User login
Clearing up confusion
“Mr. Smith seems somewhat confused today” is one of the most serious and concerning pre-visit reports you can receive from your staff or the patient’s family. Such a descriptor can be confusing—pardon the pun—not only for the patient, but to even seasoned mental health providers.
The term confusion can be code for diagnoses ranging from deliriuma to a progressive neurocognitive disorder (NCD) such as major NCD due to Alzheimer’s disease (AD), or even a more challenging problem such as beclouded dementia (delirium superimposed on dementia/NCD). It is essential for all mental health professionals to have an evidence-based approach when encountering signs or symptoms of confusion.
aICD-10 code R41.0 encompasses Confusion, Other Specified Delirium, or Unspecified Delirium.
CASE REPORT
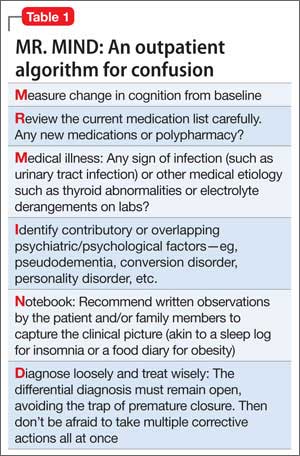
Ms. T, age 62, has hypothyroidism and bipolar I disorder, most recently depressed, with comorbid generalized anxiety disorder. She has been taking lithium, 600 mg/d, to control her mood symptoms. Her daughter-in-law reports that Ms. T has been exhibiting increasing signs of confusion. During the office evaluation, Ms. T minimizes her symptoms, only describing mild issues with forgetfulness while cooking and concern over increasing anxiety. Her daughter-in-law plays a voicemail message from earlier in the week, in which Ms. T’s speech is halting, disorganized, and in a word, confused. I decide to use the mnemonic decision chart MR. MIND (Table 1) to get to the bottom of her recent confusion.
Measure cognition
It is nice to receive advanced warning about a cognitive change or a change in activities of daily living; however, many patients present with subtle, sub-acute changes that are more difficult to assess. When encountering a broad symptom such as “confusion”—which has an equally broad differential diagnosis—systematic assessment of the current cognitive state compared with the patient’s baseline becomes the first order of business. However, this requires that the patient has had a baseline cognitive assessment.
In my practice, I often administer one of the validated neurocognitive screening instruments when a patient first begins care—even a brief test such as the Mini- Cog (3-item recall plus clock drawing test), which is comparable to longer screening tests at least for NCD/dementia.1 During a presentation for confusion, a more detailed neurocognitive assessment instrument would be recommended, allowing one to marry the clinical impression with a validated, objective measure. Formal neuropsychological testing by a clinical neuropsychologist is the gold standard, but such testing is time-consuming and expensive and often not readily available. The screening instrument I use for a more thorough evaluation depends on the clinical scenario.
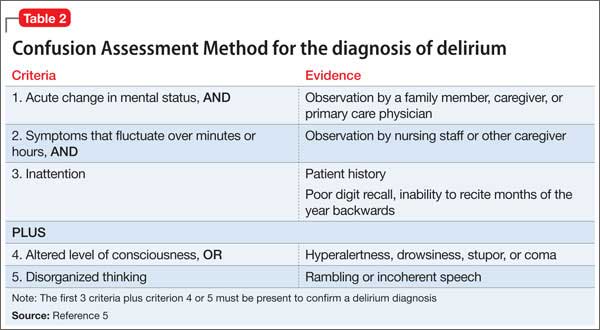
The Six-Item Screener is used in some emergency settings because it is short but boasts a higher sensitivity than the Mini- Cog (94% vs 75%) with similar specificity when screening for cognitive impairment.2 The Mini-Mental State Examination (MMSE) is a valuable instrument, although, recently, the Saint Louis University Mental Status Examination has been thought to be better at detecting mild NCD than the MMSE; more data are needed to substantiate this claim.3 The Montreal Cognitive Assessment is another validated screening tool that has been shown to be superior to the MMSE in terms of screening for mild cognitive impairment.4 The best delirium-specific assessment tool is the Confusion Assessment Method (Table 2).5
Ms. T’s MMSE score was 26/30, down from 29/30 at baseline. Her score fell below the cutoff score of 27 for mild cognitive impairment for someone with at least 8 years of completed education. Her results were abnormal mainly in the memory domain (3-item recall), raising the question of a possible prodromal state of AD although the acute nature of the change made delirium or mild NCD high in the differential.
Review medications
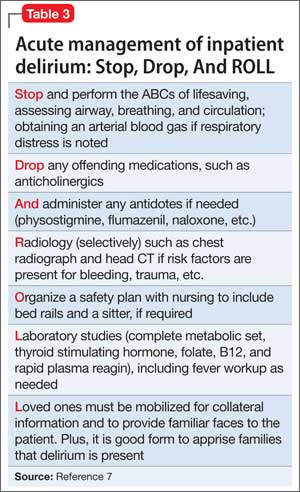
A review of the medication list is not just a Joint Commission mandate (medication reconciliation during each encounter) but is important whenever confusion is noted. Polypharmacy can be a concern, but is not as concerning as the class of medication prescribed, particularly anticholinergic and sedative medications in patients age >65. The Drug Burden Index can be helpful in assessing this risk.6 Medications such as the benzodiazepine-receptor agonists, tricyclic antidepressants, and antipsychotics should be discontinued if possible, keeping in mind that the addition or subtraction of medications must be done prudently and only after reviewing the evidence and in consultation with the patient. A detailed medication review is as important for confused outpatients as it is for an inpatient case (steps 2 and 3 of the inpatient algorithm outlined in Table 3).7
In Ms. T’s case, the primary concern on her medication list was that her medical team was prescribing levothyroxine, 112 mcg/d, and desiccated thyroid (combination thyroxine and triiodothyronine in the form of 20 mg Armour Thyroid), despite a lack of data for such combination therapy. Earlier, I had discontinued lorazepam, leaving lithium, 600 mg/d, quetiapine, 400 mg/d, and escitalopram, 10 mg/d, as her remaining psychotropics. Her other medications included atorvastatin, 40 mg/d, for hyper-lipidemia and metformin, 750 mg/d, for type 2 diabetes mellitus.
Medical illness
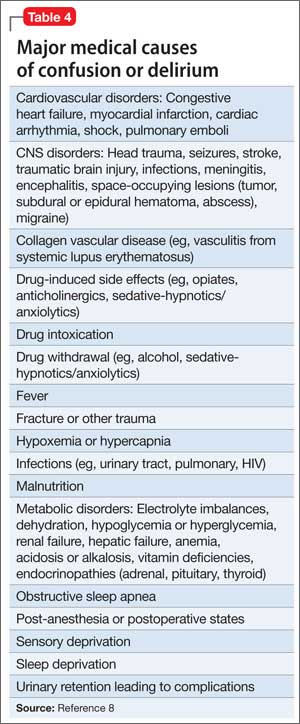
An organic basis must rank high in the differential diagnosis if medications are not the culprit. There are myriad medical disorders that can lead to confusion (Table 4).8 In an outpatient psychiatric setting, laboratory and radiology testing might not be readily available. It then becomes important to collaborate with a patient’s medical team if any of the following are met:
•there is high suspicion of a medical cause
•there could be delays in performing a medical workup
•a physical examination is needed.
Laboratory work-up should include:
•comprehensive metabolic panel (CMP) to assess for electrolyte derangements and liver or kidney disease
•urinalysis if there are signs of urinary tract infection (low threshold for testing in patients age >65 even if they are asymptomatic)
•urine drug screen or serum alcohol level if substance use is suspected
•complete blood count (CBC) if there are reports of infection (white blood cell count) or blood loss/bruising to ensure that anemia or thrombocytopenia is not playing a role
•thyroid-stimulating hormone (TSH) because thyroid disorders can cause neuropsychiatric as well as somatic symptoms.9
Other laboratory testing could be valuable depending on the clinical scenario. These include tests such as:
•drug level monitoring (lithium, valproic acid, etc.) to assess for toxicity
•HIV and rapid plasma reagin for suspected sexually transmitted infections
•vitamin levels in patients with poor nutrition or post bariatric surgery
•erythrocyte sedimentation rate or C-reactive protein, or both, if there are signs of inflammation
•bacterial culture if blood or tissue infection is a concern.
Esoteric tests include ceruloplasmin (Wilson’s disease), heavy metals screen, and even tests such as anti-gliadin antibodies because the prevalence of gluten sensitivity and celiac disease appear to be on the rise and have been associated with neuropsychiatric problems including encephalopathy.10
Brain imaging is an important consideration when a medical differential diagnosis for confusion is formulated. Unfortunately, there is little evidence-based guidance as to when brain imaging should be performed, often leading to overuse of tests such as CT, especially in emergency settings when confusion is noted. From a clinical standpoint, a head CT scan often is best ordered for patients who demonstrate an acute change in mental status, are age >70, are receiving anticoagulation, or have sustained trauma to the head. The key concern would be intracranial hemorrhage. However, some data suggest that the best use of head CT is for patients who have an impaired level of consciousness or a new focal neurologic deficit.11
Apart from more acute changes, a brain MRI study is more helpful than a head CT when evaluating the brain parenchyma for more sub-acute diagnoses such as multiple sclerosis or a brain tumor. T2-weighted hyperintensities seen on an MRI are thought to predict an increased risk of stroke, dementia, and death.
Their discovery should prompt a detailed evaluation for risk factors of stroke and dementia/NCD.12
In Ms. T’s case, she was taking lithium, so it was logical to obtain a trough lithium level 12 hours after the last dose and to check kidney function (serum creatinine to estimate the glomerular filtration rate), which were in the therapeutic/normal range. Her serum lithium level was 0.7 mEq/L. Brain imaging was not ordered, but several other labs (CMP, CBC, hemoglobin A1c [HgbA1c], and TSH) were drawn. These labs were notable for HgbA1c of 5.1% (normal <5.7%) and TSH of 0.5 mIU/L (normal level, 1.5 mIU/L), which is low for someone taking thyroid replacement.
I requested that Ms. T stop Armour Thyroid to address the suppressed TSH. I also requested that she stop metformin because, although hypoglycemia from metformin monotherapy is uncommon, it can happen in older patients. Hypoglycemia associated with metformin also can occur in situations when caloric intake is deficient or when metformin is used in combination with other drugs such as sulfonylureas (ie, glipizide), beta-adrenergic blocking drugs, angiotensin-converting enzyme inhibitors, or even nonsteroidal anti-inflammatory drugs.13
Identifying overlapping psychiatric (or psychological) illness
Symptoms of depression, anxiety, psychosis, and even dissociation can present as confusion. The term pseudodementia describes patients who exhibit cognitive symptoms consistent with NCD but could improve once the underlying mood, thought, anxiety, or personality disorder is treated.
For example, a patient with depression typically exhibits neurovegetative symptoms—such as poor sleep or appetite— amotivation, and low energy. All of these can lead to abrupt-onset cognitive changes, which are a hallmark of pseudodementia rather than the more insidious pattern of mild NCD. In cases of pseudodementia, neurocognitive testing will show impairment that often rapidly improves after the primary psychiatric (or psychological) issue is rectified. Making a diagnosis of pseudodementia at the initial presentation is difficult because neurocognitive tests such as the MMSE often fail to separate depression from true cognitive changes.14 Such a diagnosis typically requires hindsight. Yet, one must also keep in mind that pseudodementia may be part of a NCD prodrome.15
Conversion disorder as well as the dissociative disorders and substance-related disorders are notorious for causing confusion. In Ms. T’s case, pseudodementia stemming from her underlying bipolar disorder and anxiety figured prominently in the differential diagnosis, but she did not have any other overt psychopathology, personality disorder, or signs of malingering to further complicate her picture.
Notebook. I recommend that my patients keep a small notebook to record medical data ranging from blood pressure and glycemic measurements to details about sleep and dietary intake. Such data comprise the necessary metrics to properly assess target conditions and then track changes once treatment is initiated. This exercise not only yields much-needed detail about the patient’s condition for the clinician; the act of journaling also can be therapeutic for the writer through a process known as experimental disclosure, in which writing down one’s thoughts and observations has a positive impact on the writer’s physical health and psychology.16
Diagnosis. The first rule in medicine (perhaps the second, behind primum non nocere) is to determine what you are treating before beginning treatment (decernite quid tractemus, prius cura ministrandi, for Latin buffs). This means trying to fashion the best diagnostic label, even if it is merely a place-holder, while assessment of the confused state continues. DSM-5 has attempted to remove stigma from several neuropsychiatric disorders. On the cognition front, the new name for dementia is “neurocognitive disorder (NCD),” the umbrella term that focuses on the decline from a previous level of cognitive functioning. NCD has been divided into mild or major cognitive impairment headings either “with” or “without behavioral disturbance” subspecifiers.17
Aside from NCD, there are several other diagnoses in the differential for confusion. Delirium remains the most prominent and focuses on disturbances in attention and orientation that develops over a short period of time, with a change seen in an additional cognitive domain, such as memory, but not in the context of a severely reduced level of arousal such as coma. Subjective cognitive impairment (SCI) is when subjective complaints of cognitive impairment are hallmark compared with objective findings—with evidence suggesting that the presence of SCI could predict a 4.5 times higher rate of developing mild cognitive impairment (MCI) over 7 years.18 MCI was originally used to describe the early prodrome of AD, minus functional decline.
