User login
Society of Hospital Medicine Awards 3 Master in Hospital Medicine Designation
SAN DIEGO—Add three more names to the short list of individuals who’ve reached the peak of the specialty. The Master in Hospital Medicine (MHM) designation, introduced in 2010, honors “highly accomplished individuals” who have made major contributions to HM. Twenty-one people have now attained the designation.

Because Eric Howell, MD, MHM, is an introvert by personality and an engineer by training, he knows full well perfection doesn’t exist. But he tries, as evidenced by a résumé that includes being a past SHM president, current SHM board member, perennial faculty member at the society’s annual meeting, and award-winning professor.
“You’re constantly trying to achieve mastery, but no one ever really reaches it,” says Dr. Howell, director of the collaborative inpatient medicine service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore and chief of its Division of Hospital Medicine. “It’s just good to know that at least I’m viewed by others as being worthy … at least I’m on the right track.
“It’s hard as you become more experienced to find ways to assess your performance, and so getting an award like a Masters is incredibly rewarding because it verifies that your colleagues feel like your work to improve is valid and [has] paid off.”

Tina Budnitz, MPH, MHM, doesn’t see her MHM honorarium as hers alone. Sure, the designation is a nod to accomplishments made over 14 years in multiple leadership roles, including as SHM’s chief strategy and development officer. She helped the nascent specialty craft the “Core Competencies in Hospital Medicine,” design the leadership academies, and launch the now well-established Project BOOST. She developed SHM’s mentored implementation program and the SHM strategic communications plan to help guide the society into 2020.
“As the first non-physician to get this award, I am humbled and honored,” she says. “But what’s most important is the statement being made by SHM that hospital medicine will be propelled forward through the contributions of many professionals including, but not only, physicians. That’s such an important message that I want people to hear.”
Budnitz says SHM is not just a group of individuals.
“The entire team is needed to improve healthcare,” she says.

Gregory Maynard, MD, MSc, MHM, has been a clinician, educator, and quality improvement (QI) pioneer. He helped build and lead mentored-implementation programs to improve transitions of care, upgrade glycemic controls, and prevent venous thromboembolism (VTE).
And now, as chief quality officer at the University of California Davis Medical Center in Sacramento, he is a master.
So why does he still feel like the student and not the teacher?
“What I probably feel best about in hospital medicine is the collaborative approach to mentored implementation, these coaching models to educate broad groups,” he says. “When I’ve had an opportunity to try to work with other hospitalists and mentor them in terms of how to survive as a hospital medicine program or how to attack a problem in quality, be it VTE or something else … they end up teaching me a lot and mentoring me in return.” TH
Richard Quinn is a freelance writer in New Jersey.
SAN DIEGO—Add three more names to the short list of individuals who’ve reached the peak of the specialty. The Master in Hospital Medicine (MHM) designation, introduced in 2010, honors “highly accomplished individuals” who have made major contributions to HM. Twenty-one people have now attained the designation.
Because Eric Howell, MD, MHM, is an introvert by personality and an engineer by training, he knows full well perfection doesn’t exist. But he tries, as evidenced by a résumé that includes being a past SHM president, current SHM board member, perennial faculty member at the society’s annual meeting, and award-winning professor.
“You’re constantly trying to achieve mastery, but no one ever really reaches it,” says Dr. Howell, director of the collaborative inpatient medicine service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore and chief of its Division of Hospital Medicine. “It’s just good to know that at least I’m viewed by others as being worthy … at least I’m on the right track.
“It’s hard as you become more experienced to find ways to assess your performance, and so getting an award like a Masters is incredibly rewarding because it verifies that your colleagues feel like your work to improve is valid and [has] paid off.”
Tina Budnitz, MPH, MHM, doesn’t see her MHM honorarium as hers alone. Sure, the designation is a nod to accomplishments made over 14 years in multiple leadership roles, including as SHM’s chief strategy and development officer. She helped the nascent specialty craft the “Core Competencies in Hospital Medicine,” design the leadership academies, and launch the now well-established Project BOOST. She developed SHM’s mentored implementation program and the SHM strategic communications plan to help guide the society into 2020.
“As the first non-physician to get this award, I am humbled and honored,” she says. “But what’s most important is the statement being made by SHM that hospital medicine will be propelled forward through the contributions of many professionals including, but not only, physicians. That’s such an important message that I want people to hear.”
Budnitz says SHM is not just a group of individuals.
“The entire team is needed to improve healthcare,” she says.
Gregory Maynard, MD, MSc, MHM, has been a clinician, educator, and quality improvement (QI) pioneer. He helped build and lead mentored-implementation programs to improve transitions of care, upgrade glycemic controls, and prevent venous thromboembolism (VTE).
And now, as chief quality officer at the University of California Davis Medical Center in Sacramento, he is a master.
So why does he still feel like the student and not the teacher?
“What I probably feel best about in hospital medicine is the collaborative approach to mentored implementation, these coaching models to educate broad groups,” he says. “When I’ve had an opportunity to try to work with other hospitalists and mentor them in terms of how to survive as a hospital medicine program or how to attack a problem in quality, be it VTE or something else … they end up teaching me a lot and mentoring me in return.” TH
Richard Quinn is a freelance writer in New Jersey.
SAN DIEGO—Add three more names to the short list of individuals who’ve reached the peak of the specialty. The Master in Hospital Medicine (MHM) designation, introduced in 2010, honors “highly accomplished individuals” who have made major contributions to HM. Twenty-one people have now attained the designation.
Because Eric Howell, MD, MHM, is an introvert by personality and an engineer by training, he knows full well perfection doesn’t exist. But he tries, as evidenced by a résumé that includes being a past SHM president, current SHM board member, perennial faculty member at the society’s annual meeting, and award-winning professor.
“You’re constantly trying to achieve mastery, but no one ever really reaches it,” says Dr. Howell, director of the collaborative inpatient medicine service (CIMS) at Johns Hopkins Bayview Medical Center in Baltimore and chief of its Division of Hospital Medicine. “It’s just good to know that at least I’m viewed by others as being worthy … at least I’m on the right track.
“It’s hard as you become more experienced to find ways to assess your performance, and so getting an award like a Masters is incredibly rewarding because it verifies that your colleagues feel like your work to improve is valid and [has] paid off.”
Tina Budnitz, MPH, MHM, doesn’t see her MHM honorarium as hers alone. Sure, the designation is a nod to accomplishments made over 14 years in multiple leadership roles, including as SHM’s chief strategy and development officer. She helped the nascent specialty craft the “Core Competencies in Hospital Medicine,” design the leadership academies, and launch the now well-established Project BOOST. She developed SHM’s mentored implementation program and the SHM strategic communications plan to help guide the society into 2020.
“As the first non-physician to get this award, I am humbled and honored,” she says. “But what’s most important is the statement being made by SHM that hospital medicine will be propelled forward through the contributions of many professionals including, but not only, physicians. That’s such an important message that I want people to hear.”
Budnitz says SHM is not just a group of individuals.
“The entire team is needed to improve healthcare,” she says.
Gregory Maynard, MD, MSc, MHM, has been a clinician, educator, and quality improvement (QI) pioneer. He helped build and lead mentored-implementation programs to improve transitions of care, upgrade glycemic controls, and prevent venous thromboembolism (VTE).
And now, as chief quality officer at the University of California Davis Medical Center in Sacramento, he is a master.
So why does he still feel like the student and not the teacher?
“What I probably feel best about in hospital medicine is the collaborative approach to mentored implementation, these coaching models to educate broad groups,” he says. “When I’ve had an opportunity to try to work with other hospitalists and mentor them in terms of how to survive as a hospital medicine program or how to attack a problem in quality, be it VTE or something else … they end up teaching me a lot and mentoring me in return.” TH
Richard Quinn is a freelance writer in New Jersey.
Work ‘paves the way’ for platelet manufacture
in the bone marrow
Researchers in the UK have developed a new method of producing megakaryocytes from human pluripotent stem cells (hPSCs).
The team said their method generated large quantities of functional megakaryocytes that produced functional platelets.
They believe this work brings us one step closer to manufacturing platelets for transfusion.
The research was published in Nature Communications.
“Making megakaryocytes and platelets from stem cells for transfusion has been a long-standing challenge because of the sheer numbers we need to produce to make a single unit for transfusion,” said study author Cedric Ghevaert, MD, PhD, of the University of Cambridge and NHS Blood and Transplant in Cambridge, UK.
“We have found a way to ‘rewire’ the stem cells to make them become megakaryocytes a lot faster and more efficiently. It is a major step forward towards our goal to one day make blood cells in the laboratory to transfuse to patients.”
Dr Ghevaert and his colleagues employed a “forward programming” strategy in which 3 transcription factors—GATA1, FLI1, and TAL1—were used drive the differentiation of hPSCs into megakaryocytes.
The team said the forward-programmed megakaryocytes matured into platelet-producing cells that could be cryopreserved, maintained, and amplified in vitro for more than 90 days. The average yield was 200,000 megakaryocytes per hPSC.
The researchers generated platelets from the forward-programmed megakaryocytes via culture. And tests suggested these platelets were functionally similar to donor-derived platelets.
“The success of this research team in producing megakaryocytes in the laboratory has paved the way for the ultimate goal—manufacturing platelets for transfusion,” said Edwin Massey, MBChB, associate medical director for diagnostic and therapeutic services at NHS Blood and Transplant, who was not involved in this research.
“It will, however, be many years before a process for the large-scale production of platelets is developed. Donated platelets will still be needed by patients for the foreseeable future, either as part of a blood donation or by dedicated platelet donation using a machine collection process.” ![]()
in the bone marrow
Researchers in the UK have developed a new method of producing megakaryocytes from human pluripotent stem cells (hPSCs).
The team said their method generated large quantities of functional megakaryocytes that produced functional platelets.
They believe this work brings us one step closer to manufacturing platelets for transfusion.
The research was published in Nature Communications.
“Making megakaryocytes and platelets from stem cells for transfusion has been a long-standing challenge because of the sheer numbers we need to produce to make a single unit for transfusion,” said study author Cedric Ghevaert, MD, PhD, of the University of Cambridge and NHS Blood and Transplant in Cambridge, UK.
“We have found a way to ‘rewire’ the stem cells to make them become megakaryocytes a lot faster and more efficiently. It is a major step forward towards our goal to one day make blood cells in the laboratory to transfuse to patients.”
Dr Ghevaert and his colleagues employed a “forward programming” strategy in which 3 transcription factors—GATA1, FLI1, and TAL1—were used drive the differentiation of hPSCs into megakaryocytes.
The team said the forward-programmed megakaryocytes matured into platelet-producing cells that could be cryopreserved, maintained, and amplified in vitro for more than 90 days. The average yield was 200,000 megakaryocytes per hPSC.
The researchers generated platelets from the forward-programmed megakaryocytes via culture. And tests suggested these platelets were functionally similar to donor-derived platelets.
“The success of this research team in producing megakaryocytes in the laboratory has paved the way for the ultimate goal—manufacturing platelets for transfusion,” said Edwin Massey, MBChB, associate medical director for diagnostic and therapeutic services at NHS Blood and Transplant, who was not involved in this research.
“It will, however, be many years before a process for the large-scale production of platelets is developed. Donated platelets will still be needed by patients for the foreseeable future, either as part of a blood donation or by dedicated platelet donation using a machine collection process.” ![]()
in the bone marrow
Researchers in the UK have developed a new method of producing megakaryocytes from human pluripotent stem cells (hPSCs).
The team said their method generated large quantities of functional megakaryocytes that produced functional platelets.
They believe this work brings us one step closer to manufacturing platelets for transfusion.
The research was published in Nature Communications.
“Making megakaryocytes and platelets from stem cells for transfusion has been a long-standing challenge because of the sheer numbers we need to produce to make a single unit for transfusion,” said study author Cedric Ghevaert, MD, PhD, of the University of Cambridge and NHS Blood and Transplant in Cambridge, UK.
“We have found a way to ‘rewire’ the stem cells to make them become megakaryocytes a lot faster and more efficiently. It is a major step forward towards our goal to one day make blood cells in the laboratory to transfuse to patients.”
Dr Ghevaert and his colleagues employed a “forward programming” strategy in which 3 transcription factors—GATA1, FLI1, and TAL1—were used drive the differentiation of hPSCs into megakaryocytes.
The team said the forward-programmed megakaryocytes matured into platelet-producing cells that could be cryopreserved, maintained, and amplified in vitro for more than 90 days. The average yield was 200,000 megakaryocytes per hPSC.
The researchers generated platelets from the forward-programmed megakaryocytes via culture. And tests suggested these platelets were functionally similar to donor-derived platelets.
“The success of this research team in producing megakaryocytes in the laboratory has paved the way for the ultimate goal—manufacturing platelets for transfusion,” said Edwin Massey, MBChB, associate medical director for diagnostic and therapeutic services at NHS Blood and Transplant, who was not involved in this research.
“It will, however, be many years before a process for the large-scale production of platelets is developed. Donated platelets will still be needed by patients for the foreseeable future, either as part of a blood donation or by dedicated platelet donation using a machine collection process.” ![]()
Postvaccination anaphylaxis still possible with certain vaccines
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.

Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.
Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
New findings confirm that although it is rare, postvaccination anaphylaxis can still occur with certain vaccines.
Dr. Michael M. McNeil of the Centers for Disease Control and Prevention, Atlanta, and his associates identified 17,606,500 vaccination visits from Jan. 1, 2009, through Dec. 31, 2011, at which 25,173,965 vaccine doses were administered. The researchers identified 76 cases of chart-confirmed anaphylaxis; 33 anaphylaxis cases were associated with vaccination, and 43 were attributed to other causes.
Inactivated trivalent influenza vaccine (TIV) was the major contributor to vaccine-triggered anaphylaxis cases in the population, although the rate (1.35 cases per 1 million vaccine doses of TIV given alone) was similar to the rate for all vaccines. The postvaccination anaphylaxis case rate not involving TIV was 1.32 per million vaccine doses.
The study factored in race, age, gender, symptoms, and history of the patients. There were no deaths, and only 1 patient (3%) was hospitalized. A total of 28 of the 33 vaccine-triggered anaphylaxis cases involved patients with a history of atopy.
“Although anaphylaxis after immunization is rare, its immediate onset (usually within minutes) and life-threatening nature require that all personnel and facilities providing vaccinations have procedures in place for anaphylaxis management,” the investigators noted. “Additional provider education concerning current recommendations for treatment and follow-up appears to be warranted.”
Find the full story in the Journal of Allergy and Clinical Immunology (2016 Mar;137[3]:868-78).
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY

Osteoarthritis hip pain follows four distinct paths
AMSTERDAM – There are four distinct patterns of pain in patients with early presumed hip osteoarthritis, and several factors could help identify patients most likely to experience more severe pain, according to analysis from a Dutch study.
The majority of the 545 patients included in the analysis from the Cohort Hip and Knee (CHECK) study experienced a low or a mild constant hip pain over a 5-year follow-up period (231 patients, 42.4%). Around one-quarter had moderate hip pain with moderate pain progression (132 patients, 24.2%), about one in six (88 patients, 16.1%) had moderate hip pain with moderate pain regression, and the remainder (94 patients, 17.2%) had constant, severe hip pain.
Factors associated with these pain trajectories included the level of education achieved, ability to cope with pain, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function subscale, and pain experienced from internal rotation of the hip.
The findings were reported at the World Congress on Osteoarthritis sponsored by the Osteoarthritis Research Society International. They were also published online in Osteoarthritis and Cartilage (2106 Feb 5. doi: 10.1016/j.joca.2015.11.023).
Although prior studies examined progression predictors in hip OA, none looked specifically at how pain changes over time, noted study author Dr. Alex Bastick of Erasmus University Medical Center, Rotterdam, the Netherlands. Thus, the current aim was to define the trajectory of hip pain among individuals with early symptoms of hip OA, and identify any baseline factors that might help clinicians predict which pain trajectory patients may follow.
The CHECK study is a 10-year nationwide cohort study of 1,002 participants in the Netherlands with assumed early symptomatic OA of the knee, hip, or both. For the current analysis, Dr. Bastick and his associates considered only those patients with hip pain or stiffness who had completed 5 years of follow-up. At baseline, the mean age of the total population was 55.7 years, and 81% of participants were female. About one-quarter (26%) of participants had a clinical OA diagnosis according to American College of Rheumatology criteria.
Baseline radiographic severity was not associated with the various pain trajectories identified, Dr. Bastick observed, but patients who had achieved a lower level of education were roughly three times more likely to experience severe pain than mild or low constant pain. Patients experiencing severe pain were more likely to use pain transformation as a coping strategy, have higher activity limitation scores, and experience painful internal hip rotation.
Because around 60% of patients follow the mild or moderately progressing pain trajectories, conservative treatment in the early stages of hip OA appears appropriate, Dr. Bastick and his associates suggested. Their findings highlight the importance of a physical examination, and that reassessment of clinical symptoms should perhaps be undertaken in the first year of follow-up.
“Future research should be aimed at measuring symptomatic progression of hip OA with even more frequent symptom assessment,” the researchers proposed.
Reumafonds, the Dutch Arthritis Foundation, funded the study. Dr. Bastick did not have financial disclosures.
AMSTERDAM – There are four distinct patterns of pain in patients with early presumed hip osteoarthritis, and several factors could help identify patients most likely to experience more severe pain, according to analysis from a Dutch study.
The majority of the 545 patients included in the analysis from the Cohort Hip and Knee (CHECK) study experienced a low or a mild constant hip pain over a 5-year follow-up period (231 patients, 42.4%). Around one-quarter had moderate hip pain with moderate pain progression (132 patients, 24.2%), about one in six (88 patients, 16.1%) had moderate hip pain with moderate pain regression, and the remainder (94 patients, 17.2%) had constant, severe hip pain.
Factors associated with these pain trajectories included the level of education achieved, ability to cope with pain, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function subscale, and pain experienced from internal rotation of the hip.
The findings were reported at the World Congress on Osteoarthritis sponsored by the Osteoarthritis Research Society International. They were also published online in Osteoarthritis and Cartilage (2106 Feb 5. doi: 10.1016/j.joca.2015.11.023).
Although prior studies examined progression predictors in hip OA, none looked specifically at how pain changes over time, noted study author Dr. Alex Bastick of Erasmus University Medical Center, Rotterdam, the Netherlands. Thus, the current aim was to define the trajectory of hip pain among individuals with early symptoms of hip OA, and identify any baseline factors that might help clinicians predict which pain trajectory patients may follow.
The CHECK study is a 10-year nationwide cohort study of 1,002 participants in the Netherlands with assumed early symptomatic OA of the knee, hip, or both. For the current analysis, Dr. Bastick and his associates considered only those patients with hip pain or stiffness who had completed 5 years of follow-up. At baseline, the mean age of the total population was 55.7 years, and 81% of participants were female. About one-quarter (26%) of participants had a clinical OA diagnosis according to American College of Rheumatology criteria.
Baseline radiographic severity was not associated with the various pain trajectories identified, Dr. Bastick observed, but patients who had achieved a lower level of education were roughly three times more likely to experience severe pain than mild or low constant pain. Patients experiencing severe pain were more likely to use pain transformation as a coping strategy, have higher activity limitation scores, and experience painful internal hip rotation.
Because around 60% of patients follow the mild or moderately progressing pain trajectories, conservative treatment in the early stages of hip OA appears appropriate, Dr. Bastick and his associates suggested. Their findings highlight the importance of a physical examination, and that reassessment of clinical symptoms should perhaps be undertaken in the first year of follow-up.
“Future research should be aimed at measuring symptomatic progression of hip OA with even more frequent symptom assessment,” the researchers proposed.
Reumafonds, the Dutch Arthritis Foundation, funded the study. Dr. Bastick did not have financial disclosures.
AMSTERDAM – There are four distinct patterns of pain in patients with early presumed hip osteoarthritis, and several factors could help identify patients most likely to experience more severe pain, according to analysis from a Dutch study.
The majority of the 545 patients included in the analysis from the Cohort Hip and Knee (CHECK) study experienced a low or a mild constant hip pain over a 5-year follow-up period (231 patients, 42.4%). Around one-quarter had moderate hip pain with moderate pain progression (132 patients, 24.2%), about one in six (88 patients, 16.1%) had moderate hip pain with moderate pain regression, and the remainder (94 patients, 17.2%) had constant, severe hip pain.
Factors associated with these pain trajectories included the level of education achieved, ability to cope with pain, the Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function subscale, and pain experienced from internal rotation of the hip.
The findings were reported at the World Congress on Osteoarthritis sponsored by the Osteoarthritis Research Society International. They were also published online in Osteoarthritis and Cartilage (2106 Feb 5. doi: 10.1016/j.joca.2015.11.023).
Although prior studies examined progression predictors in hip OA, none looked specifically at how pain changes over time, noted study author Dr. Alex Bastick of Erasmus University Medical Center, Rotterdam, the Netherlands. Thus, the current aim was to define the trajectory of hip pain among individuals with early symptoms of hip OA, and identify any baseline factors that might help clinicians predict which pain trajectory patients may follow.
The CHECK study is a 10-year nationwide cohort study of 1,002 participants in the Netherlands with assumed early symptomatic OA of the knee, hip, or both. For the current analysis, Dr. Bastick and his associates considered only those patients with hip pain or stiffness who had completed 5 years of follow-up. At baseline, the mean age of the total population was 55.7 years, and 81% of participants were female. About one-quarter (26%) of participants had a clinical OA diagnosis according to American College of Rheumatology criteria.
Baseline radiographic severity was not associated with the various pain trajectories identified, Dr. Bastick observed, but patients who had achieved a lower level of education were roughly three times more likely to experience severe pain than mild or low constant pain. Patients experiencing severe pain were more likely to use pain transformation as a coping strategy, have higher activity limitation scores, and experience painful internal hip rotation.
Because around 60% of patients follow the mild or moderately progressing pain trajectories, conservative treatment in the early stages of hip OA appears appropriate, Dr. Bastick and his associates suggested. Their findings highlight the importance of a physical examination, and that reassessment of clinical symptoms should perhaps be undertaken in the first year of follow-up.
“Future research should be aimed at measuring symptomatic progression of hip OA with even more frequent symptom assessment,” the researchers proposed.
Reumafonds, the Dutch Arthritis Foundation, funded the study. Dr. Bastick did not have financial disclosures.
AT OARSI 2016
Key clinical point: Understanding how osteoarthritis hip pain changes over time may help manage those who experience severe pain.
Major finding: Four hip pain trajectories were identified: low, mild constant pain (42.4%, n = 231); moderate, with moderate pain progression (24.2%, n = 132); moderate, with moderate pain regression (16.1%, n = 88); and constant severe pain (17.2%, n = 94).
Data source: The Cohort Hip and Knee (CHECK) study, a Dutch, prospective, nationwide study of 1,002 participants with assumed early symptomatic osteoarthritis of the knee, hip, or both.
Disclosures: Reumafonds, the Dutch Arthritis Foundation, funded the study. Dr. Bastick did not have financial disclosures.

