User login
Newborn with desquamating rash
A 9-day-old boy was brought to the emergency department by his mother. The infant had been doing well until his most recent diaper change when his mother noticed a rash around the umbilicus (FIGURE), genitalia, and anus.
The infant was born at term via spontaneous vaginal delivery. The pregnancy was uncomplicated; the infant’s mother was group B strep negative. Following a routine postpartum course, the infant underwent an elective circumcision before hospital discharge on his second day of life. There were no interval reports of irritability, poor feeding, fevers, vomiting, or changes in urine or stool output.
The mother denied any recent unusual exposures, sick contacts, or travel. However, upon further questioning, the mother noted that she herself had several small open wounds on the torso that she attributed to untreated methicillin-resistant Staphylococcus aureus (MRSA).
On physical examination, the infant was overall well-appearing and was breastfeeding vigorously without respiratory distress or cyanosis. He was afebrile with normal vital signs. The majority of the physical examination was normal; however, there was erythematous desquamation around the umbilical stump and genitalia with no vesicles noted. The umbilical stump had a small amount of purulent drainage and necrosis centrally. The infant had a 1-cm round, peeling lesion on the left temple (FIGURE) with a small amount of dried serosanguinous drainage and similar superficial peeling lesions at the left preauricular area and anterior chest. There was no underlying fluctuance and only minimal surrounding erythema.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Staphylococcal scalded skin syndrome
Based on the age of the patient, clinical presentation, and suspected maternal MRSA infection (with possible transmission to the infant), we diagnosed staphylococcal scalded skin syndrome (SSSS) in this patient. SSSS is rare, with annual incidence of 45 cases per million US infants under the age of 2.1 Newborns with a generalized form of SSSS commonly present with fever, poor feeding, irritability, and lethargy. This is followed by a generalized erythematous rash that initially may appear on the head and neck and spread to the rest of the body. Large, fragile blisters subsequently appear. These blisters rupture on gentle pressure, which is known as a positive Nikolsky sign. Ultimately, large sheets of skin easily slough off, leaving raw, denuded skin.2
S aureus is not part of normal skin flora, yet it is found on the skin and mucous membranes of 19% to 55% of healthy adults and children.3S aureus can cause a wide range of infections ranging from abscesses to cellulitis; SSSS is caused by hematogenous spread of S aureus exfoliative toxin. Newborns and immunocompromised patients are particularly susceptible.
Neonatal patients with SSSS most commonly present at 3 to 16 days of age.2 The lack of antitoxin antibody in neonates allows the toxin to reach the epidermis where it acts locally to produce the characteristic fragile skin lesions that often rupture prior to clinical presentation.2,4 During progression of the disease, flaky skin desquamation will occur as the lesions heal.
A retrospective review of 39 cases of SSSS identified pneumonia as the most frequent complication, occurring in 74.4% of the cases.5 The mortality rate of SSSS is up to 5%, and is associated with sepsis, superinfection, electrolyte imbalances, and extensive skin involvement.2,6
If SSSS is suspected, obtain cultures from the blood, urine, eyes, nose, throat, and skin lesions to identify the primary focus of infection.7 However, the retrospective review of 39 cases (noted above) found a positive rate of S aureus isolation of only 23.5%.5 Physicians will often have to make a diagnosis based on clinical presentation and empirically initiate broad-spectrum antibiotics while considering alternative diagnoses.
Continue to: A clinical diagnosis with a large differential
A clinical diagnosis with a large differential
While biopsy rarely is required, it may be helpful to distinguish SSSS from other entities in the differential diagnosis (TABLE2,3,7-13).

Toxic epidermal necrolysis (TEN) is a rare and life-threatening desquamating disease nearly always caused by a reaction to medications, including antibiotics. TEN can occur at any age. Fever, diffuse erythema, and extensive epidermal involvement (>30% of skin) differentiate TEN from Stevens-Johnson syndrome (SJS), which affects less than 10% of the epidermis. It is worth mentioning that TEN and SJS are now considered to be a spectrum of one disease, and an overlap syndrome has been described with 10% to 30% of skin affected.8 Diagnosis is made clinically, although skin biopsy routinely is performed.7,9
Congenital syphilis features a red or pink maculopapular rash followed by desquamation. Lesions are more common on the soles.10 Desquamation or ulcerative skin lesions should be examined for spirochetes.11 A quantitative, nontreponemal test such as the rapid plasma reagin (RPR) or the Venereal Disease Research Laboratory (VDRL) will be positive in most infants if exposed through the placenta, but antibodies will disappear in uninfected infants by 6 months of age.8
Congenital cutaneous candidiasis presents with a generalized eruption of erythematous macules, papules, and/or pustules with widespread desquamating and/or erosive dermatitis. Premature neonates with extremely low birth weight are at higher risk.13 Diagnosis is confirmed on microscopy by the presence of Candida albicans spores in skin scrapings.13
Neonatal herpes simplex virus (HSV) symptoms typically appear between 1 and 3 weeks of life, with 60% to 70% of cases presenting with classic clustering vesicles on an erythematous base.14 Diagnosis is made with HSV viral culture or polymerase chain reaction (PCR).
Continue to: SSSS should be considered a pediatrics emergency
SSSS should be considered a pediatric emergency
SSSS should be considered a pediatric emergency due to potential complications. Core measures of SSSS treatment include immediate administration of intravenous (IV) antibiotics. US population studies suggest clindamycin and penicillinase-resistant penicillin as empiric therapy.15 However, local strains and resistance patterns, including the prevalence of MRSA, as well as age, comorbidities, and severity of illness should influence antibiotic selection.
IV nafcillin or oxacillin may be used with pediatric dosing of 150 mg/kg daily divided every 6 hours for methicillin-sensitive Staphylococcus aureus (MSSA). For suspected MRSA, IV vancomycin should be considered, with an infant dose of 40 to 60 mg/kg daily divided every 6 hours.16 Fluid, electrolyte, and nutritional management should be addressed immediately. Ongoing fluid losses due to exfoliated skin must be replaced, and skin care to desquamated areas also should be addressed urgently.
Our patient. Phone consultation with an infectious disease specialist at a local children’s hospital resulted in a recommendation to treat for sepsis empirically with IV vancomycin, cefotaxime, and acyclovir. Acyclovir was discontinued once the HSV PCR came back negative. The antibiotic coverage was narrowed to IV ampicillin 50 mg/kg every 8 hours when cerebrospinal fluid and blood cultures returned negative at 48 hours, wound culture sensitivity grew MSSA, and the patient’s clinical condition stabilized. Our patient received 10 days of IV antibiotics and was discharged on oral amoxicillin 50 mg/kg divided twice daily for a total of 14 days of treatment per recommendations by the infectious disease specialist. Our patient fully recovered without any residual skin findings after completion of the antibiotic course.
CORRESPONDENCE
Jennifer J. Walker, MD, MPH, Hawaii Island Family Health Center at Hilo Medical Center, 1190 Waianuenue Ave, Hilo, HI 96720; [email protected]
1. Staiman A, Hsu D, Silverberg JI. Epidemiology of staphylococcal scalded skin syndrome in US children. Br J Dermatol. 2018;178:704-708.
2. Ladhani S, Joannou CL, Lochrie DP, et al. Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. Clin Microbiol Rev. 1999;12:224-242.
3. Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clin Microbiol Rev. 1997;10:505-520.
4. Ladhani S. Understanding the mechanism of action of the exfoliative toxins of Staphylococcus aureus. FEMS Immunol Med Microbiol. 2003;39:181-189.
5. Li MY, Hua Y, Wei GH, et al. Staphylococcal scalded skin syndrome in neonates: an 8-year retrospective study in a single institution. Pediatr Dermatol. 2014;31:43-47.
6. Berk DR, Bayliss SJ. MRSA, staphylococcal scalded skin syndrome, and other cutaneous bacterial emergencies. Pediatr Ann. 2010;39:627-633.
7. Ely JW, Seabury Stone M. The generalized rash: part I. differential diagnosis. Am Fam Physician. 2010;81:726-734.
8. Bastuji-Garin SB, Stern RS, Shear NH, et al. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129:92.
9. Elias PM, Fritsch P, Epstein EH. Staphylococcal scalded skin syndrome. clinical features, pathogenesis, and recent microbiological and biochemical developments. Arch Dermatol. 1977;113:207-219.
10. O’Connor NR, McLaughlin M, Ham P. Newborn skin: part I: common rashes. Am Fam Physician. 2008;77:47-52.
11. Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8:1-21.