Treatment
After even a provisional diagnosis comes the final, all-important challenge: treating the neuropsychiatric symptoms (NPS) of the confused patient. NPS are nearly universal in NCD/delirium throughout the course of illness. There are no FDA-approved treatments for the NPS associated with these conditions. In terms of treating delirium, the best approach is to treat the underlying medical condition. For control of behavior, which can range from agitated to psychotic to hypoactive, nonpharmacotherapeutic interventions are paramount; they include making sure that the patient is at the appropriate level of care, which, for the confused outpatient, could mean hospitalization. Ensuring proper nutrition, hydration, sensory care (hearing aids, glasses, etc.), and stability in ambulation must be done before considering pharmacotherapy.
Antipsychotic use has been the mainstay of drug treatment of behavioral dyscontrol. Haloperidol has been the traditional go-to medication because there is no evidence that low-dose haloperidol (<3 mg/d) has any different efficacy compared with the atypical antipsychotics or has a greater frequency of adverse drug effects. However, high-dose haloperidol (>4.5 mg/d) was associated with a greater incidence of adverse effects, mainly parkinsonism, than atypical antipsychotics.19 Neither the typical nor atypical antipsychotics have shown mortality benefit—the real outcome measure of interest.
In terms of treating major (or minor) NCD, there are only 2 FDA-approved medication classes: cholinesterase inhibitors (donepezil, galantamine, rivastigmine, etc.) and memantine. However, these medication classes—even when combined together—have only shown marginal benefit in terms of improving cognition. Worse, even when given early in the course of illness they do not reduce the rate of NCD. For pseudodementia, selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors tend to form the mainstay of treating underlying depression or anxiety leading to cognitive changes. Preliminary data suggest that some SSRIs might improve cognition in terms of processing speed, verbal learning, and memory.20 More studies are needed before definitive conclusions can be drawn.
For the confused patient, a personalized therapeutic program, in which multiple interventions are considered at once (targeting all areas of the patient’s life) is gaining research traction. For example, a novel, comprehensive program involving multiple modalities designed to achieve metabolic enhancement for neurodegeneration (MEND) recently has shown robust benefit for patients with AD, MCI, and SCI.21 Using an individual approach to improve diet, activity, sleep, metabolic status including body mass index, and several other markers that affect neural plasticity, researchers demonstrated symptom improvement in 9 of 10 study patients.
Yet, some of the interventions, such as the use of statins for hyperlipidemia, remain controversial, with some studies suggesting that they help cognition,22,23 and others showing no association.24 The researchers caution that further research is warranted before costly dementia prevention trials with statins are undertaken. It does not appear that there are current MEND-type research projects in delirium but it’s to be hoped that we will see these in the future.
In the case of Ms. T, the cause of delirium vs mild NCD was thought to be multifactorial. Discontinuing Armour Thyroid and metformin—symptoms of hypoglycemia emerged as a leading concern—were simple adjustments that led to resolution of the most concerning elements of her confusion. She continued her other psychotropics, although there might be mild residual cognitive issues that warrant close observation.
Related Resources
• Lin JS, O’Connor E, Rossum RC, et al. Screening for cognitive impairment in older adults: an evidence update for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality (US); 2013.
• Grover S, Kate N. Assessment scales for delirium: a review. World J Psychiatry. 2012;2(4):58-70.
Drug Brand Names
Atorvastatin • Lipitor Lithium • Eskalith, Lithobid
Donepezil • Aricept Lorazepam • Ativan
Escitalopram • Lexapro Memantine • Namenda
Flumazenil • Romazicon Metformin • Glucophage
Galantamine • Razadyne Naloxone • Narcan
Glipizide • Glucotrol Physostigmine • Antilirium
Haloperidol • Haldol Quetiapine • Seroquel
Levothyroxine • Levoxyl, Synthroid Rivastigmine • Exelon
Lithium • Eskalith, Lithobid Valproic acid • Depakene
Disclosure
Dr. Raj is a speaker for Actavis Pharmaceuticals, AstraZeneca, and Merck.
1. Borson S, Scanlan JM, Chen P, et al. The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc. 2003;51(10):1451-1454.
2. Wilber ST, Lofgren SD, Mager TG, et al. An evaluation of two screening tools for cognitive impairment in older emergency department patients. Acad Emerg Med. 2005;12(7):612-616.
3. Tariq SH, Tumosa N, Chibnall JT, et al. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder—a pilot study. Am J Geriatr Psychiatry. 2006;14(11):900-910.
4. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695- 699.
5. Inouye S, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Int Med. 1990;113(12):941-948.
6. Hillmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med. 2007;167(8):781-787.
7. Raj YP. Psychiatric emergencies. In: Jiang W, Gagliardi JP, Krishnan KR, eds. Clinician’s guide to psychiatric care. New York, NY: Oxford University Press; 2009:33-40.
8. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 2nd ed. New York, NY: Oxford University Press; 2000:581-596.
9. Raj YP. Subclinical hypothyroidism: merely monitor or time to treat? Current Psychiatry. 2009;8(2):47-48.
10. Poloni N, Vender S, Bolla E, et al. Gluten encephalopathy with psychiatric onset: case report. Clin Pract Epidemiol Ment Health. 2009;5:16.
11. Naughton BJ, Moran M, Ghaly Y, et al. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
12. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi: 10.1136/bmj.c3666.
13. Zitzmann S, Reimann IR, Schmechel H. Severe hypoglycemia in an elderly patient treated with metformin. Int J Clin Pharmacol Ther. 2002;40(3):108-110.
14. Benson AD, Slavin MJ, Tran TT, et al. Screening for early Alzheimer’s Disease: is there still a role for the Mini-Mental State Examination? Prim Care Companion J Clin Psychiatry. 2005;7(2):62-69.
15. Brown WA. Pseudodementia: issues in diagnosis. Psychiatric Times. http://www.psychiatrictimes.com/ pseudodementia-issues-diagnosis. Published April 9, 2005. Accessed February 2, 2015.
16. Frattaroli J. Experimental disclosure and its moderators: a meta-analysis. Psychol Bull. 2006;132(6):823-865.
17. Stetka BS, Correll CU. A guide to DSM-5: neurocognitive disorder. Medscape. http://www.medscape.com/ viewarticle/803884_13. Published May 21, 2013. Accessed October 30, 2014.
18. Reisberg B, Sulman MD, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
19. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.
20. Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Intern Clin Psychopharmacol. 2012;27(4):215-223.
21. Bredesen DE. Reversal of cognitive decline: a novel therapeutic program. Aging (Albany NY). 2014;6(9):707-717.
22. Sparks DL, Kryscio RJ, Sabbagh MN, et al. Reduced risk of incident AD with elective statin use in a clinical trial cohort. Curr Alzheimer Res. 2008;5(4):416-421.
23. Andrade C, Radhakrishnan R. The prevention and treatment of cognitive decline and dementia: an overview of recent research on experimental treatments. Indian J Psychiatry. 2009;51(1):12-25.
24. Zandi PP, Sparks DL, Khachaturian AS, et al. Do statins reduce risk of incident dementia and Alzheimer disease? The Cache County Study. Arch Gen Psychiatry. 2005;62(2):217-224.
“Mr. Smith seems somewhat confused today” is one of the most serious and concerning pre-visit reports you can receive from your staff or the patient’s family. Such a descriptor can be confusing—pardon the pun—not only for the patient, but to even seasoned mental health providers.
The term confusion can be code for diagnoses ranging from deliriuma to a progressive neurocognitive disorder (NCD) such as major NCD due to Alzheimer’s disease (AD), or even a more challenging problem such as beclouded dementia (delirium superimposed on dementia/NCD). It is essential for all mental health professionals to have an evidence-based approach when encountering signs or symptoms of confusion.
aICD-10 code R41.0 encompasses Confusion, Other Specified Delirium, or Unspecified Delirium.
CASE REPORT
Ms. T, age 62, has hypothyroidism and bipolar I disorder, most recently depressed, with comorbid generalized anxiety disorder. She has been taking lithium, 600 mg/d, to control her mood symptoms. Her daughter-in-law reports that Ms. T has been exhibiting increasing signs of confusion. During the office evaluation, Ms. T minimizes her symptoms, only describing mild issues with forgetfulness while cooking and concern over increasing anxiety. Her daughter-in-law plays a voicemail message from earlier in the week, in which Ms. T’s speech is halting, disorganized, and in a word, confused. I decide to use the mnemonic decision chart MR. MIND (Table 1) to get to the bottom of her recent confusion.
Measure cognition
It is nice to receive advanced warning about a cognitive change or a change in activities of daily living; however, many patients present with subtle, sub-acute changes that are more difficult to assess. When encountering a broad symptom such as “confusion”—which has an equally broad differential diagnosis—systematic assessment of the current cognitive state compared with the patient’s baseline becomes the first order of business. However, this requires that the patient has had a baseline cognitive assessment.
In my practice, I often administer one of the validated neurocognitive screening instruments when a patient first begins care—even a brief test such as the Mini- Cog (3-item recall plus clock drawing test), which is comparable to longer screening tests at least for NCD/dementia.1 During a presentation for confusion, a more detailed neurocognitive assessment instrument would be recommended, allowing one to marry the clinical impression with a validated, objective measure. Formal neuropsychological testing by a clinical neuropsychologist is the gold standard, but such testing is time-consuming and expensive and often not readily available. The screening instrument I use for a more thorough evaluation depends on the clinical scenario.
The Six-Item Screener is used in some emergency settings because it is short but boasts a higher sensitivity than the Mini- Cog (94% vs 75%) with similar specificity when screening for cognitive impairment.2 The Mini-Mental State Examination (MMSE) is a valuable instrument, although, recently, the Saint Louis University Mental Status Examination has been thought to be better at detecting mild NCD than the MMSE; more data are needed to substantiate this claim.3 The Montreal Cognitive Assessment is another validated screening tool that has been shown to be superior to the MMSE in terms of screening for mild cognitive impairment.4 The best delirium-specific assessment tool is the Confusion Assessment Method (Table 2).5
Ms. T’s MMSE score was 26/30, down from 29/30 at baseline. Her score fell below the cutoff score of 27 for mild cognitive impairment for someone with at least 8 years of completed education. Her results were abnormal mainly in the memory domain (3-item recall), raising the question of a possible prodromal state of AD although the acute nature of the change made delirium or mild NCD high in the differential.
Review medications
A review of the medication list is not just a Joint Commission mandate (medication reconciliation during each encounter) but is important whenever confusion is noted. Polypharmacy can be a concern, but is not as concerning as the class of medication prescribed, particularly anticholinergic and sedative medications in patients age >65. The Drug Burden Index can be helpful in assessing this risk.6 Medications such as the benzodiazepine-receptor agonists, tricyclic antidepressants, and antipsychotics should be discontinued if possible, keeping in mind that the addition or subtraction of medications must be done prudently and only after reviewing the evidence and in consultation with the patient. A detailed medication review is as important for confused outpatients as it is for an inpatient case (steps 2 and 3 of the inpatient algorithm outlined in Table 3).7
In Ms. T’s case, the primary concern on her medication list was that her medical team was prescribing levothyroxine, 112 mcg/d, and desiccated thyroid (combination thyroxine and triiodothyronine in the form of 20 mg Armour Thyroid), despite a lack of data for such combination therapy. Earlier, I had discontinued lorazepam, leaving lithium, 600 mg/d, quetiapine, 400 mg/d, and escitalopram, 10 mg/d, as her remaining psychotropics. Her other medications included atorvastatin, 40 mg/d, for hyper-lipidemia and metformin, 750 mg/d, for type 2 diabetes mellitus.
Medical illness
An organic basis must rank high in the differential diagnosis if medications are not the culprit. There are myriad medical disorders that can lead to confusion (Table 4).8 In an outpatient psychiatric setting, laboratory and radiology testing might not be readily available. It then becomes important to collaborate with a patient’s medical team if any of the following are met:
•there is high suspicion of a medical cause
•there could be delays in performing a medical workup
•a physical examination is needed.
Laboratory work-up should include:
•comprehensive metabolic panel (CMP) to assess for electrolyte derangements and liver or kidney disease
•urinalysis if there are signs of urinary tract infection (low threshold for testing in patients age >65 even if they are asymptomatic)
•urine drug screen or serum alcohol level if substance use is suspected
•complete blood count (CBC) if there are reports of infection (white blood cell count) or blood loss/bruising to ensure that anemia or thrombocytopenia is not playing a role
•thyroid-stimulating hormone (TSH) because thyroid disorders can cause neuropsychiatric as well as somatic symptoms.9
Other laboratory testing could be valuable depending on the clinical scenario. These include tests such as:
•drug level monitoring (lithium, valproic acid, etc.) to assess for toxicity
•HIV and rapid plasma reagin for suspected sexually transmitted infections
•vitamin levels in patients with poor nutrition or post bariatric surgery
•erythrocyte sedimentation rate or C-reactive protein, or both, if there are signs of inflammation
•bacterial culture if blood or tissue infection is a concern.
Esoteric tests include ceruloplasmin (Wilson’s disease), heavy metals screen, and even tests such as anti-gliadin antibodies because the prevalence of gluten sensitivity and celiac disease appear to be on the rise and have been associated with neuropsychiatric problems including encephalopathy.10
Brain imaging is an important consideration when a medical differential diagnosis for confusion is formulated. Unfortunately, there is little evidence-based guidance as to when brain imaging should be performed, often leading to overuse of tests such as CT, especially in emergency settings when confusion is noted. From a clinical standpoint, a head CT scan often is best ordered for patients who demonstrate an acute change in mental status, are age >70, are receiving anticoagulation, or have sustained trauma to the head. The key concern would be intracranial hemorrhage. However, some data suggest that the best use of head CT is for patients who have an impaired level of consciousness or a new focal neurologic deficit.11
Apart from more acute changes, a brain MRI study is more helpful than a head CT when evaluating the brain parenchyma for more sub-acute diagnoses such as multiple sclerosis or a brain tumor. T2-weighted hyperintensities seen on an MRI are thought to predict an increased risk of stroke, dementia, and death.
