, children with underlying medical conditions such as chronic lung disease or obesity and those who are immunocompromised are more likely to be hospitalized, to be admitted to an intensive care unit, and to die of COVID-19, the statement notes. There are conflicting reports on the risk of severe COVID-19 in children and young adults with congenital heart disease, with some reports suggesting a slightly increased risk of severe COVID-19.
In terms of cardiovascular complications of COVID-19 in children, arrhythmias have included ventricular tachycardia and atrial tachycardia, as well as first-degree atrioventricular block. Although arrhythmias generally self-resolve without the need for treatment, prophylactic antiarrhythmics have been administered in some cases, and death caused by recurrent ventricular tachycardia in an adolescent with hypertrophic cardiomyopathy has been described.
Elevations of troponin, electrocardiographic abnormalities, including ST-segment changes, and delayed gadolinium enhancement on cardiac magnetic resonance imaging have been seen in those with myocardial involvement. Although death is rare, both sudden cardiac death and death after intensive medical and supportive therapies have occurred in children with severe myocardial involvement.
In a large retrospective pediatric case series of SARS-CoV-2–associated deaths in individuals under 21 years of age, the median age at death was 17 years, 63% were male, 28% were Black, and 46% were Hispanic. Of those who died, 86% had a comorbid condition, with obesity (42%) and asthma (29%) being the most common.
But the report concludes that: “Although children with comorbidities are at increased risk for symptomatic SARS-CoV-2 infection, compared with healthy children, cardiovascular complications, severe illness, and death are uncommon.”
MIS-C: Rare but severe
The authors of the statement explain that children and some young adults may develop MIS-C, a relatively rare but severe inflammatory syndrome generally occurring 2-6 weeks after infection with SARS-CoV-2 that can affect the heart and multiple organ systems.
In the first year of the pandemic, more than 2,600 cases of MIS-C were reported to the Centers for Disease Control and Prevention, at an estimated rate of 1 case per 3,164 cases of SARS-CoV-2 infection in children, with MIS-C disproportionately affecting Hispanic and Black children.
As many as 50% of children with MIS-C have myocardial involvement, including decreased left ventricular function, coronary artery dilation or aneurysms, myocarditis, elevated troponin and BNP or NT-proBNP, or pericardial effusion. Acute-phase reactants, including C-reactive protein, D-dimer, ferritin, and fibrinogen, can be significantly elevated in MIS-C, neutrophil/lymphocyte ratio may be higher, and platelet counts lower than those with non–MIS-C febrile illnesses.
Fortunately, the outcome of MIS-C is generally very good, with resolution of inflammation and cardiovascular abnormalities within 1-4 weeks of diagnosis, the report says.
However, there have been reports of progression of coronary artery aneurysms after discharge, highlighting the potential for long-term complications. Death resulting from MIS-C is rare, with a mortality rate of 1.4%-1.9%.
Compared with children and young adults who died of acute SARS-CoV-2 infection, most of the fatalities from MIS-C were in previously healthy individuals without comorbidities.
The authors recommend structured follow-up of patients with MIS-C because of concern about progression of cardiac complications and an unclear long-term prognosis.
The statement notes that the first-line treatment for MIS-C is typically intravenous immunoglobulin (IVIG) and patients with poor ventricular function may need to have IVIG in divided doses to tolerate the fluid load.
Supportive treatment for heart failure and vasoplegic shock often requires aggressive management in an ICU for administration of inotropes and vasoactive medications. Antiplatelet therapy with low-dose aspirin is considered in patients with coronary artery involvement, and anticoagulation is added, depending on the degree of coronary artery dilation.
COVID-19 vaccination
The statement notes that vaccines can prevent patients from getting COVID-19 and decrease the risk of MIS-C by 91% among children 12-18 years of age.
On vaccine-associated myocarditis, it concludes the benefits of getting the vaccines outweigh the risks.
For example, for every 1 million doses of the mRNA COVID-19 vaccines in males ages 12-29 years (the highest risk group for vaccine-associated myocarditis), it is estimated that 11,000 COVID-19 cases, 560 hospitalizations, and six deaths would be prevented, whereas 39-47 cases of myocarditis would be expected.
But it adds that the CDC is continuing to follow myocarditis in children and young adults closely, particularly a possible connection to the mRNA COVID-19 vaccines.
The statement says that more research is needed to better understand the mechanisms and optimal treatment approaches for SARS-CoV-2 infection, vaccine-associated myocarditis, the long-term outcomes of both COVID-19 and MIS-C, and the impact of these various conditions on the heart in children and young adults. In addition, any new antiviral therapies need to be tested in clinical trials focused on children.
“Although much has been learned about how the virus impacts children’s and young adult’s hearts, how to best treat cardiovascular complications, and prevent severe illness, continued clinical research trials are needed to better understand the long-term cardiovascular impacts,” Dr. Jone said. “It is also important to address health disparities that have become more apparent during the pandemic. We must work to ensure all children receive equal access to vaccination and high-quality care.”
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
Study finds discrepancies in biopsy decisions, diagnoses based on skin type
BOSTON – compared with White patients, new research shows.
“Our findings suggest diagnostic biases based on skin color exist in dermatology practice,” lead author Loren Krueger, MD, assistant professor in the department of dermatology, Emory University School of Medicine, Atlanta, said at the Annual Skin of Color Society Scientific Symposium. “A lower likelihood of biopsy of malignancy in darker skin types could contribute to disparities in cutaneous malignancies,” she added.

Disparities in dermatologic care among Black patients, compared with White patients, have been well documented. Recent evidence includes a 2020 study that showed significant shortcomings among medical students in correctly diagnosing squamous cell carcinoma, urticaria, and atopic dermatitis for patients with skin of color.
“It’s no secret that our images do not accurately or in the right quantity include skin of color,” Dr. Krueger said. “Yet few papers talk about how these biases actually impact our care. Importantly, this study demonstrates that diagnostic bias develops as early as the medical student level.”
To further investigate the role of skin color in the assessment of neoplastic and inflammatory skin conditions and decisions to perform biopsy, Dr. Krueger and her colleagues surveyed 144 dermatology residents and attending dermatologists to evaluate their clinical decisionmaking skills in assessing skin conditions for patients with lighter skin and those with darker skin. Almost 80% (113) provided complete responses and were included in the study.
For the survey, participants were shown photos of 10 neoplastic and 10 inflammatory skin conditions. Each image was matched in lighter (skin types I-II) and darker (skin types IV-VI) skinned patients in random order. Participants were asked to identify the suspected underlying etiology (neoplastic–benign, neoplastic–malignant, papulosquamous, lichenoid, infectious, bullous, or no suspected etiology) and whether they would choose to perform biopsy for the pictured condition.
Overall, their responses showed a slightly higher probability of recommending a biopsy for patients with skin types IV-V (odds ratio, 1.18; P = .054).
However, respondents were more than twice as likely to recommend a biopsy for benign neoplasms for patients with skin of color, compared with those with lighter skin types (OR, 2.57; P < .0001). They were significantly less likely to recommend a biopsy for a malignant neoplasm for patients with skin of color (OR, 0.42; P < .0001).
In addition, the correct etiology was much more commonly missed in diagnosing patients with skin of color, even after adjusting for years in dermatology practice (OR, 0.569; P < .0001).
Conversely, respondents were significantly less likely to recommend a biopsy for benign neoplasms and were more likely to recommend a biopsy for malignant neoplasms among White patients. Etiology was more commonly correct.
The findings underscore that “for skin of color patients, you’re more likely to have a benign neoplasm biopsied, you’re less likely to have a malignant neoplasm biopsied, and more often, your etiology may be missed,” Dr. Krueger said at the meeting.
Of note, while 45% of respondents were dermatology residents or fellows, 20.4% had 1-5 years of experience, and about 28% had 10 to more than 25 years of experience.
And while 75% of the dermatology residents, fellows, and attendings were White, there was no difference in the probability of correctly identifying the underlying etiology in dark or light skin types based on the provider’s self-identified race.
Importantly, the patterns in the study of diagnostic discrepancies are reflected in broader dermatologic outcomes. The 5-year melanoma survival rate is 74.1% among Black patients and 92.9% among White patients. Dr. Krueger referred to data showing that only 52.6% of Black patients have stage I melanoma at diagnosis, whereas among White patients, the rate is much higher, at 75.9%.
“We know skin malignancy can be more aggressive and late-stage in skin of color populations, leading to increased morbidity and later stage at initial diagnosis,” Dr. Krueger told this news organization. “We routinely attribute this to limited access to care and lack of awareness on skin malignancy. However, we have no evidence on how we, as dermatologists, may be playing a role.”
Furthermore, the decision to perform biopsy or not can affect the size and stage at diagnosis of a cutaneous malignancy, she noted.
Key changes needed to prevent the disparities – and their implications – should start at the training level, she emphasized. “I would love to see increased photo representation in training materials – this is a great place to start,” Dr. Krueger said.
In addition, “encouraging medical students, residents, and dermatologists to learn from skin of color experts is vital,” she said. “We should also provide hands-on experience and training with diverse patient populations.”
The first step to addressing biases “is to acknowledge they exist,” Dr. Krueger added. “I am hopeful this inspires others to continue to investigate these biases, as well as how we can eliminate them.”
The study was funded by the Rudin Resident Research Award. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – compared with White patients, new research shows.