12. Arnold SR, Ford-Jones EL. Congenital syphilis: a guide to diagnosis and management. Paediatr Child Health. 2000;5:463-469.
13. Darmstadt GL, Dinulos JG, Miller Z. Congenital cutaneous candidiasis: clinical presentation, pathogenesis, and management guidelines. Pediatrics. 2000;105:438-444.
14. Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev. 2004;17:1-13.
15. Braunstein I, Wanat KA, Abuabara K, et al. Antibiotic sensitivity and resistance patterns in pediatric staphylococcal scalded skin syndrome. Pediatr Dermatol. 2014;31:305-308.
16. Gilbert DN, Chambers HF, Eliopoulos GM, et al. The Sanford Guide to Antimicrobial Therapy. 48th ed. Sperryville, VA: Antimicrobial Therapy, Inc; 2014:56.
A 9-day-old boy was brought to the emergency department by his mother. The infant had been doing well until his most recent diaper change when his mother noticed a rash around the umbilicus (FIGURE), genitalia, and anus.
The infant was born at term via spontaneous vaginal delivery. The pregnancy was uncomplicated; the infant’s mother was group B strep negative. Following a routine postpartum course, the infant underwent an elective circumcision before hospital discharge on his second day of life. There were no interval reports of irritability, poor feeding, fevers, vomiting, or changes in urine or stool output.
The mother denied any recent unusual exposures, sick contacts, or travel. However, upon further questioning, the mother noted that she herself had several small open wounds on the torso that she attributed to untreated methicillin-resistant Staphylococcus aureus (MRSA).
On physical examination, the infant was overall well-appearing and was breastfeeding vigorously without respiratory distress or cyanosis. He was afebrile with normal vital signs. The majority of the physical examination was normal; however, there was erythematous desquamation around the umbilical stump and genitalia with no vesicles noted. The umbilical stump had a small amount of purulent drainage and necrosis centrally. The infant had a 1-cm round, peeling lesion on the left temple (FIGURE) with a small amount of dried serosanguinous drainage and similar superficial peeling lesions at the left preauricular area and anterior chest. There was no underlying fluctuance and only minimal surrounding erythema.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Staphylococcal scalded skin syndrome
Based on the age of the patient, clinical presentation, and suspected maternal MRSA infection (with possible transmission to the infant), we diagnosed staphylococcal scalded skin syndrome (SSSS) in this patient. SSSS is rare, with annual incidence of 45 cases per million US infants under the age of 2.1 Newborns with a generalized form of SSSS commonly present with fever, poor feeding, irritability, and lethargy. This is followed by a generalized erythematous rash that initially may appear on the head and neck and spread to the rest of the body. Large, fragile blisters subsequently appear. These blisters rupture on gentle pressure, which is known as a positive Nikolsky sign. Ultimately, large sheets of skin easily slough off, leaving raw, denuded skin.2
S aureus is not part of normal skin flora, yet it is found on the skin and mucous membranes of 19% to 55% of healthy adults and children.3S aureus can cause a wide range of infections ranging from abscesses to cellulitis; SSSS is caused by hematogenous spread of S aureus exfoliative toxin. Newborns and immunocompromised patients are particularly susceptible.
Neonatal patients with SSSS most commonly present at 3 to 16 days of age.2 The lack of antitoxin antibody in neonates allows the toxin to reach the epidermis where it acts locally to produce the characteristic fragile skin lesions that often rupture prior to clinical presentation.2,4 During progression of the disease, flaky skin desquamation will occur as the lesions heal.
A retrospective review of 39 cases of SSSS identified pneumonia as the most frequent complication, occurring in 74.4% of the cases.5 The mortality rate of SSSS is up to 5%, and is associated with sepsis, superinfection, electrolyte imbalances, and extensive skin involvement.2,6
If SSSS is suspected, obtain cultures from the blood, urine, eyes, nose, throat, and skin lesions to identify the primary focus of infection.7 However, the retrospective review of 39 cases (noted above) found a positive rate of S aureus isolation of only 23.5%.5 Physicians will often have to make a diagnosis based on clinical presentation and empirically initiate broad-spectrum antibiotics while considering alternative diagnoses.
Continue to: A clinical diagnosis with a large differential
A clinical diagnosis with a large differential
While biopsy rarely is required, it may be helpful to distinguish SSSS from other entities in the differential diagnosis (TABLE2,3,7-13).
Toxic epidermal necrolysis (TEN) is a rare and life-threatening desquamating disease nearly always caused by a reaction to medications, including antibiotics. TEN can occur at any age. Fever, diffuse erythema, and extensive epidermal involvement (>30% of skin) differentiate TEN from Stevens-Johnson syndrome (SJS), which affects less than 10% of the epidermis. It is worth mentioning that TEN and SJS are now considered to be a spectrum of one disease, and an overlap syndrome has been described with 10% to 30% of skin affected.8 Diagnosis is made clinically, although skin biopsy routinely is performed.7,9
Congenital syphilis features a red or pink maculopapular rash followed by desquamation. Lesions are more common on the soles.10 Desquamation or ulcerative skin lesions should be examined for spirochetes.11 A quantitative, nontreponemal test such as the rapid plasma reagin (RPR) or the Venereal Disease Research Laboratory (VDRL) will be positive in most infants if exposed through the placenta, but antibodies will disappear in uninfected infants by 6 months of age.8
Congenital cutaneous candidiasis presents with a generalized eruption of erythematous macules, papules, and/or pustules with widespread desquamating and/or erosive dermatitis. Premature neonates with extremely low birth weight are at higher risk.13 Diagnosis is confirmed on microscopy by the presence of Candida albicans spores in skin scrapings.13
Neonatal herpes simplex virus (HSV) symptoms typically appear between 1 and 3 weeks of life, with 60% to 70% of cases presenting with classic clustering vesicles on an erythematous base.14 Diagnosis is made with HSV viral culture or polymerase chain reaction (PCR).
Continue to: SSSS should be considered a pediatrics emergency
SSSS should be considered a pediatric emergency
SSSS should be considered a pediatric emergency due to potential complications. Core measures of SSSS treatment include immediate administration of intravenous (IV) antibiotics. US population studies suggest clindamycin and penicillinase-resistant penicillin as empiric therapy.15 However, local strains and resistance patterns, including the prevalence of MRSA, as well as age, comorbidities, and severity of illness should influence antibiotic selection.
IV nafcillin or oxacillin may be used with pediatric dosing of 150 mg/kg daily divided every 6 hours for methicillin-sensitive Staphylococcus aureus (MSSA). For suspected MRSA, IV vancomycin should be considered, with an infant dose of 40 to 60 mg/kg daily divided every 6 hours.16 Fluid, electrolyte, and nutritional management should be addressed immediately. Ongoing fluid losses due to exfoliated skin must be replaced, and skin care to desquamated areas also should be addressed urgently.
Our patient. Phone consultation with an infectious disease specialist at a local children’s hospital resulted in a recommendation to treat for sepsis empirically with IV vancomycin, cefotaxime, and acyclovir. Acyclovir was discontinued once the HSV PCR came back negative. The antibiotic coverage was narrowed to IV ampicillin 50 mg/kg every 8 hours when cerebrospinal fluid and blood cultures returned negative at 48 hours, wound culture sensitivity grew MSSA, and the patient’s clinical condition stabilized. Our patient received 10 days of IV antibiotics and was discharged on oral amoxicillin 50 mg/kg divided twice daily for a total of 14 days of treatment per recommendations by the infectious disease specialist. Our patient fully recovered without any residual skin findings after completion of the antibiotic course.
CORRESPONDENCE
Jennifer J. Walker, MD, MPH, Hawaii Island Family Health Center at Hilo Medical Center, 1190 Waianuenue Ave, Hilo, HI 96720; [email protected]
A 9-day-old boy was brought to the emergency department by his mother. The infant had been doing well until his most recent diaper change when his mother noticed a rash around the umbilicus (FIGURE), genitalia, and anus.
The infant was born at term via spontaneous vaginal delivery. The pregnancy was uncomplicated; the infant’s mother was group B strep negative. Following a routine postpartum course, the infant underwent an elective circumcision before hospital discharge on his second day of life. There were no interval reports of irritability, poor feeding, fevers, vomiting, or changes in urine or stool output.
The mother denied any recent unusual exposures, sick contacts, or travel. However, upon further questioning, the mother noted that she herself had several small open wounds on the torso that she attributed to untreated methicillin-resistant Staphylococcus aureus (MRSA).
