User login
Ticks use static electricity to latch onto hosts: Study
It turns out that some people really are tick magnets.
Researchers have discovered that ticks can defy gravity in their quest to latch onto people and animals. The key is static electricity, just like when someone rubs a balloon and things stick to it.
The study was published in the journal Current Biology. In the first phase of the research, scientists exposed ticks to furry rabbit feet and to acrylic surfaces that each had electrostatic charges.
“Ticks were readily attracted across air gaps of up to several millimeters or centimeters onto these statically charged surfaces,” the authors wrote.
In a second part of the study, the researchers created computer models simulating the electrostatic charges that exist in environments where both ticks and mammals are found. In one simulation, the researchers observed that the body parts of a cow with the most electric charge were the nose, tail, and legs, which are the body parts most likely to be encountered by a tick. They also found that the vegetation near the animal had a strong electric field that is just a few millimeters wide.
In a final phase of the study, the researchers conducted laboratory experiments in which they re-created the electric field conditions from the computer model and successfully lifted some ticks across an air gap, although some ticks did not make the full leap if they were observed to be resisting.
The authors noted that their findings could be applied to developing new tick prevention strategies, such as designing clothing that resists electrostatic charges or spraying livestock.
The study authors reported that they had no conflicts of interest.
A version of this article first appeared on WebMD.com.
It turns out that some people really are tick magnets.
Researchers have discovered that ticks can defy gravity in their quest to latch onto people and animals. The key is static electricity, just like when someone rubs a balloon and things stick to it.
The study was published in the journal Current Biology. In the first phase of the research, scientists exposed ticks to furry rabbit feet and to acrylic surfaces that each had electrostatic charges.
“Ticks were readily attracted across air gaps of up to several millimeters or centimeters onto these statically charged surfaces,” the authors wrote.
In a second part of the study, the researchers created computer models simulating the electrostatic charges that exist in environments where both ticks and mammals are found. In one simulation, the researchers observed that the body parts of a cow with the most electric charge were the nose, tail, and legs, which are the body parts most likely to be encountered by a tick. They also found that the vegetation near the animal had a strong electric field that is just a few millimeters wide.
In a final phase of the study, the researchers conducted laboratory experiments in which they re-created the electric field conditions from the computer model and successfully lifted some ticks across an air gap, although some ticks did not make the full leap if they were observed to be resisting.
The authors noted that their findings could be applied to developing new tick prevention strategies, such as designing clothing that resists electrostatic charges or spraying livestock.
The study authors reported that they had no conflicts of interest.
A version of this article first appeared on WebMD.com.
It turns out that some people really are tick magnets.
Researchers have discovered that ticks can defy gravity in their quest to latch onto people and animals. The key is static electricity, just like when someone rubs a balloon and things stick to it.
The study was published in the journal Current Biology. In the first phase of the research, scientists exposed ticks to furry rabbit feet and to acrylic surfaces that each had electrostatic charges.
“Ticks were readily attracted across air gaps of up to several millimeters or centimeters onto these statically charged surfaces,” the authors wrote.
In a second part of the study, the researchers created computer models simulating the electrostatic charges that exist in environments where both ticks and mammals are found. In one simulation, the researchers observed that the body parts of a cow with the most electric charge were the nose, tail, and legs, which are the body parts most likely to be encountered by a tick. They also found that the vegetation near the animal had a strong electric field that is just a few millimeters wide.
In a final phase of the study, the researchers conducted laboratory experiments in which they re-created the electric field conditions from the computer model and successfully lifted some ticks across an air gap, although some ticks did not make the full leap if they were observed to be resisting.
The authors noted that their findings could be applied to developing new tick prevention strategies, such as designing clothing that resists electrostatic charges or spraying livestock.
The study authors reported that they had no conflicts of interest.
A version of this article first appeared on WebMD.com.
FROM CURRENT BIOLOGY
FDA approves first leadless dual-chamber pacing system
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.

The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
, one based in part on an already-approved leadless single-chamber device, Abbott has announced.
The company’s AVEIR DR leadless pacing system consists of two percutaneously implanted devices, the single-chamber AVEIR VR leadless pacemaker, implanted within the right ventricle, and the novel AVEIR AR single-chamber pacemaker for implantation in the right atrium.
The AVEIR DR system relies on proprietary wireless technology to provide bidirectional, beat-to-beat communication between its two components to achieve dual-chamber synchronization, the company stated in a press release on the approval.
The system also provides real-time pacing analysis, Abbott said, allowing clinicians to assess proper device placement during the procedure and before implantation. The system is designed to be easily removed if the patient’s pacing needs evolve or its battery needs replacing.
Experienced operators achieved a 98% implantation success rate using the AVIER DR system in a 300-patient study conducted at 55 sites in Canada, Europe, and the United States. In that study, 63% of the patients had sinus-node dysfunction and 33% had AV block as their primary dual-chamber pacing indication.
The system exceeded its predefined safety and performance goals, providing AV-synchronous pacing in 97% of patients for at least 3 months, it was reported in May at the annual scientific sessions of the Heart Rhythm Society and in a simultaneous publication in The New England Journal of Medicine.
“Modern medicine has been filled with technological achievements that fundamentally changed how doctors approach patient care, and now we can officially add dual-chamber leadless pacing to that list of achievements,” coauthor Vivek Reddy, MD, director of cardiac arrhythmia services for Mount Sinai Hospital and the Mount Sinai Health System, New York, said in the press release.
A version of this article first appeared on Medscape.com.
Malaria is spreading in the U.S. for the first time in 20 years
, the Centers for Disease Control and Prevention says.
The federal health agency recently issued a nationwide warning to health providers and officials to be on the lookout for symptoms of the potentially fatal illness. Usually, people in the U.S. who get malaria get the disease during international travel.
All five people – four in Florida and one in Texas – have received treatment and are improving, according to the CDC. The case in Texas is not related to the Florida cases, and all occurred in the past 2 months.
Malaria cannot be transmitted from person to person. It is spread by the bite of an infected female mosquito. The last cases of people being infected while in the U.S. occurred 20 years ago, when there were eight cases in Palm Beach County, Fla. The Texas Department of State Health Services said the last time malaria was locally acquired in the state was 1994.
The Florida Department of Health said it was spraying for mosquitoes in the two counties surrounding Sarasota, Fla., where the four cases occurred.
The CDC said the risk of getting malaria while in the United States “remains extremely low.” The agency advised people to protect themselves by taking precautions to prevent mosquito bites, such as wearing insect repellent and wearing long-sleeved shirts and pants. People should also do things to ensure that mosquitoes aren’t around their home, such as getting rid of standing water, which is an environment for mosquitoes to lay eggs.
More than 240 million malaria cases occur annually worldwide, the CDC said, with 95% in Africa. There are 2,000 cases diagnosed annually in the U.S. that are related to international travel. Malaria symptoms are similar to those of other illnesses and include fever, chills, a headache, and muscle aches. If not treated, malaria can be fatal.
A version of this article first appeared on WebMD.com.
, the Centers for Disease Control and Prevention says.
The federal health agency recently issued a nationwide warning to health providers and officials to be on the lookout for symptoms of the potentially fatal illness. Usually, people in the U.S. who get malaria get the disease during international travel.
All five people – four in Florida and one in Texas – have received treatment and are improving, according to the CDC. The case in Texas is not related to the Florida cases, and all occurred in the past 2 months.
