User login
Study Finds Different Survival Rates for Hidradenitis Suppurativa Treatments in Children
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
results from a small single-center study showed.
A previous study found that overall drug survival of adalimumab and infliximab in adults with HS at 12 and 24 months was 56.3% and 30.5%, and 58.3% and 48.6%, respectively. “They also found that older age, longer disease duration, higher body mass index (BMI), and surgery during treatment are associated with increased drug survival,” Robyn Guo, a third-year medical student at Duke University, Durham, North Carolina, told this news organization following the annual Symposium on Hidradenitis Suppurativa Advances, where the study was presented during an oral abstract session. “To our knowledge, the drug survival of biologic therapies in pediatric HS patients has not been previously investigated.”
Adalimumab and infliximab are tumor necrosis factor blockers approved for multiple indications; adalimumab is approved for treating moderate to severe HS in patients aged 12 years or older. Infliximab is not approved for HS but is used to treat the disease.
To determine the drug survival of adalimumab and infliximab in pediatric patients with HS and whether patient comorbidities and HS lesion location are associated with length of biologic survival in pediatric patients with HS, Guo and colleagues used Kaplan-Meier survival curves to calculate biologic survival at 12 and 24 months following biologic initiation and Cox proportional hazards regression to analyze potential factors associated with biologic survival. The study population included 49 pediatric patients in the adalimumab cohort and 11 in the infliximab cohort.
The researchers found that drug survival for adalimumab was 90.6% at 12 months (95% CI, 83.0%-98.8%) and 78.3% at 24 months (95% CI, 67.7%-90.6%), while drug survival for infliximab was 54.5% at 12 months (95% CI, 31.8%-93.6%) and 36.4% at 24 months, an overall difference that reached statistical significance (P = .0009). “Our data suggests that adalimumab survival is significantly higher than infliximab survival in pediatric HS patients,” Guo said.
On univariate Cox regression analysis, gluteal HS lesions were associated with shorter adalimumab survival, and obesity was associated with longer infliximab survival.
The researchers acknowledged certain limitations of their study, including the small sample size and that unadjusted Cox regression analysis did not account for baseline HS severity, biologic therapy dosing, and concomitant medication use. Also, there were patients in both cohorts who were not biologic-naive: Two in the adalimumab cohort were previously treated with infliximab, and five patients in the infliximab cohort were previously treated with adalimumab.
“We plan on conducting further analysis using adjusted Cox regression analysis to account for baseline disease severity measured by Hurley stage, BMI, medication dosing, and concomitant medication use,” Guo said.
The researchers reported having no financial disclosures.
A version of this article appeared on Medscape.com.
FROM SDPA 24
Topical Retinoids a Key Component of Acne Treatment Regimens
LAS VEGAS —
Patients with successfully treated acne typically use an average of 2.53 different medications, Baldwin, director of the Acne Treatment & Research Center, Brooklyn, New York, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.

“Combination treatment is the name of the game, but how do we convince our patients that what we chose is carefully orchestrated?” she said. “Combination therapy is much more effective, yet we’re always told, ‘keep it simple.’ The trick is to use combination products that have two or three medications in them — fixed combinations and products with excellent vehicles.”
No matter what treatment regimen is recommended for patients with acne, she continued, it should always include a topical retinoid. Tretinoin was the first topical retinoid approved for acne treatment in 1971, followed by adapalene in 1996, tazarotene in 1997, and trifarotene in 2019. According to a review article , topical retinoids inhibit the formation of microcomedones, reduce mature comedones and inflammatory lesions, enhance penetration of other drugs, reduce and prevent scarring, reduce hyperpigmentation, and maintain remission of acne.
More recently, authors of the 2024 American Academy of Dermatology guidelines of care for the management of acne vulgaris strongly recommended the use of topical retinoids based on moderate certainty evidence in the medial literature. Strong recommendations are also made for benzoyl peroxide, topical antibiotics, and oral doxycycline.
Baldwin noted that the benefits of retinoids include their comedolytic and anti-comedogenic properties, their effectiveness in treating inflammatory lesions, and their suitability for long-term maintenance. However, their drawbacks involve the potential for irritancy, which can be concentration- and vehicle-dependent.
Irritancy “maxes out at 1-2 weeks, but the problem is you lose the patient at 2 weeks unless they know it’s coming,” she said, noting that she once heard the 2-week mark characterized as a “crisis of confidence.” Patients “came in with a bunch of pimples, and now they’re red and flaky and burning and stinging [from the retinoid], yet they still have pimples,” Baldwin said. “You really need to talk them through that 2-week mark [or] they’re going to stop the medication.”
To improve retinoid tolerability, Baldwin offered the following tips:
- Use a pea-sized amount for the entire affected area and avoid spot treatments.
- Start with every other day application.
- Moisturize regularly, possibly applying moisturizer before the retinoid.
- Consider switching to a different formulation with an alternative vehicle or retinoid delivery system. Adapalene and tazarotene are the only retinoids that have proven to be stable in the presence of benzoyl peroxide, she said.
- Be persistent. “There is no such thing as a patient who cannot tolerate a retinoid,” said Baldwin, the lead author of a review on the evolution of topical retinoids for acne. “It’s because of a provider who failed to provide a sufficient amount of information to allow the patient to eventually be able to tolerate a retinoid.”
Baldwin also referred to an independent meta-analysis of 221 trials comparing the efficacy of pharmacological therapies for acne in patients of any age, which found that the percentage reduction in total lesion count, compared with placebo, was the highest with oral isotretinoin (mean difference [MD], 48.41; P = 1.00), followed by triple therapy containing a topical antibiotic, a topical retinoid, and benzoyl peroxide (MD, 38.15; P = .95), and by triple therapy containing an oral antibiotic, a topical retinoid, and benzoyl peroxide (MD, 34.83; P = .90).
Baldwin is a former president of the American Acne & Rosacea Society and is the SDPA conference medical director. She disclosed being a speaker, consultant, and/or an advisory board member for Almirall, Arcutis, Bausch, Beiersdorf, Cutera, Galderma, Journey, Kenvue, La Roche-Posay, L’Oreal, Sanofi, Sun Pharma, and Tarsus Pharmaceuticals.
A version of this article appeared on Medscape.com.
LAS VEGAS —
Patients with successfully treated acne typically use an average of 2.53 different medications, Baldwin, director of the Acne Treatment & Research Center, Brooklyn, New York, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.
“Combination treatment is the name of the game, but how do we convince our patients that what we chose is carefully orchestrated?” she said. “Combination therapy is much more effective, yet we’re always told, ‘keep it simple.’ The trick is to use combination products that have two or three medications in them — fixed combinations and products with excellent vehicles.”
No matter what treatment regimen is recommended for patients with acne, she continued, it should always include a topical retinoid. Tretinoin was the first topical retinoid approved for acne treatment in 1971, followed by adapalene in 1996, tazarotene in 1997, and trifarotene in 2019. According to a review article , topical retinoids inhibit the formation of microcomedones, reduce mature comedones and inflammatory lesions, enhance penetration of other drugs, reduce and prevent scarring, reduce hyperpigmentation, and maintain remission of acne.
More recently, authors of the 2024 American Academy of Dermatology guidelines of care for the management of acne vulgaris strongly recommended the use of topical retinoids based on moderate certainty evidence in the medial literature. Strong recommendations are also made for benzoyl peroxide, topical antibiotics, and oral doxycycline.
Baldwin noted that the benefits of retinoids include their comedolytic and anti-comedogenic properties, their effectiveness in treating inflammatory lesions, and their suitability for long-term maintenance. However, their drawbacks involve the potential for irritancy, which can be concentration- and vehicle-dependent.
Irritancy “maxes out at 1-2 weeks, but the problem is you lose the patient at 2 weeks unless they know it’s coming,” she said, noting that she once heard the 2-week mark characterized as a “crisis of confidence.” Patients “came in with a bunch of pimples, and now they’re red and flaky and burning and stinging [from the retinoid], yet they still have pimples,” Baldwin said. “You really need to talk them through that 2-week mark [or] they’re going to stop the medication.”
To improve retinoid tolerability, Baldwin offered the following tips:
- Use a pea-sized amount for the entire affected area and avoid spot treatments.
- Start with every other day application.
- Moisturize regularly, possibly applying moisturizer before the retinoid.
- Consider switching to a different formulation with an alternative vehicle or retinoid delivery system. Adapalene and tazarotene are the only retinoids that have proven to be stable in the presence of benzoyl peroxide, she said.
- Be persistent. “There is no such thing as a patient who cannot tolerate a retinoid,” said Baldwin, the lead author of a review on the evolution of topical retinoids for acne. “It’s because of a provider who failed to provide a sufficient amount of information to allow the patient to eventually be able to tolerate a retinoid.”
Baldwin also referred to an independent meta-analysis of 221 trials comparing the efficacy of pharmacological therapies for acne in patients of any age, which found that the percentage reduction in total lesion count, compared with placebo, was the highest with oral isotretinoin (mean difference [MD], 48.41; P = 1.00), followed by triple therapy containing a topical antibiotic, a topical retinoid, and benzoyl peroxide (MD, 38.15; P = .95), and by triple therapy containing an oral antibiotic, a topical retinoid, and benzoyl peroxide (MD, 34.83; P = .90).
Baldwin is a former president of the American Acne & Rosacea Society and is the SDPA conference medical director. She disclosed being a speaker, consultant, and/or an advisory board member for Almirall, Arcutis, Bausch, Beiersdorf, Cutera, Galderma, Journey, Kenvue, La Roche-Posay, L’Oreal, Sanofi, Sun Pharma, and Tarsus Pharmaceuticals.
A version of this article appeared on Medscape.com.
LAS VEGAS —
Patients with successfully treated acne typically use an average of 2.53 different medications, Baldwin, director of the Acne Treatment & Research Center, Brooklyn, New York, said at the Society of Dermatology Physician Associates (SDPA) 22nd Annual Fall Dermatology Conference.
“Combination treatment is the name of the game, but how do we convince our patients that what we chose is carefully orchestrated?” she said. “Combination therapy is much more effective, yet we’re always told, ‘keep it simple.’ The trick is to use combination products that have two or three medications in them — fixed combinations and products with excellent vehicles.”
No matter what treatment regimen is recommended for patients with acne, she continued, it should always include a topical retinoid. Tretinoin was the first topical retinoid approved for acne treatment in 1971, followed by adapalene in 1996, tazarotene in 1997, and trifarotene in 2019. According to a review article , topical retinoids inhibit the formation of microcomedones, reduce mature comedones and inflammatory lesions, enhance penetration of other drugs, reduce and prevent scarring, reduce hyperpigmentation, and maintain remission of acne.
More recently, authors of the 2024 American Academy of Dermatology guidelines of care for the management of acne vulgaris strongly recommended the use of topical retinoids based on moderate certainty evidence in the medial literature. Strong recommendations are also made for benzoyl peroxide, topical antibiotics, and oral doxycycline.
Baldwin noted that the benefits of retinoids include their comedolytic and anti-comedogenic properties, their effectiveness in treating inflammatory lesions, and their suitability for long-term maintenance. However, their drawbacks involve the potential for irritancy, which can be concentration- and vehicle-dependent.
Irritancy “maxes out at 1-2 weeks, but the problem is you lose the patient at 2 weeks unless they know it’s coming,” she said, noting that she once heard the 2-week mark characterized as a “crisis of confidence.” Patients “came in with a bunch of pimples, and now they’re red and flaky and burning and stinging [from the retinoid], yet they still have pimples,” Baldwin said. “You really need to talk them through that 2-week mark [or] they’re going to stop the medication.”
To improve retinoid tolerability, Baldwin offered the following tips:
- Use a pea-sized amount for the entire affected area and avoid spot treatments.
- Start with every other day application.
- Moisturize regularly, possibly applying moisturizer before the retinoid.
- Consider switching to a different formulation with an alternative vehicle or retinoid delivery system. Adapalene and tazarotene are the only retinoids that have proven to be stable in the presence of benzoyl peroxide, she said.
- Be persistent. “There is no such thing as a patient who cannot tolerate a retinoid,” said Baldwin, the lead author of a review on the evolution of topical retinoids for acne. “It’s because of a provider who failed to provide a sufficient amount of information to allow the patient to eventually be able to tolerate a retinoid.”
Baldwin also referred to an independent meta-analysis of 221 trials comparing the efficacy of pharmacological therapies for acne in patients of any age, which found that the percentage reduction in total lesion count, compared with placebo, was the highest with oral isotretinoin (mean difference [MD], 48.41; P = 1.00), followed by triple therapy containing a topical antibiotic, a topical retinoid, and benzoyl peroxide (MD, 38.15; P = .95), and by triple therapy containing an oral antibiotic, a topical retinoid, and benzoyl peroxide (MD, 34.83; P = .90).
Baldwin is a former president of the American Acne & Rosacea Society and is the SDPA conference medical director. She disclosed being a speaker, consultant, and/or an advisory board member for Almirall, Arcutis, Bausch, Beiersdorf, Cutera, Galderma, Journey, Kenvue, La Roche-Posay, L’Oreal, Sanofi, Sun Pharma, and Tarsus Pharmaceuticals.
