User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Anifrolumab shows promise in refractory discoid lupus erythematosus
a small retrospective study reports.
DLE, the most common form of chronic cutaneous lupus erythematosus, can permanently scar and disfigure patients, and traditional treatments such as antimalarials, steroid-sparing immunosuppressive agents, thalidomide, retinoids, and lenalidomide don’t consistently improve refractory DLE, the authors noted.
“All patients demonstrated significant improvement in symptomatology and disease activity within 2 months of initiating anifrolumab,” lead study author Katharina Shaw, MD, of the department of dermatology of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and colleagues wrote in a research letter published in JAMA Dermatology. “These early results highlight the potential for anifrolumab to be a viable therapeutic option for patients with DLE, particularly those with severe or recalcitrant disease.”
The Food and Drug Administration approved anifrolumab (Saphnelo), a human monoclonal antibody targeting type 1 interferon receptor subunit 1, in 2021 for adults with moderate to severe systemic lupus erythematosus, but it has not been approved for the treatment of DLE.
Dr. Shaw and colleagues queried the medical records from Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, to find all cases of DLE based on biopsy, expert opinion, or both from January 2000 to October 2022.
The researchers identified eight female patients who had received anifrolumab for at least 8 weeks. The women were aged between 19 and 75 years (median, 42.5 years), and all had DLE recalcitrant to standard therapies and had been treated with hydroxychloroquine and between 1 and 10 other drugs, most commonly methotrexate and mycophenolate mofetil (MMF).
The authors looked for improvements in patient-reported symptoms and Cutaneous Lupus Erythematosus Disease Area and Severity Index scores, including CLASI A (activity) score 0-70, and CLASI-D (damage) score 0-56.
All patients showed significantly improved symptoms and disease activity within 2 months of their first infusion of the treatment. The mean decrease and mean percentage decrease in CLASI-A scores were 17.1 and 65.1%, respectively. The mean decrease and mean percentage decrease in CLASI-D scores were 0.5 and 2.9%, respectively.
The rapid clinical improvements with anifrolumab, compared with improvements with traditional medications, were striking, the authors wrote. “Given the risk for permanent scarring, dyspigmentation, and alopecia with poorly controlled DLE, the importance of rapidly mitigating disease activity cannot be overemphasized.”
They acknowledged that the results are limited by the study’s small sample size and retrospective design, and they recommend larger related prospective studies.
Asked to comment on the results, Kaveh Ardalan, MD, MS, assistant professor of pediatrics in the division of pediatric rheumatology at Duke University, Durham, N.C., said that finding new DLE therapeutics is important because of the huge impact of uncontrolled DLE on patients’ quality of life, body image, and social roles.
Dr. Ardalan noted that he sees DLE in his pediatric patients, “either as an isolated finding or in the context of systemic lupus erythematosus. Anifrolumab is not approved by the FDA to treat DLE or children.
“Randomized controlled trials, including the TULIP-1 and TULIP-2 studies of anifrolumab in systemic lupus, have indicated that lupus skin manifestations can improve in patients who receive anifrolumab,” said Dr. Ardalan, who was not involved in the study. “And we know that type I interferons are major drivers of cutaneous disease activity in patients with lupus, so targeting that mechanism with anifrolumab makes biological sense.”
The authors’ use of the validated CLASI classification system to quantify disease activity and damage over time, and their determination of the length of time for the drug to take effect are strengths of the study, he added.
Funding information was not provided. Two authors reported financial relationships with Pfizer, which does not manufacture anifrolumab. Dr. Ardalan reported no conflicts of interest with the study.
a small retrospective study reports.
DLE, the most common form of chronic cutaneous lupus erythematosus, can permanently scar and disfigure patients, and traditional treatments such as antimalarials, steroid-sparing immunosuppressive agents, thalidomide, retinoids, and lenalidomide don’t consistently improve refractory DLE, the authors noted.
“All patients demonstrated significant improvement in symptomatology and disease activity within 2 months of initiating anifrolumab,” lead study author Katharina Shaw, MD, of the department of dermatology of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and colleagues wrote in a research letter published in JAMA Dermatology. “These early results highlight the potential for anifrolumab to be a viable therapeutic option for patients with DLE, particularly those with severe or recalcitrant disease.”
The Food and Drug Administration approved anifrolumab (Saphnelo), a human monoclonal antibody targeting type 1 interferon receptor subunit 1, in 2021 for adults with moderate to severe systemic lupus erythematosus, but it has not been approved for the treatment of DLE.
Dr. Shaw and colleagues queried the medical records from Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, to find all cases of DLE based on biopsy, expert opinion, or both from January 2000 to October 2022.
The researchers identified eight female patients who had received anifrolumab for at least 8 weeks. The women were aged between 19 and 75 years (median, 42.5 years), and all had DLE recalcitrant to standard therapies and had been treated with hydroxychloroquine and between 1 and 10 other drugs, most commonly methotrexate and mycophenolate mofetil (MMF).
The authors looked for improvements in patient-reported symptoms and Cutaneous Lupus Erythematosus Disease Area and Severity Index scores, including CLASI A (activity) score 0-70, and CLASI-D (damage) score 0-56.
All patients showed significantly improved symptoms and disease activity within 2 months of their first infusion of the treatment. The mean decrease and mean percentage decrease in CLASI-A scores were 17.1 and 65.1%, respectively. The mean decrease and mean percentage decrease in CLASI-D scores were 0.5 and 2.9%, respectively.
The rapid clinical improvements with anifrolumab, compared with improvements with traditional medications, were striking, the authors wrote. “Given the risk for permanent scarring, dyspigmentation, and alopecia with poorly controlled DLE, the importance of rapidly mitigating disease activity cannot be overemphasized.”
They acknowledged that the results are limited by the study’s small sample size and retrospective design, and they recommend larger related prospective studies.
Asked to comment on the results, Kaveh Ardalan, MD, MS, assistant professor of pediatrics in the division of pediatric rheumatology at Duke University, Durham, N.C., said that finding new DLE therapeutics is important because of the huge impact of uncontrolled DLE on patients’ quality of life, body image, and social roles.
Dr. Ardalan noted that he sees DLE in his pediatric patients, “either as an isolated finding or in the context of systemic lupus erythematosus. Anifrolumab is not approved by the FDA to treat DLE or children.
“Randomized controlled trials, including the TULIP-1 and TULIP-2 studies of anifrolumab in systemic lupus, have indicated that lupus skin manifestations can improve in patients who receive anifrolumab,” said Dr. Ardalan, who was not involved in the study. “And we know that type I interferons are major drivers of cutaneous disease activity in patients with lupus, so targeting that mechanism with anifrolumab makes biological sense.”
The authors’ use of the validated CLASI classification system to quantify disease activity and damage over time, and their determination of the length of time for the drug to take effect are strengths of the study, he added.
Funding information was not provided. Two authors reported financial relationships with Pfizer, which does not manufacture anifrolumab. Dr. Ardalan reported no conflicts of interest with the study.
a small retrospective study reports.
DLE, the most common form of chronic cutaneous lupus erythematosus, can permanently scar and disfigure patients, and traditional treatments such as antimalarials, steroid-sparing immunosuppressive agents, thalidomide, retinoids, and lenalidomide don’t consistently improve refractory DLE, the authors noted.
“All patients demonstrated significant improvement in symptomatology and disease activity within 2 months of initiating anifrolumab,” lead study author Katharina Shaw, MD, of the department of dermatology of Brigham and Women’s Hospital and Harvard Medical School, both in Boston, and colleagues wrote in a research letter published in JAMA Dermatology. “These early results highlight the potential for anifrolumab to be a viable therapeutic option for patients with DLE, particularly those with severe or recalcitrant disease.”
The Food and Drug Administration approved anifrolumab (Saphnelo), a human monoclonal antibody targeting type 1 interferon receptor subunit 1, in 2021 for adults with moderate to severe systemic lupus erythematosus, but it has not been approved for the treatment of DLE.
Dr. Shaw and colleagues queried the medical records from Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, to find all cases of DLE based on biopsy, expert opinion, or both from January 2000 to October 2022.
The researchers identified eight female patients who had received anifrolumab for at least 8 weeks. The women were aged between 19 and 75 years (median, 42.5 years), and all had DLE recalcitrant to standard therapies and had been treated with hydroxychloroquine and between 1 and 10 other drugs, most commonly methotrexate and mycophenolate mofetil (MMF).
The authors looked for improvements in patient-reported symptoms and Cutaneous Lupus Erythematosus Disease Area and Severity Index scores, including CLASI A (activity) score 0-70, and CLASI-D (damage) score 0-56.
All patients showed significantly improved symptoms and disease activity within 2 months of their first infusion of the treatment. The mean decrease and mean percentage decrease in CLASI-A scores were 17.1 and 65.1%, respectively. The mean decrease and mean percentage decrease in CLASI-D scores were 0.5 and 2.9%, respectively.
The rapid clinical improvements with anifrolumab, compared with improvements with traditional medications, were striking, the authors wrote. “Given the risk for permanent scarring, dyspigmentation, and alopecia with poorly controlled DLE, the importance of rapidly mitigating disease activity cannot be overemphasized.”
They acknowledged that the results are limited by the study’s small sample size and retrospective design, and they recommend larger related prospective studies.
Asked to comment on the results, Kaveh Ardalan, MD, MS, assistant professor of pediatrics in the division of pediatric rheumatology at Duke University, Durham, N.C., said that finding new DLE therapeutics is important because of the huge impact of uncontrolled DLE on patients’ quality of life, body image, and social roles.
Dr. Ardalan noted that he sees DLE in his pediatric patients, “either as an isolated finding or in the context of systemic lupus erythematosus. Anifrolumab is not approved by the FDA to treat DLE or children.
“Randomized controlled trials, including the TULIP-1 and TULIP-2 studies of anifrolumab in systemic lupus, have indicated that lupus skin manifestations can improve in patients who receive anifrolumab,” said Dr. Ardalan, who was not involved in the study. “And we know that type I interferons are major drivers of cutaneous disease activity in patients with lupus, so targeting that mechanism with anifrolumab makes biological sense.”
The authors’ use of the validated CLASI classification system to quantify disease activity and damage over time, and their determination of the length of time for the drug to take effect are strengths of the study, he added.
Funding information was not provided. Two authors reported financial relationships with Pfizer, which does not manufacture anifrolumab. Dr. Ardalan reported no conflicts of interest with the study.
FROM JAMA DERMATOLOGY
New data forecast more oral PDE4 inhibitors for psoriasis
NEW ORLEANS – according to results of a phase 2 clinical trial presented as a late-breaker at the annual meeting of the American Academy of Dermatology.
The phase 2b data, which are prompting a phase 3 trial, suggest that the drug, called orismilast, “is a potential new addition to the psoriasis armamentarium,” reported Lars E. French, MD, professor and chair, department of dermatology, Ludwig Maximilian University of Munich (Germany).

At the same session, findings from another study supported off-label use of oral roflumilast (Daliresp and generic), a PDE4 inhibitor approved for severe chronic obstructive pulmonary disease (COPD). The only PDE4 inhibitors with an indication for psoriasis are roflumilast, approved as a cream (Zoryve), and apremilast (Otezla), approved as an oral therapy.
Phase 2 study of orismilast
In the orismilast trial, Dr. French attributed the efficacy observed to the potency of orismilast on the B and D subtypes of PDE4 associated with inflammation. One clue is that these specific subtypes are overly expressed in the skin of patients with either psoriasis or atopic dermatitis.
“When compared to apremilast, orismilast is at least two to fivefold more potent on all PDE4 isoforms and up to 39 times more potent on some of the PDE4 B and D isoforms,” said Dr. French, referring to preclinical findings in human whole blood and blood cells and in a mouse model of chronic inflammation.
The efficacy of orismilast in an immediate-release oral formulation was previously demonstrated in a recently published phase 2a trial, but the newest study tested a modified-release formulation of orismilast to test its potential to improve tolerability.
In the study, 202 adult patients with moderate to severe psoriasis (Psoriasis Area Severity Index [PASI] score ≥ 12) were randomly assigned to one of three doses of orismilast or to placebo. Each of the three doses – 20 mg, 30 mg, or 40 mg – were administered twice daily. The primary endpoint was change in PASI score at 16 weeks. Secondary endpoints included PASI 75 responses (signifying 75% clearance) and safety.
Relative to placebo, which was associated with a PASI improvement of 17%, all three of the tested orismilast doses were superior in a dose-dependent manner. The rates of response were 53%, 61%, and 64% for the 20-mg, 30-mg, and 40-mg twice-daily doses, respectively.
The PASI improvements were rapid, Dr. French said. At 4 weeks, PASI scores climbed from baseline by nearly 40% for those on all orismilast doses, which was more than double the improvement in the placebo group.
In the intention-to-treat analysis with missing data counted as nonresponders, the proportion of patients reaching PASI-75 scores at 16 weeks were 39%, 49%, 45%, and 17%, in the 20-mg, 30-mg, 40-mg, and placebo groups, respectively. The proportion of patients experiencing complete or near-complete skin clearance defined by a PASI 90 were 24%, 22%, 28%, and 8%, respectively.
The side-effect profile was consistent with other PDE4 inhibitors. The most common adverse events included gastrointestinal complaints, such as diarrhea and nausea, as well as headache and dizziness. But the majority of these events were of low grade, and they were largely confined to the first 4 weeks of treatment, which is a pattern reported with other PDE4 inhibitors in psoriasis and other chronic inflammatory diseases, such as COPD, according to Dr. French.
“There were no discontinuations for a treatment-related adverse event in the arms receiving either the 20-mg or the 30-mg doses,” Dr. French reported. There were only two serious adverse events, and neither were considered by trial investigators to be related to orismilast.
Based on the limited therapeutic gain but greater risk for adverse events on the 40-mg twice-daily dose, “the question is now whether to move forward with the 20-mg or the 30-mg dose,” said Dr. French, who said planning of a phase 3 trial is underway.
Phase 2 study of roflumilast
However, this was not the only set of data on an oral PDE4 inhibitor presented as a late-breaker at the AAD meeting. For clinicians looking for a more immediate and less expensive alternative to apremilast, another study indicated that off-label use of oral roflumilast is an option.
In an investigator-initiated, multicenter, double-blind, placebo-controlled trial conducted in Denmark, the rate of response to oral roflumilast at 24 weeks, including the clear or almost clear response, was on the same general order of magnitude as that seen in the orismilast study, reported Alexander Egeberg, MD, PhD, professor of dermatology, University of Copenhagen.
“At 24 weeks, 21.7% had achieved a PASI 90, and 8.7% achieved a PASI 100,” Dr. Egeberg said.
Oral roflumilast has been available for the treatment of COPD for more than 10 years and is now available in a generic formulation. This study was conducted independent of any pharmaceutical company involvement, and the high rate of response and low risk of adverse events suggests that patients can benefit from a PDE4 inhibitor in a very low-cost form.
“Generic oral roflumilast is cheaper than a Starbucks coffee,” Dr. Egeberg said.
