User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Rheumatologist Volunteers Make a Difference to Those in Need at Home and Overseas
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.

“There’s a language barrier no matter where you are,” Dr. Albert said.
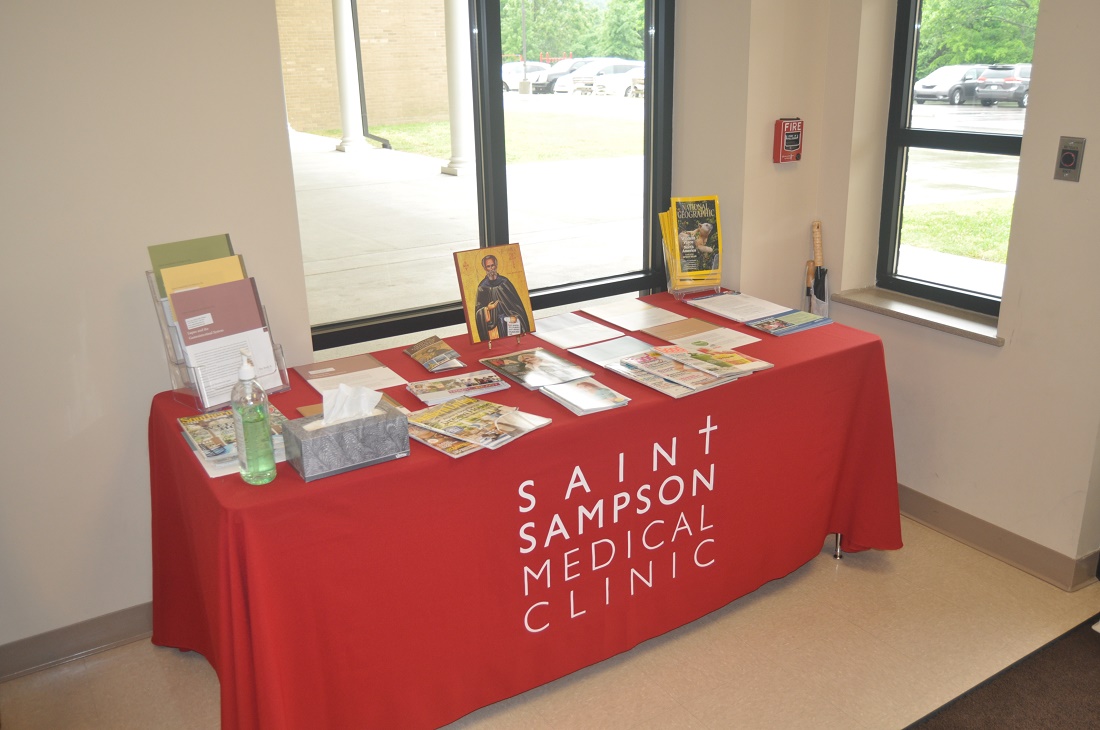
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.

Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.

The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.
“There’s a language barrier no matter where you are,” Dr. Albert said.
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.
Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.
The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.
“There’s a language barrier no matter where you are,” Dr. Albert said.
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.
Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.
The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
Ustekinumab’s ‘Egregious’ Medicare Part B and D Pricing Differences Led to Federal Intervention
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.
More Than the Paycheck: Top Non-Salary Perks for Doctors
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.
Holly Wyatt, MD, had spent 20 years in UCHealth with no plans to leave. Her home, support system, and lifestyle were all rooted in Denver. But in 2020, The University of Alabama at Birmingham (UAB) made the endocrinologist an offer she couldn’t resist.
The pay increase and a bump to full professorship weren’t enough to lure her across the country. But then UAB sweetened the deal with fewer clinic hours and paid time to create. “I didn’t have to fit into the typical ‘see patients 5 days a week, bill this many dollars,’ ” she said.
With no minimum billable hours, she could spend her time on clinical trials, designing programs, and recording podcasts. “When they offered that, I said, ‘Ooh, that’s enticing.’ ”
After a couple of visits to the campus, she began the job transition.
Doctors are looking for more than base pay. For many physicians, like Dr. Wyatt, non-salary incentives carry a lot of weight in the recruitment and job-hunting process.
“Some of the usual suspects are CME [continuing medical education] budget, signing bonuses, relocation assistance, loan repayment programs, and housing allowances,” said Jake Jorgovan, partner at Alpha Apex Group, a physician recruiting firm in Denver.
Post pandemic, doctors are vying for other benefits, perks that support their interests, work-life balance, and financial stability. “We’ve come across offers like sabbatical opportunities, paid time for research or personal projects, and even concierge services that handle things like grocery shopping or pet care,” said Mr. Jorgovan.
Amid physician shortages, doctors have more bargaining power than ever.
Money Still Talks
Financial perks are still the premiere portion of a benefits package, according to Marc Adam, physician recruiter at MASC Medical, a medical recruitment firm in Fort Lauderdale, Florida.
New data from the medical staffing company AMN Healthcare reported that the average signing bonus for physicians is $31,103. The average relocation allowance is $11,000, and the average CME allowance is $4000.
“CME budget and loan repayment programs are big because they directly impact career advancement and financial well-being,” Mr. Jorgovan said. Employers have historically been hesitant to offer these kinds of long-term benefits because of the financial commitment and planning involved, but that’s changing.
Mr. Adam said that short-term financial perks, like relocation assistance and signing bonuses, tend to be more important for younger doctors. They’re not yet financially established, so the relocation support and bonus funds have more impact as they take on a new role, he said.
Mid- and late-career doctors, on the other hand, are less beholden to these types of bonuses. Mr. Adam has recruited established doctors from across the country to Florida, and he said that the relocation allowance and singing bonus didn’t even rank in their top five priorities. Similarly, in Birmingham, Dr. Wyatt recently reread her offer letter from UAB and was surprised to find a relocation stipend that she never used. “I had no idea,” she said.
Vying for Time
Mid- and late-career doctors who have a better financial safety net tend to seek benefits that boost their quality of life.
One of Mr. Adam’s recent job-searching clients was unwilling to compromise on priorities like specific location and a 4-day workweek.
Four-day workweeks, flexible scheduling, and options for remote work are increasingly popular, especially since the pandemic. Some physicians, like those in primary care, are looking for dedicated charting hours — paid days or half-days set aside for updating the electronic medical records. Other doctors are negotiating multistate telehealth licensing paid by their employer and work-from-home telehealth hours.
“Work life has been slowly increasing over the 14 years I’ve been doing this. And post COVID, the employer’s willingness to be flexible with those types of accommodations increased,” said Mr. Adam.
Priya Jaisinghani, MD, an endocrinologist and obesity medicine specialist in her second year of practice, NYU Langone Health, New York City, said work-life balance can be a priority for young doctors, too. After training in New York during the pandemic, Dr. Jaisinghani was all too aware of the risk for burnout. So she negotiated a 4-day workweek when she took her first job out of fellowship in 2022. “I was able to prioritize work-life balance from the start,” she said.
Support for the Career You Want
When Dr. Jaisinghani signed her first contract in 2022 with NYU, her move from New Jersey to New York wasn’t far enough to warrant a relocation allowance. “There was a signing bonus, sure,” she said. But what really grabbed her attention were perks like mentorship, access to trainees, and autonomy.
Perks that support long-term growth — like CME allowance, teaching opportunities, or access to leadership tracks — are especially important to young doctors. “After dedicating so many years to medical training, you want to look for some degree of autonomy in building your practice,” she said. NYU offered her that kind of freedom and support.
On top of personal growth, young physicians are looking for perks that will allow them to build the practice they want for their patients,Dr. Jaisinghani told this news organization. A lot of young doctors don’t know that they can negotiate for schedule preferences, office space, their own exam room, and dedicated support staff. However, they can and should because these factors influence their daily work life and patient experience.
Experienced doctors are also looking for perks that support the career they want. Recruitment experts say that doctors tend to look for opportunities that accommodate their interests. One of Mr. Jorgovan’s recent clients took a position because it offered a generous CME budget and dedicated research hours. Similarly, Dr. Wyatt at UAB moved because her contract included paid time to create.
“It really comes down to the need for balance — being able to keep learning while also having time for personal life and family,” Mr. Jorgovan said.
Making and Meeting Demand
Thanks to the rising demand, doctors have more power than ever to negotiate the perks they want and need.
The existing physician shortage — driven by retiring doctors and an aging patient population — was only exacerbated by the pandemic. Now, a number of new market entries are further increasing competition for talent, according to AMN Healthcare’s report. Retail clinics, urgent care, telehealth companies, and private equity firms compete for the same doctors, driving up salaries and doctor bargaining power.
“Physicians were always in the driver’s seat, and their bargaining power has only increased,” Mr. Adam said. Healthcare systems, once reticent about flexible working arrangements or loan repayment, are reconsidering.
Even young doctors have more negotiating power than they realize, but they might need help. “It’s underrated to get a contracts lawyer as a young doctor, but I think it’s smart,” Dr. Jaisinghani said. They’re often more familiar with salaries in the area, flexibility options, and potential benefits, none of which doctors are taught in training, she said.
Mr. Adam said that the pandemic opened employers’ eyes to the fact that doctors have the bargaining power. There’s a stark need for their talent and a lot of public support for their service. So hiring managers are listening and are ready to offer “creative benefits to accommodate the market demand,” he said.
In her new position at UAB, Dr. Wyatt said that money will always matter. “When your salary is low, bumping that salary will make you happier.” But after a certain point, she said, other things become more important — like your time, the work you do, and the people you work with. Her perks at UAB offer more than money can. “I get up in the morning, and I’m excited — [the work] excites me,” she said.
A version of this article first appeared on Medscape.com.
Seated Doctors Better Satisfy Patients, Communication
During a busy day of consultations, however, it can be difficult for healthcare professionals to sit regularly with patients. Previous studies have revealed that hospital doctors sit during one out of every five meetings with patients.
A recent US study evaluated the impact of the practitioner’s seated position next to the patient on the quality of the doctor-patient interaction in an internal medicine department. This research involved a sample of 51 doctors (average age, 35 years; 51% men) and analyzed 125 clinical interviews (n = 125 patients; average age, 53 years; 55% men). Participants were not informed of the real objective of the study. The patient’s perception of medical care was also solicited.
The experimental protocol involved two distinct configurations. Either the chair was positioned near the bed (within 90 cm) before the doctor arrived or it remained visible in its usual place. Each meeting with a patient was randomized according to the chair location (intervention group: n = 60; control group: n = 65).
The primary criterion was the doctor’s binary decision to sit or not at a given moment during a meeting with a patient. Secondary criteria included patient satisfaction, time spent in the room, and the perception of time spent in the room by doctors and patients.
The chair’s location had no effect on the average duration of the interview, whether actual or estimated. When a chair was placed near the bed, the doctor sat in more than six out of 10 cases (63%), compared with fewer than one case out of 10 (8%) when the chair was less easily accessible (odds ratio, 20.7; 95% CI, 7.2-59.4; P < .001).
The chair arrangement did not lead to a significant difference in the average duration of presence in the room (10.6 min for both groups). Likewise, no notable difference was observed regarding the subjective estimation of this duration from the practitioners’ point of view (9.4 min vs 9.8 min) or from the patients’ point of view (13.1 min vs 13.5 min).
In the group in which the doctor sat to converse, patient satisfaction was significantly higher, with an overall difference of 3.9% (P = .02). Patients felt that the information provided was better (72% vs 52%; P =.03), and their confidence in the proposed care was also higher (58% vs 35%; P = .01). On the other hand, no significant difference appeared between the two groups regarding the information retained by the patient (doctor’s name and reason for hospitalization) or the doctor’s behavior.
