User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Nemolizumab Benefits for Atopic Dermatitis Maintained in Long-Term Follow-Up Study
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
(AD), revealed an interim analysis of the ARCADIA open-label extension study.
The research was presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
The results showed nemolizumab was associated with “ongoing clinically meaningful improvements in itch, skin lesions, and sleep disturbance,” said study presenter Diamant Thaçi, MD, PhD, of the Comprehensive Center for Inflammation Medicine, University of Lü̈beck in Germany.
Moreover, “patient-reported outcomes, including quality of life ... continued to improve over 56 weeks of treatment.” In addition, Thaçi added, the “safety data support the long-term use of nemolizumab for the treatment of adolescent and adult patients with moderate to severe atopic dermatitis.”
He explained that interleukin (IL) 31 is a key neuroimmune cytokine in AD, triggering itch, skin barrier disruption, and exacerbation of inflammation via its receptor. Nemolizumab inhibits IL-31 receptor binding and was shown in the ARCADIA 1 and ARCADIA 2 trials to provide, along with background topical corticosteroids, clinically meaningful improvements in itch, skin lesions, and sleep for up to weeks 48 of follow-up in adolescents and adults with moderate to severe AD.
The current open-label long-term extension study involved patients who were enrolled in both ARCADIA 1 and 2 trials, as well as those from four phase 2 and 2b studies, a phase 3b study, and adolescents who had not been included in a trial but who met the criteria for the extension study. All patients, whether they started on placebo plus background topical corticosteroids in a prior study, were treated with nemolizumab 30 mg subcutaneously every 4 weeks along with topical corticosteroids.
The interim analysis included all efficacy and safety data up to the cutoff of September 30, 2022, on 723 patients who had completed 56 weeks of treatment among the 1751 patients initially enrolled in the extension study.
The results showed that, regardless of whether patients were nemolizumab naive at enrollment or had previously taken the drug, there were increases in the proportion of patients with an Investigator Global Assessment (IGA) score of 0/1 and an Eczema Area and Severity Index (EASI) score of at least 75 (EASI-75) over the 56 weeks of the study.
In those naive to nemolizumab, the increase in the proportion with an IGA score of 0/1 increased from 17.7% at baseline to 49.0% at 56 weeks, while the proportion with an EASI-75 increased from 24.0% to 78.7%.
The increase in the proportion of patients with an IGA score 0/1 among those who had previously received nemolizumab increased from 28.5% at baseline to 47.1% at 56 weeks. The proportion with an EASI-75 was 38.1% at baseline, rising to 73.0% at 56 weeks.
Increases in the proportion of patients with an EASI score of at least 50 and at least 90 were also seen with nemolizumab, as were increases in the proportion of patients with an improvement of at least four points on the SCORing Atopic Dermatitis Pruritus visual analogue scale and Sleep loss scores.
Similarly, the proportion of patients with a reduction in Dermatology Life Quality Index of at least four points increased over the study period.
Regarding safety, Thaçi said, there appeared to be fewer adverse events than had been previously reported with nemolizumab. “We don’t see any signs of conjunctivitis,” he continued, or significant risk of infection apart from for COVID-19, but he pointed out that the study was conducted during the pandemic, which was “a very difficult time.”
The most common treatment-related adverse events were, aside from COVID-19, nasopharyngitis in about 10%-11% of patients, upper respiratory tract infection in about 6% to almost 7%, and headache in about 5%.
Among the adverse events of special interest, newly diagnosed asthma or worsening of asthma occurred in 4.7%-4.8% of patients, while peripheral edema was seen in 0.8%-1.7%.
“Besides this, the study results are really looking very good,” he said, adding: “It means, in a long-term study, we can say today that nemolizumab has revealed the [same] safety profile that was shown in the ARCADIA 1 and 2 trials.”
Alan D. Irvine, MD, DSc, professor of dermatology, Trinity College Dublin in Ireland, who was not involved in the study, underlined that the current interim assessment does not represent the complete dataset and is based on observed cases rather than a more rigorous methodology, such as net reclassification improvement analysis.
“So it makes it a little harder to interpret when you don’t know how many people are dropping out and why they’re dropping out,” he told this news organization. “That said, those who remain on drug out to 56 weeks do experience ongoing improvement in disease control.”
Consequently, “the most reliable message you can take from this interim analysis of long-term data is that there were no new safety signals,” and nemolizumab looks “safe and well-tolerated.”
Where nemolizumab would fit into the treatment pathway for moderate to severe AD remains an open question, Irvine said, although he believes that IL-13 pathway inhibitors such as dupilumab, tralokinumab, and lebrikizumab “will remain the treatment of choice for the immediate future due to prescriber familiarity and good efficacy data.”
However, for patients who are unsuitable for IL-13 inhibitors and/or Janus kinase inhibitors such as abrocitinib and upadacitinib, nemolizumab “could be an interesting alternative.”
“That’s probably where it is going to start,” Irvine said, “and then obviously that will change over time and as the data mature and prescribers become more familiar with the drug in the real world.”
Nemolizumab (Nemluvio) is approved for treating prurigo nodularis (PN) in the United States and in Japan and is under Food and Drug Administration review for treating AD. It is also under review for PN and AD in Europe, Canada, the United Kingdom, and several other countries, according to Galderma. It is also approved for treating pruritus associated with AD in pediatric, adolescent, and adult patients in Japan.
The study was funded by Galderma. Thaçi declared relationships with AbbVie, Almirall, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Galderma, Janssen-Cilag, Kyowa Kirin, LEO Pharma, L’Oréal, Eli Lilly, Novartis, Pfizer, Regeneron, Sanofi, Target RWE, and UCB. Irvine declared relationships with AbbVie, Arena Pharmaceuticals, BenevolentAl, Chugai Pharmaceutical, Dermavant, Eli Lily, Genentech, LEO Pharma, Menlo Therapeutics, Novartis, Pfizer, Regeneron, Sanofi, UCB, DS Biopharma, and Inflazome.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
Lichen Planus Responds to Treatment with Topical Ruxolitinib in Phase 2 Study
both when given twice daily and as needed, according to data from a phase 2 trial.
The research, presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress, involved 64 patients older than 18 years. Ruxolitinib cream (Opzelura) is a topical formulation of a Janus kinase (JAK)1/JAK2 inhibitor, approved by the Food and Drug Administration (FDA) for treating mild to moderate atopic dermatitis and for nonsegmental vitiligo in adults and children aged 12 years or older.

Ruxolitinib cream twice daily resulted in “significant improvements in cutaneous lichen planus disease severity vs vehicle” after 16 weeks of treatment, said the study presenter, Aaron R. Mangold, MD, a dermatologist at Mayo Clinic, Scottsdale, Arizona.
Further improvements were seen during another 16 weeks of additional open-label, as-needed application, he added, and the topical treatment was “generally well tolerated.”
Consequently, “ruxolitinib cream represents a promising potential treatment for cutaneous lichen planus,” Mangold concluded.
Asked to comment on the results, Adam Friedman, MD, Professor and Chair of Dermatology, George Washington University, Washington, DC, who was not involved with the study, said that in keeping with the characterization of lichen planus using the four Ps — purple, polygonal, pruritic, papules — it is “Pretty common, Predictably disabling and disfiguring, and Passed over again and again in the drug development world.”
He said in an interview that this chronic inflammatory skin condition, which affects roughly 2% of the population, also “lacks consensus on work-up and management, likely in part owing to the absence of sizable clinical trial data.”
A recent survey conducted at a meeting indicated that dermatologists “heavily lean on topical therapies for the management of all severity levels,” noted Friedman, one of the survey authors. “Therefore, the phase 2 data presented at EADV is a welcome addition to the mix.”
Phase 2 Study Results
At the meeting, Mangold said that a previous proof-of-concept single-arm study in 12 patients suggested that topical ruxolitinib was highly effective in treating cutaneous lichen planus.
The current phase 2 trial enrolled 64 patients with predominantly cutaneous disease who had an Investigator’s Global Assessment (IGA) score of 3 or 4 and an Itch Numeric Rating Scale (NRS) score of ≥ 4. Their median age was 57 years, and 71.9% were women. Nearly 63% were White, 28.1% were Black, and 6.3% were Asian. The median duration of disease was 4.9 years, and 90.6% had received prior treatment for their lichen planus.
They were randomized to receive 1.5% ruxolitinib cream or a vehicle cream twice daily for 16 weeks, and following a primary endpoint assessment, they were transferred to an open-label extension period, during which they used ruxolitinib cream as needed for another 16 weeks. There was an additional 30-day safety follow-up period.
At week 16, significantly more patients treated with the ruxolitinib cream (50.0%) vs vehicle cream (21.9%) achieved IGA treatment success (the primary endpoint), defined as an IGA score of 0 or 1 with ≥ 2-grade improvement from baseline (odds ratio, 4.04; P = .0129).
In the open-label extension, when all patients used the active cream as needed, the proportion achieving IGA treatment success increased to 60% among the patients originally treated with ruxolitinib cream and 60.9% among those who switched from the vehicle cream.
A similar pattern was seen with Itch NRS scores. At 16 weeks, 57.7% of those treated with the ruxolitinib cream and 19.2% of those given the vehicle cream achieved an Itch NRS score of ≥ 4 (P < .01), rising to 84.2% and 73.3%, respectively, during the open-label extension.
The time to achievement of an Itch NRS of ≥ 4 was also significantly shorter with the ruxolitinib cream than with the vehicle cream (median days, 17 vs 97; hazard ratio, 2.85; P = .0008).
In both treatment groups, Skin Pain NRS scores decreased by a mean of 3.0 with ruxolitinib cream and 1.3 with the vehicle cream at week 16. By the end of the open-label extension, scores dropped by 4.3 among those who continued on active treatment and by 3.5 among those who switched from vehicle to topical ruxolitinib.
There were few treatment-emergent adverse events, with just three ruxolitinib patients affected during the randomized phase of the trial. There was one grade ≥ 3 event considered unrelated to the study drug, and no serious treatment-emergent adverse events were reported.
The most common adverse events during the randomized period were nasopharyngitis, hypertension, and contusion, all experienced by fewer than 10% of patients, whereas sinusitis, increased blood cholesterol levels, and increased blood creatine phosphokinase were most common in the open-label extension, experienced by no more than 5% of patients.
In the interview, Friedman commented that “these data provide hope that one day soon, there will be an FDA-approved, effective, and well-tolerated approach for this condition, validating the patient and supporting the dermatologist with an evidence-based option.”
The study was funded by Incyte. Mangold declared relationships with Argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Clarivate, Incyte Corporation, Janssen, Nuvig Therapeutics, Pfizer, Regeneron Pharmaceuticals, Soligenix, Tourmaline Bio, AbbVie, Corbus, Eli Lilly, Kyowa, Merck, miRagen Therapeutics, Palvella Therapeutics, Priovant Therapeutics, and Adelphi Values. Friedman declared a relationship with Incyte, but it is not related to this topic.
A version of this article first appeared on Medscape.com.
both when given twice daily and as needed, according to data from a phase 2 trial.
The research, presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress, involved 64 patients older than 18 years. Ruxolitinib cream (Opzelura) is a topical formulation of a Janus kinase (JAK)1/JAK2 inhibitor, approved by the Food and Drug Administration (FDA) for treating mild to moderate atopic dermatitis and for nonsegmental vitiligo in adults and children aged 12 years or older.
Ruxolitinib cream twice daily resulted in “significant improvements in cutaneous lichen planus disease severity vs vehicle” after 16 weeks of treatment, said the study presenter, Aaron R. Mangold, MD, a dermatologist at Mayo Clinic, Scottsdale, Arizona.
Further improvements were seen during another 16 weeks of additional open-label, as-needed application, he added, and the topical treatment was “generally well tolerated.”
Consequently, “ruxolitinib cream represents a promising potential treatment for cutaneous lichen planus,” Mangold concluded.
Asked to comment on the results, Adam Friedman, MD, Professor and Chair of Dermatology, George Washington University, Washington, DC, who was not involved with the study, said that in keeping with the characterization of lichen planus using the four Ps — purple, polygonal, pruritic, papules — it is “Pretty common, Predictably disabling and disfiguring, and Passed over again and again in the drug development world.”
He said in an interview that this chronic inflammatory skin condition, which affects roughly 2% of the population, also “lacks consensus on work-up and management, likely in part owing to the absence of sizable clinical trial data.”
A recent survey conducted at a meeting indicated that dermatologists “heavily lean on topical therapies for the management of all severity levels,” noted Friedman, one of the survey authors. “Therefore, the phase 2 data presented at EADV is a welcome addition to the mix.”
Phase 2 Study Results
At the meeting, Mangold said that a previous proof-of-concept single-arm study in 12 patients suggested that topical ruxolitinib was highly effective in treating cutaneous lichen planus.
The current phase 2 trial enrolled 64 patients with predominantly cutaneous disease who had an Investigator’s Global Assessment (IGA) score of 3 or 4 and an Itch Numeric Rating Scale (NRS) score of ≥ 4. Their median age was 57 years, and 71.9% were women. Nearly 63% were White, 28.1% were Black, and 6.3% were Asian. The median duration of disease was 4.9 years, and 90.6% had received prior treatment for their lichen planus.
They were randomized to receive 1.5% ruxolitinib cream or a vehicle cream twice daily for 16 weeks, and following a primary endpoint assessment, they were transferred to an open-label extension period, during which they used ruxolitinib cream as needed for another 16 weeks. There was an additional 30-day safety follow-up period.
At week 16, significantly more patients treated with the ruxolitinib cream (50.0%) vs vehicle cream (21.9%) achieved IGA treatment success (the primary endpoint), defined as an IGA score of 0 or 1 with ≥ 2-grade improvement from baseline (odds ratio, 4.04; P = .0129).
In the open-label extension, when all patients used the active cream as needed, the proportion achieving IGA treatment success increased to 60% among the patients originally treated with ruxolitinib cream and 60.9% among those who switched from the vehicle cream.
A similar pattern was seen with Itch NRS scores. At 16 weeks, 57.7% of those treated with the ruxolitinib cream and 19.2% of those given the vehicle cream achieved an Itch NRS score of ≥ 4 (P < .01), rising to 84.2% and 73.3%, respectively, during the open-label extension.
The time to achievement of an Itch NRS of ≥ 4 was also significantly shorter with the ruxolitinib cream than with the vehicle cream (median days, 17 vs 97; hazard ratio, 2.85; P = .0008).
In both treatment groups, Skin Pain NRS scores decreased by a mean of 3.0 with ruxolitinib cream and 1.3 with the vehicle cream at week 16. By the end of the open-label extension, scores dropped by 4.3 among those who continued on active treatment and by 3.5 among those who switched from vehicle to topical ruxolitinib.
There were few treatment-emergent adverse events, with just three ruxolitinib patients affected during the randomized phase of the trial. There was one grade ≥ 3 event considered unrelated to the study drug, and no serious treatment-emergent adverse events were reported.
The most common adverse events during the randomized period were nasopharyngitis, hypertension, and contusion, all experienced by fewer than 10% of patients, whereas sinusitis, increased blood cholesterol levels, and increased blood creatine phosphokinase were most common in the open-label extension, experienced by no more than 5% of patients.
In the interview, Friedman commented that “these data provide hope that one day soon, there will be an FDA-approved, effective, and well-tolerated approach for this condition, validating the patient and supporting the dermatologist with an evidence-based option.”
The study was funded by Incyte. Mangold declared relationships with Argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Clarivate, Incyte Corporation, Janssen, Nuvig Therapeutics, Pfizer, Regeneron Pharmaceuticals, Soligenix, Tourmaline Bio, AbbVie, Corbus, Eli Lilly, Kyowa, Merck, miRagen Therapeutics, Palvella Therapeutics, Priovant Therapeutics, and Adelphi Values. Friedman declared a relationship with Incyte, but it is not related to this topic.
A version of this article first appeared on Medscape.com.
both when given twice daily and as needed, according to data from a phase 2 trial.
The research, presented at the European Academy of Dermatology and Venereology (EADV) 2024 Congress, involved 64 patients older than 18 years. Ruxolitinib cream (Opzelura) is a topical formulation of a Janus kinase (JAK)1/JAK2 inhibitor, approved by the Food and Drug Administration (FDA) for treating mild to moderate atopic dermatitis and for nonsegmental vitiligo in adults and children aged 12 years or older.
Ruxolitinib cream twice daily resulted in “significant improvements in cutaneous lichen planus disease severity vs vehicle” after 16 weeks of treatment, said the study presenter, Aaron R. Mangold, MD, a dermatologist at Mayo Clinic, Scottsdale, Arizona.
Further improvements were seen during another 16 weeks of additional open-label, as-needed application, he added, and the topical treatment was “generally well tolerated.”
Consequently, “ruxolitinib cream represents a promising potential treatment for cutaneous lichen planus,” Mangold concluded.
Asked to comment on the results, Adam Friedman, MD, Professor and Chair of Dermatology, George Washington University, Washington, DC, who was not involved with the study, said that in keeping with the characterization of lichen planus using the four Ps — purple, polygonal, pruritic, papules — it is “Pretty common, Predictably disabling and disfiguring, and Passed over again and again in the drug development world.”
He said in an interview that this chronic inflammatory skin condition, which affects roughly 2% of the population, also “lacks consensus on work-up and management, likely in part owing to the absence of sizable clinical trial data.”
A recent survey conducted at a meeting indicated that dermatologists “heavily lean on topical therapies for the management of all severity levels,” noted Friedman, one of the survey authors. “Therefore, the phase 2 data presented at EADV is a welcome addition to the mix.”
Phase 2 Study Results
At the meeting, Mangold said that a previous proof-of-concept single-arm study in 12 patients suggested that topical ruxolitinib was highly effective in treating cutaneous lichen planus.
The current phase 2 trial enrolled 64 patients with predominantly cutaneous disease who had an Investigator’s Global Assessment (IGA) score of 3 or 4 and an Itch Numeric Rating Scale (NRS) score of ≥ 4. Their median age was 57 years, and 71.9% were women. Nearly 63% were White, 28.1% were Black, and 6.3% were Asian. The median duration of disease was 4.9 years, and 90.6% had received prior treatment for their lichen planus.
They were randomized to receive 1.5% ruxolitinib cream or a vehicle cream twice daily for 16 weeks, and following a primary endpoint assessment, they were transferred to an open-label extension period, during which they used ruxolitinib cream as needed for another 16 weeks. There was an additional 30-day safety follow-up period.
At week 16, significantly more patients treated with the ruxolitinib cream (50.0%) vs vehicle cream (21.9%) achieved IGA treatment success (the primary endpoint), defined as an IGA score of 0 or 1 with ≥ 2-grade improvement from baseline (odds ratio, 4.04; P = .0129).
In the open-label extension, when all patients used the active cream as needed, the proportion achieving IGA treatment success increased to 60% among the patients originally treated with ruxolitinib cream and 60.9% among those who switched from the vehicle cream.
A similar pattern was seen with Itch NRS scores. At 16 weeks, 57.7% of those treated with the ruxolitinib cream and 19.2% of those given the vehicle cream achieved an Itch NRS score of ≥ 4 (P < .01), rising to 84.2% and 73.3%, respectively, during the open-label extension.
The time to achievement of an Itch NRS of ≥ 4 was also significantly shorter with the ruxolitinib cream than with the vehicle cream (median days, 17 vs 97; hazard ratio, 2.85; P = .0008).
In both treatment groups, Skin Pain NRS scores decreased by a mean of 3.0 with ruxolitinib cream and 1.3 with the vehicle cream at week 16. By the end of the open-label extension, scores dropped by 4.3 among those who continued on active treatment and by 3.5 among those who switched from vehicle to topical ruxolitinib.
There were few treatment-emergent adverse events, with just three ruxolitinib patients affected during the randomized phase of the trial. There was one grade ≥ 3 event considered unrelated to the study drug, and no serious treatment-emergent adverse events were reported.
The most common adverse events during the randomized period were nasopharyngitis, hypertension, and contusion, all experienced by fewer than 10% of patients, whereas sinusitis, increased blood cholesterol levels, and increased blood creatine phosphokinase were most common in the open-label extension, experienced by no more than 5% of patients.
In the interview, Friedman commented that “these data provide hope that one day soon, there will be an FDA-approved, effective, and well-tolerated approach for this condition, validating the patient and supporting the dermatologist with an evidence-based option.”
The study was funded by Incyte. Mangold declared relationships with Argenx, Boehringer Ingelheim, Bristol-Myers Squibb, Clarivate, Incyte Corporation, Janssen, Nuvig Therapeutics, Pfizer, Regeneron Pharmaceuticals, Soligenix, Tourmaline Bio, AbbVie, Corbus, Eli Lilly, Kyowa, Merck, miRagen Therapeutics, Palvella Therapeutics, Priovant Therapeutics, and Adelphi Values. Friedman declared a relationship with Incyte, but it is not related to this topic.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
Study Finds No Increased MACE Risk for JAK Inhibitors in Patients With Atopic Dermatitis
, suggested the results of a large, US-based, retrospective cohort study.
This holds true even in individuals aged 50 years or older, whose age puts them at increased cardiovascular (CV) risk, said Amina El Ayadi, PhD, of the University of Texas Medical Branch at Galveston. He presented the findings at the recent European Academy of Dermatology and Venereology (EADV) 2024 Congress.
Specifically, the analysis looked at treatment with the oral JAK1 inhibitors upadacitinib (Rinvoq) and abrocitinib (Cibinqo), both approved for treating AD in the United States, and found that the relative risk for MACE, such as acute myocardial infarction, cardiac arrest, stroke, or acute deep vein thrombosis, was ≤ 1.0 compared with those not treated with a JAKi.
Similarly, the relative risk for other CV safety endpoints, such as having an abnormal ECG or pericardial effusion, was also around 1.0. There was a slight increase in the relative risk for arrhythmias, peripheral edema, angina pectoris, or heart failure, but no value went > 1.6 and CIs spanned 1.0, indicating the results lack statistical significance.
Reassurance for Dermatologists?
“This suggests that oral administration of these drugs to the patient with atopic dermatitis does not increase the risk of major adverse cardiac events, and dermatologists, based on our data, can safely consider JAK inhibitors for treating moderate to severe dermatitis, even in patients with high risk for these diseases,” El Ayadi said during a late-breaking news session at the meeting.
Yolanda Gilaberte Calzada, MD, PhD, head of the Dermatology Department at Miguel Servet University Hospital in Zaragoza, Spain, who was one of the chairs for the session, said that this was “very good news for us.”
Gilaberte Calzada, president of the Spanish Academy of Dermatology and Venereology, asked if there were any data on the duration of treatment with the two JAKis included in the analysis. El Ayadi said that this was something that would be looked at in future data analyses.
Gilaberte Calzada also observed that because the CIs were wide, with more time, “we will have more defined data.”
Analyses Overview
For the two analyses — one in the overall population of patients with AD and the other in those aged 50 years or older — electronic medical record (EMR) data from the TriNetX Research Network were used. This is a global, federated health research network that contains EMRs for more than 275 million patients from over 120 healthcare organizations, El Ayadi explained.
To perform the analyses, the research team queried the TriNetX database to find all patients diagnosed with AD via the International Classification of Diseases, Tenth Revision code L20. They then determined if patients had been treated with JAKi or not, and specifically, with upadacitinib or abrocitinib. Those who had not received any JAKi treatment were the control population.
For the first analysis, no age-specific filter was applied. The investigators identified 1674 people with AD who had been treated with the JAKis and around 1.2 million who had not. Propensity score matching, based on age at diagnosis, biologic sex, and CV comorbidities, was performed to give a total of 1674 patients who had and 1674 who had not been treated with these medications.
