User login
Prescribing a winning home-exercise plan for PAD patients
CHICAGO – Following a few simple steps can help patients with peripheral artery disease (PAD) get off on the right foot with a home-based exercise program.
“There is growing evidence that PAD patients can walk for exercise at home and improve their walking performance,” Dr. Mary McDermott said at a symposium on vascular surgery sponsored by Northwestern University.

Getting them to do so, however, can be challenging. Patients with peripheral artery disease have greater functional impairment and are at higher risk for cardiovascular disease than is the general population. They also frequently limit their activity to avoid leg problems, as their PAD progresses.
“It’s hard enough to get patients without peripheral artery disease to exercise. As a general internist, I’m well aware of that,” she said. “It’s even more difficult when walking is so painful and uncomfortable.”
At present, the American College of Cardiology/American Heart Association practice guidelines for the management of patients with PAD do not recommend advising patients with PAD to go home and walk.
The guidelines were published in 2005, however, and since 2011, three of four randomized clinical trials of home-based exercise programs have shown a significant gain in walking endurance in patients with PAD, Dr. McDermott of Northwestern University in Chicago, observed.
The most hands-off of these trials showed that patients with symptomatic PAD randomized to a supervised exercise program did the best at treadmill walking, but the home-exercise group who received a step monitor and in-person feedback just once per month did significantly better than did controls assigned light resistance training. Moreover, the home-exercise group had greater change in 6-minute walk distances than either of the other groups (J Am Heart Assoc. 2014 Oct;3[5]:e001107).
“I think the reason for this is that the home-based group was walking outside or perhaps in a mall and getting better at walking over ground,” Dr. McDermott. “The treadmill group was walking only on the treadmill.”
Supervised treadmill exercise may seem like an easier prescription to write, but it faces two major barriers, she said. Most medical insurers, including Medicare, do not pay for supervised exercise for people with PAD and intermittent claudication, and most PAD patients don’t participate. The burden of traveling to an exercise center three times weekly, week after week, to participate can be overwhelming.
“For all of these reasons, we really need to develop home-based exercise programs that work,” Dr. McDermott said.
Based on the successful trials, home-based programs should include monitoring, group support, and goal setting. Dr. McDermott and her colleagues added cognitive-behavioral therapy to group support in the Group Oriented Arterial Leg Study (GOALS), resulting in significant improvement in 6-minute walk distance at 6 months, physical activity over 7 days, and self-perception of walking endurance and speed among home walkers (JAMA. 2013 Jul 3;310[1]:57-65).
Before embarking on any home-exercise program, all patients with PAD should undergo a baseline cardiac stress test to rule out coronary artery ischemia, she cautioned. This also serves to identify any coronary ischemia that may develop during the new walking program.
Once this is performed, Dr. McDermott recommends clinicians:
• Advise patients to walk 5 days per week.
“This may seem like a lot, but it’s important to have them see this as part of their daily routine; just something they get in the habit of doing,” she said.
• Start with 10-15 minutes of walking per exercise session. Tailor the program to the individual patient.
• Walk to maximal leg pain or onset of ischemic pain. Stopping to rest is acceptable.
“A lot of patients, I find, have questions, “ ‘I can’t do this.’ ‘How can this be beneficial?’ So just letting them know that if they just walk and stop, walk and stop, and start with just 10 minutes of that and increase this over time, they really can see improvement,” Dr. McDermott said.
• Increase the walk time by 5 minutes each week.
Increase the duration until the patient is walking at least 30 minutes per session and preferably 45-50 minutes per session, excluding rest periods, she said.
• Advise patients to write down their walking goals.
Specify where they will walk, when they will walk, and the duration of walking to improve compliance, which can slip following hospitalizations or when patients experience acute illness.
• Have patients self-monitor, but also check in with someone for support.
“It doesn’t have to be a nurse,” Dr. McDermott said. “In our studies, we’ve used bachelor’s degree-level people, but told them what to look for. They can do this and the patient feels there is someone they’re accountable to.”
Dr. McDermott and her colleagues are testing the boundaries of support in the ongoing HONOR trial, which includes four weekly visits to an exercise center in phase I to meet the telephone coach, learn to use a Fitbit monitor, and learn the behavioral skills necessary for long-term adherence. Phase II, however, is entirely home based and includes only Fitbit self-monitoring, regular telephone calls from the coach for feedback, use of the study website, and optional group telephone calls.
The bottom line with any program is for patients to understand it must be indefinite to maintain improvement.
“Unfortunately, if they don’t stick with it, they will slide back,” she cautioned.
Dr. McDermott reported research funding from the National Institutes of Health, the Patient-Centered Outcomes Research Institute (PCORI), and Novartis.
CHICAGO – Following a few simple steps can help patients with peripheral artery disease (PAD) get off on the right foot with a home-based exercise program.
“There is growing evidence that PAD patients can walk for exercise at home and improve their walking performance,” Dr. Mary McDermott said at a symposium on vascular surgery sponsored by Northwestern University.
Getting them to do so, however, can be challenging. Patients with peripheral artery disease have greater functional impairment and are at higher risk for cardiovascular disease than is the general population. They also frequently limit their activity to avoid leg problems, as their PAD progresses.
“It’s hard enough to get patients without peripheral artery disease to exercise. As a general internist, I’m well aware of that,” she said. “It’s even more difficult when walking is so painful and uncomfortable.”
At present, the American College of Cardiology/American Heart Association practice guidelines for the management of patients with PAD do not recommend advising patients with PAD to go home and walk.
The guidelines were published in 2005, however, and since 2011, three of four randomized clinical trials of home-based exercise programs have shown a significant gain in walking endurance in patients with PAD, Dr. McDermott of Northwestern University in Chicago, observed.
The most hands-off of these trials showed that patients with symptomatic PAD randomized to a supervised exercise program did the best at treadmill walking, but the home-exercise group who received a step monitor and in-person feedback just once per month did significantly better than did controls assigned light resistance training. Moreover, the home-exercise group had greater change in 6-minute walk distances than either of the other groups (J Am Heart Assoc. 2014 Oct;3[5]:e001107).
“I think the reason for this is that the home-based group was walking outside or perhaps in a mall and getting better at walking over ground,” Dr. McDermott. “The treadmill group was walking only on the treadmill.”
Supervised treadmill exercise may seem like an easier prescription to write, but it faces two major barriers, she said. Most medical insurers, including Medicare, do not pay for supervised exercise for people with PAD and intermittent claudication, and most PAD patients don’t participate. The burden of traveling to an exercise center three times weekly, week after week, to participate can be overwhelming.
“For all of these reasons, we really need to develop home-based exercise programs that work,” Dr. McDermott said.
Based on the successful trials, home-based programs should include monitoring, group support, and goal setting. Dr. McDermott and her colleagues added cognitive-behavioral therapy to group support in the Group Oriented Arterial Leg Study (GOALS), resulting in significant improvement in 6-minute walk distance at 6 months, physical activity over 7 days, and self-perception of walking endurance and speed among home walkers (JAMA. 2013 Jul 3;310[1]:57-65).
Before embarking on any home-exercise program, all patients with PAD should undergo a baseline cardiac stress test to rule out coronary artery ischemia, she cautioned. This also serves to identify any coronary ischemia that may develop during the new walking program.
Once this is performed, Dr. McDermott recommends clinicians:
• Advise patients to walk 5 days per week.
“This may seem like a lot, but it’s important to have them see this as part of their daily routine; just something they get in the habit of doing,” she said.
• Start with 10-15 minutes of walking per exercise session. Tailor the program to the individual patient.
• Walk to maximal leg pain or onset of ischemic pain. Stopping to rest is acceptable.
“A lot of patients, I find, have questions, “ ‘I can’t do this.’ ‘How can this be beneficial?’ So just letting them know that if they just walk and stop, walk and stop, and start with just 10 minutes of that and increase this over time, they really can see improvement,” Dr. McDermott said.
• Increase the walk time by 5 minutes each week.
Increase the duration until the patient is walking at least 30 minutes per session and preferably 45-50 minutes per session, excluding rest periods, she said.
• Advise patients to write down their walking goals.
Specify where they will walk, when they will walk, and the duration of walking to improve compliance, which can slip following hospitalizations or when patients experience acute illness.
• Have patients self-monitor, but also check in with someone for support.
“It doesn’t have to be a nurse,” Dr. McDermott said. “In our studies, we’ve used bachelor’s degree-level people, but told them what to look for. They can do this and the patient feels there is someone they’re accountable to.”
Dr. McDermott and her colleagues are testing the boundaries of support in the ongoing HONOR trial, which includes four weekly visits to an exercise center in phase I to meet the telephone coach, learn to use a Fitbit monitor, and learn the behavioral skills necessary for long-term adherence. Phase II, however, is entirely home based and includes only Fitbit self-monitoring, regular telephone calls from the coach for feedback, use of the study website, and optional group telephone calls.
The bottom line with any program is for patients to understand it must be indefinite to maintain improvement.
“Unfortunately, if they don’t stick with it, they will slide back,” she cautioned.
Dr. McDermott reported research funding from the National Institutes of Health, the Patient-Centered Outcomes Research Institute (PCORI), and Novartis.
CHICAGO – Following a few simple steps can help patients with peripheral artery disease (PAD) get off on the right foot with a home-based exercise program.
“There is growing evidence that PAD patients can walk for exercise at home and improve their walking performance,” Dr. Mary McDermott said at a symposium on vascular surgery sponsored by Northwestern University.
Getting them to do so, however, can be challenging. Patients with peripheral artery disease have greater functional impairment and are at higher risk for cardiovascular disease than is the general population. They also frequently limit their activity to avoid leg problems, as their PAD progresses.
“It’s hard enough to get patients without peripheral artery disease to exercise. As a general internist, I’m well aware of that,” she said. “It’s even more difficult when walking is so painful and uncomfortable.”
At present, the American College of Cardiology/American Heart Association practice guidelines for the management of patients with PAD do not recommend advising patients with PAD to go home and walk.
The guidelines were published in 2005, however, and since 2011, three of four randomized clinical trials of home-based exercise programs have shown a significant gain in walking endurance in patients with PAD, Dr. McDermott of Northwestern University in Chicago, observed.
The most hands-off of these trials showed that patients with symptomatic PAD randomized to a supervised exercise program did the best at treadmill walking, but the home-exercise group who received a step monitor and in-person feedback just once per month did significantly better than did controls assigned light resistance training. Moreover, the home-exercise group had greater change in 6-minute walk distances than either of the other groups (J Am Heart Assoc. 2014 Oct;3[5]:e001107).
“I think the reason for this is that the home-based group was walking outside or perhaps in a mall and getting better at walking over ground,” Dr. McDermott. “The treadmill group was walking only on the treadmill.”
Supervised treadmill exercise may seem like an easier prescription to write, but it faces two major barriers, she said. Most medical insurers, including Medicare, do not pay for supervised exercise for people with PAD and intermittent claudication, and most PAD patients don’t participate. The burden of traveling to an exercise center three times weekly, week after week, to participate can be overwhelming.
“For all of these reasons, we really need to develop home-based exercise programs that work,” Dr. McDermott said.
Based on the successful trials, home-based programs should include monitoring, group support, and goal setting. Dr. McDermott and her colleagues added cognitive-behavioral therapy to group support in the Group Oriented Arterial Leg Study (GOALS), resulting in significant improvement in 6-minute walk distance at 6 months, physical activity over 7 days, and self-perception of walking endurance and speed among home walkers (JAMA. 2013 Jul 3;310[1]:57-65).
Before embarking on any home-exercise program, all patients with PAD should undergo a baseline cardiac stress test to rule out coronary artery ischemia, she cautioned. This also serves to identify any coronary ischemia that may develop during the new walking program.
