User login
App links overdosing people to nearby volunteers with naloxone
Naloxone can reverse opioid overdoses, but time is crucial and its effectiveness wanes if medics can’t arrive right away. Now, a new app links overdose victims or their companions to trained volunteers nearby who may be able to administer the drug much faster.
Over a 1-year period, about half of 112 participants in a Philadelphia trial said they’d responded to overdoses via the app, and about half used it to report overdoses, according to a study released at the virtual annual meeting of the College on Problems of Drug Dependence.
“Thanks to the app, there may have been a life saved about twice a month that otherwise wouldn’t have been,” said public health researcher and study coauthor Stephen Lankenau, PhD, of Drexel University, Philadelphia, in an interview.
Philadelphia has the largest opioid overdose rate of any large city, Dr. Lankenau said, and people who overdose are often reluctant to call 911. “Police are often alerted when it’s determined that it’s a drug-related call. They’re concerned that police could show up and someone will get arrested.”
However, the app, called UnityPhilly, doesn’t remove professional medics from the picture. It’s designed to be a supplement to the existing first-response system – “it’s not meant to replace 911” – and allow a faster response to overdoses when minutes matter, Dr. Lankenau said.
“If someone is adamantly opposed to calling 911,” he said, “this may not be the best intervention for them.”
Here’s how the app works: Participants who overdose themselves or witness an overdose can send out an alert to nearby app users. When an alert goes out, the app also attempts to dial 911, although the participant can bypass this.
Nearby responders can reply by pressing “En route” and then go to the address of the overdose with a provided supply of naloxone (Narcan). The amateur responders, many of whom are or were opioid users themselves, are trained in how to administer the drug.
The study authors recruited 112 participants from the Philadelphia neighborhood of Kensington and tracked them from 2019 to 2020. About half (n = 57) reported using opioids within the past 30 days, and those participants had an average age of 42 years, were 54% men, and were 74% non-Hispanic white. Only 19% were employed, and 42% had been recently homeless. Nearly 80% had overdosed before, and all had witnessed overdoses.
The other participants (n = 55), defined as “community members,” had less experience with opioids (44% had misused them before), although 91% had witnessed overdoses. Their average age was 42 years, 56% were women, 53% were employed, and 16% had been recently homeless.
The percentages who reported being en route to an overdose was 47% (opioid users) and 46% (community members).
“The idea of people being trained as community responders has been around for quite a while, and there are hundreds of programs across the country. People are willing to carry naloxone and respond if they see an overdose in front of them,” Dr. Lankenau said. “Here, you have people becoming civilian responders to events they wouldn’t otherwise know about. This creates a community of individuals who can help out immediately and augment the work that emergency responders do.”
Opioid users who download the app may be drawn to the idea of responders who are nonjudgmental and supportive, compared with professional medics. “The system has not done well by people with substance abuse disorders,” said addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver. “In terms of overdose reversal, you may prefer that someone else [other than a medic] give you Narcan and support you through this experience. When it’s over after you’re reversed, you have a sudden onset of withdrawal symptoms. You feel terrible, and you don’t want to be sitting in an ambulance. You want to be in a supportive environment.”
As for adverse effects, there was concern that opioid users might take more risks with an app safety net in place. However, no one reported more risky behavior in interviews, Dr. Lankenau said.
The 3-year program costs $215,000, he said, and the next step is to get funding for a Philadelphia citywide trial.
The study was funded by the National Institute of Drug Abuse. Dr. Lankenau reported no relevant disclosures. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by NIDA.
Naloxone can reverse opioid overdoses, but time is crucial and its effectiveness wanes if medics can’t arrive right away. Now, a new app links overdose victims or their companions to trained volunteers nearby who may be able to administer the drug much faster.
Over a 1-year period, about half of 112 participants in a Philadelphia trial said they’d responded to overdoses via the app, and about half used it to report overdoses, according to a study released at the virtual annual meeting of the College on Problems of Drug Dependence.
“Thanks to the app, there may have been a life saved about twice a month that otherwise wouldn’t have been,” said public health researcher and study coauthor Stephen Lankenau, PhD, of Drexel University, Philadelphia, in an interview.
Philadelphia has the largest opioid overdose rate of any large city, Dr. Lankenau said, and people who overdose are often reluctant to call 911. “Police are often alerted when it’s determined that it’s a drug-related call. They’re concerned that police could show up and someone will get arrested.”
However, the app, called UnityPhilly, doesn’t remove professional medics from the picture. It’s designed to be a supplement to the existing first-response system – “it’s not meant to replace 911” – and allow a faster response to overdoses when minutes matter, Dr. Lankenau said.
“If someone is adamantly opposed to calling 911,” he said, “this may not be the best intervention for them.”
Here’s how the app works: Participants who overdose themselves or witness an overdose can send out an alert to nearby app users. When an alert goes out, the app also attempts to dial 911, although the participant can bypass this.
Nearby responders can reply by pressing “En route” and then go to the address of the overdose with a provided supply of naloxone (Narcan). The amateur responders, many of whom are or were opioid users themselves, are trained in how to administer the drug.
The study authors recruited 112 participants from the Philadelphia neighborhood of Kensington and tracked them from 2019 to 2020. About half (n = 57) reported using opioids within the past 30 days, and those participants had an average age of 42 years, were 54% men, and were 74% non-Hispanic white. Only 19% were employed, and 42% had been recently homeless. Nearly 80% had overdosed before, and all had witnessed overdoses.
The other participants (n = 55), defined as “community members,” had less experience with opioids (44% had misused them before), although 91% had witnessed overdoses. Their average age was 42 years, 56% were women, 53% were employed, and 16% had been recently homeless.
The percentages who reported being en route to an overdose was 47% (opioid users) and 46% (community members).
“The idea of people being trained as community responders has been around for quite a while, and there are hundreds of programs across the country. People are willing to carry naloxone and respond if they see an overdose in front of them,” Dr. Lankenau said. “Here, you have people becoming civilian responders to events they wouldn’t otherwise know about. This creates a community of individuals who can help out immediately and augment the work that emergency responders do.”
Opioid users who download the app may be drawn to the idea of responders who are nonjudgmental and supportive, compared with professional medics. “The system has not done well by people with substance abuse disorders,” said addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver. “In terms of overdose reversal, you may prefer that someone else [other than a medic] give you Narcan and support you through this experience. When it’s over after you’re reversed, you have a sudden onset of withdrawal symptoms. You feel terrible, and you don’t want to be sitting in an ambulance. You want to be in a supportive environment.”
As for adverse effects, there was concern that opioid users might take more risks with an app safety net in place. However, no one reported more risky behavior in interviews, Dr. Lankenau said.
The 3-year program costs $215,000, he said, and the next step is to get funding for a Philadelphia citywide trial.
The study was funded by the National Institute of Drug Abuse. Dr. Lankenau reported no relevant disclosures. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by NIDA.
Naloxone can reverse opioid overdoses, but time is crucial and its effectiveness wanes if medics can’t arrive right away. Now, a new app links overdose victims or their companions to trained volunteers nearby who may be able to administer the drug much faster.
Over a 1-year period, about half of 112 participants in a Philadelphia trial said they’d responded to overdoses via the app, and about half used it to report overdoses, according to a study released at the virtual annual meeting of the College on Problems of Drug Dependence.
“Thanks to the app, there may have been a life saved about twice a month that otherwise wouldn’t have been,” said public health researcher and study coauthor Stephen Lankenau, PhD, of Drexel University, Philadelphia, in an interview.
Philadelphia has the largest opioid overdose rate of any large city, Dr. Lankenau said, and people who overdose are often reluctant to call 911. “Police are often alerted when it’s determined that it’s a drug-related call. They’re concerned that police could show up and someone will get arrested.”
However, the app, called UnityPhilly, doesn’t remove professional medics from the picture. It’s designed to be a supplement to the existing first-response system – “it’s not meant to replace 911” – and allow a faster response to overdoses when minutes matter, Dr. Lankenau said.
“If someone is adamantly opposed to calling 911,” he said, “this may not be the best intervention for them.”
Here’s how the app works: Participants who overdose themselves or witness an overdose can send out an alert to nearby app users. When an alert goes out, the app also attempts to dial 911, although the participant can bypass this.
Nearby responders can reply by pressing “En route” and then go to the address of the overdose with a provided supply of naloxone (Narcan). The amateur responders, many of whom are or were opioid users themselves, are trained in how to administer the drug.
The study authors recruited 112 participants from the Philadelphia neighborhood of Kensington and tracked them from 2019 to 2020. About half (n = 57) reported using opioids within the past 30 days, and those participants had an average age of 42 years, were 54% men, and were 74% non-Hispanic white. Only 19% were employed, and 42% had been recently homeless. Nearly 80% had overdosed before, and all had witnessed overdoses.
The other participants (n = 55), defined as “community members,” had less experience with opioids (44% had misused them before), although 91% had witnessed overdoses. Their average age was 42 years, 56% were women, 53% were employed, and 16% had been recently homeless.
The percentages who reported being en route to an overdose was 47% (opioid users) and 46% (community members).
“The idea of people being trained as community responders has been around for quite a while, and there are hundreds of programs across the country. People are willing to carry naloxone and respond if they see an overdose in front of them,” Dr. Lankenau said. “Here, you have people becoming civilian responders to events they wouldn’t otherwise know about. This creates a community of individuals who can help out immediately and augment the work that emergency responders do.”
Opioid users who download the app may be drawn to the idea of responders who are nonjudgmental and supportive, compared with professional medics. “The system has not done well by people with substance abuse disorders,” said addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver. “In terms of overdose reversal, you may prefer that someone else [other than a medic] give you Narcan and support you through this experience. When it’s over after you’re reversed, you have a sudden onset of withdrawal symptoms. You feel terrible, and you don’t want to be sitting in an ambulance. You want to be in a supportive environment.”
As for adverse effects, there was concern that opioid users might take more risks with an app safety net in place. However, no one reported more risky behavior in interviews, Dr. Lankenau said.
