User login
Diagnostic role of nailfold capillaroscopy for identifying PsA in psoriasis needs further investigation
Key clinical point: Nailfold capillaroscopy (NC) outcomes could not conclusively differentiate psoriasis from psoriatic arthritis (PsA).
Major finding: In addition to altered morphology, the density of capillaries at the nailfold was significantly lower in patients with psoriasis (standardized group difference [SMD] −0.91; P = .0058; area under curve [AUC] 0.740) and PsA (SMD −1.22; P = .0432; AUC, 0.806) compared with control individuals; however, no NC outcomes conclusively differentiated between psoriasis and PsA.
Study details: Findings are from a systematic review and meta-analysis of 22 studies investigating NC as a diagnostic tool for psoriasis or PsA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lazar LT et al. Nailfold capillaroscopy as diagnostic test in patients with psoriasis and psoriatic arthritis: A systematic review. Microvasc Res. 2023;147:104476 (Jan 16). Doi: 10.1016/j.mvr.2023.104476
Key clinical point: Nailfold capillaroscopy (NC) outcomes could not conclusively differentiate psoriasis from psoriatic arthritis (PsA).
Major finding: In addition to altered morphology, the density of capillaries at the nailfold was significantly lower in patients with psoriasis (standardized group difference [SMD] −0.91; P = .0058; area under curve [AUC] 0.740) and PsA (SMD −1.22; P = .0432; AUC, 0.806) compared with control individuals; however, no NC outcomes conclusively differentiated between psoriasis and PsA.
Study details: Findings are from a systematic review and meta-analysis of 22 studies investigating NC as a diagnostic tool for psoriasis or PsA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lazar LT et al. Nailfold capillaroscopy as diagnostic test in patients with psoriasis and psoriatic arthritis: A systematic review. Microvasc Res. 2023;147:104476 (Jan 16). Doi: 10.1016/j.mvr.2023.104476
Key clinical point: Nailfold capillaroscopy (NC) outcomes could not conclusively differentiate psoriasis from psoriatic arthritis (PsA).
Major finding: In addition to altered morphology, the density of capillaries at the nailfold was significantly lower in patients with psoriasis (standardized group difference [SMD] −0.91; P = .0058; area under curve [AUC] 0.740) and PsA (SMD −1.22; P = .0432; AUC, 0.806) compared with control individuals; however, no NC outcomes conclusively differentiated between psoriasis and PsA.
Study details: Findings are from a systematic review and meta-analysis of 22 studies investigating NC as a diagnostic tool for psoriasis or PsA.
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Lazar LT et al. Nailfold capillaroscopy as diagnostic test in patients with psoriasis and psoriatic arthritis: A systematic review. Microvasc Res. 2023;147:104476 (Jan 16). Doi: 10.1016/j.mvr.2023.104476
Biologics show signs of delaying arthritis in psoriasis patients
Patients with psoriasis treated with interleukin-12/23 inhibitors or IL-23 inhibitors were less likely to develop inflammatory arthritis, compared with those treated with tumor necrosis factor (TNF) inhibitors, according to findings from a large retrospective study.
While previous retrospective cohort studies have found biologic therapies for psoriasis can reduce the risk of developing psoriatic arthritis when compared with other treatments such as phototherapy and oral nonbiologic disease-modifying antirheumatic drugs, this analysis is the first to compare classes of biologics, Shikha Singla, MD, of the Medical College of Wisconsin, Milwaukee, and colleagues wrote in The Lancet Rheumatology.

In the analysis, researchers used the TriNetX database, which contains deidentified data from electronic medical health records from health care organizations across the United States. The study included adults diagnosed with psoriasis who were newly prescribed a biologic approved by the Food and Drug Administration for the treatment of psoriasis. Biologics were defined by drug class: anti-TNF, anti-IL-17, anti-IL-23, and anti–IL-12/23. Any patient with a diagnosis of psoriatic arthritis or other inflammatory arthritis prior to receiving a biologic prescription or within 2 weeks of receiving the prescription were excluded.
The researchers identified 15,501 eligible patients diagnosed with psoriasis during Jan. 1, 2014, to June 1, 2022, with an average follow-up time of 2.4 years. The researchers chose to start the study period in 2014 because the first non–anti-TNF drug for psoriatic arthritis was approved by the FDA in 2013 – the anti–IL-12/23 drug ustekinumab. During the study period, 976 patients developed inflammatory arthritis and were diagnosed on average 528 days after their biologic prescription.
In a multivariable analysis, the researchers found that patients prescribed IL-23 inhibitors (guselkumab [Tremfya], risankizumab [Skyrizi], tildrakizumab [Ilumya]) were nearly 60% less likely (adjusted hazard ratio, 0.41; 95% confidence interval, 0.17–0.95) to develop inflammatory arthritis than were patients taking TNF inhibitors (infliximab [Remicade], adalimumab [Humira], etanercept [Enbrel], golimumab [Simponi], certolizumab pegol [Cimzia]). The risk of developing arthritis was 42% lower (aHR, 0.58; 95% CI, 0.43-0.76) with the IL-12/23 inhibitor ustekinumab (Stelara), but there was no difference in outcomes among patients taking with IL-17 inhibitors (secukinumab [Cosentyx], ixekizumab [Taltz], or brodalumab [Siliq]), compared with TNF inhibitors. For the IL-12/23 inhibitor ustekinumab, all sensitivity analyses did not change this association. For IL-23 inhibitors, the results persisted when excluding patients who developed arthritis within 3 or 6 months after first biologic prescription and when using a higher diagnostic threshold for incident arthritis.
“There is a lot of interest in understanding if treatment of psoriasis will prevent onset of psoriatic arthritis,” said Joel M. Gelfand, MD, MSCE, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania, Philadelphia, who was asked to comment on the results.
“To date, the literature is inconclusive with some studies suggesting biologics reduce risk of PsA, whereas others suggest biologic use is associated with an increased risk of PsA,” he said. “The current study is unique in that it compares biologic classes to one another and suggests that IL-12/23 and IL-23 biologics are associated with a reduced risk of PsA compared to psoriasis patients treated with TNF inhibitors and no difference was found between TNF inhibitors and IL-17 inhibitors.”
While the study posed an interesting research question, “I wouldn’t use these results to actually change treatment patterns,” Alexis R. Ogdie-Beatty, MD, an associate professor of medicine at the University of Pennsylvania, Philadelphia, said in an interview. She coauthored a commentary on the analysis. Dr. Gelfand also emphasized that this bias may have influenced the results and that these findings “should not impact clinical practice at this time.”
Although the analyses were strong, Dr. Ogdie-Beatty noted, there are inherent biases in this type of observational data that cannot be overcome. For example, if a patient comes into a dermatologist’s office with psoriasis and also has joint pain, the dermatologist may suspect that a patient could also have psoriatic arthritis and would be more likely to choose a drug that will work well for both of these conditions.
“The drugs that are known to work best for psoriatic arthritis are the TNF inhibitors and the IL-17 inhibitors,” she said. So, while the analysis found these medications were associated with higher incidence of PsA, the dermatologist was possibly treating presumptive arthritis and the patient had yet to be referred to a rheumatologist to confirm the diagnosis.
The researchers noted that they attempted to mitigate these issues by requiring that patients have at least 1 year of follow-up before receiving biologic prescription “to capture only the patients with no previous codes for any type of arthritis,” as well as conducting six sensitivity analyses.
The authors, and Dr. Ogdie-Beatty and Dr. Gelfand agreed that more research is necessary to confirm these findings. A large randomized trial may be “prohibitively expensive,” the authors noted, but pooled analyses from previous clinical trials may help with this issue. “We identified 14 published randomized trials that did head-to-head comparisons of different biologic classes with regard to effect on psoriasis, and these trials collectively contained data on more than 13,000 patients. Pooled analyses of these data could confirm the findings of the present study and would be adequately powered.”
But that approach also has limitations, as psoriatic arthritis was not assessed an outcome in these studies, Dr. Ogdie-Beatty noted. Randomizing patients who are already at a higher risk of developing PsA to different biologics could be one approach to address these questions without needing such a large patient population.
The study was conducted without outside funding or industry involvement. Dr. Singla reported no relevant financial relationships with industry, but several coauthors reported financial relationships with pharmaceutical companies that market biologics for psoriasis and psoriatic arthritis. Dr. Ogdie-Beatty reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, CorEvitas, Gilead, Happify Health, Janssen, Lilly, Novartis, Pfizer, and UCB. Dr. Gelfand reported financial relationships with Abbvie, Amgen, BMS, Boehringer Ingelheim, FIDE, Lilly, Leo, Janssen Biologics, Novartis, Pfizer, and UCB. Dr. Gelfand is a deputy editor for the Journal of Investigative Dermatology.
This article was updated 3/15/23.
Patients with psoriasis treated with interleukin-12/23 inhibitors or IL-23 inhibitors were less likely to develop inflammatory arthritis, compared with those treated with tumor necrosis factor (TNF) inhibitors, according to findings from a large retrospective study.
While previous retrospective cohort studies have found biologic therapies for psoriasis can reduce the risk of developing psoriatic arthritis when compared with other treatments such as phototherapy and oral nonbiologic disease-modifying antirheumatic drugs, this analysis is the first to compare classes of biologics, Shikha Singla, MD, of the Medical College of Wisconsin, Milwaukee, and colleagues wrote in The Lancet Rheumatology.
In the analysis, researchers used the TriNetX database, which contains deidentified data from electronic medical health records from health care organizations across the United States. The study included adults diagnosed with psoriasis who were newly prescribed a biologic approved by the Food and Drug Administration for the treatment of psoriasis. Biologics were defined by drug class: anti-TNF, anti-IL-17, anti-IL-23, and anti–IL-12/23. Any patient with a diagnosis of psoriatic arthritis or other inflammatory arthritis prior to receiving a biologic prescription or within 2 weeks of receiving the prescription were excluded.
The researchers identified 15,501 eligible patients diagnosed with psoriasis during Jan. 1, 2014, to June 1, 2022, with an average follow-up time of 2.4 years. The researchers chose to start the study period in 2014 because the first non–anti-TNF drug for psoriatic arthritis was approved by the FDA in 2013 – the anti–IL-12/23 drug ustekinumab. During the study period, 976 patients developed inflammatory arthritis and were diagnosed on average 528 days after their biologic prescription.
In a multivariable analysis, the researchers found that patients prescribed IL-23 inhibitors (guselkumab [Tremfya], risankizumab [Skyrizi], tildrakizumab [Ilumya]) were nearly 60% less likely (adjusted hazard ratio, 0.41; 95% confidence interval, 0.17–0.95) to develop inflammatory arthritis than were patients taking TNF inhibitors (infliximab [Remicade], adalimumab [Humira], etanercept [Enbrel], golimumab [Simponi], certolizumab pegol [Cimzia]). The risk of developing arthritis was 42% lower (aHR, 0.58; 95% CI, 0.43-0.76) with the IL-12/23 inhibitor ustekinumab (Stelara), but there was no difference in outcomes among patients taking with IL-17 inhibitors (secukinumab [Cosentyx], ixekizumab [Taltz], or brodalumab [Siliq]), compared with TNF inhibitors. For the IL-12/23 inhibitor ustekinumab, all sensitivity analyses did not change this association. For IL-23 inhibitors, the results persisted when excluding patients who developed arthritis within 3 or 6 months after first biologic prescription and when using a higher diagnostic threshold for incident arthritis.
“There is a lot of interest in understanding if treatment of psoriasis will prevent onset of psoriatic arthritis,” said Joel M. Gelfand, MD, MSCE, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania, Philadelphia, who was asked to comment on the results.
“To date, the literature is inconclusive with some studies suggesting biologics reduce risk of PsA, whereas others suggest biologic use is associated with an increased risk of PsA,” he said. “The current study is unique in that it compares biologic classes to one another and suggests that IL-12/23 and IL-23 biologics are associated with a reduced risk of PsA compared to psoriasis patients treated with TNF inhibitors and no difference was found between TNF inhibitors and IL-17 inhibitors.”
While the study posed an interesting research question, “I wouldn’t use these results to actually change treatment patterns,” Alexis R. Ogdie-Beatty, MD, an associate professor of medicine at the University of Pennsylvania, Philadelphia, said in an interview. She coauthored a commentary on the analysis. Dr. Gelfand also emphasized that this bias may have influenced the results and that these findings “should not impact clinical practice at this time.”
Although the analyses were strong, Dr. Ogdie-Beatty noted, there are inherent biases in this type of observational data that cannot be overcome. For example, if a patient comes into a dermatologist’s office with psoriasis and also has joint pain, the dermatologist may suspect that a patient could also have psoriatic arthritis and would be more likely to choose a drug that will work well for both of these conditions.
“The drugs that are known to work best for psoriatic arthritis are the TNF inhibitors and the IL-17 inhibitors,” she said. So, while the analysis found these medications were associated with higher incidence of PsA, the dermatologist was possibly treating presumptive arthritis and the patient had yet to be referred to a rheumatologist to confirm the diagnosis.
