User login
For MD-IQ use only
Tribal Health Officials Work To Fill Vaccination Gaps as Measles Outbreak Spreads
RAPID CITY, S.D. — Cassandra Palmier had been meaning to get her son the second and final dose of the measles vaccine. But car problems made it difficult to get to the doctor.
So she pounced on the opportunity to get him vaccinated after learning that a mobile clinic would be visiting her neighborhood.
“I was definitely concerned about the epidemic and the measles,” Palmier, a member of the Oglala Sioux Tribe, said at the June event. “I wanted to do my part.”
So did her son, Makaito Cuny.
“I’m not going to be scared,” the 5-year-old announced as he walked onto the bus containing the clinic and hopped into an exam chair.
Makaito sat still as a nurse gave him the shot in his arm. “I did it!” he said while smiling at his mother.
The vaccine clinic was hosted by the Great Plains Tribal Leaders’ Health Board, which serves tribes across Iowa, Nebraska, and the Dakotas. It’s one way Native American tribes and organizations are responding to concerns about low measles vaccination rates and patients’ difficulty accessing health care as the disease spreads across the country.
Meghan O’Connell, the board’s chief public health officer, said it is also working with tribes that want to host vaccine clinics.
Elsewhere, tribal health organizations have launched social media campaigns, are making sure health providers are vaccinated, and are reaching out to the parents of unvaccinated children.
This spring, Project ECHO at the University of New Mexico hosted an online video series about measles aimed at health care professionals and organizations that serve Native American communities. The presenters outlined the basics of measles diagnosis and treatment, discussed culturally relevant communication strategies, and shared how tribes are responding to the outbreak.
Participants also strategized about ways to improve vaccination rates, said Harry Brown, a physician and an epidemiologist for the United South and Eastern Tribes, a nonprofit that works with 33 tribes in the Atlantic Coast and Southeast regions.
“It’s a pretty hot topic right now in Indian Country and I think a lot of people are being proactive,” he said.
Measles can survive for up to two hours in the air in a space where an infected person has been, sickening up to 90% of people who aren’t vaccinated, according to the Centers for Disease Control and Prevention.
The U.S. has had 1,319 confirmed cases of measles this year as of July 23, according to the CDC. It’s the largest outbreak in the U.S. since 1992. Ninety-two percent of the 2025 cases involve unvaccinated patients or people with an unknown vaccination status. Three people had died in the U.S. and 165 had been hospitalized as of July 23.
O’Connell said data on Native Americans’ vaccination rates is imperfect but that it suggests a lower percentage of them have received measles shots than the overall U.S. population.
The limited national data on measles vaccination rates for Native Americans is based on small surveys of people who self-identify as Native American. Some show that Native Americans have slightly lower measles vaccination rates, while others show significant gaps.
Data from some states, including South Dakota and Montana, shows that Native Americans are less likely than white children to be vaccinated on schedule.
The national measles vaccination rate is significantly lower for Native Americans who use the mostly rural Indian Health Service. About 76% of children 16 to 27 months old had gotten the first shot, according to data collected by the agency during recent patient visits at 156 clinics. That’s a 10-percentage-point drop from 10 years ago.
But the IHS data shows that its patients are at least as likely as other children to have received both recommended measles shots by the time they’re 17. O’Connell said it’s unclear if currently unvaccinated patients will continue the trend of eventually getting up to date on their shots or if they will remain unvaccinated.
The immunization rate is probably higher for older children since schools require students to get vaccinated unless they have an exemption, Brown said. He said it’s important that parents get their children vaccinated on time, when they’re young and more at risk of being hospitalized or dying from the disease.
Native Americans may have lower vaccination rates due to the challenges they face in accessing shots and other health care, O’Connell said. Those on rural reservations may be an hour or more from a clinic. Or, like Palmier, they may not have reliable transportation.
Another reason, O’Connell said, is that some Native Americans distrust the Indian Health Service, which is chronically underfunded and understaffed. If the only nearby health care facility is run by the agency, patients may delay or skip care.
O’Connell and Brown said vaccine skepticism and mistrust of the entire health care system are growing in Native American communities, as has occurred elsewhere nationwide.
“Prior to social media, I think our population was pretty trustful of childhood vaccination. And American Indians have a long history of being severely impacted by infectious disease,” he said.
European colonizers’ arrival in the late 1400s brought new diseases, including measles, that killed tens of millions of Indigenous people in North and South America by the early 1600s. Native Americans have also had high mortality rates in modern pandemics, including the 1918-20 Spanish flu and COVID-19.
The Great Plains Tribal Leaders’ Health Board reacted quickly when measles cases began showing up near its headquarters in South Dakota this year. Nebraska health officials announced in late May that a child had measles in a rural part of the state, close to the Pine Ridge Indian Reservation. Then, four people from the Rapid City area got sick later that month and into the middle of June.
“Our phones really rang off the hook” once that news came out, said Darren Crowe, a vice president at the board’s Oyate Health Center in Rapid City. He said parents wanted to know if their children were up to date on their measles vaccines.
Crowe said the health board ordered extra masks, created a measles command team that meets daily, and called parents when its online database showed their children needed a shot.
Brown praised that approach.
“It takes a concerted outreach effort that goes individual to individual,” he said, adding that his organization helped the Mississippi Band of Choctaw Indians and the Alabama-Coushatta Tribe of Texas with similar efforts.
Brown said reaching specific families can be a challenge in some low-income Native American communities, where many people’s phone numbers frequently change since they use temporary prepaid plans.
Once a health worker reaches a parent, Brown said, they should listen and ask questions before sharing the importance of the vaccine against measles, mumps, and rubella.
“Rather than trying to preach to somebody and beat them over the head with data or whatever to convince them that this is what they need to do, you start out by finding out where they are,” he said. “So, ‘Tell me about your experience with vaccination. Tell me what you know about vaccination.’”
Most people agree to immunize their children when presented with helpful information in a nonjudgmental way, Brown said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
RAPID CITY, S.D. — Cassandra Palmier had been meaning to get her son the second and final dose of the measles vaccine. But car problems made it difficult to get to the doctor.
So she pounced on the opportunity to get him vaccinated after learning that a mobile clinic would be visiting her neighborhood.
“I was definitely concerned about the epidemic and the measles,” Palmier, a member of the Oglala Sioux Tribe, said at the June event. “I wanted to do my part.”
So did her son, Makaito Cuny.
“I’m not going to be scared,” the 5-year-old announced as he walked onto the bus containing the clinic and hopped into an exam chair.
Makaito sat still as a nurse gave him the shot in his arm. “I did it!” he said while smiling at his mother.
The vaccine clinic was hosted by the Great Plains Tribal Leaders’ Health Board, which serves tribes across Iowa, Nebraska, and the Dakotas. It’s one way Native American tribes and organizations are responding to concerns about low measles vaccination rates and patients’ difficulty accessing health care as the disease spreads across the country.
Meghan O’Connell, the board’s chief public health officer, said it is also working with tribes that want to host vaccine clinics.
Elsewhere, tribal health organizations have launched social media campaigns, are making sure health providers are vaccinated, and are reaching out to the parents of unvaccinated children.
This spring, Project ECHO at the University of New Mexico hosted an online video series about measles aimed at health care professionals and organizations that serve Native American communities. The presenters outlined the basics of measles diagnosis and treatment, discussed culturally relevant communication strategies, and shared how tribes are responding to the outbreak.
Participants also strategized about ways to improve vaccination rates, said Harry Brown, a physician and an epidemiologist for the United South and Eastern Tribes, a nonprofit that works with 33 tribes in the Atlantic Coast and Southeast regions.
“It’s a pretty hot topic right now in Indian Country and I think a lot of people are being proactive,” he said.
Measles can survive for up to two hours in the air in a space where an infected person has been, sickening up to 90% of people who aren’t vaccinated, according to the Centers for Disease Control and Prevention.
The U.S. has had 1,319 confirmed cases of measles this year as of July 23, according to the CDC. It’s the largest outbreak in the U.S. since 1992. Ninety-two percent of the 2025 cases involve unvaccinated patients or people with an unknown vaccination status. Three people had died in the U.S. and 165 had been hospitalized as of July 23.
O’Connell said data on Native Americans’ vaccination rates is imperfect but that it suggests a lower percentage of them have received measles shots than the overall U.S. population.
The limited national data on measles vaccination rates for Native Americans is based on small surveys of people who self-identify as Native American. Some show that Native Americans have slightly lower measles vaccination rates, while others show significant gaps.
Data from some states, including South Dakota and Montana, shows that Native Americans are less likely than white children to be vaccinated on schedule.
The national measles vaccination rate is significantly lower for Native Americans who use the mostly rural Indian Health Service. About 76% of children 16 to 27 months old had gotten the first shot, according to data collected by the agency during recent patient visits at 156 clinics. That’s a 10-percentage-point drop from 10 years ago.
But the IHS data shows that its patients are at least as likely as other children to have received both recommended measles shots by the time they’re 17. O’Connell said it’s unclear if currently unvaccinated patients will continue the trend of eventually getting up to date on their shots or if they will remain unvaccinated.
The immunization rate is probably higher for older children since schools require students to get vaccinated unless they have an exemption, Brown said. He said it’s important that parents get their children vaccinated on time, when they’re young and more at risk of being hospitalized or dying from the disease.
Native Americans may have lower vaccination rates due to the challenges they face in accessing shots and other health care, O’Connell said. Those on rural reservations may be an hour or more from a clinic. Or, like Palmier, they may not have reliable transportation.
Another reason, O’Connell said, is that some Native Americans distrust the Indian Health Service, which is chronically underfunded and understaffed. If the only nearby health care facility is run by the agency, patients may delay or skip care.
O’Connell and Brown said vaccine skepticism and mistrust of the entire health care system are growing in Native American communities, as has occurred elsewhere nationwide.
“Prior to social media, I think our population was pretty trustful of childhood vaccination. And American Indians have a long history of being severely impacted by infectious disease,” he said.
European colonizers’ arrival in the late 1400s brought new diseases, including measles, that killed tens of millions of Indigenous people in North and South America by the early 1600s. Native Americans have also had high mortality rates in modern pandemics, including the 1918-20 Spanish flu and COVID-19.
The Great Plains Tribal Leaders’ Health Board reacted quickly when measles cases began showing up near its headquarters in South Dakota this year. Nebraska health officials announced in late May that a child had measles in a rural part of the state, close to the Pine Ridge Indian Reservation. Then, four people from the Rapid City area got sick later that month and into the middle of June.
“Our phones really rang off the hook” once that news came out, said Darren Crowe, a vice president at the board’s Oyate Health Center in Rapid City. He said parents wanted to know if their children were up to date on their measles vaccines.
Crowe said the health board ordered extra masks, created a measles command team that meets daily, and called parents when its online database showed their children needed a shot.
Brown praised that approach.
“It takes a concerted outreach effort that goes individual to individual,” he said, adding that his organization helped the Mississippi Band of Choctaw Indians and the Alabama-Coushatta Tribe of Texas with similar efforts.
Brown said reaching specific families can be a challenge in some low-income Native American communities, where many people’s phone numbers frequently change since they use temporary prepaid plans.
Once a health worker reaches a parent, Brown said, they should listen and ask questions before sharing the importance of the vaccine against measles, mumps, and rubella.
“Rather than trying to preach to somebody and beat them over the head with data or whatever to convince them that this is what they need to do, you start out by finding out where they are,” he said. “So, ‘Tell me about your experience with vaccination. Tell me what you know about vaccination.’”
Most people agree to immunize their children when presented with helpful information in a nonjudgmental way, Brown said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
RAPID CITY, S.D. — Cassandra Palmier had been meaning to get her son the second and final dose of the measles vaccine. But car problems made it difficult to get to the doctor.
So she pounced on the opportunity to get him vaccinated after learning that a mobile clinic would be visiting her neighborhood.
“I was definitely concerned about the epidemic and the measles,” Palmier, a member of the Oglala Sioux Tribe, said at the June event. “I wanted to do my part.”
So did her son, Makaito Cuny.
“I’m not going to be scared,” the 5-year-old announced as he walked onto the bus containing the clinic and hopped into an exam chair.
Makaito sat still as a nurse gave him the shot in his arm. “I did it!” he said while smiling at his mother.
The vaccine clinic was hosted by the Great Plains Tribal Leaders’ Health Board, which serves tribes across Iowa, Nebraska, and the Dakotas. It’s one way Native American tribes and organizations are responding to concerns about low measles vaccination rates and patients’ difficulty accessing health care as the disease spreads across the country.
Meghan O’Connell, the board’s chief public health officer, said it is also working with tribes that want to host vaccine clinics.
Elsewhere, tribal health organizations have launched social media campaigns, are making sure health providers are vaccinated, and are reaching out to the parents of unvaccinated children.
This spring, Project ECHO at the University of New Mexico hosted an online video series about measles aimed at health care professionals and organizations that serve Native American communities. The presenters outlined the basics of measles diagnosis and treatment, discussed culturally relevant communication strategies, and shared how tribes are responding to the outbreak.
Participants also strategized about ways to improve vaccination rates, said Harry Brown, a physician and an epidemiologist for the United South and Eastern Tribes, a nonprofit that works with 33 tribes in the Atlantic Coast and Southeast regions.
“It’s a pretty hot topic right now in Indian Country and I think a lot of people are being proactive,” he said.
Measles can survive for up to two hours in the air in a space where an infected person has been, sickening up to 90% of people who aren’t vaccinated, according to the Centers for Disease Control and Prevention.
The U.S. has had 1,319 confirmed cases of measles this year as of July 23, according to the CDC. It’s the largest outbreak in the U.S. since 1992. Ninety-two percent of the 2025 cases involve unvaccinated patients or people with an unknown vaccination status. Three people had died in the U.S. and 165 had been hospitalized as of July 23.
O’Connell said data on Native Americans’ vaccination rates is imperfect but that it suggests a lower percentage of them have received measles shots than the overall U.S. population.
The limited national data on measles vaccination rates for Native Americans is based on small surveys of people who self-identify as Native American. Some show that Native Americans have slightly lower measles vaccination rates, while others show significant gaps.
Data from some states, including South Dakota and Montana, shows that Native Americans are less likely than white children to be vaccinated on schedule.
The national measles vaccination rate is significantly lower for Native Americans who use the mostly rural Indian Health Service. About 76% of children 16 to 27 months old had gotten the first shot, according to data collected by the agency during recent patient visits at 156 clinics. That’s a 10-percentage-point drop from 10 years ago.
But the IHS data shows that its patients are at least as likely as other children to have received both recommended measles shots by the time they’re 17. O’Connell said it’s unclear if currently unvaccinated patients will continue the trend of eventually getting up to date on their shots or if they will remain unvaccinated.
The immunization rate is probably higher for older children since schools require students to get vaccinated unless they have an exemption, Brown said. He said it’s important that parents get their children vaccinated on time, when they’re young and more at risk of being hospitalized or dying from the disease.
Native Americans may have lower vaccination rates due to the challenges they face in accessing shots and other health care, O’Connell said. Those on rural reservations may be an hour or more from a clinic. Or, like Palmier, they may not have reliable transportation.
Another reason, O’Connell said, is that some Native Americans distrust the Indian Health Service, which is chronically underfunded and understaffed. If the only nearby health care facility is run by the agency, patients may delay or skip care.
O’Connell and Brown said vaccine skepticism and mistrust of the entire health care system are growing in Native American communities, as has occurred elsewhere nationwide.
“Prior to social media, I think our population was pretty trustful of childhood vaccination. And American Indians have a long history of being severely impacted by infectious disease,” he said.
European colonizers’ arrival in the late 1400s brought new diseases, including measles, that killed tens of millions of Indigenous people in North and South America by the early 1600s. Native Americans have also had high mortality rates in modern pandemics, including the 1918-20 Spanish flu and COVID-19.
The Great Plains Tribal Leaders’ Health Board reacted quickly when measles cases began showing up near its headquarters in South Dakota this year. Nebraska health officials announced in late May that a child had measles in a rural part of the state, close to the Pine Ridge Indian Reservation. Then, four people from the Rapid City area got sick later that month and into the middle of June.
“Our phones really rang off the hook” once that news came out, said Darren Crowe, a vice president at the board’s Oyate Health Center in Rapid City. He said parents wanted to know if their children were up to date on their measles vaccines.
Crowe said the health board ordered extra masks, created a measles command team that meets daily, and called parents when its online database showed their children needed a shot.
Brown praised that approach.
“It takes a concerted outreach effort that goes individual to individual,” he said, adding that his organization helped the Mississippi Band of Choctaw Indians and the Alabama-Coushatta Tribe of Texas with similar efforts.
Brown said reaching specific families can be a challenge in some low-income Native American communities, where many people’s phone numbers frequently change since they use temporary prepaid plans.
Once a health worker reaches a parent, Brown said, they should listen and ask questions before sharing the importance of the vaccine against measles, mumps, and rubella.
“Rather than trying to preach to somebody and beat them over the head with data or whatever to convince them that this is what they need to do, you start out by finding out where they are,” he said. “So, ‘Tell me about your experience with vaccination. Tell me what you know about vaccination.’”
Most people agree to immunize their children when presented with helpful information in a nonjudgmental way, Brown said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Federal Health Care Data Trends 2025
Federal Health Care Data Trends 2025
.jpg)
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics.
Topics include:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics.
Topics include:
Federal Health Care Data Trends is a special supplement to Federal Practitioner, showcasing the latest research in health care for veterans and active-duty military members via compelling infographics.
Topics include:
Federal Health Care Data Trends 2025
Federal Health Care Data Trends 2025
Pedunculated Pink Papule on the Nose
THE DIAGNOSIS: Pedunculated Lipofibroma
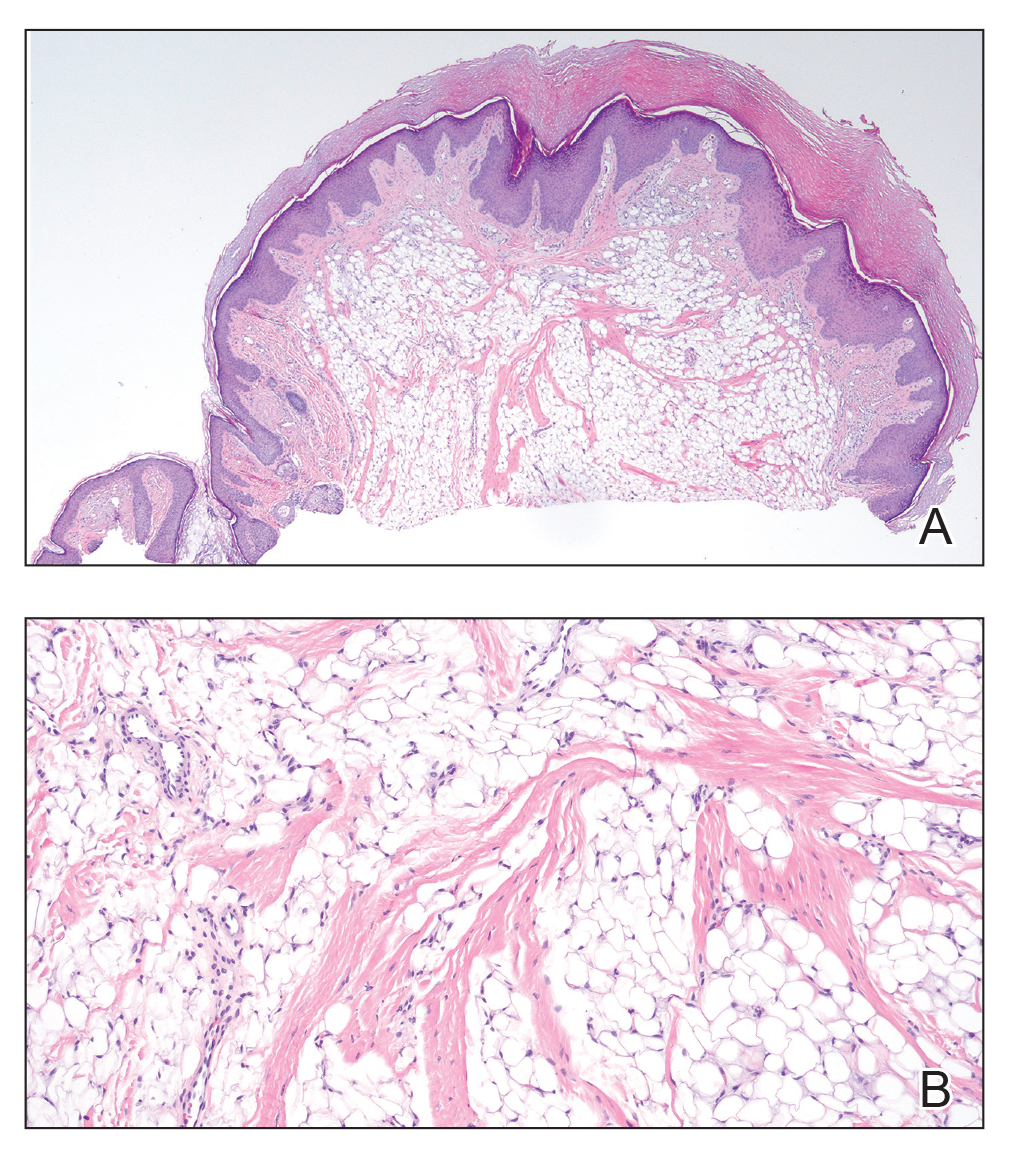
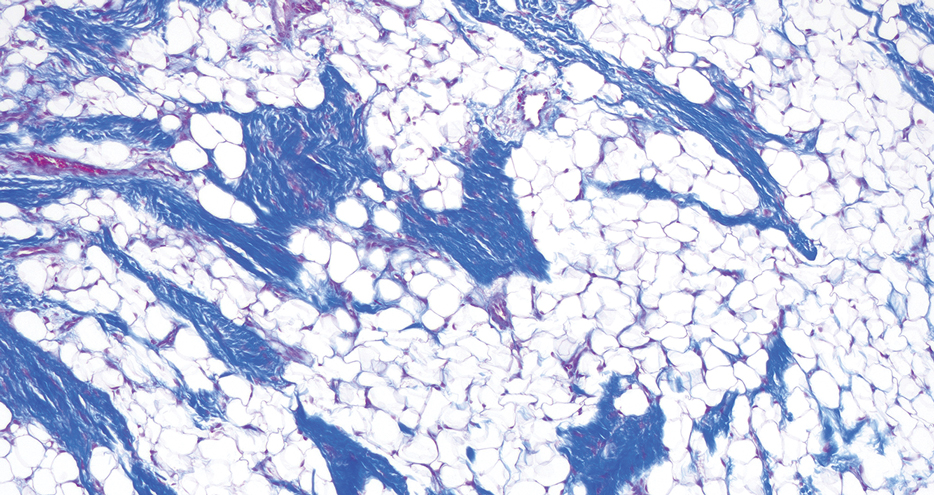
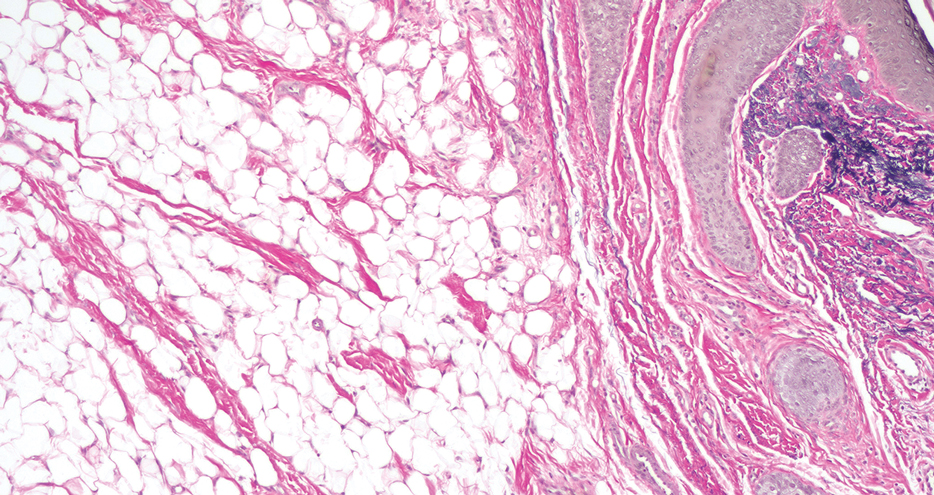
Histopathology confirmed a pedunculated/polypoid lesion with intradermal lobules of adipocytes/mature adipose tissue admixed with connective tissue bundles and vascular ectasias. Overlying epidermal acanthosis with slight papillomatosis and hyperkeratosis was present (Figure 1). Masson trichrome staining highlighted admixed collagen bundles (Figure 2). Verhoeff–van Gieson staining showed marked reduction in elastic fibers (Figure 3). Immunostaining was negative for smooth muscle actin and desmin. A diagnosis of pedunculated lipofibroma on the nose was made based on both clinical and histopathologic findings.
Pedunculated lipofibroma (or solitary lipofibroma) is the solitary form of nevus lipomatosus cutaneous superficialis (NLCS).7 First described by Hoffmann and Zurhelle1 in 1921, NLCS is an uncommon benign hamartomatous cutaneous lesion/connective tissue nevus that also has a classic multiple form.1-13 The etiology of NLCS remains unclear, but several theories have been proposed to explain its pathogenesis, including deposition of adipocytes secondary to degenerative changes in dermal connective tissue, focal/local heterotopic development of adipose tissue, and derivation from differentiating lipoblasts (preadipose tissue) originating from precursor vascular or perivascular cells.2-13
Pedunculated lipofibroma usually develops during the third to sixth decades of life and manifests as a single cutaneous lesion with a smooth surface, often on a non–pelvic girdle location.7-13 No particular predilection sites are noted, with lesions reported on the arm, axilla, back, upper thigh, knee, and sole.5,12 There are rare reports of this type of NLCS on the ear, scalp, forehead, or eyelid.7-11
In the classic form of NLCS, multiple cutaneous lesions are present at birth or develop within the first 2 to 3 decades of life.2-6 Lesions consist of soft, nontender, pedunculated, flesh-colored or yellowish papules and nodules with a verrucoid or cerebriform surface that may later coalesce to form plaques.2-6 Predilection sites include the pelvic girdle, buttocks, sacral and coccygeal regions, and upper posterior thighs, with a linear or zosteriform pattern of distribution.2-6 Rarely, the classic form can arise in elderly patients and/or at an atypical anatomic location (eg, clitoris,3 shoulder,5 thorax,5 abdomen5) and can demonstrate extension of lesions across the midline.4 Rare cases of classic NLCS on the scalp2 and face3-6 have been reported, including lesions localized to the nose3 and chin4 and others extending from the right mandible to the neck5 and right lower lip to the submandibular/posteriorateral cervical region.6 In some cases, lesions clinically resemble plane xanthoma4 and localized scleroderma.6
Adotama et al13 proposed a set of clinical features to differentiate classic NLCS, pedunculated lipofibroma (solitary NLCS), and fibroepithelial polyp with adipocytes (distinguished by their furrowed surface, hyperpigmentation, and anatomic predilection for the neck and axilla). Lesions are asymptomatic in both forms of NLCS.2-13 Family history or predominant sex involvement have not been reported in either clinical type.2-13 Reported associations with NLCS include a number of endocrinologic conditions including diabetes.7 Other coexisting skin findings can include café-au-lait macules, leukodermic (white) spots, overlying hypertrichosis, comedolike alterations, angiokeratoma, hemangioma, and folliculosebaceous cystic hamartoma.4 None of these were evident in our patient.
Lesions from both types of NLCS are indistinguishable on histopathology, characterized by the presence of a central core of ectopic mature adipocytes in the papillary/reticular dermis.2-13 Additional light microscopic features (some seen in our case) have been described, including thickened collagen bundles, reduction of elastic fibers, increased numbers of fibroblasts and/or mast cells, increased (small-vessel) vascularity, focal mucin deposition/myxoid degeneration, a mild perivascular lymphocytic infiltrate, attenuation of adnexal structures, and abnormalities of the epidermis (eg, surface ulceration).2-13
Prior to biopsy, the differential diagnosis in our patient included angiofibroma, pyogenic granuloma, and basal cell carcinoma given the exophytic, pink, papular appearance of the lesion; however, the histopathologic differential diagnosis included angiofibroma, angiomyolipoma, lymphangioma, nevus sebaceus, and spindle cell lipoma (SCL). In angiofibroma, a dermal proliferation of stellate fibroblasts, dilated blood vessels, and collagenous stroma are seen. Cutaneous angiomyolipoma demonstrates smooth muscle bundles in addition to thickened blood vessels and variable proportions of mature adipocytes. Lymphangioma is characterized by dilated lymph channels lined by flat endothelial cells. Nevus sebaceus shows superficial immature and abnormally formed pilosebaceous units, with epidermal papillomatosis.
Rare cases of SCL on the nose have been described.14 Similar to pedunculated lipofibroma, reported examples demonstrate mature univacuolar adipocytes with thick collagen fibers and bland uniform spindle cells. Unlike the lesion seen in our patient, nasal SCL may be clinically mobile and typically is localized to the subcutaneous tissue, although dermal tumors also occur.14 Variably reported histopathologic findings in nasal SCL include circumscription/encapsulation, spindle cells arranged in short fascicles with nuclear palisading, a myxoid/mucinous interstitial matrix, and/or multinucleated giant cells—all light microscopic features that were not identified in our case; however, variable proportions of adipocytic, fibrous, and myxoid components among reported examples of SCL on the nose14 can make distinction from pedunculated lipofibroma difficult, as both are benign lipomatous tumor variants.
Clinically, pedunculated lipofibroma may be confused with more common benign cutaneous lesions and must be distinguished from other fibrolipomatous lesions on the nose. Specifically, the differential diagnosis includes benign cutaneous papillomas such as acrochordon, angiofibroma, melanocytic nevi, neurofibroma, nevus sebaceus, lymphangioma, and eccrine poroma.7-13 These all can be readily excluded on histopathology. Pedunculated lipofibroma on the nose, as in our patient, must be distinguished from fibrolipoma15 and dendritic myxofibrolipoma.16 Fibrolipoma is a subcutaneous proliferation of mature adipose tissue and fibrous tissue and comprises 1.6% of all facial lipomas reported worldwide.15 Dendritic myxofibrolipoma is a recently described benign soft-tissue tumor characterized by an admixture of mature adipose tissue, spindle and stellate cells, and an abundant myxoid stroma with prominent collagenization.16
Treatment of pedunculated lipofibroma on the nose is not indicated except for cosmetic reasons, in which case simple surgical excision would be considered satisfactory. Following biopsy, no further treatment was pursued in our patient.
- Hoffmann E, Zurhelle E. Uber einen naevus lipomatodes cutaneous superficialis der linken Glutaalgegend. Arch Derm Syph. 1921;130:327-333.
- Chanoki M, Isukos S, Suzuki S, et al. Nevus lipomatosus cutaneus superficialis of the scalp. Cutis. 1989;43:143-144.
- Sáez Rodríguez M, Rodríguez-Martin M, Carnerero A, et al. Naevus lipomatosus cutaneous superficialis on the nose. J Eur Acad Dermatol Venereol. 2005;19:751-752.
- Hassab-El-Naby HMM, Rageh MA. Adult-onset nevus lipomatosus cutaneous superficialis mimicking plane xanthoma. J Clin Aesthet Dermatol. 2022;15:10-11.
- Park HJ, Park CJ, Yi JY, et al. Nevus lipomatosus superficialis on the face. Int J Dermatol. 1997;36:435-437.
- Ioannidou DJ, Stefanidou MP, Panayiotides JG, et al. Nevus lipomatosus cutaneous superficialis (Hoffman-Zurhelle) with localized scleroderma like appearance. Int J Dermatol. 2001;40:54-57.
- Nogita T, Wong TY, Hidano A, et al. Pedunculated lipofibroma. a clinicopathologic study of thirty-two cases supporting a simplified nomenclature. J Am Acad Dermatol. 1994;31(2 pt 1):235-240.
- Sawada Y. Solitary nevus lipomatosus superficialis on the forehead. Ann Plast Surg. 1986;16:356-358.
- Knoth W. Uber Naevus lipomatosus cutaneus superficialis Hoffmann-Zurhelle und uber Naevus naevocellularis partim lipomatodes. Dermatologica. 1962;125:161.
- Weitzner S. Solitary naevus lipomatosus cutaneus superficialis of scalp. Arch Dermatol. 1968;97:540-542.
- Kaw P, Carlson A, Meyer DR. Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. Ophthalmic Plast Reconstr Surg. 2005;21:74-76.
- Vano-Galvan S, Moreno C, Vano-Galvan E, et al. Solitary naevus lipomatosus cutaneous superficialis on the sole. Eur J Dermatol. 2008;18:353-354.
- Adotama P, Hutson SD, Rieder EA, et al. Revisiting solitary pedunculated lipofibromas. Am J Clin Pathol. 2021;156:954-957.
- Kubin ME, Lantto U, Lindgren O, et al. A rare, recurrent spindle cell lipoma of the nose. Acta Derm Venereol. 2021;101:adv00571.
- Jung SN, Shin JW, Kwon H, et al. Fibrolipoma of the tip of the nose. J Craniofac Surg. 2009;20:555-556.
- Han XC, Zheng LQ, Shang XL. Dendritic fibromyxolipoma on the nasal tip in an old patient. Int J Clin Exp Pathol. 2014;7:7064-7067.
THE DIAGNOSIS: Pedunculated Lipofibroma
Histopathology confirmed a pedunculated/polypoid lesion with intradermal lobules of adipocytes/mature adipose tissue admixed with connective tissue bundles and vascular ectasias. Overlying epidermal acanthosis with slight papillomatosis and hyperkeratosis was present (Figure 1). Masson trichrome staining highlighted admixed collagen bundles (Figure 2). Verhoeff–van Gieson staining showed marked reduction in elastic fibers (Figure 3). Immunostaining was negative for smooth muscle actin and desmin. A diagnosis of pedunculated lipofibroma on the nose was made based on both clinical and histopathologic findings.
Pedunculated lipofibroma (or solitary lipofibroma) is the solitary form of nevus lipomatosus cutaneous superficialis (NLCS).7 First described by Hoffmann and Zurhelle1 in 1921, NLCS is an uncommon benign hamartomatous cutaneous lesion/connective tissue nevus that also has a classic multiple form.1-13 The etiology of NLCS remains unclear, but several theories have been proposed to explain its pathogenesis, including deposition of adipocytes secondary to degenerative changes in dermal connective tissue, focal/local heterotopic development of adipose tissue, and derivation from differentiating lipoblasts (preadipose tissue) originating from precursor vascular or perivascular cells.2-13
Pedunculated lipofibroma usually develops during the third to sixth decades of life and manifests as a single cutaneous lesion with a smooth surface, often on a non–pelvic girdle location.7-13 No particular predilection sites are noted, with lesions reported on the arm, axilla, back, upper thigh, knee, and sole.5,12 There are rare reports of this type of NLCS on the ear, scalp, forehead, or eyelid.7-11
In the classic form of NLCS, multiple cutaneous lesions are present at birth or develop within the first 2 to 3 decades of life.2-6 Lesions consist of soft, nontender, pedunculated, flesh-colored or yellowish papules and nodules with a verrucoid or cerebriform surface that may later coalesce to form plaques.2-6 Predilection sites include the pelvic girdle, buttocks, sacral and coccygeal regions, and upper posterior thighs, with a linear or zosteriform pattern of distribution.2-6 Rarely, the classic form can arise in elderly patients and/or at an atypical anatomic location (eg, clitoris,3 shoulder,5 thorax,5 abdomen5) and can demonstrate extension of lesions across the midline.4 Rare cases of classic NLCS on the scalp2 and face3-6 have been reported, including lesions localized to the nose3 and chin4 and others extending from the right mandible to the neck5 and right lower lip to the submandibular/posteriorateral cervical region.6 In some cases, lesions clinically resemble plane xanthoma4 and localized scleroderma.6
Adotama et al13 proposed a set of clinical features to differentiate classic NLCS, pedunculated lipofibroma (solitary NLCS), and fibroepithelial polyp with adipocytes (distinguished by their furrowed surface, hyperpigmentation, and anatomic predilection for the neck and axilla). Lesions are asymptomatic in both forms of NLCS.2-13 Family history or predominant sex involvement have not been reported in either clinical type.2-13 Reported associations with NLCS include a number of endocrinologic conditions including diabetes.7 Other coexisting skin findings can include café-au-lait macules, leukodermic (white) spots, overlying hypertrichosis, comedolike alterations, angiokeratoma, hemangioma, and folliculosebaceous cystic hamartoma.4 None of these were evident in our patient.
Lesions from both types of NLCS are indistinguishable on histopathology, characterized by the presence of a central core of ectopic mature adipocytes in the papillary/reticular dermis.2-13 Additional light microscopic features (some seen in our case) have been described, including thickened collagen bundles, reduction of elastic fibers, increased numbers of fibroblasts and/or mast cells, increased (small-vessel) vascularity, focal mucin deposition/myxoid degeneration, a mild perivascular lymphocytic infiltrate, attenuation of adnexal structures, and abnormalities of the epidermis (eg, surface ulceration).2-13
Prior to biopsy, the differential diagnosis in our patient included angiofibroma, pyogenic granuloma, and basal cell carcinoma given the exophytic, pink, papular appearance of the lesion; however, the histopathologic differential diagnosis included angiofibroma, angiomyolipoma, lymphangioma, nevus sebaceus, and spindle cell lipoma (SCL). In angiofibroma, a dermal proliferation of stellate fibroblasts, dilated blood vessels, and collagenous stroma are seen. Cutaneous angiomyolipoma demonstrates smooth muscle bundles in addition to thickened blood vessels and variable proportions of mature adipocytes. Lymphangioma is characterized by dilated lymph channels lined by flat endothelial cells. Nevus sebaceus shows superficial immature and abnormally formed pilosebaceous units, with epidermal papillomatosis.
Rare cases of SCL on the nose have been described.14 Similar to pedunculated lipofibroma, reported examples demonstrate mature univacuolar adipocytes with thick collagen fibers and bland uniform spindle cells. Unlike the lesion seen in our patient, nasal SCL may be clinically mobile and typically is localized to the subcutaneous tissue, although dermal tumors also occur.14 Variably reported histopathologic findings in nasal SCL include circumscription/encapsulation, spindle cells arranged in short fascicles with nuclear palisading, a myxoid/mucinous interstitial matrix, and/or multinucleated giant cells—all light microscopic features that were not identified in our case; however, variable proportions of adipocytic, fibrous, and myxoid components among reported examples of SCL on the nose14 can make distinction from pedunculated lipofibroma difficult, as both are benign lipomatous tumor variants.
Clinically, pedunculated lipofibroma may be confused with more common benign cutaneous lesions and must be distinguished from other fibrolipomatous lesions on the nose. Specifically, the differential diagnosis includes benign cutaneous papillomas such as acrochordon, angiofibroma, melanocytic nevi, neurofibroma, nevus sebaceus, lymphangioma, and eccrine poroma.7-13 These all can be readily excluded on histopathology. Pedunculated lipofibroma on the nose, as in our patient, must be distinguished from fibrolipoma15 and dendritic myxofibrolipoma.16 Fibrolipoma is a subcutaneous proliferation of mature adipose tissue and fibrous tissue and comprises 1.6% of all facial lipomas reported worldwide.15 Dendritic myxofibrolipoma is a recently described benign soft-tissue tumor characterized by an admixture of mature adipose tissue, spindle and stellate cells, and an abundant myxoid stroma with prominent collagenization.16
Treatment of pedunculated lipofibroma on the nose is not indicated except for cosmetic reasons, in which case simple surgical excision would be considered satisfactory. Following biopsy, no further treatment was pursued in our patient.
THE DIAGNOSIS: Pedunculated Lipofibroma
Histopathology confirmed a pedunculated/polypoid lesion with intradermal lobules of adipocytes/mature adipose tissue admixed with connective tissue bundles and vascular ectasias. Overlying epidermal acanthosis with slight papillomatosis and hyperkeratosis was present (Figure 1). Masson trichrome staining highlighted admixed collagen bundles (Figure 2). Verhoeff–van Gieson staining showed marked reduction in elastic fibers (Figure 3). Immunostaining was negative for smooth muscle actin and desmin. A diagnosis of pedunculated lipofibroma on the nose was made based on both clinical and histopathologic findings.
Pedunculated lipofibroma (or solitary lipofibroma) is the solitary form of nevus lipomatosus cutaneous superficialis (NLCS).7 First described by Hoffmann and Zurhelle1 in 1921, NLCS is an uncommon benign hamartomatous cutaneous lesion/connective tissue nevus that also has a classic multiple form.1-13 The etiology of NLCS remains unclear, but several theories have been proposed to explain its pathogenesis, including deposition of adipocytes secondary to degenerative changes in dermal connective tissue, focal/local heterotopic development of adipose tissue, and derivation from differentiating lipoblasts (preadipose tissue) originating from precursor vascular or perivascular cells.2-13
Pedunculated lipofibroma usually develops during the third to sixth decades of life and manifests as a single cutaneous lesion with a smooth surface, often on a non–pelvic girdle location.7-13 No particular predilection sites are noted, with lesions reported on the arm, axilla, back, upper thigh, knee, and sole.5,12 There are rare reports of this type of NLCS on the ear, scalp, forehead, or eyelid.7-11
In the classic form of NLCS, multiple cutaneous lesions are present at birth or develop within the first 2 to 3 decades of life.2-6 Lesions consist of soft, nontender, pedunculated, flesh-colored or yellowish papules and nodules with a verrucoid or cerebriform surface that may later coalesce to form plaques.2-6 Predilection sites include the pelvic girdle, buttocks, sacral and coccygeal regions, and upper posterior thighs, with a linear or zosteriform pattern of distribution.2-6 Rarely, the classic form can arise in elderly patients and/or at an atypical anatomic location (eg, clitoris,3 shoulder,5 thorax,5 abdomen5) and can demonstrate extension of lesions across the midline.4 Rare cases of classic NLCS on the scalp2 and face3-6 have been reported, including lesions localized to the nose3 and chin4 and others extending from the right mandible to the neck5 and right lower lip to the submandibular/posteriorateral cervical region.6 In some cases, lesions clinically resemble plane xanthoma4 and localized scleroderma.6
Adotama et al13 proposed a set of clinical features to differentiate classic NLCS, pedunculated lipofibroma (solitary NLCS), and fibroepithelial polyp with adipocytes (distinguished by their furrowed surface, hyperpigmentation, and anatomic predilection for the neck and axilla). Lesions are asymptomatic in both forms of NLCS.2-13 Family history or predominant sex involvement have not been reported in either clinical type.2-13 Reported associations with NLCS include a number of endocrinologic conditions including diabetes.7 Other coexisting skin findings can include café-au-lait macules, leukodermic (white) spots, overlying hypertrichosis, comedolike alterations, angiokeratoma, hemangioma, and folliculosebaceous cystic hamartoma.4 None of these were evident in our patient.
Lesions from both types of NLCS are indistinguishable on histopathology, characterized by the presence of a central core of ectopic mature adipocytes in the papillary/reticular dermis.2-13 Additional light microscopic features (some seen in our case) have been described, including thickened collagen bundles, reduction of elastic fibers, increased numbers of fibroblasts and/or mast cells, increased (small-vessel) vascularity, focal mucin deposition/myxoid degeneration, a mild perivascular lymphocytic infiltrate, attenuation of adnexal structures, and abnormalities of the epidermis (eg, surface ulceration).2-13
Prior to biopsy, the differential diagnosis in our patient included angiofibroma, pyogenic granuloma, and basal cell carcinoma given the exophytic, pink, papular appearance of the lesion; however, the histopathologic differential diagnosis included angiofibroma, angiomyolipoma, lymphangioma, nevus sebaceus, and spindle cell lipoma (SCL). In angiofibroma, a dermal proliferation of stellate fibroblasts, dilated blood vessels, and collagenous stroma are seen. Cutaneous angiomyolipoma demonstrates smooth muscle bundles in addition to thickened blood vessels and variable proportions of mature adipocytes. Lymphangioma is characterized by dilated lymph channels lined by flat endothelial cells. Nevus sebaceus shows superficial immature and abnormally formed pilosebaceous units, with epidermal papillomatosis.
Rare cases of SCL on the nose have been described.14 Similar to pedunculated lipofibroma, reported examples demonstrate mature univacuolar adipocytes with thick collagen fibers and bland uniform spindle cells. Unlike the lesion seen in our patient, nasal SCL may be clinically mobile and typically is localized to the subcutaneous tissue, although dermal tumors also occur.14 Variably reported histopathologic findings in nasal SCL include circumscription/encapsulation, spindle cells arranged in short fascicles with nuclear palisading, a myxoid/mucinous interstitial matrix, and/or multinucleated giant cells—all light microscopic features that were not identified in our case; however, variable proportions of adipocytic, fibrous, and myxoid components among reported examples of SCL on the nose14 can make distinction from pedunculated lipofibroma difficult, as both are benign lipomatous tumor variants.
Clinically, pedunculated lipofibroma may be confused with more common benign cutaneous lesions and must be distinguished from other fibrolipomatous lesions on the nose. Specifically, the differential diagnosis includes benign cutaneous papillomas such as acrochordon, angiofibroma, melanocytic nevi, neurofibroma, nevus sebaceus, lymphangioma, and eccrine poroma.7-13 These all can be readily excluded on histopathology. Pedunculated lipofibroma on the nose, as in our patient, must be distinguished from fibrolipoma15 and dendritic myxofibrolipoma.16 Fibrolipoma is a subcutaneous proliferation of mature adipose tissue and fibrous tissue and comprises 1.6% of all facial lipomas reported worldwide.15 Dendritic myxofibrolipoma is a recently described benign soft-tissue tumor characterized by an admixture of mature adipose tissue, spindle and stellate cells, and an abundant myxoid stroma with prominent collagenization.16
Treatment of pedunculated lipofibroma on the nose is not indicated except for cosmetic reasons, in which case simple surgical excision would be considered satisfactory. Following biopsy, no further treatment was pursued in our patient.
- Hoffmann E, Zurhelle E. Uber einen naevus lipomatodes cutaneous superficialis der linken Glutaalgegend. Arch Derm Syph. 1921;130:327-333.
- Chanoki M, Isukos S, Suzuki S, et al. Nevus lipomatosus cutaneus superficialis of the scalp. Cutis. 1989;43:143-144.
- Sáez Rodríguez M, Rodríguez-Martin M, Carnerero A, et al. Naevus lipomatosus cutaneous superficialis on the nose. J Eur Acad Dermatol Venereol. 2005;19:751-752.
- Hassab-El-Naby HMM, Rageh MA. Adult-onset nevus lipomatosus cutaneous superficialis mimicking plane xanthoma. J Clin Aesthet Dermatol. 2022;15:10-11.
- Park HJ, Park CJ, Yi JY, et al. Nevus lipomatosus superficialis on the face. Int J Dermatol. 1997;36:435-437.
- Ioannidou DJ, Stefanidou MP, Panayiotides JG, et al. Nevus lipomatosus cutaneous superficialis (Hoffman-Zurhelle) with localized scleroderma like appearance. Int J Dermatol. 2001;40:54-57.
- Nogita T, Wong TY, Hidano A, et al. Pedunculated lipofibroma. a clinicopathologic study of thirty-two cases supporting a simplified nomenclature. J Am Acad Dermatol. 1994;31(2 pt 1):235-240.
- Sawada Y. Solitary nevus lipomatosus superficialis on the forehead. Ann Plast Surg. 1986;16:356-358.
- Knoth W. Uber Naevus lipomatosus cutaneus superficialis Hoffmann-Zurhelle und uber Naevus naevocellularis partim lipomatodes. Dermatologica. 1962;125:161.
- Weitzner S. Solitary naevus lipomatosus cutaneus superficialis of scalp. Arch Dermatol. 1968;97:540-542.
- Kaw P, Carlson A, Meyer DR. Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. Ophthalmic Plast Reconstr Surg. 2005;21:74-76.
- Vano-Galvan S, Moreno C, Vano-Galvan E, et al. Solitary naevus lipomatosus cutaneous superficialis on the sole. Eur J Dermatol. 2008;18:353-354.
- Adotama P, Hutson SD, Rieder EA, et al. Revisiting solitary pedunculated lipofibromas. Am J Clin Pathol. 2021;156:954-957.
- Kubin ME, Lantto U, Lindgren O, et al. A rare, recurrent spindle cell lipoma of the nose. Acta Derm Venereol. 2021;101:adv00571.
- Jung SN, Shin JW, Kwon H, et al. Fibrolipoma of the tip of the nose. J Craniofac Surg. 2009;20:555-556.
- Han XC, Zheng LQ, Shang XL. Dendritic fibromyxolipoma on the nasal tip in an old patient. Int J Clin Exp Pathol. 2014;7:7064-7067.
- Hoffmann E, Zurhelle E. Uber einen naevus lipomatodes cutaneous superficialis der linken Glutaalgegend. Arch Derm Syph. 1921;130:327-333.
- Chanoki M, Isukos S, Suzuki S, et al. Nevus lipomatosus cutaneus superficialis of the scalp. Cutis. 1989;43:143-144.
- Sáez Rodríguez M, Rodríguez-Martin M, Carnerero A, et al. Naevus lipomatosus cutaneous superficialis on the nose. J Eur Acad Dermatol Venereol. 2005;19:751-752.
- Hassab-El-Naby HMM, Rageh MA. Adult-onset nevus lipomatosus cutaneous superficialis mimicking plane xanthoma. J Clin Aesthet Dermatol. 2022;15:10-11.
- Park HJ, Park CJ, Yi JY, et al. Nevus lipomatosus superficialis on the face. Int J Dermatol. 1997;36:435-437.
- Ioannidou DJ, Stefanidou MP, Panayiotides JG, et al. Nevus lipomatosus cutaneous superficialis (Hoffman-Zurhelle) with localized scleroderma like appearance. Int J Dermatol. 2001;40:54-57.
- Nogita T, Wong TY, Hidano A, et al. Pedunculated lipofibroma. a clinicopathologic study of thirty-two cases supporting a simplified nomenclature. J Am Acad Dermatol. 1994;31(2 pt 1):235-240.
- Sawada Y. Solitary nevus lipomatosus superficialis on the forehead. Ann Plast Surg. 1986;16:356-358.
- Knoth W. Uber Naevus lipomatosus cutaneus superficialis Hoffmann-Zurhelle und uber Naevus naevocellularis partim lipomatodes. Dermatologica. 1962;125:161.
- Weitzner S. Solitary naevus lipomatosus cutaneus superficialis of scalp. Arch Dermatol. 1968;97:540-542.
- Kaw P, Carlson A, Meyer DR. Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. Ophthalmic Plast Reconstr Surg. 2005;21:74-76.
- Vano-Galvan S, Moreno C, Vano-Galvan E, et al. Solitary naevus lipomatosus cutaneous superficialis on the sole. Eur J Dermatol. 2008;18:353-354.
- Adotama P, Hutson SD, Rieder EA, et al. Revisiting solitary pedunculated lipofibromas. Am J Clin Pathol. 2021;156:954-957.
- Kubin ME, Lantto U, Lindgren O, et al. A rare, recurrent spindle cell lipoma of the nose. Acta Derm Venereol. 2021;101:adv00571.
- Jung SN, Shin JW, Kwon H, et al. Fibrolipoma of the tip of the nose. J Craniofac Surg. 2009;20:555-556.
- Han XC, Zheng LQ, Shang XL. Dendritic fibromyxolipoma on the nasal tip in an old patient. Int J Clin Exp Pathol. 2014;7:7064-7067.
A 60-year-old woman presented to the dermatology department with a 6-mm, firm, pink, nonulcerated, nonmobile papule on the right nasal side wall of 1 year’s duration. It had grown slowly and was asymptomatic with no tenderness or bleeding. No other skin lesions were noted on physical examination, and her medical history was otherwise unremarkable. A shave biopsy was performed.


What Effect Can a ‘Caring Message’ Intervention Have?
What Effect Can a ‘Caring Message’ Intervention Have?
Caring messages to veterans at risk for suicide come in many forms: cards, letters, phone calls, email, and text messages. Each message can have a major impact on the veteran’s mental health and their decision to use health care provided by the US Department of Veterans Affairs (VA). A recent study outlined ways to centralize that impact, ensuring the caring message reaches those who need it most.
The study examined the impact of the VA Veterans Crisis Line (VCL) caring letters intervention among veterans at increased psychiatric risk. It focused on veterans with ≥ 2 Veterans Health Administration (VHA) health service encounters within 24 months prior to VCL contact. The primary outcome was suicide-related events (SRE), including suicide attempts, intentional self-harm, and suicidal self-directed violence. Secondary outcomes included VHA health care use (all-cause inpatient and outpatient, mental health outpatient, mental health inpatient, and emergency department).
Of 186,514 VCL callers, 8.3% had a psychiatric hospitalization, 4.8% were flagged as high-risk by the REACH VET program, 6.2% had an SRE, and 12.9% met any of these criteria in the year prior to initial VCL contact. There was no association between caring letters and all-cause mortality or SRE, even though caring letters is one of the only interventions to demonstrate a reduction in suicide mortality as a randomized controlled trial.
While reducing suicide has not been the expected result, caring letters have consistently been associated with increased use of outpatient mental health services. The analysis found that veterans with and without indicators of elevated psychiatric risk were using services more. That, the researchers suggest, is more evidence that caring letters might prompt engagement with VHA care, even among veterans not identified as high risk.
Psychiatrist Jerome A. Motto, MD believed long-term supportive but nondemanding contact could reduce a suicidal person’s sense of isolation and enhance feelings of connectedness. His 1976 intervention established a plan to “exert a suicide prevention influence on high-risk persons who decline to enter the health care system.” In Motto’s 5-year follow-up study of 3,006 psychiatric inpatients, half of those who were not following their postdischarge treatment plan received calls or letters expressing interest in their well-being. Suicidal deaths were found to “diverge progressively,” leading Motto to claim the study showed “tentative evidence” that a high-risk population for suicide can be identified and that risk might be reduced through a systematic approach.
Despite those findings, the results of studies on repeated follow-up contact have been mixed. One review outlined how 5 studies showed a statistically significant reduction in suicidal behavior, 4 showed mixed results with trends toward a preventive effect, and 2 studies did not show a preventive effect.
In 2020, the VA launched an intervention for veterans who contacted the VCL. In the first 12 months, CLs were sent to > 100,000 veterans. In feedback interviews, participants described feeling appreciated, cared for, encouraged, and connected. They also said that the CLs helped them engage with community resources and made them more likely to seek VA care. Even veterans who were skeptical of the utility of the caring letters sometimes admitted keeping them.
Finding effective ways to prevent suicide among veterans has been a top priority for the VA. In 2021, then-US Surgeon General Jerome Adams issued a Call to Action that recommended using caring letters when gaps in care may exist, including following crisis line calls.
Caring messages to veterans at risk for suicide come in many forms: cards, letters, phone calls, email, and text messages. Each message can have a major impact on the veteran’s mental health and their decision to use health care provided by the US Department of Veterans Affairs (VA). A recent study outlined ways to centralize that impact, ensuring the caring message reaches those who need it most.
The study examined the impact of the VA Veterans Crisis Line (VCL) caring letters intervention among veterans at increased psychiatric risk. It focused on veterans with ≥ 2 Veterans Health Administration (VHA) health service encounters within 24 months prior to VCL contact. The primary outcome was suicide-related events (SRE), including suicide attempts, intentional self-harm, and suicidal self-directed violence. Secondary outcomes included VHA health care use (all-cause inpatient and outpatient, mental health outpatient, mental health inpatient, and emergency department).
Of 186,514 VCL callers, 8.3% had a psychiatric hospitalization, 4.8% were flagged as high-risk by the REACH VET program, 6.2% had an SRE, and 12.9% met any of these criteria in the year prior to initial VCL contact. There was no association between caring letters and all-cause mortality or SRE, even though caring letters is one of the only interventions to demonstrate a reduction in suicide mortality as a randomized controlled trial.
While reducing suicide has not been the expected result, caring letters have consistently been associated with increased use of outpatient mental health services. The analysis found that veterans with and without indicators of elevated psychiatric risk were using services more. That, the researchers suggest, is more evidence that caring letters might prompt engagement with VHA care, even among veterans not identified as high risk.
Psychiatrist Jerome A. Motto, MD believed long-term supportive but nondemanding contact could reduce a suicidal person’s sense of isolation and enhance feelings of connectedness. His 1976 intervention established a plan to “exert a suicide prevention influence on high-risk persons who decline to enter the health care system.” In Motto’s 5-year follow-up study of 3,006 psychiatric inpatients, half of those who were not following their postdischarge treatment plan received calls or letters expressing interest in their well-being. Suicidal deaths were found to “diverge progressively,” leading Motto to claim the study showed “tentative evidence” that a high-risk population for suicide can be identified and that risk might be reduced through a systematic approach.
Despite those findings, the results of studies on repeated follow-up contact have been mixed. One review outlined how 5 studies showed a statistically significant reduction in suicidal behavior, 4 showed mixed results with trends toward a preventive effect, and 2 studies did not show a preventive effect.
In 2020, the VA launched an intervention for veterans who contacted the VCL. In the first 12 months, CLs were sent to > 100,000 veterans. In feedback interviews, participants described feeling appreciated, cared for, encouraged, and connected. They also said that the CLs helped them engage with community resources and made them more likely to seek VA care. Even veterans who were skeptical of the utility of the caring letters sometimes admitted keeping them.
Finding effective ways to prevent suicide among veterans has been a top priority for the VA. In 2021, then-US Surgeon General Jerome Adams issued a Call to Action that recommended using caring letters when gaps in care may exist, including following crisis line calls.
Caring messages to veterans at risk for suicide come in many forms: cards, letters, phone calls, email, and text messages. Each message can have a major impact on the veteran’s mental health and their decision to use health care provided by the US Department of Veterans Affairs (VA). A recent study outlined ways to centralize that impact, ensuring the caring message reaches those who need it most.
The study examined the impact of the VA Veterans Crisis Line (VCL) caring letters intervention among veterans at increased psychiatric risk. It focused on veterans with ≥ 2 Veterans Health Administration (VHA) health service encounters within 24 months prior to VCL contact. The primary outcome was suicide-related events (SRE), including suicide attempts, intentional self-harm, and suicidal self-directed violence. Secondary outcomes included VHA health care use (all-cause inpatient and outpatient, mental health outpatient, mental health inpatient, and emergency department).
Of 186,514 VCL callers, 8.3% had a psychiatric hospitalization, 4.8% were flagged as high-risk by the REACH VET program, 6.2% had an SRE, and 12.9% met any of these criteria in the year prior to initial VCL contact. There was no association between caring letters and all-cause mortality or SRE, even though caring letters is one of the only interventions to demonstrate a reduction in suicide mortality as a randomized controlled trial.
While reducing suicide has not been the expected result, caring letters have consistently been associated with increased use of outpatient mental health services. The analysis found that veterans with and without indicators of elevated psychiatric risk were using services more. That, the researchers suggest, is more evidence that caring letters might prompt engagement with VHA care, even among veterans not identified as high risk.
Psychiatrist Jerome A. Motto, MD believed long-term supportive but nondemanding contact could reduce a suicidal person’s sense of isolation and enhance feelings of connectedness. His 1976 intervention established a plan to “exert a suicide prevention influence on high-risk persons who decline to enter the health care system.” In Motto’s 5-year follow-up study of 3,006 psychiatric inpatients, half of those who were not following their postdischarge treatment plan received calls or letters expressing interest in their well-being. Suicidal deaths were found to “diverge progressively,” leading Motto to claim the study showed “tentative evidence” that a high-risk population for suicide can be identified and that risk might be reduced through a systematic approach.
Despite those findings, the results of studies on repeated follow-up contact have been mixed. One review outlined how 5 studies showed a statistically significant reduction in suicidal behavior, 4 showed mixed results with trends toward a preventive effect, and 2 studies did not show a preventive effect.
In 2020, the VA launched an intervention for veterans who contacted the VCL. In the first 12 months, CLs were sent to > 100,000 veterans. In feedback interviews, participants described feeling appreciated, cared for, encouraged, and connected. They also said that the CLs helped them engage with community resources and made them more likely to seek VA care. Even veterans who were skeptical of the utility of the caring letters sometimes admitted keeping them.
Finding effective ways to prevent suicide among veterans has been a top priority for the VA. In 2021, then-US Surgeon General Jerome Adams issued a Call to Action that recommended using caring letters when gaps in care may exist, including following crisis line calls.
What Effect Can a ‘Caring Message’ Intervention Have?
What Effect Can a ‘Caring Message’ Intervention Have?
Military Service May Increase Risk for Early Menopause
Military Service May Increase Risk for Early Menopause
Traumatic and environmental exposures during military service may put women veterans at risk for early menopause, a recent longitudinal analysis of data from 668 women in the Gulf War Era Cohort Study found.
The study examined associations between possible early menopause (aged < 45 years) and participants’ Gulf War deployment, military environmental exposures (MEEs), Gulf War Illness, military sexual trauma (MST) and posttraumatic stress disorder (PTSD).
Of 384 Gulf War–deployed veterans, 63% reported MEEs and 26% reported MST during deployment. More than half (57%) of study participants (both Gulf War veterans and nondeployed veterans) met criteria for Gulf War Illness, and 23% met criteria for probable PTSD.
At follow-up, 15% of the women had possible early menopause—higher than population estimates for early menopause in the US, which range from 5% to 10%.
Gulf War deployment, Gulf War–related environmental exposures, and MST during deployment were not significantly associated with early menopause. However, both Gulf War Illness (odds ratio [OR], 1.83; 95% CI, 1.14 to 2.95) and probable PTSD (OR, 2.45; 95% CI, 1.54 to 3.90) were strongly associated with early menopause. Women with probable PTSD at baseline had more than double the odds of possible early menopause.
Previous research suggests that deployment, MEEs, and Gulf War Illness are broadly associated with adverse reproductive health conditions in women veterans. Exposure to persistent organic pollutants and combustion byproducts (eg, from industrial processes and burn pits) have been linked to ovarian dysfunction and oocyte destruction presumed to contribute to accelerated ovarian aging.
The average age for menopause in the US is 52 years. About 5% of women go through early menopause naturally. Early and premature (< 40 years) menopause may also result from a medical or surgical cause, such as a hysterectomy. Regardless the cause, early menopause can have a profound impact on a woman’s physical, emotional, and mental health. It is associated with premature mortality, poor bone health, sexual dysfunction, a 50% increased risk of cardiovascular disease, and 2-fold increased odds of depression.
“Sometimes we talk about menopause symptoms thinking that they're just sort of 1 brief point in time, but we're also talking about things that may affect women's health and functioning for a third or half of a lifespan,” Carolyn Gibson, PhD, MPH, said at the 2024 Spotlight on Women's Health Cyberseminar Series.
Gibson, a staff psychologist at the San Francisco Veterans Affairs (VA) Women’s Mental Health Program and lead author on the recent early-menopause study, pointed to some of the chronic physical health issues that might develop, such as cardiovascular disease, but also the psychological effects.
“It's just important,” she said during the Cyberseminar Series. “To think about the number of things that women in midlife tend to be juggling and managing, all of which may turn up the volume on symptom experience, effect of vulnerability to health and mental health challenges during this period.”
The findings of the study have clinical implications. Midlife women veterans (aged 45 to 64 years) are the largest group of women veterans enrolled in VA health care. Early menopause brings additional age-related care considerations. The authors advise prioritizing support for routine screening for menopause status and symptoms as well as gender-sensitive training, resources, and staffing to provide comprehensive, trauma-informed, evidence-based menopause care for women at any age.
Traumatic and environmental exposures during military service may put women veterans at risk for early menopause, a recent longitudinal analysis of data from 668 women in the Gulf War Era Cohort Study found.
The study examined associations between possible early menopause (aged < 45 years) and participants’ Gulf War deployment, military environmental exposures (MEEs), Gulf War Illness, military sexual trauma (MST) and posttraumatic stress disorder (PTSD).
Of 384 Gulf War–deployed veterans, 63% reported MEEs and 26% reported MST during deployment. More than half (57%) of study participants (both Gulf War veterans and nondeployed veterans) met criteria for Gulf War Illness, and 23% met criteria for probable PTSD.
At follow-up, 15% of the women had possible early menopause—higher than population estimates for early menopause in the US, which range from 5% to 10%.
Gulf War deployment, Gulf War–related environmental exposures, and MST during deployment were not significantly associated with early menopause. However, both Gulf War Illness (odds ratio [OR], 1.83; 95% CI, 1.14 to 2.95) and probable PTSD (OR, 2.45; 95% CI, 1.54 to 3.90) were strongly associated with early menopause. Women with probable PTSD at baseline had more than double the odds of possible early menopause.
Previous research suggests that deployment, MEEs, and Gulf War Illness are broadly associated with adverse reproductive health conditions in women veterans. Exposure to persistent organic pollutants and combustion byproducts (eg, from industrial processes and burn pits) have been linked to ovarian dysfunction and oocyte destruction presumed to contribute to accelerated ovarian aging.
The average age for menopause in the US is 52 years. About 5% of women go through early menopause naturally. Early and premature (< 40 years) menopause may also result from a medical or surgical cause, such as a hysterectomy. Regardless the cause, early menopause can have a profound impact on a woman’s physical, emotional, and mental health. It is associated with premature mortality, poor bone health, sexual dysfunction, a 50% increased risk of cardiovascular disease, and 2-fold increased odds of depression.
“Sometimes we talk about menopause symptoms thinking that they're just sort of 1 brief point in time, but we're also talking about things that may affect women's health and functioning for a third or half of a lifespan,” Carolyn Gibson, PhD, MPH, said at the 2024 Spotlight on Women's Health Cyberseminar Series.
Gibson, a staff psychologist at the San Francisco Veterans Affairs (VA) Women’s Mental Health Program and lead author on the recent early-menopause study, pointed to some of the chronic physical health issues that might develop, such as cardiovascular disease, but also the psychological effects.
“It's just important,” she said during the Cyberseminar Series. “To think about the number of things that women in midlife tend to be juggling and managing, all of which may turn up the volume on symptom experience, effect of vulnerability to health and mental health challenges during this period.”
The findings of the study have clinical implications. Midlife women veterans (aged 45 to 64 years) are the largest group of women veterans enrolled in VA health care. Early menopause brings additional age-related care considerations. The authors advise prioritizing support for routine screening for menopause status and symptoms as well as gender-sensitive training, resources, and staffing to provide comprehensive, trauma-informed, evidence-based menopause care for women at any age.
Traumatic and environmental exposures during military service may put women veterans at risk for early menopause, a recent longitudinal analysis of data from 668 women in the Gulf War Era Cohort Study found.
The study examined associations between possible early menopause (aged < 45 years) and participants’ Gulf War deployment, military environmental exposures (MEEs), Gulf War Illness, military sexual trauma (MST) and posttraumatic stress disorder (PTSD).
Of 384 Gulf War–deployed veterans, 63% reported MEEs and 26% reported MST during deployment. More than half (57%) of study participants (both Gulf War veterans and nondeployed veterans) met criteria for Gulf War Illness, and 23% met criteria for probable PTSD.
At follow-up, 15% of the women had possible early menopause—higher than population estimates for early menopause in the US, which range from 5% to 10%.
Gulf War deployment, Gulf War–related environmental exposures, and MST during deployment were not significantly associated with early menopause. However, both Gulf War Illness (odds ratio [OR], 1.83; 95% CI, 1.14 to 2.95) and probable PTSD (OR, 2.45; 95% CI, 1.54 to 3.90) were strongly associated with early menopause. Women with probable PTSD at baseline had more than double the odds of possible early menopause.
Previous research suggests that deployment, MEEs, and Gulf War Illness are broadly associated with adverse reproductive health conditions in women veterans. Exposure to persistent organic pollutants and combustion byproducts (eg, from industrial processes and burn pits) have been linked to ovarian dysfunction and oocyte destruction presumed to contribute to accelerated ovarian aging.
The average age for menopause in the US is 52 years. About 5% of women go through early menopause naturally. Early and premature (< 40 years) menopause may also result from a medical or surgical cause, such as a hysterectomy. Regardless the cause, early menopause can have a profound impact on a woman’s physical, emotional, and mental health. It is associated with premature mortality, poor bone health, sexual dysfunction, a 50% increased risk of cardiovascular disease, and 2-fold increased odds of depression.
“Sometimes we talk about menopause symptoms thinking that they're just sort of 1 brief point in time, but we're also talking about things that may affect women's health and functioning for a third or half of a lifespan,” Carolyn Gibson, PhD, MPH, said at the 2024 Spotlight on Women's Health Cyberseminar Series.
Gibson, a staff psychologist at the San Francisco Veterans Affairs (VA) Women’s Mental Health Program and lead author on the recent early-menopause study, pointed to some of the chronic physical health issues that might develop, such as cardiovascular disease, but also the psychological effects.
“It's just important,” she said during the Cyberseminar Series. “To think about the number of things that women in midlife tend to be juggling and managing, all of which may turn up the volume on symptom experience, effect of vulnerability to health and mental health challenges during this period.”
The findings of the study have clinical implications. Midlife women veterans (aged 45 to 64 years) are the largest group of women veterans enrolled in VA health care. Early menopause brings additional age-related care considerations. The authors advise prioritizing support for routine screening for menopause status and symptoms as well as gender-sensitive training, resources, and staffing to provide comprehensive, trauma-informed, evidence-based menopause care for women at any age.
Military Service May Increase Risk for Early Menopause
Military Service May Increase Risk for Early Menopause
Stay Alert to Sleep Apnea Burden in the Military
Obstructive sleep apnea (OSA) was associated with a significantly increased risk for adverse health outcomes and health care resource use among military personnel in the US, according to data from about 120,000 active-duty service members.
OSA and other clinical sleep disorders are common among military personnel, driven in part by demanding, nontraditional work schedules that can exacerbate sleep problems, but OSA’s impact in this population has not been well-studied, Emerson M. Wickwire, PhD, of the University of Maryland School of Medicine, Baltimore, and colleagues wrote in a new paper published in Chest.
In the current health economic climate of increasing costs and limited resources, the economic aspects of sleep disorders have never been more important, Wickwire said in an interview. The data in this study are the first to quantify the health and utilization burden of OSA in the US military and can support military decision-makers regarding allocation of scarce resources, he said.
To assess the burden of OSA in the military, they reviewed fully de-identified data from 59,203 active-duty military personnel with diagnoses of OSA and compared them with 59,203 active-duty military personnel without OSA. The participants ranged in age from 18 to 64 years; 7.4% were women and 64.5% were white individuals. Study outcomes included new diagnoses of physical and psychological health conditions, as well as health care resource use in the first year after the index date.
About one third of the participants were in the Army (38.7%), 25.6% were in the Air Force, 23.5% were in the Navy, 5.8% were in the Marines, 5.7% were in the Coast Guard, and 0.7% were in the Public Health Service.
Over the 1-year study period, military personnel with OSA diagnoses were significantly more likely to experience new physical and psychological adverse events than control individuals without OSA, based on proportional hazards models. The physical conditions with the greatest increased risk in the OSA group were traumatic brain injury and cardiovascular disease (which included acute myocardial infarction, atrial fibrillation, ischemic heart disease, and peripheral procedures), with hazard ratios (HRs) 3.27 and 2.32, respectively. The psychological conditions with the greatest increased risk in the OSA group vs control individuals were posttraumatic stress disorder (PTSD) and anxiety (HR, 4.41, and HR, 3.35, respectively).
Individuals with OSA also showed increased use of healthcare resources compared with control individuals without OSA, with an additional 170,511 outpatient visits, 66 inpatient visits, and 1,852 emergency department visits.
Don’t Discount OSA in Military Personnel
“From a clinical perspective, these findings underscore the importance of recognizing OSA as a critical risk factor for a wide array of physical and psychological health outcomes,” the researchers wrote in their discussion.
The results highlight the need for more clinical attention to patient screening, triage, and delivery of care, but efforts are limited by the documented shortage of sleep specialists in the military health system, they noted.
Key limitations of the study include the use of an administrative claims data source, which did not include clinical information such as disease severity or daytime symptoms, and the nonrandomized, observational study design, Wickwire told this news organization.
Looking ahead, the researchers at the University of Maryland School of Medicine and the Uniformed Services University, Bethesda, Maryland, are launching a new trial to assess the clinical effectiveness and cost-effectiveness of telehealth visits for military beneficiaries diagnosed with OSA as a way to manage the shortage of sleep specialists in the military health system, according to a press release from the University of Maryland.
“Although the association between poor sleep and traumatic stress is well-known, present results highlight striking associations between sleep apnea and posttraumatic stress disorder, traumatic brain injury, and musculoskeletal injuries, which are key outcomes from the military perspective,” Wickwire told this news organization.
“Our most important clinical recommendation is for healthcare providers to be on alert for signs and symptoms of OSA, including snoring, daytime sleepiness, and morning dry mouth,” said Wickwire. “Primary care and mental health providers should be especially attuned,” he added.
Results Not Surprising, but Research Gaps Remain
“The sleep health of active-duty military personnel is not only vital for optimal military performance but also impacts the health of Veterans after separation from the military,” said Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, Michigan, in an interview.
The current study identifies increased utilization of healthcare resources by active-duty personnel with sleep apnea, and outcomes were not surprising, said Shamim-Uzzaman, who is employed by the Veterans’ Health Administration, but was not involved in the current study.
The association between untreated OSA and medical and psychological comorbidities such as cardiovascular disease, diabetes, and mood disorders such as depression and anxiety is well-known, Shamim-Uzzaman said. “Patients with depression who also have sleep disturbances are at higher risk for suicide — the strength of this association is such that it led the Veterans’ Health Administration to mandate suicide screening for Veterans seen in its sleep clinics,” he added.
“We also know that untreated OSA is associated with excessive daytime sleepiness, slowed reaction times, and increased risk of motor vehicle accidents, all of which can contribute to sustaining injuries such as traumatic brain injury,” said Shamim-Uzzaman. “Emerging evidence also suggests that sleep disruption prior to exposure to trauma increases the risk of developing PTSD. Therefore, it is not surprising that patients with sleep apnea would have higher healthcare utilization for non-OSA conditions than those without sleep apnea,” he noted.
In clinical practice, the study underscores the importance of identifying and managing sleep health in military personnel, who frequently work nontraditional schedules with long, sustained shifts in grueling conditions not conducive to healthy sleep, Shamim-Uzzaman told this news organization. “Although the harsh work environments that our active-duty military endure come part and parcel with the job, clinicians caring for these individuals should ask specifically about their sleep and working schedules to optimize sleep as best as possible; this should include, but not be limited to, screening and testing for sleep disordered breathing and insomnia,” he said.
The current study has several limitations, including the inability to control for smoking or alcohol use, which are common in military personnel and associated with increased morbidity, said Shamim-Uzzaman. The study also did not assess the impact of other confounding factors, such as sleep duration and daytime sleepiness, that could impact the results, especially the association of OSA and traumatic brain injury, he noted. “More research is needed to assess the impact of these factors as well as the effect of treatment of OSA on comorbidities and healthcare utilization,” he said.
This study was supported by the Military Health Services Research Program.
Wickwire’s institution had received research funding from the American Academy of Sleep Medicine Foundation, Department of Defense, Merck, National Institutes of Health/National Institute on Aging, ResMed, the ResMed Foundation, and the SRS Foundation. Wickwire disclosed serving as a scientific consultant to Axsome Therapeutics, Dayzz, Eisai, EnsoData, Idorsia, Merck, Nox Health, Primasun, Purdue, and ResMed and is an equity shareholder in Well Tap.
Shamim-Uzzaman is an employee of the Veterans’ Health Administration.
A version of this article first appeared on Medscape.com.
Obstructive sleep apnea (OSA) was associated with a significantly increased risk for adverse health outcomes and health care resource use among military personnel in the US, according to data from about 120,000 active-duty service members.
OSA and other clinical sleep disorders are common among military personnel, driven in part by demanding, nontraditional work schedules that can exacerbate sleep problems, but OSA’s impact in this population has not been well-studied, Emerson M. Wickwire, PhD, of the University of Maryland School of Medicine, Baltimore, and colleagues wrote in a new paper published in Chest.
In the current health economic climate of increasing costs and limited resources, the economic aspects of sleep disorders have never been more important, Wickwire said in an interview. The data in this study are the first to quantify the health and utilization burden of OSA in the US military and can support military decision-makers regarding allocation of scarce resources, he said.
To assess the burden of OSA in the military, they reviewed fully de-identified data from 59,203 active-duty military personnel with diagnoses of OSA and compared them with 59,203 active-duty military personnel without OSA. The participants ranged in age from 18 to 64 years; 7.4% were women and 64.5% were white individuals. Study outcomes included new diagnoses of physical and psychological health conditions, as well as health care resource use in the first year after the index date.
About one third of the participants were in the Army (38.7%), 25.6% were in the Air Force, 23.5% were in the Navy, 5.8% were in the Marines, 5.7% were in the Coast Guard, and 0.7% were in the Public Health Service.
Over the 1-year study period, military personnel with OSA diagnoses were significantly more likely to experience new physical and psychological adverse events than control individuals without OSA, based on proportional hazards models. The physical conditions with the greatest increased risk in the OSA group were traumatic brain injury and cardiovascular disease (which included acute myocardial infarction, atrial fibrillation, ischemic heart disease, and peripheral procedures), with hazard ratios (HRs) 3.27 and 2.32, respectively. The psychological conditions with the greatest increased risk in the OSA group vs control individuals were posttraumatic stress disorder (PTSD) and anxiety (HR, 4.41, and HR, 3.35, respectively).
Individuals with OSA also showed increased use of healthcare resources compared with control individuals without OSA, with an additional 170,511 outpatient visits, 66 inpatient visits, and 1,852 emergency department visits.
Don’t Discount OSA in Military Personnel
“From a clinical perspective, these findings underscore the importance of recognizing OSA as a critical risk factor for a wide array of physical and psychological health outcomes,” the researchers wrote in their discussion.
The results highlight the need for more clinical attention to patient screening, triage, and delivery of care, but efforts are limited by the documented shortage of sleep specialists in the military health system, they noted.
Key limitations of the study include the use of an administrative claims data source, which did not include clinical information such as disease severity or daytime symptoms, and the nonrandomized, observational study design, Wickwire told this news organization.
Looking ahead, the researchers at the University of Maryland School of Medicine and the Uniformed Services University, Bethesda, Maryland, are launching a new trial to assess the clinical effectiveness and cost-effectiveness of telehealth visits for military beneficiaries diagnosed with OSA as a way to manage the shortage of sleep specialists in the military health system, according to a press release from the University of Maryland.
“Although the association between poor sleep and traumatic stress is well-known, present results highlight striking associations between sleep apnea and posttraumatic stress disorder, traumatic brain injury, and musculoskeletal injuries, which are key outcomes from the military perspective,” Wickwire told this news organization.
“Our most important clinical recommendation is for healthcare providers to be on alert for signs and symptoms of OSA, including snoring, daytime sleepiness, and morning dry mouth,” said Wickwire. “Primary care and mental health providers should be especially attuned,” he added.
Results Not Surprising, but Research Gaps Remain
“The sleep health of active-duty military personnel is not only vital for optimal military performance but also impacts the health of Veterans after separation from the military,” said Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, Michigan, in an interview.
The current study identifies increased utilization of healthcare resources by active-duty personnel with sleep apnea, and outcomes were not surprising, said Shamim-Uzzaman, who is employed by the Veterans’ Health Administration, but was not involved in the current study.
The association between untreated OSA and medical and psychological comorbidities such as cardiovascular disease, diabetes, and mood disorders such as depression and anxiety is well-known, Shamim-Uzzaman said. “Patients with depression who also have sleep disturbances are at higher risk for suicide — the strength of this association is such that it led the Veterans’ Health Administration to mandate suicide screening for Veterans seen in its sleep clinics,” he added.
“We also know that untreated OSA is associated with excessive daytime sleepiness, slowed reaction times, and increased risk of motor vehicle accidents, all of which can contribute to sustaining injuries such as traumatic brain injury,” said Shamim-Uzzaman. “Emerging evidence also suggests that sleep disruption prior to exposure to trauma increases the risk of developing PTSD. Therefore, it is not surprising that patients with sleep apnea would have higher healthcare utilization for non-OSA conditions than those without sleep apnea,” he noted.
In clinical practice, the study underscores the importance of identifying and managing sleep health in military personnel, who frequently work nontraditional schedules with long, sustained shifts in grueling conditions not conducive to healthy sleep, Shamim-Uzzaman told this news organization. “Although the harsh work environments that our active-duty military endure come part and parcel with the job, clinicians caring for these individuals should ask specifically about their sleep and working schedules to optimize sleep as best as possible; this should include, but not be limited to, screening and testing for sleep disordered breathing and insomnia,” he said.
The current study has several limitations, including the inability to control for smoking or alcohol use, which are common in military personnel and associated with increased morbidity, said Shamim-Uzzaman. The study also did not assess the impact of other confounding factors, such as sleep duration and daytime sleepiness, that could impact the results, especially the association of OSA and traumatic brain injury, he noted. “More research is needed to assess the impact of these factors as well as the effect of treatment of OSA on comorbidities and healthcare utilization,” he said.
This study was supported by the Military Health Services Research Program.
Wickwire’s institution had received research funding from the American Academy of Sleep Medicine Foundation, Department of Defense, Merck, National Institutes of Health/National Institute on Aging, ResMed, the ResMed Foundation, and the SRS Foundation. Wickwire disclosed serving as a scientific consultant to Axsome Therapeutics, Dayzz, Eisai, EnsoData, Idorsia, Merck, Nox Health, Primasun, Purdue, and ResMed and is an equity shareholder in Well Tap.
Shamim-Uzzaman is an employee of the Veterans’ Health Administration.
A version of this article first appeared on Medscape.com.
Obstructive sleep apnea (OSA) was associated with a significantly increased risk for adverse health outcomes and health care resource use among military personnel in the US, according to data from about 120,000 active-duty service members.
OSA and other clinical sleep disorders are common among military personnel, driven in part by demanding, nontraditional work schedules that can exacerbate sleep problems, but OSA’s impact in this population has not been well-studied, Emerson M. Wickwire, PhD, of the University of Maryland School of Medicine, Baltimore, and colleagues wrote in a new paper published in Chest.
In the current health economic climate of increasing costs and limited resources, the economic aspects of sleep disorders have never been more important, Wickwire said in an interview. The data in this study are the first to quantify the health and utilization burden of OSA in the US military and can support military decision-makers regarding allocation of scarce resources, he said.
To assess the burden of OSA in the military, they reviewed fully de-identified data from 59,203 active-duty military personnel with diagnoses of OSA and compared them with 59,203 active-duty military personnel without OSA. The participants ranged in age from 18 to 64 years; 7.4% were women and 64.5% were white individuals. Study outcomes included new diagnoses of physical and psychological health conditions, as well as health care resource use in the first year after the index date.
About one third of the participants were in the Army (38.7%), 25.6% were in the Air Force, 23.5% were in the Navy, 5.8% were in the Marines, 5.7% were in the Coast Guard, and 0.7% were in the Public Health Service.
Over the 1-year study period, military personnel with OSA diagnoses were significantly more likely to experience new physical and psychological adverse events than control individuals without OSA, based on proportional hazards models. The physical conditions with the greatest increased risk in the OSA group were traumatic brain injury and cardiovascular disease (which included acute myocardial infarction, atrial fibrillation, ischemic heart disease, and peripheral procedures), with hazard ratios (HRs) 3.27 and 2.32, respectively. The psychological conditions with the greatest increased risk in the OSA group vs control individuals were posttraumatic stress disorder (PTSD) and anxiety (HR, 4.41, and HR, 3.35, respectively).
Individuals with OSA also showed increased use of healthcare resources compared with control individuals without OSA, with an additional 170,511 outpatient visits, 66 inpatient visits, and 1,852 emergency department visits.
Don’t Discount OSA in Military Personnel
“From a clinical perspective, these findings underscore the importance of recognizing OSA as a critical risk factor for a wide array of physical and psychological health outcomes,” the researchers wrote in their discussion.
The results highlight the need for more clinical attention to patient screening, triage, and delivery of care, but efforts are limited by the documented shortage of sleep specialists in the military health system, they noted.
Key limitations of the study include the use of an administrative claims data source, which did not include clinical information such as disease severity or daytime symptoms, and the nonrandomized, observational study design, Wickwire told this news organization.
Looking ahead, the researchers at the University of Maryland School of Medicine and the Uniformed Services University, Bethesda, Maryland, are launching a new trial to assess the clinical effectiveness and cost-effectiveness of telehealth visits for military beneficiaries diagnosed with OSA as a way to manage the shortage of sleep specialists in the military health system, according to a press release from the University of Maryland.
“Although the association between poor sleep and traumatic stress is well-known, present results highlight striking associations between sleep apnea and posttraumatic stress disorder, traumatic brain injury, and musculoskeletal injuries, which are key outcomes from the military perspective,” Wickwire told this news organization.
“Our most important clinical recommendation is for healthcare providers to be on alert for signs and symptoms of OSA, including snoring, daytime sleepiness, and morning dry mouth,” said Wickwire. “Primary care and mental health providers should be especially attuned,” he added.
Results Not Surprising, but Research Gaps Remain
“The sleep health of active-duty military personnel is not only vital for optimal military performance but also impacts the health of Veterans after separation from the military,” said Q. Afifa Shamim-Uzzaman, MD, an associate professor and a sleep medicine specialist at the University of Michigan, Ann Arbor, Michigan, in an interview.
The current study identifies increased utilization of healthcare resources by active-duty personnel with sleep apnea, and outcomes were not surprising, said Shamim-Uzzaman, who is employed by the Veterans’ Health Administration, but was not involved in the current study.
The association between untreated OSA and medical and psychological comorbidities such as cardiovascular disease, diabetes, and mood disorders such as depression and anxiety is well-known, Shamim-Uzzaman said. “Patients with depression who also have sleep disturbances are at higher risk for suicide — the strength of this association is such that it led the Veterans’ Health Administration to mandate suicide screening for Veterans seen in its sleep clinics,” he added.
“We also know that untreated OSA is associated with excessive daytime sleepiness, slowed reaction times, and increased risk of motor vehicle accidents, all of which can contribute to sustaining injuries such as traumatic brain injury,” said Shamim-Uzzaman. “Emerging evidence also suggests that sleep disruption prior to exposure to trauma increases the risk of developing PTSD. Therefore, it is not surprising that patients with sleep apnea would have higher healthcare utilization for non-OSA conditions than those without sleep apnea,” he noted.
In clinical practice, the study underscores the importance of identifying and managing sleep health in military personnel, who frequently work nontraditional schedules with long, sustained shifts in grueling conditions not conducive to healthy sleep, Shamim-Uzzaman told this news organization. “Although the harsh work environments that our active-duty military endure come part and parcel with the job, clinicians caring for these individuals should ask specifically about their sleep and working schedules to optimize sleep as best as possible; this should include, but not be limited to, screening and testing for sleep disordered breathing and insomnia,” he said.
The current study has several limitations, including the inability to control for smoking or alcohol use, which are common in military personnel and associated with increased morbidity, said Shamim-Uzzaman. The study also did not assess the impact of other confounding factors, such as sleep duration and daytime sleepiness, that could impact the results, especially the association of OSA and traumatic brain injury, he noted. “More research is needed to assess the impact of these factors as well as the effect of treatment of OSA on comorbidities and healthcare utilization,” he said.
This study was supported by the Military Health Services Research Program.
Wickwire’s institution had received research funding from the American Academy of Sleep Medicine Foundation, Department of Defense, Merck, National Institutes of Health/National Institute on Aging, ResMed, the ResMed Foundation, and the SRS Foundation. Wickwire disclosed serving as a scientific consultant to Axsome Therapeutics, Dayzz, Eisai, EnsoData, Idorsia, Merck, Nox Health, Primasun, Purdue, and ResMed and is an equity shareholder in Well Tap.
Shamim-Uzzaman is an employee of the Veterans’ Health Administration.
A version of this article first appeared on Medscape.com.
Atypical Skin Bronzing in Response to Belumosudil for Graft-vs-Host Disease
Atypical Skin Bronzing in Response to Belumosudil for Graft-vs-Host Disease
To the Editor:
Drug-induced hyperpigmentation is a common cause of an acquired increase in pigmentation. Belumosudil is an oral selective inhibitor of Rho-associated coiled-coil containing protein kinase (ROCK2) that is approved for the treatment of chronic graft-vs-host disease (GVHD). We describe a patient who developed diffuse skin bronzing 3 weeks after initiation of belumosudil treatment.
A 64-year-old fair-skinned woman presented to the dermatology clinic with bronzing of the skin and dystrophic nails 3 weeks after starting belumosudil for treatment of chronic GVHD. Six months prior to presentation, the patient had received a bone marrow transplant for chronic lymphoid leukemia. She presented to dermatology 6 months after the transplant with a new-onset rash that was suspicious for GVHD. Physical examination revealed pruritic pink papules diffusely scattered on the legs and forearms (Figure 1). The patient declined biopsy at that time and later followed up with oncology. The patient’s oncologist supported a diagnosis of GVHD, and the patient began treatment with belumosudil 200 mg/d which was intended to be taken until treatment failure due to progression of chronic GVHD.
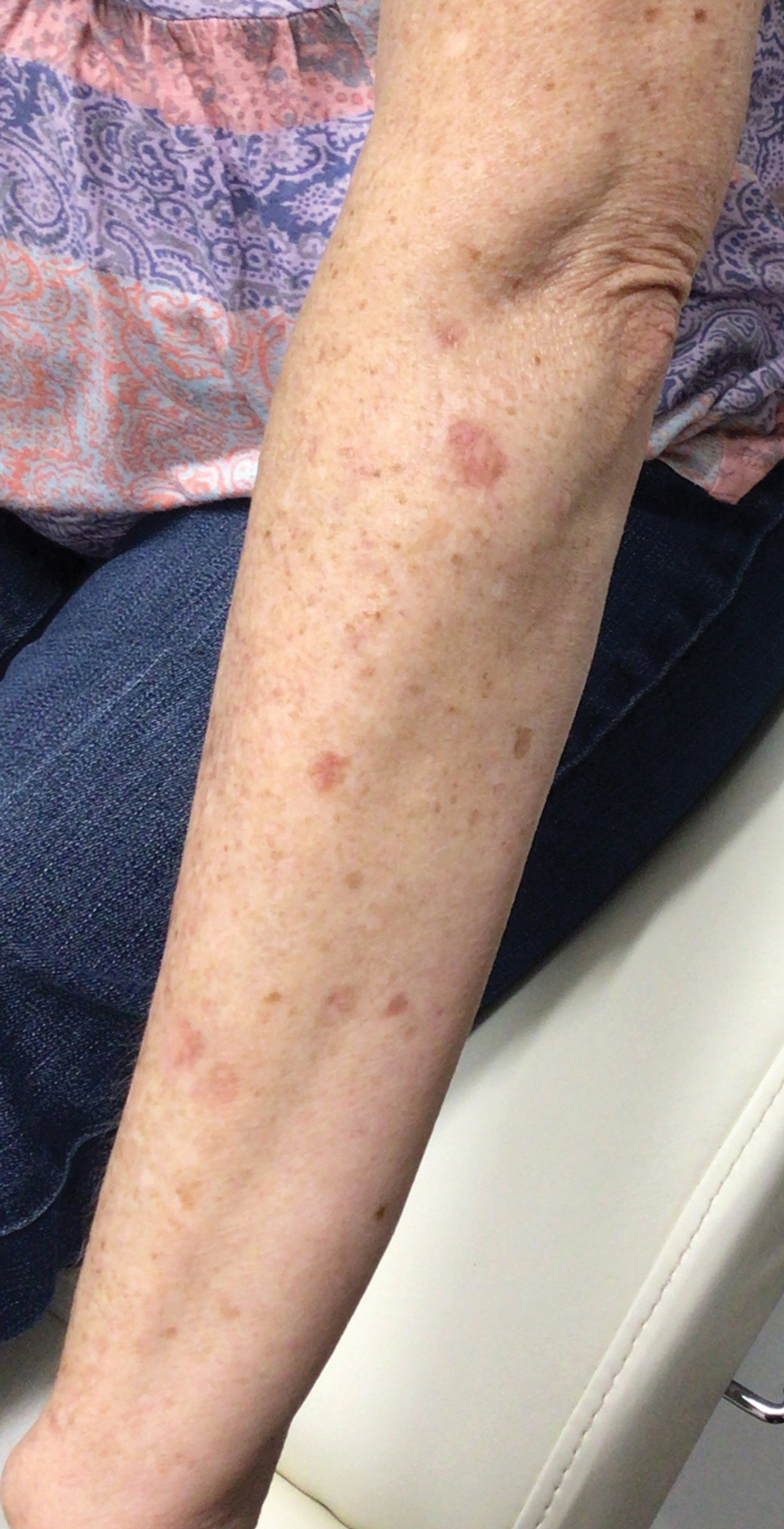
Three weeks after starting belumosudil, the patient developed diffuse bronzing of the skin and brown, evenly colored patches scattered on the trunk, back, and upper and lower extremities on a background of the presumed GVHD rash (Figure 2). The hyperpigmentation was abrupt, starting on the chest and spreading to the abdomen, extremities, and back (Figure 3).

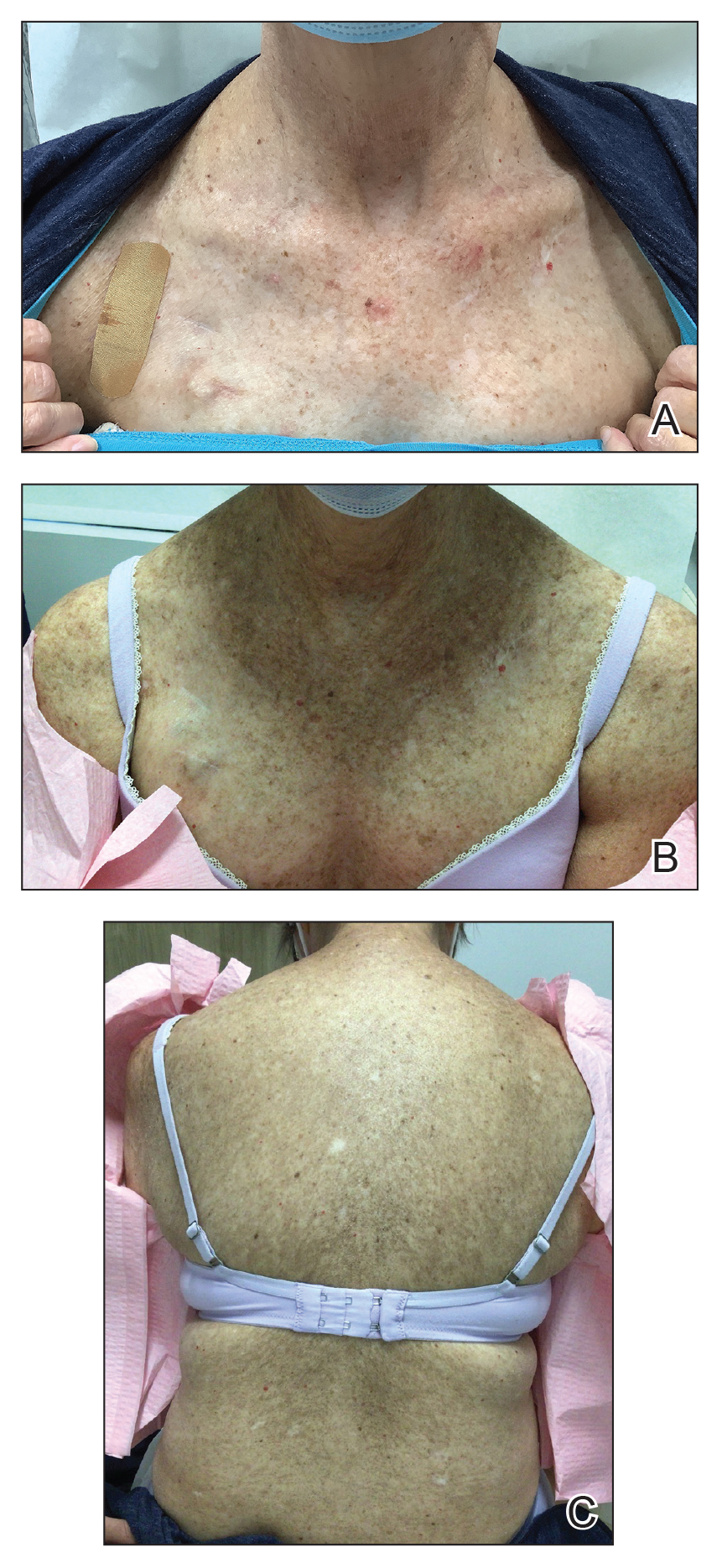
developed on the patient’s chest and back within 3 weeks of initiating treatment with belumosudil.
Again, the patient was offered biopsy for the new-onset pigmentation but declined. During this time, she had no notable sun exposure and primarily stayed indoors despite living in a region with a sunny semi-arid climate. Her medication and supplement list were reviewed and included acalabrutinib, a multivitamin, lutein, biotin, and a fish oil supplement. A compete blood cell count as well as ferritin, transferrin, cortisol, and adrenocorticotropic hormone levels were unremarkable.
The patient continued to take belumosudil for treatment of GVHD. The hyperpigmentation faded slightly by a 2-month follow-up visit but persisted and was stable. She has not tried other treatments for GVHD to manage the hyperpigmentation.
Conditions known to cause diffuse bronzing of the skin include Addison disease, hemochromatosis, Cushing disease, and medication adverse events. Our patient presented with an absence of systemic symptoms, normal laboratory results, and no clinical indicators suggesting alternate causes. Given that the onset of the hyperpigmentation was 3 weeks after she started a new medication, we hypothesized that the bronzing was an adverse effect of the belumosudil—though this correlation cannot be definitively proven by this case.
The most common offending agents for drug-induced skin hyperpigmentation are nonsteroidal anti- inflammatory drugs, antimalarials, amiodarone, cytotoxic drugs, and tetracyclines.1,2 Our patient’s medication list included the cytotoxic agent acalabrutinib, a Bruton tyrosine kinase inhibitor used for the treatment of non-Hodgkin lymphoma. It has been associated with dermatologic findings of ecchymosis, bruising, panniculitis, and cellulitis, but there are no known reports of hyperpigmentation.3 Our patient had been taking acalabrutinib for 6 months when the GVHD rash developed. At the time, she also was taking a multivitamin and lutein, biotin, and fish oil supplements, none of which have been associated with hyperpigmentation.
Polypharmacy adds a layer of difficulty in identifying the inciting cause of pigmentary change. In our case, symptoms began 3 weeks after the initiation of belumosudil. There were no cutaneous reactions observed in the ROCKstar study of belumosudil; the most common adverse events were upper respiratory tract infection, diarrhea, fatigue, nausea, increased liver enzymes, and dyspnea.4,5 Patients on belumosudil have developed aggressive cutaneous squamous cell carcinoma.6 However, a search of PubMed articles indexed for MEDLINE using the search terms acalabrutinib or belumosudil with hyperpigmentation or cutaneous reaction returned no reports of these medications causing hyperpigmentation or cutaneous deposits.
Treatment of drug-induced hyperpigmentation is difficult because discontinuation of the offending agent typically confirms diagnosis, but interruption of treatment is not always possible, as in our patient. The skin changes can fade over time, but effects typically are long lasting.
Dermatologists play a key role in the identification of drug-induced skin hyperpigmentation. After endocrine or metabolic causes of skin hyperpigmentation have been ruled out, a thorough review of the patient’s medication list should be done to assess for a drug-induced cause. Treatment is limited to sun avoidance, as interruption of treatment may not be possible, and lesions typically do fade over time. These chronic skin changes can have a psychosocial effect on patients and regular follow-up is recommended.
- Giménez García RM, Carrasco Molina S. Drug-induced hyperpigmentation: review and case series. J Am Board Fam Med. 2019;32:628-638. doi:10.3122/jabfm.2019.04.180212
- Dereure O. Drug-induced skin pigmentation. epidemiology, diagnosis and treatment. Am J Clin Dermatol. 2001;2:253-62. doi:10.2165/00128071-200102040-00006
- Sibaud V, Beylot-Barry M, Protin C, et al. Dermatological toxicities of Bruton’s tyrosine kinase inhibitors. Am J Clin Dermatol. 2020; 21:799-812. doi:10.1007/s40257-020-00535-x
- Cutler C, Lee SJ, Arai S, et al. Belumosudil for chronic graft-versus-host disease after 2 or more prior lines of therapy: the ROCKstar Study. Blood. 2021;138:2278-2289. doi:10.1182/blood.2021012021
- Jagasia M, Lazaryan A, Bachier CR, et al. ROCK2 inhibition with belumosudil (KD025) for the treatment of chronic graftversus- host disease. J Clin Oncol. 2021;39:1888-1898. doi:10.1200 /JCO.20.02754
- Lee GH, Guzman AK, Divito SJ, et al. Cutaneous squamous-cell carcinoma after treatment with ruxolitinib or belumosudil. N Engl J Med. 2023;389:188-190. doi:10.1056/NEJMc2304157
To the Editor:
Drug-induced hyperpigmentation is a common cause of an acquired increase in pigmentation. Belumosudil is an oral selective inhibitor of Rho-associated coiled-coil containing protein kinase (ROCK2) that is approved for the treatment of chronic graft-vs-host disease (GVHD). We describe a patient who developed diffuse skin bronzing 3 weeks after initiation of belumosudil treatment.
A 64-year-old fair-skinned woman presented to the dermatology clinic with bronzing of the skin and dystrophic nails 3 weeks after starting belumosudil for treatment of chronic GVHD. Six months prior to presentation, the patient had received a bone marrow transplant for chronic lymphoid leukemia. She presented to dermatology 6 months after the transplant with a new-onset rash that was suspicious for GVHD. Physical examination revealed pruritic pink papules diffusely scattered on the legs and forearms (Figure 1). The patient declined biopsy at that time and later followed up with oncology. The patient’s oncologist supported a diagnosis of GVHD, and the patient began treatment with belumosudil 200 mg/d which was intended to be taken until treatment failure due to progression of chronic GVHD.
Three weeks after starting belumosudil, the patient developed diffuse bronzing of the skin and brown, evenly colored patches scattered on the trunk, back, and upper and lower extremities on a background of the presumed GVHD rash (Figure 2). The hyperpigmentation was abrupt, starting on the chest and spreading to the abdomen, extremities, and back (Figure 3).
developed on the patient’s chest and back within 3 weeks of initiating treatment with belumosudil.
Again, the patient was offered biopsy for the new-onset pigmentation but declined. During this time, she had no notable sun exposure and primarily stayed indoors despite living in a region with a sunny semi-arid climate. Her medication and supplement list were reviewed and included acalabrutinib, a multivitamin, lutein, biotin, and a fish oil supplement. A compete blood cell count as well as ferritin, transferrin, cortisol, and adrenocorticotropic hormone levels were unremarkable.
The patient continued to take belumosudil for treatment of GVHD. The hyperpigmentation faded slightly by a 2-month follow-up visit but persisted and was stable. She has not tried other treatments for GVHD to manage the hyperpigmentation.
Conditions known to cause diffuse bronzing of the skin include Addison disease, hemochromatosis, Cushing disease, and medication adverse events. Our patient presented with an absence of systemic symptoms, normal laboratory results, and no clinical indicators suggesting alternate causes. Given that the onset of the hyperpigmentation was 3 weeks after she started a new medication, we hypothesized that the bronzing was an adverse effect of the belumosudil—though this correlation cannot be definitively proven by this case.
The most common offending agents for drug-induced skin hyperpigmentation are nonsteroidal anti- inflammatory drugs, antimalarials, amiodarone, cytotoxic drugs, and tetracyclines.1,2 Our patient’s medication list included the cytotoxic agent acalabrutinib, a Bruton tyrosine kinase inhibitor used for the treatment of non-Hodgkin lymphoma. It has been associated with dermatologic findings of ecchymosis, bruising, panniculitis, and cellulitis, but there are no known reports of hyperpigmentation.3 Our patient had been taking acalabrutinib for 6 months when the GVHD rash developed. At the time, she also was taking a multivitamin and lutein, biotin, and fish oil supplements, none of which have been associated with hyperpigmentation.
Polypharmacy adds a layer of difficulty in identifying the inciting cause of pigmentary change. In our case, symptoms began 3 weeks after the initiation of belumosudil. There were no cutaneous reactions observed in the ROCKstar study of belumosudil; the most common adverse events were upper respiratory tract infection, diarrhea, fatigue, nausea, increased liver enzymes, and dyspnea.4,5 Patients on belumosudil have developed aggressive cutaneous squamous cell carcinoma.6 However, a search of PubMed articles indexed for MEDLINE using the search terms acalabrutinib or belumosudil with hyperpigmentation or cutaneous reaction returned no reports of these medications causing hyperpigmentation or cutaneous deposits.
Treatment of drug-induced hyperpigmentation is difficult because discontinuation of the offending agent typically confirms diagnosis, but interruption of treatment is not always possible, as in our patient. The skin changes can fade over time, but effects typically are long lasting.
Dermatologists play a key role in the identification of drug-induced skin hyperpigmentation. After endocrine or metabolic causes of skin hyperpigmentation have been ruled out, a thorough review of the patient’s medication list should be done to assess for a drug-induced cause. Treatment is limited to sun avoidance, as interruption of treatment may not be possible, and lesions typically do fade over time. These chronic skin changes can have a psychosocial effect on patients and regular follow-up is recommended.
To the Editor:
Drug-induced hyperpigmentation is a common cause of an acquired increase in pigmentation. Belumosudil is an oral selective inhibitor of Rho-associated coiled-coil containing protein kinase (ROCK2) that is approved for the treatment of chronic graft-vs-host disease (GVHD). We describe a patient who developed diffuse skin bronzing 3 weeks after initiation of belumosudil treatment.
A 64-year-old fair-skinned woman presented to the dermatology clinic with bronzing of the skin and dystrophic nails 3 weeks after starting belumosudil for treatment of chronic GVHD. Six months prior to presentation, the patient had received a bone marrow transplant for chronic lymphoid leukemia. She presented to dermatology 6 months after the transplant with a new-onset rash that was suspicious for GVHD. Physical examination revealed pruritic pink papules diffusely scattered on the legs and forearms (Figure 1). The patient declined biopsy at that time and later followed up with oncology. The patient’s oncologist supported a diagnosis of GVHD, and the patient began treatment with belumosudil 200 mg/d which was intended to be taken until treatment failure due to progression of chronic GVHD.
Three weeks after starting belumosudil, the patient developed diffuse bronzing of the skin and brown, evenly colored patches scattered on the trunk, back, and upper and lower extremities on a background of the presumed GVHD rash (Figure 2). The hyperpigmentation was abrupt, starting on the chest and spreading to the abdomen, extremities, and back (Figure 3).
developed on the patient’s chest and back within 3 weeks of initiating treatment with belumosudil.
Again, the patient was offered biopsy for the new-onset pigmentation but declined. During this time, she had no notable sun exposure and primarily stayed indoors despite living in a region with a sunny semi-arid climate. Her medication and supplement list were reviewed and included acalabrutinib, a multivitamin, lutein, biotin, and a fish oil supplement. A compete blood cell count as well as ferritin, transferrin, cortisol, and adrenocorticotropic hormone levels were unremarkable.
The patient continued to take belumosudil for treatment of GVHD. The hyperpigmentation faded slightly by a 2-month follow-up visit but persisted and was stable. She has not tried other treatments for GVHD to manage the hyperpigmentation.
Conditions known to cause diffuse bronzing of the skin include Addison disease, hemochromatosis, Cushing disease, and medication adverse events. Our patient presented with an absence of systemic symptoms, normal laboratory results, and no clinical indicators suggesting alternate causes. Given that the onset of the hyperpigmentation was 3 weeks after she started a new medication, we hypothesized that the bronzing was an adverse effect of the belumosudil—though this correlation cannot be definitively proven by this case.
The most common offending agents for drug-induced skin hyperpigmentation are nonsteroidal anti- inflammatory drugs, antimalarials, amiodarone, cytotoxic drugs, and tetracyclines.1,2 Our patient’s medication list included the cytotoxic agent acalabrutinib, a Bruton tyrosine kinase inhibitor used for the treatment of non-Hodgkin lymphoma. It has been associated with dermatologic findings of ecchymosis, bruising, panniculitis, and cellulitis, but there are no known reports of hyperpigmentation.3 Our patient had been taking acalabrutinib for 6 months when the GVHD rash developed. At the time, she also was taking a multivitamin and lutein, biotin, and fish oil supplements, none of which have been associated with hyperpigmentation.
Polypharmacy adds a layer of difficulty in identifying the inciting cause of pigmentary change. In our case, symptoms began 3 weeks after the initiation of belumosudil. There were no cutaneous reactions observed in the ROCKstar study of belumosudil; the most common adverse events were upper respiratory tract infection, diarrhea, fatigue, nausea, increased liver enzymes, and dyspnea.4,5 Patients on belumosudil have developed aggressive cutaneous squamous cell carcinoma.6 However, a search of PubMed articles indexed for MEDLINE using the search terms acalabrutinib or belumosudil with hyperpigmentation or cutaneous reaction returned no reports of these medications causing hyperpigmentation or cutaneous deposits.
Treatment of drug-induced hyperpigmentation is difficult because discontinuation of the offending agent typically confirms diagnosis, but interruption of treatment is not always possible, as in our patient. The skin changes can fade over time, but effects typically are long lasting.
Dermatologists play a key role in the identification of drug-induced skin hyperpigmentation. After endocrine or metabolic causes of skin hyperpigmentation have been ruled out, a thorough review of the patient’s medication list should be done to assess for a drug-induced cause. Treatment is limited to sun avoidance, as interruption of treatment may not be possible, and lesions typically do fade over time. These chronic skin changes can have a psychosocial effect on patients and regular follow-up is recommended.
- Giménez García RM, Carrasco Molina S. Drug-induced hyperpigmentation: review and case series. J Am Board Fam Med. 2019;32:628-638. doi:10.3122/jabfm.2019.04.180212
- Dereure O. Drug-induced skin pigmentation. epidemiology, diagnosis and treatment. Am J Clin Dermatol. 2001;2:253-62. doi:10.2165/00128071-200102040-00006
- Sibaud V, Beylot-Barry M, Protin C, et al. Dermatological toxicities of Bruton’s tyrosine kinase inhibitors. Am J Clin Dermatol. 2020; 21:799-812. doi:10.1007/s40257-020-00535-x
- Cutler C, Lee SJ, Arai S, et al. Belumosudil for chronic graft-versus-host disease after 2 or more prior lines of therapy: the ROCKstar Study. Blood. 2021;138:2278-2289. doi:10.1182/blood.2021012021
- Jagasia M, Lazaryan A, Bachier CR, et al. ROCK2 inhibition with belumosudil (KD025) for the treatment of chronic graftversus- host disease. J Clin Oncol. 2021;39:1888-1898. doi:10.1200 /JCO.20.02754
- Lee GH, Guzman AK, Divito SJ, et al. Cutaneous squamous-cell carcinoma after treatment with ruxolitinib or belumosudil. N Engl J Med. 2023;389:188-190. doi:10.1056/NEJMc2304157
- Giménez García RM, Carrasco Molina S. Drug-induced hyperpigmentation: review and case series. J Am Board Fam Med. 2019;32:628-638. doi:10.3122/jabfm.2019.04.180212
- Dereure O. Drug-induced skin pigmentation. epidemiology, diagnosis and treatment. Am J Clin Dermatol. 2001;2:253-62. doi:10.2165/00128071-200102040-00006
- Sibaud V, Beylot-Barry M, Protin C, et al. Dermatological toxicities of Bruton’s tyrosine kinase inhibitors. Am J Clin Dermatol. 2020; 21:799-812. doi:10.1007/s40257-020-00535-x
- Cutler C, Lee SJ, Arai S, et al. Belumosudil for chronic graft-versus-host disease after 2 or more prior lines of therapy: the ROCKstar Study. Blood. 2021;138:2278-2289. doi:10.1182/blood.2021012021
- Jagasia M, Lazaryan A, Bachier CR, et al. ROCK2 inhibition with belumosudil (KD025) for the treatment of chronic graftversus- host disease. J Clin Oncol. 2021;39:1888-1898. doi:10.1200 /JCO.20.02754
- Lee GH, Guzman AK, Divito SJ, et al. Cutaneous squamous-cell carcinoma after treatment with ruxolitinib or belumosudil. N Engl J Med. 2023;389:188-190. doi:10.1056/NEJMc2304157
Atypical Skin Bronzing in Response to Belumosudil for Graft-vs-Host Disease
Atypical Skin Bronzing in Response to Belumosudil for Graft-vs-Host Disease
PRACTICE POINTS
- Drug-induced hyperpigmentation is a common cause of acquired hyperpigmentation and should be evaluated after metabolic or endocrine causes are ruled out.
- Belumosudil for chronic graft-vs-host disease can induce rapid-onset diffuse bronzing hyperpigmentation, even in the absence of other systemic or laboratory abnormalities.
- Treatment entails discontinuation of the offending agent and limitation of exacerbating factors such as sun exposure.

The Aftermath of Kennedy vs. Braidwood
In our June issue, I highlighted the potentially seismic clinical implications of the U.S. Supreme Court’s then-pending decision in the Kennedy vs. Braidwood Management, Inc., case. That ruling, recently released at the conclusion of the Court’s term, ultimately affirmed the Affordable Care Act’s mandate requiring insurers to cover certain preventive services, including colorectal cancer screening tests, without cost-sharing.

In doing so, however, the court determined that members of the U.S. Preventive Services Task Force (USPSTF), which recommends these services, are “inferior officers” appropriately appointed by the Secretary of Health and Human Services (HHS), rather than needing Senate confirmation. Thus, the decision reinforced the HHS Secretary’s authority to oversee and potentially influence USPSTF recommendations in the future. While the decision represented a victory in upholding a key provision of the ACA, it also signaled a potential threat to the scientific independence of the body charged with making those preventive care recommendations in a scientifically rigorous, unbiased manner.
As anticipated, the HHS Secretary responded to the Supreme Court’s ruling by abruptly canceling the USPSTF’s scheduled July meeting. This decision, coupled with his recent disbanding of the entire 17-member Advisory Committee on Immunization Practices — the group responsible for shaping evidence-based vaccine policy — has raised serious concerns across the healthcare field. On July 9th, AGA joined a coalition of 104 health organizations in submitting a letter to the Chair and Ranking Members of the Senate Committee on Health, Education, Labor and Pensions and the House Committee on Energy and Commerce, urging them to protect the integrity of the USPSTF.
The fight to protect science-based health policy is far from over — effective advocacy necessitates that clinicians use their professional platforms to push back against the politicization of science – not only for the integrity of the medical profession, but for the health and future of the patients we serve.
Megan A. Adams, MD, JD, MSc
Editor in Chief
In our June issue, I highlighted the potentially seismic clinical implications of the U.S. Supreme Court’s then-pending decision in the Kennedy vs. Braidwood Management, Inc., case. That ruling, recently released at the conclusion of the Court’s term, ultimately affirmed the Affordable Care Act’s mandate requiring insurers to cover certain preventive services, including colorectal cancer screening tests, without cost-sharing.
In doing so, however, the court determined that members of the U.S. Preventive Services Task Force (USPSTF), which recommends these services, are “inferior officers” appropriately appointed by the Secretary of Health and Human Services (HHS), rather than needing Senate confirmation. Thus, the decision reinforced the HHS Secretary’s authority to oversee and potentially influence USPSTF recommendations in the future. While the decision represented a victory in upholding a key provision of the ACA, it also signaled a potential threat to the scientific independence of the body charged with making those preventive care recommendations in a scientifically rigorous, unbiased manner.
As anticipated, the HHS Secretary responded to the Supreme Court’s ruling by abruptly canceling the USPSTF’s scheduled July meeting. This decision, coupled with his recent disbanding of the entire 17-member Advisory Committee on Immunization Practices — the group responsible for shaping evidence-based vaccine policy — has raised serious concerns across the healthcare field. On July 9th, AGA joined a coalition of 104 health organizations in submitting a letter to the Chair and Ranking Members of the Senate Committee on Health, Education, Labor and Pensions and the House Committee on Energy and Commerce, urging them to protect the integrity of the USPSTF.
The fight to protect science-based health policy is far from over — effective advocacy necessitates that clinicians use their professional platforms to push back against the politicization of science – not only for the integrity of the medical profession, but for the health and future of the patients we serve.
Megan A. Adams, MD, JD, MSc
Editor in Chief
In our June issue, I highlighted the potentially seismic clinical implications of the U.S. Supreme Court’s then-pending decision in the Kennedy vs. Braidwood Management, Inc., case. That ruling, recently released at the conclusion of the Court’s term, ultimately affirmed the Affordable Care Act’s mandate requiring insurers to cover certain preventive services, including colorectal cancer screening tests, without cost-sharing.
In doing so, however, the court determined that members of the U.S. Preventive Services Task Force (USPSTF), which recommends these services, are “inferior officers” appropriately appointed by the Secretary of Health and Human Services (HHS), rather than needing Senate confirmation. Thus, the decision reinforced the HHS Secretary’s authority to oversee and potentially influence USPSTF recommendations in the future. While the decision represented a victory in upholding a key provision of the ACA, it also signaled a potential threat to the scientific independence of the body charged with making those preventive care recommendations in a scientifically rigorous, unbiased manner.
As anticipated, the HHS Secretary responded to the Supreme Court’s ruling by abruptly canceling the USPSTF’s scheduled July meeting. This decision, coupled with his recent disbanding of the entire 17-member Advisory Committee on Immunization Practices — the group responsible for shaping evidence-based vaccine policy — has raised serious concerns across the healthcare field. On July 9th, AGA joined a coalition of 104 health organizations in submitting a letter to the Chair and Ranking Members of the Senate Committee on Health, Education, Labor and Pensions and the House Committee on Energy and Commerce, urging them to protect the integrity of the USPSTF.
The fight to protect science-based health policy is far from over — effective advocacy necessitates that clinicians use their professional platforms to push back against the politicization of science – not only for the integrity of the medical profession, but for the health and future of the patients we serve.
Megan A. Adams, MD, JD, MSc
Editor in Chief
At-Home Alzheimer’s Testing Is Here: Are Physicians Ready?
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
Given the opportunity, 90% of Americans say they would take a blood biomarker test for Alzheimer’s disease (AD) — even in the absence of symptoms. Notably, 80% say they wouldn’t wait for a physician to order a test, they’d request one themselves.
The findings, from a recent nationwide survey by the Alzheimer’s Association, suggest a growing desire to predict the risk for or show evidence of AD and related dementias with a simple blood test. For consumers with the inclination and the money, that desire can now become reality.
Once limited to research settings or only available via a physician’s order, blood-based diagnostics for specific biomarkers — primarily pTau-217 and beta-amyloid 42/20 — are now offered by at least four companies in the US. Several others sell blood-based “dementia” panels without those biomarkers and screens for apolipoprotein (APOE) genes, including APOE4, a variant that confers a higher risk for AD.
The companies promote testing to all comers, not just those with a family history or concerns about cognitive symptoms. Test prices range from hundreds to thousands of dollars, depending on whether they are included in a company membership, often designed to encourage repeat testing. Blood draws are conducted at home or at certified labs. Buyers don’t need a prescription or to consult with a physician after receiving results.
Knowing results of such tests could be empowering and may encourage people to prepare for their illness, Jessica Mozersky, PhD, assistant professor of medicine at the Bioethics Research Center at Washington University in St. Louis, told this news organization. A direct-to-consumer (DTC) test also eliminates potential physician-created barriers to testing, she added.
But there are also potential harms.
Based on results, individuals may interpret everyday forgetfulness — like misplacing keys — as a sign that dementia is inevitable. This can lead them to change life plans, rethink the way they spend their time, or begin viewing their future negatively. “It creates unnecessary worry and anxiety,” Mozersky said.
The growing availability of DTC tests — heralded by some experts and discouraged by others — comes as AD and dementia specialists continue to debate whether AD diagnostic and staging criteria should be based only on biomarkers or on criteria that includes both pathology and symptomology.
For many, it raises a fundamental concern: If experts haven’t reached a consensus on blood-based AD biomarker testing, how can consumers be expected to interpret at-home test results?
Growing Demand
In 2024, the number of people living with AD passed 7 million. A recent report from the Alzheimer’s Association estimates that number will nearly double by 2060.
The demand for testing also appears to be rising. Similar to the findings in the Alzheimer’s Association’s survey, a small observational study published last year showed that 90% of patients who received a cerebrospinal fluid AD biomarker test ordered by a physician said the decision to get the test was “easy.” For 82%, getting results was positive because it allowed them to plan ahead and to adopt or continue healthy behaviors such as exercise and cognitive activities.
Until now, blood biomarker tests for AD have primarily been available only through a doctor. The tests measure beta-amyloid 42/20 and pTau-217, both of which are strong biomarkers of AD. Some other blood-based biomarkers under investigation include neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP).
As reported by Medscape Medical News, the FDA approved the first blood-based AD diagnostic test in May. The Lumipulse G pTau 217/Beta-Amyloid 1-42 is for the early detection of amyloid plaques associated with AD in adults aged 55 years or older who show signs and symptoms of the disease. But it is only available by prescription.
Quest Diagnostics tested the DTC market in 2023, promoting a consumer-initiated test for beta-amyloid 42/40 that had previously been available only through physicians. It was not well-received by clinicians and ethicists. The company withdrew it later that year but continues to sell beta-amyloid 42/20 and pTau-217 tests through physicians, as does its competitor Labcorp.
Today, at least a handful of companies in the US market AD biomarkers directly to the public: Apollo Health, BetterBrain, Function Health, Neurogen Biomarking, and True Health Labs. None of the companies have disclosed ties to pharmaceutical or device companies or test developers.
What Can Consumers Get?
Some companies direct customers to a lab for blood sample collection, whereas others send a technician to customers’ homes. The extent of biomarker testing and posttest consultation also vary by company.
Apollo Health customers can order a “BrainScan” for $799, which includes screens for pTau-217, GFAP, and NfL. Buyers get a detailed report that explains each test, the result (in nanograms per liter) and optimal range (ng/L) and potential next steps. A pTau-217 result in the normal range, for instance, would come with a recommendation for repeat testing every 2 years. If someone receives an abnormal result, they are contacted by a health coach who can make a physician referral.
At Function Health, members pay $499 a year to have access to hundreds of tests and a written summary of results by a clinician. All of its “Brain Health” tests, including “Beta-Amyloid 42/40 Ratio,” pTau-217, APOE, MTHFR, DNA, and NfL, are available for an additional undisclosed charge.
BetterBrain has a $399 membership that covers an initial 75-minute consultation with cognitive tests, a “personalized brain health plan,” and a blood test that is a basic panel without AD biomarkers. A $499 membership includes all of that plus an APOE test. A pTau-217 test is available for an additional undisclosed fee.
At Neurogen Biomarking, which started in January, a consumer orders an at-home test kit, and a phlebotomist comes to their home for a blood draw. The consumer then fills out an online cognitive assessment. Test results are reviewed by a board-certified neurologist and discussed with the consumer via a virtual visit. If the person is at low-risk, they are given some educational material. Those at higher risk are referred to Neurogen’s “team of specialty-trained neurologists” for continuing care. Testing costs were not provided by the company.
Consumers can order “Beta-Amyloid 42/40” for $749 and pTau-217 for $229 directly through True Health Labs. No consultations or services are offered.
DTC Testing Raises Alarms
It’s unclear where DTC tests fall in terms of regulation. The FDA does not usually review at-home tests for low-risk medical purposes but will generally do so for diagnostics that are for higher-risk conditions “to determine the validity of test claims,” according to the agency’s website.
Consumers, however, don’t usually have easy access to information on biomarker tests’ sensitivity, specificity, or other characteristics that would be used by clinicians or regulatory authorities to assess a test’s validity.
The lack of regulation of consumer-initiated AD testing is one issue cited by critics of at-home tests, including the Alzheimer’s Association.
“None of these tests have been scientifically proven to be accurate,” the association noted in a statement, adding that “the tests can have false positive results, meaning that individuals can have results saying they have dementia when in fact they do not.”
“For these and other reasons, the Alzheimer’s Association believes that home screening tests cannot and should not be used as a substitute for a thorough examination by a skilled physician. The whole process of assessment and diagnosis should be carried out within the context of an ongoing relationship with a responsible and qualified healthcare professional,” the statement said.
The association also said that biomarker tests should not be ordered — even by physicians — for asymptomatic individuals.
The American Academy of Neurology (AAN) does not have a position on DTC tests for AD biomarkers, a spokesperson told this news organization. In a 2021 paper on ethical considerations for diagnosis and care, an AAN committee said that biomarker testing could be clinically useful for some symptomatic patients, but testing asymptomatic individuals is “recommended solely in a research setting” because of potential harms “and the absence of interventions capable of favorably altering the natural history of the disease.”
Eric Topol, MD, chair of the Department of Translational Medicine at Scripps Research in La Jolla, California, is bullish on the potential for blood-based biomarker tests. In a blog post, he called the pTau-217 biomarker “one of the most exciting advances in neurology for decades, giving us a new opportunity to accurately predict and potentially prevent (or at least substantially delay) mild cognitive impairment and Alzheimer’s.”
But, wrote Topol, who is the former editor in chief of MedscapeMedical News, “I don’t think these biomarkers are going to be useful in people at low risk.” He wrote that testing should not be used by people who are “cognitively intact” or to tell someone they have pre-AD. “More work needs to be done to determine whether lowering one’s pTau-217 will alter the brain plaque progression and be seen as a disease-modifier,” wrote Topol.
The Risks of Knowing
Some people don’t want to know their biomarker status. In a study in May in JAMA Network Open, Mozersky and colleagues reported that while 81% of a group of cognitively normal participants in a longitudinal study of dementia said they wanted to see results, only 60% ultimately opted to get results after testing. Participants said they did not want to know because they didn’t want to become a burden on their family or that they felt fine; others had concerns about whether the tests were accurate.
That low number “surprised us,” said Mozersky. “Our study certainly suggests that when you’re really faced with knowing, that your answer is more likely to possibly be no,” she added.
DTC companies tell buyers that results could motivate them to change their lifestyle to reduce their future risk for AD and dementia. But some participants in Mozersky’s study said they didn’t want to know their status because there were no preventive treatments. Test results weren’t seen as “actionable,” she said.
Some studies have shown a degree of fatalism in individuals after receiving a test result, whether it’s positive or negative.
A group of Israeli researchers studied responses of people given PET scans to detect beta-amyloid. Before testing, all participants said they were motivated to adopt lifestyle changes to fight dementia. However, after testing, both those who had elevated beta-amyloid and those who did not reported a much lower desire to change their lifestyle. Those with normal scans probably felt relieved, wrote the researchers. The group with abnormal scans was too small to fully understand their reaction, they wrote.
Concerns about insurance coverage might also deter potential test-takers. Overall, 44% of those responding to the Alzheimer’s Association survey said they were worried that insurers might not cover healthcare costs in the future if they had received a positive test earlier. Respondents also worried about test accuracy, the cost of testing, and whether a positive test might lead to a prohibition on some activities, like driving.
What About the Doctors?
The DTC companies promise buyers that results will be private and won’t be shared with insurers — or with clinicians. And that raises another issue for many who are concerned about the lack of a physician intermediary with at-home testing.
“You remove the opportunity for clinicians to both review the result and figure out how to interpret it before it’s communicated to the patient,” Jalayne J. Arias, JD, a bioethicist and associate professor of Health Policy and Behavioral Sciences at Georgia State University, Atlanta, told this news organization.
Many in the field have been “thinking really carefully about how do we provide guidance to clinicians about biomarker testing,” she said. “Those issues are just heightened when we put it into a direct-to-consumer model,” Arias said.
Arias — who with colleagues published an analysis of potential insurance issues with biomarker tests in JAMA Neurology — said that prohibitions against discrimination based on preexisting conditions means that most likely, health insurers could not use testing data to deny coverage or increase premiums.
But, she said, “there are some question marks around the discrimination risks.” This is especially true for people seeking long-term care, disability or life insurance, she added.
If a test result is not documented in a medical record, it’s not clear whether the individual has an obligation to disclose the result to an insurer, said Arias.
Given all the unanswered questions about how results should be interpreted, to whom the results should be disclosed, and when and how to have discussions with patients, “it’s hard for me to imagine that we’re quite ready for a direct-to-consumer” test, Arias said.
Mozersky noted that Washington University has a financial stake in C2N Diagnostics, which makes the PrecivityAD — biomarker tests for AD. Arias reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.

First New PTSD Drug in Two Decades On the Horizon?
The Psychopharmacologic Drugs Advisory Committee of the FDA is set to meet on July 18 to consider a supplemental new drug application for brexpiprazole (Rexulti, Otsuka Pharmaceutical Co., Ltd.), in combination with sertraline, for the treatment of adults with posttraumatic stress disorder (PTSD).
If approved, it would be the first new treatment for PTSD in more than 20 years.
“It is my hope that the FDA does approve this treatment for two related reasons — the data look positive and compelling, and there’s a tremendous unmet need in PTSD,” Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the Mood Disorders Psychopharmacology Unit, University of Toronto, Toronto, Ontario, Canada, told this news organization.
What’s in the Treatment Toolbox Now?
PTSD is a “common, severe, and nonremitting condition,” McIntyre noted. According to the National Center for PTSD, the condition affects roughly 13 million adults in the US in any given year. This represents about 5% of the adult population.
PTSD can develop following exposure to traumatic events such as combat, assault, disasters, or severe accidents. Core symptoms of PTSD include intrusive memories and flashbacks, avoidance behaviors, negative alterations in mood and cognition, and hyperarousal.
Currently, the selective serotonin reuptake inhibitors (SSRI), sertraline and paroxetine, are the only FDA-approved medications for PTSD, and while these medications can be effective, many patients fail to achieve remission or discontinue treatment due to adverse effects or lack of response.
Other medications used off-label to treat PTSD — including prazosin, mirtazapine, atypical antipsychotics, and mood stabilizers — have shown variable efficacy.
There has not been a new FDA-approved drug for PTSD in over two decades, underscoring the need for better therapeutic options, particularly for patients who do not fully respond to SSRI alone.
Why Brexpiprazole Plus Sertraline?
Brexpiprazole is an atypical antipsychotic currently approved as adjunctive treatment of major depressive disorder (MDD) in adults; treatment of schizophrenia in adults and adolescents aged 13 years or older; and treatment of agitation associated with Alzheimer’s dementia.
The combination of brexpiprazole and sertraline could address the limitations of SSRI alone by working synergistically to treat PTSD.
Sertraline increases serotonin levels in the brain to improve mood and reduce anxiety. Brexpiprazole has a complex mechanism of action involving multiple neurotransmitter systems, including but not limited to serotonin and dopamine.
Together, they may target different aspects of PTSD, potentially leading to a more comprehensive reduction in symptoms.
What Do the Phase 3 Data Show?
In a pivotal, double-blind, randomized controlled, phase 3 trial, brexpiprazole plus sertraline provided significantly greater relief of PTSD symptoms than sertraline plus placebo.
The results were published late last year in JAMA Psychiatry and reported by this news organization at that time.
The trial enrolled 416 adults (mean age, 37 years; 75% women) aged 18-65 years with a Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnosis of PTSD and symptoms for at least 6 months prior to screening.
At baseline, participants had a mean Clinician Administered PTSD Scale (CAPS-5) for DSM-5 total score of 38.4, indicating moderate to high severity PTSD. The average time from the index traumatic event was 4 years, and three fourths had no prior exposure to PTSD prescription medications.
Participants underwent a 1-week placebo run-in period followed by randomization to daily oral brexpiprazole 2-3 mg plus sertraline 150 mg or daily sertraline 150 mg plus placebo for 11 weeks.
At week 10, brexpiprazole plus sertraline demonstrated statistically significant greater improvement in the CAPS-5 total score (primary outcome) than sertraline plus placebo (mean change, -19.2 points vs -13.6 points; P < .001).
Brexpiprazole plus sertraline also led to statistically significant greater improvement on all key secondary and other efficacy endpoints, both clinician-reported and patient-reported, including measures of anxiety, depression, intrusive symptoms, hyperarousal, and overall functioning.
Combining an atypical antipsychotic with an antidepressant for PTSD “builds on what we’ve been doing in depression,” Elspeth Ritchie, MD, chair of Psychiatry, MedStar Washington Hospital Center, Washington, DC, noted in an interview with this news organization.
“We have found that a combination of a low-dose antipsychotic and an antidepressant is helpful for depression, so it makes sense that it will be helpful for PTSD. However, this has been mostly based on clinical decisions, without a heavy research background. Good science is always helpful to support those clinical decisions,” Ritchie told this news organization.
What About Safety?
In the phase 3 trial, brexpiprazole plus sertraline had a safety profile consistent with that of brexpiprazole in approved indications. The rate of discontinuation due to adverse events was low (3.9% for brexpiprazole plus sertraline vs 10.2% for sertraline plus placebo), indicating that most participants tolerated the brexpiprazole and sertraline combination treatment, the study team said.
In both treatment groups, the only treatment-emergent adverse event (TEAE) with incidence greater than 10% was nausea, a known adverse effect of sertraline treatment.
Weight gain was greater in participants receiving the combination. At the last visit, a weight gain of 7% or greater from week 1 was experienced by 8% of participants taking brexpiprazole with the sertraline group and 5% of those taking the sertraline plus placebo. Previous analyses in schizophrenia and MDD show that brexpiprazole is associated with moderate weight gain (+3 to 4 kg over 1 year).
The incidence of sedating TEAEs (a concern with some antipsychotics) was generally low, although fatigue (7% vs 4%) and somnolence (5% vs 3%) were more common with brexpiprazole plus sertraline than with sertraline alone.
There were no clinically meaningful between-group differences in changes in laboratory test parameters, vital signs, or ECG and participant-reported TEAEs related to suicidality.
Potential Concerns
As with any new drug application, several questions and issues are likely to be raised by the advisory committee. They could include whether the clinical benefit is substantial enough to warrant approval and how the observed effect sizes compare to existing approved therapies and evidence-based psychotherapies.
McIntyre told this news organization what’s particularly noteworthy is that the magnitude of the improvement in PTSD symptoms with brexpiprazole plus sertraline is greater than with sertraline alone. “That’s a very important statement. And this high level of efficacy was consistent on the secondary outcome measures, and the overall tolerability and safety seemed very acceptable,” he said.
What’s equally important, said McIntyre, is that most people with PTSD have depression and anxiety, and the brexpiprazole plus sertraline combination was more helpful than sertraline alone on the measures of anxiety and depression. “This is really important, especially in light of the fact that this medication [brexpiprazole] is already approved for adults living with major depressive disorder and inadequate response to antidepressants,” McIntyre said.
McIntyre added he suspects some questions the committee may have could relate to the extent to which it’s the case that brexpiprazole is effective in PTSD regardless of the antidepressant that is prescribed with it.
“There also will be the inevitable questions about the absence of long-term data which I think will need to be addressed given how chronic and relapse prone this condition is,” McIntyre said.
The committee may ask how trauma and PTSD will be screened in primary care and how outcomes related to this therapy will be evaluated in everyday clinical practice, McIntyre said.
Overall, McIntyre said brexpiprazole plus sertraline in PTSD is a “very positive” development for the field.
“PTSD is a terrible condition. It’s so darn common, and we just don’t have enough treatments for it. The data look good for my perspective. My fingers are crossed for the patients with PTSD and their families,” said McIntyre.
Ritchie reported having no relevant disclosures. McIntyre received speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and atai Life Sciences. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
The Psychopharmacologic Drugs Advisory Committee of the FDA is set to meet on July 18 to consider a supplemental new drug application for brexpiprazole (Rexulti, Otsuka Pharmaceutical Co., Ltd.), in combination with sertraline, for the treatment of adults with posttraumatic stress disorder (PTSD).
If approved, it would be the first new treatment for PTSD in more than 20 years.
“It is my hope that the FDA does approve this treatment for two related reasons — the data look positive and compelling, and there’s a tremendous unmet need in PTSD,” Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the Mood Disorders Psychopharmacology Unit, University of Toronto, Toronto, Ontario, Canada, told this news organization.
What’s in the Treatment Toolbox Now?
PTSD is a “common, severe, and nonremitting condition,” McIntyre noted. According to the National Center for PTSD, the condition affects roughly 13 million adults in the US in any given year. This represents about 5% of the adult population.
PTSD can develop following exposure to traumatic events such as combat, assault, disasters, or severe accidents. Core symptoms of PTSD include intrusive memories and flashbacks, avoidance behaviors, negative alterations in mood and cognition, and hyperarousal.
Currently, the selective serotonin reuptake inhibitors (SSRI), sertraline and paroxetine, are the only FDA-approved medications for PTSD, and while these medications can be effective, many patients fail to achieve remission or discontinue treatment due to adverse effects or lack of response.
Other medications used off-label to treat PTSD — including prazosin, mirtazapine, atypical antipsychotics, and mood stabilizers — have shown variable efficacy.
There has not been a new FDA-approved drug for PTSD in over two decades, underscoring the need for better therapeutic options, particularly for patients who do not fully respond to SSRI alone.
Why Brexpiprazole Plus Sertraline?
Brexpiprazole is an atypical antipsychotic currently approved as adjunctive treatment of major depressive disorder (MDD) in adults; treatment of schizophrenia in adults and adolescents aged 13 years or older; and treatment of agitation associated with Alzheimer’s dementia.
The combination of brexpiprazole and sertraline could address the limitations of SSRI alone by working synergistically to treat PTSD.
Sertraline increases serotonin levels in the brain to improve mood and reduce anxiety. Brexpiprazole has a complex mechanism of action involving multiple neurotransmitter systems, including but not limited to serotonin and dopamine.
Together, they may target different aspects of PTSD, potentially leading to a more comprehensive reduction in symptoms.
What Do the Phase 3 Data Show?
In a pivotal, double-blind, randomized controlled, phase 3 trial, brexpiprazole plus sertraline provided significantly greater relief of PTSD symptoms than sertraline plus placebo.
The results were published late last year in JAMA Psychiatry and reported by this news organization at that time.
The trial enrolled 416 adults (mean age, 37 years; 75% women) aged 18-65 years with a Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnosis of PTSD and symptoms for at least 6 months prior to screening.
At baseline, participants had a mean Clinician Administered PTSD Scale (CAPS-5) for DSM-5 total score of 38.4, indicating moderate to high severity PTSD. The average time from the index traumatic event was 4 years, and three fourths had no prior exposure to PTSD prescription medications.
Participants underwent a 1-week placebo run-in period followed by randomization to daily oral brexpiprazole 2-3 mg plus sertraline 150 mg or daily sertraline 150 mg plus placebo for 11 weeks.
At week 10, brexpiprazole plus sertraline demonstrated statistically significant greater improvement in the CAPS-5 total score (primary outcome) than sertraline plus placebo (mean change, -19.2 points vs -13.6 points; P < .001).
Brexpiprazole plus sertraline also led to statistically significant greater improvement on all key secondary and other efficacy endpoints, both clinician-reported and patient-reported, including measures of anxiety, depression, intrusive symptoms, hyperarousal, and overall functioning.
Combining an atypical antipsychotic with an antidepressant for PTSD “builds on what we’ve been doing in depression,” Elspeth Ritchie, MD, chair of Psychiatry, MedStar Washington Hospital Center, Washington, DC, noted in an interview with this news organization.
“We have found that a combination of a low-dose antipsychotic and an antidepressant is helpful for depression, so it makes sense that it will be helpful for PTSD. However, this has been mostly based on clinical decisions, without a heavy research background. Good science is always helpful to support those clinical decisions,” Ritchie told this news organization.
What About Safety?
In the phase 3 trial, brexpiprazole plus sertraline had a safety profile consistent with that of brexpiprazole in approved indications. The rate of discontinuation due to adverse events was low (3.9% for brexpiprazole plus sertraline vs 10.2% for sertraline plus placebo), indicating that most participants tolerated the brexpiprazole and sertraline combination treatment, the study team said.
In both treatment groups, the only treatment-emergent adverse event (TEAE) with incidence greater than 10% was nausea, a known adverse effect of sertraline treatment.
Weight gain was greater in participants receiving the combination. At the last visit, a weight gain of 7% or greater from week 1 was experienced by 8% of participants taking brexpiprazole with the sertraline group and 5% of those taking the sertraline plus placebo. Previous analyses in schizophrenia and MDD show that brexpiprazole is associated with moderate weight gain (+3 to 4 kg over 1 year).
The incidence of sedating TEAEs (a concern with some antipsychotics) was generally low, although fatigue (7% vs 4%) and somnolence (5% vs 3%) were more common with brexpiprazole plus sertraline than with sertraline alone.
There were no clinically meaningful between-group differences in changes in laboratory test parameters, vital signs, or ECG and participant-reported TEAEs related to suicidality.
Potential Concerns
As with any new drug application, several questions and issues are likely to be raised by the advisory committee. They could include whether the clinical benefit is substantial enough to warrant approval and how the observed effect sizes compare to existing approved therapies and evidence-based psychotherapies.
McIntyre told this news organization what’s particularly noteworthy is that the magnitude of the improvement in PTSD symptoms with brexpiprazole plus sertraline is greater than with sertraline alone. “That’s a very important statement. And this high level of efficacy was consistent on the secondary outcome measures, and the overall tolerability and safety seemed very acceptable,” he said.
What’s equally important, said McIntyre, is that most people with PTSD have depression and anxiety, and the brexpiprazole plus sertraline combination was more helpful than sertraline alone on the measures of anxiety and depression. “This is really important, especially in light of the fact that this medication [brexpiprazole] is already approved for adults living with major depressive disorder and inadequate response to antidepressants,” McIntyre said.
McIntyre added he suspects some questions the committee may have could relate to the extent to which it’s the case that brexpiprazole is effective in PTSD regardless of the antidepressant that is prescribed with it.
“There also will be the inevitable questions about the absence of long-term data which I think will need to be addressed given how chronic and relapse prone this condition is,” McIntyre said.
The committee may ask how trauma and PTSD will be screened in primary care and how outcomes related to this therapy will be evaluated in everyday clinical practice, McIntyre said.
Overall, McIntyre said brexpiprazole plus sertraline in PTSD is a “very positive” development for the field.
“PTSD is a terrible condition. It’s so darn common, and we just don’t have enough treatments for it. The data look good for my perspective. My fingers are crossed for the patients with PTSD and their families,” said McIntyre.
Ritchie reported having no relevant disclosures. McIntyre received speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and atai Life Sciences. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
The Psychopharmacologic Drugs Advisory Committee of the FDA is set to meet on July 18 to consider a supplemental new drug application for brexpiprazole (Rexulti, Otsuka Pharmaceutical Co., Ltd.), in combination with sertraline, for the treatment of adults with posttraumatic stress disorder (PTSD).
If approved, it would be the first new treatment for PTSD in more than 20 years.
“It is my hope that the FDA does approve this treatment for two related reasons — the data look positive and compelling, and there’s a tremendous unmet need in PTSD,” Roger McIntyre, MD, professor of psychiatry and pharmacology and head of the Mood Disorders Psychopharmacology Unit, University of Toronto, Toronto, Ontario, Canada, told this news organization.
What’s in the Treatment Toolbox Now?
PTSD is a “common, severe, and nonremitting condition,” McIntyre noted. According to the National Center for PTSD, the condition affects roughly 13 million adults in the US in any given year. This represents about 5% of the adult population.
PTSD can develop following exposure to traumatic events such as combat, assault, disasters, or severe accidents. Core symptoms of PTSD include intrusive memories and flashbacks, avoidance behaviors, negative alterations in mood and cognition, and hyperarousal.
Currently, the selective serotonin reuptake inhibitors (SSRI), sertraline and paroxetine, are the only FDA-approved medications for PTSD, and while these medications can be effective, many patients fail to achieve remission or discontinue treatment due to adverse effects or lack of response.
Other medications used off-label to treat PTSD — including prazosin, mirtazapine, atypical antipsychotics, and mood stabilizers — have shown variable efficacy.
There has not been a new FDA-approved drug for PTSD in over two decades, underscoring the need for better therapeutic options, particularly for patients who do not fully respond to SSRI alone.
Why Brexpiprazole Plus Sertraline?
Brexpiprazole is an atypical antipsychotic currently approved as adjunctive treatment of major depressive disorder (MDD) in adults; treatment of schizophrenia in adults and adolescents aged 13 years or older; and treatment of agitation associated with Alzheimer’s dementia.
The combination of brexpiprazole and sertraline could address the limitations of SSRI alone by working synergistically to treat PTSD.
Sertraline increases serotonin levels in the brain to improve mood and reduce anxiety. Brexpiprazole has a complex mechanism of action involving multiple neurotransmitter systems, including but not limited to serotonin and dopamine.
Together, they may target different aspects of PTSD, potentially leading to a more comprehensive reduction in symptoms.
What Do the Phase 3 Data Show?
In a pivotal, double-blind, randomized controlled, phase 3 trial, brexpiprazole plus sertraline provided significantly greater relief of PTSD symptoms than sertraline plus placebo.
The results were published late last year in JAMA Psychiatry and reported by this news organization at that time.
The trial enrolled 416 adults (mean age, 37 years; 75% women) aged 18-65 years with a Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnosis of PTSD and symptoms for at least 6 months prior to screening.
At baseline, participants had a mean Clinician Administered PTSD Scale (CAPS-5) for DSM-5 total score of 38.4, indicating moderate to high severity PTSD. The average time from the index traumatic event was 4 years, and three fourths had no prior exposure to PTSD prescription medications.
Participants underwent a 1-week placebo run-in period followed by randomization to daily oral brexpiprazole 2-3 mg plus sertraline 150 mg or daily sertraline 150 mg plus placebo for 11 weeks.
At week 10, brexpiprazole plus sertraline demonstrated statistically significant greater improvement in the CAPS-5 total score (primary outcome) than sertraline plus placebo (mean change, -19.2 points vs -13.6 points; P < .001).
Brexpiprazole plus sertraline also led to statistically significant greater improvement on all key secondary and other efficacy endpoints, both clinician-reported and patient-reported, including measures of anxiety, depression, intrusive symptoms, hyperarousal, and overall functioning.
Combining an atypical antipsychotic with an antidepressant for PTSD “builds on what we’ve been doing in depression,” Elspeth Ritchie, MD, chair of Psychiatry, MedStar Washington Hospital Center, Washington, DC, noted in an interview with this news organization.
“We have found that a combination of a low-dose antipsychotic and an antidepressant is helpful for depression, so it makes sense that it will be helpful for PTSD. However, this has been mostly based on clinical decisions, without a heavy research background. Good science is always helpful to support those clinical decisions,” Ritchie told this news organization.
What About Safety?
In the phase 3 trial, brexpiprazole plus sertraline had a safety profile consistent with that of brexpiprazole in approved indications. The rate of discontinuation due to adverse events was low (3.9% for brexpiprazole plus sertraline vs 10.2% for sertraline plus placebo), indicating that most participants tolerated the brexpiprazole and sertraline combination treatment, the study team said.
In both treatment groups, the only treatment-emergent adverse event (TEAE) with incidence greater than 10% was nausea, a known adverse effect of sertraline treatment.
Weight gain was greater in participants receiving the combination. At the last visit, a weight gain of 7% or greater from week 1 was experienced by 8% of participants taking brexpiprazole with the sertraline group and 5% of those taking the sertraline plus placebo. Previous analyses in schizophrenia and MDD show that brexpiprazole is associated with moderate weight gain (+3 to 4 kg over 1 year).
The incidence of sedating TEAEs (a concern with some antipsychotics) was generally low, although fatigue (7% vs 4%) and somnolence (5% vs 3%) were more common with brexpiprazole plus sertraline than with sertraline alone.
There were no clinically meaningful between-group differences in changes in laboratory test parameters, vital signs, or ECG and participant-reported TEAEs related to suicidality.
Potential Concerns
As with any new drug application, several questions and issues are likely to be raised by the advisory committee. They could include whether the clinical benefit is substantial enough to warrant approval and how the observed effect sizes compare to existing approved therapies and evidence-based psychotherapies.
McIntyre told this news organization what’s particularly noteworthy is that the magnitude of the improvement in PTSD symptoms with brexpiprazole plus sertraline is greater than with sertraline alone. “That’s a very important statement. And this high level of efficacy was consistent on the secondary outcome measures, and the overall tolerability and safety seemed very acceptable,” he said.
What’s equally important, said McIntyre, is that most people with PTSD have depression and anxiety, and the brexpiprazole plus sertraline combination was more helpful than sertraline alone on the measures of anxiety and depression. “This is really important, especially in light of the fact that this medication [brexpiprazole] is already approved for adults living with major depressive disorder and inadequate response to antidepressants,” McIntyre said.
McIntyre added he suspects some questions the committee may have could relate to the extent to which it’s the case that brexpiprazole is effective in PTSD regardless of the antidepressant that is prescribed with it.
“There also will be the inevitable questions about the absence of long-term data which I think will need to be addressed given how chronic and relapse prone this condition is,” McIntyre said.
The committee may ask how trauma and PTSD will be screened in primary care and how outcomes related to this therapy will be evaluated in everyday clinical practice, McIntyre said.
Overall, McIntyre said brexpiprazole plus sertraline in PTSD is a “very positive” development for the field.
“PTSD is a terrible condition. It’s so darn common, and we just don’t have enough treatments for it. The data look good for my perspective. My fingers are crossed for the patients with PTSD and their families,” said McIntyre.
Ritchie reported having no relevant disclosures. McIntyre received speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, and atai Life Sciences. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.