In this trial, 46 patients were randomly assigned to placebo or to the COPD-approved roflumilast dose of 500 mcg once daily. The primary endpoint was change in PASI scores from baseline to week 12, which Dr. Egeberg pointed out is a shorter time frame than the 16 weeks more typical of psoriasis treatment studies.
At week 12, the median improvement in PASI was 34.8% in the roflumilast group versus 0% in the placebo group. Patients were then followed for an additional 12 weeks, but those randomized to placebo were switched to the active treatment. By week 24, the switch patients had largely caught up to those initiated on roflumilast for median PASI improvement (39.1% vs. 43.5%).
Similar to orismilast, roflumilast “was generally well tolerated,” Dr. Egeberg said. The adverse events were consistent with those associated with PDE4 inhibitors in previous trials, whether in psoriasis or COPD. There was only one serious adverse event, and it was not considered treatment related. Discontinuations for adverse events “were very low.”
In a population with a relatively high rate of smoking, Dr. Egeberg further reported, lung function was improved, a remark initially interpreted as a joke by some attending the presentation. However, Dr. Egeberg confirmed that lung function was monitored, and objective improvements were recorded.
By Danish law, the investigators were required to inform the manufacturers of roflumilast. Despite the results of this study, he is not aware of any plans to seek an indication for roflumilast in psoriasis, but he noted that the drug is readily available at a low price.
For those willing to offer this therapy off label, “you can start using it tomorrow if you’d like,” he said.
Dr. French reports financial relationships with Almirall, Amgen, Biotest, Galderma, Janssen Cilag, Leo Pharma, Pincell, Regeneron, UCB, and UNION Therapeutics, which provided funding for this trial. Dr. Egeberg reports financial relationships with Eli Lilly, Galderma, Janssen-Cilag, Novartis, and Pfizer.
A version of this article first appeared on Medscape.com.
NEW ORLEANS – according to results of a phase 2 clinical trial presented as a late-breaker at the annual meeting of the American Academy of Dermatology.
The phase 2b data, which are prompting a phase 3 trial, suggest that the drug, called orismilast, “is a potential new addition to the psoriasis armamentarium,” reported Lars E. French, MD, professor and chair, department of dermatology, Ludwig Maximilian University of Munich (Germany).
At the same session, findings from another study supported off-label use of oral roflumilast (Daliresp and generic), a PDE4 inhibitor approved for severe chronic obstructive pulmonary disease (COPD). The only PDE4 inhibitors with an indication for psoriasis are roflumilast, approved as a cream (Zoryve), and apremilast (Otezla), approved as an oral therapy.
Phase 2 study of orismilast
In the orismilast trial, Dr. French attributed the efficacy observed to the potency of orismilast on the B and D subtypes of PDE4 associated with inflammation. One clue is that these specific subtypes are overly expressed in the skin of patients with either psoriasis or atopic dermatitis.
“When compared to apremilast, orismilast is at least two to fivefold more potent on all PDE4 isoforms and up to 39 times more potent on some of the PDE4 B and D isoforms,” said Dr. French, referring to preclinical findings in human whole blood and blood cells and in a mouse model of chronic inflammation.
The efficacy of orismilast in an immediate-release oral formulation was previously demonstrated in a recently published phase 2a trial, but the newest study tested a modified-release formulation of orismilast to test its potential to improve tolerability.
In the study, 202 adult patients with moderate to severe psoriasis (Psoriasis Area Severity Index [PASI] score ≥ 12) were randomly assigned to one of three doses of orismilast or to placebo. Each of the three doses – 20 mg, 30 mg, or 40 mg – were administered twice daily. The primary endpoint was change in PASI score at 16 weeks. Secondary endpoints included PASI 75 responses (signifying 75% clearance) and safety.
Relative to placebo, which was associated with a PASI improvement of 17%, all three of the tested orismilast doses were superior in a dose-dependent manner. The rates of response were 53%, 61%, and 64% for the 20-mg, 30-mg, and 40-mg twice-daily doses, respectively.
The PASI improvements were rapid, Dr. French said. At 4 weeks, PASI scores climbed from baseline by nearly 40% for those on all orismilast doses, which was more than double the improvement in the placebo group.
In the intention-to-treat analysis with missing data counted as nonresponders, the proportion of patients reaching PASI-75 scores at 16 weeks were 39%, 49%, 45%, and 17%, in the 20-mg, 30-mg, 40-mg, and placebo groups, respectively. The proportion of patients experiencing complete or near-complete skin clearance defined by a PASI 90 were 24%, 22%, 28%, and 8%, respectively.
The side-effect profile was consistent with other PDE4 inhibitors. The most common adverse events included gastrointestinal complaints, such as diarrhea and nausea, as well as headache and dizziness. But the majority of these events were of low grade, and they were largely confined to the first 4 weeks of treatment, which is a pattern reported with other PDE4 inhibitors in psoriasis and other chronic inflammatory diseases, such as COPD, according to Dr. French.
“There were no discontinuations for a treatment-related adverse event in the arms receiving either the 20-mg or the 30-mg doses,” Dr. French reported. There were only two serious adverse events, and neither were considered by trial investigators to be related to orismilast.
Based on the limited therapeutic gain but greater risk for adverse events on the 40-mg twice-daily dose, “the question is now whether to move forward with the 20-mg or the 30-mg dose,” said Dr. French, who said planning of a phase 3 trial is underway.
Phase 2 study of roflumilast
However, this was not the only set of data on an oral PDE4 inhibitor presented as a late-breaker at the AAD meeting. For clinicians looking for a more immediate and less expensive alternative to apremilast, another study indicated that off-label use of oral roflumilast is an option.
In an investigator-initiated, multicenter, double-blind, placebo-controlled trial conducted in Denmark, the rate of response to oral roflumilast at 24 weeks, including the clear or almost clear response, was on the same general order of magnitude as that seen in the orismilast study, reported Alexander Egeberg, MD, PhD, professor of dermatology, University of Copenhagen.
“At 24 weeks, 21.7% had achieved a PASI 90, and 8.7% achieved a PASI 100,” Dr. Egeberg said.
Oral roflumilast has been available for the treatment of COPD for more than 10 years and is now available in a generic formulation. This study was conducted independent of any pharmaceutical company involvement, and the high rate of response and low risk of adverse events suggests that patients can benefit from a PDE4 inhibitor in a very low-cost form.
“Generic oral roflumilast is cheaper than a Starbucks coffee,” Dr. Egeberg said.
In this trial, 46 patients were randomly assigned to placebo or to the COPD-approved roflumilast dose of 500 mcg once daily. The primary endpoint was change in PASI scores from baseline to week 12, which Dr. Egeberg pointed out is a shorter time frame than the 16 weeks more typical of psoriasis treatment studies.
At week 12, the median improvement in PASI was 34.8% in the roflumilast group versus 0% in the placebo group. Patients were then followed for an additional 12 weeks, but those randomized to placebo were switched to the active treatment. By week 24, the switch patients had largely caught up to those initiated on roflumilast for median PASI improvement (39.1% vs. 43.5%).
Similar to orismilast, roflumilast “was generally well tolerated,” Dr. Egeberg said. The adverse events were consistent with those associated with PDE4 inhibitors in previous trials, whether in psoriasis or COPD. There was only one serious adverse event, and it was not considered treatment related. Discontinuations for adverse events “were very low.”
In a population with a relatively high rate of smoking, Dr. Egeberg further reported, lung function was improved, a remark initially interpreted as a joke by some attending the presentation. However, Dr. Egeberg confirmed that lung function was monitored, and objective improvements were recorded.
By Danish law, the investigators were required to inform the manufacturers of roflumilast. Despite the results of this study, he is not aware of any plans to seek an indication for roflumilast in psoriasis, but he noted that the drug is readily available at a low price.
For those willing to offer this therapy off label, “you can start using it tomorrow if you’d like,” he said.
Dr. French reports financial relationships with Almirall, Amgen, Biotest, Galderma, Janssen Cilag, Leo Pharma, Pincell, Regeneron, UCB, and UNION Therapeutics, which provided funding for this trial. Dr. Egeberg reports financial relationships with Eli Lilly, Galderma, Janssen-Cilag, Novartis, and Pfizer.
A version of this article first appeared on Medscape.com.
NEW ORLEANS – according to results of a phase 2 clinical trial presented as a late-breaker at the annual meeting of the American Academy of Dermatology.
The phase 2b data, which are prompting a phase 3 trial, suggest that the drug, called orismilast, “is a potential new addition to the psoriasis armamentarium,” reported Lars E. French, MD, professor and chair, department of dermatology, Ludwig Maximilian University of Munich (Germany).
At the same session, findings from another study supported off-label use of oral roflumilast (Daliresp and generic), a PDE4 inhibitor approved for severe chronic obstructive pulmonary disease (COPD). The only PDE4 inhibitors with an indication for psoriasis are roflumilast, approved as a cream (Zoryve), and apremilast (Otezla), approved as an oral therapy.
Phase 2 study of orismilast
In the orismilast trial, Dr. French attributed the efficacy observed to the potency of orismilast on the B and D subtypes of PDE4 associated with inflammation. One clue is that these specific subtypes are overly expressed in the skin of patients with either psoriasis or atopic dermatitis.
“When compared to apremilast, orismilast is at least two to fivefold more potent on all PDE4 isoforms and up to 39 times more potent on some of the PDE4 B and D isoforms,” said Dr. French, referring to preclinical findings in human whole blood and blood cells and in a mouse model of chronic inflammation.
The efficacy of orismilast in an immediate-release oral formulation was previously demonstrated in a recently published phase 2a trial, but the newest study tested a modified-release formulation of orismilast to test its potential to improve tolerability.
In the study, 202 adult patients with moderate to severe psoriasis (Psoriasis Area Severity Index [PASI] score ≥ 12) were randomly assigned to one of three doses of orismilast or to placebo. Each of the three doses – 20 mg, 30 mg, or 40 mg – were administered twice daily. The primary endpoint was change in PASI score at 16 weeks. Secondary endpoints included PASI 75 responses (signifying 75% clearance) and safety.
Relative to placebo, which was associated with a PASI improvement of 17%, all three of the tested orismilast doses were superior in a dose-dependent manner. The rates of response were 53%, 61%, and 64% for the 20-mg, 30-mg, and 40-mg twice-daily doses, respectively.
The PASI improvements were rapid, Dr. French said. At 4 weeks, PASI scores climbed from baseline by nearly 40% for those on all orismilast doses, which was more than double the improvement in the placebo group.
In the intention-to-treat analysis with missing data counted as nonresponders, the proportion of patients reaching PASI-75 scores at 16 weeks were 39%, 49%, 45%, and 17%, in the 20-mg, 30-mg, 40-mg, and placebo groups, respectively. The proportion of patients experiencing complete or near-complete skin clearance defined by a PASI 90 were 24%, 22%, 28%, and 8%, respectively.
The side-effect profile was consistent with other PDE4 inhibitors. The most common adverse events included gastrointestinal complaints, such as diarrhea and nausea, as well as headache and dizziness. But the majority of these events were of low grade, and they were largely confined to the first 4 weeks of treatment, which is a pattern reported with other PDE4 inhibitors in psoriasis and other chronic inflammatory diseases, such as COPD, according to Dr. French.
“There were no discontinuations for a treatment-related adverse event in the arms receiving either the 20-mg or the 30-mg doses,” Dr. French reported. There were only two serious adverse events, and neither were considered by trial investigators to be related to orismilast.
Based on the limited therapeutic gain but greater risk for adverse events on the 40-mg twice-daily dose, “the question is now whether to move forward with the 20-mg or the 30-mg dose,” said Dr. French, who said planning of a phase 3 trial is underway.
Phase 2 study of roflumilast
However, this was not the only set of data on an oral PDE4 inhibitor presented as a late-breaker at the AAD meeting. For clinicians looking for a more immediate and less expensive alternative to apremilast, another study indicated that off-label use of oral roflumilast is an option.
In an investigator-initiated, multicenter, double-blind, placebo-controlled trial conducted in Denmark, the rate of response to oral roflumilast at 24 weeks, including the clear or almost clear response, was on the same general order of magnitude as that seen in the orismilast study, reported Alexander Egeberg, MD, PhD, professor of dermatology, University of Copenhagen.
“At 24 weeks, 21.7% had achieved a PASI 90, and 8.7% achieved a PASI 100,” Dr. Egeberg said.
Oral roflumilast has been available for the treatment of COPD for more than 10 years and is now available in a generic formulation. This study was conducted independent of any pharmaceutical company involvement, and the high rate of response and low risk of adverse events suggests that patients can benefit from a PDE4 inhibitor in a very low-cost form.
“Generic oral roflumilast is cheaper than a Starbucks coffee,” Dr. Egeberg said.
In this trial, 46 patients were randomly assigned to placebo or to the COPD-approved roflumilast dose of 500 mcg once daily. The primary endpoint was change in PASI scores from baseline to week 12, which Dr. Egeberg pointed out is a shorter time frame than the 16 weeks more typical of psoriasis treatment studies.
At week 12, the median improvement in PASI was 34.8% in the roflumilast group versus 0% in the placebo group. Patients were then followed for an additional 12 weeks, but those randomized to placebo were switched to the active treatment. By week 24, the switch patients had largely caught up to those initiated on roflumilast for median PASI improvement (39.1% vs. 43.5%).
Similar to orismilast, roflumilast “was generally well tolerated,” Dr. Egeberg said. The adverse events were consistent with those associated with PDE4 inhibitors in previous trials, whether in psoriasis or COPD. There was only one serious adverse event, and it was not considered treatment related. Discontinuations for adverse events “were very low.”
In a population with a relatively high rate of smoking, Dr. Egeberg further reported, lung function was improved, a remark initially interpreted as a joke by some attending the presentation. However, Dr. Egeberg confirmed that lung function was monitored, and objective improvements were recorded.
By Danish law, the investigators were required to inform the manufacturers of roflumilast. Despite the results of this study, he is not aware of any plans to seek an indication for roflumilast in psoriasis, but he noted that the drug is readily available at a low price.
For those willing to offer this therapy off label, “you can start using it tomorrow if you’d like,” he said.
Dr. French reports financial relationships with Almirall, Amgen, Biotest, Galderma, Janssen Cilag, Leo Pharma, Pincell, Regeneron, UCB, and UNION Therapeutics, which provided funding for this trial. Dr. Egeberg reports financial relationships with Eli Lilly, Galderma, Janssen-Cilag, Novartis, and Pfizer.
A version of this article first appeared on Medscape.com.
AT AAD 2023
Poor bone health is a ‘robust’ dementia risk factor
After adjusting for relevant factors, adults with the lowest versus highest BMD at the femoral neck were 42% more likely to develop dementia over roughly 10 years.
“Our research has found a link between bone loss and dementia, but further studies are needed to better understand this connection between bone density and memory loss,” study investigator Mohammad Arfan Ikram, MD, PhD, with Erasmus University Medical Center in Rotterdam, the Netherlands, said in a statement.
“It’s possible that bone loss may occur already in the earliest phases of dementia, years before any clinical symptoms manifest themselves. If that were the case, bone loss could be an indicator of risk for dementia and people with bone loss could be targeted for screening and improved care,” Dr. Ikram added.