The researchers noted that they attempted to mitigate these issues by requiring that patients have at least 1 year of follow-up before receiving biologic prescription “to capture only the patients with no previous codes for any type of arthritis,” as well as conducting six sensitivity analyses.
The authors, and Dr. Ogdie-Beatty and Dr. Gelfand agreed that more research is necessary to confirm these findings. A large randomized trial may be “prohibitively expensive,” the authors noted, but pooled analyses from previous clinical trials may help with this issue. “We identified 14 published randomized trials that did head-to-head comparisons of different biologic classes with regard to effect on psoriasis, and these trials collectively contained data on more than 13,000 patients. Pooled analyses of these data could confirm the findings of the present study and would be adequately powered.”
But that approach also has limitations, as psoriatic arthritis was not assessed an outcome in these studies, Dr. Ogdie-Beatty noted. Randomizing patients who are already at a higher risk of developing PsA to different biologics could be one approach to address these questions without needing such a large patient population.
The study was conducted without outside funding or industry involvement. Dr. Singla reported no relevant financial relationships with industry, but several coauthors reported financial relationships with pharmaceutical companies that market biologics for psoriasis and psoriatic arthritis. Dr. Ogdie-Beatty reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, CorEvitas, Gilead, Happify Health, Janssen, Lilly, Novartis, Pfizer, and UCB. Dr. Gelfand reported financial relationships with Abbvie, Amgen, BMS, Boehringer Ingelheim, FIDE, Lilly, Leo, Janssen Biologics, Novartis, Pfizer, and UCB. Dr. Gelfand is a deputy editor for the Journal of Investigative Dermatology.
This article was updated 3/15/23.
Patients with psoriasis treated with interleukin-12/23 inhibitors or IL-23 inhibitors were less likely to develop inflammatory arthritis, compared with those treated with tumor necrosis factor (TNF) inhibitors, according to findings from a large retrospective study.
While previous retrospective cohort studies have found biologic therapies for psoriasis can reduce the risk of developing psoriatic arthritis when compared with other treatments such as phototherapy and oral nonbiologic disease-modifying antirheumatic drugs, this analysis is the first to compare classes of biologics, Shikha Singla, MD, of the Medical College of Wisconsin, Milwaukee, and colleagues wrote in The Lancet Rheumatology.
In the analysis, researchers used the TriNetX database, which contains deidentified data from electronic medical health records from health care organizations across the United States. The study included adults diagnosed with psoriasis who were newly prescribed a biologic approved by the Food and Drug Administration for the treatment of psoriasis. Biologics were defined by drug class: anti-TNF, anti-IL-17, anti-IL-23, and anti–IL-12/23. Any patient with a diagnosis of psoriatic arthritis or other inflammatory arthritis prior to receiving a biologic prescription or within 2 weeks of receiving the prescription were excluded.
The researchers identified 15,501 eligible patients diagnosed with psoriasis during Jan. 1, 2014, to June 1, 2022, with an average follow-up time of 2.4 years. The researchers chose to start the study period in 2014 because the first non–anti-TNF drug for psoriatic arthritis was approved by the FDA in 2013 – the anti–IL-12/23 drug ustekinumab. During the study period, 976 patients developed inflammatory arthritis and were diagnosed on average 528 days after their biologic prescription.
In a multivariable analysis, the researchers found that patients prescribed IL-23 inhibitors (guselkumab [Tremfya], risankizumab [Skyrizi], tildrakizumab [Ilumya]) were nearly 60% less likely (adjusted hazard ratio, 0.41; 95% confidence interval, 0.17–0.95) to develop inflammatory arthritis than were patients taking TNF inhibitors (infliximab [Remicade], adalimumab [Humira], etanercept [Enbrel], golimumab [Simponi], certolizumab pegol [Cimzia]). The risk of developing arthritis was 42% lower (aHR, 0.58; 95% CI, 0.43-0.76) with the IL-12/23 inhibitor ustekinumab (Stelara), but there was no difference in outcomes among patients taking with IL-17 inhibitors (secukinumab [Cosentyx], ixekizumab [Taltz], or brodalumab [Siliq]), compared with TNF inhibitors. For the IL-12/23 inhibitor ustekinumab, all sensitivity analyses did not change this association. For IL-23 inhibitors, the results persisted when excluding patients who developed arthritis within 3 or 6 months after first biologic prescription and when using a higher diagnostic threshold for incident arthritis.
“There is a lot of interest in understanding if treatment of psoriasis will prevent onset of psoriatic arthritis,” said Joel M. Gelfand, MD, MSCE, director of the Psoriasis and Phototherapy Treatment Center at the University of Pennsylvania, Philadelphia, who was asked to comment on the results.
“To date, the literature is inconclusive with some studies suggesting biologics reduce risk of PsA, whereas others suggest biologic use is associated with an increased risk of PsA,” he said. “The current study is unique in that it compares biologic classes to one another and suggests that IL-12/23 and IL-23 biologics are associated with a reduced risk of PsA compared to psoriasis patients treated with TNF inhibitors and no difference was found between TNF inhibitors and IL-17 inhibitors.”
While the study posed an interesting research question, “I wouldn’t use these results to actually change treatment patterns,” Alexis R. Ogdie-Beatty, MD, an associate professor of medicine at the University of Pennsylvania, Philadelphia, said in an interview. She coauthored a commentary on the analysis. Dr. Gelfand also emphasized that this bias may have influenced the results and that these findings “should not impact clinical practice at this time.”
Although the analyses were strong, Dr. Ogdie-Beatty noted, there are inherent biases in this type of observational data that cannot be overcome. For example, if a patient comes into a dermatologist’s office with psoriasis and also has joint pain, the dermatologist may suspect that a patient could also have psoriatic arthritis and would be more likely to choose a drug that will work well for both of these conditions.
“The drugs that are known to work best for psoriatic arthritis are the TNF inhibitors and the IL-17 inhibitors,” she said. So, while the analysis found these medications were associated with higher incidence of PsA, the dermatologist was possibly treating presumptive arthritis and the patient had yet to be referred to a rheumatologist to confirm the diagnosis.
The researchers noted that they attempted to mitigate these issues by requiring that patients have at least 1 year of follow-up before receiving biologic prescription “to capture only the patients with no previous codes for any type of arthritis,” as well as conducting six sensitivity analyses.
The authors, and Dr. Ogdie-Beatty and Dr. Gelfand agreed that more research is necessary to confirm these findings. A large randomized trial may be “prohibitively expensive,” the authors noted, but pooled analyses from previous clinical trials may help with this issue. “We identified 14 published randomized trials that did head-to-head comparisons of different biologic classes with regard to effect on psoriasis, and these trials collectively contained data on more than 13,000 patients. Pooled analyses of these data could confirm the findings of the present study and would be adequately powered.”
But that approach also has limitations, as psoriatic arthritis was not assessed an outcome in these studies, Dr. Ogdie-Beatty noted. Randomizing patients who are already at a higher risk of developing PsA to different biologics could be one approach to address these questions without needing such a large patient population.
The study was conducted without outside funding or industry involvement. Dr. Singla reported no relevant financial relationships with industry, but several coauthors reported financial relationships with pharmaceutical companies that market biologics for psoriasis and psoriatic arthritis. Dr. Ogdie-Beatty reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, CorEvitas, Gilead, Happify Health, Janssen, Lilly, Novartis, Pfizer, and UCB. Dr. Gelfand reported financial relationships with Abbvie, Amgen, BMS, Boehringer Ingelheim, FIDE, Lilly, Leo, Janssen Biologics, Novartis, Pfizer, and UCB. Dr. Gelfand is a deputy editor for the Journal of Investigative Dermatology.
This article was updated 3/15/23.
FROM LANCET RHEUMATOLOGY
Psoriatic arthritis: An independent risk factor for reduced bone density and fractures
Key clinical point: Regular assessment of bone mineral density and initiation of primary prevention should be considered in patients with psoriatic arthritis (PsA) as they are predisposed to falls and fractures because of reduced bone density, particularly those with late-onset psoriasis involving scalp.
Major finding: Patients with PsA were at a significantly higher risk for osteopenia or osteoporosis (odds ratio [OR] 21.9; CI 7.1-67.7) and prevalent fractures (OR 3.42; P = .002) compared with control individuals, with scalp involvement (P = .0049) and late onset of psoriasis (P = .029) being significantly associated with greater number of prevalent fractures.
Study details: Findings are from an observational cohort study including 61 patients with PsA and 69 age-matched control individuals.
Disclosures: This study did not report the source of funding. The authors reported no conflicts of interest.
Source: Halasi A et al. Psoriatic arthritis and its special features predispose not only for osteoporosis but also for fractures and falls. J Dermatol. 2023 (Jan 17). Doi: 10.1111/1346-8138.16710
Key clinical point: Regular assessment of bone mineral density and initiation of primary prevention should be considered in patients with psoriatic arthritis (PsA) as they are predisposed to falls and fractures because of reduced bone density, particularly those with late-onset psoriasis involving scalp.
Major finding: Patients with PsA were at a significantly higher risk for osteopenia or osteoporosis (odds ratio [OR] 21.9; CI 7.1-67.7) and prevalent fractures (OR 3.42; P = .002) compared with control individuals, with scalp involvement (P = .0049) and late onset of psoriasis (P = .029) being significantly associated with greater number of prevalent fractures.
Study details: Findings are from an observational cohort study including 61 patients with PsA and 69 age-matched control individuals.
Disclosures: This study did not report the source of funding. The authors reported no conflicts of interest.
Source: Halasi A et al. Psoriatic arthritis and its special features predispose not only for osteoporosis but also for fractures and falls. J Dermatol. 2023 (Jan 17). Doi: 10.1111/1346-8138.16710
Key clinical point: Regular assessment of bone mineral density and initiation of primary prevention should be considered in patients with psoriatic arthritis (PsA) as they are predisposed to falls and fractures because of reduced bone density, particularly those with late-onset psoriasis involving scalp.
Major finding: Patients with PsA were at a significantly higher risk for osteopenia or osteoporosis (odds ratio [OR] 21.9; CI 7.1-67.7) and prevalent fractures (OR 3.42; P = .002) compared with control individuals, with scalp involvement (P = .0049) and late onset of psoriasis (P = .029) being significantly associated with greater number of prevalent fractures.
Study details: Findings are from an observational cohort study including 61 patients with PsA and 69 age-matched control individuals.
Disclosures: This study did not report the source of funding. The authors reported no conflicts of interest.
Source: Halasi A et al. Psoriatic arthritis and its special features predispose not only for osteoporosis but also for fractures and falls. J Dermatol. 2023 (Jan 17). Doi: 10.1111/1346-8138.16710
PsA: Guselkumab demonstrates consistent safety profile irrespective of prior TNFi exposure
Key clinical point: A dose of 100 mg guselkumab every 4 or 8 weeks (Q4W/Q8W) demonstrated a favorable and consistent safety profile for up to 2 years in both tumor necrosis factor-α inhibitor (TNFi)-naive and TNFi-experienced patients with active psoriatic arthritis (PsA).
Major finding: In TNFi-naive vs TNFi-experienced patients receiving guselkumab, adverse events rates were consistent through 24 weeks (220.8/100 person-years [PY] vs 251.6/100 PY) and remained low through 2 years (139.69/100 PY vs 174.0/100 PY).
Study details: This pooled safety analysis of four phase 2/3 trials included 1554 TNFi-naive and TNFi-experienced patients with active PsA who were randomly assigned to receive 100 mg guselkumab Q4W or Q8W for ≤2 years or placebo with a crossover at week 24 to guselkumab Q4W or Q8W.
Disclosures: The four trials were funded by Janssen Research & Development, LLC. Seven authors declared being current or former employees of Janssen or owning stock or stock options in Johnson & Johnson. Several authors reported ties with Janssen and other sources.
Source: Rahman P et al. Safety of guselkumab with and without prior TNF-α inhibitor treatment: Pooled results across four studies in patients with psoriatic arthritis. J Rheumatol. 2023 (Jan 15). Doi: 10.3899/jrheum.220928
Key clinical point: A dose of 100 mg guselkumab every 4 or 8 weeks (Q4W/Q8W) demonstrated a favorable and consistent safety profile for up to 2 years in both tumor necrosis factor-α inhibitor (TNFi)-naive and TNFi-experienced patients with active psoriatic arthritis (PsA).
Major finding: In TNFi-naive vs TNFi-experienced patients receiving guselkumab, adverse events rates were consistent through 24 weeks (220.8/100 person-years [PY] vs 251.6/100 PY) and remained low through 2 years (139.69/100 PY vs 174.0/100 PY).
Study details: This pooled safety analysis of four phase 2/3 trials included 1554 TNFi-naive and TNFi-experienced patients with active PsA who were randomly assigned to receive 100 mg guselkumab Q4W or Q8W for ≤2 years or placebo with a crossover at week 24 to guselkumab Q4W or Q8W.
