User login
PBC patients show brain abnormalities before cirrhosis occurs
Brain abnormalities associated with primary biliary cholangitis (PBC) can be observed via magnetic resonance imaging before significant liver damage occurs, according to V.B.P. Grover, MD, and associates at the Liver Unit and Robert Steiner MRI Unit, MRC Clinical Sciences Centre, Imperial College London.
In a study of 13 newly diagnosed precirrhotic PBC patients and 17 healthy volunteers, mean magnetization transfer ratios (MTR) were lower in the thalamus, putamen, and head of caudate in PBC patients, compared with the control group, with the greatest difference seen in the thalamus. Severity of PBC symptoms did not have any significant effect on MTR.
An increase in the apparent diffusion coefficient was seen in the thalamus of PBC patients; however, no significant difference in cerebral metabolite ratios or pallidal index was observed. No correlation between neuroimaging data, lab data, symptom severity scores, or age was observed.
“Larger scale, and in particular linear studies, will be needed to explore the relationship of this change to symptoms and its response to therapies such as UDCA [ursodeoxycholic acid] and OCA [obeticholic acid]. The presence of brain change so early in the disease process would, however, suggest that the current step-up approach to therapy in which treatment change follows failure of a therapy type may allow the progressive accumulation of brain injury whilst waiting for adequate therapeutic response,” the investigators concluded.
Find the full study in Alimentary Pharmacology & Therapeutics (doi: 10.1111/apt.13797).
Brain abnormalities associated with primary biliary cholangitis (PBC) can be observed via magnetic resonance imaging before significant liver damage occurs, according to V.B.P. Grover, MD, and associates at the Liver Unit and Robert Steiner MRI Unit, MRC Clinical Sciences Centre, Imperial College London.
In a study of 13 newly diagnosed precirrhotic PBC patients and 17 healthy volunteers, mean magnetization transfer ratios (MTR) were lower in the thalamus, putamen, and head of caudate in PBC patients, compared with the control group, with the greatest difference seen in the thalamus. Severity of PBC symptoms did not have any significant effect on MTR.
An increase in the apparent diffusion coefficient was seen in the thalamus of PBC patients; however, no significant difference in cerebral metabolite ratios or pallidal index was observed. No correlation between neuroimaging data, lab data, symptom severity scores, or age was observed.
“Larger scale, and in particular linear studies, will be needed to explore the relationship of this change to symptoms and its response to therapies such as UDCA [ursodeoxycholic acid] and OCA [obeticholic acid]. The presence of brain change so early in the disease process would, however, suggest that the current step-up approach to therapy in which treatment change follows failure of a therapy type may allow the progressive accumulation of brain injury whilst waiting for adequate therapeutic response,” the investigators concluded.
Find the full study in Alimentary Pharmacology & Therapeutics (doi: 10.1111/apt.13797).
Brain abnormalities associated with primary biliary cholangitis (PBC) can be observed via magnetic resonance imaging before significant liver damage occurs, according to V.B.P. Grover, MD, and associates at the Liver Unit and Robert Steiner MRI Unit, MRC Clinical Sciences Centre, Imperial College London.
In a study of 13 newly diagnosed precirrhotic PBC patients and 17 healthy volunteers, mean magnetization transfer ratios (MTR) were lower in the thalamus, putamen, and head of caudate in PBC patients, compared with the control group, with the greatest difference seen in the thalamus. Severity of PBC symptoms did not have any significant effect on MTR.
An increase in the apparent diffusion coefficient was seen in the thalamus of PBC patients; however, no significant difference in cerebral metabolite ratios or pallidal index was observed. No correlation between neuroimaging data, lab data, symptom severity scores, or age was observed.
“Larger scale, and in particular linear studies, will be needed to explore the relationship of this change to symptoms and its response to therapies such as UDCA [ursodeoxycholic acid] and OCA [obeticholic acid]. The presence of brain change so early in the disease process would, however, suggest that the current step-up approach to therapy in which treatment change follows failure of a therapy type may allow the progressive accumulation of brain injury whilst waiting for adequate therapeutic response,” the investigators concluded.
Find the full study in Alimentary Pharmacology & Therapeutics (doi: 10.1111/apt.13797).
FROM ALIMENTARY PHARMACOLOGY & THERAPEUTICS
Doctors have at least seven APM options in 2017
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.

For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
AGA supports physician-focused payment models (PFPMs) tailored to the practice and goals of GIs through the development of episodes of care. We appreciate that CMS has provided flexibility to allow more physicians to be eligible to participate in APMs and are hopeful that there will be new options in the future for gastroenterologists to demonstrate their value and maximize their earnings under APMs.
[email protected]
On Twitter @legal_med
AGA Resource
AGA is committed to preparing you for success in possible new reimbursement environments. Learn more about bundled and episode payment models at http://www.gastro.org/practice-management/quality/bundled-payment-options.
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.
For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
AGA supports physician-focused payment models (PFPMs) tailored to the practice and goals of GIs through the development of episodes of care. We appreciate that CMS has provided flexibility to allow more physicians to be eligible to participate in APMs and are hopeful that there will be new options in the future for gastroenterologists to demonstrate their value and maximize their earnings under APMs.
[email protected]
On Twitter @legal_med
AGA Resource
AGA is committed to preparing you for success in possible new reimbursement environments. Learn more about bundled and episode payment models at http://www.gastro.org/practice-management/quality/bundled-payment-options.
Physicians will have several options to choose from when it comes to advanced alternative payment models (APMs) in 2017.
In an Oct. 25 release, the Centers for Medicare & Medicaid Services announced seven models that will be considered advanced APMs in 2017, including the new Oncology Care Model with two-sided risk. Other advanced APM choices will include:
• Comprehensive Primary Care Plus (CPC+).
• Comprehensive ESRD Care Model (Large Dialysis Organization [LDO] arrangement).
• Comprehensive ESRD Care Model (non-LDO arrangement).
• Medicare Shared Savings Program Accountable Care Organizations (ACOs) – Track 2.
• Medicare Shared Savings Program ACOs – Track 3.
• Next Generation ACO Model.
For the 2017 performance year, CMS estimates that 70,000-120,000 clinicians will participate in an advanced APM. In 2018, more than 125,000 clinicians will likely participate, according to CMS. The agency plans to reopen applications for new practices in the Comprehensive Primary Care Plus (CPC+) model and the Next Generation ACO model for the 2018 performance year.
Other models available for the 2018 performance year will include:
• ACO – Track 1+.
• New voluntary bundled payment model.
• Comprehensive Care for Joint Replacement Payment Model (Certified Electronic Health Record Technology [CEHRT] track).
• Advancing Care Coordination through Episode Payment Models – Track 1 (CEHRT).
For performance years 2017 and 2018, participation requirements will apply only to Medicare payments and physicians who treat Medicare patients. Starting in 2019, clinicians may also meet an alternative standard for advanced APMs that will include non-Medicare payments and patients.
“With these new opportunities, CMS expects that by the 2018 performance period, 25% of clinicians in the Quality Payment Program will earn incentive payments by being a part of these advanced models,” Patrick Conway, MD, CMS deputy administrator said in a statement. “Thanks to MACRA and the Innovation Center, we’re striving to see more Medicare patients benefit from better care when they visit their doctor for a knee replacement, receive cancer treatment, or have a coordinated care team manage their complex conditions.”
CMS is accepting feedback from physicians on the Quality Payment Program final rule until Dec. 17. Doctors can submit their comments and suggestions electronically through the CMS e-Regulation website.
AGA supports physician-focused payment models (PFPMs) tailored to the practice and goals of GIs through the development of episodes of care. We appreciate that CMS has provided flexibility to allow more physicians to be eligible to participate in APMs and are hopeful that there will be new options in the future for gastroenterologists to demonstrate their value and maximize their earnings under APMs.
[email protected]
On Twitter @legal_med
AGA Resource
AGA is committed to preparing you for success in possible new reimbursement environments. Learn more about bundled and episode payment models at http://www.gastro.org/practice-management/quality/bundled-payment-options.
Mitral valve disease often missed in pulmonary hypertension
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.

Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.
Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
LOS ANGELES – Dyspnea in pulmonary hypertension is caused by mitral valve disease until proven otherwise, according to Paul Forfia, MD, director of pulmonary hypertension, right heart failure, and pulmonary thromboendarterectomy at Temple University, Philadelphia.
Although mitral valve disease is a well-recognized cause of pulmonary hypertension, its significance is often underestimated in practice.
“Whether the valve is regurgitant or stenotic makes absolutely no difference. When you delay” repair or replacement, “the patient keeps getting sicker,” he said. In time, “everyone is standing around wringing their hands going, ‘Oh my god, what are we going to do? Are you serious? Fix the valve.’ We see this type of patient a couple times a month,” Dr. Forfia said at the American College of Chest Physicians annual meeting.
