User login
HM16 AUDIO: Alyssa Stephany, MD, Talks about the HM16 RIV Scientific Abstract Competition
Alyssa Stephany, MD, then assistant professor at Duke and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, talks about the evolution in training stemming from her experience in the HM16 RIV competition. This year, she oversaw a study for which resident
Jennifer Ladd, MD, won an award for pediatric clinical vignette.
Alyssa Stephany, MD, then assistant professor at Duke and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, talks about the evolution in training stemming from her experience in the HM16 RIV competition. This year, she oversaw a study for which resident
Jennifer Ladd, MD, won an award for pediatric clinical vignette.
Alyssa Stephany, MD, then assistant professor at Duke and now section chief of pediatric hospital medicine at Children’s Hospital of Wisconsin, talks about the evolution in training stemming from her experience in the HM16 RIV competition. This year, she oversaw a study for which resident
Jennifer Ladd, MD, won an award for pediatric clinical vignette.
HM16 AUDIO: Vineet Chopra, MD, MSc, Chats up His Research on Costs and Complications with PICC Line Usage
RIV winner Vineet Chopra, MD, MSc, assistant professor at the University of Michigan in Ann Arbor, talks about his research on the costs and complications associated with PICC line use.
RIV winner Vineet Chopra, MD, MSc, assistant professor at the University of Michigan in Ann Arbor, talks about his research on the costs and complications associated with PICC line use.
RIV winner Vineet Chopra, MD, MSc, assistant professor at the University of Michigan in Ann Arbor, talks about his research on the costs and complications associated with PICC line use.
HM16 AUDIO: Jordan Romano Discusses Getting Published, Hospitalist Burnout
Jordan Romano, DO, a hospitalist at Massachusetts General Hospital, talks about lessons gleaned at HM16 on the importance of taking small steps toward your goals of getting published and how burnout can be relative.
Jordan Romano, DO, a hospitalist at Massachusetts General Hospital, talks about lessons gleaned at HM16 on the importance of taking small steps toward your goals of getting published and how burnout can be relative.
Jordan Romano, DO, a hospitalist at Massachusetts General Hospital, talks about lessons gleaned at HM16 on the importance of taking small steps toward your goals of getting published and how burnout can be relative.
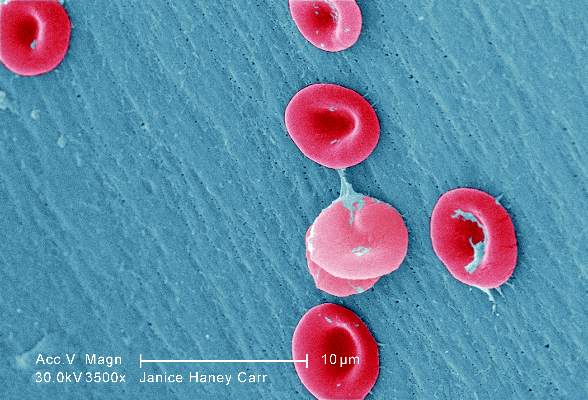
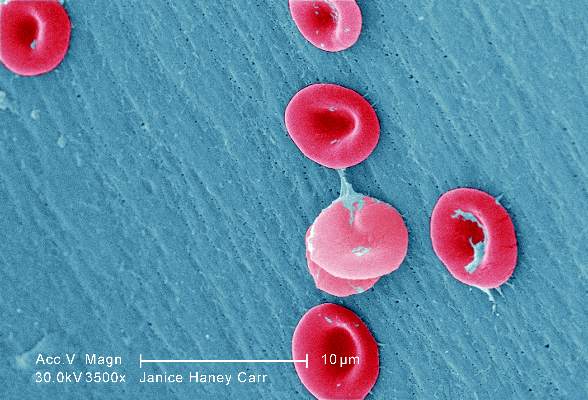
Sickle cell anemia: Stroke screening still underused
Children and adolescents with sickle cell anemia still are not being screened for stroke risk using transcranial Doppler, despite clinical guidelines that strongly recommend annual screening and despite these patients’ frequent health care encounters, according to a report published online April 11 in JAMA Pediatrics.
Approximately 10% of children and adolescents with sickle cell anemia experience stroke before the age of 20 years, unless those at high risk are identified and treated preemptively with blood transfusions, which reduces stroke risk by 92%. The National Heart, Lung, and Blood Institute clinical practice guideline on treating sickle cell disease calls for patients aged 2-16 years to undergo transcranial Doppler every year to detect any elevated velocity of cerebral blood flow, which indicates high stroke risk, said Sarah L. Reeves, Ph.D., of the Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor, and her associates.
To assess screening rates, the investigators performed a retrospective cross-sectional analysis of administrative claims data for 4,775 affected children and adolescents treated during a 5-year period in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas. This yielded 10,787 person-years of data.
Overall, screening rates increased somewhat across all six states during the study period – from 22% to 44% – but “even the highest rates we report are suboptimal,” Dr. Reeves and her associates noted (JAMA Ped. 2016 Apr 11. doi: 10.1001/jamapediatrics.2015.4859).
This is especially true given that the average patient had 20.0 disease-related outpatient visits, 2.1 disease-related hospitalizations, 3.7 emergency department visits, and 1 well-child visit each year – numerous missed opportunities when they could have been referred for screening.
One way to improve screening rates would be to integrate transcranial Doppler exams into comprehensive sickle-cell healthcare, rather than requiring separate scheduled appointments at imaging facilities, they added.
This study was funded by the Agency for Healthcare Research and Quality and the Centers for Medicare & Medicaid Services. Dr. Reeves and her associates reported having no relevant financial disclosures.
Children and adolescents with sickle cell anemia still are not being screened for stroke risk using transcranial Doppler, despite clinical guidelines that strongly recommend annual screening and despite these patients’ frequent health care encounters, according to a report published online April 11 in JAMA Pediatrics.
Approximately 10% of children and adolescents with sickle cell anemia experience stroke before the age of 20 years, unless those at high risk are identified and treated preemptively with blood transfusions, which reduces stroke risk by 92%. The National Heart, Lung, and Blood Institute clinical practice guideline on treating sickle cell disease calls for patients aged 2-16 years to undergo transcranial Doppler every year to detect any elevated velocity of cerebral blood flow, which indicates high stroke risk, said Sarah L. Reeves, Ph.D., of the Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor, and her associates.
To assess screening rates, the investigators performed a retrospective cross-sectional analysis of administrative claims data for 4,775 affected children and adolescents treated during a 5-year period in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas. This yielded 10,787 person-years of data.
Overall, screening rates increased somewhat across all six states during the study period – from 22% to 44% – but “even the highest rates we report are suboptimal,” Dr. Reeves and her associates noted (JAMA Ped. 2016 Apr 11. doi: 10.1001/jamapediatrics.2015.4859).
This is especially true given that the average patient had 20.0 disease-related outpatient visits, 2.1 disease-related hospitalizations, 3.7 emergency department visits, and 1 well-child visit each year – numerous missed opportunities when they could have been referred for screening.
One way to improve screening rates would be to integrate transcranial Doppler exams into comprehensive sickle-cell healthcare, rather than requiring separate scheduled appointments at imaging facilities, they added.
This study was funded by the Agency for Healthcare Research and Quality and the Centers for Medicare & Medicaid Services. Dr. Reeves and her associates reported having no relevant financial disclosures.
Children and adolescents with sickle cell anemia still are not being screened for stroke risk using transcranial Doppler, despite clinical guidelines that strongly recommend annual screening and despite these patients’ frequent health care encounters, according to a report published online April 11 in JAMA Pediatrics.
Approximately 10% of children and adolescents with sickle cell anemia experience stroke before the age of 20 years, unless those at high risk are identified and treated preemptively with blood transfusions, which reduces stroke risk by 92%. The National Heart, Lung, and Blood Institute clinical practice guideline on treating sickle cell disease calls for patients aged 2-16 years to undergo transcranial Doppler every year to detect any elevated velocity of cerebral blood flow, which indicates high stroke risk, said Sarah L. Reeves, Ph.D., of the Child Health Evaluation and Research Unit, University of Michigan, Ann Arbor, and her associates.
To assess screening rates, the investigators performed a retrospective cross-sectional analysis of administrative claims data for 4,775 affected children and adolescents treated during a 5-year period in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas. This yielded 10,787 person-years of data.
