User login
Latest data on COVID-19 patients with rheumatic diseases revealed in registry
An international registry of adult and pediatric rheumatology patients is beginning to identify trends in the types of patients with COVID-19 and who is recovering.

The COVID-19 Global Rheumatology Alliance (GRA) has created pediatric and adult registries for health care providers to enter information on their rheumatology patients with COVID-19. The adult registry is hosted by the University of California, San Francisco, Research Electronic Data Capture system, while the Childhood Arthritis and Rheumatology Research Alliance is supporting the pediatric registry. A separate path for data entry of both adult and pediatric cases has been established through the European League Against Rheumatism for European countries and countries with EULAR member organizations.
Prior to the creation of the registries, there were no data available to guide rheumatologists in clinical decision making for their patients, noted Jinoos Yazdany, MD, MPH, COVID-19 GRA steering committee member and chief of the division of rheumatology at Zuckerberg San Francisco General Hospital. “COVID-19 has potential to severely affect those with rheumatologic diseases or those taking immunosuppressive drugs,” she said in an interview. “The GRA registries were designed to answer critical questions that will inform the medical care of this population.”
The GRA began on Twitter, with conversations between Leonard H. Calabrese, DO, of the Cleveland Clinic; Paul Sufka, MD, of HealthPartners in St. Paul, Minn.; Philip Robinson, MBChB, PhD, of the Royal Brisbane (Australia) Hospital; and herself, Dr. Yazdany said. Dr. Robinson started work on the governance of the GRA, Dr. Yazdany designed the data infrastructure, and Dr. Sufka approached his professional networks and social media followings to promote the effort and ask for support. The COVID-19 GRA steering committee representatives include patients, private practice rheumatologists, and international investigators. Listed among official supporters of the alliance are the American College of Rheumatology and EULAR along with more than 290 medical societies, institutions, journals, and other organizations in rheumatology.
The goal of the registries is to examine the health outcomes of patients with rheumatic diseases and COVID-19 based on sociodemographic factors, comorbidities, and clinical presentations of COVID-19 as well as what role taking immunosuppressive drugs prior to a COVID-19 infection play in helping or hindering outcomes. Hydroxychloroquine, used to treat lupus and arthritis, is a potential treatment candidate for COVID-19. Biologics such as tocilizumab (Actemra) and sarilumab (Kevzara), which target interleukin-6, and anakinra (Kineret), which targets IL-1, are treatment candidates for patients who have experienced COVID-related cytokine storm syndrome, which researchers believe may contribute to worsening or fatal cases.
Dr. Yazdany, who is also vice chair of real-world data infrastructure, registry, and institutional review board/ethics for the GRA, said that there are some important high-level trends in the data thus far. “People with lupus and those taking hydroxychloroquine are becoming infected with SARS-CoV-2, which is counter to misinformation on social media. Most people with rheumatic diseases on immunosuppression are recovering, which is great news for our patients.”
One of the major strengths of the registries is that each case is entered by the rheumatologist treating the patient and contains detailed clinical information, Dr. Yazdany said. However, the registry has no control group, it is not a population surveillance study, and it may contain selection bias through rheumatologists omitting milder, undiagnosed cases.
“The Global Alliance case reporting registry represents the collective effort of hundreds of rheumatologists across the world. I have never been more inspired by the strength and collaboration of the rheumatology community,” Dr. Yazdany said.
According to a paper published in the Lancet Rheumatology, which references data on 110 cases from the combined databases up to April 1, about three-fourths of cases presented with fever (79%) and cough (77%), and about half presented with shortness of breath (50%) and myalgia (45%).
Results from the global and UCSF registries
As of April 18, 334 cases were in the global and UCSF registries, with 121 patients (36%) in the database having both COVID-19 and RA, 33 patients (10%) with psoriatic arthritis, 58 patients (17%) with systemic lupus erythematosus, 28 patients (8%) with axial spondyloarthritis, 27 patients (8%) with vasculitis, and 19 patients (6%) with Sjögren’s syndrome. There were less than five cases reported for patients with the following rheumatic diseases: inflammatory myopathy, ocular inflammation, other inflammatory arthritis, polymyalgia rheumatica, sarcoidosis, systemic sclerosis, osteoporosis, psoriasis, isolated pulmonary capillaritis, gout, and autoinflammatory disease. A majority of the patients in the registries are women (74%) aged younger than 65 years (78%) and are white (52%).
The most common comorbid conditions among patients in the registry are hypertension (33%), lung disease (18%), diabetes (11%), cardiovascular disease (10%), chronic renal insufficiency or end-stage renal disease (7%), morbid obesity (7%), and cancer (4%). Before being diagnosed with COVID-19, 219 patients (66%) in the registry were taking conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), which included antimalarials, azathioprine, cyclophosphamide, cyclosporine, leflunomide, methotrexate, mycophenolate mofetil/mycophenolic acid, sulfasalazine, and tacrolimus. A total of 122 patients (37%) were taking biologic DMARDs, 101 patients were taking glucocorticoids (30%), 86 patients (26%) were taking hydroxychloroquine, 41 patients (12%) were taking NSAIDs, and 18 patients (5%) were taking a Janus kinase inhibitor.
The most recent data from the registry show that 128 patients (38%) have been hospitalized for COVID-19, and 19 patients (6%) have died. Although 104 patients (31%) resolved their infections, 177 patients (53%) have a COVID-19 infection status of “unresolved,” and 53 patients (16%) have an unknown infection status.
EULAR registry results
As of April 21, 249 cases were in the EULAR registry, including 110 hospitalizations (44%) and 37 deaths (15%). Overall, 64% of these patients were women, and they had a median age of 60 years.
The top five diagnoses of these patients were RA (39%), psoriatic arthritis (15%), spondyloarthritis (9%), systemic lupus erythematosus (9%), and gout (5%). A total of 27% had no reported comorbidities, while lung disease occurred in 26%, hypertension in 34%, diabetes in 11%, and cardiovascular disease on 11%. The registry also reported use of any DMARD in 80%, including 62% on csDMARDs, 31% on biologics, and 2% on targeted synthetic DMARDs.
Ten authors in the Lancet Rheumatology paper reported personal and institutional relationships in the form of grants, corporate sponsorships, advisory board memberships, investigator appointments, speaker’s bureau positions, personal fees, and consultancies for a variety of pharmaceutical companies, agencies, societies, and other organizations. The other authors reported no relevant conflicts of interest.
An international registry of adult and pediatric rheumatology patients is beginning to identify trends in the types of patients with COVID-19 and who is recovering.
The COVID-19 Global Rheumatology Alliance (GRA) has created pediatric and adult registries for health care providers to enter information on their rheumatology patients with COVID-19. The adult registry is hosted by the University of California, San Francisco, Research Electronic Data Capture system, while the Childhood Arthritis and Rheumatology Research Alliance is supporting the pediatric registry. A separate path for data entry of both adult and pediatric cases has been established through the European League Against Rheumatism for European countries and countries with EULAR member organizations.
Prior to the creation of the registries, there were no data available to guide rheumatologists in clinical decision making for their patients, noted Jinoos Yazdany, MD, MPH, COVID-19 GRA steering committee member and chief of the division of rheumatology at Zuckerberg San Francisco General Hospital. “COVID-19 has potential to severely affect those with rheumatologic diseases or those taking immunosuppressive drugs,” she said in an interview. “The GRA registries were designed to answer critical questions that will inform the medical care of this population.”
The GRA began on Twitter, with conversations between Leonard H. Calabrese, DO, of the Cleveland Clinic; Paul Sufka, MD, of HealthPartners in St. Paul, Minn.; Philip Robinson, MBChB, PhD, of the Royal Brisbane (Australia) Hospital; and herself, Dr. Yazdany said. Dr. Robinson started work on the governance of the GRA, Dr. Yazdany designed the data infrastructure, and Dr. Sufka approached his professional networks and social media followings to promote the effort and ask for support. The COVID-19 GRA steering committee representatives include patients, private practice rheumatologists, and international investigators. Listed among official supporters of the alliance are the American College of Rheumatology and EULAR along with more than 290 medical societies, institutions, journals, and other organizations in rheumatology.
The goal of the registries is to examine the health outcomes of patients with rheumatic diseases and COVID-19 based on sociodemographic factors, comorbidities, and clinical presentations of COVID-19 as well as what role taking immunosuppressive drugs prior to a COVID-19 infection play in helping or hindering outcomes. Hydroxychloroquine, used to treat lupus and arthritis, is a potential treatment candidate for COVID-19. Biologics such as tocilizumab (Actemra) and sarilumab (Kevzara), which target interleukin-6, and anakinra (Kineret), which targets IL-1, are treatment candidates for patients who have experienced COVID-related cytokine storm syndrome, which researchers believe may contribute to worsening or fatal cases.
Dr. Yazdany, who is also vice chair of real-world data infrastructure, registry, and institutional review board/ethics for the GRA, said that there are some important high-level trends in the data thus far. “People with lupus and those taking hydroxychloroquine are becoming infected with SARS-CoV-2, which is counter to misinformation on social media. Most people with rheumatic diseases on immunosuppression are recovering, which is great news for our patients.”
One of the major strengths of the registries is that each case is entered by the rheumatologist treating the patient and contains detailed clinical information, Dr. Yazdany said. However, the registry has no control group, it is not a population surveillance study, and it may contain selection bias through rheumatologists omitting milder, undiagnosed cases.
“The Global Alliance case reporting registry represents the collective effort of hundreds of rheumatologists across the world. I have never been more inspired by the strength and collaboration of the rheumatology community,” Dr. Yazdany said.
According to a paper published in the Lancet Rheumatology, which references data on 110 cases from the combined databases up to April 1, about three-fourths of cases presented with fever (79%) and cough (77%), and about half presented with shortness of breath (50%) and myalgia (45%).
Results from the global and UCSF registries
As of April 18, 334 cases were in the global and UCSF registries, with 121 patients (36%) in the database having both COVID-19 and RA, 33 patients (10%) with psoriatic arthritis, 58 patients (17%) with systemic lupus erythematosus, 28 patients (8%) with axial spondyloarthritis, 27 patients (8%) with vasculitis, and 19 patients (6%) with Sjögren’s syndrome. There were less than five cases reported for patients with the following rheumatic diseases: inflammatory myopathy, ocular inflammation, other inflammatory arthritis, polymyalgia rheumatica, sarcoidosis, systemic sclerosis, osteoporosis, psoriasis, isolated pulmonary capillaritis, gout, and autoinflammatory disease. A majority of the patients in the registries are women (74%) aged younger than 65 years (78%) and are white (52%).
The most common comorbid conditions among patients in the registry are hypertension (33%), lung disease (18%), diabetes (11%), cardiovascular disease (10%), chronic renal insufficiency or end-stage renal disease (7%), morbid obesity (7%), and cancer (4%). Before being diagnosed with COVID-19, 219 patients (66%) in the registry were taking conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), which included antimalarials, azathioprine, cyclophosphamide, cyclosporine, leflunomide, methotrexate, mycophenolate mofetil/mycophenolic acid, sulfasalazine, and tacrolimus. A total of 122 patients (37%) were taking biologic DMARDs, 101 patients were taking glucocorticoids (30%), 86 patients (26%) were taking hydroxychloroquine, 41 patients (12%) were taking NSAIDs, and 18 patients (5%) were taking a Janus kinase inhibitor.
The most recent data from the registry show that 128 patients (38%) have been hospitalized for COVID-19, and 19 patients (6%) have died. Although 104 patients (31%) resolved their infections, 177 patients (53%) have a COVID-19 infection status of “unresolved,” and 53 patients (16%) have an unknown infection status.
EULAR registry results
As of April 21, 249 cases were in the EULAR registry, including 110 hospitalizations (44%) and 37 deaths (15%). Overall, 64% of these patients were women, and they had a median age of 60 years.
The top five diagnoses of these patients were RA (39%), psoriatic arthritis (15%), spondyloarthritis (9%), systemic lupus erythematosus (9%), and gout (5%). A total of 27% had no reported comorbidities, while lung disease occurred in 26%, hypertension in 34%, diabetes in 11%, and cardiovascular disease on 11%. The registry also reported use of any DMARD in 80%, including 62% on csDMARDs, 31% on biologics, and 2% on targeted synthetic DMARDs.
Ten authors in the Lancet Rheumatology paper reported personal and institutional relationships in the form of grants, corporate sponsorships, advisory board memberships, investigator appointments, speaker’s bureau positions, personal fees, and consultancies for a variety of pharmaceutical companies, agencies, societies, and other organizations. The other authors reported no relevant conflicts of interest.
An international registry of adult and pediatric rheumatology patients is beginning to identify trends in the types of patients with COVID-19 and who is recovering.
The COVID-19 Global Rheumatology Alliance (GRA) has created pediatric and adult registries for health care providers to enter information on their rheumatology patients with COVID-19. The adult registry is hosted by the University of California, San Francisco, Research Electronic Data Capture system, while the Childhood Arthritis and Rheumatology Research Alliance is supporting the pediatric registry. A separate path for data entry of both adult and pediatric cases has been established through the European League Against Rheumatism for European countries and countries with EULAR member organizations.
Prior to the creation of the registries, there were no data available to guide rheumatologists in clinical decision making for their patients, noted Jinoos Yazdany, MD, MPH, COVID-19 GRA steering committee member and chief of the division of rheumatology at Zuckerberg San Francisco General Hospital. “COVID-19 has potential to severely affect those with rheumatologic diseases or those taking immunosuppressive drugs,” she said in an interview. “The GRA registries were designed to answer critical questions that will inform the medical care of this population.”
The GRA began on Twitter, with conversations between Leonard H. Calabrese, DO, of the Cleveland Clinic; Paul Sufka, MD, of HealthPartners in St. Paul, Minn.; Philip Robinson, MBChB, PhD, of the Royal Brisbane (Australia) Hospital; and herself, Dr. Yazdany said. Dr. Robinson started work on the governance of the GRA, Dr. Yazdany designed the data infrastructure, and Dr. Sufka approached his professional networks and social media followings to promote the effort and ask for support. The COVID-19 GRA steering committee representatives include patients, private practice rheumatologists, and international investigators. Listed among official supporters of the alliance are the American College of Rheumatology and EULAR along with more than 290 medical societies, institutions, journals, and other organizations in rheumatology.