“I have seen lifesaving mitral valve surgery put off for many years in patients with pulmonary hypertension, when all they needed was to have their valve fixed,” he said.
Whatever the case, pulmonologists who want the valve fixed often end up playing patient ping pong with cardiologists who want the hypertension controlled beforehand, but “if I treat the pulmonary circulation first, all I am going to do is unmask the left heart failure. There will be no functional improvement whatsoever,” Dr. Forfia said.
Surgery is the best solution as long as patients are well enough to recover. “With pulmonary hypertension in the setting of severe mitral valve regurgitation or stenosis, whether the pulmonary hypertension is related to passive left heart congestion or associated with pulmonary arteriopathy, the only sensible option is to correct the underlying valvular abnormality,” he said. The surgery should be done at an institution capable of managing postop pulmonary arteriopathy, if present.
The ping pong solution is to send patients to an expert pulmonology center; the mitral valve problem will be spotted right away.
“There is no pulmonary pressure cutoff that should prohibit surgery” in patients able to recover. “There is no such thing as a pulmonary artery pressure too high to be explained by mitral valve disease. The pulmonary pressure can be as high as it wants to be. You will get nowhere by thinking the pressure is too high to address the valve,” Dr. Forfia said.
Often “you hear, ‘I’m afraid the person is going to die on the table.’ I always say ‘if the patient is not going to die on the table, they are going to die in their living room of progressive heart failure because you [didn’t] fix their valve. I have never had a patient with pulmonary hypertension not separate from cardiopulmonary bypass. It’s a myth,” he said.
When there’s a “question if the dyspnea is coming from the mitral valve, we routinely use exercise right heart catheterization to probe the situation. We have a recumbent bike in the cath lab. You’ll often provoke significant left heart congestion with a low workload. It’s very revealing to the significance of mitral valve disease,” he said.
Aortic valve disease is also missed in pulmonary hypertension. “It’s not [a] similar” problem; “it’s the same” problem, Dr. Forfia said.
Dr. Forfia is a consultant for Bayer, Actelion, and United Therapeutics.
EXPERT ANALYSIS FROM CHEST 2016
Weight loss procedure is linked to subsequent substance misuse
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
NEW ORLEANS – Severely obese patients who undergo Roux-en-Y gastric bypass surgery are subsequently at sharply increased risk for new-onset alcohol use disorder as well as for treatment of substance use disorder, compared with others who opt for a laparoscopic adjustable banding procedure for weight loss, Wendy C. King, PhD, reported at a meeting presented by the Obesity Society of America and the American Society for Metabolic and Bariatric Surgery.
This new finding from the NIH-sponsored Longitudinal Assessment of Bariatric Surgery–2 study (LABS-2) has important implications for clinical practice.
“Patients considering bariatric surgery really should be informed of this surgery-specific risk. Also, alcohol use disorder screening, evaluation, intervention, and referral should be incorporated as part of regular presurgical and definitely also postoperative care. And because many patients don’t return to their surgeon for long-term postoperative care, it’s important that clinicians in primary care and other specialties are really looking for this problem in long-term follow-up,” said Dr. King, an epidemiologist at the University of Pittsburgh.
LABS-2 is an observational cohort study of patients undergoing first-time bariatric surgery at 10 participating U.S. hospitals, all of which have academic ties and are rated as bariatric surgery centers of excellence. Dr. King presented 5-year postsurgical follow-up data on 1,481 patients who had Roux-en-Y gastric bypass (RYGB) and 522 with laparoscopic adjustable gastric banding (LAGB). Independently of their regular clinical care visits, participants were assessed annually for their alcohol use and its consequences using the Alcohol Use Disorders Identification Test (AUDIT), use of illicit drugs within the past year, and whether they had undergone hospitalization or counseling for alcohol or drug problems. A score of 8 or more points on the AUDIT was deemed an indication of symptoms of alcohol use disorder (AUD),
After eliminating from consideration the 7% of patients with AUD symptoms at baseline, the cumulative incidence of AUD symptoms in the RYGB patients climbed from zero to 20.8% by the end of the fifth year of follow-up. Treatment for a substance use disorder occurred in 3.5% of RYGB patients during their first 5 years postsurgery, and 7.5% admitted to illicit drug use, said Dr. King.
In contrast, the cumulative incidence of AUD symptoms through 5 years in the LAGB patients was only 11.3%, less than 1% underwent treatment for a substance use disorder, and 4.9% said they had used illicit drugs.
But LABS-2 is not a randomized trial. Patients chose their bariatric procedure together with their surgeon. For this reason, it was important to perform a multivariate regression analysis adjusted for sociodemographics, social support, psychiatric treatment, lifetime history of psychiatric hospitalization, baseline smoking and alcohol consumption, and other potential confounders.
After performing this statistical exercise, the RYGB patients remained at an adjusted 2.05-fold increased risk of AUD symptoms, compared with the LAGB patients, as well as at 3.83-fold greater risk of treatment for a substance use disorder.
The 1.6-fold increased rate of illicit drug use in the RYGB group didn’t achieve statistical significance. Moreover, on closer examination, most of this illicit drug use involved marijuana, and its use in the post–bariatric surgery population appeared to mirror secular trends in the United States as a whole, according to Dr. King.
With her coinvestigators, Dr. King searched for presurgical risk factors that might predict postsurgical substance misuse. Perhaps the most interesting finding concerned the factors that weren’t predictive, including education, unemployment, score on the Beck Depression Inventory, SF-36 mental component summary score, race, marital status, binge eating, loss of control eating, and body mass index.
Lower social support prior to surgery was associated with increased risk for developing AUD symptoms during the first 5 years after bariatric surgery. Younger age and smoking at baseline were associated with increased rates of postoperative AUD symptoms, substance use disorder treatment, and illicit drug use. A history of psychiatric treatment was associated with increased rates of substance use disorder treatment and illicit drug use.
“That could indicate greater medical surveillance among those patients or greater willingness to get treatment, since they’d had treatment for other psychiatric issues in the past,” Dr. King speculated.
She described the study’s strengths as its large size, geographically diverse patient population, unusually high retention over time, compared with other bariatric surgery studies, and the use of AUDIT, a validated and reliable screening tool. The major limitations are that investigators didn’t inquire about illicit use of opioids and benzodiazepines, and recipients of gastric sleeve procedures weren’t included in the long-term follow-up analysis because LABS-2 began before the gastric sleeve boomed in popularity.
John M. Morton, MD, a former president of the American Society for Metabolic and Bariatric Surgery, predicted that a similar study that included gastric sleeve patients would show them to have the same unremarkable postoperative rates of substance misuse as the LAGB group.
“I want to emphasize that this increased incidence of alcohol problems in the Roux-en-Y gastric bypass patients is maybe not so much a psychological issue as it is a physiologic one,” added Dr. Morton, chief of bariatric and minimally invasive surgery at Stanford (Calif.) School of Medicine.
Dr. King agreed. “Just in the last year and a half there have been some great pharmacokinetic studies showing that the Roux-en-Y affects alcohol metabolism and absorption, as well as studies in rodent models that suggest alcohol produces increased neurobiologic reward,” she noted.
The LABS-2 study is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. King reported having no relevant financial interests.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: In the first 5 years following bariatric surgery, patients who underwent Roux-en-Y gastric bypass were twice as likely to develop new-onset alcohol use disorder and nearly four times more likely to be treated for substance use disorder, compared with recipients of laparoscopic gastric banding.
Data source: The LABS-2 study is an observational cohort study involving more than 2,000 patients in long-term follow-up after undergoing Roux-en-Y gastric bypass or laparoscopic adjustable banding.
Disclosures: LABS-2 is funded by the National Institute of Diabetes and Digestive and Kidney Diseases. The presenter reported having no relevant financial interests.
Bezlotoxumab reduces CDI recurrence across antibiotic subgroups
NEW ORLEANS – The monoclonal antibody bezlotoxumab significantly reduces the risk of Clostridium difficile infection (CDI) recurrence in adults receiving standard of care antibiotic treatment, regardless of whether that treatment is with metronidazole, vancomycin, or fidaxomicin, according to an analysis of data from the MODIFY I and II trials.
The global, randomized, double-blind, placebo-controlled trials demonstrated that bezlotoxumab was safe and effective for preventing CDI recurrence, and the current prespecified analysis further showed that choice of standard of care antibiotic therapy did not affect the outcomes, Erik R. Dubberke, MD, of Washington University in St. Louis, reported at IDWeek, an annual scientific meeting on infectious diseases.

Consistent with the overall study results, clinical cure rates were similar with bezlotoxumab and placebo, regardless of the standard of care antibiotic received (80% vs. 80.3%, respectively, overall; 81% vs. 81.3% in the metronidazole group; 78.5% vs. 79.6% in the vancomycin group; and 86.7% vs. 76.9% in the fidaxomicin group), he said.