Overall, screening rates increased somewhat across all six states during the study period – from 22% to 44% – but “even the highest rates we report are suboptimal,” Dr. Reeves and her associates noted (JAMA Ped. 2016 Apr 11. doi: 10.1001/jamapediatrics.2015.4859).
This is especially true given that the average patient had 20.0 disease-related outpatient visits, 2.1 disease-related hospitalizations, 3.7 emergency department visits, and 1 well-child visit each year – numerous missed opportunities when they could have been referred for screening.
One way to improve screening rates would be to integrate transcranial Doppler exams into comprehensive sickle-cell healthcare, rather than requiring separate scheduled appointments at imaging facilities, they added.
This study was funded by the Agency for Healthcare Research and Quality and the Centers for Medicare & Medicaid Services. Dr. Reeves and her associates reported having no relevant financial disclosures.
FROM JAMA PEDIATRICS
Key clinical point: Transcranial Doppler screening for stroke risk is still underused among children and adolescents with sickle cell anemia, despite clinical guidelines that strongly recommend annual screening.
Major finding: Screening rates increased somewhat across all six states studied, from 22% to 44%, but even the highest rates were suboptimal.
Data source: A retrospective cross-sectional analysis of administrative claims data for 4,775 pediatric patients treated in a 5-year period.
Disclosures: This study was funded by the Agency for Healthcare Research and Quality and the Centers for Medicare & Medicaid Services. Dr. Reeves and her associates reported having no relevant financial disclosures.
In myelodysplastic syndrome, improved tool for predicting death after HCT
A new risk-stratification tool goes one better than the standard tools used to predict survival in those undergoing allogeneic hematopoietic cell transplantation (allo HCT) for myelodysplastic syndrome, based on a study published online April 4 in the Journal of Clinical Oncology.
The concordance index for the new risk-stratification tool was modestly better at 0.575, compared with 0.538 for the standard International Prognostic Scoring System (IPSS) and 0.554 for the revised IPSS (IPSS-R), according to Dr. Brian C. Shaffer of Memorial Sloan Kettering Cancer Center, New York, and his colleagues who participate in the Center for International Blood and Marrow Transplant Research (CIBMTR) network.

“The proposed system generally agrees with the IPSS-R in the very high–risk subcategory; however, a significant portion of patients in high- and very high–risk IPSS-R groups were represented in the low- and intermediate-risk proposed scoring subcategories. The 3-year survival in patients classified as high risk with the IPSS-R was 75%; it was 57% in those classified as low or intermediate risk with the proposed system,” the researchers wrote.
Further, the “scoring system uses readily available clinical data and can be calculated quickly, facilitating patient consultation with respect to allo HCT, and may also be used to identify high-risk populations where interventions such as post–allo HCT maintenance therapies may be of benefit,” they wrote (J Clin Oncol. 2016 April 4. doi: 10.1200/JCO.2015.65.0515).
The data were obtained from the CIBMTR, a combined research program of the Medical College of Wisconsin and the National Marrow Donor Program. The CIBMTR comprises a voluntary network of more than 450 transplantation centers worldwide that contribute data on consecutive allo and autologous HCTs to a centralized statistical center.
The researchers applied the prognostic tool to 2,133 patients with MDS undergoing HLA-matched (n = 1,728) or -mismatched (n = 405) allo HCT. Factors prognostic of mortality were identified in a training subset (n = 1,151) of the HLA-matched cohort. A weighted score using these factors was then assigned to the validation cohort of 577 remaining patients undergoing HLA-matched allo HCT as well as to patients undergoing HLA-mismatched allo HCT. The training data set was used to develop a prognostic scoring system, and the validation data set was used to assess the prognostic ability of the scoring system, the researchers noted.
In the scoring system, 1 point was assigned for the following factors: Blood blasts greater than 3%, platelet levels of 50 × 109/L or less at transplantation, Karnofsky performance status less than 90%, comprehensive cytogenetic risk score of poor or very poor, and age 30-49 years. Two points were assigned for monosomal karyotype and age 50 years or older.
Based on the scoring system, 3-year overall survival after transplantation was 71% in patients with scores of 1 point, 49% with scores of 2-3, 41% with scores of 4-5, and 25% with scores of 6 or more. Increasing score was predictive of increased relapse and treatment-related mortality in the HLA-matched set and of relapse in the HLA-mismatched cohort.
To develop the scoring system, the researchers used a model that weighed patient age; sex; and Karnofsky performance status; disease stage at transplantation; comprehensive cytogenetic risk status; bone marrow and peripheral blood blast percentages; hemoglobin, neutrophil, and platelet counts at diagnosis and pretransplantation; lactate dehydrogenase at transplantation; pretransplantation therapy (hypomethylating agents, chemotherapy, neither, or both); time from diagnosis to transplantation; year of transplantation; conditioning regimen and regimen intensity (myeloablative v reduced intensity); donor–recipient sex match or mismatch; graft-versus-host disease prophylaxis; graft type (bone marrow vs. peripheral blood); presence of secondary myelodysplastic syndrome; and unrelated donor vs. related donor.
There were no significant differences in overall survival at 1, 3, and 5 years or in the 3-year incidences of relapse and treatment-related mortality in the training subset and the validation cohort.
Data on somatic mutations have become relevant in myelodysplastic syndrome prognostication and were missing from this analysis, the researchers wrote. “The next generation of prognostic tools will need to account for this information.”
Dr. Shaffer had no relevant financial disclosures.
On Twitter @maryjodales
A new risk-stratification tool goes one better than the standard tools used to predict survival in those undergoing allogeneic hematopoietic cell transplantation (allo HCT) for myelodysplastic syndrome, based on a study published online April 4 in the Journal of Clinical Oncology.
The concordance index for the new risk-stratification tool was modestly better at 0.575, compared with 0.538 for the standard International Prognostic Scoring System (IPSS) and 0.554 for the revised IPSS (IPSS-R), according to Dr. Brian C. Shaffer of Memorial Sloan Kettering Cancer Center, New York, and his colleagues who participate in the Center for International Blood and Marrow Transplant Research (CIBMTR) network.
“The proposed system generally agrees with the IPSS-R in the very high–risk subcategory; however, a significant portion of patients in high- and very high–risk IPSS-R groups were represented in the low- and intermediate-risk proposed scoring subcategories. The 3-year survival in patients classified as high risk with the IPSS-R was 75%; it was 57% in those classified as low or intermediate risk with the proposed system,” the researchers wrote.
Further, the “scoring system uses readily available clinical data and can be calculated quickly, facilitating patient consultation with respect to allo HCT, and may also be used to identify high-risk populations where interventions such as post–allo HCT maintenance therapies may be of benefit,” they wrote (J Clin Oncol. 2016 April 4. doi: 10.1200/JCO.2015.65.0515).
The data were obtained from the CIBMTR, a combined research program of the Medical College of Wisconsin and the National Marrow Donor Program. The CIBMTR comprises a voluntary network of more than 450 transplantation centers worldwide that contribute data on consecutive allo and autologous HCTs to a centralized statistical center.
The researchers applied the prognostic tool to 2,133 patients with MDS undergoing HLA-matched (n = 1,728) or -mismatched (n = 405) allo HCT. Factors prognostic of mortality were identified in a training subset (n = 1,151) of the HLA-matched cohort. A weighted score using these factors was then assigned to the validation cohort of 577 remaining patients undergoing HLA-matched allo HCT as well as to patients undergoing HLA-mismatched allo HCT. The training data set was used to develop a prognostic scoring system, and the validation data set was used to assess the prognostic ability of the scoring system, the researchers noted.
In the scoring system, 1 point was assigned for the following factors: Blood blasts greater than 3%, platelet levels of 50 × 109/L or less at transplantation, Karnofsky performance status less than 90%, comprehensive cytogenetic risk score of poor or very poor, and age 30-49 years. Two points were assigned for monosomal karyotype and age 50 years or older.
Based on the scoring system, 3-year overall survival after transplantation was 71% in patients with scores of 1 point, 49% with scores of 2-3, 41% with scores of 4-5, and 25% with scores of 6 or more. Increasing score was predictive of increased relapse and treatment-related mortality in the HLA-matched set and of relapse in the HLA-mismatched cohort.