Once this is performed, Dr. McDermott recommends clinicians:
• Advise patients to walk 5 days per week.
“This may seem like a lot, but it’s important to have them see this as part of their daily routine; just something they get in the habit of doing,” she said.
• Start with 10-15 minutes of walking per exercise session. Tailor the program to the individual patient.
• Walk to maximal leg pain or onset of ischemic pain. Stopping to rest is acceptable.
“A lot of patients, I find, have questions, “ ‘I can’t do this.’ ‘How can this be beneficial?’ So just letting them know that if they just walk and stop, walk and stop, and start with just 10 minutes of that and increase this over time, they really can see improvement,” Dr. McDermott said.
• Increase the walk time by 5 minutes each week.
Increase the duration until the patient is walking at least 30 minutes per session and preferably 45-50 minutes per session, excluding rest periods, she said.
• Advise patients to write down their walking goals.
Specify where they will walk, when they will walk, and the duration of walking to improve compliance, which can slip following hospitalizations or when patients experience acute illness.
• Have patients self-monitor, but also check in with someone for support.
“It doesn’t have to be a nurse,” Dr. McDermott said. “In our studies, we’ve used bachelor’s degree-level people, but told them what to look for. They can do this and the patient feels there is someone they’re accountable to.”
Dr. McDermott and her colleagues are testing the boundaries of support in the ongoing HONOR trial, which includes four weekly visits to an exercise center in phase I to meet the telephone coach, learn to use a Fitbit monitor, and learn the behavioral skills necessary for long-term adherence. Phase II, however, is entirely home based and includes only Fitbit self-monitoring, regular telephone calls from the coach for feedback, use of the study website, and optional group telephone calls.
The bottom line with any program is for patients to understand it must be indefinite to maintain improvement.
“Unfortunately, if they don’t stick with it, they will slide back,” she cautioned.
Dr. McDermott reported research funding from the National Institutes of Health, the Patient-Centered Outcomes Research Institute (PCORI), and Novartis.
EXPERT ANALYSIS FROM THE NORTHWESTERN VASCULAR SYMPOSIUM

A microfluidic biochip for blood cell counts

Researchers say they have created a biosensor capable of counting blood cells electrically using only a drop of blood.
The microfluidic device can measure red blood cell, platelet, and white blood cell counts using as little as 11 µL of blood.
The device electrically counts the different types of blood cells based on their size and membrane properties.
To count leukocyte and its differentials, red blood cells are selectively lysed, and the remaining white blood cells are individually counted. Specific cells like neutrophils can be counted using multi-frequency analysis, which probes the membrane properties of the cells.
For red blood cells and platelets, 1 µL of whole blood is diluted with PBS on-chip, and the cells are counted electrically. The total time for measurement is under 20 minutes.
The researchers described this device in TECHNOLOGY.
“Our biosensor exhibits the potential to improve patient care in a spectrum of settings,” said Rashid Bashir, PhD, of the University of Illinois at Urbana-Champaign.
He noted that the device could be particularly useful in resource-limited settings where laboratory tests are often inaccessible due to costs, poor prevalence of laboratory facilities, and the difficulty of follow-up upon receiving results that take days to process.
“There exists a huge potential to translate our biosensor commercially for blood cell count applications,” added Umer Hassan, PhD, of the University of Illinois at Urbana-Champaign.
“The translation of our technology will result in minimal to no experience requirement for device operation. Even patients can perform the test at the comfort of their home and share the results with their primary care physicians via electronic means too.”
“The technology is scalable, and, in future, we plan to apply it to many other potential applications in the areas of animal diagnostics, blood transfusion analysis, ER/ICU applications, and blood cell counting for chemotherapy management,” Dr Bashir said.
The researchers are now working to further develop a portable prototype of the cell counter.
“The cartridges will be disposable and the size of a credit card,” Dr Umer said. “The base unit or the reader will be portable and possibly hand-held. Our technology has the potential to reduce the cost of the test to less than $10, as compared to $100 or more currently charged.” ![]()
Researchers say they have created a biosensor capable of counting blood cells electrically using only a drop of blood.
The microfluidic device can measure red blood cell, platelet, and white blood cell counts using as little as 11 µL of blood.
The device electrically counts the different types of blood cells based on their size and membrane properties.
To count leukocyte and its differentials, red blood cells are selectively lysed, and the remaining white blood cells are individually counted. Specific cells like neutrophils can be counted using multi-frequency analysis, which probes the membrane properties of the cells.
For red blood cells and platelets, 1 µL of whole blood is diluted with PBS on-chip, and the cells are counted electrically. The total time for measurement is under 20 minutes.
The researchers described this device in TECHNOLOGY.
“Our biosensor exhibits the potential to improve patient care in a spectrum of settings,” said Rashid Bashir, PhD, of the University of Illinois at Urbana-Champaign.
He noted that the device could be particularly useful in resource-limited settings where laboratory tests are often inaccessible due to costs, poor prevalence of laboratory facilities, and the difficulty of follow-up upon receiving results that take days to process.
“There exists a huge potential to translate our biosensor commercially for blood cell count applications,” added Umer Hassan, PhD, of the University of Illinois at Urbana-Champaign.
“The translation of our technology will result in minimal to no experience requirement for device operation. Even patients can perform the test at the comfort of their home and share the results with their primary care physicians via electronic means too.”
“The technology is scalable, and, in future, we plan to apply it to many other potential applications in the areas of animal diagnostics, blood transfusion analysis, ER/ICU applications, and blood cell counting for chemotherapy management,” Dr Bashir said.
The researchers are now working to further develop a portable prototype of the cell counter.
“The cartridges will be disposable and the size of a credit card,” Dr Umer said. “The base unit or the reader will be portable and possibly hand-held. Our technology has the potential to reduce the cost of the test to less than $10, as compared to $100 or more currently charged.” ![]()
Researchers say they have created a biosensor capable of counting blood cells electrically using only a drop of blood.
The microfluidic device can measure red blood cell, platelet, and white blood cell counts using as little as 11 µL of blood.
The device electrically counts the different types of blood cells based on their size and membrane properties.
To count leukocyte and its differentials, red blood cells are selectively lysed, and the remaining white blood cells are individually counted. Specific cells like neutrophils can be counted using multi-frequency analysis, which probes the membrane properties of the cells.
For red blood cells and platelets, 1 µL of whole blood is diluted with PBS on-chip, and the cells are counted electrically. The total time for measurement is under 20 minutes.
The researchers described this device in TECHNOLOGY.
“Our biosensor exhibits the potential to improve patient care in a spectrum of settings,” said Rashid Bashir, PhD, of the University of Illinois at Urbana-Champaign.
He noted that the device could be particularly useful in resource-limited settings where laboratory tests are often inaccessible due to costs, poor prevalence of laboratory facilities, and the difficulty of follow-up upon receiving results that take days to process.
“There exists a huge potential to translate our biosensor commercially for blood cell count applications,” added Umer Hassan, PhD, of the University of Illinois at Urbana-Champaign.
“The translation of our technology will result in minimal to no experience requirement for device operation. Even patients can perform the test at the comfort of their home and share the results with their primary care physicians via electronic means too.”
“The technology is scalable, and, in future, we plan to apply it to many other potential applications in the areas of animal diagnostics, blood transfusion analysis, ER/ICU applications, and blood cell counting for chemotherapy management,” Dr Bashir said.
The researchers are now working to further develop a portable prototype of the cell counter.
“The cartridges will be disposable and the size of a credit card,” Dr Umer said. “The base unit or the reader will be portable and possibly hand-held. Our technology has the potential to reduce the cost of the test to less than $10, as compared to $100 or more currently charged.” ![]()
Myeloma drug could treat sickle cell disease, team says

and a normal one
Image by Betty Pace
Preclinical research suggests a drug used to treat multiple myeloma (MM) might also prove effective in the treatment of sickle cell disease (SCD).
Researchers say this study is the first to reveal how the drug, pomalidomide, increases the production of fetal hemoglobin, which is known to interfere with the sickling of red blood cells.
“We knew the drug would make fetal hemoglobin, but we didn’t know to what extent or how,” said Lionel Blanc, PhD, of the Feinstein Institute for Medical Research in Manhasset, New York.
He and his colleagues reported their findings in Blood.
The researchers’ in vitro experiments revealed that pomalidomide reverses γ-globin silencing during adult erythropoiesis, and the drug delays the maturation of early erythroid precursors without impairing terminal differentiation.
The team also found that pomalidomide selectively targets BCL11A and SOX6 to induce γ-globin synthesis, the drug’s mechanism of action during erythropoiesis is independent of IKZF1 degradation, and pomalidomide partially reprograms adult erythroid progenitors to a fetal-like state.
Finally, the researchers discovered that pomalidomide’s mechanism of action is conserved in cells from SCD patients, and treatment with pomalidomide leads to γ-globin production in MM patients.
“We can also say something else—that hydroxyurea, the only FDA-approved drug for sickle cell anemia, was less effective than pomalidomide and appeared to act through a different mechanism of action,” Dr Blanc said.
“The current therapy is good, but not everyone responds equally to hydroxyurea, and what we hope with pomalidomide is to improve this.”
Dr Blanc and his colleagues plan to launch a clinical trial in the near future to test pomalidomide in young adults with SCD. ![]()
and a normal one
Image by Betty Pace
Preclinical research suggests a drug used to treat multiple myeloma (MM) might also prove effective in the treatment of sickle cell disease (SCD).
Researchers say this study is the first to reveal how the drug, pomalidomide, increases the production of fetal hemoglobin, which is known to interfere with the sickling of red blood cells.
“We knew the drug would make fetal hemoglobin, but we didn’t know to what extent or how,” said Lionel Blanc, PhD, of the Feinstein Institute for Medical Research in Manhasset, New York.
He and his colleagues reported their findings in Blood.
The researchers’ in vitro experiments revealed that pomalidomide reverses γ-globin silencing during adult erythropoiesis, and the drug delays the maturation of early erythroid precursors without impairing terminal differentiation.
The team also found that pomalidomide selectively targets BCL11A and SOX6 to induce γ-globin synthesis, the drug’s mechanism of action during erythropoiesis is independent of IKZF1 degradation, and pomalidomide partially reprograms adult erythroid progenitors to a fetal-like state.
Finally, the researchers discovered that pomalidomide’s mechanism of action is conserved in cells from SCD patients, and treatment with pomalidomide leads to γ-globin production in MM patients.
“We can also say something else—that hydroxyurea, the only FDA-approved drug for sickle cell anemia, was less effective than pomalidomide and appeared to act through a different mechanism of action,” Dr Blanc said.
“The current therapy is good, but not everyone responds equally to hydroxyurea, and what we hope with pomalidomide is to improve this.”
Dr Blanc and his colleagues plan to launch a clinical trial in the near future to test pomalidomide in young adults with SCD. ![]()
and a normal one
Image by Betty Pace
Preclinical research suggests a drug used to treat multiple myeloma (MM) might also prove effective in the treatment of sickle cell disease (SCD).
Researchers say this study is the first to reveal how the drug, pomalidomide, increases the production of fetal hemoglobin, which is known to interfere with the sickling of red blood cells.
“We knew the drug would make fetal hemoglobin, but we didn’t know to what extent or how,” said Lionel Blanc, PhD, of the Feinstein Institute for Medical Research in Manhasset, New York.
He and his colleagues reported their findings in Blood.
The researchers’ in vitro experiments revealed that pomalidomide reverses γ-globin silencing during adult erythropoiesis, and the drug delays the maturation of early erythroid precursors without impairing terminal differentiation.