Malaria cannot be transmitted from person to person. It is spread by the bite of an infected female mosquito. The last cases of people being infected while in the U.S. occurred 20 years ago, when there were eight cases in Palm Beach County, Fla. The Texas Department of State Health Services said the last time malaria was locally acquired in the state was 1994.
The Florida Department of Health said it was spraying for mosquitoes in the two counties surrounding Sarasota, Fla., where the four cases occurred.
The CDC said the risk of getting malaria while in the United States “remains extremely low.” The agency advised people to protect themselves by taking precautions to prevent mosquito bites, such as wearing insect repellent and wearing long-sleeved shirts and pants. People should also do things to ensure that mosquitoes aren’t around their home, such as getting rid of standing water, which is an environment for mosquitoes to lay eggs.
More than 240 million malaria cases occur annually worldwide, the CDC said, with 95% in Africa. There are 2,000 cases diagnosed annually in the U.S. that are related to international travel. Malaria symptoms are similar to those of other illnesses and include fever, chills, a headache, and muscle aches. If not treated, malaria can be fatal.
A version of this article first appeared on WebMD.com.
, the Centers for Disease Control and Prevention says.
The federal health agency recently issued a nationwide warning to health providers and officials to be on the lookout for symptoms of the potentially fatal illness. Usually, people in the U.S. who get malaria get the disease during international travel.
All five people – four in Florida and one in Texas – have received treatment and are improving, according to the CDC. The case in Texas is not related to the Florida cases, and all occurred in the past 2 months.
Malaria cannot be transmitted from person to person. It is spread by the bite of an infected female mosquito. The last cases of people being infected while in the U.S. occurred 20 years ago, when there were eight cases in Palm Beach County, Fla. The Texas Department of State Health Services said the last time malaria was locally acquired in the state was 1994.
The Florida Department of Health said it was spraying for mosquitoes in the two counties surrounding Sarasota, Fla., where the four cases occurred.
The CDC said the risk of getting malaria while in the United States “remains extremely low.” The agency advised people to protect themselves by taking precautions to prevent mosquito bites, such as wearing insect repellent and wearing long-sleeved shirts and pants. People should also do things to ensure that mosquitoes aren’t around their home, such as getting rid of standing water, which is an environment for mosquitoes to lay eggs.
More than 240 million malaria cases occur annually worldwide, the CDC said, with 95% in Africa. There are 2,000 cases diagnosed annually in the U.S. that are related to international travel. Malaria symptoms are similar to those of other illnesses and include fever, chills, a headache, and muscle aches. If not treated, malaria can be fatal.
A version of this article first appeared on WebMD.com.
Peripartum cardiomyopathy raises risks at future pregnancy despite LV recovery
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study suggests.
Researchers looked at the long-term outcomes in a cohort of women who had developed PPCM and became pregnant again several years later, comparing those with LV function that had “normalized” in the interim against those with persisting LV dysfunction.
In their analysis, adverse maternal outcomes 5 years after an index pregnancy were significantly worse among those in whom LV dysfunction had persisted, compared with those with recovered LV function. The risk of relapsed PPCM persisted out to 8 years. Mortality remained high in both groups through the follow-up.
The study suggests that “women with PPCM need long-term follow-up by cardiology, as mortality does not abate over time,” Kalgi Modi, MD, Louisiana State University, Shreveport, said in an interview.
Women with a history of PPCM, she said, need “multidisciplinary and shared decision-making for family planning, because normalization of left ventricular function after index pregnancy does not guarantee a favorable outcome in the subsequent pregnancies.”
Dr. Modi is senior author on the study published online in the Journal of the American College of Cardiology.
The current findings are important to women with a history of PPCM who are “contemplating future pregnancy,” Afshan Hameed, MD, a maternal-fetal medicine specialist and cardiologist at the University of California, Irvine, said in an interview. The investigators suggest that “complete recovery of cardiac function after PPCM does not guarantee a favorable outcome in future pregnancy,” agreed Dr. Hameed, who was not involved in the current study. Future pregnancies must therefore “be highly discouraged or considered with caution even in patients who have recovered their cardiac function.”
To investigate the impact of PPCM on risk at subsequent pregnancies, the researchers studied 45 patients with PPCM who had gone on to have at least one more pregnancy, the first a median of 28 months later. Their mean age was 27 and 80% were Black; they were followed a median of 8 years.
Peripartum cardiomyopathy, defined as idiopathic heart failure with LV ejection fraction (LVEF) 45% or less in the last month of pregnancy through the following 5 months, was diagnosed post partum in 93.3% and antepartum in the remaining 6.7% (mean time of diagnosis, 6 weeks post partum).
The mean LVEF fell from 45.1% at the index pregnancy to 41.2% (P = .009) at subsequent pregnancies. The “recovery group” included the 30 women with LVEF recovery to 50% or higher after the index pregnancy, and the remaining 15 with persisting LV dysfunction – defined as LVEF < 50% – made up the “nonrecovery group.”
Recovery of LVEF was associated with a reduced risk of persisting LV dysfunction, the report states, at a hazard ratio of 0.08 (95% CI, 0.01-0.64; P = .02) after adjustment for hypertension, diabetes, and history of preeclampsia. But that risk went up sharply in association with illicit drug use, similarly adjusted, with an HR of 9.08 (95% CI, 1.38-59.8; P = .02).
The nonrecovery group, compared with the recovery group, experienced significantly higher rates of adverse maternal outcomes (53.3% vs. 20.0%; P = .04) – a composite endpoint that included relapse PPCM (33.3% vs. 3.3%; P = .01), HF (53.3% vs. 20.0%; P = .03), cardiogenic shock, thromboembolic events, and death – at 5 years. However, all-cause mortality was nonsignificantly different between the two groups (13.3% vs. 3.3%; P = .25)
All-cause mortality was nonsignificantly different between the two groups at a median of 8 years (20.0% vs. 20.0%; P = 1.00), and the difference in overall adverse maternal outcomes had gone from significant to nonsignificant (53.3% vs. 33.3%; P = .20). The difference in relapse PPCM between groups remained significant after 8 years (53.3% vs. 23.3%; P = .04)
The study is limited by its retrospective nature, a relatively small population, and lack of racial diversity, the report notes.
Indeed, most of the study’s subjects were Black, and previous studies have demonstrated a “different phenotypic presentation and outcome in African American women with PPCM, compared with non–African American women,” an accompanying editorial states.
Therefore, applicability of its findings to other populations “needs to be examined by urgently needed national prospective registries with long-term follow-up,” writes Uri Elkayam, MD, University of Southern California, Los Angeles.
Moreover, the study questions “whether the reverse remodeling and improvement of [LVEF] in women with PPCM represent a true recovery.” Prior studies “have shown an impaired contractile reserve as well as abnormal myocardial strain and reduced exercise capacity and even mortality in women with PPCM after RLV,” Dr. Elkayam notes.
It’s therefore possible – as with other forms of dilated cardiomyopathy – that LVEF normalization “does not represent a true recovery but a new steady state with subclinical myocardial dysfunction that is prone to development of recurrent [LV dysfunction] and clinical deterioration in response to various triggers such as long-standing hypertension, obesity, diabetes, illicit drug use,” and, “more importantly,” subsequent pregnancies.
The study points to “the need for a close long-term follow-up of women with PPCM” and provides “a rationale for early initiation of guideline-directed medical therapy after the diagnosis of PPCM and possible continuation even after improvement of LVEF.”
No funding source was reported. Dr. Modi and coauthors, Dr. Elkayam, and Dr. Hameed declare no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Postacute effects of COVID on par with those of sepsis, flu
A large observational study examined population-wide data for 13 postacute conditions in patients who had been hospitalized with a COVID-19 infection and found that all but one of these conditions, venous thromboembolism, occurred at comparable rates in those hospitalized for sepsis and influenza.