The study authors acknowledged the study’s methodological limitations, which included a sample size that was lower than initially projected and the restriction to a single hospital setting. In addition, they noted that all patients were housed in individual rooms, which could be a source of bias. Despite these reservations, they suggested that even minimal environmental changes, such as the thoughtful placement of a chair, can significantly affect patients’ perceptions of the quality of care provided.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
During a busy day of consultations, however, it can be difficult for healthcare professionals to sit regularly with patients. Previous studies have revealed that hospital doctors sit during one out of every five meetings with patients.
A recent US study evaluated the impact of the practitioner’s seated position next to the patient on the quality of the doctor-patient interaction in an internal medicine department. This research involved a sample of 51 doctors (average age, 35 years; 51% men) and analyzed 125 clinical interviews (n = 125 patients; average age, 53 years; 55% men). Participants were not informed of the real objective of the study. The patient’s perception of medical care was also solicited.
The experimental protocol involved two distinct configurations. Either the chair was positioned near the bed (within 90 cm) before the doctor arrived or it remained visible in its usual place. Each meeting with a patient was randomized according to the chair location (intervention group: n = 60; control group: n = 65).
The primary criterion was the doctor’s binary decision to sit or not at a given moment during a meeting with a patient. Secondary criteria included patient satisfaction, time spent in the room, and the perception of time spent in the room by doctors and patients.
The chair’s location had no effect on the average duration of the interview, whether actual or estimated. When a chair was placed near the bed, the doctor sat in more than six out of 10 cases (63%), compared with fewer than one case out of 10 (8%) when the chair was less easily accessible (odds ratio, 20.7; 95% CI, 7.2-59.4; P < .001).
The chair arrangement did not lead to a significant difference in the average duration of presence in the room (10.6 min for both groups). Likewise, no notable difference was observed regarding the subjective estimation of this duration from the practitioners’ point of view (9.4 min vs 9.8 min) or from the patients’ point of view (13.1 min vs 13.5 min).
In the group in which the doctor sat to converse, patient satisfaction was significantly higher, with an overall difference of 3.9% (P = .02). Patients felt that the information provided was better (72% vs 52%; P =.03), and their confidence in the proposed care was also higher (58% vs 35%; P = .01). On the other hand, no significant difference appeared between the two groups regarding the information retained by the patient (doctor’s name and reason for hospitalization) or the doctor’s behavior.
The study authors acknowledged the study’s methodological limitations, which included a sample size that was lower than initially projected and the restriction to a single hospital setting. In addition, they noted that all patients were housed in individual rooms, which could be a source of bias. Despite these reservations, they suggested that even minimal environmental changes, such as the thoughtful placement of a chair, can significantly affect patients’ perceptions of the quality of care provided.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
During a busy day of consultations, however, it can be difficult for healthcare professionals to sit regularly with patients. Previous studies have revealed that hospital doctors sit during one out of every five meetings with patients.
A recent US study evaluated the impact of the practitioner’s seated position next to the patient on the quality of the doctor-patient interaction in an internal medicine department. This research involved a sample of 51 doctors (average age, 35 years; 51% men) and analyzed 125 clinical interviews (n = 125 patients; average age, 53 years; 55% men). Participants were not informed of the real objective of the study. The patient’s perception of medical care was also solicited.
The experimental protocol involved two distinct configurations. Either the chair was positioned near the bed (within 90 cm) before the doctor arrived or it remained visible in its usual place. Each meeting with a patient was randomized according to the chair location (intervention group: n = 60; control group: n = 65).
The primary criterion was the doctor’s binary decision to sit or not at a given moment during a meeting with a patient. Secondary criteria included patient satisfaction, time spent in the room, and the perception of time spent in the room by doctors and patients.
The chair’s location had no effect on the average duration of the interview, whether actual or estimated. When a chair was placed near the bed, the doctor sat in more than six out of 10 cases (63%), compared with fewer than one case out of 10 (8%) when the chair was less easily accessible (odds ratio, 20.7; 95% CI, 7.2-59.4; P < .001).
The chair arrangement did not lead to a significant difference in the average duration of presence in the room (10.6 min for both groups). Likewise, no notable difference was observed regarding the subjective estimation of this duration from the practitioners’ point of view (9.4 min vs 9.8 min) or from the patients’ point of view (13.1 min vs 13.5 min).
In the group in which the doctor sat to converse, patient satisfaction was significantly higher, with an overall difference of 3.9% (P = .02). Patients felt that the information provided was better (72% vs 52%; P =.03), and their confidence in the proposed care was also higher (58% vs 35%; P = .01). On the other hand, no significant difference appeared between the two groups regarding the information retained by the patient (doctor’s name and reason for hospitalization) or the doctor’s behavior.
The study authors acknowledged the study’s methodological limitations, which included a sample size that was lower than initially projected and the restriction to a single hospital setting. In addition, they noted that all patients were housed in individual rooms, which could be a source of bias. Despite these reservations, they suggested that even minimal environmental changes, such as the thoughtful placement of a chair, can significantly affect patients’ perceptions of the quality of care provided.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Risk for Giant Cell Arteritis Rises With Air Pollution Levels
TOPLINE:
Exposure to environmental particulate matter ≤ 10 μm in diameter (PM10) is associated with an increased risk for giant cell arteritis, particularly in older individuals aged ≥ 70 years and those with prolonged exposure to high levels of air pollution.
METHODOLOGY:
- Researchers conducted a retrospective case-crossover study to examine the association between exposure to airborne PM10 and the risk for giant cell arteritis and its ischemic complications.
- They included 232 patients with giant cell arteritis (median age at diagnosis, 73 years; 69% women) from three hospitals in northern Italy between June 2013 to December 2021.
- The hourly and daily average concentrations of PM10 were collected from the Italian monitoring network; patients’ exposure to PM10 was calculated using a space-time statistical model, incorporating meteorological variables, elevation, and proximity to main roads.
- The mean follow-up time of this cohort was 38 months.
TAKEAWAY:
- Every 10 μg/m3 increase in PM10 exposure in the preceding 60 days increased the incremental risk (IR) for giant cell arteritis by 27.1% (95% CI, 5.8-52.6).
- This association was more pronounced (IR, 38.8%; 95% CI, 9.2-76.3) in the subgroup of patients aged ≥ 70 years.
- The positive association between incident giant cell arteritis and concentrations of PM10 was seen only when patients were exposed to high concentrations of PM10 (26.9 ± 13.8 μg/m3) but not low concentrations (11.9 ± 7.9 μg/m3).
- This study did not show any significant association between exposure to PM10 and ischemic complications.
IN PRACTICE:
“Exposure to PM10 in the 60 days preceding [giant cell arteritis] symptoms onset seems to be associated with an increased risk of developing the disease, especially in older individuals with prolonged exposure to high levels of air pollution,” the authors wrote.
SOURCE:
The study was led by Milena Bond, MD, Hospital of Bruneck, Teaching Hospital of the Paracelsus Medical University, Brunico, Italy, and was published online in Arthritis Care & Research.
LIMITATIONS:
The retrospective nature of the study may have introduced recall bias. The study did not include data for other particulate matter fractions or gaseous pollutants, which may have impacted the findings. The use of residential addresses at the time of diagnosis precluded assessment of potential recent relocations.
DISCLOSURES:
This study did not disclose any funding source. Some authors reported having financial relationships with multiple pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Exposure to environmental particulate matter ≤ 10 μm in diameter (PM10) is associated with an increased risk for giant cell arteritis, particularly in older individuals aged ≥ 70 years and those with prolonged exposure to high levels of air pollution.
METHODOLOGY:
- Researchers conducted a retrospective case-crossover study to examine the association between exposure to airborne PM10 and the risk for giant cell arteritis and its ischemic complications.
- They included 232 patients with giant cell arteritis (median age at diagnosis, 73 years; 69% women) from three hospitals in northern Italy between June 2013 to December 2021.
- The hourly and daily average concentrations of PM10 were collected from the Italian monitoring network; patients’ exposure to PM10 was calculated using a space-time statistical model, incorporating meteorological variables, elevation, and proximity to main roads.
- The mean follow-up time of this cohort was 38 months.
TAKEAWAY:
- Every 10 μg/m3 increase in PM10 exposure in the preceding 60 days increased the incremental risk (IR) for giant cell arteritis by 27.1% (95% CI, 5.8-52.6).
- This association was more pronounced (IR, 38.8%; 95% CI, 9.2-76.3) in the subgroup of patients aged ≥ 70 years.
- The positive association between incident giant cell arteritis and concentrations of PM10 was seen only when patients were exposed to high concentrations of PM10 (26.9 ± 13.8 μg/m3) but not low concentrations (11.9 ± 7.9 μg/m3).
- This study did not show any significant association between exposure to PM10 and ischemic complications.
IN PRACTICE:
“Exposure to PM10 in the 60 days preceding [giant cell arteritis] symptoms onset seems to be associated with an increased risk of developing the disease, especially in older individuals with prolonged exposure to high levels of air pollution,” the authors wrote.
SOURCE:
The study was led by Milena Bond, MD, Hospital of Bruneck, Teaching Hospital of the Paracelsus Medical University, Brunico, Italy, and was published online in Arthritis Care & Research.
LIMITATIONS:
The retrospective nature of the study may have introduced recall bias. The study did not include data for other particulate matter fractions or gaseous pollutants, which may have impacted the findings. The use of residential addresses at the time of diagnosis precluded assessment of potential recent relocations.
DISCLOSURES:
This study did not disclose any funding source. Some authors reported having financial relationships with multiple pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Exposure to environmental particulate matter ≤ 10 μm in diameter (PM10) is associated with an increased risk for giant cell arteritis, particularly in older individuals aged ≥ 70 years and those with prolonged exposure to high levels of air pollution.
METHODOLOGY:
- Researchers conducted a retrospective case-crossover study to examine the association between exposure to airborne PM10 and the risk for giant cell arteritis and its ischemic complications.
- They included 232 patients with giant cell arteritis (median age at diagnosis, 73 years; 69% women) from three hospitals in northern Italy between June 2013 to December 2021.
- The hourly and daily average concentrations of PM10 were collected from the Italian monitoring network; patients’ exposure to PM10 was calculated using a space-time statistical model, incorporating meteorological variables, elevation, and proximity to main roads.
- The mean follow-up time of this cohort was 38 months.
TAKEAWAY:
- Every 10 μg/m3 increase in PM10 exposure in the preceding 60 days increased the incremental risk (IR) for giant cell arteritis by 27.1% (95% CI, 5.8-52.6).
- This association was more pronounced (IR, 38.8%; 95% CI, 9.2-76.3) in the subgroup of patients aged ≥ 70 years.
- The positive association between incident giant cell arteritis and concentrations of PM10 was seen only when patients were exposed to high concentrations of PM10 (26.9 ± 13.8 μg/m3) but not low concentrations (11.9 ± 7.9 μg/m3).
- This study did not show any significant association between exposure to PM10 and ischemic complications.
IN PRACTICE:
“Exposure to PM10 in the 60 days preceding [giant cell arteritis] symptoms onset seems to be associated with an increased risk of developing the disease, especially in older individuals with prolonged exposure to high levels of air pollution,” the authors wrote.
SOURCE:
The study was led by Milena Bond, MD, Hospital of Bruneck, Teaching Hospital of the Paracelsus Medical University, Brunico, Italy, and was published online in Arthritis Care & Research.