The goal of the registries is to examine the health outcomes of patients with rheumatic diseases and COVID-19 based on sociodemographic factors, comorbidities, and clinical presentations of COVID-19 as well as what role taking immunosuppressive drugs prior to a COVID-19 infection play in helping or hindering outcomes. Hydroxychloroquine, used to treat lupus and arthritis, is a potential treatment candidate for COVID-19. Biologics such as tocilizumab (Actemra) and sarilumab (Kevzara), which target interleukin-6, and anakinra (Kineret), which targets IL-1, are treatment candidates for patients who have experienced COVID-related cytokine storm syndrome, which researchers believe may contribute to worsening or fatal cases.
Dr. Yazdany, who is also vice chair of real-world data infrastructure, registry, and institutional review board/ethics for the GRA, said that there are some important high-level trends in the data thus far. “People with lupus and those taking hydroxychloroquine are becoming infected with SARS-CoV-2, which is counter to misinformation on social media. Most people with rheumatic diseases on immunosuppression are recovering, which is great news for our patients.”
One of the major strengths of the registries is that each case is entered by the rheumatologist treating the patient and contains detailed clinical information, Dr. Yazdany said. However, the registry has no control group, it is not a population surveillance study, and it may contain selection bias through rheumatologists omitting milder, undiagnosed cases.
“The Global Alliance case reporting registry represents the collective effort of hundreds of rheumatologists across the world. I have never been more inspired by the strength and collaboration of the rheumatology community,” Dr. Yazdany said.
According to a paper published in the Lancet Rheumatology, which references data on 110 cases from the combined databases up to April 1, about three-fourths of cases presented with fever (79%) and cough (77%), and about half presented with shortness of breath (50%) and myalgia (45%).
Results from the global and UCSF registries
As of April 18, 334 cases were in the global and UCSF registries, with 121 patients (36%) in the database having both COVID-19 and RA, 33 patients (10%) with psoriatic arthritis, 58 patients (17%) with systemic lupus erythematosus, 28 patients (8%) with axial spondyloarthritis, 27 patients (8%) with vasculitis, and 19 patients (6%) with Sjögren’s syndrome. There were less than five cases reported for patients with the following rheumatic diseases: inflammatory myopathy, ocular inflammation, other inflammatory arthritis, polymyalgia rheumatica, sarcoidosis, systemic sclerosis, osteoporosis, psoriasis, isolated pulmonary capillaritis, gout, and autoinflammatory disease. A majority of the patients in the registries are women (74%) aged younger than 65 years (78%) and are white (52%).
The most common comorbid conditions among patients in the registry are hypertension (33%), lung disease (18%), diabetes (11%), cardiovascular disease (10%), chronic renal insufficiency or end-stage renal disease (7%), morbid obesity (7%), and cancer (4%). Before being diagnosed with COVID-19, 219 patients (66%) in the registry were taking conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), which included antimalarials, azathioprine, cyclophosphamide, cyclosporine, leflunomide, methotrexate, mycophenolate mofetil/mycophenolic acid, sulfasalazine, and tacrolimus. A total of 122 patients (37%) were taking biologic DMARDs, 101 patients were taking glucocorticoids (30%), 86 patients (26%) were taking hydroxychloroquine, 41 patients (12%) were taking NSAIDs, and 18 patients (5%) were taking a Janus kinase inhibitor.
The most recent data from the registry show that 128 patients (38%) have been hospitalized for COVID-19, and 19 patients (6%) have died. Although 104 patients (31%) resolved their infections, 177 patients (53%) have a COVID-19 infection status of “unresolved,” and 53 patients (16%) have an unknown infection status.
EULAR registry results
As of April 21, 249 cases were in the EULAR registry, including 110 hospitalizations (44%) and 37 deaths (15%). Overall, 64% of these patients were women, and they had a median age of 60 years.
The top five diagnoses of these patients were RA (39%), psoriatic arthritis (15%), spondyloarthritis (9%), systemic lupus erythematosus (9%), and gout (5%). A total of 27% had no reported comorbidities, while lung disease occurred in 26%, hypertension in 34%, diabetes in 11%, and cardiovascular disease on 11%. The registry also reported use of any DMARD in 80%, including 62% on csDMARDs, 31% on biologics, and 2% on targeted synthetic DMARDs.
Ten authors in the Lancet Rheumatology paper reported personal and institutional relationships in the form of grants, corporate sponsorships, advisory board memberships, investigator appointments, speaker’s bureau positions, personal fees, and consultancies for a variety of pharmaceutical companies, agencies, societies, and other organizations. The other authors reported no relevant conflicts of interest.
Management of infants born to mothers with COVID-19
Initial guidance for pediatric hospitalists
Clinical question: How should we care for newborns born to mothers with COVID-19?

Background: Around the United States, the SARS-CoV-2 virus is infecting pregnant mothers and causing COVID-19. Current limited data demonstrates that children under the age of 1 year are at risk for severe disease. Clinicians are caring for infants born to mothers with COVID-19 during the pandemic with minimal guidance.
Study design: Clinical practice guidelines.
Synopsis: The American Academy of Pediatrics’ Committee on Fetus and Newborn, Section on Neonatal and Perinatal Medicine and Committee of Infectious Diseases developed guidelines of care for infants born to COVID-19 mothers to help clinicians care for newborns using limited data published before March 30, 2020.
- Neonates should be considered persons under investigation (PUIs) if they are born to mothers with diagnosed COVID-19 or with COVID-19 tests pending at the time of delivery.
- Neonatal clinicians should attend deliveries based on their center’s policies. If clinicians are required to perform stabilization they should use airborne, droplet, and contact personal protective equipment (PPE). This includes, gown, gloves, eye protection (goggles or face shield), and N95 respirator mask or an air-purifying respirator.
- Mother and newborn should be separated to minimize the infant’s risk of postnatal infection.
- Well newborns born at or near term may be admitted to areas physically separated from newborns unaffected by maternal COVID-19. Alternatively, a mother may room-in with her infant with 6 feet of separation between mother and infant. Newborn PUIs should be bathed as soon as possible.
- Newborns requiring intensive care should be admitted to a single negative-pressure room. Alternatively, COVID-19–exposed infants should be grouped with a minimum of 6 feet of separation, or placed in air temperature-controlled isolettes.
- Until the newborn PUI’s virologic status is known, clinical staff caring for the infant should use droplet and contact PPE. This includes gown, gloves, eye protection (goggles or face shield), and a standard surgical mask. Airborne, droplet, and contact precautions should be used for infants requiring CPAP or any form of mechanical ventilation.
- COVID-19–positive mothers who want to breastfeed may feed expressed breast milk using proper breast and hand hygiene or directly breastfeed their infants wearing a mask while practicing proper breast and hand hygiene.
- If testing is available, newborns should be tested for SARS-CoV-2 using molecular arrays. If testing is unavailable, clinicians may monitor newborns clinically. Infants should be tested if they require prolonged intensive care.
- Optimal timing and extent of testing is unknown. Tests should be performed around 24 hours of life and 48 hours of life. If discharge is planned for a well appearing infant before 48 hours of life, the clinician may choose not to do the 48-hour test. A single swab should be taken from the throat followed by the nasopharynx to perform the test.
- Newborns should receive all newborn care, including circumcision if requested.
- Infants who are asymptomatic with positive or pending SARS-CoV-2 tests may be discharged home with plans for frequent outpatient follow-up through 14 days after birth. Infants with negative SARS-CoV-2 testing should be discharged to the care of a noninfected caregiver. If the mother lives in the same household, she must keep a distance of 6 feet as often as possible. When not possible, the mother should wear a mask and practice hand hygiene. The mother may resume caring for her infant normally when she has been afebrile for more than 72 hours (without antipyretics) and has been asymptomatic for 7 days. Alternatively, the mother may resume care if she has two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.
- Visitation to infants requiring intensive care should be limited for mothers with COVID-19 until her fever has resolved for more than 72 hours and has improvement of respiratory symptoms and has had two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.

Bottom line: Clinicians should protect themselves with contact and droplet PPE at all times until the infant’s viral status is known. Clinicians should use airborne, contact, and droplet PPE when resuscitating the infant and/or when using CPAP/mechanical ventilation. Mothers should be encouraged to feed their infants expressed breast milk while practicing proper hygiene or directly breastfeed while wearing a mask and practicing proper hygiene. Viral testing of every infant born to a mother with COVID-19 should be performed after the infant is 24 hours old. Mothers should resume caring for their infants normally after they have met criteria suggesting they are no longer actively infected.
Article citation: Puopolo KM, Hudak ML, Kimberlin DW, Cummings J. Initial Guidance: Management of Infants born to Mothers with COVID-19. 2020 Apr 2. https://downloads.aap.org/AAP/PDF/COVID%2019%20Initial%20Newborn%20Guidance.pdf. Accessed Apr 2, 2020.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, Cleveland, and serves as the Pediatrics Editor for The Hospitalist.
Initial guidance for pediatric hospitalists
Initial guidance for pediatric hospitalists
Clinical question: How should we care for newborns born to mothers with COVID-19?
Background: Around the United States, the SARS-CoV-2 virus is infecting pregnant mothers and causing COVID-19. Current limited data demonstrates that children under the age of 1 year are at risk for severe disease. Clinicians are caring for infants born to mothers with COVID-19 during the pandemic with minimal guidance.
Study design: Clinical practice guidelines.
Synopsis: The American Academy of Pediatrics’ Committee on Fetus and Newborn, Section on Neonatal and Perinatal Medicine and Committee of Infectious Diseases developed guidelines of care for infants born to COVID-19 mothers to help clinicians care for newborns using limited data published before March 30, 2020.
- Neonates should be considered persons under investigation (PUIs) if they are born to mothers with diagnosed COVID-19 or with COVID-19 tests pending at the time of delivery.
- Neonatal clinicians should attend deliveries based on their center’s policies. If clinicians are required to perform stabilization they should use airborne, droplet, and contact personal protective equipment (PPE). This includes, gown, gloves, eye protection (goggles or face shield), and N95 respirator mask or an air-purifying respirator.
- Mother and newborn should be separated to minimize the infant’s risk of postnatal infection.
- Well newborns born at or near term may be admitted to areas physically separated from newborns unaffected by maternal COVID-19. Alternatively, a mother may room-in with her infant with 6 feet of separation between mother and infant. Newborn PUIs should be bathed as soon as possible.
- Newborns requiring intensive care should be admitted to a single negative-pressure room. Alternatively, COVID-19–exposed infants should be grouped with a minimum of 6 feet of separation, or placed in air temperature-controlled isolettes.
- Until the newborn PUI’s virologic status is known, clinical staff caring for the infant should use droplet and contact PPE. This includes gown, gloves, eye protection (goggles or face shield), and a standard surgical mask. Airborne, droplet, and contact precautions should be used for infants requiring CPAP or any form of mechanical ventilation.
- COVID-19–positive mothers who want to breastfeed may feed expressed breast milk using proper breast and hand hygiene or directly breastfeed their infants wearing a mask while practicing proper breast and hand hygiene.
- If testing is available, newborns should be tested for SARS-CoV-2 using molecular arrays. If testing is unavailable, clinicians may monitor newborns clinically. Infants should be tested if they require prolonged intensive care.
- Optimal timing and extent of testing is unknown. Tests should be performed around 24 hours of life and 48 hours of life. If discharge is planned for a well appearing infant before 48 hours of life, the clinician may choose not to do the 48-hour test. A single swab should be taken from the throat followed by the nasopharynx to perform the test.
- Newborns should receive all newborn care, including circumcision if requested.
- Infants who are asymptomatic with positive or pending SARS-CoV-2 tests may be discharged home with plans for frequent outpatient follow-up through 14 days after birth. Infants with negative SARS-CoV-2 testing should be discharged to the care of a noninfected caregiver. If the mother lives in the same household, she must keep a distance of 6 feet as often as possible. When not possible, the mother should wear a mask and practice hand hygiene. The mother may resume caring for her infant normally when she has been afebrile for more than 72 hours (without antipyretics) and has been asymptomatic for 7 days. Alternatively, the mother may resume care if she has two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.
- Visitation to infants requiring intensive care should be limited for mothers with COVID-19 until her fever has resolved for more than 72 hours and has improvement of respiratory symptoms and has had two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.
Bottom line: Clinicians should protect themselves with contact and droplet PPE at all times until the infant’s viral status is known. Clinicians should use airborne, contact, and droplet PPE when resuscitating the infant and/or when using CPAP/mechanical ventilation. Mothers should be encouraged to feed their infants expressed breast milk while practicing proper hygiene or directly breastfeed while wearing a mask and practicing proper hygiene. Viral testing of every infant born to a mother with COVID-19 should be performed after the infant is 24 hours old. Mothers should resume caring for their infants normally after they have met criteria suggesting they are no longer actively infected.
Article citation: Puopolo KM, Hudak ML, Kimberlin DW, Cummings J. Initial Guidance: Management of Infants born to Mothers with COVID-19. 2020 Apr 2. https://downloads.aap.org/AAP/PDF/COVID%2019%20Initial%20Newborn%20Guidance.pdf. Accessed Apr 2, 2020.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, Cleveland, and serves as the Pediatrics Editor for The Hospitalist.
Clinical question: How should we care for newborns born to mothers with COVID-19?
Background: Around the United States, the SARS-CoV-2 virus is infecting pregnant mothers and causing COVID-19. Current limited data demonstrates that children under the age of 1 year are at risk for severe disease. Clinicians are caring for infants born to mothers with COVID-19 during the pandemic with minimal guidance.
Study design: Clinical practice guidelines.
Synopsis: The American Academy of Pediatrics’ Committee on Fetus and Newborn, Section on Neonatal and Perinatal Medicine and Committee of Infectious Diseases developed guidelines of care for infants born to COVID-19 mothers to help clinicians care for newborns using limited data published before March 30, 2020.
- Neonates should be considered persons under investigation (PUIs) if they are born to mothers with diagnosed COVID-19 or with COVID-19 tests pending at the time of delivery.
- Neonatal clinicians should attend deliveries based on their center’s policies. If clinicians are required to perform stabilization they should use airborne, droplet, and contact personal protective equipment (PPE). This includes, gown, gloves, eye protection (goggles or face shield), and N95 respirator mask or an air-purifying respirator.