Disclosures: The four trials were funded by Janssen Research & Development, LLC. Seven authors declared being current or former employees of Janssen or owning stock or stock options in Johnson & Johnson. Several authors reported ties with Janssen and other sources.
Source: Rahman P et al. Safety of guselkumab with and without prior TNF-α inhibitor treatment: Pooled results across four studies in patients with psoriatic arthritis. J Rheumatol. 2023 (Jan 15). Doi: 10.3899/jrheum.220928
Key clinical point: A dose of 100 mg guselkumab every 4 or 8 weeks (Q4W/Q8W) demonstrated a favorable and consistent safety profile for up to 2 years in both tumor necrosis factor-α inhibitor (TNFi)-naive and TNFi-experienced patients with active psoriatic arthritis (PsA).
Major finding: In TNFi-naive vs TNFi-experienced patients receiving guselkumab, adverse events rates were consistent through 24 weeks (220.8/100 person-years [PY] vs 251.6/100 PY) and remained low through 2 years (139.69/100 PY vs 174.0/100 PY).
Study details: This pooled safety analysis of four phase 2/3 trials included 1554 TNFi-naive and TNFi-experienced patients with active PsA who were randomly assigned to receive 100 mg guselkumab Q4W or Q8W for ≤2 years or placebo with a crossover at week 24 to guselkumab Q4W or Q8W.
Disclosures: The four trials were funded by Janssen Research & Development, LLC. Seven authors declared being current or former employees of Janssen or owning stock or stock options in Johnson & Johnson. Several authors reported ties with Janssen and other sources.
Source: Rahman P et al. Safety of guselkumab with and without prior TNF-α inhibitor treatment: Pooled results across four studies in patients with psoriatic arthritis. J Rheumatol. 2023 (Jan 15). Doi: 10.3899/jrheum.220928
Causal link found between childhood obesity and adult-onset diabetes
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
FROM DIABETOLOGIA
Midwife-led care linked to positive outcomes across medical risk levels
Midwives provide safe primary care for pregnant women who are at various levels of medical risk in British Columbia, Canada, new data suggest.
In most cases, for midwifery clients, birth outcomes were similar to or were better than birth outcomes of patients who had physician-led or obstetrician-led care.
In addition, midwifery clients were less likely to experience preterm births or have low-birth-weight babies and to experience cesarean deliveries or births involving instruments.
“Based on previous research, we know that midwives provide safe care for healthy childbearing people or those with no or few risk factors that might complicate the pregnancy or birth,” lead author Kathrin Stoll, PhD, a research associate in the University of British Columbia’s department of family practice, told this news organization.
“What we didn’t know until now is whether midwives provide safe care to people with moderate and high medical risks and what proportion of B.C. [British Columbia] midwifery clients are low, moderate, and high risk,” she said. “This is important to know because of the misperception that midwives only look after low-risk people. This misperception is sometimes used against midwives to justify giving them fewer resources and supports.”
The study was published in the Canadian Medical Association Journal.
Increasing demand
Registered midwives have been part of the health care system in British Columbia since 1998, according to the study authors. The number of pregnant people who are attended by midwives during birth has steadily increased from 4.8% in 2004-2005 to 15.6% in 2019-2020.
The investigators analyzed 2008-2018 data from the British Columbia Perinatal Data Registry, which contains data for 99% of births, including home births. Their analysis included 425,056 births for which a family physician, an obstetrician, or a midwife was listed as the most responsible provider (MRP). The investigators assessed pregnancy risk status (low, moderate, or high), which was determined on the basis of an adapted perinatal risk scoring system used by the Alberta Perinatal Health Program. They estimated the differences in neonatal and maternal outcomes between MRP groups by calculating adjusted absolute and relative risks.
Among the 425,056 births, 63,151 (14.9%) had a midwife as the MRP, 189,679 (44.6%) had a family physician, and 172,226 (40.5%) had an obstetrician. The antenatal risk score ranged from 0 to 23 (median score, 2).
The proportion of births with midwife-led care increased from 9.2% to 19.8% from 2008-2018. In 2018, midwives were listed as the MRP for 24.3% of low-risk, 14.3% of moderate-risk, and 7.9% of high-risk births in the province. This represented an absolute increase of 9.1% for low-risk, 7.7% for moderate-risk, and 5.7% for high-risk births during the study period.
Among the 12,169 at-home births that took place during the study period, 9,776 (80.3%) were low-risk, 2,329 (19.1%) were moderate-risk, and 64 (0.5%) were high-risk births. As the risk score increased, so did the proportion of midwifery and family physician clients who were delivered by obstetricians. Across all risk strata, more family physician clients than midwifery clients underwent deliveries by obstetricians.
Overall, the risk of perinatal death for midwifery clients was similar to the risk for those under the care of family physicians across all risk levels. Low- and moderate-risk clients with midwife-led care were significantly less likely to experience a perinatal death, compared with those with obstetrician-led care, although the adjusted absolute risk differences were small. In the high-risk group, there was no significant difference in the rate of perinatal deaths between midwife-led and physician-led care.
In addition, clients with midwife-led care were significantly less likely to experience preterm birth and have a low-birth-weight baby regardless of medical risk level. The adjusted relative risk of an Apgar score of less than 7 at 5 minutes was significantly lower for midwife-led care than for physician-led care for nearly all comparisons.
The cesarean delivery rate among midwifery clients in the low-risk group was 7.2%, compared with 12.2% for family physicians and 42.3% for obstetrician clients. Cesarean delivery rates increased for midwifery clients as medical risk increased but were significantly lower than the physician rates across all medical risk levels.
Among low-risk clients, the absolute risk reduction for cesarean delivery was 34.4% with midwife-led care, compared with obstetrician-led care. The absolute risk difference increased to 55.3% for moderate-risk clients and to 42.2% for high-risk clients.
Labor induction varied
Although low-risk midwifery clients were significantly less likely to experience labor induction with oxytocin, high-risk midwifery clients were more than twice as likely to undergo induction with oxytocin than obstetrician clients (adjusted absolute difference, 11.3%).
For most risk levels, midwifery clients were less likely to have an assisted vaginal birth than physician clients, and they were significantly more likely to have a spontaneous vaginal birth. Low-risk clients who had a midwife as the MRP were nearly twice as likely to have a spontaneous vaginal birth than obstetricians’ clients, and moderate-risk clients were nearly four times as likely to have a spontaneous vaginal birth.
The rates of vaginal birth after cesarean delivery (VBAC) were significantly higher when a midwife was the MRP. In comparing midwifery clients with family physician clients, the relative and absolute differences were small, but they were larger when comparing midwifery clients with obstetrician clients. Among low-risk clients, the VBAC rate was 85.3% among midwifery clients, compared with 78.6% among family physician clients and 51.5% among obstetrician clients.
In general, the prevalence rates of adverse maternal outcomes (including blood transfusion, intensive care admissions, uterine rupture, and postpartum wound infection) were low for midwifery clients across all risk levels.
Breast- or chest-feeding at birth was significantly more common among midwifery clients across all risk levels as well.
Today, nearly 1 in 4 childbearing people in British Columbia receive care from a midwife at some point during pregnancy, birth, or the postpartum period, the study authors write. During the past 20 years, the profile of clients has evolved to include more moderate- and high-risk patients.
“Clients with more complex medical needs take more time and need more support,” said Dr. Stoll. “This means that midwives continue to stay on call, responding to pages and urgent medical concerns for their clients with no pay for being on call, no days off even for sick days, and unsafe working hours, often working more than 24 hours at a time. If we want to expand midwifery to communities where they are needed most, we need to provide an enabling environment.”
Additional studies are needed as to how different practice and remuneration models affect clinical outcomes, health care costs, and client and provider experiences, the study authors write. At the same time, there are several barriers to obtaining funding, conducting studies, and publishing research by and about midwives in Canada, Dr. Stoll said – barriers that she and her co-authors faced.
Seeking broader access
Alixandra Bacon, a registered midwife and president of the Canadian Association of Midwives, said, “These findings demonstrate that pregnant people at any level of medical risk can benefit from midwifery care. This is a testament both to the benefits of the Canadian midwifery model of care and to the seamless integration of midwifery into collaborative teams and the health system.” Ms. Bacon wasn’t involved with this study.
“If we can realize our goal of equitable access to midwifery care for all families in Canada, we can help to decrease rates of unnecessary medical intervention, preterm labor, and stillbirth,” she added.
“Midwifery is well established across most of Canada. This is yet one more piece of evidence that shows the clinical benefits of midwifery care,” Jasmin Tecson, a registered midwife and president of the Association of Ontario Midwives, said in an interview.
Ms. Tecson, who wasn’t involved with this study, noted the increasing number of clients with more complex health and social needs in Ontario. “It is time to think about how the skills and knowledge of midwives can be used with clients of different risk profiles and how the current scope of practice of midwives can be optimized and expanded,” she said. “For example, Ontario midwives are still required to prescribe medications from a limited list, despite the potential additional clinical risks and health system costs that this creates.”
The study received financial support from the University of British Columbia Stollery Fund and the University of British Columbia Work Learn Program. Dr. Stoll has an unpaid role with the Midwives Association Contract Negotiation Advisory Council. Ms. Bacon and Ms. Tecson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Midwives provide safe primary care for pregnant women who are at various levels of medical risk in British Columbia, Canada, new data suggest.
In most cases, for midwifery clients, birth outcomes were similar to or were better than birth outcomes of patients who had physician-led or obstetrician-led care.
In addition, midwifery clients were less likely to experience preterm births or have low-birth-weight babies and to experience cesarean deliveries or births involving instruments.
“Based on previous research, we know that midwives provide safe care for healthy childbearing people or those with no or few risk factors that might complicate the pregnancy or birth,” lead author Kathrin Stoll, PhD, a research associate in the University of British Columbia’s department of family practice, told this news organization.
“What we didn’t know until now is whether midwives provide safe care to people with moderate and high medical risks and what proportion of B.C. [British Columbia] midwifery clients are low, moderate, and high risk,” she said. “This is important to know because of the misperception that midwives only look after low-risk people. This misperception is sometimes used against midwives to justify giving them fewer resources and supports.”
The study was published in the Canadian Medical Association Journal.
Increasing demand
Registered midwives have been part of the health care system in British Columbia since 1998, according to the study authors. The number of pregnant people who are attended by midwives during birth has steadily increased from 4.8% in 2004-2005 to 15.6% in 2019-2020.
The investigators analyzed 2008-2018 data from the British Columbia Perinatal Data Registry, which contains data for 99% of births, including home births. Their analysis included 425,056 births for which a family physician, an obstetrician, or a midwife was listed as the most responsible provider (MRP). The investigators assessed pregnancy risk status (low, moderate, or high), which was determined on the basis of an adapted perinatal risk scoring system used by the Alberta Perinatal Health Program. They estimated the differences in neonatal and maternal outcomes between MRP groups by calculating adjusted absolute and relative risks.
Among the 425,056 births, 63,151 (14.9%) had a midwife as the MRP, 189,679 (44.6%) had a family physician, and 172,226 (40.5%) had an obstetrician. The antenatal risk score ranged from 0 to 23 (median score, 2).
The proportion of births with midwife-led care increased from 9.2% to 19.8% from 2008-2018. In 2018, midwives were listed as the MRP for 24.3% of low-risk, 14.3% of moderate-risk, and 7.9% of high-risk births in the province. This represented an absolute increase of 9.1% for low-risk, 7.7% for moderate-risk, and 5.7% for high-risk births during the study period.
Among the 12,169 at-home births that took place during the study period, 9,776 (80.3%) were low-risk, 2,329 (19.1%) were moderate-risk, and 64 (0.5%) were high-risk births. As the risk score increased, so did the proportion of midwifery and family physician clients who were delivered by obstetricians. Across all risk strata, more family physician clients than midwifery clients underwent deliveries by obstetricians.
Overall, the risk of perinatal death for midwifery clients was similar to the risk for those under the care of family physicians across all risk levels. Low- and moderate-risk clients with midwife-led care were significantly less likely to experience a perinatal death, compared with those with obstetrician-led care, although the adjusted absolute risk differences were small. In the high-risk group, there was no significant difference in the rate of perinatal deaths between midwife-led and physician-led care.
In addition, clients with midwife-led care were significantly less likely to experience preterm birth and have a low-birth-weight baby regardless of medical risk level. The adjusted relative risk of an Apgar score of less than 7 at 5 minutes was significantly lower for midwife-led care than for physician-led care for nearly all comparisons.
The cesarean delivery rate among midwifery clients in the low-risk group was 7.2%, compared with 12.2% for family physicians and 42.3% for obstetrician clients. Cesarean delivery rates increased for midwifery clients as medical risk increased but were significantly lower than the physician rates across all medical risk levels.
