User login
Biomarkers linked to elevated T2D MACE risk in DECLARE-TIMI 58

The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.

“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.
“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
The researchers found that N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity cardiac troponin T (hsTnT) levels helped identify a subset of T2D patients at higher risk of major adverse cardiovascular events who would benefit most from dapagliflozin.
“We’ve shown previously that these two biomarkers are very robust risk indicators for cardiovascular death and heart failure events,” senior study author David A. Morrow, MD, of Harvard University, Boston, said in an interview. “In this study, we now show that the two biomarkers also yield important prognostic information for MACE [major adverse cardiovascular events].”
Although NT-proBNP is typically measured to diagnose heart failure, and hsTnT to diagnose acute MI, Dr. Morrow pointed out that this analysis demonstrated the potential for using the two tests to evaluate risks in T2D patients.
Study results
The secondary analysis included 14,565 patients in the DECLARE-TIMI 58 trial. The patients had T2D and multiple risk factors for atherosclerotic cardiovascular disease (about 60%) or established ASCVD (about 40%). All patients had available blood samples and the data were collected from May 2013 to September 2018. The primary outcome was MACE, a composite of MI, ischemic stroke, and cardiovascular death. The results were reported online in JAMA Cardiology.
The analysis found that higher baseline concentrations of NT-proBNP increased MACE risks by 62% (95% confidence interval, 1.49-1.76) and hsTnT elevated those risks by 59% (95% CI, 1.46-1.74).
Among placebo patients, when divided into risk quartiles, those in the highest quartile had significantly higher risk with both elevated NT-proBNP and hsTnT, compared with those with low concentrations. For example, patients with established ASCVD had a 22.9% risk vs. 9.5% with elevated NT-proBNP (P < .001) and a 24.2% vs. 7.2% risk with elevated hsTnT (P < .001). The gap was similar for patients with multiple risk factors.
Dr. Morrow noted that the main DECLARE-TIMI 58 trial showed that dapagliflozin reduced the rates of cardiovascular death or hospitalization for heart failure in patients with T2D, when compared to placebo, but didn’t reach statistical significance for MACE (N Engl J Med. 2019;380:347-57).
“We have previously shown that among patients with T2D who have high risk indicators, such as prior MI or long-standing diabetes, dapagliflozin also appeared to reduce MACE,” Dr. Morrow said. “In this study, we find that these two widely available biomarkers also identify a high-risk group who may have even more potential benefits from treatment with an SGLT2i.”
Dr. Morrow noted that the study design – a nested prospective biomarker study within a randomized, double-blind, placebo-controlled clinical trial – “is a particular strength.”
Results clarify which patients will benefit
This secondary analysis of DECLARE-TIMI 58 brings more clarity to the types of T2D patients who will get the most cardiovascular benefits from dapagliflozin, said Matthew J. Budoff, MD, professor of medicine at University of California, Los Angeles, and Endowed Chair of Preventive Cardiology at the Lundquist Institute in Torrance, Calif.
“The big picture is, we’ve known for some time from epidemiologic studies that these biomarkers, when they’re elevated, mean that the patient is at higher risk of having a cardiovascular event,” he said, “but I think what it helps us with is in knowing in whom to use dapagliflozin for prevention of ASCVD. The effect in the DECLARE-TIMI 58 trial was quite modest, but if you can subgroup it, in these high-risk people there’s a more profound effect. It helps in risk stratification because the absolute benefit is larger.”
The specific biomarkers, NT-proBNP and hsTnT, “haven’t been explored very much in clinical trials,” Dr. Budoff said, “so I do think that it’s nice that in a randomized trial it plays out the way we might expect.”
He added that “for many clinicians this is novel, because I don’t think they were aware of the biomarker data, so I think that this does add some clinical benefit in that context.” The findings also strengthen the case to get T2D patients with higher ASCVD risk onto SGLT2 inhibitors if they’re not already, he said.
Dr. Morrow disclosed relationships with AstraZeneca, Roche Diagnostics, Abbott Laboratories, Anthos Therapeutics, ARCA Biopharma, Merck, Novartis, Pfizer, Regeneron, Siemens, and InCarda outside the reported work.
Dr. Budoff has no relevant disclosures.
FROM JAMA CARDIOLOGY
BIOVASC: Immediate complete revascularization beneficial in ACS
Immediate complete revascularization during the index procedure might become the new treatment paradigm in patients with an acute coronary syndrome (ACS) and multivessel disease, based on results of the BIOVASC trial.
In the trial, in patients presenting with ACS and multivessel disease, immediate complete revascularization was noninferior to staged complete revascularization for the primary composite outcome and was associated with a reduction in myocardial infarction and unplanned ischemia-driven revascularization.
The BIOVASC trial was presented on March 5 by Roberto Diletti, MD, Erasmus University Medical Center, Rotterdam, the Netherlands, at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The study was simultaneously published online in The Lancet.
“We did not detect an early safety signal against an immediate complete revascularization strategy,” the authors state in the Lancet paper, adding: “Treating physicians should not be concerned about potential risks associated with immediate treatment of nonculprit lesions.”
They note, “This strategy might be particularly effective in patients with only two-vessel disease and reasonably simple lesions, with a high likelihood of procedural success without excessive use of radiation, contrast dye, or other resources.”
The trial also showed a shorter hospital stay with an immediate complete revascularization strategy.
“Immediate complete revascularization might have potential health economic benefits because of the lower rate of myocardial infarction, including spontaneous myocardial infarction, and unplanned revascularizations, and the shorter overall hospital stay,” the researchers conclude.
Introducing his presentation, Dr. Diletti explained that multiple studies have established the clinical benefit of complete coronary revascularization as compared with exclusive reperfusion of the culprit lesion, but the optimal timing for nonculprit lesion revascularization remains unclear.
The BIOVASC trial, conducted in Belgium, Italy, the Netherlands, and Spain, involved 1,525 patients with ST-segment elevation MI (STEMI) or non-STEMI ACS and multivessel coronary artery disease with a clearly identifiable culprit lesion.
They were randomly assigned to undergo immediate complete revascularization (percutaneous coronary intervention [PCI] of the culprit lesion first, followed by other nonculprit lesions deemed to be clinically significant by the operator during the index procedure) or staged complete revascularization (PCI of only the culprit lesion during the index procedure and PCI of all nonculprit lesions deemed to be clinically significant within 6 weeks after the index procedure).
The primary outcome was the composite of all-cause mortality, MI, any unplanned ischemia-driven revascularization, or cerebrovascular events at 1 year after the index procedure.
The trial had a noninferiority design, with noninferiority of immediate to staged complete revascularization considered to be met if the upper boundary of the 95% confidence interval of the hazard ratio for the primary outcome did not exceed 1.39.
Among the trial population, 40% of patients had STEMI, 52% had non-STEMI, and 8% had unstable angina.
In the immediate complete revascularization group, 16 patients did not receive complete revascularization during the index procedure primarily because of prolonged procedure time, procedural complexity, or excessive contrast dye use.
In the staged group, 30% of patients underwent all subsequent procedures during the index hospitalization.
Results showed that the primary composite outcome at 1 year occurred in 7.6% of the immediate revascularization group and in 9.4% of the staged group, meeting the noninferiority criteria (HR, 0.78; 95% CI, 0.55-1.11; P for noninferiority = .0011).
Superiority of the immediate over the staged complete revascularization strategy was not met at 1-year follow-up (P for superiority = .17).
However, in the prespecified analysis of clinical events at 30 days after the index procedure, immediate complete revascularization was superior to staged revascularization in terms of the composite primary outcome (2.2% vs. 5.8%; HR, 0.38; P for superiority = .0007).
One-year results showed no difference in all-cause death between the two groups, but the immediate complete revascularization group appeared to have a reduction in MI (1.9% vs. 4.5%) and fewer unplanned ischemia-driven revascularizations (4.2% vs. 6.7%).
The difference in MI was mainly driven by spontaneous MIs (not procedure related) that predominantly occurred in the time window between the index procedure and the planned date for the staged intervention, and an originally nonculprit lesion was identified as the cause for these events in almost all cases.
Subgroup analysis showed similar results across the patient population, including age, sex, and STEMI vs. non-STEMI presentation.
High rate of MI in staged group
Discussant of the study at the ACC session, Dipti Itchhaporia, MD, University of California, Irvine, said this was a “very important trial.”
She expressed surprise over the “remarkably high rate” of MI in the staged procedure group and asked Dr. Diletti why that might have occurred.
He responded that the operator may have misjudged the culprit lesion or that patients with ACS may have multiple unstable plaques and “treating the culprit lesion alone does not do the job.”
He added: “We need to look at the data more thoroughly to better understand this, but in both scenarios, immediate complete revascularization would prevent these events.”
Dr. Itchhaporia also pointed out a low rate of functional imaging used in the study.
Dr. Diletti replied that this reflected current European practice, but he acknowledged that, “in my opinion this reduces our ability to detect the culprit lesion.”
Commenting at an ACC press conference, David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., said the trial poses the question “Can we fix it all at once?” and the results suggest “Yes, we can.”
He said this approach had the advantage of removing any uncertainly as to which was the culprit lesion. “We just fix everything – leave no blockage behind.”
But he pointed out that for some patients this may not be appropriate, such as those with compromised renal function, in whom excessive amounts of contrast material should be avoided.
CABG still needs to be considered
In a comment accompanying the Lancet publication, Tobias Pustjens, MD, Pieter Vriesendorp, MD, and Arnoud W.J. van’t Hof, MD, Cardiovascular Research Institute Maastricht (the Netherlands), note that more than half of the patients presenting with an ACS have multivessel coronary disease.
They say the trial results suggest that “pursuing an immediate complete revascularisation strategy, especially in times of reduced hospital capacity and staff scarcity, not only benefits the individual patient in clinical outcomes but can also safely reduce the pressure on health care systems.”
But they also point out that the possibility of coronary artery bypass grafting (CABG) should not be omitted, and that CABG is still the treatment of choice in patients with diabetes or complex coronary artery disease.
They conclude: “The results of the BIOVASC study move clinical practice forward from culprit-only to an immediate, complete revascularisation strategy. … However, further fine tuning of this treatment strategy to substantiate a role for intracoronary physiology assessment, intracoronary imaging, and guidance of the heart team decision is needed.”
The BIOVASC trial was supported by an unrestricted research grant from Biotronik AG. Dr. Diletti has received institutional research grants from Biotronik, Medtronic, ACIST Medical Systems, and Boston Scientific. Dr. van’t Hof has received institutional research grants from Biotronik.
A version of this article first appeared on Medscape.com.
Immediate complete revascularization during the index procedure might become the new treatment paradigm in patients with an acute coronary syndrome (ACS) and multivessel disease, based on results of the BIOVASC trial.
In the trial, in patients presenting with ACS and multivessel disease, immediate complete revascularization was noninferior to staged complete revascularization for the primary composite outcome and was associated with a reduction in myocardial infarction and unplanned ischemia-driven revascularization.
