User login
Expanded UCB product can stand alone

SALT LAKE CITY—The expanded umbilical cord blood (UCB) product NiCord can be used as a stand-alone graft, according to research presented at the 2018 BMT Tandem Meetings.
Researchers found that a single NiCord unit provided “robust” engraftment in a phase 1/2 study of patients with high-risk hematologic malignancies.
NiCord recipients had quicker neutrophil and platelet engraftment than matched control subjects who received standard myeloablative UCB transplant (single or double).
Mitchell Horwitz, MD, of the Duke University Medical Center in Durham, North Carolina, presented these results at the meeting as abstract 49.* The research was sponsored by Gamida Cell, the company developing NiCord.
“[NiCord] is an ex vivo expanded cell product that’s derived from an entire unit of umbilical cord blood,” Dr Horwitz explained. “It’s manufactured starting with a CD133-positive selection, which is the progenitor cell population that’s cultured, and a T-cell containing CD133-negative fraction that is provided also at the time of transplant.”
“The culture system contains nicotinamide—that’s the active ingredient in the culture. And that’s supplemented with cytokines—thrombopoietin, IL-6, FLT-3 ligand, and stem cell factor. The culture is 21 days.”
Previous research showed that double UCB transplant including a NiCord unit could provide benefits over standard double UCB transplant. This led Dr Horwitz and his colleagues to wonder if NiCord could be used as a stand-alone graft.
So the team evaluated the safety and efficacy of NiCord alone in 36 adolescents/adults with high-risk hematologic malignancies.
Patients had acute myelogenous leukemia (n=17), acute lymphoblastic leukemia (n=9), myelodysplastic syndrome (n=7), chronic myelogenous leukemia (n=2), and Hodgkin lymphoma (n=1).
Most patients had intermediate (n=15) or high-risk (n=13) disease. They had a median age of 44 (range, 13-63) and a median weight of 75 kg (range, 41-125).
Treatment
For conditioning, 19 patients received thiotepa, busulfan, and fludarabine. Fifteen patients received total body irradiation and fludarabine with or without cyclophosphamide or thiotepa. And 2 patients received clofarabine, fludarabine, and busulfan.
Most patients had a 4/6 human leukocyte antigen (HLA) match (n=26), 8 had a 5/6 HLA match, and 2 had a 6/6 HLA match.
The median total nucleated cell dose was 2.4 x 107/kg prior to expansion of the UCB unit and 3.7 x 107/kg after expansion. The median CD34+ cell dose was 0.2 x 106/kg and 6.3 x 106/kg, respectively.
“CD34 cells were expanded 33-fold in the 3-week culture system,” Dr Horwitz noted. “That translated to a median CD34 dose of 6.3 x 106/kg, a dose comparable to what would be obtained from an adult donor graft.”
Engraftment
There was 1 case of primary graft failure and 2 cases of secondary graft failure. One case of secondary graft failure was associated with an HHV-6 infection, and the other was due to a lethal adenovirus infection.
Of those patients who engrafted, 97% achieved full donor chimerism, and 3% had mixed chimerism.
Dr Horwitz and his colleagues compared engraftment results in the NiCord recipients to results in a cohort of patients from the CIBMTR registry who underwent UCB transplants from 2010 to 2013. They had similar characteristics as the NiCord patients—age, conditioning regimen, disease status, etc.
In total, there were 148 CIBMTR registry patients, 20% of whom received a single UCB unit.
The median time to neutrophil engraftment was 11.5 days (range, 6-26) with NiCord and 21 days in the CIBMTR matched control cohort (P<0.001). The cumulative incidence of neutrophil engraftment was 94.4% and 89.7%, respectively.
The median time to platelet engraftment was 34 days (range, 25-96) with NiCord and 46 days in the CIBMTR controls (P<0.001). The cumulative incidence of platelet engraftment was 80.6% and 67.1%, respectively.
“There’s a median 10-day reduction in neutrophil recovery [and] 12-day reduction in time to platelet recovery [with NiCord],” Dr Horwitz noted. “There is evidence of robust and durable engraftment with a NiCord unit, with one patient now over 7 years from his first transplant on the pilot trial.”
Relapse, survival, and GVHD
Dr Horwitz reported other outcomes in the NiCord recipients without making comparisons to the CIBMTR matched controls.
The estimated 2-year rate of non-relapse mortality in NiCord recipients was 23.8%, and the estimated 2-year incidence of relapse was 33.2%.
The estimated disease-free survival was 49.1% at 1 year and 43.0% at 2 years. The estimated overall survival was 51.2% at 1 year and 2 years.
At 100 days, the rate of grade 2-4 acute GVHD was 44.0%, and the rate of grade 3-4 acute GVHD was 11.1%.
The estimated 1-year rate of mild to severe chronic GVHD was 40.5%, and the estimated 2-year rate of moderate to severe chronic GVHD was 9.8%.
Dr Horwitz said these “promising results” have led to the launch of a phase 3 registration trial in which researchers are comparing NiCord to standard single or double UCB transplant. The trial is open for accrual.
*Information in the abstract differs from the presentation.
SALT LAKE CITY—The expanded umbilical cord blood (UCB) product NiCord can be used as a stand-alone graft, according to research presented at the 2018 BMT Tandem Meetings.
Researchers found that a single NiCord unit provided “robust” engraftment in a phase 1/2 study of patients with high-risk hematologic malignancies.
NiCord recipients had quicker neutrophil and platelet engraftment than matched control subjects who received standard myeloablative UCB transplant (single or double).
Mitchell Horwitz, MD, of the Duke University Medical Center in Durham, North Carolina, presented these results at the meeting as abstract 49.* The research was sponsored by Gamida Cell, the company developing NiCord.
“[NiCord] is an ex vivo expanded cell product that’s derived from an entire unit of umbilical cord blood,” Dr Horwitz explained. “It’s manufactured starting with a CD133-positive selection, which is the progenitor cell population that’s cultured, and a T-cell containing CD133-negative fraction that is provided also at the time of transplant.”
“The culture system contains nicotinamide—that’s the active ingredient in the culture. And that’s supplemented with cytokines—thrombopoietin, IL-6, FLT-3 ligand, and stem cell factor. The culture is 21 days.”
Previous research showed that double UCB transplant including a NiCord unit could provide benefits over standard double UCB transplant. This led Dr Horwitz and his colleagues to wonder if NiCord could be used as a stand-alone graft.
So the team evaluated the safety and efficacy of NiCord alone in 36 adolescents/adults with high-risk hematologic malignancies.
Patients had acute myelogenous leukemia (n=17), acute lymphoblastic leukemia (n=9), myelodysplastic syndrome (n=7), chronic myelogenous leukemia (n=2), and Hodgkin lymphoma (n=1).
Most patients had intermediate (n=15) or high-risk (n=13) disease. They had a median age of 44 (range, 13-63) and a median weight of 75 kg (range, 41-125).
Treatment
For conditioning, 19 patients received thiotepa, busulfan, and fludarabine. Fifteen patients received total body irradiation and fludarabine with or without cyclophosphamide or thiotepa. And 2 patients received clofarabine, fludarabine, and busulfan.
Most patients had a 4/6 human leukocyte antigen (HLA) match (n=26), 8 had a 5/6 HLA match, and 2 had a 6/6 HLA match.
The median total nucleated cell dose was 2.4 x 107/kg prior to expansion of the UCB unit and 3.7 x 107/kg after expansion. The median CD34+ cell dose was 0.2 x 106/kg and 6.3 x 106/kg, respectively.
“CD34 cells were expanded 33-fold in the 3-week culture system,” Dr Horwitz noted. “That translated to a median CD34 dose of 6.3 x 106/kg, a dose comparable to what would be obtained from an adult donor graft.”
Engraftment
There was 1 case of primary graft failure and 2 cases of secondary graft failure. One case of secondary graft failure was associated with an HHV-6 infection, and the other was due to a lethal adenovirus infection.
Of those patients who engrafted, 97% achieved full donor chimerism, and 3% had mixed chimerism.
Dr Horwitz and his colleagues compared engraftment results in the NiCord recipients to results in a cohort of patients from the CIBMTR registry who underwent UCB transplants from 2010 to 2013. They had similar characteristics as the NiCord patients—age, conditioning regimen, disease status, etc.
In total, there were 148 CIBMTR registry patients, 20% of whom received a single UCB unit.
The median time to neutrophil engraftment was 11.5 days (range, 6-26) with NiCord and 21 days in the CIBMTR matched control cohort (P<0.001). The cumulative incidence of neutrophil engraftment was 94.4% and 89.7%, respectively.
The median time to platelet engraftment was 34 days (range, 25-96) with NiCord and 46 days in the CIBMTR controls (P<0.001). The cumulative incidence of platelet engraftment was 80.6% and 67.1%, respectively.
“There’s a median 10-day reduction in neutrophil recovery [and] 12-day reduction in time to platelet recovery [with NiCord],” Dr Horwitz noted. “There is evidence of robust and durable engraftment with a NiCord unit, with one patient now over 7 years from his first transplant on the pilot trial.”
Relapse, survival, and GVHD
Dr Horwitz reported other outcomes in the NiCord recipients without making comparisons to the CIBMTR matched controls.
The estimated 2-year rate of non-relapse mortality in NiCord recipients was 23.8%, and the estimated 2-year incidence of relapse was 33.2%.
The estimated disease-free survival was 49.1% at 1 year and 43.0% at 2 years. The estimated overall survival was 51.2% at 1 year and 2 years.
At 100 days, the rate of grade 2-4 acute GVHD was 44.0%, and the rate of grade 3-4 acute GVHD was 11.1%.
The estimated 1-year rate of mild to severe chronic GVHD was 40.5%, and the estimated 2-year rate of moderate to severe chronic GVHD was 9.8%.
Dr Horwitz said these “promising results” have led to the launch of a phase 3 registration trial in which researchers are comparing NiCord to standard single or double UCB transplant. The trial is open for accrual.
*Information in the abstract differs from the presentation.
SALT LAKE CITY—The expanded umbilical cord blood (UCB) product NiCord can be used as a stand-alone graft, according to research presented at the 2018 BMT Tandem Meetings.
Researchers found that a single NiCord unit provided “robust” engraftment in a phase 1/2 study of patients with high-risk hematologic malignancies.