Among low-risk clients, the absolute risk reduction for cesarean delivery was 34.4% with midwife-led care, compared with obstetrician-led care. The absolute risk difference increased to 55.3% for moderate-risk clients and to 42.2% for high-risk clients.
Labor induction varied
Although low-risk midwifery clients were significantly less likely to experience labor induction with oxytocin, high-risk midwifery clients were more than twice as likely to undergo induction with oxytocin than obstetrician clients (adjusted absolute difference, 11.3%).
For most risk levels, midwifery clients were less likely to have an assisted vaginal birth than physician clients, and they were significantly more likely to have a spontaneous vaginal birth. Low-risk clients who had a midwife as the MRP were nearly twice as likely to have a spontaneous vaginal birth than obstetricians’ clients, and moderate-risk clients were nearly four times as likely to have a spontaneous vaginal birth.
The rates of vaginal birth after cesarean delivery (VBAC) were significantly higher when a midwife was the MRP. In comparing midwifery clients with family physician clients, the relative and absolute differences were small, but they were larger when comparing midwifery clients with obstetrician clients. Among low-risk clients, the VBAC rate was 85.3% among midwifery clients, compared with 78.6% among family physician clients and 51.5% among obstetrician clients.
In general, the prevalence rates of adverse maternal outcomes (including blood transfusion, intensive care admissions, uterine rupture, and postpartum wound infection) were low for midwifery clients across all risk levels.
Breast- or chest-feeding at birth was significantly more common among midwifery clients across all risk levels as well.
Today, nearly 1 in 4 childbearing people in British Columbia receive care from a midwife at some point during pregnancy, birth, or the postpartum period, the study authors write. During the past 20 years, the profile of clients has evolved to include more moderate- and high-risk patients.
“Clients with more complex medical needs take more time and need more support,” said Dr. Stoll. “This means that midwives continue to stay on call, responding to pages and urgent medical concerns for their clients with no pay for being on call, no days off even for sick days, and unsafe working hours, often working more than 24 hours at a time. If we want to expand midwifery to communities where they are needed most, we need to provide an enabling environment.”
Additional studies are needed as to how different practice and remuneration models affect clinical outcomes, health care costs, and client and provider experiences, the study authors write. At the same time, there are several barriers to obtaining funding, conducting studies, and publishing research by and about midwives in Canada, Dr. Stoll said – barriers that she and her co-authors faced.
Seeking broader access
Alixandra Bacon, a registered midwife and president of the Canadian Association of Midwives, said, “These findings demonstrate that pregnant people at any level of medical risk can benefit from midwifery care. This is a testament both to the benefits of the Canadian midwifery model of care and to the seamless integration of midwifery into collaborative teams and the health system.” Ms. Bacon wasn’t involved with this study.
“If we can realize our goal of equitable access to midwifery care for all families in Canada, we can help to decrease rates of unnecessary medical intervention, preterm labor, and stillbirth,” she added.
“Midwifery is well established across most of Canada. This is yet one more piece of evidence that shows the clinical benefits of midwifery care,” Jasmin Tecson, a registered midwife and president of the Association of Ontario Midwives, said in an interview.
Ms. Tecson, who wasn’t involved with this study, noted the increasing number of clients with more complex health and social needs in Ontario. “It is time to think about how the skills and knowledge of midwives can be used with clients of different risk profiles and how the current scope of practice of midwives can be optimized and expanded,” she said. “For example, Ontario midwives are still required to prescribe medications from a limited list, despite the potential additional clinical risks and health system costs that this creates.”
The study received financial support from the University of British Columbia Stollery Fund and the University of British Columbia Work Learn Program. Dr. Stoll has an unpaid role with the Midwives Association Contract Negotiation Advisory Council. Ms. Bacon and Ms. Tecson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Midwives provide safe primary care for pregnant women who are at various levels of medical risk in British Columbia, Canada, new data suggest.
In most cases, for midwifery clients, birth outcomes were similar to or were better than birth outcomes of patients who had physician-led or obstetrician-led care.
In addition, midwifery clients were less likely to experience preterm births or have low-birth-weight babies and to experience cesarean deliveries or births involving instruments.
“Based on previous research, we know that midwives provide safe care for healthy childbearing people or those with no or few risk factors that might complicate the pregnancy or birth,” lead author Kathrin Stoll, PhD, a research associate in the University of British Columbia’s department of family practice, told this news organization.
“What we didn’t know until now is whether midwives provide safe care to people with moderate and high medical risks and what proportion of B.C. [British Columbia] midwifery clients are low, moderate, and high risk,” she said. “This is important to know because of the misperception that midwives only look after low-risk people. This misperception is sometimes used against midwives to justify giving them fewer resources and supports.”
The study was published in the Canadian Medical Association Journal.
Increasing demand
Registered midwives have been part of the health care system in British Columbia since 1998, according to the study authors. The number of pregnant people who are attended by midwives during birth has steadily increased from 4.8% in 2004-2005 to 15.6% in 2019-2020.
The investigators analyzed 2008-2018 data from the British Columbia Perinatal Data Registry, which contains data for 99% of births, including home births. Their analysis included 425,056 births for which a family physician, an obstetrician, or a midwife was listed as the most responsible provider (MRP). The investigators assessed pregnancy risk status (low, moderate, or high), which was determined on the basis of an adapted perinatal risk scoring system used by the Alberta Perinatal Health Program. They estimated the differences in neonatal and maternal outcomes between MRP groups by calculating adjusted absolute and relative risks.
Among the 425,056 births, 63,151 (14.9%) had a midwife as the MRP, 189,679 (44.6%) had a family physician, and 172,226 (40.5%) had an obstetrician. The antenatal risk score ranged from 0 to 23 (median score, 2).
The proportion of births with midwife-led care increased from 9.2% to 19.8% from 2008-2018. In 2018, midwives were listed as the MRP for 24.3% of low-risk, 14.3% of moderate-risk, and 7.9% of high-risk births in the province. This represented an absolute increase of 9.1% for low-risk, 7.7% for moderate-risk, and 5.7% for high-risk births during the study period.
Among the 12,169 at-home births that took place during the study period, 9,776 (80.3%) were low-risk, 2,329 (19.1%) were moderate-risk, and 64 (0.5%) were high-risk births. As the risk score increased, so did the proportion of midwifery and family physician clients who were delivered by obstetricians. Across all risk strata, more family physician clients than midwifery clients underwent deliveries by obstetricians.
Overall, the risk of perinatal death for midwifery clients was similar to the risk for those under the care of family physicians across all risk levels. Low- and moderate-risk clients with midwife-led care were significantly less likely to experience a perinatal death, compared with those with obstetrician-led care, although the adjusted absolute risk differences were small. In the high-risk group, there was no significant difference in the rate of perinatal deaths between midwife-led and physician-led care.
In addition, clients with midwife-led care were significantly less likely to experience preterm birth and have a low-birth-weight baby regardless of medical risk level. The adjusted relative risk of an Apgar score of less than 7 at 5 minutes was significantly lower for midwife-led care than for physician-led care for nearly all comparisons.
The cesarean delivery rate among midwifery clients in the low-risk group was 7.2%, compared with 12.2% for family physicians and 42.3% for obstetrician clients. Cesarean delivery rates increased for midwifery clients as medical risk increased but were significantly lower than the physician rates across all medical risk levels.
Among low-risk clients, the absolute risk reduction for cesarean delivery was 34.4% with midwife-led care, compared with obstetrician-led care. The absolute risk difference increased to 55.3% for moderate-risk clients and to 42.2% for high-risk clients.
Labor induction varied
Although low-risk midwifery clients were significantly less likely to experience labor induction with oxytocin, high-risk midwifery clients were more than twice as likely to undergo induction with oxytocin than obstetrician clients (adjusted absolute difference, 11.3%).
For most risk levels, midwifery clients were less likely to have an assisted vaginal birth than physician clients, and they were significantly more likely to have a spontaneous vaginal birth. Low-risk clients who had a midwife as the MRP were nearly twice as likely to have a spontaneous vaginal birth than obstetricians’ clients, and moderate-risk clients were nearly four times as likely to have a spontaneous vaginal birth.
The rates of vaginal birth after cesarean delivery (VBAC) were significantly higher when a midwife was the MRP. In comparing midwifery clients with family physician clients, the relative and absolute differences were small, but they were larger when comparing midwifery clients with obstetrician clients. Among low-risk clients, the VBAC rate was 85.3% among midwifery clients, compared with 78.6% among family physician clients and 51.5% among obstetrician clients.
In general, the prevalence rates of adverse maternal outcomes (including blood transfusion, intensive care admissions, uterine rupture, and postpartum wound infection) were low for midwifery clients across all risk levels.
Breast- or chest-feeding at birth was significantly more common among midwifery clients across all risk levels as well.
Today, nearly 1 in 4 childbearing people in British Columbia receive care from a midwife at some point during pregnancy, birth, or the postpartum period, the study authors write. During the past 20 years, the profile of clients has evolved to include more moderate- and high-risk patients.
“Clients with more complex medical needs take more time and need more support,” said Dr. Stoll. “This means that midwives continue to stay on call, responding to pages and urgent medical concerns for their clients with no pay for being on call, no days off even for sick days, and unsafe working hours, often working more than 24 hours at a time. If we want to expand midwifery to communities where they are needed most, we need to provide an enabling environment.”
Additional studies are needed as to how different practice and remuneration models affect clinical outcomes, health care costs, and client and provider experiences, the study authors write. At the same time, there are several barriers to obtaining funding, conducting studies, and publishing research by and about midwives in Canada, Dr. Stoll said – barriers that she and her co-authors faced.
Seeking broader access
Alixandra Bacon, a registered midwife and president of the Canadian Association of Midwives, said, “These findings demonstrate that pregnant people at any level of medical risk can benefit from midwifery care. This is a testament both to the benefits of the Canadian midwifery model of care and to the seamless integration of midwifery into collaborative teams and the health system.” Ms. Bacon wasn’t involved with this study.
“If we can realize our goal of equitable access to midwifery care for all families in Canada, we can help to decrease rates of unnecessary medical intervention, preterm labor, and stillbirth,” she added.
“Midwifery is well established across most of Canada. This is yet one more piece of evidence that shows the clinical benefits of midwifery care,” Jasmin Tecson, a registered midwife and president of the Association of Ontario Midwives, said in an interview.
Ms. Tecson, who wasn’t involved with this study, noted the increasing number of clients with more complex health and social needs in Ontario. “It is time to think about how the skills and knowledge of midwives can be used with clients of different risk profiles and how the current scope of practice of midwives can be optimized and expanded,” she said. “For example, Ontario midwives are still required to prescribe medications from a limited list, despite the potential additional clinical risks and health system costs that this creates.”
The study received financial support from the University of British Columbia Stollery Fund and the University of British Columbia Work Learn Program. Dr. Stoll has an unpaid role with the Midwives Association Contract Negotiation Advisory Council. Ms. Bacon and Ms. Tecson disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Modified ECT lowers dental, skeletal fracture risk

“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”

Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”
Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“ECT is associated with a very low risk of skeletal fractures, even in high-risk patients, and is also associated with a low risk of dental fractures,” said study investigator Chittaranjan Andrade, MD, noting that preexisting bone and dental disease increase this risk.
Overall, clinicians who provide ECT “need to be aware of rare adverse effects, as well as the common ones,” Dr. Andrade, senior professor of clinical psychopharmacology and neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India, told this news organization. He added they also “need data to be able to provide reassurance.”
The findings were published online in The Journal of Clinical Psychiatry.
Avoid unmodified ECT
Dr. Andrade conducted the study because the risk of skeletal and dental fractures associated with ECT is “not commonly discussed.”
Although ECT is perhaps the most effective available treatment for major mental illness, it is associated with several adverse effects, including those associated with delivery of an electrical stimulus to the brain, which results in central and peripheral seizure, he noted.
“The central seizure is essential for the efficacy of ECT,” said Dr. Andrade. In contrast, “the motor seizure has no therapeutic value, is cosmetically displeasing, and may rarely be associated with peripheral adverse effects affecting muscles, joints, teeth, and bones,” he added.
The musculoskeletal and dental injuries are caused by stretching, twisting, compression, or direct injury. Particularly during the motor seizure, the “sudden jerk” associated with the tonic contraction of muscles as well as the repeated jerks associated with each clonic contraction can result in injuries, including skeletal and dental fractures.
To address this concern, the motor seizure is “modified” or attenuated through use of an intravenous muscle relaxant administered with other ECT premedication.
“How effectively the musculoskeletal and dental adverse effects are minimized depends on how well the motor seizure is modified,” Dr. Andrade said. He emphasized that the “use of unmodified ECT is strongly discouraged.”
Dr. Andrade reviewed prior research into the skeletal and dental risks of ECT. The infrequency of cases and ethical difficulties in conducting randomized clinical trials with such patients require reliance on anecdotal reports, he said.
