User login
Thinking Outside the Checkbox
A 34-year-old, previously healthy Japanese man developed a dry cough. He did not have dyspnea, nasal discharge, sore throat, facial pain, nasal congestion, or postnasal drip. His symptoms persisted despite several courses of antibiotics (from different physicians), including clarithromycin, minocycline, and levofloxacin. A chest x-ray after 2 months of symptoms and a noncontrast chest computed tomography (CT) after 4 months of symptoms were normal, and bacterial and mycobacterial sputum cultures were sterile. Treatment with salmeterol and fluticasone was ineffective.
The persistence of a cough for longer than 8 weeks constitutes chronic cough. The initial negative review of systems argues against several of the usual etiologies. The lack of nasal discharge, sore throat, facial pain, nasal congestion, and postnasal drip lessens the probability of upper airway cough syndrome. The absence of dyspnea decreases the likelihood of congestive heart failure, asthma, or chronic obstructive pulmonary disease. Additional history should include whether the patient has orthopnea, paroxysmal nocturnal dyspnea, or a reduced exercise tolerance.
The persistence of symptoms despite multiple courses of antibiotics suggests that the process is inflammatory but not infectious, that the infection is not susceptible to the selected antibiotics, that the antibiotics cannot penetrate the site of infection, or that the ongoing symptoms are related to the antibiotics themselves. Pathogens that may cause chronic cough for months include mycobacteria, fungi (eg, Aspergillus , endemic mycoses), and parasites (eg, Strongyloides , Paragonimus ). Even when appropriately treated, many infections may result in a prolonged cough (eg, pertussis). The fluoroquinolone and macrolide exposure may have suppressed the mycobacterial cultures. The lack of response to salmeterol and fluticasone lessens the probability of asthma.
After 4 months of symptoms, his cough worsened, and he developed dysphagia and odynophagia, particularly when he initiated swallowing. He experienced daily fevers with temperatures between 38.0°C and 38.5°C. A repeat chest x-ray was normal. His white blood cell count was 14,200 per μL, and the C-reactive protein (CRP) was 12.91 mg/dL (normal <0.24 mg/dL). His symptoms did not improve with additional courses of clarithromycin, levofloxacin, or moxifloxacin. After 5 months of symptoms, he was referred to the internal medicine clinic of a teaching hospital in Japan.
The patient’s fevers, leukocytosis, and elevated CRP signal an inflammatory process, but whether it is infectious or not remains uncertain. The normal repeat chest x-ray lessens the likelihood of a pulmonary infection. Difficulty with initiating a swallow characterizes oropharyngeal dysphagia which features coughing or choking with oral intake and is typically caused by neuromuscular conditions like stroke, amyotrophic lateral sclerosis, or myasthenia gravis. The coexistence of oropharyngeal dysphagia and odynophagia may indicate pharyngitis, a retropharyngeal or parapharyngeal abscess, or oropharyngeal cancer.
Esophageal dysphagia occurs several seconds following swallow initiation and may arise with mucosal, smooth muscle, or neuromuscular diseases of the esophagus. Concomitant dysphagia and odynophagia may indicate esophageal spasm or esophagitis. Causes of esophagitis include infection (eg, candidiasis, herpes simplex virus [HSV], cytomegalovirus [CMV], or human immunodeficiency virus [HIV]), infiltration (eg, eosinophilic esophagitis), or irritation (eg, from medication, caustic ingestion, or gastroesophageal reflux). He is at risk for esophageal candidiasis following multiple courses of antibiotics. Esophageal dysphagia occurring with liquids and solids may indicate disordered motility, as opposed to dysphagia with solids alone, which may signal endoluminal obstruction.
At his outpatient evaluation, he denied headache, vision changes, chest pain, hemoptysis, palpitations, abdominal pain, dysuria, musculoskeletal symptoms, anorexia, or symptoms of gastroesophageal reflux. He did not have chills, rigors, or night sweats, but he had lost 3.4 kg in 5 months. He had not traveled within or outside of Japan in many years and was not involved in outdoor activities. He was engaged to and monogamous with his female partner of 5 years. He smoked 10 cigarettes per day for 14 years but stopped smoking during the last 2 months on account of his symptoms. He drank 6 beers per month and worked as a researcher at a chemical company but did not have any inhalational exposures.
His weight loss could be from reduced caloric intake due to dysphagia and odynophagia or may reflect an energy deficit related to chronic illness and inflammatory state. His smoking history increases his risk of bronchopulmonary infection and malignancy. Bronchogenic carcinoma may present with chronic cough, fevers, weight loss, or dysphagia from external compression by lymphadenopathy or mediastinal disease; however, his young age and recent chest CT results make lung cancer unlikely.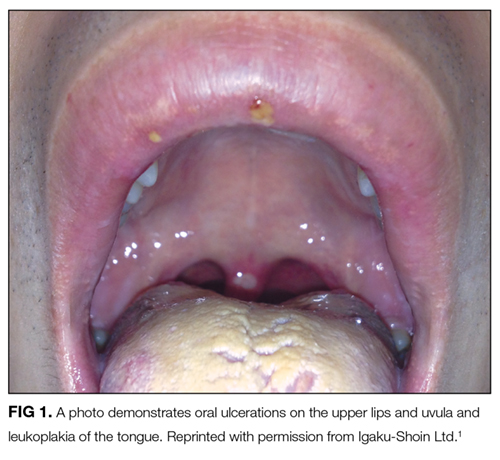
The white coating on his tongue could reflect oral leukoplakia, a reactive and potentially precancerous process that typically manifests as patches or plaques on oral mucosa. It can be distinguished from candidiasis, which scrapes off using a tongue blade. The extensive tongue coating is consistent with oral candidiasis. Potential predispositions include inhaled corticosteroids, antibiotic exposure, and/or an undiagnosed immunodeficiency syndrome (eg, HIV).
The initial diagnostic branch point for nontraumatic oral ulcers is infectious versus noninfectious. Infections that cause oral ulcers include HSV, CMV, and syphilis. The appearance and occurrence of the ulcers on freely moveable mucosa are consistent with aphthous stomatitis. Recurrent aphthous ulcers may occur in autoimmune diseases, including Behçet disease, Crohn disease, celiac sprue, and reactive arthritis. An endoscopy should be considered to detect esophageal ulcerations or esophageal candidiasis.
The rash may indicate folliculitis, usually attributable to Staphylococcus aureus or to Pseudomonas in the setting of recreational water exposure. Broad-spectrum antibiotics or immunodeficiency predisposes to candida folliculitis, while systemic candidiasis may cause metastatic skin lesions. The most common cutaneous manifestation of Behçet disease is erythema nodosum, but follicular and papulopustular lesions are also characteristic.

Pulmonary nodules are caused by infections, noninfectious inflammation, and malignancy. Infectious causes of pulmonary nodules include septic emboli, bacterial abscesses, and mycobacterial and fungal infection; noninfectious inflammatory causes include vasculitis (eg, granulomatosis with polyangiitis), rheumatoid arthritis, sarcoidosis, and lymphomatoid granulomatosis. Although additional culture data, serologic testing, and tuberculin skin testing or an interferon-gamma release assay may help to exclude these infections, the chronicity of symptoms, and lack of response to multiple antibiotic courses favor a noninfectious etiology.
Thickening of the aorta and left pulmonary artery may arise from an infectious, infiltrative, or inflammatory process. Arterial infections arise from direct inoculation, such as catheterization, trauma, or a contiguous site of infection, or from embolic seeding of atherosclerotic plaques or aneurysms. Malignant and nonmalignant processes, including sarcomas, lymphomas, histiocytoses (eg, Erdheim–Chester disease), and IgG4-related disease, may infiltrate the vascular walls. He has no evidence of visceral organ involvement to suggest these multisystem diagnoses.
The combined involvement of the aorta and pulmonary artery suggest a large-vessel vasculitis. Giant cell arteritis is exceedingly rare in patients younger than 50. Takayasu arteritis is a large-vessel vasculitis that predominantly affects women and may present with hypertension, arterial bruits, or discrepant blood pressure between arms, none of which were reported in this case. Behçet disease affects blood vessels of all sizes, including the aorta and pulmonary vasculature. His fevers, oral ulcers, perifollicular rash, and lymphadenopathy are consistent with this diagnosis, although he lacks the genital ulcers that occur in the majority of patients. Pulmonary nodules in Behçet disease arise from pulmonary or pleural vasculitis, resulting in focal inflammation, hemorrhage, or infarction. An ophthalmologic examination for uveitis and a pathergy test would support this diagnosis.
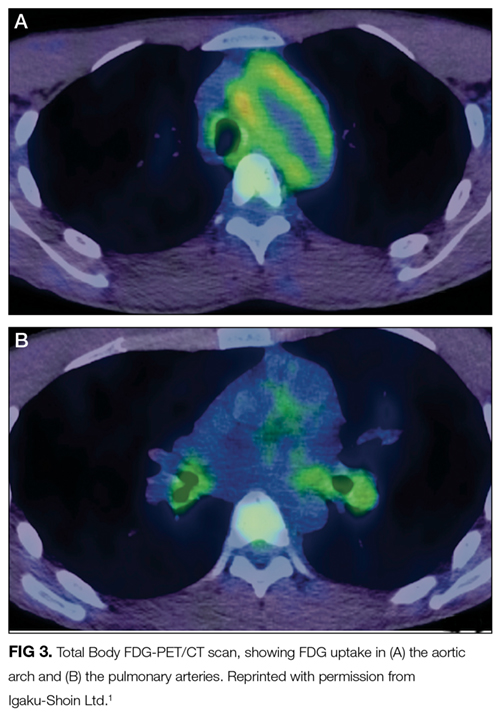
FDG accumulation in the aorta and pulmonary arteries signals large-vessel inflammation. The lack of FDG-avidity of the ground-glass opacities and nodular lesion suggests that these are not metabolically active tumors or infections but may be sequelae of the underlying disease, such as a hemorrhage or infarction from vasculitis. Sarcoidosis could account for the lung findings, but large-vessel vasculopathy would be exceedingly uncommon. Microscopic polyangiitis and granulomatosis with polyangiitis also cause pulmonary and vascular inflammation, but the nonreactive ANCA, absence of sinus disease, and normal urinalysis and kidney function make pauci-immune vasculitis unlikely. While the large-vessel involvement is consistent with Takayasu arteritis, the oral ulcers and rash are not.
Despite the absence of uveitis and the negative pathergy test, his oral aphthosis, papulopustular rash, and large-vessel vasculitis make Behçet disease the likely diagnosis. Behçet disease is most strongly associated with HLA B51, although other HLA haplotypes (including HLA A26 and HLA B52) are frequent in Behçet disease as well. As aortitis and pulmonary vasculitis can be associated with substantial morbidity and mortality, an urgent consultation with a rheumatologist regarding the initiation of immunosuppression is warranted.
Based on the mucocutaneous lesions, radiologic findings consistent with large-vessel vasculitis, and positive HLA A26 and HLA B52, he was diagnosed with Behçet disease. After 1 week of treatment with prednisolone 60 mg daily, his cough resolved and the oral aphthous ulcers and papulopustular rash improved. One month later, a chest CT showed significant reduction of the wall thickening of the aorta, its branches, and of the left pulmonary artery. The nodular lesion in the left lower lobe was unchanged, but the ground-glass opacities in the left upper lobe had disappeared.
When prednisolone was tapered down to 17.5 mg, his dry cough and low-grade fevers recurred, along with a slight elevation of inflammatory markers, and a ground-glass opacity appeared on the periphery of the left upper lobe. A sputum culture and fungal antigens were negative. His cough improved with the resumption of the previous dose of prednisolone. He remained symptom-free after 2 years of treatment with azathioprine 150 mg daily and prednisolone 2 mg daily and is now only treated with azathioprine.
DISCUSSION
Behçet disease is a multisystem vasculitis involving blood vessels of all sizes in the arterial and venous circulation that presents with oral and genital ulcers, ocular abnormalities (uveitis, retinitis), skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”), pathergy, and vascular lesions (thrombophlebitis, thrombosis, and aneurysm).
This patient presented with a chronic cough from pulmonary involvement by Behçet disease. The most common presenting symptom in a study of 47 patients with Behçet disease with pulmonary arteriopathy was hemoptysis followed by a nonbloody cough.2 Among these patients with pulmonary artery aneurysm, thrombosis, or both, 40 (85%) had nodules caused by infarction or inflammation and 21 (45%) had ground-glass opacities attributed to intraparenchymal hemorrhage. There are several case reports of chronic cough attributed to large-vessel vasculitis.3-5 Although the pathology of vasculitis-related cough is not fully understood, the inflammation of large vessels (aorta and pulmonary arteries) adjacent to the tracheobronchial tree may irritate regional cough receptors.3
Disease classification criteria are common in rheumatologic diseases; these criteria are developed to categorize patients for research studies and are not intended to diagnose individual patients.6 The classification criteria favor increased specificity at the expense of sensitivity to avoid misclassifying patients as having a disease, which would compromise the results of research studies. For instance, a study assessing a treatment for Behçet disease must exclude patients with inflammatory bowel disease, as these distinct patient populations may demonstrate discrepant responses to the investigative therapy. The specificity and homogeneity favored by classification criteria make those criteria inappropriate to rely on exclusively for the diagnosis of individual patients.7 The symptoms of many autoimmune diseases develop sequentially over time. Waiting for a patient with active, multisystem vasculitis to fulfill all of the Behçet disease classification criteria can lead to the harmful withholding of disease-modifying treatment.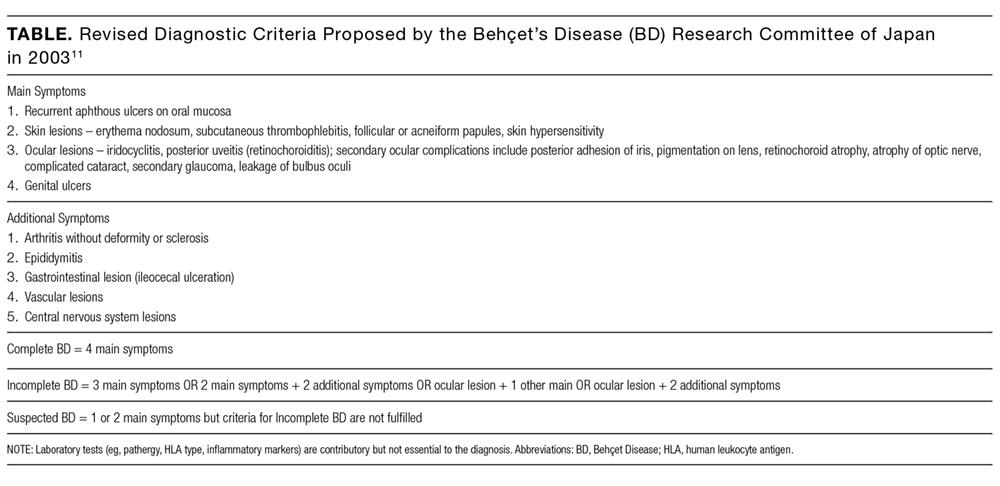
The diagnosis of Behçet disease is made on clinical grounds; there is no gold standard test or histopathologic finding, and classification criteria remain imperfect. Although classification criteria help clinicians understand cardinal disease features, they cannot substitute for the more complex clinical reasoning required to establish a working diagnosis. The clinician must understand the pretest probability of disease, consider the presence or absence of characteristic features, exclude competing diagnoses, and decipher the risk-to-benefit ratio of therapeutic options and the urgency of treatment when assigning a diagnostic label. This patient’s pneumonitis, mucocutaneous changes, aortopathy, and compatible HLA typing (coupled with the exclusion of infectious diseases) were sufficient to diagnose Behçet disease. This case reminds us that classification criteria serve as a starting point, not as an end point, and that clinicians must ultimately make diagnoses and initiate treatment by thinking outside the checkbox.
TEACHING POINTS
- Large-vessel vasculitis is a rare cause of chronic cough.
- Although the most well-recognized signs of Behçet disease include genital and oral ulcers and uveitis, patients may also present with less common manifestations such as skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”) and vascular lesions of the artery (arteritis and aneurysm) and veins (thrombophlebitis and thrombosis).
- Classification criteria capture cardinal features of a disease but favor specificity over sensitivity and should not serve as a checklist for diagnosing a patient.
Acknowledgment
A brief version of this case was published as a case report in the Journal of Integrated Medicine 2013;23(12):1014-1017. Images from that publication were republished here with the permission of the publisher (Igaku-Shoin Ltd).
Disclosure
Dr. Dhaliwal reports receiving honoraria from ISMIE Mutual Insurance Company and Physicians’ Reciprocal Insurers. All other authors have nothing to disclose.
1. Kanamori M, Kubo T, Sakemi H. What’s your diagnosis? [in Japanese] J Integrated Med. 2013; 23 (12):1014-1017.
2. Seyahi E, Melikoglu M, Akman C, et al. Pulmonary artery involvement and associated lung disease in Behçet disease: a series of 47 patients. Medicine (Baltimore). 2012;91(1):35-48. PubMed
3. Olopade CO, Sekosan M, Schraufnagel DE. Giant cell arteritis manifesting as chronic cough and fever of unknown origin. Mayo Clin Proc. 1997;72(11):1048-1050. PubMed
4. Hellmann DB. Temporal arteritis: a cough, toothache, and tongue infarction. JAMA. 2002;287(22):2996-3000. PubMed
5. Karagiannis A, Mathiopoulou L, Tziomalos K, et al. Dry cough as first manifestation of giant-cell arteritis. J Am Geriatr Soc. 2006;54(12):1957-1958. PubMed
6. Aggarwal R, Ringold S, Khanna D, et al. Distinctions between diagnostic and classification criteria? Arthritis Care Res (Hoboken). 2015;67(7):891-897. PubMed
7. Rao JK, Allen NB, Pincus T. Limitations of the 1990 American College of Rheumatology classification criteria in the diagnosis of vasculitis. Ann Intern Med. 1998;129(5):345-352. PubMed
8. Davatchi F, Sadeghi Abdollahi B, Shahram F, Chams-Davatchi C, Shams H, Nadji A. Classification and Diagnosis Criteria for Behçet’s Disease. In: Emmi L, ed. Behçet’s Syndrome. From Pathogenesis to Treatment. Milan, Italy: Springer; 2014:189-198.
9. Criteria for diagnosis of Behcet’s disease. International Study Group for Behçet’s Disease. Lancet. 1990;335(8697):1078-1080. PubMed
10. Davatchi F, Assaad-Khalil S, Calamia KT, et al. The International Criteria for Behçet’s Disease (ICBD): a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014;28(3):338–347. PubMed
11. Suzuki Kurokawa M, Suzuki N. Behçet’s disease. Clin Exp Med. 2004;4(1):10-20. PubMed
A 34-year-old, previously healthy Japanese man developed a dry cough. He did not have dyspnea, nasal discharge, sore throat, facial pain, nasal congestion, or postnasal drip. His symptoms persisted despite several courses of antibiotics (from different physicians), including clarithromycin, minocycline, and levofloxacin. A chest x-ray after 2 months of symptoms and a noncontrast chest computed tomography (CT) after 4 months of symptoms were normal, and bacterial and mycobacterial sputum cultures were sterile. Treatment with salmeterol and fluticasone was ineffective.
The persistence of a cough for longer than 8 weeks constitutes chronic cough. The initial negative review of systems argues against several of the usual etiologies. The lack of nasal discharge, sore throat, facial pain, nasal congestion, and postnasal drip lessens the probability of upper airway cough syndrome. The absence of dyspnea decreases the likelihood of congestive heart failure, asthma, or chronic obstructive pulmonary disease. Additional history should include whether the patient has orthopnea, paroxysmal nocturnal dyspnea, or a reduced exercise tolerance.
The persistence of symptoms despite multiple courses of antibiotics suggests that the process is inflammatory but not infectious, that the infection is not susceptible to the selected antibiotics, that the antibiotics cannot penetrate the site of infection, or that the ongoing symptoms are related to the antibiotics themselves. Pathogens that may cause chronic cough for months include mycobacteria, fungi (eg, Aspergillus , endemic mycoses), and parasites (eg, Strongyloides , Paragonimus ). Even when appropriately treated, many infections may result in a prolonged cough (eg, pertussis). The fluoroquinolone and macrolide exposure may have suppressed the mycobacterial cultures. The lack of response to salmeterol and fluticasone lessens the probability of asthma.
After 4 months of symptoms, his cough worsened, and he developed dysphagia and odynophagia, particularly when he initiated swallowing. He experienced daily fevers with temperatures between 38.0°C and 38.5°C. A repeat chest x-ray was normal. His white blood cell count was 14,200 per μL, and the C-reactive protein (CRP) was 12.91 mg/dL (normal <0.24 mg/dL). His symptoms did not improve with additional courses of clarithromycin, levofloxacin, or moxifloxacin. After 5 months of symptoms, he was referred to the internal medicine clinic of a teaching hospital in Japan.
The patient’s fevers, leukocytosis, and elevated CRP signal an inflammatory process, but whether it is infectious or not remains uncertain. The normal repeat chest x-ray lessens the likelihood of a pulmonary infection. Difficulty with initiating a swallow characterizes oropharyngeal dysphagia which features coughing or choking with oral intake and is typically caused by neuromuscular conditions like stroke, amyotrophic lateral sclerosis, or myasthenia gravis. The coexistence of oropharyngeal dysphagia and odynophagia may indicate pharyngitis, a retropharyngeal or parapharyngeal abscess, or oropharyngeal cancer.
Esophageal dysphagia occurs several seconds following swallow initiation and may arise with mucosal, smooth muscle, or neuromuscular diseases of the esophagus. Concomitant dysphagia and odynophagia may indicate esophageal spasm or esophagitis. Causes of esophagitis include infection (eg, candidiasis, herpes simplex virus [HSV], cytomegalovirus [CMV], or human immunodeficiency virus [HIV]), infiltration (eg, eosinophilic esophagitis), or irritation (eg, from medication, caustic ingestion, or gastroesophageal reflux). He is at risk for esophageal candidiasis following multiple courses of antibiotics. Esophageal dysphagia occurring with liquids and solids may indicate disordered motility, as opposed to dysphagia with solids alone, which may signal endoluminal obstruction.
At his outpatient evaluation, he denied headache, vision changes, chest pain, hemoptysis, palpitations, abdominal pain, dysuria, musculoskeletal symptoms, anorexia, or symptoms of gastroesophageal reflux. He did not have chills, rigors, or night sweats, but he had lost 3.4 kg in 5 months. He had not traveled within or outside of Japan in many years and was not involved in outdoor activities. He was engaged to and monogamous with his female partner of 5 years. He smoked 10 cigarettes per day for 14 years but stopped smoking during the last 2 months on account of his symptoms. He drank 6 beers per month and worked as a researcher at a chemical company but did not have any inhalational exposures.
His weight loss could be from reduced caloric intake due to dysphagia and odynophagia or may reflect an energy deficit related to chronic illness and inflammatory state. His smoking history increases his risk of bronchopulmonary infection and malignancy. Bronchogenic carcinoma may present with chronic cough, fevers, weight loss, or dysphagia from external compression by lymphadenopathy or mediastinal disease; however, his young age and recent chest CT results make lung cancer unlikely.
The white coating on his tongue could reflect oral leukoplakia, a reactive and potentially precancerous process that typically manifests as patches or plaques on oral mucosa. It can be distinguished from candidiasis, which scrapes off using a tongue blade. The extensive tongue coating is consistent with oral candidiasis. Potential predispositions include inhaled corticosteroids, antibiotic exposure, and/or an undiagnosed immunodeficiency syndrome (eg, HIV).
The initial diagnostic branch point for nontraumatic oral ulcers is infectious versus noninfectious. Infections that cause oral ulcers include HSV, CMV, and syphilis. The appearance and occurrence of the ulcers on freely moveable mucosa are consistent with aphthous stomatitis. Recurrent aphthous ulcers may occur in autoimmune diseases, including Behçet disease, Crohn disease, celiac sprue, and reactive arthritis. An endoscopy should be considered to detect esophageal ulcerations or esophageal candidiasis.
The rash may indicate folliculitis, usually attributable to Staphylococcus aureus or to Pseudomonas in the setting of recreational water exposure. Broad-spectrum antibiotics or immunodeficiency predisposes to candida folliculitis, while systemic candidiasis may cause metastatic skin lesions. The most common cutaneous manifestation of Behçet disease is erythema nodosum, but follicular and papulopustular lesions are also characteristic.
Pulmonary nodules are caused by infections, noninfectious inflammation, and malignancy. Infectious causes of pulmonary nodules include septic emboli, bacterial abscesses, and mycobacterial and fungal infection; noninfectious inflammatory causes include vasculitis (eg, granulomatosis with polyangiitis), rheumatoid arthritis, sarcoidosis, and lymphomatoid granulomatosis. Although additional culture data, serologic testing, and tuberculin skin testing or an interferon-gamma release assay may help to exclude these infections, the chronicity of symptoms, and lack of response to multiple antibiotic courses favor a noninfectious etiology.
Thickening of the aorta and left pulmonary artery may arise from an infectious, infiltrative, or inflammatory process. Arterial infections arise from direct inoculation, such as catheterization, trauma, or a contiguous site of infection, or from embolic seeding of atherosclerotic plaques or aneurysms. Malignant and nonmalignant processes, including sarcomas, lymphomas, histiocytoses (eg, Erdheim–Chester disease), and IgG4-related disease, may infiltrate the vascular walls. He has no evidence of visceral organ involvement to suggest these multisystem diagnoses.
The combined involvement of the aorta and pulmonary artery suggest a large-vessel vasculitis. Giant cell arteritis is exceedingly rare in patients younger than 50. Takayasu arteritis is a large-vessel vasculitis that predominantly affects women and may present with hypertension, arterial bruits, or discrepant blood pressure between arms, none of which were reported in this case. Behçet disease affects blood vessels of all sizes, including the aorta and pulmonary vasculature. His fevers, oral ulcers, perifollicular rash, and lymphadenopathy are consistent with this diagnosis, although he lacks the genital ulcers that occur in the majority of patients. Pulmonary nodules in Behçet disease arise from pulmonary or pleural vasculitis, resulting in focal inflammation, hemorrhage, or infarction. An ophthalmologic examination for uveitis and a pathergy test would support this diagnosis.
FDG accumulation in the aorta and pulmonary arteries signals large-vessel inflammation. The lack of FDG-avidity of the ground-glass opacities and nodular lesion suggests that these are not metabolically active tumors or infections but may be sequelae of the underlying disease, such as a hemorrhage or infarction from vasculitis. Sarcoidosis could account for the lung findings, but large-vessel vasculopathy would be exceedingly uncommon. Microscopic polyangiitis and granulomatosis with polyangiitis also cause pulmonary and vascular inflammation, but the nonreactive ANCA, absence of sinus disease, and normal urinalysis and kidney function make pauci-immune vasculitis unlikely. While the large-vessel involvement is consistent with Takayasu arteritis, the oral ulcers and rash are not.