NiCord recipients had quicker neutrophil and platelet engraftment than matched control subjects who received standard myeloablative UCB transplant (single or double).
Mitchell Horwitz, MD, of the Duke University Medical Center in Durham, North Carolina, presented these results at the meeting as abstract 49.* The research was sponsored by Gamida Cell, the company developing NiCord.
“[NiCord] is an ex vivo expanded cell product that’s derived from an entire unit of umbilical cord blood,” Dr Horwitz explained. “It’s manufactured starting with a CD133-positive selection, which is the progenitor cell population that’s cultured, and a T-cell containing CD133-negative fraction that is provided also at the time of transplant.”
“The culture system contains nicotinamide—that’s the active ingredient in the culture. And that’s supplemented with cytokines—thrombopoietin, IL-6, FLT-3 ligand, and stem cell factor. The culture is 21 days.”
Previous research showed that double UCB transplant including a NiCord unit could provide benefits over standard double UCB transplant. This led Dr Horwitz and his colleagues to wonder if NiCord could be used as a stand-alone graft.
So the team evaluated the safety and efficacy of NiCord alone in 36 adolescents/adults with high-risk hematologic malignancies.
Patients had acute myelogenous leukemia (n=17), acute lymphoblastic leukemia (n=9), myelodysplastic syndrome (n=7), chronic myelogenous leukemia (n=2), and Hodgkin lymphoma (n=1).
Most patients had intermediate (n=15) or high-risk (n=13) disease. They had a median age of 44 (range, 13-63) and a median weight of 75 kg (range, 41-125).
Treatment
For conditioning, 19 patients received thiotepa, busulfan, and fludarabine. Fifteen patients received total body irradiation and fludarabine with or without cyclophosphamide or thiotepa. And 2 patients received clofarabine, fludarabine, and busulfan.
Most patients had a 4/6 human leukocyte antigen (HLA) match (n=26), 8 had a 5/6 HLA match, and 2 had a 6/6 HLA match.
The median total nucleated cell dose was 2.4 x 107/kg prior to expansion of the UCB unit and 3.7 x 107/kg after expansion. The median CD34+ cell dose was 0.2 x 106/kg and 6.3 x 106/kg, respectively.
“CD34 cells were expanded 33-fold in the 3-week culture system,” Dr Horwitz noted. “That translated to a median CD34 dose of 6.3 x 106/kg, a dose comparable to what would be obtained from an adult donor graft.”
Engraftment
There was 1 case of primary graft failure and 2 cases of secondary graft failure. One case of secondary graft failure was associated with an HHV-6 infection, and the other was due to a lethal adenovirus infection.
Of those patients who engrafted, 97% achieved full donor chimerism, and 3% had mixed chimerism.
Dr Horwitz and his colleagues compared engraftment results in the NiCord recipients to results in a cohort of patients from the CIBMTR registry who underwent UCB transplants from 2010 to 2013. They had similar characteristics as the NiCord patients—age, conditioning regimen, disease status, etc.
In total, there were 148 CIBMTR registry patients, 20% of whom received a single UCB unit.
The median time to neutrophil engraftment was 11.5 days (range, 6-26) with NiCord and 21 days in the CIBMTR matched control cohort (P<0.001). The cumulative incidence of neutrophil engraftment was 94.4% and 89.7%, respectively.
The median time to platelet engraftment was 34 days (range, 25-96) with NiCord and 46 days in the CIBMTR controls (P<0.001). The cumulative incidence of platelet engraftment was 80.6% and 67.1%, respectively.
“There’s a median 10-day reduction in neutrophil recovery [and] 12-day reduction in time to platelet recovery [with NiCord],” Dr Horwitz noted. “There is evidence of robust and durable engraftment with a NiCord unit, with one patient now over 7 years from his first transplant on the pilot trial.”
Relapse, survival, and GVHD
Dr Horwitz reported other outcomes in the NiCord recipients without making comparisons to the CIBMTR matched controls.
The estimated 2-year rate of non-relapse mortality in NiCord recipients was 23.8%, and the estimated 2-year incidence of relapse was 33.2%.
The estimated disease-free survival was 49.1% at 1 year and 43.0% at 2 years. The estimated overall survival was 51.2% at 1 year and 2 years.
At 100 days, the rate of grade 2-4 acute GVHD was 44.0%, and the rate of grade 3-4 acute GVHD was 11.1%.
The estimated 1-year rate of mild to severe chronic GVHD was 40.5%, and the estimated 2-year rate of moderate to severe chronic GVHD was 9.8%.
Dr Horwitz said these “promising results” have led to the launch of a phase 3 registration trial in which researchers are comparing NiCord to standard single or double UCB transplant. The trial is open for accrual.
*Information in the abstract differs from the presentation.
FDA approves abemaciclib plus aromatase inhibitor as initial therapy
Abemaciclib (Verzenio) in combination with an aromatase inhibitor has been approved as initial endocrine-based therapy for postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer, the US Food and Drug Administration announced in a press release.

Approval was based on the results of the MONARCH 3 study, a randomized, double-blind, placebo-controlled, multicenter clinical trial in postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer. A total of 493 patients were randomized to receive either abemaciclib 150 mg or placebo orally twice daily, plus the treating physician’s choice of letrozole or anastrozole. The estimated median progression-free survival (PFS) (RECIST 1.1) was 28.2 months (95% CI: 23.5, not reached) for patients receiving abemaciclib and 14.8 months (95% CI: 11.2, 19.2) for those receiving placebo (HR 0.540; 95% CI: 0.418, 0.698; p<0.0001).
The most common adverse reactions that were seen in at least 20% of patients receiving abemaciclib in MONARCH 3 and were reported at a rate more than 2% higher than the rates seen in the placebo arm were diarrhea, neutropenia, fatigue, infections, nausea, abdominal pain, anemia, vomiting, alopecia, decreased appetite, and leukopenia.
The recommended starting dose of abemaciclib in combination with an aromatase inhibitor is 150 mg twice daily orally with or without food.
Abemaciclib (Verzenio) is manufactured by Eli Lilly.
Full prescribing information is available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208855s000lbl.pdf.
Abemaciclib (Verzenio) in combination with an aromatase inhibitor has been approved as initial endocrine-based therapy for postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer, the US Food and Drug Administration announced in a press release.
Approval was based on the results of the MONARCH 3 study, a randomized, double-blind, placebo-controlled, multicenter clinical trial in postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer. A total of 493 patients were randomized to receive either abemaciclib 150 mg or placebo orally twice daily, plus the treating physician’s choice of letrozole or anastrozole. The estimated median progression-free survival (PFS) (RECIST 1.1) was 28.2 months (95% CI: 23.5, not reached) for patients receiving abemaciclib and 14.8 months (95% CI: 11.2, 19.2) for those receiving placebo (HR 0.540; 95% CI: 0.418, 0.698; p<0.0001).
The most common adverse reactions that were seen in at least 20% of patients receiving abemaciclib in MONARCH 3 and were reported at a rate more than 2% higher than the rates seen in the placebo arm were diarrhea, neutropenia, fatigue, infections, nausea, abdominal pain, anemia, vomiting, alopecia, decreased appetite, and leukopenia.
The recommended starting dose of abemaciclib in combination with an aromatase inhibitor is 150 mg twice daily orally with or without food.
Abemaciclib (Verzenio) is manufactured by Eli Lilly.
Full prescribing information is available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208855s000lbl.pdf.
Abemaciclib (Verzenio) in combination with an aromatase inhibitor has been approved as initial endocrine-based therapy for postmenopausal women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced or metastatic breast cancer, the US Food and Drug Administration announced in a press release.
Approval was based on the results of the MONARCH 3 study, a randomized, double-blind, placebo-controlled, multicenter clinical trial in postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer. A total of 493 patients were randomized to receive either abemaciclib 150 mg or placebo orally twice daily, plus the treating physician’s choice of letrozole or anastrozole. The estimated median progression-free survival (PFS) (RECIST 1.1) was 28.2 months (95% CI: 23.5, not reached) for patients receiving abemaciclib and 14.8 months (95% CI: 11.2, 19.2) for those receiving placebo (HR 0.540; 95% CI: 0.418, 0.698; p<0.0001).
The most common adverse reactions that were seen in at least 20% of patients receiving abemaciclib in MONARCH 3 and were reported at a rate more than 2% higher than the rates seen in the placebo arm were diarrhea, neutropenia, fatigue, infections, nausea, abdominal pain, anemia, vomiting, alopecia, decreased appetite, and leukopenia.
The recommended starting dose of abemaciclib in combination with an aromatase inhibitor is 150 mg twice daily orally with or without food.
Abemaciclib (Verzenio) is manufactured by Eli Lilly.
Full prescribing information is available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208855s000lbl.pdf.
HCV infection tied to premature ovarian senescence and a high miscarriage rate
Premenopausal women with hepatitis C virus (HCV) showed increased ovarian senescence, which was associated with a lower chance of live birth. Such women also had a greater risk of infertility, as reported in the Journal of Hepatology.
Researchers examined three cohort studies, which comprised an age-matched prospectively enrolled cohort study of 100 women who were HCV positive and had chronic liver disease, 50 women who were HBV positive and had CLD, and 100 healthy women; 1,998 HCV-infected women enrolled in the Platform for the Study of Viral Hepatitis Therapies (PITER) trial from Italy; and 6,085 women infected with HCV plus 20,415 uninfected women from a United States database, according to Aimilia Karampatou, MD, of the University of Bologna, Modena, Italy, and colleagues.
In the second group examined, the women from the PITER trial, miscarriages occurred in 42% of the HCV-infected women with 44.6% of these women experiencing multiple miscarriages. The total fertility rate, defined as the average number of children that would be born in a lifetime, was 0.7 for the HCV-infected women, compared with 1.37 in the general Italian population.
Infertility data from the large U.S. study was assessed from a total of 27,525 women (20,415 HCV negative and HIV negative; 6,805 HCV positive; and 305 HCV positive/HIV positive). Women with HCV showed a significantly higher probability of infertility compared with uninfected controls (odds ratio, 2.44), and those women dually infected with HCV and HIV were affected even more (OR, 3.64).
Primarily based on the observations of AMH, which in many of the HCV-positive women fell into the menopausal range, the researchers suggested that “the reduced reproductive capacity of women who are HCV positive is related to failing ovarian function and subsequent follicular depletion in the context of a more generalized dysfunction of other fertility-related factors.”