- Mother and newborn should be separated to minimize the infant’s risk of postnatal infection.
- Well newborns born at or near term may be admitted to areas physically separated from newborns unaffected by maternal COVID-19. Alternatively, a mother may room-in with her infant with 6 feet of separation between mother and infant. Newborn PUIs should be bathed as soon as possible.
- Newborns requiring intensive care should be admitted to a single negative-pressure room. Alternatively, COVID-19–exposed infants should be grouped with a minimum of 6 feet of separation, or placed in air temperature-controlled isolettes.
- Until the newborn PUI’s virologic status is known, clinical staff caring for the infant should use droplet and contact PPE. This includes gown, gloves, eye protection (goggles or face shield), and a standard surgical mask. Airborne, droplet, and contact precautions should be used for infants requiring CPAP or any form of mechanical ventilation.
- COVID-19–positive mothers who want to breastfeed may feed expressed breast milk using proper breast and hand hygiene or directly breastfeed their infants wearing a mask while practicing proper breast and hand hygiene.
- If testing is available, newborns should be tested for SARS-CoV-2 using molecular arrays. If testing is unavailable, clinicians may monitor newborns clinically. Infants should be tested if they require prolonged intensive care.
- Optimal timing and extent of testing is unknown. Tests should be performed around 24 hours of life and 48 hours of life. If discharge is planned for a well appearing infant before 48 hours of life, the clinician may choose not to do the 48-hour test. A single swab should be taken from the throat followed by the nasopharynx to perform the test.
- Newborns should receive all newborn care, including circumcision if requested.
- Infants who are asymptomatic with positive or pending SARS-CoV-2 tests may be discharged home with plans for frequent outpatient follow-up through 14 days after birth. Infants with negative SARS-CoV-2 testing should be discharged to the care of a noninfected caregiver. If the mother lives in the same household, she must keep a distance of 6 feet as often as possible. When not possible, the mother should wear a mask and practice hand hygiene. The mother may resume caring for her infant normally when she has been afebrile for more than 72 hours (without antipyretics) and has been asymptomatic for 7 days. Alternatively, the mother may resume care if she has two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.
- Visitation to infants requiring intensive care should be limited for mothers with COVID-19 until her fever has resolved for more than 72 hours and has improvement of respiratory symptoms and has had two consecutive negative SARS-CoV-2 nasopharyngeal swabs taken more than 24 hours apart.
Bottom line: Clinicians should protect themselves with contact and droplet PPE at all times until the infant’s viral status is known. Clinicians should use airborne, contact, and droplet PPE when resuscitating the infant and/or when using CPAP/mechanical ventilation. Mothers should be encouraged to feed their infants expressed breast milk while practicing proper hygiene or directly breastfeed while wearing a mask and practicing proper hygiene. Viral testing of every infant born to a mother with COVID-19 should be performed after the infant is 24 hours old. Mothers should resume caring for their infants normally after they have met criteria suggesting they are no longer actively infected.
Article citation: Puopolo KM, Hudak ML, Kimberlin DW, Cummings J. Initial Guidance: Management of Infants born to Mothers with COVID-19. 2020 Apr 2. https://downloads.aap.org/AAP/PDF/COVID%2019%20Initial%20Newborn%20Guidance.pdf. Accessed Apr 2, 2020.
Dr. Kumar is a pediatric hospitalist at Cleveland Clinic Children’s. She is a clinical assistant professor of pediatrics at Case Western Reserve University, Cleveland, and serves as the Pediatrics Editor for The Hospitalist.
European cancer centers restructure care in the era of COVID-19
Delivering cancer care during the COVID-19 pandemic has proved particularly challenging, as minimizing the risk of infection must be balanced with maintaining optimal outcomes.
Healthcare systems and oncologists have had to reorganize standard oncologic care in order to protect vulnerable patients from exposure to COVID-19 as well as deal with pandemic-related issues of equipment and staffing shortages.
A new article now describes how seven cancer centers in Europe rapidly reorganized their oncologic services and are tackling this crisis, as well as offering guidance to other institutions.
This was a major undertaking, to work out a system where patients can still get care but in a safer manner, explained coauthor Emile Voest, MD, medical director of the Netherlands Cancer Institute in Amsterdam.
“Decisions needed to be taken based on availability of personnel, protective materials, and urgencies,” he told Medscape Medical News. “Because every country had its own speed of development of the COVID pandemic, there were different scenarios in all institutions, but all with a common factor of key expertise on how to de-escalate in a safe manner.”
The article was published April 16 in Nature Medicine.
The Netherlands Cancer Institute (the Netherlands), Karolinska Institute (Sweden), Institute Gustave Roussy (France), Cambridge Cancer Center (United Kingdom), Istituto Nazionale dei Tumori di Milano (Italy), German Cancer Research Center (Germany), and Vall d’Hebron Institute of Oncology (Spain) have been working closely together in a legal entity since 2014, and have created ‘Cancer Core Europe’ (CCE). The goal is to “maximize coherence and critical mass in cancer research,” the authors note.
The consortium represents roughly 60,000 patients with newly diagnosed cancer, delivers approximately 300,000 treatment courses, and conducts about 1.2 million consultations annually, with more than 1,500 ongoing clinical trials. In a joint effort, the centers collected, translated, and compared the guidelines that had been put in place to treat patients with cancer during the COVID-19 pandemic.
Cancer treatment is multidisciplinary and involves many specialties including surgery, radiology, pathology, radiation oncology, and medical oncology. Coordinating care among disciplines is a very complex process, Voest noted.
“Changing treatment also means that you need to reconsider capacities and requirements,” he said. “Hospitals have installed crisis teams that were very good at coordinating these efforts.”
Restructuring care
Cancer care had to be reorganized on multiple levels, and the CCE centers looked at several aspects that needed to be accounted for, to ensure continuity in cancer care.
“The biggest challenge for the NHS and other healthcare systems is the surge of patients requiring oxygen and/or intensive care, and the nature and infectiousness of the virus,” said coauthor Carlos Caldas, MD, FMedSci, professor of cancer medicine at the University of Cambridge, United Kingdom. “In hospitals that are mostly run close to capacity, and where all kinds of patients are treated, this has created major resource and logistical problems.”
For regular clinical activities, the institutions with dedicated cancer centers (German Cancer Research Center, Institute Gustave Roussy, Istituto Nazionale dei Tumori di Milano, and Netherlands Cancer Institute) have attempted to stay COVID-19 free. This policy would in turn help ensure that sufficient clinical and intensive-care capacity could be reserved for critical cancer surgeries or management of treatment-related side effects, and allow hospitals outside of the CCE to transfer patients with cancer to these centers. The general hospitals can then focus on caring for patients with COVID-19, as well as other illnesses/injuries that require inpatient care.
As the CCE centers located within general hospitals (Cambridge Cancer Center, Vall d’Hebron Institute of Oncology and Karolinska Institute) have to admit patients with suspected and positive cases of COVID-19, being “COVID-19 free” was never a realistic or pursued goal.
The authors note that it is the responsibility of all healthcare professionals to ensure patients are not exposed to COVID-19, and this has meant minimizing hospital visits and person-to-person contact. For example, whenever possible, consultations take place via telephone calls or over the Internet, and nonurgent appointments that would require a patient’s physical presence at the clinic have been postponed. Visitors are also not permitted to accompany patients when admitted to the hospital or during procedures.
Standard-of-care treatment regimens have been adapted across all centers to minimize the number of hospital visits and hospitalizations and prevent “anticancer treatment-induced” complications of COVID-19.
To minimize visits and hospitalizations, strategies include converting intravenous treatments to oral or subcutaneous regimens when possible; switching from cytotoxic chemotherapy to a less-toxic approach to minimize the risk of complications requiring hospitalization; or to pause therapies when possible (stable disease reached or better). In addition, nonemergency surgeries have been postponed or replaced by radiotherapy.
To prevent anticancer treatment-induced complications of COVID-19, most centers use the paradigm that the added benefit for tumor control should be weighed against the potential risk for COVID-19–related morbidity and mortality. To prevent or reduce the risk of neutropenia and lymphopenia, for example, all centers have suggested a de-escalation of cytotoxic chemotherapy or targeted treatment strategies, or to forgo second or subsequent lines of palliative treatments if response rates from up-front therapy are low.
Some of these changes may be here to stay, noted Caldas. “One of the positive messages that comes out of this is that, clearly, care can be delivered in a safe and compassionate manner without requiring as many hospital visits as in the pre-COVID-19 era,” he said. “In the future, we will take heed of the COVID-19 experience to improve delivery of cancer care.”
Capacity of facilities
Many healthcare systems have become overwhelmed as the pandemic has intensified, thus making it necessary to prioritize. To prepare for this possibility, CCE centers have established protocols to categorize and prioritize patients for systemic treatment or surgery. While the protocols vary by center, they are comparable with one another as they prioritize on the basis of anticipated treatment outcome, the authors note.
The guidelines in CCE centers unanimously recommend that neoadjuvant therapies and curative surgeries be the top priority, for the times when operating room and/or ICU capacity is limited. As an alternative, neoadjuvant systemic treatments may be initiated or extended to postpone surgery, and other nonsurgical interventions can be considered.
In addition, some centers agree that certain elective surgeries can be safely delayed if backed by scientific evidence. As an example, an 11-week deferment of surgery may be acceptable for patients with rectal cancer after downstaging.
Cancer centers may also need to upscale and downscale quickly, depending on how the pandemic evolves, and many have already outlined scenarios to prepare for increasing or decreasing their capacity using phased approaches.
The Netherlands Cancer Institute, for example, has defined four phases of increasing severity; in Germany, capacity planning has been coordinated among 18 hospitals and the federal ministry of health, in order to prevent shortages of cancer services.
“We note that the optimal downscaling strategies depend on country- and center-specific capacities and preferences,” they write. “Therefore, it is difficult to propose a common schedule, and it will be most effective if hospitals outline their own phase-specific downscaling strategies based on the prioritization schemes and practical handles discussed above.”
Future research
Better strategies will be needed to reduce the impact of COVID-19 in cancer care, and four research priorities were identified to allow for evidence-based adjustments of cancer care protocols while the pandemic continues:
- Collect real-world data about the effects of adjustment and de-escalation of treatment regimens on outcomes
- Determine the incidence of COVID-19 in both the general population and among patients with cancer who have received systemic therapies, with large-scale serological testing
- Develop an epidemiological model that will allow estimates of the cumulative incidence of COVID-19 for a patient with cancer, within a specific time frame
- Determine COVID-19 related morbidity and mortality in patients with cancer who have been treated with systemic therapies and/or granulocyte colony-stimulating factor (G-CSF). Several projects are currently underway, such as the UK Coronavirus Cancer Monitoring Project.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Delivering cancer care during the COVID-19 pandemic has proved particularly challenging, as minimizing the risk of infection must be balanced with maintaining optimal outcomes.
Healthcare systems and oncologists have had to reorganize standard oncologic care in order to protect vulnerable patients from exposure to COVID-19 as well as deal with pandemic-related issues of equipment and staffing shortages.
A new article now describes how seven cancer centers in Europe rapidly reorganized their oncologic services and are tackling this crisis, as well as offering guidance to other institutions.
This was a major undertaking, to work out a system where patients can still get care but in a safer manner, explained coauthor Emile Voest, MD, medical director of the Netherlands Cancer Institute in Amsterdam.
“Decisions needed to be taken based on availability of personnel, protective materials, and urgencies,” he told Medscape Medical News. “Because every country had its own speed of development of the COVID pandemic, there were different scenarios in all institutions, but all with a common factor of key expertise on how to de-escalate in a safe manner.”
The article was published April 16 in Nature Medicine.
The Netherlands Cancer Institute (the Netherlands), Karolinska Institute (Sweden), Institute Gustave Roussy (France), Cambridge Cancer Center (United Kingdom), Istituto Nazionale dei Tumori di Milano (Italy), German Cancer Research Center (Germany), and Vall d’Hebron Institute of Oncology (Spain) have been working closely together in a legal entity since 2014, and have created ‘Cancer Core Europe’ (CCE). The goal is to “maximize coherence and critical mass in cancer research,” the authors note.
The consortium represents roughly 60,000 patients with newly diagnosed cancer, delivers approximately 300,000 treatment courses, and conducts about 1.2 million consultations annually, with more than 1,500 ongoing clinical trials. In a joint effort, the centers collected, translated, and compared the guidelines that had been put in place to treat patients with cancer during the COVID-19 pandemic.
Cancer treatment is multidisciplinary and involves many specialties including surgery, radiology, pathology, radiation oncology, and medical oncology. Coordinating care among disciplines is a very complex process, Voest noted.
“Changing treatment also means that you need to reconsider capacities and requirements,” he said. “Hospitals have installed crisis teams that were very good at coordinating these efforts.”
Restructuring care
Cancer care had to be reorganized on multiple levels, and the CCE centers looked at several aspects that needed to be accounted for, to ensure continuity in cancer care.
“The biggest challenge for the NHS and other healthcare systems is the surge of patients requiring oxygen and/or intensive care, and the nature and infectiousness of the virus,” said coauthor Carlos Caldas, MD, FMedSci, professor of cancer medicine at the University of Cambridge, United Kingdom. “In hospitals that are mostly run close to capacity, and where all kinds of patients are treated, this has created major resource and logistical problems.”
For regular clinical activities, the institutions with dedicated cancer centers (German Cancer Research Center, Institute Gustave Roussy, Istituto Nazionale dei Tumori di Milano, and Netherlands Cancer Institute) have attempted to stay COVID-19 free. This policy would in turn help ensure that sufficient clinical and intensive-care capacity could be reserved for critical cancer surgeries or management of treatment-related side effects, and allow hospitals outside of the CCE to transfer patients with cancer to these centers. The general hospitals can then focus on caring for patients with COVID-19, as well as other illnesses/injuries that require inpatient care.
As the CCE centers located within general hospitals (Cambridge Cancer Center, Vall d’Hebron Institute of Oncology and Karolinska Institute) have to admit patients with suspected and positive cases of COVID-19, being “COVID-19 free” was never a realistic or pursued goal.