However, CDI recurrence rates were lower among those who received bezlotoxumab, compared with those who received placebo in all three standard of care subgroups, with 10%, 15%, and 12% fewer bezlotoxumab vs. placebo patients experiencing recurrence in the metronidazole, vancomycin, and fidaxomicin groups, respectively, and 12% fewer experiencing recurrence overall.
The primary endpoint of CDI recurrence was defined in the studies as a new episode of diarrhea (at least three unformed stools in 24 hours) and a positive stool test for toxigenic C. difficile after clinical cure of the baseline CDI episode. Clinical cure was defined as standard of care antibiotics given for 14 days or less and no diarrhea for 2 consecutive days after completing standard of care treatment.
Of note, the patients in the vancomycin group were older and sicker, and had more risk factors for CDI, he said, noting, for example, that 57% of vancomycin patients were aged at least 65 years and 33% were aged at least 75 years, vs. 46% and 26% for metronidazole, respectively, and 46% and 18% for fidaxomicin; 72% of vancomycin patients were inpatients, compared with 65% and 50% of metronidazole and fidaxomicin patients.
Further, 19% of vancomycin patients, vs. 13% and 14% of metronidazole and fidaxomicin patients met criteria for severe CDI.
The findings of the current analysis are important, because the incidence of CDI recurrence is about 25%, and the risk increases with each subsequent recurrence, Dr. Dubberke said, concluding that this novel, nonantibiotic approach to prevention of CDI recurrence using bezlotoxumab, which recently received Food and Drug Administration approval for this indication, is of benefit for reducing that risk, regardless of the antibiotic used as part of standard of care therapy for CDI.
Dr. Dubberke reported serving as an investigator, adviser and/or consultant for Merck, Rebiotix, Sanofi Pasteur, and Summit, and receiving consultant fees and/or grant/research support from these companies.
NEW ORLEANS – The monoclonal antibody bezlotoxumab significantly reduces the risk of Clostridium difficile infection (CDI) recurrence in adults receiving standard of care antibiotic treatment, regardless of whether that treatment is with metronidazole, vancomycin, or fidaxomicin, according to an analysis of data from the MODIFY I and II trials.
The global, randomized, double-blind, placebo-controlled trials demonstrated that bezlotoxumab was safe and effective for preventing CDI recurrence, and the current prespecified analysis further showed that choice of standard of care antibiotic therapy did not affect the outcomes, Erik R. Dubberke, MD, of Washington University in St. Louis, reported at IDWeek, an annual scientific meeting on infectious diseases.
Consistent with the overall study results, clinical cure rates were similar with bezlotoxumab and placebo, regardless of the standard of care antibiotic received (80% vs. 80.3%, respectively, overall; 81% vs. 81.3% in the metronidazole group; 78.5% vs. 79.6% in the vancomycin group; and 86.7% vs. 76.9% in the fidaxomicin group), he said.
However, CDI recurrence rates were lower among those who received bezlotoxumab, compared with those who received placebo in all three standard of care subgroups, with 10%, 15%, and 12% fewer bezlotoxumab vs. placebo patients experiencing recurrence in the metronidazole, vancomycin, and fidaxomicin groups, respectively, and 12% fewer experiencing recurrence overall.
The primary endpoint of CDI recurrence was defined in the studies as a new episode of diarrhea (at least three unformed stools in 24 hours) and a positive stool test for toxigenic C. difficile after clinical cure of the baseline CDI episode. Clinical cure was defined as standard of care antibiotics given for 14 days or less and no diarrhea for 2 consecutive days after completing standard of care treatment.
Of note, the patients in the vancomycin group were older and sicker, and had more risk factors for CDI, he said, noting, for example, that 57% of vancomycin patients were aged at least 65 years and 33% were aged at least 75 years, vs. 46% and 26% for metronidazole, respectively, and 46% and 18% for fidaxomicin; 72% of vancomycin patients were inpatients, compared with 65% and 50% of metronidazole and fidaxomicin patients.
Further, 19% of vancomycin patients, vs. 13% and 14% of metronidazole and fidaxomicin patients met criteria for severe CDI.
The findings of the current analysis are important, because the incidence of CDI recurrence is about 25%, and the risk increases with each subsequent recurrence, Dr. Dubberke said, concluding that this novel, nonantibiotic approach to prevention of CDI recurrence using bezlotoxumab, which recently received Food and Drug Administration approval for this indication, is of benefit for reducing that risk, regardless of the antibiotic used as part of standard of care therapy for CDI.
Dr. Dubberke reported serving as an investigator, adviser and/or consultant for Merck, Rebiotix, Sanofi Pasteur, and Summit, and receiving consultant fees and/or grant/research support from these companies.
NEW ORLEANS – The monoclonal antibody bezlotoxumab significantly reduces the risk of Clostridium difficile infection (CDI) recurrence in adults receiving standard of care antibiotic treatment, regardless of whether that treatment is with metronidazole, vancomycin, or fidaxomicin, according to an analysis of data from the MODIFY I and II trials.
The global, randomized, double-blind, placebo-controlled trials demonstrated that bezlotoxumab was safe and effective for preventing CDI recurrence, and the current prespecified analysis further showed that choice of standard of care antibiotic therapy did not affect the outcomes, Erik R. Dubberke, MD, of Washington University in St. Louis, reported at IDWeek, an annual scientific meeting on infectious diseases.
Consistent with the overall study results, clinical cure rates were similar with bezlotoxumab and placebo, regardless of the standard of care antibiotic received (80% vs. 80.3%, respectively, overall; 81% vs. 81.3% in the metronidazole group; 78.5% vs. 79.6% in the vancomycin group; and 86.7% vs. 76.9% in the fidaxomicin group), he said.
However, CDI recurrence rates were lower among those who received bezlotoxumab, compared with those who received placebo in all three standard of care subgroups, with 10%, 15%, and 12% fewer bezlotoxumab vs. placebo patients experiencing recurrence in the metronidazole, vancomycin, and fidaxomicin groups, respectively, and 12% fewer experiencing recurrence overall.
The primary endpoint of CDI recurrence was defined in the studies as a new episode of diarrhea (at least three unformed stools in 24 hours) and a positive stool test for toxigenic C. difficile after clinical cure of the baseline CDI episode. Clinical cure was defined as standard of care antibiotics given for 14 days or less and no diarrhea for 2 consecutive days after completing standard of care treatment.
Of note, the patients in the vancomycin group were older and sicker, and had more risk factors for CDI, he said, noting, for example, that 57% of vancomycin patients were aged at least 65 years and 33% were aged at least 75 years, vs. 46% and 26% for metronidazole, respectively, and 46% and 18% for fidaxomicin; 72% of vancomycin patients were inpatients, compared with 65% and 50% of metronidazole and fidaxomicin patients.
Further, 19% of vancomycin patients, vs. 13% and 14% of metronidazole and fidaxomicin patients met criteria for severe CDI.
The findings of the current analysis are important, because the incidence of CDI recurrence is about 25%, and the risk increases with each subsequent recurrence, Dr. Dubberke said, concluding that this novel, nonantibiotic approach to prevention of CDI recurrence using bezlotoxumab, which recently received Food and Drug Administration approval for this indication, is of benefit for reducing that risk, regardless of the antibiotic used as part of standard of care therapy for CDI.
Dr. Dubberke reported serving as an investigator, adviser and/or consultant for Merck, Rebiotix, Sanofi Pasteur, and Summit, and receiving consultant fees and/or grant/research support from these companies.
AT IDWEEK 2016
Key clinical point:
Major finding: 12% fewer bezlotoxumab vs. placebo patients experienced CDI recurrence.
Data source: A prespecified analysis of data from 1,554 subjects from the MODIFY I and II trials.
Disclosures: Dr. Dubberke reported serving as an investigator, adviser, and/or consultant for Merck, Rebiotix, Sanofi Pasteur, and Summit, and receiving consultant fees and/or grant/research support from these companies.
Diabetes, stroke linked to recurrent C. difficile
LAS VEGAS – Diabetes and stroke are risk factors for recurrent Clostridium difficile infection (CDI), with stroke patients at about 10 times the risk of recurrence.
The underlying cause for the association is a mystery, but one-sided paralysis is one possibility. “A lot of stroke patients may be hemiplegic, and they may be bedridden, so that may be a risk factor by itself. It’s something that may need to be studied in the future,” Alan Putrus, MD, a gastroenterology fellow at St. John Providence Hospital, Detroit, said in an interview.
CDI recurrence rates range from 5% to 47%, depending on the institution. Although risk factors of initial CDI have been well defined, few studies have looked at risk factors associated with recurrence.