The team also found that pomalidomide selectively targets BCL11A and SOX6 to induce γ-globin synthesis, the drug’s mechanism of action during erythropoiesis is independent of IKZF1 degradation, and pomalidomide partially reprograms adult erythroid progenitors to a fetal-like state.
Finally, the researchers discovered that pomalidomide’s mechanism of action is conserved in cells from SCD patients, and treatment with pomalidomide leads to γ-globin production in MM patients.
“We can also say something else—that hydroxyurea, the only FDA-approved drug for sickle cell anemia, was less effective than pomalidomide and appeared to act through a different mechanism of action,” Dr Blanc said.
“The current therapy is good, but not everyone responds equally to hydroxyurea, and what we hope with pomalidomide is to improve this.”
Dr Blanc and his colleagues plan to launch a clinical trial in the near future to test pomalidomide in young adults with SCD. ![]()
2014 sets U.S. record for drug overdose deaths
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
In 2014, 47,055 people in the United States died from drug overdoses – more deaths than attributed to this cause in any previous year on record, according to data from the National Vital Statistics System.
Opioids, primarily prescription pain relievers and heroin, were the main drugs associated with overdose deaths. In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths, Rose A. Rudd of the Centers for Disease Control and Prevention and her colleagues wrote (MMWR. 2015 Dec 18;64[Early release]:1-5).
The rate of opioid overdoses has tripled since 2000; the 15-year trend data implicate prescription opioid pain relievers and a recent surge in illicit opioid overdose deaths, driven largely by heroin.
From 2013 to 2014, synthetic opioids other than methadone (e.g., fentanyl and tramadol) drove the largest increase in the rate of drug overdose deaths. The rate nearly doubled from 1 per 100,000 persons to 1.8 per 100,000 persons. In 2014, the rate of drug overdose deaths involving natural and semisynthetic opioids (for example, morphine, oxycodone, and hydrocodone) was 3.8 per 100,000. The rate of drug overdose deaths involving methadone, a synthetic opioid classified separately from other synthetic opioids, was similar in 2013 and 2014.
The five states with the highest rates of drug overdose deaths in 2014 were West Virginia (35.5 deaths per 100,000), New Mexico (27.3), New Hampshire (26.2), Kentucky (24.7), and Ohio (24.6).
States with statistically significant increases in the rate of drug overdose deaths from 2013 to 2014 included Alabama, Georgia, Illinois, Indiana, Maine, Maryland, Massachusetts, Michigan, New Hampshire, New Mexico, North Dakota, Ohio, Pennsylvania, and Virginia.
The rates were noted in all adult age groups. From 2013 to 2014, statistically significant increases in drug overdose death rates were seen for both males and females, persons aged 25-34 years, 35-44 years, 55-64 years, and 65 years and older. Based on ethnicity, increases were seen in non-Hispanic whites and non-Hispanic blacks. Based on residency, increases were most common in the Northeast, Midwest, and South.
The authors noted three limitations of the data: First, the substances tested for and circumstances under which toxicologic tests are performed vary by jurisdiction; in 2013 and 2014, 22% and 19% of drug overdose deaths, respectively, did not include information on the death certificate about the specific types of drugs involved, and the percent of overdose deaths with specific drugs identified on the death certificate varies widely by state. Second, an increase from 2013 to 2014 in reporting of specific drugs involved in drug overdose deaths might have contributed to some of the observed increases in drug overdose death rates involving different types of opioids. Finally, some heroin deaths might be misclassified or underreported because morphine and heroin are similarly metabolized.
Efforts to encourage safer prescribing of opioid pain relievers should be strengthened, according to the authors. CDC has developed a draft guideline for the prescribing of opioids for chronic pain to address this need. The guideline is available at www.cdc.gov/drugoverdose/prescribing/guideline.html.
On Twitter @maryjodales
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
Key clinical point: Efforts to encourage safer prescribing of opioid pain relievers should be strengthened.
Major finding: In 2014, opioids were involved in 28,647 deaths, or 61% of all drug overdose deaths.
Data source: The National Vital Statistics System multiple cause-of-death mortality files.
Disclosures: The authors had no relevant financial disclosures.
Flu activity increases slightly across U.S.
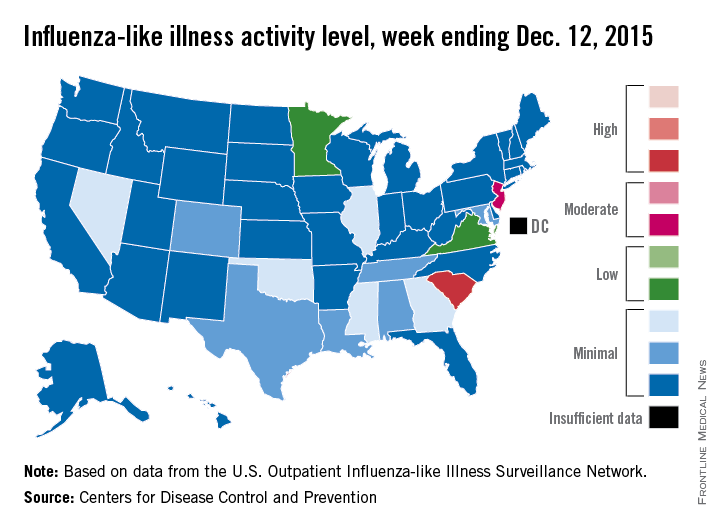
Influenza activity dropped slightly in South Carolina, but remained high enough to make it the nation’s hot spot during week 9 of the 2015-2016 U.S. flu season, the Centers for Disease Control and Prevention reported Dec. 18.
The activity of influenza-like illness (ILI) in South Carolina went from level 9 down to level 8 for the week ending Dec. 12 (week 9), but that kept it in the “high” range, according to the CDC report.
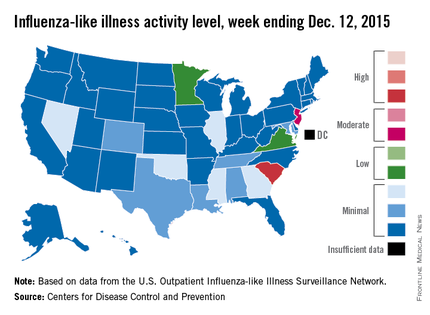
The rest of the United States saw a slight increase in activity, with 15 states at level 2 or higher, compared with 13 the week before. New Jersey had the next-highest level of activity after South Carolina, rising from level 5 last week to level 6, which moved it into the “moderate” range.
Minnesota had the largest increase in ILI activity from the previous week, going from level 1 to level 4, and other states with increased activity were Alabama, Colorado, Georgia, Illinois, Nevada, Tennessee, and Virginia. States besides South Carolina with decreased activity were Arizona, Hawaii, Louisiana, Mississippi, and Texas, the CDC data show.
The proportion of outpatient visits nationwide for ILI – defined as a temperature of 100° F or greater and cough and/or sore throat – was 1.9%, continuing to stay below the national baseline of 2.1%, the CDC said.
Outside of the fifty states, Guam reported widespread activity, Puerto Rico reported “moderate” (level 7) activity, and the District of Columbia and the U.S. Virgin Islands reported sporadic activity, the CDC noted.
Influenza activity dropped slightly in South Carolina, but remained high enough to make it the nation’s hot spot during week 9 of the 2015-2016 U.S. flu season, the Centers for Disease Control and Prevention reported Dec. 18.
The activity of influenza-like illness (ILI) in South Carolina went from level 9 down to level 8 for the week ending Dec. 12 (week 9), but that kept it in the “high” range, according to the CDC report.
The rest of the United States saw a slight increase in activity, with 15 states at level 2 or higher, compared with 13 the week before. New Jersey had the next-highest level of activity after South Carolina, rising from level 5 last week to level 6, which moved it into the “moderate” range.
Minnesota had the largest increase in ILI activity from the previous week, going from level 1 to level 4, and other states with increased activity were Alabama, Colorado, Georgia, Illinois, Nevada, Tennessee, and Virginia. States besides South Carolina with decreased activity were Arizona, Hawaii, Louisiana, Mississippi, and Texas, the CDC data show.
The proportion of outpatient visits nationwide for ILI – defined as a temperature of 100° F or greater and cough and/or sore throat – was 1.9%, continuing to stay below the national baseline of 2.1%, the CDC said.
Outside of the fifty states, Guam reported widespread activity, Puerto Rico reported “moderate” (level 7) activity, and the District of Columbia and the U.S. Virgin Islands reported sporadic activity, the CDC noted.
Influenza activity dropped slightly in South Carolina, but remained high enough to make it the nation’s hot spot during week 9 of the 2015-2016 U.S. flu season, the Centers for Disease Control and Prevention reported Dec. 18.
The activity of influenza-like illness (ILI) in South Carolina went from level 9 down to level 8 for the week ending Dec. 12 (week 9), but that kept it in the “high” range, according to the CDC report.
The rest of the United States saw a slight increase in activity, with 15 states at level 2 or higher, compared with 13 the week before. New Jersey had the next-highest level of activity after South Carolina, rising from level 5 last week to level 6, which moved it into the “moderate” range.
Minnesota had the largest increase in ILI activity from the previous week, going from level 1 to level 4, and other states with increased activity were Alabama, Colorado, Georgia, Illinois, Nevada, Tennessee, and Virginia. States besides South Carolina with decreased activity were Arizona, Hawaii, Louisiana, Mississippi, and Texas, the CDC data show.
The proportion of outpatient visits nationwide for ILI – defined as a temperature of 100° F or greater and cough and/or sore throat – was 1.9%, continuing to stay below the national baseline of 2.1%, the CDC said.
Outside of the fifty states, Guam reported widespread activity, Puerto Rico reported “moderate” (level 7) activity, and the District of Columbia and the U.S. Virgin Islands reported sporadic activity, the CDC noted.
New agents effectively target CLL’s molecular Achilles
SAN FRANCISCO – Novel targeted agents offer more options for treating chronic lymphocytic leukemia (CLL), and if properly leveraged, may be able to shorten the time on treatment, improving acceptability to patients and possibly reducing treatment costs, according to Dr. William G. Wierda.
BTK inhibitors
Agents that inhibit Bruton tyrosine kinase (BTK) block signaling through the B-cell receptor in CLL, triggering apoptosis, said Dr. Wierda, professor and medical director, department of leukemia, division of cancer medicine, at the University of Texas MD Anderson Cancer Center in Houston. One such agent, ibrutinib (Imbruvica), is approved by the Food and Drug Administration for treatment of relapsed CLL and for treatment of newly diagnosed CLL having 17p deletion, a high-risk factor.

Results from RESONATE-2, a randomized trial comparing ibrutinib with chlorambucil as frontline therapy in older adults with CLL or small lymphocytic lymphoma, will be reported later this year. “We don’t know the details of that publicly yet, but we do know from a press release that it is a positive trial and showed improvement in outcomes for ibrutinib-treated patients. With that data, we will likely have an expanded label for ibrutinib into the frontline setting, at least for the elderly population,” he said at the NCCN Annual Congress: Hematologic Malignancies.
Longer-term data, collected 3 years after patients started ibrutinib monotherapy, have been very good, with overall response rates of 90% in those with relapsed or refractory disease and 87% in those with treatment-naive disease (ASCO 2014. Abstract 7014). “The last time I saw these data updated, the complete remission portions have increased. So as patients remain on the treatment, responses do improve,” Dr. Wierda noted. Complete remission rates now are about 14% and 24%, respectively. Median progression-free survival has not been reached in either group.
