User login
Guidelines Help Hospitalists Manage Acute Coronary Syndrome Patients

Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
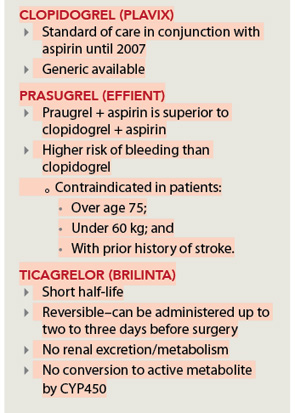
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Acute coronary syndrome (ACS) accounts for more than 1.4 million hospital admissions per year, and as many as 1 in 5 ACS patients die in the first six months after diagnosis, according to the American Academy of Family Physicians. With that in mind, Bruce Darrow, MD, PhD, presented the seminar “Acute Coronary Syndrome (ACS): Keys to Treatment and New Advances” for more than 150 hospitalists at the seventh annual Mid-Atlantic Hospital Medicine Symposium in October at Mount Sinai Medical Center in New York City.
“ACS patients are being admitted to a hospitalist’s care, although these physicians are not coronary service-line providers,” said Dr. Darrow, Mount Sinai’s director of telemetry services. “Often they work with cardiologists, but there are things hospitalists should be comfortable doing without consulting a specialist.”
Dr. Darrow spent the majority of his presentation reviewing the American College of Cardiology Foundation/American Heart Association (ACCF/AHA) 2012 update of the 2007 guidelines for managing patients with myocardial infarction (MI).
Three Phases of Treatment
To achieve the comfort level he believes hospitalists require, Dr. Darrow explained three phases of ACS care: initial medical treatment, reperfusion therapy, and transitional management.1,2 Hospitalists who see patients within the first 24 hours of their hospital stay are providing
initial treatment.
Once the physician determines that the patient is experiencing an acute myocardial infarction, treatment should begin with:
- Aspirin;
- Low-molecular-weight heparin (or heparin if the patient will be heading to the cath lab); and
- Antiplatelet agents (clopidogrel or ticagrelor for this “upstream” portion of therapy).
—Bruce Darrow, MD, PhD, director of telemetry services, Mount Sinai Medical Center, New York
Other medications to consider are intravenous IIb/IIIa inhibitors, such as abciximab, that often were used for patients going to the cath lab. Beta-blockers, although no longer required, can be included in the arsenal. Similarly, anti-ischemics may be employed, despite a lack of evidence to support their use (e.g. oxygen can be a good idea, and morphine will certainly benefit someone in pain).
In cases with ST elevation, after initial treatment, the patient is generally sent to reperfusion therapy, unless it is contraindicated. Primary percutaneous coronary intervention (PCI) is recommended in facilities with a 24/7 cath lab, or in cases for which the patient can be transferred to a hospital with an available cath lab within three hours. Otherwise, thrombolysis is the route to take, and all hospitals should be capable of that procedure, Dr. Darrow said.
After reperfusion or conservative management measures are taken, the patient is transitioned to post-MI care, which includes:
- Aspirin (except where contraindicated);
- Antiplatelet agents (clopidogrel, ticagrelor, and prasugruel, depending on patient risk factors; see Figure 1, right);
- Beta-blockers;
- Statins;
- ACE inhibitors (for patients with systolic dysfunction); and
- Eplerenone/spironolactone (for patients with systolic dysfunction and respiratory conditions).
Core Measures
Dr. Darrow also addressed the ACS Core Measures, performance measurement, and improvement initiatives set by The Joint Commission and the Centers for Medicare & Medicaid Services (CMS).3
Upon arrival, patients should be given:
- Aspirin (Joint Commission-required; voluntary according to CMS);
- Thrombolyis within 30 minutes (if applicable); and
- Primary PCI within 90 minutes (if applicable).
At discharge, patients should be given:
- Aspirin;
- Beta-blockers (Joint Commission-required; voluntary according to CMS);
- ACE/ARB for systolic heart failure (Joint Commission-required;
- voluntary according to CMS); and
- Statins.
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update). a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-681.
- Darrow B. Acute coronary syndrome (ACS): Keys to treatment and new advances. Paper presented at the seventh annual Mid-Atlantic Hospital Medicine Symposium; Oct. 19, 2012; New York, NY.
- Joint Commission and the Centers for Medicare & Medicaid Services. Specifications Manual for National Hospital Inpatient Quality Measures. The Joint Commission website. Available at: http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed Oct. 22, 2012.
Hospitalists on the Move

Bassam Kret, MD, has been named Physician of the Year at 227-bed Licking Memorial Hospital (LMH) in Newark, Ohio. Dr. Kret, who joined LMH in 2002, helped found the hospitalist program. Dr. Kret received the hospital’s MVP award in 2008 and practices with nine other hospitalists as part of the 24-hour HM service.
Louay Shawesh, MD, has been promoted to chief medical officer of Glendale, Calif.-based hospitalist services provider Apollo Medical Holdings (ApolloMed). Prior to his new position, he served as ApolloMed’s regional medical director. As CMO, Dr. Shawesh will be focused on improving efficiency and quality of healthcare delivery throughout ApolloMed’s network of 27 hospitalist programs.

Tony Rino is the new executive director for IPC: The Hospitalist Company’s New England region of operations. He is the first to serve in this new position, which oversees operations at acute-care and post-acute-care facilities throughout New England. Rino, a veteran hospital administrator, previously served as vice president of physician services for national hospital company Vanguard Health Systems. IPC is based in North Hollywood, Calif., and provides hospitalist services in 28 states.
Daniel Hilton, MD, has been named regional hospitalist medical director for ApolloMed’s new Orange County, Calif., division. Dr. Hilton will oversee all hospitalist operations at four Orange County hospitals; he already holds administrative positions at three of those facilities. A board-certified internal-medicine physician and veteran hospitalist, Dr. Hilton is especially focused on palliative care.

Mark Rudolph, MD, SFHM, is the new vice president of patient experience and physician development for Tacoma, Wash.-based Sound Physicians. He will focus on improving patient experience in all 70 of Sound’s hospitalist programs across the country. Prior to this role, Dr. Rudolph served as CMO of Sound’s Northwest region. Since joining the company in 2002, he has served as chief hospitalist at Highline Medical Center in Burien, Wash., and he helped pilot the development of SoundInstitute, a Web-based physician learning system.

Hospitalist Brian Harte, MD, SFHM, has been appointed president of Cleveland Clinic’s South Pointe Hospital in Warrensville Heights, Ohio. Dr. Harte previously served as chief operating officer at Hillcrest Hospital in Mayfield Heights, Ohio. He is a member of SHM’s board of directors and a deputy editor of the Journal of Hospital Medicine. At Cleveland Clinic, he also serves as medical director of Enterprise Business Intelligence.

Deepak Pahuja, MD, FACP, recently received the American College of Physicians’ (ACP) Illinois Downstate and Pennsylvania Leadership Development Achievement Award for completing ACP’s Leadership Seminars for Young Physicians. Dr Pahuja is a hospitalist and CEO of Aerolib Healthcare Solutions, a medical device innovation firm. He is a physician reviewer for Medical Audit and Review Solutions and Intercede Health for concurrent and retrospective patient reviews. He is pursuing his MBA with a focus in medical management from the Isenberg School of Management at the University of Massachusetts in Amherst, Mass.
Business Moves
Apollo Medical Holdings (ApolloMed) has begun providing hospitalists services at 22 Los Angeles County hospitals in the L.A. Care Health Plan. L.A. Care serves more than 1 million people in Los Angeles County, making it the largest public healthcare plan in the country.

IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced its acquisition of Elder Medical Services, P.C. Based in New York’s Syracuse and Buffalo areas, Elder provides post-acute care to patients in nursing homes and assisted living facilities. Elder’s doctors and nurse practitioners focus on safe and efficient transitions between inpatient care and these facilities.
IPC also has announced the acquisition of Valley Hospital Doctors (VHD) in McAllen, Texas. All five of VHD’s co-owner physicians will stay on as practicing hospitalists.
Brentwood, Tenn.-based Cogent HMG now provides full-service hospitalist accommodations at the 65-bed Atlanta Memorial Hospital in Atlanta, Texas. Atlanta Memorial serves the Cass and Atlanta counties’ area. Cogent provides services at more than 100 hospitals throughout the U.S.
Private equity group Sverica International has announced plans to invest in Akron, Ohio-based Inpatient Medical Services (IMS). Sverica officials say they were impressed with IMS’ exceptional growth in the Midwest over the past several years. IMS currently provides hospitalist services to hundreds of thousands of patients in the Northern Ohio region.

Sound Physicians, based in Tacoma, Wash., has announced plans to take over management of hospitalist services at 659-bed Baystate Medical Center in Springfield, Mass. Baystate’s hospitalist program already employs 45 physicians.
Antelope Valley Hospital (AVH) in Lancaster, Calif., has launched its new hospitalist program for adult inpatients. The 420-bed facility already provides pediatric and OBGYN hospitalist services to their respective patients. Hospitalist and medical director Ferdinand Panoussi, DO, will lead a team of six full-time clinicians.
—Michael O’Neal
Bassam Kret, MD, has been named Physician of the Year at 227-bed Licking Memorial Hospital (LMH) in Newark, Ohio. Dr. Kret, who joined LMH in 2002, helped found the hospitalist program. Dr. Kret received the hospital’s MVP award in 2008 and practices with nine other hospitalists as part of the 24-hour HM service.
Louay Shawesh, MD, has been promoted to chief medical officer of Glendale, Calif.-based hospitalist services provider Apollo Medical Holdings (ApolloMed). Prior to his new position, he served as ApolloMed’s regional medical director. As CMO, Dr. Shawesh will be focused on improving efficiency and quality of healthcare delivery throughout ApolloMed’s network of 27 hospitalist programs.
Tony Rino is the new executive director for IPC: The Hospitalist Company’s New England region of operations. He is the first to serve in this new position, which oversees operations at acute-care and post-acute-care facilities throughout New England. Rino, a veteran hospital administrator, previously served as vice president of physician services for national hospital company Vanguard Health Systems. IPC is based in North Hollywood, Calif., and provides hospitalist services in 28 states.
Daniel Hilton, MD, has been named regional hospitalist medical director for ApolloMed’s new Orange County, Calif., division. Dr. Hilton will oversee all hospitalist operations at four Orange County hospitals; he already holds administrative positions at three of those facilities. A board-certified internal-medicine physician and veteran hospitalist, Dr. Hilton is especially focused on palliative care.
Mark Rudolph, MD, SFHM, is the new vice president of patient experience and physician development for Tacoma, Wash.-based Sound Physicians. He will focus on improving patient experience in all 70 of Sound’s hospitalist programs across the country. Prior to this role, Dr. Rudolph served as CMO of Sound’s Northwest region. Since joining the company in 2002, he has served as chief hospitalist at Highline Medical Center in Burien, Wash., and he helped pilot the development of SoundInstitute, a Web-based physician learning system.
