User login
Common newborn hearing test promising for early detection of autism
new research shows.
Results from one of the largest studies of its kind show the auditory brainstem response (ABR) test, which is carried out on most newborns, represents “a huge untapped potential” to detect autism, lead author Oren Miron, research associate, department of biomedical informatics, Harvard Medical School, Boston, and a PhD candidate at Ben Gurion University in Beersheba, Israel, said in an interview.
“The findings further reinforce our understanding that autism, in many cases, has a sensorial and auditory aspect to it,” said Mr. Miron, adding that an adverse response to sound is one of the earliest behavioral signs of autism.
The research was published online Oct. 31 in Autism Research.
Early intervention critical
Autism spectrum disorder (ASD), which involves problems in social communication and interaction, affects an estimated 1 in 59 children. Early identification and intervention are critical for improving outcomes and decreasing the economic burden associated with ASD.
The ABR test, which is used for Universal Newborn Hearing Screening (UNHS), uses surface electrodes to measure auditory nerve and brainstem responses to sound.
Previous studies identified abnormal ABR amplitude in children with ASD. However, it’s unclear whether healthy newborns who later develop autism also show ABR differences vs those who don’t develop the disorder.
Researchers used UNHS data, which allowed them to examine a larger, younger, and healthier sample compared with previous studies. The study included 321 newborns later diagnosed with ASD and 138,844 controls without a subsequent ASD diagnosis.
The mean ABR testing age was 1.76 days for newborns later diagnosed with ASD and 1.86 for those in the non-ASD group.
The ASD group was 77% male and the non-ASD group was 51% male. The rate of neonatal intensive care unit admission was 8% in the ASD group and 10% in the non-ASD group.
The hearing test involves placing an earpiece in the baby’s ear and delivering a click sound at 35 dB above normal hearing level (nHL) at a rate of 77 clicks per second in the right ear and 79 clicks per second in the left ear.
Brainstem abnormalities?
The clicks create electrical activity, which is recorded by a surface electrode and used to extract the ABR waveform. When a sound reaches the brain stem, it creates five consecutive waveforms – waves I, II, III, IV, and V.
Previous studies focused on wave V, which is easiest to detect. The current study used low intensity sound that resulted in a weaker signal.
To overcome this low intensity issue, researchers focused on the negative drop (latency) after the wave V (Vn), which is easier to detect, and on the ABR phase, or entire waveform. They illustrated the differences between the ASD and non-ASD groups in a series of graphs.
Results showed that the ABR phase in the right ear was significantly prolonged in the ASD vs non-ASD group (P < .001). ABR phase in the left ear was also significantly prolonged in the ASD group (P = .021)
Vn latency in the right ear was significantly prolonged in the ASD group compared with the non-ASD group (P = .048); however, this was not the case in the left ear.
The prolongation could mean that the V-negative wave might appear after 8 ms in normally developing children compared with 8.5 or 9 ms in children with autism, said Mr. Miron.
The new study is the first to show V-negative and phase abnormalities are associated with ASD, the authors note. The brainstem prolongation could be due to anatomical abnormalities in the brainstem in individuals with ASD, the researchers added.
Present before birth?
The presence of ABR biomarkers of ASD in the first weeks after birth suggests the disorder is likely present before birth in a large group of these individuals, the researchers note.
It’s possible the ABR test could be modified to use lower intensities not only to detect hearing impairment but autism risk, said Mr. Miron. “The test has been optimized to detect hearing impairment, and it does so brilliantly and helps thousands of children. We want to do the same kind of optimization for autism.”
This could lead to earlier behavioral diagnoses, which, in turn, could lead to earlier treatment and better outcomes for children with ASD, said Mr. Miron.
At this time, the level of prolongation to detect ASD is unclear. “I would think a lot of people would want to make it one standard deviation, but it depends on a lot of factors, including for example, whether a baby is preterm,” said Mr. Miron.
More research and better accuracy and specificity are needed before the newborn hearing test is clinically useful.
He noted that the hearing test is only one marker of autism and that it could potentially be combined with other behavioral signs and genetic markers to facilitate earlier diagnosis and treatment and improve outcomes for patients with ASD.
Future research by his group will investigate whether the degree of auditory prolongation relates to autism severity. They also plan to research ASD subgroups including children with comorbid epilepsy.
Terrific, clever research
Jeremy Veenstra-VanderWeele, MD, professor, child and adolescent psychiatry, Columbia University, New York, said in an interview that the study is “terrific” and a “clever use” of an existing dataset.
“They showed a difference between a large group of kids with autism and a large group of kids without.”
However, he added, more research is needed before the test can be used as an autism screening tool.
“In order for this to be a screening test that could be broadly applied you would need to identify a cutoff where you’d think a child was at risk for autism, and if you look at the graphs in the article, there are no clear cutoffs,” said Dr. Veenstra-VanderWeele.
To turn this into a useful test, “you would have to establish sensitivity and specificity, you would have to look not just at the comparison of kids with autism and kids without but apply it in a predictive way in a second population.”
The study authors and Dr. Veenstra-VanderWeele have reported no relevant financial relationships. Veenstra-VanderWeele is an associate editor at Autism Research, which published the article, but he did not handle or view it before being interviewed.
A version of this article originally appeared on Medscape.com.
new research shows.
Results from one of the largest studies of its kind show the auditory brainstem response (ABR) test, which is carried out on most newborns, represents “a huge untapped potential” to detect autism, lead author Oren Miron, research associate, department of biomedical informatics, Harvard Medical School, Boston, and a PhD candidate at Ben Gurion University in Beersheba, Israel, said in an interview.
“The findings further reinforce our understanding that autism, in many cases, has a sensorial and auditory aspect to it,” said Mr. Miron, adding that an adverse response to sound is one of the earliest behavioral signs of autism.
The research was published online Oct. 31 in Autism Research.
Early intervention critical
Autism spectrum disorder (ASD), which involves problems in social communication and interaction, affects an estimated 1 in 59 children. Early identification and intervention are critical for improving outcomes and decreasing the economic burden associated with ASD.
The ABR test, which is used for Universal Newborn Hearing Screening (UNHS), uses surface electrodes to measure auditory nerve and brainstem responses to sound.
Previous studies identified abnormal ABR amplitude in children with ASD. However, it’s unclear whether healthy newborns who later develop autism also show ABR differences vs those who don’t develop the disorder.
Researchers used UNHS data, which allowed them to examine a larger, younger, and healthier sample compared with previous studies. The study included 321 newborns later diagnosed with ASD and 138,844 controls without a subsequent ASD diagnosis.
The mean ABR testing age was 1.76 days for newborns later diagnosed with ASD and 1.86 for those in the non-ASD group.
The ASD group was 77% male and the non-ASD group was 51% male. The rate of neonatal intensive care unit admission was 8% in the ASD group and 10% in the non-ASD group.
The hearing test involves placing an earpiece in the baby’s ear and delivering a click sound at 35 dB above normal hearing level (nHL) at a rate of 77 clicks per second in the right ear and 79 clicks per second in the left ear.
Brainstem abnormalities?
The clicks create electrical activity, which is recorded by a surface electrode and used to extract the ABR waveform. When a sound reaches the brain stem, it creates five consecutive waveforms – waves I, II, III, IV, and V.
Previous studies focused on wave V, which is easiest to detect. The current study used low intensity sound that resulted in a weaker signal.
To overcome this low intensity issue, researchers focused on the negative drop (latency) after the wave V (Vn), which is easier to detect, and on the ABR phase, or entire waveform. They illustrated the differences between the ASD and non-ASD groups in a series of graphs.
Results showed that the ABR phase in the right ear was significantly prolonged in the ASD vs non-ASD group (P < .001). ABR phase in the left ear was also significantly prolonged in the ASD group (P = .021)
Vn latency in the right ear was significantly prolonged in the ASD group compared with the non-ASD group (P = .048); however, this was not the case in the left ear.
The prolongation could mean that the V-negative wave might appear after 8 ms in normally developing children compared with 8.5 or 9 ms in children with autism, said Mr. Miron.
The new study is the first to show V-negative and phase abnormalities are associated with ASD, the authors note. The brainstem prolongation could be due to anatomical abnormalities in the brainstem in individuals with ASD, the researchers added.
Present before birth?
The presence of ABR biomarkers of ASD in the first weeks after birth suggests the disorder is likely present before birth in a large group of these individuals, the researchers note.
It’s possible the ABR test could be modified to use lower intensities not only to detect hearing impairment but autism risk, said Mr. Miron. “The test has been optimized to detect hearing impairment, and it does so brilliantly and helps thousands of children. We want to do the same kind of optimization for autism.”
This could lead to earlier behavioral diagnoses, which, in turn, could lead to earlier treatment and better outcomes for children with ASD, said Mr. Miron.
At this time, the level of prolongation to detect ASD is unclear. “I would think a lot of people would want to make it one standard deviation, but it depends on a lot of factors, including for example, whether a baby is preterm,” said Mr. Miron.
More research and better accuracy and specificity are needed before the newborn hearing test is clinically useful.
He noted that the hearing test is only one marker of autism and that it could potentially be combined with other behavioral signs and genetic markers to facilitate earlier diagnosis and treatment and improve outcomes for patients with ASD.
Future research by his group will investigate whether the degree of auditory prolongation relates to autism severity. They also plan to research ASD subgroups including children with comorbid epilepsy.
Terrific, clever research
Jeremy Veenstra-VanderWeele, MD, professor, child and adolescent psychiatry, Columbia University, New York, said in an interview that the study is “terrific” and a “clever use” of an existing dataset.
“They showed a difference between a large group of kids with autism and a large group of kids without.”
However, he added, more research is needed before the test can be used as an autism screening tool.
“In order for this to be a screening test that could be broadly applied you would need to identify a cutoff where you’d think a child was at risk for autism, and if you look at the graphs in the article, there are no clear cutoffs,” said Dr. Veenstra-VanderWeele.
To turn this into a useful test, “you would have to establish sensitivity and specificity, you would have to look not just at the comparison of kids with autism and kids without but apply it in a predictive way in a second population.”
The study authors and Dr. Veenstra-VanderWeele have reported no relevant financial relationships. Veenstra-VanderWeele is an associate editor at Autism Research, which published the article, but he did not handle or view it before being interviewed.
A version of this article originally appeared on Medscape.com.
new research shows.
Results from one of the largest studies of its kind show the auditory brainstem response (ABR) test, which is carried out on most newborns, represents “a huge untapped potential” to detect autism, lead author Oren Miron, research associate, department of biomedical informatics, Harvard Medical School, Boston, and a PhD candidate at Ben Gurion University in Beersheba, Israel, said in an interview.
“The findings further reinforce our understanding that autism, in many cases, has a sensorial and auditory aspect to it,” said Mr. Miron, adding that an adverse response to sound is one of the earliest behavioral signs of autism.
The research was published online Oct. 31 in Autism Research.
Early intervention critical
Autism spectrum disorder (ASD), which involves problems in social communication and interaction, affects an estimated 1 in 59 children. Early identification and intervention are critical for improving outcomes and decreasing the economic burden associated with ASD.
The ABR test, which is used for Universal Newborn Hearing Screening (UNHS), uses surface electrodes to measure auditory nerve and brainstem responses to sound.
Previous studies identified abnormal ABR amplitude in children with ASD. However, it’s unclear whether healthy newborns who later develop autism also show ABR differences vs those who don’t develop the disorder.
Researchers used UNHS data, which allowed them to examine a larger, younger, and healthier sample compared with previous studies. The study included 321 newborns later diagnosed with ASD and 138,844 controls without a subsequent ASD diagnosis.
The mean ABR testing age was 1.76 days for newborns later diagnosed with ASD and 1.86 for those in the non-ASD group.
The ASD group was 77% male and the non-ASD group was 51% male. The rate of neonatal intensive care unit admission was 8% in the ASD group and 10% in the non-ASD group.
The hearing test involves placing an earpiece in the baby’s ear and delivering a click sound at 35 dB above normal hearing level (nHL) at a rate of 77 clicks per second in the right ear and 79 clicks per second in the left ear.
Brainstem abnormalities?
The clicks create electrical activity, which is recorded by a surface electrode and used to extract the ABR waveform. When a sound reaches the brain stem, it creates five consecutive waveforms – waves I, II, III, IV, and V.
Previous studies focused on wave V, which is easiest to detect. The current study used low intensity sound that resulted in a weaker signal.
To overcome this low intensity issue, researchers focused on the negative drop (latency) after the wave V (Vn), which is easier to detect, and on the ABR phase, or entire waveform. They illustrated the differences between the ASD and non-ASD groups in a series of graphs.
Results showed that the ABR phase in the right ear was significantly prolonged in the ASD vs non-ASD group (P < .001). ABR phase in the left ear was also significantly prolonged in the ASD group (P = .021)
Vn latency in the right ear was significantly prolonged in the ASD group compared with the non-ASD group (P = .048); however, this was not the case in the left ear.
The prolongation could mean that the V-negative wave might appear after 8 ms in normally developing children compared with 8.5 or 9 ms in children with autism, said Mr. Miron.
The new study is the first to show V-negative and phase abnormalities are associated with ASD, the authors note. The brainstem prolongation could be due to anatomical abnormalities in the brainstem in individuals with ASD, the researchers added.
Present before birth?
The presence of ABR biomarkers of ASD in the first weeks after birth suggests the disorder is likely present before birth in a large group of these individuals, the researchers note.
It’s possible the ABR test could be modified to use lower intensities not only to detect hearing impairment but autism risk, said Mr. Miron. “The test has been optimized to detect hearing impairment, and it does so brilliantly and helps thousands of children. We want to do the same kind of optimization for autism.”
This could lead to earlier behavioral diagnoses, which, in turn, could lead to earlier treatment and better outcomes for children with ASD, said Mr. Miron.
At this time, the level of prolongation to detect ASD is unclear. “I would think a lot of people would want to make it one standard deviation, but it depends on a lot of factors, including for example, whether a baby is preterm,” said Mr. Miron.
More research and better accuracy and specificity are needed before the newborn hearing test is clinically useful.
He noted that the hearing test is only one marker of autism and that it could potentially be combined with other behavioral signs and genetic markers to facilitate earlier diagnosis and treatment and improve outcomes for patients with ASD.
Future research by his group will investigate whether the degree of auditory prolongation relates to autism severity. They also plan to research ASD subgroups including children with comorbid epilepsy.
Terrific, clever research
Jeremy Veenstra-VanderWeele, MD, professor, child and adolescent psychiatry, Columbia University, New York, said in an interview that the study is “terrific” and a “clever use” of an existing dataset.
“They showed a difference between a large group of kids with autism and a large group of kids without.”
However, he added, more research is needed before the test can be used as an autism screening tool.
“In order for this to be a screening test that could be broadly applied you would need to identify a cutoff where you’d think a child was at risk for autism, and if you look at the graphs in the article, there are no clear cutoffs,” said Dr. Veenstra-VanderWeele.
To turn this into a useful test, “you would have to establish sensitivity and specificity, you would have to look not just at the comparison of kids with autism and kids without but apply it in a predictive way in a second population.”
The study authors and Dr. Veenstra-VanderWeele have reported no relevant financial relationships. Veenstra-VanderWeele is an associate editor at Autism Research, which published the article, but he did not handle or view it before being interviewed.
A version of this article originally appeared on Medscape.com.
Experts disagree with USPSTF’s take on pediatric blood pressure screening
Current evidence is insufficient to assess the balance of benefits and harms of screening for high blood pressure in children and adolescents, the U.S. Preventive Services Task Force reported in JAMA.

However, two experts in this area suggested there is evidence if you know where to look, and pediatric BP testing is crucial now.
In this update to the 2013 statement, the USPSTF’s systematic review focused on evidence surrounding the benefits of screening, test accuracy, treatment effectiveness and harms, and links between hypertension and cardiovascular disease (CVD) markers in childhood and adulthood.
Limited information was available on the accuracy of screening tests. No studies were found that directly evaluated screening for pediatric high BP or reported effectiveness in delayed onset or risk reduction for cardiovascular outcomes related to hypertension. Additionally, no studies were found that addressed screening for secondary hypertension in asymptomatic pediatric patients. No studies were found that evaluated the treatment of primary childhood hypertension and BP reduction or other outcomes in adulthood. The panel also was unable to identify any studies that reported on harms of screening and treatment.
When the adult framework for cardiovascular risk reduction is extended in pediatric patients, there are methodological challenges that make it harder to determine how much of the potential burden can actually be prevented, the panel said. The clinical and epidemiologic significance of percentile thresholds that are used to determine their ties to adult CVD has limited supporting evidence. Inconsistent performance characteristics of current diagnostic methods, of which there are few, tend to yield unfavorable high false-positive rates. Such false positives are potentially harmful, because they lead to “unnecessary secondary evaluations or treatments.” Because pharmacologic management of pediatric hypertension is continued for a much longer period, it is the increased likelihood of adverse events that should be cause for concern.
Should the focus for screening be shifted to significant risk factors?
In an accompanying editorial, Joseph T. Flynn, MD, MS, of Seattle Children’s Hospital, said that the outcome of the latest statement is expected, “given how the key questions were framed and the analysis performed.” To begin, he suggested restating the question: “What is the best approach to assess whether childhood BP measurement is associated with adult CVD or whether treatment of high BP in childhood is associated with reducing the burden of adult CVD?” The answer is to tackle these questions with randomized clinical trials that compare screening to no screening and treatment to no treatment. But such studies are likely infeasible, partly because of the required length of follow-up of 5-6 decades.
Perhaps a better question would be: “Does BP measurement in childhood identify children and adolescents who already have markers of CVD or who are at risk of developing them as adults?” Were these youth to be identified, they would become candidates for approaches that seek to prevent disease progression. Reframing the question in this manner better positions physicians to focus on prevention and sidestep “the requirement that the only acceptable outcome is prevention of CVD events in adulthood,” he explained.
The next step would be to identify data already available to address the reframed question. Cross-sectional studies could be used to make the association between BP levels and cardiovascular risk markers already present. For example, several publications from the multicenter Study of High Blood Pressure in Pediatrics: Adult Hypertension Onset in Youth (SHIP-AHOY), which enrolled roughly 400 youth, provided data that reinforce prior single-center studies that essentially proved there are adverse consequences for youth with high BP, and they “set the stage for the institution of measures designed to reverse target-organ damage and reduce cardiovascular risk in youth,” said Dr. Flynn.
More specifically, results from SHIP-AHOY “have demonstrated that increased left ventricular mass can be demonstrated at BP levels currently classified as normotensive and that abnormal left ventricular function can be seen at similar BP levels,” Dr. Flynn noted. In addition, “they have established a substantial association between an abnormal metabolic phenotype and several forms of target-organ damage associated with high BP.”
One approach is to analyze longitudinal cohort studies
Because there is a paucity of prospective clinical trials, Dr. Flynn suggested that analyzing longitudinal cohort studies would be the most effective approach for evaluating the potential link between current BP levels and future CVD. Such studies already have “data that address an important point raised in the USPSTF statement, namely whether the pediatric percentile-based BP cut points, such as those in the 2017 AAP [American Academy of Pediatrics] guideline, are associated with adult hypertension and CVD,” noted Dr. Flynn. “In the International Childhood Cardiovascular Cohort Consortium study, the specific childhood BP levels that were associated with increased adult carotid intima-medial thickness were remarkably similar to the BP percentile cut points in the AAP guideline for children of similar ages.”
Analysis of data from the Bogalusa Heart Study found looking at children classified as having high BP by the 2017 AAP guideline had “increased relative risks of having hypertension, left ventricular hypertrophy, or metabolic syndrome as adults 36 years later.”
“The conclusions of the USPSTF statement underscore the need for additional research on childhood high BP and its association with adult CVD. The starting points for such research can be deduced from currently available cross-sectional and longitudinal data, which demonstrate the detrimental outcomes associated with high BP in youth. Using these data to reframe and answer the questions raised by the USPSTF should point the way toward effective prevention of adult CVD,” concluded Dr. Flynn.