Data from the randomized RESONATE trial, which led to ibrutinib’s approval in relapsed CLL, showed benefit relative to ofatumumab across subgroups, including patients who had disease that was refractory to purine analogs, who had the 17p deletion and who had received at least three prior regimens (ASCO 2014. Abstract LBA7008).
The main grade 3 or 4 toxicity of ibrutinib in patients with CLL is infections, but atrial fibrillation and bleeding/hemorrhage are each seen in about 5% of patients. “The trials all excluded patients on warfarin, so we do not recommend treating patients with ibrutinib who are on warfarin,” Dr. Wierda commented. “If patients are anticoagulated on warfarin and we want to put them on ibrutinib, I will usually switch them over to something like Xarelto [rivaroxaban],” he said. Toxicity generally declines with longer treatment.
Discontinuations because of toxicity or Richter transformation usually occur within the first 18 months (JAMA Oncol. 2015;1[1]:80-7). “The concerning [point] for me though is the patients who develop refractory disease. … The incidence starts to go up significantly as you go out beyond 30 or 36 months,” he said. “We are reviewing our data right now to see if we make a similar observation. But that suggests to me that the longer the patients stay on treatment, the more at risk they are for progressing and developing refractory disease.”
The HELIOS trial tested addition of ibrutinib to bendamustine (Treanda) and rituximab (Rituxan) (ASCO 2015. Abstract LBA7005). Results showed superior progression-free survival with the three-drug combination. “But the question that always comes up when this data is presented is, well, how would it compare with ibrutinib monotherapy? Until that question for me is adequately addressed … I would probably be inclined to give patients ibrutinib monotherapy over the combination,” Dr. Wierda said.
Trials are testing a wide range of other combinations. “To me, this suggests that we really don’t have a direction or a rational strategy for combinations with these agents. … Right now, I’m excited about combining ibrutinib with venetoclax. … They seem clinically complementary, and there is some laboratory data that suggests as well that there will be a complementary mechanism of action.”
PI3 kinase inhibitors
Inhibitors of PI3 kinase also block signaling through the B-cell receptor. In this drug class, idelalisib (Zydelig) is approved for treating relapsed CLL in combination with rituximab.
The phase III trial establishing efficacy of this combination showed that it improved both progression-free and overall survival over rituximab alone (ASH 2014. Abstract 330). Median progression-free survival was 19.4 months. There was similar benefit across various subgroups, including patients with 17p deletion or an unmutated IGHV gene, another high-risk factor.
One of the main toxicities of idelalisib, elevation of liver function test results, typically occurs early and is usually not treatment limiting. Colitis occurs with two predominant patterns: early onset and late onset. “The early colitis in my experience hasn’t necessarily been treatment limiting. We can usually get those patients through their diarrhea [by] withholding the drug; sometimes we’ll give budesonide, and can restart the drug at a lower dose,” Dr. Wierda said. “It’s the late colitis that we have difficulty with – colitis that occurs after patients have been on 3 months, 6 months. And in my experience, those patients have had more severe colitis, and it’s been more treatment limiting.”
Ongoing trials are testing idelalisib in combinations for CLL as well. “Certainly, there’s a number of strategies, and as with ibrutinib, it’s difficult for me to identify a rational combination or a clear combination that I think is going to be superior or a significant advance,” he said. Trials are also testing other PI3 kinase inhibitors, such as duvelisib (IPI-145), now in a phase III registration trial in patients with relapsed or refractory disease.
BCL-2 inhibitors
The investigational agent venetoclax (formerly ABT-199/GDC-199) inhibits BCL-2, which is overexpressed in CLL and renders the cells resistant to apoptosis. It has advanced to a pair of phase III trials, one testing it when combined with rituximab and the other when combined with obinutuzumab (Gazyva).
When used as monotherapy for patients with relapsed disease, venetoclax achieved an overall response rate of 77% and a complete response rate of 23% (EHA 2014. Abstract S702). Benefit was similar among high-risk groups, including patients with the 17p deletion or fludarabine-refractory disease. With a median follow-up of 5.3 months, median progression-free survival for patients treated at the full dose has not been reached.
In earlier trials, venetoclax was associated with a problematic tumor lysis syndrome, according to Dr. Wierda. But that issue has largely been resolved by starting at a low dose and escalating gradually to a full dose; in the trial, it was seen in 7% of patients. The most common grade 3 or 4 adverse event was neutropenia, seen in 33% of patients; however, this toxicity can usually be managed with growth factors and dose reduction, he said.
The combination of venetoclax with rituximab in relapsed CLL yields an 88% overall response rate and a 31% complete response rate (ASH 2014. Abstract 325). Respective values were 78% and 22% in patients with 17p deletion. Moreover, some patients were found to have become negative for minimal residual disease on the combination, although it was not systematically assessed, Dr. Wierda noted.
“Venetoclax is a drug we will hear more about. … It has activity. I think it has a future in treating CLL, and it will be approved in time,” he said.
Leveraging targeted therapies
These new targeted agents, and others in the pipeline, could potentially be leveraged in several ways to improve CLL treatment strategies, according to Dr. Wierda.
Importantly, if ibrutinib becomes approved for universal frontline therapy, a large share of patients are likely to achieve partial remission. “We know if patients are in partial remission, you can’t really stop their treatment on ibrutinib; they will progress. And there was some data reported at ASH [American Society of Hematology] this past year that patients who were on a lower dose or patients who had dose interruption did poorer,” he said. Furthermore, most patients don’t like to be on treatment indefinitely.
“So we’re working on trials to expand our options for consolidation strategies in patients who have been on ibrutinib. We are trying to push them over into a complete remission by adding additional agents,” he explained.
For example, an ongoing trial is testing addition of nivolumab (Opdivo), an immune checkpoint inhibitor, in patients who have been on ibrutinib for at least 9 months and still have a partial remission. “The strategy with that is to try to consolidate them and to get them into a deep remission, where we can have a discussion about holding their treatment or stopping their treatment, or at least to the point where we are comfortable doing that,” he said.
Dr. Wierda disclosed that he has various relationships with AbbVie, Ascerta, Celgene, Emergent BioSolutions, Genentech, Genzyme, Gilead Sciences, GlaxoSmithKline, Juno Therapeutics, Karyopharm, Kite Pharma, Merck, Novartis Pharmaceuticals, Pharmacyclics, Roche Laboratories, and Sanofi-Aventis U.S.
SAN FRANCISCO – Novel targeted agents offer more options for treating chronic lymphocytic leukemia (CLL), and if properly leveraged, may be able to shorten the time on treatment, improving acceptability to patients and possibly reducing treatment costs, according to Dr. William G. Wierda.
BTK inhibitors
Agents that inhibit Bruton tyrosine kinase (BTK) block signaling through the B-cell receptor in CLL, triggering apoptosis, said Dr. Wierda, professor and medical director, department of leukemia, division of cancer medicine, at the University of Texas MD Anderson Cancer Center in Houston. One such agent, ibrutinib (Imbruvica), is approved by the Food and Drug Administration for treatment of relapsed CLL and for treatment of newly diagnosed CLL having 17p deletion, a high-risk factor.
Results from RESONATE-2, a randomized trial comparing ibrutinib with chlorambucil as frontline therapy in older adults with CLL or small lymphocytic lymphoma, will be reported later this year. “We don’t know the details of that publicly yet, but we do know from a press release that it is a positive trial and showed improvement in outcomes for ibrutinib-treated patients. With that data, we will likely have an expanded label for ibrutinib into the frontline setting, at least for the elderly population,” he said at the NCCN Annual Congress: Hematologic Malignancies.
Longer-term data, collected 3 years after patients started ibrutinib monotherapy, have been very good, with overall response rates of 90% in those with relapsed or refractory disease and 87% in those with treatment-naive disease (ASCO 2014. Abstract 7014). “The last time I saw these data updated, the complete remission portions have increased. So as patients remain on the treatment, responses do improve,” Dr. Wierda noted. Complete remission rates now are about 14% and 24%, respectively. Median progression-free survival has not been reached in either group.
Data from the randomized RESONATE trial, which led to ibrutinib’s approval in relapsed CLL, showed benefit relative to ofatumumab across subgroups, including patients who had disease that was refractory to purine analogs, who had the 17p deletion and who had received at least three prior regimens (ASCO 2014. Abstract LBA7008).
The main grade 3 or 4 toxicity of ibrutinib in patients with CLL is infections, but atrial fibrillation and bleeding/hemorrhage are each seen in about 5% of patients. “The trials all excluded patients on warfarin, so we do not recommend treating patients with ibrutinib who are on warfarin,” Dr. Wierda commented. “If patients are anticoagulated on warfarin and we want to put them on ibrutinib, I will usually switch them over to something like Xarelto [rivaroxaban],” he said. Toxicity generally declines with longer treatment.
Discontinuations because of toxicity or Richter transformation usually occur within the first 18 months (JAMA Oncol. 2015;1[1]:80-7). “The concerning [point] for me though is the patients who develop refractory disease. … The incidence starts to go up significantly as you go out beyond 30 or 36 months,” he said. “We are reviewing our data right now to see if we make a similar observation. But that suggests to me that the longer the patients stay on treatment, the more at risk they are for progressing and developing refractory disease.”
The HELIOS trial tested addition of ibrutinib to bendamustine (Treanda) and rituximab (Rituxan) (ASCO 2015. Abstract LBA7005). Results showed superior progression-free survival with the three-drug combination. “But the question that always comes up when this data is presented is, well, how would it compare with ibrutinib monotherapy? Until that question for me is adequately addressed … I would probably be inclined to give patients ibrutinib monotherapy over the combination,” Dr. Wierda said.
Trials are testing a wide range of other combinations. “To me, this suggests that we really don’t have a direction or a rational strategy for combinations with these agents. … Right now, I’m excited about combining ibrutinib with venetoclax. … They seem clinically complementary, and there is some laboratory data that suggests as well that there will be a complementary mechanism of action.”
PI3 kinase inhibitors
Inhibitors of PI3 kinase also block signaling through the B-cell receptor. In this drug class, idelalisib (Zydelig) is approved for treating relapsed CLL in combination with rituximab.
The phase III trial establishing efficacy of this combination showed that it improved both progression-free and overall survival over rituximab alone (ASH 2014. Abstract 330). Median progression-free survival was 19.4 months. There was similar benefit across various subgroups, including patients with 17p deletion or an unmutated IGHV gene, another high-risk factor.
One of the main toxicities of idelalisib, elevation of liver function test results, typically occurs early and is usually not treatment limiting. Colitis occurs with two predominant patterns: early onset and late onset. “The early colitis in my experience hasn’t necessarily been treatment limiting. We can usually get those patients through their diarrhea [by] withholding the drug; sometimes we’ll give budesonide, and can restart the drug at a lower dose,” Dr. Wierda said. “It’s the late colitis that we have difficulty with – colitis that occurs after patients have been on 3 months, 6 months. And in my experience, those patients have had more severe colitis, and it’s been more treatment limiting.”
Ongoing trials are testing idelalisib in combinations for CLL as well. “Certainly, there’s a number of strategies, and as with ibrutinib, it’s difficult for me to identify a rational combination or a clear combination that I think is going to be superior or a significant advance,” he said. Trials are also testing other PI3 kinase inhibitors, such as duvelisib (IPI-145), now in a phase III registration trial in patients with relapsed or refractory disease.
BCL-2 inhibitors
The investigational agent venetoclax (formerly ABT-199/GDC-199) inhibits BCL-2, which is overexpressed in CLL and renders the cells resistant to apoptosis. It has advanced to a pair of phase III trials, one testing it when combined with rituximab and the other when combined with obinutuzumab (Gazyva).
