User login
Internists’ use of ultrasound can reduce radiology referrals
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.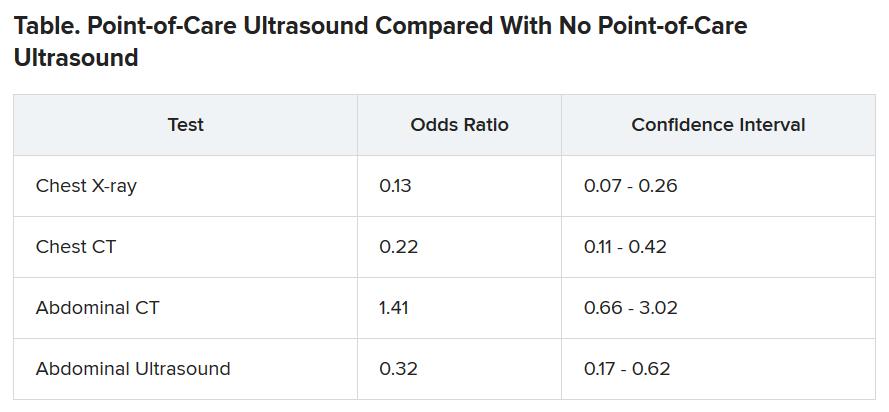
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
researchers say.
“It’s a safe and very useful tool,” Marco Barchiesi, MD, an internal medicine resident at Luigi Sacco Hospital in Milan, said in an interview. “We had a great reduction in chest x-rays because of the use of ultrasound.”
The finding addresses concerns that ultrasound used in primary care could consume more health care resources or put patients at risk.
Dr. Barchiesi and colleagues published their findings July 20 in the European Journal of Internal Medicine.
Point-of-care ultrasound has become increasingly common as miniaturization of devices has made them more portable. The approach has caught on particularly in emergency departments where quick decisions are of the essence.
Its use in internal medicine has been more controversial, with concerns raised that improperly trained practitioners may miss diagnoses or refer patients for unnecessary tests as a result of uncertainty about their findings.
To measure the effect of point-of-care ultrasound in an internal medicine hospital ward, Dr. Barchiesi and colleagues alternated months when point-of-care ultrasound was allowed with months when it was not allowed, for a total of 4 months each, on an internal medicine unit. They allowed the ultrasound to be used for invasive procedures and excluded patients whose critical condition made point-of-care ultrasound crucial.
The researchers analyzed data on 263 patients in the “on” months when point-of-care ultrasound was used, and 255 in the “off” months when it wasn’t used. The two groups were well balanced in age, sex, comorbidity, and clinical impairment.
During the on months, the internists ordered 113 diagnostic tests (0.43 per patient). During the off months they ordered 329 tests (1.29 per patient).
The odds of being referred for a chest x-ray were 87% less in the “on” months, compared with the off months, a statistically significant finding (P < .001). The risk for a chest CT scan and abdominal ultrasound were also reduced during the on months, but the risk for an abdominal CT was increased.
Nineteen patients died during the o” months and 10 during the off months, a difference that was not statistically significant (P = .15). The median length of stay in the hospital was almost the same for the two groups: 9 days for the on months and 9 days for the off months. The difference was also not statistically significant (P = .094).
Point-of-care ultrasound is particularly accurate in identifying cardiac abnormalities and pleural fluid and pneumonia, and it can be used effectively for monitoring heart conditions, the researchers wrote. This could explain the reduction in chest x-rays and CT scans.
On the other hand, ultrasound cannot address such questions as staging in an abdominal malignancy, and unexpected findings are more common with abdominal than chest ultrasound. This could explain why the point-of-care ultrasound did not reduce the use of abdominal CT, the researchers speculated.
They acknowledged that the patients in their sample had an average age of 81 years, raising questions about how well their data could be applied to a younger population. And they noted that they used point-of-care ultrasound frequently, so they were particularly adept with it. “We use it almost every day in our clinical practice,” said Dr. Barchiesi.
Those factors may have played a key role in the success of point-of-care ultrasound in this study, said Michael Wagner, MD, an assistant professor of medicine at the University of South Carolina, Greenville, who has helped colleagues incorporate ultrasound into their practices.
Elderly patients often present with multiple comorbidities and atypical signs and symptoms, he said. “Sometimes they can be very confusing as to the underlying clinical picture. Ultrasound is being used frequently to better assess these complicated patients.”
Dr. Wagner said extensive training is required to use point-of-care ultrasound accurately.
Dr. Barchiesi also acknowledged that the devices used in this study were large portable machines, not the simpler and less expensive hand-held versions that are also available for similar purposes.
Point-of-care ultrasound is a promising innovation, said Thomas Melgar, MD, a professor of medicine at Western Michigan University, Kalamazoo. “The advantage is that the exam is being done by someone who knows the patient and specifically what they’re looking for. It’s done at the bedside so you don’t have to move the patient.”
The study could help address opposition to internal medicine residents being trained in the technique, he said, adding that “I think it’s very exciting.”
The study was partially supported by Philips, which provided the ultrasound devices. Dr. Barchiesi, Dr. Melgar, and Dr. Wagner disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Used together, troponin and coronary calcium improve CV risk assessment
If either high sensitivity cardiac troponin (hs-cTnT) or coronary artery calcium (CAC) are elevated, the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) climbs substantially, which suggests these biomarkers yield more prognostic information when they are used together, according to a cohort study with a median 15 years of follow-up.
Among those with a double negative result, meaning hs-cTnT was less than the limit of detection (<3 ng/L) and the CAC score was zero, only 2.8% developed ASCVD within 10 years, but the rates climbed to 4.6% if hs-cTnT was detectable and to 9.8% if the CAC score exceeded zero even when the other biomarker was negative.
“The increased risk for ASCVD among those with discordant results indicate that their prognostic information is complementary, favoring their conjoined use for risk prediction,” reported a multicenter team of investigators led by Allan S. Jaffe, MD, professor of laboratory medicine and pathology, Mayo Clinic, Rochester, Minn.
The study was performed with data from 6,749 participants in the Multi-Ethnic Study of Atherosclerosis (MESA), which is a longitudinal, community-based study funded by the National Heart, Lung, and Blood Institute. Over the course of long-term follow-up in a patient population that was about half female, 39% non-Hispanic white, 28% Black, 22% Hispanic American, and 12% Asian, ASCVD events were evaluated in relation to both biomarkers measured at baseline.
At baseline, both biomarkers were negative in 22%, both positive in 40%, and discordant in 38%.
After a median follow-up of 15 years, when 1,002 ASCVD events had occurred, the crude rate of ASCVD was 2.8 per 1,000 person-years in the double-negative group. When compared with this, the adjusted hazard ratio for ASCVD among those with double positive biomarkers was 3.5 (P < .00001). Increased risk was also highly significant if just hs-cTnT was positive (HR, 1.59; P = .003) or if just CAC was positive (HR, 2.74; P < .00001).
The added value of using both biomarkers to identify individuals at very low risk of ASCVD makes sense, according to the authors of an accompanying editorial. Written by a team led by John W. McEvoy, MB, BCh, National University of Ireland, Galway, the editorial explained why the information is complementary.
“CAC indicates subclinical atherosclerosis, whereas hs-cTnT indicates myocardial ischemia or damage, not just from coronary stenosis but also due to other conditions like hypertensive heart and left ventricular hypertrophy,” the authors stated.
Although they maintained that adding N-terminal pro-brain natriuretic peptide, which could be drawn from the same blood sample as hs-cTnT, might prove to be an even better but still simple strategy to identify low-risk patients, they praised the concept of combining biomarkers.
“If one’s wish is to identify truly low-risk individuals, then it appears that it takes two negative ASCVD biomarkers to make that wish come true,” the authors of the editorial concluded.
Relative to alternative methods of ASCVD risk assessment, measurement of these biomarkers might be useful for sparing patients from interventions, such as lipid lowering with statin therapy, being considered on the basis of conventional risk factors alone.
Dr. Jaffe said in an interview that he considers the two-biomarker assessment to be a useful tool in the low-risk population that he studied, but he does not consider this strategy as a substitute for other methods, such as those outline in the 2019 ACC/AHA guidelines that address the entire spectrum of risk, although work is planned to see if this approach can be extended to this broader group.*
“The data we have presented now is a good start and suggests that these two objective measures can identify those who are at very low risk and avoid adding individuals who may not be at as low risk if only one of the two tests is used,” Dr. Jaffe explained.
“Given there are now techniques to measure coronary calcium from any chest CT study, and that high sensitivity cardiac troponin is a relatively inexpensive test, putting them together should really help risk stratify patients,” he added.
When asked whether this approach will eventually replace conventional methods of ASCVD risk assessment, such as those proposed in the 2019 American College of Cardiology/American Heart Association guidelines for the primary prevention of cardiovascular disease (Circulation. 2019;140:e596-e646), he said maybe.
“The answer is that we will probe that question in our ongoing studies using continuous data in an attempt to evaluate how to use this approach to risk stratify larger numbers of individuals,” Dr. Jaffe replied.
The senior investigator, Dr. Jaffe, has consulting relationships with many pharmaceutical companies. The editorial authors had no relevant disclosures.
SOURCE: Sandoval Y et al. J Am Coll Cardiol. 2020;76:357-370.
*Correction, 7/27/20: An earlier version of this article mischaracterized Dr. Jaffe's statement.
If either high sensitivity cardiac troponin (hs-cTnT) or coronary artery calcium (CAC) are elevated, the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) climbs substantially, which suggests these biomarkers yield more prognostic information when they are used together, according to a cohort study with a median 15 years of follow-up.
Among those with a double negative result, meaning hs-cTnT was less than the limit of detection (<3 ng/L) and the CAC score was zero, only 2.8% developed ASCVD within 10 years, but the rates climbed to 4.6% if hs-cTnT was detectable and to 9.8% if the CAC score exceeded zero even when the other biomarker was negative.
“The increased risk for ASCVD among those with discordant results indicate that their prognostic information is complementary, favoring their conjoined use for risk prediction,” reported a multicenter team of investigators led by Allan S. Jaffe, MD, professor of laboratory medicine and pathology, Mayo Clinic, Rochester, Minn.
The study was performed with data from 6,749 participants in the Multi-Ethnic Study of Atherosclerosis (MESA), which is a longitudinal, community-based study funded by the National Heart, Lung, and Blood Institute. Over the course of long-term follow-up in a patient population that was about half female, 39% non-Hispanic white, 28% Black, 22% Hispanic American, and 12% Asian, ASCVD events were evaluated in relation to both biomarkers measured at baseline.
At baseline, both biomarkers were negative in 22%, both positive in 40%, and discordant in 38%.
After a median follow-up of 15 years, when 1,002 ASCVD events had occurred, the crude rate of ASCVD was 2.8 per 1,000 person-years in the double-negative group. When compared with this, the adjusted hazard ratio for ASCVD among those with double positive biomarkers was 3.5 (P < .00001). Increased risk was also highly significant if just hs-cTnT was positive (HR, 1.59; P = .003) or if just CAC was positive (HR, 2.74; P < .00001).
The added value of using both biomarkers to identify individuals at very low risk of ASCVD makes sense, according to the authors of an accompanying editorial. Written by a team led by John W. McEvoy, MB, BCh, National University of Ireland, Galway, the editorial explained why the information is complementary.
“CAC indicates subclinical atherosclerosis, whereas hs-cTnT indicates myocardial ischemia or damage, not just from coronary stenosis but also due to other conditions like hypertensive heart and left ventricular hypertrophy,” the authors stated.