In a separate interview, Kristen Sexson Tejtel, MD, PhD, MPH, medical director of the preventive cardiology clinic at Texas Children’s Hospital and Baylor College of Medicine, both in Houston, noted that in spite of USPSTF’s findings, there is actually an association between children with high blood pressure and intermediate outcomes in adults.
“Dr. Flynn suggests reframing the question. In fact, evidence exists that children with high blood pressure are at higher risk of left ventricular hypertrophy, increased arterial stiffness, and changes in retinal arteries,” noted Dr. Sexson Tejtel.
Evidence of pediatric heart damage has been documented in autopsies
“It is imperative that children have blood pressure evaluation,” she urged. “There is evidence that there are changes similar to those seen in adults with cardiovascular compromise. It has been shown that children dying of other causes [accidents] who have these problems also have more plaque on autopsy, indicating that those with high blood pressure are more likely to have markers of CVD already present in childhood.
“One of the keys of pediatric medicine is prevention and the counseling for prevention of adult diseases. The duration of study necessary to objectively determine whether treatment of hypertension in childhood reduces the risk of adult cardiac problems is extensive. If nothing is done now, we are putting more future generations in danger. We must provide appropriate counseling for children and their families regarding lifestyle improvements, to have a chance to improve cardiovascular risk factors in adults, including hypertension, hyperlipidemia and/or obesity,” urged Dr. Sexson Tejtel.
All members of the USPSTF received travel reimbursement and honoraria. Dr. Barry received grants and personal fees from Healthwise. The U.S. Congress mandates that the Agency for Healthcare Research and Quality support the operations of the USPSTF. Dr. Flynn reported receiving grants from the National Institutes of Health and royalties from UpToDate and Springer outside the submitted work. Dr. Sexson Tejtel said she had no relevant financial disclosures or conflicts of interest.
SOURCE: USPSTF. JAMA. 2020 Nov 10. doi: 10.1001/jama.2020.20122.
Current evidence is insufficient to assess the balance of benefits and harms of screening for high blood pressure in children and adolescents, the U.S. Preventive Services Task Force reported in JAMA.
However, two experts in this area suggested there is evidence if you know where to look, and pediatric BP testing is crucial now.
In this update to the 2013 statement, the USPSTF’s systematic review focused on evidence surrounding the benefits of screening, test accuracy, treatment effectiveness and harms, and links between hypertension and cardiovascular disease (CVD) markers in childhood and adulthood.
Limited information was available on the accuracy of screening tests. No studies were found that directly evaluated screening for pediatric high BP or reported effectiveness in delayed onset or risk reduction for cardiovascular outcomes related to hypertension. Additionally, no studies were found that addressed screening for secondary hypertension in asymptomatic pediatric patients. No studies were found that evaluated the treatment of primary childhood hypertension and BP reduction or other outcomes in adulthood. The panel also was unable to identify any studies that reported on harms of screening and treatment.
When the adult framework for cardiovascular risk reduction is extended in pediatric patients, there are methodological challenges that make it harder to determine how much of the potential burden can actually be prevented, the panel said. The clinical and epidemiologic significance of percentile thresholds that are used to determine their ties to adult CVD has limited supporting evidence. Inconsistent performance characteristics of current diagnostic methods, of which there are few, tend to yield unfavorable high false-positive rates. Such false positives are potentially harmful, because they lead to “unnecessary secondary evaluations or treatments.” Because pharmacologic management of pediatric hypertension is continued for a much longer period, it is the increased likelihood of adverse events that should be cause for concern.
Should the focus for screening be shifted to significant risk factors?
In an accompanying editorial, Joseph T. Flynn, MD, MS, of Seattle Children’s Hospital, said that the outcome of the latest statement is expected, “given how the key questions were framed and the analysis performed.” To begin, he suggested restating the question: “What is the best approach to assess whether childhood BP measurement is associated with adult CVD or whether treatment of high BP in childhood is associated with reducing the burden of adult CVD?” The answer is to tackle these questions with randomized clinical trials that compare screening to no screening and treatment to no treatment. But such studies are likely infeasible, partly because of the required length of follow-up of 5-6 decades.
Perhaps a better question would be: “Does BP measurement in childhood identify children and adolescents who already have markers of CVD or who are at risk of developing them as adults?” Were these youth to be identified, they would become candidates for approaches that seek to prevent disease progression. Reframing the question in this manner better positions physicians to focus on prevention and sidestep “the requirement that the only acceptable outcome is prevention of CVD events in adulthood,” he explained.
The next step would be to identify data already available to address the reframed question. Cross-sectional studies could be used to make the association between BP levels and cardiovascular risk markers already present. For example, several publications from the multicenter Study of High Blood Pressure in Pediatrics: Adult Hypertension Onset in Youth (SHIP-AHOY), which enrolled roughly 400 youth, provided data that reinforce prior single-center studies that essentially proved there are adverse consequences for youth with high BP, and they “set the stage for the institution of measures designed to reverse target-organ damage and reduce cardiovascular risk in youth,” said Dr. Flynn.
More specifically, results from SHIP-AHOY “have demonstrated that increased left ventricular mass can be demonstrated at BP levels currently classified as normotensive and that abnormal left ventricular function can be seen at similar BP levels,” Dr. Flynn noted. In addition, “they have established a substantial association between an abnormal metabolic phenotype and several forms of target-organ damage associated with high BP.”
One approach is to analyze longitudinal cohort studies
Because there is a paucity of prospective clinical trials, Dr. Flynn suggested that analyzing longitudinal cohort studies would be the most effective approach for evaluating the potential link between current BP levels and future CVD. Such studies already have “data that address an important point raised in the USPSTF statement, namely whether the pediatric percentile-based BP cut points, such as those in the 2017 AAP [American Academy of Pediatrics] guideline, are associated with adult hypertension and CVD,” noted Dr. Flynn. “In the International Childhood Cardiovascular Cohort Consortium study, the specific childhood BP levels that were associated with increased adult carotid intima-medial thickness were remarkably similar to the BP percentile cut points in the AAP guideline for children of similar ages.”
Analysis of data from the Bogalusa Heart Study found looking at children classified as having high BP by the 2017 AAP guideline had “increased relative risks of having hypertension, left ventricular hypertrophy, or metabolic syndrome as adults 36 years later.”
“The conclusions of the USPSTF statement underscore the need for additional research on childhood high BP and its association with adult CVD. The starting points for such research can be deduced from currently available cross-sectional and longitudinal data, which demonstrate the detrimental outcomes associated with high BP in youth. Using these data to reframe and answer the questions raised by the USPSTF should point the way toward effective prevention of adult CVD,” concluded Dr. Flynn.
In a separate interview, Kristen Sexson Tejtel, MD, PhD, MPH, medical director of the preventive cardiology clinic at Texas Children’s Hospital and Baylor College of Medicine, both in Houston, noted that in spite of USPSTF’s findings, there is actually an association between children with high blood pressure and intermediate outcomes in adults.
“Dr. Flynn suggests reframing the question. In fact, evidence exists that children with high blood pressure are at higher risk of left ventricular hypertrophy, increased arterial stiffness, and changes in retinal arteries,” noted Dr. Sexson Tejtel.
Evidence of pediatric heart damage has been documented in autopsies
“It is imperative that children have blood pressure evaluation,” she urged. “There is evidence that there are changes similar to those seen in adults with cardiovascular compromise. It has been shown that children dying of other causes [accidents] who have these problems also have more plaque on autopsy, indicating that those with high blood pressure are more likely to have markers of CVD already present in childhood.
“One of the keys of pediatric medicine is prevention and the counseling for prevention of adult diseases. The duration of study necessary to objectively determine whether treatment of hypertension in childhood reduces the risk of adult cardiac problems is extensive. If nothing is done now, we are putting more future generations in danger. We must provide appropriate counseling for children and their families regarding lifestyle improvements, to have a chance to improve cardiovascular risk factors in adults, including hypertension, hyperlipidemia and/or obesity,” urged Dr. Sexson Tejtel.
All members of the USPSTF received travel reimbursement and honoraria. Dr. Barry received grants and personal fees from Healthwise. The U.S. Congress mandates that the Agency for Healthcare Research and Quality support the operations of the USPSTF. Dr. Flynn reported receiving grants from the National Institutes of Health and royalties from UpToDate and Springer outside the submitted work. Dr. Sexson Tejtel said she had no relevant financial disclosures or conflicts of interest.
SOURCE: USPSTF. JAMA. 2020 Nov 10. doi: 10.1001/jama.2020.20122.
Current evidence is insufficient to assess the balance of benefits and harms of screening for high blood pressure in children and adolescents, the U.S. Preventive Services Task Force reported in JAMA.
However, two experts in this area suggested there is evidence if you know where to look, and pediatric BP testing is crucial now.
In this update to the 2013 statement, the USPSTF’s systematic review focused on evidence surrounding the benefits of screening, test accuracy, treatment effectiveness and harms, and links between hypertension and cardiovascular disease (CVD) markers in childhood and adulthood.
Limited information was available on the accuracy of screening tests. No studies were found that directly evaluated screening for pediatric high BP or reported effectiveness in delayed onset or risk reduction for cardiovascular outcomes related to hypertension. Additionally, no studies were found that addressed screening for secondary hypertension in asymptomatic pediatric patients. No studies were found that evaluated the treatment of primary childhood hypertension and BP reduction or other outcomes in adulthood. The panel also was unable to identify any studies that reported on harms of screening and treatment.
When the adult framework for cardiovascular risk reduction is extended in pediatric patients, there are methodological challenges that make it harder to determine how much of the potential burden can actually be prevented, the panel said. The clinical and epidemiologic significance of percentile thresholds that are used to determine their ties to adult CVD has limited supporting evidence. Inconsistent performance characteristics of current diagnostic methods, of which there are few, tend to yield unfavorable high false-positive rates. Such false positives are potentially harmful, because they lead to “unnecessary secondary evaluations or treatments.” Because pharmacologic management of pediatric hypertension is continued for a much longer period, it is the increased likelihood of adverse events that should be cause for concern.
Should the focus for screening be shifted to significant risk factors?
In an accompanying editorial, Joseph T. Flynn, MD, MS, of Seattle Children’s Hospital, said that the outcome of the latest statement is expected, “given how the key questions were framed and the analysis performed.” To begin, he suggested restating the question: “What is the best approach to assess whether childhood BP measurement is associated with adult CVD or whether treatment of high BP in childhood is associated with reducing the burden of adult CVD?” The answer is to tackle these questions with randomized clinical trials that compare screening to no screening and treatment to no treatment. But such studies are likely infeasible, partly because of the required length of follow-up of 5-6 decades.
Perhaps a better question would be: “Does BP measurement in childhood identify children and adolescents who already have markers of CVD or who are at risk of developing them as adults?” Were these youth to be identified, they would become candidates for approaches that seek to prevent disease progression. Reframing the question in this manner better positions physicians to focus on prevention and sidestep “the requirement that the only acceptable outcome is prevention of CVD events in adulthood,” he explained.
The next step would be to identify data already available to address the reframed question. Cross-sectional studies could be used to make the association between BP levels and cardiovascular risk markers already present. For example, several publications from the multicenter Study of High Blood Pressure in Pediatrics: Adult Hypertension Onset in Youth (SHIP-AHOY), which enrolled roughly 400 youth, provided data that reinforce prior single-center studies that essentially proved there are adverse consequences for youth with high BP, and they “set the stage for the institution of measures designed to reverse target-organ damage and reduce cardiovascular risk in youth,” said Dr. Flynn.
More specifically, results from SHIP-AHOY “have demonstrated that increased left ventricular mass can be demonstrated at BP levels currently classified as normotensive and that abnormal left ventricular function can be seen at similar BP levels,” Dr. Flynn noted. In addition, “they have established a substantial association between an abnormal metabolic phenotype and several forms of target-organ damage associated with high BP.”
One approach is to analyze longitudinal cohort studies
Because there is a paucity of prospective clinical trials, Dr. Flynn suggested that analyzing longitudinal cohort studies would be the most effective approach for evaluating the potential link between current BP levels and future CVD. Such studies already have “data that address an important point raised in the USPSTF statement, namely whether the pediatric percentile-based BP cut points, such as those in the 2017 AAP [American Academy of Pediatrics] guideline, are associated with adult hypertension and CVD,” noted Dr. Flynn. “In the International Childhood Cardiovascular Cohort Consortium study, the specific childhood BP levels that were associated with increased adult carotid intima-medial thickness were remarkably similar to the BP percentile cut points in the AAP guideline for children of similar ages.”
Analysis of data from the Bogalusa Heart Study found looking at children classified as having high BP by the 2017 AAP guideline had “increased relative risks of having hypertension, left ventricular hypertrophy, or metabolic syndrome as adults 36 years later.”
“The conclusions of the USPSTF statement underscore the need for additional research on childhood high BP and its association with adult CVD. The starting points for such research can be deduced from currently available cross-sectional and longitudinal data, which demonstrate the detrimental outcomes associated with high BP in youth. Using these data to reframe and answer the questions raised by the USPSTF should point the way toward effective prevention of adult CVD,” concluded Dr. Flynn.
In a separate interview, Kristen Sexson Tejtel, MD, PhD, MPH, medical director of the preventive cardiology clinic at Texas Children’s Hospital and Baylor College of Medicine, both in Houston, noted that in spite of USPSTF’s findings, there is actually an association between children with high blood pressure and intermediate outcomes in adults.
“Dr. Flynn suggests reframing the question. In fact, evidence exists that children with high blood pressure are at higher risk of left ventricular hypertrophy, increased arterial stiffness, and changes in retinal arteries,” noted Dr. Sexson Tejtel.
Evidence of pediatric heart damage has been documented in autopsies
“It is imperative that children have blood pressure evaluation,” she urged. “There is evidence that there are changes similar to those seen in adults with cardiovascular compromise. It has been shown that children dying of other causes [accidents] who have these problems also have more plaque on autopsy, indicating that those with high blood pressure are more likely to have markers of CVD already present in childhood.
“One of the keys of pediatric medicine is prevention and the counseling for prevention of adult diseases. The duration of study necessary to objectively determine whether treatment of hypertension in childhood reduces the risk of adult cardiac problems is extensive. If nothing is done now, we are putting more future generations in danger. We must provide appropriate counseling for children and their families regarding lifestyle improvements, to have a chance to improve cardiovascular risk factors in adults, including hypertension, hyperlipidemia and/or obesity,” urged Dr. Sexson Tejtel.
All members of the USPSTF received travel reimbursement and honoraria. Dr. Barry received grants and personal fees from Healthwise. The U.S. Congress mandates that the Agency for Healthcare Research and Quality support the operations of the USPSTF. Dr. Flynn reported receiving grants from the National Institutes of Health and royalties from UpToDate and Springer outside the submitted work. Dr. Sexson Tejtel said she had no relevant financial disclosures or conflicts of interest.
SOURCE: USPSTF. JAMA. 2020 Nov 10. doi: 10.1001/jama.2020.20122.
FROM JAMA

Myocarditis rare, macrophage infiltration common at COVID autopsy
An international autopsy study of 21 patients who died from COVID-19 has shown the presence of multifocal lymphocytic myocarditis in three patients (14%). In an additional six patients, focally increased interstitial T-lymphocytes within the myocardium were noted, with only focal or no myocyte injury.
However, increased interstitial macrophage infiltration, possibly related to cytokine infiltration, was seen in 86% of patients.
“One way to think about this is that, if these patients were having biopsies and not autopsies, there would be myocardial injury in the patients with myocarditis, even after they recovered. But with interstitial macrophages, there may or may not be any injury,” said cardiovascular pathologist James R. Stone, MD, PhD, Massachusetts General Hospital, Boston.
Dr. Stone and colleagues from Mass General, two hospitals in Italy, the University of Amsterdam, and the Mayo Clinic in Rochester, Minn., conducted the autopsies in March and April. The results were published in the October 14 issue of the European Heart Journal.
Their technique was rigorous: a median of 20 full-thickness blocks of myocardium were examined histologically (range, 5-29 blocks).
The presence of myocarditis, defined by the presence of multiple foci of inflammation with associated myocyte injury, was determined, and the inflammatory cell composition analyzed by immunohistochemistry.
“I think one of the take-homes from this study is that you have to do a thorough sampling of the heart in order to exclude myocardial injury. You cannot exclude myocarditis with just a biopsy or two,” said Dr. Stone in an interview.
“We looked at multiple different sections of tissue preserved in paraffin for every case and found only 14% had myocarditis. The vast majority of autopsies done on patients dying from COVID-19 have short-changed the autopsy and not been done in a way to exclude myocarditis,” he added.
For all patients, COVID-19 was the underlying cause of death, but the mechanisms of death were acute respiratory distress syndrome in 15, viral pneumonia in 4, cardiogenic shock in 1, and cardiac arrest in 1. Seven patients had a history of cardiovascular disease, including atrial fibrillation in four, coronary artery disease in three, left ventricular hypertrophy in one, and previous valve replacement in one. A total of 16 had hypertension, 7 had diabetes mellitus, and 1 had chronic obstructive pulmonary disease. In four cases, mild pericarditis was present. Acute myocyte injury in the right ventricle, most probably from strain or overload, was also present in four cases.
A nonsignificant trend was seen toward higher serum troponin levels in the patients with myocarditis compared with those without myocarditis. There were no reports of disrupted coronary artery plaques, coronary artery aneurysms, or large pulmonary emboli.
Macrophage infiltration rather than myocarditis, myocardial injury?
The study sheds more light on previous cardiac magnetic resonance (CMR) imaging findings that have suggested that many patients who recover from COVID-19 show signs suggestive of myocarditis. These earlier studies include a recent one in competitive athletes and the earlier Puntmann and colleagues study of relatively young COVID-19 patients, which showed ongoing myocardial involvement in a majority of patients.
“It would not surprise me if some or all of the cardiac MR changes seen in some of these recent imaging studies are due to the macrophages,” said Dr. Stone.
“What we saw was not a routine pathology by any means. It was a huge amount of macrophages, higher that what we saw in SARS and more similar to a study published in 2007 that looked at patients with bacterial sepsis,” said Dr. Stone.
In an older study of SARS patients, 35% had the virus detected in myocardial tissue by polymerase chain reaction. In that subset, the degree of myocardial macrophage infiltrate was comparable to that seen in 86% of the COVID-19 cases described in this series.
Another possibility is that the macrophage infiltration reflects underlying disease rather than COVID-19. All but one of the patients had known underlying medical conditions associated with cardiac remodeling, said Nikolaos G. Frangogiannis, MD, a cardiologist who studies the mechanisms of cardiac injury, repair, and remodeling.
Frangogiannis, from Albert Einstein College of Medicine, New York, wrote an editorial that accompanied the autopsy study.
“The problem with this finding of increased macrophage infiltration is that it’s very hard to interpret because as we age, and especially in a less healthy population, the numbers and the density of macrophages in the heart increase, so it’s impossible to interpret as an effect of the infection itself unless you have an appropriate control population that matches the same characteristics, which is almost impossible to ask for,” he said.
“I’ve observed since the beginning of the pandemic that there seemed to be some people who wanted every single case to be myocarditis and others who had a bias toward not wanting COVID-19 to be a cause of myocarditis. I think what we’re seeing is it’s not either/or for anything with this virus, it’s a bit of everything,” said Dr. Stone.
Dr. Stone and Dr. Frangogiannis reported no conflict of interest.
A version of this article originally appeared on Medscape.com.
An international autopsy study of 21 patients who died from COVID-19 has shown the presence of multifocal lymphocytic myocarditis in three patients (14%). In an additional six patients, focally increased interstitial T-lymphocytes within the myocardium were noted, with only focal or no myocyte injury.
However, increased interstitial macrophage infiltration, possibly related to cytokine infiltration, was seen in 86% of patients.
“One way to think about this is that, if these patients were having biopsies and not autopsies, there would be myocardial injury in the patients with myocarditis, even after they recovered. But with interstitial macrophages, there may or may not be any injury,” said cardiovascular pathologist James R. Stone, MD, PhD, Massachusetts General Hospital, Boston.
Dr. Stone and colleagues from Mass General, two hospitals in Italy, the University of Amsterdam, and the Mayo Clinic in Rochester, Minn., conducted the autopsies in March and April. The results were published in the October 14 issue of the European Heart Journal.