When used as monotherapy for patients with relapsed disease, venetoclax achieved an overall response rate of 77% and a complete response rate of 23% (EHA 2014. Abstract S702). Benefit was similar among high-risk groups, including patients with the 17p deletion or fludarabine-refractory disease. With a median follow-up of 5.3 months, median progression-free survival for patients treated at the full dose has not been reached.
In earlier trials, venetoclax was associated with a problematic tumor lysis syndrome, according to Dr. Wierda. But that issue has largely been resolved by starting at a low dose and escalating gradually to a full dose; in the trial, it was seen in 7% of patients. The most common grade 3 or 4 adverse event was neutropenia, seen in 33% of patients; however, this toxicity can usually be managed with growth factors and dose reduction, he said.
The combination of venetoclax with rituximab in relapsed CLL yields an 88% overall response rate and a 31% complete response rate (ASH 2014. Abstract 325). Respective values were 78% and 22% in patients with 17p deletion. Moreover, some patients were found to have become negative for minimal residual disease on the combination, although it was not systematically assessed, Dr. Wierda noted.
“Venetoclax is a drug we will hear more about. … It has activity. I think it has a future in treating CLL, and it will be approved in time,” he said.
Leveraging targeted therapies
These new targeted agents, and others in the pipeline, could potentially be leveraged in several ways to improve CLL treatment strategies, according to Dr. Wierda.
Importantly, if ibrutinib becomes approved for universal frontline therapy, a large share of patients are likely to achieve partial remission. “We know if patients are in partial remission, you can’t really stop their treatment on ibrutinib; they will progress. And there was some data reported at ASH [American Society of Hematology] this past year that patients who were on a lower dose or patients who had dose interruption did poorer,” he said. Furthermore, most patients don’t like to be on treatment indefinitely.
“So we’re working on trials to expand our options for consolidation strategies in patients who have been on ibrutinib. We are trying to push them over into a complete remission by adding additional agents,” he explained.
For example, an ongoing trial is testing addition of nivolumab (Opdivo), an immune checkpoint inhibitor, in patients who have been on ibrutinib for at least 9 months and still have a partial remission. “The strategy with that is to try to consolidate them and to get them into a deep remission, where we can have a discussion about holding their treatment or stopping their treatment, or at least to the point where we are comfortable doing that,” he said.
Dr. Wierda disclosed that he has various relationships with AbbVie, Ascerta, Celgene, Emergent BioSolutions, Genentech, Genzyme, Gilead Sciences, GlaxoSmithKline, Juno Therapeutics, Karyopharm, Kite Pharma, Merck, Novartis Pharmaceuticals, Pharmacyclics, Roche Laboratories, and Sanofi-Aventis U.S.
SAN FRANCISCO – Novel targeted agents offer more options for treating chronic lymphocytic leukemia (CLL), and if properly leveraged, may be able to shorten the time on treatment, improving acceptability to patients and possibly reducing treatment costs, according to Dr. William G. Wierda.
BTK inhibitors
Agents that inhibit Bruton tyrosine kinase (BTK) block signaling through the B-cell receptor in CLL, triggering apoptosis, said Dr. Wierda, professor and medical director, department of leukemia, division of cancer medicine, at the University of Texas MD Anderson Cancer Center in Houston. One such agent, ibrutinib (Imbruvica), is approved by the Food and Drug Administration for treatment of relapsed CLL and for treatment of newly diagnosed CLL having 17p deletion, a high-risk factor.
Results from RESONATE-2, a randomized trial comparing ibrutinib with chlorambucil as frontline therapy in older adults with CLL or small lymphocytic lymphoma, will be reported later this year. “We don’t know the details of that publicly yet, but we do know from a press release that it is a positive trial and showed improvement in outcomes for ibrutinib-treated patients. With that data, we will likely have an expanded label for ibrutinib into the frontline setting, at least for the elderly population,” he said at the NCCN Annual Congress: Hematologic Malignancies.
Longer-term data, collected 3 years after patients started ibrutinib monotherapy, have been very good, with overall response rates of 90% in those with relapsed or refractory disease and 87% in those with treatment-naive disease (ASCO 2014. Abstract 7014). “The last time I saw these data updated, the complete remission portions have increased. So as patients remain on the treatment, responses do improve,” Dr. Wierda noted. Complete remission rates now are about 14% and 24%, respectively. Median progression-free survival has not been reached in either group.
Data from the randomized RESONATE trial, which led to ibrutinib’s approval in relapsed CLL, showed benefit relative to ofatumumab across subgroups, including patients who had disease that was refractory to purine analogs, who had the 17p deletion and who had received at least three prior regimens (ASCO 2014. Abstract LBA7008).
The main grade 3 or 4 toxicity of ibrutinib in patients with CLL is infections, but atrial fibrillation and bleeding/hemorrhage are each seen in about 5% of patients. “The trials all excluded patients on warfarin, so we do not recommend treating patients with ibrutinib who are on warfarin,” Dr. Wierda commented. “If patients are anticoagulated on warfarin and we want to put them on ibrutinib, I will usually switch them over to something like Xarelto [rivaroxaban],” he said. Toxicity generally declines with longer treatment.
Discontinuations because of toxicity or Richter transformation usually occur within the first 18 months (JAMA Oncol. 2015;1[1]:80-7). “The concerning [point] for me though is the patients who develop refractory disease. … The incidence starts to go up significantly as you go out beyond 30 or 36 months,” he said. “We are reviewing our data right now to see if we make a similar observation. But that suggests to me that the longer the patients stay on treatment, the more at risk they are for progressing and developing refractory disease.”
The HELIOS trial tested addition of ibrutinib to bendamustine (Treanda) and rituximab (Rituxan) (ASCO 2015. Abstract LBA7005). Results showed superior progression-free survival with the three-drug combination. “But the question that always comes up when this data is presented is, well, how would it compare with ibrutinib monotherapy? Until that question for me is adequately addressed … I would probably be inclined to give patients ibrutinib monotherapy over the combination,” Dr. Wierda said.
Trials are testing a wide range of other combinations. “To me, this suggests that we really don’t have a direction or a rational strategy for combinations with these agents. … Right now, I’m excited about combining ibrutinib with venetoclax. … They seem clinically complementary, and there is some laboratory data that suggests as well that there will be a complementary mechanism of action.”
PI3 kinase inhibitors
Inhibitors of PI3 kinase also block signaling through the B-cell receptor. In this drug class, idelalisib (Zydelig) is approved for treating relapsed CLL in combination with rituximab.
The phase III trial establishing efficacy of this combination showed that it improved both progression-free and overall survival over rituximab alone (ASH 2014. Abstract 330). Median progression-free survival was 19.4 months. There was similar benefit across various subgroups, including patients with 17p deletion or an unmutated IGHV gene, another high-risk factor.
One of the main toxicities of idelalisib, elevation of liver function test results, typically occurs early and is usually not treatment limiting. Colitis occurs with two predominant patterns: early onset and late onset. “The early colitis in my experience hasn’t necessarily been treatment limiting. We can usually get those patients through their diarrhea [by] withholding the drug; sometimes we’ll give budesonide, and can restart the drug at a lower dose,” Dr. Wierda said. “It’s the late colitis that we have difficulty with – colitis that occurs after patients have been on 3 months, 6 months. And in my experience, those patients have had more severe colitis, and it’s been more treatment limiting.”
Ongoing trials are testing idelalisib in combinations for CLL as well. “Certainly, there’s a number of strategies, and as with ibrutinib, it’s difficult for me to identify a rational combination or a clear combination that I think is going to be superior or a significant advance,” he said. Trials are also testing other PI3 kinase inhibitors, such as duvelisib (IPI-145), now in a phase III registration trial in patients with relapsed or refractory disease.
BCL-2 inhibitors
The investigational agent venetoclax (formerly ABT-199/GDC-199) inhibits BCL-2, which is overexpressed in CLL and renders the cells resistant to apoptosis. It has advanced to a pair of phase III trials, one testing it when combined with rituximab and the other when combined with obinutuzumab (Gazyva).
When used as monotherapy for patients with relapsed disease, venetoclax achieved an overall response rate of 77% and a complete response rate of 23% (EHA 2014. Abstract S702). Benefit was similar among high-risk groups, including patients with the 17p deletion or fludarabine-refractory disease. With a median follow-up of 5.3 months, median progression-free survival for patients treated at the full dose has not been reached.
In earlier trials, venetoclax was associated with a problematic tumor lysis syndrome, according to Dr. Wierda. But that issue has largely been resolved by starting at a low dose and escalating gradually to a full dose; in the trial, it was seen in 7% of patients. The most common grade 3 or 4 adverse event was neutropenia, seen in 33% of patients; however, this toxicity can usually be managed with growth factors and dose reduction, he said.
The combination of venetoclax with rituximab in relapsed CLL yields an 88% overall response rate and a 31% complete response rate (ASH 2014. Abstract 325). Respective values were 78% and 22% in patients with 17p deletion. Moreover, some patients were found to have become negative for minimal residual disease on the combination, although it was not systematically assessed, Dr. Wierda noted.
“Venetoclax is a drug we will hear more about. … It has activity. I think it has a future in treating CLL, and it will be approved in time,” he said.
Leveraging targeted therapies
These new targeted agents, and others in the pipeline, could potentially be leveraged in several ways to improve CLL treatment strategies, according to Dr. Wierda.
Importantly, if ibrutinib becomes approved for universal frontline therapy, a large share of patients are likely to achieve partial remission. “We know if patients are in partial remission, you can’t really stop their treatment on ibrutinib; they will progress. And there was some data reported at ASH [American Society of Hematology] this past year that patients who were on a lower dose or patients who had dose interruption did poorer,” he said. Furthermore, most patients don’t like to be on treatment indefinitely.
“So we’re working on trials to expand our options for consolidation strategies in patients who have been on ibrutinib. We are trying to push them over into a complete remission by adding additional agents,” he explained.
For example, an ongoing trial is testing addition of nivolumab (Opdivo), an immune checkpoint inhibitor, in patients who have been on ibrutinib for at least 9 months and still have a partial remission. “The strategy with that is to try to consolidate them and to get them into a deep remission, where we can have a discussion about holding their treatment or stopping their treatment, or at least to the point where we are comfortable doing that,” he said.
Dr. Wierda disclosed that he has various relationships with AbbVie, Ascerta, Celgene, Emergent BioSolutions, Genentech, Genzyme, Gilead Sciences, GlaxoSmithKline, Juno Therapeutics, Karyopharm, Kite Pharma, Merck, Novartis Pharmaceuticals, Pharmacyclics, Roche Laboratories, and Sanofi-Aventis U.S.
EXPERT ANALYSIS FROM NCCN ANNUAL CONGRESS: HEMATOLOGIC MALIGNANCIES

HIV-positive patients may be at greater risk of atherosclerosis
HIV-infected individuals without any traditional cardiovascular disease risk factors still show signs of vascular thickening, compared with HIV-negative controls, researchers reported in a British study.
A team led by Dr. Kathleen A.M. Rose of the cardiovascular biomedical research unit at London’s Royal Brompton Hospital performed carotid cardiovascular magnetic resonance imaging on 33 HIV-infected patients and 35 HIV-negative controls, with both groups being at low cardiovascular risk. The study showed HIV infection was associated with a significantly greater ratio of carotid wall to outer wall thickness (36.7% vs. 32.5%, P less than .0001) – an indicator of carotid intima-media thickening that has been shown in HIV-negative populations to be predictive of future cardiovascular events.