Stem cells show heart failure benefits in phase II trial
CHICAGO – After rattling around in early-stage clinical studies for more than a decade, stem cell therapy for heart failure may have finally gained the efficacy evidence to send it to the next level: large-scale, phase III trials.
Patients with ischemic cardiomyopathy and severe heart failure showed a statistically significant 37% relative reduction in their combined rate of death and cardiovascular hospitalization during 1 year of follow-up after autologous stem cell injections to their left ventricular myocardium in a multicenter, fully blinded control, phase II trial with 109 North American patients.

The treatment used a technique in commercial development by Vericel that selectively expands ex vivo bone marrow cells taken from the heart failure patient. Clinicians inject 0.4 mL aliquots of the expanded cells – enriched for mesenchymal stem cells and M2 macrophages – via a transcatheter approach into the left ventricular myocardium using 12-17 injections per patient. The bone marrow preparation during ex vivo expansion is called ixmyelocel-T.
This treatment now needs testing in more patients, Dr. Timothy D. Henry said at the annual meeting of the American College of Cardiology. “We need a new generation of cell trials in larger studies with completely double-blind, placebo controls using a more uniform preparation of cells,” said Dr. Henry.
“To the best of our knowledge, ixCELL-DCM is the largest randomized, double-blind clinical trial to date for cell therapy use in congestive heart failure,” said Dr. Henry and his associates in their report. The concept of stem cell therapy to replace damaged myocardium “has been very attractive, but most clinical trials to date have been small and unblinded, and used unselected bone marrow cells,” explained Dr. Henry, director of cardiology at the Cedars-Sinai Heart Institute in Los Angeles.
The ixCELL-DCM study ran at 31 sites in the United States and Canada. About 90% of patients had New York Heart Association class III disease, the average left ventricular ejection fraction was about 25%, patients on average would cover about 310 m during a 6-minute walk test, and the average serum level of NT-ProBNP was about 1,900 pg/L. Patients in the control arm all underwent the same bone marrow retrieval and transcatheter injection into the left ventricle, but the injections only contained carrier material without active cells.
The primary endpoint of death or a cardiovascular event, primarily hospitalization, occurred at a rate of 110 events per 100 patient years during 1-year follow-up of 51 patients in the sham-treatment group. In the active-treatment arm, the endpoint occurred at a rate of 70 events per 100 patient years among 58 patients. The difference was primarily driven by a 3% death rate with cell therapy, compared with a 14% rate in the controls, and a 38% hospitalization rate, compared with a 47% rate among controls.
The study results appeared online concurrent with Dr. Henry’s report (Lancet. 2016 Apr 5. doi: 10.1016/S0140-6736[16]30137-4).
The results showed no significant differences between the active and sham groups for changes in left ventricular size, ejection fraction, and 6-minute walk distance.
“This trial was designed to look at events. It is not a cause for concern that we did not see effects on heart function,” Dr. Henry said. The current results were also generally consistent with results from two earlier, controlled, phase II studies with a total of 61 patients (Circ Res. 2014 Sep 26;115[8]:730-7).
In the safety analysis, done in 114 patients, the rates of all adverse events and major adverse cardiovascular events were similar in the two arms. The rate of serious adverse events was significantly reduced in the patients treated with expanded bone marrow cells, compared with the controls.
The high rate of death and hospitalization of patients with severe heart failure “is a very large, unmet need, so it’s a natural to go to a larger trial,” Dr. Henry said. “The cell preparation was very safe and easy to do.”
Another pressing research issue is to try to understand the mechanism by which the cell treatment improves clinical outcomes, with improved heart function or improved exercise capacity apparently excluded as mechanisms.
The trial was sponsored by Vericel, the company developing the ex vivo protocol for selective marrow cell expansion. Dr. Henry has been a consultant to or received honoraria from Abbott Vascular, Baxter, Capricor, Cytori, Eli Lilly, and the Medicines Company, and he has received research grants from Aastrom, Baxter International, Mesoblast, and Vericel.
On Twitter @mitchelzoler
The results reported by Dr. Henry come from one of the first trials of stem cell or bone marrow treatment of failing hearts that used clinical outcomes as the primary endpoint. In contrast, prior studies focused on changes in functional characteristics of patients, such as 6-minute walk distance or left ventricular ejection fraction or size. What makes Dr. Henry’s study distinctive is that it showed benefit for a clinical outcome: the rate of death or cardiovascular hospitalization.
Another distinct difference, compared with the vast majority of earlier trials, was the way the bone marrow was handled prior to placement in a heart. The bone marrow cells underwent a 12-day period of ex vivo treatment designed to expand the content of certain mesenchymal stem cells and macrophages.
The current study was also larger than most prior reported studies, with 114 randomized patients available for the safety analysis and 109 for the efficacy analysis. But by no means was this a large study; in fact, it is relatively small. Although it produced a statistically significant result for the primary endpoint, the efficacy needs expanded testing in larger numbers.
It’s currently unclear how the expanded bone marrow cell injections improve clinical status and lead to reduced deaths and hospitalization. The results show essentially no impact from the treatment on ejection fraction or 6-minute walk distance, raising the question of what alternative mechanisms link this treatment to improved clinical outcomes.
Until now, it has not been possible to move beyond early-stage trial designs for cell therapy of failing hearts. Now, for the first time, we have study results that suggest a phase III trial is indicated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. John A. Jarcho is a deputy editor of the New England Journal of Medicine and a cardiologist at Brigham and Women’s Hospital, both in Boston. He had no disclosures. He made these comments as a discussant of Dr. Henry’s report and in an interview.
The results reported by Dr. Henry come from one of the first trials of stem cell or bone marrow treatment of failing hearts that used clinical outcomes as the primary endpoint. In contrast, prior studies focused on changes in functional characteristics of patients, such as 6-minute walk distance or left ventricular ejection fraction or size. What makes Dr. Henry’s study distinctive is that it showed benefit for a clinical outcome: the rate of death or cardiovascular hospitalization.
Another distinct difference, compared with the vast majority of earlier trials, was the way the bone marrow was handled prior to placement in a heart. The bone marrow cells underwent a 12-day period of ex vivo treatment designed to expand the content of certain mesenchymal stem cells and macrophages.
The current study was also larger than most prior reported studies, with 114 randomized patients available for the safety analysis and 109 for the efficacy analysis. But by no means was this a large study; in fact, it is relatively small. Although it produced a statistically significant result for the primary endpoint, the efficacy needs expanded testing in larger numbers.
It’s currently unclear how the expanded bone marrow cell injections improve clinical status and lead to reduced deaths and hospitalization. The results show essentially no impact from the treatment on ejection fraction or 6-minute walk distance, raising the question of what alternative mechanisms link this treatment to improved clinical outcomes.
Until now, it has not been possible to move beyond early-stage trial designs for cell therapy of failing hearts. Now, for the first time, we have study results that suggest a phase III trial is indicated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. John A. Jarcho is a deputy editor of the New England Journal of Medicine and a cardiologist at Brigham and Women’s Hospital, both in Boston. He had no disclosures. He made these comments as a discussant of Dr. Henry’s report and in an interview.
The results reported by Dr. Henry come from one of the first trials of stem cell or bone marrow treatment of failing hearts that used clinical outcomes as the primary endpoint. In contrast, prior studies focused on changes in functional characteristics of patients, such as 6-minute walk distance or left ventricular ejection fraction or size. What makes Dr. Henry’s study distinctive is that it showed benefit for a clinical outcome: the rate of death or cardiovascular hospitalization.
Another distinct difference, compared with the vast majority of earlier trials, was the way the bone marrow was handled prior to placement in a heart. The bone marrow cells underwent a 12-day period of ex vivo treatment designed to expand the content of certain mesenchymal stem cells and macrophages.
The current study was also larger than most prior reported studies, with 114 randomized patients available for the safety analysis and 109 for the efficacy analysis. But by no means was this a large study; in fact, it is relatively small. Although it produced a statistically significant result for the primary endpoint, the efficacy needs expanded testing in larger numbers.
It’s currently unclear how the expanded bone marrow cell injections improve clinical status and lead to reduced deaths and hospitalization. The results show essentially no impact from the treatment on ejection fraction or 6-minute walk distance, raising the question of what alternative mechanisms link this treatment to improved clinical outcomes.