Despite the absence of uveitis and the negative pathergy test, his oral aphthosis, papulopustular rash, and large-vessel vasculitis make Behçet disease the likely diagnosis. Behçet disease is most strongly associated with HLA B51, although other HLA haplotypes (including HLA A26 and HLA B52) are frequent in Behçet disease as well. As aortitis and pulmonary vasculitis can be associated with substantial morbidity and mortality, an urgent consultation with a rheumatologist regarding the initiation of immunosuppression is warranted.
Based on the mucocutaneous lesions, radiologic findings consistent with large-vessel vasculitis, and positive HLA A26 and HLA B52, he was diagnosed with Behçet disease. After 1 week of treatment with prednisolone 60 mg daily, his cough resolved and the oral aphthous ulcers and papulopustular rash improved. One month later, a chest CT showed significant reduction of the wall thickening of the aorta, its branches, and of the left pulmonary artery. The nodular lesion in the left lower lobe was unchanged, but the ground-glass opacities in the left upper lobe had disappeared.
When prednisolone was tapered down to 17.5 mg, his dry cough and low-grade fevers recurred, along with a slight elevation of inflammatory markers, and a ground-glass opacity appeared on the periphery of the left upper lobe. A sputum culture and fungal antigens were negative. His cough improved with the resumption of the previous dose of prednisolone. He remained symptom-free after 2 years of treatment with azathioprine 150 mg daily and prednisolone 2 mg daily and is now only treated with azathioprine.
DISCUSSION
Behçet disease is a multisystem vasculitis involving blood vessels of all sizes in the arterial and venous circulation that presents with oral and genital ulcers, ocular abnormalities (uveitis, retinitis), skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”), pathergy, and vascular lesions (thrombophlebitis, thrombosis, and aneurysm).
This patient presented with a chronic cough from pulmonary involvement by Behçet disease. The most common presenting symptom in a study of 47 patients with Behçet disease with pulmonary arteriopathy was hemoptysis followed by a nonbloody cough.2 Among these patients with pulmonary artery aneurysm, thrombosis, or both, 40 (85%) had nodules caused by infarction or inflammation and 21 (45%) had ground-glass opacities attributed to intraparenchymal hemorrhage. There are several case reports of chronic cough attributed to large-vessel vasculitis.3-5 Although the pathology of vasculitis-related cough is not fully understood, the inflammation of large vessels (aorta and pulmonary arteries) adjacent to the tracheobronchial tree may irritate regional cough receptors.3
Disease classification criteria are common in rheumatologic diseases; these criteria are developed to categorize patients for research studies and are not intended to diagnose individual patients.6 The classification criteria favor increased specificity at the expense of sensitivity to avoid misclassifying patients as having a disease, which would compromise the results of research studies. For instance, a study assessing a treatment for Behçet disease must exclude patients with inflammatory bowel disease, as these distinct patient populations may demonstrate discrepant responses to the investigative therapy. The specificity and homogeneity favored by classification criteria make those criteria inappropriate to rely on exclusively for the diagnosis of individual patients.7 The symptoms of many autoimmune diseases develop sequentially over time. Waiting for a patient with active, multisystem vasculitis to fulfill all of the Behçet disease classification criteria can lead to the harmful withholding of disease-modifying treatment.
The diagnosis of Behçet disease is made on clinical grounds; there is no gold standard test or histopathologic finding, and classification criteria remain imperfect. Although classification criteria help clinicians understand cardinal disease features, they cannot substitute for the more complex clinical reasoning required to establish a working diagnosis. The clinician must understand the pretest probability of disease, consider the presence or absence of characteristic features, exclude competing diagnoses, and decipher the risk-to-benefit ratio of therapeutic options and the urgency of treatment when assigning a diagnostic label. This patient’s pneumonitis, mucocutaneous changes, aortopathy, and compatible HLA typing (coupled with the exclusion of infectious diseases) were sufficient to diagnose Behçet disease. This case reminds us that classification criteria serve as a starting point, not as an end point, and that clinicians must ultimately make diagnoses and initiate treatment by thinking outside the checkbox.
TEACHING POINTS
- Large-vessel vasculitis is a rare cause of chronic cough.
- Although the most well-recognized signs of Behçet disease include genital and oral ulcers and uveitis, patients may also present with less common manifestations such as skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”) and vascular lesions of the artery (arteritis and aneurysm) and veins (thrombophlebitis and thrombosis).
- Classification criteria capture cardinal features of a disease but favor specificity over sensitivity and should not serve as a checklist for diagnosing a patient.
Acknowledgment
A brief version of this case was published as a case report in the Journal of Integrated Medicine 2013;23(12):1014-1017. Images from that publication were republished here with the permission of the publisher (Igaku-Shoin Ltd).
Disclosure
Dr. Dhaliwal reports receiving honoraria from ISMIE Mutual Insurance Company and Physicians’ Reciprocal Insurers. All other authors have nothing to disclose.
A 34-year-old, previously healthy Japanese man developed a dry cough. He did not have dyspnea, nasal discharge, sore throat, facial pain, nasal congestion, or postnasal drip. His symptoms persisted despite several courses of antibiotics (from different physicians), including clarithromycin, minocycline, and levofloxacin. A chest x-ray after 2 months of symptoms and a noncontrast chest computed tomography (CT) after 4 months of symptoms were normal, and bacterial and mycobacterial sputum cultures were sterile. Treatment with salmeterol and fluticasone was ineffective.
The persistence of a cough for longer than 8 weeks constitutes chronic cough. The initial negative review of systems argues against several of the usual etiologies. The lack of nasal discharge, sore throat, facial pain, nasal congestion, and postnasal drip lessens the probability of upper airway cough syndrome. The absence of dyspnea decreases the likelihood of congestive heart failure, asthma, or chronic obstructive pulmonary disease. Additional history should include whether the patient has orthopnea, paroxysmal nocturnal dyspnea, or a reduced exercise tolerance.
The persistence of symptoms despite multiple courses of antibiotics suggests that the process is inflammatory but not infectious, that the infection is not susceptible to the selected antibiotics, that the antibiotics cannot penetrate the site of infection, or that the ongoing symptoms are related to the antibiotics themselves. Pathogens that may cause chronic cough for months include mycobacteria, fungi (eg, Aspergillus , endemic mycoses), and parasites (eg, Strongyloides , Paragonimus ). Even when appropriately treated, many infections may result in a prolonged cough (eg, pertussis). The fluoroquinolone and macrolide exposure may have suppressed the mycobacterial cultures. The lack of response to salmeterol and fluticasone lessens the probability of asthma.
After 4 months of symptoms, his cough worsened, and he developed dysphagia and odynophagia, particularly when he initiated swallowing. He experienced daily fevers with temperatures between 38.0°C and 38.5°C. A repeat chest x-ray was normal. His white blood cell count was 14,200 per μL, and the C-reactive protein (CRP) was 12.91 mg/dL (normal <0.24 mg/dL). His symptoms did not improve with additional courses of clarithromycin, levofloxacin, or moxifloxacin. After 5 months of symptoms, he was referred to the internal medicine clinic of a teaching hospital in Japan.
The patient’s fevers, leukocytosis, and elevated CRP signal an inflammatory process, but whether it is infectious or not remains uncertain. The normal repeat chest x-ray lessens the likelihood of a pulmonary infection. Difficulty with initiating a swallow characterizes oropharyngeal dysphagia which features coughing or choking with oral intake and is typically caused by neuromuscular conditions like stroke, amyotrophic lateral sclerosis, or myasthenia gravis. The coexistence of oropharyngeal dysphagia and odynophagia may indicate pharyngitis, a retropharyngeal or parapharyngeal abscess, or oropharyngeal cancer.
Esophageal dysphagia occurs several seconds following swallow initiation and may arise with mucosal, smooth muscle, or neuromuscular diseases of the esophagus. Concomitant dysphagia and odynophagia may indicate esophageal spasm or esophagitis. Causes of esophagitis include infection (eg, candidiasis, herpes simplex virus [HSV], cytomegalovirus [CMV], or human immunodeficiency virus [HIV]), infiltration (eg, eosinophilic esophagitis), or irritation (eg, from medication, caustic ingestion, or gastroesophageal reflux). He is at risk for esophageal candidiasis following multiple courses of antibiotics. Esophageal dysphagia occurring with liquids and solids may indicate disordered motility, as opposed to dysphagia with solids alone, which may signal endoluminal obstruction.
At his outpatient evaluation, he denied headache, vision changes, chest pain, hemoptysis, palpitations, abdominal pain, dysuria, musculoskeletal symptoms, anorexia, or symptoms of gastroesophageal reflux. He did not have chills, rigors, or night sweats, but he had lost 3.4 kg in 5 months. He had not traveled within or outside of Japan in many years and was not involved in outdoor activities. He was engaged to and monogamous with his female partner of 5 years. He smoked 10 cigarettes per day for 14 years but stopped smoking during the last 2 months on account of his symptoms. He drank 6 beers per month and worked as a researcher at a chemical company but did not have any inhalational exposures.
His weight loss could be from reduced caloric intake due to dysphagia and odynophagia or may reflect an energy deficit related to chronic illness and inflammatory state. His smoking history increases his risk of bronchopulmonary infection and malignancy. Bronchogenic carcinoma may present with chronic cough, fevers, weight loss, or dysphagia from external compression by lymphadenopathy or mediastinal disease; however, his young age and recent chest CT results make lung cancer unlikely.
The white coating on his tongue could reflect oral leukoplakia, a reactive and potentially precancerous process that typically manifests as patches or plaques on oral mucosa. It can be distinguished from candidiasis, which scrapes off using a tongue blade. The extensive tongue coating is consistent with oral candidiasis. Potential predispositions include inhaled corticosteroids, antibiotic exposure, and/or an undiagnosed immunodeficiency syndrome (eg, HIV).
The initial diagnostic branch point for nontraumatic oral ulcers is infectious versus noninfectious. Infections that cause oral ulcers include HSV, CMV, and syphilis. The appearance and occurrence of the ulcers on freely moveable mucosa are consistent with aphthous stomatitis. Recurrent aphthous ulcers may occur in autoimmune diseases, including Behçet disease, Crohn disease, celiac sprue, and reactive arthritis. An endoscopy should be considered to detect esophageal ulcerations or esophageal candidiasis.
The rash may indicate folliculitis, usually attributable to Staphylococcus aureus or to Pseudomonas in the setting of recreational water exposure. Broad-spectrum antibiotics or immunodeficiency predisposes to candida folliculitis, while systemic candidiasis may cause metastatic skin lesions. The most common cutaneous manifestation of Behçet disease is erythema nodosum, but follicular and papulopustular lesions are also characteristic.
Pulmonary nodules are caused by infections, noninfectious inflammation, and malignancy. Infectious causes of pulmonary nodules include septic emboli, bacterial abscesses, and mycobacterial and fungal infection; noninfectious inflammatory causes include vasculitis (eg, granulomatosis with polyangiitis), rheumatoid arthritis, sarcoidosis, and lymphomatoid granulomatosis. Although additional culture data, serologic testing, and tuberculin skin testing or an interferon-gamma release assay may help to exclude these infections, the chronicity of symptoms, and lack of response to multiple antibiotic courses favor a noninfectious etiology.
Thickening of the aorta and left pulmonary artery may arise from an infectious, infiltrative, or inflammatory process. Arterial infections arise from direct inoculation, such as catheterization, trauma, or a contiguous site of infection, or from embolic seeding of atherosclerotic plaques or aneurysms. Malignant and nonmalignant processes, including sarcomas, lymphomas, histiocytoses (eg, Erdheim–Chester disease), and IgG4-related disease, may infiltrate the vascular walls. He has no evidence of visceral organ involvement to suggest these multisystem diagnoses.
The combined involvement of the aorta and pulmonary artery suggest a large-vessel vasculitis. Giant cell arteritis is exceedingly rare in patients younger than 50. Takayasu arteritis is a large-vessel vasculitis that predominantly affects women and may present with hypertension, arterial bruits, or discrepant blood pressure between arms, none of which were reported in this case. Behçet disease affects blood vessels of all sizes, including the aorta and pulmonary vasculature. His fevers, oral ulcers, perifollicular rash, and lymphadenopathy are consistent with this diagnosis, although he lacks the genital ulcers that occur in the majority of patients. Pulmonary nodules in Behçet disease arise from pulmonary or pleural vasculitis, resulting in focal inflammation, hemorrhage, or infarction. An ophthalmologic examination for uveitis and a pathergy test would support this diagnosis.
FDG accumulation in the aorta and pulmonary arteries signals large-vessel inflammation. The lack of FDG-avidity of the ground-glass opacities and nodular lesion suggests that these are not metabolically active tumors or infections but may be sequelae of the underlying disease, such as a hemorrhage or infarction from vasculitis. Sarcoidosis could account for the lung findings, but large-vessel vasculopathy would be exceedingly uncommon. Microscopic polyangiitis and granulomatosis with polyangiitis also cause pulmonary and vascular inflammation, but the nonreactive ANCA, absence of sinus disease, and normal urinalysis and kidney function make pauci-immune vasculitis unlikely. While the large-vessel involvement is consistent with Takayasu arteritis, the oral ulcers and rash are not.
Despite the absence of uveitis and the negative pathergy test, his oral aphthosis, papulopustular rash, and large-vessel vasculitis make Behçet disease the likely diagnosis. Behçet disease is most strongly associated with HLA B51, although other HLA haplotypes (including HLA A26 and HLA B52) are frequent in Behçet disease as well. As aortitis and pulmonary vasculitis can be associated with substantial morbidity and mortality, an urgent consultation with a rheumatologist regarding the initiation of immunosuppression is warranted.
Based on the mucocutaneous lesions, radiologic findings consistent with large-vessel vasculitis, and positive HLA A26 and HLA B52, he was diagnosed with Behçet disease. After 1 week of treatment with prednisolone 60 mg daily, his cough resolved and the oral aphthous ulcers and papulopustular rash improved. One month later, a chest CT showed significant reduction of the wall thickening of the aorta, its branches, and of the left pulmonary artery. The nodular lesion in the left lower lobe was unchanged, but the ground-glass opacities in the left upper lobe had disappeared.
When prednisolone was tapered down to 17.5 mg, his dry cough and low-grade fevers recurred, along with a slight elevation of inflammatory markers, and a ground-glass opacity appeared on the periphery of the left upper lobe. A sputum culture and fungal antigens were negative. His cough improved with the resumption of the previous dose of prednisolone. He remained symptom-free after 2 years of treatment with azathioprine 150 mg daily and prednisolone 2 mg daily and is now only treated with azathioprine.
DISCUSSION
Behçet disease is a multisystem vasculitis involving blood vessels of all sizes in the arterial and venous circulation that presents with oral and genital ulcers, ocular abnormalities (uveitis, retinitis), skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”), pathergy, and vascular lesions (thrombophlebitis, thrombosis, and aneurysm).
This patient presented with a chronic cough from pulmonary involvement by Behçet disease. The most common presenting symptom in a study of 47 patients with Behçet disease with pulmonary arteriopathy was hemoptysis followed by a nonbloody cough.2 Among these patients with pulmonary artery aneurysm, thrombosis, or both, 40 (85%) had nodules caused by infarction or inflammation and 21 (45%) had ground-glass opacities attributed to intraparenchymal hemorrhage. There are several case reports of chronic cough attributed to large-vessel vasculitis.3-5 Although the pathology of vasculitis-related cough is not fully understood, the inflammation of large vessels (aorta and pulmonary arteries) adjacent to the tracheobronchial tree may irritate regional cough receptors.3
Disease classification criteria are common in rheumatologic diseases; these criteria are developed to categorize patients for research studies and are not intended to diagnose individual patients.6 The classification criteria favor increased specificity at the expense of sensitivity to avoid misclassifying patients as having a disease, which would compromise the results of research studies. For instance, a study assessing a treatment for Behçet disease must exclude patients with inflammatory bowel disease, as these distinct patient populations may demonstrate discrepant responses to the investigative therapy. The specificity and homogeneity favored by classification criteria make those criteria inappropriate to rely on exclusively for the diagnosis of individual patients.7 The symptoms of many autoimmune diseases develop sequentially over time. Waiting for a patient with active, multisystem vasculitis to fulfill all of the Behçet disease classification criteria can lead to the harmful withholding of disease-modifying treatment.
The diagnosis of Behçet disease is made on clinical grounds; there is no gold standard test or histopathologic finding, and classification criteria remain imperfect. Although classification criteria help clinicians understand cardinal disease features, they cannot substitute for the more complex clinical reasoning required to establish a working diagnosis. The clinician must understand the pretest probability of disease, consider the presence or absence of characteristic features, exclude competing diagnoses, and decipher the risk-to-benefit ratio of therapeutic options and the urgency of treatment when assigning a diagnostic label. This patient’s pneumonitis, mucocutaneous changes, aortopathy, and compatible HLA typing (coupled with the exclusion of infectious diseases) were sufficient to diagnose Behçet disease. This case reminds us that classification criteria serve as a starting point, not as an end point, and that clinicians must ultimately make diagnoses and initiate treatment by thinking outside the checkbox.
TEACHING POINTS
- Large-vessel vasculitis is a rare cause of chronic cough.
- Although the most well-recognized signs of Behçet disease include genital and oral ulcers and uveitis, patients may also present with less common manifestations such as skin lesions (erythema nodosum, nonfollicular papulopustular lesions, or “pseudofolliculitis”) and vascular lesions of the artery (arteritis and aneurysm) and veins (thrombophlebitis and thrombosis).
- Classification criteria capture cardinal features of a disease but favor specificity over sensitivity and should not serve as a checklist for diagnosing a patient.
Acknowledgment
A brief version of this case was published as a case report in the Journal of Integrated Medicine 2013;23(12):1014-1017. Images from that publication were republished here with the permission of the publisher (Igaku-Shoin Ltd).
Disclosure
Dr. Dhaliwal reports receiving honoraria from ISMIE Mutual Insurance Company and Physicians’ Reciprocal Insurers. All other authors have nothing to disclose.
1. Kanamori M, Kubo T, Sakemi H. What’s your diagnosis? [in Japanese] J Integrated Med. 2013; 23 (12):1014-1017.
2. Seyahi E, Melikoglu M, Akman C, et al. Pulmonary artery involvement and associated lung disease in Behçet disease: a series of 47 patients. Medicine (Baltimore). 2012;91(1):35-48. PubMed
3. Olopade CO, Sekosan M, Schraufnagel DE. Giant cell arteritis manifesting as chronic cough and fever of unknown origin. Mayo Clin Proc. 1997;72(11):1048-1050. PubMed
4. Hellmann DB. Temporal arteritis: a cough, toothache, and tongue infarction. JAMA. 2002;287(22):2996-3000. PubMed
5. Karagiannis A, Mathiopoulou L, Tziomalos K, et al. Dry cough as first manifestation of giant-cell arteritis. J Am Geriatr Soc. 2006;54(12):1957-1958. PubMed
6. Aggarwal R, Ringold S, Khanna D, et al. Distinctions between diagnostic and classification criteria? Arthritis Care Res (Hoboken). 2015;67(7):891-897. PubMed
7. Rao JK, Allen NB, Pincus T. Limitations of the 1990 American College of Rheumatology classification criteria in the diagnosis of vasculitis. Ann Intern Med. 1998;129(5):345-352. PubMed
8. Davatchi F, Sadeghi Abdollahi B, Shahram F, Chams-Davatchi C, Shams H, Nadji A. Classification and Diagnosis Criteria for Behçet’s Disease. In: Emmi L, ed. Behçet’s Syndrome. From Pathogenesis to Treatment. Milan, Italy: Springer; 2014:189-198.
9. Criteria for diagnosis of Behcet’s disease. International Study Group for Behçet’s Disease. Lancet. 1990;335(8697):1078-1080. PubMed
10. Davatchi F, Assaad-Khalil S, Calamia KT, et al. The International Criteria for Behçet’s Disease (ICBD): a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014;28(3):338–347. PubMed
11. Suzuki Kurokawa M, Suzuki N. Behçet’s disease. Clin Exp Med. 2004;4(1):10-20. PubMed
1. Kanamori M, Kubo T, Sakemi H. What’s your diagnosis? [in Japanese] J Integrated Med. 2013; 23 (12):1014-1017.
2. Seyahi E, Melikoglu M, Akman C, et al. Pulmonary artery involvement and associated lung disease in Behçet disease: a series of 47 patients. Medicine (Baltimore). 2012;91(1):35-48. PubMed
3. Olopade CO, Sekosan M, Schraufnagel DE. Giant cell arteritis manifesting as chronic cough and fever of unknown origin. Mayo Clin Proc. 1997;72(11):1048-1050. PubMed
4. Hellmann DB. Temporal arteritis: a cough, toothache, and tongue infarction. JAMA. 2002;287(22):2996-3000. PubMed
5. Karagiannis A, Mathiopoulou L, Tziomalos K, et al. Dry cough as first manifestation of giant-cell arteritis. J Am Geriatr Soc. 2006;54(12):1957-1958. PubMed
6. Aggarwal R, Ringold S, Khanna D, et al. Distinctions between diagnostic and classification criteria? Arthritis Care Res (Hoboken). 2015;67(7):891-897. PubMed
7. Rao JK, Allen NB, Pincus T. Limitations of the 1990 American College of Rheumatology classification criteria in the diagnosis of vasculitis. Ann Intern Med. 1998;129(5):345-352. PubMed
8. Davatchi F, Sadeghi Abdollahi B, Shahram F, Chams-Davatchi C, Shams H, Nadji A. Classification and Diagnosis Criteria for Behçet’s Disease. In: Emmi L, ed. Behçet’s Syndrome. From Pathogenesis to Treatment. Milan, Italy: Springer; 2014:189-198.
9. Criteria for diagnosis of Behcet’s disease. International Study Group for Behçet’s Disease. Lancet. 1990;335(8697):1078-1080. PubMed
10. Davatchi F, Assaad-Khalil S, Calamia KT, et al. The International Criteria for Behçet’s Disease (ICBD): a collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014;28(3):338–347. PubMed
11. Suzuki Kurokawa M, Suzuki N. Behçet’s disease. Clin Exp Med. 2004;4(1):10-20. PubMed
© 2018 Society of Hospital Medicine
Oral Corticosteroids for Acute Lower Respiratory Infection: Are We Ready to Drop This Practice?
Study Overview
Objective. To assess the effects of oral corticosteroids for acute lower respiratory tract infection in adults without asthma or COPD.
Design. Multi-center, placebo-controlled, randomized clinical trial.
Setting and participants. This study was conducted at 4 UK centers (the Universities of Bristol, Southampton, Nottingham, and Oxford) between July 2013 and October 2014. Patients with acute cough (≤ 28 days) and at least 1 of the following lower respiratory tract symptoms (phlegm, chest pain, wheezing, or shortness of breath) were recruited by family physicians and nurses. Patients with chronic pulmonary disease, who had received asthma medication in the past 5 years, required hospital admission, or required same-day antibiotics were excluded. Patients were randomized by variable block size into prednisolone or placebo groups in a 1:1 ratio, stratified by center.
Intervention. Participants were asked to take 2 tablets of either 20-mg oral prednisolone or placebo tablets once daily for 5 days. The medications, which looked and tasted identical, were packaged into numbered packs by an independent pharmacist and were delivered to the family practices to be distributed to the enrolled patients. Participants were invited to report daily, using web or paper version, the severity of symptoms using a scale 0 to 6, along with twice-daily peak flow, for 28 days or until symptom resolution. Participants received shopping vouchers. Medical notes were reviewed at 3 months for new diagnosis of asthma, chronic obstructive pulmonary disease, whooping cough, and lung cancer.
Main outcome measures. The primary outcomes were the duration of moderately bad or worse cough (defined as the number of days from randomization to the last day with a score of at least 3 points prior to at least 2 consecutive days with a score of less than 3, up to a maximum of 28 days); and the mean severity score (range 0–6) of the 6 main symptoms (cough, phlegm, shortness of breath, sleep disturbance, feeling generally unwell, and activity disturbance) on days 2 to 4.
Main results. 401 patients were randomized; 25 patients were lost to follow-up, leaving 173 in prednisolone group and 161 in placebo group for analysis. The prednisolone group was slightly more likely to be male, older, and to have received an influenza vaccine. 96% were white. Symptom diaries were returned by 94% of patients. For primary outcome 1, duration of moderately bad or worse cough, the median time to recovery from moderately bad or worse cough was 5 days (interquartile range, 3–8 days) in both groups. There was no difference after sensitivity analysis (multiple imputation of missing data, per-protocol analysis, and adjusting for day of recruitment). Primary outcome 2, the mean symptom severity score, after adjustment for center and baseline measure, was lower (hazard ratio, –0.20) in the prednisolone group compared with the placebo group; however, after secondary additional adjustment for age, sex, influenza vaccine, and smoking, the difference was not statistically significant. Secondary outcomes included total duration and severity of each symptom up to 28 days, duration of abnormal peak flow up to 28 days, cough duration of any severity up to 56 days, antibiotic use, patient satisfaction, adverse events were not different between the two groups. There were no new urinary or visual symptoms and none of the patients reporting fatigue, thirst, or dry throat had diabetes.
Conclusion. Oral corticosteroids should not be used for acute lower respiratory tract infection symptoms in adults without asthma because they do not reduce symptom duration or severity.
Commentary
This study by Hay et al prospectively recruited patients with acute respiratory illness presenting to an outpatient setting within multiple centers for a placebo-controlled randomized study to evaluate the effectiveness of oral corticosteroids for acute lower respiratory tract infection. Patients with pre-existing lung disease such as asthma or COPD were excluded. This study showed moderate-dose oral prednisolone (20 mg twice a day for 5 days) did not reduce the duration of cough, and there was no statistically significant differences in primary and secondary outcomes between the 2 groups.
The beneficial effect of corticosteroids is thought to be due to its anti-inflammatory effect and decreasing harmful cytokines, which can be elevated during acute respiratory illness. In patients with severe pneumonia, patients potentially benefitted from corticosteroids by achieving clinical stability faster, reducing risk for treatment failure or ARDS and reducing hospital length of stay. However, corticosteroids are associated with hyperglycemia, myopathy, superinfection, osteopenia, and increased risk for gastrointestinal bleeding [1]. Corticosteroids have shown benefit repeatedly in patients with pneumonia severe enough to require hospitalization or intensive care unit stay [2–7].
The use of oral corticosteroids in non-critical acute respiratory tract illness without underlying obstructive lung disease has been a somewhat common practice (15%) [8]. However, no study to date firmly supports the use of oral corticosteroids in this patient group. A recently published randomized study attempted to determine if there is a benefit of oral dexamethasone in patients with acute sore throat, and found none [9]. No randomized controlled data has been published on the outpatient use of oral corticosteroids for acute lower respiratory illness.