With regard to the effect of antiviral therapy, AMH levels remained stable in women who attained a sustained virologic response but continued to fall in those for whom the therapy was a failure.
“HCV infection significantly and negatively affects many aspects of fertility. It remains to be assessed whether antiviral therapy at a very early age can positively influence the occurrence of miscarriages and can prevent ovarian senescence because the latter has broader health implications than simply preserving fertility,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Karampatou A et al. J Hepatology. 2018;68:33-41.
Premenopausal women with hepatitis C virus (HCV) showed increased ovarian senescence, which was associated with a lower chance of live birth. Such women also had a greater risk of infertility, as reported in the Journal of Hepatology.
Researchers examined three cohort studies, which comprised an age-matched prospectively enrolled cohort study of 100 women who were HCV positive and had chronic liver disease, 50 women who were HBV positive and had CLD, and 100 healthy women; 1,998 HCV-infected women enrolled in the Platform for the Study of Viral Hepatitis Therapies (PITER) trial from Italy; and 6,085 women infected with HCV plus 20,415 uninfected women from a United States database, according to Aimilia Karampatou, MD, of the University of Bologna, Modena, Italy, and colleagues.
In the second group examined, the women from the PITER trial, miscarriages occurred in 42% of the HCV-infected women with 44.6% of these women experiencing multiple miscarriages. The total fertility rate, defined as the average number of children that would be born in a lifetime, was 0.7 for the HCV-infected women, compared with 1.37 in the general Italian population.
Infertility data from the large U.S. study was assessed from a total of 27,525 women (20,415 HCV negative and HIV negative; 6,805 HCV positive; and 305 HCV positive/HIV positive). Women with HCV showed a significantly higher probability of infertility compared with uninfected controls (odds ratio, 2.44), and those women dually infected with HCV and HIV were affected even more (OR, 3.64).
Primarily based on the observations of AMH, which in many of the HCV-positive women fell into the menopausal range, the researchers suggested that “the reduced reproductive capacity of women who are HCV positive is related to failing ovarian function and subsequent follicular depletion in the context of a more generalized dysfunction of other fertility-related factors.”
With regard to the effect of antiviral therapy, AMH levels remained stable in women who attained a sustained virologic response but continued to fall in those for whom the therapy was a failure.
“HCV infection significantly and negatively affects many aspects of fertility. It remains to be assessed whether antiviral therapy at a very early age can positively influence the occurrence of miscarriages and can prevent ovarian senescence because the latter has broader health implications than simply preserving fertility,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Karampatou A et al. J Hepatology. 2018;68:33-41.
Premenopausal women with hepatitis C virus (HCV) showed increased ovarian senescence, which was associated with a lower chance of live birth. Such women also had a greater risk of infertility, as reported in the Journal of Hepatology.
Researchers examined three cohort studies, which comprised an age-matched prospectively enrolled cohort study of 100 women who were HCV positive and had chronic liver disease, 50 women who were HBV positive and had CLD, and 100 healthy women; 1,998 HCV-infected women enrolled in the Platform for the Study of Viral Hepatitis Therapies (PITER) trial from Italy; and 6,085 women infected with HCV plus 20,415 uninfected women from a United States database, according to Aimilia Karampatou, MD, of the University of Bologna, Modena, Italy, and colleagues.
In the second group examined, the women from the PITER trial, miscarriages occurred in 42% of the HCV-infected women with 44.6% of these women experiencing multiple miscarriages. The total fertility rate, defined as the average number of children that would be born in a lifetime, was 0.7 for the HCV-infected women, compared with 1.37 in the general Italian population.
Infertility data from the large U.S. study was assessed from a total of 27,525 women (20,415 HCV negative and HIV negative; 6,805 HCV positive; and 305 HCV positive/HIV positive). Women with HCV showed a significantly higher probability of infertility compared with uninfected controls (odds ratio, 2.44), and those women dually infected with HCV and HIV were affected even more (OR, 3.64).
Primarily based on the observations of AMH, which in many of the HCV-positive women fell into the menopausal range, the researchers suggested that “the reduced reproductive capacity of women who are HCV positive is related to failing ovarian function and subsequent follicular depletion in the context of a more generalized dysfunction of other fertility-related factors.”
With regard to the effect of antiviral therapy, AMH levels remained stable in women who attained a sustained virologic response but continued to fall in those for whom the therapy was a failure.
“HCV infection significantly and negatively affects many aspects of fertility. It remains to be assessed whether antiviral therapy at a very early age can positively influence the occurrence of miscarriages and can prevent ovarian senescence because the latter has broader health implications than simply preserving fertility,” the researchers concluded.
The authors reported that they had no conflicts of interest.
SOURCE: Karampatou A et al. J Hepatology. 2018;68:33-41.
FROM THE JOURNAL OF HEPATOLOGY
Key clinical point: HCV-positive women appear to undergo increased ovarian senescence.
Major finding: The fertility rate of HCV-positive women was 0.7 vs. 1.37 in the general population.
Study details: Three separate studies together comprising more than 30,000 HCV-infected and -uninfected women.
Disclosures: The authors reported that they had no conflicts of interest.
Source: Karampatou A et al. J Hepatology. 2018;68:33-41.
How to integrate mental health care into primary care
During my training as a child and adolescent psychiatry fellow, I “lived” down the hall from 10 other people just like me who had similar offices and training. Our pace was tailored to pediatric psychiatry. Appointments were 30 minutes or more. Our goal was to provide the most comprehensive mental health care for the families whom we grew to know and love.

The impetus to create an integrated mental health care approach has been well elucidated by the American Academy of Child and Adolescent Psychiatry (AACAP) in its report, Collaborative mental health care in pediatric primary care. It is based on some telling statistics: Fifty percent of all cases of mental illness begin before age 14 years and 75% begin by age 24. Half of all pediatric office visits involve behavioral, psychosocial, or educational concerns. The American Academy of Pediatrics’ Task Force on Mental Health similarly has stated that primary care clinicians can and should be able to provide mental health services to children and adolescents in a primary care setting.
Integrative psychiatry and primary care treatment comes in three forms: classic consultation, in which a specialist sees a patient and refers back to the PCP with recommendations; colocation, in which mental health specialists practice in the same office but essentially are “ships crossing in the night” with PCPs; and the most-lauded form, collaborative/integrative care, in which back-and-forth consultation and discussions of a case occur between mental health specialists and PCPs, with in-person follow-up as needed.
Several institutions offer programs to address the AACAP and AAP imperatives, most prominently the University of Washington, Seattle, and the University of Massachusetts, Worcester. Both offer resources on how to create an integrated care model (University of Washington AIMS Resource Center; The University of Massachusetts Center for Integrated Care).
What can one do in a busy pediatric primary care practice to address mental health imperatives on the individual provider level? Often PCPs can, as I do, offer families some resources by having a set of mental health handouts and resources. I have gathered useful handouts for families throughout my residency to use as shortcuts and visual aids to promote mental health. I use the AACAP Facts for Families for handouts on mental health diagnoses and topics. I use the National Sleep Foundation for its sleep hygiene tips. I also offer some low-cost mindfulness resources to help kids and parents with their anxiety, such as the Calm app and Headspace app. If parents have difficulty with access to parent management training (the first-line treatment to manage aggression in children), I often recommend “The Defiant Child: A Parent’s Guide to Oppositional Defiant Disorder” (Lanham, Md.: Taylor Trade Publishing, 1997), which shows how to create a rewards system in the home to promote positive behavior. “How to Talk So Kids Will Listen & Listen So Kids Will Talk” (New York: Scribner, 2012 ) is a beloved book for parents (and there is a teenager version) that I recommend when parents launch into questions about how to talk to kids and teens about difficult topics so that, ultimately, they can improve their relationship.

Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. Email her at [email protected].
Resources
The AACAP website has materials to help clinicians develop a collaborative mental health care model in the primary care setting: Search for “collaboration with primary care.”
The journal Pediatrics also has a useful resource: Improving mental health services in primary care: Reducing administrative and financial barriers to access and collaboration. (2009;123;1248-51).
During my training as a child and adolescent psychiatry fellow, I “lived” down the hall from 10 other people just like me who had similar offices and training. Our pace was tailored to pediatric psychiatry. Appointments were 30 minutes or more. Our goal was to provide the most comprehensive mental health care for the families whom we grew to know and love.
The impetus to create an integrated mental health care approach has been well elucidated by the American Academy of Child and Adolescent Psychiatry (AACAP) in its report, Collaborative mental health care in pediatric primary care. It is based on some telling statistics: Fifty percent of all cases of mental illness begin before age 14 years and 75% begin by age 24. Half of all pediatric office visits involve behavioral, psychosocial, or educational concerns. The American Academy of Pediatrics’ Task Force on Mental Health similarly has stated that primary care clinicians can and should be able to provide mental health services to children and adolescents in a primary care setting.
Integrative psychiatry and primary care treatment comes in three forms: classic consultation, in which a specialist sees a patient and refers back to the PCP with recommendations; colocation, in which mental health specialists practice in the same office but essentially are “ships crossing in the night” with PCPs; and the most-lauded form, collaborative/integrative care, in which back-and-forth consultation and discussions of a case occur between mental health specialists and PCPs, with in-person follow-up as needed.
Several institutions offer programs to address the AACAP and AAP imperatives, most prominently the University of Washington, Seattle, and the University of Massachusetts, Worcester. Both offer resources on how to create an integrated care model (University of Washington AIMS Resource Center; The University of Massachusetts Center for Integrated Care).
What can one do in a busy pediatric primary care practice to address mental health imperatives on the individual provider level? Often PCPs can, as I do, offer families some resources by having a set of mental health handouts and resources. I have gathered useful handouts for families throughout my residency to use as shortcuts and visual aids to promote mental health. I use the AACAP Facts for Families for handouts on mental health diagnoses and topics. I use the National Sleep Foundation for its sleep hygiene tips. I also offer some low-cost mindfulness resources to help kids and parents with their anxiety, such as the Calm app and Headspace app. If parents have difficulty with access to parent management training (the first-line treatment to manage aggression in children), I often recommend “The Defiant Child: A Parent’s Guide to Oppositional Defiant Disorder” (Lanham, Md.: Taylor Trade Publishing, 1997), which shows how to create a rewards system in the home to promote positive behavior. “How to Talk So Kids Will Listen & Listen So Kids Will Talk” (New York: Scribner, 2012 ) is a beloved book for parents (and there is a teenager version) that I recommend when parents launch into questions about how to talk to kids and teens about difficult topics so that, ultimately, they can improve their relationship.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. Email her at [email protected].
