User login
VIDEO: How to recognize and treat nonalcoholic fatty liver disease
PHILADELPHIA – Nonalcoholic fatty liver disease is on the rise worldwide, but many clinicians are unaware of how to recognize this potentially fatal condition, in part because it can be difficult to separate from common comorbidities such as obesity and diabetes.
In an interview at the Digestive Diseases: New Advances 2016 meeting, held by Global Academy for Medical Education and Rutgers, the State University of New Jersey, Dr. Zobair M. Younossi, chairman of the department of medicine at Inova Fairfax (Va.) Hospital, discussed what clinicians should know in order to screen for and treat this disease.
Dr. Younossi said he is a consultant to Conatus Pharmaceuticals, Enterome Bioscience, and Gilead, and on the advisory boards of Janssen, Salix Pharmaceuticals, and Vertex Pharmaceuticals.
Global Academy and this news organization are owned by the same company.
On Twitter @whitneymcknight
PHILADELPHIA – Nonalcoholic fatty liver disease is on the rise worldwide, but many clinicians are unaware of how to recognize this potentially fatal condition, in part because it can be difficult to separate from common comorbidities such as obesity and diabetes.
In an interview at the Digestive Diseases: New Advances 2016 meeting, held by Global Academy for Medical Education and Rutgers, the State University of New Jersey, Dr. Zobair M. Younossi, chairman of the department of medicine at Inova Fairfax (Va.) Hospital, discussed what clinicians should know in order to screen for and treat this disease.
Dr. Younossi said he is a consultant to Conatus Pharmaceuticals, Enterome Bioscience, and Gilead, and on the advisory boards of Janssen, Salix Pharmaceuticals, and Vertex Pharmaceuticals.
Global Academy and this news organization are owned by the same company.
On Twitter @whitneymcknight
PHILADELPHIA – Nonalcoholic fatty liver disease is on the rise worldwide, but many clinicians are unaware of how to recognize this potentially fatal condition, in part because it can be difficult to separate from common comorbidities such as obesity and diabetes.
In an interview at the Digestive Diseases: New Advances 2016 meeting, held by Global Academy for Medical Education and Rutgers, the State University of New Jersey, Dr. Zobair M. Younossi, chairman of the department of medicine at Inova Fairfax (Va.) Hospital, discussed what clinicians should know in order to screen for and treat this disease.
Dr. Younossi said he is a consultant to Conatus Pharmaceuticals, Enterome Bioscience, and Gilead, and on the advisory boards of Janssen, Salix Pharmaceuticals, and Vertex Pharmaceuticals.
Global Academy and this news organization are owned by the same company.
On Twitter @whitneymcknight
AT DIGESTIVE DISEASES: NEW ADVANCES 2016

Adding chemo to radiation boosts survival from low-grade gliomas
Adding a chemotherapy combination to radiation therapy for initial treatment of low-grade gliomas significantly improved overall survival and progression-free survival, regardless of the tumor type, investigators report in the New England Journal of Medicine.
Grade 2 glioma patients who received radiation plus the combination of procarbazine, lomustine (also called CCNU), and vincristine (PCV) had a longer median overall survival than those who received radiation alone (13.3 vs. 7.8 years; hazard ratio for death, 0.59; P = .003). Of those who received radiation plus chemotherapy, the progression-free survival rate at 10 years was 51%, compared with 21% for the group who received radiation alone, Dr. Jan Buckner and his colleagues report (N Engl J Med. 2016;374:1344-55. doi: 10.1056/NEJMoa1500925).
“The magnitude of treatment benefit from combined chemotherapy plus radiation therapy is substantial, but the toxic effects are greater than those observed with radiation therapy alone,” wrote Dr. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minn., and associates. Patients who received radiation plus PCV had more toxic side effects from their therapy, though most effects were grade 1 and 2.
For this study, 254 patients were randomized, with 128 assigned to radiotherapy alone, and 126 assigned to radiotherapy plus PCV. A total of 126 patients in the radiotherapy arm were included in the analysis, with one patient not receiving the intervention and 14 patients lost to follow-up at some point during the 10 years of the study. In the radiotherapy plus PCV arm, 125 patients were eligible for evaluation, and all of those patients were included in the analysis. Twenty-six patients in this arm were lost to follow-up, and 72 patients discontinued the intervention in this arm (this figure included four patients who died).
Tumor types included in the study were grade 2 astrocytoma, oligoastrocytoma, or oligodendroglioma.
Patients were included if they were between 18 and 39 years of age and had received a subtotal resection or biopsy of their tumor, or if they were 40 years of age or older and had any resection or biopsy of their tumor. Exclusion criteria included previous radiation to the head or neck, any previous chemotherapy, significant pulmonary disease, and a 5-year history of other cancers except cervical cancer in situ and non-melanoma skin cancer. Tumors could not have spread to noncontiguous leptomeninges, and patients could not have gliomatosis cerebri. Patients had to have a Karnofsky performance score of 60 or higher, and a neurological function score of 3 or less.
Dr. Buckner and his collaborators also assessed tumors for IDH1 mutational status by performing immunostaining with the mutation-specific monoclonal antibody IDH1 R132H; appropriate tissue was available for testing in slightly less than half of the patients in each study arm. The mutation was present in 35/57 patients (61%) in the radiotherapy-only arm, and 36/56 patients (64%) in the radiotherapy plus PCV arm. Patients with oligodendroglioma were most likely to have IDH1 R132H mutations. Sample sizes were too small to determine the effect of other IDH mutations or co-deletion of chromosome arms 1p and 19q.
In multivariable analysis, the presence of the IDH1 R132H mutation was identified as an independent prognostic factor for better overall survival (OS) and progression-free survival (PFS), regardless of the treatment administered. Those with the mutation still benefited significantly from receiving radiotherapy plus PCV rather than radiotherapy alone (P = .02 for OS, P less than .001 for PFS).
Exploratory analysis that broke down OS and PFS by cancer type showed that “the superiority of radiation therapy plus chemotherapy over radiation therapy alone was seen with all histologic diagnoses, although the difference did not reach significance among patients with astrocytoma,” wrote Dr. Buckner and his collaborators.
When all patients lost to follow-up in both groups were assessed as having died, the sensitivity analysis still showed benefit for radiotherapy plus PCV (HR for death, compared with radiotherapy alone, 0.72; P = .03).
The value of the long-term follow-up, wrote Dr. Buckner and his colleagues, was that “The separation of the progression-free survival curves of the two treatment groups did not begin until 2 to 3 years after randomization, although approximately 25% of the patients in each group had disease progression by then.”
Dr. Buckner and his collaborators emphasized that the patient-physician team should consider all factors in making treatment decisions, saying, “Patients and their physicians will have to weigh whether the longer survival justified the more toxic therapeutic approach.“
On Twitter @karioakes
Adding a chemotherapy combination to radiation therapy for initial treatment of low-grade gliomas significantly improved overall survival and progression-free survival, regardless of the tumor type, investigators report in the New England Journal of Medicine.
Grade 2 glioma patients who received radiation plus the combination of procarbazine, lomustine (also called CCNU), and vincristine (PCV) had a longer median overall survival than those who received radiation alone (13.3 vs. 7.8 years; hazard ratio for death, 0.59; P = .003). Of those who received radiation plus chemotherapy, the progression-free survival rate at 10 years was 51%, compared with 21% for the group who received radiation alone, Dr. Jan Buckner and his colleagues report (N Engl J Med. 2016;374:1344-55. doi: 10.1056/NEJMoa1500925).
“The magnitude of treatment benefit from combined chemotherapy plus radiation therapy is substantial, but the toxic effects are greater than those observed with radiation therapy alone,” wrote Dr. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minn., and associates. Patients who received radiation plus PCV had more toxic side effects from their therapy, though most effects were grade 1 and 2.
For this study, 254 patients were randomized, with 128 assigned to radiotherapy alone, and 126 assigned to radiotherapy plus PCV. A total of 126 patients in the radiotherapy arm were included in the analysis, with one patient not receiving the intervention and 14 patients lost to follow-up at some point during the 10 years of the study. In the radiotherapy plus PCV arm, 125 patients were eligible for evaluation, and all of those patients were included in the analysis. Twenty-six patients in this arm were lost to follow-up, and 72 patients discontinued the intervention in this arm (this figure included four patients who died).
Tumor types included in the study were grade 2 astrocytoma, oligoastrocytoma, or oligodendroglioma.
Patients were included if they were between 18 and 39 years of age and had received a subtotal resection or biopsy of their tumor, or if they were 40 years of age or older and had any resection or biopsy of their tumor. Exclusion criteria included previous radiation to the head or neck, any previous chemotherapy, significant pulmonary disease, and a 5-year history of other cancers except cervical cancer in situ and non-melanoma skin cancer. Tumors could not have spread to noncontiguous leptomeninges, and patients could not have gliomatosis cerebri. Patients had to have a Karnofsky performance score of 60 or higher, and a neurological function score of 3 or less.
Dr. Buckner and his collaborators also assessed tumors for IDH1 mutational status by performing immunostaining with the mutation-specific monoclonal antibody IDH1 R132H; appropriate tissue was available for testing in slightly less than half of the patients in each study arm. The mutation was present in 35/57 patients (61%) in the radiotherapy-only arm, and 36/56 patients (64%) in the radiotherapy plus PCV arm. Patients with oligodendroglioma were most likely to have IDH1 R132H mutations. Sample sizes were too small to determine the effect of other IDH mutations or co-deletion of chromosome arms 1p and 19q.
In multivariable analysis, the presence of the IDH1 R132H mutation was identified as an independent prognostic factor for better overall survival (OS) and progression-free survival (PFS), regardless of the treatment administered. Those with the mutation still benefited significantly from receiving radiotherapy plus PCV rather than radiotherapy alone (P = .02 for OS, P less than .001 for PFS).
Exploratory analysis that broke down OS and PFS by cancer type showed that “the superiority of radiation therapy plus chemotherapy over radiation therapy alone was seen with all histologic diagnoses, although the difference did not reach significance among patients with astrocytoma,” wrote Dr. Buckner and his collaborators.
When all patients lost to follow-up in both groups were assessed as having died, the sensitivity analysis still showed benefit for radiotherapy plus PCV (HR for death, compared with radiotherapy alone, 0.72; P = .03).
The value of the long-term follow-up, wrote Dr. Buckner and his colleagues, was that “The separation of the progression-free survival curves of the two treatment groups did not begin until 2 to 3 years after randomization, although approximately 25% of the patients in each group had disease progression by then.”