Bite blocks, seizure modifiers
Population-based data showed that the fracture risk with modified ECT is two events per 100,000 ECTs. However, the risk may be as low as 0.36 events per 100,000 ECTs if calculated only with recent data, Dr. Andrade noted.
Population-based studies also suggest that the dental fracture risk with modified ECT is .02% per ECT and .17% per ECT course.
Although fractures have been reported under “unusual circumstances” among patients receiving modified ECT, many other reports point to the safety of this treatment, even in ultrahigh-risk patients.
Such patients include those with severe osteoporosis, metastatic bone disease, osteogenesis imperfecta, Ehlers-Danlos syndrome, Harrington rod implants, recent long bone fractures, multiple bone fractures, surgical repair of hip fracture, vertebroplasty, and maxillofacial repair.
Dr. Andrade noted that oral health is “poor” among patients with major mental illness for multiple reasons, including poor nutrition, self-neglect, and decreased salivation caused by the anticholinergic effects of medications.
This places these patients at increased risk for dental adverse effects during ECT because the muscles of the jaw contract forcefully during the motor seizure, causing sudden impact and, subsequently, sustained pressure on the teeth, Dr. Andrade said.
Moreover, because ECT is typically administered through repeated sessions, dental injuries may accumulate over the course of treatment.
ECT-associated skeletal risks arise from the tonic-clonic contractions of the muscles of the trunk and limbs, which need to be addressed via use of succinylcholine or other muscle relaxants included in ECT premedication.
Dr. Andrade noted that succinylcholine is effective at modifying the motor seizure at the common dose of 0.5-1.0 mg/kg. However, about 5% of patients require a higher dose (>1.5 mg/kg). If the dose is 1-2 mg/kg for patients at high risk for orthopedic complications, “muscle relaxation during ECT could be expected to be reasonably complete,” he said.
“Because of wide interpersonal variation, a neurostimulator may need to be used to identify the ideal dose for an individual patient,” he added.
In addition, use of bite blocks and effective jaw immobilization during ECT can reduce the risk. “Careful assessment of preexisting risk and good ECT practice can minimize the risk of skeletal and dental complications during ECT,” Dr. Andrade said.
Risks vs. benefits
Commenting on the study, Mark S. George, MD, distinguished professor of psychiatry, radiology, and neurology, and director of the brain stimulation division, Medical University of South Carolina, Charleston, said this was a “well-written review of how frequently patients who are undergoing modern ECT have bone fractures or dental fractures during the procedure.”
Dr. George, who was not involved with the research, added that modern medications and management “make ECT a truly safe procedure.”
“It is not without some risk, but these risks are low, especially when compared to the risks of untreated or undertreated depression or catatonia, like suicide,” he said.
Dr. Andrade publishes an e-newsletter supported by Sun Pharmaceuticals, with payments made directly to registered charities, but does not benefit financially from the relationship. His travel expenses for delivering lectures and workshops have been supported by the organizers themselves or pharmaceutical companies at the behest of the organizers. He has provided advice to various pharmaceutical companies and has received “nominal compensation.” He has also received payments for developing educational materials for scientific initiatives and programs, such as for the Behavioral and Neurosciences Foundation of India, PsyBase India, Texas Tech University USA, the Nordic Association for Convulsive Therapy, and the American Society of Clinical Psychopharmacology. Dr. George reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
We have seen the future of healthy muffins, and its name is Roselle
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
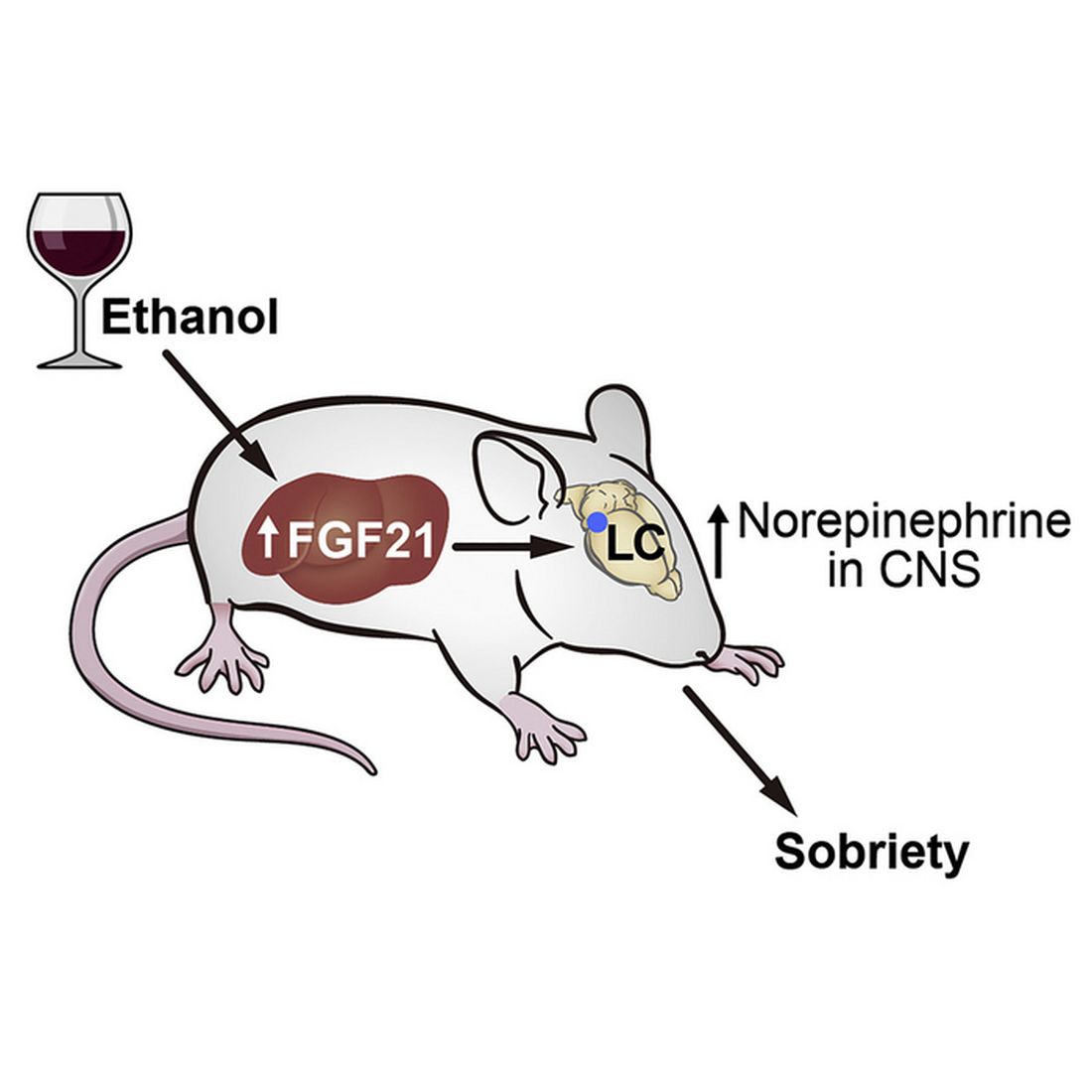
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.

The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Effect of the COVID-19 Pandemic on Resources, Other Diseases, and Healthcare Workers’ Experience

Introduction
The COVID-19 pandemic has changed the healthcare system in a multitude of ways, affecting healthcare capacity, treatment of other illnesses, and wellness as well as professional retention of healthcare workers.1-3 During the peak of the COVID-19 pandemic, healthcare capacity was tested and resources were used up quickly.1 As the pandemic has progressed, healthcare systems have had to decide how to proceed with lessons learned, reassessing the environment of care delivery, healthcare supply chains, workforce structures, communication systems, and scientific collaboration as well as policy frameworks in healthcare.4
There have been both immediate effects and long-term consequences of the delay in care for other conditions.2,5 One stark example of this is in cancer care, where screening and procedures were postponed or canceled due to the pandemic with a resulting predicted 2% increase in cancer mortality in the next 10 years.2 The care of heart disease, chronic illnesses, and other viruses has also been similarly negatively impacted by the COVID-19 pandemic due to similar delays in diagnosis and treatment.5-7
The impact on healthcare workers has also been profound.3 Occupational stress from the pandemic has correlated with increased depression and posttraumatic stress disorder (PTSD) among other mental health diseases in healthcare workers.3 In a survey of neurosurgery residents, 26.1% of physicians reported feeling burnt out, and 65.8% were worried that they would not be able to reach surgical milestones.8,9 Among respiratory therapists, a hard hit group during this time, 79% reported burnout.10 Additionally, more healthcare workers left the field during the pandemic, with 15 million lost jobs. Future recovery of jobs looks bleak in some settings, like long-term care and among assistants and aides.11 Overall, the long-term outcomes of these resource, disease, and mental health disruptions need to be assessed and solutions created to maintain a quality and effective healthcare system, with ample resources and measures to account for disease increases and address the impact on providers.
Healthcare Capacity and Resources
With COVID-19 affecting over 100 million in the United States as of March 1, 2023, the impact on healthcare resources since the start of the pandemic has been immense.12 With 5% to 38% of hospitalized patients being admitted to the intensive care unit (ICU) and 75% to 88% of those patients requiring mechanical ventilation, a huge strain was placed on resources during and after the pandemic.1
The question of balancing resources for other hospital needs while tending to patients with COVID-19 has been an ongoing discussion at many levels.1 One core resource concern is the lack of staff. In a survey of 77 different countries, including physicians (41%), nurses (40%), respiratory therapists (11%), and advanced practice providers (8%), 15% reported insufficient intensivists and 32% reported insufficient ICU nursing staff during March and April of 2020.1 A lack of hospital and care space that led to reallocation of limited-care acute care space was a concern. Thirteen percent reported a shortage of hospital ICU beds, while others reported the conversion of postoperative recovery rooms (20%) and operating rooms (12%) for patients with COVID-19.1
Along with staff and care space concerns, hospital survey respondents reported that healthcare equipment was also challenged. Access to COVID-19 testing was one concern, with only 35% of respondents reporting availability for all patients at the beginning of the pandemic, and 56% reporting availability for only select patients based on symptom severity.1 Access to personal protective equipment (PPE) was also affected, with PPE always available according to 83% to 95% of respondents but just 35% having access to N95 masks.1 Additionally, 26% reported that there were no respirators in their hospital, and 11% reported limited ventilators.1
Although resource depletion is a problem, studies have looked at public health measures that helped to mitigate this issue. With proper public health planning and implementation, such as physical distancing, aggressive testing, contact tracing, and increased hospital capacity, by freeing up existing resources or adding additional support, public health modeling showed that resources may be able to withstand the increase.13 Development of reallocation models at local, state, national, and international levels is an important step to be able to deal with future public health crises.14
The long-term impact from the pandemic includes disruption in the physical environment of healthcare, production, supply chain, staff structure, and workforce alterations.4 For example, the physical shape of healthcare facilities is changing to accommodate increasing volumes and decrease the risk of spreading disease.4 To accommodate the burden on staffing structure and workforce alteration, telehealth gained a prominent role.4 All in all, the pandemic has changed the healthcare system; however, institutions, organizations, and policy makers need to evaluate which measures were impactful and should be considered for long-term inclusion in healthcare practice.
Impact on Other Diseases: Cancer, Heart Disease, Chronic Illnesses, and Other Viruses
The treatment of other new and existing conditions has also been affected by the pandemic. Cancer, especially, is a disease of concern. Elective surgeries and screening were halted or altered during the pandemic, which is modeled to lead to higher cancer mortality in years to come.2 The most affected cancers were breast, lung, and colorectal cancer.2 A study of colorectal cancer screening showed that colonoscopies were delayed due to COVID-19 and that gastroenterology visits declined by 49% to 61%.15 This will likely lead to delayed cancer diagnoses and possible increases in mortality.15 Breast cancer screening was also delayed and many patients continued to avoid it for various reasons such as fears of contracting COVID-19 infection in healthcare facilities, and the economic effects of the pandemic such as job loss and healthcare coverage loss.16 These delays will result in an estimated potential 0.52% overall increase in breast cancer deaths by 2030.17
A study of 368 patients from Spain showed a 56.5% decrease in hospital admissions, usually related to heart attacks, in March and April of 2020, compared to January and February 2020.18,19 For other chronic illnesses, the pandemic resulted in decreased preventative care and management.20 The care of other infections similarly suffered. The World Health Organization announced that the number of patients receiving treatment for tuberculosis (TB) dropped by 1 million, setting the disease mitigation back considerably.20 An estimated 500,000 more people died in 2020 from TB.21 The drastic shift in focus to COVID-19 care during this period will continue to have a profound impact on other diseases like these for many years post-pandemic.