The study was published online in Neurology.
Common bedfellows
Low BMD and dementia commonly co-occur in the older population, with bone loss accelerating in dementia patients because of physical inactivity and poor nutrition. However, the extent to which bone loss already exists prior to the onset of dementia remains unclear.
The new findings are based on 3,651 adults (mean age 72 years, 58% women) in the Rotterdam Study who were free of dementia between 2002 and 2005. At that time, BMD at the femoral neck, lumbar spine, and total body were obtained using dual-energy radiography absorptiometry (DXA) and the trabecular bone score, which offers further details such as bone microarchitecture, was calculated. Participants were followed up until Jan. 1, 2020.
Analyses were adjusted for age, sex, education, physical activity, smoking status, body mass index, blood pressure, cholesterol, history of comorbidities (stroke and diabetes), and apolipoprotein E genotype.
During follow-up, 688 (19%) participants developed dementia, mostly Alzheimer’s disease (77%).
Throughout the entire follow-up period, lower BMD at the femoral neck (per standard deviation), but not at other bone sites, correlated with a higher risk for all-cause dementia (hazard ratio, 1.12; 95% confidence interval, 1.02-1.23) and Alzheimer’s disease (HR, 1.14; 95% CI, 1.02-1.28).
Within the first 10 years after baseline, the risk for dementia was greatest in individuals with the lowest BMD at the femoral neck (HR, 2.03; 95% CI, 1.39-2.96) and total body (HR, 1.42; 95% CI, 1.01-2.02) and lowest trabecular bone score (HR, 1.59; 95% CI, 1.11-2.28).
Only BMD at the femoral neck was related to incident all-cause dementia in the first 5 years of follow-up (HR, 2.13; 95% CI, 1.28-3.57).
These findings add “extra knowledge to previous findings that associations change with time, with the strength of the effect decreasing with increasing follow-up time,” the investigators noted.
They suggest that total BMD and trabecular bone score might occur as “prodromal features instead of causes of dementia and related toxic protein accumulation in the brain. In other words, persons with subclinical, incipient dementia may have poor bone health due to the dementia process instead of vice versa.”
The investigators noted that further research focusing on the predictive ability of BMD for dementia is necessary. “As an indicator of dementia risk, intervening in BMD may improve clinical care of these persons, especially considering the multicomorbidities and polypharmacy that are highly preventive in this group,” they concluded.
Little known bone-brain axis to blame?
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, noted that “bone health is increasingly becoming front of mind in older adults. This study confirms an association between poor bone health – low bone mineral density and bone scores – and poor brain health.”
However, it’s unclear whether the link is causal – that is, whether poor bone health actually leads to poor brain health, and whether that can be staved off by directly supporting bone density,” Dr. Lakhan said.
“The link may very well be the little known ‘brain-bone axis’ – where our bones actually regulate our brain,” he added.
“Take for example the bone-generated hormone osteocalcin that crosses the blood-brain barrier and regulates brain functions like memory and cognition. Mice who don’t express the osteocalcin gene or are injected with antibodies that block osteocalcin actually have poor memory and worse anxiety,” Dr. Lakhan said.
“In any event, good bone health begins with healthy habits: a diet with plenty of calcium, vitamin D, and protein; a regimen of not just cardio, but also weight-bearing exercises; and staying clear of smoking and heavy alcohol intake,” he concluded.
The study was funded by Erasmus Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research, the Netherlands Organization for Health Research and Development, the Research Institute for Diseases in the Elderly, the Netherlands Genomics Initiative, the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports, the European Commission, and the Municipality of Rotterdam. Dr. Ikram and Dr. Lakhan report no relevant disclosures.
A version of this article first appeared on Medscape.com.
After adjusting for relevant factors, adults with the lowest versus highest BMD at the femoral neck were 42% more likely to develop dementia over roughly 10 years.
“Our research has found a link between bone loss and dementia, but further studies are needed to better understand this connection between bone density and memory loss,” study investigator Mohammad Arfan Ikram, MD, PhD, with Erasmus University Medical Center in Rotterdam, the Netherlands, said in a statement.
“It’s possible that bone loss may occur already in the earliest phases of dementia, years before any clinical symptoms manifest themselves. If that were the case, bone loss could be an indicator of risk for dementia and people with bone loss could be targeted for screening and improved care,” Dr. Ikram added.
The study was published online in Neurology.
Common bedfellows
Low BMD and dementia commonly co-occur in the older population, with bone loss accelerating in dementia patients because of physical inactivity and poor nutrition. However, the extent to which bone loss already exists prior to the onset of dementia remains unclear.
The new findings are based on 3,651 adults (mean age 72 years, 58% women) in the Rotterdam Study who were free of dementia between 2002 and 2005. At that time, BMD at the femoral neck, lumbar spine, and total body were obtained using dual-energy radiography absorptiometry (DXA) and the trabecular bone score, which offers further details such as bone microarchitecture, was calculated. Participants were followed up until Jan. 1, 2020.
Analyses were adjusted for age, sex, education, physical activity, smoking status, body mass index, blood pressure, cholesterol, history of comorbidities (stroke and diabetes), and apolipoprotein E genotype.
During follow-up, 688 (19%) participants developed dementia, mostly Alzheimer’s disease (77%).
Throughout the entire follow-up period, lower BMD at the femoral neck (per standard deviation), but not at other bone sites, correlated with a higher risk for all-cause dementia (hazard ratio, 1.12; 95% confidence interval, 1.02-1.23) and Alzheimer’s disease (HR, 1.14; 95% CI, 1.02-1.28).
Within the first 10 years after baseline, the risk for dementia was greatest in individuals with the lowest BMD at the femoral neck (HR, 2.03; 95% CI, 1.39-2.96) and total body (HR, 1.42; 95% CI, 1.01-2.02) and lowest trabecular bone score (HR, 1.59; 95% CI, 1.11-2.28).
Only BMD at the femoral neck was related to incident all-cause dementia in the first 5 years of follow-up (HR, 2.13; 95% CI, 1.28-3.57).
These findings add “extra knowledge to previous findings that associations change with time, with the strength of the effect decreasing with increasing follow-up time,” the investigators noted.
They suggest that total BMD and trabecular bone score might occur as “prodromal features instead of causes of dementia and related toxic protein accumulation in the brain. In other words, persons with subclinical, incipient dementia may have poor bone health due to the dementia process instead of vice versa.”
The investigators noted that further research focusing on the predictive ability of BMD for dementia is necessary. “As an indicator of dementia risk, intervening in BMD may improve clinical care of these persons, especially considering the multicomorbidities and polypharmacy that are highly preventive in this group,” they concluded.
Little known bone-brain axis to blame?
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, noted that “bone health is increasingly becoming front of mind in older adults. This study confirms an association between poor bone health – low bone mineral density and bone scores – and poor brain health.”
However, it’s unclear whether the link is causal – that is, whether poor bone health actually leads to poor brain health, and whether that can be staved off by directly supporting bone density,” Dr. Lakhan said.
“The link may very well be the little known ‘brain-bone axis’ – where our bones actually regulate our brain,” he added.
“Take for example the bone-generated hormone osteocalcin that crosses the blood-brain barrier and regulates brain functions like memory and cognition. Mice who don’t express the osteocalcin gene or are injected with antibodies that block osteocalcin actually have poor memory and worse anxiety,” Dr. Lakhan said.
“In any event, good bone health begins with healthy habits: a diet with plenty of calcium, vitamin D, and protein; a regimen of not just cardio, but also weight-bearing exercises; and staying clear of smoking and heavy alcohol intake,” he concluded.
The study was funded by Erasmus Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research, the Netherlands Organization for Health Research and Development, the Research Institute for Diseases in the Elderly, the Netherlands Genomics Initiative, the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports, the European Commission, and the Municipality of Rotterdam. Dr. Ikram and Dr. Lakhan report no relevant disclosures.
A version of this article first appeared on Medscape.com.
After adjusting for relevant factors, adults with the lowest versus highest BMD at the femoral neck were 42% more likely to develop dementia over roughly 10 years.
“Our research has found a link between bone loss and dementia, but further studies are needed to better understand this connection between bone density and memory loss,” study investigator Mohammad Arfan Ikram, MD, PhD, with Erasmus University Medical Center in Rotterdam, the Netherlands, said in a statement.
“It’s possible that bone loss may occur already in the earliest phases of dementia, years before any clinical symptoms manifest themselves. If that were the case, bone loss could be an indicator of risk for dementia and people with bone loss could be targeted for screening and improved care,” Dr. Ikram added.
The study was published online in Neurology.
Common bedfellows
Low BMD and dementia commonly co-occur in the older population, with bone loss accelerating in dementia patients because of physical inactivity and poor nutrition. However, the extent to which bone loss already exists prior to the onset of dementia remains unclear.
The new findings are based on 3,651 adults (mean age 72 years, 58% women) in the Rotterdam Study who were free of dementia between 2002 and 2005. At that time, BMD at the femoral neck, lumbar spine, and total body were obtained using dual-energy radiography absorptiometry (DXA) and the trabecular bone score, which offers further details such as bone microarchitecture, was calculated. Participants were followed up until Jan. 1, 2020.
Analyses were adjusted for age, sex, education, physical activity, smoking status, body mass index, blood pressure, cholesterol, history of comorbidities (stroke and diabetes), and apolipoprotein E genotype.
During follow-up, 688 (19%) participants developed dementia, mostly Alzheimer’s disease (77%).
Throughout the entire follow-up period, lower BMD at the femoral neck (per standard deviation), but not at other bone sites, correlated with a higher risk for all-cause dementia (hazard ratio, 1.12; 95% confidence interval, 1.02-1.23) and Alzheimer’s disease (HR, 1.14; 95% CI, 1.02-1.28).
Within the first 10 years after baseline, the risk for dementia was greatest in individuals with the lowest BMD at the femoral neck (HR, 2.03; 95% CI, 1.39-2.96) and total body (HR, 1.42; 95% CI, 1.01-2.02) and lowest trabecular bone score (HR, 1.59; 95% CI, 1.11-2.28).
Only BMD at the femoral neck was related to incident all-cause dementia in the first 5 years of follow-up (HR, 2.13; 95% CI, 1.28-3.57).
These findings add “extra knowledge to previous findings that associations change with time, with the strength of the effect decreasing with increasing follow-up time,” the investigators noted.
They suggest that total BMD and trabecular bone score might occur as “prodromal features instead of causes of dementia and related toxic protein accumulation in the brain. In other words, persons with subclinical, incipient dementia may have poor bone health due to the dementia process instead of vice versa.”
The investigators noted that further research focusing on the predictive ability of BMD for dementia is necessary. “As an indicator of dementia risk, intervening in BMD may improve clinical care of these persons, especially considering the multicomorbidities and polypharmacy that are highly preventive in this group,” they concluded.
Little known bone-brain axis to blame?
In a comment, Shaheen Lakhan, MD, a neurologist and researcher in Boston, noted that “bone health is increasingly becoming front of mind in older adults. This study confirms an association between poor bone health – low bone mineral density and bone scores – and poor brain health.”
However, it’s unclear whether the link is causal – that is, whether poor bone health actually leads to poor brain health, and whether that can be staved off by directly supporting bone density,” Dr. Lakhan said.
“The link may very well be the little known ‘brain-bone axis’ – where our bones actually regulate our brain,” he added.
“Take for example the bone-generated hormone osteocalcin that crosses the blood-brain barrier and regulates brain functions like memory and cognition. Mice who don’t express the osteocalcin gene or are injected with antibodies that block osteocalcin actually have poor memory and worse anxiety,” Dr. Lakhan said.
“In any event, good bone health begins with healthy habits: a diet with plenty of calcium, vitamin D, and protein; a regimen of not just cardio, but also weight-bearing exercises; and staying clear of smoking and heavy alcohol intake,” he concluded.
The study was funded by Erasmus Medical Center and Erasmus University Rotterdam, the Netherlands Organization for Scientific Research, the Netherlands Organization for Health Research and Development, the Research Institute for Diseases in the Elderly, the Netherlands Genomics Initiative, the Ministry of Education, Culture and Science, the Ministry of Health, Welfare and Sports, the European Commission, and the Municipality of Rotterdam. Dr. Ikram and Dr. Lakhan report no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
CT results in myositis inform cancer screening strategies
Targeting cancer screenings based on idiopathic inflammatory myositis (IIM) subtype, autoantibodies, and age may help to maximize cancer detection while limiting false positives.
In a retrospective, single-center study conducted at Johns Hopkins University in Baltimore, researchers found that when screening patients with IIM for cancer via CT imaging, the diagnostic yield (number of cancers detected/tests performed) was highest in patients with dermatomyositis and the autoantibody anti–TIF1-gamma. Screening patients below age 40 years was associated with lower diagnostic yields and higher false positives, regardless of subtype.
Because of the well-known association between IIM and contemporaneous cancer, newly diagnosed patients with IIM often undergo screening. Yet, there is little research on the most efficient assessment approaches, Christopher Mecoli, MD, an assistant professor of medicine at John Hopkins University School of Medicine and lead author of the study, told this news organization. “There has been a lot written about how these patients should be evaluated for cancer. Unfortunately, the majority of literature is based on eminence,” he said. This study is “one of the first pieces of real data to inform that conversation,” he added.
The research was published online in Arthritis Care & Research.
In the study, Dr. Mecoli and colleagues looked at 1,086 patients enrolled in the center’s Myositis Research Registry from 2003 through 2020. The analysis included patients with a diagnosis of dermatomyositis, polymyositis, immune-mediated necrotizing myopathy (IMNM), and antisynthetase syndrome (ASyS). The researchers also looked at myositis-specific autoantibodies, including anti–TIF1-gamma, –Jo1, and –HMGCR. Patients were excluded from the analysis if they had a cancer diagnosis prior to their IIM onset.
Among patients included in the analysis, the average age of IIM onset was 49 years, and median follow-up duration was 5.3 years. Most patients were female (71%), 68% were white, 21% were Black, 3.6% were Asian, and 7.4% had a listed race of other or unknown. About 66% of all patients received a chest CT scan within 3 years of IIM onset, and 51% received an abdomen/pelvis CT in that same time frame. False positives were defined as the percentage of scans that led to a noncancerous biopsy.
During the study period, 62 patients had a cancer diagnosis within the first 3 years of IIM onset, with the most common cancers being breast (19%), melanoma (13%), and cervical/uterine (10%). Of 1,011 chest scans performed, 9 led to a cancer diagnosis (0.9%), compared with 12 of the 657 abdomen/pelvis (a/p) CT scans (1.8%). Patients with the dermatomyositis-specific autoantibody anti–TIF1-gamma had the highest diagnostic yield (2.9% in chest CT and 2.4% in a/p CT). Regardless of autoantibodies, dermatomyositis patients above 40 years of age had a diagnostic yield of 1.4% in chest CT and 2.7% in a/p CT. For patients under the age of 40 with polymyositis, IMNM, and ASyS, the diagnostic yield for all CT scans was 0.0%. The diagnostic yield in patients under 40 with dermatomyositis was also low (0.0% in chest CT, 0.8% in a/p CT).