Hospitalist Brian Harte, MD, SFHM, has been appointed president of Cleveland Clinic’s South Pointe Hospital in Warrensville Heights, Ohio. Dr. Harte previously served as chief operating officer at Hillcrest Hospital in Mayfield Heights, Ohio. He is a member of SHM’s board of directors and a deputy editor of the Journal of Hospital Medicine. At Cleveland Clinic, he also serves as medical director of Enterprise Business Intelligence.
Deepak Pahuja, MD, FACP, recently received the American College of Physicians’ (ACP) Illinois Downstate and Pennsylvania Leadership Development Achievement Award for completing ACP’s Leadership Seminars for Young Physicians. Dr Pahuja is a hospitalist and CEO of Aerolib Healthcare Solutions, a medical device innovation firm. He is a physician reviewer for Medical Audit and Review Solutions and Intercede Health for concurrent and retrospective patient reviews. He is pursuing his MBA with a focus in medical management from the Isenberg School of Management at the University of Massachusetts in Amherst, Mass.
Business Moves
Apollo Medical Holdings (ApolloMed) has begun providing hospitalists services at 22 Los Angeles County hospitals in the L.A. Care Health Plan. L.A. Care serves more than 1 million people in Los Angeles County, making it the largest public healthcare plan in the country.
IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced its acquisition of Elder Medical Services, P.C. Based in New York’s Syracuse and Buffalo areas, Elder provides post-acute care to patients in nursing homes and assisted living facilities. Elder’s doctors and nurse practitioners focus on safe and efficient transitions between inpatient care and these facilities.
IPC also has announced the acquisition of Valley Hospital Doctors (VHD) in McAllen, Texas. All five of VHD’s co-owner physicians will stay on as practicing hospitalists.
Brentwood, Tenn.-based Cogent HMG now provides full-service hospitalist accommodations at the 65-bed Atlanta Memorial Hospital in Atlanta, Texas. Atlanta Memorial serves the Cass and Atlanta counties’ area. Cogent provides services at more than 100 hospitals throughout the U.S.
Private equity group Sverica International has announced plans to invest in Akron, Ohio-based Inpatient Medical Services (IMS). Sverica officials say they were impressed with IMS’ exceptional growth in the Midwest over the past several years. IMS currently provides hospitalist services to hundreds of thousands of patients in the Northern Ohio region.
Sound Physicians, based in Tacoma, Wash., has announced plans to take over management of hospitalist services at 659-bed Baystate Medical Center in Springfield, Mass. Baystate’s hospitalist program already employs 45 physicians.
Antelope Valley Hospital (AVH) in Lancaster, Calif., has launched its new hospitalist program for adult inpatients. The 420-bed facility already provides pediatric and OBGYN hospitalist services to their respective patients. Hospitalist and medical director Ferdinand Panoussi, DO, will lead a team of six full-time clinicians.
—Michael O’Neal
Bassam Kret, MD, has been named Physician of the Year at 227-bed Licking Memorial Hospital (LMH) in Newark, Ohio. Dr. Kret, who joined LMH in 2002, helped found the hospitalist program. Dr. Kret received the hospital’s MVP award in 2008 and practices with nine other hospitalists as part of the 24-hour HM service.
Louay Shawesh, MD, has been promoted to chief medical officer of Glendale, Calif.-based hospitalist services provider Apollo Medical Holdings (ApolloMed). Prior to his new position, he served as ApolloMed’s regional medical director. As CMO, Dr. Shawesh will be focused on improving efficiency and quality of healthcare delivery throughout ApolloMed’s network of 27 hospitalist programs.
Tony Rino is the new executive director for IPC: The Hospitalist Company’s New England region of operations. He is the first to serve in this new position, which oversees operations at acute-care and post-acute-care facilities throughout New England. Rino, a veteran hospital administrator, previously served as vice president of physician services for national hospital company Vanguard Health Systems. IPC is based in North Hollywood, Calif., and provides hospitalist services in 28 states.
Daniel Hilton, MD, has been named regional hospitalist medical director for ApolloMed’s new Orange County, Calif., division. Dr. Hilton will oversee all hospitalist operations at four Orange County hospitals; he already holds administrative positions at three of those facilities. A board-certified internal-medicine physician and veteran hospitalist, Dr. Hilton is especially focused on palliative care.
Mark Rudolph, MD, SFHM, is the new vice president of patient experience and physician development for Tacoma, Wash.-based Sound Physicians. He will focus on improving patient experience in all 70 of Sound’s hospitalist programs across the country. Prior to this role, Dr. Rudolph served as CMO of Sound’s Northwest region. Since joining the company in 2002, he has served as chief hospitalist at Highline Medical Center in Burien, Wash., and he helped pilot the development of SoundInstitute, a Web-based physician learning system.
Hospitalist Brian Harte, MD, SFHM, has been appointed president of Cleveland Clinic’s South Pointe Hospital in Warrensville Heights, Ohio. Dr. Harte previously served as chief operating officer at Hillcrest Hospital in Mayfield Heights, Ohio. He is a member of SHM’s board of directors and a deputy editor of the Journal of Hospital Medicine. At Cleveland Clinic, he also serves as medical director of Enterprise Business Intelligence.
Deepak Pahuja, MD, FACP, recently received the American College of Physicians’ (ACP) Illinois Downstate and Pennsylvania Leadership Development Achievement Award for completing ACP’s Leadership Seminars for Young Physicians. Dr Pahuja is a hospitalist and CEO of Aerolib Healthcare Solutions, a medical device innovation firm. He is a physician reviewer for Medical Audit and Review Solutions and Intercede Health for concurrent and retrospective patient reviews. He is pursuing his MBA with a focus in medical management from the Isenberg School of Management at the University of Massachusetts in Amherst, Mass.
Business Moves
Apollo Medical Holdings (ApolloMed) has begun providing hospitalists services at 22 Los Angeles County hospitals in the L.A. Care Health Plan. L.A. Care serves more than 1 million people in Los Angeles County, making it the largest public healthcare plan in the country.
IPC: The Hospitalist Company, based in North Hollywood, Calif., has announced its acquisition of Elder Medical Services, P.C. Based in New York’s Syracuse and Buffalo areas, Elder provides post-acute care to patients in nursing homes and assisted living facilities. Elder’s doctors and nurse practitioners focus on safe and efficient transitions between inpatient care and these facilities.
IPC also has announced the acquisition of Valley Hospital Doctors (VHD) in McAllen, Texas. All five of VHD’s co-owner physicians will stay on as practicing hospitalists.
Brentwood, Tenn.-based Cogent HMG now provides full-service hospitalist accommodations at the 65-bed Atlanta Memorial Hospital in Atlanta, Texas. Atlanta Memorial serves the Cass and Atlanta counties’ area. Cogent provides services at more than 100 hospitals throughout the U.S.
Private equity group Sverica International has announced plans to invest in Akron, Ohio-based Inpatient Medical Services (IMS). Sverica officials say they were impressed with IMS’ exceptional growth in the Midwest over the past several years. IMS currently provides hospitalist services to hundreds of thousands of patients in the Northern Ohio region.
Sound Physicians, based in Tacoma, Wash., has announced plans to take over management of hospitalist services at 659-bed Baystate Medical Center in Springfield, Mass. Baystate’s hospitalist program already employs 45 physicians.
Antelope Valley Hospital (AVH) in Lancaster, Calif., has launched its new hospitalist program for adult inpatients. The 420-bed facility already provides pediatric and OBGYN hospitalist services to their respective patients. Hospitalist and medical director Ferdinand Panoussi, DO, will lead a team of six full-time clinicians.
—Michael O’Neal
We Welcome the Newest SHM Members
Enter text here
Enter text here
Enter text here
The Hospital Home Team: Physicians Increase Focus on Inpatient Care

For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
For most of my medical career, the hospital functioned more as a swap meet, where every physician had his or her own booth, than as an integrated, community health resource with a focused mission. Although the innovation of HM might be counted as the beginning of a new, more aligned approach between physicians and the hospital as an institution, the rapidly evolving employment of physicians by hospitals and the focusing of physician practice primarily on inpatient care has taken this to another level.
The New Paradigm
A number of recent surveys by physician recruitment firms and physician management companies have found that less than 25% of physicians are self-employed. Planned changes to insurance and Medicare reimbursement for healthcare have driven cardiologists, orthopedists, surgeons, and many other physicians, who want to protect their flow of patients and dollars, to readily become hospital or large-group-practice employees. The entrance of accountable-care organizations (ACOs) to the landscape and the greater need for physician and hospital alignment have only accelerated this trend.
At the same time, the growth of all sorts of hospitalist specialties has further changed the medical staff of the hospital. Internal-medicine and family-practice hospitalists now number more than 35,000. There are probably more than 2,000 pediatric hospitalists. The newly formed Society of OB/GYN Hospitalists (SOGH) estimates there are more than 1,500 so-called laborists in the U.S., and there are several hundred neurohospitalists, orthopedic hospitalists, and acute-care surgeons.
It is clear to me that a “home team” for the hospital of the future is developing, and it includes hospitalists, ED physicians, critical-care physicians, and the growing panoply of hospital-employed cardiologists and surgeons. There is an opportunity for alignment and integration in what has been a fragmented delivery of healthcare.
On the commercial side of the equation, this new opportunity for physician-hospital alignment might allow for a new distribution of compensation. It already is common for hospitals to be transferring some of “their” Medicare Part A dollars to hospitalists. With penalties or additional payments in the ACO model (e.g. shared savings) or in value-based purchasing, there certainly are mechanisms to redistribute funding to new physician compensation models, based more on performance than on volume of services (i.e. the old productivity model).
On another level, where compensation and performance merge, the new medical staff has the ability to deliver a safer hospital experience to our patients and to improve performance. This could take the form of reduction in hospital-acquired infections (HAIs) or reducing unnecessary DVTs and PEs. It could take the form of a better discharge process that leads to fewer unnecessary readmissions or fewer preventable ED visits. On the OB side, 24-hour on-site availability of OB hospitalists has been shown to reduce adverse birth events and, therefore, reduce liability risk and malpractice premiums. On-site availability for patients with fractures and trauma cases by orthopedic hospitalists or hospital-employed orthopedists also can reduce expenses and adverse events for these acutely ill patients.
HM’s Role
With all these changes occurring so rapidly and with all these new players being thrown into the stew at the hospital, it may be worth a few minutes for the “traditional” hospitalist on the medical service to step back and see how our role may evolve. We already have an increasing role in comanagement of surgical and subspecialty patients, as well as a more integrated role at the ED-hospitalist interface. As hospitals look for hospital-focused physicians, there is a potential for scope creep that must be thoughtfully managed.
This may require “rules of engagement” with other key services. While it may be appropriate for a patient with an acute abdomen to be admitted to the hospitalist service, if the hospitalist determines that this patient needs surgery sooner rather than later, there needs to be a straightforward way to get the surgeon in house and on the case and the patient to the operating room. To this point, medical hospitalists can help manage the medical aspects of a neurosurgical case, but we don’t do burr holes. And if there is to be pushback from the surgeon, this can’t happen at 2 a.m. over the telephone; it must be handled by the service leaders at their weekly meeting.
