User login
Cancer, heart disease vaccines may be ready by 2030, Moderna says
The announcement is yet another sign of what many are calling “the golden age” of vaccine development, which is largely credited to the pandemic’s use of mRNA technology to create COVID-19 vaccines.
“I think what we have learned in recent months is that if you ever thought that mRNA was just for infectious diseases, or just for COVID, the evidence now is that that’s absolutely not the case,” Moderna Chief Medical Officer Paul Burton, MD, PhD, told The Guardian. “It can be applied to all sorts of disease areas; we are in cancer, infectious disease, cardiovascular disease, autoimmune diseases, rare disease. We have studies in all of those areas, and they have all shown tremendous promise.”
The U.S. Food and Drug Administration recently designated two new Moderna vaccines as breakthrough therapies: a shot that prevents respiratory syncytial virus (RSV) in older people and a shot that helps prevent the recurrence of melanoma. The FDA’s breakthrough designation is given when a new treatment’s early trial results are substantially better than an existing therapy.
The mRNA vaccine technology that made headlines for its role in COVID-19 vaccines works by teaching the body how to make a specific protein to help the immune system prevent or target a certain disease.
Dr. Burton anticipates that mRNA technology will result in breakthroughs such as a cancer vaccine that can be personalized based on the features of a specific tumor.
“I think we will have mRNA-based therapies for rare diseases that were previously undruggable, and I think that 10 years from now, we will be approaching a world where you truly can identify the genetic cause of a disease and, with relative simplicity, go and edit that out and repair it using mRNA-based technology,” he said.
The Moderna executive made the statements before its annual update on its vaccine pipeline projects, which the company calls “Vaccines Day.” The Massachusetts-based drugmaker said it has given someone the first dose of a “next-generation” COVID-19 vaccine in a phase III trial, has made progress on a Lyme disease shot, and is developing a vaccine for the highly contagious norovirus.
In all, Moderna expects “six major vaccine product launches in the next few years,” the company said in a statement, adding that it expects the COVID-19 booster market alone to be valued at $15 billion.
A version of this article first appeared on WebMD.com.
The announcement is yet another sign of what many are calling “the golden age” of vaccine development, which is largely credited to the pandemic’s use of mRNA technology to create COVID-19 vaccines.
“I think what we have learned in recent months is that if you ever thought that mRNA was just for infectious diseases, or just for COVID, the evidence now is that that’s absolutely not the case,” Moderna Chief Medical Officer Paul Burton, MD, PhD, told The Guardian. “It can be applied to all sorts of disease areas; we are in cancer, infectious disease, cardiovascular disease, autoimmune diseases, rare disease. We have studies in all of those areas, and they have all shown tremendous promise.”
The U.S. Food and Drug Administration recently designated two new Moderna vaccines as breakthrough therapies: a shot that prevents respiratory syncytial virus (RSV) in older people and a shot that helps prevent the recurrence of melanoma. The FDA’s breakthrough designation is given when a new treatment’s early trial results are substantially better than an existing therapy.
The mRNA vaccine technology that made headlines for its role in COVID-19 vaccines works by teaching the body how to make a specific protein to help the immune system prevent or target a certain disease.
Dr. Burton anticipates that mRNA technology will result in breakthroughs such as a cancer vaccine that can be personalized based on the features of a specific tumor.
“I think we will have mRNA-based therapies for rare diseases that were previously undruggable, and I think that 10 years from now, we will be approaching a world where you truly can identify the genetic cause of a disease and, with relative simplicity, go and edit that out and repair it using mRNA-based technology,” he said.
The Moderna executive made the statements before its annual update on its vaccine pipeline projects, which the company calls “Vaccines Day.” The Massachusetts-based drugmaker said it has given someone the first dose of a “next-generation” COVID-19 vaccine in a phase III trial, has made progress on a Lyme disease shot, and is developing a vaccine for the highly contagious norovirus.
In all, Moderna expects “six major vaccine product launches in the next few years,” the company said in a statement, adding that it expects the COVID-19 booster market alone to be valued at $15 billion.
A version of this article first appeared on WebMD.com.
The announcement is yet another sign of what many are calling “the golden age” of vaccine development, which is largely credited to the pandemic’s use of mRNA technology to create COVID-19 vaccines.
“I think what we have learned in recent months is that if you ever thought that mRNA was just for infectious diseases, or just for COVID, the evidence now is that that’s absolutely not the case,” Moderna Chief Medical Officer Paul Burton, MD, PhD, told The Guardian. “It can be applied to all sorts of disease areas; we are in cancer, infectious disease, cardiovascular disease, autoimmune diseases, rare disease. We have studies in all of those areas, and they have all shown tremendous promise.”
The U.S. Food and Drug Administration recently designated two new Moderna vaccines as breakthrough therapies: a shot that prevents respiratory syncytial virus (RSV) in older people and a shot that helps prevent the recurrence of melanoma. The FDA’s breakthrough designation is given when a new treatment’s early trial results are substantially better than an existing therapy.
The mRNA vaccine technology that made headlines for its role in COVID-19 vaccines works by teaching the body how to make a specific protein to help the immune system prevent or target a certain disease.
Dr. Burton anticipates that mRNA technology will result in breakthroughs such as a cancer vaccine that can be personalized based on the features of a specific tumor.
“I think we will have mRNA-based therapies for rare diseases that were previously undruggable, and I think that 10 years from now, we will be approaching a world where you truly can identify the genetic cause of a disease and, with relative simplicity, go and edit that out and repair it using mRNA-based technology,” he said.
The Moderna executive made the statements before its annual update on its vaccine pipeline projects, which the company calls “Vaccines Day.” The Massachusetts-based drugmaker said it has given someone the first dose of a “next-generation” COVID-19 vaccine in a phase III trial, has made progress on a Lyme disease shot, and is developing a vaccine for the highly contagious norovirus.
In all, Moderna expects “six major vaccine product launches in the next few years,” the company said in a statement, adding that it expects the COVID-19 booster market alone to be valued at $15 billion.
A version of this article first appeared on WebMD.com.
Self-fitted and audiologist-fitted hearing aids equal for mild to moderate hearing loss
Self-fitted over-the-counter (OTC) hearing aids may be an effective option for individuals with mild to moderate hearing loss, a small randomized effectiveness trial reports. OTC devices yielded 6-week patient-perceived and clinical outcomes comparable to those with audiologist-fitted hearing aids, In fact, at week 2, the self-fitted group had a small but meaningful advantage on two of the four study outcome measures.
“After support and fine-tuning were provided to the self-fitting (remote support) and audiologist-fitted groups, no clinically meaningful differences were evident in any outcome measures at the end of the 6-week trial,” wrote researchers led by Karina C. De Sousa, PhD, a postdoctoral researcher in the department of speech-language pathology and audiology at the University of Pretoria, South Africa.

Their findings appear in JAMA Otolaryngology–Head & Neck Surgery.
Hearing aid uptake is low even in populations with adequate access to audiological resources, the authors noted, with hearing aid use in U.S. adults who could benefit estimated at about 20%. Currently, an estimated 22.9 million older Americans with audiometric hearing loss do not use hearing aids.
Major barriers have been access and affordability, Dr. De Sousa and associates wrote, and until recently, people with hearing loss could obtain hearing aids only after consultation with a credentialed dispenser. “The World Health Organization estimates that over 2.5 billion people will experience some degree of hearing loss by 2050,” Dr. De Sousa said in an interview. “This new category of self-fitting hearing aids opens up newer care pathways for people with mild to moderate hearing loss.”
The study
From April to August 2022 the trial recruited 68 participants (51.6% men) with mild-to-moderate self-reported hearing loss, a mean age of 63.6 years, and no ear disease within the past 90 days. They were randomized to a self-fitted commercially available device (Lexi Lumen), with instructional material on set-up and remote support, or to the same unit fitted by an audiologist. The majority in both arms were new users and were similar in age and baseline hearing scores.
The primary outcome measure was patient-reported hearing aid benefit, measured by the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire. This scale evaluates auditory acuity before and after amplification by such criteria as ease of communication, background noise, reverberation, aversiveness, and global hearing status.
Secondary measures included the International Outcome Inventory for Hearing Aids (IOI-HA) and speech recognition in noise measured using an abbreviated speech-in-noise test and a digits-in-noise test. Measures were taken at baseline, week 2, and week 6 after fitting. After the 2-week field trial, the self-fitting arm had an initial advantage on the self-reported APHAB: difference, Cohen d = −.5 (95% confidence interval [CI], −1.0 to 0). It also fared better on the IOI-HA: effect size, r = 0.3 (95% CI, .0 to –.5), but not on speech recognition in noise.
One member of the self-fitting arm withdrew owing to an unrelated middle-ear infection.
“While these results are promising, it is essential to note that OTC hearing aids are not a one-size-fits-all approach,” Dr. De Sousa said. “If a person has ear disease symptoms or hearing loss that is too severe, they have to consult a trained hearing health care professional.” She added that proper use of a self-fitted OTC hearing aid requires a degree of digital proficiency, as many devices are set up using a smartphone.
This study was supported by the National Institutes of Health and by the hearX Group, which provided the Lexie Lumen devices and software support for data collection. Dr. De Sousa reported nonfinancial support from hearX as well as consulting fees from hearX outside of the submitted work. A coauthor reported grant support from the UK’s National Institute for Health and Care Research Manchester Biomedical Research Centre, and fees from hearX during and outside of the study. Another coauthor disclosed fees, equity, and grant support from hearX during the conduct of the study.
Self-fitted over-the-counter (OTC) hearing aids may be an effective option for individuals with mild to moderate hearing loss, a small randomized effectiveness trial reports. OTC devices yielded 6-week patient-perceived and clinical outcomes comparable to those with audiologist-fitted hearing aids, In fact, at week 2, the self-fitted group had a small but meaningful advantage on two of the four study outcome measures.
“After support and fine-tuning were provided to the self-fitting (remote support) and audiologist-fitted groups, no clinically meaningful differences were evident in any outcome measures at the end of the 6-week trial,” wrote researchers led by Karina C. De Sousa, PhD, a postdoctoral researcher in the department of speech-language pathology and audiology at the University of Pretoria, South Africa.
Their findings appear in JAMA Otolaryngology–Head & Neck Surgery.
Hearing aid uptake is low even in populations with adequate access to audiological resources, the authors noted, with hearing aid use in U.S. adults who could benefit estimated at about 20%. Currently, an estimated 22.9 million older Americans with audiometric hearing loss do not use hearing aids.
Major barriers have been access and affordability, Dr. De Sousa and associates wrote, and until recently, people with hearing loss could obtain hearing aids only after consultation with a credentialed dispenser. “The World Health Organization estimates that over 2.5 billion people will experience some degree of hearing loss by 2050,” Dr. De Sousa said in an interview. “This new category of self-fitting hearing aids opens up newer care pathways for people with mild to moderate hearing loss.”
The study
From April to August 2022 the trial recruited 68 participants (51.6% men) with mild-to-moderate self-reported hearing loss, a mean age of 63.6 years, and no ear disease within the past 90 days. They were randomized to a self-fitted commercially available device (Lexi Lumen), with instructional material on set-up and remote support, or to the same unit fitted by an audiologist. The majority in both arms were new users and were similar in age and baseline hearing scores.
The primary outcome measure was patient-reported hearing aid benefit, measured by the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire. This scale evaluates auditory acuity before and after amplification by such criteria as ease of communication, background noise, reverberation, aversiveness, and global hearing status.
Secondary measures included the International Outcome Inventory for Hearing Aids (IOI-HA) and speech recognition in noise measured using an abbreviated speech-in-noise test and a digits-in-noise test. Measures were taken at baseline, week 2, and week 6 after fitting. After the 2-week field trial, the self-fitting arm had an initial advantage on the self-reported APHAB: difference, Cohen d = −.5 (95% confidence interval [CI], −1.0 to 0). It also fared better on the IOI-HA: effect size, r = 0.3 (95% CI, .0 to –.5), but not on speech recognition in noise.
One member of the self-fitting arm withdrew owing to an unrelated middle-ear infection.
“While these results are promising, it is essential to note that OTC hearing aids are not a one-size-fits-all approach,” Dr. De Sousa said. “If a person has ear disease symptoms or hearing loss that is too severe, they have to consult a trained hearing health care professional.” She added that proper use of a self-fitted OTC hearing aid requires a degree of digital proficiency, as many devices are set up using a smartphone.