LIMITATIONS:
The retrospective nature of the study may have introduced recall bias. The study did not include data for other particulate matter fractions or gaseous pollutants, which may have impacted the findings. The use of residential addresses at the time of diagnosis precluded assessment of potential recent relocations.
DISCLOSURES:
This study did not disclose any funding source. Some authors reported having financial relationships with multiple pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Pooled Trial Data Support Lower Uveitis Rate With Bimekizumab for Axial Spondyloarthritis
TOPLINE:
Patients with axial spondyloarthritis (axSpA) treated with bimekizumab had a lower incidence of uveitis than those receiving placebo in pooled clinical trial data.
METHODOLOGY:
- Researchers pooled data from two phase 3 trials, one phase 2b trial, and their open-label extensions to evaluate the incidence of uveitis in patients with radiographic and nonradiographic axSpA who were treated with bimekizumab.
- Patients received either bimekizumab 160 mg (n = 349) or placebo (n = 237) every 4 weeks in the pooled phase 3 data during a 16-week, double-blind treatment period, while 848 patients (mean age, 40.3 years; 71.5% men) received at least one dose of 160 mg bimekizumab in the overall phase 2b/3 pool.
- Outcomes included the incidence of uveitis events reported as exposure-adjusted incidence rates (EAIRs) and exposure-adjusted event rates reported per 100 patient-years.
TAKEAWAY:
- The proportion of patients experiencing uveitis was lower in those treated with bimekizumab than in those receiving placebo over 16 weeks (0.6% vs 4.6%; nominal P = .001).
- In patients with a history of uveitis, incidence was lower with bimekizumab than with placebo (6.2 vs 70.4 per 100 patient-years).
- Among patients receiving bimekizumab, the EAIR of uveitis was lower among those without a history of uveitis than in those with a history of the condition (0.6 vs 4.6 per 100 patient-years).
- A higher proportion of patients who experienced uveitis had a history of uveitis, compared with those who did not (56.0% vs 14.1%).
IN PRACTICE:
“These data suggest that [bimekizumab], a dual IL [interleukin]-17A/F inhibitor, may confer protective effects for uveitis in patients with axSpA,” the authors wrote.
SOURCE:
The study, led by Matthew A. Brown, Genomics England, London, England, and Martin Rudwaleit, Klinikum Bielefeld, University of Bielefeld, Germany, was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The reporting of uveitis in the trials relied on the spontaneous reporting of adverse events, and not all events were evaluated by an ophthalmologist. The duration of the double-blind treatment period was relatively short, and the total number of patients with acute anterior uveitis was limited. Moreover, long-term placebo comparisons extending beyond 16 weeks were lacking.
DISCLOSURES:
The studies included in the pooled data were supported by UCB Pharma. Some authors reported financial ties with UCB and other pharmaceutical companies. Some authors reported being employees and shareholders of UCB Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) treated with bimekizumab had a lower incidence of uveitis than those receiving placebo in pooled clinical trial data.
METHODOLOGY:
- Researchers pooled data from two phase 3 trials, one phase 2b trial, and their open-label extensions to evaluate the incidence of uveitis in patients with radiographic and nonradiographic axSpA who were treated with bimekizumab.
- Patients received either bimekizumab 160 mg (n = 349) or placebo (n = 237) every 4 weeks in the pooled phase 3 data during a 16-week, double-blind treatment period, while 848 patients (mean age, 40.3 years; 71.5% men) received at least one dose of 160 mg bimekizumab in the overall phase 2b/3 pool.
- Outcomes included the incidence of uveitis events reported as exposure-adjusted incidence rates (EAIRs) and exposure-adjusted event rates reported per 100 patient-years.
TAKEAWAY:
- The proportion of patients experiencing uveitis was lower in those treated with bimekizumab than in those receiving placebo over 16 weeks (0.6% vs 4.6%; nominal P = .001).
- In patients with a history of uveitis, incidence was lower with bimekizumab than with placebo (6.2 vs 70.4 per 100 patient-years).
- Among patients receiving bimekizumab, the EAIR of uveitis was lower among those without a history of uveitis than in those with a history of the condition (0.6 vs 4.6 per 100 patient-years).
- A higher proportion of patients who experienced uveitis had a history of uveitis, compared with those who did not (56.0% vs 14.1%).
IN PRACTICE:
“These data suggest that [bimekizumab], a dual IL [interleukin]-17A/F inhibitor, may confer protective effects for uveitis in patients with axSpA,” the authors wrote.
SOURCE:
The study, led by Matthew A. Brown, Genomics England, London, England, and Martin Rudwaleit, Klinikum Bielefeld, University of Bielefeld, Germany, was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The reporting of uveitis in the trials relied on the spontaneous reporting of adverse events, and not all events were evaluated by an ophthalmologist. The duration of the double-blind treatment period was relatively short, and the total number of patients with acute anterior uveitis was limited. Moreover, long-term placebo comparisons extending beyond 16 weeks were lacking.
DISCLOSURES:
The studies included in the pooled data were supported by UCB Pharma. Some authors reported financial ties with UCB and other pharmaceutical companies. Some authors reported being employees and shareholders of UCB Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Patients with axial spondyloarthritis (axSpA) treated with bimekizumab had a lower incidence of uveitis than those receiving placebo in pooled clinical trial data.
METHODOLOGY:
- Researchers pooled data from two phase 3 trials, one phase 2b trial, and their open-label extensions to evaluate the incidence of uveitis in patients with radiographic and nonradiographic axSpA who were treated with bimekizumab.
- Patients received either bimekizumab 160 mg (n = 349) or placebo (n = 237) every 4 weeks in the pooled phase 3 data during a 16-week, double-blind treatment period, while 848 patients (mean age, 40.3 years; 71.5% men) received at least one dose of 160 mg bimekizumab in the overall phase 2b/3 pool.
- Outcomes included the incidence of uveitis events reported as exposure-adjusted incidence rates (EAIRs) and exposure-adjusted event rates reported per 100 patient-years.
TAKEAWAY:
- The proportion of patients experiencing uveitis was lower in those treated with bimekizumab than in those receiving placebo over 16 weeks (0.6% vs 4.6%; nominal P = .001).
- In patients with a history of uveitis, incidence was lower with bimekizumab than with placebo (6.2 vs 70.4 per 100 patient-years).
- Among patients receiving bimekizumab, the EAIR of uveitis was lower among those without a history of uveitis than in those with a history of the condition (0.6 vs 4.6 per 100 patient-years).
- A higher proportion of patients who experienced uveitis had a history of uveitis, compared with those who did not (56.0% vs 14.1%).
IN PRACTICE:
“These data suggest that [bimekizumab], a dual IL [interleukin]-17A/F inhibitor, may confer protective effects for uveitis in patients with axSpA,” the authors wrote.
SOURCE:
The study, led by Matthew A. Brown, Genomics England, London, England, and Martin Rudwaleit, Klinikum Bielefeld, University of Bielefeld, Germany, was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The reporting of uveitis in the trials relied on the spontaneous reporting of adverse events, and not all events were evaluated by an ophthalmologist. The duration of the double-blind treatment period was relatively short, and the total number of patients with acute anterior uveitis was limited. Moreover, long-term placebo comparisons extending beyond 16 weeks were lacking.
DISCLOSURES:
The studies included in the pooled data were supported by UCB Pharma. Some authors reported financial ties with UCB and other pharmaceutical companies. Some authors reported being employees and shareholders of UCB Pharma.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
What Are the Best Supplements for Patients With Kidney Disease? A Few Stand Out
The global dietary supplement industry generates more than $400 billion a year. Supplements are alleged to treat many health concerns, from immune conditions and cognition to sexual dysfunction and premature wrinkles. Although some supplements have been proven to be helpful, others have no scientific basis.
I can preach all day that a healthy diet rarely needs supplementation. But even as a dietitian, I find it difficult to consistently eat a diet that is both sufficiently varied and adequate to provide for all my nutrition needs. Our patients with kidney disease, surely, are not immune to this plight. They may even be more inclined to nutrient deficiencies, as poor diet is linked to increased incidence and progression of chronic kidney disease (CKD).
I find that patients with kidney disease often have an interest in dietary supplementation, even those with a well-rounded diet. Though we can discourage the use of supplements, or at the very least encourage patient transparency regarding supplement use, many will continue dietary supplementation at the suggestion of their friends, family, or even their preferred daytime talk show host.
What these patients truly require is education on using supplements that are most beneficial to them. By recommending supplements that address patients’ pain points like inflammation, dyslipidemia, cardiovascular health, and reduced progression to end-stage renal disease (ESRD), we can improve patient health and, hopefully, decrease use of questionable supplements.
Probiotics
Although probiotics have been used in the treatment of digestive issues for many years, the gut-kidney axis is only recently being explored. Studies show that the microbiota of patients with CKD is altered, even in the early stages of disease, producing additional inflammation and metabolic dysfunction. This can be remedied, or at least alleviated, by introducing a probiotic supplement.
Some probiotics have been shown to decrease inflammation, decrease fasting blood glucose, decrease low-density lipoprotein cholesterol, triglycerides, and total cholesterol, increase estimated glomerular filtration rate (eGFR), decrease blood urea nitrogen and urea, and decrease uric acid
Probiotic-rich foods like kimchi or fermented pickles may not be appropriate because of excessive sodium content or simply because of patient preference — kombucha isn’t for everyone. However, adding a probiotic supplement can improve gut microbiota without undermining dietary concerns.
When recommending probiotics, patients should be educated to ensure that their probiotic has strains that have been proven to be beneficial for kidney health. Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium species, and Streptococcus thermophilus have been shown to have a positive effect on kidney health and decreasing progression of CKD at a dosage of 109 colony-forming units per day.
Fish Oil
Though nephrology and cardiology are separate fields, it cannot be overstated that kidney patients are also heart patients.
Patients with CKD and an eGFR < 60 mL/min per 1.73 m2 are most likely to die from cardiovascular causes, and this likelihood increases as eGFR decreases. CKD-associated dyslipidemia results in elevated triglycerides and reduced high-density lipoprotein cholesterol often accompanied by proteinuria, and has been linked to an increase in atherosclerosis.
A simple fish oil supplement can work to decrease oxidative stress, relieve inflammation, and improve serum lipids, leading to improved kidney and cardiovascular health. One meta-analysis found that high-dose fish oil supplementation, though it had no effect on serum creatinine or eGFR, was associated with a lower risk for proteinuria and progression to ESRD.
Fish oil’s popularity in recent years bodes well for the kidney patient. It is now easily obtained over the counter in high doses to meet the recommended adequate intake of omega-3s, which is 1100 mg/d for women and 1600 mg/d for men. There are also more burpless varieties of these supplements to increase compliance.
Vitamin D
Patients with renal disease are prone to vitamin D deficiency through inadequate intake and limited sunlight, which is exacerbated by the diseased kidney’s inability to effectively convert calcidiol to calcitriol. Vitamin D deficiency is linked to poor bone health, fatigue, muscle pain, impaired wound healing, and depression. Low vitamin D status has also been linked to poor outcomes in cancer, multiple sclerosis, cardiovascular disease, type 2 diabetes, and weight loss.
A meta-analysis of over 6000 patients with CKD found that high levels of 25-hydroxy vitamin D (25[OH]D) are associated with significantly improved survival rates regardless of CKD or ESRD status.
Kidney Disease: Improving Global Outcomes guidelines recommend supplementing with ergocalciferol or cholecalciferol to correct (OH)D deficiency. This ensures adequate supply for conversion to calcitriol, but it cannot affect bone and mineral metabolism without further intervention in the form of calcitriol supplementation. By supplementing with ergocalciferol or cholecalciferol to meet the recommended daily allowance of 15 µg (600 IU) for adults under 70 years and 20 µg (800 IU) for adults over 70 years, the primary care team can ensure that the body has all the building blocks required for the nephrology team to then address mineral and bone disorder in CKD without the fear of promoting hypercalcemia.