Their technique was rigorous: a median of 20 full-thickness blocks of myocardium were examined histologically (range, 5-29 blocks).
The presence of myocarditis, defined by the presence of multiple foci of inflammation with associated myocyte injury, was determined, and the inflammatory cell composition analyzed by immunohistochemistry.
“I think one of the take-homes from this study is that you have to do a thorough sampling of the heart in order to exclude myocardial injury. You cannot exclude myocarditis with just a biopsy or two,” said Dr. Stone in an interview.
“We looked at multiple different sections of tissue preserved in paraffin for every case and found only 14% had myocarditis. The vast majority of autopsies done on patients dying from COVID-19 have short-changed the autopsy and not been done in a way to exclude myocarditis,” he added.
For all patients, COVID-19 was the underlying cause of death, but the mechanisms of death were acute respiratory distress syndrome in 15, viral pneumonia in 4, cardiogenic shock in 1, and cardiac arrest in 1. Seven patients had a history of cardiovascular disease, including atrial fibrillation in four, coronary artery disease in three, left ventricular hypertrophy in one, and previous valve replacement in one. A total of 16 had hypertension, 7 had diabetes mellitus, and 1 had chronic obstructive pulmonary disease. In four cases, mild pericarditis was present. Acute myocyte injury in the right ventricle, most probably from strain or overload, was also present in four cases.
A nonsignificant trend was seen toward higher serum troponin levels in the patients with myocarditis compared with those without myocarditis. There were no reports of disrupted coronary artery plaques, coronary artery aneurysms, or large pulmonary emboli.
Macrophage infiltration rather than myocarditis, myocardial injury?
The study sheds more light on previous cardiac magnetic resonance (CMR) imaging findings that have suggested that many patients who recover from COVID-19 show signs suggestive of myocarditis. These earlier studies include a recent one in competitive athletes and the earlier Puntmann and colleagues study of relatively young COVID-19 patients, which showed ongoing myocardial involvement in a majority of patients.
“It would not surprise me if some or all of the cardiac MR changes seen in some of these recent imaging studies are due to the macrophages,” said Dr. Stone.
“What we saw was not a routine pathology by any means. It was a huge amount of macrophages, higher that what we saw in SARS and more similar to a study published in 2007 that looked at patients with bacterial sepsis,” said Dr. Stone.
In an older study of SARS patients, 35% had the virus detected in myocardial tissue by polymerase chain reaction. In that subset, the degree of myocardial macrophage infiltrate was comparable to that seen in 86% of the COVID-19 cases described in this series.
Another possibility is that the macrophage infiltration reflects underlying disease rather than COVID-19. All but one of the patients had known underlying medical conditions associated with cardiac remodeling, said Nikolaos G. Frangogiannis, MD, a cardiologist who studies the mechanisms of cardiac injury, repair, and remodeling.
Frangogiannis, from Albert Einstein College of Medicine, New York, wrote an editorial that accompanied the autopsy study.
“The problem with this finding of increased macrophage infiltration is that it’s very hard to interpret because as we age, and especially in a less healthy population, the numbers and the density of macrophages in the heart increase, so it’s impossible to interpret as an effect of the infection itself unless you have an appropriate control population that matches the same characteristics, which is almost impossible to ask for,” he said.
“I’ve observed since the beginning of the pandemic that there seemed to be some people who wanted every single case to be myocarditis and others who had a bias toward not wanting COVID-19 to be a cause of myocarditis. I think what we’re seeing is it’s not either/or for anything with this virus, it’s a bit of everything,” said Dr. Stone.
Dr. Stone and Dr. Frangogiannis reported no conflict of interest.
A version of this article originally appeared on Medscape.com.
An international autopsy study of 21 patients who died from COVID-19 has shown the presence of multifocal lymphocytic myocarditis in three patients (14%). In an additional six patients, focally increased interstitial T-lymphocytes within the myocardium were noted, with only focal or no myocyte injury.
However, increased interstitial macrophage infiltration, possibly related to cytokine infiltration, was seen in 86% of patients.
“One way to think about this is that, if these patients were having biopsies and not autopsies, there would be myocardial injury in the patients with myocarditis, even after they recovered. But with interstitial macrophages, there may or may not be any injury,” said cardiovascular pathologist James R. Stone, MD, PhD, Massachusetts General Hospital, Boston.
Dr. Stone and colleagues from Mass General, two hospitals in Italy, the University of Amsterdam, and the Mayo Clinic in Rochester, Minn., conducted the autopsies in March and April. The results were published in the October 14 issue of the European Heart Journal.
Their technique was rigorous: a median of 20 full-thickness blocks of myocardium were examined histologically (range, 5-29 blocks).
The presence of myocarditis, defined by the presence of multiple foci of inflammation with associated myocyte injury, was determined, and the inflammatory cell composition analyzed by immunohistochemistry.
“I think one of the take-homes from this study is that you have to do a thorough sampling of the heart in order to exclude myocardial injury. You cannot exclude myocarditis with just a biopsy or two,” said Dr. Stone in an interview.
“We looked at multiple different sections of tissue preserved in paraffin for every case and found only 14% had myocarditis. The vast majority of autopsies done on patients dying from COVID-19 have short-changed the autopsy and not been done in a way to exclude myocarditis,” he added.
For all patients, COVID-19 was the underlying cause of death, but the mechanisms of death were acute respiratory distress syndrome in 15, viral pneumonia in 4, cardiogenic shock in 1, and cardiac arrest in 1. Seven patients had a history of cardiovascular disease, including atrial fibrillation in four, coronary artery disease in three, left ventricular hypertrophy in one, and previous valve replacement in one. A total of 16 had hypertension, 7 had diabetes mellitus, and 1 had chronic obstructive pulmonary disease. In four cases, mild pericarditis was present. Acute myocyte injury in the right ventricle, most probably from strain or overload, was also present in four cases.
A nonsignificant trend was seen toward higher serum troponin levels in the patients with myocarditis compared with those without myocarditis. There were no reports of disrupted coronary artery plaques, coronary artery aneurysms, or large pulmonary emboli.
Macrophage infiltration rather than myocarditis, myocardial injury?
The study sheds more light on previous cardiac magnetic resonance (CMR) imaging findings that have suggested that many patients who recover from COVID-19 show signs suggestive of myocarditis. These earlier studies include a recent one in competitive athletes and the earlier Puntmann and colleagues study of relatively young COVID-19 patients, which showed ongoing myocardial involvement in a majority of patients.
“It would not surprise me if some or all of the cardiac MR changes seen in some of these recent imaging studies are due to the macrophages,” said Dr. Stone.
“What we saw was not a routine pathology by any means. It was a huge amount of macrophages, higher that what we saw in SARS and more similar to a study published in 2007 that looked at patients with bacterial sepsis,” said Dr. Stone.
In an older study of SARS patients, 35% had the virus detected in myocardial tissue by polymerase chain reaction. In that subset, the degree of myocardial macrophage infiltrate was comparable to that seen in 86% of the COVID-19 cases described in this series.
Another possibility is that the macrophage infiltration reflects underlying disease rather than COVID-19. All but one of the patients had known underlying medical conditions associated with cardiac remodeling, said Nikolaos G. Frangogiannis, MD, a cardiologist who studies the mechanisms of cardiac injury, repair, and remodeling.
Frangogiannis, from Albert Einstein College of Medicine, New York, wrote an editorial that accompanied the autopsy study.
“The problem with this finding of increased macrophage infiltration is that it’s very hard to interpret because as we age, and especially in a less healthy population, the numbers and the density of macrophages in the heart increase, so it’s impossible to interpret as an effect of the infection itself unless you have an appropriate control population that matches the same characteristics, which is almost impossible to ask for,” he said.
“I’ve observed since the beginning of the pandemic that there seemed to be some people who wanted every single case to be myocarditis and others who had a bias toward not wanting COVID-19 to be a cause of myocarditis. I think what we’re seeing is it’s not either/or for anything with this virus, it’s a bit of everything,” said Dr. Stone.
Dr. Stone and Dr. Frangogiannis reported no conflict of interest.
A version of this article originally appeared on Medscape.com.
Painful ethical choices in 2020 vs. 2010: How has thinking changed?
Much has changed in the 10 years since Medscape’s first survey on what physicians would do when faced with painful choices in patient care.
A new report, Ethics 2020: Life, Death, and Painful Dilemmas, shows that physicians’ value judgments have shifted in many respects, sometimes as a result of increased regulations and fears of litigation.
End-of-life decisions
Several of the questions in the survey revolved around end-of-life decisions, and in some cases, the differences seen in just a decade were striking. One example concerned life support decisions in the context of a family’s choices.
Age also seemed to play a role in the 2020 answers to that question: Physicians younger than 45 were more likely (28%) to answer “yes” (that they would withdraw life support in that instance) than were those 45 and older (16%).
A critical care physician said, “If the family appears to have an underlying motivation that may not be in the patient’s best interest, I might be inclined to pursue a legal decision prior to withdrawing support.”
A cardiologist had a more pointed response to the question: “To me, that would be murder.”
Another example of how perspectives have changed over the past 10 years concerns whether physician-aided dying should be legal for terminally ill patients. The practice is now mandated by law in eight states and the District of Columbia, and it is mandated by court ruling in two additional states.
In 2010, 41% said “no.” That number dropped to 28% in 2020.
On legalization, a psychiatrist said, “Yes, when there is truly no hope and the quality of remaining life is too poor. We show more compassion to our sick animals than we do to our human population.”
Conversely, a neurologist answered, “No, I see younger physicians already becoming comfortable with the idea of deciding ASAP whether there is a reasonable chance of survival and then pressing for the right code status. This change would make things worse.”
Assisted death and incurable suffering
Far fewer physicians supported physician-assisted death for those who had years to live but faced incurable suffering: Thirty-seven percent said “yes,” 34% said “no,” and 29% said “it depends.”
However, support was significantly higher than it was just 2 years ago, in 2018, when only 27% supported the concept, the report authors noted.
“The shift reflects movements by many states to legalize assisted dying for the terminally ill,” Arthur Caplan, PhD, director of the division of medical ethics, New York University, said in the report. “Legalization has not been abused, so some doctors are more willing to press further beyond terminal illness as a trigger to suffering.”
Conversely, many more physicians (44% vs. 24% a decade ago) said they would provide life-sustaining therapy if the family requested it, even if the physician thought it was futile.
“Concerns over a malpractice lawsuit and potential negative patient/family online reviews are factors that play into this change,” the survey authors wrote.
Shared decision making also increased in the past decade.
Would you undertreat pain?
Primary care physicians fear the consequences of what they consider adequate pain management more than specialists do (24% vs. 17%), the survey authors noted.
Ten years ago, Medscape asked physicians whether they would undertreat a patient’s pain because of fear of repercussions or the patient’s becoming addicted: Eighty-four percent said “no,” and 6% said “yes.” The rest said “it depends.”
In 2020, the question was asked slightly differently: “Would you undertreat a patient’s pain for fear of addiction or Drug Enforcement Administration or medical board scrutiny?” This year, three times as many said “yes” (18%); 63% said “no.”
“Respondents this year talked about investigations and reprimands by medical boards, and how much they wanted to avoid that,” the survey authors wrote.
Should physicians be required to treat COVID-19 patients?
Some questions were new this year, including one on whether physicians should be required to treat COVID-19 patients. Fewer than half (47%) answered “yes,” 24% said “no,” and 29% answered “it depends.”
Doctors’ answers to this question differed slightly by gender: Fifty percent of men and 43% of women said “yes.” In their responses, many physicians said consideration should be given to risk factors, such as age, underlying conditions, risk of family members, and availability of personal protective equipment (PPE).
Another pandemic-related question asked whether physicians felt they should correct physicians who post misinformation about the pandemic on social media. Half (50%) said “yes,” 19% said “no,” and 31% said “it depends.”
Speaking out against the workplace
This year, many physicians have felt betrayed when they didn’t have adequate PPE during the pandemic.
Asked, “Is it right to speak out against your hospital or workplace when they don’t give you what you need?” 53% of physicians said “yes,” 8% said “no,” and 40% said “it depends.”
A cardiologist made the value judgment this way: “Speaking out just because you had an argument with your boss is inappropriate. Bringing to the public repeated failures to correct situations that have been brought through the proper channels is necessary to incite change.”
Random drug testing for physicians?
Another question in the survey asked whether physicians should be subjected to random drug testing for alcohol and drug abuse. About one-third (34%) said yes, 43% said no, and 23% said “it depends.” A study found that between 10% and 15% of physicians have abused a substance at some point in their careers.
The subject continues to hit a nerve in medicine.
A family physician wrote, “This should not be done unless a particular physician had a problem with drug or alcohol abuse and shows signs of impairment.”
An internist took a different view, saying, “Military service men and women, police, firefighters, airline pilots, and other professions that have responsibilities affecting people’s lives are subject to testing; why not physicians?”
A version of this article originally appeared on Medscape.com.
Much has changed in the 10 years since Medscape’s first survey on what physicians would do when faced with painful choices in patient care.
A new report, Ethics 2020: Life, Death, and Painful Dilemmas, shows that physicians’ value judgments have shifted in many respects, sometimes as a result of increased regulations and fears of litigation.
End-of-life decisions
Several of the questions in the survey revolved around end-of-life decisions, and in some cases, the differences seen in just a decade were striking. One example concerned life support decisions in the context of a family’s choices.
Age also seemed to play a role in the 2020 answers to that question: Physicians younger than 45 were more likely (28%) to answer “yes” (that they would withdraw life support in that instance) than were those 45 and older (16%).
A critical care physician said, “If the family appears to have an underlying motivation that may not be in the patient’s best interest, I might be inclined to pursue a legal decision prior to withdrawing support.”
A cardiologist had a more pointed response to the question: “To me, that would be murder.”
Another example of how perspectives have changed over the past 10 years concerns whether physician-aided dying should be legal for terminally ill patients. The practice is now mandated by law in eight states and the District of Columbia, and it is mandated by court ruling in two additional states.
In 2010, 41% said “no.” That number dropped to 28% in 2020.
On legalization, a psychiatrist said, “Yes, when there is truly no hope and the quality of remaining life is too poor. We show more compassion to our sick animals than we do to our human population.”
Conversely, a neurologist answered, “No, I see younger physicians already becoming comfortable with the idea of deciding ASAP whether there is a reasonable chance of survival and then pressing for the right code status. This change would make things worse.”
Assisted death and incurable suffering
Far fewer physicians supported physician-assisted death for those who had years to live but faced incurable suffering: Thirty-seven percent said “yes,” 34% said “no,” and 29% said “it depends.”
However, support was significantly higher than it was just 2 years ago, in 2018, when only 27% supported the concept, the report authors noted.
“The shift reflects movements by many states to legalize assisted dying for the terminally ill,” Arthur Caplan, PhD, director of the division of medical ethics, New York University, said in the report. “Legalization has not been abused, so some doctors are more willing to press further beyond terminal illness as a trigger to suffering.”
Conversely, many more physicians (44% vs. 24% a decade ago) said they would provide life-sustaining therapy if the family requested it, even if the physician thought it was futile.
“Concerns over a malpractice lawsuit and potential negative patient/family online reviews are factors that play into this change,” the survey authors wrote.
Shared decision making also increased in the past decade.
Would you undertreat pain?
Primary care physicians fear the consequences of what they consider adequate pain management more than specialists do (24% vs. 17%), the survey authors noted.
Ten years ago, Medscape asked physicians whether they would undertreat a patient’s pain because of fear of repercussions or the patient’s becoming addicted: Eighty-four percent said “no,” and 6% said “yes.” The rest said “it depends.”
In 2020, the question was asked slightly differently: “Would you undertreat a patient’s pain for fear of addiction or Drug Enforcement Administration or medical board scrutiny?” This year, three times as many said “yes” (18%); 63% said “no.”
“Respondents this year talked about investigations and reprimands by medical boards, and how much they wanted to avoid that,” the survey authors wrote.
Should physicians be required to treat COVID-19 patients?
Some questions were new this year, including one on whether physicians should be required to treat COVID-19 patients. Fewer than half (47%) answered “yes,” 24% said “no,” and 29% answered “it depends.”
Doctors’ answers to this question differed slightly by gender: Fifty percent of men and 43% of women said “yes.” In their responses, many physicians said consideration should be given to risk factors, such as age, underlying conditions, risk of family members, and availability of personal protective equipment (PPE).
Another pandemic-related question asked whether physicians felt they should correct physicians who post misinformation about the pandemic on social media. Half (50%) said “yes,” 19% said “no,” and 31% said “it depends.”
Speaking out against the workplace
This year, many physicians have felt betrayed when they didn’t have adequate PPE during the pandemic.
Asked, “Is it right to speak out against your hospital or workplace when they don’t give you what you need?” 53% of physicians said “yes,” 8% said “no,” and 40% said “it depends.”
A cardiologist made the value judgment this way: “Speaking out just because you had an argument with your boss is inappropriate. Bringing to the public repeated failures to correct situations that have been brought through the proper channels is necessary to incite change.”
Random drug testing for physicians?
Another question in the survey asked whether physicians should be subjected to random drug testing for alcohol and drug abuse. About one-third (34%) said yes, 43% said no, and 23% said “it depends.” A study found that between 10% and 15% of physicians have abused a substance at some point in their careers.
The subject continues to hit a nerve in medicine.
A family physician wrote, “This should not be done unless a particular physician had a problem with drug or alcohol abuse and shows signs of impairment.”
An internist took a different view, saying, “Military service men and women, police, firefighters, airline pilots, and other professions that have responsibilities affecting people’s lives are subject to testing; why not physicians?”
A version of this article originally appeared on Medscape.com.
Much has changed in the 10 years since Medscape’s first survey on what physicians would do when faced with painful choices in patient care.
A new report, Ethics 2020: Life, Death, and Painful Dilemmas, shows that physicians’ value judgments have shifted in many respects, sometimes as a result of increased regulations and fears of litigation.
End-of-life decisions
Several of the questions in the survey revolved around end-of-life decisions, and in some cases, the differences seen in just a decade were striking. One example concerned life support decisions in the context of a family’s choices.
Age also seemed to play a role in the 2020 answers to that question: Physicians younger than 45 were more likely (28%) to answer “yes” (that they would withdraw life support in that instance) than were those 45 and older (16%).
A critical care physician said, “If the family appears to have an underlying motivation that may not be in the patient’s best interest, I might be inclined to pursue a legal decision prior to withdrawing support.”
A cardiologist had a more pointed response to the question: “To me, that would be murder.”
Another example of how perspectives have changed over the past 10 years concerns whether physician-aided dying should be legal for terminally ill patients. The practice is now mandated by law in eight states and the District of Columbia, and it is mandated by court ruling in two additional states.
In 2010, 41% said “no.” That number dropped to 28% in 2020.
On legalization, a psychiatrist said, “Yes, when there is truly no hope and the quality of remaining life is too poor. We show more compassion to our sick animals than we do to our human population.”
Conversely, a neurologist answered, “No, I see younger physicians already becoming comfortable with the idea of deciding ASAP whether there is a reasonable chance of survival and then pressing for the right code status. This change would make things worse.”
Assisted death and incurable suffering
Far fewer physicians supported physician-assisted death for those who had years to live but faced incurable suffering: Thirty-seven percent said “yes,” 34% said “no,” and 29% said “it depends.”
However, support was significantly higher than it was just 2 years ago, in 2018, when only 27% supported the concept, the report authors noted.
“The shift reflects movements by many states to legalize assisted dying for the terminally ill,” Arthur Caplan, PhD, director of the division of medical ethics, New York University, said in the report. “Legalization has not been abused, so some doctors are more willing to press further beyond terminal illness as a trigger to suffering.”
Conversely, many more physicians (44% vs. 24% a decade ago) said they would provide life-sustaining therapy if the family requested it, even if the physician thought it was futile.
“Concerns over a malpractice lawsuit and potential negative patient/family online reviews are factors that play into this change,” the survey authors wrote.
Shared decision making also increased in the past decade.
Would you undertreat pain?
Primary care physicians fear the consequences of what they consider adequate pain management more than specialists do (24% vs. 17%), the survey authors noted.