Although they maintained that adding N-terminal pro-brain natriuretic peptide, which could be drawn from the same blood sample as hs-cTnT, might prove to be an even better but still simple strategy to identify low-risk patients, they praised the concept of combining biomarkers.
“If one’s wish is to identify truly low-risk individuals, then it appears that it takes two negative ASCVD biomarkers to make that wish come true,” the authors of the editorial concluded.
Relative to alternative methods of ASCVD risk assessment, measurement of these biomarkers might be useful for sparing patients from interventions, such as lipid lowering with statin therapy, being considered on the basis of conventional risk factors alone.
Dr. Jaffe said in an interview that he considers the two-biomarker assessment to be a useful tool in the low-risk population that he studied, but he does not consider this strategy as a substitute for other methods, such as those outline in the 2019 ACC/AHA guidelines that address the entire spectrum of risk, although work is planned to see if this approach can be extended to this broader group.*
“The data we have presented now is a good start and suggests that these two objective measures can identify those who are at very low risk and avoid adding individuals who may not be at as low risk if only one of the two tests is used,” Dr. Jaffe explained.
“Given there are now techniques to measure coronary calcium from any chest CT study, and that high sensitivity cardiac troponin is a relatively inexpensive test, putting them together should really help risk stratify patients,” he added.
When asked whether this approach will eventually replace conventional methods of ASCVD risk assessment, such as those proposed in the 2019 American College of Cardiology/American Heart Association guidelines for the primary prevention of cardiovascular disease (Circulation. 2019;140:e596-e646), he said maybe.
“The answer is that we will probe that question in our ongoing studies using continuous data in an attempt to evaluate how to use this approach to risk stratify larger numbers of individuals,” Dr. Jaffe replied.
The senior investigator, Dr. Jaffe, has consulting relationships with many pharmaceutical companies. The editorial authors had no relevant disclosures.
SOURCE: Sandoval Y et al. J Am Coll Cardiol. 2020;76:357-370.
*Correction, 7/27/20: An earlier version of this article mischaracterized Dr. Jaffe's statement.
If either high sensitivity cardiac troponin (hs-cTnT) or coronary artery calcium (CAC) are elevated, the 10-year risk of atherosclerotic cardiovascular disease (ASCVD) climbs substantially, which suggests these biomarkers yield more prognostic information when they are used together, according to a cohort study with a median 15 years of follow-up.
Among those with a double negative result, meaning hs-cTnT was less than the limit of detection (<3 ng/L) and the CAC score was zero, only 2.8% developed ASCVD within 10 years, but the rates climbed to 4.6% if hs-cTnT was detectable and to 9.8% if the CAC score exceeded zero even when the other biomarker was negative.
“The increased risk for ASCVD among those with discordant results indicate that their prognostic information is complementary, favoring their conjoined use for risk prediction,” reported a multicenter team of investigators led by Allan S. Jaffe, MD, professor of laboratory medicine and pathology, Mayo Clinic, Rochester, Minn.
The study was performed with data from 6,749 participants in the Multi-Ethnic Study of Atherosclerosis (MESA), which is a longitudinal, community-based study funded by the National Heart, Lung, and Blood Institute. Over the course of long-term follow-up in a patient population that was about half female, 39% non-Hispanic white, 28% Black, 22% Hispanic American, and 12% Asian, ASCVD events were evaluated in relation to both biomarkers measured at baseline.
At baseline, both biomarkers were negative in 22%, both positive in 40%, and discordant in 38%.
After a median follow-up of 15 years, when 1,002 ASCVD events had occurred, the crude rate of ASCVD was 2.8 per 1,000 person-years in the double-negative group. When compared with this, the adjusted hazard ratio for ASCVD among those with double positive biomarkers was 3.5 (P < .00001). Increased risk was also highly significant if just hs-cTnT was positive (HR, 1.59; P = .003) or if just CAC was positive (HR, 2.74; P < .00001).
The added value of using both biomarkers to identify individuals at very low risk of ASCVD makes sense, according to the authors of an accompanying editorial. Written by a team led by John W. McEvoy, MB, BCh, National University of Ireland, Galway, the editorial explained why the information is complementary.
“CAC indicates subclinical atherosclerosis, whereas hs-cTnT indicates myocardial ischemia or damage, not just from coronary stenosis but also due to other conditions like hypertensive heart and left ventricular hypertrophy,” the authors stated.
Although they maintained that adding N-terminal pro-brain natriuretic peptide, which could be drawn from the same blood sample as hs-cTnT, might prove to be an even better but still simple strategy to identify low-risk patients, they praised the concept of combining biomarkers.
“If one’s wish is to identify truly low-risk individuals, then it appears that it takes two negative ASCVD biomarkers to make that wish come true,” the authors of the editorial concluded.
Relative to alternative methods of ASCVD risk assessment, measurement of these biomarkers might be useful for sparing patients from interventions, such as lipid lowering with statin therapy, being considered on the basis of conventional risk factors alone.
Dr. Jaffe said in an interview that he considers the two-biomarker assessment to be a useful tool in the low-risk population that he studied, but he does not consider this strategy as a substitute for other methods, such as those outline in the 2019 ACC/AHA guidelines that address the entire spectrum of risk, although work is planned to see if this approach can be extended to this broader group.*
“The data we have presented now is a good start and suggests that these two objective measures can identify those who are at very low risk and avoid adding individuals who may not be at as low risk if only one of the two tests is used,” Dr. Jaffe explained.
“Given there are now techniques to measure coronary calcium from any chest CT study, and that high sensitivity cardiac troponin is a relatively inexpensive test, putting them together should really help risk stratify patients,” he added.
When asked whether this approach will eventually replace conventional methods of ASCVD risk assessment, such as those proposed in the 2019 American College of Cardiology/American Heart Association guidelines for the primary prevention of cardiovascular disease (Circulation. 2019;140:e596-e646), he said maybe.
“The answer is that we will probe that question in our ongoing studies using continuous data in an attempt to evaluate how to use this approach to risk stratify larger numbers of individuals,” Dr. Jaffe replied.
The senior investigator, Dr. Jaffe, has consulting relationships with many pharmaceutical companies. The editorial authors had no relevant disclosures.
SOURCE: Sandoval Y et al. J Am Coll Cardiol. 2020;76:357-370.
*Correction, 7/27/20: An earlier version of this article mischaracterized Dr. Jaffe's statement.
FROM JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Cardiac CT scans can be used for osteoporosis screening
A new study has determined a benefit of cardiac CT scans beyond assessing heart health: Evaluating fracture rate and potential osteoporosis through the bone mineral density (BMD) of thoracic vertebrae.
“Our results represent a step toward appraisal and recognition of the clinical utility of opportunistic BMD screening from cardiac CT,” wrote Josephine Therkildsen, MD, of Hospital Unit West in Herning, Denmark, and coauthors. The study was published July 14 in Radiology.
To determine if further analysis of cardiac CT could help determine BMD and its association with fracture rate, the investigators launched a prospective observational study of 1,487 Danish patients with potential coronary artery disease who underwent cardiac CT scans between September 2014 and March 2016. Their mean age was 57 years (standard deviation, 9; range, 40-80). Nearly all of the patients were white, and 52.5% (n = 781) were women.
All participants underwent a noncontrast-enhanced cardiac CT, from which volumetric BMD of three thoracic vertebrae was measured via commercially available semiautomatic software. Their mean BMD was 119 mg/cm3 (SD, 34) with no significant difference noted between male and female patients. Of the 1,487 participants, 695 were defined as having normal BMD (> 120 mg/cm3), 613 as having low BMD (80-120 mg/cm3), and 179 as having very low BMD (< 80 mg/cm3). Median follow-up was 3.1 years (interquartile range, 2.7-3.4).
Incident fracture occurred in 80 patients (5.4%), of whom 48 were women and 32 were men. Patients who suffered fractures were significantly older than patients with no fractures (mean 59 years vs. 57 years; P = .03). Of the 80 patients with fractures, 31 were osteoporosis related.
In an unadjusted analysis, participants with very low BMD had a greater rate of any fracture (hazard ratio [HR], 2.6; 95% confidence interval, 1.4-4.7; P = .002) and of osteoporosis-related fracture (HR, 8.1; 95% CI, 2.4-27.0; P = .001). After adjustment for age and sex, their rates remained significantly greater for any fracture (HR, 2.1; 95% CI, 1.1-4.2; P = .03) and for osteoporosis-related fracture (HR, 4.0; 95% CI, 1.1-15.0; P = .04).
“Opportunistic” use of scans benefits both physicians and patients
“The concept of using a CT scan that was done for a different purpose allows you to be opportunistic,” Ethel S. Siris, MD, the Madeline C. Stabile Professor of Clinical Medicine in the department of medicine at Columbia University and director of the Toni Stabile Osteoporosis Center of the Columbia University Medical Center, New York–Presbyterian Hospital, New York, said in an interview. “If you’re dealing with older patients, and if you have the software for your radiologist to use to reanalyze the CT scan and say something about the bone, it’s certainly a way of estimating who may be at risk of future fractures.

“From a practical point of view, it’s hard to imagine that it would ever replace conventional bone mineral density testing via DXA [dual-energy x-ray absorptiometry],” she added. “That said, osteoporosis is woefully underdiagnosed because people don’t get DXA tested. This study showed that, if you have access to the scan of the thoracic or even the lumbar spine and if you have the necessary software, you can make legitimate statements about the numbers being low or very low. What that would lead to, I would hope, is some internists to say, ‘This could be a predictor of fracture risk. We should put you on treatment.’ And then follow up with a conventional DXA test.
“Is that going to happen? I don’t know. But the bottom line of the study is: Anything that may enhance the physician’s drive to evaluate a patient for fracture risk is good.”
Whatever the reason for the scan, CT can help diagnose osteoporosis
This study reinforces that CT exams – of the chest, in particular – can serve a valuable dual purpose as osteoporosis screenings, Miriam A. Bredella, MD, professor of radiology at Harvard Medical School and vice chair of the department of radiology at Massachusetts General Hospital, Boston, wrote in an accompanying editorial.

“In the United States, more than 80 million CT examinations are performed each year, many of which could be used to screen for osteoporosis without additional costs or radiation exposure,” she wrote. And thanks to the findings of the study by Therkildsen et al., which relied on both established and new BMD thresholds, the link between thoracic spine BMD and fracture risk is clearer than ever.
“I hope this study will ignite interest in using chest CT examinations performed for other purposes, such as lung cancer screening, for opportunistic osteoporosis screening and prediction of fractures in vulnerable populations,” she added.
The authors acknowledged their study’s limitations, including a small number of fracture events overall and the inability to evaluate associations between BMD and fracture rate at specific locations. In addition, their cohort was largely made up of white participants with a certain coronary artery disease risk profile; because of ethnical differences in BMD measurements, their results “cannot be extrapolated to other ethnical groups.”
Several of the study’s authors reported potential conflicts of interest, including receiving grants and money for consultancies and board memberships from various councils, associations, and pharmaceutical companies. Dr. Bredella reported no conflicts of interest. Dr. Siris has no relevant disclosures.
SOURCE: Therkildsen J et al. Radiology. 2020 Jul 14. doi: 10.1148/radiol.2020192706.
A new study has determined a benefit of cardiac CT scans beyond assessing heart health: Evaluating fracture rate and potential osteoporosis through the bone mineral density (BMD) of thoracic vertebrae.