On another level, hospitalists need to be careful that the hospital doesn’t just hand us the administrative functions of other physicians’ care. Hospitalists are not the default to do H&Ps on surgical cases or handle their discharges, even if this falls into the hospital strategy to be able to employ fewer high-priced surgeons and subspecialists by handing off some of their work to their hospitalists.
On the other hand, it is totally appropriate for many of the hospital-focused physicians to come together, possibly under the leadership of the hospital CMO, to look at the workflow and to set up a new way to deliver healthcare that not only redefines the workload, but also involves the rest of the team, including nursing, pharmacy, case management, and social services. Medical hospitalists will need to consider whether we should be the hub of the new physician enterprise and what that would mean for workload, FTEs, and scope of practice.
Such organizations as SHM and the American Hospital Association (AHA) are thinking how best to support and convene the hospital-based physician. AHA has developed a Physician Forum with more than 6,000 members who now have their practices aligned with their hospital. SHM has held meetings of the leaders of hospital-focused practice and is developing virtual forums on Hospital Medicine Exchange to keep the discussion going. Through the Hospital Care Collaborative (HCC), SHM is engaging the leadership of pharmacy, nursing, case management, social services, and respiratory therapy.
Although we are still early in creating the direction for the new medical staff, the water is rising and the current is moving rapidly. The strong forces that are driving new payment paradigms are leading to changes in compensation and an emphasis on definable, measureable outcomes of performance and safety. Hospitalists, who have been thinking in this way and who have some experience in the new ways, should be well positioned to lead and participate actively in the formation of the new hospital home team.
When opportunity knocks, you still have to get up and answer the door. It’s time to get ready to step up.
Dr. Wellikson is CEO of SHM.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Burnout among physicians and the general workforce
- Effects of clopidogrel added to aspirin in patients with recent lacunar stroke
- Performance of the HEMORR2AGES, ATRIA, and HAS-BLED bleeding risk prediction scores in patients with atrial fibrillation undergoing anticoagulation
- Probiotics for secondary prevention of hepatic encephalopathy
- Capsule endoscopy for acute obscure GI bleeding
- Perceptions of readmitted patients transitioning from hospital to home
- Thirty-day readmissions after acute myocardial infarction
- One-hour rule-out or rule-in for AMI patients in chest pain
- Aspirin increases bleed risk without reducing risk of stroke in CKD and NVAF patients
Burnout among Physicians and the General Workforce
Clinical question: What is the degree and distribution of burnout within the physician workforce, and how does that compare to the general U.S. workforce?
Background: Professional burnout, work satisfaction, and work-life balance are critical elements to understand in the physician workforce. It is well documented that physicians are at high risk for burnout; however, few extensive studies have looked at rates and the identification of high-risk subpopulations.
Study design: Cross-sectional survey.
Setting: U.S. workforce.
Synopsis: This study included 7,288 physicians (26.7% response rate) and 5,930 controls from the general U.S. population. Validated survey instruments were employed to assess the degree and presence of burnout, depression, and satisfaction with work-life balance.
In aggregate, using a validated, two-item burnout measure, 35.2% of physicians were characterized as having burnout, compared with 27.6% of the general population (P<0.001). Within the physician community, the specialties with the highest risk of burnout included emergency medicine, general internal medicine, family medicine, and neurology.
Important limitations of this study include that the physician and general population surveys were performed at different times (six months apart), that the groups were not ideally matched (age and sex, for example), and the overall response rate of the physician survey was low.
This study sheds light on an important topic for hospitalists. Future studies should continue to probe the problem of burnout and look for creative solutions to mitigate risks that might threaten professional longevity.
Bottom line: Burnout is prevalent among physicians, especially when compared to the general workforce. Physician specialties in front-line patient care are at highest risk.
Citation: Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;20 [Epub ahead of print].
Effects of Clopidogrel Added to Aspirin in Patients with Recent Lacunar Stroke
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
Bleeding Risk Prediction Scores in Patients with Atrial Fibrillation Undergoing Anticoagulation
Clinical question: What are the relative predictive values of the HEMORR2AGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best to predict clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORRAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867
Probiotics for Secondary Prevention of Hepatic Encephalopathy
Clinical question: Are probiotics as effective as lactulose for secondary prevention of hepatic encephalopathy (HE)?
Background: Probiotics alter the gut flora, resulting in decreased ammonia production and absorption. Probiotics have been shown to reduce the incidence of low-grade HE. However, studies on probiotics usage for secondary prevention of HE are lacking.
Study design: Prospective, randomized, controlled, nonblinded, single-center study.
Setting: Tertiary-care center, New Delhi.
Synopsis: Three hundred sixty patients who had recovered from HE from October 2008 to December 2009 were screened; 235 met the inclusion criteria. They were randomized to receive either lactulose (Gp-L), probiotics (Gp-P), or no therapy (Gp-N). The Gp-L group received 30 to 60 ml of lactulose in two to three divided doses; the Gp-P group received three capsules per day containing lactobacillus, bifidobacterium, and Streptococcus salivarius strains.
The primary endpoints were the development of overt HE (assessed by the West Haven Criteria) or a follow-up of 12 months. Lactulose therapy was significantly more effective in secondary prophylaxis than no therapy (26.2% vs. 56.9%, P=0.001), as was probiotics therapy compared with no therapy (34.4% vs. 56.9%, P=0.02), but no significant difference was found between lactulose and probiotics therapy (26.2% vs. 34.4%, P=0.349).
The major limitation of the study was its open-label design. The study also used a high concentration of probiotics, and the results could be strain-specific and hence require validation with other probiotics combinations. The Gp-N group continued the previous therapy (excluding lactulose), with an unknown number on rifaximin.
Bottom line: Lactulose and probiotics are equally effective in secondary prophylaxis of hepatic encephalopathy.
Citation: Agrawal A, Sharma BC, Sharma P, Sarin SK. Secondary prophylaxis of hepatic encephalopathy in cirrhosis: an open-label, randomized controlled trial of lactulose, probiotics and no therapy. Am J Gastroenterol. 2012;107:1043-1050.
Capsule Endoscopy for Acute Obscure GI Bleeding
Clinical question: What testing modality is most appropriate for acute obscure GI bleeding: capsule endoscopy (CE) or angiography?
Background: Acute obscure GI bleeding (OGIB): remains a diagnostic challenge, accounting for 7% to 8% of patients presenting with GI bleeding. CE enables direct visualization of small bowel mucosa but lacks the ability for therapeutic intervention. Angiography is frequently chosen for massive bleeding; however, it is invasive and does not enable visualization of the bowel.
Study design: Prospective, randomized, controlled, blinded, single-center study.
Setting: Prince of Wales Hospital, Hong Kong.
Synopsis: Ninety-one patients with active OGIB from June 2005 to November 2007 were assessed for eligibility; 60 met the criteria and were randomized to either CE or angiography. Overt OGIB was defined as patients who had nondiagnostic upper endoscopy and colonoscopy.
The primary outcome was diagnostic yield of CE or mesenteric angiography in identifying the bleeding source. Secondary outcomes were long-term rebleeding rates, readmissions for bleeding or anemia, blood transfusions, and death.
CE was positive in 16 patients (53.3%) and angiography was positive in six patients (20%). The diagnostic yield of CE was significantly higher than angiography (difference=33.3%, 95% CI 8.9-52.8%, P=0.016). The mean follow-up period was 48.5 months. The cumulative risk of rebleeding was higher in the angiography group, but this was not statistically significant. There was no significant difference in rates of subsequent hospitalization, death, or transfusions between the two groups.
The study based the sample-size estimation on the diagnostic yield rather than clinical outcomes and, hence, was underpowered to detect any significant differences in clinical outcomes.
Bottom line: CE has a higher diagnostic yield than angiography in patients with active overt OGIB.
Citation: Leung WK, Ho S, Suen B, et al. Capsule endoscopy of angiography in patients with acute overt gastrointestinal bleeding: a prospective randomized study with long term follow up. Am J Gastroenterol. 2012;107:1370-1376.
Perceptions of Readmitted Patients Transitioning from Hospital to Home
Clinical question: What are patient-reported reasons for readmission to the hospital after discharge?
Background: Reducing readmissions is a critical component to improving the value of healthcare. While readmission reduction is a goal of all hospitals, there is much to be gleaned from evaluating patients’ view of the problem. This study used a survey to assess the patient’s viewpoint.
Study design: Cross-sectional survey.
Setting: The Hospital of the University of Pennsylvania and Penn Presbyterian Medical Center, Philadelphia.
Synopsis: A survey of 36 questions was posed to 1,084 patients who were readmitted within 30 days of discharge from November 2010 to July 2011 (32% of eligible patients). The data were subdivided based on socioeconomic status and medical versus surgical patients.
Some issues patients raised regarding discharge planning included difficulty with paying for medications, challenges with travel to pharmacies, and concern over medication side effects.
Patients with low socioeconomic status had more difficulty taking medications and following instructions, had more depression, and had less social support.
Bottom line: Readmission rates are affected by a patient’s social situation. A team approach to discharge planning might mitigate some of these factors.
Citation: Kangovi S, Grande D, Meehan P, Mitra N, Shannon R, Long JA. Perceptions of readmitted patients on the transition from hospital to home. J Hosp Med. 2012 [Epub ahead of print].
30-Day Readmissions after Acute Myocardial Infarction
Clinical question: What are potential predictors of 30-day readmissions after acute myocardial infarction (MI)?
Background: Much attention has been given to evaluate the causes of readmissions of heart failure, acute MI, and pneumonia. This study looked at 30-day readmissions after an acute myocardial infarction (AMI).
Study design: Retrospective cohort study.
Setting: Olmstead County Hospital, Rochester, Minn.
Synopsis: A chart review of AMI based on ICD-9 codes from 1987 to 2010 identified 3,010 patients. Patients were verified using symptoms, cardiac enzymes, and EKG changes at the time of event. Interventions evaluated included fibrinolytic therapy, CABG, or primary PCI.
Survival increased to 96% from 89% during the period from 1987 to 2010. Researchers also noted more comorbid conditions, such as diabetes mellitus, COPD, and hypertension, noted over time. Of the patients evaluated, 643 readmissions occurred for 561 patients (18.6%). Of these, the most frequent causes were ischemic heart disease, respiratory symptoms, and heart failure. Comorbid conditions, such as diabetes, COPD, anemia, higher killip class on initial admission, duration of prior hospitalization, and procedural complications, independently increased the risk of readmission.
Bottom line: In addition to factors unrelated to an AMI, a patient’s comorbid conditions, post-procedure complications, and duration of hospitalization influence the risk of readmission.
Citation: Dunlay SM, Weston SA, Killian JM, et al. Thirty-day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157(1):11-18.
One-Hour Rule-Out or Rule-In for AMI in Chest Pain
Clinical question: How can we use the newly developed high-sensitivity cardiac troponin (hs-cTnT) to shorten the time to rule in and rule out AMI?
Background: The hs-cTnT assays available appear to improve the early diagnosis of AMI when compared to the regular cardiac troponins, but no clear guidelines are available as how to best use them in clinical practice.