The authors note that it is the responsibility of all healthcare professionals to ensure patients are not exposed to COVID-19, and this has meant minimizing hospital visits and person-to-person contact. For example, whenever possible, consultations take place via telephone calls or over the Internet, and nonurgent appointments that would require a patient’s physical presence at the clinic have been postponed. Visitors are also not permitted to accompany patients when admitted to the hospital or during procedures.
Standard-of-care treatment regimens have been adapted across all centers to minimize the number of hospital visits and hospitalizations and prevent “anticancer treatment-induced” complications of COVID-19.
To minimize visits and hospitalizations, strategies include converting intravenous treatments to oral or subcutaneous regimens when possible; switching from cytotoxic chemotherapy to a less-toxic approach to minimize the risk of complications requiring hospitalization; or to pause therapies when possible (stable disease reached or better). In addition, nonemergency surgeries have been postponed or replaced by radiotherapy.
To prevent anticancer treatment-induced complications of COVID-19, most centers use the paradigm that the added benefit for tumor control should be weighed against the potential risk for COVID-19–related morbidity and mortality. To prevent or reduce the risk of neutropenia and lymphopenia, for example, all centers have suggested a de-escalation of cytotoxic chemotherapy or targeted treatment strategies, or to forgo second or subsequent lines of palliative treatments if response rates from up-front therapy are low.
Some of these changes may be here to stay, noted Caldas. “One of the positive messages that comes out of this is that, clearly, care can be delivered in a safe and compassionate manner without requiring as many hospital visits as in the pre-COVID-19 era,” he said. “In the future, we will take heed of the COVID-19 experience to improve delivery of cancer care.”
Capacity of facilities
Many healthcare systems have become overwhelmed as the pandemic has intensified, thus making it necessary to prioritize. To prepare for this possibility, CCE centers have established protocols to categorize and prioritize patients for systemic treatment or surgery. While the protocols vary by center, they are comparable with one another as they prioritize on the basis of anticipated treatment outcome, the authors note.
The guidelines in CCE centers unanimously recommend that neoadjuvant therapies and curative surgeries be the top priority, for the times when operating room and/or ICU capacity is limited. As an alternative, neoadjuvant systemic treatments may be initiated or extended to postpone surgery, and other nonsurgical interventions can be considered.
In addition, some centers agree that certain elective surgeries can be safely delayed if backed by scientific evidence. As an example, an 11-week deferment of surgery may be acceptable for patients with rectal cancer after downstaging.
Cancer centers may also need to upscale and downscale quickly, depending on how the pandemic evolves, and many have already outlined scenarios to prepare for increasing or decreasing their capacity using phased approaches.
The Netherlands Cancer Institute, for example, has defined four phases of increasing severity; in Germany, capacity planning has been coordinated among 18 hospitals and the federal ministry of health, in order to prevent shortages of cancer services.
“We note that the optimal downscaling strategies depend on country- and center-specific capacities and preferences,” they write. “Therefore, it is difficult to propose a common schedule, and it will be most effective if hospitals outline their own phase-specific downscaling strategies based on the prioritization schemes and practical handles discussed above.”
Future research
Better strategies will be needed to reduce the impact of COVID-19 in cancer care, and four research priorities were identified to allow for evidence-based adjustments of cancer care protocols while the pandemic continues:
- Collect real-world data about the effects of adjustment and de-escalation of treatment regimens on outcomes
- Determine the incidence of COVID-19 in both the general population and among patients with cancer who have received systemic therapies, with large-scale serological testing
- Develop an epidemiological model that will allow estimates of the cumulative incidence of COVID-19 for a patient with cancer, within a specific time frame
- Determine COVID-19 related morbidity and mortality in patients with cancer who have been treated with systemic therapies and/or granulocyte colony-stimulating factor (G-CSF). Several projects are currently underway, such as the UK Coronavirus Cancer Monitoring Project.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Delivering cancer care during the COVID-19 pandemic has proved particularly challenging, as minimizing the risk of infection must be balanced with maintaining optimal outcomes.
Healthcare systems and oncologists have had to reorganize standard oncologic care in order to protect vulnerable patients from exposure to COVID-19 as well as deal with pandemic-related issues of equipment and staffing shortages.
A new article now describes how seven cancer centers in Europe rapidly reorganized their oncologic services and are tackling this crisis, as well as offering guidance to other institutions.
This was a major undertaking, to work out a system where patients can still get care but in a safer manner, explained coauthor Emile Voest, MD, medical director of the Netherlands Cancer Institute in Amsterdam.
“Decisions needed to be taken based on availability of personnel, protective materials, and urgencies,” he told Medscape Medical News. “Because every country had its own speed of development of the COVID pandemic, there were different scenarios in all institutions, but all with a common factor of key expertise on how to de-escalate in a safe manner.”
The article was published April 16 in Nature Medicine.
The Netherlands Cancer Institute (the Netherlands), Karolinska Institute (Sweden), Institute Gustave Roussy (France), Cambridge Cancer Center (United Kingdom), Istituto Nazionale dei Tumori di Milano (Italy), German Cancer Research Center (Germany), and Vall d’Hebron Institute of Oncology (Spain) have been working closely together in a legal entity since 2014, and have created ‘Cancer Core Europe’ (CCE). The goal is to “maximize coherence and critical mass in cancer research,” the authors note.
The consortium represents roughly 60,000 patients with newly diagnosed cancer, delivers approximately 300,000 treatment courses, and conducts about 1.2 million consultations annually, with more than 1,500 ongoing clinical trials. In a joint effort, the centers collected, translated, and compared the guidelines that had been put in place to treat patients with cancer during the COVID-19 pandemic.
Cancer treatment is multidisciplinary and involves many specialties including surgery, radiology, pathology, radiation oncology, and medical oncology. Coordinating care among disciplines is a very complex process, Voest noted.
“Changing treatment also means that you need to reconsider capacities and requirements,” he said. “Hospitals have installed crisis teams that were very good at coordinating these efforts.”
Restructuring care
Cancer care had to be reorganized on multiple levels, and the CCE centers looked at several aspects that needed to be accounted for, to ensure continuity in cancer care.
“The biggest challenge for the NHS and other healthcare systems is the surge of patients requiring oxygen and/or intensive care, and the nature and infectiousness of the virus,” said coauthor Carlos Caldas, MD, FMedSci, professor of cancer medicine at the University of Cambridge, United Kingdom. “In hospitals that are mostly run close to capacity, and where all kinds of patients are treated, this has created major resource and logistical problems.”
For regular clinical activities, the institutions with dedicated cancer centers (German Cancer Research Center, Institute Gustave Roussy, Istituto Nazionale dei Tumori di Milano, and Netherlands Cancer Institute) have attempted to stay COVID-19 free. This policy would in turn help ensure that sufficient clinical and intensive-care capacity could be reserved for critical cancer surgeries or management of treatment-related side effects, and allow hospitals outside of the CCE to transfer patients with cancer to these centers. The general hospitals can then focus on caring for patients with COVID-19, as well as other illnesses/injuries that require inpatient care.
As the CCE centers located within general hospitals (Cambridge Cancer Center, Vall d’Hebron Institute of Oncology and Karolinska Institute) have to admit patients with suspected and positive cases of COVID-19, being “COVID-19 free” was never a realistic or pursued goal.
The authors note that it is the responsibility of all healthcare professionals to ensure patients are not exposed to COVID-19, and this has meant minimizing hospital visits and person-to-person contact. For example, whenever possible, consultations take place via telephone calls or over the Internet, and nonurgent appointments that would require a patient’s physical presence at the clinic have been postponed. Visitors are also not permitted to accompany patients when admitted to the hospital or during procedures.
Standard-of-care treatment regimens have been adapted across all centers to minimize the number of hospital visits and hospitalizations and prevent “anticancer treatment-induced” complications of COVID-19.
To minimize visits and hospitalizations, strategies include converting intravenous treatments to oral or subcutaneous regimens when possible; switching from cytotoxic chemotherapy to a less-toxic approach to minimize the risk of complications requiring hospitalization; or to pause therapies when possible (stable disease reached or better). In addition, nonemergency surgeries have been postponed or replaced by radiotherapy.
To prevent anticancer treatment-induced complications of COVID-19, most centers use the paradigm that the added benefit for tumor control should be weighed against the potential risk for COVID-19–related morbidity and mortality. To prevent or reduce the risk of neutropenia and lymphopenia, for example, all centers have suggested a de-escalation of cytotoxic chemotherapy or targeted treatment strategies, or to forgo second or subsequent lines of palliative treatments if response rates from up-front therapy are low.
Some of these changes may be here to stay, noted Caldas. “One of the positive messages that comes out of this is that, clearly, care can be delivered in a safe and compassionate manner without requiring as many hospital visits as in the pre-COVID-19 era,” he said. “In the future, we will take heed of the COVID-19 experience to improve delivery of cancer care.”
Capacity of facilities
Many healthcare systems have become overwhelmed as the pandemic has intensified, thus making it necessary to prioritize. To prepare for this possibility, CCE centers have established protocols to categorize and prioritize patients for systemic treatment or surgery. While the protocols vary by center, they are comparable with one another as they prioritize on the basis of anticipated treatment outcome, the authors note.
The guidelines in CCE centers unanimously recommend that neoadjuvant therapies and curative surgeries be the top priority, for the times when operating room and/or ICU capacity is limited. As an alternative, neoadjuvant systemic treatments may be initiated or extended to postpone surgery, and other nonsurgical interventions can be considered.
In addition, some centers agree that certain elective surgeries can be safely delayed if backed by scientific evidence. As an example, an 11-week deferment of surgery may be acceptable for patients with rectal cancer after downstaging.
Cancer centers may also need to upscale and downscale quickly, depending on how the pandemic evolves, and many have already outlined scenarios to prepare for increasing or decreasing their capacity using phased approaches.
The Netherlands Cancer Institute, for example, has defined four phases of increasing severity; in Germany, capacity planning has been coordinated among 18 hospitals and the federal ministry of health, in order to prevent shortages of cancer services.
“We note that the optimal downscaling strategies depend on country- and center-specific capacities and preferences,” they write. “Therefore, it is difficult to propose a common schedule, and it will be most effective if hospitals outline their own phase-specific downscaling strategies based on the prioritization schemes and practical handles discussed above.”
Future research
Better strategies will be needed to reduce the impact of COVID-19 in cancer care, and four research priorities were identified to allow for evidence-based adjustments of cancer care protocols while the pandemic continues:
- Collect real-world data about the effects of adjustment and de-escalation of treatment regimens on outcomes
- Determine the incidence of COVID-19 in both the general population and among patients with cancer who have received systemic therapies, with large-scale serological testing
- Develop an epidemiological model that will allow estimates of the cumulative incidence of COVID-19 for a patient with cancer, within a specific time frame
- Determine COVID-19 related morbidity and mortality in patients with cancer who have been treated with systemic therapies and/or granulocyte colony-stimulating factor (G-CSF). Several projects are currently underway, such as the UK Coronavirus Cancer Monitoring Project.
The authors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Want to keep cancer patients and providers safe during the pandemic? Here’s how
according to the authors of a special feature article in the Journal of the National Comprehensive Cancer Network.

Prescreening, telemedicine, and limiting procedures top the authors’ list of 10 recommendations for ensuring patient safety in U.S. oncology practices. Assuring appropriate personal proctective equipment (PPE), encouraging telecommuting, and providing wellness/stress management are a few of the ways to look out for health care worker safety during the crisis.
These recommendations were drafted to provide guidance during the rapidly evolving global pandemic that, in some cases, has deluged health care delivery systems and strained the ability of providers to assure safe and effective care, said lead author Pelin Cinar, MD, of the Hellen Diller Family Comprehensive Cancer Center at the University of California, San Francisco.
“I think we have been so overwhelmed that sometimes it’s difficult to get organized in our thought processes,” Dr. Cinar said in an interview. “So this [article] was really trying to provide some structure to each of the different steps that we should be addressing at minimum.”
Screening patients
Prescreening systems are a critical first step to ensure cancer centers are helping control community spread of the virus, according to the article. Whether done by phone or online, prescreening 1-2 days before a patient’s visit can help identify COVID-19 symptoms and exposure history, guiding whether patients need to be evaluated, monitored, or referred to an ED.
Next, screening clinics can help ensure cancer patients with COVID-19 symptoms are evaluated and tested in a unit with dedicated staff, according to the article.
“If symptomatic patients present to the cancer center for treatment after a negative prescreening assessment, they must be provided with a mask and directed to a screening clinic for evaluation and potential testing before moving forward with any cancer-directed therapy,” the article states.
Telemedicine and treatment
Telemedicine visits should be done whenever possible to avoid in-person visits, according to the article. Dr. Cinar said that her center, like other cancer centers, has seen a major uptick in these visits, which are typically done over video. In February, there were a total of 232 video visits at her center, which jumped to 1,702 in March, or an approximate 600% increase.
“Even though we had a relatively robust presence [before the pandemic], we still weren’t at a level where we are now,” Dr. Cinar said.
When it comes to cancer treatment, surgeries and procedures should be limited to essential or urgent cases, and, if possible, chemotherapy and systemic therapy regimens can be modified to allow for fewer visits to the cancer center or infusion center, according to the article.
Transitions to outpatient care can help further reduce the need for in-person visits, while intervals between scans can be increased, or biochemical markers can be used instead of scans.
Protecting providers
Health care workers providing cancer care should be assured appropriate PPE, and websites or other centralized resources should be in place to make sure workers are aware of current PPE guidelines and changes in workflow, according to the article.
The authors note that daily screening tools or temperature checks of symptomatic workers can help decrease the risk of exposure to others. The authors also recommend establishing clear rules for when health care workers with suspected or confirmed COVID-19 should be staying at home and returning to the job.
Telecommuting should be encouraged, with limited staff participating in onsite rotations to further reduce exposure risks, the article states.
Anxiety, insomnia, and distress have been reported among frontline health care workers managing patients with COVID-19, according to the article, which recommends wellness and stress management resources be available as an “invaluable resource” in cancer centers.
“We have to take care of ourselves to be able to take care of others,” Dr. Cinar said. “With PPE, you’re physically protecting yourself, while self-care, stress management, and wellness are also a big component of protecting ourselves.”