A version of this article appeared on Medscape.com.
FROM SDPA 2024
Nemolizumab Benefits for Atopic Dermatitis Maintained in Long-Term Follow-Up Study
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
IBS: Understanding a Common Yet Misunderstood Condition
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
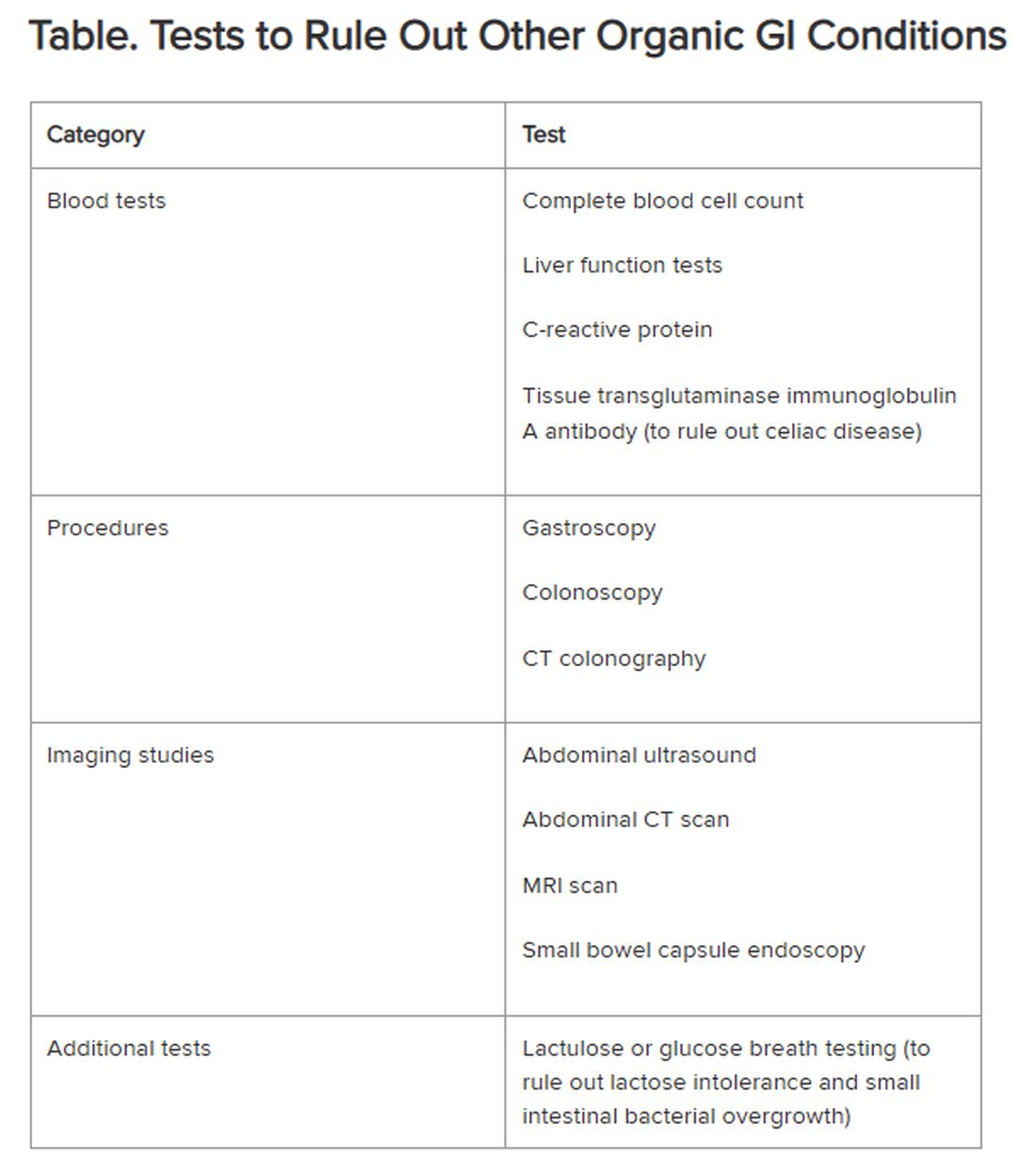
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Cannabis Use Linked to Brain Thinning in Adolescents
, research in mice and humans suggested.
The multilevel study demonstrated that tetrahydrocannabinol (THC), an active substance in cannabis, causes shrinkage of dendritic arborization — the neurons’ network of antennae that play a critical role in communication between brain cells.
The connection between dendritic arborization and cortical thickness was hinted at in an earlier study by Tomáš Paus, MD, PhD, professor of psychiatry and addictology at the University of Montreal, Quebec, Canada, and colleagues, who found that cannabis use in early adolescence was associated with lower cortical thickness in boys with a high genetic risk for schizophrenia.
“We speculated at that time that the differences in cortical thickness might be related to differences in dendritic arborization, and our current study confirmed it,” Paus said.
That confirmation came in the mouse part of the study, when coauthor Graciela Piñeyro, MD, PhD, also of the University of Montreal, counted the dendritic branches of mice exposed to THC and compared the total with the number of dendritic branches in unexposed mice. “What surprised me was finding that THC in the mice was targeting the same type of cells and structures that Dr. Paus had predicted would be affected from the human studies,” she said. “Structurally, they were mostly the neurons that contribute to synapses in the cortex, and their branching was reduced.”
Paus explained that in humans, a decrease in input from the affected dendrites “makes it harder for the brain to learn new things, interact with people, cope with new situations, et cetera. In other words, it makes the brain more vulnerable to everything that can happen in a young person’s life.”
The study was published online on October 9 in the Journal of Neuroscience.
Of Mice, Men, and Cannabis
Although associations between cannabis use by teenagers and variations in brain maturation have been well studied, the cellular and molecular underpinnings of these associations were unclear, according to the authors.
To investigate further, they conducted this three-step study. First, they exposed adolescent male mice to THC or a synthetic cannabinoid (WIN 55,212-2) and assessed differentially expressed genes, spine numbers, and the extent of dendritic complexity in the frontal cortex of each mouse.
Next, using MRI, they examined differences in cortical thickness in 34 brain regions in 140 male adolescents who experimented with cannabis before age 16 years and 327 who did not.
Then, they again conducted experiments in mice and found that 13 THC-related genes correlated with variations in cortical thickness. Virtual histology revealed that these 13 genes were coexpressed with cell markers of astrocytes, microglia, and a type of pyramidal cell enriched in genes that regulate dendritic expression.
Similarly, the WIN-related genes correlated with differences in cortical thickness and showed coexpression patterns with the same three cell types.
Furthermore, the affected genes were also found in humans, particularly in the thinner cortical regions of the adolescents who experimented with cannabis.
By acting on microglia, THC seems to promote the removal of synapses and, eventually, the reduction of the dendritic tree in mice, Piñeyro explained. That’s important not only because a similar mechanism may be at work in humans but also because “we now might have a model to test different types of cannabis products to see which ones are producing the greatest effect on neurons and therefore greater removal of synapses through the microglia. This could be a way of testing drugs that are out in the street to see which would be the most or least dangerous to the synapses in the brain.”
‘Significant Implications’
Commenting on the study, Yasmin Hurd, PhD, Ward-Coleman chair of translational neuroscience at the Icahn School of Medicine at Mount Sinai and director of the Addiction Institute of Mount Sinai in New York City, said, “These findings are in line with previous results, so they are feasible. This study adds more depth by showing that cortical genes that were differentially altered by adolescent THC correlated with cannabis-related changes in cortical thickness based on human neuroimaging data.” Hurd did not participate in the research.
“The results emphasize that consumption of potent cannabis products during adolescence can impact cortical function, which has significant implications for decision-making and risky behavior as well. It also can increase vulnerability to psychiatric disorders such as schizophrenia.”
Although a mouse model is “not truly the same as the human condition, the fact that the animal model also showed evidence of the morphological changes indicative of reduced cortical thickness, [like] the humans, is strong,” she said.
Additional research could include women and assess potential sex differences, she added.
Ronald Ellis, MD, PhD, an investigator in the Center for Medicinal Cannabis Research at the University of California, San Diego School of Medicine, said, “The findings are plausible and extend prior work showing evidence of increased risk for psychotic disorders later in life in adolescents who use cannabis.” Ellis did not participate in the research.
“Future studies should explore how these findings might vary across different demographic groups, which could provide a more inclusive understanding of how cannabis impacts the brain,” he said. “Additionally, longitudinal studies to track changes in the brain over time could help to establish causal relationships more robustly.
“The take-home message to clinicians at this point is to discuss cannabis use history carefully and confidentially with adolescent patients to better provide advice on its potential risks,” he concluded.
Paus added that he would tell patients, “If you’re going to use cannabis, don’t start early. If you have to, then do so in moderation. And if you have family history of mental illness, be very careful.”
No funding for the study was reported. Paus, Piñeyro, Hurd, and Ellis declared having no relevant financial relationships.
A version of this article appeared on Medscape.com.
, research in mice and humans suggested.
The multilevel study demonstrated that tetrahydrocannabinol (THC), an active substance in cannabis, causes shrinkage of dendritic arborization — the neurons’ network of antennae that play a critical role in communication between brain cells.
The connection between dendritic arborization and cortical thickness was hinted at in an earlier study by Tomáš Paus, MD, PhD, professor of psychiatry and addictology at the University of Montreal, Quebec, Canada, and colleagues, who found that cannabis use in early adolescence was associated with lower cortical thickness in boys with a high genetic risk for schizophrenia.
“We speculated at that time that the differences in cortical thickness might be related to differences in dendritic arborization, and our current study confirmed it,” Paus said.
That confirmation came in the mouse part of the study, when coauthor Graciela Piñeyro, MD, PhD, also of the University of Montreal, counted the dendritic branches of mice exposed to THC and compared the total with the number of dendritic branches in unexposed mice. “What surprised me was finding that THC in the mice was targeting the same type of cells and structures that Dr. Paus had predicted would be affected from the human studies,” she said. “Structurally, they were mostly the neurons that contribute to synapses in the cortex, and their branching was reduced.”
Paus explained that in humans, a decrease in input from the affected dendrites “makes it harder for the brain to learn new things, interact with people, cope with new situations, et cetera. In other words, it makes the brain more vulnerable to everything that can happen in a young person’s life.”
The study was published online on October 9 in the Journal of Neuroscience.
Of Mice, Men, and Cannabis
Although associations between cannabis use by teenagers and variations in brain maturation have been well studied, the cellular and molecular underpinnings of these associations were unclear, according to the authors.
To investigate further, they conducted this three-step study. First, they exposed adolescent male mice to THC or a synthetic cannabinoid (WIN 55,212-2) and assessed differentially expressed genes, spine numbers, and the extent of dendritic complexity in the frontal cortex of each mouse.
Next, using MRI, they examined differences in cortical thickness in 34 brain regions in 140 male adolescents who experimented with cannabis before age 16 years and 327 who did not.
Then, they again conducted experiments in mice and found that 13 THC-related genes correlated with variations in cortical thickness. Virtual histology revealed that these 13 genes were coexpressed with cell markers of astrocytes, microglia, and a type of pyramidal cell enriched in genes that regulate dendritic expression.
Similarly, the WIN-related genes correlated with differences in cortical thickness and showed coexpression patterns with the same three cell types.
Furthermore, the affected genes were also found in humans, particularly in the thinner cortical regions of the adolescents who experimented with cannabis.
By acting on microglia, THC seems to promote the removal of synapses and, eventually, the reduction of the dendritic tree in mice, Piñeyro explained. That’s important not only because a similar mechanism may be at work in humans but also because “we now might have a model to test different types of cannabis products to see which ones are producing the greatest effect on neurons and therefore greater removal of synapses through the microglia. This could be a way of testing drugs that are out in the street to see which would be the most or least dangerous to the synapses in the brain.”
‘Significant Implications’
Commenting on the study, Yasmin Hurd, PhD, Ward-Coleman chair of translational neuroscience at the Icahn School of Medicine at Mount Sinai and director of the Addiction Institute of Mount Sinai in New York City, said, “These findings are in line with previous results, so they are feasible. This study adds more depth by showing that cortical genes that were differentially altered by adolescent THC correlated with cannabis-related changes in cortical thickness based on human neuroimaging data.” Hurd did not participate in the research.
“The results emphasize that consumption of potent cannabis products during adolescence can impact cortical function, which has significant implications for decision-making and risky behavior as well. It also can increase vulnerability to psychiatric disorders such as schizophrenia.”
Although a mouse model is “not truly the same as the human condition, the fact that the animal model also showed evidence of the morphological changes indicative of reduced cortical thickness, [like] the humans, is strong,” she said.
Additional research could include women and assess potential sex differences, she added.
Ronald Ellis, MD, PhD, an investigator in the Center for Medicinal Cannabis Research at the University of California, San Diego School of Medicine, said, “The findings are plausible and extend prior work showing evidence of increased risk for psychotic disorders later in life in adolescents who use cannabis.” Ellis did not participate in the research.