To develop the scoring system, the researchers used a model that weighed patient age; sex; and Karnofsky performance status; disease stage at transplantation; comprehensive cytogenetic risk status; bone marrow and peripheral blood blast percentages; hemoglobin, neutrophil, and platelet counts at diagnosis and pretransplantation; lactate dehydrogenase at transplantation; pretransplantation therapy (hypomethylating agents, chemotherapy, neither, or both); time from diagnosis to transplantation; year of transplantation; conditioning regimen and regimen intensity (myeloablative v reduced intensity); donor–recipient sex match or mismatch; graft-versus-host disease prophylaxis; graft type (bone marrow vs. peripheral blood); presence of secondary myelodysplastic syndrome; and unrelated donor vs. related donor.
There were no significant differences in overall survival at 1, 3, and 5 years or in the 3-year incidences of relapse and treatment-related mortality in the training subset and the validation cohort.
Data on somatic mutations have become relevant in myelodysplastic syndrome prognostication and were missing from this analysis, the researchers wrote. “The next generation of prognostic tools will need to account for this information.”
Dr. Shaffer had no relevant financial disclosures.
On Twitter @maryjodales
A new risk-stratification tool goes one better than the standard tools used to predict survival in those undergoing allogeneic hematopoietic cell transplantation (allo HCT) for myelodysplastic syndrome, based on a study published online April 4 in the Journal of Clinical Oncology.
The concordance index for the new risk-stratification tool was modestly better at 0.575, compared with 0.538 for the standard International Prognostic Scoring System (IPSS) and 0.554 for the revised IPSS (IPSS-R), according to Dr. Brian C. Shaffer of Memorial Sloan Kettering Cancer Center, New York, and his colleagues who participate in the Center for International Blood and Marrow Transplant Research (CIBMTR) network.
“The proposed system generally agrees with the IPSS-R in the very high–risk subcategory; however, a significant portion of patients in high- and very high–risk IPSS-R groups were represented in the low- and intermediate-risk proposed scoring subcategories. The 3-year survival in patients classified as high risk with the IPSS-R was 75%; it was 57% in those classified as low or intermediate risk with the proposed system,” the researchers wrote.
Further, the “scoring system uses readily available clinical data and can be calculated quickly, facilitating patient consultation with respect to allo HCT, and may also be used to identify high-risk populations where interventions such as post–allo HCT maintenance therapies may be of benefit,” they wrote (J Clin Oncol. 2016 April 4. doi: 10.1200/JCO.2015.65.0515).
The data were obtained from the CIBMTR, a combined research program of the Medical College of Wisconsin and the National Marrow Donor Program. The CIBMTR comprises a voluntary network of more than 450 transplantation centers worldwide that contribute data on consecutive allo and autologous HCTs to a centralized statistical center.
The researchers applied the prognostic tool to 2,133 patients with MDS undergoing HLA-matched (n = 1,728) or -mismatched (n = 405) allo HCT. Factors prognostic of mortality were identified in a training subset (n = 1,151) of the HLA-matched cohort. A weighted score using these factors was then assigned to the validation cohort of 577 remaining patients undergoing HLA-matched allo HCT as well as to patients undergoing HLA-mismatched allo HCT. The training data set was used to develop a prognostic scoring system, and the validation data set was used to assess the prognostic ability of the scoring system, the researchers noted.
In the scoring system, 1 point was assigned for the following factors: Blood blasts greater than 3%, platelet levels of 50 × 109/L or less at transplantation, Karnofsky performance status less than 90%, comprehensive cytogenetic risk score of poor or very poor, and age 30-49 years. Two points were assigned for monosomal karyotype and age 50 years or older.
Based on the scoring system, 3-year overall survival after transplantation was 71% in patients with scores of 1 point, 49% with scores of 2-3, 41% with scores of 4-5, and 25% with scores of 6 or more. Increasing score was predictive of increased relapse and treatment-related mortality in the HLA-matched set and of relapse in the HLA-mismatched cohort.
To develop the scoring system, the researchers used a model that weighed patient age; sex; and Karnofsky performance status; disease stage at transplantation; comprehensive cytogenetic risk status; bone marrow and peripheral blood blast percentages; hemoglobin, neutrophil, and platelet counts at diagnosis and pretransplantation; lactate dehydrogenase at transplantation; pretransplantation therapy (hypomethylating agents, chemotherapy, neither, or both); time from diagnosis to transplantation; year of transplantation; conditioning regimen and regimen intensity (myeloablative v reduced intensity); donor–recipient sex match or mismatch; graft-versus-host disease prophylaxis; graft type (bone marrow vs. peripheral blood); presence of secondary myelodysplastic syndrome; and unrelated donor vs. related donor.
There were no significant differences in overall survival at 1, 3, and 5 years or in the 3-year incidences of relapse and treatment-related mortality in the training subset and the validation cohort.
Data on somatic mutations have become relevant in myelodysplastic syndrome prognostication and were missing from this analysis, the researchers wrote. “The next generation of prognostic tools will need to account for this information.”
Dr. Shaffer had no relevant financial disclosures.
On Twitter @maryjodales
FROM JCO
Key clinical point: A portion of patients with myelodysplastic syndrome in high- and very high–risk groups of the revised International Prognostic Scoring System (IPSS-R) were represented in the low- and intermediate-risk groups of the proposed scoring subcategories.
Major finding: The 3-year survival in patients classified as high risk with the IPSS-R was 75%; it was 57% in those classified as low or intermediate risk with the proposed system.
Data source: The Center for International Blood and Marrow Transplant Research (CIBMTR), a combined research program of the Medical College of Wisconsin and the National Marrow Donor Program. The CIBMTR comprises a voluntary network of more than 450 transplantation centers worldwide that contribute data on consecutive allo and autologous HCTs to a centralized statistical center.
Disclosures: Dr. Shaffer had no relevant financial disclosures.
Proactive endocrine screening urged for pediatric brain tumor survivors
BOSTON – More than a third of 419 children treated for brain tumors at Cincinnati Children’s Hospital Medical Center later developed endocrine problems, according to a review presented at the Endocrine Society annual meeting.
Over 60% of the 96 suprasellar tumor patients developed endocrine dysfunction, which isn’t surprising considering the location of the tumor, but wide-ranging endocrine problems were also common in the 145 posterior fossa, 158 supratentorial, and 20 spinal cord cases, ranging from 14% in the spinal cord group to 42% in the posterior fossa group, after some combination of radiation, chemotherapy, and surgery based on tumor location and other factors.

“Even with tumors that aren’t supposed to be high risk, there was a high risk of endocrinopathies. We need yearly screening of these patients” for about 6 years, after which symptom-based screening may be sufficient. The clock should be restarted if there’s a recurrence. “Not everyone does this” at Cincinnati Children’s and probably most other institutions, said investigator and endocrinology fellow Dr. Vincent Horne.
The findings are “changing how our oncology department is thinking about [screening]; there’s a concentrated effort to increase proactive screening and follow these patients long term,” he said.
“Even within our specialized, multidisciplinary center,” endocrinopathy screening referrals were low, about 61% overall and only 80% in the suprasellar group. “Patients at highest risk” – those with craniopharyngioma – “are being seen early by us,” but others aren’t being referred. It’s possible that the extent of endocrine problems after pediatric brain tumor treatment is simply unrecognized, he said.
Endocrine abnormalities were found in 114 (45%) of the 254 patients evaluated, which translated to problems in more than a third of all patients.
More than half of the children had more than one problem, and most of the issues occurred within 6 years of treatment. Central hypothyroidism was found in 53% of the children, probably because Cincinnati Children’s already has thyroid screening in place.
About 40% were growth hormone deficient, and almost a third had precocious puberty. About 30% were gonadotropin-releasing hormone deficient, over 20% had primary hypothyroidism, and about the same had diabetes insipidus. Just over 6% were hyperprolactinemic.
Of the 151 patients who completed adrenocorticotropic hormone (ACTH) testing, 14.6% were deficient. ACTH deficient children were about evenly split between the suprasellar and supratentorial groups, with the remaining in the posterior fossa cohort.
“We are probably not thinking about” the risk of radiation “to locations like the posterior fossa. That group actually had the highest risk of primary hypothyroidism [20%] because of the spinal radiation. The supratentorial group is also receiving radiation; even though we think we are missing the hypothalamus, obviously that’s not necessarily the case,” Dr. Horne said.
His team looked into endocrine screening because previous studies “were limited and done years ago.” People are living longer now after treatment, “so we need to think about how to screen for endocrine disease. This is an attempt to clarify how we should do it,” he said.
Children were a median of 8 years old at diagnosis, and the median radiation dose was 54 Gy.
There was no industry funding for the work, and the investigators had no disclosures.