The current study offers further evidence against the use of oral corticosteroids for acute, non-critical inflammation of the respiratory tract in nonasthmatic patients. Strengths of the study include its blinded and randomized study design and large number of patients. However, there are some limitations. Acute lower respiratory infection is associated with a wide spectrum of causative organisms and severity. It is possible that the beneficial effects of corticosteroids are only measurable when disease severity is high and there will be a systemic inflammatory response. In addition, outcome measurement was limited to a few items, namely patient-reported symptom score and duration. Furthermore, they measured the peak flow adjunctively. Without underlying airway hyperreactivity, substantial differences in peak flow are unlikely to be evident, limiting the usefulness of this as an indicator of disease in patients without chronic pulmonary disease.
Other study limitations include low patient recruitment rate, a large number of patients who did not have moderately bad cough at presentation or during the first 2 days, absence of baseline biomarkers (such as inflammatory, microbiological, spirometric or radiographic) and patient-reported outcome measures, and a sample largely homogenous in ethnicity with a small number of smokers. It is unclear whether similar results could be achieved in a more diverse population and with a greater percentage of smokers. In addition, although overall both groups were well balanced, including the number of patients taking over-the-counter cough suppressants and delayed antibiotics, the tracking of other concurrent therapies such as NSAIDs or acetaminophen was not included in the study design and the type of antibiotic was not tabulated. Such concurrent drugs could have masked a true benefit of oral corticosteroids.
Applications for Clinical Practice
This study will help prevent excessive prescription of oral corticosteroids for acute minor lower respiratory infection that requires only outpatient treatment. However, the evidence is limited to patients in stable condition. Patients with more severe acute lower respiratory infection, such as patients requiring hospitalization, may still benefit from a short course of oral corticosteroids. Furthermore, patients with underlying obstructive airways disease such as asthma or COPD should still be considered for oral corticosteroid therapy depending on their clinical circumstances.
—Minkyung Kwon, MD, Joel Roberson, MD, and Jack Leventhal, MD,
Pulmonary and Critical Care Medicine,Mayo Clini c Florida, Jacksonville, FL (Drs. Kwon andLeventhal), and Department of Radiology, Oakland University Beaumont Hospital, Royal Oak, MI (Dr. Roberson)
1. Prina E, Ceccato A, Torres A. New aspects in the management of pneumonia. Crit Care 2016;20:267.
2. Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med 2005;171:242–8.
3. Mikami K, Suzuki M, Kitagawa H, et al. Efficacy of corticosteroids in the treatment of community-acquired pneumonia requiring hospitalization. Lung 2007;185:249–55.
4. Fernandez-Serrano S, Dorca J, Garcia-Vidal C, et al. Effect of corticosteroids on the clinical course of community-acquired pneumonia: a randomized controlled trial. Crit Care 2011;15:R96.
5. Meijvis SC, Hardeman H, Remmelts HH, et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: a randomised, double-blind, placebo-controlled trial. Lancet 2011;377:2023–30.
6. Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015;385:1511–8.
7. Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 2015;163:519–28.
8. Ebell MH, Radke T. Antibiotic use for viral acute respiratory tract infections remains common. Am J Manag Care 2015;21:e567–75.
9. Hayward GN, Hay AD, Moore MV, et al. Effect of oral dexamethasone without immediate antibiotics vs placebo on acute sore throat in adults: a randomized clinical trial. JAMA 2017;317:1535–43.
Study Overview
Objective. To assess the effects of oral corticosteroids for acute lower respiratory tract infection in adults without asthma or COPD.
Design. Multi-center, placebo-controlled, randomized clinical trial.
Setting and participants. This study was conducted at 4 UK centers (the Universities of Bristol, Southampton, Nottingham, and Oxford) between July 2013 and October 2014. Patients with acute cough (≤ 28 days) and at least 1 of the following lower respiratory tract symptoms (phlegm, chest pain, wheezing, or shortness of breath) were recruited by family physicians and nurses. Patients with chronic pulmonary disease, who had received asthma medication in the past 5 years, required hospital admission, or required same-day antibiotics were excluded. Patients were randomized by variable block size into prednisolone or placebo groups in a 1:1 ratio, stratified by center.
Intervention. Participants were asked to take 2 tablets of either 20-mg oral prednisolone or placebo tablets once daily for 5 days. The medications, which looked and tasted identical, were packaged into numbered packs by an independent pharmacist and were delivered to the family practices to be distributed to the enrolled patients. Participants were invited to report daily, using web or paper version, the severity of symptoms using a scale 0 to 6, along with twice-daily peak flow, for 28 days or until symptom resolution. Participants received shopping vouchers. Medical notes were reviewed at 3 months for new diagnosis of asthma, chronic obstructive pulmonary disease, whooping cough, and lung cancer.
Main outcome measures. The primary outcomes were the duration of moderately bad or worse cough (defined as the number of days from randomization to the last day with a score of at least 3 points prior to at least 2 consecutive days with a score of less than 3, up to a maximum of 28 days); and the mean severity score (range 0–6) of the 6 main symptoms (cough, phlegm, shortness of breath, sleep disturbance, feeling generally unwell, and activity disturbance) on days 2 to 4.
Main results. 401 patients were randomized; 25 patients were lost to follow-up, leaving 173 in prednisolone group and 161 in placebo group for analysis. The prednisolone group was slightly more likely to be male, older, and to have received an influenza vaccine. 96% were white. Symptom diaries were returned by 94% of patients. For primary outcome 1, duration of moderately bad or worse cough, the median time to recovery from moderately bad or worse cough was 5 days (interquartile range, 3–8 days) in both groups. There was no difference after sensitivity analysis (multiple imputation of missing data, per-protocol analysis, and adjusting for day of recruitment). Primary outcome 2, the mean symptom severity score, after adjustment for center and baseline measure, was lower (hazard ratio, –0.20) in the prednisolone group compared with the placebo group; however, after secondary additional adjustment for age, sex, influenza vaccine, and smoking, the difference was not statistically significant. Secondary outcomes included total duration and severity of each symptom up to 28 days, duration of abnormal peak flow up to 28 days, cough duration of any severity up to 56 days, antibiotic use, patient satisfaction, adverse events were not different between the two groups. There were no new urinary or visual symptoms and none of the patients reporting fatigue, thirst, or dry throat had diabetes.
Conclusion. Oral corticosteroids should not be used for acute lower respiratory tract infection symptoms in adults without asthma because they do not reduce symptom duration or severity.
Commentary
This study by Hay et al prospectively recruited patients with acute respiratory illness presenting to an outpatient setting within multiple centers for a placebo-controlled randomized study to evaluate the effectiveness of oral corticosteroids for acute lower respiratory tract infection. Patients with pre-existing lung disease such as asthma or COPD were excluded. This study showed moderate-dose oral prednisolone (20 mg twice a day for 5 days) did not reduce the duration of cough, and there was no statistically significant differences in primary and secondary outcomes between the 2 groups.
The beneficial effect of corticosteroids is thought to be due to its anti-inflammatory effect and decreasing harmful cytokines, which can be elevated during acute respiratory illness. In patients with severe pneumonia, patients potentially benefitted from corticosteroids by achieving clinical stability faster, reducing risk for treatment failure or ARDS and reducing hospital length of stay. However, corticosteroids are associated with hyperglycemia, myopathy, superinfection, osteopenia, and increased risk for gastrointestinal bleeding [1]. Corticosteroids have shown benefit repeatedly in patients with pneumonia severe enough to require hospitalization or intensive care unit stay [2–7].
The use of oral corticosteroids in non-critical acute respiratory tract illness without underlying obstructive lung disease has been a somewhat common practice (15%) [8]. However, no study to date firmly supports the use of oral corticosteroids in this patient group. A recently published randomized study attempted to determine if there is a benefit of oral dexamethasone in patients with acute sore throat, and found none [9]. No randomized controlled data has been published on the outpatient use of oral corticosteroids for acute lower respiratory illness.
The current study offers further evidence against the use of oral corticosteroids for acute, non-critical inflammation of the respiratory tract in nonasthmatic patients. Strengths of the study include its blinded and randomized study design and large number of patients. However, there are some limitations. Acute lower respiratory infection is associated with a wide spectrum of causative organisms and severity. It is possible that the beneficial effects of corticosteroids are only measurable when disease severity is high and there will be a systemic inflammatory response. In addition, outcome measurement was limited to a few items, namely patient-reported symptom score and duration. Furthermore, they measured the peak flow adjunctively. Without underlying airway hyperreactivity, substantial differences in peak flow are unlikely to be evident, limiting the usefulness of this as an indicator of disease in patients without chronic pulmonary disease.
Other study limitations include low patient recruitment rate, a large number of patients who did not have moderately bad cough at presentation or during the first 2 days, absence of baseline biomarkers (such as inflammatory, microbiological, spirometric or radiographic) and patient-reported outcome measures, and a sample largely homogenous in ethnicity with a small number of smokers. It is unclear whether similar results could be achieved in a more diverse population and with a greater percentage of smokers. In addition, although overall both groups were well balanced, including the number of patients taking over-the-counter cough suppressants and delayed antibiotics, the tracking of other concurrent therapies such as NSAIDs or acetaminophen was not included in the study design and the type of antibiotic was not tabulated. Such concurrent drugs could have masked a true benefit of oral corticosteroids.
Applications for Clinical Practice
This study will help prevent excessive prescription of oral corticosteroids for acute minor lower respiratory infection that requires only outpatient treatment. However, the evidence is limited to patients in stable condition. Patients with more severe acute lower respiratory infection, such as patients requiring hospitalization, may still benefit from a short course of oral corticosteroids. Furthermore, patients with underlying obstructive airways disease such as asthma or COPD should still be considered for oral corticosteroid therapy depending on their clinical circumstances.
—Minkyung Kwon, MD, Joel Roberson, MD, and Jack Leventhal, MD,
Pulmonary and Critical Care Medicine,Mayo Clini c Florida, Jacksonville, FL (Drs. Kwon andLeventhal), and Department of Radiology, Oakland University Beaumont Hospital, Royal Oak, MI (Dr. Roberson)
Study Overview
Objective. To assess the effects of oral corticosteroids for acute lower respiratory tract infection in adults without asthma or COPD.
Design. Multi-center, placebo-controlled, randomized clinical trial.
Setting and participants. This study was conducted at 4 UK centers (the Universities of Bristol, Southampton, Nottingham, and Oxford) between July 2013 and October 2014. Patients with acute cough (≤ 28 days) and at least 1 of the following lower respiratory tract symptoms (phlegm, chest pain, wheezing, or shortness of breath) were recruited by family physicians and nurses. Patients with chronic pulmonary disease, who had received asthma medication in the past 5 years, required hospital admission, or required same-day antibiotics were excluded. Patients were randomized by variable block size into prednisolone or placebo groups in a 1:1 ratio, stratified by center.
Intervention. Participants were asked to take 2 tablets of either 20-mg oral prednisolone or placebo tablets once daily for 5 days. The medications, which looked and tasted identical, were packaged into numbered packs by an independent pharmacist and were delivered to the family practices to be distributed to the enrolled patients. Participants were invited to report daily, using web or paper version, the severity of symptoms using a scale 0 to 6, along with twice-daily peak flow, for 28 days or until symptom resolution. Participants received shopping vouchers. Medical notes were reviewed at 3 months for new diagnosis of asthma, chronic obstructive pulmonary disease, whooping cough, and lung cancer.
Main outcome measures. The primary outcomes were the duration of moderately bad or worse cough (defined as the number of days from randomization to the last day with a score of at least 3 points prior to at least 2 consecutive days with a score of less than 3, up to a maximum of 28 days); and the mean severity score (range 0–6) of the 6 main symptoms (cough, phlegm, shortness of breath, sleep disturbance, feeling generally unwell, and activity disturbance) on days 2 to 4.
Main results. 401 patients were randomized; 25 patients were lost to follow-up, leaving 173 in prednisolone group and 161 in placebo group for analysis. The prednisolone group was slightly more likely to be male, older, and to have received an influenza vaccine. 96% were white. Symptom diaries were returned by 94% of patients. For primary outcome 1, duration of moderately bad or worse cough, the median time to recovery from moderately bad or worse cough was 5 days (interquartile range, 3–8 days) in both groups. There was no difference after sensitivity analysis (multiple imputation of missing data, per-protocol analysis, and adjusting for day of recruitment). Primary outcome 2, the mean symptom severity score, after adjustment for center and baseline measure, was lower (hazard ratio, –0.20) in the prednisolone group compared with the placebo group; however, after secondary additional adjustment for age, sex, influenza vaccine, and smoking, the difference was not statistically significant. Secondary outcomes included total duration and severity of each symptom up to 28 days, duration of abnormal peak flow up to 28 days, cough duration of any severity up to 56 days, antibiotic use, patient satisfaction, adverse events were not different between the two groups. There were no new urinary or visual symptoms and none of the patients reporting fatigue, thirst, or dry throat had diabetes.
Conclusion. Oral corticosteroids should not be used for acute lower respiratory tract infection symptoms in adults without asthma because they do not reduce symptom duration or severity.
Commentary
This study by Hay et al prospectively recruited patients with acute respiratory illness presenting to an outpatient setting within multiple centers for a placebo-controlled randomized study to evaluate the effectiveness of oral corticosteroids for acute lower respiratory tract infection. Patients with pre-existing lung disease such as asthma or COPD were excluded. This study showed moderate-dose oral prednisolone (20 mg twice a day for 5 days) did not reduce the duration of cough, and there was no statistically significant differences in primary and secondary outcomes between the 2 groups.
The beneficial effect of corticosteroids is thought to be due to its anti-inflammatory effect and decreasing harmful cytokines, which can be elevated during acute respiratory illness. In patients with severe pneumonia, patients potentially benefitted from corticosteroids by achieving clinical stability faster, reducing risk for treatment failure or ARDS and reducing hospital length of stay. However, corticosteroids are associated with hyperglycemia, myopathy, superinfection, osteopenia, and increased risk for gastrointestinal bleeding [1]. Corticosteroids have shown benefit repeatedly in patients with pneumonia severe enough to require hospitalization or intensive care unit stay [2–7].
The use of oral corticosteroids in non-critical acute respiratory tract illness without underlying obstructive lung disease has been a somewhat common practice (15%) [8]. However, no study to date firmly supports the use of oral corticosteroids in this patient group. A recently published randomized study attempted to determine if there is a benefit of oral dexamethasone in patients with acute sore throat, and found none [9]. No randomized controlled data has been published on the outpatient use of oral corticosteroids for acute lower respiratory illness.
The current study offers further evidence against the use of oral corticosteroids for acute, non-critical inflammation of the respiratory tract in nonasthmatic patients. Strengths of the study include its blinded and randomized study design and large number of patients. However, there are some limitations. Acute lower respiratory infection is associated with a wide spectrum of causative organisms and severity. It is possible that the beneficial effects of corticosteroids are only measurable when disease severity is high and there will be a systemic inflammatory response. In addition, outcome measurement was limited to a few items, namely patient-reported symptom score and duration. Furthermore, they measured the peak flow adjunctively. Without underlying airway hyperreactivity, substantial differences in peak flow are unlikely to be evident, limiting the usefulness of this as an indicator of disease in patients without chronic pulmonary disease.
Other study limitations include low patient recruitment rate, a large number of patients who did not have moderately bad cough at presentation or during the first 2 days, absence of baseline biomarkers (such as inflammatory, microbiological, spirometric or radiographic) and patient-reported outcome measures, and a sample largely homogenous in ethnicity with a small number of smokers. It is unclear whether similar results could be achieved in a more diverse population and with a greater percentage of smokers. In addition, although overall both groups were well balanced, including the number of patients taking over-the-counter cough suppressants and delayed antibiotics, the tracking of other concurrent therapies such as NSAIDs or acetaminophen was not included in the study design and the type of antibiotic was not tabulated. Such concurrent drugs could have masked a true benefit of oral corticosteroids.
Applications for Clinical Practice
This study will help prevent excessive prescription of oral corticosteroids for acute minor lower respiratory infection that requires only outpatient treatment. However, the evidence is limited to patients in stable condition. Patients with more severe acute lower respiratory infection, such as patients requiring hospitalization, may still benefit from a short course of oral corticosteroids. Furthermore, patients with underlying obstructive airways disease such as asthma or COPD should still be considered for oral corticosteroid therapy depending on their clinical circumstances.
—Minkyung Kwon, MD, Joel Roberson, MD, and Jack Leventhal, MD,
Pulmonary and Critical Care Medicine,Mayo Clini c Florida, Jacksonville, FL (Drs. Kwon andLeventhal), and Department of Radiology, Oakland University Beaumont Hospital, Royal Oak, MI (Dr. Roberson)
1. Prina E, Ceccato A, Torres A. New aspects in the management of pneumonia. Crit Care 2016;20:267.
2. Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med 2005;171:242–8.
3. Mikami K, Suzuki M, Kitagawa H, et al. Efficacy of corticosteroids in the treatment of community-acquired pneumonia requiring hospitalization. Lung 2007;185:249–55.
4. Fernandez-Serrano S, Dorca J, Garcia-Vidal C, et al. Effect of corticosteroids on the clinical course of community-acquired pneumonia: a randomized controlled trial. Crit Care 2011;15:R96.
5. Meijvis SC, Hardeman H, Remmelts HH, et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: a randomised, double-blind, placebo-controlled trial. Lancet 2011;377:2023–30.
6. Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015;385:1511–8.
7. Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 2015;163:519–28.
8. Ebell MH, Radke T. Antibiotic use for viral acute respiratory tract infections remains common. Am J Manag Care 2015;21:e567–75.
9. Hayward GN, Hay AD, Moore MV, et al. Effect of oral dexamethasone without immediate antibiotics vs placebo on acute sore throat in adults: a randomized clinical trial. JAMA 2017;317:1535–43.
1. Prina E, Ceccato A, Torres A. New aspects in the management of pneumonia. Crit Care 2016;20:267.
2. Confalonieri M, Urbino R, Potena A, et al. Hydrocortisone infusion for severe community-acquired pneumonia: a preliminary randomized study. Am J Respir Crit Care Med 2005;171:242–8.
3. Mikami K, Suzuki M, Kitagawa H, et al. Efficacy of corticosteroids in the treatment of community-acquired pneumonia requiring hospitalization. Lung 2007;185:249–55.
4. Fernandez-Serrano S, Dorca J, Garcia-Vidal C, et al. Effect of corticosteroids on the clinical course of community-acquired pneumonia: a randomized controlled trial. Crit Care 2011;15:R96.
5. Meijvis SC, Hardeman H, Remmelts HH, et al. Dexamethasone and length of hospital stay in patients with community-acquired pneumonia: a randomised, double-blind, placebo-controlled trial. Lancet 2011;377:2023–30.
6. Blum CA, Nigro N, Briel M, et al. Adjunct prednisone therapy for patients with community-acquired pneumonia: a multicentre, double-blind, randomised, placebo-controlled trial. Lancet 2015;385:1511–8.
7. Siemieniuk RA, Meade MO, Alonso-Coello P, et al. Corticosteroid therapy for patients hospitalized with community-acquired pneumonia: a systematic review and meta-analysis. Ann Intern Med 2015;163:519–28.
8. Ebell MH, Radke T. Antibiotic use for viral acute respiratory tract infections remains common. Am J Manag Care 2015;21:e567–75.
9. Hayward GN, Hay AD, Moore MV, et al. Effect of oral dexamethasone without immediate antibiotics vs placebo on acute sore throat in adults: a randomized clinical trial. JAMA 2017;317:1535–43.
EMR-Based Tool for Identifying Type 2 Diabetic Patients at High Risk for Hypoglycemia
Study Overview
Objective. To develop and validate a risk stratification tool to categorize 12-month risk of hypoglycemia-related emergency department (ED) or hospital use among patients with type 2 diabetes (T2D).
Design. Prospective cohort study.
Setting and participants. Patients with T2D from Kaiser Permanente Northern California were identified using electronic medical records (EMR). Patients had to be 21 years of age or older as of the baseline date of 1 January 2014, with continuous health plan membership for 24 months prebaseline and pharmacy benefits for 12 months prebaseline. Of the 233,330 adults identified, 24,719 were excluded for unknown diabetes type, and 3614 were excluded for type 1 diabetes. The remaining 206,435 eligible patients with T2D were randomly split into an 80% derivation sample (n = 165,148) for tool development and 20% internal validation sample (n = 41,287). Using similar eligibility criteria, 2 external validation samples were derived from the Veterans Administration Diabetes Epidemiology Cohort (VA) (n = 1,335,966 adults) as well as from Group Health Cooperative (GH) (n = 14,972).
Main outcome measure. The primary outcome was the occurrence of any hypoglycemia-related ED visit or hospital use during the 12 months postbaseline. A primary diagnosis of hypoglycemia was ascertained using the following International Classification of Diseases, Ninth Revision (ICD-9) codes: 251.0, 251.1, 251.2, 962.3, or 250.8, without concurrent 259.3, 272.7, 681.xx, 686.9x, 707.a-707.9, 709.3, 730.0-730.2, or 731.8 codes [1]. Secondary discharge diagnoses for hypoglycemia were not used because they are often attributable to events that occurred during the ED or hospital encounter.
Main results. Beginning with 156 (122 categorical and 34 continuous) candidate clinical, demographic, and behavioral predictor variables for model development, the final classification tree was based on 6 patient-specific variables: total number of prior episodes of hypoglycemia-related ED or hospital utilization (0, 1–2, ≥ 3 times), number of ED encounters for any reason in the prior 12 months (< 2, ≥ 2 times), insulin use (yes/no), sulfonylurea use (yes/no), presence of severe or end-stage kidney disease (dialysis or chronic kidney disease stage 4 or 5 determined by estimated glomerular filtration rate of ≤ 29 mL/min/1.73 m² (yes/no), and age younger than 77 years (yes/no). This classification tree resulted in 10 mutually exclusive leaf nodes, each yielding an estimated annual risk of hypoglycemia-related utilization, which were categorized as high (> 5%), intermediate (1%–5%), or low (< 1%).
The above classification model was then transcribed into a checklist-style hypoglycemia risk stratification tool by mapping the combination of risk factors to high, intermediate, or low risk of having any hypoglycemia-related utilization in the following 12 months.
Regarding patient characteristics, there were no significant differences in the distribution of the 6 predictors between the Kaiser derivation vs. validation samples, but there were significant differences across external validation samples. For example, the VA sample was predominantly men, with a higher proportion of patients older than 77 years, and had the highest proportion of patients with severe or end-stage kidney disease. Regarding model validation, the tool performed well in both internal validation (C statistic = 0.83) and external validation samples (VA C statistic = 0.81; GH C statistic = 0.79).
Conclusion. This hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions to reduce hypoglycemia risk and improve patient safety.
Commentary
It is estimated that 25 million people in the United States have diabetes [2]. Hypoglycemia is a frequent adverse event in patients with T2D, being more common than acute hyperglycemic emergencies such as hyperosmolar hyperglycemic state [3]. Iatrogenic hypoglycemia due to glucose-lowering medication can result in hypoglycemic crisis that requires administration of carbohydrates, glucagon, or other resuscitative actions in the ED or in hospital [4,5]. The estimated total annual direct medical costs of hypoglycemia-related utilization were estimated at approximately $1.8 billion in the United States in 2009.
The risk of hypoglycemia varies widely in patients with T2D and there are no validated methods to target interventions to the at-risk population. In this article, Karter and colleagues developed and validated a pragmatic hypoglycemia risk stratification tool that uses 6 factors to categorize the 12-month risk of hypoglycemia-related ED or hospital utilization.
Identifying patients at high-risk for hypoglycemia-related utilization provides an opportunity to mobilize resources to target this minority of patients with T2D, including deintensifying or simplifying medication regimens, prescribing glucagon kits or continuous glucose monitors, making referrals to clinical pharmacists or nurse care managers, and regularly asking about hypoglycemia events occurring outside the medical setting. This is important, as more than 95% of severe hypoglycemia events may go clinically unrecognized because they did not result in ED or hospital use [6]. In addition, as the 6 inputs were identified by EMR, intervention can include automated clinical alert flags in the EMR and automated messaging to patients with elevated risk.
Several limitations exist. The study excluded secondary discharge diagnoses for hypoglycemia as these may occur due to sepsis, acute renal failure, trauma, or other causes. In addition, the external validation populations had different distributions of disease severity and case mix. The authors attribute some of the inconsistent findings to sparse data in the GH validation sample (n = 14,972). Finally, this tool was developed to stratify the population into 3 levels of risk, and it should not be used to estimate the probability of hypoglycemic-related utilization for an individual patient.
Applications for Clinical Practice
The EMR-based hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions, including integration into existing EMR as clinical decision aid, to reduce hypoglycemia risk and improve patient safety.
—Ka Ming Gordon Ngai, MD, MPH
1. Ginde AA, Blanc PG, Lieberman RM, et al. Validation of ICD-9-CM coding algorithm for improved identification of hypoglycemia visits. BMC Endocr Disord 2008;8:4.
2. Gregg EW, Li Y, Wang J, et al. Change in diabetes-related complications in the United States, 1990-2010. N Engl J Med 2014; 370:1514–23.
3. Lipska KJ, Ross JS, Wang Y, et al. National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011. JAMA Intern Med 2014:174: 1116–24.
4. Pogach L, Aron D. Balancing hypoglycemia and glycemic control: a public health approach for insulin safety. JAMA 2010;303:2076–7.
5. Lee SJ. So much insulin, so much hypoglycemia. JAMA Intern Med 2014;174:686–8.
6. Sarkar U, Karter AJ, Liu JY, et al. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: the Diabetes Study of Northern California (DISTANCE). J Gen Intern Med 2010;25:962–8.
Study Overview
Objective. To develop and validate a risk stratification tool to categorize 12-month risk of hypoglycemia-related emergency department (ED) or hospital use among patients with type 2 diabetes (T2D).
Design. Prospective cohort study.
Setting and participants. Patients with T2D from Kaiser Permanente Northern California were identified using electronic medical records (EMR). Patients had to be 21 years of age or older as of the baseline date of 1 January 2014, with continuous health plan membership for 24 months prebaseline and pharmacy benefits for 12 months prebaseline. Of the 233,330 adults identified, 24,719 were excluded for unknown diabetes type, and 3614 were excluded for type 1 diabetes. The remaining 206,435 eligible patients with T2D were randomly split into an 80% derivation sample (n = 165,148) for tool development and 20% internal validation sample (n = 41,287). Using similar eligibility criteria, 2 external validation samples were derived from the Veterans Administration Diabetes Epidemiology Cohort (VA) (n = 1,335,966 adults) as well as from Group Health Cooperative (GH) (n = 14,972).