“Our results represent a step toward appraisal and recognition of the clinical utility of opportunistic BMD screening from cardiac CT,” wrote Josephine Therkildsen, MD, of Hospital Unit West in Herning, Denmark, and coauthors. The study was published July 14 in Radiology.
To determine if further analysis of cardiac CT could help determine BMD and its association with fracture rate, the investigators launched a prospective observational study of 1,487 Danish patients with potential coronary artery disease who underwent cardiac CT scans between September 2014 and March 2016. Their mean age was 57 years (standard deviation, 9; range, 40-80). Nearly all of the patients were white, and 52.5% (n = 781) were women.
All participants underwent a noncontrast-enhanced cardiac CT, from which volumetric BMD of three thoracic vertebrae was measured via commercially available semiautomatic software. Their mean BMD was 119 mg/cm3 (SD, 34) with no significant difference noted between male and female patients. Of the 1,487 participants, 695 were defined as having normal BMD (> 120 mg/cm3), 613 as having low BMD (80-120 mg/cm3), and 179 as having very low BMD (< 80 mg/cm3). Median follow-up was 3.1 years (interquartile range, 2.7-3.4).
Incident fracture occurred in 80 patients (5.4%), of whom 48 were women and 32 were men. Patients who suffered fractures were significantly older than patients with no fractures (mean 59 years vs. 57 years; P = .03). Of the 80 patients with fractures, 31 were osteoporosis related.
In an unadjusted analysis, participants with very low BMD had a greater rate of any fracture (hazard ratio [HR], 2.6; 95% confidence interval, 1.4-4.7; P = .002) and of osteoporosis-related fracture (HR, 8.1; 95% CI, 2.4-27.0; P = .001). After adjustment for age and sex, their rates remained significantly greater for any fracture (HR, 2.1; 95% CI, 1.1-4.2; P = .03) and for osteoporosis-related fracture (HR, 4.0; 95% CI, 1.1-15.0; P = .04).
“Opportunistic” use of scans benefits both physicians and patients
“The concept of using a CT scan that was done for a different purpose allows you to be opportunistic,” Ethel S. Siris, MD, the Madeline C. Stabile Professor of Clinical Medicine in the department of medicine at Columbia University and director of the Toni Stabile Osteoporosis Center of the Columbia University Medical Center, New York–Presbyterian Hospital, New York, said in an interview. “If you’re dealing with older patients, and if you have the software for your radiologist to use to reanalyze the CT scan and say something about the bone, it’s certainly a way of estimating who may be at risk of future fractures.
“From a practical point of view, it’s hard to imagine that it would ever replace conventional bone mineral density testing via DXA [dual-energy x-ray absorptiometry],” she added. “That said, osteoporosis is woefully underdiagnosed because people don’t get DXA tested. This study showed that, if you have access to the scan of the thoracic or even the lumbar spine and if you have the necessary software, you can make legitimate statements about the numbers being low or very low. What that would lead to, I would hope, is some internists to say, ‘This could be a predictor of fracture risk. We should put you on treatment.’ And then follow up with a conventional DXA test.
“Is that going to happen? I don’t know. But the bottom line of the study is: Anything that may enhance the physician’s drive to evaluate a patient for fracture risk is good.”
Whatever the reason for the scan, CT can help diagnose osteoporosis
This study reinforces that CT exams – of the chest, in particular – can serve a valuable dual purpose as osteoporosis screenings, Miriam A. Bredella, MD, professor of radiology at Harvard Medical School and vice chair of the department of radiology at Massachusetts General Hospital, Boston, wrote in an accompanying editorial.
“In the United States, more than 80 million CT examinations are performed each year, many of which could be used to screen for osteoporosis without additional costs or radiation exposure,” she wrote. And thanks to the findings of the study by Therkildsen et al., which relied on both established and new BMD thresholds, the link between thoracic spine BMD and fracture risk is clearer than ever.
“I hope this study will ignite interest in using chest CT examinations performed for other purposes, such as lung cancer screening, for opportunistic osteoporosis screening and prediction of fractures in vulnerable populations,” she added.
The authors acknowledged their study’s limitations, including a small number of fracture events overall and the inability to evaluate associations between BMD and fracture rate at specific locations. In addition, their cohort was largely made up of white participants with a certain coronary artery disease risk profile; because of ethnical differences in BMD measurements, their results “cannot be extrapolated to other ethnical groups.”
Several of the study’s authors reported potential conflicts of interest, including receiving grants and money for consultancies and board memberships from various councils, associations, and pharmaceutical companies. Dr. Bredella reported no conflicts of interest. Dr. Siris has no relevant disclosures.
SOURCE: Therkildsen J et al. Radiology. 2020 Jul 14. doi: 10.1148/radiol.2020192706.
A new study has determined a benefit of cardiac CT scans beyond assessing heart health: Evaluating fracture rate and potential osteoporosis through the bone mineral density (BMD) of thoracic vertebrae.
“Our results represent a step toward appraisal and recognition of the clinical utility of opportunistic BMD screening from cardiac CT,” wrote Josephine Therkildsen, MD, of Hospital Unit West in Herning, Denmark, and coauthors. The study was published July 14 in Radiology.
To determine if further analysis of cardiac CT could help determine BMD and its association with fracture rate, the investigators launched a prospective observational study of 1,487 Danish patients with potential coronary artery disease who underwent cardiac CT scans between September 2014 and March 2016. Their mean age was 57 years (standard deviation, 9; range, 40-80). Nearly all of the patients were white, and 52.5% (n = 781) were women.
All participants underwent a noncontrast-enhanced cardiac CT, from which volumetric BMD of three thoracic vertebrae was measured via commercially available semiautomatic software. Their mean BMD was 119 mg/cm3 (SD, 34) with no significant difference noted between male and female patients. Of the 1,487 participants, 695 were defined as having normal BMD (> 120 mg/cm3), 613 as having low BMD (80-120 mg/cm3), and 179 as having very low BMD (< 80 mg/cm3). Median follow-up was 3.1 years (interquartile range, 2.7-3.4).
Incident fracture occurred in 80 patients (5.4%), of whom 48 were women and 32 were men. Patients who suffered fractures were significantly older than patients with no fractures (mean 59 years vs. 57 years; P = .03). Of the 80 patients with fractures, 31 were osteoporosis related.
In an unadjusted analysis, participants with very low BMD had a greater rate of any fracture (hazard ratio [HR], 2.6; 95% confidence interval, 1.4-4.7; P = .002) and of osteoporosis-related fracture (HR, 8.1; 95% CI, 2.4-27.0; P = .001). After adjustment for age and sex, their rates remained significantly greater for any fracture (HR, 2.1; 95% CI, 1.1-4.2; P = .03) and for osteoporosis-related fracture (HR, 4.0; 95% CI, 1.1-15.0; P = .04).
“Opportunistic” use of scans benefits both physicians and patients
“The concept of using a CT scan that was done for a different purpose allows you to be opportunistic,” Ethel S. Siris, MD, the Madeline C. Stabile Professor of Clinical Medicine in the department of medicine at Columbia University and director of the Toni Stabile Osteoporosis Center of the Columbia University Medical Center, New York–Presbyterian Hospital, New York, said in an interview. “If you’re dealing with older patients, and if you have the software for your radiologist to use to reanalyze the CT scan and say something about the bone, it’s certainly a way of estimating who may be at risk of future fractures.
“From a practical point of view, it’s hard to imagine that it would ever replace conventional bone mineral density testing via DXA [dual-energy x-ray absorptiometry],” she added. “That said, osteoporosis is woefully underdiagnosed because people don’t get DXA tested. This study showed that, if you have access to the scan of the thoracic or even the lumbar spine and if you have the necessary software, you can make legitimate statements about the numbers being low or very low. What that would lead to, I would hope, is some internists to say, ‘This could be a predictor of fracture risk. We should put you on treatment.’ And then follow up with a conventional DXA test.
“Is that going to happen? I don’t know. But the bottom line of the study is: Anything that may enhance the physician’s drive to evaluate a patient for fracture risk is good.”
Whatever the reason for the scan, CT can help diagnose osteoporosis
This study reinforces that CT exams – of the chest, in particular – can serve a valuable dual purpose as osteoporosis screenings, Miriam A. Bredella, MD, professor of radiology at Harvard Medical School and vice chair of the department of radiology at Massachusetts General Hospital, Boston, wrote in an accompanying editorial.
“In the United States, more than 80 million CT examinations are performed each year, many of which could be used to screen for osteoporosis without additional costs or radiation exposure,” she wrote. And thanks to the findings of the study by Therkildsen et al., which relied on both established and new BMD thresholds, the link between thoracic spine BMD and fracture risk is clearer than ever.
“I hope this study will ignite interest in using chest CT examinations performed for other purposes, such as lung cancer screening, for opportunistic osteoporosis screening and prediction of fractures in vulnerable populations,” she added.
The authors acknowledged their study’s limitations, including a small number of fracture events overall and the inability to evaluate associations between BMD and fracture rate at specific locations. In addition, their cohort was largely made up of white participants with a certain coronary artery disease risk profile; because of ethnical differences in BMD measurements, their results “cannot be extrapolated to other ethnical groups.”
Several of the study’s authors reported potential conflicts of interest, including receiving grants and money for consultancies and board memberships from various councils, associations, and pharmaceutical companies. Dr. Bredella reported no conflicts of interest. Dr. Siris has no relevant disclosures.
SOURCE: Therkildsen J et al. Radiology. 2020 Jul 14. doi: 10.1148/radiol.2020192706.
FROM RADIOLOGY
How to reboot elective CV procedures after COVID-19 lockdown
With the COVID-19 pandemic winding down in some parts of the United States, attention has turned to figuring out how to safely reboot elective cardiovascular (CV) services, which, for the most part, shut down in order to combat the virus and flatten the curve.
To aid in this effort, top cardiology societies have published a series of guidance documents. One, entitled Multimodality Cardiovascular Imaging in the Midst of the COVID-19 Pandemic: Ramping Up Safely to a New Normal, was initiated by the editors of JACC Cardiovascular Imaging and was developed in collaboration with the ACC Cardiovascular Imaging Council.
“As we enter a deceleration or indolent phase of the disease and a return to a ‘new normal’ for the foreseeable future, cardiovascular imaging laboratories will adjust to a different work flow and safety precautions for patients and staff alike,” write William Zoghbi, MD, of the department of cardiology at Houston Methodist DeBakey Heart and Vascular Center, and colleagues.
Minimize risk, maximize clinical benefit
The group outlined strategies and considerations on how to safely ramp up multimodality CV imaging laboratories in an environment of an abating but continuing pandemic.
The authors provide detailed advice on reestablishing echocardiography, transthoracic echocardiography, transesophageal echocardiography, stress testing modalities, treadmill testing, nuclear cardiology, cardiac CT, and cardiac MRI.
The advice is designed to “minimize risk, reduce resource utilization and maximize clinical benefit,” the authors wrote. They address patient and societal health; safety of healthcare professionals; choice of CV testing; and scheduling considerations.
Dr. Zoghbi and colleagues said that integrated communication among patients, referring physicians, the imaging teams, and administrative staff are key to reestablishing a more normal clinical operation.
“Recognizing that practice patterns and policies vary depending on institution and locale, the recommendations are not meant to be restrictive but rather to serve as a general framework during the COVID-19 pandemic and its recovery phase,” the writing group said.
Ultimately, the goal is to offer the necessary CV tests and information for the clinical team to provide the best care for patients, they added.
“To be successful in this new safety-driven modus operandi, innovation, coordination and adaptation among clinicians, staff and patients is necessary till herd immunity or control of COVID-19 is achieved,” they concluded.