Ten years ago, Medscape asked physicians whether they would undertreat a patient’s pain because of fear of repercussions or the patient’s becoming addicted: Eighty-four percent said “no,” and 6% said “yes.” The rest said “it depends.”
In 2020, the question was asked slightly differently: “Would you undertreat a patient’s pain for fear of addiction or Drug Enforcement Administration or medical board scrutiny?” This year, three times as many said “yes” (18%); 63% said “no.”
“Respondents this year talked about investigations and reprimands by medical boards, and how much they wanted to avoid that,” the survey authors wrote.
Should physicians be required to treat COVID-19 patients?
Some questions were new this year, including one on whether physicians should be required to treat COVID-19 patients. Fewer than half (47%) answered “yes,” 24% said “no,” and 29% answered “it depends.”
Doctors’ answers to this question differed slightly by gender: Fifty percent of men and 43% of women said “yes.” In their responses, many physicians said consideration should be given to risk factors, such as age, underlying conditions, risk of family members, and availability of personal protective equipment (PPE).
Another pandemic-related question asked whether physicians felt they should correct physicians who post misinformation about the pandemic on social media. Half (50%) said “yes,” 19% said “no,” and 31% said “it depends.”
Speaking out against the workplace
This year, many physicians have felt betrayed when they didn’t have adequate PPE during the pandemic.
Asked, “Is it right to speak out against your hospital or workplace when they don’t give you what you need?” 53% of physicians said “yes,” 8% said “no,” and 40% said “it depends.”
A cardiologist made the value judgment this way: “Speaking out just because you had an argument with your boss is inappropriate. Bringing to the public repeated failures to correct situations that have been brought through the proper channels is necessary to incite change.”
Random drug testing for physicians?
Another question in the survey asked whether physicians should be subjected to random drug testing for alcohol and drug abuse. About one-third (34%) said yes, 43% said no, and 23% said “it depends.” A study found that between 10% and 15% of physicians have abused a substance at some point in their careers.
The subject continues to hit a nerve in medicine.
A family physician wrote, “This should not be done unless a particular physician had a problem with drug or alcohol abuse and shows signs of impairment.”
An internist took a different view, saying, “Military service men and women, police, firefighters, airline pilots, and other professions that have responsibilities affecting people’s lives are subject to testing; why not physicians?”
A version of this article originally appeared on Medscape.com.
Liver-related deaths decline after Medicaid expansion under ACA
Liver-related deaths declined and liver transplant waitlist inequities decreased in states that implemented Medicaid expansion under the Affordable Care Act (ACA), results of an innovative study showed.
About 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality in 18 states that took advantage of expanded coverage began to decline, whereas the rate of liver-related deaths in 14 states that did not expand Medicaid continued to climb, reported Nabeel Wahid, MD, a resident at Weill Cornell Medicine, New York.
The differences in liver-related mortality between Medicaid expansion and nonexpansion states was particularly pronounced in people of Asian background, in Whites, and in African Americans, he said in an oral abstract presentation during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“The expansion of government health care programs such as Medicaid may improve liver-related mortality and liver transplant waitlist placement,” he said.
The implementation of the ACA, also known as Obamacare, resulted in “a pretty dramatic increase in the number of Americans with health insurance today, and there’s a lot of literature out there looking at a variety of domains throughout health care that have found that Medicaid expansion increased access and decreased disparities in care,” he added.
For example, a report published in 2019 by the nonpartisan National Bureau of Economic Research Priorities showed a significant reduction in disease-related deaths in Americans aged 55-64 in Medicaid expansion states compared with nonexpansion states.
In addition as previously reported, before Medicaid expansion African Americans were 4.8% less likely than were Whites to receive timely cancer treatment, defined as treatment starting within 30 days of diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups had dwindled to just 0.8% and was no longer statistically significant.
“However, specifically in the realm of liver transplantation and liver disease, there’s very limited literature showing any sort of significant impact on care resulting from Medicaid expansion,” Dr. Wahid said.
Listing-to-death ratio
To test their hypothesis that Medicaid expansion decreased racial disparities and improved liver-related deaths and transplant waitlist placement, Dr. Wahid and colleagues compared liver-related deaths and liver transplants listings between Medicaid expansion and nonexpansion states in the 5 years before expansion (2009-2013) and in the 5 years after expansion (2014-2018). They excluded all states without transplant centers as well as patients younger than 25 or older than 64, who were likely to be covered by other types of insurance.
They obtained data for listing from the United Network for Organ Sharing (UNOS) and on end-stage liver disease from the Centers for Disease Control and Prevention’s WONDER database.
They also used a novel measure called the listing-to-death ratio (LDR), a surrogate endpoint for waitlist placement calculated as the ratio of listings for liver transplantation relative to the number of deaths from liver disease, with a higher LDR score corresponding to improved waitlist placement.
They found that throughout the entire study period, Medicaid expansion states had lower liver-related deaths, higher liver transplant listings, and higher LDR.
Using joinpoint regression to examine changes at a specific time point, the investigators determined that the annual percentage change in liver-related deaths increased in both nonexpansion states (mean 4.3%) and expansion states (3.0%) before 2014. However, beginning around 2015, liver-related deaths began to decline in expansion states by a mean of –0.6%, while they continued on an upward trajectory in the nonexpansion states, albeit at a somewhat slower pace (mean APC 2% from 2014 through 2018).
Among all racial and ethnic groups (Whites, African Americans, Hispanics, and Asians) liver-related deaths increased from 2014 to 2018 in nonexpansion states, with the highest annual percentage change in Asians, at slightly more than 8%.
In contrast, among Asians in the expansion states, liver-related deaths over the same period increased by less than 1%, and in both Whites and African Americans liver-related deaths declined.
In addition, starting in 2015, the annual percent change in LDR increased only in expansion states primarily because of fewer end-stage liver disease deaths (the denominator in the LDR equation) rather than increased listings (the numerator).
‘No-brainer’
A gastroenterologist who was not involved in the study said that there are two key points in favor of the study.
“The obvious message is that transplant is costly, and patients need to be insured to get a liver transplant, because nobody is paying for this out of pocket. So if more candidates are insured that will reduce disparities and improve access to liver transplant for those who need it,” said Elliot Benjamin Tapper, MD, of the University of Michigan, Ann Arbor.
“It’s a no-brainer that the lack of insurance accessibility for the most vulnerable people in the United States meant that they were dying of cirrhosis instead of being transplanted,” he said in an interview.
He also commended the authors on their use of population-based data to identify outcomes.
“We know how many people are listed for liver transplant, but we don’t know how many people could have been listed. We know how many people are transplanted, but we don’t know how many people with decompensated cirrhosis should have been given that chance. We lacked that denominator,” he said.
“The innovation that makes this particular paper worthwhile is that in the absence of that denominator, they were able to construct it, so we can know from other data sources distinct from the waitlist rolls how many people are dying of cirrhosis,” he added.
No study funding source was reported. Dr. Wahid and Dr. Tapper reported no conflicts of interest.
SOURCE: Wahid N et al. AASLD 2020. Abstract 153.
Liver-related deaths declined and liver transplant waitlist inequities decreased in states that implemented Medicaid expansion under the Affordable Care Act (ACA), results of an innovative study showed.
About 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality in 18 states that took advantage of expanded coverage began to decline, whereas the rate of liver-related deaths in 14 states that did not expand Medicaid continued to climb, reported Nabeel Wahid, MD, a resident at Weill Cornell Medicine, New York.
The differences in liver-related mortality between Medicaid expansion and nonexpansion states was particularly pronounced in people of Asian background, in Whites, and in African Americans, he said in an oral abstract presentation during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“The expansion of government health care programs such as Medicaid may improve liver-related mortality and liver transplant waitlist placement,” he said.
The implementation of the ACA, also known as Obamacare, resulted in “a pretty dramatic increase in the number of Americans with health insurance today, and there’s a lot of literature out there looking at a variety of domains throughout health care that have found that Medicaid expansion increased access and decreased disparities in care,” he added.
For example, a report published in 2019 by the nonpartisan National Bureau of Economic Research Priorities showed a significant reduction in disease-related deaths in Americans aged 55-64 in Medicaid expansion states compared with nonexpansion states.
In addition as previously reported, before Medicaid expansion African Americans were 4.8% less likely than were Whites to receive timely cancer treatment, defined as treatment starting within 30 days of diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups had dwindled to just 0.8% and was no longer statistically significant.
“However, specifically in the realm of liver transplantation and liver disease, there’s very limited literature showing any sort of significant impact on care resulting from Medicaid expansion,” Dr. Wahid said.
Listing-to-death ratio
To test their hypothesis that Medicaid expansion decreased racial disparities and improved liver-related deaths and transplant waitlist placement, Dr. Wahid and colleagues compared liver-related deaths and liver transplants listings between Medicaid expansion and nonexpansion states in the 5 years before expansion (2009-2013) and in the 5 years after expansion (2014-2018). They excluded all states without transplant centers as well as patients younger than 25 or older than 64, who were likely to be covered by other types of insurance.
They obtained data for listing from the United Network for Organ Sharing (UNOS) and on end-stage liver disease from the Centers for Disease Control and Prevention’s WONDER database.
They also used a novel measure called the listing-to-death ratio (LDR), a surrogate endpoint for waitlist placement calculated as the ratio of listings for liver transplantation relative to the number of deaths from liver disease, with a higher LDR score corresponding to improved waitlist placement.
They found that throughout the entire study period, Medicaid expansion states had lower liver-related deaths, higher liver transplant listings, and higher LDR.
Using joinpoint regression to examine changes at a specific time point, the investigators determined that the annual percentage change in liver-related deaths increased in both nonexpansion states (mean 4.3%) and expansion states (3.0%) before 2014. However, beginning around 2015, liver-related deaths began to decline in expansion states by a mean of –0.6%, while they continued on an upward trajectory in the nonexpansion states, albeit at a somewhat slower pace (mean APC 2% from 2014 through 2018).
Among all racial and ethnic groups (Whites, African Americans, Hispanics, and Asians) liver-related deaths increased from 2014 to 2018 in nonexpansion states, with the highest annual percentage change in Asians, at slightly more than 8%.
In contrast, among Asians in the expansion states, liver-related deaths over the same period increased by less than 1%, and in both Whites and African Americans liver-related deaths declined.
In addition, starting in 2015, the annual percent change in LDR increased only in expansion states primarily because of fewer end-stage liver disease deaths (the denominator in the LDR equation) rather than increased listings (the numerator).
‘No-brainer’
A gastroenterologist who was not involved in the study said that there are two key points in favor of the study.
“The obvious message is that transplant is costly, and patients need to be insured to get a liver transplant, because nobody is paying for this out of pocket. So if more candidates are insured that will reduce disparities and improve access to liver transplant for those who need it,” said Elliot Benjamin Tapper, MD, of the University of Michigan, Ann Arbor.
“It’s a no-brainer that the lack of insurance accessibility for the most vulnerable people in the United States meant that they were dying of cirrhosis instead of being transplanted,” he said in an interview.
He also commended the authors on their use of population-based data to identify outcomes.
“We know how many people are listed for liver transplant, but we don’t know how many people could have been listed. We know how many people are transplanted, but we don’t know how many people with decompensated cirrhosis should have been given that chance. We lacked that denominator,” he said.
“The innovation that makes this particular paper worthwhile is that in the absence of that denominator, they were able to construct it, so we can know from other data sources distinct from the waitlist rolls how many people are dying of cirrhosis,” he added.
No study funding source was reported. Dr. Wahid and Dr. Tapper reported no conflicts of interest.
SOURCE: Wahid N et al. AASLD 2020. Abstract 153.
Liver-related deaths declined and liver transplant waitlist inequities decreased in states that implemented Medicaid expansion under the Affordable Care Act (ACA), results of an innovative study showed.
About 1 year after Medicaid expansion began on Jan. 1, 2014, the rate of liver-related mortality in 18 states that took advantage of expanded coverage began to decline, whereas the rate of liver-related deaths in 14 states that did not expand Medicaid continued to climb, reported Nabeel Wahid, MD, a resident at Weill Cornell Medicine, New York.
The differences in liver-related mortality between Medicaid expansion and nonexpansion states was particularly pronounced in people of Asian background, in Whites, and in African Americans, he said in an oral abstract presentation during the virtual annual meeting of the American Association for the Study of Liver Diseases.
“The expansion of government health care programs such as Medicaid may improve liver-related mortality and liver transplant waitlist placement,” he said.
The implementation of the ACA, also known as Obamacare, resulted in “a pretty dramatic increase in the number of Americans with health insurance today, and there’s a lot of literature out there looking at a variety of domains throughout health care that have found that Medicaid expansion increased access and decreased disparities in care,” he added.
For example, a report published in 2019 by the nonpartisan National Bureau of Economic Research Priorities showed a significant reduction in disease-related deaths in Americans aged 55-64 in Medicaid expansion states compared with nonexpansion states.
In addition as previously reported, before Medicaid expansion African Americans were 4.8% less likely than were Whites to receive timely cancer treatment, defined as treatment starting within 30 days of diagnosis of an advanced or metastatic solid tumor. After Medicaid expansion, however, the difference between the racial groups had dwindled to just 0.8% and was no longer statistically significant.
“However, specifically in the realm of liver transplantation and liver disease, there’s very limited literature showing any sort of significant impact on care resulting from Medicaid expansion,” Dr. Wahid said.
Listing-to-death ratio
To test their hypothesis that Medicaid expansion decreased racial disparities and improved liver-related deaths and transplant waitlist placement, Dr. Wahid and colleagues compared liver-related deaths and liver transplants listings between Medicaid expansion and nonexpansion states in the 5 years before expansion (2009-2013) and in the 5 years after expansion (2014-2018). They excluded all states without transplant centers as well as patients younger than 25 or older than 64, who were likely to be covered by other types of insurance.
They obtained data for listing from the United Network for Organ Sharing (UNOS) and on end-stage liver disease from the Centers for Disease Control and Prevention’s WONDER database.
They also used a novel measure called the listing-to-death ratio (LDR), a surrogate endpoint for waitlist placement calculated as the ratio of listings for liver transplantation relative to the number of deaths from liver disease, with a higher LDR score corresponding to improved waitlist placement.
They found that throughout the entire study period, Medicaid expansion states had lower liver-related deaths, higher liver transplant listings, and higher LDR.
Using joinpoint regression to examine changes at a specific time point, the investigators determined that the annual percentage change in liver-related deaths increased in both nonexpansion states (mean 4.3%) and expansion states (3.0%) before 2014. However, beginning around 2015, liver-related deaths began to decline in expansion states by a mean of –0.6%, while they continued on an upward trajectory in the nonexpansion states, albeit at a somewhat slower pace (mean APC 2% from 2014 through 2018).
Among all racial and ethnic groups (Whites, African Americans, Hispanics, and Asians) liver-related deaths increased from 2014 to 2018 in nonexpansion states, with the highest annual percentage change in Asians, at slightly more than 8%.
In contrast, among Asians in the expansion states, liver-related deaths over the same period increased by less than 1%, and in both Whites and African Americans liver-related deaths declined.
In addition, starting in 2015, the annual percent change in LDR increased only in expansion states primarily because of fewer end-stage liver disease deaths (the denominator in the LDR equation) rather than increased listings (the numerator).
‘No-brainer’
A gastroenterologist who was not involved in the study said that there are two key points in favor of the study.
“The obvious message is that transplant is costly, and patients need to be insured to get a liver transplant, because nobody is paying for this out of pocket. So if more candidates are insured that will reduce disparities and improve access to liver transplant for those who need it,” said Elliot Benjamin Tapper, MD, of the University of Michigan, Ann Arbor.
“It’s a no-brainer that the lack of insurance accessibility for the most vulnerable people in the United States meant that they were dying of cirrhosis instead of being transplanted,” he said in an interview.
He also commended the authors on their use of population-based data to identify outcomes.
“We know how many people are listed for liver transplant, but we don’t know how many people could have been listed. We know how many people are transplanted, but we don’t know how many people with decompensated cirrhosis should have been given that chance. We lacked that denominator,” he said.
“The innovation that makes this particular paper worthwhile is that in the absence of that denominator, they were able to construct it, so we can know from other data sources distinct from the waitlist rolls how many people are dying of cirrhosis,” he added.
No study funding source was reported. Dr. Wahid and Dr. Tapper reported no conflicts of interest.
SOURCE: Wahid N et al. AASLD 2020. Abstract 153.
FROM THE LIVER MEETING DIGITAL EXPERIENCE
Liver injury linked to COVID-19–related coagulopathy
There is a link between liver injury and a tendency toward excessive clotting in patients with COVID-19, and the organ’s own blood vessels could be responsible, new research shows.
Cells that line the liver’s blood vessels produce high levels of factor VIII, a coagulation factor, when they are exposed to interleukin-6, an inflammatory molecule associated with COVID-19.
These findings “center the liver in global coagulopathy of COVID-19 and define a mechanism for increased coagulation factor levels that may be treatment targets,” said investigator Matthew McConnell, MD, from the Yale University, New Haven, Conn.
The effect of IL-6 on the liver sinusoidal endothelial cells lining the liver blood vessels creates a prothrombotic environment that includes the release of factor VIII, said Dr. McConnell, who presented the results at the virtual annual meeting of the American Association for the Study of Liver Diseases.
These associations offer insights into why COVID-19 patients with underlying liver disease can experience “devastating complications” related to improper blood vessel function in the organ, he added.
For their study, Dr. McConnell and colleagues analyzed data on ALT and hypercoagulability from 68 adults treated at the Yale–New Haven Hospital. The liver and coagulation tests were administered within 5 days of each other.
The team set the ALT cutoff for liver injury at three times the upper limit of normal. Patients with two or more parameters indicating excessive clotting were considered to have a hypercoagulable profile, which Dr. McConnell called “a signature clinical finding of COVID-19 infection.”
Patients with high levels of ALT also experienced elevations in clotting-related factors, such as fibrinogen levels and the activity of factor VIII and factor II. Furthermore, liver injury was significantly associated with hypercoagulability (P < .05).
Because COVID-19 is linked to the proinflammatory IL-6, the investigators examined how this cytokine and its receptor affect human liver sinusoidal cells. Cells exposed to IL-6 and its receptor pumped out factor VIII at levels that were significantly higher than in unexposed cells (P < .01). Exposed cells also produced significantly more von Willebrand factor (P < .05), another prothrombotic molecule, and showed increased expression of genes that induce the expression of factor VIII.
“As we learn more about COVID-19, we find that it is as much a coagulatory as a respiratory disease,” said Tien Dong, MD, PhD, from the University of California, Los Angeles, who was not involved in the study.
These findings are in line with a lot of other COVID-19-related research that suggests a link between hepatocyte injury and clotting disorders, he added.
One important factor is existing liver disease, said Dr. Dong. “If you have COVID-19 on top of that, you’re probably at risk of developing acute liver injury from the infection itself.”
That said, it’s still a good idea to check liver function in patients with COVID-19 and no known liver disease, he advised. Staying on top of these measures will keep the odds of long-term problems “a lot lower.”
There is utility in the findings beyond COVID-19, said Dr. McConnell. They provide “insights into complications of critical illness, in general, in the liver blood vessels” of patients with underlying liver disease.
Dr. McConnell and Dr. Dong have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
There is a link between liver injury and a tendency toward excessive clotting in patients with COVID-19, and the organ’s own blood vessels could be responsible, new research shows.
Cells that line the liver’s blood vessels produce high levels of factor VIII, a coagulation factor, when they are exposed to interleukin-6, an inflammatory molecule associated with COVID-19.
These findings “center the liver in global coagulopathy of COVID-19 and define a mechanism for increased coagulation factor levels that may be treatment targets,” said investigator Matthew McConnell, MD, from the Yale University, New Haven, Conn.
The effect of IL-6 on the liver sinusoidal endothelial cells lining the liver blood vessels creates a prothrombotic environment that includes the release of factor VIII, said Dr. McConnell, who presented the results at the virtual annual meeting of the American Association for the Study of Liver Diseases.
These associations offer insights into why COVID-19 patients with underlying liver disease can experience “devastating complications” related to improper blood vessel function in the organ, he added.