Safe Purchasing Practices
Patients should be reminded to purchase dietary supplements from reputable dealers, especially when purchasing online. Retailers like Amazon are increasing the barriers required to sell supplements to improve the quality of products sold on the site. But other online retailers may sell products from outside of the United States that fall outside of the Food and Drug Administration’s jurisdiction.
Patients should also be reminded that “more is not always better” and counseled on appropriate dosages for individual needs.
In Summary
Patients will probably continue to lean on dietary supplements, regardless of our approval. Transparency and education are important when working with patients with CKD, especially in regard to dietary supplements.
When recommended appropriately, however, the supplements discussed can lead to better outcomes with improvements in kidney health by addressing inflammation, serum lipids, glycemic control, and cardiovascular health.
Ms. Winfree Root is a renal dietitian in private practice in Mary Esther, Florida. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The global dietary supplement industry generates more than $400 billion a year. Supplements are alleged to treat many health concerns, from immune conditions and cognition to sexual dysfunction and premature wrinkles. Although some supplements have been proven to be helpful, others have no scientific basis.
I can preach all day that a healthy diet rarely needs supplementation. But even as a dietitian, I find it difficult to consistently eat a diet that is both sufficiently varied and adequate to provide for all my nutrition needs. Our patients with kidney disease, surely, are not immune to this plight. They may even be more inclined to nutrient deficiencies, as poor diet is linked to increased incidence and progression of chronic kidney disease (CKD).
I find that patients with kidney disease often have an interest in dietary supplementation, even those with a well-rounded diet. Though we can discourage the use of supplements, or at the very least encourage patient transparency regarding supplement use, many will continue dietary supplementation at the suggestion of their friends, family, or even their preferred daytime talk show host.
What these patients truly require is education on using supplements that are most beneficial to them. By recommending supplements that address patients’ pain points like inflammation, dyslipidemia, cardiovascular health, and reduced progression to end-stage renal disease (ESRD), we can improve patient health and, hopefully, decrease use of questionable supplements.
Probiotics
Although probiotics have been used in the treatment of digestive issues for many years, the gut-kidney axis is only recently being explored. Studies show that the microbiota of patients with CKD is altered, even in the early stages of disease, producing additional inflammation and metabolic dysfunction. This can be remedied, or at least alleviated, by introducing a probiotic supplement.
Some probiotics have been shown to decrease inflammation, decrease fasting blood glucose, decrease low-density lipoprotein cholesterol, triglycerides, and total cholesterol, increase estimated glomerular filtration rate (eGFR), decrease blood urea nitrogen and urea, and decrease uric acid
Probiotic-rich foods like kimchi or fermented pickles may not be appropriate because of excessive sodium content or simply because of patient preference — kombucha isn’t for everyone. However, adding a probiotic supplement can improve gut microbiota without undermining dietary concerns.
When recommending probiotics, patients should be educated to ensure that their probiotic has strains that have been proven to be beneficial for kidney health. Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium species, and Streptococcus thermophilus have been shown to have a positive effect on kidney health and decreasing progression of CKD at a dosage of 109 colony-forming units per day.
Fish Oil
Though nephrology and cardiology are separate fields, it cannot be overstated that kidney patients are also heart patients.
Patients with CKD and an eGFR < 60 mL/min per 1.73 m2 are most likely to die from cardiovascular causes, and this likelihood increases as eGFR decreases. CKD-associated dyslipidemia results in elevated triglycerides and reduced high-density lipoprotein cholesterol often accompanied by proteinuria, and has been linked to an increase in atherosclerosis.
A simple fish oil supplement can work to decrease oxidative stress, relieve inflammation, and improve serum lipids, leading to improved kidney and cardiovascular health. One meta-analysis found that high-dose fish oil supplementation, though it had no effect on serum creatinine or eGFR, was associated with a lower risk for proteinuria and progression to ESRD.
Fish oil’s popularity in recent years bodes well for the kidney patient. It is now easily obtained over the counter in high doses to meet the recommended adequate intake of omega-3s, which is 1100 mg/d for women and 1600 mg/d for men. There are also more burpless varieties of these supplements to increase compliance.
Vitamin D
Patients with renal disease are prone to vitamin D deficiency through inadequate intake and limited sunlight, which is exacerbated by the diseased kidney’s inability to effectively convert calcidiol to calcitriol. Vitamin D deficiency is linked to poor bone health, fatigue, muscle pain, impaired wound healing, and depression. Low vitamin D status has also been linked to poor outcomes in cancer, multiple sclerosis, cardiovascular disease, type 2 diabetes, and weight loss.
A meta-analysis of over 6000 patients with CKD found that high levels of 25-hydroxy vitamin D (25[OH]D) are associated with significantly improved survival rates regardless of CKD or ESRD status.
Kidney Disease: Improving Global Outcomes guidelines recommend supplementing with ergocalciferol or cholecalciferol to correct (OH)D deficiency. This ensures adequate supply for conversion to calcitriol, but it cannot affect bone and mineral metabolism without further intervention in the form of calcitriol supplementation. By supplementing with ergocalciferol or cholecalciferol to meet the recommended daily allowance of 15 µg (600 IU) for adults under 70 years and 20 µg (800 IU) for adults over 70 years, the primary care team can ensure that the body has all the building blocks required for the nephrology team to then address mineral and bone disorder in CKD without the fear of promoting hypercalcemia.
Safe Purchasing Practices
Patients should be reminded to purchase dietary supplements from reputable dealers, especially when purchasing online. Retailers like Amazon are increasing the barriers required to sell supplements to improve the quality of products sold on the site. But other online retailers may sell products from outside of the United States that fall outside of the Food and Drug Administration’s jurisdiction.
Patients should also be reminded that “more is not always better” and counseled on appropriate dosages for individual needs.
In Summary
Patients will probably continue to lean on dietary supplements, regardless of our approval. Transparency and education are important when working with patients with CKD, especially in regard to dietary supplements.
When recommended appropriately, however, the supplements discussed can lead to better outcomes with improvements in kidney health by addressing inflammation, serum lipids, glycemic control, and cardiovascular health.
Ms. Winfree Root is a renal dietitian in private practice in Mary Esther, Florida. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The global dietary supplement industry generates more than $400 billion a year. Supplements are alleged to treat many health concerns, from immune conditions and cognition to sexual dysfunction and premature wrinkles. Although some supplements have been proven to be helpful, others have no scientific basis.
I can preach all day that a healthy diet rarely needs supplementation. But even as a dietitian, I find it difficult to consistently eat a diet that is both sufficiently varied and adequate to provide for all my nutrition needs. Our patients with kidney disease, surely, are not immune to this plight. They may even be more inclined to nutrient deficiencies, as poor diet is linked to increased incidence and progression of chronic kidney disease (CKD).
I find that patients with kidney disease often have an interest in dietary supplementation, even those with a well-rounded diet. Though we can discourage the use of supplements, or at the very least encourage patient transparency regarding supplement use, many will continue dietary supplementation at the suggestion of their friends, family, or even their preferred daytime talk show host.
What these patients truly require is education on using supplements that are most beneficial to them. By recommending supplements that address patients’ pain points like inflammation, dyslipidemia, cardiovascular health, and reduced progression to end-stage renal disease (ESRD), we can improve patient health and, hopefully, decrease use of questionable supplements.
Probiotics
Although probiotics have been used in the treatment of digestive issues for many years, the gut-kidney axis is only recently being explored. Studies show that the microbiota of patients with CKD is altered, even in the early stages of disease, producing additional inflammation and metabolic dysfunction. This can be remedied, or at least alleviated, by introducing a probiotic supplement.
Some probiotics have been shown to decrease inflammation, decrease fasting blood glucose, decrease low-density lipoprotein cholesterol, triglycerides, and total cholesterol, increase estimated glomerular filtration rate (eGFR), decrease blood urea nitrogen and urea, and decrease uric acid
Probiotic-rich foods like kimchi or fermented pickles may not be appropriate because of excessive sodium content or simply because of patient preference — kombucha isn’t for everyone. However, adding a probiotic supplement can improve gut microbiota without undermining dietary concerns.
When recommending probiotics, patients should be educated to ensure that their probiotic has strains that have been proven to be beneficial for kidney health. Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium species, and Streptococcus thermophilus have been shown to have a positive effect on kidney health and decreasing progression of CKD at a dosage of 109 colony-forming units per day.
Fish Oil
Though nephrology and cardiology are separate fields, it cannot be overstated that kidney patients are also heart patients.
Patients with CKD and an eGFR < 60 mL/min per 1.73 m2 are most likely to die from cardiovascular causes, and this likelihood increases as eGFR decreases. CKD-associated dyslipidemia results in elevated triglycerides and reduced high-density lipoprotein cholesterol often accompanied by proteinuria, and has been linked to an increase in atherosclerosis.
A simple fish oil supplement can work to decrease oxidative stress, relieve inflammation, and improve serum lipids, leading to improved kidney and cardiovascular health. One meta-analysis found that high-dose fish oil supplementation, though it had no effect on serum creatinine or eGFR, was associated with a lower risk for proteinuria and progression to ESRD.
Fish oil’s popularity in recent years bodes well for the kidney patient. It is now easily obtained over the counter in high doses to meet the recommended adequate intake of omega-3s, which is 1100 mg/d for women and 1600 mg/d for men. There are also more burpless varieties of these supplements to increase compliance.
Vitamin D
Patients with renal disease are prone to vitamin D deficiency through inadequate intake and limited sunlight, which is exacerbated by the diseased kidney’s inability to effectively convert calcidiol to calcitriol. Vitamin D deficiency is linked to poor bone health, fatigue, muscle pain, impaired wound healing, and depression. Low vitamin D status has also been linked to poor outcomes in cancer, multiple sclerosis, cardiovascular disease, type 2 diabetes, and weight loss.
A meta-analysis of over 6000 patients with CKD found that high levels of 25-hydroxy vitamin D (25[OH]D) are associated with significantly improved survival rates regardless of CKD or ESRD status.
Kidney Disease: Improving Global Outcomes guidelines recommend supplementing with ergocalciferol or cholecalciferol to correct (OH)D deficiency. This ensures adequate supply for conversion to calcitriol, but it cannot affect bone and mineral metabolism without further intervention in the form of calcitriol supplementation. By supplementing with ergocalciferol or cholecalciferol to meet the recommended daily allowance of 15 µg (600 IU) for adults under 70 years and 20 µg (800 IU) for adults over 70 years, the primary care team can ensure that the body has all the building blocks required for the nephrology team to then address mineral and bone disorder in CKD without the fear of promoting hypercalcemia.
Safe Purchasing Practices
Patients should be reminded to purchase dietary supplements from reputable dealers, especially when purchasing online. Retailers like Amazon are increasing the barriers required to sell supplements to improve the quality of products sold on the site. But other online retailers may sell products from outside of the United States that fall outside of the Food and Drug Administration’s jurisdiction.
Patients should also be reminded that “more is not always better” and counseled on appropriate dosages for individual needs.
In Summary
Patients will probably continue to lean on dietary supplements, regardless of our approval. Transparency and education are important when working with patients with CKD, especially in regard to dietary supplements.
When recommended appropriately, however, the supplements discussed can lead to better outcomes with improvements in kidney health by addressing inflammation, serum lipids, glycemic control, and cardiovascular health.
