User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
FDA OKs emergency use of Pfizer COVID-19 vaccine
The much-anticipated emergency use authorization (EUA) of this vaccine — the first such approval in the United States — was greeted with optimism by infectious disease and pulmonary experts, although unanswered questions remain regarding use in people with allergic hypersensitivity, safety in pregnant women, and how smooth distribution will be.
“I am delighted. This is a first, firm step on a long path to getting this COVID pandemic under control,” William Schaffner, MD, professor of infectious diseases at the Vanderbilt University School of Medicine in Nashville, Tennessee, said in an interview.
The FDA gave the green light after the December 10 recommendation from the agency’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting. The committee voted 17-4 in favor of the emergency authorization.

The COVID-19 vaccine is “going to have a major impact here in the US. I’m very optimistic about it,” Dial Hewlett, MD, a spokesperson for the Infectious Diseases Society of American (IDSA), told this news organization.
Daniel Culver, DO, chair of medicine at the Cleveland Clinic in Ohio, is likewise hopeful. “My understanding is that supplies of the vaccine are already in place in hubs and will be shipped relatively quickly. The hope would be we can start vaccinating people as early as next week.”
Allergic reactions reported in the UK
After vaccinations with the Pfizer vaccine began in the UK on December 8, reports surfaced of two healthcare workers who experienced allergic reactions. They have since recovered, but officials warned that people with a history of severe allergic reactions should not receive the Pfizer vaccine at this time.
“For the moment, they are asking people who have had notable allergic reactions to step aside while this is investigated. It shows you that the system is working,” Schaffner said.
Both vaccine recipients who experienced anaphylaxis carried EpiPens, as they were at high risk for allergic reactions, Hewlett said. Also, if other COVID-19 vaccines are approved for use in the future, people allergic to the Pfizer vaccine might have another option, he added.
Reassuring role models
Schaffner supports the CDC Advisory Committee on Immunization Practices (ACIP) decision to start vaccinations with healthcare workers and residents of long-term care facilities.
“Vaccinating healthcare workers, in particular, will be a model for the general public,” said Schaffner, who is also a former member of the IDSA board of directors. “If they see those of us in white coats and blue scrubs lining up for the vaccine, that will provide confidence.”
To further increase acceptance of the COVID-19 vaccine, public health officials need to provide information and reassure the general public, Schaffner said.
Hewlett agreed. “I know there are a lot of people in the population who are very hesitant about vaccines. As infection disease specialists and people in public health, we are trying to allay a lot of concerns people have.”
Reassurance will be especially important in minority communities. “They have been disproportionately affected by the virus, and they have a traditional history of not being optimally vaccinated,” Schaffner said. “We need to reach them in particular with good information and reassurance…so they can make good decisions for themselves and their families.”
No vaccine is 100% effective or completely free of side effects. “There is always a chance there can be adverse reactions, but we think for the most part this is going to be a safe and effective vaccine,” said Hewlett, medical director at the Division of Disease Control and deputy to commissioner of health at the Westchester County Department of Health in White Plains, New York.
Distribution: Smooth or full of strife?
In addition to the concern that some people will not take advantage of vaccination against COVID-19, there could be vaccine supply issues down the road, Schaffner said.
Culver agreed. “In the early phases, I expect that there will be some kinks to work out, but because the numbers are relatively small, this should be okay,” he said.
“I think when we start to get into larger-scale vaccination programs — the supply chain, transport, and storage will be a Herculean undertaking,” Culver added. “It will take careful coordination between healthcare providers, distributors, suppliers, and public health officials to pull this off.”
Planning and distribution also should focus beyond US borders. Any issues in vaccine distribution or administration in the United States “will only be multiplied in several other parts of the world,” Culver said. Because COVID-19 is a pandemic, “we need to think about vaccinating globally.”
Investigating adverse events
Adverse events common to vaccinations in general — injection site pain, headaches, and fever — would not be unexpected with the COVID-19 vaccines. However, experts remain concerned that other, unrelated adverse events might be erroneously attributed to vaccination. For example, if a fall, heart attack, or death occurs within days of immunization, some might immediately blame the vaccine product.
“It’s important to remember that any new, highly touted medical therapy like this will receive a lot of scrutiny, so it would be unusual not to hear about something happening to somebody,” Culver said. Vaccine companies and health agencies will be carefully evaluating any reported adverse events to ensure no safety signal was missed in the trials.
“Fortunately, there are systems in place to investigate these events immediately,” Schaffner said.
Pregnancy recommendations pending
One question still looms: Is the COVID-19 vaccination safe for pregnant women? This isn’t just a question for the general public, either, Schaffner said. He estimated that about 70 percent of healthcare workers are women, and data suggests about 300,000 of these healthcare workers are pregnant.
“The CDC’s Advisory Committee on Immunization Practices will speak to that just as soon as the EUA is issued,” he added.
Patients are asking Culver about the priority order for vaccination. He said it’s difficult to provide firm guidance at this point.
People also have “lingering skepticism” about whether vaccine development was done in a prudent way, Culver said. Some people question whether the Pfizer vaccine and others were rushed to market. “So we try to spend time with the patients, reassuring them that all the usual safety evaluations were carefully done,” he said.
Another concern is whether mRNA vaccines can interact with human DNA. “The quick, short, and definitive answer is no,” Schaffner said. The m stands for messenger — the vaccines transmit information. "Once it gets into a cell, the mRNA does not go anywhere near the DNA, and once it transmits its information to the cell appropriately, it gets metabolized, and we excrete all the remnants."
Hewlett pointed out that investigations and surveillance will continue. Because this is an EUA and not full approval, “that essentially means they will still be obligated to collect a lot more data than they would ordinarily,” he said.
How long immunoprotection will last also remains an unknown. “The big question left on the table now is the durability,” Culver said. “Of course, we won’t know the answer to that for quite some time.”
Schaffner and Culver have disclosed no relevant financial relationships. Hewlett was an employee of Pfizer until mid-2019. His previous work as Pfizer’s senior medical director of global medical product evaluation was not associated with development of the COVID-19 vaccine.
This article first appeared on Medscape.com.
The much-anticipated emergency use authorization (EUA) of this vaccine — the first such approval in the United States — was greeted with optimism by infectious disease and pulmonary experts, although unanswered questions remain regarding use in people with allergic hypersensitivity, safety in pregnant women, and how smooth distribution will be.
“I am delighted. This is a first, firm step on a long path to getting this COVID pandemic under control,” William Schaffner, MD, professor of infectious diseases at the Vanderbilt University School of Medicine in Nashville, Tennessee, said in an interview.
The FDA gave the green light after the December 10 recommendation from the agency’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting. The committee voted 17-4 in favor of the emergency authorization.
The COVID-19 vaccine is “going to have a major impact here in the US. I’m very optimistic about it,” Dial Hewlett, MD, a spokesperson for the Infectious Diseases Society of American (IDSA), told this news organization.
Daniel Culver, DO, chair of medicine at the Cleveland Clinic in Ohio, is likewise hopeful. “My understanding is that supplies of the vaccine are already in place in hubs and will be shipped relatively quickly. The hope would be we can start vaccinating people as early as next week.”
Allergic reactions reported in the UK
After vaccinations with the Pfizer vaccine began in the UK on December 8, reports surfaced of two healthcare workers who experienced allergic reactions. They have since recovered, but officials warned that people with a history of severe allergic reactions should not receive the Pfizer vaccine at this time.
“For the moment, they are asking people who have had notable allergic reactions to step aside while this is investigated. It shows you that the system is working,” Schaffner said.
Both vaccine recipients who experienced anaphylaxis carried EpiPens, as they were at high risk for allergic reactions, Hewlett said. Also, if other COVID-19 vaccines are approved for use in the future, people allergic to the Pfizer vaccine might have another option, he added.
Reassuring role models
Schaffner supports the CDC Advisory Committee on Immunization Practices (ACIP) decision to start vaccinations with healthcare workers and residents of long-term care facilities.
“Vaccinating healthcare workers, in particular, will be a model for the general public,” said Schaffner, who is also a former member of the IDSA board of directors. “If they see those of us in white coats and blue scrubs lining up for the vaccine, that will provide confidence.”
To further increase acceptance of the COVID-19 vaccine, public health officials need to provide information and reassure the general public, Schaffner said.
Hewlett agreed. “I know there are a lot of people in the population who are very hesitant about vaccines. As infection disease specialists and people in public health, we are trying to allay a lot of concerns people have.”
Reassurance will be especially important in minority communities. “They have been disproportionately affected by the virus, and they have a traditional history of not being optimally vaccinated,” Schaffner said. “We need to reach them in particular with good information and reassurance…so they can make good decisions for themselves and their families.”
No vaccine is 100% effective or completely free of side effects. “There is always a chance there can be adverse reactions, but we think for the most part this is going to be a safe and effective vaccine,” said Hewlett, medical director at the Division of Disease Control and deputy to commissioner of health at the Westchester County Department of Health in White Plains, New York.
Distribution: Smooth or full of strife?
In addition to the concern that some people will not take advantage of vaccination against COVID-19, there could be vaccine supply issues down the road, Schaffner said.
Culver agreed. “In the early phases, I expect that there will be some kinks to work out, but because the numbers are relatively small, this should be okay,” he said.
“I think when we start to get into larger-scale vaccination programs — the supply chain, transport, and storage will be a Herculean undertaking,” Culver added. “It will take careful coordination between healthcare providers, distributors, suppliers, and public health officials to pull this off.”
Planning and distribution also should focus beyond US borders. Any issues in vaccine distribution or administration in the United States “will only be multiplied in several other parts of the world,” Culver said. Because COVID-19 is a pandemic, “we need to think about vaccinating globally.”
Investigating adverse events
Adverse events common to vaccinations in general — injection site pain, headaches, and fever — would not be unexpected with the COVID-19 vaccines. However, experts remain concerned that other, unrelated adverse events might be erroneously attributed to vaccination. For example, if a fall, heart attack, or death occurs within days of immunization, some might immediately blame the vaccine product.
“It’s important to remember that any new, highly touted medical therapy like this will receive a lot of scrutiny, so it would be unusual not to hear about something happening to somebody,” Culver said. Vaccine companies and health agencies will be carefully evaluating any reported adverse events to ensure no safety signal was missed in the trials.
“Fortunately, there are systems in place to investigate these events immediately,” Schaffner said.
Pregnancy recommendations pending
One question still looms: Is the COVID-19 vaccination safe for pregnant women? This isn’t just a question for the general public, either, Schaffner said. He estimated that about 70 percent of healthcare workers are women, and data suggests about 300,000 of these healthcare workers are pregnant.
“The CDC’s Advisory Committee on Immunization Practices will speak to that just as soon as the EUA is issued,” he added.
Patients are asking Culver about the priority order for vaccination. He said it’s difficult to provide firm guidance at this point.
People also have “lingering skepticism” about whether vaccine development was done in a prudent way, Culver said. Some people question whether the Pfizer vaccine and others were rushed to market. “So we try to spend time with the patients, reassuring them that all the usual safety evaluations were carefully done,” he said.
Another concern is whether mRNA vaccines can interact with human DNA. “The quick, short, and definitive answer is no,” Schaffner said. The m stands for messenger — the vaccines transmit information. "Once it gets into a cell, the mRNA does not go anywhere near the DNA, and once it transmits its information to the cell appropriately, it gets metabolized, and we excrete all the remnants."
Hewlett pointed out that investigations and surveillance will continue. Because this is an EUA and not full approval, “that essentially means they will still be obligated to collect a lot more data than they would ordinarily,” he said.
How long immunoprotection will last also remains an unknown. “The big question left on the table now is the durability,” Culver said. “Of course, we won’t know the answer to that for quite some time.”
Schaffner and Culver have disclosed no relevant financial relationships. Hewlett was an employee of Pfizer until mid-2019. His previous work as Pfizer’s senior medical director of global medical product evaluation was not associated with development of the COVID-19 vaccine.
This article first appeared on Medscape.com.
The much-anticipated emergency use authorization (EUA) of this vaccine — the first such approval in the United States — was greeted with optimism by infectious disease and pulmonary experts, although unanswered questions remain regarding use in people with allergic hypersensitivity, safety in pregnant women, and how smooth distribution will be.
“I am delighted. This is a first, firm step on a long path to getting this COVID pandemic under control,” William Schaffner, MD, professor of infectious diseases at the Vanderbilt University School of Medicine in Nashville, Tennessee, said in an interview.
The FDA gave the green light after the December 10 recommendation from the agency’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting. The committee voted 17-4 in favor of the emergency authorization.
The COVID-19 vaccine is “going to have a major impact here in the US. I’m very optimistic about it,” Dial Hewlett, MD, a spokesperson for the Infectious Diseases Society of American (IDSA), told this news organization.
Daniel Culver, DO, chair of medicine at the Cleveland Clinic in Ohio, is likewise hopeful. “My understanding is that supplies of the vaccine are already in place in hubs and will be shipped relatively quickly. The hope would be we can start vaccinating people as early as next week.”
Allergic reactions reported in the UK
After vaccinations with the Pfizer vaccine began in the UK on December 8, reports surfaced of two healthcare workers who experienced allergic reactions. They have since recovered, but officials warned that people with a history of severe allergic reactions should not receive the Pfizer vaccine at this time.
“For the moment, they are asking people who have had notable allergic reactions to step aside while this is investigated. It shows you that the system is working,” Schaffner said.
Both vaccine recipients who experienced anaphylaxis carried EpiPens, as they were at high risk for allergic reactions, Hewlett said. Also, if other COVID-19 vaccines are approved for use in the future, people allergic to the Pfizer vaccine might have another option, he added.
Reassuring role models
Schaffner supports the CDC Advisory Committee on Immunization Practices (ACIP) decision to start vaccinations with healthcare workers and residents of long-term care facilities.
“Vaccinating healthcare workers, in particular, will be a model for the general public,” said Schaffner, who is also a former member of the IDSA board of directors. “If they see those of us in white coats and blue scrubs lining up for the vaccine, that will provide confidence.”
To further increase acceptance of the COVID-19 vaccine, public health officials need to provide information and reassure the general public, Schaffner said.
Hewlett agreed. “I know there are a lot of people in the population who are very hesitant about vaccines. As infection disease specialists and people in public health, we are trying to allay a lot of concerns people have.”
Reassurance will be especially important in minority communities. “They have been disproportionately affected by the virus, and they have a traditional history of not being optimally vaccinated,” Schaffner said. “We need to reach them in particular with good information and reassurance…so they can make good decisions for themselves and their families.”
No vaccine is 100% effective or completely free of side effects. “There is always a chance there can be adverse reactions, but we think for the most part this is going to be a safe and effective vaccine,” said Hewlett, medical director at the Division of Disease Control and deputy to commissioner of health at the Westchester County Department of Health in White Plains, New York.
Distribution: Smooth or full of strife?
In addition to the concern that some people will not take advantage of vaccination against COVID-19, there could be vaccine supply issues down the road, Schaffner said.
Culver agreed. “In the early phases, I expect that there will be some kinks to work out, but because the numbers are relatively small, this should be okay,” he said.
“I think when we start to get into larger-scale vaccination programs — the supply chain, transport, and storage will be a Herculean undertaking,” Culver added. “It will take careful coordination between healthcare providers, distributors, suppliers, and public health officials to pull this off.”
Planning and distribution also should focus beyond US borders. Any issues in vaccine distribution or administration in the United States “will only be multiplied in several other parts of the world,” Culver said. Because COVID-19 is a pandemic, “we need to think about vaccinating globally.”
Investigating adverse events
Adverse events common to vaccinations in general — injection site pain, headaches, and fever — would not be unexpected with the COVID-19 vaccines. However, experts remain concerned that other, unrelated adverse events might be erroneously attributed to vaccination. For example, if a fall, heart attack, or death occurs within days of immunization, some might immediately blame the vaccine product.
“It’s important to remember that any new, highly touted medical therapy like this will receive a lot of scrutiny, so it would be unusual not to hear about something happening to somebody,” Culver said. Vaccine companies and health agencies will be carefully evaluating any reported adverse events to ensure no safety signal was missed in the trials.
“Fortunately, there are systems in place to investigate these events immediately,” Schaffner said.
Pregnancy recommendations pending
One question still looms: Is the COVID-19 vaccination safe for pregnant women? This isn’t just a question for the general public, either, Schaffner said. He estimated that about 70 percent of healthcare workers are women, and data suggests about 300,000 of these healthcare workers are pregnant.
“The CDC’s Advisory Committee on Immunization Practices will speak to that just as soon as the EUA is issued,” he added.
Patients are asking Culver about the priority order for vaccination. He said it’s difficult to provide firm guidance at this point.
People also have “lingering skepticism” about whether vaccine development was done in a prudent way, Culver said. Some people question whether the Pfizer vaccine and others were rushed to market. “So we try to spend time with the patients, reassuring them that all the usual safety evaluations were carefully done,” he said.
Another concern is whether mRNA vaccines can interact with human DNA. “The quick, short, and definitive answer is no,” Schaffner said. The m stands for messenger — the vaccines transmit information. "Once it gets into a cell, the mRNA does not go anywhere near the DNA, and once it transmits its information to the cell appropriately, it gets metabolized, and we excrete all the remnants."
Hewlett pointed out that investigations and surveillance will continue. Because this is an EUA and not full approval, “that essentially means they will still be obligated to collect a lot more data than they would ordinarily,” he said.
How long immunoprotection will last also remains an unknown. “The big question left on the table now is the durability,” Culver said. “Of course, we won’t know the answer to that for quite some time.”
Schaffner and Culver have disclosed no relevant financial relationships. Hewlett was an employee of Pfizer until mid-2019. His previous work as Pfizer’s senior medical director of global medical product evaluation was not associated with development of the COVID-19 vaccine.
This article first appeared on Medscape.com.
Consider this Rx for patients with high triglycerides?
ILLUSTRATIVE CASE
A 63-year-old man with a medical history significant for myocardial infarction (MI) 5 years ago presents to you for an annual exam. His medications include a daily aspirin, angiotensin-converting enzyme inhibitor, beta-blocker, and a high-intensity statin for coronary artery disease (CAD). On his fasting lipid panel, his low-density lipoprotein (LDL) level is 70 mg/dL, but his triglycerides remain elevated at 200 mg/dL despite dietary changes.
In addition to lifestyle modifications, what can be done to reduce his risk of another MI?
Patients with known cardiovascular disease (CVD) or multiple risk factors for CVD are at high risk of cardiovascular events, even when taking primary or secondary preventive medications such as statins.2,3 In these patients, elevated triglycerides are an independent risk factor for increased rates of cardiovascular events.4,5
The 2018 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the treatment of blood cholesterol recommend statin therapy for moderate (175-499 mg/dL) to severe (≥ 500 mg/dL) hypertriglyceridemia in appropriate patients with atherosclerotic CVD risk ≥ 7.5%, after appropriately addressing secondary causes of hypertriglycidemia.6
Previous studies have shown no benefit from combination therapy with triglyceride-lowering medications (eg, extended-release niacin and fibrates) and statins, compared with statin monotherapy.7 A recent meta-analysis concluded that omega-3 fatty acid supplements offer no reduction in cardiovascular morbidity or mortality, whether taken with or without statins.8
Interestingly, the randomized controlled Japan EPA Lipid Intervention Study (JELIS) demonstrated fewer major coronary events in patients with elevated cholesterol, with or without CAD, who took eicosapentaenoic acid (EPA)—a subtype of omega-3 fatty acids—plus a statin, compared with statin monotherapy.9
The REDUCE-IT trial evaluated icosapent ethyl, a highly purified EPA that has been shown to reduce triglycerides and, at the time this study was conducted, was approved for use solely for the reduction of triglyceride levels in adults with severe hypertriglyceridemia.10,11
Continue to: Study Summary
STUDY SUMMARY
Patients with known CVD had fewercardiovascular events on icosapent ethyl
The multicenter, randomized controlled REDUCE-IT trial evaluated the effectiveness of icosapent ethyl, 2 g orally twice daily, on cardiovascular outcomes.1 A total of 8179 patients, ≥ 45 years of age with hypertriglyceridemia and known CVD or ≥ 50 years with diabetes and at least 1 additional risk factor and no known CVD, were enrolled at 473 participating sites in 11 countries, including the United States.