The BIOVASC trial was presented on March 5 by Roberto Diletti, MD, Erasmus University Medical Center, Rotterdam, the Netherlands, at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The study was simultaneously published online in The Lancet.
“We did not detect an early safety signal against an immediate complete revascularization strategy,” the authors state in the Lancet paper, adding: “Treating physicians should not be concerned about potential risks associated with immediate treatment of nonculprit lesions.”
They note, “This strategy might be particularly effective in patients with only two-vessel disease and reasonably simple lesions, with a high likelihood of procedural success without excessive use of radiation, contrast dye, or other resources.”
The trial also showed a shorter hospital stay with an immediate complete revascularization strategy.
“Immediate complete revascularization might have potential health economic benefits because of the lower rate of myocardial infarction, including spontaneous myocardial infarction, and unplanned revascularizations, and the shorter overall hospital stay,” the researchers conclude.
Introducing his presentation, Dr. Diletti explained that multiple studies have established the clinical benefit of complete coronary revascularization as compared with exclusive reperfusion of the culprit lesion, but the optimal timing for nonculprit lesion revascularization remains unclear.
The BIOVASC trial, conducted in Belgium, Italy, the Netherlands, and Spain, involved 1,525 patients with ST-segment elevation MI (STEMI) or non-STEMI ACS and multivessel coronary artery disease with a clearly identifiable culprit lesion.
They were randomly assigned to undergo immediate complete revascularization (percutaneous coronary intervention [PCI] of the culprit lesion first, followed by other nonculprit lesions deemed to be clinically significant by the operator during the index procedure) or staged complete revascularization (PCI of only the culprit lesion during the index procedure and PCI of all nonculprit lesions deemed to be clinically significant within 6 weeks after the index procedure).
The primary outcome was the composite of all-cause mortality, MI, any unplanned ischemia-driven revascularization, or cerebrovascular events at 1 year after the index procedure.
The trial had a noninferiority design, with noninferiority of immediate to staged complete revascularization considered to be met if the upper boundary of the 95% confidence interval of the hazard ratio for the primary outcome did not exceed 1.39.
Among the trial population, 40% of patients had STEMI, 52% had non-STEMI, and 8% had unstable angina.
In the immediate complete revascularization group, 16 patients did not receive complete revascularization during the index procedure primarily because of prolonged procedure time, procedural complexity, or excessive contrast dye use.
In the staged group, 30% of patients underwent all subsequent procedures during the index hospitalization.
Results showed that the primary composite outcome at 1 year occurred in 7.6% of the immediate revascularization group and in 9.4% of the staged group, meeting the noninferiority criteria (HR, 0.78; 95% CI, 0.55-1.11; P for noninferiority = .0011).
Superiority of the immediate over the staged complete revascularization strategy was not met at 1-year follow-up (P for superiority = .17).
However, in the prespecified analysis of clinical events at 30 days after the index procedure, immediate complete revascularization was superior to staged revascularization in terms of the composite primary outcome (2.2% vs. 5.8%; HR, 0.38; P for superiority = .0007).
One-year results showed no difference in all-cause death between the two groups, but the immediate complete revascularization group appeared to have a reduction in MI (1.9% vs. 4.5%) and fewer unplanned ischemia-driven revascularizations (4.2% vs. 6.7%).
The difference in MI was mainly driven by spontaneous MIs (not procedure related) that predominantly occurred in the time window between the index procedure and the planned date for the staged intervention, and an originally nonculprit lesion was identified as the cause for these events in almost all cases.
Subgroup analysis showed similar results across the patient population, including age, sex, and STEMI vs. non-STEMI presentation.
High rate of MI in staged group
Discussant of the study at the ACC session, Dipti Itchhaporia, MD, University of California, Irvine, said this was a “very important trial.”
She expressed surprise over the “remarkably high rate” of MI in the staged procedure group and asked Dr. Diletti why that might have occurred.
He responded that the operator may have misjudged the culprit lesion or that patients with ACS may have multiple unstable plaques and “treating the culprit lesion alone does not do the job.”
He added: “We need to look at the data more thoroughly to better understand this, but in both scenarios, immediate complete revascularization would prevent these events.”
Dr. Itchhaporia also pointed out a low rate of functional imaging used in the study.
Dr. Diletti replied that this reflected current European practice, but he acknowledged that, “in my opinion this reduces our ability to detect the culprit lesion.”
Commenting at an ACC press conference, David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., said the trial poses the question “Can we fix it all at once?” and the results suggest “Yes, we can.”
He said this approach had the advantage of removing any uncertainly as to which was the culprit lesion. “We just fix everything – leave no blockage behind.”
But he pointed out that for some patients this may not be appropriate, such as those with compromised renal function, in whom excessive amounts of contrast material should be avoided.
CABG still needs to be considered
In a comment accompanying the Lancet publication, Tobias Pustjens, MD, Pieter Vriesendorp, MD, and Arnoud W.J. van’t Hof, MD, Cardiovascular Research Institute Maastricht (the Netherlands), note that more than half of the patients presenting with an ACS have multivessel coronary disease.
They say the trial results suggest that “pursuing an immediate complete revascularisation strategy, especially in times of reduced hospital capacity and staff scarcity, not only benefits the individual patient in clinical outcomes but can also safely reduce the pressure on health care systems.”
But they also point out that the possibility of coronary artery bypass grafting (CABG) should not be omitted, and that CABG is still the treatment of choice in patients with diabetes or complex coronary artery disease.
They conclude: “The results of the BIOVASC study move clinical practice forward from culprit-only to an immediate, complete revascularisation strategy. … However, further fine tuning of this treatment strategy to substantiate a role for intracoronary physiology assessment, intracoronary imaging, and guidance of the heart team decision is needed.”
The BIOVASC trial was supported by an unrestricted research grant from Biotronik AG. Dr. Diletti has received institutional research grants from Biotronik, Medtronic, ACIST Medical Systems, and Boston Scientific. Dr. van’t Hof has received institutional research grants from Biotronik.
A version of this article first appeared on Medscape.com.
Immediate complete revascularization during the index procedure might become the new treatment paradigm in patients with an acute coronary syndrome (ACS) and multivessel disease, based on results of the BIOVASC trial.
In the trial, in patients presenting with ACS and multivessel disease, immediate complete revascularization was noninferior to staged complete revascularization for the primary composite outcome and was associated with a reduction in myocardial infarction and unplanned ischemia-driven revascularization.
The BIOVASC trial was presented on March 5 by Roberto Diletti, MD, Erasmus University Medical Center, Rotterdam, the Netherlands, at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The study was simultaneously published online in The Lancet.
“We did not detect an early safety signal against an immediate complete revascularization strategy,” the authors state in the Lancet paper, adding: “Treating physicians should not be concerned about potential risks associated with immediate treatment of nonculprit lesions.”
They note, “This strategy might be particularly effective in patients with only two-vessel disease and reasonably simple lesions, with a high likelihood of procedural success without excessive use of radiation, contrast dye, or other resources.”
The trial also showed a shorter hospital stay with an immediate complete revascularization strategy.
“Immediate complete revascularization might have potential health economic benefits because of the lower rate of myocardial infarction, including spontaneous myocardial infarction, and unplanned revascularizations, and the shorter overall hospital stay,” the researchers conclude.
Introducing his presentation, Dr. Diletti explained that multiple studies have established the clinical benefit of complete coronary revascularization as compared with exclusive reperfusion of the culprit lesion, but the optimal timing for nonculprit lesion revascularization remains unclear.
The BIOVASC trial, conducted in Belgium, Italy, the Netherlands, and Spain, involved 1,525 patients with ST-segment elevation MI (STEMI) or non-STEMI ACS and multivessel coronary artery disease with a clearly identifiable culprit lesion.
They were randomly assigned to undergo immediate complete revascularization (percutaneous coronary intervention [PCI] of the culprit lesion first, followed by other nonculprit lesions deemed to be clinically significant by the operator during the index procedure) or staged complete revascularization (PCI of only the culprit lesion during the index procedure and PCI of all nonculprit lesions deemed to be clinically significant within 6 weeks after the index procedure).
The primary outcome was the composite of all-cause mortality, MI, any unplanned ischemia-driven revascularization, or cerebrovascular events at 1 year after the index procedure.
The trial had a noninferiority design, with noninferiority of immediate to staged complete revascularization considered to be met if the upper boundary of the 95% confidence interval of the hazard ratio for the primary outcome did not exceed 1.39.
Among the trial population, 40% of patients had STEMI, 52% had non-STEMI, and 8% had unstable angina.
In the immediate complete revascularization group, 16 patients did not receive complete revascularization during the index procedure primarily because of prolonged procedure time, procedural complexity, or excessive contrast dye use.
In the staged group, 30% of patients underwent all subsequent procedures during the index hospitalization.
Results showed that the primary composite outcome at 1 year occurred in 7.6% of the immediate revascularization group and in 9.4% of the staged group, meeting the noninferiority criteria (HR, 0.78; 95% CI, 0.55-1.11; P for noninferiority = .0011).
Superiority of the immediate over the staged complete revascularization strategy was not met at 1-year follow-up (P for superiority = .17).
However, in the prespecified analysis of clinical events at 30 days after the index procedure, immediate complete revascularization was superior to staged revascularization in terms of the composite primary outcome (2.2% vs. 5.8%; HR, 0.38; P for superiority = .0007).
One-year results showed no difference in all-cause death between the two groups, but the immediate complete revascularization group appeared to have a reduction in MI (1.9% vs. 4.5%) and fewer unplanned ischemia-driven revascularizations (4.2% vs. 6.7%).
The difference in MI was mainly driven by spontaneous MIs (not procedure related) that predominantly occurred in the time window between the index procedure and the planned date for the staged intervention, and an originally nonculprit lesion was identified as the cause for these events in almost all cases.
Subgroup analysis showed similar results across the patient population, including age, sex, and STEMI vs. non-STEMI presentation.
High rate of MI in staged group
Discussant of the study at the ACC session, Dipti Itchhaporia, MD, University of California, Irvine, said this was a “very important trial.”
She expressed surprise over the “remarkably high rate” of MI in the staged procedure group and asked Dr. Diletti why that might have occurred.
He responded that the operator may have misjudged the culprit lesion or that patients with ACS may have multiple unstable plaques and “treating the culprit lesion alone does not do the job.”
He added: “We need to look at the data more thoroughly to better understand this, but in both scenarios, immediate complete revascularization would prevent these events.”
Dr. Itchhaporia also pointed out a low rate of functional imaging used in the study.
Dr. Diletti replied that this reflected current European practice, but he acknowledged that, “in my opinion this reduces our ability to detect the culprit lesion.”
Commenting at an ACC press conference, David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., said the trial poses the question “Can we fix it all at once?” and the results suggest “Yes, we can.”
