User login
How BMI over time impacts GI cancer risk
according to new data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial.
The researchers found that being overweight or obese in early and middle adulthood was associated with an increased risk for colorectal cancer (CRC) and noncolorectal GI cancers. Maintaining or increasing BMI over time among overweight or obese individuals was also associated with an increased GI cancer risk.
Aspirin use did not significantly modify these associations, suggesting that aspirin may not be as effective for cancer prevention among overweight or obese individuals.
The results provide “relatively consistent messaging that overweight or obesity from early to later adulthood as well as BMI increases throughout adulthood were associated with increased risk of GI cancers, especially CRC,” the authors of an editorial accompanying the study wrote.
These “important findings highlight the unmet need to identify the critical time window linking adiposity and GI cancer,” said editorialists Mengyao Shi, MBBS, MPD, and Yin Cao, ScD, MPH, of Washington University in St. Louis.
The analysis was published online in JAMA Network Open.
A growing body of evidence has revealed a strong association between obesity and GI cancers, with chronic inflammation being a likely cause. As rates of overweight and obesity continue to grow, better understanding of the association between obesity and cancer has become increasingly important.
In the analysis, Holli A. Loomans-Kropp, PhD, MPH, with Ohio State University, Columbus, and Asad Umar, PhD, DVM, with the National Cancer Institute, Rockville, Md., explored associations between BMI in early adulthood (age 20), middle adulthood (age 50) and later adulthood (age 55 and over) and GI cancer risk in 135,161 adults from the PLCO Cancer Screening Trial.
BMI was determined using self-reported height and weight at each age time point. The median age at enrollment was 62 years, and 50% of participants were women. Overweight BMI was 25.0-29.9 kg/m2 and obese BMI was 30 or higher.
During as many as 21 years of follow-up, 2,803 individuals developed CRC and 2,285 developed non-CRC GI cancers (esophageal, liver, gastric, and pancreatic).
Overweight BMI in early, middle, and later adulthood was associated with an increased risk of CRC (hazard ratio, 1.23 for early and middle years; HR, 1.21 for later years). Obese BMI in middle and later adulthood was also associated with increased risk of CRC (HR, 1.55 and 1.39, respectively).
The authors observed similar associations between BMI in middle and later adulthood and overall GI and non-CRC GI risk.
“When modeled continuously, we observed 2%-4% increased risk of both CRC and noncolorectal GI cancer with each 1-unit increase in BMI across all time points,” the researchers said.
Their data also suggest that BMI over time may be associated with GI cancer risk. Adults who exhibited no change in overweight or obese BMIs between early and later adulthood and those who exhibited increases in BMI from underweight or normal in early adulthood to overweight or obese BMI in later adulthood had a significantly higher risk for CRC and noncolorectal GI cancer.
Among frequent aspirin users, those with overweight or obese BMIs in early, middle, and later adulthood still had an increased risk for CRC and noncolorectal GI cancer (hazard ratios, 1.44, 1.45, and 1.43, respectively).
The finding that regular weekly aspirin use did not modify GI cancer risk suggests that obesity may alter the cancer-preventive effect of aspirin, the researchers suggested. Individuals with obesity may need to increase aspirin frequency or dosage to see an effect, but upping the dose comes with its own risks, including GI bleeding.
Overall, until now, most epidemiologic studies have examined BMI at one time point, “missing the opportunity to delineate the contribution of adiposity throughout the life course,” Dr. Shi and Dr. Cao wrote.
“As we continue to investigate precision-based interventions to intercept the link between obesity and cancer, it is imperative to reiterate the importance of maintaining a healthy weight and lifestyle from an early age and incorporate it widely into cancer prevention strategies at all levels with immediate implementation,” the editorialists concluded.
This study was supported in part by funds from Ohio State University and the NIH. The study authors reported no relevant financial relationships. Dr. Cao has received personal fees from Geneoscopy for consulting.
A version of this article originally appeared on Medscape.com.
according to new data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial.
The researchers found that being overweight or obese in early and middle adulthood was associated with an increased risk for colorectal cancer (CRC) and noncolorectal GI cancers. Maintaining or increasing BMI over time among overweight or obese individuals was also associated with an increased GI cancer risk.
Aspirin use did not significantly modify these associations, suggesting that aspirin may not be as effective for cancer prevention among overweight or obese individuals.
The results provide “relatively consistent messaging that overweight or obesity from early to later adulthood as well as BMI increases throughout adulthood were associated with increased risk of GI cancers, especially CRC,” the authors of an editorial accompanying the study wrote.
These “important findings highlight the unmet need to identify the critical time window linking adiposity and GI cancer,” said editorialists Mengyao Shi, MBBS, MPD, and Yin Cao, ScD, MPH, of Washington University in St. Louis.
The analysis was published online in JAMA Network Open.
A growing body of evidence has revealed a strong association between obesity and GI cancers, with chronic inflammation being a likely cause. As rates of overweight and obesity continue to grow, better understanding of the association between obesity and cancer has become increasingly important.
In the analysis, Holli A. Loomans-Kropp, PhD, MPH, with Ohio State University, Columbus, and Asad Umar, PhD, DVM, with the National Cancer Institute, Rockville, Md., explored associations between BMI in early adulthood (age 20), middle adulthood (age 50) and later adulthood (age 55 and over) and GI cancer risk in 135,161 adults from the PLCO Cancer Screening Trial.
BMI was determined using self-reported height and weight at each age time point. The median age at enrollment was 62 years, and 50% of participants were women. Overweight BMI was 25.0-29.9 kg/m2 and obese BMI was 30 or higher.
During as many as 21 years of follow-up, 2,803 individuals developed CRC and 2,285 developed non-CRC GI cancers (esophageal, liver, gastric, and pancreatic).
Overweight BMI in early, middle, and later adulthood was associated with an increased risk of CRC (hazard ratio, 1.23 for early and middle years; HR, 1.21 for later years). Obese BMI in middle and later adulthood was also associated with increased risk of CRC (HR, 1.55 and 1.39, respectively).
The authors observed similar associations between BMI in middle and later adulthood and overall GI and non-CRC GI risk.
“When modeled continuously, we observed 2%-4% increased risk of both CRC and noncolorectal GI cancer with each 1-unit increase in BMI across all time points,” the researchers said.
Their data also suggest that BMI over time may be associated with GI cancer risk. Adults who exhibited no change in overweight or obese BMIs between early and later adulthood and those who exhibited increases in BMI from underweight or normal in early adulthood to overweight or obese BMI in later adulthood had a significantly higher risk for CRC and noncolorectal GI cancer.
Among frequent aspirin users, those with overweight or obese BMIs in early, middle, and later adulthood still had an increased risk for CRC and noncolorectal GI cancer (hazard ratios, 1.44, 1.45, and 1.43, respectively).
The finding that regular weekly aspirin use did not modify GI cancer risk suggests that obesity may alter the cancer-preventive effect of aspirin, the researchers suggested. Individuals with obesity may need to increase aspirin frequency or dosage to see an effect, but upping the dose comes with its own risks, including GI bleeding.
Overall, until now, most epidemiologic studies have examined BMI at one time point, “missing the opportunity to delineate the contribution of adiposity throughout the life course,” Dr. Shi and Dr. Cao wrote.
“As we continue to investigate precision-based interventions to intercept the link between obesity and cancer, it is imperative to reiterate the importance of maintaining a healthy weight and lifestyle from an early age and incorporate it widely into cancer prevention strategies at all levels with immediate implementation,” the editorialists concluded.
This study was supported in part by funds from Ohio State University and the NIH. The study authors reported no relevant financial relationships. Dr. Cao has received personal fees from Geneoscopy for consulting.
A version of this article originally appeared on Medscape.com.
according to new data from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial.
The researchers found that being overweight or obese in early and middle adulthood was associated with an increased risk for colorectal cancer (CRC) and noncolorectal GI cancers. Maintaining or increasing BMI over time among overweight or obese individuals was also associated with an increased GI cancer risk.
Aspirin use did not significantly modify these associations, suggesting that aspirin may not be as effective for cancer prevention among overweight or obese individuals.
The results provide “relatively consistent messaging that overweight or obesity from early to later adulthood as well as BMI increases throughout adulthood were associated with increased risk of GI cancers, especially CRC,” the authors of an editorial accompanying the study wrote.
These “important findings highlight the unmet need to identify the critical time window linking adiposity and GI cancer,” said editorialists Mengyao Shi, MBBS, MPD, and Yin Cao, ScD, MPH, of Washington University in St. Louis.
The analysis was published online in JAMA Network Open.
A growing body of evidence has revealed a strong association between obesity and GI cancers, with chronic inflammation being a likely cause. As rates of overweight and obesity continue to grow, better understanding of the association between obesity and cancer has become increasingly important.
In the analysis, Holli A. Loomans-Kropp, PhD, MPH, with Ohio State University, Columbus, and Asad Umar, PhD, DVM, with the National Cancer Institute, Rockville, Md., explored associations between BMI in early adulthood (age 20), middle adulthood (age 50) and later adulthood (age 55 and over) and GI cancer risk in 135,161 adults from the PLCO Cancer Screening Trial.
BMI was determined using self-reported height and weight at each age time point. The median age at enrollment was 62 years, and 50% of participants were women. Overweight BMI was 25.0-29.9 kg/m2 and obese BMI was 30 or higher.
During as many as 21 years of follow-up, 2,803 individuals developed CRC and 2,285 developed non-CRC GI cancers (esophageal, liver, gastric, and pancreatic).
Overweight BMI in early, middle, and later adulthood was associated with an increased risk of CRC (hazard ratio, 1.23 for early and middle years; HR, 1.21 for later years). Obese BMI in middle and later adulthood was also associated with increased risk of CRC (HR, 1.55 and 1.39, respectively).
The authors observed similar associations between BMI in middle and later adulthood and overall GI and non-CRC GI risk.
“When modeled continuously, we observed 2%-4% increased risk of both CRC and noncolorectal GI cancer with each 1-unit increase in BMI across all time points,” the researchers said.
Their data also suggest that BMI over time may be associated with GI cancer risk. Adults who exhibited no change in overweight or obese BMIs between early and later adulthood and those who exhibited increases in BMI from underweight or normal in early adulthood to overweight or obese BMI in later adulthood had a significantly higher risk for CRC and noncolorectal GI cancer.
Among frequent aspirin users, those with overweight or obese BMIs in early, middle, and later adulthood still had an increased risk for CRC and noncolorectal GI cancer (hazard ratios, 1.44, 1.45, and 1.43, respectively).
The finding that regular weekly aspirin use did not modify GI cancer risk suggests that obesity may alter the cancer-preventive effect of aspirin, the researchers suggested. Individuals with obesity may need to increase aspirin frequency or dosage to see an effect, but upping the dose comes with its own risks, including GI bleeding.
Overall, until now, most epidemiologic studies have examined BMI at one time point, “missing the opportunity to delineate the contribution of adiposity throughout the life course,” Dr. Shi and Dr. Cao wrote.
“As we continue to investigate precision-based interventions to intercept the link between obesity and cancer, it is imperative to reiterate the importance of maintaining a healthy weight and lifestyle from an early age and incorporate it widely into cancer prevention strategies at all levels with immediate implementation,” the editorialists concluded.
This study was supported in part by funds from Ohio State University and the NIH. The study authors reported no relevant financial relationships. Dr. Cao has received personal fees from Geneoscopy for consulting.
A version of this article originally appeared on Medscape.com.
FROM JAMA NETWORK OPEN
AHA urges action against racial inequities in stroke care
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
Stroke is a “disease of disparities,” with racial and ethnic inequities in incidence, prevalence, treatment, and outcomes, and research is needed to identify structural or “upstream” interventions to address the problem, the American Heart Association says in a new scientific statement.
including Black, Hispanic, and Indigenous peoples,” writing group chair Amytis Towfighi, MD, professor of neurology, University of Southern California, Los Angeles, says in a news release.
“While research has historically focused on describing these inequities, it is critical to develop and test interventions to address them,” Dr. Towfighi adds.
The scientific statement was published online in the journal Stroke.
It follows a 2020 AHA presidential advisory that declared structural racism a fundamental driver of poor health and early death from heart disease and stroke.
Dr. Towfighi and colleagues reviewed the literature on interventions to address racial and ethnic inequities to identify gaps and areas for future research.
They note that various interventions have shown promise in reducing inequities across the stroke continuum of care.
For example, data suggest that careful attention to stroke preparedness among patients, caregivers, and emergency medical services can reduce inequities in getting people suspected of having a stroke to the emergency department quickly, with delivery of prompt treatment.
However, insufficient research attention has been paid to reducing inequities in rehabilitation, recovery, and social reintegration, the writing group says.
In addition, most studies have addressed patient-level factors, such as medication adherence, health literacy, and health behaviors, but not upstream social factors such as structural racism, housing, income, food security, and access to care, which also affect stroke incidence, care, and outcomes.
“Combating the effects of systemic racism will involve upstream interventions, including policy changes, place-based interventions, and engaging with the health care systems that serve predominantly historically disenfranchised populations and the communities they serve, understanding the barriers, and collaboratively developing solutions to address barriers,” the writing group says.
Further research is needed across the stroke continuum of care to tackle racial and ethnic inequities in stroke care and improve outcomes, they say.
“It’s critical for historically disenfranchised communities to participate in research so that researchers may collaborate in addressing the communities’ needs and concerns,” Bernadette Boden-Albala, DrPH, MPH, vice chair of the writing group, says in the news release.
“Opportunities include working with community stakeholder groups and community organizations to advocate for partnerships with hospitals, academic medical centers, local colleges and universities; or joining community advisory boards and volunteering with the American Heart Association,” Dr. Boden-Albala adds.
Dr. Towfighi encourages health care professionals to “think outside the ‘stroke box.’ Sustainable, effective interventions to address inequities will likely require collaboration with patients, their communities, policymakers, and other sectors.”
The scientific statement was prepared by the volunteer writing group on behalf of the AHA Stroke Council, the Council on Cardiovascular and Stroke Nursing, the Council on Cardiovascular Radiology and Intervention, the Council on Clinical Cardiology, the Council on Hypertension, the Council on the Kidney in Cardiovascular Disease, and the Council on Peripheral Vascular Disease.
The research had no commercial funding.
A version of this article first appeared on Medscape.com.
FROM STROKE
Pruritus and swelling
The history and findings in this case are suggestive of chronic kidney disease (CKD).