“Future studies should explore how these findings might vary across different demographic groups, which could provide a more inclusive understanding of how cannabis impacts the brain,” he said. “Additionally, longitudinal studies to track changes in the brain over time could help to establish causal relationships more robustly.
“The take-home message to clinicians at this point is to discuss cannabis use history carefully and confidentially with adolescent patients to better provide advice on its potential risks,” he concluded.
Paus added that he would tell patients, “If you’re going to use cannabis, don’t start early. If you have to, then do so in moderation. And if you have family history of mental illness, be very careful.”
No funding for the study was reported. Paus, Piñeyro, Hurd, and Ellis declared having no relevant financial relationships.
A version of this article appeared on Medscape.com.
, research in mice and humans suggested.
The multilevel study demonstrated that tetrahydrocannabinol (THC), an active substance in cannabis, causes shrinkage of dendritic arborization — the neurons’ network of antennae that play a critical role in communication between brain cells.
The connection between dendritic arborization and cortical thickness was hinted at in an earlier study by Tomáš Paus, MD, PhD, professor of psychiatry and addictology at the University of Montreal, Quebec, Canada, and colleagues, who found that cannabis use in early adolescence was associated with lower cortical thickness in boys with a high genetic risk for schizophrenia.
“We speculated at that time that the differences in cortical thickness might be related to differences in dendritic arborization, and our current study confirmed it,” Paus said.
That confirmation came in the mouse part of the study, when coauthor Graciela Piñeyro, MD, PhD, also of the University of Montreal, counted the dendritic branches of mice exposed to THC and compared the total with the number of dendritic branches in unexposed mice. “What surprised me was finding that THC in the mice was targeting the same type of cells and structures that Dr. Paus had predicted would be affected from the human studies,” she said. “Structurally, they were mostly the neurons that contribute to synapses in the cortex, and their branching was reduced.”
Paus explained that in humans, a decrease in input from the affected dendrites “makes it harder for the brain to learn new things, interact with people, cope with new situations, et cetera. In other words, it makes the brain more vulnerable to everything that can happen in a young person’s life.”
The study was published online on October 9 in the Journal of Neuroscience.
Of Mice, Men, and Cannabis
Although associations between cannabis use by teenagers and variations in brain maturation have been well studied, the cellular and molecular underpinnings of these associations were unclear, according to the authors.
To investigate further, they conducted this three-step study. First, they exposed adolescent male mice to THC or a synthetic cannabinoid (WIN 55,212-2) and assessed differentially expressed genes, spine numbers, and the extent of dendritic complexity in the frontal cortex of each mouse.
Next, using MRI, they examined differences in cortical thickness in 34 brain regions in 140 male adolescents who experimented with cannabis before age 16 years and 327 who did not.
Then, they again conducted experiments in mice and found that 13 THC-related genes correlated with variations in cortical thickness. Virtual histology revealed that these 13 genes were coexpressed with cell markers of astrocytes, microglia, and a type of pyramidal cell enriched in genes that regulate dendritic expression.
Similarly, the WIN-related genes correlated with differences in cortical thickness and showed coexpression patterns with the same three cell types.
Furthermore, the affected genes were also found in humans, particularly in the thinner cortical regions of the adolescents who experimented with cannabis.
By acting on microglia, THC seems to promote the removal of synapses and, eventually, the reduction of the dendritic tree in mice, Piñeyro explained. That’s important not only because a similar mechanism may be at work in humans but also because “we now might have a model to test different types of cannabis products to see which ones are producing the greatest effect on neurons and therefore greater removal of synapses through the microglia. This could be a way of testing drugs that are out in the street to see which would be the most or least dangerous to the synapses in the brain.”
‘Significant Implications’
Commenting on the study, Yasmin Hurd, PhD, Ward-Coleman chair of translational neuroscience at the Icahn School of Medicine at Mount Sinai and director of the Addiction Institute of Mount Sinai in New York City, said, “These findings are in line with previous results, so they are feasible. This study adds more depth by showing that cortical genes that were differentially altered by adolescent THC correlated with cannabis-related changes in cortical thickness based on human neuroimaging data.” Hurd did not participate in the research.
“The results emphasize that consumption of potent cannabis products during adolescence can impact cortical function, which has significant implications for decision-making and risky behavior as well. It also can increase vulnerability to psychiatric disorders such as schizophrenia.”
Although a mouse model is “not truly the same as the human condition, the fact that the animal model also showed evidence of the morphological changes indicative of reduced cortical thickness, [like] the humans, is strong,” she said.
Additional research could include women and assess potential sex differences, she added.
Ronald Ellis, MD, PhD, an investigator in the Center for Medicinal Cannabis Research at the University of California, San Diego School of Medicine, said, “The findings are plausible and extend prior work showing evidence of increased risk for psychotic disorders later in life in adolescents who use cannabis.” Ellis did not participate in the research.
“Future studies should explore how these findings might vary across different demographic groups, which could provide a more inclusive understanding of how cannabis impacts the brain,” he said. “Additionally, longitudinal studies to track changes in the brain over time could help to establish causal relationships more robustly.
“The take-home message to clinicians at this point is to discuss cannabis use history carefully and confidentially with adolescent patients to better provide advice on its potential risks,” he concluded.
Paus added that he would tell patients, “If you’re going to use cannabis, don’t start early. If you have to, then do so in moderation. And if you have family history of mental illness, be very careful.”
No funding for the study was reported. Paus, Piñeyro, Hurd, and Ellis declared having no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM THE JOURNAL OF NEUROSCIENCE
Atopic Dermatitis: Upadacitinib Effectiveness Maintained Through 76 weeks Among Adolescents
TOPLINE:
across three phase 3 trials.
METHODOLOGY:
- Researchers conducted three double-blind, placebo-controlled phase 3 randomized clinical trials (Measure Up 1, Measure Up 2, and AD Up) involving 542 adolescents aged 12-17 years with moderate to severe AD.
- Participants were randomized to receive the oral Janus kinase inhibitor upadacitinib (15 mg or 30 mg once daily) or placebo, with or without topical corticosteroids, for 16 weeks, followed by rerandomization of patients in the placebo group to upadacitinib for up to 76 weeks.
- Study endpoints were at least a 75%, 90%, or 100% reduction in the Eczema Area and Severity Index (EASI-75, EASI-90, and EASI-100, respectively), Validated Investigator Global Assessment for AD (vIGA-AD) score of 0 or 1, and a ≥ 4-point improvement in the Worst Pruritus Numerical Rating Scale (WP-NRS).
- Adverse events were monitored, including serious infections, herpes zoster, and creatine kinase elevation.
TAKEAWAY:
- Among those who continued treatment on upadacitinib, 15 mg and 30 mg, EASI-75 response rates were maintained or improved through week 76 in all three studies. Patients who switched from placebo to upadacitinib also experienced improvements in EASI-75 through week 76.
- The proportion of patients who achieved EASI-90 and EASI-100 responses increased, and in general, were maintained from week 16 through week 76 in all three studies; the proportion was numerically higher among patients on 30 mg for all three studies.
- The proportion of adolescents achieving vIGA-AD score of 0 or 1 and WP-NRS improvement of ≥ 4 points was sustained or improved through 76 weeks.
- Serious infections were reported in five patients or fewer in each treatment group for all three studies. All opportunistic infections were eczema herpeticum; most cases were not serious, or were mild or moderate, and in general, did not require stopping treatment.
IN PRACTICE:
“These results through 76 weeks demonstrated that upadacitinib, with a favorable benefit-risk profile, was an effective long-term treatment option for adolescents with moderate to severe AD,” the authors wrote.
SOURCE:
The study was led by Amy S. Paller, MD, professor and chair of dermatology, Northwestern University, Chicago, and was published online on October 23 in JAMA Dermatology.
LIMITATIONS:
The study limitations included a small sample size, and the findings did not extend to patients under 12 years or those weighing < 40 kg.
DISCLOSURES:
This study was supported by AbbVie. Paller received grants and personal fees from pharmaceutical companies including AbbVie during the conduct of the study. Several authors reported financial ties with various sources, including AbbVie.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
across three phase 3 trials.
METHODOLOGY:
- Researchers conducted three double-blind, placebo-controlled phase 3 randomized clinical trials (Measure Up 1, Measure Up 2, and AD Up) involving 542 adolescents aged 12-17 years with moderate to severe AD.
- Participants were randomized to receive the oral Janus kinase inhibitor upadacitinib (15 mg or 30 mg once daily) or placebo, with or without topical corticosteroids, for 16 weeks, followed by rerandomization of patients in the placebo group to upadacitinib for up to 76 weeks.
- Study endpoints were at least a 75%, 90%, or 100% reduction in the Eczema Area and Severity Index (EASI-75, EASI-90, and EASI-100, respectively), Validated Investigator Global Assessment for AD (vIGA-AD) score of 0 or 1, and a ≥ 4-point improvement in the Worst Pruritus Numerical Rating Scale (WP-NRS).
- Adverse events were monitored, including serious infections, herpes zoster, and creatine kinase elevation.
TAKEAWAY:
- Among those who continued treatment on upadacitinib, 15 mg and 30 mg, EASI-75 response rates were maintained or improved through week 76 in all three studies. Patients who switched from placebo to upadacitinib also experienced improvements in EASI-75 through week 76.
- The proportion of patients who achieved EASI-90 and EASI-100 responses increased, and in general, were maintained from week 16 through week 76 in all three studies; the proportion was numerically higher among patients on 30 mg for all three studies.
- The proportion of adolescents achieving vIGA-AD score of 0 or 1 and WP-NRS improvement of ≥ 4 points was sustained or improved through 76 weeks.
- Serious infections were reported in five patients or fewer in each treatment group for all three studies. All opportunistic infections were eczema herpeticum; most cases were not serious, or were mild or moderate, and in general, did not require stopping treatment.
IN PRACTICE:
“These results through 76 weeks demonstrated that upadacitinib, with a favorable benefit-risk profile, was an effective long-term treatment option for adolescents with moderate to severe AD,” the authors wrote.
SOURCE:
The study was led by Amy S. Paller, MD, professor and chair of dermatology, Northwestern University, Chicago, and was published online on October 23 in JAMA Dermatology.
LIMITATIONS:
The study limitations included a small sample size, and the findings did not extend to patients under 12 years or those weighing < 40 kg.
DISCLOSURES:
This study was supported by AbbVie. Paller received grants and personal fees from pharmaceutical companies including AbbVie during the conduct of the study. Several authors reported financial ties with various sources, including AbbVie.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
across three phase 3 trials.
METHODOLOGY:
- Researchers conducted three double-blind, placebo-controlled phase 3 randomized clinical trials (Measure Up 1, Measure Up 2, and AD Up) involving 542 adolescents aged 12-17 years with moderate to severe AD.
- Participants were randomized to receive the oral Janus kinase inhibitor upadacitinib (15 mg or 30 mg once daily) or placebo, with or without topical corticosteroids, for 16 weeks, followed by rerandomization of patients in the placebo group to upadacitinib for up to 76 weeks.
- Study endpoints were at least a 75%, 90%, or 100% reduction in the Eczema Area and Severity Index (EASI-75, EASI-90, and EASI-100, respectively), Validated Investigator Global Assessment for AD (vIGA-AD) score of 0 or 1, and a ≥ 4-point improvement in the Worst Pruritus Numerical Rating Scale (WP-NRS).
- Adverse events were monitored, including serious infections, herpes zoster, and creatine kinase elevation.
TAKEAWAY:
- Among those who continued treatment on upadacitinib, 15 mg and 30 mg, EASI-75 response rates were maintained or improved through week 76 in all three studies. Patients who switched from placebo to upadacitinib also experienced improvements in EASI-75 through week 76.
- The proportion of patients who achieved EASI-90 and EASI-100 responses increased, and in general, were maintained from week 16 through week 76 in all three studies; the proportion was numerically higher among patients on 30 mg for all three studies.
- The proportion of adolescents achieving vIGA-AD score of 0 or 1 and WP-NRS improvement of ≥ 4 points was sustained or improved through 76 weeks.
- Serious infections were reported in five patients or fewer in each treatment group for all three studies. All opportunistic infections were eczema herpeticum; most cases were not serious, or were mild or moderate, and in general, did not require stopping treatment.
IN PRACTICE:
“These results through 76 weeks demonstrated that upadacitinib, with a favorable benefit-risk profile, was an effective long-term treatment option for adolescents with moderate to severe AD,” the authors wrote.
SOURCE:
The study was led by Amy S. Paller, MD, professor and chair of dermatology, Northwestern University, Chicago, and was published online on October 23 in JAMA Dermatology.
LIMITATIONS:
The study limitations included a small sample size, and the findings did not extend to patients under 12 years or those weighing < 40 kg.
DISCLOSURES:
This study was supported by AbbVie. Paller received grants and personal fees from pharmaceutical companies including AbbVie during the conduct of the study. Several authors reported financial ties with various sources, including AbbVie.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
A New, Easily Identifiable Sign of Concussion?