Dr. Buckner and his collaborators emphasized that the patient-physician team should consider all factors in making treatment decisions, saying, “Patients and their physicians will have to weigh whether the longer survival justified the more toxic therapeutic approach.“
On Twitter @karioakes
Adding a chemotherapy combination to radiation therapy for initial treatment of low-grade gliomas significantly improved overall survival and progression-free survival, regardless of the tumor type, investigators report in the New England Journal of Medicine.
Grade 2 glioma patients who received radiation plus the combination of procarbazine, lomustine (also called CCNU), and vincristine (PCV) had a longer median overall survival than those who received radiation alone (13.3 vs. 7.8 years; hazard ratio for death, 0.59; P = .003). Of those who received radiation plus chemotherapy, the progression-free survival rate at 10 years was 51%, compared with 21% for the group who received radiation alone, Dr. Jan Buckner and his colleagues report (N Engl J Med. 2016;374:1344-55. doi: 10.1056/NEJMoa1500925).
“The magnitude of treatment benefit from combined chemotherapy plus radiation therapy is substantial, but the toxic effects are greater than those observed with radiation therapy alone,” wrote Dr. Buckner, professor of oncology at the Mayo Clinic, Rochester, Minn., and associates. Patients who received radiation plus PCV had more toxic side effects from their therapy, though most effects were grade 1 and 2.
For this study, 254 patients were randomized, with 128 assigned to radiotherapy alone, and 126 assigned to radiotherapy plus PCV. A total of 126 patients in the radiotherapy arm were included in the analysis, with one patient not receiving the intervention and 14 patients lost to follow-up at some point during the 10 years of the study. In the radiotherapy plus PCV arm, 125 patients were eligible for evaluation, and all of those patients were included in the analysis. Twenty-six patients in this arm were lost to follow-up, and 72 patients discontinued the intervention in this arm (this figure included four patients who died).
Tumor types included in the study were grade 2 astrocytoma, oligoastrocytoma, or oligodendroglioma.
Patients were included if they were between 18 and 39 years of age and had received a subtotal resection or biopsy of their tumor, or if they were 40 years of age or older and had any resection or biopsy of their tumor. Exclusion criteria included previous radiation to the head or neck, any previous chemotherapy, significant pulmonary disease, and a 5-year history of other cancers except cervical cancer in situ and non-melanoma skin cancer. Tumors could not have spread to noncontiguous leptomeninges, and patients could not have gliomatosis cerebri. Patients had to have a Karnofsky performance score of 60 or higher, and a neurological function score of 3 or less.
Dr. Buckner and his collaborators also assessed tumors for IDH1 mutational status by performing immunostaining with the mutation-specific monoclonal antibody IDH1 R132H; appropriate tissue was available for testing in slightly less than half of the patients in each study arm. The mutation was present in 35/57 patients (61%) in the radiotherapy-only arm, and 36/56 patients (64%) in the radiotherapy plus PCV arm. Patients with oligodendroglioma were most likely to have IDH1 R132H mutations. Sample sizes were too small to determine the effect of other IDH mutations or co-deletion of chromosome arms 1p and 19q.
In multivariable analysis, the presence of the IDH1 R132H mutation was identified as an independent prognostic factor for better overall survival (OS) and progression-free survival (PFS), regardless of the treatment administered. Those with the mutation still benefited significantly from receiving radiotherapy plus PCV rather than radiotherapy alone (P = .02 for OS, P less than .001 for PFS).
Exploratory analysis that broke down OS and PFS by cancer type showed that “the superiority of radiation therapy plus chemotherapy over radiation therapy alone was seen with all histologic diagnoses, although the difference did not reach significance among patients with astrocytoma,” wrote Dr. Buckner and his collaborators.
When all patients lost to follow-up in both groups were assessed as having died, the sensitivity analysis still showed benefit for radiotherapy plus PCV (HR for death, compared with radiotherapy alone, 0.72; P = .03).
The value of the long-term follow-up, wrote Dr. Buckner and his colleagues, was that “The separation of the progression-free survival curves of the two treatment groups did not begin until 2 to 3 years after randomization, although approximately 25% of the patients in each group had disease progression by then.”
Dr. Buckner and his collaborators emphasized that the patient-physician team should consider all factors in making treatment decisions, saying, “Patients and their physicians will have to weigh whether the longer survival justified the more toxic therapeutic approach.“
On Twitter @karioakes
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Adding chemotherapy to radiotherapy improved progression-free survival and overall survival in patients with low-grade glioma.
Major finding: Median overall survival was 13.3 years for those receiving radiotherapy plus chemotherapy, compared with 7.8 years for radiotherapy alone (hazard ratio for death, 0.59; P = .003).
Data source: Longitudinal study of 254 patients with grade 2 gliomas receiving radiation therapy alone or radiation therapy plus procarbazine, lomustine, and vincristine.
Disclosures: The study was supported by the National Cancer Institute and did not receive funding from commercial sources. Dr. Bell and Dr. Chakravarti reported a planned patent application related to this work. Dr. Buckner, Dr. Gilbert, Dr. Mehta, and Dr. Suh reported support from pharmaceutical companies outside the scope of this study.
Morning cortisol rules out adrenal insufficiency
BOSTON – A random morning serum cortisol above 11.1 mcg/dL safely rules out adrenal insufficiency in both inpatients and outpatients, according to a review of 3,300 adrenal insufficiency work-ups at the Edinburgh Centre for Endocrinology and Diabetes.
The finding could help eliminate the cost and hassle of unnecessary adrenocorticotropic hormone (ACTH) stimulation tests; the investigators estimated that the cut point would eliminate almost half of them without any ill effects. “You can be very confident that patients aren’t insufficient if they are above that line,” with more than 99% sensitivity. If they are below it, “they may be normal, and they may be abnormal.” Below 1.8 mcg/dL, adrenal insufficiency is almost certain, but between the cutoffs, ACTH stimulation is necessary, said lead investigator Dr. Scott Mackenzie, a trainee at the center.

In short, “basal serum cortisol as a screening test ... offers a convenient and accessible means of identifying patients who require further assessment,” he said at the annual meeting of the Endocrine Society.
Similar cut points have been suggested by previous studies, but the Scottish investigation is the first to validate its findings both inside and outside of the hospital.
The team arrived at the 11.1 mcg/dL morning cortisol cut point by comparing basal cortisol levels and synacthen results in 1,628 outpatients. They predefined a sensitivity of more than 99% for adrenal sufficiency to avoid missing anyone with true disease. The cut point’s predictive power was then validated in 875 outpatients and 797 inpatients. Morning basal cortisol levels proved superior to afternoon levels.
The investigators were thinking about cost-effectiveness, but they also wanted to increase screening. “We may be able to reduce the number of adrenal insufficiency cases we are missing because [primary care is] reluctant to send people to the clinic for synacthen tests” due to the cost and inconvenience. As with many locations in the United States, “our practice is to do [ACTH on] everyone.” If there was “a quick and easy 9 a.m. blood test” instead, it would help, Dr. Mackenzie said.
Adrenal insufficiency was on the differential for a wide variety of reasons, including hypogonadism, pituitary issues, prolactinemia, fatigue, hypoglycemia, postural hypotension, and hyponatremia. Most of the patients were middle aged, and they were about evenly split between men and women.
There was no outside funding for the work, and the investigators had no disclosures.
BOSTON – A random morning serum cortisol above 11.1 mcg/dL safely rules out adrenal insufficiency in both inpatients and outpatients, according to a review of 3,300 adrenal insufficiency work-ups at the Edinburgh Centre for Endocrinology and Diabetes.
The finding could help eliminate the cost and hassle of unnecessary adrenocorticotropic hormone (ACTH) stimulation tests; the investigators estimated that the cut point would eliminate almost half of them without any ill effects. “You can be very confident that patients aren’t insufficient if they are above that line,” with more than 99% sensitivity. If they are below it, “they may be normal, and they may be abnormal.” Below 1.8 mcg/dL, adrenal insufficiency is almost certain, but between the cutoffs, ACTH stimulation is necessary, said lead investigator Dr. Scott Mackenzie, a trainee at the center.
In short, “basal serum cortisol as a screening test ... offers a convenient and accessible means of identifying patients who require further assessment,” he said at the annual meeting of the Endocrine Society.
Similar cut points have been suggested by previous studies, but the Scottish investigation is the first to validate its findings both inside and outside of the hospital.
The team arrived at the 11.1 mcg/dL morning cortisol cut point by comparing basal cortisol levels and synacthen results in 1,628 outpatients. They predefined a sensitivity of more than 99% for adrenal sufficiency to avoid missing anyone with true disease. The cut point’s predictive power was then validated in 875 outpatients and 797 inpatients. Morning basal cortisol levels proved superior to afternoon levels.
The investigators were thinking about cost-effectiveness, but they also wanted to increase screening. “We may be able to reduce the number of adrenal insufficiency cases we are missing because [primary care is] reluctant to send people to the clinic for synacthen tests” due to the cost and inconvenience. As with many locations in the United States, “our practice is to do [ACTH on] everyone.” If there was “a quick and easy 9 a.m. blood test” instead, it would help, Dr. Mackenzie said.
Adrenal insufficiency was on the differential for a wide variety of reasons, including hypogonadism, pituitary issues, prolactinemia, fatigue, hypoglycemia, postural hypotension, and hyponatremia. Most of the patients were middle aged, and they were about evenly split between men and women.
There was no outside funding for the work, and the investigators had no disclosures.
BOSTON – A random morning serum cortisol above 11.1 mcg/dL safely rules out adrenal insufficiency in both inpatients and outpatients, according to a review of 3,300 adrenal insufficiency work-ups at the Edinburgh Centre for Endocrinology and Diabetes.
The finding could help eliminate the cost and hassle of unnecessary adrenocorticotropic hormone (ACTH) stimulation tests; the investigators estimated that the cut point would eliminate almost half of them without any ill effects. “You can be very confident that patients aren’t insufficient if they are above that line,” with more than 99% sensitivity. If they are below it, “they may be normal, and they may be abnormal.” Below 1.8 mcg/dL, adrenal insufficiency is almost certain, but between the cutoffs, ACTH stimulation is necessary, said lead investigator Dr. Scott Mackenzie, a trainee at the center.