CKD affects between 8% and 16% of the population worldwide. Risk factors for CKD are numerous and include T2D, hypertension, and prediabetes. Diabetes is the leading cause of CKD. Up to 40% of patients with diabetes develop diabetic kidney disease, which can progress to end-stage renal disease (ESRD) requiring dialysis or kidney transplantation. In fact, diabetic kidney disease is the top cause of ESRD in the United States.
Diagnostic criteria for CKD include elevated urinary albumin excretion (albuminuria) and/or eGFR < 60 mL/1.73 m2 that persists for more than 3 months. The normal presentation of diabetic kidney disease includes long-standing diabetes, retinopathy, albuminuria without gross hematuria, and gradually progressive decline of eGFR. However, signs of diabetic kidney disease may be present in patients at diagnosis or without retinopathy in T2D. Reduced eGFR without albuminuria has been frequently reported in both type 1 diabetes (T1D) and T2D and is becoming increasingly common as the prevalence of diabetes rises in the United States.
Chronic kidney disease is usually identified through routine screening with serum chemistry profile and urine studies or as an incidental finding. Less often, patients may present with symptoms, such as gross hematuria, "foamy urine" (a sign of albuminuria), nocturia, flank pain, or decreased urine output. In advanced cases, patients may report fatigue, poor appetite, nausea, vomiting, a metallic taste, unintentional weight loss, pruritus, changes in mental status, dyspnea, and/or peripheral edema.
The American Diabetes Association (ADA) 2023 Standards of Care in Diabetes describes five stages of CKD. Stages 1-2 are defined by evidence of high albuminuria with eGFR ≥ 60 mL/min/1.73 m2, while stages 3-5 are defined by progressively lower ranges of eGFR. Of note, at any eGFR, the degree of albuminuria is associated with risk for cardiovascular disease, CKD progression, and mortality. Thus, as noted by the ADA Standards, both eGFR and albuminuria should be used to guide treatment decisions; additionally, eGFR levels are essential for modifying drug dosages or restrictions of use, and the degree of albuminuria should influence selection of antihypertensive agents and glucose-lowering medications.
According to the ADA 2023 Standards of Care in Diabetes, for people with non–dialysis-dependent CKD, dietary protein intake should be ∼0.8 g/kg body weight per day (the recommended daily allowance), as this level has been shown to slow GFR decline compared with higher levels of dietary protein intake, with evidence of a greater effect over time. Conversely, higher levels of dietary protein intake (> 20% of daily calories from protein or > 1.3 g/kg/d) have been associated with increased albuminuria, more rapid kidney function loss, and cardiovascular disease mortality. For patients on dialysis, higher levels of dietary protein intake should be considered, because malnutrition is a significant problem in some of these patients.
Urinary excretion of sodium and potassium may be impaired in patients with reduced eGFR. Thus, restriction of dietary sodium to < 2300 mg/d may help to control blood pressure and reduce cardiovascular risk, and restriction of dietary potassium may be necessary to control serum potassium concentration.
Intensive glycemic control with the goal of achieving near-normoglycemia has been shown to delay the onset and progression of albuminuria and reduced eGFR in patients with diabetes. Insulin alone was used to lower blood glucose in the Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) study of T1D while a variety of agents were used in clinical trials of T2D, supporting the conclusion that glycemic control itself helps prevent CKD and its progression. However, the presence of CKD affects the risks and benefits of intensive glycemic control and several glucose-lowering medications. In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial of T2D, increased adverse effects of intensive glycemic control (hypoglycemia and mortality) were seen among patients with kidney disease at baseline. Moreover, it may take at least 2 years to see improved eGFR outcomes as an effect of intensive glycemic control. Therefore, in some patients with prevalent CKD and substantial comorbidity, target A1c levels may be less intensive.
According to guidance from the US Food and Drug Administration, eGFR should be monitored while taking metformin and metformin is contraindicated in patients with an eGFR < 30 mL/min/1.73 m2. Clinicians should assess the benefits and risks of continuing treatment when eGFR falls to < 45 mL/min/1.73 m2.
The ADA recommends that sodium–glucose cotransporter 2 inhibitors be given to all patients with stage 3 CKD or higher and T2D, regardless of glycemic control, as they have been shown to delay CKD progression and reduce heart failure risk independent of glycemic control. Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) also have direct effects on the kidney and have been reported to improve renal outcomes compared with placebo. In patients for whom cardiovascular risk is a predominant problem, the ADA suggests using GLP-1 RAs for cardiovascular risk reduction.
Comprehensive guidance on the management of CKD in patients with T2D is available in the ADA 2023 Standards of Care in Diabetes.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of chronic kidney disease (CKD).
CKD affects between 8% and 16% of the population worldwide. Risk factors for CKD are numerous and include T2D, hypertension, and prediabetes. Diabetes is the leading cause of CKD. Up to 40% of patients with diabetes develop diabetic kidney disease, which can progress to end-stage renal disease (ESRD) requiring dialysis or kidney transplantation. In fact, diabetic kidney disease is the top cause of ESRD in the United States.
Diagnostic criteria for CKD include elevated urinary albumin excretion (albuminuria) and/or eGFR < 60 mL/1.73 m2 that persists for more than 3 months. The normal presentation of diabetic kidney disease includes long-standing diabetes, retinopathy, albuminuria without gross hematuria, and gradually progressive decline of eGFR. However, signs of diabetic kidney disease may be present in patients at diagnosis or without retinopathy in T2D. Reduced eGFR without albuminuria has been frequently reported in both type 1 diabetes (T1D) and T2D and is becoming increasingly common as the prevalence of diabetes rises in the United States.
Chronic kidney disease is usually identified through routine screening with serum chemistry profile and urine studies or as an incidental finding. Less often, patients may present with symptoms, such as gross hematuria, "foamy urine" (a sign of albuminuria), nocturia, flank pain, or decreased urine output. In advanced cases, patients may report fatigue, poor appetite, nausea, vomiting, a metallic taste, unintentional weight loss, pruritus, changes in mental status, dyspnea, and/or peripheral edema.
The American Diabetes Association (ADA) 2023 Standards of Care in Diabetes describes five stages of CKD. Stages 1-2 are defined by evidence of high albuminuria with eGFR ≥ 60 mL/min/1.73 m2, while stages 3-5 are defined by progressively lower ranges of eGFR. Of note, at any eGFR, the degree of albuminuria is associated with risk for cardiovascular disease, CKD progression, and mortality. Thus, as noted by the ADA Standards, both eGFR and albuminuria should be used to guide treatment decisions; additionally, eGFR levels are essential for modifying drug dosages or restrictions of use, and the degree of albuminuria should influence selection of antihypertensive agents and glucose-lowering medications.
According to the ADA 2023 Standards of Care in Diabetes, for people with non–dialysis-dependent CKD, dietary protein intake should be ∼0.8 g/kg body weight per day (the recommended daily allowance), as this level has been shown to slow GFR decline compared with higher levels of dietary protein intake, with evidence of a greater effect over time. Conversely, higher levels of dietary protein intake (> 20% of daily calories from protein or > 1.3 g/kg/d) have been associated with increased albuminuria, more rapid kidney function loss, and cardiovascular disease mortality. For patients on dialysis, higher levels of dietary protein intake should be considered, because malnutrition is a significant problem in some of these patients.
Urinary excretion of sodium and potassium may be impaired in patients with reduced eGFR. Thus, restriction of dietary sodium to < 2300 mg/d may help to control blood pressure and reduce cardiovascular risk, and restriction of dietary potassium may be necessary to control serum potassium concentration.
Intensive glycemic control with the goal of achieving near-normoglycemia has been shown to delay the onset and progression of albuminuria and reduced eGFR in patients with diabetes. Insulin alone was used to lower blood glucose in the Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) study of T1D while a variety of agents were used in clinical trials of T2D, supporting the conclusion that glycemic control itself helps prevent CKD and its progression. However, the presence of CKD affects the risks and benefits of intensive glycemic control and several glucose-lowering medications. In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial of T2D, increased adverse effects of intensive glycemic control (hypoglycemia and mortality) were seen among patients with kidney disease at baseline. Moreover, it may take at least 2 years to see improved eGFR outcomes as an effect of intensive glycemic control. Therefore, in some patients with prevalent CKD and substantial comorbidity, target A1c levels may be less intensive.
According to guidance from the US Food and Drug Administration, eGFR should be monitored while taking metformin and metformin is contraindicated in patients with an eGFR < 30 mL/min/1.73 m2. Clinicians should assess the benefits and risks of continuing treatment when eGFR falls to < 45 mL/min/1.73 m2.
The ADA recommends that sodium–glucose cotransporter 2 inhibitors be given to all patients with stage 3 CKD or higher and T2D, regardless of glycemic control, as they have been shown to delay CKD progression and reduce heart failure risk independent of glycemic control. Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) also have direct effects on the kidney and have been reported to improve renal outcomes compared with placebo. In patients for whom cardiovascular risk is a predominant problem, the ADA suggests using GLP-1 RAs for cardiovascular risk reduction.
Comprehensive guidance on the management of CKD in patients with T2D is available in the ADA 2023 Standards of Care in Diabetes.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The history and findings in this case are suggestive of chronic kidney disease (CKD).
CKD affects between 8% and 16% of the population worldwide. Risk factors for CKD are numerous and include T2D, hypertension, and prediabetes. Diabetes is the leading cause of CKD. Up to 40% of patients with diabetes develop diabetic kidney disease, which can progress to end-stage renal disease (ESRD) requiring dialysis or kidney transplantation. In fact, diabetic kidney disease is the top cause of ESRD in the United States.
Diagnostic criteria for CKD include elevated urinary albumin excretion (albuminuria) and/or eGFR < 60 mL/1.73 m2 that persists for more than 3 months. The normal presentation of diabetic kidney disease includes long-standing diabetes, retinopathy, albuminuria without gross hematuria, and gradually progressive decline of eGFR. However, signs of diabetic kidney disease may be present in patients at diagnosis or without retinopathy in T2D. Reduced eGFR without albuminuria has been frequently reported in both type 1 diabetes (T1D) and T2D and is becoming increasingly common as the prevalence of diabetes rises in the United States.
Chronic kidney disease is usually identified through routine screening with serum chemistry profile and urine studies or as an incidental finding. Less often, patients may present with symptoms, such as gross hematuria, "foamy urine" (a sign of albuminuria), nocturia, flank pain, or decreased urine output. In advanced cases, patients may report fatigue, poor appetite, nausea, vomiting, a metallic taste, unintentional weight loss, pruritus, changes in mental status, dyspnea, and/or peripheral edema.
The American Diabetes Association (ADA) 2023 Standards of Care in Diabetes describes five stages of CKD. Stages 1-2 are defined by evidence of high albuminuria with eGFR ≥ 60 mL/min/1.73 m2, while stages 3-5 are defined by progressively lower ranges of eGFR. Of note, at any eGFR, the degree of albuminuria is associated with risk for cardiovascular disease, CKD progression, and mortality. Thus, as noted by the ADA Standards, both eGFR and albuminuria should be used to guide treatment decisions; additionally, eGFR levels are essential for modifying drug dosages or restrictions of use, and the degree of albuminuria should influence selection of antihypertensive agents and glucose-lowering medications.
According to the ADA 2023 Standards of Care in Diabetes, for people with non–dialysis-dependent CKD, dietary protein intake should be ∼0.8 g/kg body weight per day (the recommended daily allowance), as this level has been shown to slow GFR decline compared with higher levels of dietary protein intake, with evidence of a greater effect over time. Conversely, higher levels of dietary protein intake (> 20% of daily calories from protein or > 1.3 g/kg/d) have been associated with increased albuminuria, more rapid kidney function loss, and cardiovascular disease mortality. For patients on dialysis, higher levels of dietary protein intake should be considered, because malnutrition is a significant problem in some of these patients.
Urinary excretion of sodium and potassium may be impaired in patients with reduced eGFR. Thus, restriction of dietary sodium to < 2300 mg/d may help to control blood pressure and reduce cardiovascular risk, and restriction of dietary potassium may be necessary to control serum potassium concentration.
Intensive glycemic control with the goal of achieving near-normoglycemia has been shown to delay the onset and progression of albuminuria and reduced eGFR in patients with diabetes. Insulin alone was used to lower blood glucose in the Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) study of T1D while a variety of agents were used in clinical trials of T2D, supporting the conclusion that glycemic control itself helps prevent CKD and its progression. However, the presence of CKD affects the risks and benefits of intensive glycemic control and several glucose-lowering medications. In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial of T2D, increased adverse effects of intensive glycemic control (hypoglycemia and mortality) were seen among patients with kidney disease at baseline. Moreover, it may take at least 2 years to see improved eGFR outcomes as an effect of intensive glycemic control. Therefore, in some patients with prevalent CKD and substantial comorbidity, target A1c levels may be less intensive.
According to guidance from the US Food and Drug Administration, eGFR should be monitored while taking metformin and metformin is contraindicated in patients with an eGFR < 30 mL/min/1.73 m2. Clinicians should assess the benefits and risks of continuing treatment when eGFR falls to < 45 mL/min/1.73 m2.
The ADA recommends that sodium–glucose cotransporter 2 inhibitors be given to all patients with stage 3 CKD or higher and T2D, regardless of glycemic control, as they have been shown to delay CKD progression and reduce heart failure risk independent of glycemic control. Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) also have direct effects on the kidney and have been reported to improve renal outcomes compared with placebo. In patients for whom cardiovascular risk is a predominant problem, the ADA suggests using GLP-1 RAs for cardiovascular risk reduction.
Comprehensive guidance on the management of CKD in patients with T2D is available in the ADA 2023 Standards of Care in Diabetes.