The false-positive rate for all chest CT scans was 2.8%, with patients with IMNM and ASyS having the highest frequency of false positivity (both 4.4%). “Based on our data, CT chest imaging in ASyS and IMNM patients are associated with the most harm from a cancer screening perspective,” the authors write. In a/p CT, patients with dermatomyositis under 40 and patients with ASyS had the highest false-positive rates (4.9% and 3.8%, respectively).
“Age was a really big deal in terms of predicting diagnostic yield and false-positivity rate,” Dr. Mecoli said, particularly in patients with dermatomyositis. “This subgroup has historically been thought to have the biggest dissociation with cancer,” he said, but in patients under 40, “it doesn’t look like CT scans were that helpful. They were not picking up a lot of cancers, and they were leading to a lot of false-positive results.”
Still, Rohit Aggarwal, MD, of the division of rheumatology and clinical immunology at the University of Pittsburgh, Pennsylvania, noted that the diagnostic yields of 1%-2% and even 2%-4% in higher-risk populations were high. By comparison, lung cancer screening trials had a diagnostic yield of about 1%, and trials examining CT screening for colorectal cancers had diagnostic yields of 0.5%, the authors write.
“The key message for me is that we should definitely perform CT scans of the chest, abdomen, and pelvis within 3 years of diagnosis – typically at presentation – if the patient has any risk factor for increased risk of cancer, which include dermatomyositis and age above 40,” Dr. Aggarwal toldthis news organization. He was not involved with the research. There are also other clinical factors to consider that were not included in the study, he added, such as severe dysphagia, patients with refractory treatment, and male sex.
Both Dr. Aggarwal and Dr. Mecoli agreed that there are limitations to this single-center, retrospective study that make it difficult to generalize the results. Similar studies should be conducted at other institutions to see if these associations hold true, Dr. Mecoli said. A prospective study could also help control for factors such as selection bias, Dr. Aggarwal added. “I don’t think these are definitive data, but I think these data were needed at retrospective levels” to plan future research, he said.
The study was supported in part by grants from the National Institutes of Health, the Jerome L. Greene Foundation, the Donald B. and Dorothy L. Stabler Foundation, the Huayi and Siuling Zhang Discovery Fund, and Dr. Peter Buck. Dr. Mecoli and Dr. Aggarwal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Targeting cancer screenings based on idiopathic inflammatory myositis (IIM) subtype, autoantibodies, and age may help to maximize cancer detection while limiting false positives.
In a retrospective, single-center study conducted at Johns Hopkins University in Baltimore, researchers found that when screening patients with IIM for cancer via CT imaging, the diagnostic yield (number of cancers detected/tests performed) was highest in patients with dermatomyositis and the autoantibody anti–TIF1-gamma. Screening patients below age 40 years was associated with lower diagnostic yields and higher false positives, regardless of subtype.
Because of the well-known association between IIM and contemporaneous cancer, newly diagnosed patients with IIM often undergo screening. Yet, there is little research on the most efficient assessment approaches, Christopher Mecoli, MD, an assistant professor of medicine at John Hopkins University School of Medicine and lead author of the study, told this news organization. “There has been a lot written about how these patients should be evaluated for cancer. Unfortunately, the majority of literature is based on eminence,” he said. This study is “one of the first pieces of real data to inform that conversation,” he added.
The research was published online in Arthritis Care & Research.
In the study, Dr. Mecoli and colleagues looked at 1,086 patients enrolled in the center’s Myositis Research Registry from 2003 through 2020. The analysis included patients with a diagnosis of dermatomyositis, polymyositis, immune-mediated necrotizing myopathy (IMNM), and antisynthetase syndrome (ASyS). The researchers also looked at myositis-specific autoantibodies, including anti–TIF1-gamma, –Jo1, and –HMGCR. Patients were excluded from the analysis if they had a cancer diagnosis prior to their IIM onset.
Among patients included in the analysis, the average age of IIM onset was 49 years, and median follow-up duration was 5.3 years. Most patients were female (71%), 68% were white, 21% were Black, 3.6% were Asian, and 7.4% had a listed race of other or unknown. About 66% of all patients received a chest CT scan within 3 years of IIM onset, and 51% received an abdomen/pelvis CT in that same time frame. False positives were defined as the percentage of scans that led to a noncancerous biopsy.
During the study period, 62 patients had a cancer diagnosis within the first 3 years of IIM onset, with the most common cancers being breast (19%), melanoma (13%), and cervical/uterine (10%). Of 1,011 chest scans performed, 9 led to a cancer diagnosis (0.9%), compared with 12 of the 657 abdomen/pelvis (a/p) CT scans (1.8%). Patients with the dermatomyositis-specific autoantibody anti–TIF1-gamma had the highest diagnostic yield (2.9% in chest CT and 2.4% in a/p CT). Regardless of autoantibodies, dermatomyositis patients above 40 years of age had a diagnostic yield of 1.4% in chest CT and 2.7% in a/p CT. For patients under the age of 40 with polymyositis, IMNM, and ASyS, the diagnostic yield for all CT scans was 0.0%. The diagnostic yield in patients under 40 with dermatomyositis was also low (0.0% in chest CT, 0.8% in a/p CT).
The false-positive rate for all chest CT scans was 2.8%, with patients with IMNM and ASyS having the highest frequency of false positivity (both 4.4%). “Based on our data, CT chest imaging in ASyS and IMNM patients are associated with the most harm from a cancer screening perspective,” the authors write. In a/p CT, patients with dermatomyositis under 40 and patients with ASyS had the highest false-positive rates (4.9% and 3.8%, respectively).
“Age was a really big deal in terms of predicting diagnostic yield and false-positivity rate,” Dr. Mecoli said, particularly in patients with dermatomyositis. “This subgroup has historically been thought to have the biggest dissociation with cancer,” he said, but in patients under 40, “it doesn’t look like CT scans were that helpful. They were not picking up a lot of cancers, and they were leading to a lot of false-positive results.”
Still, Rohit Aggarwal, MD, of the division of rheumatology and clinical immunology at the University of Pittsburgh, Pennsylvania, noted that the diagnostic yields of 1%-2% and even 2%-4% in higher-risk populations were high. By comparison, lung cancer screening trials had a diagnostic yield of about 1%, and trials examining CT screening for colorectal cancers had diagnostic yields of 0.5%, the authors write.
“The key message for me is that we should definitely perform CT scans of the chest, abdomen, and pelvis within 3 years of diagnosis – typically at presentation – if the patient has any risk factor for increased risk of cancer, which include dermatomyositis and age above 40,” Dr. Aggarwal toldthis news organization. He was not involved with the research. There are also other clinical factors to consider that were not included in the study, he added, such as severe dysphagia, patients with refractory treatment, and male sex.
Both Dr. Aggarwal and Dr. Mecoli agreed that there are limitations to this single-center, retrospective study that make it difficult to generalize the results. Similar studies should be conducted at other institutions to see if these associations hold true, Dr. Mecoli said. A prospective study could also help control for factors such as selection bias, Dr. Aggarwal added. “I don’t think these are definitive data, but I think these data were needed at retrospective levels” to plan future research, he said.
The study was supported in part by grants from the National Institutes of Health, the Jerome L. Greene Foundation, the Donald B. and Dorothy L. Stabler Foundation, the Huayi and Siuling Zhang Discovery Fund, and Dr. Peter Buck. Dr. Mecoli and Dr. Aggarwal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Targeting cancer screenings based on idiopathic inflammatory myositis (IIM) subtype, autoantibodies, and age may help to maximize cancer detection while limiting false positives.
In a retrospective, single-center study conducted at Johns Hopkins University in Baltimore, researchers found that when screening patients with IIM for cancer via CT imaging, the diagnostic yield (number of cancers detected/tests performed) was highest in patients with dermatomyositis and the autoantibody anti–TIF1-gamma. Screening patients below age 40 years was associated with lower diagnostic yields and higher false positives, regardless of subtype.
Because of the well-known association between IIM and contemporaneous cancer, newly diagnosed patients with IIM often undergo screening. Yet, there is little research on the most efficient assessment approaches, Christopher Mecoli, MD, an assistant professor of medicine at John Hopkins University School of Medicine and lead author of the study, told this news organization. “There has been a lot written about how these patients should be evaluated for cancer. Unfortunately, the majority of literature is based on eminence,” he said. This study is “one of the first pieces of real data to inform that conversation,” he added.
The research was published online in Arthritis Care & Research.
In the study, Dr. Mecoli and colleagues looked at 1,086 patients enrolled in the center’s Myositis Research Registry from 2003 through 2020. The analysis included patients with a diagnosis of dermatomyositis, polymyositis, immune-mediated necrotizing myopathy (IMNM), and antisynthetase syndrome (ASyS). The researchers also looked at myositis-specific autoantibodies, including anti–TIF1-gamma, –Jo1, and –HMGCR. Patients were excluded from the analysis if they had a cancer diagnosis prior to their IIM onset.
Among patients included in the analysis, the average age of IIM onset was 49 years, and median follow-up duration was 5.3 years. Most patients were female (71%), 68% were white, 21% were Black, 3.6% were Asian, and 7.4% had a listed race of other or unknown. About 66% of all patients received a chest CT scan within 3 years of IIM onset, and 51% received an abdomen/pelvis CT in that same time frame. False positives were defined as the percentage of scans that led to a noncancerous biopsy.
During the study period, 62 patients had a cancer diagnosis within the first 3 years of IIM onset, with the most common cancers being breast (19%), melanoma (13%), and cervical/uterine (10%). Of 1,011 chest scans performed, 9 led to a cancer diagnosis (0.9%), compared with 12 of the 657 abdomen/pelvis (a/p) CT scans (1.8%). Patients with the dermatomyositis-specific autoantibody anti–TIF1-gamma had the highest diagnostic yield (2.9% in chest CT and 2.4% in a/p CT). Regardless of autoantibodies, dermatomyositis patients above 40 years of age had a diagnostic yield of 1.4% in chest CT and 2.7% in a/p CT. For patients under the age of 40 with polymyositis, IMNM, and ASyS, the diagnostic yield for all CT scans was 0.0%. The diagnostic yield in patients under 40 with dermatomyositis was also low (0.0% in chest CT, 0.8% in a/p CT).
The false-positive rate for all chest CT scans was 2.8%, with patients with IMNM and ASyS having the highest frequency of false positivity (both 4.4%). “Based on our data, CT chest imaging in ASyS and IMNM patients are associated with the most harm from a cancer screening perspective,” the authors write. In a/p CT, patients with dermatomyositis under 40 and patients with ASyS had the highest false-positive rates (4.9% and 3.8%, respectively).
“Age was a really big deal in terms of predicting diagnostic yield and false-positivity rate,” Dr. Mecoli said, particularly in patients with dermatomyositis. “This subgroup has historically been thought to have the biggest dissociation with cancer,” he said, but in patients under 40, “it doesn’t look like CT scans were that helpful. They were not picking up a lot of cancers, and they were leading to a lot of false-positive results.”
Still, Rohit Aggarwal, MD, of the division of rheumatology and clinical immunology at the University of Pittsburgh, Pennsylvania, noted that the diagnostic yields of 1%-2% and even 2%-4% in higher-risk populations were high. By comparison, lung cancer screening trials had a diagnostic yield of about 1%, and trials examining CT screening for colorectal cancers had diagnostic yields of 0.5%, the authors write.
“The key message for me is that we should definitely perform CT scans of the chest, abdomen, and pelvis within 3 years of diagnosis – typically at presentation – if the patient has any risk factor for increased risk of cancer, which include dermatomyositis and age above 40,” Dr. Aggarwal toldthis news organization. He was not involved with the research. There are also other clinical factors to consider that were not included in the study, he added, such as severe dysphagia, patients with refractory treatment, and male sex.
Both Dr. Aggarwal and Dr. Mecoli agreed that there are limitations to this single-center, retrospective study that make it difficult to generalize the results. Similar studies should be conducted at other institutions to see if these associations hold true, Dr. Mecoli said. A prospective study could also help control for factors such as selection bias, Dr. Aggarwal added. “I don’t think these are definitive data, but I think these data were needed at retrospective levels” to plan future research, he said.
The study was supported in part by grants from the National Institutes of Health, the Jerome L. Greene Foundation, the Donald B. and Dorothy L. Stabler Foundation, the Huayi and Siuling Zhang Discovery Fund, and Dr. Peter Buck. Dr. Mecoli and Dr. Aggarwal have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS CARE & RESEARCH
Tofacitinib may have possible protective effect against ILD in RA
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) were 69% less likely to develop interstitial lung disease (ILD), compared with those treated with adalimumab (Humira), according to a new retrospective study.
About 10% of RA patients develop ILD, but data on how different biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) may affect the risk of developing ILD is lacking, the authors wrote. Identifying treatments that may have protective effects could be useful when prescribing treatments for patients with RA who are at higher risk for ILD, first author Matthew C. Baker, MD, clinical chief in the division of immunology and rheumatology at Stanford (Calif.) University, said in an interview.
In the analysis, published in JAMA Network Open researchers used the Optum Clinformatics Data Mart to identify claims data for patients with RA who were taking b/tsDMARDs from December 2003 to December 2019. Patients were excluded if they had a preexisting diagnosis of ILD or if they had less than 1 year of continuous enrollment in the data set.
The researchers identified 28,559 patients with RA who were treated with adalimumab (13,326), abatacept (Orencia; 5,676), rituximab (Rituxan; 5,444), tocilizumab (Actemra; 2,548), and tofacitinib (1,565). More than three-fourths of patients were female (78%), and their average age was 55.6 years old. During the study period, 276 developed ILD. An adjusted model showed a 69% lower incidence of ILD in patients treated with tofacitinib, compared with those treated with adalimumab (adjusted hazard ratio, 0.31; 95% confidence interval, 0.12-0.78; P = .009). An additional sensitivity analysis also showed a similar reduction in ILD risk in those taking tofacitinib, compared with adalimumab (aHR, 0.32; 95% CI, 0.13-0.82; P < .001). There was no significant difference in risk of developing ILD in the abatacept, rituximab, or tocilizumab groups, compared with the adalimumab group.
“Patients who generally looked similar with RA, but were given different treatments, had different risks of developing ILD,” Dr. Baker said. “Based on what we found, most of the biologic therapies had similar rates of developing ILD, but the JAK inhibitor tofacitinib had a reduced risk.” Additional research is necessary to see if tofacitinib shows the same benefit in prospective studies, he said.
“Even though this wasn’t a clinical trial, it suggested that one of the medications that we use to treat RA could potentially prevent the development of ILD,” Elizabeth Volkmann, MD, codirector of the Connective Tissue Disease-Related Interstitial Lung Disease Program at the University of California, Los Angeles, told this news organization. She was not involved with the study.
