User login
Should intravascular imaging be almost routine in PCI?
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.

And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”

Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.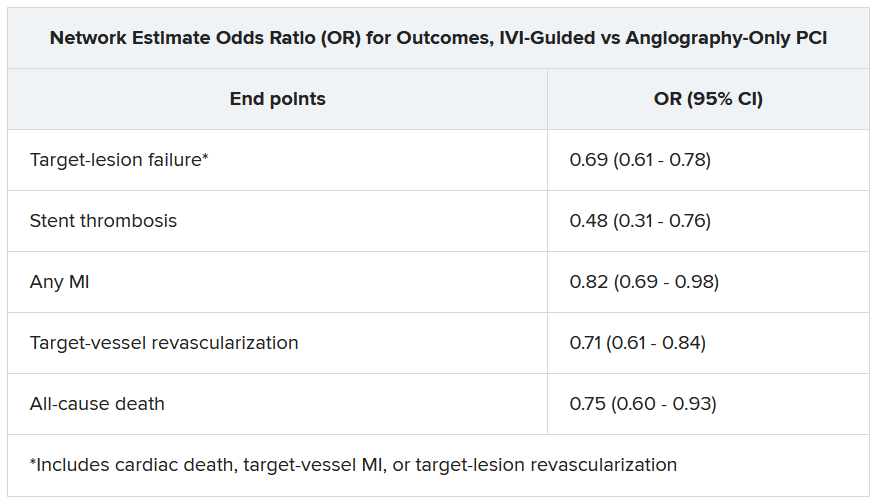
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.
And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”
Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A routine role for intravascular imaging (IVI) guidance for percutaneous coronary intervention (PCI) has long been favored by many of the technology’s researchers and enthusiasts. Now evidence from large, randomized trials may be catching up with such aspirations, though not without caveats.
One way IVI guidance may achieve that, the research suggests, albeit more speculatively, is by cutting risk for stent thrombosis, compared with the risk associated with angiography-only PCI.
The new studies, two large randomized IVI trials plus a meta-analysis of 20 such studies, were presented at the annual congress of the European Society of Cardiology.
In one, called ILUMIEN-4, PCI guided by optical coherence tomography (OCT) was associated with fewer procedural complications and better acute results – that is, larger post-PCI minimum stent area (MSA) – than in angiography-only procedures (P < .001). Poststenting MSA, an established predictor of clinical outcomes, was the primary imaging endpoint of the trial with almost 2,500 patients.
Yet the OCT group’s greater post-PCI MSA did not translate to reduced risk for the primary clinical endpoint of 2-year target-vessel failure. Among secondary endpoints, however, stent thrombosis at some point during the follow-up was 64% less likely (P = .02) with OCT guidance than angiography-only PCI.
ILUMIEN-4, despite its neutral clinical result, still “strongly advocates” for PCI guidance by OCT, at least among patients like those in the trial, said principal investigator Ziad Ali, MD, DPhil. He based that largely on the strategy’s greater postprocedure lumen areas in the trials, which are among “the strongest independent predictors for long term outcomes,” said Dr. Ali, of St. Francis Hospital & Heart Center, Roslyn, N.Y., at a press conference on IVI trials during the ESC Congress.
Selected complex lesion type
In contrast, the OCTOBER trial, presented at the sessions back to back with ILUMIEN-4, saw OCT guidance lead to better clinical outcomes than angiography alone after PCI of bifurcation lesions, which normally can be a special challenge for operators.
In the trial, which entered about 1,200 patients with such complex lesions, the 2-year risk for major adverse cardiac events (MACE) fell 60% after OCT-guided PCI, compared with angiography-only procedures (P = .035).
The finding is novel for showing that OCT guidance in bifurcation PCI can make a significant clinical difference, said OCTOBER investigator Niels R. Holm, MD, at the same media presentation on IVI trials.
“Multiple studies have shown that OCT allows for optimization of bifurcation PCI, and our results confirm that such optimization may improve the patient’s prognosis,” said Dr. Holm of Aarhus (Denmark) University Hospital.
ILUMIEN-4 and OCTOBER, both of which prespecified the Xience (Abbott) everolimus-eluting stent for the procedures, were published in the New England Journal of Medicine in tandem with their respective presentations at the ESC sessions.
Covering the spectrum
A meta-analysis presented at the same ESC session compared IVI using either OCT or intravascular ultrasound (IVUS) with angiography-only PCI across 20 randomized trials with a total of more than 12,000 patients.
Significant outcomes for IVI guidance versus angiography alone included a 31% drop in risk for target-lesion failure, the primary endpoint. And this study, as well, showed a steep 52% reduction in risk for in-stent thrombosis with the IVI-guided approach.
And “for the first time” in IVI studies, “we demonstrated reductions in all-myocardial-infarction and all-cause death, the latter by 25%,” Gregg Stone, MD, Icahn School of Medicine at Mount Sinai, New York, said in presenting the meta-analysis. Dr. Stone is also the ILUMIEN-4 study chairperson.
“The routine use of OCT or IVUS to guide most PCI procedures will substantially improve patient event-free survival,” he predicted, “enhancing both the long-term safety and effectiveness of the procedure.”
Dr. Stone said that IVI guidance “should be standard of care, if not in all patients, then in most patients.” Part of the rationale: PCI is unlikely to be improved much further by incremental gains in drug-eluting stent design. “That technology has almost plateaued.” But there’s yet room for “substantially improved outcomes” from adjunctive treatments and techniques such as IVI guidance.
The 20 studies in the meta-analysis encompassed an array of patients and lesions both complex and noncomplex, Dr. Stone observed, including bifurcation lesions, chronic total occlusions, left-main coronary stenoses, and MI culprit lesions.
“They really covered the spectrum of PCI,” he said. “I’m not recommending that intravascular imaging be used in every single case. But I do think it should be used in the majority of patients” and be standard of care for PCI in left-main lesions and “complex coronary disease, high-risk patients, and high-risk lesions.”
Unique advantage
The IVI-guidance groups in both ILUMIEN-4 and the meta-analysis showed a significant drop in risk for stent thrombosis – that is, abrupt thrombotic vessel closure, which typically occurs in 1% or fewer PCI cases but can trigger an MI and pose a mortality risk up to 45%.
Those risk reductions are consistent with a unique IVI advantage: the ability to guide optimization of stent deployments. When formally presenting ILUMIEN-4 at the ESC sessions, Ali observed that IVUS and OCT imaging allows operators to identify and often correct less-than-ideal results of an initial stent delivery – such as residual gaps between stent struts and vessel wall – that may encroach on the lumen, with possible clinical consequences.
Such imaging, said Dr. Ali, “lets you identify tissue protrusions, malappositions, dissections, and untreated reference-segment disease” that may potentially trigger thrombosis. That makes a strong argument for giving IVI guidance a more common, perhaps even routine role in PCI procedures.
Selling routine IVI-guided PCI in practice
“I think the study results are quite clear,” said Deepak L. Bhatt, MD, MPH, as session comoderator following the OCTOBER presentation. “The challenge, though, will be convincing the average interventional cardiologist worldwide that it was specifically the imaging and not the extra care that the patient getting OCT also inherently receives.”
Did OCT’s better trial outcomes stem from IVI itself or from greater operator attentiveness to procedural results – such as, for example, more high-pressure expansions to optimize stent placement, “the sort of thing that tends to occur when invasive imaging is added on to just plain old angiography?” Dr. Bhatt asked of Lene N. Andreasen, MD, who had just presented the OCTOBER trial. “There’s no way of uncoupling the two things.”
What can be said, “at this point, to convince interventional cardiologists that the extra time, energy, expense, is truly indicated,” that the data are “sufficient to change global practice?” asked Dr. Bhatt, Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai.
That remains an open question,” acknowledged Dr. Andreasen of Aarhus University Hospital. The best argument in favor of selective IVI-guided PCI is that “we actually see a clinical benefit” in the trials. “But of course, it comes with a cost. It comes with longer procedures and more contrast.” How clinical practice responds to the new data remains to be seen, she proposed.
ILUMIEN-4 and OCTOBER in detail
Conducted at 80 centers in 18 countries, ILUMIEN-4 randomly assigned patients with diabetes or complex coronary lesions to undergo PCI guided by OCT or using standard angiography only, 1,233 and 1,254 patients, respectively.
Post-PCI MSA averaged 5.72 mm2 with OCT guidance and 5.36 mm2 in the angiography-only group (P < .001).
Their rates of target-vessel failure at 2 years were not significantly different at 7.4% and 8.2%, respectively. The 2-year composite endpoint included cardiac death, target vessel–related MI, or ischemia-driven target-vessel revascularization.
Definite or probable stent thrombosis was observed over 2 years in 0.5% of the OCT group and 1.4% of those with angiography-only PCI (hazard ratio, 0.36; 95% confidence interval, 0.14-0.91; P = .02) favoring OCT.
The OCTOBER trial, conducted at 38 centers in Europe, entered 1201 patients with stable angina or acute coronary syndromes and angiographically identified complex bifurcation lesions. They involved the left-main coronary artery in about one-fifth of cases.
Patients were randomly assigned to bifurcation PCI guided by OCT or under standard angiography, 600 and 601 patients, respectively. Rates for procedure-related complications were similar at 6.8% and 5.7%, respectively.
Over a median of 2 years, 10.1% of the OCT group and 14.1% of angiography-only patients developed a MACE event, including cardiac death, target-lesion MI, or ischemia-driven target-lesion revascularization. The adjusted HR was 0.71 (95% CI, 0.51-0.98; P = .035) in favor of OCT.
Meta-analysis, trials to date
The meta-analysis presented by Dr. Stone included ILUMIEN-4, OCTOBER, and 18 earlier outcomes trials comparing PCI guided by IVI, either OCT or IVUS, and angiography-only PCI. It covered 12,428 patients with chronic or acute coronary disease and followed them a mean of 26 months; the longest follow-up was 5 years. They were assigned to IVI-guided or angiography-only PCI, 7,038 and 5,390 patients, respectively.