He said this approach had the advantage of removing any uncertainly as to which was the culprit lesion. “We just fix everything – leave no blockage behind.”
But he pointed out that for some patients this may not be appropriate, such as those with compromised renal function, in whom excessive amounts of contrast material should be avoided.
CABG still needs to be considered
In a comment accompanying the Lancet publication, Tobias Pustjens, MD, Pieter Vriesendorp, MD, and Arnoud W.J. van’t Hof, MD, Cardiovascular Research Institute Maastricht (the Netherlands), note that more than half of the patients presenting with an ACS have multivessel coronary disease.
They say the trial results suggest that “pursuing an immediate complete revascularisation strategy, especially in times of reduced hospital capacity and staff scarcity, not only benefits the individual patient in clinical outcomes but can also safely reduce the pressure on health care systems.”
But they also point out that the possibility of coronary artery bypass grafting (CABG) should not be omitted, and that CABG is still the treatment of choice in patients with diabetes or complex coronary artery disease.
They conclude: “The results of the BIOVASC study move clinical practice forward from culprit-only to an immediate, complete revascularisation strategy. … However, further fine tuning of this treatment strategy to substantiate a role for intracoronary physiology assessment, intracoronary imaging, and guidance of the heart team decision is needed.”
The BIOVASC trial was supported by an unrestricted research grant from Biotronik AG. Dr. Diletti has received institutional research grants from Biotronik, Medtronic, ACIST Medical Systems, and Boston Scientific. Dr. van’t Hof has received institutional research grants from Biotronik.
A version of this article first appeared on Medscape.com.
FROM ACS 2023
When intravascular imaging guides complex PCI, MACE risk is lowered
NEW ORLEANS – In patients undergoing percutaneous intervention (PCI) for complex coronary lesions, intravascular imaging is superior to angiography for reducing the risk of target lesion failure (TLF), according to results of a randomized trial.
Previous studies have produced the same conclusion, but the advantage was demonstrated this time in a multicenter well-powered randomized trial, principal investigator Joo Yong Hahn, MD, PhD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The earlier studies “were not definitive,” said Dr. Hahn, pointing out that even those that were randomized lacked sufficient duration of follow-up or were not inclusive of a broad array of types of complex PCI.
In this clinical outcomes–driven study, called RENOVATE-COMPLEX-PCI, 1,639 patients undergoing complex PCI in 20 South Korean treatment centers were randomized in a 2:1 ratio to PCI guided by intravascular imaging or angiography alone. There were nine types of complex PCI eligible for trial entry, including bifurcated lesions, long lesions (expected stent length ≥ 38 mm), total coronary occlusions, lesions requiring multiple stents, severely calcified lesions, and lesions in multiple vessels.
Intravascular imaging in the experimental arm could be performed with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT), according to Dr. Hahn. Because one might be better than the other for specific patient and lesions characteristics, the type of intravascular imaging in the experimental group was selected at the discretion of the treating investigator, reported Dr. Hahn, of the Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University, Seoul.
The primary TLF endpoint was defined as death from cardiovascular causes, target-vessel-related MI, and target-vessel revascularization.
Risk reduction of > 35% observed
After a median of 2.1 years of follow-up, the lower TLF incidence in the group with PCI guided by intravascular imaging (7.7% vs. 12.3%) translated into a 36% reduction in risk (hazard ratio, 0.64; P = .008).
Intravascular imaging was associated with a numerical reduction of each component of TLF. In the case of death from cardiovascular causes, the confidence interval remained below the line of unity (HR 0.47; 95% CI, 0.24-0.93).
Although this was not true for target vessel–related MI (HR, 0.74, 95% CI, 0.45-1.22) or target vessel revascularization (HR, 0.66; 95% CI, 0.36-1.22), it was also true of TLF without procedural-related MI (HR, 0.59; 95% CI, 0.39-0.90) and cardiac death or target vessel–related MI (HR, 0.63; 95% CI, 0.42-0.93).
With few exceptions, all of the secondary outcomes “moved in the right direction” to favor intravascular imaging, including death from any cause (HR 0.71, 95% CI, 0.44-1.15), reported Dr. Hahn, who noted that the results were simultaneously published in the New England Journal of Medicine.
When compared, there were no major baseline differences in the 1,092 patients with PCI guided by intravascular imaging relative to the 547 guided by angiography. The median age was 65.5 years. Most (79%) were male. About half (51%) had an acute coronary syndrome and the remainder had stable ischemic heart disease. The proportions of patients with hypertension (61%), dyslipidemia (51%), and diabetes (38%) were substantial. About 18% of patients were current smokers, 24% had a previous PCI, and 7% had a previous MI.
Stent types were similar in the two groups, and they were delivered by radial access. Procedural success was achieved in about 98% of both groups. Almost all patients were discharged on a statin, aspirin, and a P2Y12 inhibitor, and the other specific postprocedural medications were comparable in the two groups.
Advantage of intravascular imaging consistent
Of the complex lesions, most (55%) had diffuse long coronary artery lesions, but other types of complex PCI, including bifurcated lesions (22%), chronic total occlusions (20%), severely calcified lesions (14%), and ostial lesions of a major coronary artery (15%) were represented. Across these lesion types, intravascular imaging was favored over angiography for TLF at least numerically. The potential exceptions were lesions requiring at least three stents (HR, 1.24; 95% CI, 0.49-3.18), but confidence intervals were wide.
The trial was unblinded, but Dr. Hahn reported that imaging analyses were performed at a core laboratory and events were adjudicated by a committee with members unaware of trial group assignments.
One unanswered question is cost. Because intravascular imaging adds cost to PCI relative to angiography, cost-effectiveness analyses are needed to provide context for the decision to use this approach in all complex PCI patients. These analyses are planned.
Based on the consistency of these trial results with previous studies, almost all of which showed the same thing, “the intravascular imaging world has spoken,” said Wayne B. Batchelor, MD, director of interventional cardiology, Inova Heart and Vascular Institute, Fairfax, Va. “The only question now is when will the interventional community is going to listen.”
Dr. Batchelor predicted that these data will change the mindset of many practitioners “to shift the debate to why not do it [intravascular imaging] from why do it.”
“Only about 15% of PCI is performed with intravascular imaging in the United States, and these [results] argue that this number needs to go up,” Dr. Batchelor said. Although he said there are technical reasons, such as diffuse lesions or small vessels, that prevent intravascular imaging from being used in every complex patient, he suggested the data are compelling.
“If you apply this to the one million patients undergoing PCI in the United States, this will translate potentially into tens of thousands of patients protected from the TVF endpoint,” Dr. Batchelor said.
Dr. Hahn reports no potential conflicts of interest, but this investigator-initiated trial received funding from Boston Scientific and Abbott Vascular. Dr. Batchelor reports financial relationships with Abbott Vascular, Boston Scientific, Idorsia, Medtronic, and V-Wave Medical.
NEW ORLEANS – In patients undergoing percutaneous intervention (PCI) for complex coronary lesions, intravascular imaging is superior to angiography for reducing the risk of target lesion failure (TLF), according to results of a randomized trial.
Previous studies have produced the same conclusion, but the advantage was demonstrated this time in a multicenter well-powered randomized trial, principal investigator Joo Yong Hahn, MD, PhD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The earlier studies “were not definitive,” said Dr. Hahn, pointing out that even those that were randomized lacked sufficient duration of follow-up or were not inclusive of a broad array of types of complex PCI.
In this clinical outcomes–driven study, called RENOVATE-COMPLEX-PCI, 1,639 patients undergoing complex PCI in 20 South Korean treatment centers were randomized in a 2:1 ratio to PCI guided by intravascular imaging or angiography alone. There were nine types of complex PCI eligible for trial entry, including bifurcated lesions, long lesions (expected stent length ≥ 38 mm), total coronary occlusions, lesions requiring multiple stents, severely calcified lesions, and lesions in multiple vessels.
Intravascular imaging in the experimental arm could be performed with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT), according to Dr. Hahn. Because one might be better than the other for specific patient and lesions characteristics, the type of intravascular imaging in the experimental group was selected at the discretion of the treating investigator, reported Dr. Hahn, of the Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University, Seoul.
The primary TLF endpoint was defined as death from cardiovascular causes, target-vessel-related MI, and target-vessel revascularization.
Risk reduction of > 35% observed
After a median of 2.1 years of follow-up, the lower TLF incidence in the group with PCI guided by intravascular imaging (7.7% vs. 12.3%) translated into a 36% reduction in risk (hazard ratio, 0.64; P = .008).
Intravascular imaging was associated with a numerical reduction of each component of TLF. In the case of death from cardiovascular causes, the confidence interval remained below the line of unity (HR 0.47; 95% CI, 0.24-0.93).
Although this was not true for target vessel–related MI (HR, 0.74, 95% CI, 0.45-1.22) or target vessel revascularization (HR, 0.66; 95% CI, 0.36-1.22), it was also true of TLF without procedural-related MI (HR, 0.59; 95% CI, 0.39-0.90) and cardiac death or target vessel–related MI (HR, 0.63; 95% CI, 0.42-0.93).
With few exceptions, all of the secondary outcomes “moved in the right direction” to favor intravascular imaging, including death from any cause (HR 0.71, 95% CI, 0.44-1.15), reported Dr. Hahn, who noted that the results were simultaneously published in the New England Journal of Medicine.
When compared, there were no major baseline differences in the 1,092 patients with PCI guided by intravascular imaging relative to the 547 guided by angiography. The median age was 65.5 years. Most (79%) were male. About half (51%) had an acute coronary syndrome and the remainder had stable ischemic heart disease. The proportions of patients with hypertension (61%), dyslipidemia (51%), and diabetes (38%) were substantial. About 18% of patients were current smokers, 24% had a previous PCI, and 7% had a previous MI.
Stent types were similar in the two groups, and they were delivered by radial access. Procedural success was achieved in about 98% of both groups. Almost all patients were discharged on a statin, aspirin, and a P2Y12 inhibitor, and the other specific postprocedural medications were comparable in the two groups.
Advantage of intravascular imaging consistent
Of the complex lesions, most (55%) had diffuse long coronary artery lesions, but other types of complex PCI, including bifurcated lesions (22%), chronic total occlusions (20%), severely calcified lesions (14%), and ostial lesions of a major coronary artery (15%) were represented. Across these lesion types, intravascular imaging was favored over angiography for TLF at least numerically. The potential exceptions were lesions requiring at least three stents (HR, 1.24; 95% CI, 0.49-3.18), but confidence intervals were wide.
The trial was unblinded, but Dr. Hahn reported that imaging analyses were performed at a core laboratory and events were adjudicated by a committee with members unaware of trial group assignments.
One unanswered question is cost. Because intravascular imaging adds cost to PCI relative to angiography, cost-effectiveness analyses are needed to provide context for the decision to use this approach in all complex PCI patients. These analyses are planned.