Romesh K. Khardori, MD, PhD, Professor, Department of Internal Medicine, Division of Diabetes, Endocrine, and Metabolic Disorders, Eastern Virginia Medical School; EVMS Medical Group, Norfolk, Virginia
Romesh K. Khardori, MD, PhD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
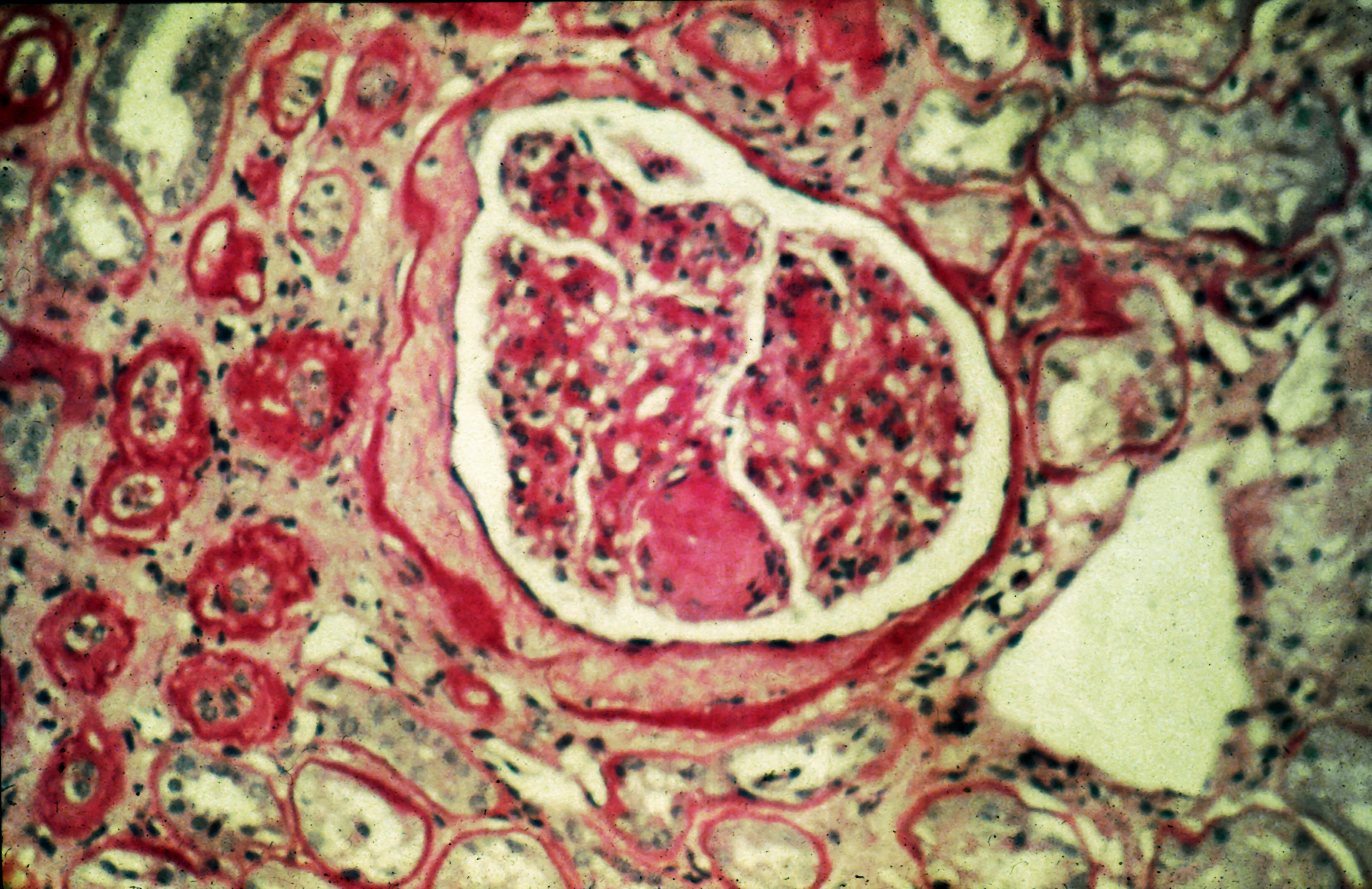
A 56-year-old Hispanic man presents and reports a 2-month history of fatigue, loss of appetite, pruritus, and swelling of the legs, ankles, and feet. The patient was diagnosed with type 2 diabetes (T2D), hypertension, and hyperlipidemia 7 years ago after an ophthalmologist diagnosed him with diabetic retinopathy and referred him for medical care. Since then, he has been inconsistent with attending regular follow-up visits. He is a current smoker (40-pack/year history).
At today's visit, the patient's blood pressure is 150/95 mm Hg, heart rate is 97 beats/min, and respiration rate is 29 breaths/min. He is 5 ft 9 in and weighs 210 lb (BMI 31). Current medications include metformin ER 1000 mg/d, atorvastatin 40 mg/d, amlodipine 10 mg/d, and hydrochlorothiazide 25 mg/d. At a routine visit 4 months ago, the patient's estimated glomerular filtration rate (eGFR) was 59 mL/min/1.73 m2; at a subsequent follow-up visit, his eGFR was 57 mL/min/1.73 m2.
Pertinent laboratory findings today include eGFR 56 mL/min/1.73 m2, serum creatinine 2.7 g/dL, serum albumin 3.3 g/dL, A1c 8.8%, glucose 189 mg/dL, and an albumin-creatinine ratio of 225 mg/g. All other findings are within normal ranges.

Genomic assay changes minds on HER2+ BC treatment
The prospective pilot study is small, and the researchers didn’t report on how the patients fared, according to a poster presented at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress. Plus, the test itself hasn’t been analyzed prospectively. But the study’s lead author, Olga Martínez-Sáez, MD, PhD, said in an interview that the 56% number is significant.
“We consider this percentage to be clinically very relevant,” said Dr. Martínez-Sáez, an oncologist at Hospital Clinic of Barcelona and the University of Barcelona. “HER2DX can change practice.”
Also in an interview, Kent Hoskins, MD, associate chief of hematology/oncology at University of Illinois at Chicago, described HER2DX as a next-generation genomic test that builds on assays developed 2 decades ago to help identify patients who would benefit – or not – from adjuvant chemotherapy.
Dr. Hoskins, who isn’t connected to the new study but has studied genomic tests for breast cancer, said the HER2DX test seeks to provide guidance to oncologists about which of several treatments are most effective in treating patients with HER2+ breast cancer.
“The overall trend in the HER2+ space is escalating therapy, and the cure rates have improved quite substantially,” he said. “But do they all need that much therapy? That’s the clinical question that this assay is addressing.”
The assay examines clinical features and the expression of 4 gene signatures, Dr. Martínez-Sáez said. It provides a risk score estimating the likelihood of recurrence plus a score that estimates the likelihood of achieving pathological complete response (pCR) with trastuzumab-based neoadjuvant therapy and an ERBB2 mRNA score.
In a retrospective 2022 study published in eBioMedicine, researchers reported that the assay “predicts response following neoadjuvant letrozole in combination with dual HER2 blockade with trastuzumab and pertuzumab in early-stage HER2-positive/hormone receptor–positive breast cancer.”
In the 2022 study, researchers wrote that assay results and other scores “might help better tailor systemic therapy in this context and identify candidates for avoiding chemotherapy, a therapy associated with short- and long-term toxicities and impact in quality of life.”
For the new study, a decision-impact analysis, researchers tracked 89 patients with HER2+ breast cancer (median age = 53 years, range 30-79, and 52% postmenopausal), the poster says. Most had T1-2 tumors (87%), negative nodes (64%), grade 2 (56%) or 3 (41%) tumors, and ductal histology (87%). And most were hormone receptor positive (65%). Seventy-eight percent of patients received neoadjuvant therapy (NAT), and 22% underwent upfront surgery.
In 56% of cases, oncologists changed their treatment decisions after getting the results of the HER2DX assays. In 59% of these cases, oncologists de-escalated therapy; in 41%, they escalated therapy, opting for more intense chemotherapy 65% of the time, according to the poster.
Clinician confidence in their decisions improved in 67% of cases, the researchers reported in their poster. Among 56 patients treated with neoadjuvant therapy who could be evaluated, “HER2DX pCR score was significantly associated with pCR (81% in pCR-medium/high and 32% in pCR-low; odds ratio=9.3, P = 0.001) independently of the rest of variables.”
Dr. Hoskins said the new report suggests that the assay can change treatment decisions, although he cautioned that “this study does not in itself establish its place in standard of care.” Large, prospective, randomized research is still needed, he said.
Dr. Martínez-Sáez said, in an interview, that the HER2DX assay should cost about as much as genomic assays for other breast cancer subtypes. These kinds of tests have cost several thousand dollars each in recent years.
What’s next? The decision impact study is ongoing. As for research into the assay itself, “prospective clinical trials are planned to demonstrate its clinical utility to de-escalate and guide therapy,” Dr. Martínez-Sáez said.
No funding is reported. Reveal Genomics is the developer of the HER2DX assay. Dr. Martinez- Saez reports financial relationships with Novartis, Eisai, Roche, and Reveal Genomics. Other study authors report multiple disclosures. Dr. Hoskins discloses non-financial research support from Agendia, which makes the MammaPrint early-breast-cancer assay.
The prospective pilot study is small, and the researchers didn’t report on how the patients fared, according to a poster presented at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress. Plus, the test itself hasn’t been analyzed prospectively. But the study’s lead author, Olga Martínez-Sáez, MD, PhD, said in an interview that the 56% number is significant.
“We consider this percentage to be clinically very relevant,” said Dr. Martínez-Sáez, an oncologist at Hospital Clinic of Barcelona and the University of Barcelona. “HER2DX can change practice.”
Also in an interview, Kent Hoskins, MD, associate chief of hematology/oncology at University of Illinois at Chicago, described HER2DX as a next-generation genomic test that builds on assays developed 2 decades ago to help identify patients who would benefit – or not – from adjuvant chemotherapy.
Dr. Hoskins, who isn’t connected to the new study but has studied genomic tests for breast cancer, said the HER2DX test seeks to provide guidance to oncologists about which of several treatments are most effective in treating patients with HER2+ breast cancer.
“The overall trend in the HER2+ space is escalating therapy, and the cure rates have improved quite substantially,” he said. “But do they all need that much therapy? That’s the clinical question that this assay is addressing.”
The assay examines clinical features and the expression of 4 gene signatures, Dr. Martínez-Sáez said. It provides a risk score estimating the likelihood of recurrence plus a score that estimates the likelihood of achieving pathological complete response (pCR) with trastuzumab-based neoadjuvant therapy and an ERBB2 mRNA score.
In a retrospective 2022 study published in eBioMedicine, researchers reported that the assay “predicts response following neoadjuvant letrozole in combination with dual HER2 blockade with trastuzumab and pertuzumab in early-stage HER2-positive/hormone receptor–positive breast cancer.”
In the 2022 study, researchers wrote that assay results and other scores “might help better tailor systemic therapy in this context and identify candidates for avoiding chemotherapy, a therapy associated with short- and long-term toxicities and impact in quality of life.”
For the new study, a decision-impact analysis, researchers tracked 89 patients with HER2+ breast cancer (median age = 53 years, range 30-79, and 52% postmenopausal), the poster says. Most had T1-2 tumors (87%), negative nodes (64%), grade 2 (56%) or 3 (41%) tumors, and ductal histology (87%). And most were hormone receptor positive (65%). Seventy-eight percent of patients received neoadjuvant therapy (NAT), and 22% underwent upfront surgery.
In 56% of cases, oncologists changed their treatment decisions after getting the results of the HER2DX assays. In 59% of these cases, oncologists de-escalated therapy; in 41%, they escalated therapy, opting for more intense chemotherapy 65% of the time, according to the poster.
Clinician confidence in their decisions improved in 67% of cases, the researchers reported in their poster. Among 56 patients treated with neoadjuvant therapy who could be evaluated, “HER2DX pCR score was significantly associated with pCR (81% in pCR-medium/high and 32% in pCR-low; odds ratio=9.3, P = 0.001) independently of the rest of variables.”
Dr. Hoskins said the new report suggests that the assay can change treatment decisions, although he cautioned that “this study does not in itself establish its place in standard of care.” Large, prospective, randomized research is still needed, he said.
Dr. Martínez-Sáez said, in an interview, that the HER2DX assay should cost about as much as genomic assays for other breast cancer subtypes. These kinds of tests have cost several thousand dollars each in recent years.
What’s next? The decision impact study is ongoing. As for research into the assay itself, “prospective clinical trials are planned to demonstrate its clinical utility to de-escalate and guide therapy,” Dr. Martínez-Sáez said.
No funding is reported. Reveal Genomics is the developer of the HER2DX assay. Dr. Martinez- Saez reports financial relationships with Novartis, Eisai, Roche, and Reveal Genomics. Other study authors report multiple disclosures. Dr. Hoskins discloses non-financial research support from Agendia, which makes the MammaPrint early-breast-cancer assay.
The prospective pilot study is small, and the researchers didn’t report on how the patients fared, according to a poster presented at the European Society for Medical Oncology (ESMO) Breast Cancer annual congress. Plus, the test itself hasn’t been analyzed prospectively. But the study’s lead author, Olga Martínez-Sáez, MD, PhD, said in an interview that the 56% number is significant.
“We consider this percentage to be clinically very relevant,” said Dr. Martínez-Sáez, an oncologist at Hospital Clinic of Barcelona and the University of Barcelona. “HER2DX can change practice.”
Also in an interview, Kent Hoskins, MD, associate chief of hematology/oncology at University of Illinois at Chicago, described HER2DX as a next-generation genomic test that builds on assays developed 2 decades ago to help identify patients who would benefit – or not – from adjuvant chemotherapy.
Dr. Hoskins, who isn’t connected to the new study but has studied genomic tests for breast cancer, said the HER2DX test seeks to provide guidance to oncologists about which of several treatments are most effective in treating patients with HER2+ breast cancer.
“The overall trend in the HER2+ space is escalating therapy, and the cure rates have improved quite substantially,” he said. “But do they all need that much therapy? That’s the clinical question that this assay is addressing.”
The assay examines clinical features and the expression of 4 gene signatures, Dr. Martínez-Sáez said. It provides a risk score estimating the likelihood of recurrence plus a score that estimates the likelihood of achieving pathological complete response (pCR) with trastuzumab-based neoadjuvant therapy and an ERBB2 mRNA score.
In a retrospective 2022 study published in eBioMedicine, researchers reported that the assay “predicts response following neoadjuvant letrozole in combination with dual HER2 blockade with trastuzumab and pertuzumab in early-stage HER2-positive/hormone receptor–positive breast cancer.”
In the 2022 study, researchers wrote that assay results and other scores “might help better tailor systemic therapy in this context and identify candidates for avoiding chemotherapy, a therapy associated with short- and long-term toxicities and impact in quality of life.”
For the new study, a decision-impact analysis, researchers tracked 89 patients with HER2+ breast cancer (median age = 53 years, range 30-79, and 52% postmenopausal), the poster says. Most had T1-2 tumors (87%), negative nodes (64%), grade 2 (56%) or 3 (41%) tumors, and ductal histology (87%). And most were hormone receptor positive (65%). Seventy-eight percent of patients received neoadjuvant therapy (NAT), and 22% underwent upfront surgery.