Women with HIV had an even greater increase in carotid intima-media thickening, compared with men with HIV, according to the study results (JAIDS. 2015 Nov 16. doi: 10.1097/QAI.0000000000000900)
While there were no significant differences between the cases and controls in total carotid lumen volume, carotid artery volume, and carotid wall volume, total wall volume was higher in HIV-infected individuals, and there was a nonsignificant decrease in carotid artery distensibility in the HIV-infected group.
“Although traditional cardiovascular risk factors are highly prevalent and accepted to play a role in HIV-associated cardiovascular disease, the role of long-term cART [combination antiretroviral therapy] and HIV infection itself remains controversial,” wrote Dr. Rose and her coauthors.
The researchers cited earlier studies linking the antiretroviral agents indinavir, abacavir, and lopinavir with increased cardiovascular risk, although they pointed out there was conflicting evidence of a link with type of antiretroviral therapy.
The HIV-infected participants were all stable on combination antiretroviral therapy for a median duration of 7 years (2-21 years), and all had a plasma HIV-1 RNA viral load below 50 copies/mL.
Years of antiretroviral therapy and use of nonnucleoside reverse transcriptase inhibitors or protease inhibitors did not significantly impact carotid intima-media thickness, although patients taking abacavir – which is associated with increased cardiovascular risk – had a lower wall/outer wall ratio than those on zidovudine.
“This result may also reflect a channeling bias whereby clinicians only use abacavir in subjects they consider to have very low cardiovascular risk,” the authors wrote.
Other parameters such as age, ethnicity, CD4 cell count, nadir CD4 cell count, and years since HIV diagnosis did not impact atherosclerosis in HIV-positive subjects.
“Although our study has not followed up patients or controls longitudinally, the diverging lines between the groups with increasing age suggests that HIV infection and/or its treatment may be associated with progression of vascular wall thickening beyond that normally seen with age,” the authors reported.
“As increasing C-IMT [carotid intima-media thickness] has been found to be independently predictive of future stroke and myocardial infarction in HIV-uninfected populations, the findings of this study suggest that the rate of vascular events is likely to remain elevated in HIV-patients despite aggressive treatment of cardiovascular risk factors, highlighting the need for improved patient and health care provider education to detect and manage aggressively early signs of cardiovascular disease.”
The study was supported by the National Institute of Health Research cardiovascular biomedical research unit at Royal Brompton and Harefield NHS Foundation Trust, and Imperial College London. Three authors declared honoraria, grants, sponsorship, and consultancies from the pharmaceutical industry.
HIV-infected individuals without any traditional cardiovascular disease risk factors still show signs of vascular thickening, compared with HIV-negative controls, researchers reported in a British study.
A team led by Dr. Kathleen A.M. Rose of the cardiovascular biomedical research unit at London’s Royal Brompton Hospital performed carotid cardiovascular magnetic resonance imaging on 33 HIV-infected patients and 35 HIV-negative controls, with both groups being at low cardiovascular risk. The study showed HIV infection was associated with a significantly greater ratio of carotid wall to outer wall thickness (36.7% vs. 32.5%, P less than .0001) – an indicator of carotid intima-media thickening that has been shown in HIV-negative populations to be predictive of future cardiovascular events.
Women with HIV had an even greater increase in carotid intima-media thickening, compared with men with HIV, according to the study results (JAIDS. 2015 Nov 16. doi: 10.1097/QAI.0000000000000900)
While there were no significant differences between the cases and controls in total carotid lumen volume, carotid artery volume, and carotid wall volume, total wall volume was higher in HIV-infected individuals, and there was a nonsignificant decrease in carotid artery distensibility in the HIV-infected group.
“Although traditional cardiovascular risk factors are highly prevalent and accepted to play a role in HIV-associated cardiovascular disease, the role of long-term cART [combination antiretroviral therapy] and HIV infection itself remains controversial,” wrote Dr. Rose and her coauthors.
The researchers cited earlier studies linking the antiretroviral agents indinavir, abacavir, and lopinavir with increased cardiovascular risk, although they pointed out there was conflicting evidence of a link with type of antiretroviral therapy.
The HIV-infected participants were all stable on combination antiretroviral therapy for a median duration of 7 years (2-21 years), and all had a plasma HIV-1 RNA viral load below 50 copies/mL.
Years of antiretroviral therapy and use of nonnucleoside reverse transcriptase inhibitors or protease inhibitors did not significantly impact carotid intima-media thickness, although patients taking abacavir – which is associated with increased cardiovascular risk – had a lower wall/outer wall ratio than those on zidovudine.
“This result may also reflect a channeling bias whereby clinicians only use abacavir in subjects they consider to have very low cardiovascular risk,” the authors wrote.
Other parameters such as age, ethnicity, CD4 cell count, nadir CD4 cell count, and years since HIV diagnosis did not impact atherosclerosis in HIV-positive subjects.
“Although our study has not followed up patients or controls longitudinally, the diverging lines between the groups with increasing age suggests that HIV infection and/or its treatment may be associated with progression of vascular wall thickening beyond that normally seen with age,” the authors reported.
“As increasing C-IMT [carotid intima-media thickness] has been found to be independently predictive of future stroke and myocardial infarction in HIV-uninfected populations, the findings of this study suggest that the rate of vascular events is likely to remain elevated in HIV-patients despite aggressive treatment of cardiovascular risk factors, highlighting the need for improved patient and health care provider education to detect and manage aggressively early signs of cardiovascular disease.”
The study was supported by the National Institute of Health Research cardiovascular biomedical research unit at Royal Brompton and Harefield NHS Foundation Trust, and Imperial College London. Three authors declared honoraria, grants, sponsorship, and consultancies from the pharmaceutical industry.
HIV-infected individuals without any traditional cardiovascular disease risk factors still show signs of vascular thickening, compared with HIV-negative controls, researchers reported in a British study.
A team led by Dr. Kathleen A.M. Rose of the cardiovascular biomedical research unit at London’s Royal Brompton Hospital performed carotid cardiovascular magnetic resonance imaging on 33 HIV-infected patients and 35 HIV-negative controls, with both groups being at low cardiovascular risk. The study showed HIV infection was associated with a significantly greater ratio of carotid wall to outer wall thickness (36.7% vs. 32.5%, P less than .0001) – an indicator of carotid intima-media thickening that has been shown in HIV-negative populations to be predictive of future cardiovascular events.
Women with HIV had an even greater increase in carotid intima-media thickening, compared with men with HIV, according to the study results (JAIDS. 2015 Nov 16. doi: 10.1097/QAI.0000000000000900)
While there were no significant differences between the cases and controls in total carotid lumen volume, carotid artery volume, and carotid wall volume, total wall volume was higher in HIV-infected individuals, and there was a nonsignificant decrease in carotid artery distensibility in the HIV-infected group.
“Although traditional cardiovascular risk factors are highly prevalent and accepted to play a role in HIV-associated cardiovascular disease, the role of long-term cART [combination antiretroviral therapy] and HIV infection itself remains controversial,” wrote Dr. Rose and her coauthors.
The researchers cited earlier studies linking the antiretroviral agents indinavir, abacavir, and lopinavir with increased cardiovascular risk, although they pointed out there was conflicting evidence of a link with type of antiretroviral therapy.
The HIV-infected participants were all stable on combination antiretroviral therapy for a median duration of 7 years (2-21 years), and all had a plasma HIV-1 RNA viral load below 50 copies/mL.
Years of antiretroviral therapy and use of nonnucleoside reverse transcriptase inhibitors or protease inhibitors did not significantly impact carotid intima-media thickness, although patients taking abacavir – which is associated with increased cardiovascular risk – had a lower wall/outer wall ratio than those on zidovudine.
“This result may also reflect a channeling bias whereby clinicians only use abacavir in subjects they consider to have very low cardiovascular risk,” the authors wrote.
Other parameters such as age, ethnicity, CD4 cell count, nadir CD4 cell count, and years since HIV diagnosis did not impact atherosclerosis in HIV-positive subjects.
“Although our study has not followed up patients or controls longitudinally, the diverging lines between the groups with increasing age suggests that HIV infection and/or its treatment may be associated with progression of vascular wall thickening beyond that normally seen with age,” the authors reported.
“As increasing C-IMT [carotid intima-media thickness] has been found to be independently predictive of future stroke and myocardial infarction in HIV-uninfected populations, the findings of this study suggest that the rate of vascular events is likely to remain elevated in HIV-patients despite aggressive treatment of cardiovascular risk factors, highlighting the need for improved patient and health care provider education to detect and manage aggressively early signs of cardiovascular disease.”
The study was supported by the National Institute of Health Research cardiovascular biomedical research unit at Royal Brompton and Harefield NHS Foundation Trust, and Imperial College London. Three authors declared honoraria, grants, sponsorship, and consultancies from the pharmaceutical industry.
Key clinical point: HIV infection and/or treatment are associated with significantly greater vascular thickening, even in the absence of other cardiovascular risk factors.
Major finding: HIV-infected patients had a significantly greater ratio of carotid wall to outer wall thickness, compared with HIV-negative controls.
Data source: An observational study of 33 HIV-infected patients and 35 HIV-negative controls.
Disclosures: The study was supported by the National Institute of Health Research cardiovascular biomedical research unit at Royal Brompton and Harefield NHS Foundation Trust, and Imperial College London. Three authors declared honoraria, grants, sponsorship, and consultancies from the pharmaceutical industry.
Resolutions
For many, the making and breaking of New Year’s resolutions has become a humorless cliché. Still, the beginning of a new year is as good a time as any for reflection and inspiration; and if you restrict your fix-it list to a few realistic promises that can actually be kept, resolution time does not have to be such an exercise in futility.
I can’t presume to know what needs improving in your practice, much less your life; but I do know the office issues I get the most questions about. Perhaps the following examples will provide inspiration for assembling a realistic list of your own:

1. Review your October, November, and December claim payments. That is, all payments since ICD-10 launched. Overall, the transition has been surprisingly smooth; the Centers for Medicare & Medicaid Services says the claim denial rate has not increased significantly, and very few rejections are due to incorrect diagnosis coding. But each private payer has its own procedure, so make sure that none of your payers has dropped the ball. The most common problem so far seems to be inconsistent handling of “Z” codes, such as skin cancer screening (Z12.83), so pay particular attention to those.
2. Do a HIPAA risk assessment. The new HIPAA rules have been in effect for more than a year. Is your office up to speed? Review every procedure that involves confidential information; make sure there are no violations. Penalties for carelessness are a lot stiffer now.
3. Encrypt your mobile devices. This is really a subset of No. 2. The biggest HIPAA vulnerability in many practices is laptops and tablets carrying confidential patient information; losing one could be a disaster. Encryption software is cheap and readily available, and a lost or stolen mobile device will probably not be treated as a HIPAA breach if it is properly encrypted.
4. Reduce your accounts receivable by keeping a credit card number on file for each patient, and charging patient-owed balances as they come in. A series of my past columns in the archive at www.edermatologynews.com explains exactly how to do this. Every hotel in the world does it; you should too.
5. Clear your “horizontal file cabinet.” That’s the mess on your desk, all the paperwork you never seem to get to (probably because you’re tweeting or answering e-mail). Set aside an hour or two and get it all done. You’ll find some interesting stuff in there. Then, for every piece of paper that arrives on your desk from now on, follow the DDD Rule: Do it, Delegate it, or Destroy it. Don’t start a new mess.
6. Keep a closer eye on your office finances. Most physicians delegate the bookkeeping, and that’s fine. But ignoring the financial side creates an atmosphere that facilitates embezzlement. Set aside a couple of hours each month to review the books personally. And make sure your employees know you’re doing it.