For their study, Dr. McConnell and colleagues analyzed data on ALT and hypercoagulability from 68 adults treated at the Yale–New Haven Hospital. The liver and coagulation tests were administered within 5 days of each other.
The team set the ALT cutoff for liver injury at three times the upper limit of normal. Patients with two or more parameters indicating excessive clotting were considered to have a hypercoagulable profile, which Dr. McConnell called “a signature clinical finding of COVID-19 infection.”
Patients with high levels of ALT also experienced elevations in clotting-related factors, such as fibrinogen levels and the activity of factor VIII and factor II. Furthermore, liver injury was significantly associated with hypercoagulability (P < .05).
Because COVID-19 is linked to the proinflammatory IL-6, the investigators examined how this cytokine and its receptor affect human liver sinusoidal cells. Cells exposed to IL-6 and its receptor pumped out factor VIII at levels that were significantly higher than in unexposed cells (P < .01). Exposed cells also produced significantly more von Willebrand factor (P < .05), another prothrombotic molecule, and showed increased expression of genes that induce the expression of factor VIII.
“As we learn more about COVID-19, we find that it is as much a coagulatory as a respiratory disease,” said Tien Dong, MD, PhD, from the University of California, Los Angeles, who was not involved in the study.
These findings are in line with a lot of other COVID-19-related research that suggests a link between hepatocyte injury and clotting disorders, he added.
One important factor is existing liver disease, said Dr. Dong. “If you have COVID-19 on top of that, you’re probably at risk of developing acute liver injury from the infection itself.”
That said, it’s still a good idea to check liver function in patients with COVID-19 and no known liver disease, he advised. Staying on top of these measures will keep the odds of long-term problems “a lot lower.”
There is utility in the findings beyond COVID-19, said Dr. McConnell. They provide “insights into complications of critical illness, in general, in the liver blood vessels” of patients with underlying liver disease.
Dr. McConnell and Dr. Dong have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
There is a link between liver injury and a tendency toward excessive clotting in patients with COVID-19, and the organ’s own blood vessels could be responsible, new research shows.
Cells that line the liver’s blood vessels produce high levels of factor VIII, a coagulation factor, when they are exposed to interleukin-6, an inflammatory molecule associated with COVID-19.
These findings “center the liver in global coagulopathy of COVID-19 and define a mechanism for increased coagulation factor levels that may be treatment targets,” said investigator Matthew McConnell, MD, from the Yale University, New Haven, Conn.
The effect of IL-6 on the liver sinusoidal endothelial cells lining the liver blood vessels creates a prothrombotic environment that includes the release of factor VIII, said Dr. McConnell, who presented the results at the virtual annual meeting of the American Association for the Study of Liver Diseases.
These associations offer insights into why COVID-19 patients with underlying liver disease can experience “devastating complications” related to improper blood vessel function in the organ, he added.
For their study, Dr. McConnell and colleagues analyzed data on ALT and hypercoagulability from 68 adults treated at the Yale–New Haven Hospital. The liver and coagulation tests were administered within 5 days of each other.
The team set the ALT cutoff for liver injury at three times the upper limit of normal. Patients with two or more parameters indicating excessive clotting were considered to have a hypercoagulable profile, which Dr. McConnell called “a signature clinical finding of COVID-19 infection.”
Patients with high levels of ALT also experienced elevations in clotting-related factors, such as fibrinogen levels and the activity of factor VIII and factor II. Furthermore, liver injury was significantly associated with hypercoagulability (P < .05).
Because COVID-19 is linked to the proinflammatory IL-6, the investigators examined how this cytokine and its receptor affect human liver sinusoidal cells. Cells exposed to IL-6 and its receptor pumped out factor VIII at levels that were significantly higher than in unexposed cells (P < .01). Exposed cells also produced significantly more von Willebrand factor (P < .05), another prothrombotic molecule, and showed increased expression of genes that induce the expression of factor VIII.
“As we learn more about COVID-19, we find that it is as much a coagulatory as a respiratory disease,” said Tien Dong, MD, PhD, from the University of California, Los Angeles, who was not involved in the study.
These findings are in line with a lot of other COVID-19-related research that suggests a link between hepatocyte injury and clotting disorders, he added.
One important factor is existing liver disease, said Dr. Dong. “If you have COVID-19 on top of that, you’re probably at risk of developing acute liver injury from the infection itself.”
That said, it’s still a good idea to check liver function in patients with COVID-19 and no known liver disease, he advised. Staying on top of these measures will keep the odds of long-term problems “a lot lower.”
There is utility in the findings beyond COVID-19, said Dr. McConnell. They provide “insights into complications of critical illness, in general, in the liver blood vessels” of patients with underlying liver disease.
Dr. McConnell and Dr. Dong have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
One-third of critical illness survivors emerge from ICU with functional deterioration
More patients are surviving critical illnesses requiring ICU care but many emerge with physical debility that may or may not eventually resolve.
Over the past decade, functional status deterioration after critical illness has become more common and of greater magnitude, despite concurrent efforts to reduce post–intensive care syndrome, based on a retrospective analysis of more than 100,000 patients.
Almost one-third of patients who survived nonsurgical ICU admission had evidence of functional status decline, reported lead author Nicholas E. Ingraham, MD, of the University of Minnesota, Minneapolis, and colleagues.
“Increasing capacity and decreasing mortality have created an evolving and diverse population of ICU survivors,” the investigators wrote in Critical Care Medicine. “Today’s survivors of critical illness are increasingly burdened by extensive physical and psychological comorbidities, often resulting in reduced quality of life.”
To determine trends in post–intensive care syndrome from 2008 to 2016, Dr. Ingraham and colleagues analyzed data from the Cerner Acute Physiology and Chronic Health Evaluation outcomes database, a national prospective cohort. Out of 202,786 adult patients admitted to the ICU, 129,917 were eligible for the study. Patients were excluded because of surgical admission, death, lack of functional status documentation, or inadequate hospital size or duration of participation. The final dataset had a median age of 63 years, with a slight predominance of male patients (54.0%). Most patients (80.9%) were White.
The primary outcome was defined as presence or absence of functional status deterioration, based on functional status at admission versus time of discharge. The secondary outcome was magnitude of deterioration over time.
The analysis, which controlled for age and severity of illness, revealed concerning trends for both outcomes.
Across the entire cohort 38,116 patients (29.3%) had functional status deterioration, with a 15% increase in prevalence over the course of the decade that spanned all disease categories (prevalence rate ratio, 1.15; 95% confidence interval, 1.13-1.17; P < .001). The magnitude of functional status decline also increased by 4% (odds ratio, 1.04; P < .001), with all but nonsurgical trauma patients showing greater deterioration over time.
“However, despite the decreasing magnitude of functional status deterioration in nonsurgical trauma, many admission diagnoses in this category remain in the top quartile of higher risk for functional status deterioration,” the investigators noted.
Functional status decline was most common among patients with head and polytrauma (OR, 3.39), followed closely by chest and spine trauma (OR, 3.38), and spine trauma (OR, 3.19). The top quartile of categories for prevalence of deterioration included nonsurgical trauma, neurologic, pulmonary, and gastrointestinal diseases.
Functional status decline was least common among patients diagnosed with diabetic ketoacidosis (OR, 0.27) or asthma (OR, 0.35).
“We believe our study provides important information that can be used in beginning to identify patients at high risk of functional status decline,” the investigators concluded. “Improving the identification of these patients and targeting appropriate interventions to mitigate this decline will be important directions for future studies in this area.”

According to David L. Bowton, MD, FCCP, professor emeritus, section on critical care, Wake Forest Baptist Health, Winston-Salem, N.C., the findings show just how common functional decline is after critical illness, and may actually underestimate prevalence.
“Because the authors employed a course evaluation tool employing only three categories of ability/disability and abstracted the level of disability from the medical record, they likely underestimated the frequency of clinically important, though not detected, disability at the time of hospital discharge,” Dr. Bowton said. “The study did not address cognitive impairment which can be detected in half of patients at 3 months following critical illness, and which significantly affects patients’ quality of life (Am J Respir Crit Care Med. 2020;202[2]:193-201).”
Dr. Bowton suggested that evidence-based methods of preventing post–intensive care syndrome are limited.
“Current efforts to improve post-ICU functional and cognitive outcomes suffer from the lack of proven effective interventions (Crit Care Med. 2019;47[11]:1607-18),” he said. “Observational data indicates that compliance with the ABCDEF bundle decreases the duration and incidence of delirium, ICU length of stay, duration of mechanical ventilation, and mortality (Crit Care Med. 2019;47[1]:3-14). However, the implications of these improvements on postdischarge functional outcomes are unknown as area the relative importance of individual elements of the bundle. Early mobility and patient and family diaries appear to improve functional status at discharge and postdischarge anxiety and depression, though the evidence supporting this is thin.”
Appropriate intervention may be especially challenging during the COVID-19 pandemic, he added.
“The impact of COVID on ICU staffing adequacy and stress is significant and the impact on quality bundle compliance and the availability of support services is currently not clear, but likely to be detrimental, especially to support services such as physical therapy that are already commonly understaffed,” Dr. Bowton said.
The study was supported by grants from the University of Minnesota’s Critical Care Research and Programmatic Development Program; the National Heart, Lung, and Blood Institute; and the University of Minnesota Clinical and Translational Science via the National Center for Advancing Translational Sciences. The investigators reported financial relationships with no other relevant organizations. Dr. Bowton reported no conflicts of interest.
SOURCE: Ingraham NE et al. Crit Care Med. 2020 Nov. doi: 10.1097/CCM.0000000000004524.
More patients are surviving critical illnesses requiring ICU care but many emerge with physical debility that may or may not eventually resolve.
Over the past decade, functional status deterioration after critical illness has become more common and of greater magnitude, despite concurrent efforts to reduce post–intensive care syndrome, based on a retrospective analysis of more than 100,000 patients.
Almost one-third of patients who survived nonsurgical ICU admission had evidence of functional status decline, reported lead author Nicholas E. Ingraham, MD, of the University of Minnesota, Minneapolis, and colleagues.
“Increasing capacity and decreasing mortality have created an evolving and diverse population of ICU survivors,” the investigators wrote in Critical Care Medicine. “Today’s survivors of critical illness are increasingly burdened by extensive physical and psychological comorbidities, often resulting in reduced quality of life.”
To determine trends in post–intensive care syndrome from 2008 to 2016, Dr. Ingraham and colleagues analyzed data from the Cerner Acute Physiology and Chronic Health Evaluation outcomes database, a national prospective cohort. Out of 202,786 adult patients admitted to the ICU, 129,917 were eligible for the study. Patients were excluded because of surgical admission, death, lack of functional status documentation, or inadequate hospital size or duration of participation. The final dataset had a median age of 63 years, with a slight predominance of male patients (54.0%). Most patients (80.9%) were White.
The primary outcome was defined as presence or absence of functional status deterioration, based on functional status at admission versus time of discharge. The secondary outcome was magnitude of deterioration over time.
The analysis, which controlled for age and severity of illness, revealed concerning trends for both outcomes.
Across the entire cohort 38,116 patients (29.3%) had functional status deterioration, with a 15% increase in prevalence over the course of the decade that spanned all disease categories (prevalence rate ratio, 1.15; 95% confidence interval, 1.13-1.17; P < .001). The magnitude of functional status decline also increased by 4% (odds ratio, 1.04; P < .001), with all but nonsurgical trauma patients showing greater deterioration over time.
“However, despite the decreasing magnitude of functional status deterioration in nonsurgical trauma, many admission diagnoses in this category remain in the top quartile of higher risk for functional status deterioration,” the investigators noted.
Functional status decline was most common among patients with head and polytrauma (OR, 3.39), followed closely by chest and spine trauma (OR, 3.38), and spine trauma (OR, 3.19). The top quartile of categories for prevalence of deterioration included nonsurgical trauma, neurologic, pulmonary, and gastrointestinal diseases.
Functional status decline was least common among patients diagnosed with diabetic ketoacidosis (OR, 0.27) or asthma (OR, 0.35).
“We believe our study provides important information that can be used in beginning to identify patients at high risk of functional status decline,” the investigators concluded. “Improving the identification of these patients and targeting appropriate interventions to mitigate this decline will be important directions for future studies in this area.”
According to David L. Bowton, MD, FCCP, professor emeritus, section on critical care, Wake Forest Baptist Health, Winston-Salem, N.C., the findings show just how common functional decline is after critical illness, and may actually underestimate prevalence.
“Because the authors employed a course evaluation tool employing only three categories of ability/disability and abstracted the level of disability from the medical record, they likely underestimated the frequency of clinically important, though not detected, disability at the time of hospital discharge,” Dr. Bowton said. “The study did not address cognitive impairment which can be detected in half of patients at 3 months following critical illness, and which significantly affects patients’ quality of life (Am J Respir Crit Care Med. 2020;202[2]:193-201).”
Dr. Bowton suggested that evidence-based methods of preventing post–intensive care syndrome are limited.
“Current efforts to improve post-ICU functional and cognitive outcomes suffer from the lack of proven effective interventions (Crit Care Med. 2019;47[11]:1607-18),” he said. “Observational data indicates that compliance with the ABCDEF bundle decreases the duration and incidence of delirium, ICU length of stay, duration of mechanical ventilation, and mortality (Crit Care Med. 2019;47[1]:3-14). However, the implications of these improvements on postdischarge functional outcomes are unknown as area the relative importance of individual elements of the bundle. Early mobility and patient and family diaries appear to improve functional status at discharge and postdischarge anxiety and depression, though the evidence supporting this is thin.”
Appropriate intervention may be especially challenging during the COVID-19 pandemic, he added.
“The impact of COVID on ICU staffing adequacy and stress is significant and the impact on quality bundle compliance and the availability of support services is currently not clear, but likely to be detrimental, especially to support services such as physical therapy that are already commonly understaffed,” Dr. Bowton said.
The study was supported by grants from the University of Minnesota’s Critical Care Research and Programmatic Development Program; the National Heart, Lung, and Blood Institute; and the University of Minnesota Clinical and Translational Science via the National Center for Advancing Translational Sciences. The investigators reported financial relationships with no other relevant organizations. Dr. Bowton reported no conflicts of interest.
SOURCE: Ingraham NE et al. Crit Care Med. 2020 Nov. doi: 10.1097/CCM.0000000000004524.
More patients are surviving critical illnesses requiring ICU care but many emerge with physical debility that may or may not eventually resolve.
Over the past decade, functional status deterioration after critical illness has become more common and of greater magnitude, despite concurrent efforts to reduce post–intensive care syndrome, based on a retrospective analysis of more than 100,000 patients.
Almost one-third of patients who survived nonsurgical ICU admission had evidence of functional status decline, reported lead author Nicholas E. Ingraham, MD, of the University of Minnesota, Minneapolis, and colleagues.
“Increasing capacity and decreasing mortality have created an evolving and diverse population of ICU survivors,” the investigators wrote in Critical Care Medicine. “Today’s survivors of critical illness are increasingly burdened by extensive physical and psychological comorbidities, often resulting in reduced quality of life.”
To determine trends in post–intensive care syndrome from 2008 to 2016, Dr. Ingraham and colleagues analyzed data from the Cerner Acute Physiology and Chronic Health Evaluation outcomes database, a national prospective cohort. Out of 202,786 adult patients admitted to the ICU, 129,917 were eligible for the study. Patients were excluded because of surgical admission, death, lack of functional status documentation, or inadequate hospital size or duration of participation. The final dataset had a median age of 63 years, with a slight predominance of male patients (54.0%). Most patients (80.9%) were White.
The primary outcome was defined as presence or absence of functional status deterioration, based on functional status at admission versus time of discharge. The secondary outcome was magnitude of deterioration over time.
The analysis, which controlled for age and severity of illness, revealed concerning trends for both outcomes.
Across the entire cohort 38,116 patients (29.3%) had functional status deterioration, with a 15% increase in prevalence over the course of the decade that spanned all disease categories (prevalence rate ratio, 1.15; 95% confidence interval, 1.13-1.17; P < .001). The magnitude of functional status decline also increased by 4% (odds ratio, 1.04; P < .001), with all but nonsurgical trauma patients showing greater deterioration over time.
“However, despite the decreasing magnitude of functional status deterioration in nonsurgical trauma, many admission diagnoses in this category remain in the top quartile of higher risk for functional status deterioration,” the investigators noted.
Functional status decline was most common among patients with head and polytrauma (OR, 3.39), followed closely by chest and spine trauma (OR, 3.38), and spine trauma (OR, 3.19). The top quartile of categories for prevalence of deterioration included nonsurgical trauma, neurologic, pulmonary, and gastrointestinal diseases.
Functional status decline was least common among patients diagnosed with diabetic ketoacidosis (OR, 0.27) or asthma (OR, 0.35).
“We believe our study provides important information that can be used in beginning to identify patients at high risk of functional status decline,” the investigators concluded. “Improving the identification of these patients and targeting appropriate interventions to mitigate this decline will be important directions for future studies in this area.”
According to David L. Bowton, MD, FCCP, professor emeritus, section on critical care, Wake Forest Baptist Health, Winston-Salem, N.C., the findings show just how common functional decline is after critical illness, and may actually underestimate prevalence.
“Because the authors employed a course evaluation tool employing only three categories of ability/disability and abstracted the level of disability from the medical record, they likely underestimated the frequency of clinically important, though not detected, disability at the time of hospital discharge,” Dr. Bowton said. “The study did not address cognitive impairment which can be detected in half of patients at 3 months following critical illness, and which significantly affects patients’ quality of life (Am J Respir Crit Care Med. 2020;202[2]:193-201).”
Dr. Bowton suggested that evidence-based methods of preventing post–intensive care syndrome are limited.
“Current efforts to improve post-ICU functional and cognitive outcomes suffer from the lack of proven effective interventions (Crit Care Med. 2019;47[11]:1607-18),” he said. “Observational data indicates that compliance with the ABCDEF bundle decreases the duration and incidence of delirium, ICU length of stay, duration of mechanical ventilation, and mortality (Crit Care Med. 2019;47[1]:3-14). However, the implications of these improvements on postdischarge functional outcomes are unknown as area the relative importance of individual elements of the bundle. Early mobility and patient and family diaries appear to improve functional status at discharge and postdischarge anxiety and depression, though the evidence supporting this is thin.”
Appropriate intervention may be especially challenging during the COVID-19 pandemic, he added.
“The impact of COVID on ICU staffing adequacy and stress is significant and the impact on quality bundle compliance and the availability of support services is currently not clear, but likely to be detrimental, especially to support services such as physical therapy that are already commonly understaffed,” Dr. Bowton said.
The study was supported by grants from the University of Minnesota’s Critical Care Research and Programmatic Development Program; the National Heart, Lung, and Blood Institute; and the University of Minnesota Clinical and Translational Science via the National Center for Advancing Translational Sciences. The investigators reported financial relationships with no other relevant organizations. Dr. Bowton reported no conflicts of interest.
SOURCE: Ingraham NE et al. Crit Care Med. 2020 Nov. doi: 10.1097/CCM.0000000000004524.
FROM CRITICAL CARE MEDICINE
Boston Scientific bails on Lotus Edge aortic valve system
Boston Scientific said it is voluntarily recalling all unused inventory of the Lotus Edge transcatheter aortic valve replacement system effective immediately.
In making the announcement today, Boston Scientific chair and CEO Mike Mahoney said the company has been increasingly challenged by the intricacies of the delivery system required to allow physicians to fully reposition and recapture the valve – key features of the system.
“The complexity of the delivery system, manufacturing challenges, the continued need for further technical enhancements, and current market adoption rates led us to the difficult decision to stop investing in the Lotus Edge platform,” Mr. Mahoney said.
Instead, the company will focus on the ACURATE neo2 aortic valve system, the Sentinel cerebral embolic protection device, and other high-growth areas, he noted.
The decision is expected to result in a $225 million to $300 million pretax charge, with $100 million to $150 million of these charges to impact the company’s adjusted results.
The Lotus device was approved in the United States in April 2019 for use in patients with severe aortic stenosis at high surgical risk based on the REPRISE 3 trial.