Dr. Stone and colleagues conducted a network meta-analysis of the 20 studies, that is, a combined analysis that allowed both direct and indirect comparisons of standard angiography-only procedures to each of the other studied comparator interventions including OCT, IVUS, and either OCT or IVUS. They then derived network-estimate odds ratios for IVI-guided PCI vs angiography-only procedures.
“Hopefully, this will impact the guidelines,” Dr. Stone said of the meta-analysis. Procedures guided by IVI might become more common in clinical practice if they were to garner a Class-I guideline recommendation, the strongest recommendation category.
“That would make a difference, but we’d also need to work to remove impediments to increasing intravascular imaging guidance” for most patients undergoing PCI, he said, referring to challenges in obtaining reimbursement for IVI-guided PCI and training enough operators to handle the projected demand.
ILUMIEN-4 was funded by Abbott. OCTOBER was supported by grants from Abbott Vascular, St. Jude Medical, and Aarhus University. The network meta-analysis received statistical support from Abbott. Dr. Ali disclosed institutional grant support from Abbott, Abiomed, Acist Medical, Boston Scientific, Cardiovascular Systems, Medtronic, the National Institutes of Health, Opsens Medical, Philips, and Teleflex; consulting fees from Astra Zeneca, Philips, Shockwave; and holding equity in Elucid, Spectrawave, Shockwave, and VitalConnect. Dr. Holm and Dr. Bhatt reported numerous conflicts of interest. Dr. Andreasen disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE ESC CONGRESS 2023
Dietary nitrates reduce contrast-induced nephropathy in ACS
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AMSTERDAM –
In the NITRATE-CIN Study, non-ST segment elevation myocardial infarction acute coronary syndrome (ACS) patients at risk of renal injury from coronary angiography who received dietary inorganic nitrates had a 70% reduction in CIN compared with those given placebo.
The nitrate group also showed an impressive reduction in periprocedural myocardial infarction (MI) and improved renal function at 3 months, as well as a halving of major adverse cardiovascular events and major adverse kidney events at 1 year.
The trial was presented by Dan Jones, MD, Barts Health NHS Trust, London, at the annual congress of the European Society of Cardiology.
“Currently, aside from intravenous hydration, there is no proven treatment that reduces contrast-induced nephropathy. We feel that dietary inorganic nitrate shows huge promise in this study, and these findings could have important implications in reducing this serious complication of coronary angiography,” Dr. Jones concluded.
He explained that the product used was a formulation of dietary inorganic nitrates given as potassium nitrate capsules, which the study investigators produced specifically for this trial.
At this point, “the only way to get inorganic nitrate is in the diet – specifically by consuming beetroot juice or green leafy vegetables such as spinach and rocket. From a clinician perspective, while these results suggest this is an effective therapy and has great potential, it is not currently possible to prescribe the medication we used in our study, although we are working on producing a commercial product,” he said in an interview.
However, Dr. Jones noted that it is possible to buy beetroot shots, which contain 7 mmol of potassium nitrate in each shot, from health food shops and websites, and two such shots per day for 5 days would give a dose similar to that used in this study, starting the day before angiography.
“While we need a larger multicenter study to confirm these results, studies so far suggest no signal at all that there is any harm in this approach, and there could be a great deal of benefit in taking a couple of beetroot shots prior to and for a few days after an angiogram,” he said.
Dietary nitrates “make sense”
Designated discussant of the NITRATE-CIN trial at the ESC Hotline session, Roxanna Mehran, MD, Icahn School of Medicine at Mount Sinai, New York, said the study was well designed, and the “interesting and plausible” hypothesis to raise nitric oxide levels by dietary nitrates “makes sense.”
On the main findings of a major significant 50% reduction in acute kidney injury, Dr. Mehran said, “It is difficult to imagine such a reduction is possible.”
She pointed out that the large reduction in major adverse cardiac events and major adverse kidney events at 1 year also suggests that there is a sustained benefit in protecting the kidney.
“We’re all going to get on beet juice after this,” she quipped.
Still, Dr. Mehran questioned whether the results were “too good to be true,” adding that a larger trial actually powered for longer term outcome events is needed, as well as a better understanding of whether CIN has a causative role in mortality.
Responding to questions about whether such a large effect could actually be achieved with dietary nitrates, Dr. Jones said he thought there would definitely be some benefits, but maybe not quite as large as those seen in this study.
“From our pilot data we thought nitrate may be effective in preventing CIN,” he said in an interview. “We recruited a higher risk group than we thought, which is why the control event rates were higher than we expected, but the acute kidney injury reduction is roughly what we had estimated, and makes sense biologically.”
Dr. Jones acknowledged that the large reductions in long-term major adverse cardiovascular and kidney events were unexpected.
“The trial was not powered to see reductions in these outcomes, so we need to see if those event reductions can be replicated in larger multicenter trials,” he said. “But this was a double-blind placebo-controlled trial so in this trial the effects are real, and I think the effect size in this trial is too large for there not to be a beneficial effect.
“But I’m not so sure that we would see the same magnitude of effect when we have a larger study with tighter confidence intervals but perhaps a 20%-25% reduction in cardiovascular and kidney may be more realistic, which would still be amazing for such an easy and cost-effective intervention,” Dr. Jones added.
A larger trial is now being planned.
The researchers are also working on the development of a commercial form of dietary inorganic nitrate that would be needed for larger multicenter studies and would then be generally available. “We want this to be a low-cost product that would be available to all,” Dr. Jones said.
He noted that other studies have shown that dietary inorganic nitrates in the form of beetroot juice lower blood pressure; there are suggestions it may also lower cholesterol and prevent stent restenosis, and athletes sometimes take it to increase their aerobic capacity.
“There appears to be many benefits of dietary nitrates, and the one thing we can do at this time is to encourage people to increase their dietary nitrate consumption by eating large quantities of green leafy vegetables and beetroot,” Dr. Jones said.
Replacing lost nitric oxide
In his presentation, Dr. Jones noted that CIN is a serious complication after coronary angiography and is associated with longer hospital stays, worse long-term kidney function, and increased risk of MI and death.
The incidence varies depending on patient risk and definitions used, but it can affect up to 50% of high-risk ACS patients – older patients and/or those with heart failure, chronic kidney disease, or diabetes.
“We don’t really understand the mechanisms that cause CIN, but multiple proposed mechanisms exist, and we know from previous studies that a deficiency of nitric oxide is crucial to the development of CIN,” he explained. “We also know that [nitric oxide] is crucial for normal renal hemostasis. Therefore, a potential therapeutic target to prevent CIN would be to replace this lost nitric oxide.”
The inorganic nitrate evaluated in this trial is found in the diet, is produced endogenously, and is different from medicinally synthesized organic nitrates such as isosorbide mononitrate, he said.
“Isosorbide mononitrate/dinitrate tablets contain organic nitrates and while they are good for angina, we know that they do not have the same beneficial effects on the sustained generation of nitric oxide as inorganic nitrates,” Dr. Jones added.
NITRATE-CIN study
NITRATE-CIN was a double-blind, randomized, placebo-controlled trial conducted at Queen Mary University of London and St. Bartholomew’s Hospital in London, which tested the effectiveness of inorganic nitrate in preventing contrast-induced nephropathy in 640 patients with non-ST elevation ACS referred for invasive coronary angiography.
To be eligible for the trial, patients had to be at risk of contrast-induced nephropathy with an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m2 or have two of the following significant risk factors: diabetes, liver failure, over 70 years of age, exposure to contrast within 7 days, heart failure, or on concomitant renally acting drugs.
Patients were randomly assigned to a formulation of potassium nitrate (12 mmol/744 mg nitrate) per day given as capsules for a 5-day course with the first dose administered prior to angiography or to a control group that received potassium chloride with a matched potassium concentration.
The patient population had a mean age of 71 years, 73% were male, 75% were White, 46% had diabetes, and 56% had chronic kidney disease. There was a 13% loss to follow-up, which was attributed to the COVID pandemic.
The amount of contrast administration was 180 mL in the placebo and 170 mL in the nitrate arm, with 50% of patients undergoing some sort of revascularization.
The primary endpoint was the incidence of CIN as defined by KDIGO criteria – a series of stages of acute kidney injury defined by changes in serum creatinine within 72 hours and up to 1 week.
Results showed that this primary CIN endpoint was reduced significantly from 30% in the placebo arm to 9.1% in the nitrate group, a 70% relative risk reduction (P < .0001). The majority (90%) of this CIN was stage 1, but 10% was stage 2.
Consistent results were seen when an alternative definition of CIN (Mehran) was used, although the rates in both arms were lower than when the KDIGO definition was used.
The benefit was seen across prespecified subgroups including diabetes status, troponin positivity, and Mehran risk. But the benefit seemed to be attenuated in patients on preexisting organic nitrate therapy, although the numbers in these groups were too small to draw definitive conclusions.
As would be expected, there were significant elevations in both systemic nitrate and nitrite levels both up to 72 hours after the procedure, which was consistent with the 5-day course. This was associated with reductions in systolic and diastolic blood pressure, but not associated with any adverse events, Dr. Jones reported.
Rates of procedural MI, a prespecified secondary endpoint, were reduced from 12.5% to 4.1% in those on inorganic nitrates (P = .003).
Looking at longer term outcomes, kidney function was improved at 3 months as measured by change in eGFR, which showed a 10% relative improvement of 5.2 mL/min per 1.73 m2 (10%) in the nitrate group vs. the placebo group. Serum creatinine levels were also significantly increased in the nitrate group.
At 12 months, there was a significant 50% relative reduction in major adverse cardiovascular events – including all-cause mortality, recurrent MI, and recurrent revascularization – which were reduced from 18.1% in the placebo group to 9.1% in the nitrate group, with a reduction in all three of the constituent components of the composite endpoint including all-cause mortality.