Study design: Prospective, multicenter study.
Setting: Switzerland hospitals.
Synopsis: The study enrolled 872 unselected patients presenting to the ED with acute chest pain. Hs-cTnT level was measured in a blinded fashion at presentation and after one hour. Two independent cardiologists using all available medical records adjudicated the final AMI diagnosis. Optimal thresholds for rule-out were selected to allow for 100% sensitivity and negative predictive value. Rule-out criteria were defined as baseline hs-cTnT level <12 ng/L and an absolute change within the first hour of <3 ng/L. Rule-in criteria was defined as baseline hs-cTnT >52 ng/L or an absolute increase within the first hour of >5 ng/L.
AMI was the final diagnosis in 17% of patients; AMI was ruled out in 60%; and the remaining 23% were placed in observation.
Primary prognostic endpoint was 30-day mortality rate, which was 0.2% in the rule-out group, validating the suitability of these patients for early discharge.
Study limitations were that it was an observational study not used for clinical decision-making, no dialysis patients were included, and only one specific hs-cTnT assay was tested.
Bottom line: Using hs-cTnT levels at presentation and absolute changes within the first hour, a safe rule-out or rule-in of AMI can be performed in 77% of patients presenting with chest pain.
Citation: Reichlin T, Schindler C, Drexler B, et al. One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch Intern Med. 2012;172(16):1-8.
Aspirin Increases Bleed Risk without Reducing Risk of Stroke in CKD and NVAF Patients
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular afib (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34) with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Burnout among physicians and the general workforce
- Effects of clopidogrel added to aspirin in patients with recent lacunar stroke
- Performance of the HEMORR2AGES, ATRIA, and HAS-BLED bleeding risk prediction scores in patients with atrial fibrillation undergoing anticoagulation
- Probiotics for secondary prevention of hepatic encephalopathy
- Capsule endoscopy for acute obscure GI bleeding
- Perceptions of readmitted patients transitioning from hospital to home
- Thirty-day readmissions after acute myocardial infarction
- One-hour rule-out or rule-in for AMI patients in chest pain
- Aspirin increases bleed risk without reducing risk of stroke in CKD and NVAF patients
Burnout among Physicians and the General Workforce
Clinical question: What is the degree and distribution of burnout within the physician workforce, and how does that compare to the general U.S. workforce?
Background: Professional burnout, work satisfaction, and work-life balance are critical elements to understand in the physician workforce. It is well documented that physicians are at high risk for burnout; however, few extensive studies have looked at rates and the identification of high-risk subpopulations.
Study design: Cross-sectional survey.
Setting: U.S. workforce.
Synopsis: This study included 7,288 physicians (26.7% response rate) and 5,930 controls from the general U.S. population. Validated survey instruments were employed to assess the degree and presence of burnout, depression, and satisfaction with work-life balance.
In aggregate, using a validated, two-item burnout measure, 35.2% of physicians were characterized as having burnout, compared with 27.6% of the general population (P<0.001). Within the physician community, the specialties with the highest risk of burnout included emergency medicine, general internal medicine, family medicine, and neurology.
Important limitations of this study include that the physician and general population surveys were performed at different times (six months apart), that the groups were not ideally matched (age and sex, for example), and the overall response rate of the physician survey was low.
This study sheds light on an important topic for hospitalists. Future studies should continue to probe the problem of burnout and look for creative solutions to mitigate risks that might threaten professional longevity.
Bottom line: Burnout is prevalent among physicians, especially when compared to the general workforce. Physician specialties in front-line patient care are at highest risk.
Citation: Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;20 [Epub ahead of print].
Effects of Clopidogrel Added to Aspirin in Patients with Recent Lacunar Stroke
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
Bleeding Risk Prediction Scores in Patients with Atrial Fibrillation Undergoing Anticoagulation
Clinical question: What are the relative predictive values of the HEMORR2AGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best to predict clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORRAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867
Probiotics for Secondary Prevention of Hepatic Encephalopathy
Clinical question: Are probiotics as effective as lactulose for secondary prevention of hepatic encephalopathy (HE)?
Background: Probiotics alter the gut flora, resulting in decreased ammonia production and absorption. Probiotics have been shown to reduce the incidence of low-grade HE. However, studies on probiotics usage for secondary prevention of HE are lacking.
Study design: Prospective, randomized, controlled, nonblinded, single-center study.
Setting: Tertiary-care center, New Delhi.
Synopsis: Three hundred sixty patients who had recovered from HE from October 2008 to December 2009 were screened; 235 met the inclusion criteria. They were randomized to receive either lactulose (Gp-L), probiotics (Gp-P), or no therapy (Gp-N). The Gp-L group received 30 to 60 ml of lactulose in two to three divided doses; the Gp-P group received three capsules per day containing lactobacillus, bifidobacterium, and Streptococcus salivarius strains.
The primary endpoints were the development of overt HE (assessed by the West Haven Criteria) or a follow-up of 12 months. Lactulose therapy was significantly more effective in secondary prophylaxis than no therapy (26.2% vs. 56.9%, P=0.001), as was probiotics therapy compared with no therapy (34.4% vs. 56.9%, P=0.02), but no significant difference was found between lactulose and probiotics therapy (26.2% vs. 34.4%, P=0.349).
The major limitation of the study was its open-label design. The study also used a high concentration of probiotics, and the results could be strain-specific and hence require validation with other probiotics combinations. The Gp-N group continued the previous therapy (excluding lactulose), with an unknown number on rifaximin.
Bottom line: Lactulose and probiotics are equally effective in secondary prophylaxis of hepatic encephalopathy.
Citation: Agrawal A, Sharma BC, Sharma P, Sarin SK. Secondary prophylaxis of hepatic encephalopathy in cirrhosis: an open-label, randomized controlled trial of lactulose, probiotics and no therapy. Am J Gastroenterol. 2012;107:1043-1050.
Capsule Endoscopy for Acute Obscure GI Bleeding
Clinical question: What testing modality is most appropriate for acute obscure GI bleeding: capsule endoscopy (CE) or angiography?
Background: Acute obscure GI bleeding (OGIB): remains a diagnostic challenge, accounting for 7% to 8% of patients presenting with GI bleeding. CE enables direct visualization of small bowel mucosa but lacks the ability for therapeutic intervention. Angiography is frequently chosen for massive bleeding; however, it is invasive and does not enable visualization of the bowel.
Study design: Prospective, randomized, controlled, blinded, single-center study.
Setting: Prince of Wales Hospital, Hong Kong.
Synopsis: Ninety-one patients with active OGIB from June 2005 to November 2007 were assessed for eligibility; 60 met the criteria and were randomized to either CE or angiography. Overt OGIB was defined as patients who had nondiagnostic upper endoscopy and colonoscopy.
The primary outcome was diagnostic yield of CE or mesenteric angiography in identifying the bleeding source. Secondary outcomes were long-term rebleeding rates, readmissions for bleeding or anemia, blood transfusions, and death.
CE was positive in 16 patients (53.3%) and angiography was positive in six patients (20%). The diagnostic yield of CE was significantly higher than angiography (difference=33.3%, 95% CI 8.9-52.8%, P=0.016). The mean follow-up period was 48.5 months. The cumulative risk of rebleeding was higher in the angiography group, but this was not statistically significant. There was no significant difference in rates of subsequent hospitalization, death, or transfusions between the two groups.
The study based the sample-size estimation on the diagnostic yield rather than clinical outcomes and, hence, was underpowered to detect any significant differences in clinical outcomes.
Bottom line: CE has a higher diagnostic yield than angiography in patients with active overt OGIB.
Citation: Leung WK, Ho S, Suen B, et al. Capsule endoscopy of angiography in patients with acute overt gastrointestinal bleeding: a prospective randomized study with long term follow up. Am J Gastroenterol. 2012;107:1370-1376.
Perceptions of Readmitted Patients Transitioning from Hospital to Home
Clinical question: What are patient-reported reasons for readmission to the hospital after discharge?
Background: Reducing readmissions is a critical component to improving the value of healthcare. While readmission reduction is a goal of all hospitals, there is much to be gleaned from evaluating patients’ view of the problem. This study used a survey to assess the patient’s viewpoint.
Study design: Cross-sectional survey.
Setting: The Hospital of the University of Pennsylvania and Penn Presbyterian Medical Center, Philadelphia.
Synopsis: A survey of 36 questions was posed to 1,084 patients who were readmitted within 30 days of discharge from November 2010 to July 2011 (32% of eligible patients). The data were subdivided based on socioeconomic status and medical versus surgical patients.
Some issues patients raised regarding discharge planning included difficulty with paying for medications, challenges with travel to pharmacies, and concern over medication side effects.
Patients with low socioeconomic status had more difficulty taking medications and following instructions, had more depression, and had less social support.
Bottom line: Readmission rates are affected by a patient’s social situation. A team approach to discharge planning might mitigate some of these factors.
Citation: Kangovi S, Grande D, Meehan P, Mitra N, Shannon R, Long JA. Perceptions of readmitted patients on the transition from hospital to home. J Hosp Med. 2012 [Epub ahead of print].
30-Day Readmissions after Acute Myocardial Infarction
Clinical question: What are potential predictors of 30-day readmissions after acute myocardial infarction (MI)?
Background: Much attention has been given to evaluate the causes of readmissions of heart failure, acute MI, and pneumonia. This study looked at 30-day readmissions after an acute myocardial infarction (AMI).
Study design: Retrospective cohort study.
Setting: Olmstead County Hospital, Rochester, Minn.
Synopsis: A chart review of AMI based on ICD-9 codes from 1987 to 2010 identified 3,010 patients. Patients were verified using symptoms, cardiac enzymes, and EKG changes at the time of event. Interventions evaluated included fibrinolytic therapy, CABG, or primary PCI.
Survival increased to 96% from 89% during the period from 1987 to 2010. Researchers also noted more comorbid conditions, such as diabetes mellitus, COPD, and hypertension, noted over time. Of the patients evaluated, 643 readmissions occurred for 561 patients (18.6%). Of these, the most frequent causes were ischemic heart disease, respiratory symptoms, and heart failure. Comorbid conditions, such as diabetes, COPD, anemia, higher killip class on initial admission, duration of prior hospitalization, and procedural complications, independently increased the risk of readmission.
Bottom line: In addition to factors unrelated to an AMI, a patient’s comorbid conditions, post-procedure complications, and duration of hospitalization influence the risk of readmission.
Citation: Dunlay SM, Weston SA, Killian JM, et al. Thirty-day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157(1):11-18.
One-Hour Rule-Out or Rule-In for AMI in Chest Pain
Clinical question: How can we use the newly developed high-sensitivity cardiac troponin (hs-cTnT) to shorten the time to rule in and rule out AMI?
Background: The hs-cTnT assays available appear to improve the early diagnosis of AMI when compared to the regular cardiac troponins, but no clear guidelines are available as how to best use them in clinical practice.
Study design: Prospective, multicenter study.
Setting: Switzerland hospitals.