Resources
The AACAP website has materials to help clinicians develop a collaborative mental health care model in the primary care setting: Search for “collaboration with primary care.”
The journal Pediatrics also has a useful resource: Improving mental health services in primary care: Reducing administrative and financial barriers to access and collaboration. (2009;123;1248-51).
During my training as a child and adolescent psychiatry fellow, I “lived” down the hall from 10 other people just like me who had similar offices and training. Our pace was tailored to pediatric psychiatry. Appointments were 30 minutes or more. Our goal was to provide the most comprehensive mental health care for the families whom we grew to know and love.
The impetus to create an integrated mental health care approach has been well elucidated by the American Academy of Child and Adolescent Psychiatry (AACAP) in its report, Collaborative mental health care in pediatric primary care. It is based on some telling statistics: Fifty percent of all cases of mental illness begin before age 14 years and 75% begin by age 24. Half of all pediatric office visits involve behavioral, psychosocial, or educational concerns. The American Academy of Pediatrics’ Task Force on Mental Health similarly has stated that primary care clinicians can and should be able to provide mental health services to children and adolescents in a primary care setting.
Integrative psychiatry and primary care treatment comes in three forms: classic consultation, in which a specialist sees a patient and refers back to the PCP with recommendations; colocation, in which mental health specialists practice in the same office but essentially are “ships crossing in the night” with PCPs; and the most-lauded form, collaborative/integrative care, in which back-and-forth consultation and discussions of a case occur between mental health specialists and PCPs, with in-person follow-up as needed.
Several institutions offer programs to address the AACAP and AAP imperatives, most prominently the University of Washington, Seattle, and the University of Massachusetts, Worcester. Both offer resources on how to create an integrated care model (University of Washington AIMS Resource Center; The University of Massachusetts Center for Integrated Care).
What can one do in a busy pediatric primary care practice to address mental health imperatives on the individual provider level? Often PCPs can, as I do, offer families some resources by having a set of mental health handouts and resources. I have gathered useful handouts for families throughout my residency to use as shortcuts and visual aids to promote mental health. I use the AACAP Facts for Families for handouts on mental health diagnoses and topics. I use the National Sleep Foundation for its sleep hygiene tips. I also offer some low-cost mindfulness resources to help kids and parents with their anxiety, such as the Calm app and Headspace app. If parents have difficulty with access to parent management training (the first-line treatment to manage aggression in children), I often recommend “The Defiant Child: A Parent’s Guide to Oppositional Defiant Disorder” (Lanham, Md.: Taylor Trade Publishing, 1997), which shows how to create a rewards system in the home to promote positive behavior. “How to Talk So Kids Will Listen & Listen So Kids Will Talk” (New York: Scribner, 2012 ) is a beloved book for parents (and there is a teenager version) that I recommend when parents launch into questions about how to talk to kids and teens about difficult topics so that, ultimately, they can improve their relationship.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and an assistant professor of psychiatry at UVM, both in Burlington. Email her at [email protected].
Resources
The AACAP website has materials to help clinicians develop a collaborative mental health care model in the primary care setting: Search for “collaboration with primary care.”
The journal Pediatrics also has a useful resource: Improving mental health services in primary care: Reducing administrative and financial barriers to access and collaboration. (2009;123;1248-51).
Teens are all about the sexting
More teenagers are sending and receiving sexts than in previous years, based on data from a meta-analysis of 39 studies including 110,380 individuals younger than 18 years.
Published rates of sexting in teens range from 1% to 60%, wrote Sheri Madigan, PhD, of the University of Calgary, Alberta, Canada, and her colleagues. “However, the true public health importance of youth sexting is unclear at present because the field is handicapped by inconsistent information regarding its prevalence.”
“Higher prevalence rates were found in more recent studies, with older youth, and with youth using a mobile device to sext,” the researchers said.
The increase in sexting among teens should inform sexting legislation, the researchers noted. However, given the increasing use of smartphones among children and the possibility that sexting may be a normal part of sexual behavior in the smartphone era, “efforts and resources to criminalize sexts should be redirected to educational programs on digital citizenship and healthy relationships,” they said. “Given that the mean age of first smartphone acquisition is 10.3 years, it is important for middle school educators, pediatricians, and parents to have ongoing conversations with tweens regarding sexting and digital citizenship.”
The meta-analysis’s results were limited by several factors, such as the focus on frequency of sexting alone and not on elements that might influence sexting behavior, as well as inclusion of relatively few studies on nonconsensual sexting.
The mean age was 15 years (range, 12-17 years). More than half of the studies were from the United States, followed by 12 from Europe, 2 from Australia, 1 from Canada, 1 from South Africa , and 1 study from South Korea.
The researchers had no relevant financial disclosures. The study was supported by the Alberta Children’s Hospital Foundation and the Canada Research Chairs Program.
SOURCE: Madigan S et al. JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5314.
“Sexting is a new behavior that is evolving rapidly, as technology changes and awareness increases,” Elizabeth Englander, PhD, and Meghan McCoy, EdD, wrote.
The current study adds to the limited knowledge about sexting in children and teens and also identifies areas in need of additional study, including the lack of a consistent definition of sexting and differences in sexting activity between males and females. Another challenge is determining the context of sexting, with the recognition that sexting within relationships is different than sexting between unattached individuals, they said. In addition, the study by Madigan et al. emphasized the concern for sexting behaviors among children younger than 12 years of age because children this age are increasingly likely to own cell phones.
Dr. Englander and Dr. McCoy concluded that the current study represents “an important step forward in understanding prevalence, including the prevalence of unauthorized distribution of sexts.”
Dr. Englander and Dr. McCoy are affiliated with the Massachusetts Aggression Reduction Center at Bridgewater (Mass.) State University. They commented in an editorial accompanying the meta-analysis by Madigan et al. (JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5682). They had no relevant financial disclosures.
“Sexting is a new behavior that is evolving rapidly, as technology changes and awareness increases,” Elizabeth Englander, PhD, and Meghan McCoy, EdD, wrote.
The current study adds to the limited knowledge about sexting in children and teens and also identifies areas in need of additional study, including the lack of a consistent definition of sexting and differences in sexting activity between males and females. Another challenge is determining the context of sexting, with the recognition that sexting within relationships is different than sexting between unattached individuals, they said. In addition, the study by Madigan et al. emphasized the concern for sexting behaviors among children younger than 12 years of age because children this age are increasingly likely to own cell phones.
Dr. Englander and Dr. McCoy concluded that the current study represents “an important step forward in understanding prevalence, including the prevalence of unauthorized distribution of sexts.”
Dr. Englander and Dr. McCoy are affiliated with the Massachusetts Aggression Reduction Center at Bridgewater (Mass.) State University. They commented in an editorial accompanying the meta-analysis by Madigan et al. (JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5682). They had no relevant financial disclosures.
“Sexting is a new behavior that is evolving rapidly, as technology changes and awareness increases,” Elizabeth Englander, PhD, and Meghan McCoy, EdD, wrote.
The current study adds to the limited knowledge about sexting in children and teens and also identifies areas in need of additional study, including the lack of a consistent definition of sexting and differences in sexting activity between males and females. Another challenge is determining the context of sexting, with the recognition that sexting within relationships is different than sexting between unattached individuals, they said. In addition, the study by Madigan et al. emphasized the concern for sexting behaviors among children younger than 12 years of age because children this age are increasingly likely to own cell phones.
Dr. Englander and Dr. McCoy concluded that the current study represents “an important step forward in understanding prevalence, including the prevalence of unauthorized distribution of sexts.”
Dr. Englander and Dr. McCoy are affiliated with the Massachusetts Aggression Reduction Center at Bridgewater (Mass.) State University. They commented in an editorial accompanying the meta-analysis by Madigan et al. (JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5682). They had no relevant financial disclosures.
More teenagers are sending and receiving sexts than in previous years, based on data from a meta-analysis of 39 studies including 110,380 individuals younger than 18 years.
Published rates of sexting in teens range from 1% to 60%, wrote Sheri Madigan, PhD, of the University of Calgary, Alberta, Canada, and her colleagues. “However, the true public health importance of youth sexting is unclear at present because the field is handicapped by inconsistent information regarding its prevalence.”
“Higher prevalence rates were found in more recent studies, with older youth, and with youth using a mobile device to sext,” the researchers said.
The increase in sexting among teens should inform sexting legislation, the researchers noted. However, given the increasing use of smartphones among children and the possibility that sexting may be a normal part of sexual behavior in the smartphone era, “efforts and resources to criminalize sexts should be redirected to educational programs on digital citizenship and healthy relationships,” they said. “Given that the mean age of first smartphone acquisition is 10.3 years, it is important for middle school educators, pediatricians, and parents to have ongoing conversations with tweens regarding sexting and digital citizenship.”
The meta-analysis’s results were limited by several factors, such as the focus on frequency of sexting alone and not on elements that might influence sexting behavior, as well as inclusion of relatively few studies on nonconsensual sexting.
The mean age was 15 years (range, 12-17 years). More than half of the studies were from the United States, followed by 12 from Europe, 2 from Australia, 1 from Canada, 1 from South Africa , and 1 study from South Korea.
The researchers had no relevant financial disclosures. The study was supported by the Alberta Children’s Hospital Foundation and the Canada Research Chairs Program.
SOURCE: Madigan S et al. JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5314.
More teenagers are sending and receiving sexts than in previous years, based on data from a meta-analysis of 39 studies including 110,380 individuals younger than 18 years.
Published rates of sexting in teens range from 1% to 60%, wrote Sheri Madigan, PhD, of the University of Calgary, Alberta, Canada, and her colleagues. “However, the true public health importance of youth sexting is unclear at present because the field is handicapped by inconsistent information regarding its prevalence.”
“Higher prevalence rates were found in more recent studies, with older youth, and with youth using a mobile device to sext,” the researchers said.