Main outcome measure. The primary outcome was the occurrence of any hypoglycemia-related ED visit or hospital use during the 12 months postbaseline. A primary diagnosis of hypoglycemia was ascertained using the following International Classification of Diseases, Ninth Revision (ICD-9) codes: 251.0, 251.1, 251.2, 962.3, or 250.8, without concurrent 259.3, 272.7, 681.xx, 686.9x, 707.a-707.9, 709.3, 730.0-730.2, or 731.8 codes [1]. Secondary discharge diagnoses for hypoglycemia were not used because they are often attributable to events that occurred during the ED or hospital encounter.
Main results. Beginning with 156 (122 categorical and 34 continuous) candidate clinical, demographic, and behavioral predictor variables for model development, the final classification tree was based on 6 patient-specific variables: total number of prior episodes of hypoglycemia-related ED or hospital utilization (0, 1–2, ≥ 3 times), number of ED encounters for any reason in the prior 12 months (< 2, ≥ 2 times), insulin use (yes/no), sulfonylurea use (yes/no), presence of severe or end-stage kidney disease (dialysis or chronic kidney disease stage 4 or 5 determined by estimated glomerular filtration rate of ≤ 29 mL/min/1.73 m² (yes/no), and age younger than 77 years (yes/no). This classification tree resulted in 10 mutually exclusive leaf nodes, each yielding an estimated annual risk of hypoglycemia-related utilization, which were categorized as high (> 5%), intermediate (1%–5%), or low (< 1%).
The above classification model was then transcribed into a checklist-style hypoglycemia risk stratification tool by mapping the combination of risk factors to high, intermediate, or low risk of having any hypoglycemia-related utilization in the following 12 months.
Regarding patient characteristics, there were no significant differences in the distribution of the 6 predictors between the Kaiser derivation vs. validation samples, but there were significant differences across external validation samples. For example, the VA sample was predominantly men, with a higher proportion of patients older than 77 years, and had the highest proportion of patients with severe or end-stage kidney disease. Regarding model validation, the tool performed well in both internal validation (C statistic = 0.83) and external validation samples (VA C statistic = 0.81; GH C statistic = 0.79).
Conclusion. This hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions to reduce hypoglycemia risk and improve patient safety.
Commentary
It is estimated that 25 million people in the United States have diabetes [2]. Hypoglycemia is a frequent adverse event in patients with T2D, being more common than acute hyperglycemic emergencies such as hyperosmolar hyperglycemic state [3]. Iatrogenic hypoglycemia due to glucose-lowering medication can result in hypoglycemic crisis that requires administration of carbohydrates, glucagon, or other resuscitative actions in the ED or in hospital [4,5]. The estimated total annual direct medical costs of hypoglycemia-related utilization were estimated at approximately $1.8 billion in the United States in 2009.
The risk of hypoglycemia varies widely in patients with T2D and there are no validated methods to target interventions to the at-risk population. In this article, Karter and colleagues developed and validated a pragmatic hypoglycemia risk stratification tool that uses 6 factors to categorize the 12-month risk of hypoglycemia-related ED or hospital utilization.
Identifying patients at high-risk for hypoglycemia-related utilization provides an opportunity to mobilize resources to target this minority of patients with T2D, including deintensifying or simplifying medication regimens, prescribing glucagon kits or continuous glucose monitors, making referrals to clinical pharmacists or nurse care managers, and regularly asking about hypoglycemia events occurring outside the medical setting. This is important, as more than 95% of severe hypoglycemia events may go clinically unrecognized because they did not result in ED or hospital use [6]. In addition, as the 6 inputs were identified by EMR, intervention can include automated clinical alert flags in the EMR and automated messaging to patients with elevated risk.
Several limitations exist. The study excluded secondary discharge diagnoses for hypoglycemia as these may occur due to sepsis, acute renal failure, trauma, or other causes. In addition, the external validation populations had different distributions of disease severity and case mix. The authors attribute some of the inconsistent findings to sparse data in the GH validation sample (n = 14,972). Finally, this tool was developed to stratify the population into 3 levels of risk, and it should not be used to estimate the probability of hypoglycemic-related utilization for an individual patient.
Applications for Clinical Practice
The EMR-based hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions, including integration into existing EMR as clinical decision aid, to reduce hypoglycemia risk and improve patient safety.
—Ka Ming Gordon Ngai, MD, MPH
Study Overview
Objective. To develop and validate a risk stratification tool to categorize 12-month risk of hypoglycemia-related emergency department (ED) or hospital use among patients with type 2 diabetes (T2D).
Design. Prospective cohort study.
Setting and participants. Patients with T2D from Kaiser Permanente Northern California were identified using electronic medical records (EMR). Patients had to be 21 years of age or older as of the baseline date of 1 January 2014, with continuous health plan membership for 24 months prebaseline and pharmacy benefits for 12 months prebaseline. Of the 233,330 adults identified, 24,719 were excluded for unknown diabetes type, and 3614 were excluded for type 1 diabetes. The remaining 206,435 eligible patients with T2D were randomly split into an 80% derivation sample (n = 165,148) for tool development and 20% internal validation sample (n = 41,287). Using similar eligibility criteria, 2 external validation samples were derived from the Veterans Administration Diabetes Epidemiology Cohort (VA) (n = 1,335,966 adults) as well as from Group Health Cooperative (GH) (n = 14,972).
Main outcome measure. The primary outcome was the occurrence of any hypoglycemia-related ED visit or hospital use during the 12 months postbaseline. A primary diagnosis of hypoglycemia was ascertained using the following International Classification of Diseases, Ninth Revision (ICD-9) codes: 251.0, 251.1, 251.2, 962.3, or 250.8, without concurrent 259.3, 272.7, 681.xx, 686.9x, 707.a-707.9, 709.3, 730.0-730.2, or 731.8 codes [1]. Secondary discharge diagnoses for hypoglycemia were not used because they are often attributable to events that occurred during the ED or hospital encounter.
Main results. Beginning with 156 (122 categorical and 34 continuous) candidate clinical, demographic, and behavioral predictor variables for model development, the final classification tree was based on 6 patient-specific variables: total number of prior episodes of hypoglycemia-related ED or hospital utilization (0, 1–2, ≥ 3 times), number of ED encounters for any reason in the prior 12 months (< 2, ≥ 2 times), insulin use (yes/no), sulfonylurea use (yes/no), presence of severe or end-stage kidney disease (dialysis or chronic kidney disease stage 4 or 5 determined by estimated glomerular filtration rate of ≤ 29 mL/min/1.73 m² (yes/no), and age younger than 77 years (yes/no). This classification tree resulted in 10 mutually exclusive leaf nodes, each yielding an estimated annual risk of hypoglycemia-related utilization, which were categorized as high (> 5%), intermediate (1%–5%), or low (< 1%).
The above classification model was then transcribed into a checklist-style hypoglycemia risk stratification tool by mapping the combination of risk factors to high, intermediate, or low risk of having any hypoglycemia-related utilization in the following 12 months.
Regarding patient characteristics, there were no significant differences in the distribution of the 6 predictors between the Kaiser derivation vs. validation samples, but there were significant differences across external validation samples. For example, the VA sample was predominantly men, with a higher proportion of patients older than 77 years, and had the highest proportion of patients with severe or end-stage kidney disease. Regarding model validation, the tool performed well in both internal validation (C statistic = 0.83) and external validation samples (VA C statistic = 0.81; GH C statistic = 0.79).
Conclusion. This hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions to reduce hypoglycemia risk and improve patient safety.
Commentary
It is estimated that 25 million people in the United States have diabetes [2]. Hypoglycemia is a frequent adverse event in patients with T2D, being more common than acute hyperglycemic emergencies such as hyperosmolar hyperglycemic state [3]. Iatrogenic hypoglycemia due to glucose-lowering medication can result in hypoglycemic crisis that requires administration of carbohydrates, glucagon, or other resuscitative actions in the ED or in hospital [4,5]. The estimated total annual direct medical costs of hypoglycemia-related utilization were estimated at approximately $1.8 billion in the United States in 2009.
The risk of hypoglycemia varies widely in patients with T2D and there are no validated methods to target interventions to the at-risk population. In this article, Karter and colleagues developed and validated a pragmatic hypoglycemia risk stratification tool that uses 6 factors to categorize the 12-month risk of hypoglycemia-related ED or hospital utilization.
Identifying patients at high-risk for hypoglycemia-related utilization provides an opportunity to mobilize resources to target this minority of patients with T2D, including deintensifying or simplifying medication regimens, prescribing glucagon kits or continuous glucose monitors, making referrals to clinical pharmacists or nurse care managers, and regularly asking about hypoglycemia events occurring outside the medical setting. This is important, as more than 95% of severe hypoglycemia events may go clinically unrecognized because they did not result in ED or hospital use [6]. In addition, as the 6 inputs were identified by EMR, intervention can include automated clinical alert flags in the EMR and automated messaging to patients with elevated risk.
Several limitations exist. The study excluded secondary discharge diagnoses for hypoglycemia as these may occur due to sepsis, acute renal failure, trauma, or other causes. In addition, the external validation populations had different distributions of disease severity and case mix. The authors attribute some of the inconsistent findings to sparse data in the GH validation sample (n = 14,972). Finally, this tool was developed to stratify the population into 3 levels of risk, and it should not be used to estimate the probability of hypoglycemic-related utilization for an individual patient.
Applications for Clinical Practice
The EMR-based hypoglycemia risk stratification tool categorizes the 12-month risk of hypoglycemia-related utilization in patients with T2D using 6 easily obtained inputs. This tool can facilitate efficient targeting of population management interventions, including integration into existing EMR as clinical decision aid, to reduce hypoglycemia risk and improve patient safety.
—Ka Ming Gordon Ngai, MD, MPH
1. Ginde AA, Blanc PG, Lieberman RM, et al. Validation of ICD-9-CM coding algorithm for improved identification of hypoglycemia visits. BMC Endocr Disord 2008;8:4.
2. Gregg EW, Li Y, Wang J, et al. Change in diabetes-related complications in the United States, 1990-2010. N Engl J Med 2014; 370:1514–23.
3. Lipska KJ, Ross JS, Wang Y, et al. National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011. JAMA Intern Med 2014:174: 1116–24.
4. Pogach L, Aron D. Balancing hypoglycemia and glycemic control: a public health approach for insulin safety. JAMA 2010;303:2076–7.
5. Lee SJ. So much insulin, so much hypoglycemia. JAMA Intern Med 2014;174:686–8.
6. Sarkar U, Karter AJ, Liu JY, et al. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: the Diabetes Study of Northern California (DISTANCE). J Gen Intern Med 2010;25:962–8.
1. Ginde AA, Blanc PG, Lieberman RM, et al. Validation of ICD-9-CM coding algorithm for improved identification of hypoglycemia visits. BMC Endocr Disord 2008;8:4.
2. Gregg EW, Li Y, Wang J, et al. Change in diabetes-related complications in the United States, 1990-2010. N Engl J Med 2014; 370:1514–23.
3. Lipska KJ, Ross JS, Wang Y, et al. National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011. JAMA Intern Med 2014:174: 1116–24.
4. Pogach L, Aron D. Balancing hypoglycemia and glycemic control: a public health approach for insulin safety. JAMA 2010;303:2076–7.
5. Lee SJ. So much insulin, so much hypoglycemia. JAMA Intern Med 2014;174:686–8.
6. Sarkar U, Karter AJ, Liu JY, et al. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: the Diabetes Study of Northern California (DISTANCE). J Gen Intern Med 2010;25:962–8.
British Society of Rheumatology issues first U.K. lupus guideline
From diagnosing, assessing, and managing common manifestations of nonrenal lupus, such as skin rashes and arthritis, through dealing with less common but potentially more serious problems such as kidney disease, the guideline aims to help everyone involved in the management of patients with SLE to give the best, evidenced-based care.

U.K.-specific guidance
The British Society for Rheumatology’s (BSR) guideline is the first to specifically cover lupus management in the United Kingdom, and it builds on existing European League Against Rheumatism (EULAR) guidance published almost a decade ago (Ann Rheum Dis. 2008;67:195-205), and more recent EULAR/European Renal Association–European Dialysis and Transplant Association (Ann Rheum Dis. 2012;71:1771-82) and American College of Rheumatology (Arthritis Care Res. 2012;64:797-808) recommendations on managing lupus nephritis (LN).
The BSR’s full guideline provides a summary of the EULAR/ERA-EDTA’s LN guidelines, and the degree to which their new guidelines concur.
As with all BSR guidelines, the recommendations have been developed by a multidisciplinary team. This included academic and consultant rheumatologists and nephrologists, rheumatology trainees, a primary care physician, a clinical nurse specialist, a patient representative, and a lay member. This should make the guideline relevant to anyone who may come across someone with SLE, including primary care physicians, dermatologists, and emergency medicine practitioners.
“These recommendations are based on the literature review covering the diagnosis, assessment, monitoring, and treatment of mild, moderate, and severe lupus, including neuropsychiatric disease,” the guideline authors stated. They noted that the reason they looked only at nonrenal disease was because the EULAR/ERA-EDTA recommendations for LN have been published close to the time that work was started on the guideline. Each of the recommendations the multidisciplinary team devised was carefully graded and the degree to which members of the team agreed with each recommendation was calculated.
Diagnosis recommendations
One of the key recommendations regarding the diagnosis of SLE is that a combination of clinical features and at least one relevant immunologic irregularity needs to be present. Blood tests, including serologic marker tests, should be performed if there is clinical suspicion of lupus.
Another recommendation on diagnosis is that if antinuclear antibodies are absent, then it is unlikely that the patient has lupus. This is because around 95% of SLE patients will test positive for antinuclear antibodies. Antiphospholipid antibodies should be tested in all patients with lupus at baseline, according to the guideline.
Monitoring recommendations
“Patients with SLE should be monitored on a regular basis for disease manifestations, drug toxicities, and comorbidities,” Dr. Gordon and her associates advised in one of the recommendations on monitoring patients. In another, they wrote that those with active disease need reviewing at least every 1-3 months, which should include evaluation of patients’ blood pressure, urine, renal function, anti-dsDNA antibodies, complement, a full blood count, and liver function tests.
It is also important to monitor patients for the presence of antiphospholipid antibodies, which are associated with thrombotic events, and it is always important to be on the lookout for comorbidities such as atherosclerotic disease and manage modifiable risk factors such as hypertension. The guideline does not go into detail about managing all of the potential complications of lupus, however, as these are covered by other national guidelines.
Treatment recommendations
Guidance on treatment is separated into how to treat patients with mild, moderate, and severe SLE. The guideline does not cover topical or systemic treatment for isolated cutaneous lupus, nor does it look at how to manage pediatric patients, the authors noted. General guidance is given on how to treat patients, and specific dosing regimens are beyond the scope of the guidelines.
The recommendations encourage the use of a variety of treatments to try to ensure less reliance on the use of steroids to control symptoms. The guideline authors noted that only hydroxychloroquine, corticosteroids, and belimumab are currently licensed treatments for lupus in the United Kingdom.
For mild disease, the disease-modifying antirheumatic drugs hydroxychloroquine and methotrexate are suggested, as are nonsteroidal anti-inflammatory drugs. If prednisolone is used, then it should be in low doses (7.5 mg or less per day). Patients should be encouraged to use sunscreen and sun avoidance to protect them against ultraviolet-induced skin lesions.
For moderate disease, higher steroid doses may be needed and immunosuppressives might be warranted, and in refractory cases, monoclonal antibody treatment may be necessary.
For severe disease, thorough investigation is essential to exclude other possible causes of any renal or neuropsychiatric manifestations. Immunosuppressive treatment is recommended, with biologic therapies considered on a case-by-case basis. Intravenous immunoglobulin and plasmapheresis may also be an option in certain patients.
Key standards of care
As general standards of care, Dr. Gordon and her coauthors wrote that “lupus patients should be referred to a physician with experience in managing lupus who can confirm the diagnosis, assess the level of disease activity, and provide advice on treatment and monitoring of the disease, its complications, and side effects of therapy.”
Furthermore, a multidisciplinary team approach is needed, and if a treatment is not helping get patients into a state of low disease activity within an expected time frame, “it is important to consider adherence to treatment and adjusting the therapy to reduce the accumulation of chronic damage.” It is also recommended that patients receive personalized advice, written information, and education about the disease and its drug treatment.
No specific funding was received from any organizations in the public, commercial, or not-for-profit sectors to carry out the work described in the guideline.
Dr. Gordon has undertaken consultancies and received honoraria from Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, MedImmune, Merck Serono, Parexel, Roche, and UCB. She has been a member of the speakers bureau for GlaxoSmithKline, UCB, and Eli Lilly. She also has received research grant support from Aspreva/Vifor Pharma in the past and currently receives it from UCB.
From diagnosing, assessing, and managing common manifestations of nonrenal lupus, such as skin rashes and arthritis, through dealing with less common but potentially more serious problems such as kidney disease, the guideline aims to help everyone involved in the management of patients with SLE to give the best, evidenced-based care.
U.K.-specific guidance
The British Society for Rheumatology’s (BSR) guideline is the first to specifically cover lupus management in the United Kingdom, and it builds on existing European League Against Rheumatism (EULAR) guidance published almost a decade ago (Ann Rheum Dis. 2008;67:195-205), and more recent EULAR/European Renal Association–European Dialysis and Transplant Association (Ann Rheum Dis. 2012;71:1771-82) and American College of Rheumatology (Arthritis Care Res. 2012;64:797-808) recommendations on managing lupus nephritis (LN).
The BSR’s full guideline provides a summary of the EULAR/ERA-EDTA’s LN guidelines, and the degree to which their new guidelines concur.
As with all BSR guidelines, the recommendations have been developed by a multidisciplinary team. This included academic and consultant rheumatologists and nephrologists, rheumatology trainees, a primary care physician, a clinical nurse specialist, a patient representative, and a lay member. This should make the guideline relevant to anyone who may come across someone with SLE, including primary care physicians, dermatologists, and emergency medicine practitioners.
“These recommendations are based on the literature review covering the diagnosis, assessment, monitoring, and treatment of mild, moderate, and severe lupus, including neuropsychiatric disease,” the guideline authors stated. They noted that the reason they looked only at nonrenal disease was because the EULAR/ERA-EDTA recommendations for LN have been published close to the time that work was started on the guideline. Each of the recommendations the multidisciplinary team devised was carefully graded and the degree to which members of the team agreed with each recommendation was calculated.
Diagnosis recommendations
One of the key recommendations regarding the diagnosis of SLE is that a combination of clinical features and at least one relevant immunologic irregularity needs to be present. Blood tests, including serologic marker tests, should be performed if there is clinical suspicion of lupus.
Another recommendation on diagnosis is that if antinuclear antibodies are absent, then it is unlikely that the patient has lupus. This is because around 95% of SLE patients will test positive for antinuclear antibodies. Antiphospholipid antibodies should be tested in all patients with lupus at baseline, according to the guideline.
Monitoring recommendations
“Patients with SLE should be monitored on a regular basis for disease manifestations, drug toxicities, and comorbidities,” Dr. Gordon and her associates advised in one of the recommendations on monitoring patients. In another, they wrote that those with active disease need reviewing at least every 1-3 months, which should include evaluation of patients’ blood pressure, urine, renal function, anti-dsDNA antibodies, complement, a full blood count, and liver function tests.
It is also important to monitor patients for the presence of antiphospholipid antibodies, which are associated with thrombotic events, and it is always important to be on the lookout for comorbidities such as atherosclerotic disease and manage modifiable risk factors such as hypertension. The guideline does not go into detail about managing all of the potential complications of lupus, however, as these are covered by other national guidelines.
Treatment recommendations
Guidance on treatment is separated into how to treat patients with mild, moderate, and severe SLE. The guideline does not cover topical or systemic treatment for isolated cutaneous lupus, nor does it look at how to manage pediatric patients, the authors noted. General guidance is given on how to treat patients, and specific dosing regimens are beyond the scope of the guidelines.
The recommendations encourage the use of a variety of treatments to try to ensure less reliance on the use of steroids to control symptoms. The guideline authors noted that only hydroxychloroquine, corticosteroids, and belimumab are currently licensed treatments for lupus in the United Kingdom.
For mild disease, the disease-modifying antirheumatic drugs hydroxychloroquine and methotrexate are suggested, as are nonsteroidal anti-inflammatory drugs. If prednisolone is used, then it should be in low doses (7.5 mg or less per day). Patients should be encouraged to use sunscreen and sun avoidance to protect them against ultraviolet-induced skin lesions.
For moderate disease, higher steroid doses may be needed and immunosuppressives might be warranted, and in refractory cases, monoclonal antibody treatment may be necessary.
For severe disease, thorough investigation is essential to exclude other possible causes of any renal or neuropsychiatric manifestations. Immunosuppressive treatment is recommended, with biologic therapies considered on a case-by-case basis. Intravenous immunoglobulin and plasmapheresis may also be an option in certain patients.
Key standards of care
As general standards of care, Dr. Gordon and her coauthors wrote that “lupus patients should be referred to a physician with experience in managing lupus who can confirm the diagnosis, assess the level of disease activity, and provide advice on treatment and monitoring of the disease, its complications, and side effects of therapy.”
Furthermore, a multidisciplinary team approach is needed, and if a treatment is not helping get patients into a state of low disease activity within an expected time frame, “it is important to consider adherence to treatment and adjusting the therapy to reduce the accumulation of chronic damage.” It is also recommended that patients receive personalized advice, written information, and education about the disease and its drug treatment.
No specific funding was received from any organizations in the public, commercial, or not-for-profit sectors to carry out the work described in the guideline.
Dr. Gordon has undertaken consultancies and received honoraria from Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, MedImmune, Merck Serono, Parexel, Roche, and UCB. She has been a member of the speakers bureau for GlaxoSmithKline, UCB, and Eli Lilly. She also has received research grant support from Aspreva/Vifor Pharma in the past and currently receives it from UCB.
From diagnosing, assessing, and managing common manifestations of nonrenal lupus, such as skin rashes and arthritis, through dealing with less common but potentially more serious problems such as kidney disease, the guideline aims to help everyone involved in the management of patients with SLE to give the best, evidenced-based care.
U.K.-specific guidance
The British Society for Rheumatology’s (BSR) guideline is the first to specifically cover lupus management in the United Kingdom, and it builds on existing European League Against Rheumatism (EULAR) guidance published almost a decade ago (Ann Rheum Dis. 2008;67:195-205), and more recent EULAR/European Renal Association–European Dialysis and Transplant Association (Ann Rheum Dis. 2012;71:1771-82) and American College of Rheumatology (Arthritis Care Res. 2012;64:797-808) recommendations on managing lupus nephritis (LN).
The BSR’s full guideline provides a summary of the EULAR/ERA-EDTA’s LN guidelines, and the degree to which their new guidelines concur.
As with all BSR guidelines, the recommendations have been developed by a multidisciplinary team. This included academic and consultant rheumatologists and nephrologists, rheumatology trainees, a primary care physician, a clinical nurse specialist, a patient representative, and a lay member. This should make the guideline relevant to anyone who may come across someone with SLE, including primary care physicians, dermatologists, and emergency medicine practitioners.
“These recommendations are based on the literature review covering the diagnosis, assessment, monitoring, and treatment of mild, moderate, and severe lupus, including neuropsychiatric disease,” the guideline authors stated. They noted that the reason they looked only at nonrenal disease was because the EULAR/ERA-EDTA recommendations for LN have been published close to the time that work was started on the guideline. Each of the recommendations the multidisciplinary team devised was carefully graded and the degree to which members of the team agreed with each recommendation was calculated.
Diagnosis recommendations
One of the key recommendations regarding the diagnosis of SLE is that a combination of clinical features and at least one relevant immunologic irregularity needs to be present. Blood tests, including serologic marker tests, should be performed if there is clinical suspicion of lupus.
Another recommendation on diagnosis is that if antinuclear antibodies are absent, then it is unlikely that the patient has lupus. This is because around 95% of SLE patients will test positive for antinuclear antibodies. Antiphospholipid antibodies should be tested in all patients with lupus at baseline, according to the guideline.
Monitoring recommendations
“Patients with SLE should be monitored on a regular basis for disease manifestations, drug toxicities, and comorbidities,” Dr. Gordon and her associates advised in one of the recommendations on monitoring patients. In another, they wrote that those with active disease need reviewing at least every 1-3 months, which should include evaluation of patients’ blood pressure, urine, renal function, anti-dsDNA antibodies, complement, a full blood count, and liver function tests.
It is also important to monitor patients for the presence of antiphospholipid antibodies, which are associated with thrombotic events, and it is always important to be on the lookout for comorbidities such as atherosclerotic disease and manage modifiable risk factors such as hypertension. The guideline does not go into detail about managing all of the potential complications of lupus, however, as these are covered by other national guidelines.
Treatment recommendations
Guidance on treatment is separated into how to treat patients with mild, moderate, and severe SLE. The guideline does not cover topical or systemic treatment for isolated cutaneous lupus, nor does it look at how to manage pediatric patients, the authors noted. General guidance is given on how to treat patients, and specific dosing regimens are beyond the scope of the guidelines.
The recommendations encourage the use of a variety of treatments to try to ensure less reliance on the use of steroids to control symptoms. The guideline authors noted that only hydroxychloroquine, corticosteroids, and belimumab are currently licensed treatments for lupus in the United Kingdom.
For mild disease, the disease-modifying antirheumatic drugs hydroxychloroquine and methotrexate are suggested, as are nonsteroidal anti-inflammatory drugs. If prednisolone is used, then it should be in low doses (7.5 mg or less per day). Patients should be encouraged to use sunscreen and sun avoidance to protect them against ultraviolet-induced skin lesions.
For moderate disease, higher steroid doses may be needed and immunosuppressives might be warranted, and in refractory cases, monoclonal antibody treatment may be necessary.
For severe disease, thorough investigation is essential to exclude other possible causes of any renal or neuropsychiatric manifestations. Immunosuppressive treatment is recommended, with biologic therapies considered on a case-by-case basis. Intravenous immunoglobulin and plasmapheresis may also be an option in certain patients.
Key standards of care
As general standards of care, Dr. Gordon and her coauthors wrote that “lupus patients should be referred to a physician with experience in managing lupus who can confirm the diagnosis, assess the level of disease activity, and provide advice on treatment and monitoring of the disease, its complications, and side effects of therapy.”
Furthermore, a multidisciplinary team approach is needed, and if a treatment is not helping get patients into a state of low disease activity within an expected time frame, “it is important to consider adherence to treatment and adjusting the therapy to reduce the accumulation of chronic damage.” It is also recommended that patients receive personalized advice, written information, and education about the disease and its drug treatment.
No specific funding was received from any organizations in the public, commercial, or not-for-profit sectors to carry out the work described in the guideline.
Dr. Gordon has undertaken consultancies and received honoraria from Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, MedImmune, Merck Serono, Parexel, Roche, and UCB. She has been a member of the speakers bureau for GlaxoSmithKline, UCB, and Eli Lilly. She also has received research grant support from Aspreva/Vifor Pharma in the past and currently receives it from UCB.