In short, “basal serum cortisol as a screening test ... offers a convenient and accessible means of identifying patients who require further assessment,” he said at the annual meeting of the Endocrine Society.
Similar cut points have been suggested by previous studies, but the Scottish investigation is the first to validate its findings both inside and outside of the hospital.
The team arrived at the 11.1 mcg/dL morning cortisol cut point by comparing basal cortisol levels and synacthen results in 1,628 outpatients. They predefined a sensitivity of more than 99% for adrenal sufficiency to avoid missing anyone with true disease. The cut point’s predictive power was then validated in 875 outpatients and 797 inpatients. Morning basal cortisol levels proved superior to afternoon levels.
The investigators were thinking about cost-effectiveness, but they also wanted to increase screening. “We may be able to reduce the number of adrenal insufficiency cases we are missing because [primary care is] reluctant to send people to the clinic for synacthen tests” due to the cost and inconvenience. As with many locations in the United States, “our practice is to do [ACTH on] everyone.” If there was “a quick and easy 9 a.m. blood test” instead, it would help, Dr. Mackenzie said.
Adrenal insufficiency was on the differential for a wide variety of reasons, including hypogonadism, pituitary issues, prolactinemia, fatigue, hypoglycemia, postural hypotension, and hyponatremia. Most of the patients were middle aged, and they were about evenly split between men and women.
There was no outside funding for the work, and the investigators had no disclosures.
AT ENDO 2016
Key clinical point: Skip ACTH stimulation if morning serum cortisol is above 11.1 mcg/dL.
Major finding: A morning serum cortisol above 11.1 mcg/dL is a test of adrenal function with 99% sensitivity.
Data source: Review of 3,300 adrenal insufficiency work-ups.
Disclosures: There was no outside funding for the work, and the investigators had no disclosures.

Fetal malformation risk not increased after exposure to lamotrigine
A new analysis of registry data from European countries does not support a risk of orofacial cleft and clubfoot with exposure to lamotrigine monotherapy, in contrast to signals from previous studies of the antiepileptic drug.
First author Helen Dolk, Dr.P.H., professor of epidemiology and health services research and the head of the center for maternal, fetal, and infant research at the University of Ulster in Coleraine, Northern Ireland, and her colleagues analyzed data from 10.1 million births exposed to antiepileptic drugs including lamotrigine (Lamictal) as a monotherapy during the first trimester between 1995 and 2011. The births were recorded in 21 population-based registries from 16 European countries. The outcomes of interest were major congenital malformations in general, as well as orofacial clefts and clubfoot (Neurology. 2016 April 6. doi: 10.1212/WNL.0000000000002540).

Assessment of all antiepileptic drug-exposed congenital malformation registrations revealed that 12% of pregnant registrants were exposed to lamotrigine monotherapy, with an additional 7% exposed to lamotrigine as part of polytherapy. A total of 77.1% of pregnant women exposed to lamotrigine monotherapy had records indicative of a diagnosis of epilepsy. The proportion of lamotrigine monotherapy exposures was observed to have increased over the study period, likely based on a movement away from the traditional use of valproate because of teratogenic concerns.
A total of 147 lamotrigine monotherapy-exposed babies with congenital malformations not attributable to chromosomal irregularities were identified from the total sample. The odds ratio for having a child with orofacial clefts after exposure to lamotrigine monotherapy was 1.31 (95% confidence interval, 0.73-2.33). Based on these data, the authors said they estimated exposure to lamotrigine would result in orofacial clefts in fewer than 1 in every 550 exposed babies.
The odds ratio for having a child with clubfoot after exposure to lamotrigine monotherapy was 1.83 (95% CI, 1.01-3.31). Although the study results confirmed the statistically significant signal for an overall excess of clubfoot risk found in a previous study conducted by this research team that analyzed births during 1995-2005, the investigators could not reproduce this result in an independent study population of 6.3 million births during 2005-2011(odds ratio, 1.43; 95% CI, 0.66-3.08). There were no significant differences in the risk for developing any other congenital malformations associated with lamotrigine monotherapy, the investigators said.
The authors said their results were in accord with those from several previous studies that did not detect an increased risk of orofacial clefts. In addition, they said statistically significant independent evidence of a clubfoot excess was not detected in the current study, despite findings from their previous study suggesting an increased risk.
The EUROCAT Central Database was funded by the EU Public Health Programme. GlaxoSmithKline, which markets lamotrigine, provided a grant for additional funding of this study. Dr. Dolk and her coauthors reported that their institutions received funding from GlaxoSmithKline for data or staff time contributed to this study.
A new analysis of registry data from European countries does not support a risk of orofacial cleft and clubfoot with exposure to lamotrigine monotherapy, in contrast to signals from previous studies of the antiepileptic drug.
First author Helen Dolk, Dr.P.H., professor of epidemiology and health services research and the head of the center for maternal, fetal, and infant research at the University of Ulster in Coleraine, Northern Ireland, and her colleagues analyzed data from 10.1 million births exposed to antiepileptic drugs including lamotrigine (Lamictal) as a monotherapy during the first trimester between 1995 and 2011. The births were recorded in 21 population-based registries from 16 European countries. The outcomes of interest were major congenital malformations in general, as well as orofacial clefts and clubfoot (Neurology. 2016 April 6. doi: 10.1212/WNL.0000000000002540).
Assessment of all antiepileptic drug-exposed congenital malformation registrations revealed that 12% of pregnant registrants were exposed to lamotrigine monotherapy, with an additional 7% exposed to lamotrigine as part of polytherapy. A total of 77.1% of pregnant women exposed to lamotrigine monotherapy had records indicative of a diagnosis of epilepsy. The proportion of lamotrigine monotherapy exposures was observed to have increased over the study period, likely based on a movement away from the traditional use of valproate because of teratogenic concerns.
A total of 147 lamotrigine monotherapy-exposed babies with congenital malformations not attributable to chromosomal irregularities were identified from the total sample. The odds ratio for having a child with orofacial clefts after exposure to lamotrigine monotherapy was 1.31 (95% confidence interval, 0.73-2.33). Based on these data, the authors said they estimated exposure to lamotrigine would result in orofacial clefts in fewer than 1 in every 550 exposed babies.
The odds ratio for having a child with clubfoot after exposure to lamotrigine monotherapy was 1.83 (95% CI, 1.01-3.31). Although the study results confirmed the statistically significant signal for an overall excess of clubfoot risk found in a previous study conducted by this research team that analyzed births during 1995-2005, the investigators could not reproduce this result in an independent study population of 6.3 million births during 2005-2011(odds ratio, 1.43; 95% CI, 0.66-3.08). There were no significant differences in the risk for developing any other congenital malformations associated with lamotrigine monotherapy, the investigators said.
The authors said their results were in accord with those from several previous studies that did not detect an increased risk of orofacial clefts. In addition, they said statistically significant independent evidence of a clubfoot excess was not detected in the current study, despite findings from their previous study suggesting an increased risk.
The EUROCAT Central Database was funded by the EU Public Health Programme. GlaxoSmithKline, which markets lamotrigine, provided a grant for additional funding of this study. Dr. Dolk and her coauthors reported that their institutions received funding from GlaxoSmithKline for data or staff time contributed to this study.
A new analysis of registry data from European countries does not support a risk of orofacial cleft and clubfoot with exposure to lamotrigine monotherapy, in contrast to signals from previous studies of the antiepileptic drug.
First author Helen Dolk, Dr.P.H., professor of epidemiology and health services research and the head of the center for maternal, fetal, and infant research at the University of Ulster in Coleraine, Northern Ireland, and her colleagues analyzed data from 10.1 million births exposed to antiepileptic drugs including lamotrigine (Lamictal) as a monotherapy during the first trimester between 1995 and 2011. The births were recorded in 21 population-based registries from 16 European countries. The outcomes of interest were major congenital malformations in general, as well as orofacial clefts and clubfoot (Neurology. 2016 April 6. doi: 10.1212/WNL.0000000000002540).
Assessment of all antiepileptic drug-exposed congenital malformation registrations revealed that 12% of pregnant registrants were exposed to lamotrigine monotherapy, with an additional 7% exposed to lamotrigine as part of polytherapy. A total of 77.1% of pregnant women exposed to lamotrigine monotherapy had records indicative of a diagnosis of epilepsy. The proportion of lamotrigine monotherapy exposures was observed to have increased over the study period, likely based on a movement away from the traditional use of valproate because of teratogenic concerns.
A total of 147 lamotrigine monotherapy-exposed babies with congenital malformations not attributable to chromosomal irregularities were identified from the total sample. The odds ratio for having a child with orofacial clefts after exposure to lamotrigine monotherapy was 1.31 (95% confidence interval, 0.73-2.33). Based on these data, the authors said they estimated exposure to lamotrigine would result in orofacial clefts in fewer than 1 in every 550 exposed babies.
The odds ratio for having a child with clubfoot after exposure to lamotrigine monotherapy was 1.83 (95% CI, 1.01-3.31). Although the study results confirmed the statistically significant signal for an overall excess of clubfoot risk found in a previous study conducted by this research team that analyzed births during 1995-2005, the investigators could not reproduce this result in an independent study population of 6.3 million births during 2005-2011(odds ratio, 1.43; 95% CI, 0.66-3.08). There were no significant differences in the risk for developing any other congenital malformations associated with lamotrigine monotherapy, the investigators said.
The authors said their results were in accord with those from several previous studies that did not detect an increased risk of orofacial clefts. In addition, they said statistically significant independent evidence of a clubfoot excess was not detected in the current study, despite findings from their previous study suggesting an increased risk.
The EUROCAT Central Database was funded by the EU Public Health Programme. GlaxoSmithKline, which markets lamotrigine, provided a grant for additional funding of this study. Dr. Dolk and her coauthors reported that their institutions received funding from GlaxoSmithKline for data or staff time contributed to this study.
FROM NEUROLOGY
Key clinical point:Babies born to mothers exposed to lamotrigine monotherapy do not show evidence for an increased incidence of orofacial clefts or clubfoot.
Major finding: The odds ratios for having a child with orofacial clefts or clubfoot after exposure to lamotrigine monotherapy were 1.31 and 1.83, respectively.
Data source: A 16-year, observational study comparing the rate of lamotrigine exposure among births with orofacial clefts or clubfoot in 10.1 million births recorded in 21 population-based registries from 16 European countries.