On physical examination, the infant was overall well-appearing and was breastfeeding vigorously without respiratory distress or cyanosis. He was afebrile with normal vital signs. The majority of the physical examination was normal; however, there was erythematous desquamation around the umbilical stump and genitalia with no vesicles noted. The umbilical stump had a small amount of purulent drainage and necrosis centrally. The infant had a 1-cm round, peeling lesion on the left temple (FIGURE) with a small amount of dried serosanguinous drainage and similar superficial peeling lesions at the left preauricular area and anterior chest. There was no underlying fluctuance and only minimal surrounding erythema.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Staphylococcal scalded skin syndrome
Based on the age of the patient, clinical presentation, and suspected maternal MRSA infection (with possible transmission to the infant), we diagnosed staphylococcal scalded skin syndrome (SSSS) in this patient. SSSS is rare, with annual incidence of 45 cases per million US infants under the age of 2.1 Newborns with a generalized form of SSSS commonly present with fever, poor feeding, irritability, and lethargy. This is followed by a generalized erythematous rash that initially may appear on the head and neck and spread to the rest of the body. Large, fragile blisters subsequently appear. These blisters rupture on gentle pressure, which is known as a positive Nikolsky sign. Ultimately, large sheets of skin easily slough off, leaving raw, denuded skin.2
S aureus is not part of normal skin flora, yet it is found on the skin and mucous membranes of 19% to 55% of healthy adults and children.3S aureus can cause a wide range of infections ranging from abscesses to cellulitis; SSSS is caused by hematogenous spread of S aureus exfoliative toxin. Newborns and immunocompromised patients are particularly susceptible.
Neonatal patients with SSSS most commonly present at 3 to 16 days of age.2 The lack of antitoxin antibody in neonates allows the toxin to reach the epidermis where it acts locally to produce the characteristic fragile skin lesions that often rupture prior to clinical presentation.2,4 During progression of the disease, flaky skin desquamation will occur as the lesions heal.
A retrospective review of 39 cases of SSSS identified pneumonia as the most frequent complication, occurring in 74.4% of the cases.5 The mortality rate of SSSS is up to 5%, and is associated with sepsis, superinfection, electrolyte imbalances, and extensive skin involvement.2,6
If SSSS is suspected, obtain cultures from the blood, urine, eyes, nose, throat, and skin lesions to identify the primary focus of infection.7 However, the retrospective review of 39 cases (noted above) found a positive rate of S aureus isolation of only 23.5%.5 Physicians will often have to make a diagnosis based on clinical presentation and empirically initiate broad-spectrum antibiotics while considering alternative diagnoses.
Continue to: A clinical diagnosis with a large differential
A clinical diagnosis with a large differential
While biopsy rarely is required, it may be helpful to distinguish SSSS from other entities in the differential diagnosis (TABLE2,3,7-13).
Toxic epidermal necrolysis (TEN) is a rare and life-threatening desquamating disease nearly always caused by a reaction to medications, including antibiotics. TEN can occur at any age. Fever, diffuse erythema, and extensive epidermal involvement (>30% of skin) differentiate TEN from Stevens-Johnson syndrome (SJS), which affects less than 10% of the epidermis. It is worth mentioning that TEN and SJS are now considered to be a spectrum of one disease, and an overlap syndrome has been described with 10% to 30% of skin affected.8 Diagnosis is made clinically, although skin biopsy routinely is performed.7,9
Congenital syphilis features a red or pink maculopapular rash followed by desquamation. Lesions are more common on the soles.10 Desquamation or ulcerative skin lesions should be examined for spirochetes.11 A quantitative, nontreponemal test such as the rapid plasma reagin (RPR) or the Venereal Disease Research Laboratory (VDRL) will be positive in most infants if exposed through the placenta, but antibodies will disappear in uninfected infants by 6 months of age.8
Congenital cutaneous candidiasis presents with a generalized eruption of erythematous macules, papules, and/or pustules with widespread desquamating and/or erosive dermatitis. Premature neonates with extremely low birth weight are at higher risk.13 Diagnosis is confirmed on microscopy by the presence of Candida albicans spores in skin scrapings.13
Neonatal herpes simplex virus (HSV) symptoms typically appear between 1 and 3 weeks of life, with 60% to 70% of cases presenting with classic clustering vesicles on an erythematous base.14 Diagnosis is made with HSV viral culture or polymerase chain reaction (PCR).
Continue to: SSSS should be considered a pediatrics emergency
SSSS should be considered a pediatric emergency
SSSS should be considered a pediatric emergency due to potential complications. Core measures of SSSS treatment include immediate administration of intravenous (IV) antibiotics. US population studies suggest clindamycin and penicillinase-resistant penicillin as empiric therapy.15 However, local strains and resistance patterns, including the prevalence of MRSA, as well as age, comorbidities, and severity of illness should influence antibiotic selection.
IV nafcillin or oxacillin may be used with pediatric dosing of 150 mg/kg daily divided every 6 hours for methicillin-sensitive Staphylococcus aureus (MSSA). For suspected MRSA, IV vancomycin should be considered, with an infant dose of 40 to 60 mg/kg daily divided every 6 hours.16 Fluid, electrolyte, and nutritional management should be addressed immediately. Ongoing fluid losses due to exfoliated skin must be replaced, and skin care to desquamated areas also should be addressed urgently.
Our patient. Phone consultation with an infectious disease specialist at a local children’s hospital resulted in a recommendation to treat for sepsis empirically with IV vancomycin, cefotaxime, and acyclovir. Acyclovir was discontinued once the HSV PCR came back negative. The antibiotic coverage was narrowed to IV ampicillin 50 mg/kg every 8 hours when cerebrospinal fluid and blood cultures returned negative at 48 hours, wound culture sensitivity grew MSSA, and the patient’s clinical condition stabilized. Our patient received 10 days of IV antibiotics and was discharged on oral amoxicillin 50 mg/kg divided twice daily for a total of 14 days of treatment per recommendations by the infectious disease specialist. Our patient fully recovered without any residual skin findings after completion of the antibiotic course.
CORRESPONDENCE
Jennifer J. Walker, MD, MPH, Hawaii Island Family Health Center at Hilo Medical Center, 1190 Waianuenue Ave, Hilo, HI 96720; [email protected]
1. Staiman A, Hsu D, Silverberg JI. Epidemiology of staphylococcal scalded skin syndrome in US children. Br J Dermatol. 2018;178:704-708.
2. Ladhani S, Joannou CL, Lochrie DP, et al. Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. Clin Microbiol Rev. 1999;12:224-242.
3. Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clin Microbiol Rev. 1997;10:505-520.
4. Ladhani S. Understanding the mechanism of action of the exfoliative toxins of Staphylococcus aureus. FEMS Immunol Med Microbiol. 2003;39:181-189.
5. Li MY, Hua Y, Wei GH, et al. Staphylococcal scalded skin syndrome in neonates: an 8-year retrospective study in a single institution. Pediatr Dermatol. 2014;31:43-47.
6. Berk DR, Bayliss SJ. MRSA, staphylococcal scalded skin syndrome, and other cutaneous bacterial emergencies. Pediatr Ann. 2010;39:627-633.
7. Ely JW, Seabury Stone M. The generalized rash: part I. differential diagnosis. Am Fam Physician. 2010;81:726-734.
8. Bastuji-Garin SB, Stern RS, Shear NH, et al. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129:92.
9. Elias PM, Fritsch P, Epstein EH. Staphylococcal scalded skin syndrome. clinical features, pathogenesis, and recent microbiological and biochemical developments. Arch Dermatol. 1977;113:207-219.
10. O’Connor NR, McLaughlin M, Ham P. Newborn skin: part I: common rashes. Am Fam Physician. 2008;77:47-52.
11. Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8:1-21.
12. Arnold SR, Ford-Jones EL. Congenital syphilis: a guide to diagnosis and management. Paediatr Child Health. 2000;5:463-469.
13. Darmstadt GL, Dinulos JG, Miller Z. Congenital cutaneous candidiasis: clinical presentation, pathogenesis, and management guidelines. Pediatrics. 2000;105:438-444.
14. Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev. 2004;17:1-13.
15. Braunstein I, Wanat KA, Abuabara K, et al. Antibiotic sensitivity and resistance patterns in pediatric staphylococcal scalded skin syndrome. Pediatr Dermatol. 2014;31:305-308.
16. Gilbert DN, Chambers HF, Eliopoulos GM, et al. The Sanford Guide to Antimicrobial Therapy. 48th ed. Sperryville, VA: Antimicrobial Therapy, Inc; 2014:56.