Patients had a triglyceride level of 150 to 499 mg/dL and an LDL cholesterol level of 41 to 100 mg/dL, and were taking a stable dose of a statin for at least 4 weeks. The enrollment protocol was amended to increase the lower limit of triglycerides from 150 to 200 mg/dL about one-third of the way through the study. Among the study population, 70.7% of patients were enrolled for secondary prevention (ie, had established CVD) and 29.3% of patients were enrolled for primary prevention (ie, had diabetes and at least 1 additional risk factor but no known CVD). Exclusion criteria included severe heart failure, active severe liver disease, glycated hemoglobin > 10%, a planned surgical cardiac intervention, history of pancreatitis, or allergies to fish or shellfish products.
Outcomes. The primary end point was a composite outcome of cardiovascular death, nonfatal MI, nonfatal stroke, coronary revascularization, or unstable angina.
Results. The median duration of follow-up was 4.9 years. From baseline to 1 year, the median change in triglycerides was an 18% reduction in the icosapent ethyl group but a 2% increase in the placebo group. Fewer patients in the icosapent ethyl group than the placebo group had a composite outcome event (17% vs 22%, respectively; hazard ratio [HR] = 0.75; 95% confidence interval [CI], 0.68-0.83; number needed to treat [NNT] to avoid 1 primary end point event = 21). Patients with known CVD had fewer composite outcome events in the icosapent ethyl group than the placebo group (19% vs 26%; HR = 0.73; 95% CI, 0.65-0.81; NNT = 14) but not in the primary prevention group vs the placebo group (12% vs 14%; HR = 0.88; 95% CI, 0.70-1.1).
In the entire population, all individual outcomes in the composite were significantly fewer in the icosapent ethyl group (cardiovascular death: HR = 0.8; 95% CI, 0.66-0.98; fatal or nonfatal MI: HR = 0.69; 95% CI, 0.58-0.81; revascularization: HR = 0.65; 95% CI, 0.55-0.78; unstable angina: HR = 0.68; 95% CI, 0.53-0.87; and fatal or nonfatal stroke: HR = 0.72; 95% CI, 0.55-0.93). All-cause mortality did not differ between groups (HR = 0.87; 95% CI, 0.74-1.02).
No significant differences in adverse events leading to discontinuation of the drug were reported between groups. Atrial fibrillation occurred more frequently in the icosapent ethyl group (5.3% vs 3.9%), but anemia (4.7% vs 5.8%) and gastrointestinal adverse events (33% vs 35%) were less common.
Continue to: What's New
WHAT’S NEW
First RCT to demonstrate valueof pairing icosapent ethyl with a statin
Many prior studies on use of omega-3 fatty acid supplements to treat hypertriglyceridemia did not show any benefit, possibly due to a low dose or low ratio of EPA in the study drug.8 One trial (JELIS) with favorable results was an open-label study, limited to patients in Japan. The REDUCE-IT study was the first randomized, placebo-controlled trial to show that icosapent ethyl treatment for hypertriglyceridemia in patients with known CVD who are taking a statin results in fewer cardiovascular events than statin use alone.
Also worth noting: Since publication of the REDUCE-IT study, the FDA has approved an expanded indication for icosapent ethyl for reduction of risk of cardiovascular events in statin-treated patients with hypertriglyceridemia and established CVD or diabetes and ≥ 2 additional cardiovascular risk factors.11
CAVEATS
Drug’s benefit was not linkedto triglyceride level reductions
The cardiovascular benefits of icosapent ethyl were obtained irrespective of triglyceride levels achieved. This raises the question of other potential mechanisms of action of icosapent ethyl in achieving cardiovascular benefit. However, this should not preclude the use of icosapent ethyl for secondary prevention in appropriate patients.
CHALLENGES TO IMPLEMENTATION
Medication is pricey
Icosapent ethyl is an expensive medication, currently priced at an estimated $351/month using a nationally available discount pharmacy plan, although additional manufacturer’s discounts may apply.12,13 The cost of the medication could be a consideration for widespread implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2020. The Family Physicians Inquiries Network. All rights reserved.
1. Bhatt DL, Steg PG, Miller M, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.
2. Bhatt DL, Eagle KA, Ohman EM, et al; REACH Registry Investigators. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304:1350-1357.
3. Cannon CP, Braunwald E, McCabe CH, et al; Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 Investigators. Intensive versus moderate lipid lowering with statins after acute coronary syndromes [published correction appears in N Engl J Med. 2006;354:778]. N Engl J Med. 2004;350:1495-1504.
4. Klempfner R, Erez A, Sagit BZ, et al. Elevated triglyceride level is independently associated with increased all-cause mortality in patients with established coronary heart disease: twenty-two-year follow-up of the Bezafibrate Infarction Prevention Study and Registry [published correction appears in Circ Cardiovasc Qual Outcomes. 2016;9:613]. Circ Cardiovasc Qual Outcomes. 2016;9:100-108.
5. Nichols GA, Philip S, Reynolds K, Granowitz CB, Fazio S. Increased cardiovascular risk in hypertriglyceridemic patients with statin-controlled LDL cholesterol. J Clin Endocrinol Metab. 2018;103:3019-3027.
6. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2019;73:3237-3241]. J Am Coll Cardiol. 2019;73:e285-e350.
7. Ganda OP, Bhatt DL, Mason RP, Miller M, Boden WE. Unmet need for adjunctive dyslipidemia therapy in hypertriglyceridemia management. J Am Coll Cardiol. 2018;72:330-343.
8. Aung T, Halsey J, Kromhout D, et al; Omega-3 Treatment Trialists’ Collaboration. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77 917 individuals. JAMA Cardiol. 2018;3:225-234.
9. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis [published correction appears in Lancet. 2007;370:220]. Lancet. 2007;369:1090-1098.
10. Ballantyne CM, Bays HE, Kastelein JJ, et al. Efficacy and safety of eicosapentaenoic acid ethyl ester (AMR101) therapy in statin-treated patients with persistent high triglycerides (from the ANCHOR study). Am J Cardiol. 2012;110:984-992.
11. FDA approves use of drug to reduce risk of cardiovascular events in certain adult patient groups [news release]. Silver Spring, MD: US Food and Drug Administration; December 13, 2019. www.fda.gov/news-events/press-announcements/fda-approves-use-drug-reduce-risk-cardiovascular-events-certain-adult-patient-groups. Accessed November 30, 2020.
12. Vascepa. GoodRx. www.goodrx.com/vascepa. Accessed November 30, 2020.
13. The VASCEPA Savings Program. www.vascepa.com/getting-started/savings-card/. Accessed November 30, 2020.
ILLUSTRATIVE CASE
A 63-year-old man with a medical history significant for myocardial infarction (MI) 5 years ago presents to you for an annual exam. His medications include a daily aspirin, angiotensin-converting enzyme inhibitor, beta-blocker, and a high-intensity statin for coronary artery disease (CAD). On his fasting lipid panel, his low-density lipoprotein (LDL) level is 70 mg/dL, but his triglycerides remain elevated at 200 mg/dL despite dietary changes.
In addition to lifestyle modifications, what can be done to reduce his risk of another MI?
Patients with known cardiovascular disease (CVD) or multiple risk factors for CVD are at high risk of cardiovascular events, even when taking primary or secondary preventive medications such as statins.2,3 In these patients, elevated triglycerides are an independent risk factor for increased rates of cardiovascular events.4,5
The 2018 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the treatment of blood cholesterol recommend statin therapy for moderate (175-499 mg/dL) to severe (≥ 500 mg/dL) hypertriglyceridemia in appropriate patients with atherosclerotic CVD risk ≥ 7.5%, after appropriately addressing secondary causes of hypertriglycidemia.6
Previous studies have shown no benefit from combination therapy with triglyceride-lowering medications (eg, extended-release niacin and fibrates) and statins, compared with statin monotherapy.7 A recent meta-analysis concluded that omega-3 fatty acid supplements offer no reduction in cardiovascular morbidity or mortality, whether taken with or without statins.8
Interestingly, the randomized controlled Japan EPA Lipid Intervention Study (JELIS) demonstrated fewer major coronary events in patients with elevated cholesterol, with or without CAD, who took eicosapentaenoic acid (EPA)—a subtype of omega-3 fatty acids—plus a statin, compared with statin monotherapy.9
The REDUCE-IT trial evaluated icosapent ethyl, a highly purified EPA that has been shown to reduce triglycerides and, at the time this study was conducted, was approved for use solely for the reduction of triglyceride levels in adults with severe hypertriglyceridemia.10,11
Continue to: Study Summary
STUDY SUMMARY
Patients with known CVD had fewercardiovascular events on icosapent ethyl
The multicenter, randomized controlled REDUCE-IT trial evaluated the effectiveness of icosapent ethyl, 2 g orally twice daily, on cardiovascular outcomes.1 A total of 8179 patients, ≥ 45 years of age with hypertriglyceridemia and known CVD or ≥ 50 years with diabetes and at least 1 additional risk factor and no known CVD, were enrolled at 473 participating sites in 11 countries, including the United States.
Patients had a triglyceride level of 150 to 499 mg/dL and an LDL cholesterol level of 41 to 100 mg/dL, and were taking a stable dose of a statin for at least 4 weeks. The enrollment protocol was amended to increase the lower limit of triglycerides from 150 to 200 mg/dL about one-third of the way through the study. Among the study population, 70.7% of patients were enrolled for secondary prevention (ie, had established CVD) and 29.3% of patients were enrolled for primary prevention (ie, had diabetes and at least 1 additional risk factor but no known CVD). Exclusion criteria included severe heart failure, active severe liver disease, glycated hemoglobin > 10%, a planned surgical cardiac intervention, history of pancreatitis, or allergies to fish or shellfish products.
Outcomes. The primary end point was a composite outcome of cardiovascular death, nonfatal MI, nonfatal stroke, coronary revascularization, or unstable angina.
Results. The median duration of follow-up was 4.9 years. From baseline to 1 year, the median change in triglycerides was an 18% reduction in the icosapent ethyl group but a 2% increase in the placebo group. Fewer patients in the icosapent ethyl group than the placebo group had a composite outcome event (17% vs 22%, respectively; hazard ratio [HR] = 0.75; 95% confidence interval [CI], 0.68-0.83; number needed to treat [NNT] to avoid 1 primary end point event = 21). Patients with known CVD had fewer composite outcome events in the icosapent ethyl group than the placebo group (19% vs 26%; HR = 0.73; 95% CI, 0.65-0.81; NNT = 14) but not in the primary prevention group vs the placebo group (12% vs 14%; HR = 0.88; 95% CI, 0.70-1.1).
In the entire population, all individual outcomes in the composite were significantly fewer in the icosapent ethyl group (cardiovascular death: HR = 0.8; 95% CI, 0.66-0.98; fatal or nonfatal MI: HR = 0.69; 95% CI, 0.58-0.81; revascularization: HR = 0.65; 95% CI, 0.55-0.78; unstable angina: HR = 0.68; 95% CI, 0.53-0.87; and fatal or nonfatal stroke: HR = 0.72; 95% CI, 0.55-0.93). All-cause mortality did not differ between groups (HR = 0.87; 95% CI, 0.74-1.02).
No significant differences in adverse events leading to discontinuation of the drug were reported between groups. Atrial fibrillation occurred more frequently in the icosapent ethyl group (5.3% vs 3.9%), but anemia (4.7% vs 5.8%) and gastrointestinal adverse events (33% vs 35%) were less common.
Continue to: What's New
WHAT’S NEW
First RCT to demonstrate valueof pairing icosapent ethyl with a statin
Many prior studies on use of omega-3 fatty acid supplements to treat hypertriglyceridemia did not show any benefit, possibly due to a low dose or low ratio of EPA in the study drug.8 One trial (JELIS) with favorable results was an open-label study, limited to patients in Japan. The REDUCE-IT study was the first randomized, placebo-controlled trial to show that icosapent ethyl treatment for hypertriglyceridemia in patients with known CVD who are taking a statin results in fewer cardiovascular events than statin use alone.
Also worth noting: Since publication of the REDUCE-IT study, the FDA has approved an expanded indication for icosapent ethyl for reduction of risk of cardiovascular events in statin-treated patients with hypertriglyceridemia and established CVD or diabetes and ≥ 2 additional cardiovascular risk factors.11
CAVEATS
Drug’s benefit was not linkedto triglyceride level reductions
The cardiovascular benefits of icosapent ethyl were obtained irrespective of triglyceride levels achieved. This raises the question of other potential mechanisms of action of icosapent ethyl in achieving cardiovascular benefit. However, this should not preclude the use of icosapent ethyl for secondary prevention in appropriate patients.
CHALLENGES TO IMPLEMENTATION
Medication is pricey
Icosapent ethyl is an expensive medication, currently priced at an estimated $351/month using a nationally available discount pharmacy plan, although additional manufacturer’s discounts may apply.12,13 The cost of the medication could be a consideration for widespread implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2020. The Family Physicians Inquiries Network. All rights reserved.
ILLUSTRATIVE CASE
A 63-year-old man with a medical history significant for myocardial infarction (MI) 5 years ago presents to you for an annual exam. His medications include a daily aspirin, angiotensin-converting enzyme inhibitor, beta-blocker, and a high-intensity statin for coronary artery disease (CAD). On his fasting lipid panel, his low-density lipoprotein (LDL) level is 70 mg/dL, but his triglycerides remain elevated at 200 mg/dL despite dietary changes.
In addition to lifestyle modifications, what can be done to reduce his risk of another MI?
Patients with known cardiovascular disease (CVD) or multiple risk factors for CVD are at high risk of cardiovascular events, even when taking primary or secondary preventive medications such as statins.2,3 In these patients, elevated triglycerides are an independent risk factor for increased rates of cardiovascular events.4,5
The 2018 American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the treatment of blood cholesterol recommend statin therapy for moderate (175-499 mg/dL) to severe (≥ 500 mg/dL) hypertriglyceridemia in appropriate patients with atherosclerotic CVD risk ≥ 7.5%, after appropriately addressing secondary causes of hypertriglycidemia.6
Previous studies have shown no benefit from combination therapy with triglyceride-lowering medications (eg, extended-release niacin and fibrates) and statins, compared with statin monotherapy.7 A recent meta-analysis concluded that omega-3 fatty acid supplements offer no reduction in cardiovascular morbidity or mortality, whether taken with or without statins.8
Interestingly, the randomized controlled Japan EPA Lipid Intervention Study (JELIS) demonstrated fewer major coronary events in patients with elevated cholesterol, with or without CAD, who took eicosapentaenoic acid (EPA)—a subtype of omega-3 fatty acids—plus a statin, compared with statin monotherapy.9
The REDUCE-IT trial evaluated icosapent ethyl, a highly purified EPA that has been shown to reduce triglycerides and, at the time this study was conducted, was approved for use solely for the reduction of triglyceride levels in adults with severe hypertriglyceridemia.10,11
Continue to: Study Summary
STUDY SUMMARY
Patients with known CVD had fewercardiovascular events on icosapent ethyl
The multicenter, randomized controlled REDUCE-IT trial evaluated the effectiveness of icosapent ethyl, 2 g orally twice daily, on cardiovascular outcomes.1 A total of 8179 patients, ≥ 45 years of age with hypertriglyceridemia and known CVD or ≥ 50 years with diabetes and at least 1 additional risk factor and no known CVD, were enrolled at 473 participating sites in 11 countries, including the United States.
Patients had a triglyceride level of 150 to 499 mg/dL and an LDL cholesterol level of 41 to 100 mg/dL, and were taking a stable dose of a statin for at least 4 weeks. The enrollment protocol was amended to increase the lower limit of triglycerides from 150 to 200 mg/dL about one-third of the way through the study. Among the study population, 70.7% of patients were enrolled for secondary prevention (ie, had established CVD) and 29.3% of patients were enrolled for primary prevention (ie, had diabetes and at least 1 additional risk factor but no known CVD). Exclusion criteria included severe heart failure, active severe liver disease, glycated hemoglobin > 10%, a planned surgical cardiac intervention, history of pancreatitis, or allergies to fish or shellfish products.
Outcomes. The primary end point was a composite outcome of cardiovascular death, nonfatal MI, nonfatal stroke, coronary revascularization, or unstable angina.
Results. The median duration of follow-up was 4.9 years. From baseline to 1 year, the median change in triglycerides was an 18% reduction in the icosapent ethyl group but a 2% increase in the placebo group. Fewer patients in the icosapent ethyl group than the placebo group had a composite outcome event (17% vs 22%, respectively; hazard ratio [HR] = 0.75; 95% confidence interval [CI], 0.68-0.83; number needed to treat [NNT] to avoid 1 primary end point event = 21). Patients with known CVD had fewer composite outcome events in the icosapent ethyl group than the placebo group (19% vs 26%; HR = 0.73; 95% CI, 0.65-0.81; NNT = 14) but not in the primary prevention group vs the placebo group (12% vs 14%; HR = 0.88; 95% CI, 0.70-1.1).
In the entire population, all individual outcomes in the composite were significantly fewer in the icosapent ethyl group (cardiovascular death: HR = 0.8; 95% CI, 0.66-0.98; fatal or nonfatal MI: HR = 0.69; 95% CI, 0.58-0.81; revascularization: HR = 0.65; 95% CI, 0.55-0.78; unstable angina: HR = 0.68; 95% CI, 0.53-0.87; and fatal or nonfatal stroke: HR = 0.72; 95% CI, 0.55-0.93). All-cause mortality did not differ between groups (HR = 0.87; 95% CI, 0.74-1.02).
No significant differences in adverse events leading to discontinuation of the drug were reported between groups. Atrial fibrillation occurred more frequently in the icosapent ethyl group (5.3% vs 3.9%), but anemia (4.7% vs 5.8%) and gastrointestinal adverse events (33% vs 35%) were less common.
Continue to: What's New
WHAT’S NEW
First RCT to demonstrate valueof pairing icosapent ethyl with a statin
Many prior studies on use of omega-3 fatty acid supplements to treat hypertriglyceridemia did not show any benefit, possibly due to a low dose or low ratio of EPA in the study drug.8 One trial (JELIS) with favorable results was an open-label study, limited to patients in Japan. The REDUCE-IT study was the first randomized, placebo-controlled trial to show that icosapent ethyl treatment for hypertriglyceridemia in patients with known CVD who are taking a statin results in fewer cardiovascular events than statin use alone.
Also worth noting: Since publication of the REDUCE-IT study, the FDA has approved an expanded indication for icosapent ethyl for reduction of risk of cardiovascular events in statin-treated patients with hypertriglyceridemia and established CVD or diabetes and ≥ 2 additional cardiovascular risk factors.11
CAVEATS
Drug’s benefit was not linkedto triglyceride level reductions
The cardiovascular benefits of icosapent ethyl were obtained irrespective of triglyceride levels achieved. This raises the question of other potential mechanisms of action of icosapent ethyl in achieving cardiovascular benefit. However, this should not preclude the use of icosapent ethyl for secondary prevention in appropriate patients.
CHALLENGES TO IMPLEMENTATION
Medication is pricey
Icosapent ethyl is an expensive medication, currently priced at an estimated $351/month using a nationally available discount pharmacy plan, although additional manufacturer’s discounts may apply.12,13 The cost of the medication could be a consideration for widespread implementation of this recommendation.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2020. The Family Physicians Inquiries Network. All rights reserved.
1. Bhatt DL, Steg PG, Miller M, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.
2. Bhatt DL, Eagle KA, Ohman EM, et al; REACH Registry Investigators. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304:1350-1357.