This study was supported by the National Institutes of Health and by the hearX Group, which provided the Lexie Lumen devices and software support for data collection. Dr. De Sousa reported nonfinancial support from hearX as well as consulting fees from hearX outside of the submitted work. A coauthor reported grant support from the UK’s National Institute for Health and Care Research Manchester Biomedical Research Centre, and fees from hearX during and outside of the study. Another coauthor disclosed fees, equity, and grant support from hearX during the conduct of the study.
Self-fitted over-the-counter (OTC) hearing aids may be an effective option for individuals with mild to moderate hearing loss, a small randomized effectiveness trial reports. OTC devices yielded 6-week patient-perceived and clinical outcomes comparable to those with audiologist-fitted hearing aids, In fact, at week 2, the self-fitted group had a small but meaningful advantage on two of the four study outcome measures.
“After support and fine-tuning were provided to the self-fitting (remote support) and audiologist-fitted groups, no clinically meaningful differences were evident in any outcome measures at the end of the 6-week trial,” wrote researchers led by Karina C. De Sousa, PhD, a postdoctoral researcher in the department of speech-language pathology and audiology at the University of Pretoria, South Africa.
Their findings appear in JAMA Otolaryngology–Head & Neck Surgery.
Hearing aid uptake is low even in populations with adequate access to audiological resources, the authors noted, with hearing aid use in U.S. adults who could benefit estimated at about 20%. Currently, an estimated 22.9 million older Americans with audiometric hearing loss do not use hearing aids.
Major barriers have been access and affordability, Dr. De Sousa and associates wrote, and until recently, people with hearing loss could obtain hearing aids only after consultation with a credentialed dispenser. “The World Health Organization estimates that over 2.5 billion people will experience some degree of hearing loss by 2050,” Dr. De Sousa said in an interview. “This new category of self-fitting hearing aids opens up newer care pathways for people with mild to moderate hearing loss.”
The study
From April to August 2022 the trial recruited 68 participants (51.6% men) with mild-to-moderate self-reported hearing loss, a mean age of 63.6 years, and no ear disease within the past 90 days. They were randomized to a self-fitted commercially available device (Lexi Lumen), with instructional material on set-up and remote support, or to the same unit fitted by an audiologist. The majority in both arms were new users and were similar in age and baseline hearing scores.
The primary outcome measure was patient-reported hearing aid benefit, measured by the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire. This scale evaluates auditory acuity before and after amplification by such criteria as ease of communication, background noise, reverberation, aversiveness, and global hearing status.
Secondary measures included the International Outcome Inventory for Hearing Aids (IOI-HA) and speech recognition in noise measured using an abbreviated speech-in-noise test and a digits-in-noise test. Measures were taken at baseline, week 2, and week 6 after fitting. After the 2-week field trial, the self-fitting arm had an initial advantage on the self-reported APHAB: difference, Cohen d = −.5 (95% confidence interval [CI], −1.0 to 0). It also fared better on the IOI-HA: effect size, r = 0.3 (95% CI, .0 to –.5), but not on speech recognition in noise.
One member of the self-fitting arm withdrew owing to an unrelated middle-ear infection.
“While these results are promising, it is essential to note that OTC hearing aids are not a one-size-fits-all approach,” Dr. De Sousa said. “If a person has ear disease symptoms or hearing loss that is too severe, they have to consult a trained hearing health care professional.” She added that proper use of a self-fitted OTC hearing aid requires a degree of digital proficiency, as many devices are set up using a smartphone.
This study was supported by the National Institutes of Health and by the hearX Group, which provided the Lexie Lumen devices and software support for data collection. Dr. De Sousa reported nonfinancial support from hearX as well as consulting fees from hearX outside of the submitted work. A coauthor reported grant support from the UK’s National Institute for Health and Care Research Manchester Biomedical Research Centre, and fees from hearX during and outside of the study. Another coauthor disclosed fees, equity, and grant support from hearX during the conduct of the study.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY
New COVID variant on WHO’s radar causing itchy eyes in children
A new COVID-19 variant that recently landed on the World Health Organization’s radar may cause previously unseen symptoms in children, according to a new report.
While the variant, called “Arcturus,” hasn’t yet made the Centers for Disease Control and Prevention’s watchlist, , according to The Times of India.
The new itchy eye symptom is in addition to a high fever and cough, Vipin M. Vashishtha, MD, said on Twitter, noting that pediatric COVID cases have picked up there for the first time in 6 months.
The country has also seen a rise in adenovirus cases among children with similar symptoms. COVID and adenovirus cannot be distinguished without testing, and many parents don’t want to have their children tested because the swabs are uncomfortable, The Times of India reported. One doctor told the newspaper that among every 10 children with COVID-like symptoms, 2 or 3 of them had tested positive on a COVID test taken at home.
Health officials in India are doing mock drills to check how prepared the country’s hospitals are as India sees cases rise, the BBC reported. India struggled during a COVID-19 surge in 2021, at which time sickened people were seen lying on sidewalks outside overflowing hospitals, and reports surfaced of a black market for private citizens to buy oxygen.
Arcturus (formally, Omicron subvariant XBB.1.16) made news recently as it landed on the WHO’s radar after surfacing in India. A WHO official called it “one to watch.” The Times of India reported that 234 new cases of XBB.1.16 were included in the country’s latest 5,676 new infections, meaning the subvariant accounts for 4% of new COVID cases.
A version of this article originally appeared on WebMD.com.
A new COVID-19 variant that recently landed on the World Health Organization’s radar may cause previously unseen symptoms in children, according to a new report.
While the variant, called “Arcturus,” hasn’t yet made the Centers for Disease Control and Prevention’s watchlist, , according to The Times of India.
The new itchy eye symptom is in addition to a high fever and cough, Vipin M. Vashishtha, MD, said on Twitter, noting that pediatric COVID cases have picked up there for the first time in 6 months.
The country has also seen a rise in adenovirus cases among children with similar symptoms. COVID and adenovirus cannot be distinguished without testing, and many parents don’t want to have their children tested because the swabs are uncomfortable, The Times of India reported. One doctor told the newspaper that among every 10 children with COVID-like symptoms, 2 or 3 of them had tested positive on a COVID test taken at home.
Health officials in India are doing mock drills to check how prepared the country’s hospitals are as India sees cases rise, the BBC reported. India struggled during a COVID-19 surge in 2021, at which time sickened people were seen lying on sidewalks outside overflowing hospitals, and reports surfaced of a black market for private citizens to buy oxygen.
Arcturus (formally, Omicron subvariant XBB.1.16) made news recently as it landed on the WHO’s radar after surfacing in India. A WHO official called it “one to watch.” The Times of India reported that 234 new cases of XBB.1.16 were included in the country’s latest 5,676 new infections, meaning the subvariant accounts for 4% of new COVID cases.
A version of this article originally appeared on WebMD.com.
A new COVID-19 variant that recently landed on the World Health Organization’s radar may cause previously unseen symptoms in children, according to a new report.
While the variant, called “Arcturus,” hasn’t yet made the Centers for Disease Control and Prevention’s watchlist, , according to The Times of India.
The new itchy eye symptom is in addition to a high fever and cough, Vipin M. Vashishtha, MD, said on Twitter, noting that pediatric COVID cases have picked up there for the first time in 6 months.
The country has also seen a rise in adenovirus cases among children with similar symptoms. COVID and adenovirus cannot be distinguished without testing, and many parents don’t want to have their children tested because the swabs are uncomfortable, The Times of India reported. One doctor told the newspaper that among every 10 children with COVID-like symptoms, 2 or 3 of them had tested positive on a COVID test taken at home.
Health officials in India are doing mock drills to check how prepared the country’s hospitals are as India sees cases rise, the BBC reported. India struggled during a COVID-19 surge in 2021, at which time sickened people were seen lying on sidewalks outside overflowing hospitals, and reports surfaced of a black market for private citizens to buy oxygen.
Arcturus (formally, Omicron subvariant XBB.1.16) made news recently as it landed on the WHO’s radar after surfacing in India. A WHO official called it “one to watch.” The Times of India reported that 234 new cases of XBB.1.16 were included in the country’s latest 5,676 new infections, meaning the subvariant accounts for 4% of new COVID cases.
A version of this article originally appeared on WebMD.com.
Previously unknown viral families hide in the darnedest places
You and me and baby makes 10,003
If you were a virus hunter, looking for your next big virus discovery, where would you go? The wholesale seafood market in Wuhan? A gathering of unmasked anti-vaxxers in the heartland of America? The frozen snot fields of northwest Siberia?

How about babies? Well, it’s too late now, because that’s what Dennis Sandris Nielsen, PhD, of the University of Copenhagen, and his associates did, and they hit the mother lode. Actually, it was more like the infant load, if we’re being honest here.
“We found an exceptional number of unknown viruses in the faeces of these babies,” Dr. Nielsen said in a written statement from the university. (The study was published in Nature Microbiology, so we get the English spelling of feces.)
The investigators mapped the gut “viromes” of 647 healthy Danish 1-year-old children over the course of 5 years and found 10,000 species of viruses distributed across 248 different viral families, of which only 16 were already known. Incredible stuff, but then things took a turn for the cute. “The researchers named the remaining 232 unknown viral families after the children whose diapers made the study possible. As a result, new viral families include names like Sylvesterviridae, Rigmorviridae and Tristanviridae,” the university said.
About 90% of the viruses found in the feces are bacterial viruses, aka bacteriophages, which have bacteria as their hosts and don’t attack the children’s cells, so they don’t cause disease. The other 10%, however, are eukaryotic: They use human cells as hosts, so they can be either friend or foe. “It is thought-provoking that all children run around with 10-20 of these virus types that infect human cells. So, there is a constant viral infection taking place, which apparently doesn’t make them sick,” Dr. Nielsen said.
Doesn’t make them sick? Riiiight. The thought that this gives rise to now? People love babies. Everyone wants to pick up the baby. Now we know why. Because the viruses want us to! Well, those cute little faces aren’t fooling us anymore. No more babies for us. Everyone should stay away from babies and their evil little eukaryotic viruses. STOP THE BABIES!
[Editor’s note: After a short timeout, we explained to the staff that the human species actually needs babies for its survival. They calmed down, picked up their crayons, and quietly went back to work.]
Fooled them. Stop the babies!
At least someone out there appreciates hospital food
Life in Alaska is not for the meek. It’s dark half the year. Summer is 3 weeks in July. And somehow, there’s a moose in line ahead of you at the doctor’s office. To make matters worse, it’s arguing about insurance. “What do you mean, you’ve heard the Moo Cross Moo Shield joke before?”

One might expect that Providence Alaska Health Park, located near downtown Anchorage, the largest city in Alaska by a massive margin, might be safe from ungulate invasion. Nope. In recent days, a young moose has taken to hanging around Providence campus, and it just could not find anything to eat. Remember, it may be early April, but this is Alaska. It’s still winter there. The ground’s still covered in snow.
Eventually, the gears in our young moose friend’s mind turned and it settled on a course of action: “Hey, those are some nice-looking plants behind that door over there. …” And that’s how Providence Alaska Health ended up with a moose munching on decorative potted plants in the hospital lobby.
Funnily enough, the moose didn’t even make a big scene. It just walked through the automatic doors and started chowing down. Security only found out because a tenant called them. Naturally though, once security made the announcement that a massive wild animal had been spotted in the building, the lobby was evacuated. … What do you mean, half the hospital came around to see it? Apparently, even though Alaskans have to fight moose herds on their daily commute, a lot of people wanted to see our moose friend do its thing.
“That’s crazy,” a woman in scrubs said in a video as she snapped a photo with her phone.
“This is the best. Like, what’s the code for this?” asked another bystander.
Despite security’s best efforts to shoo the moose out with barricades and offers of tasty branches, our furry friend left of its own volition, presumably irritated that his breakfast had become a spectator sport. But it didn’t go far. It hung around the front drive for a while, then went around the back of the building for a nap. What has four hooves and still doesn’t give a crap? Bob Moose-o! How you doing?
That click sounded stressed
How can people tell that you’re stressed? Maybe you get irritable and a little snappy. Some people have an inability to concentrate or focus. Eating that muffin when you weren’t really hungry could be a sign you’re not relaxed.