“Our findings suggest diagnostic biases based on skin color exist in dermatology practice,” lead author Loren Krueger, MD, assistant professor in the department of dermatology, Emory University School of Medicine, Atlanta, said at the Annual Skin of Color Society Scientific Symposium. “A lower likelihood of biopsy of malignancy in darker skin types could contribute to disparities in cutaneous malignancies,” she added.
Disparities in dermatologic care among Black patients, compared with White patients, have been well documented. Recent evidence includes a 2020 study that showed significant shortcomings among medical students in correctly diagnosing squamous cell carcinoma, urticaria, and atopic dermatitis for patients with skin of color.
“It’s no secret that our images do not accurately or in the right quantity include skin of color,” Dr. Krueger said. “Yet few papers talk about how these biases actually impact our care. Importantly, this study demonstrates that diagnostic bias develops as early as the medical student level.”
To further investigate the role of skin color in the assessment of neoplastic and inflammatory skin conditions and decisions to perform biopsy, Dr. Krueger and her colleagues surveyed 144 dermatology residents and attending dermatologists to evaluate their clinical decisionmaking skills in assessing skin conditions for patients with lighter skin and those with darker skin. Almost 80% (113) provided complete responses and were included in the study.
For the survey, participants were shown photos of 10 neoplastic and 10 inflammatory skin conditions. Each image was matched in lighter (skin types I-II) and darker (skin types IV-VI) skinned patients in random order. Participants were asked to identify the suspected underlying etiology (neoplastic–benign, neoplastic–malignant, papulosquamous, lichenoid, infectious, bullous, or no suspected etiology) and whether they would choose to perform biopsy for the pictured condition.
Overall, their responses showed a slightly higher probability of recommending a biopsy for patients with skin types IV-V (odds ratio, 1.18; P = .054).
However, respondents were more than twice as likely to recommend a biopsy for benign neoplasms for patients with skin of color, compared with those with lighter skin types (OR, 2.57; P < .0001). They were significantly less likely to recommend a biopsy for a malignant neoplasm for patients with skin of color (OR, 0.42; P < .0001).
In addition, the correct etiology was much more commonly missed in diagnosing patients with skin of color, even after adjusting for years in dermatology practice (OR, 0.569; P < .0001).
Conversely, respondents were significantly less likely to recommend a biopsy for benign neoplasms and were more likely to recommend a biopsy for malignant neoplasms among White patients. Etiology was more commonly correct.
The findings underscore that “for skin of color patients, you’re more likely to have a benign neoplasm biopsied, you’re less likely to have a malignant neoplasm biopsied, and more often, your etiology may be missed,” Dr. Krueger said at the meeting.
Of note, while 45% of respondents were dermatology residents or fellows, 20.4% had 1-5 years of experience, and about 28% had 10 to more than 25 years of experience.
And while 75% of the dermatology residents, fellows, and attendings were White, there was no difference in the probability of correctly identifying the underlying etiology in dark or light skin types based on the provider’s self-identified race.
Importantly, the patterns in the study of diagnostic discrepancies are reflected in broader dermatologic outcomes. The 5-year melanoma survival rate is 74.1% among Black patients and 92.9% among White patients. Dr. Krueger referred to data showing that only 52.6% of Black patients have stage I melanoma at diagnosis, whereas among White patients, the rate is much higher, at 75.9%.
“We know skin malignancy can be more aggressive and late-stage in skin of color populations, leading to increased morbidity and later stage at initial diagnosis,” Dr. Krueger told this news organization. “We routinely attribute this to limited access to care and lack of awareness on skin malignancy. However, we have no evidence on how we, as dermatologists, may be playing a role.”
Furthermore, the decision to perform biopsy or not can affect the size and stage at diagnosis of a cutaneous malignancy, she noted.
Key changes needed to prevent the disparities – and their implications – should start at the training level, she emphasized. “I would love to see increased photo representation in training materials – this is a great place to start,” Dr. Krueger said.
In addition, “encouraging medical students, residents, and dermatologists to learn from skin of color experts is vital,” she said. “We should also provide hands-on experience and training with diverse patient populations.”
The first step to addressing biases “is to acknowledge they exist,” Dr. Krueger added. “I am hopeful this inspires others to continue to investigate these biases, as well as how we can eliminate them.”
The study was funded by the Rudin Resident Research Award. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – compared with White patients, new research shows.
“Our findings suggest diagnostic biases based on skin color exist in dermatology practice,” lead author Loren Krueger, MD, assistant professor in the department of dermatology, Emory University School of Medicine, Atlanta, said at the Annual Skin of Color Society Scientific Symposium. “A lower likelihood of biopsy of malignancy in darker skin types could contribute to disparities in cutaneous malignancies,” she added.
Disparities in dermatologic care among Black patients, compared with White patients, have been well documented. Recent evidence includes a 2020 study that showed significant shortcomings among medical students in correctly diagnosing squamous cell carcinoma, urticaria, and atopic dermatitis for patients with skin of color.
“It’s no secret that our images do not accurately or in the right quantity include skin of color,” Dr. Krueger said. “Yet few papers talk about how these biases actually impact our care. Importantly, this study demonstrates that diagnostic bias develops as early as the medical student level.”
To further investigate the role of skin color in the assessment of neoplastic and inflammatory skin conditions and decisions to perform biopsy, Dr. Krueger and her colleagues surveyed 144 dermatology residents and attending dermatologists to evaluate their clinical decisionmaking skills in assessing skin conditions for patients with lighter skin and those with darker skin. Almost 80% (113) provided complete responses and were included in the study.
For the survey, participants were shown photos of 10 neoplastic and 10 inflammatory skin conditions. Each image was matched in lighter (skin types I-II) and darker (skin types IV-VI) skinned patients in random order. Participants were asked to identify the suspected underlying etiology (neoplastic–benign, neoplastic–malignant, papulosquamous, lichenoid, infectious, bullous, or no suspected etiology) and whether they would choose to perform biopsy for the pictured condition.
Overall, their responses showed a slightly higher probability of recommending a biopsy for patients with skin types IV-V (odds ratio, 1.18; P = .054).
However, respondents were more than twice as likely to recommend a biopsy for benign neoplasms for patients with skin of color, compared with those with lighter skin types (OR, 2.57; P < .0001). They were significantly less likely to recommend a biopsy for a malignant neoplasm for patients with skin of color (OR, 0.42; P < .0001).
In addition, the correct etiology was much more commonly missed in diagnosing patients with skin of color, even after adjusting for years in dermatology practice (OR, 0.569; P < .0001).
Conversely, respondents were significantly less likely to recommend a biopsy for benign neoplasms and were more likely to recommend a biopsy for malignant neoplasms among White patients. Etiology was more commonly correct.
The findings underscore that “for skin of color patients, you’re more likely to have a benign neoplasm biopsied, you’re less likely to have a malignant neoplasm biopsied, and more often, your etiology may be missed,” Dr. Krueger said at the meeting.
Of note, while 45% of respondents were dermatology residents or fellows, 20.4% had 1-5 years of experience, and about 28% had 10 to more than 25 years of experience.
And while 75% of the dermatology residents, fellows, and attendings were White, there was no difference in the probability of correctly identifying the underlying etiology in dark or light skin types based on the provider’s self-identified race.
Importantly, the patterns in the study of diagnostic discrepancies are reflected in broader dermatologic outcomes. The 5-year melanoma survival rate is 74.1% among Black patients and 92.9% among White patients. Dr. Krueger referred to data showing that only 52.6% of Black patients have stage I melanoma at diagnosis, whereas among White patients, the rate is much higher, at 75.9%.
“We know skin malignancy can be more aggressive and late-stage in skin of color populations, leading to increased morbidity and later stage at initial diagnosis,” Dr. Krueger told this news organization. “We routinely attribute this to limited access to care and lack of awareness on skin malignancy. However, we have no evidence on how we, as dermatologists, may be playing a role.”
Furthermore, the decision to perform biopsy or not can affect the size and stage at diagnosis of a cutaneous malignancy, she noted.
Key changes needed to prevent the disparities – and their implications – should start at the training level, she emphasized. “I would love to see increased photo representation in training materials – this is a great place to start,” Dr. Krueger said.
In addition, “encouraging medical students, residents, and dermatologists to learn from skin of color experts is vital,” she said. “We should also provide hands-on experience and training with diverse patient populations.”
The first step to addressing biases “is to acknowledge they exist,” Dr. Krueger added. “I am hopeful this inspires others to continue to investigate these biases, as well as how we can eliminate them.”
The study was funded by the Rudin Resident Research Award. The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Preterm C-sections, induced deliveries dropped during COVID-19 pandemic
Premature births from cesarean (C-section) and induced deliveries dropped abruptly by 6.5% from the projected number in the first month of the COVID-19 pandemic and stayed at the lower rate consistently throughout the year, researchers have found.
Results of the study, led by Daniel Dench, PhD, assistant professor at the Georgia Institute of Technology School of Economics in Atlanta, were published online in Pediatrics.
The authors say their findings help answer the question of whether numbers of preterm (less than 37 weeks gestation) C-sections and induced deliveries would change if women didn’t see their physicians during pregnancy as often, especially in person, and raise the question of whether some birth interventions by physicians may not be necessary. The pandemic gave researchers a natural, ethical way to study the question.
The researchers found that in March 2020 – the start of business closures and stay-at-home orders around the country – preterm births from C-sections or induced deliveries immediately fell from the forecast number for the month by 0.4 percentage points. For the rest of 2020, the number remained on average 0.35 percentage points below the numbers predicted.