3. Cannon CP, Braunwald E, McCabe CH, et al; Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 Investigators. Intensive versus moderate lipid lowering with statins after acute coronary syndromes [published correction appears in N Engl J Med. 2006;354:778]. N Engl J Med. 2004;350:1495-1504.
4. Klempfner R, Erez A, Sagit BZ, et al. Elevated triglyceride level is independently associated with increased all-cause mortality in patients with established coronary heart disease: twenty-two-year follow-up of the Bezafibrate Infarction Prevention Study and Registry [published correction appears in Circ Cardiovasc Qual Outcomes. 2016;9:613]. Circ Cardiovasc Qual Outcomes. 2016;9:100-108.
5. Nichols GA, Philip S, Reynolds K, Granowitz CB, Fazio S. Increased cardiovascular risk in hypertriglyceridemic patients with statin-controlled LDL cholesterol. J Clin Endocrinol Metab. 2018;103:3019-3027.
6. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2019;73:3237-3241]. J Am Coll Cardiol. 2019;73:e285-e350.
7. Ganda OP, Bhatt DL, Mason RP, Miller M, Boden WE. Unmet need for adjunctive dyslipidemia therapy in hypertriglyceridemia management. J Am Coll Cardiol. 2018;72:330-343.
8. Aung T, Halsey J, Kromhout D, et al; Omega-3 Treatment Trialists’ Collaboration. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77 917 individuals. JAMA Cardiol. 2018;3:225-234.
9. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis [published correction appears in Lancet. 2007;370:220]. Lancet. 2007;369:1090-1098.
10. Ballantyne CM, Bays HE, Kastelein JJ, et al. Efficacy and safety of eicosapentaenoic acid ethyl ester (AMR101) therapy in statin-treated patients with persistent high triglycerides (from the ANCHOR study). Am J Cardiol. 2012;110:984-992.
11. FDA approves use of drug to reduce risk of cardiovascular events in certain adult patient groups [news release]. Silver Spring, MD: US Food and Drug Administration; December 13, 2019. www.fda.gov/news-events/press-announcements/fda-approves-use-drug-reduce-risk-cardiovascular-events-certain-adult-patient-groups. Accessed November 30, 2020.
12. Vascepa. GoodRx. www.goodrx.com/vascepa. Accessed November 30, 2020.
13. The VASCEPA Savings Program. www.vascepa.com/getting-started/savings-card/. Accessed November 30, 2020.
1. Bhatt DL, Steg PG, Miller M, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.
2. Bhatt DL, Eagle KA, Ohman EM, et al; REACH Registry Investigators. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304:1350-1357.
3. Cannon CP, Braunwald E, McCabe CH, et al; Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 Investigators. Intensive versus moderate lipid lowering with statins after acute coronary syndromes [published correction appears in N Engl J Med. 2006;354:778]. N Engl J Med. 2004;350:1495-1504.
4. Klempfner R, Erez A, Sagit BZ, et al. Elevated triglyceride level is independently associated with increased all-cause mortality in patients with established coronary heart disease: twenty-two-year follow-up of the Bezafibrate Infarction Prevention Study and Registry [published correction appears in Circ Cardiovasc Qual Outcomes. 2016;9:613]. Circ Cardiovasc Qual Outcomes. 2016;9:100-108.
5. Nichols GA, Philip S, Reynolds K, Granowitz CB, Fazio S. Increased cardiovascular risk in hypertriglyceridemic patients with statin-controlled LDL cholesterol. J Clin Endocrinol Metab. 2018;103:3019-3027.
6. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2019;73:3237-3241]. J Am Coll Cardiol. 2019;73:e285-e350.
7. Ganda OP, Bhatt DL, Mason RP, Miller M, Boden WE. Unmet need for adjunctive dyslipidemia therapy in hypertriglyceridemia management. J Am Coll Cardiol. 2018;72:330-343.
8. Aung T, Halsey J, Kromhout D, et al; Omega-3 Treatment Trialists’ Collaboration. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77 917 individuals. JAMA Cardiol. 2018;3:225-234.
9. Yokoyama M, Origasa H, Matsuzaki M, et al; Japan EPA lipid intervention study (JELIS) Investigators. Effects of eicosapentaenoic acid on major coronary events in hypercholesterolaemic patients (JELIS): a randomised open-label, blinded endpoint analysis [published correction appears in Lancet. 2007;370:220]. Lancet. 2007;369:1090-1098.
10. Ballantyne CM, Bays HE, Kastelein JJ, et al. Efficacy and safety of eicosapentaenoic acid ethyl ester (AMR101) therapy in statin-treated patients with persistent high triglycerides (from the ANCHOR study). Am J Cardiol. 2012;110:984-992.
11. FDA approves use of drug to reduce risk of cardiovascular events in certain adult patient groups [news release]. Silver Spring, MD: US Food and Drug Administration; December 13, 2019. www.fda.gov/news-events/press-announcements/fda-approves-use-drug-reduce-risk-cardiovascular-events-certain-adult-patient-groups. Accessed November 30, 2020.
12. Vascepa. GoodRx. www.goodrx.com/vascepa. Accessed November 30, 2020.
13. The VASCEPA Savings Program. www.vascepa.com/getting-started/savings-card/. Accessed November 30, 2020.
PRACTICE CHANGER
Consider icosapent ethyl, 2 g twice daily, for secondary prevention of adverse cardiovascular events in patients with elevated triglycerides who are already taking a statin.
STRENGTH OF RECOMMENDATION
B: Based on a single, good-quality, multicenter, randomized controlled trial. Bhatt DL, Steg PG, Miller M, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.1
Bhatt DL, Steg PG, Miller M, et al; REDUCE-IT Investigators. Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia. N Engl J Med. 2019;380:11-22.1

Worsening skin lesions but no diagnosis
A 50-year-old woman presented to her family physician for a urinary tract infection (UTI) and an itchy rash. She said the rash had developed 2 years earlier and had gotten worse, with additional lesions emerging on her skin as time went on. She noted that other physicians had evaluated the rash but provided no clear diagnosis and had done no testing.
A physical exam revealed scattered erythematous papules with white centers on the patient’s trunk, arms, and legs (FIGURE 1). The patient’s medical history was significant for asthma, obstructive sleep apnea, obesity, gastroesophageal reflux disease, urinary incontinence, and depression. Her medications included montelukast, inhaled fluticasone, albuterol, tolterodine, omeprazole, and fluoxetine.

The patient was prescribed nitrofurantoin, 100 mg twice daily for 5 days, to treat her UTI, and a punch biopsy was performed on one of the patient’s lesions to determine the cause of the rash.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Atrophic papulosis
Pathology suggested a diagnosis of atrophic papulosis. A consultation with a dermatologist and additional biopsies confirmed the diagnosis. The biopsies showed wedge-shaped areas of superficial dermal sclerosis with thinning of the overlying epidermis. The superficial dermal vessels contained scattered, small thrombi at the periphery of the areas of sclerosis.
Atrophic papulosis (also known as Degos disease or Kölmeier-Degos disease) is a vasculopathy characterized by thrombotic occlusion of small arteries.1 Although rare—with fewer than 200 published case reports in the literature—it is likely underdiagnosed.1 Atrophic papulosis can be distinguished by hallmark skin findings, including 0.5- to 1-cm papular skin lesions with central porcelain-white atrophy and an erythematous, telangiectatic rim.1 It usually manifests between ages 20 to 50 but can occur in infants and children.1 The etiology is unknown, but case evidence suggests the condition is sometimes familial.1,2
Easy to confuse with common conditions
Clinical presentation of atrophic papulosis can vary, but evaluation should rule out systemic lupus erythematosus and other connective tissue diseases.1 In addition, the lesions can easily be confused with other common conditions such as molluscum contagiosum or insect bites.
The hallmark finding of molluscum contagiosum is raised papules with central umbilication, whereas atrophic papulosis lesions are characterized by white centers. While insect bites typically disappear within weeks, atrophic papulosis lesions persist for years or are even lifelong.1
Is it benign or malignant?
Benign atrophic papulosis is limited to the skin.1 The probability of a patient having benign atrophic papulosis is about 70% at the onset of skin lesions and 97% after 7 years without other symptoms.2
Malignant atrophic papulosis—although less common—is systemic and life-threatening. About 30% of patients with atrophic papulosis develop lesions manifesting both on the skin and in internal organs.1,2 Systemic involvement can develop at any time, sometimes years after the appearance of skin lesions, but the risk declines over time.2 In a case series, systemic signs were shown to develop, on average, 1 year after skin lesions.2 Some evidence suggests a mortality rate of 50% within 2 to 3 years of the onset of systemic involvement, making regular follow-up necessary.1
Continue to: Patients with malignant atrophic papulosis...
Patients with malignant atrophic papulosis may have systemic involvement in multiple organ systems. Gastrointestinal (GI) involvement can cause bowel perforation. Central nervous system (CNS) involvement may put the patient at risk for stroke, intracranial bleeding, meningitis, and encephalitis.1,3 There can also be cardiopulmonary involvement that causes pleuritis and pericarditis.1 Ocular involvement can affect the eyelids, conjunctiva, retina, sclera, and choroid plexus.1 Renal involvement has been noted in a few cases.2
In a prospective, single-center cohort study of 39 patients with atrophic papulosis, systemic involvement (malignant atrophic papulosis) was reported in 29% (n = 11) of the patients.2 In these patients, involved organ systems included the GI tract (73%; n = 8), CNS (64%; n = 7), eye (18%; n = 2), heart (18%; n = 2), and lungs (9%; n = 1); 64% (n = 7) had multiorgan involvement. Mortality was reported in 73% of the patients with systemic disease.
Ongoing testing is required
For a patient presenting with atrophic papulosis, initial and follow-up visits should include evaluation for systemic manifestations through a full skin examination, fecal occult blood test, and ocular fundus examination.1,2 If the patient shows any symptoms that suggest systemic involvement, further testing is advised, including evaluation of renal function, colonoscopy, endoscopy, magnetic resonance imaging of the brain, an echocardiogram, and chest computed tomography.
Because internal organ involvement in malignant atrophic papulosis can develop within years of (benign) cutaneous manifestations, regular follow-up is recommended.1 Research suggests evaluation of patients with benign atrophic papulosis every 6 months for the first 7 years after disease onset and then yearly between 7 and 10 years after onset.2
Treatment options are limited
Antiplatelet agents (aspirin, pentoxifylline, dipyridamole, and ticlodipine) and anticoagulants (heparin) have led to partial regression of skin lesions in case reports.1 Some lesions seem to disappear after treatment, but due to limited evidence, it is difficult to determine whether treatment leads to a reduction of future lesions.
When it comes to malignant atrophic papulosis, there is no uniformly effective treatment. Antiplatelet agents and anticoagulants are often used as initial treatment, but efficacy has not been clearly demonstrated. In case reports, eculizumab and treprostinil have shown effectiveness in treating CNS involvement, but there are no uniform dosage recommendations.3,4
In this case, the patient had mild GI symptoms. A colonoscopy showed evidence of microscopic colitis, but there was no evidence of atrophic papulosis in the GI tract.
Additional laboratory work-up was ordered to evaluate for signs of organ involvement and to rule out any associated connective tissue disease or hypercoagulable state. Her results showed a mildly elevated erythrocyte sedimentation rate (29 mm/h) and a positive antinuclear antibodies assay (1:640, speckled pattern). She was referred to a rheumatologist, who found no evidence of a connective tissue disorder. A complete blood count, comprehensive metabolic panel, urinalysis, and hypercoagulability work-up were all within normal limits. A complete eye exam was also normal.
The patient was started on aspirin 81 mg/d. Because she continued to develop new lesions, her dermatologist added pentoxifylline extended release and gradually increased the dose to 400 mg in the morning and 800 mg in the evening. About 4 years after onset of the rash, the patient showed no signs of systemic involvement, but her skin lesions were still present.
1. Theodoridis A, Makrantonaki E, Zouboulis CC, et al. Malignant atrophic papulosis (Köhlmeier-Degos disease)—a review. Orphanet J Rare Dis. 2013;8:10.
2. Theodoridis A, Konstantinidou A, Makrantonaki E, et al. Malignant and benign forms of atrophic papulosis (Köhlmeier-Degos disease): systemic involvement determines the prognosis. Br J Dermatol. 2014;170:110-115.
3. Huang YC, Wang JD, Lee FY, et al. Pediatric malignant atrophic papulosis. Pediatrics. 2018;141(suppl 5):S481-S484.
4. Shapiro LS, Toledo-Garcia AE, Farrell JF. Effective treatment of malignant atrophic papulosis (Köhlmeier-Degos disease) with treprostinil—early experience. Orphanet J Rare Dis. 2013;8:52.
A 50-year-old woman presented to her family physician for a urinary tract infection (UTI) and an itchy rash. She said the rash had developed 2 years earlier and had gotten worse, with additional lesions emerging on her skin as time went on. She noted that other physicians had evaluated the rash but provided no clear diagnosis and had done no testing.
A physical exam revealed scattered erythematous papules with white centers on the patient’s trunk, arms, and legs (FIGURE 1). The patient’s medical history was significant for asthma, obstructive sleep apnea, obesity, gastroesophageal reflux disease, urinary incontinence, and depression. Her medications included montelukast, inhaled fluticasone, albuterol, tolterodine, omeprazole, and fluoxetine.
The patient was prescribed nitrofurantoin, 100 mg twice daily for 5 days, to treat her UTI, and a punch biopsy was performed on one of the patient’s lesions to determine the cause of the rash.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Atrophic papulosis
Pathology suggested a diagnosis of atrophic papulosis. A consultation with a dermatologist and additional biopsies confirmed the diagnosis. The biopsies showed wedge-shaped areas of superficial dermal sclerosis with thinning of the overlying epidermis. The superficial dermal vessels contained scattered, small thrombi at the periphery of the areas of sclerosis.
Atrophic papulosis (also known as Degos disease or Kölmeier-Degos disease) is a vasculopathy characterized by thrombotic occlusion of small arteries.1 Although rare—with fewer than 200 published case reports in the literature—it is likely underdiagnosed.1 Atrophic papulosis can be distinguished by hallmark skin findings, including 0.5- to 1-cm papular skin lesions with central porcelain-white atrophy and an erythematous, telangiectatic rim.1 It usually manifests between ages 20 to 50 but can occur in infants and children.1 The etiology is unknown, but case evidence suggests the condition is sometimes familial.1,2
Easy to confuse with common conditions
Clinical presentation of atrophic papulosis can vary, but evaluation should rule out systemic lupus erythematosus and other connective tissue diseases.1 In addition, the lesions can easily be confused with other common conditions such as molluscum contagiosum or insect bites.
The hallmark finding of molluscum contagiosum is raised papules with central umbilication, whereas atrophic papulosis lesions are characterized by white centers. While insect bites typically disappear within weeks, atrophic papulosis lesions persist for years or are even lifelong.1
Is it benign or malignant?
Benign atrophic papulosis is limited to the skin.1 The probability of a patient having benign atrophic papulosis is about 70% at the onset of skin lesions and 97% after 7 years without other symptoms.2
Malignant atrophic papulosis—although less common—is systemic and life-threatening. About 30% of patients with atrophic papulosis develop lesions manifesting both on the skin and in internal organs.1,2 Systemic involvement can develop at any time, sometimes years after the appearance of skin lesions, but the risk declines over time.2 In a case series, systemic signs were shown to develop, on average, 1 year after skin lesions.2 Some evidence suggests a mortality rate of 50% within 2 to 3 years of the onset of systemic involvement, making regular follow-up necessary.1
Continue to: Patients with malignant atrophic papulosis...
Patients with malignant atrophic papulosis may have systemic involvement in multiple organ systems. Gastrointestinal (GI) involvement can cause bowel perforation. Central nervous system (CNS) involvement may put the patient at risk for stroke, intracranial bleeding, meningitis, and encephalitis.1,3 There can also be cardiopulmonary involvement that causes pleuritis and pericarditis.1 Ocular involvement can affect the eyelids, conjunctiva, retina, sclera, and choroid plexus.1 Renal involvement has been noted in a few cases.2
In a prospective, single-center cohort study of 39 patients with atrophic papulosis, systemic involvement (malignant atrophic papulosis) was reported in 29% (n = 11) of the patients.2 In these patients, involved organ systems included the GI tract (73%; n = 8), CNS (64%; n = 7), eye (18%; n = 2), heart (18%; n = 2), and lungs (9%; n = 1); 64% (n = 7) had multiorgan involvement. Mortality was reported in 73% of the patients with systemic disease.
Ongoing testing is required
For a patient presenting with atrophic papulosis, initial and follow-up visits should include evaluation for systemic manifestations through a full skin examination, fecal occult blood test, and ocular fundus examination.1,2 If the patient shows any symptoms that suggest systemic involvement, further testing is advised, including evaluation of renal function, colonoscopy, endoscopy, magnetic resonance imaging of the brain, an echocardiogram, and chest computed tomography.
Because internal organ involvement in malignant atrophic papulosis can develop within years of (benign) cutaneous manifestations, regular follow-up is recommended.1 Research suggests evaluation of patients with benign atrophic papulosis every 6 months for the first 7 years after disease onset and then yearly between 7 and 10 years after onset.2
Treatment options are limited
Antiplatelet agents (aspirin, pentoxifylline, dipyridamole, and ticlodipine) and anticoagulants (heparin) have led to partial regression of skin lesions in case reports.1 Some lesions seem to disappear after treatment, but due to limited evidence, it is difficult to determine whether treatment leads to a reduction of future lesions.
When it comes to malignant atrophic papulosis, there is no uniformly effective treatment. Antiplatelet agents and anticoagulants are often used as initial treatment, but efficacy has not been clearly demonstrated. In case reports, eculizumab and treprostinil have shown effectiveness in treating CNS involvement, but there are no uniform dosage recommendations.3,4
In this case, the patient had mild GI symptoms. A colonoscopy showed evidence of microscopic colitis, but there was no evidence of atrophic papulosis in the GI tract.
Additional laboratory work-up was ordered to evaluate for signs of organ involvement and to rule out any associated connective tissue disease or hypercoagulable state. Her results showed a mildly elevated erythrocyte sedimentation rate (29 mm/h) and a positive antinuclear antibodies assay (1:640, speckled pattern). She was referred to a rheumatologist, who found no evidence of a connective tissue disorder. A complete blood count, comprehensive metabolic panel, urinalysis, and hypercoagulability work-up were all within normal limits. A complete eye exam was also normal.
The patient was started on aspirin 81 mg/d. Because she continued to develop new lesions, her dermatologist added pentoxifylline extended release and gradually increased the dose to 400 mg in the morning and 800 mg in the evening. About 4 years after onset of the rash, the patient showed no signs of systemic involvement, but her skin lesions were still present.
A 50-year-old woman presented to her family physician for a urinary tract infection (UTI) and an itchy rash. She said the rash had developed 2 years earlier and had gotten worse, with additional lesions emerging on her skin as time went on. She noted that other physicians had evaluated the rash but provided no clear diagnosis and had done no testing.
A physical exam revealed scattered erythematous papules with white centers on the patient’s trunk, arms, and legs (FIGURE 1). The patient’s medical history was significant for asthma, obstructive sleep apnea, obesity, gastroesophageal reflux disease, urinary incontinence, and depression. Her medications included montelukast, inhaled fluticasone, albuterol, tolterodine, omeprazole, and fluoxetine.
The patient was prescribed nitrofurantoin, 100 mg twice daily for 5 days, to treat her UTI, and a punch biopsy was performed on one of the patient’s lesions to determine the cause of the rash.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Atrophic papulosis
Pathology suggested a diagnosis of atrophic papulosis. A consultation with a dermatologist and additional biopsies confirmed the diagnosis. The biopsies showed wedge-shaped areas of superficial dermal sclerosis with thinning of the overlying epidermis. The superficial dermal vessels contained scattered, small thrombi at the periphery of the areas of sclerosis.