In 56% of cases, oncologists changed their treatment decisions after getting the results of the HER2DX assays. In 59% of these cases, oncologists de-escalated therapy; in 41%, they escalated therapy, opting for more intense chemotherapy 65% of the time, according to the poster.
Clinician confidence in their decisions improved in 67% of cases, the researchers reported in their poster. Among 56 patients treated with neoadjuvant therapy who could be evaluated, “HER2DX pCR score was significantly associated with pCR (81% in pCR-medium/high and 32% in pCR-low; odds ratio=9.3, P = 0.001) independently of the rest of variables.”
Dr. Hoskins said the new report suggests that the assay can change treatment decisions, although he cautioned that “this study does not in itself establish its place in standard of care.” Large, prospective, randomized research is still needed, he said.
Dr. Martínez-Sáez said, in an interview, that the HER2DX assay should cost about as much as genomic assays for other breast cancer subtypes. These kinds of tests have cost several thousand dollars each in recent years.
What’s next? The decision impact study is ongoing. As for research into the assay itself, “prospective clinical trials are planned to demonstrate its clinical utility to de-escalate and guide therapy,” Dr. Martínez-Sáez said.
No funding is reported. Reveal Genomics is the developer of the HER2DX assay. Dr. Martinez- Saez reports financial relationships with Novartis, Eisai, Roche, and Reveal Genomics. Other study authors report multiple disclosures. Dr. Hoskins discloses non-financial research support from Agendia, which makes the MammaPrint early-breast-cancer assay.
FROM ESMO BREAST CANCER 2023
DLBCL: Major new treatment breakthroughs
Significant breakthroughs have come in just the past few weeks and months, through the use of CAR T-cell and immunotherapies and with the approval in April by the Food and Drug Administration of polatuzumab for frontline DLBCL.
“Until the publishing of data from the POLARIX study (NCT03274492), which led to the approval of polatuzumab vedotin plus rituximab-cyclophosphamide, doxorubicin, and prednisone (pola + R-CHP), we had not had a breakthrough in frontline DLBCL therapies since the addition of rituximab 22 years ago,” said Dr. Charalambos Andreadis, MD, of the University of California at San Francisco’s Helen Diller Family Comprehensive Cancer Center.

“Pola + R-CHP is an improvement over the standard-of-care treatment, R-CHOP (rituximab-cyclophosphamide, doxorubicin, vincristine, and prednisone), giving treatment naive patients an increase in PFS without an increase in side effects,” Dr. Andreadis said.
R-CHP-polatuzumab was approved only for patients with an International Prognostic Indices score between 2 and 5, leaving patients with IPI scores of 0 or 1 with the frontline standard of care (SoC) treatment of R-CHOP, which has a cure rate of between 60% and 70%.
“The highest likelihood of relapse is in the first year following treatment. After 2 years in remission, patients’ chance of relapsing is the same as the general populations’ chance of getting DLBCL for the first time. This is why even a slight increase in the progression-free survival rate with the addition of pola is so significant,” Dr. Andreadis noted.
Historically, patients with relapsed or refractory (RR) DLBCL who did not respond to R-CHOP or who experienced disease relapse less than a year after primary intervention were treated with alternative chemotherapy regimens, often followed by autologous stem cell transplants (ASCT). Randomized control studies have shown that CAR T-cell therapies yield higher success rates than chemotherapy and ASCT, leading to the SoC in RR patients being CAR-T cell therapy directly following failed primary treatment.
“There are many new CAR T-cell platforms in development, as well as novel combination strategies that aim to target critical genetic pathways,” Kieron Dunleavy, MD, professor of medicine at the Lombardi Comprehensive Cancer Center at Georgetown University Hospital, said in an interview. “While access to CAR T-cell therapies is becoming easier and more feasible in many centers, fast access continues to be an issue for many patients, often depending on geography and socioeconomic factors.”
Asked about the latest breakthroughs in treating DLBCL, Dr. Dunleavy said, “A significant proportion of patients with relapsed or refractory DLBCL do not have easy access to CAR T-cell therapies, so this needs to be addressed and improved. Sometimes the rapidity of clinical progression in DLBCL can make these therapies challenging to deliver, considering logistical issues like apheresis and insurance approvals, which are frequently complex. This highlights the need for alternative and ‘easier to deliver’ CAR-T cells and our continued prioritization of developing alternative effective agents for DLBCL.
“Currently, commercially approved CAR T-cells in DLBCL target the CD-19 marker on lymphoma cells but CAR T-cells targeting other and more than one antigen as well as alternative anti CD19 agents like loncastuximab and tafasitamab are similarly FDA approved and available for patients,” Dr. Dunleavy concluded.
Dr. Dunleavy is affiliated with the MedStar Georgetown Lymphoma group, where Rep. Raskin publicly announced that he had completed 4 months of chemotherapy treatment for DLBCL. On April 27, in an open letter to the U.S. public, he wrote that he rang the bell at MedStar to mark his preliminary diagnosis of being “in remission,” with a “90% prognosis of no relapse.”
Interviewed about the latest advances in treating DLBCL, Jason Westin, MD, associate professor of lymphoma and myeloma at the MD Anderson Cancer Center in Houston, said that even with improvements in overall survival possible with CAR T-cell therapies, “usually, a clinical trial should be considered strongly, as it is often the best option for patients, both in a newly diagnosed or in a relapsed setting, as they allow access to tomorrow’s breakthrough therapies today.”
Dr. Westin cited the example of bispecific T-cell engagers (BITE) as a promising therapy that is available to patients in clinical trials. These agents bind to one side to the lymphoma cell, but they also have a binding arm for T-cells, so they activate a patient’s own immune cells to kill lymphoma cells, in some cases offering a cure when CAR T-cell therapy has failed.
The first BITE to be approved, mosunetuzumab, is authorized only for the treatment of follicular lymphoma. However, data from a recent clinical study indicated that the agent yields complete responses in 24% of heavily pretreated patients with RR DLBCL.
Another BITE, glofitamab, was approved in Canada in March 2023 for use in RR DLBCL. Based on its high efficacy, it soon may be approved elsewhere.
Dr. Andreadis noted, “We are finally at a point where for both treatment naive and RR DLBCL patients, there are several promising options on the horizon that don’t involve ASCT. Furthermore, these breakthroughs reinforce each other, as there are studies in which therapies like BITE are being brought to the front line and pola to RR cases.”
The growing field of new frontline and RR DLBCL therapies lend credence to the optimism of specialists who treat DLBCL – and to the sanguine note that Congressman Raskin struck in published comments about his treatment for DLBCL.
Dr. Andreadis reported ties with BMS, Novartis, Roche, Genmab, Merck, Gilead, AbbVie, and J&J. Dr. Dunleavy disclosed relationships with ONO Pharmaceuticals, Kymera, Merck, Genentech, AstraZeneca, Amgen, ADC Therapeutics, MorphoSys and Incyte, Kite/Gilead, Cellectar. Dr. Westin reported ties with Kite/Gilead, BMS, Novartis, Genentech, AstraZeneca, Morphosys/Incyte, ADC Therapeutics, Kymera, Nurix, and MonteRosa.
Significant breakthroughs have come in just the past few weeks and months, through the use of CAR T-cell and immunotherapies and with the approval in April by the Food and Drug Administration of polatuzumab for frontline DLBCL.
“Until the publishing of data from the POLARIX study (NCT03274492), which led to the approval of polatuzumab vedotin plus rituximab-cyclophosphamide, doxorubicin, and prednisone (pola + R-CHP), we had not had a breakthrough in frontline DLBCL therapies since the addition of rituximab 22 years ago,” said Dr. Charalambos Andreadis, MD, of the University of California at San Francisco’s Helen Diller Family Comprehensive Cancer Center.
“Pola + R-CHP is an improvement over the standard-of-care treatment, R-CHOP (rituximab-cyclophosphamide, doxorubicin, vincristine, and prednisone), giving treatment naive patients an increase in PFS without an increase in side effects,” Dr. Andreadis said.
R-CHP-polatuzumab was approved only for patients with an International Prognostic Indices score between 2 and 5, leaving patients with IPI scores of 0 or 1 with the frontline standard of care (SoC) treatment of R-CHOP, which has a cure rate of between 60% and 70%.
“The highest likelihood of relapse is in the first year following treatment. After 2 years in remission, patients’ chance of relapsing is the same as the general populations’ chance of getting DLBCL for the first time. This is why even a slight increase in the progression-free survival rate with the addition of pola is so significant,” Dr. Andreadis noted.
Historically, patients with relapsed or refractory (RR) DLBCL who did not respond to R-CHOP or who experienced disease relapse less than a year after primary intervention were treated with alternative chemotherapy regimens, often followed by autologous stem cell transplants (ASCT). Randomized control studies have shown that CAR T-cell therapies yield higher success rates than chemotherapy and ASCT, leading to the SoC in RR patients being CAR-T cell therapy directly following failed primary treatment.
“There are many new CAR T-cell platforms in development, as well as novel combination strategies that aim to target critical genetic pathways,” Kieron Dunleavy, MD, professor of medicine at the Lombardi Comprehensive Cancer Center at Georgetown University Hospital, said in an interview. “While access to CAR T-cell therapies is becoming easier and more feasible in many centers, fast access continues to be an issue for many patients, often depending on geography and socioeconomic factors.”
Asked about the latest breakthroughs in treating DLBCL, Dr. Dunleavy said, “A significant proportion of patients with relapsed or refractory DLBCL do not have easy access to CAR T-cell therapies, so this needs to be addressed and improved. Sometimes the rapidity of clinical progression in DLBCL can make these therapies challenging to deliver, considering logistical issues like apheresis and insurance approvals, which are frequently complex. This highlights the need for alternative and ‘easier to deliver’ CAR-T cells and our continued prioritization of developing alternative effective agents for DLBCL.
“Currently, commercially approved CAR T-cells in DLBCL target the CD-19 marker on lymphoma cells but CAR T-cells targeting other and more than one antigen as well as alternative anti CD19 agents like loncastuximab and tafasitamab are similarly FDA approved and available for patients,” Dr. Dunleavy concluded.
Dr. Dunleavy is affiliated with the MedStar Georgetown Lymphoma group, where Rep. Raskin publicly announced that he had completed 4 months of chemotherapy treatment for DLBCL. On April 27, in an open letter to the U.S. public, he wrote that he rang the bell at MedStar to mark his preliminary diagnosis of being “in remission,” with a “90% prognosis of no relapse.”
Interviewed about the latest advances in treating DLBCL, Jason Westin, MD, associate professor of lymphoma and myeloma at the MD Anderson Cancer Center in Houston, said that even with improvements in overall survival possible with CAR T-cell therapies, “usually, a clinical trial should be considered strongly, as it is often the best option for patients, both in a newly diagnosed or in a relapsed setting, as they allow access to tomorrow’s breakthrough therapies today.”
Dr. Westin cited the example of bispecific T-cell engagers (BITE) as a promising therapy that is available to patients in clinical trials. These agents bind to one side to the lymphoma cell, but they also have a binding arm for T-cells, so they activate a patient’s own immune cells to kill lymphoma cells, in some cases offering a cure when CAR T-cell therapy has failed.
The first BITE to be approved, mosunetuzumab, is authorized only for the treatment of follicular lymphoma. However, data from a recent clinical study indicated that the agent yields complete responses in 24% of heavily pretreated patients with RR DLBCL.
Another BITE, glofitamab, was approved in Canada in March 2023 for use in RR DLBCL. Based on its high efficacy, it soon may be approved elsewhere.
Dr. Andreadis noted, “We are finally at a point where for both treatment naive and RR DLBCL patients, there are several promising options on the horizon that don’t involve ASCT. Furthermore, these breakthroughs reinforce each other, as there are studies in which therapies like BITE are being brought to the front line and pola to RR cases.”
The growing field of new frontline and RR DLBCL therapies lend credence to the optimism of specialists who treat DLBCL – and to the sanguine note that Congressman Raskin struck in published comments about his treatment for DLBCL.
Dr. Andreadis reported ties with BMS, Novartis, Roche, Genmab, Merck, Gilead, AbbVie, and J&J. Dr. Dunleavy disclosed relationships with ONO Pharmaceuticals, Kymera, Merck, Genentech, AstraZeneca, Amgen, ADC Therapeutics, MorphoSys and Incyte, Kite/Gilead, Cellectar. Dr. Westin reported ties with Kite/Gilead, BMS, Novartis, Genentech, AstraZeneca, Morphosys/Incyte, ADC Therapeutics, Kymera, Nurix, and MonteRosa.
Significant breakthroughs have come in just the past few weeks and months, through the use of CAR T-cell and immunotherapies and with the approval in April by the Food and Drug Administration of polatuzumab for frontline DLBCL.
“Until the publishing of data from the POLARIX study (NCT03274492), which led to the approval of polatuzumab vedotin plus rituximab-cyclophosphamide, doxorubicin, and prednisone (pola + R-CHP), we had not had a breakthrough in frontline DLBCL therapies since the addition of rituximab 22 years ago,” said Dr. Charalambos Andreadis, MD, of the University of California at San Francisco’s Helen Diller Family Comprehensive Cancer Center.
“Pola + R-CHP is an improvement over the standard-of-care treatment, R-CHOP (rituximab-cyclophosphamide, doxorubicin, vincristine, and prednisone), giving treatment naive patients an increase in PFS without an increase in side effects,” Dr. Andreadis said.
R-CHP-polatuzumab was approved only for patients with an International Prognostic Indices score between 2 and 5, leaving patients with IPI scores of 0 or 1 with the frontline standard of care (SoC) treatment of R-CHOP, which has a cure rate of between 60% and 70%.
“The highest likelihood of relapse is in the first year following treatment. After 2 years in remission, patients’ chance of relapsing is the same as the general populations’ chance of getting DLBCL for the first time. This is why even a slight increase in the progression-free survival rate with the addition of pola is so significant,” Dr. Andreadis noted.
Historically, patients with relapsed or refractory (RR) DLBCL who did not respond to R-CHOP or who experienced disease relapse less than a year after primary intervention were treated with alternative chemotherapy regimens, often followed by autologous stem cell transplants (ASCT). Randomized control studies have shown that CAR T-cell therapies yield higher success rates than chemotherapy and ASCT, leading to the SoC in RR patients being CAR-T cell therapy directly following failed primary treatment.