In the second analysis, only those aged 50 years or older were considered; 875 patients who had received JAKi treatment were identified and around 250,000 who had not. Propensity score matching based on the same variables gave two groups of 875 people who had or had not taken a JAKi.
Queried over the age cutoff used, El Ayadi noted, “We did an analysis looking at patients 65 and older. However, we came up with lower patient numbers. … We do have this data, and we did not see any significant risk.”
The study was independently supported. El Ayadi and Gilaberte Calzada reported no conflicts of interest in relation to the presented findings.
A version of this article first appeared on Medscape.com.
, suggested the results of a large, US-based, retrospective cohort study.
This holds true even in individuals aged 50 years or older, whose age puts them at increased cardiovascular (CV) risk, said Amina El Ayadi, PhD, of the University of Texas Medical Branch at Galveston. He presented the findings at the recent European Academy of Dermatology and Venereology (EADV) 2024 Congress.
Specifically, the analysis looked at treatment with the oral JAK1 inhibitors upadacitinib (Rinvoq) and abrocitinib (Cibinqo), both approved for treating AD in the United States, and found that the relative risk for MACE, such as acute myocardial infarction, cardiac arrest, stroke, or acute deep vein thrombosis, was ≤ 1.0 compared with those not treated with a JAKi.
Similarly, the relative risk for other CV safety endpoints, such as having an abnormal ECG or pericardial effusion, was also around 1.0. There was a slight increase in the relative risk for arrhythmias, peripheral edema, angina pectoris, or heart failure, but no value went > 1.6 and CIs spanned 1.0, indicating the results lack statistical significance.
Reassurance for Dermatologists?
“This suggests that oral administration of these drugs to the patient with atopic dermatitis does not increase the risk of major adverse cardiac events, and dermatologists, based on our data, can safely consider JAK inhibitors for treating moderate to severe dermatitis, even in patients with high risk for these diseases,” El Ayadi said during a late-breaking news session at the meeting.
Yolanda Gilaberte Calzada, MD, PhD, head of the Dermatology Department at Miguel Servet University Hospital in Zaragoza, Spain, who was one of the chairs for the session, said that this was “very good news for us.”
Gilaberte Calzada, president of the Spanish Academy of Dermatology and Venereology, asked if there were any data on the duration of treatment with the two JAKis included in the analysis. El Ayadi said that this was something that would be looked at in future data analyses.
Gilaberte Calzada also observed that because the CIs were wide, with more time, “we will have more defined data.”
Analyses Overview
For the two analyses — one in the overall population of patients with AD and the other in those aged 50 years or older — electronic medical record (EMR) data from the TriNetX Research Network were used. This is a global, federated health research network that contains EMRs for more than 275 million patients from over 120 healthcare organizations, El Ayadi explained.
To perform the analyses, the research team queried the TriNetX database to find all patients diagnosed with AD via the International Classification of Diseases, Tenth Revision code L20. They then determined if patients had been treated with JAKi or not, and specifically, with upadacitinib or abrocitinib. Those who had not received any JAKi treatment were the control population.
For the first analysis, no age-specific filter was applied. The investigators identified 1674 people with AD who had been treated with the JAKis and around 1.2 million who had not. Propensity score matching, based on age at diagnosis, biologic sex, and CV comorbidities, was performed to give a total of 1674 patients who had and 1674 who had not been treated with these medications.
In the second analysis, only those aged 50 years or older were considered; 875 patients who had received JAKi treatment were identified and around 250,000 who had not. Propensity score matching based on the same variables gave two groups of 875 people who had or had not taken a JAKi.
Queried over the age cutoff used, El Ayadi noted, “We did an analysis looking at patients 65 and older. However, we came up with lower patient numbers. … We do have this data, and we did not see any significant risk.”
The study was independently supported. El Ayadi and Gilaberte Calzada reported no conflicts of interest in relation to the presented findings.
A version of this article first appeared on Medscape.com.
, suggested the results of a large, US-based, retrospective cohort study.
This holds true even in individuals aged 50 years or older, whose age puts them at increased cardiovascular (CV) risk, said Amina El Ayadi, PhD, of the University of Texas Medical Branch at Galveston. He presented the findings at the recent European Academy of Dermatology and Venereology (EADV) 2024 Congress.
Specifically, the analysis looked at treatment with the oral JAK1 inhibitors upadacitinib (Rinvoq) and abrocitinib (Cibinqo), both approved for treating AD in the United States, and found that the relative risk for MACE, such as acute myocardial infarction, cardiac arrest, stroke, or acute deep vein thrombosis, was ≤ 1.0 compared with those not treated with a JAKi.
Similarly, the relative risk for other CV safety endpoints, such as having an abnormal ECG or pericardial effusion, was also around 1.0. There was a slight increase in the relative risk for arrhythmias, peripheral edema, angina pectoris, or heart failure, but no value went > 1.6 and CIs spanned 1.0, indicating the results lack statistical significance.
Reassurance for Dermatologists?
“This suggests that oral administration of these drugs to the patient with atopic dermatitis does not increase the risk of major adverse cardiac events, and dermatologists, based on our data, can safely consider JAK inhibitors for treating moderate to severe dermatitis, even in patients with high risk for these diseases,” El Ayadi said during a late-breaking news session at the meeting.
Yolanda Gilaberte Calzada, MD, PhD, head of the Dermatology Department at Miguel Servet University Hospital in Zaragoza, Spain, who was one of the chairs for the session, said that this was “very good news for us.”
Gilaberte Calzada, president of the Spanish Academy of Dermatology and Venereology, asked if there were any data on the duration of treatment with the two JAKis included in the analysis. El Ayadi said that this was something that would be looked at in future data analyses.
Gilaberte Calzada also observed that because the CIs were wide, with more time, “we will have more defined data.”
Analyses Overview
For the two analyses — one in the overall population of patients with AD and the other in those aged 50 years or older — electronic medical record (EMR) data from the TriNetX Research Network were used. This is a global, federated health research network that contains EMRs for more than 275 million patients from over 120 healthcare organizations, El Ayadi explained.
To perform the analyses, the research team queried the TriNetX database to find all patients diagnosed with AD via the International Classification of Diseases, Tenth Revision code L20. They then determined if patients had been treated with JAKi or not, and specifically, with upadacitinib or abrocitinib. Those who had not received any JAKi treatment were the control population.
For the first analysis, no age-specific filter was applied. The investigators identified 1674 people with AD who had been treated with the JAKis and around 1.2 million who had not. Propensity score matching, based on age at diagnosis, biologic sex, and CV comorbidities, was performed to give a total of 1674 patients who had and 1674 who had not been treated with these medications.
In the second analysis, only those aged 50 years or older were considered; 875 patients who had received JAKi treatment were identified and around 250,000 who had not. Propensity score matching based on the same variables gave two groups of 875 people who had or had not taken a JAKi.
Queried over the age cutoff used, El Ayadi noted, “We did an analysis looking at patients 65 and older. However, we came up with lower patient numbers. … We do have this data, and we did not see any significant risk.”
The study was independently supported. El Ayadi and Gilaberte Calzada reported no conflicts of interest in relation to the presented findings.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
Topical JAK Inhibitor Effective for Hand Eczema, Two Studies Suggest
suggested the results of two separate studies presented during the late-breaking sessions at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
In the 24-week, phase 3 DELTA FORCE trial, topical delgocitinib was compared head to head with oral alitretinoin for managing chronic hand eczema (CHE). Results showed that greater improvements from baseline to week 12 in Hand Eczema Severity Index (HECSI) scores could be achieved with delgocitinib cream than with alitretinoin capsules.
And in another analysis, which involved patients with the atopic subtype of CHE only, the application of topical delgocitinib was found to be as good as treatment with subcutaneous dupilumab (Dupixent) at improving both HECSI scores and the Investigator Global Assessment for CHE response (IGA-CHE).
Potentially a ‘Highly Impactful’ Therapy
“Chronic hand eczema is a common yet burdensome skin condition that poses a considerable challenge for dermatologists. Diversity in morphologic presentation and clinical etiology has been a key limitation for the development of a safe, targeted, one-size-fits-all therapeutic approach,” Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University of Medicine and Science, and the founder and director of the Center for Medical Dermatology and Immunology Research in Chicago, Illinois, said in an interview.
“These data show that delgocitinib cream is poised to be a novel and highly impactful topical therapy for the treatment of CHE,” said Chovatiya.
DELTA FORCE showed that the efficacy and safety of delgocitinib cream was “superior to alitretinoin, the only approved oral option for CHE,” he said. And the other study, a comparative analysis, showed that delgocitinib’s efficacy was “comparable to the biologic dupilumab specifically for the treatment of atopic hand eczema,” said Chovatiya, one of the authors of that study. He was not an author of the DELTA FORCE study.
DELTA FORCE
While it remains an investigational drug in the United States, where it is under Food and Drug Administration review for CHE, delgocitinib cream (Anzupgo) was recently approved by the European Commission for use in adults with moderate to severe hand eczema who do not respond to or who are unable to use topical corticosteroids. Approval was based on data from two phase 3 studies , DELTA 1 and DELTA 2, which compared delgocitinib cream against a cream vehicle, as well as an open-label, long-term extension study, DELTA 3.
In the DELTA FORCE study, 513 adults with severe CHE (IGA-CHE score of 4) were recruited at 102 clinical centers in Europe and North America and randomly allocated to topical treatment with delgocitinib cream, 20 mg/g applied twice daily, or alitretinoin capsules, 30 mg once daily. Treatment with delgocitinib was for 16 weeks, and treatment with alitretinoin was for 12 weeks. The latter’s dose could be reduced to 10 mg in the event of intolerability, and both treatments could be reintroduced if necessary, with a final follow-up at 24 weeks.
Study investigator Ana Maria Giménez-Arnau, MD, PhD, of the Hospital del Mar Research Institute, Pompeu Fabra University, Barcelona, Spain, who presented the findings, noted that alitretinoin (Toctino) is an oral systemic retinoid approved in a few European countries, Canada, Israel, and South Korea for the treatment of severe CHE.
The mean age of the participants was 45 years, almost two thirds were women, and the majority (93%) were White; 90% of patients had been recruited in Europe. The median duration of CHE was 4 years.
At baseline, the median HECSI score was recorded as 79.5 in the delgocitinib arm and 80.0 in the alitretinoin arm. At 12 weeks, the least squares mean change in HECSI score from baseline was –67.6 in the delgocitinib arm and –51.5 in the alitretinoin arm, giving a significant difference of –16.1 between the two groups (P < .001).
Giménez-Arnau reported that delgocitinib also outperformed alitretinoin for all other endpoints assessed, including the following: ≥ 90% improvement in HECSI (HECSI-90), IGA-CHE treatment success (defined as a score of 0/1 indicating clear/almost clear skin), changes in Hand Eczema Symptom Diary (HESD) itch and HESD pain scores, area under the curve for HECSI-90, change in Dermatology Life Quality Index score — which were all assessed at 12 weeks — and change in HECSI from baseline to week 24.
There was “significant improvement in the reduction of the HECSI from the first week” of treatment, Giménez-Arnau said at the meeting. Notably, that the effect increased to 12 weeks and then was sustained. A similar pattern was seen for IGA-CHE treatment success and for HESD pain. This is important as “chronic hand eczema is really painful,” she said.
As for safety, 49.4% of patients in the delgocitinib arm vs 76.1% of patients in the alitretinoin arm experienced any type of adverse event (AE). Serious AEs occurred in 2% and 4.9% of patients in each group, respectively, with fewer AEs leading to trial drug discontinuation observed in the delgocitinib arm (1.2% vs 10.1%). The proportion of AEs “probably or possibly” related to the trial drug was 9.5% in the delgocitinib group vs 54.3% in the alitretinoin group.
Comparison With Dupilumab in Another Trial
Delgocitinib is no longer just an investigational medication, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said during a separate late-breaking presentation at the EADV 2024 meeting. “I think it’s big news because now we have an important topical option for our patients with chronic hand eczema.”
Armstrong presented a matched-adjusted indirect comparison (MAIC) of delgocitinib vs dupilumab for the treatment of moderate to severe atopic hand eczema, which she described as “the next best thing” to a head-to-head trial.
MAICs are where patient level data from one or more clinical trials evaluating drug “A” are compared with aggregate data from one or more clinical trials evaluating drug “B.” In this case, individual patient data from the DELTA 1 and DELTA 2 trials of delgocitinib were compared with published aggregate data from the phase 3 LIBERTY-AD-HAFT trial of dupilumab.
A total of 201 patients with atopic hand eczema in the DELTA 1 and DELTA 2 trials were matched to 133 patients in the LIBERTY-AD-HAFT trial. Of these, 128 had been treated with delgocitinib cream, 73 with a cream vehicle, 67 with subcutaneous dupilumab, and 66 with a subcutaneous placebo.
“We’re trying to compare as much as possible apples to apples here in terms of the etiology of hand eczema,” Armstrong said. She noted that after matching and weighting based on age, sex, race, and baseline HECSI score, baseline characteristics in the two groups of patients were similar. The mean age was about 35.8 years in the two active treatment arms and 33.4 years in the two placebo arms, and mean baseline HESCI scores were about 79-80.
The endpoints compared were ≥ 75% improvement in HECSI; HECSI-90, HECSI percentage improvement, and IGA-CHE in the DELTA 1 and DELTA 2 trials; or a Hand and Foot IGA score of 0/1.
“The key message to take away from this is that there were no statistically significant differences between topical delgocitinib twice daily vs subcutaneous injection of dupilumab by week 16 in the treatment of patients with atopic hand dermatitis,” Armstrong reported. Odds ratios varied between 1.1 and 1.3 for the various endpoints.
Menno de Rie, MD, PhD, professor of dermatology and immunology at Amsterdam University Medical Center in the Netherlands, who cochaired the session, said that “I appreciate very much that you took the effort to compare these totally different compounds and showed us the methodology that you did. It’s really very impressive.”
Topical, Systemic, or Both?
Armstrong was questioned on how to manage someone with atopic hand dermatitis who developed lesions elsewhere on the body.
“I would take a really individualized approach to this patient,” she responded. If the eczema has been limited to the hands and has been there for a while, then perhaps delgocitinib would be her choice, but if they developed lesions elsewhere on the body, then a systemic treatment such as dupilumab may be preferable.
“The good thing is that this study shows that you can offer the patient either of those options and really engage the patient in a shared decision-making process.”
And with regards to whether the two might possibly be used together, Armstrong acknowledged insurance coverage restrictions could be a limiting factor in the United States, but elsewhere — and from a scientific point of view — this could make sense.
“If we have a patient, for example, who has moderate to severe atopic dermatitis involving the body, but also very severe hand eczema as well, one may possibly consider a combination of a systemic medication that’s helpful for the extensive area of involvement on the body ... and now you have a topical therapy, delgocitinib, where you can use it locally, have very deep efficacy locally, to kind of help augment that disease phenotype in that patient population.”
The studies were funded by Leo Pharma. Chovatiya, Giménez-Arnau, and Armstrong acknowledged ties to LEO Pharma, among other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
suggested the results of two separate studies presented during the late-breaking sessions at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
In the 24-week, phase 3 DELTA FORCE trial, topical delgocitinib was compared head to head with oral alitretinoin for managing chronic hand eczema (CHE). Results showed that greater improvements from baseline to week 12 in Hand Eczema Severity Index (HECSI) scores could be achieved with delgocitinib cream than with alitretinoin capsules.
And in another analysis, which involved patients with the atopic subtype of CHE only, the application of topical delgocitinib was found to be as good as treatment with subcutaneous dupilumab (Dupixent) at improving both HECSI scores and the Investigator Global Assessment for CHE response (IGA-CHE).
Potentially a ‘Highly Impactful’ Therapy
“Chronic hand eczema is a common yet burdensome skin condition that poses a considerable challenge for dermatologists. Diversity in morphologic presentation and clinical etiology has been a key limitation for the development of a safe, targeted, one-size-fits-all therapeutic approach,” Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University of Medicine and Science, and the founder and director of the Center for Medical Dermatology and Immunology Research in Chicago, Illinois, said in an interview.
“These data show that delgocitinib cream is poised to be a novel and highly impactful topical therapy for the treatment of CHE,” said Chovatiya.
DELTA FORCE showed that the efficacy and safety of delgocitinib cream was “superior to alitretinoin, the only approved oral option for CHE,” he said. And the other study, a comparative analysis, showed that delgocitinib’s efficacy was “comparable to the biologic dupilumab specifically for the treatment of atopic hand eczema,” said Chovatiya, one of the authors of that study. He was not an author of the DELTA FORCE study.
DELTA FORCE
While it remains an investigational drug in the United States, where it is under Food and Drug Administration review for CHE, delgocitinib cream (Anzupgo) was recently approved by the European Commission for use in adults with moderate to severe hand eczema who do not respond to or who are unable to use topical corticosteroids. Approval was based on data from two phase 3 studies , DELTA 1 and DELTA 2, which compared delgocitinib cream against a cream vehicle, as well as an open-label, long-term extension study, DELTA 3.
In the DELTA FORCE study, 513 adults with severe CHE (IGA-CHE score of 4) were recruited at 102 clinical centers in Europe and North America and randomly allocated to topical treatment with delgocitinib cream, 20 mg/g applied twice daily, or alitretinoin capsules, 30 mg once daily. Treatment with delgocitinib was for 16 weeks, and treatment with alitretinoin was for 12 weeks. The latter’s dose could be reduced to 10 mg in the event of intolerability, and both treatments could be reintroduced if necessary, with a final follow-up at 24 weeks.
Study investigator Ana Maria Giménez-Arnau, MD, PhD, of the Hospital del Mar Research Institute, Pompeu Fabra University, Barcelona, Spain, who presented the findings, noted that alitretinoin (Toctino) is an oral systemic retinoid approved in a few European countries, Canada, Israel, and South Korea for the treatment of severe CHE.
The mean age of the participants was 45 years, almost two thirds were women, and the majority (93%) were White; 90% of patients had been recruited in Europe. The median duration of CHE was 4 years.
At baseline, the median HECSI score was recorded as 79.5 in the delgocitinib arm and 80.0 in the alitretinoin arm. At 12 weeks, the least squares mean change in HECSI score from baseline was –67.6 in the delgocitinib arm and –51.5 in the alitretinoin arm, giving a significant difference of –16.1 between the two groups (P < .001).
Giménez-Arnau reported that delgocitinib also outperformed alitretinoin for all other endpoints assessed, including the following: ≥ 90% improvement in HECSI (HECSI-90), IGA-CHE treatment success (defined as a score of 0/1 indicating clear/almost clear skin), changes in Hand Eczema Symptom Diary (HESD) itch and HESD pain scores, area under the curve for HECSI-90, change in Dermatology Life Quality Index score — which were all assessed at 12 weeks — and change in HECSI from baseline to week 24.
There was “significant improvement in the reduction of the HECSI from the first week” of treatment, Giménez-Arnau said at the meeting. Notably, that the effect increased to 12 weeks and then was sustained. A similar pattern was seen for IGA-CHE treatment success and for HESD pain. This is important as “chronic hand eczema is really painful,” she said.
As for safety, 49.4% of patients in the delgocitinib arm vs 76.1% of patients in the alitretinoin arm experienced any type of adverse event (AE). Serious AEs occurred in 2% and 4.9% of patients in each group, respectively, with fewer AEs leading to trial drug discontinuation observed in the delgocitinib arm (1.2% vs 10.1%). The proportion of AEs “probably or possibly” related to the trial drug was 9.5% in the delgocitinib group vs 54.3% in the alitretinoin group.
Comparison With Dupilumab in Another Trial
Delgocitinib is no longer just an investigational medication, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said during a separate late-breaking presentation at the EADV 2024 meeting. “I think it’s big news because now we have an important topical option for our patients with chronic hand eczema.”
Armstrong presented a matched-adjusted indirect comparison (MAIC) of delgocitinib vs dupilumab for the treatment of moderate to severe atopic hand eczema, which she described as “the next best thing” to a head-to-head trial.
MAICs are where patient level data from one or more clinical trials evaluating drug “A” are compared with aggregate data from one or more clinical trials evaluating drug “B.” In this case, individual patient data from the DELTA 1 and DELTA 2 trials of delgocitinib were compared with published aggregate data from the phase 3 LIBERTY-AD-HAFT trial of dupilumab.
A total of 201 patients with atopic hand eczema in the DELTA 1 and DELTA 2 trials were matched to 133 patients in the LIBERTY-AD-HAFT trial. Of these, 128 had been treated with delgocitinib cream, 73 with a cream vehicle, 67 with subcutaneous dupilumab, and 66 with a subcutaneous placebo.
“We’re trying to compare as much as possible apples to apples here in terms of the etiology of hand eczema,” Armstrong said. She noted that after matching and weighting based on age, sex, race, and baseline HECSI score, baseline characteristics in the two groups of patients were similar. The mean age was about 35.8 years in the two active treatment arms and 33.4 years in the two placebo arms, and mean baseline HESCI scores were about 79-80.
The endpoints compared were ≥ 75% improvement in HECSI; HECSI-90, HECSI percentage improvement, and IGA-CHE in the DELTA 1 and DELTA 2 trials; or a Hand and Foot IGA score of 0/1.
“The key message to take away from this is that there were no statistically significant differences between topical delgocitinib twice daily vs subcutaneous injection of dupilumab by week 16 in the treatment of patients with atopic hand dermatitis,” Armstrong reported. Odds ratios varied between 1.1 and 1.3 for the various endpoints.
Menno de Rie, MD, PhD, professor of dermatology and immunology at Amsterdam University Medical Center in the Netherlands, who cochaired the session, said that “I appreciate very much that you took the effort to compare these totally different compounds and showed us the methodology that you did. It’s really very impressive.”
Topical, Systemic, or Both?
Armstrong was questioned on how to manage someone with atopic hand dermatitis who developed lesions elsewhere on the body.
“I would take a really individualized approach to this patient,” she responded. If the eczema has been limited to the hands and has been there for a while, then perhaps delgocitinib would be her choice, but if they developed lesions elsewhere on the body, then a systemic treatment such as dupilumab may be preferable.
“The good thing is that this study shows that you can offer the patient either of those options and really engage the patient in a shared decision-making process.”
And with regards to whether the two might possibly be used together, Armstrong acknowledged insurance coverage restrictions could be a limiting factor in the United States, but elsewhere — and from a scientific point of view — this could make sense.
“If we have a patient, for example, who has moderate to severe atopic dermatitis involving the body, but also very severe hand eczema as well, one may possibly consider a combination of a systemic medication that’s helpful for the extensive area of involvement on the body ... and now you have a topical therapy, delgocitinib, where you can use it locally, have very deep efficacy locally, to kind of help augment that disease phenotype in that patient population.”
The studies were funded by Leo Pharma. Chovatiya, Giménez-Arnau, and Armstrong acknowledged ties to LEO Pharma, among other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
suggested the results of two separate studies presented during the late-breaking sessions at the European Academy of Dermatology and Venereology (EADV) 2024 Congress.
In the 24-week, phase 3 DELTA FORCE trial, topical delgocitinib was compared head to head with oral alitretinoin for managing chronic hand eczema (CHE). Results showed that greater improvements from baseline to week 12 in Hand Eczema Severity Index (HECSI) scores could be achieved with delgocitinib cream than with alitretinoin capsules.