Their discovery should prompt a detailed evaluation for risk factors of stroke and dementia/NCD.12
In Ms. T’s case, she was taking lithium, so it was logical to obtain a trough lithium level 12 hours after the last dose and to check kidney function (serum creatinine to estimate the glomerular filtration rate), which were in the therapeutic/normal range. Her serum lithium level was 0.7 mEq/L. Brain imaging was not ordered, but several other labs (CMP, CBC, hemoglobin A1c [HgbA1c], and TSH) were drawn. These labs were notable for HgbA1c of 5.1% (normal <5.7%) and TSH of 0.5 mIU/L (normal level, 1.5 mIU/L), which is low for someone taking thyroid replacement.
I requested that Ms. T stop Armour Thyroid to address the suppressed TSH. I also requested that she stop metformin because, although hypoglycemia from metformin monotherapy is uncommon, it can happen in older patients. Hypoglycemia associated with metformin also can occur in situations when caloric intake is deficient or when metformin is used in combination with other drugs such as sulfonylureas (ie, glipizide), beta-adrenergic blocking drugs, angiotensin-converting enzyme inhibitors, or even nonsteroidal anti-inflammatory drugs.13
Identifying overlapping psychiatric (or psychological) illness
Symptoms of depression, anxiety, psychosis, and even dissociation can present as confusion. The term pseudodementia describes patients who exhibit cognitive symptoms consistent with NCD but could improve once the underlying mood, thought, anxiety, or personality disorder is treated.
For example, a patient with depression typically exhibits neurovegetative symptoms—such as poor sleep or appetite— amotivation, and low energy. All of these can lead to abrupt-onset cognitive changes, which are a hallmark of pseudodementia rather than the more insidious pattern of mild NCD. In cases of pseudodementia, neurocognitive testing will show impairment that often rapidly improves after the primary psychiatric (or psychological) issue is rectified. Making a diagnosis of pseudodementia at the initial presentation is difficult because neurocognitive tests such as the MMSE often fail to separate depression from true cognitive changes.14 Such a diagnosis typically requires hindsight. Yet, one must also keep in mind that pseudodementia may be part of a NCD prodrome.15
Conversion disorder as well as the dissociative disorders and substance-related disorders are notorious for causing confusion. In Ms. T’s case, pseudodementia stemming from her underlying bipolar disorder and anxiety figured prominently in the differential diagnosis, but she did not have any other overt psychopathology, personality disorder, or signs of malingering to further complicate her picture.
Notebook. I recommend that my patients keep a small notebook to record medical data ranging from blood pressure and glycemic measurements to details about sleep and dietary intake. Such data comprise the necessary metrics to properly assess target conditions and then track changes once treatment is initiated. This exercise not only yields much-needed detail about the patient’s condition for the clinician; the act of journaling also can be therapeutic for the writer through a process known as experimental disclosure, in which writing down one’s thoughts and observations has a positive impact on the writer’s physical health and psychology.16
Diagnosis. The first rule in medicine (perhaps the second, behind primum non nocere) is to determine what you are treating before beginning treatment (decernite quid tractemus, prius cura ministrandi, for Latin buffs). This means trying to fashion the best diagnostic label, even if it is merely a place-holder, while assessment of the confused state continues. DSM-5 has attempted to remove stigma from several neuropsychiatric disorders. On the cognition front, the new name for dementia is “neurocognitive disorder (NCD),” the umbrella term that focuses on the decline from a previous level of cognitive functioning. NCD has been divided into mild or major cognitive impairment headings either “with” or “without behavioral disturbance” subspecifiers.17
Aside from NCD, there are several other diagnoses in the differential for confusion. Delirium remains the most prominent and focuses on disturbances in attention and orientation that develops over a short period of time, with a change seen in an additional cognitive domain, such as memory, but not in the context of a severely reduced level of arousal such as coma. Subjective cognitive impairment (SCI) is when subjective complaints of cognitive impairment are hallmark compared with objective findings—with evidence suggesting that the presence of SCI could predict a 4.5 times higher rate of developing mild cognitive impairment (MCI) over 7 years.18 MCI was originally used to describe the early prodrome of AD, minus functional decline.
Treatment
After even a provisional diagnosis comes the final, all-important challenge: treating the neuropsychiatric symptoms (NPS) of the confused patient. NPS are nearly universal in NCD/delirium throughout the course of illness. There are no FDA-approved treatments for the NPS associated with these conditions. In terms of treating delirium, the best approach is to treat the underlying medical condition. For control of behavior, which can range from agitated to psychotic to hypoactive, nonpharmacotherapeutic interventions are paramount; they include making sure that the patient is at the appropriate level of care, which, for the confused outpatient, could mean hospitalization. Ensuring proper nutrition, hydration, sensory care (hearing aids, glasses, etc.), and stability in ambulation must be done before considering pharmacotherapy.
Antipsychotic use has been the mainstay of drug treatment of behavioral dyscontrol. Haloperidol has been the traditional go-to medication because there is no evidence that low-dose haloperidol (<3 mg/d) has any different efficacy compared with the atypical antipsychotics or has a greater frequency of adverse drug effects. However, high-dose haloperidol (>4.5 mg/d) was associated with a greater incidence of adverse effects, mainly parkinsonism, than atypical antipsychotics.19 Neither the typical nor atypical antipsychotics have shown mortality benefit—the real outcome measure of interest.
In terms of treating major (or minor) NCD, there are only 2 FDA-approved medication classes: cholinesterase inhibitors (donepezil, galantamine, rivastigmine, etc.) and memantine. However, these medication classes—even when combined together—have only shown marginal benefit in terms of improving cognition. Worse, even when given early in the course of illness they do not reduce the rate of NCD. For pseudodementia, selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors tend to form the mainstay of treating underlying depression or anxiety leading to cognitive changes. Preliminary data suggest that some SSRIs might improve cognition in terms of processing speed, verbal learning, and memory.20 More studies are needed before definitive conclusions can be drawn.
For the confused patient, a personalized therapeutic program, in which multiple interventions are considered at once (targeting all areas of the patient’s life) is gaining research traction. For example, a novel, comprehensive program involving multiple modalities designed to achieve metabolic enhancement for neurodegeneration (MEND) recently has shown robust benefit for patients with AD, MCI, and SCI.21 Using an individual approach to improve diet, activity, sleep, metabolic status including body mass index, and several other markers that affect neural plasticity, researchers demonstrated symptom improvement in 9 of 10 study patients.
Yet, some of the interventions, such as the use of statins for hyperlipidemia, remain controversial, with some studies suggesting that they help cognition,22,23 and others showing no association.24 The researchers caution that further research is warranted before costly dementia prevention trials with statins are undertaken. It does not appear that there are current MEND-type research projects in delirium but it’s to be hoped that we will see these in the future.
In the case of Ms. T, the cause of delirium vs mild NCD was thought to be multifactorial. Discontinuing Armour Thyroid and metformin—symptoms of hypoglycemia emerged as a leading concern—were simple adjustments that led to resolution of the most concerning elements of her confusion. She continued her other psychotropics, although there might be mild residual cognitive issues that warrant close observation.
Related Resources
• Lin JS, O’Connor E, Rossum RC, et al. Screening for cognitive impairment in older adults: an evidence update for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality (US); 2013.
• Grover S, Kate N. Assessment scales for delirium: a review. World J Psychiatry. 2012;2(4):58-70.
Drug Brand Names
Atorvastatin • Lipitor Lithium • Eskalith, Lithobid
Donepezil • Aricept Lorazepam • Ativan
Escitalopram • Lexapro Memantine • Namenda
Flumazenil • Romazicon Metformin • Glucophage
Galantamine • Razadyne Naloxone • Narcan
Glipizide • Glucotrol Physostigmine • Antilirium
Haloperidol • Haldol Quetiapine • Seroquel
Levothyroxine • Levoxyl, Synthroid Rivastigmine • Exelon
Lithium • Eskalith, Lithobid Valproic acid • Depakene
Disclosure
Dr. Raj is a speaker for Actavis Pharmaceuticals, AstraZeneca, and Merck.
“Mr. Smith seems somewhat confused today” is one of the most serious and concerning pre-visit reports you can receive from your staff or the patient’s family. Such a descriptor can be confusing—pardon the pun—not only for the patient, but to even seasoned mental health providers.
The term confusion can be code for diagnoses ranging from deliriuma to a progressive neurocognitive disorder (NCD) such as major NCD due to Alzheimer’s disease (AD), or even a more challenging problem such as beclouded dementia (delirium superimposed on dementia/NCD). It is essential for all mental health professionals to have an evidence-based approach when encountering signs or symptoms of confusion.
aICD-10 code R41.0 encompasses Confusion, Other Specified Delirium, or Unspecified Delirium.
CASE REPORT
Ms. T, age 62, has hypothyroidism and bipolar I disorder, most recently depressed, with comorbid generalized anxiety disorder. She has been taking lithium, 600 mg/d, to control her mood symptoms. Her daughter-in-law reports that Ms. T has been exhibiting increasing signs of confusion. During the office evaluation, Ms. T minimizes her symptoms, only describing mild issues with forgetfulness while cooking and concern over increasing anxiety. Her daughter-in-law plays a voicemail message from earlier in the week, in which Ms. T’s speech is halting, disorganized, and in a word, confused. I decide to use the mnemonic decision chart MR. MIND (Table 1) to get to the bottom of her recent confusion.
Measure cognition
It is nice to receive advanced warning about a cognitive change or a change in activities of daily living; however, many patients present with subtle, sub-acute changes that are more difficult to assess. When encountering a broad symptom such as “confusion”—which has an equally broad differential diagnosis—systematic assessment of the current cognitive state compared with the patient’s baseline becomes the first order of business. However, this requires that the patient has had a baseline cognitive assessment.
In my practice, I often administer one of the validated neurocognitive screening instruments when a patient first begins care—even a brief test such as the Mini- Cog (3-item recall plus clock drawing test), which is comparable to longer screening tests at least for NCD/dementia.1 During a presentation for confusion, a more detailed neurocognitive assessment instrument would be recommended, allowing one to marry the clinical impression with a validated, objective measure. Formal neuropsychological testing by a clinical neuropsychologist is the gold standard, but such testing is time-consuming and expensive and often not readily available. The screening instrument I use for a more thorough evaluation depends on the clinical scenario.
The Six-Item Screener is used in some emergency settings because it is short but boasts a higher sensitivity than the Mini- Cog (94% vs 75%) with similar specificity when screening for cognitive impairment.2 The Mini-Mental State Examination (MMSE) is a valuable instrument, although, recently, the Saint Louis University Mental Status Examination has been thought to be better at detecting mild NCD than the MMSE; more data are needed to substantiate this claim.3 The Montreal Cognitive Assessment is another validated screening tool that has been shown to be superior to the MMSE in terms of screening for mild cognitive impairment.4 The best delirium-specific assessment tool is the Confusion Assessment Method (Table 2).5
Ms. T’s MMSE score was 26/30, down from 29/30 at baseline. Her score fell below the cutoff score of 27 for mild cognitive impairment for someone with at least 8 years of completed education. Her results were abnormal mainly in the memory domain (3-item recall), raising the question of a possible prodromal state of AD although the acute nature of the change made delirium or mild NCD high in the differential.
Review medications
A review of the medication list is not just a Joint Commission mandate (medication reconciliation during each encounter) but is important whenever confusion is noted. Polypharmacy can be a concern, but is not as concerning as the class of medication prescribed, particularly anticholinergic and sedative medications in patients age >65. The Drug Burden Index can be helpful in assessing this risk.6 Medications such as the benzodiazepine-receptor agonists, tricyclic antidepressants, and antipsychotics should be discontinued if possible, keeping in mind that the addition or subtraction of medications must be done prudently and only after reviewing the evidence and in consultation with the patient. A detailed medication review is as important for confused outpatients as it is for an inpatient case (steps 2 and 3 of the inpatient algorithm outlined in Table 3).7
In Ms. T’s case, the primary concern on her medication list was that her medical team was prescribing levothyroxine, 112 mcg/d, and desiccated thyroid (combination thyroxine and triiodothyronine in the form of 20 mg Armour Thyroid), despite a lack of data for such combination therapy. Earlier, I had discontinued lorazepam, leaving lithium, 600 mg/d, quetiapine, 400 mg/d, and escitalopram, 10 mg/d, as her remaining psychotropics. Her other medications included atorvastatin, 40 mg/d, for hyper-lipidemia and metformin, 750 mg/d, for type 2 diabetes mellitus.
Medical illness
An organic basis must rank high in the differential diagnosis if medications are not the culprit. There are myriad medical disorders that can lead to confusion (Table 4).8 In an outpatient psychiatric setting, laboratory and radiology testing might not be readily available. It then becomes important to collaborate with a patient’s medical team if any of the following are met:
•there is high suspicion of a medical cause
•there could be delays in performing a medical workup
•a physical examination is needed.