That means 350 fewer preterm C-sections and induced deliveries per 100,000 live births, or 10,000 fewer overall, the authors said.
Dr. Dench told this publication the numbers for those births had been steady from January 2010 to February 2020, but the pattern “diverges from this trend very clearly beginning exactly in March 2020 and does not return to trend by December 2020.”
Meanwhile, during the study period, the number of full-term cesarean and induced deliveries stayed steady and started to increase slightly in 2020. Researchers also adjusted for seasonality as, for example, preterm births are higher on average in February than in March.
So far, Dr. Dench said in a press release, it’s not clear whether the lower numbers mean physicians didn’t deliver babies that ended up surviving in the womb anyway or if they missed some that would die in the womb without intervention.
To better understand those implications, Dr. Dench says he is turning to fetal death records for March-December 2020 and he said he expects to have those results analyzed by the end of the year.
If there was no change in fetal deaths at the same time as the drop in preterm births, Dr. Dench said, that could point to physician interventions that may not have been necessary.
Mya R. Zapata, MD, an obstetrician-gynecologist with UCLA Health, who was not involved with the study, told this publication that checking the fetal deaths is a good start and an objective outcome in answering the question, but she points out there are other outcomes that will take a deeper analysis, such as whether there are differences later in developmental outcomes after fewer physician visits.
“It’s always a good question for health care,” she said, “are we doing more than we need to?”
Dr. Zapata is the obstetrics service chief for UCLA’s labor and delivery unit and was an integral part of decision-making as to what services were essential and for which patients. She said the fewer visits and fewer ultrasounds the researchers describe fit with what ob.gyns. at UCLA experienced as the pandemic hit.
“We really tried to hone in on people who were at highest risk for an adverse outcome,” she said. “I still have the question of whether there were things we missed in low-risk people. It will take time to get the entire answer. But it does make us reflect that perhaps less intervention could be better for patients and easier. It’s our job in medicine to keep asking the question of what is essential and safe and not just continue with current practice because that’s what we’ve always done.”
The amount of data gave the researchers an unusual view. They studied 38,891,271 singleton births in the United States from 2010 to 2020 with data from the National Center for Health Statistics.
“If you look at 1,000 births in a single hospital, or even at 30,000 births across a hospital system, you wouldn’t be able to see the drop as clearly,” Dr. Dench said. “The drop we detected is a huge change, but you might miss it in a small sample.”
The researchers acknowledge a limitation of the study is that half of all preterm C-sections and induced deliveries happen because of a ruptured membrane, a spontaneous cause. Those instances can’t be distinguished from the ones caused by doctors’ interventions in this study.
“Still, these findings are significant because the causes for preterm births are not always known,” the authors wrote in the press release.
The study authors and Dr. Zapata reported no relevant financial relationships.
Premature births from cesarean (C-section) and induced deliveries dropped abruptly by 6.5% from the projected number in the first month of the COVID-19 pandemic and stayed at the lower rate consistently throughout the year, researchers have found.
Results of the study, led by Daniel Dench, PhD, assistant professor at the Georgia Institute of Technology School of Economics in Atlanta, were published online in Pediatrics.
The authors say their findings help answer the question of whether numbers of preterm (less than 37 weeks gestation) C-sections and induced deliveries would change if women didn’t see their physicians during pregnancy as often, especially in person, and raise the question of whether some birth interventions by physicians may not be necessary. The pandemic gave researchers a natural, ethical way to study the question.
The researchers found that in March 2020 – the start of business closures and stay-at-home orders around the country – preterm births from C-sections or induced deliveries immediately fell from the forecast number for the month by 0.4 percentage points. For the rest of 2020, the number remained on average 0.35 percentage points below the numbers predicted.
That means 350 fewer preterm C-sections and induced deliveries per 100,000 live births, or 10,000 fewer overall, the authors said.
Dr. Dench told this publication the numbers for those births had been steady from January 2010 to February 2020, but the pattern “diverges from this trend very clearly beginning exactly in March 2020 and does not return to trend by December 2020.”
Meanwhile, during the study period, the number of full-term cesarean and induced deliveries stayed steady and started to increase slightly in 2020. Researchers also adjusted for seasonality as, for example, preterm births are higher on average in February than in March.
So far, Dr. Dench said in a press release, it’s not clear whether the lower numbers mean physicians didn’t deliver babies that ended up surviving in the womb anyway or if they missed some that would die in the womb without intervention.
To better understand those implications, Dr. Dench says he is turning to fetal death records for March-December 2020 and he said he expects to have those results analyzed by the end of the year.
If there was no change in fetal deaths at the same time as the drop in preterm births, Dr. Dench said, that could point to physician interventions that may not have been necessary.
Mya R. Zapata, MD, an obstetrician-gynecologist with UCLA Health, who was not involved with the study, told this publication that checking the fetal deaths is a good start and an objective outcome in answering the question, but she points out there are other outcomes that will take a deeper analysis, such as whether there are differences later in developmental outcomes after fewer physician visits.
“It’s always a good question for health care,” she said, “are we doing more than we need to?”
Dr. Zapata is the obstetrics service chief for UCLA’s labor and delivery unit and was an integral part of decision-making as to what services were essential and for which patients. She said the fewer visits and fewer ultrasounds the researchers describe fit with what ob.gyns. at UCLA experienced as the pandemic hit.
“We really tried to hone in on people who were at highest risk for an adverse outcome,” she said. “I still have the question of whether there were things we missed in low-risk people. It will take time to get the entire answer. But it does make us reflect that perhaps less intervention could be better for patients and easier. It’s our job in medicine to keep asking the question of what is essential and safe and not just continue with current practice because that’s what we’ve always done.”
The amount of data gave the researchers an unusual view. They studied 38,891,271 singleton births in the United States from 2010 to 2020 with data from the National Center for Health Statistics.
“If you look at 1,000 births in a single hospital, or even at 30,000 births across a hospital system, you wouldn’t be able to see the drop as clearly,” Dr. Dench said. “The drop we detected is a huge change, but you might miss it in a small sample.”
The researchers acknowledge a limitation of the study is that half of all preterm C-sections and induced deliveries happen because of a ruptured membrane, a spontaneous cause. Those instances can’t be distinguished from the ones caused by doctors’ interventions in this study.
“Still, these findings are significant because the causes for preterm births are not always known,” the authors wrote in the press release.
The study authors and Dr. Zapata reported no relevant financial relationships.
Premature births from cesarean (C-section) and induced deliveries dropped abruptly by 6.5% from the projected number in the first month of the COVID-19 pandemic and stayed at the lower rate consistently throughout the year, researchers have found.
Results of the study, led by Daniel Dench, PhD, assistant professor at the Georgia Institute of Technology School of Economics in Atlanta, were published online in Pediatrics.
The authors say their findings help answer the question of whether numbers of preterm (less than 37 weeks gestation) C-sections and induced deliveries would change if women didn’t see their physicians during pregnancy as often, especially in person, and raise the question of whether some birth interventions by physicians may not be necessary. The pandemic gave researchers a natural, ethical way to study the question.
The researchers found that in March 2020 – the start of business closures and stay-at-home orders around the country – preterm births from C-sections or induced deliveries immediately fell from the forecast number for the month by 0.4 percentage points. For the rest of 2020, the number remained on average 0.35 percentage points below the numbers predicted.
That means 350 fewer preterm C-sections and induced deliveries per 100,000 live births, or 10,000 fewer overall, the authors said.
Dr. Dench told this publication the numbers for those births had been steady from January 2010 to February 2020, but the pattern “diverges from this trend very clearly beginning exactly in March 2020 and does not return to trend by December 2020.”
Meanwhile, during the study period, the number of full-term cesarean and induced deliveries stayed steady and started to increase slightly in 2020. Researchers also adjusted for seasonality as, for example, preterm births are higher on average in February than in March.
So far, Dr. Dench said in a press release, it’s not clear whether the lower numbers mean physicians didn’t deliver babies that ended up surviving in the womb anyway or if they missed some that would die in the womb without intervention.
To better understand those implications, Dr. Dench says he is turning to fetal death records for March-December 2020 and he said he expects to have those results analyzed by the end of the year.
If there was no change in fetal deaths at the same time as the drop in preterm births, Dr. Dench said, that could point to physician interventions that may not have been necessary.
Mya R. Zapata, MD, an obstetrician-gynecologist with UCLA Health, who was not involved with the study, told this publication that checking the fetal deaths is a good start and an objective outcome in answering the question, but she points out there are other outcomes that will take a deeper analysis, such as whether there are differences later in developmental outcomes after fewer physician visits.
“It’s always a good question for health care,” she said, “are we doing more than we need to?”
Dr. Zapata is the obstetrics service chief for UCLA’s labor and delivery unit and was an integral part of decision-making as to what services were essential and for which patients. She said the fewer visits and fewer ultrasounds the researchers describe fit with what ob.gyns. at UCLA experienced as the pandemic hit.
“We really tried to hone in on people who were at highest risk for an adverse outcome,” she said. “I still have the question of whether there were things we missed in low-risk people. It will take time to get the entire answer. But it does make us reflect that perhaps less intervention could be better for patients and easier. It’s our job in medicine to keep asking the question of what is essential and safe and not just continue with current practice because that’s what we’ve always done.”