Until now, it has not been possible to move beyond early-stage trial designs for cell therapy of failing hearts. Now, for the first time, we have study results that suggest a phase III trial is indicated.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. John A. Jarcho is a deputy editor of the New England Journal of Medicine and a cardiologist at Brigham and Women’s Hospital, both in Boston. He had no disclosures. He made these comments as a discussant of Dr. Henry’s report and in an interview.
CHICAGO – After rattling around in early-stage clinical studies for more than a decade, stem cell therapy for heart failure may have finally gained the efficacy evidence to send it to the next level: large-scale, phase III trials.
Patients with ischemic cardiomyopathy and severe heart failure showed a statistically significant 37% relative reduction in their combined rate of death and cardiovascular hospitalization during 1 year of follow-up after autologous stem cell injections to their left ventricular myocardium in a multicenter, fully blinded control, phase II trial with 109 North American patients.
The treatment used a technique in commercial development by Vericel that selectively expands ex vivo bone marrow cells taken from the heart failure patient. Clinicians inject 0.4 mL aliquots of the expanded cells – enriched for mesenchymal stem cells and M2 macrophages – via a transcatheter approach into the left ventricular myocardium using 12-17 injections per patient. The bone marrow preparation during ex vivo expansion is called ixmyelocel-T.
This treatment now needs testing in more patients, Dr. Timothy D. Henry said at the annual meeting of the American College of Cardiology. “We need a new generation of cell trials in larger studies with completely double-blind, placebo controls using a more uniform preparation of cells,” said Dr. Henry.
“To the best of our knowledge, ixCELL-DCM is the largest randomized, double-blind clinical trial to date for cell therapy use in congestive heart failure,” said Dr. Henry and his associates in their report. The concept of stem cell therapy to replace damaged myocardium “has been very attractive, but most clinical trials to date have been small and unblinded, and used unselected bone marrow cells,” explained Dr. Henry, director of cardiology at the Cedars-Sinai Heart Institute in Los Angeles.
The ixCELL-DCM study ran at 31 sites in the United States and Canada. About 90% of patients had New York Heart Association class III disease, the average left ventricular ejection fraction was about 25%, patients on average would cover about 310 m during a 6-minute walk test, and the average serum level of NT-ProBNP was about 1,900 pg/L. Patients in the control arm all underwent the same bone marrow retrieval and transcatheter injection into the left ventricle, but the injections only contained carrier material without active cells.
The primary endpoint of death or a cardiovascular event, primarily hospitalization, occurred at a rate of 110 events per 100 patient years during 1-year follow-up of 51 patients in the sham-treatment group. In the active-treatment arm, the endpoint occurred at a rate of 70 events per 100 patient years among 58 patients. The difference was primarily driven by a 3% death rate with cell therapy, compared with a 14% rate in the controls, and a 38% hospitalization rate, compared with a 47% rate among controls.
The study results appeared online concurrent with Dr. Henry’s report (Lancet. 2016 Apr 5. doi: 10.1016/S0140-6736[16]30137-4).
The results showed no significant differences between the active and sham groups for changes in left ventricular size, ejection fraction, and 6-minute walk distance.
“This trial was designed to look at events. It is not a cause for concern that we did not see effects on heart function,” Dr. Henry said. The current results were also generally consistent with results from two earlier, controlled, phase II studies with a total of 61 patients (Circ Res. 2014 Sep 26;115[8]:730-7).
In the safety analysis, done in 114 patients, the rates of all adverse events and major adverse cardiovascular events were similar in the two arms. The rate of serious adverse events was significantly reduced in the patients treated with expanded bone marrow cells, compared with the controls.
The high rate of death and hospitalization of patients with severe heart failure “is a very large, unmet need, so it’s a natural to go to a larger trial,” Dr. Henry said. “The cell preparation was very safe and easy to do.”
Another pressing research issue is to try to understand the mechanism by which the cell treatment improves clinical outcomes, with improved heart function or improved exercise capacity apparently excluded as mechanisms.
The trial was sponsored by Vericel, the company developing the ex vivo protocol for selective marrow cell expansion. Dr. Henry has been a consultant to or received honoraria from Abbott Vascular, Baxter, Capricor, Cytori, Eli Lilly, and the Medicines Company, and he has received research grants from Aastrom, Baxter International, Mesoblast, and Vericel.
On Twitter @mitchelzoler
CHICAGO – After rattling around in early-stage clinical studies for more than a decade, stem cell therapy for heart failure may have finally gained the efficacy evidence to send it to the next level: large-scale, phase III trials.
Patients with ischemic cardiomyopathy and severe heart failure showed a statistically significant 37% relative reduction in their combined rate of death and cardiovascular hospitalization during 1 year of follow-up after autologous stem cell injections to their left ventricular myocardium in a multicenter, fully blinded control, phase II trial with 109 North American patients.
The treatment used a technique in commercial development by Vericel that selectively expands ex vivo bone marrow cells taken from the heart failure patient. Clinicians inject 0.4 mL aliquots of the expanded cells – enriched for mesenchymal stem cells and M2 macrophages – via a transcatheter approach into the left ventricular myocardium using 12-17 injections per patient. The bone marrow preparation during ex vivo expansion is called ixmyelocel-T.
This treatment now needs testing in more patients, Dr. Timothy D. Henry said at the annual meeting of the American College of Cardiology. “We need a new generation of cell trials in larger studies with completely double-blind, placebo controls using a more uniform preparation of cells,” said Dr. Henry.
“To the best of our knowledge, ixCELL-DCM is the largest randomized, double-blind clinical trial to date for cell therapy use in congestive heart failure,” said Dr. Henry and his associates in their report. The concept of stem cell therapy to replace damaged myocardium “has been very attractive, but most clinical trials to date have been small and unblinded, and used unselected bone marrow cells,” explained Dr. Henry, director of cardiology at the Cedars-Sinai Heart Institute in Los Angeles.
The ixCELL-DCM study ran at 31 sites in the United States and Canada. About 90% of patients had New York Heart Association class III disease, the average left ventricular ejection fraction was about 25%, patients on average would cover about 310 m during a 6-minute walk test, and the average serum level of NT-ProBNP was about 1,900 pg/L. Patients in the control arm all underwent the same bone marrow retrieval and transcatheter injection into the left ventricle, but the injections only contained carrier material without active cells.
The primary endpoint of death or a cardiovascular event, primarily hospitalization, occurred at a rate of 110 events per 100 patient years during 1-year follow-up of 51 patients in the sham-treatment group. In the active-treatment arm, the endpoint occurred at a rate of 70 events per 100 patient years among 58 patients. The difference was primarily driven by a 3% death rate with cell therapy, compared with a 14% rate in the controls, and a 38% hospitalization rate, compared with a 47% rate among controls.
The study results appeared online concurrent with Dr. Henry’s report (Lancet. 2016 Apr 5. doi: 10.1016/S0140-6736[16]30137-4).
The results showed no significant differences between the active and sham groups for changes in left ventricular size, ejection fraction, and 6-minute walk distance.
“This trial was designed to look at events. It is not a cause for concern that we did not see effects on heart function,” Dr. Henry said. The current results were also generally consistent with results from two earlier, controlled, phase II studies with a total of 61 patients (Circ Res. 2014 Sep 26;115[8]:730-7).
In the safety analysis, done in 114 patients, the rates of all adverse events and major adverse cardiovascular events were similar in the two arms. The rate of serious adverse events was significantly reduced in the patients treated with expanded bone marrow cells, compared with the controls.
The high rate of death and hospitalization of patients with severe heart failure “is a very large, unmet need, so it’s a natural to go to a larger trial,” Dr. Henry said. “The cell preparation was very safe and easy to do.”
Another pressing research issue is to try to understand the mechanism by which the cell treatment improves clinical outcomes, with improved heart function or improved exercise capacity apparently excluded as mechanisms.
The trial was sponsored by Vericel, the company developing the ex vivo protocol for selective marrow cell expansion. Dr. Henry has been a consultant to or received honoraria from Abbott Vascular, Baxter, Capricor, Cytori, Eli Lilly, and the Medicines Company, and he has received research grants from Aastrom, Baxter International, Mesoblast, and Vericel.
On Twitter @mitchelzoler
AT ACC 16
Key clinical point: Severe, ischemic heart failure patients had a significant cut in death and cardiovascular hospitalizations 1 year after endovascular myocardial injection with selectively expanded autologous bone marrow cells in a fully blinded, placebo-controlled phase II study.
Major finding: Cell-treated patients had a 37% drop in death and cardiovascular hospitalization relative to controls in 1-year follow-up.
Data source: A multicenter, fully blinded study with 109 patients for the per protocol efficacy analysis, and 114 patients for the safety analysis.
Disclosures: The trial was sponsored by Vericel, the company developing the ex vivo protocol for selective marrow cell expansion. Dr. Henry has been a consultant to or received honoraria from Abbott Vascular, Baxter, Capricor, Cytori, Eli Lilly, and the Medicines Company, and he has received research grants from Aastrom, Baxter International, Mesoblast, and Vericel.

