User login
Sunscreens with DNA repair enzymes might lessen AK progression
Patients with actinic keratosis who used UPF 50 sunscreen containing DNA repair enzymes improved significantly more on two measures of malignant progression than did those who used sunscreen alone, according to research published in the Journal of Drugs in Dermatology.
At 6 months, improvements in field cancerization and levels of cyclobutane pyrimidine dimers were significantly greater (P less than .001) for the sunscreen-plus-enzymes group compared with sunscreen-only patients, wrote Dr. Mauro Carducci of Centro Ortopedico di Quadrante in Omegna, Italy, and his associates.
The study is the first of its type to directly compare the clinical effects of two such topicals, the investigators wrote. The findings set the stage for longer, larger trials that are powered to assess the risk of progression to squamous cell carcinoma, they added.

For the study, 28 patients with AK were randomly assigned to use SPF 50 sunscreen alone or a formula that contained 1% photolyase from Anacystis nidulans and 1% endonuclease from Micrococcus luteus. Patients applied 2 mg/cm2 of sunscreen to treatment areas that contained 4-10 AKs. They were not allowed to use other topicals during the trial or for 2 weeks beforehand.
All of the patients were white and aged older than 65 years; three-quarters were men. The investigators used fluorescence diagnostics with methylaminolaevulinate to measure field cancerization, and analyzed skin biopsies to quantify CPD levels (J Drugs Dermatol. 2015;14[9]:986-90.).
Hyperkeratosis improved the same amount in both groups at month 6, according to the researchers. But field cancerizations dropped 29% from baseline in the sunscreen-plus-enzymes group, compared with a 10% decrease with sunscreen alone (P less than .0001). Likewise, CPD levels fell 61% from baseline in the sunscreen-plus-enzymes group compared with a 35% drop with sunscreen alone (P less than .0001).
Despite those significant differences, the study was not powered to detect differences in the risk of transformation to SCC, the researchers cautioned.
Biodue S.p.A. provided the methyl aminolevulinate used in the study. Dr. Enzo Emanuele, the study’s senior author, is a major shareholder of Living Research S.A.S., a privately held biomedical research organization that provided funding for the work. The other researchers reported no conflicts of interest.
Patients with actinic keratosis who used UPF 50 sunscreen containing DNA repair enzymes improved significantly more on two measures of malignant progression than did those who used sunscreen alone, according to research published in the Journal of Drugs in Dermatology.
At 6 months, improvements in field cancerization and levels of cyclobutane pyrimidine dimers were significantly greater (P less than .001) for the sunscreen-plus-enzymes group compared with sunscreen-only patients, wrote Dr. Mauro Carducci of Centro Ortopedico di Quadrante in Omegna, Italy, and his associates.
The study is the first of its type to directly compare the clinical effects of two such topicals, the investigators wrote. The findings set the stage for longer, larger trials that are powered to assess the risk of progression to squamous cell carcinoma, they added.
For the study, 28 patients with AK were randomly assigned to use SPF 50 sunscreen alone or a formula that contained 1% photolyase from Anacystis nidulans and 1% endonuclease from Micrococcus luteus. Patients applied 2 mg/cm2 of sunscreen to treatment areas that contained 4-10 AKs. They were not allowed to use other topicals during the trial or for 2 weeks beforehand.
All of the patients were white and aged older than 65 years; three-quarters were men. The investigators used fluorescence diagnostics with methylaminolaevulinate to measure field cancerization, and analyzed skin biopsies to quantify CPD levels (J Drugs Dermatol. 2015;14[9]:986-90.).
Hyperkeratosis improved the same amount in both groups at month 6, according to the researchers. But field cancerizations dropped 29% from baseline in the sunscreen-plus-enzymes group, compared with a 10% decrease with sunscreen alone (P less than .0001). Likewise, CPD levels fell 61% from baseline in the sunscreen-plus-enzymes group compared with a 35% drop with sunscreen alone (P less than .0001).
Despite those significant differences, the study was not powered to detect differences in the risk of transformation to SCC, the researchers cautioned.
Biodue S.p.A. provided the methyl aminolevulinate used in the study. Dr. Enzo Emanuele, the study’s senior author, is a major shareholder of Living Research S.A.S., a privately held biomedical research organization that provided funding for the work. The other researchers reported no conflicts of interest.
Patients with actinic keratosis who used UPF 50 sunscreen containing DNA repair enzymes improved significantly more on two measures of malignant progression than did those who used sunscreen alone, according to research published in the Journal of Drugs in Dermatology.
At 6 months, improvements in field cancerization and levels of cyclobutane pyrimidine dimers were significantly greater (P less than .001) for the sunscreen-plus-enzymes group compared with sunscreen-only patients, wrote Dr. Mauro Carducci of Centro Ortopedico di Quadrante in Omegna, Italy, and his associates.
The study is the first of its type to directly compare the clinical effects of two such topicals, the investigators wrote. The findings set the stage for longer, larger trials that are powered to assess the risk of progression to squamous cell carcinoma, they added.
For the study, 28 patients with AK were randomly assigned to use SPF 50 sunscreen alone or a formula that contained 1% photolyase from Anacystis nidulans and 1% endonuclease from Micrococcus luteus. Patients applied 2 mg/cm2 of sunscreen to treatment areas that contained 4-10 AKs. They were not allowed to use other topicals during the trial or for 2 weeks beforehand.
All of the patients were white and aged older than 65 years; three-quarters were men. The investigators used fluorescence diagnostics with methylaminolaevulinate to measure field cancerization, and analyzed skin biopsies to quantify CPD levels (J Drugs Dermatol. 2015;14[9]:986-90.).
Hyperkeratosis improved the same amount in both groups at month 6, according to the researchers. But field cancerizations dropped 29% from baseline in the sunscreen-plus-enzymes group, compared with a 10% decrease with sunscreen alone (P less than .0001). Likewise, CPD levels fell 61% from baseline in the sunscreen-plus-enzymes group compared with a 35% drop with sunscreen alone (P less than .0001).
Despite those significant differences, the study was not powered to detect differences in the risk of transformation to SCC, the researchers cautioned.
Biodue S.p.A. provided the methyl aminolevulinate used in the study. Dr. Enzo Emanuele, the study’s senior author, is a major shareholder of Living Research S.A.S., a privately held biomedical research organization that provided funding for the work. The other researchers reported no conflicts of interest.
FROM THE JOURNAL OF DRUGS IN DERMATOLOGY
Key clinical point:Sunscreen containing DNA repair enzymes might prevent malignant progression of actinic keratosis better than sunscreen alone.
Major finding: Field cancerization and cyclobutane pyrimidine dimer levels improved significantly more with sunscreen plus enzymes than with sunscreen only (P less than .0001 for each).
Data source: Six-month randomized trial of 28 patients with actinic keratosis.
Disclosures: Biodue S.p.A. provided the methyl aminolevulinate used in the study. Dr. Enzo Emanuele, the study’s senior author, is a major shareholder of Living Research S.A.S., a privately held biomedical research organization that provided funding for the work. The other researchers reported no conflicts of interest.

Management of dysplastic nevi varies widely
PARK CITY, UTAH – When you ask clinicians why they elect to reexcise dysplastic nevi, you’re likely to get a variety of answers, according to Dr. Douglas Grossman.
“Sometimes they have no reason all,” Dr. Grossman, professor of dermatology at the University of Utah, Salt Lake City, said at the annual meeting of the Pacific Dermatologic Association. “Sometimes the answer is ‘to prevent recurrence.’ Sometimes it’s to ensure complete removal of the lesion, to confirm the diagnosis, to rule out melanoma, or for ‘therapeutic’ purposes.”

Dysplastic nevus margins are often positive, “because the melanocytes in these lesions tend to extend up to 2 mm beyond clinical margins,” Dr. Grossman said. “I always try to remove the entire clinical lesion as well as 1-2 mm around the lesion to avoid positive margins.”
A survey of 101 Chicago Dermatological Society members found wide variation in clinical practice concerning how clinicians manage dysplastic nevi if the margins are clear vs. positive, and based on the degree of atypia (Arch Dermatol. 2012;148[2]:259-60). The greatest quantitative shift in decision making (from observe to reexcise) was seen for dysplastic nevi with moderate dysplasia. Specifically, the decision to reexcise dysplastic nevi with moderate dysplasia ranged from 9% (for clear margins) to 81% (for positive margins) of respondents. “The margin status is driving the management,” said Dr. Grossman, who was not involved with the study.
In his opinion, two “unspoken fears” are also impacting the way clinicians treat dysplastic nevi. The first is that the nevus will recur in the scar years later and be indistinguishable from melanoma – the so-called pseudomelanoma phenomenon. The second fear is that residual nevus cells left behind will transform to melanoma. Evidence for these two possibilities, however, is lacking, Dr. Grossman said. According to a large study of pseudomelanoma phenomena, recurrence was rare and easily distinguishable from cases of melanoma with regression (Modern Pathol. 2009;22:611-7). “Almost all of them had recurred within a year, so if a nevus is going to recur, it’s usually going to recur within that first year,” he said.
As for the issue of recurrence, Dr. Grossman led a research team that evaluated 271 nevus biopsy sites in 115 patients (J Am Acad Dermatol. 2010;62[4]:591-6). At greater than 2 years of follow-up they observed a recurrence rate of 3.6% for dysplastic nevi, compared with 3.3% for nondysplastic nevi, “which is similar,” he said. In terms of melanoma development, one study of 28 incompletely removed dysplastic nevi found that no melanomas developed during 5 years of follow-up (Am J Dermatopathol. 1985;7 Suppl:93-7).
Dr. Grossman referenced four cases in the medical literature in which the diagnosis was changed upon reexcision from dysplastic nevus to melanoma. “The question here is whether the initial biopsy or the reexcision was the correct diagnosis,” he said. “Development of melanoma at the site of a previously biopsied dysplastic nevus is exceedingly rare, and has not been described beyond a few case reports. The most likely explanation for how this could occur would be sampling error. If you have a melanoma arising at the site, maybe it was melanoma to start with, and the diagnosis was missed on the original biopsy. It could also be the case of pseudomelanoma phenomenon where it’s a nevus to start with but it comes back looking more atypical, so it’s incorrectly diagnosed as melanoma. A final possibility, which is the least likely, is that the few nevus cells left behind transformed into melanoma.”
According to a recent consensus statement from the Pigmented Lesion Subcommittee of the Melanoma Prevention Working Group, mild/moderate dysplastic nevi with clear margins do not need reexcision (JAMA Dermatol. 2015;151[2]:212-8). The working group also recommends that mild dysplastic nevi with positive margins may be safely observed and that observation for moderately dysplastic nevi with positive margins “may be a reasonable option.”
Dr. Grossman reported having no financial disclosures.
PARK CITY, UTAH – When you ask clinicians why they elect to reexcise dysplastic nevi, you’re likely to get a variety of answers, according to Dr. Douglas Grossman.
“Sometimes they have no reason all,” Dr. Grossman, professor of dermatology at the University of Utah, Salt Lake City, said at the annual meeting of the Pacific Dermatologic Association. “Sometimes the answer is ‘to prevent recurrence.’ Sometimes it’s to ensure complete removal of the lesion, to confirm the diagnosis, to rule out melanoma, or for ‘therapeutic’ purposes.”
Dysplastic nevus margins are often positive, “because the melanocytes in these lesions tend to extend up to 2 mm beyond clinical margins,” Dr. Grossman said. “I always try to remove the entire clinical lesion as well as 1-2 mm around the lesion to avoid positive margins.”
A survey of 101 Chicago Dermatological Society members found wide variation in clinical practice concerning how clinicians manage dysplastic nevi if the margins are clear vs. positive, and based on the degree of atypia (Arch Dermatol. 2012;148[2]:259-60). The greatest quantitative shift in decision making (from observe to reexcise) was seen for dysplastic nevi with moderate dysplasia. Specifically, the decision to reexcise dysplastic nevi with moderate dysplasia ranged from 9% (for clear margins) to 81% (for positive margins) of respondents. “The margin status is driving the management,” said Dr. Grossman, who was not involved with the study.
In his opinion, two “unspoken fears” are also impacting the way clinicians treat dysplastic nevi. The first is that the nevus will recur in the scar years later and be indistinguishable from melanoma – the so-called pseudomelanoma phenomenon. The second fear is that residual nevus cells left behind will transform to melanoma. Evidence for these two possibilities, however, is lacking, Dr. Grossman said. According to a large study of pseudomelanoma phenomena, recurrence was rare and easily distinguishable from cases of melanoma with regression (Modern Pathol. 2009;22:611-7). “Almost all of them had recurred within a year, so if a nevus is going to recur, it’s usually going to recur within that first year,” he said.
As for the issue of recurrence, Dr. Grossman led a research team that evaluated 271 nevus biopsy sites in 115 patients (J Am Acad Dermatol. 2010;62[4]:591-6). At greater than 2 years of follow-up they observed a recurrence rate of 3.6% for dysplastic nevi, compared with 3.3% for nondysplastic nevi, “which is similar,” he said. In terms of melanoma development, one study of 28 incompletely removed dysplastic nevi found that no melanomas developed during 5 years of follow-up (Am J Dermatopathol. 1985;7 Suppl:93-7).
Dr. Grossman referenced four cases in the medical literature in which the diagnosis was changed upon reexcision from dysplastic nevus to melanoma. “The question here is whether the initial biopsy or the reexcision was the correct diagnosis,” he said. “Development of melanoma at the site of a previously biopsied dysplastic nevus is exceedingly rare, and has not been described beyond a few case reports. The most likely explanation for how this could occur would be sampling error. If you have a melanoma arising at the site, maybe it was melanoma to start with, and the diagnosis was missed on the original biopsy. It could also be the case of pseudomelanoma phenomenon where it’s a nevus to start with but it comes back looking more atypical, so it’s incorrectly diagnosed as melanoma. A final possibility, which is the least likely, is that the few nevus cells left behind transformed into melanoma.”
According to a recent consensus statement from the Pigmented Lesion Subcommittee of the Melanoma Prevention Working Group, mild/moderate dysplastic nevi with clear margins do not need reexcision (JAMA Dermatol. 2015;151[2]:212-8). The working group also recommends that mild dysplastic nevi with positive margins may be safely observed and that observation for moderately dysplastic nevi with positive margins “may be a reasonable option.”
Dr. Grossman reported having no financial disclosures.
PARK CITY, UTAH – When you ask clinicians why they elect to reexcise dysplastic nevi, you’re likely to get a variety of answers, according to Dr. Douglas Grossman.
“Sometimes they have no reason all,” Dr. Grossman, professor of dermatology at the University of Utah, Salt Lake City, said at the annual meeting of the Pacific Dermatologic Association. “Sometimes the answer is ‘to prevent recurrence.’ Sometimes it’s to ensure complete removal of the lesion, to confirm the diagnosis, to rule out melanoma, or for ‘therapeutic’ purposes.”
Dysplastic nevus margins are often positive, “because the melanocytes in these lesions tend to extend up to 2 mm beyond clinical margins,” Dr. Grossman said. “I always try to remove the entire clinical lesion as well as 1-2 mm around the lesion to avoid positive margins.”
A survey of 101 Chicago Dermatological Society members found wide variation in clinical practice concerning how clinicians manage dysplastic nevi if the margins are clear vs. positive, and based on the degree of atypia (Arch Dermatol. 2012;148[2]:259-60). The greatest quantitative shift in decision making (from observe to reexcise) was seen for dysplastic nevi with moderate dysplasia. Specifically, the decision to reexcise dysplastic nevi with moderate dysplasia ranged from 9% (for clear margins) to 81% (for positive margins) of respondents. “The margin status is driving the management,” said Dr. Grossman, who was not involved with the study.
In his opinion, two “unspoken fears” are also impacting the way clinicians treat dysplastic nevi. The first is that the nevus will recur in the scar years later and be indistinguishable from melanoma – the so-called pseudomelanoma phenomenon. The second fear is that residual nevus cells left behind will transform to melanoma. Evidence for these two possibilities, however, is lacking, Dr. Grossman said. According to a large study of pseudomelanoma phenomena, recurrence was rare and easily distinguishable from cases of melanoma with regression (Modern Pathol. 2009;22:611-7). “Almost all of them had recurred within a year, so if a nevus is going to recur, it’s usually going to recur within that first year,” he said.
As for the issue of recurrence, Dr. Grossman led a research team that evaluated 271 nevus biopsy sites in 115 patients (J Am Acad Dermatol. 2010;62[4]:591-6). At greater than 2 years of follow-up they observed a recurrence rate of 3.6% for dysplastic nevi, compared with 3.3% for nondysplastic nevi, “which is similar,” he said. In terms of melanoma development, one study of 28 incompletely removed dysplastic nevi found that no melanomas developed during 5 years of follow-up (Am J Dermatopathol. 1985;7 Suppl:93-7).
Dr. Grossman referenced four cases in the medical literature in which the diagnosis was changed upon reexcision from dysplastic nevus to melanoma. “The question here is whether the initial biopsy or the reexcision was the correct diagnosis,” he said. “Development of melanoma at the site of a previously biopsied dysplastic nevus is exceedingly rare, and has not been described beyond a few case reports. The most likely explanation for how this could occur would be sampling error. If you have a melanoma arising at the site, maybe it was melanoma to start with, and the diagnosis was missed on the original biopsy. It could also be the case of pseudomelanoma phenomenon where it’s a nevus to start with but it comes back looking more atypical, so it’s incorrectly diagnosed as melanoma. A final possibility, which is the least likely, is that the few nevus cells left behind transformed into melanoma.”
According to a recent consensus statement from the Pigmented Lesion Subcommittee of the Melanoma Prevention Working Group, mild/moderate dysplastic nevi with clear margins do not need reexcision (JAMA Dermatol. 2015;151[2]:212-8). The working group also recommends that mild dysplastic nevi with positive margins may be safely observed and that observation for moderately dysplastic nevi with positive margins “may be a reasonable option.”
Dr. Grossman reported having no financial disclosures.
EXPERT ANALYSIS FROM PDA 2015

An Analysis of the Clinical Trial Landscape for Cutaneous Melanoma
The incidence of cutaneous melanoma, the deadliest form of skin cancer, has been steadily increasing over the last several decades.1 Currently, there are 73,870 new diagnoses of melanoma anticipated in the United States in 2015 alone.2 Many cases of melanoma are caught at early, actionable, and curable stages thanks in part to patient education and screening by dermatologists.3 However, until recently, few options existed for the treatment of locally advanced and metastatic melanomas, with a median survival rate of less than 1 year.4
Clinical trials represent the most reliable method for advancing treatment and improving outcomes for patients with disease; however, patient accrual and access to clinical trials remain formidable barriers. Studies have suggested that patients in rural areas perceive both an increased distance to clinical trial sites and a lack of awareness of available trials compared to their urban counterparts. Additionally, studies have shown that provider awareness of actively enrolling clinical trials in their respective fields is a key determinate in patient enrollment.5 Finally, insufficient funding and lack of collaboration has resulted in many small phase 1 or phase 2 single-center trials, which are less likely to quickly impact clinical care.6 Increased awareness of the ClinicalTrials.gov registry, a publicly available and easily accessible database, can facilitate referral, enrollment, and collaboration among physicians, patients, and researchers alike.
Using the ClinicalTrials.gov database, we sought to analyze the clinical trial landscape for cutaneous melanoma to understand the current state of melanoma research, future direction, and potential barriers that may impede success.
Methods
The primary objective was to provide a snapshot of the melanoma clinical research landscape from 2005 to 2013, including the number of registered trials, phase distribution, recruitment status, location of trials, type of intervention, and disease state being studied. Secondary objectives included describing patterns of clinical trial distribution within the United States in the context of melanoma mortality and examining changing trends in interventions studied in trials over time.
ClinicalTrials.gov is a comprehensive online registry of clinical trials conducted in the United States and abroad that is maintained by the National Library of Medicine.7 Although the initiative was launched in 2000, the registry became effectively comprehensive in September 2005 when the International Committee of Medical Journal Editors declared prospective registration of clinical trials as a prerequisite for publication. The US Food and Drug Administration followed suit in September 2007, expanding the requirements for registration and declaring penalties for parties who did not comply.8 Each registered trial can be found through searchable keywords, and each study page contains details of study design, principal investigators, and inclusion and exclusion criteria, as well as contact information for enrollment.
Study Selection
Clinical trials registered between September 15, 2005, and December 31, 2013, were evaluated; a total of 138,312 trials were found to be registered on ClinicalTrials.gov during that time period. We limited our study selection to interventional studies, which were filtered by topic to yield only those pertaining to melanoma patients. To minimize reporting bias, trials registered prior to the implementation of the International Committee of Medical Journal Editors’ reporting requirements were excluded. To focus specifically on the landscape of trials in cutaneous melanoma, trials investigating multiple advanced malignancies, uveal or ocular melanoma, and mucosal melanoma were manually excluded.