In order to get at the question, the researchers conducted a study of 108 initial CDIs and 113 recurrences at two urban and one suburban hospital. Patients who experienced recurrence were matched 1:1 to age- and gender-matched controls with no recurrent CDI.
CDI recurrence rates were 16.5% and 15.9% in the two urban hospitals, and 14.9% in the suburban hospital.
Logistic regression revealed risk factors associated with CDI recurrence, including diabetes (odds ratio, 1.91; 95% confidence interval, 1.05-3.47; P = .04), stroke (OR, 9.73; 95% CI, 1.15-82.35; P = .04), exposure to proton pump inhibitors in the past 3 months (OR, 1.82; 95% CI, 1.03-3.23; P = .04), and admission to an intensive care unit in the past 3 months (OR, 1.95; 95% CI, 1.0-3.83; P = .04).
The results suggest that diabetes and especially stroke may be important risk factors for CDI recurrence, and their presence should prompt physicians to alter patient care accordingly, according to Dr. Putrus.
He stressed the importance of antibiotic stewardship. “Once you find a certain bug or pathogen, try to deescalate the antibiotics as soon as you can. If a patient is diabetic, controlling their blood sugar may also help,” Dr. Putrus said.
Finally, physicians should consider whether proton pump inhibitors are really necessary. Some patients start on PPIs but remain on the drugs long after symptoms have abated. “A lot of patients just have some discomfort in their abdomen, and they never stop taking it. They keep refilling it. So that’s a problem,” said Dr. Putrus.
Dr. Putrus has declared no conflicts of interest.
AGA Resource
AGA offers information to educate your patients about C. difficile and fecal microbiota transplant. Learn more at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
LAS VEGAS – Diabetes and stroke are risk factors for recurrent Clostridium difficile infection (CDI), with stroke patients at about 10 times the risk of recurrence.
The underlying cause for the association is a mystery, but one-sided paralysis is one possibility. “A lot of stroke patients may be hemiplegic, and they may be bedridden, so that may be a risk factor by itself. It’s something that may need to be studied in the future,” Alan Putrus, MD, a gastroenterology fellow at St. John Providence Hospital, Detroit, said in an interview.
CDI recurrence rates range from 5% to 47%, depending on the institution. Although risk factors of initial CDI have been well defined, few studies have looked at risk factors associated with recurrence.
In order to get at the question, the researchers conducted a study of 108 initial CDIs and 113 recurrences at two urban and one suburban hospital. Patients who experienced recurrence were matched 1:1 to age- and gender-matched controls with no recurrent CDI.
CDI recurrence rates were 16.5% and 15.9% in the two urban hospitals, and 14.9% in the suburban hospital.
Logistic regression revealed risk factors associated with CDI recurrence, including diabetes (odds ratio, 1.91; 95% confidence interval, 1.05-3.47; P = .04), stroke (OR, 9.73; 95% CI, 1.15-82.35; P = .04), exposure to proton pump inhibitors in the past 3 months (OR, 1.82; 95% CI, 1.03-3.23; P = .04), and admission to an intensive care unit in the past 3 months (OR, 1.95; 95% CI, 1.0-3.83; P = .04).
The results suggest that diabetes and especially stroke may be important risk factors for CDI recurrence, and their presence should prompt physicians to alter patient care accordingly, according to Dr. Putrus.
He stressed the importance of antibiotic stewardship. “Once you find a certain bug or pathogen, try to deescalate the antibiotics as soon as you can. If a patient is diabetic, controlling their blood sugar may also help,” Dr. Putrus said.
Finally, physicians should consider whether proton pump inhibitors are really necessary. Some patients start on PPIs but remain on the drugs long after symptoms have abated. “A lot of patients just have some discomfort in their abdomen, and they never stop taking it. They keep refilling it. So that’s a problem,” said Dr. Putrus.
Dr. Putrus has declared no conflicts of interest.
AGA Resource
AGA offers information to educate your patients about C. difficile and fecal microbiota transplant. Learn more at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
LAS VEGAS – Diabetes and stroke are risk factors for recurrent Clostridium difficile infection (CDI), with stroke patients at about 10 times the risk of recurrence.
The underlying cause for the association is a mystery, but one-sided paralysis is one possibility. “A lot of stroke patients may be hemiplegic, and they may be bedridden, so that may be a risk factor by itself. It’s something that may need to be studied in the future,” Alan Putrus, MD, a gastroenterology fellow at St. John Providence Hospital, Detroit, said in an interview.
CDI recurrence rates range from 5% to 47%, depending on the institution. Although risk factors of initial CDI have been well defined, few studies have looked at risk factors associated with recurrence.
In order to get at the question, the researchers conducted a study of 108 initial CDIs and 113 recurrences at two urban and one suburban hospital. Patients who experienced recurrence were matched 1:1 to age- and gender-matched controls with no recurrent CDI.
CDI recurrence rates were 16.5% and 15.9% in the two urban hospitals, and 14.9% in the suburban hospital.
Logistic regression revealed risk factors associated with CDI recurrence, including diabetes (odds ratio, 1.91; 95% confidence interval, 1.05-3.47; P = .04), stroke (OR, 9.73; 95% CI, 1.15-82.35; P = .04), exposure to proton pump inhibitors in the past 3 months (OR, 1.82; 95% CI, 1.03-3.23; P = .04), and admission to an intensive care unit in the past 3 months (OR, 1.95; 95% CI, 1.0-3.83; P = .04).
The results suggest that diabetes and especially stroke may be important risk factors for CDI recurrence, and their presence should prompt physicians to alter patient care accordingly, according to Dr. Putrus.
He stressed the importance of antibiotic stewardship. “Once you find a certain bug or pathogen, try to deescalate the antibiotics as soon as you can. If a patient is diabetic, controlling their blood sugar may also help,” Dr. Putrus said.
Finally, physicians should consider whether proton pump inhibitors are really necessary. Some patients start on PPIs but remain on the drugs long after symptoms have abated. “A lot of patients just have some discomfort in their abdomen, and they never stop taking it. They keep refilling it. So that’s a problem,” said Dr. Putrus.
Dr. Putrus has declared no conflicts of interest.
AGA Resource
AGA offers information to educate your patients about C. difficile and fecal microbiota transplant. Learn more at http://www.gastro.org/patient-care/conditions-diseases/clostridium-difficile-infection.
AT ACG 2016
Key clinical point:
Major finding: Diabetes, stroke, and a history of PPI use were all associated with higher risks of recurrence.
Data source: Case-control, retrospective study.
Disclosures: Dr. Putrus has declared no conflicts of interest.
Ozanimod has lasting effect on ulcerative colitis
LAS VEGAS – Ozanimod, an oral agent that selectively modulates the sphingosine 1-phosphate (S1P) 1 and 5 receptor, has a lasting effect on symptoms of ulcerative colitis, according to results from an open-label extension study.
The study extends the phase II TOUCHSTONE trial, in which patients with ulcerative colitis showed significant clinical improvement out to 32 weeks. The current study showed those improvements lasting out to at least 1 year, with about 80% of patients staying on the drug at the end of the study.
With other drug regimens, “the loss rates are at least 50% of the patients, so this is a remarkable level of durability over time,” William Sandborn, MD, chief of gastroenterology at the University of California at San Diego, said at the annual meeting of the American College of Gastroenterology. “With biologics, if you follow patients out for a year or 2, you see a fair amount of loss of response and some of that probably has to do with the formation of antidrug antibodies and immunogenicity,” Dr. Sandborn added.

In the original TOUCHSTONE study, 197 patients were randomized to placebo, ozanimod 0.5 mg, or ozanimod 1.0 mg, and followed out to week 32. Twenty-one percent of those in the 1.0-mg group achieved clinical remission, compared with 26% in the 0.5-mg group and 6% of those receiving placebo. Clinical response rates were 51%, 35%, and 20%, respectively.
In the open-label study, patients from all arms who did not respond to treatment after the induction phase, or relapsed during the maintenance phase, or completed the maintenance phase (170 patients in total) entered the open-label study with a dose of 1.0 mg ozanimod. At the time of the cut-off, patients in the extension study had been taking ozanimod for at least 1 year.
At the start of the extension study, the partial Mayo Score (pMS) for patients on placebo, ozanimod 0.5 mg, and 1.0 mg were 4.6, 4.5, and 3.3, respectively. All groups showed improvement in pMS by week 44 (1.7, 1.7, and 1.9, respectively)
At week 44, 90.9% of patients had little or no active disease (physician global assessment 0 or 1), 98.4% had little or no blood in their stools, and 84.7% had no blood in their stools.