Based on the consistency of these trial results with previous studies, almost all of which showed the same thing, “the intravascular imaging world has spoken,” said Wayne B. Batchelor, MD, director of interventional cardiology, Inova Heart and Vascular Institute, Fairfax, Va. “The only question now is when will the interventional community is going to listen.”
Dr. Batchelor predicted that these data will change the mindset of many practitioners “to shift the debate to why not do it [intravascular imaging] from why do it.”
“Only about 15% of PCI is performed with intravascular imaging in the United States, and these [results] argue that this number needs to go up,” Dr. Batchelor said. Although he said there are technical reasons, such as diffuse lesions or small vessels, that prevent intravascular imaging from being used in every complex patient, he suggested the data are compelling.
“If you apply this to the one million patients undergoing PCI in the United States, this will translate potentially into tens of thousands of patients protected from the TVF endpoint,” Dr. Batchelor said.
Dr. Hahn reports no potential conflicts of interest, but this investigator-initiated trial received funding from Boston Scientific and Abbott Vascular. Dr. Batchelor reports financial relationships with Abbott Vascular, Boston Scientific, Idorsia, Medtronic, and V-Wave Medical.
NEW ORLEANS – In patients undergoing percutaneous intervention (PCI) for complex coronary lesions, intravascular imaging is superior to angiography for reducing the risk of target lesion failure (TLF), according to results of a randomized trial.
Previous studies have produced the same conclusion, but the advantage was demonstrated this time in a multicenter well-powered randomized trial, principal investigator Joo Yong Hahn, MD, PhD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The earlier studies “were not definitive,” said Dr. Hahn, pointing out that even those that were randomized lacked sufficient duration of follow-up or were not inclusive of a broad array of types of complex PCI.
In this clinical outcomes–driven study, called RENOVATE-COMPLEX-PCI, 1,639 patients undergoing complex PCI in 20 South Korean treatment centers were randomized in a 2:1 ratio to PCI guided by intravascular imaging or angiography alone. There were nine types of complex PCI eligible for trial entry, including bifurcated lesions, long lesions (expected stent length ≥ 38 mm), total coronary occlusions, lesions requiring multiple stents, severely calcified lesions, and lesions in multiple vessels.
Intravascular imaging in the experimental arm could be performed with either intravascular ultrasound (IVUS) or optical coherence tomography (OCT), according to Dr. Hahn. Because one might be better than the other for specific patient and lesions characteristics, the type of intravascular imaging in the experimental group was selected at the discretion of the treating investigator, reported Dr. Hahn, of the Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University, Seoul.
The primary TLF endpoint was defined as death from cardiovascular causes, target-vessel-related MI, and target-vessel revascularization.
Risk reduction of > 35% observed
After a median of 2.1 years of follow-up, the lower TLF incidence in the group with PCI guided by intravascular imaging (7.7% vs. 12.3%) translated into a 36% reduction in risk (hazard ratio, 0.64; P = .008).
Intravascular imaging was associated with a numerical reduction of each component of TLF. In the case of death from cardiovascular causes, the confidence interval remained below the line of unity (HR 0.47; 95% CI, 0.24-0.93).
Although this was not true for target vessel–related MI (HR, 0.74, 95% CI, 0.45-1.22) or target vessel revascularization (HR, 0.66; 95% CI, 0.36-1.22), it was also true of TLF without procedural-related MI (HR, 0.59; 95% CI, 0.39-0.90) and cardiac death or target vessel–related MI (HR, 0.63; 95% CI, 0.42-0.93).
With few exceptions, all of the secondary outcomes “moved in the right direction” to favor intravascular imaging, including death from any cause (HR 0.71, 95% CI, 0.44-1.15), reported Dr. Hahn, who noted that the results were simultaneously published in the New England Journal of Medicine.
When compared, there were no major baseline differences in the 1,092 patients with PCI guided by intravascular imaging relative to the 547 guided by angiography. The median age was 65.5 years. Most (79%) were male. About half (51%) had an acute coronary syndrome and the remainder had stable ischemic heart disease. The proportions of patients with hypertension (61%), dyslipidemia (51%), and diabetes (38%) were substantial. About 18% of patients were current smokers, 24% had a previous PCI, and 7% had a previous MI.
Stent types were similar in the two groups, and they were delivered by radial access. Procedural success was achieved in about 98% of both groups. Almost all patients were discharged on a statin, aspirin, and a P2Y12 inhibitor, and the other specific postprocedural medications were comparable in the two groups.
Advantage of intravascular imaging consistent
Of the complex lesions, most (55%) had diffuse long coronary artery lesions, but other types of complex PCI, including bifurcated lesions (22%), chronic total occlusions (20%), severely calcified lesions (14%), and ostial lesions of a major coronary artery (15%) were represented. Across these lesion types, intravascular imaging was favored over angiography for TLF at least numerically. The potential exceptions were lesions requiring at least three stents (HR, 1.24; 95% CI, 0.49-3.18), but confidence intervals were wide.
The trial was unblinded, but Dr. Hahn reported that imaging analyses were performed at a core laboratory and events were adjudicated by a committee with members unaware of trial group assignments.
One unanswered question is cost. Because intravascular imaging adds cost to PCI relative to angiography, cost-effectiveness analyses are needed to provide context for the decision to use this approach in all complex PCI patients. These analyses are planned.
Based on the consistency of these trial results with previous studies, almost all of which showed the same thing, “the intravascular imaging world has spoken,” said Wayne B. Batchelor, MD, director of interventional cardiology, Inova Heart and Vascular Institute, Fairfax, Va. “The only question now is when will the interventional community is going to listen.”
Dr. Batchelor predicted that these data will change the mindset of many practitioners “to shift the debate to why not do it [intravascular imaging] from why do it.”
“Only about 15% of PCI is performed with intravascular imaging in the United States, and these [results] argue that this number needs to go up,” Dr. Batchelor said. Although he said there are technical reasons, such as diffuse lesions or small vessels, that prevent intravascular imaging from being used in every complex patient, he suggested the data are compelling.
“If you apply this to the one million patients undergoing PCI in the United States, this will translate potentially into tens of thousands of patients protected from the TVF endpoint,” Dr. Batchelor said.
Dr. Hahn reports no potential conflicts of interest, but this investigator-initiated trial received funding from Boston Scientific and Abbott Vascular. Dr. Batchelor reports financial relationships with Abbott Vascular, Boston Scientific, Idorsia, Medtronic, and V-Wave Medical.
AT ACC 2023
Viability-guided PCI doubted in stable severe CAD: REVIVED-BCIS2
There is no magical amount of viable ventricular myocardium that makes percutaneous coronary intervention (PCI) an effective addition to optimal medical therapy (OMT) in stable patients with coronary disease and poor ventricular function, suggests an analysis from a major trial.
The REVIVED-BCIS2 trial recently made waves when it showed no clinical advantage from adding PCI to OMT in stable patients with severe ischemic left ventricular (LV) dysfunction. All the patients had shown viable but dysfunctional myocardium that could potentially be revascularized.
But in a secondary analysis, extent of such hibernating heart muscle was not a good predictor of clinical outcomes, which in the trial meant death from any cause or hospitalization for heart failure (HHF).
Burden of myocardial scar tissue, however, turned out to be a potent predictor of clinical risk regardless of coronary disease severity or even LV ejection fraction (LVEF).
Because myocardial viability tracks poorly with outcomes in patients like those enrolled in the trial, as the new analysis suggests, conventional viability testing isn’t an effective guide for deciding who among them should get PCI, Divaka Perera, MD, said in an interview.
Dr. Perera, of King’s College London and the trial’s principal investigator, presented the REVIVED-BCIS2 secondary results at the joint scientific sessions of the American College of Cardiology and the World Heart Federation..
Viability testing for ischemia, he noted, is often used in practice to aid revascularization decisions. As the extent of myocardial viability can vary, it’s been asked – ever since the trial’s primary publication – whether there could be “a sweet spot or Goldilocks zone of viability that would allow prediction of which patients will do better with PCI compared to medical therapy,” Dr. Perera said. “The trial conclusively shows that is not the case.”
That the extent of hibernating myocardium, which is viable but dysfunctional, didn’t predict clinical outcomes or LV functional recovery “is disruptive of current practice and challenges a view that’s been held for decades.”
The trial’s 700 patients receiving OMT had been randomly assigned to undergo PCI or not, 347 and 353 patients, respectively. About 12% of the total were women.
About 70% of patients underwent baseline and follow-up myocardial viability testing using cardiac magnetic resonance (CMR) imaging with late gadolinium enhancement for estimation of scar burden; the remainder underwent dobutamine-stress echocardiography. All imaging assessments were conducted at independent core laboratories, Dr. Perera reported.
Extent of myocardial viability was defined three ways: volume of hibernating heart muscle, total volume of viable myocardium, and scar burden – all expressed as a percentage of total LV volume.
Every 10% increment in LV volume found to be hibernating related to a hazard ratio of 0.98 (95% confidence interval, 0.93-1.04; P = .56) for all-cause mortality or HHF at a median of 3.3 years. The analysis was adjusted for age, sex, diabetes, previous HHF, chronic renal failure, extent of CAD, type of viability testing, and baseline LVEF.
The adjusted HR for the same percentage increment in total viable myocardium was marginally significantly reduced at 0.93 (95% CI, 0.87-1.00; P = .048).
The correlation with scar burden was stronger. The adjusted composite-endpoint HR per 10% increment in scar burden was significantly increased at 1.18 (95% CI, 1.04-1.33; P = .009).
Extent of myocardial viability by tertiles, regardless of viability definition, did not highlight any group with a reduced risk for death or HHF, or group with better LV functional recovery, from OMT plus PCI, compared with OMT alone.
The findings appear to suggest that scar burden, but not extent of viability as it’s usually measured, may effectively guide PCI decisions in such patients, Dr. Perera said.
“I would say that viability testing as we understand it now, based on the paradigm of hibernating myocardium, is very useful,” he said, “but that is not the only information we can get from a viability test.”
Scar burden can also be determined from the same tests but isn’t typically looked at. “We’re actually collecting this information but not using it,” Dr. Perera said. “When we do, it is really powerfully predictive” of both clinical outcomes and LV functional recovery. “Yet scar burden is not in any of the guidelines for stratifying risk.”
REVIVED-BCIS2 was funded by the National Institute for Health and Care Research Health Technology Assessment Program. Dr. Perera had no disclosures.
A version of this article first appeared on Medscape.com.
There is no magical amount of viable ventricular myocardium that makes percutaneous coronary intervention (PCI) an effective addition to optimal medical therapy (OMT) in stable patients with coronary disease and poor ventricular function, suggests an analysis from a major trial.
The REVIVED-BCIS2 trial recently made waves when it showed no clinical advantage from adding PCI to OMT in stable patients with severe ischemic left ventricular (LV) dysfunction. All the patients had shown viable but dysfunctional myocardium that could potentially be revascularized.