“There are many new CAR T-cell platforms in development, as well as novel combination strategies that aim to target critical genetic pathways,” Kieron Dunleavy, MD, professor of medicine at the Lombardi Comprehensive Cancer Center at Georgetown University Hospital, said in an interview. “While access to CAR T-cell therapies is becoming easier and more feasible in many centers, fast access continues to be an issue for many patients, often depending on geography and socioeconomic factors.”
Asked about the latest breakthroughs in treating DLBCL, Dr. Dunleavy said, “A significant proportion of patients with relapsed or refractory DLBCL do not have easy access to CAR T-cell therapies, so this needs to be addressed and improved. Sometimes the rapidity of clinical progression in DLBCL can make these therapies challenging to deliver, considering logistical issues like apheresis and insurance approvals, which are frequently complex. This highlights the need for alternative and ‘easier to deliver’ CAR-T cells and our continued prioritization of developing alternative effective agents for DLBCL.
“Currently, commercially approved CAR T-cells in DLBCL target the CD-19 marker on lymphoma cells but CAR T-cells targeting other and more than one antigen as well as alternative anti CD19 agents like loncastuximab and tafasitamab are similarly FDA approved and available for patients,” Dr. Dunleavy concluded.
Dr. Dunleavy is affiliated with the MedStar Georgetown Lymphoma group, where Rep. Raskin publicly announced that he had completed 4 months of chemotherapy treatment for DLBCL. On April 27, in an open letter to the U.S. public, he wrote that he rang the bell at MedStar to mark his preliminary diagnosis of being “in remission,” with a “90% prognosis of no relapse.”
Interviewed about the latest advances in treating DLBCL, Jason Westin, MD, associate professor of lymphoma and myeloma at the MD Anderson Cancer Center in Houston, said that even with improvements in overall survival possible with CAR T-cell therapies, “usually, a clinical trial should be considered strongly, as it is often the best option for patients, both in a newly diagnosed or in a relapsed setting, as they allow access to tomorrow’s breakthrough therapies today.”
Dr. Westin cited the example of bispecific T-cell engagers (BITE) as a promising therapy that is available to patients in clinical trials. These agents bind to one side to the lymphoma cell, but they also have a binding arm for T-cells, so they activate a patient’s own immune cells to kill lymphoma cells, in some cases offering a cure when CAR T-cell therapy has failed.
The first BITE to be approved, mosunetuzumab, is authorized only for the treatment of follicular lymphoma. However, data from a recent clinical study indicated that the agent yields complete responses in 24% of heavily pretreated patients with RR DLBCL.
Another BITE, glofitamab, was approved in Canada in March 2023 for use in RR DLBCL. Based on its high efficacy, it soon may be approved elsewhere.
Dr. Andreadis noted, “We are finally at a point where for both treatment naive and RR DLBCL patients, there are several promising options on the horizon that don’t involve ASCT. Furthermore, these breakthroughs reinforce each other, as there are studies in which therapies like BITE are being brought to the front line and pola to RR cases.”
The growing field of new frontline and RR DLBCL therapies lend credence to the optimism of specialists who treat DLBCL – and to the sanguine note that Congressman Raskin struck in published comments about his treatment for DLBCL.
Dr. Andreadis reported ties with BMS, Novartis, Roche, Genmab, Merck, Gilead, AbbVie, and J&J. Dr. Dunleavy disclosed relationships with ONO Pharmaceuticals, Kymera, Merck, Genentech, AstraZeneca, Amgen, ADC Therapeutics, MorphoSys and Incyte, Kite/Gilead, Cellectar. Dr. Westin reported ties with Kite/Gilead, BMS, Novartis, Genentech, AstraZeneca, Morphosys/Incyte, ADC Therapeutics, Kymera, Nurix, and MonteRosa.
Teledermatology follow-up after Mohs surgery gets a thumbs up from patients
SEATTLE – The , according to new findings.
In addition, nearly all patients surveyed (91.4%) were willing to go through electronic follow-up again.
“A big takeaway from our study is that streamlining this process is really essential for successful implementation,” said study author Laura Rezac, MD, a PGY IV dermatology resident at the University of Mississippi, Jackson. “This study demonstrated the flexibility and convenience for both patients and surgeons and can serve as a prototype for future innovation.”
The study results were presented at the annual meeting of the American College of Mohs Surgery.
The role of telehealth has rapidly expanded over the past decade, with its use accelerating during the COVID-19 pandemic and transforming into an indispensable resource. It can be synchronous, Dr. Rezac explained, which is when telehealth happens in live, real-time settings where the patient interacts with a clinician. This usually occurs via phone or video, and providers and patients communicate directly.
Conversely, asynchronous telehealth, also known as “store-and-forward,” is often used for patient intake or follow-up care. For example, in dermatology, a patient can send a photo of a skin condition that is then reviewed by a dermatologist later.
“A pilot survey regarding the adoption of telemedicine in Mohs surgery found that, although most dermatologic surgeons felt that it can play a role, most said that they didn’t plan on using it after the pandemic,” said Dr. Rezac.
The survey, which was reported by this news organization, found that 80% of surveyed surgeons said that they turned to telemedicine during the pandemic, compared with just 23% who relied on the technology prior to the pandemic.
There were numerous perceived barriers to the use of telemedicine, and the one most commonly cited was the uncertainty of how telemedicine fits in the workflow of clinical practice. Other limitations reported were for physical exams (88%), patient response and training (57%), reimbursement concerns (50%), implementation of the technology (37%), regulations such as HIPAA (24%), training of staff (17%), and licensing (8%).
“The survey did identify one key use of telemedicine in Mohs and that was for [postoperative] visits,” she said. “But thus far, a postoperative evaluation after Mohs via an integrated asynchronous ‘store and forward’ teledermatology platform has not yet been evaluated.”
In the study, Dr. Rezac and colleagues sought to evaluate feasibility and efficacy, as well as patient attitudes, using a telemedicine platform for postoperative follow-up. A total of 163 patients who were treated with Mohs at a single academic institution during the 9-month study period (December 2021 through August 2022) responded to a survey and elected to participate in postoperative follow-up using telemedicine.
Dr. Rezac explained how their procedure was implemented for the patient. “On the day of the follow-up, the patient receives a text with a link that takes them to the MyChart website or app on their phone,” she said. “Once they log in, they see that they have a message telling them that they have a teledermatology message waiting for them. When they view it, they are taken to the curated message with instructions and a phone call if they need assistance, and then at the bottom, it shows they have a task to complete, which is the questionnaire.”
The patient will then be prompted to upload photos, which can be taken with their phone camera. The next step is to answer questions regarding the surgical site or pain concerns, and finally, patients are asked to respond to a few short questions about this type of follow-up. Once submitted, then they wait to be contacted by the surgeon.
On the surgeon’s side, these answers come into their EPIC inbox, and they can respond via a MyChart message.
Patient response was overwhelmingly positive, Dr. Rezac noted. Of the patients, 80.4% found the electronic surgery follow-up process to be “easy” or “very easy,” while only 4% found it “difficult” or “very difficult,” she said. “Also, 75.5% preferred electronic follow-up while 17.2% preferred in-person follow-up.”
There were limitations to this study, primarily that the asynchronous method does reduce live interaction, which could be an issue, depending on person’s needs, she pointed out. “But it is easy to schedule a phone call or video call or office visit.”
“The universal barrier is how to adopt it into the workflow, which includes training of staff,” she continued, “But this was a very streamlined process and gave very detailed instructions to the staff. Additionally, widespread use is limited to dermatological proficiency and access, and patients have to be amenable to it, so there is a selection bias since these patients chose to participate.”
Asked to comment on the study, Vishal Patel, MD, director of cutaneous oncology at George Washington University in Washington, said: “The COVID pandemic changed how practices and providers considered follow-up visits for small routine matters. Postoperative visits are often simple and do not require an in-depth, in-person evaluation.” Dr. Patel was not involved with this research.
“This study highlights the comfort of the vast majority of patients to have follow-up postoperative visits conducted via teledermatology – an approach that can help cut overall costs and also increase access for patients who are more in need of in-office care,” he added.
No external funding of the study was reported. Dr. Rezac reported no relevant financial relationships. Dr. Patel is a consultant for Sanofi, Regeneron, and Almirall.
A version of this article originally appeared on Medscape.com.
SEATTLE – The , according to new findings.
In addition, nearly all patients surveyed (91.4%) were willing to go through electronic follow-up again.
“A big takeaway from our study is that streamlining this process is really essential for successful implementation,” said study author Laura Rezac, MD, a PGY IV dermatology resident at the University of Mississippi, Jackson. “This study demonstrated the flexibility and convenience for both patients and surgeons and can serve as a prototype for future innovation.”
The study results were presented at the annual meeting of the American College of Mohs Surgery.
The role of telehealth has rapidly expanded over the past decade, with its use accelerating during the COVID-19 pandemic and transforming into an indispensable resource. It can be synchronous, Dr. Rezac explained, which is when telehealth happens in live, real-time settings where the patient interacts with a clinician. This usually occurs via phone or video, and providers and patients communicate directly.
Conversely, asynchronous telehealth, also known as “store-and-forward,” is often used for patient intake or follow-up care. For example, in dermatology, a patient can send a photo of a skin condition that is then reviewed by a dermatologist later.
“A pilot survey regarding the adoption of telemedicine in Mohs surgery found that, although most dermatologic surgeons felt that it can play a role, most said that they didn’t plan on using it after the pandemic,” said Dr. Rezac.
The survey, which was reported by this news organization, found that 80% of surveyed surgeons said that they turned to telemedicine during the pandemic, compared with just 23% who relied on the technology prior to the pandemic.
There were numerous perceived barriers to the use of telemedicine, and the one most commonly cited was the uncertainty of how telemedicine fits in the workflow of clinical practice. Other limitations reported were for physical exams (88%), patient response and training (57%), reimbursement concerns (50%), implementation of the technology (37%), regulations such as HIPAA (24%), training of staff (17%), and licensing (8%).
“The survey did identify one key use of telemedicine in Mohs and that was for [postoperative] visits,” she said. “But thus far, a postoperative evaluation after Mohs via an integrated asynchronous ‘store and forward’ teledermatology platform has not yet been evaluated.”
In the study, Dr. Rezac and colleagues sought to evaluate feasibility and efficacy, as well as patient attitudes, using a telemedicine platform for postoperative follow-up. A total of 163 patients who were treated with Mohs at a single academic institution during the 9-month study period (December 2021 through August 2022) responded to a survey and elected to participate in postoperative follow-up using telemedicine.
Dr. Rezac explained how their procedure was implemented for the patient. “On the day of the follow-up, the patient receives a text with a link that takes them to the MyChart website or app on their phone,” she said. “Once they log in, they see that they have a message telling them that they have a teledermatology message waiting for them. When they view it, they are taken to the curated message with instructions and a phone call if they need assistance, and then at the bottom, it shows they have a task to complete, which is the questionnaire.”
The patient will then be prompted to upload photos, which can be taken with their phone camera. The next step is to answer questions regarding the surgical site or pain concerns, and finally, patients are asked to respond to a few short questions about this type of follow-up. Once submitted, then they wait to be contacted by the surgeon.
On the surgeon’s side, these answers come into their EPIC inbox, and they can respond via a MyChart message.
Patient response was overwhelmingly positive, Dr. Rezac noted. Of the patients, 80.4% found the electronic surgery follow-up process to be “easy” or “very easy,” while only 4% found it “difficult” or “very difficult,” she said. “Also, 75.5% preferred electronic follow-up while 17.2% preferred in-person follow-up.”
There were limitations to this study, primarily that the asynchronous method does reduce live interaction, which could be an issue, depending on person’s needs, she pointed out. “But it is easy to schedule a phone call or video call or office visit.”
“The universal barrier is how to adopt it into the workflow, which includes training of staff,” she continued, “But this was a very streamlined process and gave very detailed instructions to the staff. Additionally, widespread use is limited to dermatological proficiency and access, and patients have to be amenable to it, so there is a selection bias since these patients chose to participate.”
Asked to comment on the study, Vishal Patel, MD, director of cutaneous oncology at George Washington University in Washington, said: “The COVID pandemic changed how practices and providers considered follow-up visits for small routine matters. Postoperative visits are often simple and do not require an in-depth, in-person evaluation.” Dr. Patel was not involved with this research.
“This study highlights the comfort of the vast majority of patients to have follow-up postoperative visits conducted via teledermatology – an approach that can help cut overall costs and also increase access for patients who are more in need of in-office care,” he added.
No external funding of the study was reported. Dr. Rezac reported no relevant financial relationships. Dr. Patel is a consultant for Sanofi, Regeneron, and Almirall.
A version of this article originally appeared on Medscape.com.
SEATTLE – The , according to new findings.
In addition, nearly all patients surveyed (91.4%) were willing to go through electronic follow-up again.
“A big takeaway from our study is that streamlining this process is really essential for successful implementation,” said study author Laura Rezac, MD, a PGY IV dermatology resident at the University of Mississippi, Jackson. “This study demonstrated the flexibility and convenience for both patients and surgeons and can serve as a prototype for future innovation.”
The study results were presented at the annual meeting of the American College of Mohs Surgery.
The role of telehealth has rapidly expanded over the past decade, with its use accelerating during the COVID-19 pandemic and transforming into an indispensable resource. It can be synchronous, Dr. Rezac explained, which is when telehealth happens in live, real-time settings where the patient interacts with a clinician. This usually occurs via phone or video, and providers and patients communicate directly.
Conversely, asynchronous telehealth, also known as “store-and-forward,” is often used for patient intake or follow-up care. For example, in dermatology, a patient can send a photo of a skin condition that is then reviewed by a dermatologist later.
“A pilot survey regarding the adoption of telemedicine in Mohs surgery found that, although most dermatologic surgeons felt that it can play a role, most said that they didn’t plan on using it after the pandemic,” said Dr. Rezac.
The survey, which was reported by this news organization, found that 80% of surveyed surgeons said that they turned to telemedicine during the pandemic, compared with just 23% who relied on the technology prior to the pandemic.
There were numerous perceived barriers to the use of telemedicine, and the one most commonly cited was the uncertainty of how telemedicine fits in the workflow of clinical practice. Other limitations reported were for physical exams (88%), patient response and training (57%), reimbursement concerns (50%), implementation of the technology (37%), regulations such as HIPAA (24%), training of staff (17%), and licensing (8%).