Disclosures: The EUROCAT Central Database was funded by the EU Public Health Programme. GlaxoSmithKline, which markets lamotrigine, provided a grant for additional funding of this study. Dr. Dolk and her coauthors reported that their institutions received funding from GlaxoSmithKline for data or staff time contributed to this study.

Phase III dupilumab data show significant improvements in atopic dermatitis
Treatment with dupilumab resulted in significant clinical improvements in adults with inadequately controlled moderate to-severe atopic dermatitis, in two phase III studies evaluating the biologic agent, according to Regeneron and Sanofi.
The phase III results of the two 16-week studies, SOLO 1 and SOLO 2, in nearly 1,400 adults with baseline Investigator’s Global Assessment (IGA) scores of 3 (moderate disease) or 4 (severe), were announced by Regeneron and Sanofi. The companies are codeveloping dupilumab, which inhibits signaling of interleukin-4 and IL-13, “two key cytokines required for the T helper 2 (Th2) immune response,” according to Regeneron.

In the studies, patients were randomized to treatment with 300 mg subcutaneously of dupilumab once a week or every 2 weeks (after a 600-mg loading dose) or placebo, for 16 weeks.
At 16 weeks, significantly more of those in the two treatment groups achieved clearing or near clearing of skin lesions – a primary endpoint – compared with placebo: In SOLO 1 and SOLO 2, respectively, an IGA score of 0 (clear) or 1 (almost clear) was achieved by 37% and 36% of those treated with 300 mg weekly, and 38% and 36% of those treated every 2 weeks, compared with 10% and 8.5% of those on placebo (P less than .0001).
Improvement from baseline in the Eczema Area and Severity Index (EASI) score in the SOLO 1 and SOLO 2 studies, respectively, were 72% and 69% of those treated with 300 mg weekly and 72% and 67% of those treated every 2 weeks, compared with 38% and 31% of those on placebo (P less than .0001).
The rates of adverse events ranged from 65% to 73% for those on dupilumab, and from 65% to 72% for those on placebo. The rates of serious adverse events were 1%-3% among those on dupilumab and 5%-6% for placebo; serious and severe infections were more common among those on placebo. Compared with placebo, injection site reactions were higher among those on dupilumab (10%-20% vs. 7%-8%). Conjunctivitis was more common among dupilumab-treated patients (7%-12% vs. 2% for placebo). One patient stopped treatment because of conjunctivitis.
The phase III results, which were announced in an April 1 press release, will be presented at a future medical meeting, and the companies plan to file for approval with the Food and Drug Administration in the third quarter of 2016.
Treatment with dupilumab resulted in significant clinical improvements in adults with inadequately controlled moderate to-severe atopic dermatitis, in two phase III studies evaluating the biologic agent, according to Regeneron and Sanofi.
The phase III results of the two 16-week studies, SOLO 1 and SOLO 2, in nearly 1,400 adults with baseline Investigator’s Global Assessment (IGA) scores of 3 (moderate disease) or 4 (severe), were announced by Regeneron and Sanofi. The companies are codeveloping dupilumab, which inhibits signaling of interleukin-4 and IL-13, “two key cytokines required for the T helper 2 (Th2) immune response,” according to Regeneron.
In the studies, patients were randomized to treatment with 300 mg subcutaneously of dupilumab once a week or every 2 weeks (after a 600-mg loading dose) or placebo, for 16 weeks.
At 16 weeks, significantly more of those in the two treatment groups achieved clearing or near clearing of skin lesions – a primary endpoint – compared with placebo: In SOLO 1 and SOLO 2, respectively, an IGA score of 0 (clear) or 1 (almost clear) was achieved by 37% and 36% of those treated with 300 mg weekly, and 38% and 36% of those treated every 2 weeks, compared with 10% and 8.5% of those on placebo (P less than .0001).
Improvement from baseline in the Eczema Area and Severity Index (EASI) score in the SOLO 1 and SOLO 2 studies, respectively, were 72% and 69% of those treated with 300 mg weekly and 72% and 67% of those treated every 2 weeks, compared with 38% and 31% of those on placebo (P less than .0001).
The rates of adverse events ranged from 65% to 73% for those on dupilumab, and from 65% to 72% for those on placebo. The rates of serious adverse events were 1%-3% among those on dupilumab and 5%-6% for placebo; serious and severe infections were more common among those on placebo. Compared with placebo, injection site reactions were higher among those on dupilumab (10%-20% vs. 7%-8%). Conjunctivitis was more common among dupilumab-treated patients (7%-12% vs. 2% for placebo). One patient stopped treatment because of conjunctivitis.
The phase III results, which were announced in an April 1 press release, will be presented at a future medical meeting, and the companies plan to file for approval with the Food and Drug Administration in the third quarter of 2016.
Treatment with dupilumab resulted in significant clinical improvements in adults with inadequately controlled moderate to-severe atopic dermatitis, in two phase III studies evaluating the biologic agent, according to Regeneron and Sanofi.
The phase III results of the two 16-week studies, SOLO 1 and SOLO 2, in nearly 1,400 adults with baseline Investigator’s Global Assessment (IGA) scores of 3 (moderate disease) or 4 (severe), were announced by Regeneron and Sanofi. The companies are codeveloping dupilumab, which inhibits signaling of interleukin-4 and IL-13, “two key cytokines required for the T helper 2 (Th2) immune response,” according to Regeneron.
In the studies, patients were randomized to treatment with 300 mg subcutaneously of dupilumab once a week or every 2 weeks (after a 600-mg loading dose) or placebo, for 16 weeks.
At 16 weeks, significantly more of those in the two treatment groups achieved clearing or near clearing of skin lesions – a primary endpoint – compared with placebo: In SOLO 1 and SOLO 2, respectively, an IGA score of 0 (clear) or 1 (almost clear) was achieved by 37% and 36% of those treated with 300 mg weekly, and 38% and 36% of those treated every 2 weeks, compared with 10% and 8.5% of those on placebo (P less than .0001).
Improvement from baseline in the Eczema Area and Severity Index (EASI) score in the SOLO 1 and SOLO 2 studies, respectively, were 72% and 69% of those treated with 300 mg weekly and 72% and 67% of those treated every 2 weeks, compared with 38% and 31% of those on placebo (P less than .0001).
The rates of adverse events ranged from 65% to 73% for those on dupilumab, and from 65% to 72% for those on placebo. The rates of serious adverse events were 1%-3% among those on dupilumab and 5%-6% for placebo; serious and severe infections were more common among those on placebo. Compared with placebo, injection site reactions were higher among those on dupilumab (10%-20% vs. 7%-8%). Conjunctivitis was more common among dupilumab-treated patients (7%-12% vs. 2% for placebo). One patient stopped treatment because of conjunctivitis.
The phase III results, which were announced in an April 1 press release, will be presented at a future medical meeting, and the companies plan to file for approval with the Food and Drug Administration in the third quarter of 2016.

Intralymphatic Histiocytosis Associated With an Orthopedic Metal Implant
To the Editor:
|
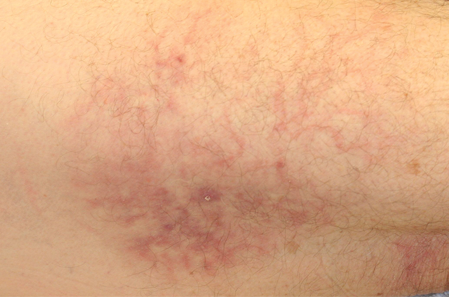
| Figure 1. A 30-cm pink and violaceous, asymmetric, reticulated patch on the lateral aspect of the right thigh. |
|
|
|
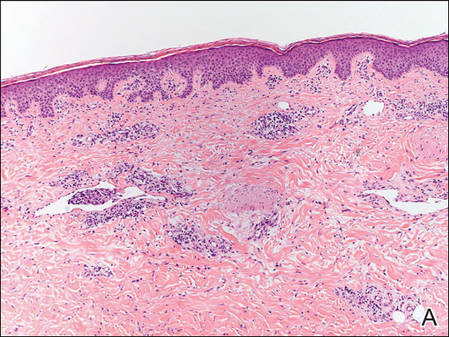
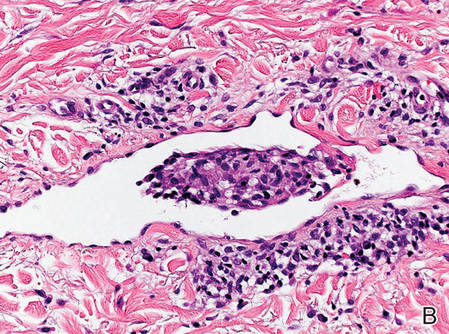
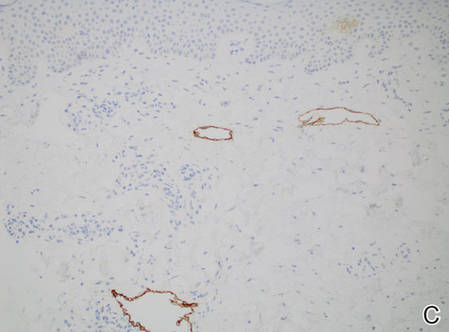
Figure 2. Histopathology revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis with adjacent features of chronic lymphedema (A)(H&E, original magnification ×10) as well as a collection of histiocytes in a dilated lymphatic channel (B)(H&E, original magnification ×40). D2-40 staining demonstrated ectatic lymphatic vessels in the upper dermins (C)(original magnification ×20).
|
A 70-year-old white man presented with an asymptomatic patch on the lateral aspect of the right thigh of 15 months’ duration. The patient believed the patch correlated with a hip replacement 3 years prior; however, it was 6 inches inferior to the incision site. Physical examination revealed a 30-cm pink and violaceous, asymmetric, reticulated patch (Figure 1). The patch was unresponsive to topical corticosteroids as well as a short course of oral prednisone. The patient’s medical history was notable for type 2 diabetes mellitus. Histopathologic examination revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis. In addition, adjacent features of chronic lymphedema were present, namely interstitial fibroplasia with dilated lymphatic vessels and a lymphoplasmacytic infiltrate (Figure 2). These findings were consistent with intralymphatic histiocytosis, a rare disease most commonly associated with rheumatoid arthritis. Our patient did not have a history or clinical symptoms of rheumatoid arthritis.