Study Variables
Information on each clinical trial was extracted from ClinicalTrials.gov. Each trial was manually reviewed by an investigator to determine the disease state and type of intervention being studied. Studies investigating multiple modalities concurrently were classified as “other.”
Data Analysis
Study variables were first analyzed among the entire cohort as a whole. Using each trial location and a python script based on open-source code, the number of actively recruiting melanoma trials in each US county was identified and mapped. County-level, melanoma-specific mortality data from 2001 to 2010 was extracted from the Centers for Disease Control and Prevention’s WONDER (Wide-ranging Online Data for Epidemiologic Research) mortality database (wonder.cdc.gov). Finally, to analyze changing trends in cutaneous melanoma investigation, trials were grouped into 3 categories based on the date they were received on ClinicalTrials.gov: (1) 2005-2007, (2) 2008-2010, and (3) 2011-2013. Disease state and type of intervention were analyzed and compared among each group using the χ2 statistic.
Results
Of the 138,312 trials registered on ClinicalTrials.gov between September 15, 2005, and December 31, 2013, only 931 were identified as interventional studies pertaining to melanoma patients. Of these, 154 were excluded because of a focus on uveal, ocular, or mucosal melanoma or because of the inclusion of participants with multiple types of advanced malignancies. The final analysis included 777 trials specifically focusing on cutaneous melanoma.
Characteristics of these 777 trials were varied. Many interventions were in the early stages of development, with 339 (44%) trials classified as phase 0, phase 1, or phase 1/phase 2; 306 (39%) as phase 2; and 71 (9%) as nonpharmacologic (nonphase) trials. Only 58 trials (8%) were classified as phase 3 or phase 4. The majority of the trials were actively recruiting (225 [29%]), active but not yet recruiting (172 [22%]), or completed (255 [33%]); however, 98 trials (13%) had been suspended, terminated, or withdrawn. Additionally, 22 trials (3%) were not yet recruiting and 5 (<1%) were classified as “other” because they did not have a recruitment status listed.
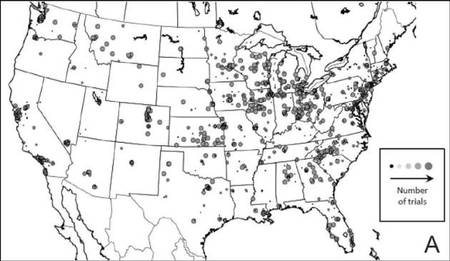
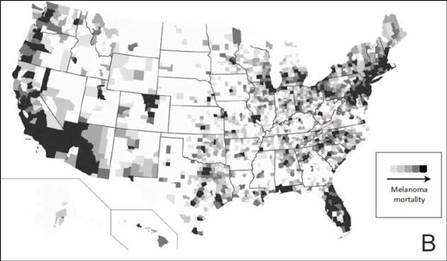
The distribution of actively enrolling clinical trials corresponds to major metropolitan areas within the Northeast, Upper Midwest, and Coastal California (Figure 1A). Figure 1B demonstrates the melanoma-specific mortality across the United States. Areas in the Southwest and Florida shared some of the greatest disease burden.
|
| Figure 1. Geographical representation of US clinical trial enrollment with the number of actively recruiting trials for each unique US zip code presented. The circle size corresponds to the number of trials. The largest circles indicate more than 5 trials within a given zip code (A). County-level melanoma-specific mortality data are presented for 2001 to 2010 (B). Darkest areas represent the highest numbers of melanoma deaths.
|
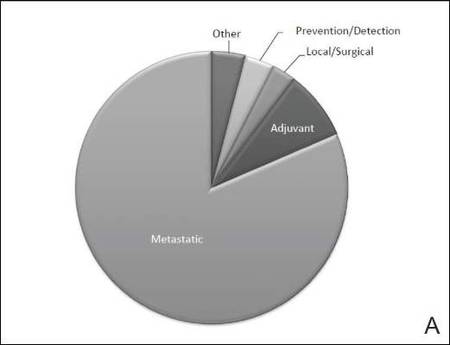
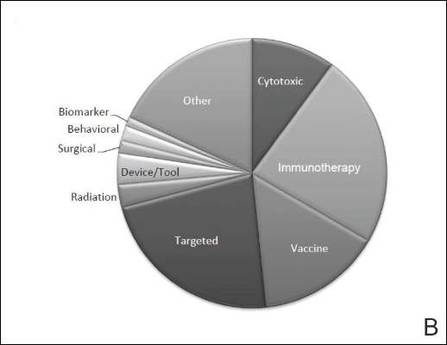
The disease state and type of intervention for all the included trials are summarized in Figure 2. The vast majority of trials (633/777 [82%]) enrolled participants with metastatic melanoma. Unlike many other tumor types, only 64 (8%) trials enrolled patients specifically in the adjuvant setting. Most trials focused on targeted (175 [23%]), immune (180 [23%]), and vaccine (117 [15%]) therapy.
|
| Figure 2. Trial distribution stratified by disease state (A) and type of intervention (B). Trial distribution is shown for 777 interventional clinical trials including melanoma patients. The majority of clinical trials involved patients with metastatic melanoma. The majority of trials investigated targeted therapy, immunotherapy, and vaccine therapy. |
We subsequently analyzed changes in trial characteristics over time. We noted a decrease in the number of trials investigating cytotoxic and vaccine-based therapies, and increasing numbers of trials investigating immunotherapy (P=.041). Between 2005 and 2007, 14% (27/201) of all trials investigated cytotoxic therapies compared to just 7% (20/294) of trials between 2011 and 2013. With the approval of ipilimumab, 29% (85/294) of all clinical trials between 2011 and 2013 investigated immunotherapies, which comprised only 18% (37/201) of clinical trials between 2005 and 2007. The majority of trials continued to enroll patients in the metastatic setting where outcomes remain poor. Importantly, only 6% (49/777) of all clinical trials have focused on prevention, early detection, and local management of melanoma, which has remained constant over time.
Comment
Cutaneous melanoma remains an area of active investigation, interdisciplinary collaboration, and great promise. The ClinicalTrials.gov registry serves not only to increase transparency among interested parties but also as a rich resource to study the clinical research landscape as demonstrated in this study.
Greater understanding of the underlying genetic and immunogenic properties of melanoma tissues has led to the US Food and Drug Administration approval of several novel agents to treat metastatic disease. BRAF inhibitors such as vemurafenib and dabrafenib target more than 50% of all melanoma tumors harboring mutations in the BRAF gene and have shown unparalleled efficacy in clinical trials; however, durability of response and adverse effects still remain a concern.4,9-11 Ipilimumab, a CTLA-4 inhibitor, enhances antitumor immunity and demonstrated improved survival in clinical trials.12,13 Nivolumab, a fully human IgG4 programmed death 1 (PD-1) immune-checkpoint inhibitor antibody, also demonstrated improved overall and progression-free survival.14 Finally, trametinib, a MEK inhibitor, used in combination with BRAF inhibitors has demonstrated improved response over BRAF inhibitors alone.15
Although traditional cytotoxic chemotherapy was one of the few available treatment options before 2011, response was infrequent.16 Our data indicate that the melanoma research landscape has shifted to follow advances in targeted therapy and immunotherapy. We noted a decrease in the study of cytotoxic chemotherapy in metastatic melanoma, with a compensatory increase in immunotherapy trials and a continued commitment to targeted therapy. Further, with the approval of BRAF inhibitors, CTLA-4 inhibitors, and PD-1 inhibitors for metastatic disease, some have pushed to move these agents into the adjuvant setting to prevent micrometastases from evolving into clinically significant disease.17 Early results from EORTC (European Organisation for Research and Treatment of Cancer) 18071 comparing adjuvant ipilimumab to placebo demonstrated a 26.1-month versus 17.1-month improvement in relapse-free survival, respectively.18 However, this finding has important implications for clinical dermatologists. Patients treated with BRAF inhibitors are at increased risk for keratoacanthomas, invasive squamous cell carcinomas, and secondary primary melanomas.19,20 Caring for these patients requires increased vigilance and collaboration between dermatologists and oncologists.
Our study also highlights the dynamic nature of the field. For example, novel vaccine therapies have demonstrated promise in the metastatic/ unresectable tumor setting, with some herpes simplex virus–based vaccines generating durable antitumor immune responses in patients with melanoma.21 Combination therapy with CTLA-4 and PD-1 inhibitors has demonstrated improved objective response rates and progression-free survival over monotherapy.22 As the status of actively recruiting trials changes on a regular basis, we encourage physicians to access ClinicalTrials.gov to find details and contact information for actively recruiting trials and results on completed trials.
Early detection and management, however, still remain our primary option for cure, and the role of community dermatologists cannot be overstated.23 Patients with stage I and stage II disease have excellent long-term survival rates, yet only 6% of all clinical trials in cutaneous melanoma have focused on patient education, disease prevention, early detection, and local management. With an increasing incidence of melanoma among an aging population, the disease burden remains of substantial concern.24 Optimizing disease prevention, appropriate screening, and early detection are critical roles for dermatologists.
Finally, our data offer some insight into accrual barriers often faced by clinical trials. Actively enrolling clinical trials cluster within major metropolitan areas, presumably with large academic medical centers; however, areas in the southwestern United States and Florida, for example, have some of the highest burden of disease, likely secondary to sun exposure and aging populations.25 Integration of community dermatologists and oncologists may decrease both actual and patient-perceived barriers to care, which requires further exploration.6
Conclusion
Melanoma incidence and disease burden is increasing, and the field of melanoma research is incredibly dynamic. Going forward, we believe dermatologists will continue to play a critical role both in primary disease prevention and detection as well as in detection of secondary treatment-related skin toxicities. ClinicalTrials.gov is an invaluable resource to keep interested parties informed, foster collaboration, identify potential barriers to success, and suggest future directions.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64:252-271.
2. American Cancer Society. Cancer Facts and Figures 2015. American Cancer Society Web site. http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed August 26, 2015.
3. Cheng MY, Moreau JF, McGuire ST, et al. Melanoma depth in patients with an established dermatologist. J Am Acad Dermatol. 2014;70:841-846.
4. Jang S, Atkins MB. Which drug, and when, for patients with BRAF-mutant melanoma? Lancet Oncol. 2013;14:e60-e69.
5. Kim SH, Tanner A, Friedman DB, et al. Barriers to clinical trial participation: a comparison of rural and urban communities in South Carolina. J Community Health. 2014;39:562-571.
6. Gregg JR, Horn L, Davidson MA, et al. Patient enrollment onto clinical trials: the role of physician knowledge. J Cancer Educ. 2014;29:74-79.
7. Galsky MD, Hendricks R, Svatek R, et al. Critical analysis of contemporary clinical research in muscle-invasive and metastatic urothelial cancer: a report from the
Bladder Cancer Advocacy Network Clinical Trials Working Group. Cancer. 2013;119:1994-1998.
8. Zarin DA, Tse T, Williams RJ, et al. The ClinicalTrials.gov results database—update and key issues. N Engl J Med. 2011;364:852-860.
9. Luke JJ, Hodi FS. Ipilimumab, vemurafenib, dabrafenib, and trametinib: synergistic competitors in the clinical management of BRAF mutant malignant melanoma. Oncologist. 2013;18:717-725.
10. McArthur GA, Chapman PB, Robert C, et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014;15:323-332.
11. Swaika A, Crozier JA, Joseph RW. Vemurafenib: an evidence-based review of its clinical utility in the treatment of metastatic melanoma. Drug Des Devel Ther. 2014;8:775-787.
12. Lacouture ME, Wolchok JD, Yosipovitch G, et al. Ipilimumab in patients with cancer and the management of dermatologic adverse events. J Am Acad Dermatol. 2014;71:161-169.
13. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723.
14. Robert C, Long G, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320-330.
15. Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372:30-39.
16. Espinosa E, Berrocal A, López Martin JA, et al. Advances in cutaneous melanoma. Clin Transl Oncol. 2012;14:325-332.
17. Chapman PB. Treating metastatic melanoma in 2014: what just happened and what is next? Am Soc Clin Oncol Educ Book. 2014:16-19.
18. Eggermont A, Chiarion-Sileni V, Grob JJ, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16:522-530.
19. Curry JL, Tetzlaff MT, Nicholson K, et al. Histological features associated with vemurafenib-induced skin toxicities: examination of 141 cutaneous lesions biopsied during therapy. Am J Dermatopathol. 2014; 36:557-561.
20. Perier-Muzet M, Thomas L, Poulalhon N, et al. Melanoma patients under vemurafenib: prospective follow-up of melanocytic lesions by digital dermoscopy. J Invest Dermatol. 2014;134:1351-1358.
21. Ross MI, Andtbacka RI, Puzanov I, et al. Patterns of durable response with intralesional talimogene laherparepvec (T-VEC): results from a phase III trial in patients with stage IIIb-IV melanoma. Paper presented at: ASCO Annual Meeting; June 2, 2014; Boston, MA.
22. Postow MA, Chesney J, Pavlick AC, et al. Novolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372:2006-2017.
23. Gorantla VC, Kirkwood JM. State of melanoma: an historic overview of a field in transition. Hematol Oncol Clin North Am. 2014;28:415-435.
24. Coit DG, Olszanski AJ. Progress in the management of melanoma in 2013. J Natl Compr Canc Netw. 2013; 11(5 suppl):645-648.
25. Watson M, Johnson CJ, Chen VW, et al. Melanoma surveillance in the United States: overview of methods. J Am Acad Dermatol. 2011;65(5, suppl 1):S6-S16.
The incidence of cutaneous melanoma, the deadliest form of skin cancer, has been steadily increasing over the last several decades.1 Currently, there are 73,870 new diagnoses of melanoma anticipated in the United States in 2015 alone.2 Many cases of melanoma are caught at early, actionable, and curable stages thanks in part to patient education and screening by dermatologists.3 However, until recently, few options existed for the treatment of locally advanced and metastatic melanomas, with a median survival rate of less than 1 year.4
Clinical trials represent the most reliable method for advancing treatment and improving outcomes for patients with disease; however, patient accrual and access to clinical trials remain formidable barriers. Studies have suggested that patients in rural areas perceive both an increased distance to clinical trial sites and a lack of awareness of available trials compared to their urban counterparts. Additionally, studies have shown that provider awareness of actively enrolling clinical trials in their respective fields is a key determinate in patient enrollment.5 Finally, insufficient funding and lack of collaboration has resulted in many small phase 1 or phase 2 single-center trials, which are less likely to quickly impact clinical care.6 Increased awareness of the ClinicalTrials.gov registry, a publicly available and easily accessible database, can facilitate referral, enrollment, and collaboration among physicians, patients, and researchers alike.
Using the ClinicalTrials.gov database, we sought to analyze the clinical trial landscape for cutaneous melanoma to understand the current state of melanoma research, future direction, and potential barriers that may impede success.
Methods
The primary objective was to provide a snapshot of the melanoma clinical research landscape from 2005 to 2013, including the number of registered trials, phase distribution, recruitment status, location of trials, type of intervention, and disease state being studied. Secondary objectives included describing patterns of clinical trial distribution within the United States in the context of melanoma mortality and examining changing trends in interventions studied in trials over time.
ClinicalTrials.gov is a comprehensive online registry of clinical trials conducted in the United States and abroad that is maintained by the National Library of Medicine.7 Although the initiative was launched in 2000, the registry became effectively comprehensive in September 2005 when the International Committee of Medical Journal Editors declared prospective registration of clinical trials as a prerequisite for publication. The US Food and Drug Administration followed suit in September 2007, expanding the requirements for registration and declaring penalties for parties who did not comply.8 Each registered trial can be found through searchable keywords, and each study page contains details of study design, principal investigators, and inclusion and exclusion criteria, as well as contact information for enrollment.
Study Selection
Clinical trials registered between September 15, 2005, and December 31, 2013, were evaluated; a total of 138,312 trials were found to be registered on ClinicalTrials.gov during that time period. We limited our study selection to interventional studies, which were filtered by topic to yield only those pertaining to melanoma patients. To minimize reporting bias, trials registered prior to the implementation of the International Committee of Medical Journal Editors’ reporting requirements were excluded. To focus specifically on the landscape of trials in cutaneous melanoma, trials investigating multiple advanced malignancies, uveal or ocular melanoma, and mucosal melanoma were manually excluded.
Study Variables
Information on each clinical trial was extracted from ClinicalTrials.gov. Each trial was manually reviewed by an investigator to determine the disease state and type of intervention being studied. Studies investigating multiple modalities concurrently were classified as “other.”
Data Analysis
Study variables were first analyzed among the entire cohort as a whole. Using each trial location and a python script based on open-source code, the number of actively recruiting melanoma trials in each US county was identified and mapped. County-level, melanoma-specific mortality data from 2001 to 2010 was extracted from the Centers for Disease Control and Prevention’s WONDER (Wide-ranging Online Data for Epidemiologic Research) mortality database (wonder.cdc.gov). Finally, to analyze changing trends in cutaneous melanoma investigation, trials were grouped into 3 categories based on the date they were received on ClinicalTrials.gov: (1) 2005-2007, (2) 2008-2010, and (3) 2011-2013. Disease state and type of intervention were analyzed and compared among each group using the χ2 statistic.
Results
Of the 138,312 trials registered on ClinicalTrials.gov between September 15, 2005, and December 31, 2013, only 931 were identified as interventional studies pertaining to melanoma patients. Of these, 154 were excluded because of a focus on uveal, ocular, or mucosal melanoma or because of the inclusion of participants with multiple types of advanced malignancies. The final analysis included 777 trials specifically focusing on cutaneous melanoma.
Characteristics of these 777 trials were varied. Many interventions were in the early stages of development, with 339 (44%) trials classified as phase 0, phase 1, or phase 1/phase 2; 306 (39%) as phase 2; and 71 (9%) as nonpharmacologic (nonphase) trials. Only 58 trials (8%) were classified as phase 3 or phase 4. The majority of the trials were actively recruiting (225 [29%]), active but not yet recruiting (172 [22%]), or completed (255 [33%]); however, 98 trials (13%) had been suspended, terminated, or withdrawn. Additionally, 22 trials (3%) were not yet recruiting and 5 (<1%) were classified as “other” because they did not have a recruitment status listed.
The distribution of actively enrolling clinical trials corresponds to major metropolitan areas within the Northeast, Upper Midwest, and Coastal California (Figure 1A). Figure 1B demonstrates the melanoma-specific mortality across the United States. Areas in the Southwest and Florida shared some of the greatest disease burden.
|
|
| Figure 1. Geographical representation of US clinical trial enrollment with the number of actively recruiting trials for each unique US zip code presented. The circle size corresponds to the number of trials. The largest circles indicate more than 5 trials within a given zip code (A). County-level melanoma-specific mortality data are presented for 2001 to 2010 (B). Darkest areas represent the highest numbers of melanoma deaths.
|
The disease state and type of intervention for all the included trials are summarized in Figure 2. The vast majority of trials (633/777 [82%]) enrolled participants with metastatic melanoma. Unlike many other tumor types, only 64 (8%) trials enrolled patients specifically in the adjuvant setting. Most trials focused on targeted (175 [23%]), immune (180 [23%]), and vaccine (117 [15%]) therapy.
|
|
| Figure 2. Trial distribution stratified by disease state (A) and type of intervention (B). Trial distribution is shown for 777 interventional clinical trials including melanoma patients. The majority of clinical trials involved patients with metastatic melanoma. The majority of trials investigated targeted therapy, immunotherapy, and vaccine therapy. |
We subsequently analyzed changes in trial characteristics over time. We noted a decrease in the number of trials investigating cytotoxic and vaccine-based therapies, and increasing numbers of trials investigating immunotherapy (P=.041). Between 2005 and 2007, 14% (27/201) of all trials investigated cytotoxic therapies compared to just 7% (20/294) of trials between 2011 and 2013. With the approval of ipilimumab, 29% (85/294) of all clinical trials between 2011 and 2013 investigated immunotherapies, which comprised only 18% (37/201) of clinical trials between 2005 and 2007. The majority of trials continued to enroll patients in the metastatic setting where outcomes remain poor. Importantly, only 6% (49/777) of all clinical trials have focused on prevention, early detection, and local management of melanoma, which has remained constant over time.
Comment
Cutaneous melanoma remains an area of active investigation, interdisciplinary collaboration, and great promise. The ClinicalTrials.gov registry serves not only to increase transparency among interested parties but also as a rich resource to study the clinical research landscape as demonstrated in this study.