Did you know that your computer can be an indicator of your stress levels?
We tend to be working when we’re using computers, right? That can be a stressor in itself. Well, some researchers at ETH Zürich decided to have a look at the situation. Surprisingly, at least to us, one in three Swiss employees experience workplace stress, which makes us wonder what the percentage is in this country.
The Swiss researchers developed a model that tells how stressed someone is just by the way they use their computer mouse or type. The results of their study showed that those who were stressed clicked and tapped differently than participants who were more relaxed.
Stressed people click “more often and less precisely and cover longer distances on the screen,” while the relaxed take “shorter, more direct routes to reach their destination and take more time doing so,” study author Mara Nägelin explained in a written statement from ETH (Eidgenössische Technische Hochschule, or Swiss Federal Institute of Technology) Zürich.
Ever find when you’re frustrated and in a rush you end up making more mistakes? Same deal. Coauthor Jasmine Kerr noted that “increased levels of stress negatively impact our brain’s ability to process information.” Which totally is going to affect how we move.
Hopefully, these results can give insight to companies on how stressed their employees are and the effect it has on their work performance, eventually leading to, guess what, more research on how to alleviate workplace stress in general, which can benefit us all.
So if you find yourself in the office working on your computer like it’s a game of Perfection and time is running out, take a beat. Maybe try a stress-relieving breathing technique. Nonstressed people, according to the study, take fewer and longer pauses on their computers. Perfection on the job may mean relaxing first.
You and me and baby makes 10,003
If you were a virus hunter, looking for your next big virus discovery, where would you go? The wholesale seafood market in Wuhan? A gathering of unmasked anti-vaxxers in the heartland of America? The frozen snot fields of northwest Siberia?
How about babies? Well, it’s too late now, because that’s what Dennis Sandris Nielsen, PhD, of the University of Copenhagen, and his associates did, and they hit the mother lode. Actually, it was more like the infant load, if we’re being honest here.
“We found an exceptional number of unknown viruses in the faeces of these babies,” Dr. Nielsen said in a written statement from the university. (The study was published in Nature Microbiology, so we get the English spelling of feces.)
The investigators mapped the gut “viromes” of 647 healthy Danish 1-year-old children over the course of 5 years and found 10,000 species of viruses distributed across 248 different viral families, of which only 16 were already known. Incredible stuff, but then things took a turn for the cute. “The researchers named the remaining 232 unknown viral families after the children whose diapers made the study possible. As a result, new viral families include names like Sylvesterviridae, Rigmorviridae and Tristanviridae,” the university said.
About 90% of the viruses found in the feces are bacterial viruses, aka bacteriophages, which have bacteria as their hosts and don’t attack the children’s cells, so they don’t cause disease. The other 10%, however, are eukaryotic: They use human cells as hosts, so they can be either friend or foe. “It is thought-provoking that all children run around with 10-20 of these virus types that infect human cells. So, there is a constant viral infection taking place, which apparently doesn’t make them sick,” Dr. Nielsen said.
Doesn’t make them sick? Riiiight. The thought that this gives rise to now? People love babies. Everyone wants to pick up the baby. Now we know why. Because the viruses want us to! Well, those cute little faces aren’t fooling us anymore. No more babies for us. Everyone should stay away from babies and their evil little eukaryotic viruses. STOP THE BABIES!
[Editor’s note: After a short timeout, we explained to the staff that the human species actually needs babies for its survival. They calmed down, picked up their crayons, and quietly went back to work.]
Fooled them. Stop the babies!
At least someone out there appreciates hospital food
Life in Alaska is not for the meek. It’s dark half the year. Summer is 3 weeks in July. And somehow, there’s a moose in line ahead of you at the doctor’s office. To make matters worse, it’s arguing about insurance. “What do you mean, you’ve heard the Moo Cross Moo Shield joke before?”
One might expect that Providence Alaska Health Park, located near downtown Anchorage, the largest city in Alaska by a massive margin, might be safe from ungulate invasion. Nope. In recent days, a young moose has taken to hanging around Providence campus, and it just could not find anything to eat. Remember, it may be early April, but this is Alaska. It’s still winter there. The ground’s still covered in snow.
Eventually, the gears in our young moose friend’s mind turned and it settled on a course of action: “Hey, those are some nice-looking plants behind that door over there. …” And that’s how Providence Alaska Health ended up with a moose munching on decorative potted plants in the hospital lobby.
Funnily enough, the moose didn’t even make a big scene. It just walked through the automatic doors and started chowing down. Security only found out because a tenant called them. Naturally though, once security made the announcement that a massive wild animal had been spotted in the building, the lobby was evacuated. … What do you mean, half the hospital came around to see it? Apparently, even though Alaskans have to fight moose herds on their daily commute, a lot of people wanted to see our moose friend do its thing.
“That’s crazy,” a woman in scrubs said in a video as she snapped a photo with her phone.
“This is the best. Like, what’s the code for this?” asked another bystander.
Despite security’s best efforts to shoo the moose out with barricades and offers of tasty branches, our furry friend left of its own volition, presumably irritated that his breakfast had become a spectator sport. But it didn’t go far. It hung around the front drive for a while, then went around the back of the building for a nap. What has four hooves and still doesn’t give a crap? Bob Moose-o! How you doing?
That click sounded stressed
How can people tell that you’re stressed? Maybe you get irritable and a little snappy. Some people have an inability to concentrate or focus. Eating that muffin when you weren’t really hungry could be a sign you’re not relaxed.
Did you know that your computer can be an indicator of your stress levels?
We tend to be working when we’re using computers, right? That can be a stressor in itself. Well, some researchers at ETH Zürich decided to have a look at the situation. Surprisingly, at least to us, one in three Swiss employees experience workplace stress, which makes us wonder what the percentage is in this country.
The Swiss researchers developed a model that tells how stressed someone is just by the way they use their computer mouse or type. The results of their study showed that those who were stressed clicked and tapped differently than participants who were more relaxed.
Stressed people click “more often and less precisely and cover longer distances on the screen,” while the relaxed take “shorter, more direct routes to reach their destination and take more time doing so,” study author Mara Nägelin explained in a written statement from ETH (Eidgenössische Technische Hochschule, or Swiss Federal Institute of Technology) Zürich.
Ever find when you’re frustrated and in a rush you end up making more mistakes? Same deal. Coauthor Jasmine Kerr noted that “increased levels of stress negatively impact our brain’s ability to process information.” Which totally is going to affect how we move.
Hopefully, these results can give insight to companies on how stressed their employees are and the effect it has on their work performance, eventually leading to, guess what, more research on how to alleviate workplace stress in general, which can benefit us all.
So if you find yourself in the office working on your computer like it’s a game of Perfection and time is running out, take a beat. Maybe try a stress-relieving breathing technique. Nonstressed people, according to the study, take fewer and longer pauses on their computers. Perfection on the job may mean relaxing first.
You and me and baby makes 10,003
If you were a virus hunter, looking for your next big virus discovery, where would you go? The wholesale seafood market in Wuhan? A gathering of unmasked anti-vaxxers in the heartland of America? The frozen snot fields of northwest Siberia?
How about babies? Well, it’s too late now, because that’s what Dennis Sandris Nielsen, PhD, of the University of Copenhagen, and his associates did, and they hit the mother lode. Actually, it was more like the infant load, if we’re being honest here.
“We found an exceptional number of unknown viruses in the faeces of these babies,” Dr. Nielsen said in a written statement from the university. (The study was published in Nature Microbiology, so we get the English spelling of feces.)
The investigators mapped the gut “viromes” of 647 healthy Danish 1-year-old children over the course of 5 years and found 10,000 species of viruses distributed across 248 different viral families, of which only 16 were already known. Incredible stuff, but then things took a turn for the cute. “The researchers named the remaining 232 unknown viral families after the children whose diapers made the study possible. As a result, new viral families include names like Sylvesterviridae, Rigmorviridae and Tristanviridae,” the university said.
About 90% of the viruses found in the feces are bacterial viruses, aka bacteriophages, which have bacteria as their hosts and don’t attack the children’s cells, so they don’t cause disease. The other 10%, however, are eukaryotic: They use human cells as hosts, so they can be either friend or foe. “It is thought-provoking that all children run around with 10-20 of these virus types that infect human cells. So, there is a constant viral infection taking place, which apparently doesn’t make them sick,” Dr. Nielsen said.
Doesn’t make them sick? Riiiight. The thought that this gives rise to now? People love babies. Everyone wants to pick up the baby. Now we know why. Because the viruses want us to! Well, those cute little faces aren’t fooling us anymore. No more babies for us. Everyone should stay away from babies and their evil little eukaryotic viruses. STOP THE BABIES!
[Editor’s note: After a short timeout, we explained to the staff that the human species actually needs babies for its survival. They calmed down, picked up their crayons, and quietly went back to work.]
Fooled them. Stop the babies!
At least someone out there appreciates hospital food
Life in Alaska is not for the meek. It’s dark half the year. Summer is 3 weeks in July. And somehow, there’s a moose in line ahead of you at the doctor’s office. To make matters worse, it’s arguing about insurance. “What do you mean, you’ve heard the Moo Cross Moo Shield joke before?”
One might expect that Providence Alaska Health Park, located near downtown Anchorage, the largest city in Alaska by a massive margin, might be safe from ungulate invasion. Nope. In recent days, a young moose has taken to hanging around Providence campus, and it just could not find anything to eat. Remember, it may be early April, but this is Alaska. It’s still winter there. The ground’s still covered in snow.
Eventually, the gears in our young moose friend’s mind turned and it settled on a course of action: “Hey, those are some nice-looking plants behind that door over there. …” And that’s how Providence Alaska Health ended up with a moose munching on decorative potted plants in the hospital lobby.
Funnily enough, the moose didn’t even make a big scene. It just walked through the automatic doors and started chowing down. Security only found out because a tenant called them. Naturally though, once security made the announcement that a massive wild animal had been spotted in the building, the lobby was evacuated. … What do you mean, half the hospital came around to see it? Apparently, even though Alaskans have to fight moose herds on their daily commute, a lot of people wanted to see our moose friend do its thing.
“That’s crazy,” a woman in scrubs said in a video as she snapped a photo with her phone.
“This is the best. Like, what’s the code for this?” asked another bystander.
Despite security’s best efforts to shoo the moose out with barricades and offers of tasty branches, our furry friend left of its own volition, presumably irritated that his breakfast had become a spectator sport. But it didn’t go far. It hung around the front drive for a while, then went around the back of the building for a nap. What has four hooves and still doesn’t give a crap? Bob Moose-o! How you doing?
That click sounded stressed
How can people tell that you’re stressed? Maybe you get irritable and a little snappy. Some people have an inability to concentrate or focus. Eating that muffin when you weren’t really hungry could be a sign you’re not relaxed.
Did you know that your computer can be an indicator of your stress levels?
We tend to be working when we’re using computers, right? That can be a stressor in itself. Well, some researchers at ETH Zürich decided to have a look at the situation. Surprisingly, at least to us, one in three Swiss employees experience workplace stress, which makes us wonder what the percentage is in this country.
The Swiss researchers developed a model that tells how stressed someone is just by the way they use their computer mouse or type. The results of their study showed that those who were stressed clicked and tapped differently than participants who were more relaxed.
Stressed people click “more often and less precisely and cover longer distances on the screen,” while the relaxed take “shorter, more direct routes to reach their destination and take more time doing so,” study author Mara Nägelin explained in a written statement from ETH (Eidgenössische Technische Hochschule, or Swiss Federal Institute of Technology) Zürich.
Ever find when you’re frustrated and in a rush you end up making more mistakes? Same deal. Coauthor Jasmine Kerr noted that “increased levels of stress negatively impact our brain’s ability to process information.” Which totally is going to affect how we move.
Hopefully, these results can give insight to companies on how stressed their employees are and the effect it has on their work performance, eventually leading to, guess what, more research on how to alleviate workplace stress in general, which can benefit us all.
So if you find yourself in the office working on your computer like it’s a game of Perfection and time is running out, take a beat. Maybe try a stress-relieving breathing technique. Nonstressed people, according to the study, take fewer and longer pauses on their computers. Perfection on the job may mean relaxing first.