BOSTON – More than a third of 419 children treated for brain tumors at Cincinnati Children’s Hospital Medical Center later developed endocrine problems, according to a review presented at the Endocrine Society annual meeting.
Over 60% of the 96 suprasellar tumor patients developed endocrine dysfunction, which isn’t surprising considering the location of the tumor, but wide-ranging endocrine problems were also common in the 145 posterior fossa, 158 supratentorial, and 20 spinal cord cases, ranging from 14% in the spinal cord group to 42% in the posterior fossa group, after some combination of radiation, chemotherapy, and surgery based on tumor location and other factors.
“Even with tumors that aren’t supposed to be high risk, there was a high risk of endocrinopathies. We need yearly screening of these patients” for about 6 years, after which symptom-based screening may be sufficient. The clock should be restarted if there’s a recurrence. “Not everyone does this” at Cincinnati Children’s and probably most other institutions, said investigator and endocrinology fellow Dr. Vincent Horne.
The findings are “changing how our oncology department is thinking about [screening]; there’s a concentrated effort to increase proactive screening and follow these patients long term,” he said.
“Even within our specialized, multidisciplinary center,” endocrinopathy screening referrals were low, about 61% overall and only 80% in the suprasellar group. “Patients at highest risk” – those with craniopharyngioma – “are being seen early by us,” but others aren’t being referred. It’s possible that the extent of endocrine problems after pediatric brain tumor treatment is simply unrecognized, he said.
Endocrine abnormalities were found in 114 (45%) of the 254 patients evaluated, which translated to problems in more than a third of all patients.
More than half of the children had more than one problem, and most of the issues occurred within 6 years of treatment. Central hypothyroidism was found in 53% of the children, probably because Cincinnati Children’s already has thyroid screening in place.
About 40% were growth hormone deficient, and almost a third had precocious puberty. About 30% were gonadotropin-releasing hormone deficient, over 20% had primary hypothyroidism, and about the same had diabetes insipidus. Just over 6% were hyperprolactinemic.
Of the 151 patients who completed adrenocorticotropic hormone (ACTH) testing, 14.6% were deficient. ACTH deficient children were about evenly split between the suprasellar and supratentorial groups, with the remaining in the posterior fossa cohort.
“We are probably not thinking about” the risk of radiation “to locations like the posterior fossa. That group actually had the highest risk of primary hypothyroidism [20%] because of the spinal radiation. The supratentorial group is also receiving radiation; even though we think we are missing the hypothalamus, obviously that’s not necessarily the case,” Dr. Horne said.
His team looked into endocrine screening because previous studies “were limited and done years ago.” People are living longer now after treatment, “so we need to think about how to screen for endocrine disease. This is an attempt to clarify how we should do it,” he said.
Children were a median of 8 years old at diagnosis, and the median radiation dose was 54 Gy.
There was no industry funding for the work, and the investigators had no disclosures.
BOSTON – More than a third of 419 children treated for brain tumors at Cincinnati Children’s Hospital Medical Center later developed endocrine problems, according to a review presented at the Endocrine Society annual meeting.
Over 60% of the 96 suprasellar tumor patients developed endocrine dysfunction, which isn’t surprising considering the location of the tumor, but wide-ranging endocrine problems were also common in the 145 posterior fossa, 158 supratentorial, and 20 spinal cord cases, ranging from 14% in the spinal cord group to 42% in the posterior fossa group, after some combination of radiation, chemotherapy, and surgery based on tumor location and other factors.
“Even with tumors that aren’t supposed to be high risk, there was a high risk of endocrinopathies. We need yearly screening of these patients” for about 6 years, after which symptom-based screening may be sufficient. The clock should be restarted if there’s a recurrence. “Not everyone does this” at Cincinnati Children’s and probably most other institutions, said investigator and endocrinology fellow Dr. Vincent Horne.
The findings are “changing how our oncology department is thinking about [screening]; there’s a concentrated effort to increase proactive screening and follow these patients long term,” he said.
“Even within our specialized, multidisciplinary center,” endocrinopathy screening referrals were low, about 61% overall and only 80% in the suprasellar group. “Patients at highest risk” – those with craniopharyngioma – “are being seen early by us,” but others aren’t being referred. It’s possible that the extent of endocrine problems after pediatric brain tumor treatment is simply unrecognized, he said.
Endocrine abnormalities were found in 114 (45%) of the 254 patients evaluated, which translated to problems in more than a third of all patients.
More than half of the children had more than one problem, and most of the issues occurred within 6 years of treatment. Central hypothyroidism was found in 53% of the children, probably because Cincinnati Children’s already has thyroid screening in place.
About 40% were growth hormone deficient, and almost a third had precocious puberty. About 30% were gonadotropin-releasing hormone deficient, over 20% had primary hypothyroidism, and about the same had diabetes insipidus. Just over 6% were hyperprolactinemic.
Of the 151 patients who completed adrenocorticotropic hormone (ACTH) testing, 14.6% were deficient. ACTH deficient children were about evenly split between the suprasellar and supratentorial groups, with the remaining in the posterior fossa cohort.
“We are probably not thinking about” the risk of radiation “to locations like the posterior fossa. That group actually had the highest risk of primary hypothyroidism [20%] because of the spinal radiation. The supratentorial group is also receiving radiation; even though we think we are missing the hypothalamus, obviously that’s not necessarily the case,” Dr. Horne said.
His team looked into endocrine screening because previous studies “were limited and done years ago.” People are living longer now after treatment, “so we need to think about how to screen for endocrine disease. This is an attempt to clarify how we should do it,” he said.
Children were a median of 8 years old at diagnosis, and the median radiation dose was 54 Gy.
There was no industry funding for the work, and the investigators had no disclosures.
AT ENDO 2016
Key clinical point: Screen for endocrine dysfunction for 6 years after pediatric brain tumor treatment.
Major finding: Endocrine abnormalities were found in 114 of 254 patients (45%) evaluated, which translated to problems in more than a third of all patients.
Data source: Single-center review of 419 pediatric brain tumor cases.
Disclosures: There was no industry funding for the work, and the investigators had no disclosures.

Surgeons commonly off the mark in estimating blood loss
MONTREAL – Surgeons, nurses, and anesthesia providers were all pretty bad at estimating surgical blood loss in a small study. And more experience doesn’t improve accuracy, though experienced providers were more confident in their estimates.
These were the findings from a study that simulated operating room scenarios and asked providers to estimate blood loss. “Estimation of blood loss is inaccurate and unreliable,” Dr. Luke Rothermel said at the Central Surgical Association’s annual meeting.
Dr. Rothermel, a resident at Case Western Reserve University, Cleveland, noted that although the Joint Commission requires operative notes to contain estimated blood loss, “no study in the United States has compared the characteristics of operating room personnel or conditions associated with improved accuracy or reliability of blood loss estimation.”

Beyond the required reporting, estimating blood loss (EBL) also provides important guidance in perioperative care. Still, said Dr. Rothermel, previous studies have shown that EBL is typically inaccurate.
To assess providers’ ability to be accurate and reliable in estimating blood loss, Dr. Rothermel and his collaborator, Dr. Jeremy Lipman, assistant residency director at MetroHealth, Cleveland, designed a study to simulate three different operating room scenarios, involving high, medium, and low blood loss volumes. The materials used, such as blood-soaked sponges and suction canisters, were identical to what’s actually used in the operating room (porcine blood was used in the simulations).
Before the study, Dr. Rothermel said that he and Dr. Lipman hypothesized that those providers who had more experience and those who were working at the operating field would be more accurate in estimating blood loss. They also hypothesized that estimations in procedures with lower volumes of blood loss would be more accurate.
The study recruited providers from the surgery, anesthesia, and nursing services at an urban level 1 trauma center. Each scenario included a written description of the procedure performed and the course of surgery, and participants could handle study materials for each scenario under the supervision of study staff.
A total of 60 participants (22 from surgery, 17 from anesthesia, and 21 from nursing) participated; they had an average of 12.8 years of experience. The surgical participants included surgical scrub techs, trainees, and attending physicians. Anesthesia participants included anesthesia assistants, CRNAs, trainees, and attending physicians. Nursing participants were all RNs.
The findings? All over the board: “There was no association between specialty, years of experience, or confidence in ability with the consistency or accuracy of estimated blood loss,” said Dr. Rothermel.