Greater understanding of the underlying genetic and immunogenic properties of melanoma tissues has led to the US Food and Drug Administration approval of several novel agents to treat metastatic disease. BRAF inhibitors such as vemurafenib and dabrafenib target more than 50% of all melanoma tumors harboring mutations in the BRAF gene and have shown unparalleled efficacy in clinical trials; however, durability of response and adverse effects still remain a concern.4,9-11 Ipilimumab, a CTLA-4 inhibitor, enhances antitumor immunity and demonstrated improved survival in clinical trials.12,13 Nivolumab, a fully human IgG4 programmed death 1 (PD-1) immune-checkpoint inhibitor antibody, also demonstrated improved overall and progression-free survival.14 Finally, trametinib, a MEK inhibitor, used in combination with BRAF inhibitors has demonstrated improved response over BRAF inhibitors alone.15
Although traditional cytotoxic chemotherapy was one of the few available treatment options before 2011, response was infrequent.16 Our data indicate that the melanoma research landscape has shifted to follow advances in targeted therapy and immunotherapy. We noted a decrease in the study of cytotoxic chemotherapy in metastatic melanoma, with a compensatory increase in immunotherapy trials and a continued commitment to targeted therapy. Further, with the approval of BRAF inhibitors, CTLA-4 inhibitors, and PD-1 inhibitors for metastatic disease, some have pushed to move these agents into the adjuvant setting to prevent micrometastases from evolving into clinically significant disease.17 Early results from EORTC (European Organisation for Research and Treatment of Cancer) 18071 comparing adjuvant ipilimumab to placebo demonstrated a 26.1-month versus 17.1-month improvement in relapse-free survival, respectively.18 However, this finding has important implications for clinical dermatologists. Patients treated with BRAF inhibitors are at increased risk for keratoacanthomas, invasive squamous cell carcinomas, and secondary primary melanomas.19,20 Caring for these patients requires increased vigilance and collaboration between dermatologists and oncologists.
Our study also highlights the dynamic nature of the field. For example, novel vaccine therapies have demonstrated promise in the metastatic/ unresectable tumor setting, with some herpes simplex virus–based vaccines generating durable antitumor immune responses in patients with melanoma.21 Combination therapy with CTLA-4 and PD-1 inhibitors has demonstrated improved objective response rates and progression-free survival over monotherapy.22 As the status of actively recruiting trials changes on a regular basis, we encourage physicians to access ClinicalTrials.gov to find details and contact information for actively recruiting trials and results on completed trials.
Early detection and management, however, still remain our primary option for cure, and the role of community dermatologists cannot be overstated.23 Patients with stage I and stage II disease have excellent long-term survival rates, yet only 6% of all clinical trials in cutaneous melanoma have focused on patient education, disease prevention, early detection, and local management. With an increasing incidence of melanoma among an aging population, the disease burden remains of substantial concern.24 Optimizing disease prevention, appropriate screening, and early detection are critical roles for dermatologists.
Finally, our data offer some insight into accrual barriers often faced by clinical trials. Actively enrolling clinical trials cluster within major metropolitan areas, presumably with large academic medical centers; however, areas in the southwestern United States and Florida, for example, have some of the highest burden of disease, likely secondary to sun exposure and aging populations.25 Integration of community dermatologists and oncologists may decrease both actual and patient-perceived barriers to care, which requires further exploration.6
Conclusion
Melanoma incidence and disease burden is increasing, and the field of melanoma research is incredibly dynamic. Going forward, we believe dermatologists will continue to play a critical role both in primary disease prevention and detection as well as in detection of secondary treatment-related skin toxicities. ClinicalTrials.gov is an invaluable resource to keep interested parties informed, foster collaboration, identify potential barriers to success, and suggest future directions.
The incidence of cutaneous melanoma, the deadliest form of skin cancer, has been steadily increasing over the last several decades.1 Currently, there are 73,870 new diagnoses of melanoma anticipated in the United States in 2015 alone.2 Many cases of melanoma are caught at early, actionable, and curable stages thanks in part to patient education and screening by dermatologists.3 However, until recently, few options existed for the treatment of locally advanced and metastatic melanomas, with a median survival rate of less than 1 year.4
Clinical trials represent the most reliable method for advancing treatment and improving outcomes for patients with disease; however, patient accrual and access to clinical trials remain formidable barriers. Studies have suggested that patients in rural areas perceive both an increased distance to clinical trial sites and a lack of awareness of available trials compared to their urban counterparts. Additionally, studies have shown that provider awareness of actively enrolling clinical trials in their respective fields is a key determinate in patient enrollment.5 Finally, insufficient funding and lack of collaboration has resulted in many small phase 1 or phase 2 single-center trials, which are less likely to quickly impact clinical care.6 Increased awareness of the ClinicalTrials.gov registry, a publicly available and easily accessible database, can facilitate referral, enrollment, and collaboration among physicians, patients, and researchers alike.
Using the ClinicalTrials.gov database, we sought to analyze the clinical trial landscape for cutaneous melanoma to understand the current state of melanoma research, future direction, and potential barriers that may impede success.
Methods
The primary objective was to provide a snapshot of the melanoma clinical research landscape from 2005 to 2013, including the number of registered trials, phase distribution, recruitment status, location of trials, type of intervention, and disease state being studied. Secondary objectives included describing patterns of clinical trial distribution within the United States in the context of melanoma mortality and examining changing trends in interventions studied in trials over time.
ClinicalTrials.gov is a comprehensive online registry of clinical trials conducted in the United States and abroad that is maintained by the National Library of Medicine.7 Although the initiative was launched in 2000, the registry became effectively comprehensive in September 2005 when the International Committee of Medical Journal Editors declared prospective registration of clinical trials as a prerequisite for publication. The US Food and Drug Administration followed suit in September 2007, expanding the requirements for registration and declaring penalties for parties who did not comply.8 Each registered trial can be found through searchable keywords, and each study page contains details of study design, principal investigators, and inclusion and exclusion criteria, as well as contact information for enrollment.
Study Selection
Clinical trials registered between September 15, 2005, and December 31, 2013, were evaluated; a total of 138,312 trials were found to be registered on ClinicalTrials.gov during that time period. We limited our study selection to interventional studies, which were filtered by topic to yield only those pertaining to melanoma patients. To minimize reporting bias, trials registered prior to the implementation of the International Committee of Medical Journal Editors’ reporting requirements were excluded. To focus specifically on the landscape of trials in cutaneous melanoma, trials investigating multiple advanced malignancies, uveal or ocular melanoma, and mucosal melanoma were manually excluded.
Study Variables
Information on each clinical trial was extracted from ClinicalTrials.gov. Each trial was manually reviewed by an investigator to determine the disease state and type of intervention being studied. Studies investigating multiple modalities concurrently were classified as “other.”
Data Analysis
Study variables were first analyzed among the entire cohort as a whole. Using each trial location and a python script based on open-source code, the number of actively recruiting melanoma trials in each US county was identified and mapped. County-level, melanoma-specific mortality data from 2001 to 2010 was extracted from the Centers for Disease Control and Prevention’s WONDER (Wide-ranging Online Data for Epidemiologic Research) mortality database (wonder.cdc.gov). Finally, to analyze changing trends in cutaneous melanoma investigation, trials were grouped into 3 categories based on the date they were received on ClinicalTrials.gov: (1) 2005-2007, (2) 2008-2010, and (3) 2011-2013. Disease state and type of intervention were analyzed and compared among each group using the χ2 statistic.
Results
Of the 138,312 trials registered on ClinicalTrials.gov between September 15, 2005, and December 31, 2013, only 931 were identified as interventional studies pertaining to melanoma patients. Of these, 154 were excluded because of a focus on uveal, ocular, or mucosal melanoma or because of the inclusion of participants with multiple types of advanced malignancies. The final analysis included 777 trials specifically focusing on cutaneous melanoma.
Characteristics of these 777 trials were varied. Many interventions were in the early stages of development, with 339 (44%) trials classified as phase 0, phase 1, or phase 1/phase 2; 306 (39%) as phase 2; and 71 (9%) as nonpharmacologic (nonphase) trials. Only 58 trials (8%) were classified as phase 3 or phase 4. The majority of the trials were actively recruiting (225 [29%]), active but not yet recruiting (172 [22%]), or completed (255 [33%]); however, 98 trials (13%) had been suspended, terminated, or withdrawn. Additionally, 22 trials (3%) were not yet recruiting and 5 (<1%) were classified as “other” because they did not have a recruitment status listed.
The distribution of actively enrolling clinical trials corresponds to major metropolitan areas within the Northeast, Upper Midwest, and Coastal California (Figure 1A). Figure 1B demonstrates the melanoma-specific mortality across the United States. Areas in the Southwest and Florida shared some of the greatest disease burden.
|
|
| Figure 1. Geographical representation of US clinical trial enrollment with the number of actively recruiting trials for each unique US zip code presented. The circle size corresponds to the number of trials. The largest circles indicate more than 5 trials within a given zip code (A). County-level melanoma-specific mortality data are presented for 2001 to 2010 (B). Darkest areas represent the highest numbers of melanoma deaths.
|
The disease state and type of intervention for all the included trials are summarized in Figure 2. The vast majority of trials (633/777 [82%]) enrolled participants with metastatic melanoma. Unlike many other tumor types, only 64 (8%) trials enrolled patients specifically in the adjuvant setting. Most trials focused on targeted (175 [23%]), immune (180 [23%]), and vaccine (117 [15%]) therapy.
|
|
| Figure 2. Trial distribution stratified by disease state (A) and type of intervention (B). Trial distribution is shown for 777 interventional clinical trials including melanoma patients. The majority of clinical trials involved patients with metastatic melanoma. The majority of trials investigated targeted therapy, immunotherapy, and vaccine therapy. |
We subsequently analyzed changes in trial characteristics over time. We noted a decrease in the number of trials investigating cytotoxic and vaccine-based therapies, and increasing numbers of trials investigating immunotherapy (P=.041). Between 2005 and 2007, 14% (27/201) of all trials investigated cytotoxic therapies compared to just 7% (20/294) of trials between 2011 and 2013. With the approval of ipilimumab, 29% (85/294) of all clinical trials between 2011 and 2013 investigated immunotherapies, which comprised only 18% (37/201) of clinical trials between 2005 and 2007. The majority of trials continued to enroll patients in the metastatic setting where outcomes remain poor. Importantly, only 6% (49/777) of all clinical trials have focused on prevention, early detection, and local management of melanoma, which has remained constant over time.
Comment
Cutaneous melanoma remains an area of active investigation, interdisciplinary collaboration, and great promise. The ClinicalTrials.gov registry serves not only to increase transparency among interested parties but also as a rich resource to study the clinical research landscape as demonstrated in this study.
Greater understanding of the underlying genetic and immunogenic properties of melanoma tissues has led to the US Food and Drug Administration approval of several novel agents to treat metastatic disease. BRAF inhibitors such as vemurafenib and dabrafenib target more than 50% of all melanoma tumors harboring mutations in the BRAF gene and have shown unparalleled efficacy in clinical trials; however, durability of response and adverse effects still remain a concern.4,9-11 Ipilimumab, a CTLA-4 inhibitor, enhances antitumor immunity and demonstrated improved survival in clinical trials.12,13 Nivolumab, a fully human IgG4 programmed death 1 (PD-1) immune-checkpoint inhibitor antibody, also demonstrated improved overall and progression-free survival.14 Finally, trametinib, a MEK inhibitor, used in combination with BRAF inhibitors has demonstrated improved response over BRAF inhibitors alone.15
Although traditional cytotoxic chemotherapy was one of the few available treatment options before 2011, response was infrequent.16 Our data indicate that the melanoma research landscape has shifted to follow advances in targeted therapy and immunotherapy. We noted a decrease in the study of cytotoxic chemotherapy in metastatic melanoma, with a compensatory increase in immunotherapy trials and a continued commitment to targeted therapy. Further, with the approval of BRAF inhibitors, CTLA-4 inhibitors, and PD-1 inhibitors for metastatic disease, some have pushed to move these agents into the adjuvant setting to prevent micrometastases from evolving into clinically significant disease.17 Early results from EORTC (European Organisation for Research and Treatment of Cancer) 18071 comparing adjuvant ipilimumab to placebo demonstrated a 26.1-month versus 17.1-month improvement in relapse-free survival, respectively.18 However, this finding has important implications for clinical dermatologists. Patients treated with BRAF inhibitors are at increased risk for keratoacanthomas, invasive squamous cell carcinomas, and secondary primary melanomas.19,20 Caring for these patients requires increased vigilance and collaboration between dermatologists and oncologists.
Our study also highlights the dynamic nature of the field. For example, novel vaccine therapies have demonstrated promise in the metastatic/ unresectable tumor setting, with some herpes simplex virus–based vaccines generating durable antitumor immune responses in patients with melanoma.21 Combination therapy with CTLA-4 and PD-1 inhibitors has demonstrated improved objective response rates and progression-free survival over monotherapy.22 As the status of actively recruiting trials changes on a regular basis, we encourage physicians to access ClinicalTrials.gov to find details and contact information for actively recruiting trials and results on completed trials.
Early detection and management, however, still remain our primary option for cure, and the role of community dermatologists cannot be overstated.23 Patients with stage I and stage II disease have excellent long-term survival rates, yet only 6% of all clinical trials in cutaneous melanoma have focused on patient education, disease prevention, early detection, and local management. With an increasing incidence of melanoma among an aging population, the disease burden remains of substantial concern.24 Optimizing disease prevention, appropriate screening, and early detection are critical roles for dermatologists.
Finally, our data offer some insight into accrual barriers often faced by clinical trials. Actively enrolling clinical trials cluster within major metropolitan areas, presumably with large academic medical centers; however, areas in the southwestern United States and Florida, for example, have some of the highest burden of disease, likely secondary to sun exposure and aging populations.25 Integration of community dermatologists and oncologists may decrease both actual and patient-perceived barriers to care, which requires further exploration.6
Conclusion
Melanoma incidence and disease burden is increasing, and the field of melanoma research is incredibly dynamic. Going forward, we believe dermatologists will continue to play a critical role both in primary disease prevention and detection as well as in detection of secondary treatment-related skin toxicities. ClinicalTrials.gov is an invaluable resource to keep interested parties informed, foster collaboration, identify potential barriers to success, and suggest future directions.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64:252-271.
2. American Cancer Society. Cancer Facts and Figures 2015. American Cancer Society Web site. http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed August 26, 2015.
3. Cheng MY, Moreau JF, McGuire ST, et al. Melanoma depth in patients with an established dermatologist. J Am Acad Dermatol. 2014;70:841-846.
4. Jang S, Atkins MB. Which drug, and when, for patients with BRAF-mutant melanoma? Lancet Oncol. 2013;14:e60-e69.
5. Kim SH, Tanner A, Friedman DB, et al. Barriers to clinical trial participation: a comparison of rural and urban communities in South Carolina. J Community Health. 2014;39:562-571.
6. Gregg JR, Horn L, Davidson MA, et al. Patient enrollment onto clinical trials: the role of physician knowledge. J Cancer Educ. 2014;29:74-79.
7. Galsky MD, Hendricks R, Svatek R, et al. Critical analysis of contemporary clinical research in muscle-invasive and metastatic urothelial cancer: a report from the
Bladder Cancer Advocacy Network Clinical Trials Working Group. Cancer. 2013;119:1994-1998.
8. Zarin DA, Tse T, Williams RJ, et al. The ClinicalTrials.gov results database—update and key issues. N Engl J Med. 2011;364:852-860.
9. Luke JJ, Hodi FS. Ipilimumab, vemurafenib, dabrafenib, and trametinib: synergistic competitors in the clinical management of BRAF mutant malignant melanoma. Oncologist. 2013;18:717-725.
10. McArthur GA, Chapman PB, Robert C, et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014;15:323-332.
11. Swaika A, Crozier JA, Joseph RW. Vemurafenib: an evidence-based review of its clinical utility in the treatment of metastatic melanoma. Drug Des Devel Ther. 2014;8:775-787.
12. Lacouture ME, Wolchok JD, Yosipovitch G, et al. Ipilimumab in patients with cancer and the management of dermatologic adverse events. J Am Acad Dermatol. 2014;71:161-169.
13. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723.
14. Robert C, Long G, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320-330.
15. Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372:30-39.
16. Espinosa E, Berrocal A, López Martin JA, et al. Advances in cutaneous melanoma. Clin Transl Oncol. 2012;14:325-332.
17. Chapman PB. Treating metastatic melanoma in 2014: what just happened and what is next? Am Soc Clin Oncol Educ Book. 2014:16-19.
18. Eggermont A, Chiarion-Sileni V, Grob JJ, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16:522-530.
19. Curry JL, Tetzlaff MT, Nicholson K, et al. Histological features associated with vemurafenib-induced skin toxicities: examination of 141 cutaneous lesions biopsied during therapy. Am J Dermatopathol. 2014; 36:557-561.
20. Perier-Muzet M, Thomas L, Poulalhon N, et al. Melanoma patients under vemurafenib: prospective follow-up of melanocytic lesions by digital dermoscopy. J Invest Dermatol. 2014;134:1351-1358.
21. Ross MI, Andtbacka RI, Puzanov I, et al. Patterns of durable response with intralesional talimogene laherparepvec (T-VEC): results from a phase III trial in patients with stage IIIb-IV melanoma. Paper presented at: ASCO Annual Meeting; June 2, 2014; Boston, MA.
22. Postow MA, Chesney J, Pavlick AC, et al. Novolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372:2006-2017.
23. Gorantla VC, Kirkwood JM. State of melanoma: an historic overview of a field in transition. Hematol Oncol Clin North Am. 2014;28:415-435.
24. Coit DG, Olszanski AJ. Progress in the management of melanoma in 2013. J Natl Compr Canc Netw. 2013; 11(5 suppl):645-648.
25. Watson M, Johnson CJ, Chen VW, et al. Melanoma surveillance in the United States: overview of methods. J Am Acad Dermatol. 2011;65(5, suppl 1):S6-S16.
1. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64:252-271.
2. American Cancer Society. Cancer Facts and Figures 2015. American Cancer Society Web site. http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed August 26, 2015.
3. Cheng MY, Moreau JF, McGuire ST, et al. Melanoma depth in patients with an established dermatologist. J Am Acad Dermatol. 2014;70:841-846.
4. Jang S, Atkins MB. Which drug, and when, for patients with BRAF-mutant melanoma? Lancet Oncol. 2013;14:e60-e69.
5. Kim SH, Tanner A, Friedman DB, et al. Barriers to clinical trial participation: a comparison of rural and urban communities in South Carolina. J Community Health. 2014;39:562-571.
6. Gregg JR, Horn L, Davidson MA, et al. Patient enrollment onto clinical trials: the role of physician knowledge. J Cancer Educ. 2014;29:74-79.
7. Galsky MD, Hendricks R, Svatek R, et al. Critical analysis of contemporary clinical research in muscle-invasive and metastatic urothelial cancer: a report from the
Bladder Cancer Advocacy Network Clinical Trials Working Group. Cancer. 2013;119:1994-1998.
8. Zarin DA, Tse T, Williams RJ, et al. The ClinicalTrials.gov results database—update and key issues. N Engl J Med. 2011;364:852-860.
9. Luke JJ, Hodi FS. Ipilimumab, vemurafenib, dabrafenib, and trametinib: synergistic competitors in the clinical management of BRAF mutant malignant melanoma. Oncologist. 2013;18:717-725.
10. McArthur GA, Chapman PB, Robert C, et al. Safety and efficacy of vemurafenib in BRAF(V600E) and BRAF(V600K) mutation-positive melanoma (BRIM-3): extended follow-up of a phase 3, randomised, open-label study. Lancet Oncol. 2014;15:323-332.
11. Swaika A, Crozier JA, Joseph RW. Vemurafenib: an evidence-based review of its clinical utility in the treatment of metastatic melanoma. Drug Des Devel Ther. 2014;8:775-787.
12. Lacouture ME, Wolchok JD, Yosipovitch G, et al. Ipilimumab in patients with cancer and the management of dermatologic adverse events. J Am Acad Dermatol. 2014;71:161-169.
13. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711-723.
14. Robert C, Long G, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372:320-330.
15. Robert C, Karaszewska B, Schachter J, et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N Engl J Med. 2015;372:30-39.
16. Espinosa E, Berrocal A, López Martin JA, et al. Advances in cutaneous melanoma. Clin Transl Oncol. 2012;14:325-332.
17. Chapman PB. Treating metastatic melanoma in 2014: what just happened and what is next? Am Soc Clin Oncol Educ Book. 2014:16-19.
18. Eggermont A, Chiarion-Sileni V, Grob JJ, et al. Adjuvant ipilimumab versus placebo after complete resection of high-risk stage III melanoma (EORTC 18071): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16:522-530.
19. Curry JL, Tetzlaff MT, Nicholson K, et al. Histological features associated with vemurafenib-induced skin toxicities: examination of 141 cutaneous lesions biopsied during therapy. Am J Dermatopathol. 2014; 36:557-561.
20. Perier-Muzet M, Thomas L, Poulalhon N, et al. Melanoma patients under vemurafenib: prospective follow-up of melanocytic lesions by digital dermoscopy. J Invest Dermatol. 2014;134:1351-1358.