The report by Dr. Cinar and colleagues was an invited article from the NCCN Best Practices Committee. One coauthor reported relationships with Abbvie, Adaptive Biotechnologies, Aduro, and several other companies. Dr. Cinar and the remaining authors said they had no relevant conflicts of interest.
SOURCE: Cinar P et al. J Natl Compr Canc Netw. 2020 Apr 15. doi: 10.6004/jnccn.2020.7572.
according to the authors of a special feature article in the Journal of the National Comprehensive Cancer Network.
Prescreening, telemedicine, and limiting procedures top the authors’ list of 10 recommendations for ensuring patient safety in U.S. oncology practices. Assuring appropriate personal proctective equipment (PPE), encouraging telecommuting, and providing wellness/stress management are a few of the ways to look out for health care worker safety during the crisis.
These recommendations were drafted to provide guidance during the rapidly evolving global pandemic that, in some cases, has deluged health care delivery systems and strained the ability of providers to assure safe and effective care, said lead author Pelin Cinar, MD, of the Hellen Diller Family Comprehensive Cancer Center at the University of California, San Francisco.
“I think we have been so overwhelmed that sometimes it’s difficult to get organized in our thought processes,” Dr. Cinar said in an interview. “So this [article] was really trying to provide some structure to each of the different steps that we should be addressing at minimum.”
Screening patients
Prescreening systems are a critical first step to ensure cancer centers are helping control community spread of the virus, according to the article. Whether done by phone or online, prescreening 1-2 days before a patient’s visit can help identify COVID-19 symptoms and exposure history, guiding whether patients need to be evaluated, monitored, or referred to an ED.
Next, screening clinics can help ensure cancer patients with COVID-19 symptoms are evaluated and tested in a unit with dedicated staff, according to the article.
“If symptomatic patients present to the cancer center for treatment after a negative prescreening assessment, they must be provided with a mask and directed to a screening clinic for evaluation and potential testing before moving forward with any cancer-directed therapy,” the article states.
Telemedicine and treatment
Telemedicine visits should be done whenever possible to avoid in-person visits, according to the article. Dr. Cinar said that her center, like other cancer centers, has seen a major uptick in these visits, which are typically done over video. In February, there were a total of 232 video visits at her center, which jumped to 1,702 in March, or an approximate 600% increase.
“Even though we had a relatively robust presence [before the pandemic], we still weren’t at a level where we are now,” Dr. Cinar said.
When it comes to cancer treatment, surgeries and procedures should be limited to essential or urgent cases, and, if possible, chemotherapy and systemic therapy regimens can be modified to allow for fewer visits to the cancer center or infusion center, according to the article.
Transitions to outpatient care can help further reduce the need for in-person visits, while intervals between scans can be increased, or biochemical markers can be used instead of scans.
Protecting providers
Health care workers providing cancer care should be assured appropriate PPE, and websites or other centralized resources should be in place to make sure workers are aware of current PPE guidelines and changes in workflow, according to the article.
The authors note that daily screening tools or temperature checks of symptomatic workers can help decrease the risk of exposure to others. The authors also recommend establishing clear rules for when health care workers with suspected or confirmed COVID-19 should be staying at home and returning to the job.
Telecommuting should be encouraged, with limited staff participating in onsite rotations to further reduce exposure risks, the article states.
Anxiety, insomnia, and distress have been reported among frontline health care workers managing patients with COVID-19, according to the article, which recommends wellness and stress management resources be available as an “invaluable resource” in cancer centers.
“We have to take care of ourselves to be able to take care of others,” Dr. Cinar said. “With PPE, you’re physically protecting yourself, while self-care, stress management, and wellness are also a big component of protecting ourselves.”
The report by Dr. Cinar and colleagues was an invited article from the NCCN Best Practices Committee. One coauthor reported relationships with Abbvie, Adaptive Biotechnologies, Aduro, and several other companies. Dr. Cinar and the remaining authors said they had no relevant conflicts of interest.
SOURCE: Cinar P et al. J Natl Compr Canc Netw. 2020 Apr 15. doi: 10.6004/jnccn.2020.7572.
according to the authors of a special feature article in the Journal of the National Comprehensive Cancer Network.
Prescreening, telemedicine, and limiting procedures top the authors’ list of 10 recommendations for ensuring patient safety in U.S. oncology practices. Assuring appropriate personal proctective equipment (PPE), encouraging telecommuting, and providing wellness/stress management are a few of the ways to look out for health care worker safety during the crisis.
These recommendations were drafted to provide guidance during the rapidly evolving global pandemic that, in some cases, has deluged health care delivery systems and strained the ability of providers to assure safe and effective care, said lead author Pelin Cinar, MD, of the Hellen Diller Family Comprehensive Cancer Center at the University of California, San Francisco.
“I think we have been so overwhelmed that sometimes it’s difficult to get organized in our thought processes,” Dr. Cinar said in an interview. “So this [article] was really trying to provide some structure to each of the different steps that we should be addressing at minimum.”
Screening patients
Prescreening systems are a critical first step to ensure cancer centers are helping control community spread of the virus, according to the article. Whether done by phone or online, prescreening 1-2 days before a patient’s visit can help identify COVID-19 symptoms and exposure history, guiding whether patients need to be evaluated, monitored, or referred to an ED.
Next, screening clinics can help ensure cancer patients with COVID-19 symptoms are evaluated and tested in a unit with dedicated staff, according to the article.
“If symptomatic patients present to the cancer center for treatment after a negative prescreening assessment, they must be provided with a mask and directed to a screening clinic for evaluation and potential testing before moving forward with any cancer-directed therapy,” the article states.
Telemedicine and treatment
Telemedicine visits should be done whenever possible to avoid in-person visits, according to the article. Dr. Cinar said that her center, like other cancer centers, has seen a major uptick in these visits, which are typically done over video. In February, there were a total of 232 video visits at her center, which jumped to 1,702 in March, or an approximate 600% increase.
“Even though we had a relatively robust presence [before the pandemic], we still weren’t at a level where we are now,” Dr. Cinar said.
When it comes to cancer treatment, surgeries and procedures should be limited to essential or urgent cases, and, if possible, chemotherapy and systemic therapy regimens can be modified to allow for fewer visits to the cancer center or infusion center, according to the article.
Transitions to outpatient care can help further reduce the need for in-person visits, while intervals between scans can be increased, or biochemical markers can be used instead of scans.
Protecting providers
Health care workers providing cancer care should be assured appropriate PPE, and websites or other centralized resources should be in place to make sure workers are aware of current PPE guidelines and changes in workflow, according to the article.
The authors note that daily screening tools or temperature checks of symptomatic workers can help decrease the risk of exposure to others. The authors also recommend establishing clear rules for when health care workers with suspected or confirmed COVID-19 should be staying at home and returning to the job.
Telecommuting should be encouraged, with limited staff participating in onsite rotations to further reduce exposure risks, the article states.
Anxiety, insomnia, and distress have been reported among frontline health care workers managing patients with COVID-19, according to the article, which recommends wellness and stress management resources be available as an “invaluable resource” in cancer centers.
“We have to take care of ourselves to be able to take care of others,” Dr. Cinar said. “With PPE, you’re physically protecting yourself, while self-care, stress management, and wellness are also a big component of protecting ourselves.”
The report by Dr. Cinar and colleagues was an invited article from the NCCN Best Practices Committee. One coauthor reported relationships with Abbvie, Adaptive Biotechnologies, Aduro, and several other companies. Dr. Cinar and the remaining authors said they had no relevant conflicts of interest.
SOURCE: Cinar P et al. J Natl Compr Canc Netw. 2020 Apr 15. doi: 10.6004/jnccn.2020.7572.
FROM THE JOURNAL OF THE NATIONAL COMPREHENSIVE CANCER NETWORK
In praise of parents and children
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.

Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”

This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
The COVID-19 pandemic has changed the lives of children, teenagers, and parents worldwide. While some families are experiencing the unburdening of overly packed schedules and may be having a romantic or nostalgic “Little House on the Prairie” experience, for most it is at a minimum uncomfortable and inconvenient. For others it’s unbearable as they experience loss and feel relationship strain intensified by social distancing, seclusion, or quarantine. Some children have found respite from bullying at school, while other children have lost their only respite from being mistreated at home. Now may be as critical a time as ever for health care providers to listen carefully, empathize, validate, and proactively reach out to provide encouraging guidance and counsel, as well as express concern for families and children.
Many parents across the country are taking on an enormous, unanticipated task. Many parents have lost employment and income, while many mandatory professionals now struggle to keep up with increased work hours and work stress. Parents are trying to become multitaskers who assume the role of the music teacher, the soccer coach, the drama instructor, the friend, and of course their original role as a parent.
This seems an appropriate time to consider the work of Donald W. Winnicott, FRCP, the English pediatrician known for the concept of the “good enough parent.”1 This notion of parental competence was in part born out of a desire to defend parents against possible erosion of their confidence in following loving instincts by encroachment from professional expertise. The concept of the “good enough” parent is also related to the idea that young children who believe their parent is perfect will eventually know better. Now is a fitting time for pediatricians to buoy up imperfect but striving parents who are plenty “good enough” as they follow loving instincts to support their children during unforeseen changes associated with the pandemic.
Social distancing has led to family condensing. Many parents and children remain within the same four walls all day, every day. For many parents, the outlet of water cooler banter or yoga classes is gone. Even the commute home, with all its frustration, may have allowed decompression in the form of an audiobook, favorite music, or verbal transference of frustration onto the stranger who just cut you off. That commute might be gone too. Now, for many the good, bad, and the ugly is all happening at home. The 3-year-old may still adorably see a parent who can do no wrong, but in the end, the truth will prevail. A timely word of encouragement to parents: It’s okay to not be omnipotent. In fact, it will help children have a richer view of the world and more realistic expectations of themselves.
For children, they’ll need praise too, and the upheaval caused by the pandemic may be a fitting opportunity to make that praise more meaningful. But sports are off, the school musical is canceled, and the spelling bee is gone. The dojo is closed, the art fair is postponed, and the dance recital isn’t happening. Report cards in many schools may now transition from letter grades to pass/fail. Parents may be asking, “How on earth are we going to celebrate and praise the children?”
Research has shown us that praising the process is more valuable than praising the person.2 If Lucy participates in a soccer game and Javier gets his math results back, there are many possible approaches to praise. “You scored a goal!” or “You got an A on your math test!” is outcome- or product-focused praise. “You’re a good soccer player” or “You’re smart at math!” is person-focused praise. Instead, the most effective praise is process-focused praise: “You worked hard and ran hard even when it looked tiring” or “I noticed that you kept trying different strategies on those math problems until you figured them out.”
This may be a time when children face less comparison, less ranking, and receive less direct reward. With help, they can focus more on the process of learning and less on the outcomes of learning. They may more readily enjoy the efforts in their hobbies, not just the outcomes of their hobbies. When children receive praise for their work, effort, and actions rather than outcomes, externally validating things may be pleasantly replaced by internally validating traits. With process praise, children are more likely to feel self-confident, to set higher learning goals, and to accurately believe that intelligence is related to effort rather than a fixed trait that has been divided up among haves and have nots.3
Families currently face immense change, uncertainty, and discouragement largely unprecedented in their lifetimes. As care providers, we can look to lasting principles as we encourage parents in their provision of love. We can effectively provide praise and celebrate effort using evidence-based strategies uniquely fitted to our current circumstances. As we do this, we can provide healing of some of the less visible ailments associated with the COVID-19 pandemic.
Dr. Jackson is in the department of psychiatry at the University of Vermont, Burlington. He said he had no relevant financial disclosures. Email Dr. Jackson at [email protected].
References
1. “The Child, the Family, and the Outside World.” London: Penguin; 1973. p. 173.
2. Dev Psychol. 1999;35(3):835-47.
3. J Exp Child Psychol. 2018;173:116-35.
2019-2020 flu season ends with ‘very high’ activity in New Jersey
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
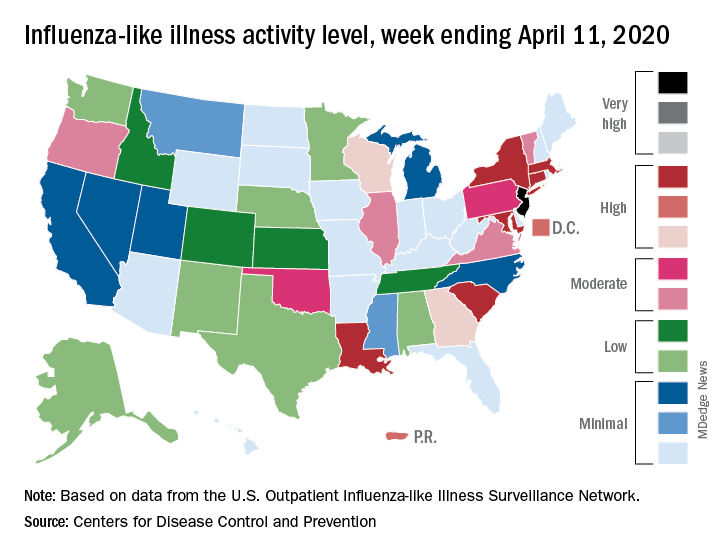
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
The 2019-2020 flu season is ending, but not without a revised map to reflect the COVID-induced new world order.
For the week ending April 11, those additions encompass only New Jersey at level 13 and New York City at level 12, the CDC reported April 17.
Eight states, plus the District of Columbia and Puerto Rico, were in the “high” range of flu activity, which runs from level 8 to level 10, for the same week. Those eight states included Connecticut, Georgia, Louisiana, Maryland, Massachusetts, New York, South Carolina, and Wisconsin.
The CDC’s influenza division included this note with its latest FluView report: “The COVID-19 pandemic is affecting healthcare seeking behavior. The number of persons and their reasons for seeking care in the outpatient and ED settings is changing. These changes impact data from ILINet [Outpatient Influenza-like Illness Surveillance Network] in ways that are difficult to differentiate from changes in illness levels, therefore ILINet data should be interpreted with caution.”
Outpatient visits for influenza-like illness made up 2.9% of all visits to health care providers for the week ending April 11, which is the 23rd consecutive week that it’s been at or above the national baseline level of 2.4%. Twenty-three weeks is longer than this has occurred during any flu season since the CDC started setting a baseline in 2007, according to ILINet data.