Adherence to oral contraceptive protocols prevents pregnancy
Combined oral contraceptives (COCs) remain a popular method of pregnancy prevention worldwide, but efficacy and failure rates can be difficult to determine, as real-word use does not always mirror clinical trials, wrote Mitchell D. Creinin, MD, of the University of California, Davis, and colleagues. Clinical trials include perfect use or method-failure rates, but data on pregnancy risk based on reported adherence alone are lacking, they said.
To assess the effects of missed pills on COC efficacy, the researchers reviewed data from a pair of parallel phase 3 trials, focusing only on adherence to the pill dosing regimen. The findings were published in Obstetrics & Gynecology.
The study population included 1,864 individuals from the United States and Canada, and 1,553 from Europe and Russia.
The participants were healthy, sexually active adults aged 16-50 years in monogamous relationships from 2016 through 2018 who agreed to used estetrol 15 mg and drospirenone 3 mg for up to 13 28-day cycles as their only contraceptive method. Condom use was permitted for protection against sexually transmitted infections if needed. The 28-day COCs included 24 hormonal tablets and 4 placebo tablets. Participants received written instructions for what to do it they missed pills.
The primary outcome was the relationship between missed pills and pregnancies.
A total of 31 pregnancies occurred across both studies; none of these occurred during cycles in which other contraception was used. Of 22 pregnancies in participants who reported taking all pills, 21 reported daily pill use during the cycle in which pregnancy occurred. One participant reported not taking one pill and one participant reported not taking two pills; neither correctly followed the instructions for missed pills.
Pregnancies occurred in .09% of cycles in which participants reported taking all pills, and in 0.25%, 0.83%, and 1.6% of cycles in which participants reported missing one pill, two pills, or more than two pills, respectively.
“Pregnancy rates exceeded 1% only in participants who did not correctly follow missed-pill instructions,” the researchers noted.
Pregnancy rates per cycle ranged from 0% to 0.21%, and 48.4% of the pregnancies occurred during the first four cycles of COC use. Approximately one-third (32.3%) of pregnancies occurred within the first week of a new pill pack.
“Fertilization does not appear to be related to the timing of missed pills within the cycle because pregnancy did not occur more frequently earlier in the cycle (after the placebo pills),” the researchers wrote in their discussion. This finding contradicts previous research suggesting that contraceptive failure rates decrease over the first year of use, they said. In addition, the formulation of the pill used may affect pregnancy rates when pills are missed, as some hormones have longer half-lives, they noted.
The study findings were limited by several factors, including the lack of adjustment for outcomes based on reported sexual activity per cycle, and by the reliance on self-reports.
However, the results were strengthened by the use of the clinical outcomes of pregnancy as the primary outcome, rather than characteristics and predictors of participants who missed pills, the researchers said.
The cycle-based methodology used in the current study may provide insight on the relationship between COC adherence and pregnancy risk that can inform future studies, they concluded.
Findings highlight the importance of options
“With increasing restrictions on abortion care, offering more contraceptive options for people is critical,” Lauren Owens, MD, associate professor of obstetrics and gynecology at the University of Washington, Seattle, said in an interview. “That’s not to say that having another pill option makes up for the harm people are experiencing as they navigate abortion bans and legal interference in their health care, but no one pill works for all people, and having more options is helpful,” she said.
Dr. Owens noted that the rates of pregnancy in the current study were lower than she traditionally associates with COCs, “although I usually discuss annual failure rates with patients, not failure rates per cycle, and the latter will clearly be lower.” In the current study, “The authors hypothesize some of this may be due to the longer half-life that estetrol has compared to ethinyl estradiol, the estrogen form more commonly found in oral contraceptive pills,” she said.
From a clinical standpoint, “I appreciated the linkage between number of missed pills and pregnancies occurring,” Dr. Owens said. “This is a good reminder to clinicians to talk to patients ahead of time about what to do when missed pills occur and to provide resources in advance that patients can reference when needed,” she said.
“The authors published other studies on this pill in the last year and it seems to work well and have a reasonable safety profile,” Dr. Owens told this news organization. However, “We still need to broaden the methods available to patients, particularly methods that people producing sperm can use. In the face of ongoing and escalating attacks on access to contraceptive care and abortion care, it’s more important than ever to do what we can to improve options for patients,” she said.
The study was supported by Estetra SRL, an affiliate company of Mithra Pharmaceuticals. Dr. Creinin disclosed relationships with multiple companies including Gedeon Richter, Mayne, and Organon. He disclosed serving on the advisory boards for Evofem, Fuji Pharma, Gedeon Richter, GlaxoSmithKline, Mayne, Merck, OLIC, Organon, and Searchlight, and serving as a consultant for Estetra SRL (including the current study), Libbs, Mayne, and Medicines360; his university department receives contraceptive research funding from Chemo Research SL, Evofem, HRA Pharma, Medicines360, Merck, and Sebela. Dr. Owens had no relevant financial conflicts to disclose.
Combined oral contraceptives (COCs) remain a popular method of pregnancy prevention worldwide, but efficacy and failure rates can be difficult to determine, as real-word use does not always mirror clinical trials, wrote Mitchell D. Creinin, MD, of the University of California, Davis, and colleagues. Clinical trials include perfect use or method-failure rates, but data on pregnancy risk based on reported adherence alone are lacking, they said.
To assess the effects of missed pills on COC efficacy, the researchers reviewed data from a pair of parallel phase 3 trials, focusing only on adherence to the pill dosing regimen. The findings were published in Obstetrics & Gynecology.
The study population included 1,864 individuals from the United States and Canada, and 1,553 from Europe and Russia.
The participants were healthy, sexually active adults aged 16-50 years in monogamous relationships from 2016 through 2018 who agreed to used estetrol 15 mg and drospirenone 3 mg for up to 13 28-day cycles as their only contraceptive method. Condom use was permitted for protection against sexually transmitted infections if needed. The 28-day COCs included 24 hormonal tablets and 4 placebo tablets. Participants received written instructions for what to do it they missed pills.
The primary outcome was the relationship between missed pills and pregnancies.
A total of 31 pregnancies occurred across both studies; none of these occurred during cycles in which other contraception was used. Of 22 pregnancies in participants who reported taking all pills, 21 reported daily pill use during the cycle in which pregnancy occurred. One participant reported not taking one pill and one participant reported not taking two pills; neither correctly followed the instructions for missed pills.
Pregnancies occurred in .09% of cycles in which participants reported taking all pills, and in 0.25%, 0.83%, and 1.6% of cycles in which participants reported missing one pill, two pills, or more than two pills, respectively.
“Pregnancy rates exceeded 1% only in participants who did not correctly follow missed-pill instructions,” the researchers noted.
Pregnancy rates per cycle ranged from 0% to 0.21%, and 48.4% of the pregnancies occurred during the first four cycles of COC use. Approximately one-third (32.3%) of pregnancies occurred within the first week of a new pill pack.
“Fertilization does not appear to be related to the timing of missed pills within the cycle because pregnancy did not occur more frequently earlier in the cycle (after the placebo pills),” the researchers wrote in their discussion. This finding contradicts previous research suggesting that contraceptive failure rates decrease over the first year of use, they said. In addition, the formulation of the pill used may affect pregnancy rates when pills are missed, as some hormones have longer half-lives, they noted.
The study findings were limited by several factors, including the lack of adjustment for outcomes based on reported sexual activity per cycle, and by the reliance on self-reports.
However, the results were strengthened by the use of the clinical outcomes of pregnancy as the primary outcome, rather than characteristics and predictors of participants who missed pills, the researchers said.
The cycle-based methodology used in the current study may provide insight on the relationship between COC adherence and pregnancy risk that can inform future studies, they concluded.
Findings highlight the importance of options
“With increasing restrictions on abortion care, offering more contraceptive options for people is critical,” Lauren Owens, MD, associate professor of obstetrics and gynecology at the University of Washington, Seattle, said in an interview. “That’s not to say that having another pill option makes up for the harm people are experiencing as they navigate abortion bans and legal interference in their health care, but no one pill works for all people, and having more options is helpful,” she said.
Dr. Owens noted that the rates of pregnancy in the current study were lower than she traditionally associates with COCs, “although I usually discuss annual failure rates with patients, not failure rates per cycle, and the latter will clearly be lower.” In the current study, “The authors hypothesize some of this may be due to the longer half-life that estetrol has compared to ethinyl estradiol, the estrogen form more commonly found in oral contraceptive pills,” she said.
From a clinical standpoint, “I appreciated the linkage between number of missed pills and pregnancies occurring,” Dr. Owens said. “This is a good reminder to clinicians to talk to patients ahead of time about what to do when missed pills occur and to provide resources in advance that patients can reference when needed,” she said.
“The authors published other studies on this pill in the last year and it seems to work well and have a reasonable safety profile,” Dr. Owens told this news organization. However, “We still need to broaden the methods available to patients, particularly methods that people producing sperm can use. In the face of ongoing and escalating attacks on access to contraceptive care and abortion care, it’s more important than ever to do what we can to improve options for patients,” she said.
The study was supported by Estetra SRL, an affiliate company of Mithra Pharmaceuticals. Dr. Creinin disclosed relationships with multiple companies including Gedeon Richter, Mayne, and Organon. He disclosed serving on the advisory boards for Evofem, Fuji Pharma, Gedeon Richter, GlaxoSmithKline, Mayne, Merck, OLIC, Organon, and Searchlight, and serving as a consultant for Estetra SRL (including the current study), Libbs, Mayne, and Medicines360; his university department receives contraceptive research funding from Chemo Research SL, Evofem, HRA Pharma, Medicines360, Merck, and Sebela. Dr. Owens had no relevant financial conflicts to disclose.
Combined oral contraceptives (COCs) remain a popular method of pregnancy prevention worldwide, but efficacy and failure rates can be difficult to determine, as real-word use does not always mirror clinical trials, wrote Mitchell D. Creinin, MD, of the University of California, Davis, and colleagues. Clinical trials include perfect use or method-failure rates, but data on pregnancy risk based on reported adherence alone are lacking, they said.
To assess the effects of missed pills on COC efficacy, the researchers reviewed data from a pair of parallel phase 3 trials, focusing only on adherence to the pill dosing regimen. The findings were published in Obstetrics & Gynecology.
The study population included 1,864 individuals from the United States and Canada, and 1,553 from Europe and Russia.
The participants were healthy, sexually active adults aged 16-50 years in monogamous relationships from 2016 through 2018 who agreed to used estetrol 15 mg and drospirenone 3 mg for up to 13 28-day cycles as their only contraceptive method. Condom use was permitted for protection against sexually transmitted infections if needed. The 28-day COCs included 24 hormonal tablets and 4 placebo tablets. Participants received written instructions for what to do it they missed pills.
The primary outcome was the relationship between missed pills and pregnancies.
A total of 31 pregnancies occurred across both studies; none of these occurred during cycles in which other contraception was used. Of 22 pregnancies in participants who reported taking all pills, 21 reported daily pill use during the cycle in which pregnancy occurred. One participant reported not taking one pill and one participant reported not taking two pills; neither correctly followed the instructions for missed pills.
Pregnancies occurred in .09% of cycles in which participants reported taking all pills, and in 0.25%, 0.83%, and 1.6% of cycles in which participants reported missing one pill, two pills, or more than two pills, respectively.
“Pregnancy rates exceeded 1% only in participants who did not correctly follow missed-pill instructions,” the researchers noted.
Pregnancy rates per cycle ranged from 0% to 0.21%, and 48.4% of the pregnancies occurred during the first four cycles of COC use. Approximately one-third (32.3%) of pregnancies occurred within the first week of a new pill pack.
“Fertilization does not appear to be related to the timing of missed pills within the cycle because pregnancy did not occur more frequently earlier in the cycle (after the placebo pills),” the researchers wrote in their discussion. This finding contradicts previous research suggesting that contraceptive failure rates decrease over the first year of use, they said. In addition, the formulation of the pill used may affect pregnancy rates when pills are missed, as some hormones have longer half-lives, they noted.
The study findings were limited by several factors, including the lack of adjustment for outcomes based on reported sexual activity per cycle, and by the reliance on self-reports.
However, the results were strengthened by the use of the clinical outcomes of pregnancy as the primary outcome, rather than characteristics and predictors of participants who missed pills, the researchers said.