The increase in sexting among teens should inform sexting legislation, the researchers noted. However, given the increasing use of smartphones among children and the possibility that sexting may be a normal part of sexual behavior in the smartphone era, “efforts and resources to criminalize sexts should be redirected to educational programs on digital citizenship and healthy relationships,” they said. “Given that the mean age of first smartphone acquisition is 10.3 years, it is important for middle school educators, pediatricians, and parents to have ongoing conversations with tweens regarding sexting and digital citizenship.”
The meta-analysis’s results were limited by several factors, such as the focus on frequency of sexting alone and not on elements that might influence sexting behavior, as well as inclusion of relatively few studies on nonconsensual sexting.
The mean age was 15 years (range, 12-17 years). More than half of the studies were from the United States, followed by 12 from Europe, 2 from Australia, 1 from Canada, 1 from South Africa , and 1 study from South Korea.
The researchers had no relevant financial disclosures. The study was supported by the Alberta Children’s Hospital Foundation and the Canada Research Chairs Program.
SOURCE: Madigan S et al. JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5314.
FROM JAMA PEDIATRICS
Key clinical point: Sexting frequency has increased among teens in recent years, and this frequency increases with age.
Major finding:
Study details: The data come from a meta-analysis of 39 studies with 110,380 participants.
Disclosures: The researchers had no financial conflicts to disclose. The study was supported by the Alberta Children’s Hospital Foundation and the Canada Research Chairs Program.
Source: Madigan S et al. JAMA Pediatr. 2018 Feb 26. doi: 10.1001/jamapediatrics.2017.5314.
How to direct refer for GI endoscopy
MAUI, HAWAII – Rheumatologists can save their patients time and the inconvenience of an unnecessary preprocedural office visit with a gastroenterologist by making a direct referral for GI endoscopy when appropriate, according to Uma Mahadevan, MD, professor of medicine at the University of California, San Francisco.
“Many health systems have access issues, and in most accountable care organizations, there’s a need to see patients within 14 days. the gastroenterologist explained at the 2018 Rheumatology Winter Clinical Symposium.

“We’re an open-access endoscopy center at UCSF, and I can’t tell you how many times a patient gets direct referred to us and – the night before the procedure, when we’re preparing for the case – we see that this patient can’t have a procedure tomorrow. Those patients have already done the bowel prep, they’re taking the day off work, they’ve arranged for someone to drive them, and they’re really mad,” said Dr. Mahadevan, who is also the medical director of the UCSF Center for Colitis and Crohn’s Disease.
Sometimes the procedure gets called off because the gastroenterologist sees that it would be inappropriate. For example, it would be inappropriate to perform an endoscopy on a patient with irritable bowel syndrome or fibromyalgia who has already had three negative endoscopic procedures in the past 5 years; alternatively, a screening colonoscopy would be inappropriate for an 80-year-old because the U.S. Preventive Services Task Force gives a class A recommendation for screening colonoscopy only during ages 50-75 years.
Sometimes the physician who made the direct referral failed to include other key information the gastroenterologist needed to have in advance of the procedure. For example, a morbidly obese patient or an individual with significant cardiovascular or pulmonary disease generally needs to have an anesthesiologist present for GI endoscopy, rather than a nurse anesthetist, since the airway is suspect. Similarly, a patient with a severe anxiety disorder or tolerance to pain medication is unlikely to be adequately sedated with the fentanyl and midazolam (Versed) used for moderate sedation in most upper endoscopy and colonoscopy procedures; those individuals are going to require deep sedation with propofol (Diprivan) and assistance in maintaining a patent airway.
“Your patient taking Oxycodone every day is not going to get sedated with fentanyl and midazolam. So you need to put that information on your direct request,” she stressed.
“If your patient has obstructive sleep apnea and is on CPAP at home, or if your patient is on home oxygen, your gastroenterologist needs to know that because those are the patients we bring into the office to evaluate the airway ahead of time,” according to the gastroenterologist.
Also, while routine direct referral for colonoscopy to rule out comorbid inflammatory bowel disease is entirely appropriate in patients with ankylosing spondylitis or other spondyloarthropathies, if they had ankylosing spondylitis in the prebiologic era, then it’s important to include that information.
“If they did, their neck is often dangerous for sedation. They’re very difficult to intubate. That’s something we need to know,” Dr. Mahadevan continued.
Other patient information gastroenterologists want included in the direct referral: Is the patient on daily aspirin and/or a thienopyridine antiplatelet agent or on oral anticoagulation with warfarin or one of the newer direct-acting oral anticoagulants? American Society for Gastrointestinal Endoscopy guidelines have detailed how to manage antithrombotic agents in patients undergoing GI endoscopy, including when and how to bridge with low-molecular-weight heparin in the days prior to the procedure (Gastrointest Endosc. 2016 Jan;83[1]:3-16). Of note, the guidelines rate diagnostic esophagogastroduodenoscopy (EGD) and colonoscopy, even with biopsies taken, as low-bleeding-risk procedures that therefore don’t require stopping antithrombotic therapy.
In addition to screening or surveillance colonoscopy, rheumatologists might also direct refer patients for GI endoscopy because they have iron-deficiency anemia, in which case evaluation by both EGD and colonoscopy is necessary. Direct referral for EGD in patients with celiac disease is appropriate. Acute GI bleeding is best handled via direct referral for colonoscopy in a patient with hematochezia and for EGD in the setting of melena. Direct referral for endoscopy is also warranted in patients with polymyalgia rheumatica or dermatomyositis, where the indication is to rule out associated malignancy.
Dr. Mahadevan reported having no financial conflicts regarding her presentation.
MAUI, HAWAII – Rheumatologists can save their patients time and the inconvenience of an unnecessary preprocedural office visit with a gastroenterologist by making a direct referral for GI endoscopy when appropriate, according to Uma Mahadevan, MD, professor of medicine at the University of California, San Francisco.
“Many health systems have access issues, and in most accountable care organizations, there’s a need to see patients within 14 days. the gastroenterologist explained at the 2018 Rheumatology Winter Clinical Symposium.
“We’re an open-access endoscopy center at UCSF, and I can’t tell you how many times a patient gets direct referred to us and – the night before the procedure, when we’re preparing for the case – we see that this patient can’t have a procedure tomorrow. Those patients have already done the bowel prep, they’re taking the day off work, they’ve arranged for someone to drive them, and they’re really mad,” said Dr. Mahadevan, who is also the medical director of the UCSF Center for Colitis and Crohn’s Disease.
Sometimes the procedure gets called off because the gastroenterologist sees that it would be inappropriate. For example, it would be inappropriate to perform an endoscopy on a patient with irritable bowel syndrome or fibromyalgia who has already had three negative endoscopic procedures in the past 5 years; alternatively, a screening colonoscopy would be inappropriate for an 80-year-old because the U.S. Preventive Services Task Force gives a class A recommendation for screening colonoscopy only during ages 50-75 years.
Sometimes the physician who made the direct referral failed to include other key information the gastroenterologist needed to have in advance of the procedure. For example, a morbidly obese patient or an individual with significant cardiovascular or pulmonary disease generally needs to have an anesthesiologist present for GI endoscopy, rather than a nurse anesthetist, since the airway is suspect. Similarly, a patient with a severe anxiety disorder or tolerance to pain medication is unlikely to be adequately sedated with the fentanyl and midazolam (Versed) used for moderate sedation in most upper endoscopy and colonoscopy procedures; those individuals are going to require deep sedation with propofol (Diprivan) and assistance in maintaining a patent airway.
“Your patient taking Oxycodone every day is not going to get sedated with fentanyl and midazolam. So you need to put that information on your direct request,” she stressed.
“If your patient has obstructive sleep apnea and is on CPAP at home, or if your patient is on home oxygen, your gastroenterologist needs to know that because those are the patients we bring into the office to evaluate the airway ahead of time,” according to the gastroenterologist.
Also, while routine direct referral for colonoscopy to rule out comorbid inflammatory bowel disease is entirely appropriate in patients with ankylosing spondylitis or other spondyloarthropathies, if they had ankylosing spondylitis in the prebiologic era, then it’s important to include that information.
“If they did, their neck is often dangerous for sedation. They’re very difficult to intubate. That’s something we need to know,” Dr. Mahadevan continued.
Other patient information gastroenterologists want included in the direct referral: Is the patient on daily aspirin and/or a thienopyridine antiplatelet agent or on oral anticoagulation with warfarin or one of the newer direct-acting oral anticoagulants? American Society for Gastrointestinal Endoscopy guidelines have detailed how to manage antithrombotic agents in patients undergoing GI endoscopy, including when and how to bridge with low-molecular-weight heparin in the days prior to the procedure (Gastrointest Endosc. 2016 Jan;83[1]:3-16). Of note, the guidelines rate diagnostic esophagogastroduodenoscopy (EGD) and colonoscopy, even with biopsies taken, as low-bleeding-risk procedures that therefore don’t require stopping antithrombotic therapy.
In addition to screening or surveillance colonoscopy, rheumatologists might also direct refer patients for GI endoscopy because they have iron-deficiency anemia, in which case evaluation by both EGD and colonoscopy is necessary. Direct referral for EGD in patients with celiac disease is appropriate. Acute GI bleeding is best handled via direct referral for colonoscopy in a patient with hematochezia and for EGD in the setting of melena. Direct referral for endoscopy is also warranted in patients with polymyalgia rheumatica or dermatomyositis, where the indication is to rule out associated malignancy.
Dr. Mahadevan reported having no financial conflicts regarding her presentation.
MAUI, HAWAII – Rheumatologists can save their patients time and the inconvenience of an unnecessary preprocedural office visit with a gastroenterologist by making a direct referral for GI endoscopy when appropriate, according to Uma Mahadevan, MD, professor of medicine at the University of California, San Francisco.
“Many health systems have access issues, and in most accountable care organizations, there’s a need to see patients within 14 days. the gastroenterologist explained at the 2018 Rheumatology Winter Clinical Symposium.
“We’re an open-access endoscopy center at UCSF, and I can’t tell you how many times a patient gets direct referred to us and – the night before the procedure, when we’re preparing for the case – we see that this patient can’t have a procedure tomorrow. Those patients have already done the bowel prep, they’re taking the day off work, they’ve arranged for someone to drive them, and they’re really mad,” said Dr. Mahadevan, who is also the medical director of the UCSF Center for Colitis and Crohn’s Disease.