Laboratory work-up should include:
•comprehensive metabolic panel (CMP) to assess for electrolyte derangements and liver or kidney disease
•urinalysis if there are signs of urinary tract infection (low threshold for testing in patients age >65 even if they are asymptomatic)
•urine drug screen or serum alcohol level if substance use is suspected
•complete blood count (CBC) if there are reports of infection (white blood cell count) or blood loss/bruising to ensure that anemia or thrombocytopenia is not playing a role
•thyroid-stimulating hormone (TSH) because thyroid disorders can cause neuropsychiatric as well as somatic symptoms.9
Other laboratory testing could be valuable depending on the clinical scenario. These include tests such as:
•drug level monitoring (lithium, valproic acid, etc.) to assess for toxicity
•HIV and rapid plasma reagin for suspected sexually transmitted infections
•vitamin levels in patients with poor nutrition or post bariatric surgery
•erythrocyte sedimentation rate or C-reactive protein, or both, if there are signs of inflammation
•bacterial culture if blood or tissue infection is a concern.
Esoteric tests include ceruloplasmin (Wilson’s disease), heavy metals screen, and even tests such as anti-gliadin antibodies because the prevalence of gluten sensitivity and celiac disease appear to be on the rise and have been associated with neuropsychiatric problems including encephalopathy.10
Brain imaging is an important consideration when a medical differential diagnosis for confusion is formulated. Unfortunately, there is little evidence-based guidance as to when brain imaging should be performed, often leading to overuse of tests such as CT, especially in emergency settings when confusion is noted. From a clinical standpoint, a head CT scan often is best ordered for patients who demonstrate an acute change in mental status, are age >70, are receiving anticoagulation, or have sustained trauma to the head. The key concern would be intracranial hemorrhage. However, some data suggest that the best use of head CT is for patients who have an impaired level of consciousness or a new focal neurologic deficit.11
Apart from more acute changes, a brain MRI study is more helpful than a head CT when evaluating the brain parenchyma for more sub-acute diagnoses such as multiple sclerosis or a brain tumor. T2-weighted hyperintensities seen on an MRI are thought to predict an increased risk of stroke, dementia, and death.
Their discovery should prompt a detailed evaluation for risk factors of stroke and dementia/NCD.12
In Ms. T’s case, she was taking lithium, so it was logical to obtain a trough lithium level 12 hours after the last dose and to check kidney function (serum creatinine to estimate the glomerular filtration rate), which were in the therapeutic/normal range. Her serum lithium level was 0.7 mEq/L. Brain imaging was not ordered, but several other labs (CMP, CBC, hemoglobin A1c [HgbA1c], and TSH) were drawn. These labs were notable for HgbA1c of 5.1% (normal <5.7%) and TSH of 0.5 mIU/L (normal level, 1.5 mIU/L), which is low for someone taking thyroid replacement.
I requested that Ms. T stop Armour Thyroid to address the suppressed TSH. I also requested that she stop metformin because, although hypoglycemia from metformin monotherapy is uncommon, it can happen in older patients. Hypoglycemia associated with metformin also can occur in situations when caloric intake is deficient or when metformin is used in combination with other drugs such as sulfonylureas (ie, glipizide), beta-adrenergic blocking drugs, angiotensin-converting enzyme inhibitors, or even nonsteroidal anti-inflammatory drugs.13
Identifying overlapping psychiatric (or psychological) illness
Symptoms of depression, anxiety, psychosis, and even dissociation can present as confusion. The term pseudodementia describes patients who exhibit cognitive symptoms consistent with NCD but could improve once the underlying mood, thought, anxiety, or personality disorder is treated.
For example, a patient with depression typically exhibits neurovegetative symptoms—such as poor sleep or appetite— amotivation, and low energy. All of these can lead to abrupt-onset cognitive changes, which are a hallmark of pseudodementia rather than the more insidious pattern of mild NCD. In cases of pseudodementia, neurocognitive testing will show impairment that often rapidly improves after the primary psychiatric (or psychological) issue is rectified. Making a diagnosis of pseudodementia at the initial presentation is difficult because neurocognitive tests such as the MMSE often fail to separate depression from true cognitive changes.14 Such a diagnosis typically requires hindsight. Yet, one must also keep in mind that pseudodementia may be part of a NCD prodrome.15
Conversion disorder as well as the dissociative disorders and substance-related disorders are notorious for causing confusion. In Ms. T’s case, pseudodementia stemming from her underlying bipolar disorder and anxiety figured prominently in the differential diagnosis, but she did not have any other overt psychopathology, personality disorder, or signs of malingering to further complicate her picture.
Notebook. I recommend that my patients keep a small notebook to record medical data ranging from blood pressure and glycemic measurements to details about sleep and dietary intake. Such data comprise the necessary metrics to properly assess target conditions and then track changes once treatment is initiated. This exercise not only yields much-needed detail about the patient’s condition for the clinician; the act of journaling also can be therapeutic for the writer through a process known as experimental disclosure, in which writing down one’s thoughts and observations has a positive impact on the writer’s physical health and psychology.16
Diagnosis. The first rule in medicine (perhaps the second, behind primum non nocere) is to determine what you are treating before beginning treatment (decernite quid tractemus, prius cura ministrandi, for Latin buffs). This means trying to fashion the best diagnostic label, even if it is merely a place-holder, while assessment of the confused state continues. DSM-5 has attempted to remove stigma from several neuropsychiatric disorders. On the cognition front, the new name for dementia is “neurocognitive disorder (NCD),” the umbrella term that focuses on the decline from a previous level of cognitive functioning. NCD has been divided into mild or major cognitive impairment headings either “with” or “without behavioral disturbance” subspecifiers.17
Aside from NCD, there are several other diagnoses in the differential for confusion. Delirium remains the most prominent and focuses on disturbances in attention and orientation that develops over a short period of time, with a change seen in an additional cognitive domain, such as memory, but not in the context of a severely reduced level of arousal such as coma. Subjective cognitive impairment (SCI) is when subjective complaints of cognitive impairment are hallmark compared with objective findings—with evidence suggesting that the presence of SCI could predict a 4.5 times higher rate of developing mild cognitive impairment (MCI) over 7 years.18 MCI was originally used to describe the early prodrome of AD, minus functional decline.
Treatment
After even a provisional diagnosis comes the final, all-important challenge: treating the neuropsychiatric symptoms (NPS) of the confused patient. NPS are nearly universal in NCD/delirium throughout the course of illness. There are no FDA-approved treatments for the NPS associated with these conditions. In terms of treating delirium, the best approach is to treat the underlying medical condition. For control of behavior, which can range from agitated to psychotic to hypoactive, nonpharmacotherapeutic interventions are paramount; they include making sure that the patient is at the appropriate level of care, which, for the confused outpatient, could mean hospitalization. Ensuring proper nutrition, hydration, sensory care (hearing aids, glasses, etc.), and stability in ambulation must be done before considering pharmacotherapy.
Antipsychotic use has been the mainstay of drug treatment of behavioral dyscontrol. Haloperidol has been the traditional go-to medication because there is no evidence that low-dose haloperidol (<3 mg/d) has any different efficacy compared with the atypical antipsychotics or has a greater frequency of adverse drug effects. However, high-dose haloperidol (>4.5 mg/d) was associated with a greater incidence of adverse effects, mainly parkinsonism, than atypical antipsychotics.19 Neither the typical nor atypical antipsychotics have shown mortality benefit—the real outcome measure of interest.
In terms of treating major (or minor) NCD, there are only 2 FDA-approved medication classes: cholinesterase inhibitors (donepezil, galantamine, rivastigmine, etc.) and memantine. However, these medication classes—even when combined together—have only shown marginal benefit in terms of improving cognition. Worse, even when given early in the course of illness they do not reduce the rate of NCD. For pseudodementia, selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors tend to form the mainstay of treating underlying depression or anxiety leading to cognitive changes. Preliminary data suggest that some SSRIs might improve cognition in terms of processing speed, verbal learning, and memory.20 More studies are needed before definitive conclusions can be drawn.
For the confused patient, a personalized therapeutic program, in which multiple interventions are considered at once (targeting all areas of the patient’s life) is gaining research traction. For example, a novel, comprehensive program involving multiple modalities designed to achieve metabolic enhancement for neurodegeneration (MEND) recently has shown robust benefit for patients with AD, MCI, and SCI.21 Using an individual approach to improve diet, activity, sleep, metabolic status including body mass index, and several other markers that affect neural plasticity, researchers demonstrated symptom improvement in 9 of 10 study patients.
Yet, some of the interventions, such as the use of statins for hyperlipidemia, remain controversial, with some studies suggesting that they help cognition,22,23 and others showing no association.24 The researchers caution that further research is warranted before costly dementia prevention trials with statins are undertaken. It does not appear that there are current MEND-type research projects in delirium but it’s to be hoped that we will see these in the future.
In the case of Ms. T, the cause of delirium vs mild NCD was thought to be multifactorial. Discontinuing Armour Thyroid and metformin—symptoms of hypoglycemia emerged as a leading concern—were simple adjustments that led to resolution of the most concerning elements of her confusion. She continued her other psychotropics, although there might be mild residual cognitive issues that warrant close observation.
Related Resources
• Lin JS, O’Connor E, Rossum RC, et al. Screening for cognitive impairment in older adults: an evidence update for the U.S. Preventive Services Task Force. Rockville, MD: Agency for Healthcare Research and Quality (US); 2013.
• Grover S, Kate N. Assessment scales for delirium: a review. World J Psychiatry. 2012;2(4):58-70.
Drug Brand Names
Atorvastatin • Lipitor Lithium • Eskalith, Lithobid
Donepezil • Aricept Lorazepam • Ativan
Escitalopram • Lexapro Memantine • Namenda
Flumazenil • Romazicon Metformin • Glucophage
Galantamine • Razadyne Naloxone • Narcan
Glipizide • Glucotrol Physostigmine • Antilirium
Haloperidol • Haldol Quetiapine • Seroquel
Levothyroxine • Levoxyl, Synthroid Rivastigmine • Exelon
Lithium • Eskalith, Lithobid Valproic acid • Depakene
Disclosure
Dr. Raj is a speaker for Actavis Pharmaceuticals, AstraZeneca, and Merck.
1. Borson S, Scanlan JM, Chen P, et al. The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc. 2003;51(10):1451-1454.
2. Wilber ST, Lofgren SD, Mager TG, et al. An evaluation of two screening tools for cognitive impairment in older emergency department patients. Acad Emerg Med. 2005;12(7):612-616.
3. Tariq SH, Tumosa N, Chibnall JT, et al. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder—a pilot study. Am J Geriatr Psychiatry. 2006;14(11):900-910.
4. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695- 699.
5. Inouye S, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Int Med. 1990;113(12):941-948.
6. Hillmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med. 2007;167(8):781-787.
7. Raj YP. Psychiatric emergencies. In: Jiang W, Gagliardi JP, Krishnan KR, eds. Clinician’s guide to psychiatric care. New York, NY: Oxford University Press; 2009:33-40.
8. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 2nd ed. New York, NY: Oxford University Press; 2000:581-596.
9. Raj YP. Subclinical hypothyroidism: merely monitor or time to treat? Current Psychiatry. 2009;8(2):47-48.
10. Poloni N, Vender S, Bolla E, et al. Gluten encephalopathy with psychiatric onset: case report. Clin Pract Epidemiol Ment Health. 2009;5:16.
11. Naughton BJ, Moran M, Ghaly Y, et al. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
12. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi: 10.1136/bmj.c3666.
13. Zitzmann S, Reimann IR, Schmechel H. Severe hypoglycemia in an elderly patient treated with metformin. Int J Clin Pharmacol Ther. 2002;40(3):108-110.
14. Benson AD, Slavin MJ, Tran TT, et al. Screening for early Alzheimer’s Disease: is there still a role for the Mini-Mental State Examination? Prim Care Companion J Clin Psychiatry. 2005;7(2):62-69.
15. Brown WA. Pseudodementia: issues in diagnosis. Psychiatric Times. http://www.psychiatrictimes.com/ pseudodementia-issues-diagnosis. Published April 9, 2005. Accessed February 2, 2015.
16. Frattaroli J. Experimental disclosure and its moderators: a meta-analysis. Psychol Bull. 2006;132(6):823-865.
17. Stetka BS, Correll CU. A guide to DSM-5: neurocognitive disorder. Medscape. http://www.medscape.com/ viewarticle/803884_13. Published May 21, 2013. Accessed October 30, 2014.
18. Reisberg B, Sulman MD, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
19. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.
20. Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Intern Clin Psychopharmacol. 2012;27(4):215-223.
21. Bredesen DE. Reversal of cognitive decline: a novel therapeutic program. Aging (Albany NY). 2014;6(9):707-717.
22. Sparks DL, Kryscio RJ, Sabbagh MN, et al. Reduced risk of incident AD with elective statin use in a clinical trial cohort. Curr Alzheimer Res. 2008;5(4):416-421.
23. Andrade C, Radhakrishnan R. The prevention and treatment of cognitive decline and dementia: an overview of recent research on experimental treatments. Indian J Psychiatry. 2009;51(1):12-25.
24. Zandi PP, Sparks DL, Khachaturian AS, et al. Do statins reduce risk of incident dementia and Alzheimer disease? The Cache County Study. Arch Gen Psychiatry. 2005;62(2):217-224.
1. Borson S, Scanlan JM, Chen P, et al. The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc. 2003;51(10):1451-1454.
2. Wilber ST, Lofgren SD, Mager TG, et al. An evaluation of two screening tools for cognitive impairment in older emergency department patients. Acad Emerg Med. 2005;12(7):612-616.
3. Tariq SH, Tumosa N, Chibnall JT, et al. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder—a pilot study. Am J Geriatr Psychiatry. 2006;14(11):900-910.
4. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695- 699.
5. Inouye S, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Int Med. 1990;113(12):941-948.
6. Hillmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med. 2007;167(8):781-787.
7. Raj YP. Psychiatric emergencies. In: Jiang W, Gagliardi JP, Krishnan KR, eds. Clinician’s guide to psychiatric care. New York, NY: Oxford University Press; 2009:33-40.