The cycle-based methodology used in the current study may provide insight on the relationship between COC adherence and pregnancy risk that can inform future studies, they concluded.
Findings highlight the importance of options
“With increasing restrictions on abortion care, offering more contraceptive options for people is critical,” Lauren Owens, MD, associate professor of obstetrics and gynecology at the University of Washington, Seattle, said in an interview. “That’s not to say that having another pill option makes up for the harm people are experiencing as they navigate abortion bans and legal interference in their health care, but no one pill works for all people, and having more options is helpful,” she said.
Dr. Owens noted that the rates of pregnancy in the current study were lower than she traditionally associates with COCs, “although I usually discuss annual failure rates with patients, not failure rates per cycle, and the latter will clearly be lower.” In the current study, “The authors hypothesize some of this may be due to the longer half-life that estetrol has compared to ethinyl estradiol, the estrogen form more commonly found in oral contraceptive pills,” she said.
From a clinical standpoint, “I appreciated the linkage between number of missed pills and pregnancies occurring,” Dr. Owens said. “This is a good reminder to clinicians to talk to patients ahead of time about what to do when missed pills occur and to provide resources in advance that patients can reference when needed,” she said.
“The authors published other studies on this pill in the last year and it seems to work well and have a reasonable safety profile,” Dr. Owens told this news organization. However, “We still need to broaden the methods available to patients, particularly methods that people producing sperm can use. In the face of ongoing and escalating attacks on access to contraceptive care and abortion care, it’s more important than ever to do what we can to improve options for patients,” she said.
The study was supported by Estetra SRL, an affiliate company of Mithra Pharmaceuticals. Dr. Creinin disclosed relationships with multiple companies including Gedeon Richter, Mayne, and Organon. He disclosed serving on the advisory boards for Evofem, Fuji Pharma, Gedeon Richter, GlaxoSmithKline, Mayne, Merck, OLIC, Organon, and Searchlight, and serving as a consultant for Estetra SRL (including the current study), Libbs, Mayne, and Medicines360; his university department receives contraceptive research funding from Chemo Research SL, Evofem, HRA Pharma, Medicines360, Merck, and Sebela. Dr. Owens had no relevant financial conflicts to disclose.
FROM OBSTETRICS & GYNECOLOGY
Price of CLL Rx rises, despite competition
In fact, the opposite has been seen: Both the price and prescribing of ibrutinib have increased markedly from 2014 to 2020, the authors of a new study say. The estimated net spending for a 30-day supply of ibrutinib increased by 46% during that period, despite the entry of several less costly and comparable products into the marketplace.
“Further research is needed to understand why oncologists have not embraced clinically superior options for CLL being sold at prices similar to, if not lower than, ibrutinib,” write the authors, led by Edward Scheffer Cliff, MBBS, MPH, from the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston.
The study was published online (2023 Apr 7. doi: 10.1001/jamanetworkopen.2023.7467) as a research letter in JAMA Network Open.
Ibrutinib is currently indicated for the treatment of mantle cell lymphoma (MCL), chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL), Waldenström’s macroglobulinemia (WM), marginal zone lymphoma (MZL), and chronic graft versus host disease. Among the top-selling drugs in the United States, ibrutinib sales by 2020 accounted for more than $2.8 billion in annual net Medicare spending.
However, since ibrutinib’s launch in 2013, there have been several new drugs approved for use in CLL, the authors note. They include acalabrutinib (Calquence), also a BTK inhibitor but associated with fewer adverse events, and venetoclax (Venclexta), the first-in-class B-cell lymphoma-2 inhibitor that offers additional clinical advantages such as time-limited therapy and the potential for complete remission. In addition, phosphatidylinositol-3 kinase inhibitors (PI3K inhibitors) were also approved for CLL, but they are less effective and associated with higher toxicity and are usually reserved for patients who relapse multiple times.
Prescribing and cost increased
With the emergence of several new oral targeted drugs for CLL, the authors hypothesized that this might lower costs as a result of competition and affect overall spending on ibrutinib.
To test their theory, they analyzed trends in Medicare Part D use and spending on these drugs from 2014 to 2020 to determine annual spending on oral CLL drugs, the number of beneficiaries who received these drugs, and the average spending per 30-day fill.
A total of six oral medications were included in their analysis: three BTK inhibitors (ibrutinib, acalabrutinib, and zanubrutinib), two PI3K inhibitors (idelalisib and duvelisib), and one B-cell lymphoma-2 inhibitor (venetoclax).
During the study period, annual net Medicare spending for all six of these drugs and across all indications increased from $254 million to $3.7 billion.
At the start of the study period in 2014, 6,180 Medicare beneficiaries were being treated with ibrutinib, and this number dramatically increased to 26,847 beneficiaries in 2020. Spending on ibrutinib constituted more than three-quarters (77%) of the total Medicare costs for these six drugs in 2020.
The estimated net spending for a 30-day supply of ibrutinib rose by 46%, from $8,206 in 2014 to $11,980 in 2020, despite the entry of the competitor drugs into the marketplace, some of which also had lower price tags: venetoclax in 2016 (2020 30-day fill price, $7,787), acalabrutinib in 2017 ($11,428) and zanubrutinib in 2020 ($12,521).
In addition, a sensitivity analysis showed a similar trend outside of the Medicare system.
Unlike for ibrutinib, net spending for other oral targeted drugs generally did not increase over time, and some drug prices even dropped slightly.
The authors note that one limitation of their study is that Medicare does not report spending by indication, so it was unknown what proportion of the cost was for CLL as opposed to the other B-cell lymphomas.
“Brand-to-brand competition may have been ineffective at lowering Medicare costs due to lags between approval and change in prescriber practices, constraints on payers’ ability to effectively use formularies to negotiate prices, and financial incentives that can encourage intermediaries such as pharmacy benefit managers to accept high prices,” they conclude.
This study was supported by a grant from Arnold Ventures. Several of the authors have reported relationships with industry.
A version of this article first appeared on Medscape.com.
In fact, the opposite has been seen: Both the price and prescribing of ibrutinib have increased markedly from 2014 to 2020, the authors of a new study say. The estimated net spending for a 30-day supply of ibrutinib increased by 46% during that period, despite the entry of several less costly and comparable products into the marketplace.
“Further research is needed to understand why oncologists have not embraced clinically superior options for CLL being sold at prices similar to, if not lower than, ibrutinib,” write the authors, led by Edward Scheffer Cliff, MBBS, MPH, from the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston.
The study was published online (2023 Apr 7. doi: 10.1001/jamanetworkopen.2023.7467) as a research letter in JAMA Network Open.
Ibrutinib is currently indicated for the treatment of mantle cell lymphoma (MCL), chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL), Waldenström’s macroglobulinemia (WM), marginal zone lymphoma (MZL), and chronic graft versus host disease. Among the top-selling drugs in the United States, ibrutinib sales by 2020 accounted for more than $2.8 billion in annual net Medicare spending.
However, since ibrutinib’s launch in 2013, there have been several new drugs approved for use in CLL, the authors note. They include acalabrutinib (Calquence), also a BTK inhibitor but associated with fewer adverse events, and venetoclax (Venclexta), the first-in-class B-cell lymphoma-2 inhibitor that offers additional clinical advantages such as time-limited therapy and the potential for complete remission. In addition, phosphatidylinositol-3 kinase inhibitors (PI3K inhibitors) were also approved for CLL, but they are less effective and associated with higher toxicity and are usually reserved for patients who relapse multiple times.
Prescribing and cost increased
With the emergence of several new oral targeted drugs for CLL, the authors hypothesized that this might lower costs as a result of competition and affect overall spending on ibrutinib.
To test their theory, they analyzed trends in Medicare Part D use and spending on these drugs from 2014 to 2020 to determine annual spending on oral CLL drugs, the number of beneficiaries who received these drugs, and the average spending per 30-day fill.
A total of six oral medications were included in their analysis: three BTK inhibitors (ibrutinib, acalabrutinib, and zanubrutinib), two PI3K inhibitors (idelalisib and duvelisib), and one B-cell lymphoma-2 inhibitor (venetoclax).
During the study period, annual net Medicare spending for all six of these drugs and across all indications increased from $254 million to $3.7 billion.
At the start of the study period in 2014, 6,180 Medicare beneficiaries were being treated with ibrutinib, and this number dramatically increased to 26,847 beneficiaries in 2020. Spending on ibrutinib constituted more than three-quarters (77%) of the total Medicare costs for these six drugs in 2020.
The estimated net spending for a 30-day supply of ibrutinib rose by 46%, from $8,206 in 2014 to $11,980 in 2020, despite the entry of the competitor drugs into the marketplace, some of which also had lower price tags: venetoclax in 2016 (2020 30-day fill price, $7,787), acalabrutinib in 2017 ($11,428) and zanubrutinib in 2020 ($12,521).
In addition, a sensitivity analysis showed a similar trend outside of the Medicare system.
Unlike for ibrutinib, net spending for other oral targeted drugs generally did not increase over time, and some drug prices even dropped slightly.
The authors note that one limitation of their study is that Medicare does not report spending by indication, so it was unknown what proportion of the cost was for CLL as opposed to the other B-cell lymphomas.
“Brand-to-brand competition may have been ineffective at lowering Medicare costs due to lags between approval and change in prescriber practices, constraints on payers’ ability to effectively use formularies to negotiate prices, and financial incentives that can encourage intermediaries such as pharmacy benefit managers to accept high prices,” they conclude.
This study was supported by a grant from Arnold Ventures. Several of the authors have reported relationships with industry.
A version of this article first appeared on Medscape.com.
In fact, the opposite has been seen: Both the price and prescribing of ibrutinib have increased markedly from 2014 to 2020, the authors of a new study say. The estimated net spending for a 30-day supply of ibrutinib increased by 46% during that period, despite the entry of several less costly and comparable products into the marketplace.
“Further research is needed to understand why oncologists have not embraced clinically superior options for CLL being sold at prices similar to, if not lower than, ibrutinib,” write the authors, led by Edward Scheffer Cliff, MBBS, MPH, from the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital, Boston.
The study was published online (2023 Apr 7. doi: 10.1001/jamanetworkopen.2023.7467) as a research letter in JAMA Network Open.
Ibrutinib is currently indicated for the treatment of mantle cell lymphoma (MCL), chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL), Waldenström’s macroglobulinemia (WM), marginal zone lymphoma (MZL), and chronic graft versus host disease. Among the top-selling drugs in the United States, ibrutinib sales by 2020 accounted for more than $2.8 billion in annual net Medicare spending.
However, since ibrutinib’s launch in 2013, there have been several new drugs approved for use in CLL, the authors note. They include acalabrutinib (Calquence), also a BTK inhibitor but associated with fewer adverse events, and venetoclax (Venclexta), the first-in-class B-cell lymphoma-2 inhibitor that offers additional clinical advantages such as time-limited therapy and the potential for complete remission. In addition, phosphatidylinositol-3 kinase inhibitors (PI3K inhibitors) were also approved for CLL, but they are less effective and associated with higher toxicity and are usually reserved for patients who relapse multiple times.
Prescribing and cost increased
With the emergence of several new oral targeted drugs for CLL, the authors hypothesized that this might lower costs as a result of competition and affect overall spending on ibrutinib.
To test their theory, they analyzed trends in Medicare Part D use and spending on these drugs from 2014 to 2020 to determine annual spending on oral CLL drugs, the number of beneficiaries who received these drugs, and the average spending per 30-day fill.
A total of six oral medications were included in their analysis: three BTK inhibitors (ibrutinib, acalabrutinib, and zanubrutinib), two PI3K inhibitors (idelalisib and duvelisib), and one B-cell lymphoma-2 inhibitor (venetoclax).
During the study period, annual net Medicare spending for all six of these drugs and across all indications increased from $254 million to $3.7 billion.
At the start of the study period in 2014, 6,180 Medicare beneficiaries were being treated with ibrutinib, and this number dramatically increased to 26,847 beneficiaries in 2020. Spending on ibrutinib constituted more than three-quarters (77%) of the total Medicare costs for these six drugs in 2020.
The estimated net spending for a 30-day supply of ibrutinib rose by 46%, from $8,206 in 2014 to $11,980 in 2020, despite the entry of the competitor drugs into the marketplace, some of which also had lower price tags: venetoclax in 2016 (2020 30-day fill price, $7,787), acalabrutinib in 2017 ($11,428) and zanubrutinib in 2020 ($12,521).