1. Staiman A, Hsu D, Silverberg JI. Epidemiology of staphylococcal scalded skin syndrome in US children. Br J Dermatol. 2018;178:704-708.
2. Ladhani S, Joannou CL, Lochrie DP, et al. Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. Clin Microbiol Rev. 1999;12:224-242.
3. Kluytmans J, van Belkum A, Verbrugh H. Nasal carriage of Staphylococcus aureus: epidemiology, underlying mechanisms, and associated risks. Clin Microbiol Rev. 1997;10:505-520.
4. Ladhani S. Understanding the mechanism of action of the exfoliative toxins of Staphylococcus aureus. FEMS Immunol Med Microbiol. 2003;39:181-189.
5. Li MY, Hua Y, Wei GH, et al. Staphylococcal scalded skin syndrome in neonates: an 8-year retrospective study in a single institution. Pediatr Dermatol. 2014;31:43-47.
6. Berk DR, Bayliss SJ. MRSA, staphylococcal scalded skin syndrome, and other cutaneous bacterial emergencies. Pediatr Ann. 2010;39:627-633.
7. Ely JW, Seabury Stone M. The generalized rash: part I. differential diagnosis. Am Fam Physician. 2010;81:726-734.
8. Bastuji-Garin SB, Stern RS, Shear NH, et al. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129:92.
9. Elias PM, Fritsch P, Epstein EH. Staphylococcal scalded skin syndrome. clinical features, pathogenesis, and recent microbiological and biochemical developments. Arch Dermatol. 1977;113:207-219.
10. O’Connor NR, McLaughlin M, Ham P. Newborn skin: part I: common rashes. Am Fam Physician. 2008;77:47-52.
11. Larsen SA, Steiner BM, Rudolph AH. Laboratory diagnosis and interpretation of tests for syphilis. Clin Microbiol Rev. 1995;8:1-21.
12. Arnold SR, Ford-Jones EL. Congenital syphilis: a guide to diagnosis and management. Paediatr Child Health. 2000;5:463-469.
13. Darmstadt GL, Dinulos JG, Miller Z. Congenital cutaneous candidiasis: clinical presentation, pathogenesis, and management guidelines. Pediatrics. 2000;105:438-444.
14. Kimberlin DW. Neonatal herpes simplex infection. Clin Microbiol Rev. 2004;17:1-13.
15. Braunstein I, Wanat KA, Abuabara K, et al. Antibiotic sensitivity and resistance patterns in pediatric staphylococcal scalded skin syndrome. Pediatr Dermatol. 2014;31:305-308.
16. Gilbert DN, Chambers HF, Eliopoulos GM, et al. The Sanford Guide to Antimicrobial Therapy. 48th ed. Sperryville, VA: Antimicrobial Therapy, Inc; 2014:56.

Poor oral health predicts children’s school problems
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.

“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.
“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
“Dental caries remains the most common chronic disease of childhood in the United States and is known to affect multiple domains of health and well-being. Academic success is an important predictor of future employment and economic performance, as well as life and health outcomes. Therefore, it is important that we understand the impact oral disease has on academic performance,” Melinda Clark, MD, said in an interview. “This study demonstrated that middle schoolers are at greatest risk of dental disease impacting school performance, with poor dental health doubling the risk of having problems at school and missing school days in children 12-14 years of age.
“Pediatricians care a great deal about the overall health and academic success of children, and the science informs us that poor oral health adversely impacts both of those domains. Pediatric primary care providers can adopt the Department of Health and Human Services Oral Health Framework to combat dental caries by integrating oral health services into practice and advocating for community water fluoridation. Application of fluoride varnish in the primary care office for all children from tooth eruption to age 6 years is recommended by the U.S. Preventive Services Task Force, the American Academy of Pediatrics, and is on the Bright Futures Periodicity schedule.
“Now is the time for action. The majority of dental disease in children is preventable with timely risk assessment, healthy diet choices, oral hygiene, and relatively simple office interventions. Future research should examine the effects of oral health changes on children’s academic outcomes to capture the full impact on children’s well-being.”
Dr. Clark is an associate professor of pediatrics at the Albany Medical Center, New York, and a member of the Pediatric News editorial advisory board. She was asked to comment on the article by Dr. Guarnizo-Herreño and associates. She has no relevant financial disclosures.
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
Poor oral health was significantly associated with poor academic performance in children aged 6-17 years, based on data from more than 45,000 children in the United States.
The study, published in the Journal of Pediatrics, updates an assessment from 2007 of a similarly representative sample of U.S. children.
“Providing an updated analysis is especially important to understand the dynamics between children’s oral health status and academic performance, given reported improvements in dental care use among children and dental treatment quality and the implementation or expansion of some state-level preventive strategies,” wrote Carol Cristina Guarnizo-Herreño, DDS, PhD, of Universidad Nacional de Colombia, Bogotá, and her colleagues.
The researchers analyzed data from the 2016 and 2017 versions of National Survey of Children’s Health that included 45,711 children aged 6-17 years. Survey data were collected from parents or other primary caregivers. In the study population, 16% of the children had a least one dental problem, defined as toothache, tooth decay or cavities, or bleeding gums, and 25% of the children had school problems: 67% missed any school, 23% missed more than 3 days of school, and 10% missed more than 6 days of school.
Overall, children with at least 1 dental problem were significantly more likely than those without dental problems to have problems at school (odds ratio, 1.56) or miss at least 1 school day (OR, 1.54) – more than 50% more likely. In addition, children with at least one dental problem were approximately 40% more likely to miss more than 3 days or more than 6 days of school (OR, 1.39 for both).
The association increased when the investigators used children’s oral health ratings; those with oral health rated as poor/fair were approximately 80% more likely to have school problems (OR, 1.77), almost 60% more likely to miss more than 3 days of school (OR, 1.56), and 90% more likely to miss more than 6 days of school, compared with children with oral health rankings of good, very good, or excellent.
Despite some variations in subgroups when the population was stratified by age, sex, race, household income, and health insurance, the associations between oral health problems and academic problems showed “remarkable stability,” across demographic and socioeconomic categories, the researchers said.
The study results were limited by several factors including the inability to identify the mechanisms behind the oral health and academic outcomes relationship, as well as the potential errors in parent or caregiver reports of children’s oral health and school performance, Dr. Guarnizo-Herreño and her associates said. However, the findings support those from an earlier study using 2007 data, and suggest that the link between poor oral health and poor academic performance has lasted for the past decade.
“The relationship between oral health and academic achievement is complex and likely involves multiple and intertwined pathways,” such as the impact of oral pain or discomfort on eating and sleeping that may affect academic performance, they said.
“These findings highlight the need for broad population-wide policies and integrated approaches to promote children’s development and reduce academic deficits that include among other components initiatives to improve oral health through prevention and treatment access strategies,” Dr. Guarnizo-Herreño and her associates concluded.
The study was supported by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
SOURCE: Guarnizo-Herreño C et al. J Pediatr. 2019. doi: 10.1016/j.jpeds.2019.01.045.
FROM THE JOURNAL OF PEDIATRICS
FDA concerned about e-cigs/seizures in youth
the agency announced April 3.

Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
the agency announced April 3.
Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
the agency announced April 3.
Between 2010 and early 2019, the FDA and poison control centers received 35 reports of seizures that mentioned the use of e-cigarettes. Most reports involved youth or young adults, and the reports have increased slightly since June 2018, the announcement says.
“We want to be clear that we don’t yet know if there’s a direct relationship between the use of e-cigarettes and a risk of seizure,” said FDA Commissioner Scott Gottlieb, MD, and Principal Deputy Commissioner Amy Abernethy, MD, PhD, in a statement. “We believe these 35 cases warrant scientific investigation into whether there is in fact a connection.”
In addition, the FDA is trying to determine whether any e-cigarette product-specific factors may be associated with the risk of seizures.
Seizures have been reported after a few puffs or up to 1 day after e-cigarette use and among first-time and experienced users. A few patients had a prior history of seizures or also used other substances, such as marijuana or amphetamines.
“While 35 cases may not seem like much compared to the total number of people using e-cigarettes, we are nonetheless concerned by these reported cases. We also recognized that not all of the cases may be reported,” Dr. Gottlieb and Dr. Abernethy said.
Although seizures are known side effects of nicotine toxicity and have been reported in the context of intentional or accidental swallowing of e-cigarette liquid, the voluntary reports of seizures occurring with vaping could represent a new safety issue, the FDA said.
The agency encouraged people to report cases via an online safety reporting portal. It also provided redacted case reports that involve vaping and seizures.