Intralymphatic histiocytosis is a rare cutaneous condition reported by O’Grady et al1 in 1994. This condition has been most frequently associated with rheumatoid arthritis2; however, there has been an emerging association in patients with orthopedic metal implants, with and without a concomitant diagnosis of rheumatoid arthritis. Cases associated with metal implants are rare.2-7
The condition presents as asymptomatic red, brown, or violaceous patches, plaques, papules, or nodules that are ill defined and tend to demonstrate a livedo reticularis–like pattern. The lesions typically are overlying or in close proximity to a joint. Histopathologic findings include dilated vascular structures in the reticular dermis, some with empty lumina and others containing collections of mononuclear histiocytes. There also may be an inflammatory infiltrate in the adjacent dermis composed of a mix of lymphocytes, plasma cells, and/or histiocytes. Endothelial cells lining the dilated lumina express immunoreactivity for CD31, CD34, D2-40, Lyve-1, and Prox-1. Intravascular histiocytes are positive for CD68 and CD31.6
The pathogenesis of intralymphatic histiocytosis remains undefined. Some hypothesize that intralymphatic histiocytosis could be the early stage of reactive angioendotheliomatosis, as these conditions share clinical and histological features.8 Reactive angioendotheliomatosis also is a rare condition that may present as erythematous to violaceous patches or plaques. The lesions are commonly found on the limbs and may be associated with constitutional symptoms. Histologic findings of reactive angioendotheliomatosis include a proliferation of epithelioid, round, or spindle-shaped cells within the lumina of dermal blood vessels, which show positivity for CD31 and CD34.9 Others suggest the lesions of intralymphatic histiocytosis arise from lymphangiectasia; obstruction of lymphatic drainage due to congenital abnormalities; or acquired damage from infection, trauma, surgery, or radiation.2 Due to the common association with rheumatoid arthritis and orthopedic implants, it is likely that lymphatic stasis secondary to chronic inflammation plays a notable role.
Therapies such as topical and systemic corticosteroids, local radiotherapy, cyclophosphamide, pentoxifylline, and arthrocentesis have been attempted without evidence of efficacy.2 Although intralymphatic histiocytosis is chronic and resistant to therapy, patients can be reassured that the condition runs a benign course.
1. O’Grady JT, Shahidullah H, Doherty VR, et al. Intravascular histiocytosis. Histopathology. 1994;24:265-268.
2. Requena L, El-Shabrawi-Caelen L, Walsh SN, et al. Intralymphatic histiocytosis. clinicopathologic study of 16 cases. Am J Dermatopathol. 2009;31:140-151.
3. Saggar S, Lee B, Krivo J, et al. Intralymphatic histiocytosis associated with orthopedic implants. J Drugs Dermatol. 2011;10:1208-1209.
4. Chiu YE, Maloney JE, Bengana C. Erythematous patch overlying a swollen knee—quiz case. intralymphatic histiocytosis. Arch Dermatol. 2010;146:1037-1042.
5. Rossari S, Scatena C, Gori A, et al. Intralymphatic histiocytosis: cutaneous nodules and metal implants. J Cutan Pathol. 2011;38:534-535.
6. Grekin S, Mesfin M, Kang S, et al. Intralymphatic histiocytosis following placement of a metal implant. J Cutan Pathol. 2011;38:351-353.
7. Watanabe T, Yamada N, Yoshida Y, et al. Intralymphatic histiocytosis with granuloma formation associated with orthopaedic metal implants. Br J Dermatol. 2008;158:402-404.
8. Rieger E, Soyer HP, Leboit PE, et al. Reactive angioendotheliomatosis or intravascular histiocytosis? an immunohistochemical and ultrastructural study in two cases of intravascular histiocytic cell proliferation. Br J Dermatol. 1999;140:497-504.
9. Rongioletti F, Rebora A. Cutaneous reactive angiomatoses: patterns and classification of reactive vascular proliferation. J Am Acad Dermatol. 2003;49:887-896.
To the Editor:
|
|
| Figure 1. A 30-cm pink and violaceous, asymmetric, reticulated patch on the lateral aspect of the right thigh. |
|
|
|
|
|
|
Figure 2. Histopathology revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis with adjacent features of chronic lymphedema (A)(H&E, original magnification ×10) as well as a collection of histiocytes in a dilated lymphatic channel (B)(H&E, original magnification ×40). D2-40 staining demonstrated ectatic lymphatic vessels in the upper dermins (C)(original magnification ×20).
|
A 70-year-old white man presented with an asymptomatic patch on the lateral aspect of the right thigh of 15 months’ duration. The patient believed the patch correlated with a hip replacement 3 years prior; however, it was 6 inches inferior to the incision site. Physical examination revealed a 30-cm pink and violaceous, asymmetric, reticulated patch (Figure 1). The patch was unresponsive to topical corticosteroids as well as a short course of oral prednisone. The patient’s medical history was notable for type 2 diabetes mellitus. Histopathologic examination revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis. In addition, adjacent features of chronic lymphedema were present, namely interstitial fibroplasia with dilated lymphatic vessels and a lymphoplasmacytic infiltrate (Figure 2). These findings were consistent with intralymphatic histiocytosis, a rare disease most commonly associated with rheumatoid arthritis. Our patient did not have a history or clinical symptoms of rheumatoid arthritis.
Intralymphatic histiocytosis is a rare cutaneous condition reported by O’Grady et al1 in 1994. This condition has been most frequently associated with rheumatoid arthritis2; however, there has been an emerging association in patients with orthopedic metal implants, with and without a concomitant diagnosis of rheumatoid arthritis. Cases associated with metal implants are rare.2-7
The condition presents as asymptomatic red, brown, or violaceous patches, plaques, papules, or nodules that are ill defined and tend to demonstrate a livedo reticularis–like pattern. The lesions typically are overlying or in close proximity to a joint. Histopathologic findings include dilated vascular structures in the reticular dermis, some with empty lumina and others containing collections of mononuclear histiocytes. There also may be an inflammatory infiltrate in the adjacent dermis composed of a mix of lymphocytes, plasma cells, and/or histiocytes. Endothelial cells lining the dilated lumina express immunoreactivity for CD31, CD34, D2-40, Lyve-1, and Prox-1. Intravascular histiocytes are positive for CD68 and CD31.6
The pathogenesis of intralymphatic histiocytosis remains undefined. Some hypothesize that intralymphatic histiocytosis could be the early stage of reactive angioendotheliomatosis, as these conditions share clinical and histological features.8 Reactive angioendotheliomatosis also is a rare condition that may present as erythematous to violaceous patches or plaques. The lesions are commonly found on the limbs and may be associated with constitutional symptoms. Histologic findings of reactive angioendotheliomatosis include a proliferation of epithelioid, round, or spindle-shaped cells within the lumina of dermal blood vessels, which show positivity for CD31 and CD34.9 Others suggest the lesions of intralymphatic histiocytosis arise from lymphangiectasia; obstruction of lymphatic drainage due to congenital abnormalities; or acquired damage from infection, trauma, surgery, or radiation.2 Due to the common association with rheumatoid arthritis and orthopedic implants, it is likely that lymphatic stasis secondary to chronic inflammation plays a notable role.
Therapies such as topical and systemic corticosteroids, local radiotherapy, cyclophosphamide, pentoxifylline, and arthrocentesis have been attempted without evidence of efficacy.2 Although intralymphatic histiocytosis is chronic and resistant to therapy, patients can be reassured that the condition runs a benign course.
To the Editor:
|
|
| Figure 1. A 30-cm pink and violaceous, asymmetric, reticulated patch on the lateral aspect of the right thigh. |
|
|
|
|
|
|
Figure 2. Histopathology revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis with adjacent features of chronic lymphedema (A)(H&E, original magnification ×10) as well as a collection of histiocytes in a dilated lymphatic channel (B)(H&E, original magnification ×40). D2-40 staining demonstrated ectatic lymphatic vessels in the upper dermins (C)(original magnification ×20).
|
A 70-year-old white man presented with an asymptomatic patch on the lateral aspect of the right thigh of 15 months’ duration. The patient believed the patch correlated with a hip replacement 3 years prior; however, it was 6 inches inferior to the incision site. Physical examination revealed a 30-cm pink and violaceous, asymmetric, reticulated patch (Figure 1). The patch was unresponsive to topical corticosteroids as well as a short course of oral prednisone. The patient’s medical history was notable for type 2 diabetes mellitus. Histopathologic examination revealed widely dilated vascular channels containing collections of histiocytes in the superficial dermis. In addition, adjacent features of chronic lymphedema were present, namely interstitial fibroplasia with dilated lymphatic vessels and a lymphoplasmacytic infiltrate (Figure 2). These findings were consistent with intralymphatic histiocytosis, a rare disease most commonly associated with rheumatoid arthritis. Our patient did not have a history or clinical symptoms of rheumatoid arthritis.
Intralymphatic histiocytosis is a rare cutaneous condition reported by O’Grady et al1 in 1994. This condition has been most frequently associated with rheumatoid arthritis2; however, there has been an emerging association in patients with orthopedic metal implants, with and without a concomitant diagnosis of rheumatoid arthritis. Cases associated with metal implants are rare.2-7
The condition presents as asymptomatic red, brown, or violaceous patches, plaques, papules, or nodules that are ill defined and tend to demonstrate a livedo reticularis–like pattern. The lesions typically are overlying or in close proximity to a joint. Histopathologic findings include dilated vascular structures in the reticular dermis, some with empty lumina and others containing collections of mononuclear histiocytes. There also may be an inflammatory infiltrate in the adjacent dermis composed of a mix of lymphocytes, plasma cells, and/or histiocytes. Endothelial cells lining the dilated lumina express immunoreactivity for CD31, CD34, D2-40, Lyve-1, and Prox-1. Intravascular histiocytes are positive for CD68 and CD31.6
The pathogenesis of intralymphatic histiocytosis remains undefined. Some hypothesize that intralymphatic histiocytosis could be the early stage of reactive angioendotheliomatosis, as these conditions share clinical and histological features.8 Reactive angioendotheliomatosis also is a rare condition that may present as erythematous to violaceous patches or plaques. The lesions are commonly found on the limbs and may be associated with constitutional symptoms. Histologic findings of reactive angioendotheliomatosis include a proliferation of epithelioid, round, or spindle-shaped cells within the lumina of dermal blood vessels, which show positivity for CD31 and CD34.9 Others suggest the lesions of intralymphatic histiocytosis arise from lymphangiectasia; obstruction of lymphatic drainage due to congenital abnormalities; or acquired damage from infection, trauma, surgery, or radiation.2 Due to the common association with rheumatoid arthritis and orthopedic implants, it is likely that lymphatic stasis secondary to chronic inflammation plays a notable role.