“For us, the main takeaway was that patients hospitalized for severe illness in general really require ongoing treatment and support after they’re discharged. That type of care is often very challenging to coordinate for people in a sometimes siloed and fragmented health care system,” study author Kieran Quinn, MD, PhD, a clinician at Sinai Health in Toronto, and assistant professor at the University of Toronto, said in an interview.
The study was published in JAMA Internal Medicine.
Postacute effects
The investigators compared clinical and health administrative data from 26,499 Ontarians hospitalized with COVID-19 with data from three additional cohorts who had been hospitalized with influenza (17,516 patients) and sepsis. The sepsis cohort was divided into two groups, those hospitalized during the COVID-19 pandemic (52,878 patients) and a historical control population (282,473 patients).
These comparators allowed the researchers to compare COVID-19 with other severe infectious illnesses and control for any changes in health care delivery that may have occurred during the pandemic. The addition of sepsis cohorts was needed for the latter purpose, since influenza rates dropped significantly after the onset of the pandemic.
The study outcomes (including cardiovascular, neurological, and mental health conditions and rheumatoid arthritis) were selected based on previous associations with COVID-19 infections, as well as their availability in the data, according to Dr. Quinn. The investigators used diagnostic codes recorded in Ontario’s Institute for Clinical Evaluative Sciences database. The investigators observed some of the studied conditions in their own patients. “Many of us on the research team are practicing clinicians who care for people living with long COVID,” said Dr. Quinn.
Compared with cohorts with other serious infections, those hospitalized with COVID-19 were not at increased risk for selected cardiovascular or neurological disorders, rheumatoid arthritis, or mental health conditions within 1 year following hospitalization. Incident venous thromboembolic disease, however, was more common after hospitalization for COVID-19 than after hospitalization for influenza (adjusted hazard ratio, 1.77).
The study results corroborate previous findings that influenza and sepsis can have serious long-term health effects, such as heart failure, dementia, and depression, and found that the same was true for COVID-19 infections. For all three infections, patients at high risk require additional support after their initial discharge.
Defining long COVID
Although there was no increased risk with COVID-19 for most conditions, these results do not mean that the postacute effects of the infection, often called “long COVID,” are not significant, Dr. Quinn emphasized. The researcher believes that it’s important to listen to the many patients reporting symptoms and validate their experiences.
There needs to be greater consensus among the global health community on what constitutes long COVID. While the research led by Dr. Quinn focuses on postacute health conditions, some definitions of long COVID, such as that of the World Health Organization, refer only to ongoing symptoms of the original infection.
While there is now a diagnostic code for treating long COVID in Ontario, the data available to the researchers did not include information on some common symptoms of post-COVID condition, like chronic fatigue. In the data used, there was not an accurate way to identify patients who had developed conditions like myalgic encephalomyelitis/chronic fatigue syndrome and postural orthostatic tachycardia syndrome, said Dr. Quinn.
In addition to creating clear definitions and determining the best treatments, prevention is essential, said Dr. Quinn. Prior studies have shown that vaccination helps prevent ICU admission for COVID-19.
‘Important questions remain’
Commenting on the finding, Aravind Ganesh, MD, DPhil, a neurologist at the University of Calgary (Alta.), said that by including control populations, the study addressed an important limitation of previous research. Dr. Ganesh, who was not involved in the study, said that the controls help to determine the cause of associations found in other studies, including his own research on long-term symptoms following outpatient care for COVID-19.
“I think what this tells us is that maybe a lot of the issues that we’ve been seeing as complications attributable to COVID are, in fact, complications attributable to serious illness,” said Dr. Ganesh. He also found the association with venous thromboembolism interesting because the condition is recognized as a key risk factor for COVID-19 outcomes.
Compared with smaller randomized control trials, the population-level data provided a much larger sample size for the study. However, this design comes with limitations as well, Dr. Ganesh noted. The study relies on the administrative data of diagnostic codes and misses symptoms that aren’t associated with a diagnosis. In addition, because the cohorts were not assigned randomly, it may not account for preexisting risk factors.
While the study demonstrates associations with physical and mental health conditions, the cause of postacute effects from COVID-19, influenza, and sepsis is still unclear. “Important questions remain,” said Dr. Ganesh. “Why is it that these patients are experiencing these symptoms?”
The study was supported by ICES and the Canadian Institutes of Health Research. Dr. Quinn reported part-time employment at Public Health Ontario and stock in Pfizer and BioNTech. Dr. Ganesh reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large observational study examined population-wide data for 13 postacute conditions in patients who had been hospitalized with a COVID-19 infection and found that all but one of these conditions, venous thromboembolism, occurred at comparable rates in those hospitalized for sepsis and influenza.
“For us, the main takeaway was that patients hospitalized for severe illness in general really require ongoing treatment and support after they’re discharged. That type of care is often very challenging to coordinate for people in a sometimes siloed and fragmented health care system,” study author Kieran Quinn, MD, PhD, a clinician at Sinai Health in Toronto, and assistant professor at the University of Toronto, said in an interview.
The study was published in JAMA Internal Medicine.
Postacute effects
The investigators compared clinical and health administrative data from 26,499 Ontarians hospitalized with COVID-19 with data from three additional cohorts who had been hospitalized with influenza (17,516 patients) and sepsis. The sepsis cohort was divided into two groups, those hospitalized during the COVID-19 pandemic (52,878 patients) and a historical control population (282,473 patients).
These comparators allowed the researchers to compare COVID-19 with other severe infectious illnesses and control for any changes in health care delivery that may have occurred during the pandemic. The addition of sepsis cohorts was needed for the latter purpose, since influenza rates dropped significantly after the onset of the pandemic.
The study outcomes (including cardiovascular, neurological, and mental health conditions and rheumatoid arthritis) were selected based on previous associations with COVID-19 infections, as well as their availability in the data, according to Dr. Quinn. The investigators used diagnostic codes recorded in Ontario’s Institute for Clinical Evaluative Sciences database. The investigators observed some of the studied conditions in their own patients. “Many of us on the research team are practicing clinicians who care for people living with long COVID,” said Dr. Quinn.
Compared with cohorts with other serious infections, those hospitalized with COVID-19 were not at increased risk for selected cardiovascular or neurological disorders, rheumatoid arthritis, or mental health conditions within 1 year following hospitalization. Incident venous thromboembolic disease, however, was more common after hospitalization for COVID-19 than after hospitalization for influenza (adjusted hazard ratio, 1.77).
The study results corroborate previous findings that influenza and sepsis can have serious long-term health effects, such as heart failure, dementia, and depression, and found that the same was true for COVID-19 infections. For all three infections, patients at high risk require additional support after their initial discharge.
Defining long COVID
Although there was no increased risk with COVID-19 for most conditions, these results do not mean that the postacute effects of the infection, often called “long COVID,” are not significant, Dr. Quinn emphasized. The researcher believes that it’s important to listen to the many patients reporting symptoms and validate their experiences.
There needs to be greater consensus among the global health community on what constitutes long COVID. While the research led by Dr. Quinn focuses on postacute health conditions, some definitions of long COVID, such as that of the World Health Organization, refer only to ongoing symptoms of the original infection.
While there is now a diagnostic code for treating long COVID in Ontario, the data available to the researchers did not include information on some common symptoms of post-COVID condition, like chronic fatigue. In the data used, there was not an accurate way to identify patients who had developed conditions like myalgic encephalomyelitis/chronic fatigue syndrome and postural orthostatic tachycardia syndrome, said Dr. Quinn.