Rebooting electrophysiology services
Uncertainty as to how to resume electrophysiology (EP) services for arrhythmia patients prompted representatives from the Heart Rhythm Society, the American Heart Association, and the ACC to develop a series of “guiding suggestions and principles” to help safely reestablish electrophysiological care.
The 28-page document is published in Circulation: Arrhythmia and Electrophysiology and the Journal of the American College of Cardiology Electrophysiology.

“Rebooting” EP services at many institutions may be more challenging than shutting down, wrote Dhanunjaya R. Lakkireddy, MD, Kansas City Heart Rhythm Institute and Research Foundation, Overland Park, Kan., and colleagues.
Topics addressed by the writing group include the role of viral screening and serologic testing, return-to-work considerations for exposed or infected health care workers, risk stratification and management strategies based on COVID-19 disease burden, institutional preparedness for resumption of elective procedures, patient preparation and communication; prioritization of procedures, and development of outpatient and periprocedural care pathways.
They suggest creating an EP COVID-19 “reboot team” made up of stakeholders involved in the EP care continuum pathway that would coordinate with institutional or hospital-level COVID-19 leadership.
The reboot team may include an electrophysiologist, an EP laboratory manager, an outpatient clinic manager, an EP nurse, advanced practice providers, a device technician, an anesthesiologist, and an imaging team to provide insights into various aspects of the work flow.
“This team can clarify, interpret, iterate and disseminate policies, and also provide the necessary operational support to plan and successfully execute the reboot process as the efforts to contain COVID-19 continue,” the writing group said.
A mandatory component of the reboot plan should be planning for a second wave of the virus.
“We will have to learn to create relatively COVID-19 safe zones within the hospitals to help isolate patients from second waves and yet be able to provide regular care for non–COVID-19 patients,” the writing group said.
“Our main goal as health care professionals, whether we serve in a clinical, teaching, research, or administrative role, is to do everything we can to create a safe environment for our patients so that they receive the excellent care they deserve,” they concluded.
Defining moment for remote arrhythmia monitoring
In a separate report, an international team of heart rhythm specialists from the Latin American Heart Rhythm Society, the HRS, the European Heart Rhythm Association, the Asia Pacific Heart Rhythm Society, the AHA, and the ACC discussed how the pandemic has fueled adoption of telehealth and remote patient management across medicine, including heart rhythm monitoring.
Their report was simultaneously published in Circulation: Arrhythmia and Electrophysiology, EP Europace, the Journal of the American College of Cardiology, the Journal of Arrhythmia, and Heart Rhythm.
The COVID-19 pandemic has “catalyzed the use of wearables and digital medical tools,” and this will likely define medicine going forward, first author Niraj Varma, MD, PhD, of the Cleveland Clinic, said in an interview.
He noted that the technology has been available for some time, but the pandemic has forced people to use it. “Necessity is the mother of invention, and this has become necessary during the pandemic when we can’t see our patients,” said Dr. Varma.
He also noted that hospitals and physicians are now realizing that telehealth and remote arrhythmia monitoring “actually work, and regulatory agencies have moved very swiftly to dissolve traditional barriers and will now reimburse for it. So it’s a win-win.”
Dr. Varma and colleagues said that the time is right to “embed and grow remote services in everyday medical practice worldwide.” In their report, they offered a list of commonly used platforms for telehealth and examples of remote electrocardiogram and heart rate monitoring devices.
Development of the three reports had no commercial funding. Complete lists of disclosures for the writing groups are available in the original articles.
A version of this article originally appeared on Medscape.com.
With the COVID-19 pandemic winding down in some parts of the United States, attention has turned to figuring out how to safely reboot elective cardiovascular (CV) services, which, for the most part, shut down in order to combat the virus and flatten the curve.
To aid in this effort, top cardiology societies have published a series of guidance documents. One, entitled Multimodality Cardiovascular Imaging in the Midst of the COVID-19 Pandemic: Ramping Up Safely to a New Normal, was initiated by the editors of JACC Cardiovascular Imaging and was developed in collaboration with the ACC Cardiovascular Imaging Council.
“As we enter a deceleration or indolent phase of the disease and a return to a ‘new normal’ for the foreseeable future, cardiovascular imaging laboratories will adjust to a different work flow and safety precautions for patients and staff alike,” write William Zoghbi, MD, of the department of cardiology at Houston Methodist DeBakey Heart and Vascular Center, and colleagues.
Minimize risk, maximize clinical benefit
The group outlined strategies and considerations on how to safely ramp up multimodality CV imaging laboratories in an environment of an abating but continuing pandemic.
The authors provide detailed advice on reestablishing echocardiography, transthoracic echocardiography, transesophageal echocardiography, stress testing modalities, treadmill testing, nuclear cardiology, cardiac CT, and cardiac MRI.
The advice is designed to “minimize risk, reduce resource utilization and maximize clinical benefit,” the authors wrote. They address patient and societal health; safety of healthcare professionals; choice of CV testing; and scheduling considerations.
Dr. Zoghbi and colleagues said that integrated communication among patients, referring physicians, the imaging teams, and administrative staff are key to reestablishing a more normal clinical operation.
“Recognizing that practice patterns and policies vary depending on institution and locale, the recommendations are not meant to be restrictive but rather to serve as a general framework during the COVID-19 pandemic and its recovery phase,” the writing group said.
Ultimately, the goal is to offer the necessary CV tests and information for the clinical team to provide the best care for patients, they added.
“To be successful in this new safety-driven modus operandi, innovation, coordination and adaptation among clinicians, staff and patients is necessary till herd immunity or control of COVID-19 is achieved,” they concluded.
Rebooting electrophysiology services
Uncertainty as to how to resume electrophysiology (EP) services for arrhythmia patients prompted representatives from the Heart Rhythm Society, the American Heart Association, and the ACC to develop a series of “guiding suggestions and principles” to help safely reestablish electrophysiological care.
The 28-page document is published in Circulation: Arrhythmia and Electrophysiology and the Journal of the American College of Cardiology Electrophysiology.
“Rebooting” EP services at many institutions may be more challenging than shutting down, wrote Dhanunjaya R. Lakkireddy, MD, Kansas City Heart Rhythm Institute and Research Foundation, Overland Park, Kan., and colleagues.
Topics addressed by the writing group include the role of viral screening and serologic testing, return-to-work considerations for exposed or infected health care workers, risk stratification and management strategies based on COVID-19 disease burden, institutional preparedness for resumption of elective procedures, patient preparation and communication; prioritization of procedures, and development of outpatient and periprocedural care pathways.
They suggest creating an EP COVID-19 “reboot team” made up of stakeholders involved in the EP care continuum pathway that would coordinate with institutional or hospital-level COVID-19 leadership.
The reboot team may include an electrophysiologist, an EP laboratory manager, an outpatient clinic manager, an EP nurse, advanced practice providers, a device technician, an anesthesiologist, and an imaging team to provide insights into various aspects of the work flow.
“This team can clarify, interpret, iterate and disseminate policies, and also provide the necessary operational support to plan and successfully execute the reboot process as the efforts to contain COVID-19 continue,” the writing group said.
A mandatory component of the reboot plan should be planning for a second wave of the virus.
“We will have to learn to create relatively COVID-19 safe zones within the hospitals to help isolate patients from second waves and yet be able to provide regular care for non–COVID-19 patients,” the writing group said.
“Our main goal as health care professionals, whether we serve in a clinical, teaching, research, or administrative role, is to do everything we can to create a safe environment for our patients so that they receive the excellent care they deserve,” they concluded.
Defining moment for remote arrhythmia monitoring
In a separate report, an international team of heart rhythm specialists from the Latin American Heart Rhythm Society, the HRS, the European Heart Rhythm Association, the Asia Pacific Heart Rhythm Society, the AHA, and the ACC discussed how the pandemic has fueled adoption of telehealth and remote patient management across medicine, including heart rhythm monitoring.
Their report was simultaneously published in Circulation: Arrhythmia and Electrophysiology, EP Europace, the Journal of the American College of Cardiology, the Journal of Arrhythmia, and Heart Rhythm.
The COVID-19 pandemic has “catalyzed the use of wearables and digital medical tools,” and this will likely define medicine going forward, first author Niraj Varma, MD, PhD, of the Cleveland Clinic, said in an interview.
He noted that the technology has been available for some time, but the pandemic has forced people to use it. “Necessity is the mother of invention, and this has become necessary during the pandemic when we can’t see our patients,” said Dr. Varma.
He also noted that hospitals and physicians are now realizing that telehealth and remote arrhythmia monitoring “actually work, and regulatory agencies have moved very swiftly to dissolve traditional barriers and will now reimburse for it. So it’s a win-win.”
Dr. Varma and colleagues said that the time is right to “embed and grow remote services in everyday medical practice worldwide.” In their report, they offered a list of commonly used platforms for telehealth and examples of remote electrocardiogram and heart rate monitoring devices.
Development of the three reports had no commercial funding. Complete lists of disclosures for the writing groups are available in the original articles.
A version of this article originally appeared on Medscape.com.
With the COVID-19 pandemic winding down in some parts of the United States, attention has turned to figuring out how to safely reboot elective cardiovascular (CV) services, which, for the most part, shut down in order to combat the virus and flatten the curve.
To aid in this effort, top cardiology societies have published a series of guidance documents. One, entitled Multimodality Cardiovascular Imaging in the Midst of the COVID-19 Pandemic: Ramping Up Safely to a New Normal, was initiated by the editors of JACC Cardiovascular Imaging and was developed in collaboration with the ACC Cardiovascular Imaging Council.
“As we enter a deceleration or indolent phase of the disease and a return to a ‘new normal’ for the foreseeable future, cardiovascular imaging laboratories will adjust to a different work flow and safety precautions for patients and staff alike,” write William Zoghbi, MD, of the department of cardiology at Houston Methodist DeBakey Heart and Vascular Center, and colleagues.
Minimize risk, maximize clinical benefit
The group outlined strategies and considerations on how to safely ramp up multimodality CV imaging laboratories in an environment of an abating but continuing pandemic.
The authors provide detailed advice on reestablishing echocardiography, transthoracic echocardiography, transesophageal echocardiography, stress testing modalities, treadmill testing, nuclear cardiology, cardiac CT, and cardiac MRI.
The advice is designed to “minimize risk, reduce resource utilization and maximize clinical benefit,” the authors wrote. They address patient and societal health; safety of healthcare professionals; choice of CV testing; and scheduling considerations.
Dr. Zoghbi and colleagues said that integrated communication among patients, referring physicians, the imaging teams, and administrative staff are key to reestablishing a more normal clinical operation.
“Recognizing that practice patterns and policies vary depending on institution and locale, the recommendations are not meant to be restrictive but rather to serve as a general framework during the COVID-19 pandemic and its recovery phase,” the writing group said.
Ultimately, the goal is to offer the necessary CV tests and information for the clinical team to provide the best care for patients, they added.
“To be successful in this new safety-driven modus operandi, innovation, coordination and adaptation among clinicians, staff and patients is necessary till herd immunity or control of COVID-19 is achieved,” they concluded.
Rebooting electrophysiology services
Uncertainty as to how to resume electrophysiology (EP) services for arrhythmia patients prompted representatives from the Heart Rhythm Society, the American Heart Association, and the ACC to develop a series of “guiding suggestions and principles” to help safely reestablish electrophysiological care.
The 28-page document is published in Circulation: Arrhythmia and Electrophysiology and the Journal of the American College of Cardiology Electrophysiology.