21. Ross MI, Andtbacka RI, Puzanov I, et al. Patterns of durable response with intralesional talimogene laherparepvec (T-VEC): results from a phase III trial in patients with stage IIIb-IV melanoma. Paper presented at: ASCO Annual Meeting; June 2, 2014; Boston, MA.
22. Postow MA, Chesney J, Pavlick AC, et al. Novolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372:2006-2017.
23. Gorantla VC, Kirkwood JM. State of melanoma: an historic overview of a field in transition. Hematol Oncol Clin North Am. 2014;28:415-435.
24. Coit DG, Olszanski AJ. Progress in the management of melanoma in 2013. J Natl Compr Canc Netw. 2013; 11(5 suppl):645-648.
25. Watson M, Johnson CJ, Chen VW, et al. Melanoma surveillance in the United States: overview of methods. J Am Acad Dermatol. 2011;65(5, suppl 1):S6-S16.
Practice Points
- The landscape of melanoma clinical trial research has shifted to follow advances in targeted therapy and immunotherapy.
- With these new treatments there is an increased risk for nonmelanoma skin toxicities requiring increased vigilance and collaboration between dermatologists and oncologists.
- Physicians are encouraged to use ClinicalTrials.gov to find details and contact information for actively recruiting clinical trials and results on completed trials.

Physician Skin Examinations for Melanoma Screening
In the United States an estimated 73,870 new cases of melanoma will be diagnosed in 2015.1 Although melanoma accounts for less than 2% of all US skin cancer cases, it is responsible for the vast majority of skin cancer deaths. From 2007 to 2011, melanoma mortality rates decreased by 2.6% per year in individuals younger than 50 years but increased by 0.6% per year among those 50 years and older.1 Reports of the direct annual treatment costs for melanoma in the United States have ranged from $44.9 million for Medicare recipients with existing cases of melanoma to $932.5 million for newly diagnosed melanomas across all age groups.2
Melanoma survival rates are inversely related to tumor thickness at the time of diagnosis.3 Melanoma can be cured if caught early and properly treated. Secondary preventative measures include physician skin examinations (PSEs), which may increase the likelihood of detecting melanomas in earlier stages, thereby potentially increasing survival rates and quality of life as well as decreasing treatment costs. Physician skin examinations are performed in the physician’s office and are safe, noninvasive, and painless. Patients with suspicious lesions should subsequently undergo a skin biopsy, which is a low-risk procedure. False-positives from biopsies do not lead to extreme patient morbidity, and false-negatives will hopefully be detected at a subsequent visit.
There is a lack of consensus regarding recommendations for PSEs for skin cancer screening. Due to a lack of randomized controlled trials on the effects of skin cancer screening on patient morbidity and mortality, the US Preventive Services Task Force (USPSTF) has concluded that there is insufficient evidence to recommend for or against such screening4; however, other organizations including the American Cancer Society and the American Academy of Dermatology recommend periodic skin cancer screening examinations.1,5 In a rapidly changing health care climate and with the rollout of the Patient Protection and Affordable Care Act, a USPSTF recommendation for skin screening with PSEs for skin cancer would have a large impact on clinical practice in the United States.
This article provides a systematic review of the current domestic and international data regarding the impact of PSEs on melanoma tumor thickness at the time of diagnosis as well as mortality from melanoma.
Methods
Search Strategy
A systematic search of PubMed articles indexed for MEDLINE and Embase for studies related to melanoma and PSEs was performed for the period from each database’s inception to November 8, 2014. One of the authors (S.L.M.) designed a broad search strategy with assistance from a medical librarian who had expertise in searching research bibliographies. Articles were excluded if they had a cross-sectional study design or were editorials or review articles. Search terms included skin neoplasm, skin cancer, or melanoma in combination with any of the following: skin examination, mass screening, screening, and secondary prevention.
Study Selection
All published studies reporting outcomes and correlations with PSEs and cutaneous melanoma in adult patients were screened. If multiple studies were published describing the same study, follow-up studies were included for data extraction, but the original study was the primary resource. Observational studies were a focus in this review, as these types of studies are much more common in this subject area.
One of the authors (S.L.M.) screened the titles and abstracts of identified studies for eligibility. If the reviewer considered a study potentially eligible based on the abstract review, a full-text review was carried out. The reference lists of eligible studies were manually searched to identify additional studies.
Data Extraction, Quality Assessment, and Data Synthesis
Data items to be extracted were agreed on before search implementation and were extracted by one investigator (S.L.M.) following criteria developed by review of the Cochrane Handbook for Systematic Reviews of Interventions.6 Study population, design, sample size, and outcomes were extracted. Risk of bias of individual articles was evaluated using a tool developed from the RTI item bank (RTI International) for determining the risk of bias and precision of eligible observational studies.7 Studies ultimately were classified into 3 categories based on the risk of bias: (1) low risk of bias, (2) medium risk of bias, and (3) high risk of bias. The strength of evidence of included studies was evaluated by the following items: risk of bias, consistency, directness, precision, and overall conclusion. Data from the included studies was synthesized qualitatively in a narrative format. This review adhered to guidelines in the Cochrane Handbook for Systematic Reviews of Interventions6 and the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines.8

Results
A total of 705 titles were screened, 98 abstracts were assessed for eligibility, 42 full-text reviews were carried out, and 5 eligible studies were identified (Figure 1). Five observational studies were included in the final review. A summary of the results is presented in Table 1.
Included studies were assessed for several types of biases, including selection bias, attrition bias, detection bias, performance bias, and response bias. The judgments were given for each domain (Table 2). There was heterogeneity in study design, reporting of total-body skin examination methods, and reporting of outcomes among all 5 studies. All 5 studies were assessed as having a medium risk of bias.
Physician Skin Examination Impact
One article by Berwick et al9 reanalyzed data from a 1996 study10 and provided no significant evidence regarding the benefits of PSEs in the reduction of melanoma mortality. Data for 650 patients with newly diagnosed melanomas were obtained from the Connecticut Tumor Registry, a site for the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, along with 549 age- and sex-frequency matched controls from the general population.10 Participants were followed biannually for a mean of 5.4 years. Of the original 650 case patients, 122 were excluded from the study with reasons provided. Physician skin examination was defined as a positive response to the following questionnaire item: “[Before your recent biopsy] did the doctor examine your skin during any of your visits?”9 Data analysis showed no significant association between PSE and death from melanoma. Upon univariate analysis, the hazard ratio for physician screening was 0.7 (95% confidence interval [CI], 0.4-1.3).9
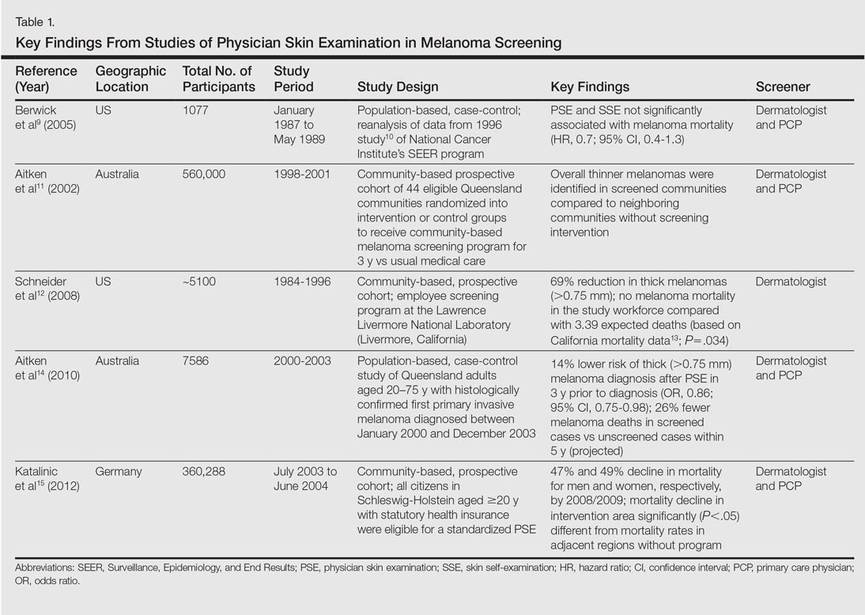
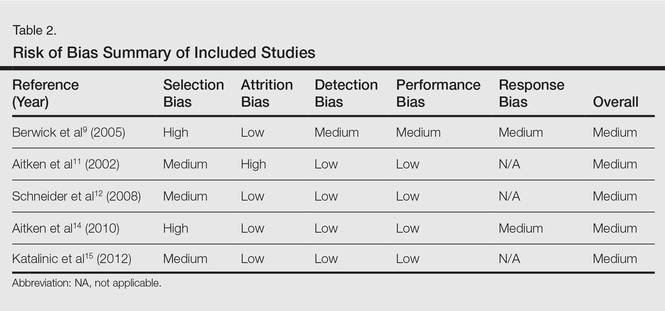
The SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, which was undertaken in Schleswig-Holstein, Germany, is the world’s largest systematic population-based skin cancer screening program.15 The participation rate was
19% (N=360,288) of the eligible population (citizens aged ≥20 years with statutory health insurance). Screening was a 2-step process performed by trained physicians: initial general practitioner whole-body skin examination followed by referral to a dermatologist for evaluation of suspicious skin findings. Five years after the SCREEN program was conducted, melanoma mortality declined by 47% per 100,000 men and by 49% per 100,000 women. The annual percentage change in the most recent 10-year period (2000-2009) was 7.5% (95% CI, –14.0 to –0.5; P<.05) for men and 7.1% for women (95% CI,
–10.5 to –2.9; P<.05). Simultaneously, the melanoma mortality rates in the 4 unscreened adjacent regions and the rest of Germany were stable, significantly (P<.05) different from the decline in mortality observed in Schleswig-Holstein.15
A community-based, prospective cohort study investigated the impact of an employee melanoma screening program at the Lawrence Livermore National Laboratory (Livermore, California) (1984-1996) demonstrated an impact on melanoma thickness and mortality rates.12 The cohort (approximately 5100 participants) was followed over 3 phases of surveillance: (1) preawareness (1969-1975), (2) early awareness of increased melanoma risk (1976-1984), and (3) screening program (1984-1996). The screening program encouraged employees to self-examine their skin for “suggestive lesions”; if a suggestive lesion was found, a full-body skin examination was performed by a physician. After being evaluated, participants with melanoma, dysplastic nevi, 50 or more moles, or a family history of melanoma were offered a periodic full-body examination every 3 to 24 months, often with
full-body photography and dermoscopy. Physician skin screening resulted in a reduction in crude incidence of thicker melanomas (defined as
>0.75 mm) during the 3 study phases. Compared with the early-awareness period (phase 2), a 69% reduction in the diagnosis of thick melanomas was reported in the screening program period (phase 3)(P=.0001). During the screening period, no eligible melanoma deaths occurred in the study population, whereas the expected number of deaths was 3.39 (P=.034) based on observed melanoma mortality in 5 San Francisco/Oakland Bay–area counties in California as reported to the SEER program from 1984 to 1996.12
The strongest evidence for reduced thickness of melanomas detected via PSEs was reported in a population-based, case-control study by Aitken et al14 of all residents in Queensland, Australia, aged 20 to 75 years with a histologically confirmed first primary invasive cutaneous melanoma diagnosed between January 2000 and December 2003. Whole-body PSE in the 3 years before diagnosis was inversely associated with tumor thickness at diagnosis (χ2=44.37; P<.001), including a 14% lower risk of diagnosis of a thick melanoma (>0.75 mm)(odds ratio [OR], 0.86; 95% CI, 0.75-0.98) and a 40% lower risk of diagnosis of a melanoma that was 3 mm or larger (OR, 0.60; 95% CI, 0.43-0.83). The investigators applied melanoma thickness-specific survival estimates to the thickness distribution of the screened and unscreened cases in their sample to estimate melanoma deaths within 5 and 10 years of diagnosis. Compared to the unscreened cases, they estimated that the screened cases would have 26% fewer melanoma deaths within 5 years of diagnosis and 23% fewer deaths within 10 years.14
Another prospective cohort study in Queensland was designed to detect a 20% reduction in mortality from melanoma during a 15-year intervention period in communities that received a screening program.11 A total of 44 communities (aggregate population, 560,000 adults aged ≥30 years) were randomized into intervention or control groups to receive a community-based melanoma screening program for 3 years versus usual medical care.Overall, thinner melanomas were identified in communities with the screening program versus neighboring communities without it.11 Of the 33 melanomas found through the screening program, 39% (13/33) were in situ lesions, 55% (18/33) were thin (<1 mm) invasive lesions, and 6% (2/33) were 1-mm thick or greater.16 Within the population of Queensland during the period from 1999 through 2002, 36% were in situ lesions, 48% were invasive thin melanomas, and 16% were invasive melanomas 1-mm thick or more, indicating that melanomas found through screening were thinner or less advanced.17
Comment
Our review identified 5 studies describing the impact of PSEs for melanoma screening on tumor thickness at diagnosis and melanoma mortality. Key findings are highlighted in Figure 2. Our findings suggest that PSEs are associated with a decline in melanoma tumor thickness and melanoma-specific mortality. Our findings are qualitatively similar to prior reviews that supported the use of PSEs to detect thinner melanomas and improve mortality outcomes.18-20
The greatest evidence for population-based screening programs was provided by the SCREEN study. This landmark study documented that screening programs utilizing primary care physicians (PCPs) and dermatologists can lead to a reduction in melanoma mortality.15 Findings from the study led to the countrywide expansion of the screening program in 2008, leading to 45 million Germans eligible for skin cancer screenings every 2 years.21 Nearly two-thirds of dermatologists (N=1348) were satisfied with routine PSE and 83% perceived a better quality of health care for skin with the 2008 expansion.22
Data suggest that physician-detected melanomas through PSEs or routine physical examinations are thinner at the time of diagnosis than those found by patients or their partners.14,23-26 Terushkin and Halpern20 analyzed 9 worldwide studies encompassing more than 7500 patients and found that physician-detected melanomas were 0.55 mm thinner than those detected by patients or their significant others. The workplace screening and education program reviewed herein also reported a reduction in thicker melanomas and melanoma mortality during the study period.12
Not all Americans have a regular dermatologist. As such, educating PCPs in skin cancer detection has been a recent area of study. The premise is that the skin examination can be integrated into routine physical examinations conducted by PCPs. The previously discussed studies, particularly Aitken et al,14 Schneider et al,12 and Katalinic et al,15 as well as the SCREEN program studies,15 suggest that integration of the skin examination into the routine physical examination may be a feasible method to reduce melanoma thickness and mortality. Furthermore, the SCREEN study15 identified participants with risk factors for melanoma, finding that approximately half of men and women (N=360,288) had at least one melanoma risk factor, which suggests that it may be more practical to design screening practices around high-risk participants.
Several studies were excluded from our analysis on the basis of study design, including cross-sectional observational studies; however, it is worth briefly commenting on the findings of the excluded studies here, as they add to the body of literature. A community-based, multi-institutional study of 566 adults with invasive melanoma assessed the role of PSEs in the year prior to diagnosis by interviewing participants in clinic within 3 months of melanoma diagnosis.24 Patients who underwent full-body PSE in the year prior to diagnosis were more than 2 times more likely to have thinner (≤1 mm) melanomas (OR, 2.51; 95% CI, 1.62-3.87]). Notably, men older than 60 years appeared to benefit the most from this practice; men in this age group contributed greatly to the observed effect, likely because they had 4 times the odds of a thinner melanoma (OR, 4.09; 95% CI, 1.88-8.89]). Thinner melanomas also were associated with an age of 60 years or younger, female sex, and higher education level.24
Pollitt et al27 analyzed the association between prediagnosis Medicaid enrollment status and melanoma tumor thickness. The study found that men and women who intermittently enrolled in Medicaid or were not enrolled until the month of diagnosis had an increased chance of late-stage melanoma when compared to other patients. Patients who continuously enrolled during the year prior to diagnosis had lower odds for thicker melanomas, suggesting that these patients had greater access to screening examinations.27
Roetzheim et al28 analyzed data from the SEER-Medicare linked dataset to investigate patterns of dermatologist and PCP visits in the 2 years before melanoma diagnosis. Medicare beneficiaries seeing both a dermatologist and a PCP prior to melanoma diagnosis had greater odds of a thinner melanoma and lower melanoma mortality compared to patients without such visits.28
Durbec et al29 conducted a retrospective, population-based study of 650 patients in France who were seen by a dermatologist for melanoma. The thinnest melanomas were reported in patients seeing a dermatologist for prospective follow-up of nevi or consulting a dermatologist for other diseases. Patients referred to a dermatologist by PCPs tended to be older and had the highest frequency of thick (>3 mm), nodular, and/or ulcerated melanomas,29 which could be interpreted as a need for greater PCP education in melanoma screening.
Rates of skin examinations have been increasing since the year 2000, both overall and among high-risk groups as reported by a recent study on skin cancer screening trends. Prevalence of having at least one total-body skin examination increased from 14.5% in 2000 to 16.5% in 2005 to 19.8% in 2010 (P<.0001).30 One study revealed a practice gap in which more than 3 in 10 PCPs and 1 in 10 dermatologists reported not screening more than half their high-risk patients for skin cancer.31 The major obstacle to narrowing the identified practice gap involves establishing a national strategy to screen high-risk individuals for skin cancer and requires partnerships among patients, PCPs, specialists, policy makers, and government sponsors.
Lack of evidence that screening for skin cancer with PSEs reduces overall mortality does not mean there is a lack of lifesaving potential of screenings. The resources required to execute a randomized controlled trial with adequate power are vast, as the USPSTF estimated 800,000 participants would be needed.4 Barriers to conducting a randomized clinical trial for skin cancer screening include the large sample size required, prolonged follow-up, and various ethical issues such as withholding screening for a cancer that is potentially curable in early stages. Lessons from screenings for breast and prostate cancers have taught us that such randomized controlled trials assessing cancer screening are costly and do not always produce definitive answers.32
Conclusion
Although proof of improved health outcomes from randomized controlled trials is still required, there is evidence to support targeted screening programs for the detection of thinner melanomas and, by proxy, reduced melanoma mortality. Amidst the health care climate change and payment reform, recommendations from national organizations on melanoma screenings are paramount. Clinicians should continue to offer regular skin examinations as the body of evidence continues to grow in support of PSEs for melanoma screening.
Acknowledgments—We are grateful to Mary Butler, PhD, and Robert Kane, MD, both from Minneapolis, Minnesota, for their guidance and consultation.
1. American Cancer Society. Cancer Facts & Figures 2015. Atlanta, GA: American Cancer Society; 2015. http: //www.cancer.org/Research/CancerFactsStatistics/cancer factsfigures2015/cancer-facts-and-figures-2015. Accessed July 6, 2015.
2. Guy G Jr, Ekwueme D, Tangka F, et al. Melanoma treatment costs: a systematic review of the literature, 1990-2011. Am J Prev. 2012;43:537-545.
3. Margolis D, Halpern A, Rebbeck T, et al. Validation of a melanoma prognostic model. Arch Dermatol. 1998;134:1597-1601.
4. Wolff T, Tai E, Miller T. Screening for skin cancer: an update of the evidence for the U.S. Preventative Services Task Force. Ann Intern Med. 2009;150:194-198.
5. American Academy of Dermatology. Melanoma
Monday. http://www.aad.org/spot-skin-cancer
/community-programs-events/melanoma-monday. Accessed August 19, 2015.
6. Higgins JPT, Green S, eds. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. http:
//www.cochrane-handbook.org. Updated March 2011. Accessed November 10, 2014.
7. Viswanathan M, Berkman N. Development of the RTI item bank on risk of bias and precision of observational studies. J Clin Epidemiol. 2012;65:163-178.
8. Moher D, Liberati A, Tetzlaff J, et al; PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement [published online ahead of print July 23, 2009]. J Clin Epidemiol. 2009;62:1006-1012.
9. Berwick M, Armstrong B, Ben-Porat L. Sun exposure and mortality from melanoma. J Natl Cancer Inst. 2005;97:195-199.
10. Berwick M, Begg C, Fine J, et al. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88:17-23.
11. Aitken J, Elwood J, Lowe J, et al. A randomised trial of population screening for melanoma. J Med Screen. 2002;9:33-37.
12. Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
13. Expert Health Data Programming Inc. Health data software and health statistics. Available from: http: //www.ehdp.com. Accessed April 1, 2001. Cited by: Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
14. Aitken J, Elwood M, Baade P, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126:450-458.
15. Katalinic A, Waldmann A, Weinstock M, et al. Does skin cancer screening save lives? an observational study comparing trends in melanoma mortality in regions with and without screening. Cancer. 2012;118:5395-5402.
16. Aitken J, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006;54:105-114.
17. Coory M, Baade P, Aitken JF, et al. Trends for in-situ and invasive melanoma in Queensland, Australia, 1982 to 2002. Cancer Causes Control. 2006;17:21-27.