The 3-year program costs $215,000, he said, and the next step is to get funding for a Philadelphia citywide trial.
The study was funded by the National Institute of Drug Abuse. Dr. Lankenau reported no relevant disclosures. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by NIDA.
FROM CPDD 2020
Take-home test strips allow drug users to detect fentanyl
Illicit drug users seem to overwhelmingly appreciate being able to use take-home test strips to detect the extremely common presence of dangerous fentanyl in opioids and other drugs, a new study finds. More than 95% said they’d use the inexpensive strips again.
said study lead author addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver, in an interview.
Dr. Klaire presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
Researchers in Vancouver distributed take-home fentanyl test strip kits at 10 sites that allow users to test their illicit drugs. The 218 participants performed 1,680 tests, mainly (73%) for opioids, over 3 months in 2019. Of the participants, 61% were male, and the average age was 36 (interquartile range, 29-47). About 30% described themselves as indigenous Canadians (First Nations).
About 90% of the opioid samples tested at home were positive for fentanyl, about the same level as samples tested at clinics. Fentanyl is very potent and linked to the huge rise in overdose deaths in the United States.
Fentanyl test strips aren’t new. According to the Harm Reduction Coalition, they originally were developed to detect fentanyl in urine samples but were jury-rigged in Vancouver to work on samples of illicit drugs. “We literally just repurposed it,” Dr. Klaire said. “It’s the same strip.”
Users test their drugs by dissolving a small sample in water. Then then dip the test strip, which provides readings similar to those in a pregnancy test. If a sample turns up positive for fentanyl, Dr. Klaire said, users may discard the drug or “be more careful with it.”
When asked what they would do if a sample turned up positive, 27% said they’d make a “positive change,” such as using less or using more slowly (n = 45) or making sure that someone else is present in case of an overdose (n = 26). But most, 71%, reported no change in behavior.
Previously, researchers in Rhode Island and North Carolina also found that some users adopted safer behaviors – such as throwing out their drugs or using less often – after testing their drugs with the strips.
The strips cost about 75 cents, Dr. Klaire said.
Harm-reduction strategies are controversial, and fentanyl test strips aren’t any exemption. “The entire approach is based on the premise that a drug user poised to use a drug is making rational choices, is weighing pros and cons, and is thinking completely logically about his or her drug use. Based on my clinical experience, I know this could not be further from the truth,” wrote Elinore F. McCance-Katz, MD, PhD, assistant secretary for Mental Health and Substance Use with the Department of Health & Human Services, in a 2018 blog post.
But Dr. Klaire said the patients in the new study are highly dependent on opioids. “The drug supply is heavily contaminated [with fentanyl],” he said, “but even when people know it’s contaminated, they still need to go ahead and use it.”
In an interview, epidemiologist Brandon Marshall, PhD, of Brown University, Providence, R.I., who has conducted fentanyl test strip research, called the study results “compelling.”
“The researchers found that the fentanyl test strips had a very high level of acceptability – over 95% said they would use the strips again – which is remarkably similar to what we found in our work here in Rhode Island,” he said. “Taken together, these studies show that take-home test strips are a feasible, acceptable, and effective strategy for people who use drugs to reduce their risk of fentanyl overdose.”
He added that “fentanyl test strips help people make more informed decisions about their drug use and reducing their risk of overdose.”
However, he said, “one of important limitations of the strips is that they do not detect all contaminants that put persons at risk of overdose. Just because a test result is negative does not mean that the drug is 100% safe.”
Kimberly Sue, MD, PhD, medical director of the National Harm Reduction Coalition, said in an interview that the research is “important,” but noted that many drug users already have been using fentanyl test strips on their own. “We should be focusing on investing in variety of other interventions that could keep more people safe against nonfatal and fatal opioid overdoses, including structural interventions such as safe supply, housing and community with appropriate supports, low barrier access to medication for opioid use disorder, and safe consumption spaces,” she said.
No study funding was reported. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by the National Institute of Drug Abuse. Dr. Sue reported no relevant disclosures. Dr. Marshall reported that he has collaborated frequently with one of the coauthors of the Vancouver study.
Illicit drug users seem to overwhelmingly appreciate being able to use take-home test strips to detect the extremely common presence of dangerous fentanyl in opioids and other drugs, a new study finds. More than 95% said they’d use the inexpensive strips again.
said study lead author addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver, in an interview.
Dr. Klaire presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
Researchers in Vancouver distributed take-home fentanyl test strip kits at 10 sites that allow users to test their illicit drugs. The 218 participants performed 1,680 tests, mainly (73%) for opioids, over 3 months in 2019. Of the participants, 61% were male, and the average age was 36 (interquartile range, 29-47). About 30% described themselves as indigenous Canadians (First Nations).
About 90% of the opioid samples tested at home were positive for fentanyl, about the same level as samples tested at clinics. Fentanyl is very potent and linked to the huge rise in overdose deaths in the United States.
Fentanyl test strips aren’t new. According to the Harm Reduction Coalition, they originally were developed to detect fentanyl in urine samples but were jury-rigged in Vancouver to work on samples of illicit drugs. “We literally just repurposed it,” Dr. Klaire said. “It’s the same strip.”
Users test their drugs by dissolving a small sample in water. Then then dip the test strip, which provides readings similar to those in a pregnancy test. If a sample turns up positive for fentanyl, Dr. Klaire said, users may discard the drug or “be more careful with it.”
When asked what they would do if a sample turned up positive, 27% said they’d make a “positive change,” such as using less or using more slowly (n = 45) or making sure that someone else is present in case of an overdose (n = 26). But most, 71%, reported no change in behavior.
Previously, researchers in Rhode Island and North Carolina also found that some users adopted safer behaviors – such as throwing out their drugs or using less often – after testing their drugs with the strips.
The strips cost about 75 cents, Dr. Klaire said.
Harm-reduction strategies are controversial, and fentanyl test strips aren’t any exemption. “The entire approach is based on the premise that a drug user poised to use a drug is making rational choices, is weighing pros and cons, and is thinking completely logically about his or her drug use. Based on my clinical experience, I know this could not be further from the truth,” wrote Elinore F. McCance-Katz, MD, PhD, assistant secretary for Mental Health and Substance Use with the Department of Health & Human Services, in a 2018 blog post.
But Dr. Klaire said the patients in the new study are highly dependent on opioids. “The drug supply is heavily contaminated [with fentanyl],” he said, “but even when people know it’s contaminated, they still need to go ahead and use it.”
In an interview, epidemiologist Brandon Marshall, PhD, of Brown University, Providence, R.I., who has conducted fentanyl test strip research, called the study results “compelling.”
“The researchers found that the fentanyl test strips had a very high level of acceptability – over 95% said they would use the strips again – which is remarkably similar to what we found in our work here in Rhode Island,” he said. “Taken together, these studies show that take-home test strips are a feasible, acceptable, and effective strategy for people who use drugs to reduce their risk of fentanyl overdose.”
He added that “fentanyl test strips help people make more informed decisions about their drug use and reducing their risk of overdose.”
However, he said, “one of important limitations of the strips is that they do not detect all contaminants that put persons at risk of overdose. Just because a test result is negative does not mean that the drug is 100% safe.”
Kimberly Sue, MD, PhD, medical director of the National Harm Reduction Coalition, said in an interview that the research is “important,” but noted that many drug users already have been using fentanyl test strips on their own. “We should be focusing on investing in variety of other interventions that could keep more people safe against nonfatal and fatal opioid overdoses, including structural interventions such as safe supply, housing and community with appropriate supports, low barrier access to medication for opioid use disorder, and safe consumption spaces,” she said.
No study funding was reported. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by the National Institute of Drug Abuse. Dr. Sue reported no relevant disclosures. Dr. Marshall reported that he has collaborated frequently with one of the coauthors of the Vancouver study.
Illicit drug users seem to overwhelmingly appreciate being able to use take-home test strips to detect the extremely common presence of dangerous fentanyl in opioids and other drugs, a new study finds. More than 95% said they’d use the inexpensive strips again.
said study lead author addiction medicine specialist Sukhpreet Klaire, MD, of the British Columbia Center on Substance Use in Vancouver, in an interview.
Dr. Klaire presented the study findings at the virtual annual meeting of the College on Problems of Drug Dependence.
Researchers in Vancouver distributed take-home fentanyl test strip kits at 10 sites that allow users to test their illicit drugs. The 218 participants performed 1,680 tests, mainly (73%) for opioids, over 3 months in 2019. Of the participants, 61% were male, and the average age was 36 (interquartile range, 29-47). About 30% described themselves as indigenous Canadians (First Nations).
About 90% of the opioid samples tested at home were positive for fentanyl, about the same level as samples tested at clinics. Fentanyl is very potent and linked to the huge rise in overdose deaths in the United States.
Fentanyl test strips aren’t new. According to the Harm Reduction Coalition, they originally were developed to detect fentanyl in urine samples but were jury-rigged in Vancouver to work on samples of illicit drugs. “We literally just repurposed it,” Dr. Klaire said. “It’s the same strip.”
Users test their drugs by dissolving a small sample in water. Then then dip the test strip, which provides readings similar to those in a pregnancy test. If a sample turns up positive for fentanyl, Dr. Klaire said, users may discard the drug or “be more careful with it.”
When asked what they would do if a sample turned up positive, 27% said they’d make a “positive change,” such as using less or using more slowly (n = 45) or making sure that someone else is present in case of an overdose (n = 26). But most, 71%, reported no change in behavior.
Previously, researchers in Rhode Island and North Carolina also found that some users adopted safer behaviors – such as throwing out their drugs or using less often – after testing their drugs with the strips.
The strips cost about 75 cents, Dr. Klaire said.
Harm-reduction strategies are controversial, and fentanyl test strips aren’t any exemption. “The entire approach is based on the premise that a drug user poised to use a drug is making rational choices, is weighing pros and cons, and is thinking completely logically about his or her drug use. Based on my clinical experience, I know this could not be further from the truth,” wrote Elinore F. McCance-Katz, MD, PhD, assistant secretary for Mental Health and Substance Use with the Department of Health & Human Services, in a 2018 blog post.