“Rebooting” EP services at many institutions may be more challenging than shutting down, wrote Dhanunjaya R. Lakkireddy, MD, Kansas City Heart Rhythm Institute and Research Foundation, Overland Park, Kan., and colleagues.
Topics addressed by the writing group include the role of viral screening and serologic testing, return-to-work considerations for exposed or infected health care workers, risk stratification and management strategies based on COVID-19 disease burden, institutional preparedness for resumption of elective procedures, patient preparation and communication; prioritization of procedures, and development of outpatient and periprocedural care pathways.
They suggest creating an EP COVID-19 “reboot team” made up of stakeholders involved in the EP care continuum pathway that would coordinate with institutional or hospital-level COVID-19 leadership.
The reboot team may include an electrophysiologist, an EP laboratory manager, an outpatient clinic manager, an EP nurse, advanced practice providers, a device technician, an anesthesiologist, and an imaging team to provide insights into various aspects of the work flow.
“This team can clarify, interpret, iterate and disseminate policies, and also provide the necessary operational support to plan and successfully execute the reboot process as the efforts to contain COVID-19 continue,” the writing group said.
A mandatory component of the reboot plan should be planning for a second wave of the virus.
“We will have to learn to create relatively COVID-19 safe zones within the hospitals to help isolate patients from second waves and yet be able to provide regular care for non–COVID-19 patients,” the writing group said.
“Our main goal as health care professionals, whether we serve in a clinical, teaching, research, or administrative role, is to do everything we can to create a safe environment for our patients so that they receive the excellent care they deserve,” they concluded.
Defining moment for remote arrhythmia monitoring
In a separate report, an international team of heart rhythm specialists from the Latin American Heart Rhythm Society, the HRS, the European Heart Rhythm Association, the Asia Pacific Heart Rhythm Society, the AHA, and the ACC discussed how the pandemic has fueled adoption of telehealth and remote patient management across medicine, including heart rhythm monitoring.
Their report was simultaneously published in Circulation: Arrhythmia and Electrophysiology, EP Europace, the Journal of the American College of Cardiology, the Journal of Arrhythmia, and Heart Rhythm.
The COVID-19 pandemic has “catalyzed the use of wearables and digital medical tools,” and this will likely define medicine going forward, first author Niraj Varma, MD, PhD, of the Cleveland Clinic, said in an interview.
He noted that the technology has been available for some time, but the pandemic has forced people to use it. “Necessity is the mother of invention, and this has become necessary during the pandemic when we can’t see our patients,” said Dr. Varma.
He also noted that hospitals and physicians are now realizing that telehealth and remote arrhythmia monitoring “actually work, and regulatory agencies have moved very swiftly to dissolve traditional barriers and will now reimburse for it. So it’s a win-win.”
Dr. Varma and colleagues said that the time is right to “embed and grow remote services in everyday medical practice worldwide.” In their report, they offered a list of commonly used platforms for telehealth and examples of remote electrocardiogram and heart rate monitoring devices.
Development of the three reports had no commercial funding. Complete lists of disclosures for the writing groups are available in the original articles.
A version of this article originally appeared on Medscape.com.
Experts publish imaging recommendations for pediatric COVID-19
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has devised recommendations for ordering imaging studies in suspected cases of the infection.
The review also included useful radiographic findings to help in the differential diagnosis of COVID-19 pneumonia from other respiratory infections. Alexandra M. Foust, DO, of Boston Children’s Hospital, and colleagues reported the summary of findings and recommendations in Pediatric Pulmonology.

“Pediatricians face numerous challenges created by increasing reports of severe COVID-19 related findings in affected children,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. “[The current review] represents a multinational collaboration to provide up to date information and key imaging findings to guide chest physicians caring for children with pneumonia symptoms during the COVID-19 pandemic.”
Clinical presentation in children
In general, pediatric patients infected with the virus show milder symptoms compared with adults, and based on the limited evidence reported to date, the most common clinical symptoms of COVID-19 in children are rhinorrhea and/or nasal congestion, fever and cough with sore throat, fatigue or dyspnea, and diarrhea.
As with other viral pneumonias in children, the laboratory parameters are usually nonspecific; however, while the complete blood count (CBC) is often normal, lymphopenia, thrombocytopenia, and neutropenia have been reported in some cases of pediatric COVID-19, the authors noted.
The current Centers for Disease Control and Prevention (CDC) recommendation for initial diagnosis of SARS-CoV-2 is obtaining a nasopharyngeal swab, followed by reverse transcription polymerase chain reaction (RT-PCR) testing, they explained.
Role of imaging in diagnosis
The researchers reported that current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as a upfront test to diagnose pediatric COVID-19, but they may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course.
The potential benefits of utilizing radiologic evaluation, such as establishing a baseline for monitoring disease progression, must be balanced with potential drawbacks, which include radiation exposure, and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Recommendations for ordering imaging studies
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia.
The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia.
“The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Dr. Cataletto. “By synthesizing the available imaging case series and guidelines, this primer provides a useful tool for the practicing pulmonologist,” she explained.
Key recommendations: CXR
“For pediatric patients with suspected or known COVID-19 infection with moderate to severe clinical symptoms requiring hospitalization (i.e., hypoxia, moderate or severe dyspnea, signs of sepsis, shock, cardiovascular compromise, altered mentation), CXR is usually indicated to establish an imaging baseline and to assess for an alternative diagnosis,” they recommended.
“Sequential CXRs may be helpful to assess pediatric patients with COVID-19 who demonstrate worsening clinical symptoms or to assess response to supportive therapy,” they wrote.
Key recommendations: CT
“Due to the increased radiation sensitivity of pediatric patients, chest CT is not recommended as an initial diagnostic test for pediatric patients with known or suspected COVID-19 pneumonia,” they explained.
The guide also included several considerations around the differential diagnosis of COVID-19 pneumonia from other pediatric lung disorders, including immune-related conditions, infectious etiologies, hematological dyscrasias, and inhalation-related lung injury.
As best practice recommendations for COVID-19 continue to evolve, the availability of practical clinical decision-making tools becomes essential to ensure optimal patient care.
No funding sources or financial disclosures were reported in the manuscript.
SOURCE: Foust AM et al. Pediatr Pulmonol. 2020 May 28. doi: 10.1002/ppul.24870.
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has devised recommendations for ordering imaging studies in suspected cases of the infection.
The review also included useful radiographic findings to help in the differential diagnosis of COVID-19 pneumonia from other respiratory infections. Alexandra M. Foust, DO, of Boston Children’s Hospital, and colleagues reported the summary of findings and recommendations in Pediatric Pulmonology.
“Pediatricians face numerous challenges created by increasing reports of severe COVID-19 related findings in affected children,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. “[The current review] represents a multinational collaboration to provide up to date information and key imaging findings to guide chest physicians caring for children with pneumonia symptoms during the COVID-19 pandemic.”
Clinical presentation in children
In general, pediatric patients infected with the virus show milder symptoms compared with adults, and based on the limited evidence reported to date, the most common clinical symptoms of COVID-19 in children are rhinorrhea and/or nasal congestion, fever and cough with sore throat, fatigue or dyspnea, and diarrhea.
As with other viral pneumonias in children, the laboratory parameters are usually nonspecific; however, while the complete blood count (CBC) is often normal, lymphopenia, thrombocytopenia, and neutropenia have been reported in some cases of pediatric COVID-19, the authors noted.
The current Centers for Disease Control and Prevention (CDC) recommendation for initial diagnosis of SARS-CoV-2 is obtaining a nasopharyngeal swab, followed by reverse transcription polymerase chain reaction (RT-PCR) testing, they explained.
Role of imaging in diagnosis
The researchers reported that current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as a upfront test to diagnose pediatric COVID-19, but they may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course.
The potential benefits of utilizing radiologic evaluation, such as establishing a baseline for monitoring disease progression, must be balanced with potential drawbacks, which include radiation exposure, and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Recommendations for ordering imaging studies
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia.
The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia.
“The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Dr. Cataletto. “By synthesizing the available imaging case series and guidelines, this primer provides a useful tool for the practicing pulmonologist,” she explained.
Key recommendations: CXR
“For pediatric patients with suspected or known COVID-19 infection with moderate to severe clinical symptoms requiring hospitalization (i.e., hypoxia, moderate or severe dyspnea, signs of sepsis, shock, cardiovascular compromise, altered mentation), CXR is usually indicated to establish an imaging baseline and to assess for an alternative diagnosis,” they recommended.
“Sequential CXRs may be helpful to assess pediatric patients with COVID-19 who demonstrate worsening clinical symptoms or to assess response to supportive therapy,” they wrote.
Key recommendations: CT
“Due to the increased radiation sensitivity of pediatric patients, chest CT is not recommended as an initial diagnostic test for pediatric patients with known or suspected COVID-19 pneumonia,” they explained.
The guide also included several considerations around the differential diagnosis of COVID-19 pneumonia from other pediatric lung disorders, including immune-related conditions, infectious etiologies, hematological dyscrasias, and inhalation-related lung injury.
As best practice recommendations for COVID-19 continue to evolve, the availability of practical clinical decision-making tools becomes essential to ensure optimal patient care.
No funding sources or financial disclosures were reported in the manuscript.
SOURCE: Foust AM et al. Pediatr Pulmonol. 2020 May 28. doi: 10.1002/ppul.24870.
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has devised recommendations for ordering imaging studies in suspected cases of the infection.
The review also included useful radiographic findings to help in the differential diagnosis of COVID-19 pneumonia from other respiratory infections. Alexandra M. Foust, DO, of Boston Children’s Hospital, and colleagues reported the summary of findings and recommendations in Pediatric Pulmonology.
“Pediatricians face numerous challenges created by increasing reports of severe COVID-19 related findings in affected children,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. “[The current review] represents a multinational collaboration to provide up to date information and key imaging findings to guide chest physicians caring for children with pneumonia symptoms during the COVID-19 pandemic.”
Clinical presentation in children
In general, pediatric patients infected with the virus show milder symptoms compared with adults, and based on the limited evidence reported to date, the most common clinical symptoms of COVID-19 in children are rhinorrhea and/or nasal congestion, fever and cough with sore throat, fatigue or dyspnea, and diarrhea.
As with other viral pneumonias in children, the laboratory parameters are usually nonspecific; however, while the complete blood count (CBC) is often normal, lymphopenia, thrombocytopenia, and neutropenia have been reported in some cases of pediatric COVID-19, the authors noted.
The current Centers for Disease Control and Prevention (CDC) recommendation for initial diagnosis of SARS-CoV-2 is obtaining a nasopharyngeal swab, followed by reverse transcription polymerase chain reaction (RT-PCR) testing, they explained.
Role of imaging in diagnosis
The researchers reported that current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as a upfront test to diagnose pediatric COVID-19, but they may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course.
The potential benefits of utilizing radiologic evaluation, such as establishing a baseline for monitoring disease progression, must be balanced with potential drawbacks, which include radiation exposure, and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Recommendations for ordering imaging studies
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia.
The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia.
“The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Dr. Cataletto. “By synthesizing the available imaging case series and guidelines, this primer provides a useful tool for the practicing pulmonologist,” she explained.
Key recommendations: CXR
“For pediatric patients with suspected or known COVID-19 infection with moderate to severe clinical symptoms requiring hospitalization (i.e., hypoxia, moderate or severe dyspnea, signs of sepsis, shock, cardiovascular compromise, altered mentation), CXR is usually indicated to establish an imaging baseline and to assess for an alternative diagnosis,” they recommended.