Synopsis: The study enrolled 872 unselected patients presenting to the ED with acute chest pain. Hs-cTnT level was measured in a blinded fashion at presentation and after one hour. Two independent cardiologists using all available medical records adjudicated the final AMI diagnosis. Optimal thresholds for rule-out were selected to allow for 100% sensitivity and negative predictive value. Rule-out criteria were defined as baseline hs-cTnT level <12 ng/L and an absolute change within the first hour of <3 ng/L. Rule-in criteria was defined as baseline hs-cTnT >52 ng/L or an absolute increase within the first hour of >5 ng/L.
AMI was the final diagnosis in 17% of patients; AMI was ruled out in 60%; and the remaining 23% were placed in observation.
Primary prognostic endpoint was 30-day mortality rate, which was 0.2% in the rule-out group, validating the suitability of these patients for early discharge.
Study limitations were that it was an observational study not used for clinical decision-making, no dialysis patients were included, and only one specific hs-cTnT assay was tested.
Bottom line: Using hs-cTnT levels at presentation and absolute changes within the first hour, a safe rule-out or rule-in of AMI can be performed in 77% of patients presenting with chest pain.
Citation: Reichlin T, Schindler C, Drexler B, et al. One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch Intern Med. 2012;172(16):1-8.
Aspirin Increases Bleed Risk without Reducing Risk of Stroke in CKD and NVAF Patients
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular afib (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34) with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Burnout among physicians and the general workforce
- Effects of clopidogrel added to aspirin in patients with recent lacunar stroke
- Performance of the HEMORR2AGES, ATRIA, and HAS-BLED bleeding risk prediction scores in patients with atrial fibrillation undergoing anticoagulation
- Probiotics for secondary prevention of hepatic encephalopathy
- Capsule endoscopy for acute obscure GI bleeding
- Perceptions of readmitted patients transitioning from hospital to home
- Thirty-day readmissions after acute myocardial infarction
- One-hour rule-out or rule-in for AMI patients in chest pain
- Aspirin increases bleed risk without reducing risk of stroke in CKD and NVAF patients
Burnout among Physicians and the General Workforce
Clinical question: What is the degree and distribution of burnout within the physician workforce, and how does that compare to the general U.S. workforce?
Background: Professional burnout, work satisfaction, and work-life balance are critical elements to understand in the physician workforce. It is well documented that physicians are at high risk for burnout; however, few extensive studies have looked at rates and the identification of high-risk subpopulations.
Study design: Cross-sectional survey.
Setting: U.S. workforce.
Synopsis: This study included 7,288 physicians (26.7% response rate) and 5,930 controls from the general U.S. population. Validated survey instruments were employed to assess the degree and presence of burnout, depression, and satisfaction with work-life balance.
In aggregate, using a validated, two-item burnout measure, 35.2% of physicians were characterized as having burnout, compared with 27.6% of the general population (P<0.001). Within the physician community, the specialties with the highest risk of burnout included emergency medicine, general internal medicine, family medicine, and neurology.
Important limitations of this study include that the physician and general population surveys were performed at different times (six months apart), that the groups were not ideally matched (age and sex, for example), and the overall response rate of the physician survey was low.
This study sheds light on an important topic for hospitalists. Future studies should continue to probe the problem of burnout and look for creative solutions to mitigate risks that might threaten professional longevity.
Bottom line: Burnout is prevalent among physicians, especially when compared to the general workforce. Physician specialties in front-line patient care are at highest risk.
Citation: Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;20 [Epub ahead of print].
Effects of Clopidogrel Added to Aspirin in Patients with Recent Lacunar Stroke
Clinical question: Does the addition of clopidogrel to aspirin reduce the risk of any type of recurrent stroke, or affect the risk of bleeding or death, in patients who recently suffered a lacunar stroke?
Background: There are no prior randomized, multicenter trials on secondary prevention of lacunar stroke; aspirin is the standard antiplatelet therapy in this setting.
Study design: Double-blind, randomized, multicenter trial.
Setting: Eighty-two clinical centers in North America, Latin America, and Spain.
Synopsis: Researchers enrolled 3,020 patients from 2003 to 2011; criteria included age >30 years old and symptomatic lacunar stroke (proven by MRI) in the preceding 180 days.
Results showed no significant difference between recurrent strokes (any type) in the aspirin-only group (2.7% per year) versus the aspirin-plus-clopidogrel group (2.5% per year). Major hemorrhage risk was much higher in the aspirin-plus-clopidogrel group (2.1% per year) versus aspirin-only group (1.1% per year). All-cause mortality also was much higher in the aspirin-plus-clopidogrel group (N=113) versus the aspirin-only group (N=77).
Bottom line: The addition of clopidogrel to aspirin for secondary prevention does not significantly reduce the risk of recurrent stroke, but it does significantly increase the risk of bleeding and death.
Citation: Benavente OR, Hart RG, McClure LA, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. N Engl J Med. 2012;367:817-825.
Bleeding Risk Prediction Scores in Patients with Atrial Fibrillation Undergoing Anticoagulation
Clinical question: What are the relative predictive values of the HEMORR2AGES, ATRIA, and HAS-BLED risk-prediction schemes?
Background: The tools predict bleeding risk in patients anticoagulated for atrial fibrillation (afib), but it is unknown which is the best to predict clinically relevant bleeding.
Study design: Post-hoc analysis.
Setting: Data previously collected for the AMADEUS trial (2,293 patients taking warfarin; 251 had at least one clinically relevant bleeding event) were used to test each of the three bleeding risk-prediction schemes on the same data set.
Synopsis: Using three analysis methods (net reclassification improvement, receiver-operating characteristic [ROC], and decision-curve analysis), the researchers compared the three schemes’ performance. HAS-BLED performed best in all three of the analysis methods.
The HAS-BLED score calculation requires the following patient information: history of hypertension, renal disease, liver disease, stroke, prior major bleeding event, and labile INR; age >65; and use of antiplatelet agents, aspirin, and alcohol.
Bottom line: HAS-BLED was the best of the three schemes, although all three had only modest ability to predict clinically relevant bleeding.
Citation: Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORRAGES, ATRIA and HAS-BLED bleeding risk-prediction scores in patients with atrial fibrillation undergoing anticoagulation. J Am Coll Cardiol. 2012;60(9):861-867
Probiotics for Secondary Prevention of Hepatic Encephalopathy
Clinical question: Are probiotics as effective as lactulose for secondary prevention of hepatic encephalopathy (HE)?
Background: Probiotics alter the gut flora, resulting in decreased ammonia production and absorption. Probiotics have been shown to reduce the incidence of low-grade HE. However, studies on probiotics usage for secondary prevention of HE are lacking.
Study design: Prospective, randomized, controlled, nonblinded, single-center study.
Setting: Tertiary-care center, New Delhi.
Synopsis: Three hundred sixty patients who had recovered from HE from October 2008 to December 2009 were screened; 235 met the inclusion criteria. They were randomized to receive either lactulose (Gp-L), probiotics (Gp-P), or no therapy (Gp-N). The Gp-L group received 30 to 60 ml of lactulose in two to three divided doses; the Gp-P group received three capsules per day containing lactobacillus, bifidobacterium, and Streptococcus salivarius strains.
The primary endpoints were the development of overt HE (assessed by the West Haven Criteria) or a follow-up of 12 months. Lactulose therapy was significantly more effective in secondary prophylaxis than no therapy (26.2% vs. 56.9%, P=0.001), as was probiotics therapy compared with no therapy (34.4% vs. 56.9%, P=0.02), but no significant difference was found between lactulose and probiotics therapy (26.2% vs. 34.4%, P=0.349).
The major limitation of the study was its open-label design. The study also used a high concentration of probiotics, and the results could be strain-specific and hence require validation with other probiotics combinations. The Gp-N group continued the previous therapy (excluding lactulose), with an unknown number on rifaximin.
Bottom line: Lactulose and probiotics are equally effective in secondary prophylaxis of hepatic encephalopathy.
Citation: Agrawal A, Sharma BC, Sharma P, Sarin SK. Secondary prophylaxis of hepatic encephalopathy in cirrhosis: an open-label, randomized controlled trial of lactulose, probiotics and no therapy. Am J Gastroenterol. 2012;107:1043-1050.
Capsule Endoscopy for Acute Obscure GI Bleeding
Clinical question: What testing modality is most appropriate for acute obscure GI bleeding: capsule endoscopy (CE) or angiography?
Background: Acute obscure GI bleeding (OGIB): remains a diagnostic challenge, accounting for 7% to 8% of patients presenting with GI bleeding. CE enables direct visualization of small bowel mucosa but lacks the ability for therapeutic intervention. Angiography is frequently chosen for massive bleeding; however, it is invasive and does not enable visualization of the bowel.
Study design: Prospective, randomized, controlled, blinded, single-center study.
Setting: Prince of Wales Hospital, Hong Kong.
Synopsis: Ninety-one patients with active OGIB from June 2005 to November 2007 were assessed for eligibility; 60 met the criteria and were randomized to either CE or angiography. Overt OGIB was defined as patients who had nondiagnostic upper endoscopy and colonoscopy.
The primary outcome was diagnostic yield of CE or mesenteric angiography in identifying the bleeding source. Secondary outcomes were long-term rebleeding rates, readmissions for bleeding or anemia, blood transfusions, and death.
CE was positive in 16 patients (53.3%) and angiography was positive in six patients (20%). The diagnostic yield of CE was significantly higher than angiography (difference=33.3%, 95% CI 8.9-52.8%, P=0.016). The mean follow-up period was 48.5 months. The cumulative risk of rebleeding was higher in the angiography group, but this was not statistically significant. There was no significant difference in rates of subsequent hospitalization, death, or transfusions between the two groups.
The study based the sample-size estimation on the diagnostic yield rather than clinical outcomes and, hence, was underpowered to detect any significant differences in clinical outcomes.
Bottom line: CE has a higher diagnostic yield than angiography in patients with active overt OGIB.
Citation: Leung WK, Ho S, Suen B, et al. Capsule endoscopy of angiography in patients with acute overt gastrointestinal bleeding: a prospective randomized study with long term follow up. Am J Gastroenterol. 2012;107:1370-1376.
Perceptions of Readmitted Patients Transitioning from Hospital to Home
Clinical question: What are patient-reported reasons for readmission to the hospital after discharge?
Background: Reducing readmissions is a critical component to improving the value of healthcare. While readmission reduction is a goal of all hospitals, there is much to be gleaned from evaluating patients’ view of the problem. This study used a survey to assess the patient’s viewpoint.
Study design: Cross-sectional survey.
Setting: The Hospital of the University of Pennsylvania and Penn Presbyterian Medical Center, Philadelphia.
Synopsis: A survey of 36 questions was posed to 1,084 patients who were readmitted within 30 days of discharge from November 2010 to July 2011 (32% of eligible patients). The data were subdivided based on socioeconomic status and medical versus surgical patients.
Some issues patients raised regarding discharge planning included difficulty with paying for medications, challenges with travel to pharmacies, and concern over medication side effects.
Patients with low socioeconomic status had more difficulty taking medications and following instructions, had more depression, and had less social support.
Bottom line: Readmission rates are affected by a patient’s social situation. A team approach to discharge planning might mitigate some of these factors.