Major adverse kidney events (all-cause mortality, renal replacement therapy, or persistent renal dysfunction) were also reduced at 12 months from 28.4% in the placebo group to 10.7% in the nitrate group (P < .0001), a 60% relative reduction. This was driven by lower rates of all-cause mortality and persistent renal dysfunction.
While Dr. Jones said these results on major cardiovascular and kidney outcomes should be viewed as hypothesis-generating at the present time, he said there were biological mechanisms that could explain these benefits.
“We saw a reduction in procedural MI, and we know there is a lot of similar biology in preventing procedural MI and subsequent cardiac events in the acute phase. This, in combination with the large reduction in acute kidney injury, could explain why there’s improved outcomes out to 12 months.”
In her comments, Dr. Mehran congratulated the investigators on having conducted the first study to have shown benefit in the prevention of contrast-associated acute kidney injury as well as major adverse cardiovascular and kidney events associated with the condition.
She used the term “contrast-associated acute kidney injury” rather than “contrast-induced nephropathy” because, she said, it has not been proven that the acute kidney injury seen after angiography is actually caused by the contrast and “so many other things are occurring during procedures when these patients are presenting with different syndromes.”
Dr. Mehran pointed out some weaknesses in the NITRATE-CIN study including the single-center design, the large volume of contrast administered, 13% of patients missing the primary endpoint blood draw, and an imbalance in relevant baseline characteristics despite randomization.
The NITRATE-CIN study was funded by Heart Research UK. Dr. Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT THE ESC CONGRESS 2023
People still want their medical intelligence in human form
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.

And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”

This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.

Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.
And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”
This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.
Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Doctors or AI? Lukewarm vote of confidence goes to …
Well, we’ve got some good news for the physicians out there, and we’ve got some bad news. Which do you want first? Okay, we’re mostly hearing good news, so here goes: Most people would choose a human doctor over artificial intelligence for the diagnosis and treatment of their medical conditions.
And the bad news? In the survey we’re talking about, “most” was 53%, so not exactly a huge victory for the carbon-based life forms. Yup, about 47% of the 2,472 respondents said they would prefer an AI-based clinic over a human specialist, and that number went up if individuals were told that their primary care physicians were on board with AI, “or otherwise nudged to consider AI as good,” the research team said in a written statement released by the University of Arizona, Tucson.
They went on to add that “this signaled the significance of the human physician in guiding a patient’s decision.” So patients will still need their doctors in the future to … um … this is a bit awkward … tell them how good the AI is?
And yes, we know that ChatGPT is already doing the same thing to journalists, but could it write a medical-humor column? Not a chance. Probably can’t even tell a joke.
How do ghosts get rid of wrinkles? Boo-tox. There, let’s see ChatGPT do that.
Explaining the joke makes it funnier, right?
Here at LOTME headquarters, we live by one simple rule, passed down directly from the Buddha himself: “Never let a good presurgical assessment of refractory epilepsy go to waste. Also, don’t believe everything you read on the Internet.”
This human-created joke has been brought to you by the leading theory of humor, which states that comedy stems from our brain reacting to an incongruous part of reality in a positive way. These positive emotions light up our neurons in a specific fashion, and boom, comedy is achieved.
Previous studies into the science of comedy have typically used functional MRI to analyze the brain while it was gripped in the throes of a comedic reaction. Unfortunately, fMRI cannot detect the entirety of the electromagnetic spectrum generated by the brain during these moments, so observing scientists have been, quite literally, missing out on some of the joke. And that’s where a new study from France comes in.
In the study, the researchers showed a group of patients with epilepsy who were hooked up to deep brain electrodes and a high-tech neuroimaging machine – part of the aforementioned presurgical assessment – a 3-minute excerpt from a Charlie Chaplin movie and analyzed their brain activity. Why Charlie Chaplin? Simple. Slapstick is perhaps the most accessible form of comedy across cultures. We can all appreciate a man getting hit in the head with a coconut. The world’s oldest bar joke or whatever this is? Not so much.
During the funniest scenes, all study participants showed increased high-frequency gamma waves (indicating high cognitive engagement) and a decrease in low-frequency waves (indicating reduced inattention and introspection). During unfunny scenes, such as transition moments, the opposite occurred. Importantly, this inverse relationship occurred in the temporal lobe but not in other regions, supporting previous research that indicated humor was mainly processed in the temporal lobe.
The investigators suggested future research should focus on longer videos with more complex forms of comedy, such as jokes, irony, sarcasm, or reference humor. So, uh, a guy getting hit in the head with two coconuts? That’s high-brow stuff right there.
Hot take: Humans aren’t that special
We humans have always prided ourselves on being different from “the animals” in an exceptional way. News flash! We aren’t. We may be the apex predator, but new research shows that humans, as part of the animal kingdom, just aren’t special.
Not special? How can they say that? Are gorillas doing open-heart surgery? Do wolverines tell jokes? At a more basic level, though, the way we operate as mammals in societies is not unique or even new. Elephants are known to mourn their deceased and to have funeral-like practices, ants invented agriculture, and we’re certainly not the only species that has figured out how to use tools.
This new research just demonstrates another way we aren’t exceptional, and that’s in our mating practices and outcomes.
“Humans appear to resemble mammals that live in monogamous partnerships and to some extent, those classified as cooperative breeders, where breeding individuals have to rely on the help of others to raise their offspring,” Monique Borgerhoff Mulder, PhD, professor emerita of anthropology at the University of California, Davis, said in a written statement.
The research team, which consisted of over 100 investigators, looked at 90 human populations based on data from over 80,000 people globally and compared the human data with 49 different nonhuman mammal species. In polygynous societies in which men take several wives, they found, women have more access to resources like food, shelter, and parenting help. Monogamy, on the other hand, “can drive significant inequalities among women,” Dr. Borgerhoff Mulder said, by promoting large differences in the number of children couples produce.
Human day-to-day behavior and child-rearing habits – one parent taking a daughter to ballet class and fixing dinner so the other parent can get to exercise class before picking up the son from soccer practice – may have us thinking that we are part of an evolved society, but really we are not much different than other mammals that hunt, forage for food, and rear and teach their children, the researchers suggested.
So, yes, humans can travel to the moon, create a vaccine for smallpox, and hit other humans with coconuts, but when it comes to simply having offspring or raising them, we’re not all that special. Get over it.
Video-based AI tool estimates LVEF from angiograms
a new study suggests.
In the test dataset, the video-based algorithm, called a deep neural network (DNN), discriminated reduced LVEF (< 40%) with an area under the receiver operating characteristic curve of 0.911.
In the external validation dataset, the DNN discriminated reduced LVEF with an AUROC of 0.906. However, the DNN tended to overestimate low LVEFs and to underestimate high LVEFs.
“We know the findings will be unexpected for cardiologists who don’t typically expect to get an estimate of systolic function or pump function just from an angiogram,” principal investigator Geoffrey H. Tison, MD, of the University of California, San Francisco, said in an interview.
In fact, he noted, “one of the challenges we face is a lack of trust by the health care community. They may not understand what drives the predictions behind our models. We have to translate that information in such a way that physicians trust that the algorithm is using the right features from the data they feed in to make the predictions.”
To help bolster that trust, “we display the ‘Model Facts,’ a nutrition-style label that describes how we train the algorithm, how it was validated, and the inclusion and exclusion criteria,” added lead author Robert Avram, MD, of the University of Montreal.
Model Facts is a safeguard against inappropriate use of the algorithm, Dr. Avram said. For example, if the algorithm was trained on patients between the ages of 40 and 90 and a clinician fed in data for a 35-year-old, a pop-up would appear warning the physician that the data being inputted are different from the data the algorithm was trained and validated on, and so any prediction “should be taken with a grain of salt.”
The study was published online in JAMA Cardiology.
Additional procedure
LVEF can be determined before coronary angiography with transthoracic echocardiography, but that is not always available, particularly for patients being seen emergently for acute coronary syndromes, the researchers wrote. LVEF can also be assessed using left ventriculography, an additional procedure that requires insertion of a pigtail catheter into the left ventricle and injection of more contrast and longer radiation exposure.
“Novel methods to assess LVEF at the point of care during coronary angiography would expand the available options to perform this important physiologic determination,” they wrote. “Video-based deep neural networks can learn subtle patterns from medical data to accomplish certain tasks beyond what physicians can achieve with that data, providing an opportunity to assess cardiac systolic function in real time from standard angiographic images without additional cost or procedures.”
The investigators conducted a cross-sectional study using UCSF patient data from 2012 to 2019. Data were randomly categorized into training, development, and test datasets.
External validation data were obtained from the University of Ottawa Heart Institute.
All adult patients who received a coronary angiogram and a transthoracic echocardiogram (TTE) within 3 months before or 1 month after receiving the angiogram were included.
A total of 4,042 angiograms with corresponding TTE LVEF from 3,679 UCSF patients were included in the analysis. The mean age of the patients was 64.3 years, and 65% were men.
The researchers’ video-based DNN, called CathEF, was used to discriminate reduced LVEF and to predict a continuous LVEF percentage from standard angiogram videos of the left coronary artery.
In the UCSF test dataset, CathEF discriminated reduced LVEF with an AUROC of 0.911; the diagnostic odds ratio for reduced LVEF was 22.7.
Furthermore, the CathEF-predicted that LVEF had a mean absolute error (MAE) of 8.5%, compared with TTE LVEF.
The CathEF-predicted LVEF differed 5% or less in comparison with the TTE LVEF in 38% of the test dataset studies; however, differences greater than 15% were seen in 15.2% of cases.
In the external validation, CathEF discriminated reduced LVEF with an AUROC of 0.906 and an MAE of 7%.