7. Make sure your long range financial planning is on track. This is another task physicians tend to “set and forget,” but the Great Recession was an eye opener for many of us. Once a year, sit down with your accountant and planner and make sure your investments are well diversified and all other aspects of your finances – budgets, credit ratings, insurance coverage, tax situations, college savings, estate plans, retirement accounts – are in the best shape possible. January is a good time.
8. Back up your data. Now is also an excellent time to verify that the information on your office and personal computers is being backed up – locally and online – on a regular schedule. Don’t wait until something crashes.
9. Take more vacations. Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.” This is the year to start spending more time enjoying your life, your friends and family, and the world. As John Lennon said, “Life is what happens to you while you’re busy making other plans.”
10. Look at yourself. A private practice lives or dies on the personalities of its physicians, and your staff copies your personality and style. Take a hard, honest look at yourself. Identify your negative personality traits and work to eliminate them. If you have any difficulty finding habits that need changing … ask your spouse. He or she will be happy to explain them in excruciating detail.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
For many, the making and breaking of New Year’s resolutions has become a humorless cliché. Still, the beginning of a new year is as good a time as any for reflection and inspiration; and if you restrict your fix-it list to a few realistic promises that can actually be kept, resolution time does not have to be such an exercise in futility.
I can’t presume to know what needs improving in your practice, much less your life; but I do know the office issues I get the most questions about. Perhaps the following examples will provide inspiration for assembling a realistic list of your own:
1. Review your October, November, and December claim payments. That is, all payments since ICD-10 launched. Overall, the transition has been surprisingly smooth; the Centers for Medicare & Medicaid Services says the claim denial rate has not increased significantly, and very few rejections are due to incorrect diagnosis coding. But each private payer has its own procedure, so make sure that none of your payers has dropped the ball. The most common problem so far seems to be inconsistent handling of “Z” codes, such as skin cancer screening (Z12.83), so pay particular attention to those.
2. Do a HIPAA risk assessment. The new HIPAA rules have been in effect for more than a year. Is your office up to speed? Review every procedure that involves confidential information; make sure there are no violations. Penalties for carelessness are a lot stiffer now.
3. Encrypt your mobile devices. This is really a subset of No. 2. The biggest HIPAA vulnerability in many practices is laptops and tablets carrying confidential patient information; losing one could be a disaster. Encryption software is cheap and readily available, and a lost or stolen mobile device will probably not be treated as a HIPAA breach if it is properly encrypted.
4. Reduce your accounts receivable by keeping a credit card number on file for each patient, and charging patient-owed balances as they come in. A series of my past columns in the archive at www.edermatologynews.com explains exactly how to do this. Every hotel in the world does it; you should too.
5. Clear your “horizontal file cabinet.” That’s the mess on your desk, all the paperwork you never seem to get to (probably because you’re tweeting or answering e-mail). Set aside an hour or two and get it all done. You’ll find some interesting stuff in there. Then, for every piece of paper that arrives on your desk from now on, follow the DDD Rule: Do it, Delegate it, or Destroy it. Don’t start a new mess.
6. Keep a closer eye on your office finances. Most physicians delegate the bookkeeping, and that’s fine. But ignoring the financial side creates an atmosphere that facilitates embezzlement. Set aside a couple of hours each month to review the books personally. And make sure your employees know you’re doing it.
7. Make sure your long range financial planning is on track. This is another task physicians tend to “set and forget,” but the Great Recession was an eye opener for many of us. Once a year, sit down with your accountant and planner and make sure your investments are well diversified and all other aspects of your finances – budgets, credit ratings, insurance coverage, tax situations, college savings, estate plans, retirement accounts – are in the best shape possible. January is a good time.
8. Back up your data. Now is also an excellent time to verify that the information on your office and personal computers is being backed up – locally and online – on a regular schedule. Don’t wait until something crashes.
9. Take more vacations. Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.” This is the year to start spending more time enjoying your life, your friends and family, and the world. As John Lennon said, “Life is what happens to you while you’re busy making other plans.”
10. Look at yourself. A private practice lives or dies on the personalities of its physicians, and your staff copies your personality and style. Take a hard, honest look at yourself. Identify your negative personality traits and work to eliminate them. If you have any difficulty finding habits that need changing … ask your spouse. He or she will be happy to explain them in excruciating detail.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
For many, the making and breaking of New Year’s resolutions has become a humorless cliché. Still, the beginning of a new year is as good a time as any for reflection and inspiration; and if you restrict your fix-it list to a few realistic promises that can actually be kept, resolution time does not have to be such an exercise in futility.
I can’t presume to know what needs improving in your practice, much less your life; but I do know the office issues I get the most questions about. Perhaps the following examples will provide inspiration for assembling a realistic list of your own:
1. Review your October, November, and December claim payments. That is, all payments since ICD-10 launched. Overall, the transition has been surprisingly smooth; the Centers for Medicare & Medicaid Services says the claim denial rate has not increased significantly, and very few rejections are due to incorrect diagnosis coding. But each private payer has its own procedure, so make sure that none of your payers has dropped the ball. The most common problem so far seems to be inconsistent handling of “Z” codes, such as skin cancer screening (Z12.83), so pay particular attention to those.
2. Do a HIPAA risk assessment. The new HIPAA rules have been in effect for more than a year. Is your office up to speed? Review every procedure that involves confidential information; make sure there are no violations. Penalties for carelessness are a lot stiffer now.
3. Encrypt your mobile devices. This is really a subset of No. 2. The biggest HIPAA vulnerability in many practices is laptops and tablets carrying confidential patient information; losing one could be a disaster. Encryption software is cheap and readily available, and a lost or stolen mobile device will probably not be treated as a HIPAA breach if it is properly encrypted.
4. Reduce your accounts receivable by keeping a credit card number on file for each patient, and charging patient-owed balances as they come in. A series of my past columns in the archive at www.edermatologynews.com explains exactly how to do this. Every hotel in the world does it; you should too.
5. Clear your “horizontal file cabinet.” That’s the mess on your desk, all the paperwork you never seem to get to (probably because you’re tweeting or answering e-mail). Set aside an hour or two and get it all done. You’ll find some interesting stuff in there. Then, for every piece of paper that arrives on your desk from now on, follow the DDD Rule: Do it, Delegate it, or Destroy it. Don’t start a new mess.
6. Keep a closer eye on your office finances. Most physicians delegate the bookkeeping, and that’s fine. But ignoring the financial side creates an atmosphere that facilitates embezzlement. Set aside a couple of hours each month to review the books personally. And make sure your employees know you’re doing it.
7. Make sure your long range financial planning is on track. This is another task physicians tend to “set and forget,” but the Great Recession was an eye opener for many of us. Once a year, sit down with your accountant and planner and make sure your investments are well diversified and all other aspects of your finances – budgets, credit ratings, insurance coverage, tax situations, college savings, estate plans, retirement accounts – are in the best shape possible. January is a good time.
8. Back up your data. Now is also an excellent time to verify that the information on your office and personal computers is being backed up – locally and online – on a regular schedule. Don’t wait until something crashes.
9. Take more vacations. Remember Eastern’s First Law: Your last words will NOT be, “I wish I had spent more time in the office.” This is the year to start spending more time enjoying your life, your friends and family, and the world. As John Lennon said, “Life is what happens to you while you’re busy making other plans.”
10. Look at yourself. A private practice lives or dies on the personalities of its physicians, and your staff copies your personality and style. Take a hard, honest look at yourself. Identify your negative personality traits and work to eliminate them. If you have any difficulty finding habits that need changing … ask your spouse. He or she will be happy to explain them in excruciating detail.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Chemo quadruples risk for myeloid cancers
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.

“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
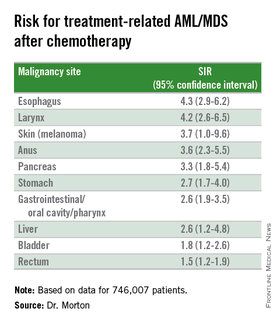
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.
“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
ORLANDO – Patients who undergo cytotoxic chemotherapy, even in the modern era, are at increased risk for developing myeloid neoplasms, based on data from a cohort of nearly 750,000 adults who were initially treated with chemotherapy and survived at least 1 year after diagnosis.
In the cohort, the standardized incidence ratio (SIR) for treatment-related acute myeloid leukemia (tAML) or myelodysplastic syndrome (MDS) was four times greater than would be expected in the general population, reported Lindsay M. Morton, Ph.D., of the division of cancer epidemiology and genetics at the National Cancer Institute in Bethesda, Md.
“We now demonstrate that there are elevated risks for treatment-related leukemia after treatment for a broad spectrum of first primary malignancies that are generally consistent with what we know about changing treatment practices,” she said at the American Society of Hematology annual meeting.
“The number of cancer survivors in the United States has increased dramatically, to reach nearly 14 million individuals today, and in just the next few years the number is expected to reach more than 18 million people, which means that the long-term health of this population is of great clinical importance as well as public health importance,” Dr. Morton emphasized.
The link between cytotoxic chemotherapy and leukemia risk has been known since the 1960s, with certain classes of agents carrying higher risks than others, including platinum-containing compounds, alkylating agents (for example, cyclophosphamide, melphalan, chlorambucil), topoisomerase II inhibitors (doxorubicin, daunorubicin, epirubicin, etc.), and antimetabolites (5-fluorauracil, capecitabine, gemcitabine, et al.).
Treatment-related leukemias are associated with higher doses of these agents, and the trend in contemporary medicine is to use more of these agents upfront for the treatment of primary malignancies. Yet estimates of the risk of tAML, MDS, or other malignancies have been hard to come by because of the relative rarity of cases and the sporadic reports in the literature, Dr. Morton said.
The investigators previously reported that risk for tAML and other myeloid neoplasms changed over time, and showed that since the 1990s there was an uptick in risk for patients treated with chemotherapy for cancers of bone, joints, and endometrium, and since 2000 for patients treated with chemotherapy for cancers of the esophagus, cervix and prostate.
For example, risks for tAML were higher in the 1970s for patients with ovarian cancer treated with melphalan, a highly leukemogenic agent, but dropped somewhat with the switch to platinum-based agents. Similarly, women with breast cancer had a comparatively high risk with the use of melphalan, a decline in risk with the introduction of cyclophosphamide, and then an increase with the addition of anthracyclines and dose-dense regimens.
Risk update
To get a better idea of the magnitude of risk in the modern era, Dr. Morton and colleagues sifted through Surveillance, Epidemiology, and End Results (SEER) data to identify a cohort of 746,007 adults who were initially treated with chemotherapy and survived for at least 1 year following a diagnosis with a first primary malignancy from 2000 through 2012. They calculated SIRs based on variables that included age, race, sex, malignancy type and treatment period.
They looked at four categories of myeloid neoplasms as defined by World Health Organization criteria: AML/MDS, chronic myeloid leukemia, myeloproliferative neoplasms (MPN) negative for BCR-ABL (Philadelphia-negative), and chronic myelomonocytic leukemia (CMML).
They found that 2,071 patients developed treatment-related AML/MDS, translating into a fourfold incidence compared with the general population (SIR 4.1, 95% confidence interval [CI] 3.9-4.2), 106 were diagnosed with CMML
They also identified novel risk for tAML/MDS after chemotherapy by malignancy (see table).
The investigators found that breast cancer, non-Hodgkin lymphoma, and lung cancer were most commonly associated with tAML/MDS (SIRs 4.1, 7.3, and 4.1, respectively, all significant).
In addition, although the overall numbers of cases were small, the investigators noted “strikingly elevated” risks for cancers of bone (SIR 35.1, CI. 16.9-64.6). testes (15.6, CI, 9.2-24.6), and soft tissue (12.6, CI=7.7-19.4),
Risk for tAML/MD was more modestly elevated for cancers of the brain, ovaries, endometrium, cervix, and prostate, and for Hodgkin lymphoma, chronic lymphocytic leukemia, and multiple myeloma.