8. Liptzin B. Clinical diagnosis and management of delirium. In: Stoudemire A, Fogel BS, Greenberg DB, eds. Psychiatric care of the medical patient. 2nd ed. New York, NY: Oxford University Press; 2000:581-596.
9. Raj YP. Subclinical hypothyroidism: merely monitor or time to treat? Current Psychiatry. 2009;8(2):47-48.
10. Poloni N, Vender S, Bolla E, et al. Gluten encephalopathy with psychiatric onset: case report. Clin Pract Epidemiol Ment Health. 2009;5:16.
11. Naughton BJ, Moran M, Ghaly Y, et al. Computed tomography scanning and delirium in elder patients. Acad Emerg Med. 1997;4(12):1107-1110.
12. Debette S, Markus HS. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: systematic review and meta-analysis. BMJ. 2010;341:c3666. doi: 10.1136/bmj.c3666.
13. Zitzmann S, Reimann IR, Schmechel H. Severe hypoglycemia in an elderly patient treated with metformin. Int J Clin Pharmacol Ther. 2002;40(3):108-110.
14. Benson AD, Slavin MJ, Tran TT, et al. Screening for early Alzheimer’s Disease: is there still a role for the Mini-Mental State Examination? Prim Care Companion J Clin Psychiatry. 2005;7(2):62-69.
15. Brown WA. Pseudodementia: issues in diagnosis. Psychiatric Times. http://www.psychiatrictimes.com/ pseudodementia-issues-diagnosis. Published April 9, 2005. Accessed February 2, 2015.
16. Frattaroli J. Experimental disclosure and its moderators: a meta-analysis. Psychol Bull. 2006;132(6):823-865.
17. Stetka BS, Correll CU. A guide to DSM-5: neurocognitive disorder. Medscape. http://www.medscape.com/ viewarticle/803884_13. Published May 21, 2013. Accessed October 30, 2014.
18. Reisberg B, Sulman MD, Torossian C, et al. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010;6(1):11-24.
19. Lonergan E, Britton AM, Luxenberg J, et al. Antipsychotics for delirium. Cochrane Database Syst Rev. 2007;(2):CD005594.
20. Katona C, Hansen T, Olsen CK. A randomized, double-blind, placebo-controlled, duloxetine-referenced, fixed-dose study comparing the efficacy and safety of Lu AA21004 in elderly patients with major depressive disorder. Intern Clin Psychopharmacol. 2012;27(4):215-223.
21. Bredesen DE. Reversal of cognitive decline: a novel therapeutic program. Aging (Albany NY). 2014;6(9):707-717.
22. Sparks DL, Kryscio RJ, Sabbagh MN, et al. Reduced risk of incident AD with elective statin use in a clinical trial cohort. Curr Alzheimer Res. 2008;5(4):416-421.
23. Andrade C, Radhakrishnan R. The prevention and treatment of cognitive decline and dementia: an overview of recent research on experimental treatments. Indian J Psychiatry. 2009;51(1):12-25.
24. Zandi PP, Sparks DL, Khachaturian AS, et al. Do statins reduce risk of incident dementia and Alzheimer disease? The Cache County Study. Arch Gen Psychiatry. 2005;62(2):217-224.
The 10,000-hour rule
In 2002, the Accreditation Council for Graduate Medical Education, or ACGME, rocked traditional residency training paradigms by proposing a regulated residency call schedule.1 Revised standards were implemented in 2011 throughout the United States prohibiting first-year residents from spending more than 16 consecutive hours in the hospital and restricting senior residents from working more than 80 hr/week averaged over the month.2 In Canada, there is no national agreement on residency restriction hours; however, in 2011, the province of Quebec mandated that 24-hour in-hospital call represents a violation of Canadian Charter of Rights and Freedoms and implemented a 16-hour call duty schedule for all Quebec trainees.3
JAMA recently published two observational cohort studies that included over 2 million hospitalized adults across the United States from 2009 to 2012.4,5 Patient outcomes (including 30-day mortality and readmissions) were compared before the 2011 reforms in duty hours and after 2011.
The key finding from these studies, albeit from a retrospective observational standpoint, demonstrated that even with the introduction of resident restriction duty hours there has been no effect on these patient outcomes. The authors wrote that such an observational study lacks the power to produce the highest level of scientific evidence that will guide practice and policy decisions. But it remains astonishing, that without any evidence in place to support, inform, or implement decisions, a change to the entire paradigm of residency training was made despite the considerable time, effort, and cost involved in implementation of these actions.
Unfortunately, the implementation of these guidelines puts evidence-based medicine to shame.
Now, after a few years of integrating these duty-hour reforms, the observational and longitudinal evidence has failed to demonstrate improved patient safety. If the primary goal was to demonstrate that the imposition of duty-hour restriction would improve patient safety, it has been unsuccessful to date.
Putting the debate aside, we currently work and live in an era of restricted resident duty hours. Looking ahead 10-15 years, we have to question what type of physicians we will be with the current duty-hour restrictions in place, and then reflect on the type of physicians we want and strive to be.
Especially in surgical residency training programs, the overarching goal is for programs to train a safe, competent, and independent surgeon within 5 years. With the current work-hour restrictions, I am not confident this can be achieved.
Many eloquent debates have been written on lack of patient ownership, professionalism, and clinical judgment in our current training paradigm that I won’t belabor. Malcolm Gladwell’s book “Outliers” repeatedly mentioned the “10,000-hour rule” and the principle holds that 10,000 hours of “deliberate practice” are needed to become world-class in any field.
This speaks volumes to surgical trainees who will be required to master complex technical skills and even more multifaceted appropriate judgments, which I doubt can be achieved in the current work-hour restrictions. I am from the camp that if we remain in our present work-hour restriction schedules, there will be a need to modify training to conform to these duty-hour restrictions in order to prepare residents optimally for practice.
Perhaps moving toward a competency-based curriculum would ensure that a surgical trainee is in fact, safe and proficient and ready to transition into practice.
So we now find ourselves working backward trying to validate the system we are presently working in. To that effect, a multicenter randomized controlled trial (The Flexibility in Duty Hour Requirements for Surgical Trainees trial) is underway with study end date projected for June 2015.
FIRST aims to determine if increasing flexibility of surgical resident duty-hour requirements affects patient care, surgical outcomes, and resident perceptions. Hospitals or programs will be randomized to either an intervention group with flexibility of duty-hour restrictions with the elimination of current duty-hour requirements or a control group with continued adherence to current requirements.
I cannot foresee what the future may hold, but I will continue to strive for excellence and hope that when my time comes to transition from trainee into independent practice, I will be ready.
References
1. JAMA 2002;288:1112-4.
2. ACGME Duty Hours. Accreditation Council for Graduate Medical Education, 2014 (www.acgme.org/acgmeweb/tabid/271/GraduateMedicalEducation/DutyHours.aspx).
3. Towards a Pan-Canadian Consensus on Resident Duty Hours. Royal College of Physicians and Surgeons of Canada, 2014 (www.royalcollege.ca/portal/page/portal/rc/advocacy/educational_initiatives/resident_duty_hours).
4. JAMA 2014;312:2364-73.5. JAMA 2014;312:2374-84.
In 2002, the Accreditation Council for Graduate Medical Education, or ACGME, rocked traditional residency training paradigms by proposing a regulated residency call schedule.1 Revised standards were implemented in 2011 throughout the United States prohibiting first-year residents from spending more than 16 consecutive hours in the hospital and restricting senior residents from working more than 80 hr/week averaged over the month.2 In Canada, there is no national agreement on residency restriction hours; however, in 2011, the province of Quebec mandated that 24-hour in-hospital call represents a violation of Canadian Charter of Rights and Freedoms and implemented a 16-hour call duty schedule for all Quebec trainees.3
JAMA recently published two observational cohort studies that included over 2 million hospitalized adults across the United States from 2009 to 2012.4,5 Patient outcomes (including 30-day mortality and readmissions) were compared before the 2011 reforms in duty hours and after 2011.
The key finding from these studies, albeit from a retrospective observational standpoint, demonstrated that even with the introduction of resident restriction duty hours there has been no effect on these patient outcomes. The authors wrote that such an observational study lacks the power to produce the highest level of scientific evidence that will guide practice and policy decisions. But it remains astonishing, that without any evidence in place to support, inform, or implement decisions, a change to the entire paradigm of residency training was made despite the considerable time, effort, and cost involved in implementation of these actions.
Unfortunately, the implementation of these guidelines puts evidence-based medicine to shame.
Now, after a few years of integrating these duty-hour reforms, the observational and longitudinal evidence has failed to demonstrate improved patient safety. If the primary goal was to demonstrate that the imposition of duty-hour restriction would improve patient safety, it has been unsuccessful to date.
Putting the debate aside, we currently work and live in an era of restricted resident duty hours. Looking ahead 10-15 years, we have to question what type of physicians we will be with the current duty-hour restrictions in place, and then reflect on the type of physicians we want and strive to be.
Especially in surgical residency training programs, the overarching goal is for programs to train a safe, competent, and independent surgeon within 5 years. With the current work-hour restrictions, I am not confident this can be achieved.
Many eloquent debates have been written on lack of patient ownership, professionalism, and clinical judgment in our current training paradigm that I won’t belabor. Malcolm Gladwell’s book “Outliers” repeatedly mentioned the “10,000-hour rule” and the principle holds that 10,000 hours of “deliberate practice” are needed to become world-class in any field.
This speaks volumes to surgical trainees who will be required to master complex technical skills and even more multifaceted appropriate judgments, which I doubt can be achieved in the current work-hour restrictions. I am from the camp that if we remain in our present work-hour restriction schedules, there will be a need to modify training to conform to these duty-hour restrictions in order to prepare residents optimally for practice.
Perhaps moving toward a competency-based curriculum would ensure that a surgical trainee is in fact, safe and proficient and ready to transition into practice.
So we now find ourselves working backward trying to validate the system we are presently working in. To that effect, a multicenter randomized controlled trial (The Flexibility in Duty Hour Requirements for Surgical Trainees trial) is underway with study end date projected for June 2015.
FIRST aims to determine if increasing flexibility of surgical resident duty-hour requirements affects patient care, surgical outcomes, and resident perceptions. Hospitals or programs will be randomized to either an intervention group with flexibility of duty-hour restrictions with the elimination of current duty-hour requirements or a control group with continued adherence to current requirements.
I cannot foresee what the future may hold, but I will continue to strive for excellence and hope that when my time comes to transition from trainee into independent practice, I will be ready.
References
1. JAMA 2002;288:1112-4.
2. ACGME Duty Hours. Accreditation Council for Graduate Medical Education, 2014 (www.acgme.org/acgmeweb/tabid/271/GraduateMedicalEducation/DutyHours.aspx).
3. Towards a Pan-Canadian Consensus on Resident Duty Hours. Royal College of Physicians and Surgeons of Canada, 2014 (www.royalcollege.ca/portal/page/portal/rc/advocacy/educational_initiatives/resident_duty_hours).
4. JAMA 2014;312:2364-73.5. JAMA 2014;312:2374-84.
In 2002, the Accreditation Council for Graduate Medical Education, or ACGME, rocked traditional residency training paradigms by proposing a regulated residency call schedule.1 Revised standards were implemented in 2011 throughout the United States prohibiting first-year residents from spending more than 16 consecutive hours in the hospital and restricting senior residents from working more than 80 hr/week averaged over the month.2 In Canada, there is no national agreement on residency restriction hours; however, in 2011, the province of Quebec mandated that 24-hour in-hospital call represents a violation of Canadian Charter of Rights and Freedoms and implemented a 16-hour call duty schedule for all Quebec trainees.3
JAMA recently published two observational cohort studies that included over 2 million hospitalized adults across the United States from 2009 to 2012.4,5 Patient outcomes (including 30-day mortality and readmissions) were compared before the 2011 reforms in duty hours and after 2011.
The key finding from these studies, albeit from a retrospective observational standpoint, demonstrated that even with the introduction of resident restriction duty hours there has been no effect on these patient outcomes. The authors wrote that such an observational study lacks the power to produce the highest level of scientific evidence that will guide practice and policy decisions. But it remains astonishing, that without any evidence in place to support, inform, or implement decisions, a change to the entire paradigm of residency training was made despite the considerable time, effort, and cost involved in implementation of these actions.
Unfortunately, the implementation of these guidelines puts evidence-based medicine to shame.
Now, after a few years of integrating these duty-hour reforms, the observational and longitudinal evidence has failed to demonstrate improved patient safety. If the primary goal was to demonstrate that the imposition of duty-hour restriction would improve patient safety, it has been unsuccessful to date.
Putting the debate aside, we currently work and live in an era of restricted resident duty hours. Looking ahead 10-15 years, we have to question what type of physicians we will be with the current duty-hour restrictions in place, and then reflect on the type of physicians we want and strive to be.
Especially in surgical residency training programs, the overarching goal is for programs to train a safe, competent, and independent surgeon within 5 years. With the current work-hour restrictions, I am not confident this can be achieved.
Many eloquent debates have been written on lack of patient ownership, professionalism, and clinical judgment in our current training paradigm that I won’t belabor. Malcolm Gladwell’s book “Outliers” repeatedly mentioned the “10,000-hour rule” and the principle holds that 10,000 hours of “deliberate practice” are needed to become world-class in any field.
This speaks volumes to surgical trainees who will be required to master complex technical skills and even more multifaceted appropriate judgments, which I doubt can be achieved in the current work-hour restrictions. I am from the camp that if we remain in our present work-hour restriction schedules, there will be a need to modify training to conform to these duty-hour restrictions in order to prepare residents optimally for practice.