18. Mayer JE, Swetter SM, Fu T, et al. Screening, early detection, education, and trends for melanoma: current status (2007-2013) and future directions: part II. screening, education, and future directions. J Am Acad Dermatol. 2014;71:611.e1-611.e10; quiz, 621-622.
19. Curiel-Lewandrowski C, Chen S, Swetter S, et al. Screening and prevention measures for melanoma: is there a survival advantage? Curr Oncol Rep. 2012;14:458-467.
20. Terushkin V, Halpern A. Melanoma early detection. Hematol Oncol Clin North Am. 2009;23:481-500.
21. Geller A, Greinert R, Sinclair C, et al. A nationwide population-based skin cancer screening in Germany: proceedings of the first meeting of the International Task Force on Skin Cancer Screening and Prevention (September 24 and 25, 2009) [published online ahead of print April 8, 2010]. Cancer Epidemiol. 2010;34:355-358.
22. Kornek T, Schafer I, Reusch M, et al. Routine skin cancer screening in Germany: four years of experience from the dermatologists’ perspective. Dermatology. 2012;225:289-293.
23. De Giorgi V, Grazzini M, Rossari S, et al. Is skin self-examination for cutaneous melanoma detection still adequate? a retrospective study. Dermatology. 2012;225:31-36.
24. Swetter S, Johnson T, Miller D, et al. Melanoma in middle-aged and older men: a multi-institutional survey study of factors related to tumor thickness. Arch Dermatol. 2009;145:397-404.
25. Kantor J, Kantor D. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145:873-876.
26. Kovalyshyn I, Dusza S, Siamas K, et al. The impact of physician screening on melanoma detection. Arch Dermatol. 2011;147:1269-1275.
27. Pollitt R, Clarke C, Shema S, et al. California Medicaid enrollment and melanoma stage at diagnosis: a population-based study. Am J Prev Med. 2008;35:7-13.
28. Roetzheim R, Lee J, Ferrante J, et al. The influence of dermatologist and primary care physician visits on melanoma outcomes among Medicare beneficiaries. J Am Board Fam Med. 2013;26:637-647.
29. Durbec F, Vitry F, Granel-Brocard F, et al. The role of circumstances of diagnosis and access to dermatological care in early diagnosis of cutaneous melanoma: a population-based study in France. Arch Dermatol. 2010;146:240-246.
30. Lakhani N, Saraiya M, Thompson T, et al. Total body skin examination for skin cancer screening among U.S. adults from 2000 to 2010. Prev Med. 2014;61:75-80.
31. Oliveria SA, Heneghan MK, Cushman LF, et al. Skin cancer screening by dermatologists, family practitioners, and internists: barriers and facilitating factors. Arch Dermatol. 2011;147:39-44.
32. Bigby M. Why the evidence for skin cancer screening is insufficient: lessons from prostate cancer screening. Arch Dermatol. 2010;146:322-324.
In the United States an estimated 73,870 new cases of melanoma will be diagnosed in 2015.1 Although melanoma accounts for less than 2% of all US skin cancer cases, it is responsible for the vast majority of skin cancer deaths. From 2007 to 2011, melanoma mortality rates decreased by 2.6% per year in individuals younger than 50 years but increased by 0.6% per year among those 50 years and older.1 Reports of the direct annual treatment costs for melanoma in the United States have ranged from $44.9 million for Medicare recipients with existing cases of melanoma to $932.5 million for newly diagnosed melanomas across all age groups.2
Melanoma survival rates are inversely related to tumor thickness at the time of diagnosis.3 Melanoma can be cured if caught early and properly treated. Secondary preventative measures include physician skin examinations (PSEs), which may increase the likelihood of detecting melanomas in earlier stages, thereby potentially increasing survival rates and quality of life as well as decreasing treatment costs. Physician skin examinations are performed in the physician’s office and are safe, noninvasive, and painless. Patients with suspicious lesions should subsequently undergo a skin biopsy, which is a low-risk procedure. False-positives from biopsies do not lead to extreme patient morbidity, and false-negatives will hopefully be detected at a subsequent visit.
There is a lack of consensus regarding recommendations for PSEs for skin cancer screening. Due to a lack of randomized controlled trials on the effects of skin cancer screening on patient morbidity and mortality, the US Preventive Services Task Force (USPSTF) has concluded that there is insufficient evidence to recommend for or against such screening4; however, other organizations including the American Cancer Society and the American Academy of Dermatology recommend periodic skin cancer screening examinations.1,5 In a rapidly changing health care climate and with the rollout of the Patient Protection and Affordable Care Act, a USPSTF recommendation for skin screening with PSEs for skin cancer would have a large impact on clinical practice in the United States.
This article provides a systematic review of the current domestic and international data regarding the impact of PSEs on melanoma tumor thickness at the time of diagnosis as well as mortality from melanoma.
Methods
Search Strategy
A systematic search of PubMed articles indexed for MEDLINE and Embase for studies related to melanoma and PSEs was performed for the period from each database’s inception to November 8, 2014. One of the authors (S.L.M.) designed a broad search strategy with assistance from a medical librarian who had expertise in searching research bibliographies. Articles were excluded if they had a cross-sectional study design or were editorials or review articles. Search terms included skin neoplasm, skin cancer, or melanoma in combination with any of the following: skin examination, mass screening, screening, and secondary prevention.
Study Selection
All published studies reporting outcomes and correlations with PSEs and cutaneous melanoma in adult patients were screened. If multiple studies were published describing the same study, follow-up studies were included for data extraction, but the original study was the primary resource. Observational studies were a focus in this review, as these types of studies are much more common in this subject area.
One of the authors (S.L.M.) screened the titles and abstracts of identified studies for eligibility. If the reviewer considered a study potentially eligible based on the abstract review, a full-text review was carried out. The reference lists of eligible studies were manually searched to identify additional studies.
Data Extraction, Quality Assessment, and Data Synthesis
Data items to be extracted were agreed on before search implementation and were extracted by one investigator (S.L.M.) following criteria developed by review of the Cochrane Handbook for Systematic Reviews of Interventions.6 Study population, design, sample size, and outcomes were extracted. Risk of bias of individual articles was evaluated using a tool developed from the RTI item bank (RTI International) for determining the risk of bias and precision of eligible observational studies.7 Studies ultimately were classified into 3 categories based on the risk of bias: (1) low risk of bias, (2) medium risk of bias, and (3) high risk of bias. The strength of evidence of included studies was evaluated by the following items: risk of bias, consistency, directness, precision, and overall conclusion. Data from the included studies was synthesized qualitatively in a narrative format. This review adhered to guidelines in the Cochrane Handbook for Systematic Reviews of Interventions6 and the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines.8
Results
A total of 705 titles were screened, 98 abstracts were assessed for eligibility, 42 full-text reviews were carried out, and 5 eligible studies were identified (Figure 1). Five observational studies were included in the final review. A summary of the results is presented in Table 1.
Included studies were assessed for several types of biases, including selection bias, attrition bias, detection bias, performance bias, and response bias. The judgments were given for each domain (Table 2). There was heterogeneity in study design, reporting of total-body skin examination methods, and reporting of outcomes among all 5 studies. All 5 studies were assessed as having a medium risk of bias.
Physician Skin Examination Impact
One article by Berwick et al9 reanalyzed data from a 1996 study10 and provided no significant evidence regarding the benefits of PSEs in the reduction of melanoma mortality. Data for 650 patients with newly diagnosed melanomas were obtained from the Connecticut Tumor Registry, a site for the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, along with 549 age- and sex-frequency matched controls from the general population.10 Participants were followed biannually for a mean of 5.4 years. Of the original 650 case patients, 122 were excluded from the study with reasons provided. Physician skin examination was defined as a positive response to the following questionnaire item: “[Before your recent biopsy] did the doctor examine your skin during any of your visits?”9 Data analysis showed no significant association between PSE and death from melanoma. Upon univariate analysis, the hazard ratio for physician screening was 0.7 (95% confidence interval [CI], 0.4-1.3).9
The SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, which was undertaken in Schleswig-Holstein, Germany, is the world’s largest systematic population-based skin cancer screening program.15 The participation rate was
19% (N=360,288) of the eligible population (citizens aged ≥20 years with statutory health insurance). Screening was a 2-step process performed by trained physicians: initial general practitioner whole-body skin examination followed by referral to a dermatologist for evaluation of suspicious skin findings. Five years after the SCREEN program was conducted, melanoma mortality declined by 47% per 100,000 men and by 49% per 100,000 women. The annual percentage change in the most recent 10-year period (2000-2009) was 7.5% (95% CI, –14.0 to –0.5; P<.05) for men and 7.1% for women (95% CI,
–10.5 to –2.9; P<.05). Simultaneously, the melanoma mortality rates in the 4 unscreened adjacent regions and the rest of Germany were stable, significantly (P<.05) different from the decline in mortality observed in Schleswig-Holstein.15
A community-based, prospective cohort study investigated the impact of an employee melanoma screening program at the Lawrence Livermore National Laboratory (Livermore, California) (1984-1996) demonstrated an impact on melanoma thickness and mortality rates.12 The cohort (approximately 5100 participants) was followed over 3 phases of surveillance: (1) preawareness (1969-1975), (2) early awareness of increased melanoma risk (1976-1984), and (3) screening program (1984-1996). The screening program encouraged employees to self-examine their skin for “suggestive lesions”; if a suggestive lesion was found, a full-body skin examination was performed by a physician. After being evaluated, participants with melanoma, dysplastic nevi, 50 or more moles, or a family history of melanoma were offered a periodic full-body examination every 3 to 24 months, often with
full-body photography and dermoscopy. Physician skin screening resulted in a reduction in crude incidence of thicker melanomas (defined as
>0.75 mm) during the 3 study phases. Compared with the early-awareness period (phase 2), a 69% reduction in the diagnosis of thick melanomas was reported in the screening program period (phase 3)(P=.0001). During the screening period, no eligible melanoma deaths occurred in the study population, whereas the expected number of deaths was 3.39 (P=.034) based on observed melanoma mortality in 5 San Francisco/Oakland Bay–area counties in California as reported to the SEER program from 1984 to 1996.12
The strongest evidence for reduced thickness of melanomas detected via PSEs was reported in a population-based, case-control study by Aitken et al14 of all residents in Queensland, Australia, aged 20 to 75 years with a histologically confirmed first primary invasive cutaneous melanoma diagnosed between January 2000 and December 2003. Whole-body PSE in the 3 years before diagnosis was inversely associated with tumor thickness at diagnosis (χ2=44.37; P<.001), including a 14% lower risk of diagnosis of a thick melanoma (>0.75 mm)(odds ratio [OR], 0.86; 95% CI, 0.75-0.98) and a 40% lower risk of diagnosis of a melanoma that was 3 mm or larger (OR, 0.60; 95% CI, 0.43-0.83). The investigators applied melanoma thickness-specific survival estimates to the thickness distribution of the screened and unscreened cases in their sample to estimate melanoma deaths within 5 and 10 years of diagnosis. Compared to the unscreened cases, they estimated that the screened cases would have 26% fewer melanoma deaths within 5 years of diagnosis and 23% fewer deaths within 10 years.14
Another prospective cohort study in Queensland was designed to detect a 20% reduction in mortality from melanoma during a 15-year intervention period in communities that received a screening program.11 A total of 44 communities (aggregate population, 560,000 adults aged ≥30 years) were randomized into intervention or control groups to receive a community-based melanoma screening program for 3 years versus usual medical care.Overall, thinner melanomas were identified in communities with the screening program versus neighboring communities without it.11 Of the 33 melanomas found through the screening program, 39% (13/33) were in situ lesions, 55% (18/33) were thin (<1 mm) invasive lesions, and 6% (2/33) were 1-mm thick or greater.16 Within the population of Queensland during the period from 1999 through 2002, 36% were in situ lesions, 48% were invasive thin melanomas, and 16% were invasive melanomas 1-mm thick or more, indicating that melanomas found through screening were thinner or less advanced.17
Comment
Our review identified 5 studies describing the impact of PSEs for melanoma screening on tumor thickness at diagnosis and melanoma mortality. Key findings are highlighted in Figure 2. Our findings suggest that PSEs are associated with a decline in melanoma tumor thickness and melanoma-specific mortality. Our findings are qualitatively similar to prior reviews that supported the use of PSEs to detect thinner melanomas and improve mortality outcomes.18-20
The greatest evidence for population-based screening programs was provided by the SCREEN study. This landmark study documented that screening programs utilizing primary care physicians (PCPs) and dermatologists can lead to a reduction in melanoma mortality.15 Findings from the study led to the countrywide expansion of the screening program in 2008, leading to 45 million Germans eligible for skin cancer screenings every 2 years.21 Nearly two-thirds of dermatologists (N=1348) were satisfied with routine PSE and 83% perceived a better quality of health care for skin with the 2008 expansion.22
Data suggest that physician-detected melanomas through PSEs or routine physical examinations are thinner at the time of diagnosis than those found by patients or their partners.14,23-26 Terushkin and Halpern20 analyzed 9 worldwide studies encompassing more than 7500 patients and found that physician-detected melanomas were 0.55 mm thinner than those detected by patients or their significant others. The workplace screening and education program reviewed herein also reported a reduction in thicker melanomas and melanoma mortality during the study period.12
Not all Americans have a regular dermatologist. As such, educating PCPs in skin cancer detection has been a recent area of study. The premise is that the skin examination can be integrated into routine physical examinations conducted by PCPs. The previously discussed studies, particularly Aitken et al,14 Schneider et al,12 and Katalinic et al,15 as well as the SCREEN program studies,15 suggest that integration of the skin examination into the routine physical examination may be a feasible method to reduce melanoma thickness and mortality. Furthermore, the SCREEN study15 identified participants with risk factors for melanoma, finding that approximately half of men and women (N=360,288) had at least one melanoma risk factor, which suggests that it may be more practical to design screening practices around high-risk participants.
Several studies were excluded from our analysis on the basis of study design, including cross-sectional observational studies; however, it is worth briefly commenting on the findings of the excluded studies here, as they add to the body of literature. A community-based, multi-institutional study of 566 adults with invasive melanoma assessed the role of PSEs in the year prior to diagnosis by interviewing participants in clinic within 3 months of melanoma diagnosis.24 Patients who underwent full-body PSE in the year prior to diagnosis were more than 2 times more likely to have thinner (≤1 mm) melanomas (OR, 2.51; 95% CI, 1.62-3.87]). Notably, men older than 60 years appeared to benefit the most from this practice; men in this age group contributed greatly to the observed effect, likely because they had 4 times the odds of a thinner melanoma (OR, 4.09; 95% CI, 1.88-8.89]). Thinner melanomas also were associated with an age of 60 years or younger, female sex, and higher education level.24
Pollitt et al27 analyzed the association between prediagnosis Medicaid enrollment status and melanoma tumor thickness. The study found that men and women who intermittently enrolled in Medicaid or were not enrolled until the month of diagnosis had an increased chance of late-stage melanoma when compared to other patients. Patients who continuously enrolled during the year prior to diagnosis had lower odds for thicker melanomas, suggesting that these patients had greater access to screening examinations.27
Roetzheim et al28 analyzed data from the SEER-Medicare linked dataset to investigate patterns of dermatologist and PCP visits in the 2 years before melanoma diagnosis. Medicare beneficiaries seeing both a dermatologist and a PCP prior to melanoma diagnosis had greater odds of a thinner melanoma and lower melanoma mortality compared to patients without such visits.28
Durbec et al29 conducted a retrospective, population-based study of 650 patients in France who were seen by a dermatologist for melanoma. The thinnest melanomas were reported in patients seeing a dermatologist for prospective follow-up of nevi or consulting a dermatologist for other diseases. Patients referred to a dermatologist by PCPs tended to be older and had the highest frequency of thick (>3 mm), nodular, and/or ulcerated melanomas,29 which could be interpreted as a need for greater PCP education in melanoma screening.
Rates of skin examinations have been increasing since the year 2000, both overall and among high-risk groups as reported by a recent study on skin cancer screening trends. Prevalence of having at least one total-body skin examination increased from 14.5% in 2000 to 16.5% in 2005 to 19.8% in 2010 (P<.0001).30 One study revealed a practice gap in which more than 3 in 10 PCPs and 1 in 10 dermatologists reported not screening more than half their high-risk patients for skin cancer.31 The major obstacle to narrowing the identified practice gap involves establishing a national strategy to screen high-risk individuals for skin cancer and requires partnerships among patients, PCPs, specialists, policy makers, and government sponsors.
Lack of evidence that screening for skin cancer with PSEs reduces overall mortality does not mean there is a lack of lifesaving potential of screenings. The resources required to execute a randomized controlled trial with adequate power are vast, as the USPSTF estimated 800,000 participants would be needed.4 Barriers to conducting a randomized clinical trial for skin cancer screening include the large sample size required, prolonged follow-up, and various ethical issues such as withholding screening for a cancer that is potentially curable in early stages. Lessons from screenings for breast and prostate cancers have taught us that such randomized controlled trials assessing cancer screening are costly and do not always produce definitive answers.32
Conclusion
Although proof of improved health outcomes from randomized controlled trials is still required, there is evidence to support targeted screening programs for the detection of thinner melanomas and, by proxy, reduced melanoma mortality. Amidst the health care climate change and payment reform, recommendations from national organizations on melanoma screenings are paramount. Clinicians should continue to offer regular skin examinations as the body of evidence continues to grow in support of PSEs for melanoma screening.
Acknowledgments—We are grateful to Mary Butler, PhD, and Robert Kane, MD, both from Minneapolis, Minnesota, for their guidance and consultation.
In the United States an estimated 73,870 new cases of melanoma will be diagnosed in 2015.1 Although melanoma accounts for less than 2% of all US skin cancer cases, it is responsible for the vast majority of skin cancer deaths. From 2007 to 2011, melanoma mortality rates decreased by 2.6% per year in individuals younger than 50 years but increased by 0.6% per year among those 50 years and older.1 Reports of the direct annual treatment costs for melanoma in the United States have ranged from $44.9 million for Medicare recipients with existing cases of melanoma to $932.5 million for newly diagnosed melanomas across all age groups.2
Melanoma survival rates are inversely related to tumor thickness at the time of diagnosis.3 Melanoma can be cured if caught early and properly treated. Secondary preventative measures include physician skin examinations (PSEs), which may increase the likelihood of detecting melanomas in earlier stages, thereby potentially increasing survival rates and quality of life as well as decreasing treatment costs. Physician skin examinations are performed in the physician’s office and are safe, noninvasive, and painless. Patients with suspicious lesions should subsequently undergo a skin biopsy, which is a low-risk procedure. False-positives from biopsies do not lead to extreme patient morbidity, and false-negatives will hopefully be detected at a subsequent visit.
There is a lack of consensus regarding recommendations for PSEs for skin cancer screening. Due to a lack of randomized controlled trials on the effects of skin cancer screening on patient morbidity and mortality, the US Preventive Services Task Force (USPSTF) has concluded that there is insufficient evidence to recommend for or against such screening4; however, other organizations including the American Cancer Society and the American Academy of Dermatology recommend periodic skin cancer screening examinations.1,5 In a rapidly changing health care climate and with the rollout of the Patient Protection and Affordable Care Act, a USPSTF recommendation for skin screening with PSEs for skin cancer would have a large impact on clinical practice in the United States.
This article provides a systematic review of the current domestic and international data regarding the impact of PSEs on melanoma tumor thickness at the time of diagnosis as well as mortality from melanoma.
Methods
Search Strategy
A systematic search of PubMed articles indexed for MEDLINE and Embase for studies related to melanoma and PSEs was performed for the period from each database’s inception to November 8, 2014. One of the authors (S.L.M.) designed a broad search strategy with assistance from a medical librarian who had expertise in searching research bibliographies. Articles were excluded if they had a cross-sectional study design or were editorials or review articles. Search terms included skin neoplasm, skin cancer, or melanoma in combination with any of the following: skin examination, mass screening, screening, and secondary prevention.
Study Selection
All published studies reporting outcomes and correlations with PSEs and cutaneous melanoma in adult patients were screened. If multiple studies were published describing the same study, follow-up studies were included for data extraction, but the original study was the primary resource. Observational studies were a focus in this review, as these types of studies are much more common in this subject area.
One of the authors (S.L.M.) screened the titles and abstracts of identified studies for eligibility. If the reviewer considered a study potentially eligible based on the abstract review, a full-text review was carried out. The reference lists of eligible studies were manually searched to identify additional studies.