Provider Experience and Mental Health Outcomes
The impact on provider experiences and mental health has been immense. One study of 510 healthcare providers (HCPs) and first responders found that occupational stress from the pandemic correlated with psychiatric symptoms, including depression, PTSD, insomnia, and generalized anxiety.3 Occupational stress also correlated with one’s likelihood to leave the medical field and trouble doing work they had once loved.3 Half of the healthcare workers surveyed indicated a decreased likelihood of staying in their current profession after the pandemic.3
Other studies have also looked at specific subspecialties and impact on trainees during the pandemic. In neurosurgery, for example, resident burnout is high, at 26.1%.9 Additionally, the lack of surgeries in the pandemic made 65.8% of neurosurgery residents anxious about meeting career milestones.9 Respiratory therapists, a highly impacted group, also experienced burnout, reporting higher levels in those who worked more in the ICU. Another study identified several themes in the concerns reported by healthcare workers during the pandemic era including “changes in personal life and enhanced negative affect,” “gaining experience, normalization, and adaptation to the pandemic,” and “mental health considerations.”22
Some studies have investigated ways to mitigate this dissatisfaction with the healthcare field post-pandemic. Intrapreneurship, reverse mentoring, and democratized learning all had a reported positive impact on employee experience and retention during this time.23 Intrapreneurship describes entrepreneurship within an existing organization, while reverse mentoring and democratized learning refer to newer employees teaching older employees and communicative learning on a breadth of topics. Other studies have examined the necessity of having mental health resources available, and that these resources need to be multi-stage and individualistic as well as specific to certain stressors HCPs faced during the pandemic.22
Conclusion and Future Directions
The COVID-19 pandemic had stark effects on the healthcare system, impacting resources and capacity, care of other diseases, and provider mental health and experiences.1-3 After the chaos of the pandemic, many questions remain. What needs to be done now by health systems and HCPs? How can we learn from the challenges and the effects on capacity to change the healthcare workflow in times of crisis and in the present? How do we mitigate the impact of the pandemic on diagnosis and management of diseases? And how do we continue to provide healthcare workers with proper mental health and professional resources now, not just in times of stress, and encourage the future generation to pursue careers in healthcare?
These are all the questions the pandemic has left us with, and more studies and initiatives are needed to investigate solutions to these issues. The COVID-19 pandemic left behind valuable lessons and changed the healthcare system, disease management, and staffing for many. Now is the time to pick up the pieces and strategize on how to make our existing system more effective for workers and patients post pandemic.
Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic's effect on critical care resources and health-care providers: a global survey. Chest. 2021;159(2):619-633. doi:10.1016/j.chest.2020.09.070
Malagón T, Yong JHE, Tope P, Miller WH Jr, Franco EL; McGill task force on the impact of COVID-19 on cancer control and care. Predicted long-term impact of COVID-19 pandemic-related care delays on cancer mortality in Canada. Int J Cancer. 2022;150(8):1244-1254. doi:10.1002/ijc.33884
Hendrickson RC, Slevin RA, Hoerster KD, et al. The impact of the COVID-19 pandemic on mental health, occupational functioning, and professional retention among health care workers and first responders. J Gen Intern Med. 2022;37(2):397-408. doi:10.1007/s11606-021-07252-z
Davis B, Bankhead-Kendall BK, Dumas RP. A review of COVID-19's impact on modern medical systems from a health organization management perspective. Health Technol (Berl). 2022;12(4):815-824. doi:10.1007/s12553-022-00660-z
Rosenbaum L. The untold toll - the pandemic's effects on patients without COVID-19. N Engl J Med. 2020;382(24):2368-2371. doi:10.1056/NEJMms2009984
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: the impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Jalili M, Niroomand M, Hadavand F, Zeinali K, Fotouhi A. Burnout among healthcare professionals during COVID-19 pandemic: a cross-sectional study. Int Arch Occup Environ Health. 2021;94(6):1345-1352. doi:10.1007/s00420-021-01695-x
Khalafallah AM, Lam S, Gami A, et al. A national survey on the impact of the COVID-19 pandemic upon burnout and career satisfaction among neurosurgery residents. J Clin Neurosci. 2020;80:137-142. doi:10.1016/j.jocn.2020.08.012
Miller AG, Roberts KJ, Smith BJ, et al. Prevalence of burnout among respiratory therapists amidst the COVID-19 pandemic. Respir Care. 2021;respcare.09283. doi:10.4187/respcare.09283
Frogner BK, Dill JS. Tracking turnover among health care workers during the COVID-19 pandemic: a cross-sectional study. JAMA Health Forum. 2022;3(4):e220371. doi:10.1001/jamahealthforum.2022.0371
CDC COVID data tracker. Centers for Disease Control and Prevention. Accessed December 22, 2022. http://covid-data-tracker/#datatracker-home.
Barrett K, Khan YA, Mac S, Ximenes R, Naimark DMJ, Sander B. Estimation of COVID-19-induced depletion of hospital resources in Ontario, Canada. CMAJ. 2020;192(24):E640-E646. doi:10.1503/cmaj.200715
Kaul V, Chahal J, Schrarstzhaupt IN, et al. Lessons learned from a global perspective of COVID-19. Clin Chest Med. 2022 Nov. 24. [online ahead of print]. doi:10.1016/j.ccm.2022.11.020
Issaka RB, Somsouk M. Colorectal cancer screening and prevention in the COVID-19 Era. JAMA Health Forum. 2020;1(5):e200588. doi:10.1001/jamahealthforum.2020.0588
Freer PE. The impact of the COVID-19 pandemic on breast imaging. Radiol Clin North Am. 2021;59(1):1-11. doi:10.1016/j.rcl.2020.09.008
Alagoz O, Lowry KP, Kurian AW, et al. Impact of the COVID-19 pandemic on breast cancer mortality in the US: estimates from collaborative simulation modeling. J Natl Cancer Inst. 2021;113(11):1484-1494. doi:10.1093/jnci/djab097
Jiménez-Blanco Bravo M, Cordero Pereda D, Sánchez Vega D, et al. Heart failure in the time of COVID-19. Cardiology. 2020;145(8):481-484. doi:10.1159/000509181
Frankfurter C, Buchan TA, Kobulnik J, et al. Reduced rate of hospital presentations for heart failure during the COVID-19 pandemic in Toronto, Canada. Can J Cardiol. 2020;36(10):1680-1684. doi:10.1016/j.cjca.2020.07.006
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: The impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547-554. doi:10.1016/j.ajic.2020.10.001
Jayathilake HD, Daud D, Eaw HC, Annuar N. Employee development and retention of generation-Z employees in the post-covid-19 workplace: a conceptual framework. Benchmarking: An International Journal. 2021;28(7):2343-2364. doi:10.1108/bij-06-2020-0311
Introduction
The COVID-19 pandemic has changed the healthcare system in a multitude of ways, affecting healthcare capacity, treatment of other illnesses, and wellness as well as professional retention of healthcare workers.1-3 During the peak of the COVID-19 pandemic, healthcare capacity was tested and resources were used up quickly.1 As the pandemic has progressed, healthcare systems have had to decide how to proceed with lessons learned, reassessing the environment of care delivery, healthcare supply chains, workforce structures, communication systems, and scientific collaboration as well as policy frameworks in healthcare.4
There have been both immediate effects and long-term consequences of the delay in care for other conditions.2,5 One stark example of this is in cancer care, where screening and procedures were postponed or canceled due to the pandemic with a resulting predicted 2% increase in cancer mortality in the next 10 years.2 The care of heart disease, chronic illnesses, and other viruses has also been similarly negatively impacted by the COVID-19 pandemic due to similar delays in diagnosis and treatment.5-7
The impact on healthcare workers has also been profound.3 Occupational stress from the pandemic has correlated with increased depression and posttraumatic stress disorder (PTSD) among other mental health diseases in healthcare workers.3 In a survey of neurosurgery residents, 26.1% of physicians reported feeling burnt out, and 65.8% were worried that they would not be able to reach surgical milestones.8,9 Among respiratory therapists, a hard hit group during this time, 79% reported burnout.10 Additionally, more healthcare workers left the field during the pandemic, with 15 million lost jobs. Future recovery of jobs looks bleak in some settings, like long-term care and among assistants and aides.11 Overall, the long-term outcomes of these resource, disease, and mental health disruptions need to be assessed and solutions created to maintain a quality and effective healthcare system, with ample resources and measures to account for disease increases and address the impact on providers.
Healthcare Capacity and Resources
With COVID-19 affecting over 100 million in the United States as of March 1, 2023, the impact on healthcare resources since the start of the pandemic has been immense.12 With 5% to 38% of hospitalized patients being admitted to the intensive care unit (ICU) and 75% to 88% of those patients requiring mechanical ventilation, a huge strain was placed on resources during and after the pandemic.1
The question of balancing resources for other hospital needs while tending to patients with COVID-19 has been an ongoing discussion at many levels.1 One core resource concern is the lack of staff. In a survey of 77 different countries, including physicians (41%), nurses (40%), respiratory therapists (11%), and advanced practice providers (8%), 15% reported insufficient intensivists and 32% reported insufficient ICU nursing staff during March and April of 2020.1 A lack of hospital and care space that led to reallocation of limited-care acute care space was a concern. Thirteen percent reported a shortage of hospital ICU beds, while others reported the conversion of postoperative recovery rooms (20%) and operating rooms (12%) for patients with COVID-19.1
Along with staff and care space concerns, hospital survey respondents reported that healthcare equipment was also challenged. Access to COVID-19 testing was one concern, with only 35% of respondents reporting availability for all patients at the beginning of the pandemic, and 56% reporting availability for only select patients based on symptom severity.1 Access to personal protective equipment (PPE) was also affected, with PPE always available according to 83% to 95% of respondents but just 35% having access to N95 masks.1 Additionally, 26% reported that there were no respirators in their hospital, and 11% reported limited ventilators.1
Although resource depletion is a problem, studies have looked at public health measures that helped to mitigate this issue. With proper public health planning and implementation, such as physical distancing, aggressive testing, contact tracing, and increased hospital capacity, by freeing up existing resources or adding additional support, public health modeling showed that resources may be able to withstand the increase.13 Development of reallocation models at local, state, national, and international levels is an important step to be able to deal with future public health crises.14
The long-term impact from the pandemic includes disruption in the physical environment of healthcare, production, supply chain, staff structure, and workforce alterations.4 For example, the physical shape of healthcare facilities is changing to accommodate increasing volumes and decrease the risk of spreading disease.4 To accommodate the burden on staffing structure and workforce alteration, telehealth gained a prominent role.4 All in all, the pandemic has changed the healthcare system; however, institutions, organizations, and policy makers need to evaluate which measures were impactful and should be considered for long-term inclusion in healthcare practice.
Impact on Other Diseases: Cancer, Heart Disease, Chronic Illnesses, and Other Viruses
The treatment of other new and existing conditions has also been affected by the pandemic. Cancer, especially, is a disease of concern. Elective surgeries and screening were halted or altered during the pandemic, which is modeled to lead to higher cancer mortality in years to come.2 The most affected cancers were breast, lung, and colorectal cancer.2 A study of colorectal cancer screening showed that colonoscopies were delayed due to COVID-19 and that gastroenterology visits declined by 49% to 61%.15 This will likely lead to delayed cancer diagnoses and possible increases in mortality.15 Breast cancer screening was also delayed and many patients continued to avoid it for various reasons such as fears of contracting COVID-19 infection in healthcare facilities, and the economic effects of the pandemic such as job loss and healthcare coverage loss.16 These delays will result in an estimated potential 0.52% overall increase in breast cancer deaths by 2030.17
A study of 368 patients from Spain showed a 56.5% decrease in hospital admissions, usually related to heart attacks, in March and April of 2020, compared to January and February 2020.18,19 For other chronic illnesses, the pandemic resulted in decreased preventative care and management.20 The care of other infections similarly suffered. The World Health Organization announced that the number of patients receiving treatment for tuberculosis (TB) dropped by 1 million, setting the disease mitigation back considerably.20 An estimated 500,000 more people died in 2020 from TB.21 The drastic shift in focus to COVID-19 care during this period will continue to have a profound impact on other diseases like these for many years post-pandemic.