FROM RHEUMATOLOGY
Vaccination program cut hospital-treated RV gastroenteritis in young children
under 5 years, and it more than adequately pays for itself in secondary health care costs, said Tuija Leino of the National Institute for Health and Welfare, Helsinki, and associates.
Since 2009, all Finnish children younger than 5 years have been offered an RV vaccine.
The investigators conducted a register-based study comparing the RV disease burden before and after introduction of RV vaccination, with the years 1999-2005 as the prevaccine period and the years 2010-2014 as the vaccination period. The study population was all children younger than 5 years living in Finland during the two study periods.

The relative reduction in inpatient RVGE incidence ranged from 86% in the 4-year-old children to 94% in the 0-year-old children, the researchers reported. That amounted to 843 prevented inpatient cases in children under 5 years.
The highest incidence of RVGE, which is rarely treated in hospital outpatients, was 0.4/1,000 person-years in children aged 1 year or younger. The relative reduction in outpatient RVGE incidence was 86% in the 0-year-olds and 100% in the 3- and 4-year-olds. The RV vaccination program prevented only 64 hospital outpatient cases in children younger than 5 years of age in 2014.
RV vaccination also resulted in a reduction of unspecified viral gastroenteritis (UVGE) incidence by 84%. Because the incidence of UVGE in 1-year-olds during the prevaccine era was more than twice the incidence of RVGE, the absolute reduction from 10.7 to 1.7 per 1,000 person-years “reflects a removal of a much larger disease burden than the reduction in the most specific outcome of inpatient RVGE,” the researchers said.
The annually prevented inpatient UVGE cases in children up to 4 years was 1,522, almost twice as many as the prevented inpatient RVGE cases. In the prevaccine era, the UVGE reduction was greatest among 1-year-olds, at 71%. In children younger than 5 years of age, 1,313 UVGE hospital outpatient cases were prevented in 2014.
“Considering secondary health care, the program annually pays for itself almost two times over in Finland,” the investigators concluded.
Read more in Vaccine (2017 Oct 9;35[42]:5611-7).
The researchers had no conflicts of interest.
under 5 years, and it more than adequately pays for itself in secondary health care costs, said Tuija Leino of the National Institute for Health and Welfare, Helsinki, and associates.
Since 2009, all Finnish children younger than 5 years have been offered an RV vaccine.
The investigators conducted a register-based study comparing the RV disease burden before and after introduction of RV vaccination, with the years 1999-2005 as the prevaccine period and the years 2010-2014 as the vaccination period. The study population was all children younger than 5 years living in Finland during the two study periods.
The relative reduction in inpatient RVGE incidence ranged from 86% in the 4-year-old children to 94% in the 0-year-old children, the researchers reported. That amounted to 843 prevented inpatient cases in children under 5 years.
The highest incidence of RVGE, which is rarely treated in hospital outpatients, was 0.4/1,000 person-years in children aged 1 year or younger. The relative reduction in outpatient RVGE incidence was 86% in the 0-year-olds and 100% in the 3- and 4-year-olds. The RV vaccination program prevented only 64 hospital outpatient cases in children younger than 5 years of age in 2014.
RV vaccination also resulted in a reduction of unspecified viral gastroenteritis (UVGE) incidence by 84%. Because the incidence of UVGE in 1-year-olds during the prevaccine era was more than twice the incidence of RVGE, the absolute reduction from 10.7 to 1.7 per 1,000 person-years “reflects a removal of a much larger disease burden than the reduction in the most specific outcome of inpatient RVGE,” the researchers said.
The annually prevented inpatient UVGE cases in children up to 4 years was 1,522, almost twice as many as the prevented inpatient RVGE cases. In the prevaccine era, the UVGE reduction was greatest among 1-year-olds, at 71%. In children younger than 5 years of age, 1,313 UVGE hospital outpatient cases were prevented in 2014.
“Considering secondary health care, the program annually pays for itself almost two times over in Finland,” the investigators concluded.
Read more in Vaccine (2017 Oct 9;35[42]:5611-7).
The researchers had no conflicts of interest.
under 5 years, and it more than adequately pays for itself in secondary health care costs, said Tuija Leino of the National Institute for Health and Welfare, Helsinki, and associates.
Since 2009, all Finnish children younger than 5 years have been offered an RV vaccine.
The investigators conducted a register-based study comparing the RV disease burden before and after introduction of RV vaccination, with the years 1999-2005 as the prevaccine period and the years 2010-2014 as the vaccination period. The study population was all children younger than 5 years living in Finland during the two study periods.
The relative reduction in inpatient RVGE incidence ranged from 86% in the 4-year-old children to 94% in the 0-year-old children, the researchers reported. That amounted to 843 prevented inpatient cases in children under 5 years.
The highest incidence of RVGE, which is rarely treated in hospital outpatients, was 0.4/1,000 person-years in children aged 1 year or younger. The relative reduction in outpatient RVGE incidence was 86% in the 0-year-olds and 100% in the 3- and 4-year-olds. The RV vaccination program prevented only 64 hospital outpatient cases in children younger than 5 years of age in 2014.
RV vaccination also resulted in a reduction of unspecified viral gastroenteritis (UVGE) incidence by 84%. Because the incidence of UVGE in 1-year-olds during the prevaccine era was more than twice the incidence of RVGE, the absolute reduction from 10.7 to 1.7 per 1,000 person-years “reflects a removal of a much larger disease burden than the reduction in the most specific outcome of inpatient RVGE,” the researchers said.
The annually prevented inpatient UVGE cases in children up to 4 years was 1,522, almost twice as many as the prevented inpatient RVGE cases. In the prevaccine era, the UVGE reduction was greatest among 1-year-olds, at 71%. In children younger than 5 years of age, 1,313 UVGE hospital outpatient cases were prevented in 2014.
“Considering secondary health care, the program annually pays for itself almost two times over in Finland,” the investigators concluded.
Read more in Vaccine (2017 Oct 9;35[42]:5611-7).
The researchers had no conflicts of interest.
from vaccine
Delivering Palliative Care in a Community Hospital: Experiences and Lessons Learned from the Front Lines
From the Division of Palliative Care, Butler Health System, Butler, PA (Drs. Stein, Reefer, Selvaggi, Ms. Doverspike); the University of Pittsburgh Medical Center, Pittsburgh, PA (Dr. Rajagopal); and the Duke Cancer Institute and Duke Fuqua School of Business, Durham, NC (Dr. Kamal).
Abstract
- Objective: To describe an approach to develop a community-centric palliative care program in a rural community health system and to review data collected over the program’s first year.
- Methods: We describe the underlying foundations of our program development including the health system’s prioritization of a palliative care program, funding opportunities, collaboration with community supports, and the importance of building a team and program that reflects a community’s needs. Data were collected through a program-maintained spreadsheet and a data monitoring system available through the Global Palliative Care Quality Alliance.
- Results: 516 new inpatient consultations were seen during the first year, for a penetration of 3.7%. The demographics of the patients who received consultation reflect that of the surrounding community. Over 50% of patients seen within the first year died, and hospice utilization at home and within facilities and inpatient hospice units increased. In addition, 79% of the patients seen by the palliative care team had a confirmed code status of do not resuscitate and do not intubate.
- Conclusions: Butler Health System’s approach to development of a palliative care program has resulted in increasing utilization of palliative care services in the hospital. Having hospital administration support, community support, and understanding the individualized needs of a community has been essential for the program’s expansion.
Key words: palliative care; program development; community hospital; rural.
Since its inception, palliative care has been committed to providing specialty-level consultation services to individuals with serious illness and their loved ones. The field has focused heavily on growth and acceptance, consistently moving upstream with regards to illness trajectory, across diseases, and across demographic variables such as age (eg, pediatric quality of life programs) and race (eg, community outreach programs addressing racial disparities in hospice use). An important frontier that remains challenging for much of the field is expansion into the community setting, where resources, implicit acceptance, and patient populations may vary.
As health system leaders appreciate the positive impacts palliative medicine on patient care and care quality, barriers to implementing palliative care programs in community hospitals must be addressed in ways tailored to the unique needs of smaller organizations and their communities. The goal of this paper is to outline the approach taken to develop Butler Health System’s community-centric palliative care program, describe our program’s underlying foundation rooted in community supports, and recount steps we have taken thus far to impact patient care in our hospital, health system, and community through the program’s first year.
Community Hospital Palliative Care—The Necessity and the Challenges
Palliative care has made strides in its growth and acceptance in the last decade; yet, the distribution of that growth has been skewed. Although 67% of hospitals now report access to specialist palliative care programs, most of the 148% growth over the last decade has been actualized in larger hospitals. Ninety percent of hospitals with greater than 300 beds report palliative care service availability whereas only 56% of small hospitals were identified to have this specialty care [1].
The inequity of access is also seen in other countries. A recent Canadian study retrospectively examined access to care of 23,860 deceased patients in Nova Scotia. Although they found 40.9% of study subjects were enrolled in a palliative care program at urban, academic centers, patients in a rural setting were only a third as likely to be enrolled in a palliative care program [2]. This access gap has important effects on patient-level outcomes, as evidence has consistently demonstrated that patients in rural settings who receive palliative care have decreased unnecessary hospitalizations and less in-hospital deaths [3].
While evidence of improved outcomes is strong, important barriers stand in the way. In a 2013 study, 374 health care providers at 236 rural hospitals in 7 states were interviewed to determine barriers to providing palliative care in rural settings. Barriers identified include a lack of administrative support, access to basic palliative care training for primary care physicians, and limited relationships to hospices [4]. Additional challenges include lack of access to tertiary-level specialty clinicians, access to and misconceptions about prescription medications, transportation for patients and providers, and incorporating a patient’s community supports [5–7].
Proposed Solutions
Techniques to improve palliative care access for rural and community centers that have been previously reviewed in the literature include videoconferencing with tertiary care experts in palliative care and education through small community-level lectures [8–10]. Goals of rural and suburban palliative care programs are broadly similar to programs at academic medical centers; however, few studies have identified impact of palliative medicine on patient care in community settings. In one suburban practice, a study found that patients were more likely to die at home if they had multiple caregivers, increased length of time under palliative care, and older age upon referral [11].
The United States has few large-scale pilot programs attempting to address the palliative needs of a more suburban or rural population. Of these, the Minnesota Rural Palliative Care Initiative developed by Stratis Health is perhaps the best publicized. Stratis Health developed and led an 18-month learning collaborative from October 2008 to April 2010 through which community teams developed or improved palliative care services. Through this initiative, a community-based health care practice model was developed that took advantage of the strong interrelationships within rural communities. After 18 months, 6 out of 10 rural Minnesota communities had formal palliative care programs, and 8 to 9 out of 10 had capabilities to at least address advance directives as well as provider and community education [12]. In another initiative, the NIH established a new suburban clinic with tertiary providers specifically for resource intensive, underserved patients [13]. The clinic was established by partnering with a service that was already in place in the community. Twenty-seven patients were seen within 7 months. The most common consults were patients with numerous comorbidities and chronic pain rather than terminal diagnoses. Given the intensive need of these patients, the authors felt that a consultation service and an interdisciplinary team that included psychosocial/spiritual/social work providers offered the most efficient method of delivering advanced palliative care needs.
The research regarding both solutions to challenges and novel methods of addressing the care gap remains sparse as evidenced by the conclusions of multiple systematic reviews and meta-analyses and the inability of the Cochrane review to find papers meeting inclusion criteria regarding techniques of community support in palliative care [14,15]. There remains a need to identify practical techniques of implementing palliative care in rural and suburban settings.
The Butler Health System Experience
In August 2015, we set out to start the first hospital-based palliative care consultation service in the Butler Health System. The health system is a nonprofit, single-hospital system anchored by Butler Memorial Hospital, a 294-bed community hospital located within a rural Pennsylvania county of 186,000 residents, 35 miles north of Pittsburgh. Butler County consists of a predominantly white, non-Hispanic population with over 15% of the residents being older than 65 years of age. The median household income is $61,000 earned primarily through blue collar occupations [16]. Driven by 53 employed primary care physicians, the health system provides services for 75,000 patients at sites covering an area of 4000 square miles. The hospital provides general medical, critical, surgical and subspecialty care and behavior health services as a regional referral center for 4 surrounding rural counties, accepting 12,500 inpatient admissions annually. A hospitalist service admits the majority of oncology patients, and the intensive care unit (ICU) is an open unit, where patients are admitted to the hospitalist, primary care, or surgical service.
While no formal needs assessment was performed prior to program development, perceptions of inadequate pain control, overuse of naloxone, underutilization of hospice services, and lack of consistent quality in end-of-life care were identified. These concerns were voiced at the levels of direct patient care on the floors, and by nursing and physician hospital leadership. Prior to our program, the chief medical officer attended the national Center to Advance Palliative Care conference to better understand the field of palliative care and its impact on improving quality of care. Concurrently, our health system was expanding its inpatient capabilities (eg, advanced neurologic and cardiac services), resulting in admissions with increased disease severity and illness complexity. With the vision of improved patient care, prioritizing quality end-of-life care and symptom management, the hospital board and administration overwhelmingly supported the development of the palliative care program, philosophically and financially.
Laying a Foundation—Funding, Collaboration, and Team Building
Funding and staffing are 2 important factors when building any program. Sources of funding for palliative care programs may include hospital support, billing revenue, grants, and philanthropy. Program development was a priority for the hospital and community. To help offset costs, efforts to raise financial support focused on utilizing the health system’s annual fundraising events. Through the generosity of individuals in the community, the hospital’s annual gala event, and donations from the hospital’s auxiliary, a total of $230,000 was raised prior to program initiation. Funds budgeted through direct hospital support and fundraising were allocated towards hiring palliative care team members and community marketing projects.
The hospital’s surrounding community is fortunate to have 2 local inpatient hospice facilities, and these relationships were imperative to providing quality end-of-life care preceding our palliative care program. A formal partnership was previously established with one while the other remains an important referral facility due to its proximity to the hospital. These hospice services are encouraged to participate in our weekly palliative care interdisciplinary team meetings. Their incorporation has improved coordination, continuity, and translation of care upon patient discharge from the acute hospital setting. Additionally, the relationships have been beneficial in tracking patients’ outcomes and data collection.
The standard structure of a palliative care team described by the Joint Commission and National Consensus Panel for Palliative Care consists of a physician, registered nurse or advanced practice provider, chaplaincy, and social work. Despite this recommendation, less than 40% of surveyed hospitals met the criteria, and less than 25% have dedicated funding to cover these positions [17]. Upon inception of our palliative care program, 2.6 funded full-time equivalents (FTEs) were allocated. These positions included a physician (1.0 FTE), a physician assistant (1.0 FTE), and a part time palliative care social worker (0.6 FTE). The 2015 National Palliative Care Registry found that 3.2 funded FTEs per 10,000 admissions is the average for hospitals with 150 to 299 beds [17]. The uncertainty of the utilization and consult volume, and the limited amount of qualified palliative care trained practitioners, resulted in the palliative program starting below this mean at 2.1 funded FTEs per 10,000 admissions. All the funded positions were located on site at the hospital. The pre-existing volunteer hospital chaplain service was identified as the pastoral care component for the program.
Increased FTEs have been associated with increased palliative care service penetration and ultimately in decreased time to consult [18]. In response to increasing consult volumes, concerns for delays in time to consult, and in preparation for expansion to an outpatient service, the palliative care department acquired an additional funded physician FTE (1.0). Ultimately the service reached a total of 3.6 FTE for inpatient services during its first 12 months; proportionately this resulted in an increase to 2.9 FTE per 10,000 admissions based on the yearly admission rate of 12,500 patients.
Educational Outreach
The success of a palliative care program depends on other clinicians’ acceptance and referral to the clinical program. We took a 2-pronged approach, focusing on both hospital-based and community-based education. The hospital-based nursing education included 30-minute presentations on general overviews of palliative care, differences between palliative care and hospice, and acute symptom management at the end of life. The palliative care team presented to all medical, surgical, and intensive care units and encompassed all shifts of nursing staff. These lectures included pre- and post-tests to assess for impact and feedback. Similar educational presentations, as well as an hour-long presentation on opioids and palliative care, were available for physicians for CME opportunities. We also distributed concise palliative care referral packets to outpatient primary care offices through the health system’s marketing team. The referral packets included examples of diagnoses, clinical scenarios, and symptoms to assist in the physicians’ understanding of palliative care services. The palliative care team also met with clinic office managers to discuss the program and answer questions.
There were also educational opportunities for patients and families in our community. Taking advantage of previously developed partnerships between the hospital system and local media outlets, the palliative care team performed local radio spots to educate the community on topics including an overview of palliative care, how to request palliative care, and the difference between palliative care and hospice care. We partnered with a local hospice agency and developed a well-received bereavement seminar for patients, family members, and employees and included the topic of advanced care planning.
Data Collection
We collect data using 2 different tools: a self-maintained spreadsheet shared between our palliative care clinicians, and a collective data tool (QDACT) included in our membership with and maintained by the Global Palliative Care Quality Alliance. Data collected and tracked in our spreadsheet includes date of consult, patient age, primary and secondary diagnoses, disposition, goals of care discussions, date of death, and 30-day readmissions. Through the QDACT data monitoring program, we are tracking and analyzing quality measures including symptom assessment and management and code status conversion. The QDACT database also provides financial data specific to our institution such as cost savings based on our billing, readmission rates, and length of stay.
Results
Projections, Volumes, and Penetration
Prior to the start of our program, our chief medical office used Center to Advance Palliative Care tools to project inpatient consultation volumes at our institution. Variables that are recommended by this center to guide projections include number of hospital admissions per year, hospital occupancy, disposition to hospice, as well as generalized estimations of inpatient mortality rates. Based on our data, it was expected that our program would receive 204 new inpatient consults in our first year, and 774 follow-up visits. Our actual new inpatient consults totaled 516, with 919 follow-up visits. Palliative care penetration (percentage of annual hospital admissions seen by the palliative care team) our first year was 3.7% (Table 1). 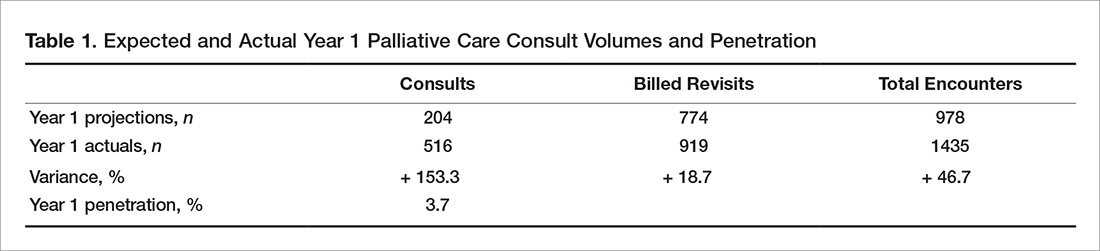
Consultation Demographics
The demographics of the patients seen by the palliative care team reflect that of Butler County’s Medicare fee-for-service (FFS) population (Table 2); however, differences were seen at the state and national level with regard to ethnicity (Table 2). 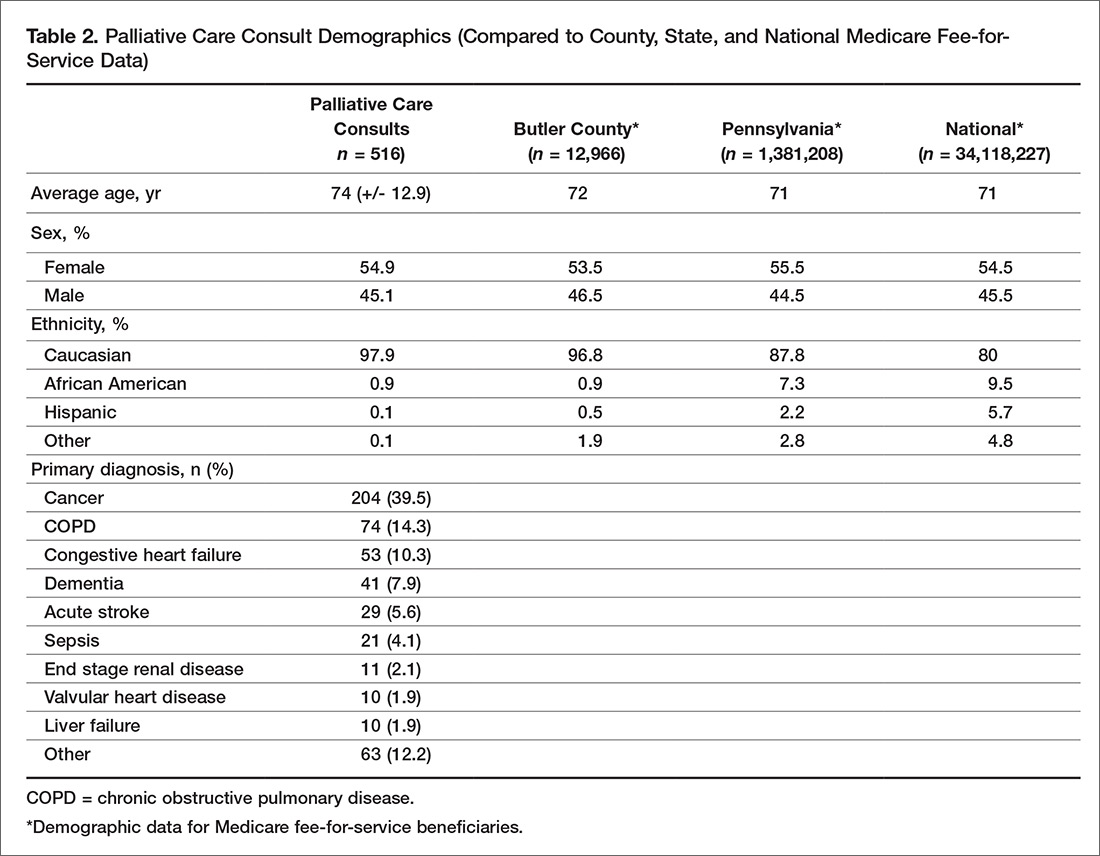
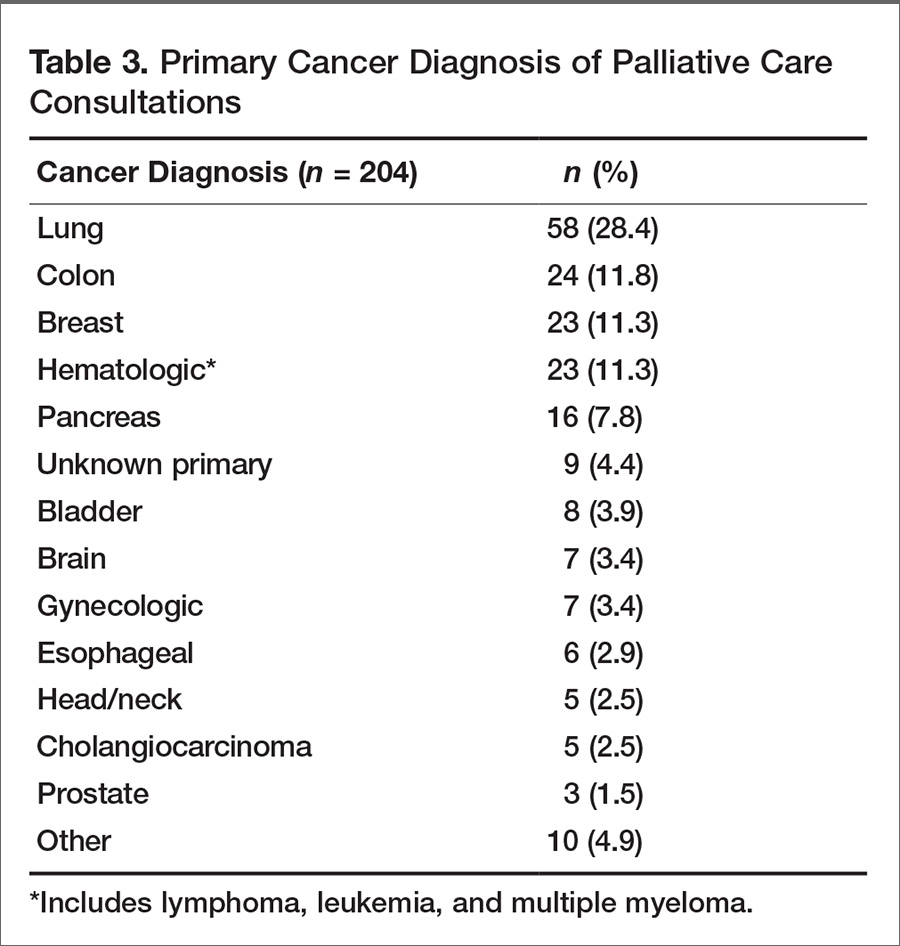
Almost half of consultations (49%) were placed by the hospitalist service. Since the ICU is an open unit, critical care consults are not adequately reflected by analysis of the ordering physician alone. Analysis of consultation location revealed that 27% of inpatient consults were located within the ICU.
Patient Outcomes and Disposition
Outcomes and discharge data from the first year were collected and reviewed. Ten percent of the patients seen by palliative care died in the hospital, and 51% of patients that were seen by palliative care died within the program’s first year. Thirty-seven percent of patients discharged from the hospital utilized hospice services at home, in residential nursing facility, or at an inpatient hospice unit. The remaining 53% were discharged without hospice services to home or facility (Figure).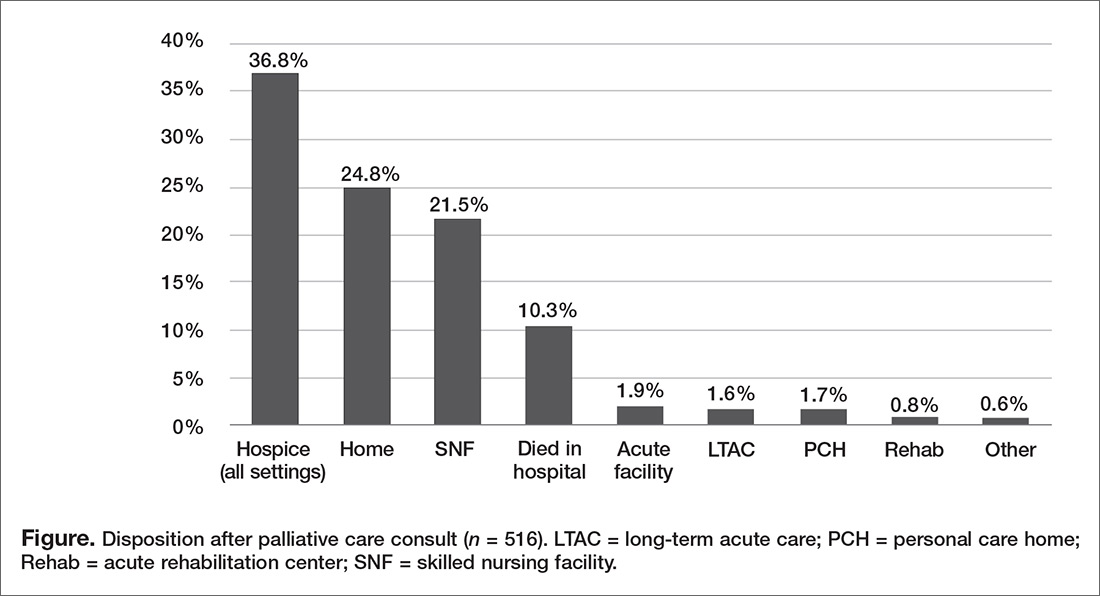
Hospice utilization by the health system increased during our first year. Compared to the 2014 calendar year, there were a total of 263 referrals for hospice services. During the first year of the palliative care program, which started August 2015, there were a total of 293 referrals. Of the 293 total hospice referrals, 190 (64.8%) of these referrals were for patients seen by the palliative care team.