In addition to creating clear definitions and determining the best treatments, prevention is essential, said Dr. Quinn. Prior studies have shown that vaccination helps prevent ICU admission for COVID-19.
‘Important questions remain’
Commenting on the finding, Aravind Ganesh, MD, DPhil, a neurologist at the University of Calgary (Alta.), said that by including control populations, the study addressed an important limitation of previous research. Dr. Ganesh, who was not involved in the study, said that the controls help to determine the cause of associations found in other studies, including his own research on long-term symptoms following outpatient care for COVID-19.
“I think what this tells us is that maybe a lot of the issues that we’ve been seeing as complications attributable to COVID are, in fact, complications attributable to serious illness,” said Dr. Ganesh. He also found the association with venous thromboembolism interesting because the condition is recognized as a key risk factor for COVID-19 outcomes.
Compared with smaller randomized control trials, the population-level data provided a much larger sample size for the study. However, this design comes with limitations as well, Dr. Ganesh noted. The study relies on the administrative data of diagnostic codes and misses symptoms that aren’t associated with a diagnosis. In addition, because the cohorts were not assigned randomly, it may not account for preexisting risk factors.
While the study demonstrates associations with physical and mental health conditions, the cause of postacute effects from COVID-19, influenza, and sepsis is still unclear. “Important questions remain,” said Dr. Ganesh. “Why is it that these patients are experiencing these symptoms?”
The study was supported by ICES and the Canadian Institutes of Health Research. Dr. Quinn reported part-time employment at Public Health Ontario and stock in Pfizer and BioNTech. Dr. Ganesh reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large observational study examined population-wide data for 13 postacute conditions in patients who had been hospitalized with a COVID-19 infection and found that all but one of these conditions, venous thromboembolism, occurred at comparable rates in those hospitalized for sepsis and influenza.
“For us, the main takeaway was that patients hospitalized for severe illness in general really require ongoing treatment and support after they’re discharged. That type of care is often very challenging to coordinate for people in a sometimes siloed and fragmented health care system,” study author Kieran Quinn, MD, PhD, a clinician at Sinai Health in Toronto, and assistant professor at the University of Toronto, said in an interview.
The study was published in JAMA Internal Medicine.
Postacute effects
The investigators compared clinical and health administrative data from 26,499 Ontarians hospitalized with COVID-19 with data from three additional cohorts who had been hospitalized with influenza (17,516 patients) and sepsis. The sepsis cohort was divided into two groups, those hospitalized during the COVID-19 pandemic (52,878 patients) and a historical control population (282,473 patients).
These comparators allowed the researchers to compare COVID-19 with other severe infectious illnesses and control for any changes in health care delivery that may have occurred during the pandemic. The addition of sepsis cohorts was needed for the latter purpose, since influenza rates dropped significantly after the onset of the pandemic.
The study outcomes (including cardiovascular, neurological, and mental health conditions and rheumatoid arthritis) were selected based on previous associations with COVID-19 infections, as well as their availability in the data, according to Dr. Quinn. The investigators used diagnostic codes recorded in Ontario’s Institute for Clinical Evaluative Sciences database. The investigators observed some of the studied conditions in their own patients. “Many of us on the research team are practicing clinicians who care for people living with long COVID,” said Dr. Quinn.
Compared with cohorts with other serious infections, those hospitalized with COVID-19 were not at increased risk for selected cardiovascular or neurological disorders, rheumatoid arthritis, or mental health conditions within 1 year following hospitalization. Incident venous thromboembolic disease, however, was more common after hospitalization for COVID-19 than after hospitalization for influenza (adjusted hazard ratio, 1.77).
The study results corroborate previous findings that influenza and sepsis can have serious long-term health effects, such as heart failure, dementia, and depression, and found that the same was true for COVID-19 infections. For all three infections, patients at high risk require additional support after their initial discharge.
Defining long COVID
Although there was no increased risk with COVID-19 for most conditions, these results do not mean that the postacute effects of the infection, often called “long COVID,” are not significant, Dr. Quinn emphasized. The researcher believes that it’s important to listen to the many patients reporting symptoms and validate their experiences.
There needs to be greater consensus among the global health community on what constitutes long COVID. While the research led by Dr. Quinn focuses on postacute health conditions, some definitions of long COVID, such as that of the World Health Organization, refer only to ongoing symptoms of the original infection.
While there is now a diagnostic code for treating long COVID in Ontario, the data available to the researchers did not include information on some common symptoms of post-COVID condition, like chronic fatigue. In the data used, there was not an accurate way to identify patients who had developed conditions like myalgic encephalomyelitis/chronic fatigue syndrome and postural orthostatic tachycardia syndrome, said Dr. Quinn.
In addition to creating clear definitions and determining the best treatments, prevention is essential, said Dr. Quinn. Prior studies have shown that vaccination helps prevent ICU admission for COVID-19.
‘Important questions remain’
Commenting on the finding, Aravind Ganesh, MD, DPhil, a neurologist at the University of Calgary (Alta.), said that by including control populations, the study addressed an important limitation of previous research. Dr. Ganesh, who was not involved in the study, said that the controls help to determine the cause of associations found in other studies, including his own research on long-term symptoms following outpatient care for COVID-19.
“I think what this tells us is that maybe a lot of the issues that we’ve been seeing as complications attributable to COVID are, in fact, complications attributable to serious illness,” said Dr. Ganesh. He also found the association with venous thromboembolism interesting because the condition is recognized as a key risk factor for COVID-19 outcomes.
Compared with smaller randomized control trials, the population-level data provided a much larger sample size for the study. However, this design comes with limitations as well, Dr. Ganesh noted. The study relies on the administrative data of diagnostic codes and misses symptoms that aren’t associated with a diagnosis. In addition, because the cohorts were not assigned randomly, it may not account for preexisting risk factors.
While the study demonstrates associations with physical and mental health conditions, the cause of postacute effects from COVID-19, influenza, and sepsis is still unclear. “Important questions remain,” said Dr. Ganesh. “Why is it that these patients are experiencing these symptoms?”
The study was supported by ICES and the Canadian Institutes of Health Research. Dr. Quinn reported part-time employment at Public Health Ontario and stock in Pfizer and BioNTech. Dr. Ganesh reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA INTERNAL MEDICINE
New ESH hypertension guidelines aim for simplified message
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
The guidelines, which are endorsed by the European Renal Association and the International Society of Hypertension, were presented during the annual European Meeting on Hypertension and Cardiovascular Protection Meeting in Milan, Italy.
The guidelines consensus document was also published online in the Journal of Hypertension. Giuseppe Mancia, MD, professor emeritus of medicine, University Milano-Bicocca, Italy, and Reinhold Kreutz, MD, PhD, Charité–University Medicine Berlin, were cochairs of the task force that created the document.
“We have tried to provide a simplified message to key topics with these new guidelines,” Dr. Kreutz said in an interview.
“We have confirmed the definition of hypertension and provide clear guidance for blood pressure monitoring and a simplified general strategy targeting similar blood pressure goals for most patients, although the treatment algorithms of how you get there may be different for different patient groups.”
Dr. Kreutz added: “Because hypertension is so prevalent and many patients have comorbidities, it is not easy to have one approach for all, but we have tried to simplify the key messages as much as possible, with a target that is more general to the whole population.”