With retrospective studies, it is difficult to account for all confounding factors, even with adjusted models, she said. For example, the authors did not have data on patients’ history of smoking, a known risk factor for ILD that could have affected which treatment was selected, they acknowledged. The tofacitinib group was also smaller than other treatment groups, which “may have contributed to a small number of events,” the authors wrote. “However, the follow-up time was similar across all groups, and we used Cox proportional hazard models to investigate the association between time-to-event and use of treatment while controlling for the other baseline characteristics.”
Both Dr. Baker and Dr. Volkmann agreed that future research could also investigate whether tofacitinib prevents the progression of ILD in patients with RA who already have the lung condition. “That’s never been looked at before,” Dr. Volkmann said.
Dr. Baker and a coauthor received support for this work from grants from the National Institutes of Health. Dr. Baker and Dr. Volkmann report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) were 69% less likely to develop interstitial lung disease (ILD), compared with those treated with adalimumab (Humira), according to a new retrospective study.
About 10% of RA patients develop ILD, but data on how different biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) may affect the risk of developing ILD is lacking, the authors wrote. Identifying treatments that may have protective effects could be useful when prescribing treatments for patients with RA who are at higher risk for ILD, first author Matthew C. Baker, MD, clinical chief in the division of immunology and rheumatology at Stanford (Calif.) University, said in an interview.
In the analysis, published in JAMA Network Open researchers used the Optum Clinformatics Data Mart to identify claims data for patients with RA who were taking b/tsDMARDs from December 2003 to December 2019. Patients were excluded if they had a preexisting diagnosis of ILD or if they had less than 1 year of continuous enrollment in the data set.
The researchers identified 28,559 patients with RA who were treated with adalimumab (13,326), abatacept (Orencia; 5,676), rituximab (Rituxan; 5,444), tocilizumab (Actemra; 2,548), and tofacitinib (1,565). More than three-fourths of patients were female (78%), and their average age was 55.6 years old. During the study period, 276 developed ILD. An adjusted model showed a 69% lower incidence of ILD in patients treated with tofacitinib, compared with those treated with adalimumab (adjusted hazard ratio, 0.31; 95% confidence interval, 0.12-0.78; P = .009). An additional sensitivity analysis also showed a similar reduction in ILD risk in those taking tofacitinib, compared with adalimumab (aHR, 0.32; 95% CI, 0.13-0.82; P < .001). There was no significant difference in risk of developing ILD in the abatacept, rituximab, or tocilizumab groups, compared with the adalimumab group.
“Patients who generally looked similar with RA, but were given different treatments, had different risks of developing ILD,” Dr. Baker said. “Based on what we found, most of the biologic therapies had similar rates of developing ILD, but the JAK inhibitor tofacitinib had a reduced risk.” Additional research is necessary to see if tofacitinib shows the same benefit in prospective studies, he said.
“Even though this wasn’t a clinical trial, it suggested that one of the medications that we use to treat RA could potentially prevent the development of ILD,” Elizabeth Volkmann, MD, codirector of the Connective Tissue Disease-Related Interstitial Lung Disease Program at the University of California, Los Angeles, told this news organization. She was not involved with the study.
With retrospective studies, it is difficult to account for all confounding factors, even with adjusted models, she said. For example, the authors did not have data on patients’ history of smoking, a known risk factor for ILD that could have affected which treatment was selected, they acknowledged. The tofacitinib group was also smaller than other treatment groups, which “may have contributed to a small number of events,” the authors wrote. “However, the follow-up time was similar across all groups, and we used Cox proportional hazard models to investigate the association between time-to-event and use of treatment while controlling for the other baseline characteristics.”
Both Dr. Baker and Dr. Volkmann agreed that future research could also investigate whether tofacitinib prevents the progression of ILD in patients with RA who already have the lung condition. “That’s never been looked at before,” Dr. Volkmann said.
Dr. Baker and a coauthor received support for this work from grants from the National Institutes of Health. Dr. Baker and Dr. Volkmann report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Patients with rheumatoid arthritis treated with tofacitinib (Xeljanz) were 69% less likely to develop interstitial lung disease (ILD), compared with those treated with adalimumab (Humira), according to a new retrospective study.
About 10% of RA patients develop ILD, but data on how different biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) may affect the risk of developing ILD is lacking, the authors wrote. Identifying treatments that may have protective effects could be useful when prescribing treatments for patients with RA who are at higher risk for ILD, first author Matthew C. Baker, MD, clinical chief in the division of immunology and rheumatology at Stanford (Calif.) University, said in an interview.
In the analysis, published in JAMA Network Open researchers used the Optum Clinformatics Data Mart to identify claims data for patients with RA who were taking b/tsDMARDs from December 2003 to December 2019. Patients were excluded if they had a preexisting diagnosis of ILD or if they had less than 1 year of continuous enrollment in the data set.
The researchers identified 28,559 patients with RA who were treated with adalimumab (13,326), abatacept (Orencia; 5,676), rituximab (Rituxan; 5,444), tocilizumab (Actemra; 2,548), and tofacitinib (1,565). More than three-fourths of patients were female (78%), and their average age was 55.6 years old. During the study period, 276 developed ILD. An adjusted model showed a 69% lower incidence of ILD in patients treated with tofacitinib, compared with those treated with adalimumab (adjusted hazard ratio, 0.31; 95% confidence interval, 0.12-0.78; P = .009). An additional sensitivity analysis also showed a similar reduction in ILD risk in those taking tofacitinib, compared with adalimumab (aHR, 0.32; 95% CI, 0.13-0.82; P < .001). There was no significant difference in risk of developing ILD in the abatacept, rituximab, or tocilizumab groups, compared with the adalimumab group.
“Patients who generally looked similar with RA, but were given different treatments, had different risks of developing ILD,” Dr. Baker said. “Based on what we found, most of the biologic therapies had similar rates of developing ILD, but the JAK inhibitor tofacitinib had a reduced risk.” Additional research is necessary to see if tofacitinib shows the same benefit in prospective studies, he said.
“Even though this wasn’t a clinical trial, it suggested that one of the medications that we use to treat RA could potentially prevent the development of ILD,” Elizabeth Volkmann, MD, codirector of the Connective Tissue Disease-Related Interstitial Lung Disease Program at the University of California, Los Angeles, told this news organization. She was not involved with the study.
With retrospective studies, it is difficult to account for all confounding factors, even with adjusted models, she said. For example, the authors did not have data on patients’ history of smoking, a known risk factor for ILD that could have affected which treatment was selected, they acknowledged. The tofacitinib group was also smaller than other treatment groups, which “may have contributed to a small number of events,” the authors wrote. “However, the follow-up time was similar across all groups, and we used Cox proportional hazard models to investigate the association between time-to-event and use of treatment while controlling for the other baseline characteristics.”
Both Dr. Baker and Dr. Volkmann agreed that future research could also investigate whether tofacitinib prevents the progression of ILD in patients with RA who already have the lung condition. “That’s never been looked at before,” Dr. Volkmann said.
Dr. Baker and a coauthor received support for this work from grants from the National Institutes of Health. Dr. Baker and Dr. Volkmann report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
New JAK inhibitor study data confirm benefit in alopecia areata
from clinical trials of two drugs presented at a late-breaker research session at the annual meeting of the American Academy of Dermatology.
Based on phase 3 studies that document robust hair growth in about one third of patients, deuruxolitinib (CTP-543), an inhibitor of the JAK1 and JAK2 enzymes, has the potential to become the second JAK inhibitor available for the treatment of alopecia areata. If approved, it will join baricitinib (Olumiant), which received U.S. approval almost 1 year ago.
In his talk on THRIVE-AA2, a phase 3 trial of the investigational medicine deuruxolitinib, the principal investigator, Brett A. King, MD, PhD, displayed several before-and-after photos and said, “The photos tell the whole story. This is why there is so much excitement about these drugs.”
THRIVE-AA2 was the second of two phase 3 studies of deuruxolitinib. King was a principal investigator for both pivotal trials, called THRIVE-AA1 and THRIVE AA-2. He characterized the results of the two THRIVE trials as “comparable.”
Dr. King also was a principal investigator for the trials with baricitinib, called BRAVE-AA1 and BRAVE AA-2, which were published last year in the New England Journal of Medicine. The trials for both drugs had similar designs and endpoints.
Deuruxolitinib and the THRIVE studies
In the THRIVE-AA2 trial, 517 adult patients were enrolled with moderate to severe alopecia areata, defined as a SALT (Severity of Alopecia Tool) score of ≥ 50%, which signifies a hair loss of at least 50%. Like THRIVE-AA1, patients participated at treatment centers in North America and Europe. About two-thirds were female. The mean age was 39 years. The majority of patients had complete or near complete hair loss at baseline.
“Many of these patients are the ones we have historically characterized as having alopecia totalis or universalis,” Dr. King said.
Participating patients were randomly assigned to 8 mg deuruxolitinib twice daily, 12 mg deuruxolitinib twice daily, or placebo. The primary endpoint was a SALT score of ≤ 20% at week 24.
At 24 weeks, almost no patients in the placebo group (1%) vs. 33% and 38% in the 8 mg and 12 mg twice-daily groups, respectively, met the primary endpoint. Each active treatment group was highly significant vs. placebo.
Of the responders, the majority achieved complete or near complete hair growth as defined by a SALT score of ≤ 10%, Dr. King reported.
Based on a graph that showed a relatively steep climb over the entire 24-week study period, deuruxolitinib “had a really fast onset of action,” Dr. King said. By week 8, which was the time of the first assessment, both doses of deuruxolitinib were superior to placebo.
The majority of patients had complete or significant loss of eyebrows and eye lashes at baseline, but more than two-thirds of these patients had regrowth by week 24, Dr. King said. Again, no significant regrowth was observed in the placebo arm.
On the Satisfaction of Hair Patient Reported Outcomes (SPRO), more than half of patients on both doses reported being satisfied or very satisfied with the improvement when evaluated at 24 weeks.
“The patient satisfaction overshot what one would expect by looking at the SALT scores, but a lot of subjects were at the precipice of the primary endpoint, sitting on SALT scores of 21, 25, or 30,” Dr. King said.
High participation in extension trial
More than 90% of the patients assigned to deuruxolitinib completed the trial and have entered an open-label extension (OLE). Dr. King credited the substantial rates of hair growth and the low rate of significant adverse events for the high rate of transition to OLE. Those who experienced the response were motivated to maintain it.
“This is a devastating disease. Patients want to get better,” Dr. King said.
There were no serious treatment-emergent adverse events associated with deuruxolitinib, including no thromboembolic events or other off-target events that have been reported previously with other JAK inhibitors in other disease states, such as rheumatoid arthritis. Although some adverse events, such as nasopharyngitis, were observed more often in those taking deuruxolitinib than placebo, there were “very few” discontinuations because of an adverse event, he said.
The data of THRIVE-AA2 are wholly compatible with the previously reported 706-patient THRIVE-AA1, according to Dr. King. In THRIVE-AA1, the primary endpoint of SALT ≤ 20% was reached by 29.6%, 41.5%, and 0.8% of the 8 mg, 12 mg, and placebo groups, respectively. Patient satisfaction scores, safety, and tolerability were also similar, according to Dr. King.
The experience with deuruxolitinib in the THRIVE-AA phase 3 program is similar to the experience with baricitinib in the BRAVE-AA trials. Although they cannot be compared directly because of potential differences between study populations, the 4-mg dose of baricitinib also achieved SALT score ≤ 20 in about 35% of patients, he said. The proportion was lower in the 2-mg group but was also superior to the placebo group.
“JAK inhibitors are changing the paradigm of alopecia areata,” Dr. King said. Responding to a question about payers reluctant to reimburse therapies for a “cosmetic” condition, Dr. King added that the effective treatments are “changing the landscape of how we think about this disease.” Dr. King believes these kinds of data show that “we are literally transforming lives forever.”
Baricitinib and the BRAVE studies
When baricitinib received regulatory approval for alopecia areata last year, it was not just the first JAK inhibitor approved for this disease, but the first systemic therapy of any kind, according to Maryanne Senna, MD, an assistant professor of dermatology at Harvard Medical School, Boston, and the director of the Lahey Hair Loss Center of Excellence, Burlington, Mass. Dr. Senna was a clinical investigator of BRAVE-AA1, as well as of THRIVE-AA2.
Providing an update on the BRAVE-AA program, Dr. Senna reported 104-week data that appear to support the idea of a life-changing benefit from JAK inhibitor therapy. This is because the effects appear durable.
In the data she presented at the AAD, responders and mixed responders at 52 weeks were followed to 104 weeks. Mixed responders were defined as those without a SALT response of ≤ 20 at week 52 but who had achieved this degree of hair regrowth at some earlier point.
Of the responders, 90% maintained their response at 104 weeks. In addition, many of the mixed responders and patients with a partial response but who never achieved a SALT score ≤ 20% gained additional hair growth, including complete or near complete hair growth, when maintained on treatment over the 2 years of follow-up.
“The follow-up suggests that, if you keep patients on treatment, you can get many of them to a meaningful response,” she said.
Meanwhile, “there have been no new safety signals,” Dr. Senna said. She based this statement not only of the 104-week data but on follow-up of up to 3.6 years among patients who have remained on treatment after participating in previous studies.
According to Dr. Senna, the off-target events that have been reported previously in other diseases with other JAK inhibitors, such as major adverse cardiovascular events and thromboembolic events, have not so far been observed in the BRAVE-AA phase 3 program.
Baricitinib, much like all but one of the JAK inhibitors with dermatologic indications, carries a black box warning that lists multiple risks for drugs in this class, based on a rheumatoid arthritis study.
The Food and Drug Administration has granted deuruxolitinib Breakthrough Therapy designation for the treatment of adult patients with moderate to severe alopecia areata and Fast Track designation for the treatment of alopecia areata, according to its manufacturer Concert Pharmaceuticals.
Dr. King reports financial relationships with more than 15 pharmaceutical companies, including Concert Pharmaceuticals, which provided the funding for the THRIVE-AA trial program, and for Eli Lilly, which provided funding for the BRAVE-AA trial program. Dr. Senna reports financial relationships with Arena pharmaceuticals, Follica, and both Concert Pharmaceuticals and Eli Lilly.
A version of this article originally appeared on Medscape.com.
from clinical trials of two drugs presented at a late-breaker research session at the annual meeting of the American Academy of Dermatology.
Based on phase 3 studies that document robust hair growth in about one third of patients, deuruxolitinib (CTP-543), an inhibitor of the JAK1 and JAK2 enzymes, has the potential to become the second JAK inhibitor available for the treatment of alopecia areata. If approved, it will join baricitinib (Olumiant), which received U.S. approval almost 1 year ago.
In his talk on THRIVE-AA2, a phase 3 trial of the investigational medicine deuruxolitinib, the principal investigator, Brett A. King, MD, PhD, displayed several before-and-after photos and said, “The photos tell the whole story. This is why there is so much excitement about these drugs.”
THRIVE-AA2 was the second of two phase 3 studies of deuruxolitinib. King was a principal investigator for both pivotal trials, called THRIVE-AA1 and THRIVE AA-2. He characterized the results of the two THRIVE trials as “comparable.”