Change of Code Status
Code status and changes in codes status data were collected. Of 462 individual patients prior to or at the time of palliative care consults, 43% were full code, 4% limited code, 8% unknown status, and 45% Do Not Resuscitate. After palliative care consult, 61% of the patients who were previously full/limited/unknown converted to do not resuscitate and do not intubate status. In total, 79% of patients seen by palliative care had a confirmed code status of Do Not Resuscitate and Do Not Intubate status after consult.
Discussion
In our first year, our palliative care program exceeded the expected number of inpatient consults, corresponding with a penetration of 3.7%. With the increase of funded FTEs, preliminary data shows that the department’s penetration continues to rise remaining consistent with the data and expectations [18]. During the second year, it is anticipated that over 600 inpatient palliative care consultations will be performed with an estimated penetration of 4%. This increasing penetration reflects the rising utilization of palliative care within our hospital. Since inception of the program, the service has expanded into an outpatient clinic 2 days per week. The palliative care clinic is staffed by a registered nurse (funded 0.6 FTE) and covered by the same physicians and physician assistant providing the inpatient services. The department acquired an unfunded but designated chaplaincy volunteer to assist with patients’ spiritual needs. We believe that the success of our program during the first year was related to multiple factors: a focus of integration and education by the palliative care department, health system administration buy-in, and identification of surrounding community needs.
In addition to patient care, our palliative care department also prioritizes “tangible” impacts to better establish our contributions to the health system. We have done this through participation on hospital committees, hospital policy revision teams, and by developing innovative solutions such as a terminal extubation protocol and order set for our ICU. The health system and its administration have recognized the importance of educating nursing and physician staff on palliative care services, and have supported these continued efforts alongside our clinical obligations.
Concurrent with administration buy-in, financial supports for our palliative care services were initially supplemented by the health system. Our department understands the importance of recognizing limitations of resources in communities and their hospitals. In efforts to minimize the department’s impact on our own health system’s financial resources, we have strived to offset our costs. We helped the hospital system meet pay-for-performance palliative care metrics set by the large local insurers resulting in financial hospital reimbursement valued at $600,000 in 2016.
The question of how the program may translate into other communities raises a major limitation: the homogeneity our population. The community surrounding the hospital is primarily Caucasian, with minimal representation of minority populations. While the patient population seen by our palliative care team is reflective of our surrounding county, it does not represent Medicare FFS beneficiaries on a national level or many other types of community hospitals across the country. Variations of ethnicity, age, diagnoses, and faith are fundamental, which highlights the importance of understanding the community in which a program is developed.
The rising trajectory of our palliative care service utilization has prompted a discussion of future endeavors for our program. Expectations for a continued shortage of hospice and palliative care physicians [19] and concerns for practitioner burnout [20] underlie our thoughtful approach to expansion of inpatient and outpatient services. At this time, potential projects include a consultation trigger system and incorporation of palliative care providers in ICU rounding, as well as possible expansion of outpatient services through implantation of an advanced practitioner into surrounding nursing homes and primary care offices.
We have found a growing utilization of our program at Butler Health System. Our first year experience has highlighted the importance of identifying community and hospital administrative champions as a foundation. Additionally, understanding the specific characteristics of one’s surrounding community may allow for improved integration and acceptance of palliative care in a community setting. Our program continues to work with the health system, community, and philanthropic organizations to expand the ever-growing need for palliative care services.
1. Dumanovsky T, Augustin R, Rogers M, et al. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
2. Lavergne MR, Lethbridge L, Johnston G, et al. Examining palliative care program use and place of death in rural and urban contexts: a Canadian population-based study using linked data. Rural Remote Health 2015;15:3134.
3. Seow H, Brazil K, Sussman J, et al. Impact of community based, specialist palliative care teams on hospitalisations and emergency department visits late in life and hospital deaths: a pooled analysis. BMJ 2014;348:g3496.
4. Fink RM, Oman KS, Youngwerth J, et al. A palliative care needs assessment of rural hospitals. J Palliat Med 2013;16:638–44.
5. Dumont S, Jacobs P, Turcotte V, et al. Palliative care costs in Canada: A descriptive comparison of studies of urban and rural patients near end of life. J Palliat Med 2015;29:908–17.
6. Kaasalainen S, Brazil K, Williams A, et al. Nurses' experiences providing palliative care to individuals living in rural communities: aspects of the physical residential setting. Rural Remote Health 2014;14:2728.
7. Ahmed N, Bestall JC, Ahmedzai SH, et al. Systematic review of the problems and issues of accessing specialist palliative care by patients, carers and health and social care professionals. J Palliat Med 2004;18:525–42.
8. Ray RA, Fried O, Lindsay D. Palliative care professional education via video conference builds confidence to deliver palliative care in rural and remote locations. BMC Health Serv Res 2014;14:272.
9. Bakitas MA, Elk R, Astin M, et al. Systematic review of palliative care in the rural setting. Cancer Control 2015;22:450–64.
10. Akiyama M, Hirai K, Takebayashi T, et al. The effects of community-wide dissemination of information on perceptions of palliative care, knowledge about opioids, and sense of security among cancer patients, their families, and the general public. Support Care Cancer 2016;24: 347–56.
11. Maida V. Factors that promote success in home palliative care: a study of a large suburban palliative care practice. J Palliat Care 2002;18:282–6.
12. Ceronsky L, Shearer J, Weng K, et al. Minnesota Rural Palliative Care Initiative: building palliative care capacity in rural Minnesota. J Palliat Med 2013;16:310–3.
13. Aggarwal SK, Ghosh A, Cheng MJ, et al. Initiating pain and palliative care outpatient services for the suburban underserved in Montgomery County, Maryland: Lessons learned at the NIH Clinical Center and MobileMed. Palliat Support Care 2015;16:1–6.
14. Rainsford S, MacLeod RD, Glasgow NJ. Place of death in rural palliative care: A systematic review. J Palliat Med 2016;30:745–63.
15. Horey D, Street AF, O'Connor M, et al. Training and supportive programs for palliative care volunteers in community settings. Cochrane Database Syst Rev 2015 Jul 20;(7):CD009500.
16. The United States Census Bureau: QuickFacts: Butler County, Pennsylvania. Accessed 10 Mar 2017 at www.census.gov/quickfacts/table/PST045216/42019,00.
17. Spetz J, Dudley N, Trupin L, et al. Few hospital palliative care programs meet national staffing recommendations. Health Aff 2016;35:1690–7.
18. Dumanovsky T, Rogers M, Spragens LH, et al. Impact of Staffing on Access to Palliative Care in U.S. Hospitals. J Palliat Med. 2015 Dec; 18(12). Pages 998-999.
19. Lupu D, American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage 2010;40:899–911.
20. Kamal AH, Bull JK, Wolf SP, et al. Prevalence and predictors of burnout among hospice and palliative care clinicians in the U.S. J Pain Symptom Manage 2016;51:690–6.
From the Division of Palliative Care, Butler Health System, Butler, PA (Drs. Stein, Reefer, Selvaggi, Ms. Doverspike); the University of Pittsburgh Medical Center, Pittsburgh, PA (Dr. Rajagopal); and the Duke Cancer Institute and Duke Fuqua School of Business, Durham, NC (Dr. Kamal).
Abstract
- Objective: To describe an approach to develop a community-centric palliative care program in a rural community health system and to review data collected over the program’s first year.
- Methods: We describe the underlying foundations of our program development including the health system’s prioritization of a palliative care program, funding opportunities, collaboration with community supports, and the importance of building a team and program that reflects a community’s needs. Data were collected through a program-maintained spreadsheet and a data monitoring system available through the Global Palliative Care Quality Alliance.
- Results: 516 new inpatient consultations were seen during the first year, for a penetration of 3.7%. The demographics of the patients who received consultation reflect that of the surrounding community. Over 50% of patients seen within the first year died, and hospice utilization at home and within facilities and inpatient hospice units increased. In addition, 79% of the patients seen by the palliative care team had a confirmed code status of do not resuscitate and do not intubate.
- Conclusions: Butler Health System’s approach to development of a palliative care program has resulted in increasing utilization of palliative care services in the hospital. Having hospital administration support, community support, and understanding the individualized needs of a community has been essential for the program’s expansion.
Key words: palliative care; program development; community hospital; rural.
Since its inception, palliative care has been committed to providing specialty-level consultation services to individuals with serious illness and their loved ones. The field has focused heavily on growth and acceptance, consistently moving upstream with regards to illness trajectory, across diseases, and across demographic variables such as age (eg, pediatric quality of life programs) and race (eg, community outreach programs addressing racial disparities in hospice use). An important frontier that remains challenging for much of the field is expansion into the community setting, where resources, implicit acceptance, and patient populations may vary.
As health system leaders appreciate the positive impacts palliative medicine on patient care and care quality, barriers to implementing palliative care programs in community hospitals must be addressed in ways tailored to the unique needs of smaller organizations and their communities. The goal of this paper is to outline the approach taken to develop Butler Health System’s community-centric palliative care program, describe our program’s underlying foundation rooted in community supports, and recount steps we have taken thus far to impact patient care in our hospital, health system, and community through the program’s first year.
Community Hospital Palliative Care—The Necessity and the Challenges
Palliative care has made strides in its growth and acceptance in the last decade; yet, the distribution of that growth has been skewed. Although 67% of hospitals now report access to specialist palliative care programs, most of the 148% growth over the last decade has been actualized in larger hospitals. Ninety percent of hospitals with greater than 300 beds report palliative care service availability whereas only 56% of small hospitals were identified to have this specialty care [1].
The inequity of access is also seen in other countries. A recent Canadian study retrospectively examined access to care of 23,860 deceased patients in Nova Scotia. Although they found 40.9% of study subjects were enrolled in a palliative care program at urban, academic centers, patients in a rural setting were only a third as likely to be enrolled in a palliative care program [2]. This access gap has important effects on patient-level outcomes, as evidence has consistently demonstrated that patients in rural settings who receive palliative care have decreased unnecessary hospitalizations and less in-hospital deaths [3].
While evidence of improved outcomes is strong, important barriers stand in the way. In a 2013 study, 374 health care providers at 236 rural hospitals in 7 states were interviewed to determine barriers to providing palliative care in rural settings. Barriers identified include a lack of administrative support, access to basic palliative care training for primary care physicians, and limited relationships to hospices [4]. Additional challenges include lack of access to tertiary-level specialty clinicians, access to and misconceptions about prescription medications, transportation for patients and providers, and incorporating a patient’s community supports [5–7].
Proposed Solutions
Techniques to improve palliative care access for rural and community centers that have been previously reviewed in the literature include videoconferencing with tertiary care experts in palliative care and education through small community-level lectures [8–10]. Goals of rural and suburban palliative care programs are broadly similar to programs at academic medical centers; however, few studies have identified impact of palliative medicine on patient care in community settings. In one suburban practice, a study found that patients were more likely to die at home if they had multiple caregivers, increased length of time under palliative care, and older age upon referral [11].
The United States has few large-scale pilot programs attempting to address the palliative needs of a more suburban or rural population. Of these, the Minnesota Rural Palliative Care Initiative developed by Stratis Health is perhaps the best publicized. Stratis Health developed and led an 18-month learning collaborative from October 2008 to April 2010 through which community teams developed or improved palliative care services. Through this initiative, a community-based health care practice model was developed that took advantage of the strong interrelationships within rural communities. After 18 months, 6 out of 10 rural Minnesota communities had formal palliative care programs, and 8 to 9 out of 10 had capabilities to at least address advance directives as well as provider and community education [12]. In another initiative, the NIH established a new suburban clinic with tertiary providers specifically for resource intensive, underserved patients [13]. The clinic was established by partnering with a service that was already in place in the community. Twenty-seven patients were seen within 7 months. The most common consults were patients with numerous comorbidities and chronic pain rather than terminal diagnoses. Given the intensive need of these patients, the authors felt that a consultation service and an interdisciplinary team that included psychosocial/spiritual/social work providers offered the most efficient method of delivering advanced palliative care needs.
The research regarding both solutions to challenges and novel methods of addressing the care gap remains sparse as evidenced by the conclusions of multiple systematic reviews and meta-analyses and the inability of the Cochrane review to find papers meeting inclusion criteria regarding techniques of community support in palliative care [14,15]. There remains a need to identify practical techniques of implementing palliative care in rural and suburban settings.
The Butler Health System Experience
In August 2015, we set out to start the first hospital-based palliative care consultation service in the Butler Health System. The health system is a nonprofit, single-hospital system anchored by Butler Memorial Hospital, a 294-bed community hospital located within a rural Pennsylvania county of 186,000 residents, 35 miles north of Pittsburgh. Butler County consists of a predominantly white, non-Hispanic population with over 15% of the residents being older than 65 years of age. The median household income is $61,000 earned primarily through blue collar occupations [16]. Driven by 53 employed primary care physicians, the health system provides services for 75,000 patients at sites covering an area of 4000 square miles. The hospital provides general medical, critical, surgical and subspecialty care and behavior health services as a regional referral center for 4 surrounding rural counties, accepting 12,500 inpatient admissions annually. A hospitalist service admits the majority of oncology patients, and the intensive care unit (ICU) is an open unit, where patients are admitted to the hospitalist, primary care, or surgical service.
While no formal needs assessment was performed prior to program development, perceptions of inadequate pain control, overuse of naloxone, underutilization of hospice services, and lack of consistent quality in end-of-life care were identified. These concerns were voiced at the levels of direct patient care on the floors, and by nursing and physician hospital leadership. Prior to our program, the chief medical officer attended the national Center to Advance Palliative Care conference to better understand the field of palliative care and its impact on improving quality of care. Concurrently, our health system was expanding its inpatient capabilities (eg, advanced neurologic and cardiac services), resulting in admissions with increased disease severity and illness complexity. With the vision of improved patient care, prioritizing quality end-of-life care and symptom management, the hospital board and administration overwhelmingly supported the development of the palliative care program, philosophically and financially.
Laying a Foundation—Funding, Collaboration, and Team Building
Funding and staffing are 2 important factors when building any program. Sources of funding for palliative care programs may include hospital support, billing revenue, grants, and philanthropy. Program development was a priority for the hospital and community. To help offset costs, efforts to raise financial support focused on utilizing the health system’s annual fundraising events. Through the generosity of individuals in the community, the hospital’s annual gala event, and donations from the hospital’s auxiliary, a total of $230,000 was raised prior to program initiation. Funds budgeted through direct hospital support and fundraising were allocated towards hiring palliative care team members and community marketing projects.
The hospital’s surrounding community is fortunate to have 2 local inpatient hospice facilities, and these relationships were imperative to providing quality end-of-life care preceding our palliative care program. A formal partnership was previously established with one while the other remains an important referral facility due to its proximity to the hospital. These hospice services are encouraged to participate in our weekly palliative care interdisciplinary team meetings. Their incorporation has improved coordination, continuity, and translation of care upon patient discharge from the acute hospital setting. Additionally, the relationships have been beneficial in tracking patients’ outcomes and data collection.
The standard structure of a palliative care team described by the Joint Commission and National Consensus Panel for Palliative Care consists of a physician, registered nurse or advanced practice provider, chaplaincy, and social work. Despite this recommendation, less than 40% of surveyed hospitals met the criteria, and less than 25% have dedicated funding to cover these positions [17]. Upon inception of our palliative care program, 2.6 funded full-time equivalents (FTEs) were allocated. These positions included a physician (1.0 FTE), a physician assistant (1.0 FTE), and a part time palliative care social worker (0.6 FTE). The 2015 National Palliative Care Registry found that 3.2 funded FTEs per 10,000 admissions is the average for hospitals with 150 to 299 beds [17]. The uncertainty of the utilization and consult volume, and the limited amount of qualified palliative care trained practitioners, resulted in the palliative program starting below this mean at 2.1 funded FTEs per 10,000 admissions. All the funded positions were located on site at the hospital. The pre-existing volunteer hospital chaplain service was identified as the pastoral care component for the program.
Increased FTEs have been associated with increased palliative care service penetration and ultimately in decreased time to consult [18]. In response to increasing consult volumes, concerns for delays in time to consult, and in preparation for expansion to an outpatient service, the palliative care department acquired an additional funded physician FTE (1.0). Ultimately the service reached a total of 3.6 FTE for inpatient services during its first 12 months; proportionately this resulted in an increase to 2.9 FTE per 10,000 admissions based on the yearly admission rate of 12,500 patients.
Educational Outreach
The success of a palliative care program depends on other clinicians’ acceptance and referral to the clinical program. We took a 2-pronged approach, focusing on both hospital-based and community-based education. The hospital-based nursing education included 30-minute presentations on general overviews of palliative care, differences between palliative care and hospice, and acute symptom management at the end of life. The palliative care team presented to all medical, surgical, and intensive care units and encompassed all shifts of nursing staff. These lectures included pre- and post-tests to assess for impact and feedback. Similar educational presentations, as well as an hour-long presentation on opioids and palliative care, were available for physicians for CME opportunities. We also distributed concise palliative care referral packets to outpatient primary care offices through the health system’s marketing team. The referral packets included examples of diagnoses, clinical scenarios, and symptoms to assist in the physicians’ understanding of palliative care services. The palliative care team also met with clinic office managers to discuss the program and answer questions.
There were also educational opportunities for patients and families in our community. Taking advantage of previously developed partnerships between the hospital system and local media outlets, the palliative care team performed local radio spots to educate the community on topics including an overview of palliative care, how to request palliative care, and the difference between palliative care and hospice care. We partnered with a local hospice agency and developed a well-received bereavement seminar for patients, family members, and employees and included the topic of advanced care planning.
Data Collection
We collect data using 2 different tools: a self-maintained spreadsheet shared between our palliative care clinicians, and a collective data tool (QDACT) included in our membership with and maintained by the Global Palliative Care Quality Alliance. Data collected and tracked in our spreadsheet includes date of consult, patient age, primary and secondary diagnoses, disposition, goals of care discussions, date of death, and 30-day readmissions. Through the QDACT data monitoring program, we are tracking and analyzing quality measures including symptom assessment and management and code status conversion. The QDACT database also provides financial data specific to our institution such as cost savings based on our billing, readmission rates, and length of stay.
Results
Projections, Volumes, and Penetration
Prior to the start of our program, our chief medical office used Center to Advance Palliative Care tools to project inpatient consultation volumes at our institution. Variables that are recommended by this center to guide projections include number of hospital admissions per year, hospital occupancy, disposition to hospice, as well as generalized estimations of inpatient mortality rates. Based on our data, it was expected that our program would receive 204 new inpatient consults in our first year, and 774 follow-up visits. Our actual new inpatient consults totaled 516, with 919 follow-up visits. Palliative care penetration (percentage of annual hospital admissions seen by the palliative care team) our first year was 3.7% (Table 1).
Consultation Demographics
The demographics of the patients seen by the palliative care team reflect that of Butler County’s Medicare fee-for-service (FFS) population (Table 2); however, differences were seen at the state and national level with regard to ethnicity (Table 2).
Almost half of consultations (49%) were placed by the hospitalist service. Since the ICU is an open unit, critical care consults are not adequately reflected by analysis of the ordering physician alone. Analysis of consultation location revealed that 27% of inpatient consults were located within the ICU.
Patient Outcomes and Disposition
Outcomes and discharge data from the first year were collected and reviewed. Ten percent of the patients seen by palliative care died in the hospital, and 51% of patients that were seen by palliative care died within the program’s first year. Thirty-seven percent of patients discharged from the hospital utilized hospice services at home, in residential nursing facility, or at an inpatient hospice unit. The remaining 53% were discharged without hospice services to home or facility (Figure).
Hospice utilization by the health system increased during our first year. Compared to the 2014 calendar year, there were a total of 263 referrals for hospice services. During the first year of the palliative care program, which started August 2015, there were a total of 293 referrals. Of the 293 total hospice referrals, 190 (64.8%) of these referrals were for patients seen by the palliative care team.
Change of Code Status
Code status and changes in codes status data were collected. Of 462 individual patients prior to or at the time of palliative care consults, 43% were full code, 4% limited code, 8% unknown status, and 45% Do Not Resuscitate. After palliative care consult, 61% of the patients who were previously full/limited/unknown converted to do not resuscitate and do not intubate status. In total, 79% of patients seen by palliative care had a confirmed code status of Do Not Resuscitate and Do Not Intubate status after consult.
Discussion
In our first year, our palliative care program exceeded the expected number of inpatient consults, corresponding with a penetration of 3.7%. With the increase of funded FTEs, preliminary data shows that the department’s penetration continues to rise remaining consistent with the data and expectations [18]. During the second year, it is anticipated that over 600 inpatient palliative care consultations will be performed with an estimated penetration of 4%. This increasing penetration reflects the rising utilization of palliative care within our hospital. Since inception of the program, the service has expanded into an outpatient clinic 2 days per week. The palliative care clinic is staffed by a registered nurse (funded 0.6 FTE) and covered by the same physicians and physician assistant providing the inpatient services. The department acquired an unfunded but designated chaplaincy volunteer to assist with patients’ spiritual needs. We believe that the success of our program during the first year was related to multiple factors: a focus of integration and education by the palliative care department, health system administration buy-in, and identification of surrounding community needs.
In addition to patient care, our palliative care department also prioritizes “tangible” impacts to better establish our contributions to the health system. We have done this through participation on hospital committees, hospital policy revision teams, and by developing innovative solutions such as a terminal extubation protocol and order set for our ICU. The health system and its administration have recognized the importance of educating nursing and physician staff on palliative care services, and have supported these continued efforts alongside our clinical obligations.
Concurrent with administration buy-in, financial supports for our palliative care services were initially supplemented by the health system. Our department understands the importance of recognizing limitations of resources in communities and their hospitals. In efforts to minimize the department’s impact on our own health system’s financial resources, we have strived to offset our costs. We helped the hospital system meet pay-for-performance palliative care metrics set by the large local insurers resulting in financial hospital reimbursement valued at $600,000 in 2016.
The question of how the program may translate into other communities raises a major limitation: the homogeneity our population. The community surrounding the hospital is primarily Caucasian, with minimal representation of minority populations. While the patient population seen by our palliative care team is reflective of our surrounding county, it does not represent Medicare FFS beneficiaries on a national level or many other types of community hospitals across the country. Variations of ethnicity, age, diagnoses, and faith are fundamental, which highlights the importance of understanding the community in which a program is developed.
The rising trajectory of our palliative care service utilization has prompted a discussion of future endeavors for our program. Expectations for a continued shortage of hospice and palliative care physicians [19] and concerns for practitioner burnout [20] underlie our thoughtful approach to expansion of inpatient and outpatient services. At this time, potential projects include a consultation trigger system and incorporation of palliative care providers in ICU rounding, as well as possible expansion of outpatient services through implantation of an advanced practitioner into surrounding nursing homes and primary care offices.
We have found a growing utilization of our program at Butler Health System. Our first year experience has highlighted the importance of identifying community and hospital administrative champions as a foundation. Additionally, understanding the specific characteristics of one’s surrounding community may allow for improved integration and acceptance of palliative care in a community setting. Our program continues to work with the health system, community, and philanthropic organizations to expand the ever-growing need for palliative care services.
From the Division of Palliative Care, Butler Health System, Butler, PA (Drs. Stein, Reefer, Selvaggi, Ms. Doverspike); the University of Pittsburgh Medical Center, Pittsburgh, PA (Dr. Rajagopal); and the Duke Cancer Institute and Duke Fuqua School of Business, Durham, NC (Dr. Kamal).
Abstract
- Objective: To describe an approach to develop a community-centric palliative care program in a rural community health system and to review data collected over the program’s first year.
- Methods: We describe the underlying foundations of our program development including the health system’s prioritization of a palliative care program, funding opportunities, collaboration with community supports, and the importance of building a team and program that reflects a community’s needs. Data were collected through a program-maintained spreadsheet and a data monitoring system available through the Global Palliative Care Quality Alliance.
- Results: 516 new inpatient consultations were seen during the first year, for a penetration of 3.7%. The demographics of the patients who received consultation reflect that of the surrounding community. Over 50% of patients seen within the first year died, and hospice utilization at home and within facilities and inpatient hospice units increased. In addition, 79% of the patients seen by the palliative care team had a confirmed code status of do not resuscitate and do not intubate.
- Conclusions: Butler Health System’s approach to development of a palliative care program has resulted in increasing utilization of palliative care services in the hospital. Having hospital administration support, community support, and understanding the individualized needs of a community has been essential for the program’s expansion.
Key words: palliative care; program development; community hospital; rural.
Since its inception, palliative care has been committed to providing specialty-level consultation services to individuals with serious illness and their loved ones. The field has focused heavily on growth and acceptance, consistently moving upstream with regards to illness trajectory, across diseases, and across demographic variables such as age (eg, pediatric quality of life programs) and race (eg, community outreach programs addressing racial disparities in hospice use). An important frontier that remains challenging for much of the field is expansion into the community setting, where resources, implicit acceptance, and patient populations may vary.
As health system leaders appreciate the positive impacts palliative medicine on patient care and care quality, barriers to implementing palliative care programs in community hospitals must be addressed in ways tailored to the unique needs of smaller organizations and their communities. The goal of this paper is to outline the approach taken to develop Butler Health System’s community-centric palliative care program, describe our program’s underlying foundation rooted in community supports, and recount steps we have taken thus far to impact patient care in our hospital, health system, and community through the program’s first year.
Community Hospital Palliative Care—The Necessity and the Challenges
Palliative care has made strides in its growth and acceptance in the last decade; yet, the distribution of that growth has been skewed. Although 67% of hospitals now report access to specialist palliative care programs, most of the 148% growth over the last decade has been actualized in larger hospitals. Ninety percent of hospitals with greater than 300 beds report palliative care service availability whereas only 56% of small hospitals were identified to have this specialty care [1].
The inequity of access is also seen in other countries. A recent Canadian study retrospectively examined access to care of 23,860 deceased patients in Nova Scotia. Although they found 40.9% of study subjects were enrolled in a palliative care program at urban, academic centers, patients in a rural setting were only a third as likely to be enrolled in a palliative care program [2]. This access gap has important effects on patient-level outcomes, as evidence has consistently demonstrated that patients in rural settings who receive palliative care have decreased unnecessary hospitalizations and less in-hospital deaths [3].