Ms. Winfree Root is a renal dietitian in private practice in Mary Esther, Florida. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
New Associations Identified Between IBD and Extraintestinal Manifestations
, according to a recent study.
For instance, antinuclear cytoplastic antibody is associated with primary sclerosing cholangitis (PSC) in Crohn’s disease, and CPEB4 genetic variation is associated with skin manifestations.
“Up to 40% of people with IBD suffer with symptoms from inflammation that occurs outside the gut, particularly affecting the liver, skin, and joints. These symptoms can often have a bigger impact on quality of life than the gut inflammation itself and can actually be life-threatening,” said senior author Dermot McGovern, MD, PhD, AGAF, director of translational medicine at the F. Widjaja Foundation Inflammatory Bowel Disease and Immunobiology Research Institute at Cedars-Sinai Medical Center, Los Angeles.
“With the advances in therapies for IBD, including availability of gut-selective agents, treatment choices often incorporate whether a patient has one of these manifestations or not,” he said. “We need to understand who is at increased risk of these and why.”
The study was published in Gastroenterology .
Analyzing Associations
Dr. McGovern and colleagues analyzed data for 12,083 unrelated European ancestry IBD cases with presence or absence of EIMs across four cohorts in the Cedars-Sinai Medical Center IBD Research Repository, National Institute for Diabetes and Digestive and Kidney Diseases IBD Genetics Consortium, Sinai Helmsley Alliance for Research Excellence Consortium, and Risk Stratification and Identification of Immunogenetic and Microbial Markers of Rapid Disease Progression in Children with Crohn’s Disease.
In particular, the researchers looked at EIM phenotypes such as ankylosing spondylitis and sacroiliitis, PSC, peripheral arthritis, and skin and ocular manifestations. They analyzed clinical and serologic parameters through regression analyses using a mixed-effects model, as well as within-case logistic regression for genetic associations.
Overall, 14% of patients had at least one EIM. Contrary to previous reports, only 2% had multiple EIMs, and most co-occurrences were negatively correlated. Nearly all EIMs were more common in Crohn’s disease, except for PSC, which was more common in ulcerative colitis.
In general, EIMs occurred more often in women, particularly with Crohn’s disease and colonic disease location, and in patients who required surgery. Jewish ancestry was associated with psoriasis and overall skin manifestations.
Smoking increased the risk for multiple EIMs, except for PSC, where there appeared to be a “protective” effect. Older age at diagnosis and a family history of IBD were associated with increased risk for certain EIMs as well.
In addition, the research team noted multiple serologic associations, such as immunoglobulin (Ig) G and IgA, perinuclear antinuclear cytoplastic antibodies, and anti–Pseudomonas fluorescens–associated sequences with any EIM, as well as particular associations with PSC, such as anti-Saccharomyces cerevisiae antibodies and anti-flagellin.
There were also genome-wide significant associations within the major histocompatibility complex and CPEB4. Genetic associations implicated tumor necrosis factor, Janus kinase-signal transducer and activator of transcription, and interleukin 6 as potential targets for EIMs.
“We are working with colleagues across the world to increase the sample size, as we believe there is more to find,” Dr. McGovern said. “Importantly, this includes non-European ancestry subjects, as there is an urgent need to increase the diversity of populations we study so advances in clinical care are available to all communities.”
Considering Target Therapies
As medicine becomes more specialized, physicians should remember to consider the whole patient while choosing treatment strategies.
“Sometimes doctors wear blinders to the whole person, and it’s important to be aware of a holistic approach, where a gastroenterologist also asks about potential joint inflammation or a rheumatologist asks about bowel inflammation,” said David Rubin, MD, AGAF, chief of the Section of Gastroenterology, Hepatology and Nutrition at the University of Chicago Medicine, Chicago.
Dr. Rubin, who wasn’t involved with this study, has researched and published on EIMs in IBD. He and colleagues analyzed the prevalence, pathophysiology, and clinical presentation of EIMs to better understand possibilities for disease management.

“As we’ve gotten a better understanding of the immune system, we’ve learned that an EIM can sometimes provide a clue to the treatment we might use,” he said. “Given a similar amount of bowel inflammation, if one patient also has joint pain and another doesn’t, we might choose different treatments based on the immune pathway that might be involved.”
In future studies, researchers may consider whether these genetic or serologic markers could predict EIM manifestation before it occurs clinically, Dr. Rubin said. He and colleagues are also studying the links between IBD and mental health associations.
“So far, we don’t have a blood test or biopsy test that tells you which treatment is more or less likely to work, so we need to think carefully as clinicians and look to other organ systems for clues,” he said. “It’s not only more efficient to pick a single therapy to treat both the skin and bowel, but it may actually be more effective if both have a particular dominant pathway.”
The study was supported by internal funds from the F. Widjaja Foundation Inflammatory Bowel and Immunobiology Research Institute. Several authors reported consultant roles or other associations with pharmaceutical companies. Dr. Rubin reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a recent study.
For instance, antinuclear cytoplastic antibody is associated with primary sclerosing cholangitis (PSC) in Crohn’s disease, and CPEB4 genetic variation is associated with skin manifestations.
“Up to 40% of people with IBD suffer with symptoms from inflammation that occurs outside the gut, particularly affecting the liver, skin, and joints. These symptoms can often have a bigger impact on quality of life than the gut inflammation itself and can actually be life-threatening,” said senior author Dermot McGovern, MD, PhD, AGAF, director of translational medicine at the F. Widjaja Foundation Inflammatory Bowel Disease and Immunobiology Research Institute at Cedars-Sinai Medical Center, Los Angeles.
“With the advances in therapies for IBD, including availability of gut-selective agents, treatment choices often incorporate whether a patient has one of these manifestations or not,” he said. “We need to understand who is at increased risk of these and why.”
The study was published in Gastroenterology .
Analyzing Associations
Dr. McGovern and colleagues analyzed data for 12,083 unrelated European ancestry IBD cases with presence or absence of EIMs across four cohorts in the Cedars-Sinai Medical Center IBD Research Repository, National Institute for Diabetes and Digestive and Kidney Diseases IBD Genetics Consortium, Sinai Helmsley Alliance for Research Excellence Consortium, and Risk Stratification and Identification of Immunogenetic and Microbial Markers of Rapid Disease Progression in Children with Crohn’s Disease.
In particular, the researchers looked at EIM phenotypes such as ankylosing spondylitis and sacroiliitis, PSC, peripheral arthritis, and skin and ocular manifestations. They analyzed clinical and serologic parameters through regression analyses using a mixed-effects model, as well as within-case logistic regression for genetic associations.
Overall, 14% of patients had at least one EIM. Contrary to previous reports, only 2% had multiple EIMs, and most co-occurrences were negatively correlated. Nearly all EIMs were more common in Crohn’s disease, except for PSC, which was more common in ulcerative colitis.
In general, EIMs occurred more often in women, particularly with Crohn’s disease and colonic disease location, and in patients who required surgery. Jewish ancestry was associated with psoriasis and overall skin manifestations.
Smoking increased the risk for multiple EIMs, except for PSC, where there appeared to be a “protective” effect. Older age at diagnosis and a family history of IBD were associated with increased risk for certain EIMs as well.
In addition, the research team noted multiple serologic associations, such as immunoglobulin (Ig) G and IgA, perinuclear antinuclear cytoplastic antibodies, and anti–Pseudomonas fluorescens–associated sequences with any EIM, as well as particular associations with PSC, such as anti-Saccharomyces cerevisiae antibodies and anti-flagellin.
There were also genome-wide significant associations within the major histocompatibility complex and CPEB4. Genetic associations implicated tumor necrosis factor, Janus kinase-signal transducer and activator of transcription, and interleukin 6 as potential targets for EIMs.
“We are working with colleagues across the world to increase the sample size, as we believe there is more to find,” Dr. McGovern said. “Importantly, this includes non-European ancestry subjects, as there is an urgent need to increase the diversity of populations we study so advances in clinical care are available to all communities.”
Considering Target Therapies
As medicine becomes more specialized, physicians should remember to consider the whole patient while choosing treatment strategies.
“Sometimes doctors wear blinders to the whole person, and it’s important to be aware of a holistic approach, where a gastroenterologist also asks about potential joint inflammation or a rheumatologist asks about bowel inflammation,” said David Rubin, MD, AGAF, chief of the Section of Gastroenterology, Hepatology and Nutrition at the University of Chicago Medicine, Chicago.
Dr. Rubin, who wasn’t involved with this study, has researched and published on EIMs in IBD. He and colleagues analyzed the prevalence, pathophysiology, and clinical presentation of EIMs to better understand possibilities for disease management.
“As we’ve gotten a better understanding of the immune system, we’ve learned that an EIM can sometimes provide a clue to the treatment we might use,” he said. “Given a similar amount of bowel inflammation, if one patient also has joint pain and another doesn’t, we might choose different treatments based on the immune pathway that might be involved.”
In future studies, researchers may consider whether these genetic or serologic markers could predict EIM manifestation before it occurs clinically, Dr. Rubin said. He and colleagues are also studying the links between IBD and mental health associations.
“So far, we don’t have a blood test or biopsy test that tells you which treatment is more or less likely to work, so we need to think carefully as clinicians and look to other organ systems for clues,” he said. “It’s not only more efficient to pick a single therapy to treat both the skin and bowel, but it may actually be more effective if both have a particular dominant pathway.”
The study was supported by internal funds from the F. Widjaja Foundation Inflammatory Bowel and Immunobiology Research Institute. Several authors reported consultant roles or other associations with pharmaceutical companies. Dr. Rubin reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a recent study.
For instance, antinuclear cytoplastic antibody is associated with primary sclerosing cholangitis (PSC) in Crohn’s disease, and CPEB4 genetic variation is associated with skin manifestations.
“Up to 40% of people with IBD suffer with symptoms from inflammation that occurs outside the gut, particularly affecting the liver, skin, and joints. These symptoms can often have a bigger impact on quality of life than the gut inflammation itself and can actually be life-threatening,” said senior author Dermot McGovern, MD, PhD, AGAF, director of translational medicine at the F. Widjaja Foundation Inflammatory Bowel Disease and Immunobiology Research Institute at Cedars-Sinai Medical Center, Los Angeles.
“With the advances in therapies for IBD, including availability of gut-selective agents, treatment choices often incorporate whether a patient has one of these manifestations or not,” he said. “We need to understand who is at increased risk of these and why.”
The study was published in Gastroenterology .
Analyzing Associations
Dr. McGovern and colleagues analyzed data for 12,083 unrelated European ancestry IBD cases with presence or absence of EIMs across four cohorts in the Cedars-Sinai Medical Center IBD Research Repository, National Institute for Diabetes and Digestive and Kidney Diseases IBD Genetics Consortium, Sinai Helmsley Alliance for Research Excellence Consortium, and Risk Stratification and Identification of Immunogenetic and Microbial Markers of Rapid Disease Progression in Children with Crohn’s Disease.
In particular, the researchers looked at EIM phenotypes such as ankylosing spondylitis and sacroiliitis, PSC, peripheral arthritis, and skin and ocular manifestations. They analyzed clinical and serologic parameters through regression analyses using a mixed-effects model, as well as within-case logistic regression for genetic associations.
Overall, 14% of patients had at least one EIM. Contrary to previous reports, only 2% had multiple EIMs, and most co-occurrences were negatively correlated. Nearly all EIMs were more common in Crohn’s disease, except for PSC, which was more common in ulcerative colitis.
In general, EIMs occurred more often in women, particularly with Crohn’s disease and colonic disease location, and in patients who required surgery. Jewish ancestry was associated with psoriasis and overall skin manifestations.