Adding radiotherapy to chemotherapy for cancers of the breast, lung, and stomach cancers showed a trend toward heightened tAML/MDS risk, but this was not significant.
An elevated risk for CMML was also seen after chemotherapy for lung cancer (SIR 2.5, CI, 1.3-4.4), breast cancer (1.8, CI, 1.3-2.5), and non-Hodgkin lymphoma (2.1, CI, 1.2-3.4). There was elevated risk for CMML following chemotherapy for breast cancer (3.0, CI. 1.7-5.0) and non-Hodgkin lymphoma (4.2, CI, 2.4-6.9).
There were no increased risks for other myeloproliferative neoplasms after chemotherapy for any first primary cancer, however.
“This reminds us that with new uses of standard agents and introduction of new agents, it’s critical to carefully weigh the risks and benefits of systemic therapy,” Dr. Morton said.
The investigators plan to quantify risks associated with specific drugs and doses, she added.
The study was supported by the National Cancer Institute. Dr. Morton reported no relevant conflicts of interest to disclose.
AT ASH 2015
Key clinical point: This study quantifies the risks for treatment-related myeloid cancers after chemotherapy.
Major finding: Chemotherapy is associated with a fourfold risk for treatment-related AML/MDS, compared with the general population.
Data source: Retrospective review of data on 746,007 adults treated with chemotherapy for a first primary malignancy.
Disclosures: The National Cancer Institute supported the study. Dr. Morton reported having no conflicts of interest to disclose.

More complete cytogenetic responses at 12 months with radotinib than imatinib
Radotinib was associated with significantly higher complete cytogenetic responses and major molecular responses than imatinib was at a minimum 12 months of follow-up in a randomized, open-label, phase III clinical trialof patients with newly diagnosed chronic myeloid leukemia-chronic phase (CML-CP).
Radotinib, an investigational BCR-ABL1 tyrosine kinase inhibitor developed by IL-YANG Pharmaceuticals, is approved in Korea for the treatment of CML-CP in patients who have failed prior TKIs.
Dr. Jae-Yong Kwak of Chonbuk National University Medical School and Hospital, Jeonju, South Korea, and his colleagues randomized 241 patients to either radotinib 300 mg twice daily (n = 79), radotinib 400 mg twice daily (n = 81), or imatinib 400 mg once daily (n = 81). All three study groups were balanced in regard to baseline age, gender, race, and Sokal risk score.
At a minimum follow-up of 12 months, the proportions of patients receiving a study drug were 86% (69/79) in the radotinib 300 mg twice-daily group, 72% (58/81) in the radotinib 400 mg twice-daily group, and 82% (66/81) in the imatinib 400 mg once-daily group.
The rates of major molecular response at 12 months were significantly higher in patients receiving radotinib 300 mg b.i.d. (52%, P = .0044) and radotinib 400 mg b.i.d. (46%, P = .0342), compared with imatinib (30%), Dr. Kwak reported at the annual meeting of the American Society of Hematology in Orlando.
Among responders, the median times to major molecular response were shorter on radotinib 300 mg b.i.d. (5.7 months) and radotinib 400 mg b.i.d. (5.6 months) than on imatinib (8.2 months). The MR4.5 rates by 12 months were also higher for both radotinib 300 mg b.i.d. (15%) and 400 mg b.i.d. (14%), compared with imatinib (9%). The complete cytogenetic response rates by 12 months were 91% for radotinib 300 mg b.i.d. (P = .0120), compared with imatinib (77%). None of the patients in the study had progressed to accelerated phase or blast crisis at 12 months.
Drug discontinuation due to adverse events (AEs) or laboratory abnormalities occurred in 9% of patients on radotinib 300 mg b.i.d., 20% on radotinib 400 mg b.i.d., and 6% on imatinib.
The major side effects included grade 3/4 thrombocytopenia in 16% of patients receiving radotinib 300 mg b.i.d., 14% on radotinib 400 mg b.i.d., and 20% receiving imatinib. Grade 3/4 neutropenia occurred in 19%, 24%, and 30% for radotinib 300 mg b.i.d., 400 mg b.i.d., and imatinib, respectively.
Overall, grade 3/4 nonlaboratory AEs were uncommon in all groups. The most common nonlaboratory AEs in the radotinib groups were skin rash (about 33% in both), nausea/vomiting (about 23% in both), headache (19% and 31%), and pruritus (19% and 30%). In the imatinib group, the most common adverse events were edema (35%), myalgia (28%), nausea/vomiting (27%), and skin rash (22%).
Dr. Kwak had no relevant disclosures. Some of his colleagues received research funding from IL-YANG Pharmaceutical Co. and Alexion Pharmaceuticals.
On Twitter @maryjodales
Radotinib was associated with significantly higher complete cytogenetic responses and major molecular responses than imatinib was at a minimum 12 months of follow-up in a randomized, open-label, phase III clinical trialof patients with newly diagnosed chronic myeloid leukemia-chronic phase (CML-CP).
Radotinib, an investigational BCR-ABL1 tyrosine kinase inhibitor developed by IL-YANG Pharmaceuticals, is approved in Korea for the treatment of CML-CP in patients who have failed prior TKIs.
Dr. Jae-Yong Kwak of Chonbuk National University Medical School and Hospital, Jeonju, South Korea, and his colleagues randomized 241 patients to either radotinib 300 mg twice daily (n = 79), radotinib 400 mg twice daily (n = 81), or imatinib 400 mg once daily (n = 81). All three study groups were balanced in regard to baseline age, gender, race, and Sokal risk score.
At a minimum follow-up of 12 months, the proportions of patients receiving a study drug were 86% (69/79) in the radotinib 300 mg twice-daily group, 72% (58/81) in the radotinib 400 mg twice-daily group, and 82% (66/81) in the imatinib 400 mg once-daily group.
The rates of major molecular response at 12 months were significantly higher in patients receiving radotinib 300 mg b.i.d. (52%, P = .0044) and radotinib 400 mg b.i.d. (46%, P = .0342), compared with imatinib (30%), Dr. Kwak reported at the annual meeting of the American Society of Hematology in Orlando.
Among responders, the median times to major molecular response were shorter on radotinib 300 mg b.i.d. (5.7 months) and radotinib 400 mg b.i.d. (5.6 months) than on imatinib (8.2 months). The MR4.5 rates by 12 months were also higher for both radotinib 300 mg b.i.d. (15%) and 400 mg b.i.d. (14%), compared with imatinib (9%). The complete cytogenetic response rates by 12 months were 91% for radotinib 300 mg b.i.d. (P = .0120), compared with imatinib (77%). None of the patients in the study had progressed to accelerated phase or blast crisis at 12 months.
Drug discontinuation due to adverse events (AEs) or laboratory abnormalities occurred in 9% of patients on radotinib 300 mg b.i.d., 20% on radotinib 400 mg b.i.d., and 6% on imatinib.
The major side effects included grade 3/4 thrombocytopenia in 16% of patients receiving radotinib 300 mg b.i.d., 14% on radotinib 400 mg b.i.d., and 20% receiving imatinib. Grade 3/4 neutropenia occurred in 19%, 24%, and 30% for radotinib 300 mg b.i.d., 400 mg b.i.d., and imatinib, respectively.
Overall, grade 3/4 nonlaboratory AEs were uncommon in all groups. The most common nonlaboratory AEs in the radotinib groups were skin rash (about 33% in both), nausea/vomiting (about 23% in both), headache (19% and 31%), and pruritus (19% and 30%). In the imatinib group, the most common adverse events were edema (35%), myalgia (28%), nausea/vomiting (27%), and skin rash (22%).
Dr. Kwak had no relevant disclosures. Some of his colleagues received research funding from IL-YANG Pharmaceutical Co. and Alexion Pharmaceuticals.
On Twitter @maryjodales
Radotinib was associated with significantly higher complete cytogenetic responses and major molecular responses than imatinib was at a minimum 12 months of follow-up in a randomized, open-label, phase III clinical trialof patients with newly diagnosed chronic myeloid leukemia-chronic phase (CML-CP).
Radotinib, an investigational BCR-ABL1 tyrosine kinase inhibitor developed by IL-YANG Pharmaceuticals, is approved in Korea for the treatment of CML-CP in patients who have failed prior TKIs.
Dr. Jae-Yong Kwak of Chonbuk National University Medical School and Hospital, Jeonju, South Korea, and his colleagues randomized 241 patients to either radotinib 300 mg twice daily (n = 79), radotinib 400 mg twice daily (n = 81), or imatinib 400 mg once daily (n = 81). All three study groups were balanced in regard to baseline age, gender, race, and Sokal risk score.
At a minimum follow-up of 12 months, the proportions of patients receiving a study drug were 86% (69/79) in the radotinib 300 mg twice-daily group, 72% (58/81) in the radotinib 400 mg twice-daily group, and 82% (66/81) in the imatinib 400 mg once-daily group.
The rates of major molecular response at 12 months were significantly higher in patients receiving radotinib 300 mg b.i.d. (52%, P = .0044) and radotinib 400 mg b.i.d. (46%, P = .0342), compared with imatinib (30%), Dr. Kwak reported at the annual meeting of the American Society of Hematology in Orlando.
Among responders, the median times to major molecular response were shorter on radotinib 300 mg b.i.d. (5.7 months) and radotinib 400 mg b.i.d. (5.6 months) than on imatinib (8.2 months). The MR4.5 rates by 12 months were also higher for both radotinib 300 mg b.i.d. (15%) and 400 mg b.i.d. (14%), compared with imatinib (9%). The complete cytogenetic response rates by 12 months were 91% for radotinib 300 mg b.i.d. (P = .0120), compared with imatinib (77%). None of the patients in the study had progressed to accelerated phase or blast crisis at 12 months.
Drug discontinuation due to adverse events (AEs) or laboratory abnormalities occurred in 9% of patients on radotinib 300 mg b.i.d., 20% on radotinib 400 mg b.i.d., and 6% on imatinib.
The major side effects included grade 3/4 thrombocytopenia in 16% of patients receiving radotinib 300 mg b.i.d., 14% on radotinib 400 mg b.i.d., and 20% receiving imatinib. Grade 3/4 neutropenia occurred in 19%, 24%, and 30% for radotinib 300 mg b.i.d., 400 mg b.i.d., and imatinib, respectively.
Overall, grade 3/4 nonlaboratory AEs were uncommon in all groups. The most common nonlaboratory AEs in the radotinib groups were skin rash (about 33% in both), nausea/vomiting (about 23% in both), headache (19% and 31%), and pruritus (19% and 30%). In the imatinib group, the most common adverse events were edema (35%), myalgia (28%), nausea/vomiting (27%), and skin rash (22%).
Dr. Kwak had no relevant disclosures. Some of his colleagues received research funding from IL-YANG Pharmaceutical Co. and Alexion Pharmaceuticals.
On Twitter @maryjodales
FROM ASH 2015
Key clinical point: Radotinib was associated with significantly higher complete cytogenetic responses and major molecular responses than was imatinib at a minimum 12 months of follow-up.
Major finding: By 12 months, the rates of major molecular response were significantly higher in patients receiving radotinib 300 mg b.i.d. (52%, P = .0044) and radotinib 400 mg b.i.d. (46%, P = .0342), compared with imatinib 400 mg/day (30%).
Data source: Randomized, open-label, phase III clinical trial involving 241 patients.
Disclosures: Dr. Kwak had no relevant disclosures. Some of his colleagues received research funding from IL-YANG Pharmaceutical Co. and Alexion Pharmaceuticals.