While evidence of improved outcomes is strong, important barriers stand in the way. In a 2013 study, 374 health care providers at 236 rural hospitals in 7 states were interviewed to determine barriers to providing palliative care in rural settings. Barriers identified include a lack of administrative support, access to basic palliative care training for primary care physicians, and limited relationships to hospices [4]. Additional challenges include lack of access to tertiary-level specialty clinicians, access to and misconceptions about prescription medications, transportation for patients and providers, and incorporating a patient’s community supports [5–7].
Proposed Solutions
Techniques to improve palliative care access for rural and community centers that have been previously reviewed in the literature include videoconferencing with tertiary care experts in palliative care and education through small community-level lectures [8–10]. Goals of rural and suburban palliative care programs are broadly similar to programs at academic medical centers; however, few studies have identified impact of palliative medicine on patient care in community settings. In one suburban practice, a study found that patients were more likely to die at home if they had multiple caregivers, increased length of time under palliative care, and older age upon referral [11].
The United States has few large-scale pilot programs attempting to address the palliative needs of a more suburban or rural population. Of these, the Minnesota Rural Palliative Care Initiative developed by Stratis Health is perhaps the best publicized. Stratis Health developed and led an 18-month learning collaborative from October 2008 to April 2010 through which community teams developed or improved palliative care services. Through this initiative, a community-based health care practice model was developed that took advantage of the strong interrelationships within rural communities. After 18 months, 6 out of 10 rural Minnesota communities had formal palliative care programs, and 8 to 9 out of 10 had capabilities to at least address advance directives as well as provider and community education [12]. In another initiative, the NIH established a new suburban clinic with tertiary providers specifically for resource intensive, underserved patients [13]. The clinic was established by partnering with a service that was already in place in the community. Twenty-seven patients were seen within 7 months. The most common consults were patients with numerous comorbidities and chronic pain rather than terminal diagnoses. Given the intensive need of these patients, the authors felt that a consultation service and an interdisciplinary team that included psychosocial/spiritual/social work providers offered the most efficient method of delivering advanced palliative care needs.
The research regarding both solutions to challenges and novel methods of addressing the care gap remains sparse as evidenced by the conclusions of multiple systematic reviews and meta-analyses and the inability of the Cochrane review to find papers meeting inclusion criteria regarding techniques of community support in palliative care [14,15]. There remains a need to identify practical techniques of implementing palliative care in rural and suburban settings.
The Butler Health System Experience
In August 2015, we set out to start the first hospital-based palliative care consultation service in the Butler Health System. The health system is a nonprofit, single-hospital system anchored by Butler Memorial Hospital, a 294-bed community hospital located within a rural Pennsylvania county of 186,000 residents, 35 miles north of Pittsburgh. Butler County consists of a predominantly white, non-Hispanic population with over 15% of the residents being older than 65 years of age. The median household income is $61,000 earned primarily through blue collar occupations [16]. Driven by 53 employed primary care physicians, the health system provides services for 75,000 patients at sites covering an area of 4000 square miles. The hospital provides general medical, critical, surgical and subspecialty care and behavior health services as a regional referral center for 4 surrounding rural counties, accepting 12,500 inpatient admissions annually. A hospitalist service admits the majority of oncology patients, and the intensive care unit (ICU) is an open unit, where patients are admitted to the hospitalist, primary care, or surgical service.
While no formal needs assessment was performed prior to program development, perceptions of inadequate pain control, overuse of naloxone, underutilization of hospice services, and lack of consistent quality in end-of-life care were identified. These concerns were voiced at the levels of direct patient care on the floors, and by nursing and physician hospital leadership. Prior to our program, the chief medical officer attended the national Center to Advance Palliative Care conference to better understand the field of palliative care and its impact on improving quality of care. Concurrently, our health system was expanding its inpatient capabilities (eg, advanced neurologic and cardiac services), resulting in admissions with increased disease severity and illness complexity. With the vision of improved patient care, prioritizing quality end-of-life care and symptom management, the hospital board and administration overwhelmingly supported the development of the palliative care program, philosophically and financially.
Laying a Foundation—Funding, Collaboration, and Team Building
Funding and staffing are 2 important factors when building any program. Sources of funding for palliative care programs may include hospital support, billing revenue, grants, and philanthropy. Program development was a priority for the hospital and community. To help offset costs, efforts to raise financial support focused on utilizing the health system’s annual fundraising events. Through the generosity of individuals in the community, the hospital’s annual gala event, and donations from the hospital’s auxiliary, a total of $230,000 was raised prior to program initiation. Funds budgeted through direct hospital support and fundraising were allocated towards hiring palliative care team members and community marketing projects.
The hospital’s surrounding community is fortunate to have 2 local inpatient hospice facilities, and these relationships were imperative to providing quality end-of-life care preceding our palliative care program. A formal partnership was previously established with one while the other remains an important referral facility due to its proximity to the hospital. These hospice services are encouraged to participate in our weekly palliative care interdisciplinary team meetings. Their incorporation has improved coordination, continuity, and translation of care upon patient discharge from the acute hospital setting. Additionally, the relationships have been beneficial in tracking patients’ outcomes and data collection.
The standard structure of a palliative care team described by the Joint Commission and National Consensus Panel for Palliative Care consists of a physician, registered nurse or advanced practice provider, chaplaincy, and social work. Despite this recommendation, less than 40% of surveyed hospitals met the criteria, and less than 25% have dedicated funding to cover these positions [17]. Upon inception of our palliative care program, 2.6 funded full-time equivalents (FTEs) were allocated. These positions included a physician (1.0 FTE), a physician assistant (1.0 FTE), and a part time palliative care social worker (0.6 FTE). The 2015 National Palliative Care Registry found that 3.2 funded FTEs per 10,000 admissions is the average for hospitals with 150 to 299 beds [17]. The uncertainty of the utilization and consult volume, and the limited amount of qualified palliative care trained practitioners, resulted in the palliative program starting below this mean at 2.1 funded FTEs per 10,000 admissions. All the funded positions were located on site at the hospital. The pre-existing volunteer hospital chaplain service was identified as the pastoral care component for the program.
Increased FTEs have been associated with increased palliative care service penetration and ultimately in decreased time to consult [18]. In response to increasing consult volumes, concerns for delays in time to consult, and in preparation for expansion to an outpatient service, the palliative care department acquired an additional funded physician FTE (1.0). Ultimately the service reached a total of 3.6 FTE for inpatient services during its first 12 months; proportionately this resulted in an increase to 2.9 FTE per 10,000 admissions based on the yearly admission rate of 12,500 patients.
Educational Outreach
The success of a palliative care program depends on other clinicians’ acceptance and referral to the clinical program. We took a 2-pronged approach, focusing on both hospital-based and community-based education. The hospital-based nursing education included 30-minute presentations on general overviews of palliative care, differences between palliative care and hospice, and acute symptom management at the end of life. The palliative care team presented to all medical, surgical, and intensive care units and encompassed all shifts of nursing staff. These lectures included pre- and post-tests to assess for impact and feedback. Similar educational presentations, as well as an hour-long presentation on opioids and palliative care, were available for physicians for CME opportunities. We also distributed concise palliative care referral packets to outpatient primary care offices through the health system’s marketing team. The referral packets included examples of diagnoses, clinical scenarios, and symptoms to assist in the physicians’ understanding of palliative care services. The palliative care team also met with clinic office managers to discuss the program and answer questions.
There were also educational opportunities for patients and families in our community. Taking advantage of previously developed partnerships between the hospital system and local media outlets, the palliative care team performed local radio spots to educate the community on topics including an overview of palliative care, how to request palliative care, and the difference between palliative care and hospice care. We partnered with a local hospice agency and developed a well-received bereavement seminar for patients, family members, and employees and included the topic of advanced care planning.
Data Collection
We collect data using 2 different tools: a self-maintained spreadsheet shared between our palliative care clinicians, and a collective data tool (QDACT) included in our membership with and maintained by the Global Palliative Care Quality Alliance. Data collected and tracked in our spreadsheet includes date of consult, patient age, primary and secondary diagnoses, disposition, goals of care discussions, date of death, and 30-day readmissions. Through the QDACT data monitoring program, we are tracking and analyzing quality measures including symptom assessment and management and code status conversion. The QDACT database also provides financial data specific to our institution such as cost savings based on our billing, readmission rates, and length of stay.
Results
Projections, Volumes, and Penetration
Prior to the start of our program, our chief medical office used Center to Advance Palliative Care tools to project inpatient consultation volumes at our institution. Variables that are recommended by this center to guide projections include number of hospital admissions per year, hospital occupancy, disposition to hospice, as well as generalized estimations of inpatient mortality rates. Based on our data, it was expected that our program would receive 204 new inpatient consults in our first year, and 774 follow-up visits. Our actual new inpatient consults totaled 516, with 919 follow-up visits. Palliative care penetration (percentage of annual hospital admissions seen by the palliative care team) our first year was 3.7% (Table 1).
Consultation Demographics
The demographics of the patients seen by the palliative care team reflect that of Butler County’s Medicare fee-for-service (FFS) population (Table 2); however, differences were seen at the state and national level with regard to ethnicity (Table 2).
Almost half of consultations (49%) were placed by the hospitalist service. Since the ICU is an open unit, critical care consults are not adequately reflected by analysis of the ordering physician alone. Analysis of consultation location revealed that 27% of inpatient consults were located within the ICU.
Patient Outcomes and Disposition
Outcomes and discharge data from the first year were collected and reviewed. Ten percent of the patients seen by palliative care died in the hospital, and 51% of patients that were seen by palliative care died within the program’s first year. Thirty-seven percent of patients discharged from the hospital utilized hospice services at home, in residential nursing facility, or at an inpatient hospice unit. The remaining 53% were discharged without hospice services to home or facility (Figure).
Hospice utilization by the health system increased during our first year. Compared to the 2014 calendar year, there were a total of 263 referrals for hospice services. During the first year of the palliative care program, which started August 2015, there were a total of 293 referrals. Of the 293 total hospice referrals, 190 (64.8%) of these referrals were for patients seen by the palliative care team.
Change of Code Status
Code status and changes in codes status data were collected. Of 462 individual patients prior to or at the time of palliative care consults, 43% were full code, 4% limited code, 8% unknown status, and 45% Do Not Resuscitate. After palliative care consult, 61% of the patients who were previously full/limited/unknown converted to do not resuscitate and do not intubate status. In total, 79% of patients seen by palliative care had a confirmed code status of Do Not Resuscitate and Do Not Intubate status after consult.
Discussion
In our first year, our palliative care program exceeded the expected number of inpatient consults, corresponding with a penetration of 3.7%. With the increase of funded FTEs, preliminary data shows that the department’s penetration continues to rise remaining consistent with the data and expectations [18]. During the second year, it is anticipated that over 600 inpatient palliative care consultations will be performed with an estimated penetration of 4%. This increasing penetration reflects the rising utilization of palliative care within our hospital. Since inception of the program, the service has expanded into an outpatient clinic 2 days per week. The palliative care clinic is staffed by a registered nurse (funded 0.6 FTE) and covered by the same physicians and physician assistant providing the inpatient services. The department acquired an unfunded but designated chaplaincy volunteer to assist with patients’ spiritual needs. We believe that the success of our program during the first year was related to multiple factors: a focus of integration and education by the palliative care department, health system administration buy-in, and identification of surrounding community needs.
In addition to patient care, our palliative care department also prioritizes “tangible” impacts to better establish our contributions to the health system. We have done this through participation on hospital committees, hospital policy revision teams, and by developing innovative solutions such as a terminal extubation protocol and order set for our ICU. The health system and its administration have recognized the importance of educating nursing and physician staff on palliative care services, and have supported these continued efforts alongside our clinical obligations.
Concurrent with administration buy-in, financial supports for our palliative care services were initially supplemented by the health system. Our department understands the importance of recognizing limitations of resources in communities and their hospitals. In efforts to minimize the department’s impact on our own health system’s financial resources, we have strived to offset our costs. We helped the hospital system meet pay-for-performance palliative care metrics set by the large local insurers resulting in financial hospital reimbursement valued at $600,000 in 2016.
The question of how the program may translate into other communities raises a major limitation: the homogeneity our population. The community surrounding the hospital is primarily Caucasian, with minimal representation of minority populations. While the patient population seen by our palliative care team is reflective of our surrounding county, it does not represent Medicare FFS beneficiaries on a national level or many other types of community hospitals across the country. Variations of ethnicity, age, diagnoses, and faith are fundamental, which highlights the importance of understanding the community in which a program is developed.
The rising trajectory of our palliative care service utilization has prompted a discussion of future endeavors for our program. Expectations for a continued shortage of hospice and palliative care physicians [19] and concerns for practitioner burnout [20] underlie our thoughtful approach to expansion of inpatient and outpatient services. At this time, potential projects include a consultation trigger system and incorporation of palliative care providers in ICU rounding, as well as possible expansion of outpatient services through implantation of an advanced practitioner into surrounding nursing homes and primary care offices.
We have found a growing utilization of our program at Butler Health System. Our first year experience has highlighted the importance of identifying community and hospital administrative champions as a foundation. Additionally, understanding the specific characteristics of one’s surrounding community may allow for improved integration and acceptance of palliative care in a community setting. Our program continues to work with the health system, community, and philanthropic organizations to expand the ever-growing need for palliative care services.
1. Dumanovsky T, Augustin R, Rogers M, et al. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
2. Lavergne MR, Lethbridge L, Johnston G, et al. Examining palliative care program use and place of death in rural and urban contexts: a Canadian population-based study using linked data. Rural Remote Health 2015;15:3134.
3. Seow H, Brazil K, Sussman J, et al. Impact of community based, specialist palliative care teams on hospitalisations and emergency department visits late in life and hospital deaths: a pooled analysis. BMJ 2014;348:g3496.
4. Fink RM, Oman KS, Youngwerth J, et al. A palliative care needs assessment of rural hospitals. J Palliat Med 2013;16:638–44.
5. Dumont S, Jacobs P, Turcotte V, et al. Palliative care costs in Canada: A descriptive comparison of studies of urban and rural patients near end of life. J Palliat Med 2015;29:908–17.
6. Kaasalainen S, Brazil K, Williams A, et al. Nurses' experiences providing palliative care to individuals living in rural communities: aspects of the physical residential setting. Rural Remote Health 2014;14:2728.
7. Ahmed N, Bestall JC, Ahmedzai SH, et al. Systematic review of the problems and issues of accessing specialist palliative care by patients, carers and health and social care professionals. J Palliat Med 2004;18:525–42.
8. Ray RA, Fried O, Lindsay D. Palliative care professional education via video conference builds confidence to deliver palliative care in rural and remote locations. BMC Health Serv Res 2014;14:272.
9. Bakitas MA, Elk R, Astin M, et al. Systematic review of palliative care in the rural setting. Cancer Control 2015;22:450–64.
10. Akiyama M, Hirai K, Takebayashi T, et al. The effects of community-wide dissemination of information on perceptions of palliative care, knowledge about opioids, and sense of security among cancer patients, their families, and the general public. Support Care Cancer 2016;24: 347–56.
11. Maida V. Factors that promote success in home palliative care: a study of a large suburban palliative care practice. J Palliat Care 2002;18:282–6.
12. Ceronsky L, Shearer J, Weng K, et al. Minnesota Rural Palliative Care Initiative: building palliative care capacity in rural Minnesota. J Palliat Med 2013;16:310–3.
13. Aggarwal SK, Ghosh A, Cheng MJ, et al. Initiating pain and palliative care outpatient services for the suburban underserved in Montgomery County, Maryland: Lessons learned at the NIH Clinical Center and MobileMed. Palliat Support Care 2015;16:1–6.
14. Rainsford S, MacLeod RD, Glasgow NJ. Place of death in rural palliative care: A systematic review. J Palliat Med 2016;30:745–63.
15. Horey D, Street AF, O'Connor M, et al. Training and supportive programs for palliative care volunteers in community settings. Cochrane Database Syst Rev 2015 Jul 20;(7):CD009500.
16. The United States Census Bureau: QuickFacts: Butler County, Pennsylvania. Accessed 10 Mar 2017 at www.census.gov/quickfacts/table/PST045216/42019,00.
17. Spetz J, Dudley N, Trupin L, et al. Few hospital palliative care programs meet national staffing recommendations. Health Aff 2016;35:1690–7.
18. Dumanovsky T, Rogers M, Spragens LH, et al. Impact of Staffing on Access to Palliative Care in U.S. Hospitals. J Palliat Med. 2015 Dec; 18(12). Pages 998-999.
19. Lupu D, American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage 2010;40:899–911.
20. Kamal AH, Bull JK, Wolf SP, et al. Prevalence and predictors of burnout among hospice and palliative care clinicians in the U.S. J Pain Symptom Manage 2016;51:690–6.
1. Dumanovsky T, Augustin R, Rogers M, et al. The growth of palliative care in U.S. hospitals: a status report. J Palliat Med 2016;19:8–15.
2. Lavergne MR, Lethbridge L, Johnston G, et al. Examining palliative care program use and place of death in rural and urban contexts: a Canadian population-based study using linked data. Rural Remote Health 2015;15:3134.
3. Seow H, Brazil K, Sussman J, et al. Impact of community based, specialist palliative care teams on hospitalisations and emergency department visits late in life and hospital deaths: a pooled analysis. BMJ 2014;348:g3496.
4. Fink RM, Oman KS, Youngwerth J, et al. A palliative care needs assessment of rural hospitals. J Palliat Med 2013;16:638–44.
5. Dumont S, Jacobs P, Turcotte V, et al. Palliative care costs in Canada: A descriptive comparison of studies of urban and rural patients near end of life. J Palliat Med 2015;29:908–17.
6. Kaasalainen S, Brazil K, Williams A, et al. Nurses' experiences providing palliative care to individuals living in rural communities: aspects of the physical residential setting. Rural Remote Health 2014;14:2728.
7. Ahmed N, Bestall JC, Ahmedzai SH, et al. Systematic review of the problems and issues of accessing specialist palliative care by patients, carers and health and social care professionals. J Palliat Med 2004;18:525–42.
8. Ray RA, Fried O, Lindsay D. Palliative care professional education via video conference builds confidence to deliver palliative care in rural and remote locations. BMC Health Serv Res 2014;14:272.
9. Bakitas MA, Elk R, Astin M, et al. Systematic review of palliative care in the rural setting. Cancer Control 2015;22:450–64.
10. Akiyama M, Hirai K, Takebayashi T, et al. The effects of community-wide dissemination of information on perceptions of palliative care, knowledge about opioids, and sense of security among cancer patients, their families, and the general public. Support Care Cancer 2016;24: 347–56.
11. Maida V. Factors that promote success in home palliative care: a study of a large suburban palliative care practice. J Palliat Care 2002;18:282–6.
12. Ceronsky L, Shearer J, Weng K, et al. Minnesota Rural Palliative Care Initiative: building palliative care capacity in rural Minnesota. J Palliat Med 2013;16:310–3.
13. Aggarwal SK, Ghosh A, Cheng MJ, et al. Initiating pain and palliative care outpatient services for the suburban underserved in Montgomery County, Maryland: Lessons learned at the NIH Clinical Center and MobileMed. Palliat Support Care 2015;16:1–6.
14. Rainsford S, MacLeod RD, Glasgow NJ. Place of death in rural palliative care: A systematic review. J Palliat Med 2016;30:745–63.
15. Horey D, Street AF, O'Connor M, et al. Training and supportive programs for palliative care volunteers in community settings. Cochrane Database Syst Rev 2015 Jul 20;(7):CD009500.
16. The United States Census Bureau: QuickFacts: Butler County, Pennsylvania. Accessed 10 Mar 2017 at www.census.gov/quickfacts/table/PST045216/42019,00.
17. Spetz J, Dudley N, Trupin L, et al. Few hospital palliative care programs meet national staffing recommendations. Health Aff 2016;35:1690–7.
18. Dumanovsky T, Rogers M, Spragens LH, et al. Impact of Staffing on Access to Palliative Care in U.S. Hospitals. J Palliat Med. 2015 Dec; 18(12). Pages 998-999.
19. Lupu D, American Academy of Hospice and Palliative Medicine Workforce Task Force. Estimate of current hospice and palliative medicine physician workforce shortage. J Pain Symptom Manage 2010;40:899–911.
20. Kamal AH, Bull JK, Wolf SP, et al. Prevalence and predictors of burnout among hospice and palliative care clinicians in the U.S. J Pain Symptom Manage 2016;51:690–6.
Does newly discovered vasoactive peptide ELABELA reveal essential mechanisms for preeclampsia development?
EXPERT COMMENTARY
Preeclampsia is a disorder of impaired placentation. ELABELA (ELA) encodes an endogenous ligand for the apelin receptor and is detected in preimplantation human blastocysts and in 2 organs in adults: the placenta and kidney. Recently, an international team of researchers described their study findings on ELA and its role in placental vascular development and preeclampsia in mice.
Details of the study
To delineate the contribution of ELA to mammalian development, Ho and colleagues generated Ela knockout mice. The investigators showed that during development, the ELA protein is first detected in the early placenta and becomes abundant later in placenta formation. They also demonstrated that ELA is a pregnancy hormone that circulates in the blood of pregnant, but not nonpregnant, mice.
Placental structure. The Ela knockout mice had placentas that demonstrated thin labyrinths, with poor vascularization, increased apoptosis, and reduced proliferation. Further, RNA analysis of ELA-lacking placentas revealed a gene expression profile indicative of hypoxia, including the upregulation of certain genes involved in blood vessel building. Placental vessels showed overall stunted architecture characterized by little or no extension and branching of angiogenic sprouts and impaired formation of the adequate labyrinth network required for proper perfusion in the placenta.
Given these gene expression findings and the fact that placental and vascular abnormalities have long been suspected to underlie preeclampsia, the investigators sought to determine if ELA-lacking mice exhibit preeclampsia. Evidence indicated they do.
Indicators of preeclampsia. Pregnant ELA-lacking mice had significantly higher levels of proteinuria and significantly higher blood pressure than either pregnant wild-type mice or nonpregnant ELA-lacking mice. Further, at the end of pregnancy, histology and transmission electron microscopy of kidney glomerular sections from ELA-lacking pregnant mice revealed signs of endotheliosis, a unique renal pathology that is also observed in women with preeclampsia. Pups of ELA-lacking mothers tended to weigh less than those of wild-type mothers, a situation that may be similar to the fetal intrauterine growth restriction commonly seen in women with preeclampsia.
Angiogenic factors. The authors then looked at levels of angiogenic proteins implicated in the pathogenesis of preeclampsia to determine if ELA is upstream. They found that ELA-lacking mice placentas had increased levels of sFlt1, Vegfa, and Plgf mRNA; these transcriptional changes, however, did not translate into significantly elevated plasma levels of the respective proteins. Thus, these findings indicate that ELA acts independently of, and possibly earlier than, angiogenic factors in the pathogenesis of preeclampsia.
Experimental treatment. The authors further showed that infusing recombinant ELA protein could alleviate symptoms of preeclampsia in mice. Injection of ELA protein in ELA-lacking mice led to reduction of blood pressure, reversal of glomerular endotheliosis, and rescue of fetal growth restriction.
Study strengths and weaknesses
This animal study contributes compelling molecular evidence of ELA’s role in mammalian placental development and angiogenesis, revealing that ELA deficiency leads to preeclampsia and placental abnormalities in pregnant mice. How ELA acts in humans and human pregnancy, however, has yet to be explored.
-- Sarosh Rana, MD, MPH
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Preeclampsia is a disorder of impaired placentation. ELABELA (ELA) encodes an endogenous ligand for the apelin receptor and is detected in preimplantation human blastocysts and in 2 organs in adults: the placenta and kidney. Recently, an international team of researchers described their study findings on ELA and its role in placental vascular development and preeclampsia in mice.
Details of the study
To delineate the contribution of ELA to mammalian development, Ho and colleagues generated Ela knockout mice. The investigators showed that during development, the ELA protein is first detected in the early placenta and becomes abundant later in placenta formation. They also demonstrated that ELA is a pregnancy hormone that circulates in the blood of pregnant, but not nonpregnant, mice.
Placental structure. The Ela knockout mice had placentas that demonstrated thin labyrinths, with poor vascularization, increased apoptosis, and reduced proliferation. Further, RNA analysis of ELA-lacking placentas revealed a gene expression profile indicative of hypoxia, including the upregulation of certain genes involved in blood vessel building. Placental vessels showed overall stunted architecture characterized by little or no extension and branching of angiogenic sprouts and impaired formation of the adequate labyrinth network required for proper perfusion in the placenta.
Given these gene expression findings and the fact that placental and vascular abnormalities have long been suspected to underlie preeclampsia, the investigators sought to determine if ELA-lacking mice exhibit preeclampsia. Evidence indicated they do.
Indicators of preeclampsia. Pregnant ELA-lacking mice had significantly higher levels of proteinuria and significantly higher blood pressure than either pregnant wild-type mice or nonpregnant ELA-lacking mice. Further, at the end of pregnancy, histology and transmission electron microscopy of kidney glomerular sections from ELA-lacking pregnant mice revealed signs of endotheliosis, a unique renal pathology that is also observed in women with preeclampsia. Pups of ELA-lacking mothers tended to weigh less than those of wild-type mothers, a situation that may be similar to the fetal intrauterine growth restriction commonly seen in women with preeclampsia.
Angiogenic factors. The authors then looked at levels of angiogenic proteins implicated in the pathogenesis of preeclampsia to determine if ELA is upstream. They found that ELA-lacking mice placentas had increased levels of sFlt1, Vegfa, and Plgf mRNA; these transcriptional changes, however, did not translate into significantly elevated plasma levels of the respective proteins. Thus, these findings indicate that ELA acts independently of, and possibly earlier than, angiogenic factors in the pathogenesis of preeclampsia.
Experimental treatment. The authors further showed that infusing recombinant ELA protein could alleviate symptoms of preeclampsia in mice. Injection of ELA protein in ELA-lacking mice led to reduction of blood pressure, reversal of glomerular endotheliosis, and rescue of fetal growth restriction.
Study strengths and weaknesses
This animal study contributes compelling molecular evidence of ELA’s role in mammalian placental development and angiogenesis, revealing that ELA deficiency leads to preeclampsia and placental abnormalities in pregnant mice. How ELA acts in humans and human pregnancy, however, has yet to be explored.
-- Sarosh Rana, MD, MPH
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Preeclampsia is a disorder of impaired placentation. ELABELA (ELA) encodes an endogenous ligand for the apelin receptor and is detected in preimplantation human blastocysts and in 2 organs in adults: the placenta and kidney. Recently, an international team of researchers described their study findings on ELA and its role in placental vascular development and preeclampsia in mice.