While there are no major surprises in the guidelines, there are multiple advances and added-value changes, including clear advice on how to measure blood pressure, an upgrade for beta-blockers in the treatment algorithms, and a new definition and treatment recommendations for “true resistant hypertension.”
Definition remains unchanged
The definition of hypertension remains unchanged from the previous guidelines – repeated office systolic blood pressure values of ≥ 140 mm Hg and/or diastolic blood pressure values of ≥ 90 mm Hg.
“The definition and classification of hypertension has not changed in these new guidelines,” Dr. Kreutz said. “While there have been suggestions that the definition/target should be changed again, particularly about blood pressure lowering being beneficial at the very low pressure range, after reviewing all the evidence we do not agree with this, and we are standing with the definition of hypertension when intervention is beneficial rather than doing nothing or causing harm.”
Clear guidance on measurement
Dr. Kreutz points out that the correct measurement of blood pressure is of key importance, and the new guidelines include a detailed algorithm on how to measure blood pressure. The preferred method is automated cuff-based blood pressure measurement.
“There are still many variations in blood pressure measurement in clinical practice, so we now have clear guidance on how to measure blood pressure in the office but also at home,” he commented.
They have upgraded the use of out-of-office blood pressure measurement, particularly home measurement, as useful in long-term management. “In future, there should be more emphasis on follow-up using technology with remote control and virtual care.”
Thresholds for starting treatment
On thresholds for initiating antihypertensive therapy, the guidelines recommend that treatment be initiated for most patients when systolic blood pressure is ≥ 140 mm Hg or diastolic blood pressure is ≥ 90 mm Hg.
The same recommendation is given for patients with grade 1 hypertension (systolic, 140-159 mm Hg; and/or diastolic, 90-99 mm Hg) irrespective of cardiovascular risk, although they add that for patients in the lower blood pressure range who have no hypertension-mediated organ damage and who are at low cardiovascular risk, consideration may be given to starting treatment with lifestyle changes only. If, however, blood pressure control is not achieved within a few months of a lifestyle-based approach alone, drug treatment is necessary.
For older patients (aged 80 or older), the task force recommends initiation of drug treatment at 160 mm Hg systolic, although a lower systolic threshold of 140-160 mm Hg may be considered. The authors note that thresholds for the initiation of drug treatment for very frail patients should be individualized.
Blood pressure targets
In the new guidelines, the blood pressure target is the same as in the previous guidelines for the general population of patients with hypertension. The goal is < 140/80 mm Hg for most patients. This accounts for the major portion of the protective effect of blood pressure lowering.
However, the consensus document notes that despite the smaller incremental benefit, an effort should be made to reach a range of 120-129/70-79 mm Hg, but only if treatment is well tolerated to avoid the risk of treatment discontinuation because of adverse events, which might offset, in part or completely, the incremental reduction in cardiovascular outcomes.
Elaborating on this, Dr. Kreutz said, “We should aim for the systolic blood pressure to be within the range of below 140 mm Hg down to 120 mm Hg, with a specific target of around 130 mm Hg for most patients and lower in patients in whom drug treatments are well tolerated and who are at high risk.
“The problem is, if we go for a target of lower that 130 mm Hg, the evidence gets weaker, the benefits diminish, and we risk losing patients because of adverse effects from using so many drugs,” he added. “But in younger and fitter patients, we would recommend the lower the better, but not below 120 mm Hg.”
Dr. Kreutz noted that the new guidelines have tried to simplify recommendations on target pressures. “We have tried to simplify guidance to focus on a target of around 130 for almost all patients. Before, it wasn’t so clear. There were different targets for different groups of patients with various comorbidities or older patients. But now we are saying the range of 120 to 139 is suitable for the vast majority of patients.”
The guidelines do allow slightly higher targets for older and very frail patients.
Drug treatments
The guidelines advise that blood pressure lowering be prioritized over the selection of specific antihypertensive drug classes. The use of any of the five major drug classes – angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), beta-blockers, calcium blockers, and thiazide/thiazidelike diuretics – and their combinations are recommended as the basis of antihypertensive treatment strategies.
They advise starting with a two-drug combination for most patients. The preferred combinations including a renin-angiotensin blocker (either an ACE inhibitor or an ARB) with a calcium blocker or a thiazide/thiazidelike diuretic, preferably in a single-pill combination to reduce pill burden and improve adherence and outcome.
If blood pressure is not controlled with the initial two-drug combination at the maximum recommended and tolerated dose of the respective components, treatment should be increased to a three-drug combination.
“We can control 60% of patients in the general hypertensive population with dual therapy, and up to 90% with triple therapy,” Dr. Kreutz said. “Only a small percentage need a fourth drug.”
A new feature of the guidelines is the upgrading of beta-blockers in the treatment algorithms.
“Beta-blockers may not have previously been considered as a first choice of antihypertensive medication, but we see that in clinical practice, many patients are actually treated with these drugs because there are so many conditions in which beta-blockers have a compelling evidence-based indication or are believed to be favorable,” he said. “So, we are now positioning beta-blockers as drugs that can be used at any step of the treatment algorithm if there is a guideline directed indication or other conditions for which they are thought to be beneficial.”
The guidelines also recommend that all drugs be given as once-daily preparations and that they be taken preferably in the morning.
“The new TIME study has established that there is no difference in outcome with morning or evening dosing, but we know that adherence is often better when drugs are taken in the morning, and it is not advisable to take diuretics in the evening,” Dr. Kreutz said.
‘True resistant hypertension’
The guidelines have introduced a new term, “true resistant hypertension,” defined as systolic blood pressure of ≥ 140 mm Hg or diastolic blood pressure of ≥ 90 mm Hg in the presence of the following conditions: the maximum recommended and tolerated doses of a three-drug combination comprising a renin-angiotensin system blocker (either an ACE inhibitor or an ARB), a calcium blocker, and a thiazide/thiazidelike diuretic were used; inadequate blood pressure control has been confirmed by ambulatory (preferable) or home blood pressure measurement; and various causes of pseudo-resistant hypertension (especially poor medication adherence) and secondary hypertension have been excluded.
“There are many patients who may appear to have resistant hypertension, but we need to screen them carefully to ensure they are adherent to treatment, and then most of these patients are found not to be truly resistant,” Dr. Kreutz explained. “We estimate that only about 5% of patients have true resistant hypertension.”
For these patients with true resistant hypertension, two treatment approaches are recommended.
For those who do not have advanced kidney disease (glomerular filtration rate > 40 mL/min), renal denervation can be considered. This is a new II B recommendation.
Dr. Kreutz noted that studies of renal denervation excluded patients with advanced kidney disease, so there are no data for this group. For these patients, the guidelines suggest that a combination diuretic approach (chlorthalidone with a loop diuretic) could be considered in light of the results of the recent CLICK study.
Differences from U.S. guidelines?
Commenting on the new European guidelines for this news organization, Paul Whelton, MD, chair of the most recent American College of Cardiology/American Heart Association hypertension guidelines committee, said: “Publication of these guidelines is important. I congratulate the European task force. It is an enormous amount of time and effort.”
Dr. Whelton, who is Show Chwan Chair in Global Public Health at Tulane University, New Orleans, and president of the World Hypertension League, added: “I would say the changes are incremental rather than major, but that is probably appropriate.”
He welcomed the greater emphasis on out-of-office blood pressure measurement, saying, “That’s where we should be headed.”
Asked how the European guidelines differ from the U.S. guidelines, Dr. Whelton commented: “There are differences, but they are not huge. The major hypertension guidelines across the world are much more alike than they are different.”