Spontaneous Headshake After a Kinematic Event (SHAAKE) refers to the rapid, back-and-forth head movement athletes exhibit following a blow to the head. This voluntary motion typically occurs within seconds to minutes after impact and is a familiar response in athletes.
In a recent survey, 7 out of 10 adult athletes recalled making this movement after a collision, and three out of four times they attributed this back-and-forth head movement to a concussion. The association was strongest among football players, who reported that over 90% of SHAAKE episodes were associated with a concussion.
The results were published online in Diagnostics.
Call to Action
“Everyone” — including sports and medical organizations — “should be adding this to their list of potential concussion signs and their protocol immediately,” study investigator Chris Nowinski, PhD, CEO and co-founder of the Concussion Legacy Foundation, told this news organization.
Nowinski said it’s “fascinating” that this concussion sign hasn’t been formally studied or added to formal concussion screening metrics before now, given that it’s been depicted in movies, television, and cartoons for decades.
Coaches, medical professionals, and concussion spotters should be trained to recognize when a SHAAKE happens, he said.
“The interesting thing is, I don’t think coaches or parents need much training other than to officially tie this to suspicion of a concussion,” Nowinski added.
The Case of Miami Dolphins QB Tua Tagovailoa
Nowinski said he was tipped off to SHAAKE as a concussion sign after Miami Dolphins quarterback Tua Tagovailoa’s controversial undiagnosed concussion during a National Football League (NFL) game in 2022.
After Tagovailoa’s head hit the ground, he rapidly shook his head side to side, indicating displaying SHAAKE, before stumbling and collapsing. At the time, a sideline doctor attributed his collapse to a prior back injury.
If Tagovailoa had been diagnosed with a concussion, he likely would not have been playing in a game just 4 days later, where he lost consciousness after suffering a suspected second concussion and was removed from the field on a stretcher.
For the survey, Nowinski and colleagues showed 347 current and former athletes, including 109 football players, video examples of SHAAKE and them asked about their experiences with this potential indicator of concussion.
Nearly 69% of athletes reported exhibiting a SHAAKE during their career, and 93% of those reported a SHAAKE in association with concussion at least once. Athletes reported SHAAKE a median of five times in their lives.
Of the athletes who reported SHAAKE, 85% linked this head-shaking movement to concussion symptoms such as disorientation (71%) and dizziness (54%).
Across all sports, SHAAKE showed a sensitivity of 49.6% and a positive predictive value (PPV) of 72.4% for diagnosing concussions.
Among football players, sensitivity improved to 52.3%, with an estimated specificity of 99.9%, a PPV of 91.9%, and an estimated negative predictive value of 99.5%.
The main limitation of the survey was the potential for recall bias due to survey participants self-reporting prior concussions. The researchers called for future prospective studies to validate SHAAKE as a sign of concussion.
Instant Replay for Brain Injury?
Experts echoed the need for validation. SHAAKE represents a “promising advance” in objective TBI assessment, particularly for sideline evaluation, said Shaheen Lakhan, MD, PhD, neurologist, and researcher based in Miami, Florida, who wasn’t involved in the research.
The potential value of SHAAKE is “particularly notable given the well-documented tendency for athletes to minimize or conceal symptoms to maintain play eligibility, a limitation that has historically challenged our reliance on subjective reporting and observational assessments,” Lakhan said.
“Moving forward, validation through prospective studies incorporating real-time video analysis, helmet sensor data, and clinician-confirmed TBI diagnoses will be essential. With appropriate validation, SHAAKE could emerge as a valuable component of our sideline assessment arsenal, complementing rather than replacing existing diagnostic approaches,” Lakhan said.
“SHAAKE could be the ‘instant replay’ for brain injuries that sports medicine has been waiting for — but like any new technology, we need to make sure it works for every player, not just some,” Lakhan added.
Also weighing in, Richard Figler, MD, director of the Concussion Center, Cleveland Clinic Sports Medicine Center, Cleveland, cautioned that the survey participants were recruited from a concussion registry and self-reported an average of 23 concussions — more than one third of which happened 5-10 years prior — which begs the question, “How much are they actually remembering?”
“Our goal is to make sure that the athletes are safe and that we’re not missing concussions, and we don’t have great tools to start off with. This study opens up the door for some prospective studies [of SHAAKE] moving forward. I think we need more data before this should be listed as a definitive marker,” said Figler, who also wasn’t involved in the study.
In any case, he said, when it comes to suspected concussion in sports, “when in doubt, you sit them out,” Figler said.
This research received no external funding. Nowinski has received travel reimbursement from the NFL Players Association (NFLPA), NFL, World Rugby, WWE, and All Elite Wrestling; served as an expert witness in cases related to concussion and chronic traumatic encephalopathy; and is compensated for speaking appearances and serving on the NFL Concussion Settlement Player Advocacy Committee. Daniel H. Daneshvar served as an expert witness in legal cases involving brain injury and concussion and received funding from the Football Players Health Study at Harvard University, which is funded by the NFLPA and evaluates patients for the MGH Brain and Body TRUST Center, sponsored in part by the NFLPA. Lakhan and Figler had no relevant disclosures.
A version of this article appeared on Medscape.com.
Spontaneous Headshake After a Kinematic Event (SHAAKE) refers to the rapid, back-and-forth head movement athletes exhibit following a blow to the head. This voluntary motion typically occurs within seconds to minutes after impact and is a familiar response in athletes.
In a recent survey, 7 out of 10 adult athletes recalled making this movement after a collision, and three out of four times they attributed this back-and-forth head movement to a concussion. The association was strongest among football players, who reported that over 90% of SHAAKE episodes were associated with a concussion.
The results were published online in Diagnostics.
Call to Action
“Everyone” — including sports and medical organizations — “should be adding this to their list of potential concussion signs and their protocol immediately,” study investigator Chris Nowinski, PhD, CEO and co-founder of the Concussion Legacy Foundation, told this news organization.
Nowinski said it’s “fascinating” that this concussion sign hasn’t been formally studied or added to formal concussion screening metrics before now, given that it’s been depicted in movies, television, and cartoons for decades.
Coaches, medical professionals, and concussion spotters should be trained to recognize when a SHAAKE happens, he said.
“The interesting thing is, I don’t think coaches or parents need much training other than to officially tie this to suspicion of a concussion,” Nowinski added.
The Case of Miami Dolphins QB Tua Tagovailoa
Nowinski said he was tipped off to SHAAKE as a concussion sign after Miami Dolphins quarterback Tua Tagovailoa’s controversial undiagnosed concussion during a National Football League (NFL) game in 2022.
After Tagovailoa’s head hit the ground, he rapidly shook his head side to side, indicating displaying SHAAKE, before stumbling and collapsing. At the time, a sideline doctor attributed his collapse to a prior back injury.
If Tagovailoa had been diagnosed with a concussion, he likely would not have been playing in a game just 4 days later, where he lost consciousness after suffering a suspected second concussion and was removed from the field on a stretcher.
For the survey, Nowinski and colleagues showed 347 current and former athletes, including 109 football players, video examples of SHAAKE and them asked about their experiences with this potential indicator of concussion.
Nearly 69% of athletes reported exhibiting a SHAAKE during their career, and 93% of those reported a SHAAKE in association with concussion at least once. Athletes reported SHAAKE a median of five times in their lives.
Of the athletes who reported SHAAKE, 85% linked this head-shaking movement to concussion symptoms such as disorientation (71%) and dizziness (54%).
Across all sports, SHAAKE showed a sensitivity of 49.6% and a positive predictive value (PPV) of 72.4% for diagnosing concussions.
Among football players, sensitivity improved to 52.3%, with an estimated specificity of 99.9%, a PPV of 91.9%, and an estimated negative predictive value of 99.5%.
The main limitation of the survey was the potential for recall bias due to survey participants self-reporting prior concussions. The researchers called for future prospective studies to validate SHAAKE as a sign of concussion.
Instant Replay for Brain Injury?
Experts echoed the need for validation. SHAAKE represents a “promising advance” in objective TBI assessment, particularly for sideline evaluation, said Shaheen Lakhan, MD, PhD, neurologist, and researcher based in Miami, Florida, who wasn’t involved in the research.
The potential value of SHAAKE is “particularly notable given the well-documented tendency for athletes to minimize or conceal symptoms to maintain play eligibility, a limitation that has historically challenged our reliance on subjective reporting and observational assessments,” Lakhan said.
“Moving forward, validation through prospective studies incorporating real-time video analysis, helmet sensor data, and clinician-confirmed TBI diagnoses will be essential. With appropriate validation, SHAAKE could emerge as a valuable component of our sideline assessment arsenal, complementing rather than replacing existing diagnostic approaches,” Lakhan said.
“SHAAKE could be the ‘instant replay’ for brain injuries that sports medicine has been waiting for — but like any new technology, we need to make sure it works for every player, not just some,” Lakhan added.
Also weighing in, Richard Figler, MD, director of the Concussion Center, Cleveland Clinic Sports Medicine Center, Cleveland, cautioned that the survey participants were recruited from a concussion registry and self-reported an average of 23 concussions — more than one third of which happened 5-10 years prior — which begs the question, “How much are they actually remembering?”
“Our goal is to make sure that the athletes are safe and that we’re not missing concussions, and we don’t have great tools to start off with. This study opens up the door for some prospective studies [of SHAAKE] moving forward. I think we need more data before this should be listed as a definitive marker,” said Figler, who also wasn’t involved in the study.
In any case, he said, when it comes to suspected concussion in sports, “when in doubt, you sit them out,” Figler said.
This research received no external funding. Nowinski has received travel reimbursement from the NFL Players Association (NFLPA), NFL, World Rugby, WWE, and All Elite Wrestling; served as an expert witness in cases related to concussion and chronic traumatic encephalopathy; and is compensated for speaking appearances and serving on the NFL Concussion Settlement Player Advocacy Committee. Daniel H. Daneshvar served as an expert witness in legal cases involving brain injury and concussion and received funding from the Football Players Health Study at Harvard University, which is funded by the NFLPA and evaluates patients for the MGH Brain and Body TRUST Center, sponsored in part by the NFLPA. Lakhan and Figler had no relevant disclosures.
A version of this article appeared on Medscape.com.
Spontaneous Headshake After a Kinematic Event (SHAAKE) refers to the rapid, back-and-forth head movement athletes exhibit following a blow to the head. This voluntary motion typically occurs within seconds to minutes after impact and is a familiar response in athletes.
In a recent survey, 7 out of 10 adult athletes recalled making this movement after a collision, and three out of four times they attributed this back-and-forth head movement to a concussion. The association was strongest among football players, who reported that over 90% of SHAAKE episodes were associated with a concussion.
The results were published online in Diagnostics.
Call to Action
“Everyone” — including sports and medical organizations — “should be adding this to their list of potential concussion signs and their protocol immediately,” study investigator Chris Nowinski, PhD, CEO and co-founder of the Concussion Legacy Foundation, told this news organization.
Nowinski said it’s “fascinating” that this concussion sign hasn’t been formally studied or added to formal concussion screening metrics before now, given that it’s been depicted in movies, television, and cartoons for decades.
Coaches, medical professionals, and concussion spotters should be trained to recognize when a SHAAKE happens, he said.
“The interesting thing is, I don’t think coaches or parents need much training other than to officially tie this to suspicion of a concussion,” Nowinski added.
The Case of Miami Dolphins QB Tua Tagovailoa
Nowinski said he was tipped off to SHAAKE as a concussion sign after Miami Dolphins quarterback Tua Tagovailoa’s controversial undiagnosed concussion during a National Football League (NFL) game in 2022.
After Tagovailoa’s head hit the ground, he rapidly shook his head side to side, indicating displaying SHAAKE, before stumbling and collapsing. At the time, a sideline doctor attributed his collapse to a prior back injury.
If Tagovailoa had been diagnosed with a concussion, he likely would not have been playing in a game just 4 days later, where he lost consciousness after suffering a suspected second concussion and was removed from the field on a stretcher.
For the survey, Nowinski and colleagues showed 347 current and former athletes, including 109 football players, video examples of SHAAKE and them asked about their experiences with this potential indicator of concussion.
Nearly 69% of athletes reported exhibiting a SHAAKE during their career, and 93% of those reported a SHAAKE in association with concussion at least once. Athletes reported SHAAKE a median of five times in their lives.
Of the athletes who reported SHAAKE, 85% linked this head-shaking movement to concussion symptoms such as disorientation (71%) and dizziness (54%).
Across all sports, SHAAKE showed a sensitivity of 49.6% and a positive predictive value (PPV) of 72.4% for diagnosing concussions.
Among football players, sensitivity improved to 52.3%, with an estimated specificity of 99.9%, a PPV of 91.9%, and an estimated negative predictive value of 99.5%.
The main limitation of the survey was the potential for recall bias due to survey participants self-reporting prior concussions. The researchers called for future prospective studies to validate SHAAKE as a sign of concussion.