Therapies such as topical and systemic corticosteroids, local radiotherapy, cyclophosphamide, pentoxifylline, and arthrocentesis have been attempted without evidence of efficacy.2 Although intralymphatic histiocytosis is chronic and resistant to therapy, patients can be reassured that the condition runs a benign course.
1. O’Grady JT, Shahidullah H, Doherty VR, et al. Intravascular histiocytosis. Histopathology. 1994;24:265-268.
2. Requena L, El-Shabrawi-Caelen L, Walsh SN, et al. Intralymphatic histiocytosis. clinicopathologic study of 16 cases. Am J Dermatopathol. 2009;31:140-151.
3. Saggar S, Lee B, Krivo J, et al. Intralymphatic histiocytosis associated with orthopedic implants. J Drugs Dermatol. 2011;10:1208-1209.
4. Chiu YE, Maloney JE, Bengana C. Erythematous patch overlying a swollen knee—quiz case. intralymphatic histiocytosis. Arch Dermatol. 2010;146:1037-1042.
5. Rossari S, Scatena C, Gori A, et al. Intralymphatic histiocytosis: cutaneous nodules and metal implants. J Cutan Pathol. 2011;38:534-535.
6. Grekin S, Mesfin M, Kang S, et al. Intralymphatic histiocytosis following placement of a metal implant. J Cutan Pathol. 2011;38:351-353.
7. Watanabe T, Yamada N, Yoshida Y, et al. Intralymphatic histiocytosis with granuloma formation associated with orthopaedic metal implants. Br J Dermatol. 2008;158:402-404.
8. Rieger E, Soyer HP, Leboit PE, et al. Reactive angioendotheliomatosis or intravascular histiocytosis? an immunohistochemical and ultrastructural study in two cases of intravascular histiocytic cell proliferation. Br J Dermatol. 1999;140:497-504.
9. Rongioletti F, Rebora A. Cutaneous reactive angiomatoses: patterns and classification of reactive vascular proliferation. J Am Acad Dermatol. 2003;49:887-896.
1. O’Grady JT, Shahidullah H, Doherty VR, et al. Intravascular histiocytosis. Histopathology. 1994;24:265-268.
2. Requena L, El-Shabrawi-Caelen L, Walsh SN, et al. Intralymphatic histiocytosis. clinicopathologic study of 16 cases. Am J Dermatopathol. 2009;31:140-151.
3. Saggar S, Lee B, Krivo J, et al. Intralymphatic histiocytosis associated with orthopedic implants. J Drugs Dermatol. 2011;10:1208-1209.
4. Chiu YE, Maloney JE, Bengana C. Erythematous patch overlying a swollen knee—quiz case. intralymphatic histiocytosis. Arch Dermatol. 2010;146:1037-1042.
5. Rossari S, Scatena C, Gori A, et al. Intralymphatic histiocytosis: cutaneous nodules and metal implants. J Cutan Pathol. 2011;38:534-535.
6. Grekin S, Mesfin M, Kang S, et al. Intralymphatic histiocytosis following placement of a metal implant. J Cutan Pathol. 2011;38:351-353.
7. Watanabe T, Yamada N, Yoshida Y, et al. Intralymphatic histiocytosis with granuloma formation associated with orthopaedic metal implants. Br J Dermatol. 2008;158:402-404.
8. Rieger E, Soyer HP, Leboit PE, et al. Reactive angioendotheliomatosis or intravascular histiocytosis? an immunohistochemical and ultrastructural study in two cases of intravascular histiocytic cell proliferation. Br J Dermatol. 1999;140:497-504.
9. Rongioletti F, Rebora A. Cutaneous reactive angiomatoses: patterns and classification of reactive vascular proliferation. J Am Acad Dermatol. 2003;49:887-896.
Practice Points
- Consider intralymphatic histiocytosis in the differential diagnosis of an asymptomatic skin lesion overlying a joint, particularly in patients with orthopedic metal implants or rheumatoid arthritis.
- Biopsy is essential for the diagnosis of intralymphatic histiocytosis; special stains highlighting dilated lymphatic vessels and intravascular histiocytes may be necessary.
- Intralymphatic histiocytosis is chronic and resistant to therapy; however, patients can be reassured that the condition runs a benign course.

Grim projections for hepatitis C disease burden in the U.S.
Although highly effective oral direct-acting antivirals (DAAs) provide clinicians with the opportunity to reduce the substantial disease burden associated with hepatitis C virus (HCV) infection in the United States, the promise of these agents cannot be realized without the expansion of HCV screening and treatment capacity, according to a report published online in Hepatology.
Working with his colleagues, Dr. Jagpreet Chhatwal of the Massachusetts General Hospital Institute for Technology Assessment and of the department of radiology at Harvard Medical School, both in Boston, utilized a validated projection model previously developed by this research team to estimate the numbers of people in the United States who will die, develop hepatocellular carcinoma, and develop decompensated cirrhosis over the next 35 years (Hepatology. 2016 Mar 25. doi: 10.1002/hep.28571).
The results of the model provided an estimate of 320,000 for the cumulative number of HCV-associated deaths in individuals treated with oral DAAs from 2015 to 2050. In addition, the projected cumulative incidence of hepatocellular carcinoma was 157,000, and the projected cumulative incidence of decompensated cirrhosis was 203,000 in individuals treated with oral DAAs from 2015 to 2050. Furthermore, the projected number of liver transplants for those on DAAs between 2015 and 2050 was 32,000.
When assessing the variables that most heavily influenced the projections, the authors said that most of the ongoing burden of HCV is related to the proportion of infected individuals who remain unaware of their infection status.
Despite such grim predictions, the research suggests hope remains, the authors said. With the same model, changing the rate of treatment from 150,000 patients per year in 2014 to 280,000 patients per year from 2015 onward would result in large reductions in the projected disease burden. For example, 8,600 cases of decompensated cirrhosis, 5,400 cases of hepatocellular carcinoma, 9,700 liver-related deaths, and 900 liver transplants would be prevented. These numbers would increase further if the annual treatment rate was increased to 500,000 patients per year from 2015 onward, preventing 12,000 cases of decompensated cirrhosis, 7,400 cases of hepatocellular carcinoma, 13,500 liver-related deaths, and 1,400 liver transplants. These model-based results emphasize the importance of expanding treatment capacity, as well as HCV screening efforts, the investigators said.
The results are important for the planning and distribution of health care resources and personnel in order to ensure that they match both current and future treatment demands, the investigators added. As an example, they highlighted their projection indicating that the number of clinicians and facilities offering HCV treatment would need to increase substantially over the next 3-4 years. Toward this end, they suggested that primary care physicians or infectious disease specialists be incorporated into HCV treatment capacity expansion.
This project was funded in part by the National Institutes of Health and Gilead Sciences. No conflicts of interest were declared.
Although highly effective oral direct-acting antivirals (DAAs) provide clinicians with the opportunity to reduce the substantial disease burden associated with hepatitis C virus (HCV) infection in the United States, the promise of these agents cannot be realized without the expansion of HCV screening and treatment capacity, according to a report published online in Hepatology.
Working with his colleagues, Dr. Jagpreet Chhatwal of the Massachusetts General Hospital Institute for Technology Assessment and of the department of radiology at Harvard Medical School, both in Boston, utilized a validated projection model previously developed by this research team to estimate the numbers of people in the United States who will die, develop hepatocellular carcinoma, and develop decompensated cirrhosis over the next 35 years (Hepatology. 2016 Mar 25. doi: 10.1002/hep.28571).
The results of the model provided an estimate of 320,000 for the cumulative number of HCV-associated deaths in individuals treated with oral DAAs from 2015 to 2050. In addition, the projected cumulative incidence of hepatocellular carcinoma was 157,000, and the projected cumulative incidence of decompensated cirrhosis was 203,000 in individuals treated with oral DAAs from 2015 to 2050. Furthermore, the projected number of liver transplants for those on DAAs between 2015 and 2050 was 32,000.
When assessing the variables that most heavily influenced the projections, the authors said that most of the ongoing burden of HCV is related to the proportion of infected individuals who remain unaware of their infection status.
Despite such grim predictions, the research suggests hope remains, the authors said. With the same model, changing the rate of treatment from 150,000 patients per year in 2014 to 280,000 patients per year from 2015 onward would result in large reductions in the projected disease burden. For example, 8,600 cases of decompensated cirrhosis, 5,400 cases of hepatocellular carcinoma, 9,700 liver-related deaths, and 900 liver transplants would be prevented. These numbers would increase further if the annual treatment rate was increased to 500,000 patients per year from 2015 onward, preventing 12,000 cases of decompensated cirrhosis, 7,400 cases of hepatocellular carcinoma, 13,500 liver-related deaths, and 1,400 liver transplants. These model-based results emphasize the importance of expanding treatment capacity, as well as HCV screening efforts, the investigators said.
The results are important for the planning and distribution of health care resources and personnel in order to ensure that they match both current and future treatment demands, the investigators added. As an example, they highlighted their projection indicating that the number of clinicians and facilities offering HCV treatment would need to increase substantially over the next 3-4 years. Toward this end, they suggested that primary care physicians or infectious disease specialists be incorporated into HCV treatment capacity expansion.
This project was funded in part by the National Institutes of Health and Gilead Sciences. No conflicts of interest were declared.
Although highly effective oral direct-acting antivirals (DAAs) provide clinicians with the opportunity to reduce the substantial disease burden associated with hepatitis C virus (HCV) infection in the United States, the promise of these agents cannot be realized without the expansion of HCV screening and treatment capacity, according to a report published online in Hepatology.
Working with his colleagues, Dr. Jagpreet Chhatwal of the Massachusetts General Hospital Institute for Technology Assessment and of the department of radiology at Harvard Medical School, both in Boston, utilized a validated projection model previously developed by this research team to estimate the numbers of people in the United States who will die, develop hepatocellular carcinoma, and develop decompensated cirrhosis over the next 35 years (Hepatology. 2016 Mar 25. doi: 10.1002/hep.28571).
The results of the model provided an estimate of 320,000 for the cumulative number of HCV-associated deaths in individuals treated with oral DAAs from 2015 to 2050. In addition, the projected cumulative incidence of hepatocellular carcinoma was 157,000, and the projected cumulative incidence of decompensated cirrhosis was 203,000 in individuals treated with oral DAAs from 2015 to 2050. Furthermore, the projected number of liver transplants for those on DAAs between 2015 and 2050 was 32,000.