Sometimes the procedure gets called off because the gastroenterologist sees that it would be inappropriate. For example, it would be inappropriate to perform an endoscopy on a patient with irritable bowel syndrome or fibromyalgia who has already had three negative endoscopic procedures in the past 5 years; alternatively, a screening colonoscopy would be inappropriate for an 80-year-old because the U.S. Preventive Services Task Force gives a class A recommendation for screening colonoscopy only during ages 50-75 years.
Sometimes the physician who made the direct referral failed to include other key information the gastroenterologist needed to have in advance of the procedure. For example, a morbidly obese patient or an individual with significant cardiovascular or pulmonary disease generally needs to have an anesthesiologist present for GI endoscopy, rather than a nurse anesthetist, since the airway is suspect. Similarly, a patient with a severe anxiety disorder or tolerance to pain medication is unlikely to be adequately sedated with the fentanyl and midazolam (Versed) used for moderate sedation in most upper endoscopy and colonoscopy procedures; those individuals are going to require deep sedation with propofol (Diprivan) and assistance in maintaining a patent airway.
“Your patient taking Oxycodone every day is not going to get sedated with fentanyl and midazolam. So you need to put that information on your direct request,” she stressed.
“If your patient has obstructive sleep apnea and is on CPAP at home, or if your patient is on home oxygen, your gastroenterologist needs to know that because those are the patients we bring into the office to evaluate the airway ahead of time,” according to the gastroenterologist.
Also, while routine direct referral for colonoscopy to rule out comorbid inflammatory bowel disease is entirely appropriate in patients with ankylosing spondylitis or other spondyloarthropathies, if they had ankylosing spondylitis in the prebiologic era, then it’s important to include that information.
“If they did, their neck is often dangerous for sedation. They’re very difficult to intubate. That’s something we need to know,” Dr. Mahadevan continued.
Other patient information gastroenterologists want included in the direct referral: Is the patient on daily aspirin and/or a thienopyridine antiplatelet agent or on oral anticoagulation with warfarin or one of the newer direct-acting oral anticoagulants? American Society for Gastrointestinal Endoscopy guidelines have detailed how to manage antithrombotic agents in patients undergoing GI endoscopy, including when and how to bridge with low-molecular-weight heparin in the days prior to the procedure (Gastrointest Endosc. 2016 Jan;83[1]:3-16). Of note, the guidelines rate diagnostic esophagogastroduodenoscopy (EGD) and colonoscopy, even with biopsies taken, as low-bleeding-risk procedures that therefore don’t require stopping antithrombotic therapy.
In addition to screening or surveillance colonoscopy, rheumatologists might also direct refer patients for GI endoscopy because they have iron-deficiency anemia, in which case evaluation by both EGD and colonoscopy is necessary. Direct referral for EGD in patients with celiac disease is appropriate. Acute GI bleeding is best handled via direct referral for colonoscopy in a patient with hematochezia and for EGD in the setting of melena. Direct referral for endoscopy is also warranted in patients with polymyalgia rheumatica or dermatomyositis, where the indication is to rule out associated malignancy.
Dr. Mahadevan reported having no financial conflicts regarding her presentation.
EXPERT ANALYSIS FROM RWCS 2018
Free testosterone linked to frailty in older men
A new study provides more evidence of a link between lower free testosterone levels and higher levels of frailty in older men, but a researcher says proof of a causal connection remains elusive.
“Our study demonstrates clear associations between testosterone and frailty progression, and, although causality and directionality of the hormone/frailty relationships require clarification, the results presented here make a strong case for large interventional trials of testosterone therapy in frail men to determine whether such treatment would be beneficial,” lead author Agnieszka Swiecicka, MD, of the andrology research unit in the division of diabetes, endocrinology, and gastroenterology at the University of Manchester (England), said in an interview.
As Dr. Swiecicka noted, “in men, testosterone levels decline with age, and it has been suggested that this phenomenon might play a role in the development of frailty.”
However, evidence is limited, and studies have offered conflicting results Dr. Swiecicka said.
For the new study, the researchers prospectively tracked 3,369 community-dwelling men aged 40-79 years from eight European centers. Hundreds were excluded for various reasons or lost to follow-up, and 2,278 men were ultimately included.
The average age was 58 years, and the average body mass index was 28 kg/m2.
Hormone measurements were performed, and frailty was tracked via frailty status (FS, n = 2,278) and frailty phenotype (FP, n = 1,980).
After adjusting their statistics to account for various factors, the researchers were able to link only free testosterone – and not testosterone or dihydrotestosterone – to changes in frailty index (FI). They linked each standard deviation improvement in free testosterone level at baseline to a –2.8% change in FI over 4 years (95% confidence interval, –4.9 to –0.3, P = .030).
“Higher free testosterone levels were associated with a lower risk of worsening frailty status. The direction of this association was consistent regardless of the frailty construct used (FI and FP),” Dr. Swiecicka said. “Higher androgen remained significantly associated with improving frailty status, as assessed by FI, despite age adjustment, suggesting that these relationships cannot be explained by age-related differences in androgen levels.”
Overall, “sex hormones are associated with the development/worsening of frailty in middle-aged and older men, but these relationships vary between different constructs of frailty assessment,” Dr. Swiecicka said. “In light of the findings, a therapeutic role for testosterone in the context of physical frailty prevention or alleviation remains an attractive possibility that should be further explored.”
The study was published in the Journal of Clinical Endocrinology and Metabolism.
In an interview, Steve Borst, PhD, of the University of Florida, questioned the study’s approach because it looks only at baseline hormone levels. “What would be much more interesting to study would be changes in hormone levels vs. changes in frailty,” he said.
Dr. Borst added that researchers already know that “the relationship between testosterone and frailty is both large in magnitude and causal in nature.”
He pointed to his group’s research that linked testosterone injections to an increase in muscle strength, and he said others have linked testosterone administration to an increase in bone density. “While these measures are not exactly the same as frailty index,” he said, “it is well established that lower body muscle strength keeps older people in an independent living state and that the changes in bone mineral density are enough to account for protection against fracture.”
John Morley, MBBCh, of Saint Louis University, said in an interview that testosterone has a role in combating frailty. “But it’s not like it’s going to turn people into super people,” he said.
He added that “we shouldn’t say ‘Let’s do testosterone before we do exercise.’ It’s better to do resistance exercise than it is to take testosterone. But most older males are loath to do any physical work to make themselves better. That’s just human nature.”
The study was funded by various European research-based organizations. The study authors reported multiple disclosures. Dr. Morley reports no disclosures.
SOURCE: Swiecicka A et al. J Clin Endocrinol Metab. 2018 Feb;103(2):701-9.
A new study provides more evidence of a link between lower free testosterone levels and higher levels of frailty in older men, but a researcher says proof of a causal connection remains elusive.
“Our study demonstrates clear associations between testosterone and frailty progression, and, although causality and directionality of the hormone/frailty relationships require clarification, the results presented here make a strong case for large interventional trials of testosterone therapy in frail men to determine whether such treatment would be beneficial,” lead author Agnieszka Swiecicka, MD, of the andrology research unit in the division of diabetes, endocrinology, and gastroenterology at the University of Manchester (England), said in an interview.
As Dr. Swiecicka noted, “in men, testosterone levels decline with age, and it has been suggested that this phenomenon might play a role in the development of frailty.”
However, evidence is limited, and studies have offered conflicting results Dr. Swiecicka said.
For the new study, the researchers prospectively tracked 3,369 community-dwelling men aged 40-79 years from eight European centers. Hundreds were excluded for various reasons or lost to follow-up, and 2,278 men were ultimately included.
The average age was 58 years, and the average body mass index was 28 kg/m2.
Hormone measurements were performed, and frailty was tracked via frailty status (FS, n = 2,278) and frailty phenotype (FP, n = 1,980).
After adjusting their statistics to account for various factors, the researchers were able to link only free testosterone – and not testosterone or dihydrotestosterone – to changes in frailty index (FI). They linked each standard deviation improvement in free testosterone level at baseline to a –2.8% change in FI over 4 years (95% confidence interval, –4.9 to –0.3, P = .030).
“Higher free testosterone levels were associated with a lower risk of worsening frailty status. The direction of this association was consistent regardless of the frailty construct used (FI and FP),” Dr. Swiecicka said. “Higher androgen remained significantly associated with improving frailty status, as assessed by FI, despite age adjustment, suggesting that these relationships cannot be explained by age-related differences in androgen levels.”
Overall, “sex hormones are associated with the development/worsening of frailty in middle-aged and older men, but these relationships vary between different constructs of frailty assessment,” Dr. Swiecicka said. “In light of the findings, a therapeutic role for testosterone in the context of physical frailty prevention or alleviation remains an attractive possibility that should be further explored.”
The study was published in the Journal of Clinical Endocrinology and Metabolism.
In an interview, Steve Borst, PhD, of the University of Florida, questioned the study’s approach because it looks only at baseline hormone levels. “What would be much more interesting to study would be changes in hormone levels vs. changes in frailty,” he said.
Dr. Borst added that researchers already know that “the relationship between testosterone and frailty is both large in magnitude and causal in nature.”
He pointed to his group’s research that linked testosterone injections to an increase in muscle strength, and he said others have linked testosterone administration to an increase in bone density. “While these measures are not exactly the same as frailty index,” he said, “it is well established that lower body muscle strength keeps older people in an independent living state and that the changes in bone mineral density are enough to account for protection against fracture.”
John Morley, MBBCh, of Saint Louis University, said in an interview that testosterone has a role in combating frailty. “But it’s not like it’s going to turn people into super people,” he said.
He added that “we shouldn’t say ‘Let’s do testosterone before we do exercise.’ It’s better to do resistance exercise than it is to take testosterone. But most older males are loath to do any physical work to make themselves better. That’s just human nature.”
The study was funded by various European research-based organizations. The study authors reported multiple disclosures. Dr. Morley reports no disclosures.
SOURCE: Swiecicka A et al. J Clin Endocrinol Metab. 2018 Feb;103(2):701-9.
A new study provides more evidence of a link between lower free testosterone levels and higher levels of frailty in older men, but a researcher says proof of a causal connection remains elusive.
“Our study demonstrates clear associations between testosterone and frailty progression, and, although causality and directionality of the hormone/frailty relationships require clarification, the results presented here make a strong case for large interventional trials of testosterone therapy in frail men to determine whether such treatment would be beneficial,” lead author Agnieszka Swiecicka, MD, of the andrology research unit in the division of diabetes, endocrinology, and gastroenterology at the University of Manchester (England), said in an interview.