The Lotus Edge valve was approved in Europe in 2016, but final testing and rollout of the valve in the United States were delayed following a 2017 global recall of all Lotus valves because of reports of premature release of a pin connecting the valve to the delivery system.
Issues with the delivery system led to other Lotus valve recalls in both 2016 and 2014.
“Given the additional time and investment required to develop and reintroduce an enhanced delivery system, the company has chosen to retire the entire Lotus product platform immediately. All related commercial, clinical, research & development and manufacturing activities will also cease,” the statement said.
There is no safety issue for patients who currently have an implanted Lotus Edge valve, the company said.
This article first appeared on Medscape.com.
Boston Scientific said it is voluntarily recalling all unused inventory of the Lotus Edge transcatheter aortic valve replacement system effective immediately.
In making the announcement today, Boston Scientific chair and CEO Mike Mahoney said the company has been increasingly challenged by the intricacies of the delivery system required to allow physicians to fully reposition and recapture the valve – key features of the system.
“The complexity of the delivery system, manufacturing challenges, the continued need for further technical enhancements, and current market adoption rates led us to the difficult decision to stop investing in the Lotus Edge platform,” Mr. Mahoney said.
Instead, the company will focus on the ACURATE neo2 aortic valve system, the Sentinel cerebral embolic protection device, and other high-growth areas, he noted.
The decision is expected to result in a $225 million to $300 million pretax charge, with $100 million to $150 million of these charges to impact the company’s adjusted results.
The Lotus device was approved in the United States in April 2019 for use in patients with severe aortic stenosis at high surgical risk based on the REPRISE 3 trial.
The Lotus Edge valve was approved in Europe in 2016, but final testing and rollout of the valve in the United States were delayed following a 2017 global recall of all Lotus valves because of reports of premature release of a pin connecting the valve to the delivery system.
Issues with the delivery system led to other Lotus valve recalls in both 2016 and 2014.
“Given the additional time and investment required to develop and reintroduce an enhanced delivery system, the company has chosen to retire the entire Lotus product platform immediately. All related commercial, clinical, research & development and manufacturing activities will also cease,” the statement said.
There is no safety issue for patients who currently have an implanted Lotus Edge valve, the company said.
This article first appeared on Medscape.com.
Boston Scientific said it is voluntarily recalling all unused inventory of the Lotus Edge transcatheter aortic valve replacement system effective immediately.
In making the announcement today, Boston Scientific chair and CEO Mike Mahoney said the company has been increasingly challenged by the intricacies of the delivery system required to allow physicians to fully reposition and recapture the valve – key features of the system.
“The complexity of the delivery system, manufacturing challenges, the continued need for further technical enhancements, and current market adoption rates led us to the difficult decision to stop investing in the Lotus Edge platform,” Mr. Mahoney said.
Instead, the company will focus on the ACURATE neo2 aortic valve system, the Sentinel cerebral embolic protection device, and other high-growth areas, he noted.
The decision is expected to result in a $225 million to $300 million pretax charge, with $100 million to $150 million of these charges to impact the company’s adjusted results.
The Lotus device was approved in the United States in April 2019 for use in patients with severe aortic stenosis at high surgical risk based on the REPRISE 3 trial.
The Lotus Edge valve was approved in Europe in 2016, but final testing and rollout of the valve in the United States were delayed following a 2017 global recall of all Lotus valves because of reports of premature release of a pin connecting the valve to the delivery system.
Issues with the delivery system led to other Lotus valve recalls in both 2016 and 2014.
“Given the additional time and investment required to develop and reintroduce an enhanced delivery system, the company has chosen to retire the entire Lotus product platform immediately. All related commercial, clinical, research & development and manufacturing activities will also cease,” the statement said.
There is no safety issue for patients who currently have an implanted Lotus Edge valve, the company said.
This article first appeared on Medscape.com.
COVID-19 burdens follow patients after discharge
COVID-19 patients who survive their hospitalization don’t leave the disease behind upon discharge, as a significant percentage died within 60 days of discharge, with an ICU admission heightening the risk, according to an observational study of 38 Michigan hospitals. What’s more, many of them were burdened with health and emotional challenges ranging from hospital readmission to job loss and financial problems.
“These data confirm that the toll of COVID-19 extends well beyond hospitalization, a finding consistent with long-term sequelae from sepsis and other severe respiratory viral illnesses,” wrote lead author Vineet Chopra, MBBS, of the University of Michigan, Ann Arbor, and colleagues (Ann Intern Med. 2020 Nov 11: doi: 10.7326/M20-5661)
The researchers found that 29.2% of all patients hospitalized for COVID-19 from March 16 to July 1 died. The observational cohort study included 1,648 COVID-19 patients hospitalized at 38 Michigan hospitals participating in a statewide collaborative.
The bulk of those deaths occurred during hospitalization: 24.2% of patients (n = 398). Of the 1,250 patients discharged, 78% (n = 975) went home and 12.6% (n = 158) went to a skilled nursing facility, with the remainder unaccounted for. Within 60 days of discharge, 6.7% (n = 84) of hospitalized survivors had died and 15.2% (n = 189) were readmitted. The researchers gathered 60-day postdischarge data via a telephone survey, contacting 41.8% (n = 488) of discharged patients.
Outcomes were even worse for discharged patients who spent time in the ICU. The death rate among this group was 10.4% (17 of 165) after discharge. That resulted in an overall study death rate of 63.5% (n = 257) for the 405 patients who were in the ICU.
While the study data were in the first wave of the novel coronavirus, the findings have relevance today, said Mary Jo Farmer, MD, PhD, FCCP, directory of pulmonary hypertension services at Baystate Health in Springfield, Mass.

“This is the best information we have to date,” she said. “We have to continue to have an open mind and expect that this information may change as the virus possibly mutates as it spreads, and we should continue doing these types of outcomes studies at 90 days, 120 days, etc.”
The median age of study patients was 62, with a range of 50-72. The three leading comorbidities among discharged patients were hypertension (n = 800, 64%), diabetes (34.9%, n = 436), and cardiovascular disease (24.1%, n = 301).
Poor postdischarge outcomes weren’t limited to mortality and readmission. Almost 19% (n = 92) reported new or worsening cardiopulmonary symptoms such as cough and dyspnea, 13.3% had a persistent loss of taste or smell, and 12% (n = 58) reported more difficulty with daily living tasks.
The after-effects were not only physical. Nearly half of discharged patients (48.7%, n = 238) reported emotional effects and almost 6% (n = 28) sought mental health care. Among the 40% (n = 195) employed before they were hospitalized, 36% (n = 78) couldn’t return to work because of health issues or layoffs. Sixty percent (n = 117) of the pre-employed discharged patients did return to work, but 25% (n = 30) did so with reduced hours or modified job duties because of health problems.
Financial problems were also a burden. More than a third, 36.7% (n = 179), reported some financial impact from their hospitalization. About 10% (n = 47) said they used most or all of their savings, and 7% (n = 35) said they resorted to rationing necessities such as food or medications.
The researchers noted that one in five patients had no primary care follow-up at 2 months post discharge. “Collectively, these findings suggest that better models to support COVID-19 survivors are necessary,” said Dr. Chopra and colleagues.
The postdischarge course for patients involves two humps, said Sachin Gupta, MD, FCCP a pulmonary and critical care specialist at Alameda Health System in Oakland, Calif.: Getting over the hospitalization itself and the recovery phase. “As you look at the median age of the survivors, elderly patients who survive a hospital stay are still going to have a period of recovery, and like any viral illness that leads to someone being hospitalized, when you have an elderly patient with comorbidities, not all of them can make it over that final hump.”

He echoed the study authors’ call for better postdischarge support for COVID-19 patients. “There’s typically, although not at every hospital, a one-size-fits-all discharge planning process,” Dr. Gupta said. “For older patients, particularly with comorbid conditions, close follow-up after discharge is important.”
Dr. Farmer noted that one challenge in discharge support may be a matter of personnel. “The providers of this care might be fearful of patients who have had COVID-19 – Do the patients remain contagious? What if symptoms of COVID-19 return such as dry cough, fever? – and of contracting the disease themselves,” she said.
The findings regarding the emotional status of discharged patients should factor into discharge planning, she added. “Providers of posthospital care need to be educated in the emotional impact of this disease (e.g., the patients may feel ostracized or that no one wants to be around them) to assist in their recovery.”
Dr. Chopra and Dr. Farmer have no financial relationships to disclose. Dr. Gupta is an employee and shareholder of Genentech.
SOURCE: Chopra V et al. Ann Intern Med. 2020 Nov 11. doi: 10.7326/M20-5661.
COVID-19 patients who survive their hospitalization don’t leave the disease behind upon discharge, as a significant percentage died within 60 days of discharge, with an ICU admission heightening the risk, according to an observational study of 38 Michigan hospitals. What’s more, many of them were burdened with health and emotional challenges ranging from hospital readmission to job loss and financial problems.
“These data confirm that the toll of COVID-19 extends well beyond hospitalization, a finding consistent with long-term sequelae from sepsis and other severe respiratory viral illnesses,” wrote lead author Vineet Chopra, MBBS, of the University of Michigan, Ann Arbor, and colleagues (Ann Intern Med. 2020 Nov 11: doi: 10.7326/M20-5661)
The researchers found that 29.2% of all patients hospitalized for COVID-19 from March 16 to July 1 died. The observational cohort study included 1,648 COVID-19 patients hospitalized at 38 Michigan hospitals participating in a statewide collaborative.
The bulk of those deaths occurred during hospitalization: 24.2% of patients (n = 398). Of the 1,250 patients discharged, 78% (n = 975) went home and 12.6% (n = 158) went to a skilled nursing facility, with the remainder unaccounted for. Within 60 days of discharge, 6.7% (n = 84) of hospitalized survivors had died and 15.2% (n = 189) were readmitted. The researchers gathered 60-day postdischarge data via a telephone survey, contacting 41.8% (n = 488) of discharged patients.
Outcomes were even worse for discharged patients who spent time in the ICU. The death rate among this group was 10.4% (17 of 165) after discharge. That resulted in an overall study death rate of 63.5% (n = 257) for the 405 patients who were in the ICU.
While the study data were in the first wave of the novel coronavirus, the findings have relevance today, said Mary Jo Farmer, MD, PhD, FCCP, directory of pulmonary hypertension services at Baystate Health in Springfield, Mass.
“This is the best information we have to date,” she said. “We have to continue to have an open mind and expect that this information may change as the virus possibly mutates as it spreads, and we should continue doing these types of outcomes studies at 90 days, 120 days, etc.”
The median age of study patients was 62, with a range of 50-72. The three leading comorbidities among discharged patients were hypertension (n = 800, 64%), diabetes (34.9%, n = 436), and cardiovascular disease (24.1%, n = 301).
Poor postdischarge outcomes weren’t limited to mortality and readmission. Almost 19% (n = 92) reported new or worsening cardiopulmonary symptoms such as cough and dyspnea, 13.3% had a persistent loss of taste or smell, and 12% (n = 58) reported more difficulty with daily living tasks.
The after-effects were not only physical. Nearly half of discharged patients (48.7%, n = 238) reported emotional effects and almost 6% (n = 28) sought mental health care. Among the 40% (n = 195) employed before they were hospitalized, 36% (n = 78) couldn’t return to work because of health issues or layoffs. Sixty percent (n = 117) of the pre-employed discharged patients did return to work, but 25% (n = 30) did so with reduced hours or modified job duties because of health problems.
Financial problems were also a burden. More than a third, 36.7% (n = 179), reported some financial impact from their hospitalization. About 10% (n = 47) said they used most or all of their savings, and 7% (n = 35) said they resorted to rationing necessities such as food or medications.
The researchers noted that one in five patients had no primary care follow-up at 2 months post discharge. “Collectively, these findings suggest that better models to support COVID-19 survivors are necessary,” said Dr. Chopra and colleagues.
The postdischarge course for patients involves two humps, said Sachin Gupta, MD, FCCP a pulmonary and critical care specialist at Alameda Health System in Oakland, Calif.: Getting over the hospitalization itself and the recovery phase. “As you look at the median age of the survivors, elderly patients who survive a hospital stay are still going to have a period of recovery, and like any viral illness that leads to someone being hospitalized, when you have an elderly patient with comorbidities, not all of them can make it over that final hump.”
He echoed the study authors’ call for better postdischarge support for COVID-19 patients. “There’s typically, although not at every hospital, a one-size-fits-all discharge planning process,” Dr. Gupta said. “For older patients, particularly with comorbid conditions, close follow-up after discharge is important.”
Dr. Farmer noted that one challenge in discharge support may be a matter of personnel. “The providers of this care might be fearful of patients who have had COVID-19 – Do the patients remain contagious? What if symptoms of COVID-19 return such as dry cough, fever? – and of contracting the disease themselves,” she said.
The findings regarding the emotional status of discharged patients should factor into discharge planning, she added. “Providers of posthospital care need to be educated in the emotional impact of this disease (e.g., the patients may feel ostracized or that no one wants to be around them) to assist in their recovery.”
Dr. Chopra and Dr. Farmer have no financial relationships to disclose. Dr. Gupta is an employee and shareholder of Genentech.
SOURCE: Chopra V et al. Ann Intern Med. 2020 Nov 11. doi: 10.7326/M20-5661.
COVID-19 patients who survive their hospitalization don’t leave the disease behind upon discharge, as a significant percentage died within 60 days of discharge, with an ICU admission heightening the risk, according to an observational study of 38 Michigan hospitals. What’s more, many of them were burdened with health and emotional challenges ranging from hospital readmission to job loss and financial problems.
“These data confirm that the toll of COVID-19 extends well beyond hospitalization, a finding consistent with long-term sequelae from sepsis and other severe respiratory viral illnesses,” wrote lead author Vineet Chopra, MBBS, of the University of Michigan, Ann Arbor, and colleagues (Ann Intern Med. 2020 Nov 11: doi: 10.7326/M20-5661)
The researchers found that 29.2% of all patients hospitalized for COVID-19 from March 16 to July 1 died. The observational cohort study included 1,648 COVID-19 patients hospitalized at 38 Michigan hospitals participating in a statewide collaborative.
The bulk of those deaths occurred during hospitalization: 24.2% of patients (n = 398). Of the 1,250 patients discharged, 78% (n = 975) went home and 12.6% (n = 158) went to a skilled nursing facility, with the remainder unaccounted for. Within 60 days of discharge, 6.7% (n = 84) of hospitalized survivors had died and 15.2% (n = 189) were readmitted. The researchers gathered 60-day postdischarge data via a telephone survey, contacting 41.8% (n = 488) of discharged patients.
Outcomes were even worse for discharged patients who spent time in the ICU. The death rate among this group was 10.4% (17 of 165) after discharge. That resulted in an overall study death rate of 63.5% (n = 257) for the 405 patients who were in the ICU.
While the study data were in the first wave of the novel coronavirus, the findings have relevance today, said Mary Jo Farmer, MD, PhD, FCCP, directory of pulmonary hypertension services at Baystate Health in Springfield, Mass.
“This is the best information we have to date,” she said. “We have to continue to have an open mind and expect that this information may change as the virus possibly mutates as it spreads, and we should continue doing these types of outcomes studies at 90 days, 120 days, etc.”
The median age of study patients was 62, with a range of 50-72. The three leading comorbidities among discharged patients were hypertension (n = 800, 64%), diabetes (34.9%, n = 436), and cardiovascular disease (24.1%, n = 301).
Poor postdischarge outcomes weren’t limited to mortality and readmission. Almost 19% (n = 92) reported new or worsening cardiopulmonary symptoms such as cough and dyspnea, 13.3% had a persistent loss of taste or smell, and 12% (n = 58) reported more difficulty with daily living tasks.
The after-effects were not only physical. Nearly half of discharged patients (48.7%, n = 238) reported emotional effects and almost 6% (n = 28) sought mental health care. Among the 40% (n = 195) employed before they were hospitalized, 36% (n = 78) couldn’t return to work because of health issues or layoffs. Sixty percent (n = 117) of the pre-employed discharged patients did return to work, but 25% (n = 30) did so with reduced hours or modified job duties because of health problems.
Financial problems were also a burden. More than a third, 36.7% (n = 179), reported some financial impact from their hospitalization. About 10% (n = 47) said they used most or all of their savings, and 7% (n = 35) said they resorted to rationing necessities such as food or medications.
The researchers noted that one in five patients had no primary care follow-up at 2 months post discharge. “Collectively, these findings suggest that better models to support COVID-19 survivors are necessary,” said Dr. Chopra and colleagues.
The postdischarge course for patients involves two humps, said Sachin Gupta, MD, FCCP a pulmonary and critical care specialist at Alameda Health System in Oakland, Calif.: Getting over the hospitalization itself and the recovery phase. “As you look at the median age of the survivors, elderly patients who survive a hospital stay are still going to have a period of recovery, and like any viral illness that leads to someone being hospitalized, when you have an elderly patient with comorbidities, not all of them can make it over that final hump.”
He echoed the study authors’ call for better postdischarge support for COVID-19 patients. “There’s typically, although not at every hospital, a one-size-fits-all discharge planning process,” Dr. Gupta said. “For older patients, particularly with comorbid conditions, close follow-up after discharge is important.”
Dr. Farmer noted that one challenge in discharge support may be a matter of personnel. “The providers of this care might be fearful of patients who have had COVID-19 – Do the patients remain contagious? What if symptoms of COVID-19 return such as dry cough, fever? – and of contracting the disease themselves,” she said.
The findings regarding the emotional status of discharged patients should factor into discharge planning, she added. “Providers of posthospital care need to be educated in the emotional impact of this disease (e.g., the patients may feel ostracized or that no one wants to be around them) to assist in their recovery.”
Dr. Chopra and Dr. Farmer have no financial relationships to disclose. Dr. Gupta is an employee and shareholder of Genentech.
SOURCE: Chopra V et al. Ann Intern Med. 2020 Nov 11. doi: 10.7326/M20-5661.
FROM ANNALS OF INTERNAL MEDICINE
Pediatric dermatology: Reflecting on 50 years
As part of the 50th anniversary of Dermatology News, it is intriguing to think about where a time machine journey 5 decades back would find the field of pediatric dermatology, and to assess the changes in the specialty during the time that Dermatology News (operating then as “Skin & Allergy News”) has been reporting on innovations and changes in the practice of dermatology.

So, starting . It was not until 3 years later, in October 1973 in Mexico City, that the first international symposium on Pediatric Dermatology was held, and the International Society for Pediatric Dermatology was founded. I reached out to Andrew Margileth, MD, 100 years old this past July, and still active voluntary faculty in pediatric dermatology at the University of Miami, to help me “reach back” to those days. Dr. Margileth commented on how the first symposium was “brilliantly orchestrated by Ramon Ruiz-Maldonado,” from the National Institute of Paediatrics in Mexico, and that it was his “Aha moment for future practice!” That meeting spurred discussions on the development of the Society for Pediatric Dermatology the next year, with Alvin Jacobs, MD; Samuel Weinberg, MD; Nancy Esterly, MD; Sidney Hurwitz, MD; William Weston, MD; and Coleman Jacobson, MD, as some of the initial “founding mothers and fathers,” and the society was officially established in 1975.
The field of pediatric dermatology was fairly “infantile” 50 years ago, with few practitioners. But the early leaders in the field recognized that up to 30% of pediatric primary care visits included skin problems, and that there was limited training for dermatologists, as well as pediatricians, about skin diseases in children. There were clearly clinical and educational needs to establish a subspecialty of pediatric dermatology, and over the next 1-2 decades, the field expanded. The journal Pediatric Dermatology was established (in 1982), the Section on Dermatology was established by the American Academy of Pediatrics (in 1986), and fellowship programs were launched at select academic centers. And it was 30 years into our timeline before the formal subspecialty of pediatric dermatology was established through the American Board of Dermatology (2000).