Citation: Kangovi S, Grande D, Meehan P, Mitra N, Shannon R, Long JA. Perceptions of readmitted patients on the transition from hospital to home. J Hosp Med. 2012 [Epub ahead of print].
30-Day Readmissions after Acute Myocardial Infarction
Clinical question: What are potential predictors of 30-day readmissions after acute myocardial infarction (MI)?
Background: Much attention has been given to evaluate the causes of readmissions of heart failure, acute MI, and pneumonia. This study looked at 30-day readmissions after an acute myocardial infarction (AMI).
Study design: Retrospective cohort study.
Setting: Olmstead County Hospital, Rochester, Minn.
Synopsis: A chart review of AMI based on ICD-9 codes from 1987 to 2010 identified 3,010 patients. Patients were verified using symptoms, cardiac enzymes, and EKG changes at the time of event. Interventions evaluated included fibrinolytic therapy, CABG, or primary PCI.
Survival increased to 96% from 89% during the period from 1987 to 2010. Researchers also noted more comorbid conditions, such as diabetes mellitus, COPD, and hypertension, noted over time. Of the patients evaluated, 643 readmissions occurred for 561 patients (18.6%). Of these, the most frequent causes were ischemic heart disease, respiratory symptoms, and heart failure. Comorbid conditions, such as diabetes, COPD, anemia, higher killip class on initial admission, duration of prior hospitalization, and procedural complications, independently increased the risk of readmission.
Bottom line: In addition to factors unrelated to an AMI, a patient’s comorbid conditions, post-procedure complications, and duration of hospitalization influence the risk of readmission.
Citation: Dunlay SM, Weston SA, Killian JM, et al. Thirty-day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157(1):11-18.
One-Hour Rule-Out or Rule-In for AMI in Chest Pain
Clinical question: How can we use the newly developed high-sensitivity cardiac troponin (hs-cTnT) to shorten the time to rule in and rule out AMI?
Background: The hs-cTnT assays available appear to improve the early diagnosis of AMI when compared to the regular cardiac troponins, but no clear guidelines are available as how to best use them in clinical practice.
Study design: Prospective, multicenter study.
Setting: Switzerland hospitals.
Synopsis: The study enrolled 872 unselected patients presenting to the ED with acute chest pain. Hs-cTnT level was measured in a blinded fashion at presentation and after one hour. Two independent cardiologists using all available medical records adjudicated the final AMI diagnosis. Optimal thresholds for rule-out were selected to allow for 100% sensitivity and negative predictive value. Rule-out criteria were defined as baseline hs-cTnT level <12 ng/L and an absolute change within the first hour of <3 ng/L. Rule-in criteria was defined as baseline hs-cTnT >52 ng/L or an absolute increase within the first hour of >5 ng/L.
AMI was the final diagnosis in 17% of patients; AMI was ruled out in 60%; and the remaining 23% were placed in observation.
Primary prognostic endpoint was 30-day mortality rate, which was 0.2% in the rule-out group, validating the suitability of these patients for early discharge.
Study limitations were that it was an observational study not used for clinical decision-making, no dialysis patients were included, and only one specific hs-cTnT assay was tested.
Bottom line: Using hs-cTnT levels at presentation and absolute changes within the first hour, a safe rule-out or rule-in of AMI can be performed in 77% of patients presenting with chest pain.
Citation: Reichlin T, Schindler C, Drexler B, et al. One-hour rule-out and rule-in of acute myocardial infarction using high-sensitivity cardiac troponin T. Arch Intern Med. 2012;172(16):1-8.
Aspirin Increases Bleed Risk without Reducing Risk of Stroke in CKD and NVAF Patients
Clinical question: Is there a difference between aspirin and warfarin in preventing thromboembolic complications and risk of bleeding in patients with chronic kidney disease (CKD) and nonvalvular afib (NVAF)?
Background: Data are lacking on risks and benefits of aspirin and warfarin in CKD, as this group of patients largely has been excluded from anticoagulation therapy trials for NVAF. This study examined the risks and benefits of aspirin and warfarin in patients with CKD with NVAF.
Study design: Retrospective, observational cohort study.
Setting: Danish National Registries.
Synopsis: Of 132,372 patients with NVAF, 2.7% had CKD and 0.7% had end-stage renal disease (ESRD). Compared to patients with no CKD, there was increased risk of stroke or systemic thromboembolism in patients with ESRD (HR, 1.83; 95% CI, 1.57-2.14) and with non-end-stage CKD (HR 1.49; 95% CI 1.38-1.59).
In patients with CKD, warfarin significantly reduced stroke risk (HR, 0.76; 95% CI, 0.64-0.91) and significantly increased bleeding risk (HR, 1.33; 95% CI, 1.16-1.53); aspirin significantly increased bleeding risk (HR, 1.17; 95% CI, 1.02-1.34) with no reduction in stroke risk.
Bottom line: CKD was associated with an increased risk of stroke among NVAF patients. While both aspirin and warfarin were associated with increased risk of bleeding, there was a reduction in the risk of stroke with warfarin, but not with aspirin.
Citation: Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med. 2012;367(7):625-635.
The Numerators: Treating Noncompliant, Medically Complicated Hospital Patients

We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
We hospitalists are scientifically minded. We understand basic statistics, including percentages, percentiles, numerators, denominators (see Figure 1, right). In healthcare, we see a lot of patients we call denominators; these denominators are generally the types of patients to whom not much happens. They come in “pre-” and they leave “post-.” They generally pass through our walls, and our lives, according to plan, without leaving an impenetrable memory of who they were or what they experienced.
The numerators, on the other hand, do have something happen to them—something unexpected, untoward, unanticipated, unlikely. Sometimes we describe numerators as “noncompliant” or “medically complicated” or “refractory to treatment.” We often find ways to rationalize and explain how the patient turned from a denominator into a numerator—something they did, or didn’t do, to nudge them above the line. They smoked, they ate too much, they didn’t take their medications “as prescribed.” Often there is a less robust discussion about what we could have done to reduce the nudge: understand their background, their literacy, their finances, their physical/cognitive limitations, their understanding of risks and benefits.
I read a powerful piece about “numerators” written by Kerry O’Connell. In this piece, she describes what it was like to cross over the line into being a numerator after acquiring a hospital-acquired infection:
Five years ago this summer while under deep anesthesia for arm surgery number 3, I drifted above the line and joined the group called Numerators. … Numerators have lost a lot to join this group; many have lost organs, and some have lost all their limbs, all have many kinds of scars from their journey. It was not our choice to leave the world of Denominators … and many will struggle the rest of their lives to understand why...
There are lots of silly rules for not counting some infected souls, as if by not counting us we might not exist. Numerators that are identified are then divided by the Denominators to create a nameless, faceless, mysteriously small number called infection rates. “Rates,” like their cousin “odds,” claim to portray hope while predicting doom for some of us. Denominators are in love with rates, for no matter how many Numerators they have sired, someone else has sired more. Rates soothe the Denominator conscious and allow them to sleep peacefully at night ...
Numerators don’t ask for much from the world. We ask that Denominators look behind the numbers to see the people, to love us, count us, respect our suffering, and help keep us out of bankruptcy, for once we were Denominators just like you. Our greatest dream is that you find the daily strength to truly care. To care enough to follow the checklists, to care enough to wash your hands, to care enough to only use virgin needles, for the saddest day for all Numerators is when another unsuspecting Denominator rises above the line to join our group.1
CB’s Story
Now think of all the numerators you have met. I am going to repeat that phrase. Think of all the numerators you have met. I have met quite a few. Now I am going to tell you about my most memorable numerator.
CB was a 36-year-old white female admitted to the hospital with a recent diagnosis of ulcerative colitis. She had a protracted hospital course on various immunosuppressant drugs, none of which relieved her symptoms. During her hospital stay, her family, including her 2-year-old twins, visited every single day. After several weeks with no improvement, the decision was made to proceed to a colectomy. The surgical procedure itself was uncomplicated, a true denominator.
Then, on post-op Day 5, the day of her anticipated discharge, a pulmonary embolus thrust her into the numerator position. A preventable, eventually fatal numerator—a numerator who “just would not keep her compression devices on” and whom the staff tried to get out of bed, “but she just wouldn’t do it.” A numerator who just so happened to be my sister.
Every year on April 2, when I call my niece and nephew to wish them a happy birthday, I think about numerators. And I think about how incredibly different life would be for those 10-year-old twins, had their mom just stayed a denominator. And every day, when I sit in conference rooms and hear from countless people about how difficult it is to prevent this and reduce that, and how zero is not feasible, I think about numerators. I don’t look at their bar chart, or their run chart, or their red line, or their blue line, or whether their line is within the control limits, or what their P-value is. I think about who represents that black dot, and about how we are going to actually convince ourselves to “First, do no harm.”
When I find myself amongst a crowd quibbling about finances, lunch breaks, workflows, accountability, and about who is going to check the box or fill out the form, I think about the numerators, and how we are truly wasting their time, their livelihood, and their ability to stay below the line.
And someday, when my niece and nephew are old enough to understand, I will try to help them tolerate and accept the fact that “preventable” and “prevented” are not interchangeable. At least not in the medical industry. At least not yet.
In memory of Colleen Conlin Bowen, May 14, 2004
Dr. Scheurer is a hospitalist and chief quality officer at the Medical University of South Carolina in Charleston. She is physician editor of The Hospitalist. Email her at [email protected].
Reference
Interfacility Transfers to Pediatric Academic EDs Often Discharged or Admitted Briefly

Clinical question: What are the characteristics of interfacility transfers to pediatric academic EDs?
Background: The majority of pediatric ED visits (89%) and hospital admissions (69%) occur via general hospital EDs, not freestanding academic children's hospitals. Pediatric hospitalists often provide consultation services in these community hospital settings and might be the primary admitting team in either setting (community hospital or children's hospital). Questions concerning the quality of pediatric ED care in community hospitals have been raised, with acknowledged improvements in post-transfer care for critically ill patients. The characteristics of less acutely ill transfers are unknown and could provide insight into opportunities for improvement.
Study design: Cross-sectional, retrospective database review.
Setting: Twenty-nine tertiary-care pediatric hospitals.
Synopsis: The Pediatric Health Information System (PHIS) database of the Child Health Corporation of America was reviewed; over a one-year period, 24,905 interfacility transfers were identified from 29 hospitals. Fifty-eight percent of patients were admitted for more than 24 hours with common respiratory illnesses (pneumonia, bronchiolitis, asthma) and surgical conditions representing the most common diagnostic categories. Among the remaining patients, 24.7% were discharged directly from the academic pediatric EDs; 17% were admitted for less than 24 hours. Among those discharged or briefly admitted, common nonsurgical diagnostic categories included abdominal pain, viral gastroenteritis/dehydration, and other gastrointestinal conditions.
The authors attempted to define areas for improvement in pediatric care in community hospital EDs. Limitations of their analysis include the use of a database without validated code for source of admission, as well as an inability to drill down further into the specifics of what additional expertise was provided at the pediatric EDs. However, this study provides a platform by which pediatric hospitalists can view and subsequently improve the value of their regional care systems.