Addiction – how are we being played?
Sometimes, you come across an article that makes you cringe. After this initial reaction – and if we are up for the challenge – we realize that this information can help us grow by pushing our clinical approach in new directions.
This is the experience I had with an article by Dr. Daniel Bouland and colleagues that explored the ways in which people struggling with addiction obtain prescription medications (J Addict Med. 2015 Jul-Aug;9[4]:281-5).

In this semiquantitative qualitative study, investigators interviewed 36 patients in a residential addiction treatment program who obtained prescriptions from clinicians in support of an addiction. Types of medications obtained by respondents were opioids (97.2%), sedative hypnotics (47.4%), and amphetamines (5.5%).
Patients reported obtaining prescriptions from clinicians because it was perceived to be “legal” – even though 75% of them faked symptoms, several falsified MRI images of an injury, and some used old or forged prescriptions. One patient paid a physician outright for the medication.
Eight percent of patients physically harmed themselves to obtain prescriptions by doing things such as cutting themselves to put blood in the urine, hitting their head against the wall to the point of unconsciousness, and undergoing unnecessary surgery.
Primary care clinicians and pain specialists were viewed as the easiest sources of medication. Most patients used “mom and pop” pharmacies, visited multiple pharmacies, and paid in cash. Importantly, 67% of patients said that an intervention could have changed their behaviors.
I think I knew this, but it challenged me to see it in writing. I appreciated the honesty of these individuals and was struck by the fact that almost two-thirds suggested that an intervention could have transformed them.
But how to start this conversation?
The last time I expressed concern about a patient’s allergy to any pain medication – except oxycodone and the potentially toxic doses of ibuprofen and acetaminophen that didn’t “touch it” – I was the recipient of seething rage and hostility.
Addiction treatment is hard, diagnosing addiction in daily primary care practice is harder, and holding up a mirror to a patient’s prescription drug habits requires protective body armor. That’s why not many of us do it.
So, now that we have guidelines for chronic opioids, we need best practices for acute visits presenting with x-rays of broken animal bones labeled with their name handwritten on duct tape.
Are we up for urine drug screens for every controlled substance prescription on nonestablished patients every time? Probably not, but we have to start somewhere.
At least it might start a conversation when we can say: “We do this for all of our patients, we are not singling you out. Is there anything you would like to talk about before we complete this test?”
Most importantly, once we make a diagnosis of prescription drug abuse, we need resources to which to refer them and health insurance to help cover the cost for this care.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Sometimes, you come across an article that makes you cringe. After this initial reaction – and if we are up for the challenge – we realize that this information can help us grow by pushing our clinical approach in new directions.
This is the experience I had with an article by Dr. Daniel Bouland and colleagues that explored the ways in which people struggling with addiction obtain prescription medications (J Addict Med. 2015 Jul-Aug;9[4]:281-5).
In this semiquantitative qualitative study, investigators interviewed 36 patients in a residential addiction treatment program who obtained prescriptions from clinicians in support of an addiction. Types of medications obtained by respondents were opioids (97.2%), sedative hypnotics (47.4%), and amphetamines (5.5%).
Patients reported obtaining prescriptions from clinicians because it was perceived to be “legal” – even though 75% of them faked symptoms, several falsified MRI images of an injury, and some used old or forged prescriptions. One patient paid a physician outright for the medication.
Eight percent of patients physically harmed themselves to obtain prescriptions by doing things such as cutting themselves to put blood in the urine, hitting their head against the wall to the point of unconsciousness, and undergoing unnecessary surgery.
Primary care clinicians and pain specialists were viewed as the easiest sources of medication. Most patients used “mom and pop” pharmacies, visited multiple pharmacies, and paid in cash. Importantly, 67% of patients said that an intervention could have changed their behaviors.
I think I knew this, but it challenged me to see it in writing. I appreciated the honesty of these individuals and was struck by the fact that almost two-thirds suggested that an intervention could have transformed them.
But how to start this conversation?
The last time I expressed concern about a patient’s allergy to any pain medication – except oxycodone and the potentially toxic doses of ibuprofen and acetaminophen that didn’t “touch it” – I was the recipient of seething rage and hostility.
Addiction treatment is hard, diagnosing addiction in daily primary care practice is harder, and holding up a mirror to a patient’s prescription drug habits requires protective body armor. That’s why not many of us do it.
So, now that we have guidelines for chronic opioids, we need best practices for acute visits presenting with x-rays of broken animal bones labeled with their name handwritten on duct tape.
Are we up for urine drug screens for every controlled substance prescription on nonestablished patients every time? Probably not, but we have to start somewhere.
At least it might start a conversation when we can say: “We do this for all of our patients, we are not singling you out. Is there anything you would like to talk about before we complete this test?”
Most importantly, once we make a diagnosis of prescription drug abuse, we need resources to which to refer them and health insurance to help cover the cost for this care.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Sometimes, you come across an article that makes you cringe. After this initial reaction – and if we are up for the challenge – we realize that this information can help us grow by pushing our clinical approach in new directions.
This is the experience I had with an article by Dr. Daniel Bouland and colleagues that explored the ways in which people struggling with addiction obtain prescription medications (J Addict Med. 2015 Jul-Aug;9[4]:281-5).
In this semiquantitative qualitative study, investigators interviewed 36 patients in a residential addiction treatment program who obtained prescriptions from clinicians in support of an addiction. Types of medications obtained by respondents were opioids (97.2%), sedative hypnotics (47.4%), and amphetamines (5.5%).
Patients reported obtaining prescriptions from clinicians because it was perceived to be “legal” – even though 75% of them faked symptoms, several falsified MRI images of an injury, and some used old or forged prescriptions. One patient paid a physician outright for the medication.
Eight percent of patients physically harmed themselves to obtain prescriptions by doing things such as cutting themselves to put blood in the urine, hitting their head against the wall to the point of unconsciousness, and undergoing unnecessary surgery.
Primary care clinicians and pain specialists were viewed as the easiest sources of medication. Most patients used “mom and pop” pharmacies, visited multiple pharmacies, and paid in cash. Importantly, 67% of patients said that an intervention could have changed their behaviors.
I think I knew this, but it challenged me to see it in writing. I appreciated the honesty of these individuals and was struck by the fact that almost two-thirds suggested that an intervention could have transformed them.
But how to start this conversation?
The last time I expressed concern about a patient’s allergy to any pain medication – except oxycodone and the potentially toxic doses of ibuprofen and acetaminophen that didn’t “touch it” – I was the recipient of seething rage and hostility.
Addiction treatment is hard, diagnosing addiction in daily primary care practice is harder, and holding up a mirror to a patient’s prescription drug habits requires protective body armor. That’s why not many of us do it.
So, now that we have guidelines for chronic opioids, we need best practices for acute visits presenting with x-rays of broken animal bones labeled with their name handwritten on duct tape.
Are we up for urine drug screens for every controlled substance prescription on nonestablished patients every time? Probably not, but we have to start somewhere.
At least it might start a conversation when we can say: “We do this for all of our patients, we are not singling you out. Is there anything you would like to talk about before we complete this test?”
Most importantly, once we make a diagnosis of prescription drug abuse, we need resources to which to refer them and health insurance to help cover the cost for this care.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.

U.S. flu activity continues to drop, but still widespread
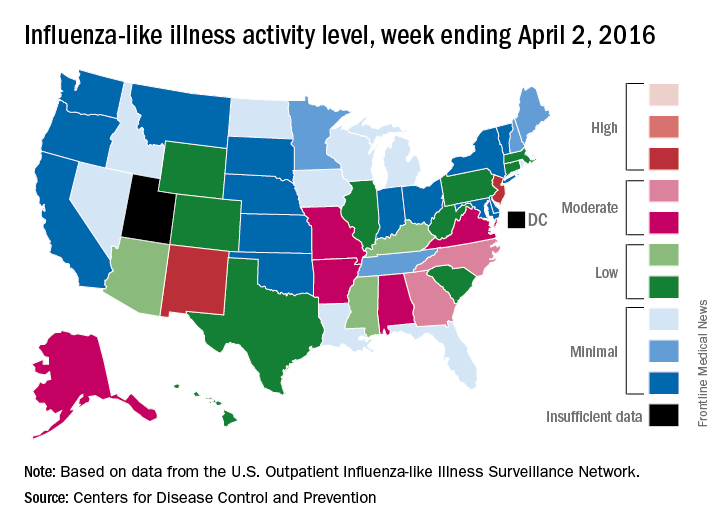
A third straight week of reduced influenza-like illness (ILI) left the U.S. with no states at the highest level of ILI activity for the first time since early February, according to the Centers for Disease Control and Prevention.
The states with the highest activity for the week ending April 2, 2016, were New Jersey and New Mexico, and both were at level 8 on the CDC’s 1-10 scale, putting them on the low end of the “high” range. States in the “moderate” range were Georgia and North Carolina at level 7 and Alabama, Alaska, Arkansas, Missouri, and Virginia at level 6, according to a report from the CDC’s Influenza-like Illness Surveillance Network (ILINet).
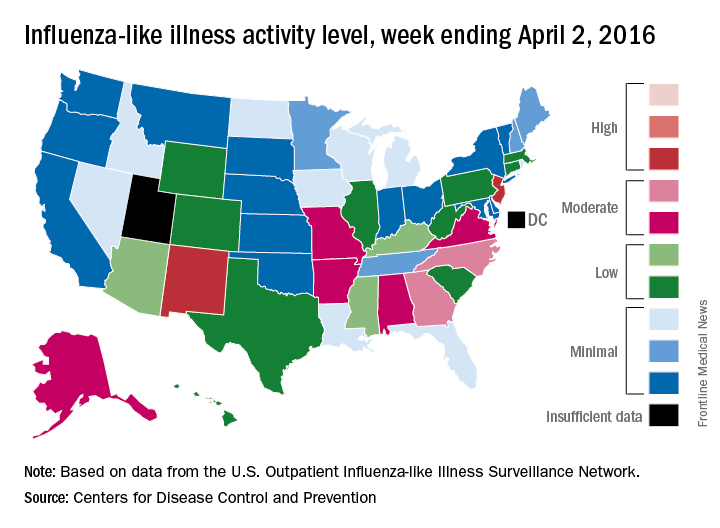
The proportion of outpatient visits for ILI was 2.4% for the week, down from 2.9% the week before but still above the national baseline of 2.1%, the CDC said. The CDC also reported a cumulative rate of 24.4 laboratory-confirmed influenza-associated hospitalizations per 100,000 population for the 2015-16 flu season.
There were seven flu-related pediatric deaths reported – all of them occurring during earlier weeks. So far, 40 flu-related pediatric deaths have been reported during the 2015-2016 season, with California having the highest number (9). The CDC said 7.4% of all deaths reported through the 122 Cities Mortality Reporting System were due to pneumonia and influenza. This percentage was above the epidemic threshold of 7.1% for week 13 of the flu season.
A third straight week of reduced influenza-like illness (ILI) left the U.S. with no states at the highest level of ILI activity for the first time since early February, according to the Centers for Disease Control and Prevention.
The states with the highest activity for the week ending April 2, 2016, were New Jersey and New Mexico, and both were at level 8 on the CDC’s 1-10 scale, putting them on the low end of the “high” range. States in the “moderate” range were Georgia and North Carolina at level 7 and Alabama, Alaska, Arkansas, Missouri, and Virginia at level 6, according to a report from the CDC’s Influenza-like Illness Surveillance Network (ILINet).
The proportion of outpatient visits for ILI was 2.4% for the week, down from 2.9% the week before but still above the national baseline of 2.1%, the CDC said. The CDC also reported a cumulative rate of 24.4 laboratory-confirmed influenza-associated hospitalizations per 100,000 population for the 2015-16 flu season.
There were seven flu-related pediatric deaths reported – all of them occurring during earlier weeks. So far, 40 flu-related pediatric deaths have been reported during the 2015-2016 season, with California having the highest number (9). The CDC said 7.4% of all deaths reported through the 122 Cities Mortality Reporting System were due to pneumonia and influenza. This percentage was above the epidemic threshold of 7.1% for week 13 of the flu season.
A third straight week of reduced influenza-like illness (ILI) left the U.S. with no states at the highest level of ILI activity for the first time since early February, according to the Centers for Disease Control and Prevention.
The states with the highest activity for the week ending April 2, 2016, were New Jersey and New Mexico, and both were at level 8 on the CDC’s 1-10 scale, putting them on the low end of the “high” range. States in the “moderate” range were Georgia and North Carolina at level 7 and Alabama, Alaska, Arkansas, Missouri, and Virginia at level 6, according to a report from the CDC’s Influenza-like Illness Surveillance Network (ILINet).
The proportion of outpatient visits for ILI was 2.4% for the week, down from 2.9% the week before but still above the national baseline of 2.1%, the CDC said. The CDC also reported a cumulative rate of 24.4 laboratory-confirmed influenza-associated hospitalizations per 100,000 population for the 2015-16 flu season.
There were seven flu-related pediatric deaths reported – all of them occurring during earlier weeks. So far, 40 flu-related pediatric deaths have been reported during the 2015-2016 season, with California having the highest number (9). The CDC said 7.4% of all deaths reported through the 122 Cities Mortality Reporting System were due to pneumonia and influenza. This percentage was above the epidemic threshold of 7.1% for week 13 of the flu season.
Tofacitinib succeeds as ulcerative colitis induction therapy
A 10-mg dose of tofacitinib twice daily significantly improved remission, mucosal healing, and clinical response in adults with active ulcerative colitis (UC), based on data from a pair of identical phase III studies including nearly 900 patients. The findings were presented at the European Crohn’s and Colitis Organisation conference in Amsterdam.
“In up to one-third of patients with UC, treatment is not completely successful or complications arise,” study coauthor Dr. Geert D’Haens of the University of Amsterdam said in an interview. The goal of the studies was to evaluate the safety and efficacy of a 10-mg dose of oral tofacitinib twice daily in inducing remission in UC patients, he added. The OCTAVE (Oral Clinical Trials for Tofacitinib in Ulcerative Colitis) Induction 1 study included 476 patients taking tofacitinib and 122 patients taking placebo; the OCTAVE Induction 2 study included 429 patients on tofacitinib and 112 patients on placebo.