He pointed out that both the U.S. and European guidelines aim for a target blood pressure of 130/80 mm Hg for most patients but have different ways of issuing that advice.
“The Europeans recommend a minimum goal of 140/90 mm Hg, and if there are no issues, then press on to get to under 130/80 mm Hg. That’s kind of a two-step process,” he said. “In the U.S., we’ve gone for a more direct approach of just recommending less than 130/80 mm Hg.
“My fear with the European approach is that by saying, get to 140/90 mm Hg first, then move on to 130/80 mm Hg, is that you’re likely to lose people. And doctors could feel that 140/90 is fine.”
More effort needed on implementation
Dr. Whelton says that where all hypertension guidelines are lacking is in the implementation of the recommendations.
“We are all falling down on implementation,” he said. “We have a huge burden of illness, and it is a very cost-effective area for management, but still, rates of blood pressure control are very bad. Generally speaking, even with a very conservative target of 140/90, the best countries only have control rates of around 30%, and this can be as low as 8% in some low/middle-income countries.”
Dr. Whelton believes the approach to blood pressure management needs to change.
“We know that the current traditional model of care, where blood pressure is managed by your local doctor, is not working. It is hopeless,” he said. “That is not an indictment of these doctors. It’s just that they have more pressing issues to deal with, so we need to look at other models.”
He suggests that the way forward is through convenient, community-based care delivered by a team in which nonphysicians assist in much of the management and in which reliable, affordable medications are given at the point of care, with patients tracked with electronic health records so as to identify those who are not adhering to their medication regimens.
“We know that using simple protocols will work for the vast majority of people. We don’t need to individualize or complicate this too much. That tends to lose people in the process.”
Dr. Whelton makes the point that it is well known how to diagnose and treat hypertension, yet this is not being done well.
“We are doing these things really badly. In routine care, blood pressure is measured horribly. Nobody would accept a pilot of a plane saying he should be doing all these procedures but he’s too busy and it’s probably okay, but that’s the way blood pressure is often measured in clinical practice,” he added. “And we can’t really do a good job if were not measuring the key variable properly that the diagnosis is based on.”
Dr. Whelton also points out that the medical profession is not making enough effort to have patients reach target levels.
“If you’re in a country where very few people are being treated and very high pressures are common, then of course you have to focus on that group first. But in most of the Western world, we are long past that, so we can move on down the chain. We then get to a lot more people with moderately high blood pressure getting exposed to increases in risk, and while this is not quite as dramatic as those with very high pressures at the individual risk level, because there are so many of them, that’s where a lot of events are occurring,” he says.
“If we get everyone to 140/90 mm Hg, we can probably prevent 60% of blood pressure–related events. But if we can get them all down to 130 mm Hg systolic, then we can prevent 75%-80% of events. It’s often quite easy to get to that target, but patients need help and encouragement.”
Going forward, he concluded, guidelines should pivot to focus more on implementation.
“We all try to make the guidelines as approachable as possible, but they are encyclopedic, and many doctors just continue doing what they are doing. That is our big challenge.”
A version of this article first appeared on Medscape.com.
Diabetes may short circuit pembrolizumab benefits in NSCLC
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators reviewed the medical records of 203 consecutive patients with metastatic NSCLC who received first-line pembrolizumab either alone or in combination with chemotherapy at a single tertiary center in Israel.
- Overall, 1 in 4 patients (n = 51) had diabetes mellitus; most (n = 42) were being treated with oral hypoglycemic agents, frequently metformin, and 7 were taking insulin.
- Rates of tumors with PD‐L1 expression above 50% were not significantly different among patients with diabetes and those without.
TAKEAWAY:
- Overall, among patients with diabetes, median progression-free survival (PFS) was significantly shorter than among patients without diabetes (5.9 vs. 7.1 months), as was overall survival (12 vs. 21 months).
- Shorter overall survival was more pronounced among those with diabetes who received pembrolizumab alone (12 vs. 27 months) in comparison with patients who received pembrolizumab plus chemotherapy (14.3 vs. 19.4 months).
- After adjusting for potential confounders, multivariate analysis confirmed that diabetes was an independent risk factor for shorter PFS (hazard ratio, 1.67) and shorter overall survival (HR, 1.73) for patients with NSCLC.
- In a validation cohort of 452 patients with metastatic NSCLC, only 19.6% of those with diabetes continued to take pembrolizumab at 12 months versus 31.7% of those without diabetes.
IN PRACTICE:
“As NSCLC patients with [diabetes] constitute a significant subgroup, there is an urgent need to validate our findings and explore whether outcomes in these patients can be improved by better glycemic control,” the authors said, adding that “chemotherapy may offset some of the deleterious effects” of diabetes.
SOURCE:
The study was led by Yasmin Leshem, MD, PhD, of the Tel Aviv Sourasky Medical Center, and was published in Cancer.
LIMITATIONS:
- Without access to blood test results outside the hospital, the researchers could not determine whether better glycemic control might have improved outcomes.
- The incidence of type 1 or 2 diabetes was not well documented.
DISCLOSURES:
- No funding source was reported.
- Two investigators reported receiving consulting and/or other fees from Bristol-Myers Squibb, Roche, Merck, Novartis, and Merck Sharp and Dohme.
A version of this article first appeared on Medscape.com.
Cannabis for cancer symptoms: Perceived or real benefit?
TOPLINE:
METHODOLOGY:
- Participants included 267 adults (mean age, 58 years; 70% women; 88% White) undergoing treatment for cancer, most commonly breast (47%) and ovarian (29%).
- Participants completed online surveys to characterize cannabis use, reasons for using it, perceived benefits and harms, and physical/psychological symptoms.
- Participants who had used cannabis for more than 1 day during the previous 30 days were compared with those who had not.
TAKEAWAY:
- Overall, 26% of respondents reported cannabis use in the past 30 days, most often edibles (65%) or smoked cannabis (51%).
- Cannabis users were more likely to be younger, male, Black, to have lower income, worse physical/psychological symptoms, and to be disabled or unable to work in comparison with nonusers.
- Cannabis was used to treat pain, cancer, sleep problems, anxiety, nausea, and poor appetite; perceived benefits were greatest with respect to sleep, nausea, pain, muscle spasms, and anxiety.
- Despite perceived benefits, cannabis users reported worse overall distress, anxiety, sleep disturbances, appetite, nausea, fatigue, and pain.
IN PRACTICE:
“The study findings indicate that patients with cancer perceived benefits to using cannabis for many symptoms” but also revealed that “those who used cannabis in the past 30 days had significantly worse symptom profiles overall than those who did not use cannabis,” the authors wrote.
SOURCE:
The study, led by Desiree R. Azizoddin, PsyD, University of Oklahoma Health Science Center, Oklahoma City, was published online in Cancer.
LIMITATIONS:
It’s not known whether adults who used cannabis had significantly worse symptoms at the outset, which may have prompted cannabis use, or whether cannabis use may have exacerbated their symptoms.
DISCLOSURES:
Funding for the study was provided by grants from the National Cancer Institute and the Oklahoma Tobacco Settlement Endowment Trust. Nine of the 10 authors have disclosed no relevant conflicts of interest. One author has relationships with various pharmaceutical companies involved in oncology.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Participants included 267 adults (mean age, 58 years; 70% women; 88% White) undergoing treatment for cancer, most commonly breast (47%) and ovarian (29%).
- Participants completed online surveys to characterize cannabis use, reasons for using it, perceived benefits and harms, and physical/psychological symptoms.
- Participants who had used cannabis for more than 1 day during the previous 30 days were compared with those who had not.