Data Extraction, Quality Assessment, and Data Synthesis
Data items to be extracted were agreed on before search implementation and were extracted by one investigator (S.L.M.) following criteria developed by review of the Cochrane Handbook for Systematic Reviews of Interventions.6 Study population, design, sample size, and outcomes were extracted. Risk of bias of individual articles was evaluated using a tool developed from the RTI item bank (RTI International) for determining the risk of bias and precision of eligible observational studies.7 Studies ultimately were classified into 3 categories based on the risk of bias: (1) low risk of bias, (2) medium risk of bias, and (3) high risk of bias. The strength of evidence of included studies was evaluated by the following items: risk of bias, consistency, directness, precision, and overall conclusion. Data from the included studies was synthesized qualitatively in a narrative format. This review adhered to guidelines in the Cochrane Handbook for Systematic Reviews of Interventions6 and the PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines.8
Results
A total of 705 titles were screened, 98 abstracts were assessed for eligibility, 42 full-text reviews were carried out, and 5 eligible studies were identified (Figure 1). Five observational studies were included in the final review. A summary of the results is presented in Table 1.
Included studies were assessed for several types of biases, including selection bias, attrition bias, detection bias, performance bias, and response bias. The judgments were given for each domain (Table 2). There was heterogeneity in study design, reporting of total-body skin examination methods, and reporting of outcomes among all 5 studies. All 5 studies were assessed as having a medium risk of bias.
Physician Skin Examination Impact
One article by Berwick et al9 reanalyzed data from a 1996 study10 and provided no significant evidence regarding the benefits of PSEs in the reduction of melanoma mortality. Data for 650 patients with newly diagnosed melanomas were obtained from the Connecticut Tumor Registry, a site for the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program, along with 549 age- and sex-frequency matched controls from the general population.10 Participants were followed biannually for a mean of 5.4 years. Of the original 650 case patients, 122 were excluded from the study with reasons provided. Physician skin examination was defined as a positive response to the following questionnaire item: “[Before your recent biopsy] did the doctor examine your skin during any of your visits?”9 Data analysis showed no significant association between PSE and death from melanoma. Upon univariate analysis, the hazard ratio for physician screening was 0.7 (95% confidence interval [CI], 0.4-1.3).9
The SCREEN (Skin Cancer Research to Provide Evidence for Effectiveness of Screening in Northern Germany) project, which was undertaken in Schleswig-Holstein, Germany, is the world’s largest systematic population-based skin cancer screening program.15 The participation rate was
19% (N=360,288) of the eligible population (citizens aged ≥20 years with statutory health insurance). Screening was a 2-step process performed by trained physicians: initial general practitioner whole-body skin examination followed by referral to a dermatologist for evaluation of suspicious skin findings. Five years after the SCREEN program was conducted, melanoma mortality declined by 47% per 100,000 men and by 49% per 100,000 women. The annual percentage change in the most recent 10-year period (2000-2009) was 7.5% (95% CI, –14.0 to –0.5; P<.05) for men and 7.1% for women (95% CI,
–10.5 to –2.9; P<.05). Simultaneously, the melanoma mortality rates in the 4 unscreened adjacent regions and the rest of Germany were stable, significantly (P<.05) different from the decline in mortality observed in Schleswig-Holstein.15
A community-based, prospective cohort study investigated the impact of an employee melanoma screening program at the Lawrence Livermore National Laboratory (Livermore, California) (1984-1996) demonstrated an impact on melanoma thickness and mortality rates.12 The cohort (approximately 5100 participants) was followed over 3 phases of surveillance: (1) preawareness (1969-1975), (2) early awareness of increased melanoma risk (1976-1984), and (3) screening program (1984-1996). The screening program encouraged employees to self-examine their skin for “suggestive lesions”; if a suggestive lesion was found, a full-body skin examination was performed by a physician. After being evaluated, participants with melanoma, dysplastic nevi, 50 or more moles, or a family history of melanoma were offered a periodic full-body examination every 3 to 24 months, often with
full-body photography and dermoscopy. Physician skin screening resulted in a reduction in crude incidence of thicker melanomas (defined as
>0.75 mm) during the 3 study phases. Compared with the early-awareness period (phase 2), a 69% reduction in the diagnosis of thick melanomas was reported in the screening program period (phase 3)(P=.0001). During the screening period, no eligible melanoma deaths occurred in the study population, whereas the expected number of deaths was 3.39 (P=.034) based on observed melanoma mortality in 5 San Francisco/Oakland Bay–area counties in California as reported to the SEER program from 1984 to 1996.12
The strongest evidence for reduced thickness of melanomas detected via PSEs was reported in a population-based, case-control study by Aitken et al14 of all residents in Queensland, Australia, aged 20 to 75 years with a histologically confirmed first primary invasive cutaneous melanoma diagnosed between January 2000 and December 2003. Whole-body PSE in the 3 years before diagnosis was inversely associated with tumor thickness at diagnosis (χ2=44.37; P<.001), including a 14% lower risk of diagnosis of a thick melanoma (>0.75 mm)(odds ratio [OR], 0.86; 95% CI, 0.75-0.98) and a 40% lower risk of diagnosis of a melanoma that was 3 mm or larger (OR, 0.60; 95% CI, 0.43-0.83). The investigators applied melanoma thickness-specific survival estimates to the thickness distribution of the screened and unscreened cases in their sample to estimate melanoma deaths within 5 and 10 years of diagnosis. Compared to the unscreened cases, they estimated that the screened cases would have 26% fewer melanoma deaths within 5 years of diagnosis and 23% fewer deaths within 10 years.14
Another prospective cohort study in Queensland was designed to detect a 20% reduction in mortality from melanoma during a 15-year intervention period in communities that received a screening program.11 A total of 44 communities (aggregate population, 560,000 adults aged ≥30 years) were randomized into intervention or control groups to receive a community-based melanoma screening program for 3 years versus usual medical care.Overall, thinner melanomas were identified in communities with the screening program versus neighboring communities without it.11 Of the 33 melanomas found through the screening program, 39% (13/33) were in situ lesions, 55% (18/33) were thin (<1 mm) invasive lesions, and 6% (2/33) were 1-mm thick or greater.16 Within the population of Queensland during the period from 1999 through 2002, 36% were in situ lesions, 48% were invasive thin melanomas, and 16% were invasive melanomas 1-mm thick or more, indicating that melanomas found through screening were thinner or less advanced.17
Comment
Our review identified 5 studies describing the impact of PSEs for melanoma screening on tumor thickness at diagnosis and melanoma mortality. Key findings are highlighted in Figure 2. Our findings suggest that PSEs are associated with a decline in melanoma tumor thickness and melanoma-specific mortality. Our findings are qualitatively similar to prior reviews that supported the use of PSEs to detect thinner melanomas and improve mortality outcomes.18-20
The greatest evidence for population-based screening programs was provided by the SCREEN study. This landmark study documented that screening programs utilizing primary care physicians (PCPs) and dermatologists can lead to a reduction in melanoma mortality.15 Findings from the study led to the countrywide expansion of the screening program in 2008, leading to 45 million Germans eligible for skin cancer screenings every 2 years.21 Nearly two-thirds of dermatologists (N=1348) were satisfied with routine PSE and 83% perceived a better quality of health care for skin with the 2008 expansion.22
Data suggest that physician-detected melanomas through PSEs or routine physical examinations are thinner at the time of diagnosis than those found by patients or their partners.14,23-26 Terushkin and Halpern20 analyzed 9 worldwide studies encompassing more than 7500 patients and found that physician-detected melanomas were 0.55 mm thinner than those detected by patients or their significant others. The workplace screening and education program reviewed herein also reported a reduction in thicker melanomas and melanoma mortality during the study period.12
Not all Americans have a regular dermatologist. As such, educating PCPs in skin cancer detection has been a recent area of study. The premise is that the skin examination can be integrated into routine physical examinations conducted by PCPs. The previously discussed studies, particularly Aitken et al,14 Schneider et al,12 and Katalinic et al,15 as well as the SCREEN program studies,15 suggest that integration of the skin examination into the routine physical examination may be a feasible method to reduce melanoma thickness and mortality. Furthermore, the SCREEN study15 identified participants with risk factors for melanoma, finding that approximately half of men and women (N=360,288) had at least one melanoma risk factor, which suggests that it may be more practical to design screening practices around high-risk participants.
Several studies were excluded from our analysis on the basis of study design, including cross-sectional observational studies; however, it is worth briefly commenting on the findings of the excluded studies here, as they add to the body of literature. A community-based, multi-institutional study of 566 adults with invasive melanoma assessed the role of PSEs in the year prior to diagnosis by interviewing participants in clinic within 3 months of melanoma diagnosis.24 Patients who underwent full-body PSE in the year prior to diagnosis were more than 2 times more likely to have thinner (≤1 mm) melanomas (OR, 2.51; 95% CI, 1.62-3.87]). Notably, men older than 60 years appeared to benefit the most from this practice; men in this age group contributed greatly to the observed effect, likely because they had 4 times the odds of a thinner melanoma (OR, 4.09; 95% CI, 1.88-8.89]). Thinner melanomas also were associated with an age of 60 years or younger, female sex, and higher education level.24
Pollitt et al27 analyzed the association between prediagnosis Medicaid enrollment status and melanoma tumor thickness. The study found that men and women who intermittently enrolled in Medicaid or were not enrolled until the month of diagnosis had an increased chance of late-stage melanoma when compared to other patients. Patients who continuously enrolled during the year prior to diagnosis had lower odds for thicker melanomas, suggesting that these patients had greater access to screening examinations.27
Roetzheim et al28 analyzed data from the SEER-Medicare linked dataset to investigate patterns of dermatologist and PCP visits in the 2 years before melanoma diagnosis. Medicare beneficiaries seeing both a dermatologist and a PCP prior to melanoma diagnosis had greater odds of a thinner melanoma and lower melanoma mortality compared to patients without such visits.28
Durbec et al29 conducted a retrospective, population-based study of 650 patients in France who were seen by a dermatologist for melanoma. The thinnest melanomas were reported in patients seeing a dermatologist for prospective follow-up of nevi or consulting a dermatologist for other diseases. Patients referred to a dermatologist by PCPs tended to be older and had the highest frequency of thick (>3 mm), nodular, and/or ulcerated melanomas,29 which could be interpreted as a need for greater PCP education in melanoma screening.
Rates of skin examinations have been increasing since the year 2000, both overall and among high-risk groups as reported by a recent study on skin cancer screening trends. Prevalence of having at least one total-body skin examination increased from 14.5% in 2000 to 16.5% in 2005 to 19.8% in 2010 (P<.0001).30 One study revealed a practice gap in which more than 3 in 10 PCPs and 1 in 10 dermatologists reported not screening more than half their high-risk patients for skin cancer.31 The major obstacle to narrowing the identified practice gap involves establishing a national strategy to screen high-risk individuals for skin cancer and requires partnerships among patients, PCPs, specialists, policy makers, and government sponsors.
Lack of evidence that screening for skin cancer with PSEs reduces overall mortality does not mean there is a lack of lifesaving potential of screenings. The resources required to execute a randomized controlled trial with adequate power are vast, as the USPSTF estimated 800,000 participants would be needed.4 Barriers to conducting a randomized clinical trial for skin cancer screening include the large sample size required, prolonged follow-up, and various ethical issues such as withholding screening for a cancer that is potentially curable in early stages. Lessons from screenings for breast and prostate cancers have taught us that such randomized controlled trials assessing cancer screening are costly and do not always produce definitive answers.32
Conclusion
Although proof of improved health outcomes from randomized controlled trials is still required, there is evidence to support targeted screening programs for the detection of thinner melanomas and, by proxy, reduced melanoma mortality. Amidst the health care climate change and payment reform, recommendations from national organizations on melanoma screenings are paramount. Clinicians should continue to offer regular skin examinations as the body of evidence continues to grow in support of PSEs for melanoma screening.
Acknowledgments—We are grateful to Mary Butler, PhD, and Robert Kane, MD, both from Minneapolis, Minnesota, for their guidance and consultation.
1. American Cancer Society. Cancer Facts & Figures 2015. Atlanta, GA: American Cancer Society; 2015. http: //www.cancer.org/Research/CancerFactsStatistics/cancer factsfigures2015/cancer-facts-and-figures-2015. Accessed July 6, 2015.
2. Guy G Jr, Ekwueme D, Tangka F, et al. Melanoma treatment costs: a systematic review of the literature, 1990-2011. Am J Prev. 2012;43:537-545.
3. Margolis D, Halpern A, Rebbeck T, et al. Validation of a melanoma prognostic model. Arch Dermatol. 1998;134:1597-1601.
4. Wolff T, Tai E, Miller T. Screening for skin cancer: an update of the evidence for the U.S. Preventative Services Task Force. Ann Intern Med. 2009;150:194-198.
5. American Academy of Dermatology. Melanoma
Monday. http://www.aad.org/spot-skin-cancer
/community-programs-events/melanoma-monday. Accessed August 19, 2015.
6. Higgins JPT, Green S, eds. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. http:
//www.cochrane-handbook.org. Updated March 2011. Accessed November 10, 2014.
7. Viswanathan M, Berkman N. Development of the RTI item bank on risk of bias and precision of observational studies. J Clin Epidemiol. 2012;65:163-178.
8. Moher D, Liberati A, Tetzlaff J, et al; PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement [published online ahead of print July 23, 2009]. J Clin Epidemiol. 2009;62:1006-1012.
9. Berwick M, Armstrong B, Ben-Porat L. Sun exposure and mortality from melanoma. J Natl Cancer Inst. 2005;97:195-199.
10. Berwick M, Begg C, Fine J, et al. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88:17-23.
11. Aitken J, Elwood J, Lowe J, et al. A randomised trial of population screening for melanoma. J Med Screen. 2002;9:33-37.
12. Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
13. Expert Health Data Programming Inc. Health data software and health statistics. Available from: http: //www.ehdp.com. Accessed April 1, 2001. Cited by: Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
14. Aitken J, Elwood M, Baade P, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126:450-458.
15. Katalinic A, Waldmann A, Weinstock M, et al. Does skin cancer screening save lives? an observational study comparing trends in melanoma mortality in regions with and without screening. Cancer. 2012;118:5395-5402.
16. Aitken J, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006;54:105-114.
17. Coory M, Baade P, Aitken JF, et al. Trends for in-situ and invasive melanoma in Queensland, Australia, 1982 to 2002. Cancer Causes Control. 2006;17:21-27.
18. Mayer JE, Swetter SM, Fu T, et al. Screening, early detection, education, and trends for melanoma: current status (2007-2013) and future directions: part II. screening, education, and future directions. J Am Acad Dermatol. 2014;71:611.e1-611.e10; quiz, 621-622.
19. Curiel-Lewandrowski C, Chen S, Swetter S, et al. Screening and prevention measures for melanoma: is there a survival advantage? Curr Oncol Rep. 2012;14:458-467.
20. Terushkin V, Halpern A. Melanoma early detection. Hematol Oncol Clin North Am. 2009;23:481-500.
21. Geller A, Greinert R, Sinclair C, et al. A nationwide population-based skin cancer screening in Germany: proceedings of the first meeting of the International Task Force on Skin Cancer Screening and Prevention (September 24 and 25, 2009) [published online ahead of print April 8, 2010]. Cancer Epidemiol. 2010;34:355-358.
22. Kornek T, Schafer I, Reusch M, et al. Routine skin cancer screening in Germany: four years of experience from the dermatologists’ perspective. Dermatology. 2012;225:289-293.
23. De Giorgi V, Grazzini M, Rossari S, et al. Is skin self-examination for cutaneous melanoma detection still adequate? a retrospective study. Dermatology. 2012;225:31-36.
24. Swetter S, Johnson T, Miller D, et al. Melanoma in middle-aged and older men: a multi-institutional survey study of factors related to tumor thickness. Arch Dermatol. 2009;145:397-404.
25. Kantor J, Kantor D. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145:873-876.
26. Kovalyshyn I, Dusza S, Siamas K, et al. The impact of physician screening on melanoma detection. Arch Dermatol. 2011;147:1269-1275.
27. Pollitt R, Clarke C, Shema S, et al. California Medicaid enrollment and melanoma stage at diagnosis: a population-based study. Am J Prev Med. 2008;35:7-13.
28. Roetzheim R, Lee J, Ferrante J, et al. The influence of dermatologist and primary care physician visits on melanoma outcomes among Medicare beneficiaries. J Am Board Fam Med. 2013;26:637-647.
29. Durbec F, Vitry F, Granel-Brocard F, et al. The role of circumstances of diagnosis and access to dermatological care in early diagnosis of cutaneous melanoma: a population-based study in France. Arch Dermatol. 2010;146:240-246.
30. Lakhani N, Saraiya M, Thompson T, et al. Total body skin examination for skin cancer screening among U.S. adults from 2000 to 2010. Prev Med. 2014;61:75-80.
31. Oliveria SA, Heneghan MK, Cushman LF, et al. Skin cancer screening by dermatologists, family practitioners, and internists: barriers and facilitating factors. Arch Dermatol. 2011;147:39-44.
32. Bigby M. Why the evidence for skin cancer screening is insufficient: lessons from prostate cancer screening. Arch Dermatol. 2010;146:322-324.
1. American Cancer Society. Cancer Facts & Figures 2015. Atlanta, GA: American Cancer Society; 2015. http: //www.cancer.org/Research/CancerFactsStatistics/cancer factsfigures2015/cancer-facts-and-figures-2015. Accessed July 6, 2015.
2. Guy G Jr, Ekwueme D, Tangka F, et al. Melanoma treatment costs: a systematic review of the literature, 1990-2011. Am J Prev. 2012;43:537-545.
3. Margolis D, Halpern A, Rebbeck T, et al. Validation of a melanoma prognostic model. Arch Dermatol. 1998;134:1597-1601.
4. Wolff T, Tai E, Miller T. Screening for skin cancer: an update of the evidence for the U.S. Preventative Services Task Force. Ann Intern Med. 2009;150:194-198.
5. American Academy of Dermatology. Melanoma
Monday. http://www.aad.org/spot-skin-cancer
/community-programs-events/melanoma-monday. Accessed August 19, 2015.
6. Higgins JPT, Green S, eds. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. http:
//www.cochrane-handbook.org. Updated March 2011. Accessed November 10, 2014.
7. Viswanathan M, Berkman N. Development of the RTI item bank on risk of bias and precision of observational studies. J Clin Epidemiol. 2012;65:163-178.
8. Moher D, Liberati A, Tetzlaff J, et al; PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement [published online ahead of print July 23, 2009]. J Clin Epidemiol. 2009;62:1006-1012.
9. Berwick M, Armstrong B, Ben-Porat L. Sun exposure and mortality from melanoma. J Natl Cancer Inst. 2005;97:195-199.
10. Berwick M, Begg C, Fine J, et al. Screening for cutaneous melanoma by skin self-examination. J Natl Cancer Inst. 1996;88:17-23.
11. Aitken J, Elwood J, Lowe J, et al. A randomised trial of population screening for melanoma. J Med Screen. 2002;9:33-37.
12. Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
13. Expert Health Data Programming Inc. Health data software and health statistics. Available from: http: //www.ehdp.com. Accessed April 1, 2001. Cited by: Schneider J, Moore D, Mendelsohn M. Screening program reduced melanoma mortality at the Lawrence Livermore National Laboratory, 1984 to 1996. J Am Acad Dermatol. 2008;58:741-749.
14. Aitken J, Elwood M, Baade P, et al. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int J Cancer. 2010;126:450-458.
15. Katalinic A, Waldmann A, Weinstock M, et al. Does skin cancer screening save lives? an observational study comparing trends in melanoma mortality in regions with and without screening. Cancer. 2012;118:5395-5402.
16. Aitken J, Janda M, Elwood M, et al. Clinical outcomes from skin screening clinics within a community-based melanoma screening program. J Am Acad Dermatol. 2006;54:105-114.
17. Coory M, Baade P, Aitken JF, et al. Trends for in-situ and invasive melanoma in Queensland, Australia, 1982 to 2002. Cancer Causes Control. 2006;17:21-27.
18. Mayer JE, Swetter SM, Fu T, et al. Screening, early detection, education, and trends for melanoma: current status (2007-2013) and future directions: part II. screening, education, and future directions. J Am Acad Dermatol. 2014;71:611.e1-611.e10; quiz, 621-622.
19. Curiel-Lewandrowski C, Chen S, Swetter S, et al. Screening and prevention measures for melanoma: is there a survival advantage? Curr Oncol Rep. 2012;14:458-467.
20. Terushkin V, Halpern A. Melanoma early detection. Hematol Oncol Clin North Am. 2009;23:481-500.
21. Geller A, Greinert R, Sinclair C, et al. A nationwide population-based skin cancer screening in Germany: proceedings of the first meeting of the International Task Force on Skin Cancer Screening and Prevention (September 24 and 25, 2009) [published online ahead of print April 8, 2010]. Cancer Epidemiol. 2010;34:355-358.
22. Kornek T, Schafer I, Reusch M, et al. Routine skin cancer screening in Germany: four years of experience from the dermatologists’ perspective. Dermatology. 2012;225:289-293.
23. De Giorgi V, Grazzini M, Rossari S, et al. Is skin self-examination for cutaneous melanoma detection still adequate? a retrospective study. Dermatology. 2012;225:31-36.