The amount of data gave the researchers an unusual view. They studied 38,891,271 singleton births in the United States from 2010 to 2020 with data from the National Center for Health Statistics.
“If you look at 1,000 births in a single hospital, or even at 30,000 births across a hospital system, you wouldn’t be able to see the drop as clearly,” Dr. Dench said. “The drop we detected is a huge change, but you might miss it in a small sample.”
The researchers acknowledge a limitation of the study is that half of all preterm C-sections and induced deliveries happen because of a ruptured membrane, a spontaneous cause. Those instances can’t be distinguished from the ones caused by doctors’ interventions in this study.
“Still, these findings are significant because the causes for preterm births are not always known,” the authors wrote in the press release.
The study authors and Dr. Zapata reported no relevant financial relationships.
FROM PEDIATRICS
‘Eye-opening’ experience on the other side of the hospital bed
The 5 days that she spent at her mother’s bedside were eye-opening for an oncologist used to being on the other side of the clinician–patient relationship.
“As a physician, I thought I had a unique perspective of things that were done well – and things that were not,” commented Pamela Kunz, MD.
Dr. Kunz, who was named the 2021 Woman Oncologist of the Year, is director of the Center for Gastrointestinal Cancers at Smilow Cancer Hospital and of the Yale Cancer Center, New Haven, Conn.
But she was propelled into quite a different role when her mother was admitted to the hospital.
Her mom, who has trouble hearing, was easily confused by jargon and by “all of the people coming in and out with no introductions,” she explained.
“She needed someone to translate what was going on because she didn’t feel well,” she added.
Seeing inpatient care through her mother’s eyes was enlightening, and at times it was “shocking to be on the other side.”
Physicians get used to “checking boxes, getting through the day,” she said. “It’s easy to forget the human side.”
“Seeing a loved one sick, [struggling] through this – I just wished I had seen things done differently,” added Dr. Kunz.
Her thread has since garnered thousands of “likes” and scores of comments and retweets.
She began the Twitter thread explaining what prompted her comments:
“I spent many hours last week observing the practice of medicine while sitting at my mom’s hospital bedside and was reminded of some important communication pearls. Some musings ...”
“1. Introduce yourself by full name, role, and team and have ID badges visible. It can get very confusing for [patients] and family members with the number of people in and out of rooms. E.g. ‘My name is Dr. X. I’m the intern on the primary internal medicine team.’
2. End your patient visit with a summary of the plan for the day.
3. Avoid medical jargon & speak slowly, clearly, and logically. Remember you are a teacher for your [patients] and their family.
4. Masks make it harder to hear, especially for [patients] with hearing loss (and they no longer have the aid of lip reading).
5. Many older [patients] get confused in the hospital. Repetition is a good thing.
6. Speak to a family member at least once per day to relay the plan.
7. Try to avoid last minute or surprise discharges – they make [patients] and family members anxious. Talk about discharge planning from day 1 and what milestones must occur prior to a safe discharge. ‘In order for you to leave the hospital, X, Y, X must happen.’
8. Talk with your [patients] about something other than what brought them to the hospital (a tip I once learned from a wise mentor).
9. When possible, sit at eye level with your patient (I love these stools from @YNHH).
10. Take time to listen.”
Dr. Kunz closed with her golden rule: “Lastly, treat your patients how you would want your own family member treated.”
Twitter user @BrunaPellini replied: “I love this, especially ‘Treat your patients how you would want your own family member treated.’ My mom and grandma always said that to me since I was a med student, and this is definitely one of my core values.”
Other clinicians shared similar experiences, and some added to Dr. Kunz’s list.
“Agree entirely, love the list – and while none of us can always practice perfectly, my experiences with my own mother’s illness taught me an enormous amount about communication,” @hoperugo responded.
Twitter user @mariejacork added: “Everyone in health care please read ... if you are lucky enough to not have had a loved one unwell in hospital, these may get forgotten. Having sat with my dad for a few days before he died a few years ago, I felt a lot of these, and it changed my practice forever.”
@bjcohenmd provided additional advice: “And use the dry erase board that should be in every room. Never start a medication without explaining it. Many docs will see the patient and then go to the computer, decide to order a med, but never go back to explain it.”
Patients also shared experiences and offered suggestions.
“As a chronic pain patient I’d add – we know it’s frustrating you can’t cure us but PLEASE do not SIGH if we say something didn’t work or [tell] us to be more positive. Just say ‘I know this is very hard, I’m here to listen.’ We don’t expect a cure, we do expect to be believed,” said @ppenguinsmt. “It makes me feel like I’m causing distress to you if I say the pain has been unrelenting. I leave feeling worse. ...You may have heard 10 [people] in pain before me but this is MY only [appointment].”
Twitter user @KatieCahoots added: “These are perfect. I wish doctors would do this not only in the hospital but in the doctor’s office, as well. I would add one caveat: When you try not to use medical jargon, don’t dumb it down as though I don’t know anything about science or haven’t done any of my own research.”
Dr. Kunz said she was taken aback but pleased by the response to her Tweet.
“It’s an example of the human side of medicine, so it resonates with physicians and with patients,” she commented. Seeing through her mom’s eyes how care was provided made her realize that medical training should include more emphasis on communication, including “real-time feedback to interns, residents, fellows, and students.”
Yes, it takes time, and “we don’t all have a lot of extra time,” she acknowledged.
“But some of these elements don’t take that much more time to do. They can help build trust and can, in the long run, actually save time if patients understand and family members feel engaged and like they are participants,” she said. “I think a little time investment will go a long way.”
In her case, she very much appreciated the one trainee who tried to call her and update her about her mother’s care each afternoon. “I really valued that,” she said.
A version of this article first appeared on Medscape.com.
The 5 days that she spent at her mother’s bedside were eye-opening for an oncologist used to being on the other side of the clinician–patient relationship.
“As a physician, I thought I had a unique perspective of things that were done well – and things that were not,” commented Pamela Kunz, MD.
Dr. Kunz, who was named the 2021 Woman Oncologist of the Year, is director of the Center for Gastrointestinal Cancers at Smilow Cancer Hospital and of the Yale Cancer Center, New Haven, Conn.
But she was propelled into quite a different role when her mother was admitted to the hospital.
Her mom, who has trouble hearing, was easily confused by jargon and by “all of the people coming in and out with no introductions,” she explained.
“She needed someone to translate what was going on because she didn’t feel well,” she added.
Seeing inpatient care through her mother’s eyes was enlightening, and at times it was “shocking to be on the other side.”
Physicians get used to “checking boxes, getting through the day,” she said. “It’s easy to forget the human side.”
“Seeing a loved one sick, [struggling] through this – I just wished I had seen things done differently,” added Dr. Kunz.
Her thread has since garnered thousands of “likes” and scores of comments and retweets.
She began the Twitter thread explaining what prompted her comments:
“I spent many hours last week observing the practice of medicine while sitting at my mom’s hospital bedside and was reminded of some important communication pearls. Some musings ...”
“1. Introduce yourself by full name, role, and team and have ID badges visible. It can get very confusing for [patients] and family members with the number of people in and out of rooms. E.g. ‘My name is Dr. X. I’m the intern on the primary internal medicine team.’
2. End your patient visit with a summary of the plan for the day.
3. Avoid medical jargon & speak slowly, clearly, and logically. Remember you are a teacher for your [patients] and their family.
4. Masks make it harder to hear, especially for [patients] with hearing loss (and they no longer have the aid of lip reading).
5. Many older [patients] get confused in the hospital. Repetition is a good thing.
6. Speak to a family member at least once per day to relay the plan.
7. Try to avoid last minute or surprise discharges – they make [patients] and family members anxious. Talk about discharge planning from day 1 and what milestones must occur prior to a safe discharge. ‘In order for you to leave the hospital, X, Y, X must happen.’
8. Talk with your [patients] about something other than what brought them to the hospital (a tip I once learned from a wise mentor).
9. When possible, sit at eye level with your patient (I love these stools from @YNHH).
10. Take time to listen.”
Dr. Kunz closed with her golden rule: “Lastly, treat your patients how you would want your own family member treated.”
Twitter user @BrunaPellini replied: “I love this, especially ‘Treat your patients how you would want your own family member treated.’ My mom and grandma always said that to me since I was a med student, and this is definitely one of my core values.”
Other clinicians shared similar experiences, and some added to Dr. Kunz’s list.
“Agree entirely, love the list – and while none of us can always practice perfectly, my experiences with my own mother’s illness taught me an enormous amount about communication,” @hoperugo responded.
Twitter user @mariejacork added: “Everyone in health care please read ... if you are lucky enough to not have had a loved one unwell in hospital, these may get forgotten. Having sat with my dad for a few days before he died a few years ago, I felt a lot of these, and it changed my practice forever.”
@bjcohenmd provided additional advice: “And use the dry erase board that should be in every room. Never start a medication without explaining it. Many docs will see the patient and then go to the computer, decide to order a med, but never go back to explain it.”
Patients also shared experiences and offered suggestions.
“As a chronic pain patient I’d add – we know it’s frustrating you can’t cure us but PLEASE do not SIGH if we say something didn’t work or [tell] us to be more positive. Just say ‘I know this is very hard, I’m here to listen.’ We don’t expect a cure, we do expect to be believed,” said @ppenguinsmt. “It makes me feel like I’m causing distress to you if I say the pain has been unrelenting. I leave feeling worse. ...You may have heard 10 [people] in pain before me but this is MY only [appointment].”