Details of the study
To delineate the contribution of ELA to mammalian development, Ho and colleagues generated Ela knockout mice. The investigators showed that during development, the ELA protein is first detected in the early placenta and becomes abundant later in placenta formation. They also demonstrated that ELA is a pregnancy hormone that circulates in the blood of pregnant, but not nonpregnant, mice.
Placental structure. The Ela knockout mice had placentas that demonstrated thin labyrinths, with poor vascularization, increased apoptosis, and reduced proliferation. Further, RNA analysis of ELA-lacking placentas revealed a gene expression profile indicative of hypoxia, including the upregulation of certain genes involved in blood vessel building. Placental vessels showed overall stunted architecture characterized by little or no extension and branching of angiogenic sprouts and impaired formation of the adequate labyrinth network required for proper perfusion in the placenta.
Given these gene expression findings and the fact that placental and vascular abnormalities have long been suspected to underlie preeclampsia, the investigators sought to determine if ELA-lacking mice exhibit preeclampsia. Evidence indicated they do.
Indicators of preeclampsia. Pregnant ELA-lacking mice had significantly higher levels of proteinuria and significantly higher blood pressure than either pregnant wild-type mice or nonpregnant ELA-lacking mice. Further, at the end of pregnancy, histology and transmission electron microscopy of kidney glomerular sections from ELA-lacking pregnant mice revealed signs of endotheliosis, a unique renal pathology that is also observed in women with preeclampsia. Pups of ELA-lacking mothers tended to weigh less than those of wild-type mothers, a situation that may be similar to the fetal intrauterine growth restriction commonly seen in women with preeclampsia.
Angiogenic factors. The authors then looked at levels of angiogenic proteins implicated in the pathogenesis of preeclampsia to determine if ELA is upstream. They found that ELA-lacking mice placentas had increased levels of sFlt1, Vegfa, and Plgf mRNA; these transcriptional changes, however, did not translate into significantly elevated plasma levels of the respective proteins. Thus, these findings indicate that ELA acts independently of, and possibly earlier than, angiogenic factors in the pathogenesis of preeclampsia.
Experimental treatment. The authors further showed that infusing recombinant ELA protein could alleviate symptoms of preeclampsia in mice. Injection of ELA protein in ELA-lacking mice led to reduction of blood pressure, reversal of glomerular endotheliosis, and rescue of fetal growth restriction.
Study strengths and weaknesses
This animal study contributes compelling molecular evidence of ELA’s role in mammalian placental development and angiogenesis, revealing that ELA deficiency leads to preeclampsia and placental abnormalities in pregnant mice. How ELA acts in humans and human pregnancy, however, has yet to be explored.
-- Sarosh Rana, MD, MPH
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Debunking Actinic Keratosis Myths: Are Patients With Darker Skin At Risk for Actinic Keratoses?
Myth: Actinic keratoses are only seen in patients with lighter skin
Actinic keratoses (AKs) are precancerous lesions that may turn into squamous cell carcinoma if left untreated. UV rays cause AKs, either from outdoor sun exposure or tanning beds. According to the American Academy of Dermatology, AKs are more likely to develop in patients 40 years or older with fair skin; hair color that is naturally blonde or red; eye color that is naturally blue, green, or hazel; skin that freckles or burns when in the sun; a weakened immune system; and occupations involving substances that contain polycyclic aromatic hydrocarbons such as coal or tar.
A 2007 study compared the most common diagnoses among patients of different racial and ethnic groups in New York City. Alexis et al found that AK was in the top 10 diagnoses in white patients but not for black patients. They postulated that photoprotective factors in darkly pigmented skin such as larger and more numerous melanosomes that contain more melanin and are more dispersed throughout the epidermis result in a lower incidence of skin cancers in the skin of color (SOC) population.
RELATED ARTICLE: Common Dermatologic Disorders in Skin of Color: A Comparative Practice Survey
However, a recent skin cancer awareness study in Cutis reported that even though SOC populations have lower incidences of skin cancer such as melanoma, basal cell carcinoma, and squamous cell carcinoma, they exhibit higher death rates. Furthermore, black individuals are more likely to present with advanced-stage melanoma and acral lentiginous melanomas compared to white individuals. Kailas et al stated, “Overall, SOC patients have the poorest skin cancer prognosis, and the data suggest that the reason for this paradox is delayed diagnosis.” They evaluated several knowledge-based interventions for increasing skin cancer awareness, knowledge, and protective behaviors in SOC populations, including the use of visuals such as photographs to allow SOC patients to visualize different skin tones, educational interventions in another language, and pamphlets.
Dermatologists should be aware that education of SOC patients is important to eradicate the common misconception that these patients do not have to worry about AKs and other skin cancers. Remind these patients that they need to protect their skin from the sun, just as patients with fair skin do. Further research in the dermatology community should focus on educational interventions that will help increase knowledge regarding skin cancer in SOC populations.
Expert Commentary
Although more common in patients with lighter skin, actinic keratosis and skin cancer can be seen in patients of all skin types. Many patients are unaware of this risk and do not use sunscreen and other sun-protective measures. We, as a specialty, have to educate our patients and the public of the risk for actinic keratosis and skin cancer in all skin types.
—Gary Goldenberg, MD (New York, New York)
Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
American Academy of Dermatology. Actinic keratosis. https://www.aad.org/public/diseases/scaly-skin/actinic-keratosis. Accessed October 17, 2017.
Kailas A, Botwin AL, Pritchett EN, et al. Assessing the effectiveness of knowledge-based interventions in increasing skin cancer awareness, knowledge, and protective behaviors in skin of color populations. Cutis. 2017;100:235-240.
Myth: Actinic keratoses are only seen in patients with lighter skin
Actinic keratoses (AKs) are precancerous lesions that may turn into squamous cell carcinoma if left untreated. UV rays cause AKs, either from outdoor sun exposure or tanning beds. According to the American Academy of Dermatology, AKs are more likely to develop in patients 40 years or older with fair skin; hair color that is naturally blonde or red; eye color that is naturally blue, green, or hazel; skin that freckles or burns when in the sun; a weakened immune system; and occupations involving substances that contain polycyclic aromatic hydrocarbons such as coal or tar.
A 2007 study compared the most common diagnoses among patients of different racial and ethnic groups in New York City. Alexis et al found that AK was in the top 10 diagnoses in white patients but not for black patients. They postulated that photoprotective factors in darkly pigmented skin such as larger and more numerous melanosomes that contain more melanin and are more dispersed throughout the epidermis result in a lower incidence of skin cancers in the skin of color (SOC) population.
RELATED ARTICLE: Common Dermatologic Disorders in Skin of Color: A Comparative Practice Survey
However, a recent skin cancer awareness study in Cutis reported that even though SOC populations have lower incidences of skin cancer such as melanoma, basal cell carcinoma, and squamous cell carcinoma, they exhibit higher death rates. Furthermore, black individuals are more likely to present with advanced-stage melanoma and acral lentiginous melanomas compared to white individuals. Kailas et al stated, “Overall, SOC patients have the poorest skin cancer prognosis, and the data suggest that the reason for this paradox is delayed diagnosis.” They evaluated several knowledge-based interventions for increasing skin cancer awareness, knowledge, and protective behaviors in SOC populations, including the use of visuals such as photographs to allow SOC patients to visualize different skin tones, educational interventions in another language, and pamphlets.
Dermatologists should be aware that education of SOC patients is important to eradicate the common misconception that these patients do not have to worry about AKs and other skin cancers. Remind these patients that they need to protect their skin from the sun, just as patients with fair skin do. Further research in the dermatology community should focus on educational interventions that will help increase knowledge regarding skin cancer in SOC populations.
Expert Commentary
Although more common in patients with lighter skin, actinic keratosis and skin cancer can be seen in patients of all skin types. Many patients are unaware of this risk and do not use sunscreen and other sun-protective measures. We, as a specialty, have to educate our patients and the public of the risk for actinic keratosis and skin cancer in all skin types.
—Gary Goldenberg, MD (New York, New York)
Myth: Actinic keratoses are only seen in patients with lighter skin
Actinic keratoses (AKs) are precancerous lesions that may turn into squamous cell carcinoma if left untreated. UV rays cause AKs, either from outdoor sun exposure or tanning beds. According to the American Academy of Dermatology, AKs are more likely to develop in patients 40 years or older with fair skin; hair color that is naturally blonde or red; eye color that is naturally blue, green, or hazel; skin that freckles or burns when in the sun; a weakened immune system; and occupations involving substances that contain polycyclic aromatic hydrocarbons such as coal or tar.
A 2007 study compared the most common diagnoses among patients of different racial and ethnic groups in New York City. Alexis et al found that AK was in the top 10 diagnoses in white patients but not for black patients. They postulated that photoprotective factors in darkly pigmented skin such as larger and more numerous melanosomes that contain more melanin and are more dispersed throughout the epidermis result in a lower incidence of skin cancers in the skin of color (SOC) population.
RELATED ARTICLE: Common Dermatologic Disorders in Skin of Color: A Comparative Practice Survey
However, a recent skin cancer awareness study in Cutis reported that even though SOC populations have lower incidences of skin cancer such as melanoma, basal cell carcinoma, and squamous cell carcinoma, they exhibit higher death rates. Furthermore, black individuals are more likely to present with advanced-stage melanoma and acral lentiginous melanomas compared to white individuals. Kailas et al stated, “Overall, SOC patients have the poorest skin cancer prognosis, and the data suggest that the reason for this paradox is delayed diagnosis.” They evaluated several knowledge-based interventions for increasing skin cancer awareness, knowledge, and protective behaviors in SOC populations, including the use of visuals such as photographs to allow SOC patients to visualize different skin tones, educational interventions in another language, and pamphlets.
Dermatologists should be aware that education of SOC patients is important to eradicate the common misconception that these patients do not have to worry about AKs and other skin cancers. Remind these patients that they need to protect their skin from the sun, just as patients with fair skin do. Further research in the dermatology community should focus on educational interventions that will help increase knowledge regarding skin cancer in SOC populations.
Expert Commentary
Although more common in patients with lighter skin, actinic keratosis and skin cancer can be seen in patients of all skin types. Many patients are unaware of this risk and do not use sunscreen and other sun-protective measures. We, as a specialty, have to educate our patients and the public of the risk for actinic keratosis and skin cancer in all skin types.
—Gary Goldenberg, MD (New York, New York)
Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
American Academy of Dermatology. Actinic keratosis. https://www.aad.org/public/diseases/scaly-skin/actinic-keratosis. Accessed October 17, 2017.
Kailas A, Botwin AL, Pritchett EN, et al. Assessing the effectiveness of knowledge-based interventions in increasing skin cancer awareness, knowledge, and protective behaviors in skin of color populations. Cutis. 2017;100:235-240.
Alexis AF, Sergay AB, Taylor SC. Common dermatologic disorders in skin of color: a comparative practice survey. Cutis. 2007;80:387-394.
American Academy of Dermatology. Actinic keratosis. https://www.aad.org/public/diseases/scaly-skin/actinic-keratosis. Accessed October 17, 2017.
Kailas A, Botwin AL, Pritchett EN, et al. Assessing the effectiveness of knowledge-based interventions in increasing skin cancer awareness, knowledge, and protective behaviors in skin of color populations. Cutis. 2017;100:235-240.

Maternally derived pneumococcal, meningococcal antibodies may affect vaccine effectiveness
, according to a new study.
That information may be useful in deciding the impact of vaccination programs that use a combination of maternal and infant vaccines and consider schedules with a delayed start, said Merryn Voysey of the University of Oxford (England) and her associates.
In this study, 5,097 children in 16 cohorts from 13 countries had pneumococcal antibody concentrations assessed from blood samples taken before their first dose of vaccine, and 2,925 infants from 5 cohorts in 4 countries had meningococcal antibody concentrations available.
At the time of their first vaccination, the children were ages 5-23 weeks and were from countries in Europe, Africa, Latin America, and South and East Asia. These populations have no routine programs of immunization in pregnancy, the researchers said. So, the maternal antibodies are passively acquired, and the decay rates may differ from those induced by maternal vaccinations.
The seroprevalence of maternal antibodies in infants was 92% for pneumococcal serotype 14 and 80% for serotype 19F; it was 30% for serotype 4 and 34% for serotype 1. Thirteen percent of infants had detectable levels of group C meningococcal antibodies prior to vaccination, and 43% had group A antibodies.
For the pneumococcal antibodies, “there was statistically significant variation in half-life estimates between country cohorts and between serotypes (both P less than .0001),” the researchers said. The half-life estimate was lowest – at 39 days – for serotype 6B, and highest – at 48 days – for serotype 5. The overall estimate across serotypes was 43 days.
“The age of the child was not significantly associated with decay rates (P = .103), confirming the assumption of exponential decay,” they said.
For the meningococcal antibodies, the half-lives were 43 days for group A and 40 days for group C.
“Substantial proportions of infants have antibodies to many vaccine serotypes of pneumococcus at the age when a vaccine program might normally commence,” the investigators noted. “Conversely, antibodies against capsular groups A and C meningococcal polysaccharides were less common, particularly for group C, which was only present in 13% of infants in the four countries contained in this analysis.
“Higher levels of group A meningococcal antibodies than group C have also been seen in unvaccinated adults of childbearing age in the Netherlands, and in mothers in the United Kingdom,” the researchers added. “Passively acquired maternal antibody has been shown to adversely affect the magnitude of the immune response to vaccination with pneumococcal conjugate vaccine, and increase the occurrence of otitis media in infants under 6 months of age.”
The proportion of infants who had maternal antipneumococcal antibodies differed between serotypes, the authors noted. Almost all infants had serotype 14 pneumococcal antibodies, and very high proportions of infants had serotype 19F antibodies.
“We have previously shown that the antibody response to vaccination with pneumococcal conjugate vaccine is adversely affected by the presence of maternal antibody,” the investigators said. “This inhibitory effect is greatest for serotype 14, with children seropositive from maternal antibodies having a response to vaccination that is only three-quarters the magnitude of those with no maternal antibody.”
Read more in Vaccine (2017 Oct 13;35[43]:5850-7).
, according to a new study.
That information may be useful in deciding the impact of vaccination programs that use a combination of maternal and infant vaccines and consider schedules with a delayed start, said Merryn Voysey of the University of Oxford (England) and her associates.
In this study, 5,097 children in 16 cohorts from 13 countries had pneumococcal antibody concentrations assessed from blood samples taken before their first dose of vaccine, and 2,925 infants from 5 cohorts in 4 countries had meningococcal antibody concentrations available.
At the time of their first vaccination, the children were ages 5-23 weeks and were from countries in Europe, Africa, Latin America, and South and East Asia. These populations have no routine programs of immunization in pregnancy, the researchers said. So, the maternal antibodies are passively acquired, and the decay rates may differ from those induced by maternal vaccinations.
The seroprevalence of maternal antibodies in infants was 92% for pneumococcal serotype 14 and 80% for serotype 19F; it was 30% for serotype 4 and 34% for serotype 1. Thirteen percent of infants had detectable levels of group C meningococcal antibodies prior to vaccination, and 43% had group A antibodies.
For the pneumococcal antibodies, “there was statistically significant variation in half-life estimates between country cohorts and between serotypes (both P less than .0001),” the researchers said. The half-life estimate was lowest – at 39 days – for serotype 6B, and highest – at 48 days – for serotype 5. The overall estimate across serotypes was 43 days.
“The age of the child was not significantly associated with decay rates (P = .103), confirming the assumption of exponential decay,” they said.
For the meningococcal antibodies, the half-lives were 43 days for group A and 40 days for group C.
“Substantial proportions of infants have antibodies to many vaccine serotypes of pneumococcus at the age when a vaccine program might normally commence,” the investigators noted. “Conversely, antibodies against capsular groups A and C meningococcal polysaccharides were less common, particularly for group C, which was only present in 13% of infants in the four countries contained in this analysis.
“Higher levels of group A meningococcal antibodies than group C have also been seen in unvaccinated adults of childbearing age in the Netherlands, and in mothers in the United Kingdom,” the researchers added. “Passively acquired maternal antibody has been shown to adversely affect the magnitude of the immune response to vaccination with pneumococcal conjugate vaccine, and increase the occurrence of otitis media in infants under 6 months of age.”
The proportion of infants who had maternal antipneumococcal antibodies differed between serotypes, the authors noted. Almost all infants had serotype 14 pneumococcal antibodies, and very high proportions of infants had serotype 19F antibodies.
“We have previously shown that the antibody response to vaccination with pneumococcal conjugate vaccine is adversely affected by the presence of maternal antibody,” the investigators said. “This inhibitory effect is greatest for serotype 14, with children seropositive from maternal antibodies having a response to vaccination that is only three-quarters the magnitude of those with no maternal antibody.”
Read more in Vaccine (2017 Oct 13;35[43]:5850-7).
, according to a new study.
That information may be useful in deciding the impact of vaccination programs that use a combination of maternal and infant vaccines and consider schedules with a delayed start, said Merryn Voysey of the University of Oxford (England) and her associates.
In this study, 5,097 children in 16 cohorts from 13 countries had pneumococcal antibody concentrations assessed from blood samples taken before their first dose of vaccine, and 2,925 infants from 5 cohorts in 4 countries had meningococcal antibody concentrations available.
At the time of their first vaccination, the children were ages 5-23 weeks and were from countries in Europe, Africa, Latin America, and South and East Asia. These populations have no routine programs of immunization in pregnancy, the researchers said. So, the maternal antibodies are passively acquired, and the decay rates may differ from those induced by maternal vaccinations.
The seroprevalence of maternal antibodies in infants was 92% for pneumococcal serotype 14 and 80% for serotype 19F; it was 30% for serotype 4 and 34% for serotype 1. Thirteen percent of infants had detectable levels of group C meningococcal antibodies prior to vaccination, and 43% had group A antibodies.
For the pneumococcal antibodies, “there was statistically significant variation in half-life estimates between country cohorts and between serotypes (both P less than .0001),” the researchers said. The half-life estimate was lowest – at 39 days – for serotype 6B, and highest – at 48 days – for serotype 5. The overall estimate across serotypes was 43 days.
“The age of the child was not significantly associated with decay rates (P = .103), confirming the assumption of exponential decay,” they said.
For the meningococcal antibodies, the half-lives were 43 days for group A and 40 days for group C.
“Substantial proportions of infants have antibodies to many vaccine serotypes of pneumococcus at the age when a vaccine program might normally commence,” the investigators noted. “Conversely, antibodies against capsular groups A and C meningococcal polysaccharides were less common, particularly for group C, which was only present in 13% of infants in the four countries contained in this analysis.
“Higher levels of group A meningococcal antibodies than group C have also been seen in unvaccinated adults of childbearing age in the Netherlands, and in mothers in the United Kingdom,” the researchers added. “Passively acquired maternal antibody has been shown to adversely affect the magnitude of the immune response to vaccination with pneumococcal conjugate vaccine, and increase the occurrence of otitis media in infants under 6 months of age.”
The proportion of infants who had maternal antipneumococcal antibodies differed between serotypes, the authors noted. Almost all infants had serotype 14 pneumococcal antibodies, and very high proportions of infants had serotype 19F antibodies.
“We have previously shown that the antibody response to vaccination with pneumococcal conjugate vaccine is adversely affected by the presence of maternal antibody,” the investigators said. “This inhibitory effect is greatest for serotype 14, with children seropositive from maternal antibodies having a response to vaccination that is only three-quarters the magnitude of those with no maternal antibody.”
Read more in Vaccine (2017 Oct 13;35[43]:5850-7).
FROM VACCINE
Vitality predicts T2DM major cardiovascular event risk
LISBON – according to the results of a primary care study.
Seldom feeling “full of pep” or not having “a lot of energy” was associated with an increased risk of a major cardiovascular event (MACE) in middle-aged (55-66 years) adults with T2DM, Marta Vergara, MD, reported at the annual meeting of the European Association for the Study of Diabetes.

“It’s well known that patients with type 2 diabetes have a high risk for developing cardiovascular disease, and it is the main cause of death,” said Dr. Vergara of Linköping (Sweden) University.
While several risk factors for cardiovascular disease are known and widely monitored for in clinical practice worldwide, including psychological aspects such as mental stress, ways to identify patients earlier are needed.
“We need more clinically useful and easy-to-manage measurement instruments,” Dr. Vergara said.
Using data from the ongoing Cardiovascular Risk Factors in Patients With Diabetes – a Prospective Study in Primary Care (CARDIPP), Dr. Vergara and colleagues identified two questions used in the 36-Item Short Form (SF-36) that might fit the bill:
- ”How much time during the past 4 weeks did you feel full of pep?”
- “How much time during the past 4 weeks did you have a lot of energy?”
Patients had answered these questions using a 6-point scale ranging from 1, all of the time, to 6 none of the time.
In addition to completing the full SF-36 at recruitment, all patients enrolled in CARDIPP underwent thorough assessment of baseline cardiovascular risk. This included asking about their duration of diabetes and smoking history, taking glycemic and anthropometric readings, and recording their systolic blood pressure. Pulse wave velocity was also used to assess patients’ carotid-femoral artery stiffness.
Over a follow-up period of 7 years, 59 (7.8%) of 761 men and women aged 55-66 years developed ischemic heart disease or had a stroke and needed hospital treatment or died.
“Our data support the use of questions about sense of vitality in order to add prognostic information about subsequent risk of MACE independently of traditional risk markers, such as diabetes duration, age, HbA1c, gender, smoking, systolic blood pressure, and carotid-femoral pulse wave velocity and sagittal abdominal diameter,” Dr. Vergara said.
“We suggest that not feeling full of pep and not having a lot of energy could be used as risk markers for MACE in patients with type 2 diabetes.” These are two easy questions that could be asked as part of the risk assessment process in primary care, she suggested. “Other questions from the SF-36, such as feeling tired or worn out, were not independent markers of MACE,” Dr. Vergara said.
She said she had no relevant financial disclosures.
LISBON – according to the results of a primary care study.
Seldom feeling “full of pep” or not having “a lot of energy” was associated with an increased risk of a major cardiovascular event (MACE) in middle-aged (55-66 years) adults with T2DM, Marta Vergara, MD, reported at the annual meeting of the European Association for the Study of Diabetes.
“It’s well known that patients with type 2 diabetes have a high risk for developing cardiovascular disease, and it is the main cause of death,” said Dr. Vergara of Linköping (Sweden) University.
While several risk factors for cardiovascular disease are known and widely monitored for in clinical practice worldwide, including psychological aspects such as mental stress, ways to identify patients earlier are needed.
“We need more clinically useful and easy-to-manage measurement instruments,” Dr. Vergara said.
Using data from the ongoing Cardiovascular Risk Factors in Patients With Diabetes – a Prospective Study in Primary Care (CARDIPP), Dr. Vergara and colleagues identified two questions used in the 36-Item Short Form (SF-36) that might fit the bill:
- ”How much time during the past 4 weeks did you feel full of pep?”
- “How much time during the past 4 weeks did you have a lot of energy?”
Patients had answered these questions using a 6-point scale ranging from 1, all of the time, to 6 none of the time.
In addition to completing the full SF-36 at recruitment, all patients enrolled in CARDIPP underwent thorough assessment of baseline cardiovascular risk. This included asking about their duration of diabetes and smoking history, taking glycemic and anthropometric readings, and recording their systolic blood pressure. Pulse wave velocity was also used to assess patients’ carotid-femoral artery stiffness.
Over a follow-up period of 7 years, 59 (7.8%) of 761 men and women aged 55-66 years developed ischemic heart disease or had a stroke and needed hospital treatment or died.
“Our data support the use of questions about sense of vitality in order to add prognostic information about subsequent risk of MACE independently of traditional risk markers, such as diabetes duration, age, HbA1c, gender, smoking, systolic blood pressure, and carotid-femoral pulse wave velocity and sagittal abdominal diameter,” Dr. Vergara said.
“We suggest that not feeling full of pep and not having a lot of energy could be used as risk markers for MACE in patients with type 2 diabetes.” These are two easy questions that could be asked as part of the risk assessment process in primary care, she suggested. “Other questions from the SF-36, such as feeling tired or worn out, were not independent markers of MACE,” Dr. Vergara said.
She said she had no relevant financial disclosures.
LISBON – according to the results of a primary care study.
Seldom feeling “full of pep” or not having “a lot of energy” was associated with an increased risk of a major cardiovascular event (MACE) in middle-aged (55-66 years) adults with T2DM, Marta Vergara, MD, reported at the annual meeting of the European Association for the Study of Diabetes.
“It’s well known that patients with type 2 diabetes have a high risk for developing cardiovascular disease, and it is the main cause of death,” said Dr. Vergara of Linköping (Sweden) University.
While several risk factors for cardiovascular disease are known and widely monitored for in clinical practice worldwide, including psychological aspects such as mental stress, ways to identify patients earlier are needed.
“We need more clinically useful and easy-to-manage measurement instruments,” Dr. Vergara said.
Using data from the ongoing Cardiovascular Risk Factors in Patients With Diabetes – a Prospective Study in Primary Care (CARDIPP), Dr. Vergara and colleagues identified two questions used in the 36-Item Short Form (SF-36) that might fit the bill:
- ”How much time during the past 4 weeks did you feel full of pep?”
- “How much time during the past 4 weeks did you have a lot of energy?”
Patients had answered these questions using a 6-point scale ranging from 1, all of the time, to 6 none of the time.
In addition to completing the full SF-36 at recruitment, all patients enrolled in CARDIPP underwent thorough assessment of baseline cardiovascular risk. This included asking about their duration of diabetes and smoking history, taking glycemic and anthropometric readings, and recording their systolic blood pressure. Pulse wave velocity was also used to assess patients’ carotid-femoral artery stiffness.
Over a follow-up period of 7 years, 59 (7.8%) of 761 men and women aged 55-66 years developed ischemic heart disease or had a stroke and needed hospital treatment or died.
“Our data support the use of questions about sense of vitality in order to add prognostic information about subsequent risk of MACE independently of traditional risk markers, such as diabetes duration, age, HbA1c, gender, smoking, systolic blood pressure, and carotid-femoral pulse wave velocity and sagittal abdominal diameter,” Dr. Vergara said.
“We suggest that not feeling full of pep and not having a lot of energy could be used as risk markers for MACE in patients with type 2 diabetes.” These are two easy questions that could be asked as part of the risk assessment process in primary care, she suggested. “Other questions from the SF-36, such as feeling tired or worn out, were not independent markers of MACE,” Dr. Vergara said.
She said she had no relevant financial disclosures.
AT EASD 2017
Key clinical point: Two simple questions about vitality could help assess the risk of major cardiovascular events in patients with type 2 diabetes mellitus.
Major finding: The hazard ratios for seldom feeling “full of pep” and seldom having “lots of energy” and MACE were a respective 1.31 (P = .003) and 1.44 (P less than .0001).
Data source: A prospective, observational primary care study of 761 patients with type 2 diabetes mellitus.
Disclosures: The presenting author had no relevant financial disclosures.