Dr. King also was a principal investigator for the trials with baricitinib, called BRAVE-AA1 and BRAVE AA-2, which were published last year in the New England Journal of Medicine. The trials for both drugs had similar designs and endpoints.
Deuruxolitinib and the THRIVE studies
In the THRIVE-AA2 trial, 517 adult patients were enrolled with moderate to severe alopecia areata, defined as a SALT (Severity of Alopecia Tool) score of ≥ 50%, which signifies a hair loss of at least 50%. Like THRIVE-AA1, patients participated at treatment centers in North America and Europe. About two-thirds were female. The mean age was 39 years. The majority of patients had complete or near complete hair loss at baseline.
“Many of these patients are the ones we have historically characterized as having alopecia totalis or universalis,” Dr. King said.
Participating patients were randomly assigned to 8 mg deuruxolitinib twice daily, 12 mg deuruxolitinib twice daily, or placebo. The primary endpoint was a SALT score of ≤ 20% at week 24.
At 24 weeks, almost no patients in the placebo group (1%) vs. 33% and 38% in the 8 mg and 12 mg twice-daily groups, respectively, met the primary endpoint. Each active treatment group was highly significant vs. placebo.
Of the responders, the majority achieved complete or near complete hair growth as defined by a SALT score of ≤ 10%, Dr. King reported.
Based on a graph that showed a relatively steep climb over the entire 24-week study period, deuruxolitinib “had a really fast onset of action,” Dr. King said. By week 8, which was the time of the first assessment, both doses of deuruxolitinib were superior to placebo.
The majority of patients had complete or significant loss of eyebrows and eye lashes at baseline, but more than two-thirds of these patients had regrowth by week 24, Dr. King said. Again, no significant regrowth was observed in the placebo arm.
On the Satisfaction of Hair Patient Reported Outcomes (SPRO), more than half of patients on both doses reported being satisfied or very satisfied with the improvement when evaluated at 24 weeks.
“The patient satisfaction overshot what one would expect by looking at the SALT scores, but a lot of subjects were at the precipice of the primary endpoint, sitting on SALT scores of 21, 25, or 30,” Dr. King said.
High participation in extension trial
More than 90% of the patients assigned to deuruxolitinib completed the trial and have entered an open-label extension (OLE). Dr. King credited the substantial rates of hair growth and the low rate of significant adverse events for the high rate of transition to OLE. Those who experienced the response were motivated to maintain it.
“This is a devastating disease. Patients want to get better,” Dr. King said.
There were no serious treatment-emergent adverse events associated with deuruxolitinib, including no thromboembolic events or other off-target events that have been reported previously with other JAK inhibitors in other disease states, such as rheumatoid arthritis. Although some adverse events, such as nasopharyngitis, were observed more often in those taking deuruxolitinib than placebo, there were “very few” discontinuations because of an adverse event, he said.
The data of THRIVE-AA2 are wholly compatible with the previously reported 706-patient THRIVE-AA1, according to Dr. King. In THRIVE-AA1, the primary endpoint of SALT ≤ 20% was reached by 29.6%, 41.5%, and 0.8% of the 8 mg, 12 mg, and placebo groups, respectively. Patient satisfaction scores, safety, and tolerability were also similar, according to Dr. King.
The experience with deuruxolitinib in the THRIVE-AA phase 3 program is similar to the experience with baricitinib in the BRAVE-AA trials. Although they cannot be compared directly because of potential differences between study populations, the 4-mg dose of baricitinib also achieved SALT score ≤ 20 in about 35% of patients, he said. The proportion was lower in the 2-mg group but was also superior to the placebo group.
“JAK inhibitors are changing the paradigm of alopecia areata,” Dr. King said. Responding to a question about payers reluctant to reimburse therapies for a “cosmetic” condition, Dr. King added that the effective treatments are “changing the landscape of how we think about this disease.” Dr. King believes these kinds of data show that “we are literally transforming lives forever.”
Baricitinib and the BRAVE studies
When baricitinib received regulatory approval for alopecia areata last year, it was not just the first JAK inhibitor approved for this disease, but the first systemic therapy of any kind, according to Maryanne Senna, MD, an assistant professor of dermatology at Harvard Medical School, Boston, and the director of the Lahey Hair Loss Center of Excellence, Burlington, Mass. Dr. Senna was a clinical investigator of BRAVE-AA1, as well as of THRIVE-AA2.
Providing an update on the BRAVE-AA program, Dr. Senna reported 104-week data that appear to support the idea of a life-changing benefit from JAK inhibitor therapy. This is because the effects appear durable.
In the data she presented at the AAD, responders and mixed responders at 52 weeks were followed to 104 weeks. Mixed responders were defined as those without a SALT response of ≤ 20 at week 52 but who had achieved this degree of hair regrowth at some earlier point.
Of the responders, 90% maintained their response at 104 weeks. In addition, many of the mixed responders and patients with a partial response but who never achieved a SALT score ≤ 20% gained additional hair growth, including complete or near complete hair growth, when maintained on treatment over the 2 years of follow-up.
“The follow-up suggests that, if you keep patients on treatment, you can get many of them to a meaningful response,” she said.
Meanwhile, “there have been no new safety signals,” Dr. Senna said. She based this statement not only of the 104-week data but on follow-up of up to 3.6 years among patients who have remained on treatment after participating in previous studies.
According to Dr. Senna, the off-target events that have been reported previously in other diseases with other JAK inhibitors, such as major adverse cardiovascular events and thromboembolic events, have not so far been observed in the BRAVE-AA phase 3 program.
Baricitinib, much like all but one of the JAK inhibitors with dermatologic indications, carries a black box warning that lists multiple risks for drugs in this class, based on a rheumatoid arthritis study.
The Food and Drug Administration has granted deuruxolitinib Breakthrough Therapy designation for the treatment of adult patients with moderate to severe alopecia areata and Fast Track designation for the treatment of alopecia areata, according to its manufacturer Concert Pharmaceuticals.
Dr. King reports financial relationships with more than 15 pharmaceutical companies, including Concert Pharmaceuticals, which provided the funding for the THRIVE-AA trial program, and for Eli Lilly, which provided funding for the BRAVE-AA trial program. Dr. Senna reports financial relationships with Arena pharmaceuticals, Follica, and both Concert Pharmaceuticals and Eli Lilly.
A version of this article originally appeared on Medscape.com.
from clinical trials of two drugs presented at a late-breaker research session at the annual meeting of the American Academy of Dermatology.
Based on phase 3 studies that document robust hair growth in about one third of patients, deuruxolitinib (CTP-543), an inhibitor of the JAK1 and JAK2 enzymes, has the potential to become the second JAK inhibitor available for the treatment of alopecia areata. If approved, it will join baricitinib (Olumiant), which received U.S. approval almost 1 year ago.
In his talk on THRIVE-AA2, a phase 3 trial of the investigational medicine deuruxolitinib, the principal investigator, Brett A. King, MD, PhD, displayed several before-and-after photos and said, “The photos tell the whole story. This is why there is so much excitement about these drugs.”
THRIVE-AA2 was the second of two phase 3 studies of deuruxolitinib. King was a principal investigator for both pivotal trials, called THRIVE-AA1 and THRIVE AA-2. He characterized the results of the two THRIVE trials as “comparable.”
Dr. King also was a principal investigator for the trials with baricitinib, called BRAVE-AA1 and BRAVE AA-2, which were published last year in the New England Journal of Medicine. The trials for both drugs had similar designs and endpoints.
Deuruxolitinib and the THRIVE studies
In the THRIVE-AA2 trial, 517 adult patients were enrolled with moderate to severe alopecia areata, defined as a SALT (Severity of Alopecia Tool) score of ≥ 50%, which signifies a hair loss of at least 50%. Like THRIVE-AA1, patients participated at treatment centers in North America and Europe. About two-thirds were female. The mean age was 39 years. The majority of patients had complete or near complete hair loss at baseline.
“Many of these patients are the ones we have historically characterized as having alopecia totalis or universalis,” Dr. King said.
Participating patients were randomly assigned to 8 mg deuruxolitinib twice daily, 12 mg deuruxolitinib twice daily, or placebo. The primary endpoint was a SALT score of ≤ 20% at week 24.
At 24 weeks, almost no patients in the placebo group (1%) vs. 33% and 38% in the 8 mg and 12 mg twice-daily groups, respectively, met the primary endpoint. Each active treatment group was highly significant vs. placebo.
Of the responders, the majority achieved complete or near complete hair growth as defined by a SALT score of ≤ 10%, Dr. King reported.
Based on a graph that showed a relatively steep climb over the entire 24-week study period, deuruxolitinib “had a really fast onset of action,” Dr. King said. By week 8, which was the time of the first assessment, both doses of deuruxolitinib were superior to placebo.
The majority of patients had complete or significant loss of eyebrows and eye lashes at baseline, but more than two-thirds of these patients had regrowth by week 24, Dr. King said. Again, no significant regrowth was observed in the placebo arm.
On the Satisfaction of Hair Patient Reported Outcomes (SPRO), more than half of patients on both doses reported being satisfied or very satisfied with the improvement when evaluated at 24 weeks.
“The patient satisfaction overshot what one would expect by looking at the SALT scores, but a lot of subjects were at the precipice of the primary endpoint, sitting on SALT scores of 21, 25, or 30,” Dr. King said.
High participation in extension trial
More than 90% of the patients assigned to deuruxolitinib completed the trial and have entered an open-label extension (OLE). Dr. King credited the substantial rates of hair growth and the low rate of significant adverse events for the high rate of transition to OLE. Those who experienced the response were motivated to maintain it.
“This is a devastating disease. Patients want to get better,” Dr. King said.
There were no serious treatment-emergent adverse events associated with deuruxolitinib, including no thromboembolic events or other off-target events that have been reported previously with other JAK inhibitors in other disease states, such as rheumatoid arthritis. Although some adverse events, such as nasopharyngitis, were observed more often in those taking deuruxolitinib than placebo, there were “very few” discontinuations because of an adverse event, he said.
The data of THRIVE-AA2 are wholly compatible with the previously reported 706-patient THRIVE-AA1, according to Dr. King. In THRIVE-AA1, the primary endpoint of SALT ≤ 20% was reached by 29.6%, 41.5%, and 0.8% of the 8 mg, 12 mg, and placebo groups, respectively. Patient satisfaction scores, safety, and tolerability were also similar, according to Dr. King.
The experience with deuruxolitinib in the THRIVE-AA phase 3 program is similar to the experience with baricitinib in the BRAVE-AA trials. Although they cannot be compared directly because of potential differences between study populations, the 4-mg dose of baricitinib also achieved SALT score ≤ 20 in about 35% of patients, he said. The proportion was lower in the 2-mg group but was also superior to the placebo group.
“JAK inhibitors are changing the paradigm of alopecia areata,” Dr. King said. Responding to a question about payers reluctant to reimburse therapies for a “cosmetic” condition, Dr. King added that the effective treatments are “changing the landscape of how we think about this disease.” Dr. King believes these kinds of data show that “we are literally transforming lives forever.”
Baricitinib and the BRAVE studies
When baricitinib received regulatory approval for alopecia areata last year, it was not just the first JAK inhibitor approved for this disease, but the first systemic therapy of any kind, according to Maryanne Senna, MD, an assistant professor of dermatology at Harvard Medical School, Boston, and the director of the Lahey Hair Loss Center of Excellence, Burlington, Mass. Dr. Senna was a clinical investigator of BRAVE-AA1, as well as of THRIVE-AA2.
Providing an update on the BRAVE-AA program, Dr. Senna reported 104-week data that appear to support the idea of a life-changing benefit from JAK inhibitor therapy. This is because the effects appear durable.
In the data she presented at the AAD, responders and mixed responders at 52 weeks were followed to 104 weeks. Mixed responders were defined as those without a SALT response of ≤ 20 at week 52 but who had achieved this degree of hair regrowth at some earlier point.
Of the responders, 90% maintained their response at 104 weeks. In addition, many of the mixed responders and patients with a partial response but who never achieved a SALT score ≤ 20% gained additional hair growth, including complete or near complete hair growth, when maintained on treatment over the 2 years of follow-up.
“The follow-up suggests that, if you keep patients on treatment, you can get many of them to a meaningful response,” she said.
Meanwhile, “there have been no new safety signals,” Dr. Senna said. She based this statement not only of the 104-week data but on follow-up of up to 3.6 years among patients who have remained on treatment after participating in previous studies.
According to Dr. Senna, the off-target events that have been reported previously in other diseases with other JAK inhibitors, such as major adverse cardiovascular events and thromboembolic events, have not so far been observed in the BRAVE-AA phase 3 program.
Baricitinib, much like all but one of the JAK inhibitors with dermatologic indications, carries a black box warning that lists multiple risks for drugs in this class, based on a rheumatoid arthritis study.
The Food and Drug Administration has granted deuruxolitinib Breakthrough Therapy designation for the treatment of adult patients with moderate to severe alopecia areata and Fast Track designation for the treatment of alopecia areata, according to its manufacturer Concert Pharmaceuticals.
Dr. King reports financial relationships with more than 15 pharmaceutical companies, including Concert Pharmaceuticals, which provided the funding for the THRIVE-AA trial program, and for Eli Lilly, which provided funding for the BRAVE-AA trial program. Dr. Senna reports financial relationships with Arena pharmaceuticals, Follica, and both Concert Pharmaceuticals and Eli Lilly.
A version of this article originally appeared on Medscape.com.
AT AAD 2023
Link between knee pain, sleep disturbance related to daily activities
DENVER – The relationship between nighttime knee pain from osteoarthritis and sleep disturbances is more complex than a simple association, according to new research presented at the Osteoarthritis Research Society International 2023 World Congress.
The findings suggested that the association between knee OA pain and sleep problems was also linked to activities of daily living, which can contribute to pain but are also affected by OA, Takahiro Sasahara, of the department of orthopedics at Juntendo University, Tokyo, and Koshigaya Municipal Hospital, Saitama, Japan, told attendees. The study also found that knee pain and mobility impairment were associated with sleep disturbances in older adults regardless of the severity of knee OA.
Luisa Cedin, a PhD student at Rush University, Chicago, who attended the presentation, noted the clinical implications of the interaction of daily activities with knee pain.
”I’m a physical therapist, and this could have a significant impact on the performance of the exercises that I’m requiring as a physical therapist,” Ms. Cedin said in an interview. “When you ask somebody who is not getting enough rest during the night – not only enough time but enough quality of rest – we know that we can expect a lower performance with any type of exercises, whether it’s less strength or force, less power, less agility, or less resistance or endurance, so this has a big impact on their quality of life.”
Mr. Sasahara cited research noting that acute pain occurs at the beginning of movement and during weight bearing and walking while chronic pain frequently occurs at night and in early morning awakenings. The prevalence of sleep disturbances in patients with chronic pain ranges from 50% to 80%, he said, and past evidence has shown the relationship between sleep and pain to be bidirectional.
For example, insomnia frequency and severity, sleep-onset problems, and sleep efficiency are all positively associated with pain sensitivity, and increasing severity of OA is linked to increasing prevalence of night knee pain and sleep problems, affecting quality of life, he said.