Perhaps moving toward a competency-based curriculum would ensure that a surgical trainee is in fact, safe and proficient and ready to transition into practice.
So we now find ourselves working backward trying to validate the system we are presently working in. To that effect, a multicenter randomized controlled trial (The Flexibility in Duty Hour Requirements for Surgical Trainees trial) is underway with study end date projected for June 2015.
FIRST aims to determine if increasing flexibility of surgical resident duty-hour requirements affects patient care, surgical outcomes, and resident perceptions. Hospitals or programs will be randomized to either an intervention group with flexibility of duty-hour restrictions with the elimination of current duty-hour requirements or a control group with continued adherence to current requirements.
I cannot foresee what the future may hold, but I will continue to strive for excellence and hope that when my time comes to transition from trainee into independent practice, I will be ready.
References
1. JAMA 2002;288:1112-4.
2. ACGME Duty Hours. Accreditation Council for Graduate Medical Education, 2014 (www.acgme.org/acgmeweb/tabid/271/GraduateMedicalEducation/DutyHours.aspx).
3. Towards a Pan-Canadian Consensus on Resident Duty Hours. Royal College of Physicians and Surgeons of Canada, 2014 (www.royalcollege.ca/portal/page/portal/rc/advocacy/educational_initiatives/resident_duty_hours).
4. JAMA 2014;312:2364-73.5. JAMA 2014;312:2374-84.

Study provides new insights regarding HSCs, FA
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
with Fanconi anemia
Image by Michael Milsom
Environmental stress is a major factor driving DNA damage in hematopoietic stem cells (HSCs), according to research published in Nature.
Investigators found that repeated exposure to such stress induces accelerated tissue aging and may cause cancer.
In examining HSCs’ response to stress, the team also gained new insight regarding Fanconi anemia.
The investigators noted that, under normal conditions, HSCs exist in a state of dormancy. They rarely divide and have very low energy demands.
“Our theory was that this state of dormancy protected hematopoietic stem cells from DNA damage and therefore protects them from premature aging,” said study author Michael Milsom, PhD, of The Heidelberg Institute for Stem Cell Technology and Experimental Medicine in Germany.
However, under conditions of stress, such as during chronic blood loss or infection, HSCs are driven into a state of rapid cell division in order to produce new blood cells and repair the damaged tissue.
“The stem cells go from a state of rest to very high activity within a short space of time, requiring them to rapidly increase their metabolic rate, synthesize new DNA, and coordinate cell division,” Dr Milsom explained. “Suddenly having to simultaneously execute these complicated functions dramatically increases the likelihood that something will go wrong.”
Indeed, the investigators’ experiments showed that the increased energy demands during stress results in elevated production of reactive metabolites that can directly damage DNA. If this happens at the same time a cell is trying to replicate its DNA, this can cause cell death or the acquisition of mutations that may cause cancer.
Normal stem cells can repair the majority of this stress-induced DNA damage, the investigators noted. However, the more HSCs are exposed to stress, the more likely they are to inefficiently repair the damage and then die or mutate.
“We believe that this model perfectly explains the gradual accumulation of DNA damage in stem cells with age and the associated reduction in the ability of a tissue to maintain and repair itself as you get older,” Dr Milsom said.
He and his colleagues also examined how this stress response impacts a mouse model of Fanconi anemia. These mice have the same DNA repair defect found in humans with the disease, but the mice never spontaneously develop the bone marrow failure observed in nearly all patients.
“We felt that stress-induced DNA damage was the missing ingredient that was required to cause hematopoietic stem cell depletion in these mice,” Dr Milsom said.
When mice with Fanconi anemia were exposed to stimulation mimicking a prolonged viral infection, they were unable to efficiently repair the resulting DNA damage, and their stem cells failed.
In the same space of time that normal mice showed a gradual decline in HSC numbers, the stem cells in Fanconi anemia mice were almost completely depleted, resulting in bone marrow failure and an inadequate production of blood cells to sustain life.
“This perfectly recapitulates what happens to Fanconi anemia patients and now gives us an opportunity to understand how this disease works and how we might better treat it,” Dr Milsom said. ![]()
How cancer patients make treatment decisions

patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
patient and her father
Photo by Rhoda Baer
A survey of more than 5000 cancer patients suggests there are a number of factors that might make a patient more likely to involve family members in treatment decisions.
A patient’s gender, age, marital status, native language, insurance status, and even past military service all appeared to impact family involvement in care decisions.
Gabriela Hobbs, MD, of Harvard Medical School in Boston, Massachusetts, and her colleagues conducted this research and reported the results in Cancer.
The researchers surveyed 5284 patients with a new diagnosis of lung or colon cancer, asking patients how they involved their families in treatment decisions.
Only 1.5% of patients reported complete family control over decisions. Nearly half of patients (49.4%) said they and family members shared decision-making responsibilities equally, 22.1% of patients reported some family input, and 28.5% reported little or no input from their families.
Asian and Hispanic patients who did not speak English were more likely than their peers to report equally shared decisions with their families. Likewise, patients who were married, female, older, and insured were more likely to share decision-making equally with their families.
Veterans were the least likely to share decision-making with their families, even when the researchers adjusted for marital status and social support.
“Understanding how patients vary in their inclusion of family members in decisions—by ethnicity, language spoken, marital status, sex, age, insurance status, and veteran status—may help physicians to better assess their patients’ preferences for engaging family members in decisions,” Dr Hobbs said.
“As we move to more patient-centered models of care, such assessments may help doctors personalize the care they offer their patients.”
Dr Hobbs noted that as therapies for cancer patients improve, they are also becoming increasingly complex, making it challenging for patients and providers to determine the optimal therapy for each patient. Therefore, knowing how patients make decisions and understanding the role families play in decision-making is crucial for optimizing patient participation in treatment decisions.
“Our study suggests that not all patients wish to include family in the same way,” Dr Hobbs said. “By raising awareness of these preferences, we hope that physicians will be aware of these variations and elicit their patient’s preference on how they wish to include, or not to include, families in decision-making.” ![]()
Look for adverse events in patients with chronic urticaria
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
HOUSTON – The risk of adverse events may be cumulative over the lifetime of patients taking oral corticosteroids for urticaria.
Dr. Dennis Ledford, professor of medicine at the University of South Florida, Tampa, and his colleagues examined records of 12,647 patients culled from a commercial claims database between January 2008 and December 2012 who had taken oral corticosteroids for chronic idiopathic or spontaneous urticaria during a 12-month period. More than half (55%) used oral corticosteroids (mean dosage of 367.5 mg) for an average of 16.2 days. At follow-up, patients displayed adverse events at a rate of 27 per 100 patient-years.
Adverse events mostly included skeletal conditions such as osteoporosis and bone fractures, but investigators also noted diabetes, hypertension, lipid disorders, depression, mania, and cataracts, Dr. Ledford said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
More concerning, “there’s a cumulative risk,” Dr. Ledford said in an interview. “The more [prednisone equivalent] you take over your lifetime, the greater the chance is that you’re going to develop the side effects we’ve listed here.”
Using time-sensitive Cox regression models, Dr. Ledford and his colleagues determined that the risk for adverse events went up by 7% for each gram dose of prednisone equivalent to which patients were exposed after adjusting for age, sex, immunomodulator use, and Charlson Comorbidity Index. Only cataracts were not subject to the cumulative effects.
“The message of this fairly large analysis is that there are cumulative side effects to prednisone that may not be evident to the physician or clinician performing day-to-day care of patients,” Dr. Ledford said. “These effects are slow to develop and often present in areas of medicine that the physician treating urticaria would not take care of.”
Patients enrolled in this study had all been diagnosed with urticaria at either of two outpatient clinic visits at least 6 weeks apart in a single calendar year, or had received one diagnosis of urticaria and one of angioedema at two separate outpatient clinics at least 6 weeks apart. Patients were followed for at least 1 year after completion of the initial 12-month study period, until end of enrollment or end of study.
Dr. Ledford stressed the need to use noncorticosteroid therapies when treating chronic urticaria, such as calcineurin inhibitors – which also carry risks of hypertension and cancer – or omalizumab.
The study was funded by Genentech and Novartis Pharma AG which market omalizumab as Xolair. Dr. Ledford disclosed that he is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
AT 2015 AAAAI ANNUAL MEETING
Key clinical point: The cumulative adverse events of oral corticosteroids may not present to the physician treating the patient for urticaria.
Major finding: The risk for adverse events went up by 7% for each gram dose of prednisone equivalent.
Data source: Retrospective cohort study of 12,647 patients selected from a commercial claims database from 2008 through 2012.
Disclosures: Study funded by Genentech and Novartis Pharma AG; Dr. Ledford is affiliated with Genentech, Novartis Pharma AG, and a number of other pharmaceutical companies.
Artemisinin-resistant malaria found across Myanmar

Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
Photo by James Gathany
Resistance to the antimalarial drug artemisinin is present in Myanmar and has reached within 25 km of the Indian border, according to research published in The Lancet Infectious Diseases.
Researchers believe the spread of artemisinin-resistant malaria parasites into neighboring India would pose a serious threat to the global control and eradication of malaria.
And if drug resistance continues to spread, millions of lives could be at risk.
Kyaw Myo Tun, MD, of the Myanmar Oxford Clinical Research Unit in Yangon, Myanmar, and colleagues uncovered artemisinin resistance by analyzing parasite samples collected at 55 malaria treatment centers across Myanmar.
The group set out to determine if the samples carried mutations in specific regions of the parasite’s kelch gene (K13)—a known genetic marker of artemisinin resistance. And they confirmed the existance of resistant parasites in Homalin, in the Sagaing Region, which is located only 25 km from the Indian border.
“Myanmar is considered the frontline in the battle against artemisinin resistance, as it forms a gateway for resistance to spread to the rest of the world,” said Charles Woodrow, MD, of the University of Oxford in the UK.
“With artemisinins, we are in the unusual position of having molecular markers for resistance before resistance has spread globally. The more we understand about the current situation in the border regions, the better prepared we are to adapt and implement strategies to overcome the spread of further drug resistance.”
The researchers obtained the DNA sequences of 940 samples of Plasmodium falciparum malaria parasites from across Myanmar and neighboring border regions in Thailand and Bangladesh between 2013 and 2014. Of those 940 samples, 371 (39%) carried a resistance-conferring K13 mutation.
“We were able to gather patient samples rapidly across Myanmar, sometimes using discarded malaria blood diagnostic tests, and then test these immediately for the K13 marker, and so generate real-time information on the spread of resistance” said Mallika Imwong, PhD, of Mahidol University in Bangkok, Thailand.
Using this information, the researchers developed maps to display the predicted extent of artemisinin resistance determined by the prevalence of K13 mutations. The maps suggested the overall prevalence of K13 mutations was greater than 10% in large areas of the east and north of Myanmar, including areas close to the border with India.
“The identification of the K13 markers of resistance has transformed our ability to monitor the spread and emergence of artemisinin resistance,” said Philippe Guerin, MD, of the Worldwide Antimalarial Resistance Network in Oxford, UK.
“However, this study highlights that the pace at which artemisinin resistance is spreading or emerging is alarming. We need a more vigorous international effort to address this issue in border regions.” ![]()
Psychotic symptoms in children and adolescents
Some of the more disturbing behavioral symptoms to present are psychotic symptoms such as auditory or visual hallucination, delusions such as paranoia, or grossly disorganized thought content. Similar to the worry many families will have that a headache is the result of a brain tumor, concern that the psychotic symptoms represent the onset of schizophrenia often creates considerable alarm for families and primary care clinicians alike. In most cases, however, further evaluation suggests causes of psychotic or psychotic-like symptoms other than primary thought disorders.

Case Summary
Ella is an 8-year-old girl who has lived with her adoptive parents for 5 years. She was removed from the care of her birth parents by child protective services because of a history of abuse and neglect. Ella has struggled for many years with a variety of emotional-behavioral problems including inattention, frequent and intense angry outbursts, anxiety, and mood instability. She currently takes a long-acting methylphenidate preparation. Her parents present to her pediatrician because Ella is now reporting that she is seeing “shadows” in her room at night that frighten her. She also has lately stated that she hears a “mean voice” in her head that tells her that she is a bad person. The parents are not aware of specific psychiatric diagnoses in the birth parents, but state that they did have a history of “mental health problems” and were homeless at times. The parents are worried that these symptoms might be early signs of schizophrenia.
Discussion
Accumulating data demonstrates that while psychotic symptoms are relatively common in children and adolescents, childhood-onset schizophrenia actually is quite rare. Estimates of psychotic symptoms in otherwise healthy children have been as high as 5%, with a recent study of adolescents reporting that 15% of the sample reported hearing a voice that commented on what the person was thinking or feeling (Schizophr. Bull. 2014;40:868-77). At the same time, the incidence of childhood-onset schizophrenia is thought to be less than 0.04% based on data from a group at the National Institute of Mental Health (Child Adolesc. Psychiatr. Clin. N. Am. 2013;22:539-55). This group has been actively evaluating and recruiting children with early onset psychosis and finds that more than 90% of their referrals end up with a diagnosis other than schizophrenia.
The differential diagnosis for psychosis is extensive. In terms of nonpsychiatric diagnoses (what in the past were referred to as “organic” causes), possible etiologies include CNS tumors, encephalitis, metabolic disorders, and various genetic conditions, among others. Some medications, such as corticosteroids, stimulants, and anticholinergic medications, also can result in psychotic symptoms, especially at higher doses. While the acute presence of psychotic symptoms in an otherwise healthy child should certainly prompt suspicion of a possible delirium or other nonpsychiatric condition, it is important to note that some of the above etiologies can be associated with other types of behavioral disturbances; thus, the presence of earlier behavioral problems does not rule out the possibility that one of these nonpsychiatric causes is present.