And in another analysis, which involved patients with the atopic subtype of CHE only, the application of topical delgocitinib was found to be as good as treatment with subcutaneous dupilumab (Dupixent) at improving both HECSI scores and the Investigator Global Assessment for CHE response (IGA-CHE).
Potentially a ‘Highly Impactful’ Therapy
“Chronic hand eczema is a common yet burdensome skin condition that poses a considerable challenge for dermatologists. Diversity in morphologic presentation and clinical etiology has been a key limitation for the development of a safe, targeted, one-size-fits-all therapeutic approach,” Raj Chovatiya, MD, PhD, clinical associate professor at Chicago Medical School, Rosalind Franklin University of Medicine and Science, and the founder and director of the Center for Medical Dermatology and Immunology Research in Chicago, Illinois, said in an interview.
“These data show that delgocitinib cream is poised to be a novel and highly impactful topical therapy for the treatment of CHE,” said Chovatiya.
DELTA FORCE showed that the efficacy and safety of delgocitinib cream was “superior to alitretinoin, the only approved oral option for CHE,” he said. And the other study, a comparative analysis, showed that delgocitinib’s efficacy was “comparable to the biologic dupilumab specifically for the treatment of atopic hand eczema,” said Chovatiya, one of the authors of that study. He was not an author of the DELTA FORCE study.
DELTA FORCE
While it remains an investigational drug in the United States, where it is under Food and Drug Administration review for CHE, delgocitinib cream (Anzupgo) was recently approved by the European Commission for use in adults with moderate to severe hand eczema who do not respond to or who are unable to use topical corticosteroids. Approval was based on data from two phase 3 studies , DELTA 1 and DELTA 2, which compared delgocitinib cream against a cream vehicle, as well as an open-label, long-term extension study, DELTA 3.
In the DELTA FORCE study, 513 adults with severe CHE (IGA-CHE score of 4) were recruited at 102 clinical centers in Europe and North America and randomly allocated to topical treatment with delgocitinib cream, 20 mg/g applied twice daily, or alitretinoin capsules, 30 mg once daily. Treatment with delgocitinib was for 16 weeks, and treatment with alitretinoin was for 12 weeks. The latter’s dose could be reduced to 10 mg in the event of intolerability, and both treatments could be reintroduced if necessary, with a final follow-up at 24 weeks.
Study investigator Ana Maria Giménez-Arnau, MD, PhD, of the Hospital del Mar Research Institute, Pompeu Fabra University, Barcelona, Spain, who presented the findings, noted that alitretinoin (Toctino) is an oral systemic retinoid approved in a few European countries, Canada, Israel, and South Korea for the treatment of severe CHE.
The mean age of the participants was 45 years, almost two thirds were women, and the majority (93%) were White; 90% of patients had been recruited in Europe. The median duration of CHE was 4 years.
At baseline, the median HECSI score was recorded as 79.5 in the delgocitinib arm and 80.0 in the alitretinoin arm. At 12 weeks, the least squares mean change in HECSI score from baseline was –67.6 in the delgocitinib arm and –51.5 in the alitretinoin arm, giving a significant difference of –16.1 between the two groups (P < .001).
Giménez-Arnau reported that delgocitinib also outperformed alitretinoin for all other endpoints assessed, including the following: ≥ 90% improvement in HECSI (HECSI-90), IGA-CHE treatment success (defined as a score of 0/1 indicating clear/almost clear skin), changes in Hand Eczema Symptom Diary (HESD) itch and HESD pain scores, area under the curve for HECSI-90, change in Dermatology Life Quality Index score — which were all assessed at 12 weeks — and change in HECSI from baseline to week 24.
There was “significant improvement in the reduction of the HECSI from the first week” of treatment, Giménez-Arnau said at the meeting. Notably, that the effect increased to 12 weeks and then was sustained. A similar pattern was seen for IGA-CHE treatment success and for HESD pain. This is important as “chronic hand eczema is really painful,” she said.
As for safety, 49.4% of patients in the delgocitinib arm vs 76.1% of patients in the alitretinoin arm experienced any type of adverse event (AE). Serious AEs occurred in 2% and 4.9% of patients in each group, respectively, with fewer AEs leading to trial drug discontinuation observed in the delgocitinib arm (1.2% vs 10.1%). The proportion of AEs “probably or possibly” related to the trial drug was 9.5% in the delgocitinib group vs 54.3% in the alitretinoin group.
Comparison With Dupilumab in Another Trial
Delgocitinib is no longer just an investigational medication, April W. Armstrong, MD, MPH, professor and chief of dermatology, University of California, Los Angeles, said during a separate late-breaking presentation at the EADV 2024 meeting. “I think it’s big news because now we have an important topical option for our patients with chronic hand eczema.”
Armstrong presented a matched-adjusted indirect comparison (MAIC) of delgocitinib vs dupilumab for the treatment of moderate to severe atopic hand eczema, which she described as “the next best thing” to a head-to-head trial.
MAICs are where patient level data from one or more clinical trials evaluating drug “A” are compared with aggregate data from one or more clinical trials evaluating drug “B.” In this case, individual patient data from the DELTA 1 and DELTA 2 trials of delgocitinib were compared with published aggregate data from the phase 3 LIBERTY-AD-HAFT trial of dupilumab.
A total of 201 patients with atopic hand eczema in the DELTA 1 and DELTA 2 trials were matched to 133 patients in the LIBERTY-AD-HAFT trial. Of these, 128 had been treated with delgocitinib cream, 73 with a cream vehicle, 67 with subcutaneous dupilumab, and 66 with a subcutaneous placebo.
“We’re trying to compare as much as possible apples to apples here in terms of the etiology of hand eczema,” Armstrong said. She noted that after matching and weighting based on age, sex, race, and baseline HECSI score, baseline characteristics in the two groups of patients were similar. The mean age was about 35.8 years in the two active treatment arms and 33.4 years in the two placebo arms, and mean baseline HESCI scores were about 79-80.
The endpoints compared were ≥ 75% improvement in HECSI; HECSI-90, HECSI percentage improvement, and IGA-CHE in the DELTA 1 and DELTA 2 trials; or a Hand and Foot IGA score of 0/1.
“The key message to take away from this is that there were no statistically significant differences between topical delgocitinib twice daily vs subcutaneous injection of dupilumab by week 16 in the treatment of patients with atopic hand dermatitis,” Armstrong reported. Odds ratios varied between 1.1 and 1.3 for the various endpoints.
Menno de Rie, MD, PhD, professor of dermatology and immunology at Amsterdam University Medical Center in the Netherlands, who cochaired the session, said that “I appreciate very much that you took the effort to compare these totally different compounds and showed us the methodology that you did. It’s really very impressive.”
Topical, Systemic, or Both?
Armstrong was questioned on how to manage someone with atopic hand dermatitis who developed lesions elsewhere on the body.
“I would take a really individualized approach to this patient,” she responded. If the eczema has been limited to the hands and has been there for a while, then perhaps delgocitinib would be her choice, but if they developed lesions elsewhere on the body, then a systemic treatment such as dupilumab may be preferable.
“The good thing is that this study shows that you can offer the patient either of those options and really engage the patient in a shared decision-making process.”
And with regards to whether the two might possibly be used together, Armstrong acknowledged insurance coverage restrictions could be a limiting factor in the United States, but elsewhere — and from a scientific point of view — this could make sense.
“If we have a patient, for example, who has moderate to severe atopic dermatitis involving the body, but also very severe hand eczema as well, one may possibly consider a combination of a systemic medication that’s helpful for the extensive area of involvement on the body ... and now you have a topical therapy, delgocitinib, where you can use it locally, have very deep efficacy locally, to kind of help augment that disease phenotype in that patient population.”
The studies were funded by Leo Pharma. Chovatiya, Giménez-Arnau, and Armstrong acknowledged ties to LEO Pharma, among other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
FROM EADV 2024
Many Patients With Cancer Visit EDs Before Diagnosis
Researchers examined Institute for Clinical Evaluative Sciences (ICES) data that had been gathered from January 1, 2014, to December 31, 2021. The study focused on patients aged 18 years or older with confirmed primary cancer diagnoses.
Factors associated with an increased likelihood of an ED visit ahead of diagnosis included having certain cancers, living in rural areas, and having less access to primary care, according to study author Keerat Grewal, MD, an emergency physician and clinician scientist at the Schwartz/Reisman Emergency Medicine Institute at Sinai Health in Toronto, Ontario, Canada, and coauthors.
“The ED is a distressing environment for patients to receive a possible cancer diagnosis,” the authors wrote. “Moreover, it is frequently ill equipped to provide ongoing continuity of care, which can lead patients down a poorly defined diagnostic pathway before receiving a confirmed diagnosis based on tissue and a subsequent treatment plan.”
The findings were published online on November 4 in CMAJ).
Neurologic Cancers Prominent
In an interview, Grewal said in an interview that the study reflects her desire as an emergency room physician to understand why so many patients with cancer get the initial reports about their disease from clinicians whom they often have just met for the first time.
Among patients with an ED visit before cancer diagnosis, 51.4% were admitted to hospital from the most recent visit.
Compared with patients with a family physician on whom they could rely for routine care, those who had no outpatient visits (odds ratio [OR], 2.09) or fewer than three outpatient visits (OR, 1.41) in the 6-30 months before cancer diagnosis were more likely to have an ED visit before their cancer diagnosis.
Other factors associated with increased odds of ED use before cancer diagnosis included rurality (OR, 1.15), residence in northern Ontario (northeast region: OR, 1.14 and northwest region: OR, 1.27 vs Toronto region), and living in the most marginalized areas (material resource deprivation: OR, 1.37 and housing stability: OR, 1.09 vs least marginalized area).
The researchers also found that patients with certain cancers were more likely to have sought care in the ED. They compared these cancers with breast cancer, which is often detected through screening.
“Patients with neurologic cancers had extremely high odds of ED use before cancer diagnosis,” the authors wrote. “This is likely because of the emergent nature of presentation, with acute neurologic symptoms such as weakness, confusion, or seizures, which require urgent assessment.” On the other hand, pancreatic, liver, or thoracic cancer can trigger nonspecific symptoms that may be ignored until they reach a crisis level that prompts an ED visit.
The limitations of the study included its inability to identify cancer-related ED visits and its narrow focus on patients in Ontario, according to the researchers. But the use of the ICES databases also allowed researchers access to a broader pool of data than are available in many other cases.
The findings in the new paper echo those of previous research, the authors noted. Research in the United Kingdom found that 24%-31% of cancer diagnoses involved the ED. In addition, a study of people enrolled in the US Medicare program, which serves patients aged 65 years or older, found that 23% were seen in the ED in the 30 days before diagnosis.
‘Unpacking the Data’
The current findings also are consistent with those of an International Cancer Benchmarking Partnership study that was published in 2022 in The Lancet Oncology, said Erika Nicholson, MHS, vice president of cancer systems and innovation at the Canadian Partnership Against Cancer. The latter study analyzed cancer registration and linked hospital admissions data from 14 jurisdictions in Australia, Canada, Denmark, New Zealand, Norway, and the United Kingdom.
“We see similar trends in terms of people visiting EDs and being diagnosed through EDs internationally,” Nicholson said. “We’re working with partners to put in place different strategies to address the challenges” that this phenomenon presents in terms of improving screening and follow-up care.
“Cancer is not one disease, but many diseases,” she said. “They present differently. We’re focused on really unpacking the data and understanding them.”
All this research highlights the need for more services and personnel to address cancer, including people who are trained to help patients cope after getting concerning news through emergency care, she said.
“That means having a system that fully supports you and helps you navigate through that diagnostic process,” Nicholson said. Addressing the added challenges for patients who don’t have secure housing is a special need, she added.
This study was supported by the Canadian Institutes of Health Research (CIHR). Grewal reported receiving grants from CIHR and the Canadian Association of Emergency Physicians. Nicholson reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Researchers examined Institute for Clinical Evaluative Sciences (ICES) data that had been gathered from January 1, 2014, to December 31, 2021. The study focused on patients aged 18 years or older with confirmed primary cancer diagnoses.
Factors associated with an increased likelihood of an ED visit ahead of diagnosis included having certain cancers, living in rural areas, and having less access to primary care, according to study author Keerat Grewal, MD, an emergency physician and clinician scientist at the Schwartz/Reisman Emergency Medicine Institute at Sinai Health in Toronto, Ontario, Canada, and coauthors.
“The ED is a distressing environment for patients to receive a possible cancer diagnosis,” the authors wrote. “Moreover, it is frequently ill equipped to provide ongoing continuity of care, which can lead patients down a poorly defined diagnostic pathway before receiving a confirmed diagnosis based on tissue and a subsequent treatment plan.”
The findings were published online on November 4 in CMAJ).
Neurologic Cancers Prominent
In an interview, Grewal said in an interview that the study reflects her desire as an emergency room physician to understand why so many patients with cancer get the initial reports about their disease from clinicians whom they often have just met for the first time.
Among patients with an ED visit before cancer diagnosis, 51.4% were admitted to hospital from the most recent visit.
Compared with patients with a family physician on whom they could rely for routine care, those who had no outpatient visits (odds ratio [OR], 2.09) or fewer than three outpatient visits (OR, 1.41) in the 6-30 months before cancer diagnosis were more likely to have an ED visit before their cancer diagnosis.
Other factors associated with increased odds of ED use before cancer diagnosis included rurality (OR, 1.15), residence in northern Ontario (northeast region: OR, 1.14 and northwest region: OR, 1.27 vs Toronto region), and living in the most marginalized areas (material resource deprivation: OR, 1.37 and housing stability: OR, 1.09 vs least marginalized area).
The researchers also found that patients with certain cancers were more likely to have sought care in the ED. They compared these cancers with breast cancer, which is often detected through screening.
“Patients with neurologic cancers had extremely high odds of ED use before cancer diagnosis,” the authors wrote. “This is likely because of the emergent nature of presentation, with acute neurologic symptoms such as weakness, confusion, or seizures, which require urgent assessment.” On the other hand, pancreatic, liver, or thoracic cancer can trigger nonspecific symptoms that may be ignored until they reach a crisis level that prompts an ED visit.
The limitations of the study included its inability to identify cancer-related ED visits and its narrow focus on patients in Ontario, according to the researchers. But the use of the ICES databases also allowed researchers access to a broader pool of data than are available in many other cases.
The findings in the new paper echo those of previous research, the authors noted. Research in the United Kingdom found that 24%-31% of cancer diagnoses involved the ED. In addition, a study of people enrolled in the US Medicare program, which serves patients aged 65 years or older, found that 23% were seen in the ED in the 30 days before diagnosis.
‘Unpacking the Data’
The current findings also are consistent with those of an International Cancer Benchmarking Partnership study that was published in 2022 in The Lancet Oncology, said Erika Nicholson, MHS, vice president of cancer systems and innovation at the Canadian Partnership Against Cancer. The latter study analyzed cancer registration and linked hospital admissions data from 14 jurisdictions in Australia, Canada, Denmark, New Zealand, Norway, and the United Kingdom.
“We see similar trends in terms of people visiting EDs and being diagnosed through EDs internationally,” Nicholson said. “We’re working with partners to put in place different strategies to address the challenges” that this phenomenon presents in terms of improving screening and follow-up care.
“Cancer is not one disease, but many diseases,” she said. “They present differently. We’re focused on really unpacking the data and understanding them.”
All this research highlights the need for more services and personnel to address cancer, including people who are trained to help patients cope after getting concerning news through emergency care, she said.
“That means having a system that fully supports you and helps you navigate through that diagnostic process,” Nicholson said. Addressing the added challenges for patients who don’t have secure housing is a special need, she added.
This study was supported by the Canadian Institutes of Health Research (CIHR). Grewal reported receiving grants from CIHR and the Canadian Association of Emergency Physicians. Nicholson reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Researchers examined Institute for Clinical Evaluative Sciences (ICES) data that had been gathered from January 1, 2014, to December 31, 2021. The study focused on patients aged 18 years or older with confirmed primary cancer diagnoses.
Factors associated with an increased likelihood of an ED visit ahead of diagnosis included having certain cancers, living in rural areas, and having less access to primary care, according to study author Keerat Grewal, MD, an emergency physician and clinician scientist at the Schwartz/Reisman Emergency Medicine Institute at Sinai Health in Toronto, Ontario, Canada, and coauthors.
“The ED is a distressing environment for patients to receive a possible cancer diagnosis,” the authors wrote. “Moreover, it is frequently ill equipped to provide ongoing continuity of care, which can lead patients down a poorly defined diagnostic pathway before receiving a confirmed diagnosis based on tissue and a subsequent treatment plan.”
The findings were published online on November 4 in CMAJ).
Neurologic Cancers Prominent
In an interview, Grewal said in an interview that the study reflects her desire as an emergency room physician to understand why so many patients with cancer get the initial reports about their disease from clinicians whom they often have just met for the first time.
Among patients with an ED visit before cancer diagnosis, 51.4% were admitted to hospital from the most recent visit.
Compared with patients with a family physician on whom they could rely for routine care, those who had no outpatient visits (odds ratio [OR], 2.09) or fewer than three outpatient visits (OR, 1.41) in the 6-30 months before cancer diagnosis were more likely to have an ED visit before their cancer diagnosis.
Other factors associated with increased odds of ED use before cancer diagnosis included rurality (OR, 1.15), residence in northern Ontario (northeast region: OR, 1.14 and northwest region: OR, 1.27 vs Toronto region), and living in the most marginalized areas (material resource deprivation: OR, 1.37 and housing stability: OR, 1.09 vs least marginalized area).
The researchers also found that patients with certain cancers were more likely to have sought care in the ED. They compared these cancers with breast cancer, which is often detected through screening.
“Patients with neurologic cancers had extremely high odds of ED use before cancer diagnosis,” the authors wrote. “This is likely because of the emergent nature of presentation, with acute neurologic symptoms such as weakness, confusion, or seizures, which require urgent assessment.” On the other hand, pancreatic, liver, or thoracic cancer can trigger nonspecific symptoms that may be ignored until they reach a crisis level that prompts an ED visit.
The limitations of the study included its inability to identify cancer-related ED visits and its narrow focus on patients in Ontario, according to the researchers. But the use of the ICES databases also allowed researchers access to a broader pool of data than are available in many other cases.
The findings in the new paper echo those of previous research, the authors noted. Research in the United Kingdom found that 24%-31% of cancer diagnoses involved the ED. In addition, a study of people enrolled in the US Medicare program, which serves patients aged 65 years or older, found that 23% were seen in the ED in the 30 days before diagnosis.
‘Unpacking the Data’
The current findings also are consistent with those of an International Cancer Benchmarking Partnership study that was published in 2022 in The Lancet Oncology, said Erika Nicholson, MHS, vice president of cancer systems and innovation at the Canadian Partnership Against Cancer. The latter study analyzed cancer registration and linked hospital admissions data from 14 jurisdictions in Australia, Canada, Denmark, New Zealand, Norway, and the United Kingdom.
“We see similar trends in terms of people visiting EDs and being diagnosed through EDs internationally,” Nicholson said. “We’re working with partners to put in place different strategies to address the challenges” that this phenomenon presents in terms of improving screening and follow-up care.
“Cancer is not one disease, but many diseases,” she said. “They present differently. We’re focused on really unpacking the data and understanding them.”
All this research highlights the need for more services and personnel to address cancer, including people who are trained to help patients cope after getting concerning news through emergency care, she said.
“That means having a system that fully supports you and helps you navigate through that diagnostic process,” Nicholson said. Addressing the added challenges for patients who don’t have secure housing is a special need, she added.
This study was supported by the Canadian Institutes of Health Research (CIHR). Grewal reported receiving grants from CIHR and the Canadian Association of Emergency Physicians. Nicholson reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM CMAJ
Pemphigus, Bullous Pemphigoid Risk Increased After COVID-19 Infection
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Rosacea: Ivermectin’s Benefits May Include Impact on Skin Microbiome
TOPLINE:
in a small study.
METHODOLOGY:
- In this single-center, open label study, 10 adults (mean age, 66.4 years) with papulopustular rosacea were treated with 1% ivermectin cream daily for 12 weeks.
- Skin swabs from lesional and nonlesional sites were collected at baseline and after 3 months of treatment to assess changes in the bacterial microbiome and the density of Demodex mites.
- The average baseline total papule count was 26.9, and the Clinician’s Erythema Assessment (CEA) score was 2 (average value on a scale of 0-4 from five locations on the face).
- For comparison, baseline swabs were taken from 10 healthy age-matched individuals.
TAKEAWAY:
- The density of Demodex mites was significantly reduced on lesional skin (P = .002) with topical ivermectin, which has anthelmintic effects against Demodex and is an effective treatment for rosacea.
- The absolute abundance of S epidermidis increased after ivermectin treatment on lesional skin (P = .039), while no changes were seen in Cutibacterium acnes.
- No changes were noted on nonlesional skin in the patients with rosacea.
- Topical ivermectin also reduced the number of papules and CEA scores (both P = .002) in individuals with rosacea.
IN PRACTICE:
“Treatment with topical ivermectin may improve the symptoms of rosacea through modulation of the skin microbiome beyond decreasing Demodex,” the authors concluded. “The results of this study,” they added, “provide valuable insights into the intricacies of the cutaneous microbiome in the pathophysiology of rosacea and highlight the potential therapeutic interventions targeting the skin microbiome.”
SOURCE:
The study was led by Teruaki Nakatsuji, PhD, of the department of dermatology, University of California, San Diego. It was published online on October 29 in the Journal of Investigative Dermatology.
LIMITATIONS:
The small sample size of 10 patients with rosacea limits the generalizability of the findings, and the study’s open-label design may introduce bias in the clinical assessments. Further research with larger sample sizes and randomized controlled trials is needed to confirm these findings.
DISCLOSURES:
This work was funded by a grant from the National Rosacea Society. One author disclosed being the cofounder and consultant, with equity interest in MatriSys Bioscience. The other authors reported no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
in a small study.
METHODOLOGY:
- In this single-center, open label study, 10 adults (mean age, 66.4 years) with papulopustular rosacea were treated with 1% ivermectin cream daily for 12 weeks.
- Skin swabs from lesional and nonlesional sites were collected at baseline and after 3 months of treatment to assess changes in the bacterial microbiome and the density of Demodex mites.
- The average baseline total papule count was 26.9, and the Clinician’s Erythema Assessment (CEA) score was 2 (average value on a scale of 0-4 from five locations on the face).
- For comparison, baseline swabs were taken from 10 healthy age-matched individuals.
TAKEAWAY:
- The density of Demodex mites was significantly reduced on lesional skin (P = .002) with topical ivermectin, which has anthelmintic effects against Demodex and is an effective treatment for rosacea.
- The absolute abundance of S epidermidis increased after ivermectin treatment on lesional skin (P = .039), while no changes were seen in Cutibacterium acnes.
- No changes were noted on nonlesional skin in the patients with rosacea.
- Topical ivermectin also reduced the number of papules and CEA scores (both P = .002) in individuals with rosacea.
IN PRACTICE:
“Treatment with topical ivermectin may improve the symptoms of rosacea through modulation of the skin microbiome beyond decreasing Demodex,” the authors concluded. “The results of this study,” they added, “provide valuable insights into the intricacies of the cutaneous microbiome in the pathophysiology of rosacea and highlight the potential therapeutic interventions targeting the skin microbiome.”
SOURCE:
The study was led by Teruaki Nakatsuji, PhD, of the department of dermatology, University of California, San Diego. It was published online on October 29 in the Journal of Investigative Dermatology.
LIMITATIONS:
The small sample size of 10 patients with rosacea limits the generalizability of the findings, and the study’s open-label design may introduce bias in the clinical assessments. Further research with larger sample sizes and randomized controlled trials is needed to confirm these findings.