Smoking increased the risk for multiple EIMs, except for PSC, where there appeared to be a “protective” effect. Older age at diagnosis and a family history of IBD were associated with increased risk for certain EIMs as well.
In addition, the research team noted multiple serologic associations, such as immunoglobulin (Ig) G and IgA, perinuclear antinuclear cytoplastic antibodies, and anti–Pseudomonas fluorescens–associated sequences with any EIM, as well as particular associations with PSC, such as anti-Saccharomyces cerevisiae antibodies and anti-flagellin.
There were also genome-wide significant associations within the major histocompatibility complex and CPEB4. Genetic associations implicated tumor necrosis factor, Janus kinase-signal transducer and activator of transcription, and interleukin 6 as potential targets for EIMs.
“We are working with colleagues across the world to increase the sample size, as we believe there is more to find,” Dr. McGovern said. “Importantly, this includes non-European ancestry subjects, as there is an urgent need to increase the diversity of populations we study so advances in clinical care are available to all communities.”
Considering Target Therapies
As medicine becomes more specialized, physicians should remember to consider the whole patient while choosing treatment strategies.
“Sometimes doctors wear blinders to the whole person, and it’s important to be aware of a holistic approach, where a gastroenterologist also asks about potential joint inflammation or a rheumatologist asks about bowel inflammation,” said David Rubin, MD, AGAF, chief of the Section of Gastroenterology, Hepatology and Nutrition at the University of Chicago Medicine, Chicago.
Dr. Rubin, who wasn’t involved with this study, has researched and published on EIMs in IBD. He and colleagues analyzed the prevalence, pathophysiology, and clinical presentation of EIMs to better understand possibilities for disease management.
“As we’ve gotten a better understanding of the immune system, we’ve learned that an EIM can sometimes provide a clue to the treatment we might use,” he said. “Given a similar amount of bowel inflammation, if one patient also has joint pain and another doesn’t, we might choose different treatments based on the immune pathway that might be involved.”
In future studies, researchers may consider whether these genetic or serologic markers could predict EIM manifestation before it occurs clinically, Dr. Rubin said. He and colleagues are also studying the links between IBD and mental health associations.
“So far, we don’t have a blood test or biopsy test that tells you which treatment is more or less likely to work, so we need to think carefully as clinicians and look to other organ systems for clues,” he said. “It’s not only more efficient to pick a single therapy to treat both the skin and bowel, but it may actually be more effective if both have a particular dominant pathway.”
The study was supported by internal funds from the F. Widjaja Foundation Inflammatory Bowel and Immunobiology Research Institute. Several authors reported consultant roles or other associations with pharmaceutical companies. Dr. Rubin reported no relevant disclosures.
A version of this article appeared on Medscape.com.
From Scrubs to Social Media: How Some Med Students Become Influencers
A medical student’s life is an endless cycle of classes, exams, clinical rotations, and residency preparation. On TikTok and Instagram, among other sites, they share medical school experiences and lessons learned in the classroom and advocate for causes such as increased diversity and gender rights in the medical field.
This news organization caught up with a few social media influencers with a large online following to learn how medical students can effectively use social media to build a professional brand and network. Most of the students interviewed said that their social media platforms offered an opportunity to educate others about significant medical developments, feel part of a community with a like-minded audience, and network with doctors who may lead them to a future residency or career path.
Many med students said that they built their large audiences by creating a platform for people of their ethnic background, nationality, race, gender, or simply what others weren’t already talking about. They said they saw a niche in social media that was missing or others hadn’t tackled in the same way.
When Joel Bervell began med school in 2020, he questioned some of the lessons he learned about how race is used in medical practice, which didn’t make sense to him. So, he began his own research. He had about 2000 followers on Instagram at the time.
Mr. Bervell read a new study about pulse oximeters and how they often produce misleading readings on patients with dark skin.
He wondered why he hadn’t learned this in medical school, so he posted it on TikTok. Within 24 hours, about 500,000 people viewed it. Most of the comments were from doctors, nurses, and physician assistants who said they weren’t aware of the disparity.
While his initial posts detailed his journey to medical school and a day-in-the-life of a medical student, he transitioned to posts primarily about race, health equity, and what he perceives as racial bias in medicine.
Now, the fourth-year Ghanaian-American student at the Elson S. Floyd College of Medicine at Washington State University Spokane has close to 1.2 million followers on Instagram and TikTok combined. He frequently visits the White House to advise on social media’s influence on healthcare and has appeared on the Kelly Clarkson Show, Good Morning America, CNN, and ABC, among others.
He said he also uses social media to translate complex medical information for a general audience, many of whom access health information online so they can manage their own healthcare. He sees his social media work as an extension of his medical education, allowing him to delve deeper into subjects and report on them as if he were publishing research in a medical journal.
“When I came to medical school, yes, I wanted to be a doctor. But I also wanted to impact people.” Social media allows him to educate many more people than individual patients, the 29-year-old told this news organization.
Inspiring Minorities
Tabhata Paulet, 27, started her TikTok presence as a premed student in 2021. She aimed to provide free resources to help low-income, first-generation Latinx students like herself study for standardized exams.
“I always looked online for guidance and resources, and the medical influencers did not share a similar background. So, I shared my story and what I had to do as a first-generation and first person in my family to become a physician. I did not have access to the same resources as my peers,” said Ms. Paulet, who was born in Peru and came to New Jersey as a child.
Students who are Hispanic, Latinx, or of Spanish origin made up 6.8% of total medical school enrollment in 2023-2024, up slightly from 6.7% in 2022-2023, according to the Association of American Medical Colleges (AAMC).
Ms. Paulet’s online presence grew when she began documenting her experiences as a first-year medical student, bridging the language barrier for Spanish-speaking patients so they could understand their diagnosis and treatment. She often posts about health disparity and barriers to care for underserved communities.
Most of her nearly 22,000 followers are Hispanic, said the now fourth-year student at Rutgers New Jersey Medical School in Newark, New Jersey. “I talk a lot about my interesting Spanish-speaking patients ... and how sometimes speaking their native language truly makes a difference in their care.”
She believes that she serves an important role in social media. “It can be very inspirational for those who come after you [in med school] to see someone from a similar culture and upbringing.”
Creating a Community
It was during a therapy session 4 years ago that Jeremy “JP” Scott decided to share Instagram posts about his experiences as a nontraditional medical student. The 37-year-old was studying at Ross University School of Medicine in Barbados and was feeling lonely as an international medical student training to be a doctor as a second career.
Before starting med school, Mr. Scott was an adjunct professor and lab supervisor at the University of Hartford Biology Department, West Hartford, Connecticut, and then a research assistant and lab manager at the Wistar Institute in Philadelphia.
Although he wanted to follow his mother’s path to becoming a doctor, it was more difficult than he envisioned, said the fourth-year student who completed clinical rotations in the United States and is now applying for residencies.
“I talked about how medical school is not what it appears to be ... There are a lot of challenges we are going through,” especially as people of color, he said.
Mr. Scott believes social media helps people feel included and less alone. He said many of his followers are med students and physicians.
His posts often focus on LGBTQIA+ pride and being a minority as a Black man in medicine.
“The pandemic spurred a lot of us. We had a racial reckoning in our country at the time. It inspired us to talk as Black creators and Black medical students.”
Black or African American medical students made up 8.5% of total med school enrollment in 2023-2024, a slight increase from 2022 to 2023, according to AAMC figures. Black men represented 7% of total enrollment in 2023-2024, while Black women represented 9.8%.
After only a handful of online posts in which Mr. Scott candidly discussed his mental health struggles and relationships, he attracted the attention of several medical apparel companies, including the popular FIGS scrubs. He’s now an ambassador for the company, which supports him and his content.
“My association with FIGS has helped attract a wider online audience, increasing my presence.” Today, he has 14,000 Instagram followers. “It opened up so many opportunities,” Mr. Scott said. One example is working with the national LGBTQIA+ community.
“The goal was never to be a social media influencer, to gain sponsorships or photo opportunities,” he said.
“My job, first, is as a medical student. Everything else is second. I am not trying to be a professional social media personality. I’m trying to be an actual physician.” He also tries to separate JP “social media” from Jeremy, the medical student.
“On Instagram, anyone can pull it up and see what you’re doing. The last thing I want is for them to think that I’m not serious about what I’m doing, that I’m not here to learn and become a doctor.”
Benefits and Drawbacks
Ms. Paulet said her social media following helped her connect with leaders in the Latinx medical community, including an obstetrics anesthesiologist, her intended specialty. “I don’t think I’d be able to do that without a social media platform.”
Her online activity also propelled her from regional to national leadership in the Latino Medical Student Association (LMSA). She now also runs their Instagram page, which has 14,000 followers.
Mr. Bervell believes social media is a great way to network. He’s connected with people he wouldn’t have met otherwise, including physicians. “I think it will help me get into a residency,” he said. “It allows people to know who you are ... They will be able to tell in a few videos the type of doctor I want to be.”
On the other hand, Mr. Bervell is aware of the negative impacts of social media on mental health. “You can get lost in social media.” For that reason, he often tries to disconnect. “I can go days without my phone.”
Posting on social media can be time-consuming, Mr. Bervell admitted. He said he spent about 2 hours a day researching, editing, and posting on TikTok when he first started building his following. Now, he spends about 2-3 hours a week creating videos. “I don’t post every day anymore. I don’t have the time.”
When she started building her TikTok presence, Ms. Paulet said she devoted 15 hours a week to the endeavor, but now she spends 10-12 hours a week posting online, including on LMSA’s Instagram page. “Whenever you are done with an exam or have a study break, this is something fun to do.” She also says you never know who you’re going to inspire when you put yourself out there.
“Talk about your journey, rotations, or your experience in your first or second year of medical school. Talk about milestones like board exams.”
Word to the Wise
Some students may be concerned that their posts might affect a potential residency program. But the medical students interviewed say they want to find programs that align with their values and accept them for who they are.
Mr. Scott said he’s not worried about someone not liking him because of who he is. “I am Black and openly gay. If it’s a problem, I don’t need to work with you or your institution.”
Mr. Bervell stressed that medical students should stay professional online. “I reach 5-10 million people a month, and I have to think: Would I want them to see this? You have to know at all times that someone is watching. I’m very careful about how I post. I script out every video.”
Mr. Scott agreed. He advises those interested in becoming medical influencers to know what they can’t post online. For example, to ensure safety and privacy, Mr. Scott doesn’t take photos in the hospital, show his medical badge, or post patient information. “You want to be respectful of your future medical profession,” he said.
“If it’s something my mother would be ashamed of, I don’t need to post about it.”
A version of this article first appeared on Medscape.com.
A medical student’s life is an endless cycle of classes, exams, clinical rotations, and residency preparation. On TikTok and Instagram, among other sites, they share medical school experiences and lessons learned in the classroom and advocate for causes such as increased diversity and gender rights in the medical field.
This news organization caught up with a few social media influencers with a large online following to learn how medical students can effectively use social media to build a professional brand and network. Most of the students interviewed said that their social media platforms offered an opportunity to educate others about significant medical developments, feel part of a community with a like-minded audience, and network with doctors who may lead them to a future residency or career path.
Many med students said that they built their large audiences by creating a platform for people of their ethnic background, nationality, race, gender, or simply what others weren’t already talking about. They said they saw a niche in social media that was missing or others hadn’t tackled in the same way.
When Joel Bervell began med school in 2020, he questioned some of the lessons he learned about how race is used in medical practice, which didn’t make sense to him. So, he began his own research. He had about 2000 followers on Instagram at the time.