In this new study examining the relationship between sleep disturbance and knee pain and mobility, the researchers focused specifically on a population of older adults with knee OA. They analyzed data from the Bunkyo Health Study, which was conducted at Juntendo University’s Sportology Center to examine the association between metabolic, cardiovascular, cognitive dysfunction, and motor organ disorders in older adults from November 2015 to September 2018.
From the initial population of 1,630 adults, aged 65-84, who did not need medical treatment because of knee pain, the researchers analyzed data from 1,145 adults who the met this study’s criteria, which included MRI imaging of medial type knee OA. A little over half (55.7%) were women, with an average age of 73 and an average body mass index (BMI) of 22.8 kg/m2.
In addition to blood and urine sampling, the researchers determined the severity of knee OA based on joint space width, femorotibial angle, and Kellgren and Lawrence (K/L) grade from x-rays in standing position. They also assessed the structure of knee OA using a whole-organ MRI score (WORMS), and pain and mobility with a visual analog scale, the Japan Knee Osteoarthritis Measure (JKOM), and the 25-question geriatric locomotive function scale.
The JKOM, based on the Western Ontario and McMaster Universities quality of life index for general knee OA, is adjusted to account for the Japanese lifestyle and covers four categories: knee pain and stiffness, a score for activities of daily living, a social activities score, and the patient’s health conditions.
Overall, 41.3% of the participants had sleep disturbances, based on a score of 6 or higher on the Pittsburgh Sleep Quality Index–Japanese. More women (55.7%) than men experienced sleep problems (P < .001), but there were no significant differences in the average age between those who did and those who did not have sleep issues. There were also no significance differences in BMI, joint space width, or femorotibial angle, which was an average 177.5 degrees in group with no sleep problems and 177.6 degrees in the group with sleep disturbances.
The proportion of participants experiencing sleep disturbances increased with increasing K/L grade of OA: 56.8% of those with K/L grade 4 had sleep problems, compared with 40.9% of those with K/L grade 3, 42.1% of those with K/L grade 2, and 33.7% of those with K/L grade 1, resulting in 30% greater odds of sleep disturbance with a higher K/L grade (odds ratio, 1.3; P = .011).
Knee pain at night was also significantly associated with severity of OA based on the K/L grade. While only 6.9% of participants reported pain at night overall, nearly 1 in 3 (29.5%) of those with K/L grade 4 reported pain at night, compared with 3.4% of those with K/L grade 1 (P < .001). (Night pain occurred in 5.4% of those with K/L grade 2 and 16.1% with K/L grade 3.)
However, after adjusting for age, gender, and BMI, the severity of knee OA was not significantly associated with sleep disturbance based on K/L grade, joint space width, femoro-tibial angle, and/or WORMS. But knee pain remained significantly associated with sleep disturbance after adjustment based on the visual analog scale and the JKOM (P < .001 for both).
Sleep problems were also significantly associated with each subcategory of the JKOM after adjustment (P < .001 for all but social activities, which was P = .014).
“Activities of daily living may affect the occurrence of knee pain at night,” Mr. Sasahara said, and “sleep disturbance may also disturb quality of life.” If sleep disturbances related to nighttime knee pain are linked to activities of daily living, then “not only knee pain but also activities of daily living need to be improved in order to improve sleep.”
He noted several of the study’s limitations, including the fact that lifestyle habits and work were not taken into account, nor did the researchers evaluate sleep disturbances potentially resulting from a medical illness. The researchers also only examined knee pain, not pain in other parts of the body.
The research was funded by Juntendo University; the Strategic Research Foundation at Private Universities; KAKENHI from the Ministry of Education, Culture, Sports, Science and Technology of Japan; the Mizuno Sports Promotion Foundation; and the Mitsui Life Social Welfare Foundation. Mr. Sasahara and Ms. Cedin had no disclosures.
DENVER – The relationship between nighttime knee pain from osteoarthritis and sleep disturbances is more complex than a simple association, according to new research presented at the Osteoarthritis Research Society International 2023 World Congress.
The findings suggested that the association between knee OA pain and sleep problems was also linked to activities of daily living, which can contribute to pain but are also affected by OA, Takahiro Sasahara, of the department of orthopedics at Juntendo University, Tokyo, and Koshigaya Municipal Hospital, Saitama, Japan, told attendees. The study also found that knee pain and mobility impairment were associated with sleep disturbances in older adults regardless of the severity of knee OA.
Luisa Cedin, a PhD student at Rush University, Chicago, who attended the presentation, noted the clinical implications of the interaction of daily activities with knee pain.
”I’m a physical therapist, and this could have a significant impact on the performance of the exercises that I’m requiring as a physical therapist,” Ms. Cedin said in an interview. “When you ask somebody who is not getting enough rest during the night – not only enough time but enough quality of rest – we know that we can expect a lower performance with any type of exercises, whether it’s less strength or force, less power, less agility, or less resistance or endurance, so this has a big impact on their quality of life.”
Mr. Sasahara cited research noting that acute pain occurs at the beginning of movement and during weight bearing and walking while chronic pain frequently occurs at night and in early morning awakenings. The prevalence of sleep disturbances in patients with chronic pain ranges from 50% to 80%, he said, and past evidence has shown the relationship between sleep and pain to be bidirectional.
For example, insomnia frequency and severity, sleep-onset problems, and sleep efficiency are all positively associated with pain sensitivity, and increasing severity of OA is linked to increasing prevalence of night knee pain and sleep problems, affecting quality of life, he said.
In this new study examining the relationship between sleep disturbance and knee pain and mobility, the researchers focused specifically on a population of older adults with knee OA. They analyzed data from the Bunkyo Health Study, which was conducted at Juntendo University’s Sportology Center to examine the association between metabolic, cardiovascular, cognitive dysfunction, and motor organ disorders in older adults from November 2015 to September 2018.
From the initial population of 1,630 adults, aged 65-84, who did not need medical treatment because of knee pain, the researchers analyzed data from 1,145 adults who the met this study’s criteria, which included MRI imaging of medial type knee OA. A little over half (55.7%) were women, with an average age of 73 and an average body mass index (BMI) of 22.8 kg/m2.
In addition to blood and urine sampling, the researchers determined the severity of knee OA based on joint space width, femorotibial angle, and Kellgren and Lawrence (K/L) grade from x-rays in standing position. They also assessed the structure of knee OA using a whole-organ MRI score (WORMS), and pain and mobility with a visual analog scale, the Japan Knee Osteoarthritis Measure (JKOM), and the 25-question geriatric locomotive function scale.
The JKOM, based on the Western Ontario and McMaster Universities quality of life index for general knee OA, is adjusted to account for the Japanese lifestyle and covers four categories: knee pain and stiffness, a score for activities of daily living, a social activities score, and the patient’s health conditions.
Overall, 41.3% of the participants had sleep disturbances, based on a score of 6 or higher on the Pittsburgh Sleep Quality Index–Japanese. More women (55.7%) than men experienced sleep problems (P < .001), but there were no significant differences in the average age between those who did and those who did not have sleep issues. There were also no significance differences in BMI, joint space width, or femorotibial angle, which was an average 177.5 degrees in group with no sleep problems and 177.6 degrees in the group with sleep disturbances.
The proportion of participants experiencing sleep disturbances increased with increasing K/L grade of OA: 56.8% of those with K/L grade 4 had sleep problems, compared with 40.9% of those with K/L grade 3, 42.1% of those with K/L grade 2, and 33.7% of those with K/L grade 1, resulting in 30% greater odds of sleep disturbance with a higher K/L grade (odds ratio, 1.3; P = .011).
Knee pain at night was also significantly associated with severity of OA based on the K/L grade. While only 6.9% of participants reported pain at night overall, nearly 1 in 3 (29.5%) of those with K/L grade 4 reported pain at night, compared with 3.4% of those with K/L grade 1 (P < .001). (Night pain occurred in 5.4% of those with K/L grade 2 and 16.1% with K/L grade 3.)
However, after adjusting for age, gender, and BMI, the severity of knee OA was not significantly associated with sleep disturbance based on K/L grade, joint space width, femoro-tibial angle, and/or WORMS. But knee pain remained significantly associated with sleep disturbance after adjustment based on the visual analog scale and the JKOM (P < .001 for both).
Sleep problems were also significantly associated with each subcategory of the JKOM after adjustment (P < .001 for all but social activities, which was P = .014).
“Activities of daily living may affect the occurrence of knee pain at night,” Mr. Sasahara said, and “sleep disturbance may also disturb quality of life.” If sleep disturbances related to nighttime knee pain are linked to activities of daily living, then “not only knee pain but also activities of daily living need to be improved in order to improve sleep.”
He noted several of the study’s limitations, including the fact that lifestyle habits and work were not taken into account, nor did the researchers evaluate sleep disturbances potentially resulting from a medical illness. The researchers also only examined knee pain, not pain in other parts of the body.
The research was funded by Juntendo University; the Strategic Research Foundation at Private Universities; KAKENHI from the Ministry of Education, Culture, Sports, Science and Technology of Japan; the Mizuno Sports Promotion Foundation; and the Mitsui Life Social Welfare Foundation. Mr. Sasahara and Ms. Cedin had no disclosures.
DENVER – The relationship between nighttime knee pain from osteoarthritis and sleep disturbances is more complex than a simple association, according to new research presented at the Osteoarthritis Research Society International 2023 World Congress.
The findings suggested that the association between knee OA pain and sleep problems was also linked to activities of daily living, which can contribute to pain but are also affected by OA, Takahiro Sasahara, of the department of orthopedics at Juntendo University, Tokyo, and Koshigaya Municipal Hospital, Saitama, Japan, told attendees. The study also found that knee pain and mobility impairment were associated with sleep disturbances in older adults regardless of the severity of knee OA.
Luisa Cedin, a PhD student at Rush University, Chicago, who attended the presentation, noted the clinical implications of the interaction of daily activities with knee pain.
”I’m a physical therapist, and this could have a significant impact on the performance of the exercises that I’m requiring as a physical therapist,” Ms. Cedin said in an interview. “When you ask somebody who is not getting enough rest during the night – not only enough time but enough quality of rest – we know that we can expect a lower performance with any type of exercises, whether it’s less strength or force, less power, less agility, or less resistance or endurance, so this has a big impact on their quality of life.”
Mr. Sasahara cited research noting that acute pain occurs at the beginning of movement and during weight bearing and walking while chronic pain frequently occurs at night and in early morning awakenings. The prevalence of sleep disturbances in patients with chronic pain ranges from 50% to 80%, he said, and past evidence has shown the relationship between sleep and pain to be bidirectional.
For example, insomnia frequency and severity, sleep-onset problems, and sleep efficiency are all positively associated with pain sensitivity, and increasing severity of OA is linked to increasing prevalence of night knee pain and sleep problems, affecting quality of life, he said.
In this new study examining the relationship between sleep disturbance and knee pain and mobility, the researchers focused specifically on a population of older adults with knee OA. They analyzed data from the Bunkyo Health Study, which was conducted at Juntendo University’s Sportology Center to examine the association between metabolic, cardiovascular, cognitive dysfunction, and motor organ disorders in older adults from November 2015 to September 2018.
From the initial population of 1,630 adults, aged 65-84, who did not need medical treatment because of knee pain, the researchers analyzed data from 1,145 adults who the met this study’s criteria, which included MRI imaging of medial type knee OA. A little over half (55.7%) were women, with an average age of 73 and an average body mass index (BMI) of 22.8 kg/m2.
In addition to blood and urine sampling, the researchers determined the severity of knee OA based on joint space width, femorotibial angle, and Kellgren and Lawrence (K/L) grade from x-rays in standing position. They also assessed the structure of knee OA using a whole-organ MRI score (WORMS), and pain and mobility with a visual analog scale, the Japan Knee Osteoarthritis Measure (JKOM), and the 25-question geriatric locomotive function scale.
The JKOM, based on the Western Ontario and McMaster Universities quality of life index for general knee OA, is adjusted to account for the Japanese lifestyle and covers four categories: knee pain and stiffness, a score for activities of daily living, a social activities score, and the patient’s health conditions.
Overall, 41.3% of the participants had sleep disturbances, based on a score of 6 or higher on the Pittsburgh Sleep Quality Index–Japanese. More women (55.7%) than men experienced sleep problems (P < .001), but there were no significant differences in the average age between those who did and those who did not have sleep issues. There were also no significance differences in BMI, joint space width, or femorotibial angle, which was an average 177.5 degrees in group with no sleep problems and 177.6 degrees in the group with sleep disturbances.
The proportion of participants experiencing sleep disturbances increased with increasing K/L grade of OA: 56.8% of those with K/L grade 4 had sleep problems, compared with 40.9% of those with K/L grade 3, 42.1% of those with K/L grade 2, and 33.7% of those with K/L grade 1, resulting in 30% greater odds of sleep disturbance with a higher K/L grade (odds ratio, 1.3; P = .011).
Knee pain at night was also significantly associated with severity of OA based on the K/L grade. While only 6.9% of participants reported pain at night overall, nearly 1 in 3 (29.5%) of those with K/L grade 4 reported pain at night, compared with 3.4% of those with K/L grade 1 (P < .001). (Night pain occurred in 5.4% of those with K/L grade 2 and 16.1% with K/L grade 3.)
However, after adjusting for age, gender, and BMI, the severity of knee OA was not significantly associated with sleep disturbance based on K/L grade, joint space width, femoro-tibial angle, and/or WORMS. But knee pain remained significantly associated with sleep disturbance after adjustment based on the visual analog scale and the JKOM (P < .001 for both).
Sleep problems were also significantly associated with each subcategory of the JKOM after adjustment (P < .001 for all but social activities, which was P = .014).
“Activities of daily living may affect the occurrence of knee pain at night,” Mr. Sasahara said, and “sleep disturbance may also disturb quality of life.” If sleep disturbances related to nighttime knee pain are linked to activities of daily living, then “not only knee pain but also activities of daily living need to be improved in order to improve sleep.”
He noted several of the study’s limitations, including the fact that lifestyle habits and work were not taken into account, nor did the researchers evaluate sleep disturbances potentially resulting from a medical illness. The researchers also only examined knee pain, not pain in other parts of the body.
The research was funded by Juntendo University; the Strategic Research Foundation at Private Universities; KAKENHI from the Ministry of Education, Culture, Sports, Science and Technology of Japan; the Mizuno Sports Promotion Foundation; and the Mitsui Life Social Welfare Foundation. Mr. Sasahara and Ms. Cedin had no disclosures.
AT OARSI 2023
Celebrity death finally solved – with locks of hair
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.