Most participants were far shy of the mark, with just 5% of study participants overall able to come within 25% accuracy in judging EBL in all scenarios. Just over a quarter were consistent in over- or underestimating blood loss.
These findings held true across scenarios, across disciplines, and regardless of the number of years of experience. “Increased years of experience trended toward increased error,” said Dr. Rothermel, though the difference was not statistically significant. However, those with more years of experience tended to be more confident of their judgments.
Dr. Rothermel noted the small study size and single institution studied as limitations. Also, “this model was not a high fidelity representation of the OR experience, “ he said, explaining that during surgery, caregivers continually assess intraoperative blood loss and may form an estimate in a different – and potentially more accurate – manner than occurs when presented with the contrived presentation of a scenario.
The study calls into question the validity of using EBL as a quality indicator in assessing physician performance and patient outcomes, said Dr. Rothermel, who had no financial disclosures.
On Twitter @karioakes
MONTREAL – Surgeons, nurses, and anesthesia providers were all pretty bad at estimating surgical blood loss in a small study. And more experience doesn’t improve accuracy, though experienced providers were more confident in their estimates.
These were the findings from a study that simulated operating room scenarios and asked providers to estimate blood loss. “Estimation of blood loss is inaccurate and unreliable,” Dr. Luke Rothermel said at the Central Surgical Association’s annual meeting.
Dr. Rothermel, a resident at Case Western Reserve University, Cleveland, noted that although the Joint Commission requires operative notes to contain estimated blood loss, “no study in the United States has compared the characteristics of operating room personnel or conditions associated with improved accuracy or reliability of blood loss estimation.”
Beyond the required reporting, estimating blood loss (EBL) also provides important guidance in perioperative care. Still, said Dr. Rothermel, previous studies have shown that EBL is typically inaccurate.
To assess providers’ ability to be accurate and reliable in estimating blood loss, Dr. Rothermel and his collaborator, Dr. Jeremy Lipman, assistant residency director at MetroHealth, Cleveland, designed a study to simulate three different operating room scenarios, involving high, medium, and low blood loss volumes. The materials used, such as blood-soaked sponges and suction canisters, were identical to what’s actually used in the operating room (porcine blood was used in the simulations).
Before the study, Dr. Rothermel said that he and Dr. Lipman hypothesized that those providers who had more experience and those who were working at the operating field would be more accurate in estimating blood loss. They also hypothesized that estimations in procedures with lower volumes of blood loss would be more accurate.
The study recruited providers from the surgery, anesthesia, and nursing services at an urban level 1 trauma center. Each scenario included a written description of the procedure performed and the course of surgery, and participants could handle study materials for each scenario under the supervision of study staff.
A total of 60 participants (22 from surgery, 17 from anesthesia, and 21 from nursing) participated; they had an average of 12.8 years of experience. The surgical participants included surgical scrub techs, trainees, and attending physicians. Anesthesia participants included anesthesia assistants, CRNAs, trainees, and attending physicians. Nursing participants were all RNs.
The findings? All over the board: “There was no association between specialty, years of experience, or confidence in ability with the consistency or accuracy of estimated blood loss,” said Dr. Rothermel.
Most participants were far shy of the mark, with just 5% of study participants overall able to come within 25% accuracy in judging EBL in all scenarios. Just over a quarter were consistent in over- or underestimating blood loss.
These findings held true across scenarios, across disciplines, and regardless of the number of years of experience. “Increased years of experience trended toward increased error,” said Dr. Rothermel, though the difference was not statistically significant. However, those with more years of experience tended to be more confident of their judgments.
Dr. Rothermel noted the small study size and single institution studied as limitations. Also, “this model was not a high fidelity representation of the OR experience, “ he said, explaining that during surgery, caregivers continually assess intraoperative blood loss and may form an estimate in a different – and potentially more accurate – manner than occurs when presented with the contrived presentation of a scenario.
The study calls into question the validity of using EBL as a quality indicator in assessing physician performance and patient outcomes, said Dr. Rothermel, who had no financial disclosures.
On Twitter @karioakes
MONTREAL – Surgeons, nurses, and anesthesia providers were all pretty bad at estimating surgical blood loss in a small study. And more experience doesn’t improve accuracy, though experienced providers were more confident in their estimates.
These were the findings from a study that simulated operating room scenarios and asked providers to estimate blood loss. “Estimation of blood loss is inaccurate and unreliable,” Dr. Luke Rothermel said at the Central Surgical Association’s annual meeting.
Dr. Rothermel, a resident at Case Western Reserve University, Cleveland, noted that although the Joint Commission requires operative notes to contain estimated blood loss, “no study in the United States has compared the characteristics of operating room personnel or conditions associated with improved accuracy or reliability of blood loss estimation.”
Beyond the required reporting, estimating blood loss (EBL) also provides important guidance in perioperative care. Still, said Dr. Rothermel, previous studies have shown that EBL is typically inaccurate.
To assess providers’ ability to be accurate and reliable in estimating blood loss, Dr. Rothermel and his collaborator, Dr. Jeremy Lipman, assistant residency director at MetroHealth, Cleveland, designed a study to simulate three different operating room scenarios, involving high, medium, and low blood loss volumes. The materials used, such as blood-soaked sponges and suction canisters, were identical to what’s actually used in the operating room (porcine blood was used in the simulations).
Before the study, Dr. Rothermel said that he and Dr. Lipman hypothesized that those providers who had more experience and those who were working at the operating field would be more accurate in estimating blood loss. They also hypothesized that estimations in procedures with lower volumes of blood loss would be more accurate.
The study recruited providers from the surgery, anesthesia, and nursing services at an urban level 1 trauma center. Each scenario included a written description of the procedure performed and the course of surgery, and participants could handle study materials for each scenario under the supervision of study staff.
A total of 60 participants (22 from surgery, 17 from anesthesia, and 21 from nursing) participated; they had an average of 12.8 years of experience. The surgical participants included surgical scrub techs, trainees, and attending physicians. Anesthesia participants included anesthesia assistants, CRNAs, trainees, and attending physicians. Nursing participants were all RNs.
The findings? All over the board: “There was no association between specialty, years of experience, or confidence in ability with the consistency or accuracy of estimated blood loss,” said Dr. Rothermel.
Most participants were far shy of the mark, with just 5% of study participants overall able to come within 25% accuracy in judging EBL in all scenarios. Just over a quarter were consistent in over- or underestimating blood loss.
These findings held true across scenarios, across disciplines, and regardless of the number of years of experience. “Increased years of experience trended toward increased error,” said Dr. Rothermel, though the difference was not statistically significant. However, those with more years of experience tended to be more confident of their judgments.
Dr. Rothermel noted the small study size and single institution studied as limitations. Also, “this model was not a high fidelity representation of the OR experience, “ he said, explaining that during surgery, caregivers continually assess intraoperative blood loss and may form an estimate in a different – and potentially more accurate – manner than occurs when presented with the contrived presentation of a scenario.
The study calls into question the validity of using EBL as a quality indicator in assessing physician performance and patient outcomes, said Dr. Rothermel, who had no financial disclosures.
On Twitter @karioakes
AT THE ANNUAL MEETING OF THE CENTRAL SURGICAL ASSOCIATION
Key clinical point: Surgery, anesthesia, and nursing providers were inaccurate and unreliable in estimating surgical blood loss.
Major finding: Only 5% of providers could come within 25% accuracy of simulated surgical blood loss.
Data source: Simulations of surgical scenarios depicting varying amounts of blood loss using porcine blood, presented to 60 providers.
Disclosures: The study authors reported no relevant disclosures.

Patient-controlled epidural analgesia similar to intravenous
Patient-controlled epidural analgesia achieves pain control similar to that of patient-controlled intravenous analgesia after spinal fusion surgery, but is associated with a higher incidence of pruritus and paresthesia, a meta-analysis published in BMC Musculoskeletal Disorders has found.
The analysis of eight randomized controlled trials involving 482 patients found that patient-controlled epidural analgesia was associated with significantly better analgesic effects on day 1 and 2 after surgery (mean difference in visual analog scale scores of −0.47 and −0.66, respectively), but this difference was no longer statistically significant on day 3.

The study, conducted by Dr. Peng Tian of Tianjin (China) Hospital and colleagues showed that patient-controlled epidural analgesia was associated with a significant 53% higher incidence of pruritus and a threefold increase in paresthesia, compared with patient-controlled intravenous analgesia, although there were no significant differences in the rates of nausea or vomiting (BMC Musculoskeletal Disorders 2015 Dec 15. doi: 10.1186/s12891-015-0849-y).