But Dr. Klaire said the patients in the new study are highly dependent on opioids. “The drug supply is heavily contaminated [with fentanyl],” he said, “but even when people know it’s contaminated, they still need to go ahead and use it.”
In an interview, epidemiologist Brandon Marshall, PhD, of Brown University, Providence, R.I., who has conducted fentanyl test strip research, called the study results “compelling.”
“The researchers found that the fentanyl test strips had a very high level of acceptability – over 95% said they would use the strips again – which is remarkably similar to what we found in our work here in Rhode Island,” he said. “Taken together, these studies show that take-home test strips are a feasible, acceptable, and effective strategy for people who use drugs to reduce their risk of fentanyl overdose.”
He added that “fentanyl test strips help people make more informed decisions about their drug use and reducing their risk of overdose.”
However, he said, “one of important limitations of the strips is that they do not detect all contaminants that put persons at risk of overdose. Just because a test result is negative does not mean that the drug is 100% safe.”
Kimberly Sue, MD, PhD, medical director of the National Harm Reduction Coalition, said in an interview that the research is “important,” but noted that many drug users already have been using fentanyl test strips on their own. “We should be focusing on investing in variety of other interventions that could keep more people safe against nonfatal and fatal opioid overdoses, including structural interventions such as safe supply, housing and community with appropriate supports, low barrier access to medication for opioid use disorder, and safe consumption spaces,” she said.
No study funding was reported. Dr. Klaire disclosed participating in a research fellowship and a research in addiction medical scholars program, both funded by the National Institute of Drug Abuse. Dr. Sue reported no relevant disclosures. Dr. Marshall reported that he has collaborated frequently with one of the coauthors of the Vancouver study.
FROM CPDD 2020
Topline results for novel intranasal med to treat opioid overdose
Topline results show positive results for the experimental intranasal nalmefene product OX125 for opioid overdose reversal, Orexo, the drug’s manufacturer, announced on June 30.
A crossover, comparative bioavailability study was conducted in healthy volunteers to assess nalmefene absorption of three development formulations of OX125. Preliminary results showed “extensive and rapid absorption” across all three formulations versus an intramuscular injection of nalmefene, Orexo reported.
“As the U.S. heroin crisis has developed to a fentanyl crisis, the medical need for novel and more powerful opioid rescue medications is vast,” Nikolaj Sørensen, president and CEO of Orexo, said in a press release.
“The need has also escalated due to the COVID-19 pandemic as the consequences of social distancing and economic weakness are expected to lead to a significant increase in mental health issues and substance use disorders,” Mr. Sørensen added.
Robert Rönn, vice president and head of research and development at Orexo, noted in the same release that the company will now be working with the Food and Drug Administration “to identify the optimal route to market.”
There were more than 31,000 fatalities from highly potent synthetic opioids in the United States in 2018, the manufacturer reported. “Like naloxone, nalmefene is an opioid antagonist that acts by blocking the effects of opioids at the opioid receptors.”
However, nalmefene has a longer half-life than naloxone. These longer-acting properties may be “of particular value to protect against renarcotization (second overdose), as the antagonist wears off,” according to an Orexo press release.
In addition to showing rapid absorption across all formulations studied, study results showed “good tolerability, supporting the viability” of the treatment as an opioid overdose rescue medication, the company said.
“This is not only a proof of concept for our wholly owned OX125 product, but also a demonstration of the value of our novel nasal technology platform,” Mr. Rönn said.
“Alongside OX124, our naloxone rescue project, OX125 will be an important lifesaving addition in our commitment to helping patients suffering from opioid addiction in all phases,” Mr. Sørensen added.
A version of this article originally appeared on Medscape.com.
Topline results show positive results for the experimental intranasal nalmefene product OX125 for opioid overdose reversal, Orexo, the drug’s manufacturer, announced on June 30.
A crossover, comparative bioavailability study was conducted in healthy volunteers to assess nalmefene absorption of three development formulations of OX125. Preliminary results showed “extensive and rapid absorption” across all three formulations versus an intramuscular injection of nalmefene, Orexo reported.
“As the U.S. heroin crisis has developed to a fentanyl crisis, the medical need for novel and more powerful opioid rescue medications is vast,” Nikolaj Sørensen, president and CEO of Orexo, said in a press release.
“The need has also escalated due to the COVID-19 pandemic as the consequences of social distancing and economic weakness are expected to lead to a significant increase in mental health issues and substance use disorders,” Mr. Sørensen added.
Robert Rönn, vice president and head of research and development at Orexo, noted in the same release that the company will now be working with the Food and Drug Administration “to identify the optimal route to market.”
There were more than 31,000 fatalities from highly potent synthetic opioids in the United States in 2018, the manufacturer reported. “Like naloxone, nalmefene is an opioid antagonist that acts by blocking the effects of opioids at the opioid receptors.”
However, nalmefene has a longer half-life than naloxone. These longer-acting properties may be “of particular value to protect against renarcotization (second overdose), as the antagonist wears off,” according to an Orexo press release.
In addition to showing rapid absorption across all formulations studied, study results showed “good tolerability, supporting the viability” of the treatment as an opioid overdose rescue medication, the company said.
“This is not only a proof of concept for our wholly owned OX125 product, but also a demonstration of the value of our novel nasal technology platform,” Mr. Rönn said.
“Alongside OX124, our naloxone rescue project, OX125 will be an important lifesaving addition in our commitment to helping patients suffering from opioid addiction in all phases,” Mr. Sørensen added.
A version of this article originally appeared on Medscape.com.
Topline results show positive results for the experimental intranasal nalmefene product OX125 for opioid overdose reversal, Orexo, the drug’s manufacturer, announced on June 30.
A crossover, comparative bioavailability study was conducted in healthy volunteers to assess nalmefene absorption of three development formulations of OX125. Preliminary results showed “extensive and rapid absorption” across all three formulations versus an intramuscular injection of nalmefene, Orexo reported.
“As the U.S. heroin crisis has developed to a fentanyl crisis, the medical need for novel and more powerful opioid rescue medications is vast,” Nikolaj Sørensen, president and CEO of Orexo, said in a press release.
“The need has also escalated due to the COVID-19 pandemic as the consequences of social distancing and economic weakness are expected to lead to a significant increase in mental health issues and substance use disorders,” Mr. Sørensen added.
Robert Rönn, vice president and head of research and development at Orexo, noted in the same release that the company will now be working with the Food and Drug Administration “to identify the optimal route to market.”
There were more than 31,000 fatalities from highly potent synthetic opioids in the United States in 2018, the manufacturer reported. “Like naloxone, nalmefene is an opioid antagonist that acts by blocking the effects of opioids at the opioid receptors.”
However, nalmefene has a longer half-life than naloxone. These longer-acting properties may be “of particular value to protect against renarcotization (second overdose), as the antagonist wears off,” according to an Orexo press release.
In addition to showing rapid absorption across all formulations studied, study results showed “good tolerability, supporting the viability” of the treatment as an opioid overdose rescue medication, the company said.
“This is not only a proof of concept for our wholly owned OX125 product, but also a demonstration of the value of our novel nasal technology platform,” Mr. Rönn said.
“Alongside OX124, our naloxone rescue project, OX125 will be an important lifesaving addition in our commitment to helping patients suffering from opioid addiction in all phases,” Mr. Sørensen added.
A version of this article originally appeared on Medscape.com.
Pursue multimodal pain management in patients taking opioids
For surgical patients on chronic opioid therapy, , according to Stephanie B. Jones, MD, professor and chair of anesthesiology at Albany Medical College, New York.
“[With] any patient coming in for any sort of surgery, you should be considering multimodal pain management. That applies to the opioid use disorder patient as well,” Dr. Jones said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
“The challenge of opioid-tolerant patients or opioid abuse patients is twofold – tolerance and hyperalgesia,” Dr. Jones said. Patient tolerance changes how patients perceive pain and respond to medication. Clinicians need to consider the “opioid debt,” defined as the daily amount of opioid medication required by opioid-dependent patients to maintain their usual prehospitalization opioid levels, she explained. Also consider hyperalgesia, a change in pain perception “resulting in an increase in pain sensitivity to painful stimuli, thereby decreasing the analgesic effects of opioids,” Dr. Jones added.
A multimodal approach to pain management in patients on chronic opioids can include some opioids as appropriate, Dr. Jones said. Modulation of pain may draw on epidurals and nerve blocks, as well as managing CNS perception of pain through opioids or acetaminophen, and also using systemic options such as alpha-2 agonists and tramadol, she said.
Studies have shown that opioid abuse or dependence were associated with increased readmission rates, length of stay, and health care costs in surgery patients, said Dr. Jones. However, switching opioids and managing equivalents is complex, and “equianalgesic conversions serve only as a general guide to estimate opioid dose equivalents,” according to UpToDate’s, “Management of acute pain in the patient chronically using opioids,” she said.
Dr. Jones also addressed the issue of using hospitalization as an opportunity to help patients with untreated opioid use disorder. Medication-assisted options include methadone, buprenorphine, and naltrexone.
“One problem with methadone is that there are a lot of medications interactions,” she said. Buprenorphine has the advantage of being long-lasting, and is formulated with naloxone which deters injection. “Because it is a partial agonist, there is a lower risk of overdose and sedation,” and it has fewer medication interactions. However, some doctors are reluctant to prescribe it and there is some risk of medication diversion, she said.
Naltrexone is newer to the role of treating opioid use disorder, Dr. Jones said. “It can cause acute withdrawal because it is a full opioid antagonist,” she noted. However, naltrexone itself causes no withdrawal if stopped, and no respiratory depression or sedation, said Dr. Jones.
“Utilize addiction services in your hospital if you suspect a patient may be at risk for opioid use disorder,” and engage these services early, she emphasized.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Dr. Jones had no financial conflicts to disclose.