In addition, a sensitivity analysis showed a similar trend outside of the Medicare system.
Unlike for ibrutinib, net spending for other oral targeted drugs generally did not increase over time, and some drug prices even dropped slightly.
The authors note that one limitation of their study is that Medicare does not report spending by indication, so it was unknown what proportion of the cost was for CLL as opposed to the other B-cell lymphomas.
“Brand-to-brand competition may have been ineffective at lowering Medicare costs due to lags between approval and change in prescriber practices, constraints on payers’ ability to effectively use formularies to negotiate prices, and financial incentives that can encourage intermediaries such as pharmacy benefit managers to accept high prices,” they conclude.
This study was supported by a grant from Arnold Ventures. Several of the authors have reported relationships with industry.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Anger in adults a red flag for childhood trauma
PARIS –
Investigators examined data on more than 2,250 individuals who were asked about trauma during childhood and a subsequent tendency toward anger or angry outbursts 4 years later.
Results showed that emotional neglect during childhood was associated with approximately a 40% increased likelihood of subsequent anger, while psychological abuse was linked to a 30% increased likelihood.
Childhood physical abuse was also significantly associated with anger in adults, with an increased risk of approximately 40%. The researchers found no link between childhood sexual abuse and adult anger.
“We can’t definitively say that the trauma causes the anger, but the link is clear,” study investigator Nienke De Bles, PhD student, department of psychiatry, Leiden (the Netherlands) University Medical Center, said in a news release.
“Being easily angered can have several consequences,” she continued. “It can make personal interactions more difficult, and it can have consequences for your mental health and well-being, but people who get angry easily also have a greater tendency to discontinue psychiatric treatment, so this anger may mean that it reduces their chances of a better life,” she added.
Ms. De Bles believes that “it should be standard practice to ask depression and anxiety sufferers about anger and past trauma, even if the patient is not exhibiting current anger.”
The findings were presented at the European Psychiatric Association 2023 Congress.
A ‘red flag’ for abuse
“Psychiatric treatments for past trauma may differ from treatments for depression, so psychiatrists need to try to understand the cause so that they can offer the correct treatment to each patient,” said Ms. De Bles.
Ms. De Bles noted that childhood trauma has many negative consequences later in life and that it is associated with a higher prevalence of adult depression and anxiety.
“There are several potential mechanisms for psychopathology in the context of childhood trauma, and emotion regulation seems to be one of the key mechanisms,” she said.
The researchers previously found that anger was highly prevalent among patients with affective disorders. It was present in 30% of those with current anxiety or depressive disorder and in 40% of those with comorbid depression and anxiety with a tendency toward anger versus 5% of healthy control persons.
Other studies have shown that anger is associated with poor treatment outcomes and dropping out of treatment.
To further investigate the link between childhood trauma and anger in adulthood, the researchers examined data on 2,271 participants in the Netherlands Study of Depression and Anxiety (NESDA).
Childhood trauma was assessed at baseline using the semistructured Childhood Trauma Interview. Anger was measured at a 4-year follow-up using the Spielberger Trait Anger Subscale, the Anger Attacks Questionnaire, and the borderline and antisocial subscales of the Personality Disorder Questionnaire 4 to identify cluster B personality traits.
Results showed that emotional neglect during childhood was significantly associated with trait anger in adulthood, at an adjusted odds ratio of 1.42 (P < .001), anger attacks (OR, 1.35; P = .004), and borderline (OR, 1.76; P < .001) and antisocial (OR, 1.88; P = .001) personality traits.
Childhood psychological abuse was also significantly associated with later trait anger (OR, 1.28; P = .002), anger attacks (OR, 1.31; P = .024), and borderline (OR, 1.77; P < .001) and antisocial (OR, 1.69; P = .011) traits.
There was also a significant association between childhood psychical abuse and trait anger in adulthood (OR, 1.37; P < .001), anger attacks (OR, 1.48; P = .004), and borderline (OR, 1.71; P < .001) and antisocial (OR, 1.98; P = .002) traits.
There was no significant association between sexual abuse experienced in childhood and later anger or personality traits.
Ms. De Bles said the findings suggest “there is indeed a relationship between childhood trauma and anger in adulthood, and this is something that might be interesting for clinicians, as anger could be a red flag for a history of childhood trauma.”
She said in an interview that anger is a “very normal human emotion” but that it has not been as widely studied as sadness and anxiety.
She suggested that future research could examine the use of trauma-based therapies for patients with a history of childhood trauma and anger.
Overlooked, neglected
Commenting on the findings, Nur Hani Zainal, PhD, department of healthcare policy, Harvard Medical School, Boston, said the findings are “very consistent with the current biopsychosocial models in psychiatry and clinical psychology.”

Dr. Zainal, who was coauthor of a recent study that showed that anger appears to mediate the relationship between childhood trauma and adult psychopathology, said the current study offers a “good, incremental contribution” to the literature.
She noted there are “good uses” for the emotion of anger, as “sometimes we need anger to set healthy boundaries for ourselves.” However, she agreed that, as an aspect of depression, anxiety, and posttraumatic stress disorder, it is often “overlooked.”
Dr. Zainal said that the findings reinforce the importance of thoroughly evaluating adult patients’ experiences during childhood.
Julian Beezhold, MD, secretary general of the EPA and a consultant psychiatrist with the Norwich (England) Medical School, University of East Anglia, commented in the release that anger is a “somewhat neglected symptom.
“The findings are in line with what we see in day-to-day clinical practice and will hopefully help increase the awareness of the importance of both anger and associated childhood trauma.”
The infrastructure for the NESDA study is funded through the Geestkracht program of the Netherlands Organization for Health Research and Development and financial contributions by participating universities and mental health care organizations. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
PARIS –
Investigators examined data on more than 2,250 individuals who were asked about trauma during childhood and a subsequent tendency toward anger or angry outbursts 4 years later.
Results showed that emotional neglect during childhood was associated with approximately a 40% increased likelihood of subsequent anger, while psychological abuse was linked to a 30% increased likelihood.
Childhood physical abuse was also significantly associated with anger in adults, with an increased risk of approximately 40%. The researchers found no link between childhood sexual abuse and adult anger.
“We can’t definitively say that the trauma causes the anger, but the link is clear,” study investigator Nienke De Bles, PhD student, department of psychiatry, Leiden (the Netherlands) University Medical Center, said in a news release.
“Being easily angered can have several consequences,” she continued. “It can make personal interactions more difficult, and it can have consequences for your mental health and well-being, but people who get angry easily also have a greater tendency to discontinue psychiatric treatment, so this anger may mean that it reduces their chances of a better life,” she added.
Ms. De Bles believes that “it should be standard practice to ask depression and anxiety sufferers about anger and past trauma, even if the patient is not exhibiting current anger.”
The findings were presented at the European Psychiatric Association 2023 Congress.
A ‘red flag’ for abuse
“Psychiatric treatments for past trauma may differ from treatments for depression, so psychiatrists need to try to understand the cause so that they can offer the correct treatment to each patient,” said Ms. De Bles.
Ms. De Bles noted that childhood trauma has many negative consequences later in life and that it is associated with a higher prevalence of adult depression and anxiety.
“There are several potential mechanisms for psychopathology in the context of childhood trauma, and emotion regulation seems to be one of the key mechanisms,” she said.
The researchers previously found that anger was highly prevalent among patients with affective disorders. It was present in 30% of those with current anxiety or depressive disorder and in 40% of those with comorbid depression and anxiety with a tendency toward anger versus 5% of healthy control persons.
Other studies have shown that anger is associated with poor treatment outcomes and dropping out of treatment.
To further investigate the link between childhood trauma and anger in adulthood, the researchers examined data on 2,271 participants in the Netherlands Study of Depression and Anxiety (NESDA).
Childhood trauma was assessed at baseline using the semistructured Childhood Trauma Interview. Anger was measured at a 4-year follow-up using the Spielberger Trait Anger Subscale, the Anger Attacks Questionnaire, and the borderline and antisocial subscales of the Personality Disorder Questionnaire 4 to identify cluster B personality traits.
Results showed that emotional neglect during childhood was significantly associated with trait anger in adulthood, at an adjusted odds ratio of 1.42 (P < .001), anger attacks (OR, 1.35; P = .004), and borderline (OR, 1.76; P < .001) and antisocial (OR, 1.88; P = .001) personality traits.
Childhood psychological abuse was also significantly associated with later trait anger (OR, 1.28; P = .002), anger attacks (OR, 1.31; P = .024), and borderline (OR, 1.77; P < .001) and antisocial (OR, 1.69; P = .011) traits.
There was also a significant association between childhood psychical abuse and trait anger in adulthood (OR, 1.37; P < .001), anger attacks (OR, 1.48; P = .004), and borderline (OR, 1.71; P < .001) and antisocial (OR, 1.98; P = .002) traits.
There was no significant association between sexual abuse experienced in childhood and later anger or personality traits.
Ms. De Bles said the findings suggest “there is indeed a relationship between childhood trauma and anger in adulthood, and this is something that might be interesting for clinicians, as anger could be a red flag for a history of childhood trauma.”
She said in an interview that anger is a “very normal human emotion” but that it has not been as widely studied as sadness and anxiety.
She suggested that future research could examine the use of trauma-based therapies for patients with a history of childhood trauma and anger.
Overlooked, neglected
Commenting on the findings, Nur Hani Zainal, PhD, department of healthcare policy, Harvard Medical School, Boston, said the findings are “very consistent with the current biopsychosocial models in psychiatry and clinical psychology.”
Dr. Zainal, who was coauthor of a recent study that showed that anger appears to mediate the relationship between childhood trauma and adult psychopathology, said the current study offers a “good, incremental contribution” to the literature.
She noted there are “good uses” for the emotion of anger, as “sometimes we need anger to set healthy boundaries for ourselves.” However, she agreed that, as an aspect of depression, anxiety, and posttraumatic stress disorder, it is often “overlooked.”
Dr. Zainal said that the findings reinforce the importance of thoroughly evaluating adult patients’ experiences during childhood.
Julian Beezhold, MD, secretary general of the EPA and a consultant psychiatrist with the Norwich (England) Medical School, University of East Anglia, commented in the release that anger is a “somewhat neglected symptom.
“The findings are in line with what we see in day-to-day clinical practice and will hopefully help increase the awareness of the importance of both anger and associated childhood trauma.”
The infrastructure for the NESDA study is funded through the Geestkracht program of the Netherlands Organization for Health Research and Development and financial contributions by participating universities and mental health care organizations. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
PARIS –
Investigators examined data on more than 2,250 individuals who were asked about trauma during childhood and a subsequent tendency toward anger or angry outbursts 4 years later.
Results showed that emotional neglect during childhood was associated with approximately a 40% increased likelihood of subsequent anger, while psychological abuse was linked to a 30% increased likelihood.
Childhood physical abuse was also significantly associated with anger in adults, with an increased risk of approximately 40%. The researchers found no link between childhood sexual abuse and adult anger.
“We can’t definitively say that the trauma causes the anger, but the link is clear,” study investigator Nienke De Bles, PhD student, department of psychiatry, Leiden (the Netherlands) University Medical Center, said in a news release.
“Being easily angered can have several consequences,” she continued. “It can make personal interactions more difficult, and it can have consequences for your mental health and well-being, but people who get angry easily also have a greater tendency to discontinue psychiatric treatment, so this anger may mean that it reduces their chances of a better life,” she added.
Ms. De Bles believes that “it should be standard practice to ask depression and anxiety sufferers about anger and past trauma, even if the patient is not exhibiting current anger.”
The findings were presented at the European Psychiatric Association 2023 Congress.
A ‘red flag’ for abuse
“Psychiatric treatments for past trauma may differ from treatments for depression, so psychiatrists need to try to understand the cause so that they can offer the correct treatment to each patient,” said Ms. De Bles.
Ms. De Bles noted that childhood trauma has many negative consequences later in life and that it is associated with a higher prevalence of adult depression and anxiety.
“There are several potential mechanisms for psychopathology in the context of childhood trauma, and emotion regulation seems to be one of the key mechanisms,” she said.