Clinical tip: From our experience at a busy outpatient child psychiatry clinic, it is often not clear whose job it is to rule out nonpsychiatric causes of behavior problems. There is a risk that the psychiatrist assumes that the pediatrician has done this work-up while the pediatrician assumes that this component is part of a psychiatric evaluation. Communication about this role is important. If a third specialist is needed, such as a pediatric neurologist or geneticist, then it is important to clarify who will initiate that consultation as well.
The differential for psychotic symptoms also includes a number of psychiatric conditions other than schizophrenia, such as bipolar or unipolar depression, obsessive-compulsive disorder, posttraumatic stress disorder, autism, or an eating disorder. Substance use, particularly cannabis, also needs to be strongly considered. A child psychiatrist or other mental health professional can be very helpful here to help decipher what are sometimes subtle differences in the nature and content of the psychotic symptoms between various diagnoses. Receptive and expressive language disorders also can be present in many youth who experience psychotic symptoms.
The decision of if and when to begin treatment with an antipsychotic medication can be a difficult one and should be made very thoughtfully and with the help of consultation. The concern that a longer duration of untreated psychosis may be related to a more protracted course needs to be weighed against other data suggesting that using as little medication as possible may predict higher levels of future functioning (JAMA Psychiatry 2013;70:913-20). It is important to note that there are many nonpharmacological interventions that also can be helpful, including individual and family psychotherapy, family education, school modifications, and other social supports.
Case follow-up
Ella was referred to a child psychologist who performed an evaluation and thought that the patient’s symptoms were most representative of posttraumatic stress disorder. She began treatment with trauma-focused cognitive-behavioral therapy (TF-CBT) which led to a reduction in both her anxiety and psychotic-sounding symptoms.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].
Some of the more disturbing behavioral symptoms to present are psychotic symptoms such as auditory or visual hallucination, delusions such as paranoia, or grossly disorganized thought content. Similar to the worry many families will have that a headache is the result of a brain tumor, concern that the psychotic symptoms represent the onset of schizophrenia often creates considerable alarm for families and primary care clinicians alike. In most cases, however, further evaluation suggests causes of psychotic or psychotic-like symptoms other than primary thought disorders.
Case Summary
Ella is an 8-year-old girl who has lived with her adoptive parents for 5 years. She was removed from the care of her birth parents by child protective services because of a history of abuse and neglect. Ella has struggled for many years with a variety of emotional-behavioral problems including inattention, frequent and intense angry outbursts, anxiety, and mood instability. She currently takes a long-acting methylphenidate preparation. Her parents present to her pediatrician because Ella is now reporting that she is seeing “shadows” in her room at night that frighten her. She also has lately stated that she hears a “mean voice” in her head that tells her that she is a bad person. The parents are not aware of specific psychiatric diagnoses in the birth parents, but state that they did have a history of “mental health problems” and were homeless at times. The parents are worried that these symptoms might be early signs of schizophrenia.
Discussion
Accumulating data demonstrates that while psychotic symptoms are relatively common in children and adolescents, childhood-onset schizophrenia actually is quite rare. Estimates of psychotic symptoms in otherwise healthy children have been as high as 5%, with a recent study of adolescents reporting that 15% of the sample reported hearing a voice that commented on what the person was thinking or feeling (Schizophr. Bull. 2014;40:868-77). At the same time, the incidence of childhood-onset schizophrenia is thought to be less than 0.04% based on data from a group at the National Institute of Mental Health (Child Adolesc. Psychiatr. Clin. N. Am. 2013;22:539-55). This group has been actively evaluating and recruiting children with early onset psychosis and finds that more than 90% of their referrals end up with a diagnosis other than schizophrenia.
The differential diagnosis for psychosis is extensive. In terms of nonpsychiatric diagnoses (what in the past were referred to as “organic” causes), possible etiologies include CNS tumors, encephalitis, metabolic disorders, and various genetic conditions, among others. Some medications, such as corticosteroids, stimulants, and anticholinergic medications, also can result in psychotic symptoms, especially at higher doses. While the acute presence of psychotic symptoms in an otherwise healthy child should certainly prompt suspicion of a possible delirium or other nonpsychiatric condition, it is important to note that some of the above etiologies can be associated with other types of behavioral disturbances; thus, the presence of earlier behavioral problems does not rule out the possibility that one of these nonpsychiatric causes is present.
Clinical tip: From our experience at a busy outpatient child psychiatry clinic, it is often not clear whose job it is to rule out nonpsychiatric causes of behavior problems. There is a risk that the psychiatrist assumes that the pediatrician has done this work-up while the pediatrician assumes that this component is part of a psychiatric evaluation. Communication about this role is important. If a third specialist is needed, such as a pediatric neurologist or geneticist, then it is important to clarify who will initiate that consultation as well.
The differential for psychotic symptoms also includes a number of psychiatric conditions other than schizophrenia, such as bipolar or unipolar depression, obsessive-compulsive disorder, posttraumatic stress disorder, autism, or an eating disorder. Substance use, particularly cannabis, also needs to be strongly considered. A child psychiatrist or other mental health professional can be very helpful here to help decipher what are sometimes subtle differences in the nature and content of the psychotic symptoms between various diagnoses. Receptive and expressive language disorders also can be present in many youth who experience psychotic symptoms.
The decision of if and when to begin treatment with an antipsychotic medication can be a difficult one and should be made very thoughtfully and with the help of consultation. The concern that a longer duration of untreated psychosis may be related to a more protracted course needs to be weighed against other data suggesting that using as little medication as possible may predict higher levels of future functioning (JAMA Psychiatry 2013;70:913-20). It is important to note that there are many nonpharmacological interventions that also can be helpful, including individual and family psychotherapy, family education, school modifications, and other social supports.
Case follow-up
Ella was referred to a child psychologist who performed an evaluation and thought that the patient’s symptoms were most representative of posttraumatic stress disorder. She began treatment with trauma-focused cognitive-behavioral therapy (TF-CBT) which led to a reduction in both her anxiety and psychotic-sounding symptoms.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].
Some of the more disturbing behavioral symptoms to present are psychotic symptoms such as auditory or visual hallucination, delusions such as paranoia, or grossly disorganized thought content. Similar to the worry many families will have that a headache is the result of a brain tumor, concern that the psychotic symptoms represent the onset of schizophrenia often creates considerable alarm for families and primary care clinicians alike. In most cases, however, further evaluation suggests causes of psychotic or psychotic-like symptoms other than primary thought disorders.
Case Summary
Ella is an 8-year-old girl who has lived with her adoptive parents for 5 years. She was removed from the care of her birth parents by child protective services because of a history of abuse and neglect. Ella has struggled for many years with a variety of emotional-behavioral problems including inattention, frequent and intense angry outbursts, anxiety, and mood instability. She currently takes a long-acting methylphenidate preparation. Her parents present to her pediatrician because Ella is now reporting that she is seeing “shadows” in her room at night that frighten her. She also has lately stated that she hears a “mean voice” in her head that tells her that she is a bad person. The parents are not aware of specific psychiatric diagnoses in the birth parents, but state that they did have a history of “mental health problems” and were homeless at times. The parents are worried that these symptoms might be early signs of schizophrenia.
Discussion
Accumulating data demonstrates that while psychotic symptoms are relatively common in children and adolescents, childhood-onset schizophrenia actually is quite rare. Estimates of psychotic symptoms in otherwise healthy children have been as high as 5%, with a recent study of adolescents reporting that 15% of the sample reported hearing a voice that commented on what the person was thinking or feeling (Schizophr. Bull. 2014;40:868-77). At the same time, the incidence of childhood-onset schizophrenia is thought to be less than 0.04% based on data from a group at the National Institute of Mental Health (Child Adolesc. Psychiatr. Clin. N. Am. 2013;22:539-55). This group has been actively evaluating and recruiting children with early onset psychosis and finds that more than 90% of their referrals end up with a diagnosis other than schizophrenia.
The differential diagnosis for psychosis is extensive. In terms of nonpsychiatric diagnoses (what in the past were referred to as “organic” causes), possible etiologies include CNS tumors, encephalitis, metabolic disorders, and various genetic conditions, among others. Some medications, such as corticosteroids, stimulants, and anticholinergic medications, also can result in psychotic symptoms, especially at higher doses. While the acute presence of psychotic symptoms in an otherwise healthy child should certainly prompt suspicion of a possible delirium or other nonpsychiatric condition, it is important to note that some of the above etiologies can be associated with other types of behavioral disturbances; thus, the presence of earlier behavioral problems does not rule out the possibility that one of these nonpsychiatric causes is present.
Clinical tip: From our experience at a busy outpatient child psychiatry clinic, it is often not clear whose job it is to rule out nonpsychiatric causes of behavior problems. There is a risk that the psychiatrist assumes that the pediatrician has done this work-up while the pediatrician assumes that this component is part of a psychiatric evaluation. Communication about this role is important. If a third specialist is needed, such as a pediatric neurologist or geneticist, then it is important to clarify who will initiate that consultation as well.
The differential for psychotic symptoms also includes a number of psychiatric conditions other than schizophrenia, such as bipolar or unipolar depression, obsessive-compulsive disorder, posttraumatic stress disorder, autism, or an eating disorder. Substance use, particularly cannabis, also needs to be strongly considered. A child psychiatrist or other mental health professional can be very helpful here to help decipher what are sometimes subtle differences in the nature and content of the psychotic symptoms between various diagnoses. Receptive and expressive language disorders also can be present in many youth who experience psychotic symptoms.
The decision of if and when to begin treatment with an antipsychotic medication can be a difficult one and should be made very thoughtfully and with the help of consultation. The concern that a longer duration of untreated psychosis may be related to a more protracted course needs to be weighed against other data suggesting that using as little medication as possible may predict higher levels of future functioning (JAMA Psychiatry 2013;70:913-20). It is important to note that there are many nonpharmacological interventions that also can be helpful, including individual and family psychotherapy, family education, school modifications, and other social supports.
Case follow-up
Ella was referred to a child psychologist who performed an evaluation and thought that the patient’s symptoms were most representative of posttraumatic stress disorder. She began treatment with trauma-focused cognitive-behavioral therapy (TF-CBT) which led to a reduction in both her anxiety and psychotic-sounding symptoms.
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Dr. Rettew said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].

EC expands indication for lenalidomide in MM

Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
Photo courtesy of Celgene
The European Commission (EC) has expanded the marketing authorization for lenalidomide (Revlimid), just 2 days after the US Food and Drug Administration did the same.
Lenalidomide is now approved in the European Union (EU) to treat adults with previously untreated multiple myeloma (MM) who are not eligible for hematopoietic stem cell transplant. These patients can receive the drug continuously until
disease progression.
Lenalidomide was already approved in the EU for use in combination with dexamethasone to treat adults with MM who have received at least 1 prior therapy.
Lenalidomide is also approved in the EU to treat patients with transfusion-dependent anemia due to low- or intermediate-1-risk myelodysplastic syndromes associated with 5q deletion when other therapeutic options are insufficient or inadequate.
“Having a new treatment option now available for patients newly diagnosed with multiple myeloma is a real step forward,” said Thierry Facon, MD, of CHRU Lille in France.
“Treating patients continuously until disease progression is supported by several clinical studies and will have an important impact on how we manage the disease over the long-term.”
The EC’s decision to extend the approved use of lenalidomide was based on the results of 2 studies: MM-015 and MM-020, also known as FIRST.
The FIRST trial
In the phase 3 FIRST trial, researchers enrolled 1623 patients who were newly diagnosed with MM and not eligible for transplant.
Patients were randomized to receive lenalidomide and dexamethasone (Rd) in 28-day cycles until disease progression (n=535), 18 cycles of lenalidomide and dexamethasone (Rd18) for 72 weeks (n=541), or melphalan, prednisone, and thalidomide (MPT) for 72 weeks (n=547).
Response rates were significantly better with continuous Rd (75%) and Rd18 (73%) than with MPT (62%, P<0.001 for both comparisons). Complete response rates were 15%, 14%, and 9%, respectively.
The median progression-free survival was 25.5 months with continuous Rd, 20.7 months with Rd18, and 21.2 months with MPT.
This resulted in a 28% reduction in the risk of progression or death for patients treated with continuous Rd compared with those treated with MPT (hazard ratio[HR]=0.72, P<0.001) and a 30% reduction compared with Rd18 (HR=0.70, P<0.001).
The pre-planned interim analysis of overall survival showed a 22% reduction in the risk of death for continuous Rd vs MPT (HR=0.78, P=0.02), but the difference did not cross the pre-specified superiority boundary (P<0.0096).
Adverse events reported in 20% or more of patients in the continuous Rd, Rd18, or MPT arms included diarrhea (45.5%, 38.5%, 16.5%), anemia (43.8%, 35.7%, 42.3%), neutropenia (35.0%, 33.0%, 60.6%), fatigue (32.5%, 32.8%, 28.5%), back pain (32.0%, 26.9%, 21.4%), insomnia (27.6%, 23.5%, 9.8%), asthenia (28.2%, 22.8%, 22.9%), rash (26.1%, 28.0%, 19.4%), decreased appetite (23.1%, 21.3%, 13.3%), cough (22.7%, 17.4%, 12.6%), pyrexia (21.4%, 18.9%, 14.0%), muscle spasms (20.5%, 18.9%, 11.3%), and abdominal pain (20.5%, 14.4%, 11.1%).