Mortality from pneumonia and influenza, at 11.7%, was well above the epidemic threshold of 7.0%, although, again, pneumonia mortality “is being driven primarily by an increase in non-influenza pneumonia deaths due to COVID-19,” the CDC wrote.
The total number of influenza-related deaths in children, with reports of two more added this week, is 168 for the season – higher than two of the last three seasons: 144 in 2018-2019, 188 in 2017-2018, and 110 in 2016-2017, according to the CDC.
N.Y. universal testing: Many COVID-19+ pregnant women are asymptomatic
based on data from 215 pregnant women in New York City.

“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.

However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.

“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
based on data from 215 pregnant women in New York City.
“The obstetrical population presents a unique challenge during this pandemic, since these patients have multiple interactions with the health care system and eventually most are admitted to the hospital for delivery,” wrote Desmond Sutton, MD, and colleagues at Columbia University Irving Medical Center, New York
In a letter published in the New England Journal of Medicine, the researchers reviewed their experiences with 215 pregnant women who delivered infants during March 22–April 4, 2020, at the New York–Presbyterian Allen Hospital and Columbia University Irving Medical Center. All the women were screened for symptoms of the COVID-19 infection on admission.
Overall, four women (1.9%) had fevers or other symptoms on admission, and all of these women tested positive for the virus that causes COVID-19. The other 211 women were afebrile and asymptomatic at admission, and 210 of them were tested via nasopharyngeal swabs. A total of 29 asymptomatic women (13.7%) tested positive for COVID-19 infection.
“Thus, 29 of the 33 patients who were positive for SARS-CoV-2 at admission (87.9%) had no symptoms of COVID-19 at presentation,” Dr. Sutton and colleagues wrote.
Three of the 29 COVID-19-positive women who were asymptomatic on admission developed fevers before they were discharged from the hospital after a median stay of 2 days. Of these, two received antibiotics for presumed endomyometritis and one patient with presumed COVID-19 infection received supportive care. In addition, one patient who was initially negative developed COVID-19 symptoms after delivery and tested positive 3 days after her initial negative test.
“Our use of universal SARS-CoV-2 testing in all pregnant patients presenting for delivery revealed that at this point in the pandemic in New York City, most of the patients who were positive for SARS-CoV-2 at delivery were asymptomatic,” Dr. Sutton and colleagues said.
Although their numbers may not be generalizable to areas with lower infection rates, they highlight the risk of COVID-19 infection in asymptomatic pregnant women, they noted.
“The potential benefits of a universal testing approach include the ability to use COVID-19 status to determine hospital isolation practices and bed assignments, inform neonatal care, and guide the use of personal protective equipment,” they concluded.
Continuing challenges
“What I have seen in our institute is the debate about rapid testing and the inherent problems with false negatives and false positives,” Catherine Cansino, MD, of the University of California, Davis, said in an interview. “I think there is definitely a role for universal testing, especially in areas with high prevalence,” and the New York clinicians have made a strong case.
However, the challenge remains of obtaining quick test results that would still be reliable, as many rapid tests have a false-negative rate of as much as 20%, noted Dr. Cansino, who was not involved in the New York study.
Her institution is using a test with a higher level of accuracy, “but it can take several hours or a day to get the results,” at which point the women may have gone through labor and delivery and been in contact with multiple health care workers who have used personal protective equipment accordingly if they don’t know a patient’s status.
To help guide policies, Dr. Cansino said that outcome data would be useful. “It’s hard to know how outcomes are different, and it would be good to know how transmission rates differ between symptomatic carriers and those who are asymptomatic.”
“As SARS-CoV-2, the virus responsible for COVID-19, continues to spread, pregnant women remain a unique population with required frequent health system contacts and ultimate need for delivery,” Iris Krishna, MD, of the Emory Healthcare Network in Atlanta, said in an interview. “This report in a high prevalence area demonstrated 1 out of 8 asymptomatic pregnant patients presenting for delivery were SARS-CoV-2 positive, illustrating a need for universal screening.
“As this pandemic evolves, we are learning more and more, and it is important to expand our understanding of asymptomatic transmission and the risk this may pose,” said Dr. Krishna, who was not part of the New York study.
“Key benefits to universal screening are the capability for labor and delivery units to implement best hospital practices in their care of mothers and babies, such as admitting positive patients to cohort units,” she noted. Such units would “allow for closer monitoring of mothers and babies, as well as ensuring proper use of personal protective equipment by health care teams” and also would help preserve supplies of personal protective equipment.
Dr. Krishna cited hospital testing capacity as an obvious barrier to universal screening of pregnant women, as well as factors including the need for additional protective equipment to be used during swab collection. Also, “If you get a negative result and there is a strong suspicion for COVID-19 infection, when do you retest?” she asked. “These are key questions or areas of assessment that should be considered before embarking on universal screening for pregnant women.” In addition, some patients may refuse testing out of fear of stigma or separation from their newborn.
“Implementing an ‘opt out’ approach to screening is encouraged, whereby a patient is informed that a test will be included in standard preventive screening, and they may decline the test,” Dr. Krishna said. “Routine, opt-out screening approaches have proven to be highly effective as it removes the stigma associated with testing, fosters earlier diagnosis and treatment, reduces risk of transmission, and has proven to be cost effective. Pregnant women should be reassured that universal screening is beneficial for their care and the care of their newborn baby,” she emphasized.
“Institutions should consider implementing universal screening on labor and delivery as several geographic areas are predicted to reach their peak time of COVID-19 transmission, and it is clear that asymptomatic individuals continue to play a role in its transmission,” Dr. Krishna concluded.
Dr. Sutton and associates had no financial conflicts to disclose. Neither Dr. Cansino nor Dr. Krishna had any financial conflicts to disclose. Dr. Cansino and Dr. Krishna are members of the Ob.Gyn. News Editorial Advisory Board.
SOURCE: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Universal COVID-19 testing for pregnant women entering hospitals for delivery could better protect patients and staff.
Major finding: Approximately 88% of 33 pregnant women who tested positive for COVID-19 infection at hospital admission were asymptomatic; about 14% of the 215 women overall tested positive for the novel coronavirus.
Study details: The data come from a review of 215 pregnant women who delivered infants between March 22 and April 4, 2020, in New York City.
Disclosures: The authors had no financial conflicts to disclose.
Source: Sutton D et al. N Engl J Med. 2020 Apr 13. doi: 10.1056/NEJMc2009316.
The necessity of being together
COVID-19 has prompted many changes in pediatric health care. They say necessity is the mother of invention. Sometimes, necessity is the motivator for the long-past-due adoption of a previous invention, such as telemedicine for minor illnesses. And sometimes necessity reminds us about what is really important in a world of high technology.

Unlike our nearly overwhelmed internal medicine, ED, and family physician colleagues, many pediatricians are in a lull that threatens the financial viability of our practices. We are postponing annual well visits. We have fewer sick visits and hospitalizations since respiratory syncytial virus (RSV) and influenza also have been reduced by social distancing. Parents are avoiding the risk of contagion in the waiting room and not bringing their children in for minor complaints. There is more telemedicine – a welcome change in financing and practice whose time has come, but was being delayed by lack of insurance coverage.
Technology has allowed clinicians to respond to the pandemic in ways that would not have been possible a few years ago. Online tools, such as subscription email lists, webinars, and electronic medical news services, provide updates when the information changes weekly on the virus’s contagiousness, asymptomatic and presymptomatic transmission, prevalence, the effectiveness of masks, and experimental treatment options. These changes have been so fast that many journal articles based on data from China were obsolete and contradicted before they appeared in print.
However, technology only helped us to more effectively do what we needed to do in the first place – come together in a world of physical distancing and work toward common goals. In many hospitals, pediatric wards were emptied by reduced RSV admissions and postponed elective surgeries. These units have been converted to accept adult patients up to age 30 or 40 years. Our med-peds colleagues quickly created webinars and online resource packages on topics pediatric hospitalists might need to care for that population. There were refresher courses on ventilator management and reminders that community pediatric hospitalists, who in the winter might have one-third of their admissions with RSV, have more experience managing viral pneumonia than the internists.
Ward teams were created with a pediatric attending and an internal medicine resident. The resident’s familiarity with the names of blood pressure medicines complemented the attending’s years of clinical judgment and bedside manner. People are stepping out of their comfort zones but initial reports from the front lines are that, with each other’s support, we’ve got this.
Mistakes in telemedicine are being made, shared, and learned from. Emergency physicians are collecting anecdotes of situations when things were missed or treatment delayed. Surgeons report seeing increased numbers of cases in which the diagnosis of appendicitis was delayed, which isn’t surprising when a pediatrician cannot lay hands on the belly. Perhaps any case in which a parent calls a second or third time should be seen in the flesh.

Some newborn nurseries are discharging mother and baby at 24 hours after birth and rediscovering what was learned about that practice, which became common in the 1990s. It works well for the vast majority of babies, but we need to be ready to detect the occasional jaundiced baby or the one where breastfeeding isn’t going well. The gray-haired pediatricians can recall those nuances.
Another key role is to help everyone process the frequent deaths during a pandemic. First, there are the families we care for. Children are losing grandparents with little warning. Parents may be overwhelmed with grief while ill themselves. That makes children vulnerable.
Our medical system in 2 months has moved heaven and earth – and significantly harmed the medical care and financial future of our children – trying to assure that every 80-year-old has the right to die while attached to a ventilator, even though only a small fraction of them will survive to discharge. Meanwhile, on the wards, visitation policies have people deteriorating and dying alone. I find this paradigm distressing and antithetical to my training.
Medicine and nursing both have long histories in which the practitioner recognized that there was little they could do to prevent the death. Their role was to compassionately guide the family through it. For some people, this connection is the most precious of the arts of medicine and nursing. We need to reexamine our values. We need to get creative. We need to involve palliative care experts and clergy with the same urgency with which we have automakers making ventilators.
Second, there are our colleagues. Pediatric caregivers, particularly trainees, rarely encounter deaths and can benefit from debriefing sessions, even short ones. There is comfort in having a colleague review the situation and say: “There was nothing you could have done.” Or even: “That minor omission did not alter the outcome.” Even when everything was done properly, deaths cause moral suffering that needs processing and healing. Even if you don’t have magic words to give, just being present aids in the healing. We are all in this, together.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
COVID-19 has prompted many changes in pediatric health care. They say necessity is the mother of invention. Sometimes, necessity is the motivator for the long-past-due adoption of a previous invention, such as telemedicine for minor illnesses. And sometimes necessity reminds us about what is really important in a world of high technology.
Unlike our nearly overwhelmed internal medicine, ED, and family physician colleagues, many pediatricians are in a lull that threatens the financial viability of our practices. We are postponing annual well visits. We have fewer sick visits and hospitalizations since respiratory syncytial virus (RSV) and influenza also have been reduced by social distancing. Parents are avoiding the risk of contagion in the waiting room and not bringing their children in for minor complaints. There is more telemedicine – a welcome change in financing and practice whose time has come, but was being delayed by lack of insurance coverage.
Technology has allowed clinicians to respond to the pandemic in ways that would not have been possible a few years ago. Online tools, such as subscription email lists, webinars, and electronic medical news services, provide updates when the information changes weekly on the virus’s contagiousness, asymptomatic and presymptomatic transmission, prevalence, the effectiveness of masks, and experimental treatment options. These changes have been so fast that many journal articles based on data from China were obsolete and contradicted before they appeared in print.
However, technology only helped us to more effectively do what we needed to do in the first place – come together in a world of physical distancing and work toward common goals. In many hospitals, pediatric wards were emptied by reduced RSV admissions and postponed elective surgeries. These units have been converted to accept adult patients up to age 30 or 40 years. Our med-peds colleagues quickly created webinars and online resource packages on topics pediatric hospitalists might need to care for that population. There were refresher courses on ventilator management and reminders that community pediatric hospitalists, who in the winter might have one-third of their admissions with RSV, have more experience managing viral pneumonia than the internists.
Ward teams were created with a pediatric attending and an internal medicine resident. The resident’s familiarity with the names of blood pressure medicines complemented the attending’s years of clinical judgment and bedside manner. People are stepping out of their comfort zones but initial reports from the front lines are that, with each other’s support, we’ve got this.
Mistakes in telemedicine are being made, shared, and learned from. Emergency physicians are collecting anecdotes of situations when things were missed or treatment delayed. Surgeons report seeing increased numbers of cases in which the diagnosis of appendicitis was delayed, which isn’t surprising when a pediatrician cannot lay hands on the belly. Perhaps any case in which a parent calls a second or third time should be seen in the flesh.
Some newborn nurseries are discharging mother and baby at 24 hours after birth and rediscovering what was learned about that practice, which became common in the 1990s. It works well for the vast majority of babies, but we need to be ready to detect the occasional jaundiced baby or the one where breastfeeding isn’t going well. The gray-haired pediatricians can recall those nuances.
Another key role is to help everyone process the frequent deaths during a pandemic. First, there are the families we care for. Children are losing grandparents with little warning. Parents may be overwhelmed with grief while ill themselves. That makes children vulnerable.
Our medical system in 2 months has moved heaven and earth – and significantly harmed the medical care and financial future of our children – trying to assure that every 80-year-old has the right to die while attached to a ventilator, even though only a small fraction of them will survive to discharge. Meanwhile, on the wards, visitation policies have people deteriorating and dying alone. I find this paradigm distressing and antithetical to my training.
Medicine and nursing both have long histories in which the practitioner recognized that there was little they could do to prevent the death. Their role was to compassionately guide the family through it. For some people, this connection is the most precious of the arts of medicine and nursing. We need to reexamine our values. We need to get creative. We need to involve palliative care experts and clergy with the same urgency with which we have automakers making ventilators.
Second, there are our colleagues. Pediatric caregivers, particularly trainees, rarely encounter deaths and can benefit from debriefing sessions, even short ones. There is comfort in having a colleague review the situation and say: “There was nothing you could have done.” Or even: “That minor omission did not alter the outcome.” Even when everything was done properly, deaths cause moral suffering that needs processing and healing. Even if you don’t have magic words to give, just being present aids in the healing. We are all in this, together.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
COVID-19 has prompted many changes in pediatric health care. They say necessity is the mother of invention. Sometimes, necessity is the motivator for the long-past-due adoption of a previous invention, such as telemedicine for minor illnesses. And sometimes necessity reminds us about what is really important in a world of high technology.