Twitter user @KatieCahoots added: “These are perfect. I wish doctors would do this not only in the hospital but in the doctor’s office, as well. I would add one caveat: When you try not to use medical jargon, don’t dumb it down as though I don’t know anything about science or haven’t done any of my own research.”
Dr. Kunz said she was taken aback but pleased by the response to her Tweet.
“It’s an example of the human side of medicine, so it resonates with physicians and with patients,” she commented. Seeing through her mom’s eyes how care was provided made her realize that medical training should include more emphasis on communication, including “real-time feedback to interns, residents, fellows, and students.”
Yes, it takes time, and “we don’t all have a lot of extra time,” she acknowledged.
“But some of these elements don’t take that much more time to do. They can help build trust and can, in the long run, actually save time if patients understand and family members feel engaged and like they are participants,” she said. “I think a little time investment will go a long way.”
In her case, she very much appreciated the one trainee who tried to call her and update her about her mother’s care each afternoon. “I really valued that,” she said.
A version of this article first appeared on Medscape.com.
The 5 days that she spent at her mother’s bedside were eye-opening for an oncologist used to being on the other side of the clinician–patient relationship.
“As a physician, I thought I had a unique perspective of things that were done well – and things that were not,” commented Pamela Kunz, MD.
Dr. Kunz, who was named the 2021 Woman Oncologist of the Year, is director of the Center for Gastrointestinal Cancers at Smilow Cancer Hospital and of the Yale Cancer Center, New Haven, Conn.
But she was propelled into quite a different role when her mother was admitted to the hospital.
Her mom, who has trouble hearing, was easily confused by jargon and by “all of the people coming in and out with no introductions,” she explained.
“She needed someone to translate what was going on because she didn’t feel well,” she added.
Seeing inpatient care through her mother’s eyes was enlightening, and at times it was “shocking to be on the other side.”
Physicians get used to “checking boxes, getting through the day,” she said. “It’s easy to forget the human side.”
“Seeing a loved one sick, [struggling] through this – I just wished I had seen things done differently,” added Dr. Kunz.
Her thread has since garnered thousands of “likes” and scores of comments and retweets.
She began the Twitter thread explaining what prompted her comments:
“I spent many hours last week observing the practice of medicine while sitting at my mom’s hospital bedside and was reminded of some important communication pearls. Some musings ...”
“1. Introduce yourself by full name, role, and team and have ID badges visible. It can get very confusing for [patients] and family members with the number of people in and out of rooms. E.g. ‘My name is Dr. X. I’m the intern on the primary internal medicine team.’
2. End your patient visit with a summary of the plan for the day.
3. Avoid medical jargon & speak slowly, clearly, and logically. Remember you are a teacher for your [patients] and their family.
4. Masks make it harder to hear, especially for [patients] with hearing loss (and they no longer have the aid of lip reading).
5. Many older [patients] get confused in the hospital. Repetition is a good thing.
6. Speak to a family member at least once per day to relay the plan.
7. Try to avoid last minute or surprise discharges – they make [patients] and family members anxious. Talk about discharge planning from day 1 and what milestones must occur prior to a safe discharge. ‘In order for you to leave the hospital, X, Y, X must happen.’
8. Talk with your [patients] about something other than what brought them to the hospital (a tip I once learned from a wise mentor).
9. When possible, sit at eye level with your patient (I love these stools from @YNHH).
10. Take time to listen.”
Dr. Kunz closed with her golden rule: “Lastly, treat your patients how you would want your own family member treated.”
Twitter user @BrunaPellini replied: “I love this, especially ‘Treat your patients how you would want your own family member treated.’ My mom and grandma always said that to me since I was a med student, and this is definitely one of my core values.”
Other clinicians shared similar experiences, and some added to Dr. Kunz’s list.
“Agree entirely, love the list – and while none of us can always practice perfectly, my experiences with my own mother’s illness taught me an enormous amount about communication,” @hoperugo responded.
Twitter user @mariejacork added: “Everyone in health care please read ... if you are lucky enough to not have had a loved one unwell in hospital, these may get forgotten. Having sat with my dad for a few days before he died a few years ago, I felt a lot of these, and it changed my practice forever.”
@bjcohenmd provided additional advice: “And use the dry erase board that should be in every room. Never start a medication without explaining it. Many docs will see the patient and then go to the computer, decide to order a med, but never go back to explain it.”
Patients also shared experiences and offered suggestions.
“As a chronic pain patient I’d add – we know it’s frustrating you can’t cure us but PLEASE do not SIGH if we say something didn’t work or [tell] us to be more positive. Just say ‘I know this is very hard, I’m here to listen.’ We don’t expect a cure, we do expect to be believed,” said @ppenguinsmt. “It makes me feel like I’m causing distress to you if I say the pain has been unrelenting. I leave feeling worse. ...You may have heard 10 [people] in pain before me but this is MY only [appointment].”
Twitter user @KatieCahoots added: “These are perfect. I wish doctors would do this not only in the hospital but in the doctor’s office, as well. I would add one caveat: When you try not to use medical jargon, don’t dumb it down as though I don’t know anything about science or haven’t done any of my own research.”
Dr. Kunz said she was taken aback but pleased by the response to her Tweet.
“It’s an example of the human side of medicine, so it resonates with physicians and with patients,” she commented. Seeing through her mom’s eyes how care was provided made her realize that medical training should include more emphasis on communication, including “real-time feedback to interns, residents, fellows, and students.”
Yes, it takes time, and “we don’t all have a lot of extra time,” she acknowledged.
“But some of these elements don’t take that much more time to do. They can help build trust and can, in the long run, actually save time if patients understand and family members feel engaged and like they are participants,” she said. “I think a little time investment will go a long way.”
In her case, she very much appreciated the one trainee who tried to call her and update her about her mother’s care each afternoon. “I really valued that,” she said.
A version of this article first appeared on Medscape.com.
Moderna reports positive COVID-19 vaccine response in kids down to 6 months
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
Moderna on March 23 released interim results indicating that its mRNA-1273 COVID vaccine produced “robust” neutralizing antibody titers in children aged 6 months to 6 years – levels similar to those seen in adults.
Vaccine efficacy against infection was 43.7% in children aged 6 months to 2 years and 37.5% among children aged 2-6 years, the new data from its phase 2/3 KidCOVE study show.
The company explained the lower efficacy numbers by noting that its study involving these younger children was conducted during the Omicron wave. The same decrease in efficacy against infection was reported in adults during the Omicron surge.
A majority of COVID-19 cases were mild in the approximately 6,900 children aged 6 months to 6 years in the study. No severe COVID-19 cases, hospitalizations, or deaths were reported.
The primary series of two 25-mcg doses of the vaccine given 28 days apart was generally well tolerated. Most adverse events were mild to moderate. For example, temperature greater than 38° C (>100.4° F) was reported for 17.0% of the 6-month-old to 2-year-old group and for 14.6% of the 2- to 6-year-old group. A few children, 0.2% of each group, experienced a temperature greater than 40° C (>104° F).
Moderna plans to include these response, efficacy, and safety data in an application to the Food and Drug Administration for emergency use authorization (EUA) of the vaccine in these younger children in the coming weeks.
“We now have clinical data on the performance of our vaccine from infants 6 months of age through older adults,” Moderna CEO Stephane Bancel said in a news release. He described the interim results as “good news for parents of children under 6 years of age.”
In other news
Moderna also announced that it began the FDA EUA submission process for a 50-μg two-dose primary series for children aged 6-12 years.
The company is also updating its EUA submission for a 100-mcg two-dose primary series for children and adolescents aged 12-18 years.
Similar to its booster research in adults, Moderna plans to evaluate the potential of a booster dose for all pediatric populations, including those aged 6 months to 6 years, 6-12 years, and adolescents. The company is evaluating both a booster dose of mRNA-1273 and its bivalent booster candidate (mRNA1273.214), which includes an Omicron variant booster and mRNA-1273.
A version of this article first appeared on Medscape.com.
What’s the future of microbiome therapies in C. diff, cancer?
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
WASHINGTON – Research on standardized microbiome-based therapies designed to prevent the recurrence of Clostridioides difficile infection (CDI) is moving “with a lot of momentum,” according to one expert, and modulation of the gut microbiome may even enhance responses to immunotherapy and/or abrogate toxicity, according to another.
Several products for prevention of CDI recurrence are poised for either phase 3 trials or upcoming Food and Drug Administration approval, Sahil Khanna, MBBS, MS, professor of medicine, gastroenterology, and hepatology at the Mayo Clinic in Rochester, Minn., reported at the annual Gut Microbiota for Health World Summit.
Jennifer A. Wargo, MD, MMSc, of the University of Texas MD Anderson Cancer Center, Houston, described her investigations of microbiome modulation’s role in cancer treatment. “I used to say yes [we can do this] somewhat enthusiastically without data, but now we have data to support this,” she said at the meeting, sponsored by the American Gastroenterological Association and the European Society for Neurogastroenterology and Motility. “The answer now is totally yes.”
New approaches for CDI
“Based on how the field is moving, we might be able to [offer our patients] earlier microbiome restoration” than is currently afforded with fecal microbiota transplantation (FMT), he said. “Right now the [Food and Drug Administration] and our clinical guidelines say we should do FMT after three or more episodes [of CDI] – that’s heartbreaking for patients.”