Adverse events with a frequency higher than 2% included ulcerative colitis flare (5.9%), anemia (3.5%), upper respiratory tract infection (4.1%), nasal pharyngitis (3.5%), back pain (2.9%), arthralgia (2.4%), and headache (2.4%). The researchers noted some transient elevation of alanine aminotransferase or aspartate aminotransferase, but these elevations were temporary and reversed during ongoing treatment; 2.4% of patients experienced ALT and AST levels higher than three times the upper limit of normal, and all were asymptomatic.
Serious adverse events that occurred in two or more patients included anemia (1.2%) and ulcerative colitis flare (2.4%).
“This is a promising oral product with a similar mechanism of action to other lymphocyte trafficking agents,” said Stephen Hanauer, MD, medical director of the digestive health center at the Northwestern University, Chicago, who attended the session.
Ozanimod and other lymphocyte trafficking agents may offer a slightly different profile than some of the other drug classes, such as the anti–tumor necrosis factor agents, according to Dr. Hanauer, because the agents don’t affect lymphocytes already in the tissues. On the other hand, once the drug has acted, its effect may linger. “The time to effect may be a little slower, but the long-term effect seems to be as good or better as other mechanisms of action.”
The drug’s real place could be in early disease, Dr. Hanauer said. “If this is truly an effective and safe agent, the real positioning should be earlier in the disease, before patients are exposed to steroids and other immune suppressants, or biologics that have an infection risk.”
Celgene funded the study. Dr. Sandborn has received funding from Receptos and Celgene and consulted for both companies. Dr. Hanauer has consulted with Receptos, Celgene, Pfizer, Jansen, and AbbVie.
AGA Resource
AGA offers an IBD Clinical Service Line that provides tools to help you become more efficient, understand quality standards, and improve the process of care for patients. Learn more at http://www.gastro.org/patient-care/conditions-diseases/ibd
LAS VEGAS – Ozanimod, an oral agent that selectively modulates the sphingosine 1-phosphate (S1P) 1 and 5 receptor, has a lasting effect on symptoms of ulcerative colitis, according to results from an open-label extension study.
The study extends the phase II TOUCHSTONE trial, in which patients with ulcerative colitis showed significant clinical improvement out to 32 weeks. The current study showed those improvements lasting out to at least 1 year, with about 80% of patients staying on the drug at the end of the study.
With other drug regimens, “the loss rates are at least 50% of the patients, so this is a remarkable level of durability over time,” William Sandborn, MD, chief of gastroenterology at the University of California at San Diego, said at the annual meeting of the American College of Gastroenterology. “With biologics, if you follow patients out for a year or 2, you see a fair amount of loss of response and some of that probably has to do with the formation of antidrug antibodies and immunogenicity,” Dr. Sandborn added.
In the original TOUCHSTONE study, 197 patients were randomized to placebo, ozanimod 0.5 mg, or ozanimod 1.0 mg, and followed out to week 32. Twenty-one percent of those in the 1.0-mg group achieved clinical remission, compared with 26% in the 0.5-mg group and 6% of those receiving placebo. Clinical response rates were 51%, 35%, and 20%, respectively.
In the open-label study, patients from all arms who did not respond to treatment after the induction phase, or relapsed during the maintenance phase, or completed the maintenance phase (170 patients in total) entered the open-label study with a dose of 1.0 mg ozanimod. At the time of the cut-off, patients in the extension study had been taking ozanimod for at least 1 year.
At the start of the extension study, the partial Mayo Score (pMS) for patients on placebo, ozanimod 0.5 mg, and 1.0 mg were 4.6, 4.5, and 3.3, respectively. All groups showed improvement in pMS by week 44 (1.7, 1.7, and 1.9, respectively)
At week 44, 90.9% of patients had little or no active disease (physician global assessment 0 or 1), 98.4% had little or no blood in their stools, and 84.7% had no blood in their stools.
Adverse events with a frequency higher than 2% included ulcerative colitis flare (5.9%), anemia (3.5%), upper respiratory tract infection (4.1%), nasal pharyngitis (3.5%), back pain (2.9%), arthralgia (2.4%), and headache (2.4%). The researchers noted some transient elevation of alanine aminotransferase or aspartate aminotransferase, but these elevations were temporary and reversed during ongoing treatment; 2.4% of patients experienced ALT and AST levels higher than three times the upper limit of normal, and all were asymptomatic.
Serious adverse events that occurred in two or more patients included anemia (1.2%) and ulcerative colitis flare (2.4%).
“This is a promising oral product with a similar mechanism of action to other lymphocyte trafficking agents,” said Stephen Hanauer, MD, medical director of the digestive health center at the Northwestern University, Chicago, who attended the session.
Ozanimod and other lymphocyte trafficking agents may offer a slightly different profile than some of the other drug classes, such as the anti–tumor necrosis factor agents, according to Dr. Hanauer, because the agents don’t affect lymphocytes already in the tissues. On the other hand, once the drug has acted, its effect may linger. “The time to effect may be a little slower, but the long-term effect seems to be as good or better as other mechanisms of action.”
The drug’s real place could be in early disease, Dr. Hanauer said. “If this is truly an effective and safe agent, the real positioning should be earlier in the disease, before patients are exposed to steroids and other immune suppressants, or biologics that have an infection risk.”
Celgene funded the study. Dr. Sandborn has received funding from Receptos and Celgene and consulted for both companies. Dr. Hanauer has consulted with Receptos, Celgene, Pfizer, Jansen, and AbbVie.
AGA Resource
AGA offers an IBD Clinical Service Line that provides tools to help you become more efficient, understand quality standards, and improve the process of care for patients. Learn more at http://www.gastro.org/patient-care/conditions-diseases/ibd
LAS VEGAS – Ozanimod, an oral agent that selectively modulates the sphingosine 1-phosphate (S1P) 1 and 5 receptor, has a lasting effect on symptoms of ulcerative colitis, according to results from an open-label extension study.
The study extends the phase II TOUCHSTONE trial, in which patients with ulcerative colitis showed significant clinical improvement out to 32 weeks. The current study showed those improvements lasting out to at least 1 year, with about 80% of patients staying on the drug at the end of the study.
With other drug regimens, “the loss rates are at least 50% of the patients, so this is a remarkable level of durability over time,” William Sandborn, MD, chief of gastroenterology at the University of California at San Diego, said at the annual meeting of the American College of Gastroenterology. “With biologics, if you follow patients out for a year or 2, you see a fair amount of loss of response and some of that probably has to do with the formation of antidrug antibodies and immunogenicity,” Dr. Sandborn added.
In the original TOUCHSTONE study, 197 patients were randomized to placebo, ozanimod 0.5 mg, or ozanimod 1.0 mg, and followed out to week 32. Twenty-one percent of those in the 1.0-mg group achieved clinical remission, compared with 26% in the 0.5-mg group and 6% of those receiving placebo. Clinical response rates were 51%, 35%, and 20%, respectively.
In the open-label study, patients from all arms who did not respond to treatment after the induction phase, or relapsed during the maintenance phase, or completed the maintenance phase (170 patients in total) entered the open-label study with a dose of 1.0 mg ozanimod. At the time of the cut-off, patients in the extension study had been taking ozanimod for at least 1 year.
At the start of the extension study, the partial Mayo Score (pMS) for patients on placebo, ozanimod 0.5 mg, and 1.0 mg were 4.6, 4.5, and 3.3, respectively. All groups showed improvement in pMS by week 44 (1.7, 1.7, and 1.9, respectively)
At week 44, 90.9% of patients had little or no active disease (physician global assessment 0 or 1), 98.4% had little or no blood in their stools, and 84.7% had no blood in their stools.
Adverse events with a frequency higher than 2% included ulcerative colitis flare (5.9%), anemia (3.5%), upper respiratory tract infection (4.1%), nasal pharyngitis (3.5%), back pain (2.9%), arthralgia (2.4%), and headache (2.4%). The researchers noted some transient elevation of alanine aminotransferase or aspartate aminotransferase, but these elevations were temporary and reversed during ongoing treatment; 2.4% of patients experienced ALT and AST levels higher than three times the upper limit of normal, and all were asymptomatic.
Serious adverse events that occurred in two or more patients included anemia (1.2%) and ulcerative colitis flare (2.4%).
“This is a promising oral product with a similar mechanism of action to other lymphocyte trafficking agents,” said Stephen Hanauer, MD, medical director of the digestive health center at the Northwestern University, Chicago, who attended the session.
Ozanimod and other lymphocyte trafficking agents may offer a slightly different profile than some of the other drug classes, such as the anti–tumor necrosis factor agents, according to Dr. Hanauer, because the agents don’t affect lymphocytes already in the tissues. On the other hand, once the drug has acted, its effect may linger. “The time to effect may be a little slower, but the long-term effect seems to be as good or better as other mechanisms of action.”
The drug’s real place could be in early disease, Dr. Hanauer said. “If this is truly an effective and safe agent, the real positioning should be earlier in the disease, before patients are exposed to steroids and other immune suppressants, or biologics that have an infection risk.”