As Dr. Swiecicka noted, “in men, testosterone levels decline with age, and it has been suggested that this phenomenon might play a role in the development of frailty.”
However, evidence is limited, and studies have offered conflicting results Dr. Swiecicka said.
For the new study, the researchers prospectively tracked 3,369 community-dwelling men aged 40-79 years from eight European centers. Hundreds were excluded for various reasons or lost to follow-up, and 2,278 men were ultimately included.
The average age was 58 years, and the average body mass index was 28 kg/m2.
Hormone measurements were performed, and frailty was tracked via frailty status (FS, n = 2,278) and frailty phenotype (FP, n = 1,980).
After adjusting their statistics to account for various factors, the researchers were able to link only free testosterone – and not testosterone or dihydrotestosterone – to changes in frailty index (FI). They linked each standard deviation improvement in free testosterone level at baseline to a –2.8% change in FI over 4 years (95% confidence interval, –4.9 to –0.3, P = .030).
“Higher free testosterone levels were associated with a lower risk of worsening frailty status. The direction of this association was consistent regardless of the frailty construct used (FI and FP),” Dr. Swiecicka said. “Higher androgen remained significantly associated with improving frailty status, as assessed by FI, despite age adjustment, suggesting that these relationships cannot be explained by age-related differences in androgen levels.”
Overall, “sex hormones are associated with the development/worsening of frailty in middle-aged and older men, but these relationships vary between different constructs of frailty assessment,” Dr. Swiecicka said. “In light of the findings, a therapeutic role for testosterone in the context of physical frailty prevention or alleviation remains an attractive possibility that should be further explored.”
The study was published in the Journal of Clinical Endocrinology and Metabolism.
In an interview, Steve Borst, PhD, of the University of Florida, questioned the study’s approach because it looks only at baseline hormone levels. “What would be much more interesting to study would be changes in hormone levels vs. changes in frailty,” he said.
Dr. Borst added that researchers already know that “the relationship between testosterone and frailty is both large in magnitude and causal in nature.”
He pointed to his group’s research that linked testosterone injections to an increase in muscle strength, and he said others have linked testosterone administration to an increase in bone density. “While these measures are not exactly the same as frailty index,” he said, “it is well established that lower body muscle strength keeps older people in an independent living state and that the changes in bone mineral density are enough to account for protection against fracture.”
John Morley, MBBCh, of Saint Louis University, said in an interview that testosterone has a role in combating frailty. “But it’s not like it’s going to turn people into super people,” he said.
He added that “we shouldn’t say ‘Let’s do testosterone before we do exercise.’ It’s better to do resistance exercise than it is to take testosterone. But most older males are loath to do any physical work to make themselves better. That’s just human nature.”
The study was funded by various European research-based organizations. The study authors reported multiple disclosures. Dr. Morley reports no disclosures.
SOURCE: Swiecicka A et al. J Clin Endocrinol Metab. 2018 Feb;103(2):701-9.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM
Key clinical point: Free testosterone levels are linked to frailty in older men.
Major finding: For each standard deviation improvement in free testosterone level at baseline, frailty index was 2.8% lower at 4 years. (95% CI, –4.9% to –0.3%, P = .030)
Study details: Prospective cohort study of 3,369 men aged 40-79 years at eight European centers.
Disclosures: The study was funded by various European research-based organizations. The investigators reported multiple disclosures.
Source: Swiecicka A et al. J Clin Endocrinol Metab. 2018 Feb;103(2):701-9.
Breast cancer deaths projected for 2018
Female breast cancer mortality is expected to be about 25.3 per 100,000 women in 2018, with the highest rate in the District of Columbia and the lowest in Utah.
Approximately 40,920 deaths from invasive female breast cancer are predicted in the United States by the American Cancer Society (ACS) in its Cancer Facts & Figures 2018, which is based on analysis of 2001-2015 data from the National Center for Health Statistics. The death rate has declined 39% since its peak in 1989, and over the last 10 years, the annual decline has been 1.8% for white women and 1.5% for black women per year, the ACS said.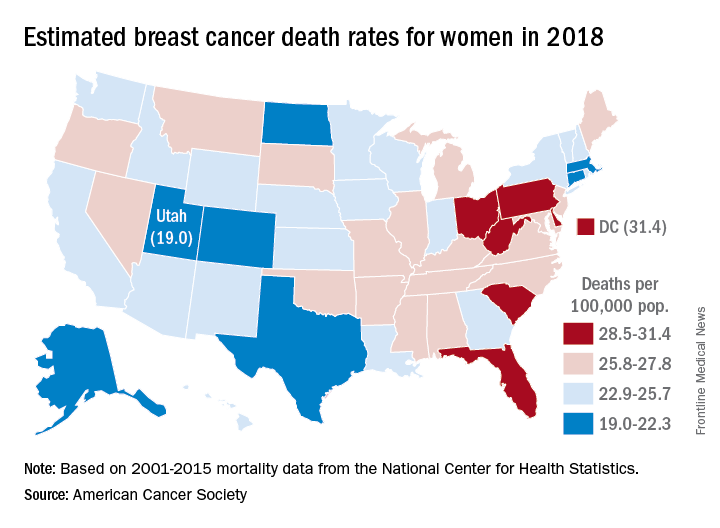
Breast cancer is the most common cancer in women, as it is expected to account for 30% of the almost 880,000 new cancer cases in 2018, compared with 13% for lung cancer, which is second. Lung cancer, however, is projected to cause more deaths among women – 70,500 – than any other cancer, the ACS reported.
Female breast cancer mortality is expected to be about 25.3 per 100,000 women in 2018, with the highest rate in the District of Columbia and the lowest in Utah.
Approximately 40,920 deaths from invasive female breast cancer are predicted in the United States by the American Cancer Society (ACS) in its Cancer Facts & Figures 2018, which is based on analysis of 2001-2015 data from the National Center for Health Statistics. The death rate has declined 39% since its peak in 1989, and over the last 10 years, the annual decline has been 1.8% for white women and 1.5% for black women per year, the ACS said.
Breast cancer is the most common cancer in women, as it is expected to account for 30% of the almost 880,000 new cancer cases in 2018, compared with 13% for lung cancer, which is second. Lung cancer, however, is projected to cause more deaths among women – 70,500 – than any other cancer, the ACS reported.
Female breast cancer mortality is expected to be about 25.3 per 100,000 women in 2018, with the highest rate in the District of Columbia and the lowest in Utah.
Approximately 40,920 deaths from invasive female breast cancer are predicted in the United States by the American Cancer Society (ACS) in its Cancer Facts & Figures 2018, which is based on analysis of 2001-2015 data from the National Center for Health Statistics. The death rate has declined 39% since its peak in 1989, and over the last 10 years, the annual decline has been 1.8% for white women and 1.5% for black women per year, the ACS said.
Breast cancer is the most common cancer in women, as it is expected to account for 30% of the almost 880,000 new cancer cases in 2018, compared with 13% for lung cancer, which is second. Lung cancer, however, is projected to cause more deaths among women – 70,500 – than any other cancer, the ACS reported.
Fluarix Quadrivalent effective in very young, simplifies flu shots for all ages
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”

The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
[email protected]
SOURCE: D-QIV-004.
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”
The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
[email protected]
SOURCE: D-QIV-004.
Fluarix Quadrivalent is highly effective against moderate and severe flu strains in children aged 6-35 months, and has the potential to simplify influenza vaccinations for all ages, according the results of a phase 3 clinical trial presented at a meeting of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices.
“Fluarix Quadrivalent, at the 0.5-mL dose in young children 6 to 35 months of age, demonstrated efficacy of 63.2% against moderate to severe influenza and 49.8% against any severity influenza disease” stated Leonard Friedland, MD, director of scientific affairs and public health, Vaccines North America, GlaxoSmithKline. Dr. Friedland, a pediatrician in Pennsylvania, said that a standard 0.5-mL dose of Fluarix Quadrivalent has practice-changing implications for physicians. “The use of a 0.5-mL dose (15 mcg per strain) for all persons aged 6 months and older potentially simplifies influenza vaccination by allowing the same vaccine dose to be used for all eligible individuals.”
The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, and in preventing moderate to severe influenza, correlated with a reduction in health care utilization by pediatric influenza patients, he said. Visits to general practitioners and emergency departments decreased by 47% and 79%, respectively, in children aged 6-35 months. Influenza-associated antibiotic use in these pediatric influenza patients also decreased by 50%.
These findings were the result of D-QIV-004, a phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months. These children were split into five cohorts, each in a different influenza season. The study spanned 13 countries and ran from October 2011 to December 2014. To determine the safety of Fluarix, the study utilized noninfluenza vaccine comparator vaccines that were age appropriate, including Prevnar 13, Havrix, and Varivax.
A majority of the children in the study (98%) were vaccine unprimed (had never received two doses of seasonal influenza vaccine) and received two doses of Fluarix. The remaining children received one dose.
On Jan. 11, 2018, the Food and Drug Administration expanded the indication of Fluarix Quadrivalent to include use in persons 6 months and older. Previously, it was approved only for persons 3 years and older.
“These study results support universal vaccination of all individuals from 6 months of age [with Fluarix] to prevent influenza.” Dr. Friedland concluded.
For live updates and information concerning influenza, visit the CDC website.
[email protected]
SOURCE: D-QIV-004.
FROM AN ACIP MEETING
Key clinical point: The high efficacy of Fluarix against almost half of all influenza strains, regardless of severity, as well as preventing moderate to severe influenza, reduced health care utilization by pediatric influenza patients.
Major finding: Fluarix Quadrivalent was effective against moderate to severe influenza in 63.2% and against any severity of influenza in 49.8% of children aged 6-35 months.
Study details: A phase 3, observer-blinded, randomized trial of 12,018 children aged 6-35 months, in which the children were split into five cohorts, each in a different influenza season from October 2011 to December 2014.
Disclosures: No disclosures were reported.
Source: The D-QIV-004 study.
Guidelines update best practices for hemorrhoid treatment
Each year, more than 2.2 million patients in the United States undergo evaluations for symptoms of hemorrhoids, according to updated guidelines on the management of hemorrhoids issued by the American Society of Colon and Rectal Surgeons.