Several of the microbiome-based therapies under investigation – including two poised for phase 3 trials – have shown efficacy after a second episode of CDI, and one of these two has also had positive results after one episode of CDI in patients 65 at older, a group at particularly high risk of recurrence, said Dr. Khanna.
The value of standardized, mostly pill-form microbiome therapies has been heightened during the pandemic. “We’ve been doing conventional FMT for recurrent C. difficile for over a decade now, and it’s probably the most effective treatment we have,” said Colleen R. Kelly, MD, associate professor of medicine at Brown University, Providence, R.I., and moderator of the session on microbiota-based therapies.
Prepandemic “it got really hard, with issues of identifying donors, and quality control and safety ... And then when COVID hit the stool banks shut down,” she said in an interview after the meeting. With stool testing for SARS-CoV-2 now in place, some stool is again available, “but it made me realize how fragile our current system is,” Dr. Kelly said. “The fact that companies are putting these products through the FDA pipeline and investigating them in rigorous, scientific randomized controlled trials is really good for the field.”
The products vary in composition; some are live multi-strain biotherapeutics derived from donor stool, for instance, while others are defined live bacterial consortia not from stool. Most are oral formulations, given one or multiple times, that do not require any bowel preparation.
One of the products most advanced in the pipeline, RBX2660 (Rebiotix, Ferring Pharmaceuticals) is stool derived and rectally administered. In phase 3 research, 70.5% of patients who received one active enema after having had two or more CDI recurrences and standard-of-care antibiotic treatment had no additional recurrence at 8 weeks compared to 58.1% in the placebo group, Dr. Khanna said.
The other product with positive phase 3 results, SER-109 (Seres Therapeutics), is a donor stool-derived oral formulation of purified Firmicutes spores that is administered after bowel prep. In results published earlier this year, the percentage of patients with recurrence of CDI up to 8 weeks after standard antibiotic treatment was 12% in the SER-109 group and 40% in the placebo group.
Patients in this trial were required to have had three episodes of CDI, and interestingly, Dr. Khanna said, the diagnosis of CDI was made only by toxin enzyme immunoassay (EIA). Earlier phase 2 research, which allowed either toxin EIA or polymerase chain reaction testing for the diagnosis of CDI (as other trials have done), produced negative results, leading investigators to surmise that some of the included patients had been colonized with C. difficile rather than being actively infected, Dr. Khanna said.
Researchers of these trials are documenting not only resolution of CDI but what they believe are positive shifts in the gut microbiota after microbiome-based therapy, he said. For instance, a phase 1 trial he led of the product RBX7455 (Rebiotix, Ferring Pharmaceuticals) – an oral capsule of lyophilized stool-based bacteria that can be kept for several days at room temperature – showed increases in Bacteroidia and Clostridia.
And other trials’ analyses of microbiome engraftment have demonstrated that “you can restore [species] even when these bacteria aren’t [included in the therapy],” he noted. “As the milieu of the gut improves, species that were not detected start coming back up.”
Asked about rates of efficacy in the trials’ placebo arms, Dr. Khanna said that “we’ve become smarter with our antibiotic regimens ... the placebo response rate is the response to newer guideline-based therapies.”
In addition to CDI, microbiome-based therapies are being studied, mostly in phase 1 research, for indications such as Crohn’s disease, ulcerative colitis, autism spectrum disorder, hepatitis B, and hepatic encephalopathy, Dr. Khanna noted.
Dr. Kelly, whose own research has focused on FMT for CDI, said she anticipates an expansion of research into other indications once products to prevent CDI recurrence are on the market. “There have been a couple of promising ulcerative colitis trials that haven’t gone anywhere clinically yet,” she said in the interview. “But will we now identify patients with UC who may be more sensitive to microbial manipulation, for whom we can use these microbial therapies along with a biologic?”
Some of her patients with IBD and CDI who are treated with FMT have not only had their CDI eradicated but have subsequently seen improvements in their IBD, she noted.
The role of traditional FMT and of stool banks will likely change in the future with new standardized oral microbiome-based therapies that can be approved and regulated by the FDA, she said. However, “we think the stool banks will still have some value,” she said, certainly for clinical research and probably for some treatment purposes as well. Regarding new therapies, “I just really hope they’re affordable,” she said.
Gut microbiome manipulation for cancer
Dr. Wargo’s research at MD Anderson has focused on metastatic breast cancer and immunotherapeutic checkpoint blockade. By sequencing microbiota samples and performing immune profiling in hundreds of patients, her team found that responders to PD-1 blockage have a greater diversity of gut bacteria and that “favorable signatures in the gut microbiome” are associated with enhanced immune responses in the tumor microenvironment.
Studies published last year in Science from investigators in Israel (2021 Feb 5;371[6529]:602-9) and Pittsburgh (2021 Feb 5;371[6529]:595-602), demonstrated that FMT promotes response in immunotherapy-refractory melanoma patients. In one study, FMT provided clinical benefit in 6 of 15 patients whose cancer had progressed on prior anti-PD-1 therapy, “which is pretty remarkable,” Dr. Wargo said.
Both research groups, she noted, saw favorable changes in the gut microbiome and immune cell infiltrates both at the level of the colon and the tumor.
Current research on FMT and other microbiome modulation strategies for cancer is guided in part by knowledge that tumors have microbial signatures – these signatures are now being identified across all tumor types – and by findings of “cross talk” between the gut and tumor microbiomes, she explained.
“Researchers are working hard to identify optimal consortia to enhance immune responses in the cancer setting, with promising work in preclinical models,” she said, and clinical trials are in progress. The role of diet in modulating the microbiome and enhancing anti-tumor immunity, with a focus on high dietary fiber intake, is also being investigated, she said.
Dr. Wargo reported that she serves on the advisory boards and is a paid speaker of numerous pharmaceutical and biotechnology companies, and is the coinventor of a patent submitted by the Texas MD Anderson Cancer Center on modulating the microbiome to enhance response to checkpoint blockade, and another related patent. Dr. Khanna reported that he is involved in research with Ferring/Rebiotix, Finch, Seres, Pfizer and Vendata, and does consulting for Immuron and several other companies. Dr. Kelly said she serves as an unpaid adviser for OpenBiome, a nonprofit stool bank, and that her site has enrolled patients in two of the trials testing products for CDI.
REPORTING FROM GMFH 2022
Excess weight over lifetime hikes risk for colorectal cancer
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.

Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
Excess weight over a lifetime may play a greater role in a person’s risk for colorectal cancer (CRC) than previously thought, according to new research.
In their paper published online March 17 in JAMA Oncology, the authors liken the cumulative effects of a lifetime with overweight or obesity to the increased risk of cancer the more people smoke over time.
This population-based, case-control study was led by Xiangwei Li, MSc, of the division of clinical epidemiology and aging research at the German Cancer Research Center in Heidelberg.
It looked at height and self-reported weight documented in 10-year increments starting at age 20 years up to the current age for 5,635 people with CRC compared with 4,515 people in a control group.
Odds for colorectal cancer increased substantially over the decades when people carried the excess weight long term compared with participants who remained within the normal weight range during the period.
Coauthor Hermann Brenner, MD, MPH, a colleague in Li’s division at the German Cancer Research Center, said in an interview that a key message in the research is that “overweight and obesity are likely to increase the risk of colorectal cancer more strongly than suggested by previous studies that typically had considered body weight only at a single point of time.”
The researchers used a measure of weighted number of years lived with overweight or obesity (WYOs) determined by multiplying excess body mass index by number of years the person carried the excess weight.
They found a link between WYOs and CRC risk, with adjusted odds ratios (ORs) increasing from 1.25 (95% confidence interval [CI], 1.09-1.44) to 2.54 (95% CI, 2.24-2.89) from the first to the fourth quartile of WYOs, compared with people who stayed within normal weight parameters.
The odds went up substantially the longer the time carrying the excess weight.
“Each SD increment in WYOs was associated with an increase of CRC risk by 55% (adjusted OR, 1.55; 95% CI, 1.46-1.64),” the authors wrote. “This OR was higher than the OR per SD increase of excess body mass index at any single point of time, which ranged from 1.04 (95% CI, 0.93-1.16) to 1.27 (95% CI 1.16-1.39).”
Dr. Brenner said that although this study focused on colorectal cancer, “the same is likely to apply for other cancers and other chronic diseases.”
Prevention of overweight and obesity to reduce burden of cancer and other chronic diseases “should become a public health priority,” he said.
Preventing overweight in childhood is important
Overweight and obesity increasingly are starting in childhood, he noted, and may be a lifelong burden.
Therefore, “efforts to prevent their development in childhood, adolescence, and young adulthood are particularly important,” Dr. Brenner said.
The average age of the patients was 68 years in both the CRC and control groups. There were more men than women in both groups: 59.7% were men in the CRC group and 61.1% were men in the control group.
“Our proposed concept of WYOs is comparable to the concept of pack-years in that WYOs can be considered a weighted measure of years lived with the exposure, with weights reflecting the intensity of exposure,” the authors wrote.
Study helps confirm what is becoming more clear to researchers
Kimmie Ng, MD, MPH, a professor at Harvard Medical School and oncologist at Dana-Farber Cancer Institute, both in Boston, said in an interview that the study helps confirm what is becoming more clear to researchers.
“We do think that exposures over the life course are the ones that will be most strongly contributing to a risk of colorectal cancer as an adult,” she said. “With obesity, what we think is happening is that it’s setting up this milieu of chronic inflammation and insulin resistance and we know those two factors can lead to higher rates of colorectal cancer development and increased tumor growth.”