Unlike our nearly overwhelmed internal medicine, ED, and family physician colleagues, many pediatricians are in a lull that threatens the financial viability of our practices. We are postponing annual well visits. We have fewer sick visits and hospitalizations since respiratory syncytial virus (RSV) and influenza also have been reduced by social distancing. Parents are avoiding the risk of contagion in the waiting room and not bringing their children in for minor complaints. There is more telemedicine – a welcome change in financing and practice whose time has come, but was being delayed by lack of insurance coverage.
Technology has allowed clinicians to respond to the pandemic in ways that would not have been possible a few years ago. Online tools, such as subscription email lists, webinars, and electronic medical news services, provide updates when the information changes weekly on the virus’s contagiousness, asymptomatic and presymptomatic transmission, prevalence, the effectiveness of masks, and experimental treatment options. These changes have been so fast that many journal articles based on data from China were obsolete and contradicted before they appeared in print.
However, technology only helped us to more effectively do what we needed to do in the first place – come together in a world of physical distancing and work toward common goals. In many hospitals, pediatric wards were emptied by reduced RSV admissions and postponed elective surgeries. These units have been converted to accept adult patients up to age 30 or 40 years. Our med-peds colleagues quickly created webinars and online resource packages on topics pediatric hospitalists might need to care for that population. There were refresher courses on ventilator management and reminders that community pediatric hospitalists, who in the winter might have one-third of their admissions with RSV, have more experience managing viral pneumonia than the internists.
Ward teams were created with a pediatric attending and an internal medicine resident. The resident’s familiarity with the names of blood pressure medicines complemented the attending’s years of clinical judgment and bedside manner. People are stepping out of their comfort zones but initial reports from the front lines are that, with each other’s support, we’ve got this.
Mistakes in telemedicine are being made, shared, and learned from. Emergency physicians are collecting anecdotes of situations when things were missed or treatment delayed. Surgeons report seeing increased numbers of cases in which the diagnosis of appendicitis was delayed, which isn’t surprising when a pediatrician cannot lay hands on the belly. Perhaps any case in which a parent calls a second or third time should be seen in the flesh.
Some newborn nurseries are discharging mother and baby at 24 hours after birth and rediscovering what was learned about that practice, which became common in the 1990s. It works well for the vast majority of babies, but we need to be ready to detect the occasional jaundiced baby or the one where breastfeeding isn’t going well. The gray-haired pediatricians can recall those nuances.
Another key role is to help everyone process the frequent deaths during a pandemic. First, there are the families we care for. Children are losing grandparents with little warning. Parents may be overwhelmed with grief while ill themselves. That makes children vulnerable.
Our medical system in 2 months has moved heaven and earth – and significantly harmed the medical care and financial future of our children – trying to assure that every 80-year-old has the right to die while attached to a ventilator, even though only a small fraction of them will survive to discharge. Meanwhile, on the wards, visitation policies have people deteriorating and dying alone. I find this paradigm distressing and antithetical to my training.
Medicine and nursing both have long histories in which the practitioner recognized that there was little they could do to prevent the death. Their role was to compassionately guide the family through it. For some people, this connection is the most precious of the arts of medicine and nursing. We need to reexamine our values. We need to get creative. We need to involve palliative care experts and clergy with the same urgency with which we have automakers making ventilators.
Second, there are our colleagues. Pediatric caregivers, particularly trainees, rarely encounter deaths and can benefit from debriefing sessions, even short ones. There is comfort in having a colleague review the situation and say: “There was nothing you could have done.” Or even: “That minor omission did not alter the outcome.” Even when everything was done properly, deaths cause moral suffering that needs processing and healing. Even if you don’t have magic words to give, just being present aids in the healing. We are all in this, together.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
Cancer patients report delays in treatment because of COVID-19
As the COVID-19 pandemic continues, many cancer patients are finding it increasingly difficult to receive the care they need and are facing financial challenges.
Half of the cancer patients and survivors who responded to a recent survey reported changes, delays, or disruptions to the care they were receiving. The survey, with 1,219 respondents, was conducted by the American Cancer Society Cancer Action Network (ACS CAN).
“The circumstances of this virus – from the fact cancer patients are at higher risk of severe complications should they be diagnosed with COVID-19, to the fact many patients are facing serious financial strain caused by the virus’ economic effect – make getting care especially difficult,” Keysha Brooks-Coley, vice president of federal advocacy for ACS CAN, told Medscape Medical News.
Nearly a quarter (24%) of survey respondents reported a delay in care or treatment. The proportion was slightly more (27%) among those currently receiving active treatment.
In addition, 12% (13% in active treatment) stated that not only was their care delayed but that they also have not been told when services would be rescheduled.
As previously reported by Medscape Medical News, many oncology groups have issued new guidelines for cancer care in reaction to the current crisis. These include recommendations to delay cancer treatment in order to avoid exposing cancer patients to the virus.
Half of those in active treatment report disruptions
The survey was initiated by ACS CAN on March 25 and was distributed over a 2-week period. The goal was to gain a better understanding of how COVID-19 was affecting cancer patients and survivors in the United States. Of the 1,219 respondents, half (51%) were cancer patients currently undergoing active treatment.
Among the patients and survivors who were currently in active treatment, 55% reported that there have been changes, delays, or disruptions in their care. The services most frequently affected included in-person provider visits (50%), supportive services (20%), and imaging procedures to monitor tumor growth (20%).
In addition, 8% reported that their treatment, including chemotherapy and immunotherapy, had been affected by the COVID-19 pandemic.
Financial concerns
Almost all of the survey respondents were covered by some type of insurance; 49% had coverage through an employer, 32% were covered by Medicare, 7% had privately purchased insurance, and 4% were covered through Medicaid.
Many cancer patients had already been having difficulty paying for their care, but for a substantial proportion of survey respondents, the COVID-19 pandemic has exacerbated the problem. More than one-third (38%) stated that COVID-19 “has had a notable impact on their financial situation that affects their ability to pay for health care.”
The most common financial problems that were related to access to care include reduced work hours (14%), reduced investment values (11%), having difficulty affording food and supplies because of staying at home to avoid contracting the virus (9%), and becoming unemployed (8%).
A reduction in work hours and job loss were of particular concern to respondents because of the possible effects these would have on their health insurance coverage. Of those who reported that they or a family member living with them had lost a job, 43% had employer-sponsored health insurance. Additionally, 58% of patients or a family member whose working hours had been reduced also had health insurance through their employer
Among the entire cohort, 28% reported that they were worried that the financial impact of COVID-19 would make it difficult to pay for the health care they need as cancer survivors. This concern was highly correlated with income. Almost half (46%) of patients who earned $30,000 or less reported that they were worried, but even in household with incomes over $110,000 per year, 21% were also concerned about the financial impact.
“Now more than ever, patients need to be able to get, keep, and afford health coverage to treat their disease,” commented Brooks-Coley.
Taking action
“ACS CAN is working every day to make clear to Congress and the administration the real and immediate challenges cancer patients and survivors face during this pandemic,” said Brooks-Coley.
With nearly 50 other professional and advocacy groups, ACS CAN has sent letters to congressional leadership and the Secretary of the Department of Health & Human Services asking them to make policy changes that would help patients.
The proposed action points include having insurers allow patients to use providers who are out of network if necessary; waiving site-specific precertification and prior authorization for cancer treatment; utilizing shared decision making between patients and providers in deciding whether to use home infusion without pressure from the insurer; allowing patients to obtain 90-day supplies of medication; increasing funding for state Medicaid programs and assistance for those who have lost employee-sponsored coverage; and improving telehealth services.
“We urge Congress and the administration to keep the needs of cancer patients and survivors in mind as they continue to address the public health crisis,” she said.
This article first appeared on Medscape.com.
As the COVID-19 pandemic continues, many cancer patients are finding it increasingly difficult to receive the care they need and are facing financial challenges.
Half of the cancer patients and survivors who responded to a recent survey reported changes, delays, or disruptions to the care they were receiving. The survey, with 1,219 respondents, was conducted by the American Cancer Society Cancer Action Network (ACS CAN).
“The circumstances of this virus – from the fact cancer patients are at higher risk of severe complications should they be diagnosed with COVID-19, to the fact many patients are facing serious financial strain caused by the virus’ economic effect – make getting care especially difficult,” Keysha Brooks-Coley, vice president of federal advocacy for ACS CAN, told Medscape Medical News.
Nearly a quarter (24%) of survey respondents reported a delay in care or treatment. The proportion was slightly more (27%) among those currently receiving active treatment.
In addition, 12% (13% in active treatment) stated that not only was their care delayed but that they also have not been told when services would be rescheduled.
As previously reported by Medscape Medical News, many oncology groups have issued new guidelines for cancer care in reaction to the current crisis. These include recommendations to delay cancer treatment in order to avoid exposing cancer patients to the virus.
Half of those in active treatment report disruptions
The survey was initiated by ACS CAN on March 25 and was distributed over a 2-week period. The goal was to gain a better understanding of how COVID-19 was affecting cancer patients and survivors in the United States. Of the 1,219 respondents, half (51%) were cancer patients currently undergoing active treatment.
Among the patients and survivors who were currently in active treatment, 55% reported that there have been changes, delays, or disruptions in their care. The services most frequently affected included in-person provider visits (50%), supportive services (20%), and imaging procedures to monitor tumor growth (20%).
In addition, 8% reported that their treatment, including chemotherapy and immunotherapy, had been affected by the COVID-19 pandemic.
Financial concerns
Almost all of the survey respondents were covered by some type of insurance; 49% had coverage through an employer, 32% were covered by Medicare, 7% had privately purchased insurance, and 4% were covered through Medicaid.
Many cancer patients had already been having difficulty paying for their care, but for a substantial proportion of survey respondents, the COVID-19 pandemic has exacerbated the problem. More than one-third (38%) stated that COVID-19 “has had a notable impact on their financial situation that affects their ability to pay for health care.”
The most common financial problems that were related to access to care include reduced work hours (14%), reduced investment values (11%), having difficulty affording food and supplies because of staying at home to avoid contracting the virus (9%), and becoming unemployed (8%).
A reduction in work hours and job loss were of particular concern to respondents because of the possible effects these would have on their health insurance coverage. Of those who reported that they or a family member living with them had lost a job, 43% had employer-sponsored health insurance. Additionally, 58% of patients or a family member whose working hours had been reduced also had health insurance through their employer
Among the entire cohort, 28% reported that they were worried that the financial impact of COVID-19 would make it difficult to pay for the health care they need as cancer survivors. This concern was highly correlated with income. Almost half (46%) of patients who earned $30,000 or less reported that they were worried, but even in household with incomes over $110,000 per year, 21% were also concerned about the financial impact.
“Now more than ever, patients need to be able to get, keep, and afford health coverage to treat their disease,” commented Brooks-Coley.
Taking action
“ACS CAN is working every day to make clear to Congress and the administration the real and immediate challenges cancer patients and survivors face during this pandemic,” said Brooks-Coley.
With nearly 50 other professional and advocacy groups, ACS CAN has sent letters to congressional leadership and the Secretary of the Department of Health & Human Services asking them to make policy changes that would help patients.
The proposed action points include having insurers allow patients to use providers who are out of network if necessary; waiving site-specific precertification and prior authorization for cancer treatment; utilizing shared decision making between patients and providers in deciding whether to use home infusion without pressure from the insurer; allowing patients to obtain 90-day supplies of medication; increasing funding for state Medicaid programs and assistance for those who have lost employee-sponsored coverage; and improving telehealth services.
“We urge Congress and the administration to keep the needs of cancer patients and survivors in mind as they continue to address the public health crisis,” she said.
This article first appeared on Medscape.com.
As the COVID-19 pandemic continues, many cancer patients are finding it increasingly difficult to receive the care they need and are facing financial challenges.
Half of the cancer patients and survivors who responded to a recent survey reported changes, delays, or disruptions to the care they were receiving. The survey, with 1,219 respondents, was conducted by the American Cancer Society Cancer Action Network (ACS CAN).
“The circumstances of this virus – from the fact cancer patients are at higher risk of severe complications should they be diagnosed with COVID-19, to the fact many patients are facing serious financial strain caused by the virus’ economic effect – make getting care especially difficult,” Keysha Brooks-Coley, vice president of federal advocacy for ACS CAN, told Medscape Medical News.
Nearly a quarter (24%) of survey respondents reported a delay in care or treatment. The proportion was slightly more (27%) among those currently receiving active treatment.
In addition, 12% (13% in active treatment) stated that not only was their care delayed but that they also have not been told when services would be rescheduled.
As previously reported by Medscape Medical News, many oncology groups have issued new guidelines for cancer care in reaction to the current crisis. These include recommendations to delay cancer treatment in order to avoid exposing cancer patients to the virus.
Half of those in active treatment report disruptions
The survey was initiated by ACS CAN on March 25 and was distributed over a 2-week period. The goal was to gain a better understanding of how COVID-19 was affecting cancer patients and survivors in the United States. Of the 1,219 respondents, half (51%) were cancer patients currently undergoing active treatment.
Among the patients and survivors who were currently in active treatment, 55% reported that there have been changes, delays, or disruptions in their care. The services most frequently affected included in-person provider visits (50%), supportive services (20%), and imaging procedures to monitor tumor growth (20%).
In addition, 8% reported that their treatment, including chemotherapy and immunotherapy, had been affected by the COVID-19 pandemic.
Financial concerns
Almost all of the survey respondents were covered by some type of insurance; 49% had coverage through an employer, 32% were covered by Medicare, 7% had privately purchased insurance, and 4% were covered through Medicaid.
Many cancer patients had already been having difficulty paying for their care, but for a substantial proportion of survey respondents, the COVID-19 pandemic has exacerbated the problem. More than one-third (38%) stated that COVID-19 “has had a notable impact on their financial situation that affects their ability to pay for health care.”
The most common financial problems that were related to access to care include reduced work hours (14%), reduced investment values (11%), having difficulty affording food and supplies because of staying at home to avoid contracting the virus (9%), and becoming unemployed (8%).