DISCLOSURES:
This work was funded by a grant from the National Rosacea Society. One author disclosed being the cofounder and consultant, with equity interest in MatriSys Bioscience. The other authors reported no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
in a small study.
METHODOLOGY:
- In this single-center, open label study, 10 adults (mean age, 66.4 years) with papulopustular rosacea were treated with 1% ivermectin cream daily for 12 weeks.
- Skin swabs from lesional and nonlesional sites were collected at baseline and after 3 months of treatment to assess changes in the bacterial microbiome and the density of Demodex mites.
- The average baseline total papule count was 26.9, and the Clinician’s Erythema Assessment (CEA) score was 2 (average value on a scale of 0-4 from five locations on the face).
- For comparison, baseline swabs were taken from 10 healthy age-matched individuals.
TAKEAWAY:
- The density of Demodex mites was significantly reduced on lesional skin (P = .002) with topical ivermectin, which has anthelmintic effects against Demodex and is an effective treatment for rosacea.
- The absolute abundance of S epidermidis increased after ivermectin treatment on lesional skin (P = .039), while no changes were seen in Cutibacterium acnes.
- No changes were noted on nonlesional skin in the patients with rosacea.
- Topical ivermectin also reduced the number of papules and CEA scores (both P = .002) in individuals with rosacea.
IN PRACTICE:
“Treatment with topical ivermectin may improve the symptoms of rosacea through modulation of the skin microbiome beyond decreasing Demodex,” the authors concluded. “The results of this study,” they added, “provide valuable insights into the intricacies of the cutaneous microbiome in the pathophysiology of rosacea and highlight the potential therapeutic interventions targeting the skin microbiome.”
SOURCE:
The study was led by Teruaki Nakatsuji, PhD, of the department of dermatology, University of California, San Diego. It was published online on October 29 in the Journal of Investigative Dermatology.
LIMITATIONS:
The small sample size of 10 patients with rosacea limits the generalizability of the findings, and the study’s open-label design may introduce bias in the clinical assessments. Further research with larger sample sizes and randomized controlled trials is needed to confirm these findings.
DISCLOSURES:
This work was funded by a grant from the National Rosacea Society. One author disclosed being the cofounder and consultant, with equity interest in MatriSys Bioscience. The other authors reported no competing interests.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Infliximab vs Adalimumab: Which Is Best for Behçet Syndrome?
TOPLINE:
Both infliximab and adalimumab are safe and effective in achieving remission in patients with severe mucocutaneous Behçet syndrome, with adalimumab demonstrating a quicker response time; both drugs also improve quality of life and disease activity scores.
METHODOLOGY:
- Researchers conducted a phase 3 prospective study to evaluate the efficacy and safety of the anti–tumor necrosis factor–alpha agents infliximab and adalimumab in patients with Behçet syndrome presenting with mucocutaneous manifestations and inadequate response to prior treatments who were recruited from four Italian tertiary referral centers specializing in Behçet syndrome.
- Patients were randomly assigned to receive either 5 mg/kg intravenous infliximab at weeks 0, 2, and 6 and then every 6-8 weeks (n = 22; mean age, 46 years; 32% women) or 40 mg subcutaneous adalimumab every 2 weeks (n = 18; mean age, 48 years; 28% women) for 24 weeks.
- Patients were followed-up for an additional 12 weeks after the treatment period, with regular assessments of disease activity, safety, and adherence to treatment.
- The primary outcome was the time to response of mucocutaneous manifestations over 6 months; the secondary outcomes included relapse rates; quality of life, assessed using the Short-Form Health Survey 36; and disease activity, assessed using the Behçet Disease Current Activity Form.
- The safety and tolerability of the drugs were evaluated as the frequency of treatment-emergent adverse events (AEs) and serious AEs, monitored every 2 weeks.
TAKEAWAY:
- The resolution of mucocutaneous manifestations was achieved significantly more quickly with adalimumab than with infliximab, with a median time to response of 42 vs 152 days (P = .001); the proportion of responders was also higher in the adalimumab group than in the infliximab group (94% vs 64%; P = .023).
- Patients in the infliximab group had a higher risk for nonresponse (adjusted hazard ratio [HR], 3.33; P = .012) and relapse (adjusted HR, 7.57; P = .036) than those in the adalimumab group.
- Both infliximab and adalimumab significantly improved the quality of life in all dimensions (P < .05 for all) and disease activity scores (P < .001 for both) from baseline to the end of the study period, with no significant differences found between the groups.
- Two AEs were reported in the adalimumab group, one of which was serious (myocardial infarction); three nonserious AEs were reported in the infliximab group.
IN PRACTICE:
“ADA [adalimumab] and IFX [infliximab] were generally well tolerated and efficacious in patients with BS [Behçet syndrome] who showed an inadequate response to prior treatments with at least AZA [azathioprine] or CyA [cyclosporine],” the authors wrote. “Although a more detailed treat-to-target profile is yet to be better defined, [the study] results are also crucial in terms of prescriptiveness (currently off label), not only in Italy but also beyond national borders, as the evidence coming from real life still needs to be confirmed by growing data from clinical trials.”
SOURCE:
The study was led by Rosaria Talarico, MD, PhD, University of Pisa in Italy, and was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The small sample size and the distinctive study design may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded through a grant from the Italian Medicines Agency. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Both infliximab and adalimumab are safe and effective in achieving remission in patients with severe mucocutaneous Behçet syndrome, with adalimumab demonstrating a quicker response time; both drugs also improve quality of life and disease activity scores.
METHODOLOGY:
- Researchers conducted a phase 3 prospective study to evaluate the efficacy and safety of the anti–tumor necrosis factor–alpha agents infliximab and adalimumab in patients with Behçet syndrome presenting with mucocutaneous manifestations and inadequate response to prior treatments who were recruited from four Italian tertiary referral centers specializing in Behçet syndrome.
- Patients were randomly assigned to receive either 5 mg/kg intravenous infliximab at weeks 0, 2, and 6 and then every 6-8 weeks (n = 22; mean age, 46 years; 32% women) or 40 mg subcutaneous adalimumab every 2 weeks (n = 18; mean age, 48 years; 28% women) for 24 weeks.
- Patients were followed-up for an additional 12 weeks after the treatment period, with regular assessments of disease activity, safety, and adherence to treatment.
- The primary outcome was the time to response of mucocutaneous manifestations over 6 months; the secondary outcomes included relapse rates; quality of life, assessed using the Short-Form Health Survey 36; and disease activity, assessed using the Behçet Disease Current Activity Form.
- The safety and tolerability of the drugs were evaluated as the frequency of treatment-emergent adverse events (AEs) and serious AEs, monitored every 2 weeks.
TAKEAWAY:
- The resolution of mucocutaneous manifestations was achieved significantly more quickly with adalimumab than with infliximab, with a median time to response of 42 vs 152 days (P = .001); the proportion of responders was also higher in the adalimumab group than in the infliximab group (94% vs 64%; P = .023).
- Patients in the infliximab group had a higher risk for nonresponse (adjusted hazard ratio [HR], 3.33; P = .012) and relapse (adjusted HR, 7.57; P = .036) than those in the adalimumab group.
- Both infliximab and adalimumab significantly improved the quality of life in all dimensions (P < .05 for all) and disease activity scores (P < .001 for both) from baseline to the end of the study period, with no significant differences found between the groups.
- Two AEs were reported in the adalimumab group, one of which was serious (myocardial infarction); three nonserious AEs were reported in the infliximab group.
IN PRACTICE:
“ADA [adalimumab] and IFX [infliximab] were generally well tolerated and efficacious in patients with BS [Behçet syndrome] who showed an inadequate response to prior treatments with at least AZA [azathioprine] or CyA [cyclosporine],” the authors wrote. “Although a more detailed treat-to-target profile is yet to be better defined, [the study] results are also crucial in terms of prescriptiveness (currently off label), not only in Italy but also beyond national borders, as the evidence coming from real life still needs to be confirmed by growing data from clinical trials.”
SOURCE:
The study was led by Rosaria Talarico, MD, PhD, University of Pisa in Italy, and was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The small sample size and the distinctive study design may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded through a grant from the Italian Medicines Agency. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Both infliximab and adalimumab are safe and effective in achieving remission in patients with severe mucocutaneous Behçet syndrome, with adalimumab demonstrating a quicker response time; both drugs also improve quality of life and disease activity scores.
METHODOLOGY:
- Researchers conducted a phase 3 prospective study to evaluate the efficacy and safety of the anti–tumor necrosis factor–alpha agents infliximab and adalimumab in patients with Behçet syndrome presenting with mucocutaneous manifestations and inadequate response to prior treatments who were recruited from four Italian tertiary referral centers specializing in Behçet syndrome.
- Patients were randomly assigned to receive either 5 mg/kg intravenous infliximab at weeks 0, 2, and 6 and then every 6-8 weeks (n = 22; mean age, 46 years; 32% women) or 40 mg subcutaneous adalimumab every 2 weeks (n = 18; mean age, 48 years; 28% women) for 24 weeks.
- Patients were followed-up for an additional 12 weeks after the treatment period, with regular assessments of disease activity, safety, and adherence to treatment.
- The primary outcome was the time to response of mucocutaneous manifestations over 6 months; the secondary outcomes included relapse rates; quality of life, assessed using the Short-Form Health Survey 36; and disease activity, assessed using the Behçet Disease Current Activity Form.
- The safety and tolerability of the drugs were evaluated as the frequency of treatment-emergent adverse events (AEs) and serious AEs, monitored every 2 weeks.
TAKEAWAY:
- The resolution of mucocutaneous manifestations was achieved significantly more quickly with adalimumab than with infliximab, with a median time to response of 42 vs 152 days (P = .001); the proportion of responders was also higher in the adalimumab group than in the infliximab group (94% vs 64%; P = .023).
- Patients in the infliximab group had a higher risk for nonresponse (adjusted hazard ratio [HR], 3.33; P = .012) and relapse (adjusted HR, 7.57; P = .036) than those in the adalimumab group.
- Both infliximab and adalimumab significantly improved the quality of life in all dimensions (P < .05 for all) and disease activity scores (P < .001 for both) from baseline to the end of the study period, with no significant differences found between the groups.
- Two AEs were reported in the adalimumab group, one of which was serious (myocardial infarction); three nonserious AEs were reported in the infliximab group.
IN PRACTICE:
“ADA [adalimumab] and IFX [infliximab] were generally well tolerated and efficacious in patients with BS [Behçet syndrome] who showed an inadequate response to prior treatments with at least AZA [azathioprine] or CyA [cyclosporine],” the authors wrote. “Although a more detailed treat-to-target profile is yet to be better defined, [the study] results are also crucial in terms of prescriptiveness (currently off label), not only in Italy but also beyond national borders, as the evidence coming from real life still needs to be confirmed by growing data from clinical trials.”
SOURCE:
The study was led by Rosaria Talarico, MD, PhD, University of Pisa in Italy, and was published online in Annals of the Rheumatic Diseases.
LIMITATIONS:
The small sample size and the distinctive study design may have limited the generalizability of the findings.
DISCLOSURES:
This study was funded through a grant from the Italian Medicines Agency. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Asymptomatic Papules on the Neck
THE DIAGNOSIS: White Fibrous Papulosis
Given the histopathology findings, location on a sun-exposed site, lack of any additional systemic signs or symptoms, and no family history of similar lesions to suggest an underlying genetic condition, a diagnosis of white fibrous papulosis (WFP) was made. White fibrous papulosis is a relatively rare cutaneous disorder that was first reported by Shimizu et al1 in 1985. It is characterized by numerous grouped, 2- to 3-mm, white to flesh-colored papules that in most cases are confined to the neck in middle-aged to elderly individuals; however, cases involving the upper trunk and axillae also have been reported.1-3 The etiology of this condition is unclear but is thought to be related to aging and chronic exposure to UV light. Although treatment is not required, various modalities including tretinoin, excision, and laser therapy have been trialed with varying success.2,4 Our patient elected not to proceed with treatment.
Histologically, WFP may manifest similarly to connective tissue nevi; the overall architecture is nonspecific with focally thickened collagen and often elastic fibers that may be normal to reduced and/or fragmented, as well as an overall decrease in superficial dermal elastic tissue.3,5 Therefore, the differential diagnosis may include connective tissue nevi and require clinical correlation to make a correct diagnosis.
Pseudoxanthoma elasticum (PXE) is an autosomalrecessive disorder most commonly related to mutations in the ATP binding cassette subfamily C member 6 (ABCC6) gene that tends to manifest clinically on the neck and flexural extremities.6 This disease affects elastic fibers, which may become calcified over time. Pseudoxanthoma elasticum is associated with ocular complications relating to the Bruch membrane of the retina and angioid streaks; choroidal neovascularization involving the damaged Bruch membrane and episodes of acute retinopathy may result in vision loss in later stages of the disease.7 Involvement of the elastic laminae of arteries can be associated with cardiovascular and cerebrovascular complications such as stroke, coronary artery disease, claudication, and aneurysms. Involvement of the gastrointestinal or genitourinary tracts also may occur and most commonly manifests with bleeding. Pathologic alterations in the elastic fibers of the lungs also have been reported in patients with PXE.8 Histologically, PXE exhibits increased abnormally clumped and fragmented elastic fibers in the superficial dermis, often with calcification (Figure 1). Pseudo-PXE related to D-penicillamine use often lacks calcification and has a bramble bush appearance.9

Fibrofolliculomas may manifest alone or in association with an underlying condition such as Birt-Hogg-Dubé syndrome, in which lesions are most frequently seen scattered on the scalp, face, ears, neck, or upper trunk.10 This condition is related to a folliculin (FLCN) gene germline mutation. Birt-Hogg-Dubé syndrome also may be associated with acrochordons, trichodiscomas, renal cancer, and lung cysts with or without spontaneous pneumothorax. Less frequently noted findings include oral papules, epidermal cysts, angiofibromas, lipomas/angiolipomas, parotid gland tumors, and thyroid neoplasms. Connective tissue nevi/collagenomas can appear clinically similar to fibrofolliculomas; true connective tissue nevi are reported less commonly in Birt-Hogg-Dubé syndrome.11 Histologically, a fibrofolliculoma manifests with epidermal strands originating from a hair follicle associated with prominent surrounding connective tissue (Figure 2).
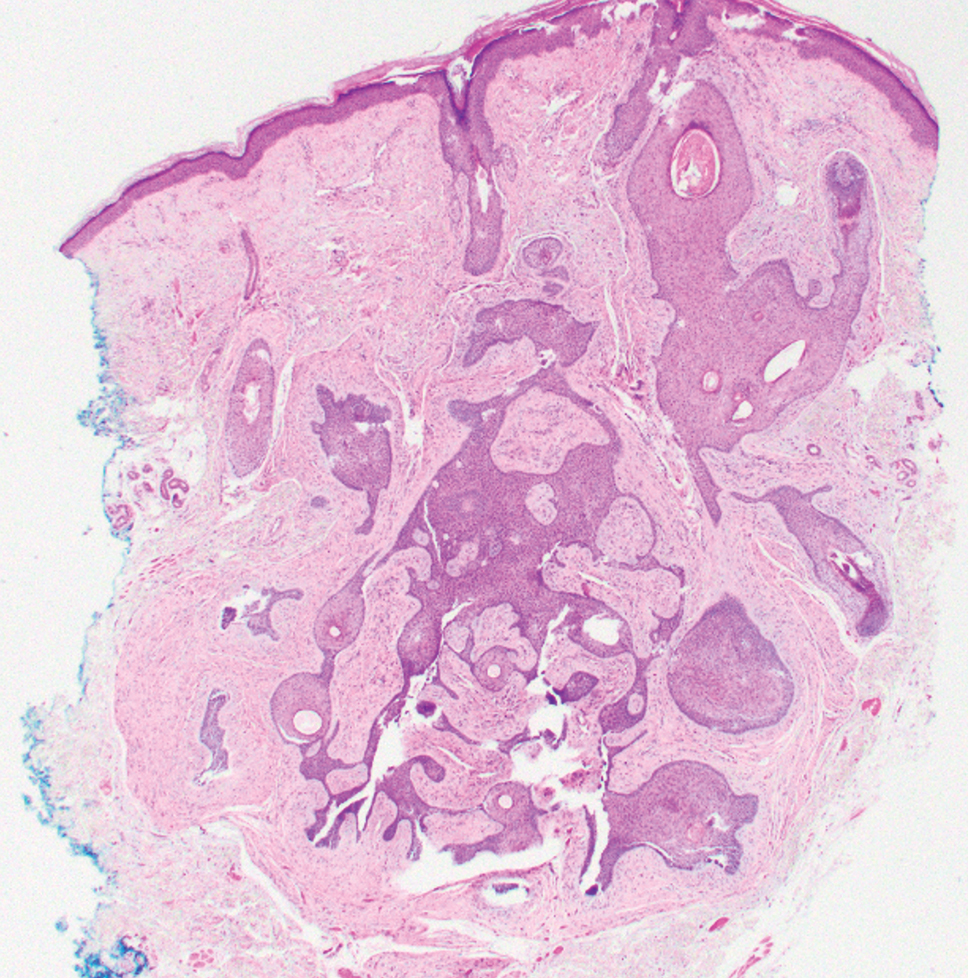
Elastofibroma dorsi is a benign tumor of connective tissue that most commonly manifests clinically as a solitary subcutaneous mass on the back near the inferior angle of the scapula; it typically develops below the rhomboid major and latissimus dorsi muscles.12 The pathogenesis is uncertain, but some patients have reported a family history of the condition or a history of repetitive shoulder movement/trauma prior to onset; the mass may be asymptomatic or associated with pain and/or swelling. Those affected tend to be older than 50 years.13 Histologically, thickened and rounded to beaded elastic fibers are seen admixed with collagen (Figure 3).
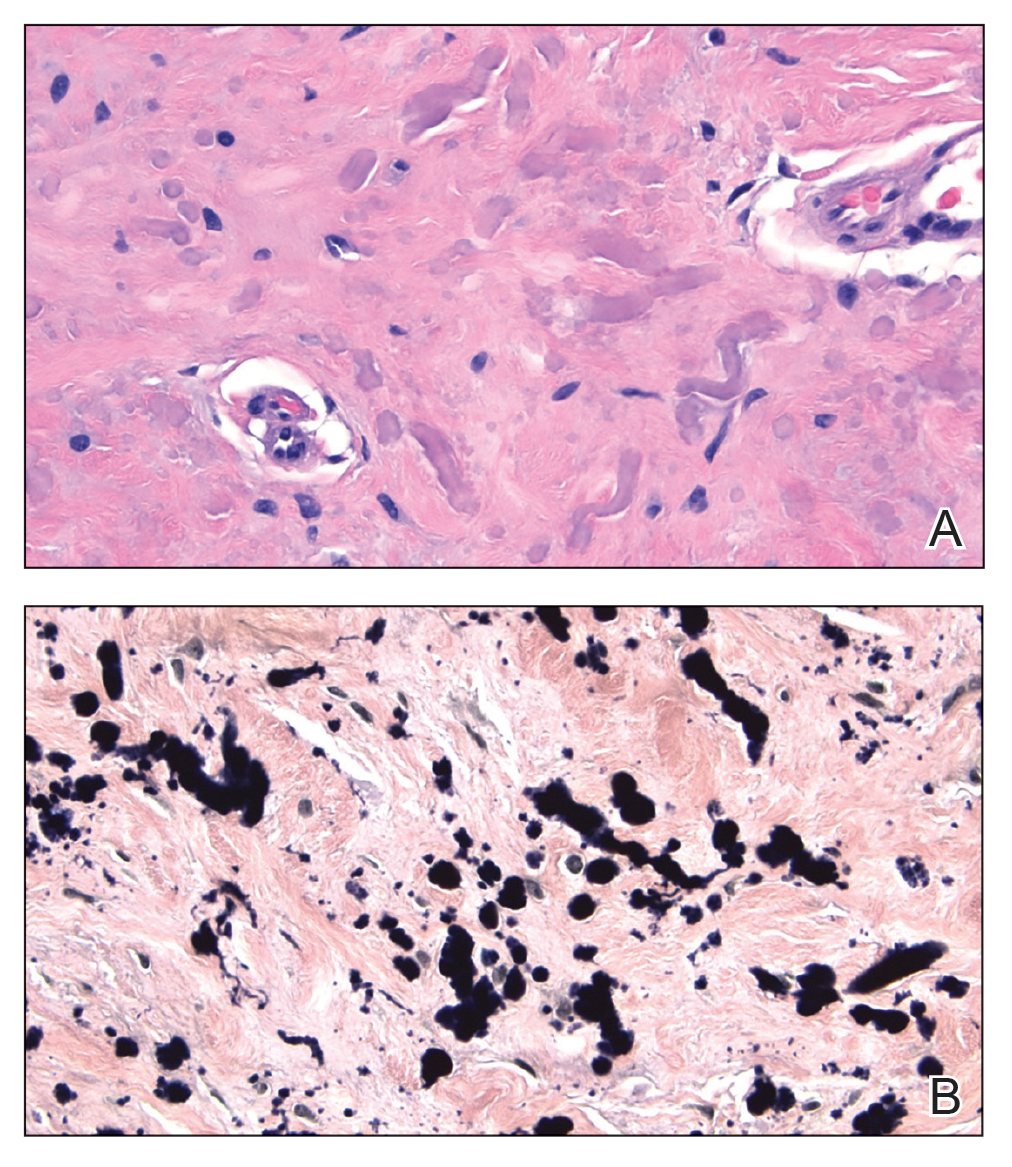
Actinic (solar) elastosis frequently is encountered in many skin biopsies and is caused by chronic photodamage. More hypertrophic variants, such as papular or nodular solar elastosis, may clinically manifest similarly to WFP.14 Histologically, actinic elastosis manifests as a considerable increase in elastic tissue in the papillary and superficial reticular dermis (Figure 4).
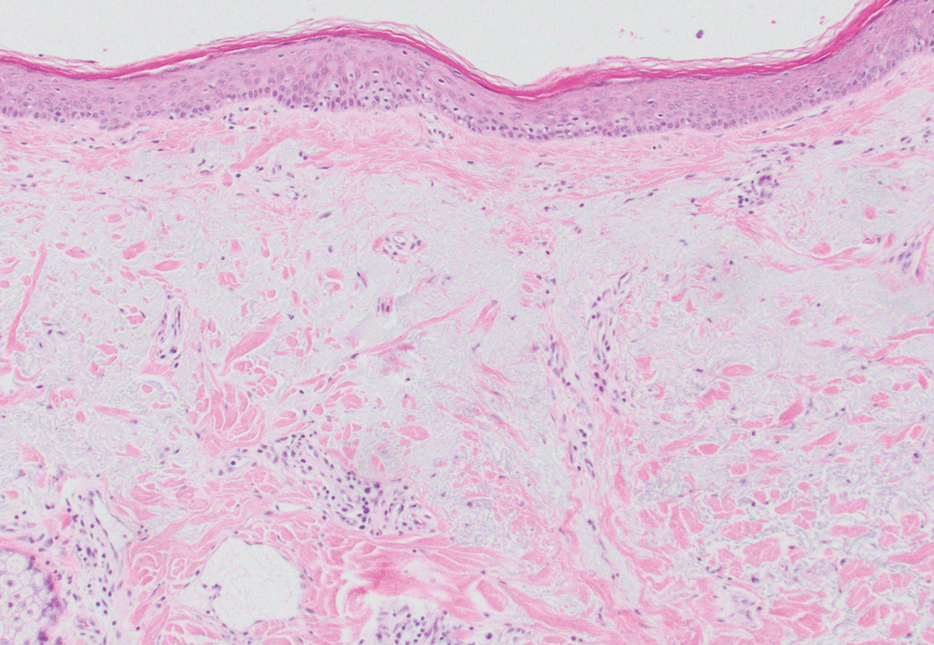
- Shimizu H, Nishikawa T, Kimura S. White fibrous papulosis of the neck: review of our 16 cases. Nihon Hifuka Gakkai Zasshi. 1985;95:1077-1084.