Provider Experience and Mental Health Outcomes
The impact on provider experiences and mental health has been immense. One study of 510 healthcare providers (HCPs) and first responders found that occupational stress from the pandemic correlated with psychiatric symptoms, including depression, PTSD, insomnia, and generalized anxiety.3 Occupational stress also correlated with one’s likelihood to leave the medical field and trouble doing work they had once loved.3 Half of the healthcare workers surveyed indicated a decreased likelihood of staying in their current profession after the pandemic.3
Other studies have also looked at specific subspecialties and impact on trainees during the pandemic. In neurosurgery, for example, resident burnout is high, at 26.1%.9 Additionally, the lack of surgeries in the pandemic made 65.8% of neurosurgery residents anxious about meeting career milestones.9 Respiratory therapists, a highly impacted group, also experienced burnout, reporting higher levels in those who worked more in the ICU. Another study identified several themes in the concerns reported by healthcare workers during the pandemic era including “changes in personal life and enhanced negative affect,” “gaining experience, normalization, and adaptation to the pandemic,” and “mental health considerations.”22
Some studies have investigated ways to mitigate this dissatisfaction with the healthcare field post-pandemic. Intrapreneurship, reverse mentoring, and democratized learning all had a reported positive impact on employee experience and retention during this time.23 Intrapreneurship describes entrepreneurship within an existing organization, while reverse mentoring and democratized learning refer to newer employees teaching older employees and communicative learning on a breadth of topics. Other studies have examined the necessity of having mental health resources available, and that these resources need to be multi-stage and individualistic as well as specific to certain stressors HCPs faced during the pandemic.22
Conclusion and Future Directions
The COVID-19 pandemic had stark effects on the healthcare system, impacting resources and capacity, care of other diseases, and provider mental health and experiences.1-3 After the chaos of the pandemic, many questions remain. What needs to be done now by health systems and HCPs? How can we learn from the challenges and the effects on capacity to change the healthcare workflow in times of crisis and in the present? How do we mitigate the impact of the pandemic on diagnosis and management of diseases? And how do we continue to provide healthcare workers with proper mental health and professional resources now, not just in times of stress, and encourage the future generation to pursue careers in healthcare?
These are all the questions the pandemic has left us with, and more studies and initiatives are needed to investigate solutions to these issues. The COVID-19 pandemic left behind valuable lessons and changed the healthcare system, disease management, and staffing for many. Now is the time to pick up the pieces and strategize on how to make our existing system more effective for workers and patients post pandemic.
Introduction
The COVID-19 pandemic has changed the healthcare system in a multitude of ways, affecting healthcare capacity, treatment of other illnesses, and wellness as well as professional retention of healthcare workers.1-3 During the peak of the COVID-19 pandemic, healthcare capacity was tested and resources were used up quickly.1 As the pandemic has progressed, healthcare systems have had to decide how to proceed with lessons learned, reassessing the environment of care delivery, healthcare supply chains, workforce structures, communication systems, and scientific collaboration as well as policy frameworks in healthcare.4
There have been both immediate effects and long-term consequences of the delay in care for other conditions.2,5 One stark example of this is in cancer care, where screening and procedures were postponed or canceled due to the pandemic with a resulting predicted 2% increase in cancer mortality in the next 10 years.2 The care of heart disease, chronic illnesses, and other viruses has also been similarly negatively impacted by the COVID-19 pandemic due to similar delays in diagnosis and treatment.5-7
The impact on healthcare workers has also been profound.3 Occupational stress from the pandemic has correlated with increased depression and posttraumatic stress disorder (PTSD) among other mental health diseases in healthcare workers.3 In a survey of neurosurgery residents, 26.1% of physicians reported feeling burnt out, and 65.8% were worried that they would not be able to reach surgical milestones.8,9 Among respiratory therapists, a hard hit group during this time, 79% reported burnout.10 Additionally, more healthcare workers left the field during the pandemic, with 15 million lost jobs. Future recovery of jobs looks bleak in some settings, like long-term care and among assistants and aides.11 Overall, the long-term outcomes of these resource, disease, and mental health disruptions need to be assessed and solutions created to maintain a quality and effective healthcare system, with ample resources and measures to account for disease increases and address the impact on providers.
Healthcare Capacity and Resources
With COVID-19 affecting over 100 million in the United States as of March 1, 2023, the impact on healthcare resources since the start of the pandemic has been immense.12 With 5% to 38% of hospitalized patients being admitted to the intensive care unit (ICU) and 75% to 88% of those patients requiring mechanical ventilation, a huge strain was placed on resources during and after the pandemic.1
The question of balancing resources for other hospital needs while tending to patients with COVID-19 has been an ongoing discussion at many levels.1 One core resource concern is the lack of staff. In a survey of 77 different countries, including physicians (41%), nurses (40%), respiratory therapists (11%), and advanced practice providers (8%), 15% reported insufficient intensivists and 32% reported insufficient ICU nursing staff during March and April of 2020.1 A lack of hospital and care space that led to reallocation of limited-care acute care space was a concern. Thirteen percent reported a shortage of hospital ICU beds, while others reported the conversion of postoperative recovery rooms (20%) and operating rooms (12%) for patients with COVID-19.1
Along with staff and care space concerns, hospital survey respondents reported that healthcare equipment was also challenged. Access to COVID-19 testing was one concern, with only 35% of respondents reporting availability for all patients at the beginning of the pandemic, and 56% reporting availability for only select patients based on symptom severity.1 Access to personal protective equipment (PPE) was also affected, with PPE always available according to 83% to 95% of respondents but just 35% having access to N95 masks.1 Additionally, 26% reported that there were no respirators in their hospital, and 11% reported limited ventilators.1
Although resource depletion is a problem, studies have looked at public health measures that helped to mitigate this issue. With proper public health planning and implementation, such as physical distancing, aggressive testing, contact tracing, and increased hospital capacity, by freeing up existing resources or adding additional support, public health modeling showed that resources may be able to withstand the increase.13 Development of reallocation models at local, state, national, and international levels is an important step to be able to deal with future public health crises.14
The long-term impact from the pandemic includes disruption in the physical environment of healthcare, production, supply chain, staff structure, and workforce alterations.4 For example, the physical shape of healthcare facilities is changing to accommodate increasing volumes and decrease the risk of spreading disease.4 To accommodate the burden on staffing structure and workforce alteration, telehealth gained a prominent role.4 All in all, the pandemic has changed the healthcare system; however, institutions, organizations, and policy makers need to evaluate which measures were impactful and should be considered for long-term inclusion in healthcare practice.
Impact on Other Diseases: Cancer, Heart Disease, Chronic Illnesses, and Other Viruses
The treatment of other new and existing conditions has also been affected by the pandemic. Cancer, especially, is a disease of concern. Elective surgeries and screening were halted or altered during the pandemic, which is modeled to lead to higher cancer mortality in years to come.2 The most affected cancers were breast, lung, and colorectal cancer.2 A study of colorectal cancer screening showed that colonoscopies were delayed due to COVID-19 and that gastroenterology visits declined by 49% to 61%.15 This will likely lead to delayed cancer diagnoses and possible increases in mortality.15 Breast cancer screening was also delayed and many patients continued to avoid it for various reasons such as fears of contracting COVID-19 infection in healthcare facilities, and the economic effects of the pandemic such as job loss and healthcare coverage loss.16 These delays will result in an estimated potential 0.52% overall increase in breast cancer deaths by 2030.17
A study of 368 patients from Spain showed a 56.5% decrease in hospital admissions, usually related to heart attacks, in March and April of 2020, compared to January and February 2020.18,19 For other chronic illnesses, the pandemic resulted in decreased preventative care and management.20 The care of other infections similarly suffered. The World Health Organization announced that the number of patients receiving treatment for tuberculosis (TB) dropped by 1 million, setting the disease mitigation back considerably.20 An estimated 500,000 more people died in 2020 from TB.21 The drastic shift in focus to COVID-19 care during this period will continue to have a profound impact on other diseases like these for many years post-pandemic.
Provider Experience and Mental Health Outcomes
The impact on provider experiences and mental health has been immense. One study of 510 healthcare providers (HCPs) and first responders found that occupational stress from the pandemic correlated with psychiatric symptoms, including depression, PTSD, insomnia, and generalized anxiety.3 Occupational stress also correlated with one’s likelihood to leave the medical field and trouble doing work they had once loved.3 Half of the healthcare workers surveyed indicated a decreased likelihood of staying in their current profession after the pandemic.3
Other studies have also looked at specific subspecialties and impact on trainees during the pandemic. In neurosurgery, for example, resident burnout is high, at 26.1%.9 Additionally, the lack of surgeries in the pandemic made 65.8% of neurosurgery residents anxious about meeting career milestones.9 Respiratory therapists, a highly impacted group, also experienced burnout, reporting higher levels in those who worked more in the ICU. Another study identified several themes in the concerns reported by healthcare workers during the pandemic era including “changes in personal life and enhanced negative affect,” “gaining experience, normalization, and adaptation to the pandemic,” and “mental health considerations.”22
Some studies have investigated ways to mitigate this dissatisfaction with the healthcare field post-pandemic. Intrapreneurship, reverse mentoring, and democratized learning all had a reported positive impact on employee experience and retention during this time.23 Intrapreneurship describes entrepreneurship within an existing organization, while reverse mentoring and democratized learning refer to newer employees teaching older employees and communicative learning on a breadth of topics. Other studies have examined the necessity of having mental health resources available, and that these resources need to be multi-stage and individualistic as well as specific to certain stressors HCPs faced during the pandemic.22
Conclusion and Future Directions
The COVID-19 pandemic had stark effects on the healthcare system, impacting resources and capacity, care of other diseases, and provider mental health and experiences.1-3 After the chaos of the pandemic, many questions remain. What needs to be done now by health systems and HCPs? How can we learn from the challenges and the effects on capacity to change the healthcare workflow in times of crisis and in the present? How do we mitigate the impact of the pandemic on diagnosis and management of diseases? And how do we continue to provide healthcare workers with proper mental health and professional resources now, not just in times of stress, and encourage the future generation to pursue careers in healthcare?
These are all the questions the pandemic has left us with, and more studies and initiatives are needed to investigate solutions to these issues. The COVID-19 pandemic left behind valuable lessons and changed the healthcare system, disease management, and staffing for many. Now is the time to pick up the pieces and strategize on how to make our existing system more effective for workers and patients post pandemic.
Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic's effect on critical care resources and health-care providers: a global survey. Chest. 2021;159(2):619-633. doi:10.1016/j.chest.2020.09.070
Malagón T, Yong JHE, Tope P, Miller WH Jr, Franco EL; McGill task force on the impact of COVID-19 on cancer control and care. Predicted long-term impact of COVID-19 pandemic-related care delays on cancer mortality in Canada. Int J Cancer. 2022;150(8):1244-1254. doi:10.1002/ijc.33884
Hendrickson RC, Slevin RA, Hoerster KD, et al. The impact of the COVID-19 pandemic on mental health, occupational functioning, and professional retention among health care workers and first responders. J Gen Intern Med. 2022;37(2):397-408. doi:10.1007/s11606-021-07252-z
Davis B, Bankhead-Kendall BK, Dumas RP. A review of COVID-19's impact on modern medical systems from a health organization management perspective. Health Technol (Berl). 2022;12(4):815-824. doi:10.1007/s12553-022-00660-z
Rosenbaum L. The untold toll - the pandemic's effects on patients without COVID-19. N Engl J Med. 2020;382(24):2368-2371. doi:10.1056/NEJMms2009984
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: the impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Jalili M, Niroomand M, Hadavand F, Zeinali K, Fotouhi A. Burnout among healthcare professionals during COVID-19 pandemic: a cross-sectional study. Int Arch Occup Environ Health. 2021;94(6):1345-1352. doi:10.1007/s00420-021-01695-x
Khalafallah AM, Lam S, Gami A, et al. A national survey on the impact of the COVID-19 pandemic upon burnout and career satisfaction among neurosurgery residents. J Clin Neurosci. 2020;80:137-142. doi:10.1016/j.jocn.2020.08.012
Miller AG, Roberts KJ, Smith BJ, et al. Prevalence of burnout among respiratory therapists amidst the COVID-19 pandemic. Respir Care. 2021;respcare.09283. doi:10.4187/respcare.09283
Frogner BK, Dill JS. Tracking turnover among health care workers during the COVID-19 pandemic: a cross-sectional study. JAMA Health Forum. 2022;3(4):e220371. doi:10.1001/jamahealthforum.2022.0371
CDC COVID data tracker. Centers for Disease Control and Prevention. Accessed December 22, 2022. http://covid-data-tracker/#datatracker-home.