Instant Replay for Brain Injury?
Experts echoed the need for validation. SHAAKE represents a “promising advance” in objective TBI assessment, particularly for sideline evaluation, said Shaheen Lakhan, MD, PhD, neurologist, and researcher based in Miami, Florida, who wasn’t involved in the research.
The potential value of SHAAKE is “particularly notable given the well-documented tendency for athletes to minimize or conceal symptoms to maintain play eligibility, a limitation that has historically challenged our reliance on subjective reporting and observational assessments,” Lakhan said.
“Moving forward, validation through prospective studies incorporating real-time video analysis, helmet sensor data, and clinician-confirmed TBI diagnoses will be essential. With appropriate validation, SHAAKE could emerge as a valuable component of our sideline assessment arsenal, complementing rather than replacing existing diagnostic approaches,” Lakhan said.
“SHAAKE could be the ‘instant replay’ for brain injuries that sports medicine has been waiting for — but like any new technology, we need to make sure it works for every player, not just some,” Lakhan added.
Also weighing in, Richard Figler, MD, director of the Concussion Center, Cleveland Clinic Sports Medicine Center, Cleveland, cautioned that the survey participants were recruited from a concussion registry and self-reported an average of 23 concussions — more than one third of which happened 5-10 years prior — which begs the question, “How much are they actually remembering?”
“Our goal is to make sure that the athletes are safe and that we’re not missing concussions, and we don’t have great tools to start off with. This study opens up the door for some prospective studies [of SHAAKE] moving forward. I think we need more data before this should be listed as a definitive marker,” said Figler, who also wasn’t involved in the study.
In any case, he said, when it comes to suspected concussion in sports, “when in doubt, you sit them out,” Figler said.
This research received no external funding. Nowinski has received travel reimbursement from the NFL Players Association (NFLPA), NFL, World Rugby, WWE, and All Elite Wrestling; served as an expert witness in cases related to concussion and chronic traumatic encephalopathy; and is compensated for speaking appearances and serving on the NFL Concussion Settlement Player Advocacy Committee. Daniel H. Daneshvar served as an expert witness in legal cases involving brain injury and concussion and received funding from the Football Players Health Study at Harvard University, which is funded by the NFLPA and evaluates patients for the MGH Brain and Body TRUST Center, sponsored in part by the NFLPA. Lakhan and Figler had no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM DIAGNOSTICS
Over 3 Years, Atopic Dermatitis Well-Controlled with Lebrikizumab
AMSTERDAM — among those followed up for an additional 2 years, according to the latest data from an extension study.
At the end of the maintenance phase of the pivotal trials at 12 months, 84% of the patients enrolled into the extension had clear or almost clear skin, as per the Investigator Global Assessment (IGA). This overall figure as well as the proportion with even better responses have persisted unchanged, reported Diamant Thaçi, MD, PhD, professor and head of the Comprehensive Center for Inflammatory Medicine, University of Lübeck in Germany.
Responses at 3 Years Maintained
“This is really quite remarkable,” Dr. Thaçi said. “Roughly all the patients maintained their response.” These results became even more remarkable when patients were assessed for their use of adjunctive therapy to control flares.
“Over the whole follow-up, 90% had no need for topical corticosteroids or any other rescue therapy,” Dr. Thaçi reported, providing data from the ADjoin lebrikizumab extension study during a late-breaking news session at the annual meeting of the European Academy of Dermatology and Venereology.
The patients in ADjoin were enrolled from the pivotal phase 3 ADvocate 1 and 2 trials completed almost 2 years ago and published together in March 2023. Lebrikizumab was approved in the United States in September 2024 for moderate to severe AD in patients aged ≥ 12 years, following previous approvals in Europe in 2023 and in Japan in January 2024.
In these two identical trials with a total of 564 patients, the primary endpoint was an IGA of 0 or 1, signifying clear or almost clear skin. At nearly 40%, the proportion of patients reaching this outcome at 16 weeks was about threefold greater (P < .001) on lebrikizumab than on placebo. The benefit was similar on secondary endpoints, such as 75% improvement in the Eczema Area and Severity Index (EASI75) score.
At the end of the double-blind, placebo-controlled 16-week phase of the ADvocate 1 and 2 trials, which enrolled adults and adolescents aged ≥ 12 years, responders were enrolled into a maintenance phase in which they were rerandomized to 250 mg lebrikizumab every 2 weeks (Q2W) or every 4 weeks (Q4W). The latter is the approved maintenance dose.
At the end of the maintenance phase, which lasted another 32 weeks (total exposure of 52 weeks for those initially randomized to lebrikizumab), patients were invited into the ADjoin extension. The only exclusions from the extension were serious adverse events related to lebrikizumab and noncompliance.
Response Curves Appear as Straight Lines
Over the next 2 years of ADjoin, response curves appeared as straight lines not only for the overall response but when patients were stratified for different levels of response at the extension study entry. Specifically, 81.5% and 83.3% had an IGA score of 0 or 1 in the Q2W and Q4W arms at completion of the ADvocate 16-week double-blind phase. At 3 years, the rates were 84.0% and 82.9%, respectively.
For the subgroup who entered ADjoin with an EASI75 or an EASI90 response, the persistence of this level of response over 2 years was similar, although there was some gain observed among those who entered the trial with an EASI75 response.
“Not only did these patients maintain their response, but the response on average slowly improved, so that there were more patients with an EASI90 response at the 3-year timepoint,” Dr. Thaçi said.
Of the 181 patients in the ADjoin extension, 82 patients were maintained on Q2W dosing and 99 were maintained on Q4W lebrikizumab. Their mean age was about 35 years, more than half were women, and nearly 40% had severe AD at the time they enrolled in the ADvocate trials. There was essentially no difference in response rates among those in the Q2W and Q4W arms over time in ADjoin.
Side Effect Profile Essentially Unchanged
The side effect and tolerability profiles, which were favorable in the original 16-week placebo-controlled study, have remained unchanged over the subsequent maintenance phase and through the additional 2 years of the ADjoin extension.
“There continued to be reports of conjunctivitis, which is very specific for anti–IL-13 therapies,” Dr. Thaçi said. However, he said that the incidence did not increase over time, and because it was easy to treat, “most patients do not discontinue lebrikizumab for this reason.” Moreover, he said the impression was that “the number of patients experiencing adverse effects has been decreasing over time.”
Calling these long-term results “very exciting,” Dr. Thaçi called lebrikizumab “a very valuable option for long-term AD care.”
Asked for his perspective on the results, Jonathan I. Silverberg, MD, PhD, Director of Clinical Research, Department of Dermatology, George Washington University, Washington, DC, said that it is important to study long-term efficacy, and these results are positive. Without direct comparisons to other biologics available for AD, nothing can be implied about the relative efficacy of monoclonal antibodies approved for AD.
“These data are important both from an efficacy and safety perspective” for those advising patients who need chronic AD treatment, said Dr. Silverberg, who was the principal investigator of the ADvocate trials.
Earlier this year, 5-year follow-up data were published for dupilumab. Of 326 patients who remained on therapy this long, 220 (67%) maintained an IGA of 0 or 1 at the end of the study. There were no unexpected adverse events, which were generally stable or declined throughout the study.
Dr. Thaçi has financial relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Leo Pharma, L’Oreal, Janssen-Cilag, New Bridge, Novartis, Pfizer, Regeneron, Roche, Sanofi, Sun Pharma, UCB, and Vichy. Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies including those that make drugs for AD.
A version of this article appeared on Medscape.com.
AMSTERDAM — among those followed up for an additional 2 years, according to the latest data from an extension study.
At the end of the maintenance phase of the pivotal trials at 12 months, 84% of the patients enrolled into the extension had clear or almost clear skin, as per the Investigator Global Assessment (IGA). This overall figure as well as the proportion with even better responses have persisted unchanged, reported Diamant Thaçi, MD, PhD, professor and head of the Comprehensive Center for Inflammatory Medicine, University of Lübeck in Germany.
Responses at 3 Years Maintained
“This is really quite remarkable,” Dr. Thaçi said. “Roughly all the patients maintained their response.” These results became even more remarkable when patients were assessed for their use of adjunctive therapy to control flares.
“Over the whole follow-up, 90% had no need for topical corticosteroids or any other rescue therapy,” Dr. Thaçi reported, providing data from the ADjoin lebrikizumab extension study during a late-breaking news session at the annual meeting of the European Academy of Dermatology and Venereology.
The patients in ADjoin were enrolled from the pivotal phase 3 ADvocate 1 and 2 trials completed almost 2 years ago and published together in March 2023. Lebrikizumab was approved in the United States in September 2024 for moderate to severe AD in patients aged ≥ 12 years, following previous approvals in Europe in 2023 and in Japan in January 2024.
In these two identical trials with a total of 564 patients, the primary endpoint was an IGA of 0 or 1, signifying clear or almost clear skin. At nearly 40%, the proportion of patients reaching this outcome at 16 weeks was about threefold greater (P < .001) on lebrikizumab than on placebo. The benefit was similar on secondary endpoints, such as 75% improvement in the Eczema Area and Severity Index (EASI75) score.
At the end of the double-blind, placebo-controlled 16-week phase of the ADvocate 1 and 2 trials, which enrolled adults and adolescents aged ≥ 12 years, responders were enrolled into a maintenance phase in which they were rerandomized to 250 mg lebrikizumab every 2 weeks (Q2W) or every 4 weeks (Q4W). The latter is the approved maintenance dose.
At the end of the maintenance phase, which lasted another 32 weeks (total exposure of 52 weeks for those initially randomized to lebrikizumab), patients were invited into the ADjoin extension. The only exclusions from the extension were serious adverse events related to lebrikizumab and noncompliance.
Response Curves Appear as Straight Lines
Over the next 2 years of ADjoin, response curves appeared as straight lines not only for the overall response but when patients were stratified for different levels of response at the extension study entry. Specifically, 81.5% and 83.3% had an IGA score of 0 or 1 in the Q2W and Q4W arms at completion of the ADvocate 16-week double-blind phase. At 3 years, the rates were 84.0% and 82.9%, respectively.
For the subgroup who entered ADjoin with an EASI75 or an EASI90 response, the persistence of this level of response over 2 years was similar, although there was some gain observed among those who entered the trial with an EASI75 response.
“Not only did these patients maintain their response, but the response on average slowly improved, so that there were more patients with an EASI90 response at the 3-year timepoint,” Dr. Thaçi said.
Of the 181 patients in the ADjoin extension, 82 patients were maintained on Q2W dosing and 99 were maintained on Q4W lebrikizumab. Their mean age was about 35 years, more than half were women, and nearly 40% had severe AD at the time they enrolled in the ADvocate trials. There was essentially no difference in response rates among those in the Q2W and Q4W arms over time in ADjoin.
Side Effect Profile Essentially Unchanged
The side effect and tolerability profiles, which were favorable in the original 16-week placebo-controlled study, have remained unchanged over the subsequent maintenance phase and through the additional 2 years of the ADjoin extension.
“There continued to be reports of conjunctivitis, which is very specific for anti–IL-13 therapies,” Dr. Thaçi said. However, he said that the incidence did not increase over time, and because it was easy to treat, “most patients do not discontinue lebrikizumab for this reason.” Moreover, he said the impression was that “the number of patients experiencing adverse effects has been decreasing over time.”
Calling these long-term results “very exciting,” Dr. Thaçi called lebrikizumab “a very valuable option for long-term AD care.”
Asked for his perspective on the results, Jonathan I. Silverberg, MD, PhD, Director of Clinical Research, Department of Dermatology, George Washington University, Washington, DC, said that it is important to study long-term efficacy, and these results are positive. Without direct comparisons to other biologics available for AD, nothing can be implied about the relative efficacy of monoclonal antibodies approved for AD.
“These data are important both from an efficacy and safety perspective” for those advising patients who need chronic AD treatment, said Dr. Silverberg, who was the principal investigator of the ADvocate trials.
Earlier this year, 5-year follow-up data were published for dupilumab. Of 326 patients who remained on therapy this long, 220 (67%) maintained an IGA of 0 or 1 at the end of the study. There were no unexpected adverse events, which were generally stable or declined throughout the study.
Dr. Thaçi has financial relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Leo Pharma, L’Oreal, Janssen-Cilag, New Bridge, Novartis, Pfizer, Regeneron, Roche, Sanofi, Sun Pharma, UCB, and Vichy. Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies including those that make drugs for AD.
A version of this article appeared on Medscape.com.
AMSTERDAM — among those followed up for an additional 2 years, according to the latest data from an extension study.
At the end of the maintenance phase of the pivotal trials at 12 months, 84% of the patients enrolled into the extension had clear or almost clear skin, as per the Investigator Global Assessment (IGA). This overall figure as well as the proportion with even better responses have persisted unchanged, reported Diamant Thaçi, MD, PhD, professor and head of the Comprehensive Center for Inflammatory Medicine, University of Lübeck in Germany.