- Teo W, Pang S. White fibrous papulosis of the chest and back. J Am Acad Dermatol. 2012;66:AB33.
- Dokic Y, Tschen J. White fibrous papulosis of the axillae and neck. Cureus. 2020;12:E7635.
- Lueangarun S, Panchaprateep R. White fibrous papulosis of the neck treated with fractionated 1550-nm erbium glass laser: a case report. J Lasers Med Sci. 2016;7:256-258.
- Rios-Gomez M, Ramos-Garibay JA, Perez-Santana ME, et al. White fibrous papulosis of the neck: a case report. Cureus. 2022;14:E25661.
- Váradi A, Szabó Z, Pomozi V, et al. ABCC6 as a target in pseudoxanthoma elasticum. Curr Drug Targets. 2011;12:671-682.
- Gliem M, Birtel J, Müller PL, et al. Acute retinopathy in pseudoxanthoma elasticum. JAMA Ophthalmol. 2019;137:1165-1173.
- Germain DP. Pseudoxanthoma elasticum. Orphanet J Rare Dis. 2017;12:85. doi:10.1186/s13023-017-0639-8
- Chisti MA, Binamer Y, Alfadley A, et al. D-penicillamine-induced pseudo-pseudoxanthoma elasticum and extensive elastosis perforans serpiginosa with excellent response to acitretin. Ann Saudi Med. 2019;39:56-60.
- Criscito MC, Mu EW, Meehan SA, et al. Dermoscopic features of a solitary fibrofolliculoma on the left cheek. J Am Acad Dermatol. 2017;76(2 suppl 1):S8-S9.
- Sattler EC, Steinlein OK. Birt-Hogg-Dubé syndrome. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews® [Internet]. Updated January 30, 2020. Accessed February 23, 2023. https://www.ncbi.nlm.nih.gov/books/NBK1522
- Patnayak R, Jena A, Settipalli S, et al. Elastofibroma: an uncommon tumor revisited. J Cutan Aesthet Surg. 2016;9:34-37. doi:10.4103/0974- 2077.178543
- Chandrasekar CR, Grimer RJ, Carter SR, et al. Elastofibroma dorsi: an uncommon benign pseudotumour. Sarcoma. 2008;2008:756565. doi:10.1155/2008/756565
- Kwittken J. Papular elastosis. Cutis. 2000;66:81-83.
THE DIAGNOSIS: White Fibrous Papulosis
Given the histopathology findings, location on a sun-exposed site, lack of any additional systemic signs or symptoms, and no family history of similar lesions to suggest an underlying genetic condition, a diagnosis of white fibrous papulosis (WFP) was made. White fibrous papulosis is a relatively rare cutaneous disorder that was first reported by Shimizu et al1 in 1985. It is characterized by numerous grouped, 2- to 3-mm, white to flesh-colored papules that in most cases are confined to the neck in middle-aged to elderly individuals; however, cases involving the upper trunk and axillae also have been reported.1-3 The etiology of this condition is unclear but is thought to be related to aging and chronic exposure to UV light. Although treatment is not required, various modalities including tretinoin, excision, and laser therapy have been trialed with varying success.2,4 Our patient elected not to proceed with treatment.
Histologically, WFP may manifest similarly to connective tissue nevi; the overall architecture is nonspecific with focally thickened collagen and often elastic fibers that may be normal to reduced and/or fragmented, as well as an overall decrease in superficial dermal elastic tissue.3,5 Therefore, the differential diagnosis may include connective tissue nevi and require clinical correlation to make a correct diagnosis.
Pseudoxanthoma elasticum (PXE) is an autosomalrecessive disorder most commonly related to mutations in the ATP binding cassette subfamily C member 6 (ABCC6) gene that tends to manifest clinically on the neck and flexural extremities.6 This disease affects elastic fibers, which may become calcified over time. Pseudoxanthoma elasticum is associated with ocular complications relating to the Bruch membrane of the retina and angioid streaks; choroidal neovascularization involving the damaged Bruch membrane and episodes of acute retinopathy may result in vision loss in later stages of the disease.7 Involvement of the elastic laminae of arteries can be associated with cardiovascular and cerebrovascular complications such as stroke, coronary artery disease, claudication, and aneurysms. Involvement of the gastrointestinal or genitourinary tracts also may occur and most commonly manifests with bleeding. Pathologic alterations in the elastic fibers of the lungs also have been reported in patients with PXE.8 Histologically, PXE exhibits increased abnormally clumped and fragmented elastic fibers in the superficial dermis, often with calcification (Figure 1). Pseudo-PXE related to D-penicillamine use often lacks calcification and has a bramble bush appearance.9
Fibrofolliculomas may manifest alone or in association with an underlying condition such as Birt-Hogg-Dubé syndrome, in which lesions are most frequently seen scattered on the scalp, face, ears, neck, or upper trunk.10 This condition is related to a folliculin (FLCN) gene germline mutation. Birt-Hogg-Dubé syndrome also may be associated with acrochordons, trichodiscomas, renal cancer, and lung cysts with or without spontaneous pneumothorax. Less frequently noted findings include oral papules, epidermal cysts, angiofibromas, lipomas/angiolipomas, parotid gland tumors, and thyroid neoplasms. Connective tissue nevi/collagenomas can appear clinically similar to fibrofolliculomas; true connective tissue nevi are reported less commonly in Birt-Hogg-Dubé syndrome.11 Histologically, a fibrofolliculoma manifests with epidermal strands originating from a hair follicle associated with prominent surrounding connective tissue (Figure 2).
Elastofibroma dorsi is a benign tumor of connective tissue that most commonly manifests clinically as a solitary subcutaneous mass on the back near the inferior angle of the scapula; it typically develops below the rhomboid major and latissimus dorsi muscles.12 The pathogenesis is uncertain, but some patients have reported a family history of the condition or a history of repetitive shoulder movement/trauma prior to onset; the mass may be asymptomatic or associated with pain and/or swelling. Those affected tend to be older than 50 years.13 Histologically, thickened and rounded to beaded elastic fibers are seen admixed with collagen (Figure 3).
Actinic (solar) elastosis frequently is encountered in many skin biopsies and is caused by chronic photodamage. More hypertrophic variants, such as papular or nodular solar elastosis, may clinically manifest similarly to WFP.14 Histologically, actinic elastosis manifests as a considerable increase in elastic tissue in the papillary and superficial reticular dermis (Figure 4).
THE DIAGNOSIS: White Fibrous Papulosis
Given the histopathology findings, location on a sun-exposed site, lack of any additional systemic signs or symptoms, and no family history of similar lesions to suggest an underlying genetic condition, a diagnosis of white fibrous papulosis (WFP) was made. White fibrous papulosis is a relatively rare cutaneous disorder that was first reported by Shimizu et al1 in 1985. It is characterized by numerous grouped, 2- to 3-mm, white to flesh-colored papules that in most cases are confined to the neck in middle-aged to elderly individuals; however, cases involving the upper trunk and axillae also have been reported.1-3 The etiology of this condition is unclear but is thought to be related to aging and chronic exposure to UV light. Although treatment is not required, various modalities including tretinoin, excision, and laser therapy have been trialed with varying success.2,4 Our patient elected not to proceed with treatment.
Histologically, WFP may manifest similarly to connective tissue nevi; the overall architecture is nonspecific with focally thickened collagen and often elastic fibers that may be normal to reduced and/or fragmented, as well as an overall decrease in superficial dermal elastic tissue.3,5 Therefore, the differential diagnosis may include connective tissue nevi and require clinical correlation to make a correct diagnosis.
Pseudoxanthoma elasticum (PXE) is an autosomalrecessive disorder most commonly related to mutations in the ATP binding cassette subfamily C member 6 (ABCC6) gene that tends to manifest clinically on the neck and flexural extremities.6 This disease affects elastic fibers, which may become calcified over time. Pseudoxanthoma elasticum is associated with ocular complications relating to the Bruch membrane of the retina and angioid streaks; choroidal neovascularization involving the damaged Bruch membrane and episodes of acute retinopathy may result in vision loss in later stages of the disease.7 Involvement of the elastic laminae of arteries can be associated with cardiovascular and cerebrovascular complications such as stroke, coronary artery disease, claudication, and aneurysms. Involvement of the gastrointestinal or genitourinary tracts also may occur and most commonly manifests with bleeding. Pathologic alterations in the elastic fibers of the lungs also have been reported in patients with PXE.8 Histologically, PXE exhibits increased abnormally clumped and fragmented elastic fibers in the superficial dermis, often with calcification (Figure 1). Pseudo-PXE related to D-penicillamine use often lacks calcification and has a bramble bush appearance.9
Fibrofolliculomas may manifest alone or in association with an underlying condition such as Birt-Hogg-Dubé syndrome, in which lesions are most frequently seen scattered on the scalp, face, ears, neck, or upper trunk.10 This condition is related to a folliculin (FLCN) gene germline mutation. Birt-Hogg-Dubé syndrome also may be associated with acrochordons, trichodiscomas, renal cancer, and lung cysts with or without spontaneous pneumothorax. Less frequently noted findings include oral papules, epidermal cysts, angiofibromas, lipomas/angiolipomas, parotid gland tumors, and thyroid neoplasms. Connective tissue nevi/collagenomas can appear clinically similar to fibrofolliculomas; true connective tissue nevi are reported less commonly in Birt-Hogg-Dubé syndrome.11 Histologically, a fibrofolliculoma manifests with epidermal strands originating from a hair follicle associated with prominent surrounding connective tissue (Figure 2).
Elastofibroma dorsi is a benign tumor of connective tissue that most commonly manifests clinically as a solitary subcutaneous mass on the back near the inferior angle of the scapula; it typically develops below the rhomboid major and latissimus dorsi muscles.12 The pathogenesis is uncertain, but some patients have reported a family history of the condition or a history of repetitive shoulder movement/trauma prior to onset; the mass may be asymptomatic or associated with pain and/or swelling. Those affected tend to be older than 50 years.13 Histologically, thickened and rounded to beaded elastic fibers are seen admixed with collagen (Figure 3).
Actinic (solar) elastosis frequently is encountered in many skin biopsies and is caused by chronic photodamage. More hypertrophic variants, such as papular or nodular solar elastosis, may clinically manifest similarly to WFP.14 Histologically, actinic elastosis manifests as a considerable increase in elastic tissue in the papillary and superficial reticular dermis (Figure 4).
- Shimizu H, Nishikawa T, Kimura S. White fibrous papulosis of the neck: review of our 16 cases. Nihon Hifuka Gakkai Zasshi. 1985;95:1077-1084.
- Teo W, Pang S. White fibrous papulosis of the chest and back. J Am Acad Dermatol. 2012;66:AB33.
- Dokic Y, Tschen J. White fibrous papulosis of the axillae and neck. Cureus. 2020;12:E7635.
- Lueangarun S, Panchaprateep R. White fibrous papulosis of the neck treated with fractionated 1550-nm erbium glass laser: a case report. J Lasers Med Sci. 2016;7:256-258.
- Rios-Gomez M, Ramos-Garibay JA, Perez-Santana ME, et al. White fibrous papulosis of the neck: a case report. Cureus. 2022;14:E25661.
- Váradi A, Szabó Z, Pomozi V, et al. ABCC6 as a target in pseudoxanthoma elasticum. Curr Drug Targets. 2011;12:671-682.
- Gliem M, Birtel J, Müller PL, et al. Acute retinopathy in pseudoxanthoma elasticum. JAMA Ophthalmol. 2019;137:1165-1173.
- Germain DP. Pseudoxanthoma elasticum. Orphanet J Rare Dis. 2017;12:85. doi:10.1186/s13023-017-0639-8
- Chisti MA, Binamer Y, Alfadley A, et al. D-penicillamine-induced pseudo-pseudoxanthoma elasticum and extensive elastosis perforans serpiginosa with excellent response to acitretin. Ann Saudi Med. 2019;39:56-60.
- Criscito MC, Mu EW, Meehan SA, et al. Dermoscopic features of a solitary fibrofolliculoma on the left cheek. J Am Acad Dermatol. 2017;76(2 suppl 1):S8-S9.
- Sattler EC, Steinlein OK. Birt-Hogg-Dubé syndrome. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews® [Internet]. Updated January 30, 2020. Accessed February 23, 2023. https://www.ncbi.nlm.nih.gov/books/NBK1522
- Patnayak R, Jena A, Settipalli S, et al. Elastofibroma: an uncommon tumor revisited. J Cutan Aesthet Surg. 2016;9:34-37. doi:10.4103/0974- 2077.178543
- Chandrasekar CR, Grimer RJ, Carter SR, et al. Elastofibroma dorsi: an uncommon benign pseudotumour. Sarcoma. 2008;2008:756565. doi:10.1155/2008/756565
- Kwittken J. Papular elastosis. Cutis. 2000;66:81-83.
- Shimizu H, Nishikawa T, Kimura S. White fibrous papulosis of the neck: review of our 16 cases. Nihon Hifuka Gakkai Zasshi. 1985;95:1077-1084.
- Teo W, Pang S. White fibrous papulosis of the chest and back. J Am Acad Dermatol. 2012;66:AB33.
- Dokic Y, Tschen J. White fibrous papulosis of the axillae and neck. Cureus. 2020;12:E7635.
- Lueangarun S, Panchaprateep R. White fibrous papulosis of the neck treated with fractionated 1550-nm erbium glass laser: a case report. J Lasers Med Sci. 2016;7:256-258.
- Rios-Gomez M, Ramos-Garibay JA, Perez-Santana ME, et al. White fibrous papulosis of the neck: a case report. Cureus. 2022;14:E25661.
- Váradi A, Szabó Z, Pomozi V, et al. ABCC6 as a target in pseudoxanthoma elasticum. Curr Drug Targets. 2011;12:671-682.
- Gliem M, Birtel J, Müller PL, et al. Acute retinopathy in pseudoxanthoma elasticum. JAMA Ophthalmol. 2019;137:1165-1173.
- Germain DP. Pseudoxanthoma elasticum. Orphanet J Rare Dis. 2017;12:85. doi:10.1186/s13023-017-0639-8
- Chisti MA, Binamer Y, Alfadley A, et al. D-penicillamine-induced pseudo-pseudoxanthoma elasticum and extensive elastosis perforans serpiginosa with excellent response to acitretin. Ann Saudi Med. 2019;39:56-60.
- Criscito MC, Mu EW, Meehan SA, et al. Dermoscopic features of a solitary fibrofolliculoma on the left cheek. J Am Acad Dermatol. 2017;76(2 suppl 1):S8-S9.
- Sattler EC, Steinlein OK. Birt-Hogg-Dubé syndrome. In: Adam MP, Everman DB, Mirzaa GM, et al, eds. GeneReviews® [Internet]. Updated January 30, 2020. Accessed February 23, 2023. https://www.ncbi.nlm.nih.gov/books/NBK1522
- Patnayak R, Jena A, Settipalli S, et al. Elastofibroma: an uncommon tumor revisited. J Cutan Aesthet Surg. 2016;9:34-37. doi:10.4103/0974- 2077.178543
- Chandrasekar CR, Grimer RJ, Carter SR, et al. Elastofibroma dorsi: an uncommon benign pseudotumour. Sarcoma. 2008;2008:756565. doi:10.1155/2008/756565
- Kwittken J. Papular elastosis. Cutis. 2000;66:81-83.
A 70-year-old woman with a history of osteoporosis and breast cancer presented for evaluation of asymptomatic, 2- to 3-mm, white to flesh-colored papules concentrated on the inferior occipital scalp and posterior neck (inset) for at least several months. She had no additional systemic signs or symptoms, and there was no family history of similar skin findings. A punch biopsy was performed.
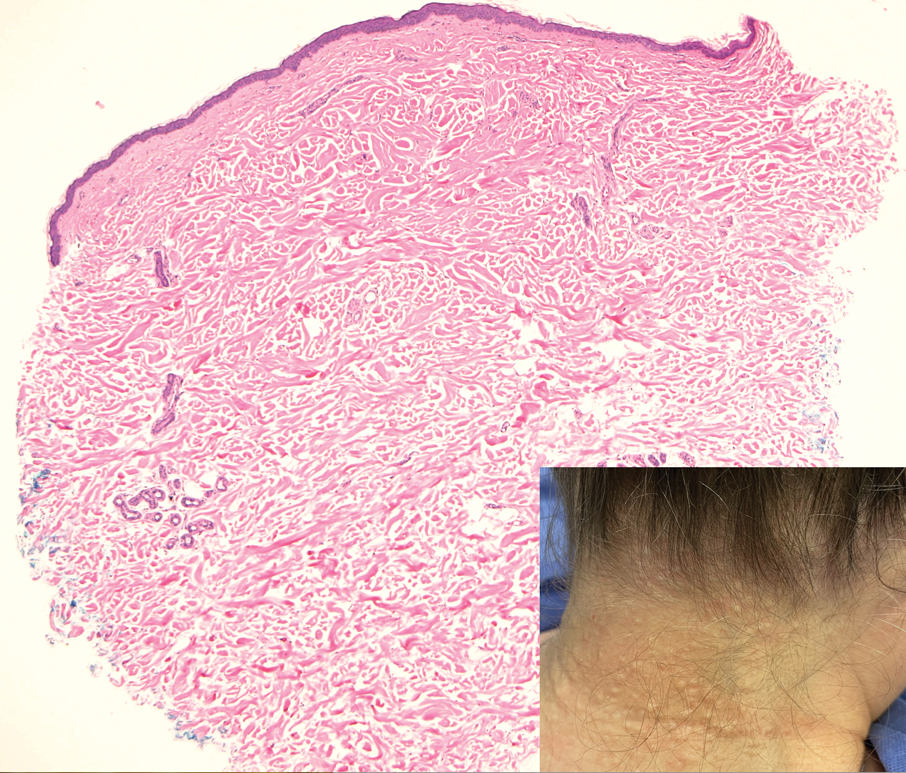
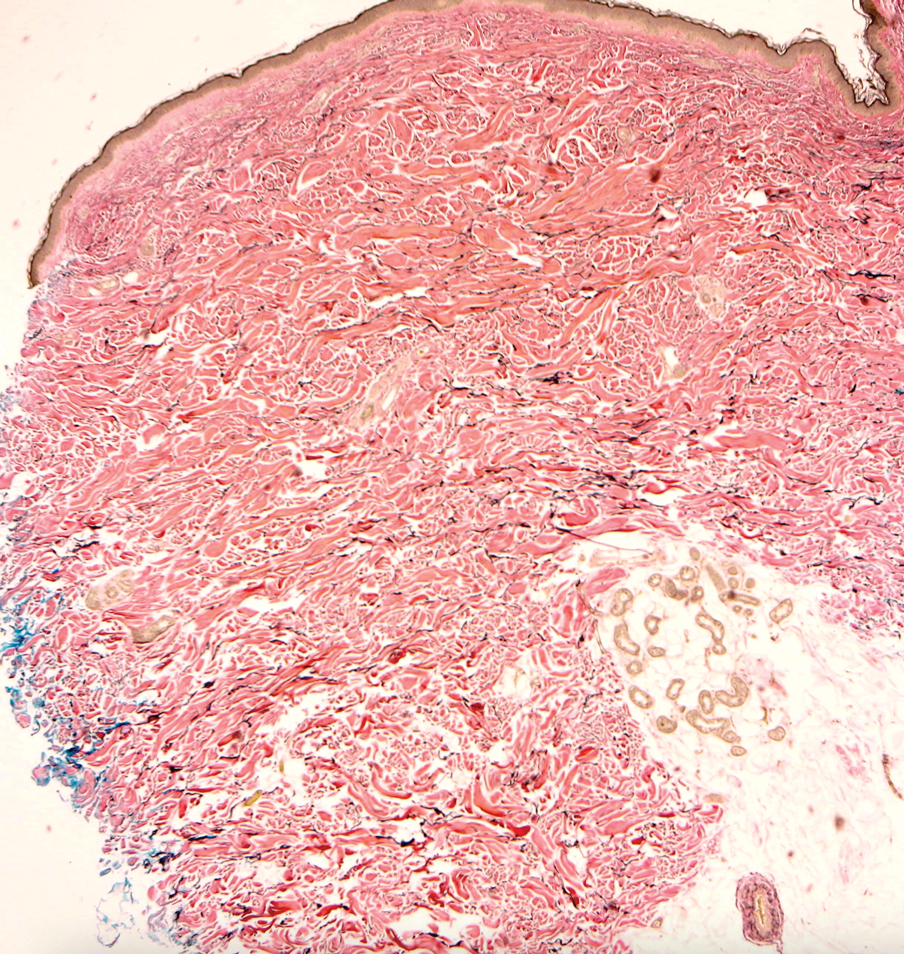
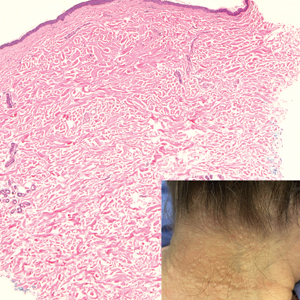
Eating Disorder Risk Factors and the Impact of Obesity in Patients With Psoriasis
Psoriasis is a chronic multisystemic inflammatory skin disease with a worldwide prevalence of 2% to 3%.1 Psoriasis can be accompanied by other conditions such as psoriatic arthritis, obesity, metabolic syndrome, diabetes mellitus, hypertension, dyslipidemia, atherosclerotic disease, inflammatory bowel disease, and anxiety/depression. It is important to manage comorbidities of psoriasis in addition to treating the cutaneous manifestations of the disease.1
Obesity is a major public health concern worldwide. Numerous observational and epidemiologic studies have reported a high prevalence of obesity among patients with psoriasis.2 Current evidence indicates that obesity may initiate or worsen psoriasis; furthermore, it is important to note that obesity may negatively impact the effectiveness of psoriasis-specific treatments or increase the incidence of adverse effects. Therefore, managing obesity is crucial in the treatment of psoriasis.3 Numerous studies have investigated the association between psoriasis and obesity, and they commonly conclude that both conditions share the same genetic metabolic pathways.2-4 However, it is important to consider environmental factors such as dietary habits, smoking, alcohol consumption, and a sedentary lifestyle—all of which are associated with psoriasis and also can contribute to the development of obesity.5 Because of the effects of obesity in psoriasis patients, factors that impact the development of obesity have become a popular research topic.
Eating disorders (EDs) are a crucial risk factor for both developing and maintaining obesity. In particular, two EDs that are associated with obesity include binge eating disorder and bulimia nervosa.6 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,7 binge eating disorder can be diagnosed when a patient has at least 1 episode of binge eating per week over a 3-month period. Bulimia nervosa can be diagnosed when a patient is excessively concerned with their body weight and shape and engages in behaviors to prevent weight gain (eg, forced vomiting, excessive use of laxatives).7 Psychiatrists who specialize in EDs make diagnoses based on these criteria. In daily practice, there are several quick and simple questionnaires available to screen for EDs that can be used by nonpsychiatrist physicians, including the commonly used 26-item Eating Attitudes Test (EAT-26).8 The EAT-26 has been used to screen for EDs in patients with inflammatory disorders.9
The aim of this study was to screen for EDs in patients with psoriasis to identify potential risk factors for development of obesity.