But in a secondary analysis, extent of such hibernating heart muscle was not a good predictor of clinical outcomes, which in the trial meant death from any cause or hospitalization for heart failure (HHF).
Burden of myocardial scar tissue, however, turned out to be a potent predictor of clinical risk regardless of coronary disease severity or even LV ejection fraction (LVEF).
Because myocardial viability tracks poorly with outcomes in patients like those enrolled in the trial, as the new analysis suggests, conventional viability testing isn’t an effective guide for deciding who among them should get PCI, Divaka Perera, MD, said in an interview.
Dr. Perera, of King’s College London and the trial’s principal investigator, presented the REVIVED-BCIS2 secondary results at the joint scientific sessions of the American College of Cardiology and the World Heart Federation..
Viability testing for ischemia, he noted, is often used in practice to aid revascularization decisions. As the extent of myocardial viability can vary, it’s been asked – ever since the trial’s primary publication – whether there could be “a sweet spot or Goldilocks zone of viability that would allow prediction of which patients will do better with PCI compared to medical therapy,” Dr. Perera said. “The trial conclusively shows that is not the case.”
That the extent of hibernating myocardium, which is viable but dysfunctional, didn’t predict clinical outcomes or LV functional recovery “is disruptive of current practice and challenges a view that’s been held for decades.”
The trial’s 700 patients receiving OMT had been randomly assigned to undergo PCI or not, 347 and 353 patients, respectively. About 12% of the total were women.
About 70% of patients underwent baseline and follow-up myocardial viability testing using cardiac magnetic resonance (CMR) imaging with late gadolinium enhancement for estimation of scar burden; the remainder underwent dobutamine-stress echocardiography. All imaging assessments were conducted at independent core laboratories, Dr. Perera reported.
Extent of myocardial viability was defined three ways: volume of hibernating heart muscle, total volume of viable myocardium, and scar burden – all expressed as a percentage of total LV volume.
Every 10% increment in LV volume found to be hibernating related to a hazard ratio of 0.98 (95% confidence interval, 0.93-1.04; P = .56) for all-cause mortality or HHF at a median of 3.3 years. The analysis was adjusted for age, sex, diabetes, previous HHF, chronic renal failure, extent of CAD, type of viability testing, and baseline LVEF.
The adjusted HR for the same percentage increment in total viable myocardium was marginally significantly reduced at 0.93 (95% CI, 0.87-1.00; P = .048).
The correlation with scar burden was stronger. The adjusted composite-endpoint HR per 10% increment in scar burden was significantly increased at 1.18 (95% CI, 1.04-1.33; P = .009).
Extent of myocardial viability by tertiles, regardless of viability definition, did not highlight any group with a reduced risk for death or HHF, or group with better LV functional recovery, from OMT plus PCI, compared with OMT alone.
The findings appear to suggest that scar burden, but not extent of viability as it’s usually measured, may effectively guide PCI decisions in such patients, Dr. Perera said.
“I would say that viability testing as we understand it now, based on the paradigm of hibernating myocardium, is very useful,” he said, “but that is not the only information we can get from a viability test.”
Scar burden can also be determined from the same tests but isn’t typically looked at. “We’re actually collecting this information but not using it,” Dr. Perera said. “When we do, it is really powerfully predictive” of both clinical outcomes and LV functional recovery. “Yet scar burden is not in any of the guidelines for stratifying risk.”
REVIVED-BCIS2 was funded by the National Institute for Health and Care Research Health Technology Assessment Program. Dr. Perera had no disclosures.
A version of this article first appeared on Medscape.com.
There is no magical amount of viable ventricular myocardium that makes percutaneous coronary intervention (PCI) an effective addition to optimal medical therapy (OMT) in stable patients with coronary disease and poor ventricular function, suggests an analysis from a major trial.
The REVIVED-BCIS2 trial recently made waves when it showed no clinical advantage from adding PCI to OMT in stable patients with severe ischemic left ventricular (LV) dysfunction. All the patients had shown viable but dysfunctional myocardium that could potentially be revascularized.
But in a secondary analysis, extent of such hibernating heart muscle was not a good predictor of clinical outcomes, which in the trial meant death from any cause or hospitalization for heart failure (HHF).
Burden of myocardial scar tissue, however, turned out to be a potent predictor of clinical risk regardless of coronary disease severity or even LV ejection fraction (LVEF).
Because myocardial viability tracks poorly with outcomes in patients like those enrolled in the trial, as the new analysis suggests, conventional viability testing isn’t an effective guide for deciding who among them should get PCI, Divaka Perera, MD, said in an interview.
Dr. Perera, of King’s College London and the trial’s principal investigator, presented the REVIVED-BCIS2 secondary results at the joint scientific sessions of the American College of Cardiology and the World Heart Federation..
Viability testing for ischemia, he noted, is often used in practice to aid revascularization decisions. As the extent of myocardial viability can vary, it’s been asked – ever since the trial’s primary publication – whether there could be “a sweet spot or Goldilocks zone of viability that would allow prediction of which patients will do better with PCI compared to medical therapy,” Dr. Perera said. “The trial conclusively shows that is not the case.”
That the extent of hibernating myocardium, which is viable but dysfunctional, didn’t predict clinical outcomes or LV functional recovery “is disruptive of current practice and challenges a view that’s been held for decades.”
The trial’s 700 patients receiving OMT had been randomly assigned to undergo PCI or not, 347 and 353 patients, respectively. About 12% of the total were women.
About 70% of patients underwent baseline and follow-up myocardial viability testing using cardiac magnetic resonance (CMR) imaging with late gadolinium enhancement for estimation of scar burden; the remainder underwent dobutamine-stress echocardiography. All imaging assessments were conducted at independent core laboratories, Dr. Perera reported.
Extent of myocardial viability was defined three ways: volume of hibernating heart muscle, total volume of viable myocardium, and scar burden – all expressed as a percentage of total LV volume.
Every 10% increment in LV volume found to be hibernating related to a hazard ratio of 0.98 (95% confidence interval, 0.93-1.04; P = .56) for all-cause mortality or HHF at a median of 3.3 years. The analysis was adjusted for age, sex, diabetes, previous HHF, chronic renal failure, extent of CAD, type of viability testing, and baseline LVEF.
The adjusted HR for the same percentage increment in total viable myocardium was marginally significantly reduced at 0.93 (95% CI, 0.87-1.00; P = .048).
The correlation with scar burden was stronger. The adjusted composite-endpoint HR per 10% increment in scar burden was significantly increased at 1.18 (95% CI, 1.04-1.33; P = .009).
Extent of myocardial viability by tertiles, regardless of viability definition, did not highlight any group with a reduced risk for death or HHF, or group with better LV functional recovery, from OMT plus PCI, compared with OMT alone.
The findings appear to suggest that scar burden, but not extent of viability as it’s usually measured, may effectively guide PCI decisions in such patients, Dr. Perera said.
“I would say that viability testing as we understand it now, based on the paradigm of hibernating myocardium, is very useful,” he said, “but that is not the only information we can get from a viability test.”
Scar burden can also be determined from the same tests but isn’t typically looked at. “We’re actually collecting this information but not using it,” Dr. Perera said. “When we do, it is really powerfully predictive” of both clinical outcomes and LV functional recovery. “Yet scar burden is not in any of the guidelines for stratifying risk.”
REVIVED-BCIS2 was funded by the National Institute for Health and Care Research Health Technology Assessment Program. Dr. Perera had no disclosures.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Bempedoic acid cuts CV events in statin-intolerant patients: CLEAR Outcomes
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.

“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.
“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
A new approach to lowering cholesterol with the use of bempedoic acid (Nexletol, Esperion) brought about a significant reduction in cardiovascular events in patients intolerant to statins in the large phase 3, placebo-controlled CLEAR Outcomes trial.
The drug lowered LDL cholesterol by 21% in the study and reduced the composite primary endpoint, including cardiovascular death, MI, stroke, or coronary revascularization, by 13%; MI was reduced by 23% and coronary revascularization, by 19%.
The drug was also well tolerated in the mixed population of primary and secondary prevention patients unable or unwilling to take statins.
“These findings establish bempedoic acid as an effective approach to reduce major cardiovascular events in statin-intolerant patients,” study chair, Steven E. Nissen, MD, of the Cleveland Clinic concluded.
Dr. Nissen presented the CLEAR Outcomes trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
The study was simultaneously published online in the New England Journal of Medicine. Top-line results were previously reported in December 2022.
Dr. Nissen pointed out that, while in the current study bempedoic acid was studied as monotherapy, he believes the drug will mainly be used in clinical practice in combination with ezetimibe, a combination shown to reduce LDL by 38%. “I think this is how it will be used in clinical practice. So, we can get an almost 40% LDL reduction – that’s about the same as 40 mg simvastatin or 20 mg atorvastatin – without giving a statin. And I think that’s where I see the potential of this therapy,” he said.
Dr. Nissen described statin intolerance as “a vexing problem” that prevents many patients from achieving LDL cholesterol levels associated with cardiovascular benefits.
He explained that bempedoic acid, an adenosine triphosphate citrate lyase inhibitor, inhibits hepatic cholesterol synthesis upstream of hydroxymethylglutaryl coenzyme A reductase, the enzyme inhibited by statins. Bempedoic acid is a prodrug activated in the liver, but not in peripheral tissues, resulting in a low incidence of muscle-related adverse events. Although bempedoic acid is approved for lowering LDL cholesterol, this is the first trial to assess its effects on cardiovascular outcomes.
CLEAR Outcomes
The CLEAR Outcomes trial included 13,970 patients (48% women) from 32 countries who were unable or unwilling to take statins owing to unacceptable adverse effects and who had, or were at high risk for, cardiovascular disease. They were randomly assigned to oral bempedoic acid, 180 mg daily, or placebo.
The mean LDL cholesterol level at baseline was 139 mg/dL in both groups, and after 6 months, the reduction in the level was greater with bempedoic acid than with placebo by 29.2 mg/dL (a 21.1% reduction).
The drug was also associated with a 22% reduction in high-sensitivity C-reactive protein.
After a median duration of follow-up of 40.6 months, the incidence of a primary endpoint (cardiovascular death, MI, stroke, or coronary revascularization) was significantly lower (by 13%) with bempedoic acid than with placebo (11.7% vs. 13.3%; hazard ratio, 0.87; P = .004).
The absolute risk reduction was 1.6 percentage points, and the number needed to treat for 40 months to prevent one event was 63.
The secondary composite endpoint of cardiovascular death/stroke/MI was reduced by 15% (8.2% vs. 9.5%; HR, 0.85; P = .006). Fatal or nonfatal MI was reduced by 23% (3.7% vs. 4.8%; HR, 0.77; P = .002), and coronary revascularization was reduced by 19% (6.2% vs. 7.6%; HR, 0.81; P = .001).