“As a result, it is important to identify symptomatic hemorrhoids as the underlying source of the anorectal symptom and to have a clear understanding of the evaluation and management of this disease process,” wrote Bradley R. Davis, MD, FACS, chief of colon and rectal surgery at the Carolinas Medical Center, Charlotte, N.C., and the fellow members of the Clinical Practice Guidelines Committee of the ASCRS.
The guidelines are based on the ASCRS Practice Parameters for the Management of Hemorrhoids published in 2011. The 2018 update was published in the Diseases of the Colon & Rectum.
The guidelines recommend evaluation of hemorrhoids based on a disease-specific history, and a physical that emphasizes the degree and duration of symptoms and identifies risk factors. But the guideline writers note that the recommendation is a grade 1C because the supporting data mainly come from observational or case studies.
“The cardinal signs of internal hemorrhoids are painless bleeding with bowel movements with intermittent protrusion,” the committee said, also emphasizing that patients should be evaluated for fecal incontinence, which could inform surgical decision making.
In addition, the guidelines call for a complete endoscopic evaluation of the colon for patients who present with symptomatic hemorrhoids and rectal bleeding; this recommendation is based on moderately strong evidence, and presented with a grade of 1B.
Medical management of hemorrhoids may include office-based procedures or surgery, according to the guidelines.
“Most patients with grade I and II and select patients with grade III internal hemorrhoidal disease who fail medical treatment can be effectively treated with office-based procedures, such as banding, sclerotherapy, and infrared coagulation,” the committee wrote, and medical office treatment received a strong grade 1A recommendation based on high-quality evidence. Although office procedures are generally well tolerated, the condition can recur. Bleeding is the most common complication, and it is more likely after rubber-band ligation than other office-based options, the guidelines state.
The guidelines offer a weak recommendation of 2C, based on the lack of quality evidence, for the use of early surgical excision to treat patients with thrombosed external hemorrhoids. “Although most patients treated nonoperatively will experience eventual resolution of their symptoms, excision of thrombosed external hemorrhoids may result in more rapid symptom resolution, lower incidence of recurrence, and longer remission intervals,” the committee noted.
Surgical hemorrhoidectomy received the strongest possible recommendation (1A, based on high-quality evidence) for the treatment of patients with external hemorrhoids or a combination of internal and external hemorrhoids with prolapse.
Surgical options described in the recommendations include surgical excision (hemorrhoidectomy), hemorrhoidopexy, and Doppler-guided hemorrhoidectomy, with citations of studies on each procedure. Data from a meta-analysis of 18 randomized prospective studies comparing hemorrhoidectomy with office-based procedures showed that hemorrhoidectomy was “the most effective treatment for patients with grade III hemorrhoids,” but it was associated with greater pain and complication rates, according to the guidelines.
However, complications in general are low after surgical hemorrhoidectomy, with reported complication rates of 1%-2% for the most common complication of postprocedure hemorrhage, the guidelines state. After surgery, the guidelines recommend with a 1B grade (moderate quality evidence) that patients use “a multimodality pain regimen to reduce narcotic usage and promote a faster recovery.”
The committee members had no financial conflicts to disclose.
AGA offers information for your patients about hemorrhoids at http://www.gastro.org/patient-care/conditions-diseases/hemorrhoids.
SOURCE: Davis BR et al. Dis Colon Rectum. 2018; 61:284-92.
Each year, more than 2.2 million patients in the United States undergo evaluations for symptoms of hemorrhoids, according to updated guidelines on the management of hemorrhoids issued by the American Society of Colon and Rectal Surgeons.
“As a result, it is important to identify symptomatic hemorrhoids as the underlying source of the anorectal symptom and to have a clear understanding of the evaluation and management of this disease process,” wrote Bradley R. Davis, MD, FACS, chief of colon and rectal surgery at the Carolinas Medical Center, Charlotte, N.C., and the fellow members of the Clinical Practice Guidelines Committee of the ASCRS.
The guidelines are based on the ASCRS Practice Parameters for the Management of Hemorrhoids published in 2011. The 2018 update was published in the Diseases of the Colon & Rectum.
The guidelines recommend evaluation of hemorrhoids based on a disease-specific history, and a physical that emphasizes the degree and duration of symptoms and identifies risk factors. But the guideline writers note that the recommendation is a grade 1C because the supporting data mainly come from observational or case studies.
“The cardinal signs of internal hemorrhoids are painless bleeding with bowel movements with intermittent protrusion,” the committee said, also emphasizing that patients should be evaluated for fecal incontinence, which could inform surgical decision making.
In addition, the guidelines call for a complete endoscopic evaluation of the colon for patients who present with symptomatic hemorrhoids and rectal bleeding; this recommendation is based on moderately strong evidence, and presented with a grade of 1B.
Medical management of hemorrhoids may include office-based procedures or surgery, according to the guidelines.
“Most patients with grade I and II and select patients with grade III internal hemorrhoidal disease who fail medical treatment can be effectively treated with office-based procedures, such as banding, sclerotherapy, and infrared coagulation,” the committee wrote, and medical office treatment received a strong grade 1A recommendation based on high-quality evidence. Although office procedures are generally well tolerated, the condition can recur. Bleeding is the most common complication, and it is more likely after rubber-band ligation than other office-based options, the guidelines state.
The guidelines offer a weak recommendation of 2C, based on the lack of quality evidence, for the use of early surgical excision to treat patients with thrombosed external hemorrhoids. “Although most patients treated nonoperatively will experience eventual resolution of their symptoms, excision of thrombosed external hemorrhoids may result in more rapid symptom resolution, lower incidence of recurrence, and longer remission intervals,” the committee noted.
Surgical hemorrhoidectomy received the strongest possible recommendation (1A, based on high-quality evidence) for the treatment of patients with external hemorrhoids or a combination of internal and external hemorrhoids with prolapse.
Surgical options described in the recommendations include surgical excision (hemorrhoidectomy), hemorrhoidopexy, and Doppler-guided hemorrhoidectomy, with citations of studies on each procedure. Data from a meta-analysis of 18 randomized prospective studies comparing hemorrhoidectomy with office-based procedures showed that hemorrhoidectomy was “the most effective treatment for patients with grade III hemorrhoids,” but it was associated with greater pain and complication rates, according to the guidelines.
However, complications in general are low after surgical hemorrhoidectomy, with reported complication rates of 1%-2% for the most common complication of postprocedure hemorrhage, the guidelines state. After surgery, the guidelines recommend with a 1B grade (moderate quality evidence) that patients use “a multimodality pain regimen to reduce narcotic usage and promote a faster recovery.”
The committee members had no financial conflicts to disclose.
AGA offers information for your patients about hemorrhoids at http://www.gastro.org/patient-care/conditions-diseases/hemorrhoids.
SOURCE: Davis BR et al. Dis Colon Rectum. 2018; 61:284-92.
Each year, more than 2.2 million patients in the United States undergo evaluations for symptoms of hemorrhoids, according to updated guidelines on the management of hemorrhoids issued by the American Society of Colon and Rectal Surgeons.
“As a result, it is important to identify symptomatic hemorrhoids as the underlying source of the anorectal symptom and to have a clear understanding of the evaluation and management of this disease process,” wrote Bradley R. Davis, MD, FACS, chief of colon and rectal surgery at the Carolinas Medical Center, Charlotte, N.C., and the fellow members of the Clinical Practice Guidelines Committee of the ASCRS.
The guidelines are based on the ASCRS Practice Parameters for the Management of Hemorrhoids published in 2011. The 2018 update was published in the Diseases of the Colon & Rectum.
The guidelines recommend evaluation of hemorrhoids based on a disease-specific history, and a physical that emphasizes the degree and duration of symptoms and identifies risk factors. But the guideline writers note that the recommendation is a grade 1C because the supporting data mainly come from observational or case studies.
“The cardinal signs of internal hemorrhoids are painless bleeding with bowel movements with intermittent protrusion,” the committee said, also emphasizing that patients should be evaluated for fecal incontinence, which could inform surgical decision making.
In addition, the guidelines call for a complete endoscopic evaluation of the colon for patients who present with symptomatic hemorrhoids and rectal bleeding; this recommendation is based on moderately strong evidence, and presented with a grade of 1B.
Medical management of hemorrhoids may include office-based procedures or surgery, according to the guidelines.
“Most patients with grade I and II and select patients with grade III internal hemorrhoidal disease who fail medical treatment can be effectively treated with office-based procedures, such as banding, sclerotherapy, and infrared coagulation,” the committee wrote, and medical office treatment received a strong grade 1A recommendation based on high-quality evidence. Although office procedures are generally well tolerated, the condition can recur. Bleeding is the most common complication, and it is more likely after rubber-band ligation than other office-based options, the guidelines state.
The guidelines offer a weak recommendation of 2C, based on the lack of quality evidence, for the use of early surgical excision to treat patients with thrombosed external hemorrhoids. “Although most patients treated nonoperatively will experience eventual resolution of their symptoms, excision of thrombosed external hemorrhoids may result in more rapid symptom resolution, lower incidence of recurrence, and longer remission intervals,” the committee noted.
Surgical hemorrhoidectomy received the strongest possible recommendation (1A, based on high-quality evidence) for the treatment of patients with external hemorrhoids or a combination of internal and external hemorrhoids with prolapse.
Surgical options described in the recommendations include surgical excision (hemorrhoidectomy), hemorrhoidopexy, and Doppler-guided hemorrhoidectomy, with citations of studies on each procedure. Data from a meta-analysis of 18 randomized prospective studies comparing hemorrhoidectomy with office-based procedures showed that hemorrhoidectomy was “the most effective treatment for patients with grade III hemorrhoids,” but it was associated with greater pain and complication rates, according to the guidelines.
However, complications in general are low after surgical hemorrhoidectomy, with reported complication rates of 1%-2% for the most common complication of postprocedure hemorrhage, the guidelines state. After surgery, the guidelines recommend with a 1B grade (moderate quality evidence) that patients use “a multimodality pain regimen to reduce narcotic usage and promote a faster recovery.”
The committee members had no financial conflicts to disclose.
AGA offers information for your patients about hemorrhoids at http://www.gastro.org/patient-care/conditions-diseases/hemorrhoids.
SOURCE: Davis BR et al. Dis Colon Rectum. 2018; 61:284-92.
FROM DISEASES OF THE COLON & RECTUM