When assessing the variables that most heavily influenced the projections, the authors said that most of the ongoing burden of HCV is related to the proportion of infected individuals who remain unaware of their infection status.
Despite such grim predictions, the research suggests hope remains, the authors said. With the same model, changing the rate of treatment from 150,000 patients per year in 2014 to 280,000 patients per year from 2015 onward would result in large reductions in the projected disease burden. For example, 8,600 cases of decompensated cirrhosis, 5,400 cases of hepatocellular carcinoma, 9,700 liver-related deaths, and 900 liver transplants would be prevented. These numbers would increase further if the annual treatment rate was increased to 500,000 patients per year from 2015 onward, preventing 12,000 cases of decompensated cirrhosis, 7,400 cases of hepatocellular carcinoma, 13,500 liver-related deaths, and 1,400 liver transplants. These model-based results emphasize the importance of expanding treatment capacity, as well as HCV screening efforts, the investigators said.
The results are important for the planning and distribution of health care resources and personnel in order to ensure that they match both current and future treatment demands, the investigators added. As an example, they highlighted their projection indicating that the number of clinicians and facilities offering HCV treatment would need to increase substantially over the next 3-4 years. Toward this end, they suggested that primary care physicians or infectious disease specialists be incorporated into HCV treatment capacity expansion.
This project was funded in part by the National Institutes of Health and Gilead Sciences. No conflicts of interest were declared.
FROM HEPATOLOGY
Key clinical point: Unless screening and treatment capacity for hepatitis C virus infection are expanded, associated disease burdens are projected to remain high, despite the availability of highly efficacious direct-acting antiviral agents.
Major Finding: Model-based projections suggest that hundreds of thousands of people will die, develop hepatocellular carcinoma, and develop decompensated cirrhosis in the United States by 2050.
Data Source: A validated hepatitis C disease burden simulation model previously developed and used to project the changing prevalence of hepatitis C virus in the United States.
Disclosures: This project was funded in part by the National Institutes of Health and Gilead Sciences. No conflicts of interest were declared.
New Sepsis Definition, Bedside Screening to Identify Patients at High-Mortality Risk
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What are the best criteria to identify sepsis and septic shock?
Bottom line: An international task force of experts has updated the definitions of sepsis and septic shock and created a new bedside scoring tool to identify patients with suspected infection who may be at high risk for poor outcomes. Based on the Sequential Organ Failure Assessment (SOFA) score, the new quickSOFA states that meeting 2 of 3 clinical criteria (respiratory rate of 22 per minute or greater, systolic blood pressure of 100 mg Hg or less, and altered mental status) identifies patients at high risk of poor outcomes from sepsis. This score will need to be validated further in multiple health care settings before it can be widely accepted in clinical practice. (LOE = 5)
References: Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801-810.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis (Sepsis-3). JAMA 2016;315(8):762-774.
Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock (Sepsis-3). JAMA 2016;315(8):775-787.
Study design: Other
Funding source: Foundation
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: Systemic inflammatory response syndrome (SIRS) criteria are present in many hospitalized patients, even those without infections or life-threatening illnesses. The use of these criteria to identify sepsis may lead to misdiagnosis. Funded by the European Society of Intensive Care Medicine and the Society of Critical Care Medicine, an international task force consisting of 19 critical care, infectious disease, surgical, and pulmonary specialists convened to update the definitions of sepsis and septic shock and identify clinical criteria that can be used to recognize patients at high risk for mortality. Researchers conducted a systematic review and meta-analysis of observational studies followed by a Delphi consensus process to determine appropriate criteria for identifying septic shock. Furthermore, they validated and confirmed the ability of different clinical criteria, including the SIRS criteria and the SOFA score, to predict poor outcomes in patients with suspected infection.
Per the task force's recommendations, sepsis should be defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis in which there is an increased risk of mortality due to profound circulatory and cellular metabolism abnormalities. Sepsis can be identified by an increase in the SOFA score of 2 points or more. This is associated with an in-hospital mortality exceeding 10%. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and a serum lactate level greater than 18 mg/dL (> 2 mmol/L) after adequate fluid resuscitation. This combination of clinical criteria is associated with a hospital mortality rate of 40%.
Using a derivation and validation cohort of approximately 75,000 patients, the group also developed a new bedside clinical measure termed quickSOFA, or qSOFA, which consists of a respiratory rate of 22 per minute or greater, altered mental status, and systolic blood pressure of 100 mm Hg or less. Patients with suspected infection who are not in the intensive care unit and have at least 2 of these 3 criteria are at higher risk of poor outcomes from sepsis (area under receiver operating characteristics curve = 0.81).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Research Reaffirms Management of Hospitalized Patients with Community-Acquired Pneumonia
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: What is the best antibiotic strategy to improve outcomes in patients hospitalized with community-acquired pneumonia?
Bottom line: For patients hospitalized with community-acquired pneumonia (CAP), start antibiotics early, use either fluoroquinolone monotherapy or beta-lactam/macrolide combination therapy, and switch to oral antibiotics as soon as patients are hemodynamically stable and can take oral medications. Although the evidence is mostly of low quality, this review reaffirms what we already do. (LOE = 2a)
Reference: Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia. JAMA 2016;315(6):593-602.
Study design: Systematic review
Funding source: Unknown/not stated
Allocation: Uncertain
Setting: Inpatient (ward only)
Synopsis: These investigators searched MEDLINE, EMBASE, and the Cochrane databases to identify studies that evaluated outcomes for patients hospitalized with CAP with regard to optimal timing of antibiotic initiation, initial antibiotic selection, and criteria for transition from intravenous to oral antibiotic therapy. Two authors independently reviewed studies for inclusion and assessed study quality.
Of 8 low-quality observational studies, 4 showed a significant association between initiating antibiotic therapy within 4 hours to 8 hours of hospital arrival and reduced mortality. When comparing 2 different antibiotic strategies, 6 of 8 observational studies showed mortality benefit with the use of beta-lactams plus macrolides as compared with beta-lactam monotherapy, though the 2 recent high-quality randomized trials had conflicting results. All three observational studies that compared fluoroquinolones with beta-lactam monotherapy for the treatment of CAP showed an association with fluoroquinolone use and decreased mortality.
Finally, one high-quality trial showed that transitioning patients to oral antibiotics once they meet clinical criteria for stability (stable vital signs, lack of confusion, ability to tolerate oral medications) leads to a shorter length of stay.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Similarities seen in rate and rhythm control for postsurgical AF
CHICAGO – Rate and rhythm control proved equally effective for treatment of new-onset post–cardiac surgery atrial fibrillation in a randomized trial that was far and away the largest ever to examine the best way to address this common and costly arrhythmia, Dr. A. Marc Gillinov said at the annual meeting of the American College of Cardiology.
Thus, either strategy is acceptable. That being said, rate control gets the edge as the initial treatment strategy because it avoids the considerable toxicities accompanying amiodarone for rhythm control, most of which arise only after patients have been discharged from the hospital. In contrast, when rate control doesn’t work, it becomes evident while the patient is still in the hospital, according to Dr. Gillinov, a cardiothoracic surgeon at the Cleveland Clinic .

Atrial fibrillation (AF) is the most common complication of cardiac surgery, with an incidence variously reported at 20%-50%. It results in lengthier hospital stays, greater cost of care, and increased risks of mortality, stroke, heart failure, and infection. Postoperative AF adds an estimated $1 billion per year to health care costs in the United States.
While current ACC/AHA/Heart Rhythm Society joint guidelines recommend rate control with a beta-blocker as first-line therapy for patients with this postoperative complication, with a class I, level-of-evidence A rating, upon closer inspection the evidence cited mainly involves extrapolation from studies looking at how to prevent postoperative AF. Because no persuasive evidence existed as to how best to treat this common and economically and medically costly condition, Dr. Gillinov and his coinvestigators in the National Institutes of Health–funded Cardiothoracic Surgical Trials Network carried out a randomized trial 10-fold larger than anything prior.
The 23-site study included 2,109 patients enrolled prior to cardiac surgery, of whom 40% underwent isolated coronary artery bypass grafting (CABG) while the other 60% had valve surgery, either alone or with CABG. These proportions reflect current cardiac surgery treatment patterns nationally. Overall, 33% of the cardiac surgery patients experienced postoperative AF. The incidence was 28% in patients who underwent isolated CABG but rose with increasing surgical complexity to nearly 50% in patients who had combined CABG and valve operations. The average time to onset of postoperative AF was 2.4 days.
A total of 523 patients with postoperative AF were randomized to rate or rhythm control. Rate control most often entailed use of a beta-blocker, while amiodarone was prescribed for rhythm control.
The primary endpoint in the trial was a measure of health care resource utilization: total days in hospital during a 60-day period starting from the time of randomization. This endpoint was a draw: a median of 5.1 days with rate control and 5.0 days with rhythm control.
At hospital discharge, 89.9% of patients in the rate control group and 93.5% in the rhythm control group had a stable heart rhythm without AF. From discharge to 60 days, 84.2% of patients in the rate control group and a similar 86.9% of the rhythm control group remained free of AF.
Rates of serious adverse events were similar in the two groups: 24.8 per 100 patient-months in the rate control arm and 26.4 per 100 patient-months in the rhythm control arm. Three patients in the rate control arm died during the 60-day study period, and two died in the rhythm control group.
Of note, roughly one-quarter of patients in each study arm crossed over to the other arm. In the rate control group, this was typically due to drug ineffectiveness, while in the rhythm control arm the switch was most often made in response to amiodarone side effects.
Roughly 43% of patients in each group were placed on anticoagulation with warfarin for 60 days according to study protocol, which called for such action if a patient remained in AF 48 hours after randomization.
There were five strokes, one case of transient ischemic attack, and four noncerebral thromboembolisms. Also, 21 bleeding events occurred, 17 of which were classified as serious; 90% of the bleeding events happened in patients on warfarin.
“I found the results very striking and very reassuring,” said discussant Hugh G. Calkins. “To me, the clinical message is clearly that rate control is the preference.”
It was troubling, however, to see that 10 thromboembolic events occurred in 523 patients over the course of just 60 days. “Should we be anticoagulating these postsurgical atrial fibrillation patients a lot more frequently?” asked Dr. Calkins, professor of medicine and of pediatrics and director of the cardiac arrhythmia service at Johns Hopkins University, Baltimore.