Bempedoic acid had no significant effects on fatal or nonfatal stroke, death from cardiovascular causes, and death from any cause.
Subgroup analysis showed similar results across all groups and no difference in treatment effect between men and women.
Adverse events were reported by 25% of patients in both groups, with adverse events leading to discontinuation reported by 10.8% of the bempedoic acid group and 10.4% of the placebo group.
Muscle disorders were reported in 15.0% of the bempedoic acid group versus 15.4% of the placebo group. And there was also no difference in new cases of diabetes (16.1% vs. 17.1%).
Bempedoic acid was associated with small increases in the incidence of gout (3.1% vs. 2.1%) and cholelithiasis (2.2% vs. 1.2%), and also small increases in serum creatinine, uric acid, and hepatic enzyme levels.
In the NEJM article, the authors pointed out that the concept of statin intolerance remains controversial. Some recent studies suggested that reported adverse effects represent an anticipation of harm, often described as the “nocebo” effect.
“Whether real or perceived, statin intolerance remains a vexing clinical problem that can prevent patients who are guideline eligible for statin treatment from reaching LDL cholesterol levels associated with clinical benefits. Accordingly, alternative nonstatin therapies are needed to manage the LDL cholesterol level in these patients,” they wrote.
“Management of patients unable or unwilling to take statins represents a challenging and frustrating clinical issue. Regardless whether this problem represents the ‘nocebo’ effect or actual intolerance, these high-risk patients need effective alternative therapies,” Dr. Nissen concluded. “The CLEAR Outcomes trial provides a sound rationale for use of bempedoic acid to reduce major adverse cardiovascular outcomes in patients intolerant to statins.”
‘Compelling findings’
Discussing the trial at the ACC late-breaking clinical trial session, Michelle O’Donoghue, MD, Brigham and Women’s Hospital, Boston, noted that this is the largest trial to date in statin-intolerant patients.
She pointed out that although the issue of statin intolerance remains controversial, adherence to statins is often not good, so this is an important patient population to study.
She said it was “quite remarkable” that 48% of the study were women, adding: “There is still much that we need to understand about why women appear to be less willing or able to tolerate statin therapy.”
Dr. O’Donoghue concluded that the study showed “compelling findings,” and the event reduction was in line with what would be expected from the LDL cholesterol reduction, further supporting the LDL cholesterol hypothesis.
She added: “Bempedoic acid is an important addition to our arsenal of nonstatin LDL-lowering therapies. And while it was overall well tolerated, it did not get a complete free pass, as there were some modest safety concerns.”
In an editorial accompanying the NEJM publication, John Alexander, MD, Duke Clinical Research Institute, Durham, N.C., wrote: “The compelling results of the CLEAR Outcomes trial will and should increase the use of bempedoic acid in patients with established atherosclerotic vascular disease and in those at high risk for vascular disease who are unable or unwilling to take statins.”
He warned, however, that it is premature to consider bempedoic acid as an alternative to statins. “Given the overwhelming evidence of the vascular benefits of statins, clinicians should continue their efforts to prescribe them at the maximum tolerated doses for appropriate patients, including those who may have discontinued statins because of presumed side effects.”.
Dr. Alexander also pointed out that although bempedoic acid also reduces the LDL cholesterol level in patients taking statins, the clinical benefits of bempedoic acid added to standard statin therapy are unknown.
On the observation that bempedoic acid had no observed effect on mortality, he noted that “Many individual trials of statins have also not shown an effect of the agent on mortality; it was only through the meta-analysis of multiple clinical trials that the effects of statins on mortality became clear.”
“Bempedoic acid has now entered the list of evidence-based alternatives to statins for primary and secondary prevention in patients at high cardiovascular risk,” Dr. Alexander concluded. “The benefits of bempedoic acid are now clearer, and it is now our responsibility to translate this information into better primary and secondary prevention for more at-risk patients, who will, as a result, benefit from fewer cardiovascular events.”
In a second editorial, John F. Keaney Jr., MD, Brigham and Women’s Hospital, said the lack of a clear association between bempedoic acid and muscle disorders, new-onset diabetes, or worsening hyperglycemia is “welcome news” for statin-intolerant patients.
But he cautioned that “these data must be interpreted cautiously, because bempedoic acid, when combined with a statin, appears to enhance the occurrence of muscle symptoms. Moreover, bempedoic acid has its own reported side effects, including tendon rupture, increased uric acid levels, gout, and reduced glomerular filtration rate, which are not seen with statin use.”
In terms of drug interactions, Dr. Keaney noted that bempedoic acid can increase the circulating levels of simvastatin and pravastatin, so it should not be used in patients who are receiving these agents at doses above 20 mg and 40 mg, respectively. Similarly, bempedoic acid should not be used with fibrates other than fenofibrate because of concerns regarding cholelithiasis.
“Available data clearly indicate that bempedoic acid can be used as an adjunct to statin and nonstatin therapies (except as noted above) to produce an additional 16%-26% reduction in the LDL cholesterol level,” he added. “However, it is not yet clear to what extent adjunctive bempedoic acid will further reduce the risk of cardiovascular events.”
The CLEAR Outcomes trial was supported by Esperion Therapeutics. Dr. Nissen reported receiving grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Esperion, Novartis, and Silence Pharmaceuticals and consultancies with Amgen and Glenmark Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
At 5 years, TAVI valves perform better than surgical ones
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.

The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”

A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.
The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”
A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
In a pooled analysis from two randomized trials, transcatheter aortic valve implantation (TAVI) was associated with significantly less bioprosthetic valve dysfunction (BVD) than a surgical prosthetic implantation, according to data presented as a late-breaker at the Cardiovascular Research Technologies conference, sponsored by MedStar Heart & Vascular Institute.
“The difference in valve performance was driven by a twofold lower SVD [structural valve deterioration] and a 3-fold lower severe PPM [prothesis-patient mismatch] for TAVI versus surgery,” reported Steven J. Yakubov, MD.
The data were pooled from the CoreValve U.S. Pivotal and SURTAVI randomized trials. Of patients participating in these two trials, 5-year follow-up data were available for 1,128 randomized to the CoreValve/Evolut TAVI and 971 randomized to surgical prosthetic valve replacement.
The major focus of the study was on the cumulative incidence of BVD, but the study also included separate analyses on the relationship between BVD and clinical outcomes. Preprocedural indicators for BVD at 5 years were also analyzed.
SVD was defined as a mean gradient increase of at least 10 mm Hg from discharge to 30 days, along with at least 20 mm Hg at last echo or new-onset aortic regurgitation. Nonstructural valve deterioration (NSVD) was defined as severe PPM at discharge or 30 days or severe paravalvular regurgitation through 5 years. In addition to these two components, the BVD endpoint also included thrombosis and endocarditis.
Surgical valve deterioration high at 5 years
On the basis of these definitions, the rate of BVD at 5 years was 14.2% in the surgery group and 7.8% in the TAVI group, translating into a 50% risk reduction in favor of TAVI (hazard ratio, 0.50; P < .001).
Thrombosis or endocarditis occurred in low rates in both groups, but every other component of BVD favored TAVI significantly, not just numerically. This included SVD (2.2% vs. 4.4%; P = .004), and the two components of NSVD, PPM (3.7% vs. 11.8%; P < .001) and severe paravalvular regurgitation (0.2% vs. 1.2%; P = .02).
When stratified by annular diameter, the relative advantage of TAVI over surgery was greatest in those valves with diameters of up to 23 mm. In this group, the lower relative rate in the TAVI group (8.6% vs. 19.7%) represented a nearly 70% reduction in risk of valve deterioration at 5 years (HR, 0.31; P < .001).
However, the advantage at 5 years also remained substantial and significant in larger valves (8.1% vs. 12.6%), translating into a 40% risk reduction in favor of TAVI (HR, 0.60; P = .002).
Independent of type of valve replacement, BVD at 5 years was associated with worse outcomes, including significantly increased risks for all-cause mortality (HR, 1.46; P = .004), cardiovascular mortality (1.84; P < .001), and hospitalization for valve disease or worsening heart failure (HR, 1.67; P = .001).
The baseline characteristics that were statistically associated with BVD at 5 years on multivariate analysis in pooled data from both the TAVI and surgical groups included age (P = .02), a creatinine clearance less than 30 mL/min per 1.73 m2 (P = .006), and a low relative baseline left ventricular ejection fraction (P < .001).
BVD criteria validated for outcome prediction
The four components of valve performance employed in this analysis (SVD, NSVD, thrombosis, and endocarditis) were drawn from consensus documents issued by the Valve Academic Research Consortium and the European Association of Percutaneous Cardiovascular Interventions, but the relative importance of these components for predicting valve survival was previously unknown, according to Dr. Yakubov.
“This is the first analysis to validate clinical criteria for valve performance and its association with clinical outcomes,” said Dr. Yakubov, medical director of cardiovascular studies, OhioHealth Research Institute at Riverside Methodist Hospital, Columbus.
This is also the first study to employ randomized data to prove an advantage of TAVI over surgery in long-term follow-up.
A 10-year follow-up is planned for the patients who participated in these two trials, but the lower rate of BVD in the TAVI arm at 5 years is already a threat to surgical repairs, acknowledged several surgeons who served as panelists in the session where these results were presented.
“I think that these data are a reflection of the fact that we [surgeons] are not being as aggressive as we should be,” said Gregory P. Fontana, MD, who is national director, cardiothoracic surgery, HCA Healthcare, and is affiliated with Los Robles Health System, Thousand Oaks, Calif. “We need to be employing larger prostheses.”
A very similar comment was made by Michael J. Reardon, MD, a professor of cardiothoracic surgery at Houston Methodist Hospital. Pointing to the higher rate of PVL as an example of a common postsurgical complication, he agreed that surgeons should be moving to bigger valve sizes.
While adjustments in valve size might address the steeper rise in NSVD subtypes of BVD observed in the surgical group, but Dr. Reardon and others pointed out that late BVD events also rose at a greater pace in the surgical group. These suggest other improvements in technique might also be needed to keep surgical valve repairs competitive.
Dr. Yakubov reported financial relationships with Medtronic and Boston Scientific, both of which provided funding for this study. Dr. Fontana reported financial relationships with Abbott and Medtronic. Dr. Reardon reported financial relationships with Abbott, Boston Scientific, Medtronic, and Gore Medical.
FROM CRT 2023
500 more steps a day tied to 14% lower CVD risk in older adults
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.

The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
Older adults who added a quarter mile of steps to their day showed a reduction in risk of cardiovascular events by 14% within 4 years, according to a study in more than 400 individuals.
“Aging is such a dynamic process, but most studies of daily steps and step goals are conducted on younger populations,” lead author Erin E. Dooley, PhD, an epidemiologist at the University of Alabama at Birmingham, said in an interview.
The impact of more modest step goals in older adults has not been well studied, Dr. Dooley said.