Atrophic papulosis (also known as Degos disease or Kölmeier-Degos disease) is a vasculopathy characterized by thrombotic occlusion of small arteries.1 Although rare—with fewer than 200 published case reports in the literature—it is likely underdiagnosed.1 Atrophic papulosis can be distinguished by hallmark skin findings, including 0.5- to 1-cm papular skin lesions with central porcelain-white atrophy and an erythematous, telangiectatic rim.1 It usually manifests between ages 20 to 50 but can occur in infants and children.1 The etiology is unknown, but case evidence suggests the condition is sometimes familial.1,2
Easy to confuse with common conditions
Clinical presentation of atrophic papulosis can vary, but evaluation should rule out systemic lupus erythematosus and other connective tissue diseases.1 In addition, the lesions can easily be confused with other common conditions such as molluscum contagiosum or insect bites.
The hallmark finding of molluscum contagiosum is raised papules with central umbilication, whereas atrophic papulosis lesions are characterized by white centers. While insect bites typically disappear within weeks, atrophic papulosis lesions persist for years or are even lifelong.1
Is it benign or malignant?
Benign atrophic papulosis is limited to the skin.1 The probability of a patient having benign atrophic papulosis is about 70% at the onset of skin lesions and 97% after 7 years without other symptoms.2
Malignant atrophic papulosis—although less common—is systemic and life-threatening. About 30% of patients with atrophic papulosis develop lesions manifesting both on the skin and in internal organs.1,2 Systemic involvement can develop at any time, sometimes years after the appearance of skin lesions, but the risk declines over time.2 In a case series, systemic signs were shown to develop, on average, 1 year after skin lesions.2 Some evidence suggests a mortality rate of 50% within 2 to 3 years of the onset of systemic involvement, making regular follow-up necessary.1
Continue to: Patients with malignant atrophic papulosis...
Patients with malignant atrophic papulosis may have systemic involvement in multiple organ systems. Gastrointestinal (GI) involvement can cause bowel perforation. Central nervous system (CNS) involvement may put the patient at risk for stroke, intracranial bleeding, meningitis, and encephalitis.1,3 There can also be cardiopulmonary involvement that causes pleuritis and pericarditis.1 Ocular involvement can affect the eyelids, conjunctiva, retina, sclera, and choroid plexus.1 Renal involvement has been noted in a few cases.2
In a prospective, single-center cohort study of 39 patients with atrophic papulosis, systemic involvement (malignant atrophic papulosis) was reported in 29% (n = 11) of the patients.2 In these patients, involved organ systems included the GI tract (73%; n = 8), CNS (64%; n = 7), eye (18%; n = 2), heart (18%; n = 2), and lungs (9%; n = 1); 64% (n = 7) had multiorgan involvement. Mortality was reported in 73% of the patients with systemic disease.
Ongoing testing is required
For a patient presenting with atrophic papulosis, initial and follow-up visits should include evaluation for systemic manifestations through a full skin examination, fecal occult blood test, and ocular fundus examination.1,2 If the patient shows any symptoms that suggest systemic involvement, further testing is advised, including evaluation of renal function, colonoscopy, endoscopy, magnetic resonance imaging of the brain, an echocardiogram, and chest computed tomography.
Because internal organ involvement in malignant atrophic papulosis can develop within years of (benign) cutaneous manifestations, regular follow-up is recommended.1 Research suggests evaluation of patients with benign atrophic papulosis every 6 months for the first 7 years after disease onset and then yearly between 7 and 10 years after onset.2
Treatment options are limited
Antiplatelet agents (aspirin, pentoxifylline, dipyridamole, and ticlodipine) and anticoagulants (heparin) have led to partial regression of skin lesions in case reports.1 Some lesions seem to disappear after treatment, but due to limited evidence, it is difficult to determine whether treatment leads to a reduction of future lesions.
When it comes to malignant atrophic papulosis, there is no uniformly effective treatment. Antiplatelet agents and anticoagulants are often used as initial treatment, but efficacy has not been clearly demonstrated. In case reports, eculizumab and treprostinil have shown effectiveness in treating CNS involvement, but there are no uniform dosage recommendations.3,4
In this case, the patient had mild GI symptoms. A colonoscopy showed evidence of microscopic colitis, but there was no evidence of atrophic papulosis in the GI tract.
Additional laboratory work-up was ordered to evaluate for signs of organ involvement and to rule out any associated connective tissue disease or hypercoagulable state. Her results showed a mildly elevated erythrocyte sedimentation rate (29 mm/h) and a positive antinuclear antibodies assay (1:640, speckled pattern). She was referred to a rheumatologist, who found no evidence of a connective tissue disorder. A complete blood count, comprehensive metabolic panel, urinalysis, and hypercoagulability work-up were all within normal limits. A complete eye exam was also normal.
The patient was started on aspirin 81 mg/d. Because she continued to develop new lesions, her dermatologist added pentoxifylline extended release and gradually increased the dose to 400 mg in the morning and 800 mg in the evening. About 4 years after onset of the rash, the patient showed no signs of systemic involvement, but her skin lesions were still present.
1. Theodoridis A, Makrantonaki E, Zouboulis CC, et al. Malignant atrophic papulosis (Köhlmeier-Degos disease)—a review. Orphanet J Rare Dis. 2013;8:10.
2. Theodoridis A, Konstantinidou A, Makrantonaki E, et al. Malignant and benign forms of atrophic papulosis (Köhlmeier-Degos disease): systemic involvement determines the prognosis. Br J Dermatol. 2014;170:110-115.
3. Huang YC, Wang JD, Lee FY, et al. Pediatric malignant atrophic papulosis. Pediatrics. 2018;141(suppl 5):S481-S484.
4. Shapiro LS, Toledo-Garcia AE, Farrell JF. Effective treatment of malignant atrophic papulosis (Köhlmeier-Degos disease) with treprostinil—early experience. Orphanet J Rare Dis. 2013;8:52.
1. Theodoridis A, Makrantonaki E, Zouboulis CC, et al. Malignant atrophic papulosis (Köhlmeier-Degos disease)—a review. Orphanet J Rare Dis. 2013;8:10.
2. Theodoridis A, Konstantinidou A, Makrantonaki E, et al. Malignant and benign forms of atrophic papulosis (Köhlmeier-Degos disease): systemic involvement determines the prognosis. Br J Dermatol. 2014;170:110-115.
3. Huang YC, Wang JD, Lee FY, et al. Pediatric malignant atrophic papulosis. Pediatrics. 2018;141(suppl 5):S481-S484.
4. Shapiro LS, Toledo-Garcia AE, Farrell JF. Effective treatment of malignant atrophic papulosis (Köhlmeier-Degos disease) with treprostinil—early experience. Orphanet J Rare Dis. 2013;8:52.

Itchy scalp with scale
An 11-year-old boy sought care at a small village’s health center in Panama for scalp itching and subtle hair loss. He was seen by a family physician (RU) and a team of medical students who were there as part of a humanitarian trip. The patient denied any hair pulling. He had a history of treatment for head lice.
Our physical examination revealed mild alopecia and scaling on the scalp (FIGURE 1), but what we saw through the dermatoscope (FIGURE 2) made the diagnosis clear.


WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tinea capitis
On dermatoscopic examination (10× magnification), there were numerous “black dots” or broken hair shafts within patches of hair loss (FIGURE 3), which is indicative of tinea capitis.1,2 This condition causes hair shafts to break, creating “comma hairs” and black dots. The hairs are uniform in thickness and color and bend distally, like a comma.3
Tinea capitis (commonly called ringworm of the scalp) is a fungal infection caused by Trichophyton and Microsporum dermatophytes. It is the most common pediatric dermatophyte infection in the world; the usual age of onset is 5 to 10 years.2 The incidence of tinea capitis in the United States is not known because cases are no longer registered by public health agencies. That said, a Northern California study that tracked occurrences in children younger than 15 years from 1998 to 2007 found that the incidence was on the decline and lower in girls compared to boys (111.9 vs 146.4, respectively, in 1998; 27.9 vs 39.9, respectively, in 2007).4 Incidence rates were calculated per 10,000 eligible children.4

Tinea capitis can spread by contact with infected individuals and contaminated objects, including combs, towels, toys, and bedding.1 Fungal spores can remain viable on these surfaces for months.
In a study of 69 patients with tinea capitis (23 females, 46 males; mean age, 12 years), the risk factors for spreading infection included participation in sports, contact with an animal, a recent haircut, and use of a swimming pool.5
4 conditions you’ll want to rule out
The following conditions should be considered as part of the differential when a patient presents with an itchy scalp and/or hair loss.
Continue to: Psoriasis of the scalp...
Psoriasis of the scalp is characterized by scaling of the scalp along with crusted plaques. It is often accompanied by similar psoriatic plaques on the elbows, knees, and other areas of the body. Examination of our patient showed no psoriatic plaques.
Seborrhea of the scalp (also known as dandruff) is a very common diagnosis. However, it is unlikely to cause hair loss. It has widespread involvement of the scalp compared to tinea capitis, which is local and patchy. Our patient’s patches of hair loss indicated that seborrhea was unlikely.
Alopecia areata. Individuals develop this condition due to an autoimmune process affecting hair follicles. However, the resulting hair loss does not cause significant scaling, inflammation, scarring, or pain in the affected area. Further, this condition can cause the loss of the entire hair shaft.
Trichotillomania is an impulse control disorder that causes patients to pull out their own hair. There is no scaling of the scalp in this condition.
A dermatoscope can beuseful in making the Dx
Although clinical appearance and patient presentation are adequate to establish the diagnosis of tinea capitis, this case demonstrates the utility of a dermatoscope in making the diagnosis of tinea capitis. Previous studies have shown that dermoscopy allows for rapid identification of the broken hair shafts, which are a key distinction from alopecia areata.3,6
Microscopic inspection. Samples from the scaling of the scalp can be examined with potassium hydroxide (KOH) on a microscope slide. Hyphae, spores, and endo/ectothrix invasion can be seen through the microsope.
Continue to: Laboratory testing is helpful, but not needed.
Laboratory testing is helpful, but not needed. Testing for tinea capitis would require that you obtain a sample from the affected area using a swab, edge of a scalpel blade, or scalp brush.7 Because treatment can require weeks of medication, diagnosis should be confirmed with a KOH or culture when possible.
Newer antifungalsprovide a Tx advantage
Oral antifungal medications are the treatment of choice for tinea capitis. Newer antifungals, such as terbinafine and fluconazole, require a 3- to 6-week course compared to the standard 6- to 8-week course of griseofulvin.1 Also, antifungal shampoos—such as those that contain selenium sulfide—may be used for topical treatment but only as adjuvant therapy.1,2
For our patient, we dispensed a 3-week course of oral fluconazole, 3 to 6 mg/kg, to be given daily by his parents. We also recommended the use of an antidandruff shampoo, if possible. The treatment outcome was not known because our team’s humanitarian global health trip had ended.
1. Usatine R, Smith MA, Mayeaux Jr EJ, Chumley HS. The Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill; 2019.
2. Handler MZ. Tinea capitis. Medscape. https://emedicine.medscape.com/article/1091351-overview. Updated February 21, 2020. Accessed November 30, 2020.
3. Hernández-Bel P, Malvehy J, Crocker A, et al. Comma hairs: a new dermoscopic marker for tinea capitis [in Spanish]. Actas Dermosifiliogr. 2012;103:836-837.
4. Mirmirani P, Lue-Yen T. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California. J Am Acad Dermatol. 2013;69:916-921.
5. Mikaeili A, Kavaoussi H, Hashemian AH, et al. Clinico-mycological profile of tinea capitis and its comparative response to griseofulvin versus terbinafine. Curr Med Mycol. 2019;5:15-20.
6. Slowinska M, Rudnicka L, Schwartz RA, et al. Comma hairs: a dermatoscopic marker for tinea capitis: a rapid diagnostic method. Journal of the American Academy of Dermatology. 2008;59(suppl 5):S77-S79.
An 11-year-old boy sought care at a small village’s health center in Panama for scalp itching and subtle hair loss. He was seen by a family physician (RU) and a team of medical students who were there as part of a humanitarian trip. The patient denied any hair pulling. He had a history of treatment for head lice.
Our physical examination revealed mild alopecia and scaling on the scalp (FIGURE 1), but what we saw through the dermatoscope (FIGURE 2) made the diagnosis clear.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tinea capitis
On dermatoscopic examination (10× magnification), there were numerous “black dots” or broken hair shafts within patches of hair loss (FIGURE 3), which is indicative of tinea capitis.1,2 This condition causes hair shafts to break, creating “comma hairs” and black dots. The hairs are uniform in thickness and color and bend distally, like a comma.3
Tinea capitis (commonly called ringworm of the scalp) is a fungal infection caused by Trichophyton and Microsporum dermatophytes. It is the most common pediatric dermatophyte infection in the world; the usual age of onset is 5 to 10 years.2 The incidence of tinea capitis in the United States is not known because cases are no longer registered by public health agencies. That said, a Northern California study that tracked occurrences in children younger than 15 years from 1998 to 2007 found that the incidence was on the decline and lower in girls compared to boys (111.9 vs 146.4, respectively, in 1998; 27.9 vs 39.9, respectively, in 2007).4 Incidence rates were calculated per 10,000 eligible children.4
Tinea capitis can spread by contact with infected individuals and contaminated objects, including combs, towels, toys, and bedding.1 Fungal spores can remain viable on these surfaces for months.
In a study of 69 patients with tinea capitis (23 females, 46 males; mean age, 12 years), the risk factors for spreading infection included participation in sports, contact with an animal, a recent haircut, and use of a swimming pool.5
4 conditions you’ll want to rule out
The following conditions should be considered as part of the differential when a patient presents with an itchy scalp and/or hair loss.
Continue to: Psoriasis of the scalp...
Psoriasis of the scalp is characterized by scaling of the scalp along with crusted plaques. It is often accompanied by similar psoriatic plaques on the elbows, knees, and other areas of the body. Examination of our patient showed no psoriatic plaques.
Seborrhea of the scalp (also known as dandruff) is a very common diagnosis. However, it is unlikely to cause hair loss. It has widespread involvement of the scalp compared to tinea capitis, which is local and patchy. Our patient’s patches of hair loss indicated that seborrhea was unlikely.
Alopecia areata. Individuals develop this condition due to an autoimmune process affecting hair follicles. However, the resulting hair loss does not cause significant scaling, inflammation, scarring, or pain in the affected area. Further, this condition can cause the loss of the entire hair shaft.
Trichotillomania is an impulse control disorder that causes patients to pull out their own hair. There is no scaling of the scalp in this condition.
A dermatoscope can beuseful in making the Dx
Although clinical appearance and patient presentation are adequate to establish the diagnosis of tinea capitis, this case demonstrates the utility of a dermatoscope in making the diagnosis of tinea capitis. Previous studies have shown that dermoscopy allows for rapid identification of the broken hair shafts, which are a key distinction from alopecia areata.3,6
Microscopic inspection. Samples from the scaling of the scalp can be examined with potassium hydroxide (KOH) on a microscope slide. Hyphae, spores, and endo/ectothrix invasion can be seen through the microsope.
Continue to: Laboratory testing is helpful, but not needed.
Laboratory testing is helpful, but not needed. Testing for tinea capitis would require that you obtain a sample from the affected area using a swab, edge of a scalpel blade, or scalp brush.7 Because treatment can require weeks of medication, diagnosis should be confirmed with a KOH or culture when possible.
Newer antifungalsprovide a Tx advantage
Oral antifungal medications are the treatment of choice for tinea capitis. Newer antifungals, such as terbinafine and fluconazole, require a 3- to 6-week course compared to the standard 6- to 8-week course of griseofulvin.1 Also, antifungal shampoos—such as those that contain selenium sulfide—may be used for topical treatment but only as adjuvant therapy.1,2
For our patient, we dispensed a 3-week course of oral fluconazole, 3 to 6 mg/kg, to be given daily by his parents. We also recommended the use of an antidandruff shampoo, if possible. The treatment outcome was not known because our team’s humanitarian global health trip had ended.
An 11-year-old boy sought care at a small village’s health center in Panama for scalp itching and subtle hair loss. He was seen by a family physician (RU) and a team of medical students who were there as part of a humanitarian trip. The patient denied any hair pulling. He had a history of treatment for head lice.
Our physical examination revealed mild alopecia and scaling on the scalp (FIGURE 1), but what we saw through the dermatoscope (FIGURE 2) made the diagnosis clear.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Tinea capitis
On dermatoscopic examination (10× magnification), there were numerous “black dots” or broken hair shafts within patches of hair loss (FIGURE 3), which is indicative of tinea capitis.1,2 This condition causes hair shafts to break, creating “comma hairs” and black dots. The hairs are uniform in thickness and color and bend distally, like a comma.3
Tinea capitis (commonly called ringworm of the scalp) is a fungal infection caused by Trichophyton and Microsporum dermatophytes. It is the most common pediatric dermatophyte infection in the world; the usual age of onset is 5 to 10 years.2 The incidence of tinea capitis in the United States is not known because cases are no longer registered by public health agencies. That said, a Northern California study that tracked occurrences in children younger than 15 years from 1998 to 2007 found that the incidence was on the decline and lower in girls compared to boys (111.9 vs 146.4, respectively, in 1998; 27.9 vs 39.9, respectively, in 2007).4 Incidence rates were calculated per 10,000 eligible children.4
Tinea capitis can spread by contact with infected individuals and contaminated objects, including combs, towels, toys, and bedding.1 Fungal spores can remain viable on these surfaces for months.
In a study of 69 patients with tinea capitis (23 females, 46 males; mean age, 12 years), the risk factors for spreading infection included participation in sports, contact with an animal, a recent haircut, and use of a swimming pool.5
4 conditions you’ll want to rule out
The following conditions should be considered as part of the differential when a patient presents with an itchy scalp and/or hair loss.
Continue to: Psoriasis of the scalp...
Psoriasis of the scalp is characterized by scaling of the scalp along with crusted plaques. It is often accompanied by similar psoriatic plaques on the elbows, knees, and other areas of the body. Examination of our patient showed no psoriatic plaques.
Seborrhea of the scalp (also known as dandruff) is a very common diagnosis. However, it is unlikely to cause hair loss. It has widespread involvement of the scalp compared to tinea capitis, which is local and patchy. Our patient’s patches of hair loss indicated that seborrhea was unlikely.
Alopecia areata. Individuals develop this condition due to an autoimmune process affecting hair follicles. However, the resulting hair loss does not cause significant scaling, inflammation, scarring, or pain in the affected area. Further, this condition can cause the loss of the entire hair shaft.
Trichotillomania is an impulse control disorder that causes patients to pull out their own hair. There is no scaling of the scalp in this condition.
A dermatoscope can beuseful in making the Dx
Although clinical appearance and patient presentation are adequate to establish the diagnosis of tinea capitis, this case demonstrates the utility of a dermatoscope in making the diagnosis of tinea capitis. Previous studies have shown that dermoscopy allows for rapid identification of the broken hair shafts, which are a key distinction from alopecia areata.3,6
Microscopic inspection. Samples from the scaling of the scalp can be examined with potassium hydroxide (KOH) on a microscope slide. Hyphae, spores, and endo/ectothrix invasion can be seen through the microsope.
Continue to: Laboratory testing is helpful, but not needed.
Laboratory testing is helpful, but not needed. Testing for tinea capitis would require that you obtain a sample from the affected area using a swab, edge of a scalpel blade, or scalp brush.7 Because treatment can require weeks of medication, diagnosis should be confirmed with a KOH or culture when possible.