24. Swetter S, Johnson T, Miller D, et al. Melanoma in middle-aged and older men: a multi-institutional survey study of factors related to tumor thickness. Arch Dermatol. 2009;145:397-404.
25. Kantor J, Kantor D. Routine dermatologist-performed full-body skin examination and early melanoma detection. Arch Dermatol. 2009;145:873-876.
26. Kovalyshyn I, Dusza S, Siamas K, et al. The impact of physician screening on melanoma detection. Arch Dermatol. 2011;147:1269-1275.
27. Pollitt R, Clarke C, Shema S, et al. California Medicaid enrollment and melanoma stage at diagnosis: a population-based study. Am J Prev Med. 2008;35:7-13.
28. Roetzheim R, Lee J, Ferrante J, et al. The influence of dermatologist and primary care physician visits on melanoma outcomes among Medicare beneficiaries. J Am Board Fam Med. 2013;26:637-647.
29. Durbec F, Vitry F, Granel-Brocard F, et al. The role of circumstances of diagnosis and access to dermatological care in early diagnosis of cutaneous melanoma: a population-based study in France. Arch Dermatol. 2010;146:240-246.
30. Lakhani N, Saraiya M, Thompson T, et al. Total body skin examination for skin cancer screening among U.S. adults from 2000 to 2010. Prev Med. 2014;61:75-80.
31. Oliveria SA, Heneghan MK, Cushman LF, et al. Skin cancer screening by dermatologists, family practitioners, and internists: barriers and facilitating factors. Arch Dermatol. 2011;147:39-44.
32. Bigby M. Why the evidence for skin cancer screening is insufficient: lessons from prostate cancer screening. Arch Dermatol. 2010;146:322-324.
Practice Points
- Current guidelines regarding melanoma screening are inconsistent.
- There is a growing pool of evidence supporting screening to improve melanoma outcomes.

Individualized Melanoma Care
Melanoma has become more diverse in terms of the patients affected and the treatment course. Dr. Lorraine L. Rosamilia discusses individualized melanoma care from the early stages of diagnosis through treatment and follow-up. She explains clear margins from excisions and management based on tumor thickness. Coordinated care also is important to evaluate the best treatment course for the patient and favorable outcomes.
Melanoma has become more diverse in terms of the patients affected and the treatment course. Dr. Lorraine L. Rosamilia discusses individualized melanoma care from the early stages of diagnosis through treatment and follow-up. She explains clear margins from excisions and management based on tumor thickness. Coordinated care also is important to evaluate the best treatment course for the patient and favorable outcomes.
Melanoma has become more diverse in terms of the patients affected and the treatment course. Dr. Lorraine L. Rosamilia discusses individualized melanoma care from the early stages of diagnosis through treatment and follow-up. She explains clear margins from excisions and management based on tumor thickness. Coordinated care also is important to evaluate the best treatment course for the patient and favorable outcomes.

Individualizing Care for Melanoma Patients
What does your patient need to know at the first visit?
Melanoma patient visits and communications are complicated. When possible, you can preview the surgical and prognostic expectations with the patient when you see the lesion clinically for the first time, especially for a lesion that you’re sure is melanoma before it even hits the specimen cup. Sometimes you have to convey important biopsy and treatment information over the telephone, or sometimes you have the luxury of an extra clinic visit to discuss it with the patient and perhaps a family member in person.
During the first set of conversations, I explain the things that are tangible: the depth of the lesion, the relationship it has to prognosis, surgical options based on staging, further testing/referrals, and known risk factors. Then I wait. The digestion phase is critical before you hang up and schedule a surgery.
Probably the most important thing I tell patients is that melanoma is unpredictable. Not everyone has the same kind of “surgery,” we don’t say “remission,” we don’t have a certain “chemo” that we know will be best, and not everyone will need “CAT scans.” I tell patients that they’re stuck with me. Skin examinations, talk of sun protection, photography of nevi, upkeep of health maintenance visits with other specialists (eg, primary care physician, optometry/ophthalmology, gynecology, dentistry), and education of family members on melanoma risk factors will be the norm.
What are your go-to treatments?
In the past, surgical management was perhaps streamlined, but as we learn more about melanoma tumor biology, the less we can form generalizable guidelines for surgery, margin control, and lymph node perusal. Wide local excision is paramount, but the evidence that guidelines for 0.5-cm, 1-cm, and 2-cm margins or greater fit for all types of tumors is lacking, and many have challenged the recommended margins, particularly for lentigo maligna subtypes (Kunishige et al).
The 0.75-mm Breslow depth threshold guides my sentinel lymph node (SLN) discussion, with upstaging based on primary tumor mitotic index and/or ulceration. But SLN biopsy is always still a discussion and not a foregone conclusion because the risk-benefit ratio and prognostic/survival data are very difficult to dissect for some cases. Certainly, mention of SLN biopsy morbidity, including lymphedema, is warranted before the patient consents. Then there is further explanation that more invasive lymphadenectomy could occur based on SLN findings. If applicable in advanced cases, options for imaging and adjuvant therapy are introduced by us but then primarily led by oncologists.
Patients are generally pleased that the approach to melanoma surgery, reconstruction, SLN biopsy, and oncologic care is increasingly becoming (almost) harmoniously multidisciplinary. Larger institutions have streamlined their melanoma providers into shared clinics or at least regional networks—dermatologists, plastic/otolaryngology/oncologic surgeons, oncologists, and radiation oncologists, for instance—and simplified patient access based on individual tumor treatment plans. Dr. Christopher J. Miller at Penn Medicine (Philadelphia, Pennsylvania) is excelling at a collaborative surgical approach for melanoma between dermatologic surgery and specialties such as otolaryngology and also spearheading the Mohs micrographic surgery approach for primary melanoma as possible standard of care for some cases (Etzkorn et al).
Also evolving is the access to clinical trials and care coordination regarding the most novel metastatic melanoma therapies, which can now be a short drive away for most patients as the National Cancer Institute broadens its clinical trial reach.
After the diagnosis of melanoma is made, care is becoming much more individualized for surgery and beyond, but true morbidity and mortality benefit for the more complicated regimens has become anybody’s guess as this research field grossly and rapidly swells. Then these discussions with the patient become longer and more open-ended.
How do you keep patients compliant with treatment?
Initial surgery and multidisciplinary management requires meticulous communication between providers to ensure that pathology reports, surgical findings, imaging, wound care, and follow-up are transparent. The easier it is for patients to navigate the medical system(s), the more likely they are to comply. Voicemail, e-mails, text messages, and/or mailings are standard for different offices for reminders, but an old-fashioned telephone call goes a long way for a patient who has melanoma on his/her mind. Adherence to sun protection, health maintenance, and skin examination appointments is then the challenge.
Sun protection strategies were well-represented in the Cutis July issue’s Practical Pearls featuring Dr. Vincent A. DeLeo. My script for sunscreen-averse patients as I leave the room is “Take a mosey through the sunscreen aisle. You may be surprised at what you find.” And sporting goods stores are chock full of UPF (UV protection factor) clothing options. I’m not a scolder, but I do utilize the power of repetition/the squeaky wheel.
Patient delay or cancellation of skin checks requires other types of surveillance. Here at Geisinger Health System (State College, Pennsylvania), when melanoma patients check out, they are placed in a “priority appointment” slot, meaning that if they cancel, their names are automatically put on an electronic list that is compiled weekly by our schedulers to ensure that patients are called for another appointment. To avert telephone tag and delay of care, melanoma patients also get our direct nurses station extension and are encouraged to use our chart e-mail system to communicate with us if they notice a new or changing skin lesion.
What do you do if they refuse treatment?
Initial consent and compliance with melanoma wide local excision are rarely challenged by a well-informed patient, but what I find more common is delay in treatment and nonadherence to periodic skin examinations.
What resources do you recommend to patients for more information?
The National Comprehensive Cancer Network clini-cal practice guideline resource in oncology (melanoma) is the place to start, as their Web site is easily naviga-ble for patients and providers (http://www.nccn.org).
The American Academy of Dermatology (http://www.aad.org) and Skin Cancer Foundation (http://www.skincancer.org) Web sites also provide useful information, and there are always copies of their key melanoma and nevi surveillance pamphlets in our office.
Most recently, my melanoma patients have been inspired by another local patient and her cause: a 28-year-old woman with metastatic melanoma on a National Cancer Institute BRAF inhibitor clinical trial who plans to run an Ironman race this year (Thomason, Ames). Her motivation to maintain her baseline health and fitness while still reaching for this further remarkable goal gives fellow melanoma patients a source for enthusiasm and hope.
Inspiration and adherence come in all shapes and sizes for patients with melanoma. I find you need to throw multiple resources and strategies at them and see what sticks.
Suggested Readings
Ames C. Local runner fights cancer. WeAreCentralPA Web site. http://www.wearecentralpa.com/news/local-runner-fights -cancer#.VZw92-pJ2AU.mailto. Published June 30, 2015. Accessed August 14, 2015.
DeLeo VA. Patient compliance with photoprotection. Cutis. 2015;96:13-14.
Etzkorn JR, Sobanko JF, Elenitsas R, et al. Low recurrence rates for in situ and invasive melanomas using Mohs micrographic surgery with melanoma antigen recognized by T cells 1 (MART-1) immunostaining: tissue processing methodology to optimize pathologic staging and margin assessment. J Am Acad Dermatol. 2015;72:840-850.
Kunishige JH, Brodland DG, Zitelli JA. Larger surgical margins are required for lentigo maligna and other melanoma in situ. J Am Acad Dermatol. 2012;67:1069-1071.
NCCN clinical practice guidelines in oncology: melanoma. National Comprehensive Cancer Network Web site. http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf. Updated March 11, 2015. Accessed August 14, 2015.
Thomason M. My story: April Salinas. Live In Our Skinz! Blog. http://blog.uvskinz.com/2015/01/30/my-story-april -salinas/#sthash.yvSRVglT.YGLDn95T.dpbs. Published January 30, 2015. Accessed August 14, 2015.
What does your patient need to know at the first visit?
Melanoma patient visits and communications are complicated. When possible, you can preview the surgical and prognostic expectations with the patient when you see the lesion clinically for the first time, especially for a lesion that you’re sure is melanoma before it even hits the specimen cup. Sometimes you have to convey important biopsy and treatment information over the telephone, or sometimes you have the luxury of an extra clinic visit to discuss it with the patient and perhaps a family member in person.
During the first set of conversations, I explain the things that are tangible: the depth of the lesion, the relationship it has to prognosis, surgical options based on staging, further testing/referrals, and known risk factors. Then I wait. The digestion phase is critical before you hang up and schedule a surgery.
Probably the most important thing I tell patients is that melanoma is unpredictable. Not everyone has the same kind of “surgery,” we don’t say “remission,” we don’t have a certain “chemo” that we know will be best, and not everyone will need “CAT scans.” I tell patients that they’re stuck with me. Skin examinations, talk of sun protection, photography of nevi, upkeep of health maintenance visits with other specialists (eg, primary care physician, optometry/ophthalmology, gynecology, dentistry), and education of family members on melanoma risk factors will be the norm.
What are your go-to treatments?
In the past, surgical management was perhaps streamlined, but as we learn more about melanoma tumor biology, the less we can form generalizable guidelines for surgery, margin control, and lymph node perusal. Wide local excision is paramount, but the evidence that guidelines for 0.5-cm, 1-cm, and 2-cm margins or greater fit for all types of tumors is lacking, and many have challenged the recommended margins, particularly for lentigo maligna subtypes (Kunishige et al).
The 0.75-mm Breslow depth threshold guides my sentinel lymph node (SLN) discussion, with upstaging based on primary tumor mitotic index and/or ulceration. But SLN biopsy is always still a discussion and not a foregone conclusion because the risk-benefit ratio and prognostic/survival data are very difficult to dissect for some cases. Certainly, mention of SLN biopsy morbidity, including lymphedema, is warranted before the patient consents. Then there is further explanation that more invasive lymphadenectomy could occur based on SLN findings. If applicable in advanced cases, options for imaging and adjuvant therapy are introduced by us but then primarily led by oncologists.
Patients are generally pleased that the approach to melanoma surgery, reconstruction, SLN biopsy, and oncologic care is increasingly becoming (almost) harmoniously multidisciplinary. Larger institutions have streamlined their melanoma providers into shared clinics or at least regional networks—dermatologists, plastic/otolaryngology/oncologic surgeons, oncologists, and radiation oncologists, for instance—and simplified patient access based on individual tumor treatment plans. Dr. Christopher J. Miller at Penn Medicine (Philadelphia, Pennsylvania) is excelling at a collaborative surgical approach for melanoma between dermatologic surgery and specialties such as otolaryngology and also spearheading the Mohs micrographic surgery approach for primary melanoma as possible standard of care for some cases (Etzkorn et al).
Also evolving is the access to clinical trials and care coordination regarding the most novel metastatic melanoma therapies, which can now be a short drive away for most patients as the National Cancer Institute broadens its clinical trial reach.
After the diagnosis of melanoma is made, care is becoming much more individualized for surgery and beyond, but true morbidity and mortality benefit for the more complicated regimens has become anybody’s guess as this research field grossly and rapidly swells. Then these discussions with the patient become longer and more open-ended.
How do you keep patients compliant with treatment?
Initial surgery and multidisciplinary management requires meticulous communication between providers to ensure that pathology reports, surgical findings, imaging, wound care, and follow-up are transparent. The easier it is for patients to navigate the medical system(s), the more likely they are to comply. Voicemail, e-mails, text messages, and/or mailings are standard for different offices for reminders, but an old-fashioned telephone call goes a long way for a patient who has melanoma on his/her mind. Adherence to sun protection, health maintenance, and skin examination appointments is then the challenge.
Sun protection strategies were well-represented in the Cutis July issue’s Practical Pearls featuring Dr. Vincent A. DeLeo. My script for sunscreen-averse patients as I leave the room is “Take a mosey through the sunscreen aisle. You may be surprised at what you find.” And sporting goods stores are chock full of UPF (UV protection factor) clothing options. I’m not a scolder, but I do utilize the power of repetition/the squeaky wheel.
Patient delay or cancellation of skin checks requires other types of surveillance. Here at Geisinger Health System (State College, Pennsylvania), when melanoma patients check out, they are placed in a “priority appointment” slot, meaning that if they cancel, their names are automatically put on an electronic list that is compiled weekly by our schedulers to ensure that patients are called for another appointment. To avert telephone tag and delay of care, melanoma patients also get our direct nurses station extension and are encouraged to use our chart e-mail system to communicate with us if they notice a new or changing skin lesion.
What do you do if they refuse treatment?
Initial consent and compliance with melanoma wide local excision are rarely challenged by a well-informed patient, but what I find more common is delay in treatment and nonadherence to periodic skin examinations.
What resources do you recommend to patients for more information?
The National Comprehensive Cancer Network clini-cal practice guideline resource in oncology (melanoma) is the place to start, as their Web site is easily naviga-ble for patients and providers (http://www.nccn.org).
The American Academy of Dermatology (http://www.aad.org) and Skin Cancer Foundation (http://www.skincancer.org) Web sites also provide useful information, and there are always copies of their key melanoma and nevi surveillance pamphlets in our office.
Most recently, my melanoma patients have been inspired by another local patient and her cause: a 28-year-old woman with metastatic melanoma on a National Cancer Institute BRAF inhibitor clinical trial who plans to run an Ironman race this year (Thomason, Ames). Her motivation to maintain her baseline health and fitness while still reaching for this further remarkable goal gives fellow melanoma patients a source for enthusiasm and hope.
Inspiration and adherence come in all shapes and sizes for patients with melanoma. I find you need to throw multiple resources and strategies at them and see what sticks.
What does your patient need to know at the first visit?
Melanoma patient visits and communications are complicated. When possible, you can preview the surgical and prognostic expectations with the patient when you see the lesion clinically for the first time, especially for a lesion that you’re sure is melanoma before it even hits the specimen cup. Sometimes you have to convey important biopsy and treatment information over the telephone, or sometimes you have the luxury of an extra clinic visit to discuss it with the patient and perhaps a family member in person.
During the first set of conversations, I explain the things that are tangible: the depth of the lesion, the relationship it has to prognosis, surgical options based on staging, further testing/referrals, and known risk factors. Then I wait. The digestion phase is critical before you hang up and schedule a surgery.
Probably the most important thing I tell patients is that melanoma is unpredictable. Not everyone has the same kind of “surgery,” we don’t say “remission,” we don’t have a certain “chemo” that we know will be best, and not everyone will need “CAT scans.” I tell patients that they’re stuck with me. Skin examinations, talk of sun protection, photography of nevi, upkeep of health maintenance visits with other specialists (eg, primary care physician, optometry/ophthalmology, gynecology, dentistry), and education of family members on melanoma risk factors will be the norm.
What are your go-to treatments?
In the past, surgical management was perhaps streamlined, but as we learn more about melanoma tumor biology, the less we can form generalizable guidelines for surgery, margin control, and lymph node perusal. Wide local excision is paramount, but the evidence that guidelines for 0.5-cm, 1-cm, and 2-cm margins or greater fit for all types of tumors is lacking, and many have challenged the recommended margins, particularly for lentigo maligna subtypes (Kunishige et al).
The 0.75-mm Breslow depth threshold guides my sentinel lymph node (SLN) discussion, with upstaging based on primary tumor mitotic index and/or ulceration. But SLN biopsy is always still a discussion and not a foregone conclusion because the risk-benefit ratio and prognostic/survival data are very difficult to dissect for some cases. Certainly, mention of SLN biopsy morbidity, including lymphedema, is warranted before the patient consents. Then there is further explanation that more invasive lymphadenectomy could occur based on SLN findings. If applicable in advanced cases, options for imaging and adjuvant therapy are introduced by us but then primarily led by oncologists.
Patients are generally pleased that the approach to melanoma surgery, reconstruction, SLN biopsy, and oncologic care is increasingly becoming (almost) harmoniously multidisciplinary. Larger institutions have streamlined their melanoma providers into shared clinics or at least regional networks—dermatologists, plastic/otolaryngology/oncologic surgeons, oncologists, and radiation oncologists, for instance—and simplified patient access based on individual tumor treatment plans. Dr. Christopher J. Miller at Penn Medicine (Philadelphia, Pennsylvania) is excelling at a collaborative surgical approach for melanoma between dermatologic surgery and specialties such as otolaryngology and also spearheading the Mohs micrographic surgery approach for primary melanoma as possible standard of care for some cases (Etzkorn et al).
Also evolving is the access to clinical trials and care coordination regarding the most novel metastatic melanoma therapies, which can now be a short drive away for most patients as the National Cancer Institute broadens its clinical trial reach.
After the diagnosis of melanoma is made, care is becoming much more individualized for surgery and beyond, but true morbidity and mortality benefit for the more complicated regimens has become anybody’s guess as this research field grossly and rapidly swells. Then these discussions with the patient become longer and more open-ended.
How do you keep patients compliant with treatment?
Initial surgery and multidisciplinary management requires meticulous communication between providers to ensure that pathology reports, surgical findings, imaging, wound care, and follow-up are transparent. The easier it is for patients to navigate the medical system(s), the more likely they are to comply. Voicemail, e-mails, text messages, and/or mailings are standard for different offices for reminders, but an old-fashioned telephone call goes a long way for a patient who has melanoma on his/her mind. Adherence to sun protection, health maintenance, and skin examination appointments is then the challenge.
Sun protection strategies were well-represented in the Cutis July issue’s Practical Pearls featuring Dr. Vincent A. DeLeo. My script for sunscreen-averse patients as I leave the room is “Take a mosey through the sunscreen aisle. You may be surprised at what you find.” And sporting goods stores are chock full of UPF (UV protection factor) clothing options. I’m not a scolder, but I do utilize the power of repetition/the squeaky wheel.
Patient delay or cancellation of skin checks requires other types of surveillance. Here at Geisinger Health System (State College, Pennsylvania), when melanoma patients check out, they are placed in a “priority appointment” slot, meaning that if they cancel, their names are automatically put on an electronic list that is compiled weekly by our schedulers to ensure that patients are called for another appointment. To avert telephone tag and delay of care, melanoma patients also get our direct nurses station extension and are encouraged to use our chart e-mail system to communicate with us if they notice a new or changing skin lesion.
What do you do if they refuse treatment?
Initial consent and compliance with melanoma wide local excision are rarely challenged by a well-informed patient, but what I find more common is delay in treatment and nonadherence to periodic skin examinations.
What resources do you recommend to patients for more information?
The National Comprehensive Cancer Network clini-cal practice guideline resource in oncology (melanoma) is the place to start, as their Web site is easily naviga-ble for patients and providers (http://www.nccn.org).
The American Academy of Dermatology (http://www.aad.org) and Skin Cancer Foundation (http://www.skincancer.org) Web sites also provide useful information, and there are always copies of their key melanoma and nevi surveillance pamphlets in our office.