For surgical patients on chronic opioid therapy, , according to Stephanie B. Jones, MD, professor and chair of anesthesiology at Albany Medical College, New York.
“[With] any patient coming in for any sort of surgery, you should be considering multimodal pain management. That applies to the opioid use disorder patient as well,” Dr. Jones said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
“The challenge of opioid-tolerant patients or opioid abuse patients is twofold – tolerance and hyperalgesia,” Dr. Jones said. Patient tolerance changes how patients perceive pain and respond to medication. Clinicians need to consider the “opioid debt,” defined as the daily amount of opioid medication required by opioid-dependent patients to maintain their usual prehospitalization opioid levels, she explained. Also consider hyperalgesia, a change in pain perception “resulting in an increase in pain sensitivity to painful stimuli, thereby decreasing the analgesic effects of opioids,” Dr. Jones added.
A multimodal approach to pain management in patients on chronic opioids can include some opioids as appropriate, Dr. Jones said. Modulation of pain may draw on epidurals and nerve blocks, as well as managing CNS perception of pain through opioids or acetaminophen, and also using systemic options such as alpha-2 agonists and tramadol, she said.
Studies have shown that opioid abuse or dependence were associated with increased readmission rates, length of stay, and health care costs in surgery patients, said Dr. Jones. However, switching opioids and managing equivalents is complex, and “equianalgesic conversions serve only as a general guide to estimate opioid dose equivalents,” according to UpToDate’s, “Management of acute pain in the patient chronically using opioids,” she said.
Dr. Jones also addressed the issue of using hospitalization as an opportunity to help patients with untreated opioid use disorder. Medication-assisted options include methadone, buprenorphine, and naltrexone.
“One problem with methadone is that there are a lot of medications interactions,” she said. Buprenorphine has the advantage of being long-lasting, and is formulated with naloxone which deters injection. “Because it is a partial agonist, there is a lower risk of overdose and sedation,” and it has fewer medication interactions. However, some doctors are reluctant to prescribe it and there is some risk of medication diversion, she said.
Naltrexone is newer to the role of treating opioid use disorder, Dr. Jones said. “It can cause acute withdrawal because it is a full opioid antagonist,” she noted. However, naltrexone itself causes no withdrawal if stopped, and no respiratory depression or sedation, said Dr. Jones.
“Utilize addiction services in your hospital if you suspect a patient may be at risk for opioid use disorder,” and engage these services early, she emphasized.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Dr. Jones had no financial conflicts to disclose.
For surgical patients on chronic opioid therapy, , according to Stephanie B. Jones, MD, professor and chair of anesthesiology at Albany Medical College, New York.
“[With] any patient coming in for any sort of surgery, you should be considering multimodal pain management. That applies to the opioid use disorder patient as well,” Dr. Jones said in a presentation at the virtual Annual Minimally Invasive Surgery Symposium sponsored by Global Academy for Medical Education.
“The challenge of opioid-tolerant patients or opioid abuse patients is twofold – tolerance and hyperalgesia,” Dr. Jones said. Patient tolerance changes how patients perceive pain and respond to medication. Clinicians need to consider the “opioid debt,” defined as the daily amount of opioid medication required by opioid-dependent patients to maintain their usual prehospitalization opioid levels, she explained. Also consider hyperalgesia, a change in pain perception “resulting in an increase in pain sensitivity to painful stimuli, thereby decreasing the analgesic effects of opioids,” Dr. Jones added.
A multimodal approach to pain management in patients on chronic opioids can include some opioids as appropriate, Dr. Jones said. Modulation of pain may draw on epidurals and nerve blocks, as well as managing CNS perception of pain through opioids or acetaminophen, and also using systemic options such as alpha-2 agonists and tramadol, she said.
Studies have shown that opioid abuse or dependence were associated with increased readmission rates, length of stay, and health care costs in surgery patients, said Dr. Jones. However, switching opioids and managing equivalents is complex, and “equianalgesic conversions serve only as a general guide to estimate opioid dose equivalents,” according to UpToDate’s, “Management of acute pain in the patient chronically using opioids,” she said.
Dr. Jones also addressed the issue of using hospitalization as an opportunity to help patients with untreated opioid use disorder. Medication-assisted options include methadone, buprenorphine, and naltrexone.
“One problem with methadone is that there are a lot of medications interactions,” she said. Buprenorphine has the advantage of being long-lasting, and is formulated with naloxone which deters injection. “Because it is a partial agonist, there is a lower risk of overdose and sedation,” and it has fewer medication interactions. However, some doctors are reluctant to prescribe it and there is some risk of medication diversion, she said.
Naltrexone is newer to the role of treating opioid use disorder, Dr. Jones said. “It can cause acute withdrawal because it is a full opioid antagonist,” she noted. However, naltrexone itself causes no withdrawal if stopped, and no respiratory depression or sedation, said Dr. Jones.
“Utilize addiction services in your hospital if you suspect a patient may be at risk for opioid use disorder,” and engage these services early, she emphasized.
Global Academy for Medical Education and this news organization are owned by the same parent company.
Dr. Jones had no financial conflicts to disclose.
FROM MISS
New York City inpatient detox unit keeps running: Here’s how
Substance use disorder and its daily consequences take no breaks even during a pandemic. The stressors created by COVID-19, including deaths of loved ones and the disruptions to normal life from policies aimed at flattening the curve, seem to have increased substance use.

I practice as a hospitalist with an internal medicine background and specialty in addiction medicine at BronxCare Health System’s inpatient detoxification unit, a 24/7, 20-bed medically-supervised unit in South Bronx in New York City. It is one of the comprehensive services provided by the BronxCare’s life recovery center and addiction services, which also includes an outpatient clinic, opioid treatment program, inpatient rehab, and a half-way house. Inpatient detoxification units like ours are designed to treat serious addictions and chemical dependency and prevent and treat life-threatening withdrawal symptoms and signs or complications. Our patients come from all over the city and its adjoining suburbs, including from emergency room referrals, referral clinics, courts and the justice system, walk-ins, and self-referrals.
At a time when many inpatient detoxification units within the city were temporarily closed due to fear of inpatient spread of the virus or to provide extra COVID beds in anticipation for the peak surge, we have been able to provide a needed service. In fact, several other inpatient detoxification programs within the city have been able to refer their patients to our facility.
Individuals with substance use disorder have historically been a vulnerable and underserved population and possess high risk for multiple health problems as well as preexisting conditions. Many have limited life options financially, educationally, and with housing, and encounter barriers to accessing primary health care services, including preventive services. The introduction of the COVID-19 pandemic into these patients’ precarious health situations only made things worse as many of the limited resources for patients with substance use disorder were diverted to battling the pandemic. Numerous inpatient and outpatient addiction services, for example, were temporarily shut down. This has led to an increase in domestic violence, and psychiatric decompensation, including psychosis, suicidal attempts, and worsening of medical comorbidities in these patients.
Our wake-up call came when the first case of COVID-19 was confirmed in New York in early March. Within a short period of time the state became the epicenter for COVID-19. With the projection of millions of cases being positive and the number of new cases doubling every third day at the onset in New York City, we knew we had a battle brewing and needed to radically transform our mode of operation fast.
Our first task was to ensure the safety of our patients and the dedicated health workers attending to them. We streamlined the patient point of entry through one screening site, while also brushing up on our history-taking to intently screen for COVID-19. This included not just focusing on travels from China, but from Europe and other parts of the world.
Yes, we did ask patients about cough, fever, shortness of breath or difficulty breathing, feeling fatigued, severe body ache, and possible contact with someone who is sick or has traveled overseas. But we were also attuned to the increased rate of community spread and the presentation of other symptoms, such as loss of taste and smell, early in the process. Hence we were able to triage patients with suspected cases to the appropriate sections of the hospital for further screening, testing, and evaluation, instead of having those patients admitted to the detox unit.
Early in the process a huddle team was instituted with daily briefing of staff lasting 30 minutes or less. This team consists of physicians, nurses, a physician assistant, a social worker, and a counselor. In addition to discussing treatment plans for the patient, they deliberate on the public health information from the hospital’s COVID-19 command center, New York State Department of Health, the Office of Mental Health, and the Centers for Disease Control and Prevention concerning the latest evidence-based information. These discussions have helped us modify our policies and practices.
We instituted a no visiting rule during a short hospital stay of 5-7 days, and this was initiated weeks in advance of many institutions, including nursing homes with vulnerable populations. Our admitting criteria was reviewed to allow for admission of only those patients who absolutely needed inpatient substance use disorder treatment, including patients with severe withdrawal symptoms and signs, comorbidities, or neuropsychiatric manifestations that made them unsafe for outpatient or home detoxification. Others were triaged to the outpatient services which was amply supported with telemedicine. Rooms and designated areas of the building were earmarked as places for isolation/quarantine if suspected COVID-19 cases were identified pending testing. To assess patients’ risk of COVID-19, we do point-of-care nasopharyngeal swab testing with polymerase chain reaction.
Regarding face masks, patients and staff were fitted with ones early in the process. Additionally, staff were trained on the importance of face mask use and how to ensure you have a tight seal around the mouth and nose and were provided with other appropriate personal protective equipment. Concerning social distancing, we reduced the patient population capacity for the unit down to 50% and offered only single room admissions. Social distancing was encouraged in the unit, including in the television and recreation room and dining room, and during small treatment groups of less than six individuals. Daily temperature checks with noncontact handheld thermometers were enforced for staff and anyone coming into the life recovery center.
Patients are continuously being educated on the presentations of COVID-19 and encouraged to report any symptoms. Any staff feeling sick or having symptoms are encouraged to stay home. Rigorous and continuous cleaning of surfaces, especially of areas subjected to common use, is done frequently by the hospital housekeeping and environmental crew and is the order of the day.

Dr. Fagbemi is a hospitalist at BronxCare Health System, a not-for-profit health and teaching hospital system serving South and Central Bronx in New York. He has no conflicts of interest to disclose.