Genetic variant increases stroke risk in childhood cancer survivors
ATLANTA – Adult survivors of childhood cancers are at significantly greater risk than the general population for late-term complications related to therapy, including secondary cancers, cardiovascular disease, and cerebrovascular complications, including ischemic and hemorrhagic strokes.
In particular, childhood cancer survivors have an approximately eightfold higher risk for stroke, compared with their siblings, with a history of cranial irradiation being a strong, dose-dependent risk factor for stroke.
Researchers at St. Jude Children’s Research Hospital in Memphis, Tenn., are conducting a retrospective cohort study with prospective clinical follow-up and ongoing enrollment of childhood cancer survivors who are 5 or more years out of therapy.
The study includes publicly available, whole-genome sequencing data on 4,500 participants. Sifting through these data, Yadav Sapkota, PhD, a clinical research scientist at St. Jude, and his colleagues have identified a genetic variant strongly associated with stroke risk in survivors of European ancestry, and they have replicated the finding in survivors of African ancestry.
In a video interview at the annual meeting of the American Association for Cancer Research, Dr. Sapkota describes his group’s findings and potential research and clinical implications.
The study was sponsored by the National Cancer Institute and ALSAC, the fundraising and awareness organization of St. Jude. Dr. Sapkota declared no conflict of interest.
ATLANTA – Adult survivors of childhood cancers are at significantly greater risk than the general population for late-term complications related to therapy, including secondary cancers, cardiovascular disease, and cerebrovascular complications, including ischemic and hemorrhagic strokes.
In particular, childhood cancer survivors have an approximately eightfold higher risk for stroke, compared with their siblings, with a history of cranial irradiation being a strong, dose-dependent risk factor for stroke.
Researchers at St. Jude Children’s Research Hospital in Memphis, Tenn., are conducting a retrospective cohort study with prospective clinical follow-up and ongoing enrollment of childhood cancer survivors who are 5 or more years out of therapy.
The study includes publicly available, whole-genome sequencing data on 4,500 participants. Sifting through these data, Yadav Sapkota, PhD, a clinical research scientist at St. Jude, and his colleagues have identified a genetic variant strongly associated with stroke risk in survivors of European ancestry, and they have replicated the finding in survivors of African ancestry.
In a video interview at the annual meeting of the American Association for Cancer Research, Dr. Sapkota describes his group’s findings and potential research and clinical implications.
The study was sponsored by the National Cancer Institute and ALSAC, the fundraising and awareness organization of St. Jude. Dr. Sapkota declared no conflict of interest.
ATLANTA – Adult survivors of childhood cancers are at significantly greater risk than the general population for late-term complications related to therapy, including secondary cancers, cardiovascular disease, and cerebrovascular complications, including ischemic and hemorrhagic strokes.
In particular, childhood cancer survivors have an approximately eightfold higher risk for stroke, compared with their siblings, with a history of cranial irradiation being a strong, dose-dependent risk factor for stroke.
Researchers at St. Jude Children’s Research Hospital in Memphis, Tenn., are conducting a retrospective cohort study with prospective clinical follow-up and ongoing enrollment of childhood cancer survivors who are 5 or more years out of therapy.
The study includes publicly available, whole-genome sequencing data on 4,500 participants. Sifting through these data, Yadav Sapkota, PhD, a clinical research scientist at St. Jude, and his colleagues have identified a genetic variant strongly associated with stroke risk in survivors of European ancestry, and they have replicated the finding in survivors of African ancestry.
In a video interview at the annual meeting of the American Association for Cancer Research, Dr. Sapkota describes his group’s findings and potential research and clinical implications.
The study was sponsored by the National Cancer Institute and ALSAC, the fundraising and awareness organization of St. Jude. Dr. Sapkota declared no conflict of interest.
REPORTING FROM AACR 2019

Mycophenolate, cyclophosphamide found equal as induction therapy in pediatric lupus nephritis
according to findings in the real-world U.K. Juvenile Systemic Lupus Erythematosus Cohort Study.

The study involved 34 patients who received mycophenolate mofetil and 17 who received IV cyclophosphamide as induction therapy for proliferative lupus nephritis in juvenile-onset systemic lupus erythematosus (JSLE). Along with her coinvestigators, first author Eve M.D. Smith, MD, PhD, of the University of Liverpool (England) and Alder Hey Children’s NHS Foundation Trust, described it as the largest study to date investigating induction treatments for proliferative lupus nephritis in JSLE.
The patients were aged 16 years or younger at diagnosis and monitored during 2006-2018 as part of the U.K. JSLE Cohort Study. They met four or more American College of Rheumatology SLE classification criteria and had a renal biopsy result demonstrating proliferative lupus nephritis, defined as class III or IV lupus nephritis by the International Society of Nephrology/Renal Pathology Society. Within the mycophenolate group, half received oral prednisolone only and half received both IV methylprednisolone and oral prednisolone, whereas 2 in the cyclophosphamide group received oral prednisolone only and 15 received both IV methylprednisolone and oral prednisolone.
All the patient demographic factors at baseline – including gender, ethnicity, age at diagnosis, and age at lupus nephritis onset – were similar in both treatment groups.
The investigators detected no significant differences between the two treatment groups at 4-8 and 10-14 months post renal biopsy and last follow-up in renal pediatric British Isles Lupus Assessment Grade scores, urine albumin/creatinine ratio, serum creatinine, erythrocyte sedimentation rate, anti-double stranded DNA antibody, Complement 3 levels, and patient/physician global scores. JSLE-related damage on the Systemic Lupus International Collaborating Clinics Standardized Damage Index also was no different between the groups after a median 13 months following renal biopsy. Lupus nephritis became inactive in 82%-85% of each group, taking a median of 262 days with mycophenolate and 151 days with IV cyclophosphamide, while flares occurred in 69% treated with mycophenolate at a median of 451 days and in 50% with cyclophosphamide at a median of 343 days.
“Results from the presented study highlight the need for prospective comparison of mycophenolate mofetil versus IV cyclophosphamide induction treatment to better inform lupus nephritis treatment protocols for children, especially given IV cyclophosphamide’s poor safety profile,” the investigators wrote.
SOURCE: Smith EMD et al. Lupus. 2019 Mar 14. doi: 10.1177/0961203319836712.
according to findings in the real-world U.K. Juvenile Systemic Lupus Erythematosus Cohort Study.
The study involved 34 patients who received mycophenolate mofetil and 17 who received IV cyclophosphamide as induction therapy for proliferative lupus nephritis in juvenile-onset systemic lupus erythematosus (JSLE). Along with her coinvestigators, first author Eve M.D. Smith, MD, PhD, of the University of Liverpool (England) and Alder Hey Children’s NHS Foundation Trust, described it as the largest study to date investigating induction treatments for proliferative lupus nephritis in JSLE.
The patients were aged 16 years or younger at diagnosis and monitored during 2006-2018 as part of the U.K. JSLE Cohort Study. They met four or more American College of Rheumatology SLE classification criteria and had a renal biopsy result demonstrating proliferative lupus nephritis, defined as class III or IV lupus nephritis by the International Society of Nephrology/Renal Pathology Society. Within the mycophenolate group, half received oral prednisolone only and half received both IV methylprednisolone and oral prednisolone, whereas 2 in the cyclophosphamide group received oral prednisolone only and 15 received both IV methylprednisolone and oral prednisolone.
All the patient demographic factors at baseline – including gender, ethnicity, age at diagnosis, and age at lupus nephritis onset – were similar in both treatment groups.
The investigators detected no significant differences between the two treatment groups at 4-8 and 10-14 months post renal biopsy and last follow-up in renal pediatric British Isles Lupus Assessment Grade scores, urine albumin/creatinine ratio, serum creatinine, erythrocyte sedimentation rate, anti-double stranded DNA antibody, Complement 3 levels, and patient/physician global scores. JSLE-related damage on the Systemic Lupus International Collaborating Clinics Standardized Damage Index also was no different between the groups after a median 13 months following renal biopsy. Lupus nephritis became inactive in 82%-85% of each group, taking a median of 262 days with mycophenolate and 151 days with IV cyclophosphamide, while flares occurred in 69% treated with mycophenolate at a median of 451 days and in 50% with cyclophosphamide at a median of 343 days.
“Results from the presented study highlight the need for prospective comparison of mycophenolate mofetil versus IV cyclophosphamide induction treatment to better inform lupus nephritis treatment protocols for children, especially given IV cyclophosphamide’s poor safety profile,” the investigators wrote.