Most recently, my melanoma patients have been inspired by another local patient and her cause: a 28-year-old woman with metastatic melanoma on a National Cancer Institute BRAF inhibitor clinical trial who plans to run an Ironman race this year (Thomason, Ames). Her motivation to maintain her baseline health and fitness while still reaching for this further remarkable goal gives fellow melanoma patients a source for enthusiasm and hope.
Inspiration and adherence come in all shapes and sizes for patients with melanoma. I find you need to throw multiple resources and strategies at them and see what sticks.
Suggested Readings
Ames C. Local runner fights cancer. WeAreCentralPA Web site. http://www.wearecentralpa.com/news/local-runner-fights -cancer#.VZw92-pJ2AU.mailto. Published June 30, 2015. Accessed August 14, 2015.
DeLeo VA. Patient compliance with photoprotection. Cutis. 2015;96:13-14.
Etzkorn JR, Sobanko JF, Elenitsas R, et al. Low recurrence rates for in situ and invasive melanomas using Mohs micrographic surgery with melanoma antigen recognized by T cells 1 (MART-1) immunostaining: tissue processing methodology to optimize pathologic staging and margin assessment. J Am Acad Dermatol. 2015;72:840-850.
Kunishige JH, Brodland DG, Zitelli JA. Larger surgical margins are required for lentigo maligna and other melanoma in situ. J Am Acad Dermatol. 2012;67:1069-1071.
NCCN clinical practice guidelines in oncology: melanoma. National Comprehensive Cancer Network Web site. http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf. Updated March 11, 2015. Accessed August 14, 2015.
Thomason M. My story: April Salinas. Live In Our Skinz! Blog. http://blog.uvskinz.com/2015/01/30/my-story-april -salinas/#sthash.yvSRVglT.YGLDn95T.dpbs. Published January 30, 2015. Accessed August 14, 2015.
Suggested Readings
Ames C. Local runner fights cancer. WeAreCentralPA Web site. http://www.wearecentralpa.com/news/local-runner-fights -cancer#.VZw92-pJ2AU.mailto. Published June 30, 2015. Accessed August 14, 2015.
DeLeo VA. Patient compliance with photoprotection. Cutis. 2015;96:13-14.
Etzkorn JR, Sobanko JF, Elenitsas R, et al. Low recurrence rates for in situ and invasive melanomas using Mohs micrographic surgery with melanoma antigen recognized by T cells 1 (MART-1) immunostaining: tissue processing methodology to optimize pathologic staging and margin assessment. J Am Acad Dermatol. 2015;72:840-850.
Kunishige JH, Brodland DG, Zitelli JA. Larger surgical margins are required for lentigo maligna and other melanoma in situ. J Am Acad Dermatol. 2012;67:1069-1071.
NCCN clinical practice guidelines in oncology: melanoma. National Comprehensive Cancer Network Web site. http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf. Updated March 11, 2015. Accessed August 14, 2015.
Thomason M. My story: April Salinas. Live In Our Skinz! Blog. http://blog.uvskinz.com/2015/01/30/my-story-april -salinas/#sthash.yvSRVglT.YGLDn95T.dpbs. Published January 30, 2015. Accessed August 14, 2015.

GM-CSF did not increase survival in high-risk melanoma
Neither adjuvant granulocyte macrophage colony-stimulating factor (GM-CSF) nor a peptide vaccination (PV) significantly improved relapse-free or overall survival in patients with high-risk stage III and IV melanoma who had already undergone surgical resection, according to a study published online Sept. 8 in the Journal of Clinical Oncology.
Findings from early clinical trials support the possible benefit of GM-CSF as adjuvant therapy for melanoma, said the authors, led by Dr. David H. Lawson of Winship Cancer Institute, Emory University, Atlanta. Some studies have also shown that combining cytokines, including GM-CSF, with melanoma vaccines yields augmented immunologic responses and clinically significant tumor responses.
However, the improvement in survival in the current study did not reach statistical significance. The median survival for patients who received GM-CSF was 69.6 months, compared to 59.3 months for the patients who received placebo. This represented a 17.4% improvement in patients who received GM-CSF, but it was less than the projected absolute increase of 13.3 months and the relative improvement of 33% required for significance (HR, 0.94; 95% repeated CI, 0.77 to 1.15; stratified log-rank P =.528).
The results for relapse-free survival also did not reach statistical significance. For patients treated with GM-CSF it was 11.4 months (95% CI,9.4 to 14.8 months) compared to 8.8 month in the placebo group (95% CI, 7.5 to 11.2 months), which was an increase of 2.6 months, or 30% (HR, 0.88; 95% CI,0.74 to 1.04; stratified log-rank P = .131).
Just over half of the cohort (53.3%) were HLA-A2–positive patients. This group was randomized to receive PV alone or with GM-CSF, or placebo. The median overall survival was 68.6 months (95% CI, 47.0 to 92.3 months) in patients who received PV and 63.3 months (95% CI,49.2 to 105.0 months) for those who received placebo (HR, 0.93; 95% CI0.71 to1.21; P = .598)
Also in this subgroup, the median relapse-free survival was only 1.7 months longer in patients who received PV than for those who got placebo (11.5 v 9.8 months, for a 17.3% improvement). This was also lower than what was expected (3 months; 33% improvement), and also did not reach statistical significance.
Even though this study did not support their hypotheses, “trials that test GM-CSF in patients with resected visceral melanoma metastases are worthy of consideration,” wrote the authors. “GM-CSF may find its greatest use in melanoma in combination with other agents” (J Clin Oncol. 2015 Sep 8. doi:10.1200/JCO.2015.62.0500).
The study was supported by grants from the Public Health Service, National Institutes of Health, and the National Cancer Institute. Several of the coauthors report financial relationships with industry.
Neither adjuvant granulocyte macrophage colony-stimulating factor (GM-CSF) nor a peptide vaccination (PV) significantly improved relapse-free or overall survival in patients with high-risk stage III and IV melanoma who had already undergone surgical resection, according to a study published online Sept. 8 in the Journal of Clinical Oncology.
Findings from early clinical trials support the possible benefit of GM-CSF as adjuvant therapy for melanoma, said the authors, led by Dr. David H. Lawson of Winship Cancer Institute, Emory University, Atlanta. Some studies have also shown that combining cytokines, including GM-CSF, with melanoma vaccines yields augmented immunologic responses and clinically significant tumor responses.
However, the improvement in survival in the current study did not reach statistical significance. The median survival for patients who received GM-CSF was 69.6 months, compared to 59.3 months for the patients who received placebo. This represented a 17.4% improvement in patients who received GM-CSF, but it was less than the projected absolute increase of 13.3 months and the relative improvement of 33% required for significance (HR, 0.94; 95% repeated CI, 0.77 to 1.15; stratified log-rank P =.528).
The results for relapse-free survival also did not reach statistical significance. For patients treated with GM-CSF it was 11.4 months (95% CI,9.4 to 14.8 months) compared to 8.8 month in the placebo group (95% CI, 7.5 to 11.2 months), which was an increase of 2.6 months, or 30% (HR, 0.88; 95% CI,0.74 to 1.04; stratified log-rank P = .131).
Just over half of the cohort (53.3%) were HLA-A2–positive patients. This group was randomized to receive PV alone or with GM-CSF, or placebo. The median overall survival was 68.6 months (95% CI, 47.0 to 92.3 months) in patients who received PV and 63.3 months (95% CI,49.2 to 105.0 months) for those who received placebo (HR, 0.93; 95% CI0.71 to1.21; P = .598)
Also in this subgroup, the median relapse-free survival was only 1.7 months longer in patients who received PV than for those who got placebo (11.5 v 9.8 months, for a 17.3% improvement). This was also lower than what was expected (3 months; 33% improvement), and also did not reach statistical significance.
Even though this study did not support their hypotheses, “trials that test GM-CSF in patients with resected visceral melanoma metastases are worthy of consideration,” wrote the authors. “GM-CSF may find its greatest use in melanoma in combination with other agents” (J Clin Oncol. 2015 Sep 8. doi:10.1200/JCO.2015.62.0500).
The study was supported by grants from the Public Health Service, National Institutes of Health, and the National Cancer Institute. Several of the coauthors report financial relationships with industry.
Neither adjuvant granulocyte macrophage colony-stimulating factor (GM-CSF) nor a peptide vaccination (PV) significantly improved relapse-free or overall survival in patients with high-risk stage III and IV melanoma who had already undergone surgical resection, according to a study published online Sept. 8 in the Journal of Clinical Oncology.
Findings from early clinical trials support the possible benefit of GM-CSF as adjuvant therapy for melanoma, said the authors, led by Dr. David H. Lawson of Winship Cancer Institute, Emory University, Atlanta. Some studies have also shown that combining cytokines, including GM-CSF, with melanoma vaccines yields augmented immunologic responses and clinically significant tumor responses.
However, the improvement in survival in the current study did not reach statistical significance. The median survival for patients who received GM-CSF was 69.6 months, compared to 59.3 months for the patients who received placebo. This represented a 17.4% improvement in patients who received GM-CSF, but it was less than the projected absolute increase of 13.3 months and the relative improvement of 33% required for significance (HR, 0.94; 95% repeated CI, 0.77 to 1.15; stratified log-rank P =.528).
The results for relapse-free survival also did not reach statistical significance. For patients treated with GM-CSF it was 11.4 months (95% CI,9.4 to 14.8 months) compared to 8.8 month in the placebo group (95% CI, 7.5 to 11.2 months), which was an increase of 2.6 months, or 30% (HR, 0.88; 95% CI,0.74 to 1.04; stratified log-rank P = .131).
Just over half of the cohort (53.3%) were HLA-A2–positive patients. This group was randomized to receive PV alone or with GM-CSF, or placebo. The median overall survival was 68.6 months (95% CI, 47.0 to 92.3 months) in patients who received PV and 63.3 months (95% CI,49.2 to 105.0 months) for those who received placebo (HR, 0.93; 95% CI0.71 to1.21; P = .598)
Also in this subgroup, the median relapse-free survival was only 1.7 months longer in patients who received PV than for those who got placebo (11.5 v 9.8 months, for a 17.3% improvement). This was also lower than what was expected (3 months; 33% improvement), and also did not reach statistical significance.
Even though this study did not support their hypotheses, “trials that test GM-CSF in patients with resected visceral melanoma metastases are worthy of consideration,” wrote the authors. “GM-CSF may find its greatest use in melanoma in combination with other agents” (J Clin Oncol. 2015 Sep 8. doi:10.1200/JCO.2015.62.0500).
The study was supported by grants from the Public Health Service, National Institutes of Health, and the National Cancer Institute. Several of the coauthors report financial relationships with industry.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Adjuvant granulocyte macrophage colony-stimulating factor and peptide vaccination did not significantly improve relapse-free or overall survival in patients with high-risk resected melanoma.
Major finding: The median overall survival with GM-CSF versus placebo treatments was 69.6 months versus 59.3 months, and relapse-free survival was 11.4 months versus 8.8 months.
Data source: A study of 815 patients with high-risk resected melanoma who were randomly assigned to receive GM-CSF, PV, both, or placebo.
Disclosures: The study was supported by grants from the Public Health Service, National Institutes of Health, and the National Cancer Institute. Several of the coauthors report financial relationships with industry.
Melanoma regression a positive prognostic indicator
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”

|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”
|
|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
The finding that patients with histologic regression have half the risk for micrometastases in sentinel lymph node biopsy, compared with patients without regression gives a clear answer to the question of whether patients with thin melanoma and regression should undergo SLNB, and that answer is “No.”
|
|
Dr. Claus Garbe |
These findings underline that fact that prognosis of patients with melanoma does not depend only on the characteristics of the tumor itself, such as tumor thickness, ulceration, and mitosis, but also on the immune response of the host.
Dr. Claus Garbe is from the Department of Dermatology, University Hospital Tübingen (Germany). These comments are taken from an accompanying editorial (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235). No conflicts of interest were declared.
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity and may serve as a prognostic factor when deciding whether to perform a sentinel lymph node biopsy, according to a study published online Sept. 2 in JAMA Dermatology.
Researchers conducted a meta-analysis of 14 studies in 10,098 patients who showed histologic regression of a primary melanoma and whose sentinel lymph node status was available. In the 14 studies combined, the analysis showed patients with histologic regression had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression, reported Dr. Simone Ribero of the University of Turin (Italy), and coauthors (JAMA Dermatol. 2015 Sep 2. doi: 10.1001/jamadermatol.2015.2235).
This figure was even lower for patients enrolled in high-quality studies, compared with lower-quality studies, they said. In the nine studies considered high quality, patients with regression had a 52% lower likelihood of having a positive sentinel lymph node, while those enrolled in the five studies considered low quality had a 27% lower likelihood of having a positive sentinel lymph node.
The prognostic significance of regression in primary melanoma has been confounded by the fact that disappearance of part of the tumor can result in an underestimation of the original Breslow thickness. Some previous studies have found an increase in sentinel lymph node positivity associated with regression, while other studies suggested that regression was in fact a protective factor against sentinel lymph node metastasis.
Although the studies used different definitions of histologic regression and all were observational (counted among the limitations of the studies), the authors concluded that regression was prognostically favorable. “The results of this meta-analysis may be useful when deciding to offer SLNB [sentinel lymph node biopsy] to patients with regressions of melanomas,” they wrote, adding: “It may help clinicians make a final selection of the most appropriate patients for this procedure.”
The authors had no conflicts of interest to declare.
FROM JAMA DERMATOLOGY
Key clinical point: Histologic regression in melanoma is associated with a significantly lower risk of sentinel lymph node positivity.
Major finding: Individuals with histologic regression in melanoma had a 44% lower likelihood of having a positive sentinel lymph node than patients without regression.
Data source: A meta-analysis evaluated 14 studies in 10,098 patients.
Disclosures: None of the authors had conflicts of interest to disclose.

Fewer moles linked with more aggressive melanoma
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.

In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.
In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
NEW YORK – Consistent with another recently published report but counterintuitive, patients with a high number of nevi prior to developing a melanoma have more favorable prognostic features than do those with fewer moles, according to data presented at the American Academy of Dermatology summer meeting.
Based on differences in numerous clinicopathologic features when patients with more than 50 nevi were compared with those with fewer than 50 nevi, “It is possible that there are different pathways that drive melanoma in these two patient groups, resulting in different degrees of aggressiveness,” reported Dr. Caroline Kim from the Pigmented Lesion Clinic and Cutaneous Oncology Program, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston.
In this study of 281 melanoma patients evaluated over 2 years at Dr. Kim’s clinic, those with a high nevi count (89 patients) were compared with those with a lower nevi count (192 patients). The investigators also performed comparisons on those who had dysplastic versus nondysplastic nevi. Of differences between the groups, the initial melanoma grade was the most surprising.
In the greater-than-50-nevi group, 21.6% had either stage III (18.2%) or stage IV (3.4%) disease at diagnosis vs. 40.2% in the fewer-than-50-nevi group (31.2% and 9.0% with stage III and IV disease, respectively). Conversely, melanoma was diagnosed at stage I in 71.6% in the greater-than-50-nevi group vs. only 41.8% in the fewer-than-50-nevi group.
Among patients in the fewer-than-50-nevi group, ulceration was more common (25.1% vs. 10.3%; P = .017) as was nodular subtype (11.2% vs. 2.9%; P = .035). The group with the lower nevi count also had a higher mitotic rate (3.7 vs. 2.3 count/mm2) and a greater Breslow’s depth (1.78 vs. 1.21 mm; P = .010). Although not significantly different, the proportion of females was higher in the lower nevi count group (56.2% vs. 46.4%) and more patients in this group developed a melanoma in the head or neck (21.6% vs. 15.3%).
There are several potential explanations for the differences observed in this study. One is that the process that drives a high nevi count is different than that which produces lower numbers of nevi. According to Dr. Kim, some of the pathologic features in the greater-than-50-nevi group were more consistent with BRAF mutation patterns than the fewer-than- 50-nevi group. Another is that a high nevi count drives a more robust immune response against melanoma growth. Dr. Kim cited published studies that support both theories.
However, it is also possible that high nevi count increases likelihood of dermatologic care and vigilance for early detection of melanomas. This might be supported by the fact that the age of diagnosis was significantly younger in the greater-than-50-nevi count group (40.1 vs. 50.1 years; P less than .001). However, a younger age at diagnosis could also be a product of different pathways of disease development and growth.
The greater likelihood of more aggressive melanoma in patients with a history of fewer than 50 nevi than in those with greater than 50 nevi has also been supported by another large series that was recently published (Int J Cancer. 2015 Oct 1;137[7]:1691-8.) Cited by Dr. Kim as consistent with her own findings, this study of 2,184 melanoma cases compared 5- and 10-year survival in those who had greater than 50 nevi, which represented 31.3% of this population, to those with fewer. The greater survival at 5 years in the greater-than-50-nevi group (91.2% vs. 86.4%) and 10 years (87.2% vs. 79%) remained significant after adjusting “for all known melanoma prognostic factors,” according to the authors.
Further studies evaluating differences in patterns of melanoma growth in those with fewer than 50 nevi vs. those with more are needed, according to Dr. Kim. She acknowledged that one limitation of her study was that all cases were drawn from a single center. However, there is support for an independent study, and the findings, if verified, “have major implications for public health screening and education.” In particular, she suggested that those with lower nevi counts might deserve the type of attention already being directed at those with high nevi counts “as they may be paradoxically at risk for more aggressive melanomas.”
Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.
This article was updated August 26, 2015.
AT THE AAD SUMMER ACADEMY 2015
Key clinical point: In patients with nevi who develop melanoma, malignancies appear to be more aggressive with a lower rather than a higher nevi count.
Major finding: Patients with fewer than 50 moles were more than twice as likely as patients with more than 50 moles to be diagnosed with stage III or IV disease.
Data source: Retrospective chart review.
Disclosures: Dr. Kim reported financial relationships with Hoffman-LaRoche, Castle Biosciences, and Shape Pharmaceuticals.

In skin lymphoma diagnosis, pathology must match clinical presentation
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.

Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.
Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
NEW YORK – Both dermatologists and pathologists can make the mistake of diagnosing a long list of pseudolymphomas as lymphomas, according to Dr. Antonio Subtil, who is an associate professor of dermatology and pathology at Yale University School of Medicine, New Haven, Connecticut.
The diagnosis is not trustworthy without agreement by a team of experts, he said. Most dermatologists do not have sufficient expertise in histopathology to interpret equivocal findings. Pathologists do not typically grasp subtleties in dermatologic presentations that may also be critical to reach an accurate diagnosis regardless of histopathology.
Mycosis fungoides (MF) represents almost 60% of cutaneous T-cell lymphomas (CTCL), but only a proportion of patients with MF have a classic presentation and the extensive array of other T-cell and B-cell lesions constitute a heterogeneous profile of lesions, according to Dr. Subtil, who spoke on skin lymphoma knowledge gaps at the summer meeting of the American Academy of Dermatology (AAD). The biases of the dermatologist and the pathologist in isolation can lead to misdiagnosis, which is the reason to insist on a clear correlation between pathologic and clinical findings.
Speaking as a dermatologist, Dr. Subtil cautioned that pathologists “do not understand our terminology” and are not facile in differentiating clinical descriptions of cutaneous lesions. Speaking as a pathologist, Dr. Subtil cautioned that “I cannot trust a pathological report by itself” without understanding the clinical context.
As an example, he recounted a case of an ulcerated nodule that proved to have a lymphoid infiltrate on biopsy. When cells in the infiltrate were found to be CD30+, the likely diagnosis appeared to be an anaplastic large cell lymphoma. Only further testing revealed molluscum contagiosum, which can have a similar appearance and also feature CD30+ cells. A course of unnecessary chemotherapy was narrowly averted.
A small sample of the pseudolymphomas that can fool the clinician include lymphomatoid drug eruption, cutaneous leishmaniasis, lymphomatoid lichenoid keratosis, and reactive lymphoid hyperplasia at the site of vaccination, according to Dr. Subtil. He outlined a series of challenges that should be recognized before settling on a diagnosis.
One of the most important of these challenges is the limited specificity and sensitivity of any clinical characteristic or diagnostic study in isolation, according to Dr. Subtil. Even tissue studies with polymerase chain reaction (PCR) are associated with false positive and false negative results and, like everything else, must be evaluated in the context of the pathological and clinical findings.
Another challenge to a definitive diagnosis is the overuse of the term “atypical” by both dermatologists and pathologists. Dr. Subtil called the propensity to use this label the “atypical syndrome” and cautioned that it may sometimes be an obstacle for seeking a more definitive description of the underlying pathology. Using a team approach, which Dr. Subtil suggested might also include a hematologist and an oncologist, to reach consensus about the diagnosis substantially reduces the risk of a misdiagnosis.
EXPERT ANALYSIS AT THE SUMMER MEETING OF THE AMERICAN ACADEMY OF DERMATOLOGY