Overall, significantly more patients receiving tofacitinib 10 mg twice daily achieved remission, mucosal healing, and clinical response in both studies, compared with the placebo, at 8 weeks. In the OCTAVE Induction 1 and Induction 2 studies, remission at 8 weeks for tofacitinib compared with placebo was 19% vs. 8% and 17% vs. 4%, respectively. Mucosal healing rates in the Induction 1 and 2 studies for tofacitinib compared with placebo were 31% vs. 16% and 28% vs. 12%, respectively, and clinical response rates were 60% vs. 33% and 55% vs. 29%, respectively. Efficacy was similar for patients previously treated with tumor necrosis factor inhibitors and those who were not.
The incidence of adverse events and serious adverse events was not significantly different between treatment and placebo groups in either study. However, tofacitinib treatment was associated with increases in serum lipid (total cholesterol, low-density and high-density lipoprotein), and creatine kinase levels.
“The clinical trial data confirm our blinded observations,” Dr. D’Haens said. “Even when all other drugs have failed, tofacitinib can be effective. Since Janus kinase inhibitors reduce the production of many proinflammatory cytokines, the clinical findings are in line with what we expected. Fortunately, adverse events were limited and allowed prolonged treatment with this agent,” he noted.
Research on tofacitinib and UC is ongoing, said Dr. D’Haens. The two studies reported here, OCTAVE Induction 1 and 2, are part of the global OCTAVE program, he said. Other related studies include a third phase III study, OCTAVE Sustain, and a long-term extension trial called OCTAVE Open. “OCTAVE Sustain is a phase III placebo-controlled study evaluating oral tofacitinib 10 mg and 5 mg b.i.d. as maintenance therapy in adult patients with moderately to severely active UC. Top-line results for this study are anticipated at the end of this year,” he said. “OCTAVE Open is an ongoing open-label extension study designed to assess the safety and tolerability of tofacitinib 10 mg and 5 mg b.i.d. in patients who have completed or who have had treatment failure in OCTAVE Sustain or who were nonresponders upon completing OCTAVE Induction 1 or 2,” he added.
The study was supported in part by Pfizer. Dr. D’Haens disclosed financial relationships with multiple companies, including Pfizer.
A 10-mg dose of tofacitinib twice daily significantly improved remission, mucosal healing, and clinical response in adults with active ulcerative colitis (UC), based on data from a pair of identical phase III studies including nearly 900 patients. The findings were presented at the European Crohn’s and Colitis Organisation conference in Amsterdam.
“In up to one-third of patients with UC, treatment is not completely successful or complications arise,” study coauthor Dr. Geert D’Haens of the University of Amsterdam said in an interview. The goal of the studies was to evaluate the safety and efficacy of a 10-mg dose of oral tofacitinib twice daily in inducing remission in UC patients, he added. The OCTAVE (Oral Clinical Trials for Tofacitinib in Ulcerative Colitis) Induction 1 study included 476 patients taking tofacitinib and 122 patients taking placebo; the OCTAVE Induction 2 study included 429 patients on tofacitinib and 112 patients on placebo.
Overall, significantly more patients receiving tofacitinib 10 mg twice daily achieved remission, mucosal healing, and clinical response in both studies, compared with the placebo, at 8 weeks. In the OCTAVE Induction 1 and Induction 2 studies, remission at 8 weeks for tofacitinib compared with placebo was 19% vs. 8% and 17% vs. 4%, respectively. Mucosal healing rates in the Induction 1 and 2 studies for tofacitinib compared with placebo were 31% vs. 16% and 28% vs. 12%, respectively, and clinical response rates were 60% vs. 33% and 55% vs. 29%, respectively. Efficacy was similar for patients previously treated with tumor necrosis factor inhibitors and those who were not.
The incidence of adverse events and serious adverse events was not significantly different between treatment and placebo groups in either study. However, tofacitinib treatment was associated with increases in serum lipid (total cholesterol, low-density and high-density lipoprotein), and creatine kinase levels.
“The clinical trial data confirm our blinded observations,” Dr. D’Haens said. “Even when all other drugs have failed, tofacitinib can be effective. Since Janus kinase inhibitors reduce the production of many proinflammatory cytokines, the clinical findings are in line with what we expected. Fortunately, adverse events were limited and allowed prolonged treatment with this agent,” he noted.
Research on tofacitinib and UC is ongoing, said Dr. D’Haens. The two studies reported here, OCTAVE Induction 1 and 2, are part of the global OCTAVE program, he said. Other related studies include a third phase III study, OCTAVE Sustain, and a long-term extension trial called OCTAVE Open. “OCTAVE Sustain is a phase III placebo-controlled study evaluating oral tofacitinib 10 mg and 5 mg b.i.d. as maintenance therapy in adult patients with moderately to severely active UC. Top-line results for this study are anticipated at the end of this year,” he said. “OCTAVE Open is an ongoing open-label extension study designed to assess the safety and tolerability of tofacitinib 10 mg and 5 mg b.i.d. in patients who have completed or who have had treatment failure in OCTAVE Sustain or who were nonresponders upon completing OCTAVE Induction 1 or 2,” he added.
The study was supported in part by Pfizer. Dr. D’Haens disclosed financial relationships with multiple companies, including Pfizer.
A 10-mg dose of tofacitinib twice daily significantly improved remission, mucosal healing, and clinical response in adults with active ulcerative colitis (UC), based on data from a pair of identical phase III studies including nearly 900 patients. The findings were presented at the European Crohn’s and Colitis Organisation conference in Amsterdam.
“In up to one-third of patients with UC, treatment is not completely successful or complications arise,” study coauthor Dr. Geert D’Haens of the University of Amsterdam said in an interview. The goal of the studies was to evaluate the safety and efficacy of a 10-mg dose of oral tofacitinib twice daily in inducing remission in UC patients, he added. The OCTAVE (Oral Clinical Trials for Tofacitinib in Ulcerative Colitis) Induction 1 study included 476 patients taking tofacitinib and 122 patients taking placebo; the OCTAVE Induction 2 study included 429 patients on tofacitinib and 112 patients on placebo.
Overall, significantly more patients receiving tofacitinib 10 mg twice daily achieved remission, mucosal healing, and clinical response in both studies, compared with the placebo, at 8 weeks. In the OCTAVE Induction 1 and Induction 2 studies, remission at 8 weeks for tofacitinib compared with placebo was 19% vs. 8% and 17% vs. 4%, respectively. Mucosal healing rates in the Induction 1 and 2 studies for tofacitinib compared with placebo were 31% vs. 16% and 28% vs. 12%, respectively, and clinical response rates were 60% vs. 33% and 55% vs. 29%, respectively. Efficacy was similar for patients previously treated with tumor necrosis factor inhibitors and those who were not.
The incidence of adverse events and serious adverse events was not significantly different between treatment and placebo groups in either study. However, tofacitinib treatment was associated with increases in serum lipid (total cholesterol, low-density and high-density lipoprotein), and creatine kinase levels.
“The clinical trial data confirm our blinded observations,” Dr. D’Haens said. “Even when all other drugs have failed, tofacitinib can be effective. Since Janus kinase inhibitors reduce the production of many proinflammatory cytokines, the clinical findings are in line with what we expected. Fortunately, adverse events were limited and allowed prolonged treatment with this agent,” he noted.
Research on tofacitinib and UC is ongoing, said Dr. D’Haens. The two studies reported here, OCTAVE Induction 1 and 2, are part of the global OCTAVE program, he said. Other related studies include a third phase III study, OCTAVE Sustain, and a long-term extension trial called OCTAVE Open. “OCTAVE Sustain is a phase III placebo-controlled study evaluating oral tofacitinib 10 mg and 5 mg b.i.d. as maintenance therapy in adult patients with moderately to severely active UC. Top-line results for this study are anticipated at the end of this year,” he said. “OCTAVE Open is an ongoing open-label extension study designed to assess the safety and tolerability of tofacitinib 10 mg and 5 mg b.i.d. in patients who have completed or who have had treatment failure in OCTAVE Sustain or who were nonresponders upon completing OCTAVE Induction 1 or 2,” he added.
The study was supported in part by Pfizer. Dr. D’Haens disclosed financial relationships with multiple companies, including Pfizer.
EXPERT ANALYSIS FROM ECCO
Key clinical point: Oral tofacitinib reduced the symptoms of moderate to severe ulcerative colitis and induced remission and healing of the diseased colonic mucosa in patients previously treated with tumor necrosis factor inhibitors and those who were not.
Major finding: In the OCTAVE Induction 1 and Induction 2 studies, remission at 8 weeks for tofacitinib patients compared with placebo patients was 19% vs. 8% and 17% vs. 4%, respectively.
Data source: A pair of identical phase III studies including nearly 900 patients.
Disclosures: The study was supported in part by Pfizer. Dr. Geert D’Haens disclosed financial relationships with multiple companies, including Pfizer.

Sustained-release steroid provides prolonged OA pain relief
AMSTERDAM – A single intra-articular injection of a novel corticosteroid formulation provided substantial and persistent pain relief for at least 12 weeks in patients with knee osteoarthritis in a phase III trial that was presented at the World Congress on Osteoarthritis.
FX006 (Zilretta), given at a dose of 40 mg, significantly (P less than .05) reduced the mean daily pain intensity score from around 2 weeks onwards in the region of 3.0 to 3.5 points on a 0-10 scale compared with a reduction of around 1.5 to 2.0 points for placebo. There were also significant reductions in additional efficacy outcomes such as Western Ontario and McMaster Universities Index (WOMAC) pain and function versus placebo and a standard formulation of triamcinolone acetate (TCA).