We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
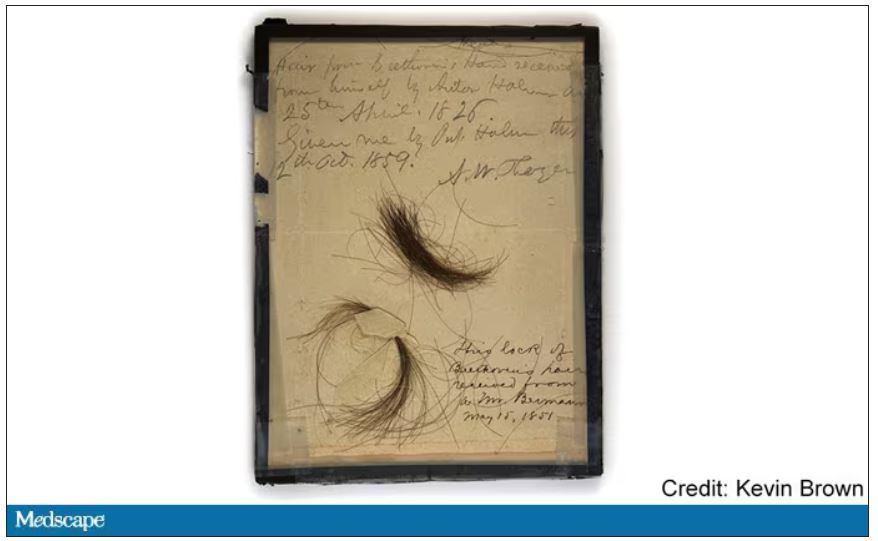
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
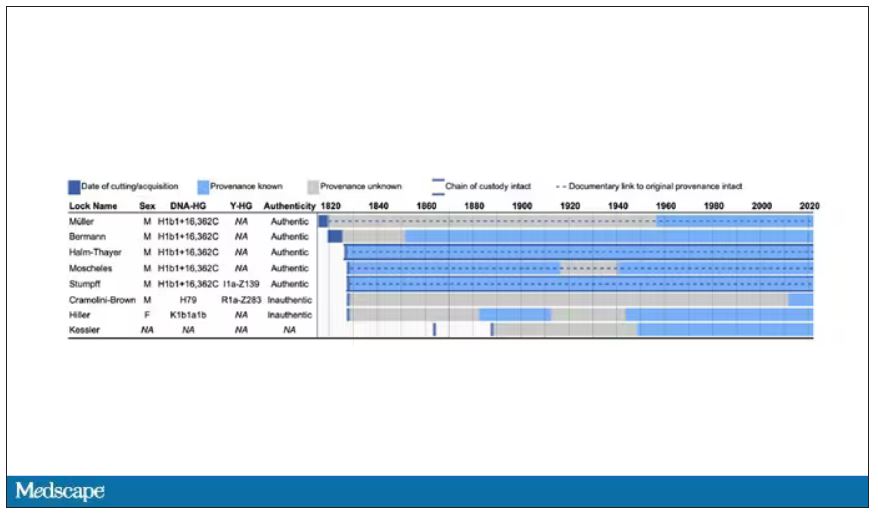
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
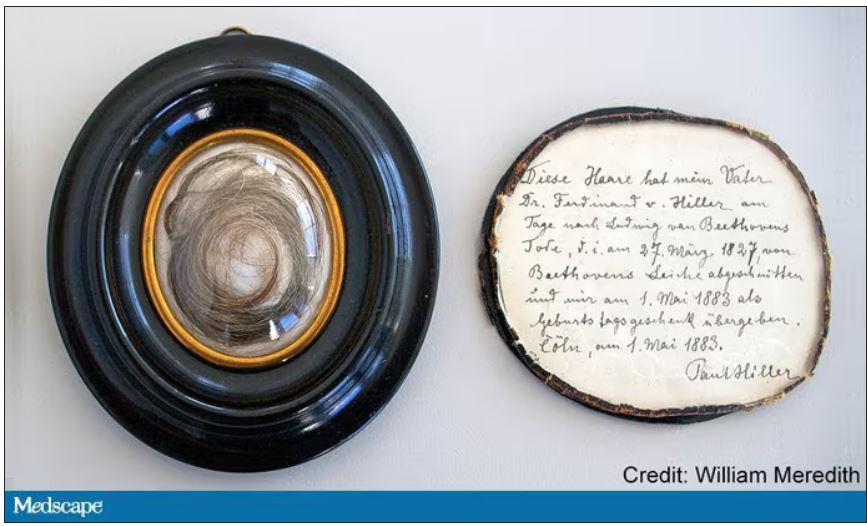
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
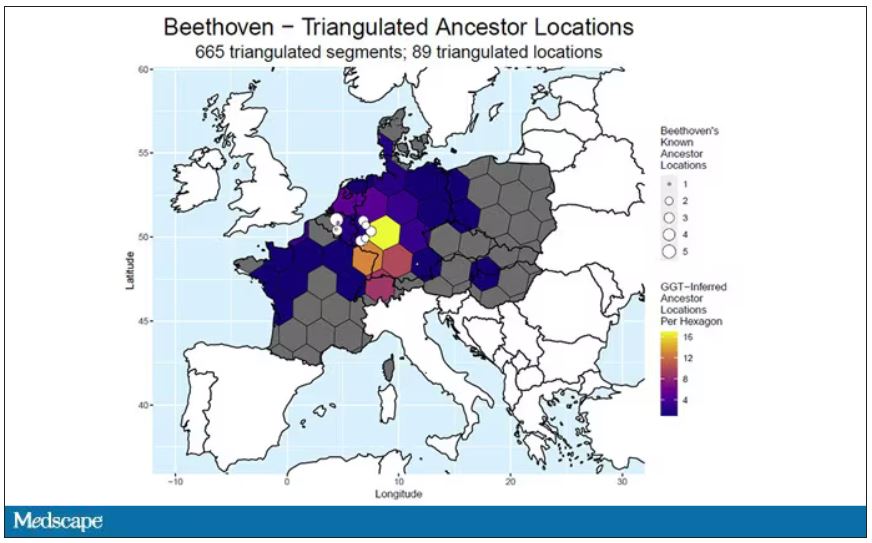
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to open this week with a case.
A 56-year-old musician presents with diffuse abdominal pain, cramping, and jaundice. His medical history is notable for years of diffuse abdominal complaints, characterized by disabling bouts of diarrhea.
In addition to the jaundice, this acute illness was accompanied by fever as well as diffuse edema and ascites. The patient underwent several abdominal paracenteses to drain excess fluid. One consulting physician administered alcohol to relieve pain, to little avail.
The patient succumbed to his illness. An autopsy showed diffuse liver injury, as well as papillary necrosis of the kidneys. Notably, the nerves of his auditory canal were noted to be thickened, along with the bony part of the skull, consistent with Paget disease of the bone and explaining, potentially, why the talented musician had gone deaf at such a young age.
An interesting note on social history: The patient had apparently developed some feelings for the niece of that doctor who prescribed alcohol. Her name was Therese, perhaps mistranscribed as Elise, and it seems that he may have written this song for her.
We’re talking about this paper in Current Biology, by Tristan Begg and colleagues, which gives us a look into the very genome of what some would argue is the world’s greatest composer.
The ability to extract DNA from older specimens has transformed the fields of anthropology, archaeology, and history, and now, perhaps, musicology as well.
The researchers identified eight locks of hair in private and public collections, all attributed to the maestro.
Four of the samples had an intact chain of custody from the time the hair was cut. DNA sequencing on these four and an additional one of the eight locks came from the same individual, a male of European heritage.
The three locks with less documentation came from three other unrelated individuals. Interestingly, analysis of one of those hair samples – the so-called Hiller Lock – had shown high levels of lead, leading historians to speculate that lead poisoning could account for some of Beethoven’s symptoms.
DNA analysis of that hair reveals it to have come from a woman likely of North African, Middle Eastern, or Jewish ancestry. We can no longer presume that plumbism was involved in Beethoven’s death. Beethoven’s ancestry turns out to be less exotic and maps quite well to ethnic German populations today.
In fact, there are van Beethovens alive as we speak, primarily in Belgium. Genealogic records suggest that these van Beethovens share a common ancestor with the virtuoso composer, a man by the name of Aert van Beethoven.
But the DNA reveals a scandal.
The Y-chromosome that Beethoven inherited was not Aert van Beethoven’s. Questions of Beethoven’s paternity have been raised before, but this evidence strongly suggests an extramarital paternity event, at least in the generations preceding his birth. That’s right – Beethoven may not have been a Beethoven.
With five locks now essentially certain to have come from Beethoven himself, the authors could use DNA analysis to try to explain three significant health problems he experienced throughout his life and death: his hearing loss, his terrible gastrointestinal issues, and his liver failure.
Let’s start with the most disappointing results, explanations for his hearing loss. No genetic cause was forthcoming, though the authors note that they have little to go on in regard to the genetic risk for otosclerosis, to which his hearing loss has often been attributed. Lead poisoning is, of course, possible here, though this report focuses only on genetics – there was no testing for lead – and as I mentioned, the lock that was strongly lead-positive in prior studies is almost certainly inauthentic.
What about his lifelong GI complaints? Some have suggested celiac disease or lactose intolerance as explanations. These can essentially be ruled out by the genetic analysis, which shows no risk alleles for celiac disease and the presence of the lactase-persistence gene which confers the ability to metabolize lactose throughout one’s life. IBS is harder to assess genetically, but for what it’s worth, he scored quite low on a polygenic risk score for the condition, in just the 9th percentile of risk. We should probably be looking elsewhere to explain the GI distress.
The genetic information bore much more fruit in regard to his liver disease. Remember that Beethoven’s autopsy showed cirrhosis. His polygenic risk score for liver cirrhosis puts him in the 96th percentile of risk. He was also heterozygous for two variants that can cause hereditary hemochromatosis. The risk for cirrhosis among those with these variants is increased by the use of alcohol. And historical accounts are quite clear that Beethoven consumed more than his share.
But it wasn’t just Beethoven’s DNA in these hair follicles. Analysis of a follicle from later in his life revealed the unmistakable presence of hepatitis B virus. Endemic in Europe at the time, this was a common cause of liver failure and is likely to have contributed to, if not directly caused, Beethoven’s demise.
It’s hard to read these results and not marvel at the fact that, two centuries after his death, our fascination with Beethoven has led us to probe every corner of his life – his letters, his writings, his medical records, and now his very DNA. What are we actually looking for? Is it relevant to us today what caused his hearing loss? His stomach troubles? Even his death? Will it help any patients in the future? I propose that what we are actually trying to understand is something ineffable: Genius of magnitude that is rarely seen in one or many lifetimes. And our scientific tools, as sharp as they may have become, are still far too blunt to probe the depths of that transcendence.
In any case, friends, no more of these sounds. Let us sing more cheerful songs, more full of joy.
For Medscape, I’m Perry Wilson.
Dr. Wilson is associate professor, department of medicine, and director, Clinical and Translational Research Accelerator, at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Nurse makes millions selling her licensing exam study sheets
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Ms. Beggs, 28, sells one-page study sheets or bundles of sheets, sometimes with colorful drawings, conversation bubbles and underlining, that boil down concepts for particular conditions into easy-to-understand language.
The biggest seller on Ms. Beggs’ online marketplace Etsy site, RNExplained, is a bundle of study guides covering eight core nursing classes. The notes range in price from $2 to $150. More than 70,000 customers have bought the $60 bundle, according to the website.
Ms. Beggs’ business developed in a “very unintentional” way when COVID hit with just months left in her nursing program at Mount Saint Mary’s University, Los Angeles, she told this news organization.
Classes had switched to Zoom, and she had no one to study with as she prepared to take her board exams.
“The best way I know how to study is to teach things out loud. But because I had nobody to teach out loud to, I would literally teach them to the wall,” Ms. Beggs said. “I would record myself so I could play it back and teach myself these topics that were hard for me to understand.”
Just for fun, she says, she posted them on TikTok and the responses started flowing in, with followers asking where she was selling the sheets. She now has more than 660,000 TikTok followers and 9 million likes.
Ms. Beggs said that every sheet highlights a condition, and she has made 308 of them.
Traditional classroom lessons typically teach one medical condition in 5-6 pages, Ms. Beggs said. “I go straight to the point.”
One reviewer on Ms. Beggs’ Etsy site appreciated the handwritten notes, calling them “simplified and concise.” Another commented: “Definitely helped me pass my last exam.”
Ms. Beggs says that her notes may seem simple, but each page represents comprehensive research.
“I have to go through not just one source of information to make sure my information is factual,” Ms. Beggs says. “What you teach in California might be a little different than what you teach in Florida. It’s very meticulous. The lab values will be a little different everywhere you go.”
She acknowledges her competition, noting that there are many other study guides for the NCLEX and nursing courses.
Nursing groups weigh in
Dawn Kappel, spokesperson for the National Council of State Boards of Nursing, which oversees NCLEX, said in an interview that “NCSBN has no issue with the current content of Stephanee Beggs’ business venture.”
For many students, the study guides will be helpful, especially for visual learners, said Carole Kenner, PhD, RN, dean and professor in the School of Nursing and Health Sciences at The College of New Jersey.
But for students “who are less confident in their knowledge, I would want to see a lot more in-depth explanation and rationale,” Dr. Kenner said.
“Since the NCLEX is moving to more cased-based scenarios, the next-gen unfolding cases, you really have to understand a lot of the rationale.”
The notes remind Dr. Kenner of traditional flash cards. “I don’t think it will work for all students, but even the fanciest of onsite review courses are useful to everyone,” she said.
‘Not cutting corners’
As an emergency nurse, Ms. Beggs said, “I have the experience as a nurse to show people that what you are learning will be seen in real life.”
“The way I teach my brand is not to take shortcuts. I love to teach to understand rather than teaching to memorize for an exam.”
She said she sees her guides as a supplement to learning, not a replacement.
“It’s not cutting corners,” she says. “I condense a medical condition that could take a very long time to understand and break it into layman’s terms.”
Ms. Beggs said when people hear about the $2 million, they often ask her whether she plans to give up her shifts in the emergency department for the more lucrative venture.
The answer is no, at least not yet.
“Aside from teaching, I genuinely love being at the bedside,” Ms. Beggs said. “I don’t foresee myself leaving that for good for as long as I can handle both.” She acknowledged, though, that her business now takes up most of her time.
“I love everything about both aspects, so it’s hard for me to choose.”
A version of this article first appeared on Medscape.com.
Disease burden is higher in women vs men with psoriatic arthritis
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3
Key clinical point: The psoriatic arthritis (PsA) disease burden had worse impact on women vs men with PsA, with women having a higher disease activity, worse function, and greater disease burden.
Major finding: Female vs male patients with PsA had a significantly higher mean patient global assessment score (P < .001), patient’s pain score (P = .003), tender joint count (P < .001), swollen joint count (P = .033), and Disease Activity Score for PsA (P < .001). Minimal disease activity was achieved by 44.0% of men vs 24.6% of women (P = .003).
Study details: Findings are from a cross-sectional analysis of 2 longitudinal cohorts including 141 male and 131 female patients with PsA who received treatment with conventional synthetic or biologic disease-modifying antirheumatic drugs for at least 6 months.
Disclosures: This study did not receive funding. The authors declared no conflicts of interest.
Source: Lubrano E et al. Psoriatic arthritis in males and females: Differences and similarities. Rheumatol Ther. 2023 (Feb 16). Doi: 10.1007/s40744-023-00535-3