A reduction in work hours and job loss were of particular concern to respondents because of the possible effects these would have on their health insurance coverage. Of those who reported that they or a family member living with them had lost a job, 43% had employer-sponsored health insurance. Additionally, 58% of patients or a family member whose working hours had been reduced also had health insurance through their employer
Among the entire cohort, 28% reported that they were worried that the financial impact of COVID-19 would make it difficult to pay for the health care they need as cancer survivors. This concern was highly correlated with income. Almost half (46%) of patients who earned $30,000 or less reported that they were worried, but even in household with incomes over $110,000 per year, 21% were also concerned about the financial impact.
“Now more than ever, patients need to be able to get, keep, and afford health coverage to treat their disease,” commented Brooks-Coley.
Taking action
“ACS CAN is working every day to make clear to Congress and the administration the real and immediate challenges cancer patients and survivors face during this pandemic,” said Brooks-Coley.
With nearly 50 other professional and advocacy groups, ACS CAN has sent letters to congressional leadership and the Secretary of the Department of Health & Human Services asking them to make policy changes that would help patients.
The proposed action points include having insurers allow patients to use providers who are out of network if necessary; waiving site-specific precertification and prior authorization for cancer treatment; utilizing shared decision making between patients and providers in deciding whether to use home infusion without pressure from the insurer; allowing patients to obtain 90-day supplies of medication; increasing funding for state Medicaid programs and assistance for those who have lost employee-sponsored coverage; and improving telehealth services.
“We urge Congress and the administration to keep the needs of cancer patients and survivors in mind as they continue to address the public health crisis,” she said.
This article first appeared on Medscape.com.
Tuberous Sclerosis With Segmental Overgrowth
To the Editor:
A 3-year-old boy with a history of tuberous sclerosis presented to our clinic for evaluation of bumps on the second and third fingers of the left hand. Physical examination revealed firm rubbery nodules on the palmar third metacarpophalangeal joint extending to the palm and the lateral aspect of the distal third dorsal finger. There also was asymmetric overgrowth of the left second and third digits consistent with bony segmental overgrowth (Figure).
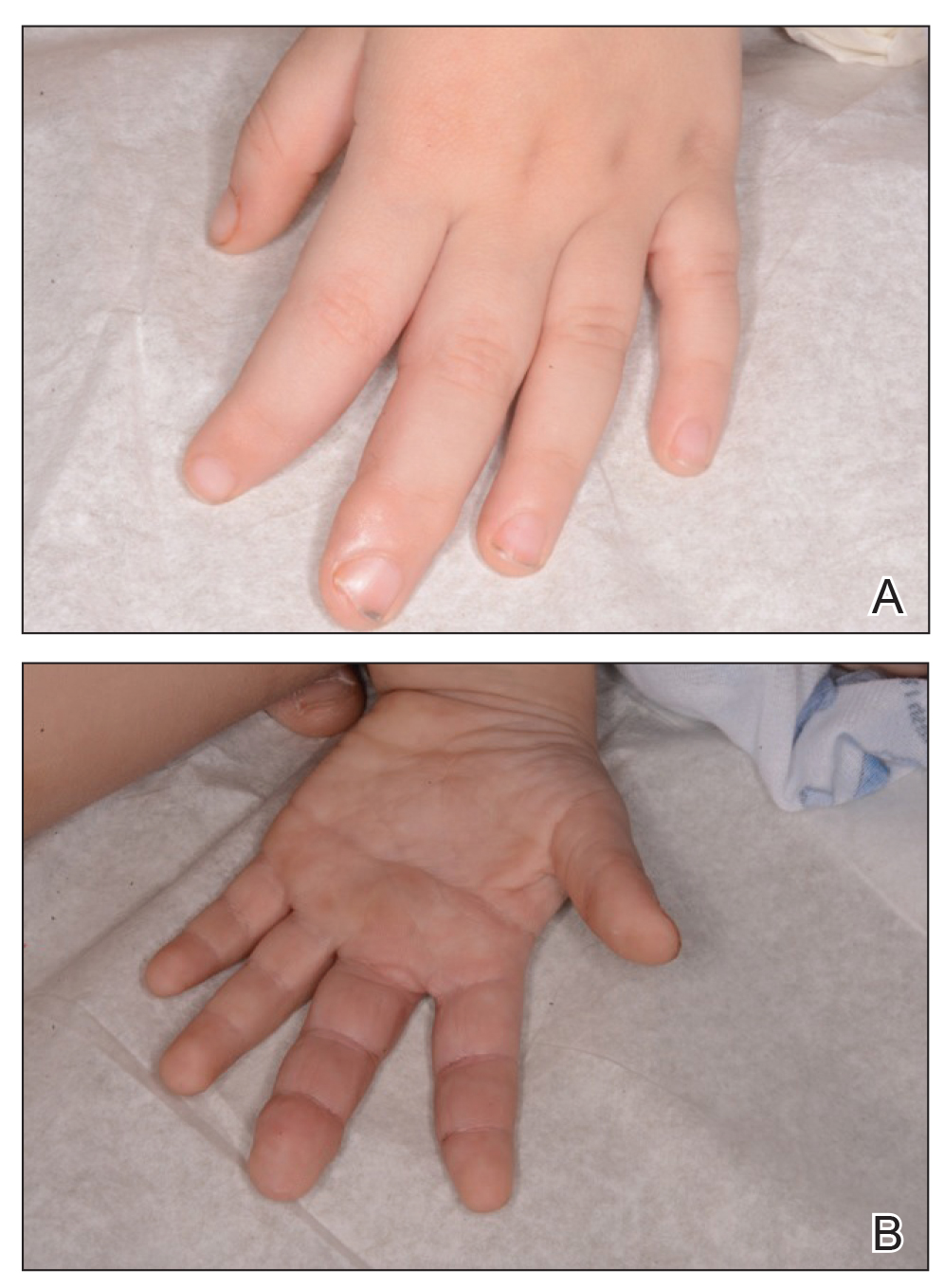
Tuberous sclerosis and overgrowth syndromes including Proteus syndrome have mutations that share a common pathway, namely the PI3K/AKT/mTOR (phosphoinositide 3-kinase/alpha serine/threonine-protein kinase/mammalian target of rapamycin) pathway.1 The mutations in tuberous sclerosis involve the loss of TSC1 (TSC complex subunit 1) on chromosome 9 or TSC2 (TSC complex subunit 2) on chromosome 16.2 The protein products of these genes, hamartin and tuberin, act together as a tumor suppressor complex.3 The inheritance pattern of tuberous sclerosis is autosomal dominant, though two-thirds of cases are due to de novo germline mutations.4 The second copy of the gene must be lost spontaneously in any particular cell for the deleterious effects of the disease to manifest. The mutation in overgrowth syndromes including Proteus syndrome involves the activation of AKT1 (AKT serine/threonine kinase 1) on chromosome 14. This mutation occurs in somatic cells as opposed to germ cells, as in tuberous sclerosis. This difference accounts for the mosaic expression of segmental overgrowth syndromes. This concept has been demonstrated in overgrowth syndromes such as Proteus syndrome, with cells from unaffected areas having different genetic makeup than those from affected tissues.5 These mutations, though different, result in the downstream effects of unchecked messenger RNA translation and dysregulated cellular growth.
In our patient, we hypothesized that a small proportion of his postfertilization somatic cells underwent a second de novo mutation in the AKT1 pathway, resulting in the bony overgrowth seen on the left hand. We suspected that this second mutation could be an activation of AKT1, the mutation seen in Proteus syndrome. Sequencing of the tissue may be performed in the future, especially if segmental overgrowth continues and necessitates therapy.
- Wu Y, Zhou BP. Kinases meet at TSC. Cell Res. 2007;17:971-973.
- Roach SE, Sparagana SP. Diagnosis of tuberous sclerosis complex. J Child Neurol. 2004;19:643-649.
- Barker KT, Houlston RS. Overgrowth syndromes: is dysfunctional PI3-kinase signaling a unifying mechanism? Eur J Hum Genet. 2003;11:665-670.
- Nothrup H, Koenig MK, Au KS. Tuberous sclerosis complex. GeneReviews. Seattle, WA: University of Washington; 1999.
- Lindhurst MJ, Parker VE, Payne F, et al. Mosaic overgrowth with fibroadipose hyperplasia is caused by somatic activating mutations in PIK3CA. Nat Genet. 2012;44:928-933.
To the Editor:
A 3-year-old boy with a history of tuberous sclerosis presented to our clinic for evaluation of bumps on the second and third fingers of the left hand. Physical examination revealed firm rubbery nodules on the palmar third metacarpophalangeal joint extending to the palm and the lateral aspect of the distal third dorsal finger. There also was asymmetric overgrowth of the left second and third digits consistent with bony segmental overgrowth (Figure).
Tuberous sclerosis and overgrowth syndromes including Proteus syndrome have mutations that share a common pathway, namely the PI3K/AKT/mTOR (phosphoinositide 3-kinase/alpha serine/threonine-protein kinase/mammalian target of rapamycin) pathway.1 The mutations in tuberous sclerosis involve the loss of TSC1 (TSC complex subunit 1) on chromosome 9 or TSC2 (TSC complex subunit 2) on chromosome 16.2 The protein products of these genes, hamartin and tuberin, act together as a tumor suppressor complex.3 The inheritance pattern of tuberous sclerosis is autosomal dominant, though two-thirds of cases are due to de novo germline mutations.4 The second copy of the gene must be lost spontaneously in any particular cell for the deleterious effects of the disease to manifest. The mutation in overgrowth syndromes including Proteus syndrome involves the activation of AKT1 (AKT serine/threonine kinase 1) on chromosome 14. This mutation occurs in somatic cells as opposed to germ cells, as in tuberous sclerosis. This difference accounts for the mosaic expression of segmental overgrowth syndromes. This concept has been demonstrated in overgrowth syndromes such as Proteus syndrome, with cells from unaffected areas having different genetic makeup than those from affected tissues.5 These mutations, though different, result in the downstream effects of unchecked messenger RNA translation and dysregulated cellular growth.
In our patient, we hypothesized that a small proportion of his postfertilization somatic cells underwent a second de novo mutation in the AKT1 pathway, resulting in the bony overgrowth seen on the left hand. We suspected that this second mutation could be an activation of AKT1, the mutation seen in Proteus syndrome. Sequencing of the tissue may be performed in the future, especially if segmental overgrowth continues and necessitates therapy.
To the Editor:
A 3-year-old boy with a history of tuberous sclerosis presented to our clinic for evaluation of bumps on the second and third fingers of the left hand. Physical examination revealed firm rubbery nodules on the palmar third metacarpophalangeal joint extending to the palm and the lateral aspect of the distal third dorsal finger. There also was asymmetric overgrowth of the left second and third digits consistent with bony segmental overgrowth (Figure).
Tuberous sclerosis and overgrowth syndromes including Proteus syndrome have mutations that share a common pathway, namely the PI3K/AKT/mTOR (phosphoinositide 3-kinase/alpha serine/threonine-protein kinase/mammalian target of rapamycin) pathway.1 The mutations in tuberous sclerosis involve the loss of TSC1 (TSC complex subunit 1) on chromosome 9 or TSC2 (TSC complex subunit 2) on chromosome 16.2 The protein products of these genes, hamartin and tuberin, act together as a tumor suppressor complex.3 The inheritance pattern of tuberous sclerosis is autosomal dominant, though two-thirds of cases are due to de novo germline mutations.4 The second copy of the gene must be lost spontaneously in any particular cell for the deleterious effects of the disease to manifest. The mutation in overgrowth syndromes including Proteus syndrome involves the activation of AKT1 (AKT serine/threonine kinase 1) on chromosome 14. This mutation occurs in somatic cells as opposed to germ cells, as in tuberous sclerosis. This difference accounts for the mosaic expression of segmental overgrowth syndromes. This concept has been demonstrated in overgrowth syndromes such as Proteus syndrome, with cells from unaffected areas having different genetic makeup than those from affected tissues.5 These mutations, though different, result in the downstream effects of unchecked messenger RNA translation and dysregulated cellular growth.
In our patient, we hypothesized that a small proportion of his postfertilization somatic cells underwent a second de novo mutation in the AKT1 pathway, resulting in the bony overgrowth seen on the left hand. We suspected that this second mutation could be an activation of AKT1, the mutation seen in Proteus syndrome. Sequencing of the tissue may be performed in the future, especially if segmental overgrowth continues and necessitates therapy.
- Wu Y, Zhou BP. Kinases meet at TSC. Cell Res. 2007;17:971-973.
- Roach SE, Sparagana SP. Diagnosis of tuberous sclerosis complex. J Child Neurol. 2004;19:643-649.
- Barker KT, Houlston RS. Overgrowth syndromes: is dysfunctional PI3-kinase signaling a unifying mechanism? Eur J Hum Genet. 2003;11:665-670.
- Nothrup H, Koenig MK, Au KS. Tuberous sclerosis complex. GeneReviews. Seattle, WA: University of Washington; 1999.
- Lindhurst MJ, Parker VE, Payne F, et al. Mosaic overgrowth with fibroadipose hyperplasia is caused by somatic activating mutations in PIK3CA. Nat Genet. 2012;44:928-933.
- Wu Y, Zhou BP. Kinases meet at TSC. Cell Res. 2007;17:971-973.
- Roach SE, Sparagana SP. Diagnosis of tuberous sclerosis complex. J Child Neurol. 2004;19:643-649.
- Barker KT, Houlston RS. Overgrowth syndromes: is dysfunctional PI3-kinase signaling a unifying mechanism? Eur J Hum Genet. 2003;11:665-670.
- Nothrup H, Koenig MK, Au KS. Tuberous sclerosis complex. GeneReviews. Seattle, WA: University of Washington; 1999.
- Lindhurst MJ, Parker VE, Payne F, et al. Mosaic overgrowth with fibroadipose hyperplasia is caused by somatic activating mutations in PIK3CA. Nat Genet. 2012;44:928-933.
Practice Points
- Tuberous sclerosis and Proteus syndrome share a common downstream effector pathway.
- For a patient to demonstrate features of both tuberous sclerosis and Proteus syndrome, he/she must have both a germline mutation (for tuberous sclerosis) as well as a postzygotic mutation (for Proteus syndrome) of this shared pathway.