CathEF performance was consistent irrespective of patient characteristics, including sex, body mass index, low estimated glomerular filtration rate (< 45), acute coronary syndromes, obstructive coronary artery disease, and left ventricular hypertrophy.
However, as noted, it tended to overestimate low LVEFs and to underestimate high LVEFs.
“Further research can improve accuracy and reduce the variability of DNNs to maximize their clinical utility,” the authors concluded.
A validation study is underway at the Montreal Heart Institute, and similar studies are planned at UCSF and McGill University, Dr. Tison said. “We expect to present preliminary findings at medical conferences either before the end of the year or maybe for the American College of Cardiology meeting in March 2024.”
Potentially improved outcomes
In a comment, Alfonso H. Waller, MD, a member of the American College of Cardiology’s Imaging Council and director of cardiac imaging at New Jersey Medical School, Newark, said that, “at some centers, in patients presenting with an acute ST-segment elevation myocardial infarction, some argue that assessment of myocardial and valvular function with [left ventriculography] grams may provide important prognostic information and in part may help guide the management of the patient.
“Therefore, this novel approach may provide information that is not usually available without performing a classic LV gram ... [and] may lead to improved delivery of care, earlier therapies, and potentially improved outcomes and quality of life.”
If the technology is available in real time, “it could enable real-time, dynamic assessment of cardiac function during coronary angiography, which may be particularly helpful in acute STEMI cases where baseline cardiac function and renal function may be unknown and additional contrast may be detrimental,” he said.
However, patients who might benefit most from the technology are those with severely reduced LVEF, “and unfortunately, the LVEF may be overestimated in this group,” he said.
Dr. Waller also noted that the model was developed using echocardiograms obtained 3 months before or up to 1 month after the angiogram, during which time “LVEF may change significantly. Typically, if someone presents with an acute coronary syndrome, there can be myocardial stunning, which can lead to regional wall motion abnormalities and lowering of LVEF.”
The validation study is evaluating patients with acute coronary syndrome for whom an echocardiogram was performed within 48 hours of the angiogram, he added.
The study was supported by grants from the Fonds de la Recherche en Santé du Québec, the Montreal Heart Institute Research Centre, the Montreal Heart Institute Foundation, the Des Groseillers-Bérard Research Chair, the National Institutes of Health, and the Heart and Stroke Foundation of Ontario. Dr. Tison, Dr. Avram, and Dr. Waller disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new study suggests.
In the test dataset, the video-based algorithm, called a deep neural network (DNN), discriminated reduced LVEF (< 40%) with an area under the receiver operating characteristic curve of 0.911.
In the external validation dataset, the DNN discriminated reduced LVEF with an AUROC of 0.906. However, the DNN tended to overestimate low LVEFs and to underestimate high LVEFs.
“We know the findings will be unexpected for cardiologists who don’t typically expect to get an estimate of systolic function or pump function just from an angiogram,” principal investigator Geoffrey H. Tison, MD, of the University of California, San Francisco, said in an interview.
In fact, he noted, “one of the challenges we face is a lack of trust by the health care community. They may not understand what drives the predictions behind our models. We have to translate that information in such a way that physicians trust that the algorithm is using the right features from the data they feed in to make the predictions.”
To help bolster that trust, “we display the ‘Model Facts,’ a nutrition-style label that describes how we train the algorithm, how it was validated, and the inclusion and exclusion criteria,” added lead author Robert Avram, MD, of the University of Montreal.
Model Facts is a safeguard against inappropriate use of the algorithm, Dr. Avram said. For example, if the algorithm was trained on patients between the ages of 40 and 90 and a clinician fed in data for a 35-year-old, a pop-up would appear warning the physician that the data being inputted are different from the data the algorithm was trained and validated on, and so any prediction “should be taken with a grain of salt.”
The study was published online in JAMA Cardiology.
Additional procedure
LVEF can be determined before coronary angiography with transthoracic echocardiography, but that is not always available, particularly for patients being seen emergently for acute coronary syndromes, the researchers wrote. LVEF can also be assessed using left ventriculography, an additional procedure that requires insertion of a pigtail catheter into the left ventricle and injection of more contrast and longer radiation exposure.
“Novel methods to assess LVEF at the point of care during coronary angiography would expand the available options to perform this important physiologic determination,” they wrote. “Video-based deep neural networks can learn subtle patterns from medical data to accomplish certain tasks beyond what physicians can achieve with that data, providing an opportunity to assess cardiac systolic function in real time from standard angiographic images without additional cost or procedures.”
The investigators conducted a cross-sectional study using UCSF patient data from 2012 to 2019. Data were randomly categorized into training, development, and test datasets.
External validation data were obtained from the University of Ottawa Heart Institute.
All adult patients who received a coronary angiogram and a transthoracic echocardiogram (TTE) within 3 months before or 1 month after receiving the angiogram were included.
A total of 4,042 angiograms with corresponding TTE LVEF from 3,679 UCSF patients were included in the analysis. The mean age of the patients was 64.3 years, and 65% were men.
The researchers’ video-based DNN, called CathEF, was used to discriminate reduced LVEF and to predict a continuous LVEF percentage from standard angiogram videos of the left coronary artery.
In the UCSF test dataset, CathEF discriminated reduced LVEF with an AUROC of 0.911; the diagnostic odds ratio for reduced LVEF was 22.7.
Furthermore, the CathEF-predicted that LVEF had a mean absolute error (MAE) of 8.5%, compared with TTE LVEF.
The CathEF-predicted LVEF differed 5% or less in comparison with the TTE LVEF in 38% of the test dataset studies; however, differences greater than 15% were seen in 15.2% of cases.
In the external validation, CathEF discriminated reduced LVEF with an AUROC of 0.906 and an MAE of 7%.
CathEF performance was consistent irrespective of patient characteristics, including sex, body mass index, low estimated glomerular filtration rate (< 45), acute coronary syndromes, obstructive coronary artery disease, and left ventricular hypertrophy.
However, as noted, it tended to overestimate low LVEFs and to underestimate high LVEFs.
“Further research can improve accuracy and reduce the variability of DNNs to maximize their clinical utility,” the authors concluded.
A validation study is underway at the Montreal Heart Institute, and similar studies are planned at UCSF and McGill University, Dr. Tison said. “We expect to present preliminary findings at medical conferences either before the end of the year or maybe for the American College of Cardiology meeting in March 2024.”
Potentially improved outcomes
In a comment, Alfonso H. Waller, MD, a member of the American College of Cardiology’s Imaging Council and director of cardiac imaging at New Jersey Medical School, Newark, said that, “at some centers, in patients presenting with an acute ST-segment elevation myocardial infarction, some argue that assessment of myocardial and valvular function with [left ventriculography] grams may provide important prognostic information and in part may help guide the management of the patient.
“Therefore, this novel approach may provide information that is not usually available without performing a classic LV gram ... [and] may lead to improved delivery of care, earlier therapies, and potentially improved outcomes and quality of life.”
If the technology is available in real time, “it could enable real-time, dynamic assessment of cardiac function during coronary angiography, which may be particularly helpful in acute STEMI cases where baseline cardiac function and renal function may be unknown and additional contrast may be detrimental,” he said.
However, patients who might benefit most from the technology are those with severely reduced LVEF, “and unfortunately, the LVEF may be overestimated in this group,” he said.
Dr. Waller also noted that the model was developed using echocardiograms obtained 3 months before or up to 1 month after the angiogram, during which time “LVEF may change significantly. Typically, if someone presents with an acute coronary syndrome, there can be myocardial stunning, which can lead to regional wall motion abnormalities and lowering of LVEF.”
The validation study is evaluating patients with acute coronary syndrome for whom an echocardiogram was performed within 48 hours of the angiogram, he added.
The study was supported by grants from the Fonds de la Recherche en Santé du Québec, the Montreal Heart Institute Research Centre, the Montreal Heart Institute Foundation, the Des Groseillers-Bérard Research Chair, the National Institutes of Health, and the Heart and Stroke Foundation of Ontario. Dr. Tison, Dr. Avram, and Dr. Waller disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
a new study suggests.
In the test dataset, the video-based algorithm, called a deep neural network (DNN), discriminated reduced LVEF (< 40%) with an area under the receiver operating characteristic curve of 0.911.
In the external validation dataset, the DNN discriminated reduced LVEF with an AUROC of 0.906. However, the DNN tended to overestimate low LVEFs and to underestimate high LVEFs.
“We know the findings will be unexpected for cardiologists who don’t typically expect to get an estimate of systolic function or pump function just from an angiogram,” principal investigator Geoffrey H. Tison, MD, of the University of California, San Francisco, said in an interview.
In fact, he noted, “one of the challenges we face is a lack of trust by the health care community. They may not understand what drives the predictions behind our models. We have to translate that information in such a way that physicians trust that the algorithm is using the right features from the data they feed in to make the predictions.”
To help bolster that trust, “we display the ‘Model Facts,’ a nutrition-style label that describes how we train the algorithm, how it was validated, and the inclusion and exclusion criteria,” added lead author Robert Avram, MD, of the University of Montreal.
Model Facts is a safeguard against inappropriate use of the algorithm, Dr. Avram said. For example, if the algorithm was trained on patients between the ages of 40 and 90 and a clinician fed in data for a 35-year-old, a pop-up would appear warning the physician that the data being inputted are different from the data the algorithm was trained and validated on, and so any prediction “should be taken with a grain of salt.”
The study was published online in JAMA Cardiology.
Additional procedure
LVEF can be determined before coronary angiography with transthoracic echocardiography, but that is not always available, particularly for patients being seen emergently for acute coronary syndromes, the researchers wrote. LVEF can also be assessed using left ventriculography, an additional procedure that requires insertion of a pigtail catheter into the left ventricle and injection of more contrast and longer radiation exposure.