The researchers previously found that anger was highly prevalent among patients with affective disorders. It was present in 30% of those with current anxiety or depressive disorder and in 40% of those with comorbid depression and anxiety with a tendency toward anger versus 5% of healthy control persons.
Other studies have shown that anger is associated with poor treatment outcomes and dropping out of treatment.
To further investigate the link between childhood trauma and anger in adulthood, the researchers examined data on 2,271 participants in the Netherlands Study of Depression and Anxiety (NESDA).
Childhood trauma was assessed at baseline using the semistructured Childhood Trauma Interview. Anger was measured at a 4-year follow-up using the Spielberger Trait Anger Subscale, the Anger Attacks Questionnaire, and the borderline and antisocial subscales of the Personality Disorder Questionnaire 4 to identify cluster B personality traits.
Results showed that emotional neglect during childhood was significantly associated with trait anger in adulthood, at an adjusted odds ratio of 1.42 (P < .001), anger attacks (OR, 1.35; P = .004), and borderline (OR, 1.76; P < .001) and antisocial (OR, 1.88; P = .001) personality traits.
Childhood psychological abuse was also significantly associated with later trait anger (OR, 1.28; P = .002), anger attacks (OR, 1.31; P = .024), and borderline (OR, 1.77; P < .001) and antisocial (OR, 1.69; P = .011) traits.
There was also a significant association between childhood psychical abuse and trait anger in adulthood (OR, 1.37; P < .001), anger attacks (OR, 1.48; P = .004), and borderline (OR, 1.71; P < .001) and antisocial (OR, 1.98; P = .002) traits.
There was no significant association between sexual abuse experienced in childhood and later anger or personality traits.
Ms. De Bles said the findings suggest “there is indeed a relationship between childhood trauma and anger in adulthood, and this is something that might be interesting for clinicians, as anger could be a red flag for a history of childhood trauma.”
She said in an interview that anger is a “very normal human emotion” but that it has not been as widely studied as sadness and anxiety.
She suggested that future research could examine the use of trauma-based therapies for patients with a history of childhood trauma and anger.
Overlooked, neglected
Commenting on the findings, Nur Hani Zainal, PhD, department of healthcare policy, Harvard Medical School, Boston, said the findings are “very consistent with the current biopsychosocial models in psychiatry and clinical psychology.”
Dr. Zainal, who was coauthor of a recent study that showed that anger appears to mediate the relationship between childhood trauma and adult psychopathology, said the current study offers a “good, incremental contribution” to the literature.
She noted there are “good uses” for the emotion of anger, as “sometimes we need anger to set healthy boundaries for ourselves.” However, she agreed that, as an aspect of depression, anxiety, and posttraumatic stress disorder, it is often “overlooked.”
Dr. Zainal said that the findings reinforce the importance of thoroughly evaluating adult patients’ experiences during childhood.
Julian Beezhold, MD, secretary general of the EPA and a consultant psychiatrist with the Norwich (England) Medical School, University of East Anglia, commented in the release that anger is a “somewhat neglected symptom.
“The findings are in line with what we see in day-to-day clinical practice and will hopefully help increase the awareness of the importance of both anger and associated childhood trauma.”
The infrastructure for the NESDA study is funded through the Geestkracht program of the Netherlands Organization for Health Research and Development and financial contributions by participating universities and mental health care organizations. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT EPA 2023
A 50-year-old White male presented with a 4- to 5-year history of progressively growing violaceous lesions on his left lower extremity
with scarce T-cells, classically presenting as rapidly progressive, plum-colored lesions on the lower extremities.1,2 CBCLs, with PCDLBCL-LT accounting for 4%, make up the minority of cutaneous lymphomas in the Western world.1-3 The leg type variant, typically demonstrating a female predominance and median age of onset in the 70s, is clinically aggressive and associated with a poorer prognosis, increased recurrence rate, and 40%-60% 5-year survival rate.1-5
Histologically, this variant demonstrates a diffuse sheet-like growth of enlarged atypical B-cells distinctively separated from the epidermis by a prominent grenz zone. Classic PCDLBCL-LT immunophenotype includes B-cell markers CD20 and IgM; triple expressor phenotype indicating c-MYC, BCL-2, and BCL-6 positivity; as well as CD10 negativity, lack of BCL-2 rearrangement, and presence of a positive MYD-88 molecular result.

Other characteristic histopathological findings include positivity for post-germinal markers IRF4/MUM-1 and FOXP-1, positivity for additional B-cell markers, including CD79 and PAX5, and negativity of t(14;18) (q32;21).1,3-5
This case is of significant interest as it falls within the approximately 10% of PCDLBCL-LT cases demonstrating weak to negative MUM-1 staining, in addition to its presentation in a younger male individual.
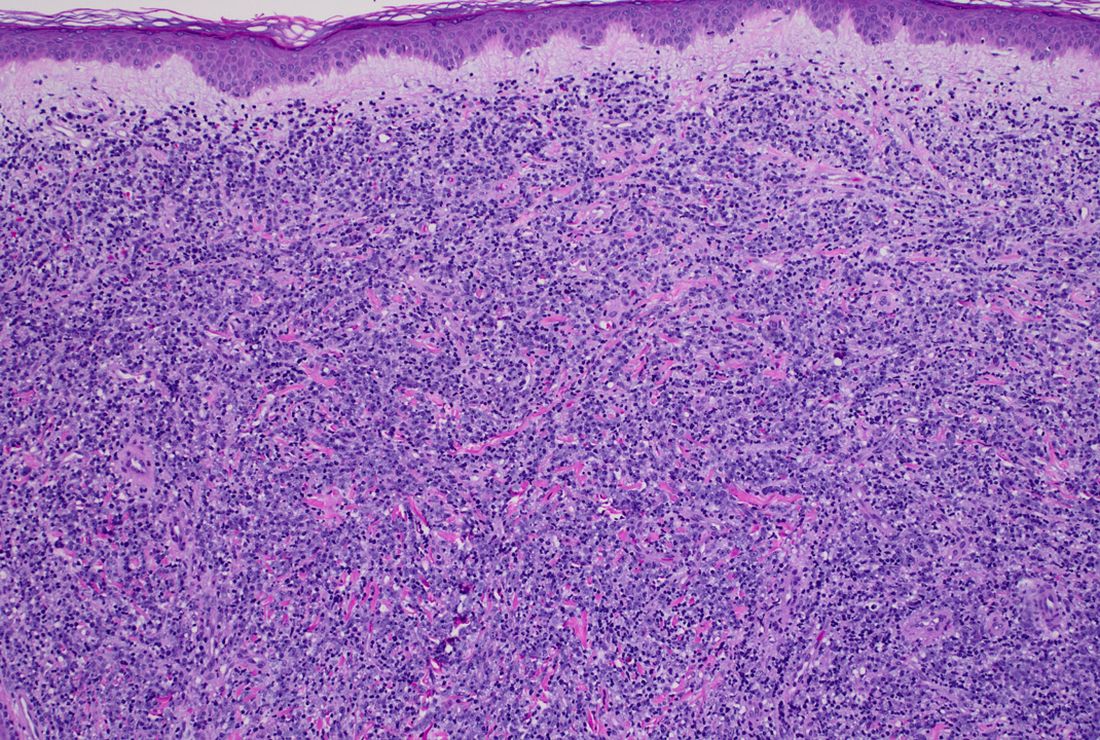
While MUM-1 positivity is common in this subtype, its presence, or lack thereof, should not be looked at in isolation when evaluating diagnostic criteria, nor has it been shown to have a statistically significant effect on survival rate – in contrast to factors like lesion location on the leg versus non-leg lesions, multiple lesions at diagnosis, and dissemination to other sites.2,6
PCDLBCL-LT can uncommonly present in non-leg locations and only 10% depict associated B-symptoms, such as fatigue, night sweats, weight loss, or lymphadenopathy.2,6 First-line treatment is with the R-CHOP chemotherapy regimen – consisting of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone – although radiotherapy is sometimes considered in patients with a single small lesion.1,2

Because of possible cutaneous involvement beyond the legs, common lack of systemic symptoms, and variable immunophenotypes, this case of MUM-1 negative PCDLBCL-LT highlights the importance of a clinicopathological approach to differentiate the subtypes of CBCLs, allowing for proper and individualized stratification of risk, prognosis, and treatment.
This case was submitted and written by Marlee Hill, BS, Michael Franzetti, MD, Jeffrey McBride, MD, and Allison Hood, MD, of the University of Oklahoma, Oklahoma City. They also provided the photos. Donna Bilu Martin, MD, edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Willemze R et al. Blood. 2019;133(16):1703-14.
2. Willemze R et al. Blood. 2005;105(10):3768-85.
3. Sukswai N et al. Pathology. 2020;52(1):53-67.
4. Hristov AC. Arch Pathol Lab Med. 2012;136(8):876-81.
5. Sokol L et al. Cancer Control. 2012;19(3):236-44.
6. Grange F et al. Arch Dermatol. 2007;143(9):1144-50.
with scarce T-cells, classically presenting as rapidly progressive, plum-colored lesions on the lower extremities.1,2 CBCLs, with PCDLBCL-LT accounting for 4%, make up the minority of cutaneous lymphomas in the Western world.1-3 The leg type variant, typically demonstrating a female predominance and median age of onset in the 70s, is clinically aggressive and associated with a poorer prognosis, increased recurrence rate, and 40%-60% 5-year survival rate.1-5
Histologically, this variant demonstrates a diffuse sheet-like growth of enlarged atypical B-cells distinctively separated from the epidermis by a prominent grenz zone. Classic PCDLBCL-LT immunophenotype includes B-cell markers CD20 and IgM; triple expressor phenotype indicating c-MYC, BCL-2, and BCL-6 positivity; as well as CD10 negativity, lack of BCL-2 rearrangement, and presence of a positive MYD-88 molecular result.
Other characteristic histopathological findings include positivity for post-germinal markers IRF4/MUM-1 and FOXP-1, positivity for additional B-cell markers, including CD79 and PAX5, and negativity of t(14;18) (q32;21).1,3-5
This case is of significant interest as it falls within the approximately 10% of PCDLBCL-LT cases demonstrating weak to negative MUM-1 staining, in addition to its presentation in a younger male individual.
While MUM-1 positivity is common in this subtype, its presence, or lack thereof, should not be looked at in isolation when evaluating diagnostic criteria, nor has it been shown to have a statistically significant effect on survival rate – in contrast to factors like lesion location on the leg versus non-leg lesions, multiple lesions at diagnosis, and dissemination to other sites.2,6
PCDLBCL-LT can uncommonly present in non-leg locations and only 10% depict associated B-symptoms, such as fatigue, night sweats, weight loss, or lymphadenopathy.2,6 First-line treatment is with the R-CHOP chemotherapy regimen – consisting of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone – although radiotherapy is sometimes considered in patients with a single small lesion.1,2
Because of possible cutaneous involvement beyond the legs, common lack of systemic symptoms, and variable immunophenotypes, this case of MUM-1 negative PCDLBCL-LT highlights the importance of a clinicopathological approach to differentiate the subtypes of CBCLs, allowing for proper and individualized stratification of risk, prognosis, and treatment.
This case was submitted and written by Marlee Hill, BS, Michael Franzetti, MD, Jeffrey McBride, MD, and Allison Hood, MD, of the University of Oklahoma, Oklahoma City. They also provided the photos. Donna Bilu Martin, MD, edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Willemze R et al. Blood. 2019;133(16):1703-14.
2. Willemze R et al. Blood. 2005;105(10):3768-85.
3. Sukswai N et al. Pathology. 2020;52(1):53-67.
4. Hristov AC. Arch Pathol Lab Med. 2012;136(8):876-81.
5. Sokol L et al. Cancer Control. 2012;19(3):236-44.
6. Grange F et al. Arch Dermatol. 2007;143(9):1144-50.
with scarce T-cells, classically presenting as rapidly progressive, plum-colored lesions on the lower extremities.1,2 CBCLs, with PCDLBCL-LT accounting for 4%, make up the minority of cutaneous lymphomas in the Western world.1-3 The leg type variant, typically demonstrating a female predominance and median age of onset in the 70s, is clinically aggressive and associated with a poorer prognosis, increased recurrence rate, and 40%-60% 5-year survival rate.1-5
Histologically, this variant demonstrates a diffuse sheet-like growth of enlarged atypical B-cells distinctively separated from the epidermis by a prominent grenz zone. Classic PCDLBCL-LT immunophenotype includes B-cell markers CD20 and IgM; triple expressor phenotype indicating c-MYC, BCL-2, and BCL-6 positivity; as well as CD10 negativity, lack of BCL-2 rearrangement, and presence of a positive MYD-88 molecular result.