Substance use disorder and its daily consequences take no breaks even during a pandemic. The stressors created by COVID-19, including deaths of loved ones and the disruptions to normal life from policies aimed at flattening the curve, seem to have increased substance use.
I practice as a hospitalist with an internal medicine background and specialty in addiction medicine at BronxCare Health System’s inpatient detoxification unit, a 24/7, 20-bed medically-supervised unit in South Bronx in New York City. It is one of the comprehensive services provided by the BronxCare’s life recovery center and addiction services, which also includes an outpatient clinic, opioid treatment program, inpatient rehab, and a half-way house. Inpatient detoxification units like ours are designed to treat serious addictions and chemical dependency and prevent and treat life-threatening withdrawal symptoms and signs or complications. Our patients come from all over the city and its adjoining suburbs, including from emergency room referrals, referral clinics, courts and the justice system, walk-ins, and self-referrals.
At a time when many inpatient detoxification units within the city were temporarily closed due to fear of inpatient spread of the virus or to provide extra COVID beds in anticipation for the peak surge, we have been able to provide a needed service. In fact, several other inpatient detoxification programs within the city have been able to refer their patients to our facility.
Individuals with substance use disorder have historically been a vulnerable and underserved population and possess high risk for multiple health problems as well as preexisting conditions. Many have limited life options financially, educationally, and with housing, and encounter barriers to accessing primary health care services, including preventive services. The introduction of the COVID-19 pandemic into these patients’ precarious health situations only made things worse as many of the limited resources for patients with substance use disorder were diverted to battling the pandemic. Numerous inpatient and outpatient addiction services, for example, were temporarily shut down. This has led to an increase in domestic violence, and psychiatric decompensation, including psychosis, suicidal attempts, and worsening of medical comorbidities in these patients.
Our wake-up call came when the first case of COVID-19 was confirmed in New York in early March. Within a short period of time the state became the epicenter for COVID-19. With the projection of millions of cases being positive and the number of new cases doubling every third day at the onset in New York City, we knew we had a battle brewing and needed to radically transform our mode of operation fast.
Our first task was to ensure the safety of our patients and the dedicated health workers attending to them. We streamlined the patient point of entry through one screening site, while also brushing up on our history-taking to intently screen for COVID-19. This included not just focusing on travels from China, but from Europe and other parts of the world.
Yes, we did ask patients about cough, fever, shortness of breath or difficulty breathing, feeling fatigued, severe body ache, and possible contact with someone who is sick or has traveled overseas. But we were also attuned to the increased rate of community spread and the presentation of other symptoms, such as loss of taste and smell, early in the process. Hence we were able to triage patients with suspected cases to the appropriate sections of the hospital for further screening, testing, and evaluation, instead of having those patients admitted to the detox unit.
Early in the process a huddle team was instituted with daily briefing of staff lasting 30 minutes or less. This team consists of physicians, nurses, a physician assistant, a social worker, and a counselor. In addition to discussing treatment plans for the patient, they deliberate on the public health information from the hospital’s COVID-19 command center, New York State Department of Health, the Office of Mental Health, and the Centers for Disease Control and Prevention concerning the latest evidence-based information. These discussions have helped us modify our policies and practices.
We instituted a no visiting rule during a short hospital stay of 5-7 days, and this was initiated weeks in advance of many institutions, including nursing homes with vulnerable populations. Our admitting criteria was reviewed to allow for admission of only those patients who absolutely needed inpatient substance use disorder treatment, including patients with severe withdrawal symptoms and signs, comorbidities, or neuropsychiatric manifestations that made them unsafe for outpatient or home detoxification. Others were triaged to the outpatient services which was amply supported with telemedicine. Rooms and designated areas of the building were earmarked as places for isolation/quarantine if suspected COVID-19 cases were identified pending testing. To assess patients’ risk of COVID-19, we do point-of-care nasopharyngeal swab testing with polymerase chain reaction.
Regarding face masks, patients and staff were fitted with ones early in the process. Additionally, staff were trained on the importance of face mask use and how to ensure you have a tight seal around the mouth and nose and were provided with other appropriate personal protective equipment. Concerning social distancing, we reduced the patient population capacity for the unit down to 50% and offered only single room admissions. Social distancing was encouraged in the unit, including in the television and recreation room and dining room, and during small treatment groups of less than six individuals. Daily temperature checks with noncontact handheld thermometers were enforced for staff and anyone coming into the life recovery center.
Patients are continuously being educated on the presentations of COVID-19 and encouraged to report any symptoms. Any staff feeling sick or having symptoms are encouraged to stay home. Rigorous and continuous cleaning of surfaces, especially of areas subjected to common use, is done frequently by the hospital housekeeping and environmental crew and is the order of the day.
Dr. Fagbemi is a hospitalist at BronxCare Health System, a not-for-profit health and teaching hospital system serving South and Central Bronx in New York. He has no conflicts of interest to disclose.
Substance use disorder and its daily consequences take no breaks even during a pandemic. The stressors created by COVID-19, including deaths of loved ones and the disruptions to normal life from policies aimed at flattening the curve, seem to have increased substance use.
I practice as a hospitalist with an internal medicine background and specialty in addiction medicine at BronxCare Health System’s inpatient detoxification unit, a 24/7, 20-bed medically-supervised unit in South Bronx in New York City. It is one of the comprehensive services provided by the BronxCare’s life recovery center and addiction services, which also includes an outpatient clinic, opioid treatment program, inpatient rehab, and a half-way house. Inpatient detoxification units like ours are designed to treat serious addictions and chemical dependency and prevent and treat life-threatening withdrawal symptoms and signs or complications. Our patients come from all over the city and its adjoining suburbs, including from emergency room referrals, referral clinics, courts and the justice system, walk-ins, and self-referrals.
At a time when many inpatient detoxification units within the city were temporarily closed due to fear of inpatient spread of the virus or to provide extra COVID beds in anticipation for the peak surge, we have been able to provide a needed service. In fact, several other inpatient detoxification programs within the city have been able to refer their patients to our facility.
Individuals with substance use disorder have historically been a vulnerable and underserved population and possess high risk for multiple health problems as well as preexisting conditions. Many have limited life options financially, educationally, and with housing, and encounter barriers to accessing primary health care services, including preventive services. The introduction of the COVID-19 pandemic into these patients’ precarious health situations only made things worse as many of the limited resources for patients with substance use disorder were diverted to battling the pandemic. Numerous inpatient and outpatient addiction services, for example, were temporarily shut down. This has led to an increase in domestic violence, and psychiatric decompensation, including psychosis, suicidal attempts, and worsening of medical comorbidities in these patients.
Our wake-up call came when the first case of COVID-19 was confirmed in New York in early March. Within a short period of time the state became the epicenter for COVID-19. With the projection of millions of cases being positive and the number of new cases doubling every third day at the onset in New York City, we knew we had a battle brewing and needed to radically transform our mode of operation fast.
Our first task was to ensure the safety of our patients and the dedicated health workers attending to them. We streamlined the patient point of entry through one screening site, while also brushing up on our history-taking to intently screen for COVID-19. This included not just focusing on travels from China, but from Europe and other parts of the world.
Yes, we did ask patients about cough, fever, shortness of breath or difficulty breathing, feeling fatigued, severe body ache, and possible contact with someone who is sick or has traveled overseas. But we were also attuned to the increased rate of community spread and the presentation of other symptoms, such as loss of taste and smell, early in the process. Hence we were able to triage patients with suspected cases to the appropriate sections of the hospital for further screening, testing, and evaluation, instead of having those patients admitted to the detox unit.
Early in the process a huddle team was instituted with daily briefing of staff lasting 30 minutes or less. This team consists of physicians, nurses, a physician assistant, a social worker, and a counselor. In addition to discussing treatment plans for the patient, they deliberate on the public health information from the hospital’s COVID-19 command center, New York State Department of Health, the Office of Mental Health, and the Centers for Disease Control and Prevention concerning the latest evidence-based information. These discussions have helped us modify our policies and practices.
We instituted a no visiting rule during a short hospital stay of 5-7 days, and this was initiated weeks in advance of many institutions, including nursing homes with vulnerable populations. Our admitting criteria was reviewed to allow for admission of only those patients who absolutely needed inpatient substance use disorder treatment, including patients with severe withdrawal symptoms and signs, comorbidities, or neuropsychiatric manifestations that made them unsafe for outpatient or home detoxification. Others were triaged to the outpatient services which was amply supported with telemedicine. Rooms and designated areas of the building were earmarked as places for isolation/quarantine if suspected COVID-19 cases were identified pending testing. To assess patients’ risk of COVID-19, we do point-of-care nasopharyngeal swab testing with polymerase chain reaction.
Regarding face masks, patients and staff were fitted with ones early in the process. Additionally, staff were trained on the importance of face mask use and how to ensure you have a tight seal around the mouth and nose and were provided with other appropriate personal protective equipment. Concerning social distancing, we reduced the patient population capacity for the unit down to 50% and offered only single room admissions. Social distancing was encouraged in the unit, including in the television and recreation room and dining room, and during small treatment groups of less than six individuals. Daily temperature checks with noncontact handheld thermometers were enforced for staff and anyone coming into the life recovery center.
Patients are continuously being educated on the presentations of COVID-19 and encouraged to report any symptoms. Any staff feeling sick or having symptoms are encouraged to stay home. Rigorous and continuous cleaning of surfaces, especially of areas subjected to common use, is done frequently by the hospital housekeeping and environmental crew and is the order of the day.
Dr. Fagbemi is a hospitalist at BronxCare Health System, a not-for-profit health and teaching hospital system serving South and Central Bronx in New York. He has no conflicts of interest to disclose.
Annual U.S. death toll from drugs, alcohol, suicide tops 150,000
Despite decreases in overall opioid overdose deaths in 2018, deaths involving synthetic opioids, cocaine, and other psychostimulants increased sharply in the United States, and alcohol and suicide deaths also rose, new data show.