TAKEAWAY:
- Overall, 26% of respondents reported cannabis use in the past 30 days, most often edibles (65%) or smoked cannabis (51%).
- Cannabis users were more likely to be younger, male, Black, to have lower income, worse physical/psychological symptoms, and to be disabled or unable to work in comparison with nonusers.
- Cannabis was used to treat pain, cancer, sleep problems, anxiety, nausea, and poor appetite; perceived benefits were greatest with respect to sleep, nausea, pain, muscle spasms, and anxiety.
- Despite perceived benefits, cannabis users reported worse overall distress, anxiety, sleep disturbances, appetite, nausea, fatigue, and pain.
IN PRACTICE:
“The study findings indicate that patients with cancer perceived benefits to using cannabis for many symptoms” but also revealed that “those who used cannabis in the past 30 days had significantly worse symptom profiles overall than those who did not use cannabis,” the authors wrote.
SOURCE:
The study, led by Desiree R. Azizoddin, PsyD, University of Oklahoma Health Science Center, Oklahoma City, was published online in Cancer.
LIMITATIONS:
It’s not known whether adults who used cannabis had significantly worse symptoms at the outset, which may have prompted cannabis use, or whether cannabis use may have exacerbated their symptoms.
DISCLOSURES:
Funding for the study was provided by grants from the National Cancer Institute and the Oklahoma Tobacco Settlement Endowment Trust. Nine of the 10 authors have disclosed no relevant conflicts of interest. One author has relationships with various pharmaceutical companies involved in oncology.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Participants included 267 adults (mean age, 58 years; 70% women; 88% White) undergoing treatment for cancer, most commonly breast (47%) and ovarian (29%).
- Participants completed online surveys to characterize cannabis use, reasons for using it, perceived benefits and harms, and physical/psychological symptoms.
- Participants who had used cannabis for more than 1 day during the previous 30 days were compared with those who had not.
TAKEAWAY:
- Overall, 26% of respondents reported cannabis use in the past 30 days, most often edibles (65%) or smoked cannabis (51%).
- Cannabis users were more likely to be younger, male, Black, to have lower income, worse physical/psychological symptoms, and to be disabled or unable to work in comparison with nonusers.
- Cannabis was used to treat pain, cancer, sleep problems, anxiety, nausea, and poor appetite; perceived benefits were greatest with respect to sleep, nausea, pain, muscle spasms, and anxiety.
- Despite perceived benefits, cannabis users reported worse overall distress, anxiety, sleep disturbances, appetite, nausea, fatigue, and pain.
IN PRACTICE:
“The study findings indicate that patients with cancer perceived benefits to using cannabis for many symptoms” but also revealed that “those who used cannabis in the past 30 days had significantly worse symptom profiles overall than those who did not use cannabis,” the authors wrote.
SOURCE:
The study, led by Desiree R. Azizoddin, PsyD, University of Oklahoma Health Science Center, Oklahoma City, was published online in Cancer.
LIMITATIONS:
It’s not known whether adults who used cannabis had significantly worse symptoms at the outset, which may have prompted cannabis use, or whether cannabis use may have exacerbated their symptoms.
DISCLOSURES:
Funding for the study was provided by grants from the National Cancer Institute and the Oklahoma Tobacco Settlement Endowment Trust. Nine of the 10 authors have disclosed no relevant conflicts of interest. One author has relationships with various pharmaceutical companies involved in oncology.
A version of this article first appeared on Medscape.com.
Necessary Updates to Skin Cancer Risk Stratification
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218


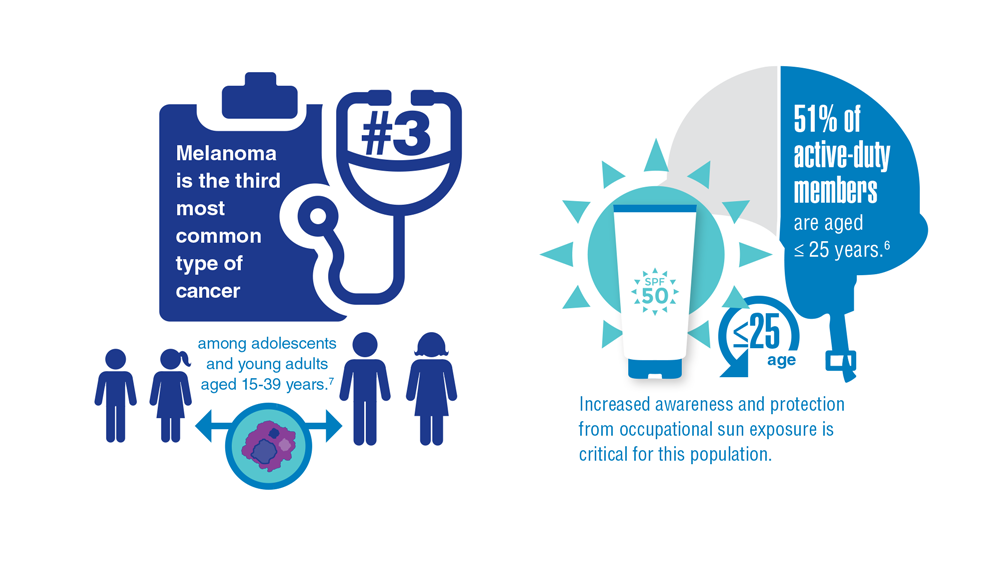



Gender Disparity in Breast Cancer Among US Veterans
1. Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: a population-based study. Cancer. 2004;101(1):51-57. doi:10.1002/cncr.20312
2. Key statistics for breast cancer in men. American Cancer Society. Updated January 12, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/about/key-statistics.html
3. Aggarwal A, Adepoju B, Yacur M, Maron D, Sharma MH. Gender disparity in breast cancer: a veteran population-based comparison. Clin Breast Cancer. 2021;21(4):e471-e478. doi:10.1016/j.clbc.2021.01.013
4. Ravandi-Kashani F, Hayes TG. Male breast cancer: a review of the literature. Eur J Cancer. 1998;34(9):1341-1347. doi:10.1016/s0959-8049(98)00028-8
5. Giordano SH. A review of diagnosis and management of male breast cancer. Oncologist. 2005;10(7):471-479. doi:10.1634/theoncologist.10-7-471
6. Midding E, Halbach SM, Kowalski C, Weber R, Würstlein R, Ernstmann N. Men with a “woman's disease”: stigmatization of male breast cancer patients—a mixed methods analysis. Am J Mens Health. 2018;12(6):2194-2207. doi:10.1177/1557988318799025
7. Key statistics for breast cancer. American Cancer Society. Updated October 6, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html
8. Male breast cancer incidence and mortality, United States—2013-2017. Centers for Disease Control and Prevention. Updated October 1, 2020. Accessed December 14, 2022. https://www.cdc.gov/cancer/uscs/about/data-briefs/no19-male-breast-cancer-incidence-mortality-UnitedStates-2013-2017.htm
9. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res Treat. 2004;83(1):77-86. doi:10.1023/B:BREA.0000010701.08825.2d 10. Pritzlaff M, Summerour P, McFarland R, et al. Male breast cancer in a multi-gene panel testing cohort: insights and unexpected results. Breast Cancer Res Treat. 2017;161(3):575-586. doi:10.1007/s10549-016-4085-4
11. Ottini L, Capalbo C, Rizzolo P, et al. HER2-positive male breast cancer: an update. Breast Cancer (Dove Med Press). 2010;2:45-58. doi:10.2147/BCTT.S6519
12. Risk factors for breast cancer in men. American Cancer Society. Updated April 27, 2018. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/causes-risks-prevention/risk-factors.html
13. Palli D, Masala G, Mariani-Constantini R, et al. A gene–environment interaction between occupation and BRCA1/BRCA2 mutations in male breast cancer? Eur J Cancer. 2004;40(16):2472-2479. doi:10.1016/j.ejca.2004.07.012