Barrett K, Khan YA, Mac S, Ximenes R, Naimark DMJ, Sander B. Estimation of COVID-19-induced depletion of hospital resources in Ontario, Canada. CMAJ. 2020;192(24):E640-E646. doi:10.1503/cmaj.200715
Kaul V, Chahal J, Schrarstzhaupt IN, et al. Lessons learned from a global perspective of COVID-19. Clin Chest Med. 2022 Nov. 24. [online ahead of print]. doi:10.1016/j.ccm.2022.11.020
Issaka RB, Somsouk M. Colorectal cancer screening and prevention in the COVID-19 Era. JAMA Health Forum. 2020;1(5):e200588. doi:10.1001/jamahealthforum.2020.0588
Freer PE. The impact of the COVID-19 pandemic on breast imaging. Radiol Clin North Am. 2021;59(1):1-11. doi:10.1016/j.rcl.2020.09.008
Alagoz O, Lowry KP, Kurian AW, et al. Impact of the COVID-19 pandemic on breast cancer mortality in the US: estimates from collaborative simulation modeling. J Natl Cancer Inst. 2021;113(11):1484-1494. doi:10.1093/jnci/djab097
Jiménez-Blanco Bravo M, Cordero Pereda D, Sánchez Vega D, et al. Heart failure in the time of COVID-19. Cardiology. 2020;145(8):481-484. doi:10.1159/000509181
Frankfurter C, Buchan TA, Kobulnik J, et al. Reduced rate of hospital presentations for heart failure during the COVID-19 pandemic in Toronto, Canada. Can J Cardiol. 2020;36(10):1680-1684. doi:10.1016/j.cjca.2020.07.006
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: The impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547-554. doi:10.1016/j.ajic.2020.10.001
Jayathilake HD, Daud D, Eaw HC, Annuar N. Employee development and retention of generation-Z employees in the post-covid-19 workplace: a conceptual framework. Benchmarking: An International Journal. 2021;28(7):2343-2364. doi:10.1108/bij-06-2020-0311
Wahlster S, Sharma M, Lewis AK, et al. The coronavirus disease 2019 pandemic's effect on critical care resources and health-care providers: a global survey. Chest. 2021;159(2):619-633. doi:10.1016/j.chest.2020.09.070
Malagón T, Yong JHE, Tope P, Miller WH Jr, Franco EL; McGill task force on the impact of COVID-19 on cancer control and care. Predicted long-term impact of COVID-19 pandemic-related care delays on cancer mortality in Canada. Int J Cancer. 2022;150(8):1244-1254. doi:10.1002/ijc.33884
Hendrickson RC, Slevin RA, Hoerster KD, et al. The impact of the COVID-19 pandemic on mental health, occupational functioning, and professional retention among health care workers and first responders. J Gen Intern Med. 2022;37(2):397-408. doi:10.1007/s11606-021-07252-z
Davis B, Bankhead-Kendall BK, Dumas RP. A review of COVID-19's impact on modern medical systems from a health organization management perspective. Health Technol (Berl). 2022;12(4):815-824. doi:10.1007/s12553-022-00660-z
Rosenbaum L. The untold toll - the pandemic's effects on patients without COVID-19. N Engl J Med. 2020;382(24):2368-2371. doi:10.1056/NEJMms2009984
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: the impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Jalili M, Niroomand M, Hadavand F, Zeinali K, Fotouhi A. Burnout among healthcare professionals during COVID-19 pandemic: a cross-sectional study. Int Arch Occup Environ Health. 2021;94(6):1345-1352. doi:10.1007/s00420-021-01695-x
Khalafallah AM, Lam S, Gami A, et al. A national survey on the impact of the COVID-19 pandemic upon burnout and career satisfaction among neurosurgery residents. J Clin Neurosci. 2020;80:137-142. doi:10.1016/j.jocn.2020.08.012
Miller AG, Roberts KJ, Smith BJ, et al. Prevalence of burnout among respiratory therapists amidst the COVID-19 pandemic. Respir Care. 2021;respcare.09283. doi:10.4187/respcare.09283
Frogner BK, Dill JS. Tracking turnover among health care workers during the COVID-19 pandemic: a cross-sectional study. JAMA Health Forum. 2022;3(4):e220371. doi:10.1001/jamahealthforum.2022.0371
CDC COVID data tracker. Centers for Disease Control and Prevention. Accessed December 22, 2022. http://covid-data-tracker/#datatracker-home.
Barrett K, Khan YA, Mac S, Ximenes R, Naimark DMJ, Sander B. Estimation of COVID-19-induced depletion of hospital resources in Ontario, Canada. CMAJ. 2020;192(24):E640-E646. doi:10.1503/cmaj.200715
Kaul V, Chahal J, Schrarstzhaupt IN, et al. Lessons learned from a global perspective of COVID-19. Clin Chest Med. 2022 Nov. 24. [online ahead of print]. doi:10.1016/j.ccm.2022.11.020
Issaka RB, Somsouk M. Colorectal cancer screening and prevention in the COVID-19 Era. JAMA Health Forum. 2020;1(5):e200588. doi:10.1001/jamahealthforum.2020.0588
Freer PE. The impact of the COVID-19 pandemic on breast imaging. Radiol Clin North Am. 2021;59(1):1-11. doi:10.1016/j.rcl.2020.09.008
Alagoz O, Lowry KP, Kurian AW, et al. Impact of the COVID-19 pandemic on breast cancer mortality in the US: estimates from collaborative simulation modeling. J Natl Cancer Inst. 2021;113(11):1484-1494. doi:10.1093/jnci/djab097
Jiménez-Blanco Bravo M, Cordero Pereda D, Sánchez Vega D, et al. Heart failure in the time of COVID-19. Cardiology. 2020;145(8):481-484. doi:10.1159/000509181
Frankfurter C, Buchan TA, Kobulnik J, et al. Reduced rate of hospital presentations for heart failure during the COVID-19 pandemic in Toronto, Canada. Can J Cardiol. 2020;36(10):1680-1684. doi:10.1016/j.cjca.2020.07.006
Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: The impact now and in the future. Prev Chronic Dis. 2021;18:E62. doi:10.5888/pcd18.210086
Roberts L. How COVID hurt the fight against other dangerous diseases. Nature. 2021;592(7855):502-504. doi:10.1038/d41586-021-01022-x
Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. 2021;49(5):547-554. doi:10.1016/j.ajic.2020.10.001
Jayathilake HD, Daud D, Eaw HC, Annuar N. Employee development and retention of generation-Z employees in the post-covid-19 workplace: a conceptual framework. Benchmarking: An International Journal. 2021;28(7):2343-2364. doi:10.1108/bij-06-2020-0311
Inclusive reminder: LGBTQ community may donate stem cells
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.
In fact, gay men have been able to donate stem cells in the United States since 2015. That’s when National Marrow Donor Program’s Be the Match registry lifted restrictions on men who have sex with men (MSM).
Physicians say advocacy is still necessary, because LGBTQ people may assume they can’t donate or be wary of clinicians. “The LGBTQIA+ population in general has experienced a lot of issues with the medical-industrial complex in terms of discrimination and inappropriate care,” said UT Southwestern Medical Center pathologist Brian Adkins, MD, who manages the blood bank at Children’s Health in Dallas, in an interview. “There’s a weariness there that may produce some hesitancy to interact with the donation process.”
An estimated 6.8 million people give blood in the United States each year, and an estimated 9 million people are registered as potential stem cell donors. A total of 22,013 hematopoietic cell transplantation procedures were performed in 2020, according to the U.S. Health Resources and Services Administration.
Expanding the number of LGBTQ donors, especially those born as biological males, could pay major dividends. As Dr. Adkins noted, the ideal stem cell donor is young – Be the Match says doctors generally prefer donors aged 18-35 – and male. According to a 2021 Gallup Poll, 21% of those born from 1997 to 2003 (Generation Z) say they’re LGBTQ, as do 11% of those born from 1981 to 1996 (Millennials).
In North America, the most extensive outreach to the LGBTQ community about stem cell donation has been launched in Canada. There, an organization called Stem Cell Club focuses on encouraging college students and other young people to register as potential stem cell donors.
Stem Cell Club has several campaigns aimed at ethnic minority groups, and its Saving Lives With Pride project focuses on MSM. The project’s web page includes testimonials from a woman whose life was saved by an unrelated gay male donor and from a gay male nurse who recovered from blood cancer thanks to a stem cell donation. The site also includes videos about stem cell donation featuring LGBTQ young people and Canadian hematologists.
“Our specialized collection center will treat donors with the highest levels of respect and courtesy, indeed as heroes of their unselfish gift that can truly save a life,” says Ottawa Hospital transplant hematologist David Allan, MD, in one of the videos.
Stem Cell Club was founded by transplant hematologist Warren Fingrut, MD, a research fellow at Memorial Sloan Kettering Cancer Center. In an interview, he said the organization’s LGBTQ project has promoted stem cell donation at several annual gay pride events and will continue the outreach this coming summer. In 2018 and 2019, advocates recruited 354 potential stem-cell donors (40% male, 42 non-White) at five pride events, Dr. Fingrut and colleagues reported last year in the journal Bone Marrow Transplantation.
For a new study, researchers interviewed 37 gay and bisexual men from five Canadian provinces about stem cell donation. Dr. Fingrut and colleagues reported the findings in February in an abstract at the Transplantation & Cellular Therapy Meetings.
Most participants didn’t know they “are eligible to donate stem cells, with many confusing stem cell versus blood donor eligibility criteria,” the researchers reported. According to Dr. Fingrut, some of the men “felt they were treated as second-class citizens, and that translated into frustration and decreased motivation to donate. There were concerns that they would be treated as though they shouldn’t be there.”
Canada has allowed gay men to donate stem cells for at least 10 years, Dr. Fingrut said. In 2022, Canadian officials said blood banks would no longer require MSM donors to have been abstinent from sex for 3 months, the BBC reported. However, donors will be asked about high-risk sexual behaviors.
The United States, where HIV spread through the blood supply during the early years of the AIDS pandemic and killed thousands of hemophiliacs, has much been slower to change its policies. For decades, starting in the 1980s, both blood banks and stem cell donation programs chose to lower the risk by turning away MSM donors.
Policies only began to change in recent years. Be the Match’s registry led the way by welcoming MSM in 2015. Stem cell donations go through more extensive testing than blood donations, Dr. Adkins said, so it’s more likely that HIV will be screened out. Also, he said, officials probably realized “it was necessary to widen the donor pool in order to best serve the patients” because it’s so hard to find matched stem-cell donors.
Be the Match has also stepped up its outreach to the LGBTQ community. “During Pride Month in 2022, Be The Match sponsored booths at events in 12 major markets from coast to coast,” said Jamie Margolis, senior vice president of Donor Services. “These efforts enabled us to increase awareness among more than 500,000 festival attendees and added more than 2,000 new members to the Be The Match Registry. We also produced a social media awareness campaign featuring one of our own employees, who is a cofounder of the Pride Employee Resource Group at Be The Match and a recent blood stem cell donor.”
In 2020 as blood banks became desperate for donations during the early days of the COVID-19 pandemic, the FDA changed its policy and required MSM to be abstinent for 3 months instead of 1 year before giving blood. (Prior to December 2014, any man who’d had sex with a man, even once, was indefinitely banned from giving blood.)
The 3-month policy instituted in 2020 drew fire from critics such as the American Medical Association, which noted the regulation treated men differently if they had unprotected sex with a single man versus with multiple women.
Now, the FDA is proposing that it once again change the policy about blood donations: It is recommending that there be no special polices regarding MSM. “All prospective donors who report having a new sexual partner or more than one sexual partner and had anal sex in the past 3 months would be deferred from donation.”
Under the proposal, anyone who’s ever had HIV will not be able to donate. (They can’t donate stem cells either.) And the FDA proposes restrictions on those who take pre-exposure prophylaxis or postexposure prophylaxis for HIV.
Margolis, of Be the Match, noted that some members of the LGBTQ community may not be able to donate to Be The Match BioTherapies, which works with cell and gene therapy developers worldwide to provide cellular starting material. “These therapies may have different requirements than those for blood stem-cell transplants. Men who have had sex with men in the past 5 years or women who have had sex with a man who has had sex with a man in the past 5 years may not be able to donate to Be The Match BioTherapies. While we understand this could be upsetting or frustrating for someone who desires to be a part of these therapies, we are committed to following medical guidelines and regulations, while also advocating for our donors and the LBGTQIA+ community as a whole.”
MSM aren’t the only target of outreach by proponents of stem cell donation. In 2019, UT Southwestern’s Dr. Adkins and colleagues wrote a commentary in Bone Marrow Transplantation that called for bone marrow donation centers to do more to be welcoming to transgender donors. “The largest age group identifying as transgender is 18-24 years of life, which overlaps considerably with the population of hematopoietic stem cell donors, which tend to be younger individuals,” the researchers wrote.
The transgender community was “simply overlooked,” Dr. Adkins said. Since then, as he pointed out, things have changed. Now, Be the Match’s website notes that “members of the LGBTQIA+ community CAN join the registry and donate.” The organization says that “for medical reasons, everyone is asked to provide their sex assigned at birth when they register. Should you be called as a match, pronouns and gender identity are respected throughout the process.”
In addition, the site says people on prescription hormone therapy are not excluded from joining the registry. Patients who have undergone surgery within the last 12 months, including sex-reassignment procedures, “will be asked about the current status of their recovery and whether they are still seeing a physician for follow-up in regards to the surgery.”
What’s next? Dr. Fingrut said he expects the lifting of strict rules about MSM and blood donation will boost stem cell donation in the community.
There seems to be plenty of room for more outreach. Cole Williams, founder of Pride & Plasma, which advocates for allowing gay men to give blood, suggested in an interview that advocates who want to increase stem cell donation in the LGBTQ community reach out to its community centers, health organizations, providers, and clinics.
So far, though, “I haven’t seen a big call for registration of any individuals unless they have a personal relation to bone marrow donation,” he said.
Dr. Fingrut and Dr. Adkins report no disclosures.