A report released May 21 by the Trust for America’s Health (TFAH) and the Well Being Trust shows that 151,964 Americans died from alcohol, drugs, and suicide. Experts warn that these “deaths of despair” may well increase in the wake of COVID-19.
A study released earlier in May estimated that an additional 75,000 Americans could die by suicide, drugs, or alcohol abuse because of the pandemic (Petterson S et al. “Projected Deaths of Despair From COVID-19,” Well Being Trust. May 8, 2020. WellBeingTrust.org).
“These data are a clarion call to action,” TFAH President and CEO John Auerbach said in a news release.
“We know what works to address deaths of despair but progress has been uneven and death rates continue to climb, with communities of color experiencing higher rates of increases in drug-induced and alcohol deaths,” he said.
“And there’s another immediate concern: The COVID-19 crisis has increased the health burdens and economic pressures on many communities of color,” said Mr. Auerbach.
According to the report, the 2018 national rate for alcohol, drug, and suicide deaths combined was only slightly lower than that reported in 2017 (46.4 vs 46.6 per 100,000).
Among the key findings in the report:
- 37,329 Americans died from alcohol-induced causes in 2018; the rate was up 4% over 2017.
- Alcohol-induced deaths were highest among American Indians (30.0 per 100,000) and adults aged 55 to 74 (27.6 per 100,000). For all population groups, rates of alcohol-related deaths were higher in 2018 than in 2017 except for people aged 17 years and younger, for whom the rate held steady.
- Despite a 4% decline in all drug-induced deaths and a 2% drop in all opioid-related deaths, 2018 saw sharp increases in deaths involving synthetic opioids (up 10%), cocaine (up 5%), and other psychostimulants, such as methamphetamine, ecstasy, amphetamine, and prescription stimulants (up 22%).
- Suicide claimed the lives of 48,344 Americans in 2018. The suicide rate in 2018 was 2% higher than in 2017 and 25% higher than in 2008.
- Suicide rates increased across all demographics except for adults aged 18-54 years, among whom the rate remained stable. Suicide death rates were highest in males (23.4 per 100,000), rural residents (19.7 per 100,000), whites (16.8 per 100,000), and American Indian/Alaska Natives (14.1 per 100,000).
- Between 2017 and 2018, 27 states had higher rates (above 0.04%) of alcohol, drug, and suicide deaths; 23 states and the District of Columbia had lower rates of deaths from those causes.
- States with the highest alcohol, drug, and suicide death rates in 2018 were West Virginia (84.9 per 100,000), New Mexico (82.8 per 100,000), New Hampshire (68.2 per 100,000), and Alaska (67.8 per 100,000).
- States with the lowest rates in 2018 were Texas (31.7 per 100,000), Mississippi (31.7 per 100,000), and Hawaii (34.6 per 100,000).
“Quite simply, too many Americans are dying from preventable causes. The profound racial health disparities seen in these data show that many ethnic minority groups are being left behind in our response efforts,” Benjamin F. Miller, PsyD, Well Being Trust chief strategy officer, said in the release.
“The nation needs a comprehensive framework for excellence in mental health and well-being, one that intentionally provides solutions for American Indians, blacks, Asians and Latinos. said Dr. Miller.
Policy recommendations outlined in the report include investing in prevention; reducing risk factors and promoting resilience in children, families, and communities; engaging all sectors of society to address mental health and substance use disorders; limiting access to lethal means of suicide; and promoting safe storage of medications and firearms.
A version of this article originally appeared on Medscape.com.
Despite decreases in overall opioid overdose deaths in 2018, deaths involving synthetic opioids, cocaine, and other psychostimulants increased sharply in the United States, and alcohol and suicide deaths also rose, new data show.
A report released May 21 by the Trust for America’s Health (TFAH) and the Well Being Trust shows that 151,964 Americans died from alcohol, drugs, and suicide. Experts warn that these “deaths of despair” may well increase in the wake of COVID-19.
A study released earlier in May estimated that an additional 75,000 Americans could die by suicide, drugs, or alcohol abuse because of the pandemic (Petterson S et al. “Projected Deaths of Despair From COVID-19,” Well Being Trust. May 8, 2020. WellBeingTrust.org).
“These data are a clarion call to action,” TFAH President and CEO John Auerbach said in a news release.
“We know what works to address deaths of despair but progress has been uneven and death rates continue to climb, with communities of color experiencing higher rates of increases in drug-induced and alcohol deaths,” he said.
“And there’s another immediate concern: The COVID-19 crisis has increased the health burdens and economic pressures on many communities of color,” said Mr. Auerbach.
According to the report, the 2018 national rate for alcohol, drug, and suicide deaths combined was only slightly lower than that reported in 2017 (46.4 vs 46.6 per 100,000).
Among the key findings in the report:
- 37,329 Americans died from alcohol-induced causes in 2018; the rate was up 4% over 2017.
- Alcohol-induced deaths were highest among American Indians (30.0 per 100,000) and adults aged 55 to 74 (27.6 per 100,000). For all population groups, rates of alcohol-related deaths were higher in 2018 than in 2017 except for people aged 17 years and younger, for whom the rate held steady.
- Despite a 4% decline in all drug-induced deaths and a 2% drop in all opioid-related deaths, 2018 saw sharp increases in deaths involving synthetic opioids (up 10%), cocaine (up 5%), and other psychostimulants, such as methamphetamine, ecstasy, amphetamine, and prescription stimulants (up 22%).
- Suicide claimed the lives of 48,344 Americans in 2018. The suicide rate in 2018 was 2% higher than in 2017 and 25% higher than in 2008.
- Suicide rates increased across all demographics except for adults aged 18-54 years, among whom the rate remained stable. Suicide death rates were highest in males (23.4 per 100,000), rural residents (19.7 per 100,000), whites (16.8 per 100,000), and American Indian/Alaska Natives (14.1 per 100,000).
- Between 2017 and 2018, 27 states had higher rates (above 0.04%) of alcohol, drug, and suicide deaths; 23 states and the District of Columbia had lower rates of deaths from those causes.
- States with the highest alcohol, drug, and suicide death rates in 2018 were West Virginia (84.9 per 100,000), New Mexico (82.8 per 100,000), New Hampshire (68.2 per 100,000), and Alaska (67.8 per 100,000).
- States with the lowest rates in 2018 were Texas (31.7 per 100,000), Mississippi (31.7 per 100,000), and Hawaii (34.6 per 100,000).
“Quite simply, too many Americans are dying from preventable causes. The profound racial health disparities seen in these data show that many ethnic minority groups are being left behind in our response efforts,” Benjamin F. Miller, PsyD, Well Being Trust chief strategy officer, said in the release.
“The nation needs a comprehensive framework for excellence in mental health and well-being, one that intentionally provides solutions for American Indians, blacks, Asians and Latinos. said Dr. Miller.
Policy recommendations outlined in the report include investing in prevention; reducing risk factors and promoting resilience in children, families, and communities; engaging all sectors of society to address mental health and substance use disorders; limiting access to lethal means of suicide; and promoting safe storage of medications and firearms.
A version of this article originally appeared on Medscape.com.
Despite decreases in overall opioid overdose deaths in 2018, deaths involving synthetic opioids, cocaine, and other psychostimulants increased sharply in the United States, and alcohol and suicide deaths also rose, new data show.
A report released May 21 by the Trust for America’s Health (TFAH) and the Well Being Trust shows that 151,964 Americans died from alcohol, drugs, and suicide. Experts warn that these “deaths of despair” may well increase in the wake of COVID-19.
A study released earlier in May estimated that an additional 75,000 Americans could die by suicide, drugs, or alcohol abuse because of the pandemic (Petterson S et al. “Projected Deaths of Despair From COVID-19,” Well Being Trust. May 8, 2020. WellBeingTrust.org).
“These data are a clarion call to action,” TFAH President and CEO John Auerbach said in a news release.
“We know what works to address deaths of despair but progress has been uneven and death rates continue to climb, with communities of color experiencing higher rates of increases in drug-induced and alcohol deaths,” he said.
“And there’s another immediate concern: The COVID-19 crisis has increased the health burdens and economic pressures on many communities of color,” said Mr. Auerbach.
According to the report, the 2018 national rate for alcohol, drug, and suicide deaths combined was only slightly lower than that reported in 2017 (46.4 vs 46.6 per 100,000).
Among the key findings in the report:
- 37,329 Americans died from alcohol-induced causes in 2018; the rate was up 4% over 2017.
- Alcohol-induced deaths were highest among American Indians (30.0 per 100,000) and adults aged 55 to 74 (27.6 per 100,000). For all population groups, rates of alcohol-related deaths were higher in 2018 than in 2017 except for people aged 17 years and younger, for whom the rate held steady.
- Despite a 4% decline in all drug-induced deaths and a 2% drop in all opioid-related deaths, 2018 saw sharp increases in deaths involving synthetic opioids (up 10%), cocaine (up 5%), and other psychostimulants, such as methamphetamine, ecstasy, amphetamine, and prescription stimulants (up 22%).
- Suicide claimed the lives of 48,344 Americans in 2018. The suicide rate in 2018 was 2% higher than in 2017 and 25% higher than in 2008.
- Suicide rates increased across all demographics except for adults aged 18-54 years, among whom the rate remained stable. Suicide death rates were highest in males (23.4 per 100,000), rural residents (19.7 per 100,000), whites (16.8 per 100,000), and American Indian/Alaska Natives (14.1 per 100,000).
- Between 2017 and 2018, 27 states had higher rates (above 0.04%) of alcohol, drug, and suicide deaths; 23 states and the District of Columbia had lower rates of deaths from those causes.
- States with the highest alcohol, drug, and suicide death rates in 2018 were West Virginia (84.9 per 100,000), New Mexico (82.8 per 100,000), New Hampshire (68.2 per 100,000), and Alaska (67.8 per 100,000).
- States with the lowest rates in 2018 were Texas (31.7 per 100,000), Mississippi (31.7 per 100,000), and Hawaii (34.6 per 100,000).