“Sequential CXRs may be helpful to assess pediatric patients with COVID-19 who demonstrate worsening clinical symptoms or to assess response to supportive therapy,” they wrote.
Key recommendations: CT
“Due to the increased radiation sensitivity of pediatric patients, chest CT is not recommended as an initial diagnostic test for pediatric patients with known or suspected COVID-19 pneumonia,” they explained.
The guide also included several considerations around the differential diagnosis of COVID-19 pneumonia from other pediatric lung disorders, including immune-related conditions, infectious etiologies, hematological dyscrasias, and inhalation-related lung injury.
As best practice recommendations for COVID-19 continue to evolve, the availability of practical clinical decision-making tools becomes essential to ensure optimal patient care.
No funding sources or financial disclosures were reported in the manuscript.
SOURCE: Foust AM et al. Pediatr Pulmonol. 2020 May 28. doi: 10.1002/ppul.24870.
FROM PEDIATRIC PULMONOLOGY
CAC scoring pinpoints stenoses in asymptomatic diabetes patients
For diabetes patients with no cardiovascular symptoms despite certain risk factors, incorporating coronary calcium scoring into a silent myocardial ischemia screening algorithm may be an effective and cost-conscious strategy that avoids missed coronary stenoses suitable for revascularization, results of a recent study suggest.
Zero patients in need of revascularization were missed in a risk stratification model in which screening for silent myocardial ischemia (SMI) was done only for patients with peripheral artery disease, severe nephropathy, or a high coronary artery calcium (CAC) score, according to investigator Paul Valensi, MD.
In practical terms, that means stress myocardial scintigraphy to detect SMI could be reserved for patients with evidence of target organ damage or a CAC score of 100 or higher, according to Dr. Valensi, head of the department of endocrinology, diabetology, and nutrition at Jean Verdier Hospital in Bondy, France.
“The strategy appears to be a good compromise, and the most cost effective strategy,” Dr. Valensi said in a presentation of the results at the virtual annual scientific sessions of the American Diabetes Association.
Utility of CAC scoring in diabetes
This algorithm proposed by Dr. Valenti and colleagues is a “reasonable” approach to guide risk stratification in asymptomatic diabetes patients, said Matthew J. Budoff, MD, professor of medicine and director of cardiac CT at Harbor-UCLA Medical Center in Torrance, Calif.

“Calcium scoring could certainly help you identify those patients (at increased risk) as a first-line test, because if their calcium score is zero, their chance of having obstructive disease is probably either zero or very close to zero,” Dr. Budoff said in an interview.
Using CAC scores to assess cardiovascular risk in asymptomatic adults with diabetes was supported by 2010 guidelines from the American College of Cardiology and the American Heart Association, Dr. Budoff said, while 2019 guidelines from the European Society of Cardiology (ESC) describe CAC score combined with CT as a potential risk modifier in the evaluation of certain asymptomatic patients with diabetes.
“We are starting to see that we might be able to understand diabetes better and the cardiovascular implications by understanding how much plaque (patients) have at the time that we see them,” Dr. Budoff said in a presentation on use of CAC scans he gave earlier at the virtual ADA meeting.
In the interview, Dr. Budoff also noted that CAC scores may be particularly useful for guiding use of statins, PCSK9 (proprotein convertase subtilisin kexin 9) inhibitors, or other treatments in patients with diabetes: “There are a lot of therapies that we can apply, if we knew somebody was at higher risk, that would potentially help them avoid a heart attack, stroke, or cardiovascular death,” he said.
CAC scoring and coronary artery stenoses
Although about 20% of patients with type 2 diabetes have SMI, screening for it is “debated,” according to Dr. Valensi.
The recent ESC guidelines state that while routine screening for coronary artery disease in asymptomatic diabetics is not recommended, stress testing or coronary angiography “may be indicated” in asymptomatic diabetics in the very-high cardiovascular risk category.
That position is based on a lack of benefit seen with a broad screening strategy, the guidelines say, possibly due in part to low event rates in randomized controlled trials that have studied the approach.
Using CAC scoring could change the equation by helping to identify a greater proportion of type 2 diabetics with SMI, according to Dr. Valensi.
“The role of the CAC score in the strategy of detection of SMI needs to be defined, and this role may depend on the a priori cardiovascular risk,” he said.
Dr. Valensi and colleagues accordingly tested several different approaches to selecting asymptomatic diabetic patients for SMI screening to see how they would perform in finding patients with coronary stenoses eligible for revascularization.
Their study included 416 diabetes patients with diabetes at very high cardiovascular risk but with no cardiac history or symptoms. A total of 40 patients (9.6%) had SMI, including 15 patients in which coronary stenoses were found; of those, 11 (73.5%) underwent a revascularization procedure.
They found that, by performing myocardial scintigraphy only in those patients with peripheral artery disease or severe nephropathy, they would have missed 6 patients with coronary stenosis suitable for revascularization among the 275 patients who did not meet those target organ damage criteria.
By contrast, zero patients would have been missed by performing myocardial scintigraphy in patients who either met those target organ damage criteria, or who had an elevated CAC score.
“We suggest screening for SMI, using stress myocardial CT scanning and coronary stenosis screening, only the patients with peripheral artery disease or severe nephropathy or with a high CAC score over 100 Agatston units,” said Dr. Valensi.
Dr. Valensi reported disclosures related to Merck Sharp Dohme, Novo Nordisk, Pierre Fabre, Eli Lilly, Bristol-Myers Squibb, AstraZeneca, Daiichi-Sankyo, and others. Coauthors provided no disclosures related to the research. Dr. Budoff reported that he has served as a paid consultant to GE.
SOURCE: Berkane N et al. ADA 2020. Abstract 8-OR.
For diabetes patients with no cardiovascular symptoms despite certain risk factors, incorporating coronary calcium scoring into a silent myocardial ischemia screening algorithm may be an effective and cost-conscious strategy that avoids missed coronary stenoses suitable for revascularization, results of a recent study suggest.
Zero patients in need of revascularization were missed in a risk stratification model in which screening for silent myocardial ischemia (SMI) was done only for patients with peripheral artery disease, severe nephropathy, or a high coronary artery calcium (CAC) score, according to investigator Paul Valensi, MD.
In practical terms, that means stress myocardial scintigraphy to detect SMI could be reserved for patients with evidence of target organ damage or a CAC score of 100 or higher, according to Dr. Valensi, head of the department of endocrinology, diabetology, and nutrition at Jean Verdier Hospital in Bondy, France.
“The strategy appears to be a good compromise, and the most cost effective strategy,” Dr. Valensi said in a presentation of the results at the virtual annual scientific sessions of the American Diabetes Association.
Utility of CAC scoring in diabetes
This algorithm proposed by Dr. Valenti and colleagues is a “reasonable” approach to guide risk stratification in asymptomatic diabetes patients, said Matthew J. Budoff, MD, professor of medicine and director of cardiac CT at Harbor-UCLA Medical Center in Torrance, Calif.
“Calcium scoring could certainly help you identify those patients (at increased risk) as a first-line test, because if their calcium score is zero, their chance of having obstructive disease is probably either zero or very close to zero,” Dr. Budoff said in an interview.
Using CAC scores to assess cardiovascular risk in asymptomatic adults with diabetes was supported by 2010 guidelines from the American College of Cardiology and the American Heart Association, Dr. Budoff said, while 2019 guidelines from the European Society of Cardiology (ESC) describe CAC score combined with CT as a potential risk modifier in the evaluation of certain asymptomatic patients with diabetes.
“We are starting to see that we might be able to understand diabetes better and the cardiovascular implications by understanding how much plaque (patients) have at the time that we see them,” Dr. Budoff said in a presentation on use of CAC scans he gave earlier at the virtual ADA meeting.
In the interview, Dr. Budoff also noted that CAC scores may be particularly useful for guiding use of statins, PCSK9 (proprotein convertase subtilisin kexin 9) inhibitors, or other treatments in patients with diabetes: “There are a lot of therapies that we can apply, if we knew somebody was at higher risk, that would potentially help them avoid a heart attack, stroke, or cardiovascular death,” he said.
CAC scoring and coronary artery stenoses
Although about 20% of patients with type 2 diabetes have SMI, screening for it is “debated,” according to Dr. Valensi.
The recent ESC guidelines state that while routine screening for coronary artery disease in asymptomatic diabetics is not recommended, stress testing or coronary angiography “may be indicated” in asymptomatic diabetics in the very-high cardiovascular risk category.
That position is based on a lack of benefit seen with a broad screening strategy, the guidelines say, possibly due in part to low event rates in randomized controlled trials that have studied the approach.
Using CAC scoring could change the equation by helping to identify a greater proportion of type 2 diabetics with SMI, according to Dr. Valensi.
“The role of the CAC score in the strategy of detection of SMI needs to be defined, and this role may depend on the a priori cardiovascular risk,” he said.
Dr. Valensi and colleagues accordingly tested several different approaches to selecting asymptomatic diabetic patients for SMI screening to see how they would perform in finding patients with coronary stenoses eligible for revascularization.
Their study included 416 diabetes patients with diabetes at very high cardiovascular risk but with no cardiac history or symptoms. A total of 40 patients (9.6%) had SMI, including 15 patients in which coronary stenoses were found; of those, 11 (73.5%) underwent a revascularization procedure.
They found that, by performing myocardial scintigraphy only in those patients with peripheral artery disease or severe nephropathy, they would have missed 6 patients with coronary stenosis suitable for revascularization among the 275 patients who did not meet those target organ damage criteria.
By contrast, zero patients would have been missed by performing myocardial scintigraphy in patients who either met those target organ damage criteria, or who had an elevated CAC score.
“We suggest screening for SMI, using stress myocardial CT scanning and coronary stenosis screening, only the patients with peripheral artery disease or severe nephropathy or with a high CAC score over 100 Agatston units,” said Dr. Valensi.
Dr. Valensi reported disclosures related to Merck Sharp Dohme, Novo Nordisk, Pierre Fabre, Eli Lilly, Bristol-Myers Squibb, AstraZeneca, Daiichi-Sankyo, and others. Coauthors provided no disclosures related to the research. Dr. Budoff reported that he has served as a paid consultant to GE.
SOURCE: Berkane N et al. ADA 2020. Abstract 8-OR.
For diabetes patients with no cardiovascular symptoms despite certain risk factors, incorporating coronary calcium scoring into a silent myocardial ischemia screening algorithm may be an effective and cost-conscious strategy that avoids missed coronary stenoses suitable for revascularization, results of a recent study suggest.
Zero patients in need of revascularization were missed in a risk stratification model in which screening for silent myocardial ischemia (SMI) was done only for patients with peripheral artery disease, severe nephropathy, or a high coronary artery calcium (CAC) score, according to investigator Paul Valensi, MD.
In practical terms, that means stress myocardial scintigraphy to detect SMI could be reserved for patients with evidence of target organ damage or a CAC score of 100 or higher, according to Dr. Valensi, head of the department of endocrinology, diabetology, and nutrition at Jean Verdier Hospital in Bondy, France.
“The strategy appears to be a good compromise, and the most cost effective strategy,” Dr. Valensi said in a presentation of the results at the virtual annual scientific sessions of the American Diabetes Association.
Utility of CAC scoring in diabetes
This algorithm proposed by Dr. Valenti and colleagues is a “reasonable” approach to guide risk stratification in asymptomatic diabetes patients, said Matthew J. Budoff, MD, professor of medicine and director of cardiac CT at Harbor-UCLA Medical Center in Torrance, Calif.