Researchers noted that patient-controlled epidural analgesia achieves a faster analgesic effect than does patient-controlled intravenous analgesia because it acts directly on the near-operative region, but the analgesic effect of the intravenous administration lasts longer.
“The most important findings of the present meta-analysis are that the application of PCEA [patient-controlled epidural analgesia] does not more effectively relieve” pain in 3 postoperative days compared with patient-controlled intravenous analgesia, “meanwhile increasing the incidence of some complications such as pruritus and paresthesia,” wrote the investigators.
The National Natural Science Foundation of China supported the study. No conflicts of interest were declared.
Patient-controlled epidural analgesia achieves pain control similar to that of patient-controlled intravenous analgesia after spinal fusion surgery, but is associated with a higher incidence of pruritus and paresthesia, a meta-analysis published in BMC Musculoskeletal Disorders has found.
The analysis of eight randomized controlled trials involving 482 patients found that patient-controlled epidural analgesia was associated with significantly better analgesic effects on day 1 and 2 after surgery (mean difference in visual analog scale scores of −0.47 and −0.66, respectively), but this difference was no longer statistically significant on day 3.
The study, conducted by Dr. Peng Tian of Tianjin (China) Hospital and colleagues showed that patient-controlled epidural analgesia was associated with a significant 53% higher incidence of pruritus and a threefold increase in paresthesia, compared with patient-controlled intravenous analgesia, although there were no significant differences in the rates of nausea or vomiting (BMC Musculoskeletal Disorders 2015 Dec 15. doi: 10.1186/s12891-015-0849-y).
Researchers noted that patient-controlled epidural analgesia achieves a faster analgesic effect than does patient-controlled intravenous analgesia because it acts directly on the near-operative region, but the analgesic effect of the intravenous administration lasts longer.
“The most important findings of the present meta-analysis are that the application of PCEA [patient-controlled epidural analgesia] does not more effectively relieve” pain in 3 postoperative days compared with patient-controlled intravenous analgesia, “meanwhile increasing the incidence of some complications such as pruritus and paresthesia,” wrote the investigators.
The National Natural Science Foundation of China supported the study. No conflicts of interest were declared.
Patient-controlled epidural analgesia achieves pain control similar to that of patient-controlled intravenous analgesia after spinal fusion surgery, but is associated with a higher incidence of pruritus and paresthesia, a meta-analysis published in BMC Musculoskeletal Disorders has found.
The analysis of eight randomized controlled trials involving 482 patients found that patient-controlled epidural analgesia was associated with significantly better analgesic effects on day 1 and 2 after surgery (mean difference in visual analog scale scores of −0.47 and −0.66, respectively), but this difference was no longer statistically significant on day 3.
The study, conducted by Dr. Peng Tian of Tianjin (China) Hospital and colleagues showed that patient-controlled epidural analgesia was associated with a significant 53% higher incidence of pruritus and a threefold increase in paresthesia, compared with patient-controlled intravenous analgesia, although there were no significant differences in the rates of nausea or vomiting (BMC Musculoskeletal Disorders 2015 Dec 15. doi: 10.1186/s12891-015-0849-y).
Researchers noted that patient-controlled epidural analgesia achieves a faster analgesic effect than does patient-controlled intravenous analgesia because it acts directly on the near-operative region, but the analgesic effect of the intravenous administration lasts longer.
“The most important findings of the present meta-analysis are that the application of PCEA [patient-controlled epidural analgesia] does not more effectively relieve” pain in 3 postoperative days compared with patient-controlled intravenous analgesia, “meanwhile increasing the incidence of some complications such as pruritus and paresthesia,” wrote the investigators.
The National Natural Science Foundation of China supported the study. No conflicts of interest were declared.
FROM BMC MUSCULOSKELETAL DISORDERS
Key clinical point: Patient-controlled epidural analgesia achieves pain control similar to that of patient-controlled intravenous analgesia after spinal fusion surgery, but with more pruritus and paresthesia.
Major finding: Patient-controlled epidural analgesia achieved greater analgesic effects on day 1 and 2 after surgery but these differences were no longer significant by day 3.
Data source: A meta-analysis of eight randomized controlled trials in 482 patients undergoing spinal fusion surgery.
Disclosures: The National Natural Science Foundation of China supported the study. No conflicts of interest were declared.

Annual Meeting Highlights Latest Research, Project Completion
One of the things that Jennifer Feighner, MD, cheerfully came away with at HM16 was how to better complete a task that is distinctly uncheerful but also important to any high-performing hospital: how to collect the data of the dead.
The quality improvement session “Reducing Inpatient Mortality: A Standardized Approach to Identify Preventable Deaths” demonstrated still evolving but, so far, well-performing projects that have been rolled out at Brigham and Women’s Hospital and the Duke University Health System.
“I was struck by the methodology for getting input from multiple providers and the nursing staff,” said Dr. Feighner, director of hospital medicine at Marcus Daly Memorial Hospital in Hamilton, Mont.
As the role of the hospitalist as agent of change and improvement continues to grow, the topic of quality improvement (QI) maintained a high profile at the annual meeting, with talks on the latest literature, sustaining motivation to complete projects, and dealing with issues such as handoffs and frequent fliers.
In the mortality review session, presenters set out to give details that could be a model to be used elsewhere. At Brigham and Women’s, all of the frontline clinicians are asked by email to fill out a report when a death occurs in any case with which they’ve been involved, with the Web-based reports to be completed within 48 to 72 hours of the death.
The number of deaths, the report completion rate, death “preventability,” and issues that arose for the patient during hospitalization are some of the data that are tracked. So far, the system has identified such themes as “alarm fatigue,” high oxygen requirements on non-intensive-care floors, handoffs, and transfers from other hospitals, said Kiran Gupta, MD, MPH, who completed her residency at Brigham and is now assistant professor of clinical medicine at the University of California San Francisco.
At Duke, where the mortality review system improvements have been led by Jonathan Bae, MD, assistant professor of medicine, self-nicknamed “Dr. Death,” inpatient deaths undergo a similarly comprehensive review, with an enhanced end-of-life section to cover issues particular to those cases and flags for cases that need independent review.
Dr. Gupta and Dr. Bae emphasized the confidentiality of the reviews and that they are non-discoverable in the event of litigation, which they hope give clinicians the freedom to fully report their observations.
Dr. Feighner said that her 23-bed hospital is far smaller than either Brigham or Duke, of course, but that the overall ideas can translate.
“I am the medical director of our hospitalist program, and our chief of staff and I’ve created a peer-review medical staff quality improvement committee,” she said. “So this obviously has a lot of interest to me.”
With only 4.2 full-time equivalents (FTEs) in her department, she said changes would be even easier to put into place.
“I think that will be really helpful for our peer-review committee and our quality and safety committee. I could see how we could take this and kind of revise it a little bit,” she said. “When you’re in charge of that few people, it’s easy to get processes implemented. We are more limited in monetary resources, but we make up for that in manpower-to-problem ratio, I guess.”
In another session, Jordan Messler, MD, SFHM, a hospitalist and former medical director of the hospitalist group at Morton Plant Hospital in Clearwater, Fla., confronted the startling statistic that 80% of initiatives in hospitals never meet their objectives. Hurdles such as burnout and disengagement, he said, often stand in the way of successful QI projects.
He emphasized the importance of intrinsic motivation (a sense of ownership and passion for the work) over extrinsic motivation (a fear of reprisal if something isn’t done). A step as simple as assigning a title (e.g., “head of readmissions”) can be a motivator, he said. But he also emphasized that project ideas need to be timed correctly and the ideas should ideally come from the physicians leading them.
Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, said he was struck by the lessons gleaned in a workshop on the I-PASS system of handoffs—a standardized system with a handoff sheet, studied prospectively, in which medical errors decreased by 23% and preventable adverse events fell by 30%.1 The system was created in pediatric departments but was deliberately made to be translatable to other settings.
“Instead of focusing on the outcome of the quality of the handoff, they focus on the quality of the feedback sessions,” Clothier said. “So it’s not the person giving the handoff or receiving the handoff that actually assesses it. It’s just the person who’s sitting there watching.”
He said the workshop underscored the importance of standardization, a concept with which he was familiar but which now seemed particularly vital.