Celgene funded the study. Dr. Sandborn has received funding from Receptos and Celgene and consulted for both companies. Dr. Hanauer has consulted with Receptos, Celgene, Pfizer, Jansen, and AbbVie.
AGA Resource
AGA offers an IBD Clinical Service Line that provides tools to help you become more efficient, understand quality standards, and improve the process of care for patients. Learn more at http://www.gastro.org/patient-care/conditions-diseases/ibd
AT ACG 2016
Key clinical point:
Major finding: Ozanimod maintains efficacy in ulcerative colitis out to 1 year, with 90% of patients having little or no evidence of active disease.
Data source: Open-label extension study following a phase II clinical trial.
Disclosures: Celgene funded the study. Dr. Sandborn has received funding from Receptos and Celgene and consulted for both companies. Dr. Hanauer has consulted with Receptos, Celgene, Pfizer, Jansen, and AbbVie.

ACR 2016 continues big buffet of basic and clinical science sessions
This year’s annual meeting of the American College of Rheumatology will feature cutting-edge research and results of studies that directly affect how attendees will manage patients once they are back in the clinical setting, according to both Richard Loeser, MD, program chair of the Annual Meeting Planning Committee (AMPC), and Gregory Gardner, MD, clinical subchair of the AMPC, who suggested special sessions of interest culled from the more than 450 sessions to be presented.
“It is an exciting time in rheumatology. Basic research is being translated into new therapies before our very eyes. Areas on the program this year that have translational potential include immunometabolism, blocking interleukin-1 (IL-1), T-cell receptor signaling, and meta-analysis of gene expression data. The meeting will also feature trials that refine and advance the management of rheumatologic diseases, including results on studies of new biologics,” Dr. Loeser said.
Hot sessions
Luke O’Neill, MD, will talk about immunometabolism Monday at 7:30 a.m. This session will explore a newly described connection between energy metabolism and the immune system and the link with inflammation.
Charles Dinarello, MD, will give the Philip Hensch Memorial Lecture Sunday at 8:30 a.m. on blocking IL-1 in inflammatory diseases. He will cover a host of diseases from gout to cancer, Dr. Loeser noted.
Another hot topic, T-cell receptor signaling in autoimmune diseases and the development of new therapies, will be discussed by Arthur Weiss, MD, Tuesday morning at 7:30 a.m.
Tuesday at 11:00 a.m., Peter Lipsky, MD, will tackle big data mining, presenting a meta-analysis of gene expression datasets to identify novel pathways and targets in systemic lupus erythematosus (SLE).
“SLE lags behind rheumatoid arthritis in therapeutic advances. A number of trials of biologics have failed in SLE, whereas they have been found effective in rheumatoid arthritis,” Dr. Loeser explained.
Clinical slant
Sunday’s Plenary session at 11:00 a.m. will feature several top-rated abstracts, among them results of a phase III study on tocilizumab in giant cell arteritis to be presented by John Stone, MD. “Tocilizumab is a major breakthrough as a steroid-sparing treatment for the most common form of vasculitis that affects older adults,” Dr. Loeser said.
At 2:30 p.m. on Sunday at The Great Debate, Paul Emery, MD, and Arthur Kavanaugh, MD, will tackle the very important clinical topic of “To Taper or Not to Taper? – Biologic DMARDs in Low Rheumatoid Arthritis Disease Activity.”
“People aren’t sure what to do. The fear with tapering is rebound, with the disease coming back even more forcefully. There is new evidence to suggest that tapering may be safe under certain circumstances. This session should inform attendees on how to make the decision to taper and on the best way to do it,” Dr. Loeser commented.
The Late-Breaking Abstract session on Tuesday at 4:30 p.m. will feature six clinical trials. Dr. Loeser singled out a study to be presented by Elaine Husni, MD, on “Vascular Safety of Celecoxib versus Ibuprofen or Naproxen” in more than 20,000 patients with osteoarthritis or rheumatoid arthritis.
“The fear is that COX-2 inhibitors have increased cardiovascular risk. The data from this study that will be presented at the meeting should answer the question of whether or not this is true in patients with arthritis,” Dr. Loeser explained.
Wednesday at 7:30 a.m. Candida Fratazzi, MD, will talk about “Emerging Biosimilars in Therapeutic Management,” a subject of great interest since they have the potential to be equally effective and less expensive than current biologics.
Two “bookends” of the meeting will frame the opening and closing. Sunday at 7:30 a.m., the “Year in Review” session will feature the best published studies on rheumatologic diseases from the past year, based on the judgment of two experts. Ingrid Lundberg, MD, will present the best clinical studies and Bruce Cronstein, MD, will present the best basic science studies. Wednesday at 7:30 a.m., John Cush, MD, and Dr. Kavanaugh will present the “Rheumatology Roundup” of the best abstracts and put them into context. “This session is usually quite entertaining,” Dr. Loeser said.

More sessions of clinical import
“In keeping with our meeting theme of fine-tuning our care of patients with rheumatic disease, I want to point out several sessions,” Dr. Gardner said.
Attendees interested in sessions on clinical applicability will have to choose between two different sessions Monday at 4:30 p.m.: one on dermatomyositis, a relatively rare but difficult-to-treat entity, and the other about treatment of the patient with rheumatoid arthritis when the patient is not well and suffering from comorbidities.
Monday at 8:30 a.m., an “Osteoporosis Update” will give listeners perspective on current and future therapies.
Sunday at 2:30 p.m., new guidelines for steroid-induced osteoporosis will be presented.
“Four or five sessions on the Tech Track will show rheumatologists how they can improve their practice by using technology,” Dr. Gardner said. “Several high-quality sessions are important to educators, including ‘Flipped Classroom, Technology, and Reflection’ [Monday at 12:30 p.m.] and ‘Year in Review’ [Sunday at 1:00 p.m.].”
Monday at 11:00 a.m., the Plenary session will feature Workforce Study results on how many rheumatologists will be needed in the year 2030, and in which geographic locations. This session will also include a discussion of the impact of part-time rheumatologists.
“Two sessions I am excited about are ‘Treat to Target in 2016,’ Tuesday at 4:30 p.m., and ‘Rheumatic Diseases in Native Americans,’ Sunday at 11:00 a.m.,” Dr. Gardner noted. “Concurrent abstract sessions throughout the meeting will feature discussions on new biologics, small molecules, and gene therapy.”
This year’s annual meeting of the American College of Rheumatology will feature cutting-edge research and results of studies that directly affect how attendees will manage patients once they are back in the clinical setting, according to both Richard Loeser, MD, program chair of the Annual Meeting Planning Committee (AMPC), and Gregory Gardner, MD, clinical subchair of the AMPC, who suggested special sessions of interest culled from the more than 450 sessions to be presented.
“It is an exciting time in rheumatology. Basic research is being translated into new therapies before our very eyes. Areas on the program this year that have translational potential include immunometabolism, blocking interleukin-1 (IL-1), T-cell receptor signaling, and meta-analysis of gene expression data. The meeting will also feature trials that refine and advance the management of rheumatologic diseases, including results on studies of new biologics,” Dr. Loeser said.
Hot sessions
Luke O’Neill, MD, will talk about immunometabolism Monday at 7:30 a.m. This session will explore a newly described connection between energy metabolism and the immune system and the link with inflammation.
Charles Dinarello, MD, will give the Philip Hensch Memorial Lecture Sunday at 8:30 a.m. on blocking IL-1 in inflammatory diseases. He will cover a host of diseases from gout to cancer, Dr. Loeser noted.
Another hot topic, T-cell receptor signaling in autoimmune diseases and the development of new therapies, will be discussed by Arthur Weiss, MD, Tuesday morning at 7:30 a.m.
Tuesday at 11:00 a.m., Peter Lipsky, MD, will tackle big data mining, presenting a meta-analysis of gene expression datasets to identify novel pathways and targets in systemic lupus erythematosus (SLE).
“SLE lags behind rheumatoid arthritis in therapeutic advances. A number of trials of biologics have failed in SLE, whereas they have been found effective in rheumatoid arthritis,” Dr. Loeser explained.
Clinical slant
Sunday’s Plenary session at 11:00 a.m. will feature several top-rated abstracts, among them results of a phase III study on tocilizumab in giant cell arteritis to be presented by John Stone, MD. “Tocilizumab is a major breakthrough as a steroid-sparing treatment for the most common form of vasculitis that affects older adults,” Dr. Loeser said.
At 2:30 p.m. on Sunday at The Great Debate, Paul Emery, MD, and Arthur Kavanaugh, MD, will tackle the very important clinical topic of “To Taper or Not to Taper? – Biologic DMARDs in Low Rheumatoid Arthritis Disease Activity.”