Newer antifungalsprovide a Tx advantage
Oral antifungal medications are the treatment of choice for tinea capitis. Newer antifungals, such as terbinafine and fluconazole, require a 3- to 6-week course compared to the standard 6- to 8-week course of griseofulvin.1 Also, antifungal shampoos—such as those that contain selenium sulfide—may be used for topical treatment but only as adjuvant therapy.1,2
For our patient, we dispensed a 3-week course of oral fluconazole, 3 to 6 mg/kg, to be given daily by his parents. We also recommended the use of an antidandruff shampoo, if possible. The treatment outcome was not known because our team’s humanitarian global health trip had ended.
1. Usatine R, Smith MA, Mayeaux Jr EJ, Chumley HS. The Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill; 2019.
2. Handler MZ. Tinea capitis. Medscape. https://emedicine.medscape.com/article/1091351-overview. Updated February 21, 2020. Accessed November 30, 2020.
3. Hernández-Bel P, Malvehy J, Crocker A, et al. Comma hairs: a new dermoscopic marker for tinea capitis [in Spanish]. Actas Dermosifiliogr. 2012;103:836-837.
4. Mirmirani P, Lue-Yen T. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California. J Am Acad Dermatol. 2013;69:916-921.
5. Mikaeili A, Kavaoussi H, Hashemian AH, et al. Clinico-mycological profile of tinea capitis and its comparative response to griseofulvin versus terbinafine. Curr Med Mycol. 2019;5:15-20.
6. Slowinska M, Rudnicka L, Schwartz RA, et al. Comma hairs: a dermatoscopic marker for tinea capitis: a rapid diagnostic method. Journal of the American Academy of Dermatology. 2008;59(suppl 5):S77-S79.
1. Usatine R, Smith MA, Mayeaux Jr EJ, Chumley HS. The Color Atlas and Synopsis of Family Medicine. 3rd ed. New York, NY: McGraw-Hill; 2019.
2. Handler MZ. Tinea capitis. Medscape. https://emedicine.medscape.com/article/1091351-overview. Updated February 21, 2020. Accessed November 30, 2020.
3. Hernández-Bel P, Malvehy J, Crocker A, et al. Comma hairs: a new dermoscopic marker for tinea capitis [in Spanish]. Actas Dermosifiliogr. 2012;103:836-837.
4. Mirmirani P, Lue-Yen T. Epidemiologic trends in pediatric tinea capitis: a population-based study from Kaiser Permanente Northern California. J Am Acad Dermatol. 2013;69:916-921.
5. Mikaeili A, Kavaoussi H, Hashemian AH, et al. Clinico-mycological profile of tinea capitis and its comparative response to griseofulvin versus terbinafine. Curr Med Mycol. 2019;5:15-20.
6. Slowinska M, Rudnicka L, Schwartz RA, et al. Comma hairs: a dermatoscopic marker for tinea capitis: a rapid diagnostic method. Journal of the American Academy of Dermatology. 2008;59(suppl 5):S77-S79.

Widespread Purple Plaques
The Diagnosis: Kaposi Sarcoma
On initial presentation, the differential diagnosis included secondary syphilis, Kaposi sarcoma (KS), lichen planus pigmentosus, sarcoidosis, and psoriasis. A laboratory workup was ordered, which included complete blood cell count, comprehensive metabolic panel, antinuclear antibodies, anti-Ro/Sjögren syndrome antigen A and anti-La/Sjögren syndrome antigen B autoantibodies, angiotensin-converting enzyme, rapid plasma reagin, and human immunodeficiency virus (HIV) antibodies. A 4-mm punch biopsy of the rash also was performed from the right upper back. Histology revealed a vascular proliferation that was diffusely positive for human herpesvirus 8 (HHV-8)(Figure 1). The patient was informed of the diagnosis, at which time he revealed he had a history of homosexual relationships, with his last sexual contact being more than 1 year prior to presentation. The laboratory workup confirmed a diagnosis of HIV, and the remainder of the tests were unremarkable.
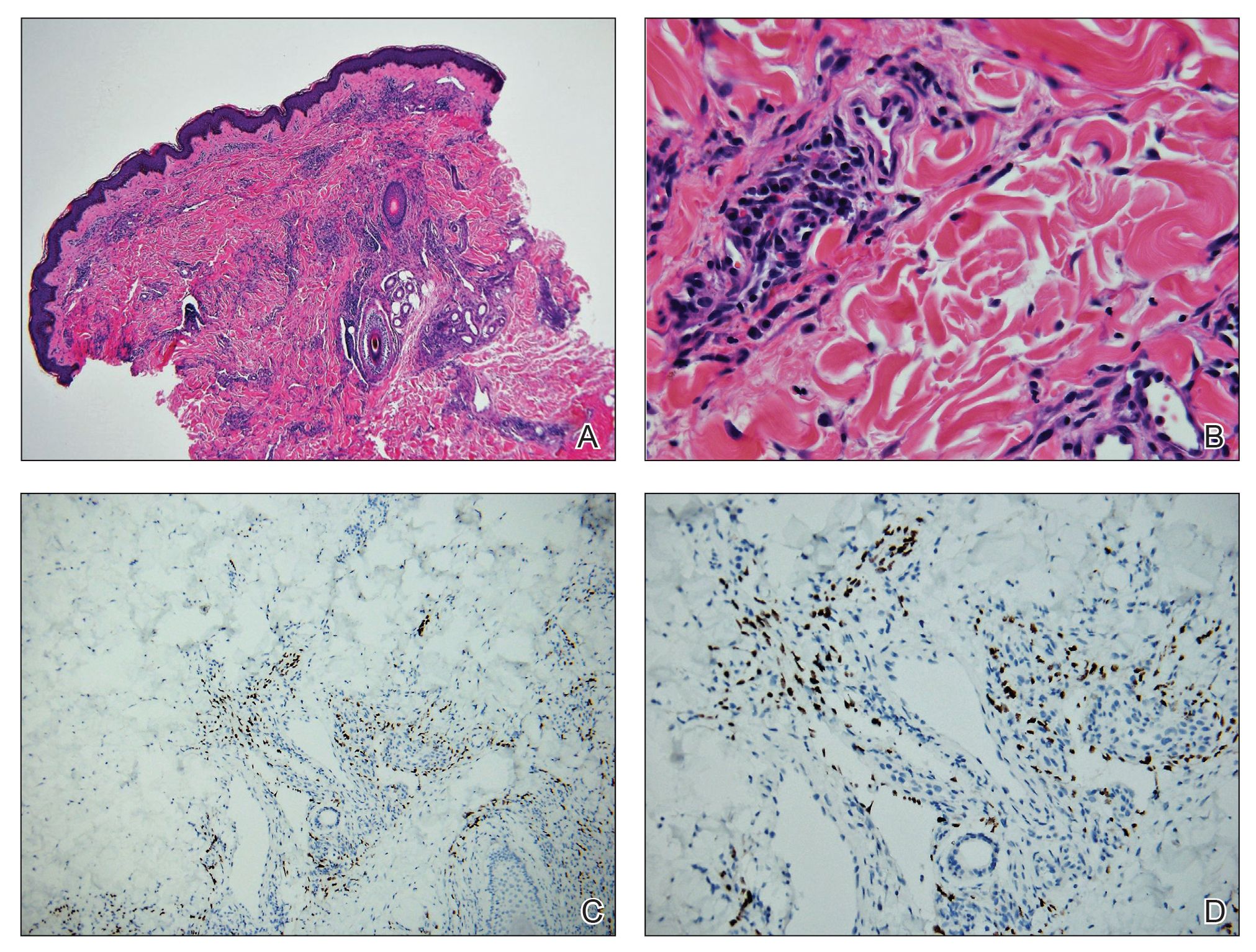
He was referred to our university's HIV clinic where he was started on highly active antiretroviral therapy (HAART). His facial swelling worsened, leading to hospital admission. Computed tomography (CT) of the chest, abdomen, and pelvis showed diffuse lymphadenopathy and lung nodules concerning for visceral involvement of KS. Hematology and oncology was consulted for further evaluation, and he was treated with 6 cycles of doxorubicin 20 mg/m2, which led to resolution of the lung nodules on CT and improvement of the rash burden. He was then started on alitretinoin gel 0.1% twice daily, which led to continued slow improvement (Figure 2).

Kaposi sarcoma is a vascular neoplasm that occurs from infection with HHV-8. It typically presents as painless, reddish to violaceous macules or patches involving the skin and mucosa that often progress to plaques or nodules with possible visceral involvement. Kaposi sarcoma is classified into 4 subtypes based on epidemiology and clinical presentation: classic, endemic, iatrogenic, and AIDS associated.1,2
Classic KS primarily affects elderly males of Mediterranean or Eastern European descent, with a mean age of 64.1 years and a male to female ratio of 3 to 1. It has an indolent course and a strong predilection for the skin of the lower extremities. The endemic form occurs mainly in Africa and has a more aggressive course, especially the lymphadenopathic type that affects children younger than 10 years.3 Iatrogenic KS develops in immunosuppressed patients, such as transplant recipients, and may regress if the immunosuppressive agent is stopped.1 Kaposi sarcoma is an AIDS-defining illness and is the most common malignancy in AIDS patients. It is strongly associated with a low CD4 count, which accounts for the notable decline in its incidence after the widespread introduction of HAART.1 Among HIV patients, KS has the highest incidence in men who have sex with men. This population has a higher seroprevalence of HHV-8, which suggests possible sexual transmission of HHV-8. AIDS-associated KS most commonly involves the lower extremities, face, and oral mucosa. It may have visceral involvement, particularly of the gastrointestinal and respiratory systems, which carries a poor prognosis.4,5
Approximately 40% of patients presenting with KS have gastrointestinal tract involvement.6 Of these patients, up to 80% are asymptomatic, with diagnosis usually being made on endoscopy.7 In contrast, pulmonary KS is less common and typically is symptomatic. It can involve the lung parenchyma, airways, or pleura and is diagnosed by chest radiography or CT scans. Glucocorticoid therapy is a known trigger for pulmonary KS exacerbation.8
All 4 subtypes share the same histopathologic findings consisting of spindled endothelial cell proliferation, inflammation, and angiogenesis. Immunohistochemistry reveals tumor cells that are CD34 and CD31 positive but are factor VIII negative. Staining for HHV-8 antigen is used to confirm the diagnosis. The inflammatory infiltrate predominantly is lymphocytic with scattered plasma cells.9
The laboratory results and histopathologic findings clearly indicated a diagnosis of KS in our patient. Other entities in the clinical differential would have shown notably different histopathologic findings and laboratory results. Lichen planus pigmentosus displays a lichenoid infiltrate and pigment dropout on histology. Histologic findings of psoriasis include psoriasiform acanthosis, dilated vessels in the dermal papillae, thinning of suprapapillary plates, and neutrophilic microabscesses. Sarcoidosis would demonstrate naked granulomas on histopathology. Syphilis displays variable but often psoriasiform or lichenoid findings on histology, and a positive rapid plasma reagin also would be noted.
First-line treatment of AIDS-related KS is HAART. For patients with severe and rapidly progressive KS or with visceral involvement, cytotoxic chemotherapy with doxorubicin or taxanes often is required. Additional therapies include radiotherapy, topical alitretinoin, and cryotherapy.1,10
- Schneider JW, Dittmer DP. Diagnosis and treatment of Kaposi sarcoma. Am J Clin Dermatol. 2017;18:529-539.
- Schwartz RA, Micali G, Nasca MR, et al. Kaposi sarcoma: a continuing conundrum. J Am Acad Dermatol. 2008;59:179-206; quiz 207-208.
- Mohanna S, Maco V, Bravo F, et al. Epidemiology and clinical characteristics of classic Kaposi’s sarcoma, seroprevalence, and variants of human herpesvirus 8 in South America: a critical review of an old disease. Int J Infect Dis. 2005;9:239-250.
- Beral V, Peterman TA, Berkelman RL, et al. Kaposi’s sarcoma among persons with AIDS: a sexually transmitted infection? Lancet. 1990;335:123-128.
- Smith NA, Sabin CA, Gopal R, et al. Serologic evidence of human herpesvirus 8 transmission by homosexual but not heterosexual sex. J Infect Dis. 1999;180:600-606.
- Arora M, Goldberg EM. Kaposi sarcoma involving the gastrointestinal tract. Gastroenterol Hepatol (N Y). 2010;6:459-462.
- Parente F, Cernuschi M, Orlando G, et al. Kaposi’s sarcoma and AIDS: frequency of gastrointestinal involvement and its effect on survival. a prospective study in a heterogeneous population. Scand J Gastroenterol. 1991;26:1007-1012.
- Gasparetto TD, Marchiori E, Lourenco S, et al. Pulmonary involvement in Kaposi sarcoma: correlation between imaging and pathology. Orphanet J Rare Dis. 2009;4:18.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294.
- Regnier-Rosencher E, Guillot B, Dupin N. Treatments for classic Kaposi sarcoma: a systematic review of the literature. J Am Acad Dermatol. 2013;68:313-331.
The Diagnosis: Kaposi Sarcoma
On initial presentation, the differential diagnosis included secondary syphilis, Kaposi sarcoma (KS), lichen planus pigmentosus, sarcoidosis, and psoriasis. A laboratory workup was ordered, which included complete blood cell count, comprehensive metabolic panel, antinuclear antibodies, anti-Ro/Sjögren syndrome antigen A and anti-La/Sjögren syndrome antigen B autoantibodies, angiotensin-converting enzyme, rapid plasma reagin, and human immunodeficiency virus (HIV) antibodies. A 4-mm punch biopsy of the rash also was performed from the right upper back. Histology revealed a vascular proliferation that was diffusely positive for human herpesvirus 8 (HHV-8)(Figure 1). The patient was informed of the diagnosis, at which time he revealed he had a history of homosexual relationships, with his last sexual contact being more than 1 year prior to presentation. The laboratory workup confirmed a diagnosis of HIV, and the remainder of the tests were unremarkable.
He was referred to our university's HIV clinic where he was started on highly active antiretroviral therapy (HAART). His facial swelling worsened, leading to hospital admission. Computed tomography (CT) of the chest, abdomen, and pelvis showed diffuse lymphadenopathy and lung nodules concerning for visceral involvement of KS. Hematology and oncology was consulted for further evaluation, and he was treated with 6 cycles of doxorubicin 20 mg/m2, which led to resolution of the lung nodules on CT and improvement of the rash burden. He was then started on alitretinoin gel 0.1% twice daily, which led to continued slow improvement (Figure 2).
Kaposi sarcoma is a vascular neoplasm that occurs from infection with HHV-8. It typically presents as painless, reddish to violaceous macules or patches involving the skin and mucosa that often progress to plaques or nodules with possible visceral involvement. Kaposi sarcoma is classified into 4 subtypes based on epidemiology and clinical presentation: classic, endemic, iatrogenic, and AIDS associated.1,2
Classic KS primarily affects elderly males of Mediterranean or Eastern European descent, with a mean age of 64.1 years and a male to female ratio of 3 to 1. It has an indolent course and a strong predilection for the skin of the lower extremities. The endemic form occurs mainly in Africa and has a more aggressive course, especially the lymphadenopathic type that affects children younger than 10 years.3 Iatrogenic KS develops in immunosuppressed patients, such as transplant recipients, and may regress if the immunosuppressive agent is stopped.1 Kaposi sarcoma is an AIDS-defining illness and is the most common malignancy in AIDS patients. It is strongly associated with a low CD4 count, which accounts for the notable decline in its incidence after the widespread introduction of HAART.1 Among HIV patients, KS has the highest incidence in men who have sex with men. This population has a higher seroprevalence of HHV-8, which suggests possible sexual transmission of HHV-8. AIDS-associated KS most commonly involves the lower extremities, face, and oral mucosa. It may have visceral involvement, particularly of the gastrointestinal and respiratory systems, which carries a poor prognosis.4,5
Approximately 40% of patients presenting with KS have gastrointestinal tract involvement.6 Of these patients, up to 80% are asymptomatic, with diagnosis usually being made on endoscopy.7 In contrast, pulmonary KS is less common and typically is symptomatic. It can involve the lung parenchyma, airways, or pleura and is diagnosed by chest radiography or CT scans. Glucocorticoid therapy is a known trigger for pulmonary KS exacerbation.8
All 4 subtypes share the same histopathologic findings consisting of spindled endothelial cell proliferation, inflammation, and angiogenesis. Immunohistochemistry reveals tumor cells that are CD34 and CD31 positive but are factor VIII negative. Staining for HHV-8 antigen is used to confirm the diagnosis. The inflammatory infiltrate predominantly is lymphocytic with scattered plasma cells.9
The laboratory results and histopathologic findings clearly indicated a diagnosis of KS in our patient. Other entities in the clinical differential would have shown notably different histopathologic findings and laboratory results. Lichen planus pigmentosus displays a lichenoid infiltrate and pigment dropout on histology. Histologic findings of psoriasis include psoriasiform acanthosis, dilated vessels in the dermal papillae, thinning of suprapapillary plates, and neutrophilic microabscesses. Sarcoidosis would demonstrate naked granulomas on histopathology. Syphilis displays variable but often psoriasiform or lichenoid findings on histology, and a positive rapid plasma reagin also would be noted.
First-line treatment of AIDS-related KS is HAART. For patients with severe and rapidly progressive KS or with visceral involvement, cytotoxic chemotherapy with doxorubicin or taxanes often is required. Additional therapies include radiotherapy, topical alitretinoin, and cryotherapy.1,10
The Diagnosis: Kaposi Sarcoma
On initial presentation, the differential diagnosis included secondary syphilis, Kaposi sarcoma (KS), lichen planus pigmentosus, sarcoidosis, and psoriasis. A laboratory workup was ordered, which included complete blood cell count, comprehensive metabolic panel, antinuclear antibodies, anti-Ro/Sjögren syndrome antigen A and anti-La/Sjögren syndrome antigen B autoantibodies, angiotensin-converting enzyme, rapid plasma reagin, and human immunodeficiency virus (HIV) antibodies. A 4-mm punch biopsy of the rash also was performed from the right upper back. Histology revealed a vascular proliferation that was diffusely positive for human herpesvirus 8 (HHV-8)(Figure 1). The patient was informed of the diagnosis, at which time he revealed he had a history of homosexual relationships, with his last sexual contact being more than 1 year prior to presentation. The laboratory workup confirmed a diagnosis of HIV, and the remainder of the tests were unremarkable.
He was referred to our university's HIV clinic where he was started on highly active antiretroviral therapy (HAART). His facial swelling worsened, leading to hospital admission. Computed tomography (CT) of the chest, abdomen, and pelvis showed diffuse lymphadenopathy and lung nodules concerning for visceral involvement of KS. Hematology and oncology was consulted for further evaluation, and he was treated with 6 cycles of doxorubicin 20 mg/m2, which led to resolution of the lung nodules on CT and improvement of the rash burden. He was then started on alitretinoin gel 0.1% twice daily, which led to continued slow improvement (Figure 2).