Data from a phase IIb trial had originally been scheduled to be presented at the meeting – which is sponsored by the Osteoarthritis Research Society International – but the phase III findings had just become available, said Dr. Philip Conaghan of the University of Leeds (England). The phase II findings showed that there was a substantial and persistent pain relieving effect of FX006 versus placebo and that there was evidence of a dose response.
These data provide “proof of concept that we can develop long-acting steroids that have real potential for changing how we might manage knee OA,” said Dr. Conaghan, professor of musculoskeletal medicine and deputy director of the Leeds Musculoskeletal Biomedical Research Unit.
Intra-articular steroids have long been used to treat OA and they can be effective, albeit for a short period of time. FX006 is an investigational formulation of TCA in polylactic-co-glycolic acid microspheres that has been designed to try to extend the analgesic effects of the steroid and to reduce overall systemic exposure and thus side effects. Each microsphere is around 45 microns in diameter.
The aim of the phase IIb study was to examine the efficacy of two doses of FX006 (20 mg and 40 mg) versus placebo in patients with moderate to severe OA knee pain. The double-blind, randomized trial involved 310 patients who were followed for 24 weeks. The primary outcome was the change from baseline to week 12 in the weekly mean of the average daily pain intensity scores, compared with placebo.
There was evidence of a dose response, with the 40-mg dose of FX006 producing statistically significantly greater changes in pain scores versus placebo. Although the primary endpoint of a statistical difference at 12 weeks was not met, there were significant differences at all other time points from week 1 to 13. WOMAC pain and function scores were also significantly reduced with the 40-mg dose versus placebo.
The phase III trial involved 484 patients who were randomized to intra-articular injections of FX006 40 mg, standard TCA 40 mg, or placebo. As in the phase IIb trial patients were well matched at baseline, with a mean overall age of 62 years, a body mass index of 30 kg/m2 and around two-thirds having OA in both knees.
Dr. Conaghan reported that there were “no unexpected safety signals” during the trials. A combined safety summary showed that treatment-emergent adverse events occurred in 42.2% and 50.9% of patients treated with FX006 20 mg and 40 mg, respectively, in 49.2% of placebo-treated patients, and in 56.5% of TCA-treated patients. Serious adverse event rates were 1%, 3%, 1.1%, and 2.5%, respectively, and were assessed as being unrelated to treatment. Adverse events related to the knee occurred in 14.7%, 16.6%, 14.1%, and 9.9%, and injection-related adverse events in 2%, 1.9%, 4.2%, and 1.9%, respectively.
The studies were funded by Flexion Therapeutics. Dr. Conaghan did not report his financial disclosures.
AMSTERDAM – A single intra-articular injection of a novel corticosteroid formulation provided substantial and persistent pain relief for at least 12 weeks in patients with knee osteoarthritis in a phase III trial that was presented at the World Congress on Osteoarthritis.
FX006 (Zilretta), given at a dose of 40 mg, significantly (P less than .05) reduced the mean daily pain intensity score from around 2 weeks onwards in the region of 3.0 to 3.5 points on a 0-10 scale compared with a reduction of around 1.5 to 2.0 points for placebo. There were also significant reductions in additional efficacy outcomes such as Western Ontario and McMaster Universities Index (WOMAC) pain and function versus placebo and a standard formulation of triamcinolone acetate (TCA).
Data from a phase IIb trial had originally been scheduled to be presented at the meeting – which is sponsored by the Osteoarthritis Research Society International – but the phase III findings had just become available, said Dr. Philip Conaghan of the University of Leeds (England). The phase II findings showed that there was a substantial and persistent pain relieving effect of FX006 versus placebo and that there was evidence of a dose response.
These data provide “proof of concept that we can develop long-acting steroids that have real potential for changing how we might manage knee OA,” said Dr. Conaghan, professor of musculoskeletal medicine and deputy director of the Leeds Musculoskeletal Biomedical Research Unit.
Intra-articular steroids have long been used to treat OA and they can be effective, albeit for a short period of time. FX006 is an investigational formulation of TCA in polylactic-co-glycolic acid microspheres that has been designed to try to extend the analgesic effects of the steroid and to reduce overall systemic exposure and thus side effects. Each microsphere is around 45 microns in diameter.
The aim of the phase IIb study was to examine the efficacy of two doses of FX006 (20 mg and 40 mg) versus placebo in patients with moderate to severe OA knee pain. The double-blind, randomized trial involved 310 patients who were followed for 24 weeks. The primary outcome was the change from baseline to week 12 in the weekly mean of the average daily pain intensity scores, compared with placebo.
There was evidence of a dose response, with the 40-mg dose of FX006 producing statistically significantly greater changes in pain scores versus placebo. Although the primary endpoint of a statistical difference at 12 weeks was not met, there were significant differences at all other time points from week 1 to 13. WOMAC pain and function scores were also significantly reduced with the 40-mg dose versus placebo.
The phase III trial involved 484 patients who were randomized to intra-articular injections of FX006 40 mg, standard TCA 40 mg, or placebo. As in the phase IIb trial patients were well matched at baseline, with a mean overall age of 62 years, a body mass index of 30 kg/m2 and around two-thirds having OA in both knees.
Dr. Conaghan reported that there were “no unexpected safety signals” during the trials. A combined safety summary showed that treatment-emergent adverse events occurred in 42.2% and 50.9% of patients treated with FX006 20 mg and 40 mg, respectively, in 49.2% of placebo-treated patients, and in 56.5% of TCA-treated patients. Serious adverse event rates were 1%, 3%, 1.1%, and 2.5%, respectively, and were assessed as being unrelated to treatment. Adverse events related to the knee occurred in 14.7%, 16.6%, 14.1%, and 9.9%, and injection-related adverse events in 2%, 1.9%, 4.2%, and 1.9%, respectively.
The studies were funded by Flexion Therapeutics. Dr. Conaghan did not report his financial disclosures.
AMSTERDAM – A single intra-articular injection of a novel corticosteroid formulation provided substantial and persistent pain relief for at least 12 weeks in patients with knee osteoarthritis in a phase III trial that was presented at the World Congress on Osteoarthritis.
FX006 (Zilretta), given at a dose of 40 mg, significantly (P less than .05) reduced the mean daily pain intensity score from around 2 weeks onwards in the region of 3.0 to 3.5 points on a 0-10 scale compared with a reduction of around 1.5 to 2.0 points for placebo. There were also significant reductions in additional efficacy outcomes such as Western Ontario and McMaster Universities Index (WOMAC) pain and function versus placebo and a standard formulation of triamcinolone acetate (TCA).
Data from a phase IIb trial had originally been scheduled to be presented at the meeting – which is sponsored by the Osteoarthritis Research Society International – but the phase III findings had just become available, said Dr. Philip Conaghan of the University of Leeds (England). The phase II findings showed that there was a substantial and persistent pain relieving effect of FX006 versus placebo and that there was evidence of a dose response.
These data provide “proof of concept that we can develop long-acting steroids that have real potential for changing how we might manage knee OA,” said Dr. Conaghan, professor of musculoskeletal medicine and deputy director of the Leeds Musculoskeletal Biomedical Research Unit.
Intra-articular steroids have long been used to treat OA and they can be effective, albeit for a short period of time. FX006 is an investigational formulation of TCA in polylactic-co-glycolic acid microspheres that has been designed to try to extend the analgesic effects of the steroid and to reduce overall systemic exposure and thus side effects. Each microsphere is around 45 microns in diameter.
The aim of the phase IIb study was to examine the efficacy of two doses of FX006 (20 mg and 40 mg) versus placebo in patients with moderate to severe OA knee pain. The double-blind, randomized trial involved 310 patients who were followed for 24 weeks. The primary outcome was the change from baseline to week 12 in the weekly mean of the average daily pain intensity scores, compared with placebo.
There was evidence of a dose response, with the 40-mg dose of FX006 producing statistically significantly greater changes in pain scores versus placebo. Although the primary endpoint of a statistical difference at 12 weeks was not met, there were significant differences at all other time points from week 1 to 13. WOMAC pain and function scores were also significantly reduced with the 40-mg dose versus placebo.
The phase III trial involved 484 patients who were randomized to intra-articular injections of FX006 40 mg, standard TCA 40 mg, or placebo. As in the phase IIb trial patients were well matched at baseline, with a mean overall age of 62 years, a body mass index of 30 kg/m2 and around two-thirds having OA in both knees.
Dr. Conaghan reported that there were “no unexpected safety signals” during the trials. A combined safety summary showed that treatment-emergent adverse events occurred in 42.2% and 50.9% of patients treated with FX006 20 mg and 40 mg, respectively, in 49.2% of placebo-treated patients, and in 56.5% of TCA-treated patients. Serious adverse event rates were 1%, 3%, 1.1%, and 2.5%, respectively, and were assessed as being unrelated to treatment. Adverse events related to the knee occurred in 14.7%, 16.6%, 14.1%, and 9.9%, and injection-related adverse events in 2%, 1.9%, 4.2%, and 1.9%, respectively.
The studies were funded by Flexion Therapeutics. Dr. Conaghan did not report his financial disclosures.
AT OARSI 2016
Key clinical point: A single intra-articular injection of FX006 provided pain relief for up to 12 weeks.
Major finding: The mean daily pain intensity score was significantly reduced by 3.0 to 3.5 points with FX006 versus 1.5 to 2.0 points for placebo.
Data source: A phase IIb (n = 310) and a phase III (n = 454) study conducted in patients with moderate to severe knee OA.
Disclosures: The studies were funded by Flexion Therapeutics. Dr. Conaghan did not report his financial disclosures.

Three things hospitalists ‘do for no reason’... and should stop
SAN DIEGO – Head CTs for patients with in-hospital delirium. Ammonia tests to check for hepatic encephalopathy in chronic liver disease. Renal ultrasounds for acute kidney injury.
Those are three low value tests highlighted in hospitalist Dr. Leonard Feldman’s latest iteration of his lecture series “Things We Do for No Reason.”