“The survey did identify one key use of telemedicine in Mohs and that was for [postoperative] visits,” she said. “But thus far, a postoperative evaluation after Mohs via an integrated asynchronous ‘store and forward’ teledermatology platform has not yet been evaluated.”
In the study, Dr. Rezac and colleagues sought to evaluate feasibility and efficacy, as well as patient attitudes, using a telemedicine platform for postoperative follow-up. A total of 163 patients who were treated with Mohs at a single academic institution during the 9-month study period (December 2021 through August 2022) responded to a survey and elected to participate in postoperative follow-up using telemedicine.
Dr. Rezac explained how their procedure was implemented for the patient. “On the day of the follow-up, the patient receives a text with a link that takes them to the MyChart website or app on their phone,” she said. “Once they log in, they see that they have a message telling them that they have a teledermatology message waiting for them. When they view it, they are taken to the curated message with instructions and a phone call if they need assistance, and then at the bottom, it shows they have a task to complete, which is the questionnaire.”
The patient will then be prompted to upload photos, which can be taken with their phone camera. The next step is to answer questions regarding the surgical site or pain concerns, and finally, patients are asked to respond to a few short questions about this type of follow-up. Once submitted, then they wait to be contacted by the surgeon.
On the surgeon’s side, these answers come into their EPIC inbox, and they can respond via a MyChart message.
Patient response was overwhelmingly positive, Dr. Rezac noted. Of the patients, 80.4% found the electronic surgery follow-up process to be “easy” or “very easy,” while only 4% found it “difficult” or “very difficult,” she said. “Also, 75.5% preferred electronic follow-up while 17.2% preferred in-person follow-up.”
There were limitations to this study, primarily that the asynchronous method does reduce live interaction, which could be an issue, depending on person’s needs, she pointed out. “But it is easy to schedule a phone call or video call or office visit.”
“The universal barrier is how to adopt it into the workflow, which includes training of staff,” she continued, “But this was a very streamlined process and gave very detailed instructions to the staff. Additionally, widespread use is limited to dermatological proficiency and access, and patients have to be amenable to it, so there is a selection bias since these patients chose to participate.”
Asked to comment on the study, Vishal Patel, MD, director of cutaneous oncology at George Washington University in Washington, said: “The COVID pandemic changed how practices and providers considered follow-up visits for small routine matters. Postoperative visits are often simple and do not require an in-depth, in-person evaluation.” Dr. Patel was not involved with this research.
“This study highlights the comfort of the vast majority of patients to have follow-up postoperative visits conducted via teledermatology – an approach that can help cut overall costs and also increase access for patients who are more in need of in-office care,” he added.
No external funding of the study was reported. Dr. Rezac reported no relevant financial relationships. Dr. Patel is a consultant for Sanofi, Regeneron, and Almirall.
A version of this article originally appeared on Medscape.com.
AT ACMS 2023
Nodule on farmer’s hand

A broad shave biopsy was performed at the base of the lesion and the results were consistent with a thick nodular melanoma with a Breslow depth of 5.5 mm.
Melanoma is the deadliest skin cancer in the United States with mortality risk corresponding with the depth of the tumor.1 Nodular melanomas grow faster than all other types of melanoma. For this reason, a concerning raised lesion with a risk of melanoma should not be observed for change over time; it should be biopsied promptly. In this case, a depth of 5.5 mm was cause for quick action. Patients with tumors > 1 mm in depth (and some tumors > 0.8 mm) should be offered sentinel lymph node biopsy (SLNB) along with wide local excision to evaluate for lymphatic spread. Patients with thinner tumors may undergo wide local excision without SLNB.
In this case, National Comprehensive Cancer Network guidelines would dictate a 2-cm margin for a wide local incision; the patient underwent a modified version of this with Surgical Oncology to accommodate maintenance of hand function. This patient’s SLNB was negative, so the melanoma was classified as Stage IIC.
In the recent past, there were no additional treatments for patients with late Stage II disease (thick tumors without evidence of metastasis). However, in December 2021, the US Food and Drug Administration approved the use of immunotherapy with pembrolizumab in patients with node-negative late Stage II melanoma after demonstration of improved recurrence-free survival in the KEYNOTE trial.2 Evidence of improved long-term survival is mixed with adjuvant therapy, and studies evaluating the best role of adjuvant therapy are ongoing.
This patient was started on a regimen of pembrolizumab 200 mg IV every 3 weeks, which he will continue for as long as 1 year. He has tolerated this regimen without difficulty and has no evidence of disease.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Epstein DS, Lange JR, Gruber SB, et al. Is physician detection associated with thinner melanomas? JAMA. 1999;281:640-643. doi: 10.1001/jama.281.7.640
2. Luke JJ, Rutkowski P, Queirolo P, et al; KEYNOTE-716 Investigators. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399:1718-1729. doi: 10.1016/S0140-6736(22)00562-1
A broad shave biopsy was performed at the base of the lesion and the results were consistent with a thick nodular melanoma with a Breslow depth of 5.5 mm.
Melanoma is the deadliest skin cancer in the United States with mortality risk corresponding with the depth of the tumor.1 Nodular melanomas grow faster than all other types of melanoma. For this reason, a concerning raised lesion with a risk of melanoma should not be observed for change over time; it should be biopsied promptly. In this case, a depth of 5.5 mm was cause for quick action. Patients with tumors > 1 mm in depth (and some tumors > 0.8 mm) should be offered sentinel lymph node biopsy (SLNB) along with wide local excision to evaluate for lymphatic spread. Patients with thinner tumors may undergo wide local excision without SLNB.
In this case, National Comprehensive Cancer Network guidelines would dictate a 2-cm margin for a wide local incision; the patient underwent a modified version of this with Surgical Oncology to accommodate maintenance of hand function. This patient’s SLNB was negative, so the melanoma was classified as Stage IIC.
In the recent past, there were no additional treatments for patients with late Stage II disease (thick tumors without evidence of metastasis). However, in December 2021, the US Food and Drug Administration approved the use of immunotherapy with pembrolizumab in patients with node-negative late Stage II melanoma after demonstration of improved recurrence-free survival in the KEYNOTE trial.2 Evidence of improved long-term survival is mixed with adjuvant therapy, and studies evaluating the best role of adjuvant therapy are ongoing.
This patient was started on a regimen of pembrolizumab 200 mg IV every 3 weeks, which he will continue for as long as 1 year. He has tolerated this regimen without difficulty and has no evidence of disease.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
A broad shave biopsy was performed at the base of the lesion and the results were consistent with a thick nodular melanoma with a Breslow depth of 5.5 mm.
Melanoma is the deadliest skin cancer in the United States with mortality risk corresponding with the depth of the tumor.1 Nodular melanomas grow faster than all other types of melanoma. For this reason, a concerning raised lesion with a risk of melanoma should not be observed for change over time; it should be biopsied promptly. In this case, a depth of 5.5 mm was cause for quick action. Patients with tumors > 1 mm in depth (and some tumors > 0.8 mm) should be offered sentinel lymph node biopsy (SLNB) along with wide local excision to evaluate for lymphatic spread. Patients with thinner tumors may undergo wide local excision without SLNB.
In this case, National Comprehensive Cancer Network guidelines would dictate a 2-cm margin for a wide local incision; the patient underwent a modified version of this with Surgical Oncology to accommodate maintenance of hand function. This patient’s SLNB was negative, so the melanoma was classified as Stage IIC.
In the recent past, there were no additional treatments for patients with late Stage II disease (thick tumors without evidence of metastasis). However, in December 2021, the US Food and Drug Administration approved the use of immunotherapy with pembrolizumab in patients with node-negative late Stage II melanoma after demonstration of improved recurrence-free survival in the KEYNOTE trial.2 Evidence of improved long-term survival is mixed with adjuvant therapy, and studies evaluating the best role of adjuvant therapy are ongoing.
This patient was started on a regimen of pembrolizumab 200 mg IV every 3 weeks, which he will continue for as long as 1 year. He has tolerated this regimen without difficulty and has no evidence of disease.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Epstein DS, Lange JR, Gruber SB, et al. Is physician detection associated with thinner melanomas? JAMA. 1999;281:640-643. doi: 10.1001/jama.281.7.640
2. Luke JJ, Rutkowski P, Queirolo P, et al; KEYNOTE-716 Investigators. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399:1718-1729. doi: 10.1016/S0140-6736(22)00562-1
1. Epstein DS, Lange JR, Gruber SB, et al. Is physician detection associated with thinner melanomas? JAMA. 1999;281:640-643. doi: 10.1001/jama.281.7.640
2. Luke JJ, Rutkowski P, Queirolo P, et al; KEYNOTE-716 Investigators. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399:1718-1729. doi: 10.1016/S0140-6736(22)00562-1

Firm nodule following tick bite

The biopsy revealed abundant lymphocytes, neutrophils, and eosinophils consistent with a diagnosis of cutaneous B cell pseudolymphoma. The pseudolymphoma was caused by an exaggerated response to a tick bite.
As the name implies, B cell pseudolymphomas clinically and histologically mimic the various patterns of cutaneous lymphoma, often appearing as a firm, pink to dark violet nodule. A biopsy is mandatory to distinguish between pseudolymphoma and true lymphoma. There is an association between pseudolymphomas and Borrelia burgdorferi, the organism responsible for Lyme disease. Thus, testing for Lyme disease is recommended for patients with pseudolymphomas who live in endemic areas. Patients who test positive should be treated with doxycycline 100 mg bid for 10 days.
In the absence of Lyme disease, a pseudolymphoma may resolve spontaneously over weeks or months. Resolution can be hastened with topical superpotent steroids, intralesional steroids, or systemic steroids. Treatment can begin with topical clobetasol 0.05% bid. If the lesion does not resolve, the next step would be intralesional triamcinolone 10 mg/mL injected directly into the nodule until it blanches slightly. Injections should be repeated every 3 to 4 weeks for a total of 2 to 3 injections.
The patient in this case had negative Lyme serology and was treated with 2 injections of triamcinolone 10 mg/mL administered 3 weeks apart. She experienced complete resolution.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Mitteldorf C, Kempf W. Cutaneous pseudolymphoma. Surg Pathol Clin. 2017;10:455-476. doi: 10.1016/j.path.2017.01.002
The biopsy revealed abundant lymphocytes, neutrophils, and eosinophils consistent with a diagnosis of cutaneous B cell pseudolymphoma. The pseudolymphoma was caused by an exaggerated response to a tick bite.
As the name implies, B cell pseudolymphomas clinically and histologically mimic the various patterns of cutaneous lymphoma, often appearing as a firm, pink to dark violet nodule. A biopsy is mandatory to distinguish between pseudolymphoma and true lymphoma. There is an association between pseudolymphomas and Borrelia burgdorferi, the organism responsible for Lyme disease. Thus, testing for Lyme disease is recommended for patients with pseudolymphomas who live in endemic areas. Patients who test positive should be treated with doxycycline 100 mg bid for 10 days.
In the absence of Lyme disease, a pseudolymphoma may resolve spontaneously over weeks or months. Resolution can be hastened with topical superpotent steroids, intralesional steroids, or systemic steroids. Treatment can begin with topical clobetasol 0.05% bid. If the lesion does not resolve, the next step would be intralesional triamcinolone 10 mg/mL injected directly into the nodule until it blanches slightly. Injections should be repeated every 3 to 4 weeks for a total of 2 to 3 injections.
The patient in this case had negative Lyme serology and was treated with 2 injections of triamcinolone 10 mg/mL administered 3 weeks apart. She experienced complete resolution.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
The biopsy revealed abundant lymphocytes, neutrophils, and eosinophils consistent with a diagnosis of cutaneous B cell pseudolymphoma. The pseudolymphoma was caused by an exaggerated response to a tick bite.
As the name implies, B cell pseudolymphomas clinically and histologically mimic the various patterns of cutaneous lymphoma, often appearing as a firm, pink to dark violet nodule. A biopsy is mandatory to distinguish between pseudolymphoma and true lymphoma. There is an association between pseudolymphomas and Borrelia burgdorferi, the organism responsible for Lyme disease. Thus, testing for Lyme disease is recommended for patients with pseudolymphomas who live in endemic areas. Patients who test positive should be treated with doxycycline 100 mg bid for 10 days.
In the absence of Lyme disease, a pseudolymphoma may resolve spontaneously over weeks or months. Resolution can be hastened with topical superpotent steroids, intralesional steroids, or systemic steroids. Treatment can begin with topical clobetasol 0.05% bid. If the lesion does not resolve, the next step would be intralesional triamcinolone 10 mg/mL injected directly into the nodule until it blanches slightly. Injections should be repeated every 3 to 4 weeks for a total of 2 to 3 injections.
The patient in this case had negative Lyme serology and was treated with 2 injections of triamcinolone 10 mg/mL administered 3 weeks apart. She experienced complete resolution.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Mitteldorf C, Kempf W. Cutaneous pseudolymphoma. Surg Pathol Clin. 2017;10:455-476. doi: 10.1016/j.path.2017.01.002
1. Mitteldorf C, Kempf W. Cutaneous pseudolymphoma. Surg Pathol Clin. 2017;10:455-476. doi: 10.1016/j.path.2017.01.002

Persistent Wounds Refractory to Broad-Spectrum Antibiotics
The Diagnosis: PASH (Pyoderma Gangrenosum, Acne, Hidradenitis Suppurativa) Syndrome
Obtaining our patient’s history of hidradenitis suppurativa (HS), a hallmark sterile neutrophilic dermatosis, was key to making the correct diagnosis of PASH (pyoderma gangrenosum, acne, HS) syndrome. In our patient, the history of HS increased the consideration of pyoderma gangrenosum (PG) due to the persistent breast and leg wounds. Additionally, it was important to consider a diagnosis of PG in lesions that were not responding to broad-spectrum antimicrobial treatment. In our patient, the concurrent presentation of draining abscesses in the axillae (Figure, A) and inflammatory nodulocystic facial acne (Figure, B) were additional diagnostic clues that suggested the triad of PASH syndrome.

Although SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome also can present with cutaneous features of acne and HS, the lack of bone and joint involvement in our patient made this diagnosis less likely. Calciphylaxis can present as ulcerations on the lower extremities, but it usually presents with a livedolike pattern with overlying black eschar and is unlikely in the absence of underlying metabolic or renal disease. PAPA (pyogenic arthritis, PG, acne) syndrome is characterized by recurrent joint involvement and lacks features of HS. Lastly, our patient was immunocompetent with no risk factors for mycobacterial infection.