Bottom line: Interfacility transfers to pediatric academic EDs might offer an opportunity for improved pediatric care in community hospital EDs.
Citation: Li J, Monuteaux MC, Bachur RG. Interfacility transfers of noncritically ill children to academic pediatric emergency departments. Pediatrics. 2012;130:83-92.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What are the characteristics of interfacility transfers to pediatric academic EDs?
Background: The majority of pediatric ED visits (89%) and hospital admissions (69%) occur via general hospital EDs, not freestanding academic children's hospitals. Pediatric hospitalists often provide consultation services in these community hospital settings and might be the primary admitting team in either setting (community hospital or children's hospital). Questions concerning the quality of pediatric ED care in community hospitals have been raised, with acknowledged improvements in post-transfer care for critically ill patients. The characteristics of less acutely ill transfers are unknown and could provide insight into opportunities for improvement.
Study design: Cross-sectional, retrospective database review.
Setting: Twenty-nine tertiary-care pediatric hospitals.
Synopsis: The Pediatric Health Information System (PHIS) database of the Child Health Corporation of America was reviewed; over a one-year period, 24,905 interfacility transfers were identified from 29 hospitals. Fifty-eight percent of patients were admitted for more than 24 hours with common respiratory illnesses (pneumonia, bronchiolitis, asthma) and surgical conditions representing the most common diagnostic categories. Among the remaining patients, 24.7% were discharged directly from the academic pediatric EDs; 17% were admitted for less than 24 hours. Among those discharged or briefly admitted, common nonsurgical diagnostic categories included abdominal pain, viral gastroenteritis/dehydration, and other gastrointestinal conditions.
The authors attempted to define areas for improvement in pediatric care in community hospital EDs. Limitations of their analysis include the use of a database without validated code for source of admission, as well as an inability to drill down further into the specifics of what additional expertise was provided at the pediatric EDs. However, this study provides a platform by which pediatric hospitalists can view and subsequently improve the value of their regional care systems.
Bottom line: Interfacility transfers to pediatric academic EDs might offer an opportunity for improved pediatric care in community hospital EDs.
Citation: Li J, Monuteaux MC, Bachur RG. Interfacility transfers of noncritically ill children to academic pediatric emergency departments. Pediatrics. 2012;130:83-92.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What are the characteristics of interfacility transfers to pediatric academic EDs?
Background: The majority of pediatric ED visits (89%) and hospital admissions (69%) occur via general hospital EDs, not freestanding academic children's hospitals. Pediatric hospitalists often provide consultation services in these community hospital settings and might be the primary admitting team in either setting (community hospital or children's hospital). Questions concerning the quality of pediatric ED care in community hospitals have been raised, with acknowledged improvements in post-transfer care for critically ill patients. The characteristics of less acutely ill transfers are unknown and could provide insight into opportunities for improvement.
Study design: Cross-sectional, retrospective database review.
Setting: Twenty-nine tertiary-care pediatric hospitals.
Synopsis: The Pediatric Health Information System (PHIS) database of the Child Health Corporation of America was reviewed; over a one-year period, 24,905 interfacility transfers were identified from 29 hospitals. Fifty-eight percent of patients were admitted for more than 24 hours with common respiratory illnesses (pneumonia, bronchiolitis, asthma) and surgical conditions representing the most common diagnostic categories. Among the remaining patients, 24.7% were discharged directly from the academic pediatric EDs; 17% were admitted for less than 24 hours. Among those discharged or briefly admitted, common nonsurgical diagnostic categories included abdominal pain, viral gastroenteritis/dehydration, and other gastrointestinal conditions.
The authors attempted to define areas for improvement in pediatric care in community hospital EDs. Limitations of their analysis include the use of a database without validated code for source of admission, as well as an inability to drill down further into the specifics of what additional expertise was provided at the pediatric EDs. However, this study provides a platform by which pediatric hospitalists can view and subsequently improve the value of their regional care systems.
Bottom line: Interfacility transfers to pediatric academic EDs might offer an opportunity for improved pediatric care in community hospital EDs.
Citation: Li J, Monuteaux MC, Bachur RG. Interfacility transfers of noncritically ill children to academic pediatric emergency departments. Pediatrics. 2012;130:83-92.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Recommendations for Antithrombotic and Thrombolytic Therapy
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
Background
Each year, 1 million people are hospitalized with a diagnosis of stroke; it was the fourth-leading cause of death in the U.S. in 2009 and 2010.1 The majority of strokes (80%) are caused by focal cerebral ischemia, and the remainder are caused by hemorrhage.1 In 2008, the direct medical costs of stroke were approximately $18.8 billion, with almost half of this amount directed toward hospitalization.1 Although stroke inpatients make up only 3% of total hospitalizations, the mortality rate is more than twice that of other patients’.1
Over the past several decades, much has been learned about the pathophysiology and treatment for ischemic stroke. The mainstays of therapies include restoring perfusion in a timely manner and targeting both clot formation and hemostasis. These therapies improve patient outcomes and reduce the risk of recurrence in appropriately selected populations.
Guideline Update
In February, the American College of Chest Physicians (ACCP) published new practice guidelines for medical patients regarding antithrombotic and thrombolytic therapy in acute ischemic stroke.2 These evidence-based guidelines are the result of new clinical trial data and a review of previous studies. They address three aspects of management decisions for stroke, including acute treatment, VTE prevention, and secondary prevention, as well as specifically address the treatment of cerebral venous sinus thrombosis.
In the management of acute ischemic stroke, several recommendations were made. In terms of IV recombinant tissue plasminogen activator (r-tPA) administration, the guidelines were expanded and allow for a less restrictive time threshold for administration. Previous recommendations limited the usage of IV r-tPA to within three hours of symptom onset in acute ischemic stroke. A science advisory from the American Heart Association/American Stroke Association (AHA/ASA) from 2009 extended that window to 4.5 hours. The 2012 ACCP guidelines have followed suit to extend this time to 4.5 hours from symptom onset as well.
In addition, intrarterial r-tPA can be given in patients not eligible for IV r-tPA within six hours of presentation of acute ischemic stroke due to proximal cerebral artery occlusion.
These updated acute stroke guidelines recommend against the use of mechanical thrombectomy based mostly on lack of data rather than lack of benefit.2
The new guidelines continue to recommend early aspirin therapy at a dosage of 160 mg to 325 mg within the first 48 hours of acute ischemic stroke. Therapeutic parenteral anticoagulation with heparin or related drugs was not recommended in patients with noncardioembolic stroke due to atrial fibrillation (afib) or in patients with stroke due to large artery stenosis or arterial dissection. In this updated analysis, there was no benefit of anticoagulation compared with antiplatelet therapy, and the risk for extracranial hemorrhage was increased. No specific recommendation regarding anticoagulation was made in patients with mechanical heart valves or intracardiac thrombus.
Updates have been made for VTE prophylaxis in patients hospitalized for acute stroke. In stroke patients with restricted mobility, prophylactic unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) and/or intermittent pneumatic compression devices should be initiated as early as possible. The panel is no longer recommending elastic compression stockings as VTE prevention given the risk of skin damage and no clear benefit in symptomatic VTE prevention. For patients with hemorrhagic stroke and restricted mobility, similar recommendations were made for VTE prevention, except to start pharmacologic treatment between days 2 and 4 of the hospital stay. However, if there is a bleeding concern, intermittent pneumatic compression devices are favored over pharmacologic prophylaxis. In all patients for whom pharmacologic prevention is utilized, prophylactic LMWH is preferred over UFH.
Secondary stroke prevention is addressed, with 2012 guidelines outlining a preference for clopidogrel or aspirin/extended-release dipyridamole rather than aspirin or cilostazol in patients with a history of noncardioembolic ischemic stroke or TIA. Oral anticoagulation is preferred in patients with a history of stroke or TIA with afib over aspirin alone, aspirin plus clopidogrel, or no antithrombotic therapy. Of the available anticoagulants, the panel recommended dabigatran 150 mg twice daily over adjusted-dose warfarin.2 This recommendation is based on results from the RE-LY trial, which showed dabigatran as noninferior to warfarin in patients with nonvalvular afib without severe renal failure or advanced liver disease.3
For patients who have contraindications or choose not to initiate anticoagulation, the combination of aspirin (ASA) and clopidogrel is a reasonable alternative. Timing of the initiation of oral anticoagulation should be between one and two weeks after the stroke. Patients with extensive infarction or hemorrhagic transformation should delay starting oral anticoagulation, with no exact timeline. Long-term antithrombotic therapy is contraindicated in patients with history of a symptomatic primary intracerebral hemorrhage.2 New guidelines also recommend full anticoagulation for patients with symptomatic cerebral venous sinus thrombosis.
The panel did not make any recommendations regarding statin usage. In several studies, findings showed that statins reduced infarct size and had improved outcome in all stroke types.4
Analysis
Prior to the 2012 update, the last guideline for antithrombotic and thrombolytic therapy for ischemic stroke was published by the ACCP in the June 2008 issue of Chest.5 Dating back to 2001, medications included r-tPA administration within three hours of stroke symptom onset, and aspirin, clopidogrel, or a com bination of aspirin and extended-release dipyridamole for stroke prophylaxis.
The management of stroke continues to focus on early intervention and secondary prevention. Thrombolytic therapy is an effective treatment of acute ischemic stroke if given within the narrow window from onset of stroke symptoms up to 4.5 hours, with the goal of treatment within a three-hour window. Beyond this time constraint, the risk outweighs the benefit of using r-tPA except in the case of intra-arterial r-tPA administration for proximal cerebral artery occlusion.
In 2010, a meta-analysis supported this by showing that the risk of death increased significantly in patients receiving r-tPA beyond 4.5 hours. Therefore, antiplatelet therapy is the best alternative for patients ineligible for thrombolytic therapy.6 Even so, that study offered little data for patients with mechanical heart valves or intracardiac thrombi. Thus, the choice for acute anticoagulation therapy is variable and uncertain. If the hemorrhagic risk is low, anticoagulation can be considered in this subgroup, but no specific guideline endorsement was made.
In 2011, the AHA/ASA published an updated treatment guideline for patients with stroke or TIA. This was an update to 2007 guidelines that outlined the early management of ischemic stroke and affirmed the benefit of IV r-tPA at 4.5 hours for the treatment of stroke.7 Of note, IV r-tPA is only FDA-approved for treatment of acute ischemic stroke within the previously recommended three-hour period from symptom onset.