Dr. Feldman, associate professor of internal medicine and pediatrics at Johns Hopkins University, Baltimore, has presented his list of usually unnecessary hospitalist practices for five years at the Society of Hospital Medicine’s annual meetings. With three new ones explained during the 2016 meeting, there are now 19 on the list and more to come, he said.
“So far, I’ve picked things that are relatively low-hanging fruit, things for which there’s good evidence we shouldn’t be doing and if you saw the evidence, you’d say ‘that’s right, we shouldn’t,’” he said.
Dr. Feldman’s intent is to help clinicians stop certain “learned behaviors,” tests and procedures which research and experience now show “are not helping people, sometimes harm people, and often result in a cascade” of further unnecessary tests and care.
The conference presentations have been so popular, the Journal of Hospital Medicine in October 2015 started a “Things We Do for No Reason” series.
Here are the three most recent tests hospitalists should avoid:
Ammonia levels for chronic liver disease
Dr. Feldman said doctors were taught in medical school that ammonia levels rise in patients with cirrhosis and when they rise too high, the patient may develop hepatic encephalopathy. They also learned that if levels are normal, the patient should not have hepatic encephalopathy.
But a number of studies have found “neither of those is true,” he said. What’s possibly worse is that “you close your mind to other possible diagnoses way too early.” Nevertheless, the practice at many hospitals is to perform multiple tests to trend those levels.”
“I had a patient who had an ammonia test sent the other day while in the emergency room, and it was elevated,” Dr. Feldman recalled in a recent phone interview. “The patient got admitted, but when we re-tested, it wasn’t.”
Part of the problem is that blood samples are often incorrectly processed. “When you draw the blood, you have to put it on ice and it needs to get to the lab very quickly. And I think we do neither of those things on a regular basis,” he said. Also, if the patient has a tourniquet or is clenching a fist, use of muscle creates ammonia.
Dr. Feldman said that at a hospital like Johns Hopkins in Baltimore, where there are high rates of hepatitis C, there might be 50 patients with chronic liver disease, or 20% of patients on medicine service. It’s not the cost of the blood test that he’s worried about because that’s probably minimal. Rather, it’s the test’s downstream provocation of more unnecessary care “and missed opportunities to intervene with a treatable diagnosis.”
In general, he said, “for patients with chronic liver disease, we shouldn’t be checking ammonia.”
Head CTs for inpatients with new onset delirium
Performing a costly head CT scan on a patient who presents in the emergency department with delirium is appropriate. But for low-risk patients who develop delirium inside the hospital without a clear reason, such as a fall or focal neurologic symptoms suggesting a stroke, a head CT is probably not necessary, Dr. Feldman said.
“But we have this knee-jerk reaction, this reflex, that when a patient becomes delirious, we probably should run a head CT on them,” he added.
Dr. Feldman acknowledged that the frequency of head CTs on inpatients with delirium has been hard to tease out.
“But all the studies indicate that patients who develop delirium while in the hospital, without any sort of risk factor, are very unlikely to have pathology found on a head CT,” he said, noting that the cause of their delirium is likely something else, like dehydration, an infection, disruption of sleep, urinary retention, or medication effect.
Of course, if patients aren’t getting better without the CT, order the CT, he said. “Even if the patient has no risk factor, there’s still a 3% chance of having an abnormality like a tumor or stroke.”
Renal ultrasound for patients with new acute kidney injury
To determine if an acute kidney injury is caused by a treatable obstruction, such as a large prostate causing urinary retention, doctors often first order a renal ultrasound, a test that can cost $300, and must be read by a radiologist.
But a much less expensive simple bladder scan, which can be performed by a nurse, is a much better substitute for the first pass, Dr. Feldman said. He said it’s logical that “a bladder scan is a much higher value test” in the early diagnostic process.
“The studies have been pretty clear. If you don’t have risk factors for having an obstruction, a history of kidney stones, it hasn’t happened before, or other reasons kidneys aren’t working, it’s extraordinarily unlikely you’re going to find anything on that renal ultrasound that could be intervened to fix that acute kidney injury,” Dr. Feldman said. He pointed to a study that found 223 renal ultrasounds were necessary to find one patient who needed an intervention.
“You can probably get a good sense from the history and physical” and start to treat them, he said, and if they’re not getting better, then order the ultrasound.
Each of the items on Feldman’s list don’t necessarily save a lot of money, but they add up. “The more we ask ‘Why are we doing this? Can we stop it if it’s not helping people, and particularly if it’s harming people?’ the more we can prevent the cascade that happens because you did one unnecessary diagnostic test,” he concluded.
SAN DIEGO – Head CTs for patients with in-hospital delirium. Ammonia tests to check for hepatic encephalopathy in chronic liver disease. Renal ultrasounds for acute kidney injury.
Those are three low value tests highlighted in hospitalist Dr. Leonard Feldman’s latest iteration of his lecture series “Things We Do for No Reason.”
Dr. Feldman, associate professor of internal medicine and pediatrics at Johns Hopkins University, Baltimore, has presented his list of usually unnecessary hospitalist practices for five years at the Society of Hospital Medicine’s annual meetings. With three new ones explained during the 2016 meeting, there are now 19 on the list and more to come, he said.
“So far, I’ve picked things that are relatively low-hanging fruit, things for which there’s good evidence we shouldn’t be doing and if you saw the evidence, you’d say ‘that’s right, we shouldn’t,’” he said.
Dr. Feldman’s intent is to help clinicians stop certain “learned behaviors,” tests and procedures which research and experience now show “are not helping people, sometimes harm people, and often result in a cascade” of further unnecessary tests and care.
The conference presentations have been so popular, the Journal of Hospital Medicine in October 2015 started a “Things We Do for No Reason” series.
Here are the three most recent tests hospitalists should avoid:
Ammonia levels for chronic liver disease
Dr. Feldman said doctors were taught in medical school that ammonia levels rise in patients with cirrhosis and when they rise too high, the patient may develop hepatic encephalopathy. They also learned that if levels are normal, the patient should not have hepatic encephalopathy.
But a number of studies have found “neither of those is true,” he said. What’s possibly worse is that “you close your mind to other possible diagnoses way too early.” Nevertheless, the practice at many hospitals is to perform multiple tests to trend those levels.”
“I had a patient who had an ammonia test sent the other day while in the emergency room, and it was elevated,” Dr. Feldman recalled in a recent phone interview. “The patient got admitted, but when we re-tested, it wasn’t.”
Part of the problem is that blood samples are often incorrectly processed. “When you draw the blood, you have to put it on ice and it needs to get to the lab very quickly. And I think we do neither of those things on a regular basis,” he said. Also, if the patient has a tourniquet or is clenching a fist, use of muscle creates ammonia.
Dr. Feldman said that at a hospital like Johns Hopkins in Baltimore, where there are high rates of hepatitis C, there might be 50 patients with chronic liver disease, or 20% of patients on medicine service. It’s not the cost of the blood test that he’s worried about because that’s probably minimal. Rather, it’s the test’s downstream provocation of more unnecessary care “and missed opportunities to intervene with a treatable diagnosis.”
In general, he said, “for patients with chronic liver disease, we shouldn’t be checking ammonia.”
Head CTs for inpatients with new onset delirium
Performing a costly head CT scan on a patient who presents in the emergency department with delirium is appropriate. But for low-risk patients who develop delirium inside the hospital without a clear reason, such as a fall or focal neurologic symptoms suggesting a stroke, a head CT is probably not necessary, Dr. Feldman said.
“But we have this knee-jerk reaction, this reflex, that when a patient becomes delirious, we probably should run a head CT on them,” he added.
Dr. Feldman acknowledged that the frequency of head CTs on inpatients with delirium has been hard to tease out.
“But all the studies indicate that patients who develop delirium while in the hospital, without any sort of risk factor, are very unlikely to have pathology found on a head CT,” he said, noting that the cause of their delirium is likely something else, like dehydration, an infection, disruption of sleep, urinary retention, or medication effect.
Of course, if patients aren’t getting better without the CT, order the CT, he said. “Even if the patient has no risk factor, there’s still a 3% chance of having an abnormality like a tumor or stroke.”
Renal ultrasound for patients with new acute kidney injury
To determine if an acute kidney injury is caused by a treatable obstruction, such as a large prostate causing urinary retention, doctors often first order a renal ultrasound, a test that can cost $300, and must be read by a radiologist.
But a much less expensive simple bladder scan, which can be performed by a nurse, is a much better substitute for the first pass, Dr. Feldman said. He said it’s logical that “a bladder scan is a much higher value test” in the early diagnostic process.
“The studies have been pretty clear. If you don’t have risk factors for having an obstruction, a history of kidney stones, it hasn’t happened before, or other reasons kidneys aren’t working, it’s extraordinarily unlikely you’re going to find anything on that renal ultrasound that could be intervened to fix that acute kidney injury,” Dr. Feldman said. He pointed to a study that found 223 renal ultrasounds were necessary to find one patient who needed an intervention.
“You can probably get a good sense from the history and physical” and start to treat them, he said, and if they’re not getting better, then order the ultrasound.
Each of the items on Feldman’s list don’t necessarily save a lot of money, but they add up. “The more we ask ‘Why are we doing this? Can we stop it if it’s not helping people, and particularly if it’s harming people?’ the more we can prevent the cascade that happens because you did one unnecessary diagnostic test,” he concluded.
SAN DIEGO – Head CTs for patients with in-hospital delirium. Ammonia tests to check for hepatic encephalopathy in chronic liver disease. Renal ultrasounds for acute kidney injury.
Those are three low value tests highlighted in hospitalist Dr. Leonard Feldman’s latest iteration of his lecture series “Things We Do for No Reason.”
Dr. Feldman, associate professor of internal medicine and pediatrics at Johns Hopkins University, Baltimore, has presented his list of usually unnecessary hospitalist practices for five years at the Society of Hospital Medicine’s annual meetings. With three new ones explained during the 2016 meeting, there are now 19 on the list and more to come, he said.
“So far, I’ve picked things that are relatively low-hanging fruit, things for which there’s good evidence we shouldn’t be doing and if you saw the evidence, you’d say ‘that’s right, we shouldn’t,’” he said.
Dr. Feldman’s intent is to help clinicians stop certain “learned behaviors,” tests and procedures which research and experience now show “are not helping people, sometimes harm people, and often result in a cascade” of further unnecessary tests and care.
The conference presentations have been so popular, the Journal of Hospital Medicine in October 2015 started a “Things We Do for No Reason” series.
Here are the three most recent tests hospitalists should avoid:
Ammonia levels for chronic liver disease
Dr. Feldman said doctors were taught in medical school that ammonia levels rise in patients with cirrhosis and when they rise too high, the patient may develop hepatic encephalopathy. They also learned that if levels are normal, the patient should not have hepatic encephalopathy.
But a number of studies have found “neither of those is true,” he said. What’s possibly worse is that “you close your mind to other possible diagnoses way too early.” Nevertheless, the practice at many hospitals is to perform multiple tests to trend those levels.”
“I had a patient who had an ammonia test sent the other day while in the emergency room, and it was elevated,” Dr. Feldman recalled in a recent phone interview. “The patient got admitted, but when we re-tested, it wasn’t.”
Part of the problem is that blood samples are often incorrectly processed. “When you draw the blood, you have to put it on ice and it needs to get to the lab very quickly. And I think we do neither of those things on a regular basis,” he said. Also, if the patient has a tourniquet or is clenching a fist, use of muscle creates ammonia.
Dr. Feldman said that at a hospital like Johns Hopkins in Baltimore, where there are high rates of hepatitis C, there might be 50 patients with chronic liver disease, or 20% of patients on medicine service. It’s not the cost of the blood test that he’s worried about because that’s probably minimal. Rather, it’s the test’s downstream provocation of more unnecessary care “and missed opportunities to intervene with a treatable diagnosis.”
In general, he said, “for patients with chronic liver disease, we shouldn’t be checking ammonia.”
Head CTs for inpatients with new onset delirium
Performing a costly head CT scan on a patient who presents in the emergency department with delirium is appropriate. But for low-risk patients who develop delirium inside the hospital without a clear reason, such as a fall or focal neurologic symptoms suggesting a stroke, a head CT is probably not necessary, Dr. Feldman said.
“But we have this knee-jerk reaction, this reflex, that when a patient becomes delirious, we probably should run a head CT on them,” he added.
Dr. Feldman acknowledged that the frequency of head CTs on inpatients with delirium has been hard to tease out.
“But all the studies indicate that patients who develop delirium while in the hospital, without any sort of risk factor, are very unlikely to have pathology found on a head CT,” he said, noting that the cause of their delirium is likely something else, like dehydration, an infection, disruption of sleep, urinary retention, or medication effect.
Of course, if patients aren’t getting better without the CT, order the CT, he said. “Even if the patient has no risk factor, there’s still a 3% chance of having an abnormality like a tumor or stroke.”
Renal ultrasound for patients with new acute kidney injury
To determine if an acute kidney injury is caused by a treatable obstruction, such as a large prostate causing urinary retention, doctors often first order a renal ultrasound, a test that can cost $300, and must be read by a radiologist.
But a much less expensive simple bladder scan, which can be performed by a nurse, is a much better substitute for the first pass, Dr. Feldman said. He said it’s logical that “a bladder scan is a much higher value test” in the early diagnostic process.
“The studies have been pretty clear. If you don’t have risk factors for having an obstruction, a history of kidney stones, it hasn’t happened before, or other reasons kidneys aren’t working, it’s extraordinarily unlikely you’re going to find anything on that renal ultrasound that could be intervened to fix that acute kidney injury,” Dr. Feldman said. He pointed to a study that found 223 renal ultrasounds were necessary to find one patient who needed an intervention.
“You can probably get a good sense from the history and physical” and start to treat them, he said, and if they’re not getting better, then order the ultrasound.
Each of the items on Feldman’s list don’t necessarily save a lot of money, but they add up. “The more we ask ‘Why are we doing this? Can we stop it if it’s not helping people, and particularly if it’s harming people?’ the more we can prevent the cascade that happens because you did one unnecessary diagnostic test,” he concluded.
FROM HOSPITAL MEDICINE 2016