14. Hansen J. Elevated risk for male breast cancer after occupational exposure to gasoline and vehicular combustion products. Am J Ind Med. 2000;37(4):349-352. doi:10.1002/(sici)1097-0274(200004)37:4<349::aid-ajim4>3.0.co;2-l
15. Sung H, DeSantis C, Jemal A. Subtype-specific breast cancer incidence rates in Black versus White men in the United States. JNCI Cancer Spectr. 2020;4(1):pkz091. doi:10.1093/jncics/pkz091
16. Breast cancer, male: statistics. Cancer.net. January 2022. Accessed December 14, 2022. https://www.cancer.net/cancer-types/breast-cancer-male/statistics
1. Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: a population-based study. Cancer. 2004;101(1):51-57. doi:10.1002/cncr.20312
2. Key statistics for breast cancer in men. American Cancer Society. Updated January 12, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/about/key-statistics.html
3. Aggarwal A, Adepoju B, Yacur M, Maron D, Sharma MH. Gender disparity in breast cancer: a veteran population-based comparison. Clin Breast Cancer. 2021;21(4):e471-e478. doi:10.1016/j.clbc.2021.01.013
4. Ravandi-Kashani F, Hayes TG. Male breast cancer: a review of the literature. Eur J Cancer. 1998;34(9):1341-1347. doi:10.1016/s0959-8049(98)00028-8
5. Giordano SH. A review of diagnosis and management of male breast cancer. Oncologist. 2005;10(7):471-479. doi:10.1634/theoncologist.10-7-471
6. Midding E, Halbach SM, Kowalski C, Weber R, Würstlein R, Ernstmann N. Men with a “woman's disease”: stigmatization of male breast cancer patients—a mixed methods analysis. Am J Mens Health. 2018;12(6):2194-2207. doi:10.1177/1557988318799025
7. Key statistics for breast cancer. American Cancer Society. Updated October 6, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html
8. Male breast cancer incidence and mortality, United States—2013-2017. Centers for Disease Control and Prevention. Updated October 1, 2020. Accessed December 14, 2022. https://www.cdc.gov/cancer/uscs/about/data-briefs/no19-male-breast-cancer-incidence-mortality-UnitedStates-2013-2017.htm
9. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res Treat. 2004;83(1):77-86. doi:10.1023/B:BREA.0000010701.08825.2d 10. Pritzlaff M, Summerour P, McFarland R, et al. Male breast cancer in a multi-gene panel testing cohort: insights and unexpected results. Breast Cancer Res Treat. 2017;161(3):575-586. doi:10.1007/s10549-016-4085-4
11. Ottini L, Capalbo C, Rizzolo P, et al. HER2-positive male breast cancer: an update. Breast Cancer (Dove Med Press). 2010;2:45-58. doi:10.2147/BCTT.S6519
12. Risk factors for breast cancer in men. American Cancer Society. Updated April 27, 2018. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/causes-risks-prevention/risk-factors.html
13. Palli D, Masala G, Mariani-Constantini R, et al. A gene–environment interaction between occupation and BRCA1/BRCA2 mutations in male breast cancer? Eur J Cancer. 2004;40(16):2472-2479. doi:10.1016/j.ejca.2004.07.012
14. Hansen J. Elevated risk for male breast cancer after occupational exposure to gasoline and vehicular combustion products. Am J Ind Med. 2000;37(4):349-352. doi:10.1002/(sici)1097-0274(200004)37:4<349::aid-ajim4>3.0.co;2-l
15. Sung H, DeSantis C, Jemal A. Subtype-specific breast cancer incidence rates in Black versus White men in the United States. JNCI Cancer Spectr. 2020;4(1):pkz091. doi:10.1093/jncics/pkz091
16. Breast cancer, male: statistics. Cancer.net. January 2022. Accessed December 14, 2022. https://www.cancer.net/cancer-types/breast-cancer-male/statistics
1. Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: a population-based study. Cancer. 2004;101(1):51-57. doi:10.1002/cncr.20312
2. Key statistics for breast cancer in men. American Cancer Society. Updated January 12, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/about/key-statistics.html
3. Aggarwal A, Adepoju B, Yacur M, Maron D, Sharma MH. Gender disparity in breast cancer: a veteran population-based comparison. Clin Breast Cancer. 2021;21(4):e471-e478. doi:10.1016/j.clbc.2021.01.013
4. Ravandi-Kashani F, Hayes TG. Male breast cancer: a review of the literature. Eur J Cancer. 1998;34(9):1341-1347. doi:10.1016/s0959-8049(98)00028-8
5. Giordano SH. A review of diagnosis and management of male breast cancer. Oncologist. 2005;10(7):471-479. doi:10.1634/theoncologist.10-7-471
6. Midding E, Halbach SM, Kowalski C, Weber R, Würstlein R, Ernstmann N. Men with a “woman's disease”: stigmatization of male breast cancer patients—a mixed methods analysis. Am J Mens Health. 2018;12(6):2194-2207. doi:10.1177/1557988318799025
7. Key statistics for breast cancer. American Cancer Society. Updated October 6, 2022. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html
8. Male breast cancer incidence and mortality, United States—2013-2017. Centers for Disease Control and Prevention. Updated October 1, 2020. Accessed December 14, 2022. https://www.cdc.gov/cancer/uscs/about/data-briefs/no19-male-breast-cancer-incidence-mortality-UnitedStates-2013-2017.htm
9. Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res Treat. 2004;83(1):77-86. doi:10.1023/B:BREA.0000010701.08825.2d 10. Pritzlaff M, Summerour P, McFarland R, et al. Male breast cancer in a multi-gene panel testing cohort: insights and unexpected results. Breast Cancer Res Treat. 2017;161(3):575-586. doi:10.1007/s10549-016-4085-4
11. Ottini L, Capalbo C, Rizzolo P, et al. HER2-positive male breast cancer: an update. Breast Cancer (Dove Med Press). 2010;2:45-58. doi:10.2147/BCTT.S6519
12. Risk factors for breast cancer in men. American Cancer Society. Updated April 27, 2018. Accessed December 14, 2022. https://www.cancer.org/cancer/breast-cancer-in-men/causes-risks-prevention/risk-factors.html
13. Palli D, Masala G, Mariani-Constantini R, et al. A gene–environment interaction between occupation and BRCA1/BRCA2 mutations in male breast cancer? Eur J Cancer. 2004;40(16):2472-2479. doi:10.1016/j.ejca.2004.07.012
14. Hansen J. Elevated risk for male breast cancer after occupational exposure to gasoline and vehicular combustion products. Am J Ind Med. 2000;37(4):349-352. doi:10.1002/(sici)1097-0274(200004)37:4<349::aid-ajim4>3.0.co;2-l
15. Sung H, DeSantis C, Jemal A. Subtype-specific breast cancer incidence rates in Black versus White men in the United States. JNCI Cancer Spectr. 2020;4(1):pkz091. doi:10.1093/jncics/pkz091
16. Breast cancer, male: statistics. Cancer.net. January 2022. Accessed December 14, 2022. https://www.cancer.net/cancer-types/breast-cancer-male/statistics