Materials and Methods
This study included patients with psoriasis who were screened for EDs at a tertiary dermatology clinic in Turkey between January 2021 and December 2023. This study was approved by the local ethics committee and was in accordance with the Declaration of Helsinki (decision number E-93471371-514.99-225000079).
Study Design and Patient Inclusion Criteria—This quantitative cross-sectional study utilized EAT-26, Dermatology Life Quality Index (DLQI), Attitude Scale for Healthy Nutrition (ASHN), and Depression Anxiety Stress Scale-21 (DASS-21) scores. All the questionnaire scales used in the study were adapted and validated in Turkey.8,10-12 The inclusion criteria consisted of being older than 18 years of age, being literate, having psoriasis for at least 1 year that was not treated topically or systemically, and having no psychiatric diseases outside an ED. The questionnaires were presented in written format following the clinical examination. Literacy was an inclusion criterion in this study due to the absence of auxiliary health personnel.
Study Variables—The study variables included age, sex, marital status (single/divorced or married), education status (primary/secondary school or high school/university), employment status (employed or unemployed/retired), body mass index (BMI), smoking status, alcohol-consumption status, Psoriasis Area Severity Index score, presence of nail psoriasis and psoriatic arthritis, duration of psoriasis, family history of psoriasis, EAT-26 score, ASHN score, DLQI score, and DASS-21 score. Body mass index was calculated by taking a participant’s weight in kilograms and dividing it by their height in meters squared. The BMI values were classified into 3 categories: normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2).13
Questionnaires—The EAT-26 questionnaire includes 26 questions that are used to detect EDs. Responses to each question include Likert-type answer options (ie, “always,” “usually,” “often,” “sometimes,” “rarely,” and “never.”) Patients with scores of 20 points or higher (range, 0–78) are classified as high risk for EDs.8 In our study, EAT-26 scores were grouped into 2 categories: patients scoring less than 20 points and those scoring 20 points or higher.
The DLQI questionnaire includes 10 questions to measure dermatologic symptoms and qualiy of life. Responses to each question include Likert-type answer options (ie, “not at all,” “a little,” “a lot,” or “very much.”) On the DLQI scale, the higher the score, the lower the quality of life (score range, 0–30).10
The ASHN questionnaire includes 21 questions that measure attitudes toward healthy nutrition with 5 possible answer options (“strongly disagree,” “disagree,” “undecided,” “agree,” and “strongly agree”). On this scale, higher scores indicate the participant is more knowledgeable about healthy nutrition (score range, 0–78).11
The DASS-21 questionnaire includes 21 questions that measure the severity of a range of symptoms common to depression, anxiety, and stress. Responses include Likert-type answer options (eg, “never,” “sometimes,” “often,” and “almost always.”) On this scale, a higher score (range of 0–21 for each) indicates higher levels of depression, anxiety, and stress.12
Statistical Analysis—Descriptive statistics were analyzed using SPSS software version 22.0 (IBM). The Shapiro-Wilk test was applied to determine whether the data were normally distributed. For categorical variables, frequency differences among groups were compared using the Pearson χ2 test. A t test was used to compare the means of 2 independent groups with a normal distribution. One-way analysis of variance and Tukey Honest Significant Difference post hoc analysis were used to test whether there was a statistically significant difference among the normally distributed means of independent groups. Pearson correlation analysis was used to determine whether there was a linear relationship between 2 numeric measurements and, if so, to determine the direction and severity of this relationship. P<.05 indicated statistical significance in this study.
Results
Study Participant Demographics—This study included 82 participants with a mean age of 44.3 years; 52.4% (43/82) were female, and 85.4% (70/82) were married. The questionnaire took an average of 4.2 minutes for participants to complete. A total of 57.3% (47/82) of patients had completed primary/secondary education and 59.8% (49/82) were employed. The mean BMI was 28.1 kg/m2. According to the BMI classification, 26.8% (22/82) participants had a normal weight, 36.6% (30/82) were overweight, and 43.9% (36/82) were obese. A total of 48.8% (40/82) of participants smoked, and 4.9% (4/82) consumed alcohol. The mean Psoriasis Area and Severity Index score was 5.4. A total of 54.9% (45/82) of participants had nail psoriasis, and 24.4% (20/82) had psoriatic arthritis. The mean duration of psoriasis was 153 months. A total of 29.3% (24/82) of participants had a positive family history of psoriasis. The mean EAT-26 score was 11.1. A total of 12.2% (10/82) of participants had an EAT-26 score of 20 points or higher and were considered at high risk for an ED. The mean ASHN score was 72.9; the mean DLQI score was 5.5; and on the DASS-21 scale, mean scores for depression, anxiety, and stress were 6.3, 8.7, and 10.0, respectively (Table).
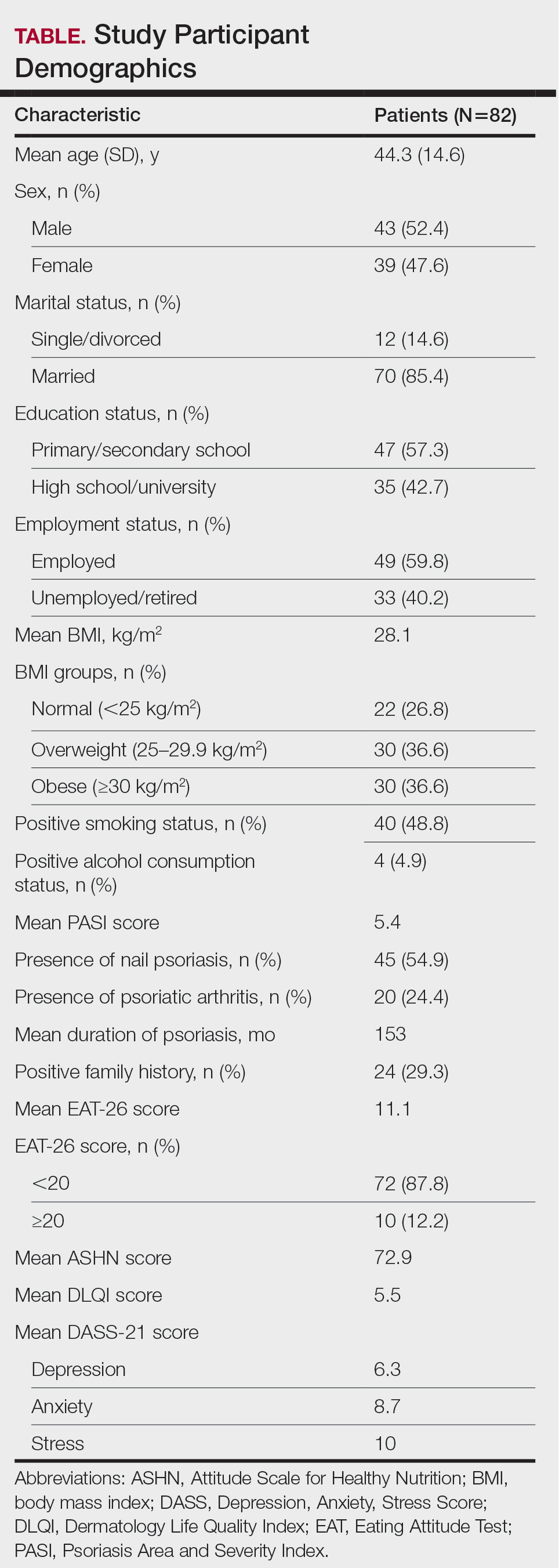
Comparative Evaluation of the BMI Groups—The only statistically significant differences among the 3 BMI groups were related to marital status, EAT-26 score, and anxiety and stress scores (P=.02, <.01, <.01, and <.01, respectively)(eTable 1). The number of single/divorced participants in the overweight group was significantly (P=.02) greater than in the normal weight group. The mean EAT-26 score for the normal weight group was significantly (P<.01) lower than for the overweight and obese groups; there was no significant difference in mean EAT-26 scores between the overweight and obese groups. The mean anxiety score was significantly (P<.01) lower in the normal weight group compared with the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean depression score. The mean stress and anxiety scores were significantly (P<.01) lower in the normal weight group than in the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean anxiety score.
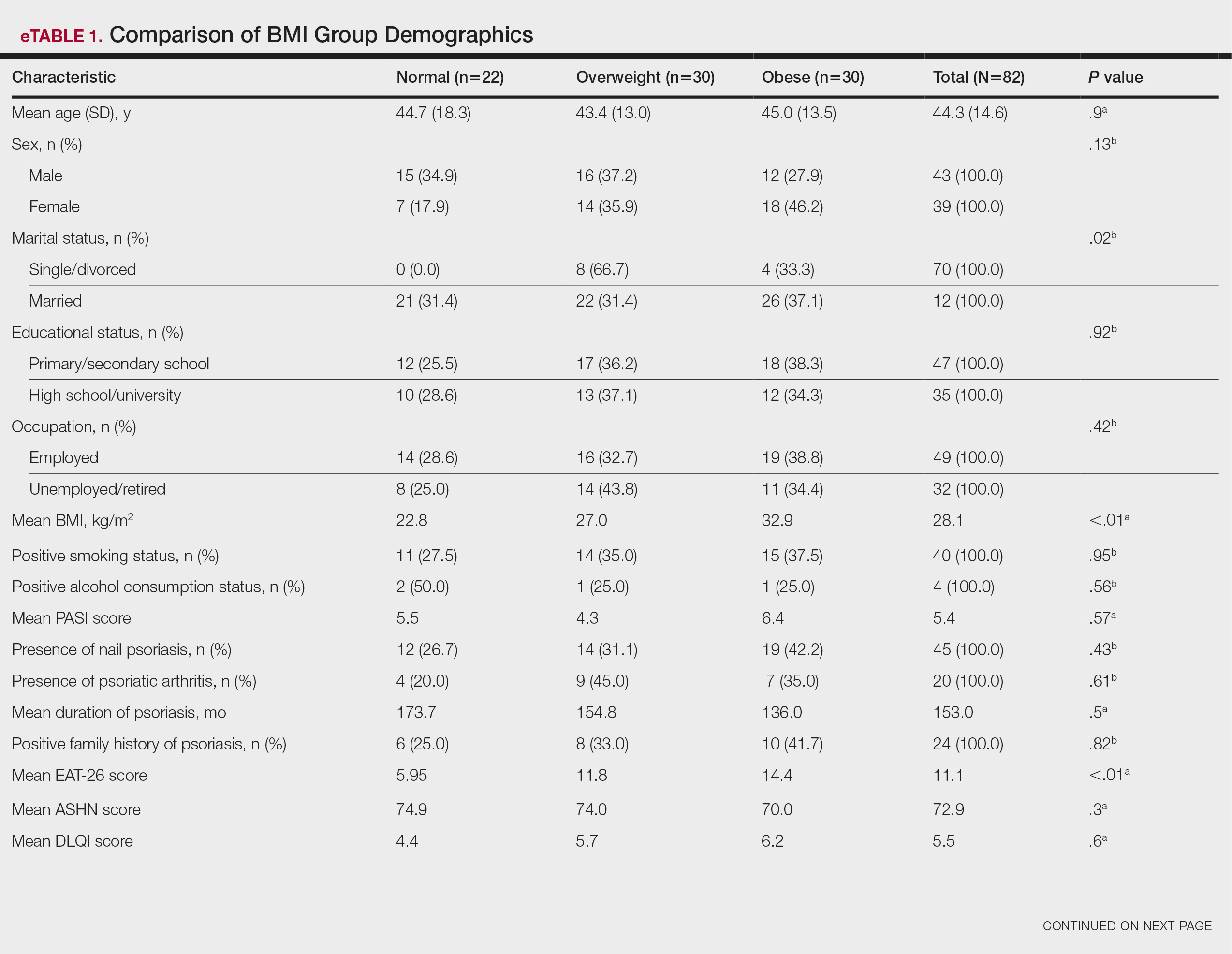
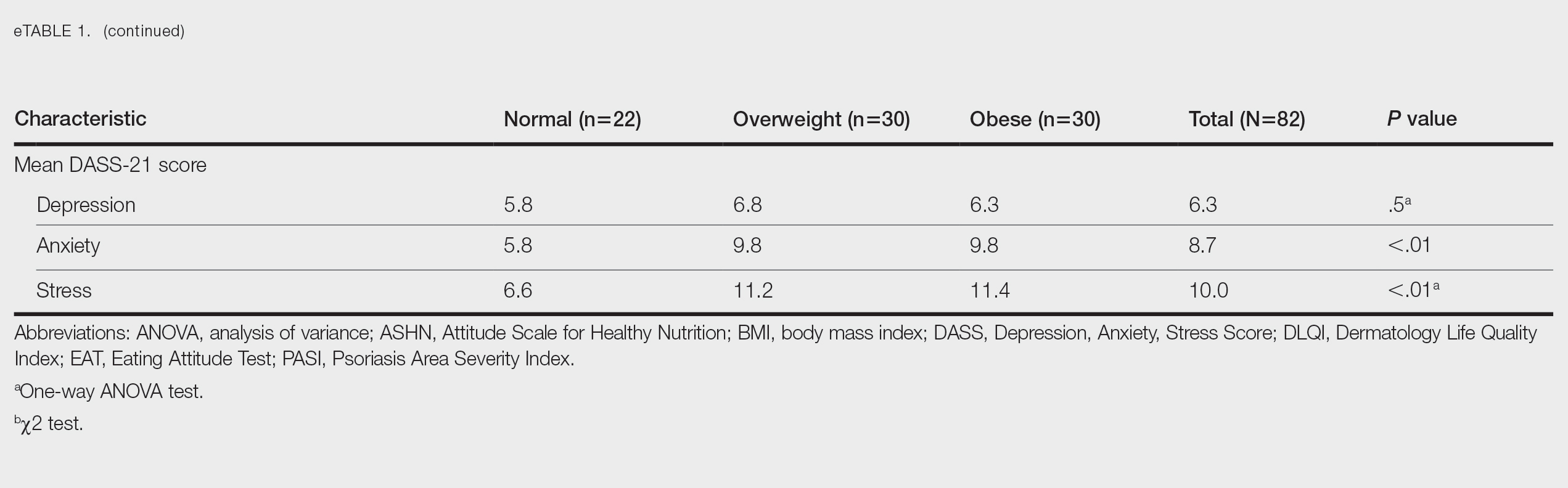
Comparative Evaluation of the EAT-26 Scores—There were statistically significant differences among the EAT-26 scores related to sex; BMI; and depression, anxiety, and stress scores (P=.04, .02, <.01, <.01, and <.01, respectively). The number of females in the group with a score of 20 points or higher was significantly (P=.04) less than that in the group scoring less than 20 points. The mean BMI in the group with a score of 20 points or higher was significantly (P=.02) greater than in group scoring less than 20 points. The mean depression, anxiety, and stress scores of the group scoring 20 points or higher were significantly (P<.01 for all) greater than in the group scoring less than 20 points (eTable 2).
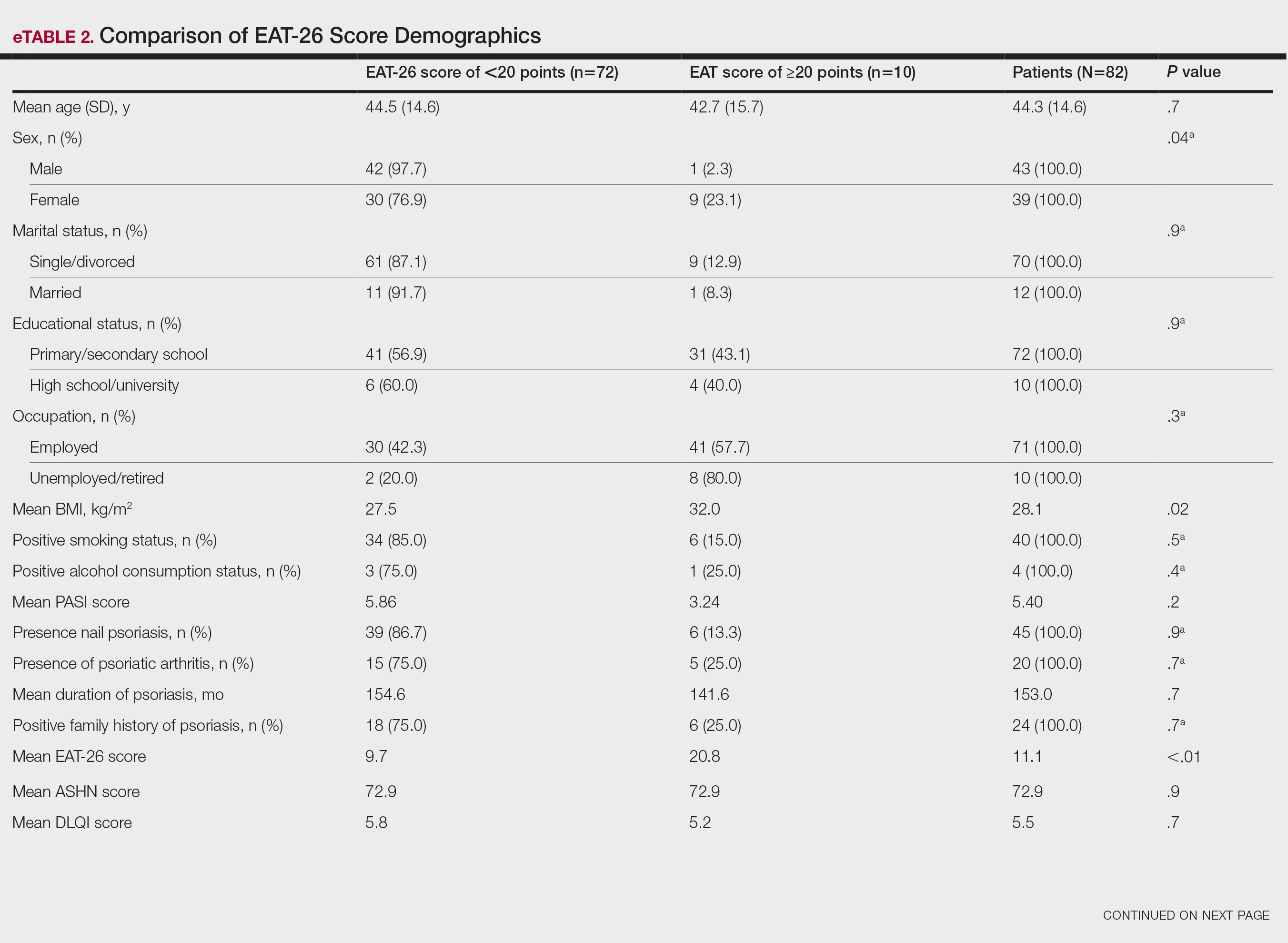
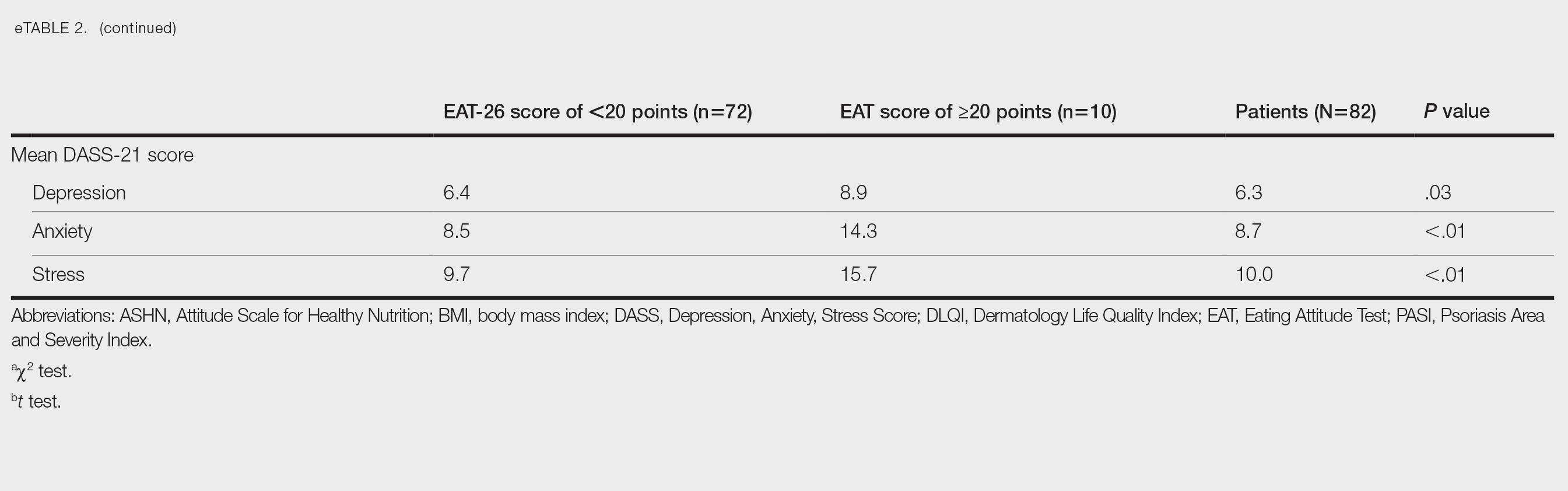
Correlation Analysis of the Study Variables—The EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress (P<.01 for all)(eTable 3).
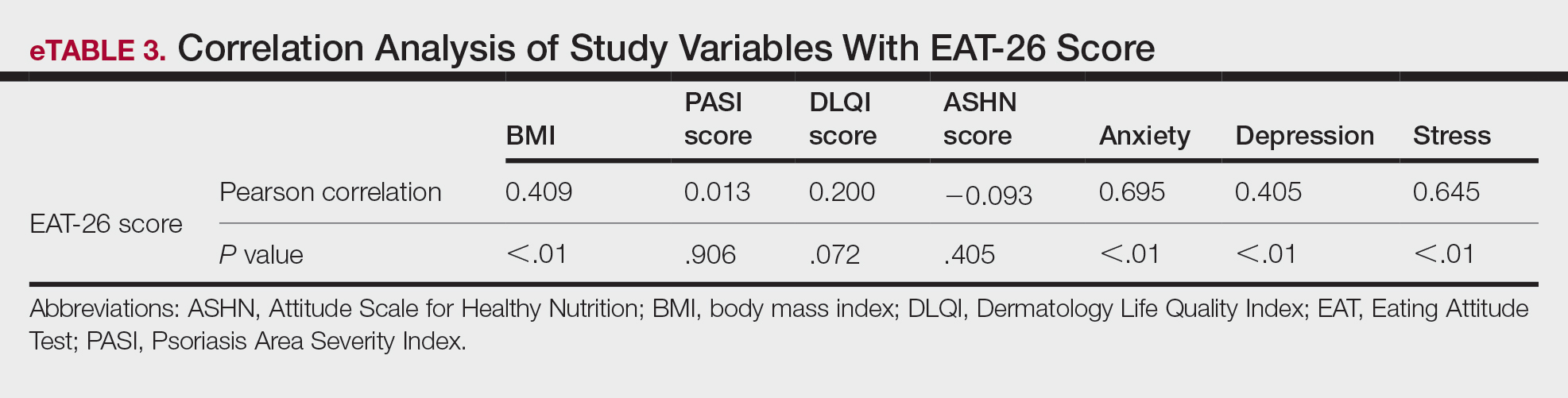
Comment
Eating disorders are psychiatric conditions that require a multidisciplinary approach. Nonpsychiatric medical departments may be involved due to the severe consequences (eg, various skin changes14) of these disorders. Psoriasis is not known to be directly affected by the presence of an ED; however, it is possible that EDs could indirectly affect patients with psoriasis by influencing obesity. Therefore, this study aimed to examine the relationship between ED risk factors and obesity in this population.