Aspirin has been found to be effective in both early treatment of acute ischemic stroke and secondary prevention. The CAST trial showed a statistically significant rate of reduction of nonfatal strokes with the use of aspirin. Other antiplatelet agents, including clopidogrel and dipyridamole, can be used. The FASTER trial compared aspirin alone versus aspirin plus clopidogrel, with no difference in outcome measures, although the MATCH trial found a larger risk of hemorrhagic and bleeding complications in the acetylsalicylic acid (ASA)-plus-clopidogrel group.6,7
In TIA or stroke patients, clopidogrel is not superior to ASA in preventing recurrent stroke. However, patients who have peripheral artery disease (PAD), previous coronary artery bypass grafting (CABG), insulin dependent diabetes mellitus (IDDM), or recurrent vascular events show a benefit of transitioning from ASA to clopidogrel for secondary long-term prevention. Clopidogrel or aspirin/extended-release dipyridamole is preferred over aspirin alone or cilostazol for long-term treatment in patients with a history of noncardioembolic ischemic stroke or TIA based on the PROFESS trial.2,7
HM Takeaways
The 2012 guidelines are a resource available to hospitalists for treating acute ischemic stroke either alone or with neurology consultation. These guidelines further define the timing of r-tPA and the use of both anticoagulation and antiplatelet therapy in the proper clinical settings.
In terms of VTE prevention, the guidelines recommend using LMWH preferentially over UH, except in patients at risk for rebleeding. The clinician should be aware of the treatment considerations for secondary prevention, noting the primary role of aspirin therapy in ischemic stroke with consideration of other agents (i.e. clopidogrel) in select populations.
Drs. Barr and Schumacher are hospitalists and assistant professors in the division of hospital medicine at The Ohio State University College of Medicine in Columbus.
References
Available at the-hospitalist.org.
John Nelson: Peformance Key to Federal Value-Based Payment Modifier Plan

For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
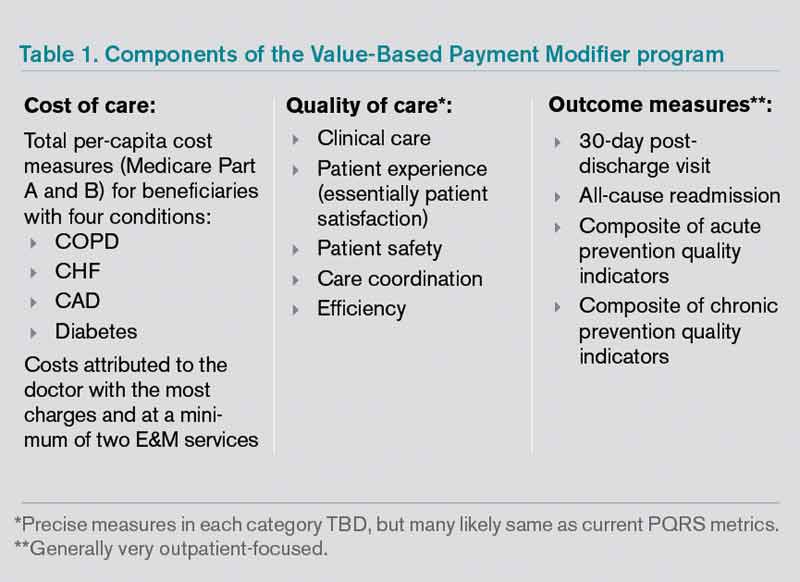
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
For years, your hospital was paid additional money by Medicare to report its performance on such things as core measures. Medicare then shared that information with the public via www.hospitalcompare.hhs.gov. Even if the hospital never gave Pneumovax when indicated, it was paid more simply for reporting that fact. (Fortunately, there were lots of reasons hospitals wanted to perform well.)
The days of hospitals being paid more simply for reporting ended a long time ago. Now performance, e.g., how often Pneumovax was given when indicated, influences payment. That is, things have transitioned from pay-for-reporting to a pay-for-performance program called hospital value-based purchasing (VBP).
I hope that at least one member of your hospitalist group is keeping up with hospital VBP. It got a lot of attention in the fall because it was the first time Medicare Part A payments to hospitals were adjusted based on performance on some core measures and patient satisfaction domains, as well as readmission rates for congestive heart failure (CHF), acute myocardial infarction (AMI), and pneumonia patients. The dollars at stake and performance metrics change will change every year, so plan to pay attention to hospital VBP on an ongoing basis.
Physicians’ Turn
Medicare payment to physicians is evolving along the same trajectory as hospitals. For several years, doctors have had the option to voluntarily participate in the Physician Quality Reporting System (PQRS). As long as a doctor reported quality performance on a sufficient portion of certain patient types, Medicare would provide a “bonus” at the end of the year. From 2012 through 2014, the “bonus” is 0.5% of that doctor’s total allowable Medicare charges. For example, if that doctor generated $150,000 of Medicare allowable charges over the calendar year, the additional payment for successful reporting PQRS would be $750 (0.5% of $150,000).
Although $750 is only a tiny fraction of collections, the right charge-capture system can make it pretty easy to achieve. And an extra payment of $750 sure is better than the 1.5% penalty for not participating; that program starts in 2015 and increases to a 2% penalty in 2016. If you are still not participating successfully in PQRS in 2015, the reimbursement for that $150,000 in charges will be reduced by $2,250 (1.5% of $150,000). So I strongly recommend that you begin reporting in 2013 so that you have time to work out the kinks well ahead of 2015. Don’t delay, but don’t panic, either, because you can still succeed in 2013 even if you don’t start capturing or reporting PQRS data until late winter or early spring.
At some point in the next year or so, data from as early as January 2013 for doctors reporting through PQRS will be made public on the Centers for Medicare & Medicaid’s (CMS) physician compare website: www.medicare.gov/find-a-doctor/provider-search.aspx. For example, should you choose to report the portion of stroke patients for whom you prescribed DVT prophylaxis, the public will be able to see your data.
The Next Wave of Physician Pay for Performance
As the name implies, PQRS is a program based on reporting. Now CMS is adding the Value-Based Payment Modifier (VBPM) program, in which performance determines payments (see Table 1). It incorporates quality measures from PQRS, but is for now a separate program. It is very similar in name and structure to the hospital VBP program mentioned above, but incorporates cost of care data as well as quality performance. So it is really about value and not just quality performance (hence the name).
For providers in groups of more than 100 that bill under the same tax ID number (they don’t have to be in the same specialty), VBPM will first influence Part B Medicare reimbursement for physician services in 2015. It will expand to include all providers in 2017.
But don’t think you have until 2015 or 2017 to learn about all of this. There is a two-year lag, so payments in 2015 are based on performance in 2013 and 2017 payments presumably will be based on 2015 performance. In the fall of 2013, CMS plans to provide group-level (not individual) performance reports to all doctors in groups of 100 or more under the same tax ID number. These performance reports are known as quality resource use reports (QRURs). QRURs were trialed on physicians in a few states who received reports in 2012 based on 2011 performance, but in 2013, reports based on 2012 performance will be distributed to all doctors who practice in groups of 100 or more.
The calculation to determine whether a doctor is due additional payment for good performance (more accurately, good value) is awfully complicated. But providers have a choice to make. They can choose to:
- Not report data and accept a 1% penalty (likely to increase in successive years and in addition to the penalty for not reporting PQRS data, for a total penalty of 2.5%);
- Report data but not compete for financial upside or downside; or
- Compete for additional payments (amount to be determined) and risk a penalty of 0.5% or 1% for poor performance.
Look for more details about the VBPM program in future columns and other articles in The Hospitalist. There are a number of good online resources, including a CMS presentation titled “CMS Proposals for the Physician Value-Based Payment Modifier under the Medicare Physician Fee Schedule.” Type “Value-Based Payment Modifier” and “CMS” into any search engine to locate the video.
Parting Recommendations
Just about every hospitalist group should:
- Designate someone in your group to keep up with evolving pay-for-performance programs. It doesn’t have to be an MD, but you do need someone local that can guide your group through it. Consider becoming the most expert physician at your hospital on this topic.
- Start reporting through PQRS in 2013 if you haven’t already.
- Support SHM’s efforts to provide feedback to CMS to ensure that the metrics are meaningful for the type of care we provide.
Dr. Nelson has been a practicing hospitalist since 1988. He is co-founder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is course co-director for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. Write to him at [email protected].
Author’s note: For helping to explain all this pay-for-performance stuff, I once again owe thanks to Dr. Pat Torcson, a hospitalist in Covington, La., and member of SHM’s Public Policy Committee. He does an amazing job of keeping up with the evolving pay-for-performance programs, advocating on behalf of hospitalists and the patients we serve, and graciously answers my tedious questions with thoughtful and informative replies. He is a really pleasant guy and a terrific asset to SHM and hospital medicine.
Consider Patient Safety, Outcomes Risk before Prescribing Off-Label Drugs

Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.
Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.
Consider Patient Safety, Outcomes Risk before Prescribing “Off-Label”
What is the story with off-label drug use? I have seen some other physicians in my group use dabigatran for VTE prophylaxis, which I know it is not an approved indication. Am I taking on risk by continuing this treatment?
—Fabian Harris, Tuscaloosa, Ala.
Dr. Hospitalist responds:
Our friends at the FDA are in the business of approving drugs for use, but they do not regulate medical practice. So the short answer to your question is that off-label drug use is perfectly acceptable. Once a drug has been approved for use, if, in your clinical judgment, there are other indications for which it could be beneficial, then you are well within your rights to prescribe it. The FDA does not dictate how you practice medicine.
However, you will still be held to the community standard when it comes to your medical practice. As an example, gabapentin is used all the time for neuropathic pain syndromes, though technically it is only approved for seizures and post-herpetic neuralgia. Although the FDA won’t restrict your prescribing, it does prohibit pharmaceutical companies from marketing their drugs for anything other than their approved indications. In fact, Pfizer settled a case in 2004 on this very drug due to the promotion of prescribing it for nonapproved indications. I think at this point it’s fairly well accepted that lots of physicians use gabapentin for neuropathic pain, so you would not be too far out on a limb in prescribing it yourself in this manner.
For newer drugs, I might proceed with a little more caution. Anyone out there remember trovofloxacin (Trovan)? It was a new antibiotic approved in the late 1990s, with a coverage spectrum similar to levofloxacin, but with even more weight toward the gram positives. A wonder drug! Oral! As a result, it got prescribed like water, but not for the serious infections it was designed for: It got prescribed “off label” for common URIs and sinusitis. Unfortunately, it also caused a fair amount of liver failure and was summarily pulled from the market.
Does this mean dabigatran is a bad drug? No, but we don’t have much history with it, either. So while it might seem to be an innocuous extension to prescribe it for VTE prevention when it has already been approved for stroke prevention in afib, I think you carry some risk by doing this. In addition, some insurers will not cover a drug being prescribed in this manner, so you might be exposing your patient to added costs as well. Additionally, there’s nothing about off-label prescribing that says you have to tell the patient that’s what you’re doing. However, if you put together the factors of not informing a patient about an off-label use, and a patient having to pay out of pocket for that medicine, with an adverse outcome ... well, let’s just say that might not end too well.
Ultimately, I think you will need to consider the safety profile of the drug, the risk for an adverse outcome, your own risk tolerance, and the current state of medical practice before you consistently agree to use a drug “off label.” Given the slow-moving jungle of FDA approval, I can understand the desire to use a newer drug in an off-label manner, but it’s probably best to stop and think about the alternatives before proceeding. If you’re practicing in a group, then it’s just as important to come to a consensus with your partners about which drugs you will comfortably use off-label and which ones you won’t, especially as newer drugs come into the marketplace.