“Novel methods to assess LVEF at the point of care during coronary angiography would expand the available options to perform this important physiologic determination,” they wrote. “Video-based deep neural networks can learn subtle patterns from medical data to accomplish certain tasks beyond what physicians can achieve with that data, providing an opportunity to assess cardiac systolic function in real time from standard angiographic images without additional cost or procedures.”
The investigators conducted a cross-sectional study using UCSF patient data from 2012 to 2019. Data were randomly categorized into training, development, and test datasets.
External validation data were obtained from the University of Ottawa Heart Institute.
All adult patients who received a coronary angiogram and a transthoracic echocardiogram (TTE) within 3 months before or 1 month after receiving the angiogram were included.
A total of 4,042 angiograms with corresponding TTE LVEF from 3,679 UCSF patients were included in the analysis. The mean age of the patients was 64.3 years, and 65% were men.
The researchers’ video-based DNN, called CathEF, was used to discriminate reduced LVEF and to predict a continuous LVEF percentage from standard angiogram videos of the left coronary artery.
In the UCSF test dataset, CathEF discriminated reduced LVEF with an AUROC of 0.911; the diagnostic odds ratio for reduced LVEF was 22.7.
Furthermore, the CathEF-predicted that LVEF had a mean absolute error (MAE) of 8.5%, compared with TTE LVEF.
The CathEF-predicted LVEF differed 5% or less in comparison with the TTE LVEF in 38% of the test dataset studies; however, differences greater than 15% were seen in 15.2% of cases.
In the external validation, CathEF discriminated reduced LVEF with an AUROC of 0.906 and an MAE of 7%.
CathEF performance was consistent irrespective of patient characteristics, including sex, body mass index, low estimated glomerular filtration rate (< 45), acute coronary syndromes, obstructive coronary artery disease, and left ventricular hypertrophy.
However, as noted, it tended to overestimate low LVEFs and to underestimate high LVEFs.
“Further research can improve accuracy and reduce the variability of DNNs to maximize their clinical utility,” the authors concluded.
A validation study is underway at the Montreal Heart Institute, and similar studies are planned at UCSF and McGill University, Dr. Tison said. “We expect to present preliminary findings at medical conferences either before the end of the year or maybe for the American College of Cardiology meeting in March 2024.”
Potentially improved outcomes
In a comment, Alfonso H. Waller, MD, a member of the American College of Cardiology’s Imaging Council and director of cardiac imaging at New Jersey Medical School, Newark, said that, “at some centers, in patients presenting with an acute ST-segment elevation myocardial infarction, some argue that assessment of myocardial and valvular function with [left ventriculography] grams may provide important prognostic information and in part may help guide the management of the patient.
“Therefore, this novel approach may provide information that is not usually available without performing a classic LV gram ... [and] may lead to improved delivery of care, earlier therapies, and potentially improved outcomes and quality of life.”
If the technology is available in real time, “it could enable real-time, dynamic assessment of cardiac function during coronary angiography, which may be particularly helpful in acute STEMI cases where baseline cardiac function and renal function may be unknown and additional contrast may be detrimental,” he said.
However, patients who might benefit most from the technology are those with severely reduced LVEF, “and unfortunately, the LVEF may be overestimated in this group,” he said.
Dr. Waller also noted that the model was developed using echocardiograms obtained 3 months before or up to 1 month after the angiogram, during which time “LVEF may change significantly. Typically, if someone presents with an acute coronary syndrome, there can be myocardial stunning, which can lead to regional wall motion abnormalities and lowering of LVEF.”
The validation study is evaluating patients with acute coronary syndrome for whom an echocardiogram was performed within 48 hours of the angiogram, he added.
The study was supported by grants from the Fonds de la Recherche en Santé du Québec, the Montreal Heart Institute Research Centre, the Montreal Heart Institute Foundation, the Des Groseillers-Bérard Research Chair, the National Institutes of Health, and the Heart and Stroke Foundation of Ontario. Dr. Tison, Dr. Avram, and Dr. Waller disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY
LAA closure outcomes improve with CCTA: Swiss-Apero subanalysis
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
Predicting BPD vs. bipolar treatment response: New imaging data
A new study identifies specific brain regions involved in treatment response in bipolar disorder (BD) and borderline personality disorder (BPD), potentially paving the way for more targeted treatment.
In a meta-analysis of 34 studies that used neuroimaging to investigate changes in brain activation following psychotherapy and pharmacotherapy for BD and BPD, investigators found most brain regions showing abnormal activation in both conditions improved after treatment. In particular, changes in brain activity after psychotherapy were found primarily in the frontal areas, whereas pharmacotherapy largely altered the limbic areas.
“,” senior investigator Xiaoming Li, PhD, professor, department of medical psychology, Anhui Medical University, Hefei, China, told this news organization.
“It may also contribute to the identification of more accurate neuroimaging biomarkers for treatment of the two disorders and to the finding of more effective therapy,” Dr. Li said.
The study was published online in the Journal of Clinical Psychiatry.
Blurred boundary
Dr. Li called BDs and BPDs “difficult to diagnose and differentiate,” noting that the comorbidity rate is “very high.” Underestimating the boundary between BD and BPD “increases the risk of improper or harmful drug exposure,” since mood stabilizing drugs are “considered to be the key therapeutic intervention for BD, while psychotherapy is the key treatment for BPD.”
The “blurred boundary between BD and BPD is one of the reasons it is important to study the relationship between these two diseases,” the authors said.
Previous studies comparing the relationship between BD and BPD “did not explore the similarities and differences in brain mechanisms between these two disorders after treatment,” they pointed out.
Patients with BD have a different disease course and response to therapy, compared to patient with BPD patients. “Misdiagnosis may result in the patients receiving ineffective treatment, so it is particularly important to explore the neural mechanisms of the treatment of these two diseases,” Dr. Li said.
To investigate, the researchers used activation likelihood estimation (ALE) – a technique that examines coordinates of neuroimaging data gleaned from published studies – after searching several databases from inception until June 2021.
This approach was used to “evaluate the similarities and differences in the activation of different brain regions in patients with BD and BPD after treatment with psychotherapy and drug therapy.”
Studies were required to focus on patients with a clinical diagnosis of BD or BPD; neuroimaging studies using functional MRI; coordinates of the peak activations in the stereotactic space of the Montreal Neurologic Institute or Talairach; treatment (pharmacologic or psychological) for patients with BD or BPD; and results of changes in brain activation after treatment, relative to a before-treatment condition.
Of 1,592 records, 34 studies (n = 912 subjects) met inclusion criteria and were selected and used in extracting the activation coordinates. The researchers extracted a total of 186 activity increase points and 90 activity decrease points. After combining these calculations, they found 12 increased activation clusters and 2 decreased activation clusters.
Of the studies, 23 focused on BD and 11 on BPD; 14 used psychotherapy, 18 used drug therapy, and 2 used a combination of both approaches.
Normalizing activation levels
Both treatments were associated with convergent activity increases and decreases in several brain regions: the anterior cingulate cortex, medial frontal gyrus, inferior frontal gyrus, cingulate gyrus, parahippocampal gyrus, and the posterior cingulate cortex.
The researchers then examined studies based on treatment method – psychotherapy or pharmacotherapy and the effect on the two disorders.
“After psychotherapy, the frontal lobe and temporal lobe were the primary brain regions in which activation changed, indicating a top-down effect of this therapy type, while after drug therapy, the limbic area was the region in which activation changed, indicating a ‘bottom-up’ effect,” said Dr. Li.
Dr. Li cited previous research pointing to functional and structural abnormalities in both disorders – especially in the default mode network (DMN) and frontolimbic network.
In particular, alterations in the amygdala and the parahippocampal gyrus are reported more frequently in BPD than in BD, whereas dysfunctional frontolimbic brain regions seem to underlie the emotional dysfunction in BPD. Several studies have also associated the impulsivity of BD with dysfunctions in the interplay of cortical-limbic circuits.
Dr. Li said the study findings suggest “that treatment may change these brain activation levels by acting on the abnormal brain circuit, such as the DMN and the frontolimbic network so as to ‘normalize’ its activity and improve symptoms.”
Specifically, brain regions with abnormally increased activation “showed decreased activation after treatment, and brain regions with abnormally decreased activation showed increased activation after treatment.”
Discrete, overlapping mechanisms
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study “provides additional support for the underlying neurobiological signature of bipolar disorder and a commonly encountered co-occurring condition – borderline personality disorder – having both discrete yet overlapping mechanisms.”

He found it interesting that “medications have a different principal target than psychosocial interventions, which has both academic and clinical implications.
“The academic implication is that we have reasons to believe that we will be in a position to parse the neurobiology of bipolar disorder or borderline personality disorder when we take an approach that isolates specific domains of psychopathology, which is what they [the authors] appear to be doing,” said Dr. McIntyre, who wasn’t associated with this research.
In addition, “from the clinical perspective, this provides a rationale for why we should be integrating pharmacotherapy with psychotherapy in people who have comorbid conditions like borderline personality disorder, which affects 20% of people living with bipolar disorder and 60% to 70% have borderline traits,” he added.
The research was supported by the Anhui Natural Science Foundation and Grants for Scientific Research from Anhui Medical University. Dr. Li and coauthors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China and the Milken Institute; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
A new study identifies specific brain regions involved in treatment response in bipolar disorder (BD) and borderline personality disorder (BPD), potentially paving the way for more targeted treatment.
In a meta-analysis of 34 studies that used neuroimaging to investigate changes in brain activation following psychotherapy and pharmacotherapy for BD and BPD, investigators found most brain regions showing abnormal activation in both conditions improved after treatment. In particular, changes in brain activity after psychotherapy were found primarily in the frontal areas, whereas pharmacotherapy largely altered the limbic areas.
“,” senior investigator Xiaoming Li, PhD, professor, department of medical psychology, Anhui Medical University, Hefei, China, told this news organization.
“It may also contribute to the identification of more accurate neuroimaging biomarkers for treatment of the two disorders and to the finding of more effective therapy,” Dr. Li said.