PASH syndrome is a rare inherited syndrome, but its constituent inflammatory conditions are ubiquitous. They share a common underlying mechanism consisting of overactivation of the innate immune systems driven by increased production of the inflammatory cytokines IL-1, IL-17, and tumor necrosis factor α, resulting in sterile neutrophilic dermatoses.1 The diagnosis is based on the clinical presentation, as laboratory investigations are nondiagnostic. Biopsies and cultures can be performed to rule out infectious etiologies. Additionally, PASH syndrome is considered part of a larger spectrum of syndromes including PAPA and PAPASH (pyogenic arthritis, acne, PG, HS) syndromes. The absence of pyogenic arthritis distinguishes PASH syndrome from PAPA and PAPASH syndromes.2 Clinically, PASH syndrome and the related sterile neutrophilic dermatoses share the characteristic of pronounced cutaneous involvement that substantially alters the patient’s quality of life. Cigarette smoking is an exacerbating factor and has a well-established association with HS.3 Therefore, smoking cessation should be encouraged in these patients to avoid exacerbation of the disease process.
Maintaining adequate immunosuppression is key to managing the underlying disease processes. Classic immunosuppressive agents such as systemic glucocorticoids and methotrexate may fail to satisfactorily control the disease.4 Treatment options currently are somewhat limited and are aimed at targeting the inflammatory cytokines that propagate the disease. The most consistent responses have been observed with anti–tumor necrosis factor α antagonists such as adalimumab, infliximab, and etanercept.5 Additionally, there is varied response to anakinra, suggesting the importance of selectively targeting IL-1β.6 Unfortunately, misdiagnosis for an infectious etiology is common, and antibiotics and debridement are of limited use for the underlying pathophysiology of PASH syndrome. Importantly, biopsy and debridement often are discouraged due to the risk of pathergy.7
Our case demonstrates the importance of maintaining a high clinical suspicion for immune-mediated lesions that are refractory to antimicrobial agents. Additionally, prior history of multiple neutrophilic dermatoses should prompt consideration for the PASH/PAPA/PAPASH disease spectrum. Early and accurate identification of neutrophilic dermatoses such as PG and HS are crucial to initiating proper cytokine-targeting treatment and achieving disease remission.
- Cugno M, Borghi A, Marzano AV. PAPA, PASH and PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562.
- Genovese G, Moltrasio C, Garcovich S, et al. PAPA spectrum disorders. G Ital Dermatol Venereol. 2020;155:542-550.
- König A, Lehmann C, Rompel R, et al. Cigarette smoking as a triggering factor of hidradenitis suppurativa. Dermatology. 1999;198:261-264.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Saint-Georges V, Peternel S, Kaštelan M, et al. Tumor necrosis factor antagonists in the treatment of pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH) syndrome. Acta Dermatovenerol Croat. 2018;26:173-178.
- Braun-Falco M, Kovnerystyy O, Lohse P, et al. Pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH)—a new autoinflammatory syndrome distinct from PAPA syndrome. J Am Acad Dermatol. 2012;66:409-415.
- Patel DK, Locke M, Jarrett P. Pyoderma gangrenosum with pathergy: a potentially significant complication following breast reconstruction. J Plast Reconstr Aesthet Surg. 2017;70:884-892.
The Diagnosis: PASH (Pyoderma Gangrenosum, Acne, Hidradenitis Suppurativa) Syndrome
Obtaining our patient’s history of hidradenitis suppurativa (HS), a hallmark sterile neutrophilic dermatosis, was key to making the correct diagnosis of PASH (pyoderma gangrenosum, acne, HS) syndrome. In our patient, the history of HS increased the consideration of pyoderma gangrenosum (PG) due to the persistent breast and leg wounds. Additionally, it was important to consider a diagnosis of PG in lesions that were not responding to broad-spectrum antimicrobial treatment. In our patient, the concurrent presentation of draining abscesses in the axillae (Figure, A) and inflammatory nodulocystic facial acne (Figure, B) were additional diagnostic clues that suggested the triad of PASH syndrome.
Although SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome also can present with cutaneous features of acne and HS, the lack of bone and joint involvement in our patient made this diagnosis less likely. Calciphylaxis can present as ulcerations on the lower extremities, but it usually presents with a livedolike pattern with overlying black eschar and is unlikely in the absence of underlying metabolic or renal disease. PAPA (pyogenic arthritis, PG, acne) syndrome is characterized by recurrent joint involvement and lacks features of HS. Lastly, our patient was immunocompetent with no risk factors for mycobacterial infection.
PASH syndrome is a rare inherited syndrome, but its constituent inflammatory conditions are ubiquitous. They share a common underlying mechanism consisting of overactivation of the innate immune systems driven by increased production of the inflammatory cytokines IL-1, IL-17, and tumor necrosis factor α, resulting in sterile neutrophilic dermatoses.1 The diagnosis is based on the clinical presentation, as laboratory investigations are nondiagnostic. Biopsies and cultures can be performed to rule out infectious etiologies. Additionally, PASH syndrome is considered part of a larger spectrum of syndromes including PAPA and PAPASH (pyogenic arthritis, acne, PG, HS) syndromes. The absence of pyogenic arthritis distinguishes PASH syndrome from PAPA and PAPASH syndromes.2 Clinically, PASH syndrome and the related sterile neutrophilic dermatoses share the characteristic of pronounced cutaneous involvement that substantially alters the patient’s quality of life. Cigarette smoking is an exacerbating factor and has a well-established association with HS.3 Therefore, smoking cessation should be encouraged in these patients to avoid exacerbation of the disease process.
Maintaining adequate immunosuppression is key to managing the underlying disease processes. Classic immunosuppressive agents such as systemic glucocorticoids and methotrexate may fail to satisfactorily control the disease.4 Treatment options currently are somewhat limited and are aimed at targeting the inflammatory cytokines that propagate the disease. The most consistent responses have been observed with anti–tumor necrosis factor α antagonists such as adalimumab, infliximab, and etanercept.5 Additionally, there is varied response to anakinra, suggesting the importance of selectively targeting IL-1β.6 Unfortunately, misdiagnosis for an infectious etiology is common, and antibiotics and debridement are of limited use for the underlying pathophysiology of PASH syndrome. Importantly, biopsy and debridement often are discouraged due to the risk of pathergy.7
Our case demonstrates the importance of maintaining a high clinical suspicion for immune-mediated lesions that are refractory to antimicrobial agents. Additionally, prior history of multiple neutrophilic dermatoses should prompt consideration for the PASH/PAPA/PAPASH disease spectrum. Early and accurate identification of neutrophilic dermatoses such as PG and HS are crucial to initiating proper cytokine-targeting treatment and achieving disease remission.
The Diagnosis: PASH (Pyoderma Gangrenosum, Acne, Hidradenitis Suppurativa) Syndrome
Obtaining our patient’s history of hidradenitis suppurativa (HS), a hallmark sterile neutrophilic dermatosis, was key to making the correct diagnosis of PASH (pyoderma gangrenosum, acne, HS) syndrome. In our patient, the history of HS increased the consideration of pyoderma gangrenosum (PG) due to the persistent breast and leg wounds. Additionally, it was important to consider a diagnosis of PG in lesions that were not responding to broad-spectrum antimicrobial treatment. In our patient, the concurrent presentation of draining abscesses in the axillae (Figure, A) and inflammatory nodulocystic facial acne (Figure, B) were additional diagnostic clues that suggested the triad of PASH syndrome.
Although SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome also can present with cutaneous features of acne and HS, the lack of bone and joint involvement in our patient made this diagnosis less likely. Calciphylaxis can present as ulcerations on the lower extremities, but it usually presents with a livedolike pattern with overlying black eschar and is unlikely in the absence of underlying metabolic or renal disease. PAPA (pyogenic arthritis, PG, acne) syndrome is characterized by recurrent joint involvement and lacks features of HS. Lastly, our patient was immunocompetent with no risk factors for mycobacterial infection.
PASH syndrome is a rare inherited syndrome, but its constituent inflammatory conditions are ubiquitous. They share a common underlying mechanism consisting of overactivation of the innate immune systems driven by increased production of the inflammatory cytokines IL-1, IL-17, and tumor necrosis factor α, resulting in sterile neutrophilic dermatoses.1 The diagnosis is based on the clinical presentation, as laboratory investigations are nondiagnostic. Biopsies and cultures can be performed to rule out infectious etiologies. Additionally, PASH syndrome is considered part of a larger spectrum of syndromes including PAPA and PAPASH (pyogenic arthritis, acne, PG, HS) syndromes. The absence of pyogenic arthritis distinguishes PASH syndrome from PAPA and PAPASH syndromes.2 Clinically, PASH syndrome and the related sterile neutrophilic dermatoses share the characteristic of pronounced cutaneous involvement that substantially alters the patient’s quality of life. Cigarette smoking is an exacerbating factor and has a well-established association with HS.3 Therefore, smoking cessation should be encouraged in these patients to avoid exacerbation of the disease process.
Maintaining adequate immunosuppression is key to managing the underlying disease processes. Classic immunosuppressive agents such as systemic glucocorticoids and methotrexate may fail to satisfactorily control the disease.4 Treatment options currently are somewhat limited and are aimed at targeting the inflammatory cytokines that propagate the disease. The most consistent responses have been observed with anti–tumor necrosis factor α antagonists such as adalimumab, infliximab, and etanercept.5 Additionally, there is varied response to anakinra, suggesting the importance of selectively targeting IL-1β.6 Unfortunately, misdiagnosis for an infectious etiology is common, and antibiotics and debridement are of limited use for the underlying pathophysiology of PASH syndrome. Importantly, biopsy and debridement often are discouraged due to the risk of pathergy.7
Our case demonstrates the importance of maintaining a high clinical suspicion for immune-mediated lesions that are refractory to antimicrobial agents. Additionally, prior history of multiple neutrophilic dermatoses should prompt consideration for the PASH/PAPA/PAPASH disease spectrum. Early and accurate identification of neutrophilic dermatoses such as PG and HS are crucial to initiating proper cytokine-targeting treatment and achieving disease remission.
- Cugno M, Borghi A, Marzano AV. PAPA, PASH and PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562.
- Genovese G, Moltrasio C, Garcovich S, et al. PAPA spectrum disorders. G Ital Dermatol Venereol. 2020;155:542-550.
- König A, Lehmann C, Rompel R, et al. Cigarette smoking as a triggering factor of hidradenitis suppurativa. Dermatology. 1999;198:261-264.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Saint-Georges V, Peternel S, Kaštelan M, et al. Tumor necrosis factor antagonists in the treatment of pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH) syndrome. Acta Dermatovenerol Croat. 2018;26:173-178.
- Braun-Falco M, Kovnerystyy O, Lohse P, et al. Pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH)—a new autoinflammatory syndrome distinct from PAPA syndrome. J Am Acad Dermatol. 2012;66:409-415.
- Patel DK, Locke M, Jarrett P. Pyoderma gangrenosum with pathergy: a potentially significant complication following breast reconstruction. J Plast Reconstr Aesthet Surg. 2017;70:884-892.
- Cugno M, Borghi A, Marzano AV. PAPA, PASH and PAPASH syndromes: pathophysiology, presentation and treatment. Am J Clin Dermatol. 2017;18:555-562.
- Genovese G, Moltrasio C, Garcovich S, et al. PAPA spectrum disorders. G Ital Dermatol Venereol. 2020;155:542-550.
- König A, Lehmann C, Rompel R, et al. Cigarette smoking as a triggering factor of hidradenitis suppurativa. Dermatology. 1999;198:261-264.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Saint-Georges V, Peternel S, Kaštelan M, et al. Tumor necrosis factor antagonists in the treatment of pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH) syndrome. Acta Dermatovenerol Croat. 2018;26:173-178.
- Braun-Falco M, Kovnerystyy O, Lohse P, et al. Pyoderma gangrenosum, acne, and suppurative hidradenitis (PASH)—a new autoinflammatory syndrome distinct from PAPA syndrome. J Am Acad Dermatol. 2012;66:409-415.
- Patel DK, Locke M, Jarrett P. Pyoderma gangrenosum with pathergy: a potentially significant complication following breast reconstruction. J Plast Reconstr Aesthet Surg. 2017;70:884-892.
A 28-year-old Black woman presented to the hospital for evaluation of worsening leg wounds as well as a similar eroding plaque on the left breast of 1 month’s duration. Broad-spectrum antibiotics prescribed during a prior emergency department visit resulted in no improvement. Her medical history was notable for hidradenitis suppurativa that previously was well controlled on adalimumab prior to discontinuation 1 year prior. A review of systems was negative for fever, chills, shortness of breath, chest pain, night sweats, and arthralgia. The patient had discontinued the antibiotics and was not taking any other medications at the time of presentation. She reported a history of smoking cigarettes (5 pack years). Physical examination revealed hyperkeratotic eroded plaques with violaceous borders circumferentially around the left breast (top) and legs with notable undermining (bottom). Inflammatory nodulocystic acne of the face as well as sinus tract formation with purulent drainage in the axillae also were present. Laboratory workup revealed an elevated erythrocyte sedimentation rate (116 mm/h [reference range, <20 mm/h]). Computed tomography of the leg wound was negative for soft-tissue infection. Aerobic and anaerobic tissue cultures demonstrated no growth.


ASCO honors Hagop Kantarjian, MD, for leukemia research
This award is the society’s “highest scientific honor, and I am extremely happy and honored to receive it,” Dr. Kantarjian commented in an interview with this news organization.
Dr. Kantarjian serves as the chair of the department of leukemia and currently holds the Samsung Distinguished University Chair in Cancer Medicine at the University of Texas MD Anderson Cancer Center, Houston.
“No doubt that this is not an individual award. It represents an award for the accomplishments of all the leukemia faculty at MD Anderson across 4 decades. It’s really a teamwork effort that led to so many discoveries and improvements in treatment and care of patients with leukemia,” he commented.
The David A. Karnofsky Memorial Award has been presented annually since 1970 to recognize oncologists who have made outstanding contributions to cancer research, diagnosis, or treatment, ASCO noted.
From Lebanon to Texas
Dr. Kantarjian received his medical degree from the American University of Beirut, in Lebanon, in 1979 and completed his residency in internal medicine at the same institution in 1981.
It was his experience at MD Anderson as a young medical student and later as a fellow that fueled his interest and career in leukemia, he said.
“In 1978, I took a 4-month elective at MD Anderson, and I soon realized how different and innovative the atmosphere at MD Anderson was, compared to where I was training in Lebanon,” Dr. Kantarjian told this news organization.