She said the ideal, but impractical, way to do the study would be to follow healthy people from childhood and document their weight over a lifetime. In this case-control study, people were asked to recall their weight at different time periods, which is a limitation and could lead to recall bias.
But the study is important, Dr. Ng said, and it adds convincing evidence that addressing the link between excess weight and CRC and chronic diseases should be a public health priority. “With the recent rise in young-onset colorectal cancer since the 1990s there has been a lot of interest in looking at whether obesity is a major contributor to that rising trend,” Dr. Ng noted. “If obesity is truly linked to colorectal cancer, these rising rates of obesity are very worrisome for potentially leading to more colorectal cancers in young adulthood and beyond.“
The study authors and Dr. Ng report no relevant financial relationships.
The new research was funded by the German Research Council, the Interdisciplinary Research Program of the National Center for Tumor Diseases, Germany, and the German Federal Ministry of Education and Research.
FROM JAMA ONCOLOGY
Hematocrit, White Blood Cells, and Thrombotic Events in the Veteran Population With Polycythemia Vera
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
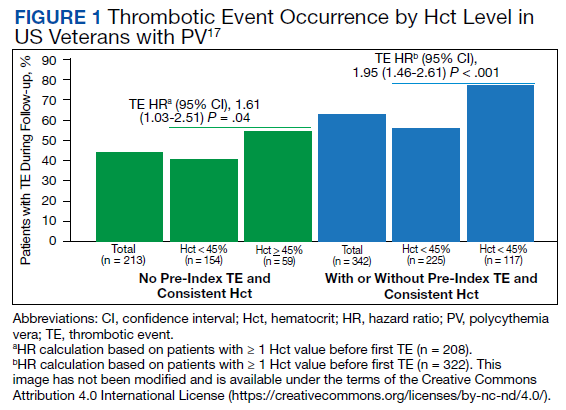
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
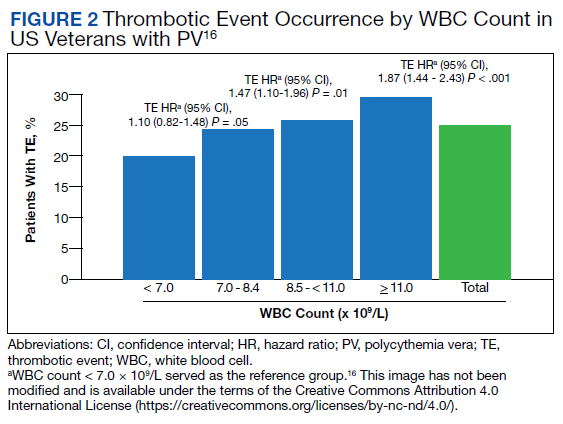
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
Polycythemia vera (PV) is a rare myeloproliferative neoplasm affecting 44 to 57 individuals per 100,000 in the United States.1,2 It is characterized by somatic mutations in the hematopoietic stem cell, resulting in hyperproliferation of mature myeloid lineage cells.2 Sustained erythrocytosis is a hallmark of PV, although many patients also have leukocytosis and thrombocytosis.2,3 These patients have increased inherent thrombotic risk with arterial events reported to occur at rates of 7 to 21/1000 person-years and venous thrombotic events at 5 to 20/1000 person-years.4-7 Thrombotic and cardiovascular events are leading causes of morbidity and mortality, resulting in a reduced overall survival of patients with PV compared with the general population.3,8-10
Blood Cell Counts and Thrombotic Events in PV
Treatment strategies for patients with PV mainly aim to prevent or manage thrombotic and bleeding complications through normalization of blood counts.11 Hematocrit (Hct) control has been reported to be associated with reduced thrombotic risk in patients with PV. This was shown and popularized by the prospective, randomized Cytoreductive Therapy in Polycythemia Vera (CYTO-PV) trial in which participants were randomized 1:1 to maintaining either a low (< 45%) or high (45%-50%) Hct for 5 years to examine the long-term effects of more- or less-intensive cytoreductive therapy.12 Patients in the low-Hct group were found to have a lower rate of death from cardiovascular events or major thrombosis (1.1/100 person-years in the low-Hct group vs 4.4 in the high-Hct group; hazard ratio [HR], 3.91; 95% confidence interval [CI], 1.45-10.53; P = .007). Likewise, cardiovascular events occurred at a lower rate in patients in the low-Hct group compared with the high-Hct group (4.4% vs 10.9% of patients, respectively; HR, 2.69; 95% CI, 1.19-6.12; P = .02).12
Leukocytosis has also been linked to elevated risk for vascular events as shown in several studies, including the real-world European Collaboration on Low-Dose Aspirin in PV (ECLAP) observational study and a post hoc subanalysis of the CYTO-PV study.13,14 In a multivariate, time-dependent analysis in ECLAP, patients with white blood cell (WBC) counts > 15 × 109/L had a significant increase in the risk of thrombosis compared with those who had lower WBC counts, with higher WBC count more strongly associated with arterial than venous thromboembolism.13 In CYTO-PV, a significant correlation between elevated WBC count (≥ 11 × 109/L vs reference level of < 7 × 109/L) and time-dependent risk of major thrombosis was shown (HR, 3.9; 95% CI, 1.24-12.3; P = .02).14 Likewise, WBC count ≥ 11 × 109/L was found to be a predictor of subsequent venous events in a separate single-center multivariate analysis of patients with PV.8
Although CYTO-PV remains one of the largest prospective landmark studies in PV demonstrating the impact of Hct control on thrombosis, it is worthwhile to note that the patients in the high-Hct group who received less frequent myelosuppressive therapy with hydroxyurea than the low-Hct group also had higher WBC counts.12,15 Work is needed to determine the relative effects of high Hct and high WBC counts on PV independent of each other.
The Veteran Population with PV
Two recently published retrospective analyses from Parasuraman and colleagues used data from the Veterans Health Administration (VHA), the largest integrated health care system in the US, with an aim to replicate findings from CYTO-PV in a real-world population.16,17 The 2 analyses focused independently on the effects of Hct control and WBC count on the risk of a thrombotic event in patients with PV.
In the first retrospective analysis, 213 patients with PV and no prior thrombosis were placed into groups based on whether Hct levels were consistently either < 45% or ≥ 45% throughout the study period.17 The mean follow-up time was 2.3 years, during which 44.1% of patients experienced a thrombotic event (Figure 1). Patients with Hct levels < 45% had a lower rate of thrombotic events compared to those with levels ≥ 45% (40.3% vs 54.2%, respectively; HR, 1.61; 95% CI, 1.03-2.51; P = .04). In a sensitivity analysis that included patients with pre-index thrombotic events (N = 342), similar results were noted (55.6% vs 76.9% between the < 45% and ≥ 45% groups, respectively; HR, 1.95; 95% CI, 1.46-2.61; P < .001).
In the second analysis, the authors investigated the relationship between WBC counts and thrombotic events.16 Evaluable patients (N = 1565) were grouped into 1 of 4 cohorts based on the last WBC measurement taken during the study period before a thrombotic event or through the end of follow-up: (1) WBC < 7.0 × 109/L, (2) 7.0 to 8.4 × 109/L, (3) 8.5 to < 11.0 × 109/L, or (4) ≥ 11.0 × 109/L. Mean follow-up time ranged from 3.6 to 4.5 years among WBC count cohorts, during which 24.9% of patients experienced a thrombotic event. Compared with the reference cohort (WBC < 7.0 × 109/L), a significant positive association between WBC counts and thrombotic event occurrence was observed among patients with WBC counts of 8.5 to < 11.0 × 109/L (HR, 1.47; 95% CI, 1.10-1.96; P < .01) and ≥ 11 × 109/L (HR, 1.87; 95% CI, 1.44-2.43; P < .001) (Figure 2).16 When including all patients in a sensitivity analysis regardless of whether they experienced thrombotic events before the index date (N = 1876), similar results were obtained (7.0-8.4 × 109/L group: HR, 1.22; 95% CI, 0.97-1.55; P = .0959; 8.5 - 11.0 × 109/L group: HR, 1.41; 95% CI, 1.10-1.81; P = .0062; ≥ 11.0 × 109/L group: HR, 1.53; 95% CI, 1.23-1.91; P < .001; compared with < 7.0 × 109/L reference group). Rates of phlebotomy and cytoreductive treatments were similar across groups.16
Some limitations to these studies are attributable to their retrospective design, reliance on health records, and the VHA population characteristics, which differ from the general population. For example, in this analysis, patients with PV in the VHA population had significantly increased risk of thrombotic events, even at a lower WBC count threshold (≥ 8.5 × 109/L) compared with those reported in CYTO-PV (≥ 11 × 109/L). Furthermore, approximately one-third of patients had elevated WBC levels, compared with 25.5% in the CYTO-PV study.14,16 This is most likely due to the unique nature of the VHA patient population, who are predominantly older adult men and generally have a higher comorbidity burden. A notable pre-index comorbidity burden was reported in the VHA population in the Hct analysis, even when compared to patients with PV in the general US population (Charlson Comorbidity Index score, 1.3 vs 0.8).6,17 Comorbid conditions such as hypertension, diabetes, and tobacco use, which are most common among the VHA population, are independently associated with higher risk of cardiovascular and thrombotic events.18,19 However, whether these higher levels of comorbidities affected the type of treatments they received was not elucidated, and the effectiveness of treatments to maintain target Hct levels was not addressed in the study.