The relationship between psoriasis and obesity has been a popular research topic in dermatology since the 1990s.15 Epidemiologic and observational studies have reported that patients with psoriasis are more likely to be overweight or have obesity, which is an independent risk factor for psoriasis.3,16 However, the causal relationship between psoriasis and obesity remains unclear. In a comprehensive review, Barros et al17 emphasized the causal relationship between obesity and psoriasis under several headings. Firstly, a higher BMI increases the risk for psoriasis by promoting cytokine release and immune system dysregulation. Secondly, a Western diet (eg, processed foods and fast food) triggers obesity and psoriasis by increasing adipose tissue. Thirdly, the alteration of the skin and gut microbiota triggers chronic inflammation as a result of bacterial translocation in patients with obesity. Fourthly, a high-fat diet and palmitic acid disrupt the intestinal integrity of the gut and increase the risk for psoriasis and obesity by triggering chronic inflammation of bacterial fragments that pass into the blood. Finally, the decrease in the amount of adiponectin and the increase in the amount of leptin in patients with obesity may cause psoriasis by increasing proinflammatory cytokines, which are similar to those involved in the pathogenesis of psoriasis.17 Additionally, psoriatic inflammation can cause insulin resistance and metabolic dysfunction, leading to obesity.18 The relationship between psoriasis and obesity cannot be solely explained by metabolic pathways. Smoking, alcohol consumption, and a sedentary lifestyle all are associated with psoriasis and also can contribute to obesity.5 Our study revealed no significant difference in smoking or alcohol consumption between the normal weight and overweight/obesity groups. Based on our data, we determined that smoking and alcohol consumption did not affect obesity in our patients with psoriasis.
Observational and epidemiologic studies have shown that patients with psoriasis experience increased rates of depression, anxiety, and stress.19 In studies of pathogenesis, a connection between depression and psoriatic inflammation has been established.20 It is known that inflammatory cytokines similar to those in psoriasis are involved in the development of obesity.18 In addition, depression and anxiety can lead to binge eating, unhealthy food choices, and a more sedentary lifestyle.5 All of these variables may contribute to the associations between depression and anxiety with psoriasis and obesity. Zafiriou et al21 conducted a study to investigate the relationship between psoriasis, obesity, and depression through inflammatory pathways with a focus on the importance of IL-17. Data showing that IL-17–producing Th17-cell subgroups play a considerable role in the development of obesity and depression prompted the authors to suggest that psoriasis, obesity, and anxiety/depression may be interconnected manifestations of immune dysregulation, potentially linked to IL-17 and its associated cells.21 Mrowietz et al22 also suggested that metabolic inflammation may contribute to obesity and depression in patients with psoriasis and highlighted the importance of several cytokines, including tumor necrosis factor α, IL-6, IL-8, IL-17, and IL-23. Our study revealed no significant differences in depression scores between BMI groups. Another meta-analysis reported conflicting findings on the incidence of depression in obese patients with psoriasis.23 Some of the studies had a small number of participants. Compared to depression, anxiety has received less attention in studies of patients with obesity with psoriasis. However, these studies have shown a positive correlation between anxiety scores and BMI in patients with psoriasis.24,25 In our study, similar to the findings of previous studies, overweight patients and those with obesitywho have psoriasis had significantly (P<.01) greater anxiety and stress scores than did normal weight patients with psoriasis.
Obesity should be assessed in patients with psoriasis via a biopsychosocial approach that takes into account genetic, behavioral, and environmental factors.26 Eating disorders are considered to be one of the factors contributing to obesity. Numerous studies in the literature have demonstrated a greater incidence of EDs in patients with obesity vs those without obesity.5,6,27 Obesity and EDs have a bidirectional relationship: individuals with obesity are at risk for EDs due to body dissatisfaction, dieting habits, and depressive states. Conversely, poor eating behaviors in individuals with a normal weight can lead to obesity.28
There are few studies in the literature exploring the relationship between psoriasis and EDs. Crosta et al29 demonstrated that patients with psoriasis had impaired results on ED screening tests and that these scores deteriorated further as BMI increased. Moreover, Altunay et al30 demonstrated that patients with psoriasis and metabolic syndrome had higher scores on the ED screening test. In this study, patients with higher scores also exhibited high levels of anxiety.30 In our study, similar to the findings of previous studies, patients with psoriasis who were overweight or had obesity had significantly (P<.01) greater EAT-26 scores than those in the normal weight group. Patients with high EAT-26 scores also exhibited elevated levels of depression, anxiety, and stress. Additionally, EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress scores. Our study as well as other studies in the literature indicate that additional research is needed to determine the associations between EDs and obesity in psoriasis.
Conclusion
Managing obesity is crucial for patients with psoriasis. This study showed that EAT-26 scores were higher in patients with psoriasis who were overweight or had obesity than in those who were normal weight. Participants with high EAT-26 scores (≥20 points) were more likely to be female and have higher anxiety and stress scores. In addition, EAT-26 scores were positively correlated with BMI as well as depression, anxiety, and stress scores. Eating disorders may contribute to the development of obesity in patients with psoriasis. Although our study was limited by a small sample size, the results suggest that there is a need for large-scale multicenter studies to investigate the relationship between psoriasis and EDs.
- Kalkan G. Comorbidities in psoriasis: the recognition of psoriasis as a systemic disease and current management. Turkderm-Turk Arch Dermatol Venereol. 2017;51:71-77.
- Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes. 2012;2:E54.
- Jensen P, Skov L. Psoriasis and obesity. Dermatology. 2016;232:633-639.
- Mirghani H, Altemani AT, Altemani ST, et al. The cross talk between psoriasis, obesity, and dyslipidemia: a meta-analysis. Cureus. 2023;15:e49253.
- Roehring M, Mashep MR, White MA, et al. The metabolic syndrome and behavioral correlates in obese patients with binge disorders. Obesity. 2009;17:481-486.
- da Luz FQ, Hay P, Touyz S, et al. Obesity with comorbid eating disorders: associated health risks and treatment approaches. Nutrients. 2018;10:829.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Association; 2013.
- Ergüney Okumus¸ FE, Sertel Berk HÖ. The psychometric properties of the Eating Attitudes Test short form (EAT-26) in a college sample. Stud Psychol. 2020;40:57-78.
- Stoleru G, Leopold A, Auerbach A, et al. Female gender, dissatisfaction with weight, and number of IBD related surgeries as independent risk factors for eating disorders among patients with inflammatory bowel diseases. BMC Gastroenterol. 2022;22:438.
- Öztürkcan S, Ermertcan AT, Eser E, et al. Cross validation of the Turkish version of dermatology life quality index. Int J Dermatol. 2006;45:1300-1307.
- Demir GT, Ciciog˘lu HI˙. Attitude scale for healthy nutrition (ASHN): validity and reliability study. Gaziantep Univ J Sport Sci. 2019;4:256-274.
- Yılmaz O, Boz H, Arslan A. The validity and reliability of depression stress and anxiety scale (DASS 21) Turkish short form. Res Financial Econ Soc Stud. 2017;2:78-91.
- Nuttall FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. 2015;50:117-128.
- Strumia R, Manzata E, Gualandi M. Is there a role for dermatologists in eating disorders? Expert Rev Dermatol. 2017; 2:109-112.
- Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol. 1995;32:982-986.
- Naldi L, Addis A, Chimenti S, et al. Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis. evidence from the Psocare project. Dermatology. 2008;217:365-373.
- Barros G, Duran P, Vera I, et al. Exploring the links between obesity and psoriasis: a comprehensive review. Int J Mol Sci. 2022;23:7499.
- Hao Y, Zhu YJ, Zou S, et al. Metabolic syndrome and psoriasis: mechanisms and future directions. Front Immunol. 2021;12:711060.
- Jing D, Xiao H, Shen M, et al. Association of psoriasis with anxiety and depression: a case–control study in Chinese patients. Front Med (Lausanne). 2021;8:771645.
- Sahi FM, Masood A, Danawar NA, et al. Association between psoriasis and depression: a traditional review. Cureus. 2020;12:E9708.
- Zafiriou E, Daponte AI, Siokas V, et al. Depression and obesity in patients with psoriasis and psoriatic arthritis: is IL-17–mediated immune dysregulation the connecting link? Front Immunol. 2021;12:699848.
- Mrowietz U, Sümbül M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Pavlova NT, Kioskli K, Smith C, et al. Psychosocial aspects of obesity in adults with psoriasis: a systematic review. Skin Health Dis. 2021;1:E33.
- Innamorati M, Quinto RM, Imperatori C, et al. Health-related quality of life and its association with alexithymia and difficulties in emotion regulation in patients with psoriasis. Compr Psychiatry. 2016;70:200-208.
- Tabolli S, Naldi L, Pagliarello C, et al. Evaluation of the impact of writing exercises interventions on quality of life in patients with psoriasis undergoing systemic treatments. Br J Dermatol. 2012;167:1254‐1264.
- Albuquerque D, Nóbrega C, Manco L, et al. The contribution of genetics and environment to obesity. Br Med Bull. 2017;123:159‐173.
- Balantekin KN, Grammer AC, Fitzsimmons-Craft EE, et al. Overweight and obesity are associated with increased eating disorder correlates and general psychopathology in university women with eating disorders. Eat Behav. 2021;41:101482.
- Jebeile H, Lister NB, Baur LA, et al. Eating disorder risk in adolescents with obesity. Obes Rev. 2021;22:E13173.
- Crosta ML, Caldarola G, Fraietta S, et al. Psychopathology and eating disorders in patients with psoriasis. G Ital Dermatol Venereol. 2014;149:355-361.
- Altunay I, Demirci GT, Ates B, et al. Do eating disorders accompany metabolic syndrome in psoriasis patients? results of a preliminary study. Clin Cosmet Investig Dermatol. 2011;4:139-143.
Psoriasis is a chronic multisystemic inflammatory skin disease with a worldwide prevalence of 2% to 3%.1 Psoriasis can be accompanied by other conditions such as psoriatic arthritis, obesity, metabolic syndrome, diabetes mellitus, hypertension, dyslipidemia, atherosclerotic disease, inflammatory bowel disease, and anxiety/depression. It is important to manage comorbidities of psoriasis in addition to treating the cutaneous manifestations of the disease.1
Obesity is a major public health concern worldwide. Numerous observational and epidemiologic studies have reported a high prevalence of obesity among patients with psoriasis.2 Current evidence indicates that obesity may initiate or worsen psoriasis; furthermore, it is important to note that obesity may negatively impact the effectiveness of psoriasis-specific treatments or increase the incidence of adverse effects. Therefore, managing obesity is crucial in the treatment of psoriasis.3 Numerous studies have investigated the association between psoriasis and obesity, and they commonly conclude that both conditions share the same genetic metabolic pathways.2-4 However, it is important to consider environmental factors such as dietary habits, smoking, alcohol consumption, and a sedentary lifestyle—all of which are associated with psoriasis and also can contribute to the development of obesity.5 Because of the effects of obesity in psoriasis patients, factors that impact the development of obesity have become a popular research topic.
Eating disorders (EDs) are a crucial risk factor for both developing and maintaining obesity. In particular, two EDs that are associated with obesity include binge eating disorder and bulimia nervosa.6 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,7 binge eating disorder can be diagnosed when a patient has at least 1 episode of binge eating per week over a 3-month period. Bulimia nervosa can be diagnosed when a patient is excessively concerned with their body weight and shape and engages in behaviors to prevent weight gain (eg, forced vomiting, excessive use of laxatives).7 Psychiatrists who specialize in EDs make diagnoses based on these criteria. In daily practice, there are several quick and simple questionnaires available to screen for EDs that can be used by nonpsychiatrist physicians, including the commonly used 26-item Eating Attitudes Test (EAT-26).8 The EAT-26 has been used to screen for EDs in patients with inflammatory disorders.9
The aim of this study was to screen for EDs in patients with psoriasis to identify potential risk factors for development of obesity.
Materials and Methods
This study included patients with psoriasis who were screened for EDs at a tertiary dermatology clinic in Turkey between January 2021 and December 2023. This study was approved by the local ethics committee and was in accordance with the Declaration of Helsinki (decision number E-93471371-514.99-225000079).
Study Design and Patient Inclusion Criteria—This quantitative cross-sectional study utilized EAT-26, Dermatology Life Quality Index (DLQI), Attitude Scale for Healthy Nutrition (ASHN), and Depression Anxiety Stress Scale-21 (DASS-21) scores. All the questionnaire scales used in the study were adapted and validated in Turkey.8,10-12 The inclusion criteria consisted of being older than 18 years of age, being literate, having psoriasis for at least 1 year that was not treated topically or systemically, and having no psychiatric diseases outside an ED. The questionnaires were presented in written format following the clinical examination. Literacy was an inclusion criterion in this study due to the absence of auxiliary health personnel.
Study Variables—The study variables included age, sex, marital status (single/divorced or married), education status (primary/secondary school or high school/university), employment status (employed or unemployed/retired), body mass index (BMI), smoking status, alcohol-consumption status, Psoriasis Area Severity Index score, presence of nail psoriasis and psoriatic arthritis, duration of psoriasis, family history of psoriasis, EAT-26 score, ASHN score, DLQI score, and DASS-21 score. Body mass index was calculated by taking a participant’s weight in kilograms and dividing it by their height in meters squared. The BMI values were classified into 3 categories: normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2).13
Questionnaires—The EAT-26 questionnaire includes 26 questions that are used to detect EDs. Responses to each question include Likert-type answer options (ie, “always,” “usually,” “often,” “sometimes,” “rarely,” and “never.”) Patients with scores of 20 points or higher (range, 0–78) are classified as high risk for EDs.8 In our study, EAT-26 scores were grouped into 2 categories: patients scoring less than 20 points and those scoring 20 points or higher.
The DLQI questionnaire includes 10 questions to measure dermatologic symptoms and qualiy of life. Responses to each question include Likert-type answer options (ie, “not at all,” “a little,” “a lot,” or “very much.”) On the DLQI scale, the higher the score, the lower the quality of life (score range, 0–30).10
The ASHN questionnaire includes 21 questions that measure attitudes toward healthy nutrition with 5 possible answer options (“strongly disagree,” “disagree,” “undecided,” “agree,” and “strongly agree”). On this scale, higher scores indicate the participant is more knowledgeable about healthy nutrition (score range, 0–78).11
The DASS-21 questionnaire includes 21 questions that measure the severity of a range of symptoms common to depression, anxiety, and stress. Responses include Likert-type answer options (eg, “never,” “sometimes,” “often,” and “almost always.”) On this scale, a higher score (range of 0–21 for each) indicates higher levels of depression, anxiety, and stress.12
Statistical Analysis—Descriptive statistics were analyzed using SPSS software version 22.0 (IBM). The Shapiro-Wilk test was applied to determine whether the data were normally distributed. For categorical variables, frequency differences among groups were compared using the Pearson χ2 test. A t test was used to compare the means of 2 independent groups with a normal distribution. One-way analysis of variance and Tukey Honest Significant Difference post hoc analysis were used to test whether there was a statistically significant difference among the normally distributed means of independent groups. Pearson correlation analysis was used to determine whether there was a linear relationship between 2 numeric measurements and, if so, to determine the direction and severity of this relationship. P<.05 indicated statistical significance in this study.
Results
Study Participant Demographics—This study included 82 participants with a mean age of 44.3 years; 52.4% (43/82) were female, and 85.4% (70/82) were married. The questionnaire took an average of 4.2 minutes for participants to complete. A total of 57.3% (47/82) of patients had completed primary/secondary education and 59.8% (49/82) were employed. The mean BMI was 28.1 kg/m2. According to the BMI classification, 26.8% (22/82) participants had a normal weight, 36.6% (30/82) were overweight, and 43.9% (36/82) were obese. A total of 48.8% (40/82) of participants smoked, and 4.9% (4/82) consumed alcohol. The mean Psoriasis Area and Severity Index score was 5.4. A total of 54.9% (45/82) of participants had nail psoriasis, and 24.4% (20/82) had psoriatic arthritis. The mean duration of psoriasis was 153 months. A total of 29.3% (24/82) of participants had a positive family history of psoriasis. The mean EAT-26 score was 11.1. A total of 12.2% (10/82) of participants had an EAT-26 score of 20 points or higher and were considered at high risk for an ED. The mean ASHN score was 72.9; the mean DLQI score was 5.5; and on the DASS-21 scale, mean scores for depression, anxiety, and stress were 6.3, 8.7, and 10.0, respectively (Table).
Comparative Evaluation of the BMI Groups—The only statistically significant differences among the 3 BMI groups were related to marital status, EAT-26 score, and anxiety and stress scores (P=.02, <.01, <.01, and <.01, respectively)(eTable 1). The number of single/divorced participants in the overweight group was significantly (P=.02) greater than in the normal weight group. The mean EAT-26 score for the normal weight group was significantly (P<.01) lower than for the overweight and obese groups; there was no significant difference in mean EAT-26 scores between the overweight and obese groups. The mean anxiety score was significantly (P<.01) lower in the normal weight group compared with the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean depression score. The mean stress and anxiety scores were significantly (P<.01) lower in the normal weight group than in the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean anxiety score.
Comparative Evaluation of the EAT-26 Scores—There were statistically significant differences among the EAT-26 scores related to sex; BMI; and depression, anxiety, and stress scores (P=.04, .02, <.01, <.01, and <.01, respectively). The number of females in the group with a score of 20 points or higher was significantly (P=.04) less than that in the group scoring less than 20 points. The mean BMI in the group with a score of 20 points or higher was significantly (P=.02) greater than in group scoring less than 20 points. The mean depression, anxiety, and stress scores of the group scoring 20 points or higher were significantly (P<.01 for all) greater than in the group scoring less than 20 points (eTable 2).
Correlation Analysis of the Study Variables—The EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress (P<.01 for all)(eTable 3).
Comment
Eating disorders are psychiatric conditions that require a multidisciplinary approach. Nonpsychiatric medical departments may be involved due to the severe consequences (eg, various skin changes14) of these disorders. Psoriasis is not known to be directly affected by the presence of an ED; however, it is possible that EDs could indirectly affect patients with psoriasis by influencing obesity. Therefore, this study aimed to examine the relationship between ED risk factors and obesity in this population.
The relationship between psoriasis and obesity has been a popular research topic in dermatology since the 1990s.15 Epidemiologic and observational studies have reported that patients with psoriasis are more likely to be overweight or have obesity, which is an independent risk factor for psoriasis.3,16 However, the causal relationship between psoriasis and obesity remains unclear. In a comprehensive review, Barros et al17 emphasized the causal relationship between obesity and psoriasis under several headings. Firstly, a higher BMI increases the risk for psoriasis by promoting cytokine release and immune system dysregulation. Secondly, a Western diet (eg, processed foods and fast food) triggers obesity and psoriasis by increasing adipose tissue. Thirdly, the alteration of the skin and gut microbiota triggers chronic inflammation as a result of bacterial translocation in patients with obesity. Fourthly, a high-fat diet and palmitic acid disrupt the intestinal integrity of the gut and increase the risk for psoriasis and obesity by triggering chronic inflammation of bacterial fragments that pass into the blood. Finally, the decrease in the amount of adiponectin and the increase in the amount of leptin in patients with obesity may cause psoriasis by increasing proinflammatory cytokines, which are similar to those involved in the pathogenesis of psoriasis.17 Additionally, psoriatic inflammation can cause insulin resistance and metabolic dysfunction, leading to obesity.18 The relationship between psoriasis and obesity cannot be solely explained by metabolic pathways. Smoking, alcohol consumption, and a sedentary lifestyle all are associated with psoriasis and also can contribute to obesity.5 Our study revealed no significant difference in smoking or alcohol consumption between the normal weight and overweight/obesity groups. Based on our data, we determined that smoking and alcohol consumption did not affect obesity in our patients with psoriasis.
Observational and epidemiologic studies have shown that patients with psoriasis experience increased rates of depression, anxiety, and stress.19 In studies of pathogenesis, a connection between depression and psoriatic inflammation has been established.20 It is known that inflammatory cytokines similar to those in psoriasis are involved in the development of obesity.18 In addition, depression and anxiety can lead to binge eating, unhealthy food choices, and a more sedentary lifestyle.5 All of these variables may contribute to the associations between depression and anxiety with psoriasis and obesity. Zafiriou et al21 conducted a study to investigate the relationship between psoriasis, obesity, and depression through inflammatory pathways with a focus on the importance of IL-17. Data showing that IL-17–producing Th17-cell subgroups play a considerable role in the development of obesity and depression prompted the authors to suggest that psoriasis, obesity, and anxiety/depression may be interconnected manifestations of immune dysregulation, potentially linked to IL-17 and its associated cells.21 Mrowietz et al22 also suggested that metabolic inflammation may contribute to obesity and depression in patients with psoriasis and highlighted the importance of several cytokines, including tumor necrosis factor α, IL-6, IL-8, IL-17, and IL-23. Our study revealed no significant differences in depression scores between BMI groups. Another meta-analysis reported conflicting findings on the incidence of depression in obese patients with psoriasis.23 Some of the studies had a small number of participants. Compared to depression, anxiety has received less attention in studies of patients with obesity with psoriasis. However, these studies have shown a positive correlation between anxiety scores and BMI in patients with psoriasis.24,25 In our study, similar to the findings of previous studies, overweight patients and those with obesitywho have psoriasis had significantly (P<.01) greater anxiety and stress scores than did normal weight patients with psoriasis.
Obesity should be assessed in patients with psoriasis via a biopsychosocial approach that takes into account genetic, behavioral, and environmental factors.26 Eating disorders are considered to be one of the factors contributing to obesity. Numerous studies in the literature have demonstrated a greater incidence of EDs in patients with obesity vs those without obesity.5,6,27 Obesity and EDs have a bidirectional relationship: individuals with obesity are at risk for EDs due to body dissatisfaction, dieting habits, and depressive states. Conversely, poor eating behaviors in individuals with a normal weight can lead to obesity.28
There are few studies in the literature exploring the relationship between psoriasis and EDs. Crosta et al29 demonstrated that patients with psoriasis had impaired results on ED screening tests and that these scores deteriorated further as BMI increased. Moreover, Altunay et al30 demonstrated that patients with psoriasis and metabolic syndrome had higher scores on the ED screening test. In this study, patients with higher scores also exhibited high levels of anxiety.30 In our study, similar to the findings of previous studies, patients with psoriasis who were overweight or had obesity had significantly (P<.01) greater EAT-26 scores than those in the normal weight group. Patients with high EAT-26 scores also exhibited elevated levels of depression, anxiety, and stress. Additionally, EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress scores. Our study as well as other studies in the literature indicate that additional research is needed to determine the associations between EDs and obesity in psoriasis.
Conclusion
Managing obesity is crucial for patients with psoriasis. This study showed that EAT-26 scores were higher in patients with psoriasis who were overweight or had obesity than in those who were normal weight. Participants with high EAT-26 scores (≥20 points) were more likely to be female and have higher anxiety and stress scores. In addition, EAT-26 scores were positively correlated with BMI as well as depression, anxiety, and stress scores. Eating disorders may contribute to the development of obesity in patients with psoriasis. Although our study was limited by a small sample size, the results suggest that there is a need for large-scale multicenter studies to investigate the relationship between psoriasis and EDs.