The study was published online in the Journal of Clinical Psychiatry.
Blurred boundary
Dr. Li called BDs and BPDs “difficult to diagnose and differentiate,” noting that the comorbidity rate is “very high.” Underestimating the boundary between BD and BPD “increases the risk of improper or harmful drug exposure,” since mood stabilizing drugs are “considered to be the key therapeutic intervention for BD, while psychotherapy is the key treatment for BPD.”
The “blurred boundary between BD and BPD is one of the reasons it is important to study the relationship between these two diseases,” the authors said.
Previous studies comparing the relationship between BD and BPD “did not explore the similarities and differences in brain mechanisms between these two disorders after treatment,” they pointed out.
Patients with BD have a different disease course and response to therapy, compared to patient with BPD patients. “Misdiagnosis may result in the patients receiving ineffective treatment, so it is particularly important to explore the neural mechanisms of the treatment of these two diseases,” Dr. Li said.
To investigate, the researchers used activation likelihood estimation (ALE) – a technique that examines coordinates of neuroimaging data gleaned from published studies – after searching several databases from inception until June 2021.
This approach was used to “evaluate the similarities and differences in the activation of different brain regions in patients with BD and BPD after treatment with psychotherapy and drug therapy.”
Studies were required to focus on patients with a clinical diagnosis of BD or BPD; neuroimaging studies using functional MRI; coordinates of the peak activations in the stereotactic space of the Montreal Neurologic Institute or Talairach; treatment (pharmacologic or psychological) for patients with BD or BPD; and results of changes in brain activation after treatment, relative to a before-treatment condition.
Of 1,592 records, 34 studies (n = 912 subjects) met inclusion criteria and were selected and used in extracting the activation coordinates. The researchers extracted a total of 186 activity increase points and 90 activity decrease points. After combining these calculations, they found 12 increased activation clusters and 2 decreased activation clusters.
Of the studies, 23 focused on BD and 11 on BPD; 14 used psychotherapy, 18 used drug therapy, and 2 used a combination of both approaches.
Normalizing activation levels
Both treatments were associated with convergent activity increases and decreases in several brain regions: the anterior cingulate cortex, medial frontal gyrus, inferior frontal gyrus, cingulate gyrus, parahippocampal gyrus, and the posterior cingulate cortex.
The researchers then examined studies based on treatment method – psychotherapy or pharmacotherapy and the effect on the two disorders.
“After psychotherapy, the frontal lobe and temporal lobe were the primary brain regions in which activation changed, indicating a top-down effect of this therapy type, while after drug therapy, the limbic area was the region in which activation changed, indicating a ‘bottom-up’ effect,” said Dr. Li.
Dr. Li cited previous research pointing to functional and structural abnormalities in both disorders – especially in the default mode network (DMN) and frontolimbic network.
In particular, alterations in the amygdala and the parahippocampal gyrus are reported more frequently in BPD than in BD, whereas dysfunctional frontolimbic brain regions seem to underlie the emotional dysfunction in BPD. Several studies have also associated the impulsivity of BD with dysfunctions in the interplay of cortical-limbic circuits.
Dr. Li said the study findings suggest “that treatment may change these brain activation levels by acting on the abnormal brain circuit, such as the DMN and the frontolimbic network so as to ‘normalize’ its activity and improve symptoms.”
Specifically, brain regions with abnormally increased activation “showed decreased activation after treatment, and brain regions with abnormally decreased activation showed increased activation after treatment.”
Discrete, overlapping mechanisms
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study “provides additional support for the underlying neurobiological signature of bipolar disorder and a commonly encountered co-occurring condition – borderline personality disorder – having both discrete yet overlapping mechanisms.”
He found it interesting that “medications have a different principal target than psychosocial interventions, which has both academic and clinical implications.
“The academic implication is that we have reasons to believe that we will be in a position to parse the neurobiology of bipolar disorder or borderline personality disorder when we take an approach that isolates specific domains of psychopathology, which is what they [the authors] appear to be doing,” said Dr. McIntyre, who wasn’t associated with this research.
In addition, “from the clinical perspective, this provides a rationale for why we should be integrating pharmacotherapy with psychotherapy in people who have comorbid conditions like borderline personality disorder, which affects 20% of people living with bipolar disorder and 60% to 70% have borderline traits,” he added.
The research was supported by the Anhui Natural Science Foundation and Grants for Scientific Research from Anhui Medical University. Dr. Li and coauthors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China and the Milken Institute; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
A new study identifies specific brain regions involved in treatment response in bipolar disorder (BD) and borderline personality disorder (BPD), potentially paving the way for more targeted treatment.
In a meta-analysis of 34 studies that used neuroimaging to investigate changes in brain activation following psychotherapy and pharmacotherapy for BD and BPD, investigators found most brain regions showing abnormal activation in both conditions improved after treatment. In particular, changes in brain activity after psychotherapy were found primarily in the frontal areas, whereas pharmacotherapy largely altered the limbic areas.
“,” senior investigator Xiaoming Li, PhD, professor, department of medical psychology, Anhui Medical University, Hefei, China, told this news organization.
“It may also contribute to the identification of more accurate neuroimaging biomarkers for treatment of the two disorders and to the finding of more effective therapy,” Dr. Li said.
The study was published online in the Journal of Clinical Psychiatry.
Blurred boundary
Dr. Li called BDs and BPDs “difficult to diagnose and differentiate,” noting that the comorbidity rate is “very high.” Underestimating the boundary between BD and BPD “increases the risk of improper or harmful drug exposure,” since mood stabilizing drugs are “considered to be the key therapeutic intervention for BD, while psychotherapy is the key treatment for BPD.”
The “blurred boundary between BD and BPD is one of the reasons it is important to study the relationship between these two diseases,” the authors said.
Previous studies comparing the relationship between BD and BPD “did not explore the similarities and differences in brain mechanisms between these two disorders after treatment,” they pointed out.
Patients with BD have a different disease course and response to therapy, compared to patient with BPD patients. “Misdiagnosis may result in the patients receiving ineffective treatment, so it is particularly important to explore the neural mechanisms of the treatment of these two diseases,” Dr. Li said.
To investigate, the researchers used activation likelihood estimation (ALE) – a technique that examines coordinates of neuroimaging data gleaned from published studies – after searching several databases from inception until June 2021.
This approach was used to “evaluate the similarities and differences in the activation of different brain regions in patients with BD and BPD after treatment with psychotherapy and drug therapy.”
Studies were required to focus on patients with a clinical diagnosis of BD or BPD; neuroimaging studies using functional MRI; coordinates of the peak activations in the stereotactic space of the Montreal Neurologic Institute or Talairach; treatment (pharmacologic or psychological) for patients with BD or BPD; and results of changes in brain activation after treatment, relative to a before-treatment condition.
Of 1,592 records, 34 studies (n = 912 subjects) met inclusion criteria and were selected and used in extracting the activation coordinates. The researchers extracted a total of 186 activity increase points and 90 activity decrease points. After combining these calculations, they found 12 increased activation clusters and 2 decreased activation clusters.
Of the studies, 23 focused on BD and 11 on BPD; 14 used psychotherapy, 18 used drug therapy, and 2 used a combination of both approaches.
Normalizing activation levels
Both treatments were associated with convergent activity increases and decreases in several brain regions: the anterior cingulate cortex, medial frontal gyrus, inferior frontal gyrus, cingulate gyrus, parahippocampal gyrus, and the posterior cingulate cortex.
The researchers then examined studies based on treatment method – psychotherapy or pharmacotherapy and the effect on the two disorders.
“After psychotherapy, the frontal lobe and temporal lobe were the primary brain regions in which activation changed, indicating a top-down effect of this therapy type, while after drug therapy, the limbic area was the region in which activation changed, indicating a ‘bottom-up’ effect,” said Dr. Li.
Dr. Li cited previous research pointing to functional and structural abnormalities in both disorders – especially in the default mode network (DMN) and frontolimbic network.
In particular, alterations in the amygdala and the parahippocampal gyrus are reported more frequently in BPD than in BD, whereas dysfunctional frontolimbic brain regions seem to underlie the emotional dysfunction in BPD. Several studies have also associated the impulsivity of BD with dysfunctions in the interplay of cortical-limbic circuits.
Dr. Li said the study findings suggest “that treatment may change these brain activation levels by acting on the abnormal brain circuit, such as the DMN and the frontolimbic network so as to ‘normalize’ its activity and improve symptoms.”
Specifically, brain regions with abnormally increased activation “showed decreased activation after treatment, and brain regions with abnormally decreased activation showed increased activation after treatment.”
Discrete, overlapping mechanisms
Commenting on the study, Roger S. McIntyre, MD, professor of psychiatry and pharmacology, University of Toronto, and head of the Mood Disorders Psychopharmacology Unit, said the study “provides additional support for the underlying neurobiological signature of bipolar disorder and a commonly encountered co-occurring condition – borderline personality disorder – having both discrete yet overlapping mechanisms.”
He found it interesting that “medications have a different principal target than psychosocial interventions, which has both academic and clinical implications.
“The academic implication is that we have reasons to believe that we will be in a position to parse the neurobiology of bipolar disorder or borderline personality disorder when we take an approach that isolates specific domains of psychopathology, which is what they [the authors] appear to be doing,” said Dr. McIntyre, who wasn’t associated with this research.
In addition, “from the clinical perspective, this provides a rationale for why we should be integrating pharmacotherapy with psychotherapy in people who have comorbid conditions like borderline personality disorder, which affects 20% of people living with bipolar disorder and 60% to 70% have borderline traits,” he added.