SOURCE: Smith EMD et al. Lupus. 2019 Mar 14. doi: 10.1177/0961203319836712.
according to findings in the real-world U.K. Juvenile Systemic Lupus Erythematosus Cohort Study.
The study involved 34 patients who received mycophenolate mofetil and 17 who received IV cyclophosphamide as induction therapy for proliferative lupus nephritis in juvenile-onset systemic lupus erythematosus (JSLE). Along with her coinvestigators, first author Eve M.D. Smith, MD, PhD, of the University of Liverpool (England) and Alder Hey Children’s NHS Foundation Trust, described it as the largest study to date investigating induction treatments for proliferative lupus nephritis in JSLE.
The patients were aged 16 years or younger at diagnosis and monitored during 2006-2018 as part of the U.K. JSLE Cohort Study. They met four or more American College of Rheumatology SLE classification criteria and had a renal biopsy result demonstrating proliferative lupus nephritis, defined as class III or IV lupus nephritis by the International Society of Nephrology/Renal Pathology Society. Within the mycophenolate group, half received oral prednisolone only and half received both IV methylprednisolone and oral prednisolone, whereas 2 in the cyclophosphamide group received oral prednisolone only and 15 received both IV methylprednisolone and oral prednisolone.
All the patient demographic factors at baseline – including gender, ethnicity, age at diagnosis, and age at lupus nephritis onset – were similar in both treatment groups.
The investigators detected no significant differences between the two treatment groups at 4-8 and 10-14 months post renal biopsy and last follow-up in renal pediatric British Isles Lupus Assessment Grade scores, urine albumin/creatinine ratio, serum creatinine, erythrocyte sedimentation rate, anti-double stranded DNA antibody, Complement 3 levels, and patient/physician global scores. JSLE-related damage on the Systemic Lupus International Collaborating Clinics Standardized Damage Index also was no different between the groups after a median 13 months following renal biopsy. Lupus nephritis became inactive in 82%-85% of each group, taking a median of 262 days with mycophenolate and 151 days with IV cyclophosphamide, while flares occurred in 69% treated with mycophenolate at a median of 451 days and in 50% with cyclophosphamide at a median of 343 days.
“Results from the presented study highlight the need for prospective comparison of mycophenolate mofetil versus IV cyclophosphamide induction treatment to better inform lupus nephritis treatment protocols for children, especially given IV cyclophosphamide’s poor safety profile,” the investigators wrote.
SOURCE: Smith EMD et al. Lupus. 2019 Mar 14. doi: 10.1177/0961203319836712.
FROM LUPUS
Improved WIC food packages reverse obesity in toddler participants
Improvements to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food package guidelines in 2009 appear responsible for reversing the upward trend in obesity prevalence among WIC toddler participants, Madeleine I.G. Daepp, of the Massachusetts Institute of Technology, Cambridge, and her associates reported in Pediatrics.

Using data.gov files from 2008, 2010, 2012, and 2014, Ms. Daepp and her colleagues conducted a quasi-experimental interrupted time series analysis to compare state-level population trends in obesity prevalence among children aged 2-4 years before and after 2009. The goal of the study was to determine whether the WIC package changes had any influence on obesity trends among program participants. Altogether, data from 2,253,471 children in 2000 and 3,152,137 children in 2012 was included in the analysis.
Among the guidelines updated to encourage healthier eating habits were the addition of cash allowances for the purchase of more fruits and vegetables, reduction by half in the allowable portions of juice, reduction in cheese, transition of toddlers aged 2-4 years to low-fat or skim milk, and replacement of refined-grain products with healthier whole grain products.
Across all states included in the study, the authors reported average obesity prevalence of 13% in 2000 and 15% in 2008. Although no change was observed in 2010, by 2014 the obesity prevalence decreased to 14%. Hawaii was excluded because of concerns about data quality.
Ms. Daepp and her associates “estimated a pre-2009 annual trend of a 0.23% increase in childhood obesity prevalence.” After the 2009 package revision, they estimated “a decline in childhood obesity of 0.34% per year [P less than .001].”
This change could not be explained by racial-ethnic makeup or child poverty, changes in maternal prepregnancy body mass indices, or prevalence of macrosomia. Speculating that “unmeasured heterogeneity in WIC populations across states” might explain the difference, the authors also suggested that variance in how effectively the package changes were implemented from state to state could be a factor.
Ms. Daepp and her associates recommended that future studies should focus on evaluating differences in how closely vendors follow the package changes, as well as considering whether any other implementation factors could have an influence on state-by-state trends in childhood obesity.
Study limitations noted included an absence of individual body mass index data and information on changes in energy intake and expenditure.
This study was funded by the National Institutes of Health. Ms. Daepp was supported by a National Science Foundation Graduate Research Fellowship grant. Three coauthors were supported by the JPB Foundation; a fourth was supported by an NIH grant.
SOURCE: Daepp MIG et al. Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2841.
Improvements to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food package guidelines in 2009 appear responsible for reversing the upward trend in obesity prevalence among WIC toddler participants, Madeleine I.G. Daepp, of the Massachusetts Institute of Technology, Cambridge, and her associates reported in Pediatrics.
Using data.gov files from 2008, 2010, 2012, and 2014, Ms. Daepp and her colleagues conducted a quasi-experimental interrupted time series analysis to compare state-level population trends in obesity prevalence among children aged 2-4 years before and after 2009. The goal of the study was to determine whether the WIC package changes had any influence on obesity trends among program participants. Altogether, data from 2,253,471 children in 2000 and 3,152,137 children in 2012 was included in the analysis.
Among the guidelines updated to encourage healthier eating habits were the addition of cash allowances for the purchase of more fruits and vegetables, reduction by half in the allowable portions of juice, reduction in cheese, transition of toddlers aged 2-4 years to low-fat or skim milk, and replacement of refined-grain products with healthier whole grain products.
Across all states included in the study, the authors reported average obesity prevalence of 13% in 2000 and 15% in 2008. Although no change was observed in 2010, by 2014 the obesity prevalence decreased to 14%. Hawaii was excluded because of concerns about data quality.
Ms. Daepp and her associates “estimated a pre-2009 annual trend of a 0.23% increase in childhood obesity prevalence.” After the 2009 package revision, they estimated “a decline in childhood obesity of 0.34% per year [P less than .001].”
This change could not be explained by racial-ethnic makeup or child poverty, changes in maternal prepregnancy body mass indices, or prevalence of macrosomia. Speculating that “unmeasured heterogeneity in WIC populations across states” might explain the difference, the authors also suggested that variance in how effectively the package changes were implemented from state to state could be a factor.
Ms. Daepp and her associates recommended that future studies should focus on evaluating differences in how closely vendors follow the package changes, as well as considering whether any other implementation factors could have an influence on state-by-state trends in childhood obesity.
Study limitations noted included an absence of individual body mass index data and information on changes in energy intake and expenditure.
This study was funded by the National Institutes of Health. Ms. Daepp was supported by a National Science Foundation Graduate Research Fellowship grant. Three coauthors were supported by the JPB Foundation; a fourth was supported by an NIH grant.
SOURCE: Daepp MIG et al. Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2841.
Improvements to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) food package guidelines in 2009 appear responsible for reversing the upward trend in obesity prevalence among WIC toddler participants, Madeleine I.G. Daepp, of the Massachusetts Institute of Technology, Cambridge, and her associates reported in Pediatrics.
Using data.gov files from 2008, 2010, 2012, and 2014, Ms. Daepp and her colleagues conducted a quasi-experimental interrupted time series analysis to compare state-level population trends in obesity prevalence among children aged 2-4 years before and after 2009. The goal of the study was to determine whether the WIC package changes had any influence on obesity trends among program participants. Altogether, data from 2,253,471 children in 2000 and 3,152,137 children in 2012 was included in the analysis.
Among the guidelines updated to encourage healthier eating habits were the addition of cash allowances for the purchase of more fruits and vegetables, reduction by half in the allowable portions of juice, reduction in cheese, transition of toddlers aged 2-4 years to low-fat or skim milk, and replacement of refined-grain products with healthier whole grain products.
Across all states included in the study, the authors reported average obesity prevalence of 13% in 2000 and 15% in 2008. Although no change was observed in 2010, by 2014 the obesity prevalence decreased to 14%. Hawaii was excluded because of concerns about data quality.
Ms. Daepp and her associates “estimated a pre-2009 annual trend of a 0.23% increase in childhood obesity prevalence.” After the 2009 package revision, they estimated “a decline in childhood obesity of 0.34% per year [P less than .001].”