“Calcium scoring could certainly help you identify those patients (at increased risk) as a first-line test, because if their calcium score is zero, their chance of having obstructive disease is probably either zero or very close to zero,” Dr. Budoff said in an interview.
Using CAC scores to assess cardiovascular risk in asymptomatic adults with diabetes was supported by 2010 guidelines from the American College of Cardiology and the American Heart Association, Dr. Budoff said, while 2019 guidelines from the European Society of Cardiology (ESC) describe CAC score combined with CT as a potential risk modifier in the evaluation of certain asymptomatic patients with diabetes.
“We are starting to see that we might be able to understand diabetes better and the cardiovascular implications by understanding how much plaque (patients) have at the time that we see them,” Dr. Budoff said in a presentation on use of CAC scans he gave earlier at the virtual ADA meeting.
In the interview, Dr. Budoff also noted that CAC scores may be particularly useful for guiding use of statins, PCSK9 (proprotein convertase subtilisin kexin 9) inhibitors, or other treatments in patients with diabetes: “There are a lot of therapies that we can apply, if we knew somebody was at higher risk, that would potentially help them avoid a heart attack, stroke, or cardiovascular death,” he said.
CAC scoring and coronary artery stenoses
Although about 20% of patients with type 2 diabetes have SMI, screening for it is “debated,” according to Dr. Valensi.
The recent ESC guidelines state that while routine screening for coronary artery disease in asymptomatic diabetics is not recommended, stress testing or coronary angiography “may be indicated” in asymptomatic diabetics in the very-high cardiovascular risk category.
That position is based on a lack of benefit seen with a broad screening strategy, the guidelines say, possibly due in part to low event rates in randomized controlled trials that have studied the approach.
Using CAC scoring could change the equation by helping to identify a greater proportion of type 2 diabetics with SMI, according to Dr. Valensi.
“The role of the CAC score in the strategy of detection of SMI needs to be defined, and this role may depend on the a priori cardiovascular risk,” he said.
Dr. Valensi and colleagues accordingly tested several different approaches to selecting asymptomatic diabetic patients for SMI screening to see how they would perform in finding patients with coronary stenoses eligible for revascularization.
Their study included 416 diabetes patients with diabetes at very high cardiovascular risk but with no cardiac history or symptoms. A total of 40 patients (9.6%) had SMI, including 15 patients in which coronary stenoses were found; of those, 11 (73.5%) underwent a revascularization procedure.
They found that, by performing myocardial scintigraphy only in those patients with peripheral artery disease or severe nephropathy, they would have missed 6 patients with coronary stenosis suitable for revascularization among the 275 patients who did not meet those target organ damage criteria.
By contrast, zero patients would have been missed by performing myocardial scintigraphy in patients who either met those target organ damage criteria, or who had an elevated CAC score.
“We suggest screening for SMI, using stress myocardial CT scanning and coronary stenosis screening, only the patients with peripheral artery disease or severe nephropathy or with a high CAC score over 100 Agatston units,” said Dr. Valensi.
Dr. Valensi reported disclosures related to Merck Sharp Dohme, Novo Nordisk, Pierre Fabre, Eli Lilly, Bristol-Myers Squibb, AstraZeneca, Daiichi-Sankyo, and others. Coauthors provided no disclosures related to the research. Dr. Budoff reported that he has served as a paid consultant to GE.
SOURCE: Berkane N et al. ADA 2020. Abstract 8-OR.
FROM ADA 2020
Radiation-associated childhood cancer quantified in congenital heart disease
Children with congenital heart disease exposed to low-dose ionizing radiation from cardiac procedures had a cancer risk more than triple that of pediatric congenital heart disease (CHD) patients without such exposures, according to a large Canadian nested case-control study presented at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
This cancer risk was dose dependent. It rose stepwise with the number of cardiac procedures involving exposure to low-dose ionizing radiation (LDIR) and the total radiation dose. Moreover, roughly 80% of the cancers were of types known to be associated with radiation exposure in children, reported Elie Ganni, a medical student at McGill University, Montreal, working with MAUDE, the McGill Adult Unit for Congenital Heart Disease.
The MAUDE group previously published the first large, population-based study analyzing the association between LDIR from cardiac procedures and incident cancer in adults with CHD. The study, which included nearly 25,000 adult CHD patients aged 18-64 years with more than 250,000 person-years of follow-up, concluded that individuals with LDIR exposure from six or more cardiac procedures had a 140% greater cancer incidence than those with no or one exposure (Circulation. 2018 Mar 27;137[13]:1334-45).
Because children are considered to be more sensitive to the carcinogenic effects of LDIR than adults, the MAUDE group next did a similar study in a pediatric CHD population included in the Quebec Congenital Heart Disease Database. This nested case-control study included 232 children with CHD who were first diagnosed with cancer at a median age of 3.9 years and 8,160 pediatric CHD controls matched for gender and birth year. About 76% of cancers were diagnosed before age 7, 20% at ages 7-12 years, and the remaining 4% at ages 13-18. Hematologic malignancies accounted for 61% of the pediatric cancers, CNS cancers for another 12.5%, and thyroid cancers 6.6%; all three types of cancer are associated with radiation exposure.
After excluding all cardiac procedures involving LDIR performed within 6 months prior to cancer diagnosis, the risk of developing a pediatric cancer was 230% greater in children with LDIR exposure from cardiac procedures than in CHD patients without such exposure. For every 4 mSv in estimated LDIR exposure from cardiac procedures, the risk of cancer rose by 15.5%. In contrast, in the earlier study in adults with CHD, cancer risk climbed by 10% per 10 mSv. Patients with six or more LDIR cardiac procedures – not at all unusual in contemporary practice – were 2.4 times more likely to have cancer than those with no or one such radiation exposure.
Current ACC guidelines on radiation exposure from cardiac procedures recommend calculating an individual’s lifetime attributable cancer incidence and mortality risks, as well as adhering to the time-honored principle of ensuring that radiation exposure is as low as reasonably achievable without sacrificing quality of care.
“Our findings strongly support these ACC recommendations and moreover suggest that radiation surveillance for patients with congenital heart disease should be considered using radiation badges. Also, cancer surveillance guidelines should be considered for CHD patients exposed to LDIR,” Mr. Ganni said.
These suggestions for creation of patient radiation passports and cancer surveillance guidelines take on greater weight in light of two trends: the increasing life expectancy of children with CHD during the past 3 decades as a result of procedural advances that entail LDIR exposure, mostly for imaging, and the growing number of such procedures performed per patient earlier and earlier in life.
He and the MAUDE group plan to confirm their latest findings in other, larger data sets and hope to identify threshold effects for LDIR for specific cancers, with hematologic malignancies as the top priority.
Mr. Ganni reported having no financial conflicts regarding his study, funded by the Heart and Stroke Foundation of Canada, the Quebec Foundation for Health Research, and the Canadian Institutes for Health Research.
Children with congenital heart disease exposed to low-dose ionizing radiation from cardiac procedures had a cancer risk more than triple that of pediatric congenital heart disease (CHD) patients without such exposures, according to a large Canadian nested case-control study presented at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
This cancer risk was dose dependent. It rose stepwise with the number of cardiac procedures involving exposure to low-dose ionizing radiation (LDIR) and the total radiation dose. Moreover, roughly 80% of the cancers were of types known to be associated with radiation exposure in children, reported Elie Ganni, a medical student at McGill University, Montreal, working with MAUDE, the McGill Adult Unit for Congenital Heart Disease.
The MAUDE group previously published the first large, population-based study analyzing the association between LDIR from cardiac procedures and incident cancer in adults with CHD. The study, which included nearly 25,000 adult CHD patients aged 18-64 years with more than 250,000 person-years of follow-up, concluded that individuals with LDIR exposure from six or more cardiac procedures had a 140% greater cancer incidence than those with no or one exposure (Circulation. 2018 Mar 27;137[13]:1334-45).
Because children are considered to be more sensitive to the carcinogenic effects of LDIR than adults, the MAUDE group next did a similar study in a pediatric CHD population included in the Quebec Congenital Heart Disease Database. This nested case-control study included 232 children with CHD who were first diagnosed with cancer at a median age of 3.9 years and 8,160 pediatric CHD controls matched for gender and birth year. About 76% of cancers were diagnosed before age 7, 20% at ages 7-12 years, and the remaining 4% at ages 13-18. Hematologic malignancies accounted for 61% of the pediatric cancers, CNS cancers for another 12.5%, and thyroid cancers 6.6%; all three types of cancer are associated with radiation exposure.
After excluding all cardiac procedures involving LDIR performed within 6 months prior to cancer diagnosis, the risk of developing a pediatric cancer was 230% greater in children with LDIR exposure from cardiac procedures than in CHD patients without such exposure. For every 4 mSv in estimated LDIR exposure from cardiac procedures, the risk of cancer rose by 15.5%. In contrast, in the earlier study in adults with CHD, cancer risk climbed by 10% per 10 mSv. Patients with six or more LDIR cardiac procedures – not at all unusual in contemporary practice – were 2.4 times more likely to have cancer than those with no or one such radiation exposure.
Current ACC guidelines on radiation exposure from cardiac procedures recommend calculating an individual’s lifetime attributable cancer incidence and mortality risks, as well as adhering to the time-honored principle of ensuring that radiation exposure is as low as reasonably achievable without sacrificing quality of care.
“Our findings strongly support these ACC recommendations and moreover suggest that radiation surveillance for patients with congenital heart disease should be considered using radiation badges. Also, cancer surveillance guidelines should be considered for CHD patients exposed to LDIR,” Mr. Ganni said.
These suggestions for creation of patient radiation passports and cancer surveillance guidelines take on greater weight in light of two trends: the increasing life expectancy of children with CHD during the past 3 decades as a result of procedural advances that entail LDIR exposure, mostly for imaging, and the growing number of such procedures performed per patient earlier and earlier in life.
He and the MAUDE group plan to confirm their latest findings in other, larger data sets and hope to identify threshold effects for LDIR for specific cancers, with hematologic malignancies as the top priority.
Mr. Ganni reported having no financial conflicts regarding his study, funded by the Heart and Stroke Foundation of Canada, the Quebec Foundation for Health Research, and the Canadian Institutes for Health Research.
Children with congenital heart disease exposed to low-dose ionizing radiation from cardiac procedures had a cancer risk more than triple that of pediatric congenital heart disease (CHD) patients without such exposures, according to a large Canadian nested case-control study presented at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
This cancer risk was dose dependent. It rose stepwise with the number of cardiac procedures involving exposure to low-dose ionizing radiation (LDIR) and the total radiation dose. Moreover, roughly 80% of the cancers were of types known to be associated with radiation exposure in children, reported Elie Ganni, a medical student at McGill University, Montreal, working with MAUDE, the McGill Adult Unit for Congenital Heart Disease.
The MAUDE group previously published the first large, population-based study analyzing the association between LDIR from cardiac procedures and incident cancer in adults with CHD. The study, which included nearly 25,000 adult CHD patients aged 18-64 years with more than 250,000 person-years of follow-up, concluded that individuals with LDIR exposure from six or more cardiac procedures had a 140% greater cancer incidence than those with no or one exposure (Circulation. 2018 Mar 27;137[13]:1334-45).
Because children are considered to be more sensitive to the carcinogenic effects of LDIR than adults, the MAUDE group next did a similar study in a pediatric CHD population included in the Quebec Congenital Heart Disease Database. This nested case-control study included 232 children with CHD who were first diagnosed with cancer at a median age of 3.9 years and 8,160 pediatric CHD controls matched for gender and birth year. About 76% of cancers were diagnosed before age 7, 20% at ages 7-12 years, and the remaining 4% at ages 13-18. Hematologic malignancies accounted for 61% of the pediatric cancers, CNS cancers for another 12.5%, and thyroid cancers 6.6%; all three types of cancer are associated with radiation exposure.