Kaposi sarcoma is a vascular neoplasm that occurs from infection with HHV-8. It typically presents as painless, reddish to violaceous macules or patches involving the skin and mucosa that often progress to plaques or nodules with possible visceral involvement. Kaposi sarcoma is classified into 4 subtypes based on epidemiology and clinical presentation: classic, endemic, iatrogenic, and AIDS associated.1,2
Classic KS primarily affects elderly males of Mediterranean or Eastern European descent, with a mean age of 64.1 years and a male to female ratio of 3 to 1. It has an indolent course and a strong predilection for the skin of the lower extremities. The endemic form occurs mainly in Africa and has a more aggressive course, especially the lymphadenopathic type that affects children younger than 10 years.3 Iatrogenic KS develops in immunosuppressed patients, such as transplant recipients, and may regress if the immunosuppressive agent is stopped.1 Kaposi sarcoma is an AIDS-defining illness and is the most common malignancy in AIDS patients. It is strongly associated with a low CD4 count, which accounts for the notable decline in its incidence after the widespread introduction of HAART.1 Among HIV patients, KS has the highest incidence in men who have sex with men. This population has a higher seroprevalence of HHV-8, which suggests possible sexual transmission of HHV-8. AIDS-associated KS most commonly involves the lower extremities, face, and oral mucosa. It may have visceral involvement, particularly of the gastrointestinal and respiratory systems, which carries a poor prognosis.4,5
Approximately 40% of patients presenting with KS have gastrointestinal tract involvement.6 Of these patients, up to 80% are asymptomatic, with diagnosis usually being made on endoscopy.7 In contrast, pulmonary KS is less common and typically is symptomatic. It can involve the lung parenchyma, airways, or pleura and is diagnosed by chest radiography or CT scans. Glucocorticoid therapy is a known trigger for pulmonary KS exacerbation.8
All 4 subtypes share the same histopathologic findings consisting of spindled endothelial cell proliferation, inflammation, and angiogenesis. Immunohistochemistry reveals tumor cells that are CD34 and CD31 positive but are factor VIII negative. Staining for HHV-8 antigen is used to confirm the diagnosis. The inflammatory infiltrate predominantly is lymphocytic with scattered plasma cells.9
The laboratory results and histopathologic findings clearly indicated a diagnosis of KS in our patient. Other entities in the clinical differential would have shown notably different histopathologic findings and laboratory results. Lichen planus pigmentosus displays a lichenoid infiltrate and pigment dropout on histology. Histologic findings of psoriasis include psoriasiform acanthosis, dilated vessels in the dermal papillae, thinning of suprapapillary plates, and neutrophilic microabscesses. Sarcoidosis would demonstrate naked granulomas on histopathology. Syphilis displays variable but often psoriasiform or lichenoid findings on histology, and a positive rapid plasma reagin also would be noted.
First-line treatment of AIDS-related KS is HAART. For patients with severe and rapidly progressive KS or with visceral involvement, cytotoxic chemotherapy with doxorubicin or taxanes often is required. Additional therapies include radiotherapy, topical alitretinoin, and cryotherapy.1,10
- Schneider JW, Dittmer DP. Diagnosis and treatment of Kaposi sarcoma. Am J Clin Dermatol. 2017;18:529-539.
- Schwartz RA, Micali G, Nasca MR, et al. Kaposi sarcoma: a continuing conundrum. J Am Acad Dermatol. 2008;59:179-206; quiz 207-208.
- Mohanna S, Maco V, Bravo F, et al. Epidemiology and clinical characteristics of classic Kaposi’s sarcoma, seroprevalence, and variants of human herpesvirus 8 in South America: a critical review of an old disease. Int J Infect Dis. 2005;9:239-250.
- Beral V, Peterman TA, Berkelman RL, et al. Kaposi’s sarcoma among persons with AIDS: a sexually transmitted infection? Lancet. 1990;335:123-128.
- Smith NA, Sabin CA, Gopal R, et al. Serologic evidence of human herpesvirus 8 transmission by homosexual but not heterosexual sex. J Infect Dis. 1999;180:600-606.
- Arora M, Goldberg EM. Kaposi sarcoma involving the gastrointestinal tract. Gastroenterol Hepatol (N Y). 2010;6:459-462.
- Parente F, Cernuschi M, Orlando G, et al. Kaposi’s sarcoma and AIDS: frequency of gastrointestinal involvement and its effect on survival. a prospective study in a heterogeneous population. Scand J Gastroenterol. 1991;26:1007-1012.
- Gasparetto TD, Marchiori E, Lourenco S, et al. Pulmonary involvement in Kaposi sarcoma: correlation between imaging and pathology. Orphanet J Rare Dis. 2009;4:18.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294.
- Regnier-Rosencher E, Guillot B, Dupin N. Treatments for classic Kaposi sarcoma: a systematic review of the literature. J Am Acad Dermatol. 2013;68:313-331.
- Schneider JW, Dittmer DP. Diagnosis and treatment of Kaposi sarcoma. Am J Clin Dermatol. 2017;18:529-539.
- Schwartz RA, Micali G, Nasca MR, et al. Kaposi sarcoma: a continuing conundrum. J Am Acad Dermatol. 2008;59:179-206; quiz 207-208.
- Mohanna S, Maco V, Bravo F, et al. Epidemiology and clinical characteristics of classic Kaposi’s sarcoma, seroprevalence, and variants of human herpesvirus 8 in South America: a critical review of an old disease. Int J Infect Dis. 2005;9:239-250.
- Beral V, Peterman TA, Berkelman RL, et al. Kaposi’s sarcoma among persons with AIDS: a sexually transmitted infection? Lancet. 1990;335:123-128.
- Smith NA, Sabin CA, Gopal R, et al. Serologic evidence of human herpesvirus 8 transmission by homosexual but not heterosexual sex. J Infect Dis. 1999;180:600-606.
- Arora M, Goldberg EM. Kaposi sarcoma involving the gastrointestinal tract. Gastroenterol Hepatol (N Y). 2010;6:459-462.
- Parente F, Cernuschi M, Orlando G, et al. Kaposi’s sarcoma and AIDS: frequency of gastrointestinal involvement and its effect on survival. a prospective study in a heterogeneous population. Scand J Gastroenterol. 1991;26:1007-1012.
- Gasparetto TD, Marchiori E, Lourenco S, et al. Pulmonary involvement in Kaposi sarcoma: correlation between imaging and pathology. Orphanet J Rare Dis. 2009;4:18.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294.
- Regnier-Rosencher E, Guillot B, Dupin N. Treatments for classic Kaposi sarcoma: a systematic review of the literature. J Am Acad Dermatol. 2013;68:313-331.

A 24-year-old Black man presented for evaluation of an asymptomatic rash on the face, chest, back, and arms that had been progressively spreading over the course of 3 months. He had some swelling of the lips prior to the onset of the rash and was prescribed prednisone 10 mg daily by an outside physician. He had no known medical problems and was taking no medications. Physical examination revealed numerous violaceous plaques scattered symmetrically on the trunk, arms, legs, and face. His family history was negative for autoimmune disease, and a review of systems was unremarkable. He denied any recent sexual contacts.

Antihistamine prescribing for AD varies by specialty
(AD), according to an analysis of a national database.
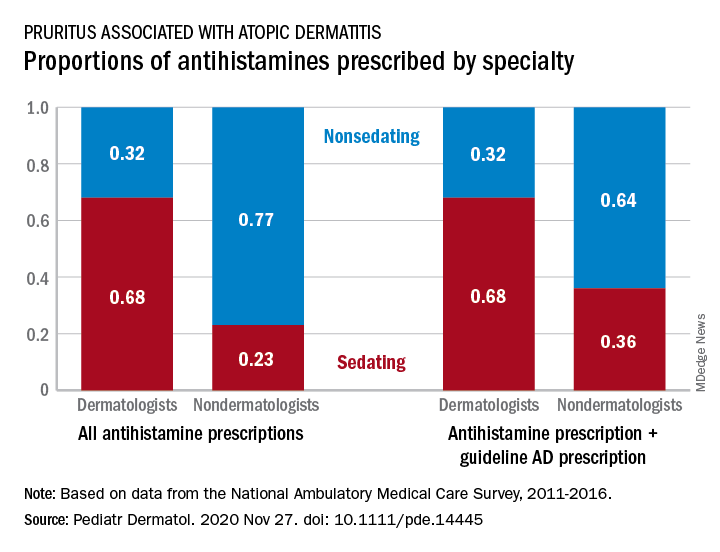
Dermatologists were more likely to prescribe sedating than nonsedating antihistamines (0.68 vs. 0.32) for patients with AD, but the reverse applied to nondermatologists, whose antihistamine distribution was 0.23 sedating and 0.77 nonsedating, based on 2011-2016 data from the National Ambulatory Medical Care Survey.
The numbers were similar for new antihistamine prescriptions, with sedating/nonsedating proportions of 0.60/0.40 for dermatologists and 0.24/0.76 for nondermatologists. Addition of guideline-recommended drugs such as topical corticosteroids and calcineurin inhibitors to the AD equation did not change the result, as dermatologists again showed a preference for sedating antihistamines, compared with nondermatologists, the investigators said.
The data also showed that Black patients with AD were more likely than were White patients to receive prescriptions for first-generation antihistamines and for therapies recommended by the AAD guidelines, and that patients under 21 years received more sedating antihistamines than did patients over age 21, they reported.
The age disparity “may be due to patient preference, as sedation effects may be less desirable to adult patients,” the investigators noted.
SOURCE: Garg S et al. Pediatr Dermatol. 2020 Nov 27. doi: 10.1111/pde.14445.
(AD), according to an analysis of a national database.
Dermatologists were more likely to prescribe sedating than nonsedating antihistamines (0.68 vs. 0.32) for patients with AD, but the reverse applied to nondermatologists, whose antihistamine distribution was 0.23 sedating and 0.77 nonsedating, based on 2011-2016 data from the National Ambulatory Medical Care Survey.
The numbers were similar for new antihistamine prescriptions, with sedating/nonsedating proportions of 0.60/0.40 for dermatologists and 0.24/0.76 for nondermatologists. Addition of guideline-recommended drugs such as topical corticosteroids and calcineurin inhibitors to the AD equation did not change the result, as dermatologists again showed a preference for sedating antihistamines, compared with nondermatologists, the investigators said.
The data also showed that Black patients with AD were more likely than were White patients to receive prescriptions for first-generation antihistamines and for therapies recommended by the AAD guidelines, and that patients under 21 years received more sedating antihistamines than did patients over age 21, they reported.
The age disparity “may be due to patient preference, as sedation effects may be less desirable to adult patients,” the investigators noted.
SOURCE: Garg S et al. Pediatr Dermatol. 2020 Nov 27. doi: 10.1111/pde.14445.
(AD), according to an analysis of a national database.
Dermatologists were more likely to prescribe sedating than nonsedating antihistamines (0.68 vs. 0.32) for patients with AD, but the reverse applied to nondermatologists, whose antihistamine distribution was 0.23 sedating and 0.77 nonsedating, based on 2011-2016 data from the National Ambulatory Medical Care Survey.
The numbers were similar for new antihistamine prescriptions, with sedating/nonsedating proportions of 0.60/0.40 for dermatologists and 0.24/0.76 for nondermatologists. Addition of guideline-recommended drugs such as topical corticosteroids and calcineurin inhibitors to the AD equation did not change the result, as dermatologists again showed a preference for sedating antihistamines, compared with nondermatologists, the investigators said.
The data also showed that Black patients with AD were more likely than were White patients to receive prescriptions for first-generation antihistamines and for therapies recommended by the AAD guidelines, and that patients under 21 years received more sedating antihistamines than did patients over age 21, they reported.
The age disparity “may be due to patient preference, as sedation effects may be less desirable to adult patients,” the investigators noted.
SOURCE: Garg S et al. Pediatr Dermatol. 2020 Nov 27. doi: 10.1111/pde.14445.
FROM PEDIATRIC DERMATOLOGY
FDA approves liraglutide for adolescents with obesity
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.

But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.
But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.
The Food and Drug Administration’s new indication for liraglutide (Saxenda) for weight loss in adolescents with obesity, announced on Dec. 4, received welcome as a milestone for advancing a field that’s seen no new drug options since 2003 and boosted by 50% the list of agents indicated for weight loss in this age group.
But liraglutide’s track record in adolescents in the key study published earlier in 2020 left some experts unconvinced that liraglutide’s modest effects would have much impact on blunting the expanding cohort of teens who are obese.
“Until now, we’ve had phentermine and orlistat with FDA approval” for adolescents with obesity, and phentermine’s label specifies only patients older than 16 years. “It’s important that the FDA deemed liraglutide’s benefits greater than its risks for adolescents,” said Aaron S. Kelly, PhD, leader of the 82-week, multicenter, randomized study of liraglutide in 251 adolescents with obesity that directly led to the FDA’s action.
“We have results from a strong, published randomized trial, and the green light from the FDA, and that should give clinicians reassurance and confidence to use liraglutide clinically,” said Dr. Kelly, professor of pediatrics and codirector of the Center for Pediatric Obesity Medicine at the University of Minnesota in Minneapolis.
An ‘unimpressive’ drop in BMI
Sonia Caprio, MD, had a more skeptical take on liraglutide’s role with its new indication: “Approval of higher-dose liraglutide is an improvement that reflects a willingness to accept adolescent obesity as a disease that needs treatment with pharmacological agents. However, the study, published in New England Journal of Medicine, was not impressive in terms of weight loss, and more importantly liraglutide was not associated with any significant changes in metabolic markers” such as insulin resistance, high-sensitivity C-reactive protein, lipoproteins and triglycerides, and hemoglobin A1c.
The observed average 5% drop in body mass index seen after a year on liraglutide treatment, compared with baseline and relative to no average change from baseline in the placebo arm, was “totally insufficient, and will not diminish any of the metabolic complications in youth with obesity,” commented Dr. Caprio, an endocrinologist and professor of pediatrics at Yale University in New Haven, Conn.
Results from the study led by Dr. Kelly also showed that liraglutide for 56 weeks cut BMI by 5% in 43% of patients, and by 10% in 26%, compared with respective rates of 19% and 8% among those in the placebo-control arm. He took a more expansive view of the potential benefits from weight loss of the caliber demonstrated by liraglutide in the study.
“In general, we wait too long with obesity in children; the earlier the intervention the better. A 3% or 4% reduction in BMI at 12 or 13 years old can pay big dividends down the road” when a typical adolescent trajectory of steadily rising weight can be flattened, he said in an interview.
Bariatric and metabolic surgery, although highly effective and usually safe, is seen by many clinicians, patients, and families as an “intervention of last resort,” and its very low level of uptake in adolescents bears witness to that reputation. It also creates an important niche for safe and effective drugs to fill as an adjunct to lifestyle changes, which are often ineffective when used by themselves. Liraglutide’s main mechanism for weight loss is depressing hunger, Dr. Kelly noted.
Existing meds have limitations
The existing medical treatments, orlistat and phentermine, both have significant drawbacks that limit their use. Orlistat (Xenical, Alli), FDA approved for adolescents 12-16 years old since 2003, limits intestinal fat absorption and as a result often produces unwanted GI effects. Phentermine’s approval for older adolescents dates from 1959 and has a weak evidence base, its label limits it to “short-term” use that’s generally taken to mean a maximum of 12 weeks. And, as a stimulant, phentermine has often been regarded as potentially dangerous, although Dr. Kelly noted that stimulants are well-accepted treatments for other disorders in children and adolescents.
“The earlier we treat obesity in youth, the better, given that it tends to track into adulthood,” agreed Dr. Caprio. “However, it remains to be seen whether weight reduction with a pharmacological agent is going to help prevent the intractable trajectories of weight and its complications. So far, it looks like surgery may be more efficacious,” she said in an interview.
Another drawback for the near future with liraglutide will likely be its cost for many patients, more than $10,000/year at full retail prices for the weight-loss formulation, given that insurers have had a poor record of covering the drug for this indication in adults, both Dr. Caprio and Dr. Kelly noted.
Compliance with liraglutide is also important. Dr. Kelly’s study followed patients for their first 26 weeks off treatment after 56 weeks on the drug, and showed that on average weights rebounded to virtually baseline levels by 6 months after treatment stopped.
Obesity treatment lasts a lifetime
“Obesity is a chronic disease, that requires chronic treatment, just like hypertension,” Dr. Kelly stressed, and cited the rebound seen in his study when liraglutide stopped as further proof of that concept. “All obesity treatment is lifelong,” he maintained.
He highlighted the importance of clinicians discussing with adolescent patients and their families the prospect of potentially remaining on liraglutide treatment for years to maintain weight loss. His experience with the randomized study convinced him that many adolescents with obesity are amenable to daily subcutaneous injection using the pen device that liraglutide comes in, but he acknowledged that some teens find this off-putting.
For the near term, Dr. Kelly foresaw liraglutide treatment of adolescents as something that will mostly be administered to patients who seek care at centers that specialize in obesity management. “I’ll think we’ll eventually see it move to more primary care settings, but that will be down the road.”
The study of liraglutide in adolescents was sponsored by Novo Nordisk, the company that markets liraglutide (Saxenda). Dr. Kelly has been a consultant to Novo Nordisk and also to Orexigen Therapeutics, Vivus, and WW, and he has received research funding from AstraZeneca. Dr. Caprio had no disclosures.

Peripheral neuropathy tied to mortality in adults without diabetes
researchers reported in Annals of Internal Medicine.

The findings do not necessarily mean that doctors should implement broader screening for peripheral neuropathy at this time, however, the investigators said.
“Doctors don’t typically screen for peripheral neuropathy in persons without diabetes,” senior author Elizabeth Selvin, PhD, MPH, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health, Baltimore, said in an interview.
“Our study shows that peripheral neuropathy – as assessed by decreased sensation in the feet – is common, even in people without diabetes,” Dr. Selvin explained. “It is not yet clear whether we should be screening people without diabetes since we don’t have clear treatments, but our study does suggest that this condition is an underrecognized condition that is associated with poor outcomes.”
Patients with diabetes typically undergo annual foot examinations that include screening for peripheral neuropathy, but that’s not the case for most adults in the absence of diabetes.
“I don’t know if we can make the jump that we should be screening people without diabetes,” said first author Caitlin W. Hicks, MD, assistant professor of surgery, division of vascular surgery and endovascular therapy, Johns Hopkins University, Baltimore. “Right now, we do not exactly know what it means in the people without diabetes, and we definitely do not know how to treat it. So, screening for it will tell us that this person has this and is at higher risk of mortality than someone who doesn’t, but we do not know what to do with that information yet.”
Nevertheless, the study raises the question of whether physicians should pay more attention to peripheral neuropathy in people without diabetes, said Dr. Hicks, director of research at the university’s diabetic foot and wound service.
Heightened risk
To examine associations between peripheral neuropathy and all-cause and cardiovascular mortality in U.S. adults, Dr. Hicks and colleagues analyzed data from 7,116 adults aged 40 years or older who participated in the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004.
The study included participants who underwent monofilament testing for peripheral neuropathy. During testing, technicians used a standard 5.07 Semmes-Weinstein nylon monofilament to apply slight pressure to the bottom of each foot at three sites. If participants could not correctly identify where pressure was applied, the test was repeated. After participants gave two incorrect or undeterminable responses for a site, the site was defined as insensate. The researchers defined peripheral neuropathy as at least one insensate site on either foot.
The researchers determined deaths and causes of death using death certificate records from the National Death Index through 2015.
In all, 13.5% of the participants had peripheral neuropathy, including 27% of adults with diabetes and 11.6% of adults without diabetes. Those with peripheral neuropathy were older, were more likely to be male, and had lower levels of education, compared with participants without peripheral neuropathy. They also had higher body mass index, were more often former or current smokers, and had a higher prevalence of hypertension, hypercholesterolemia, and cardiovascular disease.
During a median follow-up of 13 years, 2,128 participants died, including 488 who died of cardiovascular causes.
The incidence rate of all-cause mortality per 1,000 person-years was 57.6 in adults with diabetes and peripheral neuropathy, 34.3 in adults with peripheral neuropathy but no diabetes, 27.1 in adults with diabetes but no peripheral neuropathy, and 13.0 in adults without diabetes or peripheral neuropathy.
Among participants with diabetes, the leading cause of death was cardiovascular disease (31% of deaths), whereas among participants without diabetes, the leading cause of death was malignant neoplasms (27% of deaths).
After adjustment for age, sex, race, or ethnicity, and risk factors such as cardiovascular disease, peripheral neuropathy was significantly associated with all-cause mortality (hazard ratio [HR], 1.49) and cardiovascular mortality (HR, 1.66) in participants with diabetes. In participants without diabetes, peripheral neuropathy was significantly associated with all-cause mortality (HR, 1.31), but its association with cardiovascular mortality was not statistically significant.
The association between peripheral neuropathy and all-cause mortality persisted in a sensitivity analysis that focused on adults with normoglycemia.