“People aren’t sure what to do. The fear with tapering is rebound, with the disease coming back even more forcefully. There is new evidence to suggest that tapering may be safe under certain circumstances. This session should inform attendees on how to make the decision to taper and on the best way to do it,” Dr. Loeser commented.
The Late-Breaking Abstract session on Tuesday at 4:30 p.m. will feature six clinical trials. Dr. Loeser singled out a study to be presented by Elaine Husni, MD, on “Vascular Safety of Celecoxib versus Ibuprofen or Naproxen” in more than 20,000 patients with osteoarthritis or rheumatoid arthritis.
“The fear is that COX-2 inhibitors have increased cardiovascular risk. The data from this study that will be presented at the meeting should answer the question of whether or not this is true in patients with arthritis,” Dr. Loeser explained.
Wednesday at 7:30 a.m. Candida Fratazzi, MD, will talk about “Emerging Biosimilars in Therapeutic Management,” a subject of great interest since they have the potential to be equally effective and less expensive than current biologics.
Two “bookends” of the meeting will frame the opening and closing. Sunday at 7:30 a.m., the “Year in Review” session will feature the best published studies on rheumatologic diseases from the past year, based on the judgment of two experts. Ingrid Lundberg, MD, will present the best clinical studies and Bruce Cronstein, MD, will present the best basic science studies. Wednesday at 7:30 a.m., John Cush, MD, and Dr. Kavanaugh will present the “Rheumatology Roundup” of the best abstracts and put them into context. “This session is usually quite entertaining,” Dr. Loeser said.
More sessions of clinical import
“In keeping with our meeting theme of fine-tuning our care of patients with rheumatic disease, I want to point out several sessions,” Dr. Gardner said.
Attendees interested in sessions on clinical applicability will have to choose between two different sessions Monday at 4:30 p.m.: one on dermatomyositis, a relatively rare but difficult-to-treat entity, and the other about treatment of the patient with rheumatoid arthritis when the patient is not well and suffering from comorbidities.
Monday at 8:30 a.m., an “Osteoporosis Update” will give listeners perspective on current and future therapies.
Sunday at 2:30 p.m., new guidelines for steroid-induced osteoporosis will be presented.
“Four or five sessions on the Tech Track will show rheumatologists how they can improve their practice by using technology,” Dr. Gardner said. “Several high-quality sessions are important to educators, including ‘Flipped Classroom, Technology, and Reflection’ [Monday at 12:30 p.m.] and ‘Year in Review’ [Sunday at 1:00 p.m.].”
Monday at 11:00 a.m., the Plenary session will feature Workforce Study results on how many rheumatologists will be needed in the year 2030, and in which geographic locations. This session will also include a discussion of the impact of part-time rheumatologists.
“Two sessions I am excited about are ‘Treat to Target in 2016,’ Tuesday at 4:30 p.m., and ‘Rheumatic Diseases in Native Americans,’ Sunday at 11:00 a.m.,” Dr. Gardner noted. “Concurrent abstract sessions throughout the meeting will feature discussions on new biologics, small molecules, and gene therapy.”
This year’s annual meeting of the American College of Rheumatology will feature cutting-edge research and results of studies that directly affect how attendees will manage patients once they are back in the clinical setting, according to both Richard Loeser, MD, program chair of the Annual Meeting Planning Committee (AMPC), and Gregory Gardner, MD, clinical subchair of the AMPC, who suggested special sessions of interest culled from the more than 450 sessions to be presented.
“It is an exciting time in rheumatology. Basic research is being translated into new therapies before our very eyes. Areas on the program this year that have translational potential include immunometabolism, blocking interleukin-1 (IL-1), T-cell receptor signaling, and meta-analysis of gene expression data. The meeting will also feature trials that refine and advance the management of rheumatologic diseases, including results on studies of new biologics,” Dr. Loeser said.
Hot sessions
Luke O’Neill, MD, will talk about immunometabolism Monday at 7:30 a.m. This session will explore a newly described connection between energy metabolism and the immune system and the link with inflammation.
Charles Dinarello, MD, will give the Philip Hensch Memorial Lecture Sunday at 8:30 a.m. on blocking IL-1 in inflammatory diseases. He will cover a host of diseases from gout to cancer, Dr. Loeser noted.
Another hot topic, T-cell receptor signaling in autoimmune diseases and the development of new therapies, will be discussed by Arthur Weiss, MD, Tuesday morning at 7:30 a.m.
Tuesday at 11:00 a.m., Peter Lipsky, MD, will tackle big data mining, presenting a meta-analysis of gene expression datasets to identify novel pathways and targets in systemic lupus erythematosus (SLE).
“SLE lags behind rheumatoid arthritis in therapeutic advances. A number of trials of biologics have failed in SLE, whereas they have been found effective in rheumatoid arthritis,” Dr. Loeser explained.
Clinical slant
Sunday’s Plenary session at 11:00 a.m. will feature several top-rated abstracts, among them results of a phase III study on tocilizumab in giant cell arteritis to be presented by John Stone, MD. “Tocilizumab is a major breakthrough as a steroid-sparing treatment for the most common form of vasculitis that affects older adults,” Dr. Loeser said.
At 2:30 p.m. on Sunday at The Great Debate, Paul Emery, MD, and Arthur Kavanaugh, MD, will tackle the very important clinical topic of “To Taper or Not to Taper? – Biologic DMARDs in Low Rheumatoid Arthritis Disease Activity.”
“People aren’t sure what to do. The fear with tapering is rebound, with the disease coming back even more forcefully. There is new evidence to suggest that tapering may be safe under certain circumstances. This session should inform attendees on how to make the decision to taper and on the best way to do it,” Dr. Loeser commented.
The Late-Breaking Abstract session on Tuesday at 4:30 p.m. will feature six clinical trials. Dr. Loeser singled out a study to be presented by Elaine Husni, MD, on “Vascular Safety of Celecoxib versus Ibuprofen or Naproxen” in more than 20,000 patients with osteoarthritis or rheumatoid arthritis.
“The fear is that COX-2 inhibitors have increased cardiovascular risk. The data from this study that will be presented at the meeting should answer the question of whether or not this is true in patients with arthritis,” Dr. Loeser explained.
Wednesday at 7:30 a.m. Candida Fratazzi, MD, will talk about “Emerging Biosimilars in Therapeutic Management,” a subject of great interest since they have the potential to be equally effective and less expensive than current biologics.
Two “bookends” of the meeting will frame the opening and closing. Sunday at 7:30 a.m., the “Year in Review” session will feature the best published studies on rheumatologic diseases from the past year, based on the judgment of two experts. Ingrid Lundberg, MD, will present the best clinical studies and Bruce Cronstein, MD, will present the best basic science studies. Wednesday at 7:30 a.m., John Cush, MD, and Dr. Kavanaugh will present the “Rheumatology Roundup” of the best abstracts and put them into context. “This session is usually quite entertaining,” Dr. Loeser said.
More sessions of clinical import
“In keeping with our meeting theme of fine-tuning our care of patients with rheumatic disease, I want to point out several sessions,” Dr. Gardner said.
Attendees interested in sessions on clinical applicability will have to choose between two different sessions Monday at 4:30 p.m.: one on dermatomyositis, a relatively rare but difficult-to-treat entity, and the other about treatment of the patient with rheumatoid arthritis when the patient is not well and suffering from comorbidities.
Monday at 8:30 a.m., an “Osteoporosis Update” will give listeners perspective on current and future therapies.
Sunday at 2:30 p.m., new guidelines for steroid-induced osteoporosis will be presented.
“Four or five sessions on the Tech Track will show rheumatologists how they can improve their practice by using technology,” Dr. Gardner said. “Several high-quality sessions are important to educators, including ‘Flipped Classroom, Technology, and Reflection’ [Monday at 12:30 p.m.] and ‘Year in Review’ [Sunday at 1:00 p.m.].”
Monday at 11:00 a.m., the Plenary session will feature Workforce Study results on how many rheumatologists will be needed in the year 2030, and in which geographic locations. This session will also include a discussion of the impact of part-time rheumatologists.
“Two sessions I am excited about are ‘Treat to Target in 2016,’ Tuesday at 4:30 p.m., and ‘Rheumatic Diseases in Native Americans,’ Sunday at 11:00 a.m.,” Dr. Gardner noted. “Concurrent abstract sessions throughout the meeting will feature discussions on new biologics, small molecules, and gene therapy.”
FROM THE ACR ANNUAL MEETING
Study finds no increase in microcephaly with Tdap vaccine in pregnancy
The combined tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is not associated with an increased risk of microcephaly and other structural birth defects when administered during pregnancy, according to findings from a large, retrospective cohort study.