“Quite simply, too many Americans are dying from preventable causes. The profound racial health disparities seen in these data show that many ethnic minority groups are being left behind in our response efforts,” Benjamin F. Miller, PsyD, Well Being Trust chief strategy officer, said in the release.
“The nation needs a comprehensive framework for excellence in mental health and well-being, one that intentionally provides solutions for American Indians, blacks, Asians and Latinos. said Dr. Miller.
Policy recommendations outlined in the report include investing in prevention; reducing risk factors and promoting resilience in children, families, and communities; engaging all sectors of society to address mental health and substance use disorders; limiting access to lethal means of suicide; and promoting safe storage of medications and firearms.
A version of this article originally appeared on Medscape.com.
New ‘atlas’ maps links between mental disorders, physical illnesses
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
Mental illnesses are associated with a significantly increased risk of subsequent physical diseases, new research shows.
An international team of researchers has created an “atlas” that maps the relationship between specific mental disorders and the risk of subsequent physical illnesses.
The researchers found that, following the diagnosis of a mental disorder, psychiatric patients are significantly more likely than the general population to develop potentially life-threatening conditions, including heart disease and stroke.
These findings, the investigators noted, highlight the need for better medical care in this vulnerable population. They have created a website with detailed information about the risks of specific physical ailments and the link to particular mental disorders.
“We found that women with anxiety disorders have a 50% increased risk of developing a heart condition or stroke – over 15 years, one in three women with anxiety disorders will develop these medical disorders,” lead investigator John McGrath, MD, PhD, University of Queensland’s Brain Institute, Brisbane, Australia, and Aarhus (Denmark) University, said in a statement.
“We also looked at men with substance use disorders such as alcohol-related disorders and found they have a 400% increased risk of gut or liver disorders, while over 15 years, one in five of them will develop gut or liver conditions,” he added.
The study was published in the New England Journal of Medicine.
New ‘atlas’
It’s well known that patients with mental disorders have decreased quality of life, increased health care utilization, and a shorter life expectancy than individuals in the general population – about 10 years for men and 7 years for women.
However, the investigators noted, previous research examining the relationship between mental disorders and medical conditions only focused on “particular pairs or a small set of mental disorders and medical conditions.”
“We needed a comprehensive study to map the links between different types of mental disorders versus different types of general medical conditions. Our study has provided this atlas,” Dr. McGrath said in an interview.
The clinical utility of such a map could provide comprehensive data on relative and absolute risks of various medical conditions after a diagnosis of a mental disorder. This information, the researchers noted, would “help clinicians and health care planners identify the primary prevention needs of their patients.”
The study included 5.9 million people born in Denmark between 1900 and 2015 and followed them from 2000 to 2016, a total of 83.9 million person-years. The researchers followed patients for up to 17 years (2000-2016) for medical diagnoses and up to 48 years (1969-2016) for diagnoses of mental disorders.
The study’s large sample size allowed investigators to assess 10 broad types of mental disorders and 9 broad categories of medical conditions that encompassed 31 specific conditions.
Categories of medical conditions included circulatory, endocrine, pulmonary, gastrointestinal, urogenital, musculoskeletal, hematologic, neurologic, and cancer. Mental disorder categories included organic disorders such as Alzheimer’s, substance abuse disorders, schizophrenia, mood disorders, neurotic disorders, eating disorders, personality disorders, developmental disorders, behavioral/emotional disorders, and intellectual disabilities.
The researchers estimated associations between 90 pairs of mental disorders and broad-category medical conditions, as well as 310 pairs of mental disorders and specific medical conditions.
‘Curious’ finding
Individuals with mental disorders showed a higher risk of medical conditions in 76 out of 90 specific mental disorder–medical condition pairs.
After adjusting for sex, age, calendar time, and previous coexisting mental disorders, the median hazard ratio for a subsequent medical condition was 1.37 in patients with a mental disorder.
The lowest HR was 0.82 for organic mental disorders and the broad category of cancer (95% confidence interval, 0.80-0.84), and the highest was 3.62 for eating disorders and urogenital conditions (95% CI, 3.11-4.22). On the other hand, schizophrenia was associated with a reduced risk of developing musculoskeletal conditions (HR, 0.87; 95% CI, 0.84-0.91).
Dr. McGrath described this finding as “curious” and speculated it “may be related to underlying genetic risk factors.”
compared with the matched reference group without a mood disorder (40.9% vs. 32.6%, respectively).
The risk of developing subsequent medical conditions after a mental disorder diagnosis did not remain steady over time. For instance, although mood disorders were associated with an increased risk of developing circulatory problems (HR, 1.32; 95% CI, 1.31-1.34), the highest risk occurred during the first 6 months following diagnosis and gradually decreased over the next 15 years (HR, 2.39; 95% CI, 2.29-2.48 and HR, 1.18; 95% CI, 1.17-1.20, respectively).
“Many people with mental disorders have unhealthy lifestyle, including low exercise, poor diet, smoking, and alcohol, which may account for the increased risk of physical illness, and also they may not seek and/or may not get quick treatment for their health conditions,” said Dr. McGrath.
Additionally, “perhaps some genetic and early life exposures, such as trauma, may increase the risk of both medical conditions and mental disorders,” he added. “We need better treatments for mental disorders, so that they do not slip into unemployment or poverty.”
A strong case
In a comment, Roger McIntyre, MD, professor of psychiatry and pharmacology at the University of Toronto and head of the mood disorders psychopharmacology unit, University Health Network, said that the research “really makes a strong case for the fact that persons who have mental disorders are at higher risk of chronic diseases, and it’s the chronic diseases that decrease their lifespan.”
Dr. McIntyre, who is also director of the Depression and Bipolar Support Alliance, said that the “takeaway message is that mental disorders are not just brain disorders but are multisystem disorders.”
For this reason, “the most appropriate way to provide care would be to provide a holistic approach to treat and prevent the chronic diseases that lead to increase in mortality,” recommended Dr. McIntyre, who was not involved with the current study.
The study was supported by grants from the Danish National Research Foundation, the National Health and Medical Research Council, the Novo Nordisk Foundation , the European Union’s Horizon 2020 Research and Innovation Program, the Aarhus University Research Foundation, the Lundbeck Foundation, the National Institutes of Health, the European Commission, Helsefonden, the Danish Council for Independent Research, the Independent Research Fund Denmark, the National Health and Medical Research Council of Australia, and the National Institute on Drug Abuse.
Dr. McGrath has disclosed no relevant financial relationships. The other authors’ disclosures are listed on the original paper. Dr. McIntyre reports receiving grants from Stanley Medical Research Institute; the Canadian Institutes of Health Research/Global Alliance for Chronic Diseases/Chinese National Natural Research Foundation; and receiving speaking/consultation fees from Lundbeck, Janssen, Shire, Purdue, Pfizer, Otsuka, Allergan, Takeda, Neurocrine, Sunovion, and Minerva.
A version of this article originally appeared on Medscape.com.
COVID-19: An opportunity, challenge for addiction treatment, NIDA boss says
The COVID-19 pandemic is posing significant challenges while also providing unique opportunities for patients with substance use disorders (SUD), a leading expert says.

Nora Volkow, MD, director of the National Institute on Drug Abuse, said that the pandemic has accelerated the use of telemedicine, making it easier for patients with SUD to access treatment. It has also led to the proliferation of more mental health hotlines, which is critical since the vast majority of these patients have comorbid mental illness.
In addition, COVID-19 has resulted in increased availability of “alternative” peer support mechanisms via cellphones or computers to aid individuals’ sobriety.
Dr. Volkow spoke at the virtual American Psychiatric Association Spring Highlights Meeting 2020, which is replacing the organization’s canceled annual meeting.
While methadone clinics have had to close during the pandemic, making it challenging for those on medically assisted treatment to receive methadone or buprenorphine, some of the rules and regulations have been relaxed in order to make these medications accessible without the need for in-person attendance at a clinic. In addition, the Substance Abuse and Mental Health Services Administration has relaxed some of its own regulations regarding telehealth and opioid treatment programs.
Social isolation, stigma intensified
A pandemic increases anxiety in the general population, but for patients with SUD who may be also be struggling with homelessness and comorbid mental illness, the situation can further exacerbate social stigma and isolation – leading to relapse, more overdoses, and overdose deaths, Dr. Volkow said. Social interaction is “extraordinarily important” for patients and “one of the most powerful tools we have” to build resilience.
Right now, said Dr. Volkow, “we are in the dark as to how COVID infections have affected the number of overdose deaths.”
However, she noted that
“So even through this devastation, we can actually extract something that may help others in future,” she said.
Dr. Volkow noted that during the pandemic it is critical to reinforce the importance of engaging in – and remaining in – treatment to SUD patients. It’s also crucial to make patients aware of social support systems and behavioral interventions to help them cope with stress and to mitigate relapse risk.
COVID-19 and relapse
Elie G. Aoun, MD, assistant professor of psychiatry at New York University and vice chair of the APA’s Council on Addiction Psychiatry, said in an interview that Dr. Volkow’s presentation provided “exactly the kind of accessible information” clinicians need.
Dr. Aoun said he sees the impact of the COVID-19 crisis in his practice every day. Patients with SUD “are getting the short end of the stick.”
Social distancing measures prompted by the pandemic can be “very triggering” for SUD patients, he said. One of his patients told him the current isolation, loneliness, movement restrictions, and boredom remind her of the way she felt when she used drugs.
Dr. Aoun said four of his patients have relapsed since the pandemic began. Two of them had just started treatment after years of using drugs, so this was a “major setback” for them.
He and his colleagues were “not really prepared” to provide care via video link, which he believes is not as effective as in-person sessions.
In addition to disrupting patient care, said Dr. Aoun, the pandemic is forcing the medical community to face social determinants of health, such as poverty and homelessness, as they relate to addiction disorders and whether or not someone receives care.
This article originally appeared on Medscape.com.
The COVID-19 pandemic is posing significant challenges while also providing unique opportunities for patients with substance use disorders (SUD), a leading expert says.