Other characteristic histopathological findings include positivity for post-germinal markers IRF4/MUM-1 and FOXP-1, positivity for additional B-cell markers, including CD79 and PAX5, and negativity of t(14;18) (q32;21).1,3-5
This case is of significant interest as it falls within the approximately 10% of PCDLBCL-LT cases demonstrating weak to negative MUM-1 staining, in addition to its presentation in a younger male individual.
While MUM-1 positivity is common in this subtype, its presence, or lack thereof, should not be looked at in isolation when evaluating diagnostic criteria, nor has it been shown to have a statistically significant effect on survival rate – in contrast to factors like lesion location on the leg versus non-leg lesions, multiple lesions at diagnosis, and dissemination to other sites.2,6
PCDLBCL-LT can uncommonly present in non-leg locations and only 10% depict associated B-symptoms, such as fatigue, night sweats, weight loss, or lymphadenopathy.2,6 First-line treatment is with the R-CHOP chemotherapy regimen – consisting of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone – although radiotherapy is sometimes considered in patients with a single small lesion.1,2
Because of possible cutaneous involvement beyond the legs, common lack of systemic symptoms, and variable immunophenotypes, this case of MUM-1 negative PCDLBCL-LT highlights the importance of a clinicopathological approach to differentiate the subtypes of CBCLs, allowing for proper and individualized stratification of risk, prognosis, and treatment.
This case was submitted and written by Marlee Hill, BS, Michael Franzetti, MD, Jeffrey McBride, MD, and Allison Hood, MD, of the University of Oklahoma, Oklahoma City. They also provided the photos. Donna Bilu Martin, MD, edited the column.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Willemze R et al. Blood. 2019;133(16):1703-14.
2. Willemze R et al. Blood. 2005;105(10):3768-85.
3. Sukswai N et al. Pathology. 2020;52(1):53-67.
4. Hristov AC. Arch Pathol Lab Med. 2012;136(8):876-81.
5. Sokol L et al. Cancer Control. 2012;19(3):236-44.
6. Grange F et al. Arch Dermatol. 2007;143(9):1144-50.


There was no cervical, axillary, or inguinal lymphadenopathy.
New 46-week PsA data released for IL-17A inhibitor izokibep
out to 46 weeks, according to an announcement reporting some of the long-term data by the drug’s developer, Acelyrin.
Izokibep is an antibody mimetic designed to inhibit IL-17A that the company says has “high potency and the potential for robust tissue penetration due to its small molecular size, about one-tenth the size of a monoclonal antibody.”
“Patients want both rapid and meaningful improvement of their symptoms, as well as lasting – and ideally improving – resolution of disease over time. Building on the 16-week data for izokibep reported at EULAR and ACR [American College of Rheumatology] last year, the 46-week data now show not only continued but marked improvements over time in key areas of psoriatic arthritis including joint pain, skin psoriasis, and enthesitis,” Philip J. Mease, MD, director of rheumatology research at the Swedish Medical Center and clinical professor at the University of Washington, both in Seattle, and an investigator in the izokibep PsA program, said in the announcement.
The phase 2 trial tested two doses of izokibep – 40 mg and 80 mg – given by subcutaneous injection every 2 weeks – against placebo in 135 adult patients with active PsA. For inclusion in the trial, patients had to have at least three swollen and at least three tender joints and an inadequate response to prior therapy including NSAIDs, conventional synthetic disease-modifying antirheumatic drugs, or tumor necrosis factor inhibitors. At week 16, the placebo group transitioned to 80 mg izokibep every 2 weeks and the trial treatment period continued for up to 46 weeks.
The trial’s primary endpoint of a 50% or higher level of improvement in ACR response criteria (ACR 50) was achieved by 48% of those on the 40 mg dose at week 16 and by 50% at week 46. For the 80-mg group, this rate rose from 52% to 79%. In the group that went from placebo to 80 mg, the ACR 50 rose from 13% with placebo to 73% with izokibep at week 46.
Resolution of enthesitis, measured by the Leeds Enthesitis Index, among those on the 40 mg dose, was achieved by 63% at week 16 and 83% at week 46, and among those on the 80 mg dose, 88% at week 16 and 89% at week 46. Those on placebo who switched to 80 mg of izokibep at week 16 had an 80% rate of enthesitis resolution at week 46.
Total resolution of skin involvement – 100% clearance of psoriasis based on the Psoriasis Area Severity Index (PASI) – was observed at 46 weeks in 50% of those on 40 mg, 71% of those on 80 mg, and 67% of those on 80 mg after week 16.
In its announcement, Acelyrin did not report withdrawal rates from the study after 16 weeks and through 46 weeks, although the statement said that izokibep “was generally well tolerated through 46 weeks, which is in line with previous trials of izokibep.” The most common adverse event was localized injection site reactions, with the majority graded mild to moderate in severity. They were generally the size of a quarter to half-dollar, and typically presented within the first few injections, after which they declined in incidence. In the trial, a case of vulvar cancer was determined to be potentially drug related, the company said.
Acelyrin is currently conducting a phase 2b/3 trial in PsA evaluating a range of doses, including significantly higher doses than in the phase 2 trial, that the company said “could potentially result in better ACR, PASI, and enthesitis resolution responses.”
The drug has been tested at doses up to 160 mg, in some cases for up to 3 years, in more than 400 patients with psoriasis, spondyloarthritis, noninfective uveitis, and hidradenitis suppurativa.
The full 46-week data from this trial will be presented at a future scientific meeting, according to the company.
out to 46 weeks, according to an announcement reporting some of the long-term data by the drug’s developer, Acelyrin.
Izokibep is an antibody mimetic designed to inhibit IL-17A that the company says has “high potency and the potential for robust tissue penetration due to its small molecular size, about one-tenth the size of a monoclonal antibody.”
“Patients want both rapid and meaningful improvement of their symptoms, as well as lasting – and ideally improving – resolution of disease over time. Building on the 16-week data for izokibep reported at EULAR and ACR [American College of Rheumatology] last year, the 46-week data now show not only continued but marked improvements over time in key areas of psoriatic arthritis including joint pain, skin psoriasis, and enthesitis,” Philip J. Mease, MD, director of rheumatology research at the Swedish Medical Center and clinical professor at the University of Washington, both in Seattle, and an investigator in the izokibep PsA program, said in the announcement.
The phase 2 trial tested two doses of izokibep – 40 mg and 80 mg – given by subcutaneous injection every 2 weeks – against placebo in 135 adult patients with active PsA. For inclusion in the trial, patients had to have at least three swollen and at least three tender joints and an inadequate response to prior therapy including NSAIDs, conventional synthetic disease-modifying antirheumatic drugs, or tumor necrosis factor inhibitors. At week 16, the placebo group transitioned to 80 mg izokibep every 2 weeks and the trial treatment period continued for up to 46 weeks.
The trial’s primary endpoint of a 50% or higher level of improvement in ACR response criteria (ACR 50) was achieved by 48% of those on the 40 mg dose at week 16 and by 50% at week 46. For the 80-mg group, this rate rose from 52% to 79%. In the group that went from placebo to 80 mg, the ACR 50 rose from 13% with placebo to 73% with izokibep at week 46.
Resolution of enthesitis, measured by the Leeds Enthesitis Index, among those on the 40 mg dose, was achieved by 63% at week 16 and 83% at week 46, and among those on the 80 mg dose, 88% at week 16 and 89% at week 46. Those on placebo who switched to 80 mg of izokibep at week 16 had an 80% rate of enthesitis resolution at week 46.
Total resolution of skin involvement – 100% clearance of psoriasis based on the Psoriasis Area Severity Index (PASI) – was observed at 46 weeks in 50% of those on 40 mg, 71% of those on 80 mg, and 67% of those on 80 mg after week 16.
In its announcement, Acelyrin did not report withdrawal rates from the study after 16 weeks and through 46 weeks, although the statement said that izokibep “was generally well tolerated through 46 weeks, which is in line with previous trials of izokibep.” The most common adverse event was localized injection site reactions, with the majority graded mild to moderate in severity. They were generally the size of a quarter to half-dollar, and typically presented within the first few injections, after which they declined in incidence. In the trial, a case of vulvar cancer was determined to be potentially drug related, the company said.
Acelyrin is currently conducting a phase 2b/3 trial in PsA evaluating a range of doses, including significantly higher doses than in the phase 2 trial, that the company said “could potentially result in better ACR, PASI, and enthesitis resolution responses.”
The drug has been tested at doses up to 160 mg, in some cases for up to 3 years, in more than 400 patients with psoriasis, spondyloarthritis, noninfective uveitis, and hidradenitis suppurativa.
The full 46-week data from this trial will be presented at a future scientific meeting, according to the company.
out to 46 weeks, according to an announcement reporting some of the long-term data by the drug’s developer, Acelyrin.
Izokibep is an antibody mimetic designed to inhibit IL-17A that the company says has “high potency and the potential for robust tissue penetration due to its small molecular size, about one-tenth the size of a monoclonal antibody.”
“Patients want both rapid and meaningful improvement of their symptoms, as well as lasting – and ideally improving – resolution of disease over time. Building on the 16-week data for izokibep reported at EULAR and ACR [American College of Rheumatology] last year, the 46-week data now show not only continued but marked improvements over time in key areas of psoriatic arthritis including joint pain, skin psoriasis, and enthesitis,” Philip J. Mease, MD, director of rheumatology research at the Swedish Medical Center and clinical professor at the University of Washington, both in Seattle, and an investigator in the izokibep PsA program, said in the announcement.
The phase 2 trial tested two doses of izokibep – 40 mg and 80 mg – given by subcutaneous injection every 2 weeks – against placebo in 135 adult patients with active PsA. For inclusion in the trial, patients had to have at least three swollen and at least three tender joints and an inadequate response to prior therapy including NSAIDs, conventional synthetic disease-modifying antirheumatic drugs, or tumor necrosis factor inhibitors. At week 16, the placebo group transitioned to 80 mg izokibep every 2 weeks and the trial treatment period continued for up to 46 weeks.
The trial’s primary endpoint of a 50% or higher level of improvement in ACR response criteria (ACR 50) was achieved by 48% of those on the 40 mg dose at week 16 and by 50% at week 46. For the 80-mg group, this rate rose from 52% to 79%. In the group that went from placebo to 80 mg, the ACR 50 rose from 13% with placebo to 73% with izokibep at week 46.
Resolution of enthesitis, measured by the Leeds Enthesitis Index, among those on the 40 mg dose, was achieved by 63% at week 16 and 83% at week 46, and among those on the 80 mg dose, 88% at week 16 and 89% at week 46. Those on placebo who switched to 80 mg of izokibep at week 16 had an 80% rate of enthesitis resolution at week 46.
Total resolution of skin involvement – 100% clearance of psoriasis based on the Psoriasis Area Severity Index (PASI) – was observed at 46 weeks in 50% of those on 40 mg, 71% of those on 80 mg, and 67% of those on 80 mg after week 16.
In its announcement, Acelyrin did not report withdrawal rates from the study after 16 weeks and through 46 weeks, although the statement said that izokibep “was generally well tolerated through 46 weeks, which is in line with previous trials of izokibep.” The most common adverse event was localized injection site reactions, with the majority graded mild to moderate in severity. They were generally the size of a quarter to half-dollar, and typically presented within the first few injections, after which they declined in incidence. In the trial, a case of vulvar cancer was determined to be potentially drug related, the company said.
Acelyrin is currently conducting a phase 2b/3 trial in PsA evaluating a range of doses, including significantly higher doses than in the phase 2 trial, that the company said “could potentially result in better ACR, PASI, and enthesitis resolution responses.”
The drug has been tested at doses up to 160 mg, in some cases for up to 3 years, in more than 400 patients with psoriasis, spondyloarthritis, noninfective uveitis, and hidradenitis suppurativa.
The full 46-week data from this trial will be presented at a future scientific meeting, according to the company.
AHA statement targets nuance in CVD risk assessment of women
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.

“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.
“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.
“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION