User login
For MD-IQ use only
State-Mandated ‘Gold Card’ Programs to Ease Prior Authorization Burdens Offer Little Relief, Experts Say
“Gold card” programs were supposed to make it easier for frustrated physicians to deal with insurers’ burdensome prior authorization demands.
The idea: Insurers would reward doctors whose past prior authorization requests were typically approved by exempting them from red tape in the future.
At least 10 states have required insurers to establish gold card programs amid mounting concerns nationwide that overuse of prior authorization jeopardizes patient health. Last month, leading insurers joined with the White House in a voluntary pledge to reduce their use of the practice, which they contend is necessary to control costs and minimize unnecessary care.
But Texas’ experience with gold card programs may signal the limits of that approach.
Only 3% of Clinicians Qualified
The Lone Star State was an early adopter, passing a 2021 law enabling health providers with a high prior authorization success rate to earn a “gold card” exemption from insurers.
But statewide, only 3% of providers met that bar, according to a testimony provided by the Texas Department of Insurance earlier this year.
“I think it’s safe to say that the impact of this law on prior authorizations for our physicians is underwhelming,” said Ezequiel “Zeke” Silva III, MD, a San Antonio-based interventional radiologist who chairs the Texas Medical Association’s Council on Legislation. “We would have hoped for a greater percentage of our physicians to have been granted the ‘gold card’ status.”
At least nine other states have enacted gold card laws, according to the National Conference of State Legislatures (NCSL).
Care Delayed and Denied
Physicians maintain that excessive prior authorization paperwork impedes timely patient care, with clinicians and staffers devoting 13 hours weekly to documentation, according to a 2024 American Medical Association survey.
Insurers view the review as a guardrail against unnecessary care driving up costs. Studies show that restricting prior authorization could boost premiums by 5.6%-16.7%, a Texas Association of Health Plans official testified during the legislative session.
In June, Texas Gov. Greg Abbott signed a revised version of the state’s “gold card” law — part of an emerging national attempt to streamline the prior review process. Cigna, Humana, UnitedHealthcare, and other large insurers have voluntarily committed to reducing the scope of claims involved, according to the America’s Health Insurance Plans trade group.
Meanwhile, federal officials have finalized requirements that direct some insurers, including Medicaid and Medicare Advantage programs, to speed up responses to prior authorization requests, among other measures. Some of those requirements begin in 2026.
Gold Card Designs
As in other states, Texas’ “gold card” legislation applies only to state-regulated insurers, which comprise about one fifth of the state’s market. Under HB 3812, which takes effect on September 1, insurers will evaluate health providers based on a year of prior authorization requests rather than 6 months under the 2021 law.
To be evaluated, providers must have submitted at least five requests for a specific health service during that period. To achieve “gold card” status, insurers must approve at least 90% of requests, the same threshold as set by the 2021 law. But the new law stipulates that insurers review a broader pool of requests, including those made directly to the health plan as well as any related affiliates, according to the Texas Department of Insurance.
The new law continues to limit exemptions only to “top-performing physicians” who repeatedly provide cost-effective care, said Blake Hutson, director of public affairs at the Texas Association of Health Plans. “Even with the change to 1 year, and the bill also adds in a broader array of claims that will be looked at, you still have to meet 90%.”
A key addition requires insurers to release an annual report detailing how many exemptions they have granted or denied, making decisions more transparent to the public, Silva said. “Not just what’s being approved and what’s not being approved, but to potentially evaluate for trends that presently we just have no ability to evaluate,” he said.
Gold card laws vary from state to state, and some exclude prescription drugs, according to an NCSL legislative summary. Other states with gold card programs include Arkansas, Colorado, Illinois, Louisiana, Michigan, New Mexico, Vermont, West Virginia, and Wyoming.
In Illinois, legislation passed last year targeted hospital services for Medicaid patients, as denial rates were routinely higher in that population, said Dave Gross, senior vice president of Government Relations and Communications at the Illinois Health and Hospital Association, Naperville, Illinois. “We’re not seeing this problem in the commercial space,” he noted.
Real-World Implications
To some degree, the “gold card” concept makes intuitive sense, recognizing physicians who have a track record of getting their medical care requests approved, said Ravi Gupta, MD, an assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, who has studied prior authorization patterns.
But Gupta raised equity concerns. Physicians in large medical groups and hospital systems will have access to staff and other resources to better navigate the prior approval process than those in smaller private practices.
Plus, he added, there’s the potential that physicians who achieve exemptions may become “more indiscriminate” about the services that they recommend.
Insurers’ stated aim is to reduce unnecessary and low-value medical care through prior authorization gatekeeping, Gupta said. But a study he helped conduct, assessing policies across five Medicare Advantage insurers, found a significant lack of consensus on what treatments should be included. Treatments comprising only 12% of Medicare spending would have required prior authorization by all five insurers. Most of that consensus, he wrote, “was devoted to a small number of costly services.”
The administrative burdens affect patients as well. Two thirds of patients with cancer in one 2023 study become personally involved, including calling the insurer or appealing a denial. The patients also reported less trust in insurers and the health system overall, which could have worrisome downstream effects, Fumiko Chino, MD, the study’s lead author and an assistant professor of radiation oncology at Houston’s MD Anderson Cancer Center, said.
“If you don’t trust healthcare,” she said, “why on earth would you get a vaccine or get cancer screening or get your blood pressure checked?”
More Than X Percent?
Gupta views the leading health insurers’ pledge as encouraging in concept — but he notes that they are voluntary commitments without any accountability.
In the interim, gold carding remains no more than a workaround, he said.
“Gold cards aren’t really fixing that [prior authorization] problem,” he said. “They’re just rewarding certain clinicians who can demonstrate that they have been able to get through the prior authorization process successfully for X amount of time before they’re rewarded with a gold card.”
In Illinois, regulators are still hashing out gold card rules, including whether the required 90% approval threshold will be based on a specific hospital service or a broader pool of services, Gross said. The hospital association also will closely watch whether Illinois’ experience begins to mirror that in Texas, he said.
“We have some of the best hospitals in the country here in Chicago,” he said. “If we end up with a 3% approval rating of gold cards, we’re going to have to go back to the legislature.”
A version of this article first appeared on Medscape.com.
“Gold card” programs were supposed to make it easier for frustrated physicians to deal with insurers’ burdensome prior authorization demands.
The idea: Insurers would reward doctors whose past prior authorization requests were typically approved by exempting them from red tape in the future.
At least 10 states have required insurers to establish gold card programs amid mounting concerns nationwide that overuse of prior authorization jeopardizes patient health. Last month, leading insurers joined with the White House in a voluntary pledge to reduce their use of the practice, which they contend is necessary to control costs and minimize unnecessary care.
But Texas’ experience with gold card programs may signal the limits of that approach.
Only 3% of Clinicians Qualified
The Lone Star State was an early adopter, passing a 2021 law enabling health providers with a high prior authorization success rate to earn a “gold card” exemption from insurers.
But statewide, only 3% of providers met that bar, according to a testimony provided by the Texas Department of Insurance earlier this year.
“I think it’s safe to say that the impact of this law on prior authorizations for our physicians is underwhelming,” said Ezequiel “Zeke” Silva III, MD, a San Antonio-based interventional radiologist who chairs the Texas Medical Association’s Council on Legislation. “We would have hoped for a greater percentage of our physicians to have been granted the ‘gold card’ status.”
At least nine other states have enacted gold card laws, according to the National Conference of State Legislatures (NCSL).
Care Delayed and Denied
Physicians maintain that excessive prior authorization paperwork impedes timely patient care, with clinicians and staffers devoting 13 hours weekly to documentation, according to a 2024 American Medical Association survey.
Insurers view the review as a guardrail against unnecessary care driving up costs. Studies show that restricting prior authorization could boost premiums by 5.6%-16.7%, a Texas Association of Health Plans official testified during the legislative session.
In June, Texas Gov. Greg Abbott signed a revised version of the state’s “gold card” law — part of an emerging national attempt to streamline the prior review process. Cigna, Humana, UnitedHealthcare, and other large insurers have voluntarily committed to reducing the scope of claims involved, according to the America’s Health Insurance Plans trade group.
Meanwhile, federal officials have finalized requirements that direct some insurers, including Medicaid and Medicare Advantage programs, to speed up responses to prior authorization requests, among other measures. Some of those requirements begin in 2026.
Gold Card Designs
As in other states, Texas’ “gold card” legislation applies only to state-regulated insurers, which comprise about one fifth of the state’s market. Under HB 3812, which takes effect on September 1, insurers will evaluate health providers based on a year of prior authorization requests rather than 6 months under the 2021 law.
To be evaluated, providers must have submitted at least five requests for a specific health service during that period. To achieve “gold card” status, insurers must approve at least 90% of requests, the same threshold as set by the 2021 law. But the new law stipulates that insurers review a broader pool of requests, including those made directly to the health plan as well as any related affiliates, according to the Texas Department of Insurance.
The new law continues to limit exemptions only to “top-performing physicians” who repeatedly provide cost-effective care, said Blake Hutson, director of public affairs at the Texas Association of Health Plans. “Even with the change to 1 year, and the bill also adds in a broader array of claims that will be looked at, you still have to meet 90%.”
A key addition requires insurers to release an annual report detailing how many exemptions they have granted or denied, making decisions more transparent to the public, Silva said. “Not just what’s being approved and what’s not being approved, but to potentially evaluate for trends that presently we just have no ability to evaluate,” he said.
Gold card laws vary from state to state, and some exclude prescription drugs, according to an NCSL legislative summary. Other states with gold card programs include Arkansas, Colorado, Illinois, Louisiana, Michigan, New Mexico, Vermont, West Virginia, and Wyoming.
In Illinois, legislation passed last year targeted hospital services for Medicaid patients, as denial rates were routinely higher in that population, said Dave Gross, senior vice president of Government Relations and Communications at the Illinois Health and Hospital Association, Naperville, Illinois. “We’re not seeing this problem in the commercial space,” he noted.
Real-World Implications
To some degree, the “gold card” concept makes intuitive sense, recognizing physicians who have a track record of getting their medical care requests approved, said Ravi Gupta, MD, an assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, who has studied prior authorization patterns.
But Gupta raised equity concerns. Physicians in large medical groups and hospital systems will have access to staff and other resources to better navigate the prior approval process than those in smaller private practices.
Plus, he added, there’s the potential that physicians who achieve exemptions may become “more indiscriminate” about the services that they recommend.
Insurers’ stated aim is to reduce unnecessary and low-value medical care through prior authorization gatekeeping, Gupta said. But a study he helped conduct, assessing policies across five Medicare Advantage insurers, found a significant lack of consensus on what treatments should be included. Treatments comprising only 12% of Medicare spending would have required prior authorization by all five insurers. Most of that consensus, he wrote, “was devoted to a small number of costly services.”
The administrative burdens affect patients as well. Two thirds of patients with cancer in one 2023 study become personally involved, including calling the insurer or appealing a denial. The patients also reported less trust in insurers and the health system overall, which could have worrisome downstream effects, Fumiko Chino, MD, the study’s lead author and an assistant professor of radiation oncology at Houston’s MD Anderson Cancer Center, said.
“If you don’t trust healthcare,” she said, “why on earth would you get a vaccine or get cancer screening or get your blood pressure checked?”
More Than X Percent?
Gupta views the leading health insurers’ pledge as encouraging in concept — but he notes that they are voluntary commitments without any accountability.
In the interim, gold carding remains no more than a workaround, he said.
“Gold cards aren’t really fixing that [prior authorization] problem,” he said. “They’re just rewarding certain clinicians who can demonstrate that they have been able to get through the prior authorization process successfully for X amount of time before they’re rewarded with a gold card.”
In Illinois, regulators are still hashing out gold card rules, including whether the required 90% approval threshold will be based on a specific hospital service or a broader pool of services, Gross said. The hospital association also will closely watch whether Illinois’ experience begins to mirror that in Texas, he said.
“We have some of the best hospitals in the country here in Chicago,” he said. “If we end up with a 3% approval rating of gold cards, we’re going to have to go back to the legislature.”
A version of this article first appeared on Medscape.com.
“Gold card” programs were supposed to make it easier for frustrated physicians to deal with insurers’ burdensome prior authorization demands.
The idea: Insurers would reward doctors whose past prior authorization requests were typically approved by exempting them from red tape in the future.
At least 10 states have required insurers to establish gold card programs amid mounting concerns nationwide that overuse of prior authorization jeopardizes patient health. Last month, leading insurers joined with the White House in a voluntary pledge to reduce their use of the practice, which they contend is necessary to control costs and minimize unnecessary care.
But Texas’ experience with gold card programs may signal the limits of that approach.
Only 3% of Clinicians Qualified
The Lone Star State was an early adopter, passing a 2021 law enabling health providers with a high prior authorization success rate to earn a “gold card” exemption from insurers.
But statewide, only 3% of providers met that bar, according to a testimony provided by the Texas Department of Insurance earlier this year.
“I think it’s safe to say that the impact of this law on prior authorizations for our physicians is underwhelming,” said Ezequiel “Zeke” Silva III, MD, a San Antonio-based interventional radiologist who chairs the Texas Medical Association’s Council on Legislation. “We would have hoped for a greater percentage of our physicians to have been granted the ‘gold card’ status.”
At least nine other states have enacted gold card laws, according to the National Conference of State Legislatures (NCSL).
Care Delayed and Denied
Physicians maintain that excessive prior authorization paperwork impedes timely patient care, with clinicians and staffers devoting 13 hours weekly to documentation, according to a 2024 American Medical Association survey.
Insurers view the review as a guardrail against unnecessary care driving up costs. Studies show that restricting prior authorization could boost premiums by 5.6%-16.7%, a Texas Association of Health Plans official testified during the legislative session.
In June, Texas Gov. Greg Abbott signed a revised version of the state’s “gold card” law — part of an emerging national attempt to streamline the prior review process. Cigna, Humana, UnitedHealthcare, and other large insurers have voluntarily committed to reducing the scope of claims involved, according to the America’s Health Insurance Plans trade group.
Meanwhile, federal officials have finalized requirements that direct some insurers, including Medicaid and Medicare Advantage programs, to speed up responses to prior authorization requests, among other measures. Some of those requirements begin in 2026.
Gold Card Designs
As in other states, Texas’ “gold card” legislation applies only to state-regulated insurers, which comprise about one fifth of the state’s market. Under HB 3812, which takes effect on September 1, insurers will evaluate health providers based on a year of prior authorization requests rather than 6 months under the 2021 law.
To be evaluated, providers must have submitted at least five requests for a specific health service during that period. To achieve “gold card” status, insurers must approve at least 90% of requests, the same threshold as set by the 2021 law. But the new law stipulates that insurers review a broader pool of requests, including those made directly to the health plan as well as any related affiliates, according to the Texas Department of Insurance.
The new law continues to limit exemptions only to “top-performing physicians” who repeatedly provide cost-effective care, said Blake Hutson, director of public affairs at the Texas Association of Health Plans. “Even with the change to 1 year, and the bill also adds in a broader array of claims that will be looked at, you still have to meet 90%.”
A key addition requires insurers to release an annual report detailing how many exemptions they have granted or denied, making decisions more transparent to the public, Silva said. “Not just what’s being approved and what’s not being approved, but to potentially evaluate for trends that presently we just have no ability to evaluate,” he said.
Gold card laws vary from state to state, and some exclude prescription drugs, according to an NCSL legislative summary. Other states with gold card programs include Arkansas, Colorado, Illinois, Louisiana, Michigan, New Mexico, Vermont, West Virginia, and Wyoming.
In Illinois, legislation passed last year targeted hospital services for Medicaid patients, as denial rates were routinely higher in that population, said Dave Gross, senior vice president of Government Relations and Communications at the Illinois Health and Hospital Association, Naperville, Illinois. “We’re not seeing this problem in the commercial space,” he noted.
Real-World Implications
To some degree, the “gold card” concept makes intuitive sense, recognizing physicians who have a track record of getting their medical care requests approved, said Ravi Gupta, MD, an assistant professor of medicine at Johns Hopkins University School of Medicine, Baltimore, who has studied prior authorization patterns.
But Gupta raised equity concerns. Physicians in large medical groups and hospital systems will have access to staff and other resources to better navigate the prior approval process than those in smaller private practices.
Plus, he added, there’s the potential that physicians who achieve exemptions may become “more indiscriminate” about the services that they recommend.
Insurers’ stated aim is to reduce unnecessary and low-value medical care through prior authorization gatekeeping, Gupta said. But a study he helped conduct, assessing policies across five Medicare Advantage insurers, found a significant lack of consensus on what treatments should be included. Treatments comprising only 12% of Medicare spending would have required prior authorization by all five insurers. Most of that consensus, he wrote, “was devoted to a small number of costly services.”
The administrative burdens affect patients as well. Two thirds of patients with cancer in one 2023 study become personally involved, including calling the insurer or appealing a denial. The patients also reported less trust in insurers and the health system overall, which could have worrisome downstream effects, Fumiko Chino, MD, the study’s lead author and an assistant professor of radiation oncology at Houston’s MD Anderson Cancer Center, said.
“If you don’t trust healthcare,” she said, “why on earth would you get a vaccine or get cancer screening or get your blood pressure checked?”
More Than X Percent?
Gupta views the leading health insurers’ pledge as encouraging in concept — but he notes that they are voluntary commitments without any accountability.
In the interim, gold carding remains no more than a workaround, he said.
“Gold cards aren’t really fixing that [prior authorization] problem,” he said. “They’re just rewarding certain clinicians who can demonstrate that they have been able to get through the prior authorization process successfully for X amount of time before they’re rewarded with a gold card.”
In Illinois, regulators are still hashing out gold card rules, including whether the required 90% approval threshold will be based on a specific hospital service or a broader pool of services, Gross said. The hospital association also will closely watch whether Illinois’ experience begins to mirror that in Texas, he said.
“We have some of the best hospitals in the country here in Chicago,” he said. “If we end up with a 3% approval rating of gold cards, we’re going to have to go back to the legislature.”
A version of this article first appeared on Medscape.com.
Dementia Risk May Follow a Geographic Pattern
TOPLINE:
Dementia incidence varied significantly by US region in a new study, with the Southeast showing a 25% higher risk and the Northwest and Rocky Mountains each showing a 23% higher risk compared to the Mid-Atlantic. Investigators said the findings highlight the need for a geographically tailored approach to address dementia risk factors and diagnostic services.
METHODOLOGY:
- Researchers conducted a cohort study using data from the US Veterans Health Administration for more than 1.2 million older adults without dementia (mean age, 73.9 years; 98%% men) from 1999 to 2021. The average follow-up was 12.6 years.
- Ten geographical regions across the US were defined using the CDC National Center for Chronic Disease Prevention and Health Promotion definition.
- The diagnosis of dementia was made using International Classification of Diseases, Ninth and Tenth Revision codes from inpatient and outpatient visits.
TAKEAWAY:
- Dementia incidence rates per 1000 person-years were lowest in the Mid-Atlantic (11.2; 95% CI, 11.1-11.4) and highest in the Southeast (14.0; 95% CI, 13.8-14.2).
- After adjusting for demographics, compared with the Mid-Atlantic region, dementia incidence was highest in the Southeast (rate ratio [RR], 1.25), followed by the Northwest and Rocky Mountains (RR for both, 1.23), South (RR, 1.18), Southwest (RR, 1.13), and Midwest and South Atlantic (RR for both, 1.12). The Great Lakes and Northeast regions had < a 10% difference in incidence.
- Results remained consistent after adjusting for rurality and cardiovascular comorbidities, and after accounting for competing risk for death.
IN PRACTICE:
“This study provides valuable insights into the regional variation in dementia incidence among US veterans in that we observed more than 20% greater incidence in several regions compared with the Mid-Atlantic region,” the investigators wrote.
“By identifying areas with the highest incidence rates, resources can be better allocated and targeted interventions designed to mitigate the impact of dementia on vulnerable populations,” they added.
SOURCE:
This study was led by Christina S. Dintica, PhD, University of California, San Francisco. It was published online on June 9 in JAMA Neurology.
LIMITATIONS:
This study population was limited to US veterans, limiting the generalizability of the findings. Education level was defined using educational attainment rates in the participants’ zip codes rather than individual data. Additionally, because residential history was limited to a single location per participant, migration patterns could not be tracked.
DISCLOSURES:
This study was supported by grants from the Alzheimer’s Association, the National Institute on Aging, and the Department of Defense. One author reported serving on data and safety monitoring boards for studies sponsored by the National Institutes of Health, as well as holding advisory board membership and receiving personal fees from industry. Full details are listed in the original article. The other four investigators reported no relevant financial conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Dementia incidence varied significantly by US region in a new study, with the Southeast showing a 25% higher risk and the Northwest and Rocky Mountains each showing a 23% higher risk compared to the Mid-Atlantic. Investigators said the findings highlight the need for a geographically tailored approach to address dementia risk factors and diagnostic services.
METHODOLOGY:
- Researchers conducted a cohort study using data from the US Veterans Health Administration for more than 1.2 million older adults without dementia (mean age, 73.9 years; 98%% men) from 1999 to 2021. The average follow-up was 12.6 years.
- Ten geographical regions across the US were defined using the CDC National Center for Chronic Disease Prevention and Health Promotion definition.
- The diagnosis of dementia was made using International Classification of Diseases, Ninth and Tenth Revision codes from inpatient and outpatient visits.
TAKEAWAY:
- Dementia incidence rates per 1000 person-years were lowest in the Mid-Atlantic (11.2; 95% CI, 11.1-11.4) and highest in the Southeast (14.0; 95% CI, 13.8-14.2).
- After adjusting for demographics, compared with the Mid-Atlantic region, dementia incidence was highest in the Southeast (rate ratio [RR], 1.25), followed by the Northwest and Rocky Mountains (RR for both, 1.23), South (RR, 1.18), Southwest (RR, 1.13), and Midwest and South Atlantic (RR for both, 1.12). The Great Lakes and Northeast regions had < a 10% difference in incidence.
- Results remained consistent after adjusting for rurality and cardiovascular comorbidities, and after accounting for competing risk for death.
IN PRACTICE:
“This study provides valuable insights into the regional variation in dementia incidence among US veterans in that we observed more than 20% greater incidence in several regions compared with the Mid-Atlantic region,” the investigators wrote.
“By identifying areas with the highest incidence rates, resources can be better allocated and targeted interventions designed to mitigate the impact of dementia on vulnerable populations,” they added.
SOURCE:
This study was led by Christina S. Dintica, PhD, University of California, San Francisco. It was published online on June 9 in JAMA Neurology.
LIMITATIONS:
This study population was limited to US veterans, limiting the generalizability of the findings. Education level was defined using educational attainment rates in the participants’ zip codes rather than individual data. Additionally, because residential history was limited to a single location per participant, migration patterns could not be tracked.
DISCLOSURES:
This study was supported by grants from the Alzheimer’s Association, the National Institute on Aging, and the Department of Defense. One author reported serving on data and safety monitoring boards for studies sponsored by the National Institutes of Health, as well as holding advisory board membership and receiving personal fees from industry. Full details are listed in the original article. The other four investigators reported no relevant financial conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Dementia incidence varied significantly by US region in a new study, with the Southeast showing a 25% higher risk and the Northwest and Rocky Mountains each showing a 23% higher risk compared to the Mid-Atlantic. Investigators said the findings highlight the need for a geographically tailored approach to address dementia risk factors and diagnostic services.
METHODOLOGY:
- Researchers conducted a cohort study using data from the US Veterans Health Administration for more than 1.2 million older adults without dementia (mean age, 73.9 years; 98%% men) from 1999 to 2021. The average follow-up was 12.6 years.
- Ten geographical regions across the US were defined using the CDC National Center for Chronic Disease Prevention and Health Promotion definition.
- The diagnosis of dementia was made using International Classification of Diseases, Ninth and Tenth Revision codes from inpatient and outpatient visits.
TAKEAWAY:
- Dementia incidence rates per 1000 person-years were lowest in the Mid-Atlantic (11.2; 95% CI, 11.1-11.4) and highest in the Southeast (14.0; 95% CI, 13.8-14.2).
- After adjusting for demographics, compared with the Mid-Atlantic region, dementia incidence was highest in the Southeast (rate ratio [RR], 1.25), followed by the Northwest and Rocky Mountains (RR for both, 1.23), South (RR, 1.18), Southwest (RR, 1.13), and Midwest and South Atlantic (RR for both, 1.12). The Great Lakes and Northeast regions had < a 10% difference in incidence.
- Results remained consistent after adjusting for rurality and cardiovascular comorbidities, and after accounting for competing risk for death.
IN PRACTICE:
“This study provides valuable insights into the regional variation in dementia incidence among US veterans in that we observed more than 20% greater incidence in several regions compared with the Mid-Atlantic region,” the investigators wrote.
“By identifying areas with the highest incidence rates, resources can be better allocated and targeted interventions designed to mitigate the impact of dementia on vulnerable populations,” they added.
SOURCE:
This study was led by Christina S. Dintica, PhD, University of California, San Francisco. It was published online on June 9 in JAMA Neurology.
LIMITATIONS:
This study population was limited to US veterans, limiting the generalizability of the findings. Education level was defined using educational attainment rates in the participants’ zip codes rather than individual data. Additionally, because residential history was limited to a single location per participant, migration patterns could not be tracked.
DISCLOSURES:
This study was supported by grants from the Alzheimer’s Association, the National Institute on Aging, and the Department of Defense. One author reported serving on data and safety monitoring boards for studies sponsored by the National Institutes of Health, as well as holding advisory board membership and receiving personal fees from industry. Full details are listed in the original article. The other four investigators reported no relevant financial conflicts.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
A Nationwide Survey of Dermatology Faculty and Mentors on Their Advice for the Dermatology Match Process
A Nationwide Survey of Dermatology Faculty and Mentors on Their Advice for the Dermatology Match Process
While strong relationships with mentors and advisers are critical to navigating the competitive dermatology match process, the advice medical students receive from different individuals can be contradictory. Unaccredited information online—particularly on social media—as well as data reported by applicants can add to potential confusion.1 Published research has elicited comments and observations from successfully matched medical students about highly discussed topics such as presentations and publications, letters of recommendation, away rotations, and interviews.2,3 However, there currently are no published data about advice that dermatology mentors actually offer medical students. In this study, we aimed to investigate this gap in the current literature and examine the advice dermatology faculty, program directors, and other mentors at institutions accredited by the Accreditation Council for Graduate Medical Education across the United States give to medical students applying to dermatology residency.
Methods
A 14-question Johns Hopkins Qualtrics survey was sent via the Association of Professors of Dermatology (APD) listserve in June 2024 soliciting responses from members who consider themselves to be mentors to dermatology applicants across the United States. The survey included multiple-choice questions with the option to select multiple answers and a space for open-ended responses. The questions first gathered information on the respondents, including the capacity in which the mentors advised medical students (eg, program director, department chair, clinical faculty). Mentors were asked for the number of years they had been advising mentees and if they were advising students with a home dermatology program. In addition, mentors were asked what advice they give their mentees about aspects of the application process, including gap years, dual applications, research involvement, couples matching, program signaling, away rotations, internship year, letters of recommendation, geographic signaling, interviewing advice, and volunteering during medical school.
On August 18, 2024, survey results from 115 respondents were aggregated. The responses for each question were quantitatively assessed to determine whether there was consensus on specific advice offered. The open-ended responses also were qualitatively assessed to determine the most common responses.
Results
The respondents included program directors (30% [35/115]), clinical faculty (22% [25/115]), department chairs (18% [21/115]), assistant program directors (15% [17/115]), medical school clerkship directors (8% [9/115]), primary mentors (ie, faculty who did not fall into any of the aforementioned categories but still advised medical students interested in dermatology)(5% [6/115]), division chiefs (1% [1/115]), and deans (1% [1/115]). Respondents had been advising students for a median of 10 years (range, 1-40 years [25th percentile, 5.00 years; 75th percentile, 13.75 years]). The majority (90% [103/115]) of mentors surveyed were advising students with a home dermatology program.
Areas of Consensus
In some areas, there was broad consensus among the advice offered by the mentors that were surveyed (eTable).
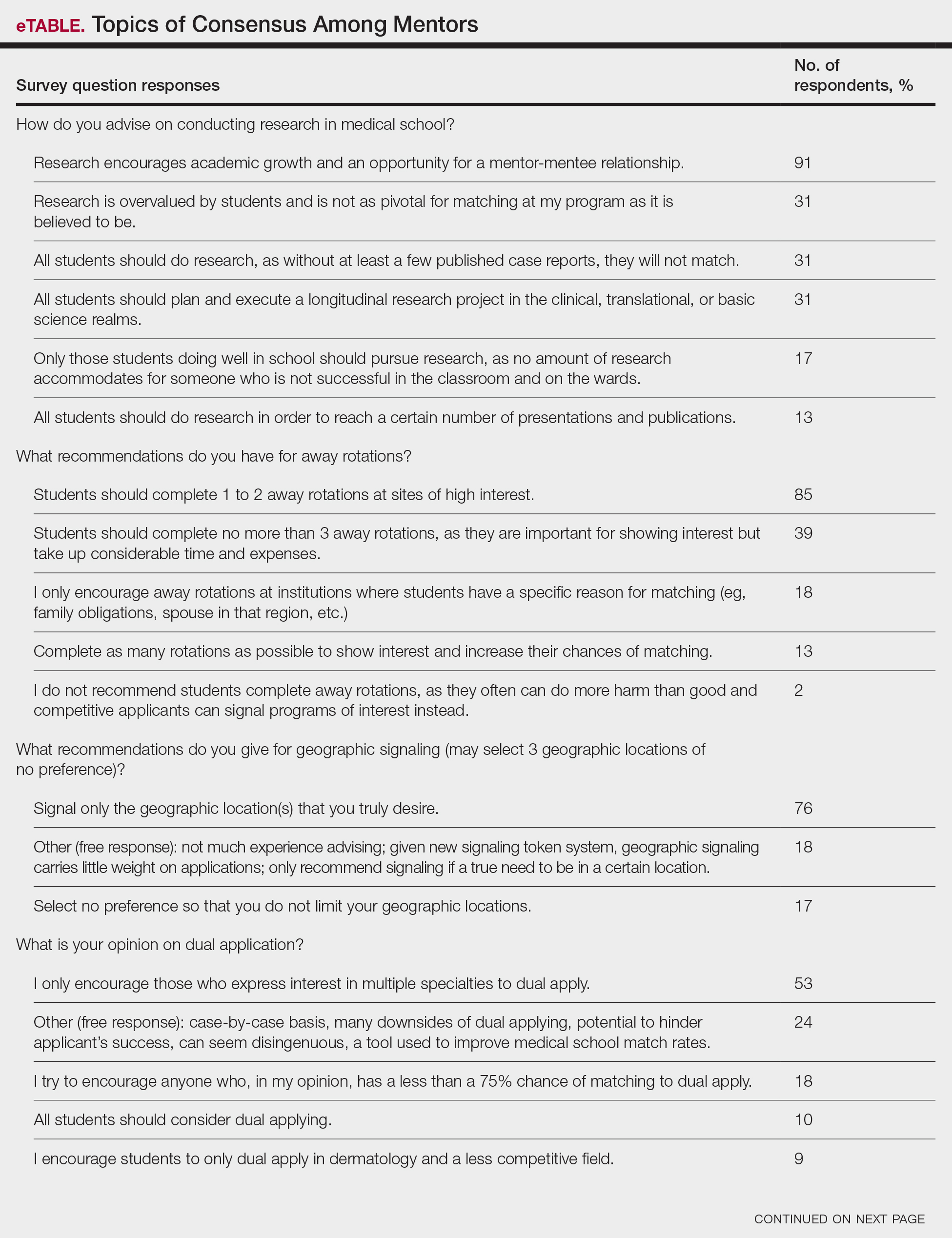
Research During Medical School—More than 91% (105/115) of the respondents recommended research to encourage academic growth and indicated that the most important reason for conducting research during medical school is to foster mentor-mentee relationships; however, more than one-third of respondents believed research is overvalued by students and research productivity is not as critical for matching as they perceive it to be. When these responses were categorized by respondent positions, 29% (15/52) of program or assistant directors indicated agreement with the statement that research is overvalued.
Away Rotations—There also was a consensus about the importance of away rotations, with 85% (98/115) of respondents advising students to complete 1 to 2 away rotations at sites of high interest, and 13% (15/115) suggesting that students complete as many away rotations as possible. It is worth noting, however, that the official APD Residency Program Directors Section’s statement on away rotations recommends no more than 2 away rotations (or no more than 3 for students with no home program).4
Reapplication Advice—Additionally, in a situation where students do not match into a dermatology residency program, the vast majority (71% [82/115]) of respondents advised students to rank competitive intern years to foster connections and improve the chance of matching on the second attempt.
Volunteering During Medical School—Seventy-seven percent (89/115) of mentors encouraged students to engage in volunteerism and advocacy during medical school to create a well-rounded application, and 69% (79/115) of mentors encouraged students to display leadership in their volunteer efforts.
Areas Without Consensus
Letters of Recommendation—Most respondents recommended submitting letters of recommendation only from dermatology professionals (55% [63/115]), with the remainder recommending students request a letter from anyone who could provide a strong recommendation regardless of specialty mix (42% [48/115]).
Dermatologic Subspecialties—For students interested in dermatologic subspecialties, 73% (84/115) of mentors advised that students be honest during interviews but keep an open mind that interests during residencies may change. Forty-three percent (49/115) of respondents encouraged students to promote a subspecialty interest during their interview only if they can demonstrate effort within that subspecialty on their application.
Couples Matching—Most respondents approach couples matching on a case-by-case basis and assess individual priorities when they do advise on this topic. Respondents often advise applicants to identify a few cities/regions and focus strongly on the programs within those regions to avoid spreading themselves too thin; however, one-third (38/115) of respondents indicated that they do not personally offer advice regarding the couples match.
Areas With Diverse Opinions
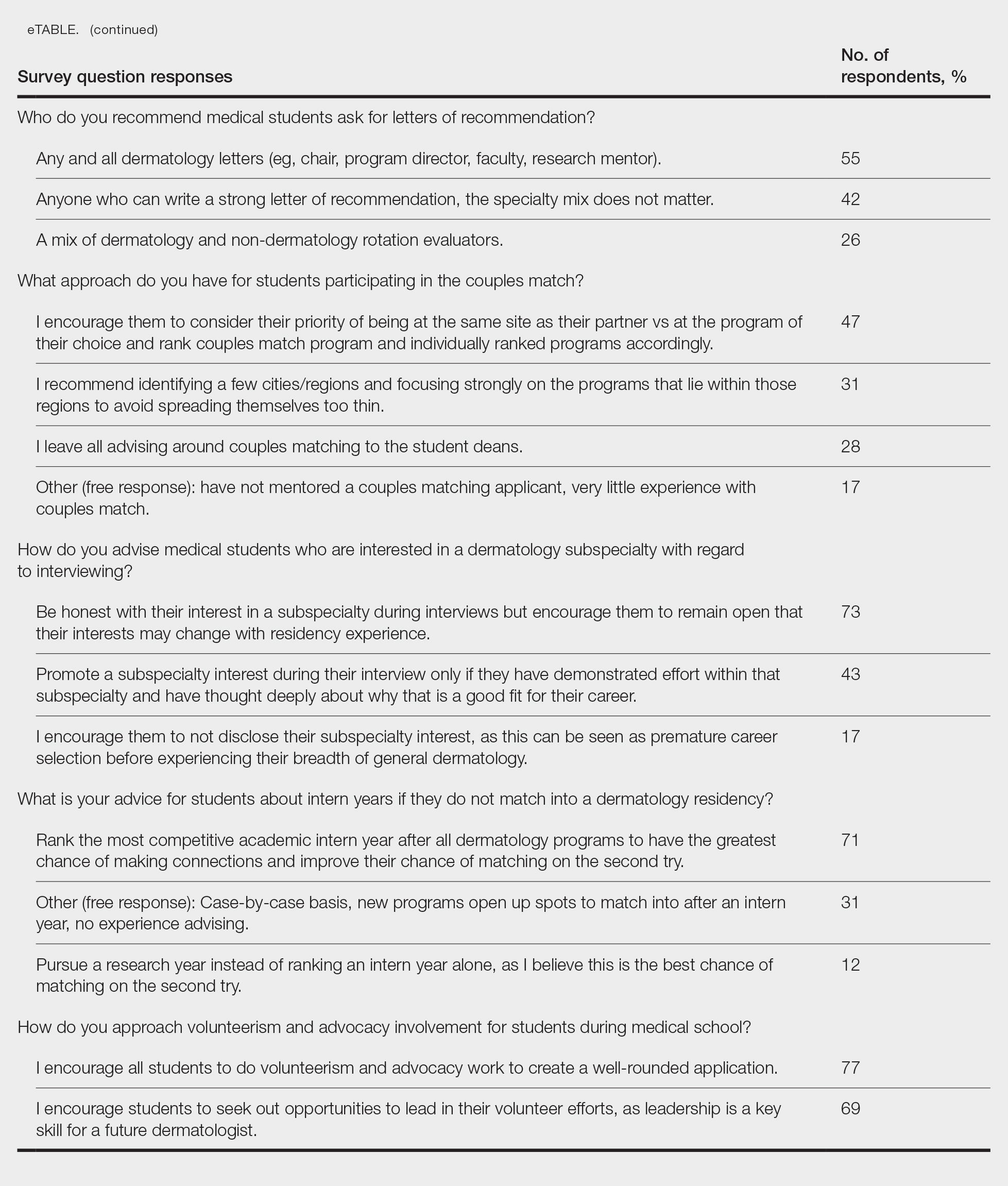
Gap Years—Nearly one-quarter (24% [28/115]) of mentors reported that they rarely recommend students take a year off and only support those who are adamant about doing so, or that they never support taking a gap year at all. A slight majority (58% [67/115]) recommend a gap year for students strongly interested in dermatologic research, and 38% (44/115) recommend a gap year for students with weaker applications (Figure 1). We received many open-ended responses to this question, with mentors frequently indicating that they advise students to take a gap year on a case-by-case basis, with 44% (51/115) of commenters recommending that students only take paid gap-year research positions.
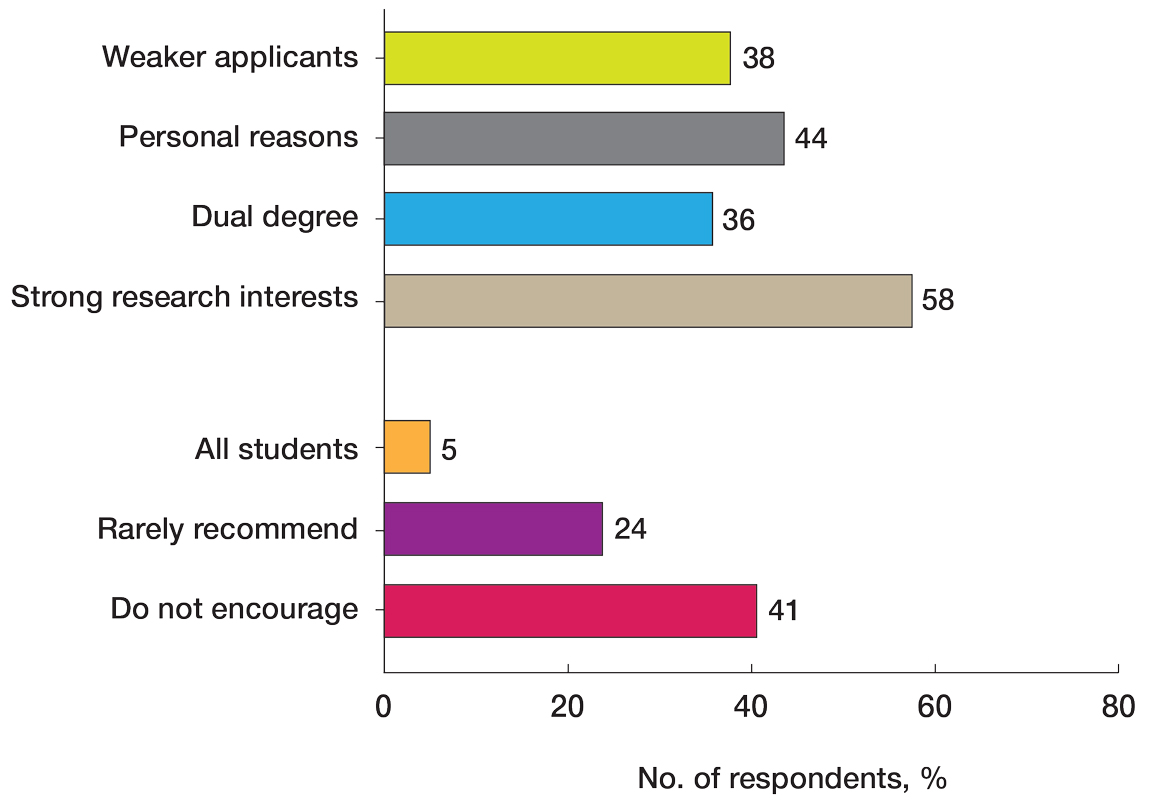
Program Signaling—The dermatology residency application process implemented a system of preference signaling tokens (PSTs) starting with the 2021-2022 cycle. Not quite half (46% [53/115]) of respondents recommend students apply only to places that they signaled, while 20% (23/115) advise responding to 10 to 15 additional programs. Very few (8% [9/115]) advise students to signal only in their stated region of interest. Approximately half (49% [56/115]) of mentors recommend students only signal based on the programs they feel would be the best fit for them without regard for perceived competitiveness—which aligns with the APD Residency Program Directors Section’s recommendation4—while 37% (43/115) recommend students distribute their signals to a wide range of programs. Sixty-three percent (72/115) of respondents recommend gold signaling to the student’s 3 most desired programs regardless of home and away rotation considerations, while 19% (22/115) recommend students give silver signals to their home and away rotation programs, as a rotation is already a signal of a strong desire to be there (Figure 2).
Dual Application—Fifty-three percent (61/115) of mentors recommended dual applying only for those truly interested in multiple specialties. Eighteen percent (21/115) of respondents advised dual applying for those with less than a 75% chance of matching. Twenty-five percent (29/115) of respondents free-wrote comments about approaching dual applying on a case-by-case basis, with many discussing the downsides of dual application and raising concerns that dual applications can hinder applicants’ success, can seem disingenuous, and seem to be a tool used to improve medical school match rates without benefit for the student.
We also stratified the data to compare overall responses from the total cohort with those from only program and assistant program directors. Across the 14 questions, responses from program and assistant program directors alone were similar to the overall cohort results
Comment
This study evaluated nationwide data on mentorship advising in dermatology, detailing mentors’ advice regarding research, gap years, dual applications, away rotations, intern year, couples matching, program signaling, and volunteering during medical school. Based on our results, most respondents agree on the importance of research during medical school, the utility of away rotations, and the value of volunteering during medical school. Similarly, respondents agreed on the importance of having strong letters of recommendation; while some advised asking only dermatology faculty to write letters, others did not have a specialty preference for the letter writers. Respondents also had varying views about sharing interest in subspecialties during residency interviews. Many of the respondents do not provide recommendations regarding geographic signaling and couples matching, expressing that these are parts of an application that are important to approach on a case-by-case basis. Lastly, respondents had diverse opinions regarding the utility of gap years, whether to encourage or discourage dual applications, and how to advise regarding program signaling.
Our results also showed that one-third of respondents believed that research is not as important as it is perceived to be by dermatology applicants. While engaging in research during medical school was almost unanimously encouraged to foster mentor-mentee relationships, respondents expressed that the number of research experiences and publications was not critical. This is an important topic of discussion, as taking a dedicated year away from medical school to complete a research fellowship is becoming a trend among dermatology applicants.5 There has been discussion both on unofficial online platforms as well as in the published literature regarding the pressure for medical students interested in dermatology to publish, which may result in a gap year for research.6 The literature on the utility of a gap year in match rates is sparse, with one study showing no difference in match rates among Mayo Clinic dermatology residents who took research years vs those who did not.7 However, this contrasts with match rates at top dermatology residency programs where 41% of applicants who took a gap year matched vs 19% who did not.7,8 These conflicting data are reflected in our study results, with respondents expressing different opinions on the utility of gap years.
There also are important equity concerns regarding the role of research years in the dermatology residency match process. Dermatology is one of the least racially diverse specialties, although there have been efforts to increase representation among residents and attending physicians.9-11 Research years can be important contributors to this lack of representation, as these often are unpaid and can discourage economically disadvantaged students from applying.9-11 Additionally, applicants may not have the flexibility to defer future salary for a year to match into dermatology; therefore, mentors should offer multiple options to individual applicants instead of solely encouraging gap years, given the conflicting feelings regarding their productivity.
Another topic of disagreement was dual application. Approximately one-third of respondents said they encourage either all students or those with less than a 75% chance of matching to dual apply, while about half only encourage students who are truly interested in multiple specialties to do so. Additionally, a large subset of respondents said they do not encourage dual applications due to concerns that they make applicants a worse candidate for each specialty and overall have negative effects on matching. Twenty-five percent of respondents opted to leave an open-ended response to this question: some offered the perspective that, if applicants feel a need to dual apply due to a weaker application, they do not advise the applicant to apply to dermatology. Many open ended responses underscored that the respondent does not encourage dual applications because they are inherently more time consuming, could hinder the applicant’s success, can seem disingenuous, and are a tool used to improve medical school match rates without being beneficial for the student. Some respondents also favored reapplying to dermatology the following year instead of dual applying. Finally, a subset of mentors indicated that they approach dual applications on a case-by-case basis, and others reported they do not have much experience advising on this topic. Currently, there are no known data in the literature on the efficacy and utility of dual applications in the dermatology match process; therefore, our study provides valuable insight for applicants interested in the impacts of the dual application. Overall, students should approach this option with mentors on an individual basis but ultimately should be aware of the concerns and mixed perceptions of the dual application process.
With regard to program signaling, previous research has shown that PSTs have a large impact on the chance of being granted an interview.12 In our study, we provide a comprehensive overview of advising regarding these signals. While mentors often responded that they did not have much experience advising in this domain—and it is too soon to tell the impact of this program signaling—many offered differing opinions. Many said they recommend that students give a gold signal to their 3 most desired programs regardless of home and away rotations and perceived competitiveness, which follows the guidelines issued by the APD; however, 19% recommend only giving silver signals to home and away rotation programs, as participation in those programs is considered a sufficient signal of interest. Additionally, about half of mentors recommended that students only apply where they signal, whereas 20% recommended applying to 10 to 15 programs beyond those signaled. Future studies should investigate the impact of PSTs on interview invitations once sufficient application cycles have occurred.
Study Limitations
This study was conducted via email to the APD listserve. The total number of faculty on this listserve is unknown; therefore, we do not know the total response rate of the survey. Additionally, we surveyed mentors in this listserve, who therefore receive more emails and overall correspondence about the dermatology match and may be more involved in these conversations. The mentors who responded to our survey may have a different approach and response to our various survey questions than a given mentor across the United States who did not respond to this survey. A final limitation of our study is that the survey responses a mentor gives may not fully match the advice that they give their students privately.
Conclusion
Our survey of dermatology mentors across the United States provides valuable insight into how mentors advise for a strong dermatology residency application. Mentors agreed on the importance of research during medical school, away rotations, strong letters of recommendation, and volunteerism and advocacy to promote a strong residency application. Important topics of disagreement include the decision for dermatology applicants to take a dedicated gap year in medical school, how to use tokens/signals effectively, and the dual application process. Our findings also underscore important application components that applicants and mentors should approach on an individual basis. Future studies should investigate the impact of signals/tokens on the match process as well as the utility of gap years and dual applications, working to standardize the advice applicants receive.
- Ramachandran V, Nguyen HY, Dao H Jr. Does it match? analyzing self-reported online dermatology match data to charting outcomes in the match. Dermatol Online J. 2020;26:13030 /qt4604h1w4.
- Kolli SS, Feldman SR, Huang WW. The dermatology residency application process. Dermatol Online J. 2021;26:13030/qt4k1570vj.
- Stratman EJ, Ness RM. Factors associated with successful matching to dermatology residency programs by reapplicants and other applicants who previously graduated from medical school. Arch Dermatol. 2011;147:196-202. doi:10.1001/archdermatol.2010.303
- Association of Professors of Dermatology Residency Program Directors Section Information Regarding the 2023-2024 Application Cycle. Published 2023. Accessed June 1, 2024. https://students-residents.aamc.org/media/12386/download
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:4.
- Wang JV, Keller M. Pressure to publish for residency applicants in dermatology. Dermatol Online J. 2016;22:13030/qt56x1t7ww.
- Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230. doi:10.1111/ijd.15964
- Yeh C, Desai AD, Wassef C, et al. The importance of mentorship during research gap years for the dermatology residency match. Int J Dermatol. 2023;62:E209-E210. doi:10.1111/ijd.16084
- Zheng DX, Gallo Marin B, Mulligan KM, et al. Inequity concerns surrounding research years and the dermatology residency match. Int J Dermatol. 2022;61:E247-E248. doi:10.1111/ijd.16179
- Vasquez R, Jeong H, Florez-Pollack S, et al. What are the barriers faced by under-represented minorities applying to dermatology? a qualitative cross-sectional study of applicants applying to a large dermatology residency program. J Am Acad Dermatol. 2020;83:1770-1773. doi:10.1016/j.jaad.2020.03.067
- Jones VA, Clark KA, Cordova A, et al. Challenging the status quo: increasing diversity in dermatology. J Am Acad Dermatol. 2020;83:E421. doi:10.1016/j.jaad.2020.04.185
- Dirr MA, Brownstone N, Zakria D, et al. Dermatology match preference signaling tokens: impact and implications. Dermatol Surg. 2022;48:1367-1368. doi:10.1097/DSS.0000000000003645
While strong relationships with mentors and advisers are critical to navigating the competitive dermatology match process, the advice medical students receive from different individuals can be contradictory. Unaccredited information online—particularly on social media—as well as data reported by applicants can add to potential confusion.1 Published research has elicited comments and observations from successfully matched medical students about highly discussed topics such as presentations and publications, letters of recommendation, away rotations, and interviews.2,3 However, there currently are no published data about advice that dermatology mentors actually offer medical students. In this study, we aimed to investigate this gap in the current literature and examine the advice dermatology faculty, program directors, and other mentors at institutions accredited by the Accreditation Council for Graduate Medical Education across the United States give to medical students applying to dermatology residency.
Methods
A 14-question Johns Hopkins Qualtrics survey was sent via the Association of Professors of Dermatology (APD) listserve in June 2024 soliciting responses from members who consider themselves to be mentors to dermatology applicants across the United States. The survey included multiple-choice questions with the option to select multiple answers and a space for open-ended responses. The questions first gathered information on the respondents, including the capacity in which the mentors advised medical students (eg, program director, department chair, clinical faculty). Mentors were asked for the number of years they had been advising mentees and if they were advising students with a home dermatology program. In addition, mentors were asked what advice they give their mentees about aspects of the application process, including gap years, dual applications, research involvement, couples matching, program signaling, away rotations, internship year, letters of recommendation, geographic signaling, interviewing advice, and volunteering during medical school.
On August 18, 2024, survey results from 115 respondents were aggregated. The responses for each question were quantitatively assessed to determine whether there was consensus on specific advice offered. The open-ended responses also were qualitatively assessed to determine the most common responses.
Results
The respondents included program directors (30% [35/115]), clinical faculty (22% [25/115]), department chairs (18% [21/115]), assistant program directors (15% [17/115]), medical school clerkship directors (8% [9/115]), primary mentors (ie, faculty who did not fall into any of the aforementioned categories but still advised medical students interested in dermatology)(5% [6/115]), division chiefs (1% [1/115]), and deans (1% [1/115]). Respondents had been advising students for a median of 10 years (range, 1-40 years [25th percentile, 5.00 years; 75th percentile, 13.75 years]). The majority (90% [103/115]) of mentors surveyed were advising students with a home dermatology program.
Areas of Consensus
In some areas, there was broad consensus among the advice offered by the mentors that were surveyed (eTable).
Research During Medical School—More than 91% (105/115) of the respondents recommended research to encourage academic growth and indicated that the most important reason for conducting research during medical school is to foster mentor-mentee relationships; however, more than one-third of respondents believed research is overvalued by students and research productivity is not as critical for matching as they perceive it to be. When these responses were categorized by respondent positions, 29% (15/52) of program or assistant directors indicated agreement with the statement that research is overvalued.
Away Rotations—There also was a consensus about the importance of away rotations, with 85% (98/115) of respondents advising students to complete 1 to 2 away rotations at sites of high interest, and 13% (15/115) suggesting that students complete as many away rotations as possible. It is worth noting, however, that the official APD Residency Program Directors Section’s statement on away rotations recommends no more than 2 away rotations (or no more than 3 for students with no home program).4
Reapplication Advice—Additionally, in a situation where students do not match into a dermatology residency program, the vast majority (71% [82/115]) of respondents advised students to rank competitive intern years to foster connections and improve the chance of matching on the second attempt.
Volunteering During Medical School—Seventy-seven percent (89/115) of mentors encouraged students to engage in volunteerism and advocacy during medical school to create a well-rounded application, and 69% (79/115) of mentors encouraged students to display leadership in their volunteer efforts.
Areas Without Consensus
Letters of Recommendation—Most respondents recommended submitting letters of recommendation only from dermatology professionals (55% [63/115]), with the remainder recommending students request a letter from anyone who could provide a strong recommendation regardless of specialty mix (42% [48/115]).
Dermatologic Subspecialties—For students interested in dermatologic subspecialties, 73% (84/115) of mentors advised that students be honest during interviews but keep an open mind that interests during residencies may change. Forty-three percent (49/115) of respondents encouraged students to promote a subspecialty interest during their interview only if they can demonstrate effort within that subspecialty on their application.
Couples Matching—Most respondents approach couples matching on a case-by-case basis and assess individual priorities when they do advise on this topic. Respondents often advise applicants to identify a few cities/regions and focus strongly on the programs within those regions to avoid spreading themselves too thin; however, one-third (38/115) of respondents indicated that they do not personally offer advice regarding the couples match.
Areas With Diverse Opinions
Gap Years—Nearly one-quarter (24% [28/115]) of mentors reported that they rarely recommend students take a year off and only support those who are adamant about doing so, or that they never support taking a gap year at all. A slight majority (58% [67/115]) recommend a gap year for students strongly interested in dermatologic research, and 38% (44/115) recommend a gap year for students with weaker applications (Figure 1). We received many open-ended responses to this question, with mentors frequently indicating that they advise students to take a gap year on a case-by-case basis, with 44% (51/115) of commenters recommending that students only take paid gap-year research positions.
Program Signaling—The dermatology residency application process implemented a system of preference signaling tokens (PSTs) starting with the 2021-2022 cycle. Not quite half (46% [53/115]) of respondents recommend students apply only to places that they signaled, while 20% (23/115) advise responding to 10 to 15 additional programs. Very few (8% [9/115]) advise students to signal only in their stated region of interest. Approximately half (49% [56/115]) of mentors recommend students only signal based on the programs they feel would be the best fit for them without regard for perceived competitiveness—which aligns with the APD Residency Program Directors Section’s recommendation4—while 37% (43/115) recommend students distribute their signals to a wide range of programs. Sixty-three percent (72/115) of respondents recommend gold signaling to the student’s 3 most desired programs regardless of home and away rotation considerations, while 19% (22/115) recommend students give silver signals to their home and away rotation programs, as a rotation is already a signal of a strong desire to be there (Figure 2).
Dual Application—Fifty-three percent (61/115) of mentors recommended dual applying only for those truly interested in multiple specialties. Eighteen percent (21/115) of respondents advised dual applying for those with less than a 75% chance of matching. Twenty-five percent (29/115) of respondents free-wrote comments about approaching dual applying on a case-by-case basis, with many discussing the downsides of dual application and raising concerns that dual applications can hinder applicants’ success, can seem disingenuous, and seem to be a tool used to improve medical school match rates without benefit for the student.
We also stratified the data to compare overall responses from the total cohort with those from only program and assistant program directors. Across the 14 questions, responses from program and assistant program directors alone were similar to the overall cohort results
Comment
This study evaluated nationwide data on mentorship advising in dermatology, detailing mentors’ advice regarding research, gap years, dual applications, away rotations, intern year, couples matching, program signaling, and volunteering during medical school. Based on our results, most respondents agree on the importance of research during medical school, the utility of away rotations, and the value of volunteering during medical school. Similarly, respondents agreed on the importance of having strong letters of recommendation; while some advised asking only dermatology faculty to write letters, others did not have a specialty preference for the letter writers. Respondents also had varying views about sharing interest in subspecialties during residency interviews. Many of the respondents do not provide recommendations regarding geographic signaling and couples matching, expressing that these are parts of an application that are important to approach on a case-by-case basis. Lastly, respondents had diverse opinions regarding the utility of gap years, whether to encourage or discourage dual applications, and how to advise regarding program signaling.
Our results also showed that one-third of respondents believed that research is not as important as it is perceived to be by dermatology applicants. While engaging in research during medical school was almost unanimously encouraged to foster mentor-mentee relationships, respondents expressed that the number of research experiences and publications was not critical. This is an important topic of discussion, as taking a dedicated year away from medical school to complete a research fellowship is becoming a trend among dermatology applicants.5 There has been discussion both on unofficial online platforms as well as in the published literature regarding the pressure for medical students interested in dermatology to publish, which may result in a gap year for research.6 The literature on the utility of a gap year in match rates is sparse, with one study showing no difference in match rates among Mayo Clinic dermatology residents who took research years vs those who did not.7 However, this contrasts with match rates at top dermatology residency programs where 41% of applicants who took a gap year matched vs 19% who did not.7,8 These conflicting data are reflected in our study results, with respondents expressing different opinions on the utility of gap years.
There also are important equity concerns regarding the role of research years in the dermatology residency match process. Dermatology is one of the least racially diverse specialties, although there have been efforts to increase representation among residents and attending physicians.9-11 Research years can be important contributors to this lack of representation, as these often are unpaid and can discourage economically disadvantaged students from applying.9-11 Additionally, applicants may not have the flexibility to defer future salary for a year to match into dermatology; therefore, mentors should offer multiple options to individual applicants instead of solely encouraging gap years, given the conflicting feelings regarding their productivity.
Another topic of disagreement was dual application. Approximately one-third of respondents said they encourage either all students or those with less than a 75% chance of matching to dual apply, while about half only encourage students who are truly interested in multiple specialties to do so. Additionally, a large subset of respondents said they do not encourage dual applications due to concerns that they make applicants a worse candidate for each specialty and overall have negative effects on matching. Twenty-five percent of respondents opted to leave an open-ended response to this question: some offered the perspective that, if applicants feel a need to dual apply due to a weaker application, they do not advise the applicant to apply to dermatology. Many open ended responses underscored that the respondent does not encourage dual applications because they are inherently more time consuming, could hinder the applicant’s success, can seem disingenuous, and are a tool used to improve medical school match rates without being beneficial for the student. Some respondents also favored reapplying to dermatology the following year instead of dual applying. Finally, a subset of mentors indicated that they approach dual applications on a case-by-case basis, and others reported they do not have much experience advising on this topic. Currently, there are no known data in the literature on the efficacy and utility of dual applications in the dermatology match process; therefore, our study provides valuable insight for applicants interested in the impacts of the dual application. Overall, students should approach this option with mentors on an individual basis but ultimately should be aware of the concerns and mixed perceptions of the dual application process.
With regard to program signaling, previous research has shown that PSTs have a large impact on the chance of being granted an interview.12 In our study, we provide a comprehensive overview of advising regarding these signals. While mentors often responded that they did not have much experience advising in this domain—and it is too soon to tell the impact of this program signaling—many offered differing opinions. Many said they recommend that students give a gold signal to their 3 most desired programs regardless of home and away rotations and perceived competitiveness, which follows the guidelines issued by the APD; however, 19% recommend only giving silver signals to home and away rotation programs, as participation in those programs is considered a sufficient signal of interest. Additionally, about half of mentors recommended that students only apply where they signal, whereas 20% recommended applying to 10 to 15 programs beyond those signaled. Future studies should investigate the impact of PSTs on interview invitations once sufficient application cycles have occurred.
Study Limitations
This study was conducted via email to the APD listserve. The total number of faculty on this listserve is unknown; therefore, we do not know the total response rate of the survey. Additionally, we surveyed mentors in this listserve, who therefore receive more emails and overall correspondence about the dermatology match and may be more involved in these conversations. The mentors who responded to our survey may have a different approach and response to our various survey questions than a given mentor across the United States who did not respond to this survey. A final limitation of our study is that the survey responses a mentor gives may not fully match the advice that they give their students privately.
Conclusion
Our survey of dermatology mentors across the United States provides valuable insight into how mentors advise for a strong dermatology residency application. Mentors agreed on the importance of research during medical school, away rotations, strong letters of recommendation, and volunteerism and advocacy to promote a strong residency application. Important topics of disagreement include the decision for dermatology applicants to take a dedicated gap year in medical school, how to use tokens/signals effectively, and the dual application process. Our findings also underscore important application components that applicants and mentors should approach on an individual basis. Future studies should investigate the impact of signals/tokens on the match process as well as the utility of gap years and dual applications, working to standardize the advice applicants receive.
While strong relationships with mentors and advisers are critical to navigating the competitive dermatology match process, the advice medical students receive from different individuals can be contradictory. Unaccredited information online—particularly on social media—as well as data reported by applicants can add to potential confusion.1 Published research has elicited comments and observations from successfully matched medical students about highly discussed topics such as presentations and publications, letters of recommendation, away rotations, and interviews.2,3 However, there currently are no published data about advice that dermatology mentors actually offer medical students. In this study, we aimed to investigate this gap in the current literature and examine the advice dermatology faculty, program directors, and other mentors at institutions accredited by the Accreditation Council for Graduate Medical Education across the United States give to medical students applying to dermatology residency.
Methods
A 14-question Johns Hopkins Qualtrics survey was sent via the Association of Professors of Dermatology (APD) listserve in June 2024 soliciting responses from members who consider themselves to be mentors to dermatology applicants across the United States. The survey included multiple-choice questions with the option to select multiple answers and a space for open-ended responses. The questions first gathered information on the respondents, including the capacity in which the mentors advised medical students (eg, program director, department chair, clinical faculty). Mentors were asked for the number of years they had been advising mentees and if they were advising students with a home dermatology program. In addition, mentors were asked what advice they give their mentees about aspects of the application process, including gap years, dual applications, research involvement, couples matching, program signaling, away rotations, internship year, letters of recommendation, geographic signaling, interviewing advice, and volunteering during medical school.
On August 18, 2024, survey results from 115 respondents were aggregated. The responses for each question were quantitatively assessed to determine whether there was consensus on specific advice offered. The open-ended responses also were qualitatively assessed to determine the most common responses.
Results
The respondents included program directors (30% [35/115]), clinical faculty (22% [25/115]), department chairs (18% [21/115]), assistant program directors (15% [17/115]), medical school clerkship directors (8% [9/115]), primary mentors (ie, faculty who did not fall into any of the aforementioned categories but still advised medical students interested in dermatology)(5% [6/115]), division chiefs (1% [1/115]), and deans (1% [1/115]). Respondents had been advising students for a median of 10 years (range, 1-40 years [25th percentile, 5.00 years; 75th percentile, 13.75 years]). The majority (90% [103/115]) of mentors surveyed were advising students with a home dermatology program.
Areas of Consensus
In some areas, there was broad consensus among the advice offered by the mentors that were surveyed (eTable).
Research During Medical School—More than 91% (105/115) of the respondents recommended research to encourage academic growth and indicated that the most important reason for conducting research during medical school is to foster mentor-mentee relationships; however, more than one-third of respondents believed research is overvalued by students and research productivity is not as critical for matching as they perceive it to be. When these responses were categorized by respondent positions, 29% (15/52) of program or assistant directors indicated agreement with the statement that research is overvalued.
Away Rotations—There also was a consensus about the importance of away rotations, with 85% (98/115) of respondents advising students to complete 1 to 2 away rotations at sites of high interest, and 13% (15/115) suggesting that students complete as many away rotations as possible. It is worth noting, however, that the official APD Residency Program Directors Section’s statement on away rotations recommends no more than 2 away rotations (or no more than 3 for students with no home program).4
Reapplication Advice—Additionally, in a situation where students do not match into a dermatology residency program, the vast majority (71% [82/115]) of respondents advised students to rank competitive intern years to foster connections and improve the chance of matching on the second attempt.
Volunteering During Medical School—Seventy-seven percent (89/115) of mentors encouraged students to engage in volunteerism and advocacy during medical school to create a well-rounded application, and 69% (79/115) of mentors encouraged students to display leadership in their volunteer efforts.
Areas Without Consensus
Letters of Recommendation—Most respondents recommended submitting letters of recommendation only from dermatology professionals (55% [63/115]), with the remainder recommending students request a letter from anyone who could provide a strong recommendation regardless of specialty mix (42% [48/115]).
Dermatologic Subspecialties—For students interested in dermatologic subspecialties, 73% (84/115) of mentors advised that students be honest during interviews but keep an open mind that interests during residencies may change. Forty-three percent (49/115) of respondents encouraged students to promote a subspecialty interest during their interview only if they can demonstrate effort within that subspecialty on their application.
Couples Matching—Most respondents approach couples matching on a case-by-case basis and assess individual priorities when they do advise on this topic. Respondents often advise applicants to identify a few cities/regions and focus strongly on the programs within those regions to avoid spreading themselves too thin; however, one-third (38/115) of respondents indicated that they do not personally offer advice regarding the couples match.
Areas With Diverse Opinions
Gap Years—Nearly one-quarter (24% [28/115]) of mentors reported that they rarely recommend students take a year off and only support those who are adamant about doing so, or that they never support taking a gap year at all. A slight majority (58% [67/115]) recommend a gap year for students strongly interested in dermatologic research, and 38% (44/115) recommend a gap year for students with weaker applications (Figure 1). We received many open-ended responses to this question, with mentors frequently indicating that they advise students to take a gap year on a case-by-case basis, with 44% (51/115) of commenters recommending that students only take paid gap-year research positions.
Program Signaling—The dermatology residency application process implemented a system of preference signaling tokens (PSTs) starting with the 2021-2022 cycle. Not quite half (46% [53/115]) of respondents recommend students apply only to places that they signaled, while 20% (23/115) advise responding to 10 to 15 additional programs. Very few (8% [9/115]) advise students to signal only in their stated region of interest. Approximately half (49% [56/115]) of mentors recommend students only signal based on the programs they feel would be the best fit for them without regard for perceived competitiveness—which aligns with the APD Residency Program Directors Section’s recommendation4—while 37% (43/115) recommend students distribute their signals to a wide range of programs. Sixty-three percent (72/115) of respondents recommend gold signaling to the student’s 3 most desired programs regardless of home and away rotation considerations, while 19% (22/115) recommend students give silver signals to their home and away rotation programs, as a rotation is already a signal of a strong desire to be there (Figure 2).
Dual Application—Fifty-three percent (61/115) of mentors recommended dual applying only for those truly interested in multiple specialties. Eighteen percent (21/115) of respondents advised dual applying for those with less than a 75% chance of matching. Twenty-five percent (29/115) of respondents free-wrote comments about approaching dual applying on a case-by-case basis, with many discussing the downsides of dual application and raising concerns that dual applications can hinder applicants’ success, can seem disingenuous, and seem to be a tool used to improve medical school match rates without benefit for the student.
We also stratified the data to compare overall responses from the total cohort with those from only program and assistant program directors. Across the 14 questions, responses from program and assistant program directors alone were similar to the overall cohort results
Comment
This study evaluated nationwide data on mentorship advising in dermatology, detailing mentors’ advice regarding research, gap years, dual applications, away rotations, intern year, couples matching, program signaling, and volunteering during medical school. Based on our results, most respondents agree on the importance of research during medical school, the utility of away rotations, and the value of volunteering during medical school. Similarly, respondents agreed on the importance of having strong letters of recommendation; while some advised asking only dermatology faculty to write letters, others did not have a specialty preference for the letter writers. Respondents also had varying views about sharing interest in subspecialties during residency interviews. Many of the respondents do not provide recommendations regarding geographic signaling and couples matching, expressing that these are parts of an application that are important to approach on a case-by-case basis. Lastly, respondents had diverse opinions regarding the utility of gap years, whether to encourage or discourage dual applications, and how to advise regarding program signaling.
Our results also showed that one-third of respondents believed that research is not as important as it is perceived to be by dermatology applicants. While engaging in research during medical school was almost unanimously encouraged to foster mentor-mentee relationships, respondents expressed that the number of research experiences and publications was not critical. This is an important topic of discussion, as taking a dedicated year away from medical school to complete a research fellowship is becoming a trend among dermatology applicants.5 There has been discussion both on unofficial online platforms as well as in the published literature regarding the pressure for medical students interested in dermatology to publish, which may result in a gap year for research.6 The literature on the utility of a gap year in match rates is sparse, with one study showing no difference in match rates among Mayo Clinic dermatology residents who took research years vs those who did not.7 However, this contrasts with match rates at top dermatology residency programs where 41% of applicants who took a gap year matched vs 19% who did not.7,8 These conflicting data are reflected in our study results, with respondents expressing different opinions on the utility of gap years.
There also are important equity concerns regarding the role of research years in the dermatology residency match process. Dermatology is one of the least racially diverse specialties, although there have been efforts to increase representation among residents and attending physicians.9-11 Research years can be important contributors to this lack of representation, as these often are unpaid and can discourage economically disadvantaged students from applying.9-11 Additionally, applicants may not have the flexibility to defer future salary for a year to match into dermatology; therefore, mentors should offer multiple options to individual applicants instead of solely encouraging gap years, given the conflicting feelings regarding their productivity.
Another topic of disagreement was dual application. Approximately one-third of respondents said they encourage either all students or those with less than a 75% chance of matching to dual apply, while about half only encourage students who are truly interested in multiple specialties to do so. Additionally, a large subset of respondents said they do not encourage dual applications due to concerns that they make applicants a worse candidate for each specialty and overall have negative effects on matching. Twenty-five percent of respondents opted to leave an open-ended response to this question: some offered the perspective that, if applicants feel a need to dual apply due to a weaker application, they do not advise the applicant to apply to dermatology. Many open ended responses underscored that the respondent does not encourage dual applications because they are inherently more time consuming, could hinder the applicant’s success, can seem disingenuous, and are a tool used to improve medical school match rates without being beneficial for the student. Some respondents also favored reapplying to dermatology the following year instead of dual applying. Finally, a subset of mentors indicated that they approach dual applications on a case-by-case basis, and others reported they do not have much experience advising on this topic. Currently, there are no known data in the literature on the efficacy and utility of dual applications in the dermatology match process; therefore, our study provides valuable insight for applicants interested in the impacts of the dual application. Overall, students should approach this option with mentors on an individual basis but ultimately should be aware of the concerns and mixed perceptions of the dual application process.
With regard to program signaling, previous research has shown that PSTs have a large impact on the chance of being granted an interview.12 In our study, we provide a comprehensive overview of advising regarding these signals. While mentors often responded that they did not have much experience advising in this domain—and it is too soon to tell the impact of this program signaling—many offered differing opinions. Many said they recommend that students give a gold signal to their 3 most desired programs regardless of home and away rotations and perceived competitiveness, which follows the guidelines issued by the APD; however, 19% recommend only giving silver signals to home and away rotation programs, as participation in those programs is considered a sufficient signal of interest. Additionally, about half of mentors recommended that students only apply where they signal, whereas 20% recommended applying to 10 to 15 programs beyond those signaled. Future studies should investigate the impact of PSTs on interview invitations once sufficient application cycles have occurred.
Study Limitations
This study was conducted via email to the APD listserve. The total number of faculty on this listserve is unknown; therefore, we do not know the total response rate of the survey. Additionally, we surveyed mentors in this listserve, who therefore receive more emails and overall correspondence about the dermatology match and may be more involved in these conversations. The mentors who responded to our survey may have a different approach and response to our various survey questions than a given mentor across the United States who did not respond to this survey. A final limitation of our study is that the survey responses a mentor gives may not fully match the advice that they give their students privately.
Conclusion
Our survey of dermatology mentors across the United States provides valuable insight into how mentors advise for a strong dermatology residency application. Mentors agreed on the importance of research during medical school, away rotations, strong letters of recommendation, and volunteerism and advocacy to promote a strong residency application. Important topics of disagreement include the decision for dermatology applicants to take a dedicated gap year in medical school, how to use tokens/signals effectively, and the dual application process. Our findings also underscore important application components that applicants and mentors should approach on an individual basis. Future studies should investigate the impact of signals/tokens on the match process as well as the utility of gap years and dual applications, working to standardize the advice applicants receive.
- Ramachandran V, Nguyen HY, Dao H Jr. Does it match? analyzing self-reported online dermatology match data to charting outcomes in the match. Dermatol Online J. 2020;26:13030 /qt4604h1w4.
- Kolli SS, Feldman SR, Huang WW. The dermatology residency application process. Dermatol Online J. 2021;26:13030/qt4k1570vj.
- Stratman EJ, Ness RM. Factors associated with successful matching to dermatology residency programs by reapplicants and other applicants who previously graduated from medical school. Arch Dermatol. 2011;147:196-202. doi:10.1001/archdermatol.2010.303
- Association of Professors of Dermatology Residency Program Directors Section Information Regarding the 2023-2024 Application Cycle. Published 2023. Accessed June 1, 2024. https://students-residents.aamc.org/media/12386/download
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:4.
- Wang JV, Keller M. Pressure to publish for residency applicants in dermatology. Dermatol Online J. 2016;22:13030/qt56x1t7ww.
- Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230. doi:10.1111/ijd.15964
- Yeh C, Desai AD, Wassef C, et al. The importance of mentorship during research gap years for the dermatology residency match. Int J Dermatol. 2023;62:E209-E210. doi:10.1111/ijd.16084
- Zheng DX, Gallo Marin B, Mulligan KM, et al. Inequity concerns surrounding research years and the dermatology residency match. Int J Dermatol. 2022;61:E247-E248. doi:10.1111/ijd.16179
- Vasquez R, Jeong H, Florez-Pollack S, et al. What are the barriers faced by under-represented minorities applying to dermatology? a qualitative cross-sectional study of applicants applying to a large dermatology residency program. J Am Acad Dermatol. 2020;83:1770-1773. doi:10.1016/j.jaad.2020.03.067
- Jones VA, Clark KA, Cordova A, et al. Challenging the status quo: increasing diversity in dermatology. J Am Acad Dermatol. 2020;83:E421. doi:10.1016/j.jaad.2020.04.185
- Dirr MA, Brownstone N, Zakria D, et al. Dermatology match preference signaling tokens: impact and implications. Dermatol Surg. 2022;48:1367-1368. doi:10.1097/DSS.0000000000003645
- Ramachandran V, Nguyen HY, Dao H Jr. Does it match? analyzing self-reported online dermatology match data to charting outcomes in the match. Dermatol Online J. 2020;26:13030 /qt4604h1w4.
- Kolli SS, Feldman SR, Huang WW. The dermatology residency application process. Dermatol Online J. 2021;26:13030/qt4k1570vj.
- Stratman EJ, Ness RM. Factors associated with successful matching to dermatology residency programs by reapplicants and other applicants who previously graduated from medical school. Arch Dermatol. 2011;147:196-202. doi:10.1001/archdermatol.2010.303
- Association of Professors of Dermatology Residency Program Directors Section Information Regarding the 2023-2024 Application Cycle. Published 2023. Accessed June 1, 2024. https://students-residents.aamc.org/media/12386/download
- Alikhan A, Sivamani RK, Mutizwa MM, et al. Advice for medical students interested in dermatology: perspectives from fourth year students who matched. Dermatol Online J. 2009;15:4.
- Wang JV, Keller M. Pressure to publish for residency applicants in dermatology. Dermatol Online J. 2016;22:13030/qt56x1t7ww.
- Costello CM, Harvey JA, Besch-Stokes JG, et al. The role research gap years play in a successful dermatology match. Int J Dermatol. 2022;61:226-230. doi:10.1111/ijd.15964
- Yeh C, Desai AD, Wassef C, et al. The importance of mentorship during research gap years for the dermatology residency match. Int J Dermatol. 2023;62:E209-E210. doi:10.1111/ijd.16084
- Zheng DX, Gallo Marin B, Mulligan KM, et al. Inequity concerns surrounding research years and the dermatology residency match. Int J Dermatol. 2022;61:E247-E248. doi:10.1111/ijd.16179
- Vasquez R, Jeong H, Florez-Pollack S, et al. What are the barriers faced by under-represented minorities applying to dermatology? a qualitative cross-sectional study of applicants applying to a large dermatology residency program. J Am Acad Dermatol. 2020;83:1770-1773. doi:10.1016/j.jaad.2020.03.067
- Jones VA, Clark KA, Cordova A, et al. Challenging the status quo: increasing diversity in dermatology. J Am Acad Dermatol. 2020;83:E421. doi:10.1016/j.jaad.2020.04.185
- Dirr MA, Brownstone N, Zakria D, et al. Dermatology match preference signaling tokens: impact and implications. Dermatol Surg. 2022;48:1367-1368. doi:10.1097/DSS.0000000000003645
A Nationwide Survey of Dermatology Faculty and Mentors on Their Advice for the Dermatology Match Process
A Nationwide Survey of Dermatology Faculty and Mentors on Their Advice for the Dermatology Match Process
PRACTICE POINTS
- Dermatology mentors should abide by Association of Professors of Dermatology guidelines when advising regarding signals and away rotations.
- Mentors agree with the utility of research during medical school, completing away rotations, and volunteering during medical school.
- There are differing opinions regarding the utility of a research year, program signaling, couples matching, and dual applying.

Antibiotics Pre-Appendectomy Don’t Lower Perforation Risk, But Reduce Infections
, according to a new study.
While the percentage of surgical site infections (SSIs) was small for both groups, patients who received antibiotics during the waiting period had lower rates of these infections.
The trial — titled PERFECT-Antibiotics — was a substudy embedded in a larger PERFECT clinical trial, which aimed to determine whether an in-hospital delay of appendectomy resulted in increased risk for appendiceal perforation when compared to emergent surgery.
The trial “concluded that appendectomy does not need to be performed promptly in acute uncomplicated appendicitis and can be scheduled within 24 hours without increasing complications,” senior author Panu Mentula, MD, of the Department of Gastroenterological Surgery, Helsinki University Hospital, Helsinki, Finland, and colleagues wrote in the study. “The next question is whether preoperatively started antibiotic treatment reduces the risk of appendiceal perforations.”
The findings were published online in JAMA Surgery on May 14, 2025.
Trial Design
PERFECT-Antibiotics was an open-label, randomized trial conducted at two hospitals in Finland and one hospital in Norway. Researchers enrolled 1774 individuals diagnosed with acute uncomplicated appendicitis, diagnosed clinically or via imaging. Patients were placed in one of two groups: The antibiotic group received intravenous (IV) cefuroxime (1500 mg) and metronidazole (500 mg) every 8 hours until surgery, while the nonantibiotic group waited for surgery without antibiotics.
All patients received one dose of IV cefuroxime (1500 mg) and metronidazole (500 mg) during anesthesia induction. The primary outcome was perforated appendicitis and secondary outcomes included complication rate and SSIs within 30 days of follow-up.
The median age of patients was 35 years (interquartile range [IQR], 28-46 years), and 55% of patients were men. Patients waited a median time of 9 hours (IQR, 4.3-15.5) from study randomization to undergoing surgery.
No Difference in Appendiceal Perforation
Of the 888 patients in the preoperative antibiotic group, 26.2% received one dose, 38.7% received two doses, 22.6% received three doses, and 11.8% received four or more doses of antibiotics, including the antibiotic dose given during anesthesia. A total of 74 patients (8.3%) in this group had a perforated appendix.
Of the 886 patients not given preoperative antibiotics, 79 (8.9%) had a perforated appendix, which met the predetermined noninferiority threshold.
The groups had similar complication rates over the 30-day follow-up, though SSIs were lower in the antibiotic group (1.6%) than the no antibiotic group (3.2%).
The researchers estimated that the number needed to treat for antibiotic therapy was 63 for SSIs, 83 for intra-abdominal SSI, and 125 for reintervention.
“Although longer preoperative antibiotic treatment resulted in slightly lower rate of postoperative infectious complications, the actual difference was very small and probably clinically not significant to justify longer preoperative antibiotic treatment,” Mentula and colleagues wrote.
Lower Infection Rates With Antibiotics
Commenting on the study for GI & Hepatology News, Theodore Pappas, MD, professor of surgery at Duke University School of Medicine in Durham, North Carolina, placed greater importance on these secondary outcomes.
Intra-abdominal infections, a subset of SSIs, were more than twice as common in the no-antibiotic group (1.9%) than in the antibiotic group (0.7%; P = .02). Positive blood cultures were also more common in the no-antibiotic group than the antibiotic group (P = .02).
While the authors qualified these results, “the reality was it was better to use antibiotics,” he said.
There was also a “big overlap between the two groups,” he said, which may have muted differences between the two groups. For example, one fourth of patients in the antibiotic group received only one dose of antibiotics, the same treatment regimen as the no-antibiotic group.
“Although protocol required prophylaxis in all patients in the induction of anesthesia, some clinicians thought that it was unnecessary, because antibiotics had already been given only a couple of hours ago” in patients in the antibiotic group, Mentula told GI & Hepatology News. She did not think that would affect the study’s results.
The PERFECT trial and the antibiotics subtrial answer two important questions that have been asked for years, Pappas continued: Whether appendectomy for uncomplicated acute appendicitis needs to be performed emergently and if antibiotics administered while waiting for surgery improve outcomes.
“Basically, the study shows that you probably should keep them on antibiotics while you’re waiting,” he said.
The study was funded by Finnish Medical Foundation, the Mary and Georg Ehrnrooth Foundation, the Biomedicum Helsinki Foundation, and The Norwegian Surveillance Programme for Antimicrobial Resistance and research funds from the Finnish government. Mentula received grants from the Finnish government during the conduct of the study and personal fees from Pfizer outside the submitted work. Pappas reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a new study.
While the percentage of surgical site infections (SSIs) was small for both groups, patients who received antibiotics during the waiting period had lower rates of these infections.
The trial — titled PERFECT-Antibiotics — was a substudy embedded in a larger PERFECT clinical trial, which aimed to determine whether an in-hospital delay of appendectomy resulted in increased risk for appendiceal perforation when compared to emergent surgery.
The trial “concluded that appendectomy does not need to be performed promptly in acute uncomplicated appendicitis and can be scheduled within 24 hours without increasing complications,” senior author Panu Mentula, MD, of the Department of Gastroenterological Surgery, Helsinki University Hospital, Helsinki, Finland, and colleagues wrote in the study. “The next question is whether preoperatively started antibiotic treatment reduces the risk of appendiceal perforations.”
The findings were published online in JAMA Surgery on May 14, 2025.
Trial Design
PERFECT-Antibiotics was an open-label, randomized trial conducted at two hospitals in Finland and one hospital in Norway. Researchers enrolled 1774 individuals diagnosed with acute uncomplicated appendicitis, diagnosed clinically or via imaging. Patients were placed in one of two groups: The antibiotic group received intravenous (IV) cefuroxime (1500 mg) and metronidazole (500 mg) every 8 hours until surgery, while the nonantibiotic group waited for surgery without antibiotics.
All patients received one dose of IV cefuroxime (1500 mg) and metronidazole (500 mg) during anesthesia induction. The primary outcome was perforated appendicitis and secondary outcomes included complication rate and SSIs within 30 days of follow-up.
The median age of patients was 35 years (interquartile range [IQR], 28-46 years), and 55% of patients were men. Patients waited a median time of 9 hours (IQR, 4.3-15.5) from study randomization to undergoing surgery.
No Difference in Appendiceal Perforation
Of the 888 patients in the preoperative antibiotic group, 26.2% received one dose, 38.7% received two doses, 22.6% received three doses, and 11.8% received four or more doses of antibiotics, including the antibiotic dose given during anesthesia. A total of 74 patients (8.3%) in this group had a perforated appendix.
Of the 886 patients not given preoperative antibiotics, 79 (8.9%) had a perforated appendix, which met the predetermined noninferiority threshold.
The groups had similar complication rates over the 30-day follow-up, though SSIs were lower in the antibiotic group (1.6%) than the no antibiotic group (3.2%).
The researchers estimated that the number needed to treat for antibiotic therapy was 63 for SSIs, 83 for intra-abdominal SSI, and 125 for reintervention.
“Although longer preoperative antibiotic treatment resulted in slightly lower rate of postoperative infectious complications, the actual difference was very small and probably clinically not significant to justify longer preoperative antibiotic treatment,” Mentula and colleagues wrote.
Lower Infection Rates With Antibiotics
Commenting on the study for GI & Hepatology News, Theodore Pappas, MD, professor of surgery at Duke University School of Medicine in Durham, North Carolina, placed greater importance on these secondary outcomes.
Intra-abdominal infections, a subset of SSIs, were more than twice as common in the no-antibiotic group (1.9%) than in the antibiotic group (0.7%; P = .02). Positive blood cultures were also more common in the no-antibiotic group than the antibiotic group (P = .02).
While the authors qualified these results, “the reality was it was better to use antibiotics,” he said.
There was also a “big overlap between the two groups,” he said, which may have muted differences between the two groups. For example, one fourth of patients in the antibiotic group received only one dose of antibiotics, the same treatment regimen as the no-antibiotic group.
“Although protocol required prophylaxis in all patients in the induction of anesthesia, some clinicians thought that it was unnecessary, because antibiotics had already been given only a couple of hours ago” in patients in the antibiotic group, Mentula told GI & Hepatology News. She did not think that would affect the study’s results.
The PERFECT trial and the antibiotics subtrial answer two important questions that have been asked for years, Pappas continued: Whether appendectomy for uncomplicated acute appendicitis needs to be performed emergently and if antibiotics administered while waiting for surgery improve outcomes.
“Basically, the study shows that you probably should keep them on antibiotics while you’re waiting,” he said.
The study was funded by Finnish Medical Foundation, the Mary and Georg Ehrnrooth Foundation, the Biomedicum Helsinki Foundation, and The Norwegian Surveillance Programme for Antimicrobial Resistance and research funds from the Finnish government. Mentula received grants from the Finnish government during the conduct of the study and personal fees from Pfizer outside the submitted work. Pappas reported no relevant disclosures.
A version of this article appeared on Medscape.com.
, according to a new study.
While the percentage of surgical site infections (SSIs) was small for both groups, patients who received antibiotics during the waiting period had lower rates of these infections.
The trial — titled PERFECT-Antibiotics — was a substudy embedded in a larger PERFECT clinical trial, which aimed to determine whether an in-hospital delay of appendectomy resulted in increased risk for appendiceal perforation when compared to emergent surgery.
The trial “concluded that appendectomy does not need to be performed promptly in acute uncomplicated appendicitis and can be scheduled within 24 hours without increasing complications,” senior author Panu Mentula, MD, of the Department of Gastroenterological Surgery, Helsinki University Hospital, Helsinki, Finland, and colleagues wrote in the study. “The next question is whether preoperatively started antibiotic treatment reduces the risk of appendiceal perforations.”
The findings were published online in JAMA Surgery on May 14, 2025.
Trial Design
PERFECT-Antibiotics was an open-label, randomized trial conducted at two hospitals in Finland and one hospital in Norway. Researchers enrolled 1774 individuals diagnosed with acute uncomplicated appendicitis, diagnosed clinically or via imaging. Patients were placed in one of two groups: The antibiotic group received intravenous (IV) cefuroxime (1500 mg) and metronidazole (500 mg) every 8 hours until surgery, while the nonantibiotic group waited for surgery without antibiotics.
All patients received one dose of IV cefuroxime (1500 mg) and metronidazole (500 mg) during anesthesia induction. The primary outcome was perforated appendicitis and secondary outcomes included complication rate and SSIs within 30 days of follow-up.
The median age of patients was 35 years (interquartile range [IQR], 28-46 years), and 55% of patients were men. Patients waited a median time of 9 hours (IQR, 4.3-15.5) from study randomization to undergoing surgery.
No Difference in Appendiceal Perforation
Of the 888 patients in the preoperative antibiotic group, 26.2% received one dose, 38.7% received two doses, 22.6% received three doses, and 11.8% received four or more doses of antibiotics, including the antibiotic dose given during anesthesia. A total of 74 patients (8.3%) in this group had a perforated appendix.
Of the 886 patients not given preoperative antibiotics, 79 (8.9%) had a perforated appendix, which met the predetermined noninferiority threshold.
The groups had similar complication rates over the 30-day follow-up, though SSIs were lower in the antibiotic group (1.6%) than the no antibiotic group (3.2%).
The researchers estimated that the number needed to treat for antibiotic therapy was 63 for SSIs, 83 for intra-abdominal SSI, and 125 for reintervention.
“Although longer preoperative antibiotic treatment resulted in slightly lower rate of postoperative infectious complications, the actual difference was very small and probably clinically not significant to justify longer preoperative antibiotic treatment,” Mentula and colleagues wrote.
Lower Infection Rates With Antibiotics
Commenting on the study for GI & Hepatology News, Theodore Pappas, MD, professor of surgery at Duke University School of Medicine in Durham, North Carolina, placed greater importance on these secondary outcomes.
Intra-abdominal infections, a subset of SSIs, were more than twice as common in the no-antibiotic group (1.9%) than in the antibiotic group (0.7%; P = .02). Positive blood cultures were also more common in the no-antibiotic group than the antibiotic group (P = .02).
While the authors qualified these results, “the reality was it was better to use antibiotics,” he said.
There was also a “big overlap between the two groups,” he said, which may have muted differences between the two groups. For example, one fourth of patients in the antibiotic group received only one dose of antibiotics, the same treatment regimen as the no-antibiotic group.
“Although protocol required prophylaxis in all patients in the induction of anesthesia, some clinicians thought that it was unnecessary, because antibiotics had already been given only a couple of hours ago” in patients in the antibiotic group, Mentula told GI & Hepatology News. She did not think that would affect the study’s results.
The PERFECT trial and the antibiotics subtrial answer two important questions that have been asked for years, Pappas continued: Whether appendectomy for uncomplicated acute appendicitis needs to be performed emergently and if antibiotics administered while waiting for surgery improve outcomes.
“Basically, the study shows that you probably should keep them on antibiotics while you’re waiting,” he said.
The study was funded by Finnish Medical Foundation, the Mary and Georg Ehrnrooth Foundation, the Biomedicum Helsinki Foundation, and The Norwegian Surveillance Programme for Antimicrobial Resistance and research funds from the Finnish government. Mentula received grants from the Finnish government during the conduct of the study and personal fees from Pfizer outside the submitted work. Pappas reported no relevant disclosures.
A version of this article appeared on Medscape.com.
Gut Microbiome Changes in Chronic Pain — Test and Treat?
A new study adds to what has been emerging in the literature — namely that — suggesting that microbiome-based diagnostics and therapeutics may one day be routine for a broad range of pain conditions.
“There is now a whole list of pain conditions that appear to have these signatures, including postoperative pain, arthritis, neuropathy and migraine to name a few,” Robert Bonakdar, MD, director of pain management, Scripps Center for Integrative Medicine, San Diego, told GI & Hepatology News.
Fibromyalgia and complex regional pain syndrome (CRPS) are also on the list.
A team led by Amir Minerbi, MD, PhD, director of the Institute for Pain Medicine, Haifa, Israel, and colleagues published one of the first articles on gut changes in fibromyalgia. They noted that the gut microbiome could be utilized to determine which individuals had the condition and which did not — with about a 90% accuracy.
The team went on to show that transplanting gut microbiota from patients with fibromyalgia into germ-free mice was sufficient to induce pain-like behaviors in the animals — “effects that were reversed when healthy human microbiota were transplanted instead,” Minerbi told GI & Hepatology News.
Further, in a pilot clinical study, the researchers showed that transplanting microbiota from healthy donors led to a reduction in pain and other symptoms in women with treatment-resistant fibromyalgia.
Most recently, they found significant differences in the composition of the gut microbiome in a cohort of patients with CRPS from Israel, compared to matched pain-free control individuals.
Notably, two species — Dialister succinatiphilus and Phascolarctobacterium faecium – were enriched in patients with CRPS, while three species — Ligilactobacillus salivarius, Bifidobacterium dentium, and Bifidobacterium adolescentis – were increased in control samples, according to their report published last month in Anesthesiology.
“Importantly,” these findings were replicated in an independent cohort of patients with CRPS from Canada, “suggesting that the observed microbiome signature is robust and consistent across different environments,” Minerbi told GI & Hepatology News.
Causal Role?
“These findings collectively suggest a causal role for the gut microbiome in at least some chronic pain conditions,” Minerbi said.
However, the co-authors of a linked editorial cautioned that it’s “unclear if D succinatiphilus or P faecium are functionally relevant to CRPS pathophysiology or if the bacteria increased in healthy control samples protect against CRPS development.”
Minerbi and colleagues also observed that fecal concentrations of all measured short chain fatty acids (SCFA) in patients with CRPS were lower on average compared to pain-free control individuals, of which butyric, hexanoic, and valeric acid showed significant depletion.
Additionally, plasma concentrations of acetic acid showed significant depletion in patients with CRPS vs control individuals, while propionate, butyrate, isobutyrate and 2-methyl-butyric acid showed a trend toward lower concentrations.
The quantification of SCFA in patient stool and serum is a “notable advance” in this study, Zulmary Manjarres, PhD; Ashley Plumb, PhD; and Katelyn Sadler, PhD; with the Center for Advanced Pain Studies at The University of Texas at Dallas, wrote in their editorial.
SCFA are produced by bacteria as a byproduct of dietary fiber fermentation and appropriate levels of these compounds are important to maintain low levels of inflammation in the colon and overall gut health, they explained.
This begs the question of whether administering probiotic bacteria — many of which are believed to exert health benefits through SCFA production — can be used to treat CRPS-associated pain. It’s something that needs to be studied, the editorialists wrote.
Yet, in their view, the “most notable achievement” of Minerbi and colleagues is the development of a machine learning model that accurately, specifically and sensitively categorized individuals as patients with CRPS or control individuals based on their fecal microbiome signature.
The model, trained on exact sequence variant data from the Israeli patients, achieved 89.5% accuracy, 90.0% sensitivity, and 88.9% specificity in distinguishing patients with CRPS from control individuals in the Canadian cohort.
Interestingly, in three patients with CRPS who underwent limb amputation and recovered from their pain, their gut microbiome signature remained unchanged, suggesting that microbiome alterations might precede or persist beyond symptomatic phases.
Test and Treat: Are We There Yet?
The gut microbiome link to chronic pain syndromes is a hot area of research, but for now gut microbial testing followed by treatment aimed at “fixing” the microbiome remains largely experimental.
At this point, comprehensive gut-microbiome sequencing is not a routine, guideline-supported part of care for fibromyalgia or any chronic pain condition.
“Unfortunately, even for doctors interested in this area, we are not quite at the state of being able to diagnose and treat pain syndrome based on microbiome data,” Bonakdar told GI & Hepatology News.
He said there are many reasons for this including that this type of microbiome analysis is not commonly available at a routine lab. If patients do obtain testing, then the results are quite complex and may not translate to a diagnosis or a simple microbiome intervention.
“I think the closest option we have now is considering supplementing with commonly beneficial probiotic in pain conditions,” Bonakdar said.
One example is a preliminary fibromyalgia trial which found that supplementing with Lactobacillus, Bifidobacterium, and Saccharomyces boulardii appeared to have benefit.
“Unfortunately, this is hit or miss as other trials such as one in low back pain did not find benefit,” Bonakdar said.
Addressing gut microbiome changes will become “more actionable when microbiome analysis is more commonplace as well as is the ability to tailor treatment to the abnormalities seen on testing in a real-world manner,” Bonakdar said.
“Until then, there is no harm in promoting an anti-inflammatory diet for our patients with pain which we know can improve components of the microbiome while also supporting pain management,” he concluded.
Minerbi, Bonakdar, and the editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
A new study adds to what has been emerging in the literature — namely that — suggesting that microbiome-based diagnostics and therapeutics may one day be routine for a broad range of pain conditions.
“There is now a whole list of pain conditions that appear to have these signatures, including postoperative pain, arthritis, neuropathy and migraine to name a few,” Robert Bonakdar, MD, director of pain management, Scripps Center for Integrative Medicine, San Diego, told GI & Hepatology News.
Fibromyalgia and complex regional pain syndrome (CRPS) are also on the list.
A team led by Amir Minerbi, MD, PhD, director of the Institute for Pain Medicine, Haifa, Israel, and colleagues published one of the first articles on gut changes in fibromyalgia. They noted that the gut microbiome could be utilized to determine which individuals had the condition and which did not — with about a 90% accuracy.
The team went on to show that transplanting gut microbiota from patients with fibromyalgia into germ-free mice was sufficient to induce pain-like behaviors in the animals — “effects that were reversed when healthy human microbiota were transplanted instead,” Minerbi told GI & Hepatology News.
Further, in a pilot clinical study, the researchers showed that transplanting microbiota from healthy donors led to a reduction in pain and other symptoms in women with treatment-resistant fibromyalgia.
Most recently, they found significant differences in the composition of the gut microbiome in a cohort of patients with CRPS from Israel, compared to matched pain-free control individuals.
Notably, two species — Dialister succinatiphilus and Phascolarctobacterium faecium – were enriched in patients with CRPS, while three species — Ligilactobacillus salivarius, Bifidobacterium dentium, and Bifidobacterium adolescentis – were increased in control samples, according to their report published last month in Anesthesiology.
“Importantly,” these findings were replicated in an independent cohort of patients with CRPS from Canada, “suggesting that the observed microbiome signature is robust and consistent across different environments,” Minerbi told GI & Hepatology News.
Causal Role?
“These findings collectively suggest a causal role for the gut microbiome in at least some chronic pain conditions,” Minerbi said.
However, the co-authors of a linked editorial cautioned that it’s “unclear if D succinatiphilus or P faecium are functionally relevant to CRPS pathophysiology or if the bacteria increased in healthy control samples protect against CRPS development.”
Minerbi and colleagues also observed that fecal concentrations of all measured short chain fatty acids (SCFA) in patients with CRPS were lower on average compared to pain-free control individuals, of which butyric, hexanoic, and valeric acid showed significant depletion.
Additionally, plasma concentrations of acetic acid showed significant depletion in patients with CRPS vs control individuals, while propionate, butyrate, isobutyrate and 2-methyl-butyric acid showed a trend toward lower concentrations.
The quantification of SCFA in patient stool and serum is a “notable advance” in this study, Zulmary Manjarres, PhD; Ashley Plumb, PhD; and Katelyn Sadler, PhD; with the Center for Advanced Pain Studies at The University of Texas at Dallas, wrote in their editorial.
SCFA are produced by bacteria as a byproduct of dietary fiber fermentation and appropriate levels of these compounds are important to maintain low levels of inflammation in the colon and overall gut health, they explained.
This begs the question of whether administering probiotic bacteria — many of which are believed to exert health benefits through SCFA production — can be used to treat CRPS-associated pain. It’s something that needs to be studied, the editorialists wrote.
Yet, in their view, the “most notable achievement” of Minerbi and colleagues is the development of a machine learning model that accurately, specifically and sensitively categorized individuals as patients with CRPS or control individuals based on their fecal microbiome signature.
The model, trained on exact sequence variant data from the Israeli patients, achieved 89.5% accuracy, 90.0% sensitivity, and 88.9% specificity in distinguishing patients with CRPS from control individuals in the Canadian cohort.
Interestingly, in three patients with CRPS who underwent limb amputation and recovered from their pain, their gut microbiome signature remained unchanged, suggesting that microbiome alterations might precede or persist beyond symptomatic phases.
Test and Treat: Are We There Yet?
The gut microbiome link to chronic pain syndromes is a hot area of research, but for now gut microbial testing followed by treatment aimed at “fixing” the microbiome remains largely experimental.
At this point, comprehensive gut-microbiome sequencing is not a routine, guideline-supported part of care for fibromyalgia or any chronic pain condition.
“Unfortunately, even for doctors interested in this area, we are not quite at the state of being able to diagnose and treat pain syndrome based on microbiome data,” Bonakdar told GI & Hepatology News.
He said there are many reasons for this including that this type of microbiome analysis is not commonly available at a routine lab. If patients do obtain testing, then the results are quite complex and may not translate to a diagnosis or a simple microbiome intervention.
“I think the closest option we have now is considering supplementing with commonly beneficial probiotic in pain conditions,” Bonakdar said.
One example is a preliminary fibromyalgia trial which found that supplementing with Lactobacillus, Bifidobacterium, and Saccharomyces boulardii appeared to have benefit.
“Unfortunately, this is hit or miss as other trials such as one in low back pain did not find benefit,” Bonakdar said.
Addressing gut microbiome changes will become “more actionable when microbiome analysis is more commonplace as well as is the ability to tailor treatment to the abnormalities seen on testing in a real-world manner,” Bonakdar said.
“Until then, there is no harm in promoting an anti-inflammatory diet for our patients with pain which we know can improve components of the microbiome while also supporting pain management,” he concluded.
Minerbi, Bonakdar, and the editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
A new study adds to what has been emerging in the literature — namely that — suggesting that microbiome-based diagnostics and therapeutics may one day be routine for a broad range of pain conditions.
“There is now a whole list of pain conditions that appear to have these signatures, including postoperative pain, arthritis, neuropathy and migraine to name a few,” Robert Bonakdar, MD, director of pain management, Scripps Center for Integrative Medicine, San Diego, told GI & Hepatology News.
Fibromyalgia and complex regional pain syndrome (CRPS) are also on the list.
A team led by Amir Minerbi, MD, PhD, director of the Institute for Pain Medicine, Haifa, Israel, and colleagues published one of the first articles on gut changes in fibromyalgia. They noted that the gut microbiome could be utilized to determine which individuals had the condition and which did not — with about a 90% accuracy.
The team went on to show that transplanting gut microbiota from patients with fibromyalgia into germ-free mice was sufficient to induce pain-like behaviors in the animals — “effects that were reversed when healthy human microbiota were transplanted instead,” Minerbi told GI & Hepatology News.
Further, in a pilot clinical study, the researchers showed that transplanting microbiota from healthy donors led to a reduction in pain and other symptoms in women with treatment-resistant fibromyalgia.
Most recently, they found significant differences in the composition of the gut microbiome in a cohort of patients with CRPS from Israel, compared to matched pain-free control individuals.
Notably, two species — Dialister succinatiphilus and Phascolarctobacterium faecium – were enriched in patients with CRPS, while three species — Ligilactobacillus salivarius, Bifidobacterium dentium, and Bifidobacterium adolescentis – were increased in control samples, according to their report published last month in Anesthesiology.
“Importantly,” these findings were replicated in an independent cohort of patients with CRPS from Canada, “suggesting that the observed microbiome signature is robust and consistent across different environments,” Minerbi told GI & Hepatology News.
Causal Role?
“These findings collectively suggest a causal role for the gut microbiome in at least some chronic pain conditions,” Minerbi said.
However, the co-authors of a linked editorial cautioned that it’s “unclear if D succinatiphilus or P faecium are functionally relevant to CRPS pathophysiology or if the bacteria increased in healthy control samples protect against CRPS development.”
Minerbi and colleagues also observed that fecal concentrations of all measured short chain fatty acids (SCFA) in patients with CRPS were lower on average compared to pain-free control individuals, of which butyric, hexanoic, and valeric acid showed significant depletion.
Additionally, plasma concentrations of acetic acid showed significant depletion in patients with CRPS vs control individuals, while propionate, butyrate, isobutyrate and 2-methyl-butyric acid showed a trend toward lower concentrations.
The quantification of SCFA in patient stool and serum is a “notable advance” in this study, Zulmary Manjarres, PhD; Ashley Plumb, PhD; and Katelyn Sadler, PhD; with the Center for Advanced Pain Studies at The University of Texas at Dallas, wrote in their editorial.
SCFA are produced by bacteria as a byproduct of dietary fiber fermentation and appropriate levels of these compounds are important to maintain low levels of inflammation in the colon and overall gut health, they explained.
This begs the question of whether administering probiotic bacteria — many of which are believed to exert health benefits through SCFA production — can be used to treat CRPS-associated pain. It’s something that needs to be studied, the editorialists wrote.
Yet, in their view, the “most notable achievement” of Minerbi and colleagues is the development of a machine learning model that accurately, specifically and sensitively categorized individuals as patients with CRPS or control individuals based on their fecal microbiome signature.
The model, trained on exact sequence variant data from the Israeli patients, achieved 89.5% accuracy, 90.0% sensitivity, and 88.9% specificity in distinguishing patients with CRPS from control individuals in the Canadian cohort.
Interestingly, in three patients with CRPS who underwent limb amputation and recovered from their pain, their gut microbiome signature remained unchanged, suggesting that microbiome alterations might precede or persist beyond symptomatic phases.
Test and Treat: Are We There Yet?
The gut microbiome link to chronic pain syndromes is a hot area of research, but for now gut microbial testing followed by treatment aimed at “fixing” the microbiome remains largely experimental.
At this point, comprehensive gut-microbiome sequencing is not a routine, guideline-supported part of care for fibromyalgia or any chronic pain condition.
“Unfortunately, even for doctors interested in this area, we are not quite at the state of being able to diagnose and treat pain syndrome based on microbiome data,” Bonakdar told GI & Hepatology News.
He said there are many reasons for this including that this type of microbiome analysis is not commonly available at a routine lab. If patients do obtain testing, then the results are quite complex and may not translate to a diagnosis or a simple microbiome intervention.
“I think the closest option we have now is considering supplementing with commonly beneficial probiotic in pain conditions,” Bonakdar said.
One example is a preliminary fibromyalgia trial which found that supplementing with Lactobacillus, Bifidobacterium, and Saccharomyces boulardii appeared to have benefit.
“Unfortunately, this is hit or miss as other trials such as one in low back pain did not find benefit,” Bonakdar said.
Addressing gut microbiome changes will become “more actionable when microbiome analysis is more commonplace as well as is the ability to tailor treatment to the abnormalities seen on testing in a real-world manner,” Bonakdar said.
“Until then, there is no harm in promoting an anti-inflammatory diet for our patients with pain which we know can improve components of the microbiome while also supporting pain management,” he concluded.
Minerbi, Bonakdar, and the editorial writers had no relevant disclosures.
A version of this article appeared on Medscape.com.
Experiencing DDW as an Early Career GI
Dear Friends,
Like many readers, I just returned from Digestive Disease Week® (DDW) in San Diego, California. For the first time in my early career, my experience was not just overwhelming and exhausting. Before, I wanted to do everything – lectures, posters, meetings with friends, prospective research collaborators, and more! This year, I acknowledged that instead of spreading myself thin and not fully engaging, I made a focused daily schedule mixed with productivity and social events, selecting only what was most important to me at this time in my career. This time, after DDW, instead of giving in to my inner introvert and holing myself in my house for a week to recover, I am invigorated by what I learned and the people I met. I can’t wait to see what’s to come next year!

In this issue’s “In Focus”, Dr. Evan Dellon describes his diagnostic approach, including a clear history, endoscopic evaluation with biopsy, and ruling out other causes of esophageal eosinophilia. He emphasizes that treatment should target both inflammation and fibrostenosis and reviews the guidelines and evidence behind first-line treatments, surveillance, and long-term maintenance.
In the second of a two-part series in the “Short Clinical Review” section, Dr. Christopher Vélez, Dr. Rosa L. Yu, and Dr. Jennifer Dimino discuss care for patients with disorders of brain-gut interaction from historically marginalized communities. They highlight ways to improve care for these patients in day-to-day clinical practice.
The transition from trainee to a practicing gastroenterologist may bring with it responsibilities of giving feedback to trainees and/or colleagues to improve. In the “Early Career” section, Dr. Michelle Baliss and Dr. Christine Hachem give practical tips on how best to deliver feedback, with a focus on creating time, building rapport, bidirectional communication, and more.
Lastly, in the “Finance/Legal” section, John S. Gardner, a financial advisor, guides trainees and early career gastroenterologists through estate planning – why it’s important, how to do it effectively, and long-term benefits to starting early.
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Danielle Kiefer ([email protected]), Communications/Managing Editor of TNG.
Until next time, I leave you with a historical fun fact because we would not be where we are now without appreciating where we were: the first case of eosinophilic esophagitis was only first described in 1978 and became a distinct entity in the early 1990s.
Yours truly,
Judy A. Trieu, MD, MPH
Editor-in-Chief
Assistant Professor of Medicine
Interventional Endoscopy, Division of Gastroenterology
Washington University School of Medicine in St. Louis
Dear Friends,
Like many readers, I just returned from Digestive Disease Week® (DDW) in San Diego, California. For the first time in my early career, my experience was not just overwhelming and exhausting. Before, I wanted to do everything – lectures, posters, meetings with friends, prospective research collaborators, and more! This year, I acknowledged that instead of spreading myself thin and not fully engaging, I made a focused daily schedule mixed with productivity and social events, selecting only what was most important to me at this time in my career. This time, after DDW, instead of giving in to my inner introvert and holing myself in my house for a week to recover, I am invigorated by what I learned and the people I met. I can’t wait to see what’s to come next year!
In this issue’s “In Focus”, Dr. Evan Dellon describes his diagnostic approach, including a clear history, endoscopic evaluation with biopsy, and ruling out other causes of esophageal eosinophilia. He emphasizes that treatment should target both inflammation and fibrostenosis and reviews the guidelines and evidence behind first-line treatments, surveillance, and long-term maintenance.
In the second of a two-part series in the “Short Clinical Review” section, Dr. Christopher Vélez, Dr. Rosa L. Yu, and Dr. Jennifer Dimino discuss care for patients with disorders of brain-gut interaction from historically marginalized communities. They highlight ways to improve care for these patients in day-to-day clinical practice.
The transition from trainee to a practicing gastroenterologist may bring with it responsibilities of giving feedback to trainees and/or colleagues to improve. In the “Early Career” section, Dr. Michelle Baliss and Dr. Christine Hachem give practical tips on how best to deliver feedback, with a focus on creating time, building rapport, bidirectional communication, and more.
Lastly, in the “Finance/Legal” section, John S. Gardner, a financial advisor, guides trainees and early career gastroenterologists through estate planning – why it’s important, how to do it effectively, and long-term benefits to starting early.
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Danielle Kiefer ([email protected]), Communications/Managing Editor of TNG.
Until next time, I leave you with a historical fun fact because we would not be where we are now without appreciating where we were: the first case of eosinophilic esophagitis was only first described in 1978 and became a distinct entity in the early 1990s.
Yours truly,
Judy A. Trieu, MD, MPH
Editor-in-Chief
Assistant Professor of Medicine
Interventional Endoscopy, Division of Gastroenterology
Washington University School of Medicine in St. Louis
Dear Friends,
Like many readers, I just returned from Digestive Disease Week® (DDW) in San Diego, California. For the first time in my early career, my experience was not just overwhelming and exhausting. Before, I wanted to do everything – lectures, posters, meetings with friends, prospective research collaborators, and more! This year, I acknowledged that instead of spreading myself thin and not fully engaging, I made a focused daily schedule mixed with productivity and social events, selecting only what was most important to me at this time in my career. This time, after DDW, instead of giving in to my inner introvert and holing myself in my house for a week to recover, I am invigorated by what I learned and the people I met. I can’t wait to see what’s to come next year!
In this issue’s “In Focus”, Dr. Evan Dellon describes his diagnostic approach, including a clear history, endoscopic evaluation with biopsy, and ruling out other causes of esophageal eosinophilia. He emphasizes that treatment should target both inflammation and fibrostenosis and reviews the guidelines and evidence behind first-line treatments, surveillance, and long-term maintenance.
In the second of a two-part series in the “Short Clinical Review” section, Dr. Christopher Vélez, Dr. Rosa L. Yu, and Dr. Jennifer Dimino discuss care for patients with disorders of brain-gut interaction from historically marginalized communities. They highlight ways to improve care for these patients in day-to-day clinical practice.
The transition from trainee to a practicing gastroenterologist may bring with it responsibilities of giving feedback to trainees and/or colleagues to improve. In the “Early Career” section, Dr. Michelle Baliss and Dr. Christine Hachem give practical tips on how best to deliver feedback, with a focus on creating time, building rapport, bidirectional communication, and more.
Lastly, in the “Finance/Legal” section, John S. Gardner, a financial advisor, guides trainees and early career gastroenterologists through estate planning – why it’s important, how to do it effectively, and long-term benefits to starting early.
If you are interested in contributing or have ideas for future TNG topics, please contact me ([email protected]) or Danielle Kiefer ([email protected]), Communications/Managing Editor of TNG.
Until next time, I leave you with a historical fun fact because we would not be where we are now without appreciating where we were: the first case of eosinophilic esophagitis was only first described in 1978 and became a distinct entity in the early 1990s.
Yours truly,
Judy A. Trieu, MD, MPH
Editor-in-Chief
Assistant Professor of Medicine
Interventional Endoscopy, Division of Gastroenterology
Washington University School of Medicine in St. Louis
Landmark 20-Year Study Reshapes Understanding of PTSD
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A large 20-year study — the longest and most detailed of its kind — shows that posttraumatic stress disorder (PTSD) symptoms can endure for decades, challenging conventional timelines for recovery and offering new insights to guide future treatment.
Researchers analyzed data from the World Trade Center Health Program (WTCHP), which is administered by the US CDC’s National Institute for Occupational Safety and Health (NIOSH), and found symptoms of PTSD persisted for as long as two decades in 10% of first responders involved in the World Trade Center disaster of September 2001.
Participation in the WTCHP is voluntary, but those who enroll receive free assessments, monitoring, and treatment, including psychiatric and behavioral healthcare. It is the longest and most detailed analysis of PTSD and includes 81,298 observations from 12,822 WTC responders.
Participants entered the WTCHP at different timepoints and were assessed annually. Not every enrollee was assessed every year, but the sheer number of participants and observations “just provides much greater density of data over that 20-year course than any previous study,” lead author Frank D. Mann, PhD, told this news organization.
The study was published online on May 27 in Nature Mental Health.
Filling the PTSD Knowledge Gap
Most PTSD research has focused on the short term, with limited insight into how symptoms evolve over the long haul. Without long-term data, it’s been difficult to understand whether PTSD resolves, persists, or worsens — hindering efforts to guide treatment and support. This study aimed to fill that gap by tracking symptom patterns over two decades.
Responders were assessed regularly using the PTSD Checklist for a Specific Stressor, a standardized tool that measures symptom severity on an 85-point scale. On average, each participant completed 6.3 assessments over the course of the study.
A score of ≥ 44 was considered indicative of clinically elevated PTSD symptoms. Between 2002 and 2022, the crude prevalence of elevated symptoms ranged from 8% to 15%. At the same time, 16% to 34% of responders each year reported little to no symptoms, scoring at or near the minimum on the scale.
The researchers found that symptom trajectories varied widely. Nearly as many participants experienced worsening symptoms as those who improved. As a result, the overall population average remained relatively flat over the 20-year period.
Among responders who met the threshold for PTSD, the median time to symptom improvement was 8.9 years — and by year 20, about 76% had shown improvement.
New Insights
Mann, a senior research scientist at Stony Brook University Renaissance School of Medicine, Stony Brook, New York, said the study not only reinforced existing knowledge about PTSD in responders but also uncovered new insights.
Most notably, it showed that PTSD symptoms tended to peak around a decade after 9/11 — significantly later than delayed-onset patterns reported in previous trauma studies.
He also noted a surprising outcome — the top 10% of responders who experienced worsening symptoms over the long term accounted for the majority of mental health costs. These individuals, Mann said, represent a critical gap in care, with current interventions proving largely ineffective for them.
Mann suggested that ongoing trauma exposure — especially for responders still in high-risk jobs — and potential genetic susceptibility may contribute to late-emerging or persistent symptoms.
“These individuals are an urgent priority for health systems, as available resources have not been effective for them,” the study authors wrote.
Mann and his colleagues also found that occupation offered the strongest protection against developing PTSD. Police officers and firefighters benefit from training designed to help them cope with trauma, and repeated exposure may build a degree of resilience.
In contrast, responders without such training — like construction workers — faced a 50% to 55% higher risk of developing PTSD symptoms. Mann emphasized that occupational status was a more powerful predictor of PTSD risk than the severity of the traumatic exposures themselves.
A Valuable Contribution
Commenting on the research for this news organization, Sandra Lowe, MD, medical director of the Mount Sinai WTCMH program, noted that while the study largely confirms what has been known about responders — such as the significant variability in symptom trajectories over time — it still makes a valuable contribution.
“Extending observations for up to 20 years is rare in any study, especially in a cohort this large,” said Lowe, an associate professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York City, who was not involved in the study.
Also commenting, James West, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, described the finding that 10% of responders continued to experience symptoms two decades after exposure as “sobering.”
However, he emphasized that it aligns with observations in the disaster recovery community, where the psychological impact “goes way beyond what most people see as the immediate aftermath and recovery.” West stressed the urgent need to develop effective treatments that enable those affected to live fuller, less impaired lives.
“We still need to be finding the effective treatments that can help these people live fuller lives without impairment from their trauma symptoms,” said West.
Lowe pointed out that the symptom peak around 10 years post-exposure is often linked to external factors. Some responders who had been managing symptoms might lose resilience due to major life changes such as retirement.
“One of the things that was able to keep them engaged is now lost,” she said. “They begin to spend more time reflecting on recollections, and symptoms can worsen.”
West agreed, adding that retirement or job loss often leads to symptom increases because it removes a primary coping mechanism. Both Lowe and Mann also highlighted that 9/11 memorial events can trigger new symptoms or exacerbate existing ones.
Lowe noted that responders with stronger coping skills tended to fare better over time. Effective coping strategies include maintaining regular schedules — especially for eating and sleeping — leading a structured life, and employing stress management techniques like meditation, yoga, or enjoyable hobbies. Social connection and being part of a community are also critical for resilience. She added that clinicians should always inquire about trauma history.
Lowe, West, and Mann all pointed out that PTSD is often accompanied by physical health issues, particularly cardiovascular problems, which tend to be worse in those with the disorder.
Responders with stronger coping skills tended to do better over time, said Lowe. Coping skills that can help make a difference include having a regular schedule, especially for eating and sleeping; having a structured life; and stress management tools, such as meditation or yoga or an enjoyable hobby. Social connection — being part of a community — is also critical, Lowe said.
Clinicians should always inquire about trauma, she said. Lowe, West, and Mann all noted that people with PTSD often have physical illness and that cardiovascular outcomes in particular are worse for those individuals.
WTCHP Future Uncertain
However, despite advances in understanding PTSD and the importance of ongoing care, the future of the program supporting World Trade Center responders remains uncertain.
Some 140,000 people are now enrolled in the WTCHP, which was established as a federal program in 2010. Congress has generally reauthorized the program whenever its funding came up for renewal.
However, earlier this year, the Trump administration dismissed two thirds of the NIOSH workforce, including John Howard, MD, the administrator of the WTCHP.
In response, members of Congress and advocates for 9/11 survivors urged the US Department of Health and Human Services (HHS) to reinstate Howard and the affected employees. Howard is listed as back on the job has since returned to his position, and HHS reportedly reinstated hundreds of NIOSH workers in May.
An HHS spokesperson told this news organization that the WTCHP continues to provide services and is actively “accepting, reviewing, and processing new enrollment applications and certification requests.”
Meanwhile, the Trump administration’s fiscal year 2026 budget proposal seeks to reduce CDC funding by $3.5 billion — approximately 40% — with a shift in focus toward infectious diseases. It remains unclear how the WTCHP will be affected by this new direction.
Mann said he is not involved in the program’s funding details but added, “Presumably, as long as some funding continues to keep the program alive, we will continue monitoring responders and providing free treatment until the very last World Trade Center responder passes.”
The study was partially funded through National Institutes of Health and CDC grants, the SUNY Research Foundation, and the CDC’s World Trade Center Health Program. Mann, Lowe, and West reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE MENTAL HEALTH

Posttraumatic Stress Disorder May Increase Morbidity Risk in Veterans With HIV
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Vital Partners in GI Care
Demand for specialized GI care has skyrocketed in recent years, eclipsing the supply of gastroenterologists and impairing patient access to high-quality GI care, particularly in rural and other underserved areas. In this environment,

Across specialties, APPs are estimated to constitute roughly a third of the US clinical workforce, and demand is only growing. A June 2024 MGMA Stat poll found that 63% of medical groups planned to add new APP roles in the next year. As the GI APP workforce grows, so too will demand for advanced training tailored to the APP role.
AGA has invested heavily in professional development opportunities for NPs and PAs, in recognition of their vital role in providing high-quality GI care. The newly formed AGA NPPA Task Force, co-chaired by Abigail Meyers (who we featured in GIHN’s April issue) and Kimberly Kearns, works closely with the Education and Training Committee to develop education programs to meet the specific needs of NPs and PAs, and advocate for more APP involvement in AGA programming. One example of this is AGA’s 2025 Principles of GI for the NP and PA course, which will be held in Chicago in early August – I encourage you to spread the word and support your APP colleagues in getting involved in these important initiatives as our vital partners in GI care delivery.
In this month’s issue of GIHN, we present the exciting results of the BOSS trial, showing no survival difference between regular and at need surveillance for Barrett’s esophagus, suggesting that at need endoscopy may be a safe alternative for low-risk patients. Continuing our coverage of potentially practice-changing research from DDW, we highlight another recent RCT challenging the use of papillary sphincterotomy as a treatment for pancreas divisum.
In our July Member Spotlight, Eric Shah, MD, MBA (University of Michigan), a past AGA Research Scholar Award recipient, highlights how this critical research support aided him in his journey to develop a now FDA-approved point-of care screening tool used to evaluate patients with chronic constipation for pelvic floor dysfunction during a routine clinic visit. In our quarterly Perspectives column, Dr. David Wan (a GI hospitalist) and Dr. Zeyed Metwalli (an interventional radiologist) discuss best practices in management of lower GI bleeding. We hope you have a restful summer!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Demand for specialized GI care has skyrocketed in recent years, eclipsing the supply of gastroenterologists and impairing patient access to high-quality GI care, particularly in rural and other underserved areas. In this environment,
Across specialties, APPs are estimated to constitute roughly a third of the US clinical workforce, and demand is only growing. A June 2024 MGMA Stat poll found that 63% of medical groups planned to add new APP roles in the next year. As the GI APP workforce grows, so too will demand for advanced training tailored to the APP role.
AGA has invested heavily in professional development opportunities for NPs and PAs, in recognition of their vital role in providing high-quality GI care. The newly formed AGA NPPA Task Force, co-chaired by Abigail Meyers (who we featured in GIHN’s April issue) and Kimberly Kearns, works closely with the Education and Training Committee to develop education programs to meet the specific needs of NPs and PAs, and advocate for more APP involvement in AGA programming. One example of this is AGA’s 2025 Principles of GI for the NP and PA course, which will be held in Chicago in early August – I encourage you to spread the word and support your APP colleagues in getting involved in these important initiatives as our vital partners in GI care delivery.
In this month’s issue of GIHN, we present the exciting results of the BOSS trial, showing no survival difference between regular and at need surveillance for Barrett’s esophagus, suggesting that at need endoscopy may be a safe alternative for low-risk patients. Continuing our coverage of potentially practice-changing research from DDW, we highlight another recent RCT challenging the use of papillary sphincterotomy as a treatment for pancreas divisum.
In our July Member Spotlight, Eric Shah, MD, MBA (University of Michigan), a past AGA Research Scholar Award recipient, highlights how this critical research support aided him in his journey to develop a now FDA-approved point-of care screening tool used to evaluate patients with chronic constipation for pelvic floor dysfunction during a routine clinic visit. In our quarterly Perspectives column, Dr. David Wan (a GI hospitalist) and Dr. Zeyed Metwalli (an interventional radiologist) discuss best practices in management of lower GI bleeding. We hope you have a restful summer!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Demand for specialized GI care has skyrocketed in recent years, eclipsing the supply of gastroenterologists and impairing patient access to high-quality GI care, particularly in rural and other underserved areas. In this environment,
Across specialties, APPs are estimated to constitute roughly a third of the US clinical workforce, and demand is only growing. A June 2024 MGMA Stat poll found that 63% of medical groups planned to add new APP roles in the next year. As the GI APP workforce grows, so too will demand for advanced training tailored to the APP role.
AGA has invested heavily in professional development opportunities for NPs and PAs, in recognition of their vital role in providing high-quality GI care. The newly formed AGA NPPA Task Force, co-chaired by Abigail Meyers (who we featured in GIHN’s April issue) and Kimberly Kearns, works closely with the Education and Training Committee to develop education programs to meet the specific needs of NPs and PAs, and advocate for more APP involvement in AGA programming. One example of this is AGA’s 2025 Principles of GI for the NP and PA course, which will be held in Chicago in early August – I encourage you to spread the word and support your APP colleagues in getting involved in these important initiatives as our vital partners in GI care delivery.
In this month’s issue of GIHN, we present the exciting results of the BOSS trial, showing no survival difference between regular and at need surveillance for Barrett’s esophagus, suggesting that at need endoscopy may be a safe alternative for low-risk patients. Continuing our coverage of potentially practice-changing research from DDW, we highlight another recent RCT challenging the use of papillary sphincterotomy as a treatment for pancreas divisum.
In our July Member Spotlight, Eric Shah, MD, MBA (University of Michigan), a past AGA Research Scholar Award recipient, highlights how this critical research support aided him in his journey to develop a now FDA-approved point-of care screening tool used to evaluate patients with chronic constipation for pelvic floor dysfunction during a routine clinic visit. In our quarterly Perspectives column, Dr. David Wan (a GI hospitalist) and Dr. Zeyed Metwalli (an interventional radiologist) discuss best practices in management of lower GI bleeding. We hope you have a restful summer!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Recommendations for Empiric Antibiotic Therapy in Hidradenitis Suppurativa
Recommendations for Empiric Antibiotic Therapy in Hidradenitis Suppurativa
Hidradenitis suppurativa (HS) is a chronic scarring inflammatory skin condition of the follicular epithelium that impacts 1% to 4% of the general population (eFigure).1-3 This statistic likely is an underrepresentation of the affected population due to missed and delayed diagnoses.1 Hidradenitis suppurativa has been identified as having one of the strongest negative impacts on patients’ lives based on studied skin diseases.4 Its recurrent nature can negatively impact both the patient’s physical and mental state.3 Due to the debilitating effects of HS, we aimed to create updated recommendations for empiric antibotics based on affected anatomic locations in an effort to improve patient quality of life.

Methods
An institutional review board–approved retrospective medical chart review of 485 patients diagnosed with HS and evaluated at the University of Texas Medical Branch in Galveston from January 2006 to December 2021 was conducted. Males and females of all ages (including pregnant and pediatric patients) were included. Only patients for whom anatomic locations of HS lesions or culture sites were not documented were excluded from the analysis. Locations of cultures were categorized into 5 groups: axilla; groin; buttocks; inframammary; and multiple sites of involvement, which included any combination of 2 or more sites. Types of bacteria collected from cultures and recorded included Escherichia coli, Enterococcus species, Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus aureus, coagulase-negative staphylococci (CoNS), and other Gram-negative species. Sensitivity profiles also were analyzed for the most commonly cultured bacteria to create recommendations on antibiotic use based on the anatomic location of the lesions. Data analysis was conducted using descriptive statistics and bivariate analysis.
Results
The analysis included 485 patients comprising 600 visits. Seventy-five percent (363/485) of the study population was female. The axilla was the most common anatomic location for HS lesions followed by multiple sites of involvement. In total, 283 cultures were performed; males were 1.1 times more likely than females to be cultured. While cultures were most frequently obtained in patients with axillary lesions only (93/262 [35%]) or from multiple sites of involvement (83/179 [46%]) as this was the most common presentation of HS in our patient population, cultures were more likely to be obtained when patients presented with only buttock (32/38 [84%]) and inframammary (20/25 [80%]) lesions (Table).
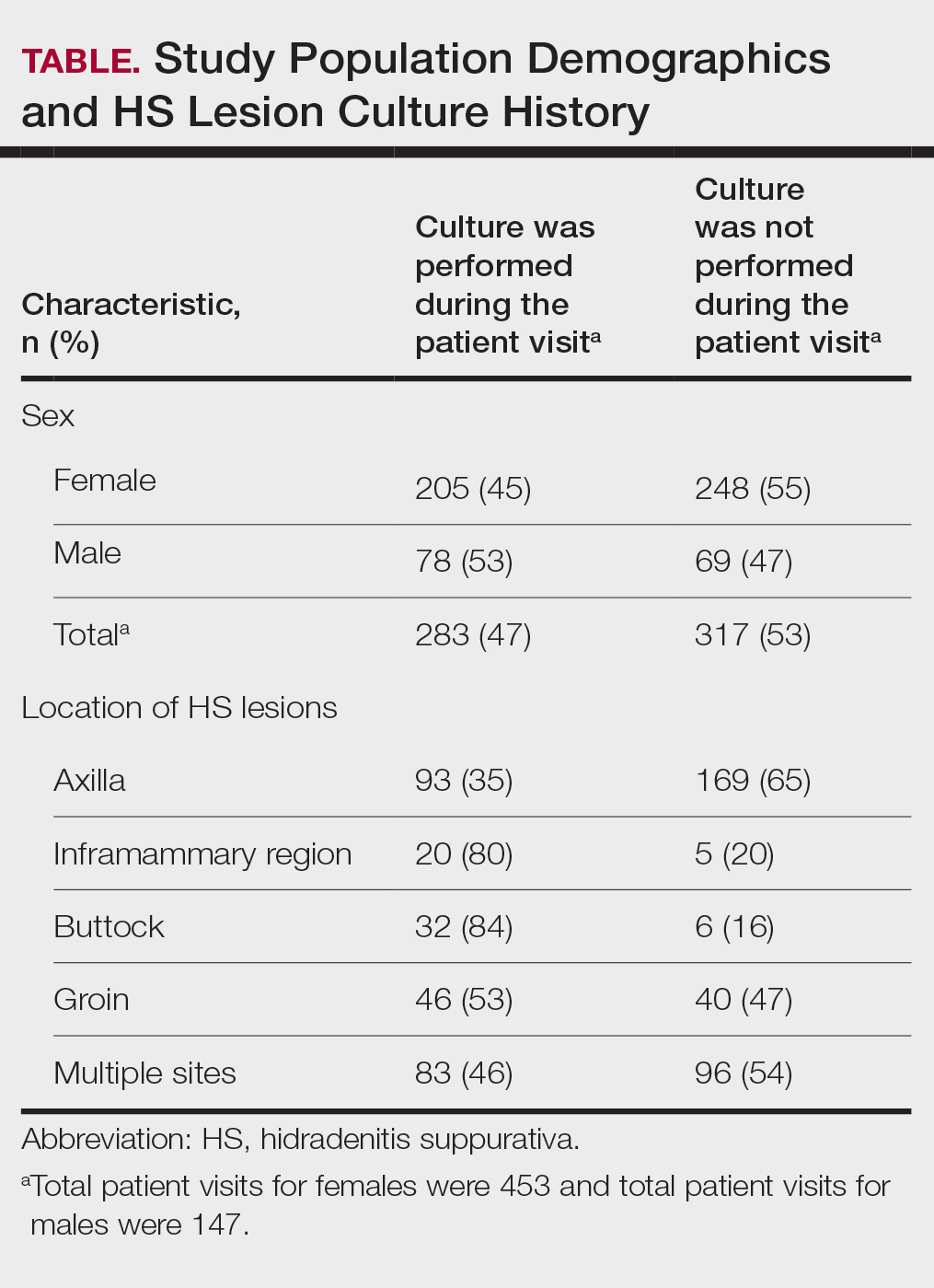
Staphylococcus aureus was the most commonly cultured bacteria in general (53/283 [19%]) as well as for HS located the axilla (24/56 [43%]) and in multiple sites (16/51 [31%]). Proteus mirabilis (29/283 [10%]) was the second most commonly cultured bacteria overall and was cultured most often in the axilla (15/56 [27%]) and inframammary region (6/14 [43%]). These were followed by beta-hemolytic Streptococcus species (26/283 [9%]) and Enterococcus species (21/283 [7%]), which was second to P mirabilis as the most commonly cultured bacteria in the inframammary region (6/14 [43%])(eTable 1).
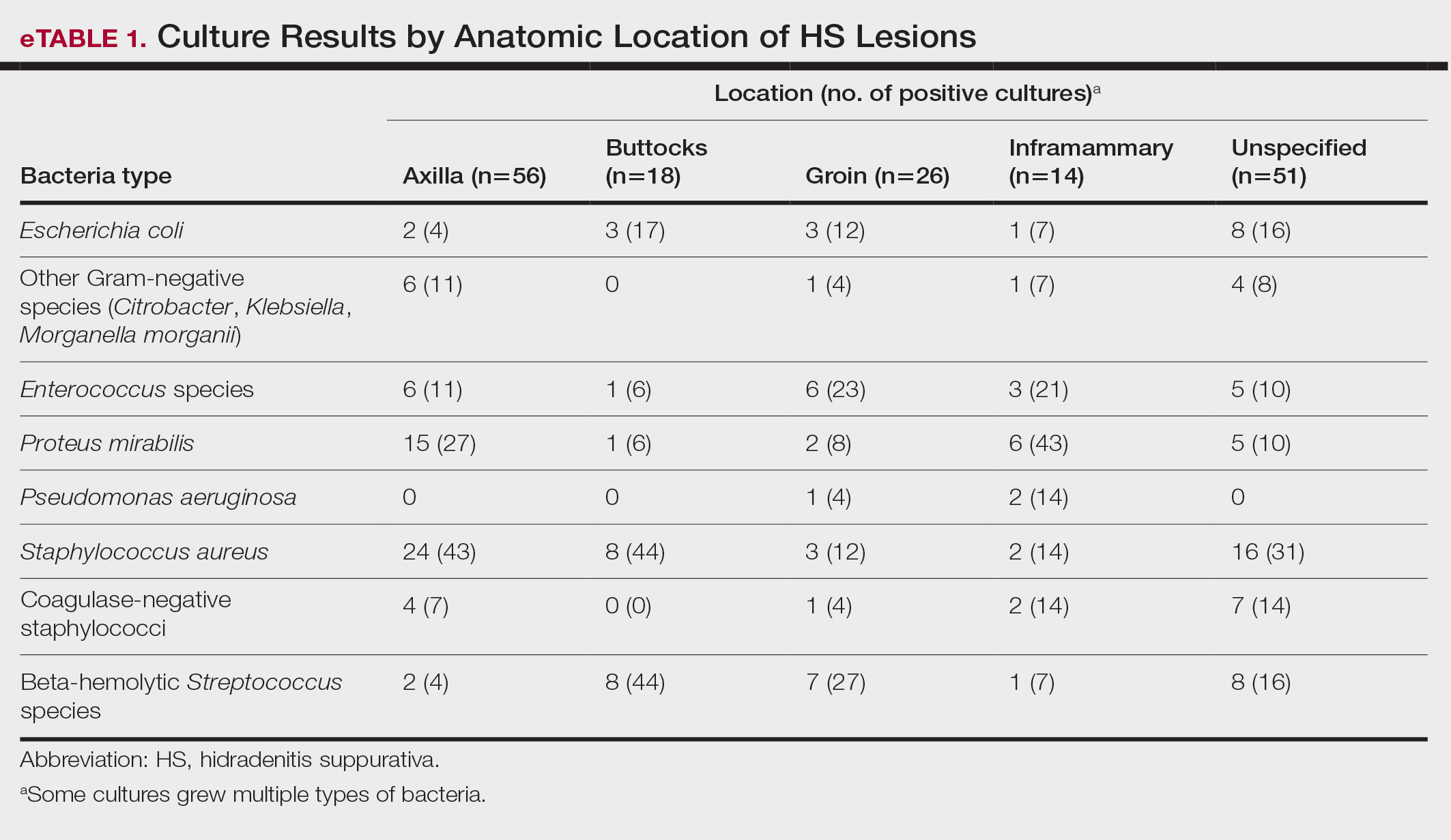
eTable 2 shows the sensitivity profiles for the most commonly cultured bacteria: S aureus, P mirabilis, and Enterococcus species. Staphylococcus aureus located in the axilla, buttocks, and groin was most sensitive to rifampin (41/44 [93%]), TMP/SMX (41/44 [93%]), and tetracycline (39/44 [89%]) and most resistant to erythromycin (26/44 [59%]) and oxacillin (24/44 [55%]). Proteus mirabilis in the inframammary region was most sensitive to ampicillin (27/27 [100%]), gentamicin (27/27 [100%]), levofloxacin (27/27 [100%]), and TMP/SMX (26/27 [96%]). Enterococcus species were most sensitive to vancomycin (20/20 [100%]) and ampicillin (19/20 [95%]) and most resistant to gentamicin (5/20 [25%]).
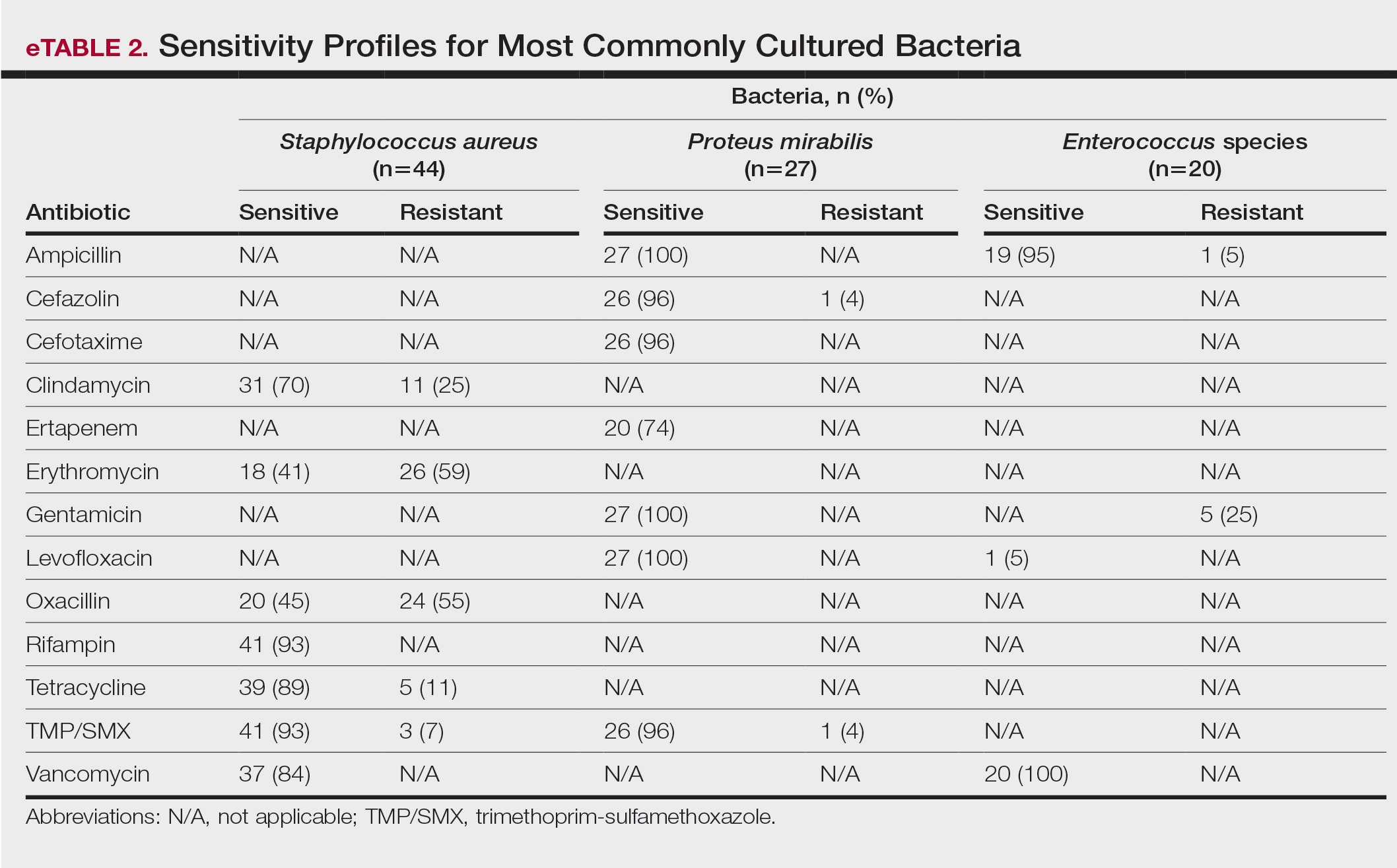
Comment
To treat HS, it is important to understand the cause of the condition. Although the pathogenesis of HS has many unknowns, bacterial colonization and biofilms are thought to play a role. Lipopolysaccharides found in the outer membrane of Gram-negative bacteria are pathogen-associated molecular patterns that present to the toll-like receptors of the human immune system. Once the toll-like receptors recognize the pathogen-associated molecular patterns, macrophages and keratinocytes are activated and release proinflammatory and anti-inflammatory cytokines and chemokines. Persistent presentation of bacteria to the immune system increases immune-cell recruitment and worsens chronic inflammation in patients with HS. Evidence has revealed that bacteria initiate and sustain the inflammation seen in patients with HS; therefore, reducing the amount of bacteria could alleviate some of the symptoms of HS.5 It is important to continue learning about the pathophysiology of this disease as well as formulating tailored treatments to minimize patient discomfort and improve quality of life.
Based on the findings of the current study and the safety profile of the medication, tetracyclines may be considered for first-line empiric therapy in patients with HS involving the axilla only, buttocks only, or multiple sites. For additional coverage of P mirabilis in the axilla or inframammary region, TMP/SMX monotherapy or tetracycline plus ampicillin may be considered. For inframammary lesions only, empiric treatment with ampicillin or TMP/ SMX is recommended. For HS lesions in the groin area, coverage of Enterococcus species with ampicillin should be considered. Patients with multiple sites of involvement that include the inframammary or groin regions similarly should receive empiric antibiotics that cover both S aureus and Gram-negative bacteria, such as TMP/SMX or tetracycline and ampicillin, respectively; if the multiple sites do not include the inframammary or groin regions, Gram-negative coverage may not be indicated. Based on our findings, standardization of treatment for patients with HS can allow for earlier and potentially more effective treatment.
In a similar study conducted in 2016, bacteria species were isolated from the axilla, groin, and gluteus/perineum in patients with HS.5 In that study, the most prominent bacteria in the axilla was CoNS; in the groin, P mirabilis and E coli; and in the gluteus/perineum, E coli and CoNS. These results differed from ours, which found S aureus as the abundant bacteria in these areas. In the 2016 study, the highest rates of resistance were found for penicillin G, erythromycin, clindamycin, and ampicillin.5 In contrast, the current study found high sensitivities for clindamycin and ampicillin, but our results support the finding of high resistance for erythromycin. These differences could be accounted for by the lower sample size of patients in the 2016 study: 68 patients were analyzed for sensitivity results, and 171 patients were analyzed for frequency of bacterial species in patients with HS.5
Our study is limited by its relatively small sample size. Additionally, all patients were seen at 1 of 2 clinic sites, located in League City and Galveston, Texas, and the data from this geographic area may not be applicable to patients seen in different climates.
Conclusion
Outcomes for patients with HS improve with early intervention; however, HS treatment may be delayed by selection of ineffective antibiotic therapy. Our study provides clinicians with recommendations for empiric antibiotic treatment based on anatomic location of HS lesions and culture sensitivity profiles. Utilizing tailored antibiotic therapy on initial clinical evaluation may increase early disease control and improve morbidity and disease outcomes, thereby increasing patient quality of life.
- Vinkel C, Thomsen SF. Hidradenitis suppurativa: causes, features, and current treatments. J Clin Aesthet Dermatol. 2018;11:17-23.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60:539-561; quiz 562-563.
- Yazdanyar S, Jemec GBE. Hidradenitis suppurativa: a review of cause and treatment. Curr Opin Infect Dis. 2011;24:118-123.
- Hessam S, Sand M, Georgas D, et al. Microbial profile and antimicrobial susceptibility of bacteria found in inflammatory hidradenitis suppurativa lesions. Skin Pharmacol Physiol. 2016; 29:161-167.
Hidradenitis suppurativa (HS) is a chronic scarring inflammatory skin condition of the follicular epithelium that impacts 1% to 4% of the general population (eFigure).1-3 This statistic likely is an underrepresentation of the affected population due to missed and delayed diagnoses.1 Hidradenitis suppurativa has been identified as having one of the strongest negative impacts on patients’ lives based on studied skin diseases.4 Its recurrent nature can negatively impact both the patient’s physical and mental state.3 Due to the debilitating effects of HS, we aimed to create updated recommendations for empiric antibotics based on affected anatomic locations in an effort to improve patient quality of life.
Methods
An institutional review board–approved retrospective medical chart review of 485 patients diagnosed with HS and evaluated at the University of Texas Medical Branch in Galveston from January 2006 to December 2021 was conducted. Males and females of all ages (including pregnant and pediatric patients) were included. Only patients for whom anatomic locations of HS lesions or culture sites were not documented were excluded from the analysis. Locations of cultures were categorized into 5 groups: axilla; groin; buttocks; inframammary; and multiple sites of involvement, which included any combination of 2 or more sites. Types of bacteria collected from cultures and recorded included Escherichia coli, Enterococcus species, Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus aureus, coagulase-negative staphylococci (CoNS), and other Gram-negative species. Sensitivity profiles also were analyzed for the most commonly cultured bacteria to create recommendations on antibiotic use based on the anatomic location of the lesions. Data analysis was conducted using descriptive statistics and bivariate analysis.
Results
The analysis included 485 patients comprising 600 visits. Seventy-five percent (363/485) of the study population was female. The axilla was the most common anatomic location for HS lesions followed by multiple sites of involvement. In total, 283 cultures were performed; males were 1.1 times more likely than females to be cultured. While cultures were most frequently obtained in patients with axillary lesions only (93/262 [35%]) or from multiple sites of involvement (83/179 [46%]) as this was the most common presentation of HS in our patient population, cultures were more likely to be obtained when patients presented with only buttock (32/38 [84%]) and inframammary (20/25 [80%]) lesions (Table).
Staphylococcus aureus was the most commonly cultured bacteria in general (53/283 [19%]) as well as for HS located the axilla (24/56 [43%]) and in multiple sites (16/51 [31%]). Proteus mirabilis (29/283 [10%]) was the second most commonly cultured bacteria overall and was cultured most often in the axilla (15/56 [27%]) and inframammary region (6/14 [43%]). These were followed by beta-hemolytic Streptococcus species (26/283 [9%]) and Enterococcus species (21/283 [7%]), which was second to P mirabilis as the most commonly cultured bacteria in the inframammary region (6/14 [43%])(eTable 1).
eTable 2 shows the sensitivity profiles for the most commonly cultured bacteria: S aureus, P mirabilis, and Enterococcus species. Staphylococcus aureus located in the axilla, buttocks, and groin was most sensitive to rifampin (41/44 [93%]), TMP/SMX (41/44 [93%]), and tetracycline (39/44 [89%]) and most resistant to erythromycin (26/44 [59%]) and oxacillin (24/44 [55%]). Proteus mirabilis in the inframammary region was most sensitive to ampicillin (27/27 [100%]), gentamicin (27/27 [100%]), levofloxacin (27/27 [100%]), and TMP/SMX (26/27 [96%]). Enterococcus species were most sensitive to vancomycin (20/20 [100%]) and ampicillin (19/20 [95%]) and most resistant to gentamicin (5/20 [25%]).
Comment
To treat HS, it is important to understand the cause of the condition. Although the pathogenesis of HS has many unknowns, bacterial colonization and biofilms are thought to play a role. Lipopolysaccharides found in the outer membrane of Gram-negative bacteria are pathogen-associated molecular patterns that present to the toll-like receptors of the human immune system. Once the toll-like receptors recognize the pathogen-associated molecular patterns, macrophages and keratinocytes are activated and release proinflammatory and anti-inflammatory cytokines and chemokines. Persistent presentation of bacteria to the immune system increases immune-cell recruitment and worsens chronic inflammation in patients with HS. Evidence has revealed that bacteria initiate and sustain the inflammation seen in patients with HS; therefore, reducing the amount of bacteria could alleviate some of the symptoms of HS.5 It is important to continue learning about the pathophysiology of this disease as well as formulating tailored treatments to minimize patient discomfort and improve quality of life.
Based on the findings of the current study and the safety profile of the medication, tetracyclines may be considered for first-line empiric therapy in patients with HS involving the axilla only, buttocks only, or multiple sites. For additional coverage of P mirabilis in the axilla or inframammary region, TMP/SMX monotherapy or tetracycline plus ampicillin may be considered. For inframammary lesions only, empiric treatment with ampicillin or TMP/ SMX is recommended. For HS lesions in the groin area, coverage of Enterococcus species with ampicillin should be considered. Patients with multiple sites of involvement that include the inframammary or groin regions similarly should receive empiric antibiotics that cover both S aureus and Gram-negative bacteria, such as TMP/SMX or tetracycline and ampicillin, respectively; if the multiple sites do not include the inframammary or groin regions, Gram-negative coverage may not be indicated. Based on our findings, standardization of treatment for patients with HS can allow for earlier and potentially more effective treatment.
In a similar study conducted in 2016, bacteria species were isolated from the axilla, groin, and gluteus/perineum in patients with HS.5 In that study, the most prominent bacteria in the axilla was CoNS; in the groin, P mirabilis and E coli; and in the gluteus/perineum, E coli and CoNS. These results differed from ours, which found S aureus as the abundant bacteria in these areas. In the 2016 study, the highest rates of resistance were found for penicillin G, erythromycin, clindamycin, and ampicillin.5 In contrast, the current study found high sensitivities for clindamycin and ampicillin, but our results support the finding of high resistance for erythromycin. These differences could be accounted for by the lower sample size of patients in the 2016 study: 68 patients were analyzed for sensitivity results, and 171 patients were analyzed for frequency of bacterial species in patients with HS.5
Our study is limited by its relatively small sample size. Additionally, all patients were seen at 1 of 2 clinic sites, located in League City and Galveston, Texas, and the data from this geographic area may not be applicable to patients seen in different climates.
Conclusion
Outcomes for patients with HS improve with early intervention; however, HS treatment may be delayed by selection of ineffective antibiotic therapy. Our study provides clinicians with recommendations for empiric antibiotic treatment based on anatomic location of HS lesions and culture sensitivity profiles. Utilizing tailored antibiotic therapy on initial clinical evaluation may increase early disease control and improve morbidity and disease outcomes, thereby increasing patient quality of life.
Hidradenitis suppurativa (HS) is a chronic scarring inflammatory skin condition of the follicular epithelium that impacts 1% to 4% of the general population (eFigure).1-3 This statistic likely is an underrepresentation of the affected population due to missed and delayed diagnoses.1 Hidradenitis suppurativa has been identified as having one of the strongest negative impacts on patients’ lives based on studied skin diseases.4 Its recurrent nature can negatively impact both the patient’s physical and mental state.3 Due to the debilitating effects of HS, we aimed to create updated recommendations for empiric antibotics based on affected anatomic locations in an effort to improve patient quality of life.
Methods
An institutional review board–approved retrospective medical chart review of 485 patients diagnosed with HS and evaluated at the University of Texas Medical Branch in Galveston from January 2006 to December 2021 was conducted. Males and females of all ages (including pregnant and pediatric patients) were included. Only patients for whom anatomic locations of HS lesions or culture sites were not documented were excluded from the analysis. Locations of cultures were categorized into 5 groups: axilla; groin; buttocks; inframammary; and multiple sites of involvement, which included any combination of 2 or more sites. Types of bacteria collected from cultures and recorded included Escherichia coli, Enterococcus species, Proteus mirabilis, Pseudomonas aeruginosa, Staphylococcus aureus, coagulase-negative staphylococci (CoNS), and other Gram-negative species. Sensitivity profiles also were analyzed for the most commonly cultured bacteria to create recommendations on antibiotic use based on the anatomic location of the lesions. Data analysis was conducted using descriptive statistics and bivariate analysis.
Results
The analysis included 485 patients comprising 600 visits. Seventy-five percent (363/485) of the study population was female. The axilla was the most common anatomic location for HS lesions followed by multiple sites of involvement. In total, 283 cultures were performed; males were 1.1 times more likely than females to be cultured. While cultures were most frequently obtained in patients with axillary lesions only (93/262 [35%]) or from multiple sites of involvement (83/179 [46%]) as this was the most common presentation of HS in our patient population, cultures were more likely to be obtained when patients presented with only buttock (32/38 [84%]) and inframammary (20/25 [80%]) lesions (Table).
Staphylococcus aureus was the most commonly cultured bacteria in general (53/283 [19%]) as well as for HS located the axilla (24/56 [43%]) and in multiple sites (16/51 [31%]). Proteus mirabilis (29/283 [10%]) was the second most commonly cultured bacteria overall and was cultured most often in the axilla (15/56 [27%]) and inframammary region (6/14 [43%]). These were followed by beta-hemolytic Streptococcus species (26/283 [9%]) and Enterococcus species (21/283 [7%]), which was second to P mirabilis as the most commonly cultured bacteria in the inframammary region (6/14 [43%])(eTable 1).
eTable 2 shows the sensitivity profiles for the most commonly cultured bacteria: S aureus, P mirabilis, and Enterococcus species. Staphylococcus aureus located in the axilla, buttocks, and groin was most sensitive to rifampin (41/44 [93%]), TMP/SMX (41/44 [93%]), and tetracycline (39/44 [89%]) and most resistant to erythromycin (26/44 [59%]) and oxacillin (24/44 [55%]). Proteus mirabilis in the inframammary region was most sensitive to ampicillin (27/27 [100%]), gentamicin (27/27 [100%]), levofloxacin (27/27 [100%]), and TMP/SMX (26/27 [96%]). Enterococcus species were most sensitive to vancomycin (20/20 [100%]) and ampicillin (19/20 [95%]) and most resistant to gentamicin (5/20 [25%]).
Comment
To treat HS, it is important to understand the cause of the condition. Although the pathogenesis of HS has many unknowns, bacterial colonization and biofilms are thought to play a role. Lipopolysaccharides found in the outer membrane of Gram-negative bacteria are pathogen-associated molecular patterns that present to the toll-like receptors of the human immune system. Once the toll-like receptors recognize the pathogen-associated molecular patterns, macrophages and keratinocytes are activated and release proinflammatory and anti-inflammatory cytokines and chemokines. Persistent presentation of bacteria to the immune system increases immune-cell recruitment and worsens chronic inflammation in patients with HS. Evidence has revealed that bacteria initiate and sustain the inflammation seen in patients with HS; therefore, reducing the amount of bacteria could alleviate some of the symptoms of HS.5 It is important to continue learning about the pathophysiology of this disease as well as formulating tailored treatments to minimize patient discomfort and improve quality of life.
Based on the findings of the current study and the safety profile of the medication, tetracyclines may be considered for first-line empiric therapy in patients with HS involving the axilla only, buttocks only, or multiple sites. For additional coverage of P mirabilis in the axilla or inframammary region, TMP/SMX monotherapy or tetracycline plus ampicillin may be considered. For inframammary lesions only, empiric treatment with ampicillin or TMP/ SMX is recommended. For HS lesions in the groin area, coverage of Enterococcus species with ampicillin should be considered. Patients with multiple sites of involvement that include the inframammary or groin regions similarly should receive empiric antibiotics that cover both S aureus and Gram-negative bacteria, such as TMP/SMX or tetracycline and ampicillin, respectively; if the multiple sites do not include the inframammary or groin regions, Gram-negative coverage may not be indicated. Based on our findings, standardization of treatment for patients with HS can allow for earlier and potentially more effective treatment.
In a similar study conducted in 2016, bacteria species were isolated from the axilla, groin, and gluteus/perineum in patients with HS.5 In that study, the most prominent bacteria in the axilla was CoNS; in the groin, P mirabilis and E coli; and in the gluteus/perineum, E coli and CoNS. These results differed from ours, which found S aureus as the abundant bacteria in these areas. In the 2016 study, the highest rates of resistance were found for penicillin G, erythromycin, clindamycin, and ampicillin.5 In contrast, the current study found high sensitivities for clindamycin and ampicillin, but our results support the finding of high resistance for erythromycin. These differences could be accounted for by the lower sample size of patients in the 2016 study: 68 patients were analyzed for sensitivity results, and 171 patients were analyzed for frequency of bacterial species in patients with HS.5
Our study is limited by its relatively small sample size. Additionally, all patients were seen at 1 of 2 clinic sites, located in League City and Galveston, Texas, and the data from this geographic area may not be applicable to patients seen in different climates.
Conclusion
Outcomes for patients with HS improve with early intervention; however, HS treatment may be delayed by selection of ineffective antibiotic therapy. Our study provides clinicians with recommendations for empiric antibiotic treatment based on anatomic location of HS lesions and culture sensitivity profiles. Utilizing tailored antibiotic therapy on initial clinical evaluation may increase early disease control and improve morbidity and disease outcomes, thereby increasing patient quality of life.
- Vinkel C, Thomsen SF. Hidradenitis suppurativa: causes, features, and current treatments. J Clin Aesthet Dermatol. 2018;11:17-23.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60:539-561; quiz 562-563.
- Yazdanyar S, Jemec GBE. Hidradenitis suppurativa: a review of cause and treatment. Curr Opin Infect Dis. 2011;24:118-123.
- Hessam S, Sand M, Georgas D, et al. Microbial profile and antimicrobial susceptibility of bacteria found in inflammatory hidradenitis suppurativa lesions. Skin Pharmacol Physiol. 2016; 29:161-167.
- Vinkel C, Thomsen SF. Hidradenitis suppurativa: causes, features, and current treatments. J Clin Aesthet Dermatol. 2018;11:17-23.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Alikhan A, Lynch PJ, Eisen DB. Hidradenitis suppurativa: a comprehensive review. J Am Acad Dermatol. 2009;60:539-561; quiz 562-563.
- Yazdanyar S, Jemec GBE. Hidradenitis suppurativa: a review of cause and treatment. Curr Opin Infect Dis. 2011;24:118-123.
- Hessam S, Sand M, Georgas D, et al. Microbial profile and antimicrobial susceptibility of bacteria found in inflammatory hidradenitis suppurativa lesions. Skin Pharmacol Physiol. 2016; 29:161-167.
Recommendations for Empiric Antibiotic Therapy in Hidradenitis Suppurativa
Recommendations for Empiric Antibiotic Therapy in Hidradenitis Suppurativa
PRACTICE POINTS
- The inflammation seen in patients with hidradenitis suppurativa (HS) is initiated and sustained by bacteria; therefore, reducing the number of bacteria may alleviate some of the symptoms of HS.
- For HS involving the axillae or buttocks, tetracyclines should be recommended as first-line empiric therapy.
- Patients with HS with multiple sites affected that include the inframammary or groin regions should receive empiric antibiotics that cover both Staphylococcus aureus and Gram-negative bacteria, such as trimethoprim-sulfamethoxazole or tetracycline plus ampicillin.