Related conditions
The study confirms findings from prior studies that examined the prevalence of loss of peripheral sensation in populations of older adults with and without diabetes, said Elsa S. Strotmeyer, PhD, MPH, associate professor of epidemiology at the University of Pittsburgh. “The clinical significance of the loss of peripheral sensation in older adults without diabetes is not fully appreciated,” she said.
A limitation of the study is that peripheral neuropathy was not a clinical diagnosis. “Monofilament testing at the foot is a quick clinical screen for decreased lower-extremity sensation that likely is a result of sensory peripheral nerve decline,” Dr. Strotmeyer said.
Another limitation is that death certificates are less accurate than medical records for determining cause of death.
“Past studies have indicated that peripheral nerve decline is related to common conditions in aging such as the metabolic syndrome and cardiovascular disease, cancer treatment, and physical function loss,” Dr. Strotmeyer said. “Therefore it is not surprising that is related to mortality as these conditions in aging are associated with increased mortality. Loss of peripheral sensation at the foot may also be related to fall injuries, and mortality from fall injuries has increased dramatically in older adults over the past several decades.”
Prior research has suggested that monofilament testing may play a role in screening for fall risk in older adults without diabetes, Dr. Strotmeyer added.
“For older adults both with and without diabetes, past studies have recommended monofilament testing be incorporated in geriatric screening for fall risk. Therefore, this article expands implications of clinical importance to understanding the pathology and consequences of loss of sensation at the foot in older patients,” she said.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Heart, Lung, and Blood Institute. Dr. Hicks, Dr. Selvin, and a coauthor, Kunihiro Matsushita, MD, PhD, disclosed NIH grants. In addition, Dr. Selvin disclosed personal fees from Novo Nordisk and grants from the Foundation for the National Institutes of Health outside the submitted work, and Dr. Matsushita disclosed grants and personal fees from Fukuda Denshi outside the submitted work. Dr. Strotmeyer receives funding from the National Institute on Aging and the National Institute of Arthritis and Musculoskeletal and Skin Diseases and is chair of the health sciences section of the Gerontological Society of America.
A version of this article originally appeared on Medscape.com.
researchers reported in Annals of Internal Medicine.
The findings do not necessarily mean that doctors should implement broader screening for peripheral neuropathy at this time, however, the investigators said.
“Doctors don’t typically screen for peripheral neuropathy in persons without diabetes,” senior author Elizabeth Selvin, PhD, MPH, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health, Baltimore, said in an interview.
“Our study shows that peripheral neuropathy – as assessed by decreased sensation in the feet – is common, even in people without diabetes,” Dr. Selvin explained. “It is not yet clear whether we should be screening people without diabetes since we don’t have clear treatments, but our study does suggest that this condition is an underrecognized condition that is associated with poor outcomes.”
Patients with diabetes typically undergo annual foot examinations that include screening for peripheral neuropathy, but that’s not the case for most adults in the absence of diabetes.
“I don’t know if we can make the jump that we should be screening people without diabetes,” said first author Caitlin W. Hicks, MD, assistant professor of surgery, division of vascular surgery and endovascular therapy, Johns Hopkins University, Baltimore. “Right now, we do not exactly know what it means in the people without diabetes, and we definitely do not know how to treat it. So, screening for it will tell us that this person has this and is at higher risk of mortality than someone who doesn’t, but we do not know what to do with that information yet.”
Nevertheless, the study raises the question of whether physicians should pay more attention to peripheral neuropathy in people without diabetes, said Dr. Hicks, director of research at the university’s diabetic foot and wound service.
Heightened risk
To examine associations between peripheral neuropathy and all-cause and cardiovascular mortality in U.S. adults, Dr. Hicks and colleagues analyzed data from 7,116 adults aged 40 years or older who participated in the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004.
The study included participants who underwent monofilament testing for peripheral neuropathy. During testing, technicians used a standard 5.07 Semmes-Weinstein nylon monofilament to apply slight pressure to the bottom of each foot at three sites. If participants could not correctly identify where pressure was applied, the test was repeated. After participants gave two incorrect or undeterminable responses for a site, the site was defined as insensate. The researchers defined peripheral neuropathy as at least one insensate site on either foot.
The researchers determined deaths and causes of death using death certificate records from the National Death Index through 2015.
In all, 13.5% of the participants had peripheral neuropathy, including 27% of adults with diabetes and 11.6% of adults without diabetes. Those with peripheral neuropathy were older, were more likely to be male, and had lower levels of education, compared with participants without peripheral neuropathy. They also had higher body mass index, were more often former or current smokers, and had a higher prevalence of hypertension, hypercholesterolemia, and cardiovascular disease.
During a median follow-up of 13 years, 2,128 participants died, including 488 who died of cardiovascular causes.
The incidence rate of all-cause mortality per 1,000 person-years was 57.6 in adults with diabetes and peripheral neuropathy, 34.3 in adults with peripheral neuropathy but no diabetes, 27.1 in adults with diabetes but no peripheral neuropathy, and 13.0 in adults without diabetes or peripheral neuropathy.
Among participants with diabetes, the leading cause of death was cardiovascular disease (31% of deaths), whereas among participants without diabetes, the leading cause of death was malignant neoplasms (27% of deaths).
After adjustment for age, sex, race, or ethnicity, and risk factors such as cardiovascular disease, peripheral neuropathy was significantly associated with all-cause mortality (hazard ratio [HR], 1.49) and cardiovascular mortality (HR, 1.66) in participants with diabetes. In participants without diabetes, peripheral neuropathy was significantly associated with all-cause mortality (HR, 1.31), but its association with cardiovascular mortality was not statistically significant.
The association between peripheral neuropathy and all-cause mortality persisted in a sensitivity analysis that focused on adults with normoglycemia.
Related conditions
The study confirms findings from prior studies that examined the prevalence of loss of peripheral sensation in populations of older adults with and without diabetes, said Elsa S. Strotmeyer, PhD, MPH, associate professor of epidemiology at the University of Pittsburgh. “The clinical significance of the loss of peripheral sensation in older adults without diabetes is not fully appreciated,” she said.
A limitation of the study is that peripheral neuropathy was not a clinical diagnosis. “Monofilament testing at the foot is a quick clinical screen for decreased lower-extremity sensation that likely is a result of sensory peripheral nerve decline,” Dr. Strotmeyer said.
Another limitation is that death certificates are less accurate than medical records for determining cause of death.
“Past studies have indicated that peripheral nerve decline is related to common conditions in aging such as the metabolic syndrome and cardiovascular disease, cancer treatment, and physical function loss,” Dr. Strotmeyer said. “Therefore it is not surprising that is related to mortality as these conditions in aging are associated with increased mortality. Loss of peripheral sensation at the foot may also be related to fall injuries, and mortality from fall injuries has increased dramatically in older adults over the past several decades.”
Prior research has suggested that monofilament testing may play a role in screening for fall risk in older adults without diabetes, Dr. Strotmeyer added.
“For older adults both with and without diabetes, past studies have recommended monofilament testing be incorporated in geriatric screening for fall risk. Therefore, this article expands implications of clinical importance to understanding the pathology and consequences of loss of sensation at the foot in older patients,” she said.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Heart, Lung, and Blood Institute. Dr. Hicks, Dr. Selvin, and a coauthor, Kunihiro Matsushita, MD, PhD, disclosed NIH grants. In addition, Dr. Selvin disclosed personal fees from Novo Nordisk and grants from the Foundation for the National Institutes of Health outside the submitted work, and Dr. Matsushita disclosed grants and personal fees from Fukuda Denshi outside the submitted work. Dr. Strotmeyer receives funding from the National Institute on Aging and the National Institute of Arthritis and Musculoskeletal and Skin Diseases and is chair of the health sciences section of the Gerontological Society of America.
A version of this article originally appeared on Medscape.com.
researchers reported in Annals of Internal Medicine.
The findings do not necessarily mean that doctors should implement broader screening for peripheral neuropathy at this time, however, the investigators said.
“Doctors don’t typically screen for peripheral neuropathy in persons without diabetes,” senior author Elizabeth Selvin, PhD, MPH, professor of epidemiology at the Johns Hopkins Bloomberg School of Public Health, Baltimore, said in an interview.
“Our study shows that peripheral neuropathy – as assessed by decreased sensation in the feet – is common, even in people without diabetes,” Dr. Selvin explained. “It is not yet clear whether we should be screening people without diabetes since we don’t have clear treatments, but our study does suggest that this condition is an underrecognized condition that is associated with poor outcomes.”
Patients with diabetes typically undergo annual foot examinations that include screening for peripheral neuropathy, but that’s not the case for most adults in the absence of diabetes.
“I don’t know if we can make the jump that we should be screening people without diabetes,” said first author Caitlin W. Hicks, MD, assistant professor of surgery, division of vascular surgery and endovascular therapy, Johns Hopkins University, Baltimore. “Right now, we do not exactly know what it means in the people without diabetes, and we definitely do not know how to treat it. So, screening for it will tell us that this person has this and is at higher risk of mortality than someone who doesn’t, but we do not know what to do with that information yet.”
Nevertheless, the study raises the question of whether physicians should pay more attention to peripheral neuropathy in people without diabetes, said Dr. Hicks, director of research at the university’s diabetic foot and wound service.
Heightened risk
To examine associations between peripheral neuropathy and all-cause and cardiovascular mortality in U.S. adults, Dr. Hicks and colleagues analyzed data from 7,116 adults aged 40 years or older who participated in the National Health and Nutrition Examination Survey (NHANES) between 1999 and 2004.
The study included participants who underwent monofilament testing for peripheral neuropathy. During testing, technicians used a standard 5.07 Semmes-Weinstein nylon monofilament to apply slight pressure to the bottom of each foot at three sites. If participants could not correctly identify where pressure was applied, the test was repeated. After participants gave two incorrect or undeterminable responses for a site, the site was defined as insensate. The researchers defined peripheral neuropathy as at least one insensate site on either foot.
The researchers determined deaths and causes of death using death certificate records from the National Death Index through 2015.
In all, 13.5% of the participants had peripheral neuropathy, including 27% of adults with diabetes and 11.6% of adults without diabetes. Those with peripheral neuropathy were older, were more likely to be male, and had lower levels of education, compared with participants without peripheral neuropathy. They also had higher body mass index, were more often former or current smokers, and had a higher prevalence of hypertension, hypercholesterolemia, and cardiovascular disease.
During a median follow-up of 13 years, 2,128 participants died, including 488 who died of cardiovascular causes.
The incidence rate of all-cause mortality per 1,000 person-years was 57.6 in adults with diabetes and peripheral neuropathy, 34.3 in adults with peripheral neuropathy but no diabetes, 27.1 in adults with diabetes but no peripheral neuropathy, and 13.0 in adults without diabetes or peripheral neuropathy.
Among participants with diabetes, the leading cause of death was cardiovascular disease (31% of deaths), whereas among participants without diabetes, the leading cause of death was malignant neoplasms (27% of deaths).
After adjustment for age, sex, race, or ethnicity, and risk factors such as cardiovascular disease, peripheral neuropathy was significantly associated with all-cause mortality (hazard ratio [HR], 1.49) and cardiovascular mortality (HR, 1.66) in participants with diabetes. In participants without diabetes, peripheral neuropathy was significantly associated with all-cause mortality (HR, 1.31), but its association with cardiovascular mortality was not statistically significant.
The association between peripheral neuropathy and all-cause mortality persisted in a sensitivity analysis that focused on adults with normoglycemia.
Related conditions
The study confirms findings from prior studies that examined the prevalence of loss of peripheral sensation in populations of older adults with and without diabetes, said Elsa S. Strotmeyer, PhD, MPH, associate professor of epidemiology at the University of Pittsburgh. “The clinical significance of the loss of peripheral sensation in older adults without diabetes is not fully appreciated,” she said.
A limitation of the study is that peripheral neuropathy was not a clinical diagnosis. “Monofilament testing at the foot is a quick clinical screen for decreased lower-extremity sensation that likely is a result of sensory peripheral nerve decline,” Dr. Strotmeyer said.
Another limitation is that death certificates are less accurate than medical records for determining cause of death.
“Past studies have indicated that peripheral nerve decline is related to common conditions in aging such as the metabolic syndrome and cardiovascular disease, cancer treatment, and physical function loss,” Dr. Strotmeyer said. “Therefore it is not surprising that is related to mortality as these conditions in aging are associated with increased mortality. Loss of peripheral sensation at the foot may also be related to fall injuries, and mortality from fall injuries has increased dramatically in older adults over the past several decades.”
Prior research has suggested that monofilament testing may play a role in screening for fall risk in older adults without diabetes, Dr. Strotmeyer added.
“For older adults both with and without diabetes, past studies have recommended monofilament testing be incorporated in geriatric screening for fall risk. Therefore, this article expands implications of clinical importance to understanding the pathology and consequences of loss of sensation at the foot in older patients,” she said.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases and the National Heart, Lung, and Blood Institute. Dr. Hicks, Dr. Selvin, and a coauthor, Kunihiro Matsushita, MD, PhD, disclosed NIH grants. In addition, Dr. Selvin disclosed personal fees from Novo Nordisk and grants from the Foundation for the National Institutes of Health outside the submitted work, and Dr. Matsushita disclosed grants and personal fees from Fukuda Denshi outside the submitted work. Dr. Strotmeyer receives funding from the National Institute on Aging and the National Institute of Arthritis and Musculoskeletal and Skin Diseases and is chair of the health sciences section of the Gerontological Society of America.
A version of this article originally appeared on Medscape.com.
Fracking sites tied to increased heart failure hospitalizations
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Living near hydraulic fracturing is associated with increased risk of hospitalization in people with heart failure (HF), a new study from Pennsylvania suggests.
The link was strongest among those with more severe heart failure but patients with either HF phenotype showed this association of increased risk with exposure to fracking activities, according to the investigators, led by Tara P. McAlexander, PhD, MPH, Drexel University Dornsife School of Public Health in Philadelphia.
“Our understanding has expanded well beyond the famous Harvard Six Cities study to know that it’s not just a short-term uptick in air pollution that›s going to send someone to the hospital a couple days later,” said Dr. McAlexander in an interview, referring to the study conducted from the mid-1970s through 1991. “We know that people who live in these environments and are exposed for long periods of time may have long-term detrimental effects.”
Although questions remain about specific mechanisms and how best to assess exposure, the evidence is mounting in a way that is consistent with the biologic hypotheses of how fracking would adversely affect health, Dr. McAlexander said. “We have many studies now on adverse pregnancy and birth outcomes, and that’s just the tip of the iceberg.”
Pennsylvania is a hot spot for fracking, also known as unconventional natural gas development (UNGD), with more than 12,000 wells drilled in the Marcellus shale since 2004. The shale extends from upstate New York in the north to northeastern Kentucky and Tennessee in the south and covers about 72,000 square miles. Last year, Pennsylvania pledged $3 million to study clusters of rare pediatric cancers and asthma near fracking operations. A recent grand jury report concluded government officials failed to protect residents from the health effects of fracking.
Fracking involves a cascade of activities that can trigger neural circuitry, sympathetic activation, and inflammation – all well-known pathways that potentiate heart failure, said Sanjay Rajagopalan, MD, who has researched the health effects of air pollution for two decades and was not involved with the study.
“If you think about it, it’s like environmental perturbation on steroids in some ways where they are pulling the trigger from a variety of different ways: noise, air pollution, social displacement, psychosocial impacts, economic disparities. So it’s not at all surprising that they saw an association,” said Dr. Rajagopalan, chief of cardiovascular medicine at University Hospitals Harrington Heart & Vascular Institute and director of the Case Western Cardiovascular Research Institute, both in Cleveland, Ohio.
As reported in the Journal of the American College of Cardiology, Dr. McAlexander and colleagues at Johns Hopkins University, Baltimore, used electronic health data from the Geisinger Health System to identify 9,054 patients with heart failure seen between 2008 and 2015. Of these, 5,839 patients had an incident HF hospitalization and 3,215 served as controls. Geisinger operates 13 hospitals and two research centers in 45 of Pennsylvania’s 67 counties, serving more than 3 million of the state’s residents.
Patients’ residential addresses were used to identify latitude and longitude coordinates that were matched with 9,669 UNGD wells in Pennsylvania and the location of major and minor roadways. The researchers also calculated a measure of community socioeconomic deprivation.
The adjusted odds of hospitalization were higher for patients in the highest quartile of exposure for three of the four UNGD phases: pad preparation (odds ratio, 1.70; 95% confidence interval, 1.35-2.13), stimulation or the actual fracking (OR, 1.80; 95% CI, 1.35-2.40), and production (OR, 1.62; 95% CI, 1.07-2.45).
Dr. McAlexander said she initially thought the lack of association with drilling (OR, 0.97; 95% CI, 0.75-1.27) was a mistake but noted that the drilling metric reflects a shorter time period than, for example, 30 days needed to clear the well pad and bring in the necessary equipment.
Stronger associations between pad preparation, fracking, and production are also consistent with the known increases in air pollution, traffic, and noise associated with these phases.
Individuals with more severe HF had greater odds of hospitalization, but the effect sizes were generally comparable between HF with preserved versus reduced ejection fraction. For those with the highest exposure to fracking, the odds ratios for hospitalization reached 2.25 (95% CI, 1.56-3.25) and 2.09 (95% CI, 1.44-3.03), respectively.
Notably, patients who could be phenotyped versus those who could not were more likely to die, to be hospitalized for HF, and to have a higher Charlson Comorbidity Index and other relevant diagnoses like myocardial infarction.
“Clinicians need to be increasingly aware that the environments their patients are in are a huge factor in their disease progression and outlook,” McAlexander said. “We know that UNGD, specifically now, is something that could be impacting a heart failure patient’s survival.”
She also suggested that the findings may also spur more advocacy work and “across-silo” collaboration between clinicians and environmental researchers.
Dr. Rajagopalan said there is increasing recognition that physicians need to be aware of environmental health links as extreme events like the California and Oregon wildfires and coastal flooding become increasingly common. “Unfortunately, unconventional is becoming the new convention.”
The problem for many physicians, however, is just having enough bandwidth to get through the day and get enough learning to keep above water, he said. Artificial intelligence could be used to seed electronic medical records with other personalized information from a bevy of sources including smartphones and the internet of things, but fundamental changes are also needed in the educational process to emphasize the environment.
“It’s going to take a huge societal shift in the way we view commodities, what we consider healthy, etc, but it can happen very quickly because all it takes is a crisis like COVID-19 to bring people to their knees and make them understand how this is going to take over our lives over the next decade,” Dr. Rajagopalan said.
The scientific community has been calling for “good” epidemiologic studies on the health effects of fracking since the early 2010s, Barrak Alahmad, MBChB, MPH, Harvard T.H. Chan School of Public Health, and Haitham Khraishah, MD, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, point out in an accompanying editorial.
The current study applied “extensive and rigorous methods” involving both the design and statistical approach, including use of a negative control analysis to assess for sources of spurious causal inference, several sensitivity analyses, and controlled for a wide range of covariates.
“Their results were consistent and robust across all these measures,” the editorialists wrote. “Most importantly, the effect size is probably too large to be explained away by an unmeasured confounder.”
Dr. Alahmad and Dr. Khraishah call for advancements in exposure assessment, citing a recent study reporting that ambient particle radioactivity near unconventional oil and gas sites could induce adverse health effects. Other unmet needs include a better understanding of racial disparities in the impacts of fracking and a fine-tuning of cause-specific cardiovascular morbidity and mortality.
The study was supported by training grants from the National Institute of Environmental Health Sciences to Dr. McAlexander and principal investigator Brian Schwartz, MD. The authors, Dr. Rajagopalan, Dr. Alahmad, and Dr. Khraishah have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Calcium burden drives CV risk whether coronary disease is obstructive or not
Coronary artery calcium (CAC) score as a measure of plaque burden more reliably predicts future cardiovascular (CV) risk in patients with suspected coronary disease (CAD) than whether or not the disease is obstructive, a large retrospective study suggests.