Responses at 3 Years Maintained
“This is really quite remarkable,” Dr. Thaçi said. “Roughly all the patients maintained their response.” These results became even more remarkable when patients were assessed for their use of adjunctive therapy to control flares.
“Over the whole follow-up, 90% had no need for topical corticosteroids or any other rescue therapy,” Dr. Thaçi reported, providing data from the ADjoin lebrikizumab extension study during a late-breaking news session at the annual meeting of the European Academy of Dermatology and Venereology.
The patients in ADjoin were enrolled from the pivotal phase 3 ADvocate 1 and 2 trials completed almost 2 years ago and published together in March 2023. Lebrikizumab was approved in the United States in September 2024 for moderate to severe AD in patients aged ≥ 12 years, following previous approvals in Europe in 2023 and in Japan in January 2024.
In these two identical trials with a total of 564 patients, the primary endpoint was an IGA of 0 or 1, signifying clear or almost clear skin. At nearly 40%, the proportion of patients reaching this outcome at 16 weeks was about threefold greater (P < .001) on lebrikizumab than on placebo. The benefit was similar on secondary endpoints, such as 75% improvement in the Eczema Area and Severity Index (EASI75) score.
At the end of the double-blind, placebo-controlled 16-week phase of the ADvocate 1 and 2 trials, which enrolled adults and adolescents aged ≥ 12 years, responders were enrolled into a maintenance phase in which they were rerandomized to 250 mg lebrikizumab every 2 weeks (Q2W) or every 4 weeks (Q4W). The latter is the approved maintenance dose.
At the end of the maintenance phase, which lasted another 32 weeks (total exposure of 52 weeks for those initially randomized to lebrikizumab), patients were invited into the ADjoin extension. The only exclusions from the extension were serious adverse events related to lebrikizumab and noncompliance.
Response Curves Appear as Straight Lines
Over the next 2 years of ADjoin, response curves appeared as straight lines not only for the overall response but when patients were stratified for different levels of response at the extension study entry. Specifically, 81.5% and 83.3% had an IGA score of 0 or 1 in the Q2W and Q4W arms at completion of the ADvocate 16-week double-blind phase. At 3 years, the rates were 84.0% and 82.9%, respectively.
For the subgroup who entered ADjoin with an EASI75 or an EASI90 response, the persistence of this level of response over 2 years was similar, although there was some gain observed among those who entered the trial with an EASI75 response.
“Not only did these patients maintain their response, but the response on average slowly improved, so that there were more patients with an EASI90 response at the 3-year timepoint,” Dr. Thaçi said.
Of the 181 patients in the ADjoin extension, 82 patients were maintained on Q2W dosing and 99 were maintained on Q4W lebrikizumab. Their mean age was about 35 years, more than half were women, and nearly 40% had severe AD at the time they enrolled in the ADvocate trials. There was essentially no difference in response rates among those in the Q2W and Q4W arms over time in ADjoin.
Side Effect Profile Essentially Unchanged
The side effect and tolerability profiles, which were favorable in the original 16-week placebo-controlled study, have remained unchanged over the subsequent maintenance phase and through the additional 2 years of the ADjoin extension.
“There continued to be reports of conjunctivitis, which is very specific for anti–IL-13 therapies,” Dr. Thaçi said. However, he said that the incidence did not increase over time, and because it was easy to treat, “most patients do not discontinue lebrikizumab for this reason.” Moreover, he said the impression was that “the number of patients experiencing adverse effects has been decreasing over time.”
Calling these long-term results “very exciting,” Dr. Thaçi called lebrikizumab “a very valuable option for long-term AD care.”
Asked for his perspective on the results, Jonathan I. Silverberg, MD, PhD, Director of Clinical Research, Department of Dermatology, George Washington University, Washington, DC, said that it is important to study long-term efficacy, and these results are positive. Without direct comparisons to other biologics available for AD, nothing can be implied about the relative efficacy of monoclonal antibodies approved for AD.
“These data are important both from an efficacy and safety perspective” for those advising patients who need chronic AD treatment, said Dr. Silverberg, who was the principal investigator of the ADvocate trials.
Earlier this year, 5-year follow-up data were published for dupilumab. Of 326 patients who remained on therapy this long, 220 (67%) maintained an IGA of 0 or 1 at the end of the study. There were no unexpected adverse events, which were generally stable or declined throughout the study.
Dr. Thaçi has financial relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Leo Pharma, L’Oreal, Janssen-Cilag, New Bridge, Novartis, Pfizer, Regeneron, Roche, Sanofi, Sun Pharma, UCB, and Vichy. Dr. Silverberg reported financial relationships with more than 40 pharmaceutical companies including those that make drugs for AD.
A version of this article appeared on Medscape.com.
FROM EADV 2024
State of Confusion: Should All Children Get Lipid Labs for High Cholesterol?
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Clinicians receive conflicting advice on whether to order blood tests to screen for lipids in children. A new study could add to the confusion. Researchers found that a combination of physical proxy measures such as hypertension and body mass index (BMI) predicted the risk for future cardiovascular events as well as the physical model plus lipid labs, questioning the value of those blood tests.
Some medical organizations advise screening only for high-risk children because more research is needed to define the harms and benefits of universal screening. Diet and behavioral changes are sufficient for most children, and universal screening could lead to false positives and unnecessary further testing, they said.
Groups that favor lipid tests for all children say these measurements detect familial hypercholesterolemia (FH) that would not otherwise be diagnosed, leading to treatment with drugs like statins and a greater chance of preventing cardiovascular disease (CVD) in adulthood.
Researchers from the new study said their findings do not address screenings for FH, which affects 1 in 250 US children and puts them at a risk for atherosclerotic CVD.
Recommending Blood Tests in Age Groups
One of the seminal guidelines on screening lipids in children came from the National Heart, Lung, and Blood Institute (NHLBI), which in 2011 recommended children undergo dyslipidemia screening between the ages of 9 and 11 years and again between 17 and 21 years. Children should receive a screening starting at age 2 years if they have a family history of CVD or dyslipidemia or have diabetes, an elevated BMI, or hypertension. The American Academy of Pediatrics shortly followed suit, issuing similar recommendations.
Screening for the two subsets of ages was an expansion from the original 1992 guidelines from the National Cholesterol Education Program, which recommended screening only for children with either a family history of early CVD or elevated total cholesterol levels.
A 2011 panel for the NHLBI said the older approach identified significantly fewer children with abnormal levels of low-density lipoprotein cholesterol (LDL-C) than the addition of two age groups for screening, adding that many children do not have a complete family history. The American College of Cardiology and American Heart Association later supported NHLBI’s stance in their joint guidelines on the management of cholesterol.
Mark Corkins, MD, chair of the AAP’s Committee on Nutrition, told Medscape Medical News that if children are screened only because they have obesity or a family history of FH, some with elevated lipid levels will be missed. For instance, studies indicate caregiver recall of FH often is inaccurate, and the genetic disorder that causes the condition is not related to obesity.
“The screening is to find familial hypercholesterolemia, to try to find the ones that need therapy,” that would not be caught by the risk-based screening earlier on in childhood, Corkins said.
Only Screen Children With Risk Factors
But other groups do not agree. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against screening for lipid disorders in asymptomatic children and teens.
The group also said it found inadequate evidence that lipid-lowering interventions in the general pediatric population lead to reductions in cardiovascular events or all-cause mortality once they reached adulthood. USPSTF also raised questions about the safety of lipid-lowering drugs in children.
“The current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger,” the panel wrote.
The American Academy of Family Physicians supports USPSTF’s recommendations.
Low Rate of Screening
While the uncertainty over screening in children continues, the practice has been adopted by a minority of clinicians.
A study published in JAMA Network Open in July found 9% of 700,000 9- to 11-year-olds had a documented result from a lipid screening. Among more than 1.3 million 17- to 21-year-olds, 13% had received a screening.
As BMI went up, so did screening rates. A little over 9% children and teens with a healthy weight were screened compared with 14.7% of those with moderate obesity and 21.9% of those with severe obesity.
Among those screened, 32.3% of 9- to 11-year-olds and 30.2% of 17- to 21-year-olds had abnormal lipid levels, defined as having one elevated measure out of five, including total cholesterol of 200 mg/dL or higher or LDL-C levels of 130 mg/dL or higher.
Justin Zachariah, MD, MPH, an associate professor of pediatrics-cardiology at Baylor College of Medicine in Houston, spoke about physicians screening children based only on factors like obesity during a presentation at the recent annual meeting of the American Academy of Pediatrics. He cited research showing roughly one in four children with abnormal lipids had a normal weight.
If a clinician is reserving a lipid screening for a child who is overweight or has obesity, “you’re missing nearly half the problem,” Zachariah said during his presentation.
One reason for the low rate of universal screening may be inattention to FH by clinicians, according to Samuel S. Gidding, MD, a professor in the Department of Genomic Health at Geisinger College of Health Sciences in Bridgewater Corners, Vermont.
For instance, a clinician has only a set amount of time during a well-child visit and other issues may take precedence, “so it doesn’t make sense to broach preventive screening for something that could happen 30 or 40 years from now, vs this [other] very immediate problem,” he said.
Clinicians “are triggered to act on the LDL level, but don’t think about FH as a possible diagnosis,” Gidding told Medscape Medical News.
Another barrier is that in some settings, caregivers must take children and teens to another facility on a different day to fulfill an order for a lipid test.
“It’s reluctance of doctors to order it, knowing patients won’t go through with it,” Gidding said.
Gidding is a consultant for Esperion Therapeutics. Other sources in this story reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Wide Availability of Naloxone and Education on Its Use Can Save Pediatric Lives
ORLANDO — More than half of youth improved after receiving a dose of naloxone by emergency medical services (EMS) after an emergency dispatch call, according to research presented at the American Academy of Pediatrics 2024 National Conference.
“Emergency responders or EMS are often the first to arrive to an opioid poisoning, and they’re often the first to give naloxone, a potentially lifesaving medication,” said Christopher E. Gaw, MD, MPH, MBE, assistant professor of pediatrics at The Ohio State University College of Medicine and an emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
“Our study highlights and underscores its safety of use in the prehospital setting, and this is also supported by other data,” Gaw said.
Additional research at the meeting showed that teens’ knowledge, attitudes, and confidence about recognizing overdoses and assisting with naloxone administration improved following a peer-to-peer training program, suggesting that teens can play an important role in reducing youth mortality from overdoses.
An average of 22 American teens died from overdose every week in 2022, and as counterfeit pill use has increased among youth, research has found that fentanyl was detected in 93% of overdose deaths with counterfeit pills, according to Talia Puzantian, PharmD, BCPP, of the Keck Graduate Institute School of Pharmacy, Claremont, California, who led the study on peer education. Yet a recent survey had found that less than a third of teens (30%) knew what naloxone was, and only 14% knew how to administer it.
“Ensuring that adolescents have easy and confidential access to naloxone is important and can save lives,” said Taylor Nichols, MD, assistant clinical professor at the University of California San Francisco and an emergency medicine and addiction medicine–certified physician. “I have had teen patients who have told me that they have had to use naloxone obtained from our clinic on friends when they have accidentally overdosed.”

Nichols, who was not involved in either study, added that all 50 states have some version of Good Samaritan laws that offer protection to individuals who attempt to aid in emergency assistance in good faith, and all except Kansas and Wyoming have laws specifically protecting people trying to help with overdose prevention.
“I tell people that everyone should carry naloxone and have naloxone available to be able to reverse an overdose, whether they personally use opioids or know people who use opioids because if they happen to come into a situation in which someone is passed out and unresponsive, that timely administration of naloxone may save their life,” Nichols said.
He added that primary care physicians, “particularly in family medicine and pediatrics, should be asking about any opioids in the home prescribed to anyone else and ensure that those patients also are prescribed or have access to naloxone to keep at home. Just as with asking about any other potential safety hazards, making sure they have naloxone available is crucial.”
EMS Naloxone Administration to Youth
EMS clinicians are often the first healthcare providers to respond to an opioid overdose or poisoning event, and evidence-based guidelines for EMS naloxone administration were developed in 2019 to support this intervention. Gaw’s team investigated the frequency and demographics of pediatric administration of naloxone.
They analyzed data from the National Emergency Medical Services Information System on EMS activations for administration of at least one dose of naloxone during 2022 to those aged 0-17. There were 6215 EMS pediatric administrations of naloxone that year, and in the vast majority of cases (82%), the patient had not received a naloxone injection prior to EMS’s arrival.
Most patients (79%) were aged 13-17 years, but 10% were in the 6-12 age group. The remaining patients included 6% infants younger than 1 year and 4% aged 6-12 years. Just over half were for males (55%), and most were dispatched to a home or residential setting (61%). One in five incidents (22%) occurred at a non-healthcare business, 9% on a street or highway, and the rest at a healthcare facility or another location.
Most of the incidents occurred in urban areas (86%), followed by rural (7%), suburban (6%), and wilderness (1.4%). More occurred in the US South (42%) than in the West (29%), Midwest (22%), or Northeast (7.5%).