“If you do the process and everybody does it the same, then it’s not only the person that’s giving the information who can do it in a very standardized way but the person who’s listening already knows what they’re going to be listening for so they hear it more clearly because they don’t have to discern what’s coming next,” Clothier said. “They already know what’s coming next.” TH
Reference
1. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371:1803-1812.
One of the things that Jennifer Feighner, MD, cheerfully came away with at HM16 was how to better complete a task that is distinctly uncheerful but also important to any high-performing hospital: how to collect the data of the dead.
The quality improvement session “Reducing Inpatient Mortality: A Standardized Approach to Identify Preventable Deaths” demonstrated still evolving but, so far, well-performing projects that have been rolled out at Brigham and Women’s Hospital and the Duke University Health System.
“I was struck by the methodology for getting input from multiple providers and the nursing staff,” said Dr. Feighner, director of hospital medicine at Marcus Daly Memorial Hospital in Hamilton, Mont.
As the role of the hospitalist as agent of change and improvement continues to grow, the topic of quality improvement (QI) maintained a high profile at the annual meeting, with talks on the latest literature, sustaining motivation to complete projects, and dealing with issues such as handoffs and frequent fliers.
In the mortality review session, presenters set out to give details that could be a model to be used elsewhere. At Brigham and Women’s, all of the frontline clinicians are asked by email to fill out a report when a death occurs in any case with which they’ve been involved, with the Web-based reports to be completed within 48 to 72 hours of the death.
The number of deaths, the report completion rate, death “preventability,” and issues that arose for the patient during hospitalization are some of the data that are tracked. So far, the system has identified such themes as “alarm fatigue,” high oxygen requirements on non-intensive-care floors, handoffs, and transfers from other hospitals, said Kiran Gupta, MD, MPH, who completed her residency at Brigham and is now assistant professor of clinical medicine at the University of California San Francisco.
At Duke, where the mortality review system improvements have been led by Jonathan Bae, MD, assistant professor of medicine, self-nicknamed “Dr. Death,” inpatient deaths undergo a similarly comprehensive review, with an enhanced end-of-life section to cover issues particular to those cases and flags for cases that need independent review.
Dr. Gupta and Dr. Bae emphasized the confidentiality of the reviews and that they are non-discoverable in the event of litigation, which they hope give clinicians the freedom to fully report their observations.
Dr. Feighner said that her 23-bed hospital is far smaller than either Brigham or Duke, of course, but that the overall ideas can translate.
“I am the medical director of our hospitalist program, and our chief of staff and I’ve created a peer-review medical staff quality improvement committee,” she said. “So this obviously has a lot of interest to me.”
With only 4.2 full-time equivalents (FTEs) in her department, she said changes would be even easier to put into place.
“I think that will be really helpful for our peer-review committee and our quality and safety committee. I could see how we could take this and kind of revise it a little bit,” she said. “When you’re in charge of that few people, it’s easy to get processes implemented. We are more limited in monetary resources, but we make up for that in manpower-to-problem ratio, I guess.”
In another session, Jordan Messler, MD, SFHM, a hospitalist and former medical director of the hospitalist group at Morton Plant Hospital in Clearwater, Fla., confronted the startling statistic that 80% of initiatives in hospitals never meet their objectives. Hurdles such as burnout and disengagement, he said, often stand in the way of successful QI projects.
He emphasized the importance of intrinsic motivation (a sense of ownership and passion for the work) over extrinsic motivation (a fear of reprisal if something isn’t done). A step as simple as assigning a title (e.g., “head of readmissions”) can be a motivator, he said. But he also emphasized that project ideas need to be timed correctly and the ideas should ideally come from the physicians leading them.
Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, said he was struck by the lessons gleaned in a workshop on the I-PASS system of handoffs—a standardized system with a handoff sheet, studied prospectively, in which medical errors decreased by 23% and preventable adverse events fell by 30%.1 The system was created in pediatric departments but was deliberately made to be translatable to other settings.
“Instead of focusing on the outcome of the quality of the handoff, they focus on the quality of the feedback sessions,” Clothier said. “So it’s not the person giving the handoff or receiving the handoff that actually assesses it. It’s just the person who’s sitting there watching.”
He said the workshop underscored the importance of standardization, a concept with which he was familiar but which now seemed particularly vital.
“If you do the process and everybody does it the same, then it’s not only the person that’s giving the information who can do it in a very standardized way but the person who’s listening already knows what they’re going to be listening for so they hear it more clearly because they don’t have to discern what’s coming next,” Clothier said. “They already know what’s coming next.” TH
Reference
1. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371:1803-1812.
One of the things that Jennifer Feighner, MD, cheerfully came away with at HM16 was how to better complete a task that is distinctly uncheerful but also important to any high-performing hospital: how to collect the data of the dead.
The quality improvement session “Reducing Inpatient Mortality: A Standardized Approach to Identify Preventable Deaths” demonstrated still evolving but, so far, well-performing projects that have been rolled out at Brigham and Women’s Hospital and the Duke University Health System.
“I was struck by the methodology for getting input from multiple providers and the nursing staff,” said Dr. Feighner, director of hospital medicine at Marcus Daly Memorial Hospital in Hamilton, Mont.
As the role of the hospitalist as agent of change and improvement continues to grow, the topic of quality improvement (QI) maintained a high profile at the annual meeting, with talks on the latest literature, sustaining motivation to complete projects, and dealing with issues such as handoffs and frequent fliers.
In the mortality review session, presenters set out to give details that could be a model to be used elsewhere. At Brigham and Women’s, all of the frontline clinicians are asked by email to fill out a report when a death occurs in any case with which they’ve been involved, with the Web-based reports to be completed within 48 to 72 hours of the death.
The number of deaths, the report completion rate, death “preventability,” and issues that arose for the patient during hospitalization are some of the data that are tracked. So far, the system has identified such themes as “alarm fatigue,” high oxygen requirements on non-intensive-care floors, handoffs, and transfers from other hospitals, said Kiran Gupta, MD, MPH, who completed her residency at Brigham and is now assistant professor of clinical medicine at the University of California San Francisco.
At Duke, where the mortality review system improvements have been led by Jonathan Bae, MD, assistant professor of medicine, self-nicknamed “Dr. Death,” inpatient deaths undergo a similarly comprehensive review, with an enhanced end-of-life section to cover issues particular to those cases and flags for cases that need independent review.
Dr. Gupta and Dr. Bae emphasized the confidentiality of the reviews and that they are non-discoverable in the event of litigation, which they hope give clinicians the freedom to fully report their observations.
Dr. Feighner said that her 23-bed hospital is far smaller than either Brigham or Duke, of course, but that the overall ideas can translate.
“I am the medical director of our hospitalist program, and our chief of staff and I’ve created a peer-review medical staff quality improvement committee,” she said. “So this obviously has a lot of interest to me.”
With only 4.2 full-time equivalents (FTEs) in her department, she said changes would be even easier to put into place.
“I think that will be really helpful for our peer-review committee and our quality and safety committee. I could see how we could take this and kind of revise it a little bit,” she said. “When you’re in charge of that few people, it’s easy to get processes implemented. We are more limited in monetary resources, but we make up for that in manpower-to-problem ratio, I guess.”
In another session, Jordan Messler, MD, SFHM, a hospitalist and former medical director of the hospitalist group at Morton Plant Hospital in Clearwater, Fla., confronted the startling statistic that 80% of initiatives in hospitals never meet their objectives. Hurdles such as burnout and disengagement, he said, often stand in the way of successful QI projects.
He emphasized the importance of intrinsic motivation (a sense of ownership and passion for the work) over extrinsic motivation (a fear of reprisal if something isn’t done). A step as simple as assigning a title (e.g., “head of readmissions”) can be a motivator, he said. But he also emphasized that project ideas need to be timed correctly and the ideas should ideally come from the physicians leading them.
Robert Clothier, RN, a practice manager for the hospitalist group at ThedaCare in Wisconsin, said he was struck by the lessons gleaned in a workshop on the I-PASS system of handoffs—a standardized system with a handoff sheet, studied prospectively, in which medical errors decreased by 23% and preventable adverse events fell by 30%.1 The system was created in pediatric departments but was deliberately made to be translatable to other settings.
“Instead of focusing on the outcome of the quality of the handoff, they focus on the quality of the feedback sessions,” Clothier said. “So it’s not the person giving the handoff or receiving the handoff that actually assesses it. It’s just the person who’s sitting there watching.”
He said the workshop underscored the importance of standardization, a concept with which he was familiar but which now seemed particularly vital.