The population in the current study ranged from 71 to 92 years, with an average age of 78 years. The older age and relatively short follow-up period show the importance of steps and physical activity in older adults, she said.
Dr. Dooley presented the study at the Epidemiology and Prevention/Lifestyle and Cardiometabolic Health meeting.
She and her colleagues analyzed a subsample of participants in Atherosclerosis Risk in Communities (ARIC) study, an ongoing study conducted by the National Heart, Lung, and Blood Institute. The study population included 452 adults for whom step data were available at visit 6 of the ARIC study between 2016 and 2017. Participants wore an accelerometer on the waist for at least 10 hours a day for at least 3 days. The mean age of the participants was 78.4 years, 59% were women, and 20% were Black.
Outcomes were measured through December 2019 and included fatal and nonfatal cardiovascular disease (CVD) events of coronary heart disease, stroke, and heart failure.
Overall, each additional 500 steps per day was linked to a 14% reduction in risk of a CVD event (hazard ratio, 0.86; 95% confidence interval, 0.76-0.98). The mean step count was 3,447 steps per day, and 34 participants (7.5%) experienced a CVD event over 1,269 person-years of follow-up.
The cumulative risk of CVD was significantly higher (11.5%) in the quartile of adults with the lowest step count (defined as fewer than 2,077 steps per day), compared with 3.5% in those with the highest step count (defined as at least 4,453 steps per day).
In addition, adults in the highest quartile of steps had a 77% reduced risk of a proximal CVD (within 3.5 years) event over the study period (HR, 0.23).
Additional research is needed to explore whether increased steps prevent or delay CVD and whether low step counts may be a biomarker for underlying disease, the researchers noted in their abstract.
However, the results support the value of even a modest increase in activity to reduce CVD risk in older adults.
Small steps may get patients started
Dr. Dooley said she was surprised at the degree of benefits on heart health from 500 steps, and noted that the findings have clinical implications.
“Steps may be a more understandable metric for physical activity for patients than talking about moderate to vigorous intensity physical activity,” she said in an interview. “While we do not want to diminish the importance of higher intensity physical activity, encouraging small increases in the number of daily steps can also have great benefits for heart health.
“Steps are counted using a variety of devices and phones, so it may be helpful for patients to show clinicians their activity during well visits,” Dr. Dooley said. “Walking may also be more manageable for people as it is low impact. Achievable goals are also important. This study suggests that, for older adults, around 3,000 steps or more was associated with reduced CVD risk,” although the greatest benefits were seen with the most active group who averaged 4,500 or more steps per day.
More research is needed to show how steps may change over time, and how this relates to CVD and heart health,” she said. “At this time, we only had a single measure of physical activity.”
Study fills research gap for older adults
“Currently, the majority of the literature exploring a relationship between physical activity and the risk for developing cardiovascular disease has evaluated all adults together, not only those who are 70 year of age and older,” Monica C. Serra, PhD, of the University of Texas, San Antonio, said in an interview. “This study allows us to start to target specific cardiovascular recommendations for older adults.”.
“It is always exciting to see results from physical activity studies that continue to support prior evidence that even small amounts of physical activity are beneficial to cardiovascular health,” said Dr. Serra, who is also vice chair of the program committee for the meeting. “These results suggest that even if only small additions in physical activity are achievable, they may have cumulative benefits in reducing cardiovascular disease risk.” For clinicians, the results also provide targets that are easy for patients to understand, said Dr. Serra. Daily step counts allow clinicians to provide specific and measurable goals to help their older patients increase physical activity.
“Small additions in total daily step counts may have clinically meaningful benefits to heart health, so promoting their patients to make any slight changes that are able to be consistently incorporated into their schedule should be encouraged. This may be best monitored by encouraging the use of an activity tracker,” she said.
Although the current study adds to the literature with objective measures of physical activity utilizing accelerometers, these devices are not as sensitive at picking up activities such as bicycling or swimming, which may be more appropriate for some older adults with mobility limitations and chronic conditions, Dr. Serra said. Additional research is needed to assess the impact of other activities on CVD in the older population.
The meeting was sponsored by the American Heart Association. The study received no outside funding. Dr. Dooley and Dr. Serra had no financial conflicts to disclose.
FROM EPI/LIFESTYLE 2023
Frequent cannabis use tied to coronary artery disease
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
In the first part, in an observational study, daily cannabis use was associated with 34% higher odds for CAD, compared with never-users, in a large population-based U.S. cohort. Less frequent use was not associated with increased odds for CAD.
In the second part, people with a genetic susceptibility to cannabis use disorder or severe cannabis dependency had an increased risk for CAD, compared with other people.
Ishan Paranjpe, MD, the study’s lead author, reported these results in a press briefing and will present the study at the upcoming joint scientific sessions of the American College of Cardiology and the World Heart Federation 2023.
“A couple of takeaway points are that daily cannabis use, but not less frequent cannabis use, was associated with CAD” in the large population-based cohort, said Dr. Paranjpe, a resident physician at Stanford (Calif.) University, during the press conference.
“This analysis was adjusted for several possible confounders including age, sex at birth, [body mass index (BMI)], race, education, cigarette use, hypertension, high cholesterol, and diabetes,” he noted, and even after accounting for these risk factors, the association with heart disease remained.
“And the next thing, using Mendelian randomization, we sort of implied that there might be a causal relationship between cannabis and heart disease. Importantly this effect is independent of alcohol and cigarette use.
“The notion that cannabis is completely benign is probably wrong, and there might be certain risk of certain cardiovascular effects of cannabis we should be more on the lookout for,” Dr. Paranjpe said in an interview.
“Our main conclusion was that prevalent CAD is associated with cannabis consumption,” he added. “Other mechanistic work published in Cell has also shown that cannabis causes vascular inflammation that may lead to CAD.
“Thus, there is growing evidence from both laboratory and population studies that cannabis consumption may be harmful for cardiovascular health,” he said. “However, we still need more work on whether it affects the risk of incident cardiovascular events (i.e., stroke, heart attack) in patient[s] with existing CAD.”
ASCVD risk
Invited to comment, Robert L. Page II, PharmD, chair of the writing group for the American Heart Association’s scientific statement Medical Marijuana, Recreational Cannabis, and Cardiovascular Health, published in 2020, said, “This adds to our hypothesis that if you are using marijuana over a longer period, greater exposure, you’re going to see an increase in the risk” for atherosclerotic cardiovascular disease (ASCVD).
“We’re seeing this increased risk for ASCVD in young adults between ages 18 to 40 – people who think that they’re invincible,” Dr. Page, a professor at the University of Colorado at Denver, Aurora, who was not involved with this research, told this news organization in an interview.
“The bottom line is that the risk that they are seeing is what has also been documented in other observational studies, and it adds fuel to the fire. We need to be paying close attention to this,” he said.
“Primary care [clinicians], cardiologists, need to address this, particularly in younger adults – because that’s where you’re seeing the highest amount of use.”
‘All of Us’ observational study
In the first part of the study, the researchers analyzed data from the “All of Us” cohort comprising adults age 18 and older from 340 inpatient and outpatient sites across the United States.
They identified 57,958 individuals who replied to a questionnaire asking about cannabis use (medicinal or recreational and whether it was edible or used by smoking or vaping) over the past 3 months.
There were 39,678 never-users, 8,749 who used it once or twice, 2,075 who used it monthly, 2,720 who used it weekly, and 4,736 who used it daily.
Of these, 3,506 individuals had CAD, based on medical records.
Only daily users had a significantly higher risk for CAD, compared with never-users (odds ratio, 1.34; P = .001) after adjusting for age, sex, hypertension, hyperlipidemia, type 2 diabetes, BMI, education, insurance status, and cigarette use.
The median age for daily users was 41, whereas the median age for never-users was 59.
GWAS analyses
The researchers then performed a Mendelian randomization analysis based on genome-wide association studies (GWAS) of cannabis use disorder and of CAD.
“Cannabis use disorder is a psychiatric diagnosis of severe cannabis dependency, equivalent to ‘alcohol use disorder’ for alcohol consumption,” Dr. Paranjpe explained. “The exact definition involves frequent use leading to significant dependence (but does not specify how often it is used).”
The GWAS data for cannabis use disorder came from a recent meta-analysis of three cohorts: the Psychiatric Genomics Consortium Substance Use Disorders working group, iPSYCH, and deCODE.
The GWAS statistics for CAD were obtained from the CARDIoGRAMplusC4D Consortium.
Cannabis use disorder was associated with significantly increased odds for CAD (OR, 1.05; P = .001), which remained after adjusting for both cigarette and alcohol use (OR, 1.04).
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Old drug verapamil may have new use in type 1 diabetes
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
In children and adolescents with new-onset type 1 diabetes, the calcium channel blocker verapamil slowed the destruction of insulin-producing pancreatic beta cells for up to a year, new data show.
Use of daily verapamil within a month of diagnosis resulted in a 30% increase in C-peptide secretion (a measure of preserved beta-cell function), compared with placebo at 52 weeks, without serious adverse events.
To put it another way, verapamil delayed the expected decline in C-peptide production from 3 months after diagnosis of type 1 diabetes to 6 months after diagnosis.
“We think this is a really, really exciting finding that’s hopefully going to impact the care for children with type 1 diabetes in the new-onset period,” lead author Gregory P. Forlenza, MD, said during his presentation of the data on Feb. 24 at the annual Advanced Technologies & Treatments for Diabetes (ATTD) meeting in Berlin.
“In view of the favorable safety profile, particularly compared with immune-suppressive agents, once-a-day oral administration, and low cost, initiation of verapamil should be a consideration for newly diagnosed patients with type 1 diabetes,” added Dr. Forlenza, a pediatric endocrinologist at the Barbara Davis Center for Diabetes, Anschutz Medical Campus, University of Colorado, Aurora.
The data were also simultaneously published in JAMA, as part of the CLVer (Hybrid Closed Loop Therapy and Verapamil for Beta Cell Preservation in New Onset Type 1 Diabetes) trial.
The randomized, double-blind, six-center trial involved 113 participants, aged 7-17 years, with newly diagnosed type 1 diabetes. They were randomized to the most advanced commercially available automated insulin delivery systems available or standard care to test the effects of intensive glucose control on C-peptide levels for 52 weeks during the COVID-19 pandemic (July 2020 to September 2022). Eighty-eight patients who weighed 30 kg (66 lb) or more were further randomized (1:1) to daily extended-release verapamil or placebo for the same duration.
The positive findings for verapamil, published in one paper, contrasted with the negative ones for the automated insulin delivery (AID) system. The latter did not prevent the expected decline in C-peptide, putting to rest a long-held hypothesis that reducing glucotoxicity might preserve beta-cell function in newly diagnosed individuals with type 1 diabetes, noted Dr. Forlenza.
Could combination therapy work?