A key takeaway of those demographic findings is that ingestions and accidental poisonings with opioids can occur in children of any age, Nichols said. “Every single home that has any opioids in the home should absolutely have naloxone immediately available as well,” he said. “Every single person who is prescribed opioids should also have naloxone available and accessible and to be sure that the naloxone is not expired or otherwise tampered with and update that every few years.” He noted that Narcan expiration was recently extended from 3 years to 4 years by the US Food and Drug Administration (FDA).
“I always advise that people who have opioid medications keep them stored safely and securely,” Nichols said. “However, I also acknowledge that even perfect systems fail and that people make mistakes and may accidentally leave medication out, within reach, or otherwise unsecured. If that happens, and someone were to intentionally or unintentionally get into that medication and potentially overdose as a result, we want to have that reversal medication immediately available to reverse the overdose.”
In nearly all cases (91%), EMS provided advanced life support, with only 7.5% patients receiving basic life support and 1.5% receiving specialty critical care. Just under a third (29%) of the dispatch calls were for “overdose/poisoning/ingestion.” Other dispatch calls included “unconscious/fainting/near-fainting” (21%) or “cardiac arrest/death” (17%), but the frequency of each dispatch label varied by age groups.
For example, 38% of calls for infants were for cardiac arrest, compared with 15% of calls for older teens and 18% of calls for 6-12 year olds. An overdose/poisoning dispatch was meanwhile more common for teens (32%) than for infants (13%), younger children (23%), and older children/tweens (18%). Other dispatch complaints included “sick person/person down/unknown problem” (12%) and “breathing problem” (5%).
A possible reason for these variations is that “an overdose might be mistaken for another medical emergency, or vice versa, because opioid poisonings can be challenging to recognize, especially in young children and in the pediatric population,” Gaw said. “Both the public and emergency responders should maintain a high level of suspicion” of possible overdose for children with the signs or symptoms of it, such as low breathing, unresponsiveness, or small pupils.
In most cases (87%), the patient was not in cardiac arrest, though the patient had entered cardiac arrest before EMS’s arrival in 11.5% of cases. Two thirds of cases only involved one dose of naloxone, while the other 33% involved two doses.
Ryan Marino, MD, an addiction medicine specialist and an associate professor of emergency medicine at Case Western Reserve University School of Medicine in Cleveland, Ohio, who was not involved in the study, took note of the high proportion of cases in which two doses were administered.
“While there is, in my professional opinion, almost no downside to giving naloxone in situations like this, and everybody should have it available and know how to use it, I would caution people on the risk of anchor bias, especially when more than two doses of naloxone are given, since we know that one should be an effective amount for any known opioid overdose,” Marino said. Anchoring bias refers to the tendency for individuals to rely more heavily on the first piece of information they receive about a topic or situation.
“For first responders and healthcare professionals, the importance of additional resuscitation measures like oxygenation and ventilation are just as crucial,” Marino said. “People should not be discouraged if someone doesn’t immediately respond to naloxone as overdose physiology can cause mental status to stay impaired for other reasons beyond direct drug effect, such as hypercarbia, but continue to seek and/or provide additional emergency care in these situations.”
Patients improved after one dose in just over half the cases (54%), and their conditions were unchanged in 46% of cases. There were only 11 cases in which the patient’s condition worsened after a naloxone dose (0.2%). Most of the cases (88%) were transported by EMS, and there were 13 total deaths at the scene (0.2%).
Nichols found the low incidence of worsening clinical status particularly striking. “This is further evidence of a critically important point — naloxone is purely an opioid antagonist, and only binds to opioid receptors, such that if a person has not overdosed on opioids or does not otherwise have opioids in their system, naloxone will not have a significant effect and will not cause them harm,” Nichols said.
“The most common causes of harm are due to rapid reversal of overdose and the potential risks involved in the rapid reversal of opioid effects and potentially precipitating withdrawal, and as this paper demonstrates, these are exceedingly rare,” he said. “Given that, we should have an incredibly low barrier to administer naloxone appropriately.”
The study was limited by inability to know how many true pediatric opioid poisonings are managed by EMS, so future research could look at linking EMS and emergency room hospital databases.
Improved Self-Efficacy in Teens
Another study showed that a peer-to-peer training program increased teens’ knowledge about overdoses from 34% before training to 79% after (P < .0001), and it substantially improved their confidence in recognizing an overdose and administering naloxone.
Nichols said the study shows the importance of ensuring “that adolescents know how to keep themselves and their friends safe in the case that they or anyone they know does end up using illicit substances which either intentionally or unintentionally contain opioids.”
This study assessed a training program with 206 students in a Los Angeles County high school who were trained by their peers between November 2023 and March 2024. The training included trends in teen overdose deaths, defining what opioids and fentanyl are, recognizing an overdose, and responding to one with naloxone.
The teens were an average 16 years old, about evenly split between boys and girls, and mostly in 11th (40%) or 12th (28%) grade, though nearly a third (29%) were 9th graders.
The students’ knowledge about fentanyl’s presence in counterfeit pills increased from 21% before the training to 68% afterward, and their correct identification of an overdose increased from 47% of participants to 90%.
The students’ confidence and attitudes toward helping with an overdose also improved substantially after the training. About two thirds agreed that non-medical people should be able to carry naloxone before the training, and that rose to 88% agreeing after the training. The proportion who agreed they would be willing to assist in an overdose rose from 77% before to 89% after training.
More dramatically, the teens’ confidence after training more than doubled in recognizing an overdose (from 31% to 81%) and more than tripled in their ability to give naloxone during an overdose (from 26% to 83%).
“The critical piece to keep in mind is that the concern about opioid overdose is respiratory depression leading to a lack of oxygen getting to the brain,” Nichols explained. “In the event of an overdose, time is brain — the longer the brain is deprived of oxygen, the lower the chance of survival. There is no specific time at which naloxone would become less effective at reversing an overdose.”
Therefore, people do not need to know the exact time that someone may have overdosed or how long they have been passed out in order to administer naloxone, he said. “The sooner naloxone is administered to someone who is unresponsive and who may have overdosed on opioids, the higher the likelihood of a successful reversal of an overdose and of saving a life.”
The peer-to-peer program was sponsored by the CARLOW Center for Medical Innovation, and the EMS study used no external funding. The authors of both studies and Marino had no disclosures. Nichols has consulted or clinically advised TV shows and health tech startup companies and has no disclosures related to naloxone or the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
ORLANDO — More than half of youth improved after receiving a dose of naloxone by emergency medical services (EMS) after an emergency dispatch call, according to research presented at the American Academy of Pediatrics 2024 National Conference.
“Emergency responders or EMS are often the first to arrive to an opioid poisoning, and they’re often the first to give naloxone, a potentially lifesaving medication,” said Christopher E. Gaw, MD, MPH, MBE, assistant professor of pediatrics at The Ohio State University College of Medicine and an emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
“Our study highlights and underscores its safety of use in the prehospital setting, and this is also supported by other data,” Gaw said.
Additional research at the meeting showed that teens’ knowledge, attitudes, and confidence about recognizing overdoses and assisting with naloxone administration improved following a peer-to-peer training program, suggesting that teens can play an important role in reducing youth mortality from overdoses.
An average of 22 American teens died from overdose every week in 2022, and as counterfeit pill use has increased among youth, research has found that fentanyl was detected in 93% of overdose deaths with counterfeit pills, according to Talia Puzantian, PharmD, BCPP, of the Keck Graduate Institute School of Pharmacy, Claremont, California, who led the study on peer education. Yet a recent survey had found that less than a third of teens (30%) knew what naloxone was, and only 14% knew how to administer it.
“Ensuring that adolescents have easy and confidential access to naloxone is important and can save lives,” said Taylor Nichols, MD, assistant clinical professor at the University of California San Francisco and an emergency medicine and addiction medicine–certified physician. “I have had teen patients who have told me that they have had to use naloxone obtained from our clinic on friends when they have accidentally overdosed.”
Nichols, who was not involved in either study, added that all 50 states have some version of Good Samaritan laws that offer protection to individuals who attempt to aid in emergency assistance in good faith, and all except Kansas and Wyoming have laws specifically protecting people trying to help with overdose prevention.
“I tell people that everyone should carry naloxone and have naloxone available to be able to reverse an overdose, whether they personally use opioids or know people who use opioids because if they happen to come into a situation in which someone is passed out and unresponsive, that timely administration of naloxone may save their life,” Nichols said.
He added that primary care physicians, “particularly in family medicine and pediatrics, should be asking about any opioids in the home prescribed to anyone else and ensure that those patients also are prescribed or have access to naloxone to keep at home. Just as with asking about any other potential safety hazards, making sure they have naloxone available is crucial.”
EMS Naloxone Administration to Youth
EMS clinicians are often the first healthcare providers to respond to an opioid overdose or poisoning event, and evidence-based guidelines for EMS naloxone administration were developed in 2019 to support this intervention. Gaw’s team investigated the frequency and demographics of pediatric administration of naloxone.
They analyzed data from the National Emergency Medical Services Information System on EMS activations for administration of at least one dose of naloxone during 2022 to those aged 0-17. There were 6215 EMS pediatric administrations of naloxone that year, and in the vast majority of cases (82%), the patient had not received a naloxone injection prior to EMS’s arrival.
Most patients (79%) were aged 13-17 years, but 10% were in the 6-12 age group. The remaining patients included 6% infants younger than 1 year and 4% aged 6-12 years. Just over half were for males (55%), and most were dispatched to a home or residential setting (61%). One in five incidents (22%) occurred at a non-healthcare business, 9% on a street or highway, and the rest at a healthcare facility or another location.
Most of the incidents occurred in urban areas (86%), followed by rural (7%), suburban (6%), and wilderness (1.4%). More occurred in the US South (42%) than in the West (29%), Midwest (22%), or Northeast (7.5%).
A key takeaway of those demographic findings is that ingestions and accidental poisonings with opioids can occur in children of any age, Nichols said. “Every single home that has any opioids in the home should absolutely have naloxone immediately available as well,” he said. “Every single person who is prescribed opioids should also have naloxone available and accessible and to be sure that the naloxone is not expired or otherwise tampered with and update that every few years.” He noted that Narcan expiration was recently extended from 3 years to 4 years by the US Food and Drug Administration (FDA).
“I always advise that people who have opioid medications keep them stored safely and securely,” Nichols said. “However, I also acknowledge that even perfect systems fail and that people make mistakes and may accidentally leave medication out, within reach, or otherwise unsecured. If that happens, and someone were to intentionally or unintentionally get into that medication and potentially overdose as a result, we want to have that reversal medication immediately available to reverse the overdose.”
In nearly all cases (91%), EMS provided advanced life support, with only 7.5% patients receiving basic life support and 1.5% receiving specialty critical care. Just under a third (29%) of the dispatch calls were for “overdose/poisoning/ingestion.” Other dispatch calls included “unconscious/fainting/near-fainting” (21%) or “cardiac arrest/death” (17%), but the frequency of each dispatch label varied by age groups.
For example, 38% of calls for infants were for cardiac arrest, compared with 15% of calls for older teens and 18% of calls for 6-12 year olds. An overdose/poisoning dispatch was meanwhile more common for teens (32%) than for infants (13%), younger children (23%), and older children/tweens (18%). Other dispatch complaints included “sick person/person down/unknown problem” (12%) and “breathing problem” (5%).
A possible reason for these variations is that “an overdose might be mistaken for another medical emergency, or vice versa, because opioid poisonings can be challenging to recognize, especially in young children and in the pediatric population,” Gaw said. “Both the public and emergency responders should maintain a high level of suspicion” of possible overdose for children with the signs or symptoms of it, such as low breathing, unresponsiveness, or small pupils.
In most cases (87%), the patient was not in cardiac arrest, though the patient had entered cardiac arrest before EMS’s arrival in 11.5% of cases. Two thirds of cases only involved one dose of naloxone, while the other 33% involved two doses.
Ryan Marino, MD, an addiction medicine specialist and an associate professor of emergency medicine at Case Western Reserve University School of Medicine in Cleveland, Ohio, who was not involved in the study, took note of the high proportion of cases in which two doses were administered.
“While there is, in my professional opinion, almost no downside to giving naloxone in situations like this, and everybody should have it available and know how to use it, I would caution people on the risk of anchor bias, especially when more than two doses of naloxone are given, since we know that one should be an effective amount for any known opioid overdose,” Marino said. Anchoring bias refers to the tendency for individuals to rely more heavily on the first piece of information they receive about a topic or situation.
“For first responders and healthcare professionals, the importance of additional resuscitation measures like oxygenation and ventilation are just as crucial,” Marino said. “People should not be discouraged if someone doesn’t immediately respond to naloxone as overdose physiology can cause mental status to stay impaired for other reasons beyond direct drug effect, such as hypercarbia, but continue to seek and/or provide additional emergency care in these situations.”
Patients improved after one dose in just over half the cases (54%), and their conditions were unchanged in 46% of cases. There were only 11 cases in which the patient’s condition worsened after a naloxone dose (0.2%). Most of the cases (88%) were transported by EMS, and there were 13 total deaths at the scene (0.2%).