The U.S. Advisory Committee on Immunization Practices currently recommends administration of the Tdap vaccine between 27 and 36 weeks’ gestation in every pregnancy. However, the overlap of the start of Brazil’s maternal Tdap immunization in November 2014 with the substantial increase in microcephaly cases in 2015 prompted concerns of an association between the vaccine and structural birth defects.
They found that Tdap immunization was not significantly associated with an increased risk for microcephaly during any week of pregnancy (adjusted prevalence ratio, 0.86; 95% CI, 0.60-1.24). They also saw no increased risk of microcephaly when vaccinations occurred before 14 weeks’ gestation (adjusted prevalence ratio, 0.96; 95% CI, 0.36-2.58), or when vaccinations were administered between 27 weeks’ and 36 weeks’ gestation (adjusted prevalence ratio, 1.01; 95% CI, 0.63-1.61). The findings were similar for other structural defects, including congenital heart defects, spina bifida, encephalocele, and anophthalmia (JAMA. 2016;316[17]:1823-5).
“These results expand upon what is known about maternal Tdap vaccination safety to include information about structural birth defects and microcephaly in offspring,” the investigators wrote. “The findings support recommendations for routine Tdap administration during pregnancy.”
However, they noted that the study findings may have been limited by incomplete data on women’s immunization status, birth defects, and defects that may have resulted in pregnancy loss or elective termination.
The study was funded by the Centers for Disease Control and Prevention. The investigators reported having no relevant financial disclosures.
The combined tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is not associated with an increased risk of microcephaly and other structural birth defects when administered during pregnancy, according to findings from a large, retrospective cohort study.
The U.S. Advisory Committee on Immunization Practices currently recommends administration of the Tdap vaccine between 27 and 36 weeks’ gestation in every pregnancy. However, the overlap of the start of Brazil’s maternal Tdap immunization in November 2014 with the substantial increase in microcephaly cases in 2015 prompted concerns of an association between the vaccine and structural birth defects.
They found that Tdap immunization was not significantly associated with an increased risk for microcephaly during any week of pregnancy (adjusted prevalence ratio, 0.86; 95% CI, 0.60-1.24). They also saw no increased risk of microcephaly when vaccinations occurred before 14 weeks’ gestation (adjusted prevalence ratio, 0.96; 95% CI, 0.36-2.58), or when vaccinations were administered between 27 weeks’ and 36 weeks’ gestation (adjusted prevalence ratio, 1.01; 95% CI, 0.63-1.61). The findings were similar for other structural defects, including congenital heart defects, spina bifida, encephalocele, and anophthalmia (JAMA. 2016;316[17]:1823-5).
“These results expand upon what is known about maternal Tdap vaccination safety to include information about structural birth defects and microcephaly in offspring,” the investigators wrote. “The findings support recommendations for routine Tdap administration during pregnancy.”
However, they noted that the study findings may have been limited by incomplete data on women’s immunization status, birth defects, and defects that may have resulted in pregnancy loss or elective termination.
The study was funded by the Centers for Disease Control and Prevention. The investigators reported having no relevant financial disclosures.
The combined tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is not associated with an increased risk of microcephaly and other structural birth defects when administered during pregnancy, according to findings from a large, retrospective cohort study.
The U.S. Advisory Committee on Immunization Practices currently recommends administration of the Tdap vaccine between 27 and 36 weeks’ gestation in every pregnancy. However, the overlap of the start of Brazil’s maternal Tdap immunization in November 2014 with the substantial increase in microcephaly cases in 2015 prompted concerns of an association between the vaccine and structural birth defects.
They found that Tdap immunization was not significantly associated with an increased risk for microcephaly during any week of pregnancy (adjusted prevalence ratio, 0.86; 95% CI, 0.60-1.24). They also saw no increased risk of microcephaly when vaccinations occurred before 14 weeks’ gestation (adjusted prevalence ratio, 0.96; 95% CI, 0.36-2.58), or when vaccinations were administered between 27 weeks’ and 36 weeks’ gestation (adjusted prevalence ratio, 1.01; 95% CI, 0.63-1.61). The findings were similar for other structural defects, including congenital heart defects, spina bifida, encephalocele, and anophthalmia (JAMA. 2016;316[17]:1823-5).
“These results expand upon what is known about maternal Tdap vaccination safety to include information about structural birth defects and microcephaly in offspring,” the investigators wrote. “The findings support recommendations for routine Tdap administration during pregnancy.”
However, they noted that the study findings may have been limited by incomplete data on women’s immunization status, birth defects, and defects that may have resulted in pregnancy loss or elective termination.
The study was funded by the Centers for Disease Control and Prevention. The investigators reported having no relevant financial disclosures.
FROM JAMA
Key clinical point:
Major finding: Tdap immunization was not significantly associated with an increased risk for microcephaly during any week of pregnancy (adjusted prevalence ratio, 0.86; 95% CI, 0.60-1.24).
Data source: A retrospective cohort study in 41,654 singleton infants born to women who received Tdap during pregnancy and a control group of 282,809 babies born to unvaccinated women.
Disclosures: The study was funded by the Centers for Disease Control and Prevention. The investigators reported having no relevant financial disclosures.
Large increase seen in number of Zika-infected pregnancies
The 288 new cases of pregnant women in the United States with laboratory evidence of Zika infection reported for the week ending Oct. 27, 2016, represent the largest weekly increase so far this year, according to new data from the Centers for Disease Control and Prevention.
The 52 new cases in the 50 states and the District of Columbia and the 236 cases in the U.S. territories bring the totals for the year to 1,005 and 2,263, respectively, and to 3,268 for the United States as a whole, the CDC reported.
The week ending Oct. 27 also brought reports of two more infants born with Zika-related birth defects in the 50 states/D.C., but there were no reports of Zika-related pregnancy losses. So far in 2016, there have been 25 liveborn infants with Zika-related birth defects and five pregnancy losses in the states.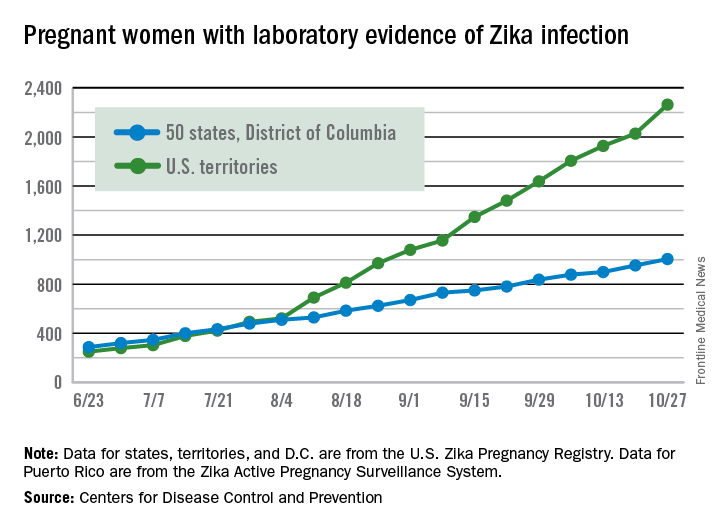
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
The 288 new cases of pregnant women in the United States with laboratory evidence of Zika infection reported for the week ending Oct. 27, 2016, represent the largest weekly increase so far this year, according to new data from the Centers for Disease Control and Prevention.
The 52 new cases in the 50 states and the District of Columbia and the 236 cases in the U.S. territories bring the totals for the year to 1,005 and 2,263, respectively, and to 3,268 for the United States as a whole, the CDC reported.
The week ending Oct. 27 also brought reports of two more infants born with Zika-related birth defects in the 50 states/D.C., but there were no reports of Zika-related pregnancy losses. So far in 2016, there have been 25 liveborn infants with Zika-related birth defects and five pregnancy losses in the states.
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
The 288 new cases of pregnant women in the United States with laboratory evidence of Zika infection reported for the week ending Oct. 27, 2016, represent the largest weekly increase so far this year, according to new data from the Centers for Disease Control and Prevention.
The 52 new cases in the 50 states and the District of Columbia and the 236 cases in the U.S. territories bring the totals for the year to 1,005 and 2,263, respectively, and to 3,268 for the United States as a whole, the CDC reported.
The week ending Oct. 27 also brought reports of two more infants born with Zika-related birth defects in the 50 states/D.C., but there were no reports of Zika-related pregnancy losses. So far in 2016, there have been 25 liveborn infants with Zika-related birth defects and five pregnancy losses in the states.
The CDC is no longer reporting adverse pregnancy outcomes for the territories because Puerto Rico is not using the same “inclusion criteria to monitor brain abnormalities and other adverse pregnancy outcomes.” As of Sept. 29 – the date of the last territorial report – there had been one liveborn infant and one pregnancy loss related to Zika.
Zika-related birth defects reported by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
The pregnancy-related figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.