Mr. Bervell read a new study about pulse oximeters and how they often produce misleading readings on patients with dark skin.
He wondered why he hadn’t learned this in medical school, so he posted it on TikTok. Within 24 hours, about 500,000 people viewed it. Most of the comments were from doctors, nurses, and physician assistants who said they weren’t aware of the disparity.
While his initial posts detailed his journey to medical school and a day-in-the-life of a medical student, he transitioned to posts primarily about race, health equity, and what he perceives as racial bias in medicine.
Now, the fourth-year Ghanaian-American student at the Elson S. Floyd College of Medicine at Washington State University Spokane has close to 1.2 million followers on Instagram and TikTok combined. He frequently visits the White House to advise on social media’s influence on healthcare and has appeared on the Kelly Clarkson Show, Good Morning America, CNN, and ABC, among others.
He said he also uses social media to translate complex medical information for a general audience, many of whom access health information online so they can manage their own healthcare. He sees his social media work as an extension of his medical education, allowing him to delve deeper into subjects and report on them as if he were publishing research in a medical journal.
“When I came to medical school, yes, I wanted to be a doctor. But I also wanted to impact people.” Social media allows him to educate many more people than individual patients, the 29-year-old told this news organization.
Inspiring Minorities
Tabhata Paulet, 27, started her TikTok presence as a premed student in 2021. She aimed to provide free resources to help low-income, first-generation Latinx students like herself study for standardized exams.
“I always looked online for guidance and resources, and the medical influencers did not share a similar background. So, I shared my story and what I had to do as a first-generation and first person in my family to become a physician. I did not have access to the same resources as my peers,” said Ms. Paulet, who was born in Peru and came to New Jersey as a child.
Students who are Hispanic, Latinx, or of Spanish origin made up 6.8% of total medical school enrollment in 2023-2024, up slightly from 6.7% in 2022-2023, according to the Association of American Medical Colleges (AAMC).
Ms. Paulet’s online presence grew when she began documenting her experiences as a first-year medical student, bridging the language barrier for Spanish-speaking patients so they could understand their diagnosis and treatment. She often posts about health disparity and barriers to care for underserved communities.
Most of her nearly 22,000 followers are Hispanic, said the now fourth-year student at Rutgers New Jersey Medical School in Newark, New Jersey. “I talk a lot about my interesting Spanish-speaking patients ... and how sometimes speaking their native language truly makes a difference in their care.”
She believes that she serves an important role in social media. “It can be very inspirational for those who come after you [in med school] to see someone from a similar culture and upbringing.”
Creating a Community
It was during a therapy session 4 years ago that Jeremy “JP” Scott decided to share Instagram posts about his experiences as a nontraditional medical student. The 37-year-old was studying at Ross University School of Medicine in Barbados and was feeling lonely as an international medical student training to be a doctor as a second career.
Before starting med school, Mr. Scott was an adjunct professor and lab supervisor at the University of Hartford Biology Department, West Hartford, Connecticut, and then a research assistant and lab manager at the Wistar Institute in Philadelphia.
Although he wanted to follow his mother’s path to becoming a doctor, it was more difficult than he envisioned, said the fourth-year student who completed clinical rotations in the United States and is now applying for residencies.
“I talked about how medical school is not what it appears to be ... There are a lot of challenges we are going through,” especially as people of color, he said.
Mr. Scott believes social media helps people feel included and less alone. He said many of his followers are med students and physicians.
His posts often focus on LGBTQIA+ pride and being a minority as a Black man in medicine.
“The pandemic spurred a lot of us. We had a racial reckoning in our country at the time. It inspired us to talk as Black creators and Black medical students.”
Black or African American medical students made up 8.5% of total med school enrollment in 2023-2024, a slight increase from 2022 to 2023, according to AAMC figures. Black men represented 7% of total enrollment in 2023-2024, while Black women represented 9.8%.
After only a handful of online posts in which Mr. Scott candidly discussed his mental health struggles and relationships, he attracted the attention of several medical apparel companies, including the popular FIGS scrubs. He’s now an ambassador for the company, which supports him and his content.
“My association with FIGS has helped attract a wider online audience, increasing my presence.” Today, he has 14,000 Instagram followers. “It opened up so many opportunities,” Mr. Scott said. One example is working with the national LGBTQIA+ community.
“The goal was never to be a social media influencer, to gain sponsorships or photo opportunities,” he said.
“My job, first, is as a medical student. Everything else is second. I am not trying to be a professional social media personality. I’m trying to be an actual physician.” He also tries to separate JP “social media” from Jeremy, the medical student.
“On Instagram, anyone can pull it up and see what you’re doing. The last thing I want is for them to think that I’m not serious about what I’m doing, that I’m not here to learn and become a doctor.”
Benefits and Drawbacks
Ms. Paulet said her social media following helped her connect with leaders in the Latinx medical community, including an obstetrics anesthesiologist, her intended specialty. “I don’t think I’d be able to do that without a social media platform.”
Her online activity also propelled her from regional to national leadership in the Latino Medical Student Association (LMSA). She now also runs their Instagram page, which has 14,000 followers.
Mr. Bervell believes social media is a great way to network. He’s connected with people he wouldn’t have met otherwise, including physicians. “I think it will help me get into a residency,” he said. “It allows people to know who you are ... They will be able to tell in a few videos the type of doctor I want to be.”
On the other hand, Mr. Bervell is aware of the negative impacts of social media on mental health. “You can get lost in social media.” For that reason, he often tries to disconnect. “I can go days without my phone.”
Posting on social media can be time-consuming, Mr. Bervell admitted. He said he spent about 2 hours a day researching, editing, and posting on TikTok when he first started building his following. Now, he spends about 2-3 hours a week creating videos. “I don’t post every day anymore. I don’t have the time.”
When she started building her TikTok presence, Ms. Paulet said she devoted 15 hours a week to the endeavor, but now she spends 10-12 hours a week posting online, including on LMSA’s Instagram page. “Whenever you are done with an exam or have a study break, this is something fun to do.” She also says you never know who you’re going to inspire when you put yourself out there.
“Talk about your journey, rotations, or your experience in your first or second year of medical school. Talk about milestones like board exams.”
Word to the Wise
Some students may be concerned that their posts might affect a potential residency program. But the medical students interviewed say they want to find programs that align with their values and accept them for who they are.
Mr. Scott said he’s not worried about someone not liking him because of who he is. “I am Black and openly gay. If it’s a problem, I don’t need to work with you or your institution.”
Mr. Bervell stressed that medical students should stay professional online. “I reach 5-10 million people a month, and I have to think: Would I want them to see this? You have to know at all times that someone is watching. I’m very careful about how I post. I script out every video.”
Mr. Scott agreed. He advises those interested in becoming medical influencers to know what they can’t post online. For example, to ensure safety and privacy, Mr. Scott doesn’t take photos in the hospital, show his medical badge, or post patient information. “You want to be respectful of your future medical profession,” he said.
“If it’s something my mother would be ashamed of, I don’t need to post about it.”
A version of this article first appeared on Medscape.com.
A medical student’s life is an endless cycle of classes, exams, clinical rotations, and residency preparation. On TikTok and Instagram, among other sites, they share medical school experiences and lessons learned in the classroom and advocate for causes such as increased diversity and gender rights in the medical field.
This news organization caught up with a few social media influencers with a large online following to learn how medical students can effectively use social media to build a professional brand and network. Most of the students interviewed said that their social media platforms offered an opportunity to educate others about significant medical developments, feel part of a community with a like-minded audience, and network with doctors who may lead them to a future residency or career path.
Many med students said that they built their large audiences by creating a platform for people of their ethnic background, nationality, race, gender, or simply what others weren’t already talking about. They said they saw a niche in social media that was missing or others hadn’t tackled in the same way.
When Joel Bervell began med school in 2020, he questioned some of the lessons he learned about how race is used in medical practice, which didn’t make sense to him. So, he began his own research. He had about 2000 followers on Instagram at the time.
Mr. Bervell read a new study about pulse oximeters and how they often produce misleading readings on patients with dark skin.
He wondered why he hadn’t learned this in medical school, so he posted it on TikTok. Within 24 hours, about 500,000 people viewed it. Most of the comments were from doctors, nurses, and physician assistants who said they weren’t aware of the disparity.
While his initial posts detailed his journey to medical school and a day-in-the-life of a medical student, he transitioned to posts primarily about race, health equity, and what he perceives as racial bias in medicine.
Now, the fourth-year Ghanaian-American student at the Elson S. Floyd College of Medicine at Washington State University Spokane has close to 1.2 million followers on Instagram and TikTok combined. He frequently visits the White House to advise on social media’s influence on healthcare and has appeared on the Kelly Clarkson Show, Good Morning America, CNN, and ABC, among others.
He said he also uses social media to translate complex medical information for a general audience, many of whom access health information online so they can manage their own healthcare. He sees his social media work as an extension of his medical education, allowing him to delve deeper into subjects and report on them as if he were publishing research in a medical journal.
“When I came to medical school, yes, I wanted to be a doctor. But I also wanted to impact people.” Social media allows him to educate many more people than individual patients, the 29-year-old told this news organization.
Inspiring Minorities
Tabhata Paulet, 27, started her TikTok presence as a premed student in 2021. She aimed to provide free resources to help low-income, first-generation Latinx students like herself study for standardized exams.
“I always looked online for guidance and resources, and the medical influencers did not share a similar background. So, I shared my story and what I had to do as a first-generation and first person in my family to become a physician. I did not have access to the same resources as my peers,” said Ms. Paulet, who was born in Peru and came to New Jersey as a child.
Students who are Hispanic, Latinx, or of Spanish origin made up 6.8% of total medical school enrollment in 2023-2024, up slightly from 6.7% in 2022-2023, according to the Association of American Medical Colleges (AAMC).
Ms. Paulet’s online presence grew when she began documenting her experiences as a first-year medical student, bridging the language barrier for Spanish-speaking patients so they could understand their diagnosis and treatment. She often posts about health disparity and barriers to care for underserved communities.
Most of her nearly 22,000 followers are Hispanic, said the now fourth-year student at Rutgers New Jersey Medical School in Newark, New Jersey. “I talk a lot about my interesting Spanish-speaking patients ... and how sometimes speaking their native language truly makes a difference in their care.”
She believes that she serves an important role in social media. “It can be very inspirational for those who come after you [in med school] to see someone from a similar culture and upbringing.”
Creating a Community
It was during a therapy session 4 years ago that Jeremy “JP” Scott decided to share Instagram posts about his experiences as a nontraditional medical student. The 37-year-old was studying at Ross University School of Medicine in Barbados and was feeling lonely as an international medical student training to be a doctor as a second career.
Before starting med school, Mr. Scott was an adjunct professor and lab supervisor at the University of Hartford Biology Department, West Hartford, Connecticut, and then a research assistant and lab manager at the Wistar Institute in Philadelphia.
Although he wanted to follow his mother’s path to becoming a doctor, it was more difficult than he envisioned, said the fourth-year student who completed clinical rotations in the United States and is now applying for residencies.
“I talked about how medical school is not what it appears to be ... There are a lot of challenges we are going through,” especially as people of color, he said.
Mr. Scott believes social media helps people feel included and less alone. He said many of his followers are med students and physicians.
His posts often focus on LGBTQIA+ pride and being a minority as a Black man in medicine.
“The pandemic spurred a lot of us. We had a racial reckoning in our country at the time. It inspired us to talk as Black creators and Black medical students.”