Psoriasis is a chronic multisystemic inflammatory skin disease with a worldwide prevalence of 2% to 3%.1 Psoriasis can be accompanied by other conditions such as psoriatic arthritis, obesity, metabolic syndrome, diabetes mellitus, hypertension, dyslipidemia, atherosclerotic disease, inflammatory bowel disease, and anxiety/depression. It is important to manage comorbidities of psoriasis in addition to treating the cutaneous manifestations of the disease.1
Obesity is a major public health concern worldwide. Numerous observational and epidemiologic studies have reported a high prevalence of obesity among patients with psoriasis.2 Current evidence indicates that obesity may initiate or worsen psoriasis; furthermore, it is important to note that obesity may negatively impact the effectiveness of psoriasis-specific treatments or increase the incidence of adverse effects. Therefore, managing obesity is crucial in the treatment of psoriasis.3 Numerous studies have investigated the association between psoriasis and obesity, and they commonly conclude that both conditions share the same genetic metabolic pathways.2-4 However, it is important to consider environmental factors such as dietary habits, smoking, alcohol consumption, and a sedentary lifestyle—all of which are associated with psoriasis and also can contribute to the development of obesity.5 Because of the effects of obesity in psoriasis patients, factors that impact the development of obesity have become a popular research topic.
Eating disorders (EDs) are a crucial risk factor for both developing and maintaining obesity. In particular, two EDs that are associated with obesity include binge eating disorder and bulimia nervosa.6 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition,7 binge eating disorder can be diagnosed when a patient has at least 1 episode of binge eating per week over a 3-month period. Bulimia nervosa can be diagnosed when a patient is excessively concerned with their body weight and shape and engages in behaviors to prevent weight gain (eg, forced vomiting, excessive use of laxatives).7 Psychiatrists who specialize in EDs make diagnoses based on these criteria. In daily practice, there are several quick and simple questionnaires available to screen for EDs that can be used by nonpsychiatrist physicians, including the commonly used 26-item Eating Attitudes Test (EAT-26).8 The EAT-26 has been used to screen for EDs in patients with inflammatory disorders.9
The aim of this study was to screen for EDs in patients with psoriasis to identify potential risk factors for development of obesity.
Materials and Methods
This study included patients with psoriasis who were screened for EDs at a tertiary dermatology clinic in Turkey between January 2021 and December 2023. This study was approved by the local ethics committee and was in accordance with the Declaration of Helsinki (decision number E-93471371-514.99-225000079).
Study Design and Patient Inclusion Criteria—This quantitative cross-sectional study utilized EAT-26, Dermatology Life Quality Index (DLQI), Attitude Scale for Healthy Nutrition (ASHN), and Depression Anxiety Stress Scale-21 (DASS-21) scores. All the questionnaire scales used in the study were adapted and validated in Turkey.8,10-12 The inclusion criteria consisted of being older than 18 years of age, being literate, having psoriasis for at least 1 year that was not treated topically or systemically, and having no psychiatric diseases outside an ED. The questionnaires were presented in written format following the clinical examination. Literacy was an inclusion criterion in this study due to the absence of auxiliary health personnel.
Study Variables—The study variables included age, sex, marital status (single/divorced or married), education status (primary/secondary school or high school/university), employment status (employed or unemployed/retired), body mass index (BMI), smoking status, alcohol-consumption status, Psoriasis Area Severity Index score, presence of nail psoriasis and psoriatic arthritis, duration of psoriasis, family history of psoriasis, EAT-26 score, ASHN score, DLQI score, and DASS-21 score. Body mass index was calculated by taking a participant’s weight in kilograms and dividing it by their height in meters squared. The BMI values were classified into 3 categories: normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30 kg/m2).13
Questionnaires—The EAT-26 questionnaire includes 26 questions that are used to detect EDs. Responses to each question include Likert-type answer options (ie, “always,” “usually,” “often,” “sometimes,” “rarely,” and “never.”) Patients with scores of 20 points or higher (range, 0–78) are classified as high risk for EDs.8 In our study, EAT-26 scores were grouped into 2 categories: patients scoring less than 20 points and those scoring 20 points or higher.
The DLQI questionnaire includes 10 questions to measure dermatologic symptoms and qualiy of life. Responses to each question include Likert-type answer options (ie, “not at all,” “a little,” “a lot,” or “very much.”) On the DLQI scale, the higher the score, the lower the quality of life (score range, 0–30).10
The ASHN questionnaire includes 21 questions that measure attitudes toward healthy nutrition with 5 possible answer options (“strongly disagree,” “disagree,” “undecided,” “agree,” and “strongly agree”). On this scale, higher scores indicate the participant is more knowledgeable about healthy nutrition (score range, 0–78).11
The DASS-21 questionnaire includes 21 questions that measure the severity of a range of symptoms common to depression, anxiety, and stress. Responses include Likert-type answer options (eg, “never,” “sometimes,” “often,” and “almost always.”) On this scale, a higher score (range of 0–21 for each) indicates higher levels of depression, anxiety, and stress.12
Statistical Analysis—Descriptive statistics were analyzed using SPSS software version 22.0 (IBM). The Shapiro-Wilk test was applied to determine whether the data were normally distributed. For categorical variables, frequency differences among groups were compared using the Pearson χ2 test. A t test was used to compare the means of 2 independent groups with a normal distribution. One-way analysis of variance and Tukey Honest Significant Difference post hoc analysis were used to test whether there was a statistically significant difference among the normally distributed means of independent groups. Pearson correlation analysis was used to determine whether there was a linear relationship between 2 numeric measurements and, if so, to determine the direction and severity of this relationship. P<.05 indicated statistical significance in this study.
Results
Study Participant Demographics—This study included 82 participants with a mean age of 44.3 years; 52.4% (43/82) were female, and 85.4% (70/82) were married. The questionnaire took an average of 4.2 minutes for participants to complete. A total of 57.3% (47/82) of patients had completed primary/secondary education and 59.8% (49/82) were employed. The mean BMI was 28.1 kg/m2. According to the BMI classification, 26.8% (22/82) participants had a normal weight, 36.6% (30/82) were overweight, and 43.9% (36/82) were obese. A total of 48.8% (40/82) of participants smoked, and 4.9% (4/82) consumed alcohol. The mean Psoriasis Area and Severity Index score was 5.4. A total of 54.9% (45/82) of participants had nail psoriasis, and 24.4% (20/82) had psoriatic arthritis. The mean duration of psoriasis was 153 months. A total of 29.3% (24/82) of participants had a positive family history of psoriasis. The mean EAT-26 score was 11.1. A total of 12.2% (10/82) of participants had an EAT-26 score of 20 points or higher and were considered at high risk for an ED. The mean ASHN score was 72.9; the mean DLQI score was 5.5; and on the DASS-21 scale, mean scores for depression, anxiety, and stress were 6.3, 8.7, and 10.0, respectively (Table).
Comparative Evaluation of the BMI Groups—The only statistically significant differences among the 3 BMI groups were related to marital status, EAT-26 score, and anxiety and stress scores (P=.02, <.01, <.01, and <.01, respectively)(eTable 1). The number of single/divorced participants in the overweight group was significantly (P=.02) greater than in the normal weight group. The mean EAT-26 score for the normal weight group was significantly (P<.01) lower than for the overweight and obese groups; there was no significant difference in mean EAT-26 scores between the overweight and obese groups. The mean anxiety score was significantly (P<.01) lower in the normal weight group compared with the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean depression score. The mean stress and anxiety scores were significantly (P<.01) lower in the normal weight group than in the overweight and obese groups. There was no significant difference between the overweight and obese groups according to the mean anxiety score.
Comparative Evaluation of the EAT-26 Scores—There were statistically significant differences among the EAT-26 scores related to sex; BMI; and depression, anxiety, and stress scores (P=.04, .02, <.01, <.01, and <.01, respectively). The number of females in the group with a score of 20 points or higher was significantly (P=.04) less than that in the group scoring less than 20 points. The mean BMI in the group with a score of 20 points or higher was significantly (P=.02) greater than in group scoring less than 20 points. The mean depression, anxiety, and stress scores of the group scoring 20 points or higher were significantly (P<.01 for all) greater than in the group scoring less than 20 points (eTable 2).
Correlation Analysis of the Study Variables—The EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress (P<.01 for all)(eTable 3).
Comment
Eating disorders are psychiatric conditions that require a multidisciplinary approach. Nonpsychiatric medical departments may be involved due to the severe consequences (eg, various skin changes14) of these disorders. Psoriasis is not known to be directly affected by the presence of an ED; however, it is possible that EDs could indirectly affect patients with psoriasis by influencing obesity. Therefore, this study aimed to examine the relationship between ED risk factors and obesity in this population.
The relationship between psoriasis and obesity has been a popular research topic in dermatology since the 1990s.15 Epidemiologic and observational studies have reported that patients with psoriasis are more likely to be overweight or have obesity, which is an independent risk factor for psoriasis.3,16 However, the causal relationship between psoriasis and obesity remains unclear. In a comprehensive review, Barros et al17 emphasized the causal relationship between obesity and psoriasis under several headings. Firstly, a higher BMI increases the risk for psoriasis by promoting cytokine release and immune system dysregulation. Secondly, a Western diet (eg, processed foods and fast food) triggers obesity and psoriasis by increasing adipose tissue. Thirdly, the alteration of the skin and gut microbiota triggers chronic inflammation as a result of bacterial translocation in patients with obesity. Fourthly, a high-fat diet and palmitic acid disrupt the intestinal integrity of the gut and increase the risk for psoriasis and obesity by triggering chronic inflammation of bacterial fragments that pass into the blood. Finally, the decrease in the amount of adiponectin and the increase in the amount of leptin in patients with obesity may cause psoriasis by increasing proinflammatory cytokines, which are similar to those involved in the pathogenesis of psoriasis.17 Additionally, psoriatic inflammation can cause insulin resistance and metabolic dysfunction, leading to obesity.18 The relationship between psoriasis and obesity cannot be solely explained by metabolic pathways. Smoking, alcohol consumption, and a sedentary lifestyle all are associated with psoriasis and also can contribute to obesity.5 Our study revealed no significant difference in smoking or alcohol consumption between the normal weight and overweight/obesity groups. Based on our data, we determined that smoking and alcohol consumption did not affect obesity in our patients with psoriasis.
Observational and epidemiologic studies have shown that patients with psoriasis experience increased rates of depression, anxiety, and stress.19 In studies of pathogenesis, a connection between depression and psoriatic inflammation has been established.20 It is known that inflammatory cytokines similar to those in psoriasis are involved in the development of obesity.18 In addition, depression and anxiety can lead to binge eating, unhealthy food choices, and a more sedentary lifestyle.5 All of these variables may contribute to the associations between depression and anxiety with psoriasis and obesity. Zafiriou et al21 conducted a study to investigate the relationship between psoriasis, obesity, and depression through inflammatory pathways with a focus on the importance of IL-17. Data showing that IL-17–producing Th17-cell subgroups play a considerable role in the development of obesity and depression prompted the authors to suggest that psoriasis, obesity, and anxiety/depression may be interconnected manifestations of immune dysregulation, potentially linked to IL-17 and its associated cells.21 Mrowietz et al22 also suggested that metabolic inflammation may contribute to obesity and depression in patients with psoriasis and highlighted the importance of several cytokines, including tumor necrosis factor α, IL-6, IL-8, IL-17, and IL-23. Our study revealed no significant differences in depression scores between BMI groups. Another meta-analysis reported conflicting findings on the incidence of depression in obese patients with psoriasis.23 Some of the studies had a small number of participants. Compared to depression, anxiety has received less attention in studies of patients with obesity with psoriasis. However, these studies have shown a positive correlation between anxiety scores and BMI in patients with psoriasis.24,25 In our study, similar to the findings of previous studies, overweight patients and those with obesitywho have psoriasis had significantly (P<.01) greater anxiety and stress scores than did normal weight patients with psoriasis.
Obesity should be assessed in patients with psoriasis via a biopsychosocial approach that takes into account genetic, behavioral, and environmental factors.26 Eating disorders are considered to be one of the factors contributing to obesity. Numerous studies in the literature have demonstrated a greater incidence of EDs in patients with obesity vs those without obesity.5,6,27 Obesity and EDs have a bidirectional relationship: individuals with obesity are at risk for EDs due to body dissatisfaction, dieting habits, and depressive states. Conversely, poor eating behaviors in individuals with a normal weight can lead to obesity.28
There are few studies in the literature exploring the relationship between psoriasis and EDs. Crosta et al29 demonstrated that patients with psoriasis had impaired results on ED screening tests and that these scores deteriorated further as BMI increased. Moreover, Altunay et al30 demonstrated that patients with psoriasis and metabolic syndrome had higher scores on the ED screening test. In this study, patients with higher scores also exhibited high levels of anxiety.30 In our study, similar to the findings of previous studies, patients with psoriasis who were overweight or had obesity had significantly (P<.01) greater EAT-26 scores than those in the normal weight group. Patients with high EAT-26 scores also exhibited elevated levels of depression, anxiety, and stress. Additionally, EAT-26 scores were positively correlated with BMI, anxiety, depression, and stress scores. Our study as well as other studies in the literature indicate that additional research is needed to determine the associations between EDs and obesity in psoriasis.
Conclusion
Managing obesity is crucial for patients with psoriasis. This study showed that EAT-26 scores were higher in patients with psoriasis who were overweight or had obesity than in those who were normal weight. Participants with high EAT-26 scores (≥20 points) were more likely to be female and have higher anxiety and stress scores. In addition, EAT-26 scores were positively correlated with BMI as well as depression, anxiety, and stress scores. Eating disorders may contribute to the development of obesity in patients with psoriasis. Although our study was limited by a small sample size, the results suggest that there is a need for large-scale multicenter studies to investigate the relationship between psoriasis and EDs.
- Kalkan G. Comorbidities in psoriasis: the recognition of psoriasis as a systemic disease and current management. Turkderm-Turk Arch Dermatol Venereol. 2017;51:71-77.
- Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes. 2012;2:E54.
- Jensen P, Skov L. Psoriasis and obesity. Dermatology. 2016;232:633-639.
- Mirghani H, Altemani AT, Altemani ST, et al. The cross talk between psoriasis, obesity, and dyslipidemia: a meta-analysis. Cureus. 2023;15:e49253.
- Roehring M, Mashep MR, White MA, et al. The metabolic syndrome and behavioral correlates in obese patients with binge disorders. Obesity. 2009;17:481-486.
- da Luz FQ, Hay P, Touyz S, et al. Obesity with comorbid eating disorders: associated health risks and treatment approaches. Nutrients. 2018;10:829.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Association; 2013.
- Ergüney Okumus¸ FE, Sertel Berk HÖ. The psychometric properties of the Eating Attitudes Test short form (EAT-26) in a college sample. Stud Psychol. 2020;40:57-78.
- Stoleru G, Leopold A, Auerbach A, et al. Female gender, dissatisfaction with weight, and number of IBD related surgeries as independent risk factors for eating disorders among patients with inflammatory bowel diseases. BMC Gastroenterol. 2022;22:438.
- Öztürkcan S, Ermertcan AT, Eser E, et al. Cross validation of the Turkish version of dermatology life quality index. Int J Dermatol. 2006;45:1300-1307.
- Demir GT, Ciciog˘lu HI˙. Attitude scale for healthy nutrition (ASHN): validity and reliability study. Gaziantep Univ J Sport Sci. 2019;4:256-274.
- Yılmaz O, Boz H, Arslan A. The validity and reliability of depression stress and anxiety scale (DASS 21) Turkish short form. Res Financial Econ Soc Stud. 2017;2:78-91.
- Nuttall FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. 2015;50:117-128.
- Strumia R, Manzata E, Gualandi M. Is there a role for dermatologists in eating disorders? Expert Rev Dermatol. 2017; 2:109-112.
- Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol. 1995;32:982-986.
- Naldi L, Addis A, Chimenti S, et al. Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis. evidence from the Psocare project. Dermatology. 2008;217:365-373.
- Barros G, Duran P, Vera I, et al. Exploring the links between obesity and psoriasis: a comprehensive review. Int J Mol Sci. 2022;23:7499.
- Hao Y, Zhu YJ, Zou S, et al. Metabolic syndrome and psoriasis: mechanisms and future directions. Front Immunol. 2021;12:711060.
- Jing D, Xiao H, Shen M, et al. Association of psoriasis with anxiety and depression: a case–control study in Chinese patients. Front Med (Lausanne). 2021;8:771645.
- Sahi FM, Masood A, Danawar NA, et al. Association between psoriasis and depression: a traditional review. Cureus. 2020;12:E9708.
- Zafiriou E, Daponte AI, Siokas V, et al. Depression and obesity in patients with psoriasis and psoriatic arthritis: is IL-17–mediated immune dysregulation the connecting link? Front Immunol. 2021;12:699848.
- Mrowietz U, Sümbül M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Pavlova NT, Kioskli K, Smith C, et al. Psychosocial aspects of obesity in adults with psoriasis: a systematic review. Skin Health Dis. 2021;1:E33.
- Innamorati M, Quinto RM, Imperatori C, et al. Health-related quality of life and its association with alexithymia and difficulties in emotion regulation in patients with psoriasis. Compr Psychiatry. 2016;70:200-208.
- Tabolli S, Naldi L, Pagliarello C, et al. Evaluation of the impact of writing exercises interventions on quality of life in patients with psoriasis undergoing systemic treatments. Br J Dermatol. 2012;167:1254‐1264.
- Albuquerque D, Nóbrega C, Manco L, et al. The contribution of genetics and environment to obesity. Br Med Bull. 2017;123:159‐173.
- Balantekin KN, Grammer AC, Fitzsimmons-Craft EE, et al. Overweight and obesity are associated with increased eating disorder correlates and general psychopathology in university women with eating disorders. Eat Behav. 2021;41:101482.
- Jebeile H, Lister NB, Baur LA, et al. Eating disorder risk in adolescents with obesity. Obes Rev. 2021;22:E13173.
- Crosta ML, Caldarola G, Fraietta S, et al. Psychopathology and eating disorders in patients with psoriasis. G Ital Dermatol Venereol. 2014;149:355-361.
- Altunay I, Demirci GT, Ates B, et al. Do eating disorders accompany metabolic syndrome in psoriasis patients? results of a preliminary study. Clin Cosmet Investig Dermatol. 2011;4:139-143.
- Kalkan G. Comorbidities in psoriasis: the recognition of psoriasis as a systemic disease and current management. Turkderm-Turk Arch Dermatol Venereol. 2017;51:71-77.
- Armstrong AW, Harskamp CT, Armstrong EJ. The association between psoriasis and obesity: a systematic review and meta-analysis of observational studies. Nutr Diabetes. 2012;2:E54.
- Jensen P, Skov L. Psoriasis and obesity. Dermatology. 2016;232:633-639.
- Mirghani H, Altemani AT, Altemani ST, et al. The cross talk between psoriasis, obesity, and dyslipidemia: a meta-analysis. Cureus. 2023;15:e49253.
- Roehring M, Mashep MR, White MA, et al. The metabolic syndrome and behavioral correlates in obese patients with binge disorders. Obesity. 2009;17:481-486.
- da Luz FQ, Hay P, Touyz S, et al. Obesity with comorbid eating disorders: associated health risks and treatment approaches. Nutrients. 2018;10:829.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. American Psychiatric Association; 2013.
- Ergüney Okumus¸ FE, Sertel Berk HÖ. The psychometric properties of the Eating Attitudes Test short form (EAT-26) in a college sample. Stud Psychol. 2020;40:57-78.
- Stoleru G, Leopold A, Auerbach A, et al. Female gender, dissatisfaction with weight, and number of IBD related surgeries as independent risk factors for eating disorders among patients with inflammatory bowel diseases. BMC Gastroenterol. 2022;22:438.
- Öztürkcan S, Ermertcan AT, Eser E, et al. Cross validation of the Turkish version of dermatology life quality index. Int J Dermatol. 2006;45:1300-1307.
- Demir GT, Ciciog˘lu HI˙. Attitude scale for healthy nutrition (ASHN): validity and reliability study. Gaziantep Univ J Sport Sci. 2019;4:256-274.
- Yılmaz O, Boz H, Arslan A. The validity and reliability of depression stress and anxiety scale (DASS 21) Turkish short form. Res Financial Econ Soc Stud. 2017;2:78-91.
- Nuttall FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. 2015;50:117-128.
- Strumia R, Manzata E, Gualandi M. Is there a role for dermatologists in eating disorders? Expert Rev Dermatol. 2017; 2:109-112.
- Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol. 1995;32:982-986.
- Naldi L, Addis A, Chimenti S, et al. Impact of body mass index and obesity on clinical response to systemic treatment for psoriasis. evidence from the Psocare project. Dermatology. 2008;217:365-373.
- Barros G, Duran P, Vera I, et al. Exploring the links between obesity and psoriasis: a comprehensive review. Int J Mol Sci. 2022;23:7499.
- Hao Y, Zhu YJ, Zou S, et al. Metabolic syndrome and psoriasis: mechanisms and future directions. Front Immunol. 2021;12:711060.
- Jing D, Xiao H, Shen M, et al. Association of psoriasis with anxiety and depression: a case–control study in Chinese patients. Front Med (Lausanne). 2021;8:771645.
- Sahi FM, Masood A, Danawar NA, et al. Association between psoriasis and depression: a traditional review. Cureus. 2020;12:E9708.
- Zafiriou E, Daponte AI, Siokas V, et al. Depression and obesity in patients with psoriasis and psoriatic arthritis: is IL-17–mediated immune dysregulation the connecting link? Front Immunol. 2021;12:699848.
- Mrowietz U, Sümbül M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37:1731-1738.
- Pavlova NT, Kioskli K, Smith C, et al. Psychosocial aspects of obesity in adults with psoriasis: a systematic review. Skin Health Dis. 2021;1:E33.
- Innamorati M, Quinto RM, Imperatori C, et al. Health-related quality of life and its association with alexithymia and difficulties in emotion regulation in patients with psoriasis. Compr Psychiatry. 2016;70:200-208.
- Tabolli S, Naldi L, Pagliarello C, et al. Evaluation of the impact of writing exercises interventions on quality of life in patients with psoriasis undergoing systemic treatments. Br J Dermatol. 2012;167:1254‐1264.
- Albuquerque D, Nóbrega C, Manco L, et al. The contribution of genetics and environment to obesity. Br Med Bull. 2017;123:159‐173.
- Balantekin KN, Grammer AC, Fitzsimmons-Craft EE, et al. Overweight and obesity are associated with increased eating disorder correlates and general psychopathology in university women with eating disorders. Eat Behav. 2021;41:101482.
- Jebeile H, Lister NB, Baur LA, et al. Eating disorder risk in adolescents with obesity. Obes Rev. 2021;22:E13173.
- Crosta ML, Caldarola G, Fraietta S, et al. Psychopathology and eating disorders in patients with psoriasis. G Ital Dermatol Venereol. 2014;149:355-361.
- Altunay I, Demirci GT, Ates B, et al. Do eating disorders accompany metabolic syndrome in psoriasis patients? results of a preliminary study. Clin Cosmet Investig Dermatol. 2011;4:139-143.
Practice Points
- Eating disorders are considered a contributing factor in obesity.
- Obesity is prevalent in patients with psoriasis, and current evidence indicates that obesity may initiate psoriasis or worsen existing disease.
- Obesity should be considered as contributory to the development of psoriasis via a biopsychosocial approach that accounts for genetic, behavioral, and environmental factors.