This change could not be explained by racial-ethnic makeup or child poverty, changes in maternal prepregnancy body mass indices, or prevalence of macrosomia. Speculating that “unmeasured heterogeneity in WIC populations across states” might explain the difference, the authors also suggested that variance in how effectively the package changes were implemented from state to state could be a factor.
Ms. Daepp and her associates recommended that future studies should focus on evaluating differences in how closely vendors follow the package changes, as well as considering whether any other implementation factors could have an influence on state-by-state trends in childhood obesity.
Study limitations noted included an absence of individual body mass index data and information on changes in energy intake and expenditure.
This study was funded by the National Institutes of Health. Ms. Daepp was supported by a National Science Foundation Graduate Research Fellowship grant. Three coauthors were supported by the JPB Foundation; a fourth was supported by an NIH grant.
SOURCE: Daepp MIG et al. Pediatrics. 2019 Apr 1. doi: 10.1542/peds.2018-2841.
FROM PEDIATRICS
Noninfected children of HIV-positive mothers have high rates of obesity
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
NEW ORLEANS – than are those with no such exposure, according to research that provides a compelling link between inflammatory activity in utero and subsequent risk of metabolic disorders.
Most supportive of that link was a near-linear inverse relationship between CD4 counts during the time of pregnancy and risk of both obesity and reactive respiratory disease more than a decade later, according to research presented by Lindsay Fourman, MD, an instructor in medicine at Massachusetts General Hospital, Boston, during the annual meeting of the Endocrine Society.
In this video interview, Dr. Fourman discusses the effort to understand the long-term health consequences of being exposed to HIV and antiretroviral therapies while in utero, a group known by the acronym HIV-exposed uninfected (HEU). With effective therapies now routinely preventing mother-to-child transmission, this population of children is growing quickly.
For this study, 50 HEU individuals were identified from a patient database. They were matched in a 3:1 ratio to a control group for a variety of demographic and socioeconomic variables. At a median age of 18 years, the HEU population was found to have a “strikingly” higher rate of obesity, compared with controls (42% vs. 25%, respectively; P = .04). The rate of reactive airway disease was similarly increased in the HEU group (40% vs. 24%; P = .04).
These data are important for considering health risks in an HEU population, but Dr. Fourman explained that it provides support for looking at metabolic risks from other in utero exposures linked to upregulated inflammation, such as gestational diabetes or obesity.
Dr Fourman and her colleagues reported no disclosures or financial conflicts of interest.
SOURCE: Fourman L et al. ENDO 2019, Session P10 (SAT-256).
REPORTING FROM ENDO 2019

Measles: Latest weekly count is the highest of the year
according to the Centers for Disease Control and Prevention.
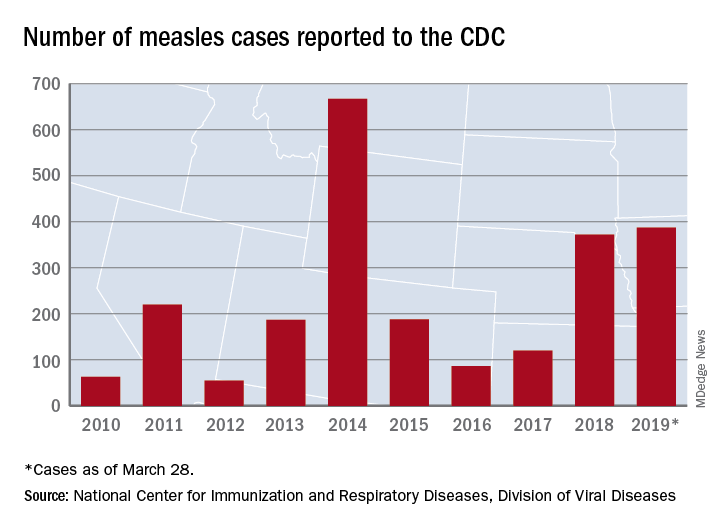
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.
according to the Centers for Disease Control and Prevention.
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.
according to the Centers for Disease Control and Prevention.
The 73 new cases of measles reported to the CDC during the week ending March 28 – more than any other single week so far in 2019 – brings the total number of cases for the year to 387, the CDC reported April 1. That surpasses the 372 reported in 2018 and is now the highest annual count since 667 cases were reported in 2014.
The ongoing outbreak in Rockland County, N.Y., which resulted in 6 new cases there last week and 52 for the year, prompted County Executive Ed Day to declare a state of emergency effective March 27 that bars unvaccinated individuals under age 18 years from public places for the next 30 days unless they receive an MMR vaccination.
“As this outbreak has continued our inspectors have begun to meet resistance from those they are trying to protect. They have been hung up on or told not to call again. They’ve been told ‘we’re not discussing this, do not come back,’ when visiting the homes of infected individuals as part of their investigations. This type of response is unacceptable and irresponsible. It endangers the health and well-being of others and displays a shocking lack of responsibility and concern for others in our community,” Mr. Day said in a written statement.
In addition to Rockland County, the CDC is currently tracking five other outbreaks: New York City, mainly Brooklyn (33 new cases last week); Washington state (74 cases for the year, but no new cases in the last week); New Jersey (10 total cases, with 8 related to an outbreak in Ocean and Monmouth Counties); and two in California (16 total cases, with 11 related to the outbreaks). One of the California outbreaks and the New Jersey outbreak are new, but the CDC is no longer reporting outbreaks in Texas and Illinois, so the total stays at six nationwide.
In related news from California, state Sen. Richard Pan (D), a pediatrician, and Assemblywoman Lorena Gonzalez (D) introduced a bill to monitor vaccine exemptions “by requiring the state health department to vet each medical exemption form written by physicians [and to] maintain a database of exemptions that would allow officials to monitor which doctors are granting the exemptions,” the Los Angeles Times reported.
Valproate, topiramate prescribed in young women despite known teratogenicity risks
results of a retrospective analysis suggest.

Topiramate, linked to increased risk of cleft palate and smaller-than-gestational-age newborns, was among the top three antiepileptic drugs (AEDs) prescribed to women 15-44 years of age in the population-based cohort study.
Valproate, linked to increases in both anatomic and behavioral teratogenicity, was less often prescribed, but nevertheless still prescribed in a considerable proportion of patients in the study, which looked at U.S. commercial, Medicare, and Medicaid claims data from 2009 to 2013.
Presence of comorbidities could be influencing whether or not a woman of childbearing age receives one of these AEDs, the investigators said. Specifically, they found valproate more often prescribed for women with epilepsy who also had mood or anxiety and dissociative disorder, while topiramate was more often prescribed in women with headaches or migraines.
Taken together, these findings suggest a lack of awareness of the teratogenic risks of valproate and topiramate, said the investigators, led by Hyunmi Kim, MD, PhD, MPH, of the department of neurology at Stanford (Calif.) University.
“To improve current practice, knowledge of the teratogenicity of certain AEDs should be disseminated to health care professionals and patients,” they wrote. The report is in JAMA Neurology.
The findings of Dr. Kim and her colleagues were based on data for 46,767 women of childbearing age: 8,003 incident (new) cases with a mean age of 27 years, and 38,764 prevalent cases with a mean age of 30 years.
Topiramate was the second- or third-most prescribed AED in the analyses, alongside levetiracetam and lamotrigine. In particular, topiramate prescriptions were found in incident cases receiving first-line monotherapy (15%), prevalent cases receiving first-line monotherapy (13%), and prevalent cases receiving polytherapy (29%).
Valproate was the fifth-most prescribed AED for incident and prevalent cases receiving first-line monotherapy (5% and 10%, respectively), and came in fourth place among prevalent cases receiving polytherapy (22%).
The somewhat lower rate of valproate prescriptions tracks with other recent analyses showing that valproate use decreased among women of childbearing age following recommendations against its use during pregnancy, according to Dr. Kim and her coauthors.
However, topiramate is another story: “Although the magnitude of risk and range of adverse reproductive outcomes associated with topiramate use appear substantially less than those associated with valproate, some reduction in the use of topiramate in this population might be expected after evidence emerged in 2008 of its association with cleft palate,” they said in their report.
UCB Pharma sponsored this study. Study authors reported disclosures related to UCB Pharma, Biogen, Eisai, SK Life Science, Brain Sentinel, UCB Pharma, and the University of Alabama at Birmingham.
SOURCE: Kim H et al. JAMA Neurol. 2019 Apr 1. doi: 10.1001/jamaneurol.2019.0447.
results of a retrospective analysis suggest.