Current PV Management and Future Implications
The National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology in myeloproliferative neoplasms recommend maintaining Hct levels < 45% in patients with PV.11 Patients with high-risk disease (age ≥ 60 years and/or history of thrombosis) are monitored for new thrombosis or bleeding and are managed for their cardiovascular risk factors. In addition, they receive low-dose aspirin (81-100 mg/day), undergo phlebotomy to maintain an Hct < 45%, and are managed with pharmacologic cytoreductive therapy. Cytoreductive therapy primarily consists of hydroxyurea or peginterferon alfa-2a for younger patients. Ruxolitinib, a Janus kinase (JAK1)/JAK2 inhibitor, is now approved by the US Food and Drug Administration as second-line treatment for those with PV that is intolerant or unresponsive to hydroxyurea or peginterferon alfa-2a treatments.11,20 However, the role of cytoreductive therapy is not clear for patients with low-risk disease (age < 60 years and no history of thrombosis). These patients are managed for their cardiovascular risk factors, undergo phlebotomy to maintain an Hct < 45%, are maintained on low-dose aspirin (81-100 mg/day), and are monitored for indications for cytoreductive therapy, which include any new thrombosis or disease-related major bleeding, frequent or persistent need for phlebotomy with poor tolerance for the procedure, splenomegaly, thrombocytosis, leukocytosis, and disease-related symptoms (eg, aquagenic pruritus, night sweats, fatigue).
Even though the current guidelines recommend maintaining a target Hct of < 45% in patients with high-risk PV, the role of Hct as the main determinant of thrombotic risk in patients with PV is still debated.21 In JAK2V617F-positive essential thrombocythemia, Hct levels are usually normal but risk of thrombosis is nevertheless still significant.22 The risk of thrombosis is significantly lower in primary familial and congenital polycythemia and much lower in secondary erythrocytosis such as cyanotic heart disease, long-term native dwellers of high altitude, and those with high-oxygen–affinity hemoglobins.21,23 In secondary erythrocytosis from hypoxia or upregulated hypoxic pathway such as hypoxia inducible factor-2α (HIF-2α) mutation and Chuvash erythrocytosis, the risk of thrombosis is more associated with the upregulated HIF pathway and its downstream consequences, rather than the elevated Hct level.24
However, most current literature supports the association of increased risk of thrombosis with higher Hct and high WBC count in patients with PV. In addition, the underlying mechanism of thrombogenesis still remains elusive; it is likely a complex process that involves interactions among multiple components, including elevated blood counts arising from clonal hematopoiesis, JAK2V617F allele burden, and platelet and WBC activation and their interaction with endothelial cells and inflammatory cytokines.25
Nevertheless, Hct control and aspirin use are current standard of care for patients with PV to mitigate thrombotic risk, and the results from the 2 analyses by Parasuraman and colleagues, using real-world data from the VHA, support the current practice guidelines to maintain Hct < 45% in these patients. They also provide additional support for considering WBC counts when determining patient risk and treatment plans. Although treatment response criteria from the European LeukemiaNet include achieving normal WBC levels to decrease the risk of thrombosis, current NCCN guidelines do not include WBC counts as a component for establishing patient risk or provide a target WBC count to guide patient management.11,26,27 Updates to these practice guidelines may be warranted. In addition, further study is needed to understand the mechanism of thrombogenesis in PV and other myeloproliferative disorders in order to develop novel therapeutic targets and improve patient outcomes.
Acknowledgments
Writing assistance was provided by Tania Iqbal, PhD, an employee of ICON (North Wales, PA), and was funded by Incyte Corporation (Wilmington, DE).
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891
1. Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. doi:10.3109/10428194.2013.813500
2. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391-2405. doi:10.1182/blood-2016-03-643544
3. Tefferi A, Rumi E, Finazzi G, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: an international study. Leukemia. 2013;27(9):1874-1881. doi:10.1038/leu.2013.163
4. Marchioli R, Finazzi G, Landolfi R, et al. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J Clin Oncol. 2005;23(10):2224-2232. doi:10.1200/JCO.2005.07.062
5. Vannucchi AM, Antonioli E, Guglielmelli P, et al. Clinical profile of homozygous JAK2 617V>F mutation in patients with polycythemia vera or essential thrombocythemia. Blood. 2007;110(3):840-846. doi:10.1182/blood-2006-12-064287
6. Goyal RK, Davis KL, Cote I, Mounedji N, Kaye JA. Increased incidence of thromboembolic event rates in patients diagnosed with polycythemia vera: results from an observational cohort study. Blood (ASH Annual Meeting Abstracts). 2014;124:4840. doi:10.1182/blood.V124.21.4840.4840
7. Barbui T, Carobbio A, Rumi E, et al. In contemporary patients with polycythemia vera, rates of thrombosis and risk factors delineate a new clinical epidemiology. Blood. 2014;124(19):3021-3023. doi:10.1182/blood-2014-07-591610 8. Cerquozzi S, Barraco D, Lasho T, et al. Risk factors for arterial versus venous thrombosis in polycythemia vera: a single center experience in 587 patients. Blood Cancer J. 2017;7(12):662. doi:10.1038/s41408-017-0035-6
9. Stein BL, Moliterno AR, Tiu RV. Polycythemia vera disease burden: contributing factors, impact on quality of life, and emerging treatment options. Ann Hematol. 2014;93(12):1965-1976. doi:10.1007/s00277-014-2205-y
10. Hultcrantz M, Kristinsson SY, Andersson TM-L, et al. Patterns of survival among patients with myeloproliferative neoplasms diagnosed in Sweden from 1973 to 2008: a population-based study. J Clin Oncol. 2012;30(24):2995-3001. doi:10.1200/JCO.2012.42.1925
11. National Comprehensive Cancer Network. NCCN clinical practice guidelines in myeloproliferative neoplasms (Version 1.2020). Accessed March 3, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
12. Marchioli R, Finazzi G, Specchia G, et al. Cardiovascular events and intensity of treatment in polycythemia vera. N Engl J Med. 2013;368(1):22-33. doi:10.1056/NEJMoa1208500
13. Landolfi R, Di Gennaro L, Barbui T, et al. Leukocytosis as a major thrombotic risk factor in patients with polycythemia vera. Blood. 2007;109(6):2446-2452. doi:10.1182/blood-2006-08-042515
14. Barbui T, Masciulli A, Marfisi MR, et al. White blood cell counts and thrombosis in polycythemia vera: a subanalysis of the CYTO-PV study. Blood. 2015;126(4):560-561. doi:10.1182/blood-2015-04-638593
15. Prchal JT, Gordeuk VR. Treatment target in polycythemia vera. N Engl J Med. 2013;368(16):1555-1556. doi:10.1056/NEJMc1301262
16. Parasuraman S, Yu J, Paranagama D, et al. Elevated white blood cell levels and thrombotic events in patients with polycythemia vera: a real-world analysis of Veterans Health Administration data. Clin Lymphoma Myeloma Leuk. 2020;20(2):63-69. doi:10.1016/j.clml.2019.11.010
17. Parasuraman S, Yu J, Paranagama D, et al. Hematocrit levels and thrombotic events in patients with polycythemia vera: an analysis of Veterans Health Administration data. Ann Hematol. 2019;98(11):2533-2539. doi:10.1007/s00277-019-03793-w
18. WHO CVD Risk Chart Working Group. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. Lancet Glob Health. 2019;7(10):e1332-e1345. doi:10.1016/S2214-109X(19)30318-3.
19. D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743-753. doi:10.1161/CIRCULATIONAHA.107.699579
20. Jakafi. Package insert. Incyte Corporation; 2020.
21. Gordeuk VR, Key NS, Prchal JT. Re-evaluation of hematocrit as a determinant of thrombotic risk in erythrocytosis. Haematologica. 2019;104(4):653-658. doi:10.3324/haematol.2018.210732
22. Carobbio A, Thiele J, Passamonti F, et al. Risk factors for arterial and venous thrombosis in WHO-defined essential thrombocythemia: an international study of 891 patients. Blood. 2011;117(22):5857-5859. doi:10.1182/blood-2011-02-339002
23. Perloff JK, Marelli AJ, Miner PD. Risk of stroke in adults with cyanotic congenital heart disease. Circulation. 1993;87(6):1954-1959. doi:10.1161/01.cir.87.6.1954
24. Gordeuk VR, Miasnikova GY, Sergueeva AI, et al. Thrombotic risk in congenital erythrocytosis due to up-regulated hypoxia sensing is not associated with elevated hematocrit. Haematologica. 2020;105(3):e87-e90. doi:10.3324/haematol.2019.216267
25. Kroll MH, Michaelis LC, Verstovsek S. Mechanisms of thrombogenesis in polycythemia vera. Blood Rev. 2015;29(4):215-221. doi:10.1016/j.blre.2014.12.002
26. Barbui T, Tefferi A, Vannucchi AM, et al. Philadelphia chromosome-negative classical myeloproliferative neoplasms: revised management recommendations from European LeukemiaNet. Leukemia. 2018;32(5):1057-1069. doi:10.1038/s41375-018-0077-1
27. Barosi G, Mesa R, Finazzi G, et al. Revised response criteria for polycythemia vera and essential thrombocythemia: an ELN and IWG-MRT consensus project. Blood. 2013;121(23):4778-4781. doi:10.1182/blood-2013-01-478891