Working with mentors that included MD Anderson heavyweights Emil Freireich, MD, Kenneth McCredie, MD, and Michael Keating, MD, helped shape his career and guide his leukemia research, he said.
Transformative impact on leukemia outcomes
The award citation notes that over the past 4 decades, Dr. Kantarjian’s research has transformed some standards of care and has dramatically improved survival in several leukemia subtypes, including chronic myeloid leukemia (CML), acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), and acute lymphocytic leukemia (ALL).
“Four decades ago, most of the leukemias were incurable. Today, most of the leukemias are potentially curable with targeted therapies. That’s what I am most proud of,” Dr. Kantarjian told this news organization.
Among Dr. Kantarjian’s contributions to the field of leukemia:
- Developing the HYPER-CVAD regimen (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone) as a standard-of-care, frontline therapy for adults with ALL.
- Establishing clinical biology parameters of CML, including definitions of CML phases and cytogenetic responses, and establishing new prognostic factors that were subsequently adopted in studies of tyrosine kinase inhibitors.
- Leading the development of decitabine and epigenetic hypomethylation therapy for MDS and for older/unfit patients with AML.
- Pioneering research with hypomethylating agents (HMAs) in combination with venetoclax, which led to FDA approval of HMA-venetoclax combinations for older/unfit patients with AML.
- Championing the development of clofarabine, conducting animal toxicology studies, and leading subsequent phase 1 and 2 trials and pivotal phase 3 and 4 trials that led to FDA approval of clofarabine for pediatric ALL.
- Developing several FLT3 inhibitors, isocitrate dehydrogenase inhibitors, and venetoclax, which all received FDA approval for the treatment of AML and its subsets.
- Developing regimens for inotuzumab and blinatumomab combined with chemotherapy for adults with pre-B ALL.
- Working on the development of imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and omacetaxine, which all received FDA approval for CML therapy.
“Dr. Kantarjian’s long list of accomplishments and groundbreaking discoveries are a testament to his lifelong commitment to impactful cancer research and patient care,” Giulio Draetta, MD, PhD, chief scientific officer at MD Anderson, said in a statement.
Giving back
Dr. Kantarjian has written more than 2,200 peer-reviewed articles and more than 100 book chapters. In 2012, he cofounded the Society of Hematologic Oncology, which has now expanded worldwide.
He has served on multiple ASCO committees throughout the years and served on the ASCO board of directors from 2010 to 2015.
Dr. Kantarjian is passionately involved in mentoring and education. In 2000 he created the MD Anderson Leukemia Fellowship, which now trains about 10 fellows in leukemia annually.
He is a nonresident fellow in health care at the Rice Baker Institute and has written extensively on important health care issues in cancer, including the importance of universal equitable health care, health care safety nets, health care as a human right, and the problem of drug shortages.
Dr. Kantarjian is a strong advocate for more affordable drug therapies. For years he has been outspoken about the high price of leukemia drugs and has written high-profile articles in medical journals. He has even appeared on a popular television program to publicize the issue.
“Drug costs have been increasing over time. If you think about it, even if you discover a drug that cures cancer, but the drug is affordable for the 1% of the patients, then you have no cure for cancer,” Dr. Kantarjian told this news organization.
“I started speaking about the issue of the cancer drug costs in 2012. Unfortunately, we have not made progress simply because of the for-profit nature of health care and the strong lobbying by drug companies,” he added. Dr. Kantarjian hopes new legislation will eventually turn the tide.
Dr. Kantarjian has received many other honors throughout his distinguished career, including the American Lebanese Medical Association’s Lifetime Achievement Award, the American Association for Cancer Research’s Joseph H. Burchenal Memorial Award, and the Leukemia Society of America’s Outstanding Service to Mankind Award. He also was named an ASCO Fellow and a Leukemia Society of America Special Fellow and Scholar.
Dr. Kantarjian will be presented with the 2023 David A. Karnofsky Memorial Award, which includes a $25,000 honorarium, and will give a scientific lecture about his research at the ASCO annual meeting in Chicago in early June.
A version of this article originally appeared on Medscape.com.
This award is the society’s “highest scientific honor, and I am extremely happy and honored to receive it,” Dr. Kantarjian commented in an interview with this news organization.
Dr. Kantarjian serves as the chair of the department of leukemia and currently holds the Samsung Distinguished University Chair in Cancer Medicine at the University of Texas MD Anderson Cancer Center, Houston.
“No doubt that this is not an individual award. It represents an award for the accomplishments of all the leukemia faculty at MD Anderson across 4 decades. It’s really a teamwork effort that led to so many discoveries and improvements in treatment and care of patients with leukemia,” he commented.
The David A. Karnofsky Memorial Award has been presented annually since 1970 to recognize oncologists who have made outstanding contributions to cancer research, diagnosis, or treatment, ASCO noted.
From Lebanon to Texas
Dr. Kantarjian received his medical degree from the American University of Beirut, in Lebanon, in 1979 and completed his residency in internal medicine at the same institution in 1981.
It was his experience at MD Anderson as a young medical student and later as a fellow that fueled his interest and career in leukemia, he said.
“In 1978, I took a 4-month elective at MD Anderson, and I soon realized how different and innovative the atmosphere at MD Anderson was, compared to where I was training in Lebanon,” Dr. Kantarjian told this news organization.
Working with mentors that included MD Anderson heavyweights Emil Freireich, MD, Kenneth McCredie, MD, and Michael Keating, MD, helped shape his career and guide his leukemia research, he said.
Transformative impact on leukemia outcomes
The award citation notes that over the past 4 decades, Dr. Kantarjian’s research has transformed some standards of care and has dramatically improved survival in several leukemia subtypes, including chronic myeloid leukemia (CML), acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), and acute lymphocytic leukemia (ALL).
“Four decades ago, most of the leukemias were incurable. Today, most of the leukemias are potentially curable with targeted therapies. That’s what I am most proud of,” Dr. Kantarjian told this news organization.
Among Dr. Kantarjian’s contributions to the field of leukemia:
- Developing the HYPER-CVAD regimen (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone) as a standard-of-care, frontline therapy for adults with ALL.
- Establishing clinical biology parameters of CML, including definitions of CML phases and cytogenetic responses, and establishing new prognostic factors that were subsequently adopted in studies of tyrosine kinase inhibitors.
- Leading the development of decitabine and epigenetic hypomethylation therapy for MDS and for older/unfit patients with AML.
- Pioneering research with hypomethylating agents (HMAs) in combination with venetoclax, which led to FDA approval of HMA-venetoclax combinations for older/unfit patients with AML.
- Championing the development of clofarabine, conducting animal toxicology studies, and leading subsequent phase 1 and 2 trials and pivotal phase 3 and 4 trials that led to FDA approval of clofarabine for pediatric ALL.
- Developing several FLT3 inhibitors, isocitrate dehydrogenase inhibitors, and venetoclax, which all received FDA approval for the treatment of AML and its subsets.
- Developing regimens for inotuzumab and blinatumomab combined with chemotherapy for adults with pre-B ALL.
- Working on the development of imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and omacetaxine, which all received FDA approval for CML therapy.
“Dr. Kantarjian’s long list of accomplishments and groundbreaking discoveries are a testament to his lifelong commitment to impactful cancer research and patient care,” Giulio Draetta, MD, PhD, chief scientific officer at MD Anderson, said in a statement.
Giving back
Dr. Kantarjian has written more than 2,200 peer-reviewed articles and more than 100 book chapters. In 2012, he cofounded the Society of Hematologic Oncology, which has now expanded worldwide.
He has served on multiple ASCO committees throughout the years and served on the ASCO board of directors from 2010 to 2015.
Dr. Kantarjian is passionately involved in mentoring and education. In 2000 he created the MD Anderson Leukemia Fellowship, which now trains about 10 fellows in leukemia annually.
He is a nonresident fellow in health care at the Rice Baker Institute and has written extensively on important health care issues in cancer, including the importance of universal equitable health care, health care safety nets, health care as a human right, and the problem of drug shortages.
Dr. Kantarjian is a strong advocate for more affordable drug therapies. For years he has been outspoken about the high price of leukemia drugs and has written high-profile articles in medical journals. He has even appeared on a popular television program to publicize the issue.
“Drug costs have been increasing over time. If you think about it, even if you discover a drug that cures cancer, but the drug is affordable for the 1% of the patients, then you have no cure for cancer,” Dr. Kantarjian told this news organization.
“I started speaking about the issue of the cancer drug costs in 2012. Unfortunately, we have not made progress simply because of the for-profit nature of health care and the strong lobbying by drug companies,” he added. Dr. Kantarjian hopes new legislation will eventually turn the tide.
Dr. Kantarjian has received many other honors throughout his distinguished career, including the American Lebanese Medical Association’s Lifetime Achievement Award, the American Association for Cancer Research’s Joseph H. Burchenal Memorial Award, and the Leukemia Society of America’s Outstanding Service to Mankind Award. He also was named an ASCO Fellow and a Leukemia Society of America Special Fellow and Scholar.
Dr. Kantarjian will be presented with the 2023 David A. Karnofsky Memorial Award, which includes a $25,000 honorarium, and will give a scientific lecture about his research at the ASCO annual meeting in Chicago in early June.
A version of this article originally appeared on Medscape.com.
This award is the society’s “highest scientific honor, and I am extremely happy and honored to receive it,” Dr. Kantarjian commented in an interview with this news organization.
Dr. Kantarjian serves as the chair of the department of leukemia and currently holds the Samsung Distinguished University Chair in Cancer Medicine at the University of Texas MD Anderson Cancer Center, Houston.
“No doubt that this is not an individual award. It represents an award for the accomplishments of all the leukemia faculty at MD Anderson across 4 decades. It’s really a teamwork effort that led to so many discoveries and improvements in treatment and care of patients with leukemia,” he commented.
The David A. Karnofsky Memorial Award has been presented annually since 1970 to recognize oncologists who have made outstanding contributions to cancer research, diagnosis, or treatment, ASCO noted.
From Lebanon to Texas
Dr. Kantarjian received his medical degree from the American University of Beirut, in Lebanon, in 1979 and completed his residency in internal medicine at the same institution in 1981.
It was his experience at MD Anderson as a young medical student and later as a fellow that fueled his interest and career in leukemia, he said.
“In 1978, I took a 4-month elective at MD Anderson, and I soon realized how different and innovative the atmosphere at MD Anderson was, compared to where I was training in Lebanon,” Dr. Kantarjian told this news organization.
Working with mentors that included MD Anderson heavyweights Emil Freireich, MD, Kenneth McCredie, MD, and Michael Keating, MD, helped shape his career and guide his leukemia research, he said.
Transformative impact on leukemia outcomes
The award citation notes that over the past 4 decades, Dr. Kantarjian’s research has transformed some standards of care and has dramatically improved survival in several leukemia subtypes, including chronic myeloid leukemia (CML), acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), and acute lymphocytic leukemia (ALL).
“Four decades ago, most of the leukemias were incurable. Today, most of the leukemias are potentially curable with targeted therapies. That’s what I am most proud of,” Dr. Kantarjian told this news organization.
Among Dr. Kantarjian’s contributions to the field of leukemia:
- Developing the HYPER-CVAD regimen (hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone) as a standard-of-care, frontline therapy for adults with ALL.
- Establishing clinical biology parameters of CML, including definitions of CML phases and cytogenetic responses, and establishing new prognostic factors that were subsequently adopted in studies of tyrosine kinase inhibitors.
- Leading the development of decitabine and epigenetic hypomethylation therapy for MDS and for older/unfit patients with AML.
- Pioneering research with hypomethylating agents (HMAs) in combination with venetoclax, which led to FDA approval of HMA-venetoclax combinations for older/unfit patients with AML.
- Championing the development of clofarabine, conducting animal toxicology studies, and leading subsequent phase 1 and 2 trials and pivotal phase 3 and 4 trials that led to FDA approval of clofarabine for pediatric ALL.
- Developing several FLT3 inhibitors, isocitrate dehydrogenase inhibitors, and venetoclax, which all received FDA approval for the treatment of AML and its subsets.
- Developing regimens for inotuzumab and blinatumomab combined with chemotherapy for adults with pre-B ALL.
- Working on the development of imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and omacetaxine, which all received FDA approval for CML therapy.
“Dr. Kantarjian’s long list of accomplishments and groundbreaking discoveries are a testament to his lifelong commitment to impactful cancer research and patient care,” Giulio Draetta, MD, PhD, chief scientific officer at MD Anderson, said in a statement.
Giving back
Dr. Kantarjian has written more than 2,200 peer-reviewed articles and more than 100 book chapters. In 2012, he cofounded the Society of Hematologic Oncology, which has now expanded worldwide.
He has served on multiple ASCO committees throughout the years and served on the ASCO board of directors from 2010 to 2015.
Dr. Kantarjian is passionately involved in mentoring and education. In 2000 he created the MD Anderson Leukemia Fellowship, which now trains about 10 fellows in leukemia annually.
He is a nonresident fellow in health care at the Rice Baker Institute and has written extensively on important health care issues in cancer, including the importance of universal equitable health care, health care safety nets, health care as a human right, and the problem of drug shortages.
Dr. Kantarjian is a strong advocate for more affordable drug therapies. For years he has been outspoken about the high price of leukemia drugs and has written high-profile articles in medical journals. He has even appeared on a popular television program to publicize the issue.
“Drug costs have been increasing over time. If you think about it, even if you discover a drug that cures cancer, but the drug is affordable for the 1% of the patients, then you have no cure for cancer,” Dr. Kantarjian told this news organization.
“I started speaking about the issue of the cancer drug costs in 2012. Unfortunately, we have not made progress simply because of the for-profit nature of health care and the strong lobbying by drug companies,” he added. Dr. Kantarjian hopes new legislation will eventually turn the tide.
Dr. Kantarjian has received many other honors throughout his distinguished career, including the American Lebanese Medical Association’s Lifetime Achievement Award, the American Association for Cancer Research’s Joseph H. Burchenal Memorial Award, and the Leukemia Society of America’s Outstanding Service to Mankind Award. He also was named an ASCO Fellow and a Leukemia Society of America Special Fellow and Scholar.
Dr. Kantarjian will be presented with the 2023 David A. Karnofsky Memorial Award, which includes a $25,000 honorarium, and will give a scientific lecture about his research at the ASCO annual meeting in Chicago in early June.
A version of this article originally appeared on Medscape.com.