Nora Volkow, MD, director of the National Institute on Drug Abuse, said that the pandemic has accelerated the use of telemedicine, making it easier for patients with SUD to access treatment. It has also led to the proliferation of more mental health hotlines, which is critical since the vast majority of these patients have comorbid mental illness.
In addition, COVID-19 has resulted in increased availability of “alternative” peer support mechanisms via cellphones or computers to aid individuals’ sobriety.
Dr. Volkow spoke at the virtual American Psychiatric Association Spring Highlights Meeting 2020, which is replacing the organization’s canceled annual meeting.
While methadone clinics have had to close during the pandemic, making it challenging for those on medically assisted treatment to receive methadone or buprenorphine, some of the rules and regulations have been relaxed in order to make these medications accessible without the need for in-person attendance at a clinic. In addition, the Substance Abuse and Mental Health Services Administration has relaxed some of its own regulations regarding telehealth and opioid treatment programs.
Social isolation, stigma intensified
A pandemic increases anxiety in the general population, but for patients with SUD who may be also be struggling with homelessness and comorbid mental illness, the situation can further exacerbate social stigma and isolation – leading to relapse, more overdoses, and overdose deaths, Dr. Volkow said. Social interaction is “extraordinarily important” for patients and “one of the most powerful tools we have” to build resilience.
Right now, said Dr. Volkow, “we are in the dark as to how COVID infections have affected the number of overdose deaths.”
However, she noted that
“So even through this devastation, we can actually extract something that may help others in future,” she said.
Dr. Volkow noted that during the pandemic it is critical to reinforce the importance of engaging in – and remaining in – treatment to SUD patients. It’s also crucial to make patients aware of social support systems and behavioral interventions to help them cope with stress and to mitigate relapse risk.
COVID-19 and relapse
Elie G. Aoun, MD, assistant professor of psychiatry at New York University and vice chair of the APA’s Council on Addiction Psychiatry, said in an interview that Dr. Volkow’s presentation provided “exactly the kind of accessible information” clinicians need.
Dr. Aoun said he sees the impact of the COVID-19 crisis in his practice every day. Patients with SUD “are getting the short end of the stick.”
Social distancing measures prompted by the pandemic can be “very triggering” for SUD patients, he said. One of his patients told him the current isolation, loneliness, movement restrictions, and boredom remind her of the way she felt when she used drugs.
Dr. Aoun said four of his patients have relapsed since the pandemic began. Two of them had just started treatment after years of using drugs, so this was a “major setback” for them.
He and his colleagues were “not really prepared” to provide care via video link, which he believes is not as effective as in-person sessions.
In addition to disrupting patient care, said Dr. Aoun, the pandemic is forcing the medical community to face social determinants of health, such as poverty and homelessness, as they relate to addiction disorders and whether or not someone receives care.
This article originally appeared on Medscape.com.
The COVID-19 pandemic is posing significant challenges while also providing unique opportunities for patients with substance use disorders (SUD), a leading expert says.
Nora Volkow, MD, director of the National Institute on Drug Abuse, said that the pandemic has accelerated the use of telemedicine, making it easier for patients with SUD to access treatment. It has also led to the proliferation of more mental health hotlines, which is critical since the vast majority of these patients have comorbid mental illness.
In addition, COVID-19 has resulted in increased availability of “alternative” peer support mechanisms via cellphones or computers to aid individuals’ sobriety.
Dr. Volkow spoke at the virtual American Psychiatric Association Spring Highlights Meeting 2020, which is replacing the organization’s canceled annual meeting.
While methadone clinics have had to close during the pandemic, making it challenging for those on medically assisted treatment to receive methadone or buprenorphine, some of the rules and regulations have been relaxed in order to make these medications accessible without the need for in-person attendance at a clinic. In addition, the Substance Abuse and Mental Health Services Administration has relaxed some of its own regulations regarding telehealth and opioid treatment programs.
Social isolation, stigma intensified
A pandemic increases anxiety in the general population, but for patients with SUD who may be also be struggling with homelessness and comorbid mental illness, the situation can further exacerbate social stigma and isolation – leading to relapse, more overdoses, and overdose deaths, Dr. Volkow said. Social interaction is “extraordinarily important” for patients and “one of the most powerful tools we have” to build resilience.
Right now, said Dr. Volkow, “we are in the dark as to how COVID infections have affected the number of overdose deaths.”
However, she noted that
“So even through this devastation, we can actually extract something that may help others in future,” she said.
Dr. Volkow noted that during the pandemic it is critical to reinforce the importance of engaging in – and remaining in – treatment to SUD patients. It’s also crucial to make patients aware of social support systems and behavioral interventions to help them cope with stress and to mitigate relapse risk.
COVID-19 and relapse
Elie G. Aoun, MD, assistant professor of psychiatry at New York University and vice chair of the APA’s Council on Addiction Psychiatry, said in an interview that Dr. Volkow’s presentation provided “exactly the kind of accessible information” clinicians need.
Dr. Aoun said he sees the impact of the COVID-19 crisis in his practice every day. Patients with SUD “are getting the short end of the stick.”
Social distancing measures prompted by the pandemic can be “very triggering” for SUD patients, he said. One of his patients told him the current isolation, loneliness, movement restrictions, and boredom remind her of the way she felt when she used drugs.
Dr. Aoun said four of his patients have relapsed since the pandemic began. Two of them had just started treatment after years of using drugs, so this was a “major setback” for them.
He and his colleagues were “not really prepared” to provide care via video link, which he believes is not as effective as in-person sessions.
In addition to disrupting patient care, said Dr. Aoun, the pandemic is forcing the medical community to face social determinants of health, such as poverty and homelessness, as they relate to addiction disorders and whether or not someone receives care.
This article originally appeared on Medscape.com.
Elderly Americans carry heavier opioid burden
according to the Agency for Healthcare Quality and Research.
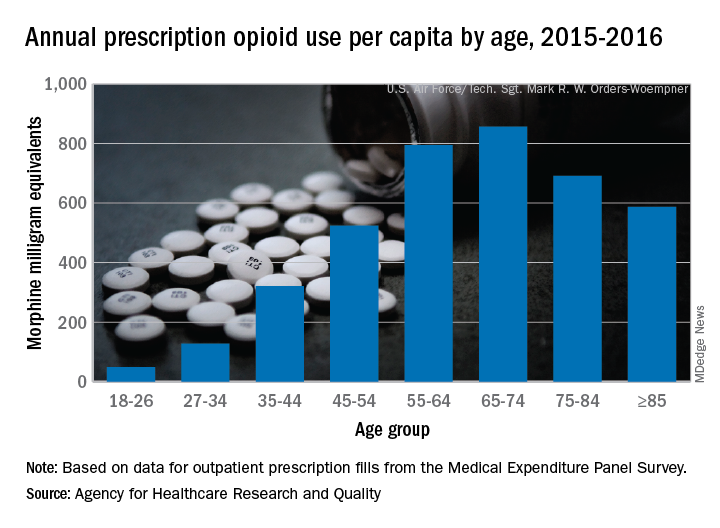
Elderly adults with chronic and acute pain obtained an average of 774 morphine milligram equivalents (MMEs) of prescription opioids annually during 2015-2016 from outpatient clinicians, compared with 376 MMEs a year for nonelderly adults, said Asako S. Moriya, PhD, and G. Edward Miller, PhD, of the AHRQ.
Narrowing the age groups shows that opioid MMEs increased with age, starting at 49 MMEs for 18- to 26-year-olds and rising to a high of 856 MMEs in the 65- to 74-year-old group, before dropping off in the oldest adults, the investigators said in a Medical Expenditure Panel Survey (MEPS) research findings report.
The analysis included “all opioid medications that are commonly used to treat pain” and excluded respiratory agents, antitussives, and drugs used for medication-assisted treatment, they noted. The MEPS data cover prescriptions purchased or obtained in outpatient settings but not those administered in inpatient settings or in clinics or physician offices.
according to the Agency for Healthcare Quality and Research.
Elderly adults with chronic and acute pain obtained an average of 774 morphine milligram equivalents (MMEs) of prescription opioids annually during 2015-2016 from outpatient clinicians, compared with 376 MMEs a year for nonelderly adults, said Asako S. Moriya, PhD, and G. Edward Miller, PhD, of the AHRQ.
Narrowing the age groups shows that opioid MMEs increased with age, starting at 49 MMEs for 18- to 26-year-olds and rising to a high of 856 MMEs in the 65- to 74-year-old group, before dropping off in the oldest adults, the investigators said in a Medical Expenditure Panel Survey (MEPS) research findings report.
The analysis included “all opioid medications that are commonly used to treat pain” and excluded respiratory agents, antitussives, and drugs used for medication-assisted treatment, they noted. The MEPS data cover prescriptions purchased or obtained in outpatient settings but not those administered in inpatient settings or in clinics or physician offices.
according to the Agency for Healthcare Quality and Research.
Elderly adults with chronic and acute pain obtained an average of 774 morphine milligram equivalents (MMEs) of prescription opioids annually during 2015-2016 from outpatient clinicians, compared with 376 MMEs a year for nonelderly adults, said Asako S. Moriya, PhD, and G. Edward Miller, PhD, of the AHRQ.
Narrowing the age groups shows that opioid MMEs increased with age, starting at 49 MMEs for 18- to 26-year-olds and rising to a high of 856 MMEs in the 65- to 74-year-old group, before dropping off in the oldest adults, the investigators said in a Medical Expenditure Panel Survey (MEPS) research findings report.
The analysis included “all opioid medications that are commonly used to treat pain” and excluded respiratory agents, antitussives, and drugs used for medication-assisted treatment, they noted. The MEPS data cover prescriptions purchased or obtained in outpatient settings but not those administered in inpatient settings or in clinics or physician offices.
New ASAM guideline released amid COVID-19 concerns
Home-based buprenorphine induction deemed safe for OUD
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.
Home-based buprenorphine induction deemed safe for OUD
Home-based buprenorphine induction deemed safe for OUD
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.