“If you do the process and everybody does it the same, then it’s not only the person that’s giving the information who can do it in a very standardized way but the person who’s listening already knows what they’re going to be listening for so they hear it more clearly because they don’t have to discern what’s coming next,” Clothier said. “They already know what’s coming next.” TH
Reference
1. Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371:1803-1812.
Study Suggests that Elderly Patients with Hip Fractures get Better Care at Smaller Hospitals
(Reuters Health) - Elderly patients with hip fractures may get better care at smaller hospitals, a new study suggests. Seniors with hip fractures waited longer for surgery and were more likely to be rehospitalized if they were treated at a major trauma center than if they went to a smaller emergency room, researchers found.
Seniors in level 1 trauma centers were also more likely to develop blood clots in their legs, compared to their peers who were treated in settings designed for less serious injuries, the researchers reported March 11 in the journal Medical Care.
Level 1 trauma centers have the resources to treat very serious injuries, said lead author Dr. David Metcalfe of Brigham and Women's Hospital in Boston.
"However, because they care for the most complex patients, these hospitals are often very busy. There is therefore a risk that some groups of patients might be disadvantaged or 'lost' in the system," Metcalfe told Reuters Health by email.
For example, patients with multiple injuries or bones breaking through skin may be treated before seniors with hip fractures.
Each year in the U.S. alone, more than 250,000 people aged 65 and older are hospitalized for hip fractures, according to the Centers for Disease Control and Prevention.
The study team used statewide data from California on 91,401 seniors hospitalized between 2007 and 2011. All were over age 65 and had surgery for hip fractures.
Overall, 6% were treated at a level 1 trauma center, 18% at a level 2 trauma center and 70% in a non-trauma center.
On average, patients stayed in the hospital for five days and waited one day for surgery.
Patients in level 1 trauma centers stayed for one day longer than those in the other settings and waited nearly eight hours longer for surgery.
Seniors treated at level 1 centers were 62% more likely to be readmitted to the hospital within a month of their surgery than seniors treated in level 2 or non-trauma settings.Seniors were also 32% more likely to develop blood clots in their legs at level 1 centers.
Patients at level 2 trauma centers had the same outcomes as those at non-trauma centers, the authors found. There was no difference between any of the groups in risk of death, bed sores, or pneumonia, however.
"We now know that it is important to treat patients with hip fractures as quickly as possible," said Metcalfe, noting that older adults who wait too long for treatment may be at risk for bed sores, blood clots, and lung infections.
"The concern is that this delay will lead to increasing length of stay in hospital as well as increased complications for the patients because they spend longer in bed waiting for surgery," said Dr. Chris Gooding, a surgeon at Addenbrookes Hospital, a level 1 trauma center in Cambridge, UK. Gooding was not involved in the study.
"This is an important subject as in developed countries we have an aging population and as a result we are seeing increasing numbers of patients with hip fractures," Gooding told Reuters Health by email.
At the same time, Gooding noted, there are also a growing number of level 1 trauma centers.
"One of the best ways to help these patients is to get their operation done quickly so that they can start walking again and return to their own homes as soon as possible," Metcalfe advised.
(Reuters Health) - Elderly patients with hip fractures may get better care at smaller hospitals, a new study suggests. Seniors with hip fractures waited longer for surgery and were more likely to be rehospitalized if they were treated at a major trauma center than if they went to a smaller emergency room, researchers found.
Seniors in level 1 trauma centers were also more likely to develop blood clots in their legs, compared to their peers who were treated in settings designed for less serious injuries, the researchers reported March 11 in the journal Medical Care.
Level 1 trauma centers have the resources to treat very serious injuries, said lead author Dr. David Metcalfe of Brigham and Women's Hospital in Boston.
"However, because they care for the most complex patients, these hospitals are often very busy. There is therefore a risk that some groups of patients might be disadvantaged or 'lost' in the system," Metcalfe told Reuters Health by email.
For example, patients with multiple injuries or bones breaking through skin may be treated before seniors with hip fractures.
Each year in the U.S. alone, more than 250,000 people aged 65 and older are hospitalized for hip fractures, according to the Centers for Disease Control and Prevention.
The study team used statewide data from California on 91,401 seniors hospitalized between 2007 and 2011. All were over age 65 and had surgery for hip fractures.
Overall, 6% were treated at a level 1 trauma center, 18% at a level 2 trauma center and 70% in a non-trauma center.
On average, patients stayed in the hospital for five days and waited one day for surgery.
Patients in level 1 trauma centers stayed for one day longer than those in the other settings and waited nearly eight hours longer for surgery.
Seniors treated at level 1 centers were 62% more likely to be readmitted to the hospital within a month of their surgery than seniors treated in level 2 or non-trauma settings.Seniors were also 32% more likely to develop blood clots in their legs at level 1 centers.
Patients at level 2 trauma centers had the same outcomes as those at non-trauma centers, the authors found. There was no difference between any of the groups in risk of death, bed sores, or pneumonia, however.
"We now know that it is important to treat patients with hip fractures as quickly as possible," said Metcalfe, noting that older adults who wait too long for treatment may be at risk for bed sores, blood clots, and lung infections.
"The concern is that this delay will lead to increasing length of stay in hospital as well as increased complications for the patients because they spend longer in bed waiting for surgery," said Dr. Chris Gooding, a surgeon at Addenbrookes Hospital, a level 1 trauma center in Cambridge, UK. Gooding was not involved in the study.
"This is an important subject as in developed countries we have an aging population and as a result we are seeing increasing numbers of patients with hip fractures," Gooding told Reuters Health by email.
At the same time, Gooding noted, there are also a growing number of level 1 trauma centers.
"One of the best ways to help these patients is to get their operation done quickly so that they can start walking again and return to their own homes as soon as possible," Metcalfe advised.
(Reuters Health) - Elderly patients with hip fractures may get better care at smaller hospitals, a new study suggests. Seniors with hip fractures waited longer for surgery and were more likely to be rehospitalized if they were treated at a major trauma center than if they went to a smaller emergency room, researchers found.
Seniors in level 1 trauma centers were also more likely to develop blood clots in their legs, compared to their peers who were treated in settings designed for less serious injuries, the researchers reported March 11 in the journal Medical Care.
Level 1 trauma centers have the resources to treat very serious injuries, said lead author Dr. David Metcalfe of Brigham and Women's Hospital in Boston.
"However, because they care for the most complex patients, these hospitals are often very busy. There is therefore a risk that some groups of patients might be disadvantaged or 'lost' in the system," Metcalfe told Reuters Health by email.
For example, patients with multiple injuries or bones breaking through skin may be treated before seniors with hip fractures.
Each year in the U.S. alone, more than 250,000 people aged 65 and older are hospitalized for hip fractures, according to the Centers for Disease Control and Prevention.
The study team used statewide data from California on 91,401 seniors hospitalized between 2007 and 2011. All were over age 65 and had surgery for hip fractures.
Overall, 6% were treated at a level 1 trauma center, 18% at a level 2 trauma center and 70% in a non-trauma center.
On average, patients stayed in the hospital for five days and waited one day for surgery.
Patients in level 1 trauma centers stayed for one day longer than those in the other settings and waited nearly eight hours longer for surgery.
Seniors treated at level 1 centers were 62% more likely to be readmitted to the hospital within a month of their surgery than seniors treated in level 2 or non-trauma settings.Seniors were also 32% more likely to develop blood clots in their legs at level 1 centers.
Patients at level 2 trauma centers had the same outcomes as those at non-trauma centers, the authors found. There was no difference between any of the groups in risk of death, bed sores, or pneumonia, however.
"We now know that it is important to treat patients with hip fractures as quickly as possible," said Metcalfe, noting that older adults who wait too long for treatment may be at risk for bed sores, blood clots, and lung infections.
"The concern is that this delay will lead to increasing length of stay in hospital as well as increased complications for the patients because they spend longer in bed waiting for surgery," said Dr. Chris Gooding, a surgeon at Addenbrookes Hospital, a level 1 trauma center in Cambridge, UK. Gooding was not involved in the study.
"This is an important subject as in developed countries we have an aging population and as a result we are seeing increasing numbers of patients with hip fractures," Gooding told Reuters Health by email.
At the same time, Gooding noted, there are also a growing number of level 1 trauma centers.
"One of the best ways to help these patients is to get their operation done quickly so that they can start walking again and return to their own homes as soon as possible," Metcalfe advised.