Black or African American medical students made up 8.5% of total med school enrollment in 2023-2024, a slight increase from 2022 to 2023, according to AAMC figures. Black men represented 7% of total enrollment in 2023-2024, while Black women represented 9.8%.
After only a handful of online posts in which Mr. Scott candidly discussed his mental health struggles and relationships, he attracted the attention of several medical apparel companies, including the popular FIGS scrubs. He’s now an ambassador for the company, which supports him and his content.
“My association with FIGS has helped attract a wider online audience, increasing my presence.” Today, he has 14,000 Instagram followers. “It opened up so many opportunities,” Mr. Scott said. One example is working with the national LGBTQIA+ community.
“The goal was never to be a social media influencer, to gain sponsorships or photo opportunities,” he said.
“My job, first, is as a medical student. Everything else is second. I am not trying to be a professional social media personality. I’m trying to be an actual physician.” He also tries to separate JP “social media” from Jeremy, the medical student.
“On Instagram, anyone can pull it up and see what you’re doing. The last thing I want is for them to think that I’m not serious about what I’m doing, that I’m not here to learn and become a doctor.”
Benefits and Drawbacks
Ms. Paulet said her social media following helped her connect with leaders in the Latinx medical community, including an obstetrics anesthesiologist, her intended specialty. “I don’t think I’d be able to do that without a social media platform.”
Her online activity also propelled her from regional to national leadership in the Latino Medical Student Association (LMSA). She now also runs their Instagram page, which has 14,000 followers.
Mr. Bervell believes social media is a great way to network. He’s connected with people he wouldn’t have met otherwise, including physicians. “I think it will help me get into a residency,” he said. “It allows people to know who you are ... They will be able to tell in a few videos the type of doctor I want to be.”
On the other hand, Mr. Bervell is aware of the negative impacts of social media on mental health. “You can get lost in social media.” For that reason, he often tries to disconnect. “I can go days without my phone.”
Posting on social media can be time-consuming, Mr. Bervell admitted. He said he spent about 2 hours a day researching, editing, and posting on TikTok when he first started building his following. Now, he spends about 2-3 hours a week creating videos. “I don’t post every day anymore. I don’t have the time.”
When she started building her TikTok presence, Ms. Paulet said she devoted 15 hours a week to the endeavor, but now she spends 10-12 hours a week posting online, including on LMSA’s Instagram page. “Whenever you are done with an exam or have a study break, this is something fun to do.” She also says you never know who you’re going to inspire when you put yourself out there.
“Talk about your journey, rotations, or your experience in your first or second year of medical school. Talk about milestones like board exams.”
Word to the Wise
Some students may be concerned that their posts might affect a potential residency program. But the medical students interviewed say they want to find programs that align with their values and accept them for who they are.
Mr. Scott said he’s not worried about someone not liking him because of who he is. “I am Black and openly gay. If it’s a problem, I don’t need to work with you or your institution.”
Mr. Bervell stressed that medical students should stay professional online. “I reach 5-10 million people a month, and I have to think: Would I want them to see this? You have to know at all times that someone is watching. I’m very careful about how I post. I script out every video.”
Mr. Scott agreed. He advises those interested in becoming medical influencers to know what they can’t post online. For example, to ensure safety and privacy, Mr. Scott doesn’t take photos in the hospital, show his medical badge, or post patient information. “You want to be respectful of your future medical profession,” he said.
“If it’s something my mother would be ashamed of, I don’t need to post about it.”
A version of this article first appeared on Medscape.com.
TYK2 Inhibitor Effective for Psoriasis in Phase 2 Study
TOPLINE:
METHODOLOGY:
- Researchers performed a phase 2b, randomized, double-blind trial to assess the efficacy, safety, and tolerability of different doses of zasocitinib in adults with moderate to severe psoriasis (mean age, 47 years; 32% women) at 47 centers in the United States and eight centers in Canada. Most (83%) were White, 7% were Black, and 8% were Asian.
- A total of 287 patients were randomly assigned to receive one of the four oral doses of zasocitinib (2 mg, 5 mg, 15 mg, or 30 mg, once daily) or a matched placebo for 12 weeks, followed by a 4-week safety monitoring period.
- The primary outcome was the proportion of patients achieving a ≥ 75% improvement in the Psoriasis Area and Severity Index score (PASI 75) from baseline at week 12.
TAKEAWAY:
- At week 12, PASI 75 was achieved by 18%, 44%, 68%, and 67% of patients receiving zasocitinib at doses of 2 mg, 5 mg, 15 mg, and 30 mg, respectively, vs 6% of patients receiving placebo.
- PASI 90 was achieved in 8%, 21%, 45%, and 46% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, and in no patients in the placebo group.
- At week 12, 10%, 27%, 49%, and 52% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, had no or mild disease (a score of 0 or 1) according to the Physician Global Assessment tool vs 4% in the placebo group.
- Treatment-emergent adverse events occurred in 53%-62% of patients in the zasocitinib groups compared with 44% in the placebo group. The most common were COVID-19, acne/acneiform dermatitis, and diarrhea. There were no reports of major adverse cardiovascular events, thromboembolic events, or opportunistic infections.
IN PRACTICE:
“Zasocitinib, an advanced, potent, and highly selective oral TYK2 inhibitor bioengineered to optimize target coverage and functional selectivity, achieved biologic-level efficacy with complete skin clearance observed after only a 12-week treatment period in up to one third of patients, with a low incidence of known tolerability issues and absence of serious toxic effects that are characteristic of [Janus kinase] 1-3 inhibition,” the authors wrote.
SOURCE:
The study was led by April W. Armstrong, MD, MPH, University of California, Los Angeles, and was published online on August 21, 2024, in JAMA Dermatology.
LIMITATIONS:
The study was limited by a relatively small sample size and a short duration. In addition, the inclusion of predominantly White patients may limit the generalizability of findings to a diverse population.
DISCLOSURES:
The study was funded by Nimbus Discovery, which includes Nimbus Therapeutics and Nimbus Lakshmi. Dr. Armstrong’s disclosures included receiving grants and/or personal fees from various pharmaceutical companies, including Nimbus Therapeutics and Nimbus. Three authors were employees of and reported holding equity, stocks, or shares in Nimbus. Several authors had disclosures related to pharmaceutical companies, including Nimbus.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers performed a phase 2b, randomized, double-blind trial to assess the efficacy, safety, and tolerability of different doses of zasocitinib in adults with moderate to severe psoriasis (mean age, 47 years; 32% women) at 47 centers in the United States and eight centers in Canada. Most (83%) were White, 7% were Black, and 8% were Asian.
- A total of 287 patients were randomly assigned to receive one of the four oral doses of zasocitinib (2 mg, 5 mg, 15 mg, or 30 mg, once daily) or a matched placebo for 12 weeks, followed by a 4-week safety monitoring period.
- The primary outcome was the proportion of patients achieving a ≥ 75% improvement in the Psoriasis Area and Severity Index score (PASI 75) from baseline at week 12.
TAKEAWAY:
- At week 12, PASI 75 was achieved by 18%, 44%, 68%, and 67% of patients receiving zasocitinib at doses of 2 mg, 5 mg, 15 mg, and 30 mg, respectively, vs 6% of patients receiving placebo.
- PASI 90 was achieved in 8%, 21%, 45%, and 46% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, and in no patients in the placebo group.
- At week 12, 10%, 27%, 49%, and 52% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, had no or mild disease (a score of 0 or 1) according to the Physician Global Assessment tool vs 4% in the placebo group.
- Treatment-emergent adverse events occurred in 53%-62% of patients in the zasocitinib groups compared with 44% in the placebo group. The most common were COVID-19, acne/acneiform dermatitis, and diarrhea. There were no reports of major adverse cardiovascular events, thromboembolic events, or opportunistic infections.
IN PRACTICE:
“Zasocitinib, an advanced, potent, and highly selective oral TYK2 inhibitor bioengineered to optimize target coverage and functional selectivity, achieved biologic-level efficacy with complete skin clearance observed after only a 12-week treatment period in up to one third of patients, with a low incidence of known tolerability issues and absence of serious toxic effects that are characteristic of [Janus kinase] 1-3 inhibition,” the authors wrote.
SOURCE:
The study was led by April W. Armstrong, MD, MPH, University of California, Los Angeles, and was published online on August 21, 2024, in JAMA Dermatology.
LIMITATIONS:
The study was limited by a relatively small sample size and a short duration. In addition, the inclusion of predominantly White patients may limit the generalizability of findings to a diverse population.
DISCLOSURES:
The study was funded by Nimbus Discovery, which includes Nimbus Therapeutics and Nimbus Lakshmi. Dr. Armstrong’s disclosures included receiving grants and/or personal fees from various pharmaceutical companies, including Nimbus Therapeutics and Nimbus. Three authors were employees of and reported holding equity, stocks, or shares in Nimbus. Several authors had disclosures related to pharmaceutical companies, including Nimbus.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers performed a phase 2b, randomized, double-blind trial to assess the efficacy, safety, and tolerability of different doses of zasocitinib in adults with moderate to severe psoriasis (mean age, 47 years; 32% women) at 47 centers in the United States and eight centers in Canada. Most (83%) were White, 7% were Black, and 8% were Asian.
- A total of 287 patients were randomly assigned to receive one of the four oral doses of zasocitinib (2 mg, 5 mg, 15 mg, or 30 mg, once daily) or a matched placebo for 12 weeks, followed by a 4-week safety monitoring period.
- The primary outcome was the proportion of patients achieving a ≥ 75% improvement in the Psoriasis Area and Severity Index score (PASI 75) from baseline at week 12.
TAKEAWAY:
- At week 12, PASI 75 was achieved by 18%, 44%, 68%, and 67% of patients receiving zasocitinib at doses of 2 mg, 5 mg, 15 mg, and 30 mg, respectively, vs 6% of patients receiving placebo.
- PASI 90 was achieved in 8%, 21%, 45%, and 46% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, and in no patients in the placebo group.
- At week 12, 10%, 27%, 49%, and 52% of patients receiving zasocitinib at 2 mg, 5 mg, 15 mg, and 30 mg, respectively, had no or mild disease (a score of 0 or 1) according to the Physician Global Assessment tool vs 4% in the placebo group.
- Treatment-emergent adverse events occurred in 53%-62% of patients in the zasocitinib groups compared with 44% in the placebo group. The most common were COVID-19, acne/acneiform dermatitis, and diarrhea. There were no reports of major adverse cardiovascular events, thromboembolic events, or opportunistic infections.
IN PRACTICE:
“Zasocitinib, an advanced, potent, and highly selective oral TYK2 inhibitor bioengineered to optimize target coverage and functional selectivity, achieved biologic-level efficacy with complete skin clearance observed after only a 12-week treatment period in up to one third of patients, with a low incidence of known tolerability issues and absence of serious toxic effects that are characteristic of [Janus kinase] 1-3 inhibition,” the authors wrote.
SOURCE:
The study was led by April W. Armstrong, MD, MPH, University of California, Los Angeles, and was published online on August 21, 2024, in JAMA Dermatology.
LIMITATIONS:
The study was limited by a relatively small sample size and a short duration. In addition, the inclusion of predominantly White patients may limit the generalizability of findings to a diverse population.
DISCLOSURES:
The study was funded by Nimbus Discovery, which includes Nimbus Therapeutics and Nimbus Lakshmi. Dr. Armstrong’s disclosures included receiving grants and/or personal fees from various pharmaceutical companies, including Nimbus Therapeutics and Nimbus. Three authors were employees of and reported holding equity, stocks, or shares in Nimbus. Several authors had disclosures related to pharmaceutical companies, including Nimbus.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.