The research was supported by the Anhui Natural Science Foundation and Grants for Scientific Research from Anhui Medical University. Dr. Li and coauthors declared no relevant financial relationships. Dr. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China and the Milken Institute; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, AbbVie, Atai Life Sciences. Dr. McIntyre is a CEO of Braxia Scientific Corp.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
New ASE guideline on interventional echocardiography training
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
Spherical heart may predict cardiomyopathy, AFib
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MED
Subclinical CAD by CT predicts MI risk, with or without stenoses
About half of middle-aged adults in the community without cardiovascular (CV) symptoms have coronary atherosclerosis by CT angiography (CTA) that puts them at substantial risk for myocardial infarction (MI), suggests a prospective cohort study.
The 10% of participants who had subclinical disease considered obstructive at CTA showed a ninefold increased risk for MI over several years. Obstructive disease seemed to elevate risk more than subclinical disease that wasn’t obstructive but still considered extensive within the coronary arteries.
The findings, based on a Copenhagen General Population Study cohort, are new for CTA but consistent with research based on coronary artery calcium (CAC) scores and other ways to assess CV risk, say researchers.
Although all participants underwent CTA, such imaging isn’t used in the general population for atherosclerosis screening. But the findings may have implications for “opportunistic screening” for subclinical coronary disease at CTA conducted for other reasons, notes the study’s report, published online in the Annals of Internal Medicine.
“Identification of luminal obstructive or extensive subclinical coronary atherosclerosis” could potentially provide “clinically relevant, incremental risk assessment” in nonischemic patients who undergo cardiac CT or electrocardiogram-gated chest CT before procedures such as arrhythmia ablation or valve repair, it states.
Such patients found with subclinical coronary atherosclerosis might potentially “benefit from referral to intensified cardiovascular primary prevention therapy,” write the authors, led by Andreas Fuchs, MD, PhD, Copenhagen University Hospital-Rigshospitalet.
The group acknowledges the findings may not entirely apply to a non-Danish population.
A screening role for CTA?
Whether CTA has a role to play in adults without symptoms “is a big, open question in the field right now,” observed Ron Blankstein, MD, not associated with the current analysis, for this news organization.
Most population studies of CV risk prediction, such as MESA, have looked at CAC scores, not CTA, and have shown that “the more plaque individuals have, the higher the risk.” The current findings are similar but novel in coming from coronary CTA in a large asymptomatic community population, said Dr. Blankstein, who is director of cardiac CT at Brigham and Women’s Hospital, Boston.
“It’s possible that patients who have obstructive plaque in general tend to have a larger amount of plaque as well,” he said. So, while the study suggests that “the more plaque individuals have, the worse their overall risk,” it also shows that the risk “is enhanced even more if they have obstructive disease.”
The Danish cohort analysis “provides a unique opportunity to study the contemporary natural history of coronary artery disease in the absence of intervention,” notes an accompanying editorial.
For example, both patients and clinicians were blinded to CTA results, and CV preventive therapies weren’t common, observe Michael McDermott, MBChB, and David E. Newby, DM, PhD, of the BHF Centre for Cardiovascular Science, University of Edinburgh.
The analysis suggests that subclinical coronary disease that is obstructive predicts MI risk more strongly than extensive coronary disease, they note, and may be present in two-thirds of MI patients. “This contrasts with symptomatic populations, where nonobstructive disease accounts for most future myocardial infarctions, presumably from plaque rupture.”
It also points to “strong associations between nonobstructive extensive disease and adverse plaque characteristics,” write Dr. McDermott and Dr. Newby. “This underscores the major importance of plaque burden” for the prediction of coronary events.
Graded risk
The analysis included 9,533 persons aged 40 and older without known ischemic heart disease or symptoms with available CTA assessments.
Obstructive disease, defined as presence of a luminal stenosis of at least 50%, was seen in 10% and nonobstructive disease in 36% of the total cohort, the report states.
Disease occupying more than one-third of the coronary tree was considered extensive and less than one-third of the coronaries nonextensive, occurring in 10.5% and 35.8% of the cohort, respectively.
There were 71 MIs and 193 deaths over a median of 3.5 years. The adjusted relative risk for MI, compared with those without coronary atherosclerosis, was:
- 7.65 (95% confidence interval, 3.53-16.57) overall in patients with extensive disease.
- 8.28 (95% CI, 3.75-18.32) in those with obstructive but nonextensive disease.
- 9.19 (95% CI, 4.49-18.82) overall in those with obstructive disease.
- 12.48 (95% CI, 5.50-28.12) in those with or obstructive and extensive disease.
The adjusted RR for the composite of death or MI was also elevated in persons with extensive disease:
- 2.70 (95% CI, 1.72-4.25) in those with extensive but nonobstructive disease.
- 3.15 (95% CI, 2.05-4.83) in those with extensive and obstructive disease.
“It’s one thing to show that the more plaque, the higher the risk,” Dr. Blankstein said. But “does the information ultimately lead to better outcomes? Do patients have fewer MIs or fewer deaths?” Several ongoing randomized trials are exploring these questions.
They include DANE-HEART (Computed Tomography Coronary Angiography for Primary Prevention), projected to enroll about 6,000 participants from the Copenhagen General Population Study cohort who have at least one CV risk factor, and SCOT-HEART 2 (second Computed Tomography Coronary Angiography for the Prevention of Myocardial Infarction), enrolling a similar cohort in Scotland.
The study was supported by grants from AP Møller og Hustru Chastine Mc-Kinney Møllers Fond, the Research Council of Rigshospitalet, and Danish Heart Foundation. Dr. Fuchs reports no relevant financial relationships. Disclosures for the other authors can be found here. Dr. Blankstein recently disclosed serving as a consultant to Amgen, Caristo Diagnostics, Novartis, and Silence Therapeutics. Disclosures for Dr. McDermott and Dr. Newby, who are SCOT-HEART 2 investigators, can be found here.
A version of this article originally appeared on Medscape.com.
About half of middle-aged adults in the community without cardiovascular (CV) symptoms have coronary atherosclerosis by CT angiography (CTA) that puts them at substantial risk for myocardial infarction (MI), suggests a prospective cohort study.
The 10% of participants who had subclinical disease considered obstructive at CTA showed a ninefold increased risk for MI over several years. Obstructive disease seemed to elevate risk more than subclinical disease that wasn’t obstructive but still considered extensive within the coronary arteries.
The findings, based on a Copenhagen General Population Study cohort, are new for CTA but consistent with research based on coronary artery calcium (CAC) scores and other ways to assess CV risk, say researchers.
Although all participants underwent CTA, such imaging isn’t used in the general population for atherosclerosis screening. But the findings may have implications for “opportunistic screening” for subclinical coronary disease at CTA conducted for other reasons, notes the study’s report, published online in the Annals of Internal Medicine.
“Identification of luminal obstructive or extensive subclinical coronary atherosclerosis” could potentially provide “clinically relevant, incremental risk assessment” in nonischemic patients who undergo cardiac CT or electrocardiogram-gated chest CT before procedures such as arrhythmia ablation or valve repair, it states.
Such patients found with subclinical coronary atherosclerosis might potentially “benefit from referral to intensified cardiovascular primary prevention therapy,” write the authors, led by Andreas Fuchs, MD, PhD, Copenhagen University Hospital-Rigshospitalet.
The group acknowledges the findings may not entirely apply to a non-Danish population.
A screening role for CTA?
Whether CTA has a role to play in adults without symptoms “is a big, open question in the field right now,” observed Ron Blankstein, MD, not associated with the current analysis, for this news organization.
Most population studies of CV risk prediction, such as MESA, have looked at CAC scores, not CTA, and have shown that “the more plaque individuals have, the higher the risk.” The current findings are similar but novel in coming from coronary CTA in a large asymptomatic community population, said Dr. Blankstein, who is director of cardiac CT at Brigham and Women’s Hospital, Boston.
“It’s possible that patients who have obstructive plaque in general tend to have a larger amount of plaque as well,” he said. So, while the study suggests that “the more plaque individuals have, the worse their overall risk,” it also shows that the risk “is enhanced even more if they have obstructive disease.”
The Danish cohort analysis “provides a unique opportunity to study the contemporary natural history of coronary artery disease in the absence of intervention,” notes an accompanying editorial.
For example, both patients and clinicians were blinded to CTA results, and CV preventive therapies weren’t common, observe Michael McDermott, MBChB, and David E. Newby, DM, PhD, of the BHF Centre for Cardiovascular Science, University of Edinburgh.
The analysis suggests that subclinical coronary disease that is obstructive predicts MI risk more strongly than extensive coronary disease, they note, and may be present in two-thirds of MI patients. “This contrasts with symptomatic populations, where nonobstructive disease accounts for most future myocardial infarctions, presumably from plaque rupture.”
It also points to “strong associations between nonobstructive extensive disease and adverse plaque characteristics,” write Dr. McDermott and Dr. Newby. “This underscores the major importance of plaque burden” for the prediction of coronary events.
Graded risk
The analysis included 9,533 persons aged 40 and older without known ischemic heart disease or symptoms with available CTA assessments.
Obstructive disease, defined as presence of a luminal stenosis of at least 50%, was seen in 10% and nonobstructive disease in 36% of the total cohort, the report states.
Disease occupying more than one-third of the coronary tree was considered extensive and less than one-third of the coronaries nonextensive, occurring in 10.5% and 35.8% of the cohort, respectively.
There were 71 MIs and 193 deaths over a median of 3.5 years. The adjusted relative risk for MI, compared with those without coronary atherosclerosis, was:
- 7.65 (95% confidence interval, 3.53-16.57) overall in patients with extensive disease.
- 8.28 (95% CI, 3.75-18.32) in those with obstructive but nonextensive disease.
- 9.19 (95% CI, 4.49-18.82) overall in those with obstructive disease.
- 12.48 (95% CI, 5.50-28.12) in those with or obstructive and extensive disease.
The adjusted RR for the composite of death or MI was also elevated in persons with extensive disease:
- 2.70 (95% CI, 1.72-4.25) in those with extensive but nonobstructive disease.
- 3.15 (95% CI, 2.05-4.83) in those with extensive and obstructive disease.