The incidence of invasive second primary malignancies was 3% in patients taking continuous Rd, 6% in patients taking Rd18, and 5% in those taking MPT. The overall incidence of solid tumors was identical in the continuous Rd and MPT arms (3%) and 5% in the Rd18 arm.
The MM-015 trial
In the phase 3 MM-015 study, researchers enrolled 459 patients who were 65 or older and newly diagnosed with MM.
The team compared melphalan-prednisone-lenalidomide induction followed by lenalidomide maintenance (MPR-R) with melphalan-prednisone-lenalidomide (MPR) or melphalan-prednisone (MP) followed by placebo maintenance.
Patients who received MPR-R or MPR had significantly better response rates than patients who received MP, at 77%, 68%, and 50%, respectively (P<0.001 and P=0.002, respectively, for the comparison with MP).
And the median progression-free survival was significantly longer with MPR-R (31 months) than with MPR (14 months, HR=0.49, P<0.001) or MP (13 months, HR=0.40, P<0.001).
During induction, the most frequent adverse events were hematologic. Grade 4 neutropenia occurred in 35% of patients in the MPR-R arm, 32% in the MPR arm, and 8% in the MP arm. The 3-year rate of second primary malignancies was 7%, 7%, and 3%, respectively. ![]()
March 2015 Quiz 2
ANSWER: B
Critique
This patient has evidence of an acute colonic pseudo-obstruction (known as Ogilvie’s syndrome). This is seen most commonly after non-GI related surgeries such as cardiac or orthopedic surgeries. The exact etiology is uncertain but increased inhibitory sympathetic and/or decreased stimulatory, parasympathetic innervations of the distal colon have been incriminated. The most appropriate first step in management of this patient is a thorough clinical evaluation to ensure there is no evidence of peritonitis to suggest a perforation complication. The next step is to exclude an obstruction and the CT had no clear evidence of obstruction. One could consider a water soluble enema to exclude obstruction but should avoid the use of barium in the event of a perforation. The next steps include restricting all possible culprit medications such as opiates and anticholinergics, encouraging ambulation (although often clinical circumstances limit ambulation), and correcting any potential electrolyte abnormalities.
Placement of a nasogastric tube to low intermittent suction, keeping the patient NPO (nothing by mouth), and placing a rectal tube to gravity are practical measure that can facilitate decompression. If the patient cannot ambulate, some clinicians also advocate rotating the patient into the right lateral decubitus position for several hours, alternating with the supine position, to facilitate gas evacuation. Such conservative measures are appropriate if there is no evidence of clinical toxicity or progression of the condition. Cecal diameters may be monitored on plain abdominal x-rays. If there is no clinical response to the above measures, then further treatments may be considered. Use of an acetylcholinesterase inhibitor has been shown to be beneficial in a placebo-controlled trial. If use of an acetylcholinesterase inhibitor is unsuccessful, colonic decompression can be considered though this typically provides only transient benefit. Finally, an emergent cecostomy can be considered if colonic decompression is unsuccessful.
References
1. De Giorgio R., Cogliandro R.F., Barbara G., Corinaldesi R., Stanghellini V. Chronic intestinal pseudo-obstruction: clinical features, diagnosis, and therapy. Gastroenterol. Clin. North Am. 2011;40:787-807.
2. Ponec R.J., Saunders M.D., KImmey M.B. Neostigmine for the treatment of acute colonic pseudo-obstruction. N. Engl. J. Med. 1999;341:137-41.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.
ANSWER: B
Critique
This patient has evidence of an acute colonic pseudo-obstruction (known as Ogilvie’s syndrome). This is seen most commonly after non-GI related surgeries such as cardiac or orthopedic surgeries. The exact etiology is uncertain but increased inhibitory sympathetic and/or decreased stimulatory, parasympathetic innervations of the distal colon have been incriminated. The most appropriate first step in management of this patient is a thorough clinical evaluation to ensure there is no evidence of peritonitis to suggest a perforation complication. The next step is to exclude an obstruction and the CT had no clear evidence of obstruction. One could consider a water soluble enema to exclude obstruction but should avoid the use of barium in the event of a perforation. The next steps include restricting all possible culprit medications such as opiates and anticholinergics, encouraging ambulation (although often clinical circumstances limit ambulation), and correcting any potential electrolyte abnormalities.
Placement of a nasogastric tube to low intermittent suction, keeping the patient NPO (nothing by mouth), and placing a rectal tube to gravity are practical measure that can facilitate decompression. If the patient cannot ambulate, some clinicians also advocate rotating the patient into the right lateral decubitus position for several hours, alternating with the supine position, to facilitate gas evacuation. Such conservative measures are appropriate if there is no evidence of clinical toxicity or progression of the condition. Cecal diameters may be monitored on plain abdominal x-rays. If there is no clinical response to the above measures, then further treatments may be considered. Use of an acetylcholinesterase inhibitor has been shown to be beneficial in a placebo-controlled trial. If use of an acetylcholinesterase inhibitor is unsuccessful, colonic decompression can be considered though this typically provides only transient benefit. Finally, an emergent cecostomy can be considered if colonic decompression is unsuccessful.
References
1. De Giorgio R., Cogliandro R.F., Barbara G., Corinaldesi R., Stanghellini V. Chronic intestinal pseudo-obstruction: clinical features, diagnosis, and therapy. Gastroenterol. Clin. North Am. 2011;40:787-807.
2. Ponec R.J., Saunders M.D., KImmey M.B. Neostigmine for the treatment of acute colonic pseudo-obstruction. N. Engl. J. Med. 1999;341:137-41.
ANSWER: B
Critique
This patient has evidence of an acute colonic pseudo-obstruction (known as Ogilvie’s syndrome). This is seen most commonly after non-GI related surgeries such as cardiac or orthopedic surgeries. The exact etiology is uncertain but increased inhibitory sympathetic and/or decreased stimulatory, parasympathetic innervations of the distal colon have been incriminated. The most appropriate first step in management of this patient is a thorough clinical evaluation to ensure there is no evidence of peritonitis to suggest a perforation complication. The next step is to exclude an obstruction and the CT had no clear evidence of obstruction. One could consider a water soluble enema to exclude obstruction but should avoid the use of barium in the event of a perforation. The next steps include restricting all possible culprit medications such as opiates and anticholinergics, encouraging ambulation (although often clinical circumstances limit ambulation), and correcting any potential electrolyte abnormalities.
Placement of a nasogastric tube to low intermittent suction, keeping the patient NPO (nothing by mouth), and placing a rectal tube to gravity are practical measure that can facilitate decompression. If the patient cannot ambulate, some clinicians also advocate rotating the patient into the right lateral decubitus position for several hours, alternating with the supine position, to facilitate gas evacuation. Such conservative measures are appropriate if there is no evidence of clinical toxicity or progression of the condition. Cecal diameters may be monitored on plain abdominal x-rays. If there is no clinical response to the above measures, then further treatments may be considered. Use of an acetylcholinesterase inhibitor has been shown to be beneficial in a placebo-controlled trial. If use of an acetylcholinesterase inhibitor is unsuccessful, colonic decompression can be considered though this typically provides only transient benefit. Finally, an emergent cecostomy can be considered if colonic decompression is unsuccessful.
References
1. De Giorgio R., Cogliandro R.F., Barbara G., Corinaldesi R., Stanghellini V. Chronic intestinal pseudo-obstruction: clinical features, diagnosis, and therapy. Gastroenterol. Clin. North Am. 2011;40:787-807.
2. Ponec R.J., Saunders M.D., KImmey M.B. Neostigmine for the treatment of acute colonic pseudo-obstruction. N. Engl. J. Med. 1999;341:137-41.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.
March 2015 Quiz 1
ANSWER: D
Critique
The patient is most likely to have Zollinger-Ellison syndrome (ZES), a condition caused by a gastrinoma. In 25% of cases, ZES is associated with multiple endocrine neoplasia type 1 (MEN-1). Clinical features of MEN-1 include gastrinoma or other islet cell tumor, hyperparathyroidism, and anterior pituitary tumors. ZES should be especially considered in a patient with multiple, refractory, or recurrent peptic ulcer disease, especially if accompanied by diarrhea or hypercalcemia. Diarrhea is often a predominant symptom and is caused by the large volume of acid that inactivates pancreatic lipase and damages the absorptive mucosa of the proximal gut. Tests to diagnose ZES include serum gastrin radioimmunoassay, secretin stimulation test, somatostatin receptor scintigraphy, and endoscopic ultrasound. Almost all gastrinomas contain somatostatin receptors on the gastrin cells and somatostatin scintigraphy using [111In-DPTA-Dphe1]-octreotide is considered the initial localization study of choice. It has 71% sensitivity and 86% specificity for primary tumors and 92% sensitivity for detection of metastatic disease.
References
1. Murugesan S.V., Varro A., Pritchard D.M. Review article: Strategies to determine whether hypergastrinaemia is due to Zollinger-Ellison syndrome rather than a more common benign cause. Aliment Pharmacol. Ther. 2009;29:1055-68.
2. Jensen R.T., Niederle B., Mitry E., et al. Frascati Consensus Conference; European Neuroendocrine Tumor Society. Gastrinoma (duodenal and pancreatic). Neuroendocrinology 2006;84:173-82.
3. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
4. Gibril F., Reynolds J.C., Doppman J.L., et al. Somatostatin receptor scintigraphy: Its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas - A prospective study. Ann. Intern. Med. 1996;125:26-34.
5. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.
ANSWER: D
Critique
The patient is most likely to have Zollinger-Ellison syndrome (ZES), a condition caused by a gastrinoma. In 25% of cases, ZES is associated with multiple endocrine neoplasia type 1 (MEN-1). Clinical features of MEN-1 include gastrinoma or other islet cell tumor, hyperparathyroidism, and anterior pituitary tumors. ZES should be especially considered in a patient with multiple, refractory, or recurrent peptic ulcer disease, especially if accompanied by diarrhea or hypercalcemia. Diarrhea is often a predominant symptom and is caused by the large volume of acid that inactivates pancreatic lipase and damages the absorptive mucosa of the proximal gut. Tests to diagnose ZES include serum gastrin radioimmunoassay, secretin stimulation test, somatostatin receptor scintigraphy, and endoscopic ultrasound. Almost all gastrinomas contain somatostatin receptors on the gastrin cells and somatostatin scintigraphy using [111In-DPTA-Dphe1]-octreotide is considered the initial localization study of choice. It has 71% sensitivity and 86% specificity for primary tumors and 92% sensitivity for detection of metastatic disease.
References
1. Murugesan S.V., Varro A., Pritchard D.M. Review article: Strategies to determine whether hypergastrinaemia is due to Zollinger-Ellison syndrome rather than a more common benign cause. Aliment Pharmacol. Ther. 2009;29:1055-68.
2. Jensen R.T., Niederle B., Mitry E., et al. Frascati Consensus Conference; European Neuroendocrine Tumor Society. Gastrinoma (duodenal and pancreatic). Neuroendocrinology 2006;84:173-82.
3. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
4. Gibril F., Reynolds J.C., Doppman J.L., et al. Somatostatin receptor scintigraphy: Its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas - A prospective study. Ann. Intern. Med. 1996;125:26-34.
5. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
ANSWER: D
Critique
The patient is most likely to have Zollinger-Ellison syndrome (ZES), a condition caused by a gastrinoma. In 25% of cases, ZES is associated with multiple endocrine neoplasia type 1 (MEN-1). Clinical features of MEN-1 include gastrinoma or other islet cell tumor, hyperparathyroidism, and anterior pituitary tumors. ZES should be especially considered in a patient with multiple, refractory, or recurrent peptic ulcer disease, especially if accompanied by diarrhea or hypercalcemia. Diarrhea is often a predominant symptom and is caused by the large volume of acid that inactivates pancreatic lipase and damages the absorptive mucosa of the proximal gut. Tests to diagnose ZES include serum gastrin radioimmunoassay, secretin stimulation test, somatostatin receptor scintigraphy, and endoscopic ultrasound. Almost all gastrinomas contain somatostatin receptors on the gastrin cells and somatostatin scintigraphy using [111In-DPTA-Dphe1]-octreotide is considered the initial localization study of choice. It has 71% sensitivity and 86% specificity for primary tumors and 92% sensitivity for detection of metastatic disease.
References
1. Murugesan S.V., Varro A., Pritchard D.M. Review article: Strategies to determine whether hypergastrinaemia is due to Zollinger-Ellison syndrome rather than a more common benign cause. Aliment Pharmacol. Ther. 2009;29:1055-68.
2. Jensen R.T., Niederle B., Mitry E., et al. Frascati Consensus Conference; European Neuroendocrine Tumor Society. Gastrinoma (duodenal and pancreatic). Neuroendocrinology 2006;84:173-82.
3. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
4. Gibril F., Reynolds J.C., Doppman J.L., et al. Somatostatin receptor scintigraphy: Its sensitivity compared with that of other imaging methods in detecting primary and metastatic gastrinomas - A prospective study. Ann. Intern. Med. 1996;125:26-34.
5. Hung, P.D., Schubert, M.L., Mihas, A.A. Zollinger-Ellison Syndrome. Current Treatment Options in Gastroenterology 2003;6:163-70.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.
- Sifrim D, Dupont L, Blondeau K, Zhang X, Tack J, Janssens J. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure, pH, and impedance monitoring. Gut 2005;54:449–54.
- Smith J, Woodcock A, Houghton L. New developments in reflux-associated cough. Lung 2010;188(Suppl1)S81-6.
- Sifrim D, Barnes N. GERD related chronic cough: How to identify patients who will respond to antireflux therapy. J. Clin. Gastroenterol. 2010;44:234-6.