The field of pediatric dermatology has evolved and matured rapidly. Standard reference textbooks have been developed in the United States and around the world (and of course, online). Pediatric dermatology is an essential part of the core curriculum for dermatologist trainees. Organizations promoting pediatric research have developed to influence basic, translational, and clinical research in conditions in neonates through adolescents, such as the Pediatric Dermatology Research Alliance (PeDRA). And meetings throughout the world now feature pediatric dermatology sessions and help to spread the advances in the diagnosis and management of pediatric skin disorders.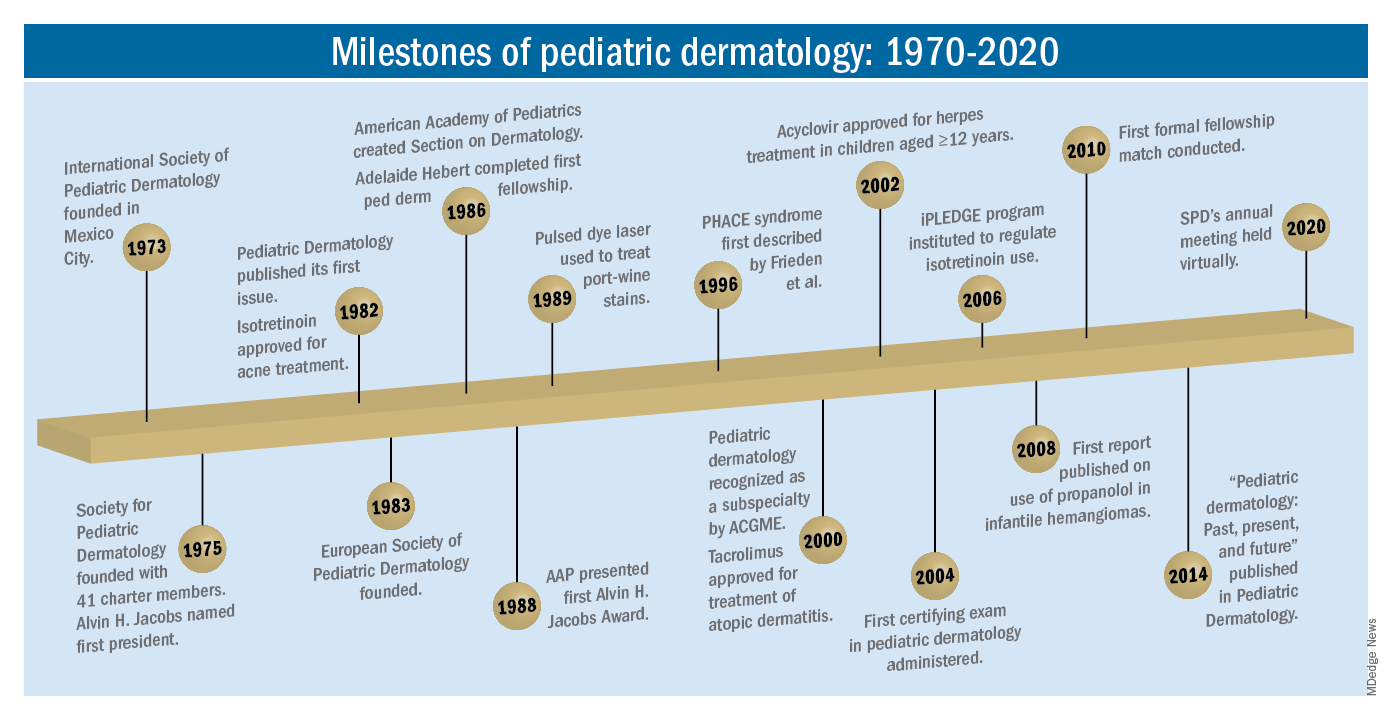
The practice of pediatric dermatology: How has it changed?
It is beyond the scope of this article to try to comprehensively review all of the changes in pediatric dermatology practice. But review of the evolution of a few disease states (choices influenced by my discussions with my 100-year old history guide, Dr. Margileth) displays examples of where we have been, and where we are going in our next 5, 10, or 50 years.
Hemangiomas and vascular malformations
Some of the first natural history studies on hemangiomas were done in the early 1960s, establishing that standard cutaneous hemangiomas had a typical clinical course of fairly rapid growth, plateau, and involution over time. Of interest, the hallmark article’s first author was Dr. Margileth, published in 1965 in JAMA!.This was still at a time when the identification of hemangiomas of infancy (or “HOI” as we say in the trade) was confused with vascular malformations, and no one had recognized the distinct variant tumors such as rapidly involuting and noninvoluting congenital hemangiomas (RICHs or NICHs), tufted angiomas, or hemangioendotheliomas. PHACE syndrome was not yet described (that was done in 1996 by Ilona Frieden, MD, and colleagues). And for a time, hemangiomas were treated with x-rays, before the negative impact of such radiation was acknowledged. It seems that, as a consequence of the use of x-ray therapy and as a backlash from the radiation therapy side effects and potential toxicities, even deforming and functionally significant lesions were “followed clinically” for natural involution, with a sensibility that doing nothing might be better than doing the wrong thing.
Over the next 15 years, the recognition of functionally significant hemangiomas, deformation associated with their proliferation, and the recognition of PHACE syndrome made hemangiomas of infancy an area of concern, with systemic steroids and occasionally chemotherapeutic agents (such as vincristine) being used for problematic lesions.
It has now been 12 years since the work of Christine Léauté-Labrèze, MD, et al., from the University of Bordeaux (France), led to the breakthrough of propranolol for hemangioma treatment, profoundly changing hemangioma management to an incredibly effective medical therapy extensively studied, tested in formal clinical trials, and approved by regulatory authorities. And how intriguing that this was pursued after the chance (but skilled) observation that a child who developed hypertension as a side effect of systemic steroids for nasal hemangioma treatment was prescribed propranolol for the hypertension and had his nasal hemangioma rapidly shrink, with a response superior and much quicker than that to corticosteroids.

The evolution of management of hemangiomas has another story within it, that of collaborative research. The Hemangioma Investigator Group was formed to take a collaborative approach to characterize and study hemangiomas and related tumors. Beginning with energetic, insightful pediatric dermatologists and little funding, they changed our knowledge base of how hemangiomas present, the risk factors for their development, and the characteristics and multiple organ findings associated with PHACE and other syndromic hemangiomas. Our knowledge of these lesions is now evidence based and broad, and the impact on care tremendous! The HIG has also influenced the practice of pediatricians and other specialists, including otorhinolaryngologists, hematologist/oncologists, and surgeons, is partnering with advocacy groups to support patients and families, and is helping guide patients and families to contribute to ongoing research.
Vascular malformations (VM) reflect an incredible change in our understanding of the developmental pathways and pathophysiology of blood vessel tumors, and, in fact, birthmarks other than vascular lesions! First, important work separated out hemangiomas of infancy and hemangiomalike tumors from vascular malformations, with the thought being that hemangiomas had a rapid growth phase, often arising from lesions that were minimally evident or not evident at birth, unlike malformations, which were “programing errors,” all present at birth and expected to be fairly static with proportionate growth over a lifetime. Approaches to vascular malformations were limited to sclerotherapy, laser, and/or surgery. While this general schema of classification is still useful, our sense of the “why and how” of vascular malformations is remarkably different. Vascular malformations – still usefully subdivided into capillary, lymphatic, venous arteriovenous, or mixed malformations – are mostly associated with inherited or somatic mutations. Mutations are most commonly found in two signal pathways: RAS/MAPK/ERK and PI3K/AKT/mTOR pathways, with specific sets of mutations seen in both localized and multifocal lesions, with or without overgrowth or other systemic anomalies. The discovery of specific mutations has led to the possibility of small-molecule inhibitors, many already existing as anticancer drugs, being utilized as targeted therapies for VM.
And similar advances in understanding of other birthmarks, with or without syndromic features, are being made steadily. The mutations in congenital melanocytic nevi, epidermal nevi, acquired tumors (pilomatricomas), and other lesions, along with steady epidemiologic, translational, and clinical work, evolves our knowledge and potential therapies.
Inflammatory skin disorders: Acne, psoriasis, and atopic dermatitis
The care of pediatric inflammatory skin disorders has evolved, but more slowly for some diseases than others. Acne vulgaris is now recognized as much more common under age 12 than previously, presumably reflecting earlier pubertal changes in our preteens. Over the past 30 years, therapy has evolved with the use of topical retinoids (still underused by pediatricians, considered a “practice gap”), hormonal therapy with combined oral contraceptives, and oral isotretinoin, a powerful but highly effective systemic agent for severe and refractory acne. Specific pediatric guidelines came much later, with expert recommendations formulated by the American Acne and Rosacea Society and endorsed by the American Academy of Pediatrics in 2013. Over the past few years, there has been a push by experts for more judicious use of antibiotics for acne (oral and topical) to minimize the emergence of bacterial resistance. There are unanswered questions as we evolve our care: How will the new topical antiandrogens be used? Will spironolactone become part of hormonal therapy under age 18? Will the insights on certain strains of Cutibacterium acnes being associated with worse acne translate to microbiome or vaccine-based strategies?
Pediatric psoriasis has suffered, being “behind in the revolution” of biologic agents because of delayed approval of any biologic agent for treatment of pediatric psoriasis in the United States until just a few years ago, and lags behind Europe and elsewhere in the world by almost a decade. Only this year have we expanded beyond one biologic agent approved for under age 12 and two for ages 12 and older, with other approvals expected including interleukin (IL)-17 and IL-23 agents. Adult psoriasis has been recognized to be associated with a broad set of comorbidities, including obesity and early heart disease, and there is now research on how children are at risk as well, with new recommendations on how to screen children with psoriasis, supplied first by PeDRA and then in the new American Academy of Dermatology-National Psoriasis Foundation pediatric psoriasis guidelines .
Pediatric atopic dermatitis (AD) is in its early years of revolution. In the 50-year period of our thought experiment, AD has increased in prevalence from 5% or less of the pediatric population to 10%-15%. Treatment of most individuals has remained the same over the decades: Good skin care, frequent moisturizers, topical corticosteroids for flares, and management of infection if noted. The topical calcineurin inhibitors (TCIs) broadened the therapeutic approach when introduced in 2000 and 2001, but the boxed warning resulted in some practitioners minimizing their use of these useful agents. But newer studies are markedly reassuring about their safe use in children.
Steroid phobia, as well as concerns about potential side effects of the TCIs, has resulted in undertreatment of childhood AD. It is quite common to see multiple children during pediatric dermatology office hours with poorly controlled eczema, high body-surface areas of eczema, compromised sleep, secondary infections, and anxiety and depression, especially in our moderate to severe adolescents. The field is “hot” with new topical and systemic agents, including our few years’ experience with topical crisaborole, a phosphodiesterase (PDE)-4 inhibitor; and dupilumab, an IL-4-alpha blocker – the first biologic agent approved for AD and the first systemic agent (other than oral corticosteroids), just extended from 12 years to 6 years of age! As dupilumab gets studied for younger children, other biologics (including IL-13 and IL-31 blockers) are undertaking pediatric and/or adolescent trials, oral and topical JAK inhibitors are including adolescents in core clinical trials, and other novel topical agents are under study, including an aryl-hydrocarbon receptor–modulating agent and other PDE-4 inhibitors.
Procedural pediatric dermatology: From liquid nitrogen to laser, surgery, and multimodal skin care
The first generation of pediatric dermatologists were considered medical dermatologist specialists. The care of the conditions discussed above, as well as genodermatoses, diagnostic dilemmas, and management of dermatologic manifestations of systemic disease and other conditions, was the “bread and butter” of pediatric dermatology care. When I was in training, my mentor Paul Honig, MD, at the Children’s Hospital of Philadelphia had a procedure half-day each week, where he would care for a few patients who needed liquid nitrogen therapy for warts, or who needed biopsies. It was uncommon to have a large procedural/surgical part of pediatric dermatology practice. But this is now a routine part of many specialists in the field. How did this change occur?

The fundamental shift began to occur with the introduction of the pulsed dye laser for treatment of port-wine birthmarks in children with minimal scarring, and a seminal article published in the New England Journal of Medicine in 1989. Vascular lesions including port-wine stains were common, and pediatric dermatologists managed these patients for both diagnosis and medical management. Also, dermatology residencies at this time offered training in cutaneous surgery, excisions (including Mohs surgery) and repairs, and trainees in pediatric dermatology were “trained up” to high levels of expertise. As lasers were incorporated into dermatology residency work and practices, pediatric dermatologists developed the exposure and skill to do this work. An added advantage was having the knowledge of how to handle children and adolescents in an age-appropriate manner, with consideration of methods to minimize the pain and anxiety of procedures. Within a few years, pediatric dermatologists were at the forefront of the use of topical anesthetics (EMLA and liposomal lidocaine) and had general anesthesia privileges for laser and excisional surgery.
So while pediatric dermatologists still do “small procedures” every hour in most practices (cryotherapy for warts, cantharidin for molluscum, shave and punch biopsies), a subset now have extensive procedural practices, which in recent years has extended to pigment lesion lasers (to treat nevus of Ota, for example), hair laser, and combinations of lasers, including fractionated CO2 technology, to treat hypertrophic, constrictive and/or deforming scars.
The future
What will pediatric dermatology be like in 10, 20, or 50 years?
I have not yet discussed some of the most challenging diseases in our field, including epidermolysis bullosa, ichthyosis, and neurocutaneous disorders and other genetic skin disorders that have an incredible impact on the lives of affected children and their families, with incredible morbidity and with many conditions that shorten lifespans. But these are the conditions where “the future is happening now,” and we are looking forward to our new gene therapy techniques helping to transform our care.
And other aspects of practice? Will we be doing a large percentage of practice over the phone (or whatever devices we have then – remember, the first iPhone was only released 13 years ago)?
Will our patients be using their own imaging systems to evaluate their nevi and skin growths, and perhaps to diagnose and manage their rashes?
Will we have prevented our inflammatory skin disorders, or “turned them off” in early life with aggressive therapy in infantile life?
I project only that all of us in dermatology will still be a resource to our pediatric patients, from neonate through young adult, through our work of preventing, caring, healing and minimizing disease impact, and hopefully enjoying the pleasures of seeing our patients healthfully develop and evolve! As will our field.
Dr. Eichenfield is professor of dermatology and pediatrics and vice-chair of the department of dermatology at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. Dr. Eichenfield reports financial relationships with 20 pharmaceutical companies that manufacture dermatologic products, including products for the diseases discussed here.
As part of the 50th anniversary of Dermatology News, it is intriguing to think about where a time machine journey 5 decades back would find the field of pediatric dermatology, and to assess the changes in the specialty during the time that Dermatology News (operating then as “Skin & Allergy News”) has been reporting on innovations and changes in the practice of dermatology.
So, starting . It was not until 3 years later, in October 1973 in Mexico City, that the first international symposium on Pediatric Dermatology was held, and the International Society for Pediatric Dermatology was founded. I reached out to Andrew Margileth, MD, 100 years old this past July, and still active voluntary faculty in pediatric dermatology at the University of Miami, to help me “reach back” to those days. Dr. Margileth commented on how the first symposium was “brilliantly orchestrated by Ramon Ruiz-Maldonado,” from the National Institute of Paediatrics in Mexico, and that it was his “Aha moment for future practice!” That meeting spurred discussions on the development of the Society for Pediatric Dermatology the next year, with Alvin Jacobs, MD; Samuel Weinberg, MD; Nancy Esterly, MD; Sidney Hurwitz, MD; William Weston, MD; and Coleman Jacobson, MD, as some of the initial “founding mothers and fathers,” and the society was officially established in 1975.
The field of pediatric dermatology was fairly “infantile” 50 years ago, with few practitioners. But the early leaders in the field recognized that up to 30% of pediatric primary care visits included skin problems, and that there was limited training for dermatologists, as well as pediatricians, about skin diseases in children. There were clearly clinical and educational needs to establish a subspecialty of pediatric dermatology, and over the next 1-2 decades, the field expanded. The journal Pediatric Dermatology was established (in 1982), the Section on Dermatology was established by the American Academy of Pediatrics (in 1986), and fellowship programs were launched at select academic centers. And it was 30 years into our timeline before the formal subspecialty of pediatric dermatology was established through the American Board of Dermatology (2000).
The field of pediatric dermatology has evolved and matured rapidly. Standard reference textbooks have been developed in the United States and around the world (and of course, online). Pediatric dermatology is an essential part of the core curriculum for dermatologist trainees. Organizations promoting pediatric research have developed to influence basic, translational, and clinical research in conditions in neonates through adolescents, such as the Pediatric Dermatology Research Alliance (PeDRA). And meetings throughout the world now feature pediatric dermatology sessions and help to spread the advances in the diagnosis and management of pediatric skin disorders.
The practice of pediatric dermatology: How has it changed?
It is beyond the scope of this article to try to comprehensively review all of the changes in pediatric dermatology practice. But review of the evolution of a few disease states (choices influenced by my discussions with my 100-year old history guide, Dr. Margileth) displays examples of where we have been, and where we are going in our next 5, 10, or 50 years.
Hemangiomas and vascular malformations
Some of the first natural history studies on hemangiomas were done in the early 1960s, establishing that standard cutaneous hemangiomas had a typical clinical course of fairly rapid growth, plateau, and involution over time. Of interest, the hallmark article’s first author was Dr. Margileth, published in 1965 in JAMA!.This was still at a time when the identification of hemangiomas of infancy (or “HOI” as we say in the trade) was confused with vascular malformations, and no one had recognized the distinct variant tumors such as rapidly involuting and noninvoluting congenital hemangiomas (RICHs or NICHs), tufted angiomas, or hemangioendotheliomas. PHACE syndrome was not yet described (that was done in 1996 by Ilona Frieden, MD, and colleagues). And for a time, hemangiomas were treated with x-rays, before the negative impact of such radiation was acknowledged. It seems that, as a consequence of the use of x-ray therapy and as a backlash from the radiation therapy side effects and potential toxicities, even deforming and functionally significant lesions were “followed clinically” for natural involution, with a sensibility that doing nothing might be better than doing the wrong thing.
Over the next 15 years, the recognition of functionally significant hemangiomas, deformation associated with their proliferation, and the recognition of PHACE syndrome made hemangiomas of infancy an area of concern, with systemic steroids and occasionally chemotherapeutic agents (such as vincristine) being used for problematic lesions.
It has now been 12 years since the work of Christine Léauté-Labrèze, MD, et al., from the University of Bordeaux (France), led to the breakthrough of propranolol for hemangioma treatment, profoundly changing hemangioma management to an incredibly effective medical therapy extensively studied, tested in formal clinical trials, and approved by regulatory authorities. And how intriguing that this was pursued after the chance (but skilled) observation that a child who developed hypertension as a side effect of systemic steroids for nasal hemangioma treatment was prescribed propranolol for the hypertension and had his nasal hemangioma rapidly shrink, with a response superior and much quicker than that to corticosteroids.
The evolution of management of hemangiomas has another story within it, that of collaborative research. The Hemangioma Investigator Group was formed to take a collaborative approach to characterize and study hemangiomas and related tumors. Beginning with energetic, insightful pediatric dermatologists and little funding, they changed our knowledge base of how hemangiomas present, the risk factors for their development, and the characteristics and multiple organ findings associated with PHACE and other syndromic hemangiomas. Our knowledge of these lesions is now evidence based and broad, and the impact on care tremendous! The HIG has also influenced the practice of pediatricians and other specialists, including otorhinolaryngologists, hematologist/oncologists, and surgeons, is partnering with advocacy groups to support patients and families, and is helping guide patients and families to contribute to ongoing research.
Vascular malformations (VM) reflect an incredible change in our understanding of the developmental pathways and pathophysiology of blood vessel tumors, and, in fact, birthmarks other than vascular lesions! First, important work separated out hemangiomas of infancy and hemangiomalike tumors from vascular malformations, with the thought being that hemangiomas had a rapid growth phase, often arising from lesions that were minimally evident or not evident at birth, unlike malformations, which were “programing errors,” all present at birth and expected to be fairly static with proportionate growth over a lifetime. Approaches to vascular malformations were limited to sclerotherapy, laser, and/or surgery. While this general schema of classification is still useful, our sense of the “why and how” of vascular malformations is remarkably different. Vascular malformations – still usefully subdivided into capillary, lymphatic, venous arteriovenous, or mixed malformations – are mostly associated with inherited or somatic mutations. Mutations are most commonly found in two signal pathways: RAS/MAPK/ERK and PI3K/AKT/mTOR pathways, with specific sets of mutations seen in both localized and multifocal lesions, with or without overgrowth or other systemic anomalies. The discovery of specific mutations has led to the possibility of small-molecule inhibitors, many already existing as anticancer drugs, being utilized as targeted therapies for VM.