Indeed, CV risk went up in tandem with growing plaque burden regardless of whether there was obstructive disease in any coronary artery, defined as a 50% or greater stenosis by computed tomographic angiography (CTA).
The findings argue for plaque burden as measured by CAC score, rather than percent-stenosis severity, for guiding further treatment decisions in such patients, researchers say.
The research was based on more than 20,000 symptomatic patients referred to diagnostic CTA in the Western Denmark Heart Registry who were then followed for about 4 years for major CV events, including death, myocardial infarction, or stroke.
“What we show is that CAC is important for prognosis, and that patients with no stenosis have similar high risk as patients with stenosis when CAC burden is similar,” Martin Bødtker Mortensen, MD, PhD, Aarhus (Denmark) University Hospital, said in an interview.
The guidelines “distinguish between primary and secondary prevention patients” based on the presence or absence of obstructive CAD, he said, but “our results challenge this long-held approach. We show that patients with nonobstructive CAD carry similar risk as patients with obstructive CAD.”
In practice, risk tends to be greater in patients with obstructive compared with nonobstructive CAD. But the reason “is simply that they normally have higher atherosclerosis burden,” Dr. Mortensen said. “When you stratify based on atherosclerosis burden, then patients with obstructive and nonobstructive CAD have similar risk.”
The analysis was published online Dec. 7 in the Journal of the American College of Cardiology with Mortensen as lead author.
Until recently, it had long been believed that CV-event risk was driven by ischemia – but “ischemia is just a surrogate for the extent of atherosclerotic disease,” Armin Arbab Zadeh, MD, PhD, MPH, who is not connected with the current study, said in an interview.
The finding that CV risk climbs with growing coronary plaque burden “essentially confirms” other recent studies, but with “added value in showing how well the calcium scores, compared to obstructive disease, track with risk. So it’s definitely a nice extension of the evidence,” said Dr. Zadeh, director of cardiac CT at Johns Hopkins University, Baltimore.
“This study clearly shows that there is no ischemia ‘threshold,’ that the risk starts from mild and goes up with the burden of atherosclerotic disease. We were essentially taught wrong for decades.”
Dr. Mortensen said that the new results “are in line with previous studies showing that atherosclerosis burden is very important for risk.” They also help explain why revascularization of patients with stable angina failed to cut the risk of MI or death in trials like COURAGE, FAME-2, and ISCHEMIA. It’s because “stenosis per se explains little of the risk compared to atherosclerosis burden.”
In the current analysis, for example, about 65% of events were in patients who did not show obstructive CAD at CTA. Its 23,759 patients with symptoms suggestive of CAD were referred for CTA from 2008 through 2017; 5,043 (21.2%) were found to have obstructive disease and 18,716 (78.8%) either had no CAD or nonobstructive disease.
About 4.4% of patients experienced a first major CV event over a median follow-up of 4.3 years. Only events occurring later than 90 days after CTA were counted in an effort to exclude any directly related to revascularization, Dr. Mortensen noted.
The risk of events went up proportionally with both CAC score and the number of coronaries with obstructive disease.
The number of major CV events per 1,000 person-years was 6.2 for patients with a CAC score of 0, of whom 87% had no CAD by CTA, 7% had nonobstructive CAD, and 6% had obstructive CAD.
The corresponding rate was 17.5 among patients with a CAC score >100-399 for a hazard ratio (HR) of 1.7 (95% confidence interval [CI] 1.4-2.1) vs. a CAC score of 0.
And it was 42.3 per 1,000 patient-years among patients with CAC score >1000, HR 3.4 (95% CI, 2.5-4.6) vs. a CAC score of 0. Among those with the highest-tier CAC score, none were without CAD by CTA, 17% had nonobstructive disease, and 83% had obstructive CAD.
The major CV event rate rose similarly by number of coronaries with obstructive disease. It was 6.1 per 1,000 person-years in patients with no CAD. But it was 12.3 in those with nonobstructive disease, HR 1.3 (95% CI 1.1-1.6), up to 34.7 in those with triple-vessel obstructive disease, HR 2.9 (95% CI 2.2-3.9), vs. no CAD.
However, in an analysis with stratification by CAC score tier (0, 1-99, 100-399, 400-1,000, and >1,000), obstructive CAD was not associated with increased major CV-event risk in any stratum. The findings were similar in each subgroup with 1-vessel, 2-vessel, or 3-vessel CAD when stratified by CAC score.
Nor did major CV event risk track with obstructive CAD in analyses by age or after excluding all patients who underwent coronary revascularization within 90 days of CTA, the group reported.
“I believe these results support the use of CTA as a first-line test in patients with symptoms suggestive of CAD, as it provides valuable information for both diagnosis and prognosis in symptomatic patients,” Dr. Mortensen said. Those found to have a higher burden of atherosclerosis, he added, should receive aggressive preventive therapy regardless of whether or not they have obstructive disease.
The evidence from this study and others “supports a CTA-based approach” in such patients, Dr. Zadeh said. “And I would go further to say that a stress test is really inadequate,” in that it “detects the disease at such a late stage, you’re missing the opportunity to identify these patients who have atherosclerotic disease while you can do something about it.”
Its continued use as a first-line test, Dr. Zadeh said, “is essentially, in my mind, dismissing the evidence.”
An accompanying editorial Todd C. Villines, MD, and Patricia Rodriguez Lozano, MD, of the University of Virginia, Charlottesville agreed that “it is time that the traditional definitions of primary and secondary prevention evolve to incorporate CAC and CTA measures of patient risk based on coronary artery plaque burden.”
But they pointed out some limitations of the current study.
“The authors compared CAC with ≥50% stenosis, not CAC to comprehensive, contemporary coronary CTA,” and so “did not assess numerous other well-validated measures of coronary plaque burden that are routinely obtained from coronary CTA that typically improve the prognostic accuracy of coronary CTA beyond stenosis alone.” Also not performed was “plaque quantification on coronary CTA, an emerging field of study.”
The editorialists noted that noncontrast CT as used in the study for CAC scoring “is generally not recommended as a standalone test in symptomatic patients. Most studies have shown that coronary CTA, a test that accurately detects stenosis and identifies all types of coronary atherosclerosis (calcified and noncalcified), has significantly higher diagnostic and prognostic accuracy than CAC when performed in symptomatic patients without known coronary artery disease.”
Dr. Mortensen has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Villines and Dr. Rodriguez Lozano have disclosed no relevant financial relationships. Dr. Zadeh disclosed receiving grant support from Canon Medical Systems.
A version of this article originally appeared on Medscape.com.
Coronary artery calcium (CAC) score as a measure of plaque burden more reliably predicts future cardiovascular (CV) risk in patients with suspected coronary disease (CAD) than whether or not the disease is obstructive, a large retrospective study suggests.
Indeed, CV risk went up in tandem with growing plaque burden regardless of whether there was obstructive disease in any coronary artery, defined as a 50% or greater stenosis by computed tomographic angiography (CTA).
The findings argue for plaque burden as measured by CAC score, rather than percent-stenosis severity, for guiding further treatment decisions in such patients, researchers say.
The research was based on more than 20,000 symptomatic patients referred to diagnostic CTA in the Western Denmark Heart Registry who were then followed for about 4 years for major CV events, including death, myocardial infarction, or stroke.
“What we show is that CAC is important for prognosis, and that patients with no stenosis have similar high risk as patients with stenosis when CAC burden is similar,” Martin Bødtker Mortensen, MD, PhD, Aarhus (Denmark) University Hospital, said in an interview.
The guidelines “distinguish between primary and secondary prevention patients” based on the presence or absence of obstructive CAD, he said, but “our results challenge this long-held approach. We show that patients with nonobstructive CAD carry similar risk as patients with obstructive CAD.”
In practice, risk tends to be greater in patients with obstructive compared with nonobstructive CAD. But the reason “is simply that they normally have higher atherosclerosis burden,” Dr. Mortensen said. “When you stratify based on atherosclerosis burden, then patients with obstructive and nonobstructive CAD have similar risk.”
The analysis was published online Dec. 7 in the Journal of the American College of Cardiology with Mortensen as lead author.
Until recently, it had long been believed that CV-event risk was driven by ischemia – but “ischemia is just a surrogate for the extent of atherosclerotic disease,” Armin Arbab Zadeh, MD, PhD, MPH, who is not connected with the current study, said in an interview.
The finding that CV risk climbs with growing coronary plaque burden “essentially confirms” other recent studies, but with “added value in showing how well the calcium scores, compared to obstructive disease, track with risk. So it’s definitely a nice extension of the evidence,” said Dr. Zadeh, director of cardiac CT at Johns Hopkins University, Baltimore.
“This study clearly shows that there is no ischemia ‘threshold,’ that the risk starts from mild and goes up with the burden of atherosclerotic disease. We were essentially taught wrong for decades.”
Dr. Mortensen said that the new results “are in line with previous studies showing that atherosclerosis burden is very important for risk.” They also help explain why revascularization of patients with stable angina failed to cut the risk of MI or death in trials like COURAGE, FAME-2, and ISCHEMIA. It’s because “stenosis per se explains little of the risk compared to atherosclerosis burden.”
In the current analysis, for example, about 65% of events were in patients who did not show obstructive CAD at CTA. Its 23,759 patients with symptoms suggestive of CAD were referred for CTA from 2008 through 2017; 5,043 (21.2%) were found to have obstructive disease and 18,716 (78.8%) either had no CAD or nonobstructive disease.
About 4.4% of patients experienced a first major CV event over a median follow-up of 4.3 years. Only events occurring later than 90 days after CTA were counted in an effort to exclude any directly related to revascularization, Dr. Mortensen noted.
The risk of events went up proportionally with both CAC score and the number of coronaries with obstructive disease.
The number of major CV events per 1,000 person-years was 6.2 for patients with a CAC score of 0, of whom 87% had no CAD by CTA, 7% had nonobstructive CAD, and 6% had obstructive CAD.
The corresponding rate was 17.5 among patients with a CAC score >100-399 for a hazard ratio (HR) of 1.7 (95% confidence interval [CI] 1.4-2.1) vs. a CAC score of 0.
And it was 42.3 per 1,000 patient-years among patients with CAC score >1000, HR 3.4 (95% CI, 2.5-4.6) vs. a CAC score of 0. Among those with the highest-tier CAC score, none were without CAD by CTA, 17% had nonobstructive disease, and 83% had obstructive CAD.
The major CV event rate rose similarly by number of coronaries with obstructive disease. It was 6.1 per 1,000 person-years in patients with no CAD. But it was 12.3 in those with nonobstructive disease, HR 1.3 (95% CI 1.1-1.6), up to 34.7 in those with triple-vessel obstructive disease, HR 2.9 (95% CI 2.2-3.9), vs. no CAD.
However, in an analysis with stratification by CAC score tier (0, 1-99, 100-399, 400-1,000, and >1,000), obstructive CAD was not associated with increased major CV-event risk in any stratum. The findings were similar in each subgroup with 1-vessel, 2-vessel, or 3-vessel CAD when stratified by CAC score.
Nor did major CV event risk track with obstructive CAD in analyses by age or after excluding all patients who underwent coronary revascularization within 90 days of CTA, the group reported.
“I believe these results support the use of CTA as a first-line test in patients with symptoms suggestive of CAD, as it provides valuable information for both diagnosis and prognosis in symptomatic patients,” Dr. Mortensen said. Those found to have a higher burden of atherosclerosis, he added, should receive aggressive preventive therapy regardless of whether or not they have obstructive disease.
The evidence from this study and others “supports a CTA-based approach” in such patients, Dr. Zadeh said. “And I would go further to say that a stress test is really inadequate,” in that it “detects the disease at such a late stage, you’re missing the opportunity to identify these patients who have atherosclerotic disease while you can do something about it.”
Its continued use as a first-line test, Dr. Zadeh said, “is essentially, in my mind, dismissing the evidence.”
An accompanying editorial Todd C. Villines, MD, and Patricia Rodriguez Lozano, MD, of the University of Virginia, Charlottesville agreed that “it is time that the traditional definitions of primary and secondary prevention evolve to incorporate CAC and CTA measures of patient risk based on coronary artery plaque burden.”
But they pointed out some limitations of the current study.
“The authors compared CAC with ≥50% stenosis, not CAC to comprehensive, contemporary coronary CTA,” and so “did not assess numerous other well-validated measures of coronary plaque burden that are routinely obtained from coronary CTA that typically improve the prognostic accuracy of coronary CTA beyond stenosis alone.” Also not performed was “plaque quantification on coronary CTA, an emerging field of study.”
The editorialists noted that noncontrast CT as used in the study for CAC scoring “is generally not recommended as a standalone test in symptomatic patients. Most studies have shown that coronary CTA, a test that accurately detects stenosis and identifies all types of coronary atherosclerosis (calcified and noncalcified), has significantly higher diagnostic and prognostic accuracy than CAC when performed in symptomatic patients without known coronary artery disease.”
Dr. Mortensen has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Villines and Dr. Rodriguez Lozano have disclosed no relevant financial relationships. Dr. Zadeh disclosed receiving grant support from Canon Medical Systems.
A version of this article originally appeared on Medscape.com.
Coronary artery calcium (CAC) score as a measure of plaque burden more reliably predicts future cardiovascular (CV) risk in patients with suspected coronary disease (CAD) than whether or not the disease is obstructive, a large retrospective study suggests.
Indeed, CV risk went up in tandem with growing plaque burden regardless of whether there was obstructive disease in any coronary artery, defined as a 50% or greater stenosis by computed tomographic angiography (CTA).
The findings argue for plaque burden as measured by CAC score, rather than percent-stenosis severity, for guiding further treatment decisions in such patients, researchers say.
The research was based on more than 20,000 symptomatic patients referred to diagnostic CTA in the Western Denmark Heart Registry who were then followed for about 4 years for major CV events, including death, myocardial infarction, or stroke.
“What we show is that CAC is important for prognosis, and that patients with no stenosis have similar high risk as patients with stenosis when CAC burden is similar,” Martin Bødtker Mortensen, MD, PhD, Aarhus (Denmark) University Hospital, said in an interview.
The guidelines “distinguish between primary and secondary prevention patients” based on the presence or absence of obstructive CAD, he said, but “our results challenge this long-held approach. We show that patients with nonobstructive CAD carry similar risk as patients with obstructive CAD.”
In practice, risk tends to be greater in patients with obstructive compared with nonobstructive CAD. But the reason “is simply that they normally have higher atherosclerosis burden,” Dr. Mortensen said. “When you stratify based on atherosclerosis burden, then patients with obstructive and nonobstructive CAD have similar risk.”
The analysis was published online Dec. 7 in the Journal of the American College of Cardiology with Mortensen as lead author.
Until recently, it had long been believed that CV-event risk was driven by ischemia – but “ischemia is just a surrogate for the extent of atherosclerotic disease,” Armin Arbab Zadeh, MD, PhD, MPH, who is not connected with the current study, said in an interview.
The finding that CV risk climbs with growing coronary plaque burden “essentially confirms” other recent studies, but with “added value in showing how well the calcium scores, compared to obstructive disease, track with risk. So it’s definitely a nice extension of the evidence,” said Dr. Zadeh, director of cardiac CT at Johns Hopkins University, Baltimore.
“This study clearly shows that there is no ischemia ‘threshold,’ that the risk starts from mild and goes up with the burden of atherosclerotic disease. We were essentially taught wrong for decades.”
Dr. Mortensen said that the new results “are in line with previous studies showing that atherosclerosis burden is very important for risk.” They also help explain why revascularization of patients with stable angina failed to cut the risk of MI or death in trials like COURAGE, FAME-2, and ISCHEMIA. It’s because “stenosis per se explains little of the risk compared to atherosclerosis burden.”
In the current analysis, for example, about 65% of events were in patients who did not show obstructive CAD at CTA. Its 23,759 patients with symptoms suggestive of CAD were referred for CTA from 2008 through 2017; 5,043 (21.2%) were found to have obstructive disease and 18,716 (78.8%) either had no CAD or nonobstructive disease.
About 4.4% of patients experienced a first major CV event over a median follow-up of 4.3 years. Only events occurring later than 90 days after CTA were counted in an effort to exclude any directly related to revascularization, Dr. Mortensen noted.
The risk of events went up proportionally with both CAC score and the number of coronaries with obstructive disease.
The number of major CV events per 1,000 person-years was 6.2 for patients with a CAC score of 0, of whom 87% had no CAD by CTA, 7% had nonobstructive CAD, and 6% had obstructive CAD.
The corresponding rate was 17.5 among patients with a CAC score >100-399 for a hazard ratio (HR) of 1.7 (95% confidence interval [CI] 1.4-2.1) vs. a CAC score of 0.
And it was 42.3 per 1,000 patient-years among patients with CAC score >1000, HR 3.4 (95% CI, 2.5-4.6) vs. a CAC score of 0. Among those with the highest-tier CAC score, none were without CAD by CTA, 17% had nonobstructive disease, and 83% had obstructive CAD.
The major CV event rate rose similarly by number of coronaries with obstructive disease. It was 6.1 per 1,000 person-years in patients with no CAD. But it was 12.3 in those with nonobstructive disease, HR 1.3 (95% CI 1.1-1.6), up to 34.7 in those with triple-vessel obstructive disease, HR 2.9 (95% CI 2.2-3.9), vs. no CAD.
However, in an analysis with stratification by CAC score tier (0, 1-99, 100-399, 400-1,000, and >1,000), obstructive CAD was not associated with increased major CV-event risk in any stratum. The findings were similar in each subgroup with 1-vessel, 2-vessel, or 3-vessel CAD when stratified by CAC score.
Nor did major CV event risk track with obstructive CAD in analyses by age or after excluding all patients who underwent coronary revascularization within 90 days of CTA, the group reported.
“I believe these results support the use of CTA as a first-line test in patients with symptoms suggestive of CAD, as it provides valuable information for both diagnosis and prognosis in symptomatic patients,” Dr. Mortensen said. Those found to have a higher burden of atherosclerosis, he added, should receive aggressive preventive therapy regardless of whether or not they have obstructive disease.
The evidence from this study and others “supports a CTA-based approach” in such patients, Dr. Zadeh said. “And I would go further to say that a stress test is really inadequate,” in that it “detects the disease at such a late stage, you’re missing the opportunity to identify these patients who have atherosclerotic disease while you can do something about it.”
Its continued use as a first-line test, Dr. Zadeh said, “is essentially, in my mind, dismissing the evidence.”
An accompanying editorial Todd C. Villines, MD, and Patricia Rodriguez Lozano, MD, of the University of Virginia, Charlottesville agreed that “it is time that the traditional definitions of primary and secondary prevention evolve to incorporate CAC and CTA measures of patient risk based on coronary artery plaque burden.”
But they pointed out some limitations of the current study.
“The authors compared CAC with ≥50% stenosis, not CAC to comprehensive, contemporary coronary CTA,” and so “did not assess numerous other well-validated measures of coronary plaque burden that are routinely obtained from coronary CTA that typically improve the prognostic accuracy of coronary CTA beyond stenosis alone.” Also not performed was “plaque quantification on coronary CTA, an emerging field of study.”
The editorialists noted that noncontrast CT as used in the study for CAC scoring “is generally not recommended as a standalone test in symptomatic patients. Most studies have shown that coronary CTA, a test that accurately detects stenosis and identifies all types of coronary atherosclerosis (calcified and noncalcified), has significantly higher diagnostic and prognostic accuracy than CAC when performed in symptomatic patients without known coronary artery disease.”
Dr. Mortensen has disclosed no relevant financial relationships. Disclosures for the other authors are in the report. Dr. Villines and Dr. Rodriguez Lozano have disclosed no relevant financial relationships. Dr. Zadeh disclosed receiving grant support from Canon Medical Systems.
A version of this article originally appeared on Medscape.com.