In recent years, immune-modulating agents have increasingly been shown to preserve beta-cell function in both new-onset and preclinical type 1 diabetes. One such agent, teplizumab (Tzield, Provention Bio), was approved by the U.S. Food and Drug Administration in November 2022 to delay type 1 diabetes onset in those at high risk.
Calcium channel blockers such as verapamil – used for years to treat hypertension and cardiac arrhythmias – may accomplish the same goal as teplizumab but in a different way, by reducing the protein overexpression that induces beta-cell apoptosis and death.
Dr. Forlenza showed a slide comparing the preservation of C-peptide, which was much lower with verapamil, at 30%, than with teplizumab, at 75%.
Asked to comment, session moderator Torben Biester, MD, a pediatric diabetologist at Auf der Bult-Zentrum Diabetes-Center for Children and Adolescents, Hanover, Germany, said: “[Verapamil] is a very cheap [daily] pill. [Teplizumab] is a very high-priced ... immune therapy in the United States ... an infusion twice for 10 days, so it’s a lot more burden for the patients and a lot more risk of side effects.”
“The future might be combination therapy,” added Dr. Biester.
And in an editorial published in JAMA and accompanying the two CLVer papers, Jennifer Couper, MD, of the University of Adelaide, agrees: “A well-tolerated, inexpensive, oral treatment such as verapamil with modest benefits on C-peptide production is relevant to practice.”
The new work “supports investigation of verapamil in combination with other effective agents during the earlier stages of type 1 diabetes before insulin dependence develops,” she noted.
Verapamil results ‘brilliant’ but more work needed
In the verapamil part of the CLVer trial, by 52 weeks, verapamil doses in the youth who received it ranged from 120-360 mg/day based on weight and tolerance.
The primary outcome, C-peptide area under the curve, stayed stable, from 0.66 pmol/mL at baseline to 0.65 pmol/mL at 52 weeks in the verapamil group, compared with a drop from 0.60 pmol/mL down to 0.44 pmol/mL with placebo, a significant difference of 0.14 pmol/mL (P = .04), representing a 30% higher C-peptide level in the verapamil group.
“For us, this is a phenomenally exciting result,” Dr. Forlenza commented during his presentation.
At 52 weeks, A1c was 6.6% in the verapamil group versus 6.9% with placebo, which was not significantly different. Daily insulin dose was 0.65 versus 0.74 units/kg per day, respectively, also not significantly different.
One severe hypoglycemic event occurred in each group, and one diabetic ketoacidosis event occurred in the placebo group. In the verapamil group, three participants experienced “nonserious” electrocardiogram abnormalities and one had hypertension.
Dr. Biester said he isn’t “that concerned” about the small number of mild ECG abnormalities seen in the study with verapamil, as this is a known side effect. But overall, he said, “I would think that for a recommendation for routine use it’s too early after one study, even though the results are brilliant.”
He noted that he is involved in a similar ongoing study of verapamil in adults with new-onset type 1 diabetes, called Ver-A-T1D.
No C-peptide effect of tight glycemic control: ‘A tough pill’
In the AID part of the study, the 113 participants were randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact (a median of 35 times) by study staff, or standard management using a continuous glucose monitor (CGM) with an insulin pump or multiple daily injections.
At 52 weeks, A1c was 6.5% for the intensive group versus 7.1% with standard care, a significant difference. Time in blood glucose range of 70-180 mg/dL was significantly longer with intensive management, at 78%, compared with standard care, at 64%.
Nonetheless, the change in C-peptide area under the curve did not differ between the two groups, decreasing from 0.57 pmol/mL at baseline to 0.45 pmol/mL at 52 weeks with the AID system, compared with a decrease from 0.60 pmol/L down to 0.50 pmol/L with standard care (P = .89).
Dr. Forlenza commented that the hypothesis that tight glycemic control would delay the decline in C-peptide secretion “is something I think a lot of endocrinologists assumed to be true and something I’ve heard lots of colleagues over the years talk about.”
Consequently, he said these findings are “a tough pill for us to swallow ... but it’s important for us in the field to understand.”
“Even with frequent contacts that are well above the level we’d be able to do in standard clinical care, and even with use of the most advanced AID systems we have ... we saw absolutely no difference in stimulated C-peptide levels at any of the timepoints throughout the first year or at 52 weeks.”
“So, in our opinion, this,” combined with a prior study from 2022, “should put this hypothesis to rest,” he said.
“Excellent glycemic control has a benefit in and of itself, but it was not a successful intervention for beta-cell preservation.”
Dr. Forlenza has reported serving as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem Diabetes Care, Insulet, Lilly, and Beta Bionics, and his institution has also received funding on his behalf for research grants from these companies. Dr. Biester has reported receiving speaker’s fees from DexCom, Medtronic, Novo Nordisk, F. Hoffmann–La Roche, Sanofi, and Ypsomed Holding; serving on advisory boards for Ascensia Diabetes Care Holdings, AstraZeneca, DexCom, and Medtronic; and receiving personal fees from SYNLAB; and is a member of the European Commission Expert Panel for Medical Devices for Endocrinology and Diabetes. Dr. Couper has reported no relevant financial relationships.
The rationale for the companion CLVer analysis of the effect of reducing glucose toxicity via tight glycemic control on C-peptide progression dates back to an inpatient study published in 1989 involving 26 adolescents using an early artificial pancreas prototype called a Biostator, in which beta-cell preservation was achieved. However, two more recent studies of this approach, including one published in late 2022, did not show a difference. The CLVer analysis involved 113 participants randomized 2:1 to one of two commercially available AID systems (Tandem t:slim X2 with Control-IQ or Medtronic 670G or 780G) plus frequent contact by study staff, or standard management using a CGM with a pump or multiple daily injections.
A version of this article originally appeared on Medscape.com.
Insomnia, short sleep linked to greater risk for MI
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.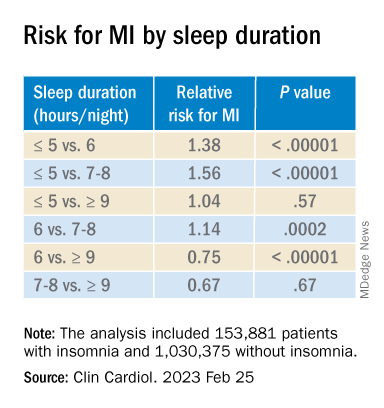
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Insomnia – difficulty falling or staying asleep – was associated with a 69% greater risk of having a myocardial infarction than among adults without insomnia, according to new research.
Those who slept 5 or fewer hours per night had the highest risk for MI, and those with both diabetes and insomnia had double the risk for MI, compared with patients without these comorbidities.
The findings are from a meta-analysis of studies in more than 1 million patients, almost all without prior MI who were, on average, in their early 50s and followed for 9 years.
Yomna E. Dean, a medical student at Alexandria (Egypt) University, reported these results in a press briefing, and the study was simultaneously published in Clinical Cardiology. It will be presented at the upcoming at the annual scientific sessions of the American College of Cardiology.
“Insomnia and ]at least] 5 hours of sleep are highly associated with increased incidence of MI, an association comparable to that of other MI risk factors and as such, it should be considered as a risk factor for MI and to be incorporated into MI prevention guidelines,” the researchers concluded.
“We believe that [insomnia] should be screened and patients should be educated about the importance of sleep because nowadays insomnia is no longer a disease – sleep deprivation could also be a life choice,” Ms, Dean told a press conference prior to the meeting.
“Clinicians must educate the patients about the importance of sleep in maintaining a healthy heart and encourage proper sleep hygiene,” Ms. Dean reiterated in an email. “And if a patient still has insomnia, other methods should be considered such as cognitive-behavior[al] therapy for insomnia [CBT-I].”
Adds to growing evidence
This study does not allow any conclusion about whether treating insomnia will reduce heart attack risk, Jennifer L. Martin, PhD, president of the American Academy of Sleep Medicine, noted in a comment. Nor does it report the diversity of study participants, since insomnia is also a health equity issue, she noted, and insomnia symptoms and comorbidities were self-reported.
However, this analysis “adds to the growing evidence that poor quality or insufficient sleep is associated with poor health,” said Dr. Martin, professor of medicine at the University of California, Los Angeles, who was not involved with this research.
The study reinforces the recommendation from the American Heart Association, which includes “Get Healthy Sleep” as one of “Life’s Essential 8” for heart health, Dr. Martin noted.
“Particularly in primary care where disease prevention and health promotion are important, clinicians should be asking all patients about their sleep – just like they ask about diet and exercise – as a key aspect of maintaining heart health,” she said.
Advice about basic sleep hygiene advice is a first step, she noted.
When improved sleep hygiene is not enough to address chronic insomnia, the AASM’s clinical practice guidelines and the guidelines of the Department of Veterans Affairs/Department of Defense, recommend first-line treatment with CBT-I, typically offered by a sleep specialist or mental health clinician.
Similarly, the American College of Physicians suggests that sleeping pills should be reserved for short-term use in patients who may not benefit sufficiently from CBT-I.
Sleeping too little, too much, equally harmful
“Studies have found that insomnia and subsequent sleep deprivation puts the body under stress,” Ms. Dean said. “This triggers cortisol release which could accelerate atherosclerosis,” and increase risk of MI.
For this analysis, the researchers identified nine observational studies, published from 1998 to 2019, with data on incident MI in adults who had insomnia.
The diagnosis of insomnia was based on ICD diagnostic codes or on the DSM‐5, which defines insomnia as the presence of any of the following three symptoms: difficulty initiating sleep, difficulty maintaining sleep, or early morning awakening with inability to return to sleep. Patients with sleep apnea were excluded.
The studies were in populations in China, Germany, Norway, Taiwan, United Kingdom, and United States, in 1.1 million adults aged 18 and older. The patients had a mean age of 52 years and 13% had insomnia.
During follow-up, 2,406 of 153,881 patients with insomnia, and 12,398 of 1,030,375 patients without insomnia had an MI.
In the pooled analysis, patients with insomnia had a significantly increased risk of MI (relative risk, 1.69; P < .00001), after adjusting for age, gender, diabetes, hypertension, high cholesterol, and smoking.
Sleeping 5 hours or less was associated with a greater risk for MI than sleeping 6 hours, or 7-8 hours, but sleeping 9 hours or more was just as harmful.
Patients who had difficulty initiating and maintaining sleep – two symptoms of insomnia – had a 13% increased risk for MI compared with other patients (RR, 1.13; P = .003).
However, patients who had nonrestorative sleep and daytime dysfunction despite adequate sleep – which is common – did not have an increased risk of MI, compared with other patients (RR, 1.06; P = .46).
Women with insomnia had a 2.24-fold greater risk for MI than other women, whereas men with insomnia had a 2.03-fold greater risk for MI than other men.
Patients with insomnia had a greater risk for MI than those without insomnia in subgroups based on patients’ age (< 65 and > 65), follow up duration (≤ 5 years and > 5 years), and comorbidities (diabetes, hypertension, and hyperlipidemia).
The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACC 2023