“It’s one thing to show that the more plaque, the higher the risk,” Dr. Blankstein said. But “does the information ultimately lead to better outcomes? Do patients have fewer MIs or fewer deaths?” Several ongoing randomized trials are exploring these questions.
They include DANE-HEART (Computed Tomography Coronary Angiography for Primary Prevention), projected to enroll about 6,000 participants from the Copenhagen General Population Study cohort who have at least one CV risk factor, and SCOT-HEART 2 (second Computed Tomography Coronary Angiography for the Prevention of Myocardial Infarction), enrolling a similar cohort in Scotland.
The study was supported by grants from AP Møller og Hustru Chastine Mc-Kinney Møllers Fond, the Research Council of Rigshospitalet, and Danish Heart Foundation. Dr. Fuchs reports no relevant financial relationships. Disclosures for the other authors can be found here. Dr. Blankstein recently disclosed serving as a consultant to Amgen, Caristo Diagnostics, Novartis, and Silence Therapeutics. Disclosures for Dr. McDermott and Dr. Newby, who are SCOT-HEART 2 investigators, can be found here.
A version of this article originally appeared on Medscape.com.
About half of middle-aged adults in the community without cardiovascular (CV) symptoms have coronary atherosclerosis by CT angiography (CTA) that puts them at substantial risk for myocardial infarction (MI), suggests a prospective cohort study.
The 10% of participants who had subclinical disease considered obstructive at CTA showed a ninefold increased risk for MI over several years. Obstructive disease seemed to elevate risk more than subclinical disease that wasn’t obstructive but still considered extensive within the coronary arteries.
The findings, based on a Copenhagen General Population Study cohort, are new for CTA but consistent with research based on coronary artery calcium (CAC) scores and other ways to assess CV risk, say researchers.
Although all participants underwent CTA, such imaging isn’t used in the general population for atherosclerosis screening. But the findings may have implications for “opportunistic screening” for subclinical coronary disease at CTA conducted for other reasons, notes the study’s report, published online in the Annals of Internal Medicine.
“Identification of luminal obstructive or extensive subclinical coronary atherosclerosis” could potentially provide “clinically relevant, incremental risk assessment” in nonischemic patients who undergo cardiac CT or electrocardiogram-gated chest CT before procedures such as arrhythmia ablation or valve repair, it states.
Such patients found with subclinical coronary atherosclerosis might potentially “benefit from referral to intensified cardiovascular primary prevention therapy,” write the authors, led by Andreas Fuchs, MD, PhD, Copenhagen University Hospital-Rigshospitalet.
The group acknowledges the findings may not entirely apply to a non-Danish population.
A screening role for CTA?
Whether CTA has a role to play in adults without symptoms “is a big, open question in the field right now,” observed Ron Blankstein, MD, not associated with the current analysis, for this news organization.
Most population studies of CV risk prediction, such as MESA, have looked at CAC scores, not CTA, and have shown that “the more plaque individuals have, the higher the risk.” The current findings are similar but novel in coming from coronary CTA in a large asymptomatic community population, said Dr. Blankstein, who is director of cardiac CT at Brigham and Women’s Hospital, Boston.
“It’s possible that patients who have obstructive plaque in general tend to have a larger amount of plaque as well,” he said. So, while the study suggests that “the more plaque individuals have, the worse their overall risk,” it also shows that the risk “is enhanced even more if they have obstructive disease.”
The Danish cohort analysis “provides a unique opportunity to study the contemporary natural history of coronary artery disease in the absence of intervention,” notes an accompanying editorial.
For example, both patients and clinicians were blinded to CTA results, and CV preventive therapies weren’t common, observe Michael McDermott, MBChB, and David E. Newby, DM, PhD, of the BHF Centre for Cardiovascular Science, University of Edinburgh.
The analysis suggests that subclinical coronary disease that is obstructive predicts MI risk more strongly than extensive coronary disease, they note, and may be present in two-thirds of MI patients. “This contrasts with symptomatic populations, where nonobstructive disease accounts for most future myocardial infarctions, presumably from plaque rupture.”
It also points to “strong associations between nonobstructive extensive disease and adverse plaque characteristics,” write Dr. McDermott and Dr. Newby. “This underscores the major importance of plaque burden” for the prediction of coronary events.
Graded risk
The analysis included 9,533 persons aged 40 and older without known ischemic heart disease or symptoms with available CTA assessments.
Obstructive disease, defined as presence of a luminal stenosis of at least 50%, was seen in 10% and nonobstructive disease in 36% of the total cohort, the report states.
Disease occupying more than one-third of the coronary tree was considered extensive and less than one-third of the coronaries nonextensive, occurring in 10.5% and 35.8% of the cohort, respectively.
There were 71 MIs and 193 deaths over a median of 3.5 years. The adjusted relative risk for MI, compared with those without coronary atherosclerosis, was:
- 7.65 (95% confidence interval, 3.53-16.57) overall in patients with extensive disease.
- 8.28 (95% CI, 3.75-18.32) in those with obstructive but nonextensive disease.
- 9.19 (95% CI, 4.49-18.82) overall in those with obstructive disease.
- 12.48 (95% CI, 5.50-28.12) in those with or obstructive and extensive disease.
The adjusted RR for the composite of death or MI was also elevated in persons with extensive disease:
- 2.70 (95% CI, 1.72-4.25) in those with extensive but nonobstructive disease.
- 3.15 (95% CI, 2.05-4.83) in those with extensive and obstructive disease.
“It’s one thing to show that the more plaque, the higher the risk,” Dr. Blankstein said. But “does the information ultimately lead to better outcomes? Do patients have fewer MIs or fewer deaths?” Several ongoing randomized trials are exploring these questions.
They include DANE-HEART (Computed Tomography Coronary Angiography for Primary Prevention), projected to enroll about 6,000 participants from the Copenhagen General Population Study cohort who have at least one CV risk factor, and SCOT-HEART 2 (second Computed Tomography Coronary Angiography for the Prevention of Myocardial Infarction), enrolling a similar cohort in Scotland.
The study was supported by grants from AP Møller og Hustru Chastine Mc-Kinney Møllers Fond, the Research Council of Rigshospitalet, and Danish Heart Foundation. Dr. Fuchs reports no relevant financial relationships. Disclosures for the other authors can be found here. Dr. Blankstein recently disclosed serving as a consultant to Amgen, Caristo Diagnostics, Novartis, and Silence Therapeutics. Disclosures for Dr. McDermott and Dr. Newby, who are SCOT-HEART 2 investigators, can be found here.
A version of this article originally appeared on Medscape.com.
COVID can mimic prostate cancer symptoms
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.
This patient has a strong likelihood of aggressive prostate cancer, right? If that same patient also presents with severe, burning bone pain with no precipitating trauma to the area and rest and over-the-counter painkillers are not helping, you’d think, “check for metastases,” right?
That patient was me in late January 2023.
As a research scientist member of the American Urological Association, I knew enough to know I had to consult my urologist ASAP.
With the above symptoms, I’ll admit I was scared. Fortunately, if that’s the right word, I was no stranger to a rapid, dramatic spike in PSA. In 2021 I was temporarily living in a new city, and I wanted to form a relationship with a good local urologist. The urologist that I was referred to gave me a thorough consultation, including a vigorous digital rectal exam (DRE) and sent me across the street for a blood draw.
To my shock, my PSA had spiked over 2 points, to 9.9 from 7.8 a few months earlier. I freaked. Had my 3-cm tumor burst out into an aggressive cancer? Research on PubMed provided an array of studies showing what could cause PSA to suddenly rise, including a DRE performed 72 hours before the blood draw.1 A week later, my PSA was back down to its normal 7.6.
But in January 2023, I had none of those previously reported experiences that could suddenly trigger a spike in PSA, like a DRE or riding on a thin bicycle seat for a few hours before the lab visit.
The COVID effect
I went back to PubMed and found a new circumstance that could cause a surge in PSA: COVID-19. A recent study2 of 91 men with benign prostatic hypertrophy by researchers in Turkey found that PSA spiked from 0 to 5 points during the COVID infection period and up to 2 points higher 3 months after the infection had cleared. I had tested positive for COVID-19 in mid-December 2022, 4 weeks before my 9.9 PSA reading.
Using Google translate, I communicated with the team in Turkey and found out that the PSA spike can last up to 6 months.
That study helps explain why my PSA dropped over 1.5 points to 8.5 just 2 weeks after the 9.9 reading, with the expectation that it would return to its previous normal of 7.8 within 6 months of infection with SARS-CoV-2. To be safe, my urologist scheduled another PSA test in May, along with an updated multiparametric MRI, which may be followed by an in-bore MRI-guided biopsy of the 3-cm tumor if the mass has enlarged.
COVID-19 pain
What about my burning bone pain in my upper right humerus and right rotator cuff that was not precipitated by trauma or strain? A radiograph found no evidence of metastasis, thank goodness. And my research showed that several studies3 have found that COVID-19 can cause burning musculoskeletal pain, including enthesopathy, which is what I had per the radiology report. So my PSA spike and searing pain were likely consequences of the infection.
To avoid the risk for a gross misdiagnosis after a radical spike in PSA, the informed urologist should ask the patient if he has had COVID-19 in the previous 6 months. Overlooking that question could lead to the wrong diagnostic decisions about a rapid jump in PSA or unexplained bone pain.
References
1. Bossens MM et al. Eur J Cancer. 1995;31A:682-5.
2. Cinislioglu AE et al. Urology. 2022;159:16-21.
3. Ciaffi J et al. Joint Bone Spine. 2021;88:105158.
Dr. Keller is founder of the Keller Research Institute, Jacksonville, Fla. He reported serving as a research scientist for the American Urological Association, serving on the advisory board of Active Surveillance Patient’s International, and serving on the boards of numerous nonprofit organizations.
A version of this article first appeared on Medscape.com.