Topiramate, linked to increased risk of cleft palate and smaller-than-gestational-age newborns, was among the top three antiepileptic drugs (AEDs) prescribed to women 15-44 years of age in the population-based cohort study.
Valproate, linked to increases in both anatomic and behavioral teratogenicity, was less often prescribed, but nevertheless still prescribed in a considerable proportion of patients in the study, which looked at U.S. commercial, Medicare, and Medicaid claims data from 2009 to 2013.
Presence of comorbidities could be influencing whether or not a woman of childbearing age receives one of these AEDs, the investigators said. Specifically, they found valproate more often prescribed for women with epilepsy who also had mood or anxiety and dissociative disorder, while topiramate was more often prescribed in women with headaches or migraines.
Taken together, these findings suggest a lack of awareness of the teratogenic risks of valproate and topiramate, said the investigators, led by Hyunmi Kim, MD, PhD, MPH, of the department of neurology at Stanford (Calif.) University.
“To improve current practice, knowledge of the teratogenicity of certain AEDs should be disseminated to health care professionals and patients,” they wrote. The report is in JAMA Neurology.
The findings of Dr. Kim and her colleagues were based on data for 46,767 women of childbearing age: 8,003 incident (new) cases with a mean age of 27 years, and 38,764 prevalent cases with a mean age of 30 years.
Topiramate was the second- or third-most prescribed AED in the analyses, alongside levetiracetam and lamotrigine. In particular, topiramate prescriptions were found in incident cases receiving first-line monotherapy (15%), prevalent cases receiving first-line monotherapy (13%), and prevalent cases receiving polytherapy (29%).
Valproate was the fifth-most prescribed AED for incident and prevalent cases receiving first-line monotherapy (5% and 10%, respectively), and came in fourth place among prevalent cases receiving polytherapy (22%).
The somewhat lower rate of valproate prescriptions tracks with other recent analyses showing that valproate use decreased among women of childbearing age following recommendations against its use during pregnancy, according to Dr. Kim and her coauthors.
However, topiramate is another story: “Although the magnitude of risk and range of adverse reproductive outcomes associated with topiramate use appear substantially less than those associated with valproate, some reduction in the use of topiramate in this population might be expected after evidence emerged in 2008 of its association with cleft palate,” they said in their report.
UCB Pharma sponsored this study. Study authors reported disclosures related to UCB Pharma, Biogen, Eisai, SK Life Science, Brain Sentinel, UCB Pharma, and the University of Alabama at Birmingham.
SOURCE: Kim H et al. JAMA Neurol. 2019 Apr 1. doi: 10.1001/jamaneurol.2019.0447.
results of a retrospective analysis suggest.
Topiramate, linked to increased risk of cleft palate and smaller-than-gestational-age newborns, was among the top three antiepileptic drugs (AEDs) prescribed to women 15-44 years of age in the population-based cohort study.
Valproate, linked to increases in both anatomic and behavioral teratogenicity, was less often prescribed, but nevertheless still prescribed in a considerable proportion of patients in the study, which looked at U.S. commercial, Medicare, and Medicaid claims data from 2009 to 2013.
Presence of comorbidities could be influencing whether or not a woman of childbearing age receives one of these AEDs, the investigators said. Specifically, they found valproate more often prescribed for women with epilepsy who also had mood or anxiety and dissociative disorder, while topiramate was more often prescribed in women with headaches or migraines.
Taken together, these findings suggest a lack of awareness of the teratogenic risks of valproate and topiramate, said the investigators, led by Hyunmi Kim, MD, PhD, MPH, of the department of neurology at Stanford (Calif.) University.
“To improve current practice, knowledge of the teratogenicity of certain AEDs should be disseminated to health care professionals and patients,” they wrote. The report is in JAMA Neurology.
The findings of Dr. Kim and her colleagues were based on data for 46,767 women of childbearing age: 8,003 incident (new) cases with a mean age of 27 years, and 38,764 prevalent cases with a mean age of 30 years.
Topiramate was the second- or third-most prescribed AED in the analyses, alongside levetiracetam and lamotrigine. In particular, topiramate prescriptions were found in incident cases receiving first-line monotherapy (15%), prevalent cases receiving first-line monotherapy (13%), and prevalent cases receiving polytherapy (29%).
Valproate was the fifth-most prescribed AED for incident and prevalent cases receiving first-line monotherapy (5% and 10%, respectively), and came in fourth place among prevalent cases receiving polytherapy (22%).
The somewhat lower rate of valproate prescriptions tracks with other recent analyses showing that valproate use decreased among women of childbearing age following recommendations against its use during pregnancy, according to Dr. Kim and her coauthors.
However, topiramate is another story: “Although the magnitude of risk and range of adverse reproductive outcomes associated with topiramate use appear substantially less than those associated with valproate, some reduction in the use of topiramate in this population might be expected after evidence emerged in 2008 of its association with cleft palate,” they said in their report.
UCB Pharma sponsored this study. Study authors reported disclosures related to UCB Pharma, Biogen, Eisai, SK Life Science, Brain Sentinel, UCB Pharma, and the University of Alabama at Birmingham.
SOURCE: Kim H et al. JAMA Neurol. 2019 Apr 1. doi: 10.1001/jamaneurol.2019.0447.
FROM JAMA NEUROLOGY
Key clinical point: Both valproate and topiramate are prescribed relatively often in women of childbearing age despite known teratogenic risks.
Major finding: Topiramate was the second- or third-most prescribed AED in the analyses. Valproate was the fifth-most prescribed AED for incident and prevalent cases receiving first-line monotherapy.
Study details: Retrospective cohort study including nearly 47,000 women of childbearing age enrolled in claims databases between 2009 and 2013.
Disclosures: UCB Pharma sponsored the study. Study authors reported disclosures related to UCB Pharma, Biogen, Eisai, SK Life Science, Brain Sentinel, UCB Pharma, and the University of Alabama at Birmingham.
Source: Kim H et al. JAMA Neurol. 2019 Apr 1. doi: 10.1001/jamaneurol.2019.0447.
Click for Credit: Suicide in Medicaid youth; persistent back pain; more
Here are 5 articles from the April issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Back pain persists in one in five patients
To take the posttest, go to: https://bit.ly/2Uiod8N
Expires January 14, 2019
2. COPD linked to higher in-hospital death rates in patients with PAD
To take the posttest, go to: https://bit.ly/2TFCeJC
Expires January 22, 2019
3. Medicaid youth suicides include more females, younger kids, hanging deaths
To take the posttest, go to: https://bit.ly/2Uleyyp
Expires January 17, 2019
4. Potential antidepressant overprescribing found in 24% of elderly cohort
To take the posttest, go to: https://bit.ly/2HWwcSq
Expires January 24, 2019
5. Perceptions of liver transplantation for ALD are evolving
To take the posttest, go to: https://bit.ly/2OCANuA
Expires January 22, 2019
Here are 5 articles from the April issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Back pain persists in one in five patients
To take the posttest, go to: https://bit.ly/2Uiod8N
Expires January 14, 2019
2. COPD linked to higher in-hospital death rates in patients with PAD
To take the posttest, go to: https://bit.ly/2TFCeJC
Expires January 22, 2019
3. Medicaid youth suicides include more females, younger kids, hanging deaths
To take the posttest, go to: https://bit.ly/2Uleyyp
Expires January 17, 2019
4. Potential antidepressant overprescribing found in 24% of elderly cohort
To take the posttest, go to: https://bit.ly/2HWwcSq
Expires January 24, 2019
5. Perceptions of liver transplantation for ALD are evolving
To take the posttest, go to: https://bit.ly/2OCANuA
Expires January 22, 2019
Here are 5 articles from the April issue of Clinician Reviews (individual articles are valid for one year from date of publication—expiration dates below):
1. Back pain persists in one in five patients
To take the posttest, go to: https://bit.ly/2Uiod8N
Expires January 14, 2019
2. COPD linked to higher in-hospital death rates in patients with PAD
To take the posttest, go to: https://bit.ly/2TFCeJC
Expires January 22, 2019
3. Medicaid youth suicides include more females, younger kids, hanging deaths
To take the posttest, go to: https://bit.ly/2Uleyyp
Expires January 17, 2019
4. Potential antidepressant overprescribing found in 24% of elderly cohort
To take the posttest, go to: https://bit.ly/2HWwcSq
Expires January 24, 2019
5. Perceptions of liver transplantation for ALD are evolving
To take the posttest, go to: https://bit.ly/2OCANuA
Expires January 22, 2019