And similar advances in understanding of other birthmarks, with or without syndromic features, are being made steadily. The mutations in congenital melanocytic nevi, epidermal nevi, acquired tumors (pilomatricomas), and other lesions, along with steady epidemiologic, translational, and clinical work, evolves our knowledge and potential therapies.
Inflammatory skin disorders: Acne, psoriasis, and atopic dermatitis
The care of pediatric inflammatory skin disorders has evolved, but more slowly for some diseases than others. Acne vulgaris is now recognized as much more common under age 12 than previously, presumably reflecting earlier pubertal changes in our preteens. Over the past 30 years, therapy has evolved with the use of topical retinoids (still underused by pediatricians, considered a “practice gap”), hormonal therapy with combined oral contraceptives, and oral isotretinoin, a powerful but highly effective systemic agent for severe and refractory acne. Specific pediatric guidelines came much later, with expert recommendations formulated by the American Acne and Rosacea Society and endorsed by the American Academy of Pediatrics in 2013. Over the past few years, there has been a push by experts for more judicious use of antibiotics for acne (oral and topical) to minimize the emergence of bacterial resistance. There are unanswered questions as we evolve our care: How will the new topical antiandrogens be used? Will spironolactone become part of hormonal therapy under age 18? Will the insights on certain strains of Cutibacterium acnes being associated with worse acne translate to microbiome or vaccine-based strategies?
Pediatric psoriasis has suffered, being “behind in the revolution” of biologic agents because of delayed approval of any biologic agent for treatment of pediatric psoriasis in the United States until just a few years ago, and lags behind Europe and elsewhere in the world by almost a decade. Only this year have we expanded beyond one biologic agent approved for under age 12 and two for ages 12 and older, with other approvals expected including interleukin (IL)-17 and IL-23 agents. Adult psoriasis has been recognized to be associated with a broad set of comorbidities, including obesity and early heart disease, and there is now research on how children are at risk as well, with new recommendations on how to screen children with psoriasis, supplied first by PeDRA and then in the new American Academy of Dermatology-National Psoriasis Foundation pediatric psoriasis guidelines .
Pediatric atopic dermatitis (AD) is in its early years of revolution. In the 50-year period of our thought experiment, AD has increased in prevalence from 5% or less of the pediatric population to 10%-15%. Treatment of most individuals has remained the same over the decades: Good skin care, frequent moisturizers, topical corticosteroids for flares, and management of infection if noted. The topical calcineurin inhibitors (TCIs) broadened the therapeutic approach when introduced in 2000 and 2001, but the boxed warning resulted in some practitioners minimizing their use of these useful agents. But newer studies are markedly reassuring about their safe use in children.
Steroid phobia, as well as concerns about potential side effects of the TCIs, has resulted in undertreatment of childhood AD. It is quite common to see multiple children during pediatric dermatology office hours with poorly controlled eczema, high body-surface areas of eczema, compromised sleep, secondary infections, and anxiety and depression, especially in our moderate to severe adolescents. The field is “hot” with new topical and systemic agents, including our few years’ experience with topical crisaborole, a phosphodiesterase (PDE)-4 inhibitor; and dupilumab, an IL-4-alpha blocker – the first biologic agent approved for AD and the first systemic agent (other than oral corticosteroids), just extended from 12 years to 6 years of age! As dupilumab gets studied for younger children, other biologics (including IL-13 and IL-31 blockers) are undertaking pediatric and/or adolescent trials, oral and topical JAK inhibitors are including adolescents in core clinical trials, and other novel topical agents are under study, including an aryl-hydrocarbon receptor–modulating agent and other PDE-4 inhibitors.
Procedural pediatric dermatology: From liquid nitrogen to laser, surgery, and multimodal skin care
The first generation of pediatric dermatologists were considered medical dermatologist specialists. The care of the conditions discussed above, as well as genodermatoses, diagnostic dilemmas, and management of dermatologic manifestations of systemic disease and other conditions, was the “bread and butter” of pediatric dermatology care. When I was in training, my mentor Paul Honig, MD, at the Children’s Hospital of Philadelphia had a procedure half-day each week, where he would care for a few patients who needed liquid nitrogen therapy for warts, or who needed biopsies. It was uncommon to have a large procedural/surgical part of pediatric dermatology practice. But this is now a routine part of many specialists in the field. How did this change occur?
The fundamental shift began to occur with the introduction of the pulsed dye laser for treatment of port-wine birthmarks in children with minimal scarring, and a seminal article published in the New England Journal of Medicine in 1989. Vascular lesions including port-wine stains were common, and pediatric dermatologists managed these patients for both diagnosis and medical management. Also, dermatology residencies at this time offered training in cutaneous surgery, excisions (including Mohs surgery) and repairs, and trainees in pediatric dermatology were “trained up” to high levels of expertise. As lasers were incorporated into dermatology residency work and practices, pediatric dermatologists developed the exposure and skill to do this work. An added advantage was having the knowledge of how to handle children and adolescents in an age-appropriate manner, with consideration of methods to minimize the pain and anxiety of procedures. Within a few years, pediatric dermatologists were at the forefront of the use of topical anesthetics (EMLA and liposomal lidocaine) and had general anesthesia privileges for laser and excisional surgery.
So while pediatric dermatologists still do “small procedures” every hour in most practices (cryotherapy for warts, cantharidin for molluscum, shave and punch biopsies), a subset now have extensive procedural practices, which in recent years has extended to pigment lesion lasers (to treat nevus of Ota, for example), hair laser, and combinations of lasers, including fractionated CO2 technology, to treat hypertrophic, constrictive and/or deforming scars.
The future
What will pediatric dermatology be like in 10, 20, or 50 years?
I have not yet discussed some of the most challenging diseases in our field, including epidermolysis bullosa, ichthyosis, and neurocutaneous disorders and other genetic skin disorders that have an incredible impact on the lives of affected children and their families, with incredible morbidity and with many conditions that shorten lifespans. But these are the conditions where “the future is happening now,” and we are looking forward to our new gene therapy techniques helping to transform our care.
And other aspects of practice? Will we be doing a large percentage of practice over the phone (or whatever devices we have then – remember, the first iPhone was only released 13 years ago)?
Will our patients be using their own imaging systems to evaluate their nevi and skin growths, and perhaps to diagnose and manage their rashes?
Will we have prevented our inflammatory skin disorders, or “turned them off” in early life with aggressive therapy in infantile life?
I project only that all of us in dermatology will still be a resource to our pediatric patients, from neonate through young adult, through our work of preventing, caring, healing and minimizing disease impact, and hopefully enjoying the pleasures of seeing our patients healthfully develop and evolve! As will our field.
Dr. Eichenfield is professor of dermatology and pediatrics and vice-chair of the department of dermatology at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. Dr. Eichenfield reports financial relationships with 20 pharmaceutical companies that manufacture dermatologic products, including products for the diseases discussed here.
As part of the 50th anniversary of Dermatology News, it is intriguing to think about where a time machine journey 5 decades back would find the field of pediatric dermatology, and to assess the changes in the specialty during the time that Dermatology News (operating then as “Skin & Allergy News”) has been reporting on innovations and changes in the practice of dermatology.
So, starting . It was not until 3 years later, in October 1973 in Mexico City, that the first international symposium on Pediatric Dermatology was held, and the International Society for Pediatric Dermatology was founded. I reached out to Andrew Margileth, MD, 100 years old this past July, and still active voluntary faculty in pediatric dermatology at the University of Miami, to help me “reach back” to those days. Dr. Margileth commented on how the first symposium was “brilliantly orchestrated by Ramon Ruiz-Maldonado,” from the National Institute of Paediatrics in Mexico, and that it was his “Aha moment for future practice!” That meeting spurred discussions on the development of the Society for Pediatric Dermatology the next year, with Alvin Jacobs, MD; Samuel Weinberg, MD; Nancy Esterly, MD; Sidney Hurwitz, MD; William Weston, MD; and Coleman Jacobson, MD, as some of the initial “founding mothers and fathers,” and the society was officially established in 1975.
The field of pediatric dermatology was fairly “infantile” 50 years ago, with few practitioners. But the early leaders in the field recognized that up to 30% of pediatric primary care visits included skin problems, and that there was limited training for dermatologists, as well as pediatricians, about skin diseases in children. There were clearly clinical and educational needs to establish a subspecialty of pediatric dermatology, and over the next 1-2 decades, the field expanded. The journal Pediatric Dermatology was established (in 1982), the Section on Dermatology was established by the American Academy of Pediatrics (in 1986), and fellowship programs were launched at select academic centers. And it was 30 years into our timeline before the formal subspecialty of pediatric dermatology was established through the American Board of Dermatology (2000).
The field of pediatric dermatology has evolved and matured rapidly. Standard reference textbooks have been developed in the United States and around the world (and of course, online). Pediatric dermatology is an essential part of the core curriculum for dermatologist trainees. Organizations promoting pediatric research have developed to influence basic, translational, and clinical research in conditions in neonates through adolescents, such as the Pediatric Dermatology Research Alliance (PeDRA). And meetings throughout the world now feature pediatric dermatology sessions and help to spread the advances in the diagnosis and management of pediatric skin disorders.
The practice of pediatric dermatology: How has it changed?
It is beyond the scope of this article to try to comprehensively review all of the changes in pediatric dermatology practice. But review of the evolution of a few disease states (choices influenced by my discussions with my 100-year old history guide, Dr. Margileth) displays examples of where we have been, and where we are going in our next 5, 10, or 50 years.
Hemangiomas and vascular malformations
Some of the first natural history studies on hemangiomas were done in the early 1960s, establishing that standard cutaneous hemangiomas had a typical clinical course of fairly rapid growth, plateau, and involution over time. Of interest, the hallmark article’s first author was Dr. Margileth, published in 1965 in JAMA!.This was still at a time when the identification of hemangiomas of infancy (or “HOI” as we say in the trade) was confused with vascular malformations, and no one had recognized the distinct variant tumors such as rapidly involuting and noninvoluting congenital hemangiomas (RICHs or NICHs), tufted angiomas, or hemangioendotheliomas. PHACE syndrome was not yet described (that was done in 1996 by Ilona Frieden, MD, and colleagues). And for a time, hemangiomas were treated with x-rays, before the negative impact of such radiation was acknowledged. It seems that, as a consequence of the use of x-ray therapy and as a backlash from the radiation therapy side effects and potential toxicities, even deforming and functionally significant lesions were “followed clinically” for natural involution, with a sensibility that doing nothing might be better than doing the wrong thing.
Over the next 15 years, the recognition of functionally significant hemangiomas, deformation associated with their proliferation, and the recognition of PHACE syndrome made hemangiomas of infancy an area of concern, with systemic steroids and occasionally chemotherapeutic agents (such as vincristine) being used for problematic lesions.
It has now been 12 years since the work of Christine Léauté-Labrèze, MD, et al., from the University of Bordeaux (France), led to the breakthrough of propranolol for hemangioma treatment, profoundly changing hemangioma management to an incredibly effective medical therapy extensively studied, tested in formal clinical trials, and approved by regulatory authorities. And how intriguing that this was pursued after the chance (but skilled) observation that a child who developed hypertension as a side effect of systemic steroids for nasal hemangioma treatment was prescribed propranolol for the hypertension and had his nasal hemangioma rapidly shrink, with a response superior and much quicker than that to corticosteroids.
The evolution of management of hemangiomas has another story within it, that of collaborative research. The Hemangioma Investigator Group was formed to take a collaborative approach to characterize and study hemangiomas and related tumors. Beginning with energetic, insightful pediatric dermatologists and little funding, they changed our knowledge base of how hemangiomas present, the risk factors for their development, and the characteristics and multiple organ findings associated with PHACE and other syndromic hemangiomas. Our knowledge of these lesions is now evidence based and broad, and the impact on care tremendous! The HIG has also influenced the practice of pediatricians and other specialists, including otorhinolaryngologists, hematologist/oncologists, and surgeons, is partnering with advocacy groups to support patients and families, and is helping guide patients and families to contribute to ongoing research.
Vascular malformations (VM) reflect an incredible change in our understanding of the developmental pathways and pathophysiology of blood vessel tumors, and, in fact, birthmarks other than vascular lesions! First, important work separated out hemangiomas of infancy and hemangiomalike tumors from vascular malformations, with the thought being that hemangiomas had a rapid growth phase, often arising from lesions that were minimally evident or not evident at birth, unlike malformations, which were “programing errors,” all present at birth and expected to be fairly static with proportionate growth over a lifetime. Approaches to vascular malformations were limited to sclerotherapy, laser, and/or surgery. While this general schema of classification is still useful, our sense of the “why and how” of vascular malformations is remarkably different. Vascular malformations – still usefully subdivided into capillary, lymphatic, venous arteriovenous, or mixed malformations – are mostly associated with inherited or somatic mutations. Mutations are most commonly found in two signal pathways: RAS/MAPK/ERK and PI3K/AKT/mTOR pathways, with specific sets of mutations seen in both localized and multifocal lesions, with or without overgrowth or other systemic anomalies. The discovery of specific mutations has led to the possibility of small-molecule inhibitors, many already existing as anticancer drugs, being utilized as targeted therapies for VM.
And similar advances in understanding of other birthmarks, with or without syndromic features, are being made steadily. The mutations in congenital melanocytic nevi, epidermal nevi, acquired tumors (pilomatricomas), and other lesions, along with steady epidemiologic, translational, and clinical work, evolves our knowledge and potential therapies.
Inflammatory skin disorders: Acne, psoriasis, and atopic dermatitis
The care of pediatric inflammatory skin disorders has evolved, but more slowly for some diseases than others. Acne vulgaris is now recognized as much more common under age 12 than previously, presumably reflecting earlier pubertal changes in our preteens. Over the past 30 years, therapy has evolved with the use of topical retinoids (still underused by pediatricians, considered a “practice gap”), hormonal therapy with combined oral contraceptives, and oral isotretinoin, a powerful but highly effective systemic agent for severe and refractory acne. Specific pediatric guidelines came much later, with expert recommendations formulated by the American Acne and Rosacea Society and endorsed by the American Academy of Pediatrics in 2013. Over the past few years, there has been a push by experts for more judicious use of antibiotics for acne (oral and topical) to minimize the emergence of bacterial resistance. There are unanswered questions as we evolve our care: How will the new topical antiandrogens be used? Will spironolactone become part of hormonal therapy under age 18? Will the insights on certain strains of Cutibacterium acnes being associated with worse acne translate to microbiome or vaccine-based strategies?
Pediatric psoriasis has suffered, being “behind in the revolution” of biologic agents because of delayed approval of any biologic agent for treatment of pediatric psoriasis in the United States until just a few years ago, and lags behind Europe and elsewhere in the world by almost a decade. Only this year have we expanded beyond one biologic agent approved for under age 12 and two for ages 12 and older, with other approvals expected including interleukin (IL)-17 and IL-23 agents. Adult psoriasis has been recognized to be associated with a broad set of comorbidities, including obesity and early heart disease, and there is now research on how children are at risk as well, with new recommendations on how to screen children with psoriasis, supplied first by PeDRA and then in the new American Academy of Dermatology-National Psoriasis Foundation pediatric psoriasis guidelines .
Pediatric atopic dermatitis (AD) is in its early years of revolution. In the 50-year period of our thought experiment, AD has increased in prevalence from 5% or less of the pediatric population to 10%-15%. Treatment of most individuals has remained the same over the decades: Good skin care, frequent moisturizers, topical corticosteroids for flares, and management of infection if noted. The topical calcineurin inhibitors (TCIs) broadened the therapeutic approach when introduced in 2000 and 2001, but the boxed warning resulted in some practitioners minimizing their use of these useful agents. But newer studies are markedly reassuring about their safe use in children.
Steroid phobia, as well as concerns about potential side effects of the TCIs, has resulted in undertreatment of childhood AD. It is quite common to see multiple children during pediatric dermatology office hours with poorly controlled eczema, high body-surface areas of eczema, compromised sleep, secondary infections, and anxiety and depression, especially in our moderate to severe adolescents. The field is “hot” with new topical and systemic agents, including our few years’ experience with topical crisaborole, a phosphodiesterase (PDE)-4 inhibitor; and dupilumab, an IL-4-alpha blocker – the first biologic agent approved for AD and the first systemic agent (other than oral corticosteroids), just extended from 12 years to 6 years of age! As dupilumab gets studied for younger children, other biologics (including IL-13 and IL-31 blockers) are undertaking pediatric and/or adolescent trials, oral and topical JAK inhibitors are including adolescents in core clinical trials, and other novel topical agents are under study, including an aryl-hydrocarbon receptor–modulating agent and other PDE-4 inhibitors.
Procedural pediatric dermatology: From liquid nitrogen to laser, surgery, and multimodal skin care
The first generation of pediatric dermatologists were considered medical dermatologist specialists. The care of the conditions discussed above, as well as genodermatoses, diagnostic dilemmas, and management of dermatologic manifestations of systemic disease and other conditions, was the “bread and butter” of pediatric dermatology care. When I was in training, my mentor Paul Honig, MD, at the Children’s Hospital of Philadelphia had a procedure half-day each week, where he would care for a few patients who needed liquid nitrogen therapy for warts, or who needed biopsies. It was uncommon to have a large procedural/surgical part of pediatric dermatology practice. But this is now a routine part of many specialists in the field. How did this change occur?
The fundamental shift began to occur with the introduction of the pulsed dye laser for treatment of port-wine birthmarks in children with minimal scarring, and a seminal article published in the New England Journal of Medicine in 1989. Vascular lesions including port-wine stains were common, and pediatric dermatologists managed these patients for both diagnosis and medical management. Also, dermatology residencies at this time offered training in cutaneous surgery, excisions (including Mohs surgery) and repairs, and trainees in pediatric dermatology were “trained up” to high levels of expertise. As lasers were incorporated into dermatology residency work and practices, pediatric dermatologists developed the exposure and skill to do this work. An added advantage was having the knowledge of how to handle children and adolescents in an age-appropriate manner, with consideration of methods to minimize the pain and anxiety of procedures. Within a few years, pediatric dermatologists were at the forefront of the use of topical anesthetics (EMLA and liposomal lidocaine) and had general anesthesia privileges for laser and excisional surgery.
So while pediatric dermatologists still do “small procedures” every hour in most practices (cryotherapy for warts, cantharidin for molluscum, shave and punch biopsies), a subset now have extensive procedural practices, which in recent years has extended to pigment lesion lasers (to treat nevus of Ota, for example), hair laser, and combinations of lasers, including fractionated CO2 technology, to treat hypertrophic, constrictive and/or deforming scars.
The future
What will pediatric dermatology be like in 10, 20, or 50 years?
I have not yet discussed some of the most challenging diseases in our field, including epidermolysis bullosa, ichthyosis, and neurocutaneous disorders and other genetic skin disorders that have an incredible impact on the lives of affected children and their families, with incredible morbidity and with many conditions that shorten lifespans. But these are the conditions where “the future is happening now,” and we are looking forward to our new gene therapy techniques helping to transform our care.
And other aspects of practice? Will we be doing a large percentage of practice over the phone (or whatever devices we have then – remember, the first iPhone was only released 13 years ago)?
Will our patients be using their own imaging systems to evaluate their nevi and skin growths, and perhaps to diagnose and manage their rashes?
Will we have prevented our inflammatory skin disorders, or “turned them off” in early life with aggressive therapy in infantile life?
I project only that all of us in dermatology will still be a resource to our pediatric patients, from neonate through young adult, through our work of preventing, caring, healing and minimizing disease impact, and hopefully enjoying the pleasures of seeing our patients healthfully develop and evolve! As will our field.
Dr. Eichenfield is professor of dermatology and pediatrics and vice-chair of the department of dermatology at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego. Dr. Eichenfield reports financial relationships with 20 pharmaceutical companies that manufacture dermatologic products, including products for the diseases discussed here.