After excluding all cardiac procedures involving LDIR performed within 6 months prior to cancer diagnosis, the risk of developing a pediatric cancer was 230% greater in children with LDIR exposure from cardiac procedures than in CHD patients without such exposure. For every 4 mSv in estimated LDIR exposure from cardiac procedures, the risk of cancer rose by 15.5%. In contrast, in the earlier study in adults with CHD, cancer risk climbed by 10% per 10 mSv. Patients with six or more LDIR cardiac procedures – not at all unusual in contemporary practice – were 2.4 times more likely to have cancer than those with no or one such radiation exposure.
Current ACC guidelines on radiation exposure from cardiac procedures recommend calculating an individual’s lifetime attributable cancer incidence and mortality risks, as well as adhering to the time-honored principle of ensuring that radiation exposure is as low as reasonably achievable without sacrificing quality of care.
“Our findings strongly support these ACC recommendations and moreover suggest that radiation surveillance for patients with congenital heart disease should be considered using radiation badges. Also, cancer surveillance guidelines should be considered for CHD patients exposed to LDIR,” Mr. Ganni said.
These suggestions for creation of patient radiation passports and cancer surveillance guidelines take on greater weight in light of two trends: the increasing life expectancy of children with CHD during the past 3 decades as a result of procedural advances that entail LDIR exposure, mostly for imaging, and the growing number of such procedures performed per patient earlier and earlier in life.
He and the MAUDE group plan to confirm their latest findings in other, larger data sets and hope to identify threshold effects for LDIR for specific cancers, with hematologic malignancies as the top priority.
Mr. Ganni reported having no financial conflicts regarding his study, funded by the Heart and Stroke Foundation of Canada, the Quebec Foundation for Health Research, and the Canadian Institutes for Health Research.
FROM ACC 2020
Coronary CT angiography gives superior MI risk prediction
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.

These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
FROM ACC 2020
Chest imaging guidelines released for pediatric COVID-19
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
ASE issues echocardiography guidance amid COVID-19 pandemic
The American Society of Echocardiography (ASE) has issued a statement on protecting patients and echocardiography service providers during the COVID-19 pandemic.
Given the risk for cardiovascular complications associated with COVID-19, echocardiographic services will likely be needed for patients with suspected or confirmed COVID-19, meaning echo providers will be exposed to SARS-CoV-2, write the statement authors, led by James N. Kirkpatrick, MD, director of the echocardiography laboratory at University of Washington Medical Center in Seattle.
The statement was published online April 6 in the Journal of the American College of Cardiology.
The authors say the statement is intended to help guide the practice of echocardiography in this “challenging time.” It was developed with input from a variety of echocardiography providers and institutions who have experience with the COVID-19, or have been “actively and thoughtfully preparing for it.”
Who, When, Where, and How
The statement covers triaging and decision pathways for handling requests for echocardiography, as well as indications and recommended procedures, in cases of suspected or confirmed COVID-19.
Among the recommendations:
- Only perform transthoracic echocardiograms (TTE), stress echocardiograms, and transesophageal echocardiograms (TEE) if they are expected to provide clinical benefit. Appropriate-use criteria represent the first decision point as to whether an echocardiographic test should be performed.
- Determine which studies are “elective” and reschedule them, performing all others. Identify “nonelective” (urgent/emergent) indications and defer all others.
- Determine the clinical benefit of echocardiography for symptomatic patients whose SARS-CoV-2 status is unknown.
- Cautiously consider the benefit of a TEE examination weighed against the risk for exposure of healthcare personnel to aerosolization in a patient with suspected or confirmed COVID-19.
- Postpone or cancel TEEs if an alternative imaging modality can provide the necessary information.
- Note that treadmill or bicycle stress echo tests in patients with COVID-19 may lead to exposure because of deep breathing and/or coughing during exercise. These tests should generally be deferred or converted to a pharmacologic stress echo.
The ASE statement also provides advice on safe imaging protocol and adequate personal protection measures.
“In addition to limiting the number of echocardiography practitioners involved in scanning, consideration should be given to limiting the exposure of staff who may be particularly susceptible to severe complications of COVID-19,” the ASE advises.
Staff who are older than 60 years, who have chronic conditions, are immunocompromised or are pregnant may wish to avoid contact with patients suspected or confirmed to have COVID-19.
It’s also important to realize the risk for transmission in reading rooms. “Keyboards, monitors, mice, chairs, phones, desktops, and door knobs should be frequently cleaned, and ventilation provided wherever possible,” the ASE advises. When the echo lab reading room is located in a high-traffic area, remote review of images or via webinar might be advisable, they suggest.
Summing up, Kirkland and colleagues say providing echocardiographic service “remains crucial in this difficult time of the SARS-CoV-2 outbreak. Working together, we can continue to provide high-quality care while minimizing risk to ourselves, our patients, and the public at large. Carefully considering ‘Whom to Image’, ‘Where to Image’ and ‘How to Image’ has the potential to reduce the risks of transmission.”
The authors note that the statements and recommendations are primarily based on expert opinion rather than on scientifically verified data and are subject to change as the COVID-19 outbreak continues to evolve and new data emerges.
This article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued a statement on protecting patients and echocardiography service providers during the COVID-19 pandemic.
Given the risk for cardiovascular complications associated with COVID-19, echocardiographic services will likely be needed for patients with suspected or confirmed COVID-19, meaning echo providers will be exposed to SARS-CoV-2, write the statement authors, led by James N. Kirkpatrick, MD, director of the echocardiography laboratory at University of Washington Medical Center in Seattle.
The statement was published online April 6 in the Journal of the American College of Cardiology.
The authors say the statement is intended to help guide the practice of echocardiography in this “challenging time.” It was developed with input from a variety of echocardiography providers and institutions who have experience with the COVID-19, or have been “actively and thoughtfully preparing for it.”
Who, When, Where, and How
The statement covers triaging and decision pathways for handling requests for echocardiography, as well as indications and recommended procedures, in cases of suspected or confirmed COVID-19.
Among the recommendations:
- Only perform transthoracic echocardiograms (TTE), stress echocardiograms, and transesophageal echocardiograms (TEE) if they are expected to provide clinical benefit. Appropriate-use criteria represent the first decision point as to whether an echocardiographic test should be performed.
- Determine which studies are “elective” and reschedule them, performing all others. Identify “nonelective” (urgent/emergent) indications and defer all others.
- Determine the clinical benefit of echocardiography for symptomatic patients whose SARS-CoV-2 status is unknown.
- Cautiously consider the benefit of a TEE examination weighed against the risk for exposure of healthcare personnel to aerosolization in a patient with suspected or confirmed COVID-19.
- Postpone or cancel TEEs if an alternative imaging modality can provide the necessary information.
- Note that treadmill or bicycle stress echo tests in patients with COVID-19 may lead to exposure because of deep breathing and/or coughing during exercise. These tests should generally be deferred or converted to a pharmacologic stress echo.
The ASE statement also provides advice on safe imaging protocol and adequate personal protection measures.
“In addition to limiting the number of echocardiography practitioners involved in scanning, consideration should be given to limiting the exposure of staff who may be particularly susceptible to severe complications of COVID-19,” the ASE advises.
Staff who are older than 60 years, who have chronic conditions, are immunocompromised or are pregnant may wish to avoid contact with patients suspected or confirmed to have COVID-19.
It’s also important to realize the risk for transmission in reading rooms. “Keyboards, monitors, mice, chairs, phones, desktops, and door knobs should be frequently cleaned, and ventilation provided wherever possible,” the ASE advises. When the echo lab reading room is located in a high-traffic area, remote review of images or via webinar might be advisable, they suggest.
Summing up, Kirkland and colleagues say providing echocardiographic service “remains crucial in this difficult time of the SARS-CoV-2 outbreak. Working together, we can continue to provide high-quality care while minimizing risk to ourselves, our patients, and the public at large. Carefully considering ‘Whom to Image’, ‘Where to Image’ and ‘How to Image’ has the potential to reduce the risks of transmission.”
The authors note that the statements and recommendations are primarily based on expert opinion rather than on scientifically verified data and are subject to change as the COVID-19 outbreak continues to evolve and new data emerges.
This article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued a statement on protecting patients and echocardiography service providers during the COVID-19 pandemic.
Given the risk for cardiovascular complications associated with COVID-19, echocardiographic services will likely be needed for patients with suspected or confirmed COVID-19, meaning echo providers will be exposed to SARS-CoV-2, write the statement authors, led by James N. Kirkpatrick, MD, director of the echocardiography laboratory at University of Washington Medical Center in Seattle.
The statement was published online April 6 in the Journal of the American College of Cardiology.
The authors say the statement is intended to help guide the practice of echocardiography in this “challenging time.” It was developed with input from a variety of echocardiography providers and institutions who have experience with the COVID-19, or have been “actively and thoughtfully preparing for it.”
Who, When, Where, and How
The statement covers triaging and decision pathways for handling requests for echocardiography, as well as indications and recommended procedures, in cases of suspected or confirmed COVID-19.
Among the recommendations:
- Only perform transthoracic echocardiograms (TTE), stress echocardiograms, and transesophageal echocardiograms (TEE) if they are expected to provide clinical benefit. Appropriate-use criteria represent the first decision point as to whether an echocardiographic test should be performed.
- Determine which studies are “elective” and reschedule them, performing all others. Identify “nonelective” (urgent/emergent) indications and defer all others.
- Determine the clinical benefit of echocardiography for symptomatic patients whose SARS-CoV-2 status is unknown.
- Cautiously consider the benefit of a TEE examination weighed against the risk for exposure of healthcare personnel to aerosolization in a patient with suspected or confirmed COVID-19.
- Postpone or cancel TEEs if an alternative imaging modality can provide the necessary information.
- Note that treadmill or bicycle stress echo tests in patients with COVID-19 may lead to exposure because of deep breathing and/or coughing during exercise. These tests should generally be deferred or converted to a pharmacologic stress echo.
The ASE statement also provides advice on safe imaging protocol and adequate personal protection measures.
“In addition to limiting the number of echocardiography practitioners involved in scanning, consideration should be given to limiting the exposure of staff who may be particularly susceptible to severe complications of COVID-19,” the ASE advises.
Staff who are older than 60 years, who have chronic conditions, are immunocompromised or are pregnant may wish to avoid contact with patients suspected or confirmed to have COVID-19.
It’s also important to realize the risk for transmission in reading rooms. “Keyboards, monitors, mice, chairs, phones, desktops, and door knobs should be frequently cleaned, and ventilation provided wherever possible,” the ASE advises. When the echo lab reading room is located in a high-traffic area, remote review of images or via webinar might be advisable, they suggest.
Summing up, Kirkland and colleagues say providing echocardiographic service “remains crucial in this difficult time of the SARS-CoV-2 outbreak. Working together, we can continue to provide high-quality care while minimizing risk to ourselves, our patients, and the public at large. Carefully considering ‘Whom to Image’, ‘Where to Image’ and ‘How to Image’ has the potential to reduce the risks of transmission.”
The authors note that the statements and recommendations are primarily based on expert opinion rather than on scientifically verified data and are subject to change as the COVID-19 outbreak continues to evolve and new data emerges.
This article first appeared on Medscape.com.