Dr. Gillinov replied that he and his colleagues in the Cardiothoracic Surgical Trials Network consider that to be the key remaining question regarding postoperative AF. They are now planning a clinical trial aimed at finding the optimal balance between stroke protection via anticoagulation and bleeding risk.
The National Institutes of Health and the Canadian Institutes of Health Research funded the work. Dr. Gillinov reported serving as a consultant to five surgical device companies, none of which played any role in the study.
Simultaneously with Dr. Gillinov’s presentation at ACC 16, the study results were published in the New England Journal of Medicine (doi: 10.1056/NEJMoa1602002).
CHICAGO – Rate and rhythm control proved equally effective for treatment of new-onset post–cardiac surgery atrial fibrillation in a randomized trial that was far and away the largest ever to examine the best way to address this common and costly arrhythmia, Dr. A. Marc Gillinov said at the annual meeting of the American College of Cardiology.
Thus, either strategy is acceptable. That being said, rate control gets the edge as the initial treatment strategy because it avoids the considerable toxicities accompanying amiodarone for rhythm control, most of which arise only after patients have been discharged from the hospital. In contrast, when rate control doesn’t work, it becomes evident while the patient is still in the hospital, according to Dr. Gillinov, a cardiothoracic surgeon at the Cleveland Clinic .
Atrial fibrillation (AF) is the most common complication of cardiac surgery, with an incidence variously reported at 20%-50%. It results in lengthier hospital stays, greater cost of care, and increased risks of mortality, stroke, heart failure, and infection. Postoperative AF adds an estimated $1 billion per year to health care costs in the United States.
While current ACC/AHA/Heart Rhythm Society joint guidelines recommend rate control with a beta-blocker as first-line therapy for patients with this postoperative complication, with a class I, level-of-evidence A rating, upon closer inspection the evidence cited mainly involves extrapolation from studies looking at how to prevent postoperative AF. Because no persuasive evidence existed as to how best to treat this common and economically and medically costly condition, Dr. Gillinov and his coinvestigators in the National Institutes of Health–funded Cardiothoracic Surgical Trials Network carried out a randomized trial 10-fold larger than anything prior.
The 23-site study included 2,109 patients enrolled prior to cardiac surgery, of whom 40% underwent isolated coronary artery bypass grafting (CABG) while the other 60% had valve surgery, either alone or with CABG. These proportions reflect current cardiac surgery treatment patterns nationally. Overall, 33% of the cardiac surgery patients experienced postoperative AF. The incidence was 28% in patients who underwent isolated CABG but rose with increasing surgical complexity to nearly 50% in patients who had combined CABG and valve operations. The average time to onset of postoperative AF was 2.4 days.
A total of 523 patients with postoperative AF were randomized to rate or rhythm control. Rate control most often entailed use of a beta-blocker, while amiodarone was prescribed for rhythm control.
The primary endpoint in the trial was a measure of health care resource utilization: total days in hospital during a 60-day period starting from the time of randomization. This endpoint was a draw: a median of 5.1 days with rate control and 5.0 days with rhythm control.
At hospital discharge, 89.9% of patients in the rate control group and 93.5% in the rhythm control group had a stable heart rhythm without AF. From discharge to 60 days, 84.2% of patients in the rate control group and a similar 86.9% of the rhythm control group remained free of AF.
Rates of serious adverse events were similar in the two groups: 24.8 per 100 patient-months in the rate control arm and 26.4 per 100 patient-months in the rhythm control arm. Three patients in the rate control arm died during the 60-day study period, and two died in the rhythm control group.
Of note, roughly one-quarter of patients in each study arm crossed over to the other arm. In the rate control group, this was typically due to drug ineffectiveness, while in the rhythm control arm the switch was most often made in response to amiodarone side effects.
Roughly 43% of patients in each group were placed on anticoagulation with warfarin for 60 days according to study protocol, which called for such action if a patient remained in AF 48 hours after randomization.
There were five strokes, one case of transient ischemic attack, and four noncerebral thromboembolisms. Also, 21 bleeding events occurred, 17 of which were classified as serious; 90% of the bleeding events happened in patients on warfarin.
“I found the results very striking and very reassuring,” said discussant Hugh G. Calkins. “To me, the clinical message is clearly that rate control is the preference.”
It was troubling, however, to see that 10 thromboembolic events occurred in 523 patients over the course of just 60 days. “Should we be anticoagulating these postsurgical atrial fibrillation patients a lot more frequently?” asked Dr. Calkins, professor of medicine and of pediatrics and director of the cardiac arrhythmia service at Johns Hopkins University, Baltimore.
Dr. Gillinov replied that he and his colleagues in the Cardiothoracic Surgical Trials Network consider that to be the key remaining question regarding postoperative AF. They are now planning a clinical trial aimed at finding the optimal balance between stroke protection via anticoagulation and bleeding risk.
The National Institutes of Health and the Canadian Institutes of Health Research funded the work. Dr. Gillinov reported serving as a consultant to five surgical device companies, none of which played any role in the study.
Simultaneously with Dr. Gillinov’s presentation at ACC 16, the study results were published in the New England Journal of Medicine (doi: 10.1056/NEJMoa1602002).
CHICAGO – Rate and rhythm control proved equally effective for treatment of new-onset post–cardiac surgery atrial fibrillation in a randomized trial that was far and away the largest ever to examine the best way to address this common and costly arrhythmia, Dr. A. Marc Gillinov said at the annual meeting of the American College of Cardiology.
Thus, either strategy is acceptable. That being said, rate control gets the edge as the initial treatment strategy because it avoids the considerable toxicities accompanying amiodarone for rhythm control, most of which arise only after patients have been discharged from the hospital. In contrast, when rate control doesn’t work, it becomes evident while the patient is still in the hospital, according to Dr. Gillinov, a cardiothoracic surgeon at the Cleveland Clinic .
Atrial fibrillation (AF) is the most common complication of cardiac surgery, with an incidence variously reported at 20%-50%. It results in lengthier hospital stays, greater cost of care, and increased risks of mortality, stroke, heart failure, and infection. Postoperative AF adds an estimated $1 billion per year to health care costs in the United States.
While current ACC/AHA/Heart Rhythm Society joint guidelines recommend rate control with a beta-blocker as first-line therapy for patients with this postoperative complication, with a class I, level-of-evidence A rating, upon closer inspection the evidence cited mainly involves extrapolation from studies looking at how to prevent postoperative AF. Because no persuasive evidence existed as to how best to treat this common and economically and medically costly condition, Dr. Gillinov and his coinvestigators in the National Institutes of Health–funded Cardiothoracic Surgical Trials Network carried out a randomized trial 10-fold larger than anything prior.
The 23-site study included 2,109 patients enrolled prior to cardiac surgery, of whom 40% underwent isolated coronary artery bypass grafting (CABG) while the other 60% had valve surgery, either alone or with CABG. These proportions reflect current cardiac surgery treatment patterns nationally. Overall, 33% of the cardiac surgery patients experienced postoperative AF. The incidence was 28% in patients who underwent isolated CABG but rose with increasing surgical complexity to nearly 50% in patients who had combined CABG and valve operations. The average time to onset of postoperative AF was 2.4 days.
A total of 523 patients with postoperative AF were randomized to rate or rhythm control. Rate control most often entailed use of a beta-blocker, while amiodarone was prescribed for rhythm control.
The primary endpoint in the trial was a measure of health care resource utilization: total days in hospital during a 60-day period starting from the time of randomization. This endpoint was a draw: a median of 5.1 days with rate control and 5.0 days with rhythm control.
At hospital discharge, 89.9% of patients in the rate control group and 93.5% in the rhythm control group had a stable heart rhythm without AF. From discharge to 60 days, 84.2% of patients in the rate control group and a similar 86.9% of the rhythm control group remained free of AF.
Rates of serious adverse events were similar in the two groups: 24.8 per 100 patient-months in the rate control arm and 26.4 per 100 patient-months in the rhythm control arm. Three patients in the rate control arm died during the 60-day study period, and two died in the rhythm control group.
Of note, roughly one-quarter of patients in each study arm crossed over to the other arm. In the rate control group, this was typically due to drug ineffectiveness, while in the rhythm control arm the switch was most often made in response to amiodarone side effects.
Roughly 43% of patients in each group were placed on anticoagulation with warfarin for 60 days according to study protocol, which called for such action if a patient remained in AF 48 hours after randomization.
There were five strokes, one case of transient ischemic attack, and four noncerebral thromboembolisms. Also, 21 bleeding events occurred, 17 of which were classified as serious; 90% of the bleeding events happened in patients on warfarin.
“I found the results very striking and very reassuring,” said discussant Hugh G. Calkins. “To me, the clinical message is clearly that rate control is the preference.”
It was troubling, however, to see that 10 thromboembolic events occurred in 523 patients over the course of just 60 days. “Should we be anticoagulating these postsurgical atrial fibrillation patients a lot more frequently?” asked Dr. Calkins, professor of medicine and of pediatrics and director of the cardiac arrhythmia service at Johns Hopkins University, Baltimore.
Dr. Gillinov replied that he and his colleagues in the Cardiothoracic Surgical Trials Network consider that to be the key remaining question regarding postoperative AF. They are now planning a clinical trial aimed at finding the optimal balance between stroke protection via anticoagulation and bleeding risk.
The National Institutes of Health and the Canadian Institutes of Health Research funded the work. Dr. Gillinov reported serving as a consultant to five surgical device companies, none of which played any role in the study.
Simultaneously with Dr. Gillinov’s presentation at ACC 16, the study results were published in the New England Journal of Medicine (doi: 10.1056/NEJMoa1602002).
AT ACC 16
Key clinical point: Rate control offers the advantage of simplicity over a rhythm control strategy in new-onset atrial fibrillation after cardiac surgery.
Major finding: Rate and rhythm control strategies for treatment of new-onset atrial fibrillation after cardiac surgery resulted in equal numbers of hospital days, similar serious complication rates, and low rates of persistent atrial fibrillation at 60 days of follow-up.
Data source: A randomized clinical trial of 523 patients with new-onset atrial fibrillation following cardiac surgery at 23 U.S. and Canadian academic medical centers.
Disclosures: The study was funded by the National Institutes of Health and the Canadian Institutes of Health Research and carried out through the Cardiothoracic Surgical Trials Network. The presenter reported having no relevant financial interests.