Nichols found the low incidence of worsening clinical status particularly striking. “This is further evidence of a critically important point — naloxone is purely an opioid antagonist, and only binds to opioid receptors, such that if a person has not overdosed on opioids or does not otherwise have opioids in their system, naloxone will not have a significant effect and will not cause them harm,” Nichols said.
“The most common causes of harm are due to rapid reversal of overdose and the potential risks involved in the rapid reversal of opioid effects and potentially precipitating withdrawal, and as this paper demonstrates, these are exceedingly rare,” he said. “Given that, we should have an incredibly low barrier to administer naloxone appropriately.”
The study was limited by inability to know how many true pediatric opioid poisonings are managed by EMS, so future research could look at linking EMS and emergency room hospital databases.
Improved Self-Efficacy in Teens
Another study showed that a peer-to-peer training program increased teens’ knowledge about overdoses from 34% before training to 79% after (P < .0001), and it substantially improved their confidence in recognizing an overdose and administering naloxone.
Nichols said the study shows the importance of ensuring “that adolescents know how to keep themselves and their friends safe in the case that they or anyone they know does end up using illicit substances which either intentionally or unintentionally contain opioids.”
This study assessed a training program with 206 students in a Los Angeles County high school who were trained by their peers between November 2023 and March 2024. The training included trends in teen overdose deaths, defining what opioids and fentanyl are, recognizing an overdose, and responding to one with naloxone.
The teens were an average 16 years old, about evenly split between boys and girls, and mostly in 11th (40%) or 12th (28%) grade, though nearly a third (29%) were 9th graders.
The students’ knowledge about fentanyl’s presence in counterfeit pills increased from 21% before the training to 68% afterward, and their correct identification of an overdose increased from 47% of participants to 90%.
The students’ confidence and attitudes toward helping with an overdose also improved substantially after the training. About two thirds agreed that non-medical people should be able to carry naloxone before the training, and that rose to 88% agreeing after the training. The proportion who agreed they would be willing to assist in an overdose rose from 77% before to 89% after training.
More dramatically, the teens’ confidence after training more than doubled in recognizing an overdose (from 31% to 81%) and more than tripled in their ability to give naloxone during an overdose (from 26% to 83%).
“The critical piece to keep in mind is that the concern about opioid overdose is respiratory depression leading to a lack of oxygen getting to the brain,” Nichols explained. “In the event of an overdose, time is brain — the longer the brain is deprived of oxygen, the lower the chance of survival. There is no specific time at which naloxone would become less effective at reversing an overdose.”
Therefore, people do not need to know the exact time that someone may have overdosed or how long they have been passed out in order to administer naloxone, he said. “The sooner naloxone is administered to someone who is unresponsive and who may have overdosed on opioids, the higher the likelihood of a successful reversal of an overdose and of saving a life.”
The peer-to-peer program was sponsored by the CARLOW Center for Medical Innovation, and the EMS study used no external funding. The authors of both studies and Marino had no disclosures. Nichols has consulted or clinically advised TV shows and health tech startup companies and has no disclosures related to naloxone or the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
ORLANDO — More than half of youth improved after receiving a dose of naloxone by emergency medical services (EMS) after an emergency dispatch call, according to research presented at the American Academy of Pediatrics 2024 National Conference.
“Emergency responders or EMS are often the first to arrive to an opioid poisoning, and they’re often the first to give naloxone, a potentially lifesaving medication,” said Christopher E. Gaw, MD, MPH, MBE, assistant professor of pediatrics at The Ohio State University College of Medicine and an emergency medicine physician at Nationwide Children’s Hospital in Columbus, Ohio.
“Our study highlights and underscores its safety of use in the prehospital setting, and this is also supported by other data,” Gaw said.
Additional research at the meeting showed that teens’ knowledge, attitudes, and confidence about recognizing overdoses and assisting with naloxone administration improved following a peer-to-peer training program, suggesting that teens can play an important role in reducing youth mortality from overdoses.
An average of 22 American teens died from overdose every week in 2022, and as counterfeit pill use has increased among youth, research has found that fentanyl was detected in 93% of overdose deaths with counterfeit pills, according to Talia Puzantian, PharmD, BCPP, of the Keck Graduate Institute School of Pharmacy, Claremont, California, who led the study on peer education. Yet a recent survey had found that less than a third of teens (30%) knew what naloxone was, and only 14% knew how to administer it.
“Ensuring that adolescents have easy and confidential access to naloxone is important and can save lives,” said Taylor Nichols, MD, assistant clinical professor at the University of California San Francisco and an emergency medicine and addiction medicine–certified physician. “I have had teen patients who have told me that they have had to use naloxone obtained from our clinic on friends when they have accidentally overdosed.”
Nichols, who was not involved in either study, added that all 50 states have some version of Good Samaritan laws that offer protection to individuals who attempt to aid in emergency assistance in good faith, and all except Kansas and Wyoming have laws specifically protecting people trying to help with overdose prevention.
“I tell people that everyone should carry naloxone and have naloxone available to be able to reverse an overdose, whether they personally use opioids or know people who use opioids because if they happen to come into a situation in which someone is passed out and unresponsive, that timely administration of naloxone may save their life,” Nichols said.
He added that primary care physicians, “particularly in family medicine and pediatrics, should be asking about any opioids in the home prescribed to anyone else and ensure that those patients also are prescribed or have access to naloxone to keep at home. Just as with asking about any other potential safety hazards, making sure they have naloxone available is crucial.”
EMS Naloxone Administration to Youth
EMS clinicians are often the first healthcare providers to respond to an opioid overdose or poisoning event, and evidence-based guidelines for EMS naloxone administration were developed in 2019 to support this intervention. Gaw’s team investigated the frequency and demographics of pediatric administration of naloxone.
They analyzed data from the National Emergency Medical Services Information System on EMS activations for administration of at least one dose of naloxone during 2022 to those aged 0-17. There were 6215 EMS pediatric administrations of naloxone that year, and in the vast majority of cases (82%), the patient had not received a naloxone injection prior to EMS’s arrival.
Most patients (79%) were aged 13-17 years, but 10% were in the 6-12 age group. The remaining patients included 6% infants younger than 1 year and 4% aged 6-12 years. Just over half were for males (55%), and most were dispatched to a home or residential setting (61%). One in five incidents (22%) occurred at a non-healthcare business, 9% on a street or highway, and the rest at a healthcare facility or another location.
Most of the incidents occurred in urban areas (86%), followed by rural (7%), suburban (6%), and wilderness (1.4%). More occurred in the US South (42%) than in the West (29%), Midwest (22%), or Northeast (7.5%).
A key takeaway of those demographic findings is that ingestions and accidental poisonings with opioids can occur in children of any age, Nichols said. “Every single home that has any opioids in the home should absolutely have naloxone immediately available as well,” he said. “Every single person who is prescribed opioids should also have naloxone available and accessible and to be sure that the naloxone is not expired or otherwise tampered with and update that every few years.” He noted that Narcan expiration was recently extended from 3 years to 4 years by the US Food and Drug Administration (FDA).
“I always advise that people who have opioid medications keep them stored safely and securely,” Nichols said. “However, I also acknowledge that even perfect systems fail and that people make mistakes and may accidentally leave medication out, within reach, or otherwise unsecured. If that happens, and someone were to intentionally or unintentionally get into that medication and potentially overdose as a result, we want to have that reversal medication immediately available to reverse the overdose.”
In nearly all cases (91%), EMS provided advanced life support, with only 7.5% patients receiving basic life support and 1.5% receiving specialty critical care. Just under a third (29%) of the dispatch calls were for “overdose/poisoning/ingestion.” Other dispatch calls included “unconscious/fainting/near-fainting” (21%) or “cardiac arrest/death” (17%), but the frequency of each dispatch label varied by age groups.
For example, 38% of calls for infants were for cardiac arrest, compared with 15% of calls for older teens and 18% of calls for 6-12 year olds. An overdose/poisoning dispatch was meanwhile more common for teens (32%) than for infants (13%), younger children (23%), and older children/tweens (18%). Other dispatch complaints included “sick person/person down/unknown problem” (12%) and “breathing problem” (5%).
A possible reason for these variations is that “an overdose might be mistaken for another medical emergency, or vice versa, because opioid poisonings can be challenging to recognize, especially in young children and in the pediatric population,” Gaw said. “Both the public and emergency responders should maintain a high level of suspicion” of possible overdose for children with the signs or symptoms of it, such as low breathing, unresponsiveness, or small pupils.
In most cases (87%), the patient was not in cardiac arrest, though the patient had entered cardiac arrest before EMS’s arrival in 11.5% of cases. Two thirds of cases only involved one dose of naloxone, while the other 33% involved two doses.
Ryan Marino, MD, an addiction medicine specialist and an associate professor of emergency medicine at Case Western Reserve University School of Medicine in Cleveland, Ohio, who was not involved in the study, took note of the high proportion of cases in which two doses were administered.
“While there is, in my professional opinion, almost no downside to giving naloxone in situations like this, and everybody should have it available and know how to use it, I would caution people on the risk of anchor bias, especially when more than two doses of naloxone are given, since we know that one should be an effective amount for any known opioid overdose,” Marino said. Anchoring bias refers to the tendency for individuals to rely more heavily on the first piece of information they receive about a topic or situation.
“For first responders and healthcare professionals, the importance of additional resuscitation measures like oxygenation and ventilation are just as crucial,” Marino said. “People should not be discouraged if someone doesn’t immediately respond to naloxone as overdose physiology can cause mental status to stay impaired for other reasons beyond direct drug effect, such as hypercarbia, but continue to seek and/or provide additional emergency care in these situations.”
Patients improved after one dose in just over half the cases (54%), and their conditions were unchanged in 46% of cases. There were only 11 cases in which the patient’s condition worsened after a naloxone dose (0.2%). Most of the cases (88%) were transported by EMS, and there were 13 total deaths at the scene (0.2%).
Nichols found the low incidence of worsening clinical status particularly striking. “This is further evidence of a critically important point — naloxone is purely an opioid antagonist, and only binds to opioid receptors, such that if a person has not overdosed on opioids or does not otherwise have opioids in their system, naloxone will not have a significant effect and will not cause them harm,” Nichols said.
“The most common causes of harm are due to rapid reversal of overdose and the potential risks involved in the rapid reversal of opioid effects and potentially precipitating withdrawal, and as this paper demonstrates, these are exceedingly rare,” he said. “Given that, we should have an incredibly low barrier to administer naloxone appropriately.”
The study was limited by inability to know how many true pediatric opioid poisonings are managed by EMS, so future research could look at linking EMS and emergency room hospital databases.
Improved Self-Efficacy in Teens
Another study showed that a peer-to-peer training program increased teens’ knowledge about overdoses from 34% before training to 79% after (P < .0001), and it substantially improved their confidence in recognizing an overdose and administering naloxone.
Nichols said the study shows the importance of ensuring “that adolescents know how to keep themselves and their friends safe in the case that they or anyone they know does end up using illicit substances which either intentionally or unintentionally contain opioids.”
This study assessed a training program with 206 students in a Los Angeles County high school who were trained by their peers between November 2023 and March 2024. The training included trends in teen overdose deaths, defining what opioids and fentanyl are, recognizing an overdose, and responding to one with naloxone.
The teens were an average 16 years old, about evenly split between boys and girls, and mostly in 11th (40%) or 12th (28%) grade, though nearly a third (29%) were 9th graders.
The students’ knowledge about fentanyl’s presence in counterfeit pills increased from 21% before the training to 68% afterward, and their correct identification of an overdose increased from 47% of participants to 90%.
The students’ confidence and attitudes toward helping with an overdose also improved substantially after the training. About two thirds agreed that non-medical people should be able to carry naloxone before the training, and that rose to 88% agreeing after the training. The proportion who agreed they would be willing to assist in an overdose rose from 77% before to 89% after training.
More dramatically, the teens’ confidence after training more than doubled in recognizing an overdose (from 31% to 81%) and more than tripled in their ability to give naloxone during an overdose (from 26% to 83%).
“The critical piece to keep in mind is that the concern about opioid overdose is respiratory depression leading to a lack of oxygen getting to the brain,” Nichols explained. “In the event of an overdose, time is brain — the longer the brain is deprived of oxygen, the lower the chance of survival. There is no specific time at which naloxone would become less effective at reversing an overdose.”
Therefore, people do not need to know the exact time that someone may have overdosed or how long they have been passed out in order to administer naloxone, he said. “The sooner naloxone is administered to someone who is unresponsive and who may have overdosed on opioids, the higher the likelihood of a successful reversal of an overdose and of saving a life.”
The peer-to-peer program was sponsored by the CARLOW Center for Medical Innovation, and the EMS study used no external funding. The authors of both studies and Marino had no disclosures. Nichols has consulted or clinically advised TV shows and health tech startup companies and has no disclosures related to naloxone or the pharmaceutical industry.
A version of this article first appeared on Medscape.com.
FROM AAP 2024